validity of newly developed appropriateness criteria for cataract surgery
TRANSCRIPT

Validity of Newly Developed AppropriatenessCriteria for Cataract Surgery
Jose M. Quintana, MD, PhD,1 Antonio Escobar, MD, PhD,2 Amaia Bilbao, MSc,3 Juan A. Blasco, MD,4
Juan R. Lacalle, MD, PhD,5 Marisa Bare, MD, PhD,6 Jose M. Begiristain, MD, PhD,7 for the IRYSS-CataractGroup
Objective: The introduction of phacoemulsification in the early 1990s significantly changed the treatment ofcataract. It is possible that appropriateness criteria for cataract extraction developed before the widespreadadoption of phacoemulsification no longer is as accurate or valid as possible. The objective of this study was tovalidate newly developed explicit appropriateness criteria.
Design: Prospective, observational cohort study.Participants: Consecutive patients with a diagnosis of cataract who were on waiting lists to undergo
cataract extraction by phacoemulsification were recruited.Methods: Newly developed explicit appropriateness criteria for cataract extraction, following Research and
Development methodology, were applied in this study conducted in 17 public teaching hospitals. Data necessaryto classify the appropriateness of the intervention, including demographic and clinical data and that related to thesurgery and complications, were recorded by previously trained ophthalmologists in all centers before theintervention and at the 6-week visit afterward.
Main Outcome Measures: Subjects completed 2 questionnaires that measure health-related quality oflife—the Short Form 36 and the Visual Function Index 14 (VF-14)—before the procedure and 3 months afterward.Also, visual acuity was recorded by ophthalmologists previous to the intervention and at 6 weeks after.
Results: Five thousand two hundred fifty-seven cases were included in the study. At 3 months after cataractextraction, 4335 (82.5%) patients had responded to the questionnaires. Patients whose procedures wereclassified as necessary or appropriate by the new appropriateness criteria had greater improvements in visualacuity and VF-14 scores than those undergoing procedures classified as inappropriate. These differencesseemed to be clinically relevant by measures such as the minimal clinically important difference and minimaldetectable change. Complications rates were similar among all appropriateness categories, except for compli-cations occurring in the peri-intervention period.
Conclusions: These results suggest a direct relationship between the newly developed explicit appropri-ateness criteria for cataract extraction and outcomes, as measured by clinical evaluation and health-relatedquality-of-life instruments. The results support the use of these criteria for clinical evaluation or the developmentof clinical guidelines.
Financial Disclosure(s): The author(s) have no proprietary or commercial interest in any materials discussedin this article. Ophthalmology 2009;116:409–417 © 2009 by the American Academy of Ophthalmology.
Cataract extraction is the most commonly performed surgi-cal intervention in developed countries.1 Given the slow,progressive development of cataract, the variability in pa-tient tolerance of the visual changes that accompany it, andthe high prevalence of the disease, clinicians, managers, andhealth payers must decide which patients are appropriatecandidates for cataract extraction. Reports of wide vari-ations in the indication of cataract extraction led to theinitiation of studies to determine if the procedure wasoverused or underused.2– 4 The ultimate aim of that earlywork was to increase the quality of care delivered topatients while improving cost effectiveness in the medi-cal system. Presumably, both of these goals are aided bythe development of appropriateness criteria on which to
base clinical decisions.© 2009 by the American Academy of OphthalmologyPublished by Elsevier Inc.
Methodology developed in the 1980s by the Researchand Development (RAND) group at the University of Cal-ifornia, Los Angeles, offers a procedure for developingexplicit appropriateness criteria with the purpose of reduc-ing unnecessary variation.5 In fact, RAND chose cataractextraction as one of the first procedures to test this meth-odology.6 In the 1990s, Tobacman et al7 used the RANDtechnique to develop and apply explicit criteria for cataractextraction. At that time, extracapsular cataract surgery wasthe primary procedure for cataract extraction; phacoemulsi-fication was just beginning to gain acceptance. Today,phacoemulsification is by far the predominant surgical tech-nique used for uncomplicated cataract extraction, at least indeveloped countries.8 Whenever a new therapeutic method
is introduced, the criteria for treating a condition may409ISSN 0161-6420/09/$–see front matterdoi:10.1016/j.ophtha.2008.07.017

Ophthalmology Volume 116, Number 3, March 2009
change. New variables should be considered in the decision-making process, whereas other previously essential vari-ables no longer may be important. Thus, it is possible thatthe appropriateness criteria developed previously7 are nolonger valid.
Visual acuity traditionally has been a main outcomemeasure for studies of cataract extraction. But in the last fewyears, patient perception of the effectiveness of cataractextraction also is being measured, generally by means ofhealth-related quality-of-life (HRQoL) questionnaires. Amongthose specifically used in the ophthalmologic field, oneHRQoL instrument that has gained widespread acceptanceand that has been validated in different languages is theVisual Function Index (VF-14).9,10
In addition to determining statistically significant changesin outcomes after medical interventions, it is also importantto determine if those changes are clinically relevant. Withthat end in mind, 2 additional parameters have been devel-oped: the minimal clinically important difference (MCID)and the minimal detectable change (MDC). The MCID wasdefined by Jaeschke et al11 as “the smallest difference inscore in the domain of interest which patients perceive asbeneficial and which would mandate, in the absence oftroublesome side effects and excessive cost, a change in thepatient’s management.” The MDC is expressed as the min-imal magnitude of change above which the observed changeis likely to be real and not just measurement error. As far asthe authors know, neither MCID nor MDC have been eval-uated so far for visual acuity or the VF-14.
This study was designed to validate, in a prospective,observational study of patients undergoing cataract extrac-tion, a previously developed set of appropriateness crite-ria,12 following the RAND methodology, for cataract ex-traction by phacoemulsification. The authors hypothesizedthat if these new appropriateness criteria did, indeed, offereffective clinical guidance, then patients undergoing cata-ract extraction that was considered to be necessary or ap-propriate would have higher HRQoL and functional im-provements than those undergoing procedures not deemedappropriate.
Patients and Methods
The authors previously described in detail how they developednew appropriateness criteria for cataract extraction by phacoemul-sification based on the RAND methodology.12 Briefly, they con-ducted an extensive literature review that focused on defining therisks and benefits of cataract surgery. This review, supplementedwith the work of clinical experts, was used to develop a detailedlist of 765 clinical scenarios, or indications, for which cataractphacoemulsification may be performed. A panel of 12 expertophthalmologists, from different regions of Spain, received thebibliography review along with the 765 clinical indications. Theythen rated the appropriateness of cataract surgery for each indica-tion. The ratings were confidential and took place in 2 rounds,using a modified Delphi process. In the first round, each participantwas asked to rate the appropriateness of each of the 765 indicationson a scale from 1 (least appropriate) to 9 (most appropriate). Anappropriate indication was defined as when the expected benefitsof the cataract surgery exceeded the risks by a sufficiently wide
margin to justify the risk of intervention. An inappropriate indi-410
cation was defined as one in for which the risks exceeded theexpected benefits. An indication was rated as appropriate if themedian score was 7, 8, or 9 and as inappropriate if the score was1, 2, or 3; uncertain indications were those with median scores of4, 5, or 6 or if there was substantial disagreement among panelmembers. Disagreement was identified when the 12 ratings in-cluded at least 4 ratings of 1, 2, or 3 and at least 4 ratings of 7, 8,or 9. With the results of the first round in hand, the panelistsrepeated the ratings, and final scores were determined.
In the final step, the panelists rated the necessity of all 252indications classified as appropriate in the second round on a9-point scale. Necessary indications were defined as those that arenot only appropriate but also are essential, such that withholdingthem would constitute improper clinical care.13 Indications with amedian necessity rating of 7 to 9 and no disagreement wereclassified as necessary. The remainders were considered appropri-ate but not necessary.
These appropriateness criteria then were applied in a prospec-tive observational study of patients scheduled for cataract phaco-emulsification between October 2004 and July 2005. Patients forthis study were drawn from 17 public teaching hospitals in differ-ent regions of Spain, all of which belong to the network of publichospitals that are part of the Spanish National Health Service,which provides free, unrestricted care to nearly 100% of thepopulation. In each hospital, consecutive patients attending oph-thalmologic units for the prescription of cataract removal byphacoemulsification were invited to participate in the study. Pa-tients with severe comorbidities, such as cancer, terminal disease,or psychiatric conditions, were excluded. Physicians in each hos-pital were blinded to the study goals.
Clinical data were collected at the visit before the interventionand approximately 6 weeks after surgery by ophthalmologists andnurses collaborating in the study. These data were demographic(gender, age, address, telephone number), data necessary to clas-sify the appropriateness of the intervention, and data related tosurgical technique and complications in the 6 weeks after surgery.Variables needed to determine appropriateness, and the summarydecision trees, are included in Appendix 1 (available at http://aaojournal.org).
At the time of the preintervention visit, 2 quality-of-life ques-tionnaires were mailed to patients: the Short Form 36 (SF-36)14
and the Visual Function Index (VF-14).15 The SF-36 covers 8domains and 2 summary scales, physical health and mental health.Scores for the 8 SF-36 domains range from 0 to 100, with higherscores indicating better health status. The SF-36 has been trans-lated into Spanish and validated in Spanish populations.16 Func-tional impairment related to vision was evaluated with the VF-14,a validated index of measures that estimate the difficulty patientshave performing 14 vision-dependent activities of daily living suchas day-time and night-time driving, reading traffic signs or smallprint, and engaging in recreational activities.17 Scores on theVF-14 range from 0 (unable to perform any activities) to 100 (ableto perform all activities without difficulty). The VF-14 has beentranslated and validated in Spanish.18
To increase the response rate to mailed questionnaires, up to 2reminder letters were mailed at scheduled times to patients whohad not returned their questionnaires; telephone calls were madewhen necessary to collect this information. Approximately 3months after the intervention, patients were sent another letter thatincluded the same questionnaires along with additional questionson the clinical aspects of their disease. Patients also were asked toanswer this transitional question about their visual improvementafter the intervention: How is your vision now compared with howit was before your cataract surgery? The possible responses were:a great deal better, quite better, somewhat better, equal, somewhat
worse, quite worse, and a great deal worse. Those who did not
Quintana et al � Outcomes and Appropriateness
reply in a timely fashion were followed up as described for thepreintervention mailing.
All study procedures were approved by the institutional reviewboards of the participating hospitals. Personal data were collectedonly for tracking patients during the period before and after sur-gery, and all data were kept confidential.
Statistical Analysis
The unit of study was the patient. In cases in which 1 patientunderwent 2 interventions during the recruitment period, the firstintervention performed was selected.
Descriptive Analysis. Descriptive statistics included fre-quency tables plus means and standard deviations. Visual acuity ispresented in decimal fraction units. Sociodemographic data, clin-ical characteristics, and SF-36 and VF-14 scores at baseline werecompared between the patients who completed the questionnaires3 months after surgery and those who did not using the chi-squareand Fisher exact tests for categorical variables and Student t test orthe nonparametric Wilcoxon test for continuous variables. In ad-dition, the effect on mean changes in visual acuity and VF-14 ofnonresponders to questionnaires after surgery was explored. To doso, data from responders were used to predict the changes in visualacuity and VF-14 scores by means of general linear models.Preintervention scores and ocular pathologic features were used asindependent variables. Predicted changes then were input for thenonresponders.
Comparison of Preintervention and Postintervention Scores.The main outcomes of the study were changes in visual acuity andscores on the VF-14 questionnaire. The results for 2 subgroupswere analyzed: patients with simple cataract and those with anyretinopathy. Preintervention and postintervention main outcomeresults were compared by means of a paired t test to assess ifchanges were significant.
Evaluation of Change of Scores, Minimal Clinically Impor-tant Difference, and Minimal Detectable Change According toAppropriateness Categories. First, the MCID and the MDC werederived. The MCID was estimated by the mean change in visualacuity scores and VF-14 for patients who declared their eyesight tobe somewhat better in response to the transitional question 3months after surgery.19 The percent MCID (%MCID) was esti-mated, which is the proportion of the sample with a change inscores exceeding the MCID.
For the estimation of MDC for the VF-14, the standard error ofmeasurement (SEM), which represents the amount of error asso-ciated with an individual subject assessment, was estimated first20
using a formula described in detail elsewhere.21 From the SEM, theMDC was derived using the following equation20: MDC � SEM� z-score � �2. A 95% confidence level for the MDC (MDC95%)corresponding to a z-value of 1.96 was established. The interpre-tation of MDC95% is that if a patient has a change in score equalto or greater than the MDC95% threshold, it is possible to state with95% confidence that this change is reliable and not the result ofmeasurement error. The proportion of the sample with a change inscore exceeding the MDC95% (%MDC95%) was estimated. TheMDC for visual acuity could not be estimated because neither areliability coefficient nor a Cronbach � value for that outcomewere available.
Then, the mean change scores, %MCID, and %MDC95% of theoutcome parameters were compared at 6 weeks after surgery forvisual acuity and 3 months after surgery for VF-14 scores betweenthe 4 appropriateness categories: necessary, appropriate, uncertain,and inappropriate. For the comparison of mean change scores, ananalysis of variance was performed with the Scheffe test for
multiple comparisons. For the comparison of proportions, chi-square tests were performed, considering the Bonferroni correctionfor multiple comparisons.
Change in Main Outcome Scores According to Appropriate-ness Categories Adjusting for Respective Baseline Scores. First,the general linear model was used to compare the mean changes invisual acuity and VF-14 scores among the 4 appropriateness cat-egories, with adjustment for baseline scores. Interaction betweenbaseline scores and appropriateness categories also was consid-ered. Multilevel analysis with mixed models also was performed totest differences among hospitals for changes in visual acuity andVF-14 scores for the 4 appropriateness categories.
Second, for the graphical representation, lowess curves wereused for each appropriateness category. The lowess curve, alsocalled locally weighted scatterplot smoothing function, fits a localregression model. This statistical technique is a modeling methodused to plot a smooth curve through a set of data points, givingmore weight to points near the point whose response is beingestimated and less weight to points further away.22
Third, in an effort to explain differences in gains among theappropriateness categories, differences between the variables thatmake up the criteria in each appropriateness category were eval-uated, and the effect of those variables on changes in visual acuityand VF-14 scores was explored.
Fourth, differences observed in changes in visual acuity andVF-14 scores among the 4 appropriateness categories after adjust-ment by other relevant variables were explored. In a multivariateanalysis, by means of the general linear models, the effect ofvariables were studied that were statistically significant on changesin visual acuity or VF-14 scores, being main independent variablethe appropriateness criteria, and adjusted by preintervention visualacuity or VF-14 score, age, level of education, preinterventionSF-36 physical summary component, and interaction between ap-propriateness and preintervention visual acuity or VF-14 score.
Figure 1. Flow chart showing the recruitment process, exclusions, and
losses during follow-up.411
Ophthalmology Volume 116, Number 3, March 2009
Evaluation of Complications According to AppropriatenessCategories. Finally, procedure-related complications were exam-ined among the 4 appropriateness categories by means of chi-square tests, considering the Bonferroni correction for multiplecomparisons. All effects were considered statistically significant atP�0.05. All statistical analyses were performed using SAS forWindows statistical software version 8.0 (SAS Inc., Cary, NC) andS-Plus 2000 (MathSoft, Inc., Cambridge, MA, 1999).
Results
A total of 7438 consecutive patients being evaluated for cataractextraction were invited to participate in the study. Of these, 907(12.2%) were excluded. Of the 6531 who fulfilled the inclusioncriteria, complete clinical information and responses to the prein-tervention HRQoL questionnaires were available for 5257(80.5%). A total of 4335 (82.5% of the preintervention population)responded to questionnaires sent by mail 3 months after theircataract extraction patients (Fig 1).
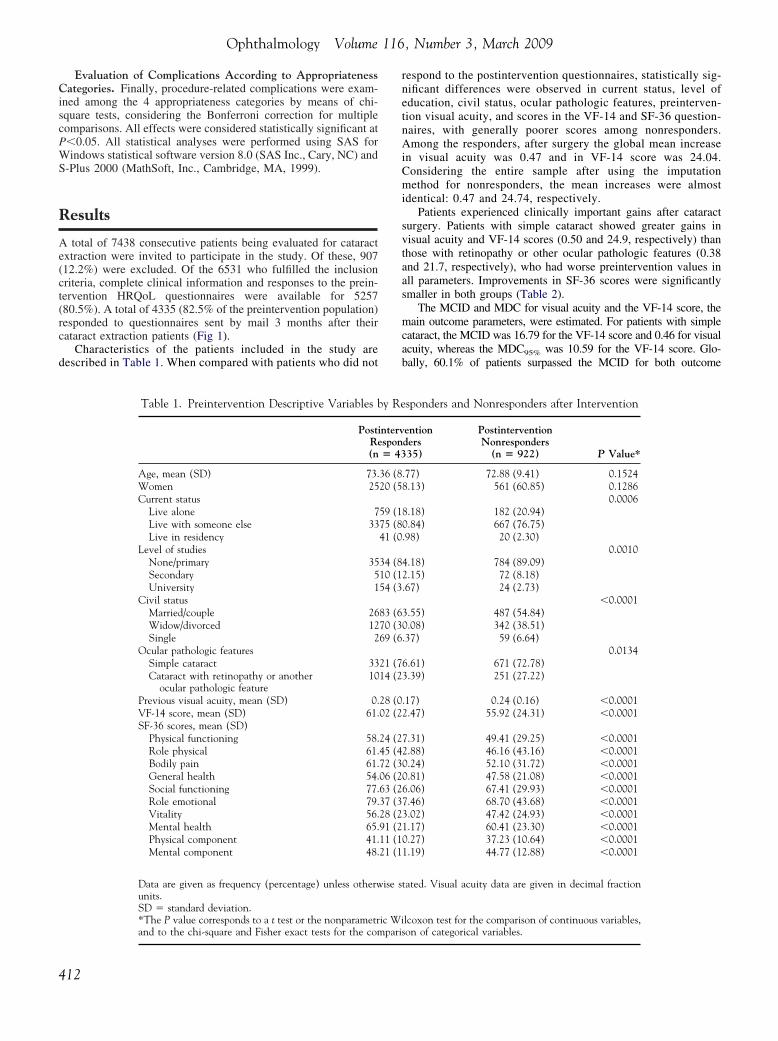
Characteristics of the patients included in the study aredescribed in Table 1. When compared with patients who did not
Table 1. Preintervention Descriptive Variables b
PostRe(n
Age, mean (SD) 73.Women 25Current status
Live alone 7Live with someone else 33Live in residency
Level of studiesNone/primary 35Secondary 5University 1
Civil statusMarried/couple 26Widow/divorced 12Single 2
Ocular pathologic featuresSimple cataract 33Cataract with retinopathy or another
ocular pathologic feature10
Previous visual acuity, mean (SD) 0.VF-14 score, mean (SD) 61.SF-36 scores, mean (SD)
Physical functioning 58.Role physical 61.Bodily pain 61.General health 54.Social functioning 77.Role emotional 79.Vitality 56.Mental health 65.Physical component 41.Mental component 48.
Data are given as frequency (percentage) unless otherwunits.SD � standard deviation.*The P value corresponds to a t test or the nonparametr
and to the chi-square and Fisher exact tests for the compari412
respond to the postintervention questionnaires, statistically sig-nificant differences were observed in current status, level ofeducation, civil status, ocular pathologic features, preinterven-tion visual acuity, and scores in the VF-14 and SF-36 question-naires, with generally poorer scores among nonresponders.Among the responders, after surgery the global mean increasein visual acuity was 0.47 and in VF-14 score was 24.04.Considering the entire sample after using the imputationmethod for nonresponders, the mean increases were almostidentical: 0.47 and 24.74, respectively.
Patients experienced clinically important gains after cataractsurgery. Patients with simple cataract showed greater gains invisual acuity and VF-14 scores (0.50 and 24.9, respectively) thanthose with retinopathy or other ocular pathologic features (0.38and 21.7, respectively), who had worse preintervention values inall parameters. Improvements in SF-36 scores were significantlysmaller in both groups (Table 2).
The MCID and MDC for visual acuity and the VF-14 score, themain outcome parameters, were estimated. For patients with simplecataract, the MCID was 16.79 for the VF-14 score and 0.46 for visualacuity, whereas the MDC95% was 10.59 for the VF-14 score. Glo-bally, 60.1% of patients surpassed the MCID for both outcome
sponders and Nonresponders after Intervention
entionders35)
PostinterventionNonresponders
(n � 922) P Value*
.77) 72.88 (9.41) 0.15248.13) 561 (60.85) 0.1286
0.00068.18) 182 (20.94)0.84) 667 (76.75).98) 20 (2.30)
0.00104.18) 784 (89.09)2.15) 72 (8.18).67) 24 (2.73)
�0.00013.55) 487 (54.84)0.08) 342 (38.51).37) 59 (6.64)
0.01346.61) 671 (72.78)3.39) 251 (27.22)
.17) 0.24 (0.16) �0.00012.47) 55.92 (24.31) �0.0001
7.31) 49.41 (29.25) �0.00012.88) 46.16 (43.16) �0.00010.24) 52.10 (31.72) �0.00010.81) 47.58 (21.08) �0.00016.06) 67.41 (29.93) �0.00017.46) 68.70 (43.68) �0.00013.02) 47.42 (24.93) �0.00011.17) 60.41 (23.30) �0.00010.27) 37.23 (10.64) �0.00011.19) 44.77 (12.88) �0.0001
tated. Visual acuity data are given in decimal fraction
lcoxon test for the comparison of continuous variables,
y Re
intervspon� 43
36 (820 (5
59 (175 (841 (0
34 (810 (154 (3
83 (670 (369 (6
21 (714 (2
28 (002 (2
24 (245 (472 (306 (263 (237 (328 (291 (211 (121 (1
ise s
ic Wi
son of categorical variables.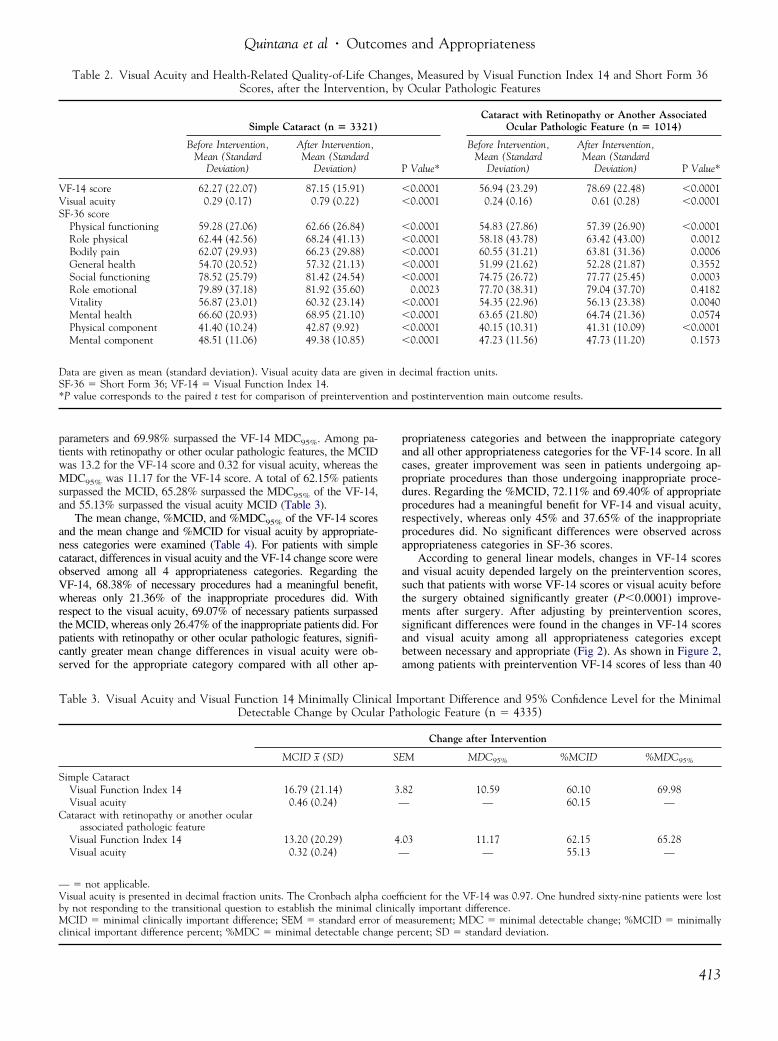
n an
Quintana et al � Outcomes and Appropriateness
parameters and 69.98% surpassed the VF-14 MDC95%. Among pa-tients with retinopathy or other ocular pathologic features, the MCIDwas 13.2 for the VF-14 score and 0.32 for visual acuity, whereas theMDC95% was 11.17 for the VF-14 score. A total of 62.15% patientssurpassed the MCID, 65.28% surpassed the MDC95% of the VF-14,and 55.13% surpassed the visual acuity MCID (Table 3).
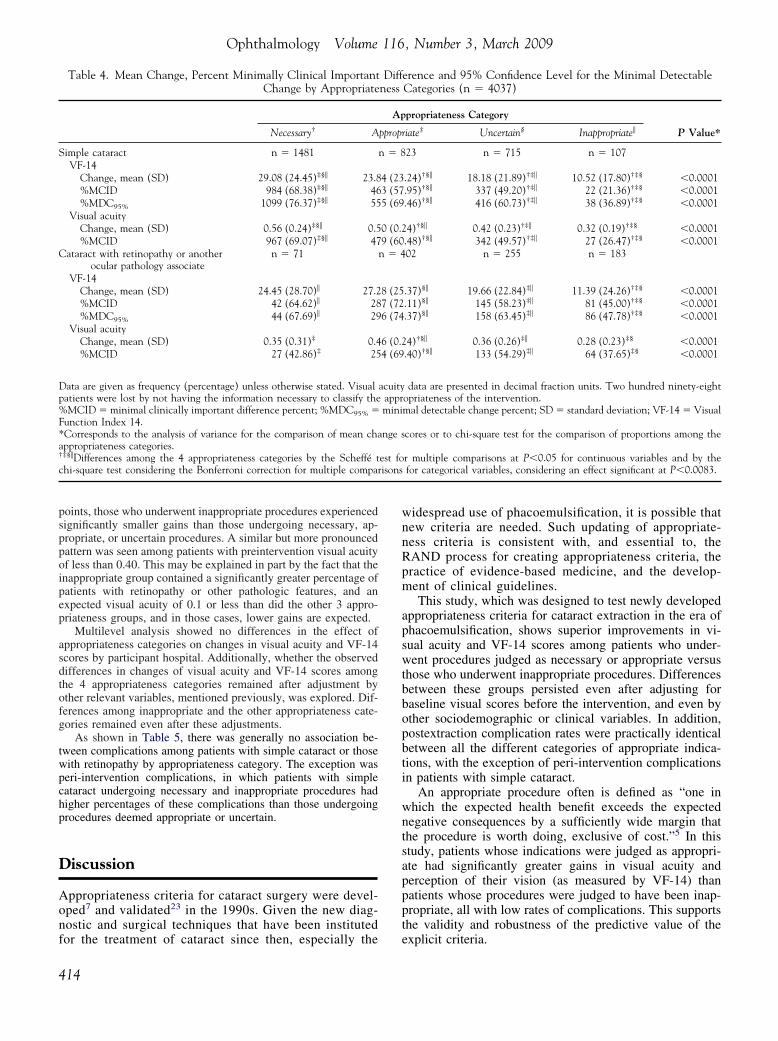
The mean change, %MCID, and %MDC95% of the VF-14 scoresand the mean change and %MCID for visual acuity by appropriate-ness categories were examined (Table 4). For patients with simplecataract, differences in visual acuity and the VF-14 change score wereobserved among all 4 appropriateness categories. Regarding theVF-14, 68.38% of necessary procedures had a meaningful benefit,whereas only 21.36% of the inappropriate procedures did. Withrespect to the visual acuity, 69.07% of necessary patients surpassedthe MCID, whereas only 26.47% of the inappropriate patients did. Forpatients with retinopathy or other ocular pathologic features, signifi-cantly greater mean change differences in visual acuity were ob-served for the appropriate category compared with all other ap-
Table 2. Visual Acuity and Health-Related Quality-of-Life ChScores, after the Interventio
Simple Cataract (n � 3321)
Before Intervention,Mean (Standard
Deviation)
After Intervention,Mean (Standard
Deviation)
VF-14 score 62.27 (22.07) 87.15 (15.91)Visual acuity 0.29 (0.17) 0.79 (0.22)SF-36 score
Physical functioning 59.28 (27.06) 62.66 (26.84)Role physical 62.44 (42.56) 68.24 (41.13)Bodily pain 62.07 (29.93) 66.23 (29.88)General health 54.70 (20.52) 57.32 (21.13)Social functioning 78.52 (25.79) 81.42 (24.54)Role emotional 79.89 (37.18) 81.92 (35.60)Vitality 56.87 (23.01) 60.32 (23.14)Mental health 66.60 (20.93) 68.95 (21.10)Physical component 41.40 (10.24) 42.87 (9.92)Mental component 48.51 (11.06) 49.38 (10.85)
Data are given as mean (standard deviation). Visual acuity data are givenSF-36 � Short Form 36; VF-14 � Visual Function Index 14.*P value corresponds to the paired t test for comparison of preinterventio
Table 3. Visual Acuity and Visual Function 14 Minimally CliniDetectable Change by Ocula
MCID x (SD)
Simple CataractVisual Function Index 14 16.79 (21.14)Visual acuity 0.46 (0.24)
Cataract with retinopathy or another ocularassociated pathologic feature
Visual Function Index 14 13.20 (20.29)Visual acuity 0.32 (0.24)
— � not applicable.Visual acuity is presented in decimal fraction units. The Cronbach alphaby not responding to the transitional question to establish the minimal cMCID � minimal clinically important difference; SEM � standard error
clinical important difference percent; %MDC � minimal detectable change ppropriateness categories and between the inappropriate categoryand all other appropriateness categories for the VF-14 score. In allcases, greater improvement was seen in patients undergoing ap-propriate procedures than those undergoing inappropriate proce-dures. Regarding the %MCID, 72.11% and 69.40% of appropriateprocedures had a meaningful benefit for VF-14 and visual acuity,respectively, whereas only 45% and 37.65% of the inappropriateprocedures did. No significant differences were observed acrossappropriateness categories in SF-36 scores.
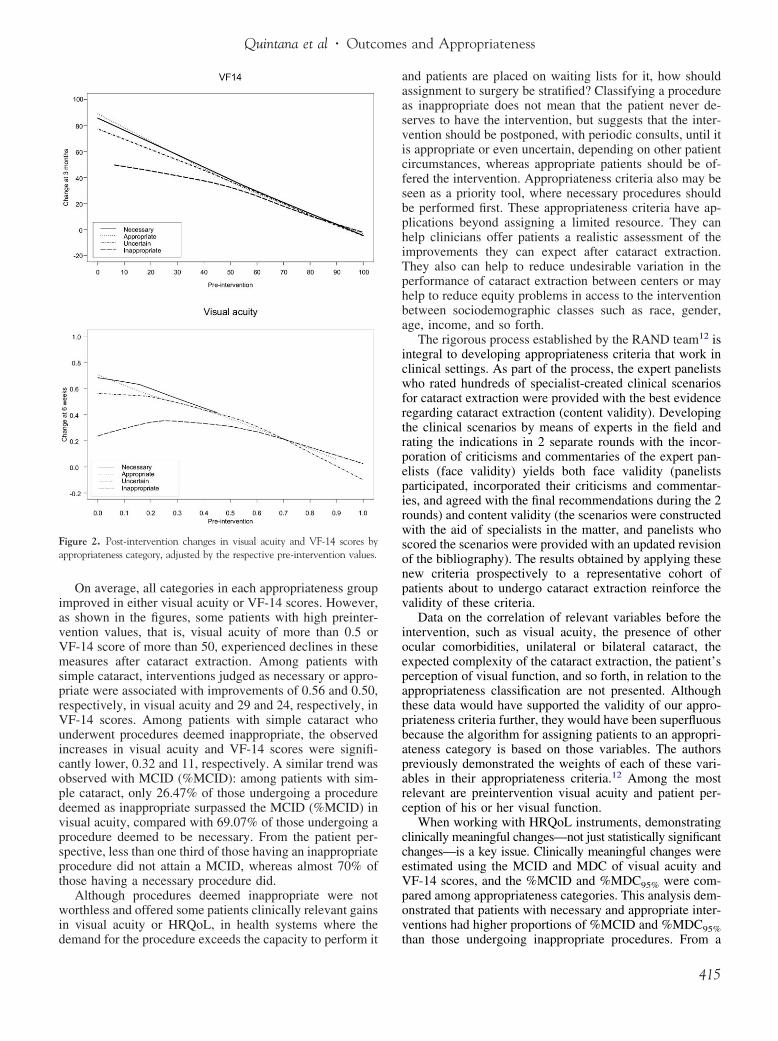
According to general linear models, changes in VF-14 scoresand visual acuity depended largely on the preintervention scores,such that patients with worse VF-14 scores or visual acuity beforethe surgery obtained significantly greater (P�0.0001) improve-ments after surgery. After adjusting by preintervention scores,significant differences were found in the changes in VF-14 scoresand visual acuity among all appropriateness categories exceptbetween necessary and appropriate (Fig 2). As shown in Figure 2,among patients with preintervention VF-14 scores of less than 40
s, Measured by Visual Function Index 14 and Short Form 36Ocular Pathologic Features
Cataract with Retinopathy or Another AssociatedOcular Pathologic Feature (n � 1014)
Value*
Before Intervention,Mean (Standard
Deviation)
After Intervention,Mean (Standard
Deviation) P Value*
0.0001 56.94 (23.29) 78.69 (22.48) �0.00010.0001 0.24 (0.16) 0.61 (0.28) �0.0001
0.0001 54.83 (27.86) 57.39 (26.90) �0.00010.0001 58.18 (43.78) 63.42 (43.00) 0.00120.0001 60.55 (31.21) 63.81 (31.36) 0.00060.0001 51.99 (21.62) 52.28 (21.87) 0.35520.0001 74.75 (26.72) 77.77 (25.45) 0.00030.0023 77.70 (38.31) 79.04 (37.70) 0.41820.0001 54.35 (22.96) 56.13 (23.38) 0.00400.0001 63.65 (21.80) 64.74 (21.36) 0.05740.0001 40.15 (10.31) 41.31 (10.09) �0.00010.0001 47.23 (11.56) 47.73 (11.20) 0.1573
ecimal fraction units.
d postintervention main outcome results.
portant Difference and 95% Confidence Level for the Minimalhologic Feature (n � 4335)
Change after Intervention
M MDC95% %MCID %MDC95%
82 10.59 60.10 69.98— 60.15 —
03 11.17 62.15 65.28— 55.13 —
cient for the VF-14 was 0.97. One hundred sixty-nine patients were lostlly important difference.easurement; MDC � minimal detectable change; %MCID � minimally
angen, by
P
��
�����
����
in d
cal Imr Pat
SE
3.—
4.—
coeffilinicaof m
ercent; SD � standard deviation.
413
risons
Ophthalmology Volume 116, Number 3, March 2009
points, those who underwent inappropriate procedures experiencedsignificantly smaller gains than those undergoing necessary, ap-propriate, or uncertain procedures. A similar but more pronouncedpattern was seen among patients with preintervention visual acuityof less than 0.40. This may be explained in part by the fact that theinappropriate group contained a significantly greater percentage ofpatients with retinopathy or other pathologic features, and anexpected visual acuity of 0.1 or less than did the other 3 appro-priateness groups, and in those cases, lower gains are expected.
Multilevel analysis showed no differences in the effect ofappropriateness categories on changes in visual acuity and VF-14scores by participant hospital. Additionally, whether the observeddifferences in changes of visual acuity and VF-14 scores amongthe 4 appropriateness categories remained after adjustment byother relevant variables, mentioned previously, was explored. Dif-ferences among inappropriate and the other appropriateness cate-gories remained even after these adjustments.
As shown in Table 5, there was generally no association be-tween complications among patients with simple cataract or thosewith retinopathy by appropriateness category. The exception wasperi-intervention complications, in which patients with simplecataract undergoing necessary and inappropriate procedures hadhigher percentages of these complications than those undergoingprocedures deemed appropriate or uncertain.
Discussion
Appropriateness criteria for cataract surgery were devel-oped7 and validated23 in the 1990s. Given the new diag-nostic and surgical techniques that have been instituted
Table 4. Mean Change, Percent Minimally Clinical ImportantChange by Appropriate
Necessary† A
Simple cataract n � 1481VF-14
Change, mean (SD) 29.08 (24.45)‡§� 23.8%MCID 984 (68.38)‡§� 46%MDC95% 1099 (76.37)‡§� 55
Visual acuityChange, mean (SD) 0.56 (0.24)‡§� 0.5%MCID 967 (69.07)‡§� 47
Cataract with retinopathy or anotherocular pathology associate
n � 71
VF-14Change, mean (SD) 24.45 (28.70)� 27.2%MCID 42 (64.62)� 28%MDC95% 44 (67.69)� 29
Visual acuityChange, mean (SD) 0.35 (0.31)‡ 0.4%MCID 27 (42.86)‡ 25
Data are given as frequency (percentage) unless otherwise stated. Visualpatients were lost by not having the information necessary to classify the%MCID � minimal clinically important difference percent; %MDC95% �Function Index 14.*Corresponds to the analysis of variance for the comparison of mean chaappropriateness categories.†‡§�Differences among the 4 appropriateness categories by the Scheffé tchi-square test considering the Bonferroni correction for multiple compa
for the treatment of cataract since then, especially the
414
widespread use of phacoemulsification, it is possible thatnew criteria are needed. Such updating of appropriate-ness criteria is consistent with, and essential to, theRAND process for creating appropriateness criteria, thepractice of evidence-based medicine, and the develop-ment of clinical guidelines.
This study, which was designed to test newly developedappropriateness criteria for cataract extraction in the era ofphacoemulsification, shows superior improvements in vi-sual acuity and VF-14 scores among patients who under-went procedures judged as necessary or appropriate versusthose who underwent inappropriate procedures. Differencesbetween these groups persisted even after adjusting forbaseline visual scores before the intervention, and even byother sociodemographic or clinical variables. In addition,postextraction complication rates were practically identicalbetween all the different categories of appropriate indica-tions, with the exception of peri-intervention complicationsin patients with simple cataract.
An appropriate procedure often is defined as “one inwhich the expected health benefit exceeds the expectednegative consequences by a sufficiently wide margin thatthe procedure is worth doing, exclusive of cost.”5 In thisstudy, patients whose indications were judged as appropri-ate had significantly greater gains in visual acuity andperception of their vision (as measured by VF-14) thanpatients whose procedures were judged to have been inap-propriate, all with low rates of complications. This supportsthe validity and robustness of the predictive value of the
erence and 95% Confidence Level for the Minimal DetectableCategories (n � 4037)
propriateness Category
P Value*riate‡ Uncertain§ Inappropriate�
23 n � 715 n � 107
.24)†§� 18.18 (21.89)†‡� 10.52 (17.80)†‡§ �0.0001
.95)†§� 337 (49.20)†‡� 22 (21.36)†‡§ �0.0001
.46)†§� 416 (60.73)†‡� 38 (36.89)†‡§ �0.0001
4)†§� 0.42 (0.23)†‡� 0.32 (0.19)†‡§ �0.0001.48)†§� 342 (49.57)†‡� 27 (26.47)†‡§ �0.000102 n � 255 n � 183
.37)§� 19.66 (22.84)‡� 11.39 (24.26)†‡§ �0.0001
.11)§� 145 (58.23)‡� 81 (45.00)†‡§ �0.0001
.37)§� 158 (63.45)‡� 86 (47.78)†‡§ �0.0001
4)†§� 0.36 (0.26)‡� 0.28 (0.23)‡§ �0.0001.40)†§� 133 (54.29)‡� 64 (37.65)‡§ �0.0001
data are presented in decimal fraction units. Two hundred ninety-eightopriateness of the intervention.mal detectable change percent; SD � standard deviation; VF-14 � Visual
cores or to chi-square test for the comparison of proportions among the
r multiple comparisons at P�0.05 for continuous variables and by thefor categorical variables, considering an effect significant at P�0.0083.
Diffness
Ap
pprop
n � 8
4 (233 (575 (69
0 (0.29 (60
n � 4
8 (257 (726 (74
6 (0.24 (69
acuityapprmini
nge s
est fo
explicit criteria.
Quintana et al � Outcomes and Appropriateness
On average, all categories in each appropriateness groupimproved in either visual acuity or VF-14 scores. However,as shown in the figures, some patients with high preinter-vention values, that is, visual acuity of more than 0.5 orVF-14 score of more than 50, experienced declines in thesemeasures after cataract extraction. Among patients withsimple cataract, interventions judged as necessary or appro-priate were associated with improvements of 0.56 and 0.50,respectively, in visual acuity and 29 and 24, respectively, inVF-14 scores. Among patients with simple cataract whounderwent procedures deemed inappropriate, the observedincreases in visual acuity and VF-14 scores were signifi-cantly lower, 0.32 and 11, respectively. A similar trend wasobserved with MCID (%MCID): among patients with sim-ple cataract, only 26.47% of those undergoing a proceduredeemed as inappropriate surpassed the MCID (%MCID) invisual acuity, compared with 69.07% of those undergoing aprocedure deemed to be necessary. From the patient per-spective, less than one third of those having an inappropriateprocedure did not attain a MCID, whereas almost 70% ofthose having a necessary procedure did.
Although procedures deemed inappropriate were notworthless and offered some patients clinically relevant gainsin visual acuity or HRQoL, in health systems where the
Figure 2. Post-intervention changes in visual acuity and VF-14 scores byappropriateness category, adjusted by the respective pre-intervention values.
demand for the procedure exceeds the capacity to perform it
and patients are placed on waiting lists for it, how shouldassignment to surgery be stratified? Classifying a procedureas inappropriate does not mean that the patient never de-serves to have the intervention, but suggests that the inter-vention should be postponed, with periodic consults, until itis appropriate or even uncertain, depending on other patientcircumstances, whereas appropriate patients should be of-fered the intervention. Appropriateness criteria also may beseen as a priority tool, where necessary procedures shouldbe performed first. These appropriateness criteria have ap-plications beyond assigning a limited resource. They canhelp clinicians offer patients a realistic assessment of theimprovements they can expect after cataract extraction.They also can help to reduce undesirable variation in theperformance of cataract extraction between centers or mayhelp to reduce equity problems in access to the interventionbetween sociodemographic classes such as race, gender,age, income, and so forth.
The rigorous process established by the RAND team12 isintegral to developing appropriateness criteria that work inclinical settings. As part of the process, the expert panelistswho rated hundreds of specialist-created clinical scenariosfor cataract extraction were provided with the best evidenceregarding cataract extraction (content validity). Developingthe clinical scenarios by means of experts in the field andrating the indications in 2 separate rounds with the incor-poration of criticisms and commentaries of the expert pan-elists (face validity) yields both face validity (panelistsparticipated, incorporated their criticisms and commentar-ies, and agreed with the final recommendations during the 2rounds) and content validity (the scenarios were constructedwith the aid of specialists in the matter, and panelists whoscored the scenarios were provided with an updated revisionof the bibliography). The results obtained by applying thesenew criteria prospectively to a representative cohort ofpatients about to undergo cataract extraction reinforce thevalidity of these criteria.
Data on the correlation of relevant variables before theintervention, such as visual acuity, the presence of otherocular comorbidities, unilateral or bilateral cataract, theexpected complexity of the cataract extraction, the patient’sperception of visual function, and so forth, in relation to theappropriateness classification are not presented. Althoughthese data would have supported the validity of our appro-priateness criteria further, they would have been superfluousbecause the algorithm for assigning patients to an appropri-ateness category is based on those variables. The authorspreviously demonstrated the weights of each of these vari-ables in their appropriateness criteria.12 Among the mostrelevant are preintervention visual acuity and patient per-ception of his or her visual function.
When working with HRQoL instruments, demonstratingclinically meaningful changes—not just statistically significantchanges—is a key issue. Clinically meaningful changes wereestimated using the MCID and MDC of visual acuity andVF-14 scores, and the %MCID and %MDC95% were com-pared among appropriateness categories. This analysis dem-onstrated that patients with necessary and appropriate inter-ventions had higher proportions of %MCID and %MDC95%
than those undergoing inappropriate procedures. From a415
Ophthalmology Volume 116, Number 3, March 2009
clinical point of view, patients who had appropriate proce-dures had greater gains in vision than those undergoinginappropriate procedures.
The SF-36 was used as a generic measure of HRQoL.11
Although the improvements reflected by this instrumentwere statistically significant (mainly because of the largesample size), they were clinically insignificant and similaramong the 4 appropriateness categories. At least in thispopulation and for this indication, the SF-36 does not seemto be an appropriate tool for capturing clinically importantchanges. Thus, the analyses were focused on changes invisual acuity and VF-14 scores.
As in any prospective study, one limitation of this workis missing data. Although the response rate after the inter-vention was quite high, 82.5%, patients who did not provideinformation 3 months after cataract extraction had poorerpreintervention HRQoL as measured by both the VF-14 andSF-36, which may suppose a bias. But, as has been pre-sented in this study, an estimation of that bias indicated thatthe error is likely to have been minor. Nevertheless, the factis that some bias exists and may have underestimated oroverestimated the results. The time established for patientfollow-up after the intervention also may limit the results ofthis study. In Spain, the ophthalmologic evaluation of pa-tients after cataract extraction routinely is carried out ap-proximately 1 to 2 months after the procedure, and it tookthe patients in this study an average of 3 months to completethe mailed questionnaires, which included the VF-14. Al-though this is similar to follow-up in some studies,24 someauthors have suggested longer follow-up.9,10 Third, strictlyspeaking, these results can be generalized only to the hos-pitals participating in this study. Nevertheless, the authorsbelieve that the results can be of value to many centers indeveloped countries that are likely to have patients with
Table 5. Complications
Necessary†
Simple cataract n � 1754Peri-intervention 199 (11.35)‡
PostinterventionSolved 339 (19.33)Some not solved 109 (6.21)
Urgent consultation required 47 (2.68)Reintervention needed 34 (1.94)
Cataract with retinopathy or other associatedocular pathologic features
n � 92
Peri-intervention 12 (13.04)Postintervention
Solved 15 (16.30)Some not solved 7 (7.61)
Urgent consultation required 3 (3.26)Reintervention needed 1 (1.09)
Data are given as frequency (percentage). Five hundred sixty-five patients wof the intervention or the postintervention clinical information.*Corresponds to the chi-square test for the comparison of proportions am†‡§�Differences among the 4 appropriateness categories by chi-square test ceffect significant at P�0.0083.
sociodemographic and clinical characteristics similar to the
416
authors’. Another limitation was that we used the sametransitional question, obtained through the patients’ opinionat 3 months, for visual function measured through the VF-14, or for visual acuity. In the case of visual acuity, theophthalmologist’s perception of visual improvement mayhave been more appropriate. Also, MCID and MDC param-eters must be used carefully and not as absolute measures19
because there are several practical problems in estimatingboth parameters. Finally, appropriateness criteria have to betaken cautiously knowing that clinician knowledge and thepatient–clinician relationship or other clinical or patientcircumstances not included in the criteria may play animportant role when making decisions on the top of theappropriateness algorithm.
In conclusion, the results of this study support the valid-ity of newly developed explicit appropriateness criteria forcataract extraction by showing greater benefits among pa-tients who underwent interventions deemed as necessary orappropriate compared with those who underwent proce-dures classified as inappropriate. These results support theuse of these criteria for the development of clinical guide-lines or to determine the degree of appropriateness of cat-aract extraction for individual patients.
References
1. Eye Diseases Prevalence Research Group. Prevalence of cat-aract and pseudophakia/aphakia among adults in the UnitedStates. Arch Ophthalmol 2004;122:487–94.
2. Goldzweig CL, Mittman BS, Carter GM, et al. Variations incataract extraction rates in Medicare prepaid and fee-for-service settings. JAMA 1997;277:1765–8.
3. Kellie SE, Kelly JT. Medicare Peer Review Organizationpreprocedure review criteria: an analysis of criteria for three
ppropriateness Category
Appropriateness
P Value*ppropriate‡ Uncertain§ Inappropriate�
n � 954 n � 795 n � 1213 (7.65)† 69 (8.68) 14 (11.57) 0.0103
0.89410 (19.92) 150 (18.87) 22 (18.18)1 (7.44) 50 (6.29) 8 (6.61)
33 (3.46) 21 (2.64) 4 (3.31) 0.654313 (1.36) 13 (1.64) 0 (0) 0.3335n � 470 n � 296 n � 210
58 (12.34) 30 (10.14) 22 (10.48) 0.72890.8565
93 (19.79) 66 (22.30) 41 (19.52)37 (7.87) 27 (9.12) 19 (9.05)17 (3.62) 12 (4.05) 5 (2.38) 0.779710 (2.13) 2 (0.68) 2 (0.95) 0.3494
ost by not having the information necessary to classify the appropriateness
the appropriateness categories.ering the Bonferroni correction for multiple comparisons, considering an
by A
A
7
197
ere l
ongonsid
procedures. JAMA 1991;265:1265–70.

Quintana et al � Outcomes and Appropriateness
4. Norregaard JC, Schein OD, Anderson GF, et al. Interna-tional variation in ophthalmologic management of patientswith cataracts: results from the International Cataract Sur-gery Outcomes Study. Arch Ophthalmol 1997;115:399 –403.
5. Brook RH, Chassin MR, Fink A, et al. A method for thedetailed assessment of the appropriateness of medical technol-ogies. Int J Technol Assess Health Care 1986;2:53–63.
6. Kahan JP, Park RE, Leape LL, et al. Variations by specialty inphysician ratings of the appropriateness and necessity of in-dications for procedures. Med Care 1996;34:512–23.
7. Tobacman JK, Lee P, Zimmerman B, et al. Assessment ofappropriateness of cataract surgery at ten academic medicalcenters in 1990. Ophthalmology 1996;103:207–15.
8. Lundstrom M, Barry P, Leite E, et al. 1998 European CataractOutcome Study: report from the European Cataract OutcomeStudy Group. J Cataract Refract Surg 2001;27:1176–84.
9. Norregaard JC, Bernth-Petersen P, Alonso J, et al. Visualfunctional outcomes of cataract surgery in the United States,Canada, Denmark, and Spain: report of the International Cat-aract Surgery Outcomes Study. J Cataract Refract Surg 2003;29:2135–42.
10. Steinberg EP, Tielsch JM, Schein OD, et al. National study ofcataract surgery outcomes: variation in 4-month postoperativeoutcomes as reflected in multiple outcome measures. Ophthal-mology 1994;101:1131–40.
11. Jaeschke R, Singer J, Guyatt GH. Measurement of healthstatus: ascertaining the minimal clinically important differ-ence. Control Clin Trials 1989;10:407–15.
12. Quintana JM, Escobar A, Arostegui I. Development of appro-priateness explicit criteria for cataract extraction by phaco-emulsification. BMC Health Serv Res [serial online] 2006;6:23. Available at: http://www.biomedcentral.com/1472-6963/6/23. Accessed July 26, 2008.
13. Kahan JP, Bernstein SJ, Leape LL, et al. Measuring the
necessity of medical procedures. Med Care 1994;32:357–65.Spain.
14. Ware JE Jr, Sherbourne CD. The MOS 36-item short-formhealth survey (SF-36): conceptual framework and item selec-tion. Med Care 1992;30:473–83.
15. Steinberg EP, Tielsch JM, Schein OD, et al. The VF-14: anindex of functional impairment in patients with cataract. ArchOphthalmol 1994;112:630–8.
16. Alonso J, Prieto L, Anto JM. The Spanish version of the SF-36Health Survey (the SF-36 health questionnaire): an instrumentfor measuring clinical results [in Spanish]. Med Clin (Barc)1995;104:771–6.
17. Cassard SD, Patrick DL, Damiano AM, et al. Reproducibility andresponsiveness of the VF-14: an index of functional impairmentin patients with cataracts. Arch Ophthalmol 1995;113:1508–13.
18. Alonso J, Espallargues M, Andersen TF, et al. Internationalapplicability of the VF-14: an index of visual function inpatients with cataracts. Ophthalmology 1997;104:799–807.
19. Hays RD, Woolley JM. The concept of clinically meaningfuldifference in health-related quality-of-life research. Howmeaningful is it? Pharmacoeconomics 2000;18:419–23.
20. Schmitt JS, Di Fabio RP. Reliable change and minimumimportant difference (MID) proportions facilitated group re-sponsiveness comparisons using individual threshold criteria.J Clin Epidemiol 2004;57:1008–18.
21. Wyrwich KW, Tierney WM, Wolinsky FD. Using the stan-dard error of measurement to identify important changes onthe Asthma Quality of Life Questionnaire. Qual Life Res2002;11:1–7.
22. Cleveland WS. Robust locally weighted regression andsmoothing scatterplots. J Am Stat Assoc 1979;74:829–36.
23. Tobacman JK, Zimmerman B, Lee P, et al. Visual acuityfollowing cataract surgeries in relation to preoperative appro-priateness ratings. Med Decis Making 2003;23:122–30.
24. Rosen PN, Kaplan RM, David K. Measuring outcomes ofcataract surgery using the Quality of Well-Being Scale andVF-14 Visual Function Index. J Cataract Refract Surg 2005;
31:369–78.Footnotes and Financial Disclosures
Originally received: February 15, 2008.Final revision: July 2, 2008.Accepted: July 31, 2008.Available online: October 30, 2008. Manuscript no. 2008-218.1 Unidad de Investigación, Hospital Galdakao-Usansolo-CIBER Epidemi-ología y Salud Pública (CIBERESP), Galdakao, Vizcaya, Spain.2 Unidad de Investigación, Hospital de Basurto-CIBER Epidemiología ySalud Pública (CIBERESP), Bilbao, Vizcaya, Spain.3 Fundación Vasca de Innovacion e Investigación Sanitarias-(BIOEF)-CIBER Epidemiología y Salud Pública (CIBERESP), Sondika, Vizcaya,Spain.4 Agencia Lain Entralgo, Madrid, Spain.5 Facultad de Medicina, Universidad de Sevilla, Spain.6 Unidad de Epidemiologia Clinica, Corporacio Parc Tauli, Barcelona,
7 Direccion Territorial de Sanidad, San Sebastián-Donostia, Guipúzcoa,Spain.
A complete listing of the members of the IRYSS-Cataract Group isavailable at http://aaojournal.org.
Financial Disclosure(s):The author(s) have no proprietary or commercial interest in any materialsdiscussed in this article.
Supported in part by the Fondo de Investigación Sanitaria - Instituto deSalud Carlos III, Madrid, Spain (grant nos.: PI03/0550, PI03/0724, PI03/0471, PI03/0828, PI04/1577); the Department of Health of the BasqueCountry, Vitoria, Spain; and the thematic networks (Red IRYSS) of theInstituto de Salud Carlos III, Madrid, Spain (G03/220).
Correspondence:José M. Quintana, MD, Unidad de Investigación, Hospital Galdakao-Usansolo, Barrio Labeaga s/n, 48960 Galdakao, Vizcaya, Spain. E-mail:
[email protected].417

Ophthalmology Volume 116, Number 3, March 2009
Appendix 1
Variables Necessary to Establish a Judgment of Appropriateness
1. Ocular comorbidities to classify the scenario as sim-ple cataract, cataract with diabetic retinopathy, orcataract with other pathologic features influencing theprognosis (glaucoma, myopia without retinopathy,vasculopathies, retinopathies, maculopathies, neurop-athies, amblyopia, corneal opacities, or dystrophia).
2. Preintervention best-corrected visual acuity in the eyewith cataract (�0.1, 0.2–0.4, �0.5).
3. Preintervention best-corrected visual acuity in thecontralateral eye (�0.1, 0.2–0.4, �0.5).
4. Surgical complexity of the cataract extraction: (1) nosurgical complications or minor complexity antici-pated (presence of narrow anterior chamber [cornealamplitude-iris, �2], deep-set eyes, extreme myopiawithout retinal involvement, posterior synechiae, or a
417.e1
small pupil); (2) medium complexity anticipated(pseudoexfoliation with mydriasis �3 mm and with-out subluxation of the crystalline lens, dense cataract,poor pupil dilatation [mydriasis �3 mm, according tothe dilatation guidelines], vitrectomized eye, poor pa-tient cooperation during examination, or the presenceof 2 or more minor factors); or (3) high complexityanticipated (subluxation of the crystalline lens, fibro-sis of the anterior capsule of the crystalline lens,brunescent cataract, posterior polar cataract, or thepresence of 2 or more factors of medium complexity).
5. Laterality of cataract (unilateral or bilateral).6. Anticipated visual acuity after intervention (�0.1,
0.2–0.4, 0.5–0.7, �0.7) for patients with diabeticretinopathy or with other ocular pathologic features.
7. Visual function (no impairment, glare, difficulty withrecreational activities, or difficulty with activities ofdaily living) collected from the patient information bythe physician or by survey.
Quintana et al � Outcomes and Appropriateness
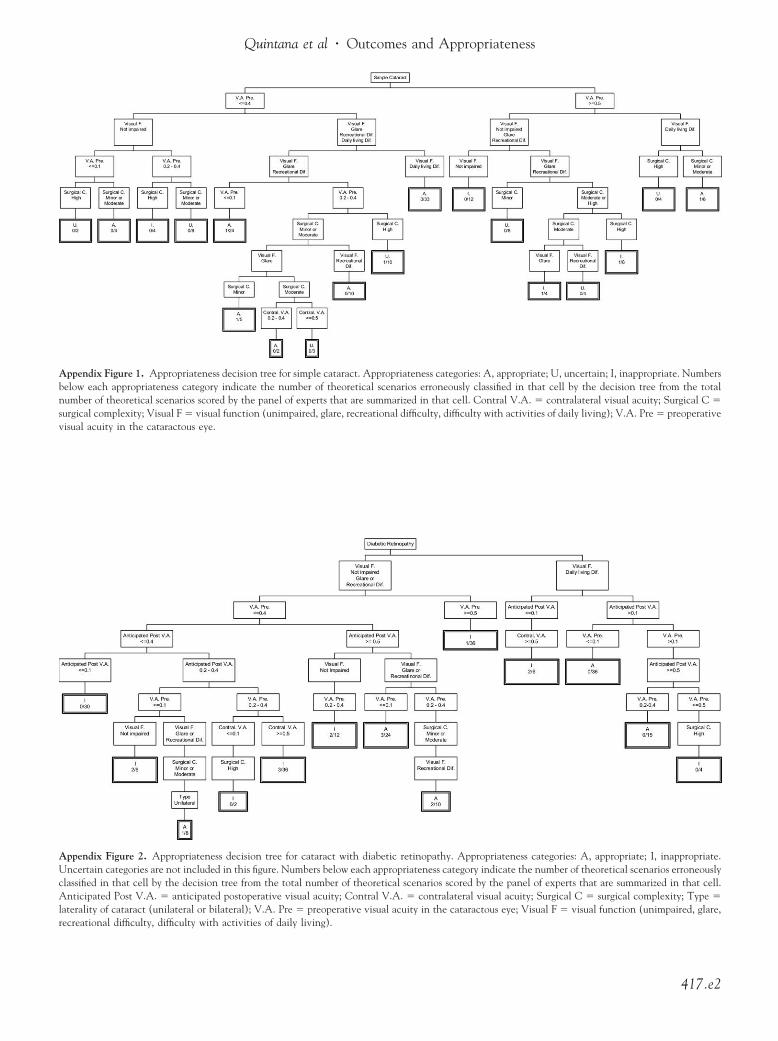
Appendix Figure 1. Appropriateness decision tree for simple cataract. Appropriateness categories: A, appropriate; U, uncertain; I, inappropriate. Numbersbelow each appropriateness category indicate the number of theoretical scenarios erroneously classified in that cell by the decision tree from the totalnumber of theoretical scenarios scored by the panel of experts that are summarized in that cell. Contral V.A. � contralateral visual acuity; Surgical C �surgical complexity; Visual F � visual function (unimpaired, glare, recreational difficulty, difficulty with activities of daily living); V.A. Pre � preoperative
visual acuity in the cataractous eye.Appendix Figure 2. Appropriateness decision tree for cataract with diabetic retinopathy. Appropriateness categories: A, appropriate; I, inappropriate.Uncertain categories are not included in this figure. Numbers below each appropriateness category indicate the number of theoretical scenarios erroneouslyclassified in that cell by the decision tree from the total number of theoretical scenarios scored by the panel of experts that are summarized in that cell.Anticipated Post V.A. � anticipated postoperative visual acuity; Contral V.A. � contralateral visual acuity; Surgical C � surgical complexity; Type �laterality of cataract (unilateral or bilateral); V.A. Pre � preoperative visual acuity in the cataractous eye; Visual F � visual function (unimpaired, glare,
recreational difficulty, difficulty with activities of daily living).417.e2
ith a
Ophthalmology Volume 116, Number 3, March 2009
The IRYSS-Cataract GroupThe IRYSS-Cataract group included the following coinvestigators:Dr Jesús Martínez-Tapias, Dr Eduardo Aguayo (Hospital Univer-sitario Virgen de las Nieves, Granada); Dr. Emilio Perea-Milla(Hospital Costa del Sol-CIBER Epidemiología y Salud Pública(CIBERESP), Málaga); Dr Eduardo Briones (Hospital Universita-rio Virgen de Valme, Sevilla); Dr Gemma Navarro (CorporacióSanitaria Parc Taulí, Sabadell); Dr Elena Andradas, Nerea Fernán-dez de Larrea (Agencia Laín Entralgo, Madrid); Dr InmaculadaArostegui (Departamento de Matemática Aplicada, UPV-CIBER
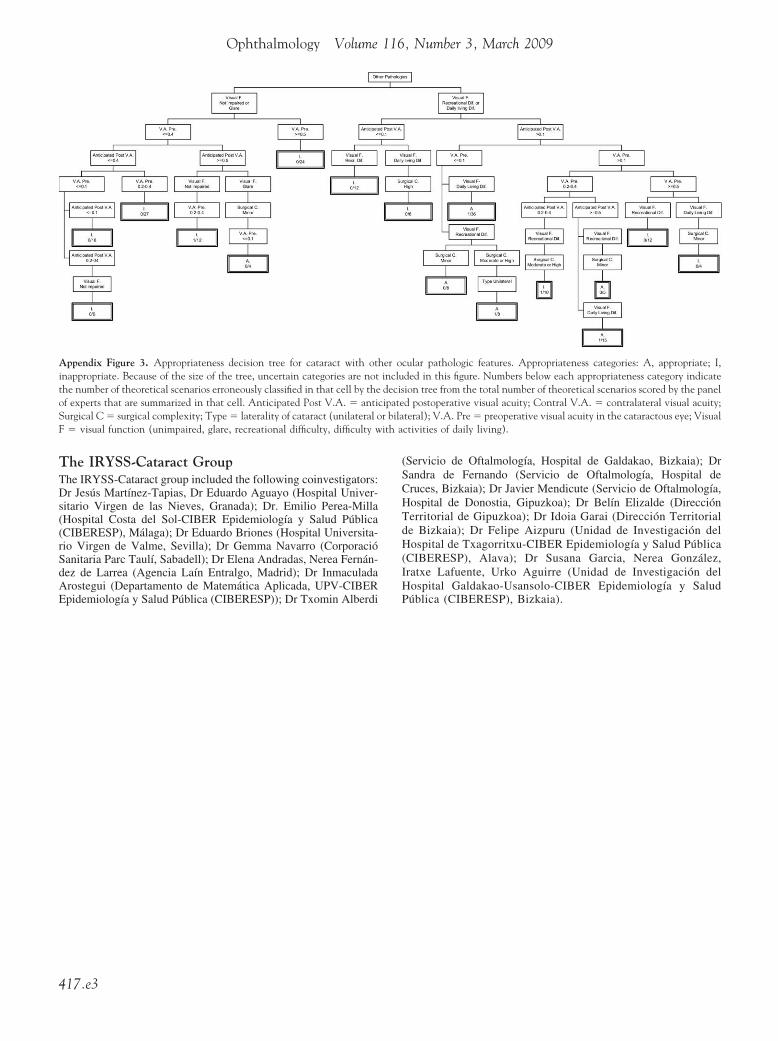
Appendix Figure 3. Appropriateness decision tree for cataract with otinappropriate. Because of the size of the tree, uncertain categories are notthe number of theoretical scenarios erroneously classified in that cell by theof experts that are summarized in that cell. Anticipated Post V.A. � antiSurgical C � surgical complexity; Type � laterality of cataract (unilateral oF � visual function (unimpaired, glare, recreational difficulty, difficulty w
Epidemiología y Salud Pública (CIBERESP)); Dr Txomin Alberdi
417.e3
(Servicio de Oftalmología, Hospital de Galdakao, Bizkaia); DrSandra de Fernando (Servicio de Oftalmología, Hospital deCruces, Bizkaia); Dr Javier Mendicute (Servicio de Oftalmología,Hospital de Donostia, Gipuzkoa); Dr Belín Elizalde (DirecciónTerritorial de Gipuzkoa); Dr Idoia Garai (Dirección Territorialde Bizkaia); Dr Felipe Aizpuru (Unidad de Investigación delHospital de Txagorritxu-CIBER Epidemiología y Salud Pública(CIBERESP), Alava); Dr Susana Garcia, Nerea González,Iratxe Lafuente, Urko Aguirre (Unidad de Investigación delHospital Galdakao-Usansolo-CIBER Epidemiología y Salud
cular pathologic features. Appropriateness categories: A, appropriate; I,ded in this figure. Numbers below each appropriateness category indicateion tree from the total number of theoretical scenarios scored by the paneld postoperative visual acuity; Contral V.A. � contralateral visual acuity;teral); V.A. Pre � preoperative visual acuity in the cataractous eye; Visualctivities of daily living).
her oincludecis
cipater bila
Pública (CIBERESP), Bizkaia).