transdermal scopolamine in the management of postparotidectomy salivary fistula
TRANSCRIPT

!
A preliminary study of the use of ultrasound in de!ning nasal fractures: Criteria for a con!dent diagnosis
A case of chronic subdural hematomafollowing lumbar drainage for the management of iatrogenic cerebrospinal "uid rhinorrhea: Pitfalls and lessons
Transdermal scopolamine in the management of postparotidectomy salivary !stula
!
A Vendome Publication
!
2013
BUYERS GUIDE

Entellus OFFICE Balloon Sinus Dilation helps you grow your practice, meet patient demand, and deliver safe, effective sinusitis treatment.
Entellus is Leading the Way in Office-based Balloon Sinus Dilation
Find out how Entellus can help you add Balloon Sinus Dilation procedures to your office. For more information, call 866-620-7615 or visit www.EntellusMedical.com
FOR IN-OFFICE TREATMENT
1738-018 rM 08/2013

Give your patients the thing they’ve been searching for.
Peace and quiet. Not too much to ask for, unless your patient has tinnitus. Arches Tinnitus Formula™ is safe, effective and affordable, and has been helping individuals with tinnitus for over 12 years. Give your patients the peace they seek and recommend Arches Tinnitus Formula today.
Get a free CD of clinical studies, physician’s booklet, and patient brochures. Call 800.486.1237 or email [email protected]
www.tinnitusformula.com
and quiet

EDITORIAL BOARD
Joseph Haddad Jr., MDMaureen T. Hannley, PhDChristopher J. Hartnick, MDMary Hawkshaw, RN, BSN,
CORLNGarett D. Herzon, MD!omas Higgins, MD, MSPHJun Steve Hou, MDJohn W. House, MDAmanda Hu, MD, FRCSCDarrell Hunsaker, MDGlenn Isaacson, MDSteven F. Isenberg, MDStephanie A. Joe, MDShruti S. Joglekar, MBBSRaleigh O. Jones, Jr., MDPetros D. Karkos, MD, AFRCS,
PhD, MPhilDavid Kennedy, MDSeungwon Kim, MDRobert Koenigsberg, DOKaren M. Kost, MD, FRCSCJamie A. Koufman, MDStilianos E. Kountakis, MD, PhDJohn Krouse, MDRonald B. Kuppersmith, MD,
MBA, FACSRande H. Lazar, MDRobert S. Lebovics, MD, FACSLevi G. Ledgerwood, MDKeat-Jin Lee, MDDonald A. Leopold, MDSteve K. Lewis, BSc, MBBS,
MRCSDaqing Li, MDCatherine Rees Lintzenich, MDRobert R. Lorenz, MDJohn M. Luckhurst, MS, CCC-AValerie Lund, FRCSA.A.S. Rifat Mannan, MDRichard Mattes, PhDWilliam A. McIntosh, MDBrian J. McKinnon, MDOleg A. Melnikov, MDAlbert L. Merati, MD, FACSJoseph P. Mirante, MD, MBA, FACSRon B. Mitchell, MDSteven Ross Mobley, MDMarcus Moody, MD!omas Murry, PhDJ. Gail Neely, MDAlan J. Nissen, MDAshli K. O’Rourke, MD
Ryan F. Osborne, MD, FACSJ. David Osguthorpe, MDRobert H. Osso", DMD, MDEnrique Palacios, MD, FACRMichael M. Paparella, MDArthur S. Patchefsky, MDMeghan Pavlick, AuDSpencer C. Payne, MDKevin D. Pereira, MD, MS (ORL)Didier Portmann, MDGregory N. Postma, MDKishore Chandra Prasad, DLO,
FACSEdmund A. Pribitkin, MD, FACSMatthew J. Provenzano, MDHassan H. Ramadan, MD, FACSRichard T. Ramsden, FRCSGabor Repassy, MD, PhDDale H. Rice, MDErnesto Ried, MDAlessandra Rinaldo, MD, FRSMAllan Maier Rubin, MD, PhD,
FACSJohn S. Rubin, MD, FACS, FRCSAmy L. Rutt, DOAnthony Sclafani, MD, FACS Raja R. Seethala, MDMichael Setzen, MD, FACS,
FAAPStanley Shapshay, MDDouglas M. Sidle, MDHerbert Silverstein, MDRaj Sindwani, MD, FACS, FRCSAristides Sismanis, MD, FACSWilliam H. Slattery III, MDLibby Smith, DO!omas C. Spalla, MDMatthew Spector, MDPaul M. Spring, MDBrendan C. Stack, Jr., MD, FACSJames A. Stankiewicz, MDJames Y. Suen, MDJun-Ichi Suzuki, MDDavid !ompson, MDLester D.R. !ompson, MD,
FASCPHelga Toriello, PhD, FACMGGaldino Valvassori, MDEmre Vural, MDDonald T. Weed, MD, FACSPaul M. Weinberger, MDNeil Weir, FRCSKenneth R. Whittemore, MDJacqueline Ann Wieneke, MD
EDITORIAL BOARD MEMBERS
Jason L. Acevedo, MD, MAJ, MC, USA
Jack B. Anon, MDSo#a Avitia, MDGregorio Babighian, MDPeter C. Belafsky, MD, PhDBruce Benjamin, MDGerald S. Berke, MDCarol R. Bradford, MDMichael J. Brenner, MDKenneth H. Brookler, MDKaren H. Calhoun, MDSteven B. Cannady, MDRicardo Carrau, MDNicholas J. Cassisi, DDS, MDSwapna Chandran, MDChien Chen, MDDewey A. Christmas, MDNicolle T. Clements, MSDavid M. Cognetti, MDJacquelynne P. Corey, MDMaura Cosetti, MDJames V. Crawford, MDDavid H. Darrow, MD, DDSRima Abraham DeFatta, MDRobert J. DeFatta, MD, PhDOlivier Deguine, MDJoseph Di Bartolomeo, MD,
FACSHamilton Dixon, MDPaul J. Donald, MD, FRCSSamer Fakhri, MD, FACS,
FRCS(C)Russell A. Faust, PhD, MDJose Fayad, MDAl#o Ferlito, MDRamón E. Figueroa, MD, FACRCharles N. Ford, MDPaul Frake, MDChristine B. Franzese, MD Marvin P. Fried, MDRichard R. Gacek, MDAndrea Gallo, MDFrank Gannon, MDToni M. Ganzel, MDEmilio Garcia-Ibanez, MDMahmood Ghaderi, MDSoha Ghossani, MDWilliam P. R. Gibson, MDDavid Goldenberg, MDJerome C. Goldstein, MDRichard L. Goode, MDSamuel Gubbels, MDReena Gupta, MD
CLINIC EDITORSClinical NuggetsMichael M. Paparella, MD
DysphagiaJamie A. Koufman, MDPeter C. Belafsky, MD, PhDGregory N. Postma, MD
Facial Plastic SurgerySteven Ross Mobley, MDDouglas M. Sidle, MD
Head and NeckRyan F. Osborne, MD, FACSPaul J. Donald, MD, FRCSReena Gupta, MD
ImagingEnrique Palacios, MD, FACRRamón E. Figueroa, MD,
FACR
LaryngoscopicRobert T. Sataloff, MD, DMA,
FACS
OtoscopicJohn W. House, MDJose Fayad, MD
PathologyLester D.R. Thompson, MD,
FASCP
Pediatric OtolaryngologyRande H. Lazar, MD
RhinoscopicEiji Yanagisawa, MD, FACSDewey A. Christmas, MDJoseph P. Mirante, MD, MBA,
FACS
Special TopicsRobert T. Sataloff, MD, DMA,
FACS
David F. Wilson, MDIan M. Windmill, PhDIan J. Witterick, MD,MSc, FRCSCRichard J. Wong, MDNaoaki Yanagihara, MDEiji Yanagisawa, MD, FACSKen Yanagisawa, MD, FACSAnthony Yonkers, MD Mark Zacharek, MDLiang Zhou, MD
Editor-in-Chief Robert T. Sataloff, MD, DMA, FACS
Professor and Chairman, Department of Otolaryngology–Head and Neck Surgery, and Senior Associate Dean for Clinical
Academic Specialties, Drexel University College of MedicinePhiladelphia, PA

1738-165 rB 08/2013
Find out how Entellus can help you Do More With Less. For more information, call 866-620-7615 or visit www.EntellusMedical.comXprESS Indications for Use: To access and treat the frontal recesses, sphenoid sinus ostia and maxillary ostia/ethmoid infundibula in adults using a trans-nasal approach. The bony sinus outflow tracts are remodeled by balloon displacement of adjacent bone and paranasal sinus structures. LED Light Fiber Indications for Use: To locate, illuminate within, and transilluminate across nasal and sinus structure in patients aged 18 and over. Refer to products’ Instructions For Use (IFU) for complete instructions.CAUTION: Federal (USA) law restricts these devices to sale by or on the order of a physician.1-2 Published references and/or data on file at Entellus Medical.
Entellus OFFICE Balloon Sinus Dilation enables you to treat more appropriate patients, more comfortably with one device. And now, you don’t need a secondary light source!
With XprESS™ LoProfile with integrated PathAssist™ LED Light Fiber™, you can:

476 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Editor-in-Chief Robert T. Sataloff, MD, DMA, FACS 1721 Pine Street, Philadelphia, PA [email protected] Ph: 215-732-6100
Managing Editor Linda ZinnManuscript Editor Martin StevensonAssociate Editor, Reader Engagement Megan RozsaCreative Director Eric CollanderArt Director Rebecca DeneauSenior Designer Suzanne Quintero
Executive Group Publisher Michael W. O’DonnellNational Sales Manager Mark C. [email protected] Ph: 216-373-1229Directory Sales Elana [email protected] Ph: 216-373-12027UDI¿F�0DQDJHU��Judi ZengPlease send IOs to DGWUDI¿F#YHQGRPHJUS�FRPAll ad materials should be sent electronically to:https://vendome/sendmyadcom
Reprints & e-Prints Erin Tyler Beirne [email protected] Ph: 216-373-1217
Customer Service/Subscriptions [email protected] Ph: 888-873-3566www.entjournal.com/subscribe
Reuse Permissions Copyright Clearance Center [email protected] Ph: 978-750-8400Fax: 978-646-8600
&KLHI�([HFXWLYH�2I¿FHU��Jane ButlerPresident Mark FriedVice President Ron Lowy&KLHI�0DUNHWLQJ�2I¿FHU Dan MeloreExecutive Director, Corporate Editorial Initiatives Charlene MariettiVice President, Finance Bill NewberryDirector, Custom Media Jennifer TurneyDirector, Digital Marketing Daniel P. TimoneyDirector, Circulation Rachel BeneventiDirector, Production and Web Development Kathryn Homenick
ENT-Ear, Nose & Throat Journal (ISSN: Print 0145-5613, Online 1942-7522) is published 10 times per year in Jan, Feb, Mar, Apr/May, June, July, Aug, Sept, Oct/Nov and Dec, by Vendome Group, LLC, 6 East 32nd, Street, 8th !oor, New York, NY 10016.
©2013 by Vendome Group, LLC. All rights reserved. No part of ENT-Ear, Nose & Throat Journal may be reproduced, distributed, transmitted, dis-played, published, or broadcast in any form or in any media without prior written permission of the publisher. To request permission to reuse this content in any form, including distribution in education, professional, or promotional contexts or to reproduce material in new works, please contact the Copyright Clearance Center at [email protected] or 978.750.8400. For custom reprints, e-prints, or logo licensing, please contact Erin Tyler Beirne at 216.373.1217 or [email protected].
EDITORIAL: The opinions expressed in the editorial and advertising material in this issue of ENT-Ear, Nose & Throat Journal are those of the authors and advertisers and do not necessarily re!ect the opinions or recom-mendations of the publisher, editors, or the staff of Vendome Group, LLC. ENT-Ear, Nose & Throat Journal is indexed in Index Medicus and Current Contents/Clinical Medicine and Science Citation Index Expanded. Edito-rial of"ces are located at 812 Huron Rd., Suite 450, Cleveland, OH 44115. Manuscripts should be submitted online at www.editorialmanager.com/entjournal. Instructions for Authors are available at www.entjournal.com.
SUBSCRIPTIONS: For questions about a subscription or to subscribe, please contact us by phone: 888-873-3566; or email: [email protected]. Individual subscriptions, U.S. and possessions: 1 year $225, 2 years $394; International: 1 year $279, 2 years $488. Institution subscriptions, U.S.: 1 year $675. Special rate for U.S. students, interns, residents, and tech-nicians $100/year. Single copies $28; outside the U.S., $40.
POSTMASTER: send address changes to Ear, Nose & Throat Journal, PO Box 397, 2865 S Eagle Rd., Newtown, PA 18940
SIGN UP FOR OUR MONTHLY
E-NEWSLETTER AT http://www.entjournal.com/e-news
Receive exclusive online content and news stories on the latest ear, nose and
throat developments as well as links to other informative
resources and events.

478 ! www.entjournal.com ENT-Ear, Nose & Throat Journal Q October/November 2013
CONTENTS OCTOBER/NOVEMBER
EDITORIAL OFFICE
ORIGINAL ARTICLES
508 A preliminary study of the use of ultrasound in de!ning nasal fractures: Criteria for a con!dent diagnosis
Farhad Ardeshirpour, MD; Keith M. Ladner, MD; Carol G. Shores, MD, PhD; William W. Shockley, MD
513 A case of chronic subdural hematoma following lumbar drainage for the management of iatrogenic cerebrospinal "uid rhinorrhea: Pitfalls and lessons
Vincent Eng-Soon Tan, MD, MRCS, MS(ORL–HNS); Donald Liew, FRACS
516 Transdermal scopolamine in the management of postparotidectomy salivary !stula
Andrea Gallo, MD, PhD; Valentina Manciocco, MD, PhD; Giulio Pagliuca, MD, PhD; Salvatore Martellucci, MD;
Marco de Vincentiis, MD
ONLINE EXCLUSIVES
E1 Synchronous verrucous carcinoma and inverted papilloma of the lacrimal sac: Case report and clinical update
Cheryl Gustafson, MD; Eugene Einhorn, MD; Mary H. Scanlon, MD; Kenneth E. Morgenstern, MD; Paul J. Howlett, MD; Noam A. Cohen, MD, PhD
E6 A case and a series of published cases of esthesioneuroblastoma (ENB) in which long-
standing paraneoplastic SIADH had preceded ENB diagnosis
Uri Gabbay, MD, MPH; Leonor Leider-Trejo, MD; Gideon Marshak, MD; Merav Gabbay, MD; Dan M. Fliss, MD E10 Glass in the frontal sinus: 28-year delayed presentation Alice K. Guidera, MBChB, BSc; Peter M. Dixon, MBBS, FRCS; Hans R. Stegehuis, MBChB, FRACS
E13 Case report: Paraneoplastic neurologic syndrome associated with squamous cell carcinoma of the tonsil
Jeffrey R. Janus, MD; Sivakumar Chinnadurai, MD; Eric J. Moore, MD E17 Diffuse sphenoid bone cavernous hemangioma
presenting during pregnancy Hugh Robertson, MD, FACR; Enrique Palacios, MD, FACR;
Sheryl Rincon, MD; Kamal R. Shah, MD
E21 Arteriovenous malformation of the neck: An unusual cause of hoarseness successfully treated
with endovascular techniques Joseph J. Gemmete, MD; Neeraj Chaudhary, MD; Aditya S. Pandey, MD; Dheeraj Gandhi, MD; Sameer A. Ansari, MD, PhD
E25 Intracranial and internal jugular vein thrombosis secondary to ENT infections: A report of 3 cases
Faruque Riffat, BSc(Med), MBBS (Hons); Martin Forer, FRACS; Andrew Wignall, FRACS; David Veivers, FRACS; Nirmal Patel, MS, FRACS
E29 Endoscopic closure of a frontocutaneous !stula Alexandros Tsikoudas, DLO, FRCS(Otol), FRCS(ORL–HNS); Christos Georgalas, PhD, MRCS, FRCS(ORL–HNS)
DEPARTMENTS
482 ENT Journal Online
486 Guest Editorial
488
490
492
496 Imaging Clinic
500
502 Head and Neck Clinic
505
506
E31
E33
E34
519 Classi!eds
528 Advertiser Index
BUYERS GUIDE
520 Introduction/Index
521

Please see Brief Summary of Full Prescribing Information on the following pages.* As listed in the Full Prescribing Information, in 3 pivotal trials, symptom relief was measured by change from baseline in the placebo-subtracted mean Total Nasal Symptom Score (TNSS) for each day (maximum score 24) averaged over the 14-day study period. Dymista provided a statistically signi! cant improvement in TNSS compared with both " uticasone propionate and azelastine HCI. The " uticasone propionate and azelastine HCI comparators used the same device and vehicle as Dymista and are not commercially marketed. Additionally, Dymista provided a statistically signi! cant, rapid improvement in TNSS as early as 30 minutes after administration when compared with placebo.1
Reference: Dymista [package insert]. Somerset, NJ: Meda Pharmaceuticals Inc; 2012.©2013 Meda Pharmaceuticals Inc. Dymista is a trademark of Meda Pharmaceuticals Inc. 9/13 DYM-13-0253
www.Dymista.com
Rapid-onset relief as early as 30 minutes vs placebo* and
More complete relief vs " uticasone propionateor azelastine HCl comparator*
from seasonal allergy symptomsfor rapid and more complete reliefFirst and Only
IndicationDymista Nasal Spray, containing an H1-receptor antagonist and a corticosteroid, is indicated for the relief of symptoms of seasonal allergic rhinitis in patients 12 years of age and older who require treatment with both azelastine hydrochloride and " uticasone propionate for symptomatic relief.
Important Safety Information Patients may experience somnolence. Caution patients against engaging in hazardous occupations requiring complete mental alertness, such as driving or operating machinery Patients should avoid concurrent use of alcohol or other central nervous system (CNS) depressants because additional reductions in alertness and additional impairment of CNS performance may occur Because of the inhibitory effect of corticosteroids on wound healing, avoid use in patients with recent nasal ulcers, nasal surgery, or nasal trauma until healed Glaucoma, cataracts, and increased intraocular pressure may be associated with nasal corticosteroid use; therefore, close monitoring is warranted in patients with a change in vision and/or with a history of increased intraocular pressure, glaucoma, and/or cataracts
Patients using corticosteroids may be susceptible to infections and may experience a more serious or even fatal course of chicken pox or measles. Dymista should be used with caution in patients with active or quiescent tuberculosis; fungal, bacterial, viral, or parasitic infections; or ocular herpes simplex Systemic corticosteroid effects, such as hypercorticism and adrenal suppression, may occur with very high dosages or at the regular dosage in susceptible individuals. If such changes occur, discontinue Dymista gradually, under medical supervision Potent inhibitors of cytochrome P450 (CYP) 3A4 may increase blood levels of " uticasone propionate Ritonavir: coadministration is not recommended Other potent CYP3A4 inhibitors, such as ketoconazole: use caution with coadministration Intranasal corticosteroids may cause a reduction in growth velocity when administered to pediatric patients. Monitor the growth routinely of pediatric patients receiving Dymista In clinical trials, the most common adverse reactions that occurred with Dymista Nasal Spray, azelastine hydrochloride nasal spray, " uticasone nasal spray, and vehicle placebo groups, respectively, were dysgeusia (4%, 5%, 1%, <1%), epistaxis (2% for each group), and headache (2%, 2%, 2%, and 1%) Pregnancy Category C: based on animal data; may cause fetal harm

DYMISTA (AZELASTINE HYDROCHLORIDE 137 MCG / FLUTICASONE PROPIONATE 50 MCG) NASAL SPRAY
Brief Summary (for Full Prescribing Information, see package insert)
1 INDICATIONS AND USAGEDymista Nasal Spray is indicated for the relief of symptoms of seasonal allergic rhinitis in patients 12 years of age and older who require treatment with both azelastine hydrochloride and !uticasone propionate for symptomatic relief.
5 WARNINGS AND PRECAUTIONS5.1 SomnolenceIn clinical trials, the occurrence of somnolence has been reported in some patients (6 of 853 patients) taking Dymista Nasal Spray [see Adverse Reactions (6.1)]. Patients should be cautioned against engaging in hazardous occupations requiring complete mental alertness and motor coordination such as operating machinery or driving a motor vehicle after administration of Dymista Nasal Spray. Concurrent use of Dymista Nasal Spray with alcohol or other central nervous system depressants should be avoided because additional reductions in alertness and additional impairment of central nervous system performance may occur [see Drug Interactions (7.1)].
5.2 Local Nasal EffectsIn clinical trials of 2 to 52 weeks’ duration, epistaxis was observed more frequently in patients 38 treated with Dymista Nasal Spray than those who received placebo [see Adverse Reactions (6)].Instances of nasal ulceration and nasal septal perforation have been reported in patients following the intranasal application of corticosteroids. There were no instances of nasal ulceration or nasal septal perforation observed in clinical trials with Dymista Nasal Spray. Because of the inhibitory effect of corticosteroids on wound healing, patients who have experienced recent nasal ulcers, nasal surgery, or nasal trauma should not use Dymista Nasal Spray until healing has occurred. In clinical trials with !uticasone propionate administered intranasally, the development of localized infections of the nose and pharynx with Candida albicans has occurred. When such an infection develops, it may require treatment with appropriate local therapy and discontinuation of treatment with Dymista Nasal Spray. Patients using Dymista Nasal Spray over several months or longer should be examined periodically for evidence of Candida infection or other signs of adverse effects on the nasal mucosa.
5.3 Glaucoma and CataractsNasal and inhaled corticosteroids may result in the development of glaucoma and/or cataracts. Therefore, close monitoring is warranted in patients with a change in vision or with a history of increased intraocular pressure, glaucoma, and/or cataracts.Glaucoma and cataract formation were evaluated with intraocular pressure measurements and slit 56 lamp examinations in a controlled 12-month study in 612 adolescent and adult patients aged 12 years and older with perennial allergic or vasomotor rhinitis (VMR). Of the 612 patients enrolled in the study, 405 were randomized to receive Dymista Nasal Spray (1 spray per nostril twice daily) and 207 were randomized to receive !uticasone propionate nasal spray (2 sprays per nostril once daily). In the Dymista Nasal Spray group, one patient had increased intraocular pressure at month 6. In addition, three patients had evidence of posterior subcapsular cataract at month 6 and one at month 12 (end of treatment). In the !uticasone propionate group, three patients had evidence of posterior subcapsular cataract at month 12 (end of treatment).
5.4 ImmunosuppressionPersons who are using drugs, such as corticosteroids, that suppress the immune system are more susceptible to infections than healthy individuals. Chickenpox and measles, for example, can have a more serious or even fatal course in susceptible children or adults using corticosteroids. In children or adults who have not had these diseases or been properly immunized, particular care should be taken to avoid exposure. How the dose, route, and duration of corticosteroid administration affect the risk of developing a disseminated infection is not known. The contribution of the underlying disease and/or prior corticosteroid treatment to the risk is also not known. If exposed to chickenpox, prophylaxis with varicella zoster immune globulin (VZIG) may be indicated. If exposed to measles, prophylaxis with pooled intramuscular immunoglobulin 74 (IG) may be indicated. (See the respective package inserts for complete VZIG and IG prescribing information.) If chickenpox develops, treatment with antiviral agents may be considered.Corticosteroids should be used with caution, if at all, in patients with active or quiescent tuberculous infections of the respiratory tract; untreated local or systemic fungal or bacterial infections; systemic viral or parasitic infections; or ocular herpes simplex because of the potential for worsening of these infections.
5.5 Hypothalamic-Pituitary-Adrenal (HPA) Axis EffectsWhen intranasal steroids are used at higher than recommended dosages or in susceptible individuals at recommended dosages, systemic corticosteroid effects such as hypercorticism and adrenal suppression may appear. If such changes occur, the dosage of Dymista Nasal Spray should be discontinued slowly, consistent with accepted procedures for discontinuing oral corticosteroid therapy. The concomitant use of intranasal corticosteroids with other inhaled corticosteroids could increase the risk of signs or symptoms of hypercorticism and/or suppression of the HPA axis. The replacement of a systemic corticosteroid with a topical corticosteroid can be accompanied by signs of adrenal insuf"ciency, and in addition some patients may experience symptoms of withdrawal, e.g., joint and/or muscular pain, lassitude, and depression. Patients previously treated for prolonged periods with systemic corticosteroids and transferred to topical corticosteroids should be carefully monitored for acute adrenal insuf"ciency in response to stress. In those patients who have asthma or
other clinical conditions requiring long-term systemic corticosteroid treatment, too rapid a decrease in systemic corticosteroids may cause a severe exacerbation of their symptoms.
5.6 Use of Cytochrome P450 3A4 InhibitorsRitonavir and other strong cytochrome P450 3A4 (CYP3A4) inhibitors can signi"cantly increase plasma !uticasone propionate exposure, resulting in signi"cantly reduced serum cortisol concentrations [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)]. During postmarketing use, there have been reports of clinically signi"cant drug interactions in patients receiving !uticasone propionate and ritonavir, resulting in systemic corticosteroid effects including Cushing syndrome and adrenal suppression. Therefore, coadministration of Dymista Nasal Spray and ritonavir is not recommended unless the potential bene"t to the patient outweighs the risk of systemic corticosteroid side effects.Use caution with the coadministration of Dymista Nasal Spray and other potent CYP3A4 inhibitors, such as ketoconazole [see Drug Interactions (7.2) and Clinical Pharmacology (12.3)].
5.7 Effect on GrowthCorticosteroids may cause a reduction in growth velocity when administered to pediatric patients. Monitor the growth routinely of pediatric patients receiving Dymista Nasal Spray [see Use in Speci!c Populations (8.4)].
6 ADVERSE REACTIONSSystemic and local corticosteroid use may result in the following:
Somnolence [see Warnings and Precautions (5.1)]Local nasal effects, including epistaxis, nasal ulceration, nasal septal perforation, impaired wound healing, and Candida albicans infection [see Warnings and Precautions (5.2)]Cataracts and glaucoma [see Warnings and Precautions (5.3)]Immunosuppression [see Warnings and Precautions (5.4)]Hypothalamic-pituitary-adrenal (HPA) axis effects, including growth reduction [see Warnings and Precautions (5.5 and 5.7), Use in Speci!c Populations (8.4)]
6.1 Clinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not re!ect rates observed in practice. The safety data described below re!ect exposure to Dymista Nasal Spray in 853 patients (12 years of age and older; 36% male and 64% female) with seasonal allergic rhinitis in 3 doubleblind, placebo-controlled clinical trials of 2-week duration. The racial distribution for the 3 clinical trials was 80% white, 16% black, 2% Asian, and 1% other. In the 12-month open-label, active-controlled clinical trial, 404 Asian patients (240 males and 164 females) with perennial allergic rhinitis or vasomotor rhinitis were treated with Dymista Nasal Spray, 1 spray per nostril twice daily.Adults and Adolescents 12 Years of Age and Older In the 3 placebo-controlled clinical trials of 2-week duration, 3411 patients with seasonal allergic rhinitis were treated with 1 spray per nostril of Dymista Nasal Spray, azelastine hydrochloride nasal spray, !uticasone propionate nasal spray, or placebo, twice daily. The azelastine hydrochloride and !uticasone propionate comparators use the same vehicle and device as Dymista Nasal Spray and are not commercially marketed. Overall, adverse reactions were 16% in the Dymista Nasal Spray treatment groups, 15% in the azelastine hydrochloride nasal spray groups, 13% in the !uticasone propionate nasal spray groups, and 12% in the placebo groups. Overall, 1% of patients in both the Dymista Nasal Spray and placebo groups discontinued due to adverse reactions.Table 1 contains adverse reactions reported with frequencies greater than or equal to 2% and more frequently than placebo in patients treated with Dymista Nasal Spray in the seasonal allergic rhinitis controlled clinical trials.
Table 1. Adverse Reactions with >2% Incidence and More Frequently than Placebo in Placebo-Controlled Trials of 2 Weeks Duration with Dymista Nasal
Spray in Adult and Adolescent Patients With Seasonal Allergic Rhinitis
1 spray per nostril twice daily
Dymista Nasal Spray
(N=853)*
Azelastine Hydrochloride Nasal Spray†
(N=851)
Fluticasone Propionate
Nasal Spray†
(N=846)
Vehicle Placebo
(N=861)
Dysgeusia 30 (4%) 44 (5%) 4 (1%) 2 (<1%)
Headache 18 (2%) 20 (2%) 20 (2%) 10 (1%)
Epistaxis 16 (2%) 14 (2%) 14 (2%) 15 (2%)
*Safety population N=853, intent-to-treat population N=848† Not commercially marketed
In the above trials, somnolence was reported in <1% of patients treated with Dymista Nasal Spray (6 of 853) or vehicle placebo (1 of 861) [see Warnings and Precautions (5.1)].Long-Term (12-Month) Safety Trial: In the 12-month, open-label, active-controlled, long-term safety trial, 404 patients (12 years of age and older) with perennial allergic rhinitis or vasomotor rhinitis were treated with Dymista Nasal Spray 1 spray per nostril twice daily and 207 patients were treated with !uticasone propionate nasal spray, 2 sprays per nostril once daily. Overall, adverse reactions were 47% in the Dymista Nasal Spray treatment group and 44% in the !uticasone propionate nasal spray group. The most frequently reported adverse reactions (# 2%) with Dymista Nasal Spray were headache, pyrexia, cough, nasal congestion, rhinitis, dysgeusia, viral infection, upper respiratory tract infection, pharyngitis, pain, diarrhea, and epistaxis. In the Dymista Nasal Spray treatment
group, 7 patients (2%) had mild epistaxis and 1 patient (<1%) had moderate epistaxis. In the !uticasone propionate nasal spray treatment group 1 patient (<1%) had mild epistaxis. No patients had reports of severe epistaxis. Focused nasal examinations were performed and no nasal ulcerations or septal perforations were observed. Eleven of 404 patients (3%) treated with Dymista Nasal Spray and 6 of 207 patients (3%) treated with !uticasone propionate nasal spray discontinued from the trial due to adverse events.
7 DRUG INTERACTIONSNo formal drug interaction studies have been performed with Dymista Nasal Spray. The drug interactions of the combination are expected to re!ect those of the individual components.
7.1 Central Nervous System DepressantsConcurrent use of Dymista Nasal Spray with alcohol or other central nervous system depressants should be avoided because somnolence and impairment of central nervous system performance may occur [see Warnings and Precautions (5.1)].
7.2 Cytochrome P450 3A4Ritonavir (a strong CYP3A4 inhibitor) signi"cantly increased plasma !uticasone propionate exposure following administration of !uticasone propionate aqueous nasal spray, resulting in signi"cantly reduced serum cortisol concentrations [see Clinical Pharmacology (12.3)]. During postmarketing use, there have been reports of clinically signi"cant drug interactions in patients receiving !uticasone propionate and ritonavir, resulting in systemic corticosteroid effects including Cushing syndrome and adrenal suppression. Therefore, coadministration of !uticasone propionate and ritonavir is not recommended unless the potential bene"t to the patient outweighs the risk of systemic corticosteroid side effects.Ketoconazole (also a strong CYP3A4 inhibitor), administered in multiple 200 mg doses to steady-state, increased plasma exposure of !uticasone propionate, reduced plasma cortisol AUC, but had no effect on urinary excretion of cortisol, following administration of a single 1000 mcg dose of !uticasone propionate by oral inhalation route.Caution should be exercised when Dymista Nasal Spray is coadministered with ketoconazole and other known strong CYP3A4 inhibitors.
8 USE IN SPECIFIC POPULATIONS8.1 PregnancyDymista Nasal Spray: Teratogenic Effects: Pregnancy Category C:There are no adequate and well-controlled clinical trials of Dymista Nasal Spray, azelastine hydrochloride only, or !uticasone propionate only in pregnant women. Animal reproductive studies of azelastine hydrochloride and !uticasone propionate in mice, rats, and/or rabbits revealed evidence of teratogenicity as well as other developmental toxic effects. Because animal reproduction studies are not always predictive of human response, Dymista Nasal Spray should be used during pregnancy only if the potential bene"t justi"es the potential risk to the fetus.Azelastine hydrochloride: Teratogenic Effects: In mice, azelastine hydrochloride caused embryo-fetal death, malformations (cleft palate; short or absent tail; fused, absent or branched ribs), delayed ossi"cation, and decreased fetal weight at an oral dose approximately 610 times the maximum recommended human daily intranasal dose (MRHDID) in adults (on a mg/m2 basis at a maternal dose of 68.6 mg/kg). This dose also caused maternal toxicity as evidenced by decreased body weight. Neither fetal nor maternal effects occurred at a dose that was approximately 26 times the MRHDID (on a mg/m2 basis at a maternal dose of 3 mg/kg).In rats, azelastine hydrochloride caused malformations (oligo- and brachydactylia), delayed ossi"cation and skeletal variations, in the absence of maternal toxicity, at an oral dose approximately 530 times the MRHDID in adults (on a mg/m2 basis at a maternal dose of 30 mg/kg). At a dose approximately 1200 times the MRHDID (on a mg/m2 basis at a maternal dose of 68.6 mg/kg), azelastine hydrochloride also caused embryo-fetal death and decreased fetal weight; however, this dose caused severe maternal toxicity. Neither fetal nor maternal effects occurred at a dose approximately 53 times the MRHDID (on a mg/m2 basis at a maternal dose of 3 mg/kg).In rabbits, azelastine hydrochloride caused abortion, delayed ossi"cation, and decreased fetal weight at oral doses approximately 1100 times the MRHDID in adults (on a mg/m2 basis at a maternal dose of 30 mg/kg); however, these doses also resulted in severe maternal toxicity. Neither fetal nor maternal effects occurred at a dose approximately 11 times the MRHDID (on a mg/m2 basis at a maternal dose of 0.3 mg/kg).Fluticasone propionate: Teratogenic Effects: Corticosteroids have been shown to be teratogenic in laboratory animals when administered systemically at relatively low dosage levels. Subcutaneous studies in the mouse and rat at doses approximately equivalent to and 4 times, respectively, the MRHDID in adults (on a mcg/m2 basis at maternal doses of 45 and 100 mcg/kg respectively), revealed fetal toxicity characteristic of potent corticosteroid compounds, including embryonic growth retardation, omphalocele, cleft palate, and retarded cranial ossi"cation.In the rabbit, fetal weight reduction and cleft palate were observed at a subcutaneous dose less than the MRHDID in adults (on a mcg/m2 basis at a maternal dose of 4 mcg/kg). However, no teratogenic effects were reported at oral doses up to approximately 25 times the MRHDID in adults (on a mcg/m2 basis at a maternal dose of 300 mcg/kg) of !uticasone propionate to the rabbit. No !uticasone propionate was detected in the plasma in this study, consistent with the established low bioavailability following oral administration [see Clinical Pharmacology (12.3)].Experience with oral corticosteroids since their introduction in pharmacologic, as opposed to physiologic, doses suggests that rodents are more prone to teratogenic effects from corticosteroids than humans. In addition, because there is a natural increase in corticosteroid production during pregnancy, most women will require a lower exogenous corticosteroid dose and many will not need corticosteroid treatment during pregnancy.
Nonteratogenic Effects: Fluticasone propionate crossed the placenta following oral administration of approximately 4 and 25 times the MRHDID in adults (on a mcg/m2 basis at maternal doses of 100 mcg/kg and 300 mcg/kg to rats and rabbits, respectively).
8.3 Nursing MothersDymista Nasal Spray: It is not known whether Dymista Nasal Spray is excreted in human breast milk. Because many drugs are excreted in human milk, caution should be exercised when Dymista Nasal Spray is administered to a nursing woman. Since there are no data from well-controlled human studies on the use of Dymista Nasal Spray by nursing mothers, based on data from the individual components, a decision should be made whether to discontinue nursing or to discontinue Dymista Nasal Spray, taking into account the importance of Dymista Nasal Spray to the mother.Azelastine hydrochloride: It is not known if azelastine hydrochloride is excreted in human milk.Fluticasone propionate: It is not known if !uticasone propionate is excreted in human milk. However, other corticosteroids are excreted in human milk. Subcutaneous administration to lactating rats of 10 mcg/kg of tritiated !uticasone propionate (less than the maximum recommended daily intranasal dose in adults on a mcg/m2 basis) resulted in measurable radioactivity in the milk.
8.4 Pediatric UseSafety and effectiveness of Dymista Nasal Spray in pediatric patients below the age of 12 years have not been established.Controlled clinical studies have shown that intranasal corticosteroids may cause a reduction in growth velocity in pediatric patients. This effect has been observed in the absence of laboratory evidence of HPA axis suppression, suggesting that growth velocity is a more sensitive indicator of systemic corticosteroid exposure in pediatric patients than some commonly used tests of HPA axis function. The long-term effects of this reduction in growth velocity associated with intranasal corticosteroids, including the impact on "nal adult height, are unknown. The potential for “catch-up” growth following discontinuation of treatment with intranasal corticosteroids has not been adequately studied. The growth of pediatric patients receiving intranasal corticosteroids, including Dymista Nasal Spray, should be monitored routinely (e.g., via stadiometry). The potential growth effects of prolonged treatment should be weighed against the clinical bene"ts obtained and the risks/bene"ts of treatment alternatives.
8.5 Geriatric UseClinical trials of Dymista Nasal Spray did not include suf"cient numbers of patients 65 years of age and older to determine whether they respond differently from younger patients. Other reported clinical experience has not identi"ed differences in responses between the elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, re!ecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
10 OVERDOSAGEDymista Nasal Spray: Dymista Nasal Spray contains both azelastine hydrochloride and !uticasone propionate; therefore, the risks associated with overdosage for the individual components described below apply to Dymista Nasal Spray.Azelastine hydrochloride: There have been no reported overdosages with azelastine hydrochloride. Acute azelastine hydrochloride overdosage by adults with this dosage form is unlikely to result in clinically signi"cant adverse events, other than increased somnolence, since one (1) 23 g bottle of Dymista Nasal Spray contains approximately 23 mg of azelastine hydrochloride. Clinical trials in adults with single doses of the oral formulation of azelastine hydrochloride (up to 16 mg) have not resulted in increased incidence of serious adverse events. General supportive measures should be employed if overdosage occurs. There is no known antidote to Dymista Nasal Spray. Oral ingestion of antihistamines has the potential to cause serious adverse effects in children. Accordingly, Dymista Nasal Spray should be kept out of the reach of children.Fluticasone propionate: Chronic !uticasone propionate overdosage may result in signs/symptoms of hypercorticism [see Warnings and Precautions (5.2)]. Intranasal administration of 2 mg (10 times the recommended dose) of !uticasone propionate twice daily for 7 days to healthy human volunteers was well tolerated. Single oral !uticasone propionate doses up to 16 mg have been studied in human volunteers with no acute toxic effects reported. Repeat oral doses up to 80 mg daily for 10 days in volunteers and repeat oral doses up to 10 mg daily for 14 days in patients were well tolerated. Adverse reactions were of mild or moderate severity, and incidences were similar in active and placebo treatment groups. Acute overdosage with this dosage form is unlikely since one (1) 23 g bottle of Dymista Nasal Spray contains approximately 8.5 mg of !uticasone propionate.
Distributed by:MEDA Pharmaceuticals® Meda Pharmaceuticals Inc. Somerset, NJ 08873-4120

482 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
ENT JOURNAL ONLINE
Ear, Nose & Throat Journal's Web site is easy to navigate and provides readers with more editorial content each month than ever before. Access to
everything on the site is free of charge to physicians and allied ENT professionals. To take advantage of all our site has to offer, go to www.entjournal.
com and click on the "Registration" link. Once you have !lled out the brief registration form, you will have full access. Explore and enjoy!
Synchronous verrucous carcinoma and inverted papilloma of the lacrimal sac: Case report and clincal updateCheryl Gustafson, MD; Eugene Einhorn, MD; Mary H. Scanlon, MD; Kenneth E. Morgenstern, MD; Paul J. Howlett, MD; Noam A. Cohen, MD, PhD Inverted papilloma is a benign epithelial tumor of the nasal cavity. It is known to coexist with malignancy in 5 to 13% of cases, with squamous cell carcinoma being the most common malignancy. Another asso-ciated malignancy, one that is extremely rare, is verru-cous carcinoma. To the best of our knowledge, no case of verrucous carcinoma occurring alone or in association with another neoplasm has been described in the nasolac-rimal system. We report a case of synchronous verrucous carcinoma and inverted papilloma of the lacrimal sac in a 47-year-old man. !e patient presented with epiphora, nasal obstruction, swelling of the le" medial canthus, and drainage of a foul-smelling #uid from the le" nostril. Computed tomography and magnetic resonance imaging detected the presence of a large mass occupying the le" nasal cavity and sinuses with extension into the nasopharynx. In addition, bony invasion of the anteroinferomedial wall of the le" orbit was noted with extension of the tumor into the orbit itself, which resulted in lateral displacement of the le" medial rectus muscle. !e patient underwent endoscopic debulking of the le" sinonasal lesion. Of note, the surgery had to be completed in stages because of excessive blood loss. Histopathologic examination of the intranasal component of the tumor identi$ed it as an inverted papilloma. One month a"er the intranasal resection, a le" dacryocystectomy was performed; histopathologic examination revealed that an invasive verrucous squamous cell carcinoma had arisen within the inverted papilloma.
A case and a series of published cases of esthesioneuroblastoma (ENB) in which long-standing paraneoplastic SIADH had preceded ENB diagnosis Uri Gabbay, MD, MPH; Leonor Leider-Trejo, MD; Gideon Marshak, MD; Merav Gabbay, MD; Dan M. Fliss, MD Esthesioneuroblastoma (ENB) is a rare tumor of the olfac-tory mucosa. We treated a 50-year-old man with an ENB
JOURNAL ONLINE www.entjournal.com
in the right ethmoid sinus who had been diagnosed 16 years earlier with syndrome of inappropriate antidiuretic hormone secretion (SIADH) of unknown cause. When the ENB was surgically removed, the patient’s osmoregu-lation returned to normal—that is, his SIADH resolved completely, which suggested that the SIADH was paraneo-plastic in nature. These events prompted us to review the literature to determine if there is an association between our patient’s ENB and his SIADH in general and between long-standing SIADH that precedes ENB in particular. Based on our review and an extrapolation of data, we have estimated that 1,300 cases of ENB have occurred since it was first described in 1924. Of these cases, SIADH was reported in 26 cases, including ours, which represents an estimated prevalence of 2% (although we believe this is actually an underestimation of the true prevalence). Of the 26 cases, SIADH had already been present in 14 patients (54%) prior to their diagnosis of EBN for a me-dian duration of 3.5 years. We recommend that patients with newly diagnosed EBN be evaluated for SIADH. In those who are SIADH-positive, a resolution of SIADH should be expected once the ENB has been removed. If this does not occur, one should suspect that the ENB was not completely removed. If SIADH resolves but later recurs during follow-up, then a relapse should be suspected. In long-standing SIADH of unknown etiology, nasal sinus imaging should be considered.
Glass in the frontal sinus: 28-year delayed presentationAlice K. Guidera, MBChB, BSc; Peter M. Dixon, MBBS, FRCS; Hans R. Stegehuis, MBChB, FRACS Reports of delayed presen-tation of foreign bodies in the frontal sinus are infre-quent and likely to become rarer with the widespread availability of computed tomography in the last 2 decades. We present a case in which glass from a road tra%c injury was found in the frontal sinus, causing symptoms of frontal sinusitis 28 years a"er the initial injury. We also present a review of the literature.
ONLINE EXCLUSIVES

RADIESSE Voice and RADIESSE Voice Gel implants are sold with ei-ther a malleable transoral needle or a non-coring percutaneous needle.
Transoral needle25 cm long overall16-gauge malleable shaft
Transoral needle tip24-gauge, 1 cm tipMarker at 5mm
1. Rosen, Clark A., et al, Vocal Fold Augmentation with Calcium Hydroxylapatite: Twelve-Month Report, Laryngoscope (2009), 119(5):1033-41
2. Amin, Milan R., Thyrohyoid Approach for Vocal Fold Augmentation, Annals of Otology, Rhinology & Laryngology (2006), 115(9):699-702
3. Rees, Cathrine J., Mouadeb, Debbie A., Belafsky, Peter C., Otolaryngology-Head and Neck Surgery (2008), 138:743-746
4. M. Boyd Gillespie, et al, Effectiveness of Calcium Hydroxylapatite Paste in Voice Rehabilitation., Annals of ORL, 118(8): 546-551
In Europe, availability of the RADIESSE Voice implant varies by country, and the RADIESSE Voice Gel implant is currently not available. Copyright © 2010 Merz Aesthetics, Inc. All rights reserved. RADIESSE is a registered trademark of Merz Aesthetics, Inc. EM00311-00
RADIESSE® Voice and RADIESSE® Voice Gel Implants for vocal fold augmentation
Clinically proven results
Proven effective – in clinical testing with 12 months follow up, the majority of patients treated with the RADIESSE Voice implant reported that their voice was greatly or signifi cantly improved.1 Proven safe – no granuloma formation or major complications have been reported.1
Proven long-lasting – results typically last more than 12 months.1,4
Convenient and easy-to-use
No fat harvesting or processingNo preparation or mixing – supplied in ready-to-use 1.0 cc syringe with injection needleNo refrigeration – store at room temperatureNo allergy testing – contains no animal or human componentsNo waiting – injection can be performed in-offi ce in 30 minutes or less
Injection techniques
RADIESSE products can be inject-ed through a 25-gauge needle in the operating room or in the of-fi ce using a trans-thyroid cartilage, trans-cricothyroid membrane or thyrohyoid approach.2,3
RADIESSE Voice Products
The RADIESSE Voice injectable implant contains synthetic Cal-cium Hydroxylapatite (CaHA) mi-crospheres, which have a diameter of 25-45 micron, suspended in an aqueous resorbable carrier gel. The product is injectable through a 25-gauge needle. RADIESSE Voice implant provides vocal fold augmentation with results that typically lasts 1 year.
The RADIESSE Voice Gel inject-able implant contains synthetically derived polymers, with no CaHA microspheres, and it is suitable for short term vocal fold augmenta-tion in patients where reversible nerve damage is suspected, or in patients wishing a short term aug-mentation before deciding to have a long term augmentation done with the RADIESSE Voice implant.
References
Merz Aesthetics, Inc. | www.radiesse-voice.com | [email protected] | North America: 1-866-862-1209
RADIESSE Voice implant (CaHA + gel carrier) initially performs as a fi ller.
Macrophages start to degrade gel carrier (2-3 months).
Macrophages dissolve gel carrier as new collagen forms.
Unique mechanism of action
Over time the RADIESSE Voice implant carrier gel is resorbed and the Calcium Hydroxylapatite par-ticles support in-growth of new collagen. The durable Calcium Hydroxylapatite microspheres degrade slowly over years for a long-lasting effect. The implant remains soft after injection and does not ossify.
In clinical testing and routine clini-cal use for over 6 years, no implant migration or evidence of granulo-ma formation has been observed.
Percutaneous needle1.5”, 25-gauge
Percutaneous needle tipNon-coring Huber point

484 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
ENT JOURNAL ONLINE
Case report: Paraneoplastic neurologic syndrome associated with squamous cell carcinoma of the tonsil Je!rey R. Janus, MD; Sivakumar Chinnadurai, MD; Eric J. Moore, MDParaneoplastic syndromes include a variety of disorders that a!ect the neurologic, endocrine, mucocutaneous, hematologic, and other sys-tems as a result of neoplastic disease. Although their pre-sentations vary, syndromes occur when tumor antigens exhibit cross-reactivity to similar antigens expressed by these systems. "e antigens in the ner-vous system are called “onconeural” antigens. Although many disorders are associated with a comparatively high incidence of paraneoplastic neurologic syndromes, only a few cases have been associated with squamous cell carcinoma (SCC) of the tonsil. We report the case of a 69-year-old man who initially presented with weakness and spastic gait. He was subsequently found to have a characteristic paraneoplastic tractopathy on thoracic magnetic resonance imaging. "e subsequent workup and operative intervention identi#ed a T2N0M0 SCC of the tonsil. Following resection, the patient’s overall symptoms were signi#cantly alleviated, and his gait improved. A thorough literature search yielded no other report of a tonsillar SCC with associated paraneoplastic thoracic spine tractopathy.
Diffuse sphenoid bone cavernous hemangioma presenting during pregnancyHugh Robertson, MD, FACR; Enrique Palacios, MD, FACR; Sheryl Rincon, MD; Kamal R. Shah, MDWe present a case of di!use sphenoid bone cavernous hem-angioma in a 22-year-old primigravid woman. Her disease #rst manifested clinically as progressively decreasing vision in her le$ eye during her third trimester of pregnancy. We also discuss the known causes and some theoretical causes of cavernous hemangioma enlargement during pregnancy.
Arteriovenous malformation of the neck: An unusual cause of hoarseness successfully treated with endovascular techniquesJoseph J. Gemmete, MD; Neeraj Chaudhary, MD; Aditya S. Pandey, MD; Dheeraj Gandhi, MD; Sameer A. Ansari, MD, PhD Hoarseness is a common presenting symptom in patients referred to the otolaryngology clinic. An arteriovenous mal-formation (AVM) in the neck is a previously unreported cause of hoarseness. We describe the case of a 61-year-old woman who presented with hoarseness and vocal fold paralysis, which was caused by an AVM. She was successfully treated with endovascular embolization. Devascularization of the AVM resulted in symptomatic relief of the hoarseness and resolution of the vocal fold paralysis, presumably secondary to interval reduction in edema and venous congestion.
Intracranial and internal jugular vein thrombosis secondary to ENT infections: A report of 3 casesFaruque Riffat, BSc(Med), MBBS (Hons); Martin Forer, FRACS; Andrew Wignall, FRACS; David Veivers, FRACS; Nirmal Patel, MS, FRACSWe report 3 cases of rare, life-threatening intracrani-al and internal jugular vein (IJV) thrombosis that were caused by common ENT infections. These infections included otitis media in a 6-year-old girl, tonsillitis in a 21-year-old woman, and odontogenic sepsis in a 56-year-old woman. All 3 patients were treated with culture-directed systemic antibiotics; 2 of them also required surgical drainage (the child and the older adult). The 2 adults also received therapeutic anticoagulation, which was continued until venous recanalization was documented; the duration of combined antibiotic and anticoagulation treatment was 6 weeks. All 3 patients made uneventful recoveries. Sig-nificant morbidities associated with intracranial and IJV thrombosis were avoided as a result of prompt diagnosis and judicious treatment.
Endoscopic closure of a frontocutaneous !stulaAlexandros Tsikoudas, DLO, FRCS(Otol), FRCS(ORL–HNS); Christos Georgalas, PhD, MRCS, FRCS(ORL–HNS)A frontocutaneous #stula is a rare sequela of frontal sinus pathology. Management via an endoscopic approach is not frequently reported in the literature. We describe such an approach with the aid of still photography and imaging plus videoendoscopy, and we discuss the current literature.
ONLINE DEPARTMENTS
Laryngoscopic Clinic:A case of cicatricial pemphigoid of the larynx successfully treated with plasmapheresis therapyTakeshi Kusunoki, MD; Katsuhisa Ikeda, MD
Otoscopic Clinic:Dehiscence of the high jugular bulbMin-Tsan Shu, MD; Yu-Chun Chen, MD; Cheng-Chien Yang, MD; Kang-Chao Wu, MD
Rhinoscopic Clinic:Endoscopic appearance of a healed skull base resection reconstructed with a pedicled nasoseptal "apHadia M. Leon, MD; Mark H. Tabor, MD

Xylitol is a natural sweetener derived
from the fibrous portions of plants and
is naturally produced in our bodies—but
this sugar is unique in that it has
significant health benefits. Research
suggests that safe, all-natural Xlear
Sinus Care System helps promote better
upper respiratory health when used
on a regular basis. And unlike many
prescription or medicated sprays with
unwanted side effects, daily usage of
Xlear Sinus Care Spray is non-addictive
and will not damage tissues. Xlear is
safe for infants, yet strong enough for
adults to soothe the most stubborn and
irritated sinus conditions. For optimal
wellness, the choice is clear!
XYLITOLTHE POWER OF
PROTECT YOUR PATIENTS’ NOSES FROM NASTY NASAL IRRITANTS AND CONTAMINANTS THIS SEASON.The Sinus Care System is clinically proven to reduce irritants and airborne contaminants in the upper respiratory tract while soothing and moisturizing the sinuses and nasal passages.
Learn more about XLEAR, the XYLITOL EXPERTS at www.xlear.com. Or contact XLEAR at 877.599.5327.
as
earch
Xlear
ote better
used
many
ys with
age of
ddictive
lear is
ugh for
born and
optimal
w.xlear.com.

DYSPHAGIA CLINIC
486 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
GUEST EDITORIAL
Immunization guidelines for cochlear implant recipients
[Editor’s note: !is Guest Editorial has been adapted with permission from an article entitled “Implants in Otology” that appeared in the Fall 2012 issue of Sound-ings, the Pennsylvania Academy of Otolaryngology–Head and Neck Surgery’s newsletter.]
Patients who have a cochlear implant are considered to be at a higher risk of developing meningitis follow-ing otitis media. Whether this occurs along the elec-trode going from the middle ear into the cochlea or through a blood-borne pathway is unclear. !e most prevalent organism in both children and adults re-mains Streptococcus pneumonia, also known as Pneu-mococcus.
Although there was a high incidence of implant- related cases of meningitis when an old implant design had a positioner placed along the intracochlear elec-trode to get it closer to the modiolus, other cochlear implant manufacturers had devices that su"ered the same complication. !is was an area of great concern that prompted international attention. In 2006, an aggressive awareness campaign was initiated by the American Academy of Otolaryngology–Head and Neck Surgery’s Implantable Device Committee with full support of the manufacturers.
A few other factors might have contributed to the high incidence of meningitis besides the positioner de-sign. For example, there was a greater number of cases in children with congenital anomalies. !ere was also a peak in the number of cases in Europe. Adoption of careful operative techniques and a vaccination pro-gram were deemed successful, resulting in fewer cases of meningitis related to cochlear implant prostheses.
Recently, the Centers for Disease Control and Pre-vention (CDC) Advisory Committee on Immunization Practices issued new recommendations for vaccina-tions in both adults and children. !e announcement
was made through the CDC Web site (www.cdc.gov/vaccines/vpd-vac/pneumo/vac-PCV13-adults.htm) in October 2012.
!e previous vaccination sequence began with pneumococcal 7-valent conjugate vaccine (PCV7) for pediatric patients and pneumococcal polysaccharide vaccine (PPSV23) for older children and adults. An updated vaccine, PCV13, contains additional anti-genic strains that were not covered by the earlier series of vaccines. It is now recommended that all pending cochlear implant patients initially receive PCV13, fol-lowed by PPSV23 8 weeks later. It is also recommended that those who have a cochlear implant and who have received PPSV23 should still get the PCV13 vaccine.
A practical problem has arisen with these updated guidelines. !e typical means for delivery of the vac-cine is through the pediatrician’s or primary care phy-sician’s o#ce. !ese critical providers may not be aware of the CDC recommendations. Our cochlear implant center has sent out a mailing to our existing cochlear implant recipients to get them updated on their immu-nization coverage. We provided a letter with an expla-nation and the link to the CDC Web site.
We understand that some facilities or providers cannot get the PCV13 vaccine or are unaware of the changes in the current guidelines. Nonetheless, we en-courage patients to follow the advice of the CDC Ad-visory Committee and persist with this request. !e CDC is taking every precaution to minimize the op-portunity for this bacterial infection to cause signi$-cant morbidity.
Barry E. Hirsch, MDChair, PAO–HNS Otology CommitteeDirector, Division of Otology–NeurotologyUniversity of Pittsburgh Medical Center

GN Otometrics, Australia.Telephone: +61 2 9743 9707Email: [email protected]
Bringing diagnostic accuracy and efficiency
into balance testing
www.futurefitting.com
www.icsimpulse.com
Advanced diagnosis using Impulse by Dr David Szmulewicz 21 August 2013, Prince Hotel, St Kilda, Victoria
RSVP by 19 August to [email protected]
Assess all 6 semi-circular
canals
RE P O RT I N G
NO
AH
EMR REA
DY
CO
UNSEL IN G
PM
M
H IT
IMMITTANCE
AU
DIO
MET
RY

RHINOSCOPIC CLINIC
488 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Endoscopic view of the sphenoid sinus seen through the posterior ethmoid sinus
RHINOSCOPIC CLINIC
From the Section of Otolaryngology, Halifax Medical Center, Daytona Beach, Fla. (Dr. Christmas and Dr. Mirante); the Department of Otolaryn-gology, University of South Florida, Tampa (Dr. Mirante); Florida State University School of Medicine, Daytona Beach (Dr. Mirante); and the Section of Otolaryngology–St. Raphael Campus; and the Section of Otolaryngology, Yale University School of Medicine, New Haven, Conn. (Dr. Yanagisawa).
Joseph P. Mirante, MD, FACS; Dewey A. Christmas, MD; Eiji Yanagisawa, MD, FACS
In functional endoscopic sinus surgery (FESS) for chronic rhinosinusitis, it is of-ten bene!cial to create a surgically enlarged opening to the sphenoid sinus. "e two stan-dard endoscopic approaches in sphenoid sinus disease are transnasal, through the an-terior wall of the sphenoid sinus, or transeth-moid, through the posterior ethmoid sinus.
An approach to the sphenoid sinus through the ethmoid sinus requires dissection of the anterior and posterior ethmoid cells (!gure, A). "e important landmark in this technique is the posterior wall of the posterior ethmoid sinus (!gure, B). "e approach to the sphe-noid sinus is then carried out through the inferior and medial portion of the posterior ethmoid sinus. "is is important because ap-proaching laterally and superiorly through the lateral portion of the ethmoid sinus could easily injure the optic nerve, or in the case of an Onodi cell, cause entry into the intracra-nial cavity.1 "e opening from the posterior ethmoid into the sphenoid sinus is shown in the !gure, image C. Once that opening has been en-larged, the lateral wall of the sphenoid sinus can be visu-alized, showing the internal carotid artery, optic nerve, and infraoptic recess (!gure, D).
"e transethmoid approach to the sphenoid sinus was described by Messerklinger.2 In an anterior-to-posterior FESS dissection, the surgeon may choose this route as an extension of the posterior ethmoid dissection, to open the sphenoid sinus. As described above, care must
be taken when entering the sphenoid sinus, to dissect inferiorly and medially to avoid injury to the vital struc-tures of the lateral wall of the sphenoid sinus.
References 1. Yanagisawa E, Yanagisawa K, Ashikawa R. "e Onodi (sphenoeth-
moid) cell. In: Yanagisawa E (ed). Atlas of Rhinoscopy. San Diego: Singular "ompson Learning; 2000:92-93.
2. Messerklinger W. Endoskgsiche diagnose und chirurgie der regidi-vierenden sinusitis. In: Krajina Z (ed). Advances in Nose Sinus Sur-gery. Zagreb: Zagreb University; 1985.
Figure. A: Telescopic view (4 mm, 0°) of le! nasal cavity shows a transethmoidal approach to the sphenoid sinus through the anterior and posterior ethmoid cells. B: "e sphenoid sinus is entered through the inferior and medial portion of the le! posterior ethmoid sinus. C: "e posterior wall opening of the posterior ethmoid sinus is enlarged, exposing the sphenoid sinus adequately. D: In the lateral portion of the le! sphenoid sinus, the internal carotid artery (ICA), the optic nerve (ON), and the infraoptic recess (IOR) can be seen.

REMODEL, sponsored by Entellus, is the first prospective, multi-center, randomized, controlled trial with sufficient statistical power to compare standalone Balloon Sinus Dilation to traditional Functional Endoscopic Sinus Surgery (FESS) for the treatment of chronic or recurrent sinusitis. The results confirm past studies on the safety and effectiveness of Entellus balloon technology, and affirm that office balloon dilation should be an integral part of the continuum of care for patients with uncomplicated sinusitis.
EfficacyBalloon dilation and FESS deliver comparable, significant long-term symptom relief and durability.
Patient ExperienceThe REMODEL study results show balloon outcomes were significantly better than FESS in terms of:
Why do REMODEL Results Matter?
effective option in the continuum of patient care
symptom relief is as effective as FESS
contribute to a better patient experience
office means a more efficient practice for you
Why Did Entellus Sponsor REMODEL?A significant number of existing studies demonstrate the safety and efficacy of balloon sinus dilation. As more and more physicians add office balloon sinus dilation to their practice, Entellus recognized the desire from many
prospective, multi-center, randomized, controlled trial comparing balloon dilation and FESS. Entellus sponsored REMODEL to be the first to help address that need.
About the StudyProspective, multi-center, open-label, randomized, controlled trialTreatment: Balloon dilation of maxillary ostia & ethmoid infundibulaControl: Maxillary antrostomy and uncinectomy with
Inclusion Criteria!
sinuses with or without anterior ethmoid disease
practice guidelines
necessary functional endoscopic sinus surgery (Anthem Coverage Guideline or BlueCross BlueShield of North Carolina Medical Policy)
Entellus Medical 3600 Holly Lane North, Suite 40Plymouth, MN 55447O 866.620.7615F 763.463.1599www.EntellusMedical.comwww.SinusSurgeryOptions.com
1738-210 rB 08/13
Request the complete REMODEL study publication at www.EntellusMedical.com/REMODELentj
RANDOMIZED, CONTROLLED STUDY REDEFINES THE CONTINUUM OF CARE
0
1
2
3
4
5
CHANGE IN SNOT-20 SCORE
p<0.0001
Mea
n SN
OT-2
0 Sc
ore
Baseline 6 months
Balloon Dilation
Control (FESS)
= -1.6 = -1.7
p<0.0001Baseline 6 months
Cutler J, Bikhazi N, Light J, Truitt T, Schwartz M. Standalone balloon dilation versus sinus surgery for chronic rhinosinusitis: A prospective, multicenter, randomized, controlled trial. Am J Rhinol Allergy doi.org/10.2500/ajra.2013.27.3970. [Epub ahead of print Aug 5, 2013].
Appropriately Powered to Compare FESS and Balloon Dilation
PARTICIPANT FLOW
53 ASSIGNED TOFESS
42 RECEIVEDFESS
42 COMPLETED6-MONTH VISIT
52 ASSIGNED TOBALLOON DILATION
50 RECEIVEDBALLOON DILATION
49 COMPLETED6-MONTH VISIT
105PATIENTS
UNDERWENT RANDOMIZATION
2 WITHDREW BEFORE TREATMENT
11 WITHDREW BEFORE TREATMENT (8 refused FESS treatment)
Summary:91/92 patients treated (99%) completed the
6-month follow-up
REMODEL
Randomized Evaluation of Maxillary Antrostomy Versus Ostial Dilation Efficacy
Through Long-Term Follow-Up

LARYNGOSCOPIC CLINIC
490 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Extrusion of hydroxyapatite ossicular prosthesis
OTOSCOPIC CLINIC
From the Department of Otolaryngology–Head and Neck Surgery, Rutgers New Jersey Medical School, Newark.
Danielle M. Blake, BA; Senja Tomovic, MD; Robert W. Jyung, MD
A 42-year-old man presented to our department with a worsening le!-sided hearing loss. He had a his-tory of a le!-sided type III tympanoplasty and had undergone placement of a hydroxyapatite total os-sicular replacement prosthesis (TORP) by an outside otolaryngologist 4 years earlier because of recurrent otitis media and hearing loss. He denied experiencing tinnitus, otalgia, otorrhea, vertigo, and imbalance. He also denied prior noise exposure or otologic trauma. He had no right-sided otologic symptoms. His medical history was signi"cant for chronic hepatitis C and type II diabetes mellitus.
Otoscopy of the le! ear revealed an intact tympanic membrane with a hydroxyapatite prosthesis tenting the tympanic membrane and partially extruding through the posterosuperior quadrant ("gure 1). #e right side showed a normal tympanic membrane with no signi"-cant "ndings. A Weber test lateralized to the le!, and
a Rinne test was positive on the right but negative on the le!, consistent with a le!-sided conductive hear-ing loss. An audiogram showed a severe, down-sloping conductive hearing loss on the le!. #e diagnosis of an extruding hydroxyapatite prosthesis was con"rmed by computed tomography (CT) ("gure 2).
#e patient underwent a le! transcanal revision type III tympanoplasty with tragal cartilage and TORP placement. Operative "ndings included an extruding le! middle ear hydroxyapatite prosthesis with com-plete absence of the incus long process and the stapes superstructure. #e stapes footplate was intact and mobile. No evidence of cholesteatoma or infection was found.
Hydroxyapatite is a calcium phosphate ceramic that resembles the mineral matrix of bone, providing a prosthesis that is bioactive, biocompatible, and osteo-conductive.1 Extrusion of hydroxyapatite prostheses
Figure 1. Endoscopic view shows the extruding hydroxyapatite pros-thesis (arrow).
Continued on page 494

GN Otometrics, North America. 1-800-289-2150. [email protected]
The first FDA cleared medical device that assesses all six semicircular canals
This breakthrough revolutionizes vestibular testing by delivering objective results in less than ten minutes. Head Impulse is a simple and precise test which allows you to quickly assess patients exhibiting dizziness and/or vertigo. Integrate ICS Impulse into your existing vestibular test battery to improve patient care and the efficiency of your practice.
Balance
Revolutionize Vestibular Assessment.
Bringing diagnostic accuracy and efficiency into balance testing
ICS Chartr 200 ICS Chartr EP 200 / VEMP ICS AirCal ICS Balance Platform
Leaders in Education
Sign-up for the expert instructed 2013 Head Impulse seminars www.otometrics.com/impulse
Sign up for the VNG/ENG course with Kamran Barin, P.h.D. www.otometrics.com/vngcourse
NEW! Exclusive distribution of MADSEN, ICS and AURICALFind your local distributor at www.otometrics.com
(VEMP - Not FDA cleared)

LARYNGOSCOPIC CLINIC
492 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Of!ce assessment of vocal fold hypomobility
LARYNGOSCOPIC CLINIC
From the Department of Otolaryngology–Head and Neck Surgery, Drexel University College of Medicine, Philadelphia.
Ronak Shah, MD; Rima A. DeFatta, MD; Robert T. Satalo!, MD, DMA, FACS
A 76-year-old woman diagnosed with idiopathic vocal fold paralysis in 1976 had complained of dys-phonia. She had been treated with Te"on vocal fold injection shortly a#er diagnosis. $e treatment was e!ective, and her voice had been stable until sev-eral months prior to presentation to us in 2009. She complained of a “gravely” voice quality, poor volume, odynophonia, and vocal fatigue a#er prolonged speak-ing. Her voice was slightly hoarse, moderately breathy, and so#. Strobovideolaryngoscopy revealed right vo-cal fold immobility with bowing, atrophy, and incom-plete glottic closure (%gure 1). A right jostle sign was present (%gure 2).
Vocal fold immobility can have a neurologic or me-chanical cause. Vocal fold paralysis results from a non-functioning recurrent laryngeal nerve (RLN), whereas vocal fold %xation usually is caused by %brosis or dis-
location of the cricoarytenoid (CA) joint. $ese condi-tions are distinct but can coexist. Patients can present with a variety of vocal complaints that range from dys-phonia to aphonia; vocal fatigue, so# voice, and short phrase length are common. Laryngeal penetration of food and drink can lead to frank aspiration, particu-larly when a supraglottic sensory de%cit is present.1,2
Laryngeal electromyography (LEMG) can con-%rm RLN compromise and determine the severity of injury. Although the correct diagnosis o#en can be made based on laryngoscopic %ndings alone, LEMG is invaluable in establishing an accurate diagnosis.3-5 A systematic approach should include assessment of CA joint mobility, vocal fold level and bulk, vocal process level and position, and laryngeal position during pho-nation. Presence of a jostle sign suggests CA joint mo-bility (passive movement of the arytenoid associated
Figure 1. Strobovideolaryngscopy shows the right vocal fold bowing and atrophy, causing incomplete glottic closure.

GREER Human Allergy PO Box 800, 639 Nuway Circle NE, Lenoir, NC 28645 800.378.3906/www.greerlabs.com © GREER 2013. All Rights Reserved. 092313H913 09.13
Many allergy patients get lost in the grass.
Request tools from a GREER Allergy Sales Consultant to identify patients who still need help.
Call 1.800.378.3906 or, for the quickest response, visit
LostInTheGrass.com
Let GREER® help you get in touch.Subcutaneous immunotherapy (SCIT) can be diffi cult for many of your grass allergy patients to accept and maintain. Previously diagnosed patients who refused or discontinued SCIT may not be coming into your practice for injections. They are not receiving the immunotherapy they need and may still be experiencing intolerable allergy symptoms.
In Touch. Within Reach®.

494 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
LARYNGOSCOPIC CLINIC
Figure 2. !e presence of a right jostle sign indicates passive move-ment of the arytenoid on the paralyzed side caused by contact with the normal arytenoid, which presses against it during adduction. It is seen most easily at the muscular process. !is image also highlights laryngeal rotation toward the paralyzed side during phonation. Contraction of the normal side pulls the laryngeal framework to the le" of the esophageal inlet, which is seen here posteriorly and to the right.
OTOSCOPIC CLINIC
is unfortunately a common complication of middle ear surgery. Reported extrusion rates range from 5 to 22%.2,3
Cartilage interposed between the prosthesis and tympanic membrane has been employed to decrease the chance of extrusion by providing a rigid autolo-gous surface that prevents scarring of the tympanic membrane to the prosthesis.4 !e addition of inter-posed cartilage decreases the rate of extrusion to just 3 to 6%, allowing long-term retention and function of these prostheses.3
References 1. Goldenberg RA, Driver M. Long-term results with hydroxylapa-
tite middle ear implants. Otolaryngol Head Neck Surg 2000;122 (5):635-42.
2. Meijer AG, Verheul J, Albers FW, Segenhout HM. Cartilage inter-position in ossiculoplasty with hydroxyapatite prostheses: A his-topathologic study in the guinea pig. Ann Otol Rhinol Laryngol 2002;111(4):364-9.
3. Shinohara T, Gyo K, Saiki T, Yanagihara N. Ossiculoplasty using hydroxyapatite prostheses: Long-term results. Clin Otolaryngol Allied Sci 2000;25(4):287-92.
4. Zöllner C. (1987). Interposed cartilage as a precaution against extrusions of ceramic ossicular replacement implants. Ann Otol Rhinol Laryngol 1987;96(2 Pt 1):207-9.
Figure 2. Axial CT demonstrates the extruding prosthesis (arrow).
Continued from page 490
with the paralyzed fold when contacted by the aryte-noid of the normal fold during adduction).
Vocal fold "ndings depend upon the location and extent of injury, as well as the degree of neural regen-eration and synkinesis. Long-standing vocal fold pa-ralysis without reinnervation usually leads to incom-plete glottic closure, vocal fold atrophy and bowing, and decreased vocal process and vocal fold heights. However, partial neural regeneration is common and can prevent muscle atrophy and bowing by maintain-ing muscle tone.
Even though abductor-adductor "ber mismatch of-ten leads to net vocal fold immobility, the preserved muscle tone sometimes permits glottic closure through compensation by the normal vocal fold. For this rea-son, early reinnervation procedures in cases with a poor prognosis may be bene"cial when performed be-fore the onset of muscle atrophy.2
References 1. Rubin AD, Satalo# RT. Vocal fold paresis and paralysis. In: Profes-
sional Voice: !e Science and Art of Clinical Care. 3rd ed. San Diego: Plural Publishing; 2005:871-86.
2. Crumley RL. Unilateral recurrent laryngeal nerve paralysis. J Voice 1994;8(1):79-83.
. Norris BK, Schweinfurth JM. Arytenoid dislocation: An analysis of the contemporary literature. Laryngoscope 2011;121(1):142-6.
4. Satalo# RT, Mandel S, Heman-Ackah Y, et al. Laryngeal Electro-myography. 2nd ed. San Diego: Plural Publishing; 2006.
5. Satalo# RT, Praneetvatakul P, Heuer RJ, et al. Laryngeal electro-myography: Clinical application. J Voice 2010;24(2):228-34.

Sinus Dynamics provide people suffering from chronic rhinosinusitis with compounded medications for a simple and seamless approach to Topical Sinus Therapy (TST). One at a time, person to person.
Your patient and customized solution is our priority.
Atomized TherapyMedicated Irrigation Therapy
Unit Dose Vials
Topical Sinus Therapies Compounded Medications
Call and experience the difference.
Phone: 877.747.4275
Services:
��6SHFLDOL]LQJ�LQ�FRPSRXQGHG�PHGLFDWLRQV� and delivery devices for CRS
��3KDUPDFLVWV�IRFXVHG�RQ�TST
��6LQJOH�XQLW�GRVH�YLDOV�IRU�DFFXracy, consistent dosing, ease of patient use and increased compliance
��'HYLFHV�WKDW�GHOLver medications to problem sinuses
��4XLFN�GHOLvery of prescription to the patients
��0DQDJH�SDWLHQW�LQVXrance and reimbursement
RHINOSCOPIC CLINIC
496 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Langerhans cell histiocytosis: Temporal bone invasion in an adult
IMAGING CLINIC
From the Department of Otolaryngology, Head and Neck Surgery (Dr. Alexander, Ms. Worthen, and Dr. May) and the Department of Pathology (Dr. Pang), Wake Forest University School of Medicine, Winston-Salem, N.C. Previous presentation: !is case was given as an oral presenta-tion at the North Carolina South Carolina Society of Otolaryngology, Head and Neck surgery in 2012.
Richard L. Alexander MD, PhD, MBA; Mary L. Worthen, BS; Changlee S. Pang, MD;John S. May, MD
B
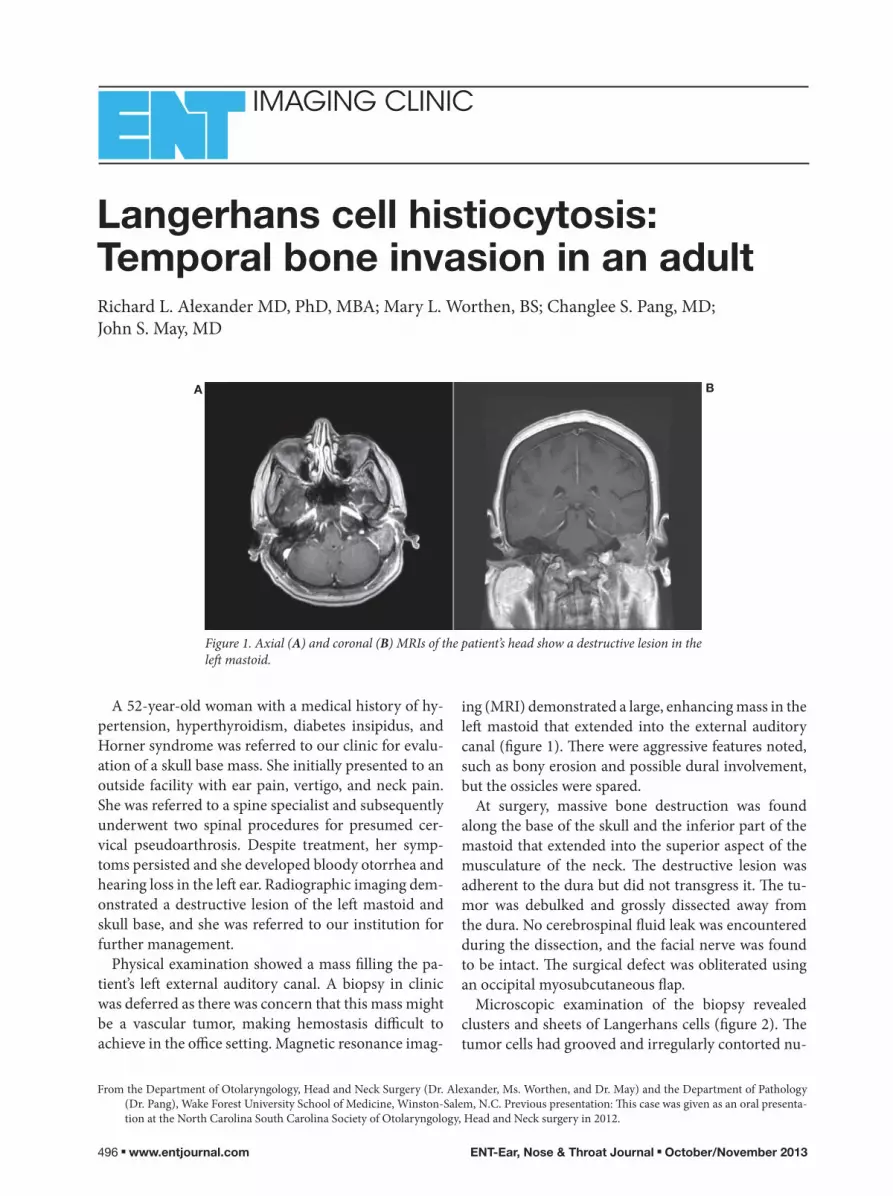
A 52-year-old woman with a medical history of hy-pertension, hyperthyroidism, diabetes insipidus, and Horner syndrome was referred to our clinic for evalu-ation of a skull base mass. She initially presented to an outside facility with ear pain, vertigo, and neck pain. She was referred to a spine specialist and subsequently underwent two spinal procedures for presumed cer-vical pseudoarthrosis. Despite treatment, her symp-toms persisted and she developed bloody otorrhea and hearing loss in the le" ear. Radiographic imaging dem-onstrated a destructive lesion of the le" mastoid and skull base, and she was referred to our institution for further management.
Physical examination showed a mass #lling the pa-tient’s le" external auditory canal. A biopsy in clinic was deferred as there was concern that this mass might be a vascular tumor, making hemostasis di$cult to achieve in the o$ce setting. Magnetic resonance imag-
A
ing (MRI) demonstrated a large, enhancing mass in the le" mastoid that extended into the external auditory canal (#gure 1). !ere were aggressive features noted, such as bony erosion and possible dural involvement, but the ossicles were spared.
At surgery, massive bone destruction was found along the base of the skull and the inferior part of the mastoid that extended into the superior aspect of the musculature of the neck. !e destructive lesion was adherent to the dura but did not transgress it. !e tu-mor was debulked and grossly dissected away from the dura. No cerebrospinal %uid leak was encountered during the dissection, and the facial nerve was found to be intact. !e surgical defect was obliterated using an occipital myosubcutaneous %ap.
Microscopic examination of the biopsy revealed clusters and sheets of Langerhans cells (#gure 2). !e tumor cells had grooved and irregularly contorted nu-
Figure 1. Axial (A) and coronal (B) MRIs of the patient’s head show a destructive lesion in the le! mastoid.


498 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
IMAGING CLINIC
clei with inconspicuous nucleoli. Admixed eosinophils were also noted. !e tumor cells showed immunoreac-tivity for S-100 protein and CD1a, con"rming a diag-nosis of Langerhans cell histiocytosis (LCH).
Radiographic imaging—including computed to-mography (CT) of the chest, abdomen, and pelvis and an osseous survey—were ordered for further evalua-tion and to determine the extent of the disease. !e imaging demonstrated disseminated disease with a destructive lesion of the right ilium and abnormal so# tissue in the bilateral perinephric space. !e oncolo-gists recommended systemic chemotherapy because further surgical debulking was no longer practical. !e patient expired several months later from compli-cations of her disease and her comorbid conditions, as well as poor compliance.
LCH is caused by the proliferation and accumula-tion of a speci"c histiocyte, the Langerhans cell. !e disease can involve any bone, but most lesions occur in the $at bones of the skull, pelvis, spine, mandible, and ribs.1 Imaging of the skull will o#en reveal lytic lesions with scalloped edges. CT is better suited for demonstrating bone detail and MRI for bone marrow and so#-tissue involvement.
Patients with limited initial involvement of the tem-poral bone have a better prognosis on long-term fol-low-up than do patients with the multisystemic form of LCH.2 Temporal bone involvement is bilateral in 31% of cases, and otologic symptoms were the initial presentation in 25% of these cases.3
Despite the characteristic of extensive destruction of the temporal bone in this disease, the facial nerve is surprisingly resistant to destruction, and facial nerve palsy is rare. If present, facial nerve palsies are likely caused by compromise of blood supply to the nerve.3
Histopathologically, LCH is characterized by prolif-eration of atypical Langerhans cells that form granu-
lomas. Langerhans cells have cytoplasmic inclusion bodies known as Birbeck granules; a de"nitive diagno-sis requires electron microscopy of Birbeck granules or CD1 antigenic determinants by immunohistochemis-try.3
Treatment of temporal bone lesions remains contro-versial. Surgery is required to make the histologic di-agnosis but does not improve outcome. Treatment op-tions include intralesional steroids, systemic steroids, systemic chemotherapy, and surgical curettage. Other authors have reported good local disease control with low-dose radiotherapy.4
LCH is rare in adults compared to the pediatric population. !e age at presentation does not appear to predict the severity or course of the disease in adults, in contrast to children. Multisystemic disease is the only known prognostic factor. Although rare in adults, LCH is an important disease process that needs to be considered in the di%erential in patients presenting with refractory otologic symptoms.
!is case report was reviewed and approved by the Institutional Review Board of Wake Forest University Baptist Medical Center.
References 1. Azouz EM, Saigal G, Rodriguez MM, Podda A. Langerhans’ cell
histiocytosis: Pathology, imaging and treatment of skeletal in-volvement. Pediatr Radiol 2005;35(2):103-15.
2. Fernandez-Latorre F, Menor-Serrano F, Alonso-Charterina S, Arenas-Jimenéz J. Langerhans’ cell histiocytosis of the tempo-ral bone in pediatric patients: Imaging and follow-up. AJR Am J Roentgenol 2000;174(1):217-21.
3. Whitaker EG, Cerenko D, Muller S, Hudgins P. Multifocal lang-erhans’ [sic] cell histiocytosis involving bilateral temporal bones, lungs, and hypothalamus in an adult. Skull Base Surg 1999;9(1): 51-6.
4. Zlodre JK, Rennie AT, Ramsden JD. Langerhans’ cell histiocytosis of the temporal bone: Successful treatment of sensorineural hear-ing loss with low-dose radiotherapy. J Laryngol Otol 2009;123(6): 676-9.
Figure 2. Pathology demonstrates di!use proliferation of Langerhans cells with nuclear folds or grooves. Hematoxylin and eosin stain shows admixed eosinophils present in the background (A; hematoxylin and eosin, original magni"cation #60). Immunohistochemistry reveals that the Langerhans cells are positive for S-100 protein (B) and CD1a (C).
A B C

Stop Suffering. Start Living.Sto
Are you recommending allergy symptom relief that’s fast* and non-sedating?
Visit Allegra.com/hcp for samples and coupons! 6007A ©2013 Chattem, Inc.
* Starts working at hour one. Applies to first dose only.†Among OTC branded antihistamines.
gives you both!ALLEGRAONLY
†
®

DYSPHAGIA CLINIC
500 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Undifferentiated thyroid carcinoma
PATHOLOGY CLINIC
From the Department of Pathology, Southern California Permanente Medical Group, Woodland Hills Medical Center, Woodland Hills, Calif.
Lester D.R. !ompson, MD
Undi"erentiated carcinoma (also known as ana-plastic carcinoma) of the thyroid gland is a highly aggressive malignant neoplasm composed of undif-ferentiated cells that exhibit immunohistochemical or ultrastructural epithelial di"erentiation. Nearly all patients report a long history of thyroid gland disease, o#en goiter or Hashimoto thyroiditis. In most cases, there is a transformation from a papillary (80%) or fol-licular carcinoma into undi"erentiated carcinoma. Ra-diation exposure is reported in about 10% of patients.
While accounting for only 2% of all thyroid gland malignancies, undi"erentiated carcinoma accounts for >60% of thyroid cancer mortality. !e majority of patients are elderly, with a slight female predilection. Patients present with a rapidly enlarging, $rm-hard neck mass, usually involving a single lobe (60%). In addition, many patients also report hoarseness, vocal fold paralysis, and pain. So#-tissue or adjacent organ
(esophagus, trachea) extension by the tumor is com-mon.
In spite of multimodality therapy, the prognosis is still grave, with >95% of patients dead from disease in <9 months. !ere is a worse prognosis for patients aged >60 years, male, with >5-cm tumors or exten-sive local disease. By de$nition, all tumors are pT4 and separated into groups IVA, IVB, and IVC based on extent of local and metastatic disease. !e tumors are %eshy to $rm, usually replacing the thyroid gland parenchyma, with an in$ltrative and irregular border. !ey nearly always show extrathyroid gland extension. !e tumors are large, with a mean size of 6 cm.
Histologically, undi"erentiated thyroid carcinomas show a variety of patterns, from sheet-like, storiform, fascicular, angiomatoid, and meningothelial to solid, exhibiting extensive lymph-vascular invasion. !ere is usually extensive coagulative-type necrosis, hem-
Figure 1. An undi!erentiated carcinoma is present in association with a papillary carcinoma (lower right). Note the osteoclastic-type giant cells.
Continued on page 504

When Your Chair Expires, Call Reliance.
Then again, why wait for a busted back or armrest? Invest in
an ultra-durable exam chair from Reliance ENT. The kind built
by hand with brutish materials, like forged iron, to live for 30 years
or more.
Go ahead. Zip up your old clunker and call Reliance, Brutishly
Durable Since 1898.
800.735.0357 or visit reliance-medical.com
Brutishly Durable.
800.735.0357reliance-medical.com
© 2
013
Relia
nce
Medic
al P
roduct
s. A
ll R
ights
Rese
rved.

HEAD AND NECK CLINIC
502 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Amyloidosis: A rare case with nodular lesions on the tongue and buccal mucosa
HEAD AND NECK CLINIC
From the Department of Otorhinolaryngology, GATA Haydarpasa Training Hospital, Istanbul, Turkey.
Evren Erkul, MD; Hakan Cincik, MD.
An 82-year-old man was referred for evaluation of nodular lesions on the tongue and le! buccal muco-sa. He had an 8-year medical history of chronic renal failure and had been treated with hemodialysis. Two months prior to presentation, the "rst nodular lesion appeared on the tip of his tongue. Seven days later, four new nodular lesions appeared in the oral cavity. #e size of the lesions gradually increased.
Physical examination revealed a lesion on the le! buccal mucosa and four lesions on the tongue. #e le-sions were nodular, approximately 1 to 2 cm in diam-eter, ulcerated, friable, "rm, white-yellow in color, and bled on touch ("gure). #ere was no macroglossia or disturbance of tongue mobility.
Incisional biopsy was performed on one of the nodules under local anesthesia for diagnosis. Light microscopic examination revealed an eosinophilic amorphous substance, and Congo red staining dem-
onstrated green birefringence under polarized light. #ese "ndings were consistent with a diagnosis of amyloidosis.
We completely excised all of the other masses and treated the patient medically with corticosteroids. #e patient died of chronic renal failure 17 days a!er the diagnosis of amyloidosis.
Amyloidosis is a disease process in which protein-aceous material is formed and deposited in so! tissues and organs in response to various cell dyscrasias or in$ammatory conditions.% #e pathogenesis of amy-loidosis appears to be multifactorial, but the common "nal pathway is identical in all forms of the disease; i.e., the production of amyloid "brils in the extracel-lular matrix.%
Dialysis-related amyloidosis (DRA) is a frequent and serious complication in patients on long-term di-alysis.& In these patients, '2-microglobulin, which is
Figure. A: Photo shows the ulcerated, friable buccal lesion. B: !e tongue nodules are rough, they bleed with touch, and they are 1 to 2 cm in diameter.
A B

LLC
NDC# AMERISOURCE BERGEN
CARDINAL HEALTH MCKESSON MORRIS &
DICKSON PRODUCT
0283-0610-11 048-855CIN
4362547 1410125 086611HurriCaine ONE® Unit Dose Non-Aerosol SprayBox of 2, 0.017 !. oz. (0.5 mL) each
0283-0610-26 048-868CIN
4363370 1411925 086629HurriCaine ONE Unit Dose Non-Aerosol SprayBox of 25, 0.017 !. oz. (0.5 mL) each
ORDERING INFORMATION
If HurriCaine ONE is not yet available through your wholesaler, request it by name and NDC Number.
*Joint Commission Standard: MM.05.01.11, EP4
SPRAY KIT ! MULTIPLE USE20% Benzocaine Oral Anesthetic
NOW YOU HAVE A CHOICE!
Spray Extension Tubes
ORDERING INFORMATION
............................................NDC 0283-0679-02
...............................NDC 0283-0679-60
..................Product number 0283-1185-20
1/2 SECOND SPRAY is all it takes!
0.5 mL each
UNIT DOSE ! PATIENT SAFETYAn Innovative Non-Aerosol Unit Dose Topical Anesthetic Spray
form available*
accommodate point-of-care scanning
medication errors, ensuring the “5 Rights” are met: " Right Drug " Right Patient " Right Dose " Right Route " Right Time
cross-contamination

HEAD AND NECK CLINIC
504 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
HEAD AND NECK CLINIC PATHOLOGY CLINIC
part of the class I major histocompatibility complex antigen, is the major protein constituent of the amy-loid !brils. It fails to cross the dialysis membrane, re-sulting in the formation of amyloid !brils."
Amyloid involvement of the oral tissues is rather rare; when it does occur, the tongue is the most fre-quent location, and amyloidosis in this area usually manifests as rubbery or !rm macroglossia.3 Amyloi-dosis of the tongue results in white-yellow nodules >1 mm in diameter and !rmer than the other parts of the tongue.4 Petechiae, ecchymoses, and hemorrhagic blisters may also be present.1,3 Zhou et al5 reported 14 patients with oral amyloidosis, 12 of whom had mac-roglossia. Our patient did not show macroglossia, but hemorrhagic and ulcerated nodules were observed on the tongue and buccal mucosa.
In one study, 8 cases of DRA were found as tongue amyloid nodules among 103 long-term (>20 years) hemodialysis patients.# Our patient had been on he-modialysis for only 8 years. $e de!nitive diagnosis is made by tissue biopsy.% Treatment of DRA has been limited to surgical removal of amyloid deposits. Clini-cal therapeutic strategies for DRA include dialysis, medical or surgical therapy, and renal transplantation to obtain normal serum levels of &2-microglobulin.'()
New high-*ux, biocompatible dialysis membranes are more permeable and are e+ective in treating amy-loidosis.4 More e+ective preventive therapy strategies will be helpful for patients with DRA. Benign epithe-lial and connective tissue neoformation—including !brosarcoma, malignant !brous histiocytoma, leio-myoma, papilloma, lipoma, lymphangioma, neuroma, hemangioma, and adenoma—must be considered in the di+erential diagnosis of oral masses.3
References 1. Gertz MA, Lacy MQ, Dispenzieri A. Amyloidosis. Hematol Oncol
Clin North Am 1999;13(6):1211-33, ix. 2. Danesh F, Ho LT. Dialysis-related amyloidosis: History and clinical
manifestations. Semin Dial 2001;14(2):80-5. 3. van der Waal RI, van de Scheur MR, Huijgens PC, et al. Amyloido-
sis of the tongue as a paraneoplastic marker of plasma cell dyscra-sia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;94(4): 444-7.
4. Yusa H, Yoshida H, Kikuchi H, Onizawa K. Dialysis-related amyloi-dosis of the tongue. J Oral Maxillofac Surg 2001;59(8):947-50.
5. Zhou Z, Lu Y, Wu L. Clinicopathological and diagnostic study of amy loidosis of oral maxillofacial area [in Chinese]. Zhonghua Kou Qiang Yi Xue Za Zhi 1998;33(5):282-4.
6. Matsuo K, Nakamoto M, Yasunaga C, et al. Dialysis-related amyloi-dosis of the tongue in long-term hemodialysis patients. Kidney Int 1997;52(3):832-8.
7. Khan MF, Falk RH. Amyloidosis. Postgrad Med J 2001;77(913):686-93.
8. Yamamoto S, Gejyo F. Historical background and clinical treatment of dialysis-related amyloidosis. Biochim Biophys Acta 2005;1753 (1):4-10.
orrhage, and degeneration. Colloid is absent, but en-trapped follicles can mimic colloid production.
$e tumor cells are poorly di+erentiated, yielding a polygonal, pleomorphic, spindle, giant, epithelioid, or squamoid appearance. Tumor giant cells and osteoclas-tic giant cells are seen (!gure 1). Mitoses are easily iden-ti!ed, are increased, and include atypical forms. Several histologic variants are recognized and include spindle cell, pleomorphic giant cell, squamoid, osteoclastic, rhabdoid, and angiomatoid variants, among others.
Because of the pleomorphic nature of the tumor, immunohistochemistry is frequently employed to con!rm a diagnosis. Most tumors exhibit vimentin, keratin, CAM5.2, EMA, &-catenin, and p63 immunore-activity, while usually negative with thyroglobulin and TTF-1 (!gure 2); p53 and Ki-67 are usually strongly positive. $e histologic di+erential diagnosis includes metastases to the thyroid gland (carcinoma, sarcoma, melanoma); primary sarcoma, lymphoma, and several primary thyroid gland malignancies (including medul-lary thyroid gland carcinoma); and Riedel thyroiditis.
Suggested readingChiacchio S, Lorenzoni A, Boni G, et al. Anaplastic thyroid cancer:
Prevalence, diagnosis and treatment. Minerva Endocrinol 2008; 33(4):341-57.
Cornett WR, Sharma AK, Day TA, et al. Anaplastic thyroid carcinoma: An overview. Curr Oncol Rep 2007;9(2):152-8.
Nikiforov YE. Genetic alterations involved in the transition from well-di+erentiated to poorly di+erentiated and anaplastic thyroid car-cinomas. Endocr Pathol 2004;15(4):319-27.
Figure 2. Le!: Numerous osteoclastic-type giant cells are present, with a pleomorphic population in the background, including mitoses. Right: !e papillary carcinoma is strongly immunoreactive with TTF-1, while the undi"erentiated carcinoma is negative.
Continued from page 500

Volume 92, Number 10-11 www.entjournal.com ! 505
PEDIATRIC OTOLARYNGOLOGY CLINIC
Tracheal bronchus in an 11-month-old infant
From the Division of Pediatric Otolaryngology–Head and Neck Surgery, Nemours Children’s Clinic, Jacksonville, Fla.
Robert Sprecher, MD, FACS, FAAP; Gary Josephson, MD, FACS, FAAP
An 11-month-old infant boy presented to the oto-laryngology service for evaluation of recurrent acute otitis media, persistent middle ear e!usions, and re-active airway disease. He was a former 33-week pre-mature infant with a cardiac history of patent foramen ovale and had been intubated for 1 week a"er birth. Over the subsequent 11 months, he had intermittent wheezing thought to be due to reactive airway disease, which was treated with nebulizers.
Given the patient’s history, a bronchoscopy was planned to be performed while he was under anesthe-sia for myringotomy tube placement. #e bronchos-copy revealed a tracheal bronchus. ($gure 1). No sig-ni$cant collapse or retained secretions were present. Postoperatively, a computed tomography (CT) scan of
his chest showed the right upper lobe bronchus aris-ing from the distal trachea, above the carina ($gure 2). #e patient has been asymptomatic for more than 2 years since his diagnosis.
A tracheal bronchus is an aberrant right upper lobe bronchus arising from the distal trachea proximal to the carina. Alternatively, it has been referred to as bronchus suis, or pig bronchus, as a tracheal bronchus is a normal $nding in swine and other ruminants. #e incidence has been reported as 0.001 to 2%, depend-ing on the means of diagnosis (bronchoscopic, radio-graphic, or cadaveric).1,2 #erefore, most otolaryngol-ogists will have diagnosed a patient with this anomaly at some time in their careers.
#ere is an association between tracheal bronchus
PEDIATRIC OTOLARYNGOLOGY CLINIC
Figure 1. Intraoperative photograph shows the right upper bronchus arising from the trachea proximal to the carina (arrow).
Figure 2. Coronal CT scan demonstrates the tracheal bronchus arising from the distal trachea (arrow).
Continued on page 512

DYSPHAGIA CLINIC
506 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Esophageal perforation in a patient with diverticulum following anterior discectomy and fusion
DYSPHAGIA CLINIC
From the Department of Otolaryngology/Head and Neck Surgery, Georgia Regents University, Augusta.
Aasif A. Kazi, PharmD; Nancy L. Solowski, MD; Gregory N. Postma, MD; Paul M. Weinberger, MD
A 42-year-old man was referred to us with a 6-month history of dysphagia and regurgitation. He reported a 38-pound weight loss, and serum prealbumin indicat-ed protein malnutrition at 17 mg/dl. He had a complex surgical history at an outside hospital, including ante-rior cervical discectomy and fusion (ACDF) in 2006 complicated by intraoperative esophageal perforation. Subsequently, multiple surgical attempts at repair were made. Recovery was prolonged by the patient’s refusal to remain NPO.
A barium swallow was obtained (!gure 1), which revealed a proximal diverticulum that did not appear like a typical Zenker diverticulum. "e patient was
taken to the operating room for endoscopic diverticu-lotomy. Endoscopic examination in the OR revealed visible cervical hardware on the anterior surface of the vertebral bodies in the pouch (!gure 2). "e procedure was aborted.
"e patient was taken back to the OR with the neu-rosurgical team for removal of the exposed hardware and closure of the anticipated defect. Examination of the hardware a#er removal showed food particles em-bedded within the cage. Tissue quality was noted to be extremely poor, and a three-layered closure was per-formed and bolstered by a sternocleidomastoid muscle $ap. Despite this, postoperative wound breakdown oc-
Figure 1. Gastrogra!n esophagogram reveals the large pharyngo-esophageal !stula. "e large “septum” in this iatrogenic diverticulum made it amenable to endoscopic treatment.
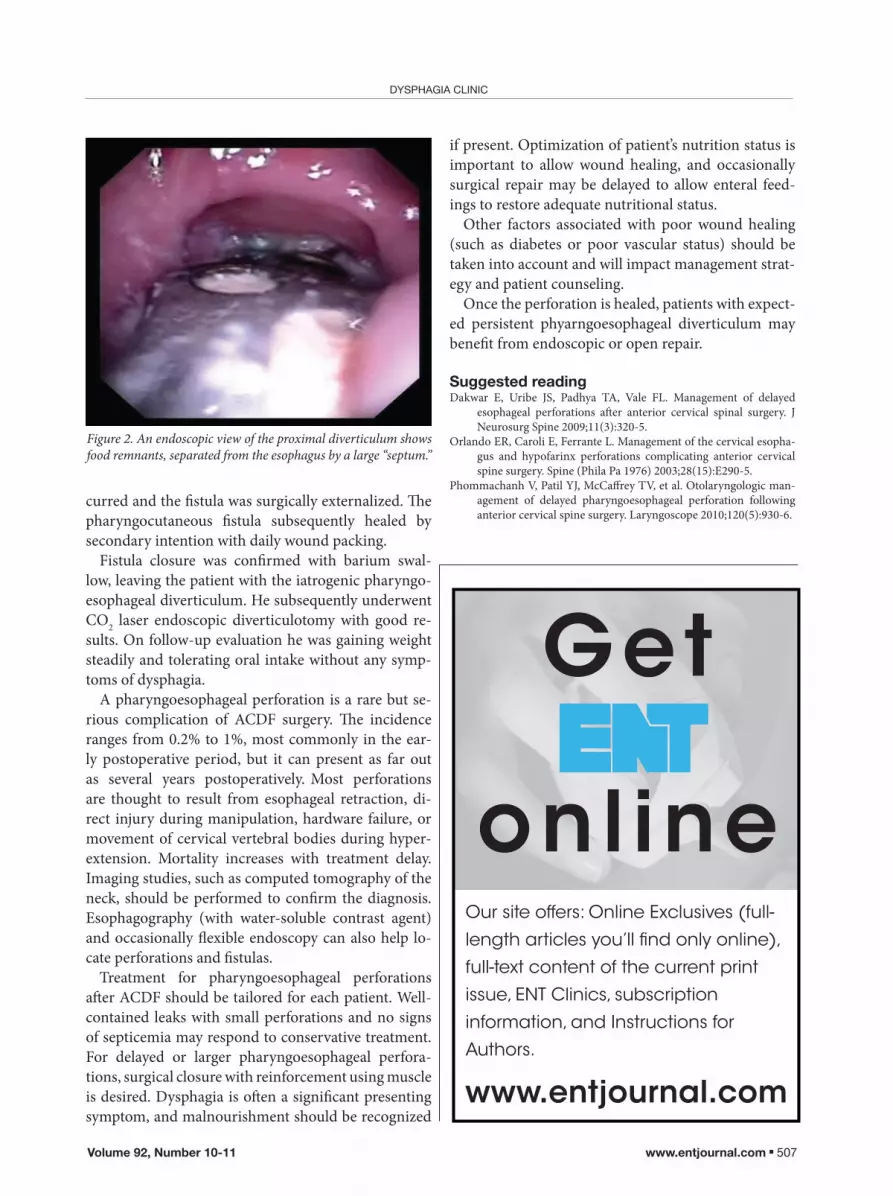
Volume 92, Number 10-11 www.entjournal.com ! 507
DYSPHAGIA CLINIC
www.entjournal.com
Get
online Our site offers: Online Exclusives (full-length articles you’ll !nd only online), full-text content of the current print issue, ENT Clinics, subscription information, and Instructions for Authors.
curred and the !stula was surgically externalized. "e pharyngocutaneous !stula subsequently healed by secondary intention with daily wound packing.
Fistula closure was con!rmed with barium swal-low, leaving the patient with the iatrogenic pharyngo-esophageal diverticulum. He subsequently underwent CO2 laser endoscopic diverticulotomy with good re-sults. On follow-up evaluation he was gaining weight steadily and tolerating oral intake without any symp-toms of dysphagia.
A pharyngoesophageal perforation is a rare but se-rious complication of ACDF surgery. "e incidence ranges from 0.2% to 1%, most commonly in the ear-ly postoperative period, but it can present as far out as several years postoperatively. Most perforations are thought to result from esophageal retraction, di-rect injury during manipulation, hardware failure, or movement of cervical vertebral bodies during hyper-extension. Mortality increases with treatment delay. Imaging studies, such as computed tomography of the neck, should be performed to con!rm the diagnosis. Esophagography (with water-soluble contrast agent) and occasionally #exible endoscopy can also help lo-cate perforations and !stulas.
Treatment for pharyngoesophageal perforations a$er ACDF should be tailored for each patient. Well-contained leaks with small perforations and no signs of septicemia may respond to conservative treatment. For delayed or larger pharyngoesophageal perfora-tions, surgical closure with reinforcement using muscle is desired. Dysphagia is o$en a signi!cant presenting symptom, and malnourishment should be recognized
if present. Optimization of patient’s nutrition status is important to allow wound healing, and occasionally surgical repair may be delayed to allow enteral feed-ings to restore adequate nutritional status.
Other factors associated with poor wound healing (such as diabetes or poor vascular status) should be taken into account and will impact management strat-egy and patient counseling.
Once the perforation is healed, patients with expect-ed persistent phyarngoesophageal diverticulum may bene!t from endoscopic or open repair.
Suggested readingDakwar E, Uribe JS, Padhya TA, Vale FL. Management of delayed
esophageal perforations a$er anterior cervical spinal surgery. J Neurosurg Spine 2009;11(3):320-5.
Orlando ER, Caroli E, Ferrante L. Management of the cervical esopha-gus and hypofarinx perforations complicating anterior cervical spine surgery. Spine (Phila Pa 1976) 2003;28(15):E290-5.
Phommachanh V, Patil YJ, McCa%rey TV, et al. Otolaryngologic man-agement of delayed pharyngoesophageal perforation following anterior cervical spine surgery. Laryngoscope 2010;120(5):930-6.
Figure 2. An endoscopic view of the proximal diverticulum shows food remnants, separated from the esophagus by a large “septum.”

ARDESHIRPOUR, LADNER, SHORES, SHOCKLEY
508 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
A preliminary study of the use of ultrasound in de!ning nasal fractures: Criteria for a con!dent diagnosis
ORIGINAL ARTICLE
Farhad Ardeshirpour, MD; Keith M. Ladner, MD; Carol G. Shores, MD, PhD; William W. Shockley, MD
From the Department of Otolaryngology–Head and Neck Surgery, Univer-sity of Washington School of Medicine, Seattle (Dr. Ardeshirpour); Ladner Facial Plastic and Reconstructive Surgery, Englewood, Colo. (Dr. Ladner); and the Department of Otolaryngology–Head and Neck Surgery, University of North Carolina School of Medicine, Chapel Hill (Dr. Shores and Dr. Shockley). !e study described in this article was conducted at the University of North Carolina.
Corresponding author: Farhad Ardeshirpour, MD, Department of Oto-laryngology–Head and Neck Surgery, University of Washington School of Medicine, 1959 NE Paci"c St., Box 356515, Seattle, WA 98195. Email: [email protected]
Previous presentation: !e information in this article has been updated from its original presentation as a poster at !e Triological Society’s Southern Section Meeting; Jan. 10-12, 2008; Naples, Fla.
Abstract Nasal fractures are usually diagnosed by clinical examina-tion, with or without the support of imaging studies. While plain-!lm radiography lacks sensitivity and speci!city for diagnosing nasal fractures, and computed tomography (CT) is not always practical or cost-e"ective, ultrasonog-raphy (US) may be useful in this regard. #e criteria by which adult nasal fractures are reliably identi!ed on US must be clear. We conducted a preliminary prospective, controlled, observational study to de!ne the appearance of nasal fractures on US. We used US to image 12 patients with a clinical or radiologic (CT or x-ray) diagnosis of nasal fracture. All patients presented within 2 weeks of their injury. For comparison purposes, we also obtained US images from 12 control subjects who had no history of nasal trauma or surgery. We found that we could con!dently diagnose nasal fractures on lateral-view US on the basis of a disruption of bone continuity and/or displacement of fracture segments. However, our !ndings were not as consistent with dorsal-view US, and we do not believe it is adequate for diagnosis. We conclude that lateral US can be used to detect nasal fractures in adults, but further studies are needed to assess its sensitivity, speci!city, cost-e"ectiveness, and practicality.
Introduction Historically, the gold standard for diagnosing nasal fractures has been the clinical examination.1 Physical "ndings typically include nasal deformity, mobility, crepitus, and edema; swelling o#en precludes a de"ni-tive diagnosis until it abates. Imaging modalities such as computed tomography (CT) and plain-"lm radiography have been used to support the diagnosis of nasal frac-ture. However, studies have shown that plain "lms are neither sensitive nor speci"c for adults in this regard, and while CT is good for imaging complex fractures, it is expensive and o#en impractical in the setting of an isolated nasal fracture.2
Ultrasonography (US) is a safe and easy imaging tool that is usually used in the head and neck region to identify pathologic changes in so# tissue. It has long been shown to be useful in the diagnosis of fractures of the larger bones, such as the skull, clavicle, and ribs. US has been used to identify fractures of the facial bones, including the zygomatic arch, orbit, and frontal sinus.3
At the time of this study, the literature contained few studies of the use of US in diagnosing nasal fractures. !iede et al4 reported that US was equal to conventional radiography, and Hong et al1 reported that US can be used as a primary diagnostic technique in children. More recent studies have further advocated the use of US in diagnosing nasal fractures.5-8
In this article, we describe our study of the useful-ness of US in diagnosing nasal fracture, and we present the criteria by which a diagnosis can be con"dently established.
Patients and methods From January to May 2007, we performed a prospec-tive, nonrandomized, controlled, observational study of the use of US in patients with a diagnosis of nasal fracture. Our exclusion criteria were a previous nasal

Volume 92, Number 10-11 www.entjournal.com ! 509
A PRELIMINARY STUDY OF THE USE OF ULTRASOUND IN DEFINING NASAL FRACTURES: CRITERIA FOR A CONFIDENT DIAGNOSIS
fracture or sinonasal surgery, including sinus surgery and septorhinoplasty, and age less than 16 years (for the purposes of this study, potential subjects aged 16 or 17 years were considered to be adults).
A total of 24 subjects were enrolled—12 patients with nasal fracture and 12 normal controls. !e fracture group was made up of 10 men and 2 women, aged 17 to 71 years (mean: 34.8); there were 10 whites and 2 blacks (table 1). !e control group included 6 men and 6 women, aged 23 to 73 years (mean: 39.4); there were 7 whites,
2 blacks, 2 Asians, and 1 American Indian (table 2). !e patients in the fracture group had been diagnosed
on the basis of a clinical examination, CT ("gure 1), and/or plain "lm radiography, and all had presented within 10 days of their injury. !e choice of imaging was made at the discretion of the treating Emergency Department physician. A#er evaluation by the Emergency Depart-ment sta$, we obtained US images with a 40-mm %at 5-12 mHz probe (Accuvix XQ; Samsung Medison USA; Cypress, Calif.).
US images were obtained in the right and le# lateral views and in the dorsal view ("gure 2). !ese images were later reviewed and discussed by a team of 4 otolar-yngologists, who determined whether nasal bones were either fractured (positive) or not fractured (negative). Controls were imaged in the same manner with the same equipment.
!e study protocol was approved by the Institutional Review Board at the University of North Carolina.
Results Ten of the 12 patients were evaluated for nasal fracture by facial CT at the time of their presentation to the Emergency Department (table 1). Of the 2 remaining patients, 1 (patient 6) was diagnosed on the basis of a clinical examination and plain "lm x-ray and the other (patient 11) underwent only a clinical examination.
!e team of 4 otolaryngologists had access to the o&cial
Table 1. Summary of cases
Left Right Pts. Age/sex Race Days* Cause CT US CT US Notes
1 37/M White 3 Assault Pos Pos Pos Pos
2 37/M White 0 Assault Pos Pos Neg Neg
3 24/M White 10 Assault Neg Pos Neg Neg CT showed no fracture
4 26/M Black 0 Assault Pos Pos Neg Neg
5 47/M White 0 Assault Pos Pos Neg Neg
6 60/M White 7 Fall N/A Pos N/A Neg Positive clinical exam and x-ray
7 71/F White 0 Fall Pos Pos Pos Pos
8 26/M White 2 Assault Pos Pos Pos Neg Fracture not seen on right US
9 31/M White 0 Assault Pos Pos Pos Pos
10 17/F Black 0 Fall Pos Pos Pos Pos
11 20/M White 6 Fall N/A Pos N/A Neg Clinical exam only
12 22/M White 0 MVA Pos Pos Pos Pos
* Number of days since injury. Key: CT = computed tomography; US = ultrasonography; Pos = positive; Neg = negative, N/A = not applicable; MVA = motor vehicle accident.
Table 2. Demographic data for the control group
Control Age/sex Race
1 26/F White
2 57/F Asian
3 27/M White
4 31/F White
5 49/F White
6 54/F White
7 28/F Black
8 31/M White
9 23/M White
10 49/M Black
11 73/M Asian
12 25/M American Indian

ARDESHIRPOUR, LADNER, SHORES, SHOCKLEY
510 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
radiology reports for all CTs and x-rays. Two members of the team had participated in the collection of the US images. !e review process involved an open discussion of the fracture and control US images, and decisions as to whether an image was su"cient to diagnose a fracture were reached by consensus.
We were able to con#dently di$erentiate between fracture and nonfracture on US images obtained in the lateral view (#gure 3). From this exercise, we were able to determine that certain criteria are su"cient to diag-nose a nasal fracture in the lateral view. !ese criteria are disruption of bone continuity and/or displacement of fracture segments. We were unable to con#dently di$erentiate between fractures and nonfractures on US images in the dorsal view (#gure 4).
Discussion Most nasal fracture patients present with signi#cant edema, which makes the physical examination di"cult for the provider and painful for the patient. In many cases, patients are asked to return in 1 week to allow time for swelling to subside. Nasal fractures more than 2 weeks old can be technically di"cult to reduce and painful for the patient, thus requiring operative intervention.
Contemporary radiographs have been shown to have low sensitivity and speci#city for nasal fracture.1,2 Al-though patients with signs of multiple and complex facial injuries may warrant CT, isolated nasal fractures do not. A reliable, e"cient, and inexpensive imaging study that does not expose the patient to radiation would be very useful in diagnosing nasal fractures. Moreover, such
imaging could prove to be very useful in the evaluation of postreduction results.
!e purpose of our study was to identify speci#c cri-teria that could be used to diagnose adult nasal fractures on US, as such guidance has been lacking. Without such criteria, one cannot be certain of the diagnosis. Based on our observations, we concluded that in order to diagnose a nasal fracture by lateral US, the practitioner must see a disruption of bone continuity and/or displacement of fracture segments. !is conclusion was arrived at by comparing the US images of normal controls with those of patients with fractures that had been diagnosed by clinical examination, CT, and/or plain-#lm radiography.
In view of the small number of participants in our study, strong statistical di$erences between the fracture and control groups could not be calculated. Our goal was to conduct a preliminary study to establish which criteria are useful to measure outcomes in future studies.
Figure 1. Coronal (A) and axial (B) CTs show bilateral nasal fractures (arrows).
A B
Figure 2. US is obtained in the lateral (A) and dorsal (B) views.
A B

Volume 92, Number 10-11 www.entjournal.com ! 511
A PRELIMINARY STUDY OF THE USE OF ULTRASOUND IN DEFINING NASAL FRACTURES: CRITERIA FOR A CONFIDENT DIAGNOSIS
Our patients and controls did not experience any discomfort from the US gel or from the pressure exerted by the probe. Examinations were performed in less than 5 minutes. While the accuracy of a US examination is dependent on the skill of the operator, in our experience this technique can be learned very easily. !e images can be interpreted by a care provider in real time or they can be reviewed later to provide a diagnosis.
In our study, the fracture locations were obvious in the vast majority of cases, and the panel of 4 otolaryn-gologists had no di"culty reaching a consensus. None of the control images showed any disruption of bony continuity or displacement. Only 1 patient (patient 8) had a fracture that could be seen on CT but not on US; however, that particular reading might have actually represented a nasal suture line that then led to a false-positive result.
We did #nd it di"cult to identify clear di$erences between the fracture patients and control subjects when
assessing the dorsal-view images. Both groups showed interruptions in bony continuity or displaced nasal seg-ments, which likely represented anatomic suture lines (#gure 4). !iede et al demonstrated that dorsal-view plain #lms were superior to dorsal-view US images, which is consistent with our #ndings.4 On the other hand, they also found that lateral-view US was superior to lateral-view x-rays.
In 2007, Hong et al demonstrated that US could be used as the primary diagnostic technique in evaluating nasal and septal fractures in children.1 Children have a higher proportion of cartilage to bone in the nasal skeleton, which makes radiologic assessment easier than it is in adults.
Since the original presentation of our study at !e Triological Society’s Southern Section Meeting in 2008, other studies have used criteria similar to ours in de#ning nasal fractures by US. !ese studies have demonstrated sensitivities and speci#cities of greater than 90% in diag-
Figure 3. Lateral-view US demonstrates a normal le! side in a control subject (A) and a fracture (arrow) in a study patient (B).
Figure 4. Dorsal-view US shows a control subject (A) and a fracture (arrows) patient (B).
A B
A B

512 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
ARDESHIRPOUR, LADNER, SHORES, SHOCKLEY PEDIATRIC OTOLARYNGOLOGY CLINIC
and other congenital malformations of the ribs and vertebrae, as well as a higher association in children with Down syndrome.3 In most cases, the diagnosis is made incidentally during routine bronchoscopy performed for other issues. While most patients are asymptomatic, it is important to remember that this anomaly may be associ-ated with signi!cant morbidity, and possibly mortality.4
"e possibility of a tracheal bronchus should be en-tertained when a patient presents with recurrent right upper lobe pneumonia or right upper lobe collapse. "e cause in these cases is thought to be retained secretions distal to the anomalous bronchus. Other presenting symptoms include stridor, respiratory distress, and symptoms indicative of foreign body aspiration or a thoracic mass.3
A tracheal bronchus also may have important im-plications for airway management and lung isolation during general anesthesia for other thoracic procedures.5 Ultimately, a right upper lobectomy may be required for management of recurrent pneumonia and atelectasis of the anomalous right upper lobe. Bronchoscopy and CT scan should be performed to con!rm the diagnosis and ensure that no other airway anomaly or pulmonary pathology exists that requires treatment.
Because tracheal bronchus, while uncommon and usually asymptomatic, may be associated with signi!-cant morbidity and possibly mortality, clinicians should keep this anomaly in mind when evaluating a patient with recurrent symptoms localized to the right upper lobe region. Persistence of recurrent or chronic airway disease may warrant diagnostic bronchoscopy to con!rm the diagnosis.
References 1. Doolittle AM, Mair EA. Tracheal bronchus: Classi!cation, endo-
scopic analysis, and airway management. Otolaryngol Head Neck Surg 2002;126(3):240-3.
2. McLaughlin FJ, Strieder DJ, Harris GB, et al. Tracheal bronchus: Association with respiratory morbidity in childhood. J Pediatr 1985;106(5):751-5.
3. Setty SP, Michaels AJ. Tracheal bronchus: Case presentation, literature review, and discussion. J Trauma 2000;49(5):943-5.
4. Hansen-Welches L, Slabach R, Landrum JE, Prahlow JA. Death of a 6-month-old due to a tracheal bronchus. Am J Forensic Med Pathol 2011;32(3):219-22.
5. Wiser SH, Hartigan PM. Challenging lung isolation secondary to aberrant tracheobronchial anatomy. Anesth Analg 2011;112 (3):688-92.
Continued from page 505nosing nasal fractures with US.5-8 Lou et al outlined an algorithm that includes ultrasonography in the workup of isolated nasal fractures.7 Furthermore, recent studies have shown US to be useful in assessing postreduction nasal contour intraoperatively,9,10 similar to its use in reducing zygomatic complex fractures.11
"is study demonstrates that ultrasonography, par-ticularly in the lateral view, can be useful in identifying fractures based on disruption of bone continuity and/or displacement of fracture segments. Ultrasound should be considered in the algorithm for assessment and treat-ment of nasal fractures.
References 1. Hong HS, Cha JG, Paik SH, et al. High-resolution sonography
for nasal fracture in children. AJR Am J Roentgenol 2007;188(1): W86-92.
2. Clayton MI, Lesser TH. "e role of radiography in the management of nasal fractures. J Laryngol Otol 1986;100(7):797-801.
3. Adeyemo WL, Akadiri OA. A systematic review of the diagnostic role of ultrasonography in maxillofacial fractures. Int J Oral Maxil-lofac Surg 2011;40(7):655-61.
4. "iede O, Krömer JH, Rudack C, et al. Comparison of ultraso-nography and conventional radiography in the diagnosis of nasal fractures. Arch Otolaryngol Head Neck Surg 2005;131(5):434-9.
5. Javadrashid R, Khatoonabad M, Shams N, et al. Comparison of ultrasonography with computed tomography in the diagnosis of nasal bone fractures. Dentomaxillofac Radiol 2011;40(8):486-91.
6. Lee MH, Cha JG, Hong HS, et al. Comparison of high-resolution ultrasonography and computed tomography in the diagnosis of nasal fractures. J Ultrasound Med 2009;28(6):717-23.
7. Lou YT, Lin HL, Lee SS, et al. Conductor-assisted nasal sonography: An innovative technique for rapid and accurate detection of nasal bone fracture. J Trauma Acute Care Surg 2012;72(1):306-11.
8. Mohammadi A, Ghasemi-Rad M. Nasal bone fracture—ultrasonog-raphy or computed tomography? Med Ultrason 2011;13(4):292-5.
9. Park CH, Joung HH, Lee JH, Hong SM. Usefulness of ultrasonography in the treatment of nasal bone fractures. J Trauma 2009;67(6):1323-6.
10. Abu-Samra M, Selmi G, Mansy H, Agha M. Role of intra-operative ultrasound-guided reduction of nasal bone fracture in patient satisfaction and patient nasal pro!le (a randomized clinical trial). Eur Arch Otorhinolaryngol 2011;268(4):541-6.
11. Gülicher D, Krimmel M, Reinert S. "e role of intraoperative ultrasonography in zygomatic complex fracture repair. Int J Oral Maxillofac Surg 2006;35(3):224-30.

Volume 92, Number 10-11 www.entjournal.com ! 513
A CASE OF CHRONIC SUBDURAL HEMATOMA FOLLOWING LUMBAR DRAINAGE FOR THE MANAGEMENT OF IATROGENIC CEREBROSPINAL FLUID RHINORRHEA: PITFALLS AND LESSONS
A case of chronic subdural hematomafollowing lumbar drainage for the management of iatrogenic cerebrospinal !uid rhinorrhea: Pitfalls and lessons
ORIGINAL ARTICLE
Vincent Eng-Soon Tan, MD, MRCS, MS(ORL–HNS); Donald Liew, FRACS
From the Department of Otorhinolaryngology–Head and Neck Surgery, Sarawak General Hospital, Sarawak, Malaysia.
Corresponding author: Dr. Vincent Eng-Soon Tan, Department of Otorhinolaryngology–Head and Neck Surgery, Sarawak General Hospital, Jalan Tun Ahmad Zaidi Adruce, Kuching, Sarawak 93400, Malaysia. Email: [email protected]
AbstractChronic subdural hematoma as a complication of lum-bar drain placement for the management of iatrogenic cerebrospinal !uid (CSF) leak has not been previously documented in the literature. We describe such a case in a 69-year-old man who presented with right nasal obstruc-tion secondary to an inverted papilloma involving the paranasal sinuses. "e patient underwent endoscopic sinus surgery, which included a medial maxillectomy. Surgery was complicated by a small CSF leak, which was repaired intraoperatively. Five days later, the patient experienced CSF rhinorrhea, and a lumbar drain was inserted. He developed overdrainage symptoms but was well when he was discharged. However, 22 days later he returned with right hemiparesis. Computed tomography of the brain showed a le# frontoparietal subdural hematoma with a mass e$ect. "e neurosurgical team performed an emergency drainage procedure, and the patient expe-rienced a complete neurologic recovery. We discuss the pitfalls of lumbar drainage, the possible pathophysiology of overdrainage, and the lessons learned from this case.
Introduction As more anterior skull base surgeries are being performed endoscopically by otorhinolaryngologists, we are faced with a greater likelihood of encountering neurosurgical
complications. Cerebrospinal !uid (CSF) rhinorrhea at the anterior skull base is a rare complication of such endoscopic endeavors. A lumbar drain is sometimes placed perioperatively as a shunt to reduce the leak.
Chronic subdural hematoma as a complication of lumbar drainage for the management of iatrogenic CSF leak has not been previously documented in the litera-ture. We describe what we believe is the "rst such case, and we discuss the pitfalls of lumbar drainage in cases of iatrogenic CSF leak, the possible pathophysiology of overdrainage, and the lessons learned from this case.
Case report A 69-year-old man presented to our ENT clinic with a 6-month history of right nasal obstruction. He was otherwise asymptomatic. Endoscopic nasal examination detected the presence of polyps "lling the right nasal cavity; the lesions were papillomatous in appearance. Biopsy analysis con"rmed inverted papilloma of the nose. Computed tomography (CT) of the paranasal sinuses demonstrated involvement of the right maxillary sinus, ostiomeatal complex, frontal recess, and ethmoid air cells.
#e patient underwent endoscopic sinus surgery, which included a medial maxillectomy. Surgery was complicated by a small CSF leak (<2 mm in diameter) over the cribriform plate. #e leak was repaired intra-operatively with a free mucoperiosteal gra$ (underlay technique) from the inferior turbinate. With help from the anesthesiologist, con"rmation of the seal was veri-"ed with the Valsalva maneuver at the conclusion of the operation. #e patient’s right nostril was packed with Merocel.
#e patient was ventilated overnight and extubated

TAN, LIEW
514 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
the next day. He was prescribed a laxative, intravenous ce!riaxone, a cough suppressant, and strict bed rest. "e Merocel was removed on postoperative day 3. "e patient was well until postoperative day 5, when he developed CSF rhinorrhea during straining. He was then referred to the neurosurgery unit for insertion of a lumbar drain, which was placed to drain at bed level.
"ree days later, the patient complained of worsening occipital headaches when he sat up to eat; the headaches abated when he would lie down. Otherwise, he remained afebrile and exhibited no clinical evidence of CSF rhi-norrhea. Daily biochemical and culture studies of the lumbar CSF ruled out any infection. "e 24-hour lumbar drain chart showed the following consecutive readings:
At that point, the drain was removed. Endoscopic
absence of CSF leakage. "e patient was discharged home in good condition on postoperative day 9.
Twenty-two days later, the patient was readmitted for evaluation of weakness in the right upper and lower limbs; the weakness had become worse over the previous few days (grade 3). He was alert and conscious, and no spontaneous CSF leak had occurred.
An urgent CT of the brain showed a le! frontopa-
normal. "e next day, the neurosurgical team placed the patient under general anesthesia and then inserted a drain through a le! parietal burr hole. Intraoperatively,
"e patient’s recovery was uneventful, his muscle power improved, and he was discharged 3 days later. Findings on a repeat CT of the brain 2 months later were normal. On review at 5 months postoperatively, the patient had regained full muscle power, and his right nasal cavity remained free of disease.
Discussion Inverted papillomas are relatively uncommon nasal tu-mors. Some long-standing lesions have been known to undergo malignant transformation. Endoscopic medial maxillectomy and sinus surgery are increasingly being used for complete removal of these lesions. As is the case with all endoscopic procedures, a possible surgical
complication of such procedures is a breach of the skull base resulting in CSF leakage; this is especially risky if important landmarks are obscured or altered by a nasal mass. In our case, the iatrogenic CSF leak was small, and
In our experience, lumbar drainage has not been used routinely. In this case, the lumbar drain was inserted only a!er the CSF leak recurred on postoperative day 5. It is di#cult to say in retrospect if the free gra! might have been displaced during removal of the intranasal packing or if there was a temporary rise in intracranial pressure during extubation.
Subdural hematoma following a lumbar drain inser-tion is exceptionally rare. While cases of subdural he-matoma a!er spinal anesthesia and ventriculoperitoneal shunt placement have been described in the literature, our case was di$erent in that the patient experienced a delayed leak accompanied by chronic subdural hema-
Menon et al reported a case in which a patient had collapsed as a result of an acute subdural hematoma following lumbar drainage for an iatrogenic CSF leak that had occurred during transsphenoid surgery; despite the drainage, the patient remained physically disabled.
Risk factors for subdural hematoma a!er lumbar
Figure. Axial CT shows the mixed subdural iso- and hyperdense collection in the le! frontoparietal area (arrow). At its widest (1.5 cm) point, the mass has caused compression of the lateral and third ventricles, with a midline shi! to the right. "e right lateral ventricle is mildly dilated

Learn from practical peer-reviewed, original scienti!c and clinical articles, as well as
insightful case reports.

Connect with those dedicated to serving the needs of practicing otolaryngologists and related
professionals with a digital subscription to
Ear, Nose & Throat Journal.
Become a Digital Subscriber Today!
Get cutting-edge original articles, informative online exclusives,
and a host of hands-on clinics.

Volume 92, Number 10-11 www.entjournal.com ! 515
A CASE OF CHRONIC SUBDURAL HEMATOMA FOLLOWING LUMBAR DRAINAGE FOR THE MANAGEMENT OF IATROGENIC CEREBROSPINAL FLUID RHINORRHEA: PITFALLS AND LESSONS
drainage are overdrainage, older age, and tension pneu-mocephalus. Overdrainage reduces the CSF volume and intraventricular pressure. !is can lead to dural separa-tion from the brain and stretching of the bridging vein, which increases the risk of rupture. Headache is the most common symptom of intracranial hypotension, and it is believed to arise as a result of the descent of the brain a"er a loss of CSF buoyancy.2 !is places traction on pain-sensitive structures such as the cerebral veins and arteries.3,4 !is would explain the postural nature of orthostatic headaches and the symptomatic relief that occurs upon lying down.
Overdrainage also creates more space for the accu-mulation of subdural #uid.5 !erefore, it is important to ensure that the drain is clamped while the patient is sitting up, because sitting up is the most common cause of overdrainage. Our patient displayed the classic symp-toms of overdrainage, as he complained of headaches that became worse when he sat up to eat and then experienced relief when he became supine. Although his symptoms abated a"er a few hours, his total CSF volume on the $nal full day of drainage was 315 ml. On retrospective analysis, a high index of suspicion might have alerted us to the possibility of an intracranial pathology, and an urgent CT of the brain might have led to an earlier diagnosis of the subdural hematoma.
Typically, the head end of the bed is elevated 30° and the receiving chamber of the lumbar drain is positioned at the level of the tragus. !e importance of clamping the drain cannot be overemphasized, even in a busy ward setting in a tertiary care hospital. With nursing assis-tance, a drain should be clamped to prevent accidental overdrainage before the patient sits up or otherwise moves around. When the patient lies down again, the nurse should readjust the level of the drip and reopen the drain. Proper attention must also be given to the positioning of the drain catheter, especially when the patient moves, and to making sure that it does not fall out unnoticed for a prolonged duration.
!e risk of subdural hematoma is higher in an ag-ing atrophic brain, so older patients should receive special attention. A tear in the dura can lead to tension pneumocephalus,6 but it is unlikely that this occurred in our patient because his leak was small and repaired immediately.
!e routine use of a lumbar drain in the repair of a CSF leak remains debatable. Some surgeons routinely use them,7 while others have achieved a high rate of success without them.8,9 Some surgeons recommend them more selectively, reserving them for patients with
a high-volume or long-standing CSF leak.10 Even though we do not routinely use a lumbar drain, it proved to be useful in our patient, although it did cause a rare late complication.
In conclusion, there is always a risk of CSF leak in skull base endoscopic surgeries, more so if important landmarks are obscured or altered by the tumor. Lumbar drainage has a role in the management of CSF leaks. It is important that proper positioning and timely clamp-ing of the drain not be taken lightly. While subdural hematoma following the placement of a lumbar drain is exceptionally rare, surgeons must be aware of the possibility. !e diagnosis of this potentially catastrophic condition would bene$t from a high index of suspicion and a low threshold for investigation.
References 1. Menon G, Bahuleyan B, Nair S. Acute subdural hematoma a"er
transsphenoidal surgery. J Clin Neurosci 2009;16(1):160-2. 2. Mokri B. Low cerebrospinal #uid pressure syndromes. Neurol Clin
2004;22(1):55-74. 3. Metafratzi Z, Argyropoulou MI, Mokou-Kanta C, et al. Spontane-
ous intracranial hypotension: Morphological $ndings and CSF #ow dynamics studied by MRI. Eur Radiol 2004;14(6):1013-16.
4. Mokri B. Spontaneous cerebrospinal #uid leaks: From intracranial hypotension to cerebrospinal #uid hypovolemia—evolution of a concept. Mayo Clin Proc 1999;74(11):1113-23.
5. Sternbach GL. Subdural hematoma in a shunted patient. J Emerg Med 2005;29(4):483-4.
6. Eloqayli H, Cappelen J, Vik A. Acute spontaneous subdural haema-toma a"er transsphenoidal surgery. Acta Neurochir (Wien) 2006; 148(5):587-90; discussion 590.
7. Anand VK, Murali RK, Glasgold MJ. Surgical decisions in the man-agement of cerebrospinal #uid rhinorrhoea. Rhinology 1995;33(4): 212-18.
8. Casiano RR, Jassir D. Endoscopic cerebrospinal #uid rhinorrhea repair: Is a lumbar drain necessary? Otolaryngol Head Neck Surg 1999;121(6):745-50.
9. Burns JA, Dodson EE, Gross CW. Transnasal endoscopic repair of cranionasal $stulae: A re$ned technique with long-term follow-up. Laryngoscope 1996;106(9 Pt 1):1080-3.
10. Wormald PJ, McDonogh M. ‘Bath plug’ technique for the endoscopic management of cerebrospinal #uid rhinorrhea. J Laryngol Otol 1997;111(11):1042-6.

GALLO, MANCIOCCO, PAGLIUCA, MARTELLUCCI, DE VINCENTIIS
516 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
Transdermal scopolamine in the management of postparotidectomy salivary !stula
ORIGINAL ARTICLE
Andrea Gallo, MD, PhD; Valentina Manciocco, MD, PhD; Giulio Pagliuca, MD, PhD; Salvatore Martellucci, MD; Marco de Vincentiis, MD
From the Department of Otorhinolaryngology, “Sapienza” University of Rome, Italy (Dr. Gallo, Dr. Pagliuca, Dr. Martellucci, and Dr. de Vincentiis); and the Department of Otolaryngology/Head and Neck Surgery, National Cancer Institute Regina Elena, Rome (Dr. Manciocco).
Corresponding author: Andrea Gallo MD, PhD, Via Adolfo Venturi 19, 00162 Rome, Italy. Email: [email protected]
AbstractParotid !stula represents an uncommon complication in parotid surgery. Its early recognition contributes to successful management. "e condition is distressing for both the patient and the surgeon, since conservative and operative treatment frequently fail. "ere is no consensus on the optimal management of parotid gland !stula. "e aim of this study is to describe a new, simple procedure in the treatment of this condition using transdermal sco-polamine. We report 3 cases of salivary !stulae occurring a#er parotidectomy. "e patients were admitted to our department with swelling in the parotid region and an output of clear drainage from the drain site during oral intake. "e patients were treated with a scopolamine trans-dermal release system applied to hairless skin overlying the parotid region. A prompt and remarkable decrease in daily salivary output was observed. Fistulae healed com-pletely within 3 days. No collateral e$ects were observed. Parotid !stulae do not generally occur as a complication of parotidectomies. "eir management can be di%cult, and several methods of treatment have been attempted. We believe that the use of transdermal scopolamine is a valid option in the treatment of parotid !stulae without causing collateral e$ects.
IntroductionParotid !stulae are connections between the skin and salivary ducts or glands, through which saliva is dis-charged.1-3 Fistulae of the parotid gland are rather un-common and result either from ductal or parenchymal injury. While in the preantibiotic era parotid gland !s-
tulae were frequently the consequence of parotid abscess drainage or suppuration associated with sialolithiasis, today the most frequent causes are gland injury during parotid surgery and penetrating trauma.4,5 Parotid !s-tulae could also be a rare complication of rhytidectomy, mastoidectomy, dental extraction, temporomandibular joint surgery, and mandibular osteotomy.6-8
Early detection of injury and prompt treatment are important, since !stulae may cause embarrassment as well as wound dehiscence and infection.8 Although numerous methods have been advocated in the treat-ment of salivary !stulae, none of these has proven to be totally satisfactory.1,2,5,9-12
We report 3 cases of salivary !stulae occurring a"er super!cial parotidectomy that were successfully treated with transdermal scopolamine.
Case reportsPatient 1. A 62-year-old man was admitted to our department complaining of unilateral swelling in the right parotid gland region. #e swelling was !rm, non-indurated, and not painful on palpation. #e size of the mass was approximately 4 $ 4 cm. A !ne-needle aspira-tion biopsy (FNAB) was suggestive of Warthin tumor.
#e patient underwent a super!cial parotidectomy with facial nerve preservation. Intraoperative !ndings con!rmed a large, !rm parotid mass. #e main facial nerve trunk was identi!ed, and the tumor was removed en bloc. A suction drain was placed and a pressure dressing applied.
#e patient did very well a"er surgery. Facial nerve function was intact in all divisions. #e pressure dressing was removed 48 hours later, and the drain was removed 72 hours later; this was possible because the amount of drainage was less than 15 ml in a 24-hour period.
#e day a"er drain removal, the patient discharged clear drainage from the drain site, which increased

Volume 92, Number 10-11 www.entjournal.com ! 517
TRANSDERMAL SCOPOLAMINE IN THE MANAGEMENT OF POSTPAROTIDECTOMY SALIVARY FISTULA
with mastication and oral intake. !is drainage caused embarrassment, thus preventing participation in social activities. !e patient was examined, and a diagnosis of parotid "stula was made. SteriStrips were placed to close the "stula but without success. In order to limit saliva production, a scopolamine transdermal release system was applied to the hairless skin overlying the parotid region. !is system is a circular, "lm-like patch with a drug reservoir containing 1.5 mg of scopolamine that is delivered into the bloodstream.
Approximately 0.5 mg of scopolamine was delivered every day for 3 days. A few hours a#er patch application, the patient noticed a prompt and remarkable decrease in the "stula output, allowing him to appear in public that same evening. !e following day the "stula did not drain, but a limited sialocele appeared in the area of the residual deep parotid gland. !e "stula healed completely a#er 3 days of scopolamine treatment. On the third day, the patch and the SteriStrips were removed. !e sialocele progressively shrank and was completely reabsorbed within 10 days from initial treatment. !e treatment was well tolerated; the patient only complained of slight xerostomia without any other side e$ects. He had no recurrence of the "stula during 5 months of follow-up.
Patient 2. A 60-year-old woman was admitted to our department because of a nodule in the right pa-rotid gland that had appeared 4 months earlier. !e size of the nodule was approximately 3 % 4 cm. FNAB revealed a mixed tumor. !e patient underwent a right parotidectomy with facial nerve monitoring. !e main facial nerve trunk was identi"ed, and the tumor was removed en bloc.
A small drain was placed and a mastoid dressing ap-plied. !e dressing and drain were removed 3 days a#er surgery. !e postoperative course was uneventful except for the formation of a small "stula that secreted saliva while the patient was eating. SteriStrips were placed to close the "stula, and oral intake was limited to reduce salivary output, but without success.
Because of severe discomfort caused by a large amount of secretion, a system of transdermal-release scopolamine was applied to the hairless skin overlying the parotid region. A prompt and remarkable decrease in the daily salivary output was observed. !e "stula healed completely a#er 2 days of scopolamine treatment. A#er 3 days the patch was removed. Treatment was well tolerated without any side e$ects. No recurrence of the "stula was observed.
Patient 3. A 58-year-old man was admitted to our department with chronic salivary drainage in the le# preauricular region. Super"cial parotidectomy for
Warthin tumor had been performed elsewhere 1 year earlier. Because of persistent sialorrhea in the preauricu-lar region, revision surgery had been performed twice under local anesthesia without success.
On physical examination, permanent preauricular sialorrhea from the incision site that increased with mastication and oral intake was noted. A diagnosis of salivary "stula was made. Placement of a scopolamine transdermal delivery system in the preauricular area relieved the patient’s symptoms within a day. A#er 3 days, the patch was removed and the "stula healed completely. Treatment was well tolerated, and the patient only complained of slight xerostomia without other side e$ects. No recurrence of the "stula was observed.
DiscussionAlthough parotid parenchymal injury is part and parcel of every super"cial parotidectomy, the reasons for the rare occurrence of postoperative salivary "stulae remain unclear. Postparotidectomy "stulae occur when the re-sected edge of the remaining gland leaks saliva, which drains through the surgical wound. Saliva secretion, par-ticularly during meals, counteracts the healing process. Moreover, the "stulous opening usually becomes coated with epithelium, thus further preventing "stula closure.2
A#er super"cial parotidectomy, the placement of an acellular human dermal matrix gra# to cover the entire parotid bed has been successfully used to prevent Frey syndrome and to obtain a better cosmesis of the surgi-cal site.13,14 It could be hypothesized that this physical interpositional barrier, separating the skin &ap from the remaining gland, may also play a role in preventing the formation of salivary "stulae.
In spite of a number of procedures advocated for the management of this condition, none of the methods is satisfactory, and there is no standard approach. Since saliva coming out through the "stula impairs wound healing, the reduction of salivary &ow plays a major role in the management of this complication.
Since the main stimulus for parotid secretion is the gustatory re&ex, a method to reduce salivary secretion is to reduce oral intake. Parekh et al obtained acceptable results in the treatment of parotid "stulae by suspend-ing oral intake, but their patients required intravenous feeding for a mean period of 15 days.3
Some authors recommend that compressive dressing alone be used to close "stulae a#er parotidectomies.4
However, some patients require long-lasting treatment (up to 1 month) and have di'culty maintaining the compression dressing for more than a few days. Other authors have proposed more aggressive approaches

GALLO, MANCIOCCO, PAGLIUCA, MARTELLUCCI, DE VINCENTIIS
518 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
when conservative treatment fails. Total parotidecto-mies and tympanic neurectomies are disadvantageous, since they represent additional and dangerous surgical procedures.1,2,4,5,9 Radiotherapy has been used but is no longer popular. Doses required for healing are high and may cause secondary malignancies.1,3,10
Since the work of Bushara, reporting on the abil-ity of botulinum toxin type A (BoNT/A) to block the cholinergic secretions in the head and neck area, many authors have experimented with this toxin in the treat-ment of salivary disorders.15 Vargas et al16 !rst performed percutaneous local injections of the residual parotid gland using BoNT/A for the treatment of postparoti-dectomy sialoceles, while Guntinas-Lichius and Sittel17 proposed botulinum toxin to treat postparotidectomy !stulae. Although local injections of botulinum toxin, as described by several researchers, appear to be an ef-fective and noninvasive strategy in the management of postparotidectomy !stulae, this approach is burdened with rare side e"ects.17-20 However, many authors perform BoNT/A injections under electromyographic control to prevent facial nerve damage. Other authors suggest the use of ultrasonographic assistance during the injec-tions to avoid blood vessel puncturing, thus preventing systemic di"usion of the toxin.20
#e use of anticholinergics as antisialogogues, alone or in combination with pressure dressings, has been reported in the treatment of parotid gland !stulae.5 How-ever, the undesirable side e"ects—such as drowsiness, blurred vision, sedation, nausea and vomiting, urinary retention, and mouth dryness—associated with high peak serum levels a$er oral or parenteral administra-tion of anticholinergics have precluded their utilization.
Scopolamine is an antimuscarinic agent with a potent action on salivary glands; it can reduce the volume of salivary secretion in human beings. #e availability of scopolamine in a transdermal delivery system provides an alternative method for the administration of antisi-alogogues and avoids collateral e"ects.21 #e system is a circular, !lm-like patch with a drug reservoir containing 1.5 mg of scopolamine. When the patch is applied to the skin, the scopolamine is released at a constant rate to maintain a steady plasma level for at least 72 hours. Ab-sorption occurs when the patch is applied to the hairless skin behind the ear. #e application of the patch in this region may have a direct e"ect on the residual parotid tissue, thus causing a reduction in salivary secretion.
Transdermal scopolamine has been described in the management of drooling in neurologically damaged patients, in the prevention of nausea and vomiting as-sociated with motion sickness, and in the prevention of
postoperative nausea and vomiting.21,22 Mouth dryness, which occurs in as many as two-thirds of patients, is the only relevant side e"ect in the use of transdermal scopolamine.21 However, other side e"ects such as som-nolence and transient disorders of ocular accommoda-tion can occasionally occur, even with the transdermal system.
In 2007, the !rst report of transdermal scopolamine in the treatment of salivary !stulae was published.23 In this study, Dessy et al !rst described a case of parotid !stula a$er a face-li$ that was treated successfully using a transdermal scopolamine patch combined with BoNT/A. Previously, a case of post-rhytidectomy sialocele was reported to have resolved in 6 days when a transdermal scopolamine patch alone was used.24 #ese cases are, to the best of our knowledge, the only two descriptions of the use of transdermal scopolamine in the management of salivary disorders a$er surgery.
Salivary !stulae a$er a face-li$ are caused by parotid injury due to the deeper dissection of the super!cial musculoaponeurotic system. #e pathogenesis of post-rhytidectomy salivary !stulae is therefore similar to that of postparotidectomy !stulae.
In the present case series, our patients were initially treated with direct closure of the !stulae using Steri-Strips and with reduction of oral intake. A$er a few days, transdermal scopolamine was applied to the region of the residual parotid gland. A prompt and remarkable decrease in the !stula output was observed. #e salivary !stulae healed completely in 2 to 3 days. #e patch was kept in place for 3 days and then replaced by a new one to maintain an adequate scopolamine plasma level for at least 3 more days a$er the resolution of salivary dis-charge. #e only adverse e"ect that 2 of our 3 patients experienced was xerostomia, which resolved a$er the end of treatment. No recurrence of the !stula was observed during follow-up.
Although our case records are limited, our experi-ence shows that transdermal scopolamine could be a minimally invasive and e"ective therapy in cases of parotid !stulae. In consideration of the cost and safety of transdermal scopolamine, this treatment could be a valid alternative to BoNT/A as primary treatment in the management of postparotidectomy !stulae.
In conclusion, postparotidectomy !stulae are uncom-mon. #eir management can be di%cult, and several methods of treatment have been used. Because of our encouraging experience, we believe that the use of transdermal scopolamine is a valid and simple option in the treatment of parotid !stulae. It is possible that the application of the patch on the preauricular region

Volume 92, Number 10-11 www.entjournal.com ! 519
TRANSDERMAL SCOPOLAMINE IN THE MANAGEMENT OF POSTPAROTIDECTOMY SALIVARY FISTULA
Advanced Techniques in Endoscopic Sinus Surgery
February 13-17, 2014
President’s Day / Valentine’s Day Weekend
Hyatt Regency Indian Wells Palm Springs, California
Lectures and Cadaver dissection with image guidance LIVE SURGERY
World-class golf, tennis, shopping, spa, outdoor activities, pools, and family fun
Honored Guest:
Richard Orlandi, MD
Course Faculty: Karen Fong, MD Winston Vaughan, MD Christopher Church, MD Nadeem Akbar, MD Kimberly Cockerham, MD Tim Haegen, MD Ed Hepworth, MD
Manish Khanna, MD Peter Killian, MD Brad Mechor, MD Ankit Patel, MD Ryan Rehl, MD Kristin Seiberling, MD Alex Stewart, MD Roy Thomas, MD Darshni Vira, MD Rhoda Wynn, MD
$200 Early Registration Discount!
before December 14,2013
www.calsinus.com/course [email protected]
Rigid & Flexible Endoscope Repair
E.C. MEDICAL PRODUCTSBRENTWOOD, TN
(615)373-3240 or (800) [email protected]
ASK FOR FRITZ
Repairs · Refurbished EquipmentVideo Camera Systems
Portable LED Endoscopic Light Sources
Refurbished Surgical Microscopes
Pre-OwnedFlexible & Rigid Scopes
SAVE MONEY!We repair ALL Makes & Models of both
Rigid & Flexible Scopes.No Models are obsolete! Substantial Savings!
with 18 month warrantyC
LASS
IFIE
DS
may have a direct e!ect on the residual parotid tissue by reducing salivary secretion and rapidly healing the "stula.
References 1. Ananthakrishnan N, Parkash S. Parotid "stulas: A review. Br J Surg
1982;69(11):641-3. 2. Arulpragasam AC. On the treatment of parotid "stulae. J Laryngol
Otol 1967;81(3):329-37. 3. Parekh D, Glezerson G, Stewart M, et al. Post-traumatic parotid
"stulae and sialoceles. A prospective study of conservative manage-ment in 51 cases. Ann Surg 1989;209(1):105-11.
4. Wax M, Tarshis L. Post-parotidectomy "stula. J Otolaryngol 1991;20 (1):10-13.
5. Cavanaugh K, Park A. Postparotidectomy "stula: A di!erent treat-ment for an old problem. Int J Pediatr Otorhinolaryngol 1999;47(3): 265-8.
6. Bailey BM. A persistent parotid "stula following the extraction of mandibular teeth. J Laryngol Otol 1984;98(10):1051-4.
7. Hutchison IL, Ryan D. A parotid "stula and sialocele complicating temporomandibular joint surgery. Br J Oral Maxillofac Surg 1989;27 (3):203-8.
8. Wolf K, Bostwick J, Dinner M, Jackson IT. Parotid salivary "stula following rhytidectomy. Plast Reconstr Surg 1996;97(3):641-2.
9. Mandour MA, El-Sheikh MM, El-Garem F. Tympanic neurectomy for parotid "stula. Arch Otolaryngol 1976;102(6):327-9.
10. Shimm DS, Berk FK, Tilsner TJ, Coulthard SW. Low-dose radiation therapy for benign salivary disorders. Am J Clin Oncol 1992;15(1): 76-8.
11. Spinell C, Ricci E, Berti P, Miccoli P. Postoperative salivary "stula: #erapeutic action of octreotide. Surgery 1995;117(1):117-18.
12. Krausen AS, Ogura JH. Sialoceles: Medical treatment "rst. Trans Sect Otolaryngol Am Acad Ophthalmol Otolaryngol 1977;84(5): ORL890-5.
13. Sachsman SM, Rice DH. Use of AlloDerm implant to improve cosmesis a$er parotidectomy. Ear Nose #roat J 2007;86(8):512-13.
14. Ye WM, Zhu HG, Zheng JW, et al. Use of allogenic acellular dermal matrix in prevention of Frey’s syndrome a$er parotidectomy. Br J Oral Maxillofac Surg 2008;46(8):649-52.
15. Bushara KO. Sialorrhea in amyotrophic lateral sclerosis: A hypothesis of a new treatment—botulinum toxin A injections of the parotid glands. Med Hypotheses 1997;48(4):337-9.
16. Vargas H, Galati LT, Parnes SM. A pilot study evaluating the treat-ment of postparotidectomy sialoceles with botulinum toxin type A. Arch Otolaryngol Head Neck Surg 2000;126(3):421-4.
17. Guntinas-Lichius O, Sittel C. Treatment of postparotidectomy salivary "stula with botulinum toxin. Ann Otol Rhinol Laryngol 2001;110(12):1162-4.
18. Marchese-Ragona R, Marioni G, Restivo DA, Sta%eri A. #e role of botulinum toxin in postparotidectomy "stula treatment. A technical note. Am J Otolaryngol 2006;27(3):221-4.
19. Lim YC, Choi EC. Treatment of an acute salivary "stula a$er parotid surgery: Botulinum toxin type A injection as primary treatment. Eur Arch Otorhinolaryngol 2008;265(2):243-5.
20. Capaccio P, Torretta S, Osio M, et al. Botulinum toxin therapy: A tempting tool in the management of salivary secretory disorders. Am J Otolaryngol 2008;29(5):333-8.
21. Talmi YP, Finkelstein Y, Zohar Y. Reduction of salivary &ow with transdermal scopolamine: A four-year experience. Otolaryngol Head Neck Surg 1990;103(4):615-18.
22. Kranke P, Morin AM, Roewer N, et al. #e e%cacy and safety of transdermal scopolamine for the prevention of postoperative nau-sea and vomiting: A quantitative systematic review. Anesth Analg 2002;95(1):133-43.
23. Dessy LA, Mazzocchi M, Monarca C, et al. Combined transdermal scopolamine and botulinum toxin A to treat a parotid "stula a$er a face-li$ in a patient with siliconomas. Int J Oral Maxillofac Surg 2007;36(10):949-52.
24. Lapid O, Kreiger Y, Sagi A. Transdermal scopolamine use for post-rhytidectomy sialocele. Aesthetic Plast Surg 2004;28(1):24-8.

520 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
BUYE RS G U IDE
INDEX
We at ENT-Ear, Nose & Throat Journal are pleased to offer readers our eighth annual Buyers Guide! Its listings give you
convenient access to useful information about companies offering products and services of interest to ENT physicians. We
hope you will also visit the online Buyers Guide at http://directory.entjournal.com, where you can contact vendors and
download additional information about many of the products/services available. We hope you !nd this resource a useful
tool when addressing your purchasing needs.
Introduction
Cameras/AccessoriesDigital Cameras .................................................................... 521
Computer Equipment/SoftwareComputer Software, Practice Management ........................... 521Electronic Medical Records ................................................... 521
Diagnostic Equipment/SuppliesAudiometers ......................................................................... 521Balance Testing Devices ....................................................... 521Microscopes ......................................................................... 522Swallowing Assessment Instrumentation .............................. 522Vestibular Assessment Devices ............................................. 522Videonystagmography (VNG) ................................................. 522Voice Analysis Equipment ..................................................... 522
Furniture, Exam/Treatment RoomCabinets, Treatment .............................................................. 522Chairs, Power ....................................................................... 523Chairs, Treatment Room ........................................................ 523Stools, Adjustable-Height ...................................................... 523
Hearing & Speech Devices/AccessoriesSpeech/Voice Analysis Instrumentation ................................. 523
Imaging Equipment/Accessories3-D Imaging Systems ........................................................... 523CT Scanners, In-Of!ce .......................................................... 523Endoscopes .......................................................................... 524Image-Capturing Devices ...................................................... 524Laryngostroboscopes ............................................................ 524Nasopharyngoscopes ............................................................ 524Transnasal Esophagoscopes ................................................. 525Video Otoscopes ................................................................... 525Videostroboscopes ................................................................ 525
ImplantsImplant Material, Soft-Tissue ................................................ 525Implants, Vocal Fold .............................................................. 525
Light SourcesHalogen Lights ...................................................................... 525Stroboscopic Lights .............................................................. 526Xenon Lights ......................................................................... 526
Patient Care ProductsEarplugs, Hearing Protection ................................................. 526Earplugs, Water Protection .................................................... 526Hearing Aid Protection .......................................................... 526Nasal Moisturizers ................................................................ 526Tinnitus Treatment ................................................................ 526Tracheostomy Speaking Valves ............................................. 526Ventilator Speaking Valves .................................................... 526
Patient Rehabilitation ProductsBalance Training Equipment .................................................. 526
Pharmaceutical ProductsAnesthetics, Topical .............................................................. 527Nasal Spray, Allergy .............................................................. 527Tinnitus Treatments .............................................................. 527
ServicesEndoscope Evaluation & Repair ............................................. 527
Surgical EquipmentLasers, Compact CO2 ............................................................ 527Surgery Tables ...................................................................... 527Surgical Microscopes ............................................................ 528Surgical Stools ...................................................................... 528
Surgical Instruments/AccessoriesBalloon Sinuplasty ................................................................ 528
Surgical SuppliesEpistaxis Packing .................................................................. 528Intranasal Splints .................................................................. 528Nasal Packing ....................................................................... 528Nasal Splints ......................................................................... 528Tracheostomy Tubes ............................................................. 528

Volume 92, Number 10-11 www.entjournal.com ! 521
BUYERS GU IDE
CAMERAS/ACCESSORIES
DIGITAL CAMERAS
HMB Endoscopy ProductsHollywood, FLContact: Harvey Buxbaum(954) 792-6522Email: [email protected]: www.hmbendoscopy.com
H.M.B. Endoscopy Products is a 24-year-old company that sells and repairs new and refurbished endoscopy instrumentation made by Olympus, Pentax, and other manufacturers, at extremely a!ordable prices. All previously owned endoscopy products are meticulously refurbished and rebuilt by factory-trained technicians and are sold with a 2-year extended warranty against defects in materials and workmanship. "e price savings are substantial, and you will #nd that there is absolutely no sacri#ce in quality compared to buying new directly from the manufacturer.
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
COMPUTER EQUIPMENT/ SOFTWARE
COMPUTER SOFTWARE, PRACTICE MANAGEMENT
AllMeds Inc.Oak Ridge, TNContact: Todd Davis(888) 343-6337Email: [email protected]: www.allmeds.com
ELECTRONIC MEDICAL RECORDS
AllMeds Inc.Oak Ridge, TNContact: Todd Davis(888) 343-6337Email: [email protected]: www.allmeds.com
ENT’s Most Widely Used EHR!Since being founded by ENT surgeons, AllMeds
has provided the most e!ective EHR speci#cally designed for Otolaryngologists. For more than 15 years, guidance from AllMeds’ ENT leadership and customers has created an EHR perfectly evolved for the unique needs of Otolaryngology practices.
AllMeds’ consistent ENT focus has produced the industry’s highest lifetime customer success rate and an EHR Incentives Rate that exceeds national performance by over 200%!
ENT is in AllMeds’ DNA.
ChartLogicSalt Lake City, UT(800) 686-9651Email: [email protected]: www.chartlogic.com
Rosch Visionary Systems, Inc.Altoona, PAContact: Heather Wallen(800) 307-3320Email: [email protected]: www.roschvisionary.com
At Rosch Visionary Systems, we’re your allergy technology specialists. Our Rosch Immunotherapy so$ware safely and e!ectively manages your allergy mixing, injections and reactions. Multiple safety features include vial bar coding and tracking a patient’s progression when vials are mixed using a dilution board.
Our Visionary Allergy Tracker sends patient noti#cations for upcoming and/or overdue shots, increasing patient compliance. Includes phone app, text messaging and email capabilities.
DIAGNOSTIC EQUIPMENT/ SUPPLIES
AUDIOMETERS
InteracousticsEden Prairie, MNContact: Richard Mitchell(800) 947-6334Email: [email protected]: www.interacoustics-us.com
Maico DiagnosticsEden Prairie, MN(888) 941-4201Email: [email protected]: www.maico-diagnostics.com
OtometricsRegents Park, NSW, AustraliaContact: Chris WebberEmail: [email protected]: www.otometrics.com
See our ad in this issue
BALANCE TESTING DEVICES
Micromedical Technologies, Inc.Chatham, ILContact: Diane Miles(800) 334-4154Email: [email protected]: www.micromedical.com
OtometricsRegents Park, NSW, AustraliaContact: Chris WebberEmail: [email protected]: www.otometrics.com
See our ad in this issue

522 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
BUYE RS G U IDE
MICROSCOPES
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
Seiler Precision MicroscopesSt. Louis, MOContact: Dane Carlson(800) 489-2282Email: [email protected]: www.seilerinst.com
SWALLOWING ASSESSMENT INSTRUMENTATION
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
VESTIBULAR ASSESSMENT DEVICES
Micromedical Technologies, Inc.Chatham, ILContact: Diane Miles(800) 334-4154Email: [email protected]: www.micromedical.com
VIDEONYSTAGMOGRAPHY (VNG)
Micromedical Technologies, Inc.Chatham, ILContact: Diane Miles(800) 334-4154Email: [email protected]: www.micromedical.com
OtometricsRegents Park, NSW, AustraliaContact: Chris WebberEmail: [email protected]: www.otometrics.com
See our ad in this issue
VOICE ANALYSIS EQUIPMENT
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
FURNITURE, EXAM/TREATMENT ROOM
CABINETS, TREATMENT
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
JEDMED has 35 years of experience providing service, sales, and extensive knowledge of all types of ENT products. As an employee-owned company, we pride ourselves in bringing innovation to customary products for practices. Our innovation has also carried over into unique products for unusual diagnostic applications. Based in St. Louis, Missouri, our company is certi!ed to ISO 13485 medical device design manufacturing standards, meaning you can be con!dent in the equipment you purchase from JEDMED.
MTISalt Lake City, UTContact: Mike BakerUS/Canada (800) 924-4655 International (801) 875-4999Email: [email protected]: www.mti.net
See our ad in this issue
Reliance Medical ProductsMason, OHContact: Chris Blizzard(800) 735-0357Email: [email protected]: www.reliance-medical.com
See our ad in this issue

Volume 92, Number 10-11 www.entjournal.com ! 523
BUYERS GU IDE
CHAIRS, POWER
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
MTISalt Lake City, UTContact: Mike BakerUS/Canada (800) 924-4655 International (801) 875-4999Email: [email protected]: www.mti.net
With more than 75 years combined industry experience, MTI designs exam chairs with ADA- compliant seat entry height and a max li! of 650 lbs., designed for many ENT procedures. When you need an exam or minor procedure chair that also provides Trendelenburg and a footrest for easy entry, the MTI 424 is your choice. "e independent power tilt provides the #exibility to contour your patient for better comfort.
See our ad in this issue
Reliance Medical ProductsMason, OHContact: Chris Blizzard(800) 735-0357Email: [email protected]: www.reliance-medical.com
See our ad in this issue
CHAIRS, TREATMENT ROOM
Reliance Medical ProductsMason, OHContact: Chris Blizzard(800) 735-0357Email: [email protected]: www.reliance-medical.com
See our ad in this issue
STOOLS, ADJUSTABLE-HEIGHT
MTISalt Lake City, UTContact: Mike BakerUS/Canada (800) 924-4655 International (801) 875-4999Email: [email protected]: www.mti.net
See our ad in this issue
Reliance Medical ProductsMason, OHContact: Chris Blizzard(800) 735-0357Email: [email protected]: www.reliance-medical.com
See our ad in this issue
HEARING & SPEECH DEVICES/ACCESSORIES
SPEECH/VOICE ANALYSIS INSTRUMENTATION
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
IMAGING EQUIPMENT/ ACCESSORIES
3-D IMAGING SYSTEMS
SOREDEXMilwaukee, WIContact: Bob Dif!n(800) 558-6120Email: [email protected]: www.soredex.com/products/3d-imaging/scanora-3d-for-ent.aspx
See our ad in this issue
CT SCANNERS, IN-OFFICE
Medkamp, LLCSt. Louis, MOContact: Robyn Gettemeyer(866) 891-9217Email: [email protected]: www.medkamp.com
Distributor of the Xoran Technologies “Mini-cat” and “Xcat.”
524 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
BUYE RS G U IDE
SOREDEXMilwaukee, WIContact: Bob Dif!n(800) 558-6120Email: [email protected]: www.soredex.com/products/3d-imaging/scanora-3d-for-ent.aspx
See our ad in this issue
Xoran Technologies, Inc.Ann Arbor, MIContact: Rachel Gajda(800) 709-6726Email: [email protected]: www.xorantech.com
ENDOSCOPES
HMB Endoscopy ProductsHollywood, FLContact: Harvey Buxbaum(954) 792-6522Email: [email protected]: www.hmbendoscopy.com
H.M.B. Endoscopy Products is a 24-year-old company that sells and repairs new and refurbished endoscopy instrumentation made by Olympus, Pentax, and other manufacturers, at extremely a!ordable prices. All previously owned endoscopy products are meticulously refurbished and rebuilt by factory-trained technicians and are sold with a 2-year extended warranty against defects in materials and workmanship. "e price savings are substantial, and you will #nd that there is absolutely no sacri#ce in quality compared to buying new directly from the manufacturer.
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
IMAGE-CAPTURING DEVICES
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
LARYNGOSTROBOSCOPES
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
NASOPHARYNGOSCOPES
HMB Endoscopy ProductsHollywood, FLContact: Harvey Buxbaum(954) 792-6522Email: [email protected]: www.hmbendoscopy.com
H.M.B. Endoscopy Products is a 24-year-old company that sells and repairs new and refurbished endoscopy instrumentation made by Olympus, Pentax, and other manufacturers, at extremely a!ordable prices. All previously owned endoscopy products are meticulously refurbished and rebuilt by factory-trained technicians and are sold with a 2-year extended warranty against defects in materials and workmanship. "e price savings are substantial, and you will #nd that there is absolutely no sacri#ce in quality compared to buying new directly from the manufacturer.
Volume 92, Number 10-11 www.entjournal.com ! 525
BUYERS GU IDE
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
Optim LLCSturbridge, MAContact: Lisa Skowyra(508) 347-5100Email: [email protected]: www.optim-llc.com
TRANSNASAL ESOPHAGOSCOPES
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
VIDEO OTOSCOPES
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
VIDEOSTROBOSCOPES
JEDMEDSt. Louis, MOContact: Technical Service(314) 845-3770Email: [email protected]: www.jedmed.com
JEDMED has 35 years of experience providing service, sales, and extensive knowledge of all types of ENT products. As an employee-owned company, we pride ourselves in bringing innovation to customary products for practices. Our innovation has also carried over into unique products for unusual diagnostic applications. Based in St. Louis, Missouri, our company is certi!ed to ISO 13485 medical device design manufacturing standards, meaning you can be con!dent in the equipment you purchase from JEDMED.
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
IMPLANTS
IMPLANT MATERIAL, SOFT-TISSUE
Merz Aesthetics, Inc. (formerly BioForm Medical)San Mateo, CA(866) 862-1209Email: [email protected]: www.radiesse-voice.com
See our ad in this issue
IMPLANTS, VOCAL FOLD
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
LIGHT SOURCES
HALOGEN LIGHTS
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com

526 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
BUYE RS G U IDE
STROBOSCOPIC LIGHTS
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
XENON LIGHTS
PENTAX MedicalMontvale, NJContact: Joyce Romano(973) 628-6200Email: [email protected]: www.kaypentax.com
PATIENT CARE PRODUCTS
EARPLUGS, HEARING PROTECTION
McKeon Products, Inc.Warren, MIContact: Elaine Masterson(586) 427-7560Email: [email protected]: www.macksearplugs.com
See our ad in this issue
EARPLUGS, WATER PROTECTION
Jaco Enterprises, Inc.Phoenix, AZContact: Scott Malkoff(866) 420-4255Email: [email protected]: www.earbandit.com
McKeon Products, Inc.Warren, MIContact: Elaine Masterson(586) 427-7560Email: [email protected]: www.macksearplugs.com
See our ad in this issue
HEARING AID PROTECTION
Hearing Aid Sweat BandWest Valley, NYContact: Scott VanBuskirk(866) 644-2500Email: [email protected]: www.hearingaidsweatband.com
NASAL MOISTURIZERS
Xlear Inc.American Fork, UT(877) 599-5327Email: [email protected]: www.xlear.com
See our ad in this issue
TINNITUS TREATMENT
Arches Tinnitus FormulasSalt Lake City, UTContact: Brent Curtis(800) 486-1237Email: [email protected]: www.tinnitusformula.com
Arches Tinnitus Formula™ is a dietary supplement whose ingredients have been proven clinically e!ective for tinnitus. Arches Tinnitus Formula is recommended by thousands of leading ENTs for their patients with tinnitus. Many tell their patients to try the Arches Tinnitus Combo Pack, a three-month supply of Arches Tinnitus, Stress and B-12 Formulas. At a minimum they advise them to take four bottles of Arches Tinnitus Formula to determine their total degree of e"cacy.
See our ad in this issue
TRACHEOSTOMY SPEAKING VALVES
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
VENTILATOR SPEAKING VALVES
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
PATIENT REHABILITATION PRODUCTS
BALANCE TRAINING EQUIPMENT
Micromedical Technologies, Inc.Chatham, ILContact: Diane Miles(800) 334-4154Email: [email protected]: www.micromedical.com

Volume 92, Number 10-11 www.entjournal.com ! 527
BUYERS GU IDE
PHARMACEUTICAL PRODUCTS
ANESTHETICS, TOPICAL
Beutlich Pharmaceuticals, LLCWaukegan, ILContact: Heather Wagner(800) 238-8542Email: [email protected]: www.beutlich.com
See our ad in this issue
NASAL SPRAY, ALLERGY
Xlear Inc.American Fork, UT(877) 599-5327Email: [email protected]: www.xlear.com
See our ad in this issue
TINNITUS TREATMENTS
Arches Tinnitus FormulasSalt Lake City, UTContact: Brent Curtis(800) 486-1237Email: [email protected]: www.tinnitusformula.com
Arches Tinnitus Formula™ is a dietary supplement whose ingredients have been proven clinically e!ective for tinnitus. Arches Tinnitus Formula is recommended by thousands of leading ENTs for their patients with tinnitus. Many tell their patients to try the Arches Tinnitus Combo Pack, a three-month supply of Arches Tinnitus, Stress and B-12 Formulas. At a minimum they advise them to take four bottles of Arches Tinnitus Formula to determine their total degree of e"cacy.
See our ad in this issue
SERVICES
ENDOSCOPE EVALUATION & REPAIR
HMB Endoscopy ProductsHollywood, FLContact: Harvey Buxbaum(954) 792-6522Email: [email protected]: www.hmbendoscopy.com
H.M.B. Endoscopy Products is a 24-year-old company that sells and repairs new and refurbished endoscopy instrumentation made by Olympus, Pentax, and other manufacturers, at extremely a!ordable prices. All previously owned endoscopy products are meticulously refurbished and rebuilt by factory-trained technicians and are sold with a 2-year extended warranty against defects in materials and workmanship. #e price savings are substantial, and you will $nd that there is absolutely no sacri$ce in quality compared to buying new directly from the manufacturer.
SURGICAL EQUIPMENT
LASERS, COMPACT CO!
LumenisSan Jose, CAContact: Susan Smith(408) 764-3013Email: [email protected]: www.lumenis.com
Introducing the new AcuPulse DUO CO2 Sur-gical Laser, coupling line-of-sight and $ber-based laser approaches to allow the greatest surgical freedom in addressing lesions that are di"cult to access. #e AcuPulse DUO addresses a broad range of clinical solutions for ear, nose and throat, gy-necology, otology and general surgery. Combined with its full range of $ber and free-beam acces-sories, it is a powerful surgical tool. Additionally, three power modes, three timed-exposure modes and the SurgiTouch scanner give surgeons the freedom to customize beam delivery and control tissue e!ect for optimal balance between surgical precision and microvascular hemostasis.
SURGERY TABLES
MTISalt Lake City, UTContact: Mike BakerUS/Canada (800) 924-4655 International (801) 875-4999Email: [email protected]: www.mti.net
See our ad in this issue

528 ! www.entjournal.com ENT-Ear, Nose & Throat Journal ! October/November 2013
BUYE RS G U IDE
SURGICAL MICROSCOPES
Seiler Precision MicroscopesSt. Louis, MOContact: Dane Carlson(800) 489-2282Email: [email protected]: www.seilerinst.com
SURGICAL STOOLS
MTISalt Lake City, UTContact: Mike BakerUS/Canada (800) 924-4655International (801) 875-4999Email: [email protected]: www.mti.net
See our ad in this issue
SURGICAL INSTRUMENTS/ ACCESSORIES
BALLOON SINUPLASTY
Entellus MedicalPlymouth, MNContact: Cheryl Schwanke(866) 620-7615Email: [email protected]: www.entellusmedical.com
See our ad in this issue
SURGICAL SUPPLIES
EPISTAXIS PACKING
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
INTRANASAL SPLINTS
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
NASAL PACKING
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
NASAL SPLINTS
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
TRACHEOSTOMY TUBES
BostonMedical Products
Boston Medical Products, Inc.Westborough, MAContact: Stuart Montgomery(800) 433-2674Email: [email protected]: www.bosmed.com
ADVERTISER INDEXArches Tinnitus Formulas ..................................................................................473Beutlich Pharmaceuticals ..................................................................................503entellus Medical ............................................................................CVR 2, 475, 489Feather Safety Razor .........................................................................................497GN Otometrics ..................................................................................................491GN ReSound Pty Ltd ..........................................................................................487GREER LABS .....................................................................................................493McKeon Products, Inc. .................................................................................. CVR 4MEDA Pharmaceuticals ............................................................................. 479-481Merz Aesthetics ................................................................................................483MTI, Inc. ...........................................................................................................477Reliance Medical Products ................................................................................501sano! aventis ...................................................................................................499SinuScience Network ........................................................................................495SOREDEX ...................................................................................................... CVR 3Xlear, Inc. ..........................................................................................................485

for ENT
Make an immediate impact on your practice. The SCANORA® 3D ENT
A!ordable ReliableWith a state-of-the-art SCANORA® 3D from Soredex, we can show you how our system will have an impact on your practice:
Generate a new revenue stream Increase case acceptance and scheduled surgeries Implement continuity of care program for your patients
Our Scanora® 3D imaging system for ENT Specialists comes with our proven accreditation support as part of our complete turnkey package including:
On site lAC accreditation support lAC compliant CME courses Accreditation support to assure fast and accurate applications for quicker certi!cation
When you combine all this with a national support system, no ongoing monthly support fees, FREE online and phone support for as long as you own your system, it equals the best solution for in-o"ce CT scanners in the market.
NO MONTHLY FEES3 YEAR WARRANTY
Call for details: 800-558-6120
Review treatment options with your patients the same day
SOREDEX®
www.soredex.com/usa
