predictive modeling news - magnacare
TRANSCRIPT

Volume 3, Number 5 May 2010
Published by Health Policy Publishing, LLC ● 209-577-4888 ● www.predictivemodelingnews.com
In This Issue 1 New ‘Prediction Market’
Aims to Aid Drug Discovery
1 Looming ICD-10 Conversion Bodes Well for PM Players
3 MagnaCare’s Predictive Analytics Tool Fuels Northeast Market Growth
4 Journals Examine Using PM for Rate Adjusting, Fraud Detecting
5 PM Permeates Managed Care Executives’ Issues List
7 Subscribers’ Corner
8 Thought Leader’s Corner
9 Industry News
12 Data Snapshots Looming ICD-10 Conversion Bodes
Well for Predictive Modeling Players Milliman Inc.’s Rong Yi shares implications, strategies and approaches by Russell A. Jackson
he switch from ICD-9 to ICD-10 won’t be easy, but it should be quite productive for the predictive modeling community. Better data, simply, mean better models and better results. Rong Yi PhD, senior consultant in the Boston office of Milliman Inc., discussed the impending switch in a recent HealthcareWebSummit presentation on “Predictive
Modeling Implications for ICD-10 Conversion.” Here, she addresses three follow-up questions.
[1] What are the major implications of ICD-10 for predictive modeling?
As we all know, ICD-10-CM will become effective on October 1, 2013. The implementation of ICD-10 is a significant advance for the healthcare industry in the United States. It’s a better analytic tool for the healthcare industry in managing and understanding risk, and it’s also a very important event for the predictive modeling community. Let me first make an observation as an economist -- by training, I’m an economist specializing in health economics. In economics, there’s a term called “menu cost,” which is the cost that a business has to incur when updating its menus or price lists -- things like brochures or other marketing materials -- as a response to changes in the market. Those market conditions could be competition that drives down costs or general inflation that increases costs or innovation that requires an updated product manual or brochure. Basically, it’s viewed as a transaction cost that may cause stickiness in business operations in response to those market changes. The changes are needed, but it takes a little time to have them in full force.
The debate around the implementation schedule for ICD-10-CM had been going on for quite some time, which is exactly what the economic theories are projecting. It’s important to remember that while there is going to be stickiness in the process, the industry overall has reached consensus that ICD-10-CM will provide richer details on medical diagnoses and procedures.
continued on page 6
T
rug devfrom the past to see the futurund
or failurD elopers are using a version of predictive modeling that relies not on data
e but on comments from live experts who put their erstanding of relevant products and services into play to predict the success
e of a new product launch. Recently, in fact, Redwood City, CA-based Crowdcast, along with faculty from MIT and Harvard University, have launched the Pharmer’s Market, a so-called “prediction market” that, according to a statement, “harnesses collective intelligence to predict the likelihood of breast cancer drugs succeeding through the three phases of drug clinical trials.”
The first of its kind, the Pharmer’s Market was created by Ragu Bharadwaj, Eric von Hippel and Fiona Murray of MIT’s Sloan School of Management, with Peter Coles of the Harvard Business School serving as an advisor. The prediction market was developed using Crowdcast’s patented Team Intelligence Platform, which, the company says, “anonymously collects intelligence from a diversified group of people who have insight into breast cancer drug trials.” In addition to helping predict the outcome of clinical trials, the Pharmer’s Market will also help doctors and patients gain insights into the safety and efficacy of specific drugs at the early stages of clinical trials, the statement says, beyond information that is publicly available.
continued on page 2
New ‘Prediction Market’ Aims to Aid Drug Discovery
Using the wisdom of crowds to forecast accurate outcomes by Russell A. Jackson

2 Predictive Modeling News May 2010
To subscribe: visit www.predictivemodelingnews.com or call 209-577-4888 page 2
Predictive Modeling News Editorial Advisory Board Swati Abbott President, MEDai Inc., Orlando, FL Ian Duncan FSA FIA FCIA MAAA President, Solucia Inc., Farmington, CT Peter N. Grant JD PhD President, Health Care Conference Administrators LLC, Partner and Co-Chair, Health Law Group, Davis Wright Tremaine LLP, Editorial Board, Health Affairs, Advisory Board, Harvard Health Policy Review, Seattle, WA Soyal Momin MBA Manager, Research and Development and Consulting, BlueCross BlueShield of Tennessee, Chattanooga, TN Jeremy J. Nobel MD MPH Adjunct Lecturer, Department of Health Policy and Management, Harvard University School of Public Health, Boston, MA Seth Serxner PhD MPH Principal, Mercer, Los Angeles, CA Jonathan P. Weiner DrPH Professor of Health Policy & Management, Johns Hopkins University Bloomberg School of Public Health, Baltimore, MD
Publisher Clive Riddle, President, MCOL Editor Russell A. Jackson Predictive Modeling News is published monthly by Health Policy Publishing, LLC. Newsletter publication administration is provided by MCOL. Predictive Modeling News 1101 Standiford Avenue, Suite C-3 Modesto, CA 95350 Phone: 209.577.4888 Fax: 209.577.3557 [email protected] www.predicitivemodelingnews.com Copyright © 2010 by Health Policy Publishing, LLC. All rights reserved. No part of this publication may be reproduced or transmitted by any means, electronic or mechanical including photocopy, fax, or electronic delivery without the prior written permission of the publisher. Subscribe to Predictive Modeling News – the only newsletter dedicated to predictive modeling in healthcare. Subscriptions are available for $39 a month or $468 a year. To subscribe, call 209-577-4888 or go to www.predictivemodelingnews.com.
New ‘Prediction Market’ Aims to Aid…continued “Today’s pharmaceutical industry is faced with exponentially rising costs, but fewer drugs than ever are approved,” comments Bharadwaj. “One cause is the lack of information sharing, and the Pharmer’s Market will redress that by allowing people to aggregate and share information and solutions based on their own experiences and knowledge, creating a superior prediction model. Our aim is to be a resource for the pharmaceutical community, so that researchers can tap existing knowledge and stop duplicating efforts and wasting resources, preventing delays in drug development.” The Pharmer’s Market launched with six drugs in clinical trials for the treatment of breast cancer, and uses the intelligence of the pharmaceutical and medical community at large to predict the success likelihoods that the drugs will progress through the phases of testing, the statement continues. The market will be open to the public; participants include drug researchers at pharmaceutical companies, chemists, researchers in academia and the government, pharmaceutical financial analysts and the greater medical community. Members of the market will also be able to participate in a community forum and provide comments on their “trades.”
Comments Leslie Fine, chief strategist at Crowdcast: “Prediction markets utilize the wisdom of the crowd to forecast future outcomes with high accuracy. The system works by aggregating and balancing collective intelligence through a prediction market, rewarding and empowering those contributing accurate forecasts. For the pharmaceutical community, prediction markets are an innovative way to harness and share information that will help speed drug development and predict outcomes of clinical trials.” The Pharmer’s Market is now live. To participate, visit: http://pharmersmarket.crowdcast.com.
Predictive Modeling News talked to Crowdcast CEO Mat Fogarty about prediction markets and their relevance to drug discovery.
Predictive Modeling News: How exactly does a “prediction market” work?
Mat Fogarty: A prediction market aggregates the insight of a group of people to bet on a forecast that represents the knowledge of the entire collective. While all bets are anonymous to allow participants to freely share their knowledge, Crowdcast’s collective intelligence technology has a built-in reward mechanism that rewards participants who offer the most insight-driven predictions. Crowdcast applies the technology to help companies tap employee insight to gather better data around key company metrics and, ultimately, make better decisions about the future. Those “employee-powered” predictions about product ship dates, budget allocation, price points and a broad range of other metrics are used to make informed planning decisions and adjustments, set goals and keep projects on track. To quickly highlight a couple of general points, Crowdcast has two distinct faces: one for decision makers and the other for market participants. For decision makers, Crowdcast is a dashboard that provides an accurate, real-time view into what’s really going on with their projects and initiatives. For participants, Crowdcast is an engaging and lightweight way to share insights about forward-looking metrics. Participants start out with a fixed amount of virtual cash they use to bet on outcomes of metrics. It provides unbiased forecasts by rewarding people for being correct and allowing them to share their insights anonymously. PMN: Where do you get contributors from? MF: The Pharmer’s Market is a public market, which means that anyone with interest or experience in the pharma space can participate. In internal enterprise markets, participants can include employees, partners and/or clients; they’re invited by the market administrator based on their expertise and area of focus. For instance, a brand manager who wishes to “crowdcast” the launch date of a new product might invite people from sales, engineering, manufacturing and marketing. In the case of the Pharmer’s Market, participation was driven by industry interest in the market as a new concept that could improve the drug discovery process. PMN: Are contributors vetted in any way? How? Who gets in?
continued on page 7

May 2010 Predictive Modeling News 3
© 2010, Health Policy Publishing, LLC. All rights reserved. No reproduction or electronic forwarding without permission. page 3
MagnaCare’s Predictive Analytics Tool Fuels Northeast Market Growth Predictive modeling helps identify company-wide and individual health issues for proactive management
ew York-based MagnaCare, a health plan services company with national reach, plans to build on its “stable customer base” and “dominant position in the fiercely competitive New York-New Jersey-Connecticut region” to expand into the broader healthcare services market. And it plans to use predictive modeling to do so. Pointing to, as it calls it, “innovative
differentiators fueling continued growth and expanded market share,” MagnaCare cites its ability to “provide exemplary customer service and offer deep discounts to Taft-Hartley funds; self-insured companies; commercial insurers for health, workers’ compensation or no-fault; third-party administrators; and government entities.”
N
Adds Joseph Berardo Jr., CEO and president at MagnaCare: “As healthcare costs continue to rise, it is no longer sufficient to rely on network discounts or disease management to control costs. It is now becoming increasingly evident that self-insured plan sponsors need to proactively manage chronic conditions – like diabetes and coronary artery disease -- so that members remain as healthy as possible and are educated and encouraged to manage their diseases.” Predictive modeling, he says, when tied to a member outreach program, “gives self-insured plan sponsors the tools necessary to identify company-wide and individual health issues, review gaps in care and proactively manage those members to get the most out of their healthcare dollars.”
The analytics enable clients to identify gaps in care and then implement coaching, wellness and health improvement initiatives at the individual level.
And MagnaCare is the company to provide those tools, he says. “With 20 years of vigorous organic growth, MagnaCare serves a diverse customer base and maintains long-standing relationships, with our top 20 customers averaging nearly 10-plus years,” he comments. “We’ve demonstrated high retention rates – averaging 95% historically -- positive pricing trends and historic investments in infrastructure support. That stellar market position is reflected in a solid financial profile with an overall compound annual growth rate of over 12%.”
Integral to that robust market position, he emphasizes, is “market receptivity for the MagnaCare Evaluaide product,” which he characterizes as “a sophisticated program that offers the best in predictive modeling combined with individualized coaching and outreach.” He explains: “We empower our clients with state-of-the-art health analysis technology that confidentially assesses the health risks of every member and their dependents. When risks are identified, Evaluaide coordinates unlimited one-on-one guidance to the individuals who need it the most.” The analytics enable clients to identify gaps in care and then implement coaching, wellness and health improvement initiatives at the individual level. “That type of product is typically not available from our competitors,” Berardo notes.
Those identified as high-risk -- the top 20% of members -- will typically receive a phone call from a health advocate, who generally is a registered nurse, who explains the program, encourages participation and offers to act as a healthcare coach in helping to manage the disease or condition.
The data that populate the predictive models come from MagnaCare’s claim systems, its pharmacy benefits management company and various labs. After the analytics are completed, the Evaluaide tool “offers a complete list of members and their risks vis a vis various conditions and diseases,” Berardo explains. “That information is forwarded to our health advocates, who stratify the population into high, medium and low risks.” Those identified as high-risk -- the top 20% of members -- will typically receive a phone call from a health advocate, who generally is a registered nurse, who explains the program, encourages participation and offers to act as a healthcare coach in helping to manage the disease or condition.
The coaching includes “effective management of the disease or condition, goal setting and measuring progress toward achieving those goals, direction to a variety of third-party information sources, arranging appropriate doctor visits and anything else the member chooses to discuss,” Berardo adds. The ultimate purpose, of course, is to increase members’ knowledge of their diseases and conditions and to teach them how to manage them and how to develop the skills necessary to make the right lifestyle choices. “Most importantly,” Berardo says, “the sessions are designed to keep members motivated to manage their diseases.” The amount of time for a coach and member to work together is unlimited. The services are also offered to medium- and low-risk members, but the initial communication in those cases is typically via mail.
Additionally, MagnaCareRx, the company’s own PBM, “effectively addresses the pharmaceutical spend with a transparent business model that meets the fiscal needs of employers and payers,” Berardo continues. “At a time when few health plans are growing, MagnaCare presents unique, highly sophisticated offerings that have enabled us to capture significant market share in the Northeast -- a platform that allows for powerful national expansion. We offer a compelling value proposition that is based on delivering value to customers, payers and providers.” He stresses that the scope of the MagnaCare provider network and its proprietary medical delivery system is “analogous to competitive offerings.”
The MagnaCare leadership team has identified numerous opportunities that could immediately enhance its product offerings, Berardo says, and has laid the groundwork for both geographic and product expansion. Plans are underway for continued development and implementation of new program offerings as the company explores additional opportunities for accelerating growth.
continued on page 6

4 Predictive Modeling News May 2010
To subscribe: visit www.predictivemodelingnews.com or call 209-577-4888 page 4
Journals Examine Using Predictive Modeling for Rate Adjusting, Fraud Detecting PM looks to play an even more important role in tomorrow’s post-reform healthcare system, and researchers are hard at work figuring out how best to apply it. Here’s what’s been in the journals lately.
Taiwanese Government Eyes PM for Setting Rates Under Nationalized Health System New investigation results are detailed in a study published in BMC Medicine called “An in-depth assessment of a diagnosis-based risk adjustment model based on national health insurance claims: The application of the Johns Hopkins Adjusted Clinical Group case-mix system in Taiwan.” BMC Medicine, its publisher says, is the flagship medical journal of the BMC series and publishes original research articles, commentaries and reviews in all areas of medical science and clinical practice. A statement from the journal notes that “diagnosis-based risk adjustment is becoming an important issue globally as a result of its implications for payment, high-risk predictive modeling and provider performance assessment. The Taiwanese National Health Insurance program provides universal coverage and maintains a single national computerized claims database, which enables the application of diagnosis-based risk adjustment.” The statement continues: “However, research regarding risk adjustment is limited. The study aims to examine the performance of the Adjusted Clinical Group case mix system using claims-based diagnosis information from the Taiwanese NHI program. A random sample of NHI enrollees was selected. Those continuously enrolled in 2002 were included for concurrent analyses (n=173,234), while those in both 2002 and 2003 were included for prospective analyses (n=164,562). Health status measures derived from 2002 diagnoses were used to explain the 2002 and 2003 health expenditure.” Further, the statement points out, “a multivariate linear regression model was adopted after comparing the performance of seven different statistical models. Split-validation was performed to avoid over-fitting. The performance measures were adjusted R2 and mean absolute prediction error of five types of expenditure at individual level and predictive ratio of total expenditure at group level. The more comprehensive models performed better when used for explaining resource utilization. Adjusted R2 of total expenditure in concurrent/prospective analyses were 4.2%/4.4% in the demographic model, 15%/10% in the ACGs or ADGs (Aggregated Diagnosis Group) model and 40%/22% in the models containing Expanded Diagnosis Cluster.” The statement adds: “When predicting expenditure for groups based on expenditure quintiles, all models under-predicted the highest expenditure group and over-predicted the four other groups. For groups based on morbidity burden, the ACGs model had the best performance overall. Given the widespread availability of claims data and the superior explanatory power of claims-based risk adjustment models over demographics-only models, Taiwan’s government should consider using claims-based models for policy-relevant applications. The performance of the ACG case mix system in Taiwan was comparable to that found in other countries, suggesting that the ACG system could be applied to Taiwan’s NHI even though it was originally developed in the USA.” The researchers concluded, according to the statement: “Many of the findings in this paper are likely to be relevant to other diagnosis-based risk adjustment methodologies.”
DecisionQ Executive, Others Look at Fraud-Fighting Using PM In an article called “Healthcare Fraud and Abuse,” in the Fall 2009 issue of Perspectives in Health Information Management, researchers William J. Rudman PhD, John S. Eberhardt III, William Pierce RHIA and Susan Hart-Hester PhD looked at ways predictive modeling can be used to fight fraud and abuse. (Eberhardt is an executive vice president at and founder of DecisionQ Corp., which provided the journal submissions.) Here are excerpts: “From our review of the literature, the following four solutions to identifying and reducing fraud and abuse are suggested:
training and education; implementation of computer-assisted coding; increased federal enforcement of fraud and abuse monitoring; and use of data modeling and data mining.
“Data modeling and mining techniques are perhaps the most valuable tools an organization can utilize in detecting fraud and abuse. Data modeling and mining techniques can be used to identify both consumer fraud and provider fraud. Both types of fraud can cost healthcare organizations millions of dollars each year. The advancement of data mining and machine learning programs gives healthcare organizations and providers the ability to predict potential fraud and abuse. Automated data mining techniques allow the organization to gain valuable insights and to detect patterns within data without predetermined bias. Statistical algorithms can be used to identify general trends or patterns of suspicious transactions in healthcare data sets. “Given the complexity of the problem and the challenge at hand, most payers have historically used a ‘threshold’ approach to claims review and fraud detection, in which a claim or payee gets referred for review when the dollar amount or number claimed exceeds a certain threshold that has been historically observed to correlate with fraud and abuse. That’s a blunt instrument: A great deal of fraud and abuse cases are too small to trigger those thresholds, many legitimate claims that are simply large are reviewed unnecessarily and most fraud occurs over long time periods. As a result, only a small portion – 3% to 5% -- of fraud is actually detected, and it is typically detected late in the cycle, resulting in only a small recovery and wasted resources that could have been used to provide care.
continued on page 5
May 2010 Predictive Modeling News 5
© 2010, Health Policy Publishing, LLC. All rights reserved. No reproduction or electronic forwarding without permission. page 5
PM Permeates Managed Care Executives’ Issues List Data Analytics and Informatics is fourth on the Top Ten list
redictive modeling is on managed care executives’ minds. When the Cleveland-based Managed Care Executive Group held its annual forum in Ft. Lauderdale recently, assembled members put together their annual Top 10 Issues list. As the organization points out in a statement, “the Top Ten is dominated by the role of government, enhancing
collaboration and working on affordability.” And peppered throughout is predictive modeling. P Indeed, Number 4 on the MCEG list was Data Analytics and Informatics, described this way: “Disease management, real-time decision support, case management, customer segmentation and protocol development will continue to drive investment in analytics. Clinical information will be broad and deep, enabling caregivers to more precisely identify diagnoses and target treatment.” Using data to drive behavior permeates much of the rest of the list as well. Numbers 1 and 2 addressed healthcare reform specifically, and Number 6 touched on consumerism, but Number 3 was ICD-10, described like this: “The impact of changing to ICD-10 for medical record coding and billing is underestimated. It will likely be as significant a project across the industry as Y2K or HIPAA 5010 and, when undertaken, will push many other HIT projects to lower priority.” Number 5, then was HIPAA 5010, described this way: “New HIPAA requirements will present substantial changes in the content of the data submitted with claims as well as the data available in response to electronic inquiries. The implementation will require changes to the software, systems and perhaps procedures that are used for billing Medicare and other payers.”
Here’s the rest of the list:
Number 7. Health Data Exchanges: “HIOs are a key component of the HITECH Act. State-level HIE efforts are addressing five critical domains identified by the Office of the National Coordinator: governance, finance, legal/privacy, technical infrastructure and business/technical operations. Finding the sustainable financial model is a core issue.”
Number 8. Automated Member Acquisition and Retention: “As participation in employer-sponsored plans decreases and the need for individual and family health insurance grows, health plans are looking to connect directly with potential members to enable them to search and select plans right for them and then purchase them online. Health plans will need enterprise application integration techniques and processes to connect their Web portals to their underwriting systems, their enrollment systems, their sales systems, their customer service systems and their billing and payment systems.”
Number 9. Providing Transparency to Health Plan Data and Operations: “The ability to allow providers and health plans to utilize secure shared data continues to expand. The need to improve patient outcomes and operational efficiency is leading to investments in quality measurement, peer grouping, provider report cards and predictive modeling.”
Number 10. Collaboration with Providers as a Business Partnership: “Prior authorization and utilization reviews are fading and in their place is a more collaborative model based on real- time eligibility, benefit verification, access, quality, safety, effectiveness and patient-centeredness. P4P is holding providers accountable, as stressed by Bridges to Excellence, Leapfrog and other initiatives.”
Attendance at the annual forum is limited to 75 executives and senior managers. MCEG is a national organization that, a statement says, “provides a forum for the open exchange of information, innovative ideas and experience among senior health plan leaders.” It was formed in 1988.
Journals Examine Using Predictive Modeling for Rate Adjusting, Fraud Detecting…continued “Data mining techniques have allowed payers to use more sophisticated techniques, such as data mining, reporting, and rules engines for fraud and abuse detection. An effective automated review and detection system has three key components:
a data curation component, which is focused on the development of appropriate data standards and methodologies (which include identifying source data for study and structuring data for analysis, as well as data cleaning and normalization);
an algorithmic component, which requires the input of experts in data mining and statistics (Many methods can be used to develop an algorithm or set of rules for detecting fraud and abuse: Bayesian belief networks, neural networks, fuzzy logic, genetic algorithms, logistic regression and others. People often have strong views about which method is appropriate, and entire books have been dedicated to the topic.); and
an implementation process, which consists of four critical elements: validation, system implementation, maintenance and policy.
A major concern physicians have in the use of data modeling and mining techniques is that they will be unfairly accused of fraud. A primary advantage of the data mining approach is that the resulting algorithms can be tested, validated and optimized to an optimal level of sensitivity and specificity that will exclude patterns of normal use. Educating physicians to understand that data modeling and mining will help alleviate suspicion of fraud and abuse should go along way to addressing their concerns.”
Visit http://www.biomedcentral.com/bmcmed and http://perspectives.ahima.org.

6 Predictive Modeling News May 2010
To subscribe: visit www.predictivemodelingnews.com or call 209-577-4888 page 6
Looming ICD-10 Conversion Bodes Well for PM Players…continued
By being more detailed and specific, it is also better-suited to documenting research and innovations in healthcare. It’s also the industry consensus that business benefits will occur downstream. ICD-10-CM is adapted from ICD-10, the WHO version. It will also better align the United States with the global healthcare community. One question is who needs to comply. Most people know that HIPAA-covered entities are all required to comply. The non-covered entities, such as workers’ compensation and auto insurance companies, are encouraged to use the new standards for their own coding. I have been doing predictive modeling for both healthcare and workers’ comp medical management; therefore, I am keeping an eye on both industries’ ICD-10-CM conversions. I think workers’ comp insurers have good incentives to move forward with ICD-10-CM because of the expanded injury codes and laterality, which shed more light on expected recovery time, return-to-work planning and medical management. There are major changes worth noting for PM, too. First and foremost: The total number of codes has increased by more than five times, from about 13,000 codes to, now, 68,000 codes. Predictive models always start by classifying clinical codes into disease categories, so that codes within a certain category represent a cluster of diseases of similar etiology, treatment and resource use. The classification systems are being maintained and updated by PM vendors on a regular basis. Now that there will be five times more codes, there will also be a lot more effort required to maintain and update the classification systems. The grouping logic of ICD-10-CM codes is believed to be better and more coherent than ICD-9-CM. Some codes are moved into other chapters. There are also new chapters created in ICD-10-CM. The new grouping logic is worth studying, and may potentially be used as the starting point for new classification systems for PM. Signs and symptoms represent precursors to clinical and financial risk. With increased specificity for signs and symptoms, models can do a better job of predicting disease progression and of identifying patients at risk in the early stages. ICD-10-CM also has combination codes, allowing for a full description of etiology, symptoms and manifestations by just one code, reducing coding effort. It saves the predictive modeler time and effort in searching for disease patterns and combinations. There are more post-procedural codes in ICD-10-CM, allowing us to track healthcare outcomes better. Other factors that may affect health status and outcomes -- lifestyle, socioeconomics and family relationships, for example – also are detailed and included in ICD-10-CM. Some of those codes already exist in the current ICD-9-CM code set, but they are not organized to be found easily. Ultimately, I think ICD-10-CM will help PM practitioners develop better models, although it will take some time to happen – not until we have mature ICD-10-CM data to work with. [2] To follow up on some of the implications you’ve touched on, what strategies and approaches to do you recommend to
address them? I mentioned that ICD-10-CM has five times more codes than ICD-9. The volume alone is a big challenge. I think PM companies should start by modifying and expanding their clinical classifications. ICD-10-CM full conversion is about two years away. When solid ICD-10-CM claim data become available, which will be about two additional years down the road, PM vendors will need to recalibrate all the models to new data. In the interim, PM companies can conduct comparative studies and impact analyses using the ICD-9-CM-to-ICD-10-CM General Equivalence Mappings. The mapping is not one-on-one, but good enough for initial studies. In anticipation of the gradual improvement of data quality, PM companies should also think about how to design robust models and classification systems so that the predictions are less sensitive to coding quality -- thereby extending the shelf life of predictive models. There might be lessons we can learn from other countries that have had a longer experience with ICD-10. [3] Do you think the new ICD-10-CM codes will improve PM accuracy or perhaps even lead to new directions in healthcare
risk prediction? Yes. I think it has a lot of potential, although it will take some time to realize. For example, predictive models using ICD-10-CM will do a better job of outcome valuations in the future, as I mentioned before. More detailed information about the patient will be documented in ICD-10-CM, which helps us better address questions like, “Which of the high-cost patients are likely to be compliant in an intervention program?” and “What resources are required to provide care to a patient in his or her home under health reform?” That type of information has been captured in patient registries and is not easily accessible. Contact Yi at 781-213-6275 or at [email protected].
MagnaCare’s Predictive Analytics Tool…continued “MagnaCare has had the good fortune of having 20 successful years in the New York and New Jersey markets,” the CEO explains. “Each product’s initial launch has been or will be there. Historically, MagnaCare has participated in a number of national conferences and works with consultants with a national client base. We have introduced Evaluaide and MagnaCareRx through those channels and will do so for our upcoming vision and dental products.” Additionally, in 2010, the company will become the business process outsource partner for several other managed care organizations and TPAs, which will “expand our reach through a private-label approach using the MagnaCare infrastructure.”
Berardo adds: “With the prospect of national healthcare reform on the horizon, our customers will continue to benefit from our cost-effective, high-quality provider network and best-in-class administrative efficiencies, as well as our industry-leading connectivity and systems. We are tracking ongoing growth in our core network access and plan administration businesses, with plans to expand complementary offerings in dental, vision, mental health and as a BPO to other payers and TPAs.” MagnaCare expects to be able to announce two or three such contracts in the next several months. Visit Magnacare at www.magnacare.com.

May 2010 Predictive Modeling News 7
© 2010, Health Policy Publishing, LLC. All rights reserved. No reproduction or electronic forwarding without permission. page 7
New ‘Prediction Market’…continued MF: In a public market, anyone can sign up and participate – vetting happens automatically, thanks to the underlying reward mechanism. All participants start out with the same amount of virtual cash for betting on outcomes. They use their cash to give weight to their insights. The more confident they are of a certain outcome, the more virtual cash they bet. Therefore, they select metrics about which they actually have knowledge. Similar to investing in stocks, you’d trade in shares of companies you actually know about. And participants don’t just make bets – they also give proof of insight, offering comments and details about not only what they think, but how they came to that conclusion. PMN: How often do they comment on the issue at hand? MF: People comment frequently because the application encourages them to do so immediately after they place a bet. In fact, that’s one of the most popular – and, indeed, valuable -- features of the product. The marriage of the quantitative predictions with supporting rationale is what leads to actionable insights. PMN: How are their comments presented to users of the site? MF: In Crowdcast prediction markets, comments are presented as a stream to give participants some context as they give their insight. PMN: Who uses the prediction the site produces? MF: In the Pharmer’s Market, the drug developers whose drugs are showcased, analysts and other researchers use the predictions. In companies, executives and other decision makers do. PMN: How do users compensate for intentionally false or otherwise malicious comments made on the site? MF: Within crowdcasts, we monitor for inappropriate content in comment sections, which are much like open forum sites where people are free to share their opinions. If someone intentionally bets “incorrectly” to disrupt the crowd forecast, it’s reflected within the metrics as such:
Other participants will see it as a money-making opportunity and respond to correct the forecast. Think of it as an undervalued stock.
The sandbagger will eventually lose all of his virtual money (participants win only by being correct) and won’t be able to participate in future markets.
If the crowd forecast has lots of bets, one or two bad apples won’t affect it that much. PMN: How will patients and physicians put the predictions to use? MF: At the highest level, they can use the insights gleaned from the Pharmer’s Market to align and fine-tune product development and marketing initiatives. Patients can, in turn, see how industry professionals and influencers have made bets and where the market is headed, where drug development stands as they purchase prescriptions and invest in the market. PMN: Have any of the first six test drugs come to market? How did the Pharmer’s Market predictions play out? MF: At the point, we are unsure as to the ultimate influence of the Pharmer’s Market, since we created it to showcase and study the theory behind prediction market and collective intelligence technology. The Pharmer’s Market is an exploration of what the future of pharma could look like, a way to gauge how information could become more easily tapped and decisions made more efficiently and effectively. PMN: A press release about the Pharmer’s Market says, “Members of the market will also be able to participate in a community forum and provide comments on their trades.” What are “trades”? How do they fit into the prediction aim of the site? MF: “Trades” is another way of describing the way participants express their beliefs and knowledge about outcomes of questions -- just like trading stocks, they buy or sell contracts on the outcomes. Each trade influences the crowd forecast. Visit Crowdcast at http://crowdcast.com.
Subscribers’ Corner Remember, you can receive each issue of Predictive Modeling News via email in an electronic pdf version, via regular mail in print version, or both. There is no additional charge for whichever option you select. The electronic version will arrive approximately seven to ten days earlier than the regular mail print version. Should you wish to confirm or change your delivery option, feel free to contact us anytime. Subscribers can access an archive of current and past issues of Predictive Modeling News, view added features, change account information and more from the Subscriber web site. To access the site, click the “Subscribers” link at www.predictivemodelingnews.com, and then click the Subscriber Login link. Should you wish to change your username/password or update your e-mail address or postal mailing address, you can use the subscriber profile change form. Subscribers can network and discuss Predictive Modeling with other health care professionals, review job opportunities and more in the LinkedIn Predictive Modeling News Group. To join, go to http://www.linkedin.com/groups?gid=1669467

8 Predictive Modeling News May 2010
To subscribe: visit www.predictivemodelingnews.com or call 209-577-4888 page 8
Thought Leader’s Corner Each month, Predictive Modeling News asks a panel of industry experts to discuss a topic suggested by a subscriber. To suggest a topic, send it to us at [email protected]. Here’s this month’s question:
Q: “Do you see predictive analytics being deployed in any new or modified ways to address any aspect of the Patient Protection and Affordable Care Act?”
“It’s likely that even before the Act was signed into law, think tanks were coordinated to consider predictive models that could be used to inform the major policy changes. I do think PM has played and will continue to play a role in healthcare on multiple fronts. Areas include reducing waste, fraud and abuse, which is spoken to directly in the bill, as are payment for quality outcomes in Medicare and development of new patient care models and interventions. Concerning fraud and abuse, the bill’s supporters point to findings by the CBO that estimate that every $1 invested to fight fraud results in approximately $1.75 in savings. Because of the potential for savings, PM may become more sophisticated in those areas, but fraud will not likely go away. PM may support the development of systematically derived best practices that guide treatment options and care plans. In addition, PM may be used to forecast, develop and implement community-based interventions that are appropriately sized and funded for the population that they will serve. Predictive analytics have improved healthcare delivery for many years. The use of well-designed models can only serve to improve the overall goal of the Patient Protection and Affordable Care Act, which is to improve the lives of the American population.”
Damon Shepherd MS Clinical Outcomes and Business Analytics Humana/LifeSynch Irving TX
“Predictive analytics will be deployed within health reform in many different ways. Moreover, health reform will also have significant implications for the field. First, within the health insurance exchanges, risk-adjusted transfer payments will be used to ensure that adverse or favorable bias selection does not lead to unfair advantages to any plans. Second, there will be a surge of new previously uninsured patients -- in the exchange-mediated plans and as a result of Medicaid expansions. All types of PM will be needed to manage the care of those individuals. Third, health plans will be far more limited in their use of PM to set premiums or exclude enrollees; instead, they will need to use PM more proactively to manage the risk once a person is enrolled. Fourth, there will be many demonstration projects where PM is key, such as medical homes, wellness programs and integrated ‘ACOs’. Lastly, the huge expansion of electronic health records as part of ‘HITECH’ will increase the availability of expanded risk information that can be used to improve PM measures and methods. In short, the field will undoubtedly become impacted in many ways. (Readers interested in more of my thoughts on the issue of PM and healthcare reform should review the feature article on the topic in the March 2010 PMN. It summarizes a related presentation I gave at a recent conference. I can also send copies of my presentation to readers. Contact me at [email protected].)”
Jonathan Weiner DrPH Professor, Health Policy and Management; Director, PhD Program in Health Services Research and Policy; Deputy Director, Health Services Research & Development Center, Johns Hopkins University Baltimore MD
“In the now-immortal words of Rep. Nancy Pelosi (D-CA): ‘We have to pass it to see what’s in it.’ So I regret that I am not familiar with the ins and outs of the bill yet. We are getting enquiries from employer clients trying to determine what the bill will mean for their future costs, and whether terminating their plans and sending employees to the Exchanges makes sense. Normally, one would say that that alternative, like other situations that offer employers opportunities to select, will create winners out of high-risk populations, so that identifying high-risk populations will become important. Despite everything that has been said, I suspect that the ‘new world’ of healthcare will end up looking like the old, just more expensive, with the same tools and techniques being deployed in the future.”
Ian Duncan FSA FIA FCIA MAAA President, Solucia Inc. Farmington CT

May 2010 Predictive Modeling News 9
© 2010, Health Policy Publishing, LLC. All rights reserved. No reproduction or electronic forwarding without permission. page 9
Thought Leader’s Corner
“There are a considerable number of ways that analytics can be used to help companies thrive in light of the new Act. We are just starting to scratch the surface, but obvious and immediate areas that we have been exploring with our clients include these:
The use of underwriting as a means to control risk is going to be minimized in one way or another. Thus, what other methods of risk control can be implemented to counteract that loss? One way is through selective marketing, sales and retention activities that do not have the same level of regulation in the Act. Those areas have traditionally focused solely on identifying individuals who are likely to purchase or likely to terminate. By combining lifestyle-based health risk analysis with the more traditional marketing analytics, companies can further refine their marketing and retention campaigns to focus on the healthiest individuals, thereby shifting adverse risks to their competitors who are not using those same advanced techniques.
Population health management will be critical whether or not wellness activities can be defined as a ‘medical expense’ item. Those companies that are successful in this area will become so through the use of predictive analytics to score and identify those in their populations who are at risk of medical conditions or events prior to their manifesting themselves through claims analysis, as well as identifying those individuals who are open to change management to reverse those at-risk characteristics.”
Chris Stehno Senior Manager, Deloitte Consulting Chicago IL
“I expect the key use of it will be what the Act itself is designed to do: bend the cost curve over time. There are plenty of predictive models that have been developed showing how certain changes in physician and hospital practices, driven by changes to the reimbursement model, will bend the cost curve. So that work will likely be utilized a lot.”
Lawrence S. Borok President Vantage Point Healthcare Information Systems New Milford CT
INDUSTRY NEWS
Cognizant Reports 2009 Results, Predicts 2010 Numbers Cognizant Technology Solutions Corp. (Nasdaq:CTSH), Teaneck, NJ, reports that revenue for the fourth quarter of 2009 rose to $902.7 million, up 20% from $753 million in the fourth quarter of 2008. “Despite a very difficult economy, Cognizant delivered strong results, with 16% annual revenue growth. The investments we made in our business leave us in an even stronger position than when we entered 2009,” comments Francisco D’Souza, CEO and president there. “During the year, we grew our workforce by more than 16,700 people, improved our employee utilization, strengthened our client partnerships and brought new services and capabilities to market.” Revenue for all of 2009 increased to $3.3 billion, up 16% from $2.8 billion for 2008. First-quarter 2010 revenue is anticipated to be at least $935 million and fiscal 2010 revenue is expected to be at least $3.9 billion, up at least 20% compared to 2009. Visit www.cognizant.com.
Veteran Executive Joins Connextions Inc. Board of Directors Connextions Inc., Orlando, has appointed Kenneth A. Burdick to its Board of Directors. Burdick is “a transformational health insurance leader with an outstanding record of management and fiscal performance with the nation’s most respected insurers, including UnitedHealth Group, Travelers and CIGNA,” a statement from his new employer says. Says Connextions’ chair and CEO Jack LeFort: “Burdick will provide the clear perspective of a health and public sector industry veteran and expert. His appointment is consistent with our plan to continue our strong momentum and market penetration as the leader in revenue-driving outsourced business process, technology and exchange solutions, particularly in the health insurance industry.” Visit www.connextions.com.
Subscribe to Predictive Modeling News – the only newsletter dedicated to predictive modeling in healthcare. Join the healthcare predictive modeling community! Subscriptions are available for $39 a month or $468 a year. To subscribe, call 209-577-4888 or order online at www.predictivemodelingnews.com.

10 Predictive Modeling News May 2010
To subscribe: visit www.predictivemodelingnews.com or call 209-577-4888 page 10
INDUSTRY NEWS
Reality Show Drives New Business to Modeling Company Ironworks, a management, Web and IT consulting firm, reports that following “an in-depth performance-tuning project for BioSignia’s Website, the site handled a 300% increase in site load during a recent airing of NBC’s popular reality show ‘The Biggest Loser’.” Since the start of the 2010 season, when the “Biggest Loser Know Your Number HealthScore” was first used by the contestants and the consumer product was mentioned on the television show as being available online, the site was challenged to meet high user demands, explains Randall Bowen, executive vice president at BioSignia. “With Ironworks’ help, after our two-week performance-tuning project, we were able to handle increased site load during and after the show, which allowed us to manage a close-to-400% increase in visits to the product order page.” BioSignia engaged Ironworks to review front- and back-end application code and server configuration and to analyze the technology stack of the “Biggest Loser Know Your Number” Website to handle the upsurge in traffic due to the show’s popularity and consumer interest in the “Biggest Loser Know Your Number HealthScore,” an at-home health test. Headquartered in Research Triangle Park, NC, BioSignia says it focuses on bringing innovative predictive modeling solutions to the preventive health and life insurance markets. Visit www.knowyournumber.com and www.ironworks.com.
University of Washington Chooses Dentra’s PatSat Analytics Tool Seattle’s Dentra, a leading provider of online quality measurement solutions, reports that the University of Washington School of Dentistry has selected PatSat to measure and monitor patient satisfaction in real time. Aimed to serve as an outcome assessment tool for the school’s entire clinical department, PatSat is, Dentra says in a statement, “a cost-effective online satisfaction measurement solution that enables dental patients to provide feedback about their experience after each visit by answering a short survey.” As an early adopter joining Dentra’s University PatSat Network, UW’s School of Dentistry provides academic leadership for quality measurement best practices in dental schools across the country, the statement adds. The school will use PatSat to collect and process satisfaction data daily and deliver benchmark reports and dashboards that faculty and students can consult at any time via an online portal.
University of Washington Chooses…continued
UW will be able to better understand how its dental patients perceive the clinic’s service performance, the statement says, and, as a result, rapidly enhance overall patient satisfaction. Significant growth in the number of patients using the clinic is expected through continuous improvement of quality best practices among faculty and students. PatSat works with the school’s axiUm practice management system, “making it easy to generate daily lists of treated patients and pre-populate and automatically send email invitations to individual satisfaction surveys,” the statement says.
“Just as healthcare came to use outcomes and analytics to look for and define best practices in quality care delivery, it is now an opportune time for dentistry to embrace and move toward transparency with regard to quality measurement,” adds Amanda Twiss, Dentra’s CEO and president. Visit www.dentra.com.
Pharsight Unveils Products Developed Under FDA Agreement St. Louis-based Pharsight, a provider of software and scientific services to improve productivity and decision-making in clinical drug development, has released two new data analysis tools, Phoenix NLME and Phoenix Connect. The pair were developed via a collaborative effort between the Food and Drug Administration and Pharsight under Pharsight’s previously announced Cooperative Research and Development Agreement with the FDA’s Center for Drug Evaluation and Research.
“When we entered into this CRADA, we agreed to provide the FDA with new software for the analysis, visualization, storage, reporting and review of pharmacokinetic and pharmacodynamic data,” says Daniel Weiner, chief technology officer at Pharsight. “With the increasing costs associated with new drug development, the FDA has recognized the importance of utilizing innovative technologies to accurately assess the safety and effectiveness of potential new therapies.”
The Phoenix suite of tools will be used by the FDA, along with software products from other suppliers, to review clinical trial data, especially for clinical pharmacology and clinical safety reviews. The goal of the collaboration is to ensure that the suite of products helps meet FDA needs for Investigational New Drug Application and New Drug Application data review and analysis. Visit www.pharsight.com.
www.healthwebsummit.com/pm2010.htm

May 2010 Predictive Modeling News 11
© 2010, Health Policy Publishing, LLC. All rights reserved. No reproduction or electronic forwarding without permission. page 11
INDUSTRY NEWS
Evolution of Life Insurance Industry to Accelerate and Engage in Predictive Modeling, Says LOMA Survey The long-term outlook for the life insurance industry: a faster pace of change, particularly in the use of technology. That’s according to a survey of top industry executives by LOMA, an international association through which more than 1,200 insurance and financial services companies from more than 80 countries engage in research and educational activities to improve company operations. The executives were asked for their opinions on what the industry will look like 10 years from now. “Over the decade, advancements in service and technology will continue to transform our industry,” comments Robert Kerzner, CEO and president at LIMRA, LOMA and LL Global. “While technology is the enabler to reach more consumers through the Internet, the ability to integrate data across the organization will afford companies the ability to engage in predictive modeling, data mining and forecasting. It will provide them a 360-degree view of their customers, which will better serve the customer and improve companies’ productivity.” Respondents to the LOMA survey highlighted advances in technology as well as companies’ ability to provide comprehensive financial solutions to their customers as the key drivers of change. Service capabilities will continue to advance, the LOMA survey found, and the industry will see the Internet become an even more important service delivery mechanism. The use of mobile devices as a communication vehicle will become standard, the survey also found, as will push technology. Telepresence and teleconference technology will enhance collaboration and communication among home office employees and the field force. The findings were published in the March issue of LOMA’s Resource magazine. Visit www.loma.org.
Predictive Modeling Web Summit Agenda Set The Healthcare Web Summit’s Third Annual Predictive Modeling Summit will include a live webinar on Thursday June 17, 2010, at 1:00 p.m. Eastern, with additional faculty podcasts and other Web Summit features available for download 24/7. The webinar agenda includes presentations by Brian T. Day EdD, director of advanced analytics, Highmark Inc., on “Utilizing Predictive Modeling to Meet the Challenges of Healthcare Reform;” Russell D. Robbins MD MBA, principal & senior clinical consultant, Mercer, on “Current Issues in Employer Use of Predictive Modeling;“ and Swati Abbott, president, MEDai, and William F. Bramble, president, Health Cost & Risk Management LLC, on “Utilizing Analytics to Create Evidence-Based Care Plans, Improve Member Compliance and Drive Down Costs.” Visit www.healthwebsummit.com/pm2010.htm.
New Firm Helps Insurers with Competitive Intelligence, Business Development
P&C carriers, reinsurers, life and health companies and wealth management firms can see their data turned into actionable information with the help of Structured Stream, a new business intelligence, data solutions and analytic services company, a statement from the start-up says. Partners Deb Cooper and Jim Hearn launched the company at a recent industry conference; it focuses on helping companies “construct the business intelligence and business development systems that are keys to sustainable revenue flows,” the statement says. In particular, it adds, “Structured Stream can provide clients with a 360o view of individual client potential through Linkage 360o, which links an individual’s consumer records to profiles of his or her owned businesses. A powerful cross-selling tool, the Linkage 360° concept has been widely used in the banking industry for more than 20 years.”
Cooper and Hearn are working with Oxxford Information Technologies to introduce the application of Linkage 360° to the insurance industry. Structured Stream’s analytic service expertise “allows the company to evaluate an insurer’s data to identify ‘sweet spots’ within its client base. That insight can then be used to assist the carrier’s marketing, distribution and underwriting leadership through deployment via Structured Stream’s Web-based dashboards. Doing so delivers clearer appetite communications to agency-facing teams and the distribution plant, driving operating efficiency through higher volumes of qualified submissions and reduced out-of-appetite churn.” Structured Stream says it will also provide consulting services designed to help firms market and sell effectively. Visit www.structuredstream.com.
Qforma Appoints Three New Business Development Executives Santa Fe, NM-based Qforma, a healthcare data analytics and predictive modeling company, reports the appointments of Carl Kunz, Keith Mangas and Chris Rofidal to business development executive positions. Kunz comes to Qforma with more than 25 years’ experience in pharmaceutical and medical device sales. Mangas has held multiple sales and marketing positions over the course of his career in the healthcare industry. “His extensive data expertise will enable Qforma clients to develop more innovative and successful strategies,” a statement says. Rofidal began his career in the pharmaceutical industry as a medical representative. Recently, he’s “brought his managed markets expertise to start-up companies,” the statement adds. Visit www.qforma.com.
12
Published by Health Policy Publishing, LLC ● 209-577-4888 ● www.predictivemodelingnews.com
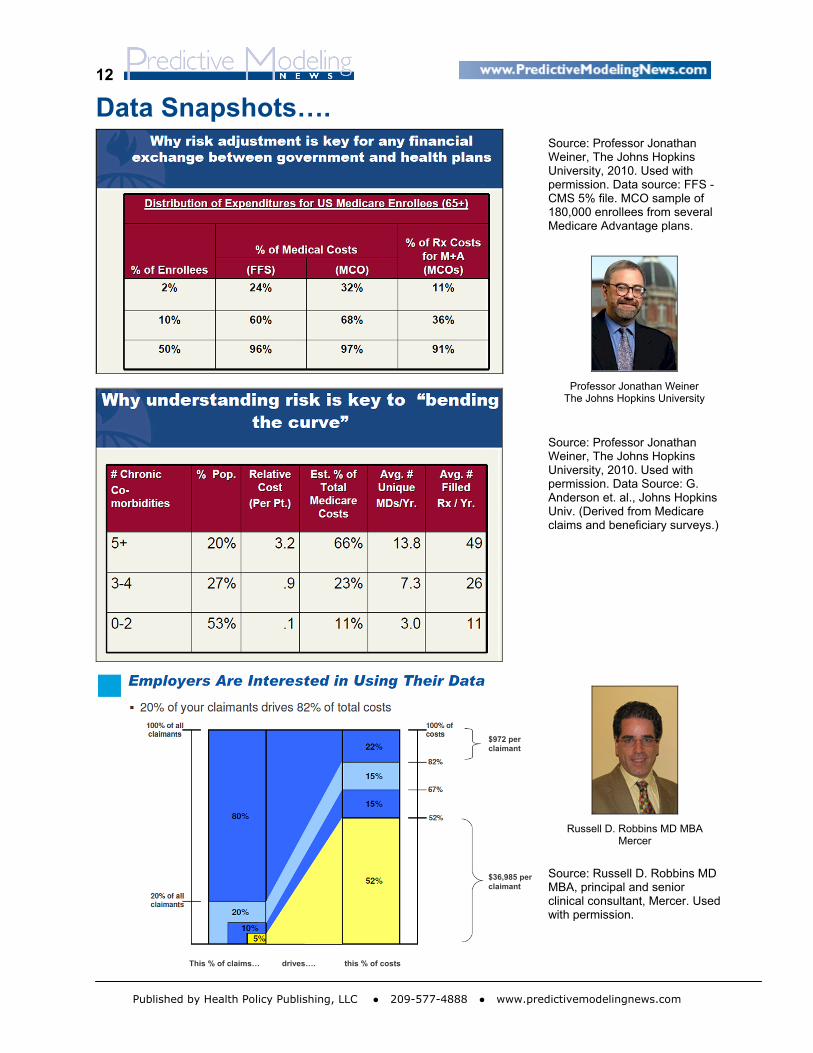
Data Snapshots….
Source: Professor Jonathan Weiner, The Johns Hopkins University, 2010. Used with permission. Data source: FFS - CMS 5% file. MCO sample of 180,000 enrollees from several Medicare Advantage plans.
Professor Jonathan Weiner
The Johns Hopkins University
Source: Professor Jonathan Weiner, The Johns Hopkins University, 2010. Used with permission. Data Source: G. Anderson et. al., Johns Hopkins Univ. (Derived from Medicare claims and beneficiary surveys.)
Russell D. Robbins MD MBA
Mercer
$972 per claimant
Source: Russell D. Robbins MD MBA, principal and senior clinical consultant, Mercer. Used with permission.
$36,985 per claimant
This % of claims… drives…. this % of costs