treatment of unstable distal radius fractures: methods and comparison of external distraction and...
TRANSCRIPT
Treatment of Unstable Distal Radius Fractures:
Methods and Comparison of External Distraction and ORIF
versus External Distraction-ORIF Neutralization
Matthew D. Putnam, MD, Mark D. Fischer, MD, Minneapolis, MN
Twenty-six closed unstable distal radius fractures were treated using a combination of inter- nal fixation, external distraction (intraoperative), and, in some cases, up to 4 weeks of post- operative external fixation (neutralization). Introperative stability check determined the need for external neutralization. This combined technique allowed a comprehensive approach to even the most unstable fracture by merging the advantages of internal and external fixation. Up to 4 weeks of external fixation (neutralization) was not associated with the complications of external fixation usually reported. (J Hand Surg 1997;22A:238-251 ).
The majority of distal radius fractures can be satis- factorily reduced by closed methods. 1,2 The unstable distal radius fracture is indicated by the presence of several properties, including pattern, number of frag- ments, intra-articular extension, and associated soft tissue injury. Unlike periarticular injuries involving many other joints, in which closed treatment is obso- lete, distal radius fractures are commonly treated by closed reduction and other indirect methods of reduction that rely on ligamentotaxis. Laboratory studies have shown ligamentotaxis to be unreliable, however, in reducing unstable distal radius fractures where cortical comminution exists. 3 Although the distal radius is not a weight-beating joint and natural
From the Department of Orthopaedic Surgery, Hand and Microvascu- lar Center, University of Minnesota Hospital and Clinic, Minneapolis, MN.
Received for publication April 22, 1994; accepted in revised form Sept. 13, 1996.
No benefits in any format have been or will be received from a com- mercial party related directly or indirectly to the subject of this article.
Reprint requests: Matthew D. Putnam, MD, Department of Ortho- paedic Surgery, University of Minnesota Hospital, 420 Delaware Street S.E., Minneapolis, MN 55455.
238 The Journal of Hand Surgery
history studies are few, 4 there is evidence to suggest that suboptimal reduction leads to abnormal force transmission through the radiocarpal articulation. 5,6 This has been shown to occur with both alterations in ulnar variance and changes in the angulation in the distal radial articular surface. In addition, intra- articular displacement has been clinically related to the occurrence of degenerative joint disease. 7
The deleterious effects of prolonged immobiliza- tion on intra-articular cartilage and the surrounding soft tissue structures have been well documented both clinically and experimentally. 8,9 For these rea- sons, we believe the optimal treatment for complex distal radius fractures includes external fixation, to faciliatate reduction and in some cases to protect the reduction against the forces of shortening; internal fixation, to accurately restore the anatomy and allow early removal of the external fixator; and early mobi- lization of all joints in the hand and wrist.
The purpose of this paper is to review the results of 26 consecutive unstable distal radius fractures that underwent a defined protocol of external distraction, internal fixation, and early removal of external fixa- tion and mobilization.
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 239
Materials and Methods
Patient Demographics
Twenty-seven patients in a 3-year period were identified and were selected for the open manage- ment of their fracture (as described below). We fol- lowed 26 patients; the average follow-up period was 14 months (range, 6-26 months). The average age was 53 years (range, 36-72 years). There were 16 women and 10 men. Ten of the 26 injuries involved the left side. The dominant hand was involved in 18 of the 26 cases. Five of the patients were heavy labor- ers, 13 were non-manual laborers, 4 were homemak- ers, and 4 were retired. Two patients were involved in workers' compensation claims.
All injuries were closed. There was one associated proximal humerus fracture. No other acute injuries to other structures in the area of the distal radius requiring repair were noted.
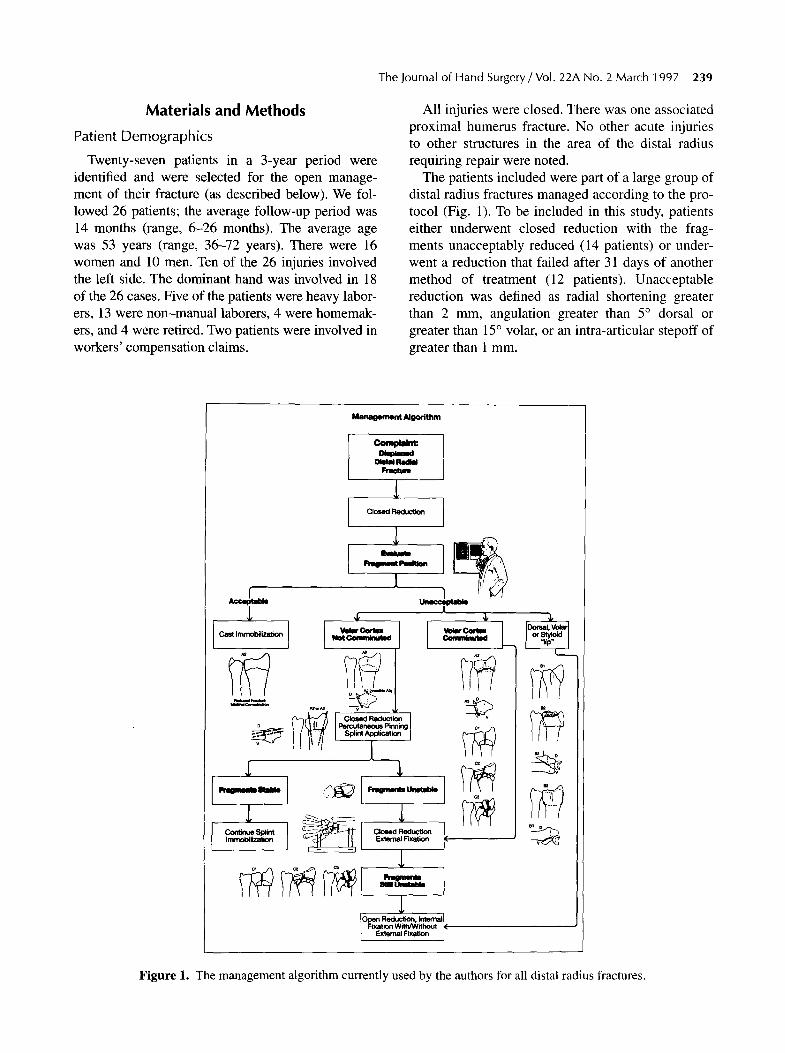
The patients included were part of a large group of distal radius fractures managed according to the pro- tocol (Fig. 1). To be included in this study, patients either underwent closed reduction with the frag- ments unacceptably reduced (14 patients) or under- went a reduction that failed after 31 days of another method of treatment (12 patients). Unacceptable reduction was defined as radial shortening greater than 2 ram, angulation greater than 5 ~ dorsal or greater than 15 ~ volar, or an intra-articular stepoff of greater than 1 ram.
Management Ng~ ' i t hm
m a a l ~
I
o laec~Jtaneous Pinning Spl ~,~0p ication
1
1
YeW r Come~utNI
r I
F ~ e t = e = U e = t ~
Closed Reduction External Fixation
Open Reduction, Internal| I Fixation With/Wit hout ~( L External Fixation j
Figure 1. The management algorithm currently used by the authors for all distal radius fractures.
240 Putnam and Fischer/Distal Radius Fractures--External Fixation
The patients treated in this study were believed not to be candidates for percutaneous pinning and/or external fixation, owing to at least one of the follow- ing factors: excessive cortical communition (all A3, C3), intra-articular malreduction (all B and C groups), fracture geometry, or age of the fracture.
Data were obtained from chart review and exami- nation of patients at least 6 months after the index procedure. Patients were questioned about pain, return to work status, and activities of daily living. Wrist and forearm active range of motion (ROM) were measured using a goniometer. Grip strength was recorded using a Jamar dynomometer (Asinow Engineering, Los Angeles, CA). Injured and unin- jured sides were recorded for all parameters. Results were scored according to the modified clinical scor- ing system of Green and O'Brien 10 and the demerit point system of Gartland and Werley.~
All preoperative, immediate postoperative, and delayed postoperative (at least 6 months) x-rays related to the index procedures were obtained. In
most cases, only posteroanterior (PA) and lateral views were available for each of the three intervals. PA radiographs were done 3 in neutral forearm rota- tion. Preoperative x-rays consisted of views taken before and after closed reduction. No additional radiographic studies were obtained. Fracture classifi- cation according to the AO/ASIF method as well as Frykman's method were used with radiographs taken both before and after reduction.~243 Measurements of the radial inclination, volar tilt, radioulnar variance, and intra-articular stepoff were performed according to methods described below. These were done on both a closed reduction, immediate postoperative and final postoperative radiographs.
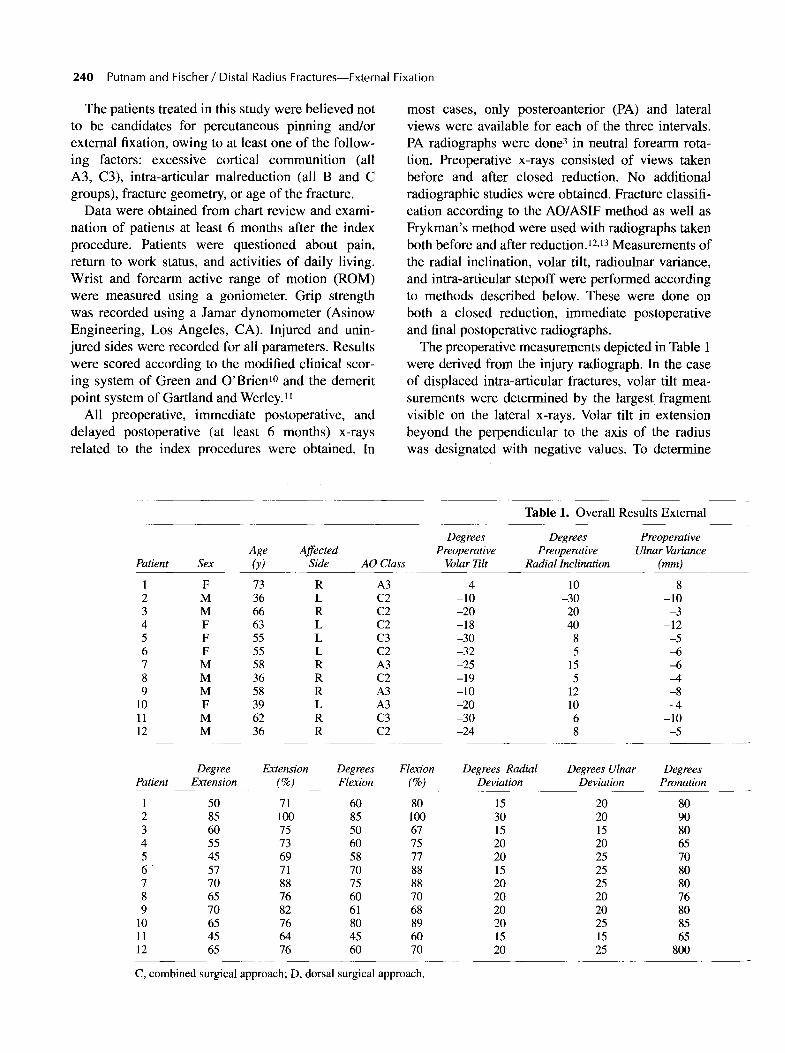
The preoperative measurements depicted in Table 1 were derived from the injury radiograph. In the case of displaced intra-articular fractures, volar tilt mea- surements were determined by the largest fragment visible on the lateral x-rays. Volar tilt in extension beyond the perpendicular to the axis of the radius was designated with negative values. To determine
Age Affected Patient Sex (y) Side AO Class
1 F 73 R A3 2 M 36 L C2 3 M 66 R C2 4 F 63 L C2 5 F 55 L C3 6 F 55 L C2 7 M 58 R A3 8 M 36 R C2 9 M 58 R A3
10 F 39 L A3 11 M 62 R C3 12 M 36 R C2
Tab le 1. Overa l l Resul ts External
Degrees Degrees Preoperative Preoperative Preoperative Ulnar Variance
Volar 771t Radial Inclination (mm)
4 10 -8 -10 -30 -10 -20 20 -3 -18 40 -12 -30 8 -5 -32 5 ~5 -25 15 --6 -19 5 --4 -10 12 -8 -20 10 -4 -30 6 -10 -24 8 -5
Degree Extension Degrees Flexion Paffent Extension (%) Flexion (%)
1 50 71 60 80 2 85 100 85 100 3 60 75 50 67 4 55 73 60 75 5 45 69 58 77 6 57 71 70 88 7 70 88 75 88 8 65 76 60 70 9 70 82 61 68
10 65 76 80 89 11 45 64 45 60 12 65 76 60 70
C, combined surgical approach; D, dorsal surgical approach.
Degrees Radial Degrees Ulnar Degrees Deviation Deviation Pronation
15 20 80 30 20 90 15 15 80 20 20 65 20 25 70 15 25 80 20 25 80 20 20 76 20 20 80 20 25 85 15 15 65 20 25 800
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 241
radial inclination, the tip of the styloid was con- nected by a line to the ulnar corner of the distal radius and intersected with a line perpendicular to the axis of the radius. Ulnar variance was measured according to a method described by Coleman et al. 14 and validated by Styers and Blair.15 The ulna was used to determine the length of the radius using Palmer's method, comparing the preoperative and final radiographs. 16 Radial intra-articular disruption was categorized according to a modification of the classification of Knirk and Jupiter. 7 That original classification is not mutually exclusive; therefore, we made the following modifications: grade 0 is less than or equal to 1-mm articular stepoff; grade I, less than or equal to 2-mm articular stepoff; grade II, less than or equal to 3-mm articular stepoff; and grade III, greater than 3-mm of articular stepoff. Radio- graphic classification using the AO method included 1 (A-2), 6 (A-3), 1 (B-3), 2 (C-I), 13 (C-2), and 3 (C-3). By the Frykman classification, there were 17 grade VIII, 5 grade VII, 3 grade VI, and 1 grade V.
Rating of the intra-articular disruption was done using the above-described system of Knirk and Jupiter with our modification in grading articular stepoff from 0 to 3. Using this classification, there were 19 intra-articular fractures: 6 grade 0, 7 grade I, 1 grade II, and 5 grade III. There were 21 fractures of the ulnar styloid out of 26 injuries.
The mean radial preoperative inclination was 7 ~ (-7~176 The volar tilt on lateral radiographs was an average of -20 ~ (ie, 20 ~ of extension beyond the neutral position with respect to the axis of the radius). The range was -3 ~ to -32 ~ with two volarly inclined fractures (4 ~ and 24 ~ ) not included in this average. Radial shortening resulted in an ulnar plus an average of 6.6 ram, ranging from an ulnar plus an average of 2.0 mm to 12.0 mm.
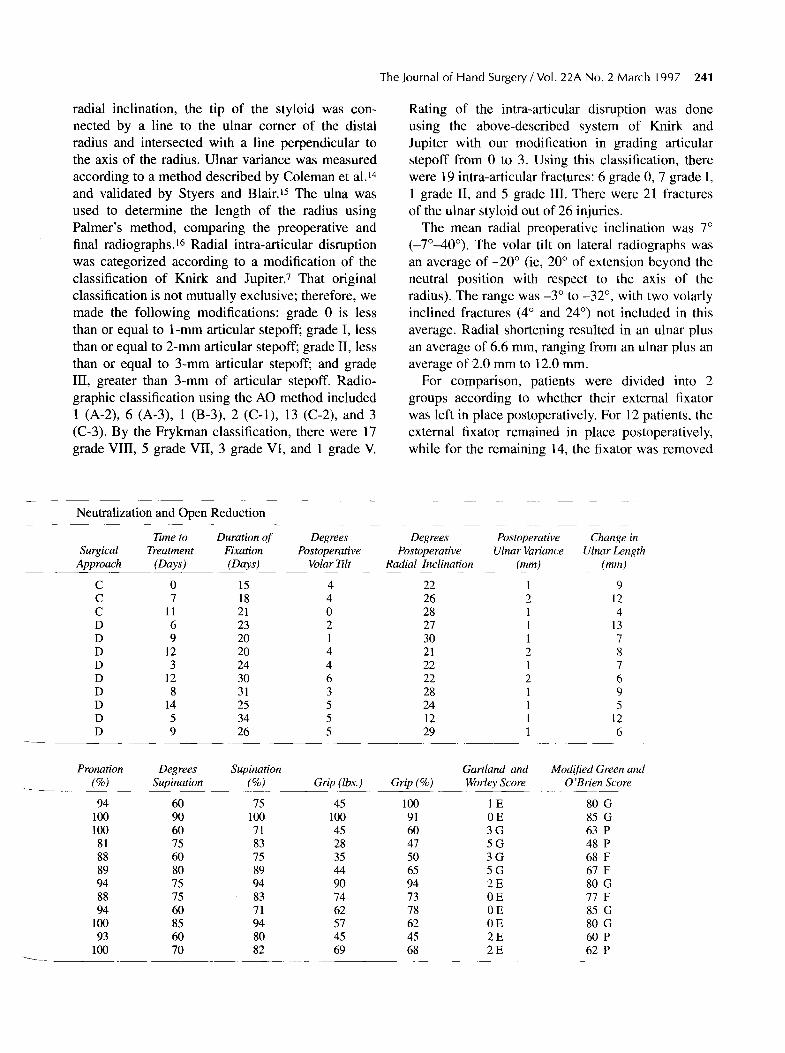
For comparison, patients were divided into 2 groups according to whether their external fixator was left in place postoperatively. For 12 patients, the external fixator remained in place postoperatively, while for the remaining 14, the fixator was removed
Neutralization and Open Reduction
~me ~ Duraffon of Degrees Degrees Postoperanve Change in Surgwal Treatment F i x a n o n Postopera~ve Postoperanve Ulnar Valance Ulnar Leng~
Approach (Days) (Days) Vo~r ~lt Radial Inclination (ram) (mm)
C 0 15 4 22 1 9 C 7 18 4 26 2 12 C 11 21 0 28 1 4 D 6 23 2 27 1 13 D 9 20 1 30 1 7 D 12 20 4 21 2 8 D 3 24 4 22 1 7 D 12 30 6 22 2 6 D 8 31 3 28 1 9 D 14 25 5 24 1 5 D 5 34 5 12 1 12 D 9 26 5 29 1 6
Pronation D e g r e e s Supination Gartland and Modified Green and (%) Supination (%) Grip (Ibs.) Grip (%) Worley Score O'Brien Score
94 60 75 45 100 1 E 80 G 100 90 100 100 91 0 E 85 G 100 60 71 45 60 3 G 63 P 81 75 83 28 47 5 G 48 P 88 60 75 35 50 3 G 68 F 89 80 89 44 65 5 G 67 F 94 75 94 90 94 2 E 80 G 88 75 83 74 73 0 E 77 F 94 60 71 62 78 0 E 85 G
100 85 94 57 62 0 E 80 G 93 60 80 45 45 2 E 60 P
100 70 82 69 68 2 E 62 P
242 Putnam and Fischer/Distal Radius Fractures--External Fixation
prior to conclusion of surgical treatment. All patient interviews, chart reviews, and follow-up postopera- tive measurements, as well as interpretation of the radiographs, were performed by one of us (M. D. F.).
Operative Techniques
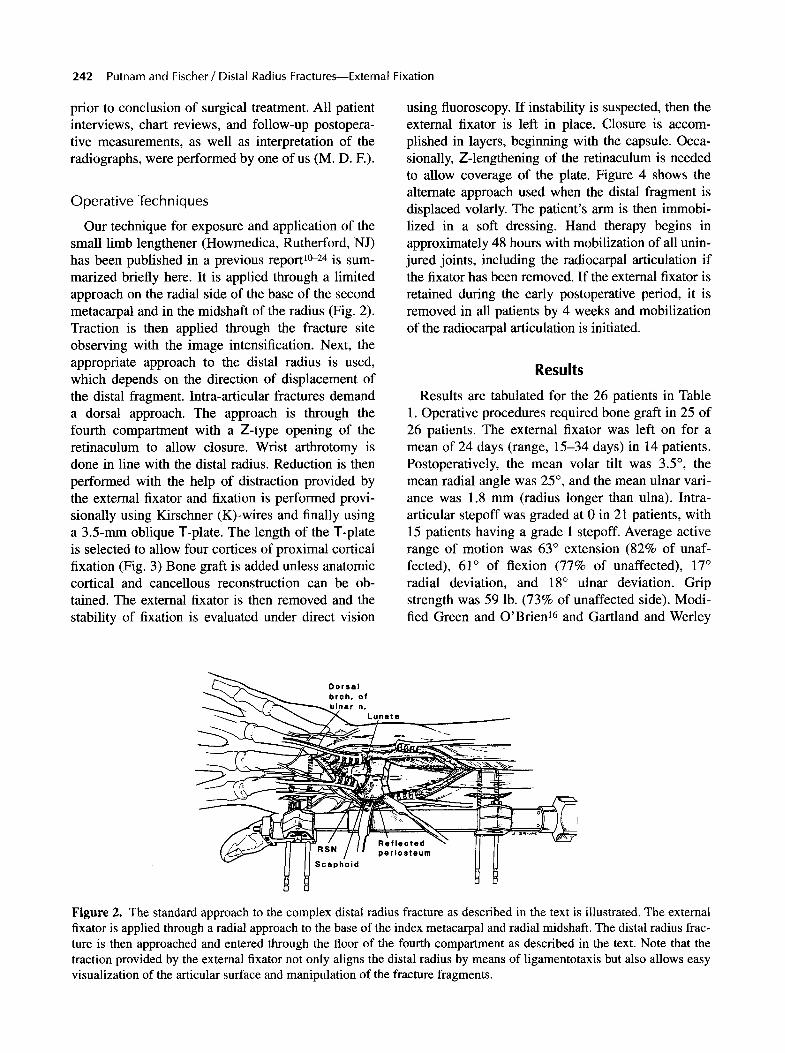
Our technique for exposure and application of the small limb lengthener (Howmedica, Rutherford, NJ) has been published in a previous report 1~ is sum- marized briefly here. It is applied through a limited approach on the radial side of the base of the second metacarpal and in the midshaft of the radius (Fig. 2). Traction is then applied through the fracture site observing with the image intensification. Next, the appropriate approach to the distal radius is used, which depends on the direction of displacement of the distal fragment. Intra-articular fractures demand a dorsal approach. The approach is through the fourth compartment with a Z-type opening of the retinaculum to allow closure. Wrist arthrotomy is done in line with the distal radius. Reduction is then performed with the help of distraction provided by the external fixator and fixation is performed provi- sionally using Kirschner (K)-wires and finally using a 3.5-mm oblique T-plate. The length of the T-plate is selected to allow four cortices of proximal cortical fixation (Fig. 3) Bone graft is added unless anatomic cortical and cancellous reconstruction can be ob- tained. The external fixator is then removed and the stability of fixation is evaluated under direct vision
using fluoroscopy. If instability is suspected, then the external fixator is left in place. Closure is accom- plished in layers, beginning with the capsule. Occa- sionally, Z-lengthening of the retinaculum is needed to allow coverage of the plate. Figure 4 shows the alternate approach used when the distal fragment is displaced volarly. The patient's ann is then immobi- lized in a soft dressing. Hand therapy begins in approximately 48 hours with mobilization of all unin- jured joints, including the radiocarpal articulation if the fixator has been removed. If the external fixator is retained during the early postoperative period, it is removed in all patients by 4 weeks and mobilization of the radiocarpal articulation is initiated.
Results
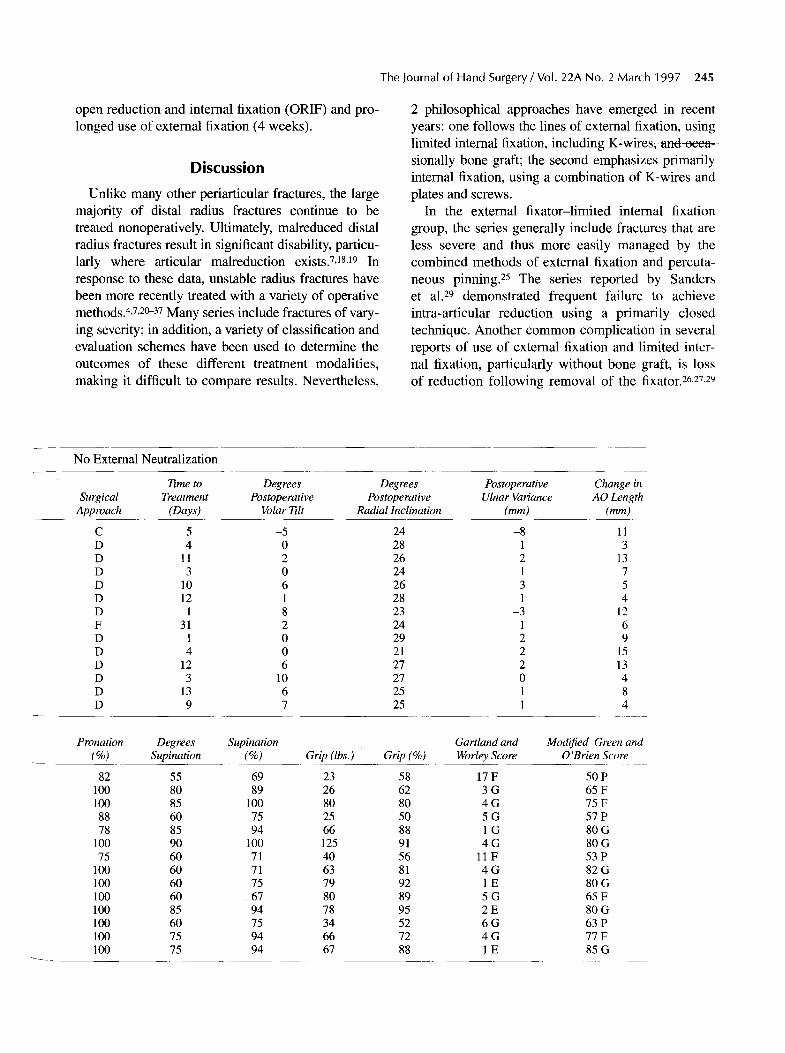
Results are tabulated for the 26 patients in Table 1. Operative procedures required bone graft in 25 of 26 patients. The external fixator was left on for a mean of 24 days (range, 15-34 days) in 14 patients. Postoperatively, the mean volar tilt was 3.5 ~ the mean radial angle was 25 ~ , and the mean ulnar vari- ance was 1.8 mm (radius longer than ulna). Intra- articular stepoff was graded at 0 in 21 patients, with 15 patients having a grade I stepoff. Average active range of motion was 63 ~ extension (82% of unaf- fected), 61 ~ of flexion (77% of unaffected), 17 ~ radial deviation, and 18 ~ ulnar deviation. Grip strength was 59 lb. (73% of unaffected side). Modi- fied Green and O'Brien 16 and Gartland and Werley
Figure 2. The standard approach to the complex distal radius fracture as described in the text is illustrated. The external fixator is applied through a radial approach to the base of the index metacarpal and radial midshafl. The distal radius frac- ture is then approached and entered through the floor of the fourth compartment as described in the text. Note that the traction provided by the extemal fixator not only aligns the distal radius by means of ligamentotaxis but also allows easy visualization of the articular surface and manipulation of the fracture fragments.
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 243
o b
, "-' ~ a. l " ~' ~-'~'
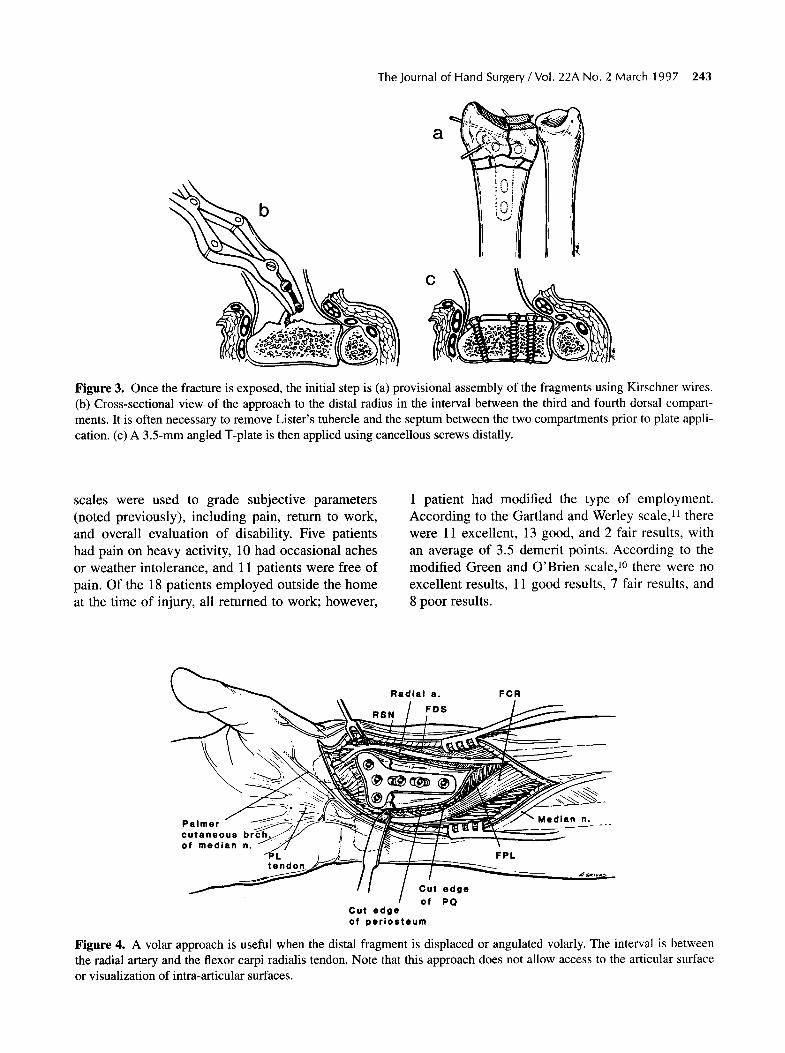
Figure 3. Once the fracture is exposed, the initial step is (a) provisional assembly of the fragments using Kirschner wires. (b) Cross-sectional view of the approach to the distal radius in the interval between the third and fourth dorsal compart- ments. It is often necessary to remove Lister's tubercle and the septum between the two compartments prior to plate appli- cation. (c) A 3.5-mm angled T-plate is then applied using cancellous screws distally.
scales were used to grade subjective parameters (noted previously), including pain, return to work, and overall evaluation of disability. Five patients had pain on heavy activity, 10 had occasional aches or weather intolerance, and 11 patients were free of pain. Of the 18 patients employed outside the home at the time of injury, all returned to work; however,
1 patient had modified the type of employment. According to the Gartland and Werley scale,U there were 11 excellent, 13 good, and 2 fair results, with an average of 3.5 demerit points. According to the modified Green and O'Brien scale, ]~ there were no excellent results, 11 good results, 7 fair results, and 8 poor results.
Radial e . FCR
~ , ~ . . . . .
Palmer
o f m e d i a n n. ~ / / ;~,J_.ll~" l----T---
! Cut edge of PQ Cut edge
of periosteum
Figure 4. A volar approach is useful when the distal fragment is displaced or angulated volarly. The interval is between the radial artery and the flexor carpi radialis tendon. Note that this approach does not allow access to the articular surface or visualization of intra-articular surfaces.
244 Putnam and Fischer/Distal Radius Fractures--External Fixation
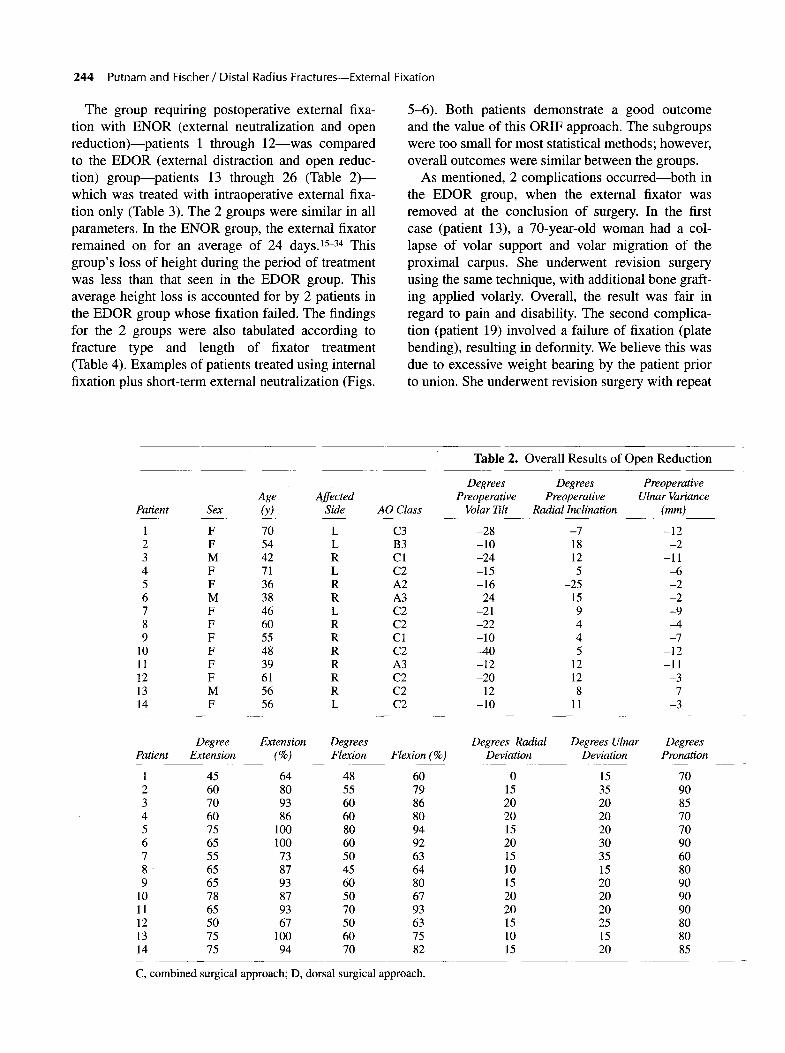
The group requiring postoperative external fixa- tion with ENOR (external neutralization and open reduct ion)--pat ients l through 12---was compared to the EDOR (external distraction and open reduc- tion) group---patients 13 through 26 (Table 2 ) - - which was treated with intraoperative external fixa- tion only (Table 3). The 2 groups were similar in all parameters. In the E N O R group, the external fixator remained on for an average of 24 days. 15-34 This
group 's loss of height during the period of treatment was less than that seen in the E D O R group. This average height loss is accounted for by 2 patients in the EDOR group whose fixation failed. The findings for the 2 groups were also tabulated according to fracture type and length of fixator treatment (Table 4). Examples of patients treated using internal fixation plus short-term external neutralization (Figs.
5-6). Both patients demonstrate a good outcome and the value of this ORIF approach. The subgroups were too small for most statistical methods; however, overall outcomes were similar between the groups.
As mentioned, 2 complications occur red- -bo th in the E D O R group, when the external fixator was removed at the conclusion of surgery. In the first case (patient 13), a 70-year-old woman had a col- lapse of volar support and volar migration of the proximal carpus. She underwent revision surgery using the same technique, with additional bone graft- ing applied volarly. Overall, the result was fair in regard to pain and disability. The second complica- tion (patient 19) involved a failure of fixation (plate bending), resulting in deformity. We believe this was due to excessive weight bearing by the patient prior to union. She underwent revision surgery with repeat
Table 2. Overall Results of Open Reduction
Degrees Degrees Preoperative Age Affected Preoperative Preoperative Ulnar Variance
Patient Sex (y) Side AO Class Volar Ti l t Radial Inclination (ram)
1 F 70 L C3 -28 -7 -12 2 F 54 L B3 -10 18 -2 3 M 42 R C1 -24 12 -11 4 F 71 L C2 -15 5 -6 5 F 36 R A2 -16 -25 -2 6 M 38 R A3 24 15 -2 7 F 46 L C2 -21 9 -9 8 F 60 R C2 -22 4 -4 9 F 55 R C1 -10 4 -7
10 F 48 R C2 -40 5 -12 11 F 39 R A3 -12 12 -11 12 F 61 R C2 -20 12 -3 13 M 56 R C2 -12 8 -7 14 F 56 L C2 -10 11 -3
Degree Extension Degrees Degrees Radial Degrees Ulnar Patient Extension (%) Flexion Flexion (%) Deviation Deviation
1 45 64 48 60 0 15 2 60 80 55 79 15 35 3 70 93 60 86 20 20 4 60 86 60 80 20 20 5 75 100 80 94 15 20 6 65 100 60 92 20 30 7 55 73 50 63 15 35 8 65 87 45 64 10 15 9 65 93 60 80 15 20
10 78 87 50 67 20 20 11 65 93 70 93 20 20 12 50 67 50 63 15 25 13 75 100 60 75 10 15 14 75 94 70 82 15 20
Degrees Pronation
70 90 85 70 70 90 60 80 90 90 90 80 80 85
C, combined surgical approach; D, dorsal surgical approach.
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 245
open reduction and internal fixation (ORIF) and pro- longed use of external fixation (4 weeks).
Discussion
Unlike many other periarticular fractures, the large majority of distal radius fractures continue to be treated nonoperatively. Ultimately, malreduced distal radius fractures result in significant disability, particu- larly where articular malreduction exists. 7,18,19 In response to these data, unstable radius fractures have been more recently treated with a variety of operative methods. 4,7,20-37 Many series include fractures of vary- ing severity; in addition, a variety of classification and evaluation schemes have been used to determine the outcomes of these different treatment modalities, making it difficult to compare results. Nevertheless,
2 philosophical approaches have emerged in recent years: one follows the lines of external fixation, using limited internal fixation, including K-wires, and occa- sionally bone graft; the second emphasizes primarily internal fixation, using a combination of K-wires and plates and screws.
In the external fixator-limited internal fixation group, the series generally include fractures that are less severe and thus more easily managed by the combined methods of external fixation and percuta- neous pinning. 25 The series reported by Sanders et al. 29 demonstrated frequent failure to achieve intra-articular reduction using a primarily closed technique. Another common complication in several reports of use of external fixation and limited inter- nal fixation, particularly without bone graft, is loss of reduction following removal of the fixator. 26,27,29
f
No Exte rna l Neu t r a l i za t ion
Time to Degrees Degrees Postoperative Change in Surgical T r e a t m e n t P o s t o p e r a t i v e Postoperative Ulnar Variance AO Length
Approach (Days) Volar 7qlt Radial Inclination (mm) (mm)
C 5 -5 24 -8 11 D 4 0 28 1 3 D 11 2 26 2 13 D 3 0 24 1 7 D 10 6 26 3 5 D 12 1 28 1 4 D 1 8 23 -3 12 F 31 2 24 1 6 D 1 0 29 2 9 D 4 0 21 2 15 D 12 6 27 2 13 D 3 10 27 0 4 D 13 6 25 1 8 D 9 7 25 1 4
Pronafion D e g r e e s Supination Ga~landand (%) Supinafion (%) Grip(~s.) Grip(%) WorleyScore
82 55 69 23 58 17 F 100 80 89 26 62 3 G 100 85 100 80 80 4 G
88 60 75 25 50 5 G 78 85 94 66 88 1 G
100 90 100 125 91 4 G 75 60 71 40 56 11F
100 60 71 63 81 4 G 100 60 75 79 92 1 E 100 60 67 80 89 5 G 100 85 94 78 95 2 E 100 60 75 34 52 6 G 100 75 94 66 72 4 G 100 75 94 67 88 1 E
Modified Green and O'Brien Score
50 P 65 F 75 F 57 P 80 G 80 G 53 P 82 G 80 G 65 F 80 G 63 P 77 F 85 G
246 Putnam and Fischer / Distal Radius Fractures--External Fixation
Finally, where relatively long periods of external fix- ation are required, there are relatively high rates of pin track problems, including superficial infection and radial sensory nerve irritation. Four of the exter- nal fixator series report at least one sympathetic dys- trophy, and 1 study documented 5 cases. 2~176
Several papers report internal fixation, using a combinat ion of pins with 3 .5-mm plates and screws. 31-37 Excellent outcomes were reported in
terms of grip strength (70%-80%) as well as ROM (70%-80%) of the opposite side. Two of the series 35,37 include a number of fractures of lesser
severity that are therefore more amenable to less rigid fixation (K-wires). The 2 series most similar to ours in terms of average morbidi ty 31,36 report
slightly better results in grip strength, although pain results were not significantly different. Series using
less rigid fixation 35,37 report loss of reduction in sig- nificant numbers during the treatment period.
When our series was broken down into fracture type (Table 3), the fracture outcomes in terms of mean functional ratings (Green and O'Brien/Gart - land and Werley) decreased as fracture complexi ty increased as described by the AO classification.
The fracture type did not specifically predict the need for external fixation. In fact, the fracture types were near equally divided (by number and type) between external neutralization and external fixation (intraoperative only) and the outcomes were similar.
What was used to gauge the need for external fix- ation postoperatively in this series was our intraoper- ative evaluation of whether internal fixation had achieved adequate fracture stabilization using fluo- roscopy. This was accurate in all but 2 cases (the 2
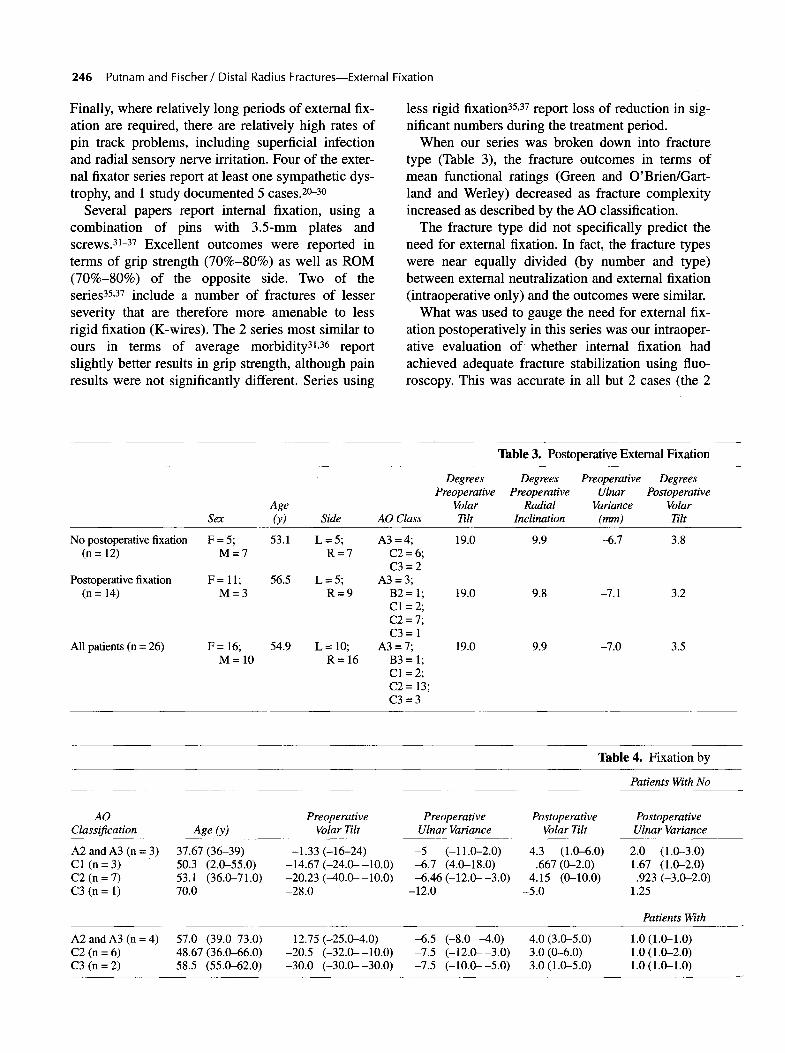
Table 3. Postoperative External Fixation
Degrees Degrees Preoperative Degrees Preoperative Preoperative Ulnar Postoperative
Age Volar Radial Variance Volar Sex (y) Side AO Class Tilt Inclination (mm) Tilt
F=5; 53.1 L=5; A3=4; 19.0 9.9 -6.7 3.8 M=7 R=7 C2=6;
C3=2 56.5 L = 5; A3 = 3;
R=9 B2= 1; 19.0 9.8 -7.1 3.2 C1 = 2; C2 = 7; C3= 1
54.9 L = 10; A3 = 7; 19.0 9.9 -7.0 3.5 R=16 B3=l;
C1 = 2; C2 = 13; C3=3
No postoperative fixation (n = 12)
Postoperative fixation F = 11; (n = 14) M = 3
All patients (n = 26) F = 16; M= 10
Table 4. Fixation by
Patients With No
AO Preoperative Preoperative Postoperative Postoperative Classification Age (y) Volar Tilt Ulnar Variance Volar Tilt Ulnar Variance
A2 andA3 (n = 3) 37.67 (36-39) -1.33 (-16-24) -5 (-11.0-2.0) 4.3 (1.0-6.0) 2.0 (1.0-3.0) C1 (n = 3) 50.3 (2.0-55.0) -14.67 (-24.0--10.0) -6.7 (4.0-18.0) .667 (0-2.0) 1.67 (1.0-2.0) C2 (n = 7) 53.1 (36.0-71.0) -20.23 (-40.0--10.0) -6.46 (-12.0--3.0) 4.15 (0-10.0) .923 (-3.0-2.0) C3 (n = l) 70.0 -28.0 -12.0 -5.0 1.25
Patients With
A2 and A3 (n = 4) 57.0 (39.0-73.0) -12.75 (-25.0---4.0) -6.5 (-8.0--4.0) 4.0 (3.0-5.0) 1.0 (1.0-1.0) C2 (n = 6) 48.67 (36.0--66.0) -20.5 (-32.0--10.0) -7.5 (-12.0--3.0) 3.0 (0-6.0) 1.0 (1.0-2.0) C3 (n = 2) 58.5 (55.0--62.0) -30.0 (-30.0--30.0) -7.5 (-10.0--5.0) 3.0 (1.0-5.0) 1.0 (1.0-1.0)
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 247
fixation failures). The fact that the outcomes for the 2 groups (intraoperative and postoperative external fixation) were similar implies that 4 weeks of post- operative external fixation added little if any morbid- ity to the overall treatment and therefore can be used with confidence when necessary.
Finally, because our outcomes are similar to those for arguably more stable fractures where limited internal or external fixation were used, it is implied that the extensile approach did not compromise over- all outcome.
We believe that this series reports a versatile technique that is capable of managing the most severe fractures in a systematic manner. The consis- tent use of bone graft as well as plates and screws in these fractures minimizes the chance of loss of reduction. In the more extreme cases, the use of an
external fixator for up to 4 weeks provides addi- tional stability. The additional support provided with rigid internal fixation allows removal of exter- nal fixation no later than 4 weeks, minimizing the possibility of pin-related problems related to over- distraction. In our opinion, fixator problems are minimized by making a direct exposure to bone prior to pin placement. 10
Clearly, the limitations in this study are similar to those faced by other surgeons. There are no clear objective means by which to identify those fractures that can be managed by less invasive techniques, such as external fixation and/or percutaneous pin- ning. Nor are there absolute indications, in our expe- rience, as to which fractures might need additional support with external fixation, along with open reduction and bone grafting.
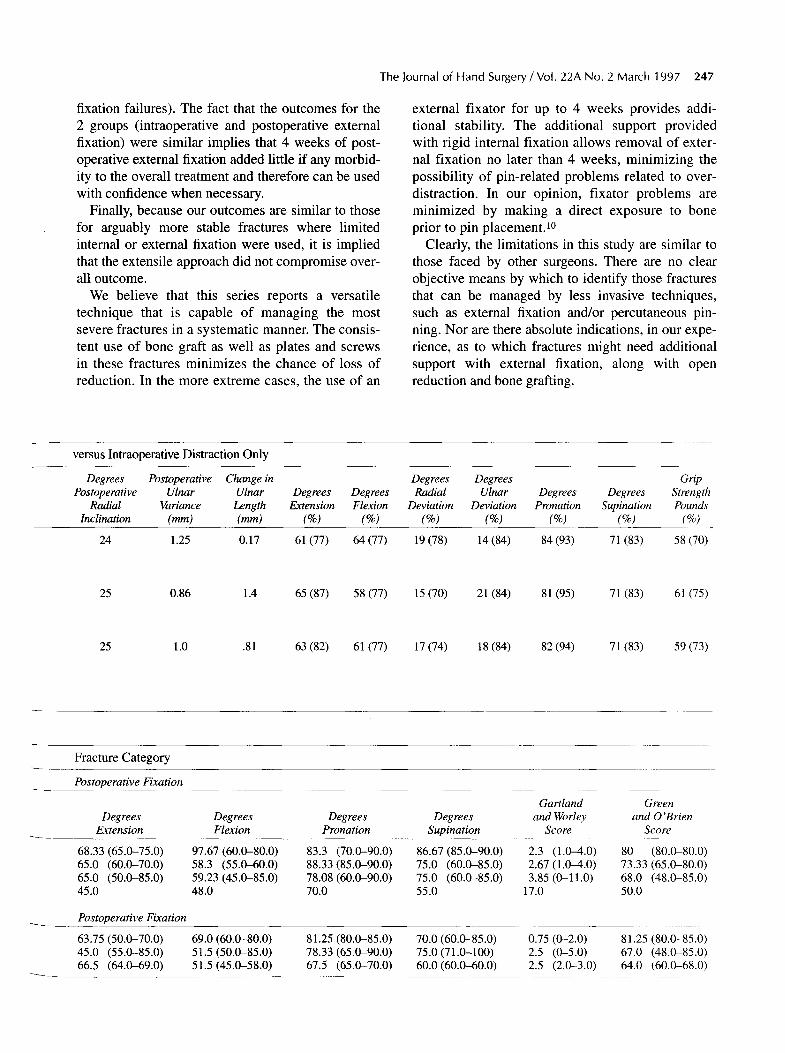
versus Intraoperative Distraction Only
Degrees Postoperative Change in Degrees Degrees Grip Postoperative Ulnar Ulnar Degrees Degrees Radial Ulnar D e g r e e s D e g r e e s Strength
Radial Variance Length Extension Flexion Deviation Deviation Pronation Supination Pounds Inclination (mm) (ram) (%) (%) (%) (%) (%) (%) (%)
24 1.25 0.17 61 (77) 64 (77) 19 (78) 14 (84) 84 (93) 71 (83) 58 (70)
25 0.86 1.4 65 (87) 58 (77) 15 (70) 21 (84) 81 (95) 71 (83) 61 (75)
25 1.0 .81 63 (82) 61 (77) 17 (74) 18 (84) 82 (94) 71 (83) 59 (73)
Fracture Category
Postoperative Fixation
Gartland Green Degrees Degrees Degrees Degrees and Worley and 0 'Brien
Extension Flexion Pronation Supination Score Score
68.33 (65.0-75.0) 97.67 (60.0-80.0) 83.3 (70.0-90.0) 86.67 (85.0-90.0) 2.3 (1.0--4.0) 80 (80.0-80.0) 65.0 (60.0-70.0) 58.3 (55.0--60.0) 88.33 (85.0-90.0) 75.0 (60.0-85.0) 2.67 (1.0--4.0) 73.33 (65.0-80.0) 65.0 (50.0-85.0) 59.23 (45.0-85.0) 78.08 (60.0-90.0) 75.0 (60.0-85.0) 3.85 (0-11.0) 68.0 (48.0-85.0) 45.0 48.0 70.0 55.0 17.0 50.0
Postoperative Fixation
63.75 (50.0-70.0) 69.0 (60.0-80.0) 81.25 (80.0-85.0) 70.0 (60.0-85.0) 0.75 (0-2.0) 81.25 (80.0-85.0) 45.0 (55.0-85.0) 51.5(50.0-85.0) 78.33(65.0-90.0) 75.0(71.0-100) 2.5 (0-5.0) 67.0 (48.0-85.0) 66.5 (64.0--69.0) 51.5(45.0-58.0) 67.5 (65.0-70.0) 60.0(60.0-60.0) 2.5 (2.0-3.0) 64.0 (60.0-68.0)
248 Putnam and Fischer/Distal Radius Fractures--External Fixation
A B C D
E F
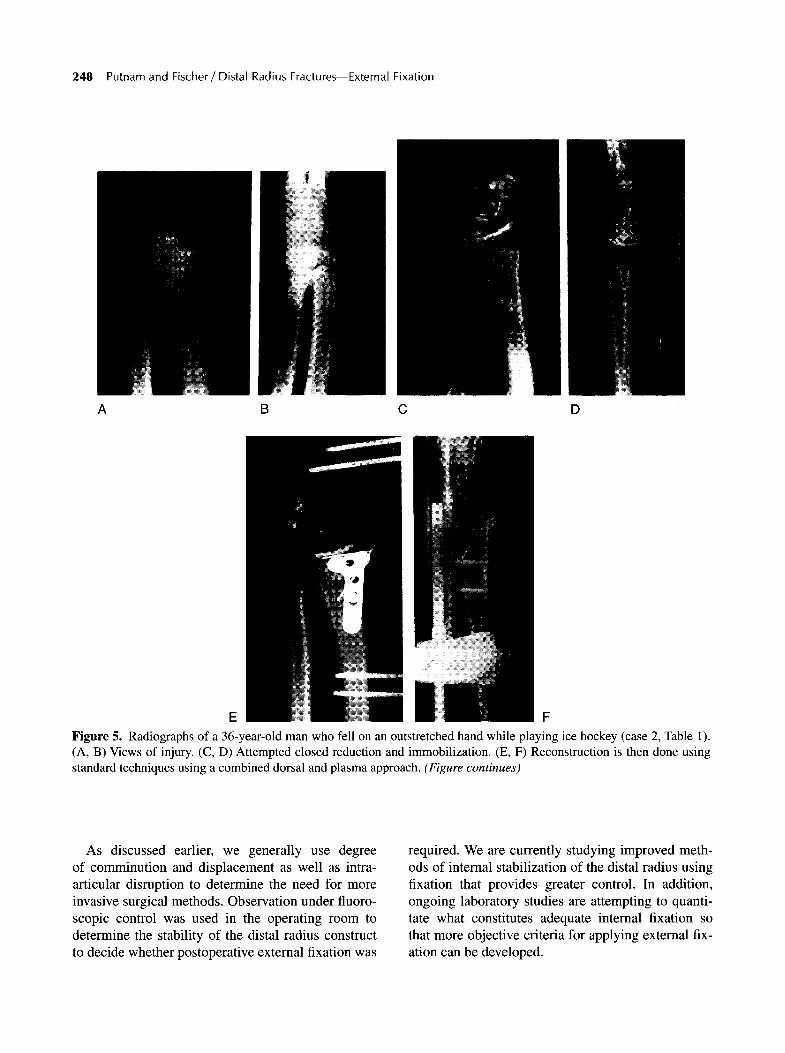
Figure 5. Radiographs of a 36-year-old man who fell on an outstretched hand while playing ice hockey (case 2, Table 1). (A, B) Views of injury. (C, D) Attempted closed reduction and immobilization. (E, F) Reconstruction is then done using standard techniques using a combined dorsal and plasma approach. (Figure continues)
As discussed earlier, we generally use degree of comminution and displacement as well as intra- articular disruption to determine the need for more invasive surgical methods. Observation under fluoro- scopic control was used in the operating room to determine the stability of the distal radius construct to decide whether postoperative external fixation was
required. We are currently studying improved meth- ods of internal stabilization of the distal radius using fixation that provides greater control. In addition, ongoing laboratory studies are attempting to quanti- tate what constitutes adequate internal fixation so that more objective criteria for applying external fix- ation can be developed.
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 249
G H I
K L
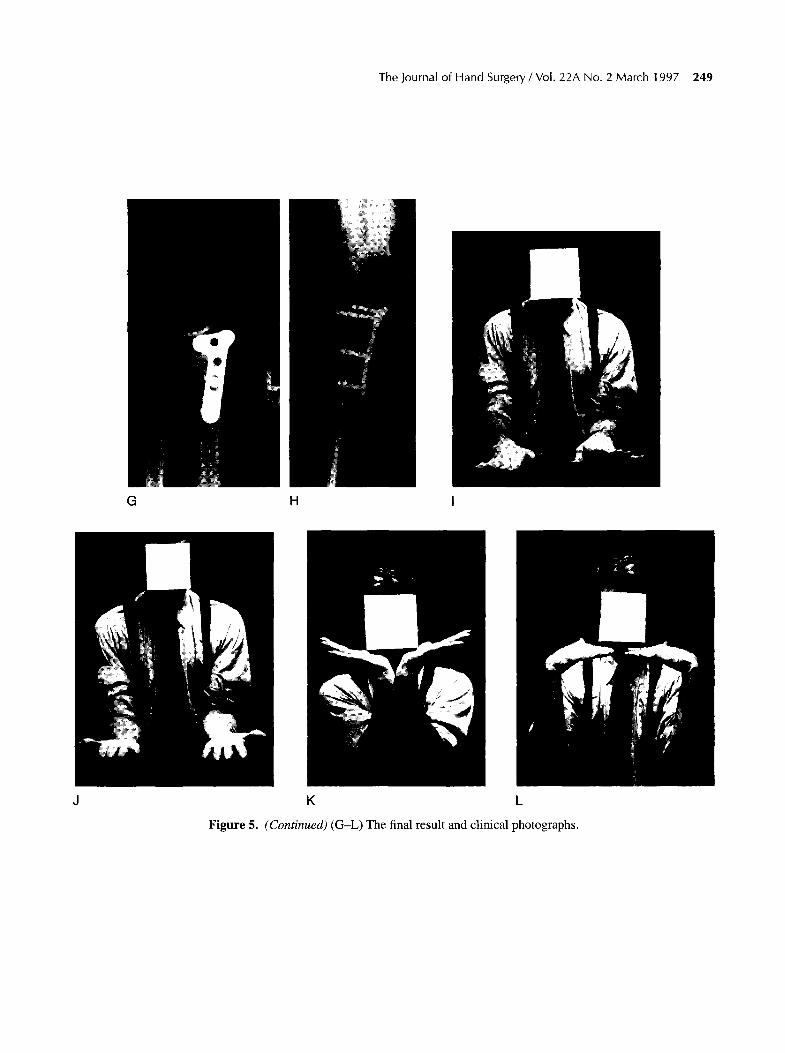
Figure 5. (Continued) (G-L) The final result and clinical photographs.
250 Putnam and Fischer/Distal Radius Fractures--External Fixation
A B
D . E F
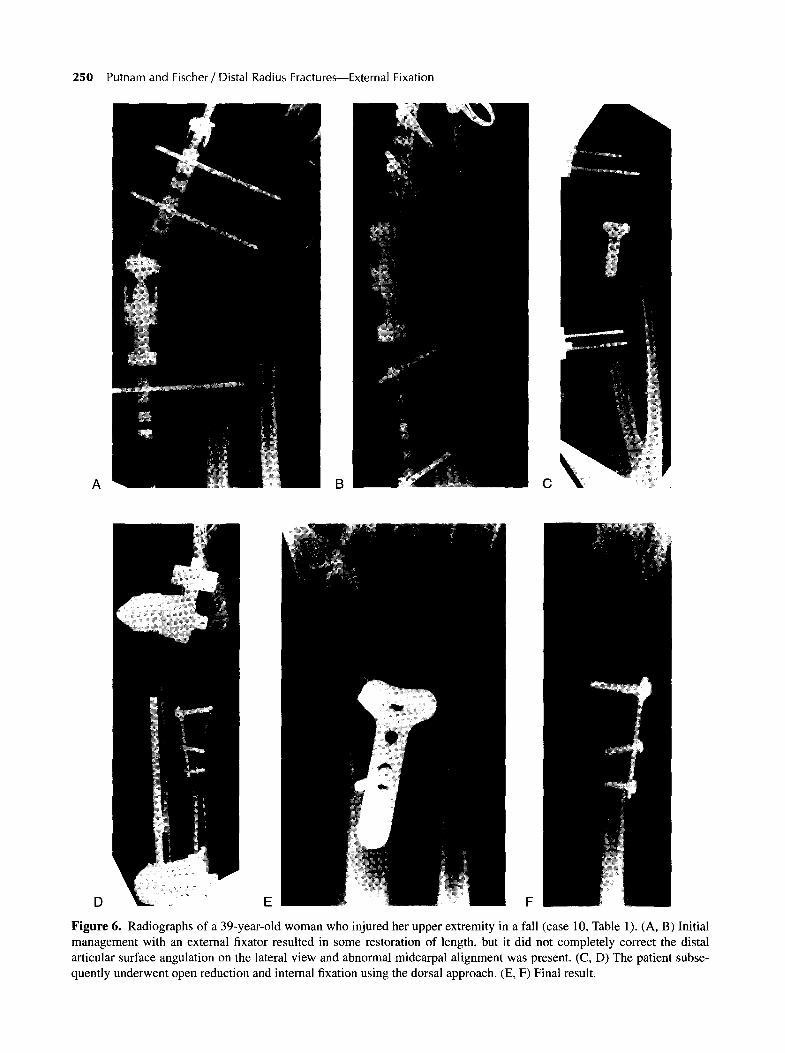
Figure 6. Radiographs of a 39-year-old woman who injured her upper extremity in a fall (case 10, Table 1). (A, B) Initial management with an external fixator resulted in some restoration of length, but it did not completely correct the distal articular surface angulation on the lateral view and abnormal midcarpal alignment was present. (C, D) The patient subse- quently underwent open reduction and internal fixation using the dorsal approach. (E, F) Final result.
The Journal of Hand Surgery / Vol. 22A No. 2 March 1997 251
References
1. Falch JA. Epidemiology of fractures of the distal forearm in Oslo, Norway. Acta Orthop Scand 1983;54:291-301.
2. Lee LW, Putnam MD. Unstable fractures of the distal radius: an algorithmic method of treatment. Orthop Trans 1988;12:357-541.
3. Bartosh RA, Saldana MI. Intra-articular fractures of the distal radius: a cadaveric study to determine if ligamento- taxis restores radiopalmar tilt. J Hand Surg 1990;15A: 18-23.
4. Parisien S. Settling in Colles fracture: a review of the liter- ature. Bull Hosp Joint Dis 1973;34:117-123.
5. Pogue DJ, Viegas SF, Patterson RM et al. Effects of distal radius fracture malunion on wrist joint mechanics. J Hand Surg 1990;15A:721-728.
6. Short WH, Palmer AK, Werner FW et al. The biomechani- cal study of distal radial fractures. J Hand Surg 1987; 12A:529-532.
7. Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg 1986; 68A:647-653.
8. Dias JJ, Wray CC, Jones JM, Gregg PH. The value of early mobilization in the treatment of Colles fractures. J Bone Joint Surg 1987;69B:463-467.
9. van Royen BJ, O'Driscoll SW, Dhert WJ, Salter RB. A comparison of the effects of immobilization and continu- ous passive motion on surgical wound healing in mature rabbits. Plast Reconstr Surg 1986;78:360-368.
10. Green DP, O'Brien ET. Open reduction of carpal disloca- tions indications and operative techniques. J Hand Surg 1978;3A:250-265.
11. Gartland JJ, Werley CW. Evaluation of healed Colles frac- tures. J Bone Joint Surg 1951;33A:895-899.
12. Mueller ME, Nazarian S, Koch P. Classification A t der fracturen. Berlin: Springer-Verlag, 1987:10-40.
13. Frykman G. Fracture of the distal radius including seque- lae: shoulder-hand-finger syndrome disturbance in the dis- tal radio-ulnar joint and impairment of nerve function. Acta Orthop Scand 1967;108(suppl.):23-30.
14. Coleman DA, Blair WF, Shurr D. Resection of the radial head for fracture of the radial head, J Bone Joint Surg 1987;69A:385-392.
15. Steyers CM, Blair WF. Measuring ulnar variance a com- parison of techniques. J Hand Surg 1989;14A:607-612.
16. Epner RA, Bowers WH, Guilford WB. Ulnar variance: the effect of wrist positioning and roentgen filming technique. J Hand Surg 1982;7A:298-305.
17. Putnam MD, Seitz WH. Advances in fracture management in the hand and distal radius. Hand Clin 1989;5:455--470.
18. Sarmiento A, Pratt GH, Berry NC, Sinclair WF. Colles fractures functional bracing in supination. J Bone Joint Surg 1975;57A:311-320.
19. Cooney WP, Dobyns JH, Linscheid RL. Complications of Colles fractures. J Bone Joint Surgery 1980;62A:613-618.
20. Weber SC, Szabo RM: Severely comminuted distal radius fracture as an unsolved problem: complications associated with external fixation and pins and plaster techniques. J Hand Surg 1986;11A: 157-161.
21. Clyburn TA. Dynamic extertnal fixation for comminuted intra-articular fractures of the distal end of the radius. J Bone Joint Surg 1987;69A:248-253.
22. Cooney WE External fixation of distal radius fractures. Clin Orthop 1983;180:44-50.
23. Schwind F, Donkerwoicke M, Rosquin C, Burney E Exter- nal fixation of fractures of the distal radius: a study of 225 cases. J Hand Surg 1989;14A:404-409.
24. Seitz WH, Putnam MD, Dick HM. Limited open surgical approach for external fixation of distal radius fractures. J Hand Surg 1990;15A:288-293.
25. McQueen MM, Michie M, Court-Brown CM: Hand and wrist function after external fixation of unstable distal radial fractures. Clin Orthop 1992;285:200--204.
26. Leung KS, Shen WY, Tsang HK. An effective treatment of comminuted fractures of the distal radius. J Hand Surg 1990;15A:11-17.
27. Sommerkamp TG, Suman M, Sillman J. Dynamic external fixation of unstable fractures of the distal part of the radius. J Bone Joint Surg 1994;76A: 1149-1165.
28. Seitz WH, Froimson AV, Leb R et al. Augmented external fixation of unstable distal radius fractures. J Hand Surg 1991;16A:1010--1016,
29. Sanders RA, Keppel FL, Waldrop JI. External fixation of distal radius fractures: results and complications. J Hand Surg 1991;16A:385-391.
30. Kaempfke FA, Wheeler DR, Peimer CA et al. Severe frac- ture of the distal radius: effect of amount and duration of external fixator distraction on outcome. J Hand Surg 1990; 15A: 11-16.
31. Axelrod T, Paley D, Green J, McMurtry RY. Limited open reduction of the lunate facet in comminuted intra-articular fractures of the distal radius. J Hand Surg 1988;13A: 372-377.
32. Bradway JK, Amadio PC, Cooney WP. Open reduction and internal fixation of displaced, comminuted intra-artic- ular fractures of the distal end of the radius. J Bone Joint Surg 1989;71A:839-845.
33. Clancy GJ. Percutaneous Kirschner wire fixation of Colles fractures. J Bone Joint Surg 1984;66A: 1008-1113.
34. Melone CP. Articular fractures of the distal radius. Orthop Clin North Am 1984;15:217-230.
35. Hastings H, Leibovic SJ. Indications and techniques of open reduction internal fixation of distal radius fractures. Orthop Clin North Am 1993;24:309-326.
36. Jupiter JB, Lipton H, The operative treatment of intraartic- ular fractures of the distal radius. Clin Orthop 1993;292: 48-61.
37. Keating JF, Court-Brown CM, McQueen MM. Internal fix- ation of volar-displaced distal radial fractures. J Bone Joint Surg 1994;76B:401-405.