hyponatraemia more than just a marker of disease severity
DESCRIPTION
HyponetremiaTRANSCRIPT

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 37
University of Colorado School of Medicine, 12700 East 19th Avenue C281, Aurora, CO 80045, USA (R. W. Schrier, S. Sharma, D. Shchekochikhin).
Correspondence to: R. W. Schrier [email protected]
Hyponatraemia: more than just a marker of disease severity?Robert W. Schrier, Shailendra Sharma and Dmitry Shchekochikhin
Abstract | Hyponatraemia—the most common serum electrolyte disorder—has also emerged as an important marker of the severity and prognosis of important diseases such as heart failure and cirrhosis. Acute hyponatraemia can cause severe encephalopathy, but the rapid correction of chronic hyponatraemia can also profoundly impair brain function and even cause death. With the expanding elderly population and the increased prevalence of hyponatraemia in this segment of society, prospective studies are needed to examine whether correcting hyponatraemia in the elderly will diminish cognitive impairment, improve balance and reduce the incidence of falls and fractures. Given that polypharmacy is also common in the elderly population, the various medications that may stimulate arginine vasopressin release and/or enhance the hormone’s action to increase water absorption must also be taken into consideration. Whether hyponatraemia in a patient with cancer is merely a marker of poor prognosis or whether its presence may alter the patient’s quality of life remains to be examined. In any case, hyponatraemia can no longer be considered as just a biochemical bystander in the ill patient. A systematic diagnostic approach is necessary to determine the specific aetiology of a patient’s hyponatraemia. Therapy must then be dictated not only by recognized reversible causes such as advanced hypothyroidism, adrenal insufficiency, diuretics or other medicines, but also by whether the hyponatraemia occurred acutely or chronically. Information is emerging that the vast majority of cases of hyponatraemia are caused by the nonosmotic release of arginine vasopressin. Now that vasopressin V2-receptor blockers are available, a new era of clinical investigation is necessary to examine whether hyponatraemia is just a marker of severe disease or whether correction of hyponatraemia could improve a patient’s quality of life. Such an approach must involve prospective randomized studies in different groups of patients with hyponatraemia, including those with advanced heart failure, those with cirrhosis, patients with cancer, and the elderly.
Schrier, R. W. et al. Nat. Rev. Nephrol. 9, 37–50 (2013); published online 20 November 2012; corrected online 28 January 2013; doi:10.1038/nrneph.2012.246
IntroductionHyponatraemia, the most frequently encountered plasma electrolyte abnormality, is defined as a serum sodium concentration of less than 135 mmol/l, indicates excessive total body water relative to total body sodium,1 and occurs when urine-diluting capacity is exceeded by electrolyte-free water intake. One study found that hyponatraemia occurred in 21% of patients on initial presentation to ambulatory hospital care and in 7.2% of patients on initial presentation to a community care centre.2 Hyponatraemia is also considered a marker of severity of illness such that mean serum sodium concentration is 5–6 mmol/l lower in hospitalized patients than in healthy outpatients.3 In a large database of 300,000 serum samples studied over 2 years, hyponatraemia (serum sodium concentration <136 mmol) was observed in 34% of the hospitalized patients.2 Another prospective cohort study of 2,907 hospitalized patients reported the incidence of hyponatraemia to be 30%.4
Critically ill patients frequently have impaired urinary dilution and are unable to excrete electrolyte-free water. One study found that 30% of patients in intensive care units (ICUs) have a serum sodium concentration of less than 134 mmol/l.5 Increasing age is also associated with impaired capacity to excrete water, which makes the elderly population more vulnerable to developing hyponatraemia, as will be discussed.
Acute hyponatraemia and the resultant extra cellular hypo-osmolality are known to cause brain oedema and raise intracranial pressure.6 Acute hyponatraemic encephalopathy is an established life-threatening medical emergency associated with an overall morbidity and mortality rate of 42%.7 In addition, cardiorespiratory arrest and hypoxia may contribute to brain damage in cases of severe hyponatraemia.6 Chronic asymptomatic hyponatraemia has also been associated with multiple poor outcomes including, but not limited to, increased mortality8 and an increased length of hospital stay.9 Wald et al. showed that patient survival is poor and that length of stay increases if hyponatraemia is present on admis-sion, is exacerbated during hospitalization, is acquired
Competing interestsR. W. Schrier declares associations with the following companies: Janssen Pharmaceuticals, Otsuka Pharmaceuticals. See the article online for full details of the relationships. The
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
38 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
while in hospital or remains uncorrected throughout the hospital stay.10 This group found a linear increase in mortality with decreases in serum sodium concentration below the normal range of 138–142 mmol/l, but other
Key points
■ Hyponatraemia is the most common electrolyte disturbance in clinical practice and its most common mediator is the nonosmotic release of arginine vasopressin
■ In the elderly, hyponatraemia predisposes to falls and fractures and may worsen cognitive impairment; in patients with heart failure, hyponatraemia reflects severe haemodynamic alterations and is associated with worse morbidity and mortality
■ In patients with liver cirrhosis, hyponatraemia is associated with increased mortality, hepatorenal syndrome, hepatic encephalopathy, and reduced quality of life
■ Hyponatraemia carries a worse prognosis in patients with chronic kidney disease, including those with end-stage renal disease
■ Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) is classified as euvolaemic hyponatraemia, and therefore hypovolaemic or hypervolaemic causes of hyponatremia need to be excluded
■ In addition to fluid restriction, vasopressin-receptor antagonists are now available in some countries to treat hyponatremia in heart failure, cirrhosis and SIADH
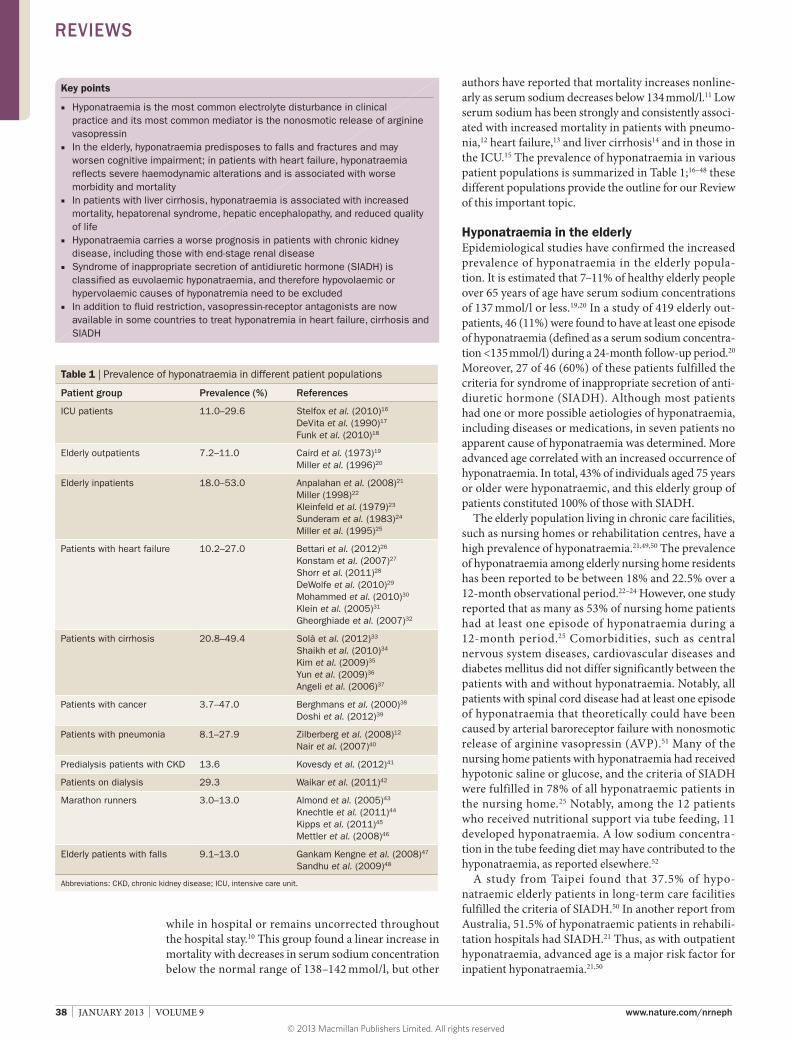
authors have reported that mortality increases nonline-arly as serum sodium decreases below 134 mmol/l.11 Low serum sodium has been strongly and consistently associ-ated with increased mortality in patients with pneumo-nia,12 heart failure,13 and liver cirrhosis14 and in those in the ICU.15 The prevalence of hyponatraemia in various patient populations is summarized in Table 1;16–48 these different populations provide the outline for our Review of this important topic.
Hyponatraemia in the elderly Epidemiological studies have confirmed the increased prevalence of hyponatraemia in the elderly popula-tion. It is estimated that 7–11% of healthy elderly people over 65 years of age have serum sodium concentrations of 137 mmol/l or less.19,20 In a study of 419 elderly out-patients, 46 (11%) were found to have at least one episode of hyponatraemia (defined as a serum sodium concentra-tion <135 mmol/l) during a 24-month follow-up period.20 Moreover, 27 of 46 (60%) of these patients fulfilled the criteria for syndrome of inappropriate secretion of anti-diuretic hormone (SIADH). Although most patients had one or more possible aetiologies of hyponatraemia, including diseases or medications, in seven patients no apparent cause of hyponatraemia was determined. More advanced age correlated with an increased occurrence of hyponatraemia. In total, 43% of individuals aged 75 years or older were hyponatraemic, and this elderly group of patients constituted 100% of those with SIADH.
The elderly population living in chronic care facilities, such as nursing homes or rehabilitation centres, have a high prevalence of hyponatraemia.21,49,50 The prevalence of hyponatraemia among elderly nursing home residents has been reported to be between 18% and 22.5% over a 12-month observational period.22–24 However, one study reported that as many as 53% of nursing home patients had at least one episode of hyponatraemia during a 12-month period.25 Comorbidities, such as central nervous system diseases, cardiovascular diseases and diabetes mellitus did not differ significantly between the patients with and without hyponatraemia. Notably, all patients with spinal cord disease had at least one episode of hyponatraemia that theoretically could have been caused by arterial baroreceptor failure with nonosmotic release of arginine vasopressin (AVP).51 Many of the nursing home patients with hyponatraemia had received hypotonic saline or glucose, and the criteria of SIADH were fulfilled in 78% of all hyponatraemic patients in the nursing home.25 Notably, among the 12 patients who received nutritional support via tube feeding, 11 developed hyponatraemia. A low sodium concentra-tion in the tube feeding diet may have contributed to the hypo natraemia, as reported elsewhere.52
A study from Taipei found that 37.5% of hypo-natraemic elderly patients in long-term care facilities fulfilled the criteria of SIADH.50 In another report from Australia, 51.5% of hyponatraemic patients in rehabili-tation hospitals had SIADH.21 Thus, as with outpatient hypo natraemia, advanced age is a major risk factor for inpatient hyponatraemia.21,50
Table 1 | Prevalence of hyponatraemia in different patient populations
Patient group Prevalence (%) References
ICU patients 11.0–29.6 Stelfox et al. (2010)16
DeVita et al. (1990)17
Funk et al. (2010)18
Elderly outpatients 7.2–11.0 Caird et al. (1973)19
Miller et al. (1996)20
Elderly inpatients 18.0–53.0 Anpalahan et al. (2008)21
Miller (1998)22
Kleinfeld et al. (1979)23
Sunderam et al. (1983)24
Miller et al. (1995)25
Patients with heart failure 10.2–27.0 Bettari et al. (2012)26
Konstam et al. (2007)27
Shorr et al. (2011)28
DeWolfe et al. (2010)29
Mohammed et al. (2010)30
Klein et al. (2005)31
Gheorghiade et al. (2007)32
Patients with cirrhosis 20.8–49.4 Solà et al. (2012)33
Shaikh et al. (2010)34
Kim et al. (2009)35
Yun et al. (2009)36
Angeli et al. (2006)37
Patients with cancer 3.7–47.0 Berghmans et al. (2000)38
Doshi et al. (2012)39
Patients with pneumonia 8.1–27.9 Zilberberg et al. (2008)12
Nair et al. (2007)40
Predialysis patients with CKD 13.6 Kovesdy et al. (2012)41
Patients on dialysis 29.3 Waikar et al. (2011)42
Marathon runners 3.0–13.0 Almond et al. (2005)43
Knechtle et al. (2011)44
Kipps et al. (2011)45
Mettler et al. (2008)46
Elderly patients with falls 9.1–13.0 Gankam Kengne et al. (2008)47
Sandhu et al. (2009)48
Abbreviations: CKD, chronic kidney disease; ICU, intensive care unit.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 39
These observations support the concept of a SIADH-like condition related to ageing.20,50,53 Hyponatraemia is generally modest in elderly patients with SIADH, but this population may be at increased risk of developing symp-tomatic hyponatraemia with intercurrent illnesses and medication use. Moreover, hyponatraemia in the elderly would predispose to falls and fractures and could worsen cognitive impairment.47,54,55 So-called ‘asymptomatic’ hyponatraemia has been shown to be associated with unstable gait and decreased reaction times.54
Another factor in the capacity to excrete solute-free water is the rate of urinary solute excretion. In a healthy individual with AVP suppressed, a minimal urinary osmolality of 50 mOsm/l and daily solute intake of 600 mOsm, 12 l of solute-free water is excreted to main-tain daily solute balance. With this maximal urinary dilu-tion, a patient with primary polydipsia would therefore have to drink more than 12 l per of water day to become hyponatraemic. By contrast, with the same minimal urinary osmolality of 50 mOsm, and a 300 mOsm daily solute intake, 6 l of water is excreted to maintain daily solute balance. Therefore, a patient with primary polydipsia and a decreased solute intake can become hyponatraemic when only drinking in excess of 6 l daily. It is known that beer drinkers, who ingest very little solute, may become hyponatraemic in spite of maximal suppression of AVP and maximal urinary dilution; this phenomenon has been termed potomania.56 Whether very elderly individuals who have lost their appetite can become hyponatraemic secondary to decreased solute intake and excretion remains unproven. More com-monly, a dry mouth secondary to use of medications with anticholinergic activity could induce thirst in the elderly, resulting in increased water intake that could cause hypo natraemia. On the other hand, hypernatraemia can also occur in the elderly secondary to a decreased thirst drive and this perturbation, like hyponatraemia, has also been shown to be associated with increased mortality.57
Thiazide diuretics are one of the most common causes of hyponatraemia in the elderly. Of note, thi-azides can cause both hypovolaemic and euvolaemic types of hyponatraemia. In a large study of hypertensive patients on a relatively low dose of thiazide in a primary care setting, hyponatraemia was present in 18% of those aged greater than 70 years and only 4% of those aged younger than 51 years.58 Moreover, polypharmacy is very common in the elderly population and an increas-ing number of other medications are also recognized to cause hyponatraemia (Box 1).59
Hyponatraemia in heart failureHyponatraemia is common in patients with advanced heart failure. One study reported that 38% of patients admitted for acute decompensated heart failure had hyponatraemia and that a further 28% developed hyponatraemia during the hospital admission.10 Hyponatraemia was associated with increased mortal-ity and hospital readmission. The authors found that the significant relationship between decreased sodium and increased mortality began with a serum sodium
concentration of less than 138 mmol/l and that the more severe the hyponatraemia, the higher the mortality. Hyponatraemia was also associated with an increased length of hospital stay. As 30% of patients with acute decompensated heart failure are readmitted within 60 days,60 hyponatraemia could be a marker indicating that a patient needs a more careful follow-up and perhaps alterations in their therapy (for example, changes in doses of renin–angiotensin–aldosterone system [RAAS] blockers, β-blockers, and/or diuretics).
The long-term effect of hyponatraemia was analysed in a large group of patients undergoing cardiac cathetheri-zation who had a left ventricular ejection fraction of less than 40% and grade II or III heart failure according to the New York Heart Association Classification.26 Patients were followed for an average of 4.5 years. In this long-term study, the presence of hyponatraemia was inde-pendently associated with increased all-cause mortality, cardiovascular mortality and rehospitalization. Another study reported that on multivariate analysis, heart failure patients with hyponatraemia had a poorer quality of life than heart failure patients with a normal plasma sodium concentration.61 Therefore, hyponatraemia is a serious risk factor in chronic, as well as acute, heart failure.
The relationship between hyponatraemia, activation of the neurohumoral axis and survival in patients with advanced heart failure is also affected by decreased renal function. This association of decreased renal function
Box 1 | Drugs associated with hyponatraemia*
Vasopressin analogues ■ Desmopressin ■ Oxytocin
Drugs that potentiate the renal action of vasopressin ■ Chlorpropamide ■ Cyclophosphamide ■ Nonsteroidal anti-inflammatory drugs ■ Acetaminophen
Drugs that enhance vasopressin release ■ Chlorpropamide ■ Clofibrate ■ Carbamazepine/oxcarbazepine ■ Vincristine ■ Nicotine ■ Narcotics ■ Antipsychotics/antidepressants ■ Ifosfamide
Drugs that cause hyponatraemia by unknown mechanisms ■ Haloperidol ■ Fluphenazine ■ Amitriptyline ■ Thioridazine ■ Fluoxetine ■ Methamphetamine ■ MDMA (ecstasy) ■ Sertraline
*Not including diuretics. Abbreviation: MDMA, 3,4-methylenedioxymethamphetamine. Permission obtained from Wolters Kluwer Health © Berl, T. & Schrier, R. Disorders of water metabolism. In Renal and Electrolyte Disorders 6th edn (ed. Schrier, R.) (Philadelphia, Lippincott Williams & Wilkins, 2003).59
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

40 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
with increased mortality in heart failure patients occurs with an increase in serum creatinine as small as 27 μmol/l.62 Of interest, a rise in blood urea nitrogen cor-relates even better with mortality than does increased serum creatinine in patients with hyponatraemia.63 This correlation with blood urea nitrogen may be due to the effect of increased AVP increasing urea reabsorption in the renal collecting duct.63
Although substantial evidence is available to show that hyponatraemia in patients with heart failure is associated with a poor prognosis, less evidence exists to show that correction of the hyponatraemia has beneficial effects. Thus, hyponatraemia may be primarily a marker of more severe disease in patients with heart failure. In this regard, hyponatraemia is known to be associated with an increased plasma concentration of plasma renin and norepinephrine, which are also known risk factors for increased mortality in heart failure.64
In 1981, a sensitive radioimmunoassay was first used to measure levels of the antidiuretic hormone, AVP, in the plasma of hyponatraemic patients with heart failure.65 The results demonstrated that hypo-osmolar plasma levels, which would maximally suppress plasma AVP in healthy individuals, did not suppress plasma AVP concentration in hyponatraemic patients with heart failure. Subsequent studies have reported similar findings of a nonosmotic stimulation of AVP in heart failure.66,67 Experimental studies have demonstrated that
the osmotic regulation of AVP can be overridden by the nonosmotic baroreceptor pathway.68
When cardiac output decreases, the arterial stretch baroreceptors in the carotid sinus and aortic arch become unloaded (Figure 1).69 Thus, the normal tonic inhibitory effect to the central nervous system via the vagus and glossopharyngeal nerves is removed, with a resultant increase in sympathetic efferent activity. This increased sympathetic activity is associated with stimulation of the RAAS and the nonosmotic release of AVP.70 The resultant systemic and renal vasoconstriction, as well as the sodium and water retention, attenuates the arterial underfilling, but ultimately at the expense of the occur-rence of hyponatraemia, pulmonary congestion and diminished kidney function.
The prevalence of hyponatraemia in patients with high-output cardiac failure, as occurs in beriberi and thyrotoxicosis, has not been well studied. The initiating event in this setting, as occurs in patients with a large arterio-venous fistula, is a decrease in systemic vascu-lar resistance.71 As with a decrease in cardiac output, primary arterial vasodilatation leads to unloading of the arterial baroreceptors, with subsequent activation of the neurohumoral axis, including the sympathetic nervous system and RAAS, as well as the nonosmotic release of AVP (Figure 1).70 Thus, hyponatraemia would be expected to be associated with worse survival in both low-output and high-output cardiac failure. Evidence also exists to show that hyponatraemia is associated with increased mortality in patients with primary pulmonary hypertension and pulmonary embolism.72,73 In addition, preoperative hyponatraemia predicts an unfavourable outcome after cardiac surgery.74
The recent availability of vasopressin V2-receptor antagonists has been used to acutely reverse hypo-natraemia in patients with advanced cardiac failure.75 However, prospective studies are needed in patients with heart failure before and after correction of hypo natraemia to assess the effects on cognitive function, which is often impaired in these patients.76 In the EVEREST study, which investigated the safety of the V2-receptor antago-nist tolvaptan in patients with heart failure, only 7.7% of patients had hyponatraemia. This 9.9-month-long randomized study demonstrated the safety of tolvaptan in patients with heart failure, and showed a decrease in body weight and improved dyspnoea in the first week of therapy,77 but no effect on survival.27
Hyponatraemia in cirrhosis The pathophysiology of hyponatraemia in patients with cirrhosis is very similar to that observed in patients with high-output heart failure. The portal hypertension that occurs in patients with cirrhosis leads to primary splanchnic arterial vasodilatation, which is the main cause of the decreased systemic vascular resistance in these patients.78,79 Several vasodilators have been pro-posed as mediators of the splanchnic vasodilatation in cirrhosis, but the most convincing results implicate increased inducible and endothelial nitric oxide synthase leading to nitric-oxide-mediated arterial vasodilatation.80
Cardiac output Primary systemic arterial vasodilation
Heart failure
Cirrhosis
Arterial under�lling
Arterial baroreceptors unloaded
Sympathetic tone Nonosmotic vasopressin stimulation RAAS stimulation
Hyponatraemia
Figure 1 | The pivotal role of vasopressin in the pathophysiology of hyponatraemia. Stimulation of the sympathetic nervous system and the RAAS increases proximal sodium and water reabsorption and thus decreases fluid delivery to the distal diluting segment, but the primary defect in the pathophysiology of hyponatraemia is the inability to dilute the urine. Urine dilution is primarily mediated by suppression of vasopressin. Abbreviation: RAAS, renin–angiotensin–aldosterone system.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 41
As in those with high-output cardiac failure, arterial baroreceptors are unloaded in patients with cirrhosis, which results in compensatory activation of the neuro-humoral axis, including the sympathetic nervous system and the RAAS, as well as nonosmotic AVP stimulation (Figure 1).70 Again, the availability of a sensitive radio-immunoassay implicated the nonosmotic AVP release in patients with hyponatraemia, cirrhosis and impaired water excretion.81 Hyponatraemia, high plasma nor-epinephrine concentration and increased renin activity have been associated with increased mortality in patients with cirrhosis.78 Hyponatraemia rarely occurs in patients with cirrhosis in the absence of ascites. In a 2002 study involving patients with cirrhosis, survival was decreased in patients who had spontaneous hyponatraemia (com-pared with survival in normonatraemic controls with cir-rhosis), but not in those who had hyponatraemia with precipitating factors.82
The presence of hyponatraemia in patients with cir-rhosis has been shown to predict the development of hepatorenal syndrome.83 Hyponatraemia has also been associated with hepatic encephalopathy and neurologi-cal disturbances in patients with cirrhosis.84 A study published in 2012 used the Medical Outcomes Study Short-Form 36 (SF-36) questionnaire to determine factors associated with health-related quality of life in 523 patients with cirrhosis and ascites.33 Multivariate analysis showed hyponatraemia to be a strong predictor of impaired mental and physical component scores on the SF-36 survey.33
These findings indicate that, as in cardiac failure, hyponatraemia is a strong predictor of morbidity and mortality in patients with advanced cirrhosis. Several studies have shown that vasopressin V2-receptor antag-onists increase serum sodium concentration in patients with cirrhosis.85,86 In a subanalysis of the SALT study, the effect of correcting the hyponatraemia in cirrhosis was assessed in the physical and mental component of the SF-12.87 The results demonstrated that correction of the low serum sodium concentration improved the mental component of this quality-of-life survey. However, no data exist on the effect of long-term reversal of hypo-natraemia on morbidity and mortality in patients with cirrhosis. Hyponatraemia has been shown to be associ-ated with worse outcomes following liver transplantation in some,88,89 but not all, studies.90
Hyponatraemia in chronic kidney disease Patients with chronic kidney disease (CKD) are more susceptible to developing hyponatraemia than are healthy individuals by virtue of their diminished ability to maintain water homeostasis in the face of decreas-ing kidney function. A 2012 study that included 655,493 patients with predialysis CKD (mean estimated glomeru-lar filtration rate 50.2 ± 14.1 ml/min/1.73 m2) revealed that 13.6% of patients were hyponatraemic at baseline and 26% had at least one episode of hyponatraemia during a median follow-up of 5.5 years.41 A U-shaped relationship was demonstrated, with both decreased and increased serum sodium concentrations being associated
with increased all-cause mortality. Moreover, these associations were linearly proportional to the severity of the underlying serum sodium abnormality and were independent of comorbid conditions, including heart failure, liver cirrhosis and cancer. Development of hypo-natraemia during follow-up had a stronger association with mortality than having hyponatraemia at baseline, but the stage of CKD did not affect the mortality risk associated with hyponatraemia.
A study in patients with end-stage renal disease (ESRD) showed that predialysis hyponatraemia was present in 29.3% of patients and was associated with increased all-cause mortality.42 Each 4 mmol/l incre-ment in baseline predialysis serum sodium concentra-tion was associated with a decrease in the risk of all-cause mortality (hazard ratio 0.84, 95% CI 0.78–0.90). The association of hyponatraemia with mortality remained after adjusting for mode of haemodialysis, ultrafiltration volume, and presence of severe volume overload and/or heart failure. It remains to be proven whether this close relationship between hyponatraemia and mortality in patients with CKD and ESRD can be reversed by avoiding or correcting hyponatraemia.
Hyponatraemia in patients with SIADH The diagnosis of SIADH is in large part a diagnosis of exclusion. In a patient presenting with hyponatraemia, a diagnosis of hypervolaemic hyponatraemia as occurs with oedematous disorders, such as advanced cardiac failure and cirrhosis, and with acute kidney injury or advanced CKD, must be eliminated. In addition, hypo-volaemic hyponatraemia must be excluded, such as occurs in patients with gastro intestinal losses, diuretics, primary adrenal insufficiency, salt- losing nephro pathy, solute diuresis with diabetes-related glucosuria, or bicarbonaturia with metabolic alkalosis.
After the exclusion of hypervolaemic and hypo-volaemic hyponatraemia, euvolaemic hyponatraemia can be considered; this category is the one in which SIADH resides. However, euvolaemic hyponatraemia can also have other causes; for example, advanced hypo-thyroidism or myxoedema.91 Nonosmotic plasma AVP concentrations are elevated in experimental advanced hypothyroidism, and the hyponatraemia is reversed by thyroid replacement.92 A study in humans, however, indicates that newly diagnosed hypothyroidism is rarely associated with clinically significant hyponatraemia.93 Glucocorticoid deficiency, as occurs in patients with hypopituitarism, may also be associated with hypo-natraemia and elevated plasma concentrations of AVP. Physiological doses of glucocorticoid hormone have been shown to reverse the hyponatraemia occurring in patients with glucocorticoid deficiency.94
SIADH has several major aetiologies including tumours, central nervous system disorders, pulmonary disorders and drugs. After tumours, central nervous system disorders are the second most common cause of SIADH. Any diffuse disorder of the central nervous system and traumatic brain injury can be associated with SIADH.95 Hyponatraemia with brain trauma is often
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

42 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
associated with increased intracranial pressure.96 Acute psychotic exacerbation has also been reported to cause SIADH,97 possibly via the activation of stimulatory path-ways or the removal of inhibitory neural pathways to the magnocellular neurons from osmoreceptors in the ante-rior hypothalamus or from cardiovascular and emetic centres in the brainstem. When the cause of the SIADH is not clear, computer tomography or magnetic resonance imaging of both the lungs and the central nervous system should be performed. As already noted, however, SIADH in the elderly is idiopathic in up to 40% of cases, perhaps secondary to cerebral atherosclerosis and/or impaired autonomic neural function.
Pulmonary disorders are a relatively common cause of SIADH and can be associated with acute pneu-monia, pulmonary or miliary tuberculosis, chronic obstructive lung diseases, cystic fibrosis and any type of respiratory failure, perhaps involving hypoxia and hyper-capnia.40,98–101 Mechanical ventilation may also worsen SIADH in patients with pulmonary diseases.102
Drug-induced hyponatraemia is also a common cause of hyponatraemia, over and above the hypovolaemic hyponatraemia associated with diuretic use. As noted earlier, a list of drugs that can cause SIADH is shown (Box 1).59 Psychopharmacological treatment may be associated with drug-induced hyponatraemia and rates are especially high with carbamazepine, oxcarbazepine and selective serotonin reuptake inhibitors (SSRIs).103 SSRI medications cause SIADH in up to 30% of elderly patients.104 SSRIs have been suggested to have a direct tubular effect that leads to enhanced water reabsorp-tion.105 All SSRIs, serotonin–norepinephrine reuptake inhibitors (for example, venlafaxine) and anti convulsants (for example, levetiracetam) can be associated with hyponatraemia. Severe hyponatraemia can also occur with the recreational drug ecstasy (3,4-methylenedi-oxymethamphetamine), which also has serotoninergic activity.106 Patients with acquired immunodeficiency syndrome (AIDS) may have hyponatraemia that fulfils the criteria of SIADH.107
A subanalysis of the patients with SIADH from the SALT study was undertaken to evaluate the safety and efficacy of the V2-receptor antagonist, tolvaptan, in this subgroup. The results demonstrated that the increased serum sodium concentration with use of tolvaptan was associated with significant improvements in the physical component of the SF-12 Health Survey in patients with SIADH. Improvements seen in the mental component of the SF-12 survey were not statistically significant.108
In patients with SIADH, the hyponatraemia must be associated with hypo-osmolality and a less-than-maximal urinary dilution. A less-than-maximal urinary dilution in general has been determined to be a urinary osmolality greater than 100 mOsm/kg H2O in the presence of hypo-osmolality. Plasma AVP concentration assessed by sensi-tive radioimmunoassay is not suppressed in those with SIADH in spite of the hypo- osmolality that would lead to maximal suppression of AVP in healthy individuals. However, in about 10% of hyponatraemic patients, who otherwise fulfil the diagnostic criteria for SIADH, plasma
AVP concentrations are not detectable. One explanation for this occurrence is that physiological levels of plasma AVP may not be detectable by the current sensitivity of the radioimmunoassay. This lack of sensitivity has been demonstrated in experimental studies in which a small AVP infusion caused an antidiuresis, but plasma concen-trations could not be detected by radio immunoassay.1 Another explanation is that a mutation of the vaso-pressin V2 receptor has activated the receptor in the absence of AVP, the so-called nephrogenic syndrome of inappropriate antidiuresis (NSIAD).109
A diagnostic algorithm for the treatment of patients with hypotonic hyponatraemia is shown (Figure 2). Before using this approach, isotonic hyponatraemia due to hyperparaproteinaemia, γ-globulin administra-tion, use of contrast media and hyperlipidaemia needs to be excluded. In addition, hypertonic hyponatraemia caused by hyperglycaemia, mannitol, sorbitol or a posi-tive anion gap need to be excluded. Thus, the diagnostic workup of a patient with hyponatraemia should include a measurement of plasma osmolality.
The pitfalls of this algorithm should be acknowledged. For example, the urinary sodium concentration is not of value if the patient is receiving diuretics. Secondly, even after a careful history and physical examina-tion is performed, the hypovolaemic and euvolaemic hypo natraemic states may be difficult to distinguish.110 Patients with hypervolaemic causes generally have oedema, severe disease and impaired kidney function.
Patients with hyponatraemia associated with primary polydipsia usually have a urine osmolality that is less that 100 mOsm/kg. However, as discussed, hypo-natraemia can be associated with low solute intake and beer potamania may have a urinary osmolality less than 100 mOsm/kg. With the increase in total body water, serum uric acid, urea and creatinine levels tend to be lower than normal in patients with SIADH.111 Uric acid excretion is increased in most patients with SIADH, and may therefore be of diagnostic value in hyponatraemic patients who are receiving diuretics.112 Serum copeptin, a stable glycopeptide derived from the same precursor peptide as arginine vasopressin in equimolar amounts, has been measured in patients with hyponatraemia and may exclude primary polydipsia.113
Normal saline infusion (0.5–1 l over 12 h) can differen-tiate hypovolaemic from euvolaemic hypo natraemia. In patients with SIADH, the sodium load will be excreted without improvement in the hyponatraemia. However, in patients with hypovolaemic hyponatraemia, volume expansion with saline should increase the serum sodium concentration.114 Among patients with SIADH with a urinary osmolality lower than 500 mOsm/kg, normal saline infusion may cause a water diuresis and an increase in serum sodium concentration.111
A prospective study in 121 consecutive patients with hyponatraemia compared the diagnostic accuracy at 24 h between inexperienced physicians using a diag-nostic algorithm (such as the one presented in Figure 2) and senior intensive care physicians not using the algo-rithm.115 After the availability of a complete work-up,
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 43
the results were compared to a reference standard of an experienced endocrinologist with expertise in hypo-natraemia. The inexperienced physicians using the algorithm had an overall agreement with the reference standard of 86%, whereas the senior intensive care phy-sicians not using the algorithm only had a 48% agree-ment with the reference standard. So, although such algorithms do have limitations in guiding the diagnos-tic approach to hyponatraemia, they do seem to be of considerable assistance to the practicing physician.
Hyponatraemia in strenuous exercise Another cause of acute hyponatraemia is endurance exercise such as marathons, ultra-marathons and tri-athlons.116–118 Among nonelite marathon runners, the reported incidence of hyponatraemia has varied from 3% to 13%.43–46 Hyponatraemia has been shown to cor-relate with increased weight gain during the race.117 Hyponatraemia in this setting can be associated with severe symptoms of cerebral oedema, convulsions, and even death.119 Evidence exists to indicate that the non-osmotic release of AVP occurs during marathons.120 This finding was demonstrated by directly measuring levels of AVP or copeptin120,121 in hyponatraemic marathon runners. Consumption of water in excess of insensible
losses (such as sweating and hyperventilation), in the presence of the nonosmotic stimulation of vaso pressin, explains why weight gain during the marathon runs correlates with hyponatraemia.43 In addition to exces-sive water intake and weight gain during the race, other risk factors for exercise-related hyponatraemia are female gender, a body mass index (BMI) of less than 20 kg/m2, and a slow race time.43
Hyponatraemia-induced encephalopathy due to strenuous exercise has been found to be associated with noncardiogenic pulmonary oedema. The noncardiogenic pulmonary oedema is a result of increased intracranial pressure, and resolution of brain oedema resolves the pulmonary oedema.122 The condition can be successfully treated with hypertonic saline.122
Hyponatraemia in cancer patients Hyponatraemia is one of the most common electro-lyte disorders associated with tumour-related condi-tions.123 Approximately 14% of cases of hyponatraemia in medical inpatients is associated with an underlying tumour-related condition.124 Such hyponatraemia usually accompanies, but can also precede, the diagnosis of the tumour.38 Hyponatraemia in patients with tumours may also be related to medical125 or surgical treatment.126
Hyponatraemia
Sodium and water de�cit Water excess Sodium and water excess
HypovolaemiaTotal body water
Total body sodium
Isotonic saline
Renal lossesDiuretic excess
Mineralocorticoidde�ciency
Salt-losing nephritisBicarbonaturia
Renal tubular acidosisKetonuria
Osmotic diuresis (glucose, urea, mannitol)
Extrarenal lossesVomitingDiarrhoea
“Third-space” burnsPancreatitis
Traumatized muscle
EuvolaemiaTotal body water
Normal total body sodium
HypervolaemiaTotal body water
Total body sodium
Water restriction Sodium and water restriction
Glucocorticoid de�ciencyHypothyroidism
PainPsychiatric disorders
DrugsSIADH
Nephrotic syndromeCardiac failure
Cirrhosis
Acute kidney injuryChronic renal failure
Urinary sodiumconcentration>30 mmol/l
Urinary sodiumconcentration<20 mmol/l
Urinary sodiumconcentration>30 mmol/l
Urinary sodiumconcentration<20 mmol/l
Urinary sodiumconcentration>30 mmol/l
Normonatraemia
Figure 2 | Diagnostic and therapeutic approach to the hypovolaemic, euvolaemic, and hypervolaemic patient with hyponatraemia. Urinary sodium concentrations in between 20 mmol/l and 30 mmol/l represent a ‘grey zone’. Abbreviation: SIADH, syndrome of inappropriate secretion of antidiuretic hormone. Permission obtained from American Society of Nephrology © Schrier, R. W. J. Am. Soc. Nephrol. 17, 1820–1832 (2006).1
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

44 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
The exact frequency of hyponatraemia in patients with cancer is uncertain, primarily because of variations in the populations evaluated and differences in the defi-nitions of hyponatraemia.127 A serum sodium concen-tration of 130 mmol/l or less was used to analyse the frequency of hyponatraemia in a prospective study per-formed at a dedicated cancer hospital in Belgium. During 11 months of observation, 3.7% of the 106 patients with cancer had hyponatraemia, which is within the range reported for general hospitals, intensive care wards, and geriatric centres.38 However, in a large study of 3,357 cancer patients in whom a serum sodium concentra-tion of less than 135 mmol/l was used to define hypo-natraemia, 47% of the patients had hyponatraemia (23% had hypo natraemia on admission and 24% developed hypo natraemia during hospitalization).39 Hyponatraemia in patients with cancer is associated with a poor prog-nosis. After adjusting for several confounding factors, including age, chemotherapy and serum creatinine concentration, the presence of hyponatraemia (versus normo natraemia) was associated with an increased hospital stay and increased 90-day mortality.39
SIADH is the most common cause of hyponatraemia in cancer patients, but anticancer treatment may also be involved. The tumours most commonly associated with SIADH are lung, breast and head and neck tumours.38 A paper published in 1957 reported the presence of hypo natraemia in two patients with lung cancer; the authors postulated that the tumours led to the inap-propriate release of antidiuretic hormone.128 This sug-gestion of SIADH in cancer patients was supported by a paper published in 1978 in which researchers found that plasma AVP was elevated in hyponatraemic patients with broncho genic carcinoma.129 The vast majority of the tumours that have been found to produce AVP are small cell lung cancers and, much less commonly, non-small-cell lung cancer.129 Studies have shown that 10–15% of patients with small cell lung carcinoma have hypo natraemia130,131 and that approximately 70% of these patients have significant elevations of plasma AVP.132 However, in one-third of patients with small cell lung cancer and hyponatraemia, no evidence of ectopic AVP production is found.
SIADH occurs in 3% of patients with head and neck cancer.38,132 Head and neck lesions associated with the development of SIADH are often located in the oral cavity, and less often in the larynx, pharynx, maxillary sinus or salivary glands.133 Other tumours that have been more rarely associated with SIADH include olfactory neuroblastoma, small cell neuroendocrine carcinomas, adenoid cystic carcinoma, undifferentiated carcinoma and sarcoma.134
Antineoplastic agents such as vincristine, vinblastine and cyclophosphamide can induce hypo natraemia,125 possibly via a central mechanism of AVP release caused by cytotoxicity of paraventricular and supra-optic neurons.127 However, direct tubular cisplatin tox-icity causing salt-wasting and volume depletion has been proposed as a cause of hyponatraemia.135 During trans urethral resection of prostate and transcervical
endometrial ablation,136–138 irrigation with large volumes of sorbitol, saline, or hypertonic glucose may contrib-ute to hyponatraemia in the presence of nonosmotic AVP release.
Postoperative hyponatraemia Hyponatraemia is the most frequent electrolyte abnor-mality observed in postoperative patients who are receiving intravenous maintenance fluid therapy. Ayus and colleagues analysed risk factors for postoperative hyponatraemic encephalopathy.139 They found that the prevalence of hyponatraemia and hyponatraemic encephalopathy was equal in male and female patients; however, when hyponatraemic encephalopathy devel-oped, young, menstruant women were about 25 times more likely to die or have permanent brain damage than either men or postmenopausal women. The patho-genesis of postoperative hyponatraemia is believed to be caused by hypotonic infusions in patients with high AVP concentrations related to surgery.
Several studies have addressed associations between type of postsurgery fluid management and the risk of developing hyponatraemia.140–142 The use of isotonic saline has been considered preferable to use of hypotonic fluids, as is the case with irrigation solutions.
Falls, osteoporosis and fractures Hyponatraemia can be associated with impaired cogni-tion, gait disturbances and falls. People over the age of 65 years have at least one fall every year on average.47 The prevalence of falls is much greater in patients with chronic ‘asymptomatic’ hyponatraemia than in normo-natraemic patients, with an adjusted odds ratio as high as 67-fold greater in those with hyponatraemia (Table 2).54
One-third of total-body sodium is stored in bone, of which 40% is exchangeable with serum. In states of chronic sodium depletion, sodium is mobilized from the bone with resultant bone matrix resorption and bone demineralization.143,144 Severe chronic hypo-natraemia has been shown to cause a 30% decrease in bone mineral density in animal models.145 Although sodium- dependent activation of osteoclasts is not clearly understood, low serum sodium concentration is associ-ated with increases in osteoclastic activity and low bone mineral density.145,146
Examination of data from NHANES III showed that mild hyponatraemia (mean serum sodium concentra-tion 133.0 mmol/l) is associated with increased osteo-porosis (T-score ≤–2.5).146 This analysis was adjusted for age, sex, BMI, physical activity, diuretic use and serum level of 25-hydroxyvitamin D. However, several studies found that hyponatraemia was associated with fractures independent of a low bone mineral density.48,147,148
An analysis of medical records of elderly patients who experienced bone fractures following falls has shown the prevalence of hyponatraemia to be between 9.1% and 13.0%,47,48 two to three times higher than in matched controls without a history of bone fracture. The authors suggested that the occurrence of falls and fractures was caused by gait instability and attention
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 45
deficits.47 Underlying causes of hyponatraemia were not studied. However, up to 24.2% of these hyponatraemic patients in one study were taking SSRIs,48 which can induce hyponatraemia and cause impaired sensorium and mobility deficits.149
Moreover, experimental chronic hyponatraemia has been found to be associated with sarcopenia.150 The presence of sarcopenia could predispose to falls by decreasing muscle mass and strength, particularly in elderly individuals.
The prospective Rotterdam study investigated the association of hyponatraemia with the risk of falls in 5,208 patients aged greater than 55 years. In total, 7.7% of individuals included in the study had hypo natraemia. The presence of hyponatraemia was associated with an increased risk of recent falls. Moreover, baseline hyponatraemia was associated with an increased inci-dence of nonvertebral fractures over 6–7 years of follow-up.148,151 No relationship, however, was found between serum sodium concentration and bone mineral density.
Although emerging evidence has revealed a close cor-relation between hyponatraemia and the risk of falls and fractures, no data are available to show whether correction of hyponatraemia decreases this risk.
Available therapies for hyponatraemia The treatment of hyponatraemia is dependent on several factors. These factors include the symptoms present, the duration of hyponatraemia, and the diagnostic category (namely hypovolaemic, hypervolaemic or euvolaemic hyponatraemia).1,152 In hyponatraemic patients with severe symptoms including obtundation, coma, sei-zures, and respiratory arrest, the treatment of choice is 3% hypertonic saline (513 mmol/l) to decrease brain oedema and avoid brainstem herniation and cardio-respiratory arrest. Although not evidence-based, a prac-tical approach is a 100 ml bolus of 3% sodium chloride to be repeated within 30 min if no clinical improvement occurs.153 This approach will increase serum sodium concentration by 2–4 mmol/l and thereby attenuate the brain oedema. In rare cases, however, this amount of hypertonic saline may be insufficient. Concomitant furosemide use could increase serum sodium concen-tration even more. In patients with transtentorial brain herniation secondary to hyponatraemia, researchers have reported the more rapid (>5 mmol/l per hour) correction of serum sodium using 23.4% saline (30–60 ml bolus).154
In most cases, such severe symptomatology occurs when acute hyponatraemia has developed over less than 24–48 h, when brain adaptation has not yet occurred. Patients with moderate neurological symptoms due to
hyponatraemia may present with confusion, disorienta-tion, nausea and alerted mental status. This scenario can occur with either acute or chronic hyponatraemia. Such moderate symptoms may progress to more severe neuro-logical abnormalities and therefore should prob ably also be treated with hypertonic saline. This approach, however, should be used with caution so as to avoid too rapid a correction of hyponatraemia. In patients with either severe or moderate symptoms, fluid restriction should be instituted and the patient followed carefully in hospital.
Minimal symptoms of hyponatraemia include head-ache, inability to concentrate, irritability, altered mood and depression. Patients with these symptoms generally have more chronic hyponatraemia and can be treated with fluid restriction. The degree of fluid restriction depends on the patient’s urine output. For example, if a patient’s daily urine output is 1,200 ml, their daily oral fluid intake should be restricted to 750 ml. The water in food generally equates to the amount of insensible loss. Such fluid restriction will generally increase the patient’s serum sodium concentration by 1–2 mmol per day. The higher the urinary-to-plasma osmolality ratio, the less effective fluid restriction becomes, and long-term compliance, particularly outside the hospital, is poor. Although some patients with mild hyponatraemia can be managed by fluid restriction alone, this strategy is insuf-ficient in some cases. In elderly females with chronic hyponatraemic encephalopathy, normal saline infusion was reported to be associated with much better outcomes than was fluid restriction alone.155
Administration of demeclocycline can result in a vas-opressin-resistant diabetes insipidus and enable more liberal fluid intake. However, owing to drug accumula-tion and toxic effects, demeclocycline is contraindicated in patients with either heart failure or cirrhosis.156 Oral urea (15–30 g per day in divided doses) has been used to treat hyponatraemia; this agent works by causing a solute diuresis (that is, increased solute-free water excretion). The main criticism associated with urea is its bitter taste.157 Because of its poor palatability, oral urea should be given with orange juice. In the inten-sive care unit setting, urea (0.5–1 g/kg per day) can be given via gastric tube.158 Soupart et al. have reported that urea has a similar efficacy and tolerance compared to vasopressin-receptor antagonists in the long-term treat-ment of patients with SIADH.159 A loop diuretic admin-istered together with increased sodium intake can also enhance solute-free water excretion.160 The US FDA has not approved demeclocycline, urea or furosemide and sodium chloride to treat hyponatraemia.
Table 2 | Risk of falls in patients with ‘asymptomatic’ hyponatraemia
Group n Individuals with falls (%)
Odds ratio Adjusted odds ratio*
‘Asymptomatic’ chronic hyponatraemia 122 21.3 9.45 (95% CI 2.64–34.09); P <0.001
67.43 (95% CI 7.48–607.42); P <0.001
Normonatraemic controls 244 5.35 1.00 1.00
*Adjusted for age, sex, and covariates. Permission obtained from Excerpta Medica Inc. © Renneborg, B. et al. Am. J. Med. 119, 71.e1–71.e8 (2006).54
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

46 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
As most hyponatraemia is primarily mediated by the nonosmotic release of AVP,161 the most direct treatment would be the use of a vasopressin- receptor blocker. Conivaptan was the first FDA-approved AVP-receptor blocker.162 Conivaptan is given only by the intra-venous route (20 mg bolus, then continuous infusion 20–40 mg/24 h) over up to 4 days in hospital. Although the drug is both a V1a and a V2 vasopressin- receptor blocker, the mechanism of the solute-free water diu-resis (aquaresis) is via the blockade of V2 receptors in the collecting duct. Tolvaptan is an orally active, selective V2-receptor blocker that must be started in hospital for safety reasons, but has been shown to be effective and safe for as long as 3 years.163 Both conivap-tan and tolvaptan are FDA approved for the treat-ment of hypervolaemic hyponatraemia (for example, in patients with heart failure or cirrhosis) and euvol-aemic hypo natraemia (for example, in patients with SIADH). Tolvaptan has been approved by the European Medicines Agency (EMA) for the treatment of SIADH and by the Japanese Health Ministry for treating diuretic resistance in heart failure. In hyponatraemic patients starting these V2-receptor blockers, fluid should not be restricted and the patient’s serum sodium concen-tration should be monitored every 6–8 h so as to avoid an excessive increase in serum sodium concentration (>12 mmol/24 h or >18 mmol/48 h). More rapid correc-tion of chronic hyponatraemia can lead to the osmotic demyelination syndrome secondary to brain dehydra-tion and blood–brain barrier disruption. The excess correction of hyponatraemia occurring secondary to a rapid water diuresis (for example, vaptan therapy) may indicate the need for interventional treatment, such as an increase in water intake and possibly administration of desmopressin.
Acutely, hyponatraemia causes brain oedema, but after approximately 48–72 h an adaptation occurs to attenu-ate this oedema. This adaptation is associated with the extrusion of cell potassium and organic osmolytes, such as myoinositol, phosphocreatinine and amino acids (for example, glutamine and taurine).164 After this adapta-tion, a rapid correction of hyponatraemia of more than 10–12 mmol/l in 24 h may lead to osmotic demyelina-tion in the brain.165 This entity can be associated with severe brain damage and even death. Osmotic demy-elination has been reported to occur mostly in patients who have an initial serum sodium level lower than 115–120 mmol/l.166 Risk factors for developing demy-elination are concomitant liver diseases, hypoxia, hypo-kalaemia, malnutrition and a change in serum sodium of more than 25 mmol/l in the initial 48 h of treatment.167 In a rat model, urea treatment was shown to protect against the negative consequences of rapid serum sodium cor-rection.168 This effect is not mediated by a urea-induced reverse osmotic shift, as observed in dialysis; it has been observed in rats with renal failure in the absence of renal replacement therapy.169 Moreover, hypoxia is known to alter brain adaptation to a change in serum sodium, and it can produce demyelinization even in the absence of hyponatraemia.170 Much less information exists on
the adaptation and consequences of hyponatraemia in the myocardium. However, experimental taurine defi-ciency has been associated with heart failure.171 This finding may be relevant as, at least in the brain, chronic hyponatraemia leads to the cellular depletion of taurine. Moreover, interstitial oedema can cause myocardial dysfunction.172,173 Experimental evidence also exists to indicate that hypo-osmolality increases the contractile response of vascular smooth muscle.174 This theoretically could increase in vivo cardiac afterload in patients with heart failure and hyponatraemia.
A consensus exists, though remains to be proven, that osmotic demyelination is more likely to occur in patients with a baseline serum sodium concentration of less than 120 mmol/l.165 The use of tolvaptan is FDA approved for patients with serum sodium concentrations of less than 125 mmol/l or patients with clinically related symptoms. Few data exist, however, on the use of tolvaptan to treat patients with serum sodium concentrations of less than 125 mmol/l.85 Large swings in serum sodium concentra-tion can occur in patients on dialysis. However, osmotic demyelination rarely occurs in this setting, probably because the increased intracellular urea may protect against brain dehydration. Patients with a chronic serum sodium concentration of less than 105 mmol/l, liver disease, malnutrition, alcoholism and hypokalaemia are at increased risk of developing osmotic demyelination. In these settings, serum sodium correction should not exceed 8 mmol in 24 h.152
Although osmotic demyelination has not been reported with use of V2-receptor antagonists (conivap-tan and tolvaptan) in all published studies, including use in more than 2,000 heart failure patients, Otsuka recently issued a warning letter concerning the occur-rence of neurological sequelae in some patients treated with tolvaptan in whom the correction of serum sodium exceeded the suggested rate.175
Adverse effects of vasopressin-receptor antagonists include dry mouth, thirst and increased urination in most patients. These agents may not be effective in patients with advanced acute or chronic renal failure such as those with serum creatinine concentrations greater than 221 μmol/l. In addition, vasopressin- receptor antagonists should not be used in patients with hypovolaemic hyponatraemia, who should instead be treated with isotonic saline. As Gross et al. have stated,176 the indications for use of vaptans need to be more firmly established and comparisons are needed with other therapies. Several unanswered questions remain relat-ing to the use of vaptans to treat hyponatraemia. For example, what symptoms of hyponatraemia should be treated? Will there be an effect on quality of life and/or mortality in various patient populations? Will the use of vaptans decrease the length of hospital stays in patients with hyponatraemia? And will these agents be proven to be cost-effective?
Conclusions Although the relationship between hyponatraemia and increased morbidity and mortality is very strong
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 47
in some patient populations, the beneficial effects of treating hyponatraemia are less clear. Evidence on the adverse effects of hyponatraemia on the central nervous function is quite convincing, but it is yet to be proven that correction of hyponatraemia will improve cogni-tion and prevent falls in the elderly, or in patients with advanced cardiac or liver disease. In addition, whether correction of hyponatraemia can improve cardiac func-tion in patients with heart failure is yet to be determined. Prospective, randomized trials are needed to examine whether hyponatraemia is just a marker of severe disease or whether correction of hyponatraemia could improve a patient’s quality of life.
Review criteria
The MEDLINE and PubMed databases were searched for English-language articles published between January 1950 and January 2012, including articles published online ahead of print. We also identified English-language abstracts in cases where the manuscript was not published in English. Search terms included “hyponatraemia”, “serum sodium”, “SIADH”, “sodium handling”, “vasopressin-receptor antagonists” and “vaptans”. In addition, we used a manual search strategy where relevant review articles were searched to identify studies that might have been missed by our database screening. Studies that have not yet been accepted for publication were excluded.
1. Schrier, R. W. Body water homeostasis: clinical disorders of urinary dilution and concentration. J. Am. Soc. Nephrol. 17, 1820–1832 (2006).
2. Hawkins, R. C. Age and gender as risk factors for hyponatremia and hypernatremia. Clin. Chim. Acta 337, 169–172 (2003).
3. Owen, J. A. & Campbell, D. G. A comparison of plasma electrolyte and urea values in healthy persons and in hospital patients. Clin. Chim. Acta 22, 611–618 (1968).
4. Hoorn, E., Lindemans, J. & Zietse, R. Development of severe hyponatraemia in hospitalized patients: treatment-related risk factors and inadequate management. Nephrol. Dial. Transplant. 21, 70–76 (2006).
5. DeVita, M. V., Gardenswartz, M. H., Konecky, A. & Zabetakis, P. Incidence and etiology of hyponatremia in an intensive care unit. Clin. Nephrol. 34, 163–166 (1990).
6. Ayus, J. C., Achinger, S. G. & Arieff, A. Brain cell volume regulation in hyponatremia: role of sex, age, vasopressin, and hypoxia. Am. J. Physiol. Renal Physiol. 295, F619–F624 (2008).
7. Bradley, E. L., Etheridge, M. S. & Arieff, A. I. Causes of brain damage in patients with severe symptomatic hyponatremia: analysis of 344 patients over 30 years [abstract]. J. Am. Soc. Nephrol. 16, 44A (2005).
8. Waikar, S. S., Mount, D. B. & Curhan, G. C. Mortality after hospitalization with mild, moderate, and severe hyponatremia. Am. J. Med. 122, 857–865 (2009).
9. Doshi, S. M., Shah, P., Lei, X., Lahoti, A. & Salahudeen, A. K. Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am. J. Kidney Dis. 59, 222–228 (2012).
10. Wald, R., Jaber, B. L., Price, L. L., Upadhyay, A. & Madias, N. E. Impact of hospital-associated hyponatremia on selected outcomes. Arch. Intern. Med. 170, 294–302 (2010).
11. Chawla, A., Sterns, R. H., Nigwekar, S. U. & Cappuccio, J. D. Mortality and serum sodium: do patients die from or with hyponatremia? Clin. J. Am. Soc. Nephrol. 6, 960–965 (2011).
12. Zilberberg, M. D. et al. Hyponatremia and hospital outcomes among patients with pneumonia: a retrospective cohort study. BMC Pulm. Med. 8, 16 (2008).
13. Klein, L. et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure. Circulation 111, 2454–2460 (2005).
14. Biggins, S. W. et al. Serum sodium predicts mortality in patients listed for liver transplantation. Hepatology 41, 32–29 (2005).
15. Pokaharel, M. & Block, C. A. Dysnatremia in the ICU. Curr. Opin. Crit. Care 17, 581–593 (2011).
16. Stelfox, H. T. et al. The epidemiology of intensive care unit-acquired hyponatraemia and hypernatraemia in medical-surgical intensive care units. Can. J. Anaesth. 57, 650–658 (2010).
17. DeVita, M. V., Gardenswartz, M. H., Konecky, A. & Zabetakis, P. M. Incidence and etiology of hyponatremia in an intensive care unit. Clin. Nephrol. 34, 163–166 (1990).
18. Funk, G. C. et al. Incidence and prognosis of dysnatremias present on ICU admission. Intensive Care Med. 36, 304–311 (2010).
19. Caird, F. I., Andrews, G. R. & Kennedy, R. D. Effect of posture on blood pressure in the elderly. Br. Heart J. 35, 527–530 (1973).
20. Miller, M., Hecker, M. S. & Friedlander, D. A. Apparent idiopathic hyponatremia in an ambulatory geriatric population. J. Am. Geriatr. Soc. 44, 404–408 (1996).
21. Anpalahan, M. Chronic idiopathic hyponatremia in older people due to syndrome of inappropriate antidiuretic hormone secretion (SIADH) possibly related to aging. Q. J. Med. 101, 583–588 (2008).
22. Miller, M. Hyponatremia: age-related risk factors and therapy decisions. Geriatrics 53, 32–48 (1998).
23. Kleinfeld, M., Casimir, M. & Borra, S. Hyponatremia as observed in a chronic disease facility. J. Am. Geriatr. Soc. 27, 156–161 (1979).
24. Sunderam, S. G. & Mankikar, G. D. Hyponatremia in the elderly. Age Ageing 12, 77–80 (1983).
25. Miller, M., Morley, J. F. & Rubinstein, L. Z. Hyponatremia in a nursing home population. J. Am. Geriatr. Soc. 43, 1410–1413 (1995).
26. Bettari, L. et al. Hyponatremia and long-term outcomes in chronic heart failure-an observational study from the Duke Databank for Cardiovascular Diseases. J. Card. Fail. 18, 74–81 (2012).
27. Konstam, M. A. et al. Effects of oral tolvaptan in patients hospitalized for worsening heart failure: the EVEREST Outcome Trial. JAMA 297, 1319–1331 (2007).
28. Shorr, A. F. et al. Burden of sodium abnormalities in patients hospitalized for heart failure. Congest. Heart Fail. 17, 1–7 (2011).
29. DeWolfe, A., Lopez, B., Arcement, L. M. & Hebert, K. Low serum sodium as a poor prognostic indicator for mortality in congestive heart failure patients. Clin. Cardiol. 33, E13–E17 (2010).
30. Mohammed, A. A. et al. Hyponatremia, natriuretic peptides, and outcomes in acutely decompensated heart failure: results from the International Collaborative of NT-proBNP Study. Circ. Heart Fail. 3, 354–361 (2010).
31. Klein, L. et al. Lower serum sodium is associated with increased short-term mortality in hospitalized patients with worsening heart failure: results from the Outcomes of a Prospective Trial of Intravenous Milrinone for Exacerbations of Chronic Heart Failure (OPTIME-CHF) study. Circulation 111, 2454–2460 (2005).
32. Gheorghiade, M. et al. Characterization and prognostic value of persistent hyponatremia in patients with severe heart failure in the ESCAPE Trial. Arch. Intern. Med. 167, 1998–2005 (2007).
33. Solà, E. et al. Factors related to quality of life in patients with cirrhosis and ascites. Relevance of serum sodium concentration and leg edema. J. Hepatol. http://dx.doi.org/10.1016/ j.jhep.2012.07.020.
34. Shaikh, S., Mal, G., Khalid, S., Baloch, G. H. & Akbar, Y. Frequency of hyponatraemia and its influence on liver cirrhosis-related complications. J. Pak. Med. Assoc. 60, 116–120 (2010).
35. Kim, J. H. et al. The association between the serum sodium level and the severity of complications in liver cirrhosis. Korean J. Intern. Med. 24, 106–112 (2009).
36. Yun, B. C. et al. Impact of pretransplant hyponatremia on outcome following liver transplantation. Hepatology 49, 1610–1615 (2009).
37. Angeli, P., Wong, F., Watson, H. & Ginès, P. Hyponatremia in cirrhosis: results of a patient population survey. Hepatology 44, 1535–1542 (2006).
38. Berghmans, T., Paesmans, M. & Body, J. J. A prospective study on hyponatraemia in medical cancer patients: epidemiology, aetiology and differential diagnosis. Support Care Cancer 8, 192–197 (2000).
39. Doshi, S. M., Shah, P., Lei, X., Lahoti, A. & Salahudeen, A. Hyponatremia in hospitalized cancer patients and its impact on clinical outcomes. Am. J. Kidney Dis. 59, 222–228 (2012).
40. Nair, V., Niederman, M. S., Masani, N. & Fishbane, S. Hyponatremia in community-acquired pneumonia. Am. J. Nephrol. 27, 184–190 (2007).
41. Kovesdy, C. P. et al. Hyponatremia, hypernatremia, and mortality in patients with chronic kidney disease with and without congestive heart failure. Circulation 125, 677–684 (2012).
42. Waikar, S. S., Curhan, G. C. & Brunelli, S. M. Mortality associated with low serum sodium concentration in maintenance hemodialysis. Am. J. Med. 124, 77–84 (2011).
43. Almond, C. S. et al. Hyponatremia among runners in the Boston Marathon. N. Engl. J. Med. 352, 1550–1556 (2005).
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved
48 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
44. Knechtle, B., Knechtle, P. & Rosemann, T. Low prevalence of exercise-associated hyponatremia in male 100 km ultra-marathon runners in Switzerland. Eur. J. Appl. Physiol. 111, 1007–1016 (2011).
45. Kipps, C., Sharma, S. & Pedoe, D. T. The incidence of exercise-associated hyponatraemia in the London marathon. Br. J. Sports Med. 45, 14–19 (2011).
46. Mettler, S. et al. Hyponatremia among runners in the Zurich Marathon. Clin. J. Sport Med. 18, 344–349 (2008).
47. Gankam Kengne, F., Andres, C., Sattar, L., Melot, C. & Decaux G. Mild hyponatremia and risk of fracture in the ambulatory elderly. QJM 101, 583–588 (2008).
48. Sandhu, H. S., Gilles, E., DeVita, M. V., Panagopoulos, G. & Michelis, M. F. Hyponatremia associated with large-bone fracture in elderly patients. Int. Urol. Nephrol. 41, 733–737 (2009).
49. Beck, L. H. Changes in renal function with aging. Clin. Geriatr. Med. 14, 199–209 (1998).
50. Chen, L. K., Lin, M. H., Hwang, A. J. & Chen, T. W. Hyponatremia among the institutionalized elderly in 2 long-term care facilities in Taipei. J. Chin. Med. Assoc. 69, 115–119 (2006).
51. Schrier, R. W., Berl, T. & Anderson, R. J. Osmotic and non-osmotic control of vasopressin release. Am. J. Physiol. 236, F321–F322 (1979).
52. Rudman, D. et al. Hyponatremia in tube-fed elderly men. J. Chronic Dis. 39, 73–80 (1986).
53. Goldstein, C. S., Braunstein, S. & Goldfarb, S. Idiopathic syndrome of inappropriate antidiuretic hormone secretion possibly related to advanced age. Ann. Intern. Med. 99, 185–188 (1983).
54. Renneborg, B., Musch, W., Vandemergel, X., Manto, M. & Decaux, G. Mild chronic hyponatremia is associated with falls, unsteadiness, and attention deficits. Am. J. Med. 119, 71.e1–71.e8 (2006).
55. Gosch, M., Joosten-Gstrein, B., Heppner, H. J. & Lechleitner, M. Hyponatremia in geriatric inhospital patients: effects on results of a comprehensive geriatric assessment. Gerontology 58, 430–440 (2012).
56. Thaler, S. M., Teitelbaum, I. & Berl, T. “Beer potomania” in non-beer drinkers: effect of low dietary solute intake. Am. J. Kidney Dis. 31, 1028–1031 (1998).
57. Kugler, J. P. & Hustead, T. Hyponatremia and hypernatremia in the elderly. Am. Fam. Physician 61, 3623–3630 (2000).
58. Clayton, J. A., Rodgers, S., Blakey, J., Avery, A. & Hall, I. P. Thiazide diuretic prescription and electrolyte abnormalities in primary care. Br. J. Clin. Pharmacol. 61, 87–95 (2006).
59. Berl, T. & Schrier, R. Disorders of water metabolism. In Renal and Electrolyte Disorders 6th edn (ed. Schrier, R.) (Philadelphia, Lippincott Williams & Wilkins, 2003).
60. Jencks, S. F., Williams, M. V. & Coleman, E. A. Rehospitalizations among patients in the Medicare fee-for-service program. N. Engl. J. Med. 360, 1418–1429 (2009).
61. Allen, L. A. et al. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ. Cardiovasc. Qual. Outcomes 4, 389–398 (2011).
62. Gottlieb, S. S. et al. The prognostic importance of different definitions of worsening renal function in congestive heart failure. J. Card. Fail. 8, 136–141 (2002).
63. Schrier, R. W. Blood urea nitrogen (BUN) and serum creatinine: not married in heart failure. Circ. Heart Fail. 1, 2–5 (2008).
64. Lilly, L., Dzau, V., Williams, G., Rydstedt, L. & Hollenberg, N. Hyponatremia in congestive heart
failure: implications for neurohumoral activation and responses to orthostasis. J. Clin. Endocrinol. Metab. 52, 924 (1984).
65. Szatalowicz, V. L. et al. Radioimmunoassay of plasma arginine vasopressin in hyponatremic patients with congestive heart failure. N. Engl. J. Med. 305, 263–266 (1981).
66. Riegger, G. A., Leibau, G. & Kochsiek, K. Antidiuretic hormone in congestive heart failure. Am. J. Med. 72, 49 (1982).
67. Goldsmith, S. R., Francis, G. S., Cowley, A. W., Levine, T. B. & Cohn, J. N. Increased plasma arginine vasopressin levels in patients with congestive heart failure. J. Am. Coll. Cardiol. 1, 1385 (1983).
68. Kim, J. K. et al. Arginine vasopressin gene expression in chronic cardiac failure in rats. Kidney Int. 38, 818–822 (1990).
69. Abraham, W. T. Hormones and hemodynamics in heart failure. N. Engl. J. Med. 341, 577–585 (1999).
70. Schrier, R. W. Body fluid regulation in health and disease: a unifying hypothesis. Ann. Intern. Med. 113, 155–159 (1990).
71. Riegger, G. A., Liebau, G., Bauer, E. & Kochsiek, K. Vasopressin and renin in high output heart failure of rats: hemodynamic effects of elevated plasma hormone levels. J. Cardiovasc. Pharmacol. 7, 1–5 (1985).
72. Forfia, P. R. et al. Hyponatremia predicts right heart failure and poor survival in pulmonary arterial hypertension. Am. J. Respir. Crit. Care Med. 177, 1364–1369 (2008).
73. Scherz, N. et al. Prognostic importance of hyponatremia in patients with acute pulmonary embolism. Am. J. Respir. Crit. Care Med. 182, 1178–1183 (2010).
74. Crestanello, J. A. et al. Preoperative hyponatremia predicts outcomes after cardiac surgery. J. Surg. Res. http://dx.doi.org/ 10.1016/j.jss.2012.06.004.
75. Abraham, W., Shamshirsaz, A., McFann, K., Oren, R. & Schrier, R. W. Aquaretic effect of lixivaptan, an oral non-peptide selective V2 receptor vasopressin antagonist, in the New York Heart Association Functional class II and III chronic failure patients. J. Am. Coll. Cardiol. 47, 1615–1621 (2006).
76. Kindermann, I. et al. Cognitive function in patients with decompensated heart failure: the Cognitive Impairment in Heart Failure (CogImpair-HF) study. Eur. J. Heart Fail. 14, 404–413 (2012).
77. Gheorghiade, M. et al. Short-term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA 297, 1332–1343 (2007).
78. Ginés, P. & Schrier, R. W. Renal failure in cirrhosis. N. Engl. J. Med. 361, 1279–1290 (2009).
79. Ginés, P. et al. Hyponatremia in cirrhosis: from pathogenesis to treatment. Hepatology 28, 851–864 (1998).
80. Martin, P. Y., Gines, P. & Schrier, R. W. Nitric oxide as a mediator of hemodynamic abnormalities and sodium and water retention in cirrhosis. N. Engl. J. Med. 339, 533–541 (1998).
81. Bichet, D., Szatalowicz, V., Chaimovitz, C. & Schrier, R. W. Role of vasopressin in abnormal water excretion in cirrhotic patients. Ann. Intern. Med. 96, 413–417 (1982).
82. Porcel, A. et al. Dilutional hyponatremia in patients with cirrhosis and ascites. Arch. Intern. Med. 162, 323–328 (2002).
83. Gines, A. et al. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in
cirrhosis with ascites. Gastroenterology 105, 229–236 (1993).
84. Guevara, M. et al. Risk factors for hepatic encephalopathy in patients with cirrhosis and refractory ascites: relevance of serum sodium concentration. Liver Int. 30, 1137–1142 (2010).
85. Schrier, R. W. et al. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N. Engl. J. Med. 355, 2099–2112 (2006).
86. Gines, P. et al. Effects of satavaptan, a selective vasopressin V(2) receptor antagonist, on ascites and serum sodium in cirrhosis with hyponatremia: a randomized trial. Hepatology 48, 204–213 (2008).
87. Cárdenas, A. et al. Tolvaptan, an oral vasopressin antagonist, in the treatment of hyponatremia in cirrhosis. J. Hepatol. 56, 571–578 (2011).
88. Hackworth, W. A. et al. Effect of hyponatraemia on outcomes following orthotopic liver transplantation. Liver Int. 29, 1071–1077 (2009).
89. Dawwas, M. F. et al. The impact of serum sodium concentration on mortality after liver transplantation: a cohort multicenter study. Liver Transpl. 13, 1115–1124 (2007).
90. Yun, B. C. et al. Impact of pretransplant hyponatremia on outcome following liver transplantation. Hepatology 49, 1610–1615 (2009).
91. DiScala, V. A. & Kinney, M. J. Effects of myxedema on the renal diluting and concentrating mechanism. Am. J. Med. 50, 325–335 (1971).
92. Chen, Y. C. et al. Nonosmotic release of vasopressin and renal aquaporins in impaired urinary dilution in hypothyroidism. Am. J. Physiol. Renal Physiol. 289, F672–F678 (2005).
93. Warner, M. H., Holding, S. & Kilpatrick, E. S. The effect of newly diagnosed hypothyroidism on serum sodium concentrations: a retrospective study. Clin. Endocrinol. (Oxf.) 64, 598–599 (2006).
94. Oelkers, W. Hyponatremia and inappropriate secretion of vasopressin (antidiuretic hormone) in patients with hypopituitarism. N. Engl. J. Med. 321, 492–496 (1989).
95. Diringer, M. N. & Zazulia, A. R. Hyponatremia in neurologic patients: consequences and approaches to treatment. Neurologist 12, 117–126 (2006).
96. Dhar, R. & Murphy-Human, T. A bolus of conivaptan lowers intracranial pressure in a patient with hyponatremia after traumatic brain injury. Neurocrit. Care 14, 97–102 (2011).
97. Dubovsky, S. L., Grabon, S., Berl, T. & Schrier, R. W. Syndrome of inappropriate secretion of antidiuretic hormone with exacerbated psychosis. Ann. Intern. Med. 79, 551–554 (1973).
98. Hill, A. R., Uribarri, J., Mann, J. & Berl, T. Altered water metabolism in tuberculosis: role of vasopressin. Am. J. Med. 88, 357–364 (1990).
99. Breuer, R. & Rubinow, A. Inappropriate secretion of antidiuretic hormone and mycoplasma pneumonia infection. Respiration 42, 217–219 (1981).
100. Farber, M. O. et al. Abnormalities of sodium and H2O handling in chronic obstructive lung disease. Arch. Intern. Med. 142, 1326–1330 (1982).
101. Kaskavage, J. & Sklansky, D. Hyponatremia-associated rhabdomyolysis following exercise in an adolescent with cystic fibrosis. Pediatrics 130, e220–e223 (2012).
102. Baratz, R. A. & Ingraham, R. C. Renal hemodynamics and antidiuretic hormone
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY VOLUME 9 | JANUARY 2013 | 49
release associated with volume regulation. Am. J. Physiol. 198, 565–570 (1960).
103. Letmaier, M. et al. Hyponatraemia during psychopharmacological treatment: results of a drug surveillance programme. Int. J. Neuropsychopharmacol. 15, 739–748 (2012).
104. Wilkinson, T. J., Begg, E. J., Winter, A. C. & Sainsbury, R. Incidence and risk factors for hyponatraemia following treatment with fluoxetine or paroxetine in elderly people. Br. J. Clin. Pharmacol. 47, 211–217 (1999).
105. Moyses, Z. P., Nakandakari, F. K. & Magaldi, A. J. Fluoxetine effect on kidney water reabsorption. Nephrol. Dial. Transplant. 23, 1173–1178 (2008).
106. Burgess, C., O’Donohoe, A. & Gill, M. Agony and ecstasy: a review of MDMA effects and toxicity. Eur. Psychiatry 15, 287–294 (2000).
107. Tang, W. W., Kaptein, E. M., Feinstein, E. I. & Massry, S. G. Hyponatremia in hospitalized patients with the acquired immunodeficiency syndrome (AIDS) and the AIDS-related complex. Am. J. Med. 94, 169–174 (1993).
108. Verbalis, J. G. et al. Efficacy and safety of oral tolvaptan therapy in patients with the syndrome of inappropriate antidiuretic hormone secretion. Eur. J. Endocrinol. 164, 725–732 (2011).
109. Rosenthal, S. M. et al. Nephrogenic syndrome of inappropriate antidiuresis. N. Engl. J. Med. 352, 1884–1890 (2005).
110. Chung, H. M., Kluge, R., Schrier, R. W. & Anderson, R. J. Clinical assessment of extracellular fluid volume in hyponatremia. Am. J. Med. 83, 905–908 (1987).
111. Decaux, G. & Musch, W. Clinical laboratory evaluation of the syndrome of inappropriate secretion of antidiuretic hormone. Clin. J. Am. Soc. Nephrol. 3, 1175–1184 (2008).
112. Fenske, W. et al. Value of fractional uric acid excretion in differential diagnosis of hyponatremic patients on diuretics. J. Clin. Endocrinol. Metab. 93, 2991–2997 (2008).
113. Fenske, W. et al. Copeptin in the differential diagnosis of hyponatremia. J. Clin. Endocrinol. Metab. 94, 123–129 (2009).
114. Ellison, D. H. & Berl, T. Clinical practice. The syndrome of inappropriate antidiuresis. N. Engl. J. Med. 356, 2064–2072 (2007).
115. Fenske, W., Maier, S. K., Blechschmidt, A., Allolio, B. & Störk, S. Utility and limitations of the traditional diagnostic approach to hyponatremia: a diagnostic study. Am. J. Med. 123, 652–657 (2010).
116. Young, M., Sciurba, F. & Rinaldo, J. Delirium and pulmonary edema after completing a marathon. Am. Rev. Respir. Dis. 136, 737–739 (1987).
117. Noakes, T. D., Goodwin, N., Rayner, B. L., Branken, T. & Taylor, R. K. Water intoxication: a possible complication during endurance exercise. Med. Sci. Sports Exerc. 17, 370–375 (1985).
118. Speedy, D. B. et al. Hyponatremia in ultradistance triathletes. Med. Sci. Sports Exerc. 31, 809–815 (1999).
119. Petzold, A., Keir, G. & Appleby, I. Marathon related death due to brainstem herniation in rehydration-related hyponatraemia: a case report. J. Med. Case Rep. 1, 186 (2007).
120. Siegel, A. J. et al. Hyponatremia in marathon runners due to inappropriate arginine vasopressin secretion. Am. J. Med. 120, 461.e11–461.e17 (2007).
121. Hew-Butler, T. et al. Changes in copeptin and bioactive vasopressin in runners with and without hyponatremia. Clin. J. Sport Med. 21, 211–217 (2011).
122. Ayus, J. C., Varon, J. & Arieff, A. I. Hyponatremia, cerebral edema, and noncardiogenic pulmonary
edema in marathon runners. Ann. Intern. Med. 132, 711–714 (2000).
123. Wakui, A. Electrolyte abnormalities associated with cancer: a review [Japanese]. Gan. To. Kagaku Ryoho 13, 2031–2038 (1986).
124. Gill, G. et al. Characteristics and mortality of severe hyponatraemia—a hospital-based study. Clin. Endocrinol. (Oxf.) 65, 246–249 (2006).
125. Berghmans, T. Hyponatremia related to medical anticancer treatment. Support Care Cancer 4, 341–350 (1996).
126. Bennett, H. E., Bishop, M., Zadik, T. D. & Lincoln, N. B. Cognitive impairment after transurethral resection of the prostate (TURP). Disabil. Rehabil. 26, 1381–1387 (2004).
127. Sorensen, J. B., Andersen, M. K. & Hansen, H. H. Syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in malignant disease. J. Intern. Med. 238, 97–110 (1995).
128. Schwartz, W. B., Bennett, W., Curelop, S. & Bartter, F. C. A syndrome of renal sodium loss and hyponatremia probably resulting from inappropriate secretion of antidiuretic hormone. Am. J. Med. 23, 529–542 (1957).
129. Morton, J. J., Kelly, P. & Padfield, P. L. Antidiuretic hormone in bronchogenic carcinoma. Clin. Endocrinol. (Oxf.) 9, 357–370 (1978).
130. Shapiro, J. & Richardson, G. E. Hyponatremia of malignancy. Crit. Rev. Oncol. Hematol. 18, 129–135 (1995).
131. List, A. F. et al. The syndrome of inappropriate secretion of antidiuretic hormone (SIADH) in small-cell lung cancer. J. Clin. Oncol. 4, 1191–1198 (1986).
132. Odell, W. D. & Wolfsen, A. R. Humoral syndromes associated with cancer. Annu. Rev. Med. 29, 379–406 (1978).
133. Ferlito, A., Rinaldo, A. & Devaney, K. O. Syndrome of inappropriate antidiuretic hormone secretion associated with head neck cancers: review of the literature. Ann. Otol. Rhinol. Laryngol. 106, 878–883 (1997).
134. Onitilo, A. A., Kio, E. & Doi, S. A. R. Tumor-Related Hyponatremia. Clin. Med. Res. 5, 228–237 (2007).
135. Hamdi, T. et al. Cisplatin-induced renal salt wasting syndrome. South Med. J. 103, 793–799 (2010).
136. Iihoshi, M., Sakuragi, T., Higa, K. & Hamada, T. Severe hyponatremia during transurethral resection of prostate [Japanese]. Masui 54, 414–417 (2005).
137. Issa, M. M., Young, M. R., Bullock, A. R., Bouet, R. & Petros, J. A. Dilutional hyponatremia of TURP syndrome: a historical event in the 21st century. Urology 64, 298–301 (2004).
138. Hwang, C. B. et al. Absorption of irrigating fluid during transcervical resection of endometrium—a report of two cases. Acta Anaesthesiol. Sin. 35, 45–50 (1997).
139. Ayus, J. C., Wheeler, J. M. & Arieff, A. I. Postoperative Hyponatremic Encephalopathy in Menstruant Women. Ann. Intern. Med. 117, 891–897 (1992).
140. Choong, K. et al. Hypotonic versus isotonic maintenance fluids after surgery for children: a randomized controlled trial. Pediatrics 128, 857–866 (2011).
141. Yung, M. & Keeley, S. Randomised controlled trial of intravenous maintenance fluids. J. Paediatr. Child. Health. 45, 9–14 (2009).
142. Moritz, M. L. & Ayus, J. C. Prevention of hospital-acquired hyponatremia: a case for using isotonic saline. Pediatrics 111, 227–230 (2003).
143. Bergstrom, W. H. The participation of bone in total body sodium metabolism in the rat. J. Clin. Invest. 34, 997–1004 (1955).
144. Bergstrom, W. H. & Wallace, W. M. Bone as a sodium and potassium reservoir. J. Clin. Invest. 33, 867–873 (1954).
145. Verbalis, J. G. et al. Hyponatremia-induced osteoporosis. J. Bone Miner. Res. 25, 554–563 (2010).
146. Barsony, J., Sugimura, Y. & Verbalis, J. F. Osteoclast response to low extracellular sodium and the mechanism of hyponatremia-induced bone loss. J. Biol. Chem. 286, 10864–10875 (2011).
147. Kinsella, S., Moran, S., Sullivan, M. O., Molloy, M. G. M. & Eustace, J. A. Hyponatremia independent of osteoporosis is associated with fracture occurrence. Clin. J. Am. Soc. Nephrol. 5, 275–280 (2010).
148. Hoorn, E. J. et al. Mild hyponatremia as a risk factor for fractures: the Rotterdam Study. J. Bone Miner. Res. 26, 1822–1828 (2011).
149. Ziere, G. et al. Selective serotonin reuptake inhibiting antidepressants are associated with an increased risk of nonvertebral fractures. J. Clin. Psychopharmacol. 28, 411–417 (2008).
150. Barsony, J., Manigrasso, M. B., Xu, Q., Tam, H. & Verbalis, J. G. Chronic hyponatremia exacerbates multiple manifestations of senescence in male rats. Age (Dordr). http://dx.doi.org/10.1007/s11357-011-9347-9.
151. Hoorn, E. J., Liamis, G., Zietse, R. & Zillikens, M. C. Hyponatremia and bone: an emerging relationship. Nat. Rev. Endocrinol. 8, 33–39 (2011).
152. Verbalis, J. G., Goldsmith, S. R., Greenberg, A., Schrier, R. W. & Sterns, R. H. Hyponatremia treatment guidelines 2007: expert panel recommendations. Am. J. Med. 120 (11 Suppl. 1), S1–S21 (2007).
153. Moritz, M. L. & Ayus, J. C. 100 cc 3% sodium chloride bolus: a novel treatment for hyponatremic encephalopathy. Metab. Brain Dis. 25, 91–96 (2010).
154. Koenig, M. A. et al. Reversal of transtentorial herniation with hypertonic saline. Neurology 70, 1023–1029 (2008).
155. Ayus, J. C. & Arieff, A. I. Chronic hyponatremic encephalopathy in postmenopausal women: association of therapies with morbidity and mortality. JAMA 281, 2299–2304 (1999).
156. Miller, P. D., Linas, S. L. & Schrier, R. W. Plasma demeclocycline levels and nephrotoxicity. Correlation in hyponatremic cirrhotic patients. JAMA 243, 2513–2515 (1980).
157. Bichet, D. G. What is the role of vaptans in routine clinical nephrology? Clin. J. Am. Soc. Nephrol. 7, 700–703 (2012).
158. Decaux, G., Andres, C., Gankam Kengne, F. & Soupart, A. Treatment of euvolemic hyponatremia in the intensive care unit by urea. Crit. Care 14, R184 (2010).
159. Soupart, A., Coffernils, M., Couturier, B., Gankam-Kengne, F. & Decaux, G. Efficacy and tolerance of urea compared with vaptans for long-term treatment of patients with SIADH. Clin. J. Am. Soc. Nephrol. 7, 742–747 (2012).
160. Hantman, D., Rossier, B., Kohlman, R. & Schrier, R. W. Rapid correction of hyponatremia in the syndrome of inappropriate secretion of antidiuretic hormone. Ann. Intern. Med. 78, 870–875 (1973).
161. Anderson, R. J., Chung, H. M., Kluge, R. & Schrier, R. W. Hyponatremia: a prospective analysis of its epidemiology and the pathogenetic role of vasopressin. Ann. Intern. Med. 102, 164–168 (1985).
162. Verbalis, J. G., Zeltser, D., Smith, N., Barve, A. & Andoh, M. Assessment of the efficacy and safety of intravenous conivaptan in patients with euvolaemic hyponatraemia: subgroup analysis
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

50 | JANUARY 2013 | VOLUME 9 www.nature.com/nrneph
of a randomized, controlled study. Clin. Endocrinol. (Oxf.) 69, 159–168 (2008).
163. Berl, T. et al. Oral tolvaptan is safe and effective in chronic hyponatremia. J. Am. Soc. Nephrol. 21, 705–712 (2010).
164. Gullans, S. R. & Verbalis, J. G. Control of brain volume during hyperosmolar and hypoosmolar conditions. Annu. Rev. Med. 44, 289–301 (1993).
165. Sterns, R. H., Cappuccio, J. D., Silver, S. M. & Cohen, E. P. Neurologic sequelae after treatment of severe hyponatremia: a multicenter perspective. J. Am. Soc. Nephrol. 4, 1522–1530 (1994).
166. Cluitmans, F. H. & Meinders, A. E. Management of severe hyponatremia: rapid or slow correction? Am. J. Med. 88, 161–166 (1990).
167. Ayus, J. C., Krothapalli, R. K. & Arieff, A. I. Treatment of symptomatic hyponatremia and its relation to brain damage. A prospective study. N. Engl. J. Med. 317, 1190–1195 (1987).
168. Soupart, A., Schroëder, B. & Decaux, G. Treatment of hyponatraemia by urea decreases
risks of brain complications in rats. Brain osmolyte contents analysis. Nephrol. Dial. Transplant. 22, 1856–1863 (2007).
169. Soupart, A., Silver, S., Schroöeder, B., Sterns, R. & Decaux, G. Rapid (24-hour) reaccumulation of brain organic osmolytes (particularly myo-inositol) in azotemic rats after correction of chronic hyponatremia. J. Am. Soc. Nephrol. 13, 1433–1441 (2002).
170. Ayus, J. C., Armstrong, D. & Arieff, A. I. Hyponatremia with hypoxia: effects on brain adaptation, perfusion, and histology in rodents. Kidney Int. 69, 1319–1325 (2006).
171. Schaffer, S., Solodushko, V., Pastukh, V., Ricci, C. & Azuma, J. Possible cause of taurine-deficient cardiomyopathy: potentiation of angiotensin II action. J. Cardiovasc. Pharmacol. 41, 751–759 (2003).
172. Desai, K. V. et al. Mechanics of the left ventricular myocardial interstitium: effects of acute and chronic myocardial edema. Am. J. Physiol. Heart Circ. Physiol. 294, H2428–H2434 (2008).
173. Dongaonkar, R. M., Stewart, R. H., Geissler, H. J. & Laine, G. A. Myocardial microvascular permeability, interstitial oedema, and compromised cardiac function. Cardiovasc. Res. 87, 331–339 (2010).
174. Okada, K., Ishikawa, S., Caramelo, C., Tsai, P. & Schrier, R. W. Enhancement of vascular action of arginine vasopressin by diminished extracellular sodium concentration. Kidney Int. 44, 755–763 (1993).
175. Otsuka Pharmaceutical Ltd. Direct Healthcare Professional Communication on the risk of increases in serum sodium with tolvaptan which are too rapid [online], http://www.mhra.gov.uk/home/groups/comms-ic/documents/websiteresources/con146921.pdf (2012).
176. Gross, P. A., Wagner, A. & Decaux, G. Vaptans are not the mainstay of treatment in hyponatremia: perhaps not yet. Kidney Int. 80, 594–600 (2011).
Author contributionsThe authors contributed equally to all aspects of this manuscript.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | NEPHROLOGY
CORRECTION
Hyponatraemia: more than just a marker of disease severity?Robert W. Schrier, Shailendra Sharma and Dmitry Shchekochikhin
Schrier, R. W. et al. Hyponatraemia: more than just a marker of disease severity? Nat. Rev. Nephrol. 9, 37–50 (2013); doi:10.1038/nrneph.2012.246
In Figure 1 of the version of this article initially published online, “Baroreceptors” was incorrectly written as “Basoreceptors”. The error has been corrected for the HTML and PDF versions of the article.
REVIEWS
© 2013 Macmillan Publishers Limited. All rights reserved