integrated care in practice laura galbreath, mpp director, center for integrated health solutions...
TRANSCRIPT

Integrated Care in PracticeLaura Galbreath, MPP
Director, Center for Integrated Health Solutions
May 15, 2013
About the Center In partnership with Health & Human Services (HHS)/Substance Abuse and Mental Health Services Administration (SAMHSA), Health Resources and Services Administration (HRSA).
Goal: To promote the planning, and development and of integration of primary and behavioral health care for those with serious mental illness and/or substance use disorders and physical health conditions, whether seen in specialty mental health or primary care safety net provider settings across the country.
Purpose: To serve as a national training and technical assistance center on the
bidirectional integration of primary and behavioral health care and related workforce development
To provide technical assistance to SAMHSA PBHCI grantees and entities funded through HRSA to address the health care needs of individuals with mental illnesses, substance use and co-occurring disorders

National Council for Community Behavioral Healthcare
Represents 2,500 community organizations that provide safety-net mental health & substance abuse treatment services to 8M adults, children &
families
National voice for legislation, regulations, and practices that protect & expand access to adequately funded, effective mental health & addictions
services
Technical Assistance Available from CIHSIndividual Technical Assistance:
Phone and video consultations, e-mail, site visits Medicaid Health Home Consultation to States
Group Learning Experiences: Regional and State Based Learning Communities Trainings and Presentations National Webinars
Tools: Web-based Resources (http://www.integration.samhsa.gov) Training Curricula White Papers and Factsheets eSolutions Newsletter

Primary and Behavioral Health Integration: The New Standard of Care
Tipping Point
Behavioral health is essential to health
Prevention/early intervention is possible
Treatment is Effective and People Recover
Primary Care Level of Behavioral Health
The Affordable Care Act: Four Key Strategies
The Future is Focused on Value Developing and implementing a
suite of value-based incentive programs that reward care providers for improvements in quality and efficiency
Supporting delivery systems as they become more integrated and accountable for cost, quality and experience outcomes
Coordination of medical and behavioral health services increases the value for payors and consumers
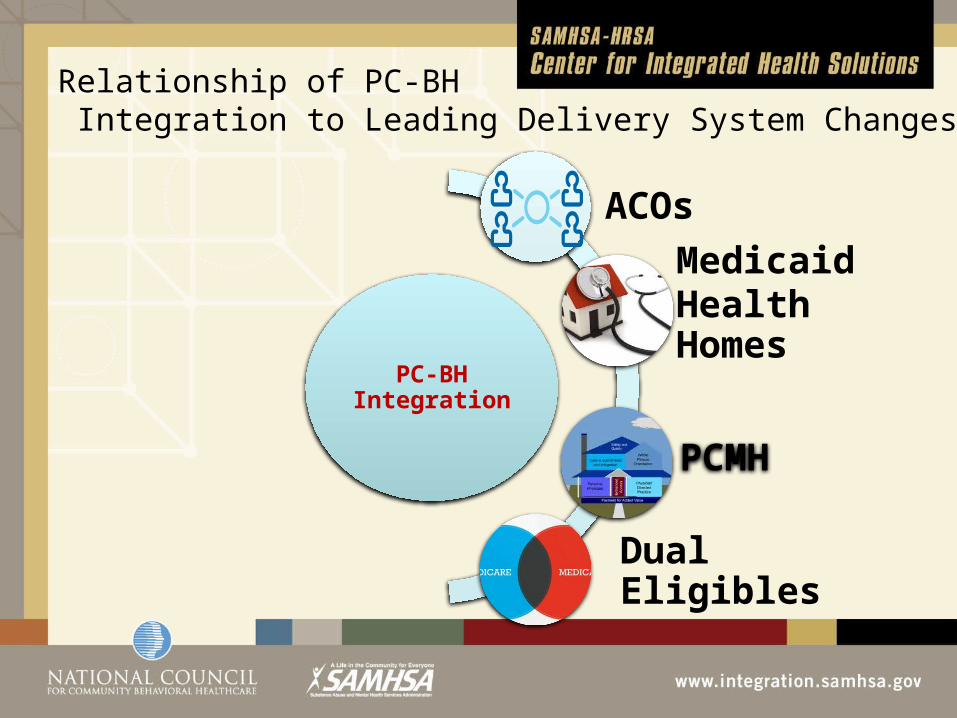
Relationship of PC-BH Integration to Leading Delivery System Changes
PC-BH Integration
Medicaid Health Homes
ACOs
Dual Eligibles
PCMH
Get to Know Your ACO
ACOs can fund community organizations to take the lead on conducting community health assessments.
ACOs can fund community stakeholder groups to develop and/or adapt health promotion and disease prevention programs for their communities; help get them up and running
ACOs can fund successful prevention programs, especially when bringing them to new populations and communities
ACOs can fund the testing of new or adapted programs to support community buy-in
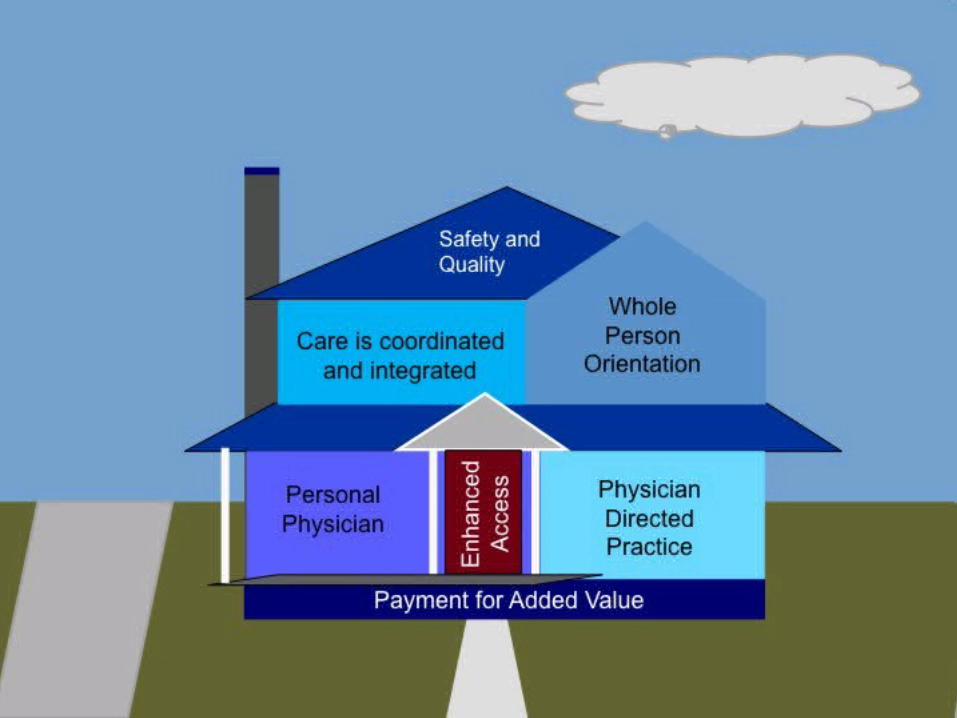
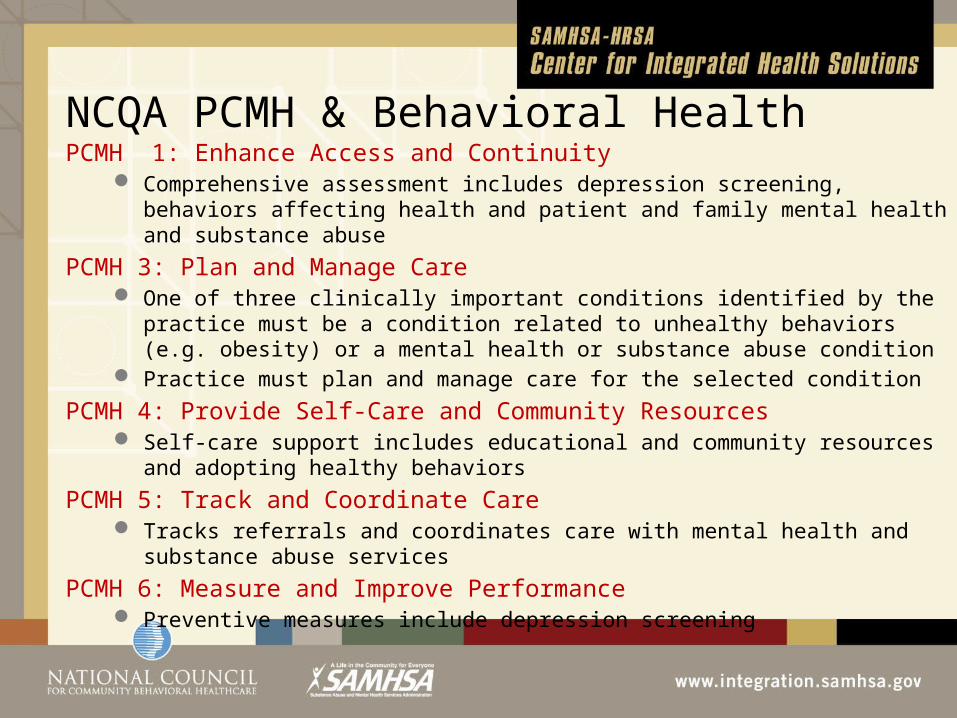
NCQA PCMH & Behavioral HealthPCMH 1: Enhance Access and Continuity
Comprehensive assessment includes depression screening, behaviors affecting health and patient and family mental health and substance abuse
PCMH 3: Plan and Manage Care One of three clinically important conditions identified by the practice must be a
condition related to unhealthy behaviors (e.g. obesity) or a mental health or substance abuse condition
Practice must plan and manage care for the selected condition
PCMH 4: Provide Self-Care and Community Resources Self-care support includes educational and community resources and adopting
healthy behaviors
PCMH 5: Track and Coordinate Care Tracks referrals and coordinates care with mental health and substance abuse
services
PCMH 6: Measure and Improve Performance Preventive measures include depression screening
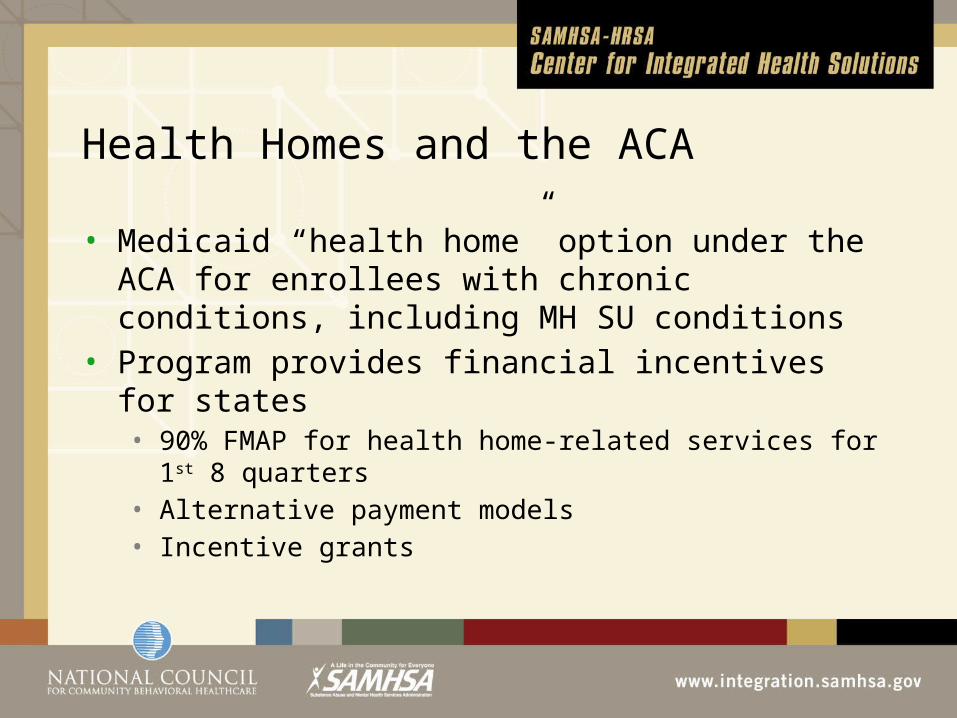
Health Homes and the ACA
• Medicaid “health home” option under the ACA for enrollees with chronic conditions, including MH SU conditions
• Program provides financial incentives for states• 90% FMAP for health home-related services for 1st 8 quarters • Alternative payment models• Incentive grants
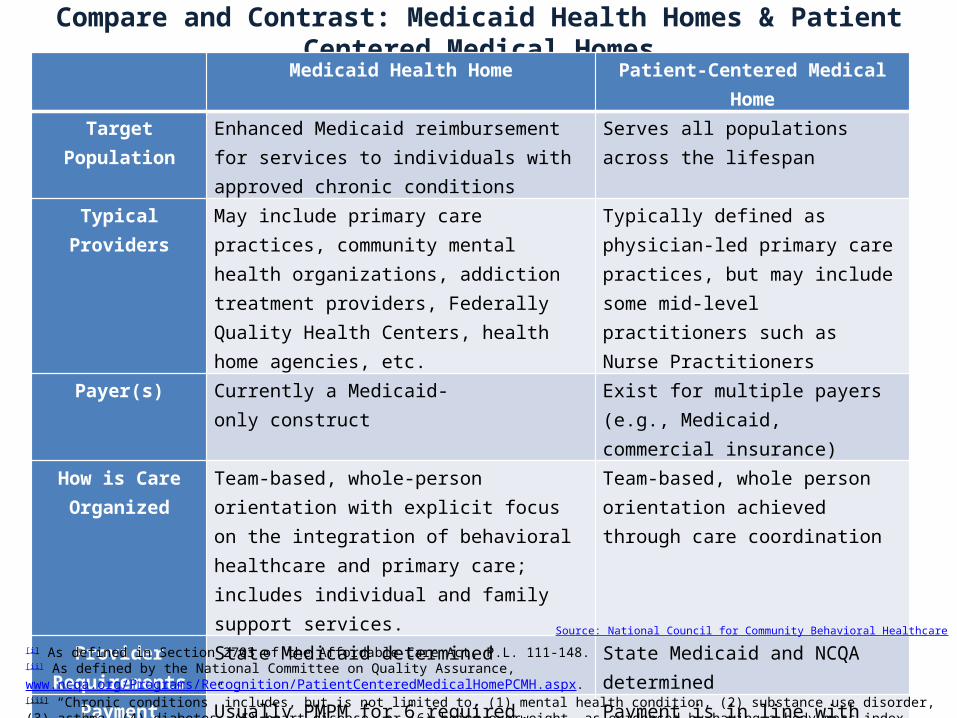
Compare and Contrast: Medicaid Health Homes & Patient Centered Medical HomesMedicaid Health Home Patient-Centered Medical Home
Target Population Enhanced Medicaid reimbursement for services to individuals with approved chronic conditions
Serves all populations across the lifespan
Typical Providers May include primary care practices, community mental health organizations, addiction treatment providers, Federally Quality Health Centers, health home agencies, etc.
Typically defined as physician-led primary care practices, but may include some mid-level practitioners such as Nurse Practitioners
Payer(s) Currently a Medicaid-only construct Exist for multiple payers (e.g., Medicaid, commercial insurance)
How is Care Organized
Team-based, whole-person orientation with explicit focus on the integration of behavioral healthcare and primary care; includes individual and family support services.
Team-based, whole person orientation achieved through care coordination
Provider Requirements
State Medicaid determined State Medicaid and NCQA determined
Payment Usually PMPM for 6 required services with more intensive care coordination and patient activation
Payment is in line with added value; usually small PMPM
Source: National Council for Community Behavioral Healthcare
[i] As defined in Section 2703 of the Affordable Care Act, P.L. 111-148.[ii] As defined by the National Committee on Quality Assurance, www.ncqa.org/Programs/Recognition/PatientCenteredMedicalHomePCMH.aspx. [iii] “Chronic conditions” includes, but is not limited to, (1) mental health condition, (2) substance use disorder, (3) asthma, (4) diabetes, (5) heart disease, or (6) being overweight, as evidenced by having a body mass index (BMI) over 25. (Section 2703 of the Affordable Care Act, P.L. 111-148).
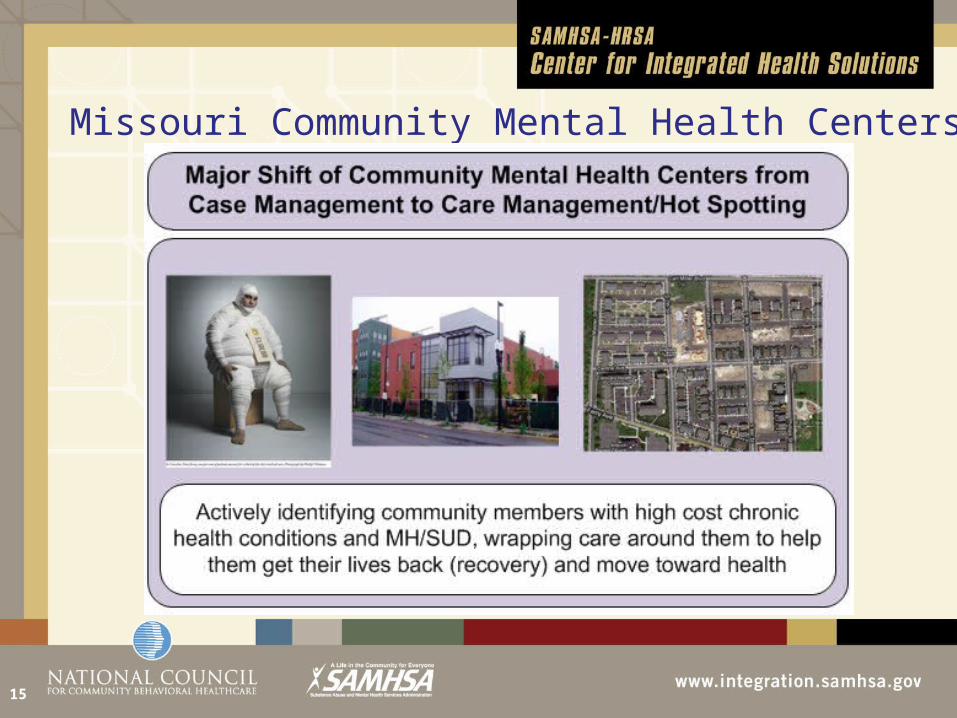
Missouri Community Mental Health Centers…
15
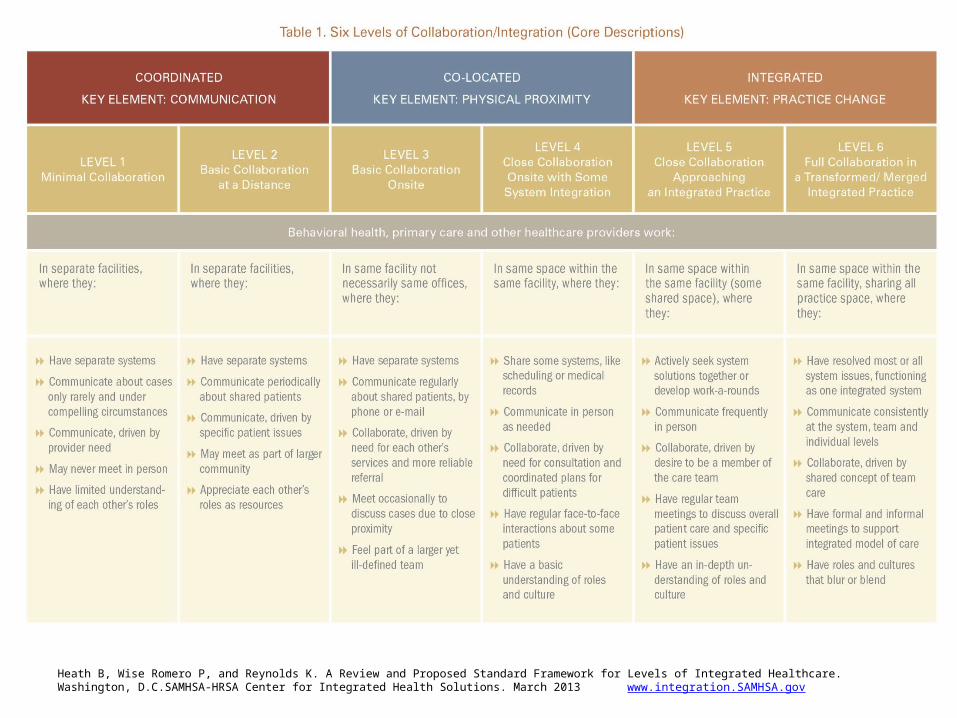
Heath B, Wise Romero P, and Reynolds K. A Review and Proposed Standard Framework for Levels of Integrated Healthcare. Washington, D.C.SAMHSA-HRSA Center for Integrated Health Solutions. March 2013 www.integration.SAMHSA.gov
SAMHSA Primary and Behavioral Health Care Integration (PBHCI)
Grant Program
PBHCI offers an important opportunity to reduce health disparities for Individuals with SMI
–Eliminate the early mortality gap–Reach people who will not access primary care– Intervene early before medical co-morbidities
develop or worsen–Reduce expensive emergency department use– Improve recovery outcomes