the effect of unilateral intravitreal bevacizumab (avastin), in the treatment of diffuse bilateral...
TRANSCRIPT
THE EFFECT OF UNILATERALINTRAVITREAL BEVACIZUMAB(AVASTIN), IN THE TREATMENTOF DIFFUSE BILATERAL DIABETICMACULAR EDEMAA Pilot StudyRAUL VELEZ-MONTOYA, MD,* JANS FROMOW-GUERRA, MD,*OCTAVIO BURGOS, MD,* MAURICE B. LANDERS, 3RD, MD,†VIRGILIO MORALES-CATON, MD,* HUGO QUIROZ-MERCADO, MD‡
Purpose: To investigate whether there are systemic effects of unilateral intravitrealadministration of bevacizumab on the untreated eye.
Methods: Twenty-three consecutive patients were enrolled in this study. All patientshad a clinical diagnosis of bilateral diffuse diabetic macular edema with a central retinalthickness greater than 275 �m by Optical Coherence Tomography. They were treated with2.5 mg bevacizumab intravitreally in the worst eye based on lines of vision, number of EarlyTreatment Diabetic Retinopathy Study letters, and central retinal thickness. The patientswere observed every 2 weeks for 4 weeks. The Best Corrected Visual Acuity, central retinalthickness (�m), and macular volume (mm3) in the untreated eye measured by OpticalCoherence Tomography were recorded at every visit.
Results: The Best Corrected Visual Acuity (mean � SD) in the untreated eye was34.46 � 17.29. Early Treatment Diabetic Retinopathy Study letters at baseline, 38.31 �14.64 at 2 weeks, and 37.38 � 14.59 at 4 weeks. The central retinal thickness in theuntreated eye was 324.77 � 76.51 �m at baseline, 319 � 75.7 �m at 2 weeks, and315.54 � 78.2 �m at 4 weeks. The macular volume in the untreated eye was 8.99 � 1.2mm3 at baseline, 9.16 � 1.26 mm3 at 2 weeks, and 8.99 � 1.09 mm3 at 4 weeks. Therewere no statistically significant differences between any of the measurements.
Conclusion: Due to the lack of significant changes in the measurements of the untreatedeye, the systemic effect of intravitreal bevacizumab seems to be unlikely. The small sample andlow confidence of this pilot study prevent us to draw concrete conclusions.
RETINA 29:20–26, 2009
Vascular endothelial growth factor (VEGF) wasfirst identified in guinea pig ascitis fluid.1,2 VEGF
is a dimeric glycoprotein whose expression increasesduring retinal hypoxia.3 It is also implicated in the
genesis of new vessels, such as in diabetic retinopa-thy,3–7 and in the increase of vascular permeabilitythrough the formation of vascular fenestrations, which
From the *Retina Department, Asociacion Para Evitar laCeguera en Mexico; and †Retina Department, University of NorthCarolina at Chapel Hill Medical School, Chapel Hill, North Caro-lina; and ‡Department of Ophthalmology, Denver Medical Center,University of Colorado, Denver, Colorado.
No conflicting relationship exists for any author or proprietaryinterest.
Clinical Trial Registration Number: NCT00496405.Reprint requests: Raul Velez-Montoya, MD, Vicente Garcıa
Torres #46. Col, San Lucas Coyoacan. Mexico DF. Del. Coyoacan04030; email: [email protected]; [email protected]
20

allow for the escape of liquid and protein deposits intothe tissue interstices.3,6,8,9
The main cause of loss of vision in patients ofworking age in developed countries is diabetic reti-nopathy,3 mainly due to the development of diabeticmacular edema (DME), with an incidence between13.9% and 25.4%.10 DME is associated with highlevels of VEGF in the vitreous.2,3,6
Time domain Optical Coherence Tomography (OCT)is a noninvasive tool,9–11 based on low-coherenceinterferometry, that provides cross-sectional retinalimages9,10,12 with a resolution of 10 �m to 15 �m,allowing for the quantitative measurement of macularthickness.9,10,11 The measurements obtained using thissystem are highly reproducible and correlate withpatient visual acuity.2,7,10–13 In macular edema, OCTdisplays low reflectivity images with increased retinalthickness.12,14
Bevacizumab (Avastin, Genetech, Inc., San Francisco,CA) is a recombinant monoclonal antibody (IgG1)that binds all forms of VEGF. It is approved by theFood and Drug Administration for the treatment ofmetastatic colorectal cancer, metastatic breast cancer,and nonsmall cell lung cancer.4,15,16 In the last fewyears its “off-label” use in the ophthalmology field hasbecome popular due to its proven safety and effective-ness for the treatment of diverse ocular diseases.2,4,5,7,8
Bevacizumab administered to patients with DME im-proves visual acuity, decreases macular thickness, andimproves angiographic patterns.6,9
There has been much speculation about the sys-temic absorption of Bevacizumab. In a study at theBascom Palmer Eye Institute, Rosenfeld and cowork-ers demonstrated the effectiveness of systemic admin-istration of 5 mg/kg bevacizumab for the treatment ofage-related macular degeneration, thus demonstratingthat the molecule passes from the systemic circulationto the eyes.9 Recently, Bakri et al at the Mayo Clinicin Rochester, MN, established that a small portion ofintravitreal bevacizumab enters the systemic circula-tion (1.6% of the injected dose) in an animal model.They also reported detectable concentrations of bev-acizumab in the vitreous of the fellow eye (11.17ng/mL) 4 weeks after the injection.17 There are alsoundocumented clinical observations of Bevacizumabapplication in one eye improving the base pathologyin the fellow eye.
The objective of the present pilot study is to deter-mine if there is an effect in the untreated eye after asingle dose of intravitreal bevacizumab, in patientswith bilateral DME by examining visual acuity, mac-ular thickness and macular volume.
Methods
The study was reviewed and approved by the insti-tutional ethics board. We screened patients older than30 years of age with pupil midriasis greater than 5mm, no significant vitreous opacities or cataract, clin-ical diagnosis of bilateral diffuse DME, confirmed bya retinal thickness greater than 275 �m and no fovealvitreous traction in OCT scan, and who had neverbeen treated with a laser for DME or with an antian-giogenic agent for at least 3 months before the start ofthe study. Patients with focal DME, macular edemadue to an etiology other than diabetes, vitreous trac-tion, macular ischemia, medical history of thrombo-embolic events, uncontrolled arterial hypertension,transient ischemic attacks, cardiac stroke, acute cere-bral vascular event, and pregnant women or lactatingwomen were excluded. All patients signed a declara-tion of informed consent.
At the baseline visit, we recorded a complete med-ical history, including general demographic data suchas age, gender, time since loss of vision, and the lastblood glucose level. The refraction and best correctedvisual acuity with an Early Treatment Diabetic Reti-nopathy Study chart (number of letters) was also re-corded. We performed a complete comprehensiveophthalmologic revision of the anterior segment andthe posterior pole and classified the grade of diabeticretinopathy and macular edema according to an inter-nationally accepted classification system.18,19
An time domain OCT scan of the macular area wasperformed with a Stratus OCT system (Carl Zeiss, Med-itec Inc., Dublin, CA) to assess the macular thickness andmacular volume with a fast macular protocol for botheyes. The eye to be treated was selected according to theseverity of the macular edema. An intravitreal dose of2.5 mg was administered, according to the AmericanAcademy of Ophthalmology guidelines for intravitrealdrug delivery.20 After the injection, a short course oftopical antibiotic was instituted.
Follow-up examinations were performed 2 and 4weeks after the injection. At each visit, Best CorrectedVisual Acuity was assessed as described above andOCT scans of both eyes were obtained. A completecomprehensive ophthalmologic examination was alsoperformed at each visit.
Statistical analyses were performed using SPSS Soft-ware, version 10.1.0 (SPSS Inc., Chicago, IL). A non-parametric Friedman/Wilcoxon test was used to deter-mine statistical significance with P � 0.05 consideredsignificant. The data are presented as means � SD.
The study has been registered as a clinical trial (moreinformation available at http://www/clinicaltrials.gov).
21BILATERAL EFFECTS OF UNILATERAL BEVACIZUMAB ● VELEZ-MONTOYA ET AL

Results
A total of 23 consecutive patients were enrolled.The relevant demographic data are summarized inTable 1. All patients met the inclusion/exclusion cri-teria and completed the 4-week follow-up. All 23subjects had clinically significant macular edema andreceived a dose of 2.5 mg/mL of intravitreal bevaci-zumab. The mean age was 62.45 � 8.5 years (range,52–80 years).
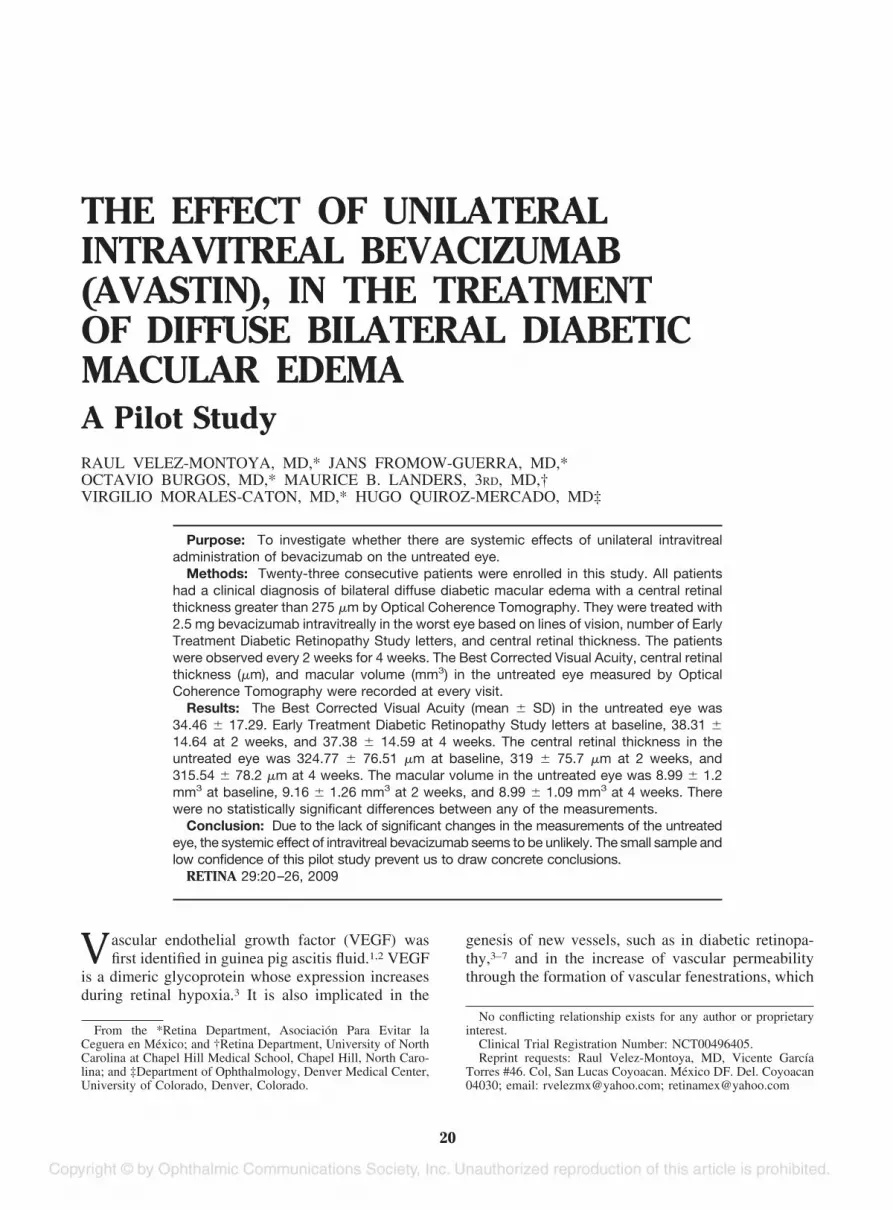
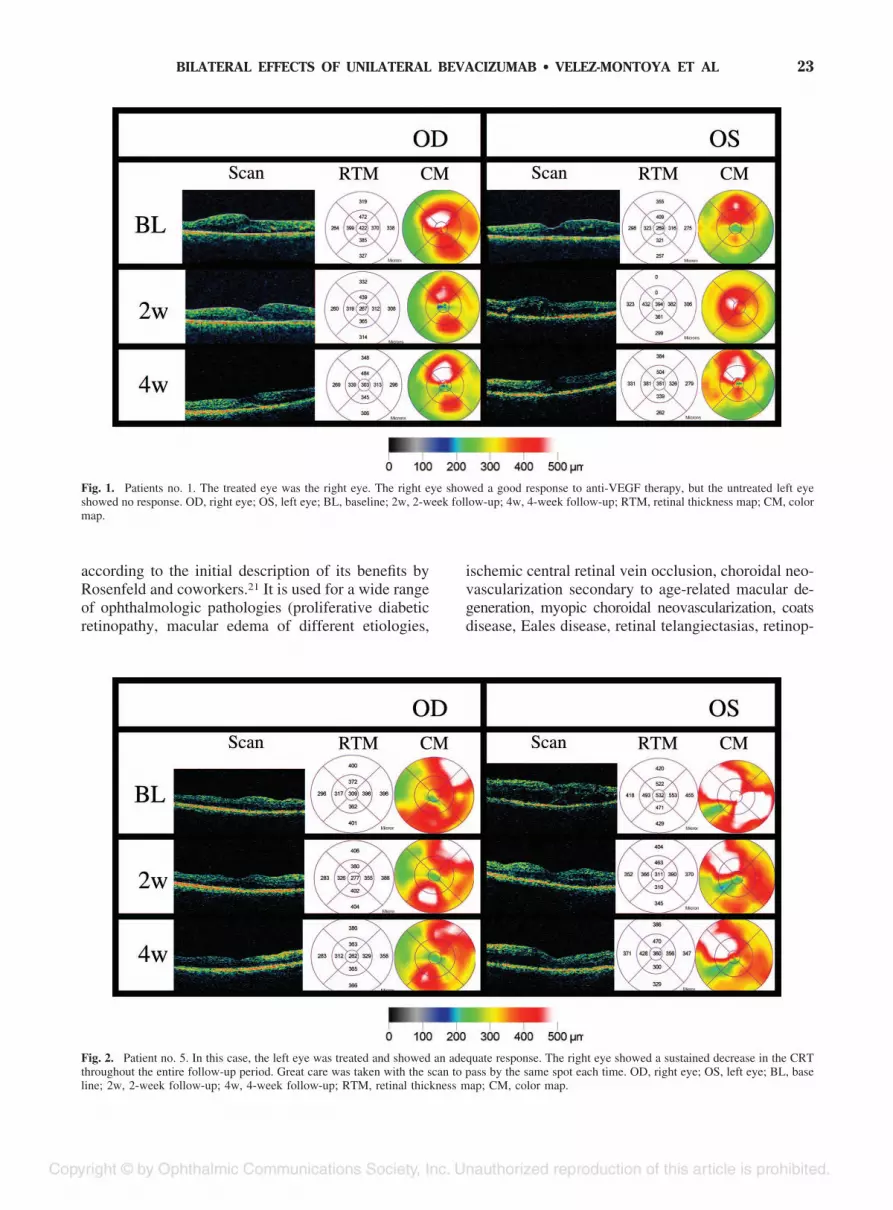
The results of Best Corrected Visual Acuity, centralretinal thickness and macular volume are summarizedin Table 2. As we can see in the Table, all parametersmeasured in the eye treated with bevacizumab, had asignificant improvement, as expected. Moreover, themeasurements in the contralateral eye showed no sig-nificant change along the 4-week follow-up. An ex-ample of two different scenarios can be reviewed inFigures 1 and 2. In the first case, the contralateral eyeshowed no response at all, and in the second case, itseems to have an effect.
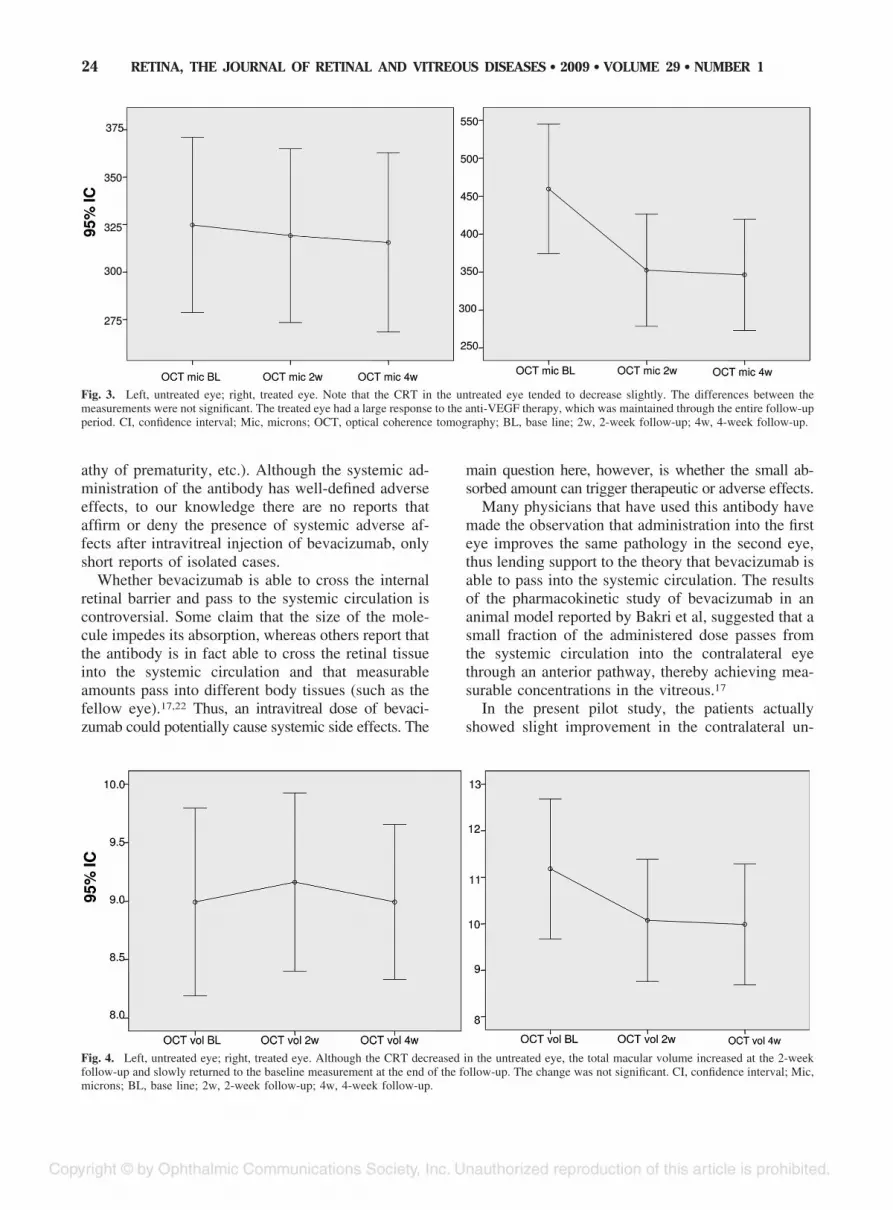
During the 4 weeks of follow-up, there was aninsignificant variation in the untreated eye in the num-ber of Early Treatment Diabetic Retinopathy Studyletters. Central retinal thickness and macular volumemeasurements in the untreated eye did not changesignificantly during the 4-week study period. (Figures3 and 4).
Discussion
Intravitreal injection with bevacizumab is a verypopular treatment for choroidal and retinal pathologies
Table 1. Patients Demographic Data
Number %
Group 13 100.00Males 5 38.46Females 8 61.54
Study eyeOD 4 30.77OS 9 69.23
Time since loss of vision�2 months 1 7.702–4 months 2 15.40�4 months 10 76.90
Diabetic retinopathyclassification
NPDR severe 7 53.80Proliferative 1 7.70Post laser 5 38.50
Blood glucose level mg/dl SDBase line 190.40 �50.164 week follow-up 141.36 �39.03
Descriptive data of only the untreated eye are included above.NPDR, none proliferative diabetic retinopathy.
Tab
le2.
Vis
ualA
cuity
,C
entr
alR
etin
alTh
ickn
ess
and
Mac
ular
Vol
ume
Res
ults
(Bas
elin
e,2
&4
Wee
ksFo
llow
-up
)
Trea
ted
Eye
Unt
reat
edE
ye
Bas
eLi
ne2
Wee
ks4
Wee
ksP
Bas
eLi
ne2
Wee
ks4
Wee
ksP
Num
ber
ofE
TDR
Sle
tter
s22
.15
�20
.21
27.1
5�
20.7
126
.31
�20
.89
0.46
34.4
6�
17.2
938
.31
�14
.64
37.3
8�
14.5
90.
098
Cen
tral
retin
alth
ickn
ess
(mic
s)45
9.46
�14
1.26
352.
38�
122.
5334
6.23
�12
1.3
0.00
232
4.77
�76
.51
319.
15�
75.7
315.
54�
78.2
0.14
2M
acul
arvo
lum
e(m
m3)
11.1
7�
2.4
10.0
7�
2.1
9.98
�2.
10.
001
8.99
�1.
329.
16�
1.26
8.99
�1.
090.
727
Res
ults
are
pre
sent
edin
term
sof
mea
n�
stan
dar
dd
evia
tion.
Non
par
amet
ricst
atis
ticw
asus
edto
anal
yze
the
dat
a.
22 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 1
according to the initial description of its benefits byRosenfeld and coworkers.21 It is used for a wide rangeof ophthalmologic pathologies (proliferative diabeticretinopathy, macular edema of different etiologies,
ischemic central retinal vein occlusion, choroidal neo-vascularization secondary to age-related macular de-generation, myopic choroidal neovascularization, coatsdisease, Eales disease, retinal telangiectasias, retinop-
Fig. 1. Patients no. 1. The treated eye was the right eye. The right eye showed a good response to anti-VEGF therapy, but the untreated left eyeshowed no response. OD, right eye; OS, left eye; BL, baseline; 2w, 2-week follow-up; 4w, 4-week follow-up; RTM, retinal thickness map; CM, colormap.
Fig. 2. Patient no. 5. In this case, the left eye was treated and showed an adequate response. The right eye showed a sustained decrease in the CRTthroughout the entire follow-up period. Great care was taken with the scan to pass by the same spot each time. OD, right eye; OS, left eye; BL, baseline; 2w, 2-week follow-up; 4w, 4-week follow-up; RTM, retinal thickness map; CM, color map.
23BILATERAL EFFECTS OF UNILATERAL BEVACIZUMAB ● VELEZ-MONTOYA ET AL
athy of prematurity, etc.). Although the systemic ad-ministration of the antibody has well-defined adverseeffects, to our knowledge there are no reports thataffirm or deny the presence of systemic adverse af-fects after intravitreal injection of bevacizumab, onlyshort reports of isolated cases.
Whether bevacizumab is able to cross the internalretinal barrier and pass to the systemic circulation iscontroversial. Some claim that the size of the mole-cule impedes its absorption, whereas others report thatthe antibody is in fact able to cross the retinal tissueinto the systemic circulation and that measurableamounts pass into different body tissues (such as thefellow eye).17,22 Thus, an intravitreal dose of bevaci-zumab could potentially cause systemic side effects. The
main question here, however, is whether the small ab-sorbed amount can trigger therapeutic or adverse effects.
Many physicians that have used this antibody havemade the observation that administration into the firsteye improves the same pathology in the second eye,thus lending support to the theory that bevacizumab isable to pass into the systemic circulation. The resultsof the pharmacokinetic study of bevacizumab in ananimal model reported by Bakri et al, suggested that asmall fraction of the administered dose passes fromthe systemic circulation into the contralateral eyethrough an anterior pathway, thereby achieving mea-surable concentrations in the vitreous.17
In the present pilot study, the patients actuallyshowed slight improvement in the contralateral un-
Fig. 3. Left, untreated eye; right, treated eye. Note that the CRT in the untreated eye tended to decrease slightly. The differences between themeasurements were not significant. The treated eye had a large response to the anti-VEGF therapy, which was maintained through the entire follow-upperiod. CI, confidence interval; Mic, microns; OCT, optical coherence tomography; BL, base line; 2w, 2-week follow-up; 4w, 4-week follow-up.
Fig. 4. Left, untreated eye; right, treated eye. Although the CRT decreased in the untreated eye, the total macular volume increased at the 2-weekfollow-up and slowly returned to the baseline measurement at the end of the follow-up. The change was not significant. CI, confidence interval; Mic,microns; BL, base line; 2w, 2-week follow-up; 4w, 4-week follow-up.
24 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 1

treated eye, but there were no statistically significantchanges in visual acuity or in the central retinal thick-ness. In fact, there was a paradoxical increase in thetotal volume of the macula at the 2-week follow-up,which returned to baseline values at the end of thestudy. Therefore under the light of this pilot study abilateral effect seems to be unlikely.
It is important to remark that the conditions underwhich this study was conducted, are very far fromreality. Since the pathophysiology of DME, alongwith frequent bad metabolic control of diabetic pa-tients; normally requires repeated injections of anti-VEGF drugs (we are treating the “effect” rather thanthe “cause” itself). Because of this, the observationsabout the bilateral effect of bevacizumab in the un-treated eye might be more influenced by the number ofconsecutive applications than just the systemic ab-sorption of a single dose.
But what is the relevance of checking if the bev-acizumab has a bilateral effect? At the Association forResearch in Vision and Ophthalmology 2007 meeting,two poster presentations, one by Maia et al (1411/B467)and the second by Alvarez-Verdusco et al (1412/B468), suggested the possibility that intravitreally ad-ministered bevacizumab accelerates the developmentof tractional retinal detachment in uncontrolled dia-betic patients with proliferative diabetic retinopathydue to a rapid regression of neovessels, contraction offibrous tissue, or due to an unknown effect of the anti-body. Because the minimum effective dose of bevaci-zumab is not known, the possibility that extremely smalldoses trigger this process is a latent risk. Therefore in ascenario in where we have a patient with a tractionalretinal detachment in one eye and DME in the other,we might think twice before injecting first the secondeye. Further investigation is critical to determine if theantibody concentrations obtained after intravitreal ad-ministration in one eye affect (therapeutically or ad-versely) the contralateral eye.
One of the limitations of our study (besides thesmall sample size, short follow-up time and, therefore,little confidence), is that the model we used (DME) isnot the best model in which to explore the possibilityof a bilateral effect of bevacizumab. Although Dr.Bakri speculates that the antibody enters the contralat-eral eye through an anterior pathway, the fact is thatthe observations of the effect of bevacizumab on theuntreated eye have been made in diseases in whichthere are major alterations in the blood-retina barrier,particularly in choroidal neovascularization secondaryto age-related macular degeneration. Whereas thereare alterations of the retinal barrier in DME, leakagefrom the neovascular membrane is likely much higher.Therefore, the bevacizumab concentrations in the un-
treated eye tissues might be even higher than thoughtand have an unexpected effect.
Another major limitation, is the lack of a largergroup. The small confidence provided by this smallgroup makes it impossible to drawn concrete conclu-sions about whether there is an effect or not in theuntreated eye. To have a 95% confidence we have to,at least, double the study group. Only then we canensure, that the changes observed in the study are trulysignificant. The short follow-up time is also an issue,but how long can we maintain the contralateral eye(who also have DME) without applying treatment?This is a delicate topic for the ethic board. Perhaps, weshould consider a different approach rather than bilat-eral DME to investigate this topic.
In summary, although the results of our study indi-cates; that the effect on the contralateral eye of bev-acizumab is unlikely, the limitations of the study pre-vents to draw conclusions about whether the resultsare final. A greater number of patients, longer follow-uptime, and probably the replacement of the model withone in which there are more alterations of the blood-retina barrier, are conditions required before morespecific conclusions can be drawn.
Key words: bevacizumab, central retinal thickness,diabetic macular edema, intravitreal injection, opticalcoherence tomography.
References
1. Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS,Dvorak HF. Tumor cells secrete a vascular permeability factorthat promotes accumulation of ascites fluid. Science 1983;219:983–985.
2. Haritoglou C, Kook D, Neubauer A, et al. Intravitreal bevaci-zumab (Avastin) therapy for persistent diffuse diabetic macu-lar edema. Retina 2006;26:999–1005.
3. Spaide RF, Fisher YL. Intravitreal bevacizumab (Avastin)treatment of proliferative diabetic retinopathy complicated byvitreous hemorrhage. Retina 2006;26:275–278.
4. Rosenfeld PJ, Moshfeghi AA, Puliafito CA. Optical coherencetomography findings after an intravitreal injection of bevaci-zumab (Avastin) for neovascular age-related macular degen-eration. Ophthalmic Surg Lasers Imaging 2005;36:331–335.
5. Manzano RP, Peyman GA, Khan P, Kivilcim M. Testingintravitreal toxicity of bevacizumab (Avastin). Retina 2006;26:257–261.
6. Iturralde D, Spaide RF, Meyerle CB, et al. Intravitreal bevaci-zumab (Avastin) treatment of macular edema in central retinalvein occlusion: a short-term study. Retina 2006;26:279–284.
7. Rosenfeld PJ, Fung AE, Puliafito CA. Optical coherence tomog-raphy findings after an intravitreal injection of bevacizumab(Avastin) for macular edema from central retinal vein occlusion.Ophthalmic Surg Lasers Imaging 2005;36:336–339.
8. Pai SA, Shetty R, Vijayan PB, et al. Clinical, anatomic, andelectrophysiologic evaluation following intravitreal bevaci-zumab for macular edema in retinal vein occlusion. Am JOphthalmol 2007;143:601–606.
9. Diabetic Retinopathy Clinical Research Network, Danis RP,
25BILATERAL EFFECTS OF UNILATERAL BEVACIZUMAB ● VELEZ-MONTOYA ET AL

Glassman AR, et al. Diurnal variation in retinal thickeningmeasurement by optical coherence tomography in center-in-volved diabetic macular edema. Arch Ophthalmol 2006;124:1701–1707.
10. Hee MR, Puliafito CA, Duker JS, et al. Topography of diabeticmacular edema with optical coherence tomography. Ophthal-mology 1998;105:360–370.
11. Frank RN, Schulz L, Abe K, Iezzi R. Temporal variation indiabetic macular edema measured by optical coherence tomog-raphy. Ophthalmology 2004;111:221–227.
12. Catier A, Tadayoni R, Paques M, et al. Characterization ofmacular edema from various etiologies by optical coherencetomography. Am J Ophthalmol 2005;140:200–206.
13. Otani T, Kishi S, Maruyama Y. Patterns of diabetic macularedema with optical coherence tomography. Am J Ophthalmol1999;127:688–693.
14. Otani T, Kishi S. Correlation between optical coherence to-mography and fluorescein angiography findings in diabeticmacular edema. Ophthalmology 2007;114:104–107.
15. Cohen MH, Gootenberg J, Keegan P, Pazdur R. FDA drugapproval summary: bevacizumab (Avastin) plus Carboplatinand Paclitaxel as first-line treatment of advanced/metastatic
recurrent nonsquamous non-small cell lung cancer. Oncologist2007;12:713–718.
16. Diabetic Retinopathy Clinical Research Network, Scott IU,Edwards AR, et al. A phase II randomized clinical trial ofintravitreal bevacizumab for diabetic macular edema. Ophthal-mology 2007;114:1860–1867.
17. Bakri SJ, Snyder MR, Reid JM, Pulido JS, Singh RJ. Pharma-cokinetics of intravitreal bevacizumab (Avastin). Ophthalmol-ogy 2007;114:855–859.
18. Bresnick GH. The Early Treatment Diabetic RetinopathyStudy: an update. J Diabet Complications 1988;2:105–108.
19. Pelzek C, Lim JI. Diabetic macular edema: review and update.Ophthalmol Clin North Am 2002;15:555–563.
20. Aiello LP, Brucker AJ, Chang S, et al. Evolving guidelines forintravitreous injections. Retina 2004;24:S3–S19.
21. Michels S, Rosenfeld PJ, Puliafito CA, Marcus EN, Venkatra-man AS. Systemic bevacizumab (Avastin) therapy for neovas-cular age-related macular degeneration twelve-week results ofan uncontrolled open-label clinical study. Ophthalmology2005;112:1035–1047.
22. Heiduschka P, Fietz H, Hofmeister S, et al. Penetration ofbevacizumab through the retina after intravitreal injection inthe monkey. Invest Ophthalmol Vis Sci 2007;48:2814–2823.
26 RETINA, THE JOURNAL OF RETINAL AND VITREOUS DISEASES ● 2009 ● VOLUME 29 ● NUMBER 1