hank hallegraeff - welkom bij de hanzehogeschool groningen · hank hallegraeff ... consequence of a...
TRANSCRIPT

Common musculoskeletal disorders in primary care
physiotherapy: assessment and intervention
Acute low back pain and nocturnal leg cramps
Hank Hallegraeff
© 2013 Hank Hallegraeff
The study presented in this thesis was performed at the SHARE Graduate School for Health Research and the
Department of Health Sciences of the University Medical Center Groningen, University of Groningen, the
Netherlands, and at the Professorship of Health Care and Nursing of Hanze University of Applied Sciences
Groningen, the Netherlands.
Dissertation for the University of Groningen, the Netherlands, with references and summary in Dutch.
Hank Hallegraeff
Common musculoskeletal disorders in primary care physiotherapy: assessment and intervention.
Dissertation University of Groningen, June 2013
ISBN/EAN: 978‐94‐6108‐445‐3
Cover and graphic design: Peter J. Reese, AAAPEX. Illustration: Sophie Reese
Layout and printed by: Gildeprint Drukkerijen – Enschede, the Netherlands
Acknowledgments
Financial support for the printing of this thesis has been kindly provided by:
‐ Professorship of Health Care and Nursing, Hanze University of Applied Sciences Groningen
‐ Rijksuniversiteit Groningen, University Medical Center Groningen, Research Institute SHARE
‐ Educational Center for Musculoskeletal Therapies (SOMT)
‐ Wetenschappelijk College Fysiotherapie (KNGF)

RIJKSUNIVERSITEIT GRONINGEN
Common musculoskeletal disorders
in primary care physiotherapy: assessment and intervention
Acute low back pain and nocturnal leg cramps
Proefschrift
ter verkrijging van het doctoraat in de
Medische wetenschappen
aan de Rijksuniversiteit Groningen op gezag van de
Rector Magnificus, dr. E. Sterken,
in het openbaar te verdedigen op
maandag 24 juni 2013
om 16.15 uur.
door
Joannes Marinus Hallegraeff
geboren op 3 november 1955
te Haarlem

Promotor: Prof. dr. C.P. van der Schans Copromotor(es): Dr. M.H.G. de Greef
Dr. W.P. Krijnen
Beoordelingscommissie: Prof. dr. I. Bautmans
Prof. dr. P.U. Dijkstra
Prof. dr. J.W. Groothoff

5
Table of contents
Table of contents ..................................................................................................................... 5
Chapter 1
Introduction ............................................................................................................................. 7
Chapter 2
Expectations about recovery from acute non‐specific low back pain predict absence
from usual work due to chronic low back pain: a systematic review .................................. 21
Journal of Physiotherapy 2012 58 (3): 165‐172
Chapter 3
Measurement of acute nonspecific low back pain perception in primary care physical
therapy: reliability and validity of the brief illness perception questionnaire ................... 47
BMC Musculoskeletal Disorders, 2013, 14(1), 53
Chapter 4
A note of caution with respect to the Low Back Pain Perception Scale in primary care
physiotherapy. Submitted. .................................................................................................... 69
Chapter 5
Manipulative therapy and clinical prediction criteria in treatment of acute nonspecific
low back pain. ........................................................................................................................ 85
Perceptual and Motor skills, 2009, 108, 196‐208
Chapter 6
Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in
older adults: a randomised trial .......................................................................................... 109
Journal of Physiotherapy 2012, 58 (1): 17‐22
Chapter 7
Summary and General discussion ........................................................................................ 129

6

7
Chapter 1
Introduction

8
A
In
In
of
re
re
pe
co
se
F
Aim
n ph
nter
f co
elev
epre
erc
ont
ee F
igu
ms
hys
rna
ont
van
ese
cep
text
Fig
ure
s a
siot
atio
tex
nt
ent
tio
tua
ure
1. I
and
the
ona
xtua
for
t on
n o
al in
e 1.
ICF
d r
erap
l C
al f
r m
ne’
of p
nflu
F m
re
py
las
fact
mu
s f
pain
uen
od
ese
hea
sifi
tor
uscu
fun
n) a
nce
el.
ea
alth
cat
rs s
ulo
ctio
and
e. T
rc
h c
tion
uch
oske
ona
d en
her
ch
care
n o
h a
ele
al h
nvi
re i
qu
e, m
of F
as p
tal
hea
ron
is a
ue
mus
Fun
pers
d
alth
nm
a co
est
scu
ctio
son
diso
h c
ent
om
tio
ulos
oni
nal
ord
on
tal
ple
on
ske
ing
an
ers
dit
(e.
ex i
ns
elet
g (IC
nd e
s.
ion
.g.
nte
9
of
tal
CF)
env
Ph
n. P
wo
era
f t
dis
), se
viro
ysi
Per
ork
ctio
thi
sord
ee
onm
cal
son
loa
on
is
der
Fig
men
a
nal
ad,
be
th
rs a
gure
nta
acti
(e
so
etw
hes
are
e 1.
al d
ivit
e.g.
ocia
wee
sis
e ex
. W
dete
y
re
al su
n a
s
xam
With
erm
an
eco
upp
all c
min
hin
min
d
ver
por
com
ned
the
nan
wo
ry e
rt)
mpo
ac
e IC
ts
ork
exp
fac
one
cco
CF,
are
k p
pec
cto
ent
rdi
the
e co
par
ctat
rs r
ts o
ng
e im
ons
rtici
tio
rep
of t
to
mp
side
ipa
ns
pres
the
o th
pact
ere
atio
an
sen
IC
he
ts
ed
on
nd
nt
F,

10
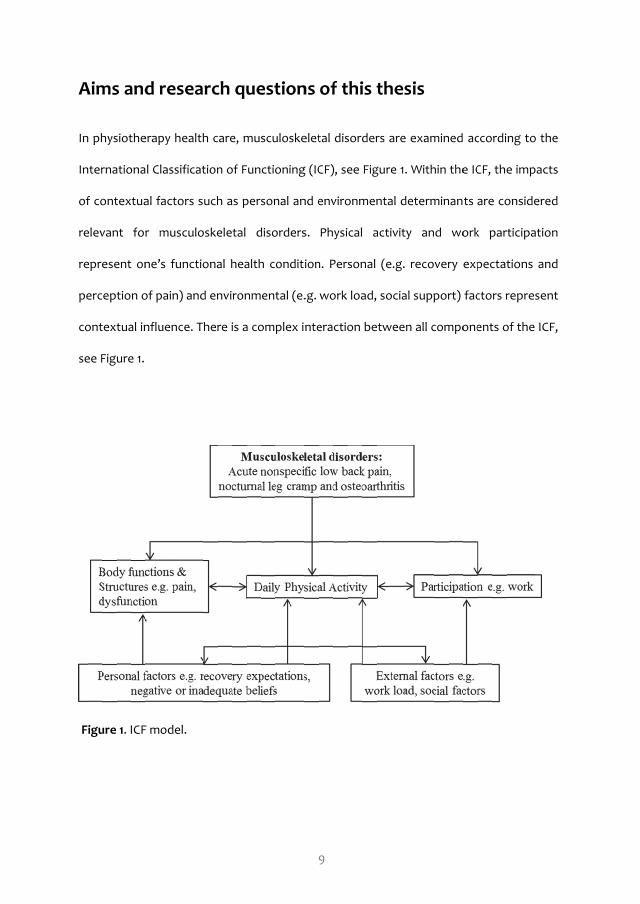
Aging and the age‐related increase of the number of patients with various
musculoskeletal disorders represent a major challenge for physiotherapists in primary
health care. As a consequence, reliable and valid measurement instruments are
necessary to assess, diagnose and evaluate the course of musculoskeletal disorders
matching the components of the ICF.
The focus of the studies in this thesis is on three common musculoskeletal disorders:
acute nonspecific low back pain and nocturnal leg cramps. These disorders can be
present within one patient.
Acute nonspecific low back pain
Nonspecific low back pain is defined as pain with a physical disorder not due to any
single known cause, such as a (previous) particular pathogen or an infection whereby
treatment is not directed against a particular agent (1). Nonspecific low back pain is
localized below the costal margin and above the inferior gluteal folds, with or without
leg pain, and not attributed to recognizable, known specific pathology or cause, e.g.
infection, tumor, osteoporosis, ankylosing spondylitis, fracture, inflammatory process,
radicular syndrome or cauda equina syndrome (2). Most patients experience their first
episode of nonspecific low back pain between 20 and 55 years of age. Within the Dutch
population, the twelve‐month period prevalence is 43.9% and point prevalence is 26.9%
with the highest prevalence in the late forties (3). In western industrialized countries,
the lifetime prevalence is 84% (4).

11
Nonspecific low back pain can be an acute or chronic condition. Acute nonspecific low
back pain is usually defined as an episode of less than 6 weeks; sub‐acute low back pain
persists between 6 and 12 weeks; and chronic low back pain persists for 12 weeks or
more. Acute nonspecific low back pain may evolve into chronic nonspecific low back
pain due to a number of personal factors like perception and poor recovery
expectations (5,6). Negative recovery expectations are prognostic for the transition
from acute to chronic nonspecific low back pain (6), however, it has not been
investigated how much more risk there is on an outcome of chronic low back pain by
negative recovery expectations.
The recurrence rate of severe nonspecific low back pain varies from 15 % to 50% (3,7).
Recurrence may strongly influence recovery expectations. Patients with less frequent
recurrence may recover more quickly than patients with more frequent recurrence.
Previous recovery may affect recovery expectations due to early treatment experience
or inadequate pain perception (8). However, there is conflicting evidence related to the
prognostic role of patients’ expectations for recovery.
Several physiotherapeutic interventions are available to improve recovery and reduce
the risk for recurrence. Spinal manipulation in the acute stage has moderate positive
effects on pain intensity and physical activity, however, there is variation on the level of
effectiveness in different studies (9,10). The choice for intervention is currently based on
clinical prediction rules. Such rules contain predictor variables obtained from patient
history, examination, and simple diagnostic tests. In daily practice, however, most
prediction rules are complicated and not easily applicable for implementation. For
12
example, a clinical prediction rule consisting of five predictor criteria: symptoms < 16
days, at least one hip > 35 degrees inner rotation, at least one hypo mobility lumbar
segment, no symptoms distal of the knee, and a FABQW score < 19 (11,12). To improve
the applicability of this five‐item rule, a two‐item rule was developed (13). However, a
limited validation of this two‐item rule was performed (13).
Cognitions and beliefs may influence recovery. The multidimensional representations of
the Common Sense Model (CSM) of self‐regulation of illness reflect five cognitive
dimensions: identity, consequences, cause, timeline, and cure or control (14). As a
consequence of a musculoskeletal disorder, beliefs are formed and result in a
perception of illness. For example, many patients may believe that the underlying cause
of their acute nonspecific low back pain is a lumbosacral radicular syndrome
(herniation). Two instruments measuring this psychological construct are available: the
Brief Illness Perception Questionnaire and the Low Back Pain Perception Scale.
However, these instruments are not validated in acute nonspecific low back pain
patients
Nocturnal leg cramps
Nocturnal leg cramps is defined as suddenly occurring, episodic, painful, sustained,
involuntary muscle contractions of the calf muscles, hamstrings or foot (15,16). The
prevalence of nocturnal leg cramps is more than 50% in the elderly (17,18). The most
frequently prescribed pharmacological treatment is (hydro) quinine having moderate
effects. Side effects of hydro quinine are high blood pressure, tinnitus,
thrombocytopenia, hepatitis, severe skin rash, and uremic syndrome. Potentially,

13
nonpharmacological treatments are also effective such as stretching. Many patients use
this technique spontaneously during cramps. Stretching may also prevent cramps.
However, there is insufficient evidence of non‐pharmacological treatment such as
preventive stretching (19).
Case example
The following case example illustrates a patient having several musculoskeletal
disorders like acute nonspecific low back pain and nocturnal leg cramps.
Case:
Mr. B, male, 59 years old, recurrent low back pain with radiating pain right hamstrings,
time since onset 11 days, absence of work since 11 days.
After ruling out serious diseases by a standardized screening procedure, a physical
examination was undertaken. Pain was not typically dermatome distributed, no pain
with coughing, and leg pain was not worse than in the lower back region, a negative
straight leg raise and negative crossed straight leg raise (20). Patient also complained
about intermittent nocturnal pain and cramps in both legs during the night and brief
morning stiffness in both groin areas and knees. Last year, the same low back pain was
treated with limited success; therefore, he expressed a negative recovery expectation.
As a result of the previous low back pain, the episode patient’s subjective interpretation
is negative about his expected recovery. The score of the Brief Illness Perception
Questionnaire indicates that the low back pain is perceived as most threatening.

14
In conclusion, a patient with severe acute low back pain intensity at onset, negative
expectations about recovery and inadequate low back pain perceptions with recurrent
acute nonspecific low back pain due to a sacroiliac joint dysfunction on the right side
(21). The brief morning stiffness could mean OA might be present.
During treatment, attention could be on the sacroiliac joint dysfunction, on the
nocturnal leg cramps and the likely presence of OA. Although the demand for
physiotherapy care of the patient is directed to reduce pain, according to the Dutch
guideline for nonspecific low back pain, it is recommended to advise, inform and to
prescribe low load exercises. Intervention with manipulative therapy is, therefore, not
the first treatment option, although evidence is present for pain reduction with
manipulative therapy, and the patient meets the two‐item criteria of the clinical
prediction rule.
In this case, example two personal prognostic factors are present: negative recovery
expectations and inadequate beliefs. They should be the first to approach with
counseling. Elimination of joint dysfunction by manipulative therapy following the
clinical prediction rule (acute low back pain and no pain extending the knee) might be
the second option in this acute stage.
Aims of this thesis
In this thesis, the first aim is to evaluate the predictive value of early patients’
expectations of recovery in acute nonspecific low back pain patients and the risk for
progression to chronic low back pain. A second aim is to investigate the psychometric

15
properties of specific illness perception questionnaires in patients with acute
nonspecific low back pain. The third aim is to evaluate the effect of manipulative
therapy in acute nonspecific low back pain patients. The fourth aim is to examine the
effect of stretching in patients with nocturnal leg cramps.
Specific research questions related to these aims are as follows.
Do negative expectations in patients after the onset of acute low back pain increase the
odds of absence from usual work due to progression to chronic low back pain?
Is the Dutch version of the Brief Illness Perception Questionnaire a reliable and valid
instrument in acute nonspecific low back pain patients in primary health care
physiotherapy?
Is the Dutch version of the Low Back Pain Perception Scale a reliable and valid
instrument in acute nonspecific low back pain patients in primary health care
physiotherapy?
Is manipulative therapy more effective than standard physical therapy in subjects with
acute (< 16 days) nonspecific low back pain without pain distal of the knee?
Is stretching of the calf and hamstring muscles each day just before sleep for six weeks
an effective strategy in older patients with nocturnal leg cramps (NLC) without quinine
use?

16
Overview of this thesis
In chapter 2, the results of a systematic review with meta‐analysis are reported to obtain
the predictive role of recovery expectations in (sub) acute nonspecific low back pain
patients with regard to absence from usual work due to progression to chronic low back
pain.
Chapter 3 addresses the test‐retest reliability and validity of the Brief Illness Perception
Questionnaire in acute nonspecific low back pain patients. Measuring perception of pain
in acute low back pain patients is widely used, however, the psychometric properties of
this instrument have never been examined.
The purpose of the study in chapter 4 is to examine reliability and validity of a specific
instrument measuring patients’ perceptions of acute nonspecific low back pain using
the Low Back Pain Perception Scale.
In chapter 5 is examined whether manipulative therapy more effective than standard
physical therapy in patients with acute (< 16 days) nonspecific low back pain without
pain distal of the knee.
Chapter 6 examines whether a pre‐sleep stretching program is effective to reduce
frequency and severity in adults with nocturnal leg cramps. Medications used to prevent
this disorder have variable efficacy and substantial side effects. A pre‐sleep stretching

17
program might be a useful alternative; it is easy to perform, has a low risk of side effects
and often relieves the after onset pain due to cramps.
Chapter 7 describes a summary, general discussion and conclusions of this thesis with
focus on implications for further research and consequences for clinical practice.
References.
1. Waddell G. The back pain revolution, 2nd edn. Churchill Livingstone, Edinburgh, 2004.
2. Chavannes AW, Mens JMA, Koes BW, Lubbers WJ, Ostelo R, Spinnewijn WEM, Kolnaar
BGM. NHG‐Standaard Aspecifieke lage rugpijn (Eerste herziening) Huisarts Wet 2005;
48(3),113‐23.
3. Picavet HSJ, Hazes JMW. Prevalence of self‐reported musculoskeletal diseases is high
Annals Rheumatic Diseases 2003; 62,644‐650.
4. Balagué F, Mannion AF, Pellisé F, Cedraschi C. Non‐specific low back pain. The Lancet
2012 (2); 379(9814),482‐91.
5. Hayden JA, Dunn KM, van der Windt DA, Shaw WS. What is the prognosis of back pain?
Best Practice & Research: Clinical Rheumatology 2010 (4); 24(2),167‐79.
6. Iles RA, Davidson M, Taylor NF, O'Halloran P. Systematic review of the ability of recovery
expectations to predict outcomes in non‐chronic non‐specific low back pain. Journal of
Occupational Rehabilitation 2009 (3); 19(1),25‐40.
7. Hestbaek L, Leboeuf‐Yde C, Manniche C. Low back pain: what is the long‐term course? A
review of studies of general patient populations. European Spine Journal 2003 (4);
12(2),149‐65.

18
8. Hancock MJ, Maher CG, Latimer J, Herbert RD, McAuley JH. Can rate of recovery be
predicted in patients with acute low back pain? Development of a clinical prediction rule.
European Journal of Pain 2009; 13(1),51‐5.
9. Rubinstein SM, Terwee CB, Assendelft WJJ, de Boer MR, van Tulder MW. Spinal
manipulative therapy for acute low‐back pain (Cochrane review). Spine 2013; (38) 3,158‐
77.
10. Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies:
the UK evidence report. Chiropractic and Osteopathy. 2010; 18,3.
11. Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D, Butler B, Garber M, Allison
S. A clinical prediction rule for classifying patients with low back pain who demonstrate
short‐term improvement with spinal manipulation. Spine 2002; 27(24), 2835‐43.
12. Childs JD, Fritz JM, Flynn TW, Irrgang JJ, Johnson KK, Majkowski GR, DelittoA. A clinical
prediction rule to identify patients with low back pain most likely to benefit from spinal
manipulation: a validation study. Annals of Internal Medicine 2004; 141(12),920‐8.
13. Fritz JM, Childs JD, Flynn TW. Pragmatic application of a clinical prediction rule in
primary care to identify patients with low back pain with a good prognosis following a
brief spinal manipulation intervention. BMC Family Practice 2005; 6(1),29.
14. Leventhal H, Brisette I, Leventhal EA: The common‐sense‐model in health and illness.
The self‐regulation of health and illness behavior, Routledge, London, 2003.
15. Monderer RS, Wu WP, Thorpy MJ. Nocturnal leg cramps. Current Neurology and
Neuroscience Reports 2010; 10(1),53‐9.
16. Sontag SJ, Wanner JN. The cause of leg cramps and knee pains: an hypothesis and
effective treatment. Medical Hypotheses 1988; 25(1),35‐41.

19
17. Abdulla AJ, Jones PW, Pearce VR. Leg cramps in the elderly: prevalence, drug and
disease associations. International Journal of Clinical Practice 1999; 53(7),494‐6.
18. Oboler SK, Prochazka AV, Meyer TJ. Leg symptoms in outpatient veterans. West Journal
Medicine 1991; 155(3),256‐9.
19. Katzberg HD, Khan AH, So YT. Assessment: symptomatic treatment for muscle cramps
(an evidence‐based review): report of the therapeutics and technology assessment
subcommittee of the American academy of neurology. Neurology 2010;74 (8), 691‐6.
20. van der Windt DA, Simons E, Riphagen II, Ammendolia C, Verhagen AP, Laslett M, Devillé
W, Deyo RA, Bouter LM, de Vet HC, Aertgeerts B. Physical examination for lumbar
radiculopathy due to disc herniation in patients with low‐back pain. Cochrane Database
Systematic Review 2010;(2).
21. Laslett M, Aprill CN, McDonald B, Young SB. Diagnosis of sacroiliac joint pain: validity of
individual provocation tests and composites of tests. Manual Therapy. 2005; 10(3),207‐
18.

20

21
Chapter 2
Expectations about recovery from acute non‐specific low
back pain predict absence from usual work due to chronic
low back pain: a systematic review
Journal of Physiotherapy 2012 Vol. 58 (3): 165‐172
Joannes M Hallegraeff
Wim P Krijnen
Cees P van der Schans
Mathieu HG de Greef

22
23
Abstract
Question: Do negative expectations in patients after the onset of acute low back pain
increase the odds of absence from usual work due to progression to chronic low back
pain?
Design: Systematic review with meta‐analysis of prospective inception cohort studies.
Participants: Adults with acute or subacute non‐specific low back pain.
Outcome measure: Absence from usual work at a given time point greater than 12
weeks after the onset of pain due to on‐going pain.
Results: Ten studies involving 4683 participants were included in the review.
Participants with acute or subacute pain and negative expectations about their recovery
had significantly greater odds of being absent from usual work at a given time point
more than 12 weeks after the onset of pain: OR 2.17 (95% CI 1.61 to 2.91). The exclusion of
five studies with the greatest risk of bias showed that the result was similar when more
rigorous quality criteria were applied: OR 2.52 (95% CI 1.47 to 4.31).
Conclusion: The odds that adults with acute or subacute non‐specific low back pain and
negative recovery expectations will remain absent from work due to progression to
chronic low back pain are two times greater than for those with more positive
expectations. These results were consistent across the included studies despite
variations in the risk of bias.

24
Introduction
Acute low back pain is defined as pain, increased muscle tonus, and stiffness localised
below the costal margin and above the inferior gluteal folds, sometimes accompanied
by radiating pain, for up to six weeks. Pain that continues but does not exceed 12 weeks
is defined as subacute, becoming chronic thereafter (1,2). The lifetime prevalence of low
back pain is greater than 70% in industrialised countries (3). Several studies have
reported that acute low back pain improves within four weeks, with 75–90% recovery
and a relapse rate of 60% (4,5). However, a small proportion of people with acute low
back pain progress to have chronic low back pain (6,7).
Low back pain may cause a person to take sick leave or it may cause disability that limits
a person’s ability to perform usual work activities. Either of these can contribute to the
period absent from usual work. Recall of sick leave is accurate over 2 to 3 months and
reliable (8,9,10).
Some psychosocial factors measured in the acute or subacute stages of low back pain
are predictors of progression, with the strength of the prediction being dependent on
the time of measurement (11). One psychosocial factor that we address in this review is
the patient’s prediction or expectations, which we define as what patients believe might
occur. These expectations may be a prognostic indicator, perhaps by affecting clinical
outcomes. The review of Iles and colleagues (12) showed that recovery expectations
measured within three weeks of the onset of low back pain are a strong predictor that
the pain will become chronic. This prognostic relationship appears to exist despite high

25
pain and disability levels in the acute phase (12,13). However, evidence to support the
premise that patients’ expectations predict the number of days absent from usual work
is inconsistent (14,15,16,17,18,19). This inconsistency can be explained by variation in the
methods used to assess the predictive relationship. Across studies there can be
heterogeneity in the populations studied, the risk statistics reported, and the predictive
measures considered. Even measurement of a single outcome can allow heterogeneity
in the measurement instrument, its cut‐off point, and the timeframe (20). The variability
in the existing studies of patients’ expectations makes it difficult to compare the results
and summarise the findings. Meta‐analysis could assess an overall effect but no meta‐
analysis has been performed concerning the predictive value of patients’ expectations
on work absenteeism due to progression of low back pain from acute to chronic.
Despite the inconsistencies in the evidence noted above, we aimed to draw a conclusion
from the available evidence using meta‐analysis about whether the recovery
expectations of adults with acute or subacute non‐specific low back pain are predictive
of progressing to chronic low back pain that is severe enough to cause on‐going
absence from usual work activities. We also aimed to examine the homogeneity of the
studies and characteristics that may modify any predictive relationship. To do this, we
sought to examine all primary data from prospective inception cohort studies of the
recovery expectations of people with acute or subacute non‐specific low back pain.
Therefore, the research question for this systematic review was:
Do negative expectations about recovery in adults with acute or subacute non‐specific
low back pain increase the odds of absence from usual work due to progression to
chronic low back pain?

26
What is already known on this topic: Acute low back pain is common and it becomes
chronic in a small proportion of people. Some psychosocial factors measured in the
acute or subacute stages of low back pain are predictors of progression to chronic low
back pain.
What this review adds: Adults with negative expectations about their recovery during
acute or subacute low back pain are more likely to remain absent from work more than
12 weeks after the onset of their pain, due to progression to chronic low back pain.
Method
Identification and selection of studies
Four electronic databases were searched: PubMed, MEDLINE, EMBASE and PEDro. The
search terms included: low back pain, back pain, patient expectations, expectations about
recovery, prognosis, prognostic, risk factors, risk, psychosocial, psychological, sick leave,
sickness, absence, absenteeism, workers’ compensation, redress, cohort studies and
longitudinal studies.
The titles and abstracts of the retrieved publications were screened by two reviewers
(JMH, MHGdeG) working independently to identify potentially eligible studies. Eligible
studies were defined by the criteria in Box 1. However, studies meeting those criteria
were excluded if they were published prior to 1999 or in a non‐English language. Studies
were also excluded if the participants had rheumatic disease, cancer, or trauma. The
two reviewers were not blinded with respect to authors, journals, and results.
Potentially eligible studies were retrieved in full text for further evaluation against the

27
criteria. When an eligible study was identified, its reference list was checked for other
potentially eligible studies. When eligible studies were identified, the same reviewers
extracted data regarding the study design, the characteristics of the participants, details
of the prognostic and outcome measures, and the duration of follow‐up. The reviewers
also extracted odds ratios or hazard ratios and their 95% CIs, or data that could be
converted into these statistics. The two reviewers discussed any disagreements, seeking
the advice of the other reviewers (WPK, CPvdS) if necessary to reach consensus.
Design
• Prospective cohort studies
• Randomised trials analysed as cohort studies
Participants
• Adults aged 18 to 65 years
• Non‐specific low back pain less than 12 weeks from onset of the pain
• Living in a Western, industrialised country
Predictor
• Expectations regarding recovery from low back pain, measured within 12 week from
onset of the pain
Outcome measure
• Continued absence from usual work at a given time point greater than 12 weeks from
onset of the pain
Analyses
• Odds ratios or hazard ratios expressing the increased risk of the outcome due to the
predictor
Box 1. Inclusion Criteria

28
Assessment of characteristics of studies
Quality: Two reviewers (JMH, MHGdeG) used the checklist of the Agency for Healthcare
Research and Quality to appraise the methodological quality of the included studies (21).
The AHRQ checklist consists of nine items, which are presented in Table 1. When
calculating the overall AHRQ score, studies that meet all nine criteria are given a score of
1, indicating the highest quality. The score for other studies is calculated by adding 1 for
each criterion that is not met. Therefore, low scores reflect high quality, whereas high
scores reflect low quality and major weaknesses. Criteria 1 to 3 and 8 assess external
validity, criteria 4 to 7 internal validity, and criterion 9 assesses the statistical method.
Scores less than 4 indicate a low risk of bias, scores of 4 to 6 indicate a medium risk of
bias, and scores of 7 and above indicate a high risk of bias. Consensus was again reached
by discussion or by intervention of a third reviewer where necessary.
Participants: The age and gender of participants were recorded for each study. The time
since onset of the low back pain was also recorded. Data were extracted from each
study regarding the recovery expectations of the participants.
Outcome measures: The numbers of days absent from work in a given period or time to
return to work were recorded as outcome measures. Use of time absent from usual
work as an outcome measure has a relatively low risk of bias (22).

29
Data analysis
Odds ratios (ORs) computed from logistic regression were used. These derived OR
values from the various studies were summarised by calculating the pooled OR using
meta‐analysis. Random variation between the studies was incorporated by using a
random effects model assuming that studies are closely related with a similar study
question and that heterogeneity has been taken into account. The studies included in
the meta‐analysis reflect a random sample of the relevant distribution of ORs as effect
sizes and the pooled OR estimates the mean effect in this distribution. Study weights
were assigned according to the inverse variance. Q values were calculated for
estimating heterogeneity as the weighted sum of squared differences between
individual study effects.
According to the classification of Hartvigsen and colleagues (23), ORs between 1.50 and
2.00 were considered moderate, and higher ORs were considered strong. ORs were
considered statistically significant if the 95% CI straddled 1.00. Publication bias was
examined through visual inspection of asymmetry in a scatter plot and Egger’s constant
of regression (24). A sensitivity analysis was conducted based on trial quality. Only
studies with a quality score < 4, ie, those with low risk of bias, were included in the
sensitivity analysis to explore how methodological quality affects the overall result (25).
The Statistical Programming Language R, version 2.14.0 was used for all analyses.

Study
Adequate
selection
of study
population
Description
of in‐ a
nd
exclusion
criteria
Description
of
potential
pro
gnostic
factors
Pro
spective
study
design
Study
size
> 100
Follo
w
up > 3
months
Loss
to
follo
w
up <
20%
Releva
nt
outcome
measures
Appro
priate
statistica
l
analysis
AHRQ
score*
Dionne et
al (20
05)
N
Y
N
Y
Y
Y
N
Y
N
5
Hag
en et al
(2005)
N
Y
N
N
Y
Y
Y
N
Y
5
Kap
oor et
al (20
06)
Y
N
Y
Y
Y
N
Y
Y
Y
3
Lotters et
al (20
06)
Y
Y
Y
Y
Y
Y
N
Y
Y
2
Reme e
t al
(2009)
N
Y
N
N
Y
Y
N
Y
Y
5
Sch
ultz et
al (20
04)
Y
Y
Y
Y
Y
N
N
Y
Y
3
Sch
ultz et
al (20
05)
Y
N
Y
Y
Y
N
N
Y
N
5
Shaw
et al
(2005)
N
N
Y
Y
Y
N
N
Y
Y
5
Steenstra
et al (20
05)
Y
N
Y
Y
Y
N
Y
Y
Y
3
Turner et al
(2006)
Y
Y
Y
Y
Y
N
N
Y
Y
3
* See text for scoring details.
Tab
le 1. A
HRQ sco
res fo
r all included studies (n = 10)
30

31
Figure 1. Identification and selection of studies for the review
Next page:
Table 2. Summary of included studies (n =10)
Titles and abstracts screened (n = 589)
MEDLINE (n = 505)
Embase (n = 60)
PEDro (n = 24)
Potentially relevant papers retrieved for evaluation of
full text (n = 154)
Records excluded after screening titles and abstracts (n = 435)
Papers excluded after
evaluation of full text (n = 146)
• not related to low back pain
• chronic low back pain
• no patients expectations
• follow‐up < 3 months
• duplicates
• retrospective cohorts
• no effect size
• trauma, rheumatic diseases,
cancer
• disability, pain level as
outcome
Papers included after searching reference lists
(n = 2)
Included studies (n = 10)

Stu
dy
Design
Part
icipants
Stage
Pro
gnostic factor
Outcome m
easure
Follo
w‐up
( months)
Dionne et al
Prospective
n = 1007
One d
ay o
ff work
Expect w
ork
ing w
ithout
Percentage chance o
f fa
ilure to
24
(2005)
cohort
Age (y) = 39 (SD 11)
restrictions w
ithin 3 m
onths:
retu
rn to w
ork w
ithin 3 m
onths
Gender = 589 M
, 418 F
su
ccess, part
ial success, failu
re
Retu
rn to w
ork in good health
after attempt, and failu
re
OR 2.08 (95% C
I 1.05 to 4.12)
Hagen et al
Secondary
n = 457
Within 4–12 weeks after
Do not belie
ve lo
w bac
k pain w
ill
Retu
rn to w
ork
(2005)
analysis of
Age (y) = 41 (SD N
/S)
onset
disappear yes/no
Univariate
data fro
m
Gender = 238 M
, 219 F
One g
roup in spine c
linic
OR 2.6 (95% C
I 1.4 to 3.8)
3
RCT
OR 2.3 (95% C
I 1.4 to 3.8)
12
Kapoor et al
Prospective
N = 300
Less then14 d
ays after
Will you b
e able to do w
ork
Retu
rn to w
ork
3
(2006)
cohort
Age (yr) = 35 (SD N
/S)
onset
without restr
ictions w
ithin 4
Univariate
Gender = 210 M
, 90 F
weeks: positive or negative
OR 3.09 (95% C
I 1.77 to 5.38)
Lo
tters et al
Prospective
n = 129
Within 2–6 w
eeks sick
Workers
’ own perception re
turn Sick leave
12
(2006)
cohort
Age (yr) = 43 (SD 9)
leave
work w
ithin 6 weeks
Univariate
Gender = 90 M
, 39 F
Scale 1–10
HR 2.43 (9
5% C
I 1.61 to 3.66)
Reme e
t al
Secondary
n = 246
Sick listed 8–12 weeks
Wheth
er they expected to retu
rn
Retu
rn to w
ork
(2009)
analysis of
Age (yr) = 41 (SD 11)
to w
ork w
ithin the n
ext
few weeks Adjusted (no m
ultivariate?)
data fro
m
Gender = 120 M
, 126 F
or not
OR 4.2 (95% C
I 1.7 to 10)
3
RCT
OR 1.9 (95% C
I 0.9 to 4.0)
12
OR 2.0 (95% C
I 0.9 to 4.3)
24
Schultz
Prospective
n = 159
Within 4–6 w
eeks after
Reco
very exp
ectations
Retu
rn to w
ork
3
et al
cohort
Age (yr) = 40 (SD 11)
onset
Retu
rn to w
ork
Multivariate
(2004)
Gender = N/S
Scale 7 items (range 7–21) lower
OR 1.27 (9
5% C
I 1.10 to1.45)
score indicate m
ore p
ositive
exp
ectations
Schultz
Prospective
n = 100
Within 4–6 w
eeks after
Exp
ecta
tions o
f recovery Scale
Retu
rn to w
ork
3
et al
cohort
Age (y) = 41 (SD 11)
onset
7 items scale (range 7–21) lower
Multivariate
(2005)
Gender = 62 M, 3
8 F
score indicates m
ore p
ositive
OR 1.21 (9
5% C
I 1.01 to 1.45)
exp
ectations
Shaw
et al
(2005)
Prospective
cohort
n = 568
Age (yr) = 36 (SD 11)
≤ 14 days, hospital care
Will you be able to work w
ithout
restrictions
four weeks from now?
Working
without
restrictions
4
weeks from now
3
Gender = 385 M 18
3 F
Definitely/probably/not sure
/ Multivariate
unlikely/no
OR 2.25 (9
5% C
I 1.52 to 3.32)
Steenstra
Prospective
n = 615
Within 2 days of work
Expected s
ick leave < 10 days o
r Sick leave in days
for at least 4
6
et al
cohort
Age (yr) = 42 (SD 9)
absence
Expected s
ick leave > 10 days
weeks
(2005)
Gender = 222 M
, 393 F
Univariate
HR 3.66 (95% C
I 2.78 to 4.76)
Tu
rner et al
Prospective
n = 1068
Within 10–58 days
Expectations about work
ing
Sick
leave (work d
isability duration)
6
(2006)
cohort
Age (yr) = 39 (SD 11)
w
ithin 6 m
onths
Very lo
w expecta
tions adjusted
Gender = 740 M
, 328 F
Scale 0–10 h
igher score is m
ore
OR 3.08 (95% C
I 1.46 to 6.48)
certain
N/S = not stated
32

33
Results
Flow of studies through the review
The electronic searches identified 589 publications, of which 154 were considered
potentially relevant and were evaluated as full‐text papers. Of these, 146 studies were
excluded. Figure 1 presents the flow of the studies through the review and the reasons
for exclusions. Searching the reference lists of the eight eligible studies identified
another two eligible studies. Therefore 10 studies were included in the review
(15,16,19,26,27,28,29,30,31,32).
Characteristics of included studies
Quality: Five studies had a low risk of bias, with AHRQ scores of 2 (31) or 3 (15,26,30,32).
The other five studies all had a moderate risk of bias, with an AHRQ score of 5. The
quality criterion related to < 20% loss to follow up was met in only three of the studies
(26,27,30). Consensus about quality interpretation was unanimous. Table 1 presents the
quality of the studies and Table 2 presents the characteristics of the studies.
Participants: The total number of participants in the 10 included studies was 4683.
Overall, 59% of the participants were male, although one study listed no gender details
(15). The mean age of participants in each study ranged from 35 to 43 years.

34
Outcome: Absence from usual work in a given period was reported using different terms
such as ‘not return to work’, ‘sick leave’, ‘work absenteeism’, ‘sickness absenteeism’,
and ‘compensated sick leave’. Follow‐up time ranged from 3 to 24 months.
Prediction of absence from work by recovery expectation
The standard error of the estimated ORs of the 10 included studies was computed from
the confidence intervals, presented in Table 2. From these weights, the weights were
computed using the inverse variance method to calculate the heterogeneity statistic Q =
96.23, p < 0.0001, df = 9 (33). Because homogeneity was rejected, the DerSimonian and
Laird random effects model was estimated yielding a tau squared equal to 0.19. The
corresponding weights and pooled OR of 2.17 (95% CI 1.61 to 2.91) are presented in
Figure 2. The 95% CIs of all but one of the studies, as well as that of the pooled result, lie
to the right of 1.00, indicating significantly greater risk of absence from usual work
among participants whose early expectations about their recovery were poor.
For the sensitivity analysis, the standard error of the estimated ORs of the 5 studies with
low risk of bias was computed from the 95% CIs. From these, the weights were
computed using the inverse variance method to calculate the heterogeneity statistic Q =
43.83, p < 0.0001, df = 4 (33). Because homogeneity was again rejected, the DerSimonian
and Laird random effects model was estimated yielding a tau squared equal to 0.34. The
corresponding weights and pooled OR of 2.52 (95 % CI 1.47 to 4.31) are presented in
Figure 3. The confidence intervals of the five studies with low risk of bias as well as that
of our pooled result all lie to the right of 1.00, again indicating significantly greater risk

35
of absence from usual work among participants whose early expectations about their
recovery were poor.

36
0,5 1 2 4 8Odds Ratio (95% CI)
0,5 1 2 4 8
Odds Ratio (95% CI)
Study OR (95% CI) Weight (%)
Dionne 2005 2.08 (1.05 to 4.12) 9
Hagen 2005 2.30 (1.40 to 3.80) 10
Kapoor 2006 3.09 (1.77 to 5.38) 10
Lotters 2006 2.43 (1.61 to 3.66) 10
Reme 2009 1.90 (0.90 to 4.00) 9
Schultz 2004 1.27 (1.10 to 1.45) 12
Schultz 2005 1.21 (1.01 to 1.45) 11
Shaw 2005 2.25 (1.52 to 3.32) 10
Steenstra 2005 3.66 (2.78 to 4.76) 11
Turner 2006 3.08 (1.46 to 6.48) 9
Pooled 2.17 (1.61 to 2.91)
Figure 2. Odds ratios (95% CI) of the association between recovery expectations during acute or
subacute non‐specific low back pain and being absent from usual work due to low back pain
beyond 12 weeks, pooling data from the 10 included studies (n = 4683). Odds ratios greater than
one indicate greater odds of absenteeism among people with more negative recovery
expectations.
Study OR (95% CI) Weight (%)
Kapoor 2006 3.09 (1.77 to 5.38) 19
Lotters 2006 2.43 (1.61 to 3.66) 20
Schultz 2004 1.27 (1.10 to 1.45) 20
Steenstra 2005 3.66 (2.78 to 4.76) 22
Turner 2006 3.08 (1.46 to 6.48) 18
Pooled 2.52 (1.47 to 4.31)
Figure 3. Odds ratios (95% CI) of the association between recovery expectations during acute or
subacute non‐specific low back pain and being absent from usual work due to low back pain
beyond 12 weeks, pooling data from the 5 included studies with higher quality (AHRQ score < 4)

37
High quality Schultz (2004)
Low quality
Schultz (2005)
Steenstra (2005)
Lotters (2006) Shaw (2005)
Hagen (2005) Kapoor (2006)
Turner (2006) Reme (2009)
Dionne (2005)
SND
(n = 2271). Odds ratios greater than one indicate greater odds of absenteeism among people
with more negative recovery expectations.
In order to detect whether publication bias might be affecting the cohort of studies we
included in the review, a regression analysis was performed using precision as a
predictor for standard normal deviates (24). The standard normal deviates were
computed by dividing the ORs with their corresponding standard error and the precision
was computed as the inverse of the standard error. A marginal t‐test of the constant (t =
–0.770) yielded a P value of 0.46 indicating no publication bias, which is in line with the
observation that there is no clear asymmetry in the scatterplot (Figure 4.)
15 10 5 0
0.2 0.4 0.6 0.8 1.0
1.2 precision
Figure 4. Scatterplot of precision versus standard normal deviates (SND) from the
Odds Ratios of the included studies (n =10).

38
Discussion
This review confirmed that the recovery expectations of patients with acute or
subacute non‐specific low back pain are a statistically significant predictor of absence
from usual work due to progression to chronic low back pain. The odds of remaining
absent from work at a given time point beyond 12 weeks after the onset of the pain
were two times higher among those with negative expectations about their recovery.
This pooled result (OR = 2.17, 95% CI 1.61 to 2.91) indicates a strong predictive value. In
addition, our analysis yielded consistent evidence of this prognostic role of patients’
expectations. That is, negative expectations about recovery were a strong predictor of
future work absence despite variations in follow‐up time and the use of different
measurement instruments. Across the individual studies, the ORs were all greater than
1.00 and almost all were statistically significant, indicating robust evidence from this
meta‐analysis (34). This result was also still evident when more rigorous eligibility
criteria were applied to ensure only high quality studies were contributing data to the
meta‐analysis.
No indication of publication bias was shown by our analysis (24). However, as a
consequence the limited number of studies on which the scatter plot was based, our
conclusion with respect to publication bias is preliminary (35). Another limitation of this
review is that, although low back pain is a multifactorial problem, only one potential
prognostic factor was examined.

39
All measures of participants’ recovery expectations were carried out within the first
three months of non‐specific low back pain. However, in contrast to Burton et al (11) and
Iles et al (13), in this review strength of prediction was not related to time of
measurement within these three months. Moreover, Steenstra et al provided the
largest effect size despite patients’ expectations being measured within two days of the
onset of the pain (26).
We recommend that physiotherapists screen patients’ expectations in the acute stage
of low back pain so that strategies can be targeted to those most at risk of absence
from work in a given period due to progression of their low back pain into the chronic
phase. For example, we suggest counselling patients with more negative expectations
and the development of guidelines to screen patients’ recovery expectations as a
psychological construct. An effective coaching strategy can affect how risk patients
handle their recovery expectations (36). A number of studies substantiated the need for
screening, and if necessary, for quick intervention by providing information directly
after onset (37,30,38,39). Thus, in future research, patients’ expectations should be
included in a core set of factors predicting chronic low back pain.
Interpreting low recovery expectations of a patient is difficult due to the complex
mental states that underlie an individual’s expectations (40,41,42). Although different
measurement tools were used in the included studies, it may be worth considering the
problems that patients encounter when describing their expectations. This might
influence the content validity of the construct and future research should be focussed
on interpretation of this construct. There is a need for further studies to develop a

40
specific measurement instrument for patients’ expectations. Determination of a sound
definition of the construct might be a first step to develop such an instrument.
In conclusion, unlike earlier systematic reviews, which reported that the recovery
expectations of people with acute low back pain are a prognostic factor for future
absence from usual work in a given period, this review and meta‐ analysis provides a
numerical estimate of the overall effect of the prognostic role of this construct and
offers consistent and conclusive evidence for predicting chronic low back pain, as
reflected in on‐going absence from work beyond 12 weeks after the onset of the pain.
References
1. Van Tulder MW, Becker A, Bekkering T, Breen A, Del Real MT, Hutchinson A. European
guidelines for the management of acute nonspecific low back pain in primary care.
European Spine Journal 2006; 15 (Suppl. 2),S169–S191.
2. Koes BW, van Tulder MW, Thomas S. Diagnosis and treatment of low back pain. British
Medical Journal 2006; 332,1430 –1434.
3. Airaksinen O, Brox JI, Cedrascki C. European Guidelines for the management of chronic
nonspecific low back pain, European Spine Journal 2006; 15 (suppl.2),192–300.
4. Coste J, Lefrancois G, Guillemin F, Pouchot J. Prognosis and quality of life in patients
with acute low back pain: insights from a comprehensive inception cohort study.
Arhtritis & Rheumatism 2004; 51,168–176.
5. Grotle M, Brox JI, Glomsrod B, Lonn JH, Vollestad NK, Vøllestad NK. Prognostic factors
in first‐time care seekers due to acute low back pain. European Journal of Pain 2007;
1,290–298.

41
6. Waddell G (2004) The back pain revolution (2nd edn). Edinburgh: Churchill
Livingstone.
7. Waddell G, Burton AK, Main CJ (2003) Screening to identify people at risk of long‐term
incapacity for work. London: Royal Society of Medicine Press.
8. Burdorf A, Post W, Bruggeling T. Reliability of a questionnaire on sickness absence
with specific attention to absence due to back pain and respiratory complaints.
Occupational and Environmental Medicine 1996; 53,58– 62.
9. Severens JL, Mulder J, Laheij RJF, Verbeek ALM. Precision and accuracy in measuring
absence from work as a basis for calculating productivity costs in The Netherlands.
Social Science & Medicine 2000; 51,243–249.
10.Fredriksson K, Toomingas A, Torgen M, Thorbjornsson CB, Kilbom A. Validity and
reliability of self‐reported retrospectively collected data on sick leave related to
musculoskeletal diseases. Scandinavian Journal of Work, Environment & Health 1998;
24,425–443.
11. Burton AK, Waddell G, Bartys S, Main CJ. Screening to identify people at risk of long‐
term incapacity: a conceptual and scientific review. Disability Medicine 2003; 3,72–83.
12. Iles RA, Davidson M, Taylor NF. Psychosocial predictors of failure to return to work in
non‐chronic non‐ specific low back pain: a systematic review. Occupational and
Environmental Medicine 2008; 65,507–517.
13. Iles RA, Davidson M, Taylor NF, O’Halloran P. Systematic review of the ability of
recovery expectations to predict outcomes in non‐chronic non‐specific low back pain.
Journal of Occupational and Rehabilitation 2009; 19,25–40.

42
14. Schultz IZ, Crook JM, Berkowitz J, Meloche GR, Milner R, Zuberbier OA. Biopsychosocial
multivariate predictive model of occupational low back disability. Spine 2002; 27,2720 –
2725.
15. Schultz IZ, Crook J, Meloche GR, Berkowitz J, Milner R, Zuberbier OA. Psychosocial
factors predictive of occupational low back disability: towards development of a return‐
to‐work model. Pain 2004; 107,77–85.
16. Dionne CE, Bourbonnais R, Frémont P, Rossignol M, Stock SR, Larocque I. A clinical
return‐to‐work rule for patients with back pain. Canadian Medical Association Journal
2005; 172,1559–1567.
17. Heymans MW, de Vet HCW, Knol DL, Bongers PM, Koes BW, van Mechelen W. Workers’
beliefs and expectations affect return to work over 12 months. Journal of Occupational
and Rehabilitation 2006; 16,685– 695.
18. Du Bois M, Szpalski M, Donceel P. Patients at risk for long‐term sick leave because of
low back pain. The Spine Journal 2009; 9,350–359.
19. Reme SE, Hagen EM, Eriksen HR. Expectations, perceptions, and physiotherapy predict
prolonged sick leave in subacute low back pain. BMC Musculoskeletal Disorders 2009;
10,139.
20. Hayden JA, Chou R, Hogg‐Johnson S, Bombardier C. Systematic reviews of low back pain
prognosis had variable methods and results: guidance for future prognosis reviews.
Journal of Clinical Epidemiology 2009; 62,781–796.
21. Agency for Healthcare Research and Quality, US Department of Health & Human
Services. The Peer Review Process. http://www.ahrq.gov/fund/peerrev/peerproc.htm
[Accessed August, 2011]

43
22. Ostelo WJG, de Vet CW. Clinically important outcomes in low back pain. Best Practice
& Research. Clinical Rheumatology 2005; 19,593– 607.
23. Hartvigsen J, Lings S, Leboeuf‐Yde C. Psychosocial factors at work in relation to low
back pain and consequences of low back pain; a systematic, critical review of
prospective cohort studies. Occupational Environmental Medicine 2004; 61,e2.
24. Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta‐analysis detected by a
simple, graphical test. British Medical Journal 1997; 315,629–34.
25. Guyatt G, Rennie D (2002) User’s guides to the medical literature. Chicago: AMA Press.
26. Steenstra IA, Koopman FS, Knol DL, Kat E, Bongers PM, de Vet HCW. Prognostic factors
for duration of sick leave due to low‐back pain in Dutch health care professionals.
Journal of Occupational Rehabilitation 2005; 15,591– 605.
27. Hagen EM, Svensen E, Eriksen HR. Predictors and modifiers of treatment effect
influencing sick leave in sub acute low back pain patients. Spine 2005; 30,2717–2723.
28. Schultz IZ, Crook J, Berkowitz J, Milner R, Meloche GR. Predicting return to work after
low back injury using the psychosocial risk for occupational disability instrument: a
validation study. Journal of Occupational Rehabilitation 2005; 15,365–736.
29. Shaw WS, Pransky G, Patterson W, Winters T. Early disability risk factors for low back
pain assessed at outpatient occupational health clinics. Spine 2005; 30,572–580.
30. Kapoor S, Shaw WS, Pransky G, Patterson W. Initial patient and clinician expectations of
return to work after acute onset of work‐related low back pain. Journal of
Occupational and Environmental Medicine 2006; 48,1173–1118.
31. Lotters F, Burdorf A. Prognostic factors for duration of sickness absence due to
musculoskeletal disorders. Clinical Journal of Pain 2006; 22,212–221.

44
32. Turner JA, Franklin G, Fulton‐Kehoe D, Sheppard L, Whickizer TM, Wu R. Worker
recovery expectations and fear‐avoidance predict work disability in a population‐based
workers’ compensation back pain sample. Spine 2006; 31,682–689.
33. Egger M, Smith GD, Altman DG (2001) Systematic reviews in health care: meta‐analysis in
context,2nd edn. BMJ Books, London, 2001.
34. Lewis S, Clarke M. Forest plots: trying to see the wood and the trees. British Medical
Journal 2001; 322,1479–1480.
35. Lau J, Ioannidis JPA, Terrin N, Schmid CH, Olkin I. The case of the misleading funnel plot.
British Medical Journal 2006; 333,597– 600.
36. Iles RA, Taylor NF, Davidson M, O’Halloran P. Telephone coaching can increase activity
levels for people with non‐ chronic low back pain: a randomised trial. Journal of
Physiotherapy 2011; 57,231–238.
37. Perrot FA, Allaert V, Concas F, Laroche F. ’When will I recover?’ A national survey on
patients’ and physicians’ expectations concerning the recovery time for acute back pain.
European Spine Journal 2009; 18,419–429.
38. Pengel LHM, Herbert RD, Maher CG, Refshauge KM. Acute low back pain: systematic
review of its prognosis. British Medical Journal 2003; 327,323.
39. Linton SJ, Hallden K. Can we screen for problematic back pain? A screening
questionnaire for predicting outcome in acute and sub acute back pain. Clinical Journal
of Pain 1998; 14,209–215.
40. Cedraschi C, Allaz AF. How to identify patients with a poor prognosis in daily clinical
practice. Best Practice & Research. Clinical Rheumatology 2005; 19:577–591.

45
41. Baxter GD, O’Donovan BGG, Doody C, Daly L Hurley DA. Doctors’ attitudes and beliefs
regarding acute low back pain management: a systematic review. Pain 2008; 36,388–
396.
42. Henschke N, Maher CG, Refshauge KM, Herbert RD, Cumming RG, Bleasel J. Prognosis in
patients with recent onset low back pain in Australian primary care: inception cohort
study. British Medical Journal 2008; 337,a171.

46

47
Chapter 3
Measurement of acute nonspecific low back pain
perception in primary care physical therapy: reliability
and validity of the brief illness perception questionnaire
BMC Musculoskeletal Disorders 2013, 14(1), 53
Joannes M Hallegraeff
Cees P van der Schans
Wim P Krijnen
Mathieu HG de Greef

48

49
Abstract
Background: The eight‐item Brief Illness Perception Questionnaire is used as a screening
instrument in physical therapy to assess mental defeat in patients with acute low back
pain, besides patient perception might determine the course and risk for chronic low
back pain. However, the psychometric properties of the Brief Illness Perception
Questionnaire in common musculoskeletal disorders like acute low back pain have not
been adequately studied. Patients’ perceptions vary across different populations and
affect coping styles. Thus, our aim was to determine the internal consistency, test‐retest
reliability, and validity of the Dutch language version of the Brief Illness Perception
Questionnaire in acute non‐specific low back pain patients in primary care physical
therapy.
Methods. A non‐experimental cross‐sectional study with two measurements was
performed. Eighty‐four acute low back pain patients, in multidisciplinary health care
center in Dutch primary care with a sample mean (SD) age of 42 (12) years, participated
in the study. Internal consistency (Cronbach’s α) and test‐retest procedures (Intraclass
Correlation Coefficients and limits of agreement) were evaluated at a one‐week interval.
The concurrent validity of the Brief Illness Perception Questionnaire was examined by
using the mental health component of the Short Form 36 Health Survey.
Results. The Cronbach’s α for internal consistency was 0.73 (95% CI 0.67 to 0.83); and
the Intraclass Correlation Coefficient test‐retest reliability was acceptable: 0.72 (95% CI
0.53 to 0.82), however, the limits of agreement were large. The Intraclass Correlation
Coefficient measuring concurrent validity was 0.65 (95% CI 0.46 to 0.80).
50
Conclusion. The Dutch version of the Brief Illness Perception Questionnaire is an
appropriate instrument for measuring patients’ perceptions in acute low back pain
patients, showing acceptable internal consistency and reliability. Concurrent validity is
adequate, however, the instrument may be unsuitable for detecting changes in low
back pain perception over time.
Background
The natural course of recovery from acute nonspecific low back pain (ANLBP) is
favorable, but recurrence within a year is high and primary care physiotherapy may be
indicated (1,2). Recurrence of ANLBP may be influenced by a patient’s behavior, as the
cognitive and emotional process of pain often translates into complaints (3).
The multidimensional representations of the Common Sense Model (CSM) of self‐
regulation of illness reflect five cognitive dimensions: identity, consequences, cause,
timeline, and cure or control (4,5,6). In the context of ANLBP, these five areas
characterize how low back pain patients view their disorder in terms of its cause, the
condition itself, their expectations about recovery, and how to formulate their coping
behavior (5,7). Although illness perceptions of patients with common musculoskeletal
disorders have not been studied adequately, it is generally recognized that patients’
illness perceptions do vary across different patient populations, and that illness
perceptions can affect coping styles and the nature of subsequent complaints (8,9).
Indeed, psychological constructs, such as a patient’s perception of pain, determine the
course and risk for chronic complaints of nonspecific low back pain (10). Hence, a
patient’s perception of ANLBP should be recognized as a potential risk factor for

51
delayed recovery, one, in addition to the biomedical approach, that is potentially
modifiable (11,12). Indeed, there is evidence that treatment outcomes for chronic low
back, such as return to work, improve after changing patients’ illness perceptions (13).
This observation was corroborated by Hagger et al, who reported a relationship
between perception of illness and mental health at several points in time (7).
These findings demonstrate the importance of assessing patients’ perceptions of their
ANLBP, as their perceptions can influence their treatment and recovery. The Brief Illness
Perception Questionnaire (IPQ‐B) has been used widely in Dutch primary care for
measuring the five cognitive representations of common musculoskeletal disorders,
with the goal of altering patients’ perception towards their ANLBP. Broadbent et al. (14)
derived the eight‐item IPQ‐B from the long 80‐item version of the IPQ (IPQ‐R) (15). The
IPQ‐R is less suitable for use in daily clinical practice due to its length (15). It is
recommended to measure illness perceptions in terms of one psychological construct,
one that can be measured repeatedly in a short period of time. The IPQ‐B is a prime
candidate for this purpose, as it quickly assesses cognitive perceptions of illness, such as
consequences, timeline, personal control, treatment control, identity for describing the
condition, the comprehensibility (coherence) of low back pain symptoms, concern, and
emotions.
The psychometric properties of the IPQ‐B have already been examined in a wide variety
of illnesses and its correlation coefficients have been reported (14). Moreover, the
content validity of the IPQ‐B and how its construct validity was measured in previous
studies have undergone intensive discussion (16,17,18). It is surprising that the

52
psychometric properties of the Dutch version of the IPQ‐B has never been assessed in
ANLBP patients in primary care physiotherapy, given its widespread use in several
musculoskeletal disorders in Dutch primary care physiotherapy and the importance of
behavior in musculoskeletal disorders, in particular in ANLBP patients and their
perception of pain. Therefore, the aim of this study was to assess the internal
consistency, test‐retest reliability, and concurrent validity of the Dutch version of the
IPQ‐B in primary care ANLBP patients.
Methods
Patients and setting
The study sample consisted of 84 patients with ANLBP consecutively recruited from
three different primary care physical therapy providers localized in two medium‐sized
towns and one of them in rural areas in the northern part of the Netherlands. General
practitioners screened all participants. Participants had a mean (SD) age of 42 (12) years;
43% were female.
Inclusion criteria: age 20–60 years, a new episode of acute non‐specific low back (time
since onset < 6 weeks) with or without radiating pain in the leg. Be capable to read and
understand Dutch language.
Exclusion criteria: specific cause of low back pain like nerve root disorders, lumbar spinal
stenosis, spondylolisthesis, after injury, infection, osteoporosis, tumour or rheumatic
diseases such as M. Bechterew.
Before patients were included in the study, we obtained oral and written informed
53
consent and explained to them the study protocol. Patient characteristics (gender, age,
height, weight) and IPQ‐B and SF‐36 responses were obtained in a separate room prior
to each patient’s scheduled standard care service. At this initial contact only anamnesis
and physical examination were carried out after the data was collected. After one‐week
interval and before the second contact moment data of IPQ‐B and SF‐36 responses were
again obtained. Physical therapists were instructed to avoid giving any information what
might influence patients’ perception of low back pain. Intervention was carried out
according to the Dutch guideline for ANLBP patients without controlling participants or
conditions as every patient with ANLBP and as a result ethical approval was not
required. All data were confidential to protect the health status of the participant and
anonymity was guaranteed in electronic database. Ethics approval was not required
because a purely observational, non‐interactive study was carried out without
interference in standard usual care and in accordance with normal practice and
approvals. Research involving tests on cognitive, diagnostic or attitude procedures does
not require ethics approval when data are completely and truly anonymous, participants
can’t be identified, data will not cause any damage and participants consented to the
use of the data. The study was performed in agreement with the directives given in the
Helsinki Declaration as revised in 1975 (19). Data collection was carried out from January
2011 to December 2011.
Design
A non‐experimental, cross‐sectional study design was performed, with two
measurement moments.

54
IPQ‐B
In 2006, Broadbent et al. constructed the briefer IPQ‐B from the longer IPQ‐R (14). They
assessed concurrent validity by examining correlations of items with the same construct
(13,14). The IPQ‐B is an eight‐item instrument that measures on an ordinal scale (0‐10) a
patient’s cognitive perceptions of his or her illness. Eight areas are examined:
consequences (item 1), timeline (item 2), personal control (item 3), treatment control
(item 4), identity for describing the condition and symptoms of low back pain (item 5),
coherence (item 7), and concern and emotions (items 6 and 8). Items 3, 4, and 7 are
reversed items. The maximum score on the IPQ‐B is 80; higher scores reflect more
negative perceptions of low back pain. To make the questionnaire suitable for ANLBP
patients, we adapted the IPQ‐B by replacing ‘illness’ with ‘low back pain’. De Raaij et al.
developed a cross‐cultural adaptation of the IPQ‐B to make this scale applicable in the
Netherlands. No minimal clinical difference or cut‐off point is obtained (20,21).
SF‐36
The SF‐36 health survey is an eight‐scale generic and comprehensive instrument that
measures physical and mental health and can be used in various musculoskeletal and
medical disorders (22). It has been intensively studied and validated for different
musculoskeletal disorders, including low back pain (22,23). Its psychometric quality is
high. The higher the score on the SF‐36, the better the status of health. In this study, we
used the ‘acute form’ of the SF‐36. There is no gold standard measure for the
assessment of concurrent validity of the IPQ‐B. Broadbent et al 2008 stated that use of

55
mental health care is high when illness perceptions are more negative (24). In contrast
with a disease‐specific health survey this generic health survey can be used across ages
with several disorders and treatment groups.
We examined the correlation of the IPQ‐B with the Mental Health Component score
(MCS) of the SF 36 consisting of the domains “mental health”, “role‐emotional”, “social
functioning” and “vitality”. The SF 36 MCS is useful to compare correlations with other
instruments measuring the same construct. Besides, this measure makes it possible to
compare results across different populations such as acute nonspecific low back pain
patients.
Cronbach ‘s alpha coefficient of the MCS summed score is 0.76.
Statistical analyses
We used SPSS 19.0. For normally distributed data, patient characteristics and descriptive
statistics were presented as means and standard deviations. Internal consistency was
assessed using Cronbach’s analysis and confidence interval (95%). We assessed the test‐
retest reliability of the IPQ‐B after a one‐week interval to measure the same entities at
two different time points and calculated intraclass correlation coefficients (ICCs) and
confidence interval (95%). An ICC value above 0.75 is indicative of good reliability,
whereas values below 0.75 are indicative of moderate reliability (23).
Pearson’s correlation coefficient was used to assess concurrent validity with the MCS of
the SF‐36.

56
We used a Bland Altman plot to show the Limits Of Agreement (LOA) between two
measurements on a ratio scale: the mean values of the test and retest assessments and
mean difference between the two assessments, considering 95% of the results vary
between the mean difference. LOAs are indicators of agreement and the plot is for
visual judgment reflecting the relationship between the mean and the difference of the
two measurements. LOA can be considered to be an assessment of measurement error.
The time interval of the test‐retest measurements is a random effect in the model.
Results
Patients’ characteristics
Twenty‐one subjects were excluded from this study due to either lost to follow‐up or
chronic lower back complaints due to nerve root disorders, rheumatic diseases, or other
specific causes. A total of 84 patients participated in this study and completed the first
assessment successfully. The data were normally distributed, as determined using the
Kolmogorov‐Smirnov test (P > 0.05), and showed no floor or ceiling effects (< 15% or >
15% of the highest or lowest score). Table 1 shows the patients’ characteristics.

57
Table 1. Patient Characteristics
Total number of
patients
84
Age (years), mean 42 (12)
Female, n (%) 36 (43%)
Relapsea – yes 28
Sportsb – yes 40
Educationc
Low 10
Intermediate 45
High 29
Height (cm), mean 178 (9)
Weight (kg), mean 81 (15)
BMI (kg/m2), mean 25 (4)
Pain (mm), mean (SD) 57 (20)
a Last previous episode was <6 months. b Organised sports. c Low = Primary school; intermediate = secondary education; high = higher
education
Internal consistency
The inter‐item consistency of the IPQ‐B was 0.73 (Cronbach’s α; 95% CI 0.67 to 0.83).
Table 2 shows internal reliability of the IPQ‐B.

58
Table 2. Items of the IPQ‐B and internal reliability
Items of the IPQ‐B
Scale means if item
deleted
Cronbach’s if item deleted
Consequences 46 0.65
Timeline 45 0.72
Personal control 46 0.68
Treatment control 44 0.73
Identity 47 0.69
Concern 45 0.66
Coherence 45 0.70
Emotional response 45 0.63
Test‐retest reliability
There was a significant difference between the first assessment and second assessment
(t=‐3.5 [P < 0.05]). This reduces the reliability of the IPQ‐B, with a mean difference of 4.1
(95% CI ‐6.4 to ‐1.7). Test‐retest over a one‐week period showed an adequate correlation,
measured by an ICC of 0.72 (95% CI 0.53 to 0.82) two‐way random effects model,
absolute agreement.

F
p
d
b
p
Th
sh
re
m
w
Figu
pat
diff
bet
pre
he
how
epe
mea
was
ure
ien
fere
twe
sen
95
wn
eate
sur
1.17
e 1.
nts
enc
een
nte
% u
in
ed
rem
7, a
. B
pa
ce b
n te
ed a
upp
th
me
men
and
lan
arti
bet
est
as f
per
e B
eas
nts
d th
nd A
icip
twe
an
flan
r an
Bla
sure
. N
he
Alt
pate
een
nd r
nkin
nd
nd
em
o s
sm
tma
ed
n te
ret
ng
low
Al
men
syst
malle
an
in
est
test
line
wer
tm
ts
tem
est
plo
th
t an
t sc
es.
r L
man
for
mat
t de
ot f
he
nd
cor
OA
pl
r ea
tic
ete
for
te
ret
res,
A w
ot,
ach
tre
ecta
r th
st‐r
test
, w
was
, se
h su
end
able
he
ret
t. T
whic
21
ee
ubj
d w
e c
tes
test
The
ch
.2 (
Fig
ect
was
han
5
st‐r
t a
e ce
wa
(‐ 4
gur
t is
vis
nge
59
rete
asse
ent
as ‐
4.1
e 1
s in
sibl
e (S
est
ess
tral
‐ 4.
± 2
. T
de
e. T
SD
t re
sme
l lin
.1, a
21.2
This
pen
The
C)
elia
ent
ne
and
2) L
s in
nde
e st
wa
bili
t. T
rep
d t
LOA
ndic
ent
tan
as 4
ity
The
pre
he
A r
cat
t of
nda
42.
of
e d
esen
95
ran
es
f th
ard
Th
f th
dott
ntin
5% l
ge
th
he
er
us,
he
ted
ng
lim
d f
at
me
ror
, a
IPQ
d li
th
its
from
the
ean
r of
cha
Q‐B
ine
e m
of
m
e v
n o
f th
ang
B. A
re
mea
f ag
‐25
vari
f th
he m
ge
A t
epr
an
gre
.3
an
he
me
in t
ota
rese
dif
em
to
ce
rep
ean
the
al o
ent
ffer
men
17.
of
pea
(S
e IP
of
ts
ren
nt a
.1 a
th
ate
EM
PQ‐
84
no
nce
are
as
he
ed
M)
‐B

60
score must exceed a value of 42 in order to reflect a true difference between test and
retest scores.
Concurrent validity
When compared with the mental health component scale (MCS) of the SF‐36,
concurrent validity of the IPQ‐B had an ICC of 0.65 (95% CI 0.46 to 0.80). The Pearson’s
correlation coefficient was r p = 0.51, (P < 0.01), indicating adequate validity between the
two instruments. Correlation coefficients of the four separate scales of the Mental
Health component of the SF‐36 with the IPQ‐B showed: Vitality: r p = 0.54**; Social
Functioning r p = 0.45**; Role Emotional r p = 0.43
**; Mental Health r p = 0.59**.
**Correlation is significant at the 0.01 level (two‐tailed).
Table 3. Pearson’s correlations between IPQ‐B items and the mental health component
of the SF‐36
Mental Health Component SF‐36
IPQ‐B 0.51**
Consequences 0.49**
Timeline 0.15
Personal control 0.35**
Treatment control 0.28*
Identity 0.23
Concern 0.48**
Coherence 0.28*
Emotional response 0.53**
*Correlation is significant at the 0.05 level (two‐tailed). **Correlation is significant at the 0.01 level (two‐tailed).

61
Discussion
This is the first study to evaluate the Dutch version of the IPQ‐B in ANLBP patients. The
internal reliability, test‐retest reliability, and concurrent validity indicate that the Dutch
IPQ‐B is of moderate psychometric quality. Even though the IPQ‐B measures a
psychological construct by means of a multidimensional scale with a few items, we
found its internal consistency of 0.73 to be adequate (25). None of the items will affect
the overall reliability if they were deleted. Kline, as well as other authors, agree that an
internal consistency of ≥ 0.60 indicates sufficient reliability for psychological constructs
(26). According Terwee et al., an acceptable test‐retest reliability must exceed an ICC
value of >0.70 (27). Although the lower limits of the 95% CI in the present study was less
than 0.60, the ICC was an acceptable 0.72 (95% CI 0.53 to 0.82). For concurrent validity,
no gold standard is available for assessing patients’ perception of acute low back pain.
Therefore, we used the criteria of Nunnally et al. to determine that in our study the
concurrent validity of the IPQ‐B with the MCS of the SF‐36 to be adequate (28).
In contrast to the ICC values, which demonstrated adequate test‐retest reliability, the
LOAs in the Bland Altman plot were large. The large LOAs might have been due to fewer
low back complaints over time resulting from intervention‐related changes in the
patients’ perception of their back pain. Participants reported more positive perceptions
on the IPQ‐B retest than test (t – 3.5, P < 0.05). Therefore, it was preferable to shorten
the test‐retest interval time in the study. Most ANLBP decreases within the first weeks
after onset, and as a result, negative perceptions concerning ANLBP also decrease (1).

62
To mitigate this phenomenon as much as possible, we instructed the examiners in the
primary care units that had contact with the patients to avoid giving patients any
information about the course of ANLBP that could influence their perception of pain. As
a consequence of the positive natural course of ANLBP recovery, patients’ perception
might also have been influenced, especially during the acute stage.
However, the maximum score of the IPQ‐B is 80. In the present study, the SDC was 42,
which means that a change in IPQ‐B score must exceed a value of 42 in order to reflect a
true difference between test and retest scores; random error also explains the decrease
of IPQ‐B score. An SDC value of 42 also indicates that there is low agreement between
the two scores, and thus moderate longitudinal responsiveness to real changed
perception of complaints. We conclude, therefore, that the instrument is not suitable
for detecting real individual changes.
For concurrent validity, Terwee et al. proposed a correlation value of ≥ 0.50 to be
acceptable (27). In our study, the Pearson’s correlation coefficient was 0.51 and the ICC
value for the IPQ‐B and the mental health subscale of the SF‐36 was 0.65 (95% CI 0.46 to
0.80). However, since the items of the IPQ‐B are derived from earlier versions of the
IPQ, the content validity of the scale might have been influenced during this derivation
process. The IPQ‐B was developed by ‘forming one question that best summarized the
items contained in each subscale of the IPQ‐R’ (13). Indeed, more recent findings
indicate that people do have difficulties understanding the items of the IPQ‐B, with
some even misinterpreting them (15). This could influence the content validity of the
instrument, leading to the question: ‘Is the scale really measuring the same construct
63
(15)?’ Nonetheless, in the present study, we did find the internal consistency of the scale
to be adequate in ANLBP patients.
The results of our study are consistent with those reporting on the psychometric
properties of the IPQ‐B for several diseases. However, our findings differ from those of
Broadbent et al., who also used the mental health component of the SF‐36 to determine
concurrent validity in myocardial patients (13). They found negative associations for four
items of the IPQ‐B when compared to the mental health subscale. A possible
explanation for this disparity is that psychological state has a greater impact on ANLBP
patients than on patients with a specific medical condition such as myocardial infarction.
Small sample size was a major limitation of the study; results must be interpreted with
caution. Another limitation was the relatively long test‐retest period, so patients could
have been influenced by the favourable natural course and a positive change in pain and
activities might have occurred. These developments changed the perception of low
back pain that might have negatively biased the test‐retest reliability results. One
problem inherent of this kind is to minimize treatment influence; hence, all data was
collected just before the two interventions. However, an explanation of the changed
IPQ‐B score might be that internal and/or external influences between both
administrations have affected patients’ perception of low back pain.
Main and George emphasized the importance of measuring a patient’s perception as
part of a more psychologically informed physical therapy practice (11). The goal of doing
so is to identify and alter the patient’s perception of musculoskeletal pain and response

64
to pain in his or her daily coping behavior, as a patient’s cognition of his or her pain and
disability might be essential for decreasing musculoskeletal disorders and for a more
rapid recovery (11). Therefore, we emphasize the need for measuring patient pain
perception for several musculoskeletal disorders. At the same time, we need to
acknowledge the complexity of this multilevel representation and the problems
patients might have interpreting the items of instruments measuring this psychological
construct. In this regard, we support the use of the IPQ‐B in primary care physical
therapy management, as it is a useful instrument to assess patients’ initial perceptions
of their disorder. Such assessments should address more negative perceptions of
patients’ back pain, with the aim of decreasing the risk of more chronic low back pain
problems.
Conclusions
On the basis of the data from this study, we conclude that the IPQ‐B is a suitable
instrument for measuring patients’ perception in acute nonspecific low back pain
patients however this measure needs further examination with another criterion
measure and with a larger patient population. The instrument may be unsuitable for
detecting changes in low back pain perception over time.
References
1. Pengel LH, Herbert RD, Maher CG, Refshauge KM: Acute low back pain: systematic
review of its prognosis. British Medical Journal 2003; 327(7410),323.

65
2. Kent PM, Keating JL: Can we predict poor recovery from recent‐onset nonspecific low
back pain? A systematic review. Manual Therapy 2007; 13,12‐28.
3. Weinman J, Petrie KJ: Illness perceptions: a new paradigm for psychosomatics? Journal
of Psychosomatic Research 1997; 42,113‐116.
4. Leventhal H, Meyer D, Nerenz D: The common sense model of illness danger. In:
Rachman S. ed. Contributions to Medical Psychology. Pergamon, New York, 1980. 17‐30.
5. Leventhal H, Nerenz DR, Steele, DJ. Illness representation and coping with health
threats. In A. Baum, S. E. Taylor, J. E. Singer (Eds.). Handbook of Psychology and Health.
Hillsdale, NJ: Lawrence Erlbaum Associates, 1984, 219‐252.
6. Leventhal H, Brisette I, Leventhal EA. The common‐sense‐model in health and illness.
The self‐regulation of health and illness behavior. Routledge, London, 2003, 42‐65.
7. Hagger MS, Orbell S: A meta‐analytic review of the common‐sense model of illness
representations. Psychology and Health 2003;18,141–184.
8. Petrie KJ, Cameron LD, Ellis, CJ Buick, D Weinman, J: Changing illness perceptions after
myocardial infarction: an early intervention randomized controlled trial. Psychosomatic
Medicine 2002; 64,580‐586.
9. Petrie, KJ, Broadbent E: Assessing illness behavior: what condition is my condition in?
Journal of Psychosomatic Research 2003; 54,415‐6.
10. Waddell G, Main CJ, Morris EW, Di Paola M, and Gray IC: Chronic low back pain,
psychological distress and illness behavior. Spine 1984; 9,209 ‐213.
11. Main, CJ, George, SZ: Psychologically informed practice for management of low back
pain: future directions in practice and research. Physical Therapy 2011; 91,820‐824.
12. Siemonsma PC, CD Schröder, CD, Roorda LD, AT Lettinga: Benefits of treatment theory
in the design of explanatory trials: cognitive treatment of illness perceptions in chronic

66
low back pain rehabilitation as an illustrative example. Journal of Rehabilitation
Medicine 2010; 42,111–116.
13. Reme SE, Hagen EM, Eriksen HR: Expectations, perceptions, and physiotherapy predict
prolonged sick leave in subacute low back pain. BMC Musculoskeletal Disorders 2009;
13,10 ‐139.
14. Broadbent E, Petrie KJ, Main J, Weinman J: The brief illness perception questionnaire.
Journal of Psychosomatic Research 2006, 60,631‐637.
15. Moss‐Morris R, Weinman, J, Petrie KJ, Horne R, Cameron LD, Buick D: The Revised
Illness Perception Questionnaire (IPQ‐R). Psychology and Health, 2003,17,1–16.
16. van Oort L, Schroder CI, French DP: What do people think about when they answer the
Brief Illness Perception Questionnaire? A 'think‐aloud' study. British Journal of Health
Psychology 2011; 16,231‐45.
17. French, DP, Cooke R, McLean N, Williams M, Sutton S: What do people think about
when they answer Theory of Planned Behavior Questionnaires? A ‘think aloud’ study.
British Journal of Health Psychology 2007; 12,672–687.
18. Broadbent E, Kaptein AA, Petrie, KJ: Double Dutch: The ‘think aloud’ Brief IPQ study
uses a Dutch translation with confusing wording and the wrong instructions. British
Journal of Health Psychology 2011; 16,246–249.
19. Goodyear MDE, Krleza‐Jeric K: The Declaration of Helsinki. British Medical Journal 2007;
335,624–625.
20. de Raaij, EJ, Schroder C, Maissan FJ, Pool JJ, Wittink H: Cross‐cultural adaptation and
measurement properties of the Brief Illness Perception Questionnaire‐Dutch Language
Version. Manual Therapy 2012; 17(4),330‐5.

67
21. de Raaij EJ, Schroder C, Kaptein AA: Ziekteperceptie vragenlijst IPQ‐K. Retrieved from
http://www.ziekteperceptie.nl/, 2007.
22. Ware JE, Snow KK, Kosinski M, Gandek B. SF‐36 health survey: manual and
interpretation guide. Boston: The Health Institute, 1993.
23. Raheleh Khorsan, MA, Coulter, ID, Cheryl Hawk, DC, Choate, CG. Measures in
chiropractic research: choosing patient‐based outcome assessments. Journal of
Manipulative and Physiological Therapeutics 2008; 31,355–375.
24. Broadbent E, Kydd R, Sanders D, VanderPyl J: Unmet needs and treatment seeking in
high users of mental health services: role of illness perceptions. Australian & New
Zealand Journal of Psychiatry 2008; 42(2),147‐53.
25. Gross Portney L, Watkins MP: Foundations of Clinical Research, applications to practice.
2nd edition, New Jersey: Prentice Hall Health, 2000.
26. Kline P: Handbook of psychological testing (2nd ed.). London: Routledge 2000.
27. Terwee CB, Bot SD, de Boer MR, van der Windt DA, Knol DL, Dekker J, Bouter LM, de Vet
HC: Quality criteria were proposed for measurement properties of health status
questionnaires. Journal of Clinical Epidemiology 2007; 60 (1),34‐42.
28. Nunnally JC. Psychometric theory (2nd ed.). New York: McGraw‐Hill, 1978.
68

69
Chapter 4
A note of caution with respect to the Low Back Pain
Perception Scale in primary care physiotherapy
Submitted
Joannes M Hallegraeff
Cees P van der Schans
Wim P Krijnen
Mathieu HG de Greef

70

71
Abstract
Background. The Low Back Pain Perception Scale is a 5‐item questionnaire and is used
as a first screening instrument to assess mental defeat in acute low back pain patients
to predict the risk of more chronic complaints. The predictive validity is determined in
two studies in general practice and showed sufficient discriminative ability, although the
psychometric properties of the scale have never been established until now. The aim of
the study is to determine the reliability and validity in acute nonspecific low back pain of
the Dutch language version of the Low Back Pain Perception Scale in physiotherapy
primary care.
Methods. The Low Back Pain Perception Scale has been authorized translated into
Dutch by two bilingual content experts. A back translation procedure into English was
executed to assess its equivalency. A sample of 84 acute low back pain patients in
physiotherapy primary care, mean age (SD) age 42 (12) years participated in this study.
Internal reliability and a test‐retest procedure within one‐week interval were evaluated.
The concurrent validity was examined by using the Brief Illness Perception
Questionnaire (IPQ‐B).
Results. The internal consistency Cronbach α = 0.38 (95% CI 0.09 to 0.56) and test–retest
reliability within one week IntraClassCorrelation coefficient = 0.50 (95% CI 0.31 to 0.64).
Minimal Detectable Change was measured 1.95. The concurrent validity demonstrates
Pearson’s r p = 0.35 (95% CI 0.14 to 0.53).
Conclusion. The Low Back Pain Perception Scale demonstrates poor internal
consistency and reliability. Concurrent validity is moderate. Extreme high or low scores

72
may be clinical relevant and can be used as a first screening instrument in acute
nonspecific low back pain patients.
Key points: perception, reliability, validity, acute low back pain, and prognosis.
Introduction
The role of illness perception in musculoskeletal disorders, which is specified in the
Common Sense Model of self‐regulation of illness (CSM), represents a number of
cognitive properties like identity, consequences, cause, timeline, cure or control and
next to other prognostic factors influence the course of nonspecific low back pain
(1,2,3). These representations are patients’ beliefs concerning cause, condition and
expectations about recovery and the possibility to underpin coping behaviour of low
back pain patients (4,5). Although, the natural course of acute nonspecific low back pain
(ANSLBP) is favourable, however, probability of recurrence within a year is high. The
latter may be influenced by patients’ perceptions of complaints (6,7). There is evidence
that the course of acute nonspecific low back pain can be improved by a change of
patients’ illness perception (8,9).
Generic scales measuring patients’ illness perception are available, however, these are
not directed towards a musculoskeletal disorder like acute nonspecific low back pain.
Miller et al (1994) developed a specific instrument, the Low Back Pain Perception Scale
(LBPPS) to assess patients’ perception of acute nonspecific low back pain, which can be
used to predict the risk of chronic complaints (10). Reis et al., 2007, determined the
predictive validity of the LBPPS evaluating the subjective interpretation of the general
practitioner (GP) measured by pain intensity, pain duration and functional status during

73
4 months follow‐up (11). Jellema et al. 2007, also determined the predictive validity of
the LBPPS in acute low back pain patients as a prognostic factor for chronic complaints
(12). Due to the simplicity of administration of the LBPPS it may also be suitable in
primary care physiotherapy.
Therefore, the aim of this study is to examine internal consistency, test‐retest reliability
and concurrent validity of the Dutch version of the LBPPS in acute nonspecific low back
pain patients in primary care physiotherapy.
Methods
Patients and setting
Inclusion criteria: age 20–60 years, a new episode of acute non‐specific low back (time
since onset < 6 weeks) with or without radiating pain in the leg and being capable to
read and understand in the Dutch language.
Exclusion criteria: specific cause of low back pain like nerve root disorders, lumbar spinal
stenosis, spondylolisthesis, after injury, infection, osteoporosis, tumour or rheumatic
diseases such as M. Bechterew.
The study sample consists of Dutch patients with acute nonspecific low back pain,
consecutively recruited by physiotherapists. After a written informed consent was
signed and verbally confirmed, patients filled in the demographic characteristics and the
procedure of the study was explained. Measurements of the LBPPS and the IPQ‐B are

74
obtained prior to the usual standard physiotherapy care service. All participants were
screened by general practitioners and referred to physiotherapists in two
multidisciplinary health care centres in the northern part of the Netherlands. At this
initial contact only history and physical examination were carried out after the data was
collected. Physiotherapists were instructed to avoid giving any information what might
influence patients’ perception of low back pain. All data were treated as confidential in
order to protect the privacy and anonymity. Participants can’t be identified, data will
not cause any damage and participants consented to the scientific use of the data. The
current purely observational, non‐interactive study was carried out without interference
in standard usual care or interfering with normal practice and approvals. The study was
performed in agreement with the directives given in the Helsinki Declaration as revised
in 1975 (14).
Scale
LBPPS components:
1. What are your expectations for recovery? (Expectations, hope)
2. Do you feel limited in your activities? (Activities, behavioural)
3. Are you worried about your low back pain? (Worrying, affective)
4. Did you find a way to deal with your low back pain? (Coping, behavioural)
5. Does your low back pain influence the most important elements of daily life? (Meaning
of pain)

75
Cross‐cultural adaptation and translation
To maintain content validity of health status self‐reported questionnaires when used in
another country or culture, the items need to be translated in a cross‐culturally adapted
way. The original authors of the LBPPS gave permission for authorised translation and
re‐validation of the LBPPS. Cross‐cultural adaptation and the authorised translation
procedure were carried out according Beaton’s guideline (15). Two bilingual translators
who achieved consensus and synthesis of the two translations performed forward
translation English into Dutch. Another two bilingual English native speakers living in
The Netherlands for 23 years performed the back translation procedure, Dutch into
English unaware of the English version; these translations were merged into one
version. This version is compared with the original English version and as a consequence
two bilingual physiotherapists obtained the translated version and reached consensus
concerning this final version of the LBBPS.
Reliability
The LBPPS, introduced by Reis et al, 2005, is used as a self‐reported, self‐administered
two point Likert scale with 5 items to express patients perceived perception towards
low back pain (total score range 5 – 10): a high score reflects high risk for not recovery
(11). A cut off point of ≥ 2 and ≥ 4 is determined (12). Assessment of test‐retest of the
LBBPS is carried out with one‐week interval to measure the same constructs at two
different points in time. Administration was executed prior to intervention.

76
Concurrent validity
The brief IPQ (IPQ‐B) is derived from the IPQ‐R by Broadbent et al, 2006, to assess
concurrent validity by examining correlations of items with the same construct (13,16).
This ordinal (0‐10) eight item instrument measures the cognitive patients’ perceptions
concerning illness like consequences (item 1), timeline (item 2), personal control (item
3), treatment control (item 4), identity for describing the condition and the symptoms
of low back pain (item 5), illness comprehensibility (item 7), concern and emotions (item
6 and 8). The Brief IPQ is a reliable and validated instrument, a three‐week test‐retest
interval show a Pearson’s r = 0.62 in a sample of renal patients, and the associations
between the cognitive perception scales in the Brief IPQ and the IPQ‐R show
appropriate correlations with the perception of personal control and treatment control
(16). De Raaij et al, 2012, applied a cross‐cultural adaptation of the Brief IPQ to make this
scale applicable in the Netherlands. No minimal clinical difference or cut off point is
obtained (17).
Statistical analyses
Statistical analyses were performed using SPSS 19.0. For internal consistency
Chronbach’s alpha was calculated. The Intraclass Correlation Coefficient (ICC) and its
confidence intervals (95%) were performed to evaluate test‐retest reliability. An ICC
value above 0.70 indicates acceptable reliability; those below 0.7 are moderate (18).
Pearson’s correlation coefficient is used to assess concurrent validity with the Brief IPQ.
A Bland Altman plot represents the limits of agreement between two measurements on
a ratio scale: mean values of two assessments and mean difference of the two
assessments considering 95% of the results vary between the mean difference.

77
Results
Patients’ characteristics
105 Participants were recruited. Excluded were 21 participants because of chronic
complaints, like nerve root disorders, rheumatic diseases or other specific causes. The
obtained sample consists of 84 acute nonspecific low back pain patients with a mean
(SD) age of 42 (11) years and complaints less than six weeks.
Individual patient data are listed in Table 1.

78
Table 1 Patients characteristics
Total number of
patients 84
Age (years), mean 42 (12)
Female, n (%) 36 (43%)
Relapsea – yes 28
Sportsb – yes 40
Educationc
Low 10
Intermediate 45
High 29
Height (cm), mean 178 (9)
Weight (kg), mean 81 (15)
BMI (kg/m2), mean 25 (4)
Pain (millimeter), 57 (20)
a Last previous episode was < 6 months.
b Organised sports.
c Low = Primary school; intermediate = secondary education; high = higher
education.

79
Internal consistency
The inter‐item consistency of the LBPPS is Cronbach’s alpha 0.38 (95% CI 0.09 to 0.56).
Except one (expectation), all individual items show a Cronbach’s alpha less than the
overall value if they were deleted, see Table 2.
Table 2. Items of the LBPPS and internal reliability
Items of the LBPPS Cronbach’s �
if item deleted
Expectations 0.51
Feels limited 0.31
Worrying 0.32
Coping 0.23
Meaning of pain 0.20
Test‐retest Reliability
Mean score at the first assessment of the LBPPS is 7.29 (1.25) and at the second
assessment mean score 6.83 (1.28). The mean difference of 0.37 (1.16) tested by the
paired t‐test is significant (t=2.86, df=81, P=0.005). There was one participant with
missing values at the first administration and another participant at the second.
The Bland Altman plot resulted in Limits of Agreement between ‐1.90 and 2.64, see
Figure 1. The coefficient from regression of the difference on the mean 0.24 (SE=0.13,
P=0.054) is not significantly different from zero. The distribution is homogenous, no
clear outliers are detectable and no systematic trend is visible.

Th
M
1.9
Co
A
IP
D
In
ba
fa
he
Mini
95.
onc
Pe
PQ‐
Dis
n th
ack
act
tw
ma
cur
ears
B, P
scu
his
k pa
tha
o‐w
al D
rren
son
Pea
us
stu
ain
at t
way
Det
nt v
n’s
ars
sio
udy
pa
the
y co
ect
val
co
ons
on
y w
atie
co
ons
tab
idit
rre
s r
n
e f
ent
ons
sist
ble
ty
elat
= 0
fou
ts. T
tru
ten
Ch
tion
0.35
nd
Thi
uct
ncy
ang
n co
5 (9
po
is m
is p
ICC
ge
oef
95%
oor
may
psy
C f
wa
ffic
% CI
r int
y b
ycho
or
as m
ien
0.
ter
be a
olo
sin
me
nt w
14 t
rna
attr
ogic
ngle
easu
was
to
l co
ribu
cal,
e m
ure
s u
0.5
ons
ute
, an
8
mea
ed (
sed
53)
sist
ed t
nd t
80
asu
(St
d to
sho
ten
to
the
res
and
o a
ow
cy
the
e lo
s eq
dar
ana
ws m
of
e m
ow n
qua
rd
lys
mod
th
mul
num
als
Err
e t
der
e L
tid
mb
0.5
ror
he
rate
LBP
ime
ber
50 (
Me
co
e v
PPS
ens
of
(95
eas
onc
valid
S in
sion
ite
5% C
sur
urr
dity
ac
nal
ems
CI 0
em
ren
y.
cute
ity
s (1
0.3
men
nt v
e n
of
9).
1 to
nt x
valid
non
f th
o 0
x √2
dty
nspe
he s
0.64
2 x
y w
eci
sca
4).
1.9
with
fic
ale,
Th
6)
th
low
th
he
=
he
w
he
81
The test‐retest reliability ICC is 0.50 (95% CI 0.32 to 0.64) and is considered moderate.
However, a test‐retest reliability of more than 0.70 is acceptable in basic research
according to Nunnally et al 1978 (18). The threshold of an ICC > 0.70 is preferable,
although such a threshold must be taken with caution and should be viewed from the
context of the study and the psychological construct being measured (20). The analysed
concurrent validity compared with the IPQ‐B revealed to be moderate.
Systematic difference within one week is significant but small from clinical perspective.
The minimal detectable change of 1.95 indicates that large differences on the scale are
clinically relevant in the sense of smaller risk for recurrence or chronic complaints. It is
crucial that physiotherapists use reliable instruments to identify perception of acute
nonspecific low back pain patients and teach patients to cope with negative beliefs.
The high correlation of the item describing “patients expectations for recovery” in the
LBPPS and the brief IPQ is remarkable. It is possible that patient understood the
implications of this item well and that it strongly appealed. In recent literature “patient
expectations for recovery” has proved to be a strong predictor for chronic complaints in
musculoskeletal disorders and in particular in acute nonspecific low back pain (21,22).
A limitation of the study was the relatively long time between test and retest so
patients could have been influenced by the favourable natural course of acute
nonspecific low back pain. Although the physiotherapists were instructed to avoid
giving any information what might affect patients’ perception of pain in a subjective
way this remains uncertain. A changed perception of pain within one week may have
82
negatively influenced the test‐retest reliability results. The Hawthorne effect may have
been present: a change to a positive result and a more positive perception of pain due
to participation in the study.
This study suggests that this short, five‐item scale must be used with caution, large
differences seem to be clinically relevant whereas small differences should not be over
interpreted. In this sense, in primary care physiotherapy, the LBPPS can be a useful first
screening instrument, which can be quickly administrated.
Conclusion
We conclude the LBPPS for use in primary care physiotherapy shows poor internal
consistency and reliability and moderate concurrent validity. Extreme high or low scores
on the LBPPS may be clinical relevant. Further research on the items of the LBPPS is
necessary to increase reliability and validity.
References
1. Pengel LH, Herbert RD, Maher CG, Refshauge, KM. Acute low back pain: systematic
review of its prognosis. British Medical Journal 2003; 327(7410),323.
2. Kent PM, Keating JL. Can we predict poor recovery from recent‐onset nonspecific low
back pain? A systematic review. Manual Therapy 2007; 13(1),12‐28.
3. Weinman J, & Petrie KJ. Illness perceptions: a new paradigm for psychosomatics?
Journal of Psychosomatic Research 1997; 42(2),113‐116.

83
4. Leventhal H, Meyer D, Nerenz D: The common sense model of illness danger. In:
Rachman S. ed. Contributions to Medical Psychology. Pergamon, New York, 1980. 17‐30.
5. Leventhal H, Nerenz DR, Steele, DJ. Illness representation and coping with health
threats. In A. Baum, S. E. Taylor, J. E. Singer (Eds.). Handbook of Psychology and Health.
Hillsdale, NJ: Lawrence Erlbaum Associates, 1984, 219‐252.
6. Leventhal H, Brisette I, Leventhal EA. The common‐sense‐model in health and illness.
The self‐regulation of health and illness behavior, Routledge, London, 2003, 42‐65.
7. Waddell G, Main, CJ, Morris EW, Di Paola M, Gray IC. Chronic low back pain,
psychological distress and illness behavior. Spine 1984; 9(2),209 ‐13.
8. Hagger MS, & Orbell S. A meta‐analytic review of the common‐sense model of illness
representations. Psychology and Health 2003; 18,141–184.
9. Petrie KJ, Cameron, LD, Ellis CJ, Buick D, Weinman J. Changing illness perceptions after
myocardial infarction: an early intervention randomized controlled trial. Psychosomatic
Medicine 2002; 64(4),580‐6.
10. Miller Miller WL, Yanoshik MK, Crabtree BF, Reymond WK. Patients, family physicians,
and pain: visions from interview narratives. Family Medicine1994; 26,179–84.
11. Reis S, Borkan J, Vanraalte R, Tamir, A, Dahan, R, Hermoni, D. The LBP patient
perception scale: a new predictor of LBP episode outcomes among primary care
patients. Patient Education and Counseling 2005; 67,1‐2,191‐5.
12. Jellema P, van der Windt DAWM, van der Horst HE, Stalman WAB, & Bouter LM.
Prediction of an unfavourable course of low back pain in general practice: comparison
of four instruments. British Journal of General Practice 2007; 57,15–22.
13. Broadbent E, Petrie KJ, Main J, & Weinman J. The brief illness perception questionnaire.
Journal of Psychosomatic Research 2006; 60,6:631‐7.

84
14. Goodyear MDE, Krleza‐Jeric K. The Declaration of Helsinki. British Medical Journal. 2007;
335,624–625.
15. Beaton, DE, Bombardier, C, Guillemin, F, & Ferraz, MB. Guidelines for the process of
cross‐cultural adaptation of self‐report measures. Spine 2000; 25,3186‐91.
16. Moss‐Morris R, Weinman J, Petrie KJ, Horne R, Cameron LD, & Buick D. The Revised
Illness Perception Questionnaire (IPQ‐R). Psychology & Health 2003; 17,1–16.
17. de Raaij, EJ, Schroder C, Maissan FJ, Pool JJ, Wittink H. Cross‐cultural adaptation and
measurement properties of the Brief Illness Perception Questionnaire‐Dutch Language
Version. Manual Therapy 2012; 17(4),330‐5.
18. Nunnally J C. Psychometric theory (2nd ed.), New York: McGraw‐Hill, 1978.
19. Kline P, The handbook of psychological testing (2nd edition). London: Routledge, 1999.
20. Gross Portney L, Watkins MP. Foundations of Clinical Research, applications to practice.
2nd ed., New Jersey: Prentice Hall Health; 2000.
21. Koes BW, van Tulder MW, &Thomas MS. Diagnosis and treatment of low back pain.
British Medical Journal 2006; 332,1430–4.
22. Pincus T, Vlaeyen JW, Kendall NA, Von Korff MR, Kalauokalani DA, & Reis S. Cognitive‐
behavioral therapy and psychosocial factors in low back pain: directions for the future.
Spine 2002; 27(5),133‐8.

85
Chapter 5
Manipulative therapy and clinical prediction criteria in
treatment of acute nonspecific low back pain
Perceptual and Motor skills, 2009, 108, 196‐208
Joannes M Hallegraeff
Mathieu HG de Greef
Jan C Winters
Cees P Lucas

86

87
Abstract
This study examines whether Manipulative therapy as part of a multidimensional
approach may be more effective than standard physical therapy in treating Acute Non
Specific Low Back Pain. Participants. 64 participants, 29 women and 35 men, with Acute
Nonspecific Low Back Pain and a mean age (sd) of 40 (9.6) were randomly assigned to
two groups: an experimental group (manipulative therapy plus physical therapy) and a
control group (only physical therapy). A multicentre, nonblinded randomised clinical
trial was conducted. Pain relief was the main performance criteria measured together
with secondary criteria, which included functional status and mobility of the lower back.
Fritz, Childs and Flynn’s clinical prediction rule ‐‐ a duration of symptoms less than 16
days, no pain distal of the knee ‐‐ was used to analyse the results. In combination with
an age > 35 years, results showed a statistical significant effect for disability, but no
statistically significant benefit of additional manipulative therapy over physical therapy
found for pain and mobility within 4 treatments. Controlled for the applied clinical
prediction rule, there were statistically significant interaction effects with low effect
size for disability and sex, but no significant effects were found for pain of mobility.
Introduction
The term „low back pain� refers to „nonspecific low back pain�, which is defined as low
back pain that does not have a specified physical cause, such as nerve root compression
(radicular syndrome), trauma, rheumatic disorders, infection or the presence of a
tumor. Pain is constantly present or comes in episodes. Croft et al 1998 determined that
of those participants with low back pain interviewed at 3 and 12 months follow‐up, only

88
21 % and 25%, respective1y, had completely recovered in terms of pain and disability (1).
They concluded that most participants will still be experiencing low back pain and
related disability one year after consultation (1). Cherkin et al, 1996 found that only 67%
of patients with low back pain reported good outcomes after 7 weeks, and only 71 %
were satisfied with their condition one year later (2).
Low back pain can be classified as acute (0‐6 weeks), subacute (6‐12 weeks), and chronic
(>12 weeks) (3). Sixty to 90% of all people will experience an episode of low back pain
during their life. In the Netherlands, the incidence of subjects with Acute NonSpecific
Low Back Pain attending their general practitioner is 36 per 1,000 subjects per year (4,
5). Clinical assessment is important to identify features of rare but serious causes of
Acute Nonspecific Low Back Pain, and in the majority of cases it is not possible to
determine a cause. Van Tulder et al, 1999 reported that most patients improve with
conservative management and do not need diagnostic assessment (6).
According to the “biopsychosocial model” of the Royal Dutch Society for Physical
Therapy (7), Acute Nonspecific Low Back Pain is the result of an interaction between
biological, mental and social factors wherein psychosocial can be contributory to
chronicity (8). Acute Nonspecific Low Back Pain is linked to depression, passive coping,
and fear of movement (9).
Fewer than 10 percent of subjects with acute low back pain are diagnosed with a
specific cause of pain. Usually there are no abnormal sensations in the lower back, with
or without radiation of pain to one or both legs related to physical disorders. For this

89
reason, it is hypothesized psychosocial factors may be increase the chance on low back
pain becoming chronic (8). Regarding the biopsychosocial model, according to the
Dutch guideline “manipulative therapy at nonspecific low back pain,” standard physical
therapy is based on a multidimensional approach with attention to posture, mild
exercises, information, and advice to subjects to stay physically active (10). Spinal
manipulative therapy is commonly used by physical therapists, chiropractors, and
osteopaths for the management of Acute Nonspecific Low Back Pain and is advocated
by the majority of national clinical guidelines (11). A number of investigators concluded
that spinal manipulation and typical physical therapy produced similar outcomes in the
first four weeks of treatment of Acute Nonspecific Low Back Pain (12,13). In contrast
with this, other investigators of acute and subacute back pain have suggested that
manipulation produced significantly better short‐term (< 6 weeks) improvement in pain
and physical activity compared to physical therapy and a placebo treatment (6,13,14,15).
They reported that exercise therapy had no additional treatment effect on pain and
functional status in the acute phase of low back pain compared to no treatment.
Consequently, research results are not consistent about the effectiveness of
manipulative therapy.
Research shows the relevance of application of a clinical prediction rule for spinal
manipulation (16,17). Childs, et al. 2004, showed that effect sizes for treatment
effectiveness increase dramatically when the spinal manipulation clinical prediction rule
is used to classify participants appropriately (17). Fritz, Childs & Flynn proposed a two‐
item clinical prediction ruIe, duration of symptoms less than 16 days and no symptoms
extending distal to the knee as an effective strategy for the decision to use spinal
90
manipulation in the treatment of Acute Nonspecific Low Back Pain (18). However, the
spinal manipulation of patients with ANSLBP in Dutch primary care is not based on the
clinical prediction rule of Childs, et al. (17) or Fritz, et al. (18).
The aim of the present study was to assess the efficacy of additional manipulative
therapy, as part of a multidimensional approach compared with standard physical
therapy care in subjects with Acute Nonspecific Low Back Pain using the following spinal
manipulation clinical prediction rule: duration of symptoms less than 16 days, no pain
distal of the knee and age greater than 35 years. It was hypothesized that four
additional manipulative sessions added to multidimensional physiotherapy would be
more effective than standard physical therapy for subjects with Acute (< 16 days)
Nonspecific Low Back Pain and with age over 35 years.
Outcome measures are pain, mobility of the lower back, and disability.
Methods
Design
A nonblinded randomised, multicentre clinical trial was used to examine the effect.
Aftereligibility was verified, written informed consent was obtained, treatment was
assigned by the Department of Clinical Epidemiology and Biostatistics of the Academic
Medical Centre in Amsterdam using a computerized randomised design with
stratification for age. An independent employee, not involved in recruitment of
participants, generated a random stratified list in which by means of a computerized

91
programme, every patient was assigned either manipulative therapy and physical
therapy or physical therapy only.
This study was carried out following the principles of the Declaration of Helsinki. All
persons involved in this study were informed about these ethical regulations and the
study protocol was approved by the Medical Ethics Committee of the Medical Centre of
the University of Amsterdam in the Netherlands.
Participants
Based on a sample size calculation with a two‐sided α of 0.05 and power of 0.8, 64
participants were needed to detect a 50% reduction of pain after four manipulation
treatments in the experimental group to be considered as a clinically relevant treatment
effect. The study was conducted in three primary health‐care centres for physical
therapy and manual therapy located in the north of the Netherlands. Inclusion criteria
are Acute Nonspecific Low Back Pain (< 16 days), age between 20 and 55 years, with or
without previous complaints, and no symptoms distal of the knee. Exclusion criteria are
specific low back pain, such as low back pain with neurological signs, specific rheumatic
diseases, signs of osteoporotic fractures or inability to fill in the research questionnaires.
Sixty‐four patients participated in the trial, 33 were assigned to the Control group
(physical therapy only) and 31 to the Experimental group (manipulative therapy and
physical therapies). In the experimental group, one patient discontinued treatment
because of increasing pain. No statistically significant difference was found on baseline

92
variables of the experimental and control groups. As shown in Table 1, the study sample
was homogeneous in terms of sex, age, duration of complaints, onset of low back pain,
relapse, physical labour, and the prescription of non‐steroidal anti‐inflammatory drugs
(NSAIDs). Only the baseline Pain scores differed significantly (P < 0.01).
There were 21 participants with previous complaints.
Procedure
Physical examination was carried out by three experienced physical therapists, all
members of the Dutch Association of Manual Therapy and registered with the Royal
Dutch Association for Physical Therapy, a member of the International Federation of
Orthopedic Manipulative Therapists. A standard physical examination was carried out
together with specific manipulative therapy tests. Inspection and physical examination
of the patient’s lumbar spine was conducted while each was standing erect (19). Their
spines were examined for symmetry of range of motion in flexion, lateral flexion (pelvic
shift/tilt) and extension, and straight leg raising.
For the manipulative therapy tests, the lumbar joints were examined by segmental joint
play techniques (20,21).
The sacroiliac joint was tested using the Thigh Trust test, Patrick sign, Gaenslen test,
distraction test, and compression test. At least two of these tests had to produce a
positive result in terms of pain provocation in order to diagnose the location of
dysfunction (22,23).

93
A total of four treatment sessions were given to the experimental group over a period
of two and a half weeks by the manual therapists.
The treatments were given to the restricted lumbosacral joints, sacroiliac joints, or both,
immediately following standard physical therapy. All therapists applied the same
diagnostic and treatment procedures. In the trial, manipulative therapy included specific
manipulations, low amplitude, range‐expanding thrust of high velocity techniques. The
acceleration of the high velocity technique is high and the amplitude is small, which
causes a cavitation followed by a palpable joint movement to improve overall joint
function and decrease any restrictions in movement at the segmental at the segmental
levels in the lumbar spine and sacroiliac joint, and to reduce pain. No other technique
was applied. The manual therapist chose the appropriate applied techniques on the
basis of the location of the dysfunction. In each treatment session only one
manipulation was applied with an added time investment of approximately four
minutes. Standard physical therapy, the control treatment, is based on the principle of
gradually increasing the level of physical activity and improving the relevant physical
functions, such as muscle strength, exercise capacity, and mobility. Also, the awareness
of each participant is increased, as is understanding of the condition, thus enabling each
to modify any biopsychosocial factors associated with an increased risk of chronicity.
Consequently, the physical conditioning of the participant is increased and participants
will be enabled to adopt an adequate coping strategy.

94
In practice, each participant took part in low intensity, low load endurance exercises to
train abdominal oblique and straight abdominal muscles for 2 min. and stretch lumbar
extensors for 2 min.; in total, approximately 5 min. twice per day as prescribed.
Information on back pain and its course were provided together with the advice to stay
active within functional limits.
This information was supported by a leaflet “Less complaints with your back” published
by the Royal Dutch Society for PhysicalTherapy (24). This information focuses on
maintaining daily activities and explains the nature of low back pain. Practical
recommendations were also given such as how to squat and to sit in a correct way and
that intensity of pain should not be the cause of physical inactivity. In this process the
therapist acts as a coach, motivates the participant, determines progress, and provides
positive feedback (25).
A participant compliance checklist was completed to verify instructions (26). This
standard physical therapy regimen was performed by the same manual therapists.
Measures
Baseline and final measurements of pain, mobility of the lower back, and disability were
recorded by the therapists at the start of treatment and after the fourth treatment, two
and a half weeks into the treatment programme.
Pain. ‐‐ Pain was assessed using a Visual Analogue Scale, a horizontal line, 100 mm in
length, anchored by descriptors at each end (0: No pain, 100: Maximum pain). The

95
participant marked on the line the point which each felt represented their perception of
pain over the last 24 hours (27,28,29,30,31). The test‐retest correlation was r p = 0.97 and
external validity is r p = 0.91 with the McGill Pain Questionnaire (31,32).
Oswestry Disability Low Back Pain Questionnaire (33,34,35,36,37) ‐‐‐‐ This questionnaire
was used to assess the extent of disability experienced by participants with low back
pain in their activities of daily living, such as to wash themselves, sitting, walking,
standing erect, sleeping, lifting, travel, and disability which influences sexual and social
life. The questionnaire contains 10 items scored on a 5‐point scale with anchors of 0 : No
complaints to 5: Many complaints. The total possible score was 50, test‐ retest reliability
is ICC= 0.90 (95% CI 5.78 to 0.96) and external validity is r p = 0.82 (36).
Mobility. ‐‐‐‐ Mobility of the lower body and spinal column was evaluated using the Sit‐
and‐Reach Test (38,39). Participants sat on the floor, legs outstretched, in front of a
box. The participant bent forward and pushed a slide as far as possible over the table
using their fingertips. A record was made of the distance the slide was pushed (cm). The
best of three trials was taken as the obtained score. According to van Heuvelen et al.,
the test‐retest reliability (ICC) is 0.98 for men and 0.96 for women (40). The Sit‐and‐
Reach test is highly correlated (r p = 0.80) with hamstring flexibility for both left and
right legs (41).

96
Statistical Analysis
All analyses were done with SPSS Version 15.0 (SPSS Inc., Chicago, Illinois), according to
the intention‐to‐treat principle. The intention‐to‐treat principle is a strategy for
analysing data in which all participants are included in the group to which they were
assigned, whether or not they completed the intervention given to the group.
Descriptive statistics, χ2 and independent groups t‐tests, are used to analyse baseline
characteristics. Multivariate analysis of variance was used for analysing the effects of
treatment on pain, disability, and mobility between the experimental and the control
groups. Interaction effects were calculated using the clinical prediction rule for
manipulation. Effect sizes were calculated according to Cohen et al., 1988; an effect size
of 0.2 is indicative of a small effect, 0.5 a medium and 0.8 a large effect (42).
Results
At baseline the Pain score in the Experimental group was 43 and in the Control group 54.
The level of disability in activities of daily life for the entire sample, according to the
Oswestry questionnaire, showed moderate disability (25.5%), 24% in the Experimental
group and 26% in the control group; the mobility of the lower spine was almost equal:
29.7 in the Experimental and 31.6 in the Control group.

97
Table 1. Baseline characteristics of 64 patients with acute, nonspecific low back pain, treated
with manual therapy (MT + PT) and physiotherapy (PT).
Total (n = 64)
MT + PT (n = 31)
PT (n = 33)
Number by group
20‐35 21 11 10
35‐50 32 15 17 50‐55
11 5 6
Sex male 35 17 18 Female
29 14 15
Durationa 1 week 20 8 12a 2 weeks 14 6 8 3 weeks 10 7 3 3<>4 weeks
20 11 9
Onset of LBPb acute 25 11 14b slow 19 11 8 Moderate
20 9 11
Relapse yes 22 11 11 No
42 20 22
Physical labour none 18 9 9 moderate 20 11 9 Heavy
26 11 15
Medicationc yes 26 16 10c no
38 15 23
Pain (mm ± sd)
48± 18.7 42.7 ±18.4 54.0±17.5d
Disability (% ± sd)e
0.26 ± 0.16 0.24 ± 0.18 0.26 ± 0.12e
Mobility (cm ± sd)f
31 ± 7.6 29.7 ±7.7 31.6 ± 6.9f
a Number of patients with complaint episode in weeks. b Acute: within a day; slow: gradually within some days; Average: combination of both. c NSAID d Severity of pain assessed by patients on a VAS (0 ‐ 100). e Functional status assessed by the Oswestry Disability Questionnaire, according to
Fairbanks between 20%‐40% a moderate disability. f Mobility of the lower back measured by means of the sit‐and‐reach test.

98
An independent t‐test analysis showed that participants feel more pain decrease in the
control group than in the experimental group; however, this difference was not
statistically significant, see Table 2. Moreover, disability decreased equally in the
experimental group and the control group. Mobility of the lower back showed no
statistically significant difference between the experimental group and the control
groups. A small difference is observed between the multivariate analysis of variance and
the t‐test results to three participants not taking a Sit‐and‐Reach Test at follow‐up.
Table 2. The values of the mean final scores of the two treatment groups and P values of the t‐
test (n = 64)
MT + PT
PT P value
Pain (mm ± sd)a
19 ± 16.9
24.8 ± 20.1
0.26
Disability (% ± sd)b 0.14 ± 0.17
0.14 ± 0.12 0.38
Mobility (cm ± sd)c 35.1 ± 8.5
35.2 ± 7.8 0.14
As indicated in Table 3, additional manipulative therapy shows a statistically significant
benefit over physical therapy on disability rating, while no statistically significant effects
were found for pain or mobility. Controlled for the applied clinical prediction rule (2 vs 3
criteria), a statistically significant interaction effect was found for disability, but not for
pain or mobility. Controlled for sex and clinical prediction rule, a statistical significant
interaction was found for disability. These results are confirmed by the patients’
statements about the effects of both interventions: 32% of those in the experimental and

99
31% of those in the control groups declared that they had no complaints in terms of pain
and disability after four treatments. The effect sizes are all small.
Table 3. MANOVA (group X time) analysis to determine the effects on pain, disability, and mobility of the lumbar spine from MT + PT and PT (n = 63).
MT + PT PT MANOVA (group x time)
Pre‐test
Post‐test
Pre‐test
Post‐test
F (1,63)
P β ES
Pain (mm ± sd)a
42.7 ± 18.4
19 ± 16.9
54.0 ±
17.6
24.8 ±
20.1 1.28
0.26
0.20
0.28
Clinical prediction
rule1
43.0 ± 24.4
17.0 ± 15.6
52.0 ±
21.3
17.4 ±
17.4 0.72
0.40
0.13
0.01
Clinical prediction
rule controlled
for gender2
male
18.0 ± 18.3
7.0 ± 18.0
48.2 ± 9.2
19.2 ± 8.9
2.99
0.17
0.07
0.03
female
48.0 ± 8.2
19.0 ± 8.0
57.0 ±
10.6
15.0 ±
10.4
Disability (% ± sd)b
0.24 ± 0.18
0.14 ± 0.17
0.26 ±
0.12
0.14 ±
0.12 15.3
0.001
0.97
0.21
Clinical prediction
rule1
0.34 ± 0.28
0.27 ± 0.23
0.35 ±
0.16
0.19 ±
0.15 11.4
0.001
0.91
0.17
Clinical prediction
rule controlled
for gender2
male 0.16 0.66 0.25 ±
0.03
0.13 ±
0.14
9.29
0.004 0.85
0.14
female
0.27 ± 0.29
0.19 ± 0.23
0.47 ± 0.18
0.27 ± 0.13
Mobility (cm ± sd)c
29.7 ± 7.7
35.1 ± 8.5
31.6 ± 6.9
35.2 ± 7.8
2.20
0.14
0.31
0.24
Clinical prediction
rule1
25.0 ± 1.4
34.0 ± 2.8
35.5 ± 6.4
37.5 ± 4.9
0.51
0.48
0.19
0.01
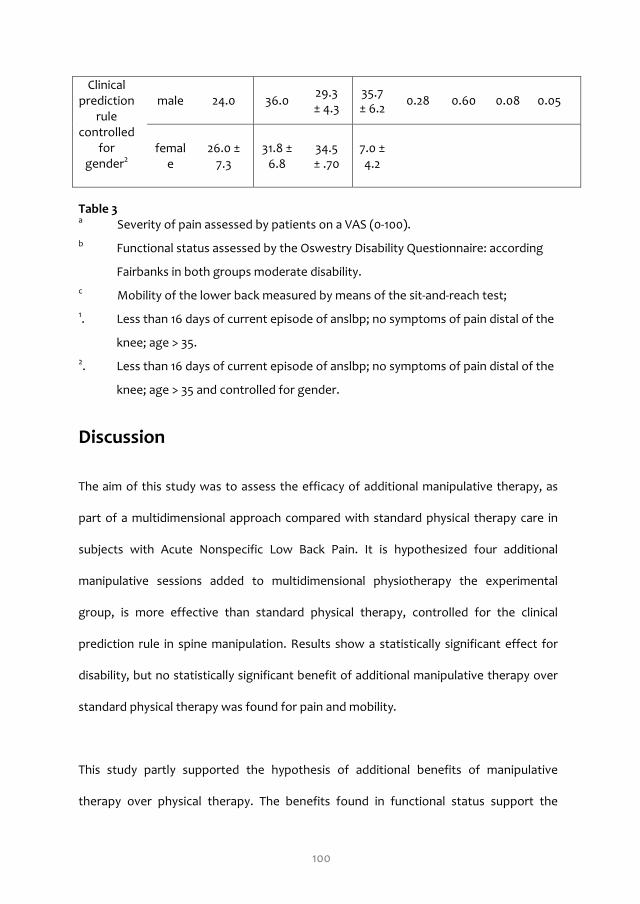
100
Clinical prediction
rule controlled
for gender2
male 24.0 36.0 29.3 ± 4.3
35.7 ± 6.2
0.28 0.60 0.08
0.05
female
26.0 ± 7.3
31.8 ± 6.8
34.5 ± .70
7.0 ± 4.2
Table 3 a Severity of pain assessed by patients on a VAS (0‐100).
b Functional status assessed by the Oswestry Disability Questionnaire: according
Fairbanks in both groups moderate disability.
c Mobility of the lower back measured by means of the sit‐and‐reach test;
1. Less than 16 days of current episode of anslbp; no symptoms of pain distal of the
knee; age > 35.
2. Less than 16 days of current episode of anslbp; no symptoms of pain distal of the
knee; age > 35 and controlled for gender.
Discussion
The aim of this study was to assess the efficacy of additional manipulative therapy, as
part of a multidimensional approach compared with standard physical therapy care in
subjects with Acute Nonspecific Low Back Pain. It is hypothesized four additional
manipulative sessions added to multidimensional physiotherapy the experimental
group, is more effective than standard physical therapy, controlled for the clinical
prediction rule in spine manipulation. Results show a statistically significant effect for
disability, but no statistically significant benefit of additional manipulative therapy over
standard physical therapy was found for pain and mobility.
This study partly supported the hypothesis of additional benefits of manipulative
therapy over physical therapy. The benefits found in functional status support the

101
results of a review study by Reid et al., (43). They found that both acute and chronic
pain and disability were only weakly correlated. They suggested that this weak
correlation is caused by a self‐serving bias: injured workers often perceive themselves to
be more disabled than their functional testing would indicates, so the overestimation of
disability is more sensitive for change than pain and limitations in mobility. This study
does not support the conclusion of Fritz, et al., wherein a clinical prediction rule based
on just two criteria, was a strong predictor for a rapid response to manipulation (18).
Most participants in their study had been recruited into health care facilities within the
U.S. Air Force, a population not similar to the current study sample. According to Childs
et al., an application of 3‐ of 5‐criteria prediction rule yielded a 7% probability of success,
compared with a 73% probability of success using 4 or 5 prediction criteria (17). Thus,
using fewer criteria, as in this study, is less likely to yield significant results, since therapy
is less well matched to patients’ needs. Another reason for not finding effects on pain
and mobility was the short treatment period.
Natural recovery within four weeks might also have influenced the result (44, 45). Pain
and disability associated with an initial episode of Acute Nonspecific Low Back Pain is
known to resolve itself spontaneously in the first three or four weeks in the majority of
cases. That no significant difference was found between the two groups may be due to
the short follow‐up period. Maybe, for those participants who still had complaints after
four weeks, a longer follow‐up might have shown differences between treatment
groups. The present results support Assendelft, et al. in concluding that spinal
manipulative therapy is not superior to physical therapy and exercise treatment in
general participants with Acute Nonspecific Low Back Pain, at least in the short term

102
(12).
A number of methodological features of this study are relevant in interpreting the
results of this study. A nonblinded design can potentially produce bias. The measures
used to assess effectiveness were administered by the same therapists performing
treatment on subjects. To prevent potential bias, a randomisation of the participants to
treatment was executed by the University of Amsterdam, and the data were
independently analysed by the coauthors. The lack of benefits found in pain and
disability are quite possibly due to low statistical power. A number of conclusions are
limited by type II error.
Finally, the self‐administered and self‐reported measures used to examine the effect of
the treatment on pain, mobility and functional status could produce self‐report bias.
References
1. Croft PA, Macfarlane GJ, Papageorgiou AC, Thomas E, Silman AJ. Outcomeof low back
pain in general practice: a prospective study. British Medical Journal 1998; 316,1356‐59.
2. Cherkin DC, Deyo RA, Street JH, Barlow W. Predicting poor outcomes for back pain seen
in primary care using patients' own criteria. Spine 1996; 21,2900‐07.
3. Hoogen HJM, Koes BW, Eijk JThM. On the course of low back pain in general practice: a
one year follow up study. Annals of the Rheumatic Diseases 1998; 57(1),13–19.

103
4. Faas A, Chavannes AW, Koes BW, Hoogen JMM van den, Mens JMA, Smeele IJM,
Romeijnders JR, Laan ACM van der. NHG‐Standaard lage rugpijn.Huisarts en
Wetenschap 1996; 39,18‐31.
5. Patel AT, Ogle AA. Diagnosis and management of acute low back pain. American Family
Physician 2000; 61,1779‐1786,1789‐1790.
6. Tulder MW van, Koes BW, Assendelft WJJ, Bouter LM (1999). The effectiveness of
conservative treatment of acute and chronic low back pain. Amsterdam; EMGO‐
Institute.
7. Hendriks HJM, Bekkering GE, Koes BW. KNGF Richtlijn Lage rugklachten. Nederlands
Tijdschrift voor Fysiotherapie 2001; 3,1‐24.
8. Linton SJ, Buer N. Working despite pain: factors associated with work attendance versus
dysfunction. International Journal Behavorial Medicine 1995; 2,252‐62.
9. Linton SJ, Vlaeyen J,Ostelo R. The back pain beliefs of health care providers: Are we
fear‐avoidant? Journal of Occupational Rehabilitation 2002; 12,223‐32.
10. Burton AK, Waddell G, Summerton N. Information and Advice to patients with back pain
can have a positive effect. Spine 1999; 24,2484‐91.
11. Koes BW, Tulder van MW, Ostelo R, Kim Burton A, Waddell, G. Clinical guidelines for the
management of low back pain in primary care: an international comparison.Spine 2001;
26,2504‐13.
12. Assendelft WJJ, Morton SC, Yu EI, Suttorp MJ, Shekelle PG. Spinal manipulative therapy
for low‐back pain (Cochrane Review). Annals of Internal Medicine 2003; 138,871‐81.
13. Ferreira ML, Ferreira PH, Latimer J. Efficacy of spinal manipulative therapy for low back
pain of less than three months´ duration. Journal of Manipulative and Physiogical
Therapeutics 2003; 26,593‐601.

104
14. Waddell, G., Feder, G., McIntosh, A., Lewis, M., & Hutchinson, A. (1996). Low back pain
evidence review. Royal College of General Practitioners, London.
15. Koes BW, Sanders RJ, Tuut MK. CBO‐richtlijn voor diagnostiek en behandeling van acute
en chronische aspecifieke lage rugklachten. Nederlands Tijdschrift voor Geneeskunde
2004; 148,310‐314.
16. Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D, Butler B, Garber M, Allison S.
A clinical prediction rule for classifying patients with low back pain who demonstrate
short‐term improvement with spinal manipulation. Spine 2002; 27,2835‐43.
17. Childs JD, Fritz JM, Flynn TW, Irrgang JR, Johnson KK, Majkowski GR, Delitto A. A Clinical
Predection Rule To Identify Patients with Low Back Pain Most Likely To Benefit from
Spinal Manipulation: A Validation Study. Annals of Internal Medicine 2004; 141,920‐928.
18. Fritz JM, Childs JD, Flynn TW. Pragmatic application of a clinical prediction rule in
primary care to identify patients with low back pain with a good prognosis following a
brief spinal manipulation intervention. BMC Family Practice 2005; 6(1),29.
19. Nachemson A. A review of the mechanics of the lumbar disc. Rheumatology and
Rehabilitation 1975; 13,129‐143.
20. El, A. van der.. Manuele diagnostiek van de wervelkolom. 1st ed. Rotterdam; Manthel,
1992.
21. Tulder MW van, Malmivaars A, Esmail R, Koes BW. Exercise therapy for low back pain
(Cochrane Review). The Cochrane Library, 1.
22. Wurff P, van der Meyne W, Hagmeijer RHM. Clinical tests of the sacroiliac joint. Manual
Therapy 2000; 5,89‐96.

105
23. Kokmeyer, DJ, Wurff P, van der Aufdemkampe G, Fickenscher TC. The reliability of
multitest regimens with sacroiliac pain provocation test. Journal of Manipulative and
Physiological Therapeutics 2002; 25,42‐8.
24. Nederlands Paramedisch Instituut (NPi). (2002; 2004). Less complaints with your back.
Amersfoort, Koninklijk Nederlands Genootschap voor Fysiotherapie.
25. Sluijs E. Therapietrouw door voorlichting; handleiding voor patiëntenvoorlichting in de
fysiotherapie. Derde druk. Amsterdam; Uitgeverij SWP, 2000.
26. Weber, CL, Dumas GA, Smith JT, Kuhnke TJN, Stevenson JM. Prediction of mild low back
pain using psycho‐social measures. Queen’s Dupont Back Study, North American
Congres of Biomechanics.
27. Price DD. The validation of visual analogue scales as ratio scale measures for chronic and
experimental pain. Pain 1983;17,45‐56.
28. Duncan G, Bushnell M, Lavigne G. Comparison of verbal and visual analogue scales for
measuring the intensity and unpleasantness of experimental pain. Pain 1989; 37,295‐303.
29. Gift A. Visual analogue scales: Measurement of subjective phenomenon. Nursing
Research 1989; 38,286‐288.
30. Price DD, Bush FM, Long S, Harkins SW. A comparison of pain measurement
characteristics of mechanical visual analogue and simple numerical rating scales. Pain
1994; 2,217‐226.
31. Bijur PE, Silver W, Gallagher MA & EJ. MD Reliability of the Visual Analog Scale for
Measurement of Acute Pain. Academic Emergency Medicine 2001; 8,1153‐1157.
32. Seymour RA, Charlton JE, Phillips ME. An evaluation of dental pain using Visual Analogue
Scales and the McGill Pain Questionnaire. Journal of Oral and Maxillofacial Surgery 1983;
41,643‐648.

106
33. Fairbanks JCT, Pynsent PB. The Oswestry Disability Index. Spine 2000; 25,2940‐53.
34. Fairbanks JCT. The Roland Morris Disability Questionnaire and the Oswestry
Disability Questionnaire. Spine 2000; 25,3115‐3124.
35. Davidson M, Keating J. A comparison of five low disability questionnaires:reliability and
Responsiveness. Physical Therapy 2001; 82:8‐24.
36. Fritz JM, Irrgang JJ. A comparison of a modified Oswestry Low back pain Disability
questionnaire and the Quebec Back Pain Disability Scale. Physical Therapy 2001; 81,776‐
88.
37. Good M, Stiller C, Zauszniewski JA, Anderson GC, Stanton‐Hicks M, Grass JA. Sensation
and Distress of Pain Scales: reliability, validity, and sensitivity. Journal of Nursing
Measurement 2001; 9,219‐238.
38. Hoeger, WWK, Hopkins DR. A comparison of the Sit and Reach and the modified Sit and
Reach in the measurement of flexibility in women. Research Quarterly for Exercise and
Sport 1992; 63,191‐195.
39. Lemmink, KA, Kemper HC, Greef MH de, Rispens P, Stevens M. The validity of the sit‐
and‐reach test and the modified sit‐and‐reach test in middle‐aged to older men and
women. Research Quarterly for Exercise and Sport 2003; 74,331‐336.
40. Heuvelen MJG, van Kempen GIJM, Ormel J, Rispens P. Physical fitness related to age and
physical activity in older persons. Medicine and Science in Sports and Exercise 1998;
30,434‐41.
41. Baltaci G, Un N, Tunay V, Besler A, Gerçeker S. Comparison of three different sit and
reach tests for measurement of hamstring flexibility in female university students.
British Journal of Sports Medicine 2003; 37,59‐61.
107
42. Cohen, J. Statistical power analysis for the behavioral sciences (2nd ed.), Hillsdale, NJ:
Erlbaum, 1988.
43. Reid S, Haugh LD, Hazard RG, Tripathi M. Occupational Low Back Pain: Recovery Curves
and Factors Associated with Disability. Journal of Occupational Rehabilitation 1997; 7,1‐
14.
44. Awad MA, Shapiro SH, Lund JP, Feine, JS. Determinants of patient�s
treatmentpreferences in a clinical trial. Community Dentistry and Oral Epidemiology
2000; 28,119‐25.
45. Scientific approach to the assessment and management of activity‐related spinal
disorders. A monograph for clinicians. Report of the Quebec Task Force on Spinal
Disorders 1987; Spine; 12(7),S1‐59.

108

109
Chapter 6
Stretching before sleep reduces the frequency and
severity of nocturnal leg cramps in older adults: a
randomised trial
Journal of Physiotherapy 2012, 58 (1): 165‐172
Johannes M Hallegraeff
Cees P van der Schans
Renee de Ruiter
Mathieu HG de Greef

110

111
Abstract
Question: In adults who experience nocturnal leg cramps, does stretching of the calf
and hamstring muscles each day just before sleep reduce the frequency and severity
of the cramps?
Design: A randomised trial with concealed allocation and intention‐to‐treat analysis.
Participants: Eighty adults aged over 55 years with nocturnal leg cramps who were
not being treated with quinine. Intervention: The experimental group performed
stretches of the calf and hamstring muscles nightly, immediately before going to
sleep, for six weeks. The control group performed no specific stretching exercises.
Both groups continued other usual activities.
Outcome measures: Participants recorded the frequency of nocturnal leg cramps in
a daily diary. Participants also recorded the severity of the pain associated with
nocturnal leg cramps on a 10‐cm visual analogue scale. Adverse events were also
recorded.
Results: All participants completed the study. At six weeks, the frequency of
nocturnal leg cramps decreased significantly more in the experimental group, mean
difference 1.2 cramps per night (95% CI 0.6 to 1.8). The severity of the nocturnal leg
cramps had also decreased significantly more in the experimental group than in the
control group, mean difference 1.3 cm (95% CI 0.9 to 1.7) on the 10‐cm visual analogue
scale.
Conclusion: Nightly stretching before going to sleep reduces the frequency and
severity of nocturnal leg cramps in older adults.

112
Introduction
Nocturnal leg cramps are suddenly occurring, episodic, painful, sustained, involuntary
muscle contractions of the calf muscles, hamstrings, or foot muscles (1,2). During the
cramp, the involved muscles are tender and hard on palpation. The pain that occurs with
these contractions is sharp and intense and may last from seconds to several minutes.
Although they are otherwise benign, nocturnal leg cramps can cause substantial distress
and can disrupt sleep. In 20% of people who experience nocturnal leg cramps, cramps
also occur during the daytime (1). The cramps sometimes occur in episodes a few days a
week, during which they repeat themselves (1,3,4). Although the insults generally
persist for no longer than ten minutes, in exceptional situations they can continue for
several hours. In approximately 2% of cases, nocturnal leg cramps occur weekly (5).
Nocturnal leg cramps occur more commonly with advancing age, affecting between 38%
and 50% of the elderly (2,5,6). Nocturnal leg cramps are more prevalent among women
and among people with comorbidities, especially those with neurological and
cardiovascular diseases (4,6).
It is important to distinguish nocturnal leg cramps from restless legs syndrome and
periodic limb movement disorder, because all are sleep disorders characterised by
abnormal leg movements and reduced sleep quality. However, restless legs syndrome
involves more continuous discomfort and the urge to move the legs, occurs during the
day also, and is relieved by movement. Periodic limb movement disorder causes
involuntary limb movements (primarily of the legs) during sleep, recurring at brief
intervals, but not necessarily waking the person (7). Therefore, the diagnosis of

113
nocturnal leg cramps can be based on reports of episodes of painful involuntary
contractions of muscles, affecting the leg, calf, or foot, which occur at night and which
recur at sporadic intervals (3,6).
What is already known on this topic: Nocturnal leg cramps are common among the
elderly, causing pain and sleep disturbance. The medications used to prevent nocturnal
leg cramps have variable efficacy and may have substantial side effects.
What this study adds: Nightly stretching of the calves and hamstrings reduces the
frequency of nocturnal leg cramps in older adults. Nightly stretching also lessens the
pain associated with any cramps that continue to occur.
The cause of nocturnal leg cramps is unknown. However, several possible causes and
precipitating factors have been hypothesised. Abnormal excitability of motor nerves,
perhaps due to electrolyte imbalance, may be a contributing mechanism (1). Diuretics,
steroids, morphine, and lithium are also reported to cause nocturnal cramps, as can
repetitive movements during sport (1,3,6). Conversely, physical inactivity has been
proposed as a cause, with inadequate stretching leading to reduced muscle and tendon
length (1,2). Although it is not fully understood how this could lead to nocturnal leg
cramps, this would be consistent with the higher prevalence of the disorder among
people with reductions in lower limb activity and joint range, such as those with
varicose veins and arthritis (2,4,5,8).

114
Quinine and hydroquinine are moderately effective in reducing the frequency and
severity of nocturnal leg cramps (9,10), perhaps by decreasing the excitability of the
motor end plate and thereby increasing the refractory period of a muscle (11). However,
quinine can have important side effects, especially for women, such as:
thrombocytopenia, hepatitis, high blood pressure, tinnitus, severe skin rash, and
haemolytic uremic syndrome (12,13). If hydroquinine is used, a trial intervention period is
advised to monitor side effects (1,13). Although other medications have been used to
treat nocturnal leg cramps such as magnesium, Vitamin B Complex Forte, calcium, and
vitamin E, none of these appears to be effective (14,15).
Muscle stretching is worth considering as an alternative therapy. It is easy to perform,
has a very low risk of side effects, and often relieves the pain when a cramp has
occurred. Moreover, stretching techniques can foster a resilient attitude toward
recovery in patients with nocturnal leg cramps by promoting a ‘bounce back and move
on’ behavioural strategy (16), because they give patients a strategy to seek immediate
relief.
Daniell examined a program of calf‐stretching exercises performed three times per day
by people with nocturnal leg cramps (15). Although the program of stretches appeared
to prevent nocturnal leg cramps, the study lacked a randomised control group for
comparison. In contrast, Coppin and colleagues performed a randomised controlled trial
in which the stretching exercises failed to decrease the frequency and severity of
nocturnal leg cramps in older adults (17). However, in this study all participants were
already taking quinine at baseline and continued taking it throughout the study, which

115
may have reduced the potential for stretching to affect the outcome. Also, the
stretching was performed three times ‘spread through each day’ without further
prescription or recording of the actual times. Because nocturnal leg cramps occur
primarily at night and may be associated with physical inactivity and muscle shortening,
stretching immediately before sleep may be a useful preventative therapy. Therefore,
the research question for this study was:
In older adults who suffer from nocturnal leg cramps, does a 6‐week program of
stretching the hamstring and calf muscles immediately before going to bed reduce the
frequency and severity of the cramps?
Method
Design
A randomised trial was conducted at a physical therapy clinic in Groningen, with
participants recruited through advertisement in local newspapers in the northern part
of the Netherlands. At baseline, each participant’s age, gender, and history of nocturnal
leg cramps were recorded. After eligibility was verified and written informed consent
was obtained, participants underwent measurement of their body mass index, daily
physical activity, and functional lower limb strength, as described in detail below.
Participants were then randomised to either an experimental (daily stretches before
sleep) or a control (no stretching) group, based on a computer‐generated assignment
schedule that was coded and concealed until after the study. An independent
researcher assigned each patient to either the experimental group or the control group.
Participants allocated to the experimental group were taught the stretches and those in

116
the control group were advised not to stretch. Other investigators and care providers
were blinded to group assignment. Outcome measures were cramp frequency and
severity, recorded by participants daily in a diary during Week 0 and Week 6.
The methods used to characterise participants at their baseline visit were as follows.
Body mass index was calculated from height and weight, which were measured on
calibrated instruments. Daily physical activity was measured by a pedometera fitted to
each participant’s belt for one week. The participants received instructions on how to
use the pedometer. The step count mechanism in this pedometer has elsewhere been
shown to give values consistently within 3% of the actual steps taken during a self‐
paced walk, with Cronbach’s Alpha of 0.99 for intra‐model reliability (18). Participants
were strongly encouraged not to make any changes to their typical daily routine of work
and leisure activity. Patients were instructed to wear the pedometer for seven days and
to record daily the number of steps and the number of minutes that they cycled, swam,
or participated in any other activity. Non‐ambulatory activities were converted into
steps based on the intensity of the physical activity calculated in metabolic equivalents
per minute (MET/min). For example, one minute of cycling or swimming translates to
about 150 steps, whereas one minute of moderate fitness‐related activity corresponds
to about 100 steps. Steps per day, including converted steps, were expressed as step
equivalents. Functional leg strength was measured with the chair‐stand test, which
assesses leg strength, and is commonly used in generally active, community‐dwelling
older adults (19). In this test, older adults stand up from a sitting position in a chair as
often as they can in 30 seconds. The chair‐stand test has a reliability (test‐retest) of r =
0.88 and a convergent validity of r = 0.75.

117
Stretch Description
Calf stretch in standing
Starting position. Standing facing a wall with the
elbows extended and both palms on the wall at chest
height. One leg is forward with the knee flexed and the
other leg is back with the knee extended. Both feet are
in full contact with the floor.
Motion to apply stretch. Flex the front knee so that the
trunk moves forward, keeping the trunk straight and
the heels in contact with the floor.
Hamstring stretch in
standing
Starting position. Standing facing a chair that is placed
against a wall. Place one heel on the chair with the knee
of that leg fully extended.
Motion to apply stretch. Flex at the hips so that the
trunk tilts forward, keeping the trunk straight. The foot
on the floor should maintain full contact and the other
heel remains in contact with the chair.
Hamstring and calf stretch
in sitting
Starting position. Sit on the floor or a firm bed with
both legs extended. Grasp toes with both hands.
Motion to apply stretch. Flex at the hips so that the
trunk tilts forward, keeping the trunk as straight as
possible. Dorsiflex at the ankles.
Box 1. Description of the stretching exercises.
Participants
To be included in the study, respondents to the study advertisement had to be over 55
years old and to experience regular episodes of nocturnal leg cramps, defined as at least
once per week. Potential participants were excluded if they were using quinine or

118
medication to assist sleep. They were also excluded if they had orthopaedic problems,
severe medical conditions, or comorbidities known to cause muscular spasms or
cramps.
Intervention
Participants in the experimental group attended a 45‐ min visit at which they were
taught a program of daily stretching exercises for the hamstring and calf muscles by one
physiotherapist, who was specially trained in the study procedures. Participants were
advised to perform the stretches in standing, as presented in Figure 1a and b and
described in Box 1. For each stretch, the participant was advised to adopt the position
shown, move to the comfortable limit of motion, move beyond this to until a
moderately intense stretch was felt and sustained for 10 seconds, and then return to the
starting position. Participants were instructed to remain calm and never to hold their
breath during the stretch. Each stretch was performed a total of three times, with 10
seconds of relaxation between each stretch. Stretching of both legs was done within
three minutes. The physiotherapist demonstrated the stretches first and then observed
the participant performing the stretches, correcting the technique if necessary. If a
participant found stretching in standing difficult, the participant was shown how to
stretch in a sitting position, as presented in Figure 1c and described in Box 1.
The control group was not taught any sham stretches and was advised not to
commence stretches.

Al
w
st
ll p
wee
tud
part
k 4
y p
tici
4, a
prot
ipa
ll p
toc
nts
part
col.
s w
tici
.
wer
pan
re e
nts
enc
s re
cou
ecei
urag
ive
ged
d a
d t
a ho
to
om
ma
me v
11
aint
visi
19
tain
t to
n a
o a
all o
sse
oth
ess
her
an
us
nd e
sua
enc
al a
cou
acti
urag
ivit
ge
ty u
ad
unc
her
cha
ren
ang
nce
ged
to
d. A
o th
At
he

120
Figure 1. Stretches used in the experimental group: (a) calf stretch in standing, (b)
hamstring stretch in standing, (c) hamstring and calf stretch in sitting.
Outcome measures
At an instruction visit prior to starting the study, participants were instructed in the daily
recording of the frequency and severity of nocturnal leg cramps. The primary outcome
was the change in the average number of nocturnal leg cramps per day over a one‐week
period. This was assessed in the week prior to starting the 6‐week stretching program
(Week 0) and again in the final week of the stretching program (Week 6).
The secondary outcome was the severity of nocturnal leg cramps. The severity was
marked by the participants on a 10‐cm visual analogue scale with 0 cm representing no
pain and 10 cm representing the worst pain the participant could imagine. Recordings
were again made in the daily diary over the same 1‐week periods before and at the end
of the 6‐week stretching program. If adverse events were present, they were recorded
daily in the diary card throughout the trial.
Data analysis
We sought to identify a difference in the average number of nocturnal leg cramps of 1
cramp per night. Anticipating a standard deviation of 1.4 cramps per night, we
calculated that we would require 32 participants per group to have 80% power to detect

th
in
Al
to
co
m
ar
Fi
his
cre
ll p
o‐tr
ont
mea
re p
gu
dif
eas
art
reat
trol
n d
pre
re
ffer
ed
ticip
t a
l gr
diff
sen
2. D
ren
th
pan
ana
rou
fere
nte
Des
nce
e t
nts
alys
ups
enc
ed w
sign
as
ota
we
sis.
s in
ce.
wit
n a
s s
al s
ere
Fo
th
Sta
h 9
nd
sign
am
e an
or e
he
atis
95%
flo
nific
mple
naly
eac
cha
stic
% co
ow
can
e si
yse
ch
ang
cal
onf
of
nt w
ize
ed a
ou
ge
sig
ide
pa
wit
to
acc
utco
fro
gnif
enc
rtic
th
80
cord
om
om
fica
e in
cipa
an
0 pa
din
me,
ba
anc
nte
ant
al
arti
ng t
th
ase
e w
erva
ts t
1
lph
icip
to t
e d
line
was
als.
thro
21
ha o
pan
the
diff
e t
s se
.
oug
of
nts.
eir g
fer
o p
et a
gh
5%
gro
enc
pos
at P
the
% (1
oup
ce
st‐
P <
e tr
17).
p al
be
int
< 0.
rial.
To
loc
etw
terv
05,
.
o a
cati
wee
ven
, so
allo
on
en
ntio
o th
ow
, ie
the
on
hes
fo
e, u
e e
wa
se m
or d
sin
exp
as c
me
dro
ng a
peri
calc
ean
op
an i
ime
cula
di
ou
inte
ent
ate
ffe
uts,
ent
tal
ed
eren
w
tion
an
as
nce
we
n‐
nd
a
es

122
Table 1. Baseline characteristics of participants.
Characteristic Randomised
Total
Exp (n = 40)
Con (n = 40)
(n = 80)
Age (yr), mean (SD) 67 (7) 72 (7) 70 (6) Gender, n males (%) 20 (50) 26 (65) 46 (58) BMI (kg/m2), mean (SD) 26.0 (3.0) 24.9 (3.8) 25.4 (3.6) ≥1 chronic disorder, n (%) 9 (23) 9 (23) 18 (23) Physical activity (steps/d), mean (SD) 7780 (2644) 7956 (3810) 7868 (3259) Site of nocturnal cramps, n (%) alf 11 (28) 9 (23) 20 (25) amstrings 2 (5) 4 (10) 6 (8) alf and hamstrings 17 (43) 17 (43) 34 (43)
whole leg 10 (25) 10 (25) 20 (25) Cramp duration (mo), mean (SD) 10 (8) 12 (14) 11 (12) Chair‐stand test (stands/30 s), mean 12 (3) 12 (3) 12 (3)
Table 2. Mean (SD) of groups, mean (SD) difference within groups, and mean (95% CI)
difference between groups for both outcomes.
Outcome Groups Difference within groups
Difference between groups
Week 0 Week 6 Week 6 minus Week 0
Week 6 minus Week 0
Exp (n = 40)
Con (n = 40)
Exp (n = 40)
Con (n = 40)
Exp Con Exp minus Con
Cramp frequency (cramps/night), mean (SD)
3.4 (1.5)
3.2 (1.9)
1.4 (1.4)
2.4 (1.7)
‐2.0 (1.3)
‐0.8 (1.3)
‐1.2 (‐0.6 to ‐1.8)
Cramp severity (0 to 10), mean (SD)
7.2 (1.4)
7.4 (1.3)
5.9 (1.4)
7.5 (1.3)
‐1.3 (1.1)
0.0 (0.9)
‐1.3 (‐0.9 to ‐1.7)

123
Results
Flow of participants through the trial
In total, 119 people responded to the study advertisement. Telephone screening of
these respondents identified 39 as ineligible or unwilling to participate. The remaining
80 participants were randomised into the experimental or control group and completed
the study, with 40 being allocated to each group. The flow of participants through the
trial and reasons for exclusion are presented in Figure 2. The baseline characteristics of
the participants are presented in Table 1 and the first two columns of Table 2.
Compliance with trial method
All participants completed their diary cards at Weeks 0 and 6 and reported that they
maintained their usual daily activities throughout the study. No participants used
quinine for the duration of the study.
Effect of intervention
Group data for all outcomes are presented in Table 2. The frequency of nocturnal leg
cramps reduced in both groups over the 6‐week intervention period. However, the
reduction in frequency was significantly greater in the experimental group, by a mean of
1.2 cramps per night (95% CI 0.6 to 1.8).
The severity of nocturnal leg cramps did not improve at all in the control group.
However, there was a substantial reduction in the experimental group. The mean

124
difference in improvement in the severity of the nocturnal leg cramps was 1.3 cm on the
10‐cm visual analogue scale.
No adverse events were reported in either group.
Discussion
Our results showed that six weeks of nightly stretching of the calf and hamstring
muscles significantly reduced the frequency and severity of nocturnal leg cramps in
older people. The best estimate of the average effect of stretching on the frequency of
cramps was a reduction of about one cramp per night. Given that participants had an
average of approximately three cramps per night at the beginning of the study, this is a
substantial effect and approximately equal to the effect we nominated as worthwhile.
Since the stretches are quick and simple to perform, some patients may even consider
the weakest effect suggested by the limit of the confidence interval (a reduction of 0.6
cramps per night) to be worthwhile.
The stretches reduced the severity of the pain that occurred with the nocturnal leg
cramps by 1.3 cm on a 10‐cm visual analogue scale. We do not know the smallest effect
on the severity of the cramps that patients typically feel would make the stretches
worthwhile. In other research using the 10‐cm visual analogue scale for pain, a change
score of 2 cm has been proposed in chronic low back pain patients (20). An effect of this
magnitude was not achieved in our study within the 6‐week intervention period.
However, the confidence interval around this result is reasonably narrow. Therefore
patients can be advised that the average effect of the stretches is to reduce the severity

125
of the pain by 1.3 cm on the 10‐cm scale (or close to this value). Patients can then decide
for themselves whether this effect – in addition to the reduced frequency of the cramps
– makes the stretches worth doing.
In this trial, stretching was performed at home and was patient‐centred. This facilitated
performance of the intervention, which may have aided adherence with the stretches
and increased the effectiveness of the intervention. In this setting, however, correct
execution of the stretching technique was not closely monitored. All the participants in
the experimental group did two exercises, regardless of whether the cramp was located
in the hamstrings or calf. Greater effects may perhaps be achievable if stretches were to
be targeted at the site(s) of each participant’s cramps. This could be investigated in a
future trial.
The results of this study are consistent with those of the uncontrolled study by Daniell
and colleagues, which suggested that stretching exercises were effective in preventing
the occurrence of nocturnal leg cramps (15). Conversely, our results differ from those of
Coppin and colleagues, who concluded that a stretching intervention failed to
significantly relieve the intensity and frequency of nocturnal leg cramps (17). Some
details of that stretching regimen, such as the exact time of day at which stretching was
performed, remain unclear. However, the different result in our study may be
attributable to differences in the time of day, the number of repetitions of the stretch,
and the different eligible populations (users versus non‐users of quinine).

126
One possible limitation of this study is that the test results were obtained using self‐
reported ‘measurements’ in a daily diary. Progress in the control group might be due to
the Hawthorne effect (21). In addition, selection bias may have affected our results due
to the preferences of the participants to participate in this study. Difference in the ages
of both groups also may have caused bias, which could have been reduced through a
pre‐stratification procedure. However, the study design incorporated several features
to reduce the risk of bias in the results, the necessary sample size was calculated and
obtained, and no dropouts occurred during the follow‐up.
Despite some potential limitations, the results of the study are promising for use in
physical therapy settings; even though it only considered the context of the increasing
number of older adults with nocturnal leg cramps, a physical therapy consultation might
be an effective option. More evidence is needed to validate the long‐term effects of
stretching on nocturnal leg cramps.
References
1. Monderer RS, Wu WP, Thorpy MJ. Nocturnal leg cramps. Current Neurology and
Neuroscience Reports 2010; 10,53–59.
2. Sontag SJ, Wanner JN. The cause of leg cramps and knee pains: a hypothesis and
effective treatment. Medical Hypothesis 1988; 25,35–41.
3. Kanaan N, Sawaya R. Nocturnal leg cramps: Clinically mysterious and painful–but
manageable. Geriatrics 2001; 56,39–42.
127
4. Stewart RB, Moore MT, Marks RG. Nocturnal leg cramps in an ambulatory elderly
population: An evaluation of risk factors. Journal of Geriatric Drug Therapy 1993; 7,
23–46.
5. Abdulla AJ, Jones PW, Pearce VR. Leg cramps in the elderly: prevalence, drug and
disease associations. International Journal of Clinical Practice 1999; 53,494–496.
6. Butler JV, Mulkerrin EC, O’Keeffe ST. Nocturnal leg cramps in older people.
Postgraduate Medical Journal 2002; 78,596–598
7. Khassawneh BY (2005) Periodic limb movement disorder. In, Lee‐Chiong T (Ed) Sleep:
A Comprehensive Handbook. Hoboken: Wiley.
8. Hirai M. Prevalence and characteristics of muscle cramps in patients with varicose
veins. Vasa 2000; 29,269–273.
9. El‐Tawil S, Al Musa T, Valli H, Lunn MPT, El‐Tawil T, Weber M. Quinine for muscle
cramps. Cochrane Database of Systematic Reviews, 2010; 12,CD005044.
10. van Kan VH, Jansen PH, Tuinte C, Smits P, Verbeek AL. Hydroquinine pharmacokinetics
after oral administration in adult patients with muscle cramps. European Journal of
Clinical Pharmacology 2000; 56,263–267.
11. Vetrugno R, D’Angelo R, Montagna P. Periodic limb movements in sleep and
periodic limb movement disorder. Neurological Sciences 2007; 28,S9–S14.
12. Aronson JK (2006) Meyler’s side effects of drugs: the international encyclopedia
of adverse drug reactions and interactions (15th edn). Amsterdam: Elsevier.
13. Inan‐Arslan N, Knuistingh Neven A, Eekhof JAH. Nachtelijke kuitkrampen. Huisarts
Wet 2006; 49,215–217.
14. Anonymous. Nocturnal leg cramps and quinine therapy. Australian Journal of Pharmacy
2007; 88,68.

128
15. Daniell HW. Simple cure for nocturnal leg cramps. New England Journal of Medicine
1979; 301,216.
16. Norris SP, Stevens B, Pfefferbaum KF, Wyche RL. Community resilience as a
metaphor, theory, set of capacities, and strategy for disaster readiness. American
Journal of Community Psychology 2008; 41,127–150.
17. Coppin RJ, Wicke DM, Little PS. Managing nocturnal leg cramps–calf‐stretching
exercises and cessation of quinine treatment: a factorial randomized controlled
trial. British Journal of General Practice 2005; 55,186–191.
18. Schneider PL, Crouter SE, Lukajic O, Bassett DR, Jr. Accuracy and reliability of 10
pedometers for measuring steps over a 400‐m walk. Medicine and Science in Sports
and Exercise 2003; 35,1779–1784.
19. Jones CJ, Rikli RE, Beam WC. A 30‐s chair‐stand test to measure lower body strength
in community‐residing older adults. Journal of Aging & Physical Activity 2000; 8,85.
20. Ostelo RW, de Vet HW. Clinically important outcomes in low back pain. Best
Practice & Research Clinical Rheumatology 2005; 19,593–607.
21. Adair G. The Hawthorne effect: a reconsideration of the methodological artefact.
Journal of Applied Psychology 1984; 2,334–345.

129
Chapter 7
Summary and General discussion

130

131
Main findings
In primary health care physiotherapy, the prevalence of patients with musculoskeletal
disorders is rising due to aging in society. The scope in this thesis concentrates
predominantly on three common musculoskeletal disorders: acute nonspecific low back
pain and nocturnal leg cramps. The main objective of this thesis was to investigate the
psychometric features of diagnostic instruments and examining the effectiveness of
interventions for these musculoskeletal disorders.
The main findings of the studies performed are summarized as answers to the research
questions formulated in the introduction. Consequently, the clinical implication will be
discussed.
Research question 1: Do negative expectations in patients after the onset of acute
nonspecific low back pain increase the odds of absence from usual work due to progression
to chronic low back pain?
A meta‐analysis was executed to answer this question. In this analysis, the prognostic
role of early recovery expectations of patients with acute low back pain for the
transition to sickness absenteeism due to chronic low back pain are highlighted. Ten
primary studies involving 4,683 participants were included in the review. Participants
with acute or sub acute pain and negative expectations about their recovery show
significantly greater odds of being absent from work after more than 12 weeks after the
onset of pain: OR 2.17 (95% CI 1.61 to 2.91). Conclusion: The odds that adults with acute

132
or sub acute nonspecific low back pain and negative recovery expectations will remain
absent from work due to the progression to chronic low back pain are two times
greater than for those with more positive expectations. These results are consistent
across the included studies. In addition, a recent review emphasized the importance of
expectations of recovery as the most consistent prognostic factor in musculoskeletal
disorders with strong evidence (1).
These results provide prompts on the daily physical therapy practice. As the assessment
of recovery expectations is a relevant issue in the diagnosis of acute non‐specific low
back pain, we recommend to add assessment and counseling to the physical therapy
repertoire. This recommendation matches with the decision to add a question of
patients’ expectations of recovery in the patient’s electronic records in Dutch primary
care physiotherapy. This does support patients in dealing with negative expectations
and perceptions in order to prevent acute nonspecific low back pain becoming chronic.
Research question 2: Is the Dutch version of the Brief Illness Perception Questionnaire a
reliable and valid instrument in acute nonspecific low back pain patients in primary health
care physiotherapy?
In this psychometric study, 83 patients with acute nonspecific low back pain filled in the
Brief Illness Perception Questionnaire (IPQ‐B), two times with a one‐week interval and
the mental health subscale of the Short Form 36 Health Survey (SF‐36). The Cronbach’s
α for internal consistency of the Brief IPQ was 0.73 (95% CI 0.67 to 0.83), indicating
acceptable.. The Intraclass Correlation Coefficient (ICC) test‐retest reliability was 0.72
(95% CI 0.53 to 0.82) indicating adequate reliability scores as a measure of a

133
psychological construct. The Pearson correlation coefficient between IPQ‐B and the SF‐
36, measuring concurrent validity was r p = 0.65 (95% CI 0.46 to 0.80) indicate an
adequate r p. Therefore, it was concluded that the Dutch version of the Brief Illness
Perception Questionnaire shows excellent concurrent validity compared with the
mental health subscale of the Short Form 36 Health Survey.
Negative perception of pain and expectation of recovery is a prognostic factor for
transition to chronic complaints. The Brief IPQ is a reliable and valid instrument
measuring the perception in acute nonspecific low back pain patients. Including the
Brief IPQ with the diagnostics of acute non‐specific low back pain supports
physiotherapists in applying an appropriate intervention, especially in patients with
negative recovery expectations, in order to limit the risk for chronic complaints.
Research question 3: Is the Dutch version of the Low Back Pain Perception Scale a reliable
and valid instrument in acute nonspecific low back pain patients in primary health care
physiotherapy?
Both the authorized translated and linguistically validated Dutch version of the Low
Back Pain Perception Scale (LBPPS) and the Brief Illness Perception Questionnaire (IPQ‐
B) were completed by 84 patients with acute nonspecific low back pain two times with
a one‐week interval. The internal consistency Cronbach’s alpha of the LBPPS was 0.38,
(95% CI 0.09 to 0.56), indicating a poor alpha. Retest reliability shows an overall ICC of
0.50 (95% CI 0.31 to 0.64) indicating a poor ICC (2). A Pearson’s correlation analysis was
134
used to examine the concurrent validity with the IPQ‐B. Pearson’s r p = 0.35 (95% CI 0.14
to 0.53) shows moderate concurrent validity.
Although the prognostic validity of the scale is already determined in primary care, the
internal consistency and retest reliability of the LBPPS both show poor psychometric
properties in physiotherapy practice. The LBPPS has moderate concurrent validity.
Consequently, the LBPPS should be used with caution in primary care physiotherapy.
Research question 4: Is manipulative therapy more effective than standard physical
therapy in subjects with acute (< 16 days) nonspecific low back pain without pain distal of
the knee?
A randomised trial, the EMPAL study (n=64), was set up in primary health care
physiotherapy to evaluate the effectiveness of four manipulative therapy interventions
compared to standard physiotherapy care according to the Dutch guideline of acute
nonspecific low back pain. Flynn’s clinical prediction rule (a duration of symptoms less
than 16 days and no pain distal of the knee) was used to analyse the results (3). Results
of this study showed a statistical significant effect for disability (P < 0.05, d = .20) in
favour of the manipulative therapy over the physiotherapy intervention. No difference
was found for pain intensity and mobility of the lower back. Therefore, it was concluded
that with regard to disability, manipulative therapy in the acute stage of nonspecific low
back pain is only slightly more effective than standard physiotherapy.
As a decision‐making instrument in clinical reasoning, the two‐item clinical prediction
rule used in this study does not include patients’ expectations about recovery in
135
nonspecific acute low back pain. According to the components of the ICF model, further
validation of this prediction model should include multiple patients’ characteristics.
In contrast with international guidelines, when recommending spinal manipulation as an
effective treatment option in the acute stage, the results of our study show an effect of
spinal manipulation on disability but not on pain intensity and mobility.
Research question 5: Is stretching of the calf and hamstring muscles each day just before
sleep for six weeks an effective strategy in older patients with nocturnal leg cramps?
To answer this question, a randomised controlled trial (n=80), was executed to evaluate
the effect of a pre‐sleep stretching procedure in older adults on the frequency and
severity of cramps during the night. All 80 participants completed the study. After six
weeks, the frequency of nocturnal leg cramps improved significantly more in the
experimental group with a mean difference of 1.2 cramps per night (95% CI ‐0.6 to ‐1.8).
Also, the severity of nocturnal leg cramps had decreased significantly in favor of the
experimental group over the control group with a mean difference 1.3 cm (95% CI ‐0.9 to
‐1.7) on the 10‐cm visual analogue scale. Nightly stretching before going to sleep reduces
the frequency and severity of nocturnal leg cramps in older adults.
As a result of this study, stretching techniques should be considered in primary health
care physiotherapy in older adults, age > 55 years with nocturnal leg cramps. It is
recommended to implement this treatment option in medical guidelines.
136
Our study shows the beneficial effect of stretching without any side effect and is,
therefore, an effective alternative for use of medication.
Strong en weak points of this thesis
The studies in this thesis are characterized by a number of strong and weak points.
Undoubtedly a strong point of all studies executed in this thesis is that the research
questions were directly addressed to clinical uncertainty in daily practice of primary care
physiotherapy. Secondly, the results of the studies that deal with specific problems like
nocturnal leg cramps and acute nonspecific low back pain contribute to the ongoing
process of improving the evidence of interventions in primary care physiotherapy. In the
meta‐analysis a personal factor like patients’ expectations in acute low back pain could
be pooled as a result of consistency in the included studies, which was suggested in
earlier reviews. In addition, psychometric studies of the Brief Illness Perception
Questionnaire and the Low Back Pain Perception Scale indicate the relevance of these
self‐reported scales for the assessment of personal factors in acute nonspecific low
back pain patients in primary health care physiotherapy. Attention for perception of
pain in this musculoskeletal disorder is of increasing interest in clinical reasoning to
invent the risk of chronic complaints.
In the other hand, based on the methodological characteristics of the studies, a number
of weaknesses can be identified. First, although the meta‐analysis in the systematic
review provides evidence about the impact of early recovery expectations of patients
with acute low back pain for the transition to sickness absenteeism, it only partially
explains the emergence of chronic low back pain. Only by modelling all the
determinants of acute low back pain in an overall model can truly understand how the
137
complex network of determinants affects the process of this nonspecific
musculoskeletal disorder. Second, both the EMPAL and NLC trails executed in this study
are relative small‐scale studies with relative low statistical power. In addition a local
newspaper recruited the respondents of the NLC trail, so response bias cannot be
excluded. Moreover, the application on the 2‐item clinical prediction rule in the EMPAL
study is a selective reduction of criteria favours spinal manipulation in low back pain.
However, the effect sizes found in the EMPAL study could be an artefact of the selected
criteria of the prediction rule.
Key messages and recommendations
‐ An easy to use instrument measuring early recovery expectations in acute nonspecific
low back pain patients must be developed.
‐ It is important to tackle patients’ negative expectations for recovery by physiotherapists
in acute nonspecific low back pain patients to decrease the risk for chronic complaints.
Advice and information about the favourable course of acute nonspecific low back pain
is essential to reassure as well as to avoid negative recovery expectations and
perceptions. Physiotherapists and manipulative therapists should be educated in a
psychosocial approach in acute nonspecific low back pain patients.
‐ In the acute stage of non‐specific acute low back pain, manipulative therapy is a suitable
treatment option.
‐ Physiotherapists and general practitioners need to underline the concern of nocturnal
leg cramps in older adults and take note of this complaint in daily practice. A nightly
stretching program in older adults with nocturnal leg cramps is strongly recommended.

138
‐ Physiotherapy is essential to teach the pre‐sleep stretching technique to decrease
frequency and severity of nocturnal leg cramps in older adults. We recommend
implementing this finding in physiotherapy and medical directives.
- The prognostic role of negative perception of pain in the transition of acute to chronic
nonspecific low back pain needs further research.
‐ Due to aging patients in primary health care physiotherapy, there is an increasing
number of patients with comorbidity and with various musculoskeletal disorders that
require other competences and insights of primary care physiotherapists.
References.
1. Laisné F, Lecomte C, Corbière M. Biopsychosocial predictors of prognosis in
musculoskeletal disorders: a systematic review of the literature. Disabil Rehabil. 2012;
34(5),355‐82.
2. Nunnally JC. Psychometric theory (2nd ed.), New York: McGraw Hil, 1978.
3. Flynn T, Fritz J, Whitman J, Wainner R, Magel J, Rendeiro D, Butler B, Garber M, Allison
S. A clinical prediction rule for classifying patients with low back pain who demonstrate
short‐term improvement with spinal manipulation. Spine 2002; 27(24),2835‐43.

139
Samenvatting

140
Dit proefschrift is gericht op twee veel voorkomende aandoeningen van het
bewegingsapparaat: acute aspecifieke lage rugpijn en nachtelijke beenkramp bij
ouderen. Door de vergrijzing in de samenleving stijgt de prevalentie van patiënten met
aandoeningen van het bewegingsapparaat in de eerstelijns gezondheidszorg
fysiotherapie. De belangrijkste doelstellingen van dit proefschrift zijn om een
persoonsgebonden factor als verwachting van patiënten over het herstel, als
prognostische factor bij acute lage rugpijn te onderzoeken, de psychometrische
eigenschappen van twee meetinstrumenten die beiden de perceptie van de patiënt
meten, te beoordelen en de effectiviteit te toetsen van twee behandelinterventies.
De belangrijkste resultaten en conclusies naar aanleiding van de onderzoeksvragen in
dit proefschrift zijn als volgt samengevat.
Onderzoeksvraag 1: Zijn negatieve verwachtingen over het herstel bij patiënten met
acute aspecifieke lage rugpijn een prognostische factor voor het ontstaan van
chronische lage rugpijn, gemeten met afwezigheid op het werk?
Een systematic review en meta‐analyse werd uitgevoerd om deze vraag te
beantwoorden. In de meta‐analyse worden de prognostische rol van herstel
verwachtingen van patiënten met acute lage rugpijn voor de overgang naar chronische
lage rugpijn gemarkeerd, gemeten met als uitkomstmaat werkabsentie. Tien primaire
studies met in totaal 4.683 patiënten zijn geïncludeerd in deze review. Patiënten met
acute of subacute lage rugpijn en met negatieve verwachtingen over het herstel hebben
een significant grotere kans op werkabsentie als gevolg van chronische lage rugpijn na

141
meer dan 12 weken sinds het ontstaan van de rugpijn: OR 2,17 (95% BI 1,61 tot 2,91).
Conclusie: De kans dat volwassenen met acute of subacute aspecifieke lage rugpijn en
met negatieve herstel verwachtingen nog niet aan het arbeidsproces deelnemen als
gevolg van progressie naar chronische lage rugpijn is twee keer groter dan voor
patiënten met meer positieve verwachtingen over het herstel. Deze resultaten zijn
consistent in de 10 geïncludeerde studies. In een recente review blijkt eveneens sterk
bewijs van negatieve verwachtingen over het herstel bij verschillende andere
aandoeningen van het bewegingsapparaat als de meest consistente prognostische
factor (1).
Aangezien de beoordeling van de verwachtingen over het herstel relevant is in de
prognostiek van acute aspecifieke lage rugpijn, raden we aan om de beoordeling en
begeleiding toe te voegen aan het repertoire van de fysiotherapeut. Deze aanbeveling
past bij de beslissing om de verwachtingen van de patiënt betreffende zijn herstel in het
elektronische patiëntendossier op te nemen in de eerstelijns fysiotherapie. Dit
ondersteunt patiënten bij het omgaan met negatieve verwachtingen en percepties en is
erop gericht om te voorkomen dat acute aspecifieke lage rugpijn zich ontwikkelt tot
chronische lage rugpijn.
Onderzoeksvraag 2: Is de Nederlandse versie van de Illness Perception Questionnaire,
korte versie, een betrouwbaar en valide instrument bij patiënten met acute aspecifieke
lage rugpijn in de eerstelijns fysiotherapie?

142
In deze psychometrische studie zijn 83 patiënten met acute aspecifieke lage rugpijn
geïncludeerd. De betrouwbaarheid van de korte versie van de Illness Perception
Questionnaire (IPQ‐B) is onderzocht en de Mental Component Scale (MCS), een
subschaal van de Short Form 36 Health Survey (SF‐36) is gebruikt om de validiteit van de
schaal in deze populatie te bepalen. De Cronbach's alpha voor de interne consistentie
van de Brief IPQ was acceptabel: 0,73 (95% BI 0,67 tot 0,83). De Intraclass Correlatie
Coëfficiënt (ICC) als maat voor de test‐hertest betrouwbaarheid was adequaat: 0,72
(95% BI 0,53 tot 0,82). De Pearson correlatiecoëfficiënt is gebruikt als maat voor de
concurrente validiteit van de IPQ‐B en de MCS van de SF‐36 Health Survey: r p = 0,65
(95% BI 0,46 tot 0,80). Dit impliceert een adequate validiteit.
Negatieve perceptie van pijn en verwachting van herstel is een prognostische factor
voor de overgang naar chronische rugpijn. De IPQ‐B is een betrouwbaar en valide
meetinstrument om de perceptie bij acute aspecifieke lage rugpijn patiënten te meten.
De IPQ‐B ondersteunt fysiotherapeuten in het klinisch redeneren om het risico op
chronische klachten in te schatten.
Onderzoeksvraag 3: Is de Nederlandse versie van de Low Back Pain Perception Scale
een betrouwbaar en valide instrument bij acute aspecifieke lage rugpijn in de eerstelijns
fysiotherapie?
De Low Back Pain Perception Scale (LBPPS) is geautoriseerd vertaald en onderzocht op
betrouwbaarheid en validiteit. De interne consistentie gemeten met Cronbach's alpha
van de LBPPS was 0,38 (95% BI 0,09 tot 0,56), dit impliceert een lage Cronbach’s alpha

143
en een slechte interne consistentie. Her‐test betrouwbaarheid gemeten met de
IntraClass Correlation coefficient (ICC): 0,50 (95% BI 0,31 tot 0,64) impliceert een matige
betrouwbaarheid (2). Een Pearson's correlatie analyse is gebruikt voor de concurrente
validiteit met de Illness Perception Questionnaire (IPQ‐B). Pearson’s r p = 0,35 (95% BI
0,14 tot 0,53) en betekent een matige concurrente validiteit.
Hoewel de predictieve validiteit van de schaal al is onderzocht bij patiënten met acute
aspecifieke lage rugpijn in de eerstelijns huisartsenzorg, blijken de interne consistentie
en de test her‐test betrouwbaarheid van de LBPPS in de eerstelijns fysiotherapie niet te
voldoen aan de criteria waardoor men terughoudend moet zijn om de LBPPS toe te
passen in de eerstelijns fysiotherapie. De LBPPS heeft bovendien een matige
concurrente validiteit.
Onderzoeksvraag 4: Is manipulatieve therapie effectiever dan standaard fysiotherapie
bij patiënten met acute (<16 dagen) aspecifieke lage rugpijn zonder pijn distaal van de
knie?
Een gerandomiseerde effectstudie, de EMPAL studie (n = 64), in de eerstelijns
fysiotherapie, is uitgevoerd om de effectiviteit van manuele therapie te vergelijken met
standaard fysiotherapeutische zorg volgens de Nederlandse Richtlijn van fysiotherapie
bij acute aspecifieke lage rugpijn. De ‘clinical prediction rule’ volgens Flynn: duur van de
symptomen minder dan 16 dagen en geen pijn distaal van de knie, is gebruikt om de
resultaten analyseren (3). De resultaten van deze studie toonden een statistisch
significant effect voor beperkingen in activiteiten (P < 0,05, d = 0,20) in het voordeel van

144
manuele therapie ten opzichte van fysiotherapeutische behandeling volgens de richtlijn.
Er werd geen verschil gevonden voor pijnintensiteit en algehele mobiliteit. Conclusie is
dat manuele therapie in de acute fase van aspecifieke lage rugpijn effectiever is dan
standaard fysiotherapie wanneer toename van activiteiten het doel van de behandeling
is.
Deze ‘twee‐item prediction rule’ kan als middel worden ingezet om het klinisch
redeneerproces verder vorm te geven en te onderbouwen. Verdere validatie van dit
voorspellingsmodel is echter noodzakelijk.
In tegenstelling tot nationale en internationale richtlijnen acute aspecifieke lage rugpijn
kan manuele therapie als een effectieve behandeling in de acute fase worden ingezet.
De resultaten van onze studie tonen een effect van manuele therapie op het gebied van
activiteiten maar niet op pijnintensiteit en mobiliteit.
Onderzoeksvraag 5: Is dagelijks rekken van de kuit en hamstrings direct voor bedrust
gedurende zes weken een effectieve strategie bij oudere volwassenen met nachtelijke
beenkramp?
Om deze vraag te beantwoorden is een gerandomiseerd gecontroleerde trial (n = 80)
uitgevoerd om het effect van rekken van de kuit en de hamstrings direct voor het slapen
bij ouderen te evalueren. De frequentie van nachtelijke beenkramp (NLC) was de
primaire uitkomstmaat. Alle 80 deelnemers voltooiden het onderzoek. Na zes weken
bleek de frequentie van NLC significant afgenomen in de experimentele groep met een
gemiddeld verschil van ‐1,2 krampaanvallen per nacht, ten opzichte van de

145
controlegroep die geen rekprocedure uitvoerden (95% BI ‐0,6 tot ‐1,8). Bovendien was
de pijn als gevolg van NLC significant verlaagd in de experimentele groep ten opzichte
van de controle groep met een gemiddeld verschil van ‐1,3 cm (95% BI ‐0,9 tot ‐1,7) op de
10‐cm visuele analoge schaal (VAS). Rekken van de kuit en hamstrings direct voor
bedrust vermindert de frequentie en de pijn van NLC bij oudere volwassenen.
Als gevolg van het resultaat van dit onderzoek, dient rekken van de kuit en hamstrings
te worden overwogen in de eerstelijns fysiotherapie bij oudere volwassenen met een
leeftijd > 55 jaar met NLC. Het wordt aanbevolen om deze behandeling te
implementeren in een richtlijn van het KNGF.
Deze studie toont het gunstige effect aan van rekken zonder enige bijwerking, en is
daarom een alternatief voor medicamenteuze behandeling.

146

147
Dankwoord

148
Dit proefschrift was nooit ontstaan zonder de begeleiding van mijn promotoren: Cees
van der Schans, Mathieu de Greef en Wim Krijnen.
Beste Cees, jij zorgde immer voor een bijzonder prettige overlegstructuur. We hebben
veel samengewerkt en ik voelde me altijd gesteund door jouw vertrouwen. Je feedback
op mijn artikelen was opbouwend en ik heb er veel van geleerd. Ik zal je heldere
commentaar op teksten tijdens de bijeenkomsten in jouw werkkamer niet snel
vergeten. Ingewikkelde statistische analyses of zinsconstructies werden bovendien
altijd afgewisseld met ontspannende momenten. Het Sinterklaasoverleg was
onvergetelijk en een historisch moment! De link tussen toegepast wetenschappelijk
onderzoek en de dagelijkse praktijk wordt door jou goed bewaakt. Bedankt dat je altijd
snel hebt gereageerd en dat iedere exercitie met voldoening tot een goed einde is
gebracht.
Beste Mathieu, jij als mijn directe begeleider en copromotor. Ik heb heel veel van je
geleerd! Onze eerste studie was gereed en tevens de start voor vervolgonderzoek met
de mogelijkheid tot promoveren, een mogelijkheid die jij destijds hebt aangegeven. De
zomer van 2008, aan een zonnig strand, heb ik benut om daar over na te denken en
hierna was het snel duidelijk dat deze uitdaging voor mij een perfecte gelegenheid zou
zijn om me met veel passie te storten op toegepast wetenschappelijk onderzoek. Je
zoekt naar oplossingen en je creativiteit om een probleem van diverse kanten te
benaderen heeft me geïnspireerd. Daar heb ik veel van geleerd. Bovendien ben je er
altijd geweest om de focus op het doel te bewaken en daar waar nodig heb je
bijgestuurd. Mijn dank is bijzonder groot voor de kans die je mij geboden hebt en me
geleerd hebt hoe met wetenschappelijk onderzoek om te gaan waardoor ik me verder

149
heb kunnen ontwikkelen als onderzoeker. Van begin tot eind ben je betrokken geweest
en zijn we samen opgetrokken. Het mag bovendien niet onvermeld dat soms een
kwinkslag onze werkzaamheden hebben begeleid!
Beste Wim, jouw uitstekende analyses hebben me doen inzien dat zuiver
wetenschappelijk onderzoek afhangt van een prachtige statistische analyse. Mijn kennis
hierover is vergroot en ik heb meer inzicht gekregen in deze boeiende materie. Wim, jij
blinkt uit in biostatistiek en in het bewaken van consistentie in een artikel. Ik ben je
dankbaar voor je adviezen.
Ik kijk uit naar een voortzetting van de samenwerking op enigerlei wijze en dat nieuwe
onderzoeksterreinen worden verkend binnen het Lectoraat.
Beste leden van de Leescommissie.
Voor het lezen en beoordelen van mijn proefschrift en inbreng van kennis en expertise
wil ik Prof. Dr. I. Bautmans, Prof. Dr. P. Dijkstra en Prof. Dr. J. Groothoff bedanken voor
hun bijdrage in de beoordelingscommissie. Ivan, wie had dat gedacht!
Het Lectoraat Transparante Zorgverlening van de Hanzehogeschool ben ik speciale
dank verschuldigd voor de mogelijkheid die ze geboden heeft om dit proefschrift te
realiseren. Ik denk hierbij aan alle mede‐onderzoekers voor de inspirerende
bijeenkomsten. Alle contacten en uitwisseling van inzichten en gegevens zijn heel
waardevol geweest en hebben bijgedragen tot de realisatie van dit proefschrift. Ik hoop
dat we elkaar nog vaak tegenkomen!
Judith van der Boom, als eerste aanspreekpunt van het Lectoraat, bedankt voor al je
ondersteuning, begrip en bijdragen.

150
Mijn dank gaat ook uit naar de faculteit Bewegingswetenschappen van de
Rijksuniversiteit en de hulp van studenten die in de NLC studie zeer vakkundig hebben
geopereerd. Zonder jullie hulp was het niet zo’n mooie studie geworden.
Kinese Fysiotherapeuten wil ik bedanken voor de mogelijkheid van dataverzameling
voor het onderzoek. Niet in de laatste plaats hulde aan alle proefpersonen die geheel
vrijwillig hun medewerking verleend hebben.
Data invoer was onmogelijk geweest zonder de hulp van Wouter, Ilse en Svenja. Alle
data is zeer nauwkeurig ingevoerd en gecontroleerd. Een kort verzoek was al
voldoende; nooit was iets te veel gevraagd. Jullie hebben voortreffelijk werk geleverd!
Bovendien Ilse, ‘your corrections in the final phase were excellent’.
Alle vrijwillige medewerkers en collega’s in Friesland in de diverse praktijken die volledig
belangeloos hun bijdrage hebben geleverd: zeer bedankt. In de EMPAL studie heeft Jan
Winters op een spontane manier zijn ideeën ingebracht, hierdoor is Jan gevraagd om als
mede auteur zijn bijdrage te leveren.
Collega’s van de SOMT ontzettend bedankt voor de vele interactiemomenten en het
delen van kennis en expertise op vakinhoudelijk gebied. We hebben veel van elkaar
geleerd en ik hoop van harte op een voortgaande samenwerking in de komende jaren.
Ook de directie mijn hartelijke dank voor de spontane support!

151
Marijke, jij verdient speciale dank voor de accurate hulp bij de afronding en opmaak van
het proefschrift.
De verzorging van de cover van het proefschrift was in prima handen van jou Peter,
bovendien heb je veel geduld moeten betrachten. Soms hebben ideeën tijd nodig om te
rijpen!
Lieve familie en vrienden. Jullie hebben dikwijls gevraagd waar ik mee bezig was. Er zijn
wat afspraken verplaatst of uitgesteld als gevolg van andere belangen! Wellicht ligt hier
voor jullie nu een tastbaar resultaat van deze inspanningen. Bob, als wetenschapper zou
hiervan genoten hebben, oprecht jammer dat hij er niet meer bij kan zijn.
Tot slot aandacht voor de belangrijkste persoon in mijn leven. Zonder jou en zonder
jouw steun was dit proefschrift nooit tot stand gekomen ondanks het feit dat de start
van het proefschrift samenviel met een belangrijke periode in ons leven. Gonny, je hebt
me de ruimte gegeven om dit promotie traject tot een goed einde te brengen ook al is
veel ten koste gegaan van tijd samen. Desondanks hebben we er veel ‘quality hours’
voor teruggekregen. Jouw adviezen heb ik altijd ter harte genomen en je support was
onmisbaar. Ik blijf je er altijd dankbaar voor!

152

153
Curriculum vitae
154
Joannes Marinus (Hank) Hallegraeff (3 november 1955, Haarlem) behaalde het bachelor
diploma fysiotherapie in 1981 aan de Hogeschool van Amsterdam. Hij heeft in 1987 het
diploma Manueel therapeut behaald aan de Stichting Opleiding Musculoskeletale
Therapie (SOMT). Gedurende deze jaren was hij werkzaam als fysiotherapeut en
manueel therapeut in de eerstelijns gezondheidszorg. Op zoek naar een nieuwe
uitdaging en ingegeven door de opkomst van EBP (evidence based practice) heeft hij in
2005 zijn Master of Science Klinische Epidemiologie behaald aan de Universiteit van
Amsterdam met als afstudeeropdracht manuele therapie bij acute lage rugpijn.
Van 2006 tot 2012 is hij als redactielid werkzaam geweest voor het Tijdschrift voor
Manuele Therapie.
Vanaf 2006 is hij naast zijn werkzaamheden in een multidisciplinaire eerstelijns
omgeving ook werkzaam als docent aan de Masteropleiding Musculoskeletale Therapie
aan de SOMT. Naast onderwijskundige taken is zijn aandacht gericht op
wetenschappelijk onderzoek en de inhoud van het curriculum van ‘Life Long Learning’.
Vanaf 2008 is hij verbonden aan de onderzoeksgroep van het Lectoraat Transparante
Zorgverlening van de Hanzehogeschool Groningen. In 2009 waren er tevens
onderwijsactiviteiten aan de Hanzehogeschool. Het promotieonderzoek ‘Common
musculoskeletal disorders in primary care physiotherapy’ is in 2008 gestart in
samenwerking met SHARE onder leiding van prof. dr. CP van der Schans.
Sinds 2012 is hij lid van het BOCK (BeleidsOrgaan Centraal Kwaliteitsregister) van het
KNGF.
Als onderzoeker, clinicus en docent is Hank overtuigd van het feit dat de
professionalisering van het vak fysiotherapie zich momenteel in een noodzakelijke
stroomversnelling bevindt en wil daar graag een bijdrage aan blijven leveren. Blijvende
155
wetenschappelijke onderbouwing van het fysiotherapeutisch handelen is een noodzaak
om de evolutie naar verdere professionalisering mogelijk te maken.
Hierin ligt een blijvende onderzoeksinteresse besloten.
Publicaties
Expectations about recovery from acute non‐specific low back pain predict absence
from usual work due to chronic low back pain: a systematic review.
Hallegraeff JM, van der Schans CP, Krijnen WP, de Greef MH
Journal of Physiotherapy 2012, 58(3)165‐172.
Measurement of acute nonspecific low back pain perception in primary care physical
therapy: reliability and validity of the brief illness perception questionnaire.
Hallegraeff JM, van der Schans CP, Krijnen WP, de Greef MH.
BMC Musculoskelet Disord. 2013 Feb 1;14:53.
Manipulative treatment and clinical prediction criteria in nonspecific acute low back
pain. Hallegraeff JM, de Greef MH. Winters JC, Lucas C.
Perceptual and Motor Skills, 2009, 108, 196‐208.
Stretching before sleep reduces the frequency and severity of nocturnal leg cramps in
older adults: a randomised trial.
Hallegraeff JM, van der Schans CP, de Ruiter R, de Greef MH.
Journal of Physiotherapy 2012, 58(1)17‐22.

156

157
Wetenschappelijk onderzoek afdeling Revalidatiegeneeskunde – Centrum voor
Revalidatie UMCG
EXPAND
Extremities, Pain and Disability
Missie: EXPAND draagt bij aan participatie en kwaliteit van leven van mensen met
aandoeningen en amputaties van de extremiteiten of met pijn aan het
bewegingsapparaat.
EXPAND omvat twee speerpunten: onderzoek naar aandoeningen aan en amputaties
van extremiteiten met nadruk op stoornissen, activiteiten en participatie en onderzoek
naar chronische pijn en arbeidsparticipatie. EXPAND draagt bij aan het UMCG‐brede
thema Healthy Ageing.
Research Department of Rehabilitation Medicine – Center for Rehabilitation UMCG
EXPAND
Extremities, Pain and Disability
Mission: EXPAND contributes to participation and quality of life of people with
conditions and amputations of the extremities and musculoskeletal pain.

158
EXPAND focuses on two spearheads: research on the conditions and amputations of the
extremities with emphasis on body functions and structures, activities and
participations, and chronic pain and work participation. EXPAND contributes to Healthy
Aging, the focus of the UMCG.

159

160
Research Institute for Health Research SHARE This thesis is published within the Research Institute SHARE of the Graduate School of Medical Sciences (embedded in the University Medical Center Groningen / University of Groningen). More recent theses can be found in the list below. Further information regarding the institute and its research can be obtained from our internetsite: www.rug.nl/share. ((co‐) supervisors are between brackets)
2013 Fortington LV. Enabling the elderly person with lower limb amputation through
surgery, rehabilitation and long term care (prof JHB Geertzen, prof PU Dijkstra, dr GM Rommers) Lako IM. Depressive symptoms in patients with schizophrenia; count symptoms
that count (prof K Taxis, prof D Wiersma) Arnardottir AH. Regulatory benefit‐risk assessment; different perspectives
(prof FM Haaijer‐Ruskamp, prof PA de Graeff, dr PGM Mol, SMJM Straus)
Meijer A. The forest trough the trees; investigating depression in patients with
cancer and patients with myocardial infarction using systematic reviews and meta‐analytic techniques (prof P de Jonge, dr HJ Conradi, dr BD Thombs)
Kuchenbecker WKH. Obesity and female infertility (prof JA Land, prof BHR Wolffenbuttel, dr A Hoek, dr H Groen) Rozenbaum MH. Costs and effectiveness of extended vaccination strategies
against pertussis and pneumococcal disease (prof MJ Postma, prof E Hak) Kingma EM. Intelligence and functional somatic symptoms and syndromes (prof JGM Rosmalen, prof J Ormel, prof P de Jonge) Kedde JH. Sexual health of people with disability and chronic illness (prof HBM van de Wiel, prof WCM Weijmar Schultz) Horst PGJ ter. Clinical pharmacology of antidepressants during pregnancy

161
(prof B Wilffert, prof LTW de Jong‐van den Berg) Sinha R. Adjustment to amputation and artificial limg, and quality of life in lower limb amputees (prof WJA van den Heuvel, prof P Arokiasamy, dr JP van Dijk) 2012 Pechlivanoglou P. Applying and extending mixed‐effects models in health in health economics and outcomes research (prof MP Postma, prof JE Wieringa, dr HH Le)
Verboom CE. Depression and role functioning; their relation during adolescence
and adulthood (prof J Ormel, prof WA Nolen, prof BWJH Penninx, dr JJ Sijtsema) Benka J. Living with rheumatoid arthritis: do personal and social resources make
a difference? (prof JW Groothoff, prof JJL van der Klink, dr JP van Dijk, dr I Rajnicova‐Nagyova)
Kalina O. Sexual risky behaviour among Slovak adolescents and young adults; social and psychological factors (prof SA Reijneveld, dr JP van Dijk, dr A Madarasova‐Geckova) Crijns HJMJ. Drug related safety issues affecting pregnancy outcome and
concerning risk minimisation measures; emphasis on pregnancy prevention programmes (prof LTW de Jong‐van den Berg, dr SMJM Straus)
Vries HJ de. Working with pain; sustainable work participation of workers with
chronic non‐specific musculoskeletal pain (prof JHB Geertzen, JW Groothoff, MF Reneman, dr S Brouwer)
Karsten J. On the threshold of disorder; definition and course of subthreshold
depression and subthreshold anxiety (prof WA Nolen, prof BWJH Penninx, dr CA Hartman)
Abma FI. Work functioning: development and evaluation of a measurement tool (prof JJL van der Klink, prof U Bültmann) Rodrigues HCML. Who’s the patient? Ethics in and around maternal‐fetal
surgery (prof PP van den Berg, prof M. Düwell) For more 2012 and earlier SHARE‐theses see our website.

162