female reproductive system imaging. female reproductive anatomy
TRANSCRIPT

Female Reproductive System IMAGING

Female Reproductive Anatomy
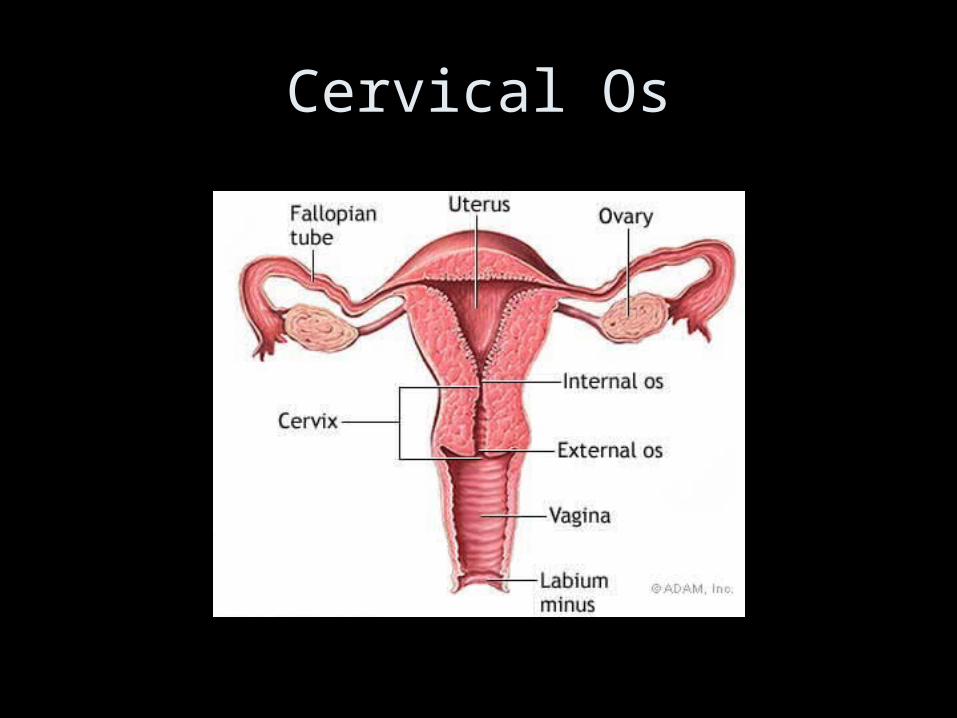
Cervical Os
Female Reproductive System Imaging and Procedures
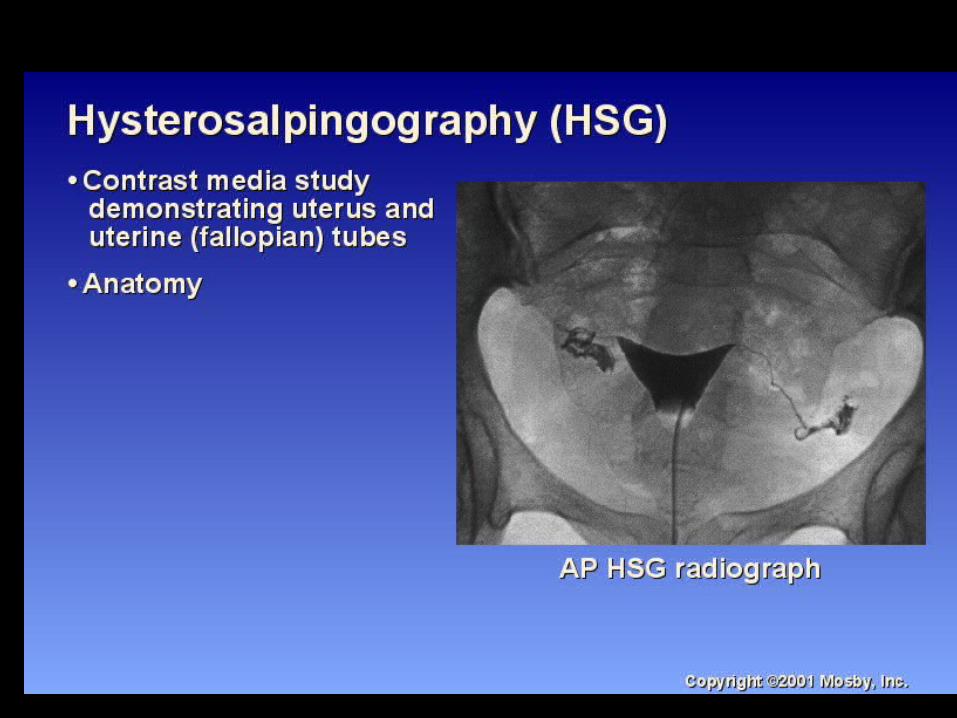

HSG


SAGITTAL T2WI MRI
U: UTERS (BIGHT ENDOMETIUM, DARK JUNCTIONAL ZONE,
LIGHT DARK MYOMETRIUM)
C: CERVIXB: BLADDERR: RECTUM

OO
U
B
CORONAL T2WI MRI
O: OVARIESU: UTERUSB: BLADDER
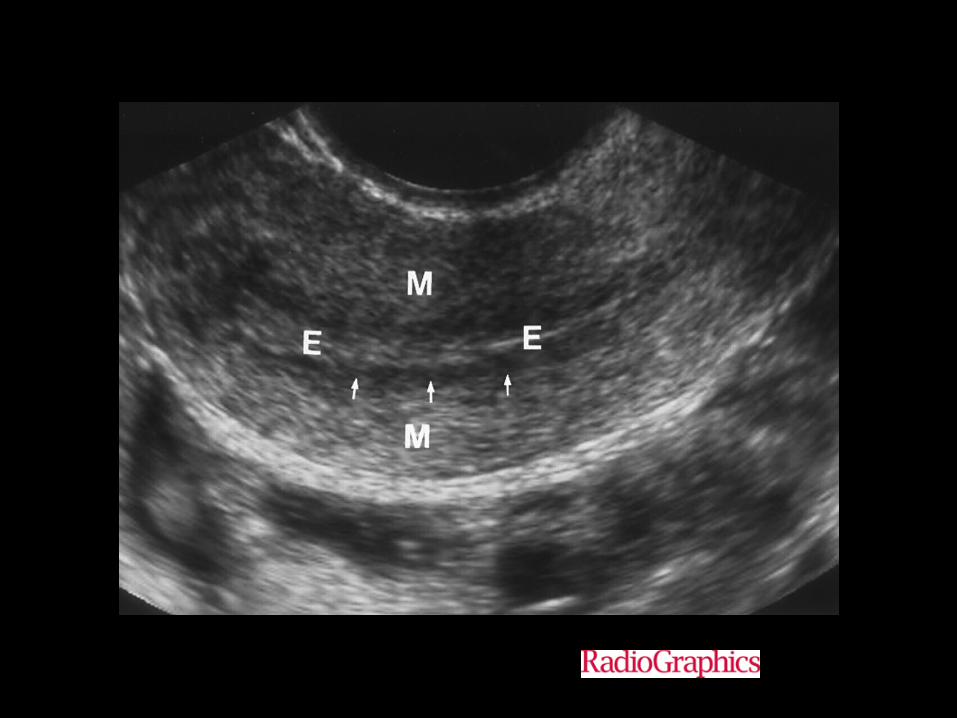
Figure 1. Normal uterus.
Reinhold C et al. Radiographics 1999;19:S147-S160
©1999 by Radiological Society of North America

Congenital Anomolies(FEMALE)

Uterus Didelphys
Unicornate Uterus
• Pathology
• There is failure of one müllerian duct to elongate while the other develops normally. The embryologic predominance of the unicornuate uterus to be on the right has not been explained. It may or may not have rudimentary horn.

• Hysterosalpingogram (HSG)
• The endometrial cavity usually assumes a fusiform (banana type) shape (except for type a where there may a small cavitatory filling defect), tapering at the apex and draining into a solitary fallopian tube. The uterus is generally shifted off the midline.

Unicornuate Uterus
MRI• unicornuate uterus appears curved and
elongated, with the external uterine contour assuming a banana shape
• uterine volume is reduced, and the configuration of the uterus is asymmetric
• normal myometrial zonal anatomy is maintained

• MRI obtained subsequent to hysterosalpingography. Axial T2 MRI shows fusiform uterine cavity with typical trilaminar appearance of high-signal endometrium (star), low-signal junctional zone (long arrow), and intermediate-signal myometrium (short arrow) of uterus seen in right side of pelvis. This corresponds to cavity opacified on

• septate uterus 12 : has a normal fundal contour but is characterized by a persistent longitudinal septum that partially divides the uterine cavity
•
Bicornate Uterus
• Pathology• It results from an abnormal development of the
paramesonephric ducts that results in a uterus divided into two horns from a partial failure of fusion.
• bicornuate bicollis : two cervical canals - central myometrium extends to external cervical os
• bicornuate unicollis : one cervical canal - central myometrium extends to internal cervical os

• Radiographic features
• General
• The external uterine contour is concave or heart shaped, and the uterine horns are widely divergent. The fundal cleft is typically more than 1cm deep and the inter-cornual distance is widened.

Fluoroscopy - Hysterosalpinogram (HSG)• Difficult to differentiate between septate and bicornuate
anomalies due to the outer uterine contour not being visible 5.
MRI• May help confirm anatomy by showing a deep (> 1 cm)
fundal cleft in the outer uterine contour and an inter-cornual distance of more than 4 cm. The uterus demonstrates normal uterine zonal anatomy.

Bicornate Uterus


Uterus Didelphys
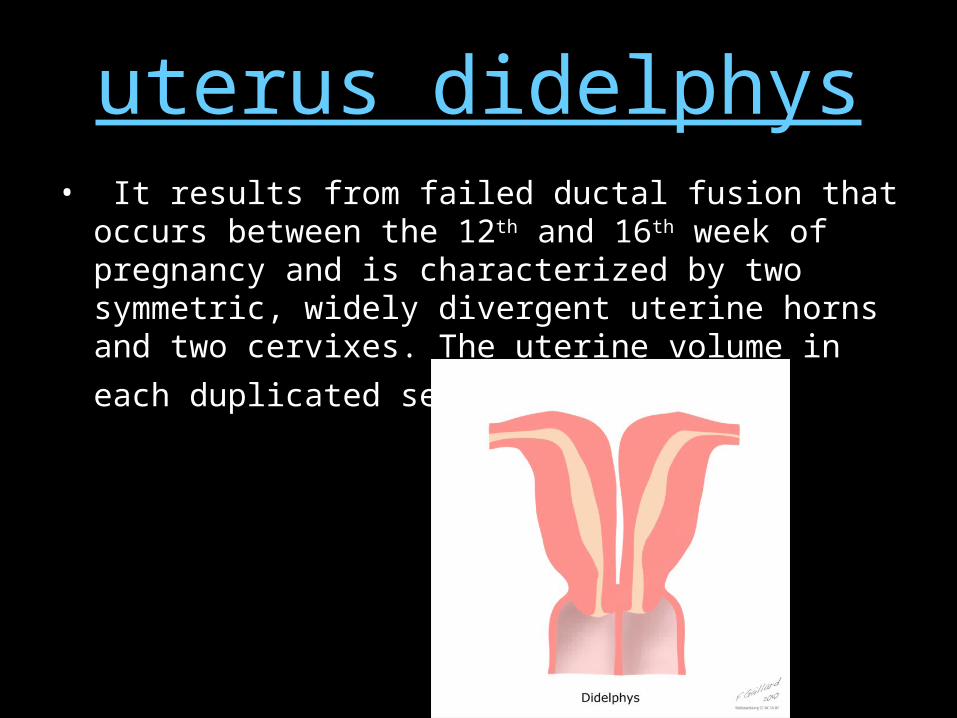
uterus didelphys• It results from failed ductal fusion that occurs between
the 12th and 16th week of pregnancy and is characterized by two symmetric, widely divergent uterine horns and two cervixes. The uterine volume in each duplicated
segment is reduced.

Hysterosalpingogram (HSG)• HSG demonstrates two separate endocervical canals that open into
separate fusiform endometrial cavities, with no communication between the two horns. Each endometrial cavity ends in a solitary fallopian tube.
• If the anomaly is associated with an obstructed longitudinal vaginal septum, only one cervical os may be depicted, and it may be cannulated with the endometrial configuration mimicking a unicornuate uterus.
• Pelvic ultrasound• Separate divergent uterine horns are identified with a
large fundal cleft. Endometrial cavities are uniformly separate, with no evidence of communication. Two separate cervices need to be documented.
• MRI• MR imaging demonstrates two separate uteri with widely
divergent apices, two separate cervices, and usually an upper vaginal longitudinal septum. In each uterus, normal uterine zonal anatomy is preserved

Neoplastic Diseases(FEMALE)
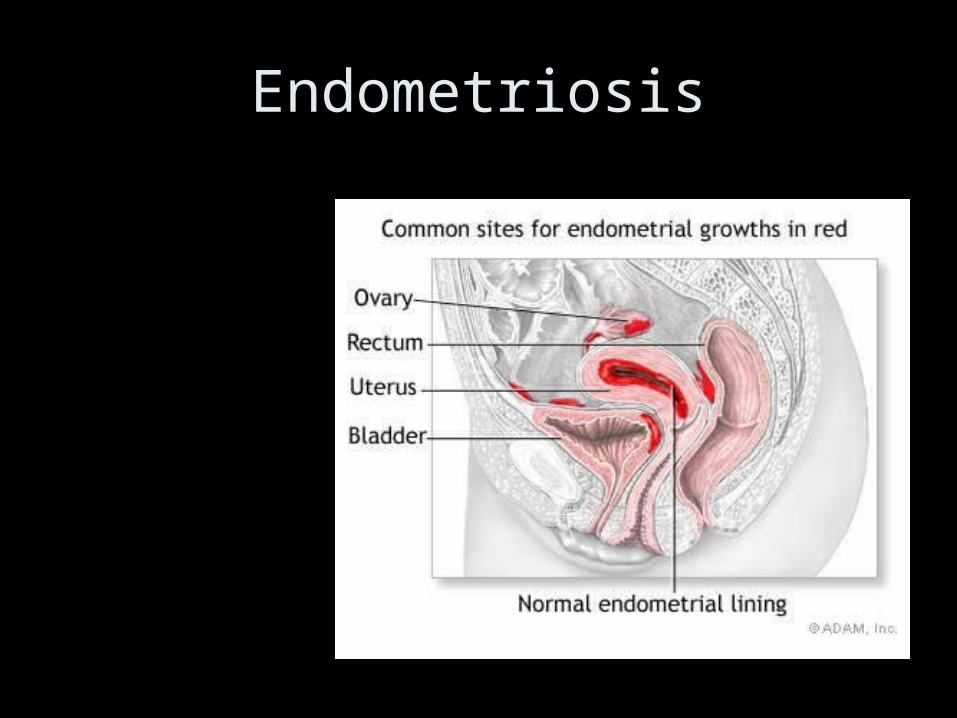
Endometriosis
• Endometriotic cysts (endometriomas or "chocolate cysts") most commonly occur in the ovaries and are the result of repeated cyclic haemorrhage within a deep implant. Often there is complete replacement of ovarian tissue. The cyst walls may become thick and fibrotic with dense adhesions, with lining that varies in contour (smooth to shaggy) and colour (pale to brown).

• haemorrhagic “powder burn” – lesions appear bright on T1 fat saturated sequences.
• small solid deep lesions – may be hyperintense on T1 and low on T2
• endometriomas – < 5 mm: early stage disease; > 15 mm: advanced disease– shading sign 25: may be less likely to respond to medical treatment 28 – low T1 and T2 due to tissue and haemosiderin laden macrophages 1 – diagnostic criteria:
• multiple cysts with T1 hyperintensity OR • one or more cysts with high T1 and shading on T2

Hemorrhagic cyst of the right ovary in a 21-year-old woman.
Patel M D et al. Radiology 1999;210:739-745
©1999 by Radiological Society of North America

Figure 15a. Bilateral endometriomas in a 27-year-old woman.
Woodward P J et al. Radiographics 2001;21:193-216
©2001 by Radiological Society of North America
ADENOMYOSIS• Adenomyosis is a nonneoplastic condition,
characterized by benign invasion of ectopic endometrium into the myometrium with hyperplasia of adjacent smooth muscle.

Figure 2a. Imaging signs of adenomyosis.
Reinhold C et al. Radiographics 1999;19:S147-S160
©1999 by Radiological Society of North America
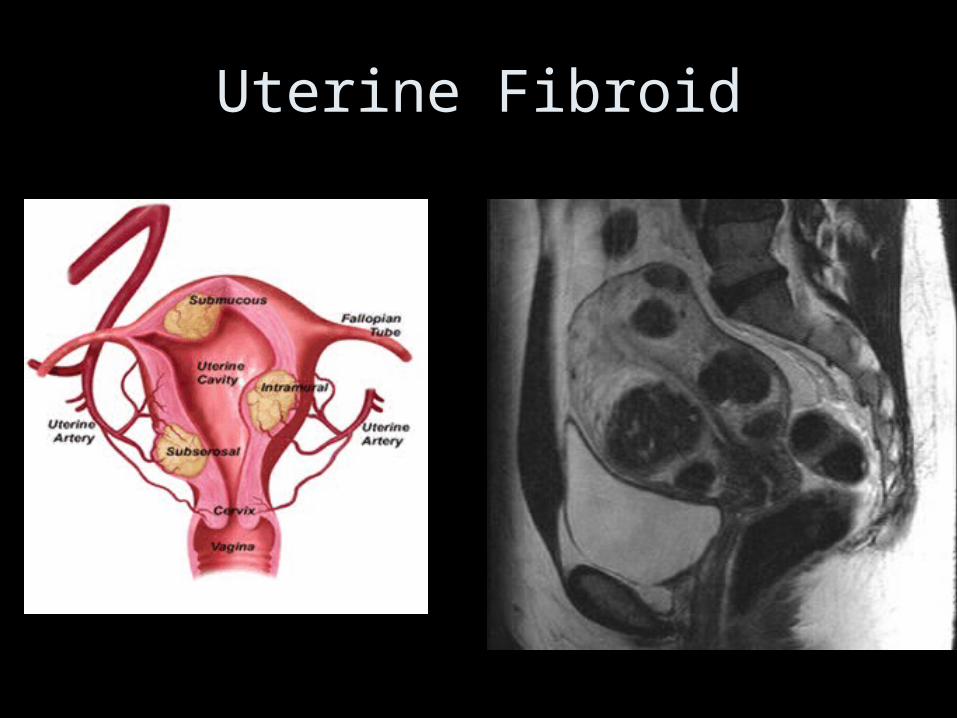
Uterine Fibroid
• A uterine leiomyoma (uterine fibroid) is a benign tumour of myometrial (smooth muscle) origin. It is the most common solid benign uterine neoplasm
• pidemiology • They occur in ~ 20 - 30% of women of
reproductive age 1 and are particularly common in the African population .
• a number of locations within or out of the uterus :• Within the uterus• intra-mural leiomyoma : most common• sub-serosal leiomyoma• sub-mucosal leiomyoma : least common : ~ 10 -
15 %
They can also undergo several types of degeneration
• hyaline degeneration, cystic degeneration• myxoid degeneration, red - carneous• extra uterine pelvic leiomyomas7
• Pelvic ultrasound• ultrasound is used to diagnose the presence and
monitor the growth of fibroids• uncomplicated leiomyomas are usually hypo-
echoic.• calcification is seen as echogenic foci with
shadowing• cystic areas of necrosis / degeneration may be
seen

• CT• on CT images, fibroids are usually of soft tissue
density but may exhibit coarse peripheral or central calcification
• they may distort the usually smooth uterine contour• enhancement pattern is variable• Pelvic MRI• Signal characteristics are variable, and include 1-2
• T1 : – non-degenerated fibroids and calcification appear as low
to intermediate signal intensity compared with the normal myometrium

• T2 : – non-degenerated fibroids and calcification appear as
low signal intensity – as they are usually hypervascular, flow voids are often
observed around them 10 – fibroids that have undergone cystic degeneration /
necrosis can have a variable appearance, usually appearing high signal on T2 sequences.
• T1 C+ (Gd) : – variable enhancement is seen with contrast
administration

LEIOMYOMA (FIBROID TUMOR)