pczf- ziz l'p~~ (i nephrotoxicity induced by cancer ... · pdf filetlons with other...
TRANSCRIPT

~ 9 - - 7 / 4 d c 7 */>/- r r r , / > . w ~ ~ c ~ ~ p h o ~ ~ - /WZ~-?JL.& 5 h p 1 p ~ A u . - PW * Cj/lF y , ~ ~ A ~ - S F M I +
c - MMM COW/ G ~ v o i J c c I 1/1 - f l M R m r m c y - A ~ N pCZF- m c Z A t M C O
Z i z - L ' p ~ ~ ec~10.c (I $ i F - /su=
Nephrotoxicity Induced by Cancer Chemotherapy With Special Emphasis on Cisplatin Toxicity
F. Ries. MD, and J. Klastersky, MD
Renaliailure in cancer patients Is a common problem in oncology; this complicatlon is frequently multlfactorial In origih. Several antineoplastlc agents are potentially nephrotoxlc; previous renal impairment as well aa comblnr. tlons with other nephrotoxic drugs may Increase the risk of nephrotoxiclty during administration of chemotherapy. Methotrexate-related renal damage most frequently occula with hlghdose therapy and can be avoldd by t o m alkaline diuresis and administration of follnlc acid. Renal dysfunction secondary to semustlne (CHACNU) 18 clearly related t o cumulative doses in excess to 1,200 mglma; the onset may be delayed and renal failure progreu despite drug discontinuation. Streptozotocin is also nephrotoxic and may cause proteinuria and renal tubular acidosis; progressive renal failu-dicted by a close monitoring of protelnuria and preventd by drug discontinuance. Mltomycin-associated renal failure frequently presents with sign8 of microanglopathlc hemolytic anemia; renal failure is usually delayed but occasionally, It may be rapidly progressive despite drug dlscontlnu. ance. Clsplatin nephrotoxicity is clearly dose-related and used to be considered dose llmltlng. Renal Insuff lc len~~ can be prevented by hydration and forced dlsuresis; in addltlon, hyperhydratlon with mannltol-Induced 8allne dluresis may allow administration of high doses and thus circumvent the dose-limiting effect of clsplatln-Induced renal toxicity. Cisplatin-induced renal magnesium wasting occurs frequently and should be supplemented. C?!-;.r approaches to reduce c~splatin nephrotoxicity are currently under investigation and are diacusOed. 9 1986 by the National Kldney Foundaton, Inc.
INDEX WORDS: Nephrotoxic drugs; chemotherapy; renal failure; cisplatln; methotrexate; mltomycin; semustine; streptozotocin; cancer.
S INCE THE KIDNEY is highly susceptible to toxic injury by a multitude of different drugs.
it is not surprising that several antineoplastic agents may exert potent nephrotoxicity. In cancer patients. however, one must always be aware of additive or synergistic efiects that may potentiate chemotherapy-induced nephrotoxicity. Cancer pa- tients are frequently treated with nephrotoxic anti- biotics (eg, aminoglycosides or amphotericin B). They may suffer from radiation-induced nephro- toxicity. or present with hypercalcemia. hyperuri- cemia. lysozymuria. cancer-related microan- giopathic hemolysis. or disseminated intravascular coagulopathy. These patients also may present with immune complex-mediated glomerulopathy or paraprotein-'felated nephropathy, and with amy- loidosis as well as minimal-change nephritis. They
contrast media may be potentially harmful to the kidney; cancer patients frequently suffer from urinary tract infections. It is. therefore, important to take into account every potentially harmful ef- fect when looking for chemotherapy-related nephrotoxicity.
The agents whose potential for nephrotoxicity has been clearly established will be discussed i:: the following review. These are methotrexate. :.. .
platin. semustine (methyl-CCNU), streptozotocrn. mithramycin. mitomycin C, and azacytidine. Cis- platin nephrotoxicity will be reviewed in greater detail. In addition. the reader is informed that the problem of chemotherapy-related nephrotoxicity has been analyzed in several review articles.'.'
METHOTREXATE may have direct infiltration of the kidney by tumdr Methotrexate (MTX), an inhibitor of folate syn- cells as well as an obstructive nephropathy caused thesis. is one of the earliest and one of the most by lower urinary tract invasion and compression. used agents in cancer chemotherapy. Used for Different radiologic investigations with iodine more than 30 years. MTX has shown activity in
From rhe Senice de Midedne lnrtrnr er Laboraroire d ' ln - great number of tumors. such as leukemia. !I -' \.esrigarion Clinique H. 7hgnon. Cenrre des Tumeurs de phoma. choriocarcinoma, osteosarcoma. and I'Universire Ljbre de Bturelles. lr~srirur Jules Border. B n u - mors of the breast, h e d and neck, and lung." elles.
Address reprinr rcquesrs ro F: Ries. MD. Imrirur Jules Bor- Since MTX is excreted primarily by the kidney.
der. I Rue Heger- order. IWO Bnuelles. Belgique. any changes in renal function will have an effect C 1986 bv rhe National Kidt~e; Fou&iion. Inc. on hfTX plasma levels arid MTX clearance, with 02 n-6386/86/08os-oo14soj. 0010 subsequent exposuro of the whole organism to per-
368 American Jourri6l of IOdn6y 3iseases. Vol Vlli. No 5 (November). 1986: pp 368-379

EPHROTOXICITY OF CYTOSTATICS
y elevated concentrations of the d r ~ g . ~ . ~ . ~ liferating or cycling cells. since those of the e marrow and gastrointestinal tract are most
usceptible to the toxic effects of MTX and intox- with MTX secondary to renal failure, pri- result in marrow hypoplaiia and severe mu-
cositis. Apart from causing important systemic toxicity, high plasma concentrations of MTX are also nephrotoxic per se, and renal failure has been implicated in 20% of the deaths associated with highdose MTX adminis t ra t i~n.~
I W'" qeveral mechanisms may contribute to MTX- :r~ated renal failure: precipitation of MTX in renal tubules, direct antimitotic effect on renal
tubular cells, and possibly, alteration of glomeru- Iar filtration rate (GFR). Among these mecha- nisms, tubular precipitation producing obstructive renal failure is the best known and the most widely accepted. MTX solubility has been shown to change with urinary pH, and the drug was shown to be two to ten times more soluble at pH 6.9 than at pH 5.7.9.'0 Precipitation of the drug may occur in concentrated and acid urine resulting in renal ~ b u l a r obstruction by an amorphous yellow mate- rial; this has been shown at autopsy examinations of MTX-treated patients dying from acute renal f a i l ~ r e . ~ The amorphous material was identified as MTX by immunofluorescent techniques. The risk of tubular MTX precipitation can be minimized by
< hydration as well as alkalinization. I - ' ) Since hy- : dration and alkalinization programs have been in-
>- troduced into clinical practice, the incidence of re- : nal toxicity has decreased dramatically.
3ther observations suggest that MTX might in- 2ce renal failure without tubular precipitation be-
1 cause oliguria or anuria are rarely found. and true obstructive nephropathy has only been reported in <. a few case repc~r ts .~ Since MTX reaches high con-
., centrations for prolonged periods in h e urine, re- nal tubular epithelialcells undergoing renewal or repair could be potentially susceptible to this con-
t - centration by time effect of the drug. l 4
A high-dose MTX-related decrease in GFR was observed in pediatric and adult patients,I5.l6 but the pathogenetic mechanism of this phenomenon is still unclear.
MTX nephrotoxicity may be predicted by , several tests: (1) ~ o w ' u r i n a r ~ pH during high-dose
I MTX infusion may be associated with impending toxicity. In high-dose MTX programs. urinary pH should be maintained above pH 7 by intravenous
(IV) or oral bicarbonate admin i~ t ra t ion .~ (2) A rise of serum creatinine value from baseline pretreat- ment value may identify patients at risk for addi- tional renal damage. For these patients, adminis- tration of leucovorin rescue as well as vigorous hydration and alkalinization should be consid- ered.9 (3) Monitoring of serum MTX levels is of primordial importance and identifies patients needing additional rescue measures. Leucovorin rescue should be provided until MTX serum levels - , fall below lo-' m o l / ~ . 17-19 i - ' i- i P '-/dl z 6 . 0 9 )
In patients with established nephrotoxicity, leucovorin rescue treatment may counteract the cytotoxic effects of MTX. Leucovorin (tetrahy- drofolate), inhibitins MTX activity by competi- tion. is administered in high-dose MTX programs at conventional doses of 15 mg, repeated at regular intervals12; since MTX concentrations are some- times extremely high in MTX-induced renal failure, the doses of leucovorin rescue should be appropriately i n c r e a ~ e d . ~ Lowering of MTX levels by means of peritoneal dialysis, hemodialysis. or hemoperfusion seems to be of marginal v a l ~ e . ~ ~ - ~ ~ Since, in most cases. patients are not oliguric or anuric in MTX-related renal failure, high fluid in- take with alkalinization should always be main- tained. Apart from vigorous hydration, alkaliniza- tion. and administration of leucovorin during high-dose MTX therapy, care should be taken to avoid the drug in patients who suffer from pre- liminary renal insufficiency or to postpone its use in patients who are dehydrated; urine acidifying agents and salicglate derivatives should be avoided before and during MTX treatment. Good knowl- edge and careful application of these efficient measures for prevention of MTX-related nephro- toxicity have been associated with the near disap- pearance of this potentially harmful complication.
SEMUSTINE (METHYL-CCNU)
Semustine. like the other nitrosourea com- pounds. is a highly lipid-soluble drug that has some clinical activity in neoplasms of the brain. gastrointestinal tract. as well as malignant mela- noma. Nephrotoxicity of this compound had been described in early preclinical toxicology experi- m e n t ~ , ~ , ' , ~ ' but evidence for possible nephrotoxic- ity in humans appeared only much later in 1978 and 1979.26.27 Since then. numerous other reports on semustine nephrotoxiciry have been p u b l i s l ~ e d . ~ ~ - ~ ~
RlES AND KLASTERSKY
The most frequent clinical manifestation is a slowly rising serum creatinine level with progres- sive irreversible renal failure. Pathologic findings are generally consistent with the presence of small and atrophic kidneys, signs of tubular atrophy, hy- alinization, glomerulosclerosis, and interstitial fibrosis. 32
Semustine nephrotoxicity is cumulative; renal dysfunction has been noted in 26% of patients who received total cumulative doses in excess of 1,400 m g / n ~ ~ . ~ I median cumulative dose at which nephrotoxicity is likely to occur has been esti- mated to be near 2,000 mg/m2.32 It is, thus, not surprising that this problem generally appears only in patients being treated for more than 1 year, which requires a prolonged survival time.
Compared to the other nitrosoureas, it can be noted that semustine nephrotoxicity totally differs from that of streptozotocin, the most nephrotoxic compound of the nitrosourea group. The other ni- trosoureas. ie, chlorozotocin, lomustine, and car- mustine. seem to be much less nephrotoxic, with only occasional cases reported.
The specific mechanisms of semustine-related nephrotoxicity remain unclear and there are no established recommendations for toxicity protec- tion. Prochlorperazine, a commonly used phenothiazine with antiemetic properties, has been reported in animal studies to reduce the frequency as well as the severity of semustine-related renal lesions33: the clinical impact of this observation has not yet been established.
STREPTOZOTOCIN
Streptozotocin is a nitrosourea that has been used successfully in. the treatment of islet cell tum0rs .~~-3~ Renal toxicity is the major dose- limiting side"effect of this drug. Nephrotoxicity seems to be dcse-related and. to some extent, cu- mulative. occurring most frequently at doses in ex- cess of 1.5 g /m2/~k.37~3a
Toxicity generally presents initially as mild pr~teinuria.'~ but with continued use, proximal re- nal tubular damage may develop.38 Fanconi syn- drome. renal tubular acidosis. hypokalemia, renal glycosuria. hypophosphatemia, and most signifi- cantly, life-threatening oliguria and anuria have been reported. Nephrogenic diabetes insipidus seems to be less frequent.*.41
The best prevention for potentially harmful nephrotoxicity should be afforded by an optimal
dosage schedule and frequent examinations for p r o t e i n ~ r i a . ~ ~ . ~ ~ The drug should be discontinued when proteinuria or other signs of renal dysfu;: - tion develop; with resolving proteinuria, drug ..:. .-. ministration might be carefully continued.
Mithramycin, a naturally occurring cytotoxic antibiotic, has shown some activity against go- nadal cancer, as well as glioblastomas*~~; how- ever, its multiple toxic side effects have precluded its widespread use. Apart from causing important hematologic and cloning abnormalities, gastroin- testinal, central nervous, and hepatic dysfunction, as well as hypocalcemia, it also induces renal tox- icity, manifested by signs of renal failure and pro- teinuria.
This renal toxic effect tends to be cumulat~: ..
and may be irreversible; drug-related deaths due ti:
renal failure have been reported in 6 of 32 patients treated with the drug.4s Histopathologic changes consist primarily of renal tubular swelling, de- generation. necrosis, and atrophy with sparing of the glomeruli. Mithramycin still has some applica- tions in refractory cancer-related hypercalcemia, where lower doses are generally effecti~e.*~.~'
Mitomycin C (MMC) is a naturally occurring alkylating agent, introduced for clinical use as early as 1958. It has been demonstrated to be ac- tive against carcinomas of the gastrointest~n.: tract; breast. prostate, and a few other carcinomas as we11.49.s0
Activation of mitomycin seems to require in vivo metabolism to form short-lived metabolites that are highly reactive. Its serum half-life varies from nine to 17 minutes, and inactivation of the drug occurs in various organs including the liver and the kidney. Renal excretion of mitomycin is negligible.49
Early reports on animal studies had shown vari- ous nephrotoxic effects in dogs, monkeys, and mice.s1-" Reports on possible renal toxicity in hu- mans occurred only much later.s4 These studies generally showed microangiopathic changes in r h ~ renal circulation with hemolytic anemia. thrombo- cytopenia. proteinuria, hematuria, renal failure. systemic hypertension, pulmonary edema, and congestive heart failure. This clinical syndrome has been variously described as microangiopathic
. . .-
NEPHROTOXICITY OF CMOSTATICS 37 1
hemolytic anemia.55 MMC-related hemolytic- tions without any effect on progressive renal uremic syndrome.56 and MMC nephrotoxicity. 57 f a i l ~ r e . ~ ~ . ~ ~ Combinations of immunosuppressive Several clinical manifestations show similarities and antiplatelet drugs, with or without plas- with cancer-related microangiopathy and coagu- mapheresis, has been shown to be only of marginal 10pathy,~~-~l and different authors have suggested a benefit.63 Temporary progression of the disease possible relation between both problem^.^^.^^ activity has been attributed to blood transfusions,
In one large series, 140 of 143 patients treated which should, therefore, be administered with with mitornycin had renal impairments7; among ~ a u t i o n . ~ ~ . ~ ' Hemodialysis may be necessary for these, 6% died of renal failure. Three patients de- life-threatening renal failure, but it will not effect veloped rapidly progressive renal disease with the underlying disease process. sharp elevations of BUN and'creatinine level. hy- For patients treated with MMC, renal and hema- penension, proteinuria, hematuria, signs of mi- tologic function should be monitored regularly af- croangiopathic hemolytic anemia. and death from ter initiation of chemotherapy. MMC should be renal failure. Several other patients in that series discontinued if early toxic manifestations, espe- presented with some degree of red-cell fragmenta- cially azoternia or hematuria, are detected. To tion, thrombocytopenia. proteinuria. and hyper- date, there are no data available to predict individ- tension, but the clinical course was generally less ual susceptibility to this complication. Further tulminant and renal failure frequently developed studies are needed to clarify the causes, preven- without signs of hemolysis. As in other stud- tion. and treatment of the renal complication. and
related to repeated doses of 10 to 20 mglm2, with a use. ., total dose-range between 40 and 115 mglm2. The
time interval between the onset of MMC therapy AZACYTIDINE
: and renal failure was 4 to 16 months. with an 5-Azacytidine, a pyrimidine analogue, is a use- average of 10 to 11 months. ful agent in acute nonlymphocytic leukemia.70
Renal toxicity of MMC is apparently not dose- This drug was shown to be associated with azote- related and the precise pathogenetic mechanism rnia and renal tubular dy~function.~' Abnormali-
.: autopsy material have shown microangiopathic le- collecting ducts, have been described. Polyuria, sions with fibrous thrombi in the glomeruli and salt wasting, defective reabsorption of phosphate.
'. small arteries.65 glomerular nuclear degeneration aminoaciduria, and renal glycosuria have also :. and thickened basement membrane.s4 intirnal hy- been do~umented.'~
CISPLATIN
In 1969, platinum compounds were reported by . tients with MMC-associated hernolytic-uremic Rosenberg et al to exen potent antitumor activity
syndrome63; these immune complexes showed in mice73; cisdiamminedichloroplatinum I1 (cis- high platelet aggregation activity in vitro. The platin) was the most active drug among these com- constituent antibody of each complex faded to p o u n d ~ . ~ ~ Cisplatin, therefore, entered toxicologic react with MMC antigen preparations, whereas in evaluation in before introduction into vitro reactivity to endodermally derived neo- phase I clinical trial^.^^-^' Since then, cisplatin has plasms could be detected. These data suggest that been studied in numerous phase 111111 trials (alone MMC might not be the only etiologic factor of this or with other agents), and it has proven to be one syndrome, but that some tumor-specific relation- of the most potent chemotherapeutic agents, being ship might exist as well. active in cancer of the ovary,84 t e ~ t i s , ~ . ~ ~ blad-
Mitomycin-associated nephrotoxic reactions der,87-89 head and neck,90 l ~ n g , ~ ' . ~ ~ endome- must be c~nsidered refractory to most treatments t r i ~ m . ~ ~ uterine cervix,94 and many others. studied until now. In small studies. steroids, anti- Several excellent reviews deal with problems such
f coagulants, and platelet inhibitors have been tried as mechanism of action, activity on diverse tu-
( u n s u c c e ~ s f u l l y . ~ ~ ~ ~ ~ ~ Plasmapheresis has shown mors. as well as toxicity of isp plat in.^^.^^^
I variable resolution of the hematologic manifesta- Since 1971, animal studies have shown a major
RlES AND KLASTERSKY
cisplatin-induced nephrot~xicity'~ that proved to be dose related.76 These and other reports with studies performed on various animal models showed a strong relationship between the adminis- tered dose and uremia, as well as dose-related structural alterations detected on microscopic kid- ney examination. These alterations consisted pre- dominantly in tubular necrosis. As could be ex- pected from animal studies, early clinical reports showed similar toxicity in humans.78-m.82.a3 In pa- tients with n&mal kidney function, rising BUN levels were noted during the second week after a bolus cisplatin administration in excess of 50 mg/ m2 of body surface area (BSA); reversible nephro- toxicity was generally noted between 50 and 75 mglm2ld, while doses 2 100 mglm21d were fre- quently followed by acute renal failure with pro- nounced tubular cell necrosis. Renal failure pro- gressing from reversible to irreversible stages was described with repeated treatment courses. These early studies were performed without particular hydration or drug-induced diuresis programs. Several authors have reviewed the problem of cisplatin-related n e p h r o t o x i ~ i t y ~ ~ ~ - ~ ~ ~ ; the conclu- sions of their articles. as well as more recent infor- mation, will be analyzed in the following discus- sion. In fact, cisplatin nephrotoxicity remains of particular interest since renal damage is one of its most critical side effects and frequently constitutes a dose-limiting factor.
Mechanism of Acrion and Implications for Renal Tox ic i~
Several studies suggest that cisplatin exerts its activity in a manner similar to aklylating agents by drug interaction with \the nucleophilic sites of pyrimidines in DNA.97.98.'06 These infrastrand DNA cross-link will occur after physiologic ac- tivation of the dnlg, which will take place in a low
u I1"Ui Cl , 103 .MIL1
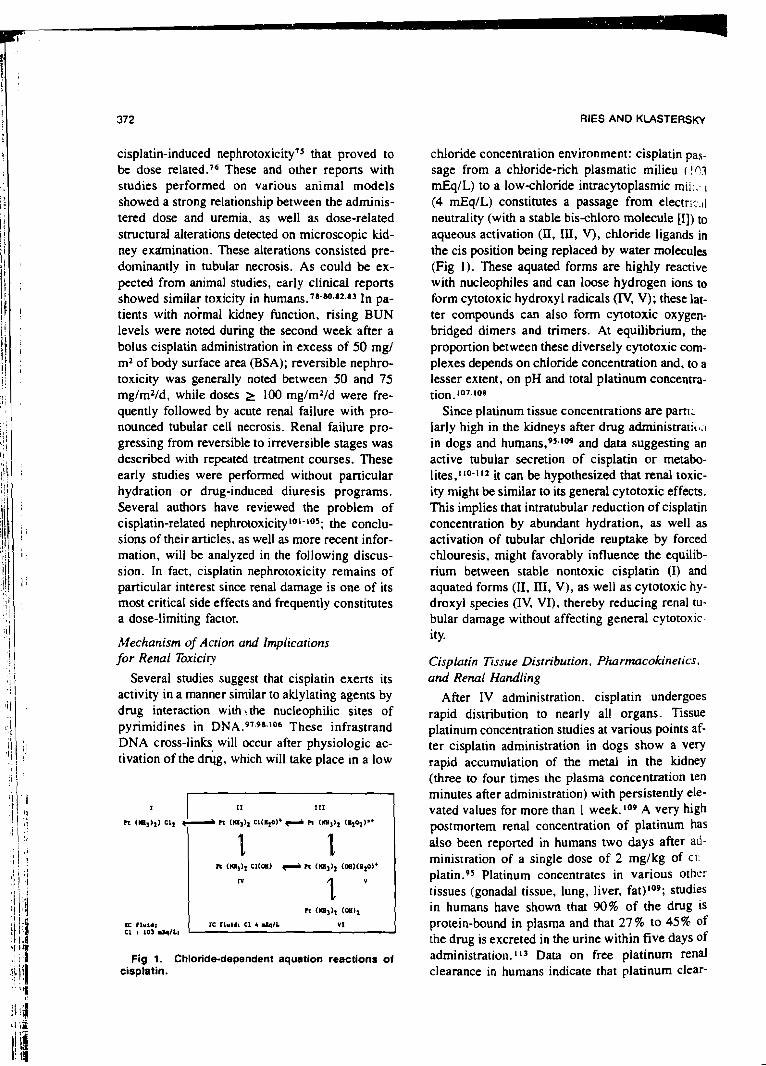
Fig 1. Chloridedependent aquation reactions of cisplatin.
chloride concentration environment: cisplatin pas- sage from a chloride-rich plasmatic milieu ( ! 03 mEq/L) to a low-chloride invacytoplasmic mii;.. I (4 mEqIL) constitutes a passage from electr:.s.,l neutrality (with a stable bis-chloro molecule [I]) to aqueous activation (II, III, V), chloride ligands in the cis position being replaced by water molecules (Fig 1). These aquated forms are highly reactive with nucleophiles and can loose hydrogen ions to form cytotoxic hydroxyl radicals (IV, V); these lat- ter compounds can also form cytotoxic oxygen- bridged dimers and trimers. At equilibrium, the proportion between these diversely cytotoxic corn- plexes depends on chloride concentration and, to a lesser extent, on pH and total platinum concentra- tion. 107.108
Since platinum tissue concentrations are panl; larly high in the kidneys after drug admini~tratit~;~ in dogs and h u r n a n ~ , ~ 5 . ' ~ ~ and data suggesting an active tubular secretion of cisplatin or metabo- lites,'10-112 it can be hypothesized that renal toxic- ity might be similar to its general cytotoxic effects. This implies that intratubular reduction of cisplatin concentration by abundant hydration, as well as activation of tubular chloride reuptake by forced chlouresis, might favorably influence the equilib- rium between stable nontoxic cisplatin 0) and aquated forms (11, III, V), as well as cytotoxic hy- droxyl species (IV, VI), thereby reducing renal tu- bular damage without affecting general cytotoxic- ity.
Cisplarin Tissue Disrriburion, Pharmacokinetics. and Renal Handling
After IV administration. cisplatin undergoes rapid distribution to nearly all organs. Tissue platinum concentration studies at various points af- ter cisplatin administration in dogs show a very rapid accumulation of the metal in the kidney (three to four times the plasma concentration ten minutes after administration) with persistently ele- vated values fbr more than 1 week. lop A very high postmortem renal concentration of platinum has also been reported in humans two days after ad- ministration of a single dose of 2 mg/kg of cii platin.95 Platinum concentrates in various other tissues (gonadal tissue, lung, liver, fat)lo9; studies in humans have shown that 90% of the drug is protein-bound in plasma and that 27 % to 45% of the drug is excreted in the urine within five days of administration. 113 Data on free platinum renal clearance in humans indicate that platinum clear-
NEPHROTOXICITY OF CYTOSTATICS
ance exceeds the GFR, suggesting active secretion [of the drug or a metab01ite.I~~ As might be ex- -petted, cisplatin pharmacokinetics are altered in i patients with renal insufficiency, and normal or i near normal values of creatinine clearance are \generally considered necessary in order to avoid jcxcessive nephrotoxici@ This general rule seems , to be of questionable importance in cases of age- related decrease in renal function and especially in cases of a unique functional kidney. In fact, both conditions generally result in a lower 24-hour creatinine clearance, but as has been shown in a recent clinical study, they are not associated with greater renal toxicity if standard hydration is per- formed and if cisplatin dosage does not exceed 60 mg/m2/d. ' I 4 This study even suggests a protective mechanism in patients with unique kidneys (14 of 43 patients studied) compared with those with two normally functioning kidneys. In fact, the reduced number of nephrons will produce a higher flow of ultrafiltrate per tubule with lower tubular cisplatin concentration and probably less tubular "contact" between the toxin and tubular epithelium. This is illustrated by a higher than normal 24-hour diure- sis, wit!! lower cisplatin urinary concentrations for an identical cisplatin dose and hydration program in these patients, compared with those with two ' normally functioning kidneys. A similar mecha- nism is thought to contnbute to the relative lack of excessive age-associated cisplatin-induced nephro- toxicity.
. Other studies (in animals and humans), based on rhythmic changes in kidney function, according to circadian rhythms, have shown that optimal renal tolerance of cisplatin occurs very near to the time of day associated with the normal circadian max- imum in urinary volume. This beneficial effect is potentiated by concurrent hydration and is corre- lated by lower urinary cisplatin concentra- tions. 15-I l 7 These studies, along with those on hy- dration and forced diuresis suggest the primordial role of reducing cisplatin urinary concentrations by high urinary output; in fact. direct tubular ex- posure for a few hours to a concentration of 200 pg/mL of cisplatin seems to be necessary for tubu- lar damage to occur.96
Parhologic Kidney Changes As documented by animal and human studies.
cisplatin induces several microscopic kidney changes that are dose-related and, to a lesser de- gree. cumu!ative. 96,102,'03.118 These changes in-
clude epithelial cell degeneration, proximal tubu- lar necrosis, dilatation and necrosis of distal tubules, interstitial edema. and lymphocytic in- filtration. Glomerular changes are generally not observed and most alterations are considered to be nonspecific. Tbbular damage is also suggested by sensitive assays for tubular enzymes, thought to be liberated by renal injury: alanine-aminopeptidase, N-acetyl-0-glucosaminidase (NAG) I l 9 . I z 0 ;
these studies support the concept that all areas of the tubule may be injured to some extent.
Studies on urinary activity of NAG, a lysosomal enzyme released into the urine from the brush bor- der of proximal tubular cells, have shown a posi- tive correlation between cisplatin nephrotoxicity and NAG urinary activity. Potentiation of cisplatin tissue uptake by NAG tissue activity has been re-
as well as a circadian rhythm of urinary NAG activity, suggesting that rhythmic changes in NAG activity may cause variations in cisplatin nephrotoxicity along with circadian rhythms. PZ- microglobulin, possibly another mediator of tubu- lar injury, was shown to be significantly elevated in the urine 12 hours after treatment with cis- platinI2l: since no patient in that report developed laboratory evidence of renal toxicity, this in- creased /32-microglobulinuria has been interpreted as reflecting subclinical renal damage.
Hypomagnesemia and renal magnesium wasting are the most prominent electrolytic disorders sec- ondary' to cisplatin administration. 122-124 Hypo- magnesemia d e v e l o e 2 % of 44 patie- h e seriesLz2 with a treatment schedule of 70 mg/ m2 cisplatin (on day l ) , repeated every 21 days. Among patients with hypomagnesemia. the nadir Mg concentration (median) was 0.92 mEq/L. usually occumng more than 2 weeks after drug administration and generally after one or two courses of cisplatin had been given. Similar hypo- magnesemia was also observed in other stud- ies1Z3.125 and is frequently complicated by hypo- calcemia that is probably secondary to diminished PTH release and/or end-organ resistance to parathyroid hormone induced by hypomagnese- mia.126 I z 7 Clinical manifestations of hypomagne- semia. including abnormalities in neuromuscular. central nervous system. and cardiac function that may appear for serum levels of less than 1 mEq/L. should be treated by parented replacement of magilesium sulfate. Associated hypocalcemia is responsive to .magnesium repletion and is unre- sponsive to calcium replacement alone. The more

RlES AND KLAST ERSKY
rarely seen hypokalemia should be treated by re- placement of both potassium and magnesium.
Prevention of' Cisplatin-Induced Nephrotoxiciry
Preexistent renal insufficiency should always be excluded before starting cisplatin therapy; dehy- dration, arterial hypeitension and hyperuricemia shouid be corrected; concomitant administration of nephrotoxic drugs, especially aminoglycoside antibiotics, should be avoided.Iz8
Numerous clinical trials proposing various hy- dration programs have been d e ~ c r i b e d . ~ ~ . ~ ~ . l ~ 9 All of these schedules are valuable, provided that hy- dration status is closely monitored. Most hydration programs are performed with normal saline solu- tion or glucose 5 % in saline and are given for vari- ous durations, before, during, and after cisplatin administration. Hydration alone can be considered sufficiently effective if cisplatin is administered as 20 mglm2ld by one- to two-hour infusion for five consecutive days.
Forceddiuresis programs, combining hydration with furosemide or mannitol administration, have proved clinically beneficial in numerous stud- ies,84.130.132 and superiority of hydration-diuretic programs compared to hydration alone has been suggested.'33 Most of the more recent programs permit administration of cisplatin at doses of 100 ro 120 mg/m2 as short daily infusions or adminis- tration of 20 to 40 mglm21d for five consecutive days. Intensive parenteral hydration with mannitol-induced diuresis even permits prevention of dose-limiting nephrotoxicity. In these patients. myelotoxicity might become a major problem134; combined with cisplatin administration in hyper- tonic saline, doses as high as 200 mglm2 have been administered, with thrombocytopenia being the most promineht toxic effect."' In a recent study, three "highdosf" regimens, with doses between 180 and 220 mglm2/d, were compared: cisplatin was dissolved in 5% saline and was administered along with a well-defined prehydration-mannitol- induced diuresis and posthydration program. In that study it was concluded that cisplatin, given at a dose of 200 mg/m2 in five daily fractions, com- bined with an appropriate hydration and diuresis program. was devoid of significant nephrotoxicity and was probably much less ototoxic than single- bolus high-dose admini~tra t i0n. l~~ High chloride diuresis may improve the therapeutic index of cis- platin by reduced nephrotoxicity without loss of antitumor activity. Animal studies have shown in-
creased nephrotoxicity in chloridedeprived rats and significantly reduced renal damage with phar- macologically induced chloriuresis; this favorabi: effect could be explained by the reduction ni highly toxic aqueous-cisplatin complexes in chloride-rich urine. lo'
Continuous infusion of cisplatin results in re- duced gastrointestinal and renal when compared with earlier studies with equal daily doses. Continuous infusion should, however, always be associated with adequate hydration pro- grams, the influence on renal toxicity of vigorous urinary output being more important than the duration of infusion.
Pharmacologic Interaction With Cisplatin Nephrotoxici~
Unlike mannitol and furosemide, which exert their activity by inducing a potent diuresis, various other compounds have been proposed on the basis of a potential for detoxification. Among these. probenecid has been studied in animals (F344 rat model) and was shown to decrease the peak values of BUN and creatinine if administered one hour prior to cisplatin; this protection has been ascribed to probenecid inhibition of active secretion of cis- platin by the p-aminohippurate system.14' WR-2721 [S-2-(3-aminopropy1amino)-
ethylphosphorothioic acid], a radioprotective agent, has been shown to exert protective activity on renal function in the same F344 rat model.IJ2 Diethyldithiocarbamate (DDTC). a potent SH- group chelator administered to F344 rats after a known nephrotoxic dose of cisplatin. may prevent renal pathologic as well as functional changes.14' This protective activity is ascribed to competition with cisplatin for protein-bound sulfhydril groups within proximal tubular cells. Protein binding of cisplatin in tubular cells, with resultant inhibition of transport enzymes, is one postulated mecha- nism of cisplatin nephrotoxicity in rats and, perhaps, in humans. The closely related disulfiram (Antabuse: Ayerst Laboratories. New York). being metabolized to diethylthiocarbarnate. might exen a similar protective effect.
Sodium thiosulfate has also been studied for its nephrotoxicity preventive effects. L 4 4 This sulhr- containing compound is thought to reacr CO-
valently with cisplatin, resulting in complexes that are neither toxic nor t ~ m o r i c i d a l . ~ ~ ~ Apart from markedly reducing general cisplatin toxicity by its systemic activity, sodium thiosulfate might exert

PERSPECTIVES AND CONCLUSIONS
;
A better knowledge of various factors contribut- ing to cisplatin nephrotoxicity, as well as optimal administration programs with hydration and dmg-
further reduction in nephrotoxicity through partic- ularly high intratubular thiosulfate to cisplatin con- centration ratios. Intravenous sodium thiosulfate seems to be a most intiresting agent when ad- ministered in combination with intraperitoneal cis- platin. eg, for ovarian cancer. In this indication. parenteral thiosulfate adniinistration allowed esca- lation of intraperitoneal cisplatin up to a dose of 270 mg/m2 without significant nephrotoxicity, thus permitting an increased activity.i4s Other sulfur compounds, eg, thiourea, L-methionine. and peni- cillarnine, might also inhibit the biologic activity
induced diuresis, have considerably changed the
of cisplatin and might, therefore, interfere with its 1 therapeutic as well as toxic effects.14C148 The carbonic anhydrase inhibitor acetazolarnide
has also been considered potentially useful for pre- vention of cisplatin nephrotoxicity. i49.1s0 A Pa* from its activity as a diuretic, this organic acid could act by competition with cisplatin for tubular reabsorption, thus promoting cisplatin excretion: however, the presence of two sulfur atoms in this molecule could also permit chemical interaction and detoxification. In an animal study (male F344 rat model), pretreatment with acetazolarnide de- creased cisplatin nephrotoxicity and diminished renal platinum content, as well as urinary platinum e ~ c r e t i 0 n . l ~ ~ Comparison of acetazolamide and mannitol in the same animal model (performed by the same authors) shows acetazolamide to be more effective than mannitol in preventing cisplatin- induced nephrotoxicity in male F344 rats. lS0 The enzyme copper-zinc superoxide dismutase (orgo- tein) has also been associated with reduction of
I nephrotoxicity in rats, thus suggesting that su- peroxide radicals may participate in the nephro- toxic effects of c i ~ p l a t i n . ~ ~ ~
Selenium. known for its ability to combine to metals such as cadmium and mercury, as well as for its resemblance to sulfur by its chemical prop- erties, shows theoretical promise as a cisplatin- precipitating agent. As shown in studies on mice. selenium is able to decrease cisplatin nephrotoxic- ity without influencing in vivo and in vitro tumor growth. This could suggest either detoxification by ligation to sites not involved in cisplatin antitu- mor activity or, perhaps, prevention of tubular reabsorption of the mo1esu:ar complex. 152
spectrum of cisplatin's potential for renal toxicity. Introduction of some of the new detoxification agents will probably prove useful as well. Dosing plasma cisplatin levels at various times after drug infusion could be helpful to predict nephrotoxicity early in the course of cisplatin infusion. I s 3 Finally, several second-generation platinum complexes are being evaluated in preclinical and clinical studies for toxicity and antitumor activity. Among these, i p r o p l a t i ~ u m (CHIP) and carboplatinurn (CBDCA) show little or no n e p h r o t o x i ~ i t y . ~ ~ ~ - ~ ~ ~ These and other platinum compounds are possibly candidates as future alternatives to cisplatin in several conditions. Until then. however, cisplatin remains one of the most potent antineoplastic agents ever developed. Further work should be performed to reduce its potential for renal toxicity.
REFERENCES I. Garnick MB. Mayer RJ: Management of acute renal
failure associated with neoplastic disease. in Yarbm J. Born- stein R (eds): Oncologic Emergencies. Management of Acute Renal Failure Associated With Neoplastic Disease. Orlando. FL. Grune & Stranon, 1981, pp 247-271
2. Weiss RB. Poster DS: The renal toxicity of cancer che- motherapeutic agents. Cancer Treat Rev 9:37-56. 1982
3. Abelson HT. Garnick MB: Renal failure induced by can- cer chemotherapy, in Rieselbach RE. Garnick MB (eds): Can- cer and the Kidney. Philadelphia. Lea & Febiger. 1982. pp 769-8 1 3
4. Bleyer WA: The clinical pharmacology of methotrexate: New applications of an old drug. Cancer 4 1 :36-5 1. 1978
5. Frei E UI. Jaffe N. Tanenall MHN. et al: New ap- proaches to cancer chemotherapy with methotrexate. N Engl J Med 292:846-85 1. 1975
6. Pran CB. Roberts D. Shanks E. et al: Response. toxicity. and pharrnacokinetics of highdose methotrexate (NSC-740) with citrovorum factor (NSC-3590) rescue for children with osteosarcorna and other malignant tumors. Cancer Chemother Rep 6: 13- 18. 1975 (suppl)
7. Stoller RG. Jacobs SA. Drake JC. et al: Pharmaco- kinetics of highdose methotrexate (NSC-740). Cancer Che- mother Rep 6: 19-24. 1975 (suppl)
8. Von Hoff DD. Penta JS. Helman U. et al: Incidence of drug-related deaths secondary to highdose of methotrexate and citrovorum factor administration. Cancer Treat Rep 61:745- 748. 1977
9. Pitman SW. Parker LM. Tattersall MHN. et al: Clinical trial of highdose methotrexate (NSC-740) with citrovorum factor (NSC-35%)-Toxicologic and therapeutic observations. Cancer Chemother Rep 6:43-49. 1975 (suppl)
10. Bratlid D. Moe PJ: Pharmacokinetics of highdose rnethotrexate treatment in children. Eur J Clin Pharmacol 14: 143-147. 1978
I I. Pitman SW. Fre~ E 111: Weekly rnethurexatetalcium leucovorin rescue: Effect of alkalinization on nephrotoxicity; pharn~acokineti:~ in the CNS: and u x in CtJS non-Hodgkin's lymphoma. Cancer Treat Rep 61 :695-701. 1977
/ I It. I;,
1: i l I I! ; I ! / i ;
!: I " I I ! i ,i j ( 11: i 8 . .
/ I / 1
. .
12. Frei E Ill. Blum RH. Pitman SW. et al: Highdose methotrexate with leucovorin rescue. Rationale and spectrum of antitumor activity. Am J Med 68:370-376. 1980
13. Romolo JL. Goldberg NH. Hande KR. et al: Effect of hydration on plasma methouexate levels. Cancer Treat Rep 61: 1393-13%. 1977
14. Pinedo HM. Chabner BA: Role of drug concentration, durationaf exposure, and endogenous metabolites in determin- ing methotrerate cytotoxicity. Cancer Treat Rep 61:709-775. 1977
15. Link DA. Fosburg MT. Ingelfinger JR. et al: Renal tox- icity of highdose-methouexate. Pediatr Res 10:455. 1976 (ab- s a 923)
16. Howell SB, Carmody J: Changes in glomerular filtration rate associated with highdose methotrexate therapy in adults. Cancer Treat Rep 6 1: 1389- 138 1. 1977
17. Abelson HT. Fosburg MT. Beardsley GP. et al: Methotrexate-induced renal impairment: Clinical studies and rescue from systemic toxicity with highdose leucovorin and thymidine. J Clin Oncol 1:208-216. 1983
18. Tanersall MHN. Parker LM. Pitman SW. et al: Clinical pharmacology of highdose methotrexatc. Cancer Chemother Rep 6:25-29. 1975
19. lsacoff WH. Townsend CM. Eibcr FR, et al: Highdose methotrexate therapy of solid tumors: Observations relating to clinical toxicity. Med Pediatr Oncol 21319-325. 1976
20. Ahmad S. Shen F. Bleyer WA: Methotrexatc-induced re- nal failure and ineffectiveness of peritoneal dialysis. Arch In- tern Mcd 138:1146-1147. 1978
2 1. Hande KR. Balow JE. Drake JC. et al: Methotrexate and hemodialysis. Ann Intern Med 87:4954%. 1977
22. Gibson TI? Reich SD. Krumlovsky FA. et al: Hemoper- fusion for methotrexate removal. Clin Pharmacol Ther 23:351-355. 1978
23. Djerassi I. Ciesielka W, Kim JS: Removal of methotrex- ate by filtration-adsorpt~on using charcoal filters or by hemo: dialysis. Cancer Treat Rep 61 :75 1-752. 1977
24. Oliverio VT: Toxicology and pharmacology of the nitro- soureas. Cancer Chemother Rep 4: 13-20. 1973
25. Denine EP, Hamson SD Jr. Peckham JC: Qualitative and quantitative toxicity of sublethal doses of methyl-CCNU in BDF, mice. Cancer Treat Rep 61:409-417. 1977
26. Schacht RG. Baldwln DS: Chronic interstitial nephritis and renal failure due to nitrosourea (NU) therapy. Kidney Int 14:661. 1978 '
27. Harmon WE. Cohen HJ. Schneegerger EE. et al: Chronic renal fai1u;e in children treated with methyl-CCNU. N Engl J Med 300: 1200-1203. 1979
28. Schacht RG. Feiner HD. Gallo GR. et al: Nephrotoxic- ity of nitroswreas. Cancer 48: 1328- 1334, 198 1
29. Nichols WC. ~Moertel CG: Nephrotoxicity of methyl CCNU. N Engl J Med 301:1181. 1979 (lener)
30. Kundaria 8. Armentrwt S. hlargileth D. et al: Nephro- toxicity of semustine. Proc Am Soc Clin Oncol 223352. 1981 (abstr C-77)
31. Micetich KC. Jensen-Akula M. Mandard JC. et al: Nephrotoxicity and semustine (methyl-CCNU) in patients with malignant melanoma receiving adjuvant chemotherapy. Am J Med 7 1 :967-972. 198 1
32. Weiss RB. Posada JG. Kramer RA. et al: Nephrotoxicity of semustine. Cancer Treat Rep 67: 1 105-1 1 12. 1983
RlES AND KLASTERSKY
33. Harrison SD Jr. Cox JL, Giles RC Jr: Effbcu of pro- chlorpcrazine on experimental nephrotoxicity. Cancer Che- mother Pharmacol 10:62-67. 1982
34. Taylor SG Ill. Schwanz TB. Zannini JJ, et al: Streptoz, twin therapy for metastatic insulinoma. Arch Intern .\I<... 126:654457. 1970
35. Schein I? Kahn R. Gordcn I? et al: Streptozotocin for malignant insulinomas and carcinoid NmOr. Arch Intern Med 132555-561. 1973
36. Weiss RB: Streptozotocin: A review of its pharmacol- ogy. efficacy, and toxicity. Cancer *at Rep 66:427438. 1982
37. Broder LE. Carter SK: Pancreatic islet cell carcinoma. Ann Intern Med 79: 108- 1 18. 1973
38. Sadoff I: Nephrotoxicity of streptozotocin (NSC- 85998). Cancer Chemother Rep 54:457459. 1970
39. Schein PS. De Lellis RA. Kahn CR, et al: Islet cell tu- mors: Currcnt concepts and management. AM Intern Med 79:239-257. 1973
40. Murray-Lyon IM. Eddleston ALWF. Williams R. et al: Treatment of multiple-hormone-producing malignant islet-cei! tumor with streptozotocin. Lancet 2:895-898, 1968
41. hloertcl CG. Hanley JA. Johnson LA: Streptozotocin alone compared with streptozotocin plus fluorouracil in the treatment of advanced islet-cell carcinoma. N Engl J Med 303:1189-1194, 1980
42. Schein P, O'Connell MI. Blom J, et al: Clinical antitu- mor activity and toxicity of streptozotocin (NSC-85998). Can- cer 3493-1000. 1974
43. Brown JH. Kennedy BJ: Mithramycin in the treatment of disseminated testicular neoplasms. N Engl J Mcd 272:111- 118, 1965
44. Ream NW, Perlia CP, Wolter J, et al: Mithramycin therapy in disseminated germinal testicular cancer. JAMA 204: 1030- 1036. 1968
45. Kennedy BJ: Meabolic and toxic effects of mithramycin during tumor therapy. Am J Med 49:494-503. 1970
46. Kennedy BJ. Brown JH. Yarbro JW: Mithramyc~n (NSC-24559) therapy for primary glioblastomas. Cancer Chs- mother Rep 4839-63. 1965
47. Elias EG. Reynoso G. Mittelman A: Control of hyper- calcemia with mithramycin. Ann Surg 175:431435. 1972
48. Mazzaferri EL. O'Dsrisio TM. LoBuglio AF: Treat- ment of hypercalcemia associated with malignancy. Semin On- col 5:141-153. 1978
49. Crooke ST, Bradner WT Mitomycin C: A review. Can- cer Treat Rev 3:121-139. 1976
50. Caner SK. Crooke ST (eds): Mitomycin C: Currcnt Sta- tus and New Developments. Orlando. FL. Academic. 1979. pp 1-4
51. Phillips FS, Schwanz HS. Sternbert SS: Pharmacology of mitomycin C: 1. Toxicity and pathologic effects. Cancer Res 20~1344-1361. 1960
52. Mrtsuyama M. Suzumori K. Nakamura T: Biological studies on anticanccr agents: I. Effects of prolonged intraperi- toneal injections of Mitomycin C on the urinary organs. J Urol 92:618-620. 1%4
53. Matsuyama M. Suzumori K. Nakamura T: Induction of hydronephrosis by prolonged intraperitoneal injections of sub- toxic dose of mitomycin C in mice. Nature 202:99-100. 1964
54. Liu K. Minelman A. Sproul EE. et al: Renal toxicity in man treated with mitomycin C. Cancer 25:1314-1320. 1971
NEPHROTOXICITY O F CYTOSTATICS
- 55. Gulati SC, Sordillo P. Kemp~n S. et al: Microangtopath~c hemolytic anerma observed after treatment of epldermoid car-
'? cinoma wirh Mitomycin C and 5-fluorouracil. Cancer 45:2252-2257. 1980 .
56. Pavy MD. Wiley EL. Abeloff MD: Hemolytic-uremic syndrome associated with mitomycin therapy. Cancer Treat Rep 6 6 : 4 5 7 4 1 . 1982 '.
,
57. Hanna W. Krauss S. Regester RF. et al: Renal disease
g after mitomycin-C therapy. Cancer 48:2583-2588. 1981 X 58. Brain MC, Azzopardi JG. Baker LRI. el al: Microan-
giopathic hemolytic anemia and mucin-forming adenocar-
#: cinoma Br J Haematol 18: 183-192. 1970 59. Lohrmann H. Adam W. Hcymer B. et al: Microan-
giopathic hemolytic anemia in metastatic carcinoma. Ann In- tern Med 79368-375, 1973
60. Sack GH. Levin J. Bell WR: Trousseau's syndrome and other manifestations of chronic dissermnated coagulopathy in patients with neoplasms: Clinical, pathophysiologic, and thera- peutic feawres. Medicine 56: 1-37. 1977
61. Antman KH. Skarln AT. Mayer RI. et al: Microan- giopathic hemolytic anemia and cancer. A review. Medicine 58:377-384. 1979
62. Kressel BR. Ryan KP. Duong AT. et al: Microan- giopathic hemolytic anemia. thrombocytopenia and renal failure in patients treated for adenocarcinoma. Cancer 48:1738-1745. 1981
63. Cantrell JE, Phillips TM, Schein PS: Carcinoma- associated hemolytic-uremic syndrome: A complicatton of mi-
l ' tomycin C chemotherapy. J Clin Oncol 3~723-734. 1985
J 64. Krauss AS. Sonada T. Soloman A: Treatment of ad- vanced gastrointestinal cancer with 5-fluorouracil and mitomy- cin C. Cancer 43: 1598-1603, 1979
55. Hamner RW. Verani R. Weinman EJ: Mitomycin- associated renal failure. Arch Intern Med 143:803-807. 1983
66. Jones BG. Newman CD. Fielding JW. et al: Intravascu- lar haemolvsis and renal impairment after blood transfusion in rwo patients on long-term 5-fluorouracil and mitomycin C.
1 Lancet 1: 1275-1276. 1980 67. Rumpf KW. Rieger J. Lankisch PG. et al: Mitomycin-
i induced haemolvsis and renal failure. Lancet 2: 1037- 1038. 1980
I 68. Ratanatharathorn V. Baker LH. Cadoapaphorchai P. rt al: Clinical and pathological swdy of mitomycin C nephrotox- icity. in Caner SK. Crooke ST (eds): Mitomycin C. Current
( S I ~ N S and New Developments. Orlando. FL. Academic 1979.
I pp 2 19-229 69. Lempen KD: Haemolysis and renal impairment syn-
drome in patients on 5-fluorouracil and mitomycin C. Lancet 2:369-370. 1980
I 70. Von Hoff DD. Slavik M. Muggia FM: 5-Azacytidine: A
1 new anticancer drug with effectiveness in acute myelogenous
I leukemia. Ann Intern Med 85:237. 1976 71. Greenberg MS: Reversible renal dysfunction due to 5-
I azacytidinc. Cancer Treat Rep 63:806. 1979
72. Peterscn BA. Collins AJ. Vogelzang NJ. et al: 5 - Azacytidine and rer~al tubular dysfunction. Blood 57: 182-:85. 198 1
73. ~ o s e n b e ; ~ 9. Van Camp L. Trosko JE. ct al: Platinum compounds. Sawre 222385-386. 1969
74. Rosenkrg B. Van Camp L: The successful regrcsson of
large solid sarcoma 180 tumors by platinum compounds. Can- cer Res 30: 1799- 1802. 1970
75. Kociba RJ. Sleight SD: Acute toxicologic and patho- logic effects of cisdiamrninedichloroplatinum (NSC-119875) in the male rat. Cancer Chemother Rep 55: 1-9. 1971
76. Leonard BJ. Eccleston E. Jones D. et al: Antileukaemic and nephrotoxic propenies of platinum compounds. Nature 234:43-45. 197 1
77. Schaeppi U. Heyman 1A. Flcischman RW. et al: Cis- dichlorodiammineplatinum (IJ) (NSC-I 19875): Preclinical tox- icologic evaluation of intravenous injection in dogs. monkeys and mtce. Toxicol Appl P h a m c o l 25:230. 1973
78. Rossof AH. Slayton RE. Perlia CP: Preliminary clinical experience with cis-diamminedichloroplatinum (11) (NSC- 1 19875. CACP). Cancer 30: 1451-1456. 1972
79. Lippman AJ. Helson C. Helson L. et al: Clinical trials of cis-diamrninedichloroplatinum (NSC-I 19875). Cancer Che- mother Rep 57:191. 1973
80 . Higby DJ. Wallace HJ Jr. Holland JF: Cis - diamm~nedichloroplatinum (NSC-1 19875): A phase I study. Cancer Chemother Rep 57:459-463. 1973
81. Talley RW. O'Bryan RM. Gutterman JU. et al: Clinical evaluation of toxic effects of cisdiamminedichloroplatinum (NSC-119875): Phase I clinical study. Cancer Chemother Rep 57:465-47 I, 1973
82. De Conti RC. Toftness BR. Lange RC. et al: Clinical and pharmacological studies with cis-diamminedichloro- platinum 111). Cancer Res 33:1310. 1973
83. Higby DJ. Wallace HJ Jr. Alben DJ. et al: Diammino- dichloroplatinum: A Phase I study showing responses In testic- ular and other tumors. Cancer 33:1219-1225. 1974
84. Young RC, Von Hoff DD. Gormley P. et al: Cis- diamminedichloroplatincm (11) for the treatment of advanced ovarian cancer. Cancer Treat Rep 63: 1539- 1544. 1979
85. Einhorn LH. Donohue J: Cis-diamminedichloro- platinum. vinblastine and bleomycin combination chemother- apy in disseminated testicular cancer. Ann Intern Med 87:293- 298. 1977
86. Garnick MB. Canellos GP. Richie JP. et al: Sequential combination chemotherapy and surgery for disseminated testic- ular cancer: Cisdiamminedichloroplatinum. vinblastine and bleomycin remission-induction followed by cyclophosphamide and adriamycin. Cancer Treat Rep 63: 1681 -1686. 1979
87. Yagoda A: Phase 11 trials with cis-diamminedi- chloroplatinum (11) in the treatment of urothelial cancer. Can- cer Treat Rep 63: 1565- 1572. 1979
88. Williams SD. Donohue JP. Einhorn LH: Advanced blad- der cancer: Therapy with cisdiamminedichloroplatinum (11). ddriamycin and 5-fluorouracil. Cancer Treat Rep 63:1573- 1576. 1979
89. Samuels ML. et al: CISCA combination chemotherapy for metastatic carcinoma of the bladder. in Johnson DE. Sam- uels ML (eds): Cancer of the Genitourinary Tract. New York. Raven. 1979. p 101
90. Hong WK. Bhutani R. Shapshay SH. el al: Induction chemotherapy of advanced previously untreated squamous cell head and neck cancer with cisplatin and bleom)c~n. in Pre- stayko AW. Crwke ST. Carter SK (eds): Cisplattn-Current Sratus and New Developments. Orlando. FL. .4cademic. 1980. p 431
91. Eagsn RT: Phase I1 study of cyclophosphamide.
RlES AND KLASTERSK
adriamycin, and cisdiamrninedichloroplatinum (11) by infusion in patients with ademcarcinoma and large cell carcinoma of the lung. Cancer Treat Rep 63: 1589. 1979
92. De Jaeger R, bngeval E. Klastersky J: Highdose cis- ptatin with fluid and rnannitol-induced diunsis in advanced lung cancer: A phase U clinical trial of the EORTC Lung Can- cer Working Party e lg ium) . Canar Treat Rep 64: 1341- 1346, 1980
93. Baker LH: Cisplatin in treatment of cervical and endo- metrial cancer patients. in Rcstayko AW, Crooke ST, Carter SK (eds): Cisplatin-Current Status and New Developments. Orlando. FL. Academic. 1980. p 403
94. Thiepn IT. Shingleton H. Homesley H. et al: Cisplatin in the treatment of advanced or recurrent cervix and uterine cancer. in Prestayko AW, Crooke ST. Caner SK (eds): Cisplatin-Current Status and New Developments. Orlando. FL. Academic. 1980. p 41 1
95. Hill JM, Loeb E, MacLcllan A, et al: Clinical studies of platinum corodination c o m p n d s in the treatment of various malignant diseases. Cancer Chemother Rep 59:647-659. 1975
96. Rozencweig M. Von Hoff DD. Slavik M, et al: Cis- diamminedichloroplatinum (In. a new anticancer drug. Ann In- tern Med 86:803-812, 1977
97. Einhorn LH, Williams SD: The role of cis-platinum in solid tumor therapy. N Engl J Med 300:289-291. 1979
98. Zwelling LA, Kohn KW: Mechanism of action of cis- diamminedichloroplatinum (11). Cancer Treat Rep 63:1439- 1444. 1979
99. Guarino AM, Miller DS. Arnold ST, et al: Platinate tox- icity: Past. present, and prospects. Cancer Treat Rep 63: 1475- 1483. 1979
100. Prestayko AW. CrookeST. Cancr SK (eds): Cisplatin- Current Status and New Developments. Orlando. FL. Aca- demic. 1980
101. Hardaker WT Jr. Stone RA. McCoy R: Platinum nephrotoxicity. Cancer 34: 1030-1032. 1974
102. Gonzalu-Vitale JC. Hayes DM, Cvitkovic E. et al: The renal pathology in clinical trials for cis-platinum (II) diam- rninedichloride. Cancer 39: 1362- 1371. 1977
103. Madias NE, Hanington JT: Platinum nephrotoxicity. Am J Med 65:307-314. 1978
104. Stark JJ. Howell SB: Nephrotoxicity of cis-platinum (11) dichlorodiammine, Clin Pharmacol Ther 23:461-466. 1978
105. Comis RL: Cisplatin nephrotoxicity: The effect of dose. schedule. and hydration scheme. in Prestayko AW, Crooke ST. Carter SK (cds): Cisplatin-Current Status and New Developments. Orlando. FL. Academic. 1980. p 485
106. Rosenberg B: Cisplatin: Its history and possible mecha- nisms of action. in Prestayko AW. Crooke ST. G n e r SK (eds): Cisplatin-Current Status and New Developmenrs. Orlando. FL. Academic. 1980. p 9
107. Lee KW. Martin DS: Ci~di~hlorodiamrnine~latinum (ID. Aquation equilibria and isotop~c exchange of chloride l i - gands with free chloride and tetrachloroplatinate (11). lnorp Chim Acta 17:105-110. 1976
108. Earhan RM, Martin PA. 'htsch KD. et al: Improve- ment in the therapeutic index of cisplatin (NSC 119875) by pharmacologically induced chloriuresis in the rat. Cancer Res 43: 1 187-1 194. 1983
109. Le Roy AF. Lutz RJ. Dedrick RL. et al: Pharmaco-
kinetic study of cis4chlorodiammineplatinum (XI) (DDP) the beagle dog: Thermodynamic and kinetic behavior of DT in a biologic milieu. Cancer Treat Rep 6359-71, 1979
110. Jacobs C, Kalrnan SM. Treaon M, et al: Rend h: dling of cisdichlodiammineplatinum 0. Cancer Trcat Rt 64:1223-1226. 1980
I I I . Patton IT, Himmelstcin KJ. Belt R. et al: Plasma level. and urinary excretion of filterable platinum species followin! bolus injection and i.v. infusion of cis-dichloro. diamrnineplatinum (I0 in man. Cancer Treat Rep 62~1359- 1362, 1978
1 12. Gonnley PE, Bull JM, LeRoy AF, et al: Kinetics of cis- dichlorodiammineplatinum. Clin Phannscol Thcr 25:351-357. 1979
113. Frick GA. Ballentine R. Driever CW. et al: Renal ex- cmion kinetics of highdose cirdichlorodiammincplatinurn (II) administered with hydration and manniwl diurcsis. Cancer M t Rep 63: 13-16, 1979
114. Hrushesky WJM. Shimp W, Kennedy BJ: Lack of arc dependent cisplatin nephrotoxicity. Am J Mcd 76:579-5.- 1984
115. Hrushesky WJM. Levi FA. Halkrg F, et al: Cisplatin lethal toxicity is circadian stagedepcndent. Cancer Res 42:945-949, 1982
116. Levi FA, Hrushesky WWJ, Blomquut CH: Reduction of cisplatin nephrotoxicity by optimal circadian drug timing. Cancer Res 42:950-955. 1982
117. Levi FA, Hrushesky WJM, Borch W, et al: Cisplatin urinary pharmacokinetics and nephmtolicity: A common cir- cadian mechanism. Cancer Treat Rep 66: 1933- 1938. 1982
118. Agganval SK. Whitehouse MW, Rvnachandran C: U1- trastructural effects of cisplatin. in Restay ko AW, Crooke ST. Caner SK (4s) : Cisplatin. Orlando. FL. Academic, 1980. p 79
119. Jones BR, Ravi BB. Mladek J. et al: Comparison of methods of evaluating nephrotoxicity of cis-platinum. C1.'-1 Pharmacol Ther 27557-562. 1980
120. Diener U. Knoll E. Langer B, et 81: Urinary excretion of N-acetyl-8-glucosaminidasc and alanine arninopcptidase in patienu receiving amikacin or cis-platinum. Clin Chim Acta 112:149-157, 1981
121. Cohen AL. Hargerg J, Citrin DL: Measurement of urinary 6, microglobulin in the detection of cisplatin nephro- toxicity. Cancer Treat Rep 65:1083-1085. 1981
122. Schilsky R, Anderson T: Hypornagnexmia and m a 1 magnesium wasting in patienu receiving cisplatin. AM Intern Med 92929-93 1, 1979
123. Anderson T, Javadpour N, Schilsky R, et al: Chemo- therapy for test~cular cancer: Current status of the National Cancer Institute combined modality trial. Cancer Treat Rep 63~1687-1695. 1979
124. Blachley JD. Hill JB: Renal and electrolyte disturb- ances associated with cisplatin. Ann Intern Med 95:628-6.':. 1981
125. Hill JB, Blachley JD. Trotter M: Hypomagnesemla. hypcalcemia, and hypokalemia with cis-platinum treatment Clin Res 26:780A, 1978 (abnr)
126. Suh SM, Tashjian AH Jr. Mauuo N, et al: pathogenesis of hypocalcernia in primary hypomagnescmia: Normal end- organ responsiveness to parathyroid hormone impaired parathyroid gland function. J Clin Invest 52:153-160. 1973

127. Connor TB. Toskes P, Mahaffey J. et al: Parathyroid funcrion during chronic magnesium deficiency. Johns Hopluns \fed J 131:100-117, 1972
128. Haas A. ~ n d e r s o n L. Lad T: The influence of aminoglycosides on the nephrotoxicity of cis-dichloro- diammineplatinum in cancer patients. J Infect Dis 147:3634, 1983
129. Salem P. Hall SW. Benjamin RS. et al: Clinical phase I- II study of cisdichlorodiammine platinum (ID given by con- tinuous IV inhion. Cancer Treat Rep 62:1553-1555. 1978
130. Chary KK, Higby DJ. Henderson ES. et al: Phase 1 study of high dose cisdichlorodiammineplatinum (iI) with forced diuresis. Cancer T m t Rep 6 1 :367-370. 1977
131. Merrin C. Beckley S, Takita H: MultimoQl treatment of advanced testicular tuMr with radical reductive surgery and multisequential chemotherapy with cis-platinum. bleomycin. vinblastine. vincristine and actinomycin D. J Urol 120:73-76. 1978
132. Hayes DM. Cvitkovic E. Golbey RB. et al: High dose ,-1s-platinum diammine dichloride. Amelioration of renal toxic- :ty by mannitol diuresis. Cancer 39: 1372-1381. 1977
133. Al-Sarraf M. Fletcher W. Oishi N. et al: Cisplatin hy- dration with and without mannitol diuresis in refractory dis- seminated malignant melanoma: A Swthwcst Oncology Group study. Cancer Treat Rep 66:3 1-35, 1982
134. Chary KK. Higby DJ. Henderson ES. et al: Phase I study of high dose cisdichlorodiammineplatinum (11) with forced diuresis. Cancer Treat Rep 61:367-370. 1977
135. Ozols RF. Corden BJ. Jacob J. et al: High dose cis- platin in hypenonic saline. Ann Intern Med 100: 19-24, 1984
136. Blumemich MS. Woodcock TM. Jones M. et al: Highdose cisplatin in patients with advanced malignancies. C.mcer 55: 11 18-1 122. 1985
137. Jacobs C. Benino JR, Goffinet DR. et al: 24-hour infu- sion of cis-platinum in head and neck cancers. Cancer 42:2135-2140. 1978
138. Kuhn JA. Argy Wi? Barnard W. et al: Lessening of cis- dichlorodiammineplatinum nephrotox~ciry by protracted infu- sion. Clin Res 28:837A, 1980 (abstr)
139. Lokich JJ: Phase I study of cis-dichloro- diammineplatinum (11) administered as a conswt 5-day infu- sion. Cancer Treat Rep 64:905-908. 1980
140. Carlson RW, Sikic BI: Conttnuous infusion or bolus injection in cancer chemotherapy. AM Intern Med 99:823- 833. 1983
141. Ross DA. Gale GR: Reduction of the renal toxicity of cis-dichlorodiammineplatinum (11) by probenecid. Cancer Treat Rep 63:781-787. 1979
142. Yuhas JM. Culo F: Selective inhibition of the nephro- toxicity of cisdichlorodiammineplattnum (LI) by WR-27-21 without altering its antitumor propenies. Cancer Treat Rep 64:57-64. 1980
143. Borch RF. Pleasants ME: Inhibition of cis-platinum
nephrotoxicity by diethyldithiocarbamatc rescue in a rat model. Roc Natl Acad Sci 76561 1-6614. 1979
144. Howell SB. Taetle R: Effect of sodium thiosulfate on cisdichlorodiammineplatinum (11) toxicity and antitumor ac- tivity in L1210 leukemia. Cancer Treat Rep 64:611-616. 1980
145. Howell SB. Pfeifle CL. Wung WE, et al: Intraprite neal cisplatin with systemic thiosulfate protection. AM intern Med 97:845-851. 1982
146. Filipski J. Kohn KW. Prather R. et al: Thiourea m- verses cross-links and restores biological activity in DNA treated with dichlorodiammineplatinum (LI). Science 204: 181- 183, 1979
147. Newman AD. Ridgway H. Spoor RI. et al: Inhibition of biological activity of cisplatin by thiourea and L-methionire. J Clin Hematol Oncol 9:208-209. 1979
148. Higby DJ. Wallace HI Jr. &kcsi JG: Reduction of cis- dichlorodiammineplatinum U toxicity by penicillamine com- pounds in animal models and humans. Proc Am Assa: Cancer Res 16:131. 1975
149. Osrnan NM. Copley Mi? Litterst CL: Amelioration of cisplatin-induced nephrotoxicity by the diuretic acerazolamide in F344 rats. Cancer Treat Rep 68:999- 1004. 1984
150. Osman NM. Copley MI? Lincnt CL: Effms of the diumtics mannitol or acetazolamide on nephroroxicity and physiological disposition of cisplatin in rats. Cancer Che- mother Pharmacol 1358-62. 1984
I5 I. McGinness JE, Proctor PH, Demopoulos HB: Ame- liontion of cis-platinum nephrotoxicity by orgotein (suprox- ide dismutase). Physiol Chem Phys 10:267-277. 1978
152. Beny JP. Pauwells C. l lwzcau S. et al: Effect of sele- nium in combination with cis-dichlorodiammineplatinum (u) in the treatment of murine fibrosarcoma. Cancer Res 44:2864- 2868, 1984
153. Campbell B. Kalrnan SM, Jacobs C: Plasma platinum levels: Relationship to cisplatin dose and nephrotoxicity. Can- cer Treat Rep 67: 169-172. 1983
154. Mihich G. Bullard G. Pavelic Z, et al: Preclinical stud- ies of dihydroxycisdichlorc+bis-isopropylarnine platinum IV (CHIP). Proc Am Soc Clin Oncol 20:426. 1979 (abstr C-559)
155. Atassi G. Rozencweig M: Cisdichloro I . I . di(amine methyl)cyclohexane platinum (II) (DDCP: NSC 26%08): A new platinum complex with no renal toxicity. Proc Am Soc Clin Oncol 21:260. 1980 (abstr 1044)
156. Creaven PJ. Madajewicz S. Pendyala C. et al: Phase I clinical trial of cis-dichloro-trans-dihydroxy-bis- isopropylamine platinum (IV) (CHIP). Cancer Treat Rep 67:795-800. 1983
157. Rose WC. Schurig JE. Huftalen JB. et al: Antitumor activity and toxicity of cisplatin analogs. Cancer Treat Rep 66: 135- 146, 1982
158. Rozencweiq M. Nicaise C. Beer M. et al: Phase I study of carboplatin given on a five day intravenous schedule. J Clin Oncol 1 :62 1-626, 1983