sustained efficacy of virtual reality distraction
TRANSCRIPT
Sustained Efficacy of Virtual Reality Distraction
Charles E. Rutter1,2, Lynnda M. Dahlquist1, and Karen E. Weiss1
1Department of Psychology; University of Maryland, Baltimore County2University of Maryland, School of Medicine
AbstractThe current study tested whether the effectiveness of distraction using virtual reality (VR)technology in reducing cold pressor pain would maintain over the course of eight weeklyexposures. Twenty-eight adults, 18 to 23 years of age, underwent one baseline cold pressor trialand one VR distraction trial in randomized order each week. VR distraction led to significantincreases in pain threshold and pain tolerance, and significant decreases in pain intensity, timespent thinking about pain, and self-reported anxiety, relative to baseline. Repeated exposure didnot appear to affect the benefits of VR. Implications for the long-term use of VR distraction as anon-pharmacological analgesic are discussed.
KeywordsDistraction; Virtual Reality; Habituation; Pain
IntroductionThe use of Virtual Reality (VR) technology to enhance distraction is a relatively newapproach to acute pain management. Although definitions of VR distraction in the literaturevary considerably, most VR interventions involve a human-computer interface in which theuser interacts with a responsive, multi-sensory virtual environment. VR applicationstypically utilize a head-mounted wide-angle display and headphones to present the virtualenvironment. The user interacts with the virtual environment by manipulating a joystick ormouse, or via head- or hand-motion-sensitive tracking devices, resulting in a sense of beingmore or less “present” in the virtual environment17,19. VR distraction is presumed to affectpain perception by competing for finite attentional resources and by blocking externalstimulation associated with the real environment and the painful stimulus20.
In their 2005 review, Wismeijer and Vingerhoots identified 10 studies of VR distraction foranalgesia involving a total of 108 participants. Although they documented encouraginganalgesic effects for VR distraction for a wide range of medical procedures and laboratorypain, the findings were limited by the small samples (6 of the studies were case studies; twoinvolved 7–12 subjects) and methodological weaknesses20. More recent, larger scale studies
© 2011 The American Pain Society. Published by Elsevier Inc. All rights reservedPlease direct correspondence to Lynnda M. Dahlquist, Ph.D. Department of Psychology University of Maryland, Baltimore County1000 Hilltop Circle Baltimore, MD 21250 Phone: (410) 455 - 2411 Fax: (410) 455 - 1055 [email protected]'s Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to ourcustomers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review ofthe resulting proof before it is published in its final citable form. Please note that during the production process errors may bediscovered which could affect the content, and all legal disclaimers that apply to the journal pertain.The authors are not aware of any potential conflicts of interest.
NIH Public AccessAuthor ManuscriptJ Pain. Author manuscript; available in PMC 2011 July 20.
Published in final edited form as:J Pain. 2009 April ; 10(4): 391–397. doi:10.1016/j.jpain.2008.09.016.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

provide additional support for the effectiveness of VR analgesia for cold pressor pain inchildren3 and burn patients ages 9–4012.
Despite evidence of the efficacy of VR- distraction, uncertainty about the real-world valueof VR distraction remains due to the concern that the distractive properties of VR conferringit such success may attenuate with repeated exposure. Because distraction interventions arethought to work by competing for attention otherwise directed towards the painful stimulus,the analgesic effect observed may diminish with repeated exposure as the novelty of the VRdecreases10,15. Infants, for example, will show a decrement in orientation toward a distractorafter repeated exposure to the stimulus13.
This process, known as habituation, has been understudied in the VR literature. Only a fewinvestigators have exposed participants to more than one VR distraction trial. Hoffman et al.implemented VR distraction in seven burn patients during three daily physical therapysessions11. Pain ratings were significantly lower in the VR condition relative to baseline.More importantly, a within-subjects analysis of this effect showed that pain reductions didnot diminish over the three trials. In a case study of a 32-year-old male burn patient,Hoffman et al. showed significant reductions in patient ratings of time spent thinking aboutpain, pain bothersomeness and unpleasantness, worst pain, and average pain during a VRcondition relative to baseline, which were maintained over five daily physical therapysessions10. In a second case study, Hoffman et al. showed similar reductions in pain andanxiety during a VR condition relative to another active distraction condition in two maleyouth9. Repeated VR exposure was only reported for one patient, whose pain ratingsremained lower during the VR condition, but to a lesser degree than in the first exposure.However, these findings are difficult to interpret because the VR and non-VR conditionswere administered during different clinical procedures each day. To our knowledge, thereare no published laboratory studies of repeated exposure to VR distraction.
While the findings of Hoffman and colleagues are significant, the case study nature andlimited sample size of these studies substantially limits the generalizability of the findings.Thus it is important that the hypotheses and results of the aforementioned studies be testedin a larger-scaled, controlled experimental design. The present study examined the effects ofdistraction via VR technology over eight weekly trials with a larger sample size than hasbeen reported in the literature, and in a controlled laboratory environment.
Materials and MethodsParticipants
Participants were recruited from a university campus using flyers and online posts. Thirty-five adults initially agreed to participate in the study; however one participant did not keepthe initial appointment and three participants stopped attending sessions in the first threeweeks. Three participants were dropped from the study because their baseline pain tolerancescores for the first four sessions reached the 4-minute safety ceiling, thus making itimpossible to detect any improvements in pain tolerance due to VR distraction. Anadditional three participants demonstrated pain tolerance ceiling effects (i.e., tolerancescores greater than 240 sec.) in three or more of the later baseline sessions. Theseparticipants were retained in the study, but their data were excluded from the pain toleranceanalyses. One subject's pain threshold data were excluded from analyses because of similarceiling effects during baseline trials. Comparable rates of baseline ceiling effects, rangingfrom 10–19 percent of the total sample, have been reported by other researchers usingsimilar cold pressor paradigms and the standard 4-minute maximum immersion time6,14.
Rutter et al. Page 2
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
The final sample consisted of 28 participants, 17 (60.7%) of which were male. Participantages ranged from 18 to 23 years of age, with a mean of 18.86 years (SD = 1.27). No race orethnicity information was collected.
DesignA within-subjects design was used, eliminating inter-subject variability from week to week,thus increasing statistical power. Each study session consisted of two conditions, a baseline(control) condition in which the participant immersed his/her hand in the cold-pressorwithout distraction, and a VR distraction condition in which the participant interacted withthe VR environment while immersing his/her hand in the cold-pressor. During the VRdistraction condition, participants used a Playstation-2® controller (Model SCPH-10010U,Sony, Oradell, NJ) anchored to a table to play the videogame, which was viewed through avirtual reality head mounted display with integrated headphones. Condition order wasrandomized to control for order effects. Randomization was performed separately for eachparticipant.
Materials and EquipmentCold-pressor Apparatus—A Thermo NESLAB (Newington, NH) RTE-10 Digital OneRefrigerated Bath was used as the cold-pressor apparatus. The RTE-10 was chosen due to itsability to circulate the water, which is necessary to maintain a constant water temperatureand to avoid local pockets of heat near the hand of the participant. As noted in Mitchell,MacDonald, & Brodie, circulation is also needed to ensure comparable and reliable paininduction across multiple uses16. Also, because the RTE-10 is a digital apparatus,temperature can be set to a tenth of a degree and maintained automatically by the machine.The water temperature was maintained at 1 °C. This temperature was selected to limitceiling effects which can occur at higher temperatures, as well as to ensure an intense painstimulus which mimics as closely as possible those incurred in the clinical environment.
Stopwatch—A stopwatch was used to measure pain threshold and pain tolerance times toa tenth of a second.
Thermal Feedback System—A Thermal Feedback System, manufactured by Bio-Feedback Systems, Inc. of Boulder, Colorado (Model DT-100; Power ID-91), was used tomeasure hand temperature before and after each trial to a tenth of a degree.
Video Game Equipment—The Sony Playstation 2® Finding Nemo® “Catch Dory”game was chosen for this study. The game is played from a third-person perspective as theparticipant controls “Marlin,” chasing “Dory” as she rapidly swims away. This game waschosen because the time for completion of the game was greater than four minutes (i.e. themaximum allowed immersion in the cold pressor), it required active interaction by theparticipant throughout the trial, and it allowed for one-handed game play, freeing the otherhand to be immersed in the cold pressor. The game is suitable for ages six and above, asdetermined by the Entertainment Software Rating Board (ESRB) and has been used withchildren aged 5–13 in similar laboratory pain studies without difficulty3. The SonyPlaystation 2® controller was mounted to a base and anchored to a table to allowparticipants to manipulate the controller with one hand while the other hand was in the coldwater. The equipment was connected to a portable Ground Fault Circuit Interrupter (GFCI)at the receptacle outlet, as recommended by OSHA for construction sites using high voltagepower tools. The GFCI device was tested each day prior to use. All cords were secured toprevent tripping and were inspected daily for damage or fraying.
Rutter et al. Page 3
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Head-mounted Display Helmet—In the VR distraction condition a 5DT 800 HMDVirtual Reality Helmet adjustable head-mounted display with integrated headphones wasused. The head mounted display (HMD), made by Fifth Dimension Technologies (Irvine,CA), was connected to the Sony Playstation 2® through a Sony RDR-6×7 DVD player/recorder and Impact Acoustics (Dayton, Ohio) S-Video to VGA converter (product numberK0227).
ProcedureThis study was approved by the university Institutional Review Board (IRB). At the time ofenlistment in the study, participants selected a convenient half-hour timeslot during whichthey attended a weekly study session. Informed consent was obtained from the participantduring the first study session. All sessions were conducted in the same 4.9 m × 3.7 mcarpeted laboratory room maintained between 22 and 23 °C. The same procedure wasfollowed in all study sessions.
The first author, three graduate students and eight undergraduate students served asexperimenters. To minimize experimenter bias, each participant underwent trials conductedby several different experimenters.
Upon entering the laboratory room, the participant was asked to sit, with the cold-pressor onhis/her non-dominant side, the Playstation 2® controller on his/her dominant side, and theHMD and audio-visual equipment in front of him/her. At this time, the baseline handtemperature of the participant was measured by attaching the temperature sensor to the tip ofthe index finger of the non-dominant hand.
Before each trial, the participant was instructed to immerse his/her non-dominant hand in thecold-pressor bath up to the wrist, palm-side down, and to leave his/her hand open (non-fisted). This was done to avoid the formation of heat pockets around the fingertips whichcan influence pain stimulus. The participant was told to report when they began to feel painby saying “Pain now” and to remove their hand from the cold-pressor when the pain becameunbearable. Finally, the participant was asked if they understood the directions.
In each trial, the participant immersed his/her hand in the cold-pressor up to the wrist.Timing began once the hand was immersed and ended when the hand was removed. Thetime read when the participant said “Pain now” was recorded as pain threshold, and the timeread when the participant removed their hand from the water was recorded as pain tolerance.Following the participant's removal of their hand from the water, the hand was quickly driedwith a towel and the hand temperature was measured as in the baseline measurement.During this time, several 100 mm visual analog scales were issued, as described below.Next, the participant was asked to place his/her hand in a warm water bath (35 °C) forapproximately five minutes, or until the participant felt his/her hand had returned tobaseline. The hand temperature was again measured, ensuring it was within 1 °C of the firstbaseline temperature taken upon entering the laboratory.
Baseline (Control) Condition—The experimenter read the directions above to theparticipant, and subsequently asked the participant to immerse his/her hand in the cold-pressor bath. The participant's pain threshold and pain tolerance times were recorded to atenth of a second.
VR Distraction Condition—Before commencing the VR distraction condition, theparticipant was shown how to play the game by one of the experimenters. Approximately 3–5 minutes were devoted to teaching game play to the participant. The HMD was placed onthe participant's head and adjusted to ensure a comfortable and secure fit. The participant's
Rutter et al. Page 4
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

non-dominant hand was placed above the cold-pressor bath, and the dominant hand abovethe Playstation 2® controller. The participant was read the above instructions. Next, thegame was commenced and the participant immersed his/her hand in the cold-pressor bath, asinstructed. The participant's pain threshold and pain tolerance times were recorded to a tenthof a second as described above.
As compensation for participation in any number of study sessions, extra credit was issuedin undergraduate psychology courses, where applicable. Also, as compensation forcompleting all eight study sessions, participants were given a ticket for a raffle of an Apple(Cupertino, CA) iPod® and several smaller prizes. The latter compensation was intended tolimit participant attrition over the course of the eight weekly sessions.
MeasuresPain threshold was defined as the number of seconds of immersion in the cold-pressor bathuntil the participant reported pain. Pain tolerance was defined as the number of seconds ofimmersion in the cold-pressor bath until the participant removed his/her hand from thewater.
Visual analog scales were used to measure the intensity of the participant's pain duringimmersion, the participant's anxiety during immersion, the amount of time the participantspent thinking about his/her pain during immersion, and the participant's level of enjoymentof the VR game (if applicable). Each scale consisted of a 100 mm line, with the left terminuslabeled as the total absence of the variable (i.e. no pain, no anxiety, no time spent thinkingabout pain), and the right terminus labeled as the complete presence of the variable (i.e.worst possible pain, very anxious, 100% of time spent thinking about pain). These scaleswere scored by measuring the distance in millimeters from the left terminus of the scale tothe mark made by the participant, indicating the degree to which the participant experiencedeach variable. Visual analog scales yield reliable and precise measurements of severalaspects of the pain experience, and have been applied throughout the existing VR distractionliterature9,10. Visual analog scales have also been shown to be a valid way to estimate stateanxiety1.
ResultsHypothesis Testing
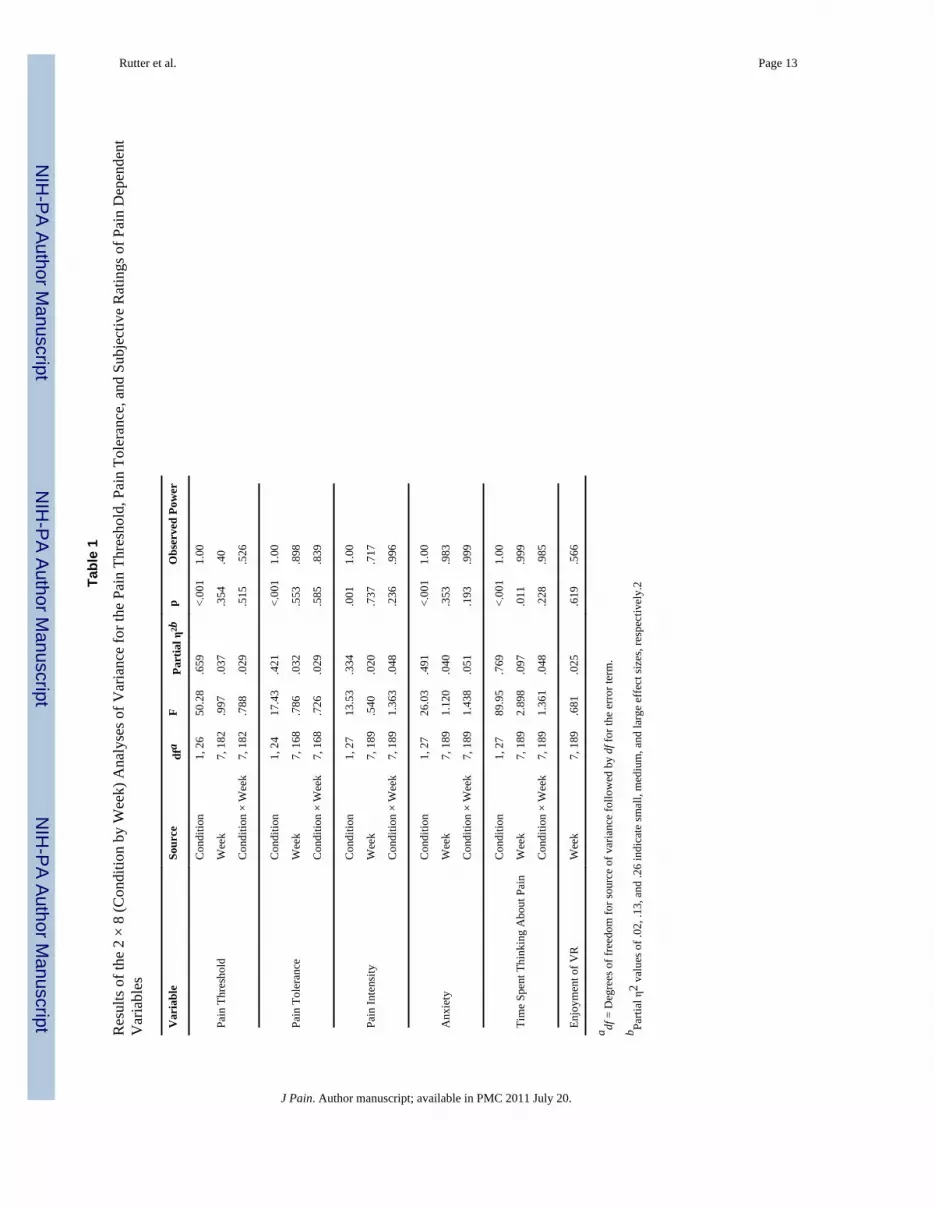
A series of (2 × 8) within-subjects analyses of variance (ANOVA) were conducted toascertain the effects of condition (i.e., VR distraction vs. baseline) and week on painthreshold, pain tolerance, pain intensity, anxiety, and time spent thinking about pain over theeight weeks of the study. The ANOVA results are presented in Table 1. Median values forpain threshold and pain tolerance in both experimental conditions are shown in Table 2. Asseen in Figures 1 and 2 respectively, VR distraction led to significant increases in painthreshold and pain tolerance relative to baseline. VR distraction also led to significantdecreases in pain intensity, anxiety, and time spent thinking about pain (see Table 1). Poweranalyses conducted using G*Power (version 3.0)5 indicated that adequate power (greaterthan .80, according to Cohen, 1988)2 was obtained for the pain tolerance, pain intensity,anxiety, and time spent thinking about pain analyses (See Table 1). However, lower power (.53 to .57) was obtained for the pain threshold and level of enjoyment of VR analyses.Therefore, these analyses should be interpreted with caution. Pain tolerance and painthreshold were significantly correlated at each time point, with correlations ranging from .53to .77 (ps < .01).
Analyses of condition by week effects were not significant for any of the dependentvariables. As shown in Figure 3, the standard mean difference (SMD, calculated by taking
Rutter et al. Page 5
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
the difference between the mean of pain tolerance during intervention and baseline anddividing this by the square root of the pooled standard deviation) effect sizes for the primarydependent variables (pain tolerance, pain threshold, and pain intensity) across the 8 weeks ofthe study demonstrate some scatter, but only slightly negative slopes (slopes = −0.0063,−0.0011, and 0.0133 for pain tolerance, pain threshold, and pain intensity, respectively).Effect sizes for pain tolerance fell within the moderate range, effect sizes for pain thresholdfell in the small to moderate range, and effect sizes for pain intensity fell in the small range,according to Cohen's (1988) standards2.
DiscussionThe virtual reality distraction intervention appeared to be very effective for this sample of18- to 23-year-old adults. Participants demonstrated increases in pain tolerance and painthreshold during the VR condition relative to their baseline, showing the largest and moststable effects for pain tolerance. Moreover, VR distraction led to significant decreases inparticipant ratings of pain intensity, anxiety, and time spent thinking about pain. The overallfindings of this study are consistent with studies currently in the literature7,9,10,11. However,the magnitude of effects in the current study exceeds those of other studies. To the best ofour knowledge, this study is the only of its kind to find significant improvements due to VRdistraction in all of the aforementioned indices of the pain experience within a singlesample. Furthermore, none of the above effects diminished significantly over the course ofthe eight weekly exposures to VR, as indicated by the absence of condition by week effectsin all of the variables and the absence of meaningful degradation in effect sizes over time.This suggests that participants did not habituate to the distracting properties of VR.
The finding that participants did not habituate to the distracting properties of VR is inagreement with the limited existing literature, but with a larger sample size and moreextended timeline of exposures than previous studies in the literature10,11. This finding is ofspecial importance because it addresses the concern noted by Hoffman et al. that if thenovelty of VR wears off with repeated exposure, the efficacy of VR distraction from painwould decrease10. Moreover, this finding suggests that VR distraction interventions mayhave the potential to be clinically effective over an extended course of exposures.
LimitationsAlthough the observed effects of VR distraction in this study were impressive, laboratorypain differs from clinical pain in many ways. First, the participants knew they were incomplete control of the pain experience, meaning they could remove their hands from thewater at any time. Secondly, the duration of the pain experience was limited to a maximumof four minutes. Also, because many patient populations may require the use of centralnervous system depressants, such as opioids, a patient's ability to interact with a complexVR environment may be decreased significantly. This may limit the efficacy of VRintervention during these periods of a patient's treatment. Finally, the participantsexperienced pain in a more subdued atmosphere than that of a hospital, which may haveimportant implications on the clinical use of VR distraction in highly anxious patients.However, we chose to study experimental pain for the present study in order to avoid themany uncontrolled factors influencing pain in the clinical setting. This allowed for astandardized pain stimulus to be delivered to all participants over the course of the eightweekly trials. Had clinical pain been studied instead, variations in the same clinicalprocedure among trials would have varied the intensity of the pain stimulus from week toweek, thus adding considerable error variance. As noted by Edens & Gil, studies utilizingexperimental pain in the laboratory setting allow for closer control of the experimentalenvironment than in the clinic4. Many experimental pain stimuli are also safe to implementrepeatedly within a single, short laboratory visit, thereby allowing for within-subject
Rutter et al. Page 6
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

experimental design that avoids problems of inter-subject variability in pain tolerance andthreshold. Thus, the use of experimental pain stimuli allows for the careful study ofclinically-related phenomena and processes in a more controlled and constantenvironment1,4.
Secondly, the age range of the participants used in this study was limited. Age differences incognition and attention may affect the efficacy of VR over repeated exposures and/or therate at which participants habituate. However, the existing literature on VR habituationemploys several different age populations, all with converging results consistent with thisstudy. Therefore, the effect of age may be relatively minor, given that age-appropriate VRequipment and software can be provided to patients of different ages. Replication of thecurrent study in both younger and older populations would expand the generalizability of thefindings.
It is possible that participants' expectancy effects may have influenced the results of thisstudy. That is, although the participants were not directly told what the hypotheses of thisstudy were, they might have guessed the hypotheses and subsequently tried harder to keeptheir hand in the water while playing the videogame.
Several participants were not included in the pain tolerance analyses because of repeatedceiling effects during baseline. Thus, these findings are not necessarily generalizable toindividuals with exceptionally high pain threshold and/or pain tolerance. Also, becauseresearch assistants involved in running study sessions had prior knowledge of VR distractiontheory and the hypothesis of this individual study, the potential for experimenter bias exists.However, the risk of bias was mitigated by ensuring that several different research assistantsserved as experimenters for each participant over the course of the eight week study.
Although pain threshold was correlated with pain tolerance, pain threshold proved to be aless sensitive, more erratic dependent variable in this study. However, this issue may beunavoidable. In order to reliably report the onset of pain, participants would need to directtheir attention to pain sensations, which is incompatible with the goals of a distractionintervention. The same concern applies to pain intensity. Thus, it may be advisable to relyprimarily on pain threshold as a dependent variable for laboratory studies of distraction-based pain management.
Finally, this study employed a third person rather than first person perspective (i.e., theparticipant saw the game character, Marlin, as he/she manipulated his movements in thevirtual environment, rather than viewing the virtual environment as if through Marlin'seyes). As noted in Schubert et al. and Schuemie et al., a first person perspective is thought toprovide a superior sense of presence relative to third person, although third personperspectives also can induce presence18,19. Thus, the VR software used in the present studymay not have achieved the optimal level of presence, relative to more elaborate andexpensive variations on this technology. It is possible that a virtual reality intervention witha first person perspective could be even more efficacious over repeated exposures than thethird person perspective virtual reality stimuli used in the current study.
Future DirectionsThe maintained efficacy of VR distraction over repeated exposures observed in the currentstudy indicates that VR distraction is a viable pain intervention, capable of sustaining itspowerful analgesic effects over an extended period of time. To the best of our knowledge,the current study is the only study of VR habituation to use an extended period of exposuresin a sample larger than seven participants11. However, further study is needed to evaluatethe long-term effectiveness of VR distraction using repeated clinical, rather than laboratory-
Rutter et al. Page 7
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
based pain stimuli, with a comparable or larger sample size. In addition, as recommended byGlantz et al., future studies of VR habituation in clinical populations should also address thecost effectiveness of VR distraction relative to other, less expensive distraction techniques8.
AcknowledgmentsThe authors thank the following undergraduate research assistants who aided in experimental procedures and datamanagement: Victoria Grossi, Joseph Keller, Cyrus Mistry, Jessica Wentling, and Monica Jimeno. The authorswould also like to thank several graduate students for their support and collaboration: Emily Kastelic, ClaireAckerman, Soumitri Sil, and Lindsay Dillinger. Finally, the authors would like to thank Dr. Lynanne McGuire,Ph.D. for her assistance in reviewing this manuscript in preparation for publication.
This study was supported in part by a University of Maryland, Baltimore County Undergraduate research award tothe first author and by grant No. R01HD050385 from the National Institute for Child Health and Development,National Institutes of Health.
References1. Bond A, Shine P, Bruce M. Validation of visual analogue scales in anxiety. Int J Methods Psychiatr
Res. 1995; 5:1–9.2. Cohen, J. Statistical power analysis for the behavioral sciences. 2nd Edition. Lawrence Erlbaum
Associates; Hillsdale, NJ: 1988.3. Dahlquist LM, McKenna KD, Jones KK, Dillinger L, Weiss KE, Sonntag C. Active and passive
distraction using a head-mounted display helmet: Effects on cold pressor pain in children. HealthPsychol. 2007; 26:794–801. [PubMed: 18020853]
4. Edens JL, Gil KM. Experimental induction of pain: Utility in the study of clinical pain. Behav Ther.1995; 26:197–216.
5. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: A flexible statistical power analysis programfor the social, behavioral, and biomedical sciences. Behav Res Methods. 2007; 39:175–191.[PubMed: 17695343]
6. Forys KL, Dahlquist LM. The influence of preferred coping style and cognitive strategy onlaboratory-induced pain. Health Psychol. 2007; 26:22–29. [PubMed: 17209694]
7. Gershon J, Zimand E, Lemos R, Rothbaum BO, Hodges L. Use of virtual reality as a distractor forpainful procedures in a patient with pediatric cancer: A case study. CyberPsychol. 2003; 6:657–661.
8. Glantz K, Rizzo A, Graap K. Virtual reality for psychotherapy: Current reality and futurepossibilities. Psychotherapy. 2003; 40(1/2):55–67.
9. Hoffman HG, Doctor JN, Patterson DR, Carrougher GJ, Furness TA III. Virtual reality as anadjunctive pain control during burn wound care in adolescent patients. Pain. 2000; 85:305–309.[PubMed: 10692634]
10. Hoffman HG, Patterson DR, Carrougher GJ, Nakamura D, Moore M, Garcia-Palacios A, FurnessTA III. The effectiveness of virtual reality pain control with multiple treatments of longerdurations: A case study. Int J Hum Comput Interact. 2001; 13(1):1–12.
11. Hoffman HG, Patterson DR, Carrougher GJ, Sharar SR. The effectiveness of virtual reality basedpain control with multiple treatments. Clin J Pain. 2001; 17:229–235. [PubMed: 11587113]
12. Hoffman HG, Patterson DR, Seibel E, Soltani M, Jewett-Leahy L, Sharar SR. Virtual reality paincontrol during burn wound debridement in the hydrotank. Clin J Pain. 2008; 24(4):299–304.[PubMed: 18427228]
13. Houston-Price C, Nakai S. Distinguishing novelty and familiarity effects in infant preferenceprocedures. Inf Child Dev. 2004; 13:341–348.
14. Jones A, Spindler H, Jorgensen MM, Zachariae R. The effect of situation-evoked anxiety andgender on pain report using the cold pressor test. Scand J Psychol. 2002; 43:307–313. [PubMed:12361099]
15. McCaul KD, Malott JM. Distraction and coping with pain. Psychol Bull. 1984; 95:516–533.[PubMed: 6399756]
Rutter et al. Page 8
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
16. Mitchell LA, MacDonald RA, Brodie EE. Temperature and the cold pressor test. J Pain. 2004;5(4):233–237. [PubMed: 15162346]
17. Regenbrecht H, Schubert T, Friedman F. Measuring the sense of presence and its relations to fearof heights in virtual environments. Int J Hum Comput Interact. 1998; 10(3):233–249.
18. Schubert T, Friedmann F, Regenbrecht HT. The experience of presence: Factor analytic insights.Presence. 2001; 10:266–281.
19. Schuemie M, van der Straaten P, Krijn M, van der Mast C. Research on presence in virtual reality:A survey. Cyberpsychol Behav. 2001; 4(2):183–201. [PubMed: 11710246]
20. Wismeijer A, Vingerhoets A. The use of virtual reality and audiovisual eyeglass systems as adjunctanalgesis techniques: A review of the literature. Ann Behav Med. 2005; 30(3):268–278. [PubMed:16336078]
Rutter et al. Page 9
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 1.Pain Tolerance during Baseline and VR Distraction Trials Across Weekly Sessions (n = 25).Note: Error bars represent standard deviations (SD). To avoid overlap of error bars, +.5 SDis graphed for the VR Distraction condition and −.5 SD is graphed for the Baselinecondition.
Rutter et al. Page 10
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 2.Pain Threshold during Baseline and VR Distraction Trials Across Weekly Sessions (n = 27).Note: Error bars represent the standard deviations (SD). To avoid overlap of error bars, +.5SD is graphed for the VR Distraction condition and −.5 SD is graphed for the Baselinecondition.
Rutter et al. Page 11
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Figure 3.Standardized Mean Difference Scores Across Weekly Sessions
Rutter et al. Page 12
J Pain. Author manuscript; available in PMC 2011 July 20.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Rutter et al. Page 13
Tabl
e 1
Res
ults
of t
he 2
× 8
(Con
ditio
n by
Wee
k) A
naly
ses o
f Var
ianc
e fo
r the
Pai
n Th
resh
old,
Pai
n To
lera
nce,
and
Sub
ject
ive
Rat
ings
of P
ain
Dep
ende
ntV
aria
bles
Var
iabl
eSo
urce
dfa
FPa
rtia
l η2b
pO
bser
ved
Pow
er
Pain
Thr
esho
ld
Con
ditio
n1,
26
50.2
8.6
59<.
001
1.00
Wee
k7,
182
.997
.037
.354
.40
Con
ditio
n ×
Wee
k7,
182
.788
.029
.515
.526
Pain
Tol
eran
ce
Con
ditio
n1,
24
17.4
3.4
21<.
001
1.00
Wee
k7,
168
.786
.032
.553
.898
Con
ditio
n ×
Wee
k7,
168
.726
.029
.585
.839
Pain
Inte
nsity
Con
ditio
n1,
27
13.5
3.3
34.0
011.
00
Wee
k7,
189
.540
.020
.737
.717
Con
ditio
n ×
Wee
k7,
189
1.36
3.0
48.2
36.9
96
Anx
iety
Con
ditio
n1,
27
26.0
3.4
91<.
001
1.00
Wee
k7,
189
1.12
0.0
40.3
53.9
83
Con
ditio
n ×
Wee
k7,
189
1.43
8.0
51.1
93.9
99
Tim
e Sp
ent T
hink
ing
Abo
ut P
ain
Con
ditio
n1,
27
89.9
5.7
69<.
001
1.00
Wee
k7,
189
2.89
8.0
97.0
11.9
99
Con
ditio
n ×
Wee
k7,
189
1.36
1.0
48.2
28.9
85
Enjo
ymen
t of V
RW
eek
7, 1
89.6
81.0
25.6
19.5
66
a df =
Deg
rees
of f
reed
om fo
r sou
rce
of v
aria
nce
follo
wed
by
df fo
r the
err
or te
rm.
b Parti
al η
2 va
lues
of .
02, .
13, a
nd .2
6 in
dica
te sm
all,
med
ium
, and
larg
e ef
fect
size
s, re
spec
tivel
y.2
J Pain. Author manuscript; available in PMC 2011 July 20.