enfermedad renal
DESCRIPTION
articulo en ingles de daño renal,diagnostico y manejoTRANSCRIPT
Hematuria, 844History and Review of Systems, 845Physical Examination, 845Laboratory Tests, 845Imaging, 847
Nephritic Syndrome, 847History and Review of Systems, 848Physical Examination, 848Laboratory Tests, 848Imaging, 849Renal Biopsy, 849
Nephrotic Syndrome, 850History and Review of Systems, 850Physical Examination, 851Laboratory Tests, 852Imaging, 853Renal Biopsy, 853
Obstructive Uropathy, 853History and Review of Systems, 853Physical Examination, 854
Laboratory Tests, 854Imaging, 854
Hypertension, 854History and Review of Systems, 855Physical Examination, 855Laboratory Tests, 856Imaging, 856Other Studies, 856
Nephrolithiasis, 856History and Review of Systems, 856Physical Examination, 857Laboratory Tests, 857Imaging, 858Differential Diagnosis, 858Initial Treatment, 858
Acute Kidney Injury, 859History and Review of
Systems, 860Physical Examination, 860Laboratory Tests, 860
Imaging, 861Renal Biopsy, 861
Chronic Kidney Disease and Chronic Kidney Failure, 861History and Review of Symptoms, 862Physical Examination, 863Laboratory Tests, 863Imaging, 864
Urinary Tract Infection, 864History and Review of Systems, 864Physical Examination, 865Laboratory Tests, 865Imaging, 865
Approach to the Patient with Kidney DiseaseMichael Emmett, Andrew Z. Fenves, and John C. Schwartz
Chapter
24
844
Readers of this chapter are assumed already to be competent medical historians and to be very familiar with the essentials of the general physical examination. Furthermore, many of the topics that are briefly reviewed in this chapter are addressed in much greater detail in other parts of this textbook. Con-sequently, the focus here is on certain features of the history, physical examination, and laboratory testing that might be of specific utility to nephrologists and nephrology trainees. The chapter is divided into nine broad areas of kidney disorder and addresses those features of greatest importance to the early diagnostic and therapeutic phases of the patient’s workup.
Hematuria
Hematuria is the excretion of abnormal amounts of red blood cells (RBCs) into the urine. Normal individuals excrete about 1 million RBCs per day in their urine. When translated to the sediment of a spun urine specimen, this equates to about 1 to 3 RBCs per high-power field (HPF). Therefore excretion of more than 3 RBCs per HPF is abnormal and may warrant
further evaluation. Asymptomatic “microscopic hematuria” is very common; it may be detected in up to 13% of adults.1 Although it is most often of no consequence, hematuria can be a sign of serious disease and should never be ignored. Gross hematuria occurs when enough blood is present in the urine to turn it red or brown. Although microscopic and gross hema-turia are generally caused by the same conditions, there are marked differences in the relative frequencies with which vari-ous pathologic conditions manifest these two presentations. Therefore, the diagnostic approaches to these two conditions are different. Routine screening of healthy individuals for the presence of hematuria is not recommended by the U.S. Preventive Services Task Force.2 However, asymptomatic microscopic hematuria may be detected when a urinalysis is performed during the evaluation of a patient for nonurinary complaints. Furthermore, despite official recommendations, urinalyses are nonetheless frequently ordered as a screening test. When such testing reveals hematuria, the person’s age, gender, race, medical history, and physical findings should be considered in deciding whether to further evaluate this find-ing and, if so, in determining the most appropriate diagnostic

Chapter 24 Approach to the Patient with Kidney Disease 845
studies and the sequence in which they should be performed. Asymptomatic microscopic hematuria should be confirmed in at least two of three midstream clean-catch voidings before the physician embarks on a potentially expensive workup, which can have significant adverse impact and complications. If microscopic hematuria spontaneously resolves, evaluation decisions are strongly influenced by the clinician’s index of suspicion (see later). Microscopic hematuria associated with symptoms such as urinary frequency or pain is more worri-some and mandates further evaluation. Gross hematuria, especially if clots are passed, usually indicates a urologic source of bleeding. Even a single episode of gross hematuria man-dates evaluation. The most common cause of gross hematuria in young women (<40 years of age) is urinary tract infection (UTI). Malignancy must be strongly considered and ruled out by appropriate studies in older patients.3 Brown, “Coca-Cola”–colored, or smoky urine with RBCs present on micros-copy is very suggestive of a glomerular source of bleeding.
History and Review of Systems
Three major factors influencing the workup are the patient’s gender, race, and age. The common causes of hematuria in chil-dren and young adults are much different than those in older individuals. Hematuria in adults older than 40 years (some experts propose an age cutoff of older than 50 years) must be considered a sign of malignancy (of the bladder, upper urinary tract, or kidney) until proved otherwise. Although malignancy is much less frequent in young patients with hematuria, a Wilms’ tumor should be considered. Bladder cancer is much more common in men and in whites. Hypercalciuria, and less commonly hyperuricosuria, cause hematuria frequently in children but less commonly in adults. Hematuria due to UTI is much more common in women, whereas older men may bleed from the prostate. In women, cyclic gross hematu-ria concurrent with the menses raises the strong possibility of genitourinary (GU) tract endometriosis. The combination of hematuria with fever, dysuria, or flank pain, or a prior history of these symptoms raises the likelihood of infection, stones, or malignancy. Colicky pain suggests ureteral obstruction from a stone, blood clot, or sloughed renal papilla. This is especially the case if the pain radiates to the testicle or labia. A family history of renal dysfunction or renal stones should be sought. When a patient with hematuria has family members with renal failure, polycystic kidney disease or Alport’s disease should be considered. Familial hearing loss, especially in male relatives, also suggests Alport’s disease. A very common cause of otherwise unexplained asymptomatic familial hematuria is thin basement membrane disease.4 Sickle cell trait is a very common cause of hematuria in African Americans. Sickle cell anemia can also cause hematuria.5
Hematuria sometimes occurs after vigorous exercise or participation in contact or noncontact sports.6 Mechanisms include direct recurrent trauma to the bladder or kidneys and pathologic renal hemodynamic effects. However, the fact that hematuria occurs after completing a long bicycle ride or running a marathon does not exclude the possibil-ity of other potentially serious pathologic conditions, and generally a complete evaluation is necessary. Exercise-related hemoglobinuria, such as march hemoglobinuria, and postex-ercise myoglobinuria result in excretion of globin pigments
and positive results on dipstick testing without RBCs in the urine.
Travel history may be very important as, for example, when hematuria develops in patients who have traveled to areas where Schistosoma haematobium infection or tuberculo-sis is endemic. Although otherwise unexplained bleeding into the urine can occur in patients with hereditary or acquired coagulation disorders or in patients who take therapeutic anti-coagulants, these conditions and drugs should not preclude consideration of other important underlying etiologies. Bleed-ing disorders and anticoagulants will cause any pathologic GU structures such as malignancies to bleed more readily. This is especially common in older patients.7 A history of cigarette smoking (or second-hand smoke exposure) increases the risk of bladder cancer twofold to fourfold.8 Occupational exposure to aniline dyes and aromatic amines and amides; treatment with some chemotherapeutic agents such as cyclophospha-mide and mitotane; and radiation to the pelvis increase the risk for uroepithelial cancers. In the past, long-term use of analgesics did increase the risk of bladder cancer, but this was probably due to the presence of phenacetin, which has now been removed from these medications. Indeed, the use of aspi-rin and other nonsteroidal antiinflammatory drugs (NSAIDs) has been shown to reduce the likelihood of bladder cancer in some epidemiologic studies.9
A recent history of pharyngitis followed by hematuria raises the possibility of glomerulonephritis with synpharyn-gitic bleeding. Chronic glomerulonephritis, most commonly immunoglobulin A (IgA) nephropathy, is often exacerbated by an upper respiratory tract infection and may result in gross hematuria. This is distinct from poststreptococcal glomerulo-nephritis, which occurs 2 to 6 weeks following the infection.
With gross hematuria, it is useful to determine if the bleed-ing is more pronounced at the very beginning or at the termina-tion of voiding. Although formal “three-glass” urine collections are rarely performed, a history of initiation hematuria suggests a urethral source, whereas termination hematuria is suggestive of bladder neck or prostatic urethra pathology. Blood clots in some the urine usually denote structural urologic pathology.
Physical Examination
Evaluation of blood pressure and volume status is especially important when glomerulonephritis is a consideration. If pal-pation of the abdomen reveals a mass, a renal tumor or hydro-nephrosis may exist. A palpable bladder after voiding indicates obstruction or retention. Atrial fibrillation raises the possibil-ity of renal embolic infarction, especially if the patient has flank pain. Costovertebral angle tenderness is also suggestive of pyelonephritis, nephrolithiasis, or ureteropelvic junction obstruction. A bruit over the kidney suggests a vascular cause. Careful genital and rectal examination is necessary to diag-nose prostatitis, prostate cancer, epididymitis, meatal stenosis, and other structural causes of hematuria.
Laboratory Tests
A diagnosis of gross hematuria is suggested by red or brown urine. Only about 1 mL of blood causes 1 L of urine to become red. However, many substances other than RBCs can produce

846 Section IV Evaluation of the Patient with Kidney Disease
red or brown urine. Many chemicals, medications, and food metabolites can produce a spectrum of urine colors. A chemi-cal test for hemoglobin is very helpful in distinguishing among these possibilities. The most commonly used method of test-ing the urine for blood is the urine test strip or dipstick, which utilizes the peroxidase-like activity of hemoglobin to gener-ate a color change. The test strip does not react with most nonhemoglobin pigments that can color the urine. In addi-tion to detecting the hemoglobin within RBCs, however, the test reaction yields a positive result with free hemoglobin and myoglobin. Also, hypochlorite solutions, which are sometimes used to clean urine collection containers, can produce a false-positive test strip reaction for blood. Therefore, a positive test strip result must be followed by a microscopic examination of the urine to confirm the presence of RBCs. Some of the causes of red or brown urine are shown in Table 24-1.
It is crucial to separate hematuria caused by glomerular abnormalities from bleeding due to other pathologic kidney conditions (tumors or cysts) or pathologic processes distal to the glomerulus (interstitial disease, stones, or tumors, or other processes affecting the renal pelvis, ureters, bladder, urethra, prostate, or other lower GU system structures). When blood originates from glomeruli, the RBCs pass through the length of the renal tubules, where they are subjected to marked changes in osmolality, ionic strength, pH, and other forces. Compres-sion of the RBCs together with urine proteins creates RBC casts (Figure 24-1), and identification of these casts on micro-scopic examination is excellent evidence of glomerular bleed-ing. Although quite specific, RBC casts often are not seen even with definite glomerular bleeding. A more common helpful finding in glomerular bleeding is the identification of dysmor-phic RBCs of varying shape and sizes with blebs, budding, and especially the vesicle-shaped protrusions that characterize acanthocytes (i.e., “Mickey Mouse ears”; see Figure 24-1). For dysmorphic RBCs to be an excellent indicator of glomerular bleeding, most of the urine RBCs should be affected.10 Acan-thocytes are quite specific, however, and if they represent more
TABLE 24-1 Causes of Red or Brown Urine
ENDOGENOUS SUBSTANCES FOODS DRUGS
Red blood cells Artificial food coloring Adriamycin
Hemoglobin Beets Chloroquine
Myoglobin Blackberries Deferoxamine
Bilirubin Blueberries Levodopa
Porphyrins Fava beans Methyldopa
Melanin Paprika Metronidazole
Rhubarb Nitrofurantoin
Phenazopyridine (Pyridium)
Phenolphthalein
Phenytoin
Prochlorperazine
Quinine
Rifampin
Sulfonamides
than 5% of the RBCs, this is very a suggestive sign of glomeru-lar bleeding. Another indication that bleeding is more likely of glomerular origin is coexistent significant proteinuria (>0.5 g/day or >0.5 g protein per gram of creatinine). The presence of pyuria with hematuria suggests inflammation or infection and warrants a urine culture. Table 24-2 highlights some of the features that can be used to differentiate glomerular and non-glomerular, or urologic, hematuria. Urine cytologic analysis is indicated when otherwise unexplained hematuria is docu-mented. It has good specificity when results are positive and a sensitivity of about 80% for bladder cancer but a much lower sensitivity for upper tract malignancy.11
FIGURE 24-1 Red blood cell cast and acanthocytes consistent with glomerular bleeding (diffusion interference contrast optics). (Courtesy of Dr. Rajiv Agarwal, Nephrology Division, Indiana University School of Medicine.)
TABLE 24-2 Differentiation of Glomerular from Urologic Bleeding
GLOMERULAR HEMATURIA
NONGLOMERULAR/ UROTHELIAL/ UROLOGIC HEMATURIA
Urine color Dark red, brown, cola colored, smoky
Bright red
Clots − +
Proteinuria + −
Red blood cell morphology
Dysmorphic (espe-cially acanthocytes)
Isomorphic
Hypertension + −
Edema + −
Urinary voiding symptoms
− +
Back pain, flank pain + +
Renal function Reduced Normal
Family history + +
Trauma − +
Upper respiratory tract infection
+ −
Fever, rash + −
Cha
Imaging
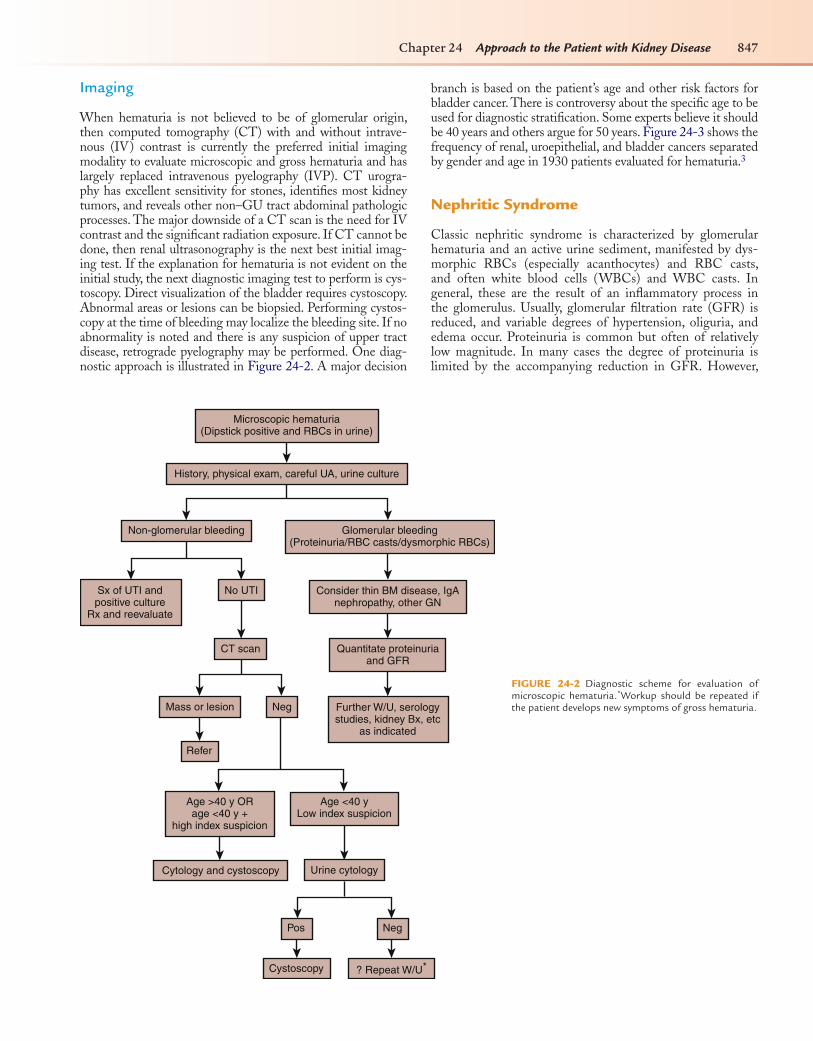
When hematuria is not believed to be of glomerular origin, then computed tomography (CT) with and without intrave-nous (IV) contrast is currently the preferred initial imaging modality to evaluate microscopic and gross hematuria and has largely replaced intravenous pyelography (IVP). CT urogra-phy has excellent sensitivity for stones, identifies most kidney tumors, and reveals other non–GU tract abdominal pathologic processes. The major downside of a CT scan is the need for IV contrast and the significant radiation exposure. If CT cannot be done, then renal ultrasonography is the next best initial imag-ing test. If the explanation for hematuria is not evident on the initial study, the next diagnostic imaging test to perform is cys-toscopy. Direct visualization of the bladder requires cystoscopy. Abnormal areas or lesions can be biopsied. Performing cystos-copy at the time of bleeding may localize the bleeding site. If no abnormality is noted and there is any suspicion of upper tract disease, retrograde pyelography may be performed. One diag-nostic approach is illustrated in Figure 24-2. A major decision
pter 24 Approach to the Patient with Kidney Disease 847
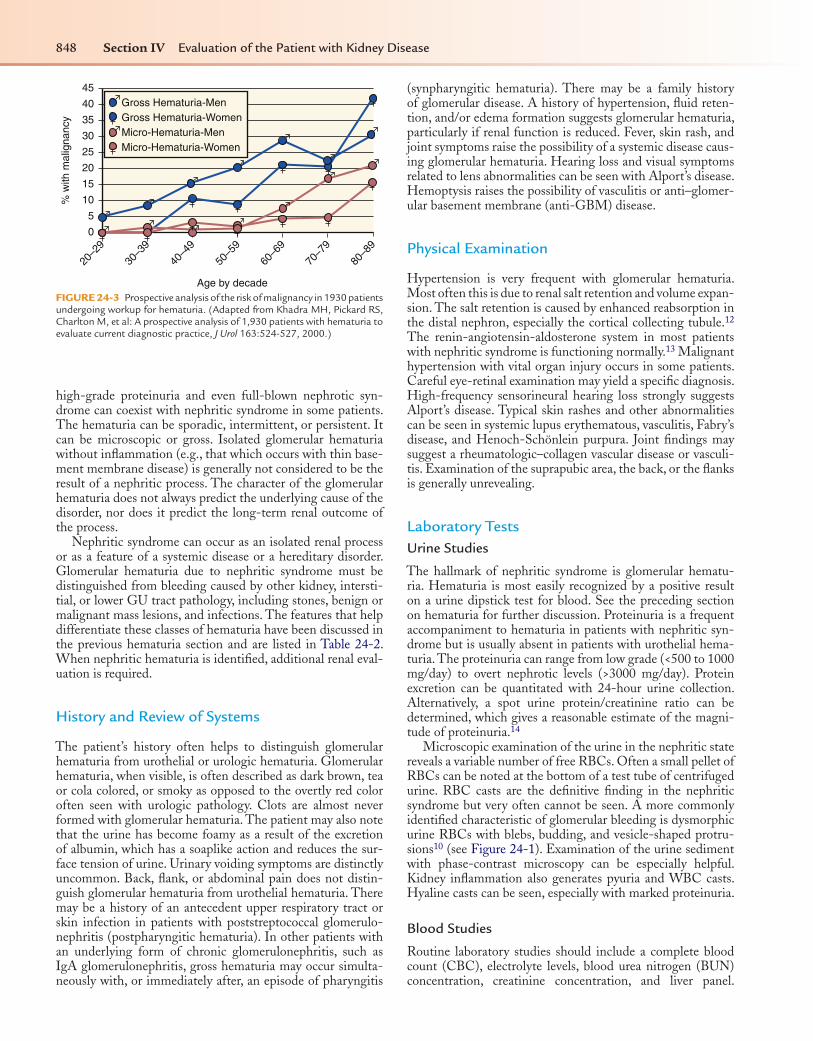
branch is based on the patient’s age and other risk factors for bladder cancer. There is controversy about the specific age to be used for diagnostic stratification. Some experts believe it should be 40 years and others argue for 50 years. Figure 24-3 shows the frequency of renal, uroepithelial, and bladder cancers separated by gender and age in 1930 patients evaluated for hematuria.3
Nephritic Syndrome
Classic nephritic syndrome is characterized by glomerular hematuria and an active urine sediment, manifested by dys-morphic RBCs (especially acanthocytes) and RBC casts, and often white blood cells (WBCs) and WBC casts. In general, these are the result of an inflammatory process in the glomerulus. Usually, glomerular filtration rate (GFR) is reduced, and variable degrees of hypertension, oliguria, and edema occur. Proteinuria is common but often of relatively low magnitude. In many cases the degree of proteinuria is limited by the accompanying reduction in GFR. However,
Microscopic hematuria(Dipstick positive and RBCs in urine)
History, physical exam, careful UA, urine culture
Non-glomerular bleeding
Sx of UTI andpositive culture
Rx and reevaluate
No UTI
CT scan
Mass or lesion
Refer
Neg Further W/U, serologystudies, kidney Bx, etc
as indicated
Age >40 y ORage <40 y +
high index suspicion
Age <40 yLow index suspicion
Urine cytology
Pos
Cystoscopy ? Repeat W/U*
Neg
Cytology and cystoscopy
Quantitate proteinuriaand GFR
Consider thin BM disease, IgAnephropathy, other GN
Glomerular bleeding(Proteinuria/RBC casts/dysmorphic RBCs)
FIGURE 24-2 Diagnostic scheme for evaluation of microscopic hematuria.*Workup should be repeated if the patient develops new symptoms of gross hematuria.
848 Section IV Evaluation of the Patient with Kidney Disease
high-grade proteinuria and even full-blown nephrotic syn-drome can coexist with nephritic syndrome in some patients. The hematuria can be sporadic, intermittent, or persistent. It can be microscopic or gross. Isolated glomerular hematuria without inflammation (e.g., that which occurs with thin base-ment membrane disease) is generally not considered to be the result of a nephritic process. The character of the glomerular hematuria does not always predict the underlying cause of the disorder, nor does it predict the long-term renal outcome of the process.
Nephritic syndrome can occur as an isolated renal process or as a feature of a systemic disease or a hereditary disorder. Glomerular hematuria due to nephritic syndrome must be distinguished from bleeding caused by other kidney, intersti-tial, or lower GU tract pathology, including stones, benign or malignant mass lesions, and infections. The features that help differentiate these classes of hematuria have been discussed in the previous hematuria section and are listed in Table 24-2. When nephritic hematuria is identified, additional renal eval-uation is required.
History and Review of Systems
The patient’s history often helps to distinguish glomerular hematuria from urothelial or urologic hematuria. Glomerular hematuria, when visible, is often described as dark brown, tea or cola colored, or smoky as opposed to the overtly red color often seen with urologic pathology. Clots are almost never formed with glomerular hematuria. The patient may also note that the urine has become foamy as a result of the excretion of albumin, which has a soaplike action and reduces the sur-face tension of urine. Urinary voiding symptoms are distinctly uncommon. Back, flank, or abdominal pain does not distin-guish glomerular hematuria from urothelial hematuria. There may be a history of an antecedent upper respiratory tract or skin infection in patients with poststreptococcal glomerulo-nephritis (postpharyngitic hematuria). In other patients with an underlying form of chronic glomerulonephritis, such as IgA glomerulonephritis, gross hematuria may occur simulta-neously with, or immediately after, an episode of pharyngitis
20–2
9
30–3
9
40–4
9
50–5
9
60–6
9
70–7
9
80–8
90
5
10
15
20
25
30
% w
ith m
alig
nanc
y 35
40
45
Age by decade
Gross Hematuria-MenGross Hematuria-WomenMicro-Hematuria-MenMicro-Hematuria-Women
FIGURE 24-3 Prospective analysis of the risk of malignancy in 1930 patients undergoing workup for hematuria. (Adapted from Khadra MH, Pickard RS, Charlton M, et al: A prospective analysis of 1,930 patients with hematuria to evaluate current diagnostic practice, J Urol 163:524-527, 2000.)
(synpharyngitic hematuria). There may be a family history of glomerular disease. A history of hypertension, fluid reten-tion, and/or edema formation suggests glomerular hematuria, particularly if renal function is reduced. Fever, skin rash, and joint symptoms raise the possibility of a systemic disease caus-ing glomerular hematuria. Hearing loss and visual symptoms related to lens abnormalities can be seen with Alport’s disease. Hemoptysis raises the possibility of vasculitis or anti–glomer-ular basement membrane (anti-GBM) disease.
Physical Examination
Hypertension is very frequent with glomerular hematuria. Most often this is due to renal salt retention and volume expan-sion. The salt retention is caused by enhanced reabsorption in the distal nephron, especially the cortical collecting tubule.12 The renin-angiotensin-aldosterone system in most patients with nephritic syndrome is functioning normally.13 Malignant hypertension with vital organ injury occurs in some patients. Careful eye-retinal examination may yield a specific diagnosis. High-frequency sensorineural hearing loss strongly suggests Alport’s disease. Typical skin rashes and other abnormalities can be seen in systemic lupus erythematous, vasculitis, Fabry’s disease, and Henoch-Schönlein purpura. Joint findings may suggest a rheumatologic–collagen vascular disease or vasculi-tis. Examination of the suprapubic area, the back, or the flanks is generally unrevealing.
Laboratory TestsUrine Studies
The hallmark of nephritic syndrome is glomerular hematu-ria. Hematuria is most easily recognized by a positive result on a urine dipstick test for blood. See the preceding section on hematuria for further discussion. Proteinuria is a frequent accompaniment to hematuria in patients with nephritic syn-drome but is usually absent in patients with urothelial hema-turia. The proteinuria can range from low grade (<500 to 1000 mg/day) to overt nephrotic levels (>3000 mg/day). Protein excretion can be quantitated with 24-hour urine collection. Alternatively, a spot urine protein/creatinine ratio can be determined, which gives a reasonable estimate of the magni-tude of proteinuria.14
Microscopic examination of the urine in the nephritic state reveals a variable number of free RBCs. Often a small pellet of RBCs can be noted at the bottom of a test tube of centrifuged urine. RBC casts are the definitive finding in the nephritic syndrome but very often cannot be seen. A more commonly identified characteristic of glomerular bleeding is dysmorphic urine RBCs with blebs, budding, and vesicle-shaped protru-sions10 (see Figure 24-1). Examination of the urine sediment with phase-contrast microscopy can be especially helpful. Kidney inflammation also generates pyuria and WBC casts. Hyaline casts can be seen, especially with marked proteinuria.
Blood Studies
Routine laboratory studies should include a complete blood count (CBC), electrolyte levels, blood urea nitrogen (BUN) concentration, creatinine concentration, and liver panel.

Chapter 24 Approach to the Patient with Kidney Disease 849
Sedimentation rate and C-reactive protein level are often ele-vated regardless of the cause of nephritic syndrome. A deter-mination of the GFR is required. Usually this is accomplished with a quantitative urine collection for measurement of cre-atinine clearance. Iothalamate clearance, if available, provides the most accurate measurement. Various formulas, such as the Cockcroft-Gault equation or one of the equations developed by the Modification of Diet in Renal Disease (MDRD) study, can estimate the GFR based on a single and presumably sta-ble serum creatinine measurement (Table 24-3). However, all methods that rely on a single serum creatinine measurement will give erroneous results when renal function is rapidly changing and the serum creatinine concentration is not relatively stable.
Measurements of complement levels can be very helpful in patients with nephritic syndrome.15 It is generally best to begin with a measure of total hemolytic complement (CH50) and then proceed to measurement of C3 (a component of both the classic and alternative complement pathways) and C4 (a component of the classic pathway only). Table 24-4 separates the various forms of acute nephritic glomerulonephritis into those with normal and those with reduced complement levels. Low C3 with normal C4 levels suggest poststreptococcal glo-merulonephritis or membranoproliferative glomerulonephri-tis, whereas low C3 and C4 levels are more consistent with postinfectious glomerulonephritis, systemic lupus erythema-tous, hepatitis C–associated membranoproliferative glomeru-lonephritis (type I), or mixed cryoglobulinemia.
Other serologic studies, mainly to measure various autoanti-bodies, are ordered when specific underlying systemic diseases are considered the possible cause. The antinuclear antibody (ANA) and anti-DNA, anti-Smith, and anti-Rho antibodies help confirm the diagnosis of systemic lupus erythematosus and other collagen vascular diseases. The perinuclear anti-neutrophil cytoplasmic antibody (P-ANCA) and cytoplasmic antineutrophil cytoplasmic antibody (C-ANCA) tests help to establish a diagnosis of vasculitis. Anti-GBM antibodies are seen in patients with Goodpasture’s syndrome. A number of infectious diseases can produce an acute nephritic syndrome. It is also important to consider viral hepatitis, both B and C, as well as human immunodeficiency virus (HIV) infection and syphilis and, if plausible, to send blood specimens for diagnostic studies. Other infectious diseases that must always be considered are infectious endocarditis or another persis-tent bacterial infection such as an abscess or infected vascular
TABLE 24-3 Glomerular Filtration Rate (GFR)/Creatinine Clearance Estimating Formulas
Cockcroft-Gault Equation
(estimates creatinine clearance)
eGFR =(140 − age) × wt (kg)
Cr × 72× .85 (if female)
Abbreviated MDRD Equation
(estimates body surface area–corrected GFR in mL/min/1.73 m2)
eGFR = 186 × Cr − 1.154 × Age − 0.203 × 1.21 (if black)× .742 (if female)
Cr, Serum creatinine concentration (measured as mg/dL); eGFR, estimated glomerular filtration rate; MDRD, Modification of Diet in Renal Disease study.
Data from National Kidney Foundation: K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification, Am J Kidney Dis 39(2 suppl 1):S1-S266, 2002.
shunt. Blood cultures must be ordered for all patients with otherwise unexplained fever, heart murmurs, or leukocytosis.
The commonly ordered laboratory studies for patients with nephritic syndrome are shown in Table 24-5.
Imaging
Renal size is a very important parameter to define in patients with nephritic syndrome. This is most easily accomplished with renal ultrasonography. Although normal-sized kidneys do not definitively predict reversibility (even irreversible end-stage kid-neys can be of normal size as a result of swelling or infiltration in patients with diabetes mellitus or amyloidosis), small kidneys do indicate that irreversible fibrosis and atrophy are probably pres-ent. The assessment of renal size is therefore especially important for determining renal prognosis and making decisions regarding renal biopsy. If the kidneys are small (<9 cm in a normal-sized adult) the likelihood of reversible disease decreases markedly, and the difficulty and risk of the biopsy procedure increase.
Renal Biopsy
Patients with glomerular hematuria who have normal blood pressure, normal renal function, and minimal proteinuria rarely require a renal biopsy unless the clinical presentation
TABLE 24-4 Complement Levels in Acute Nephritic Syndromes
Low Serum Complement Levels
Systemic Diseases (Low C3 and C4)
Systemic lupus erythematosus
Cryoglobulinemia (hepatitis C)
Bacterial endocarditis
Shunt nephritis
Renal Localized Diseases
Acute poststreptococcal glomerulonephritis (low C3; normal C4)
Membranoproliferative glomerulonephritis
Type I (low C3 and C4)
Type II (dense deposit disease) (low C3; normal C4)
Normal Serum Complement Levels
Systemic Diseases
Polyarteritis nodosa
Antineutrophil cytoplasmic antibody–positive granulomatosis vasculitis (Wegener’s granulomatosis)
Hypersensitivity vasculitis
Henoch-Schönlein purpura
Goodpasture’s syndrome
Renal Localized Diseases
Immunoglobulin A nephropathy
Rapidly progressive glomerulonephritis
Anti–glomerular basement membrane disease isolated to kidney
Pauci-immune glomerulonephritis (kidney localized)
850 Section IV Evaluation of the Patient with Kidney Disease
suggests an underlying systemic illness causing secondary glo-merular disease. Renal biopsy may be helpful when glomeru-lar hematuria is associated with abnormal renal function and is especially so when it is important to establish the specific diagnosis to guide therapy.16 When renal function is decreas-ing rapidly (rapidly progressive glomerulonephritis) and a nephritic picture exists, the biopsy may need to be obtained very rapidly.
Nephrotic Syndrome
Nephrotic syndrome has historically been considered to include five principal clinical findings: 1. High-grade, albumin-dominant proteinuria (generally >3
to 3.5 g/day or spot urine protein/creatinine ratio of >3 to 3.5 [grams of protein per gram of creatinine])
2. Hypoalbuminemia 3. Edema 4. Hyperlipidemia 5. Lipiduria
However, milder and earlier forms of many clinical dis-orders that can generate the full nephrotic syndrome may produce lower degrees of albuminuria in the range between 30 mg/day to 3500 mg/day with or without the other fea-tures. Also, the full spectrum of nephrotic syndrome may not develop in some patients despite high-grade albumin-uria. The principal underlying abnormality responsible for all the other clinical features of nephrotic syndrome is increased permeability of the glomerular capillaries. Nephrotic syndrome may occur as an idiopathic and iso-lated condition, may be an inherited disorder, or may be a complication of an underlying systemic disease or allergic or immunologic disorder. It is always imperative to identify any underlying cause, when one exists (Table 24-6). This is accomplished by recognizing clues from the history and physical examination, reviewing a routine set of laboratory studies, and performing more specific tests suggested by the initial findings.
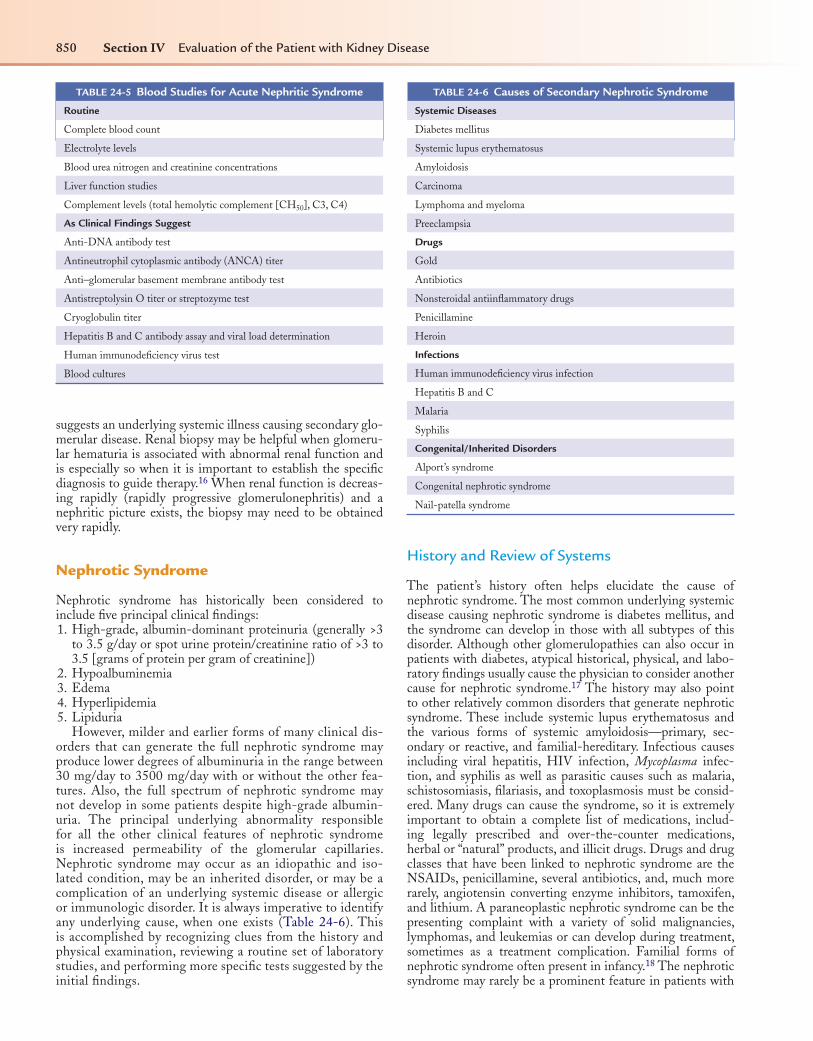
TABLE 24-5 Blood Studies for Acute Nephritic Syndrome
Routine
Complete blood count
Electrolyte levels
Blood urea nitrogen and creatinine concentrations
Liver function studies
Complement levels (total hemolytic complement [CH50], C3, C4)
As Clinical Findings Suggest
Anti-DNA antibody test
Antineutrophil cytoplasmic antibody (ANCA) titer
Anti–glomerular basement membrane antibody test
Antistreptolysin O titer or streptozyme test
Cryoglobulin titer
Hepatitis B and C antibody assay and viral load determination
Human immunodeficiency virus test
Blood cultures
History and Review of Systems
The patient’s history often helps elucidate the cause of nephrotic syndrome. The most common underlying systemic disease causing nephrotic syndrome is diabetes mellitus, and the syndrome can develop in those with all subtypes of this disorder. Although other glomerulopathies can also occur in patients with diabetes, atypical historical, physical, and labo-ratory findings usually cause the physician to consider another cause for nephrotic syndrome.17 The history may also point to other relatively common disorders that generate nephrotic syndrome. These include systemic lupus erythematosus and the various forms of systemic amyloidosis—primary, sec-ondary or reactive, and familial-hereditary. Infectious causes including viral hepatitis, HIV infection, Mycoplasma infec-tion, and syphilis as well as parasitic causes such as malaria, schistosomiasis, filariasis, and toxoplasmosis must be consid-ered. Many drugs can cause the syndrome, so it is extremely important to obtain a complete list of medications, includ-ing legally prescribed and over-the-counter medications, herbal or “natural” products, and illicit drugs. Drugs and drug classes that have been linked to nephrotic syndrome are the NSAIDs, penicillamine, several antibiotics, and, much more rarely, angiotensin converting enzyme inhibitors, tamoxifen, and lithium. A paraneoplastic nephrotic syndrome can be the presenting complaint with a variety of solid malignancies, lymphomas, and leukemias or can develop during treatment, sometimes as a treatment complication. Familial forms of nephrotic syndrome often present in infancy.18 The nephrotic syndrome may rarely be a prominent feature in patients with
TABLE 24-6 Causes of Secondary Nephrotic Syndrome
Systemic Diseases
Diabetes mellitus
Systemic lupus erythematosus
Amyloidosis
Carcinoma
Lymphoma and myeloma
Preeclampsia
Drugs
Gold
Antibiotics
Nonsteroidal antiinflammatory drugs
Penicillamine
Heroin
Infections
Human immunodeficiency virus infection
Hepatitis B and C
Malaria
Syphilis
Congenital/Inherited Disorders
Alport’s syndrome
Congenital nephrotic syndrome
Nail-patella syndrome

Cha
Alport’s disease and nail-patella syndrome. Some patients can date the onset of major proteinuria, because they notice that their urine has become foamy. This phenomenon, which is most readily noticed by men, occurs because albumin has a soaplike effect that reduces the surface tension of urine. This can be a very useful sign in patients with recurring episodes of nephrotic syndrome.
Physical Examination
Edema is a major characteristic of nephrotic syndrome. The development of hypoalbuminemia reduces the oncotic pressure within the capillaries, and this favors the net translocation of fluid into the interstitial spaces. To the extent that this occurs, intravascular volume and blood pressure fall, and this triggers the sympathetic nervous system, activates the renin-angioten-sin-aldosterone axis, elevates vasopressin levels, and modulates many other control systems that act together to promote net renal salt and water retention. This pathogenic sequence has been termed the underfill mechanism of salt and water retention in nephrotic syndrome. However, edema formation in many, perhaps most, nephrotic patients cannot be fully explained by underfill mechanisms. Although reduced intravascular oncotic pressures certainly exist in nephrotic patients, the net hydro-static gradient for water movement across capillary beds is also influenced by the interstitial oncotic pressure, and this generally falls in parallel with reductions in plasma oncotic pressure. Consequently, the net hydrostatic pressure gradient from the intravascular compartment to the interstitial space may not significantly increase. Edema formation under these conditions may be the consequence of a primary form of renal salt and water retention. This pathogenic sequence for edema formation is called the overfill mechanism. Undoubtedly each of these mechanisms plays a role in various phases and forms of nephrotic syndrome. The mechanism that predominates is probably related to the specific renal lesion causing the nephrotic syndrome.19,20 Also, these mechanisms may evolve from one form to the other. Regardless of which mechanism occurs initially, either will likely progress to a steady-state con-dition in which the initial effective arterial volume status is difficult or impossible to discern. Whether the initiating event is “underfill” of the effective arterial space leading to renal salt and water retention or “overfill” of this compartment causing excess salt and water to enter the interstitial spaces, the devel-opment of clinically apparent edema in an adult requires the net retention of about 8 to 10 pounds of fluid, which is equiva-lent to more than 4 L of normal saline.
Nephrotic edema is a form of pitting edema. When the thumb is pushed against a bony structure such as the tibia or sacrum, the resulting “pit” remains visible for a short period of time. Pitting edema is graded on a scale of 1 to 4 (from very slight to more apparent to deep pitting that persists for longer than 2 minutes).
Nephrotic edema is diffuse and to some degree probably affects virtually all tissues, but it is not equally distributed. The interstitial pressure in various locations has a major impact on edema formation. Thus the low ambient interstitial pressure often results in prominent periorbital edema. Gravitational force also causes nephrotic edema to accumulate in dependent body parts. Edema is generally worse in the lower legs and feet at the end of the day and becomes more prominent in the face after
pter 24 Approach to the Patient with Kidney Disease 851
nocturnal recumbency. Bedfast patients accumulate edema fluid in their back and sacral areas. The diurnal variation of edema formation becomes less prominent when the degree of edema worsens. Edema that is massive and generalized is termed ana-sarca. Dropsy is a historical term for generalized edema.
Nephrotic edema is usually symmetric (after adjustment for gravitational dependency), and unilateral edema should raise the possibility of edema due to local anatomic abnor-malities such as venous thromboses, varicosities, or lym-phatic obstruction. However, asymmetric nephrotic edema can be caused by upon an anatomic condition that generates greater local or asymmetrical edema. Severe edema can result in skin breakdown, blisters, weeping, and superinfection. Chronic (months to years) severe edema of any cause, includ-ing nephrotic syndrome, can produce fibrosis of the skin and subcutaneous tissues. The resulting “brawny” edema is usually pigmented, is very firm, and often will not pit.
Physical clues to other disorders that produce generalized edema should be sought during physical examination. The neck veins must be carefully evaluated to determine whether right-sided cardiac pressures are increased due to cardiac, pul-monary, or pericardial abnormalities. Elevated jugular venous pressures, pericardial knock, Kussmaul’s sign (absence of inspiratory decline in jugular pressure), and prominent x and y descents suggest pericardial disease. Pulsus paradoxus (an exaggerated fall in systemic blood pressure of 10 mm Hg or more with inspiration) suggests pericardial or pulmonary dis-ease. Although prominent ascites often indicates liver disease, whereas pulmonary congestion and pleural effusions suggest cardiac or pulmonary pathology, fluid may accumulate in these locations in patients with severe nephrotic syndrome in the absence of cardiac or liver abnormalities.
Many skin findings other than edema are associated with nephrotic syndrome itself and some suggest underlying primary diseases. Xanthelasma palpebrarum (periorbital-eyelid xantho-mas) is associated with hypercholesterolemia about 50% of the time and may become very prominent in nephrotic patients. Eruptive xanthomas, usually associated with extreme hyper-triglyceridemia, are much rarer but may also occur in patients with nephrotic syndrome. A number of relatively specific skin, nail, and scalp abnormalities are associated with various rheu-matolgic conditions. These include a malar facial rash, scarring alopecia, mat telangiectasia, nail bed telangiectasia and nail fold capillary loops and vascular infarcts, and erythema nodosum. Sarcoidosis is also frequently associated with erythema nodo-sum and skin papules. Jaundice, angiomata, telangiectasia, and palmar erythema raise the likelihood of hepatic disorders. The vasculitides produce a number of skin manifestations, includ-ing leukocytoclastic rashes and skin infarctions.
Several nail findings occur in nephrotic patients. Transverse white lines, or leukonychia (sometimes called Muehrcke’s lines) can develop during periods of marked hypoalbuminemia. Chronic hypoalbuminemia may cause more diffuse white nails (Terry’s or half-and-half nails) or yellow nails.21 None of these nail findings is specific, however, and they can also occur with other debilitating diseases, after chemotherapy, and so on. Nail-patella syndrome—characterized by dystro-phic nails, hypoplastic patellae, and iliac horns—may present with nephrotic syndrome.
The eyes, in addition to being swollen, may be inflamed or show evidence of scleritis with systemic vasculitic disease. Of course the heart and liver must be carefully examined and the

852 Section IV Evaluation of the Patient with Kidney Disease
extremities must be carefully evaluated for evidence of arthri-tis and for deep vein thrombi, which occur with increased fre-quency in these patients.22
Laboratory TestsUrine Studies
Proteinuria is readily detected using a semiquantitative urine dipstick test. The protein-detecting pad is impregnated with a protein-sensitive pH indicator dye and a strong pH buffer (which keeps the pad’s pH constant independent of the actual urine pH). The pH indicator changes color when moistened with urine containing dissolved proteins (the phenomenon is called the protein error of pH indicators). Dipstick protein tests are most sensitive to albumin and react poorly to urine globulins and immunoglobulin light chains (Bence Jones pro-tein). The dipstick results have the following approximate cor-relations with protein concentration:Negative:<15mg/dL Trace: 15-30 mg/dL1+: 30-100 mg/dL2+: 100-300 mg/dL3+: 300-1000 mg/dL4+: >1000 mg/dLExtremely alkaline urine (i.e., infected urine) can overwhelm the acid buffer and thereby produce a false-positive dipstick protein test.
More recently albumin-specific urine dipstick tests have been marketed specifically to detect low-grade albuminuria (i.e., microalbuminuria). Some can simultaneously measure creatinine concentrations so that the albumin/creatinine ratio can be determined.
Albumin-specific dipstick tests are generally not used to diagnosis or follow patients with overt (macro) albuminuria or nephrotic syndrome. Sulfosalicylic acid precipitates most urine proteins, and the resulting turbidity is proportional to the protein concentration. The sulfosalicylic acid turbid-ity test detects albumin, globulins, and Bence Jones proteins. Although it was a very useful test, environmental safety con-cerns have eliminated it from most physician’s offices.
If a high urine protein concentration is documented, a quantitative measurement of protein excretion will be required. This is usually achieved with a 24-hour urine col-lection. Alternatively, the protein/creatinine ratio (grams pro-tein/gram creatinine) in a single morning specimen may be used.14 If the creatinine excretion rate is assumed to be about 1 g/day, then the ratio of grams protein to 1 gram of creatinine will approximate the 24-hour protein excretion. Approximate corrections can be made depending on the patient’s gender and body habitus. A timed quantitative urine collection has the advantage of permitting measurement of creatinine clear-ance, and this may be very useful.
The urine dipstick protein test, sulfosalicylic acid turbidity test, 24-hour protein excretion, and protein/creatinine ratio are all measures of total protein concentration or excretion. None of these will characterize the specific urine proteins (except that the urine dipstick tests are more sensitive to albumin, and the albumin sticks are specific to that class). Agarose gel protein electrophoresis of the urine defines the urine protein classes (i.e., albumin, α1-globulin, α2-globulin, β-globulin, γ-globulin), and monoclonal immunoglobulins and light chains can be
identified. Electrophoresis results also allow stratification of nephrotic patients into those with selective proteinuria (mainly albumin) and those with nonselective proteinuria (both heavy albuminuria and globulinuria). This differentiation may have prognostic implications. Characterization of intact immuno-globulins, heavy chains, and light chains is also accomplished with either immunoelectrophoresis or immunofixation.
Hyaline casts are common in patients with nephrotic syn-drome and represent precipitated Tamm-Horsfall protein together with abnormally filtered and excreted serum pro-teins.23,24 Cellular casts are usually indicative of renal infection and/or interstitial inflammation (WBC casts) or glomerular inflammation, proliferation, and/or necrosis (when RBC casts are seen; see Figure 24-1). Such disorders may be idiopathic and isolated to the kidney, associated with systemic vasculitis, or related to another systemic inflammatory disease process such as systemic lupus erythematosus.
Lipiduria is a characteristic feature of nephrotic syndrome. The lipids in the urine sediment can be found in excreted tubule cells (oval fat bodies), within fatty casts, and/or as free-floating lipid globules. Some, but not all, of the urinary lipid is esterified cholesterol, and this component is birefringent and therefore is best seen with a polarizing microscope, which demonstrates their characteristic bright crosslike appearance25 (Figure 24-4). Much of the urine fat originates from filtered high-density lipoprotein. The high-density lipoprotein is small enough to be filtered by “leaky” glomerular epithelial and is then partially reabsorbed by renal tubule epithelial cells, which subsequently degenerate and slough into the urine.26
Blood Studies
Initial studies should include a routine chemical profile (elec-trolytes, glucose, BUN, creatinine, total protein, albumin, calcium, phosphate, and liver enzymes), a lipid panel (total cholesterol, triglycerides, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol), and a CBC. The
FIGURE 24-4 Lipiduria. Birefringent cholesterol crystals seen with polar-izing light microscopy.

Chapter 24 Approach to the Patient with Kidney Disease 853
sodium concentration may be artifactually reduced (pseudo-hyponatremia) as a result of a displacement error caused by hyperlipidemia. This error occurs with flame photometry and with indirect potentiometry but not with direct potentiom-etry. The calcium concentration must also be corrected for the low albumin concentration, and measurement of ionized calcium concentration may be helpful. Additional testing is directed by the patient’s clinical presentation and findings and the suspicions of the physician. Testing for syphilis and HIV and screening studies for viral hepatitis (hepatitis B and C) are generally performed. If a collagen vascular disease is sus-pected, then an ANA assay, anti–double-stranded DNA anti-body assay, complement levels, and other more specific tests for autoimmune disorders are indicated. Although determina-tion of sedimentation rate is sometimes helpful, it is usually elevated in all patients with nephrotic syndrome, regardless of cause.27 If a paraproteinemia disorder (including primary amyloidosis) is suspected, a serum immunoelectrophoresis or immunofixation study should be performed (in addition to qualitative and quantitative urine protein studies). When clinical and historical features are suggestive, cryoglobulin and antistreptolysin O titers are obtained. Assessment of the GFR is mandatory and is usually accomplished with a timed urine collection for calculation of the creatinine clearance. Although estimation of GFR from the serum creatinine concentration using one of several equations, such as the MDRD equation, can be very helpful, collection of a timed urine specimen for measurement of protein and creatinine excretion is indicated in all nephrotic patients who are considered to be compliant and who can understand the instructions for accurate col-lection of such a specimen. When available, an iothalamate clearance may be very helpful; this remains the “gold standard” measure for GFR.
Imaging
A chest radiograph (CXR) is required to assess cardiac size and evaluate for pericardial disease, pleural effusions, and so on. A renal sonogram with Doppler study is required to determine the renal anatomy and status of the collection sys-tem and renal vasculature. Special attention is directed to the possibility of renal vein thrombosis. The finding of a single kidney, asymmetrical kidney size, or bilaterally small kidneys will direct subsequent evaluation. Patients should have routine age-indicated screening studies for malignancy such as mam-mography and colonoscopy. However, extensive studies to rule out occult malignancy are not indicated.
Renal Biopsy
Renal biopsy is not always indicated in patients with nephrotic syndrome. If the cause seems apparent, then treatment can be initiated without histologic confirmation. For example, biopsy is not usually required in a patient with long-standing diabetes mellitus who develops nephrotic syndrome after the expected time period. However, if atypical features exist, such as very active sediment with RBC casts, a very short time course, or absence of retinopathy and other end-organ involvement, then a biopsy may be required to rule out other causes of the syn-drome. In young children with a classic clinical presentation,
the diagnosis of minimal change disease can be assumed and therapy initiated without histologic confirmation. This diag-nosis is not as frequent in adults, and empiric therapy is less commonly initiated. Nonetheless, this course may be appro-priate when contraindications to a biopsy exist or the patient is very reluctant to undergo an invasive procedure, and the clini-cal features are consistent with minimal change nephropathy. In the majority of adults with nephrotic syndrome, however, a biopsy is appropriate to define the disease, improve prognosti-cation, and direct therapeutic intervention.
Obstructive Uropathy
Obstructive uropathy refers to structural or functional interfer-ence with normal urine flow anywhere from the renal pelvis to the urethra. The resultant increase in pressure within the urinary tract proximal to the obstruction leads to a number of structural and physiologic changes. The anatomic outcome of an obstructive process often includes dilatation of the calyces and renal pelvis, termed hydronephrosis, and, if the obstruction is distal to the ureteropelvic junction, hydroureter.
Obstructive uropathy is a common cause of acute or sub-acute renal failure. The early recognition of this clinical entity is essential both to improve prognosis and to identify the most appropriate therapy, which is quite different than that used to treat other forms of acute kidney injury. Untreated obstructive uropathy can result in a progressive and irrevers-ible loss of renal function and eventually lead to end-stage renal disease. However, early recognition and treatment can allow a potentially full renal recovery. Obstructive uropathy is often described as acute (hours to a few days), subacute (several days to weeks), and chronic (months to years). The obstruction may be unilateral or bilateral, and either partial or complete. The clinician should establish the severity and chronicity of the condition so that appropriate therapy can be instituted. This is accomplished by means of careful his-tory taking and physical examination, appropriate laboratory tests, and selected imaging studies depending on the clinical circumstances.
History and Review of Systems
Patients with acute obstructive uropathy may report abrupt onset of severe flank pain (if the obstruction is at the level of the ureter or above) or suprapubic pain and fullness (if there is lower-level obstruction). The pain is often colicky when the intraluminal process is due to nephrolithiasis or papillary necrosis. The pain may be accompanied by urinary frequency and urgency if there is partial urinary tract obstruction. Occa-sionally, nausea and even vomiting may occur when severe pain is present. A history of complete anuria should always alert the physician to the possibility of obstruction, especially in the appropriate clinical setting, for example, in an elderly man with a history of prostate cancer or prostatic hypertrophy. Gross hematuria may occur when obstructive uropathy is due to nephrolithiasis, papillary necrosis, or neoplasms of the uri-nary tract. Rarely, patients may report the passage of renal cal-culi or small pieces of tissue with the sudden cessation of pain after such an event. The history in patients with subacute or chronic obstruction is often negative or vague, but symptoms

854 Section IV Evaluation of the Patient with Kidney Disease
can include suprapubic fullness, frequency, polyuria, or noctu-ria. Patients may also complain of difficulty with initiating or stopping micturition if bladder outlet obstruction is present. Occasionally, urinary tract obstruction leads to an infection such as pyelonephritis, with accompanying high fever, flank pain, and dysuria.
Physical Examination
The physical examination can be very informative when blad-der obstruction exists. The enlarged bladder may be detected with palpation and percussion. In rare cases a flank mass may be palpable from a hydronephrotic kidney. Prostatic enlargement and other prostatic pathology that may produce obstruction, such as malignancy or infection, can be detected via rectal examination. The physical examination is usually of limited value, however, for detecting obstruction of the ureters or pelvis of the kidney. Hypertension is occasionally caused by urinary tract obstruction. Several mechanisms have been proposed for this development. In acute, unilateral obstruc-tion there can be activation of the renin-angiotensin system, with increased renin secretion by the obstructed kidney.28,29 The plasma renin activity is typically normal with bilateral obstruction or with chronic unilateral obstruction. The hyper-tension that may occur in this setting has been attributed to renal failure with extracellular fluid (ECF) volume expan-sion.30 In these instances, the diuresis that follows the correc-tion of the obstruction often, but not always, eliminates the hypertension. Fever may be present if infection complicates obstruction.
Laboratory Tests
The initial laboratory evaluation may provide clues to the presence of obstructive uropathy. The urinalysis may reveal a few RBCs and WBCs. There may be evidence of impaired renal function in patients with complete or severe partial bilateral obstruction or in those with obstruction of a soli-tary kidney. The plasma creatinine concentration is usually normal in patients with unilateral obstruction due to the presence of the normal contralateral kidney. However, uni-lateral renal obstruction can very rarely lead to anuria and acute renal failure. This has been attributed to vascular or ureteral spasm.31 Renal tubular acidosis with hyperkale-mia is well described with obstructive uropathy.32 Multiple defects in renin, aldosterone, and distal tubule function have been described. In some patients renin and aldosterone lev-els are reduced and the electrolyte abnormalities resolve in response to exogenous mineralocorticoids. In others, distal tubule injury diminishes sodium reabsorption and potas-sium secretion. The hyperchloremic acidosis is due to both hyperkalemia-induced suppression of ammoniagenesis and directly impaired proton secretion. Consequently, obstruc-tive uropathy is a common cause of hyperkalemia and type 4 renal tubular acidosis.32,33 Often, maximal urine concentrat-ing capacity is also reduced.33
Acute obstruction causes an initial increase in renal blood flow, but this is soon followed by a reduction attributed to vasoconstriction.33 This can sometimes increase the BUN/creatinine ratio similar to that seen in prerenal azotemia.
Imaging
Renal ultrasonography is the test of choice to diagnose obstructive uropathy. This modality avoids IV contrast expo-sure. It has an extremely high sensitivity (>95%) and very good specificity (75%) for the diagnosis of hydronephrosis.34,35 In early obstruction (first 1 to 3 days), however, the collecting system can be relatively noncompliant, and therefore overt hydronephrosis may not occur. Furthermore, when extrin-sic compression of the ureter exists, obstructive uropathy can develop without overt dilation of the ureter or the renal pel-vis. This most often occurs in elderly men with malignancy involving the retroperitoneum or prostate or when retroperi-toneal fibrosis exists.36 Furthermore, hydronephrosis or hydro-ureter should not be equated with obstruction. Nonobstructive hydronephrosis can occur as a result of neuromuscular abnor-malities of the bladder and/or ureters (megacystis-megaureter syndrome) and in other conditions such as vesicoureteral reflux and pregnancy.37 Examination of the resistive index of the renal vasculature (vasoconstriction occurs with obstruction) and the response of the resistive index to a diuretic challenge can be a very helpful differentiator.37 As Ellenbogen and colleagues stated, “It should be clear that the degree of hydronephrosis does not always correspond with the degree of obstruction.”35 When ultrasonographic results are inconclusive or the suspi-cion of obstruction is very high despite a nondiagnostic sono-gram, CT scanning should be performed. The combination of renal ultrasonography and CT of the kidneys will establish the diagnosis of obstructive uropathy in the overwhelming major-ity of cases.34,37 CT scans have generally replaced the IVP.
In some cases a retrograde study or percutaneous nephros-tomy is necessary. Although much more invasive studies, they do not require IV contrast material, have a very high diag-nostic yield, and also often treat the obstruction. Whenever a high degree of clinical suspicion of bladder obstruction exists, bladder catheterization, both a diagnostic and a therapeutic procedure, should be performed.
Hypertension
Systemic hypertension is one of the most common disorders seen in clinical practice. In the United States it affects about 20% of white adults, 40% of African American adults, and more than 80% of those older than 80 years of age. In addi-tion, it is extremely common in patients with virtually any type of renal disease. The nephrologist must be an expert in the diagnosis and treatment of this disease and should have a rigorous and systematic approach for the diagnosis and treat-ment of hypertension. Over time the definition and classifica-tion of adult hypertension has been a moving target. The most recent diagnostic classification and therapeutic guidelines were published in the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treat-ment of High Blood Pressure.38 Table 24-7 shows how this report classifies blood pressure, but these guidelines should always be viewed in the context of the individual patient’s history and clinical circumstances. Also these blood pres-sure levels are for patients who are not acutely ill and are not taking antihypertensive medications. A patient with a con-sistently elevated blood pressure and no comorbid conditions is obviously treated quite differently than an individual with
Chapter 24 Approach to the Patient with Kidney Disease 855
a similar degree of hypertension but with coexistent diabetes mellitus or other cardiovascular or renal disease. Chronic sys-temic hypertension is also associated with the development of cardiovascular disease, congestive heart failure, stroke, and chronic kidney disease (CKD). Appropriate treatment of the hypertension clearly reduces the risk of development of these complications, and it is therefore imperative to carefully evaluate and classify hypertensive patients so that appropriate therapy can be rendered.
History and Review of Systems
The evaluation of patients with hypertension should include an assessment of target organ function and/or damage, con-comitant risk factors, and comorbid conditions, as well as a search to detect causes of secondary forms of hypertension, especially reversible conditions.39 Obviously, a complete and detailed medical history is the first step in the evaluation. Particular attention should be paid to the presence of other cardiovascular risk factors such as age, African American ethnicity, underlying CKD, dyslipidemia, history of smok-ing, obesity, microalbuminuria, left ventricular hypertrophy, a family history of a myocardial infarction before age 50, and coincident arterial disease. The clinician should determine the duration and degree of hypertension and assess for any symp-toms of severe hypertension such as blurry vision, visual loss, headaches, encephalopathy, or nausea. A thorough dietary his-tory is also essential and should include an estimate of sodium, potassium, calcium, and fat intake. Other important factors to identify include tobacco use, alcohol consumption, all pre-scribed and over-the-counter medications taken, illicit drug use, the efficacy of previous antihypertensive drug therapy and any adverse effects, and the presence (or absence) of sexual dysfunction. It is remarkable that patients (and many physi-cians) remain unaware of the potential hypertensive effects of many over-the-counter medications, particularly the NSAID class of drugs. A family history of hypertension is also very important for the diagnosis of both familial monogenetic forms of hypertension and essential hypertension.
Nephrologists are very often asked to evaluate and treat hypertensive patients who are referred for a second opinion, particularly those with poor blood pressure control. In this population it is particularly important to identify any poten-tial primary (and hopefully reversible) cause for secondary hypertension (Table 24-8). In this regard, symptoms charac-teristic of certain underlying causes of hypertension should be sought. Examples include paroxysmal hypertension, sweating, palpitations, and severe headache for pheochromocytomas; sweating, palpitations, and weight loss for thyrotoxicosis; and weight gain, edema, and polyuria for Cushing’s syndrome.
TABLE 24-7 Classification of Blood Pressure in Adults
HYPERTENSION CLASSIFICATION
SYSTOLIC PRES-SURE (mm Hg)
DIASTOLIC PRES-SURE (mm Hg)
Normal <120 and <80
Prehypertension 120-139 or 80-89
Stage 1 hypertension 140-159 or 90-99
Stage 2 hypertension ≥160 or ≥100
A common form of secondary hypertension is that due to atherosclerotic renal artery stenosis. These patients may relate a history of recent worsening of their blood pressure control despite adherence to the antihypertensive medication regi-men. They also very frequently have a history of generalized vascular disease. Primary hyperaldosteronism is now recog-nized as a very common condition, especially in patients with difficult to control or severe hypertension. Prevalence among hypertensive patients may be as high as 10%. Although spon-taneous or drug-related hypokalemia suggests this diagnosis, it often presents with normal electrolytes.
Physical Examination
The physical examination begins with careful blood pressure measurement in the office setting. Patients should not smoke or ingest caffeine for at least 30 minutes prior to the examina-tion. They should be comfortably seated in a chair with back support with the arm resting at heart level. An appropriately sized cuff must be used. Its width should be at least 40 percent of arm circumference and its length at least 80 percent of arm circumference.40 Two or more readings should be taken 2 to 5 minutes apart and averaged. Blood pressure should also be measured in the supine and standing position if orthostatic hypotension is likely. When a coarctation is considered, blood pressure should be measured in each arm and also in the legs. Use of incorrect cuff size in obese individuals causes an over-estimation of blood pressure. Although the use of mercury manometers is encouraged, these have largely been eliminated due to the environmental toxicity of mercury. A regularly cali-brated aneroid or electronic device is acceptable. Overestima-tion of systolic blood pressure is common in elderly patients who have calcified and stiff arteries that cannot be com-pressed. This condition, called pseudohypertension, is suspected when the radial artery remains palpable after the cuff has been inflated above systolic blood pressure.
TABLE 24-8 Causes of Secondary Hypertension
Renal parenchymal disease
Renovascular hypertension
Fibromuscular dysplasia
Atherosclerotic renal artery disease
Renal vasculitis
Renal infarction
Primary hyperaldosteronism
Renin-secreting tumor
Pheochromocytoma
Cushing’s syndrome
Liddle’s syndrome
Apparent mineralocorticoid excess
Geller’s syndrome
Aortic coarctation
Thyroid disease
Drugs (e.g., corticosteroids, cocaine, amphetamines, oral contraceptives)
Sleep apnea

856 Section IV Evaluation of the Patient with Kidney D
The next very important element of the physical examina-tion is a thorough funduscopic evaluation. The presence and severity of hypertensive retinopathy provides an important clue to the duration and severity of the hypertension. Spe-cial note should be made of hemorrhage, arteriolar narrowing, papilledema, and/or cotton-wool spots.
The cardiovascular and pulmonary examination may reveal evidence of carotid and/or peripheral vascular disease, left ventricular hypertrophy (e.g., hyperdynamic precordium and the presence of a fourth heart sound), or congestive heart fail-ure (e.g., jugular venous distention, peripheral edema, third heart sound, and/or rales). Coarctation of the aorta is sug-gested by differences in the intensity of the radial pulses or a radial-femoral arterial pulsation difference or temporal delay.
The abdominal and flank examination may reveal abdomi-nal bruits suggesting renal artery stenosis. Neurologic exami-nation in severely hypertensive patients may reveal findings consistent with encephalopathy. Abnormal findings on thy-roid examination may suggest otherwise occult thyroid dis-ease. The presence of hyperpigmentation and striae raises the possibility of Cushing’s syndrome. Neurofibroma and café au lait spots suggest the possibility of neurofibromatosis (and either pheochromocytoma or renal vascular disease).
Laboratory Tests
The extent of laboratory evaluation depends on the clinical circumstances of the individual patient. The initial evaluation of a person with stage 1 hypertension includes measurement of serum electrolytes, BUN, creatinine, calcium, and glucose; a lipid profile; urinalysis; and CBC. If warranted by the clinical history and physical examination findings, additional testing such as thyroid studies, urine albumin/creatinine ratio, and quantitation of GFR with a timed urine collection for mea-surement of creatinine clearance or iothalamate clearance are measured. When a pheochromocytoma is suspected, 24-hour urine catecholamines and fractionated metanephrines, or frac-tionated plasma catecholamines or free metanephrines should be measured. A plasma aldosterone/plasma renin activity ratio is a reasonable screening test for the detection of primary hyperaldosteronism if this condition is clinically suspected. This test should be ordered for patients with unprovoked hypokalemia; those with severe diuretic-induced hypoka-lemia, unexpected metabolic alkalosis, or severe or resistant hypertension; or hypertensive patients with an incidentally discovered adrenal mass (“incidentaloma”).
Imaging
A baseline CXR is appropriate for all hypertensive patients. Other imaging modalities are required when the history, physical examination, and laboratory results suggest that the hypertension may be secondary to anatomic abnormalities or when pathologic end-organ changes due to the hypertension must be determined. Renal sonography is an excellent non-invasive test for assessing renal size, identifying cysts, and detecting hydronephrosis. It is obviously indicated whenever enlarged kidneys or a mass can be palpated. When there is strong clinical suspicion of renovascular hypertension, several options are available to establish the diagnosis. They include
isease
spiral CT angiography, magnetic resonance angiography, and duplex Doppler ultrasonography. Which screening test is best is determined by the specific features of each patient and the skill of the imaging center that is used. Renal artery Doppler studies are very operator dependent, and results are often sub-optimal in large patients. CT angiography of the renal arteries is an excellent diagnostic tool but carries the risk of contrast-related kidney injury in susceptible patients as well as consid-erable radiation exposure. Gadolinium-enhanced magnetic resonance angiography also yields excellent results, but is con-traindicated in patients with reduced kidney function because of concerns about nephrogenic systemic fibrosis. Also it can-not be used when patients are claustrophobic or have metallic implants. Captopril renal perfusion scans are no longer recom-mended as a screening test because of their relatively low pre-dictive value. It should be emphasized that one should proceed directly to catheter angiography if the clinical suspicion is very high, no matter what any screening tests show.
Other Studies
An electrocardiogram is necessary to screen for left ventricular hypertrophy and cardiac arrhythmias and to provide a baseline for future comparison.
Nephrolithiasis
Nephrolithiasis, or kidney stones, is an increasingly prevalent medical problem. Over 5% of the U.S. population is affected, and the lifetime risk of developing a stone is between 10% and 15%.41 Patients who develop a first stone are very likely to have a second one (50% within 5 years and 80% within 20 years).41 Therefore, every physician is likely to encounter patients with this problem.
History and Review of Systems
Kidney stones are strongly suspected when patients present with classic signs and symptoms such as gross hematuria associated with waves of flank and/or lower abdominal pain (colic), which may radiate into the genital region. However, symptoms are sometimes very vague. Either gross hematu-ria or microscopic hematuria is usually, but not always, pres-ent. The absence of hematuria does not exclude a diagnosis of nephrolithiasis.42 Poorly localized abdominal pain, nausea, vomiting, and urinary frequency may occur. Often, patients are entirely asymptomatic, and the stones are noted inciden-tally when an imaging study is done for a different reason. When painful symptoms do develop, they generally indicate that an asymptomatic stone has passed from the renal pel-vis into the ureter where it has caused obstruction, inflam-mation, and/or bleeding. These symptoms often first occur during the night or in the early morning, beginning abruptly with rapidly worsening pain. The paroxysms of pain prob-ably reflect hyperperistalsis of the renal calyces, pelvis, and ureter. The site of pain and its referral pattern are clues to the stone’s location. Upper ureteral obstruction usually produces flank pain and tenderness, and anterior abdominal radiation of pain. Lower ureteral obstruction produces lower abdominal

Cha
pain, which frequently radiates into the testicle or labia. Very often stones lodge near the ureterovesical junction where they irritate the bladder, which produces urinary frequency, uri-nary urgency, suprapubic tenderness, and dysuria. If the stone enters the bladder and then obstructs its outlet, suprapubic pain and anuria may develop.
Potential kidney stone risk factors should be identified. The patient should be questioned about unusual dietary hab-its. Does the patient consume large amounts of oxalate-rich foods such as spinach, rhubarb, beets, or black tea? Is intake of animal protein, which reduces urine citrate excretion, excessive? High salt ingestion increases urine calcium excre-tion. Sardines, anchovies, and organ meat are rich sources of purines and thereby increase urine uric acid excretion. The medication history may reveal other important clues to stone pathogenesis. Some medications increase the risk of stones by reducing urine citrate excretion—carbonic anhydrase inhibi-tors such as acetazolamide and topiramate are important examples. Other medications that may directly precipitate as stones are the protease inhibitor indinavir, triamterene, and some sulfonamides.43 Dietary supplements, vitamins, and minerals such as calcium salts and vitamin D can produce hypercalciuria.
A number of underlying medical conditions can generate kidney stones. These include most chronic disorders associ-ated with hypercalciuria, such as hyperparathyroidism and sarcoidosis. Hypercalcemia-hypercalciuria of malignancy usually does not result in kidney stones because of its acute presentation and relatively short course. Any medical or sur-gical condition associated with significant steatorrhea (short gut disorders, cystic fibrosis, bile salt depletion from ileal dis-ease, gastrointestinal bypass) may generate stones as a result of hyperoxaluria and reduced urine volume. Chronic diarrhea without steatorrhea causes chronic metabolic acidosis and persistent aciduria—a risk factor for uric acid stones. Strong epidemiologic associations with both calcium and uric acid kidney stones have been demonstrated for obesity, weight gain, diabetes mellitus, and metabolic syndrome.44 The impact of occupations associated with reduced fluid intake and/or excessive sweating should be considered, because low urine volume is a major risk factor for stone formation. A his-tory of recurrent kidney infections raises concern for infec-tion (struvite) stones (see later). The age when the first kidney stone develops is also a clue to the etiologic diagnosis. Kidney stones associated with inherited disorders such as cystinuria and congenital hyperoxaluria often present in the young. Eth-nicity has a major impact on risk. Over a 6-year period (1988 to 1994) in the United States, whites had the highest risk of kidney stones (5.9%), African Americans the lowest risk (1.7%), and Mexican Americans intermediate risk (2.6%).41 The family history also may be helpful; first-degree relatives of patients with stones very often also have had stones.45
Physical Examination
The presence of fever is a sign of possible infection, which must be rapidly addressed. It is of critical importance to rec-ognize an infection proximal to an obstructing stone. This is a medical-urologic emergency requiring urgent drainage of the renal pelvis (surgically or via interventional radiology) and appropriate antibiotic therapy. Fever and/or leukocytosis,
pter 24 Approach to the Patient with Kidney Disease 857
which do not usually occur with uncomplicated kidney stones, are red flags for this condition. The skin is generally pale and cool, and often clammy. The patient should be examined for costovertebral angle tenderness. Hypoactive bowel sounds and ileus may develop in these patients, but abdominal tenderness is unusual, and if rebound tenderness is present another cause should be sought. Bruits over the abdominal aorta and iliac vessels may be indicative of a leaking aortic abdominal aneu-rysm, which can mimic the symptoms of renal colic. In men, a rectal examination may reveal prostatitis, and in women, a pelvic examination may suggest ovarian pathology or an ecto-pic pregnancy.
Laboratory Tests
The routine initial laboratory battery includes a CBC. The WBC count may be slightly increased with an uncompli-cated stone, but leukocytosis of more than 15,000 cells/mm3 and a left shift suggests a complicating infection. The BUN and creatinine values are important markers of GFR, espe-cially if renal mass is reduced, severe obstruction exists, or the patient is volume depleted. An electrolyte panel may provide clues that distal renal tubular acidosis exists (hyperchloremic acidosis and hypokalemia). The serum calcium, phosphate, and uric acid levels can indicate the existence of a hypercal-cemic-hypercalciuric condition, renal phosphate wasting, or a hyperuricosuric condition. In women of childbearing age a pregnancy test must be performed.
Urine Studies
Hematuria with isomorphic RBCs is very common but not universal.42 RBC casts should not be seen. Proteinuria should be absent or low grade. Although pyuria may occur without infection, it should always raise suspicion, and a urine culture should be performed. The urine pH may provide a helpful clue. A very high pH of freshly voided urine (i.e., >7.5) almost always indicates the existence of a UTI. Chronic UTIs may lead to the development of struvite stones, also called triple phosphate, urease-related, or infection stones. When the infecting bacteria produce the enzyme urease, the urea in urine is split into two molecules of NH3 and one of CO2. The CO2 escapes from the urine, whereas each NH3 molecule binds a proton and thereby elevates the urine pH above that under usual physiologic con-ditions. Abundant ammonium in an alkaline urine tends to precipitate with magnesium and phosphate to form struvite (MgNH4PO4 · 6H2O). Note that struvite is really a double phosphate crystal. The term triple phosphate derives from the fact that carbonate-apatite (Ca10[PO4]6 · CO3) commonly coprecipitates with struvite, which results in a combination of three cations—calcium, magnesium, and ammonium—and the phosphate anion. Struvite stones often grow to large stag-horn shapes. Urease-producing bacteria include Ureaplasma urealyticum, most Proteus species, and many Staphylococcus, Klebsiella, and Pseudomonas species. Escherichia coli does not generate urease.
A urine pH that is not appropriately acidic (<5.5) in a patient with hyperchloremic acidosis suggests distal renal tubular acidosis, a disorder often associated with calcium phosphate stones. Conversely, persistently acidic urine is associated with uric acid stones (because uric acid becomes

858 Section IV Evaluation of the Patient with Kidney D
increasingly insoluble as the pH falls below 6.5). When bac-teriuria is identified, a urine sample must be sent for culture. If overt signs of infection exist, then hospital admission for additional evaluation is generally required.
Identification of crystals in the urine sediment can be helpful and sometimes diagnostic. Recognition of the “ben-zene ring” cysteine is virtually diagnostic of cystinuria. The “coffin lid” crystals of struvite are also very characteristic and indicate that an infection-related stone is likely. Although uric acid and calcium oxalate crystals are very common and relatively nonspecific, they may be helpful clues to etiology when kidney stones are recognized.46 Twenty-four-hour urine collection for quantitation of nephrolithiasis-relevant chemicals can be very helpful. Several commercial laborato-ries offer stone risk profile or metabolic stone risk testing. These studies may identify abnormally high (e.g., calcium, oxalate, urate) and/or low (e.g., citrate) chemical concen-trations and excretion rates. The saturation-supersaturation state of the urine for various stone-forming crystals is also routinely calculated. In general at least two samples should be collected for such studies because of significant day-to-day variation in excretion rates. Specimens should be sent for these studies whenever recurrent stones develop or when a first stone is documented in a patient with a higher than usual risk for recurrence (e.g., those with a family history of stones, patients with gastrointestinal disorders). Some suggest that 24-hour urine studies should be performed after the first kid-ney stone in all patients.
Imaging
The imaging procedure of choice is a noncontrast helical CT scan with relatively thin (3- to 5-mm) cuts. This modality has replaced IVP as the preferred imaging procedure. Although a plain radiograph of the abdomen (kidneys, ureters, bladder) is very inexpensive and may be diagnostic, it has generally also been replaced by the CT scan as the initial screening test.47 The CT scan can detect radiopaque calculi as small as 1 mm in diameter. Calcium stones are opaque; cysteine and struvite stones are slightly radiopaque; and pure uric acid stones are radiolucent. Stones comprised of indinavir or triamterene are also radiolucent. The CT scan will also reveal renal anatomy, the presence of hydronephrosis, other abdominal and pelvic pathology, and other potential causes of the patient’s symp-toms. Although a renal-abdominal sonogram will demon-strate renal anatomy and reveal the presence of hydronephrosis and most stones in the renal pelvis, it will miss most ureteral stones. Therefore sonography is generally used to follow the progress of known stone disease but not as an initial study. However, sonography is indicated as the initial procedure in pregnant women and others for whom radiation exposure must be minimized. Magnetic resonance imaging (MRI) is generally not very good for the diagnosis of kidney stones.
Differential Diagnosis
Many conditions can mimic nephrolithiasis. Any form of renal bleeding associated with blood clots can cause ure-teral obstruction and produce symptoms identical to those of a kidney stone. Other clinical mimics of kidney stones
isease
are acute abdominal aneurysm, pyelonephritis, renal can-cer, renal tuberculosis, papillary necrosis, renal infarction, and renal vein thrombosis. Papillary necrosis, which is more likely in patients with diabetes or sickle cell disease, can cause true renal colic when sloughed papillae obstruct the ureter. Ectopic pregnancy, appendicitis, and bowel obstruc-tion must be considered. Finally, some patients complain of kidney stone symptoms because they are seeking anal-gesic drugs. Table 24-9 shows the differential diagnosis of urolithiasis-like pain.
Initial Treatment
Patients with renal colic can often be managed conserva-tively as outpatients with analgesics and fluids. However, admission and urgent urologic consultation is required if the patient is septic, has an infection proximal to an obstruc-tion, has obstruction of a solitary kidney (including a renal transplant) or bilateral kidney obstruction, has high-grade obstruction with a large (> 7-mm) stone, has acute kidney failure, has urine extravasation, or has unrelenting pain despite analgesic use or pain responsive only to parenteral analgesics.
The most important determinant of the likelihood that a stone will pass is its size. Most kidney stones smaller than
TABLE 24-9 Differential Diagnosis of Urolithiasis-Like Pain
CATEGORY DISORDERS
Renal PyelonephritisBlood clotRenal infarctionTumor (kidney or pelvis)Papillary necrosis
Ureteral TumorBlood clotStricture
Bladder TumorBlood clotUrinary retention
Intraabdominal PeritonitisAppendicitisBiliary diseaseBowel obstructionVascular disorderAortic aneurysmMesenteric insufficiency
Retroperitoneal LymphadenopathyFibrosisTumor
Gynecologic Ectopic or tubal pregnancyOvarian torsion/cyst rupturePelvic inflammatory diseaseCervical cancerEndometriosisOvarian vein syndrome
Neuromuscular Muscle painRib fractureRadiculitis
Infectious Herpes zosterPleuritis/pneumoniaFungal bezoar

Chapter 24 Approach to the Patient with Kidney Disease 859
4 mm in diameter will pass spontaneously. As stone size increases beyond a diameter of 4 mm, the chance of pass-ing falls progressively until it becomes very unlikely at a diameter of 10 mm. Consequently, conservative outpatient therapy becomes less likely to be successful as the stone size increases beyond 4 to 5 mm.48,49 Narcotics and/or NSAIDs are used for analgesia. If the patient is to be managed as an outpatient then NSAIDs are the preferred agents. If nau-sea and vomiting are prominent, a parenteral NSAID such as ketorolac can be used.50 For severe pain IV morphine is generally given.51 If the stone has a reasonable chance of passing without urologic intervention, then glucocorticoste-roids, calcium channel blockers (usually nifedipine), and/or α1-adrenergic antagonists (usually tamsulosin, which is used to treat benign prostatic hyperplasia) are often employed to relax ureteral muscles and thereby assist stone passage. Patients should always attempt to retrieve the passed stone for analysis. This can be accomplished by urinating through a filter or fine screen (an aquarium net is a good option). If none is available, the patient can urinate through a fine gauze pad or simply void into a glass jar so the calculus will be visible.
Acute Kidney Injury
Acute kidney injury (AKI) is a clinical syndrome broadly defined as an abrupt decline in renal function occurring over a period of hours to days resulting in the retention of nitrog-enous and metabolic waste products and ECF volume. Very often, electrolyte and acid-base disorders also develop (hyper-kalemia, hyponatremia, and metabolic acidosis). AKI develops as a result of a variety of pathophysiologic influences and may lead to varying degrees of damage to one or more anatomic divisions of the nephron with subsequent adverse functional consequences. Although the initial clinical manifestation of AKI may be oliguria, urine volume can remain normal or even increase, and patients can be completely asymptomatic. The diagnosis is often made when routine biochemical screen-ing reveals a recent increase in serum creatinine and/or BUN concentrations.
There is no universally accepted operational defini-tion of AKI, and more than 30 different criteria have been employed in various clinical studies.52 Commonly used definitions include an absolute increase in serum creatinine
c2firthc
pplaUic5wra
ehiitraa
TABLE 24-10 RIFLE Criteria for Acute Kidney Injury (AKI)
CLASS GFR URINE OUTPUT
Risk Creatinine increase ×1.5 or GFR fall of >25%
<0.5 mL/kg/hr >6 hr
Injury Creatinine increase ×2 or GFR fall of >50%
<0.5 mL/kg/hr >12 hr
Failure Creatinine increase ×3 or GFR fall of >75%
orCreatinine ≥4 mg% (acute
increase ≥0.5 mg%)
<0.3 mL/kg/hr >24 hr
orAnuria >12 hr
Loss Persistent AKI = complete loss of renal function >4 wk
End stage End-stage renal disease >3 mo
GFR, Glomerular filtration rate.
oncentration of 0.5 to 1.0 mg/dL, and relative increases of 5% to 100% over a period of 1 to several days. Although ar from perfect, these approaches have proved to be useful n identifying patients with AKI in clinical practice. More ecently a new classification and diagnostic system known by he acronym RIFLE (Risk, Injury, Failure, Loss, End stage) as been introduced.52 Table 24-10 shows this diagnostic and lassification system.
The incidence of AKI depends greatly on the patient opulation studied and the criteria used to identify affected atients. The incidence of AKI in ambulatory patients is very
ow, but AKI develops in up to 7% of hospitalized patients nd about 30% of those admitted to intensive care units.53,54 nited Kingdom population studies report that the annual
ncidence of AKI is between 486 and 620 per million.54 Out-omes associated with AKI have changed little over the past 0 years. The in-hospital mortality rate of critically ill patients ith AKI is higher than 50%. Older age, female gender, respi-
atory failure, liver failure, sepsis, and impaired consciousness ll correlate with higher in-hospital mortality rates.
The causes of AKI can be broadly divided into three cat-gories: prerenal azotemia (a disorder characterized by renal ypoperfusion in which renal parenchymal tissue integrity
s preserved), intrinsic renal failure with parenchymal tissue njury, and postrenal failure (dysfunction due to acute obstruc-ion of the urinary tract) (Table 24-11). Appropriate catego-ization of AKI requires the clinician to integrate the findings nd results from a careful history, physical examination, and ppropriate laboratory and imaging studies.
TABLE 24-11 Causes of Acute Kidney Injury
Prerenal
Gastrointestinal hemorrhage
Burns
Pancreatitis
Capillary leak
Diarrhea, vomiting, nasogastric suction, fistula fluid loss
Excessive sweating
Diuretics, nonsteroidal antiinflammatory drugs
Congestive heart failure
Cirrhosis
Intrinsic
Ischemia (e.g., postoperative acute tubular necrosis)
Nephrotoxins (e.g., radiocontrast agents, aminoglycosides)
Sepsis
Acute interstitial nephritis
Acute glomerulonephritis
Acute vascular syndrome (e.g., bilateral renal artery thromboembolism or dissection)
Atheroembolic disease
Postrenal
Bilateral upper tract obstruction (e.g., nephrolithiasis, papillary necrosis) or obstruction of solitary functioning kidney
Lower tract obstruction (e.g., prostatic hypertrophy, urethral stricture, bladder mass or stone, obstructed urinary catheter)

860 Section IV Evaluation of the Patient with Kidney D
History and Review of Systems
The initial goal of history taking is to establish whether the patient actually has AKI. In this regard, a careful review of clinical, pharmacy, nursing, and radiologic records is necessary. A relatively recent serum creatinine determination is invalu-able but not always available. In some cases the clinician must make a presumptive diagnosis of AKI pending further data collection and investigation. A diagnosis of AKI can usually be more readily established when it occurs during a hospital-ization because urine output is often recorded and laboratory values are measured frequently.
A history of anuria should raise the possibility of obstruc-tive uropathy. The historical features that assist in the differ-entiation of AKI into the categories shown in Table 24-11 should be identified. One of the risk factors that most strongly predicts the development of AKI is the presence of CKD.55 A history of salt and fluid losses such as occur with diarrhea, vomiting, or ECF loss into a third space as is seen with exten-sive burns, pancreatitis, or leaky capillaries suggests a prerenal etiology. NSAIDs, angiotensin converting enzyme inhibitors, and angiotensin receptor blockers, especially when combined with diuretics, can generate a renal hypoperfusion state and AKI. Therefore medication review is essential to identify such drugs and also any other potential nephrotoxic agents.
A history of heart failure or liver disease increases the like-lihood that AKI is the result of reduced effective arterial vol-ume. Often, the cause of AKI is multifactorial (e.g., a patient with a gastrointestinal hemorrhage may undergo a radiologic study with IV contrast). It is also critically important to iden-tify any history of underlying CKD. Often, such patients develop superimposed AKI due to a variety of renal insults. A history of decreased urine output or anuria is important, but, as noted earlier, many patients have normal urine output despite AKI.
A history of voiding symptoms such as urinary frequency, hesitancy, or incontinence suggests the possibility of obstruc-tive uropathy. Many patients with renal artery emboli and some with bilateral renal vein thrombosis may present with flank pain and a history of hematuria. It is also important to elicit any history of a recent interventional procedure, which raises the possibility of AKI as a result of IV or intraarterial contrast infusion or atheroembolic disease. A history of fever, skin rash, arthralgias, sinusitis, and/or hemoptysis raises the possibility of glomerulonephritis related to infection, collagen vascular disease, or vasculitis.
Physical Examination
An extremely important aspect of the physical examination in every patient with AKI is an assessment of ECF and effec-tive arterial volume status. Overt hypotension is the strongest indicator of potential renal underperfusion. Less severe vol-ume depletion is suggested by an orthostatic pulse increase of more than 30 beats/min (measured 1 minute after standing). Of note, orthostatic hypotension, defined as a drop in systolic blood pressure of more than 20 mm Hg after standing, is less helpful because it occurs in 10% of normal subjects.56 Dry axillae and dry mucous membranes with a furrowed tongue are useful signs of volume depletion. However, poor skin tur-gor and slow capillary refill have not been shown to be helpful
isease
signs in adults.56 The neck veins are usually flat when volume contraction exists.
Renal perfusion is reduced as a result of heart failure or hepatic cirrhosis. Signs of the former condition include dis-tended neck veins, pulmonary rales, an S3 gallop, and pitting peripheral edema. Stigmata of chronic liver disease, includ-ing jaundice, hepatosplenomegaly, ascites, gynecomastia, nail clubbing, palmar erythema, vascular spiders, and testicular atrophy, should be sought. The presence of either true ECF volume depletion or reduced effective arterial volume raises the very strong possibility of a prerenal (and potentially readily reversible) cause of the AKI.
The physical examination may suggest a systemic disease associated with an intrinsic AKI, such as vasculitis, endocar-ditis, thrombotic thrombocytopenic purpura and hemolytic uremic syndrome, and so on. An important cause of AKI in the hospitalized or recently hospitalized patient is athero-embolic (cholesterol embolic) disease. This often overlooked condition generally occurs following an invasive procedure that requires intraarterial catheterization (e.g., cardiac cath-eterization, angiography) or cardiac or aortic surgeries. Skin findings include livedo reticularis, ulcers, purpura, petechiae, painful erythematous nodules, cyanosis, and gangrene. Retinal examination may reveal arterial atheroemboli (Hollenhorst plaques).
Flank tenderness or an enlarged palpable bladder indicates possible postrenal causes for AKI. A digital examination of the prostate should be performed in all men with AKI, and a bimanual pelvic examination to detect pelvic masses should be considered in women. If lower tract obstruction is a seri-ous consideration in-and-out diagnostic postvoid bladder catheterization should be done. The normal postvoid residual urine volume is less than 50 mL. Any urine collected should be saved for potential additional studies.
Laboratory Tests
Initial testing in AKI must include urinalysis and an estimate of the GFR. ECF volume contraction causes marked urine concentration, which increases the urine specific gravity and may generate positive dipstick protein results. Microscopy often reveals hyaline casts, but there should be few cells and no cellular casts. Quantitative protein excretion is relatively low (<1 g/day). A “bland” finding on urinalysis is also consistent with an obstructive or postrenal cause for AKI, unless a com-plicating infection produces pyuria and bacteriuria, or hema-turia results from stone disease. AKI due to intrinsic damage such as tubular necrosis will generate a “dirty” urinalysis with many epithelial cells and muddy brown granular and epithe-lial cell casts. The urine is generally isosthenuric (i.e., specific gravity is 1.010). Rhabdomyolysis causes myoglobinuria, and pigmented granular casts are seen. Acute glomerulonephritis produces proteinuria, hematuria, and RBC casts. Acute inter-stitial nephritis causes pyuria and white cell casts. If it is due to an allergic reaction, then urine eosinophils are often seen, but this is not a specific finding.57
Estimation of the GFR gives an approximate measure of the number of functioning nephrons. In the setting of AKI the GFR is, by definition, not in a steady state. This makes GFR estimates, especially those based on plasma cre-atinine, unreliable. However, a rising creatinine concentration
Chapter 24 Approach to the Patient with Kidney Disease 861
indicates that the renal injury is stable or worsening, whereas a falling creatinine concentration is indicative of improve-ment. A daily rise in creatinine concentration of more than 1 mg/dL is usually associated with a GFR of less than 10 mL/min. A timed urine collection for determination of cre-atinine and/or urea clearance can be very helpful (but even here tubular secretion of creatinine can lead to overestimation of the GFR). When available, clearance values for radioiso-topes such as iothalamate can be used as the most accurate measurement of GFR.
Routine studies of electrolytes, BUN, calcium, and phos-phorus should be performed. Potentially life-threatening hyperkalemia and severe metabolic acidosis must be identified and treated. Table 24-12 lists a number of urine and plasma chemical measurements and calculations that help differenti-ate prerenal AKI from intrinsic renal injury. Although mea-surement of the urine sodium concentration can be helpful in distinguishing these disorders, the fractional excretion of sodium and/or urea is a better indicator. Important exceptions include AKI due to contrast nephropathy, rhabdomyolysis, acute myeloma kidney, and acute urate nephropathy in which the fractional excretion of sodium and urea are often very low despite the absence of an apparent prerenal cause.
Imaging
Imaging of the urinary tract by ultrasonography is an extremely helpful and important test in the setting of AKI. It will gen-erally diagnose obstruction. However, it is not 100% sensi-tive nor specific; ultrasonography can produce negative results immediately following obstruction or in patients with ureteric encasement. Renal ultrasonography also provides an excellent measurement of kidney size. This helps to distinguish chronic renal failure (in which the kidneys are often small and echo-genic) from AKI (in which renal size is expected to be nor-mal). If contrast nephropathy is suspected, a plain radiograph of the abdomen (kidneys, ureters, bladder [KUB]) may reveal
TABLE 24-12 Tests to Differentiate Prerenal from Intrinsic Kidney Damage
MEASUREPRERENAL AKI
INTRINSIC KIDNEY DAMAGE (ATN, ETC.)
Urine Na (mEq/L) <20 >40
Urine osmolality (mOsm/kg H2O)
>500 <350
Serum BUN/creatinine (Cr) ratio
>20 10-15*
Fractional excretion of Na[UNa × PCr][PNa × UCr]
× 100
<1† >2
Fractional excretion of urea[UUrea × PCr]
[PUrea × UCr]× 100
<30† >50
*A BUN/Cr ratio of <10 may occur with rhabdomyolysis because the Cr concentration increases sharply as a result of increased release from necrotic muscle. A low BUN/Cr ratio can also develop in malnourished individuals due to very low BUN.
†The fractional excretion of Na and fractional excretion of urea are often also very low with contrast nephropathy, rhabdomyolysis, acute myeloma kidney, and acute urate nephropathy.
AKI, Acute kidney injury; ATN, acute tubular necrosis; BUN, blood urea nitrogen; P, plasma; U, urinary.
a persistent nephrogram due to retained IV contrast material. Doppler ultrasonography can also be useful in the assessment of renal arterial and venous patency when vascular obstruc-tion is suspected. Although CT, MRI, and angiography can be used when ultrasonography is insufficient, these modalities are limited because renal injury restricts the use of contrast agents.
Renal Biopsy
Renal biopsy is generally not necessary in the setting of AKI. However, renal biopsy can be useful when vasculitis, glomeru-lonephritis, or allergic interstitial nephritis is considered a possible cause of the AKI.58
Chronic Kidney Disease and Chronic Kidney Failure
CKD, regardless of the specific cause, is defined as an irre-versible and usually progressive decline in nephron function and number generally quantitated as a reduction in GFR. As GFR falls from 90 mL/min to approximately 30 mL/min, retention in the plasma of substances that are handled pri-marily by glomerular filtration develops. The plasma concen-trations of urea nitrogen and creatinine, two such substances that are routinely measured, increase. As the GFR falls from 30 to 15 mL/min, additional alterations in plasma composi-tion develop, and additional pathophysiologic disturbances, including anemia, altered calcium and phosphate metabolism, and nutritional changes, occur. Although overt symptoms may be absent, careful evaluation generally reveals a wide spectrum of abnormalities in these patients. Then, as GFR falls below 10 mL/min, overt uremic signs and symptoms develop, and if the decline is irreversible, the patient will have reached end-stage kidney failure (ESKD). Uremic syndrome is the result of severely reduced excretory function with reten-tion of metabolic products, fluid and acid-base derangements, hormonal abnormalities, and other consequences of the loss of renal function.
In 2002 the National Kidney Foundation proposed a new classification system for CKD based on the severity of GFR reduction and made recommendations for appropriate actions to be taken at each disease stage.59 This system, known as the Kidney Disease Outcomes Quality Initiative (KDOQI) Classifi-cation, is shown in Table 24-13. Also shown in the table are the number of adults in the United States with each stage of chronic kidney disease (CKD). Most individuals with CKD have stage 1 or 2 disease. Patients with stage 3 CKD, number-ing almost 8 million, comprise the most rapidly expanding group. In 2007 the incidence of ESKD in the United States was approximately 355,000 and the prevalence was 1665 per million population.60,61 Mortality in patients with CKD is high, and in patients with stage 3 CKD the risk of death (usu-ally from cardiovascular disease) is at least 10 times higher than the risk of progression to ESKD. Patients with ESKD have a mortality rate of about 50% after 3 years and 65% to 75% at 5 years. At least 60% of these deaths are also related to cardiovascular disease. CKD has manifestations and com-plications affecting virtually every organ system, including the central and peripheral nervous, neuropsychiatric, endo-crine, hematologic, cardiovascular, gastrointestinal, peripheral
862 Section IV Evaluation of the Patient with Kidney Disease
TABLE 24-13 National Kidney Foundation Kidney Disease Outcomes Quality Initiative (KDOQI) Classification System, Disease Prevalence, and Action Plan
STAGE DESCRIPTION GFR (mL/min/1.73 m2)PREVALENCE (IN MILLIONS)* ACTION
At increased risk ≥90 (with CKD risk factors) Reduction of CKD risk factors
1 Kidney damage with normal or ↑ GFR
≥90 3.6 Treatment of comorbid conditions and reduction of CVD risks
2 Kidney damage with mild ↓ GFR 60-89 6.5 Estimation of progression rate
3 Moderate ↓ GFR 30-59 15.5 Evaluation and treatment of complications
4 Severe ↓ GFR 15-29 0.7 Preparation for kidney replacement therapy
5 Kidney failure (end-stage kidney disease)
<15 (or dialysis) 0.6 Kidney replacement (if uremic)
Chronic kidney disease is defined as kidney damage for ≥3 months defined by structural or functional abnormalities of the kidney, with or without decreased GFR. Damage may be documented as a pathologic abnormality or the presence of markers of kidney damage. These include abnormalities on blood or urine tests, abnormalities on kidney imaging tests, or a GFR of <60 mL/min/1.73 m2.
CKD, Chronic kidney disease; CVD, cardiovascular disease; GFR, glomerular filtration rate.Prevalence data from National Kidney Foundation,59 United States Renal Data System,60 and Coresh et al.61 Data are for adults aged ≥20 years.
vascular, and skeletal systems. Consequently the diagnosis and treatment of CKD requires a broad, multifaceted approach.
The most common renal diseases that progress to ESKD (in order of both incidence and prevalence) are diabetic nephrop-athy, hypertensive nephrosclerosis, polycystic kidney disease, and chronic glomerulonephritis. The focus of the history, physical examination, and laboratory studies in these patients is establish the specific diagnosis, determine the severity of kidney dysfunction, identify any reversible component, iden-tify and quantitate any comorbid conditions and complica-tions, assess the risk for continued loss of kidney function, and assess the risk for cardiovascular disease.
History and Review of Symptoms
Patients are often referred to a nephrologist for evaluation of CKD when the BUN and creatinine concentrations are noted to be elevated on routine laboratory testing. The patient may have no knowledge of any kidney disorder or abnormal kidney function. Other patients may have had an extensive prior renal evaluation. In some the kidney disease is an isolated abnor-mality; in others an underlying disease known to be associated with kidney involvement such as systemic lupus erythemato-sus, hepatitis B or C, scleroderma, or vasculitis may exist. The duration of the kidney disease and the rate of progression must be established whenever possible. The patient might know of a specific diagnosis, the severity or stage of the kidney disease, and its pace. Any available laboratory data, biopsy reports, and imaging results should be obtained. Prior urologic interven-tions should be reviewed. Any previous discussions regarding treatment or renal replacement therapy should be discussed, and the patient’s adherence to prior nephrologic recommen-dations should be determined.
A detailed family history of kidney disease can be extremely informative. Monogenic familial kidney diseases include poly-cystic kidney disease, Alport’s disease, medullary cystic disease, certain forms of membranoproliferative glomerulonephri-tis, and Fabry’s disease. Polygenic familial disorders include diabetes mellitus, hypertension, obesity, hyperlipidemia, and premature vascular disease. The patient’s general health, abil-ity to perform activities of daily living, energy level, appetite,
and any recent weight changes should be assessed. Mental acuity, memory, mood, and any change in sleep pattern must be evaluated. Sometimes family members can provide a more accurate assessment of these parameters than the patient.
Many symptoms do not become apparent until very late in the disease course. Patients with CKD may exhibit amaz-ing adaptive ability. GU symptomatology should be identified. This includes voiding symptoms such as polyuria, nocturia, hesitancy, and frequency and any history of UTIs; back, flank, abdominal, or pelvic pain; renal calculi; or urologic manipula-tion. Any history of GU malignancy, including cancer of the bladder, prostate, kidney, or cervix, and any renal imaging pro-cedures should be reviewed. Cardiovascular, peripheral vascular, and cerebrovascular disease history should be elicited. Coronary artery disease is the most important vascular complication in patients with CKD.62 A history of myocardial infarction and/or congestive heart failure should be noted and left ventricular function assessed. A history of coronary artery interventions, significant arrhythmias, or insertion of a pacemaker or defi-brillator should be identified. It is imperative that any history of resting or exertional chest pain and/or shortness of breath be recognized. Peripheral vascular disease is also very common in patients with CKD. A history of claudication, peripheral ulcers, revascularization, gangrenous extremities, or extrem-ity amputation must be documented. Symptoms secondary to autonomic and sensorimotor neuropathy should be identified.
Nutritional status, appetite, and weight changes should be determined. The interpretation of weight change is compli-cated, however, because loss of body mass may be masked by fluid accumulation. Food may taste bad, and foul breath may develop. With overt uremia, anorexia, nausea, and vomit-ing develop. Occasionally diarrhea is present. In the diabetic patient with ESKD it may be difficult to distinguish between uremic symptoms and those of diabetic neuropathy and enter-opathy. Musculoskeletal complaints occur frequently with CKD. Muscle cramps are often related to diuretic use. Muscle wasting and loss of muscle strength occur. Bone and joint pain may be due to osteodystrophy. Spontaneous fractures can occur.
All medications should be carefully reviewed and docu-mented. The review should include current and prior medica-tions, and over-the-counter and nonprescription medications. Medications should be reviewed for potential nephrotoxic

Chapter 24 Approach to the Patient with Kidney Disease 863
effects and appropriate dosing. Calcineurin inhibitors (cyclo-sporine, tacrolimus), lithium, pamidronate, chemotherapy agents (cisplatin, mitomycin C), and various analgesics are sev-eral examples of drugs that can damage the kidneys. Recently, use of sodium phosphate bowel preparations before colonos-copy or surgical procedures has been found to cause irreversible renal disease.63 Therefore, this has become an important line of questioning in patients with otherwise unexplained CKD.
Ophthalmic complications, largely related to diabetes and hypertension, are common in CKD. Lens abnormalities may occur in patients with Alport’s disease. When diabetes exists, the date of onset, type of treatments, results of microalbumin-uria studies, adequacy of control, hemoglobin A1C levels, and so on, should be ascertained. In general, the onset of type 2 diabetes is difficult to determine, because it may be clinically silent for years. Hypertensive nephrosclerosis is the second leading cause of CKD resulting in ESKD, and hypertension is also a very common complication of virtually all forms of CKD. Differentiating primary hypertension that has caused CKD from a kidney disease complicated by hypertension is frequently very difficult. The duration of hypertension may also be difficult to establish. Hospitalization for an acute car-diovascular event may lead to recognition of hypertension. A history of high or low blood pressure extremes, as well as response to and adherence to antihypertensive medica-tion regimens, should be documented. A history of gross or microscopic hematuria, proteinuria, or foamy urine suggests glomerulonephritis, the third most common cause of CKD progressing to ESKD. Back or flank pain may be presenting or prominent complaints. Fever, skin rash, inflammation of the eyes or sinuses, and joint pains raise the possibility of second-ary forms of glomerulonephritis. Occasionally a family history of glomerulonephritis can be elicited.
Polycystic kidney disease is often diagnosed from the family history. Occasionally polycystic kidney disease is first recog-nized after an abdominal imaging procedure reveals the diag-nosis. Shoulder, back, flank, and/or pelvic pain occur frequently. Abdominal fullness, bloating, and episodes of hematuria are often described. Sometimes the patient feels the enlarged kid-neys. The multiple extrarenal manifestations of polycystic kid-ney disease include cerebral aneurysms, which are by far the most life-threatening extrarenal complication. Because they occur more commonly within families, a history of cerebral aneurysms, stroke, or sudden death at a young age among rela-tives should be sought. Colonic diverticula and abdominal wall or inguinal hernias are also common in these patients.
Physical Examination
Assessment of vital signs should include supine and upright pulse and blood pressure measurements. One primary focus of the physical examination in patients with CKD is the assess-ment of ECF and effective intraarterial volume status. This is not always straightforward. Physical findings that indicate volume depletion are also discussed in the section on acute kidney injury. Although overt hypotension is the strongest indicator of potential renal underperfusion, an orthostatic pulse increase of more than 30 beats/min (measured 1 min-ute after standing) is indicative of less severe volume deple-tion.56 Orthostatic hypotension, defined as a drop in systolic blood pressure of more than 20 mm Hg after standing, is less
helpful because it is seen in 10% of normal subjects. Auto-nomic neuropathy also complicates the assessment of ortho-static hypotension. Dry axillae and dry mucous membranes with a furrowed tongue are useful signs of volume depletion. However, poor skin turgor and slow capillary refill have not been shown to be helpful signs in adults.56 The neck veins are usually flat in the volume-contracted patient. If volume deple-tion is possible, a trial of ECF expansion with crystalloid solu-tions is indicated to determine if a reversible component of kidney dysfunction exists. At the other extreme, hypertension, peripheral edema, pleural effusions, and pulmonary rales may indicate volume overload and require treatment with diuretics or ultrafiltration. However, edema and effusions may also be the result of nephrotic syndrome. Heart failure and cirrhosis also generate total body salt and water expansion with effec-tive intraarterial volume contraction.
Advanced CKD produces a sallow appearance. General-ized muscle wasting may be observed. Current body weight should be noted and compared with prior known weights.
Thorough evaluation of the cardiovascular system is man-datory. Retinal examination may reveal hypertensive or dia-betic retinopathy. Carotid pulse should be evaluated and the presence of bruits identified. Cardiac examination may reveal left ventricular hypertrophy or decompensation. Flank or abdominal bruits may suggest renovascular disease.
Palpation of the abdomen may reveal an enlarged bladder or large kidneys. Costovertebral tenderness indicates possible inflammatory or infectious kidney disease.
Motor and/or sensory neuropathy can occur with CKD as well as diabetes. Muscle wasting is common. Neuromuscu-lar irritability with tremor and myoclonic jerks can be seen when CKD is advanced or is complicated by hypocalcemia or hypomagnesemia.
Skin changes common in CKD include pallor related to anemia, hyperpigmentation, and scratch marks and excoria-tions produced as a result of pruritus. Uremic frost, represent-ing residue from evaporated urea-rich sweat, occurs in severe untreated ESKD. Skin necrosis due to calcific arteriopathy and calciphylaxis is a dreaded complication.
Laboratory Tests
The urinalysis can provide important clues to the diagnosis. Hematuria with high-grade proteinuria suggests a glomerular process, either glomerulonephritis or diabetes, whereas low-grade proteinuria is consistent with nephrosclerosis, an inter-stitial disease, or polycystic disease. When the urine sediment reveals RBCs, their appearance as acanthocytes (see Figure 24-1) or RBC casts supports a glomerular origin.
The urine protein/creatinine ratio provides an estimate of protein excretion. With the assumption that urine creatinine excretion is about 1 g/day, this ratio, expressed as grams of protein per gram of creatinine, represent the daily protein excretion in grams per day. Adjustments can be made for very small or very large patients. Excretion of more than 3 g/day of protein (primarily albumin) is most consistent with a glomer-ular process. True quantitative measurement of protein and creatinine excretion may be very helpful in selected patients.
Blood studies should include a CBC, BUN and creatinine concentrations, electrolyte panel, calcium level, phosphate level, liver function studies, and a lipid panel. Sedimentation

864 Section IV Evaluation of the Patient with Kidney Disease
rate and C-reactive protein level provide information about the patient’s inflammatory state. Based on the results of these tests and the patient’s underlying conditions, the iron stor-age status, vitamin B12 and folate levels, and hemoglobin A1C levels are often measured. Serologic testing to evaluate for the presence of systemic lupus erythematosus or other collagen vascular diseases, HIV infection, hepatitis B or C, and mul-tiple myeloma is often done. Evaluation of complement levels may be helpful with certain types of glomerulonephritis.
An assessment of the GFR is an essential component of the evaluation of the patient with CKD. GFR can be estimated from the serum creatinine concentration using one of several standard formulas (see Table 24-3). These formulas produce inaccurate results for the very old, the very large, and patients with a relatively high GFR (normal serum creatinine concen-tration). In addition, the serum creatinine concentration must be relatively stable. A timed urine collection to measure creati-nine clearance is the standard method for documenting renal function. A radioisotope clearance study (usually iothalmate) is the most accurate, gold standard method for determining GFR. Serum cystatin C level has recently been proposed as a better marker of renal function, but this test is not routinely done in most facilities. It may have some advantage relative to creatinine concentration, but this remains unproven.
Imaging
Renal ultrasonography should be done for all patients being evaluated for CKD. The sonogram provides a kidney size assessment, supplies information on cortical width and echo-genicity, and demonstrates the presence or absence of scars and hydronephrosis as well as renal stones or masses. Renal Doppler ultrasound imaging is used to assess renovascular flow. If there is any suspicion of coexistent heart disease, an echocardiogram can be done to assess cardiac size, left ven-tricular function, regional wall motion abnormalities, pulmo-nary pressures, valvular function, and pericardial fluid.
Urinary Tract Infection
UTI is one of the most frequent infectious illnesses occurring in humans and is probably the most common bacterial infec-tion.64 It can occur in those of all ages, from the very young to the very old. It most often affects women in the reproductive age group. UTI presents in multiple ways, from asymptom-atic bacteriuria, to bothersome local symptoms of pelvic pain and dysuria, to severe local symptoms of back or flank pain and fever, to severe overwhelming infection with septic shock and multiorgan failure.
It is useful to separate UTIs on an anatomic basis. Pyelone-phritis represents an upper urinary tract infection of the kid-ney itself. Lower urinary tract infections may be separated into those of the bladder (cystitis), prostate, and urethra.
History and Review of Systems
The most common complaint of patients with an acute UTI is urinary frequency and dysuria. Other voiding symptoms such as difficulty voiding, polyuria, halting voiding symptoms, or
frequent small voids also occur. Sometimes a change in the appearance of the urine is the presenting complaint. The patient may complain of grossly purulent, foul-smelling, and/or blood-tinged or frankly bloody urine. Passage of a stone or tissue debris may be reported. Patients with UTIs (other than asymptomatic bacteriuria) also often present with some localizing symptom. Back, flank, abdominal, and/or pelvic pain may be the presenting complaint. Fever, with or without chills, suggests a more serious illness.
A past history of similar symptoms associated with a doc-umented UTI can often be elicited. The frequency of prior UTIs should be established. The patient’s report of specific antibiotics used for treatment of previous UTIs is helpful. Some patients can describe prior infecting organisms as dem-onstrated on urine culture.
In addition to localizing symptoms of pain, with or without fever, some patients have constitutional symptoms of fatigue, malaise, and weight loss. Gastrointestinal symptoms of nausea and vomiting, constipation, or diarrhea may be present. With severe UTIs, symptoms of hypotension with orthostatic diz-ziness may be seen.
Asymptomatic bacteriuria can occur as the initial presen-tation. It must be distinguished from urinary contamination at the time of urine culture. It is often identified in patients with a history of UTIs and is sometimes noted when urine cultures are performed during follow-up of previously treated symptomatic UTIs. Most often it is detected in patients at high risk for UTIs in whom surveillance urine cultures are performed. High-risk groups include pregnant women; sexually active young women; elderly men and women, par-ticularly in a nursing home setting; patients with indwelling urinary catheters or other drainage devices; patients with dia-betes; and patients with spinal cord injury. However, current recommendations are that only pregnant women should be screened (and treated) for asymptomatic bacteriuria.64 There is currently no evidence that the benefits of screening out-weigh its potential negative impact in any other adult patient group.65
It is important to identify underlying risk factors for the development of the current UTI as well as previous episodes of UTI. Most young and middle-aged women have no appar-ent anatomic abnormality that might predispose them to UTIs. Recurrent UTIs in this group should prompt a discus-sion regarding the timing of the UTI with respect to sexual activity. The use of diaphragms and spermicides as well as delayed postcoital micturition has been associated with UTI. Vaginitis is an important risk factor for UTI in women, so a history of associated symptoms should be elicited. There is lit-tle evidence that tampon use or the method (direction of wip-ing) of cleansing after defecation have a significant impact on the risk of developing UTI. The frequency of UTI increases during pregnancy and is probably related to a combination of physiologic and anatomic changes, frequent glucosuria, and hormonal effects.
UTIs in men raise concern for an anatomic abnormal-ity. The most common abnormalities that predispose men to UTI are prostatic enlargement and prostatitis. Sexual history regarding homosexual activity, and specifically anal inter-course, which increases UTI risk in men, is also important. Other anatomic abnormalities that predispose patients to UTI include bladder pathology (neurogenic bladder, espe-cially in the setting of spinal cord injury; bladder cancer with

Chapter 24 Approach to the Patient with Kidney Disease 865
disruption of the urothelium; bladder diverticula); enterovesi-cal fistula; polycystic kidney disease; prostate cancer; urinary drainage devices and procedures (indwelling transurethral or suprapubic bladder catheters, percutaneous nephrostomy, ure-teral stent, ileal conduit); renal calculi with or without urinary obstruction; vesicoureteral reflux; and urinary obstruction at any level.
Certain medical conditions also place patients at increased risk for developing UTIs and complications of these infec-tions. These include pregnancy, diabetes, renal transplanta-tion, and long-term immunosuppression.
Physical Examination
Physical examination findings in the setting of UTI are often nonspecific.66 Fever may indicate a more serious or compli-cated UTI, as does hypotension and tachycardia. The patient with a severe systemic infection of urinary origin may have a toxic appearance and altered mentation. Careful attention should be given to the back, flank, abdomen, and pelvic areas to detect localized tenderness or palpable mass. The patient should be inspected for urinary drainage devices. In men a rectal examination for assessment of the prostate is important.
Laboratory Tests
The urinalysis results often confirm the presence of an active UTI.67 Gross visual inspection of the urine may reveal tur-bidity or blood, and the urine often has a foul smell. On the urine dipstick test, the pH can be markedly alkaline (supra-physiologic level, i.e., >7.5) when the urine is infected with urea-splitting bacteria (see section on laboratory evaluation of nephrolithiasis). The dipstick result is often positive for occult blood. The nitrite test result is positive when the urine is infected with Enterobacteriaceae. These gram-negative bacilli have an enzyme that reduces urinary nitrate to nitrite. A false-negative nitrite test result can occur when the urine is very dilute (e.g., the patient is taking a diuretic) or the infecting bac-teria do not produce the nitrate reductase enzyme (Staphylococ-cus or Enterococcus species or Pseudomonas aeruginosa). Urine granulocytes generally indicate inflammation, which may or may not be due to infection. They can be detected by a dipstick test for leukocyte esterase, an enzyme contained in the gran-ules of neutrophils. More than 5 WBCs per HPF is needed for a positive test finding. In rare cases false-positive results are produced by strong oxidants in the urine collection container. High-grade proteinuria or glucosuria, some antibiotics, and high levels of ascorbic acid can produce false-negative results.
Simultaneous positive test results for nitrite and leuko-cyte esterase virtually guarantee the presence of a UTI. A finding of marked proteinuria raises the possibility of reflux nephropathy complicated by focal glomerulosclerosis, whereas moderate proteinuria (in the range of 1 to 1.5 g/day or less) can occur with chronic interstitial nephritis. The spun urine sediment shows neutrophils, often in clumps, and occasion-ally neutrophil casts. RBCs are also usually seen. Bacteria are generally easily observed when significant bacteriuria exists. A Gram-stained smear of either unspun urine or spun sediment can aid in identification of the bacteria and help target empiric therapy.
Urine culture will verify an active UTI. Good urine col-lection and culture techniques are necessary to avoid con-tamination. Midstream urine should be collected after careful washing of external genitalia followed by voiding into a sterile container. Bladder catheterization, suprapubic needle blad-der aspiration, or sterile aspiration of urine from the tube of a closed catheter drainage system is sometimes required. Most true UTIs are caused by a single organism. Therefore dem-onstration of multiple organisms on urine culture strongly suggests contamination. A colony count of more than 105 organisms/mL (from voided specimens) correlates with active infection. However, colony counts of less than 105/mL may be significant in a symptomatic patient.
The vast majority (80% to 90%) of positive urine cultures in the outpatient setting grow E. coli. The presence of other gram-negative bacteria on urine culture suggests a compli-cated UTI possibly related to renal calculi or obstruction. Pro-teus infections occur in patients with staghorn calculi. Urine culture findings for hospitalized patients are much more diverse. UTIs caused by gram-positive cocci (usually Entero-coccus) are uncommon, and those due to Staphylococcus spe-cies are extremely rare. Staphylococcus aureus UTI may suggest staphylococcal bacteremia, and UTI caused by coagulase-neg-ative staphylococci can occur after instrumentation in elderly men. Mycobacterial and fungal UTIs are very rare. Candida infections may develop in immunocompromised patients or those with long-standing catheters. Anaerobic bacteria almost never cause UTIs.
An assessment of baseline renal function should be done. This is most commonly accomplished using a serum creatinine measurement and any one of several standard predictive formu-las (see Table 24-3). If renal function is reduced, this may be an acute or chronic process. Acute renal failure occurs in patients with volume depletion and sepsis syndromes with hypoten-sion. Infection with bilateral urinary obstruction or obstruc-tion in a solitary functional kidney can present with AKI or kidney failure. Chronic renal dysfunction and failure can occur with vesicoureteral reflux, chronic pyelonephritis, or chronic urinary obstruction. In all patients with persistently reduced estimates of kidney function, formal measurements should be obtained using either a timed urine collection to assess creati-nine clearance or an isotopic measurement of GFR.
A number of acid-base and potassium abnormalities may occur in patients with UTI. If UTI causes nausea and vomiting then metabolic alkalosis and hypokalemia ensue. Hyperkalemia can be caused by renal dysfunction or may be a component of type 4 renal tubular acidosis due to chronic renal interstitial disease or obstruction. Metabolic acidosis can be caused by lactic acidosis associated with sepsis or renal tubular acidosis.
Imaging
Kidney and GU tract imaging is usually done to diagnosis ves-icoureteral reflux, renal calculi, and other lesions that obstruct urine flow or otherwise cause stasis. In general, imaging stud-ies are not required in adult women with an uncomplicated UTI that responds rapidly to antibiotic treatment. Imaging is generally recommended for all men with their first UTI. Imaging should also be done when patients have a compli-cated UTI, when bacteremia has developed, when the UTI
866 Section IV Evaluation of the Patient with Kidney Disease
has failed to respond to appropriate antibiotic therapy, and when urinary obstruction or stones are suspected. Women with unexplained recurrent UTIs and all patients with pyelo-nephritis serious enough to warrant hospitalization should undergo imaging. Also, if hematuria persists following resolu-tion of a UTI, imaging is indicated.
Renal ultrasonography has now replaced IV urography as the standard renal imaging procedure in patients with UTI. Renal size, cortical width and echogenicity, obstruction, and stones can be readily determined with ultrasonography. Blad-der and prostate anatomy can be assessed. CT with contrast infusion permits further assessment of renal and ureteral anat-omy and pathology. Pyelonephritis in an obstructed kidney requires emergent intervention for drainage, and detection of a perinephric abscess usually also calls for surgical intervention.
Some patients require cystoscopy, retrograde pyelography, and/or voiding cystography to detect vesicoureteral reflux.
References
1. Mohr DN, Offord KP, Owen RA, Melton 3rd LJ. Asymptomatic microhematuria and urologic disease. A population-based study. JAMA. 1986;256:224-229.
2. U. S. Preventive Services Task Force. Screening for bladder cancer in adults: recommendation statement. June 2004. Available at http://www.uspreventiveservicestaskforce.org/3rduspstf/bladder/blacanrs.htm.Accessed March 12, 2011.
3. Khadra MH, Pickard RS, Charlton M, et al. A prospective analysis of 1,930 patients with hematuria to evaluate current diagnostic practice. J Urol. 2000;163:524-527.
4. Karl Tryggvason. Jaakko Patrakka: Thin basement membrane nephropathy. J Am Soc Nephrol. 2006;17:813-822.
5. Kiryluk K, Jadoon A, Gupta M, et al. Sickle cell trait and gross hematuria. Kidney Int. 2007;71:706-710.
6. Abarbanel J, Benet AE, Lask D, et al. Sports hematuria. J Urol. 1990;143:887-890.
7. Culclasure TF, Bray VJ, Hasbargen JA. The significance of hematuria in the anticoagulated patient. Arch Intern Med. 1994;154:649-652.
8. Brennan P, Bogillot O, Cordier S, et al. Cigarette smoking and bladder cancer in men: a pooled analysis of 11 case-control studies. Int J Cancer. 2000;86:289-294.
9. Fortuny J, Kogevinas M, Garcia-Closas M, et al. Use of analgesics and nonsteroidal anti-inflammatory drugs, genetic predisposition, and bladder cancer risk in Spain. Cancer Epidemiol Biomarkers Prev. 2006;15:1696-1702.
10. Pollock C, Liu PL, Gyory AZ, et al. Dysmorphism of urinary RBCs—value in diagnosis. Kidney Int. 1989;36:1045-1049.
11. Koss LG, Deitch D, Ramanathan R, et al. Diagnostic value of cytology of voided urine. Acta Cytol. 1985;29:810-816.
12. Juncos LI. Intrarenal mechanisms of salt and water retention in the nephritic syndrome. Kidney Int. 2002;61:1182-1195.
13. Rodríguez-Iturbe B, Baggio B, Colina-Chourio J, et al. Studies on the renin-aldosterone system in the acute nephritic syndrome. Kidney Int. 1981;19:445-453.
14. Ruggenenti P, Gaspari F, Perna A, et al. Cross sectional longitudinal study of spot morning urine protein:creatinine ratio, 24 hour urine protein excretion rate, glomerular filtration rate, and end stage renal failure in chronic renal disease in patients without diabetes. BMJ. 1998;316:504-509.
15. Brown KM, Sacks SH, Sheerin NS. Mechanisms of disease: the complement system in renal injury—new ways of looking at an old foe. Nat Clin Pract Nephrol. 2007;3:277-286.
16. Madaio MP, Harrington JT. Current concepts: the diagnosis of acute glomerulonephritis. N Engl J Med. 1983;309:1299-1302.
17. Olsen S. Identification of non-diabetic glomerular disease in renal biopsies from diabetics—a dilemma. Nephrol Dial Transplant. 1999;14:1846-1849.
18. Niaudet P. Genetic forms of nephrotic syndrome. Pediatr Nephrol. 2004;19:1313-1318.
19. Schrier RW, Fassett RG. A critique of the overfill hypothesis of sodium and water retention in the nephrotic syndrome. Kidney Int. 1998;53:1111-1117.
20. Koomans HA, Kortlandt W, Geers AB, et al. Lowered protein content of tissue fluid in patients with the nephrotic syndrome: observations during disease and recovery. Nephron. 1985;40:391-395.
21. Cockram CS, Richards P. Yellow nails and nephrotic syndrome. Br J Dermatol. 1979;101:707-709.
22. Llach F. Hypercoagulability, renal vein thrombosis, and other thrombotic complications of nephrotic syndrome. Kidney Int. 1985;28:429-439.
23. Venkataseshan VS, Faraggiana T, Grishman E, et al. Renal failure due to tubular obstruction by large protein casts in patients with massive proteinuria. Clin Nephrol. 1993;39:321-326.
24. Cohen AH. Morphology of renal tubular hyaline casts. Lab Invest. 1981;44:280-287.
25. Martin RS, Small DM. Physicochemical characterization of the urinary lipid from humans with nephrotic syndrome. J Lab Clin Med. 1984;103:798-810.
26. Blackburn V, Grignani S, Fogazzi GB. Lipiduria as seen by transmission electron microscopy. Nephrol Dial Transplant. 1998;13:2682-2684.
27. Liverman PC, Tucker FL, Bolton WK. Erythrocyte sedimentation rate in glomerular disease: association with urinary protein. Am J Nephrol. 1988;8:363-367.
28. Weidmann P, Beretta-Piccoli C, Hirsch D, et al. Curable hypertension with unilateral hydronephrosis. Studies on the role of circulating renin. Ann Intern Med. 1977;87:437-440.
29. Wanner C, Lüscher TF, Schollmeyer P, et al. Unilateral hydronephrosis and hypertension: cause or coincidence? Nephron. 1987;45:236-241.
30. Vaughn Jr ED, Bubler FR, Laragh JH. Normal renin secretion in hypertensive patients with primarily unilateral chronic hydronephrosis. J Urol. 1974;112:153.
31. Maletz R, Beman D, Peelle K, et al. Reflex anuria and uremia from unilateral ureteral obstruction. Am J Kidney Dis. 1993;22:870-873.
32. Batlle DC, Arruda JA, Kurtzman NA. Hyperkalemic distal renal tubular acidosis associated with obstructive uropathy. N Engl J Med. 1981;304:373-380.
33. Klahr S. Nephrology forum: pathophysiology of obstructive nephropathy. Kidney Int. 1983;23:414-426.
34. Webb JA. Ultrasonography and Doppler studies in the diagnosis of renal obstruction. BJU Int. 2000;86(suppl 1):25-32.
35. Ellenbogen PH, Scheible FW, Talner LB, et al. Sensitivity of gray-scale ultrasound in detecting urinary tract obstruction. AJR Am J Roentgenol. 1978;130:730-733.
36. Spital A, Valvo JR, Segal AJ. Nondilated obstructive uropathy. Urology. 1988;31:478-482.
37. Mostbeck GH, Zontsich T, Turetschek K. Ultrasound of the kidney: obstruction and medical diseases. Eur Radiol. 2001;11:1878-1889.
38. Chobanian AV, Bakris GL, Black HR, et al. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood PressureNational High Blood Pressure Education Program Coordinating Committee, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289:2560-2572.
39. Ram V, Fenves A. Hypertension. In: Rakel RE, ed. Conn’s current therapy 2000. Philadelphia: Saunders; 1999:303-315.
40. Frolich ED, Grim C, Laberthe DR, et al. Recommendations for human blood pressure determination by sphygmomanometers; report of special task force appointed by the Steering Committee. Circulation. 1988;77:502A-514A.
41. Stamatelou KK, Francis ME, Jones CA, et al. Time trends in reported prevalence of kidney stones in the United States. Kidney Int. 2003;63:1951-1952.
42. Luchs JS, Katz DS, Lane MJ, et al. Utility of hematuria testing in patients with suspected renal colic: correlation with unenhanced helical CT results. Urology. 2002;59:839-842.
43. Daudon M, Jungers P. Drug-induced renal calculi: epidemiology, prevention and management. Drugs. 2004;64:245-275.
44. Taylor EN, Stampler MJ, Curhan GC. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005;293:455-462.
45. Ljunghall S, Danielson BG, Fellstrom B, et al. Family history of renal stones in recurrent stone patients. Br J Urol. 1985;57:370-374.
46. Daudon M, Jungers P. Clinical value of crystalluria and quantitative morphoconstitutional analysis of urinary calculi. Nephron Physiol. 2004;98:31-36.
47. Longo J, Akbar SA, Schaff T, et al. A prospective comparative study of noncontrast helical computed tomography and intravenous urogram for the assessment of renal colic. Emerg Radiol. 2001;8:285-292.
48. National Institutes of Health Consensus Development Conference on Prevention and Treatment of Kidney Stones, Bethesda, Maryland. JAMA. 1988;260:977-981.
49. Preminger GM, Tiselius HG, Assimos DG, et al. EAU/AUA Nephrolithiasis Guideline Panel: 2007 Guideline for the management of ureteral calculi. J Urol. 2007;178:2418-2434.
50. Larkin GL, Peacock 4th WF, Pearl SM, et al. Efficacy of ketorolac tromethamine versus meperidine in the ED treatment of acute renal colic. Am J Emerg Med. 1999;17:6-10.

Chapter 24 Approach to the Patient with Kidney Disease 867
51. Safdar B, Degutis LC, Landry K, et al. Intravenous morphine plus ketorolac is superior to either drug alone for treatment of acute renal colic. Ann Emerg Med. 2006;48:173-181.
52. Bellomo R, Ronco C, Kellum JA, et al. Acute Dialysis Quality Initiative workgroup: Acute renal failure—definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care. 2004;8:R204-R212.
53. Nash K, Hafeez A, Hon S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930-936.
54. Khan IH, Catto GR, Edward N, et al. Acute renal failure: factors influencing nephrology referral and outcome. QJM. 1997;90:781-785.
55. Hsu CY, Ordoñez JD, Chertow GM, et al. The risk of acute renal failure in patients with chronic kidney disease. Kidney Int. 2008;74:101-107.
56. McGee S, Abernethy 3rd WB, Simel DL. The rational clinical examination. Is this patient hypovolemic? JAMA. 1999;281:1022-1029.
57. Nolan 3rd CR, Anger MS, Kelleher SP. Eosinophiluria—a new method of detection and definition of the clinical spectrum. N Engl J Med. 1986;315:1516-1519.
58. Solez K, Racusen LC. Role of the renal biopsy in acute renal failure. Contrib Nephrol. 2001;132:68-75.
59. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(Suppl 1):S1-S266.
60. United States Renal Data System. USRDS 2009 annual data report: atlas of chronic kidney disease and end-stage renal disease in the united states. Bethesda, Md: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2009, Available at: http://www.usrds.org/adr.htm. Accessed March 17, 2011.
61. Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States. JAMA. 2007;298:2038-2047.
62. Dikow R, Zeier M, Ritz E. Pathophysiology of cardiovascular disease and renal failure. Cardiol Clin. 2005;23:311-317.
63. Markowitz GS, Stokes MB, Radhakrishnan J, et al. Acute phosphate nephropathy following oral sodium phosphate bowel purgative: an under recognized cause of chronic renal failure. J Am Soc Nephrol. 2005;16:3389-3396.
64. Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med. 2002;113(suppl 1A):5S-13S.
65. Lin K, Fajardo K. U.S. Preventive Services Task Force: Screening for asymptomatic bacteriuria in adults: evidence for the U.S. Preventive Services Task Force reaffirmation recommendation statement. Ann Intern Med. 2008;149:W20-W24.
66. Bent S, Nallamothu BK, Simel DL, et al. Does this woman have an acute uncomplicated urinary tract infection? JAMA. 2002;287:2701-2710.
67. Young JL, Soper DE. Urinalysis and urinary tract infection: update for clinicians. Infect Dis Obstet Gynecol. 2001;9:249-255.