drug induced akf
TRANSCRIPT

Tauhid Ahmed Bhuiyan, PharmDPGY-1 Resident
King Faisal Specialist Hospital & Research Center
Drug-Induced Acute Kidney Injury: A Contemporary Overview and Prevention Strategies
King Faisal Specialist Hospital and Research Center (KFSHRC) is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. (UAN# 0833-0000-14-006-L01-P, 0833-0000-14-006-L01-T)
A Knowledge Based Activity

You have a heart murmur and I’m starting
to hear your liver and kidneys complain, too

Objectives
Familiarize with the background, epidemiology, and general overview of acute kidney injury (AKI)
Recognize diagnostic criteria and laboratory parameters of AKI
Review pathogenic mechanisms and practical prevention strategies of drug-induced AKI (DI-AKI)
Evaluate implications of computerized Clinical Decision Support System (CDSS) for medication dosing in patients with renal insufficiency
I do not have financial relationship and no actual or potential conflict of interest in relation to this activity

ACUTE KIDNEY INJURY (AKI)

Renal System
Blood flow to the glomeruli
Formation and processing of ultrafiltrate
Excretion
Basic physiology:
Plasma filtration: 120 mL/min
http://patients.uroweb.org/kidney-ureteral-stones/symptoms

Epidemiology
In US, the reported incidence of AKI in all hospital admission: 1% (community-acquired) 7.1% (hospital-acquired)
About 5-20% of critically ill patients experience an episode of AKI during the course of their illness
AKI receiving renal replacement therapy (RRT) has been reported in 4.9% of all admission to intensive-care unit (ICU)
Prognosis: Mortality range ≈10%-80% depending on patient population
Lewington A., et al. Clinical practice guideline 2010; www.renal.org/guidelines

Definition
Clinical characterization:
Abrupt decrease in renal function
Accumulation of nitrogenous waste products (azotemia)
Inability to maintain and regulate fluid, electrolytes, and acid-base balance

Clinical Course
Three distinct phases:
• Generally occurs over 1 to 2 days• Characterized by progressive decrease in urine production
(UO <400mL/day)• Lasts from days to weeks• Worse prognosis than nonoliguric patients• Strict fluid and electrolyte monitoring and management are
required
Oliguric
• Period of increased urine production over several days immediately after oliguric phase
• Signals the initial repair of the kidney insult• Patients may remain markedly azotemic for several days
Diuretic
• Occurs over several weeks to months depending on the severity
• Signals the return to the patient’s baseline kidney function, normalization of urine production
Recovery

Pathogenesis
Acute Kidney Failure (AKF)
Classification Causes
Prerenal azotemia
Intravascular volume depletion Decreased effective circulating volume Hypotension, shock syndrome Increased renal vascular occlusion or constriction
Functional Afferent arteriole vasoconstrictors Efferent arteriole vasodilators
Intrinsic Glomerular disorders Acute tubular necrosis (ATN) Acute interstitial nephritis (AIN)
Postrenal Ureter obstruction
Donald FB. Acute Renal Failure. Applied Therapeutics: The Clinical Use Of Drugs. 2009;30:1-11

Risk Factors
Age >75 Sepsis Heart failure Diabetes mellitus Liver disease Use of nephrotoxic agents/medications Urinary tract obstruction

Objectives
Familiarize with the background, epidemiology, and general overview of acute kidney injury (AKI)
Recognize diagnostic criteria and laboratory parameters of AKI
Review pathogenic mechanisms and practical prevention strategies of drug-induced AKI (DI-AKI)
Evaluate implications of computerized Clinical Decision Support System (CDSS) for medication dosing in patients with renal insufficiency

Diagnosis
Clinical assessment Comprehensive history and physical examination Volume status AKI risk factors
Assessment of kidney function RIFLE vs. AKIN ?
Laboratory findings

Assessment of Kidney Function
Acute Kidney Injury Network
Stage Serum Creatinine (Scr)Urine Output
(UO)
1 Scr increase 1.5 to 2 fold OR ≥26.5 µmol/L from baseline
<0.5 mL/kg/h ≥6 hours
2 Scr increase >2 to 3 fold from baseline<0.5 mL/kg/h ≥12 hours
3Scr increase >3 fold from baseline OR ≥354 µmol/L with an acute rise of at least >44 µmol/L OR on RRT
<0.3 mL/kg/h ≥24 hours OR anuria ≥12 hours
This staging system is accepted by Kidney Disease Improving Global Outcome (KDIGO) clinical practice guideline of AKI
−Diagnosis Kellum JA., et al. Kidney International Supplements 2012; 2:124-138

Assessment of Kidney Function
Risk, Injury, Failure, Loss, and ESRD
Serum Creatinine (Scr) Urine Output (UO)
R Scr increase 1.5 fold OR GFR decrease >25%
<0.5 mL/kg/h ≥6 hours
I Scr increase 2 fold OR GFR decrease >50%
<0.5 mL/kg/h ≥12 hours
FScr increase 3 fold OR GFR decrease >75%; Scr >354 µmol/L with an acute rise >44 µmol/L
<0.3 mL/kg/h ≥24 hours OR anuria ≥12 hours
LPersistent acute renal failure = complete loss of kidney function >4 weeks
E ESRD >3 months
−Diagnosis Kellum JA., et al. Kidney International Supplements 2012; 2:124-138

Laboratory Evaluation
Quantitative measurements Urine output: direct evaluation of kidney function
Measured over 24hrs as I/O’s Glomerular Filtration Rate (GFR)
Cockcroft-Gault vs. MDRD (Modification of Diet in Renal Disease)
Qualitative measurements Urinanalysis (UA): GOLD standard Specific to differentiating AKF
−Diagnosis

Laboratory Evaluation Cont.
UA
Component Prerenal Azotemia
Acute Tubular Necrosis
Postrenal Obstruction
Urine Na+
(mEq/l)<20 >40 >40
FENa+ <1% >2% >1%
Urine/plasma creatinine
>40 <20 <20
Specific gravity >1.010 <1.010 Variable
Urine osmolality
(mOsm/kg) Up to 1200 <300 <300
[Urinary indices in acute kidney failure]
Donald FB. Acute Renal Failure. Applied Therapeutics: The Clinical Use Of Drugs. 2009;30:1-11

Objectives
Familiarize with the background, epidemiology, and general overview of acute kidney injury (AKI)
Recognize diagnostic criteria and laboratory parameters of AKI
Review pathogenic mechanisms and practical prevention strategies of drug-induced AKI (DI-AKI)
Evaluate implications of computerized Clinical Decision Support System (CDSS) for medication dosing in patients with renal insufficiency

DRUG-INDUCED ACUTE KIDNEY INJURY (DI-AKI)

Epidemiology
Drug-induced kidney injury causes 7% of all drug toxicities 18%—20% of AKI in hospitals 1%—5% of nonsteroidal anti-inflammatory drugs (NSAIDs) users in
community
Most implicated medications
Aminoglycosides (AG) Amphotericin B (Amp B) Radiocontrast media
Angiotensin Converting Enzyme Inhibitor (ACEI)
Angiotensin Receptor Blockers (ARBs)
NSAIDs
Howell HR., et al. US Pharm 2007;32(3): 45-50Lewington A., et al. Clinical practice guideline 2010; www.renal.org/guidelines

Pathogenic Mechanisms
Altered intraglomerular hemodynamics
Acute Tubular Necrosis (ATN) or tubular cell toxicity
Acute Interstitial Nephritis (AIN)
Crystal nephropathy

Altered Intraglomerular Hemodynamics
Pathogenesis is via reducing the volume OR pressure OR both of blood delivered to the kidney
Common medications NSAIDs ACEI, ARBs Calcineurin inhibitors (e.g.
cyclosporine, tacrolimus)
Prostaglandins (PGs) Angiotensin II
Vasodilation Vasoconstriction
http://biologigonz.blogspot.com/2010/02/mengenal-ginjal.html
−Functional

In most circumstances, do not pose significant risk to patients with normal renal function
In patients with decreased renal perfusion Inhibition of PGs vasoconstrictions ↓ blood flow & ischemic injury
Indomethacin poses the highest risk
Altered Intraglomerular Hemodynamics−NSAIDs
Pannu N., et al. Crit Care Med. 2008;36(4):216-22

Frequent cause of AKI in patient with Severe renal artery stenosis Chronic kidney disease (CKD) Congestive heart failure
“Double-edged sword”
Exerts a predictable dose-related reduction in GFR
Nephrotoxicity is due to vasoconstrictive effect on efferent arteriole in the absence of “absolute” or “effective” circulatory volume
Altered Intraglomerular Hemodynamics−ACEI/ARBs
Pannu N., et al. Crit Care Med. 2008;36(4):216-22
Altered Intraglomerular Hemodynamics−Calcineurin inhibitors
Despite improved allograft half-life and patient survival Nephrotoxicity often limits the clinical use
Severity Acute (reversible) Chronic (irreversible)
Mechanism of nephrotoxicity has not been clearly established Experimental model
Exerts preglomerular vasoconstriction significant reduction of renal plasma flow and GFR tissue ischemia
Pannu N., et al. Crit Care Med. 2008;36(4):216-22

Prevention Strategies
Drugs Practical Prevention
NSAIDs, ACEIs/ARBs
Use analgesics with lesser PG activity (e.g. acetaminophen, aspirin)
Avoid ACEIs/ARBs in patients with hypovolemia or bilateral renal artery stenosis
Calcineurin inhibitors
Use lowest effective dose For cyclosporine
Use micronized form Avoid strong CYP3A4 inhibitors Calcium channel blockers may
ameliorate or provide early protection
Pannu N., et al. Crit Care Med. 2008;36(4):216-22Guo X., et al. CLEV CLIN J MED. 2002;69(4):289312

Pathogenic Mechanisms
Altered intraglomerular hemodynamics
Acute Tubular Necrosis (ATN) or tubular cell toxicity
Acute Interstitial Nephritis (AIN)
Crystal nephropathy

Acute Tubular Necrosis (ATN)
Most common drug-induced kidney disease in the inpatient settings
Proposed mechanisms of toxicity Impairing mitochondrial function Interfering with tubular transport Increase oxidative stress or forming free radicals
Common medications Antibiotics: Amp B, AGs , Vancomycin Antivirals: Adefovir, Cidofovir, Tenofovir, Foscarnet Antineoplastics: Cisplatin Bisphosphonate: Zoledronate Radiocontrast media
Pannu N., et al. Crit Care Med. 2008;36(4):216-22Naughton CA., et al. Am Fam Physician. 2008;78(6)743-50
−Intrinsic

Approximately 80% of patients experience some renal dysfunction with amp B treatment (> 4g dose)
Proposed pathogenic mechanisms Direct proximal and distal tubular toxicity Afferent arterial vasoconstriction
Risk factors Pre-existing renal insufficiency Volume depletion Hypokalemia High average daily dose Diuretic use Concomitant nephrotoxin use Rapid infusion
Acute Tubular Necrosis−Amp B
Pannu N., et al. Crit Care Med. 2008;36(4):216-22

Variable incidence of nephrotoxicity 1.7%—58%
Proposed pathogenic mechanisms Cationic charge binding and uptake
by tubular epithelial cells disrupt normal cellular function cellular death
Stimulate calcium sensing receptor on the apical membrane induction of cellular signaling and cell death
Risk factors Prolonged therapy Trough concentration >2 μg/mL
(except amikacin) Previous AG therapy (recent) Concurrent use of other
nephrotoxins Patient related factors
Acute Tubular Necrosis−AGs
Pannu N., et al. Crit Care Med. 2008;36(4):216-22
Relative toxicities (in descending order)
Neomycin > Gentamycin > Tobramicin > Amikacin > Streptomycin

Mostly contributed to the early formulations “Mississippi mud” (~70% pure)
Variable incidence of nephrotoxicity Monotherapy: 5-7% Concomitant aminoglycoside:
7-35%
Proposed mechanisms Stimulates oxygen consumption
and ATP in proximal tubule Oxidative stress damages glomeruli
and proximal tubule
Independent risk factors Concomitant nephrotoxins use Age Duration of therapy Trough >15 μg/mL
Informative reading: “Vancomycin nephrotoxicity: myths and facts”
Acute Tubular Necrosis−Vancomycin
Rybak M, et al. Am J Health Syst Pharm. ‐ 2009;82-98

Third leading cause of inpatient AKI
Associated with a high (34%) inpatient mortality rate
Complex pathogenic mechanism Started with renal vasodilation and an osmotic diuresis to intense
vasoconstriction ischemia
Risk factors Underlying diabetic nephropathy or chronic renal insufficiency Age >75 years Congestive heart failure Volume depletion Patient receiving aggressive diuretic regimens
Acute Tubular Necrosis−Radiocontrast media
Donald, Brophy F. Acute Renal Failure. Applied Therapeutics: The Clinical Use of Drugs. 2009; 30-41

Drugs Practical Prevention
Amp B
Use sodium loading before and after therapy initiation Use lipid-based formulation Consider alternate day administration or continuous
infusion over 24h Consider alternative agents in high-risk patients with renal
impairment
AGs
Avoid use if possible in high-risk population Limit prolonged therapy Use extended interval dosing Adjust dosage for renal function Maintain trough levels ≤ 1 μg/mL
Prevention Strategies
Pannu N., et al. Crit Care Med. 2008;36(4):216-22Guo X., et al. CLEV CLIN J MED. 2002;69(4):289312
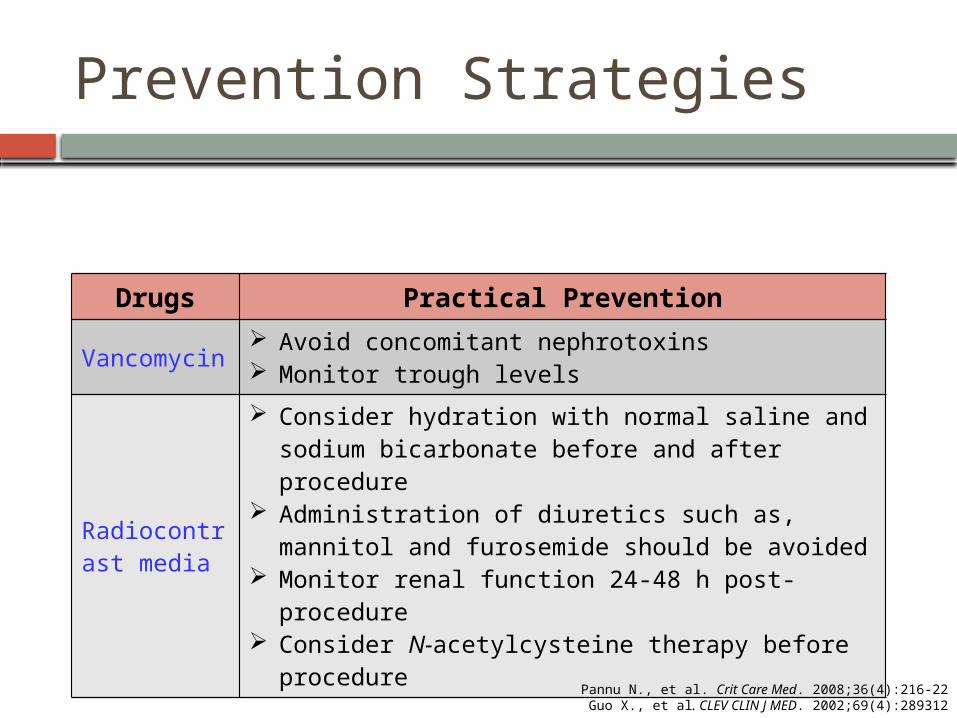
Prevention Strategies
Drugs Practical Prevention
Vancomycin Avoid concomitant nephrotoxins Monitor trough levels
Radiocontrast media
Consider hydration with normal saline and sodium bicarbonate before and after procedure
Administration of diuretics such as, mannitol and furosemide should be avoided
Monitor renal function 24-48 h post-procedure Consider N-acetylcysteine therapy before procedure
Pannu N., et al. Crit Care Med. 2008;36(4):216-22Guo X., et al. CLEV CLIN J MED. 2002;69(4):289312

Pathogenic Mechanisms
Altered intraglomerular hemodynamics
Acute Tubular Necrosis (ATN) a.k.a tubular cell toxicity
Acute Interstitial Nephritis (AIN)
Crystal nephropathy

Acute Interstitial Nephritis (AIN)
Cause of up to 3% of all AKI cases
Etiology Drugs (antibiotics responsible for one-third of these cases) – 75% Infections – 5%-10% Tubulointerstitial nephritis and uveitis (TINU) syndrome – 5%-10% Autoimmune/Systemic disease (e.g. sarcoidosis, SLE) – 5%-10%
Inflammatory changes Glomerulus, renal tubular cells, and the surrounding interstitium
Fibrosis and renal scarring
Pannu N., et al. Crit Care Med. 2008;36(4):216-22
−Intrinsic

Acute Interstitial Nephritis (AIN)
Common medications NSAIDs Penicillin (methicillin) and cephalosporin Lithium Rifampin Quinolones Diuretics (loops, thiazides) Hydralazine Interferon-alfa
May need kidney biopsy to confirm diagnosis
Pannu N., et al. Crit Care Med. 2008;36(4):216-22

Prevention Strategies
Drugs Practical Prevention
NSAIDs Avoid long term use, particularly of more than one analgesic Use alternate agents in patients with chronic pain
Lithium Avoid volume depletion Monitor drug levels
Naughton CA., et al. Am Fam Physician. 2008;78(6)743-50

Pathogenic Mechanisms
Altered intraglomerular hemodynamics
Acute Tubular Necrosis (ATN) a.k.a tubular cell toxicity
Acute Interstitial Nephritis (AIN)
Crystal nephropathy

Crystal Nephropathy
Renal impairment results from drugs that produce crystals that are insoluble in human urine
Pathogenic mechanism Precipitation of crystals in distal
tubular lumen obstruct urine flow and elicit interstitial reaction
Common medications Antibiotics: Ampicillin,
Ciprofloxacin, Sulfonamides Antivirals: Acyclovir, Foscarnet,
Ganciclovir, Indinavir, Methotrexate
Triamterene
Risk factors Volume depletion Underlying renal insufficiency Excessive dose Intravenous (IV) administration
Naughton CA., et al. Am Fam Physician. 2008;78(6)743-50
−Postrenal

Prevention Strategies
Drugs Practical PreventionAcyclovir, methotrexate, sulfa antibiotics, triamterene
Discontinue or reduce dose Ensure adequate hydration Establish high urine flow Administer orally
Naughton CA., et al. Am Fam Physician. 2008;78(6)743-50

Goals Short term: stop the progression of kidney damage Long term: restore normal kidney function
In general Stopping the offending agent Avoid concomitant nephrotoxins Maintain adequate hydration RRT
Management of DI-AKI

General Preventative Measures
Assess baseline renal function using MDRD
Dose adjustment based on renal function
Correct modifiable risk factors of nephrotoxicity before initiation of drug therapy
Ensure adequate hydration before and during therapy with potential nephrotoxins
Use equally effective non-nephrotoxic drugs whenever possible

Objectives
Familiarize with the background, epidemiology, and general overview of acute kidney injury (AKI)
Recognize diagnostic criteria and laboratory parameters of AKI
Review pathogenic mechanisms and practical prevention strategies of drug-induced AKI (DI-AKI)
Evaluate implications of computerized Clinical Decision Support System (CDSS) for medication dosing in patients with renal insufficiency
Clinical Decision Support System (CDSS)
First introduced in clinical practice in the 1970s
Designed to improve clinical decision making at the point of care
Implementation provided Improved medication related clinical outcomes, and Reduced medication related errors and adverse events
Guided Medication Dosing for Inpatients With Renal Insufficiency Study objective
Incorporation of guided dosing algorithms for inpatients with renal insufficiency into existing computerized physician order entry system would result in: Larger proportion of appropriate dosing and frequency orders Shorter hospital length of stay (LOS) Lower cost Lower frequency of worsening renal function
Study design Study population: all patients admitted to the medical, surgical, neurology,
and obstetrics and gynecology services at Brigham and Women’s Hospital between September 1997 and April 1998
Study periods: 4 alternating 8-weeks blocks of intervention and control subperiods
Chertow GM., et al. JAMA. 2001;286(22):2839-44

Screen Displays
Chertow GM., et al. JAMA. 2001;286(22):2839-44

Chertow GM., et al. JAMA. 2001;286(22):2839-44

Results
Chertow GM., et al. JAMA. 2001;286(22):2839-44

Authors’ Conclusion
“The application intervention led to a statistically significant and clinically meaningful increase in the proportion of prescriptions considered appropriate for inpatients with renal insufficiency”
Chertow GM., et al. JAMA. 2001;286(22):2839-44

Pharmacist Role
Vigilance
Early intervention Identify patient and drug related risk factors Recommend specific dosing or safer alternatives
Suggest and help implement CDSS
Summary
AKI is an abrupt decrease in renal function that leads to azotemia, and imbalance of fluid, acid-base, and electrolytes
Almost all cases of AKI are hospital-acquired and drug related etiologies are being the most common
Diagnosis of AKI is based on clinical presentations, assessment of kidney function, and laboratory findings especially UA
Pathogenic mechanisms of DI-AKI include altered intraglomerular hemodynamics, ATN, AIN, and crystal nephropathy

Summary Cont. Management of DI-AKI is common across all drugs:
Correcting volume and electrolyte depletion Stopping the offending agents, and Maintaining adequate hydration
Implementation of CDSS had shown to have clinically meaningful appropriate dose and frequency of drug orders, and decrease length of stay in patients with renal insufficiency

THANK YOU

References Pannu N., Nadim MK. An overview of drug-induced acute kidney injury. Crit Care Med. 2008;36(4):216-
223 Donald FB. Acute Renal Failure. In: Koda-kimble MA., Young LY., Alldredge BK., et al., ed. Applied
Therapeutics: The Clinical Use Of Drugs. Baltimore, Lippincott Williams & Wilkins; 2009: 30(1-11) Guo X., Nzerue C. How to prevent, recognize, and treat drug-induced nephrotoxicity. Clev Clin J Med.
2002; 69(4):289-312 Lewington A., Kanagasundaram S. Module 5 - acute kidney injury clinical practice guideline. UK renal
association. www.renal.org/guidelines. Published March 08, 2011. Accessed January 12, 2014 Howell HR., Brundige ML. et al. Drug-Induced Acute Renal Failure. US Pharm. 2007;32(3):45-50 Schetz M., Dasta J., et al. Drug-induced acute kidney injury. Curr Opin Crit Care. 2005;11:555-65 Singh NP., Ganguli A., et al. Drug-induced Kidney Disease. JAPI. 2003; 51:970-79 Rybak M, Lomaestro B, Rotschafer JC., et al. Therapeutic monitoring of vancomycin in adult patients: A
consensus review of the American Society of Health-System Pharmacists, the Infectious Disease Society of America, and the Society of Infectious Disease Pharmacists. Am J Health-Syst Pharm. 2009; 66: 82-98
Kellum JA., Aspelin P., Barsoum RS., et al. Clinical practice guideline for acute kidney injury. Kidney International Supplements. 2012; 2:124-138
Chertow GM., Lee J., Kuperman GJ., et al. Guided medication dosing for inpatients with renal insufficiency. JAMA 2001;286(22):2839-44

Self Assessment Questions

Question 1
What is the CORRECT sequence of clinical course of AKI?
a) Recovery Diuretic Oliguricb) Diuretic Recovery Oliguricc) Oliguric Diuretic Recoveryd) None of the above

Question 2
How do NSAIDs alter intraglomerular hemodynamics?
a) Vasoconstriction of afferent arteriole by blocking PG activity
b) Vasodilation of efferent arteriole by blocking Angiotnesin II
c) Vasoconstriction of efferent arteriole by blocking Angiotnesin II
d) Vasodilation of afferent arteriole by blocking PG activity

Question 3
Which of the following pharmacologic agents has been shown to decrease radiocontrast media induced AKI when given concurrently with other fluid therapies?
a) N-acetylcysteine
b) Furosemidec) Mannitold) Calcium channel blockers

Question 4
Which of the following aminoglycosides have relatively the highest risk of nephrotoxicity?
a) Neomycin b) Gentamycin c) Amikacin d) Streptomycin

Question 5
Prophylactic measures to reduce amphotericin B induced nephrotoxicity include:
a) Ensure adequate hydration before and after therapy initiation
b) Use lipid-based formulationc) Consider alternate day administration or continuous
infusion over 24hd) All of the above