management of hypokalaemia - wasd · management of hypokalaemia 37 z estimating fl uid replacement...
TRANSCRIPT

WASD
ABC of Intravenous Fluids, Electrolyte Disorders and AKI Management in Adults
MANAGEMENT OFHYPOKALAEMIA
5
Hypokalaemia (HoK) is a serum potassium concentration (s[K]) ,3.5mmol/L. This is the commonest electrolyte disorder in hospitalised patients; most cases are mild. It can be life-threatening if severe[1–4].
HoK-related Symptoms and Signs (S/S)[1–7]
Often asymptomatic. S/S are prominent when the reduction in s[K] occurs rapidly or is large.
Muscle weakness – ascending, can involve respiratory muscles, ileus, rhabdomyolysis secondary to decreased muscle blood fl ow.
Cardiac: ECG changes – fl attening T, ST depression, increased amplitude U waves (V4–V6), prolonged QT, arrhythmias – Sinus Bradycardia, A/VEs, AVB, VT, and VF. The progression of ECG changes varies widely between patients; VF can be the fi rst presentation.
Glucose Intolerance; Metabolic Alkalosis; Polyurea
31
S/S develop usually when s[K] is ,3 and resolvewith correction of HoK
C05-Hypokalaemia.indd 31C05-Hypokalaemia.indd 31 26/3/2017 12:07:47 AM26/3/2017 12:07:47 AM

ABC of Intravenous Fluids32
Common Causes
The cause is usually clear from the history[1–6]
a. K depletion (the commonest cause): Renal loss: u[K].20mmol/L – diuretics, mineralocorticoid
excess, glucocorticoid therapy, Mg depletion, Renal Tubular Disease; also occurs secondary to GI fl uid loss and volume depletion
Extra-renal loss: u[K],20mmol/L – gastro-intestinal fl uid loss; skin
b. Intracellular shift (redistributive HoK): insulin or bicarbonate treatment, theophylline, β2 agonists, periodic paralysis, chloroquine intoxication, rapid blood cell proliferation –e.g. GCSF therapy
c. Reduced intake (rare): anorexia nervosa
Investigations[1–6,8]
It is fundamental to understand K distribution for a selective investigation approach
Immediate:
If s[K],3: check ECG, and s[Mg] Repeat urgent K on plasma sample (lithium heparin) as release of
K1 from cells during clotting may give a falsely higher level in serum FBC/glucose
Further, if cause unclear, select as clinically indicated: [Serum HCO3, Cl2, Mg21, PO4, Ca and Urine (paired spot sample with serum) K, Cl, PH (RTA), Ca (BS), P AR (CS, LS]
HCO3, if: 1. Normal: anorexia nervosa, laxatives 2. Metabolic acidosis in absence of diarrhoea: consider RTA,
refer to Renal team 3. Metabolic alkalosis: indicates chronic depletion (see table)
u[K]: if cause not obvious
Abbreviations: A/VEs5Atrial/Ventricular Ectopics; AVB5Atrio-Ventricular Block; VT5Ventricular Tachycardia; VF5Ventricular Fibrillation; u[K]5Urine Potassium concentration; s[Mg]5Serum Magnesium concentration; GCSF5Granulocyte Colony Stimulating Factor; RTA5Renal Tubular Acidosis; BS5Barter’s Syndrome;P AR5Plasma Aldosterone and Renin; CS5Cushing’s Syndrome; LS5Liddle’s Syndrome.
Treatment is shown on the next page.
Beware of blood taken from drip arm!If cause not obvious, refer to Renal or Endocrine Team
for further evaluation
HoK: many patients, up to 40%, are also Mg defi cient. Hypomagnesaemia can induce renal K wasting. Combined defi ciency may potentiate the risk of cardiac arrhythmias – both arepro-arrhythmic. Simultaneous repletion of the Mg stores will facilitate more rapid correction of hypokalaemia and is recommended in severe cases of hypokalaemia[4,8]
C05-Hypokalaemia.indd 32C05-Hypokalaemia.indd 32 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM
Management of Hypokalaemia33
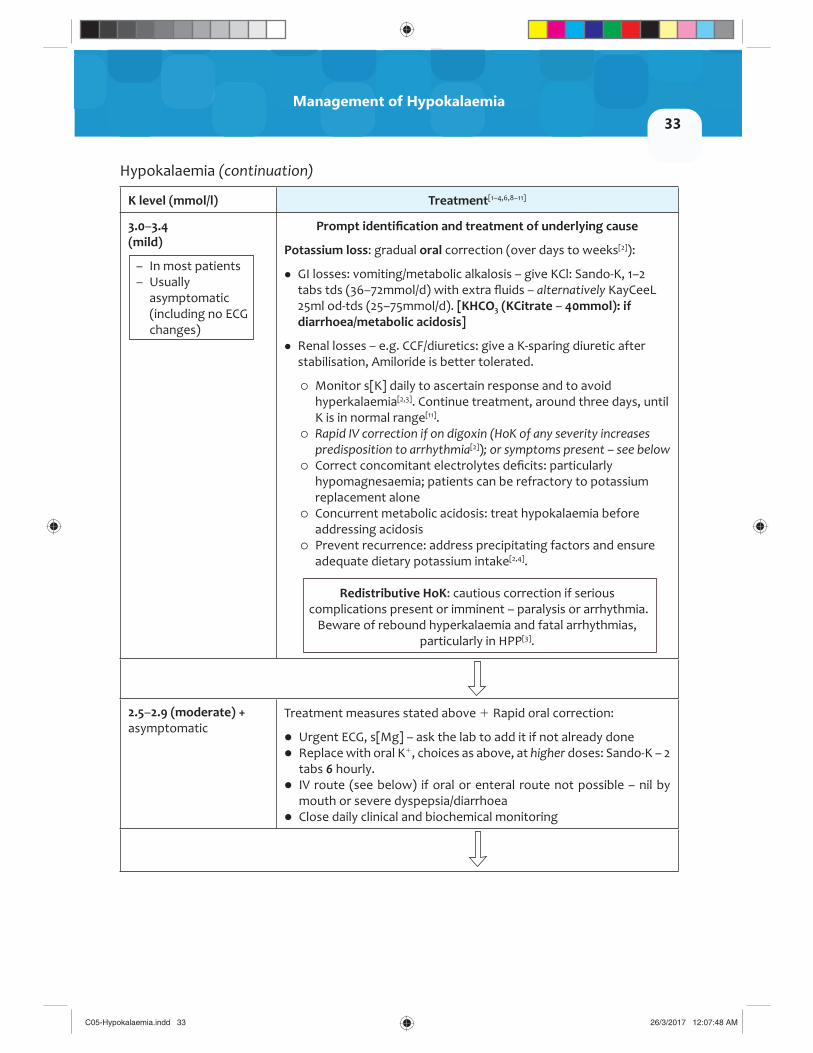
Hypokalaemia (continuation)
K level (mmol/l) Treatment[1–4,6,8–11]
3.0–3.4(mild)
– In most patients– Usually
asymptomatic (including no ECG changes)
Prompt identifi cation and treatment of underlying cause
Potassium loss: gradual oral correction (over days to weeks[2]):
GI losses: vomiting/metabolic alkalosis – give KCl: Sando-K, 1–2 tabs tds (36–72mmol/d) with extra fl uids – alternatively KayCeeL 25ml od-tds (25–75mmol/d). [KHCO3 (KCitrate – 40mmol): if diarrhoea/metabolic acidosis]
Renal losses – e.g. CCF/diuretics: give a K-sparing diuretic after stabilisation, Amiloride is better tolerated.
Monitor s[K] daily to ascertain response and to avoid hyperkalaemia[2,3]. Continue treatment, around three days, until K is in normal range[11].
Rapid IV correction if on digoxin (HoK of any severity increases predisposition to arrhythmia[2]); or symptoms present – see below
Correct concomitant electrolytes defi cits: particularly hypomagnesaemia; patients can be refractory to potassium replacement alone
Concurrent metabolic acidosis: treat hypokalaemia before addressing acidosis
Prevent recurrence: address precipitating factors and ensure adequate dietary potassium intake[2,4].
Redistributive HoK: cautious correction if serious complications present or imminent – paralysis or arrhythmia.
Beware of rebound hyperkalaemia and fatal arrhythmias,particularly in HPP[3].
2.5–2.9 (moderate) + asymptomatic
Treatment measures stated above 1 Rapid oral correction:
Urgent ECG, s[Mg] – ask the lab to add it if not already done Replace with oral K1, choices as above, at higher doses: Sando-K – 2
tabs 6 hourly. IV route (see below) if oral or enteral route not possible – nil by
mouth or severe dyspepsia/diarrhoea Close daily clinical and biochemical monitoring
C05-Hypokalaemia.indd 33C05-Hypokalaemia.indd 33 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM

ABC of Intravenous Fluids34
< 2.5 (severe)
Severe if:,2.5 and/orSymptomatic: Paralysis, arrhythmia -(or pre-existing cardiac disease e.g. ACS, Digoxin toxicity …)
Treatment measures stated above1IV correction:
Continuous ECG monitoring or telemetry Secure proper IV access: large veins, or CV line if access poor. Use
infusion pump to prevent overly rapid potassium administration. Give 1L NS 0.9%/40mmol KCl IV, over 4hrs. Do not use 5% Dextrose.
[Use 1L 0.45% saline/40mmol KCl in DKA/HHS] It is not recommended to exceed 2–3mmol K/kg/BWT/24hrs[11]. Monitor s[K] levels after every 40–80mmol K, and daily to ascertain
the response, as it is diffi cult to predict. Avoid volume overload. Close monitoring until S/S resolved and K level .3; then switch to
oral therapy as per the mild/moderate regime above.
If life threatening/intractable cardiac arrhythmia: double infusion rate, up to 40mmol/hr[3], and contact resuscitation team. If life threatening cardiac arrhythmia: add IV MgSO4, 10mmol over 30 minutes, even before the s[Mg] is known[4].
Renal impairment: cautious K replacement – risk of overcorrection (hyperkalaemia) – contact renal team if severe renal failure or patient on dialysis Use pre-mixed infusion fl uid. NEVER add KCl to infusion bags[9]
Abbreviations: CCF5Congestive Cardiac Failure; HPP5Hypokalaemic Periodic Paralysis; CV5Central Venous; DKA5Diabetic Ketoacidosis; HHS5Hyperosmolar Hyperglycaemic State; BWT5Body Weight; Hr(s)5Hour(s)
Hypokalaemia: further evaluation if the cause is unclear:
Hypokalaemia: further evaluation if the cause is unclear:[1–6]
Extra-renal loss: metabolic (M)acid-base status
Renal loss: metabolicacid-base status
Normal M Acidosis M Alkalosis M Alkalosis M Acidosis Variable
AN Laxative abuse
RTA, DKA MgDepletion
C05-Hypokalaemia.indd 34C05-Hypokalaemia.indd 34 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM

Management of Hypokalaemia35
Metabolic Alkalosis
Low u[Cl]<10mmol/L (low u[K])
High u[Cl] (.10mmol/L) – (high u[K])
Normotensive Normotensive Hypertensive
Volumecontraction: due tosurreptitious vomiting
Diuretics use, BS, GS: (1/2 low Mg)
High (P)Aldosterone (A)
Normal (P)A and R
Low (P)A and R
a. Low R: Conn’s (CS)b. High R: RVD
Cushing’s – U Cortisol, LD-DST: refer to endocrine
AME – (liquorice ingestion),CAH, LS
Abbreviations: AN5anorexia nervosa; u[Cl]5urine chloride concentration; BS5Barter’s syndrome; GS5Gitleman’s syndrome; P5Plasma; R5Renin; LD-DST5low dose dexamethasone Suppression test; RVD5Reno-vascular Disease; AME5apparent mineralocorticoid excess; CAH5congenitaladrenal hyperplasia
CONCLUSION
Due concern and appropriate management should be given to patients’ with hypokalaemia as it can be fatal.
C05-Hypokalaemia.indd 35C05-Hypokalaemia.indd 35 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM

ABC of Intravenous Fluids36
PRACTICAL EXERCISE
All units are in mmol/L unless stated otherwise
A 74-year-old male was admitted with fever, vomiting, diarrhoea and shortness of breath for three days. He was confused, with dry mucus membranes, reduced skin turgor, supine BP 95/55, 75/50mmHg on sitting up, tachycardia, tacchypnoea, fever and body weight 70Kg. s[Na] 158, s[K] 2.8, sCr 119μmol/L, sUrea 12mmol/L, s glucose 9mmol/L, s osmolality 333mOsm/Kg and a spot urine – u[Na] 7, u[K] 26, urine osmolality 846mOsm/Kg. A clinical diagnosis of acute confusion secondary to pneumonia was made.
Q1: What is the cause of hypokalaemia?
A1: Hypokalaemia is due to a combination of:
a. Vomiting: Main factor is the increased Distal Tubular (DT) renal potassium loss
due to increased bicarbonate delivery to DTs, in addition hypovolaemia stimulates aldosterone secretion.
Upper GI K loss/reduced intake b. Diarrhoea: Lower GI loss/reduced intake Increased DT renal K loss due to hypovolaemia-induced RAAS activation
Q 2. What is the cause of hypernatraemia?
A 2. Chronic hypernatraemia is due to:
a. Hypotonic sodium and potassium loss secondary to vomiting and diarrhoea b. Pure water loss secondary to fever and tacchypnoea
Q 3. How would you correct hypokalaemia, hypernatraemia and hypovolaemia?
A 3. Therapeutic approach:
a. The fi rst aim is to correct hypovolaemia. He became haemodynamically stable after receiving 1.5L of NS (120mmol KCl per litre) within three hours, the repeat s[Na] was 158, s[K] was 3.
b. The second aim is to correct hypokalaemia and gradual correction of hypernatraemia over 2–3 days.
C05-Hypokalaemia.indd 36C05-Hypokalaemia.indd 36 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM

Management of Hypokalaemia37
Estimating fl uid replacement using Formula 2, see chapter on hyponatraemia, to correct hypokalaemia and hypernatraemia: the desired water replacement in the fi rst 24 hours to reduce s[Na] by~ 10mmol/L using (5% D10.18% saline110mmol KCl per L) is:
1L of (0.18% saline+10mmol KCl) will reduce s[Na] by 3.3mmol/l, obtained from the equation (formula 2): (402166)/(35 11). Therefore, the volume required to reduce s[Na] by 10mmol/l510/3.353L, Plus 1.5L to compensate for 24 hour obligatory water losses5Total of 4.5L over 24 hours. 3L were given IV at 125ml/hr, he became more lucid during the day and managed to take 1.5L orally.
Close monitoring: UOP; s[Na], s[K], and serum glucose every 2 hours.
REFERENCES
[1] Unwin, R.J., Luft, F.C. and Shirley, D.G. Pathophysiology and management of hypokalemia:a clinical perspective. Nature Reviews Nephrology (2011), Vol. 7, pp.75–84. doi:10.1038/nrneph.2010.175.
[2] Gennari, F.J. Hypokalemia. New England Journal of Medicine (1998), pp.339:451.
[3] Uptodate. Clinical manifestations and treatment of hypokalemia in adults (Accessed 04.2015).
[4] Alfonzo, A., Isles, C., Geddes, C. and Deighan, C.. Potassium disorders – clinical spectrum and emergency treatment. Resuscitation (2006), Vol. 70, pp.10–25.
[5] Rastegar, A. and Soleimani, M. Fluid, Electrolytes and Acid-Base Disturbances. Nephrology Self-Assessment Program, ASN, (2015), Vol. 14, No. 1.
[6] The British Medical Journal Best Practice. Assessment of Hypokalaemia. 08.2014. http://bestpractice.bmj.com/best-practice/monograph/59/diagnosis.html
[7] Moore, R. and Stuart, L.L. Hypokalaemia and Hyperkalaemia. Nephrology Secrets, 3rd Edition, 2012.
[8] Cohn, J.N., Kowey, P.R., Whelton, P.K. and Prisant, L.M. New guidelines for potassium replacement in clinical practice. Archives of Internal Medicine (2000), Vol. 160, pp.2429–36.
[9] NPSA Patient safety alert. Potassium chloride concentrates solution Alert 01. 2002. London: National Patient Safety Agency.
[10] Guideline for the management of hypokalaemia in adults. Produced by Medicines Information, CGH: August 2010 http://www.gloshospitals.nhs.uk/SharePoint110/Antibiotics%20Web%20Documents/ TG/Hypokalaemia%20Guidelines.pdf
[11] Guidelines for potassium replacement in hypokalaemia. Nottingham City Hospital NHS Trust. Update 05.2013b. https://www.nuh.nhs.uk/handlers/downloads.ashx?id=35682
C05-Hypokalaemia.indd 37C05-Hypokalaemia.indd 37 26/3/2017 12:07:48 AM26/3/2017 12:07:48 AM