toxicological assessment of orally delivered nanoparticulate insulin
TRANSCRIPT

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Reis, Catarina Pinto]On: 12 October 2008Access details: Access Details: [subscription number 903535462]Publisher Informa HealthcareInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
NanotoxicologyPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t716100760
Toxicological assessment of orally delivered nanoparticulate insulinCatarina P. Reis a; Isabel V. Figueiredo a; Rui A. Carvalho b; John Jones c; Patrícia Nunes bc; Ana F. Soares ab;Cristina F. Silva d; António J. Ribeiro a; Francisco J. Veiga a; Christiane Damgé e; António M. S. Cabrita f;Ronald J. Neufeld g
a Faculty of Pharmacy, University of Coimbra, b FCTUC, University of Coimbra, c Neurosciences Center ofCoimbra, d Labesfal-Grupo Fresenius Kabi, Campo de Besteiros, Tondela, Portugal e Institute of Physiology,Faculty of Medicine, University Louis Pasteur, Strasbourg, France f Faculty of Medicine, University ofCoimbra, Coimbra, Portugal g Department of Chemical Engineering, Queen's University, Kingston, Ontario,Canada
First Published on: 10 October 2008
To cite this Article Reis, Catarina P., Figueiredo, Isabel V., Carvalho, Rui A., Jones, John, Nunes, Patrícia, Soares, Ana F., Silva,Cristina F., Ribeiro, António J., Veiga, Francisco J., Damgé, Christiane, Cabrita, António M. S. and Neufeld, RonaldJ.(2008)'Toxicological assessment of orally delivered nanoparticulate insulin',Nanotoxicology,To link to this Article: DOI: 10.1080/17435390802398309URL: http://dx.doi.org/10.1080/17435390802398309
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Toxicological assessment of orally delivered nanoparticulate insulin
CATARINA P. REIS1, ISABEL V. FIGUEIREDO1, RUI A. CARVALHO2, JOHN JONES3,
PATRICIA NUNES2,3, ANA F. SOARES1,2, CRISTINA F. SILVA4, ANTONIO J. RIBEIRO1,
FRANCISCO J. VEIGA1, CHRISTIANE DAMGE5, ANTONIO M. S. CABRITA6, &
RONALD J. NEUFELD7
1Faculty of Pharmacy, University of Coimbra, 2FCTUC, University of Coimbra, 3Neurosciences Center of Coimbra,4Labesfal-Grupo Fresenius Kabi, Campo de Besteiros, Tondela, Portugal, 5Institute of Physiology, Faculty of Medicine,
University Louis Pasteur, Strasbourg, France, 6Faculty of Medicine, University of Coimbra, Coimbra, Portugal &7Department of Chemical Engineering, Queen’s University, Kingston, Ontario, Canada
(Received 13 May 2008; accepted 8 August 2008)
AbstractSubacute toxicological assessment on diabetic rats was conducted after 15 days of daily oral administration ofnanoparticulate insulin. Haematological and biochemical analyses were conducted on blood and urine, biopsies performedon organs and tissues, and histology analysed by optical microscopy. Insulin-loaded nanoparticles alone did not change liveror kidney functions. The increase of some hepatic parameters was attributed to diabetes physiopathology and to chemicalinducement of diabetes and not to the nanoparticle composition since diabetic controls showed the same variations. Interms of kidney function, parameters such as urea nitrogen and creatinine, were also similar to normal rats with theexception of glycosuria. This single effect was due to diabetes physiopathology and the method of induction, and not to thenanoparticle composition, since non-dosed diabetic rats showed the same alteration. Even so, glycosuria levels of animalsdosed with insulin-loaded nanoparticles were lower than control diabetic rats which may indicate an effective hypoglycaemicresponse. Nanoparticles did not exhibit toxicity in haematological parameters. Finally, organ histology was similar betweendosed animals and normal rats with the exception of pancreas histology.
Keywords: Insulin, nanoencapsulation, oral delivery, nanoparticles, toxicology
Introduction
Diabetes mellitus is a chronic disease requiring strictglycemic control to reduce its progression andcomplications and thus insulin replacement therapyprovides the most successful means for glycemiccontrol. Subcutaneous administration is still the onlymethod to administer insulin. While peroral is themost convenient and physiological, peroral bioavail-ability of insulin is relatively low mainly due to highproteolytic activity in the gut and low permeability ofthe intestinal epithelium (Delie and Blanco-Prıeto2005). A promising strategy is the use of insulin-loaded nanoparticles consisting of biodegradablepolymers, which exhibit a strong intestinal permea-tion enhancing effect and intestinal mucoadhesiveproperties (Damge et al. 2007).The recent shift in the focus of developing
polymeric drug-loaded particles from micro- tonanoscale is critical to future advances in medicineand pharmacy. In fact, particle size reduction has
been shown to be an efficient and reliable tool forimproving the bioavailability of a gene or drugdelivery system (Kim et al. 2006). However, whilenanotechnology is used in a growing range ofapplications, concerns are being raised as to whethernanoparticulate components or the nanoparticlesthemselves, might have unintended consequencesto humans or even to the environment. The lack ofinformation regarding the toxicity of nanoparticlesand their components, poses serious problems(Kabanov 2006). Therefore, it is necessary thatspecialists and researchers in toxicology, chemistry,and other fields explore the novel applications ofnanomaterials while being aware of potential toxiceffects (Kim et al. 2006). Nanoparticles are poly-meric submicron carriers, which should be biode-gradable for purposes of drug delivery (Reis et al.2006a). A polymer used in controlled drug deliveryformulations, should be chemically inert, non-toxicand free of leachable impurities (Jacobson-Kram and
Correspondence: Catarina Pinto Reis, Laboratory of Pharmaceutical Technology, Faculty of Pharmacy, University of Coimbra, Rua do
Norte, 3000-295 Coimbra, Portugal. Tel: !351 239855085. Fax: !351 239855099. E-mail: [email protected]
Nanotoxicology2008, 1"13, iFirst article
ISSN 1743-5390 print/ISSN 1743-5404 online # 2008 Informa UK Ltd.
DOI: 10.1080/17435390802398309
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

McGovern 2007). It must also have an appropriate
physical structure, with minimal undesired aging,and be readily processable (Nanopharmaceuticals
2007). But even if biodegradable, and absorbed,
polymeric nanoparticles are still foreign bodies to thehost organism. Ideally, the oral administration of
nanoparticles is followed by rapid uptake through
intestinal mucosa and then other tissues. Never-theless, it is unknown whether its prolonged admin-
istration can lead to damage to the liver, kidney or
other cells. Beside polymer toxicity, another concernis related to products of polymer degradation
(Jacobson-Kram and McGovern 2007). In the case
of the present study, all components of the nano-particles are biodegradable and their degradation
products are non-toxic. Finally, the last concern is
related to other reagents used to prepare nanopar-ticles. There are now numerous preparation meth-
ods available (Reis et al. 2006a) and recent progress
has been especially noted by the need for less toxicreagents (Reis et al. 2006a). Residual solvents must
be quantified on the final product and its level must
be in agreement with FDA limits (FDA 2007). In thenanoparticles described in the present study, resi-
dual solvents were quantified previously by gas
chromatography and were under FDA limits.This study evaluates polymeric insulin-loaded
nanoparticles, for subacute toxicity, after 15 days
of oral daily administration to diabetic rats. Thetime course was based on previous studies with
polyalkylcyanoacrylate nanoparticles on rats
(Fernandez-Urrusuno et al. 1995). The novel oraldosage form of insulin used in the present study is
composed of a composite of natural polymers
consisting of an insulin-loaded alginate-dextransulfate core, complexed with a bilayer chitosan-
polyethylene glycol (PEG) coat, followed by an
albumin coat, as described previously (Reis et al.2006c, 2008). All excipients are well accepted in the
pharmaceutical field. Nanoparticles preserved insu-
lin bioactivity and exerted a strong antidiabeticeffect when orally administered (higher than 75%
reduction of basal glycemia values after 14 h) and
demonstrated a pharmacological availability of 42%,the highest value reported for an oral dosage
formulation by a wide margin. However, toxicolo-
gical effects of these nanoparticles are unknown.Several parameters were analysed such as weight
variation, mortality and histology of collected organ/
tissues. We also evaluated blood biochemistry,haematology and urine parameters since toxicologi-
cal damage may be accompanied by an alteration of
blood cells, hepatic function enzymes and kidneyfunction parameters.
Materials and methods
Materials
Low viscosity sodium alginate (viscosity of 2%solution at 258C, 250 cps) was purchased fromSigma (St Louis, MO, USA). Chitosan (50 kDa),albumin, pepsin and streptozotocin (STZ) werepurchased from Sigma-Aldrich Chimie (L’Isled’Abeau Chesnes, France). Setacarb calcium car-bonate was obtained from Omya (Orgon, France).Paraffin oil was supplied by Vaz Pereira (Lisbon,Portugal). The emulsifier, Span 80, dextran sulfate(5 kDa) and PEG 4000 were purchased from Fluka,Chemie GmbH (Buchs, Switzerland). Insulin waskindly donated by Hospitais da Universidade deCoimbra (Actrapid Insulin† from Novo Nordisk,Bagsvaerd, Denmark).
Nanoparticle preparation
Nanoparticle preparation involved nanoemulsiondispersion followed by triggered instantaneous par-ticle gelation (Reis et al. 2007). A sodium alginate(2%, w/v), dextran sulfate (0.75%, w/v) solution wasprepared by stirring (100 rpm) overnight. Followingstationary deaeration for 1 h, insulin was added anddissolved (100 IU/ml, 10 ml). An aqueous suspen-sion of ultrafine calcium carbonate (5%, w/v) wasadded at calcium-alginate ratio of 7% (w/w), and thedispersion was emulsified within paraffin oil facili-tated by Span 80 emulsifier (1.5% v/v) at high speed(1600 rpm). After 15 min, gelation was induced byaddition of 20 ml paraffin oil containing glacialacetic acid (acid-calcium molar ratio, 3) to solubilizecalcium salt. After 60 min, an acetate buffer solution(pH 4.5, United States Pharmacopeia, USPXXVIII) with dehydrating solvents (acetate buffersolution, acetone, isopropanol, hexane in ratio 70:15: 10: 5 (v/v)) was added to the oil-nanoparticlesuspension and nanoparticles recovered by centrifu-gation (12,500 g during 10 min) (Reis et al. 2006c).Chitosan-PEG coating at pH 4.5 (PEG-chitosanmass ratio of 5 with high calcium level at 1.5%(w/v)) was applied under magnetic stirring during 30min. Then, the supernatant containing unboundpolymer was removed by vacuum, and albumin-coating (1% albumin (w/v) in 100 ml at pH 5.1)applied under magnetic stirring during 30 min.Unbound-coating protein contained in the super-natant was also removed by vacuum. Empty nano-particles lacking insulin were also prepared. Residualsolvents were quantified by gas chromatography andlevels obtained were: acetone and isopropanol with25 ppm and n-hexane with 10 ppm. Levels obtainedwere lower than the limits from FDA (5000 ppm for
2 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

acetone and isopropanol and 290 ppm for n-hexane).
Determination of insulin content
Insulin content was determined by HPLC afterdissolution of a 1 ml nanoparticle suspension with5 ml of sodium citrate (55 mM) in phosphate bufferpH 7.4 (USPXXVIII). Protein released from nano-particles was assayed using HPLC where the mobilephase was water (A): acetonitrile (B) with 0.04%trifluoroacetic acid with linear gradient B 30"40%over 5 min, flow rate 1.2 ml/min at 258C. Areversed-phase X-Terra C-18 column, 5 mm, 4.6#250 mm (Waters, USA), with a Purospher† STARRP-18 precolumn, 5 mm, 4#4 mm (Merck, Ger-many) was employed. The UV detector was set at210 nm and HPLC analysis was carried out at 278C.An insulin retention time around 5 min wasobtained.
In vivo trials of insulin-loaded nanoparticles
Male Wistar rats (250 g) obtained from CharlesRiver (Barcelona, Spain) were housed in a 12 h-12 hlight-dark cycle, constant temperature environmentof 228C, relative humidity 55% and allowed freeaccess to water and food during acclimatization. Alltreatments were carried out in accordance with theEuropean Community Council Directive (86/609/EEC).Diabetes was induced with intravenous injection
of 65 mg/kg streptozotocin (STZ) in citrate buffer(pH 4.5) except for one group (normal rats withoutdiabetes, control 1). Ten days after the treatment,rats with frequent urination, loss of weight and bloodglucose levels higher than 300 mg/dl were includedin experiments. Blood glucose levels were deter-mined by glucose oxidase/peroxidase method using aglucometer (Accu-Chek Aviva, Roche, Lisboa, Por-tugal). Animals were randomized in groups as shownin Table I and dosed daily over a 15-day period bygavage with approximately 2 ml of aqueous disper-sion medium. Insulin dosage (50 IU/kg) was basedon drug content results obtained by HPLC. After 15days, animals were sacrificed and blood, urine,tissues and organs collected for analysis.
Evaluation of changes in weight and mortality
Weight and mortality of all animal groups weremonitored over the 15-day experiment.
Clinical signs
Each rat was examined for lack of movement, ataxia,hunched posture, ruffled fur, hypothermia, dehydra-tion, dyspnea, tachypnea, seizure and sustainedrapid movement around the cage, over a 15-dayperiod. A 0 to 3 scale was used where 0$noindication, 1$slight indication, 2$serious indica-tion, and 3$extreme indication of the problem.Glycemia was measured during the 15-day assay.
Analysis of urine parameters
Urine of all animal groups was collected on day 16and urine density, pH, bilirubin, uribilinogen, blood,glycosuria, proteinuria and ketonic bodies wereanalysed using Sticks Combur (Roche, Portugal).
Evaluation of haematological and biochemicalparameters
The blood of all animals after day 16 was taken bycardiac puncture. Whole blood was collected intotwo tubes containing ethylenediaminetetraaceticacid (EDTA) as anticoagulant. One tube was usedfor analysis of haematological parameters: Erythro-cyte counts (RBC), mean corpuscular volumes(MCV), mean corpuscular haemoglobin (MCH),mean corpuscular haemoglobin concentrations(MCHC), leukocyte counts (WBC), neutrophils(NEU, %), eosinophils (EO, %), basophils (BAS,%), monocytes (MO, %) and lymphocytes (LYM,%), and haematocrit and haemoglobin (Hb) con-centrations were measured spectrophotometricallyusing a haematology flow cytometer (CoulterMaxM, Beckman Coulter, UK). Another portionof the blood was centrifuged (2500 g during 10 min)and plasma analysed (Synchron CX4, BeckmanCoulter, Bucks, UK). Biochemical parameters ana-lysed were aspartate aminotransferase (AST), ala-nine aminotransferase (ALT), alkaline phosphatase(ALP), cholesterol (CHOL), glutamil transferase(GGT), urea (UR), azoto nitrogen (BUN), totalbilirubin (T-BIL), direct bilirubin (D-Bil) and crea-tinine (CR).
Histopathologic examination
In addition to haematological and biochemicalparameters, histopathologic examination was per-formed on day 16. Biopsy specimens from liver,kidney, heart, skeletal muscle (biceps femoris), small
Table I. Design of toxicological 15-day study.
Groups Status Treatment
Number
animals (n)
Test Diabetic Insulin-loaded nanoparticles 10
Control 1 Normal Water 5
Control 2 Diabetic Water 10
Control 3 Diabetic Free insulin 10Control 4 Diabetic Empty nanoparticles 10
Orally delivered insulin 3
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008
and large intestine, eye, lungs, pancreas, spleen,veins (vena cava) and arteries (abdominal aorta)were collected, fixed in formaldehyde at 10% withphosphate buffer (pH$7.2) and then post-fixed for24 h, dehydrated and embedded in paraffin. Sec-tions, with 3"4 mm of thickness, were cut with amicrotome (microtome AS 325/Shadon, Waltham,MA, USA), then stained with haematoxylin/eosinand observed with a photonic microscope (micro-scope Nikon Eclipse E600, Tokyo, Japan).
Statistical analysis of in vivo data
Results were expressed as means9standard errors ofmeans (SEM). An analysis of variance with a one-way layout was applied. For multiple comparisongroup tests, a Dunnett multicomparison test wasapplied, using Graph Prisma Version 3.0 (GraphPadSoftware, San Diego, California, USA). The differ-ences were considered significant when pB0.05.
Results
Evaluation of changes in weight and mortality
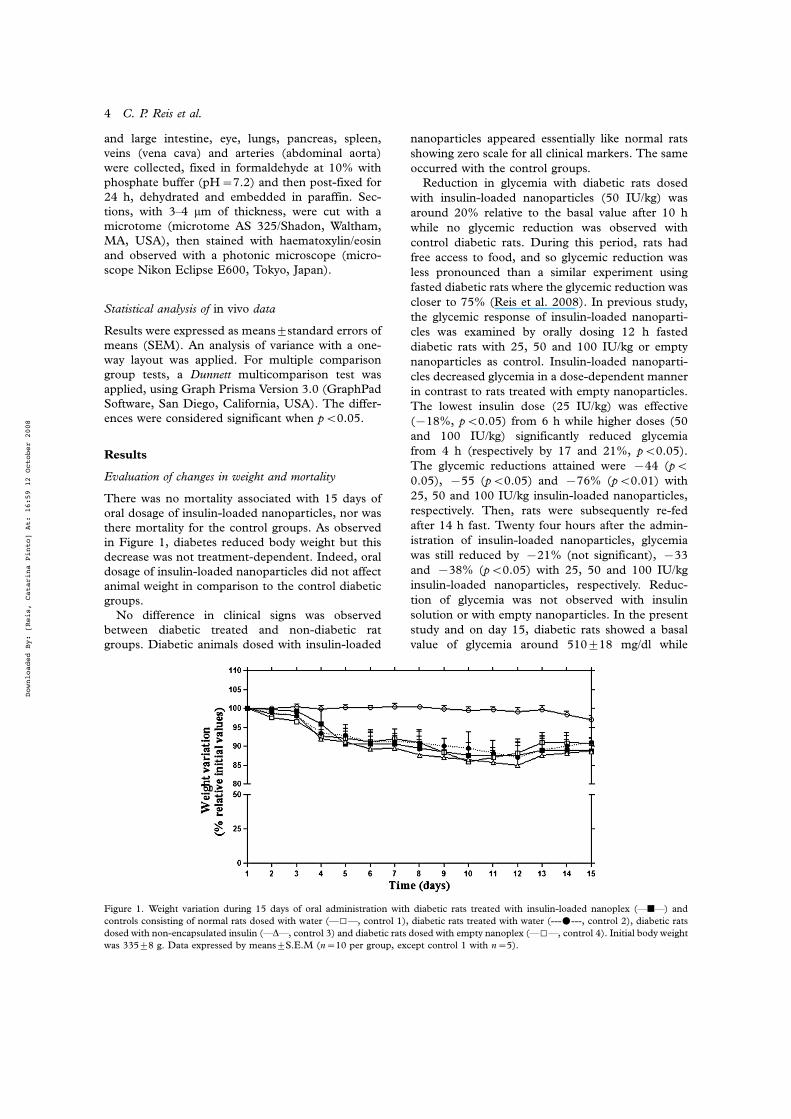
There was no mortality associated with 15 days oforal dosage of insulin-loaded nanoparticles, nor wasthere mortality for the control groups. As observedin Figure 1, diabetes reduced body weight but thisdecrease was not treatment-dependent. Indeed, oraldosage of insulin-loaded nanoparticles did not affectanimal weight in comparison to the control diabeticgroups.No difference in clinical signs was observed
between diabetic treated and non-diabetic ratgroups. Diabetic animals dosed with insulin-loaded
nanoparticles appeared essentially like normal ratsshowing zero scale for all clinical markers. The sameoccurred with the control groups.
Reduction in glycemia with diabetic rats dosedwith insulin-loaded nanoparticles (50 IU/kg) wasaround 20% relative to the basal value after 10 hwhile no glycemic reduction was observed withcontrol diabetic rats. During this period, rats hadfree access to food, and so glycemic reduction wasless pronounced than a similar experiment usingfasted diabetic rats where the glycemic reduction wascloser to 75% (Reis et al. 2008). In previous study,the glycemic response of insulin-loaded nanoparti-cles was examined by orally dosing 12 h fasteddiabetic rats with 25, 50 and 100 IU/kg or emptynanoparticles as control. Insulin-loaded nanoparti-cles decreased glycemia in a dose-dependent mannerin contrast to rats treated with empty nanoparticles.The lowest insulin dose (25 IU/kg) was effective(%18%, pB0.05) from 6 h while higher doses (50and 100 IU/kg) significantly reduced glycemiafrom 4 h (respectively by 17 and 21%, pB0.05).The glycemic reductions attained were %44 (pB0.05), %55 (pB0.05) and %76% (pB0.01) with25, 50 and 100 IU/kg insulin-loaded nanoparticles,respectively. Then, rats were subsequently re-fedafter 14 h fast. Twenty four hours after the admin-istration of insulin-loaded nanoparticles, glycemiawas still reduced by %21% (not significant), %33and %38% (pB0.05) with 25, 50 and 100 IU/kginsulin-loaded nanoparticles, respectively. Reduc-tion of glycemia was not observed with insulinsolution or with empty nanoparticles. In the presentstudy and on day 15, diabetic rats showed a basalvalue of glycemia around 510918 mg/dl while
Figure 1. Weight variation during 15 days of oral administration with diabetic rats treated with insulin-loaded nanoplex (*j*) and
controls consisting of normal rats dosed with water (*I*, control 1), diabetic rats treated with water (---m---, control 2), diabetic rats
dosed with non-encapsulated insulin (*D*, control 3) and diabetic rats dosed with empty nanoplex (*I*, control 4). Initial body weightwas 33598 g. Data expressed by means9S.E.M (n$10 per group, except control 1 with n$5).
4 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

normal rats showed a lower basal value of glycemiaaround 159926 mg/dl. These values decreased to7794 mg/dl, 270972 mg/dl, 180925 mg/dl, 210944 mg/dl, 120917 mg/dl for normal rats, diabeticrats dosed with water, diabetic rats dosed with free-insulin, diabetic rats dosed with empty nanoparticlesand insulin-loaded nanoparticles, respectively, after10 h of treatment.Urine analysis of the nanoparticle dosed group is
presented in Table II and levels were similar tocontrol 1 with normal rats except glycosuria. Asexpected, glucose was present in urine but less sothan other diabetic rats. Glycosuria was observed inall animal groups in the order control 3!control4]control 2!test group and was almost non-existent in normal rat control 1. Urine bilirubin,leukocytes or ketonic bodies were not detected in thetest group and uribilinogen levels were normal.Urine pH and density were similar for all groups.Urine analysis of control groups 2 and 3 wasdifferent from normal animals (control 1) andanimals from the test group.Haematological parameters are summarized in
Table III. Animals from the test group showedsimilarity of haematological parameters with normalrats except EO, MCV, MCH, MCHC or platelets.However, the same observations except EO weremade with all other diabetic groups which mayindicate that this change was not attributed to thenanoparticle composition.Biochemical parameters summarized in Table IV
showed that some were elevated in the test group incomparison with normal rats, namely CHOL, GGT,BUN and urea, but this was also the case with thediabetic control rats. However, some parametersfrom the test group were similar to normal valuessuch as AST, ALT and ALP.Diabetic animals (test and control groups) showed
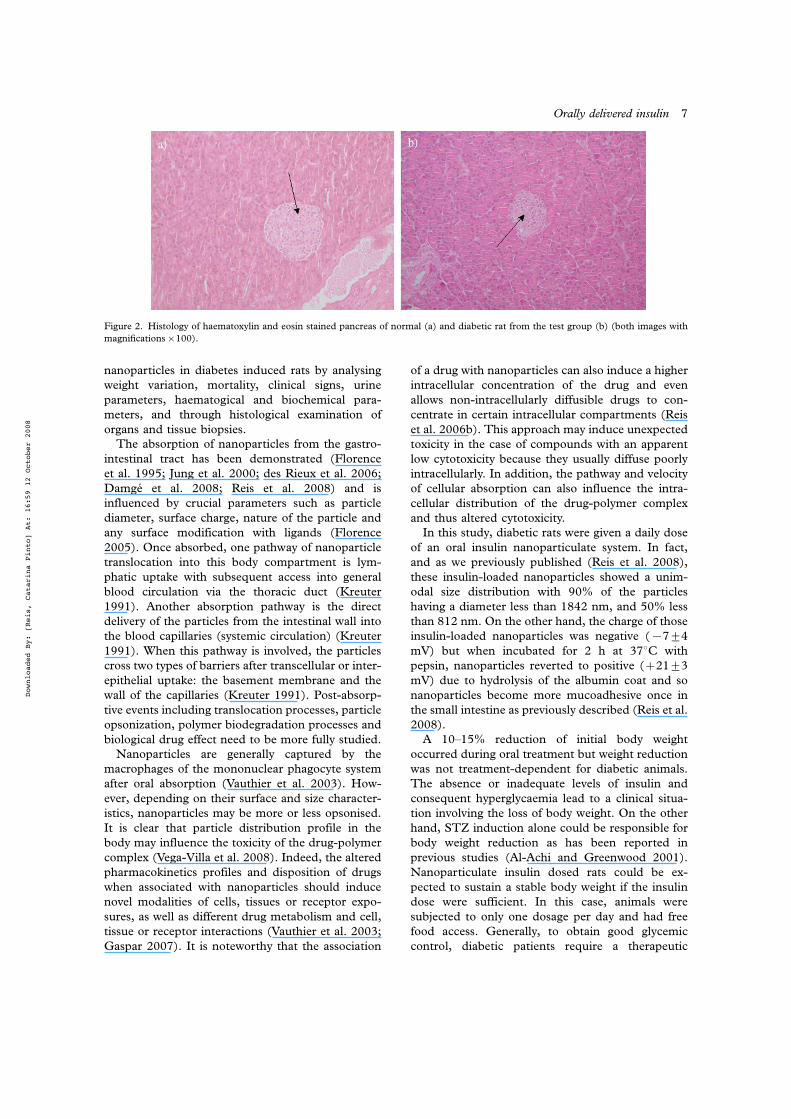
lower islet cell density and fewer cells (arrow inFigure 2b) in the endocrine pancreas as seen inFigure 2b. An example of normal pancreas histologyis illustrated in Figure 2a, taken from control group1. The density of islets cells was typical for theWistar rat (arrow in Figure 2a). An example of hearthistology is illustrated in Figure 3a. Histology was
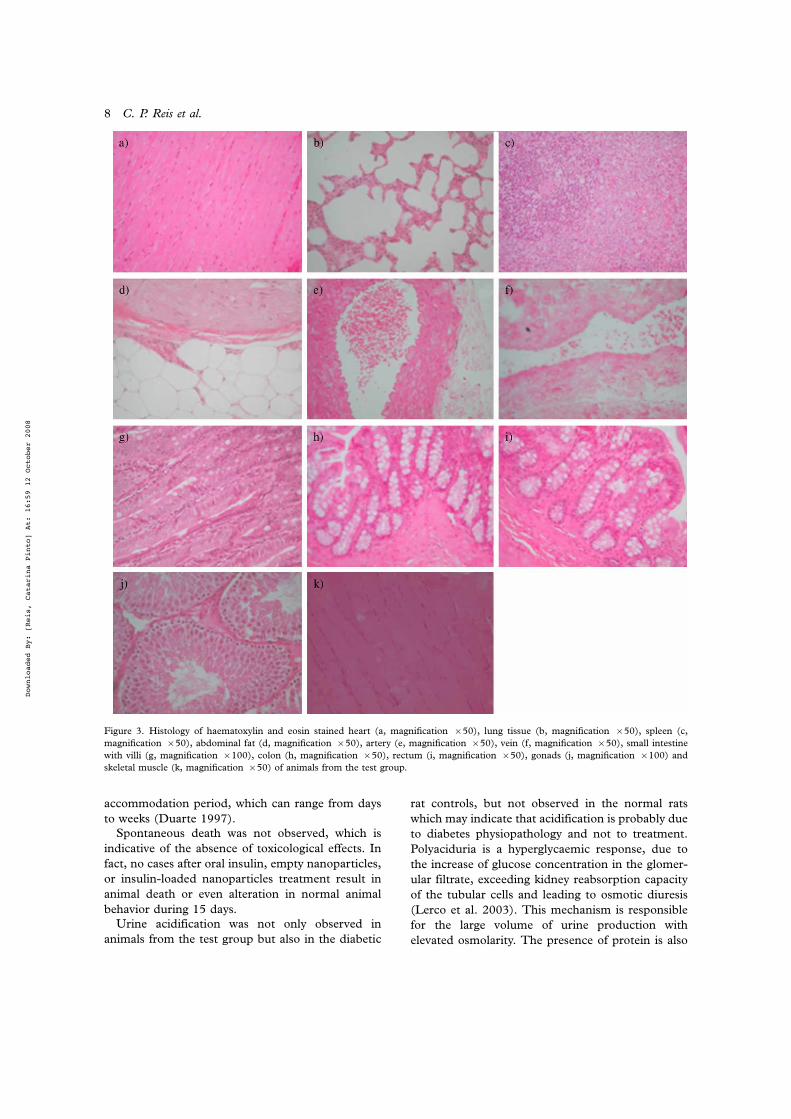
normal for all animals of the test group. Lung imagesdemonstrated thicker alveolar septa as shown inFigure 3b but this was also observed for all diabeticand non-diabetic animals tested comparing toimages extracted from a previous work (Fazzariet al. 2007). Spleen histology of animals from thetest group was also normal as shown in Figure 3c. Aswell, no differences in abdominal fat between testand control groups were observed. Microscopicexamination showed an absence of morphologicalterations in fat tissue such as inflammatory pro-cesses or necrosis. However, histological analysisshowed the presence of conjunctive vases and septalwalls as shown in Figure 3d, which is not attributedto pathological effect, but related with the randomi-zation. Concerning arteries (Figure 3e) and veins(Figure 3f), histological samples did not demon-strate pathological or morphologic alterations in thetest group or any of the control groups. In terms ofthe small (Figure 3g) and large intestine pathology(both colon with Figure 3h and rectal regions Figure3i), morphological or pathological alterations wereabsent in the test and control groups. In the case ofgonads, histopathologic analysis did not disclose anymorphologic or pathological alterations in the dif-ferent groups as shown in Figure 3j as was the casewith skeletal muscle histology as seen in Figure 3k.Microscopic analysis of the liver from the test groupdemonstrated an absence of morphologic alterations(Figure 4a) or pathological evidences. Degenerativealterations, infiltrated inflammation, haemorrhage ornecrosis were not observed. In contrast, one of theanimals of control 2 showed necrosis and smallhaemorrhages as seen in Figure 4b and necrosis wasobserved in one animal of control group 3. Anothersituation of necrosis was observed in one animalfrom control 3 (Figure 4c). Eye histology of thetest group was normal as seen in Figure 5a. Incontrast, two isolated cases were detected with a newformation of thick vessel wall (Figure 5b) as well as acase in which a new vessel appeared in one animalfrom each of control group 2 and 3 (Figure 5c).Finally, kidney histology of animals from the testgroup was normal as shown in Figure 6 except basalmembranes of blood vessels which were thickener
Table II. Table II. Urine analysis.
Group Bilirubin Leukocytes Uribilinogen Ketonic bodies Ascorbic acid Glucose (mg/dl) Proteinuria pH Density
Insulin"loadedNanoparticles
" " N " " 3009200 1 Positive case 5.5 1.02
Control 1 " " N " " 33917 1 Positive case 6.3 1.01
Control 2 " " N " 2 Positive cases 4259106 1 Positive case 5 1.02
Control 3 " " N 2 Positive cases " 5509112 3 Positive cases 5.7 1.02
Control 4 " " N " " 4339130 1 Positive case 5.5 1.02
" indicates result is not detected; N, within normal range.
Orally delivered insulin 5
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

around the glomerulus capsule in comparison tonormal rats. This change was also observed for otherdiabetic control groups. Histopathological analysis issummarized in Table V.
Discussion
Diabetes mellitus is a syndrome that disturbs themetabolism of carbohydrates, fat and protein andresults from shortage or lack of insulin secretion orreduced sensitivity of the tissues to insulin (Akbar-zadeh et al. 2007). Insulin is a key regulator ofmetabolism. Without insulin to move glucose intocells, blood glucose levels become excessively high, acondition known as hyperglycaemia. Because thebody cannot utilize the sugar, it is excreted in theurine and thus is lost. Weakness, weight loss, andexcessive hunger and thirst result, and thus patientsbecome dependent on administered insulin forglycemic control, necessary for survival. Inadequate
control may lead to serious complications such asamputation, blindness, diabetic ketoacidosis, neuro-pathy, retinopathy, eating disorders, erectile dys-function, foot problems, gastroparesis, gum disease,heart problems, high blood pressure, infertility,kidney problems, lactic acidosis, seizures andcoma, peripherical arterial disease, urologic pro-blems and high susceptibility to infections. Appro-priate therapeutic insulin delivery and replacementmay delay the progression of diabetic complications.
A variety of nanoparticles are being developed forinsulin delivery (Oppenheim et al. 1982; Damgeet al. 1988, 2007, 2008; Pan et al. 2002; Cui et al.2004; Ma et al. 2005; Sajeesh and Sharma 2006;Reis et al. 2008), however little information isavailable about the toxicological effect of theseparticles in vivo. Generally, in vitro studies are notable to reproduce the effects of chronic administra-tion (Fernandez-Urrusuno et al. 1995). This studyevaluated the potential toxicity of insulin-loaded
Table III. Haematological parameters after 15 days of oral administration. Data expressed by mean9SEM (n$10 per group, except
control 1 with n$5).
Haematological parameters
Test group (diabetic
!insulin nanoparticles)
Control 1
(normal!water)
Control 2
(diabetic!water)
Control 3 (diabetic
!free-insulin)
Control 4 (diabetic
!empty nanoparticles)
RBC (#1012/l) 8.390.2 9.392 8.290.2 7.490.2** 8.190.4
Hb (g/dl) 15.390.4 13.692.0 14.990.3 13.790.4 15.390.5Haematocrit 0.590.0 0.590.0 0.590.0 0.490.0** 0.590.0
WBC (#109/l) 2.290.3 1.990.3 2.490.4 1.290.2 1.390.4
MO (%) 2.790.5 2.990.1 4.190.3 3.491.1 2.290.9
NEU (%) 31.1914.7 11.892.0 36.393.0 29.895.8 18.298.1EO (%) 0.990.3*,# 1.990.1 1.390.2 1.290.2 2.190.2
BAS (%) 0.290.1 1.090.1 1.691.0 0.190.0 2.991.2
LYM (%) 65.1914.5 82.492.0 56.393.2 65.995.1 72.897.1
Platelets (gpt/l) 656.3996.3 103.092.0 471.89105.3 409.39125.2 486.39140.6MCV (fl) 54.190.8** 55.092.0 54.790.6 54.990.6 55.590.4
MCH (pg) 18.590.4** 14.792 18.190.3** 18.690.1** 18.890.3**
MCHC (g/l) 341.393.6** 266.092.0 331.292.9** 338.591.8** 338.393.0**
*Statistically different from control 1 with pB0.05. **Statistically different from control 1 with pB0.01. #Statistically different from control
4 with pB0.05.
Table IV. Biochemical parameters after 15 days of oral administration. Data expressed by means9SEM (n$10 per group, except control 1
with n$5).
Biochemical parameters
Test group
(diabetic!insulin
nanoparticles)
Control 1
(normal!water)
Control 2
(diabetic!water)
Control 3 (diabetic
!free-insulin)
Control 4 (diabetic
!empty nanoparticles)
CHOL (mg/dl) 50.291.3*,# 27.092.0 43.696.5* 37.494.7 41.893.8
AST (UI/l) 88.0910.8 125.590.5 167.6947.9 115.4916.9 139.8925.9
ALT (U/Il) 42.097.4 40.093.0 50.094.8 45.095.8 54.299.7GGT (UI/l) 4.490.6* 0.590.1 3.690.8* 4.290.6* 3.290.5*
ALP (UI/l) 3.591.6# 4.090.0# 22.394.5 31.8910.3 3.391.9#
Urea (mg/dl) 94.995.2* 56.094.3 115.194.9**, # 97.7912.0* 107.498.8*, #
BUN (mg/dl) 44.392.4* 26.192.0 53.892.3**,# 45.695.6* 50.194.1*,#
CR (mg/dl) 0.790.1 0.690.1 0.6290.1 0.690.1 0.690.0
T-Bil (mg/dl) 0.890.1 0.990.1 0.690.1 0.690.1 0.790.1
D-Bil (mg/dl) 0.390.4 0.390.1 0.390.1 0.290.0 0.390.1
*Statistically different from control 1 with pB0.05. **Statistically different from control 1 with pB0.01. #Statistically different from control
3 with pB0.05.
6 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008
nanoparticles in diabetes induced rats by analysingweight variation, mortality, clinical signs, urineparameters, haematogical and biochemical para-meters, and through histological examination oforgans and tissue biopsies.The absorption of nanoparticles from the gastro-
intestinal tract has been demonstrated (Florenceet al. 1995; Jung et al. 2000; des Rieux et al. 2006;Damge et al. 2008; Reis et al. 2008) and isinfluenced by crucial parameters such as particlediameter, surface charge, nature of the particle andany surface modification with ligands (Florence2005). Once absorbed, one pathway of nanoparticletranslocation into this body compartment is lym-phatic uptake with subsequent access into generalblood circulation via the thoracic duct (Kreuter1991). Another absorption pathway is the directdelivery of the particles from the intestinal wall intothe blood capillaries (systemic circulation) (Kreuter1991). When this pathway is involved, the particlescross two types of barriers after transcellular or inter-epithelial uptake: the basement membrane and thewall of the capillaries (Kreuter 1991). Post-absorp-tive events including translocation processes, particleopsonization, polymer biodegradation processes andbiological drug effect need to be more fully studied.Nanoparticles are generally captured by the
macrophages of the mononuclear phagocyte systemafter oral absorption (Vauthier et al. 2003). How-ever, depending on their surface and size character-istics, nanoparticles may be more or less opsonised.It is clear that particle distribution profile in thebody may influence the toxicity of the drug-polymercomplex (Vega-Villa et al. 2008). Indeed, the alteredpharmacokinetics profiles and disposition of drugswhen associated with nanoparticles should inducenovel modalities of cells, tissues or receptor expo-sures, as well as different drug metabolism and cell,tissue or receptor interactions (Vauthier et al. 2003;Gaspar 2007). It is noteworthy that the association
of a drug with nanoparticles can also induce a higherintracellular concentration of the drug and evenallows non-intracellularly diffusible drugs to con-centrate in certain intracellular compartments (Reiset al. 2006b). This approach may induce unexpectedtoxicity in the case of compounds with an apparentlow cytotoxicity because they usually diffuse poorlyintracellularly. In addition, the pathway and velocityof cellular absorption can also influence the intra-cellular distribution of the drug-polymer complexand thus altered cytotoxicity.
In this study, diabetic rats were given a daily doseof an oral insulin nanoparticulate system. In fact,and as we previously published (Reis et al. 2008),these insulin-loaded nanoparticles showed a unim-odal size distribution with 90% of the particleshaving a diameter less than 1842 nm, and 50% lessthan 812 nm. On the other hand, the charge of thoseinsulin-loaded nanoparticles was negative (%794mV) but when incubated for 2 h at 378C withpepsin, nanoparticles reverted to positive (!2193mV) due to hydrolysis of the albumin coat and sonanoparticles become more mucoadhesive once inthe small intestine as previously described (Reis et al.2008).
A 10"15% reduction of initial body weightoccurred during oral treatment but weight reductionwas not treatment-dependent for diabetic animals.The absence or inadequate levels of insulin andconsequent hyperglycaemia lead to a clinical situa-tion involving the loss of body weight. On the otherhand, STZ induction alone could be responsible forbody weight reduction as has been reported inprevious studies (Al-Achi and Greenwood 2001).Nanoparticulate insulin dosed rats could be ex-pected to sustain a stable body weight if the insulindose were sufficient. In this case, animals weresubjected to only one dosage per day and had freefood access. Generally, to obtain good glycemiccontrol, diabetic patients require a therapeutic
Figure 2. Histology of haematoxylin and eosin stained pancreas of normal (a) and diabetic rat from the test group (b) (both images with
magnifications#100).
Orally delivered insulin 7
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008
accommodation period, which can range from days
to weeks (Duarte 1997).Spontaneous death was not observed, which is
indicative of the absence of toxicological effects. In
fact, no cases after oral insulin, empty nanoparticles,or insulin-loaded nanoparticles treatment result in
animal death or even alteration in normal animal
behavior during 15 days.Urine acidification was not only observed in
animals from the test group but also in the diabetic
rat controls, but not observed in the normal rats
which may indicate that acidification is probably dueto diabetes physiopathology and not to treatment.
Polyaciduria is a hyperglycaemic response, due to
the increase of glucose concentration in the glomer-ular filtrate, exceeding kidney reabsorption capacity
of the tubular cells and leading to osmotic diuresis
(Lerco et al. 2003). This mechanism is responsiblefor the large volume of urine production with
elevated osmolarity. The presence of protein is also
Figure 3. Histology of haematoxylin and eosin stained heart (a, magnification #50), lung tissue (b, magnification #50), spleen (c,
magnification #50), abdominal fat (d, magnification #50), artery (e, magnification #50), vein (f, magnification #50), small intestine
with villi (g, magnification #100), colon (h, magnification #50), rectum (i, magnification #50), gonads (j, magnification #100) and
skeletal muscle (k, magnification #50) of animals from the test group.
8 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

a consequence of hyperglycaemic status, leading tomicrovascular alterations, which are responsible forthe diabetic nephropathy, presence of persistentproteinuria and other renal problems (Barbas1997). Ketonic bodies were only present in diabeticcontrol 3 dosed with free-insulin which can predict amore advanced diabetes state. Without insulin,animals cannot use glucose normally, and thusutilize other energy reserves such as lipids. The liverthen produces ketonic bodies, which reach thekidneys and may pass to urine with glucose (Barbas1997).The effect of insulin-loaded nanoparticles on
biochemical parameters was also analyzed. It iscommonly known that the metabolites of polymerbiodegradation can be responsible for hepatoxicity(Fernandez-Urrusuno et al. 1995) and increase ofliver enzymes in the blood. Plasma analysis showedthat only some biochemical parameters had beenaffected. The CHOL value was higher in animalsfrom test groups but also in other diabetic rats, butthe observed value was always lower than normaland healthy values reported (57.190.8 mg/dl)(Karakilcik et al. 2005). In terms of hepatic enzymes(ALT and AST), the observed values were lowerthan the normal healthy rat levels (44.494.7 IU/l(Inal et al. 2006) and 232.0950.6 IU/l (Inal et al.2006), respectively). The AST of animals from thetest group dosed with insulin-loaded nanoparticleswas slightly lower than other diabetic and normal
rats. This value shows benefits in terms of hepatictoxicity because when liver functionally is damaged,the level of this enzyme consequently increases(Lopes 2007). Other enzymes whose cellular loca-tion is on the membrane and where high levelsgenerally mean colestasis (such as ALP) weredifferent in diabetic rats. The lowest value wasobtained with the group of animals dosed withempty and insulin-loaded nanoparticles where ALPwas the same as for normal rats. ALP describes onegroup of phosphohydrolases and is located in tissuesincluding the liver, epithelial biliary and bone,among other tissues and organs (Lopes 2007). Inthe liver, ALP is secreted by hepatocytes and biliarycells (Lopes 2007). Generally, any active hepato-pathy increases ALP values (Lopes 2007). Thehighest ALP improvement is generally observed inthe presence of intra or extra-hepatic biliary obstruc-tion. In hepatic tumours, hepatitis and in response tosome hepatotoxic drugs, changes in this enzyme areless pronounced compared to extra or intra-hepaticbiliary (Lopes 2007). Considering the present re-sults, it seems that nanoparticles, whether empty orwith insulin, should be not hepatotoxic. The in-crease of this enzyme in control 2 and 3 could berelated to STZ hepatoxicity (Cancercare 2007) butalso to individual treatment. On the other hand, thelevels of GGT were elevated in animals dosedwith insulin-loaded nanoparticles but also wereelevated in control diabetic rats groups. This fact
Figure 4. Histology of haematoxylin and eosin stained liver of animal from the test group (a), liver of an animal of control 2 with necrosisand small haemorrhages (b), and liver of an animal of control 3 with necrosis (c). Magnification #50.
Figure 5. Histology of haematoxylin and eosin stained retina of test group (a), retina of an animal of control 2 with neovascularization (b),
and retina of an animal of control 3 with new blood vessel (c). Magnification #50.
Orally delivered insulin 9
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

corroborates the conclusion that nanoparticles werenot hepatotoxic. The GGT level can be related tothe induction method of diabetes as previouslydescribed (Al-Achi and Greenwood 2001; Cancer-care 2007). Kidney function was slightly alteredsince urea and BUN levels were significantly chan-ged, possibly indicating kidney modification. How-ever CR values were normal as previously reportedfor healthy animals (CaparrozAssef et al. 2005)which may indicate that biochemical change wasrelated to extra-kidney damage (Healthbanks 2007).This damage can be explained by abnormal proteincatabolism in diabetic rats and not to individualtreatment.This study also evaluated haematological para-
meters. Most of all parameters were similar exceptthe percentage of EO in animals dosed with insulin-loaded nanoparticles. The decrease of EO is gen-erally related with glucocorticoid therapy which wasnot the case in this situation, and this value could be
related to other undetermined factors. The otherhaematological parameters of diabetic rats from thetest group were slightly different compared tonormal rats in terms of RBC, MCH and MCHCand platelet numbers, as was the case with controlrats. Most haematological parameters, even modi-fied, still ranged between normal healthy levels forrats, namely RBC with normal healthy rat levels of7.291.4#1012/l (Priya et al. 1997), MCH with 19"23 pg (Sayim et al. 2005), and, MCHC with37.3092.4 gHb/dl (Priya et al. 1997). Plateletnumbers were elevated in animals from the testgroup but also in diabetic controls, however withoutstatistical significance. Thrombocytosis could berelated to diabetes physiopathology (Martin et al.1995) or possibly to the induction method ofdiabetes (Al-Achi and Greenwood 2001). Generallyin diabetes, an increase in platelet aggregation,appearance of blood clots, reduction in platelet life,reduction of the fibrinolytic activity and increase ofthe Factor of von Willebrand is observed (Lopes2007; Medicina 2007). Physiologically, an improve-ment of platelet activity (Yngen et al. 2001) seems tobe related to arachidonic acid metabolism, reductionof prostacyclins and increase of expression of theglycoproteins GPIb and GPIIb/IIIa (Quintana et al.2001). On the other hand, studies have reported thatthe induction method of diabetes can be associatedwith platelet dysfunction (Tschope et al. 1992; Al-Achi and Greenwood 2001). In the group dosedwith insulin-loaded nanoparticles, platelet valueswere higher than those of other diabetic rats, eventhrough the differences were not statistically signifi-cant. Some previous studies described insulin actionon platelet activity (Umeda et al. 1982; Hamet et al.1983; Valentovic and Lubawy 1983; Tschope et al.1992; Morinelli 1993; Yngen et al. 2001). In general
Figure 6. Histology of haematoxylin and eosin stained kidney of
test group. Magnification #50.
Table V. Histopathological analysis after 15 days of oral administration (n$10 per group, except control 1 with n$5).
Histology Test group (insulin
nanoparticles)
Control 1
(normal!water)
Control 2
(diabetic!water)
Control 3 (diabetic
!free-insulin)
Control 4 (diabetic
!empty nanoparticles)
Pancreas Lower islet cell
density
Normal islet cell
density
Lower islet cell
density
Lower islet cell
density
Lower islet cell
density
Heart % % % % %Lung ! ! ! ! !Spleen % % % % %Abdominal fat % % % % %Arteries and veins % % % % %Upper intestine % % % % %Small intestine % % % % %Gonads % % % % %Liver % % !/% !/% %Eye % % !/% !/% %Kidney ! % ! ! !
% indicates an absence of pathological or morphologic alterations; !, presence of pathological or morphologic alterations; !/%, some
animals demonstrated pathological or morphologic alterations.
10 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

and as is the case with other cells, platelets haveinsulin-like receptors (Yngen et al. 2001). Insulininfluences platelet turnover (Hamet et al. 1983), andthus insulin released from nanoparticles could affectplatelet values (Tschope et al. 1992). The animalgroup dosed with free insulin showed the sameplatelet levels as other diabetic controls, mainlydue to the ineffective action of free insulin whenadministered orally. As previously described, freeinsulin is fully degraded when orally administeredalong the gastrointestinal tract by proteolytic andacidic attack. Degraded insulin is not bioactive andcannot act on insulin-like receptors. Thus plateletlevels were not increased as seen in animals dosedwith insulin-loaded nanoparticles. Histological studydisclosed an absence of toxicological effects ob-served in collected tissues and organs. The fewabnormalities occurred in isolated cases and inrandom form and were not associated with thenanoparticle composition. The observed minor dif-ferences can be associated with the evolution ofdiabetes and/or toxicity of STZ. In particular, somehepatic dysfunction was observed in isolated casesfrom controls 2 and 3, possibly due to STZhepatoxicity (Kume et al. 2005; Wijkstrom et al.2005; Cancercare 2007). On the other hand, kidneychanges were also independent of treatment type,which suggests that nanoparticles were not nephro-toxic and the observed alterations may be related toSTZ action as previously demonstrated (Wijkstromet al. 2005; Cancercare 2007) but also to diabetes.Kidney dysfunction occurs with some pathologicalsituations during the course of diabetes, at both theinitial and advanced stages (Barbas 1997). Kidneydamage caused by diabetes most often involvesthickening and hardening of the internal kidneystructures. Patients with type 1 or type 2 diabetesare at high risk of developing diabetic nephropathy.The risk is even higher if blood-glucose levels arepoorly controlled. Another important observationwas associated with the proliferation of new bloodvessels in the retina of some diabetic animals, namelydosed with water and with free insulin. This changecan be indicative of a more advanced diabetic stateand not to toxicity associated with each treatment.Generally, patients with diabetes are more likely todevelop retinopathy. Over the years, high sugar levelcan damage the tiny blood vessels (Gabbay 1975).Chemically, constant hyperglycaemia status pro-vokes an increase of polyols and the reduction ofinositol through aldose-reductase action (Duarteet al. 1997). Another potentially pathogenic me-chanism involving retinopathy is associated with theaccumulation of particular products (Duarte et al.1997). The earliest phase is known as background
diabetic retinopathy, in which arteries in the retinabecome weakened and leak, forming small, dot-likehaemorrhages or micro aneurisms. These leakingvessels often lead to swelling or oedema in the retinaand decreased vision. The next stage is known asproliferative diabetic retinopathy. In this stage,circulation problems cause areas of the retina tobecome oxygen-deprived or ischemic. New abnor-mal blood vessels form and grow on the surface ofthe retina as the circulatory system attempts tomaintain adequate oxygen levels within the retinasuch as is observed with animals from controls 2 and3, in a condition known as neovascularization.Unfortunately, these vessels haemorrhage easilyand blood leaking into the retina and vitreous,causes spots or floaters, along with decreased vision,which can lead to blindness (Duarte et al. 1997).
It may be concluded that the insulin-loadednanoparticles were not toxic during a 15-day periodof oral administration. The next stage will be toexamine the toxicity of nanoparticulate insulinfollowing chronic exposure.
Conclusions
A toxicological study using biochemical, haematolo-gical and urine-based parameters as well as organand tissue histology, demonstrated the absence oftoxicological effects of insulin-loaded nanoparticlescomposed of natural and biodegradable polymers.Observed changes were attributed to diabetes phy-siopathology and/or STZ inducement of diabetesand/or diabetes evolution status. The lack of nano-particulate insulin toxicity was also demonstrated byan absence of mortality during a 15-day period oforal administration. The overall objective of thiswork is to develop a nanoparticulate system aspotential oral delivery for insulin but also for otherpeptidic therapeutic drugs.
Acknowledgements
The authors are grateful for financial support fromthe Fundacao para a Ciencia e Tecnologia, Portugal(SFRH/BD/13673/2003) and from the NaturalSciences and Engineering Research Council of Canada.The authors would like to thank to Dr LucıliaSilveira and Dr Ana Donato for their collaborativehelp haematological and biochemical parametersstudies.
Declaration of interest: The authors report noconflicts of interest. The authors alone are respon-sible for the content and writing of the paper.
Orally delivered insulin 11
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

References
Akbarzadeh A, Noruzian D, Jamshidi S, Farhangi A, Mehrabi
MR, B. Lame Rad, Mofidian M, Allahverdi A. 2007. Treat-
ment of streptozotocin induced diabetes in male rats by
immunoisolated transplantation of islet cells. Ind J Clin
Biochem 22:71"76.Al-Achi A, Greenwood R. 2001. A brief report on some
physiological parameters of streptozotocin-diabetic rat. Drug
Dev Ind Pharm 27:465"468.Barbas J. 1997. Nefropatia diabetica. In: Duarte R, editor.
Diabetologia Clınica. Lisboa: Lidel-Edicoes Tecnicas, Lda.
pp 255"269.Cancercare. 2007. Toronto, Canada: Cancer Care Ontario; 2007
June 5; Available from the website: http://www.cancercare.
on.ca/pdfdrugs/STREPTOZ.pdfCaparrozAssef SM, Grespan R, Batista RCF, BersaniAmado FA,
Baroni S, Dantas JA, Cuman RKN, Bersani-Amado CA. 2005.
Toxicity studies of Cordia salicifolia extract. Acta Sci Health
Sci 27:4141"4144.Cui F, Zhang L, Zheng J, Kawashima Y. 2004. A study of insulin-
chitosan complex nanoparticles used for oral administration. J
Drug Del Sci Tech 14:435"439.Damge C, Reis CP, Maincent P. 2008. Nanoparticle strategies for
the oral delivery of insulin. Expert Opin. Drug Deliv 5:45"68.Damge C, Maincent P, Ubrich N. 2007. Oral delivery of insulin
associated to polymeric nanoparticles in diabetic rats. J Control
Rel 117:163"170.Damge C, Michel C, Aprahamian M, Couvreur P. 1988. New
approach for oral administration of insulin with polyalkylcya-
noacrylate nanocapsules as drug carrier. Diabetes 37:246"251.Delie F, Blanco-Prıeto MJ. 2005. Polymeric particulates to
improve oral bioavailability of peptide drugs. Molecules
10:65"80.des Rieux A, Fievez V, Garinot M, Schneider Y-J, Preat V. 2006.
Nanoparticles as potential oral delivery systems of proteins and
vaccines: A mechanistic approach. J Control Rel 116:1"27.Duarte R. 1997. Insulina. In: Duarte R, editor. Diabetologia
Clınica. Lisboa: Lidel-Edicoes Tecnicas, Lda. pp 139"151.Duarte R, Zeller PV, Lisboa PE. 1997. Alteracoes oculares na
Diabetes. In: Duarte R, editor. Diabetologia Clınica. Lisboa:
Lidel-Edicoes Tecnicas, Lda. pp 242"254.Fazzari P, Penachioni J, Gianola S, Rossi F, Eickholt BJ, Maina F,
Alexopoulou L, Sottile A, Comoglio PM, Flavell RA, et al.
2007. Plexin-B1 plays a redundant role during mouse devel-
opment and in tumour angiogenesis. BMC Dev Biol 7:55.
FDA. 2007. Guidance for Industry, Q3C-Tables and List. FDA.
2007 July 5; Available from the website: http://www.fda.gov/
ohrms/dockets/98fr/01b-0431-gdl0001.doc
Fernandez-Urrusuno R, Fatal E, Porquet D, Feger J, Couvreur P.
1995. Evaluation of liver toxicological effects induced by
polyalkylcyanoacrylate nanoparticles. Toxicol Appl Pharmacol
130:272"279.Florence AT. 2005. Nanoparticle uptake by the oral route:
Fulfilling its potential? Drug Discovery Today: Technologies
2:75"81.Florence AT, Hillery AM, Hussain N, Jani PU. 1995. Nanopar-
ticles as carriers for oral peptide absorption: Studies on particle
uptake and fate. J Control Rel 36:39"46.Gabbay K. 1975. Hyperglycemia, polyol metabolism, and com-
plication of diabetes mellitus. Ann Rev Med 26:521"536.Gaspar R. 2007. Regulatory issues surrounding nanomedicines:
Setting the scene for the next generation of nanopharmaceu-
ticals. Future Nanomed 2:143"147.Hamet P, Sugimoto H, Umeda F, Franks DJ. 1983. Platelets and
vascular smooth muscle: abnormalities of phosphodiesterase,
aggregation, and cell growth in experimental and human
diabetes. Metabolism 32:124"130.Healthbanks. 2007. Blood urea nitrogen. Healthbanks. 2007 July
5; Available from the website: http://www.healthbanks.com/
PatientPortal/Public/LinkPublic.do?ArticleID$HW5aa36271
Inal S, Yilmaz N, Nisbet C, Guvenc T, Samsun T. 2006.
Biochemical and histopathological findings of N-butyl-2-cya-
noacrylate in oral surgery: An experimental study. Oral Surg
Oral Med Oral Pathol Oral Radiol Endod 102:e14"17.Jacobson-Kram D, McGovern T. 2007. Toxicological overview of
impurities in pharmaceutical products. Adv Drug Del Rev
59:38"42.Jung T, KammW, Breitenbach A, Kaiserling E, Xiao JX, Kissel T.
2000. Biodegradable nanoparticles for oral delivery of peptides:
Is there a role for polymers to affect mucosal uptake? Eur J
Pharm Biopharm 50:147"160.Kabanov AV. 2006. Polymer genomics: An insight into pharma-
cology and toxicology of nanomedicines. Adv Drug Del Rev
Supplementary Non-Thematic Collection 58:1597"1621.Karakilcik AZ, Hayat A, Aydilek N, Zerin M, Cay M. 2005.
Effects of vitamin C on liver enzymes and biochemical
parameters in rats anesthetized with halothane. Gen Physiol
Biophys 24:47"55.Kim JS, Yoon T-J, Yu KN, Kim BG, Park SJ, Kim HW, Lee KH,
Park SB, Lee J-K, Cho MH. 2006. Toxicity and tissue
distribution of magnetic nanoparticles in mice. Toxicol Sci
89:338"347.Kreuter J. 1991. Peroral administration of nanoparticles. Adv
Drug Deliv Rev 7:71"86.Kume E, Aruga C, Ishizuka Y, Takahashi K, Miwa S, Itoh M,
Fujimura H, Toriumi W, Kitamura K, Doi K. 2005. Gene
expression profiling in streptozotocin treated mouse liver using
DNA microarray. Exp Toxicol Pathol 56:235"244.Lerco MM, Spadella CT, Machado JLM, Schellini SA, Pavodini
CR. 2003. Caracterizacao de um modelo experimental de
Diabetes Mellitus, induzido pela aloxana em ratos. Estudo
clınico e laboratorial. Acta Cirurg. Bras 18:136"142.Lopes HJJ. 2007. Enzimas no laboratorio clınico. Aplicacoes
diagnosticas. 2007 July 2; Available from the website: www.golda
nalisa.com.br/publicacoes/Enzimas_no_Laboratorio_Clinico.pdf,Ma Z, Lim TM, Lim L-Y. 2005. Pharmacological activity of
peroral chitosan-insulin nanoparticles in diabetic rats. Int J
Pharm 293:271"280.Martin FJ, Miguez JM, Aldegunde M, Atienza G. 1995. Platelet
serotonin transport is altered in streptozotocin-induced dia-
betic rats. Life Sci 56:1807"1815.medicina.fm.usp.br. 2007. Sao Paulo, Brasil; Faculdade de
Medicina da Universidade de Sao Paulo; 2007 June 18;
Available from the website: http://medicina.fm.usp.br/endore
sidentes/roteiro/diabetes_mellitus_roteiro.pdf.Morinelli TA, Tempel GE, Jaffa AA, Silva RH, Naka M, Folger
W, Halushka PV. 1993. Thromboxane A2/prostaglandin H2
receptors in streptozotocin-induced diabetes: Effects of insulin
therapy in the rat. Prostaglandins 45:427"438.Nanopharmaceuticals. 2007. NanoPharmaceuticals.org; Available
from the website: http://www.nanopharmaceuticals.org/Poly
meric_nanoparticles.htmlOppenheim RC, Stewart NF, Gordon L, Patel HM. 1982.
Production and evaluation of orally administered insulin
nanoparticles. Drug Dev Ind Pharm 8:531"546.Pan Y, Li Y, Zhao H, Zheng J, Xu H, Wei G, Hao J, Cui F. 2002.
Bioadhesive polysaccharide in protein delivery system: Chit-
osan nanoparticles improve the intestinal absorption of insulin
in vivo. Int J Pharm 249:139"147.Priya CAYB, Anitha K, Mohan EM, Pillai KS, Murthy PB, Nadu
T. 1997. Toxicity of fluoride to diabetic rats. Fluoride 30:
51"58.
12 C. P. Reis et al.
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008

Quintana XG, Rodrıguez MN, Sabo AG. 2001. Las plaquetas en
la diabetes mellitus. Rev Cub Hematol Inmunol Hemoter17:19"24.
Reis C, Veiga F, Ribeiro A, Neufeld R, Damge C. 2008.
Nanoparticulate biopolymers deliver insulin orally eliciting
pharmacological response. J Pharm Sci [ePub March 27,2008] DOI: 10.1002/jps.21363.
Reis CP, Neufeld RJ, Ribeiro, Antonio J, Veiga F. 2006a.
Nanoencapsulation I. Methods for preparation of drug-loadedpolymeric nanoparticles. Nanomed: Nanotechnol, Biol Med
2:8"21.Reis CP, Neufeld RJ, Ribeiro AJ, Veiga F. 2006b. Nanoencapsula-
tion II. Biomedical applications and current status of peptideand protein nanoparticulate delivery systems. Nanomed: Na-
notechnol, Biol Med 2:53"65.Reis CP, Ribeiro AJ, Houng S, Veiga F, Neufeld RJ. 2007.
Nanoparticulate delivery system for insulin: Design, character-ization and in vitro/in vivo bioactivity. Eur J Pharm Sci 30:392"397.
Reis CP, Ribeiro AJ, Neufeld RJ, Veiga F. 2006c. Alginate
microparticles as novel carrier for oral insulin delivery. Bio-technol Bioeng 96:977"989.
Sajeesh S, Sharma CP. 2006. Cyclodextrin-insulin complex
encapsulated polymethacrylic acid based nanoparticles fororal insulin delivery. Int J Pharm 325:147"154.
Sayim F, Yavasoglu NUK, Uyanikgil Y, Aktug H, Yavasoglu A,
Turgut M. 2005. Neurotoxic effects of cypermethrin in Wistar
rats: A haematological, biochemical and histophathologic
study. J Health Sci 51:300"307.Tschope D, Schwippert B, Schettler B, Kiesel U, Rothe H,
Roesen P, Gries FA. 1992. Increased GPIIB/IIIA expression
and altered DNA-ploidy pattern in megakaryocytes of diabetic
BB-rats. Eur J Clin Invest 22:591"598.Umeda F, Adnot S, Franks DJ, Hamet P. 1982. Cyclic nucleotide
phosphodiesterase and aggregation in platelets from diabetic
rats. Metabolism 31:704"709.Valentovic MA, Lubawy WC. 1983. Impact of insulin or
tolbutamide treatment on 14C-arachidonic acid conversion to
prostacyclin and/or thromboxane in lungs, aortas, and platelets
of streptozotocin-induced diabetic rats. Diabetes 32:846"851.Vauthier C, Dubernet C, Fattal E, Pinto-Alphandary H, Couvreur
P. 2003. Poly(alkylcyanoacrylates) as biodegradable materials
for biomedical applications. Adv Drug Deliv Rev 55:519"548.Vega-Villa KR, Takemoto JK, Yanez JA, Remsberg CM, Forrest
ML, Davies NM. 2008. Clinical toxicities of nanocarrier
systems. Adv Drug Deliv Rev 60:929"938.Wijkstrom M, Kirchhof N, Graham M, Ingulli E, Colvin RB,
Christians U, Hering BJ, Schuurman H-J. 2005. Cyclosporine
toxicity in immunosuppressed streptozotocin-diabetic nonhu-
man primates. Toxicology 207:117"127.Yngen M, Li N, Hjemdahl P, Wallen NH. 2001. Insulin enhances
platelet activation in vitro. Thromb Res 104:85"91.
Orally delivered insulin 13
Downloaded By: [Reis, Catarina Pinto] At: 16:59 12 October 2008