patient and public involvement committee involved... · 2 patient & public involvement...
TRANSCRIPT

1
Patient and Public Involvement Committee
Thursday 9 January 2020, 5.30pm–7.30pm
City and Hackney CCG, 3rd Floor, A Block, St Leonard’s Hospital
Nuttall Street, London, N1 5LZ
AGENDA
Item
Number
Agenda Item Led By Timing
1. Welcome and introductions
Chair’s updates
Matters arising
Ann Sanders, (Chair), CCG Lay
Member for PPI, City & Hackney
Clinical Commissioning Group
5.30pm
2. Verbal Update on single
CCG
David Maher, Managing Director, City
and Hackney Clinical Commissioning
Group
5.45pm
3. Prevention review and
Social Prescribing
procurement update
Jayne Taylor, Workstream Director,
Prevention Workstream, Integrated
Commissioning Programme, London
Borough Hackney & City of London
Corporation
Kate Wignall, Prevention Workstream
Programme Manager, Integrated
Commissioning Programme, London
Borough Hackney & City of London
Corporation
6.00pm
4. GP Confederation update Laura Sharpe, CEO, City & Hackney GP Confederation
6.25pm
5. Equality & Diversity update
and sustainability update
Catherine Macadam, CCG Associate
Member, Equality and Diversity,
Sustainability and Primary Care, City
& Hackney Clinical Commissioning
Group
6.45pm
6. Round the table updates All 7.10pm
7. AOB
All 7.25pm
8. Close
Chair 7.30pm

2
Patient & Public Involvement Committee Minutes
Thursday 12th December 2019, 17.30–19.30
Hoxton Room, City and Hackney CCG, 3rd Floor, A Block, St Leonard’s Hospital
Nuttall Street, London N1 5LZ
In Attendance:
Ann Sanders (AS) PPI Chair, Governing Body Lay Member
Tim Wiseman (TW) CCG Head of Operations
Ali Aksoy (AA) Director, Hackney Migrant and Refugee Forum
Michael Vidal (MV) Integrated Commissioning Workstream Representative for
Planned Care, Medicines Management and Estates
Ida Scoullos (IS) Integrated Commissioning workstream representative for
Prevention
Eeva Huoviala Head of Public Engagement – PPI & Personalised Care
Catherine Perez- Phillips (CPP)Director, Healthwatch Hackney
Anu Kumar (AK) GP Clinical Lead for PPI, Equality, Diversity and Sustainability
Cynthia White (CW) Chair, Older People’s Reference Group and Neaman Practice
PPG
Jackie Brett (JB) Director of Programmes and VCS Strategy, HCVS
Rosemary Jawara (RJ) Patient representative, Long-term Conditions representative
Shirley Murgraff (SM) PPG member, Well Street Practice
Sarah Weiss (SW) Interlink, Maternity Programme representative
John Bailey (JB) Hoxton Practice PPG
Apologies:
Lola Njoku (LN) Involvement Alliance Co-ordinator
Jamal Wallace (JW) Engagement and Co-production Manager, City and Hackney
Integrated Commissioning
Tony Harms (TH) PPG member, Stratham Grove Practice
Steve Stephenson (SS) Healthwatch City of London

3
Clancy Etienne (CE) Patient representative for Equality, Diversity and Sustainability
Jon Williams (JW) Director, Healthwatch Hackney
Maureen Brewster (MB) Advocacy project
Ismael Kaehid Aibrahy Advocacy Project
(IKA)
Guests:
Amy Wilkinson Director, Children, Young People, Maternity and Families
Workstream
Sarah Darcy Programme Manager, Children, Young People, Maternity and
Families Workstream
Jenny Zienau Programme Manager, Children, Young People, Maternity and
Families Workstream
Action tracker:
Number Action By Deadline/action
by
Status
1. Find out whether a
service similar to
Homerton ‘Transfer
of care for
medicines’ is in
place at ELFT.
RE RE awaiting for a
further response
from ELFT who
have told that this
is on their ‘to do’
list
Pending
2. PUEG update to
next PPI Committee
JWa February PPI
committee
Pending
3. Submit GP Confed
related questions
All to EH On-going Pending
4. Regular Co-
production Council
Updates to PPI
Committee
JS Update Dec PPI
Committee
On-going
5. E&D Committee to
feedback to PPI
Committee
Jan PPI Committee Pending
6. Circulate information
about the ICS
evaluation process
EH Jan PPI Committee Pending
7. Share positive
feedback about
JSNA engagement
and gathering
demographic data
AK January Clinical
Executive
Committee
Pending

4
with Clinical
Executive
Committee
8. Circulate a link to
the Migrant and
Refugee health
information on the
CCG’s clinical
website
EH January Pending
1. Chair’s Welcome - Introductions and matters arising
The Chair (AS) introduced herself and welcomed attendees to the meeting. Members
introduced themselves and apologies were noted. The following amendments to
November minutes, and matters arising were noted:
- CW is a representative of Neaman Practice
- AA represents Hackney Migrant an Refugee Forum
- MV said that there will be patient workshop at UCL partners
- SW had mentioned a positive planned care experience
- SH was thanked for providing the mortality figures requested at November
meeting
- P. 9 should refer to JM instead of JS
Chair told members she was still in the process of settling into her role. A key area of
work so far has been to input into the City and Hackney ICS evaluation. It was
agreed that information about the evaluation process would be circulated to members
who felt it was important that patients were involved in the work.
LBH JSNA involvement and focus groups were mentioned as examples of good
practice when it comes to engagement. JB also mentioned that the policy team at
LBH provide good quality demographic data but that overall data could be structured
in a way that would enable voluntary sector organisations to better make use of it in
their funding applications.
Action: AK to update Clinical Executive Committee about the positive JSNA
feedback and the comments about the quality of data.
Action: EH to circulate information about the evaluation process and explore the
opportunities for PPI representatives to get involved and bring an update to February
PPI meeting
2. Round table updates (All)
5
Round table updates commenced with a progress update from NHS Community
Voice provided by CPP. A set of slides was tabled to support the update.
CPP provided context and background to NHS Community Voice and told members
that the patient led steering group was a crucial part of the service, although would
have to be reinvigorated in 2020. Half of the meeting topics should be set by the
steering group although this has not been the case during 2019 due to the NHS Long
Term Plan engagement dominating the agenda. The other half of the topics should
come from the ICS workstreams.
CPP told members that Andrew Mitchelson who was the previous service manager
had left in October and that CPP is leading the service delivery until a new manager
will start in February.
The committee proceeded to discuss the NHSCV events that had taken place during
19/20 to date. It was noted that the majority of the events and engagement activities
have been well attended and have attracted a mixed audience. The recent
hypertension event was not attended as well as it was hoped, and the reasons for
this have been discussed as part of a debrief process.
Members agreed that it was crucial to be able to demonstrate the impact of the
service and close the feedback loop. AK provided additional background to how the
NHS Community Voice came to be following the Super PPGs and requested that the
events be more widely advertised which she felt they had been previously.
MV suggested that if NHSCV had any issues hearing back from workstreams they
could consider copying in the relevant patient representatives. SM said that practice
screens should be used to promote the service. CW requested a quarterly
engagement bulletin or similar, to ensure people can find all information in once
place as opposed to scattergun approach. EH told members that there are plans for
reinstating the newsletter but that this was put on hold due to lack of resourcing.
RJ raised her concerns about the fact that she felt something had happened during
the course of Healthwatch and NHSCV being co-located with HCVS.
Chair suggested that the rest of the round table updates would be done after item 3.
3. Children, Young People (CYP) and Families update (Amy Wilkinson, Sarah
Darcy, Jenny Zienau)
AW provided an overview of work using the slides that had been circulated to
members beforehand. She outlined some of the engagement related priorities for
20/21, which include learning disabilities and autism, developing CYP engagement,
refreshing the local offer and developing the parents’ advisory forum. The team
welcomed members’ thoughts on how to gather patient feedback when it comes to
CYP.

6
Plans for refreshing the parents advisory group
The team want to reach out to all parent groups to promote a workshop that takes place on 30 Jan;
Initial meetings have taken place with parents who have been able to attend;
The goal is to have a group of 12 parents involved on on-going basis
Autism
CCG has responsibility to identify people with learning disabilities and /or autism who are at risk of being admitted a specialist hospital;
SD told members that an enhanced support register has been established and this includes consent from the young person and their family to have them in the register to help co-ordinate care in the community;
The register is reviewed every three months.
Local offer
The team want to co-produce the local offer and this will be taken forward with NHSCV
Comments and questions from members included:
MV suggested that the team could try contacting school governors association to develop a closer working relationship with schools; crucial to co-ordinate work with Learning Trust;
RJ pointed out the importance of looking at CYP in the youth justice system and asked about the age at which children were usually diagnosed with autism. SW responded and said that a key issue they are looking at is the fact that autism is often diagnosed too late and earlier intervention would result in better outcomes;
CW asked about the links that the team have with safeguarding. AW said that they have a huge range of statutory responsibilities regarding safeguarding and have designated safeguarding nurses. She also mentioned that JZ who has recently joined the team has a background in children’s social care. AW reassured members that safeguarding has been made part of policies and processes etc;
AA wanted to emphasise the importance of good equality and diversity monitoring. AW responded and said that the team are fairly ‘data rich’. All data is evidence based and ethnicity monitoring is in place. Their main priorities based on this data are 1) improving emotional health, 2) strengthening health services and support for vulnerable groups. Work is taking place around young black men and youth in justice;
Maternity performance at Homerton Hospital is improving. SW added that some negative feedback recently relates to patients not feeling confident administering their blood thinning medication. She also said that there are some great examples or maternity support programmes from the Orthodox Jewish community;
SW stated that people may be asked to leave the maternity unit after 6 hours if they are fit and healthy. Members felt this was too soon. SD added that she had heard similar feedback from other sources and people being discharged as quickly as after 3 hours. The team will be looking into this;
CW thanked SW for her continuous service as a maternity representative;

7
SM suggested working with children and young people to develop life skills (link to PHSE) and made a point about working more closely with schools. It was agreed that the team would follow this up.
2. Round table updates (CONT)
AA told members that the Migrant Support Network is going well;
AK said that there is now useful information related to migrant and refugee health included on the CCG’s website for clinicians ACTION: EH to circulate the link
AK emphasised the importance of a correct number being recorded on patient records;
CW updated members and said that City of London have just embarked on a 6 month project to support homeless people with medical health;
CW told that she had taken part in a group meeting about developing the co-production council with JW, RJ, Jonathan McShane and EH. The outcome of the meeting was that it is important to maintain the dual function of the PPI committee/ Co-production Council, keep the feedback function and maintain the authentic voice of community representatives with minimal silos. SM requested being involved in the next meeting.
SM provided members with an update on the Neighbourhoods Resident Involvement Group.
JB said that there is now a voluntary sector representative at the Safeguarding Group. This group covers every death that occurs on the street. With regards to Neighbourhood work the Well St common training has taken place. Work is also taking place with residents for a website for Well St.
MV told people that he had been at a eUCLH workshop in November on virtual reviews and virtual clinics and that there are two types of virtual clinics: one is a skype consultation and the other the other GP speaks to consultant and then to the patients.
IS attended a special allocation service review panel and had first primary care enabler group meeting (engagement re strategy)
SW said she has been busy with her paid role and input into safeguarding work;
RJ told members that her patient group is looking at wider determinants of health with particular focus on the issues that affect African Caribbean community. She has been able to secure some funding from the local authority and will be putting on 6 x conferences and engaging with African Caribbean communities.
MV suggested that the January meeting could start early to allow for sufficient time to discuss NEL 2021 (i.e. the single CCG proposal);
EH outlined the PPI assurance process for 19/20 and said she would contact members for input into it. The assurance template is due to be submitted to Jane Milligan at the end of January 2020 and then to NHSE in early February.
EH also said that the committee had planned to discuss the NEL 2021 at today’s meeting covering the following questions:
o What are things that could work better ‘at scale’ (e.g. when done at a larger scale across NEL) when it comes to a) services, b) data and information and c) engagement and involvement d) anything else?
o How do you feel the single CCG could best support local systems with a) services, b) data and information, c) engagement and involvement and d)anything else?

8
However, due to lack of time it was decided that this item be covered in January in more detail.
SM suggested that the PPI team review the membership list and get in touch with people who are no longer attending.

9

10

11

12

13

14

15

16

17

18
19

20

21

22
23

24
25
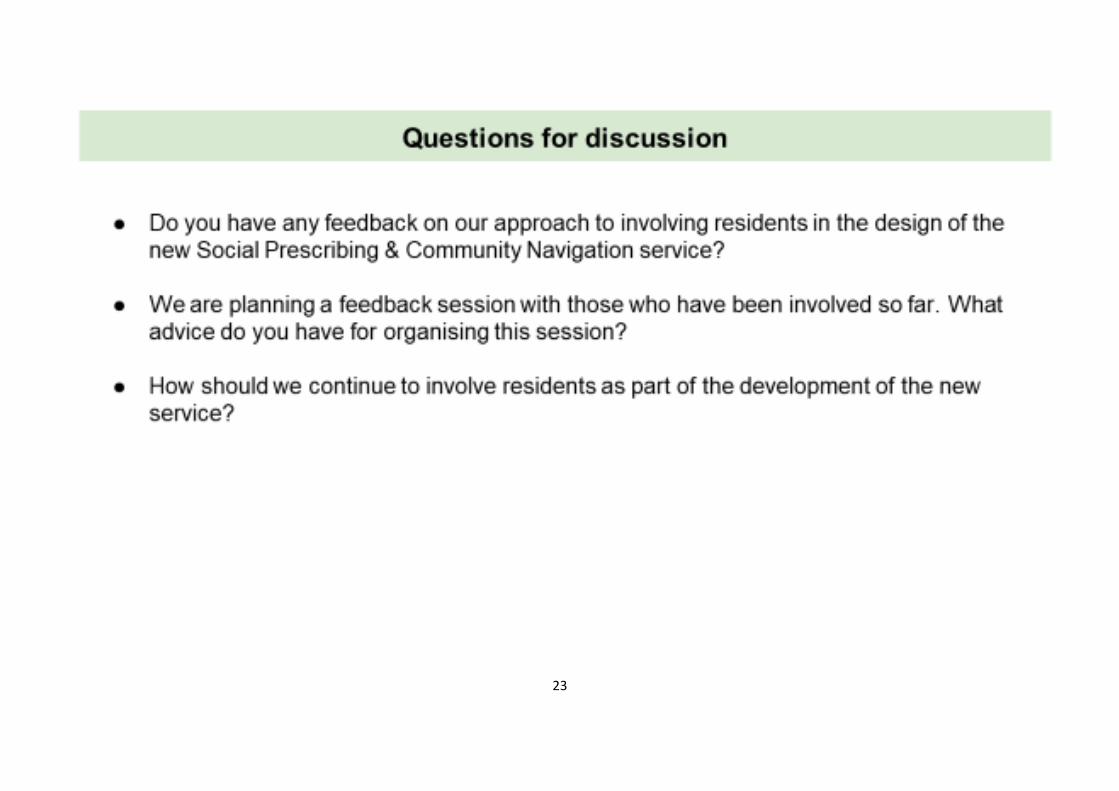
Briefing note for the City & Hackney CCG PPI Committee, meeting on 9 January 2020
A. What is the GP Confederation?
We are a community interest company set up in 2014 to act as an umbrella support organisation for all our
GP member practices. Each practice holds a 1p share in the organisation and our governance is GP led. We
have a Clinical Board, in company terms this is the Board of Directors, and this is composed of:
- A GP Chair (Dr Deborah Colvin of the Lawson practice)
- Four GPs, one from each Quadrant of C&H
- A practice manager
- A practice nurse
- 2 lay members, one who comes from a finance and audit background
- Laura Sharpe, the CEO
- The Director of Finance
The key roles of the GP Confederation are to help the practices to deliver more services by winning service
contracts for them to deliver, to support the practices with workforce recruitment and training, to support
anything else the practices want us to do for them, eg they asked us to help them with the legislation on
data protection requirements.
1. The service contracts that we then sub-contract to the practices
This is the majority of our work and totals about £14m per year. We sub contract with each practice to
deliver the CCG LTC contract, duty doctor, extended access, end of life, mental health, proactive care and
also from LBH sexual health and health checks. We also directly provide a few services ourselves – the stop
smoking service linked to GP practices and the special childhood immunisation clinics in the Stamford Hill
area.
Many of these contracts require practices to identify people and pro-actively call them in. So no longer do
C&H practices just respond to people coming to them when they are ill – they are actually running searches
to find all the people, for example, with diabetes or at risk of getting diabetes, and then asking those people
to come in and see them. This is not the case in many other parts of the country.
2. Top of the QOF!!!!
QOF is the national evidence-based Quality Outcomes Framework which measures all GP practices’
performance against quality standards. The work that practices have done under these contracts over the
last 4 years has led to C&H being TOP IN THE COUNTRY on a significant number of these QOF scores. C&H is
first on four measures of Diabetes management, first on 5 measure of Cardio- Vascular Disease
management, first on two measures of Chronic Obstructive Pulmonary Disease (COPD) management. People
are healthier and living longer in C&H because of this work.
3. Stop Smoking Service
Have you heard of this? Every year our team of smoking cessation advisers (6 staff plus 3 sessional workers)
support 750 to stop smoking. This is one of the best quit rates in the country and we get asked a lot about
how we achieve this – answer – LOTS of referrals from GPs and a really supportive team who help people on
their quit journey. We operate out of a range of practices – please use your PPI connections to tell people
about this – they can just self-refer.
4. Patient Engagement

26
We have a small commission from Richard Bull to do two things: to pilot the use of something called Care
Opinion – an online platform for patients to submit views and to run a pilot on how one of the new Primary
Care Networks might develop a patient participation group at network level.
Care Opinion is really interesting because it shows practices that the vast majority of patients are really
happy with primary care, and this in and of itself is a great driver for breaking down some of the
defensiveness that exists in some practices about hearing what patients have to say. Healthwatch have a
free licence to look at all the Care Opinion data each month from the pilot practices. It would be interesting
to hear their views.
Sam Meikle has been commissioned by the GP Confed to support the Hackney Downs Primary Care Network
in developing patient participation. This is slow, steady work. I will get more info from Sam in time for the
meeting. If this work proceeds well then it is likely that the CCG will ask us to do similar work with a second
network.
5. Access and Duty Doctor
All practices struggle with access. They have to constantly balance those people for whom continuity of care
is vital with those who want speedy access and a one off consultation. In addition, there are three different
access sources of funding: normal GMS expects practices to be open and to treat people who turn up,
extended access appointments (evenings and weekends) commissioned by the CCG via the Confed, and the
PCN extended access scheme. It does not help that these last two operate independently of each other
(there is talk that they might come together in 21/22).
The GP Confed has tried to help relieve access problems by helping practices to look at how they run their
internal systems and through all the workforce initiatives below. But it does remain a constant challenge for
practices.
Duty doctor was brought in 4 years ago by the CCG with the aim of enabling those with an urgent medical
need to be able to get a call back from a doctor within 2 hours and, if needed, a same day appointment. Duty
doctor offers lots of additional access slots and is a very valuable service. It is under review right now by the
CCG, due to report to the Unplanned Care Board in January or February, and we want to then follow that up
with some work on communications with practices. We would very much like your help with this.
6. The CCG Primary Care Strategy refresh
We have a number of key comments about this thinking so far. The first is we think that there should be an
agreed aim for where we want primary care to be by 2014. We suggest something on the lines of:
“Properly staff primary care with strong teams and leaders, GPs being used for their medical skills
with the right staff around them to support, eg an LTC team, a care navigation team, volunteers.
Efficient and effective back office functions in place, and staff enjoying their work. Time for teams to
reflect and review. Strong patient input that is truly representative of the practice population.”
We think the strategy should focus on the evidence around best quality of care and continuity of care –
there is very strong evidence that continuity keeps people out of hospital. Sadly because of the pressures on
staffing, continuity is becoming harder and harder. We wonder if the CCG could do some work to look at
how to maximise continuity of team as the next best thing.

27
Because workforce is such a problem we think also that the strategy should invest in more staff and differing
roles.
We also support the concept in the strategy of practices being given support to think and work differently,
with some time to just reflect on things, and skilled coaches to help them to make changes.
Finally we think that there is a need to get the basics right in general practice – wifi, computers, and printers.
It sounds boring but it is fundamental.
B. What is GMS?
However, this is only one part of primary care – the GP confederation is not responsible for the other part,
which is called GMS (General Medical Services). This is the national contract that GPs work to and which is
commissioned locally by Richard Bull. This is how GPs are contracted to open premises, take people onto
their practice list, treat those who turn up, make referrals on to other services.
So we have to be really careful that we as a Confed don’t overstep the mark with our practices and stray into
this GMS world.
C. What else is the GP Confederation doing?
We currently have two other major obsessions:
1. Workforce
Almost all of our practices are crying out for extra staff. We have the second highest number of GPs in
London (Camden is highest) but we are providing one third again of work over and above a normal GP
practice, so we actually still need more GPs. We are very low on practice nurses, we have quite a lot of really
good Health Care Assistants, we have shortages in reception and admin staff, plus we need to bring in new
roles like pharmacy, physiotherapy in the surgery, community paramedics. Practices ask us to help with this
and with staff training – they cannot do all of this themselves.
2. The wider determinants of health
Deborah can describe to you many patients whose lives and health are so complex that they need far more
time than the 10-minute appointment slot, and indeed for many, their problems around debt, housing,
mental ill health, overshadow everything else. GPs want the system to really invest in supporting such
people so that they can go on a journey towards wellbeing. GPs simply do not have the time to do this, so we
are supporting the recruitment of social prescribers across the system and we are also piloting Wellbeing
Practitioners in 6 practices to work alongside patients to help them get things in their lives back on track. We
call it the “do what needs to be done, do it with unremitting kindness” job. We are very excited about this.
This is just a high level flavour about the world of the GP Confederation and what we are doing to support
our member practices. Deborah and I are looking forward to talking informally with you about all of this and
more!
Laura Sharpe
CEO, GP Confederation
28

29
City and Hackney CCG PPI Committee 9th January 2020 Discussion Paper from the Associate Lay Member for E&D and Sustainable Development
Purpose and summary To seek PPI Committee views on: - the overall focus of the new Associate Lay Member Role - The CCGs Equalities Objectives and Priorities - The approach to developing Sustainable Development Principles for City and Hackney
Discussion Questions 1. The CCG created a new Associate Lay Member role starting in September 2019. • I am keen to hear the committee’s thoughts about how to make sure that this role can
add the most value and help the CCG and the systems we are part of to improve how we respond to the challenges (in the NHS Long Term Plan and more widely) around equalities and sustainability?
• Do you think that combining the focus on Equalities with our work on Quality Improvement (and Performance) would help us to do this better?
Please see: Appendix 1 Associate Lay Member E&D and Sustainable Development - Overview of role and areas of work 2. The CCG’s equalities duties include the requirement to publish equality
information and set out and publish equality objectives. • What are the committee’s thought about the focus for our equalities objectives and
priorities? • Who else do we need to talk to (how/where/when) about this? Please see Appendix 2 City and Hackney CCG Draft Equalities and Diversity priorities 3. The Governing Body agreed a series of recommendations in relation to its
approach to Sustainable Development earlier this year. A working group has started to work on an Action Plan which will be reporting in due course.
• Any thoughts about the overall approach set out here and the scope for this work to produce a “City and Hackney Way" along the lines of the “Wigan Deal”? 1
• Do the ‘pillars’ of sustainable development (and high-level drivers and priorities) make sense
from a health and care perspective and from a City & Hackney perspective? • Any thoughts about what the principles of Sustainable Development might look like for C&H? Please see Appendix 3 Sustainable Development Principles; City & Hackney: ‘This is how we do things around here’
1 https://www.wigan.gov.uk/Council/The-Deal/The-Deal.aspx; https://www.kingsfund.org.uk/projects/lessons-wigan-deal

30
Appendix 1 Associate Lay Member E&D and Sustainable Development
Overview or role and areas of work
Equality & Diversity Sustainable
Development Primary Care contracts
Me
etin
gs a
nd
ag
en
das
CCG’s E&D working group: Quarterly meetings agenda includes CCG’s E&D plan, EDS2 (revised Equality Delivery System for the NHS), Workforce Race Equality Standard (WRES) and Workforce Disability Standard (WDES) and other monitoring and reporting mechanisms; Develop thinking around approach to tackling health inequalities through Prevention Investment Standard Place-base approaches (Neighbourhoods and PCNs)
CCG Sustainable Development working group overseeing the SD Action Plan Co-creating sustainable development ‘Principles’ for local health and care commissioning – building on the co-production charter
PCCC and GP PCC (Part 2) Proposals for commissioned services from GP providers will deliver outcomes and performance, achieve health improvement and represent value for money; Contracts for commissioned services from providers have proper regard for E&D and SD requirements. Primary Care Strategy development
Rep
ortin
g
Report to the GB, the Clinical Executive Committee (CEC) and the Public & Patient Involvement (PPI) Committee on E&D Plan Agree links with reporting on Quality Improvement and performance reporting
Report on progress with the SD Plan for the CCG to GB, CEC and PPI Committee and to the Integrated Care System
Report to GB for approval of decisions/ recommendations
Sy
ste
m le
ve
l Rela
tion
sh
ips
Develop relationships with other E&D leads across the Health and Care system in C&H and in NEL to promote and align the E&D agenda, learn from each other and disseminate good practice NEL WRES workshop and follow-up Co-production Council proposals Mechanisms for discussing E&D at system level
Involvement in Sustainability work for C&H ICS and NEL
Input to the planning and development of primary care and out of hospital provision by C&H ICB and NEL/STP
Co
mm
s a
nd
En
gag
em
en
t
Working with IC Comms and Engagement Enabler Group to ensure that staff, residents and stakeholders are properly informed and updated about E&D and SD work in relation to Integrated Commissioning, and that opportunities to involve staff/patients/service users/public in the work are maximised; Specific engagement around Equalities objectives and priorities Sustainable development principles and Primary Care Strategy

31
Appendix 2 City & Hackney CCG Draft Equalities and Diversity priorities
Strategic Objective
Equalities Strategic Objective
Focus of this work
1. Shift resource and focus onto prevention and address health inequalities
Improve health outcomes for those with protected characteristics under the EA and other vulnerable groups
- Understand key gaps in terms of health outcomes for those with protected characteristics and other vulnerable groups to determine priorities for action in terms of inequalities in health outcomes
- Work with partners to develop Prevention Investment Standard and other initiatives designed to shift resource and focus to prevention targeted at these priorities
- Use place-based and asset-based community development approaches to generate solutions
2. Deliver proactive, community-based care close-to-home, rather than institutional settings, where appropriate
Improve access to and engagement with health and care services for those with protected characteristics under the EA and other vulnerable groups
- Understand key gaps in terms of access to and engagement with health and care services for those with protected characteristics and other vulnerable groups, to determine priorities for action.
- Work with partners to ensure that work e.g. on Neighbourhoods and NHCS is targeted towards addressing these priorities
- Use place-based and asset-based community development approaches to generate solutions
3. Ensure we maintain financial balance as a system and achieve our financial plans
Target resources and processes to ensure that commissioning properly addresses equality priorities
- Understand impact of current financial plans on addressing key equality priorities and consider what changes might be needed to how resources are targeted and any savings that could be generated by addressing gaps in health outcomes, access and engagement and maximising benefits of good use of services
- Consider how CCG’s commissioning, contracting and procurement processes can be targeted at addressing key equalities priorities and making sure that services are delivered equitably
4. Deliver integrated care which meets the physical, mental health and social needs of our diverse communities
Ensure that integrated care system design and delivery and workforce plan is informed by an understanding of and targeted at addressing the needs of all our communities
- Embed co-production approach to service design and delivery and ensure voices of marginalised groups are properly heard to inform decision-making within the ICS
- Address workforce inequality issues across the system that limit our ability to delivery effective, holistic, integrated care (WRES and WDES action plans)
- Organisational development at system level to support cultural competence and prioritise achievement of equalities goals
5. Empower patients and residents
Ensure all residents are empowered to be proactively involved in their own health and care and barriers to self-care in particular groups are addressed
- Identify groups who are least able to play a proactive role in their care and to engage in self-care activities
- Target PPI/engagement activities to address these barriers and investment to support other organisations to work with marginalised communities
- Make sure safeguarding work empowers people in vulnerable groups to take action to stay safe/keep each other safe/engage with services

32
Appendix 3 Sustainable Development Principles
City & Hackney: ‘This is how we do things around here’
Aim:
To co-create a set of principles for ‘sustainable health and care’ in City & Hackney.
To develop tools and guidelines to embed the principles into the partnership culture.
Introduction
Sustainable development is traditionally it is described as three pillars – environmental, social and
economic. In reality, it is complex, multifaceted, has many connecting parts and often confusing
terminologies. For example:
Sustainability is often though to focus solely on ‘environmental sustainability’, but in the
health sector the word has been used to drive ‘financial sustainability’.
‘Social value’ is a vague term, because ‘value’ is subjective. What is beneficial to Hackney
residents will be different to those in Wigan, and what is valuable to residents in the City of
London will differ to those in Kings Park (Hackney).
Many aspects of ‘economic’ value overlap with ‘social’ value – especially around access to
employment and meaningful work.
The word sustainability simply means ‘the ability to sustain’. It is about creating a balance between
many elements that are essential or ‘of value’ to a community/system/society, in a way that ensures
longevity.
But what does this mean for a local health and care system? What elements will underpin the core
services and help to achieve the best possible health and wellbeing outcomes for residents?
This is not a new subject for the system - many principles of sustainable development align to the
marmot principles – but it is rarely understood in the same way by all parties.
Other programmes also align strongly to and overlap with sustainable development, in the way that
they unpin quality improvement in service delivery. Co-production2 is one, Equality and Diversity
a second, and a parallel programme researching Anchor3 Institutions and their ability to build
community wealth, a third.
The immediate challenge, therefore, is to break down these elements and define their value in a
way that makes sense to the partners, patients and residents within City & Hackney, and to bring
these often-dispersed programmes under one banner, with clear tools and guidelines for
implementation.
2 www.healthwatchhackney.co.uk/wp-content/uploads/2018/03/Co-production-Charter_Hackney-City_Final.pdf 3 www.health.org.uk/news-and-comment/charts-and-infographics/the-nhs-as-an-anchor-institution

33
The Approach
An initial review has been undertaken with Catherine Macadam (Lay CCG GB Member for Equality
& Diversity and Sustainability) Jamal Wallace (Engagement & Co-Production Manager, City &
Hackney HCCCP) and Briony Pete (External Sustainable Development Consultant) with input from
the Sustainable Development Working Group.
Under the umbrella term ‘Sustainable Health and Care’ we have begun to redefine the ‘pillars’ of
sustainable development so that they make sense from a health and care perspective and from a
City & Hackney perspective. Underneath these pillars sit several high-level drivers and priorities
that will help to shape the sort of principles that underpin our work to create a sustainable local
system. Diagram 1 sets out a ‘starter for 10’ with further engagement and development planned
over the coming months throughout the C&H CCP.
Patient and Resident Identified Themes
In a separate piece of work, discussions have been held with over 1,200 residents and patients of Hackney and the City of London about what they want integrated care to deliver. This was consolidated into eight Patient and Resident Identified Themes around which we will encourage conversations, about what sustainable principles might look like (Table 2)
Developing Principles & Guidelines
From April 2020 we plan to engage with system partners, patients and residents to co-develop a set of principles for sustainable healthcare that will be used to guide delivery across the system.
Alongside these principles we will create tools and guidelines to help embed them into practical everyday action – for every role. This process will include:
1. Discussions/workshops with stakeholders to find out what they think the principles should be, how they could be implemented and what support they might need.
2. Public comms and engagement to share thinking and seek endorsement from wider range of people/perspectives
3. Alignment to the City and Hackney Integrated Care Outcomes Framework and Governance Structures
4. Agreement by partnership on the Principles and identify support needs to help embed them into the partnership culture and develop tools and guidelines for implementation.
Next Steps
This discussion document has been created to allow partners to help shape the process by which we carry out engagement from April 2020. It will be discussed at many partnership meetings, the first planned being the Comms and Engagement Enabler Group.

34
Diagram 1
Empowerment: Staff, patients, residents

35
Table 2. Patient and Resident Identified Themes with examples of what
sustainable principles might look like in blue
1. Making sure all children and young people have a good start in life
‘Value’ from procurement can support low income families (e.g. Real Living Wage)
2. Reducing the present inequity in health and well-being, while contributing towards reducing
inequity in other areas outside the remit of the Integrated Commissioning Programme. This
includes closing the health and well-being gap for people with long-term conditions and co-
morbidities.
Sustainable health and care will drive quality and efficiency in the local system
3. Increasing the length of a healthy life, so that local people have longer lives and more years
spent free of ill-health and disability
4. Tackling the causes of poor health and well-being at an earlier stage and putting better
prevention measures in place
An active partnership (staff and residents) is healthier and lowers carbon
5. Creating ‘services that work for me’, or services that are more joined-up and person-
centred
We value and utilise patient, resident, staff and partner insight
6. Improving the mental health and well-being of the local population, including ensuring
better access to mental healthcare
Sustainable ‘thinking’ and sustainable ‘doing’ will enhance the wellbeing and life-opportunities for
residents
Nature heals – we support the use of green spaces and encourage biodiversity
7. Helping local people to become resilient and empowered, increasing people’s sense of
control, autonomy and self-efficacy. This includes encouraging people to become involved
in their own care and to understand and manage their own health better
Autonomy for staff to act on change.
Reciprocity: working together between patients and all partners

36
8. Tackling the wiser determinants of health, e.g. Reducing social isolation, increasing
employment, creating a safe environment for everyone to live in
Wealth and opportunity circulate locally (e.g. C&H Pound)
Urgent climate action is necessary to preserve the planets boundaries
Value in measurement, especially around prevention
Additional principles outside of the Patient Identified Themes
Capacity and resource: if we deem something of value it must be resourced sufficiently
Accountability: ownership and responsibility from each organisation
Reciprocity: share resources and insight and encourage innovation