the influence of media campaigns on vesico vaginal fistula
TRANSCRIPT
i
Department of Mass Communication
Digitally Signed by: Content manager’s Name
DN : CN = Weabmaster’s name
O= University of Nigeria, Nsukka
OU = Innovation Centre
THE INFLUENCE OF MEDIA CAMPAIGNS ON VESICO
VAGINAL FISTULA PREVENTION AND CONTROL IN
NORTH WEST NIGERIA
Odimba Rita
Faculty of Arts
UDEH, KENNETH
PG/MA/11/61257
ii
TITLE PAGE
THE INFLUENCE OF MEDIA CAMPAIGNS ON VESICO VAGINAL
FISTULA PREVENTION AND CONTROL IN NORTH WEST NIGERIA
BY
UDEH, KENNETH
PG/MA/11/61257
A RESEARCH PROJECT SUBMITTED TO THE DEPARTMENT OF
MASS COMMUNICATION, UNIVERSITY OF NIGERIA, NSUKKA, IN
PARTIAL FULFILLMENT OF THE REQIREMENTS FOR THE AWARD
OF MASTER OF ARTS (M.A) DEGREE IN MASS COMMUNICATION
iii
CERTIFICATION
This research project is an original work of Udeh Kenneth, with registration
number PG/MA/11/61257. It satisfies the requirement for presentation of research
to the department of Mass Communication University of Nigeria.
………………… ……………… …. ……………… …………
Mr.L.I Anorue Date Dr. Ray. Udeajah Date
Supervisor Head of Department
…………………………. …………………..
External Supervisor Date
iv
DEDICATION
This work is dedicated to God Almighty for being my source of inspiration
throughout the period of this study.
v
ACKNOWLEDGEMENTS
This work wouldn’t have been successful without the contributions of the
finest people around me. First, I must commend my father-figure-supervisor, Dr
L.I. Anorue, for his immense contributions throughout the period that this work
lasted. His courage to break new grounds pulled out the idea of this work in the
first place. His intelligence and moral clarity was unshaken. Let me also;
appreciate my Head of Department, Dr. Ray. Udeajah, for his contribution
throughout my stay in the Department. He is a role model. For other lecturers in
the Department; Prof.C. Okigbo, Prof. I.S. Ndolo, Dr. Church Akpan, Dr.
Nnanyelugo Okoro, Dr.G. Ezeah, U.J. Ohaja and others, I appreciate you all.
The contribution of Philip Amune, Okwudili Ekwe, Emmanuel Eze,
Geoffrey Akhile, Mavis Onojeghene Okeoghene, Chinemelum Oguine,
Okechukwu Chukwuma, and Ifeanyi Onyike can’t be expressed in few words. I
thank God for having you by my side.
Also to my mother Josephine Udeh, my siblings: Obioma, Chinelo,
Ukamaka, Chinedu, Chidiebere and my Aunty, Mrs. Esther Agbo who will always
call me and ask me how I am going with my project. Those calls were
inspirational. I thank you all.
I sincerely thank all the staff of Prudence Computer, for their efforts when I
was out of office for this work: Eze Martha, Okagbue Chinonso, and Eze Edith. I
thank you all for typesetting this work.
Finally, thanks to Mallam Ali Wada for taking me around Jigawa state and
translating my questionnaire into Hausa language. Dr. Aminu and Kenneth of
MSF Jahun, Jigawa State. Big thanks to all of you.
Udeh, Kenneth
PG/MA/11/61257
Department of Mass Communication
University of Nigeria Nsukka.
vi
TABLE OF CONTENTS
Title Page ........................................................................................................i
Certification ....................................................................................................ii
Dedication .......................................................................................................iii
Acknowledgements.........................................................................................iv
Table of Content .............................................................................................v
Abstract ...........................................................................................................viii
CHAPTER ONE: INTRODUCTION
1.1 Background of the study ............................................................................1
1.2 Statement of the Research Problem ...........................................................4
1.3 Objectives of the Study ..............................................................................6
1.4 Research Questions ....................................................................................6
1.5 Significance of the Study ...........................................................................7
1.6 Scope of the Study .....................................................................................8
1.7 Operational Definition of Terms ................................................................8
References ..................................................................................................10
CHAPTER TWO: LITERATURE REVIEW
2.0 Focus of the Review ...................................................................................12
2.1 An Overview of Vesico Vaginal Fistula ....................................................12
2.2 Causes of Vesico Vaginal Fistula ..............................................................15
2.3 Psycho-Social Consequences of VVF on its Victim .................................24
2.4 Empirical Studies .......................................................................................27
2.5 Theoretical Frame work .............................................................................38
References .................................................................................................41
CHAPTER THREE: METHODOLOGY
3.1 Research Design .........................................................................................47
3.2 Population of the Study ..............................................................................49
3.3 Sample Size ................................................................................................49
3.5 Measuring Instruments ...............................................................................55
3.6 Validity and Reliability of Measuring Instrument .....................................56
3.7 Methods of Data Presentation and Analysis ..............................................57
References ............................................................................................. 58
vii
CHAPTER FOUR: DATA PRESENTATION AND ANALYSIS
4.1 Data Presentation and Analysis .................................................................59
4.2 Discussion of Findings ...............................................................................99
References .................................................................................................104
CHAPTER FIVE: SUMMARY, CONCLUSION AND
RECOMMENDATIONS
5.1 Summary ....................................................................................................105
5.2 Conclusion .................................................................................................107
5.3 Recommendations ......................................................................................107
Biography ..................................................................................................110
Appendix ...................................................................................................I-VII
viii
LIST OF TABLES
Table 1: Sex of Respondents .............................................................................................................. 59
Table 2: Age of Respondents ............................................................................................................. 61
Table 3: Marital status of the Respondents ........................................................................................ 62
Table 4:Educational Qualification of Respondents ............................................................................ 63
Table 5: Occupation of Respondents .................................................................................................. 64
Table 6: Responses on Access to media of Communication .............................................................. 66
Table 7: Frequency of Exposure to media of Communication ........................................................... 67
Table 8: Access to VVF Campaigns .................................................................................................. 68
Table 9: Frequency of Exposure to VVF Campaigns......................................................................... 69
Table 10: Responses on the awareness level on VVF Campaigns ..................................................... 73
Table 11: Sources of Information ....................................................................................................... 74
Table 12: Analysing Causes of VVF ................................................................................................. 75
Table 13: Analyzing What VVF is Associated with .......................................................................... 77
Table 14: Analysis of those who Have Seen VVF Patient ................................................................. 78
Table 15: Analysis of how the respondents know VVF Patient ......................................................... 79
Table 16: Responses on the major source of Information .................................................................. 82
Table 17: Responses on the influence of the campaigns on the necessity of Antenatal Care ............ 86
Table 18: Responses on the influence of the campaigns in stopping Early Marriage ...................... 87
Table 19: Responses on the influence of the campaigns in stopping Female Genital Mutilation ..... 89
Table 20: Responses on the influence of the Campaigns on the Preventive Measures on VVF
Condition ............................................................................................................................................ 90
Table 21: Responses on the influence of campaigns in handling cases that can lead to VVF with
serious care. ........................................................................................................................................ 91
Table 22: Responses on the influence of the campaigns on the way VVF can be best Prevented ..... 92
Table 23: Responses on the influence of the campaigns on what to do with VVF Patients ............... 94
Table 24: Responses on influence of the campaigns on experience of Reported VVF Cases ......... 95
Table 25: Responses on the influence of the campaigns on the way VVF can be best
Controlled ........................................................................................................................... 96
ix
LIST OF FIGURES
Figure 1: Sex of Respondents ............................................................................................................. 60
Figure 2: Age of Respondents ............................................................................................................ 61
Figure 3: Marital status of the Respondents ....................................................................................... 62
Figure 4: Educational Qualification of Respondents .......................................................................... 63
Figure 5: Occupation of Respondents ................................................................................................ 65
Figure 6: Responses on Access to media of Communication............................................................. 66
Figure 7: Frequency of Exposure to media of Communication ......................................................... 67
Figure 8: Access to VVF Campaigns ................................................................................................. 68
Figure 9: Frequency of Exposure to VVF Campaigns ....................................................................... 69
Figure 10: Responses on the awareness level on VVF Campaigns .................................................... 73
Figure 11: Sources of Information ..................................................................................................... 74
Figure 12: Analysing Causes of VVF ............................................................................................... 76
Figure 13: Analyzing What VVF is Associated with ......................................................................... 77
Figure 14: Analysis of those who Have Seen VVF Patient ................................................................ 78
Figure 15: Analysis of how the respondents know VVF Patient ....................................................... 79
Figure 16: Responses on the major source of Information ................................................................. 82
Figure 17: Responses on the influence of the campaigns on the necessity of Antenatal Care ........... 86
Figure 18: Responses on the influence of the campaigns in stopping Early Marriage ..................... 88
Figure 19: Responses on the influence of the campaigns in stopping Female Genital Mutilation .... 89
Figure 20: Responses on the influence of the Campaigns on the Preventive Measures on VVF
Condition ............................................................................................................................................ 90
Figure 21: Responses on the influence of campaigns in handling cases that can lead to VVF with
serious care. ........................................................................................................................................ 91
Figure 22: Responses on the influence of the campaigns on the way VVF can be best Prevented .... 93
Figure 23: Responses on the influence of the campaigns on what to do with VVF Patients ............. 94
Figure 24: Responses on influence of the campaigns on experience of Reported VVF Cases ........ 97
Figure 25: Responses on the influence of the campaigns on the ways VVF can be best
Controlled ........................................................................................................................... 97

x
ABSTRACT
Vesico Vaginal Fistula is an abnormal communication between the urinary
bladder and the vagina that result into constant involuntary discharge of urine
into the vagina. This research work evaluated the influence of media campaigns
on Vesico Vaginal Fistula prevention and control in North West Nigeria. In
executing this study the researcher used explanatory mixed research method.
Australian National Statistical Services (NSS) online calculator was used to draw
a manageable sample size of 428 from the entire population of North Western
Nigeria (35, 786, 944). Three measuring instrument: questionnaire, interview and
observation were used to generate both qualitative and quantitative data. Five
research questions were raised and findings revealed that respondents are
exposed to VVF campaigns in the region. However, the level of exposure seem to
be relatively high. It was equally found out that the knowledge level of the people
of North West Nigeria on VVF is high. From the study it was also found that radio
and seminar /workshop forms the major sources of information to the people. The
challenges associated with the use of the media in campaigns against VVF were as
well discovered to include: language, frequency of the awareness campaigns and
boring awareness progammes. The level of the influence of the campaigns on VVF
prevention and control is moderately high. Based on the findings the study
recommends that the campaigns planners should ensure they use local languages
during the campaigns, skilled counselors should be used during the seminars, the
awareness campaign should inform the people on the consequences of early
marriage.
1
CHAPTER ONE
INTRODUCTION
1.1 Background of the Study
Vesico-Vaginal Fistula (VVF) is a sub type of Obstetric Fistula. It is an
abnormal disorder that occurs between the urinary bladder and the vagina. This
can lead to constant/involuntary discharge of urine into the vagina. It is associated
with women alone; and can be caused by severe birth morbidity resulting from
prolonged labour (Obstetric Fistula), severe sexual violence (Traumatic Fistula) or
surgical errors (Iatrogenic Fistula).This disorder in the urinary track causes
deterioration in the tissues between the vagina and the bladder or rectum. This
deterioration subjects women to great discomfort, pains and embarrasses women
in the control of their urine or faeces. However, while some women find
support/help from families and friends, many others suffer from social isolation
and most of these women are the impoverished members of the society (USAID,
2003, p. 1).
In addition to this, the report of the National Foundation on Vesico- Vagina
Fistulae (2003,p.19) enumerates major causes of VVF in Nigeria which includes,
prolonged labour due to cephalopelvic disproportion, the pelvic of the teenage not
being fully developed as at pregnancy, making the pelvis often two small for the
baby. Prolonged labour of the baby’s head against the back of the pelvic bone
produces ischemic necrosis of the intervening soft tissues (Andrew, 2011, p.13).
2
Early marriage is also, one of the major causes of VVF. Most of the Vesico
Vaginal Fistula patients in Northern Nigeria had early marriages, 93.6% of Sokoto
patients were married before or at 18years of age and 81.5% of Kano patients and
52% of Maiduguri fistula patients got married by 15years of age (Benjamin, 2010,
p.294). It must also be noted that early marriage notwithstanding, it is not the only
socio-cultural practices that leads to VVF. Female Genital Mutilations is a twin
sister which is practiced everywhere in North Western Nigeria. The insertion of
various herbs and medication for traditional treatment of various conditions such
as, Dysperunia, Infertility, Congenital Vaginal Septum, Vaginal Infections,
Amenorrhea, Vaginal discharge and to procure abortion. However, the preparation
rather than the content of the herb damages the wall of the vagina (Lawson, 1998,
p.15).
The physical, psychological and social consequences of this disorder are
enormous. Robertson (1957, p.7) pointed out that, the misery of this condition has
one of the most frightful affliction of human kind, “ hour by hour, night and day
the leakage wet, excoriate and hurts the victim of this misfortune. Clothes are
ruined, the bed becomes a night mare, sexual intercourse stops, a pariah is made
and the family house is an outcast”. National foundation on Vesico Vaginal Fistula
(2003.p.10)
Globally, over two million women are estimated to be living with VVF and
majority of them are in Sub-Sahara Africa and South Asia. The Fistula in West
3
Africa ranges between 1-4 /1,000 deliveries. An annual obstetric fistula incidence
is estimated at 2:11 per 1000 birth (Benjamin, 2010, p. 294).
In 2008, Nigeria Demographic and Health Survey (NDHS) revealed that,
Nigeria has about 545/100,000 maternal morbidity ratio, thereby contributing
about 10% of the global burden. Similarly, majority of delivery occurs at home,
while births attended by skilled Birth Attendants are estimated to be only 39%
with very low contraceptives utilization rate (NDHS, 2008, p. 32).
In a recent report by the United Nation Population Fund Agency (2010, p.
22), it notes that, VVF and maternal death are immensely associated with
complications related to pregnancies, and childbirth, and this has continued to
pose a threat to women. The prevalence in Nigeria ranges from 100,000 to
1,000,000 cases, while the incidence is recently estimated at 20,000 cases per
annum (UNPFA, 2010, p. 23). However, it is evident that Vesico Vagina Fistula is
rampart in the Northern part of Nigeria due to several prevailing social-cultural
factors such as, early marriage /pregnancies and low status of woman coupled with
poor access and utilization of antenatal services (UNPFA, 2010, p. 23).
The Federal Government of Nigeria through the Federal Ministry of Health
(FMH) in conjunction with United Nation Population Fund Agency (UNFPA)
recognized that Vesico Vagina Fistula cannot be addressed in isolation but as part
of an integrated effort to improve sexual and reproductive health, including the
aim of reducing maternal mortality and morbidity and as such, National Strategic
Frame Work for Eradication of fistula in Nigeria was developed to ensure a
4
holistic approach for fistula intervention, prevention, treatment and care as well as
rehabilitation and reintegration campaign to end fistula( Lawrence, 2010, p.9).
In other to address this issue, a lot of awareness campaigns (e.g. Campaign to
End Fistula, sponsored by UNPFA) are on by the government, NGOs, private
individuals and organizations. The mass media, particularly the radio tends to be
the major carriers of the VVF campaign messages in the North West Nigeria.
Despite all the campaigns going on in North Western Nigeria, the problem of
VVF is still at an alarming rate. For instance, Medicine San Frontier (Doctors
without borders) is vigorously battling VVF in all the states of the North Western
Nigeria with numerous awareness campaigns, free treatment of VVF patients and
rehabilitation / reintegration programmes. Despite all these, many people are still
left in the dark in what actually causes VVF, its prevention and control.
(Lawrence, 2010, p.9).
Given the above scenario, it becomes imperative to investigate the
influence of media campaigns on Vesico Vagina Fistula prevention and control in
North West Nigeria.
1.2 Statement of Problem
Wall (2001, p. 896) in his work,’Urinary incontinent in the developing
world: The Obstetric Fistula” discovered that Vesico Vagina Fistula is relatively
rare in developed and industrialized nations, but remains a nightmare in
developing nations most especially Africa. It is one of the worst morbidities
associated with delivery in this part of the world. WHO (2005, p.2) reveals that
5
more than 2 million women and young girls live with VVF worldwide, and Africa
has the largest number of those affected with VVF in the globe. Also, UNFPA’s
Report in 2010 (p.34), states that there are over one million newborn children
deaths yearly and for every woman who dies in childbirth, at least 20 percent
suffered injuries, infections or disabilities. Tragically, an estimate of more than 2
million women and young girls in developing nations are affected, with not less
than 100,000 new cases occurring yearly (UNFPA, 2010, p. 47). Comparing
UNFPA’s Report of 2010 with the earlier report made by WHO in 2005, it
becomes clear that there is an increase in this fistula problem. This condition
leaves affected women and young girls in a state of despair; some are subjected to
social humiliation as a result of the condition.
This reality can be averted, and efforts have been on by various
organizations across the globe such as, Fistula Foundation of Nigeria, Women’s
Missionary Society, WHO, White Ribbon Alliance, UNFPA, Human Right Watch,
International Women’s Health Coalition, United Nations Foundation, Family Care
International, and others have in one form or the other supported the campaigns on
this, gave free treatment and aid to people that are affected.
The media have been employed to create awareness about the disease and
as a major step towards preventing and controlling the disease. The extent to
which these awareness campaigns have influenced the people to take preventive
and control measures is the focus of this study. Therefore, this study examined the
6
influence of Media Campaigns on Vesico Vagina prevention and control in North
West Nigeria.
1.3 Objectives of the Study
Generally, every research is goal-oriented; the goal must be stated in clear
terms to enable its realization. The broad objective of this study therefore is to find
out the influence of media campaigns on Vesico Vagina prevention and control in
North West Nigeria . Specifically, the research sought:
1. To find the level of exposure of the people in North-Western Nigeria on
Vesico Vagina Fistula campaigns.
2. To ascertain the knowledge level of the people in North-Western Nigeria
on Vesico Vagina Fistula.
3. To find out their major sources of information.
4. To find out the challenges associated with the use of the media in
campaign against VVF
5. To ascertain the level of influence of these campaigns in the prevention and
control of VVF in North West Nigeria
1.4 Research Questions
The following research questions are formulated to guide the proper
investigation of this research work. They are:
1. What is the level of exposure on VVF campaigns among the people of
North-Western Nigeria?
7
2. What is the level of knowledge on VVF among the people of North-
Western Nigeria?
3. What is the major source(s) of information about VVF among the people of
North West Nigeria?
4. What are the challenges associated with the use of the media in campaign
against VVF?
5. What is the level of the influence of the campaigns in the prevention and
control of VVF?
1.5 Significance of the Study
It is a fact that health matters are key issues that must not be toyed with in
any nation. At the same time, a healthy society is a wealthy society. The impact of
this study will be felt positively in various fields, such as the health sector,
governments, private individuals, NGOs, academics and others.
Academically, this research work will advance knowledge. The academic
community will use this work as a reference point and in the execution of similar
studies.
Professionals, NGO and other bodies like, WHO, UNICEF, UNFPA, USAID,
MSF etc who are core partners in the campaign on VVF will find this study very
useful in the implementations of some programmes, and decisions.
It will also be of immense help to the government, most especially those in
the health sector. The outcome of the study will motivate government and non-
governmental organization that are interested in women and child development to
8
formulate health policies that will help rehabilitate VVF patients as well as
eradicate the disease in Nigeria.
Theoretically, this study will serve as a platform to test the postulation of
the theory used in the study.
1.6 Scope of the Study
This study is carried out in North-Western Nigeria. This region is made up
of, Jigawa State, Kaduna State, Kastina State, Kano State, Kebbi State, Sokoto
State and Zamfara State. The indigenes of these states are mostly Muslims.
1.7 Operational Definition of Terms.
For the purpose of clarity, key variables were defined operationally.
Vesico Vaginal Fistula: Vesico Vaginal Fistula (VVF) is a subtype of female
urogenital fistula (UGF). VVF is an abnormal fistulous tract extending between
the bladder and the vagina that allows the continuous involuntary discharge of
urine into the Vagina.When it occurs there is always the wetting of the victims
clothing leading to a tear or wear off of the skin around the already damaged
vagina.
Campaigns: These are media programmes that are aimed at fighting Vesico
Vaginal Fistula by informing the people of North West Nigeria on the danger of
VVF and how it can be prevented, detected or treated.
Influence: This refers to how the campaigns change the attitude, knowledge and
behaviour of people of North Western Nigeria.
9
Knowledge: The level of information known to the people of North Western
Nigeria on VVF.
VVF Prevetion: All conscious effort meant to limit or regulate Vesico Vaginal
fistula in North Western Nigeria
VVF Control: All conscious effort meant to stop Vesico Vaginal Fistula
occurrence in North West Nigeria
North Western Nigeria: This refers to the seven states of North Western Nigeria
namely: Jigawa, Kaduna, Kastina, Kano, Kebbi, Sokoto and Zamfara.
References
Andrew, O. (2011). Africa: The effect of VVF in Africa. International Journal of
Gynecology and Obstetrics.2, 6
Benjamin, G. (2010). Fistula in developing nations. Lagos: Kemi Press.
Lawrence, P. (2010). Vesico-vagina fistula: A tropical disease. London: Edward
Arold
10
Lawson, J. (1998). Urinary Tract Injuries in Obstetrics and gynecology in the
tropics and developing countries. London: Arnold
Nigeria Demographic Health Survey (NDHS). Religion, Gender and Educational
Level of Nigerians. Retrieved March 23, 2012 from
www.unicef.org/nigeria/ng_publicati
ions _Nigeria_2008_final_rep
The National Foundation on Vesico-Vaginal Fistula (2003). Report of the rapid
assessment of vesico-vaginal fistula in Nigeria. Retrieved March 20, 2013
from http://www.endfitsula .org
United Nation Population Fund. (2010) Campaign to End Fistula. Retrieved
March 3, 2012from http://www.endfistula.com/publications.htm
United States Agency for International Development (USAID) (2003). Mid Term
Evaluation of Fistula Care Project. Retrieved February 21, 2012 from
http://www.ghtechproject.com/.../nigeria%20mch-
Wall.L.L (2001) Urinary Incontinence in the Developing World: The Obstetric
Fistula. Retrieved January 12,2013 from www.fistulafoundation.org
WHO (2005). Obstetric fistula, guiding principles for clinical management and
programme development. Geneva, Switzerland.
11
CHAPTER TWO
LITERATURE REVIEW
2.0 Focus of the Review
The review of literature consists of both conceptual and empirical review.
The conceptual review provides background for the understanding of the study,
while the empirical review helped redirect the focus of this study by showing what
other researchers have done in regards to VVF. The review is done in the
following order:
� An Overview of Vesico Vaginal Fistula.
� Causes of Vesico Vaginal Fistula.
� Psycho -Social Consequences of VVF on its Victims
� Review of Empirical Studies
� Theoretical Framework
12
Conceptual Review
2.1 An Overview of Vesico Vaginal Fistula.
Vesico Vagina Fistula (VVF) is an abnormal fistulous tract extending
between the bladder and the vagina. The abnormality allows for the continuous
and involuntary discharge of urine into the Vagina vault (Forsgren, Lundholm, &
Johansson, 2009, p. 8). In a report by Villey (2006 p.3), “VVF is an abnormal
communication between the urinary bladder and the vagina that results in the
continuous involuntary discharge of urine into the vaginal vault”
Tracing the earliest discovery and oldest evidence of obstructed fistula,
Zacharin (1988, p.5) noted that in 1923 in Cairo, the remains of Queen Henhenit
the wife of King Mentuhotep 11 of Egypt (2050 BC) was discovered and detailed
clinical examination was carried out on it and the vagina was normal but there was
a tear in the bladder which links the vagina. The medical doctor concluded that
this must be the cause of her death.
The above has clearly shown that VVF is not new in the globe. Wall
(2001, p.895) discovered that “The growth in science and technology mostly in
Europe and North America has made the scourge relatively unknown in these
geographical regions of the world. Here in Africa, many lives are lost on a daily
bases as a result of VVF”. Metro (2006, p.13) observed that,” Fistula is almost
oblivion in countries where there is universal health care which takes woman’s
health more seriously”. Metro further stated that the causes of VVF in most third
13
world countries centre on obstetric difficulties. He noted that, 90% of such cases
are caused by advent bladder trauma during surgery with hysterectomy.
On the contrary, Wall and Lancer (2006, p.1408) observed that, there are
cases of VVF in industrialized countries and to a large extent these are due to
“radiation therapy or surgery thus distinguishing the etiology from that of
developing countries which result mainly from neglect of obstetric compared from
that of developed countries, which occur under very different circumstance”.
Most discussions about VVF centres in Africa and this is because Africans
are the most affected. In Nigeria alone, according to Villey (2006, p .3),
There is a Vesico-Vaginal Fistula rate of 350 cases
per100,000 deliveries at a University Teaching
Hospital. This condition is enormous and thus
ravages Nigeria women that the country’s Federal
Ministry for Women Affair and Youth Development,
has estimated that the number of untreated VVF
Nigerian’s stands between 800,000 and 1,000,000.
The above report depicts that NigerianWomen are under serious siege of
VVF and as such only quick intervention by Government, International
Organizations, NGOs, etc can free the Nigerian women. Giving more credence to
the above report, the Nigeria Ministry of Health as was recorded by Kari (2007,
p.7) estimated that 800,000 women are plagued by the scourge of VVF, a majority
of them live in the rural areas. In Nigeria, majority of her rural areas lack good
health care facilities. The country accounts for 40% of the global burden of VVF.
The presence of VVF patients becomes offensive to others because of the
stinky smell that constantly oozes out of the victims; some of the victims are very
young and are not even privileged to have basic elementary school education. A
14
clear picture of the agony victims of VVF go through was noted by Matsamura
Evelyn, thus:
(March 2004) Martina Nakamya (not her real name)
was having her first baby after having left school at
age 16 because of her pregnancy. Preparations were
made with the birth attendant in the village.
Nakamya’s labour lasted almost four days. When she
finally pushed the baby out, it was dead, and Nakamya
was not well. She ‘leaked’ and smelled of urine and
faeces all day, every day (Matsamura, 2004, p.1)
Similarly, Magashi (2006, p.40) pointed out that in most rural parts of the
country, women in labour usually stay at home for three days trying to push, and if
not successful, the family may decide to take her to the closest obstetric centre
around.
Hamlin and Nicholson were the founders of the second Fistula Hospital in
Addis Ababa, Ethiopia. They described VVF patient thus: “Constantly in pains,…
ashamed of the offensive smell that comes out of them, abandoned therefore by
their husbands, outcasts of society, unemployable except in the fields, they live,
they exist without friends and without hope” (Hamlin and Nicholson, 1974, in
Akpeji, 2012, p. 12).
Magashi (2006, p.42) also reports that Nigeria’s maternal mortality ratio of
948 per 100,000 live births with range of 339 to 1716 ranks among the highest in
the world. In every maternal morbidity in Nigeria, 15 to 20 women suffer short or
long term maternal morbidities and prominent among these morbidities is
Obstetric Fistula. Incidence of Obstetric Fistula is directly connected to maternal
15
mortality (WHO, 2006, p.1407). This clearly gives a good grasp on the miserable
life most of the women and young girls with VVF are faced with.
2.2 Causes of Vesico Vaginal Fistula
It is very difficult to associate a particular cause to VVF. However, this
study looks at the problem from both physical and socio-cultural perspective. The
physical causes are referred to as the direct causes, while the socio-cultural causes
are termed the underlying or the contributing factor to the problem. However, the
symptoms of VVF include constant urine leakage from the vagina, irritation at the
vulva, frequent urinary tract infections and others.
2.2.1 Physical Causes
This can also be referred to as direct causes of VVF. This means the young
lady or woman is exposed to the scourge of VVF. It is predominantly caused by
prolonged labour. This can last for days and in most cases if good medical care is
not received immediately, the patient can die as a result of complications.
According to Kees’ report (2006, p.3), approximately 80 percent of fistula cases
reported in Nigeria are due to unresolved obstructed labour during child delivery.
Also, WHO (2006, p.4) added that:
If labour remains obstructed, the unrelenting pressure of the
baby’s head against the pelvis can greatly reduce the flow of
blood to the soft tissue surrounding the bladder, vagina and
rectum. This situation often leaves the pelvic tissue with
injury which may rotten away, thus, creating a hole or a
fistula between the bladder and the urethra
Obstructed labour is also directly related to early marriage in Nigeria. Early
marriage no doubt leads to early sexual intercourse and as such can lead to
16
pregnancy. It becomes dangerous when the young girl is not physically developed
to permit the passage of the baby with ease (Moir, 1997, p.129). He added that,
“the common form of obstetric fistula is caused by pressure necrosis following
prolonged labour; often this situation may be unnoticed until many days after a
woman delivers her child.”
To Ward (1998, p, 7), 15 percent of fistula cases of VVF in Nigeria is
caused by the harmful practice of female genital mutilation. For instance, in the
Northern part of Nigeria, the “gishiri” cut, and a form of female genital mutilation
is common among the Hausas. Most often, this traditional practice is performed by
untrained traditional birth attendants.
Zacharin (1988, p.127) added that, other forms of fistula occurs as a result
of the poor and improper obstetric instruments used, such as perforator which may
slip and damage the vaginal wall and bladder. He also, pointed out that, in some
cases, incorrect applications of obstetric substances into the urethra may cause the
bladder to extend abnormally, thereby causing eruption, hence urethra injury.
Still on the causes of VVF, a study carried out in Zaria, Nigeria by The
National Foundation on Vesico-Vaginal Fistulae (2003, p.31), revealed that
infection can cause VVF.The study shows that ten cases of various types of
infections such as, lymphogranuloma venereum, diphtheria, measles, boil in the
vagina that had ruptured and schistosoma haemotobium can cause VVF.
17
The Report (The National Foundation on Vesico-Vaginal Fistulae, 2003,
p.32), also mentioned sexual intercourse as another cause of VVF. The Report
reads:
In the Zaria study, there were six lesions due to sexual
intercourse. All the patients were under 16 years of
age, apart from one prostitute who had a lesion due to
coitus at 18 years of age and subsequently she had
repeated coital breakdown of the lesion after it was
repaired twice. There was one suspected case of rape
of a 9-year-old child, and one case of a fistula in a
single unmarried girl; otherwise the others were all
married. The age of the patients ranging from 10 to 14
is noteworthy (The National Foundation on Vesico-
Vaginal Fistulae, 2003, p.32).
In developing countries, according to Wall (2001, p.895) there are several
cases on this disease (VVF). Majority of these cases originate from obstetric
complications during child birth. The inadequate maternity facilities or complete
lack of it in some communities has worsened and increased the cases of VVF in
the part of the globe. He noted that in Nigeria, northern Nigeria still remains the
most affected part of the nation. On the other hand, women from developed
nations have adequate access to well equipped maternity centres, and as such, they
have little or no worries over the incidence of VVF resulting from obstructed
labour. The adequacy of maternal care facilities in these developed countries, have
been a plus to these nations as an endangered baby or mother can be saved
through caesarean section with ease, a method which is still very new in some
developing nations. Wall (2001, p.896).
18
Hilton, (2003, p. 286) also added that VVF can be caused as a result of
abortion. Abortions done in the hands of quack medical personnel most times
leave the woman or young girl involved with series of cuts. In Hilton’s words:
Most criminal abortions are clandestinely practiced by
untrained individuals who claim to be knowledgeable
in the act. Through the use of wrong instrument, some
girls have had their birth canal unknowingly damaged.
If not repaired on time and adequately, this may result
in VVF. (Hilton, 2003, p. 286)
In Africa, majority of the pregnant women do have their child birth at
home. In the case of complications, traditional birth attendants are sometimes
called on. To a large extent, most of these traditional birth attendants lack
comprehensive knowledge or have little knowledge on how to handle complicated
issues. An immeasurable population of pregnant women in developing nations
lack access to basic obstetric care. Adequate obstetric care before, during and after
labour no doubt goes a long way in preventing or correcting difficulties in child
birth; and since the most women in poor-resource setting of the lack access to
adequate obstetric care before, during and after delivery, it is expected that infant
and maternal mortality during after delivering would be very high in such regions
of the world (Benjamin, 2010, p. 280).
United Nations Populations Fund Agency (2004, p.43) reports that, if
mothers are at risk of maternal death or illness, their children are at risk too.
Neonatal and infants deaths can result from poor maternal health and inadequate
care during pregnancy, delivery and the critical immediate postpartum period.
WHO (2005, p. 23) also notes that, physical causes of fistula problems emanates
19
mainly from, inaccessibility to basic maternity care and lack of knowledge about
facilities for fistula repair
2.2.2 Socio -Cultural Causes
In Nigeria there are underlying behaviours that causes VVF and
intimidation on affected victims. Some of these common socio-cultural conditions
in our society include but are not limited to the followings; culture and tradition,
early marriage, poverty, illiteracy, gender discrimination etc.
Culture and Tradition
Nigeria is a nation with different cultures and tradition. In some cultures the
traditional birth attendants are still preferred to modern methods of child birth.
Mohammed (2009, p.3) assert that, “a high percentage (87 %) of rural childbirth
takes place at home. Problems occur when complications arise and there is an
absence of attendants adequately qualified to identify these complications”.
Ngoma (2010, p. 4) noted that female circumcision and the practice of
some crude traditional methods such as ‘gishiri cut’ increases the chance of getting
VVF. Mkuma and Kasonka, (2003, p.4), explained this cut as:
A traditional cure consisting of surgical cut into the
interior vaginal wall of the woman who has been
diagnosed by a traditional healer to suffer from gishiri
disease (a wide range of conditions and symptoms,
such as itching of the vulva, amenorrhea-lack of
menstrual periods. Infertility obstructed labuor,
anemic headaches, malaria, and fainting e.t.c.)And the
insertion of caustic substances into the vagina with
intent to treat a gynecologic condition or to help the
vagina to return to its nulliparous state.
20
Early Marriage
Ajuwon (1997.p.27) stated that “in most parts of the nation, particularly
northern part of Nigeria, early marriage is encouraged. Conception at a tender age
often between the age of 11, 12, 13 and even 14 when the female genital organ has
not fully developed (i.e. most often, full pelvic growth has not been achieved at
this stage of growth). Early marriage, leads to early introduction to sexual
activities and at times early childbirth, however, when the growth of the pelvis is
not complete; this situation can lead to caphalopelvic disproportion, a condition
where by the baby’s head or body is too big to fit through the mother’s pelvic”
(Ajuwon, 1997. p.27). He added that, “since the birth canal is too narrow for the
baby to come out, a prolonged and obstructed labour occurs, threatening both the
life of the mother and the child at the same time”.
WHO, 2006, p.140). reports that, in Ethiopia and Nigeria, over 25% of
fistula patients had become pregnant before the age of 15, and over 50% had
become pregnant before the age of 18, early marriage no doubt affects pregnancy
and labour complications among Nigeria women, hence a likelihood of VVF.
Poverty
21
It is not new to say majority of Nigerians live in abject poverty. Poverty is
linked to, malnutrition, poor living condition, accessibility to good obstetric care
and so on. WHO reports that women suffering from fistula came exclusively from
poor families with subsistence farming background (WHO,1997, p. 13). Also, two
thirds of fistulas caused by difficulties in labour were due to contracted pelvis of
the flat type which resulted from poor nutrition, and infections. Due to poverty, it
is difficult for people especially in the rural areas to afford good nutrition; most
times they live on nutritional diets that do not make them achieve full body
growth. Many victims of VVF are malnourished resulting in abnormal growth of
the pelvic bones (WHO, 1997, p. 13).
Poverty has made some parents in Nigeria to find it difficult to send their
children to school; some are even withdrawn from school so as to be given out in
marriage to attract high bride prices, especially if they are still virgins (Balogun,
1995, p. 29). Poverty has also made it very difficult for women/girls to seek better
medical treatment and as such, they resolve to quack/cheaper means of treatment.
For instance, pregnant young ladies a times are sent to their parent’s home to
deliver and during childbirth should there arise any complications, the cost of
procuring immediate and good obstetric care might be too exorbitant for parents
and as such they seek alternatives and most of these alternatives are quacks.
Poverty has made it difficult for VVF victims to afford medical services for
repairs (Balogun, 1995, p. 29).
Illiteracy
22
In a research work conducted by The National Foundation on Vesico-
Vaginal Fistulae (2003, p. 36), the report shows that only 0.2 % of the VVF
patients in the Zaria study had received some rudimentary conventional education,
compared to 7 % of all women delivered in the area. The study also shows that
only 12 % of the VVF patients had received secondary education and 33 %
primary education. There is a nexus between the high level of VVF and formal
education. In Northern Nigeria, the level of education is low and to a large extent
educated women are at an advantage because they are well informed on cases like
this.
Female Genital Mutilation
Another important underlying factor to the problem of VVF in Nigeria is
the customary birth practices. Most prominent is the female genital mutilation or
simply put female circumcision. For instance, the gishiri cut which is very popular
in Northern part of Nigeria involves the incision of parts of the vagina with razor
blade or large curved knife, the cut is made against the pubic bone endangering
both bladder and urethra. The cuts are often handled by traditional birth attendants
to prevent or treat numerous conditions including prolonged obstructed labour,
infertility, goiter, backaches, dysuria coital difficulties, others are to prevent
promiscuity and premarital pregnancy, to guarantee marriage with subsequent
economic and social security for a daughter’s future. (Ajuwon, 1997, p.30).WHO
reports that there is a version of circumcision which includes pricking, piercing of
23
the clitoris and surrounding tissue; scrapping of the vagina to cause bleeding; or to
cause tightening or narrowing (WHO, 2006, p.20).
Moir (1997, p.156) observed that, about 10% of fistula seen at a particular
hospital in Zaria region of Nigeria was directly attributed to the traditional practice
of female circumcision, with a further 30% following a combination of genital
cutting with obstructed labour. Circumcised women often faced lots of health
consequences such as the type of procedure performed, the extent of the cutting,
the skill of the practitioner, the hygiene of the instruments, the environment of the
operation, and more importantly, the physical condition of the girls to be
circumcised (Chalmers &Omer – Hash, 2003, p.2)
2.3 Psycho -Social Consequences of VVF on its Victims
The psycho-social consequence of VVF on its victim’s is worse than that of
HIV/AIDS. Due to high cost of treatment involved, a majority of the victims are
unable to afford the cost for the treatment, in this case, their physical, social and
mental conditions are worsened. Victims of VVF suffer from urinary incontinence,
which makes them stink of urine, exposes their vulnerability to tract infection,
virginities, and excoriation of valve (i.e. injury to the surface of the skin or
mucous membrane caused by physical abrasion, such as scratching). Structure of
the Vagina which narrows the vagina, secondary amenorrhea, possible future of
inability to carry a child even after repair of VVF, and a low child survival rate are
also related to VVF. Considering the nature of VVF victims often find it very
difficult to keep themselves clean and hygienic (WHO, 2006, p. 23).
24
The devastating complication of VVF is the psycho-social consequence
victims have to put up with, the major problems being incontinence, childlessness,
divorce, poverty. WHO (2006, p.23) noted that, if a victim of VVF is fortunate
enough to be in the same compound with her husband, they obviously do not share
the same bed. This situation makes the sexual desire between the couple die out.
Since victims can neither satisfy their husband’s sexual urge nor produce
offspring, they become useless in the eyes of their husbands and even the society.
In Nigeria, there is virtually no social welfare programme put in place by
the government, thus the only hope parents have for coping at old age is their
children. In traditional Nigeria society, any married woman who has no child for
her husband has no contribution to the socio-economic and political development
of her family, and the society in general. This is usually the case of a VVF victim
with no child. In this case, the future becomes disastrous for both the wife and the
husband, because men still have the capacity to father many children, many men
find it easier to rid themselves of their damaged wives and seek other fertile
spouses. Women in this condition are left to live their lives in quietness and shame
(WHO, 2006, 25).
Another view to the setback VVF victims face in the society is seen from
the perspective of their economic irrelevances. Since the majority of VVF victims
come from the rural areas where farming is the mainstay of economy and
subsistence for each household, it is expected that women should contribute their
labour in cultivating the family land. However, and due to the VVF conditions,
25
victims are no longer able to contribute to the economic productivity of their
household; instead they become an economic burden. The inability of the victims
to satisfy their husband’s sexual desires, produce offspring and contribute to the
economy of their household ultimately lead to the collapse of the marriage (WHO,
2006, p. 27). Ajuwon (1997, p.42) pointed out that, according to Islamic belief,
cleanliness is considered as an important ritual while praying and during sexual
intercourse, whoever is afflicted with VVF is considered unclean and therefore
cannot pray, however, she could be granted a permission to pray only when her
condition is considered as incurable. Because of the magnanimity of the stigma
involved and its consequences, families and sufferers alike may decide not to
reveal the existence of VVF, thus they are denied access to treatment (Moir, 1997,
p.37).
Wall (2006, p. 31), notes that, in North Western Nigeria, women (wives)
often live under a system of seclusion as a result of their religion, they only have
contact with their immediate family and female neighbours alone. This system is
referred to as purdah, the women and young girls are provided with special
clothing designed to cover their head and to keep them away from public view. In
some cases, they are provided with separate rooms in the household to prevent
them from intermingling with strangers or visitors. Women with VVF suffer a lot,
WHO (2006, p. 34) described it thus:
In a situation whereby a wife is afflicted with the VVF
condition, the repulsive smell that accompanies total
urinary incontinence usually curtails even the limited
26
opportunity for social interaction. For the family to
deal with this problem of offensive smell of the
incontinence urine, the afflicted women is often
removed from the main household into separate hut,
though within the same compound, but as time goes
on, they are often forced out of the family compound
(WHO 2006).
Murphy (1992), added that , “ the victims goes to sleep at night and wakes up to
find their beddings wet and soaked, and that they feel so ashamed and humiliated”
(Murphy, 1992 in Muhammad, 2010, p.4)
2.4 Empirical Studies
The empirical review of literature on the other hand, reviewed the
following related literatures in other to help the understanding of this research
work. These literatures include the following but not limited to these alone:
Muhammad (2011); UNFPA (2005); Ngoma (2010); Njoku (2006); Sambo
(1994); Ijaiya (2010); The National Foundation on Vesico- Vaginal Fistulae
(2003); Murphy (2009); Johnson (2007); Shaikh (2011); Ahmed and Holtz (2007);
WHO (2006); Akpeji (2012); Agwu, Umeora,and Obuna (2010);Onwunali
(2012);Mahendeka (2007);Ramsey,Illiyasu and Idoko (2007); Orji, Aduloju and
Orji (2007); Moir (1997); Umoiyoho,and Inyang-Eboh (2012); Rassen,
Verdaasdonk and Vierhout (2007);Fasakin (2007) etc. However, their studies were
all discussed in-line with this research study.
27
Muhammad (2011,p.1) conducted a study on Perceived causes, prevalence
and effect of Vesico Vagina Fistula among Hausa/Fulani women in Kano State.
The study looked at the stigmatization effects on the women, as well as the
treatment facilities of VVF in the state. The Ex-post Facto research design method
was used in the study. The population of the study comprised of 300 victims of
VVF and there was focus group for health personals. Major findings revealed that,
the use of traditional birth attendants and prolonged obstetric labour are the
primary causes of VVF in Kano State. The finding also shows that victims
suffered from divorce and neglect as a result of this disease. Muhammad
recommended that female education should be encouraged in the state and
community mobilization should be used to sensitize the women on the issue of
VVF.
Akpeji (2012,p.4) carried out a study to determine the knowledge of
patients who have developed VVF and their attitude towards it. Data were
collected through the instrumentality of a questionnaire and focus group
discussions were held with the maternity staff. The findings revealed that majority
(70%) of the patients knew the causes of VVF; however 30% of the respondents
would still not change from risking obstetric measures despite still knowing it.
In a study on the awareness of VVF carried out by Mohammed (2007,p.5)
titled, A community program for women’s health and development: Implications
for the long-term care of women with fistulas. Mohammed documented the
activities of the women’s health and development project (FOWARD) in
28
Nigeria.The project was set up to improve the social, economic, and health status
of women affected by Vesico-Vaginal Fistulas. The program takes a holistic
approach not only by providing surgical repair and rehabilitation, but also through
the development of skills that will help women improve their physical and
economic well-being. In addition, to prevent VVF in young women, the project
organizes campaigns to bring about a culture fostering the education and
empowerment of women.
Still on the level of exposure of VVF, Agwu, Umeora, and Obuna
(2010,p.4 ), in a study titled, After the Repair: Voices of Vesico Vaginal Fistula
(VVF) Patients in South East Nigeria. The researchers assess patients’ knowledge
of the causes of fistula and their attitude towards future pregnancy. The
researchers interviewed patients of VVF in Abakaliki and a focus group discussion
was held with the nurses in charge of the patients. The result revealed that 96.6%
of VVF occurred as a result of prolonged obstructed labour. Other causes noted
includes caesarean section, crude delivery method etc. Majority (60 %) of the
respondents said they will want to get pregnant again.
Sambo (1994, p.2) in his work, Vesico Vagina Fistula ( VVf Campaign, A
vision Realised .The study identified the causes of VVF raging from direct to
indirect. It looked at preventive measures taken in Nigeria to control VVF and
reviewed various campaigns strategies used in Nigeria like the National Task
Force on VVF organized in Kano state and women in Nigeria (WIN) supported by
Ford Foundation. It as well identified early marriage and age at birth,
29
nuclearization of house hold, women status in house hold as indirect causes of
VVF. She finally identified the followings strategies for prevention of VVF: Ante-
natal care, intra- partum care and training of traditional birth attendants. She
concluded that campaign on VVF has come along way. In her word “I am happy
now to acknowledge the fact that the country is now fully aware of the problem
afflicting VVF victims.” (Sambo, 1994. p.45)
Ramsey, Illiyasu and Idoko (2007,p.136) organized a fortnight treatment
on VVF as part of the global campaign to End Fistula. The treatment was carried
out in northern Nigeria. The campaign aimed at treating VVF victims and creating
awareness regarding to VVF, surgical treatment were carried out on obstetric
fistula victims. A total of 569 women received VVF treatment, (i.e. 87.8 % rate of
success). The campaign was highly publicized among the people in that locality.
UNPFA (2006, p.23) Fistula in Brief: Campaign to End Fistula. The study
gave a comprehensive definition, causes; medical and psychosocial consequences;
prevention; prevalence and treatment of obstetric fistula. The success rate of a
simple surgery repair is high (90 percent for experienced surgeons). The study
noted that, at least 2 million women in Africa, Asia and the Arab region are living
with VVF. It was also pointed out that this disease is common mostly among rural
dwellers that live far from medical centres.
Also, Donnay and Ramsey (2007, p.1). In a study entitled, Eliminating
obstetric fistula: Progress in partnerships. The study describes the various
strategies and progress used in the global campaign to end fistula. The global
30
campaign brings a variety of actors together to create awareness on the prevention
and treatment of VVF, during the campaign comprehensive treatment for women
living with fistula was done.
In an experimental study done by Murphy (2006), four sets of patients were
used; hundred fistula patients in a gynecological clinic in Zaria, 52 long term
patients formed the first control group. The second control group was provided
from records of 207 patients with post partum cardiac failure. The result shows
that fistula patients were much younger than the controls, 69% of the new patients
and over 50 % of the long-term patients were aged 19 and under as against 13 %
and 22 % in control groups (The National Foundation on Vesico-Vagina Fistulae,
2003, p. 23).
In regards to the attitude of people towards VVF, Fasakin (2007, p.1)
carried out a research on the Effect of Vesico Vaginal Fistula on the Psychosocial
Well-being of Victims in Nigeria. The study assesses the effect of VVF on the
psychosocial-well-being of victims in Nigeria. The research questions were
logically coined to address the emotional effects of VVF on patients, their family
attitude towards victims and public attitude towards them. Six selected VVF
Centres/Hospitals were used, one from each geographical zone of the country. In
all 506 respondents were used. The result shows that VVF has adverse significant
effect on the psycho-social well-being of victims.
Still on the attitude, Wall (2005, p.2). Ethical issues in Vesico-Vaginal
Fistula care and research pointed out the plight of women in poor nations who
31
have incurred catastrophic childbirth injuries, such as Vesico-Vaginal and Recto-
Vaginal Fistulas, from prolonged obstructed labor. The work emphasizes the
vulnerability to exploitation of women with obstetric fistulas and reviews the basic
principles of medical ethics relevant to fistula care.
Also, in a recent study conducted by Umoiyoho and Inyang-Eboh (2012,
p.2) on Community Conception about the Aetiopathogenesis and Treatment of
Vesico Vaginal Fistula in Northern Nigeria. The study seeks to gain insight into
the perception of people in northern Nigeria on VVF. The research method used
was focus group discussion (FGD) . The result collected from group discussion
shows that majority of the women with obstetric fistula see their situation as a
result of negligence on the part of the traditional birth attendants.
Orji, Aduloju and Orji (2007, p.25) worked on Correlation and Impact of
Obstetric Fistula on Motherhood; the study investigates the impact of obstetric
fistula on mother hood. 72 cases of VVF were examined over a period of 9 years
(January, 1994 to December 2003) at Obafemi Awolowo University Teaching
Hospital, Ile-Ife, Nigeria. The result shows that obstetric VVF accounted for
94.4% of all the types of VVF. This means obstetric VVF is common and the
major cause of this was attributed to prolong labour.
UNFPA (2005, p.1) conducted a research on VVF. The study shows that
one out of 18 women in Nigeria die from complications during child birth. The
study also, revealed that there is acute shortage of medical personnel who are
specialized in treating VVF and the nation lack ultra modern facilities for the
32
treatment of VVF, thereby resulting in a back log of patients in need of treatment
(UNFPA, 2005)
Raassen, Verdaasdonk and Vierhout (2007,p.5) carried out a study on
VVF victims and only patients who received surgery for the first time and whose
fistula was caused by obstructed labour were included in the study. The study was
conducted for a period of two years (January 2001 and August 2003). Of the 581
women (91%) out of 647 patients who underwent fistula treatment and care during
the duration, 45% of the women lived apart from their partner at one time of the
other. Women operated on within three months had slightly better surgical
outcome 94% than those operated several months after discovering the disease
(87%).
Ngoma (2010, p.22), Prevention of Vesico Vagina Fistula. She collected
existing articles and books relating to the prevention of VVF. The study sought for
preventive measures of VVF and how these measures could be implemented. The
secondary method of collection was used. Various literatures were reviewed and
compared. The works were analyzed and the findings show that, direct prevention
of VVF can occur during delivery when skilled medical personnel identify women
and young girls at risk of having VVF. It was also observed that prevention should
involve alleviation of poverty. Furthermore, it was observed that accessible
emergency obstetric care is necessary to decrease the burden of obstetric fistula in
Africa at large. It could be accomplished through increased and improved health
care facilities and education of health care providers and patients.
33
Recommendations were made, such as improvement in education and community-
based programmes should be encouraged and it should be on creating awareness
on VVF.
Ahmed and Holtz (2007, p.8), in a study, Social and Economic
consequences of obstetric fistula: Life changed forever? Took a look at obstetric
fistula from the social and economic perspective with a major focus on the
consequences of this disease. The study summarizes the social, economic,
emotional, and psychological consequences incurred by women with obstetric
fistula. Based on the results, two major consequences were noted,
divorce/separation and parental loss. The study recommends that there should be
more social support and counseling on women to enable them reintegrate socially
with families and friends.
Also, The National Foundation on Vesico-Vaginal Fistula (2003, p.8) did
an assessment of VVF in Nigeria. The aim of the rapid assessment is to provide
relevant data on the magnitude and distribution of VVF and to ascertain the
resources available for the treatment and control of VVF.
Shaikh (2011, p.5) conducted a study on Vesico- Vaginal Fistula, in the
study, he evaluated the outcome of Vesico-Vaginal Fistulae (VVF) repair done by
abdominal and vaginal route. Patients were divided into two groups for the study.
Group 1 are made up of patients who had low or uncomplicated fistulae issue
while Group 2 are made up of those who have complicated issues. The study
34
included 32 cases, the result indicates that, the major cause of VVF is obstetrical
and iatrogenic gynecological.
Dodson, Gutman and Mostwin (2007,p.13). Complications of treatment of
obstetric fistula in the developing world: Gynatresia, urinary incontinence, and
urinary diversion. The study did a comprehensive review of the pathophysiology,
evaluation, and treatment of gynatresia and urinary incontinence, two conditions
that can arise following the repair of obstetric fistulas. Relevant issues with respect
to urinary diversion in the treatment of obstetrical fistula and associated urinary
incontinence were full discussed in the work. Finding shows that, gynatresia and
urinary incontinence develop in approximately 10% and 16% of patients,
respectively, after the first repair. The result also reveals that in some cases,
urinary diversion may be necessary when fistulas cannot be closed vaginally or in
cases of severe urinary diversion are all associated with morbidity. The researchers
noted that in cases like this, surgical and nonsurgical expertise is required for
proper management and treatment.
Also, a retrospective study was conducted by Mahendeka (2007, p.15 ) on
the management of Vesico and/or recto-vaginal fistulae at Bugando (East Africa),
in the study a modified management of the vesico and/or recto-vaginal fistulae
was compared to a usual modified management method, two groups were used, off
the 100 patients (first group) with a vesico and/or recto-vaginal fistula of 21 days –
37years duration, 92 (92%) were closed after the first operative attempt carried out
for 30 days, while in the second group using the usual method, out of 100 patients
35
with a vesico and/or recto-vaginal fistula of 97 days – 37 years, 90 (90%) were
closed after the first operative attempt that lasted for 10 months. The modified
management has lesser cost when compared to the second method.
Johnson (2007, p.21) in a study Incontinence in Malawi: Analysis of a
proxy measure of vaginal fistula in national survey. The objective of the study
aimed at documenting the first effort to collect national lifetime prevalence data on
vaginal fistulas and discern the usefulness of the measure. The results show that
the relationships between fistula symptoms and wealth and fistula symptoms and
education were negative and monotonic. Rural women were 40% more likely than
urban women to report the symptoms, and those who had experienced a stillbirth
were 66% more likely to report the symptoms. Those who had experienced sexual
violence were 71% more likely to report the symptoms. A crude fistula rate of
15.6 per 1000 live births was found for Malawi.
Similarly, Sulaiman (2003, p.1) carried out a study on Socio-Economic and
Cultural Roots of Reproductive Health Care problems in North-Western Nigeria.
The study used participatory and qualitative tools and it was carried out in eight
communities. The study revealed that people were generally dissatisfied with the
availability and quality of health care facilities. Maternal mortality and morbidity,
arising from pregnancy and childbirth were found to be very prevalent in all the
communities studied. The immediate underlying factor is the non-availability or
poor access to and utilization of modern maternal health care services. Economic
and cultural factors also play very crucial role in deepening the reproductive health
36
crises. The study recommends that there is an urgent need for increased public and
private sector investment in the provision of health care services in rural
community. There is also an urgent need for increased public and private sector
investment in the provision of health care services in rural area.
According to Fasakin, (2007,p.5) in his study Vesico-Vaginal Fistula and
Psycho-social well being of women in Northern Nigeria, the study however
discusses the socio-cultural and psychological consequences of the disease.
Locally and internationally, attempts are being made to eradicate the problem of
VVF, however, if the Nigeria government does not recognize the incidence of
VVF as a major public health issue, it will continue to ravage lives of Nigerian
women, hence increasing maternal mortality in the country. The study found out
that it is difficult to attribute VVF to a particular factor; respondents reported the
following as possible causes prolong labour, early marriage, female genital
mutilation, illiteracy, poverty and poor obstetric care. The study further
recommended free education, provision of adequate health facilities, economic
empowerment, free repair or treatment.
Wall, Karshima, and Kirschner (2004, p.12) also conducted a research on
The Obstetric Vesico- Vaginal Fistula in the Developing Word. The study, fished
out the level of evidence concerning obstetric fistulas, the relationship of obstetric
fistulas to maternal morality, epidemiology of the obstetric fistula, the obstructed
labour injury complex, the classification of obstetric fistulas, early care of the
fistula patient, surgical technique for fistula closure, complicated cases and
37
technical surgical questions, prevention of obstetric fistulas and dealing with the
backlog of surgical cases were all discussed in the study. The study made the
following conclusions and recommendations: The precise extent of the fistula
problem in developing countries is unknown. The available evidence suggest that
at a minimum hundred of thousands (if not several millions) of women are
afflicted with the condition worldwide, most especially in sub Sahara Africa.
In theory, obstetric fistula is completely preventable by the provision of
adequate, timely obstetric care. The presence of obstetric fistulas in any country,
therefore, is an indictment of the quality and effectiveness of its health care
delivery system. When obstetric fistulas do occur, they should be curable
(closeable) in over 90% cases using appropriate low-technology medical and
surgical services (Akpeji, 2012, p.14).
To Fasakin, there is a great need for village-based community studies of the
incidence and prevalence of obstructed labour and fistula formation. It is clear that
most fistula arise from the combination of obstructed labour and obstructed
transportation, but much work is needed to understand the sexual context in which
obstructed emergency arise and how they are dealt with in developing countries.
(Fasakin, 2007, p 54). He further stated that, the urgent needs of pregnant women
should not be sacrificed on the altar of epidemiological research, rather, more
attention should be paid to improving emergency treatment for obstetric
complications at existing referral facilities, to upgrading peripheral facilities to
provide access to obstetric facilities (Fasakin, 2007, p 24).
38
2.4 Theoretical Frame work
To give a theoretical footing to this study, the researcher used the Planned
Behaviour theory. This theory was proposed by Icek Ajzen. It started as theory of
Reasoned Action in 1980. According to Ajzen and Fishbein (1980, p.15), an
individual’s intention to engage in a behaviour at a specific time and place forms
the crux of the theory.It is a theory which predicts deliberate behaviour, because
behaviour can be deliberative and planned. The core assumptions of the theory is
that a person’s behaviour is determined by his or her intention to perform the
behaviour and the intention is a function of his or her attitude towards the
behaviour which is also influenced by the person’s subjective norm. The best
predictor of behaviour is intention. The intention is the cognitive representation of
a person’s readiness to perform a given behaviour, and it is considered the
immediate antecedent of behaviour. Ajzen and Fishbein ( p.15)
Ajzen (1988) added that this intention is determined by three things: the
attitude towards the specific behaviour, the subjective norms and the perceived
behavioural control.(p.7). He noted that the Theory of Planned Behaviour holds
that only specific attitudes towards the behaviour in question can be expected to
predict that behaviour. He noted that the main construct of theory of planned
behaviour are attitudes, behavioural intention, subjective norms, social norms,
perceived power and perceived behavioural control.(p.7)
For instance, the construct of attitude refers to an individual’s positive or
negative evaluation of self-performance of a particular behaviour. The concept is
39
the degree to which performance of behaviour is positively or negatively valued. It
is determined by the total set of accessible behavioural beliefs linking the
behaviour to various outcomes and other attitudes. Behavioural Intention refers to
motivation factor that influences a given behaviour. Where the stronger the
intention to perform the behaviour, the more likely the behaviour will be
performed.Subjective Norms refers to the belief whether most people approve or
disapprove a particular behaviour. It relates to a person’s beliefs about whether
peers and people of importance approve the behaviour or not. In the same
direction, Social Norms refer to the customary codes of behaviour in a group or
people or larger cultural context. Social norms are considered normative, or
standard in a group of people. Ajzen (1988. p.18)
Perceived power on the other hand, refers to the perceived presence of
factors that may facilitate or impede performances of a behavior. Perceived power
contributes to person’s perceived behavioural control over each of those factors.
Perceived behavioural control refers to a person’s perceptions of behavioral
control depending on the situation. Ajzen ( 1988.p.23)
This theory is relevant to the study under investigation because it centres on
behavioural decisions that bring about good health. For example if one already
know that early marriage/early pregnancy will lead to VVF he or she will not
engage in early marriage.
A cursory look at the major constructs of this theory shows that the attitude
of an individual can help him/her to be careful of the seriousness of the
40
unfavourable behaviour (early marriage, early pregnancy and female genital
mutilation) that could lead to fistula. On the other hand, behavioral intention can
also help one to go for antenatal care knowing fully well that it is the only way one
can prevent obstructed labour.
Perceived power refers to perceived presence of factors that can facilitate
the performance of a given behaviour. For instance, factors like being abandoned
by one’s husband, inability to control urine, smelling and becoming unemployable
will facilitate the earlier behaviour therefore, behaviour that will make a woman to
live a life free from VVF . Perceived behavioural control can be of help to let
people know that fistula patients can access fistula treatment and can be re-
integrate in the society.
References
Ahmed, S, Creenga, A. & Tsui, A. (2007). The role of delayed child bearing in the
prevention of obstetric fistulas. International Journal of Gynecology and
Obstetrics.2(3)5
41
Ahmed, S. & Holtz, S.A. (2007). Social and Economic Consequence of Obstetric
Fistula: Life changed forever? International Journal of Gynecology and
obstetrics. 2,10
Ajuwon, A. (1997). Visco Vaginal Fistula in Nigeria, extent of the problem &
strategies for prevention and control. In Owumi,I. (Ed). Primary Health
care in Nigeria. Ibadan: Taiwo Press
Ajzen,I.(1988) Attitude, personality and change.Chikago:Dorsey Press
Ajzen,I & Fishein,M.(1980)Understanding attitudes and predicting social
behaviour ,Prentice-Hall:Englewood Cliffs,NJ.
Akpeji, F. (2012). Vesico- Vaginal Fistula in northern Nigeria. Urogynaecologia
International Journal, 2, 5.
Balogun, S. (1995). The VVF victims. Ibadan: Stirling-Horden:
Chalmers, B & Omer-Hashi, K. (2000). 432 Somali women’s birth experience in
Canada after earlier female genital mutilation. Retrieved March 24, 2012
from www.ncbi.nlm.gov/pubmed/1121507
Dodson, J.L, Gutman, R, &Mostwin, J. L. (2007). Complications of treatment of
obstetric fistula in developing world: Gynastresia, urinary incontinence and
urinary diversion. International Journal of Gynecology and Obstetrics
4,(2)223-225
Fasakin, G. (2007). Vesico virginal fistula & psycho-social well being of women in
northern Nigeria: unpublished masters project work.
42
Forsgren, C, Lundholm, C & Johansson, N. (2009). Hysterectomy for benign
indications and risk of pelvic organ fistula disease. Obstetrics and
Gynecology, 114, 3
Hilton, P. (2003). Vesico-vaginal fistula in developing counties. International
Journal of Gynastresia and Obstetric. 2(3)12
Ijaiya, M. (2010) Vesico vaginal fistula: A review of Nigeria experience. West
African Journal of Medicine, 10(5), 293-298. Retrieved January 12, 2013
from http://www.ncbi.nlm.nih.gov/pubmed/21089013
Kari,J. (2007, September, 9) Easing the scourge of VVF. Nigeria Guardian
Newspapers, p.7
Johnson, K. (2007). Incontinence in Malawi: Analysis of proxy measure of vaginal
fistula in national survey. International Journal of Gynecology and
Obstetrics 3,9.
Kees, W. (2006). Prevalence of Obstetric Fistulae in northern Nigeria
(Report).Retrived February 3 2013 from http:// www.fistularepair .com.
Magashi, A. (2006). Female genital mutilation and our societies. Retrieved on 18th
February 2012 from http://www.nigerianmasterweb.com/paperfrms.html
Mahendeka, M (2007). The management of vesico and/ or recto-vaginal fistula: A
retrospective study. Tanzania: Liventus Publishers
Matsamura, E. (2004). Uganda’s fistula patients lack knowledge of prevention and
treatment.Retrievedfromhttp://www//pro.org/articles/2004/ugandasfistulapa
tientslackknowledge of prevention and treatment.aspx
43
Metro, M. (2006). Modification of O’ Connor’s technique for the treatment of
VVF repair described. Retrieved Jan 3, 2013 from
www.newsmedical.net/news /2006/03/30/16974.aspx
Mkuma, G. & Kasonka, L. (2003). Obstetric fistula situation Analysis in zambia.
Ministry of health, Zambia
Mohammed, R. (2007). A community programe for women’s health and
development: Implications for the long term care of women with fistula.
International Journal of Gynecology and Obstetrics.2(5)12-15
Moir, J.C (1997). The Vesico-Vagina Fistula. London: Baillore Tin dall & Casell
Muhammad, J. (2011). Perceived causes, prevalence and effect of Vesico Vagina
Fistula among Hausa/Fulani women in Kano state (Being an Unpublished
Masters Degree Thesis, Department of Physical and Health Education,
Ahmadu Bello University, Zaria, Nigeria)
National Demographic Health Survey (2008) Religion, Gender and Educational
Level of Nigerians. National Demographic Health Survey
National strategic frame work for eradication of fistula in Nigeria (2005-2011).
Retrieved March 3,2012 fromhttp://www.maternal-health.org/.../unfpa-
evaluierungsbericht-ueber-die-en.
Ngoma, J. (2010). Prevention of Vesico-Vaginal Fistula. (Being a Thesis, Turku
University of Applied Sciences, Zambia)
Orji, E, Aduloju, O & Orji, V. (2007). Correlation and impact of obstetric fistula
on motherhood. Journal of Chinese Clinical Medicine. 2 (8), August, 2007
44
Raassen T, Verdaasdonk,E&Vierhout,M (2007). Perspective results after first time
survey for obstetric fistulas in east African women. International
Urogynecology Journal, 19, pp.73-79
Ramsey, K, Illiyasu, Z. & Idoko, L. (2007). Fistula fortnight: Innovative
partnership brings mass treatment and public awareness towards ending
obstetric fistula. International Journal of Gynecology and Obstetrics.9,9,
doi: 10.1016/j-ijgo.2007.06.034
Sambo, A.E. (1994.) Vesico Vaginal Fistula (VVF) A vision realized.Retrived
from
www.ghononline.org/Vesico%20Vaginal%20Fistula%20 (VVF)
%20Cam...
Sheikh.R (2011). Vesico- vaginal fistula: Abdominal Repair Versus Repair via
Vaginal route. Professional Medical Journal. 1,4
The National Foundation on Vesico-Vaginal Fistula (2003). Report of the rapid
assessment of vesico-vaginal fistula in Nigeria. Retrieved March 20, 2013
from http://www.endfitsula .org
The thematic evaluation of national programme and UNFPA experience in the
campaign to end fistula: Assessment of global/regional activity (2010).
Retrieved January 13, 2013 from http://www.end fistula.org
UNFPA (2007). Family care International. Risk and resilience. Obstetric fistula in
Zambia. Women dignity project. Zambia and Engender Health. USA:
Procures
45
United Nation Population Fund. (2010) Campaign to End Fistula. Retrieved from
http://www.endfistula.com/publications.htm
United State Agency for International Development (USAID) (2003). Mid Term
Evaluation of Fistula Care Project. Retrieved February 21, 2012 from
http://www.ghtechproject.com/.../nigeria%20mch-
Villey, T (2006). The VVF patients. Stirling-Horden . Ibadan
Wall.L. (2001) Urinary Incontinence in the Developing World: The Obstetric
Fistula. Retrieved January 12,2013 from www.fistulafoundation.org
Wall, L. (2005). Ethical issues in vesico-vaginal fistula care and research.
International Journal of Gynecology and Obstetrics. 5,17
Wall, L, Arrowsmith, S, Lassey A, & Danso K. (2003). Humanitarian ventures or
‘fistula tourism? The ethical perils of pelvic surgery in the developing
world. International Urogynecol Journal, 17, 559-62.
Wall, L. & Lancer, T. (2006) Obstetric Vesico-Vaginal Fistula as an international
health problem. American Journal of Obstetric & Gnecology, 9 (4)190.
Wall, L., Karshima, J. & Kirschner,G. (2004). The obstetric vesico vaginal fistula:
characteristics of 889 patients from Jos, Nigeria. American Journal of
Obstetric & Gnecology, 9 (4)192.
WHO (2005). Obstetric fistula, guiding principles for clinical management and
programme development. Geneva, Switzerland.
Zacharin R.F. (1988). Obstetric Fistula. New York: Springer Verlag.
46
CHAPTER THREE
METHODOLOGY
3.1 Research Design
To effectively evaluate the influence of Media campaigns on Vesico
Vaginal Fistula prevention and control in North Western Nigeria, the researcher
used explanatory mixed method. This approach enabled the researcher to generate
both quantitative and qualitative data and generalize the result on the entire
population. Another rationale for this approach, according to Creswell (2002. p
565), is that “one data collection form supplies strengths to offset the weakness of
the other form.” With this design, the researcher gathered both quantitative and
qualitative data, compared results from the analysis of both data and made
statistical interpretations.
The cross-sectional survey method was used to generate quantitative data
while critical ethnography was used to generate qualitative data. This research
design is very important to this work because it addresses the various research
questions in the study and it also provides a platform for the researcher to study
the people of North Western Nigeria in their natural settings in order to ascertain
47
their responses and dispositions towards Vesico Vaginal Fistula. This to a large
extent, reduced incidences of respondent manipulating the outcome of the study.
To this end, research question one,two,three and five were answered using the
two methods, however, only research question four was answered using interview,
the justification for this is based on the fact that the researcher tend to have an
indept interview with th campaign planners alone (Health Workers).
The questionnaire was used to collect quantitative data generated for the
survey aspect of the study and it addresses the research questions raised in the
study. Consequently, qualitative data generated through ethnography (interviews
and observations) complemented the quantitative data collected
The justification for the use of ethnography research method in this study is
because the researcher had to generate qualitative data that complement
quantitative data that is used in the study since ethnography research method calls
for researchers to spend considerable amount of time living with and observing the
people. This method availed the researcher the opportunity of studying the people
of North Western Nigeria by spending time with them and observing them in their
natural environment by living with them (Wimmer and Dominick, 2011, p.145).
Critical ethnography, according to Creswell (2002, p.483), examines shared
patterns of communication among marginalized (VVF patients) group with the
aim of making a case for them. This design provided the researcher with two data
collection instruments-interview and observation.
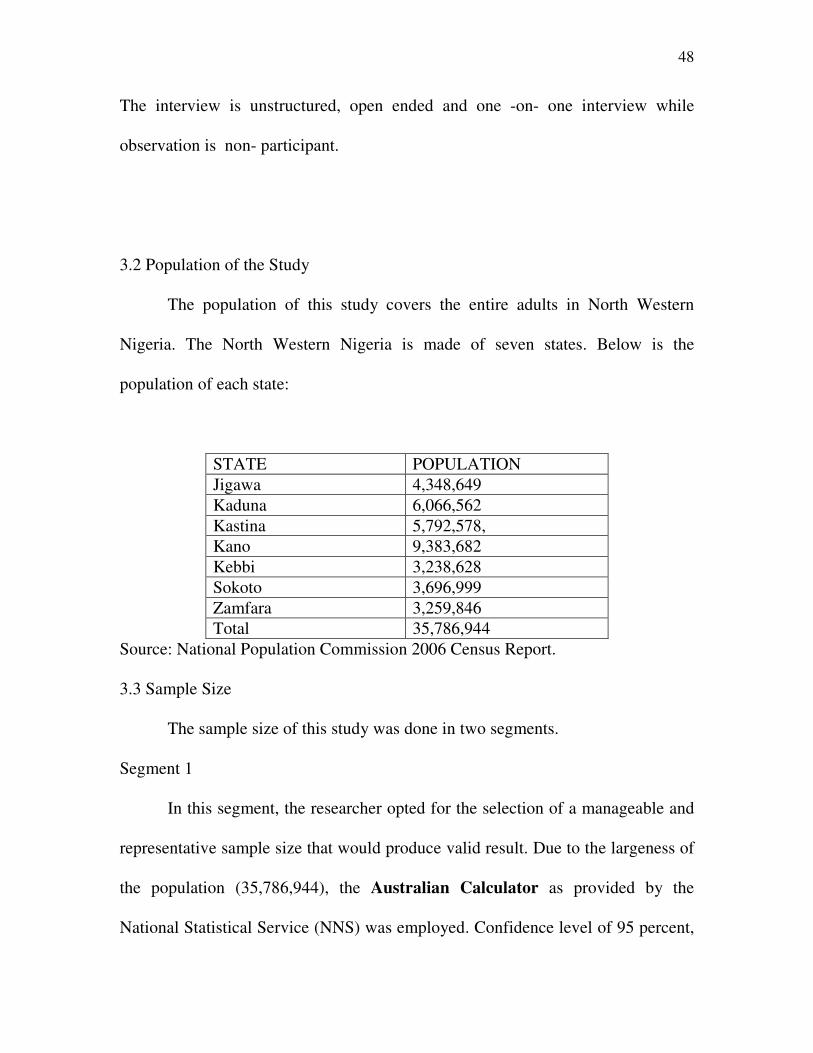
48
The interview is unstructured, open ended and one -on- one interview while
observation is non- participant.
3.2 Population of the Study
The population of this study covers the entire adults in North Western
Nigeria. The North Western Nigeria is made of seven states. Below is the
population of each state:
STATE POPULATION
Jigawa 4,348,649
Kaduna 6,066,562
Kastina 5,792,578,
Kano 9,383,682
Kebbi 3,238,628
Sokoto 3,696,999
Zamfara 3,259,846
Total 35,786,944
Source: National Population Commission 2006 Census Report.
3.3 Sample Size
The sample size of this study was done in two segments.
Segment 1
In this segment, the researcher opted for the selection of a manageable and
representative sample size that would produce valid result. Due to the largeness of
the population (35,786,944), the Australian Calculator as provided by the
National Statistical Service (NNS) was employed. Confidence level of 95 percent,
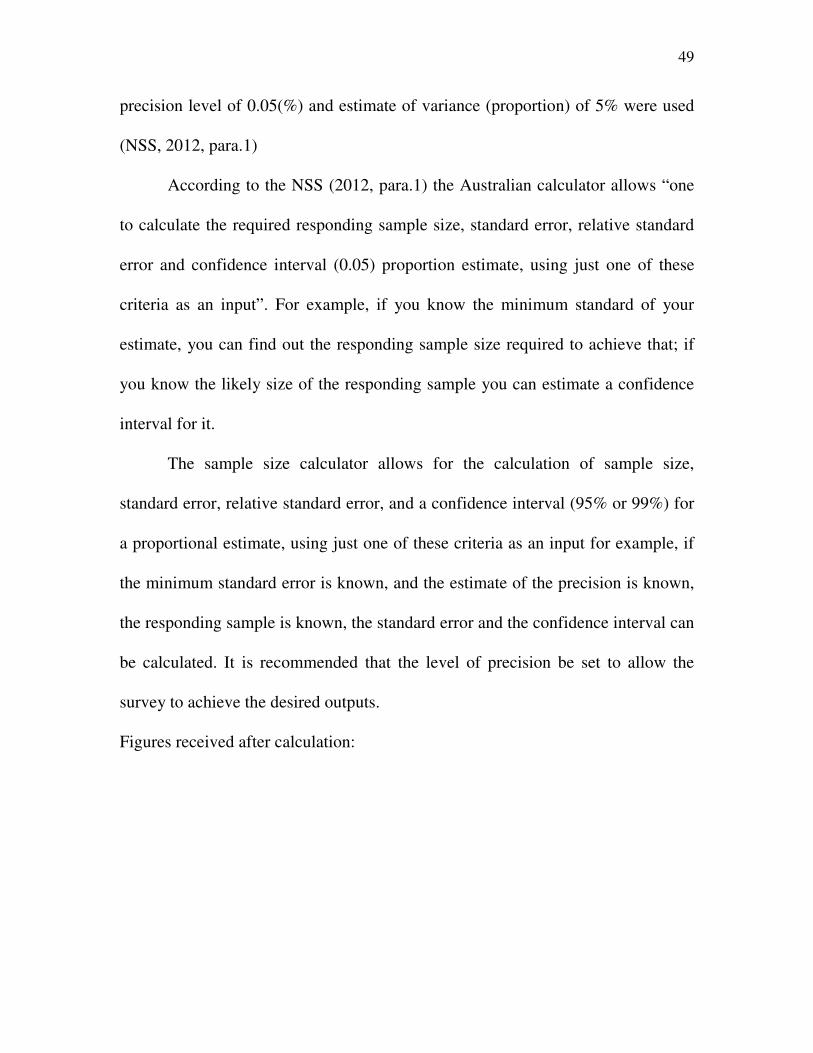
49
precision level of 0.05(%) and estimate of variance (proportion) of 5% were used
(NSS, 2012, para.1)
According to the NSS (2012, para.1) the Australian calculator allows “one
to calculate the required responding sample size, standard error, relative standard
error and confidence interval (0.05) proportion estimate, using just one of these
criteria as an input”. For example, if you know the minimum standard of your
estimate, you can find out the responding sample size required to achieve that; if
you know the likely size of the responding sample you can estimate a confidence
interval for it.
The sample size calculator allows for the calculation of sample size,
standard error, relative standard error, and a confidence interval (95% or 99%) for
a proportional estimate, using just one of these criteria as an input for example, if
the minimum standard error is known, and the estimate of the precision is known,
the responding sample is known, the standard error and the confidence interval can
be calculated. It is recommended that the level of precision be set to allow the
survey to achieve the desired outputs.
Figures received after calculation:
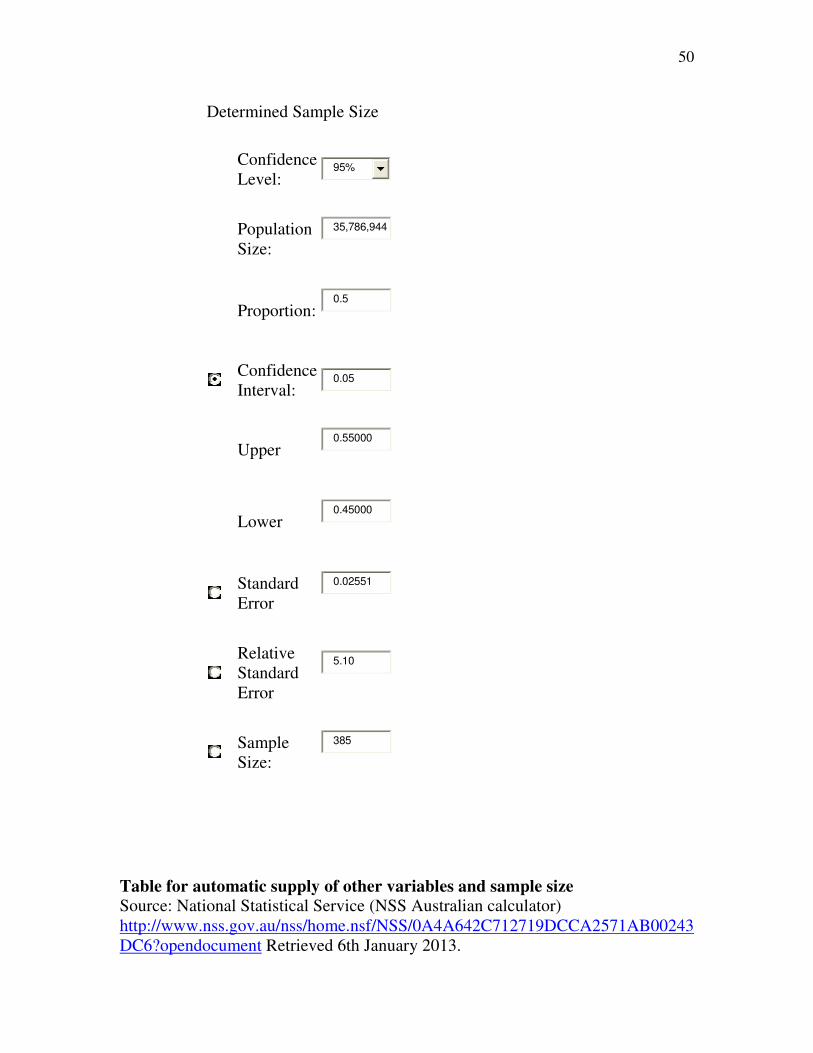
50
Determined Sample Size
Confidence
Level: 95%
Population
Size:
35,786,944
Proportion: 0.5
Confidence
Interval: 0.05
Upper 0.55000
Lower 0.45000
Standard
Error
0.02551
Relative
Standard
Error
5.10
Sample
Size:
385
Table for automatic supply of other variables and sample size
Source: National Statistical Service (NSS Australian calculator)
http://www.nss.gov.au/nss/home.nsf/NSS/0A4A642C712719DCCA2571AB00243
DC6?opendocument Retrieved 6th January 2013.
51
From this calculation, it is given that the basic sample size of the study is
385.
However, NSS (2012, para.8) states that “the sample size require to be selected
from your population will need to take into account the number of individuals or
groups that will not respond to your survey. For example, if the sample size
calculator indicates that you need a sample size of 500 and from previous
experience the number of individuals or groups that has responded to your survey
is 50 percent then the total sample required from the population would be 1000.
This simply means that an over sampling calculation is required.
Bertlett, Kotrlik and Higgins (2001, p.46) citing salkind (1997,p.107)Fink
(1995,p.36) and Cochran (1977,p.396) recommended oversampling when they
noted that “if you are mailing out surveys or questionnaires count on increasing
your sample size by 10%-50% to account for lost mails and uncooperative
subjects”. Berthett, Kotrlik and Higgins (2001,p.46) further opined that “if
researcher decided to use oversampling, let him estimate the response rate as a
means of calculating for it”. To calculate for the oversampling procedure, a
response rate estimate of 90% was adopted. The calculation for the contingency is
represented below:
n2 =
atedresponserAuticipate
plesizeMinimumsam
Where anticipated return rate = 90%
Where n2 = sample size adjusted for response rate.
52
Where minimum sample size = 385
Therefore:
atedresponserAuticipate
plesizeMinimumsam =
%90
385
n2 = 385/0.90 = 427.777778 approximately 428
The sample size for the survey aspect of the study is 428
Segment 2
To determine the sample size for the second segment of the population the
researcher purposively sampled 6 heath workers (from VVF centres/ Hospitals) in
the North Western Nigeria. These health workers were selected based on their
accomplishments in battling VVF in North Western Nigeria. More also the
researcher saw their willingness to interact with him.
Segment 3
The researcher also observed the selected areas for the duration of 6 weeks.
That is, two weeks in each of the three states. Patients and indigenes of the
communities were observed and the outcomes were recorded in the observation
dairy.
3.4 Sampling Technique
The research used multi-stage sampling technique as the sampling
technique for the study. This technique, according to Chukwuemeka (2002, p.111)
requires the use of several sampling techniques or/and stages in a particular
53
method for ensuring true presentation, especially when the population is large and
complex.
Stage 1
First, the researcher used cluster technique; the North Western Geo-
Political Zone which the research studied has seven states (Jigawa, Kano, Kaduna,
Katsina, Kebbi, Sokoto and Zamfara State). These states are regarded as clusters,
from these 7 states/ clusters, the researcher randomly selected three states namely,
Jigawa , Kano and Kebbi states. These states have VVF treatment centres.
Stage 2
Due to the large nature of the three selected states, occasioned by the
remote area where the population lives, the researcher purposively selected two
local government areas from the selected three states (a L.G.A where VVF centres
are located and the local government area in which the state capital falls under
were also selected, the justification for this is that, the researcher deemd it
necessary to observe the VVF patients from these VVF centres, and for this to be
achieved, he had to visit the VVF centres. The justification for the selection of
Local Government Areas where the state capital is located is as a result of the fact
that such local government areas are usually the centre of activities in the states).
States Selected L.G.A
54
Jigawa Jahun, Dutse
Kano Dambatta, Kano municipal
Kebbi Birnin kebbi, koko/Besse
3.5 Measuring Instruments
Questionnaire was used in this study as the measuring instrument that
would generate quantitative data for the survey aspect of the study. Interview and
observation served as instruments for the generation of qualitative data for the
ethnographic aspect of the study.
The questionnaire, which was designed in a very simple form was
administered to the respondents in their various home with the help of health
workers. Interview and observation served as instruments for the generation of
qualitative data for the ethnographic aspect of the study. Diary of all activities
observed by the researcher was used for qualitative analysis.
3.6 Validity and Reliability of Measuring Instrument.
The validity of the questionnaire, interview questions and observation diary
were done using face validity technique. The instruments were given to the project
supervisor and three communication scholars who are Senior Lecturers in the
Department of Mass Communication, University of Nigeria, Nsukka. First it was
tested if the questions in the questionnaire were related to the topic under study. It
was tested for clarity and ambiguity the question in the interview schedule and the
55
observation dairy equally passed through the same process, corrections were made
thereafter.
In checking for the reliability of the questionnaire, a pretest was conducted
in Jahun L.G.A Jigawa state using test-re-test strategy. A total of 28 respondents
were drawn for the purpose. The reason was to determine whether responses
would be in line with result expected form the instrument. The instrument was
employed twice and the data collected were compared to see if they met the
expected reliability rate. After the instrument had been administered an interval of
one week was given for the re-administration of the instruments. The data
obtained from the two tests were then subjected to the main reliability test using
Parsons Correlational Coefficient Statistical procedure
In the test of reliability using correlational Coefficient, Osuala (p.149)
opined that “high reliability is indicated by high correlation coefficient. It is
difficult to say how high the correlation should be before accepting the measure as
reliable. But for most measures, the correlation would probably be at least +0.80”.
Since the test re-test result shows a correlation coefficient of 0.90, it means that
the reliability of the instrument is high.
3.7 Methods of data Presentation and Analysis
The quantitative data generated from the use of questionnaire were
presented using simple frequency distribution tables, percentages and numbers to
ascertain the influence of media campaigns on VVF prevention and control. These
data were analyzed using Statistical Package for Social Science (SPSS).

56
The qualitative data generated through interview and observations were
used to complement the quantitative data generated through questionnaire.
References
Bertlett, J., Kotrlik, J. & Higgins, C. (2001). Organizational Research:
Determining appropriate sample size in survey research. Information
Technology, Learning and Performance Journal. 19(1), 43-50
Chukwuemeka, E.E (2002). Research methods and thesis writing:
A multidisciplinary approach. Enugu : Hope Rising venture
Creswell, J. (2002). Educational research: Planning, conducting and evaluating
quantitative and qualitative research. New Jersey: Pearson Education Inc.
National Statistical Service (2012). Sample size calculator. Retrieved April 26,
form htp//www.nss.gov.au/nss/home.rsf/nss/oa4a642c712719dcca25
Osuala, E.C. (2005). Introduction to research methodology (3rd
ed.). Onitsha:
Africana.First Publishers Limited
Wimmer, R, & Dominick, J. (2011).Mass media research. An introduction
(9th
ed). Canada: Wadsworth Cengage Learning
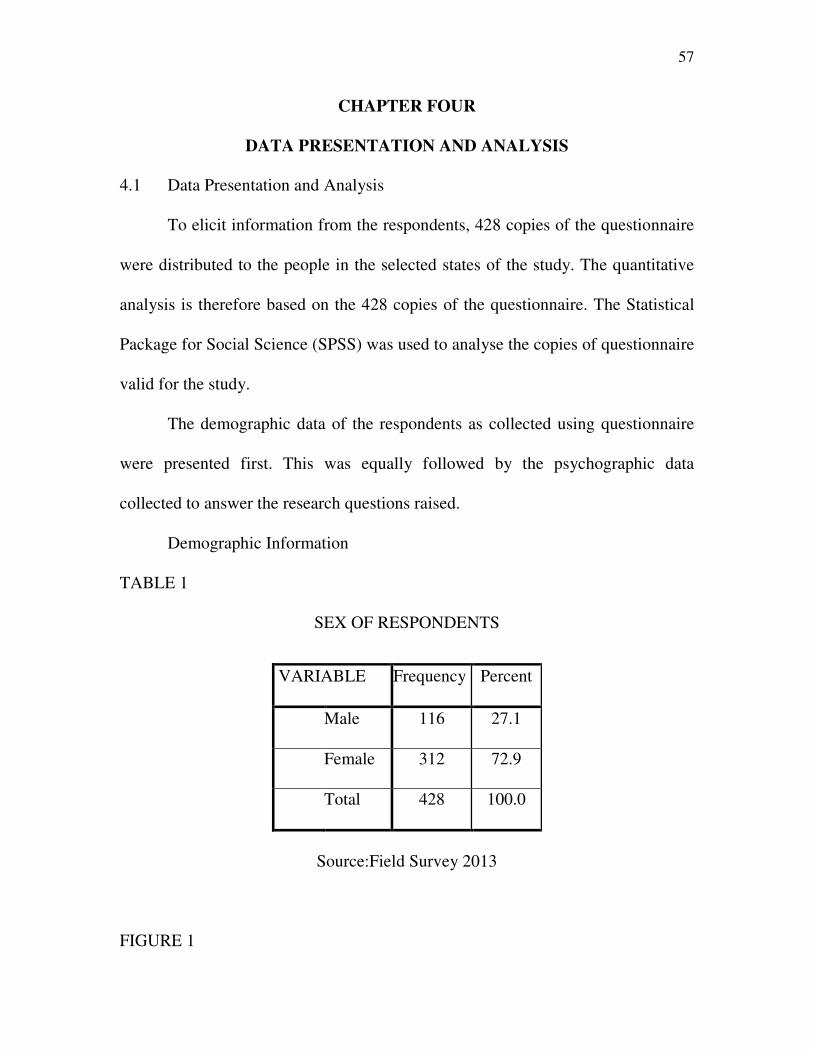
57
CHAPTER FOUR
DATA PRESENTATION AND ANALYSIS
4.1 Data Presentation and Analysis
To elicit information from the respondents, 428 copies of the questionnaire
were distributed to the people in the selected states of the study. The quantitative
analysis is therefore based on the 428 copies of the questionnaire. The Statistical
Package for Social Science (SPSS) was used to analyse the copies of questionnaire
valid for the study.
The demographic data of the respondents as collected using questionnaire
were presented first. This was equally followed by the psychographic data
collected to answer the research questions raised.
Demographic Information
TABLE 1
SEX OF RESPONDENTS
Source:Field Survey 2013
FIGURE 1
VARIABLE Frequency Percent
Male 116 27.1
Female 312 72.9
Total 428 100.0
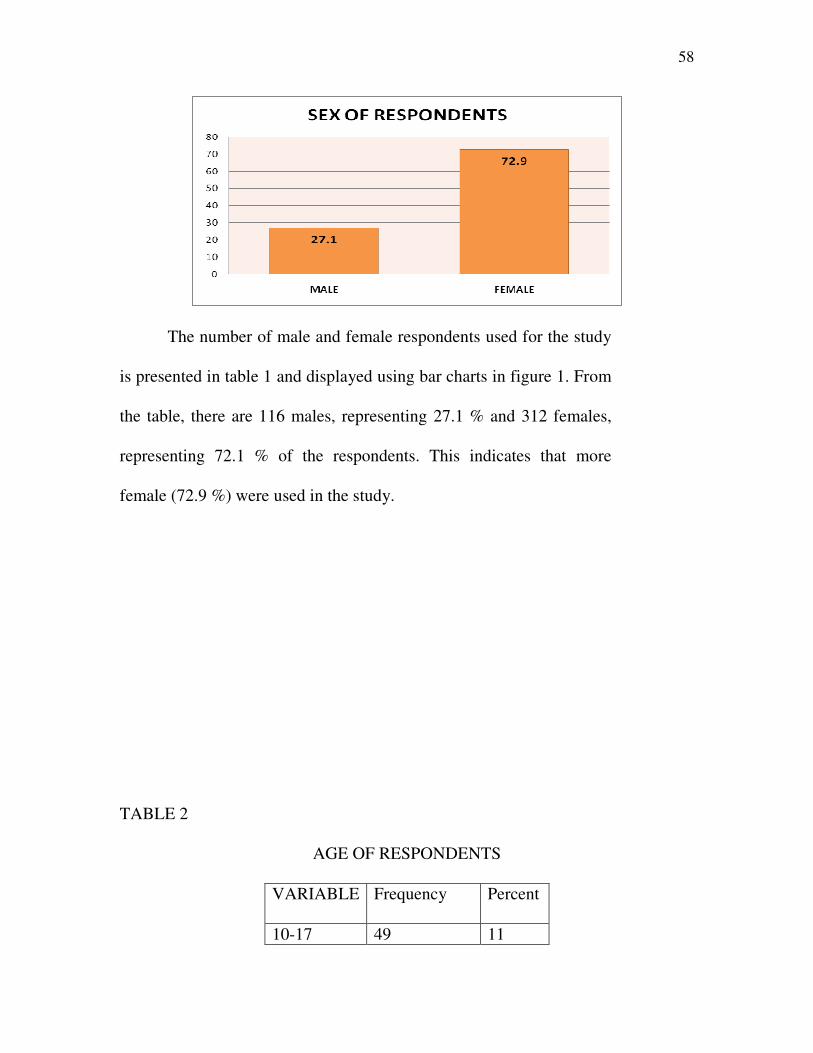
58
The number of male and female respondents used for the study
is presented in table 1 and displayed using bar charts in figure 1. From
the table, there are 116 males, representing 27.1 % and 312 females,
representing 72.1 % of the respondents. This indicates that more
female (72.9 %) were used in the study.
TABLE 2
AGE OF RESPONDENTS
VARIABLE Frequency Percent
10-17 49 11
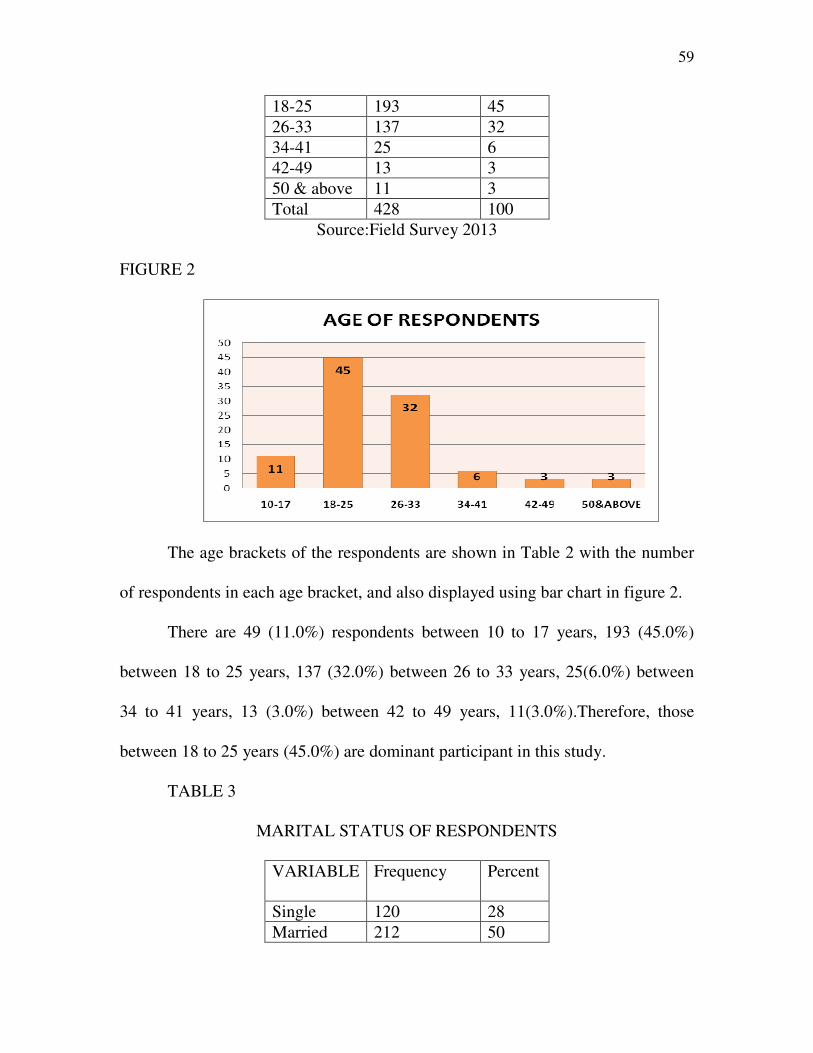
59
18-25 193 45
26-33 137 32
34-41 25 6
42-49 13 3
50 & above 11 3
Total 428 100
Source:Field Survey 2013
FIGURE 2
The age brackets of the respondents are shown in Table 2 with the number
of respondents in each age bracket, and also displayed using bar chart in figure 2.
There are 49 (11.0%) respondents between 10 to 17 years, 193 (45.0%)
between 18 to 25 years, 137 (32.0%) between 26 to 33 years, 25(6.0%) between
34 to 41 years, 13 (3.0%) between 42 to 49 years, 11(3.0%).Therefore, those
between 18 to 25 years (45.0%) are dominant participant in this study.
TABLE 3
MARITAL STATUS OF RESPONDENTS
VARIABLE Frequency Percent
Single 120 28
Married 212 50
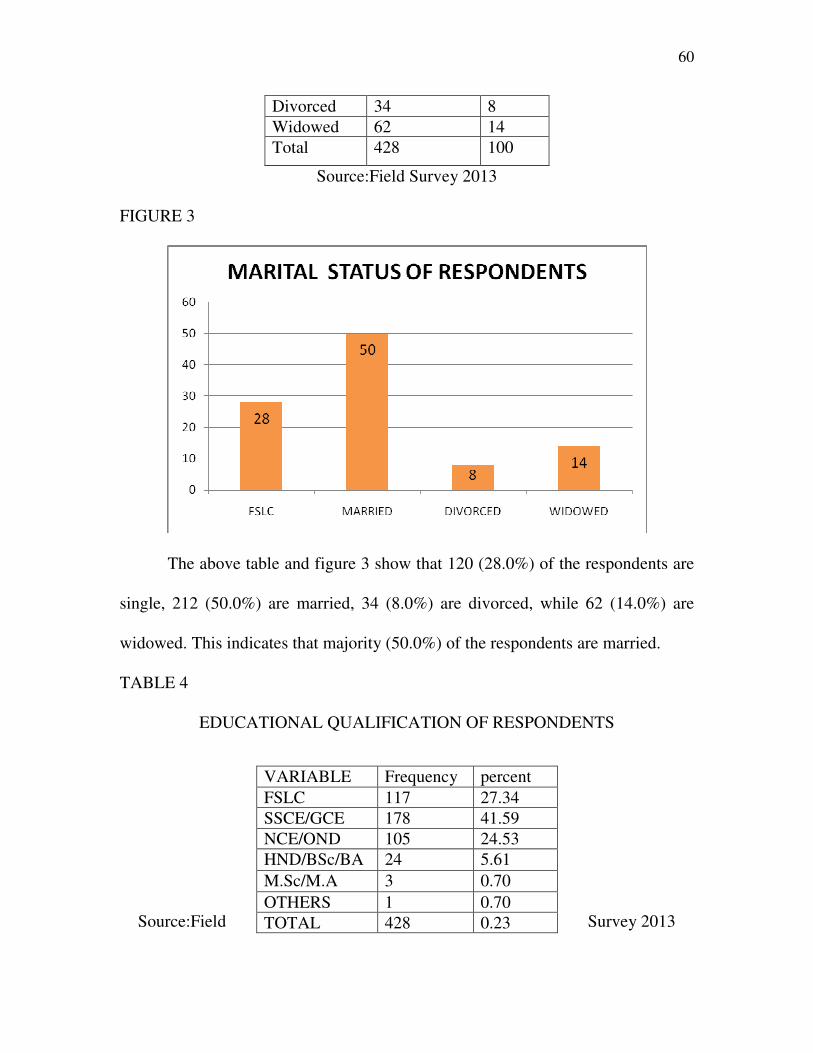
60
Divorced 34 8
Widowed 62 14
Total 428 100
Source:Field Survey 2013
FIGURE 3
The above table and figure 3 show that 120 (28.0%) of the respondents are
single, 212 (50.0%) are married, 34 (8.0%) are divorced, while 62 (14.0%) are
widowed. This indicates that majority (50.0%) of the respondents are married.
TABLE 4
EDUCATIONAL QUALIFICATION OF RESPONDENTS
Source:Field Survey 2013
VARIABLE Frequency percent
FSLC 117 27.34
SSCE/GCE 178 41.59
NCE/OND 105 24.53
HND/BSc/BA 24 5.61
M.Sc/M.A 3 0.70
OTHERS 1 0.70
TOTAL 428 0.23
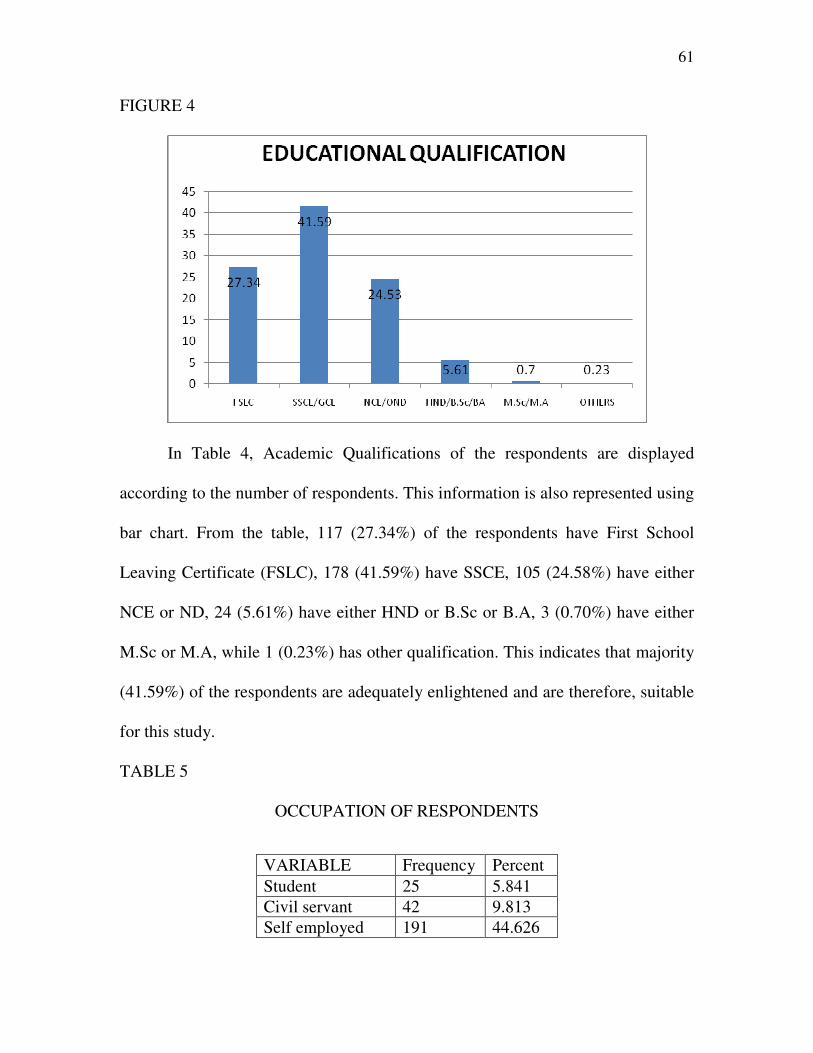
61
FIGURE 4
In Table 4, Academic Qualifications of the respondents are displayed
according to the number of respondents. This information is also represented using
bar chart. From the table, 117 (27.34%) of the respondents have First School
Leaving Certificate (FSLC), 178 (41.59%) have SSCE, 105 (24.58%) have either
NCE or ND, 24 (5.61%) have either HND or B.Sc or B.A, 3 (0.70%) have either
M.Sc or M.A, while 1 (0.23%) has other qualification. This indicates that majority
(41.59%) of the respondents are adequately enlightened and are therefore, suitable
for this study.
TABLE 5
OCCUPATION OF RESPONDENTS
VARIABLE Frequency Percent
Student 25 5.841
Civil servant 42 9.813
Self employed 191 44.626
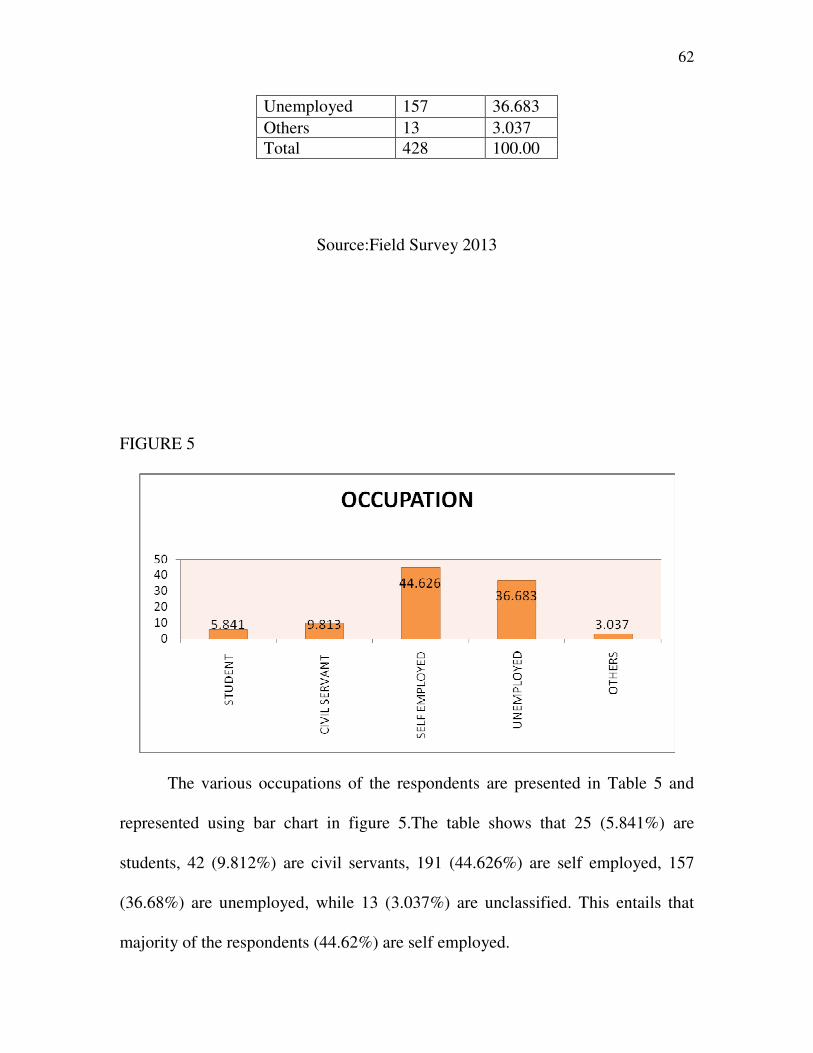
62
Source:Field Survey 2013
FIGURE 5
The various occupations of the respondents are presented in Table 5 and
represented using bar chart in figure 5.The table shows that 25 (5.841%) are
students, 42 (9.812%) are civil servants, 191 (44.626%) are self employed, 157
(36.68%) are unemployed, while 13 (3.037%) are unclassified. This entails that
majority of the respondents (44.62%) are self employed.
Unemployed 157 36.683
Others 13 3.037
Total 428 100.00
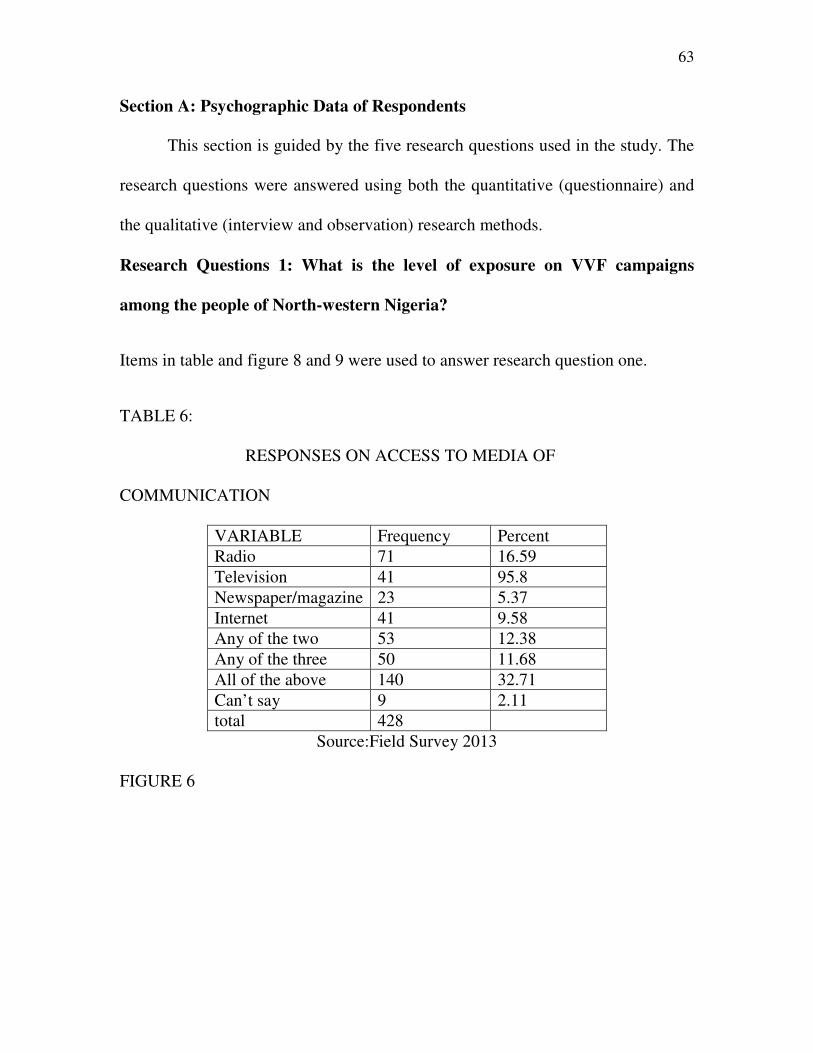
63
Section A: Psychographic Data of Respondents
This section is guided by the five research questions used in the study. The
research questions were answered using both the quantitative (questionnaire) and
the qualitative (interview and observation) research methods.
Research Questions 1: What is the level of exposure on VVF campaigns
among the people of North-western Nigeria?
Items in table and figure 8 and 9 were used to answer research question one.
TABLE 6:
RESPONSES ON ACCESS TO MEDIA OF
COMMUNICATION
VARIABLE Frequency Percent
Radio 71 16.59
Television 41 95.8
Newspaper/magazine 23 5.37
Internet 41 9.58
Any of the two 53 12.38
Any of the three 50 11.68
All of the above 140 32.71
Can’t say 9 2.11
total 428
Source:Field Survey 2013
FIGURE 6
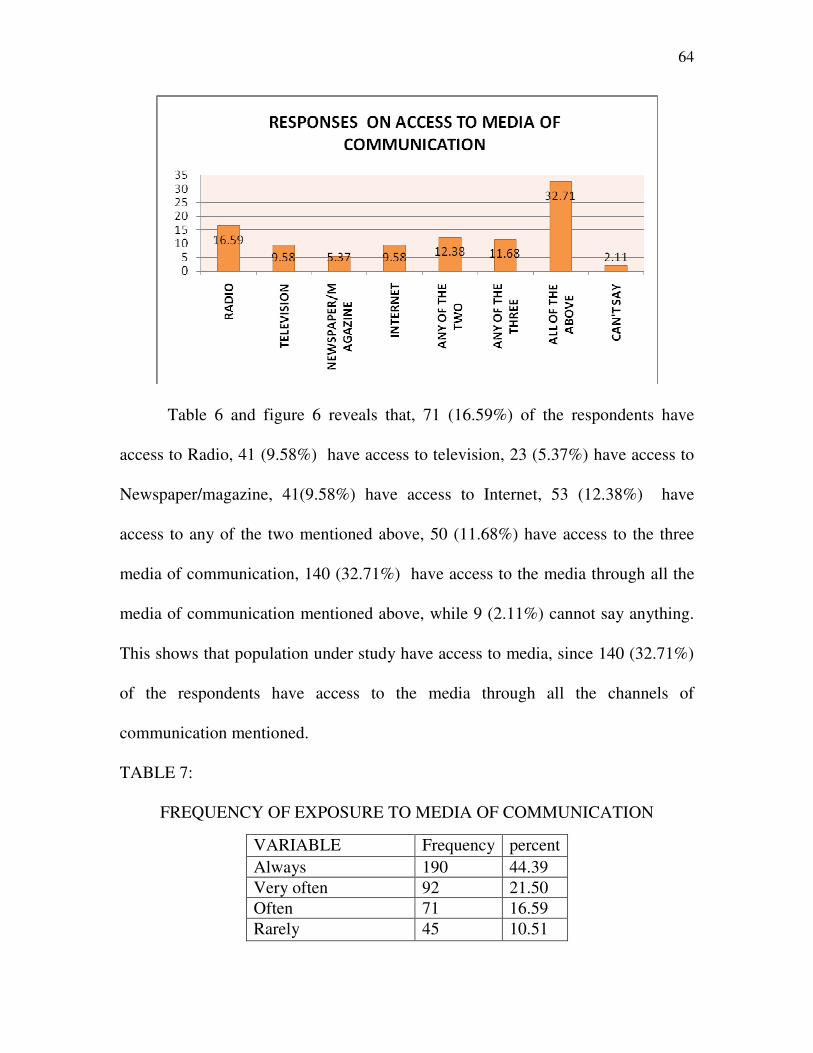
64
Table 6 and figure 6 reveals that, 71 (16.59%) of the respondents have
access to Radio, 41 (9.58%) have access to television, 23 (5.37%) have access to
Newspaper/magazine, 41(9.58%) have access to Internet, 53 (12.38%) have
access to any of the two mentioned above, 50 (11.68%) have access to the three
media of communication, 140 (32.71%) have access to the media through all the
media of communication mentioned above, while 9 (2.11%) cannot say anything.
This shows that population under study have access to media, since 140 (32.71%)
of the respondents have access to the media through all the channels of
communication mentioned.
TABLE 7:
FREQUENCY OF EXPOSURE TO MEDIA OF COMMUNICATION
VARIABLE Frequency percent
Always 190 44.39
Very often 92 21.50
Often 71 16.59
Rarely 45 10.51
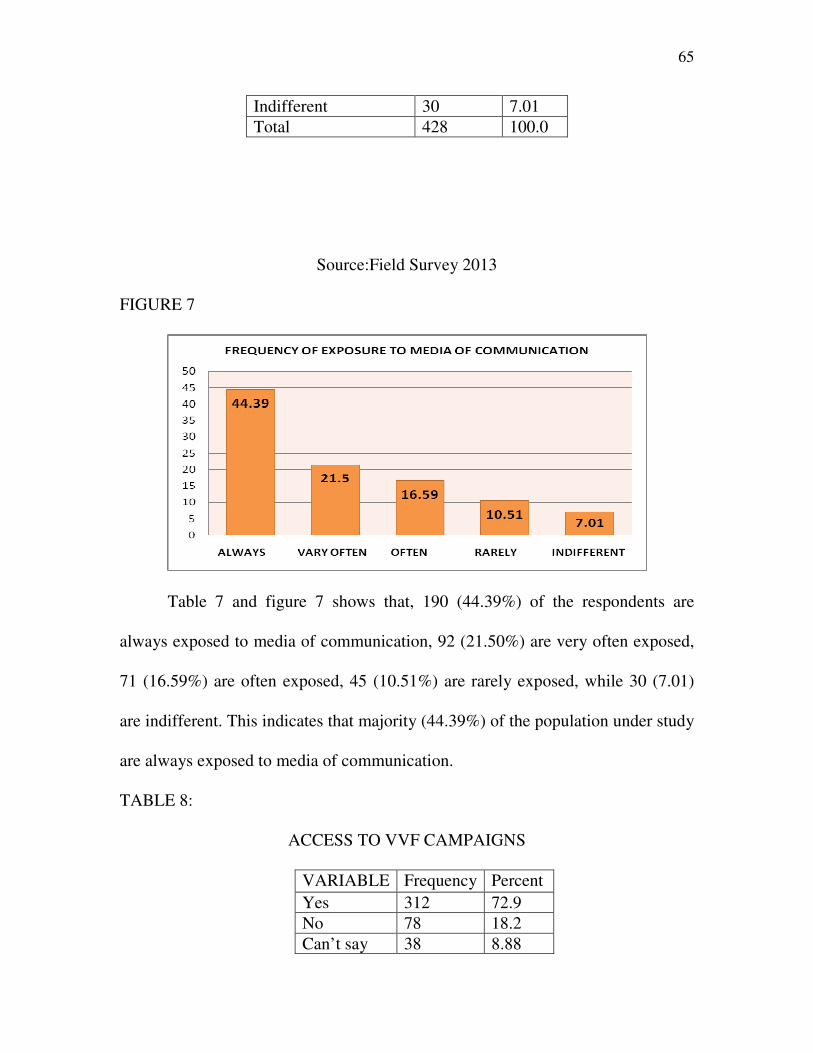
65
Source:Field Survey 2013
FIGURE 7
Table 7 and figure 7 shows that, 190 (44.39%) of the respondents are
always exposed to media of communication, 92 (21.50%) are very often exposed,
71 (16.59%) are often exposed, 45 (10.51%) are rarely exposed, while 30 (7.01)
are indifferent. This indicates that majority (44.39%) of the population under study
are always exposed to media of communication.
TABLE 8:
ACCESS TO VVF CAMPAIGNS
VARIABLE Frequency Percent
Yes 312 72.9
No 78 18.2
Can’t say 38 8.88
Indifferent 30 7.01
Total 428 100.0
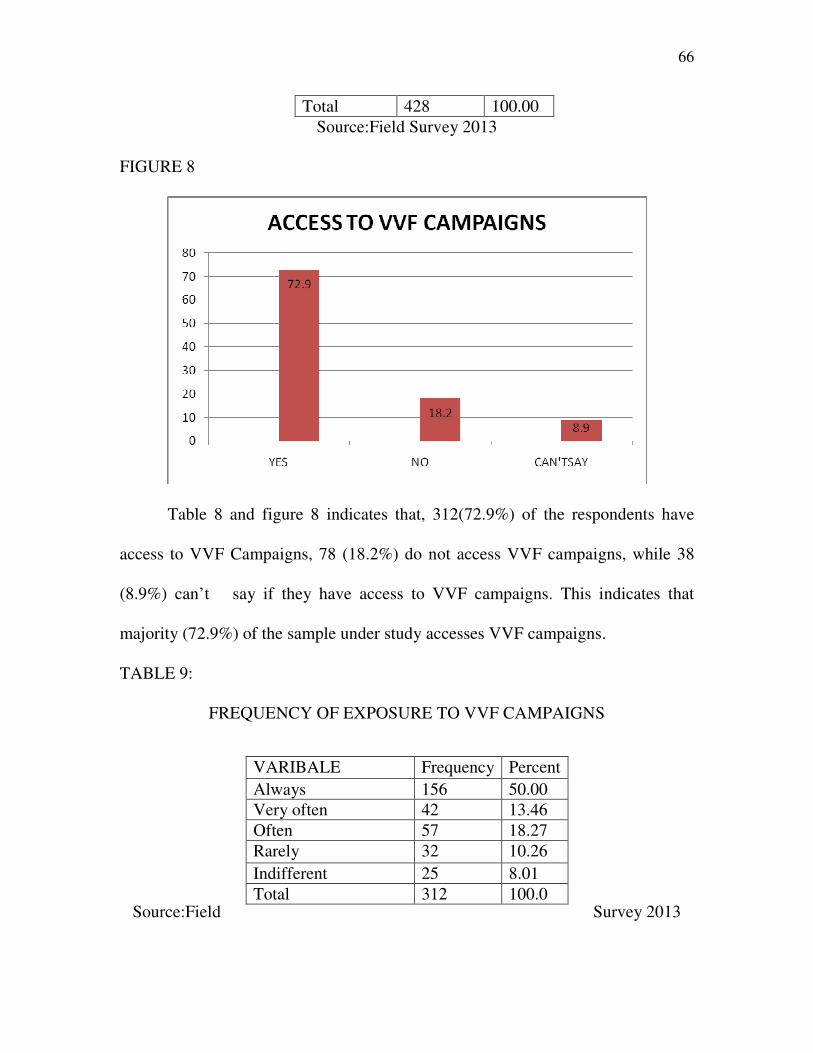
66
Total 428 100.00
Source:Field Survey 2013
FIGURE 8
Table 8 and figure 8 indicates that, 312(72.9%) of the respondents have
access to VVF Campaigns, 78 (18.2%) do not access VVF campaigns, while 38
(8.9%) can’t say if they have access to VVF campaigns. This indicates that
majority (72.9%) of the sample under study accesses VVF campaigns.
TABLE 9:
FREQUENCY OF EXPOSURE TO VVF CAMPAIGNS
Source:Field Survey 2013
VARIBALE Frequency Percent
Always 156 50.00
Very often 42 13.46
Often 57 18.27
Rarely 32 10.26
Indifferent 25 8.01
Total 312 100.0
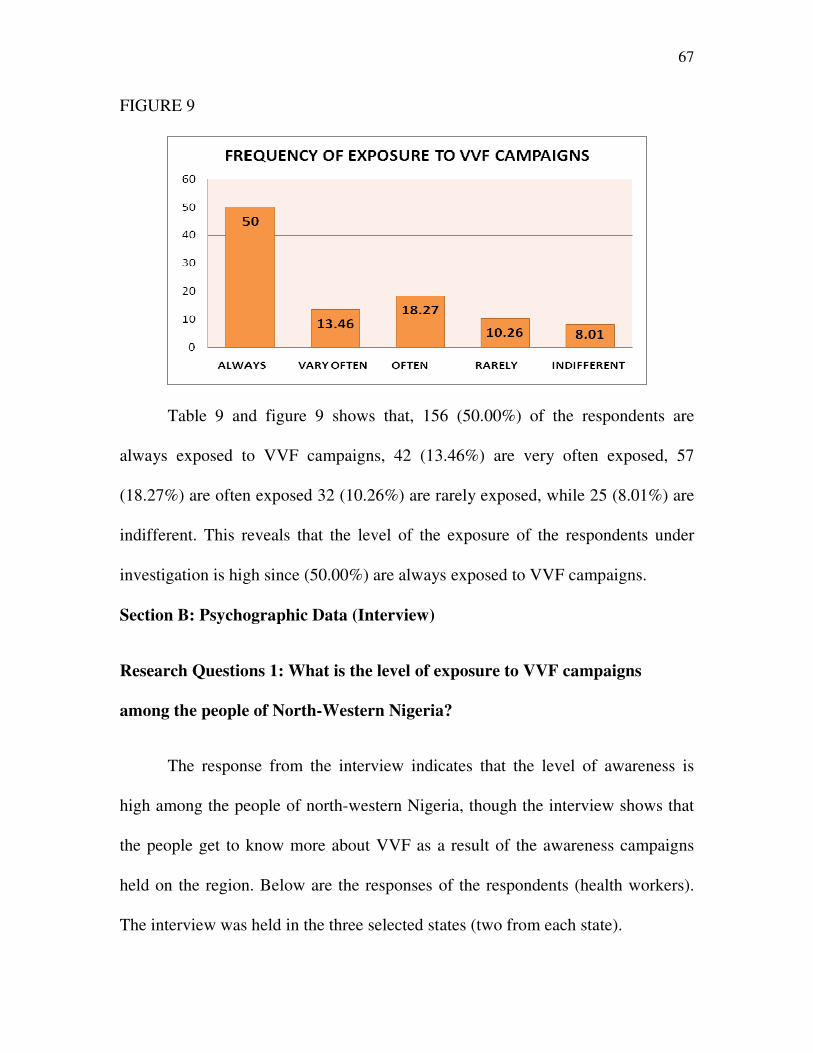
67
FIGURE 9
Table 9 and figure 9 shows that, 156 (50.00%) of the respondents are
always exposed to VVF campaigns, 42 (13.46%) are very often exposed, 57
(18.27%) are often exposed 32 (10.26%) are rarely exposed, while 25 (8.01%) are
indifferent. This reveals that the level of the exposure of the respondents under
investigation is high since (50.00%) are always exposed to VVF campaigns.
Section B: Psychographic Data (Interview)
Research Questions 1: What is the level of exposure to VVF campaigns
among the people of North-Western Nigeria?
The response from the interview indicates that the level of awareness is
high among the people of north-western Nigeria, though the interview shows that
the people get to know more about VVF as a result of the awareness campaigns
held on the region. Below are the responses of the respondents (health workers).
The interview was held in the three selected states (two from each state).
68
Respondent A: Yes, people in this part of the country are fully aware of VVF,
however, thanks to the government and NGOs that helped in creating this
awareness.
Respondent B: The level of awareness is very high, compared to 10 years ago.
Children, youths and adults are all aware of VVF.
Respondent C:Vesico Virginal Fistula, well I will not call it a disease; it is an
abnormality in the virgina. It is mostly caused by female genital mutilation; in
Hausa we call it “yankigishiri”. The level of exposure has increased ever since the
government discovered that majority of the girls in the north die during this act.
There have been massive campaigns on it.
Respondent D: Early marriage, poverty, poor health facilities all reduces a
woman’s chance of getting timely obstetric care. The awareness have increased,
at least better than before, we now have VVF centres to take care of VVF patients.
Respondent E: Young man, you can see for yourself that the level of exposure is
high.
Respondent F: The awareness campaigns on VVF I must confess has helped a lot.
Most people here are aware of the dangers of female child mutilation, which is a
major cause of VVF.
Section C: Psychographic Data (Observation)
69
The observation lasted for two weeks in each of the states. The report here
is the general outcome of the researcher’s observation which lasted for 6 weeks in
all. From the three states, the researcher observed that majority of the people in the
selected states are already taking measures such as educating the young and old on
VVF. The researcher also discovered that there are very few traditional child
delivery centres in the states. In those traditional health centres, two patients were
seen in one of the villages in Jigawa state. Both patients were there for child
delivery, however, the traditional child birth attendant said there has been low
turn-up ever since the campaigns on VVF started in the state. The researcher also
interacted with pupils in some schools in the states and most of the pupils said
their parents seek modern health centres for medical attention. Based on the
observations made in these three states, the researcher draws a conclusion that the
masses are fully aware of the vesico vaginal fistula campaign, although some of
the respondents knows and refer to VVF as “yankigishiri” an Hausa word for
female genital mutilation.
Research Questions 2: What is the knowledge level on VVF among the people
of North-Western Nigeria?
Items in table and figure 10, 11,12,13,14 and 15 were used to answer research
question two.
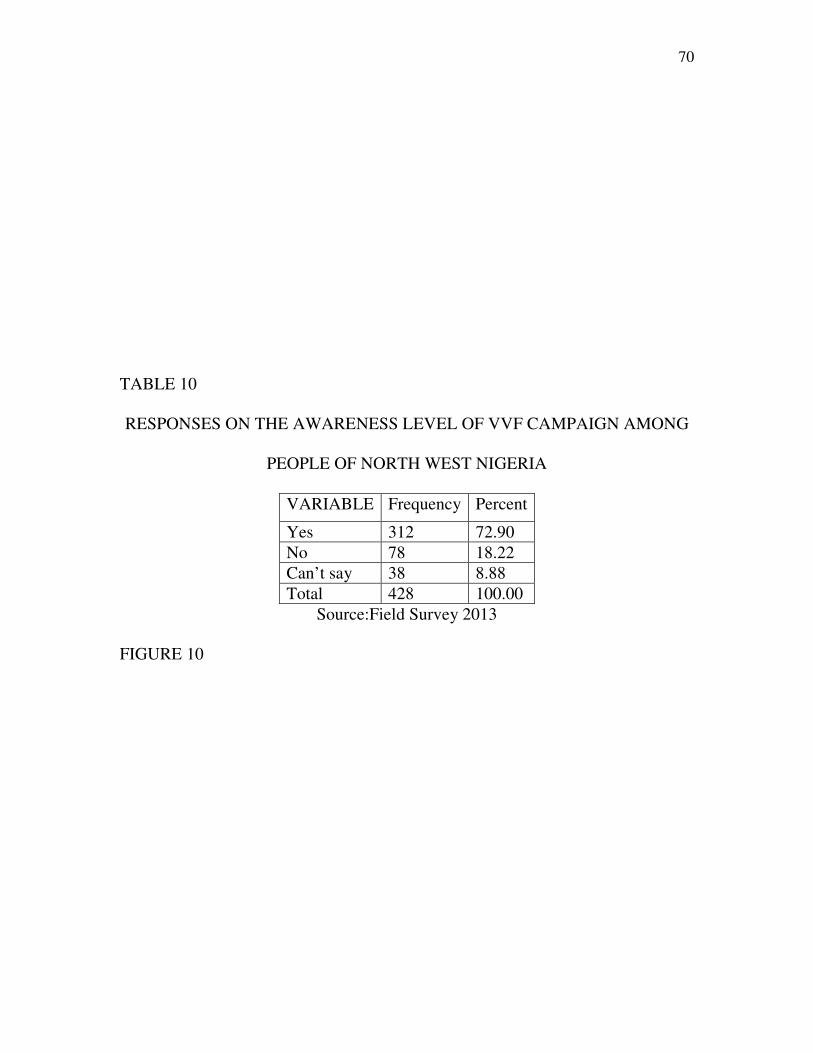
70
TABLE 10
RESPONSES ON THE AWARENESS LEVEL OF VVF CAMPAIGN AMONG
PEOPLE OF NORTH WEST NIGERIA
VARIABLE Frequency Percent
Yes 312 72.90
No 78 18.22
Can’t say 38 8.88
Total 428 100.00
Source:Field Survey 2013
FIGURE 10
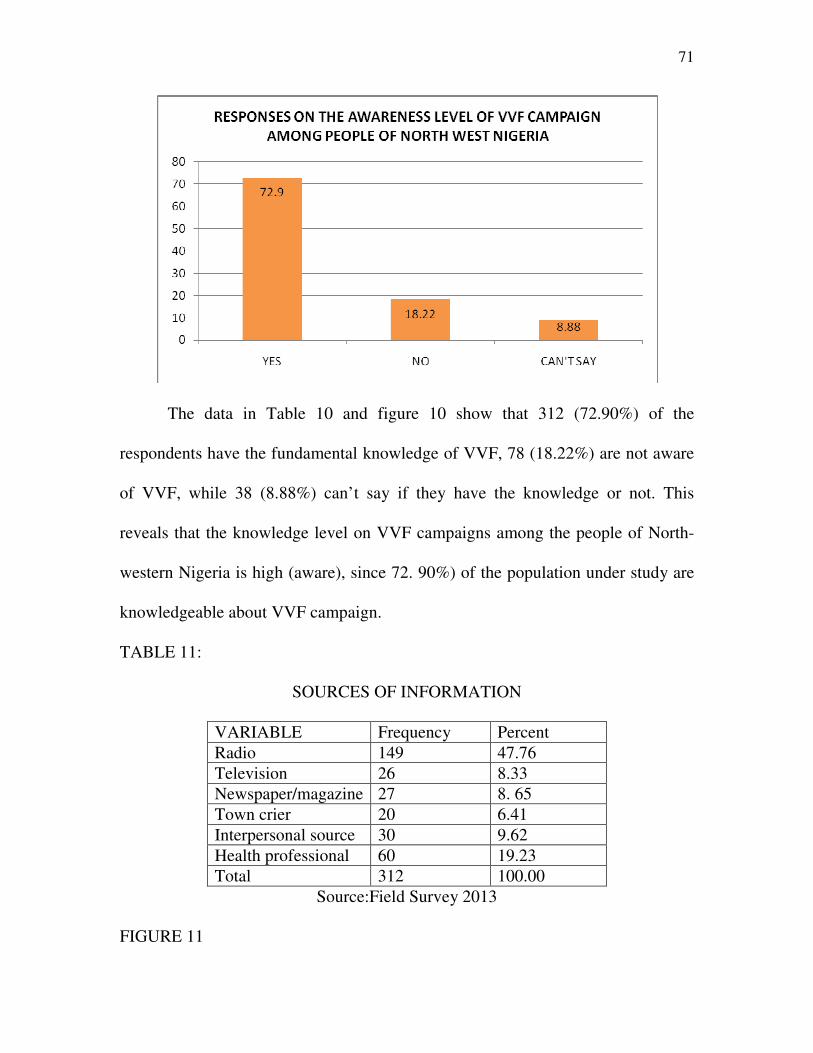
71
The data in Table 10 and figure 10 show that 312 (72.90%) of the
respondents have the fundamental knowledge of VVF, 78 (18.22%) are not aware
of VVF, while 38 (8.88%) can’t say if they have the knowledge or not. This
reveals that the knowledge level on VVF campaigns among the people of North-
western Nigeria is high (aware), since 72. 90%) of the population under study are
knowledgeable about VVF campaign.
TABLE 11:
SOURCES OF INFORMATION
VARIABLE Frequency Percent
Radio 149 47.76
Television 26 8.33
Newspaper/magazine 27 8. 65
Town crier 20 6.41
Interpersonal source 30 9.62
Health professional 60 19.23
Total 312 100.00
Source:Field Survey 2013
FIGURE 11
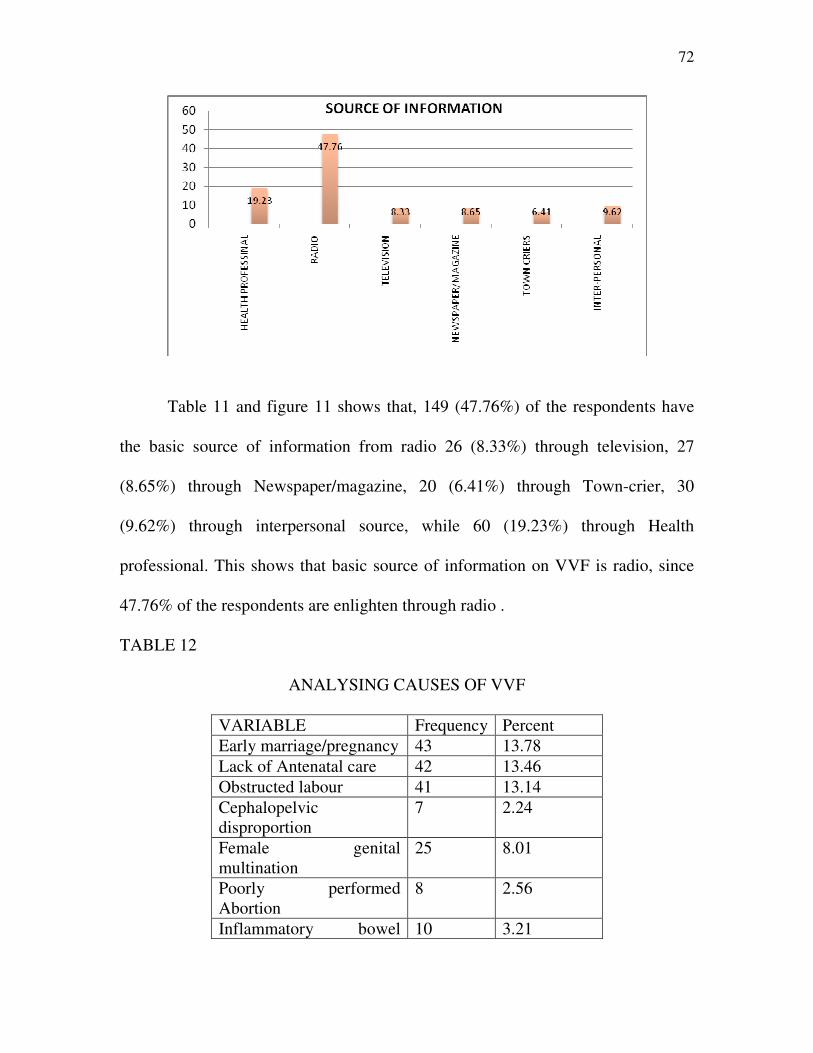
72
Table 11 and figure 11 shows that, 149 (47.76%) of the respondents have
the basic source of information from radio 26 (8.33%) through television, 27
(8.65%) through Newspaper/magazine, 20 (6.41%) through Town-crier, 30
(9.62%) through interpersonal source, while 60 (19.23%) through Health
professional. This shows that basic source of information on VVF is radio, since
47.76% of the respondents are enlighten through radio .
TABLE 12
ANALYSING CAUSES OF VVF
VARIABLE Frequency Percent
Early marriage/pregnancy 43 13.78
Lack of Antenatal care 42 13.46
Obstructed labour 41 13.14
Cephalopelvic
disproportion
7 2.24
Female genital
multination
25 8.01
Poorly performed
Abortion
8 2.56
Inflammatory bowel 10 3.21
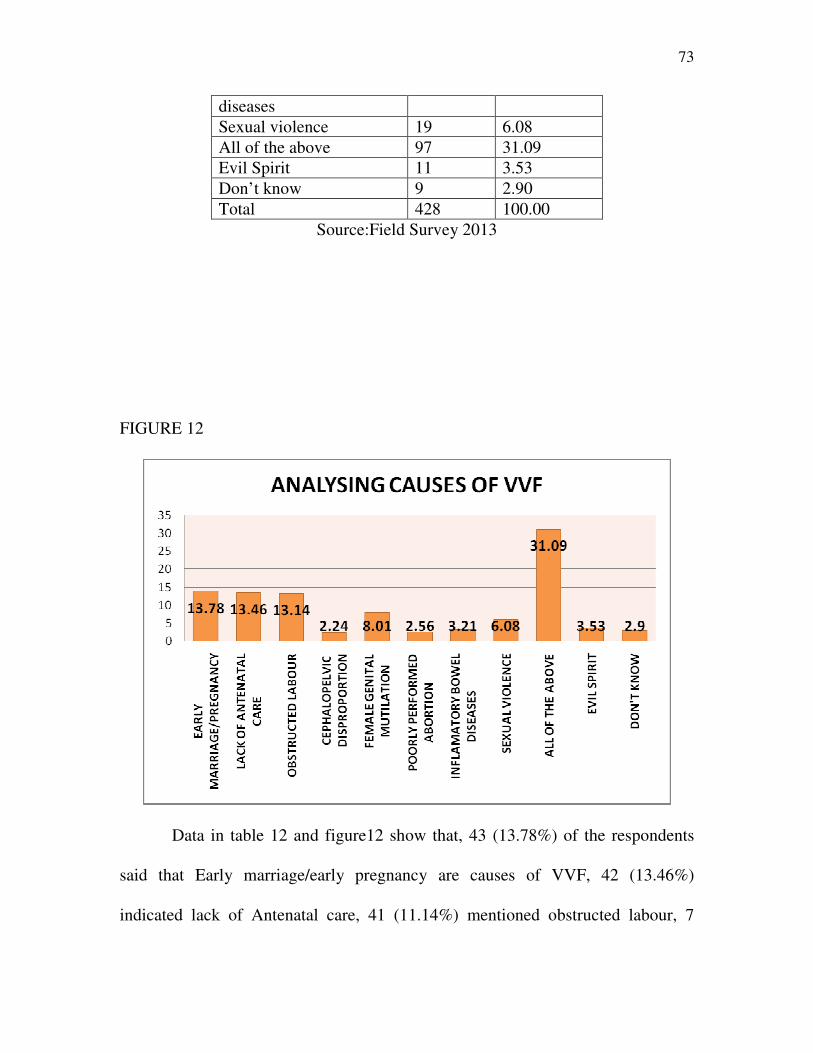
73
diseases
Sexual violence 19 6.08
All of the above 97 31.09
Evil Spirit 11 3.53
Don’t know 9 2.90
Total 428 100.00
Source:Field Survey 2013
FIGURE 12
Data in table 12 and figure12 show that, 43 (13.78%) of the respondents
said that Early marriage/early pregnancy are causes of VVF, 42 (13.46%)
indicated lack of Antenatal care, 41 (11.14%) mentioned obstructed labour, 7
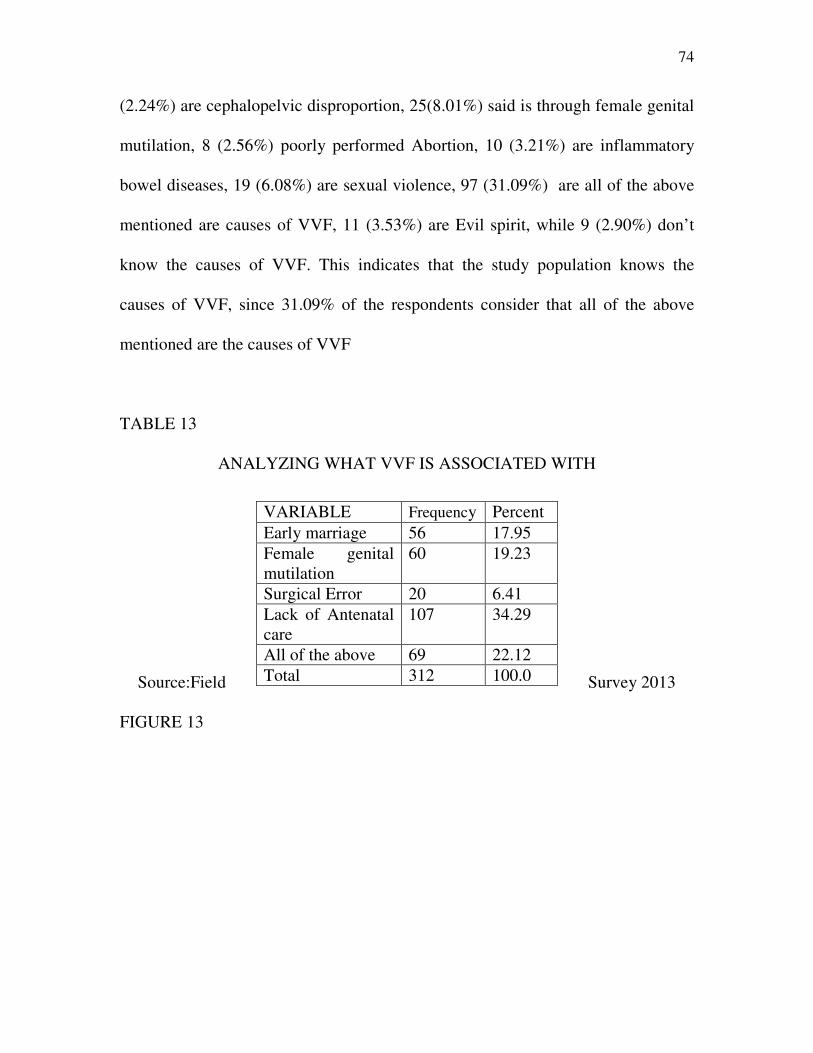
74
(2.24%) are cephalopelvic disproportion, 25(8.01%) said is through female genital
mutilation, 8 (2.56%) poorly performed Abortion, 10 (3.21%) are inflammatory
bowel diseases, 19 (6.08%) are sexual violence, 97 (31.09%) are all of the above
mentioned are causes of VVF, 11 (3.53%) are Evil spirit, while 9 (2.90%) don’t
know the causes of VVF. This indicates that the study population knows the
causes of VVF, since 31.09% of the respondents consider that all of the above
mentioned are the causes of VVF
TABLE 13
ANALYZING WHAT VVF IS ASSOCIATED WITH
Source:Field Survey 2013
FIGURE 13
VARIABLE Frequency Percent
Early marriage 56 17.95
Female genital
mutilation
60 19.23
Surgical Error 20 6.41
Lack of Antenatal
care
107 34.29
All of the above 69 22.12
Total 312 100.0
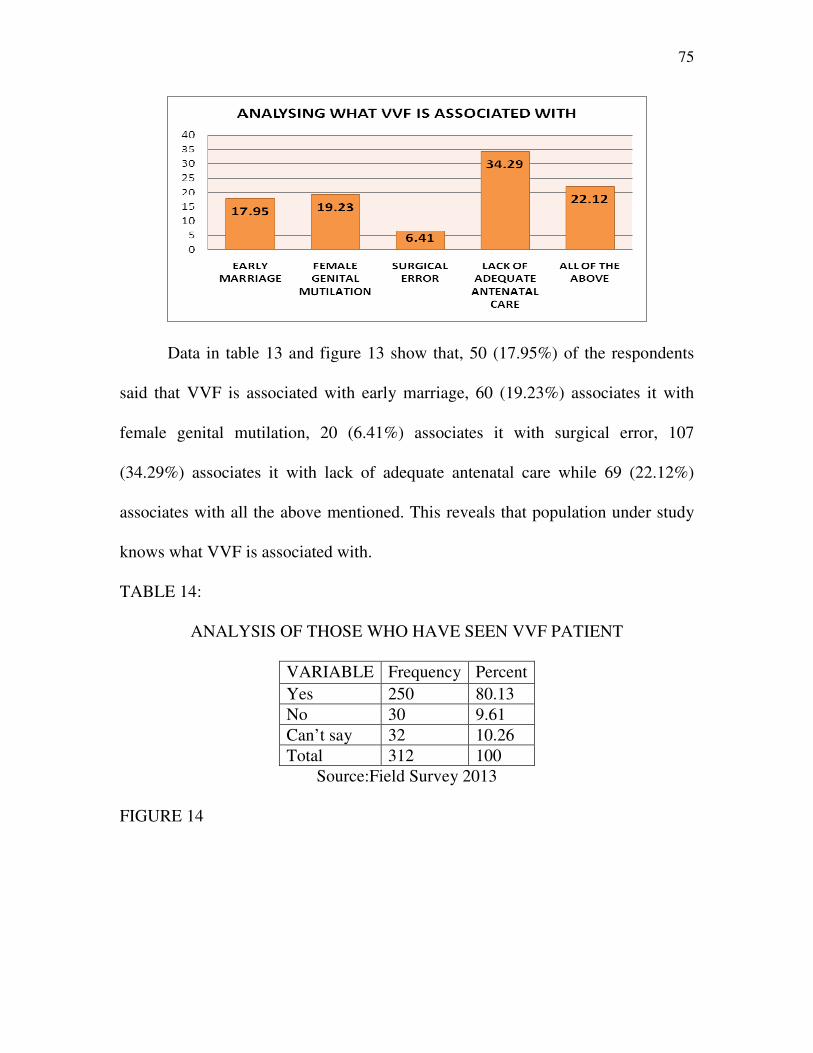
75
Data in table 13 and figure 13 show that, 50 (17.95%) of the respondents
said that VVF is associated with early marriage, 60 (19.23%) associates it with
female genital mutilation, 20 (6.41%) associates it with surgical error, 107
(34.29%) associates it with lack of adequate antenatal care while 69 (22.12%)
associates with all the above mentioned. This reveals that population under study
knows what VVF is associated with.
TABLE 14:
ANALYSIS OF THOSE WHO HAVE SEEN VVF PATIENT
VARIABLE Frequency Percent
Yes 250 80.13
No 30 9.61
Can’t say 32 10.26
Total 312 100
Source:Field Survey 2013
FIGURE 14
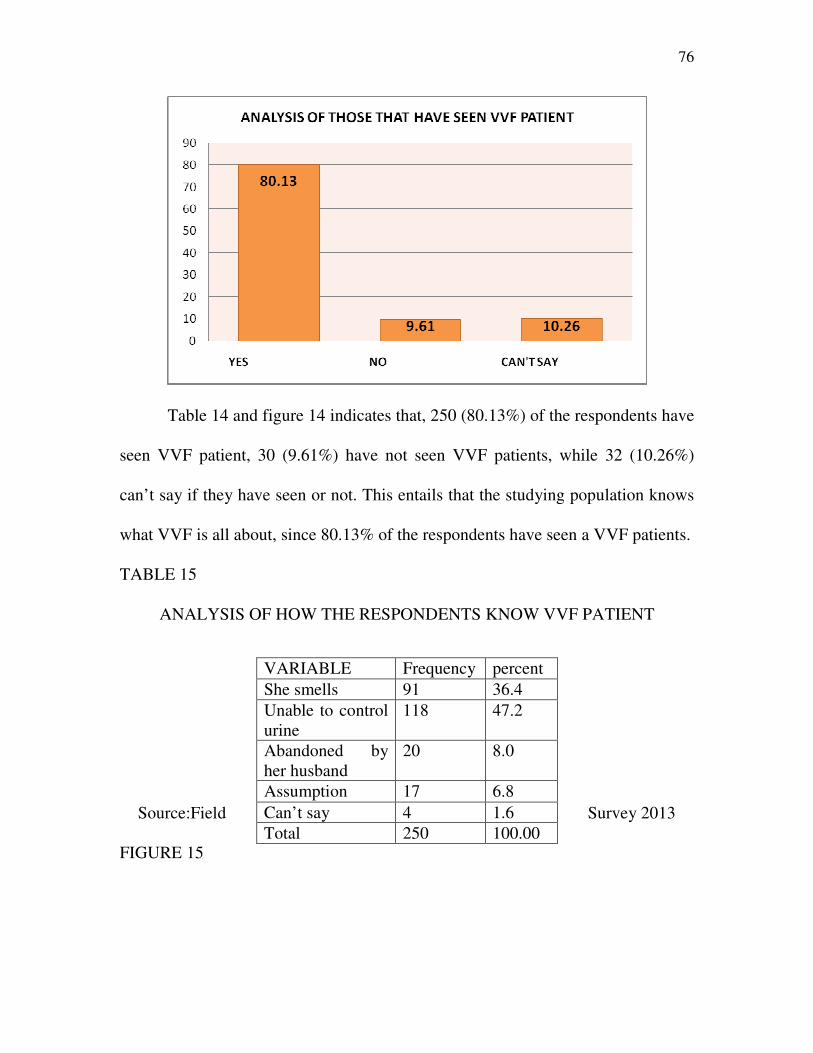
76
Table 14 and figure 14 indicates that, 250 (80.13%) of the respondents have
seen VVF patient, 30 (9.61%) have not seen VVF patients, while 32 (10.26%)
can’t say if they have seen or not. This entails that the studying population knows
what VVF is all about, since 80.13% of the respondents have seen a VVF patients.
TABLE 15
ANALYSIS OF HOW THE RESPONDENTS KNOW VVF PATIENT
Source:Field Survey 2013
FIGURE 15
VARIABLE Frequency percent
She smells 91 36.4
Unable to control
urine
118 47.2
Abandoned by
her husband
20 8.0
Assumption 17 6.8
Can’t say 4 1.6
Total 250 100.00
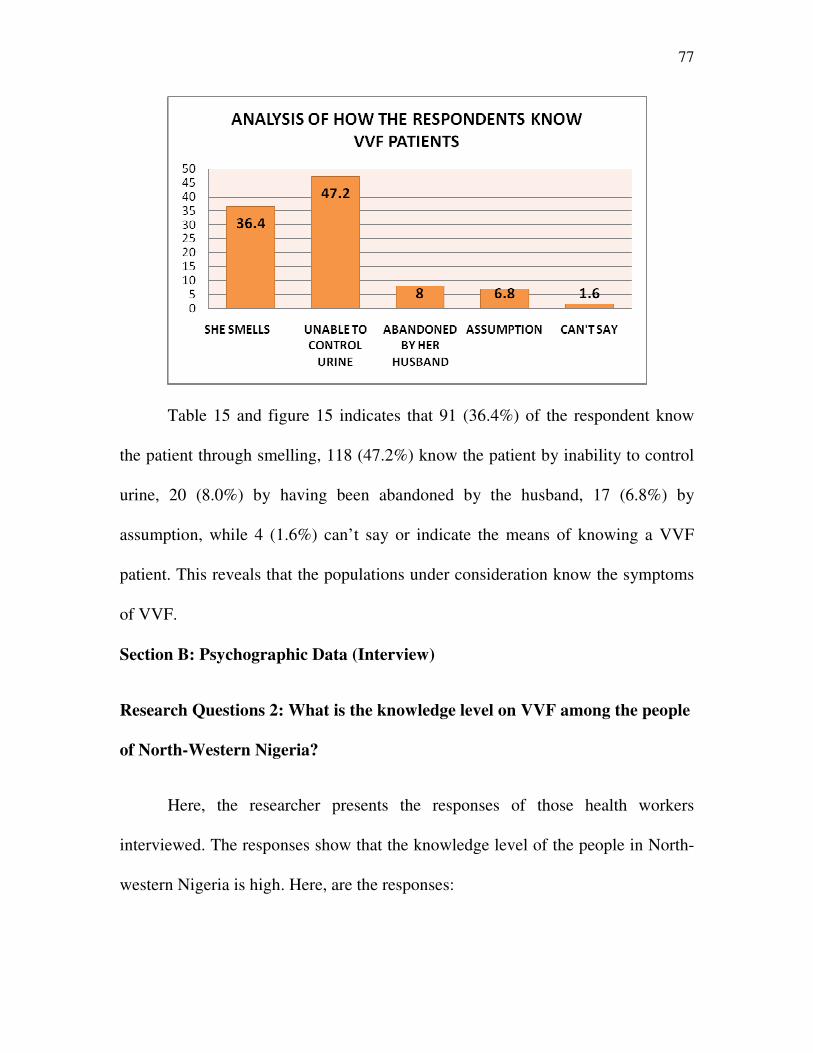
77
Table 15 and figure 15 indicates that 91 (36.4%) of the respondent know
the patient through smelling, 118 (47.2%) know the patient by inability to control
urine, 20 (8.0%) by having been abandoned by the husband, 17 (6.8%) by
assumption, while 4 (1.6%) can’t say or indicate the means of knowing a VVF
patient. This reveals that the populations under consideration know the symptoms
of VVF.
Section B: Psychographic Data (Interview)
Research Questions 2: What is the knowledge level on VVF among the people
of North-Western Nigeria?
Here, the researcher presents the responses of those health workers
interviewed. The responses show that the knowledge level of the people in North-
western Nigeria is high. Here, are the responses:
78
Respondent A: To say that the people in this region have no knowledge of VVF
will be unfair. They know what VVF is all about, although not to a very large
extent, but the cause and how to avoid this is known by the people. The campaigns
on VVF have been an eye opener to them. Most of them no longer patronise local
health services again.
Respondent B: I will not be wrong to say the knowledge level is slightly above
average. The knowledge level is high, let say 55 percent.
Respondent C: Initially, their knowledge level is low because they lack access to
obstetric care facilities but now the facilities are there as you can see, the
government has helped in providing this facilities and couple with the campaign
on VVF, all these have increased their knowledge level of the disease.
Respondent D: Well, their knowledge level has increased. We now have more
patients coming for treatment and child birth, unlike before where most of them
prefer traditional birth attendants.
Respondent E: What I know is that they are aware of the disease, but as for the
knowledge level, that one I can’t say if it has increased or not.
Respondent F: I think their knowledge level has grown. In the past early marriage
was common, infant mortality rate was high and death as a result of child delivery
was also high, but since this VVF campaign came up, the community no longer
79
record high rate of child death and maternal mortality rate has dropped
significantly. In a nutshell, the knowledge is there.
Section C: Psychographic Data (Observation)
In regards to the people’s knowledge level, the researcher observed that the
women in these states attend antenatal classes. In one of the communities in Kano
State, the researcher saw a man reminding the wife of her antenatal class. In
Jigawa state, the researcher observed that VVF patients were kept in a separate
place in the community. The researcher observed that after every three days the
isolated patients were moved to the nearest VVF centres in the state. That is to say
they know the symptoms of this disease based on their knowledge of it.
Research Question 3: what is the major source of information on Vesico
Vaginal Fistula among people of North West Nigeria?
Items in table and figure 16 were used to answer research question three.
TABLE 16:
RESPONSES ON THE MAJOR SOURCE OF INFORMATION ON VVF
VARIABLE Frequency Percent
Radio 101 32.372
Television 40 12.820
Newspaper/magazine 30 9.615
Internet 25 8.012
Interpersonal source 47 15.064
Bill Board 7 2.245
Seminar/workshop 62 19.872
Total 312 100.00
Source:Field Survey 2013
FIGURE 16
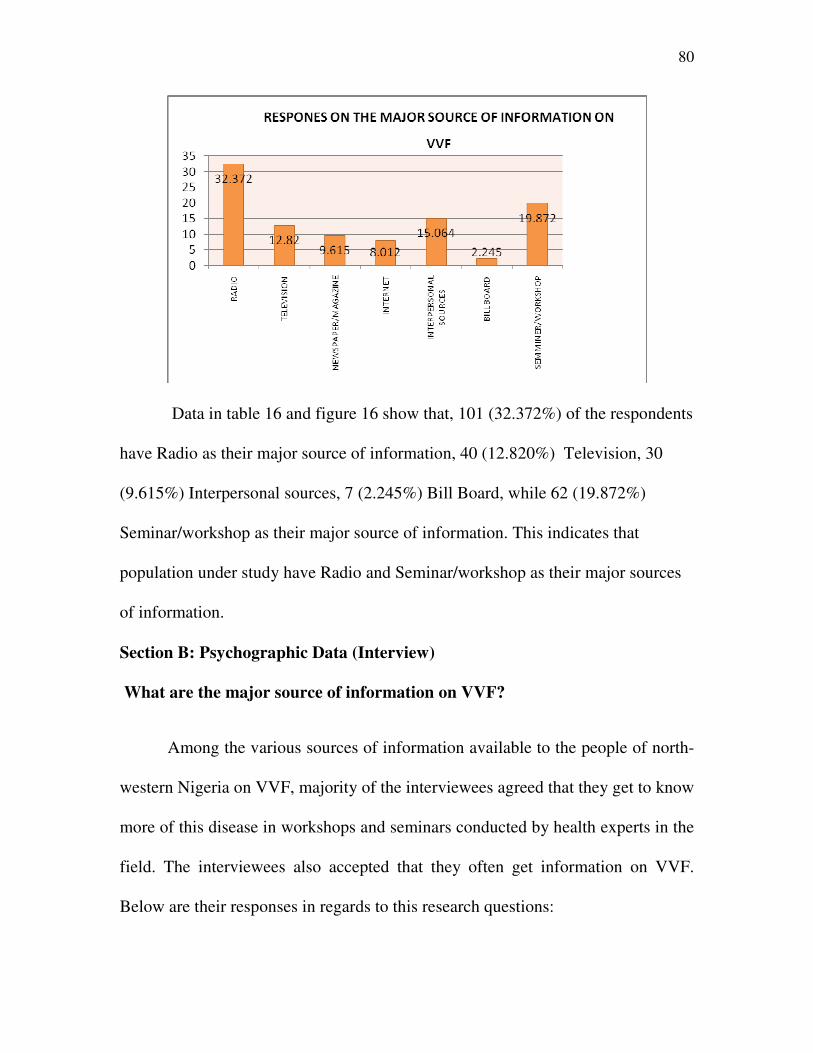
80
Data in table 16 and figure 16 show that, 101 (32.372%) of the respondents
have Radio as their major source of information, 40 (12.820%) Television, 30
(9.615%) Interpersonal sources, 7 (2.245%) Bill Board, while 62 (19.872%)
Seminar/workshop as their major source of information. This indicates that
population under study have Radio and Seminar/workshop as their major sources
of information.
Section B: Psychographic Data (Interview)
What are the major source of information on VVF?
Among the various sources of information available to the people of north-
western Nigeria on VVF, majority of the interviewees agreed that they get to know
more of this disease in workshops and seminars conducted by health experts in the
field. The interviewees also accepted that they often get information on VVF.
Below are their responses in regards to this research questions:
81
Respondent A: Seminars, workshops and conferences organized by experts serves
as the main source of information on VVF. Although there are other sources such
as health journals but the most effective and more interactive one are the seminars
and workshops organized in the community by VVF experts. They often organize
it.
Respondent B: I think, seminars form the major source of information in this area
when it comes to VVF issues.
Respondent C: There are various sources, I can’t say which is the major source,
what I know is that more than one source of information is used here.
Respondent D: It is obvious that workshops and seminars are the primary source
of information used in the dissemination of information on VVF. Virtually every
month seminars and workshops are organized on VVF.
Respondent E: I will not say internet is the major source here unlike developed
cities and nations, also newspapers are not because we hardly get papers here and
very few will sacrifice their money for it, in short radio is the main source of
dissemination of VVF messages.
Respondent F: The main source of information I think is community town crier.
This is because the town crier informs the people of latest development on VVF.
Whenever there is a need for meetings, etc, we the health workers tell the town
crier to announce it to the people.
82
Section C: Psychographic Data (Observation)
The researcher observed that majority of the people in this states have
portable radio. Most often information was aired in Hausa language. The
knowledge of the language (Hausa) was an added advantage to the researcher as
most of the information aired on VVF was centred on creating awareness,
preventive methods, symptoms and available facilities for victims. The researcher
also witnessed two seminars/workshops on VVF. The first was in Dambatta (Kano
state), two days after his arrival and the last was in Koko (Kebbi State). The
seminars were mainly on sensitizing the people on VVF.
Research Questions 4: What are the challenges associated with the use of the
media in campaigns against VVF?
The researcher used only interview to address this question. The reason for
this was stated earlier in chapter three. The followings are extracts from the
interview conducted:
Respondent A: There are no challenges as such. In fact the media has been of
tremendous benefits to the awareness campaigns.
Respondent B: One of the major challenges confronting us here is language,
although Hausa language is understood by majority but there are other dialects
that the awareness campaigns failed to communicate with.
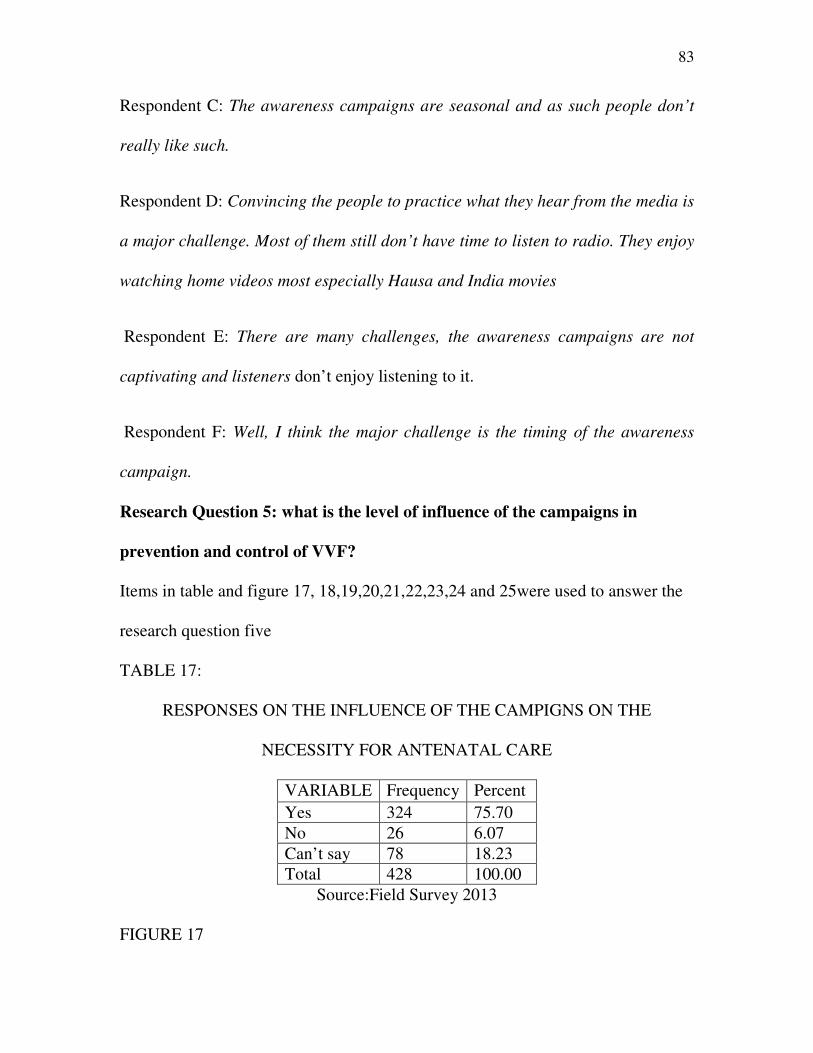
83
Respondent C: The awareness campaigns are seasonal and as such people don’t
really like such.
Respondent D: Convincing the people to practice what they hear from the media is
a major challenge. Most of them still don’t have time to listen to radio. They enjoy
watching home videos most especially Hausa and India movies
Respondent E: There are many challenges, the awareness campaigns are not
captivating and listeners don’t enjoy listening to it.
Respondent F: Well, I think the major challenge is the timing of the awareness
campaign.
Research Question 5: what is the level of influence of the campaigns in
prevention and control of VVF?
Items in table and figure 17, 18,19,20,21,22,23,24 and 25were used to answer the
research question five
TABLE 17:
RESPONSES ON THE INFLUENCE OF THE CAMPIGNS ON THE
NECESSITY FOR ANTENATAL CARE
VARIABLE Frequency Percent
Yes 324 75.70
No 26 6.07
Can’t say 78 18.23
Total 428 100.00
Source:Field Survey 2013
FIGURE 17
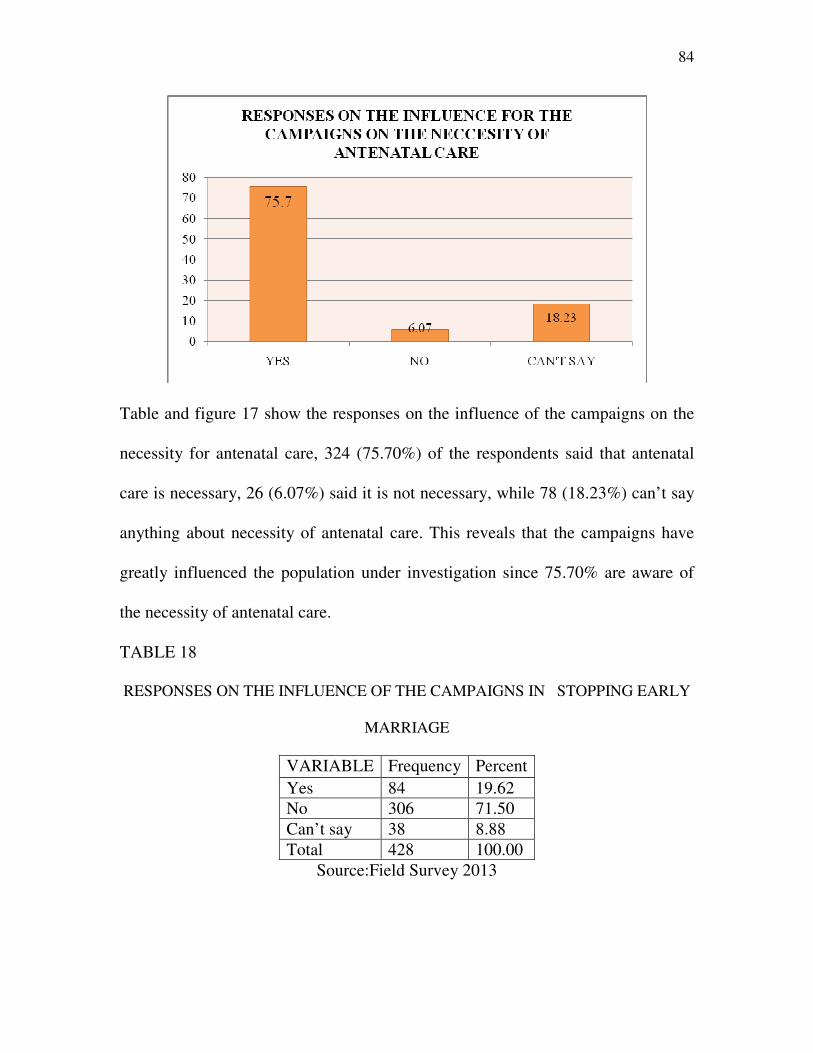
84
Table and figure 17 show the responses on the influence of the campaigns on the
necessity for antenatal care, 324 (75.70%) of the respondents said that antenatal
care is necessary, 26 (6.07%) said it is not necessary, while 78 (18.23%) can’t say
anything about necessity of antenatal care. This reveals that the campaigns have
greatly influenced the population under investigation since 75.70% are aware of
the necessity of antenatal care.
TABLE 18
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS IN STOPPING EARLY
MARRIAGE
VARIABLE Frequency Percent
Yes 84 19.62
No 306 71.50
Can’t say 38 8.88
Total 428 100.00
Source:Field Survey 2013
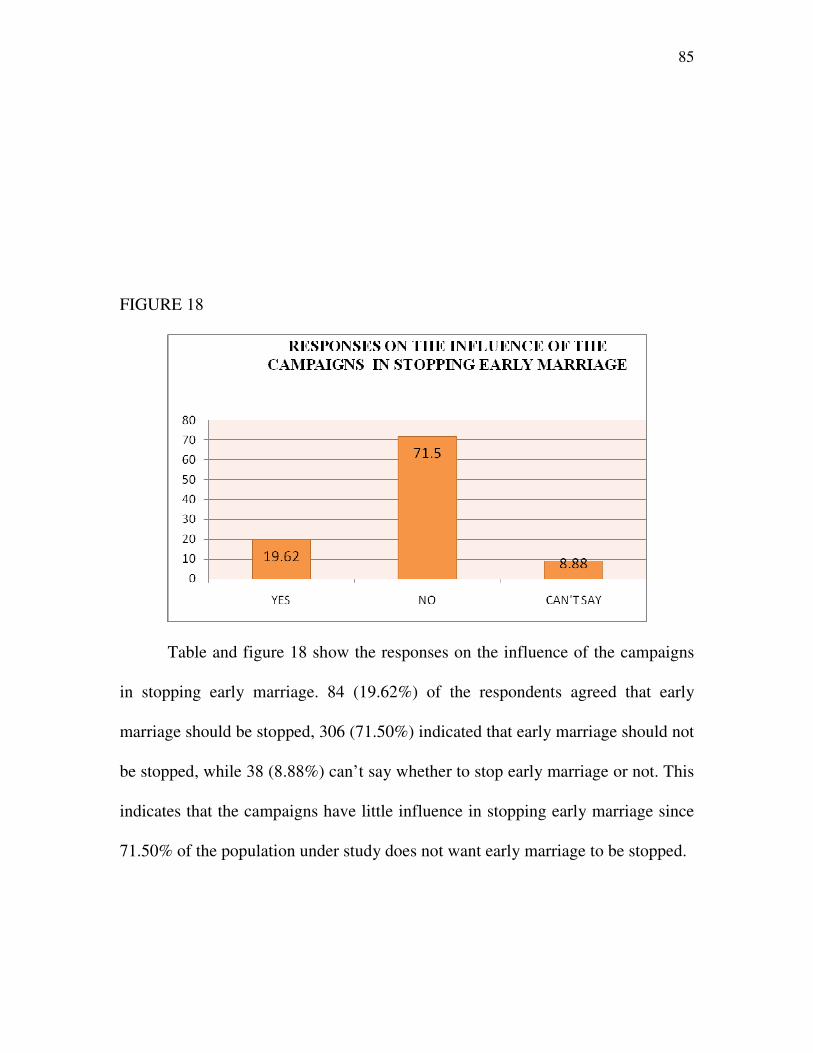
85
FIGURE 18
Table and figure 18 show the responses on the influence of the campaigns
in stopping early marriage. 84 (19.62%) of the respondents agreed that early
marriage should be stopped, 306 (71.50%) indicated that early marriage should not
be stopped, while 38 (8.88%) can’t say whether to stop early marriage or not. This
indicates that the campaigns have little influence in stopping early marriage since
71.50% of the population under study does not want early marriage to be stopped.
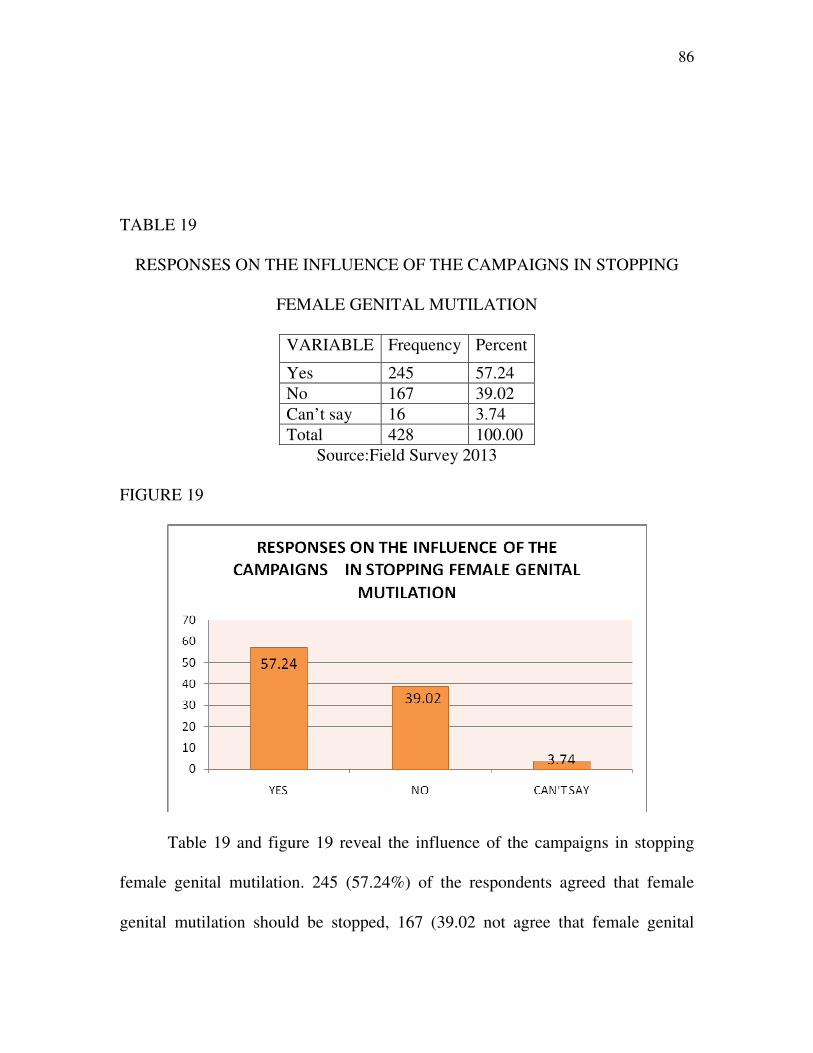
86
TABLE 19
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS IN STOPPING
FEMALE GENITAL MUTILATION
VARIABLE Frequency Percent
Yes 245 57.24
No 167 39.02
Can’t say 16 3.74
Total 428 100.00
Source:Field Survey 2013
FIGURE 19
Table 19 and figure 19 reveal the influence of the campaigns in stopping
female genital mutilation. 245 (57.24%) of the respondents agreed that female
genital mutilation should be stopped, 167 (39.02 not agree that female genital
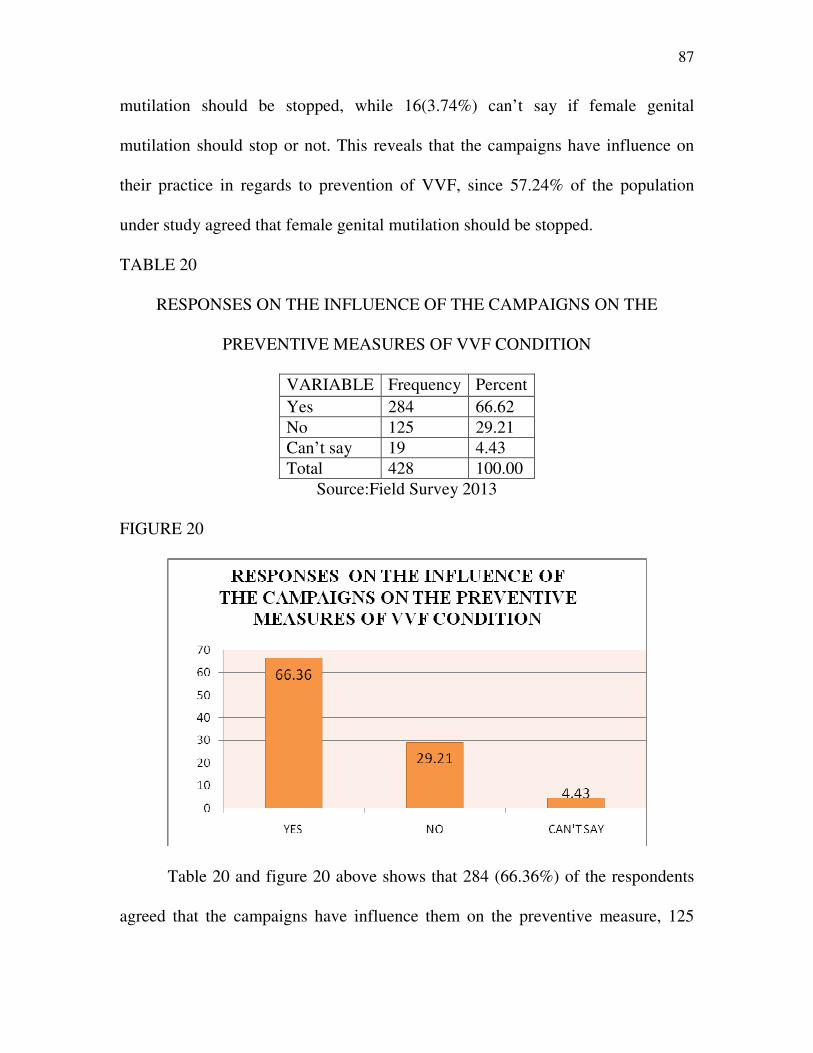
87
mutilation should be stopped, while 16(3.74%) can’t say if female genital
mutilation should stop or not. This reveals that the campaigns have influence on
their practice in regards to prevention of VVF, since 57.24% of the population
under study agreed that female genital mutilation should be stopped.
TABLE 20
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS ON THE
PREVENTIVE MEASURES OF VVF CONDITION
VARIABLE Frequency Percent
Yes 284 66.62
No 125 29.21
Can’t say 19 4.43
Total 428 100.00
Source:Field Survey 2013
FIGURE 20
Table 20 and figure 20 above shows that 284 (66.36%) of the respondents
agreed that the campaigns have influence them on the preventive measure, 125
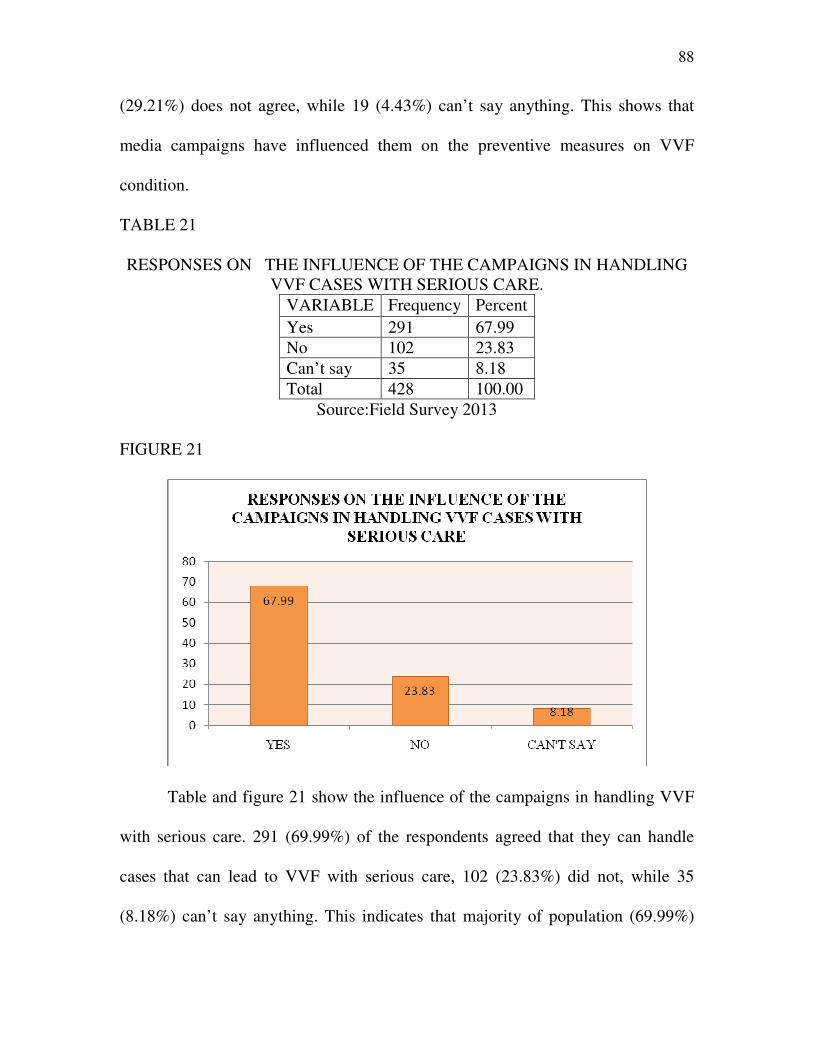
88
(29.21%) does not agree, while 19 (4.43%) can’t say anything. This shows that
media campaigns have influenced them on the preventive measures on VVF
condition.
TABLE 21
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS IN HANDLING
VVF CASES WITH SERIOUS CARE.
VARIABLE Frequency Percent
Yes 291 67.99
No 102 23.83
Can’t say 35 8.18
Total 428 100.00
Source:Field Survey 2013
FIGURE 21
Table and figure 21 show the influence of the campaigns in handling VVF
with serious care. 291 (69.99%) of the respondents agreed that they can handle
cases that can lead to VVF with serious care, 102 (23.83%) did not, while 35
(8.18%) can’t say anything. This indicates that majority of population (69.99%)
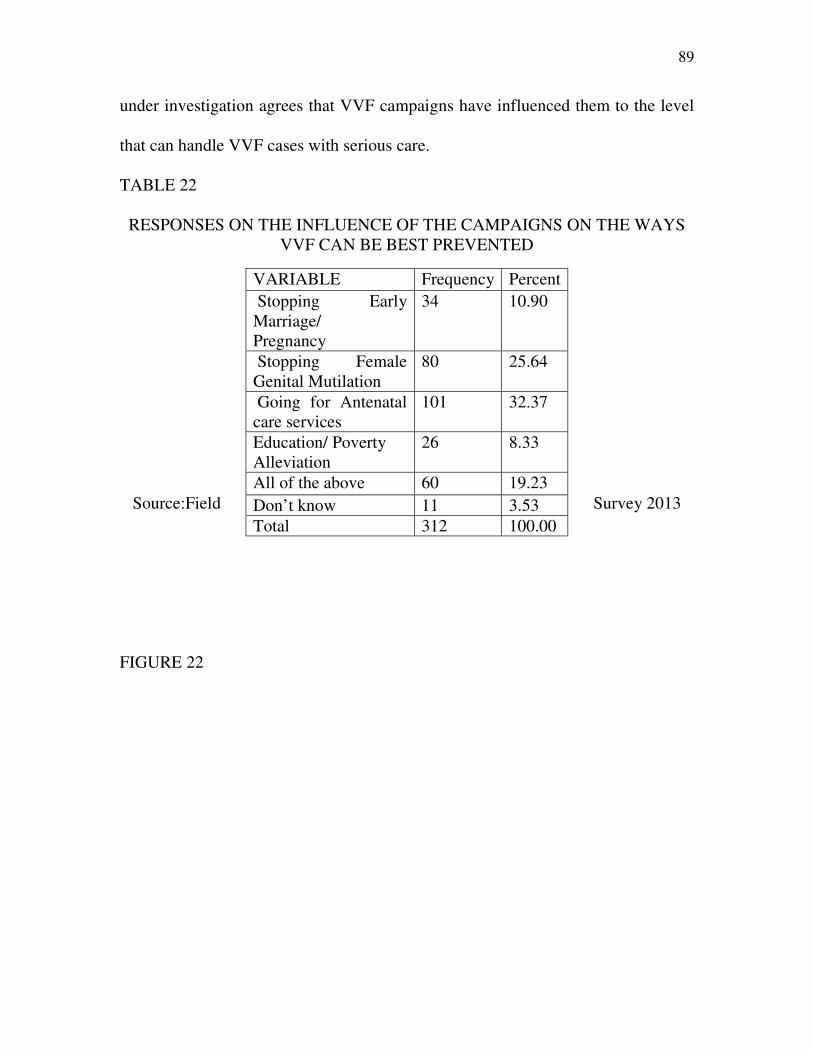
89
under investigation agrees that VVF campaigns have influenced them to the level
that can handle VVF cases with serious care.
TABLE 22
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS ON THE WAYS
VVF CAN BE BEST PREVENTED
Source:Field Survey 2013
FIGURE 22
VARIABLE Frequency Percent
Stopping Early
Marriage/
Pregnancy
34 10.90
Stopping Female
Genital Mutilation
80 25.64
Going for Antenatal
care services
101 32.37
Education/ Poverty
Alleviation
26 8.33
All of the above 60 19.23
Don’t know 11 3.53
Total 312 100.00
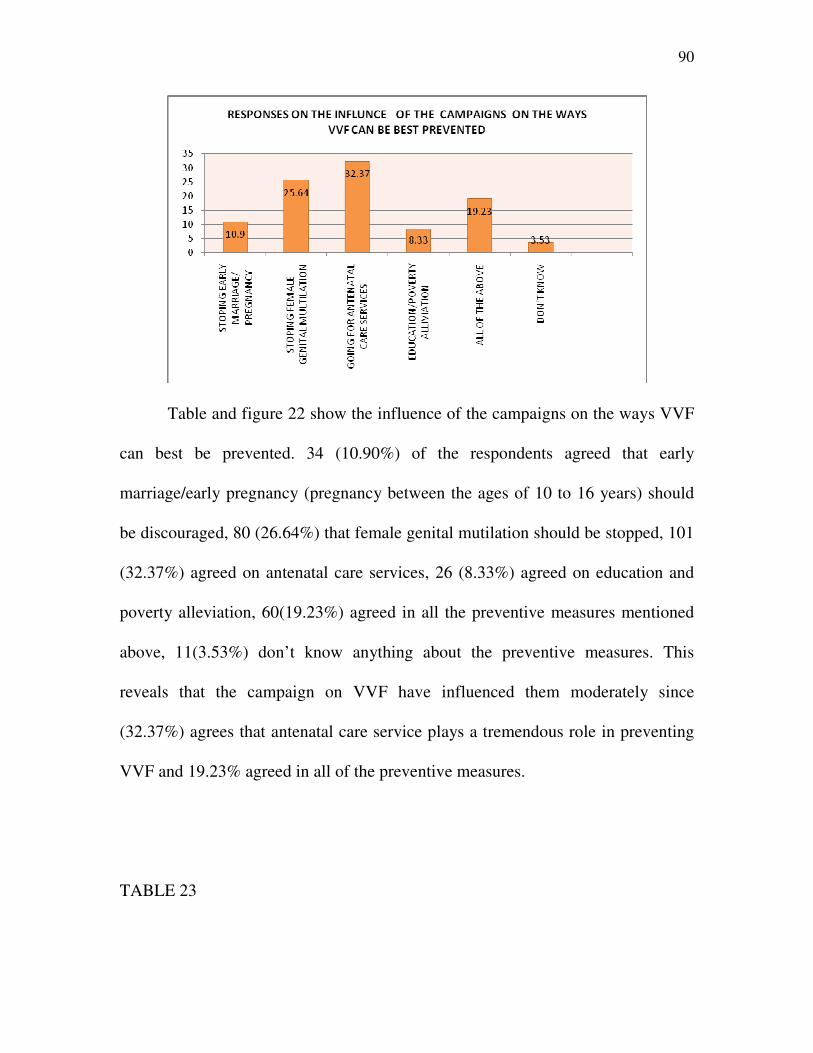
90
Table and figure 22 show the influence of the campaigns on the ways VVF
can best be prevented. 34 (10.90%) of the respondents agreed that early
marriage/early pregnancy (pregnancy between the ages of 10 to 16 years) should
be discouraged, 80 (26.64%) that female genital mutilation should be stopped, 101
(32.37%) agreed on antenatal care services, 26 (8.33%) agreed on education and
poverty alleviation, 60(19.23%) agreed in all the preventive measures mentioned
above, 11(3.53%) don’t know anything about the preventive measures. This
reveals that the campaign on VVF have influenced them moderately since
(32.37%) agrees that antenatal care service plays a tremendous role in preventing
VVF and 19.23% agreed in all of the preventive measures.
TABLE 23
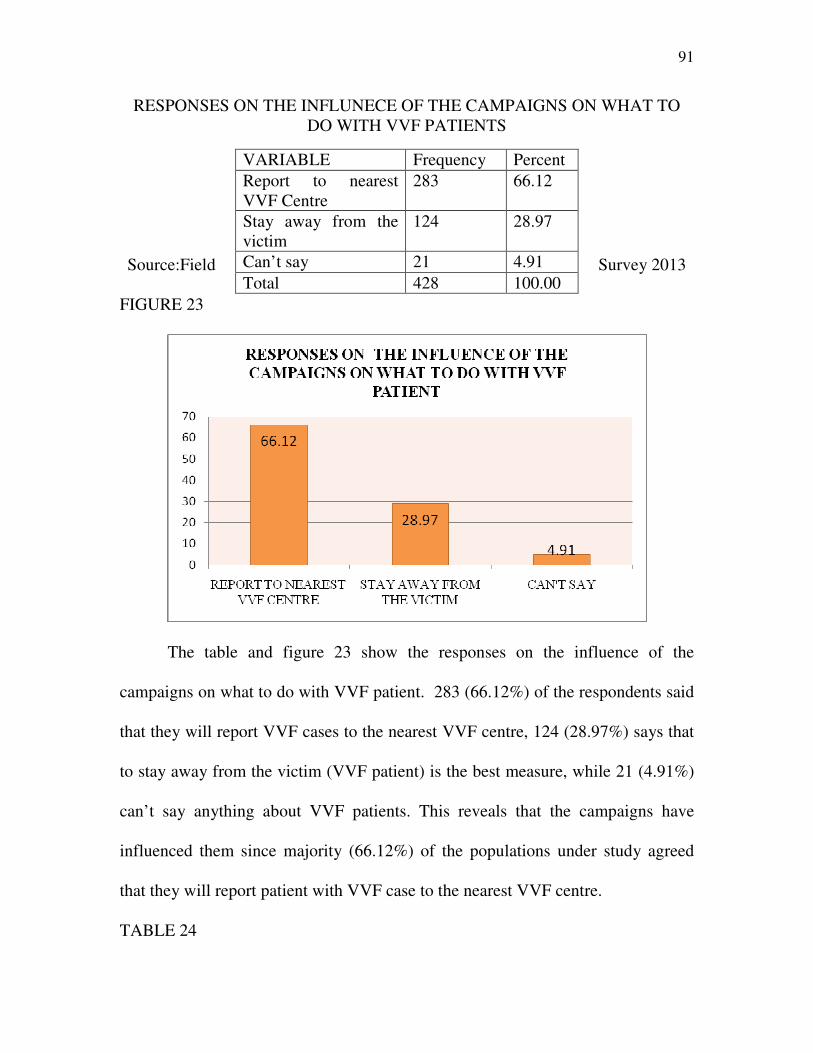
91
RESPONSES ON THE INFLUNECE OF THE CAMPAIGNS ON WHAT TO
DO WITH VVF PATIENTS
Source:Field Survey 2013
FIGURE 23
The table and figure 23 show the responses on the influence of the
campaigns on what to do with VVF patient. 283 (66.12%) of the respondents said
that they will report VVF cases to the nearest VVF centre, 124 (28.97%) says that
to stay away from the victim (VVF patient) is the best measure, while 21 (4.91%)
can’t say anything about VVF patients. This reveals that the campaigns have
influenced them since majority (66.12%) of the populations under study agreed
that they will report patient with VVF case to the nearest VVF centre.
TABLE 24
VARIABLE Frequency Percent
Report to nearest
VVF Centre
283 66.12
Stay away from the
victim
124 28.97
Can’t say 21 4.91
Total 428 100.00
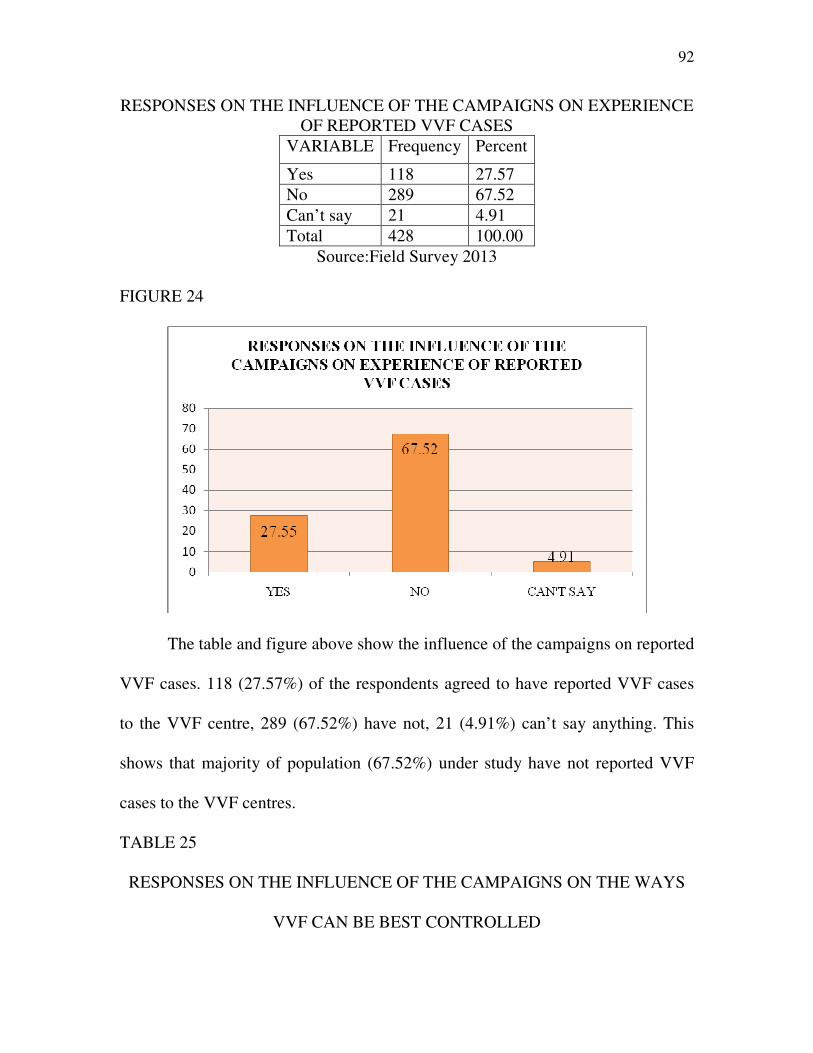
92
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS ON EXPERIENCE
OF REPORTED VVF CASES
VARIABLE Frequency Percent
Yes 118 27.57
No 289 67.52
Can’t say 21 4.91
Total 428 100.00
Source:Field Survey 2013
FIGURE 24
The table and figure above show the influence of the campaigns on reported
VVF cases. 118 (27.57%) of the respondents agreed to have reported VVF cases
to the VVF centre, 289 (67.52%) have not, 21 (4.91%) can’t say anything. This
shows that majority of population (67.52%) under study have not reported VVF
cases to the VVF centres.
TABLE 25
RESPONSES ON THE INFLUENCE OF THE CAMPAIGNS ON THE WAYS
VVF CAN BE BEST CONTROLLED
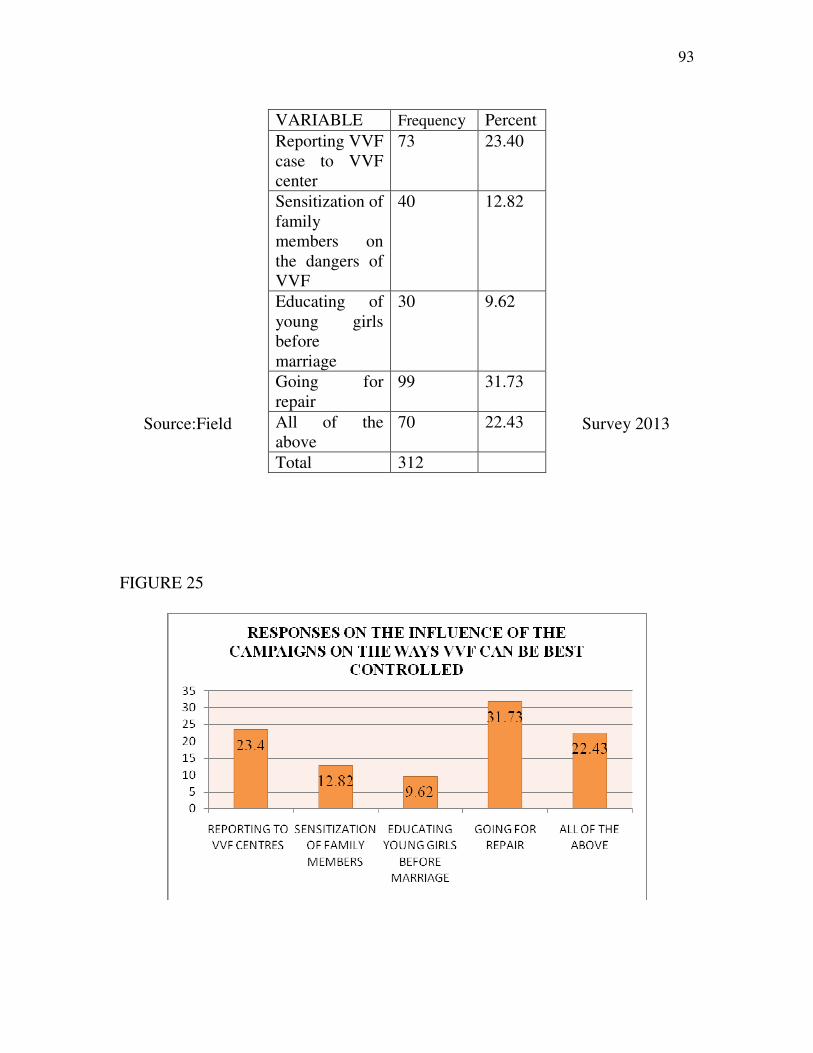
93
Source:Field Survey 2013
FIGURE 25
VARIABLE Frequency Percent
Reporting VVF
case to VVF
center
73 23.40
Sensitization of
family
members on
the dangers of
VVF
40 12.82
Educating of
young girls
before
marriage
30 9.62
Going for
repair
99 31.73
All of the
above
70 22.43
Total 312
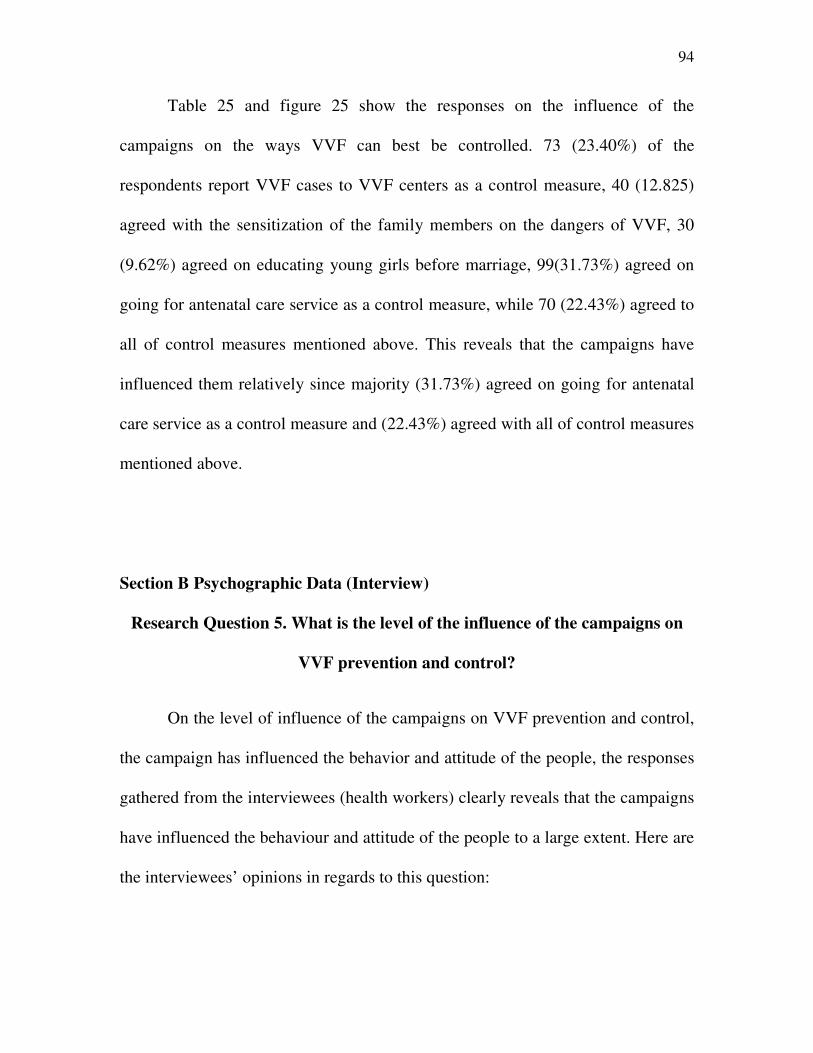
94
Table 25 and figure 25 show the responses on the influence of the
campaigns on the ways VVF can best be controlled. 73 (23.40%) of the
respondents report VVF cases to VVF centers as a control measure, 40 (12.825)
agreed with the sensitization of the family members on the dangers of VVF, 30
(9.62%) agreed on educating young girls before marriage, 99(31.73%) agreed on
going for antenatal care service as a control measure, while 70 (22.43%) agreed to
all of control measures mentioned above. This reveals that the campaigns have
influenced them relatively since majority (31.73%) agreed on going for antenatal
care service as a control measure and (22.43%) agreed with all of control measures
mentioned above.
Section B Psychographic Data (Interview)
Research Question 5. What is the level of the influence of the campaigns on
VVF prevention and control?
On the level of influence of the campaigns on VVF prevention and control,
the campaign has influenced the behavior and attitude of the people, the responses
gathered from the interviewees (health workers) clearly reveals that the campaigns
have influenced the behaviour and attitude of the people to a large extent. Here are
the interviewees’ opinions in regards to this question:
95
Respondent A: The campaign has influenced the behaviour and attitude of the
people here. We have little records of those who deliver at home.
Respondent B: Well, it has influenced their behaviour; most of them no longer
encourage traditional child birth delivery. Their behavior has changed as they all
want their children to benefit from the modern facilities we have here.
Respondent C: It has influenced their behaviour but not to a large extent. Why
because early marriage and pregnancy is still practiced everywhere especially
here in the village. But there is high attendance of antenatal classes.
Respondent D: the campaign influenced them to a great extent, majority do not
practice female genital mutilation.
Respondent E: Yes, it has. They now know that VVF is treatable, if you walk down
you will see that we have so many patients more than we can manage. Initially we
have “out reach unit” that goes to the village in search of the victims but now we
have more than we can manage.
Respondent F: The campaigns have changed many things here, it has influenced
them, it has given them more knowledge on the need to patronize modern health
centres, in short, and the campaign has helped a lot.
Section C: Psychographic Data (Observation)
96
The researcher observed that they (the victims) no more visit traditional
birth attendants. He saw a traditional birth attendant complaining for low turnover
in Koko Besse L.G.A. They are now visiting modern medical centre. They now
send young girls to school unlike before. The status of women is increasing; good
numbers of women were seen as practicing nurses, teachers and in other important
area of life. The campaigns have influenced them to the extent that VVF centers
in the states are filled up with VVF patients. Despite the influence of the
campaigns, majority especially in villages still practice early marriage/pregnancy
and female genital mutilation.
4.2 Discussion of Findings
Using the results that emerged from the research an attempt was made to
answer the research questions in chapter one of this work.
RESEARCH QUESTION 1 seeks to know the level of exposure to VVF
campaigns among people of north western Nigeria
This research question was addressed using questionnaire, interview and
observation. Table and figure 8 and 9 were used to answer this question on
exposure. 72.9% agreed in table 8 that they have access to VVF campaigns, while
50% agreed in table 9 that they are always exposed to VVF campaigns. Based on
this, the results indicate that the respondents are exposed to VVF campaigns in the
region, infact, the level of exposure is said to be relatively high. From the
interview section, those interviewed (health workers at VVF centres) also attest to
the result gotten from the administered copies of questionnaires, the observation
97
carried out was not far from the above result as the researcher’s observation shows
that there is a high level of exposure among the people of north-western Nigeria.
This result is in line with Sambo (1994) Vesico Vaginal Fistula (VVF) A vision
realized. She found that VVF campaign has come a long way. In her words “I am
happy to now acknowledge the fact that the country is now fully aware of the
problem afflicting VVF victims” (p.45)
RESEARCH QUESTION 2: The following table and figure 10,11 12, 13,
14, and 15 were used to answer this research question on respondents’ knowledge
level on VVF. The results indicate that, 72.9 % of the respondents know what
VVF is all about, 93.67% know the causes of VVF. The result also reveals that
radio is their major source of information (on the causes of VVF) to the people in
this zone. Also, large number of the respondents agreed that VVF is associated
with all of the followings, early marriage, female genital mutilation, lack of
antenatal care and surgical error. The analysis also shows that, 80.30 % of the
respondents have seen a VVF patient and 47.2% of the respondents accepted that
uncontrollable urine flow is the major symptom of VVF.
Both the interview and the observation carried out were all in-line with the
results obtained from the administered copies of the questionnaire. This means that
their knowledge level is high, and this can be attributed to a large extent, as the
result of the massive campaigns carried out in the region.
The finding here is in consonance with a study done by Akpeji (2012) on
the knowledge of patients who have VVF. Akpeji’s finding revealed that 70 % of
98
the patients knew the causes of VVF; this means that their knowledge level is
high.
RESEARCH QUESTION 3:Table 16 and figure16 were used to seek
answers to the research question on the sources of information to respondents on
VVF. The result findings reveal that 32.372 % of the respondents said they got to
know about VVF through the radio while 19.872 got to know through
workshops/seminars.
On the other hand, three out of the six health workers interviewed said the
major source of information on VVF is seminars and workshops, while the other
three choose between radio and community meetings as their main source. The
observation carried out revealed that radio and seminars/workshops formed the
primary source of information on VVF.
Based on this, the researcher concludes that both radio and
seminars/workshops form the principal sources of information to the people in the
North-Western Nigeria on VVF.
RESAECH QUESTION 4: Only interview was used here. Health workers
were interviewed; they all said there are challenges associated with the use of the
media in the campaign against VVF. Some of the challenges are language, timing
of the awareness campaign and boring awareness programmes.
RESEARCH QUESTION 5: The research question seek to know the level of
influence of the campaigns on VVF prevention and control. Table and figure 17 to
99
25 answered the research question. 75.70% of the respondents agreed that
antenatal care is necessary as a preventive measure in table and figure 17, while
19.62% agreed that early marriage should be stopped in table and figure 18. In the
same direction, 57.24% agreed that female genital mutilation should be stopped in
table and figure19. In table and figure 20, majority (66.36) agreed that the
campaigns have influenced them to the level that they can take preventive
measures. In table and figure 21, majority (67.99%) agreed that they can handle
VVF cases with serious care. In table and figure 22, good number of the
respondents (32.7%) identified going for antenatal care as one of the ways VVF
can be best prevented, while 19.23% identified all the preventive measure
mentioned. 66.12% agreed to report VVF cases to the nearest VVF centre in table
and figure 23. Though in the table and figure 24, majority (67.52%) agreed that
they have never reported VVF cases. 31.73% identified going for repair as one of
the ways VVF can be best controlled in table and figure 25, while 22.43%
identified all of the control measures. The result obtained from the interview and
observation attests to the above. The interview shows that the campaigns have
influenced them (respondents) to the point that they seek modern medical
attention, go for antenatal classes and as well know that VVF is repairable. One of
the interviewees stated that despite the influence of the campaigns that they still
engage in early marriage and pregnancy. The observation is also in line with the
above. The researcher observed that they do not patronize traditional child birth
delivery centres and are all going for antenatal classes, but are still involved in
100
early marriage and pregnancy. Based on the above, the researcher concludes that
the level of the influence of the campaigns in prevention and control of VVF is
moderately high.
The finding is in line with Ngoma ((2010), Prevention of Vesico Vagina Fistula.It
was also observed that prevention should involve alleviation of poverty.
Furthermore, it was observed that accessible emergency obstetric care is necessary
to decrease the burden of obstetric fistula in Africa at large. It could be
accomplished through increased and improved health care facilities and education
of health care providers and patients.
References
Akpeji, F. (2012). Vesico- Vaginal Fistula in northern Nigeria. Urogynaecologia
International Journal, 2 (5)
Fasakin, G. (2009). Vesico virginal fistula & psycho-social well being of women in
northern Nigeria: Zumi Press
101
Mohammed, R. (2007). A community programme for women’s health and
development: Implications for the long term care of women with fistula.
International Journal of Gynecology and Obstetrics. 2(5)12-15
Ngoma, J. (2010). Prevention of vesico-vaginal fistula. (Being a Thesis, Turku
University of Applied Sciences, Zambia)
Ramsey, K, Illiyasu, Z. &Idoko, L. (2007). Fistula fortnight: Innovative
partnership brings mass treatment and public awareness towards ending
obstetric fistula. International Journal of Gynecology and Obstetrics.9,9
doi: 10.1016/j-ijgo.2007.06.034
Sambo, A.E. (1994.) Vesico Vaginal Fistula (VVF) A vision realized.Retrived
from
www.ghononline.org/Vesico%20Vaginal%20Fistula%20 (VVF) %20Cam...
Wall, L (2005). Ethical issues in vesico-vaginal fistula care and research.
International Journal of Gynecology and Obstetrics. 5,17
CHAPTER FIVE
SUMMARY, CONCLUSION AND RECOMMENDATIONS
5.1 Summary
In summary, this study analysed the influence of media campaigns on the
prevention and control of Vesico Vaginal Fistula among people of north-western
Nigeria. In conducting this research, three research instruments were used to
collect data. Research questions raised were analysed using Statistical Package for
102
Social Science (SPSS). The data were presented in tables, percentage and bar
charts. At the end of the analysis, various findings were made, below is the
summary of the major findings:
Research Question one sought to know the level of exposure of respondents
to VVF campaigns. The results indicate that the respondents are aware of VVF
campaigns in the region, however, the level of exposure is said to be relatively
high, in addition to this, both the interview section and the observation made were
also in-line with the above finding. This implies that the level of exposure of
respondents in respect to the subject of discuss is relatively high.
On the knowledge level of respondents, the results indicates that VVF is
associated with all of the followings, early marriage, female genital mutilation,
lack of antenatal care and surgical error. Both the interview and the observation
carried out were all in-line with the results gotten from the administered copies of
questionnaire. This means that their knowledge level is high, and this can be
attributed to a large extent as a result of the massive campaigns carried out in the
region.
In regards to the major source of information, findings reveals that the
repondents got to know about VVF through workshops/seminars, on the other
hand, three out of the six health workers interviewed said the major source of their
information on VVF is seminars/workshops, the observation carried out revealed
that radio and seminars/workshops formed the primary source of information on
103
VVF. Based on this, radio and seminars/workshops formed their major source of
information.
In research question four, only interview was used. Health workers were
interviewed; they all said there are challenges associated with the use of the media
in the campaign against VVF. Some of the challenges are language, timing of the
awareness campaign and boring awareness programmes. etc.
The research five questions seek to know the level of influence of the
campaigns on VVF prevention and control. The respondents agreed that the
campaigns have influenced them to the level that they can take the following
preventive measures; going for antenatal care, stopping early marriage and
stopping female genital mutilation. The result gotten from the interview and
observation attests to the above. The interview shows that the campaigns have
influenced them to the point that they seek modern medical attention, go for
antenatal classes and as well know that VVF is repairable. One of the interviewees
stated that despite the influence of the campaigns that they still engage in early
marriage and pregnancy. The observation is also in line with the above. The
researcher observed that they do not patronize traditional child birth delivery
centers and are all going for antenatal classes. But are still involved in early
marriage and pregnancy. Based on the above, the researcher concludes that the
level of the influence of the campaigns in prevention and control of VVF is
moderately high.
5.2 Conclusion
104
Vesico Vaginal Fistula remains a major public health problem in northern
Nigeria. From the findings of this study, the researcher therefore concludes that:
The level of exposure on VVF is high among the people of north-western Nigeria.
However, this can be attributed to the massive campaigns carried out in the region
by government and NGOs.
Their knowledge level of the disease is high; this can also be linked to the
campaigns carried out in the north-western Nigeria on VVF.
Both radio and seminars/workshops formed the major sources of information to
the
people in the North-western Nigeria on VVF.
Challenges associated with the use of the media in the campaign against VVF
includes language, timing of the awareness campaigns, boring awareness
programmes, etc.
The influence of the campaigns on VVF on prevention and control is moderately
high among people of north western Nigeria.
5.3 Recommendations
Over the years, VVF has remained a medical and social problem especially
to the people of the north; it has also remained a surgical challenge to those in the
health sector. However, the good news is that, VVF is treatable and preventable.
Going by the findings, this study therefore recommends the following:
The awareness campaigns should include women from different communities in
north-western Nigeria and the campaign planners should ensure they use local
105
language during the campaigns; this will aid better understanding of the campaign
message.
During the cause of the campaigns, skilled counselors should be used to sensitize
and provide adequate information and education to VVF patients and their
relatives, so that they in turn can serve as agents of change to their communities.
The campaign should be intensified more on the prevention of prolonged and
obstructed labour since it’s the main and commonest cause of VVF.
The campaign will be of tremendous benefit to the communities if it can also
cover health education, free antenatal care and free child delivery.
The awareness campaigns should be in the form of community mobilization in
which the communities will be made to know the consequences of early marriage,
the importance of attending antenatal care should be encouraged and traditional
childbirth delivery should be discouraged.
The campaign should strive to renew the hopes and dreams of those who suffer
from VVF. The campaign should also aim at reducing the stigma associated with
VVF.
More health workers should be trained on how to educate the people on the
prevention and treatment of fistula. More specialized centres dedicated exclusively
for VVF care with ultra modern facilities should be built in various communities
in the north-western Nigeria
There should be an assessment before providing financial backing for the planning
of campaigns on VVF and executing the campaigns in the various northern states.
106
International support should be sought for; agencies like the World- Wide Fund
for Mother Injured in Childbirth can provide support for the campaign, treatment
and rehabilitation of affected women.
Education can also be very effective in reducing cases of VVF.
The Government should legislate against some traditional practices such as female
child circumcision (gishiri cut) and they should improve the socio-economic
condition of the populace.
The launch by UNFPA to stop fistula is a welcome idea, but it should not only
stop there, more progress will be made if political office holders put this issue as
their priority in their national health care agenda.
Finally, further research works on VVF can be carried out to cover the entire
northern states of Nigeria.
107
BIBLOGRAPHY
Journals Ahmed, S, Creenga, A. & Tsui, A. (2007). The role of delayed child bearing in the
prevention of obstetric fistulas. International Journal of Gynecology and
Obstetrics.2(3)5
Ahmed, S. & Holtz, S.A. (2007). Social and Economic Consequence of Obstetric
Fistula: Life changed forever? International Journal of Gynecology and
obstetrics. . 2,10
Akpeji, F. (2012). Vesico- Vaginal Fistula in northern Nigeria. Urogynaecologia
International Journal, 2, 5
Andrew, O. (2011). Africa: The effect of VVF in Africa. International Journal of
Gynecology and Obstetrics.2, 6
Dodson, J.L, Gutman, R, &Mostwin, J. L. (2007). Complications of treatment of
obstetric fistula in developing world: Gynastresia, urinary incontinence and
urinary diversion. International Journal of Gynecology and Obstetrics
4,(2)223-225
Donnay, F. & Ramsey, K, (2007). Eliminating obstetric fistula: Progress in
partnerships. International Journal of Gynecology and Obstetrics.
4,(2)227-230 Forsgren, C, Lundholm, C & Johansson, N. (2009). Hysterectomy for benign indications
and risk of pelvic organ fistula disease. Obstetrics and Gynecology. 114, 3
Hilton, P. (2003). Vesico-vaginal fistula in developing counties. International
Journa of Gynastresia and Obstetric. 2(3)12
Ijaiya, M. (2010) Vesico Vaginal Fistula: A review of Nigeria experience. West
African Journal of Medicine, 10(5), 293-298. Retrieved January 12, 2013
from http://www.ncbi.nlm.nih.gov/pubmed/21089013
Johnson, K. (2007). Incontinence in Malawi: Analysis of proxy measure of vaginal
fistula in national survey. International Journal of Gynecology and
Obstetrics. 3,9.
Mohammed, R. (2007). A community programe for women’s health and
development: Implications for the long term care of women with fistula.
International Journal of Gynecology and Obstetrics. 2(5)12-15
Orji, E, Aduloju, O & Orji, V. (2007). Correlation and impact of obstetric fistula
on motherhood. Journal of Chinese Clinical Medicine. 2 ,8
Raasen,T,Verdaasdonke,E & Vierhout,M (2007). Perspective results after first
time survey for obstetric fistulas in east African women. International
Urogynecology Journal, 19, pp.73-79
Ramsey, K, Illiyasu, Z. &Idoko, L. (2007). Fistula fortnight: Innovative
partnership brings mass treatment and public awareness towards ending
obstetric fistula. International Journal of Gynecology and Obstetrics.9,9
doi: 10.1016/j-ijgo.2007.06.034 Sheikh, A. Gulzer, A.& Hassan,T (2011). Vesico- vaginal fistula: Abdominal Repair via
vaginal route. Professional Medical Journal.1,4
108
Wall, L.L (2005). Ethical issues in vesico-vaginal fistula care and research. International
Journal of Gynecology and Obstetrics. 5,17 Wall, L, Arrowsmith, S, Lassey A, &Danso K. (2003). Humanitarian ventures or ‘fistula
tourism? The ethical perils of pelvic surgery in the developing world.
International Urogynecol Journal, 17, 559-62.
Wall, L. & Lancer,T. (2006) Obstetric Vesico-Vaginal Fistula as an international health
problem. American Journal of Obstetric & Gnecology, 190 (4).
Wall, L., Karshima, J. &Kirschner, (2004). The obstetric vesico vaginal fistula:
characteristics of 889 patients from Jos, Nigeria. American Journal of Obstetric
&Gnecology, 9 (4)190.. Internet materials
Chalmers, B & Omer-Hashi, K. (2000). 432 Somali women’s birth experience in
Canada after earlier female genital mutilation. Retrieved March 24, 2012
from www.ncbi.nlm.gov/pubmed/1121507 Magashi, A. (2006). Female genital mutilation and our societies. Retrieved on 18
th
February 2012 from http://www.nigerianmasterweb.com/paperfrms.html
Matsamura, E. (2004). Uganda’s fistula patients lack knowledge of prevention and
treatment. Retrieved from
http://www//pro.org/articles/2004/ugandasfistulapatientslackknowledge of
prevention and treatment.aspx
Metro.M (2006). Modification of O’ Connor’s technique for the treatment of VVF repair
described. Retrieved from
www.medicalnewstoday.com/medicalnews.php?newsid
National Statistical Service (2012). Sample size calculator. Retrieved April 26,
from htp//www.nss.gov.au/nss/home.rsf/nss/oa4a642c712719dcca25 National strategic frame work for eradication of fistula in Nigeria (2005-2011). Retrieved
March 3, 2012 from http://www.maternal-health.org/.../unfpa-
evaluierungsbericht-ueber-die-en
Nigeria Demographic Health Survey (NDHS). Religion, Gender and Educational
Level of Nigerians. Retrieved March 23, 2012 from
www.unicef.org/nigeria/ng_publicati
ions _Nigeria_2008_final_rep The National Foundation on Vesico-Vaginal Fistula (2003). Report of the rapid
assessment of vesico-vaginal fistula in Nigeria. Retrieved March 20, 2013 from
http://www.endfitsula .org
The thematic evaluation of national programme and UNFPA experience in the campaign
to end fistula: Assessment of global/regional activity (2010). Retrieved January
13, 2013 from http://www.end fistula.org
United Nations Population Fund. (2010) Campaign to End Fistula. Retrieved March 3,
2012 from http://www.endfistula.com/publications.htm
United States Agency for International Development (USAID) (2003). Mid Term
Evaluation of Fistula Care Project. Retrieved February 21, 2012 from
http:www.ghtechproject.com/…/
nigeria %20mch-

109
Wall.L (2001) Urinary Incontinence in the Developing World: The Obstetric
Fistula. Retrieved January 12,2013 from www.fistulafoundation.org
Sambo, A.E. (1994.) Vesico Vaginal Fistula (VVF) A vision realized.Retrived
from
www.ghononline.org/Vesico%20Vaginal%20Fistula%20 (VVF)
%20Cam... Books
Ajuwon, A. (1997). Visco Vaginal Fistula in Nigeria, extent of the problem & strategies
for prevention and control. In Owumi, (Ed). Primary Health care in Nigeria.
Ibadan: Taiwo Press
Ajzen,I.(1988) Attitude, personality and change.Chikago:Dorsey Press
Ajzen,I & Fishein,M.(1980)Understanding attitudes and predicting social
behaviour ,Prentice-Hall:Englewood Cliffs,NJ. Balogun, S. (1995). The VVF victims. Ibadan :Stirling-Horden.
Benjamin, G. (2010). Fistula in developing nations. Lagos: Kemi Press.
Chukwuemeka, E.E (2002). Research methods and thesis writing: A multi disciplinar
Approach: Enugu: Hope Rising venture
Creswell, J. (2002). Educational research: Planning, conducting and evaluating
quantitative
and qualitative research. New Jersey: Pearson Education Inc. Kees,W. (2006). Prevalence of Obstetric Fistulae in northern Nigeria (Report).
).Retrived February 3
2013 from http:// www.fistularepair .com. Lawrence, P. (2010). Vesico-vagina fistula: A tropical disease. London: Edward Amold
Lawson, J. (1998). Urinary Tract Injuries in Obstetrics and gynecology in the tropics and
developing countries. London: Edward Arnold
Lawson, J. (1998). Urinary Tract Injuries in Obstetrics and gynecology in the tropics and
developing countries. London: Arnold
Mahendeka, M (2007). The management of vesico and/ or recto-vaginal fistula: A
retrospective study. Tanzania: Liventus Publishers
Mkuma, G. &Kasonka, L. (2003). Obstetric fistula situation Analysis in Zambia.
Ministry of health, Zambia .
Moir, J.C (1997). The vesico-vagina fistula. London: Baillore Tin dall&Casell
National Demographic Health Survey (2008). Religion, Gender and Educational Level of
Nigerians. National Demographic Health Survey
Osuala, E.C. (2005). Introduction to research methodology (3rd
ed.). Onitsha: Pearson
Education Inc.
UNFPA (2007). Family care International. Risk and resilience. Obstetric fistula in
Zambia. Women dignity project. Zambia and Engender Health. USA: Procures
WHO (2005). Obstetric fistula, guiding principles for clinical management and
programme development. Geneva, Switzerland.
Wimmer, R, & Dominick, J. (2011).Mass media research. An introduction (9th
ed).
Belmont, CA: Wadsworth Publishing Company. Zacharin R.F. (1988). Obstetric Fistula. New York: Springer Verlag.

110
Newspaper material
John Kari. (2007, September, 9) Easing the scourge of VVF. Nigeria Guardian
Newspapers, p.7
Unpublished Materials
Muhammad, J. (2011). Perceived causes, prevalence and effect of vesico vagina fistula
among Hausa/Fulani women in Kano state (Being an Unpublished Master’s
Degree Thesis, Department of Physical and Health Education, Ahmadu Bello
University, Zaria, Nigeria)
Ngoma, J. (2010). Prevention of vesico-vaginal fistula. (Being a Master’s Degree
Thesis, Turku University of Applied Sciences, Zambia)
Fasakin, G.(2007) Vesico Vaginal Fistula and psychological well-being of women in
nigeria (being an unpublished thesis Linkoping’s University TEMA Institute of
health & Society Department of Health & Society)