learning and teaching about risk communication
TRANSCRIPT

Learning and teachingabout riskcommunicationJill Thistlethwaite,1 Rodney Nan Tie,2 1University of Sydney, Sydney, Australia;2James Cook University, Townsville, Australia
Risk communication is afundamental skill in theconsultation between health
professionals and patients. Suchcommunication is part of theprocess leading to shareddecision-making and involves theclinician discussing advantagesand disadvantages of treatment,while specific numerical dataabout potential outcomes may begiven.1 Risk communication is theopen two-way exchange ofinformation and opinion aboutrisk, which should lead to betterunderstanding and betterdecisions about clinicalmanagement.2 This exchange ofinformation and opinion isimportant if treatment decisionsare to reflect the attitudes torisk of the patients who will livewith the outcomes.3 Informedconsent to investigations or
treatment is impossible withoutan understanding of risk. Goodrisk communication reduces thepossibility of litigation.
Helping patients understandrisk in the context ofdecision-making about lifestyleand management is of paramountimportance to ensure thatpatients make the correctdecision in relation to theirongoing treatment in partnershipwith their doctors. During theircommunication skillsdevelopment, medical studentsneed to learn to conveysometimes quite technicalinformation and to decide on thequantity and quality of thatinformation, including concreteevidence, but probably alsoincluding conjecture. Theevidence-based practice approach
is also fundamental to theprocess. However, studentsshould have some understandingof why patients make certainchoices that may be more risky orthat the clinician does notconsider the optimum choice.Suggested learning outcomes forrisk communication are in Box 1.
THE DEFINITION OF RISK
A good start to a session on riskcommunication is to ask studentswhat they understand by risk.What risks have they taken in lifeand why?
Risk is the possibility ofsuffering harm or loss;danger; the chances thata hazard will give rise toharm.
Good riskcommunicationreduces thepossibility oflitigation
Practicalteaching
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140 135

People take risks all the timeand for various reasons: forpleasure (including sexualgratification), for endorphinrelease, to save time, to lookgood, because of addiction, etc.They balance the risk of pleasure/gain against the risk of pain/loss,and where this balance lies differsbetween people and in individualsover time. Previous experience ofthe outcomes of risk behaviourcolours people’s subsequentbehaviour – if they are told thattheir behaviour is dangerous butindulge several times withoutadverse effect, they are likely toindulge again. An understandingof risk behaviour is important.Without some insight into howpatients make decisions aboutrisk, counselling and shareddecision-making are difficult.
Ask the students what theythink influences patients abouttaking risks with regard totreatment and lifestyle decisions.Risk evidence rarely includespsychosocial outcomes, althoughthese are important to individualpatients.4 For some, short-termgain is often a more powerfulmotivator than long-termbenefits.5 This type of balancingof risks is a fundamental processin human behaviour. There are anumber of other influencingfactors, as shown in Box 2.6 Thetrust that patients have for theirdoctors is thus of paramountimportance in the process of riskcommunication. Such trust
develops over time and in relationto the skill and professionalismof the doctor. Students areunlikely to have built up such arelationship based on trust withpatients. They should be asked todiscuss how trust is developedand maintained in theircommunication skills sessions.
How much of the conceptualbasis of risk behaviour and deci-sion-making is required by stu-dents is open to debate. Studentsshould certainly be aware of thehealth belief model7 frombehavioural sciences courses andmay have covered the five stagesof change model8 when learningabout motivational interviewing.
THE LANGUAGE OF RISK
As patients understand differentmethods of presenting risk tovarying extents,9 students shoulddiscuss the language that theywould use with patients. As withall information that is impartedby a doctor, the language may bemisunderstood or misinterpreted.
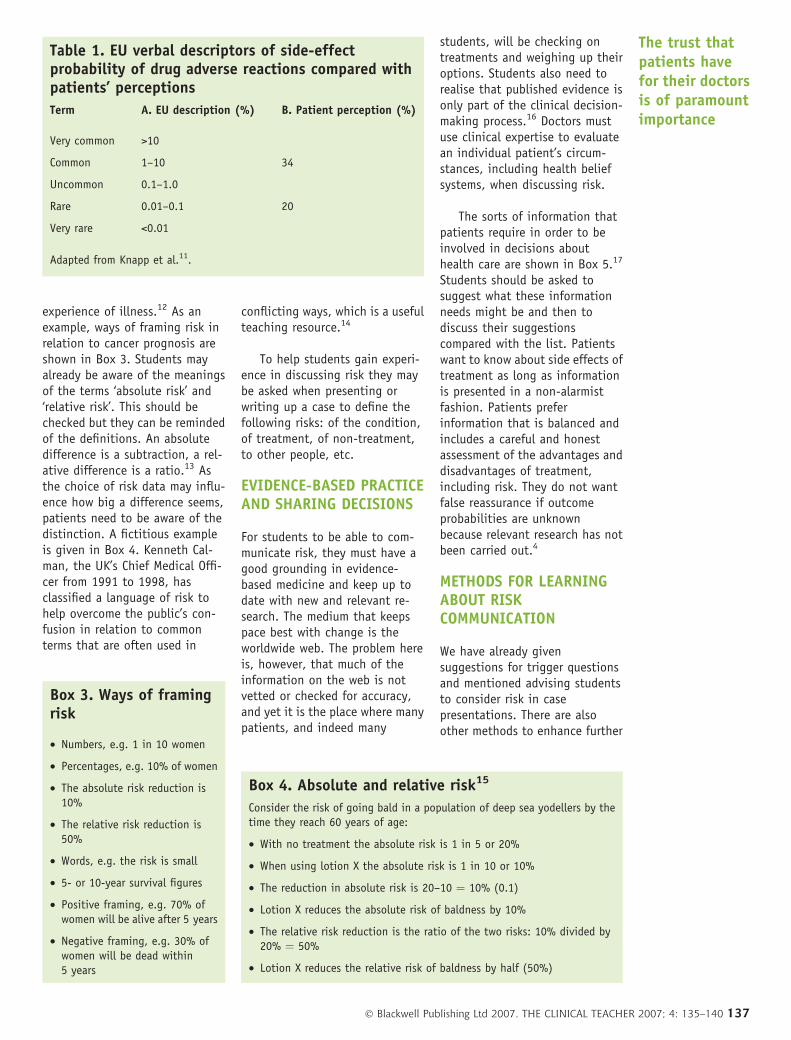
In particular risk language isoften ambiguous. Students can begiven the list of descriptors inTable 3 and asked to say what thewords mean and what patientsthink they might mean in relationto potential side effects of med-icines. The European Union de-fined these words in 1999(column A in Table 1) advisingthat they be used on patientinformation leaflets inserted intodrug packaging.10 However,patients’ interpretations of thewords are very different (column Bin Table 1).11 Patients interpretthe words in a way that results inthem considering side effects asmuch more frequent than theyactually are, affecting the waythat they may adhere to drugregimens.
Risk is generally defined interms of numerical odds orprobabilities, yet research hasshown that patients find suchterms difficult to understand, andthat their understanding isaffected by their age, educationallevel, health status and recent
Box 2. Influences on response to information aboutrisk6
• The extent to which the source of information is trusted
• The relevance of the information for everyday life and decision-making
• The relation to other perceived risks
• The fit with previous knowledge and experience
• The difficulty and importance of the choices and decisions
People takerisks all thetime and for
variousreasons
Box 1. Learning outcomes for risk communication
• The definition of risk
• An understanding of the language of risk
• Evidence-based practice and sharing decisions with patients
• ‘Differentiation of absolute risk, relative risk and number needed to treat’
• Knowledge of what patients want to know about treatment options and what influences their choices
• Placing risk into context for the patient
• Ability to transfer technical information to patients relating to risk of management options
• Ability to help patients weigh up risks versus benefits, ensuring their preferences are based on fact and notmisconception
• Familiarity with the use of decision aids for facilitating choice
136 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140
experience of illness.12 As anexample, ways of framing risk inrelation to cancer prognosis areshown in Box 3. Students mayalready be aware of the meaningsof the terms ‘absolute risk’ and‘relative risk’. This should bechecked but they can be remindedof the definitions. An absolutedifference is a subtraction, a rel-ative difference is a ratio.13 Asthe choice of risk data may influ-ence how big a difference seems,patients need to be aware of thedistinction. A fictitious exampleis given in Box 4. Kenneth Cal-man, the UK’s Chief Medical Offi-cer from 1991 to 1998, hasclassified a language of risk tohelp overcome the public’s con-fusion in relation to commonterms that are often used in
conflicting ways, which is a usefulteaching resource.14
To help students gain experi-ence in discussing risk they maybe asked when presenting orwriting up a case to define thefollowing risks: of the condition,of treatment, of non-treatment,to other people, etc.
EVIDENCE-BASED PRACTICEAND SHARING DECISIONS
For students to be able to com-municate risk, they must have agood grounding in evidence-based medicine and keep up todate with new and relevant re-search. The medium that keepspace best with change is theworldwide web. The problem hereis, however, that much of theinformation on the web is notvetted or checked for accuracy,and yet it is the place where manypatients, and indeed many
students, will be checking ontreatments and weighing up theiroptions. Students also need torealise that published evidence isonly part of the clinical decision-making process.16 Doctors mustuse clinical expertise to evaluatean individual patient’s circum-stances, including health beliefsystems, when discussing risk.
The sorts of information thatpatients require in order to beinvolved in decisions abouthealth care are shown in Box 5.17
Students should be asked tosuggest what these informationneeds might be and then todiscuss their suggestionscompared with the list. Patientswant to know about side effects oftreatment as long as informationis presented in a non-alarmistfashion. Patients preferinformation that is balanced andincludes a careful and honestassessment of the advantages anddisadvantages of treatment,including risk. They do not wantfalse reassurance if outcomeprobabilities are unknownbecause relevant research has notbeen carried out.4
METHODS FOR LEARNINGABOUT RISKCOMMUNICATION
We have already givensuggestions for trigger questionsand mentioned advising studentsto consider risk in casepresentations. There are alsoother methods to enhance further
Table 1. EU verbal descriptors of side-effectprobability of drug adverse reactions compared withpatients’ perceptions
Term A. EU description (%) B. Patient perception (%)
Very common >10
Common 1–10 34
Uncommon 0.1–1.0
Rare 0.01–0.1 20
Very rare <0.01
Adapted from Knapp et al.11.
Box 3. Ways of framingrisk
• Numbers, e.g. 1 in 10 women
• Percentages, e.g. 10% of women
• The absolute risk reduction is10%
• The relative risk reduction is50%
• Words, e.g. the risk is small
• 5- or 10-year survival figures
• Positive framing, e.g. 70% ofwomen will be alive after 5 years
• Negative framing, e.g. 30% ofwomen will be dead within5 years
Box 4. Absolute and relative risk15
Consider the risk of going bald in a population of deep sea yodellers by thetime they reach 60 years of age:
• With no treatment the absolute risk is 1 in 5 or 20%
• When using lotion X the absolute risk is 1 in 10 or 10%
• The reduction in absolute risk is 20–10 ¼ 10% (0.1)
• Lotion X reduces the absolute risk of baldness by 10%
• The relative risk reduction is the ratio of the two risks: 10% divided by20% ¼ 50%
• Lotion X reduces the relative risk of baldness by half (50%)
The trust thatpatients havefor their doctorsis of paramountimportance
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140 137
learning. As adult learners,students learn best through use ofreal case materials andexperience. In small groups theycan be given information aboutthe absolute and relative risks ofvarious treatments (e.g. hormonereplacement therapy/HRT), testresults that use probabilities(e.g. Down syndrome prenatalscreening) and test results thatdo not have clear-cut diagnosticreadings (e.g. the prostate-specific antigen/PSA test). Theydiscuss the meanings of theinformation and how they wouldcommunicate these to patients.This combination of learningusing their medical statisticsknowledge (often taught in thefirst 2 years of medical school),clinical material and communica-tion skills is an example oflearning in context and istherefore likely to appear more
relevant to students thanstatistical data alone.18
If video-tapes of suitableconsultations with real patientsare available, these may be usedas other triggers for discussion, inline with best practice for thelearning and teaching ofcommunication skills.19 The maindrawback with videos, however, isthat the patient perspective islost. Therefore the next stage inthe learning process is workingwith simulated patients.
WORKING WITHSIMULATED PATIENTS
Students may work through one ormore scenarios with simulatedpatients. The efficacy of experi-ential learning with simulatedpatients has a rich evidence baseand we have worked extensively
with simulated patients over theyears. The simulated patient rolesmay be adapted to the clinicalexperience of the students. Theexamples above can be adaptedfor use: e.g. woman aged 52 yearsrequesting information about thebenefits and risk of HRT, man age55 requesting PSA screening, wo-man aged 35 wishing to discussantenatal screening for Downsyndrome. In the last two cases,the students could follow up thepatients with their test results.
Experienced simulatedpatients are able to givefeedback, in role, on how wellthey understand the risk beingconveyed and ways in which thestudents could improve theircommunication. The facilitatorchecks that the patients haveunderstood the implications ofthe risk and are actually making adecision based on a correctinterpretation of the discussion.In the scenarios the patients maydecide not to follow the advice ofthe student, if offered. They mayrun the roles in various ways –choosing the lower risk or thehigher risk option and givingreasons for their choice.
LEARNING ABOUT RISKTABLES
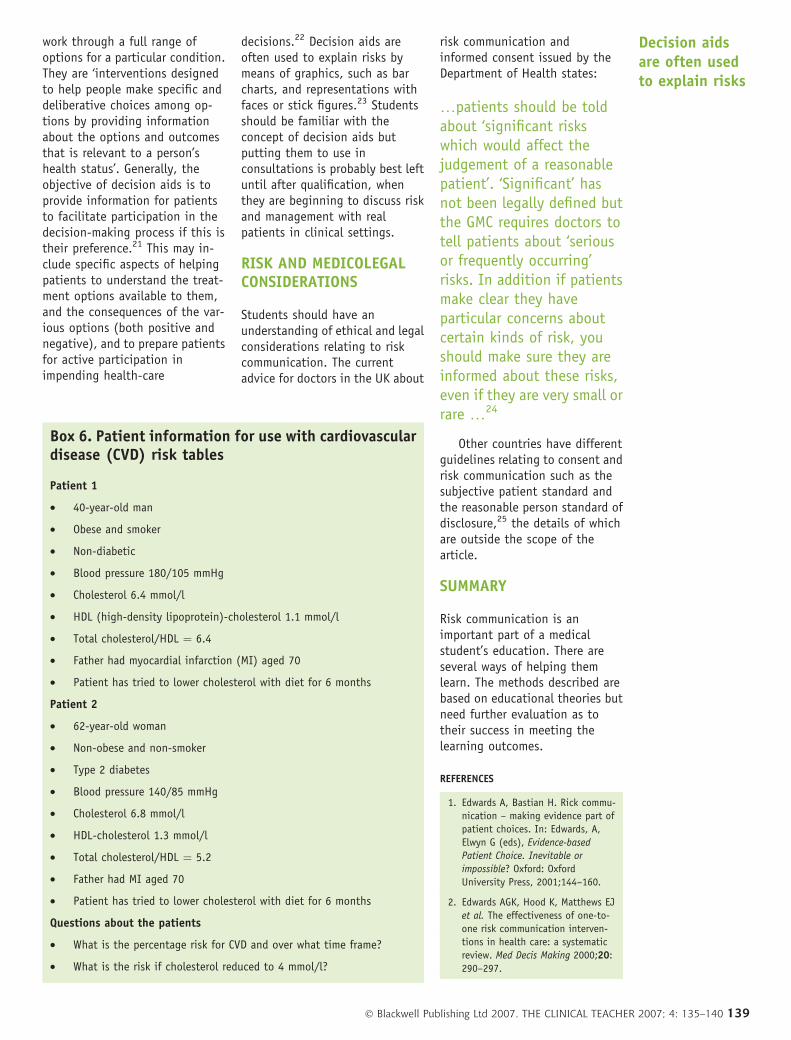
A learning exercise that has beenused successfully for many yearsat James Cook University isthrough the use of the NewZealand risk tables for cardiovas-cular disease (CVD).20 In thesesessions students are given anumber of case scenarios andasked about each patient: what isthe absolute risk of CVD and wouldyou prescribe lipid-loweringdrugs? Students then have toexplain their reasoning and howthey would communicate the riskto patients. Examples of patientdetails are given in Box 6.
THE USE OF DECISION AIDS
Decision aids are means ofhelping both doctors and patients
Box 5. Information needs of patients15
• Understanding what is wrong
• A realistic idea of prognosis
• The processes and likely outcomes of possible tests and treatments
• How to assist in self-care
• Available services and sources of help
• Reassurance and help to cope
• Helping others understand
• Legitimising seeking help and their concerns
• How to prevent further illness
• How to identify further information and self-help groups
Much of theinformation onthe web is not
vetted
138 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140
work through a full range ofoptions for a particular condition.They are ‘interventions designedto help people make specific anddeliberative choices among op-tions by providing informationabout the options and outcomesthat is relevant to a person’shealth status’. Generally, theobjective of decision aids is toprovide information for patientsto facilitate participation in thedecision-making process if this istheir preference.21 This may in-clude specific aspects of helpingpatients to understand the treat-ment options available to them,and the consequences of the var-ious options (both positive andnegative), and to prepare patientsfor active participation inimpending health-care
decisions.22 Decision aids areoften used to explain risks bymeans of graphics, such as barcharts, and representations withfaces or stick figures.23 Studentsshould be familiar with theconcept of decision aids butputting them to use inconsultations is probably best leftuntil after qualification, whenthey are beginning to discuss riskand management with realpatients in clinical settings.
RISK AND MEDICOLEGALCONSIDERATIONS
Students should have anunderstanding of ethical and legalconsiderations relating to riskcommunication. The currentadvice for doctors in the UK about
risk communication andinformed consent issued by theDepartment of Health states:
…patients should be toldabout ‘significant riskswhich would affect thejudgement of a reasonablepatient’. ‘Significant’ hasnot been legally defined butthe GMC requires doctors totell patients about ‘seriousor frequently occurring’risks. In addition if patientsmake clear they haveparticular concerns aboutcertain kinds of risk, youshould make sure they areinformed about these risks,even if they are very small orrare …24
Other countries have differentguidelines relating to consent andrisk communication such as thesubjective patient standard andthe reasonable person standard ofdisclosure,25 the details of whichare outside the scope of thearticle.
SUMMARY
Risk communication is animportant part of a medicalstudent’s education. There areseveral ways of helping themlearn. The methods described arebased on educational theories butneed further evaluation as totheir success in meeting thelearning outcomes.
REFERENCES
1. Edwards A, Bastian H. Rick commu-
nication – making evidence part of
patient choices. In: Edwards, A,
Elwyn G (eds), Evidence-based
Patient Choice. Inevitable or
impossible? Oxford: Oxford
University Press, 2001;144–160.
2. Edwards AGK, Hood K, Matthews EJ
et al. The effectiveness of one-to-
one risk communication interven-
tions in health care: a systematic
review. Med Decis Making 2000;20:
290–297.
Box 6. Patient information for use with cardiovasculardisease (CVD) risk tables
Patient 1
• 40-year-old man
• Obese and smoker
• Non-diabetic
• Blood pressure 180/105 mmHg
• Cholesterol 6.4 mmol/l
• HDL (high-density lipoprotein)-cholesterol 1.1 mmol/l
• Total cholesterol/HDL ¼ 6.4
• Father had myocardial infarction (MI) aged 70
• Patient has tried to lower cholesterol with diet for 6 months
Patient 2
• 62-year-old woman
• Non-obese and non-smoker
• Type 2 diabetes
• Blood pressure 140/85 mmHg
• Cholesterol 6.8 mmol/l
• HDL-cholesterol 1.3 mmol/l
• Total cholesterol/HDL ¼ 5.2
• Father had MI aged 70
• Patient has tried to lower cholesterol with diet for 6 months
Questions about the patients
• What is the percentage risk for CVD and over what time frame?
• What is the risk if cholesterol reduced to 4 mmol/l?
Decision aidsare often usedto explain risks
� Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140 139
3. Edwards A, Elwyn G, Muller A.
Explaining risks: turning numerical
data into meaningful pictures. BMJ
2002;324:827–830.
4. Godolphin W. The role of risk
communication in shared decision
making. BMJ 2003;327:692–693.
5. Tversky A, Kahnemann D. The
framing of decisions and the
psychology of choice. Science
1981;211:453–458.
6. Alaszewski A, Horlick-Jones T. How
can doctors communicate informa-
tion about risk more effectively?
BMJ 2003;327:728–731.
7. Becker M. The Health Belief Model
and Personal Health Behaviour.
Thorofare, NJ: Slack, 1974.
8. Prochaska JO, DiClemente CC,
Norcross JC. In search of how people
change. Am Psychol 1992;47:1102–
1104.
9. Say RE, Thomson R. The importance
of patient preferences in treatment
decisions – challenges for doctors.
BMJ 2003;327:542–545.
10. European Commission. A guideline on
the readability on the label and
package leaflet of medicinal products
for human use. Brussels: EC Pharma-
ceuticals Committee, 1998.
11. Knapp P, Raynor DK, Berry DC.
Comparison of two methods of
presenting risk information to
patients about the side effects of
medication. Quality Safety in Health
2004;13:176–180.
12. Mazur DJ, Merz JF. Patients’
interpretations of verbal expressions
of probability – implications for
securing informed consent to
medical interventions. Behavioural
Sciences and the Law 1994;12:
417–426.
13. American College of Physicians:
http://www.acponline.org/journals/
ecp/janfeb00/primer.htm (accessed
February 2007).
14. Calman KC. Cancer: science and
society and the communication of
risk. BMJ 1996;313:799–803.
15. Thistlethwaite JE, Ridgway G.
Making it real. A practical guide to
experiential learning. Oxford:
Radcliffe Medical Press, 2006.
16. Shaughnessy AF, Slawson DC, Becker
L. Clinical jazz: harmonising clinical
experience and evidence-based
medicine. J Fam Pract 1998;47:
425–428.
17. Coulter A, Entwistle V, Gilbert D.
Sharing decisions with patients: is
the information good enough? BMJ
1999;318:318–322.
18. Sedgwick P, Hall, A. Teaching
medical students and doctors how to
communicate risk. BMJ 2003;327:
694–695.
19. Kurtz S, Silverman J, Draper J.
Teaching and Learning Communica-
tion Skills in Medicine, 2nd edn.
Oxford: Radcliffe Medical Press,
2004.
20. http://www.nzgg.org.nz/guide-
lines/0035/CVD_Risk_Full.pdf
(accessed February 2007).
21. Edwards A, Elwyn G. The potential
benefits of decision aids in clinical
medicine. JAMA 1999;282:779–780.
22. O’Connor A, Edwards A. The role of
decision aids in promoting evidence-
based patient choice. In: Edwards A,
Elwyn G (eds), Evidence-based
Patient Choice: Inevitable or impos-
sible? New York: Oxford University
Press, 2001; 220–242.
23. Edwards A, Elwyn G, Mulley AI.
Explaining risks: turning numerical
data into meaningful pictures. BMJ
2002;324:827–830.
24. Stauch M, Wheat K, Tingle J. Source
Book on Medical Law, 2nd edn.
London: Cavendish Publishing, 2002,
160.
25. Kerridge I, Lowe M, McPhee, J. Ethics
and Law for the Health Professions,
2nd edn. Sydney: Federation Press,
2005.
140 � Blackwell Publishing Ltd 2007. THE CLINICAL TEACHER 2007; 4: 135–140