toxicological aspects and analysis of phenylalkylamine and
TRANSCRIPT

Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Medical University of Sofia, 2 Dunav Str, Sofia 1000, Bulgaria
Department of Pharmacology and Clinical pharmacology, Faculty of Medicine, Medical University of Plovdiv, 15A Vasil Aprilov Str., Plovdiv 4002,Bulgaria
Department of Chemistry, Faculty of Pharmacy, Medical University of Sofia, 2 Dunav Str, Sofia 1000, Bulgaria
Department of Pharmacology and Drug Toxicology, Faculty of Pharmacy, Medical University of Plovdiv, 15A Vasil Aprilov Str., Plovdiv 4002, Bulgaria
Clinic of Internal Diseases UMHATEM ”N. I. Pirogov”-Sofia, Bulgaria College of Pharmacy, Medical University-Plovdiv, 15A Vasil Aprilov Str., Plovdiv
4002, Bulgaria
Introduction Hallucinogens are substances which alter thought, perception and mood without affecting memory, producing intellectual impairment or leading to addiction. They also have negligible autonomic side effects. This definition is often considered too limited because besides the two main hallucinogenic classes’ indolylalkyl amines and phenylalkylamines other classes like
cannabinoids and N-methyl-d-aspartate (NMDA) antagonists, which are not classified as hallucinogens and possess different mechanism of action may produce similar and overlapping effects. Therefore the definition was expanded by Glennon (1996) who added that ‘the halluci-nogens are also agents that with an affinity for the 5-HT2A receptors’[1] (Fig. 1).
32 Review articles
PHARMACO - TOXICOLOGICAL ASPECTS AND ANALYSIS OFPHENYLALKYLAMINE AND INDOLYLALKYLAMINE
HALLUCINOGENS(REVIEW)
D. Obreshkova , I. Kandilarov , V. T. Angelova , Y. Iliev , P. Atanasov , P. S. Fotev
1
2
3
4
5
6
Abstract: The classical hallucinogens having an affinity towards 5HT2A recep-tors are discussed, along with their common behavioral effects, toxicity and psychiatric complications which could have long-term consequences on individuals. A survey has been done on the various analytical methods used for determination and quantification of hallucinogens: colorimetrical reactions (Marquis, Ehrlich tests), gas chromatography with mass spectrometry (when the substances are not thermo labile), tandem mass spec-trometry, high-performance liquid chromatography with UV detection and IR spectros-copy. Methods most often used to analyze biological samples like urine, blood or plasma immunological methods for quick detection, which results are confirmed later by the other methods mentioned above have been also discussed.
Key words: hallucinogens, analysis, LSD, Mescaline, DMT
1,6 2 3 4 5 6

Fig. 1 Hallucinations arise from agonism at 5-HT2A receptors[1].
These drugs are also known as classical or serotonergic hallucinogens [2]. Phenylalkyl-amines contain a phenetyl amine group similar to endogenous neurotransmitters dopamine and noradrenaline. Mescaline, 2,5-dimethoxy-4-me-thylamphetamine (DOM) and 2,5-dime-thoxy-4-iodoamphetamine (DOI) are examples of phenylalkilamines. Indolylalkylamines possess an indole nucleus similar structurally to 5-hydroxytryptamine or serotonin. They are divided into two subgroups – simple triptamines like N,N-dimethyltryptamine (DMT), bufotenin and psilocybin and ergolines like LSD [3]. The research into the psychopharmacology of hallu-cinations is conducted in two directions: first, hallucinogenic agents are investigating to deter-
mine their molecular effect on the brain [4, 5]; second, psychosis-associated diseases, which commonly include hallucinations, are success-fully treat using specific molecular approaches as well as another diseases [6, 7]. Because of the growing importance of the hallucinogens as drugs of abuse, analytical methods are needed in forensic and clinical toxicology, which allow reliable screening and quantification of these substances in biological matrices [8]. The aim of the current review is to sum-marize current information related to the analy-sis, pharmacology and toxicology of some clas-sic hallucinogens with phenylalkylamine and indolylalkylamine structure.
33PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
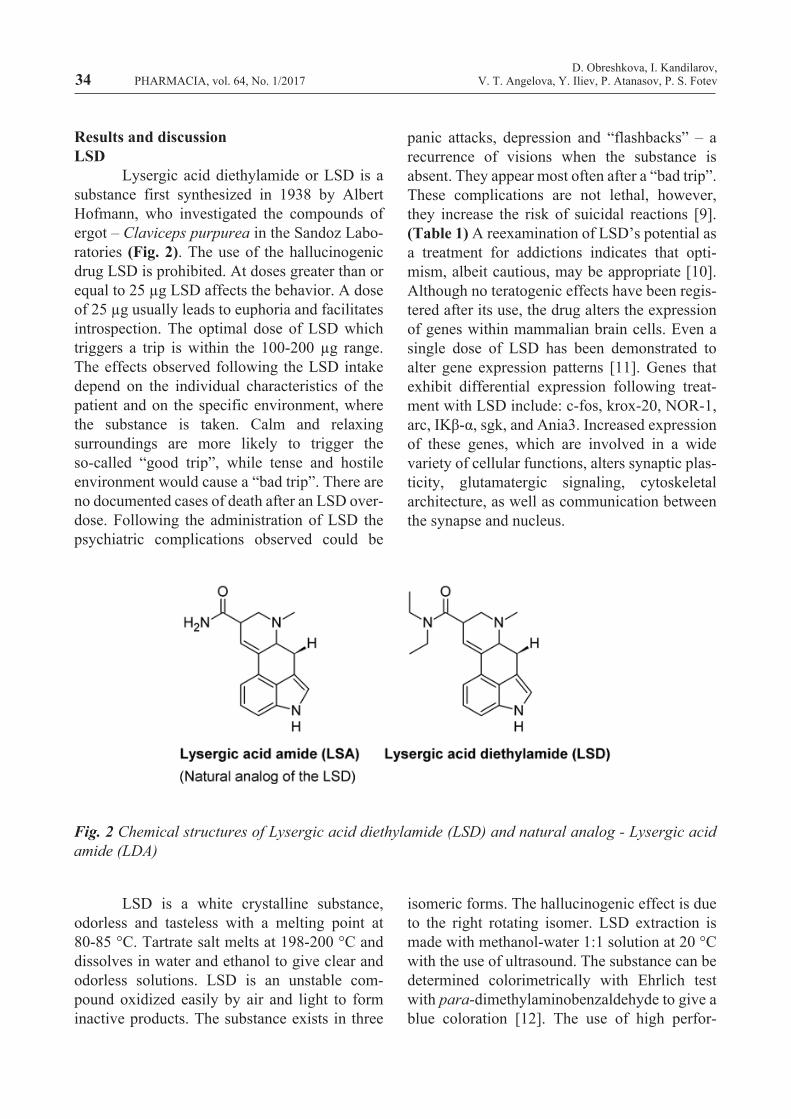
Fig. 2 Chemical structures of Lysergic acid diethylamide (LSD) and natural analog - Lysergic acid amide (LDA)
Results and discussionLSD Lysergic acid diethylamide or LSD is a substance first synthesized in 1938 by Albert Hofmann, who investigated the compounds of ergot – Claviceps purpurea in the Sandoz Labo-ratories (Fig. 2). The use of the hallucinogenic drug LSD is prohibited. At doses greater than or equal to 25 µg LSD affects the behavior. A dose of 25 µg usually leads to euphoria and facilitates introspection. The optimal dose of LSD which triggers a trip is within the 100-200 µg range. The effects observed following the LSD intake depend on the individual characteristics of the patient and on the specific environment, where the substance is taken. Calm and relaxing surroundings are more likely to trigger the so-called “good trip”, while tense and hostile environment would cause a “bad trip”. There are no documented cases of death after an LSD over-dose. Following the administration of LSD the psychiatric complications observed could be
panic attacks, depression and “flashbacks” – a recurrence of visions when the substance is absent. They appear most often after a “bad trip”. These complications are not lethal, however, they increase the risk of suicidal reactions [9]. (Table 1) A reexamination of LSD’s potential as a treatment for addictions indicates that opti-mism, albeit cautious, may be appropriate [10]. Although no teratogenic effects have been regis-tered after its use, the drug alters the expression of genes within mammalian brain cells. Even a single dose of LSD has been demonstrated to alter gene expression patterns [11]. Genes that exhibit differential expression following treat-ment with LSD include: c-fos, krox-20, NOR-1, arc, IΚβ-α, sgk, and Ania3. Increased expression of these genes, which are involved in a wide variety of cellular functions, alters synaptic plas-ticity, glutamatergic signaling, cytoskeletal architecture, as well as communication between the synapse and nucleus.
LSD is a white crystalline substance, odorless and tasteless with a melting point at 80-85 °C. Tartrate salt melts at 198-200 °C and dissolves in water and ethanol to give clear and odorless solutions. LSD is an unstable com-pound oxidized easily by air and light to form inactive products. The substance exists in three
isomeric forms. The hallucinogenic effect is due to the right rotating isomer. LSD extraction is made with methanol-water 1:1 solution at 20 °C with the use of ultrasound. The substance can be determined colorimetrically with Ehrlich test with para-dimethylaminobenzaldehyde to give a blue coloration [12]. The use of high perfor-
34D. Obreshkova, I. Kandilarov,
V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
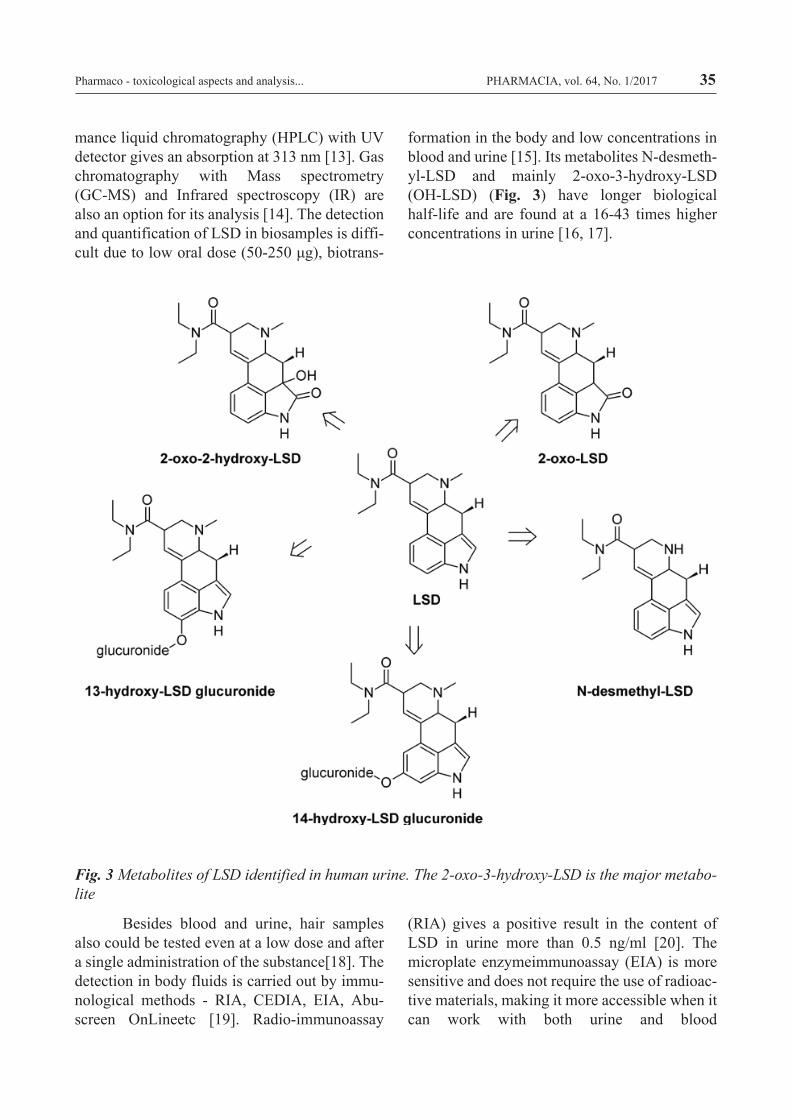
Fig. 3 Metabolites of LSD identified in human urine. The 2-oxo-3-hydroxy-LSD is the major metabo-lite
mance liquid chromatography (HPLC) with UV detector gives an absorption at 313 nm [13]. Gas chromatography with Mass spectrometry (GC-MS) and Infrared spectroscopy (IR) are also an option for its analysis [14]. The detection and quantification of LSD in biosamples is diffi-cult due to low oral dose (50-250 μg), biotrans-
formation in the body and low concentrations in blood and urine [15]. Its metabolites N-desmeth-yl-LSD and mainly 2-oxo-3-hydroxy-LSD (OH-LSD) (Fig. 3) have longer biological half-life and are found at a 16-43 times higher concentrations in urine [16, 17].
Besides blood and urine, hair samples also could be tested even at a low dose and after a single administration of the substance[18]. The detection in body fluids is carried out by immu-nological methods - RIA, CEDIA, EIA, Abu-screen OnLineetc [19]. Radio-immunoassay
(RIA) gives a positive result in the content of LSD in urine more than 0.5 ng/ml [20]. The microplate enzymeimmunoassay (EIA) is more sensitive and does not require the use of radioac-tive materials, making it more accessible when it can work with both urine and blood
35PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
36
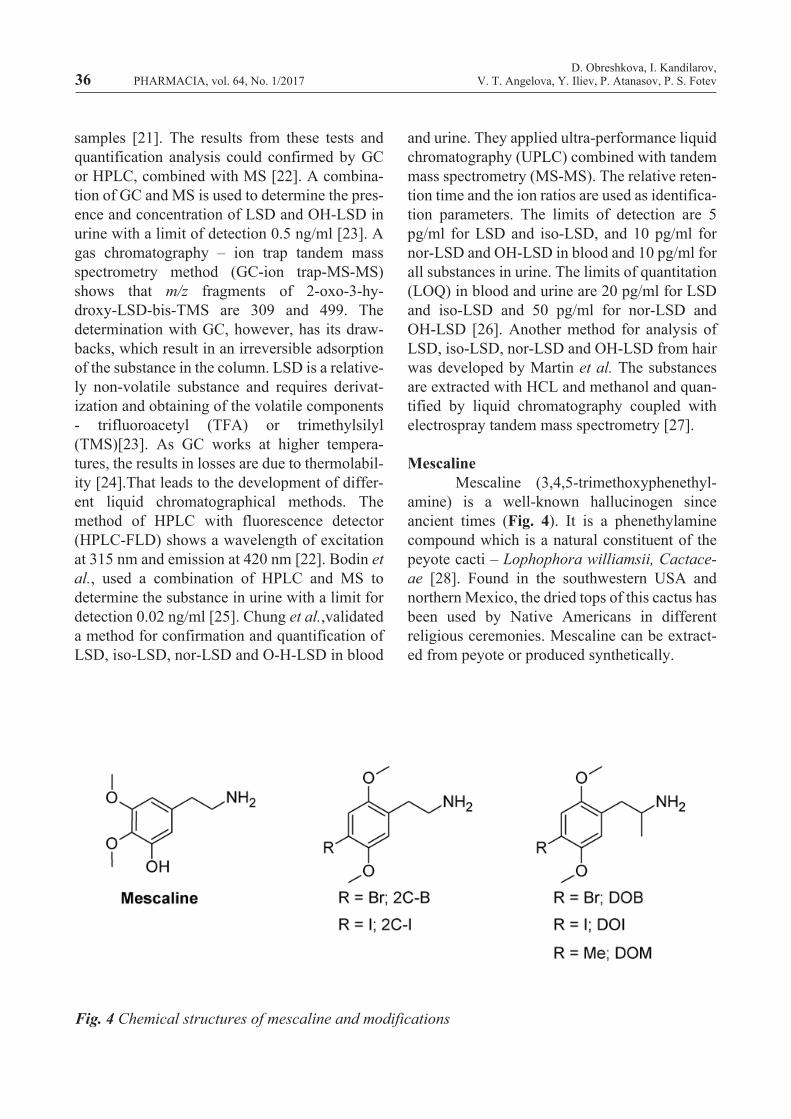
Fig. 4 Chemical structures of mescaline and modifications
samples [21]. The results from these tests and quantification analysis could confirmed by GC or HPLC, combined with MS [22]. A combina-tion of GC and MS is used to determine the pres-ence and concentration of LSD and OH-LSD in urine with a limit of detection 0.5 ng/ml [23]. A gas chromatography – ion trap tandem mass spectrometry method (GC-ion trap-MS-MS) shows that m/z fragments of 2-oxo-3-hy-droxy-LSD-bis-TMS are 309 and 499. The determination with GC, however, has its draw-backs, which result in an irreversible adsorption of the substance in the column. LSD is a relative-ly non-volatile substance and requires derivat-ization and obtaining of the volatile components - trifluoroacetyl (TFA) or trimethylsilyl (TMS)[23]. As GC works at higher tempera-tures, the results in losses are due to thermolabil-ity [24].That leads to the development of differ-ent liquid chromatographical methods. The method of HPLC with fluorescence detector (HPLC-FLD) shows a wavelength of excitation at 315 nm and emission at 420 nm [22]. Bodin et al., used a combination of HPLC and MS to determine the substance in urine with a limit for detection 0.02 ng/ml [25]. Chung et al.,validated a method for confirmation and quantification of LSD, iso-LSD, nor-LSD and O-H-LSD in blood
and urine. They applied ultra-performance liquid chromatography (UPLC) combined with tandem mass spectrometry (MS-MS). The relative reten-tion time and the ion ratios are used as identifica-tion parameters. The limits of detection are 5 pg/ml for LSD and iso-LSD, and 10 pg/ml for nor-LSD and OH-LSD in blood and 10 pg/ml for all substances in urine. The limits of quantitation (LOQ) in blood and urine are 20 pg/ml for LSD and iso-LSD and 50 pg/ml for nor-LSD and OH-LSD [26]. Another method for analysis of LSD, iso-LSD, nor-LSD and OH-LSD from hair was developed by Martin et al. The substances are extracted with HCL and methanol and quan-tified by liquid chromatography coupled with electrospray tandem mass spectrometry [27].
Mescaline Mescaline (3,4,5-trimethoxyphenethyl-amine) is a well-known hallucinogen since ancient times (Fig. 4). It is a phenethylamine compound which is a natural constituent of the peyote cacti – Lophophora williamsii, Cactace-ae [28]. Found in the southwestern USA and northern Mexico, the dried tops of this cactus has been used by Native Americans in different religious ceremonies. Mescaline can be extract-ed from peyote or produced synthetically.
D. Obreshkova, I. Kandilarov,V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
Mescaline is used primarily as a recre-ational drug and is also used to supplement vari-ous types of meditation and psychedelic therapy. The use of peyote is illegal and its consumption leads to a hallucinogenic effect similar to those of LSD, but 4000 times weaker although the duration of the trip is longer [29, 30]. Although mescaline does not lead to addiction, it could provoke a lot of adverse reactions like tachycar-dia, hypertension, nausea, psychosis and para-noia [29]. Some death cases are reported after the consumption of peyote but on extremely rare occasions. In one of them, a 32 year-old Native American having drunk peyote tea died due to Mallory-Weiss esophageal laceration caused by vomiting which mescaline had induced [31].With continued drug use, the long term effects of mescaline take the form of addiction where a person’s lifestyle revolves around getting and using the drug. Mescaline interacts with the brain’s cognitive and emotion-based centers, oftentimes bringing users to vulnerable and even helpless states of mind. With frequent drug use, the long term effects of mescaline can compromise severely the psychological well-be-ing of a person (Table 1). Mescaline is a white crystalline substance with melting point of 35-36 °C, boil-ing at 180 °C. It is moderately soluble in water and soluble in ethanol, chloroform and benzene [32]. The usual dose of mescaline which provokes a hallucinogenic reaction is within the range of 200 to 500 mg [30] (equals to 5-10 peyote buttons) [33]. Mescaline could be detect-ed by a colorimetric test, e.g. Marquis test which is used for alkaloids and amphetamines. The reagent is a mixture of 100 ml of concentrated sulfuric acid and 1 ml of 40 % solution of form-aldehyde dripped onto the tested substance. The test is quick and does not require specific equip-ment. Mescaline gives orange color and its limit of detection is 1 µg [34]. Froehde reagent could also be used to identify mescaline. It consists of molybdic acid or sodium molybdate and concen-trated sulfuric acid, mixed, heated and then added dropwise on the substance tested. If mes-caline is available, it gives a greenish to brown
color [35]. Detection of mescaline could be made with GC combined with MS [36, 37]. The m/z top peak is 30, m/z 2nd highest is 182 and m/z 3rd highest is 166. MS-MS peaks are m/z 180, m/z 195 and m/z 179(35)(25).The quantification of mescaline is carried out by HPLC with UV detector. The UV absorbance maximum for mes-caline is 205 nm [34]. Urine could be screened for mescaline using biochip array immunoassay as it is done by Battal et al. They validate GC-MS by an electron impact ionization method for quantification of the substance [38]. LC-MS-MS method was developed by Bjorns-tad et al.,in order to confirm the presence of mes-caline in urine samples. The limit of detection in a urine matrix is 3-5 µg/l. Separation is made on a HyPURITY C18 column using methanol gradient in ammonium acetate buffer. The observed transitions in the MS-MS analysis are m/z 212.3 to m/z 180.3 for mescaline and m/z 221.3 to m/z 186.3 for the deutered internal stan-dard – mescaline-d9 [39]. Peyote tea, hair sam-ples and urine from boy suspected in mescaline abuse were analyzed using GC-MS and GC-MS-MS methods, validated by Gambelung-he et al.,[40]. GC-MS analysis detected mesca-line in the tea but not in the urine (because it was already excreted) and GC-MS-MS analysis found mescaline in the proximal segments of the hair where the substance accumulated for longer periods.
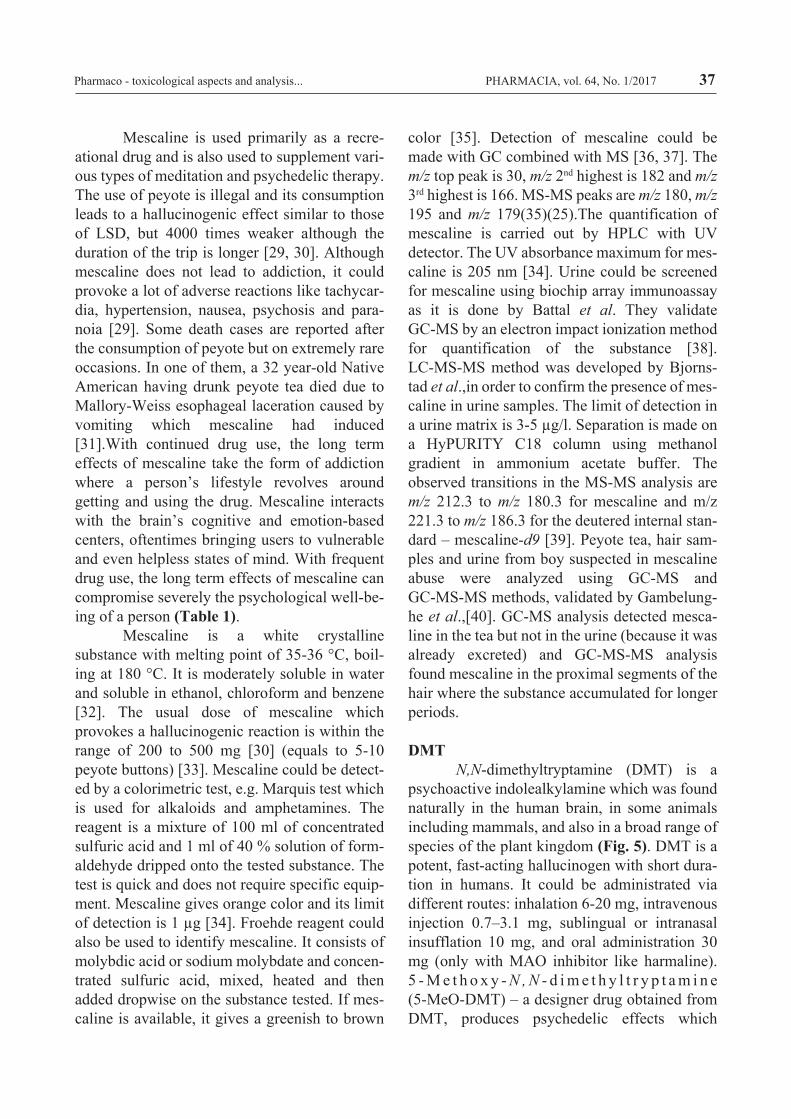
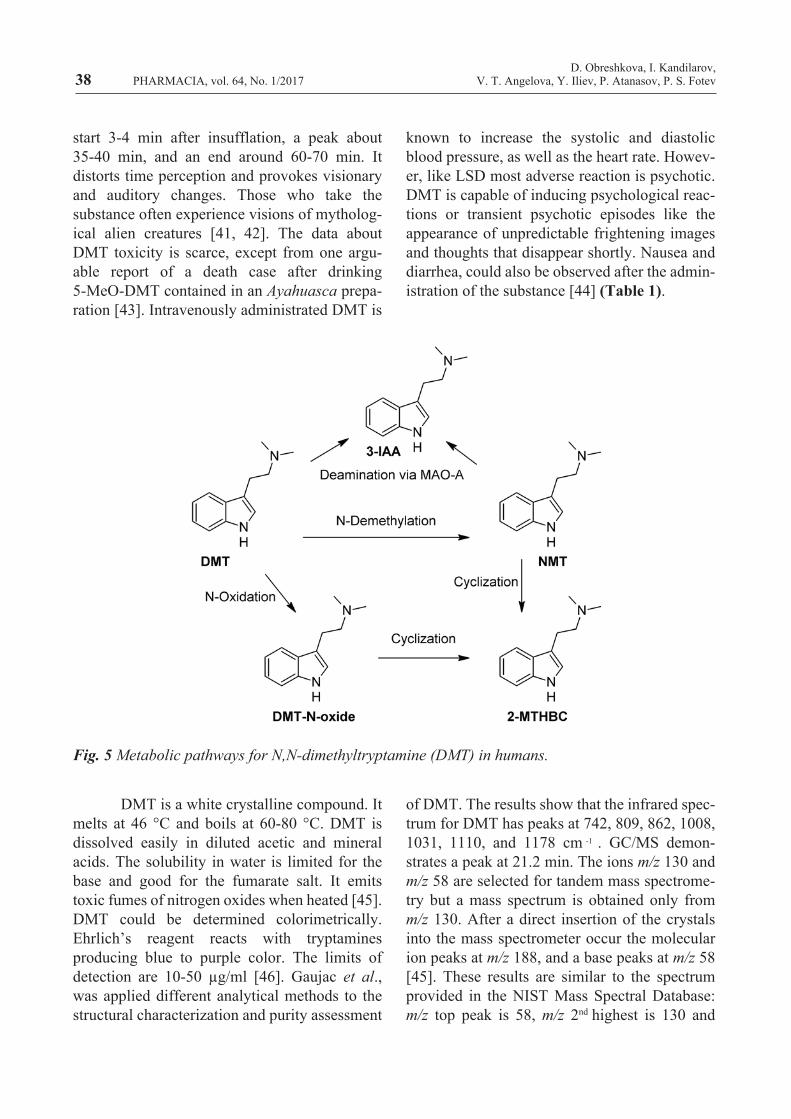
DMT N,N-dimethyltryptamine (DMT) is a psychoactive indolealkylamine which was found naturally in the human brain, in some animals including mammals, and also in a broad range of species of the plant kingdom (Fig. 5). DMT is a potent, fast-acting hallucinogen with short dura-tion in humans. It could be administrated via different routes: inhalation 6-20 mg, intravenous injection 0.7–3.1 mg, sublingual or intranasal insufflation 10 mg, and oral administration 30 mg (only with MAO inhibitor like harmaline). 5 - M e t h o x y - N , N - d i m e t h y l t r y p t a m i n e (5-MeO-DMT) – a designer drug obtained from DMT, produces psychedelic effects which
37PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
DMT is a white crystalline compound. It melts at 46 °C and boils at 60-80 °C. DMT is dissolved easily in diluted acetic and mineral acids. The solubility in water is limited for the base and good for the fumarate salt. It emits toxic fumes of nitrogen oxides when heated [45]. DMT could be determined colorimetrically. Ehrlich’s reagent reacts with tryptamines producing blue to purple color. The limits of detection are 10-50 µg/ml [46]. Gaujac et al., was applied different analytical methods to the structural characterization and purity assessment
of DMT. The results show that the infrared spec-trum for DMT has peaks at 742, 809, 862, 1008, 1031, 1110, and 1178 cm . GC/MS demon-strates a peak at 21.2 min. The ions m/z 130 and m/z 58 are selected for tandem mass spectrome-try but a mass spectrum is obtained only from m/z 130. After a direct insertion of the crystals into the mass spectrometer occur the molecular ion peaks at m/z 188, and a base peaks at m/z 58 [45]. These results are similar to the spectrum provided in the NIST Mass Spectral Database: m/z top peak is 58, m/z 2nd highest is 130 and
Fig. 5 Metabolic pathways for N,N-dimethyltryptamine (DMT) in humans.
start 3-4 min after insufflation, a peak about 35-40 min, and an end around 60-70 min. It distorts time perception and provokes visionary and auditory changes. Those who take the substance often experience visions of mytholog-ical alien creatures [41, 42]. The data about DMT toxicity is scarce, except from one argu-able report of a death case after drinking 5-MeO-DMT contained in an Ayahuasca prepa-ration [43]. Intravenously administrated DMT is
known to increase the systolic and diastolic blood pressure, as well as the heart rate. Howev-er, like LSD most adverse reaction is psychotic. DMT is capable of inducing psychological reac-tions or transient psychotic episodes like the appearance of unpredictable frightening images and thoughts that disappear shortly. Nausea and diarrhea, could also be observed after the admin-istration of the substance [44] (Table 1).
38
-1
D. Obreshkova, I. Kandilarov,V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
m/z 3rd highest is 188. The UV absorbance maxi-mum for DMT is at 280 nm [47]. Ishii at al.,[48] used GC with surface ionization detection (SID) for identification and quantization of DMT in whole blood and urine using gramine as an inter-nal standard. Solid-phase extraction of the sam-ples is carried out with Sep-Pak C18 cartrige before the analysis. The limit of detection of DMT is 0.5 ng/ml. The retention times are 7.9 min for gramine and 9.4 min for DMT. The intensity of the peaks is similar, regardless of the different quantity - 500 ng for gramine and 10 ng for DMT thus the response of SID to DMT is higher [48]. Another method for the analysis of designer triptamines and phenetylamines in blood and urine was developed by Vorce and Sklerov. They used a screening method based on GC/MS with electrospray ionization (ESI), opti-mizing the separation of the substances. The retention time for DMT is 10.-14 min. The different drugs are identified of - by selected ion monitoring (SIM). The SIM ions for DMT is m/z 58.129 and 180 [49]. There are other analytical methods for identification and quantization of DMT as a component of the Ayahuasca prepara-tion such as: analysis of plasma with GC with a nitrogen-phosphorus detection after liquid-liquid extraction with diphenhydramine as an internal standard [50]; or with n-pentane [51]; analysis of urine with LC-ESI-MS/MS [52].
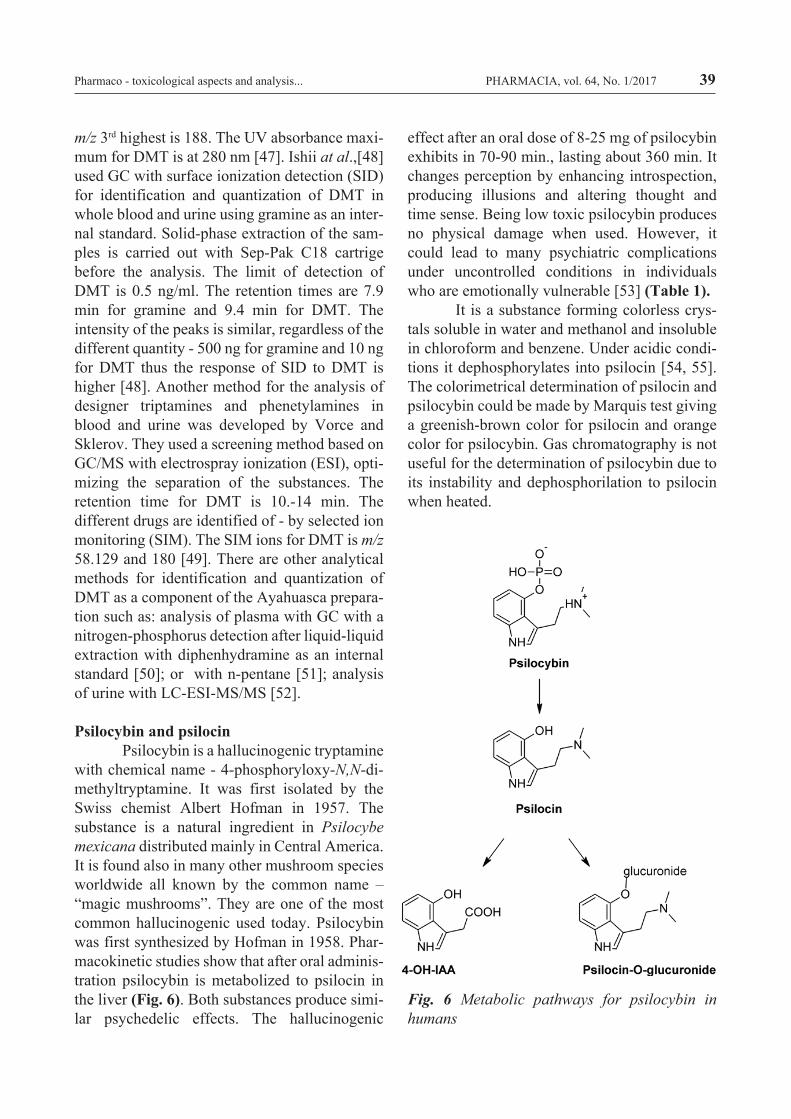
Psilocybin and psilocin Psilocybin is a hallucinogenic tryptamine with chemical name - 4-phosphoryloxy-N,N-di-methyltryptamine. It was first isolated by the Swiss chemist Albert Hofman in 1957. The substance is a natural ingredient in Psilocybe mexicana distributed mainly in Central America. It is found also in many other mushroom species worldwide all known by the common name – “magic mushrooms”. They are one of the most common hallucinogenic used today. Psilocybin was first synthesized by Hofman in 1958. Phar-macokinetic studies show that after oral adminis-tration psilocybin is metabolized to psilocin in the liver (Fig. 6). Both substances produce simi-lar psychedelic effects. The hallucinogenic
effect after an oral dose of 8-25 mg of psilocybin exhibits in 70-90 min., lasting about 360 min. It changes perception by enhancing introspection, producing illusions and altering thought and time sense. Being low toxic psilocybin produces no physical damage when used. However, it could lead to many psychiatric complications under uncontrolled conditions in individuals who are emotionally vulnerable [53] (Table 1). It is a substance forming colorless crys-tals soluble in water and methanol and insoluble in chloroform and benzene. Under acidic condi-tions it dephosphorylates into psilocin [54, 55]. The colorimetrical determination of psilocin and psilocybin could be made by Marquis test giving a greenish-brown color for psilocin and orange color for psilocybin. Gas chromatography is not useful for the determination of psilocybin due to its instability and dephosphorilation to psilocin when heated.
Fig. 6 Metabolic pathways for psilocybin in humans
39PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
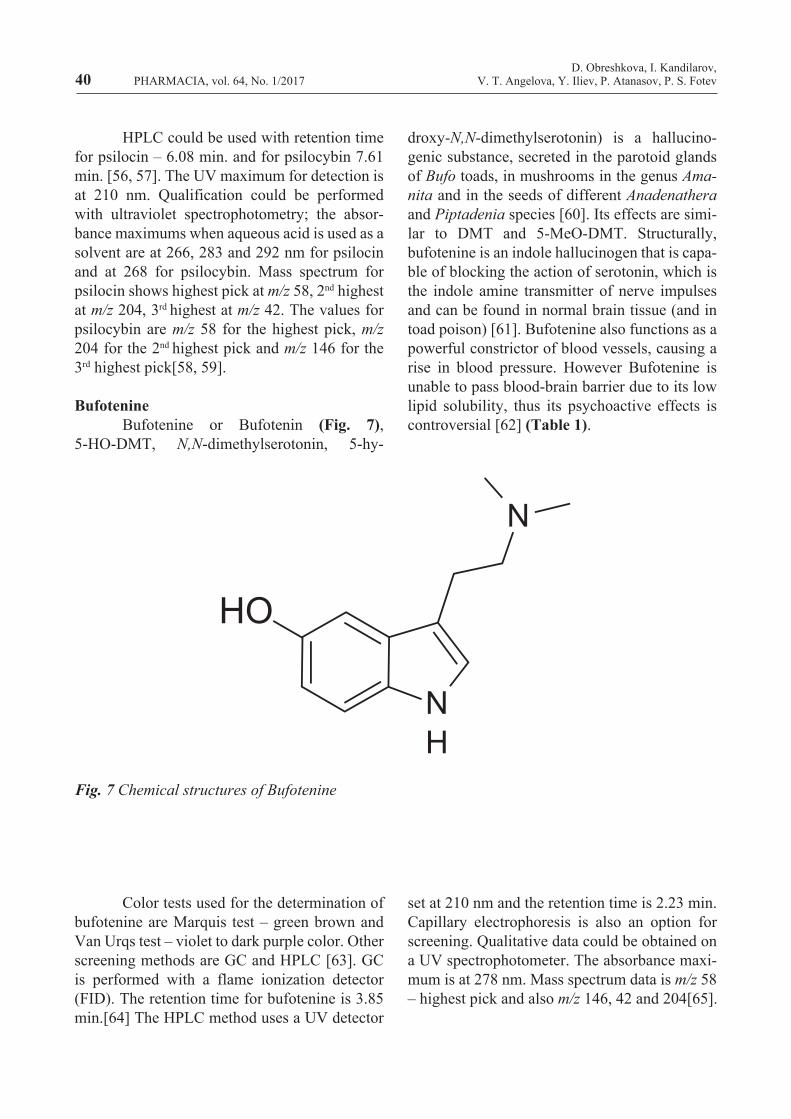
Fig. 7 Chemical structures of Bufotenine
HPLC could be used with retention time for psilocin – 6.08 min. and for psilocybin 7.61 min. [56, 57]. The UV maximum for detection is at 210 nm. Qualification could be performed with ultraviolet spectrophotometry; the absor-bance maximums when aqueous acid is used as a solvent are at 266, 283 and 292 nm for psilocin and at 268 for psilocybin. Mass spectrum for psilocin shows highest pick at m/z 58, 2nd highest at m/z 204, 3rd highest at m/z 42. The values for psilocybin are m/z 58 for the highest pick, m/z 204 for the 2nd highest pick and m/z 146 for the 3rd highest pick[58, 59].
Bufotenine Bufotenine or Bufotenin (Fig. 7), 5-HO-DMT, N,N-dimethylserotonin, 5-hy-
droxy-N,N-dimethylserotonin) is a hallucino-genic substance, secreted in the parotoid glands of Bufo toads, in mushrooms in the genus Ama-nita and in the seeds of different Anadenathera and Piptadenia species [60]. Its effects are simi-lar to DMT and 5-MeO-DMT. Structurally, bufotenine is an indole hallucinogen that is capa-ble of blocking the action of serotonin, which is the indole amine transmitter of nerve impulses and can be found in normal brain tissue (and in toad poison) [61]. Bufotenine also functions as a powerful constrictor of blood vessels, causing a rise in blood pressure. However Bufotenine is unable to pass blood-brain barrier due to its low lipid solubility, thus its psychoactive effects is controversial [62] (Table 1).
Color tests used for the determination of bufotenine are Marquis test – green brown and Van Urqs test – violet to dark purple color. Other screening methods are GC and HPLC [63]. GC is performed with a flame ionization detector (FID). The retention time for bufotenine is 3.85 min.[64] The HPLC method uses a UV detector
set at 210 nm and the retention time is 2.23 min. Capillary electrophoresis is also an option for screening. Qualitative data could be obtained on a UV spectrophotometer. The absorbance maxi-mum is at 278 nm. Mass spectrum data is m/z 58 – highest pick and also m/z 146, 42 and 204[65].
40D. Obreshkova, I. Kandilarov,
V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
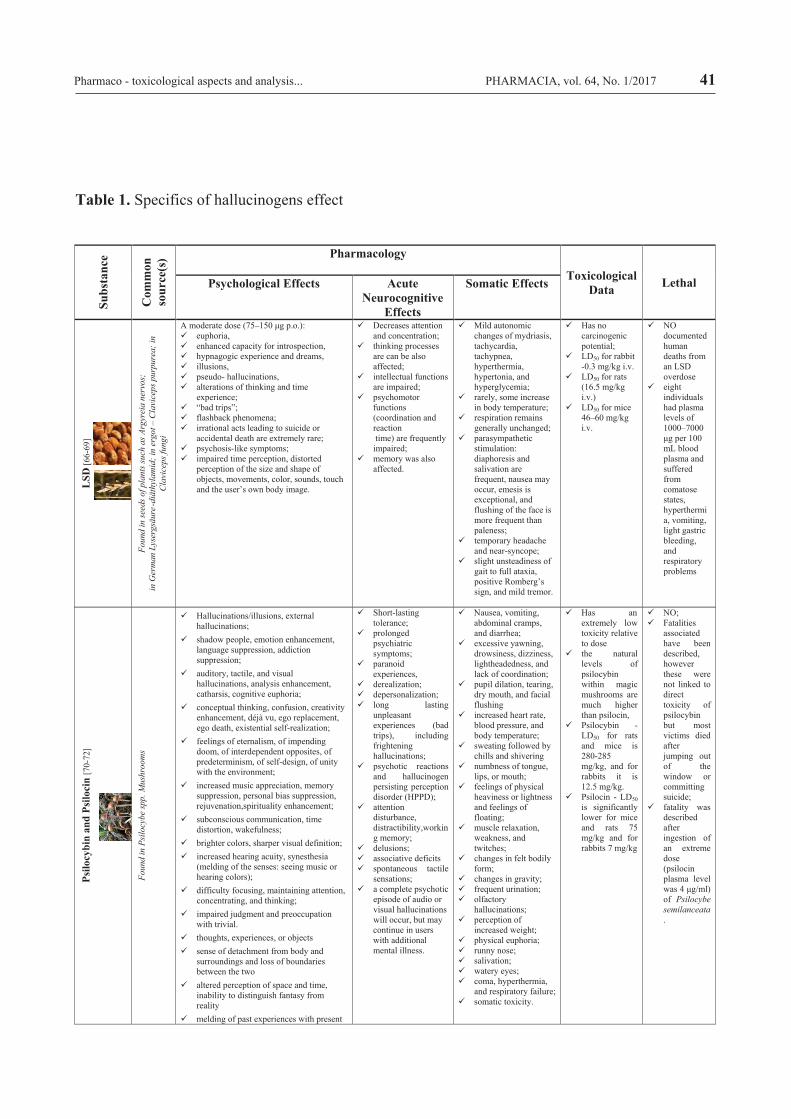
Table 1. Specifics of hallucinogens effect
41Su
bsta
nce
Com
mon
so
urce
(s) Pharmacology
Toxicological Data LethalPsychological Effects Acute
Neurocognitive Effects
Somatic Effects
LSD
[66-
69]
Fo
und
in se
eds o
f pla
nts s
uch
as A
rgyr
eia
nerv
os;
inG
erm
an L
yser
gsäu
re-d
iäth
ylam
id;i
n er
got –
Cla
vice
ps p
urpu
rea;
inC
lavi
ceps
fung
i
A moderate dose (75–150 μg p.o.): euphoria, enhanced capacity for introspection, hypnagogic experience and dreams, illusions, pseudo- hallucinations, alterations of thinking and time
experience; “bad trips”; flashback phenomena; irrational acts leading to suicide or
accidental death are extremely rare; psychosis-like symptoms; impaired time perception, distorted
perception of the size and shape of objects, movements, color, sounds, touch and the user’s own body image.
Decreases attention and concentration;
thinking processes are can be also affected;
intellectual functions are impaired;
psychomotor functions (coordination and reactiontime) are frequently
impaired; memory was also
affected.
Mild autonomic changes of mydriasis, tachycardia, tachypnea,hyperthermia, hypertonia, and hyperglycemia;
rarely, some increase in body temperature;
respiration remains generally unchanged;
parasympathetic stimulation: diaphoresis and salivation are frequent, nausea may occur, emesis is exceptional, and flushing of the face is more frequent than paleness;
temporary headache and near-syncope;
slight unsteadiness of gait to full ataxia, positive Romberg’s sign, and mild tremor.
Has no carcinogenic potential;
LD50 for rabbit -0.3 mg/kg i.v.
LD50 for rats (16.5 mg/kg i.v.)
LD50 for mice 46–60 mg/kg i.v.
NOdocumented human deaths from an LSD overdose
eight individuals had plasma levels of 1000–7000 μg per 100 mL blood plasma and suffered from comatose states, hyperthermia, vomiting, light gastric bleeding, and respiratory problems
Psilo
cybi
nan
d Ps
iloci
n[7
0-72
]
Foun
d in
Psi
locy
be sp
p. M
ushr
oom
s
Hallucinations/illusions, external hallucinations;
shadow people, emotion enhancement, language suppression, addiction suppression;
auditory, tactile, and visual hallucinations, analysis enhancement, catharsis, cognitive euphoria;
conceptual thinking, confusion, creativity enhancement, déjà vu, ego replacement, ego death, existential self-realization;
feelings of eternalism, of impending doom, of interdependent opposites, of predeterminism, of self-design, of unity with the environment;
increased music appreciation, memory suppression, personal bias suppression, rejuvenation,spirituality enhancement;
subconscious communication, time distortion, wakefulness;
brighter colors, sharper visual definition; increased hearing acuity, synesthesia
(melding of the senses: seeing music or hearing colors);
difficulty focusing, maintaining attention, concentrating, and thinking;
impaired judgment and preoccupation with trivial.
thoughts, experiences, or objects sense of detachment from body and
surroundings and loss of boundaries between the two
altered perception of space and time, inability to distinguish fantasy from reality
melding of past experiences with present
Short-lasting tolerance;
prolonged psychiatric symptoms;
paranoid experiences,
derealization; depersonalization; long lasting
unpleasant experiences (bad trips), including frightening hallucinations;
psychotic reactions and hallucinogen persisting perception disorder (HPPD);
attention disturbance, distractibility,working memory;
delusions; associative deficits spontaneous tactile
sensations; a complete psychotic
episode of audio or visual hallucinations will occur, but may continue in users with additional mental illness.
Nausea, vomiting, abdominal cramps, and diarrhea;
excessive yawning, drowsiness, dizziness, lightheadedness, and lack of coordination;
pupil dilation, tearing, dry mouth, and facial flushing
increased heart rate, blood pressure, and body temperature;
sweating followed by chills and shivering
numbness of tongue, lips, or mouth;
feelings of physical heaviness or lightness and feelings of floating;
muscle relaxation, weakness, and twitches;
changes in felt bodily form;
changes in gravity; frequent urination; olfactory
hallucinations; perception of
increased weight; physical euphoria; runny nose; salivation; watery eyes; coma, hyperthermia,
and respiratory failure; somatic toxicity.
Has anextremely low toxicity relative to dose
the natural levels of psilocybin within magic mushrooms are much higher than psilocin,
Psilocybin -LD50 for rats and mice is 280-285 mg/kg, and for rabbits it is 12.5 mg/kg.
Psilocin - LD50is significantly lower for mice and rats 75 mg/kg and for rabbits 7 mg/kg
NO; Fatalities
associatedhave been described, however these were not linked to direct toxicity of psilocybin but most victims died after jumping out of the window or committing suicide;
fatality was described after ingestion of an extreme dose (psilocin plasma level was 4 μg/ml) of Psilocybe semilanceata.
PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
Conclusion Most hallucinogens are found as natural ingredients in many plants, mushrooms or animals and have been known to man since ancient times. Nowadays with the discovery of novel synthetic and semi-synthetic substances, they are still used despite of the unpredictable consequences that might occur as a result of their application. Most of the substances exhibit low
toxicity but the risks of damaging mental health or causing physical traumas during the halluci-nogenic trips should not be underestimated. Moreover, hallucinogenic substances are illegal in most countries worldwide, thus it is important to know different sensitive analytical methods for their determination and quantification in different biological matrices such as blood, plasma, urine and hair.
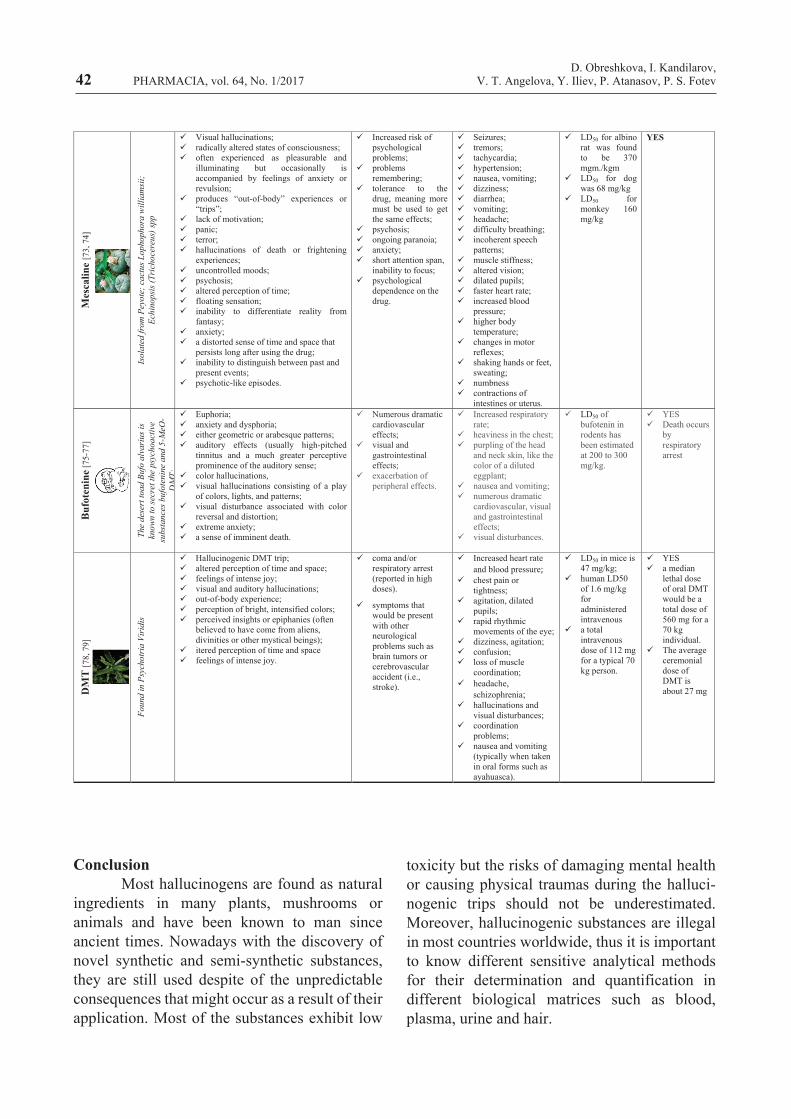
42M
esca
line
[73,
74]
Isol
ated
from
Pey
ote;
cact
us L
opho
phor
a w
illia
msi
i;Ec
hino
psis
(Tric
hoce
reus
) spp
Visual hallucinations; radically altered states of consciousness; often experienced as pleasurable and
illuminating but occasionally is accompanied by feelings of anxiety or revulsion;
produces “out-of-body” experiences or “trips”;
lack of motivation; panic; terror; hallucinations of death or frightening
experiences; uncontrolled moods; psychosis; altered perception of time; floating sensation; inability to differentiate reality from
fantasy; anxiety; a distorted sense of time and space that
persists long after using the drug; inability to distinguish between past and
present events; psychotic-like episodes.
Increased risk of psychological problems;
problems remembering;
tolerance to the drug, meaning more must be used to get the same effects;
psychosis; ongoing paranoia; anxiety; short attention span,
inability to focus; psychological
dependence on the drug.
Seizures; tremors; tachycardia; hypertension; nausea, vomiting; dizziness; diarrhea; vomiting; headache; difficulty breathing; incoherent speech
patterns; muscle stiffness; altered vision; dilated pupils; faster heart rate; increased blood
pressure; higher body
temperature; changes in motor
reflexes; shaking hands or feet,
sweating; numbness contractions of
intestines or uterus.
LD50 for albino rat was found to be 370 mgm./kgm
LD50 for dog was 68 mg/kg
LD50 formonkey 160mg/kg
YES
Buf
oten
ine [
75-7
7]
The
dese
rt to
ad B
ufo
alva
rius
is
know
n to
secr
et th
e ps
ycho
activ
e su
bsta
nces
buf
oten
ine
and
5-M
eO-
DM
T;
Euphoria; anxiety and dysphoria; either geometric or arabesque patterns; auditory effects (usually high-pitched
tinnitus and a much greater perceptive prominence of the auditory sense;
color hallucinations, visual hallucinations consisting of a play
of colors, lights, and patterns; visual disturbance associated with color
reversal and distortion; extreme anxiety; a sense of imminent death.
Numerous dramatic cardiovascular effects;
visual and gastrointestinaleffects;
exacerbation of peripheral effects.
Increased respiratory rate;
heaviness in the chest; purpling of the head
and neck skin, like the color of a diluted eggplant;
nausea and vomiting; numerous dramatic
cardiovascular, visual and gastrointestinal effects;
visual disturbances.
LD50 of bufotenin in rodents has been estimated at 200 to 300mg/kg.
YES Death occurs
by respiratory arrest
DM
T[7
8, 7
9]
Foun
d in
Psyc
hotr
ia V
irid
is
Hallucinogenic DMT trip; altered perception of time and space; feelings of intense joy; visual and auditory hallucinations; out-of-body experience; perception of bright, intensified colors; perceived insights or epiphanies (often
believed to have come from aliens, divinities or other mystical beings);
itered perception of time and space feelings of intense joy.
coma and/or respiratory arrest (reported in high doses).
symptoms that would be present with other neurological problems such as brain tumors or cerebrovascular accident (i.e., stroke).
Increased heart rateand blood pressure;
chest pain or tightness;
agitation, dilated pupils;
rapid rhythmicmovements of the eye;
dizziness, agitation; confusion; loss of muscle
coordination; headache,
schizophrenia; hallucinations and
visual disturbances; coordination
problems; nausea and vomiting
(typically when taken in oral forms such asayahuasca).
LD50 in mice is 47 mg/kg;
human LD50 of 1.6 mg/kg for administered intravenous
a total intravenous dose of 112 mg for a typical 70 kg person.
YES a median
lethal dose of oral DMT would be a total dose of 560 mg for a 70 kg individual.
The average ceremonial dose of DMT is about 27 mg
D. Obreshkova, I. Kandilarov,V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
References 1. Lowe NG, Rapagnani MP, Mattei C, Stahl SM. The Psychopharmacology of Halluci-nations: Ironic Insights into Mechanisms of Action. The Neuroscience of Hallucinations: Springer; 2013. p. 471-92. 2. Araújo AM, Carvalho F, de Lourdes Bastos M, de Pinho PG, Carvalho M. The hallu-cinogenic world of tryptamines: an updated review. Archives of toxicology. 2015;89(8):1151-73. 3. Fantegrossi WE, Murnane KS, Reissig CJ. The behavioral pharmacology of hallucino-gens. Biochemical pharmacology. 2008;75(1):17-33. 4. dos Santos RG, Osório FL, Crippa JAS, Hallak JE. Classical hallucinogens and neuroimaging: A systematic review of human studies: Hallucinogens and neuroimaging. Neu-roscience & Biobehavioral Reviews. 2016;71:715-28. 5. Ibarra-Laclette E, Zamudio-Hernán-dez F, Pérez-Torres CA, Albert VA, Ramírez-Chávez E, Molina-Torres J, et al. De novo sequencing and analysis of Lophophora williamsii transcriptome, and searching for puta-tive genes involved in mescaline biosynthesis. BMC genomics. 2015;16(1):657. 6. Grob CS, Bossis AP, Griffiths RR. Use of the classic hallucinogen psilocybin for treatment of existential distress associated with cancer. Psychological aspects of cancer: Spring-er; 2013. p. 291-308. 7. Vigerelli H, Sciani JM, Jared C, Anto-niazzi MM, Caporale GMM, da Silva AdCR, et al. Bufotenine is able to block rabies virus infec-tion in BHK-21 cells. Journal of Venomous Animals and Toxins including Tropical Diseas-es. 2014;20(1):1. 8. Habrdova V, Peters FT, Theobald DS, Maurer HH. Screening for and validated quanti-fication of phenethylamine‐type designer drugs and mescaline in human blood plasma by gas chromatography/mass spectrometry. Journal of mass spectrometry. 2005;40(6):785-95. 9. Passie T, Halpern JH, Stichtenoth DO, Emrich HM, Hintzen A. The pharmacology of
lysergic acid diethylamide: a review. CNS Neu-roscience & Therapeutics. 2008;14(4):295-314. 10. B Liester M. A review of lysergic acid diethylamide (LSD) in the treatment of addictions: historical perspectives and future prospects. Current drug abuse reviews. 2014;7(3):146-56. 11. Nichols CD, Sanders-Bush E. A single dose of lysergic acid diethylamide influ-ences gene expression patterns within the mam-malian brain. 2002. 12. Ghysel M-H, Trotin F, editors. Les substances hallucinogènes provenant de l'ergot de seigle et des volubilis. Annales de Toxicolo-gie Analytique; 2004: EDP Sciences. 13. Veress T. Study of the extraction of LSD from illicit blotters for HPLC determina-tion. Journal of Forensic Science. 1993;38(5):1105-10. 14. Harris HA, Kane T. A method for identification of Lysergic acid diethylamide (LSD) using a microscope sampling device with Fourier Transform Infrared (FT/IR) spectrosco-py. Journal of Forensic Science. 1991;36(4):1186-91. 15. Schneider S, Kuffer P, Wennig R. Determination of lysergide (LSD) and phency-clidine in biosamples. Journal of Chromatogra-phy B: Biomedical Sciences and Applications. 1998;713(1):189-200. 16. Horn CK, Klette KL, Stout PR. LC-MS Analysis of 2-Oxo-3-Hydroxy LSD from Urine Using a Speedisk® Positive-Pressure Processor with Cerex® PolyChrom™ CLIN II Columns. Journal of analytical toxicology. 2003;27(7):459-63. 17. Klette KL, Anderson CJ, Poch GK, Nimrod AC, ElSohly MA. Metabolism of lyser-gic acid diethylamide (LSD) to 2-oxo-3-hydroxy LSD (OH-LSD) in human liver microsomes and cryopreserved human hepatocytes. Journal of analytical toxicology. 2000;24(7):550-6. 18. Nakahara Y, Kikura R, Takahashi K, Foltz RL, Mieczkowski T. Detection of LSD and metabolite in rat hair and human hair. Journal of analytical toxicology. 1996;20(5):323-9. 19. McNally A, Goc-Szkutnicka K, Li Z,
43PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
Pilcher I, Polakowski S, Salamone S. An online immunoassay for LSD: Comparison with GC-MS and the abuscreen® RIA. Journal of analytical toxicology. 1996;20(6):404-8. 20. Alan H, Feng Y-J, Pajor A, Gornet TG, Wong SS, Forte E, et al. Detection and inter-pretation of lysergic acid diethylamide results by immunoassay screening of urine in various testing groups. Journal of analytical toxicology. 1997;21(3):181-4. 21. Cassells NP, Craston DH, Hand CW, Baldwin D. Development and Validation of a Nonisotopic Immunoassay for the Detection of LSD in Human Urine. Journal of analytical toxi-cology. 1996;20(6):409-15. 22. Grobosch T, Lemm-Ahlers U. Immu-noassay screening of lysergic acid diethylamide (LSD) and its confirmation by HPLC and fluo-rescence detection following LSD immunelute extraction. Journal of analytical toxicology. 2002;26(3):181-6. 23. Burnley B, George S. The develop-ment and application of a gas chromatogra-phy-mass spectrometric (GC-MS) assay to determine the presence of 2-oxo-3-hy-droxy-LSD in urine. Journal of analytical toxi-cology. 2003;27(4):249-52. 24. Libong D, Bouchonnet S, Ricordel I. A selective and sensitive method for quantitation of lysergic acid diethylamide (LSD) in whole blood by gas chromatography-ion trap tandem mass spectrometry. Journal of analytical toxicol-ogy. 2003;27(1):24-9. 25. Bodin K, Svensson J-O. Determina-tion of LSD in Urine With High-Performance Liquid Chromatography–Mass Spectrometry. Therapeutic drug monitoring. 2001;23(4):389-93. 26. Jang M, Kim J, Han I, Yang W. Simultaneous determination of LSD and 2-oxo-3-hydroxy LSD in hair and urine by LC–MS/MS and its application to forensic cases. Journal of pharmaceutical and biomedical analy-sis. 2015;115:138-43. 27. Martin R, Schürenkamp J, Gasse A, Pfeiffer H, Köhler H. Analysis of Psilocin, Bufo-tenine and LSD in Hair. Journal of analytical
toxicology. 2015;39(2):126-9. 28. Kyzar EJ, Collins C, Gaikwad S, Green J, Roth A, Monnig L, et al. Effects of hallucinogenic agents mescaline and phencycli-dine on zebrafish behavior and physiology. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2012;37(1):194-202. 29. Carstairs SD, Cantrell FL. Peyote and mescaline exposures: a 12-year review of a state-wide poison center database. Clinical toxicolo-gy. 2010;48(4):350-3. 30. Casado R, Uriarte I, Cavero RY, Calvo MI. LC-PAD determination of mescaline in cactus “peyote”(Lophophora williamsii). Chromatographia. 2008;67(7-8):665-7. 31. Nolte KB, Zumwalt RE. Fatal peyote ingestion associated with Mallory-Weiss lacera-tions. Western journal of medicine. 1999;170(6):328. 32. Tsao MU. A new synthesis of mesca-line. Journal of the American Chemical Society. 1951;73(11):5495-6. 33. Albaugh BJ, Anderson PO. Peyote in the treatment of alcoholism among American Indians. American journal of Psychiatry. 1974;131(11):1247-50. 34. Cooper G, Negrusz A. Clarke's analytical forensic toxicology: Pharmaceutical Press; 2013. 35. Sushma K, Ghosh S, Banji D. Role of Chemical and Analytical Reagents in Colorimet-ric Estimation of Pharmaceuticals-A Review. International Journal of Medicine and Pharma-ceutical Research. 2013;1(5):433-45. 36. Ogunbodede O, McCombs D, Trout K, Daley P, Terry M. New mescaline concentra-tions from 14 taxa/cultivars of Echinopsis spp.(-Cactaceae)(“San Pedro”) and their relevance to shamanic practice. Journal of ethnopharmacolo-gy. 2010;131(2):356-62. 37. Valentine JL, Middleton R. GC-MS identification of sympathomimetic amine drugs in urine: rapid methodology applicable for emer-gency clinical toxicology. Journal of analytical toxicology. 2000;24(3):211-22. 38. Battal D, Barnes AJ, Castaneto MS, Martin TM, Klette KL, Huestis MA.
44D. Obreshkova, I. Kandilarov,
V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
45
Urine Mescaline Screening With a Biochip Array Immunoassay and Quantification by Gas Chromatography–Mass Spectrometry. Thera-peutic drug monitoring. 2015;37(6):805-11. 39. Björnstad K, Helander A, Beck O. Development and clinical application of an LC-MS-MS method for mescaline in urine. Jour-nal of analytical toxicology. 2008;32(3):227-31. 40. Gambelunghe C, Marsili R, Aroni K, Bacci M, Rossi R. GC‐MS and GC‐MS/MS in PCI Mode Determination of Mescaline in Peyote Tea and in Biological Matrices. Journal of foren-sic sciences. 2013;58(1):270-8. 41. Shen H-W, Jiang X-L, C Winter J, Yu A-M. Psychedelic 5-methoxy-N, N-dimeth-yltryptamine: metabolism, pharmacokinetics, drug interactions, and pharmacological actions. Current drug metabolism. 2010;11(8):659-66. 42. Luke D. Discarnate entities and dimethyltryptamine (DMT): Psychopharmacol-ogy, phenomenology and ontology. Journal of the Society for Psychical Research. 2011;75(902):26. 43. Sklerov J, Levine B, Moore KA, King T, Fowler D. A fatal intoxication following the ingestion of 5-methoxy-N, N-dimethyltrypt-amine in an ayahuasca preparation. Journal of analytical toxicology. 2005;29(8):838-41. 44. Gable RS. Risk assessment of ritual use of oral dimethyltryptamine (DMT) and harmala alkaloids. Addiction. 2007;102(1):24-34. 45. Gaujac A, Martinez ST, Gomes AA, de Andrade SJ, da Cunha Pinto A, David JM, et al. Application of analytical methods for the structural characterization and purity assessment of N, N-dimethyltryptamine, a potent psychedel-ic agent isolated from Mimosa tenuiflora inner barks. Microchemical Journal. 2013;109:78-83. 46. Namera A, Nakamoto A, Saito T, Nagao M. Colorimetric detection and chromato-graphic analyses of designer drugs in biological materials: a comprehensive review. Forensic Toxicology. 2011;29(1):1-24. 47. Wang M-J, Tsai C-H, Hsu W-Y, Liu J-T, Lin C-H. Original Paper Optimization of separation and online sample concentration of N,
N-dimethyltryptamine and related compounds using MEKC. J Sep Sci. 2009;32:441-5. 48. Ishii A, Seno H, Suzuki O, Hattori H, Kumazawa T. A simple and sensitive quantita-tion of N, N-dimethyltryptamine by gas chroma-tography with surface ionization detection. Jour-nal of analytical toxicology. 1997;21(1):36-40. 49. Vorce SP, Sklerov JH. A general screening and confirmation approach to the anal-ysis of designer tryptamines and phenethyl-amines in blood and urine using GC-EI-MS and HPLC-electrospray-MS. Journal of analytical toxicology. 2004;28(6):407-10. 50. Callaway JC, Raymon LP, Hearn WL, McKenna DJ, Grob CS, Brito GS, et al. Quantitation of N, N-dimethyltryptamine and harmala alkaloids in human plasma after oral dosing with ayahuasca. Journal of Analytical Toxicology. 1996;20(6):492-7. 51. Yritia M, Riba J, Ortuno J, Ramirez A, Castillo A, Alfaro Y, et al. Determination of N, N-dimethyltryptamine and β-carboline alka-loids in human plasma following oral adminis-tration of ayahuasca. Journal of Chromatography B. 2002;779(2):271-81. 52. McIlhenny EH, Riba J, Barbanoj MJ, Strassman R, Barker SA. Methodology for and the determination of the major constituents and metabolites of the Amazonian botanical medi-cine ayahuasca in human urine. Biomedical Chromatography. 2011;25(9):970-84. 53. Passie T, Seifert J, Schneider U, Emrich HM. The pharmacology of psilocybin. Addiction biology. 2002;7(4):357-64. 54. Kysilka R, Wurst M. A novel extraction procedure for psilocybin and psilocin determination in mushroom samples. Planta medica. 1990;56(03):327-8. 55. Gartz J. Extraction and analysis of indole derivatives from fungal biomass. Journal of basic microbiology. 1994;34(1):17-22. 56. Perkal M, Blackman GL, Ottrey A, Turner L. Determination of hallucinogenic com-ponents of Psilocybe mushrooms using high-performance liquid chromatography. Jour-nal of Chromatography A. 1980;196(1):180-4. 57. White P. Analysis of extracts from
PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...
Psilocybe semilanceata mushrooms by high-pressure liquid chromatography. Journal of Chromatography A. 1979;169:453-6. 58. Grieshaber AF, Levine B, Moore KA. The detection of psilocin in human urine. Journal of Forensic Science. 2001;46(3):627-30. 59. Hasler F, Bourquin D, Brenneisen R, Bär T, Vollenweider F. Determination of psilocin and 4-hydroxyindole-3-acetic acid in plasma by HPLC-ECD and pharmacokinetic profiles of oral and intravenous psilocybin in man. Pharmaceutica Acta Helvetiae. 1997;72(3):175-84. 60. Takeda N, Ikeda R, Ohba K, Kondo M. Bufotenine reconsidered as a diagnostic indi-cator of psychiatric disorders. Neuroreport. 1995;6(17):2378-80. 61. Wieczorek PP, Witkowska D, Jasic-ka-Misiak I, Poliwoda A, Oterman M, Zielinska K. Bioactive alkaloids of hallucinogenic mush-rooms: Elsevier; 2015. 62. Lyttle T, Goldstein D, Gartz J. Bufo toads and bufotenine: fact and fiction surround-ing an alleged psychedelic. Journal of psychoac-tive drugs. 1996;28(3):267-90. 63. Forsström JT, J. Kärkkäinen, T. Determination of potentially hallucinogenic N-dimethylated indoleamines in human urine by HPLC/ESI-MS-MS. Scandinavian journal of clinical and laboratory investigation. 2001;61(7):547-56. 64. Takahashi M, Nagashima M, Suzuki J, Seto T, Yasuda I, Yoshida T. Creation and application of psychoactive designer drugs data library using liquid chromatography with photo-diode array spectrophotometry detector and gas chromatography–mass spectrometry. Talanta. 2009;77(4):1245-72. 65. Shen H-W, Jiang X-L, Yu A-M. Development of a LC-MS/MS method to analyze 5-methoxy-N, N-dimethyltryptamine and bufotenine: application to pharmacokinetic study. 2009;1(1):87-95. 66. Passie T, Halpern JH, Stichtenoth DO, Emrich HM, & Hintzen A. The pharmacol-ogy of lysergic acid diethylamide: a review. CNS Neuroscience & Therapeutics.
2008;14(4):295-314. 67. De Gregorio D, Comai S, Posa L, & Gobbi G. D-Lysergic Acid Diethylamide (LSD) as a Model of Psychosis: Mechanism of Action and Pharmacology. International Journal of Molecular Sciences. 2016;17(11):1953. 68. Das S, Barnwal P, Ramasamy A, Sen S., & Mondal S. Lysergic acid diethylamide: a drug of ‘use’?. Therapeutic Advances in Psycho-pharmacology, 6(3): 214-228: a review. CNS Neuroscience &Therapeutics. 2016;14(4): 295-314. 69. Carhart-Harris RL, Kaelen M, Bolstridge M, Williams TM, Williams LT, Underwood R, ... & Nutt DJ. The paradoxical psychological effects of lysergic acid diethylam-ide (LSD). Psycholog cal medicine 2016;46(07):1379-1390. 70. Tylš F, Páleníček T, Horáček J. Psilo-cybin–summary of knowledge and new perspec-tives. European Neuropsychopharmacology. 2014; 24(3):42-356. 71. de Veen BT, Schellekens AF, Verheij MM, & Homberg JR. Psilocybin for treating substance use disorders? Expert Review of Neu-rotherapeutics. 2017;17(2):203-212. 72. Dinis-Oliveira, Ricardo Jorge. METABOLISM OF PSILOCYBIN AND PSILOCIN: CLINICAL AND FORENSIC TOXICOLOGICAL RELEVANCE. Drug Metabolism Reviews, just-accepted 2016:1-21. 73. Davis WM, Bedford JA, Buelke, J. L., Guinn, M. M., Hatoum, H. T., Waters, I. W., ... & Braude, M. C. Acute toxicity and gross behavioral effects of amphetamine, four methoxyamphetamines, and mescaline in rodents, dogs, and monkeys. Toxicology and applied pharmacology. 1978;45(1):49-62. 74. Speck LB. Toxicity and effects of increasing doses of mescaline. Journal of Phar-macology and Experimental Therapeu-tics.1957;119(1):78-84. 75. McBride MC. Bufotenine: toward an understanding of possible psychoactive mecha-nisms. Journal of psychoactive drugs. 2000;32(3):321-331. 76. Repke DB, Torres CM. Anadenan-
46D. Obreshkova, I. Kandilarov,
V. T. Angelova, Y. Iliev, P. Atanasov, P. S. FotevPHARMACIA, vol. 64, No. 1/2017
Corresponding author:V. T. AngelovaMedical University of Sofia,2 Dunav str., Sofia 1000, BULGARIA,Tel: +359 2 9236 586E-mail address: [email protected]
thera: visionary plant of ancient South America. New York: Haworth Herbal Press. 2006; ISBN 0-7890-2642-2. 77. Ott J. Pharmanopo-psychonautics: human intranasal, sublingual, intrarectal, pulmo-nary and oral pharmacology of bufotenine. Jour-nal of psychoactive drugs. 2001; 33(3):273. 78. Gable RS. Risk assessment of ritual
use of oral dimethyltryptamine (DMT) and harmala alkaloids. Addiction .2007;102(1):24-34. 79. Ujváry I. Psychoactive natural prod-ucts: overview of recent developments. Annali dell'Istituto Superiore di Sanità. 2014;50(1):12-27.
47PHARMACIA, vol. 64, No. 1/2017Pharmaco - toxicological aspects and analysis...