Download - Pneumothorax Lapsus Fix
PNEUMOTHORAX
Shintya Nanda CaritaDina Fauziah
Supervisor : dr. Ali Haedar, Sp.EM
BACKGROUND
• Definition: Pneumothorax is defined as accumulation of air in the pleural space with secondary lung collapse (Al-Qudah, 2006).
• Pneumothoraces can be classified according to their cause and clinical presentation: Spontaneous, traumatic, or iatrogenic (Al-Qudah, 2006).
• Spontaneous pneumothorax (SP) can be a medical emergency requiring early diagnosis and treatment to prevent subsequent respiratory failure and death (Saiphoklang, 2013).
• Spontaneous Pneumothorax clasified into 2 types: PSP and SSP The distinction between PSP and SSP should be made at the time of diagnosis to guide appropriate management
• Etiology: Secondary pneumothorax develops in patients with known clinical and/or radiographic lung disease (Al-Qudah, 2006)
Saiphoklang N1, Kanitsap A2. 2013. Prevalence, clinical manifestations and mortality rate in patients with spontaneous pneumothorax in Thammasat University Hospital. J Med Assoc Thai. Oct;96(10):1290-7.
Al-Qudah, Abdullah. 2006. Treatment Options of Spontaneous Pneumothorax. Indian J Chest Dis Allied Sci 2006; 48: 191-200.
• Causes of secondary SP were pulmonary tuberculosis (19/34, 55.9%), chronic obstructive pulmonary disease (14/34, 41.2%), and pneumonia (8/34, 23.5%) (Saiphoklang, 2013).
• Mortality and Morbidity Rate: Studey in Thailand use one hundred patients with SP were identified (66 primary, 34 secondary SP), for a prevalence of 76.3 per 100,000 hospital admissions. There were 12 deaths (12%), 11 with secondary SP (Saiphoklang, 2013).
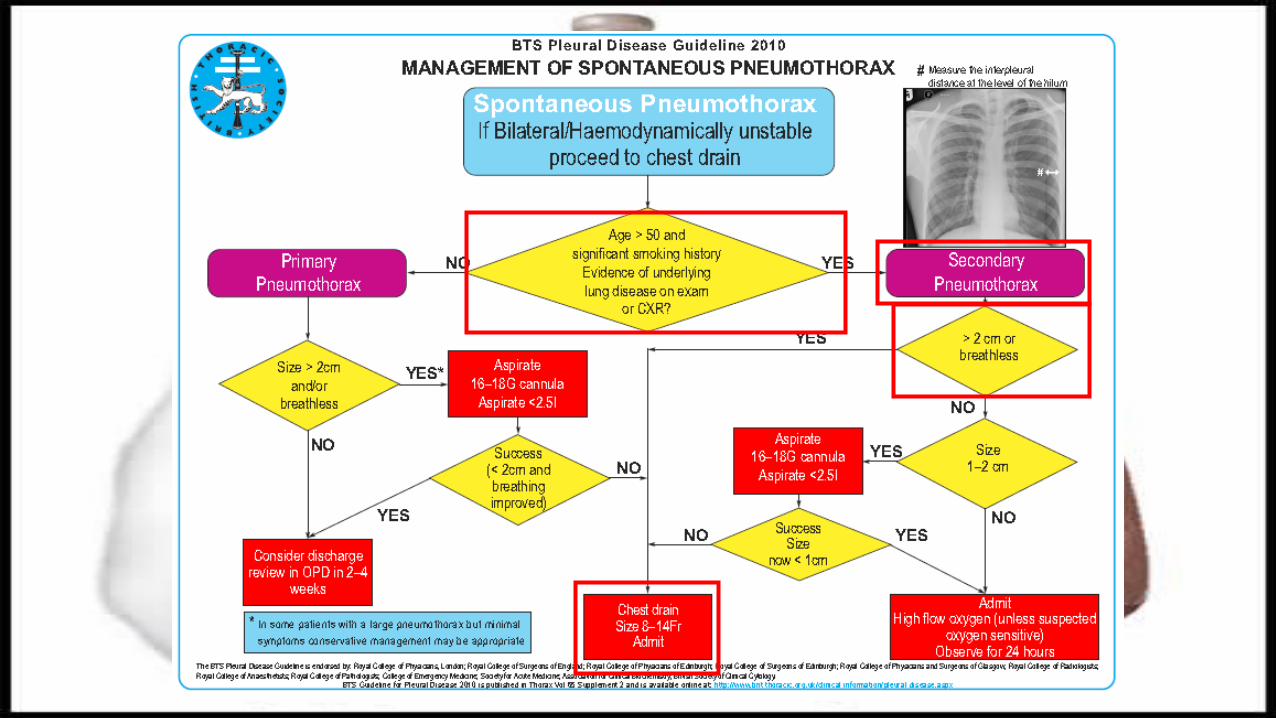
• The size of the pneumothorax determines the rate of resolution and is a relative indication for active intervention (BTS guideline,2010).
• Needle (14e16 G) aspiration (NA) is as effective as large-bore (>20 F) chest drains and may be associated with reduced hospitalisation and length of stay. (BTS guideline,2010). Following failed NA, small-bore (<14F) chest drain insertion is recommended
Saiphoklang N1, Kanitsap A2. 2013. Prevalence, clinical manifestations and mortality rate in patients with spontaneous pneumothorax in Thammasat University Hospital. J Med Assoc Thai. Oct;96(10):1290-7.
BACKGROUND
CASE REPORT
Patient Identity
Name : Mr. GSex : MaleAge : 64 years oldAdress : Sukun Pondok Indah K-16, MalangEducation : Junior High SchoolOccupation : RetiredBody Weight : 60 kgAdmitted to ER on January 17th, 2015
A : PatenB : Unsymmetrical chest movement, RR 30x/mnt, retraction (-), SpO2 88%C : BP 149/84 mmHg, PR 106x/mnt, warm acral
(Tax : 36,8°C), CRT < 2 sD : Round and isochoric pupils, GCS 456
Triage : Red ZoneTwo BLS vital sign measurements that are helpful in assessing and monitoring the degree of respiratory distress are respiratory rate and oxygen saturation. Tachypnea in adults is generally defined as a respiratory rate greater than 25 breaths per minute. Lastly, when pulse oximetry is used to monitor a patient in respiratory distress and saturations are normal (94–98%), desaturation is a warning of decompensation.
McEvoy, Mike. 2013. How to Assess and Treat Acute Respiratory DistressA rapid and thorough assessment is critical for patients with acute respiratory distress. Article from Journal of Emergency Medical Service
Primary Survey
Initial Treatment
A : -B : Semi-fowler position, O2 NRBM 10 lpm-Sat 90%C : IVFD NaCl 0,9% lifeline D : -
Primary Survey
AnamnesaChief complain: shortness of breath
• Patient suffered from shortness of breath since one day before admission. Patient feels shortness of breath while he did activity or rest, but it decreased while he rest. Patient also complaint pain on left chest that get worse with breathing. Patient went to doctor and got some medicine but the shortness of breath was persist.
• Patient has also been having little cough since 4 months ago, with no sputum and blood. The cough worst since 3 days before admission. He also suffered weakness since a month ago. Patient denied night sweating, fever or decreased of body weight. Patient didn’t go to the doctor for treat his cough.
• Past medical history: There was no history of shortness of breath before and TB. There was no history of 6 months drug consuming. No history of hypertension and diabetes mellitus
• Family history: There was no family with same complain. No history of diabetes mellitus, hypertension, TB and malingnancy in his family.
• Social history: Patient was a smoker since he was 20 years old, 5-10 sticks a day. But he already stop smoking since one year ago. He lives at home with his wife. There was a neighbor that had cough since more than 6 month.
Anamnesa
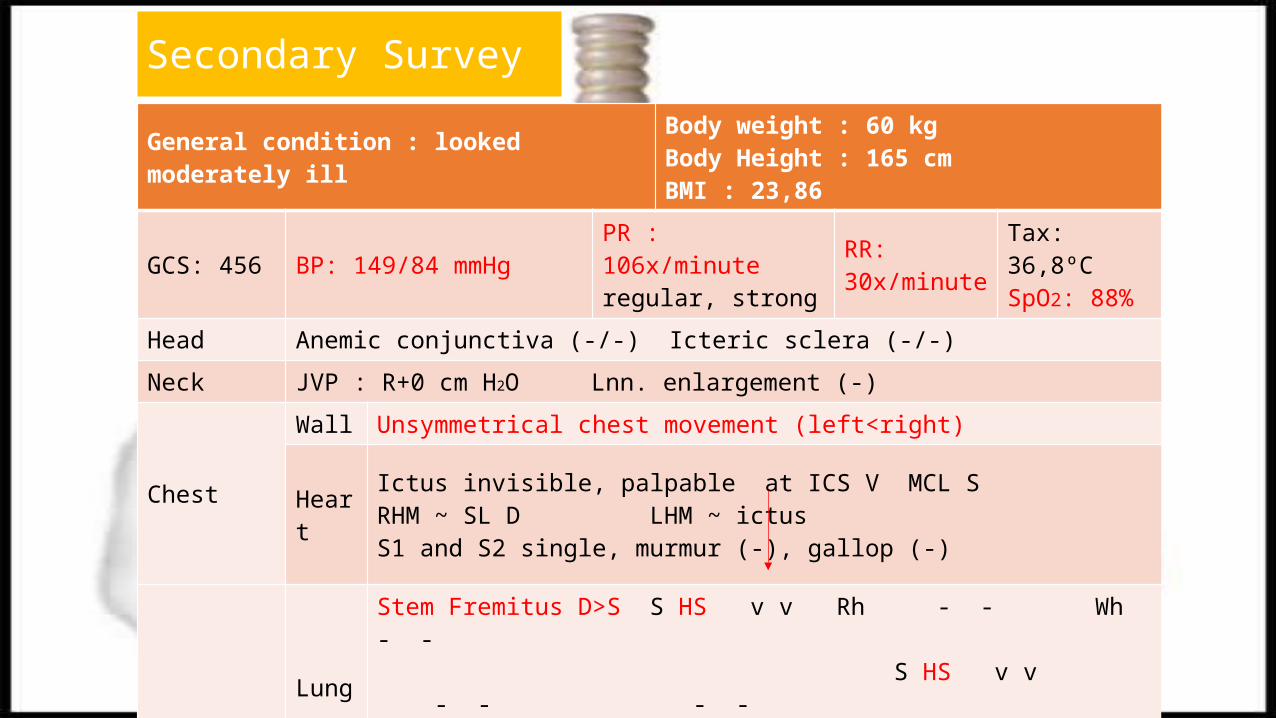
General condition : looked moderately ill Body weight : 60 kgBody Height : 165 cm BMI : 23,86
GCS: 456 BP: 149/84 mmHg PR : 106x/minute regular, strong
RR: 30x/minute
Tax: 36,8ºC SpO2: 88%
Head Anemic conjunctiva (-/-) Icteric sclera (-/-)
Neck JVP : R+0 cm H2O Lnn. enlargement (-)
Chest
Wall Unsymmetrical chest movement (left<right)
HeartIctus invisible, palpable at ICS V MCL S RHM ~ SL D LHM ~ ictusS1 and S2 single, murmur (-), gallop (-)
LungStem Fremitus D>S S HS v v Rh - - Wh - - S HS v v - - - - S HS v v - - - -
Abdomen Flat, Bowel sound (+) normal, soefl, liver span 8 cm, traube’s space tympani, shifting dulness (-)
Extremities Warm; edema -/- -/-
Secondary Survey
Laboratory Result Normal Value Unit
Hb 17,30 11,4-15,1 g/dL
Leucocyte 11.450 4.700-11.300 /µL
Thrombocyte 349.000 142.000-420.000 /µL
MCV 86,30 80-93 fL
MCH 29,20 27-31 Pg
MCHC 33,90 32-36 g/dL
Differential count 0,0/0,3/82,9/11,7/5,1 0-4/0-1/51-67/25-33/2-5 %
SGOT 22 0-32 U/L
SGPT 21 0-32 U/L
RBS 127 <200 mg/dL
Ureum 20,20 16,6-48,5 mg/dL
Creatinine 1,11 <1,2 mg/dL
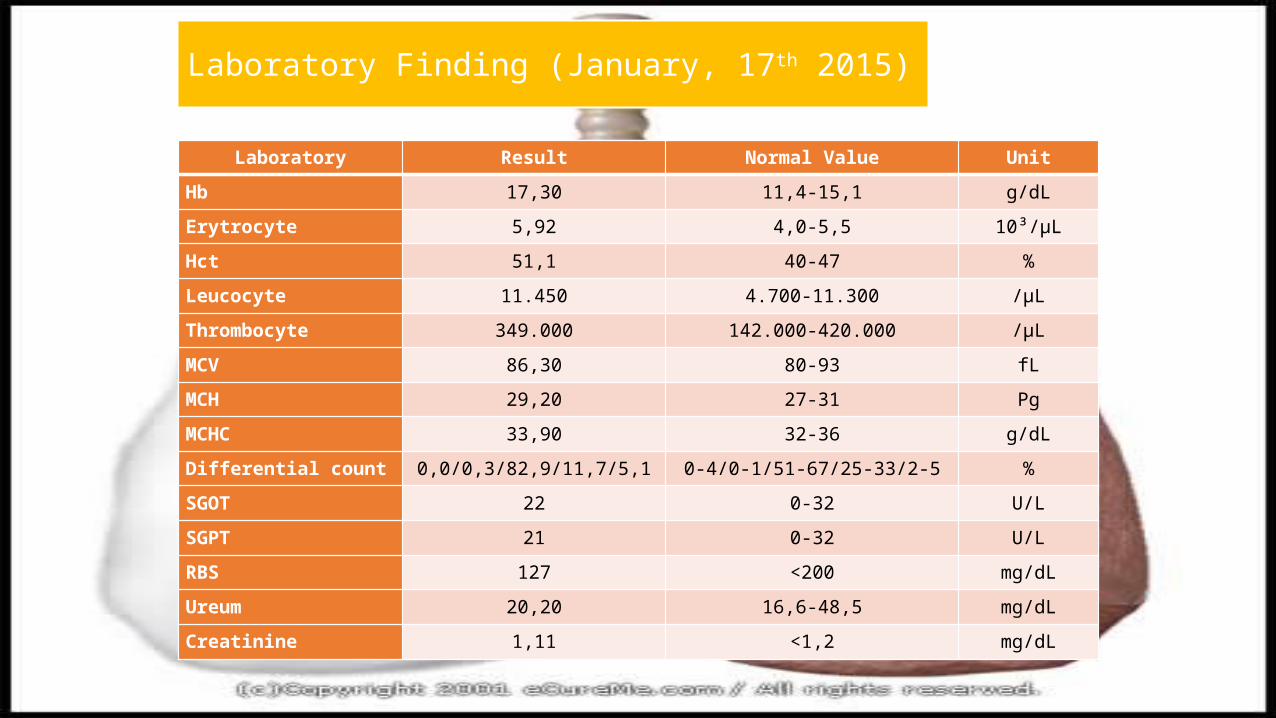
Laboratory Result Normal Value Unit
Hb 17,30 11,4-15,1 g/dL
Erytrocyte 5,92 4,0-5,5 10³/µL
Hct 51,1 40-47 %
Leucocyte 11.450 4.700-11.300 /µL
Thrombocyte 349.000 142.000-420.000 /µL
MCV 86,30 80-93 fL
MCH 29,20 27-31 Pg
MCHC 33,90 32-36 g/dL
Differential count 0,0/0,3/82,9/11,7/5,1 0-4/0-1/51-67/25-33/2-5 %
SGOT 22 0-32 U/L
SGPT 21 0-32 U/L
RBS 127 <200 mg/dL
Ureum 20,20 16,6-48,5 mg/dL
Creatinine 1,11 <1,2 mg/dL
Laboratory Finding (January, 17th 2015)
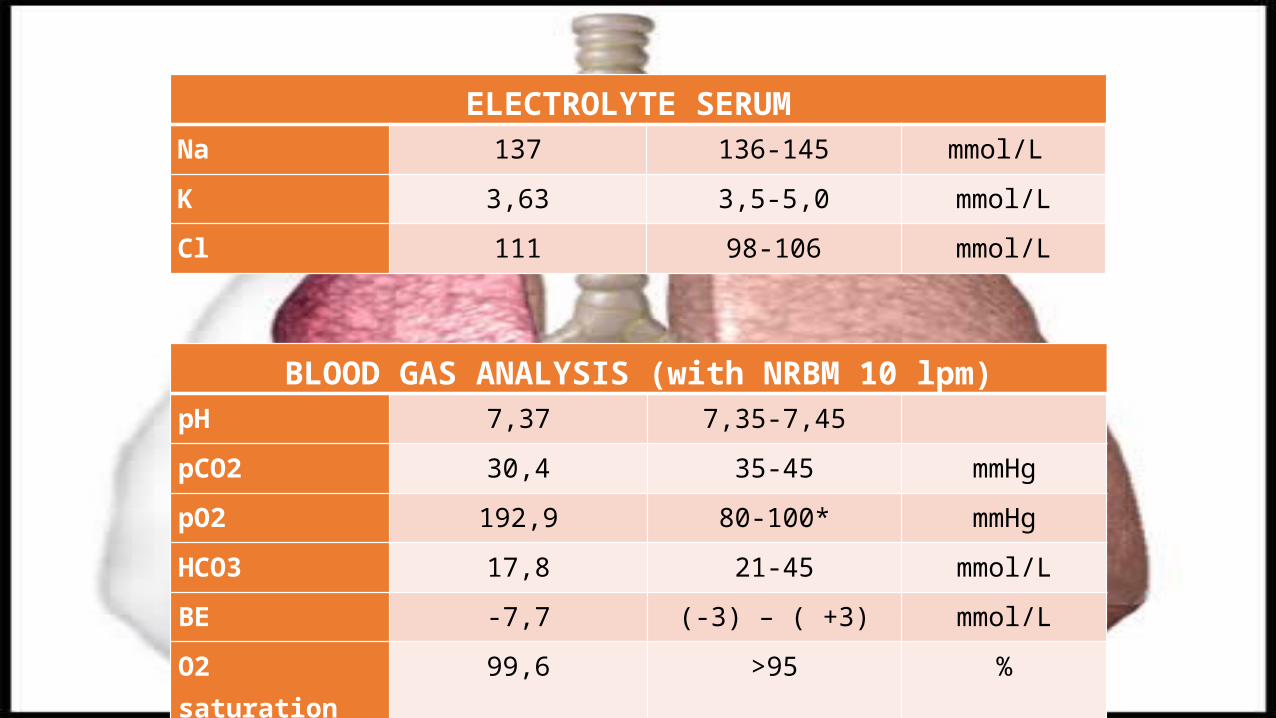
BLOOD GAS ANALYSIS (with NRBM 10 lpm)pH 7,37 7,35-7,45
pCO2 30,4 35-45 mmHg
pO2 192,9 80-100* mmHg
HCO3 17,8 21-45 mmol/L
BE -7,7 (-3) – ( +3) mmol/L
O2 saturation 99,6 >95 %
ELECTROLYTE SERUM Na 137 136-145 mmol/L
K 3,63 3,5-5,0 mmol/L
Cl 111 98-106 mmol/L
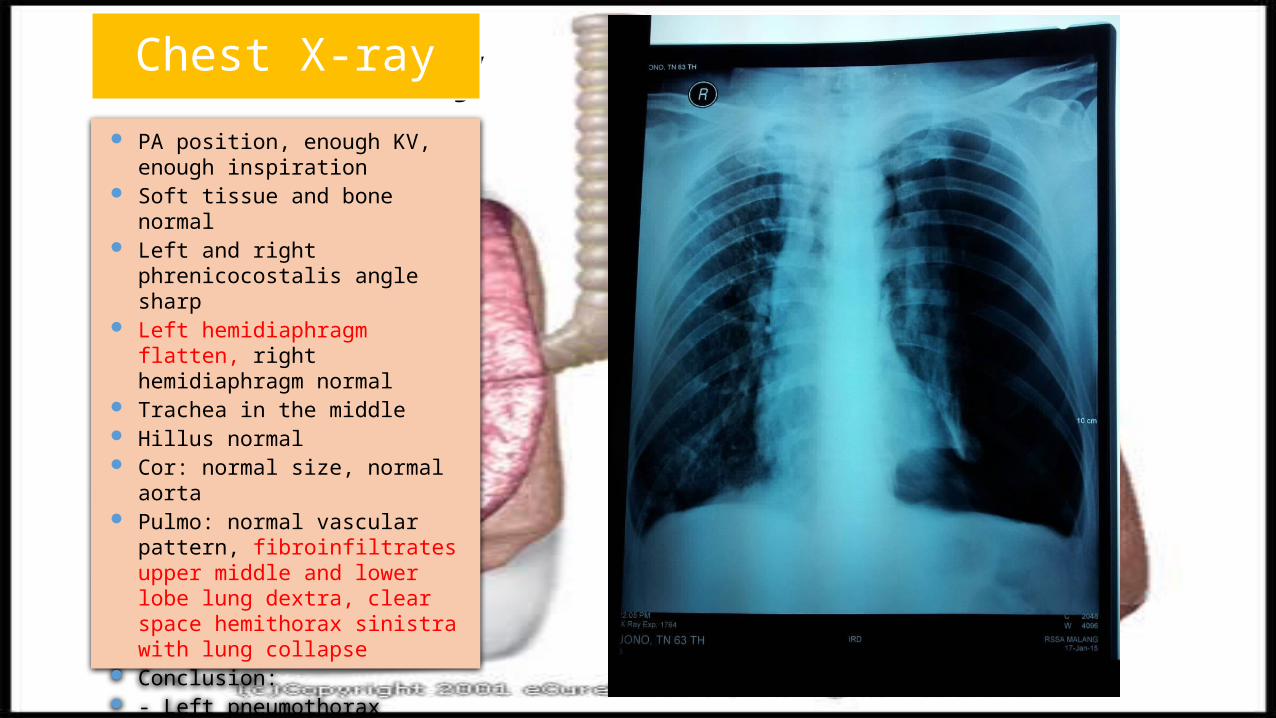
Chest X-Ray PA position, enough KV,
enough inspiration Soft tissue and bone normal Left and right phrenicocostalis
angle sharp Left hemidiaphragm flatten,
right hemidiaphragm normal Trachea in the middle Hillus normal Cor: normal size, normal aorta Pulmo: normal vascular
pattern, fibroinfiltrates upper middle and lower lobe lung dextra, clear space hemithorax sinistra with lung collapse
Conclusion: - Left pneumothorax -TB active far advance lesion
Chest X-ray
ECG
Conclusion: sinus rhythm 98 bpm
ECG
• SOB dt Spontaneous Secondary pneumothorax• Lung TB•Pneumonia
Working Diagnosis
Management
• Semi-fowler position• O2 NRBM 10 lpm• IVFD NS 0,9% lifeline• Chest tube insertion
DispositionPulmonary
Department
Management
• Semi-fowler position• O2 NRBM 10 lpm• IVFD NS 0,9% lifeline• Chest tube insertion
Discussion
Secondary pneumothorax develops in patients with known clinical and/or radiographic lung disease (Al-Qudah, 2006). Causes of secondary SP were pulmonary tuberculosis (19/34, 55.9%), chronic obstructive pulmonary disease (14/34, 41.2%), and pneumonia (8/34, 23.5%) (Saiphoklang, 2013).
Etiology
Symptoms of Pneumothorax
Saiphoklang N1, Kanitsap A2. 2013. Prevalence, clinical manifestations and mortality rate in patients with spontaneous pneumothorax in Thammasat University Hospital. J Med Assoc Thai. Oct;96(10):1290-7.
The common presenting symptoms were dyspnea (73%), chest pain or discomfort (68%), pleuritic pain (46%), cough (20%), and fever (13%) (Saiphoklang, 2013)
Symptoms of Lung TBPrimary TB infection may be asymptomatic, cause fever and pleuritic pain. Cough, arthralgia and occur rarely.Older individual more likely to present with non specific finding of dyspnea and fatigue (Hoffmann dan Churcyard, 2009)
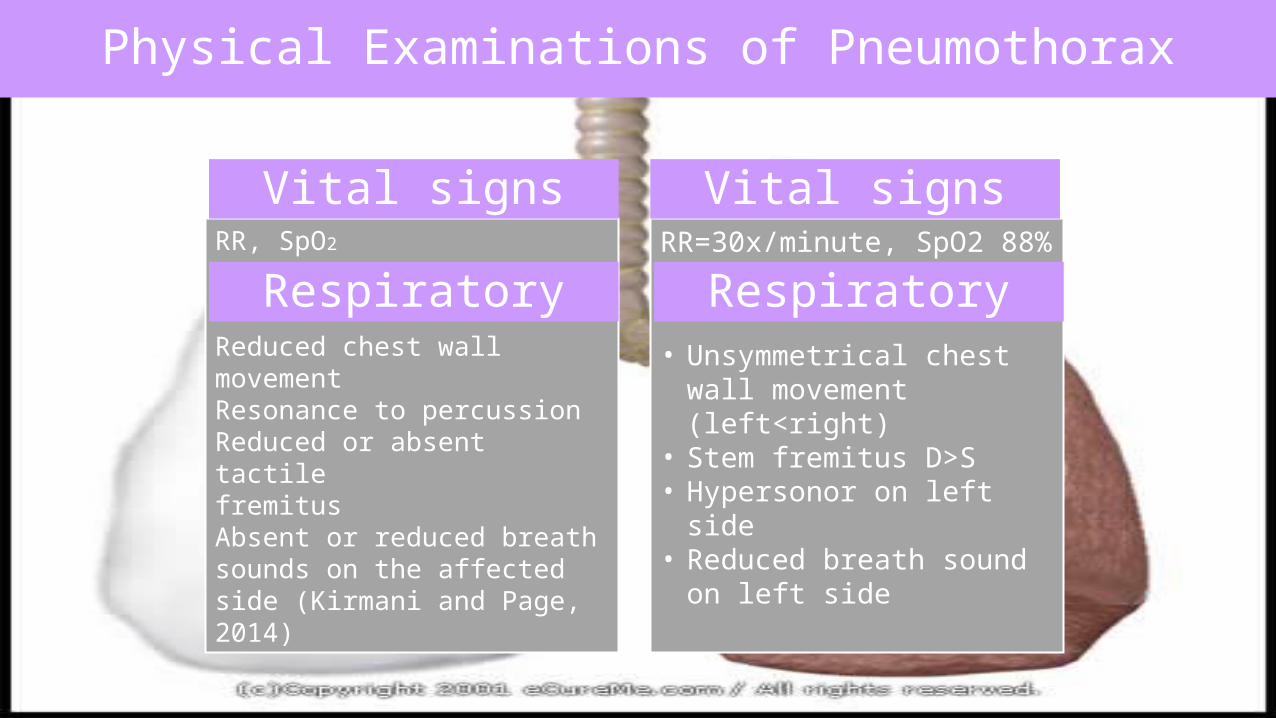
• Unsymmetrical chest wall movement (left<right)
• Stem fremitus D>S• Hypersonor on left
sideReduced breath sound on left side
RR, SpO2
Reduced chest wallmovementResonance to percussionReduced or absent tactilefremitusAbsent or reduced breath sounds on the affectedside (Kirmani and Page, 2014)
Vital signs
RespiratoryRR=30x/minute, SpO2 88%
• Unsymmetrical chest wall movement (left<right)
• Stem fremitus D>S• Hypersonor on left side• Reduced breath sound on
left side
Vital signs
Respiratory
Physical Examinations of Pneumothorax
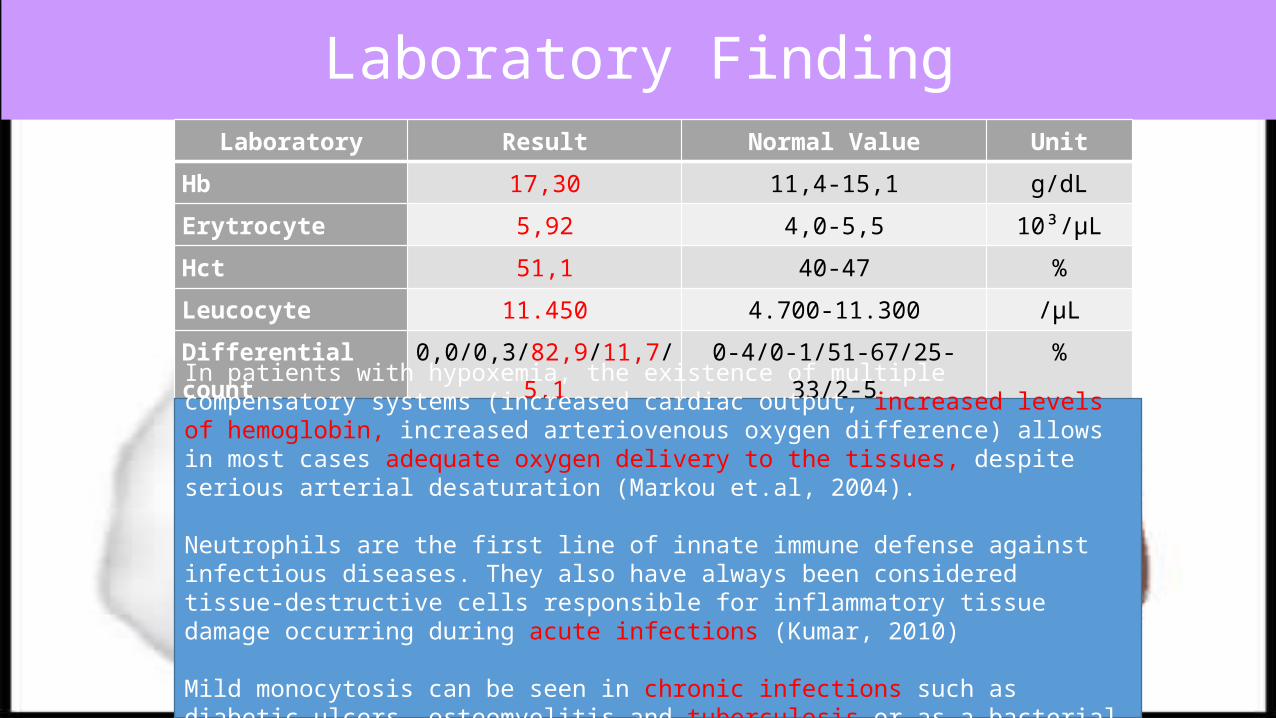
Laboratory FindingLaboratory Result Normal Value Unit
Hb 17,30 11,4-15,1 g/dL
Erytrocyte 5,92 4,0-5,5 10³/µL
Hct 51,1 40-47 %
Leucocyte 11.450 4.700-11.300 /µL
Differential count 0,0/0,3/82,9/11,7/5,1 0-4/0-1/51-67/25-33/2-5 %
In patients with hypoxemia, the existence of multiple compensatory systems (increased cardiac output, increased levels of hemoglobin, increased arteriovenous oxygen difference) allows in most cases adequate oxygen delivery to the tissues, despite serious arterial desaturation (Markou et.al, 2004).
Neutrophils are the first line of innate immune defense against infectious diseases. They also have always been considered tissue-destructive cells responsible for inflammatory tissue damage occurring during acute infections (Kumar, 2010)
Mild monocytosis can be seen in chronic infections such as diabetic ulcers, osteomyelitis and tuberculosis or as a bacterial infection is resolving (Thomas, 2007).
TB IRIS
• Immune Reconstitution Inflammatory Syndrome (IRIS) refers to :
• a phenomenon experienced by people living with HIV who have recently initiated antiretroviral therapy.
• a paradoxical inflammatory reaction against a foreign antigen (alive or dead) in patients who have started antiretroviral therapy and who have undergone a reconstitution of their immune responses against this antigen. (Colebunders, 2010)
Pathophysiology
• The partial reconstitution of the immune system following initiation of antiretroviral therapy in these patients can result in an exaggerated inflammatory response against any concurrent opportunistic infection. Sometimes the opportunistic infection pathogen against which the inflammatory response is directed remains clinically 'silent' prior to initiation of antiretroviral therapy, such that antiretroviral therapy 'unmasks' a previously undiagnosed disease.
Pathophysiology
Tuberculosis - Immune Reconstitution Inflammatory Syndrome (TB-IRIS) refers specifically to IRIS that occurs in the context of a patient with active Mycobacterium tuberculosis infection, and is a relatively common complication for HIV-infected persons who initiate antiretroviral therapy in resource-limited settings, particularly in regions that have a high TB prevalence.
Pathogenesis
• Increased lymphoproliferative response to mycobacterium antigens in vitro
• Restoration of cutaneous response to Tuberculin• Increased [Il-6], activation markers (CD38)• Associated with TNFA-308*1, IL6-174*G
(Colebunders, 2010)
Pathogenesis
• Starting ARV’s within 6 weeks of TB treatment• Disseminated, extra-pulmonary disease• Low base line CD4 count (have a CD4 count < 100
cells/mm3)• have a prompt rise in CD4 count in the initial 3 months
of HAART• Fall in viral load• High bacillary burden (?)
Risk Factors for TB/IRIS
Recommendations to prevent TB IRIS
• Exclude TB before starting antiretroviral therapy • Treat first the TB and start antiretroviral treatment
only once the patient has clinically improved, is tolerating very well his TB treatment
• Increase awareness about TB IRIS
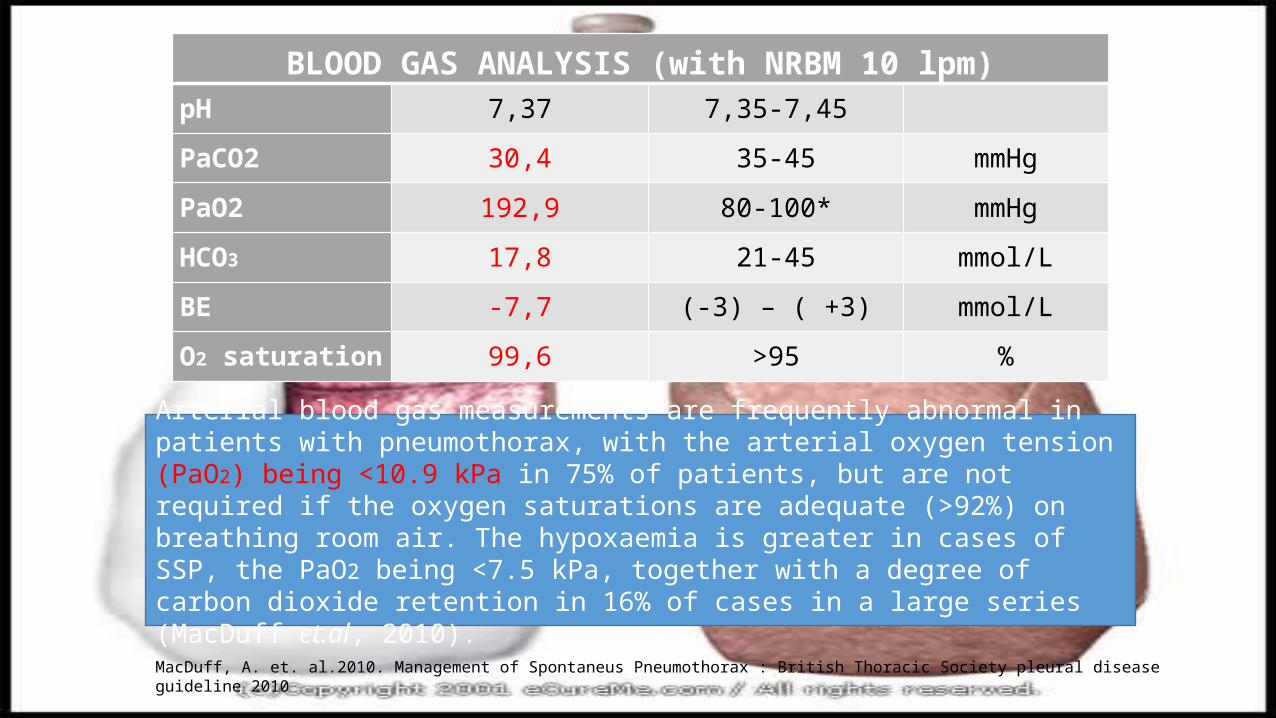
BLOOD GAS ANALYSIS (with NRBM 10 lpm)pH 7,37 7,35-7,45
PaCO2 30,4 35-45 mmHg
PaO2 192,9 80-100* mmHg
HCO3 17,8 21-45 mmol/L
BE -7,7 (-3) – ( +3) mmol/L
O2 saturation 99,6 >95 %
Arterial blood gas measurements are frequently abnormal in patients with pneumothorax, with the arterial oxygen tension (PaO2) being <10.9 kPa in 75% of patients, but are not required if the oxygen saturations are adequate (>92%) on breathing room air. The hypoxaemia is greater in cases of SSP, the PaO2 being <7.5 kPa, together with a degree of carbon dioxide retention in 16% of cases in a large series (MacDuff et.al, 2010).
MacDuff, A. et. al.2010. Management of Spontaneus Pneumothorax : British Thoracic Society pleural disease guideline 2010
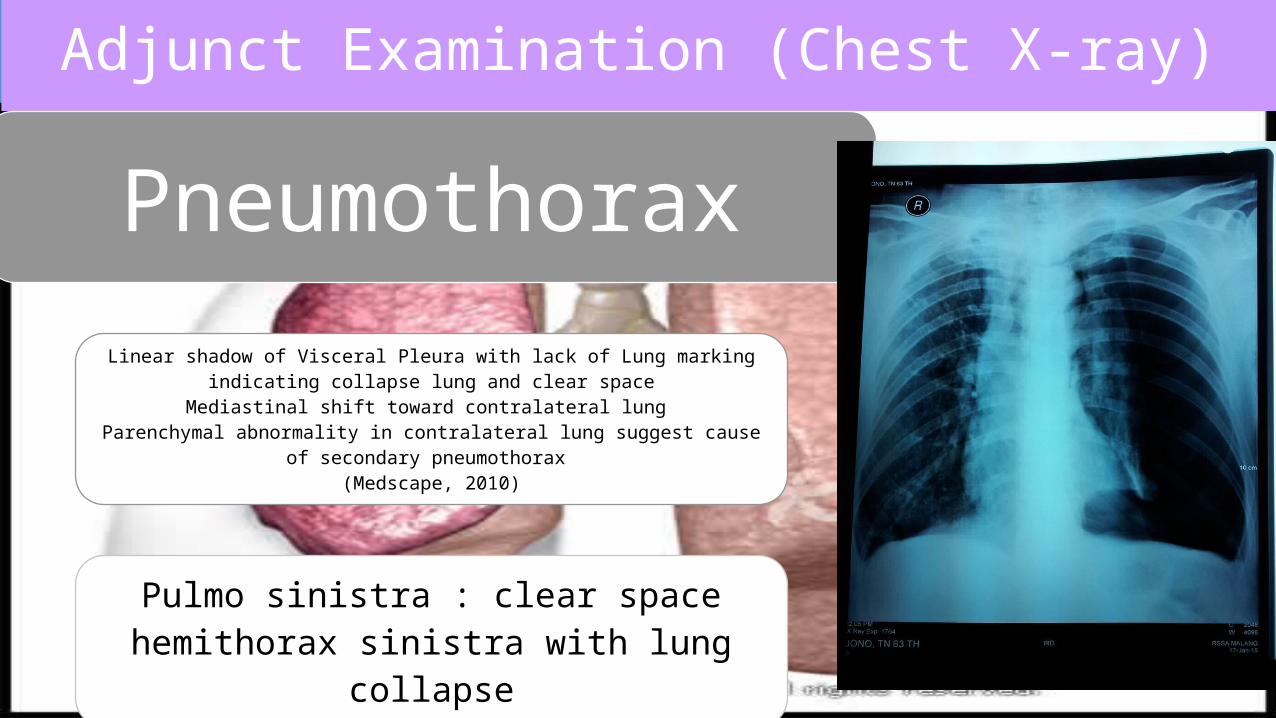
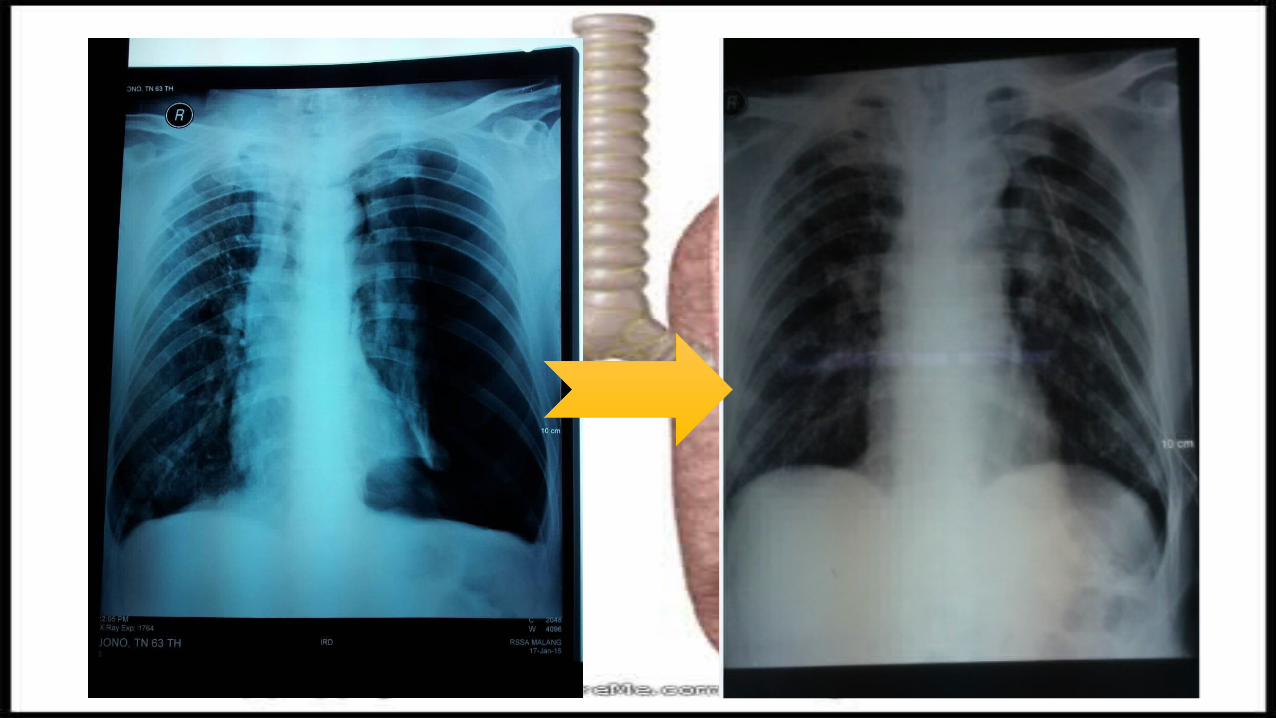
Adjunct ExaminationAdjunct Examination (Chest X-ray)
Pneumothorax
Linear shadow of Visceral Pleura with lack of Lung marking indicating collapse lung and clear space
Mediastinal shift toward contralateral lung Parenchymal abnormality in contralateral lung suggest cause of secondary pneumothorax
(Medscape, 2010)
Pulmo sinistra : clear space hemithorax sinistra with lung
collapse
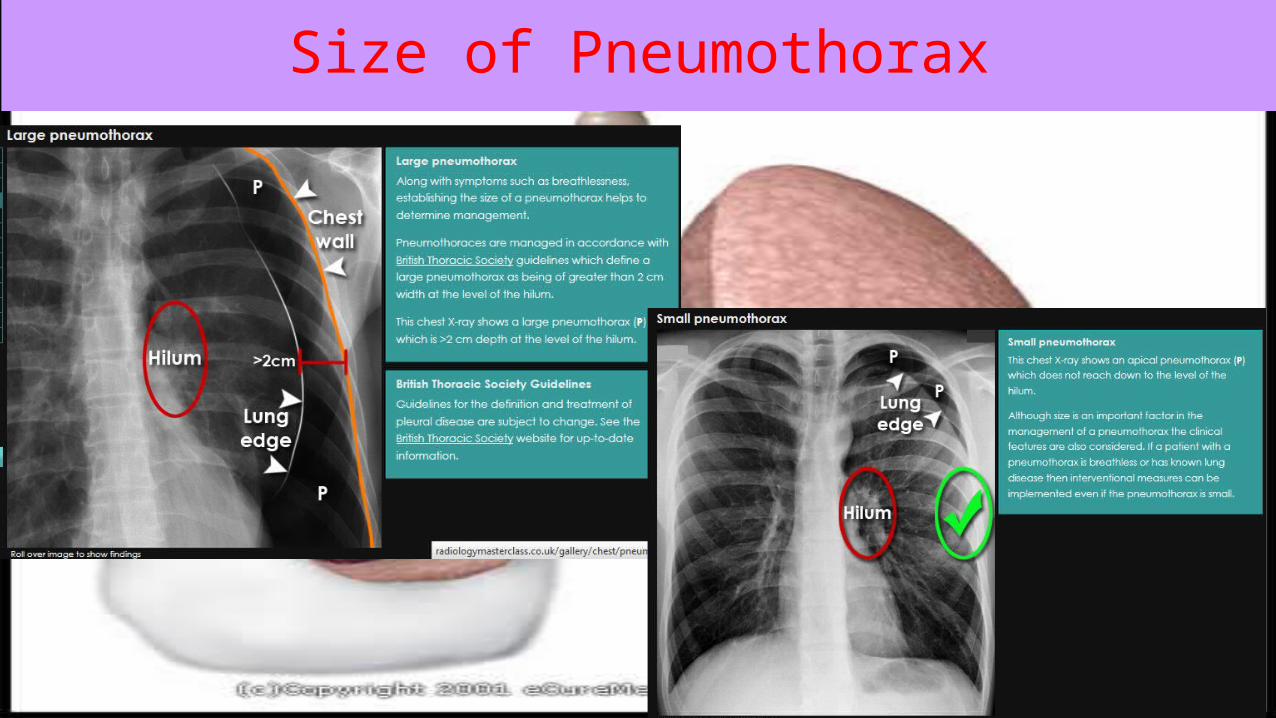
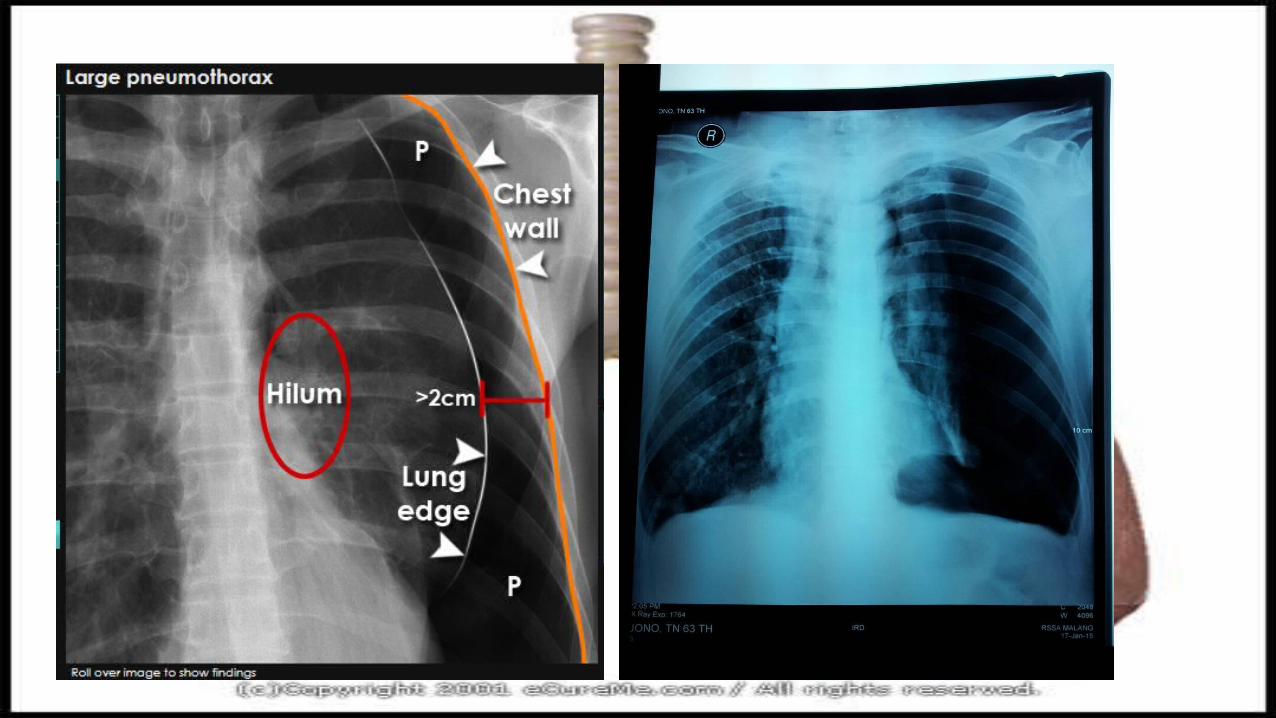
Size of Pneumothorax
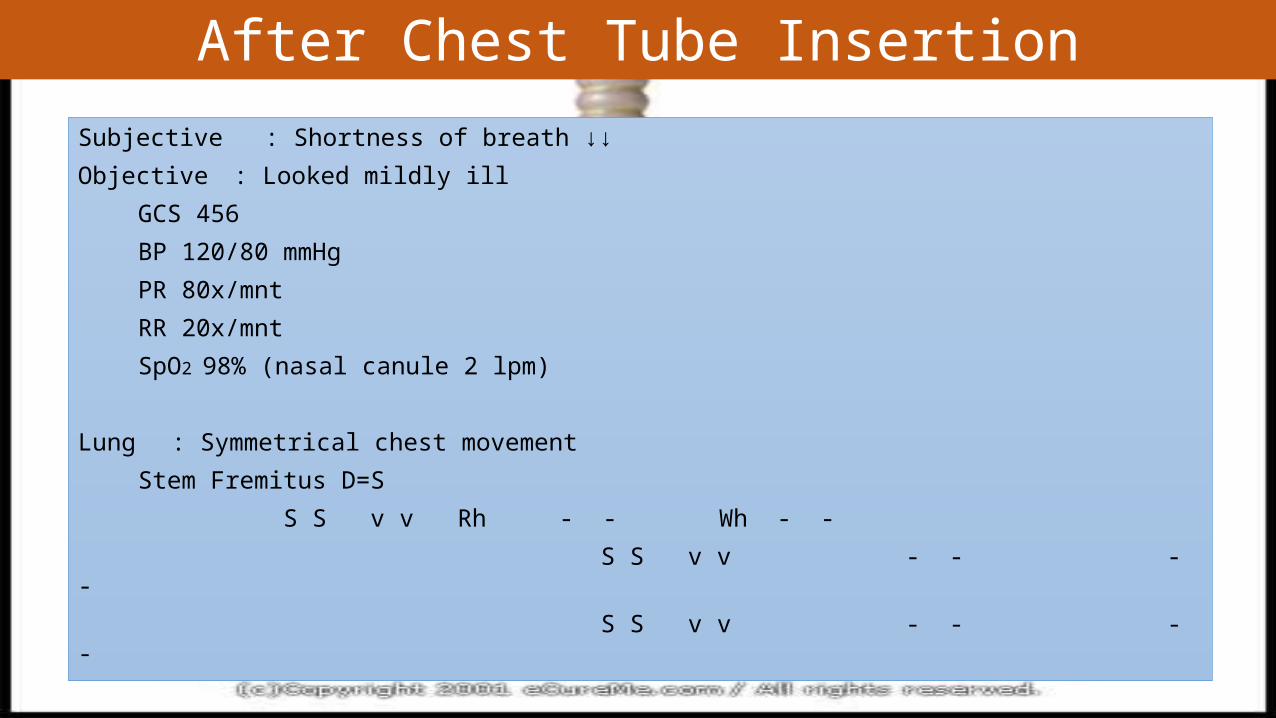
After Chest Tube InsertionSubjective : Shortness of breath ↓↓Objective : Looked mildly ill
GCS 456 BP 120/80 mmHg PR 80x/mnt RR 20x/mnt SpO2 98% (nasal canule 2 lpm)
Lung : Symmetrical chest movement Stem Fremitus D=S S S v v Rh - - Wh - -
S S v v - - - - S S v v - - - -
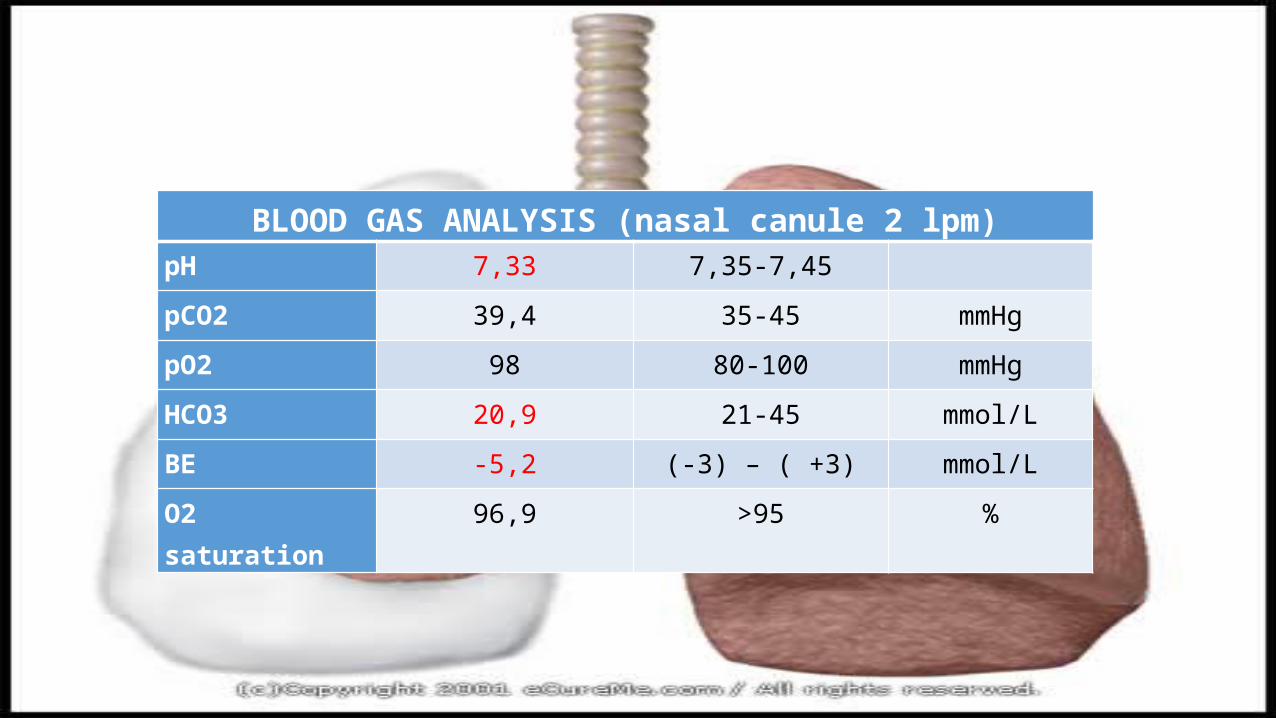
BLOOD GAS ANALYSIS (nasal canule 2 lpm)pH 7,33 7,35-7,45
pCO2 39,4 35-45 mmHg
pO2 98 80-100 mmHg
HCO3 20,9 21-45 mmol/L
BE -5,2 (-3) – ( +3) mmol/L
O2 saturation 96,9 >95 %
Lessons Learnt
When we got patient with shortness of breath, we should do appropriate first aid treatment and diagnose the underlying causes of it from good history taking, physical examination, and adjunction examination interpretation.
There are 3 major underlying diseases (TB, COPD, and Pneumonia) that can cause Spontaneous Secondary Pneumothorax. So we should keep in our mind the possibility of SSP occur when we treat patient with these diseases.
Pneumothorax is one of Pulmonary Emergency that need fast and precise treatment based on the underlying causes, size of pneumothorax, and clinical manifestation.

http://www.jems.com/article/patient-care/how-assess-and-treat-acute-respiratory-d
The pathogenesis of pneumonia in each etiologic agent may be different; in general, patients with typical bacterial pneumonia manifest more toxic clinical symptoms with leukocytosis, neutrophilia with band form neutrophils, and bacteremia. In initial pneumonia lesions, mainly activated neutrophils and mononuclear phagocytes are predominantly observed, and mediators such as proteolytic enzymes, oxygen radicals, and cytokines from these cells may be associated with host lung injury.
Mycoplasma pneumoniae pneumonia, bacterial pneumonia and viral pneumonia Kyung-Yil LeeI; You-Sook YounII; Jae-Wook LeeII; Jin-Han KangI
IMD. PhD. Departments of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Republic of KoreaIIMD. Departments of Pediatrics, College of Medicine, The Catholic University of Korea, Seoul, Republic of KoreaJornal de PediatriaPrint version ISSN 0021-7557J. Pediatr. (Rio J.) vol.86 no.6 Porto Alegre Nov./Dec. 2010http://dx.doi.org/10.1590/S0021-75572010000600002
Most instances of neutrophilia are secondary to a pathologic process outside the marrow. It can occur in infectious diseases, especially acute bacterial infections; neoplasia, either affecting the myeloid system (chronic myelogenous leukemia and other myeloproliferative disorders) or secondary to a solid tumor (paraneoplastic syndrome); inflammation secondary to tissue necrosis, metabolic and collagen diseases, hypersensitivity reactions; hemorrhage; hemolysis; and stress.
Monocytosis can follow chronic infectious disorders (tuberculosis, brucellosis), rheumatic diseases (lupus, rheumatoid arthritis), chronic inflammatory bowel disease, and some malignant processes (Hodgkin's and non-Hodgkin's lymphoma). Monocytes play an important role in other chronic granulomatous diseases: sarcoidosis, histiocytosis X, and storage diseases (Gaucher's disease, Niemann–Pick disease).
Lymphocytopenia can be seen mainly in association with several congenital diseases of the immune system or following treatment with corticosteroids, antineoplastic agents, or radiation.
NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.Walker HK, Hall WD, Hurst JW, editors. Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition. Boston: Butterworths; 1990.
Clinical Methods: The History, Physical, and Laboratory Examinations. 3rd edition.







