tracheoesophageal fistula “”
TRANSCRIPT

12/01/2022 1
TRACHEOESOPHAGEAL FISTULA
NWAFORNSO, CHIAZOR I.NELSON CLUB PRESENTATION.DEPARTMENT OF PAEDIATRICS.
FEDERAL MEDICAL CENTRE, KEFFI.14th SEPTEMBER 2015

12/01/2022 2
OUTLINE• INTRODUCTION• EMBRYOLGY• CLASSIFICATION• EPIDEMIOLOGY• EMRYOLOGY• AETIOLOGY/ RISK FACTORS• CLINICAL FEATURES• DIFFERNTIAL DIAGNOSIS• WORKUP• MANAGEMENT• COMPLICATION• PROGNOSIS• PREVENTION• CONCLUSION.
12/01/2022 3
INTRODUCTION
• Tracheoesophageal fistula(TEF) is a congenital or acquired communication between the trachea and esophagus.
• Esophageal atresia(EA) occurs in association with TEF in about 90% of instances.
• TEF most likely leads to fatal pulmonary complications.
12/01/2022 4
Introduction
• Most congenital TEFs are diagnosed immediately following birth or in infancy.
• They are commonly associated with other congenital anomalies.
• Acquired TEF occur secondary to malignant disease, infection,, trauma, etc.
12/01/2022 5
EMBRYOLOGY
• The esophagus and trachea both develop from the primitive foregut.
• During 4 – 6 weeks of life the caudal part of the foregut forms the ventral diverticular which gives rise to the trachea.

12/01/2022 6
Embryology - 1
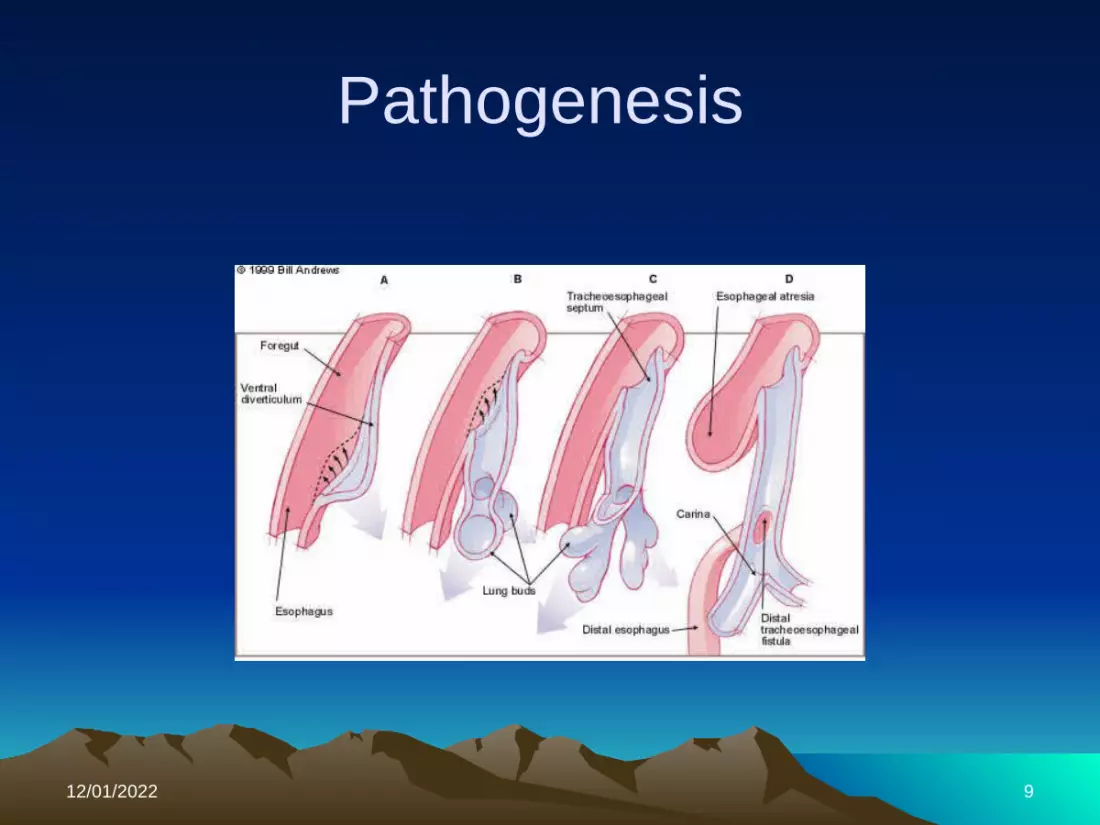
• The longitudinal tracheoesophageal fold fuses to form a septum, dividing the foregut into a ventral laryngotracheal tube and a dorsal esophagus.
• Posterior deviation of the septum causes incomplete separation of the esophagus from the laryngo tracheal tube resulting in TEF.

12/01/2022 7
Embryology - 2
12/01/2022 8
Embryology - 3
• Isolated esophageal atresia can occur when the esophagus fails to recannalize by the 8th week.
12/01/2022 9
Pathogenesis

12/01/2022 10
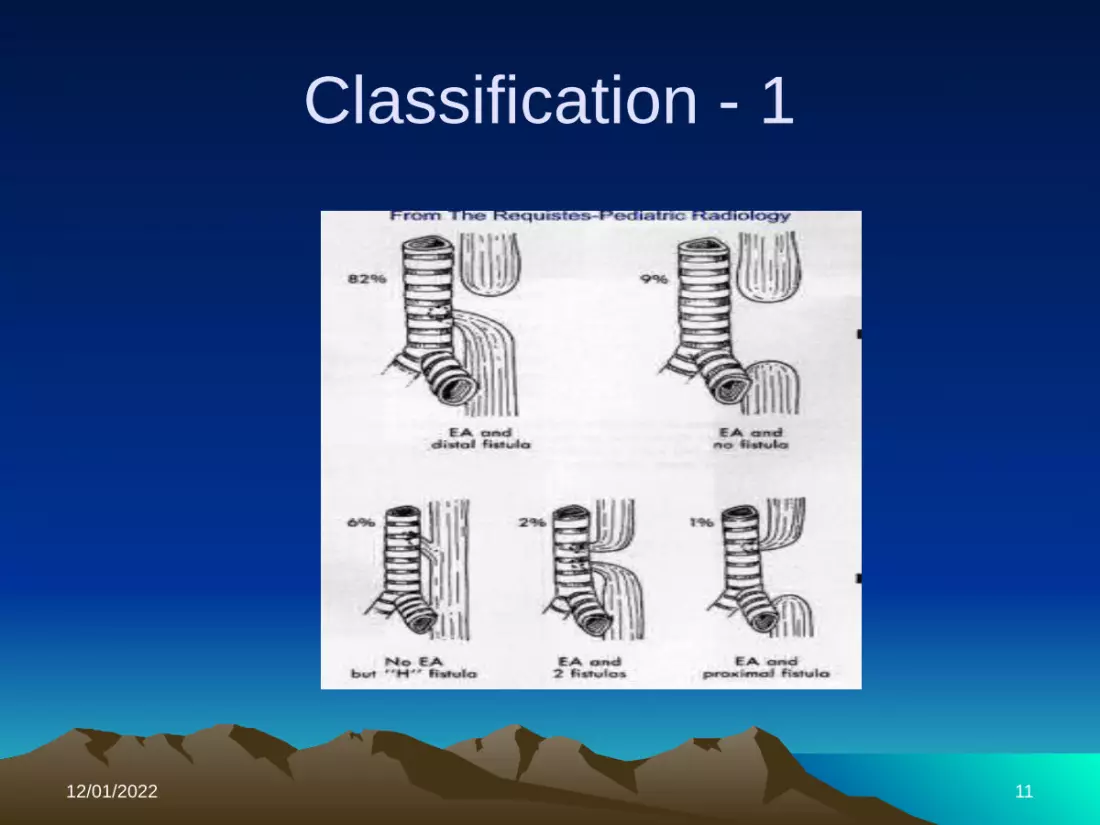
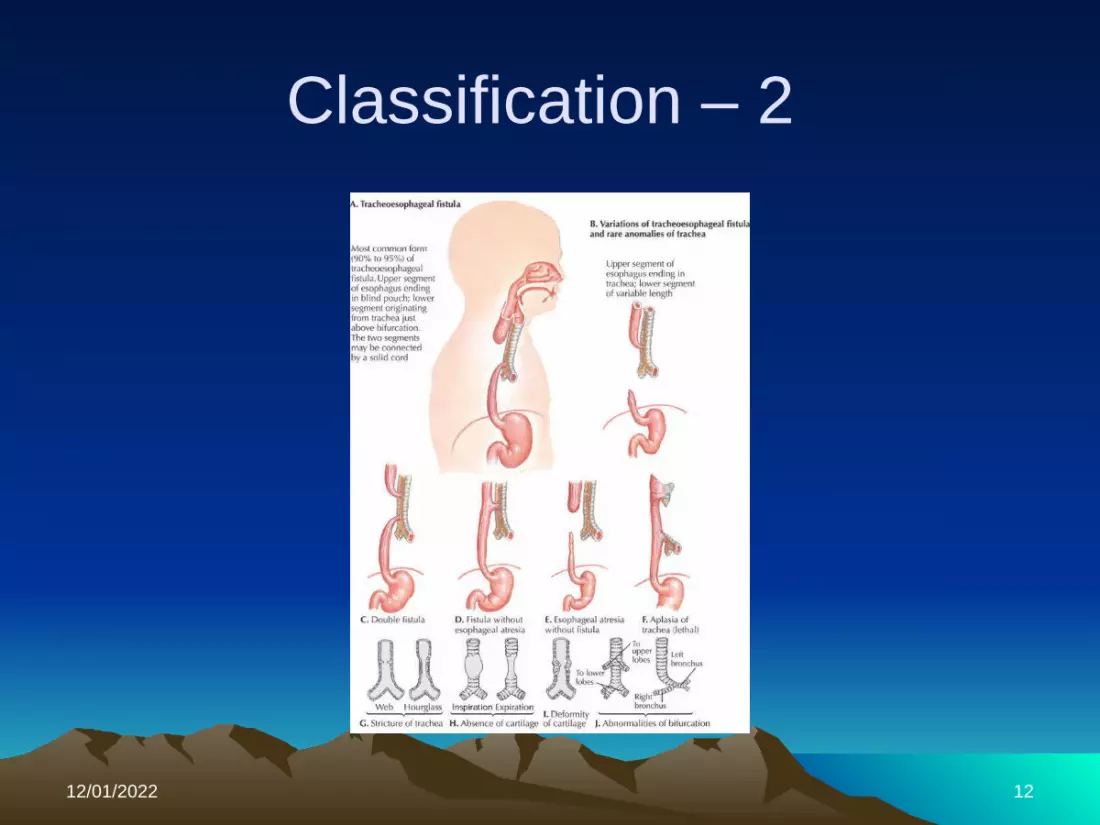
Classification of Tracheoesophageal fistula
Anatomic characteristics Percentage of cases Esophageal atresia with distal TEF 87%
Isolated esophageal atresia without TEF
8%
Isolated TEF (H type). 4%
Esophageal atresia with proximal TEF 1%
Esophageal atresia with proximal and distal TEF
1%
12/01/2022 11
Classification - 1
12/01/2022 12
Classification – 2
12/01/2022 13
Epidemiology
• Common congenital anomaly with an incidence of 1/2000- 4000 live births.
• Acquired TEF is rare.• No racial predilection• Commonly observed in neonates and
during the first year of life.• No data recorded in FMC Keffi from 2013
till date.
12/01/2022 14
AETIOLOGY
• Exact aetiology of TEF is unclear.• Embryologically believed to be due to
incomplete closure of laryngotracheal groove.
• Observed in mothers that used imidazole containing decongestants in the first trimester of pregnancy.
• Association with trisomies 18, 21, 13.
12/01/2022 15
Aetiology - 1
• Associated risk factors• Advanced maternal age• European ethnicity• Obesity• Low socioeconomic status• Tobacco smoking• Infants < 1500g ( highest mortality).
12/01/2022 16
Aetiology - 2
• Approximately 50% affected infants have associated anomalies.
• Syndromes include VATER/VACTERL( vertebral, anorectal, cardiac, tracheal, esophageal, renal, radial).
• Some genetic factors have been implicated with discrete mutations in syndromic cases.
12/01/2022 17
Aetiology - 3
• Examples : Feingold syndrome(N –MYC), CHARGE syndrome (chd7), anorectal- esophageal –genital syndrome(SOX2).
12/01/2022 18
CLINICAL FEATURES
• Approximately 80 -90% of affected infants have respiratory decompensation within the first hour of life.
• Neonates present with frothing, bubbling at the mouth and nose after birth.
• Episodes of coughing, cyanosis and respiratory distress.
• Feeding exacerbates symptoms.

12/01/2022 19
Clinical features - 2
• About 10-20% of older children present late in life with chronic respiratory problems – refractory bronchospasm, recurrent pneumonia.
12/01/2022 20
Clinical features - 3
• Clinically they have the following features.• Funnel shaped chest• Mediastinal shift• Absent breath sounds• Presence of peristaltic sound on affected
side.• Displaced heart sounds• Scaphoid abdomen
12/01/2022 21
DIAGNOSIS
• Prenatal diagnosis• Maternal ultrasound after 14 weeks G.A-
polyhydramnios, absence of fluid filled stomach, small abdomen, distended esophageal pouch.
12/01/2022 22
Diagnosis - 2
• Post natal diagnosis.• Plain chest radiograph tracheal compression,Absence of gastric bubble.(EA + proximal
TEF, isolated EA).Aspiration pneumonia opacity in the
posterior segment of upper lung zone.Insertion of NG tube-coiling in the
mediastinum(associated TEF).

12/01/2022 23
Plain radiograph – coiled NG tube, absent gastric bubble.
12/01/2022 24
Plain abdominal radiograpgh – gaseous stomach distention in
EA + distal fistula.
12/01/2022 25
Diagnosis - 3
• Contrast studies. 1 – 2 mls of barium instilled in the esophagus, and a plain lateral decubitus chest radiograph shows spilling of content in lungs.
• N.B rarely done due to risk of aspiration and pulmonary injury.
12/01/2022 26
Diagnosis - 4
• Multisector CT scans• Flexible esophagoscopy• Flexible bronchoscopy.
12/01/2022 27
DIFFERENTIAL DIAGNOSIS
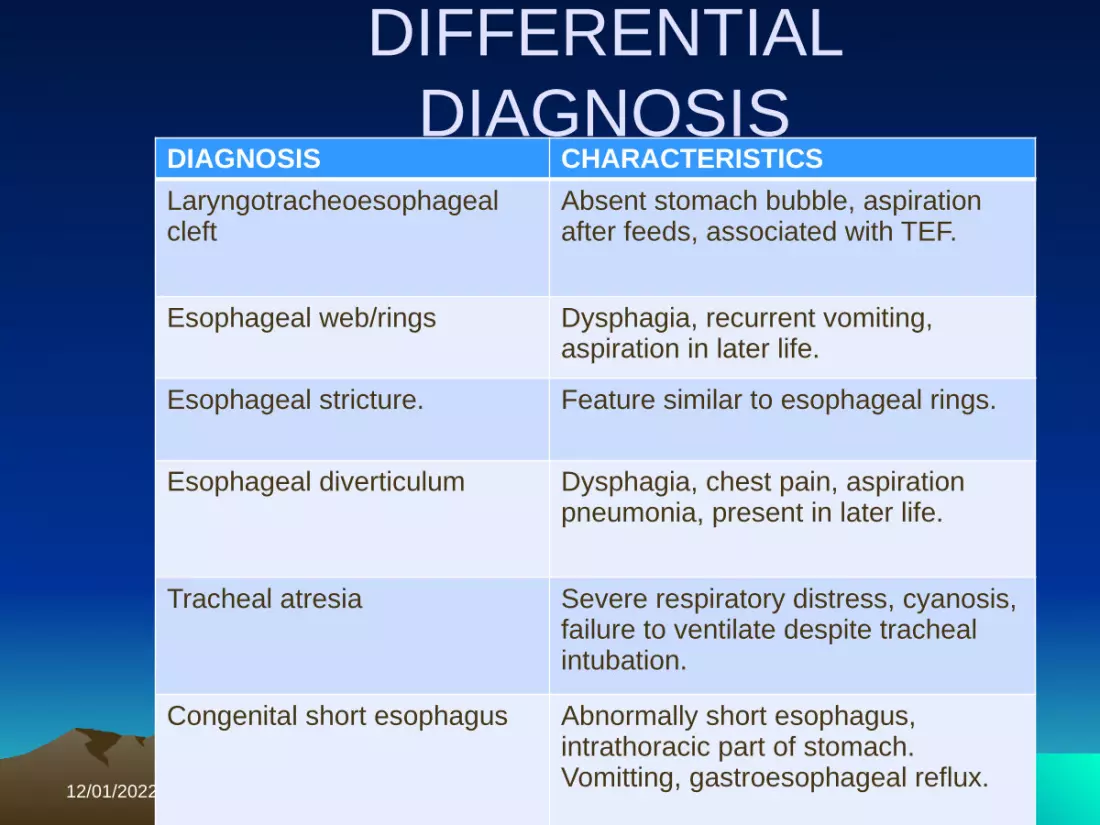
DIAGNOSIS CHARACTERISTICSLaryngotracheoesophageal cleft
Absent stomach bubble, aspiration after feeds, associated with TEF.
Esophageal web/rings Dysphagia, recurrent vomiting, aspiration in later life.
Esophageal stricture. Feature similar to esophageal rings.
Esophageal diverticulum Dysphagia, chest pain, aspiration pneumonia, present in later life.
Tracheal atresia Severe respiratory distress, cyanosis, failure to ventilate despite tracheal intubation.
Congenital short esophagus Abnormally short esophagus, intrathoracic part of stomach. Vomitting, gastroesophageal reflux.
12/01/2022 28
MANAGEMENT
• A multidisciplinary approach involving the paediatric gastroenterologist, pulmonologist, and cardiothoracic surgeon.

12/01/2022 29
Management - 1
• Stabilization of the patient.• Maintain a patent airway• Prevent aspiration of secretions• Prone positioning of patient to prevent
secretion from a distal fistula.• Esophageal suctioning to minimize
aspiration from a blind pouch.

12/01/2022 30
Management - 2
• In healthy infants without pulmonary complications, primary repair done in first few days of life.
• Delay is done in low birth weight infants, presence of pulmonary infection, or other anomalies.
• Conservative management- parenteral nutrition, gastrostomy,upper pouch suctioning.

12/01/2022 31
Management - 3
• Broad spectrum antibiotics are also commenced for lower respiratory tract infection.
• Forgarty balloon catheter may be used in patients with RDS to obliterate the TEF while awaiting surgery.
• Tracheostomy is considered only if a staged repair is planned.
12/01/2022 32
Management - 4
• Surgical repair involves surgical ligation of TEF and end to end anastomosis of esophagus.
• If the gap between the atretic ends is> 3-4 cm, a neoesophagus is created.
• Thoracoscopic surgical repair is now feasible with good outcome.
12/01/2022 33
Management - 5
• Feeding • After surgery baby is placed on I.v fluids
for 48 hours.• Feeding through gastrotomy tube
commenced on 3rd day post operatively.• Oral feeding commenced on the 10th day if
general condition is stable.

12/01/2022 34
COMPLICATIONS
• Recurrent pneumonia• Acute lung injury• Acute RDS• Lung abscess• Poor nutrition• Bronchiectasis• Respiratory failure• Death .

12/01/2022 35
Complications - 2
• Post op complications:• Tracheal stenosis• Recurrent fistula.o Others • Abnormal esophageal motility• Hiatal hernia• Barret esophagus• Gastro esophageal reflux disease
12/01/2022 36
Follow up
• Very essential• Evaluation by barium studies.

12/01/2022 37
OUTCOME
• Survival rate in healthy infants undergoing surgery may be >100%, and 80 – 95% in unfit patients.
• In a study done at UNTH Enugu by Nwosu and Onyekwulu, a total of 10 cases were seen over a 12 year period with only one survival after surgery.
12/01/2022 38
Outcome
• Delay in arriving at diagnosis, late presentation, associated congenital anomalies, and co morbidities contribute to poor outcome.
12/01/2022 39
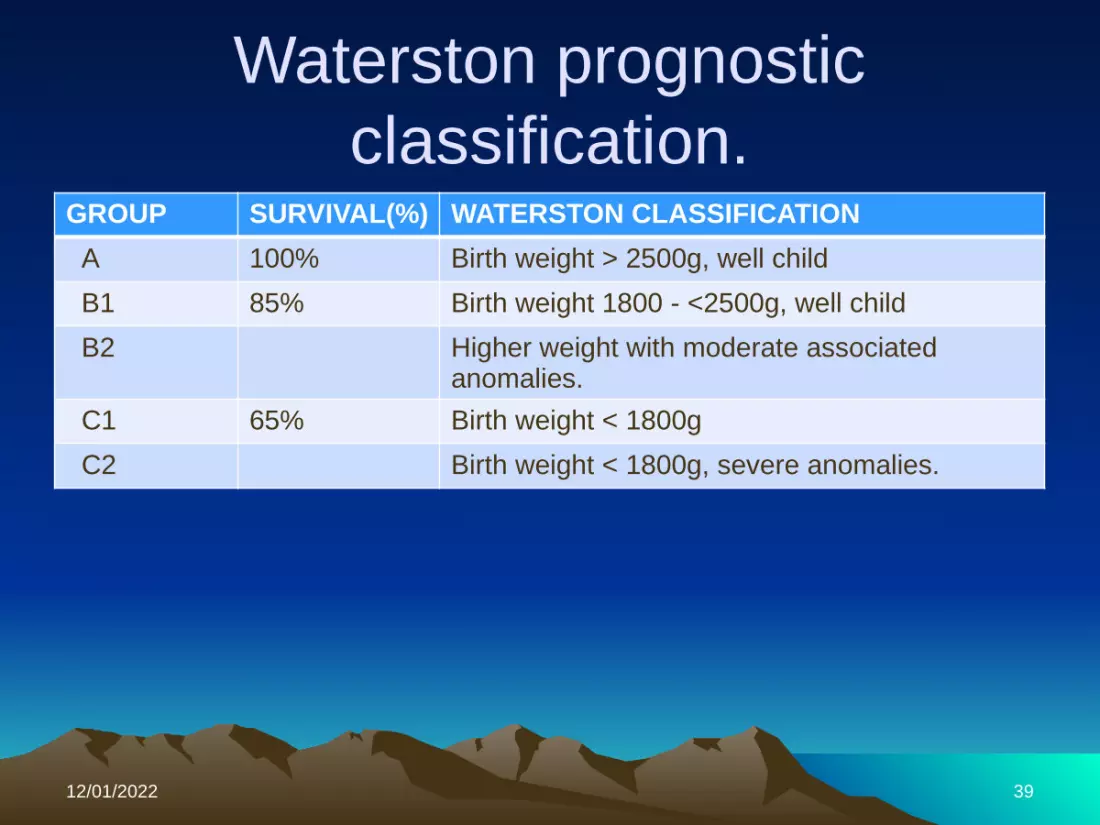
Waterston prognostic classification.
GROUP SURVIVAL(%) WATERSTON CLASSIFICATION A 100% Birth weight > 2500g, well child
B1 85% Birth weight 1800 - <2500g, well child
B2 Higher weight with moderate associated anomalies.
C1 65% Birth weight < 1800g
C2 Birth weight < 1800g, severe anomalies.

12/01/2022 40
Conclusion
• Tracheoesophageal fistula is a common congenital anomaly with fatal lung complications if not managed on time.
• It is a surgical emergency.• Early presentation and diagnosis helps
improve survival rate and outcome

12/01/2022 41
Refernces
• Langfield embryology, by Sadler, 5th edition. Chapter 13, pages 290 – 293.
• Nelson textbook of paediatrics, by R. Behrman et al, 19th edition, pages 4648 – 4650.
• Nigerian journal of medicine. ISSN 1115- 2613. volume 22. Number 4, October – December 2013.page 295-297.
12/01/2022 42
References .
• The short textbook of paediatrics, by Suraj Gupte, 11th edition. Chapter 40, page 695 – 696.

12/01/2022 43
• THANK YOU FOR YOUR TIME.
Giant post-traumatic parotid gland sialocele and fistula: A case report and review of the literature
Interventions for treating oro-antral communications and fistula due to dental procedures (Protocol)