the biologic window for chimeric l6 radioimmunotherapy
TRANSCRIPT

1023
The Biologic Window for Chimeric L6 Radioimmunotherapy Sally J. DeNardo, M.D.,* G a y R. Mirick, B.A.,* Linda A. Kroger, M.S.,* Lois F. O’Grady, M.D.,* Kent 1. Erickson, Ph.D.,* Aina Yuan, Ph.D.,* Kathleen R. Lamborn, Ph.D.,t Ingegerd Hellsfrom, M.D.,$ Karl Erik Hellstrom, M.D.,S and Gerald L. DeNardo, M.D.*
Background. There has been little success in using radioimmunotherapy in patients with adenocarcinoma, partly because of the low tumor uptake of the adminis- tered monoclonal antibody (MoAb). The authors recently reported therapeutic response in advanced cancer pa- tients who received 1311 chimeric-16 MoAb. The L6 MoAb identifies abundant, nonshed antigen that is expressed in many human carcinomas, including carcinomas of the lung, breast, colon, and ovary. In vitro both mouse L6 (L6) and chimeric L6 (ChL6) mediate complement-dependent tumor cytolysis with human serum, and antibody-depen- dent tumor cell cytolysis with normal human peripheral blood mononuclear cells. The authors have used L6 or ChL6 for radioimmunotherapy to exploit their biologic activity to create a “therapeutic window” of increased vascular permeability, allowing more 1311 MoAb to reach the tumor. A reactive target is present in the vascular endothelium but can be covered by unlabeled L6 or ChL6.
Methods. Nine patients with metastatic breast cancer were treated on a therapy protocol and received imaging and therapy doses of 1311 ChL6 on two sequential days at 4 week intervals. During each treatment cycle, serum cytokines, complement, albumin, and 1311 ChL6 blood clearance were monitored, peripheral blood mono- nuclear cell activation was assessed, and tumor uptake and response were documented.
Results. After L6 or ChL6 was infused, patients dem- onstrated immediate serum-complement activation,
- Presented at the Fourth Conference on Radioimmunodetection
and Radioimmunotherapy of Cancer, Princeton, New Jersey, Sep- tember 17-19, 1992.
From the *University of California at Davis Medical Center, Sac- ramento, California; tQuintilles Pacific, Mountain View, California; and SBristol-Myers Squibb Pharmaceutical Research Institute, Seattle Washington.
Supported by grants from the Department of Energy (DE-FG03- 84ER-60233) and the National Cancer Institute (PHS CA 47829).
The authors thank Joyce Steeves for her assistance in prepara- tion of this manuscript.
Address for reprints: Sally J. DeNardo, M.D., 1508 Alhambra Boulevard, Sacramento, CA 95816.
Accepted for publication September 24, 1993.
manifested by rapidly decreasing levels of serum comple- ments 3 and 4. Tumor uptake of the second 1311 MoAb (therapeutic) injection, given after the second daily injec- tions of 200 mg MoAb, was usually higher than the tumor uptake of the first 1311 MoAb (imaging) dose given after a single 200 mg infusion of MoAb. Although serum comple- ment frequently decreased after the first 50-100 mg dose of L6 or ChL6, elevation of soluble interleukin-2 receptor (IL-ZR) in serum was seen only in patients who received 150 mg or more of L6 or ChL6. In the nine treated pa- tients, with only one exception, the higher grade of thera- peutic tumor response was seen in patients with a greater increase in IL-ZR levels.
Conclusions. The clinical importance of understand- ing these mechanisms is emphasized by the occurrence of measurable tumor regressions in five of the first nine ad- vanced metastatic breast cancer patients treated in this manner. Absence of pulmonary edema and delayed re- lease of dose-dependent IL-ZR suggest that targeting of the pulmonary endothelium by L6 or ChL6 is not the ma- jor cause of the observed biologic effects. This unique response of a solid tumor to radioimmunoconjugate ther- apy may be secondary to both the increased delivery of the radioimmunoconjugate to tumor cells caused by en- hanced vascular permeability, and to synergistic effects of radiation and activated effector cell mechanisms. Cancer 1994; 73:1023-32.
Key words: chimeric antibody, radioimmunotherapy, bio- logic response modifiers, interlukin-2 receptor.
The mouse monoclonal antibody (MoAb) L6 and its chimeric counterpart (ChL6) were chosen for radioim- munotherapy of breast cancer because they target a tu- mor-related antigen that is expressed on breast, lung, colon, and ovarian cancers and is not processed or shed.’,’ In vitro evidence for biologic activity of L6 and ChL6 with potent complement activation leading to tu- mor cell lysis of antigen-positive cell lines (CDC) and antibody-dependent cellular cytotoxicity (ADCC) with

1024 CANCER Supplement February I , 2994, Volume 73, No. 3
human peripheral blood mononuclear cells were equally important in their s e l e c t i ~ n . ~ , ~
The nature of the cell surface antigen target of L6 and ChL6 has been elusive. Earlier reports described the antigen as either a glycolipid' or prone~rophysin,~ but recently a cDNA clone encoding the L6 antigen was isolated and the putative L6-defined antigen described by using expression cloning te~hnology.~ The antigen is a protein of approximately 24 kilodaltons (KD) belong- ing to a family of integral membrane proteins that in- cludes two tumor-related growth regulator proteins, CD63 (ME491)6,7 and C0-029.* Our previous work has demonstrated that the L6-defined target is present on vascular endothelial cells as well as on adenocarcinoma cells.' A Phase I clinical study in patients with recurrent cancer of either the breast, colon, lung, or ovary showed that murine L6 used as a single agent with multi-day sequential infusions of several hundred milligrams was well tolerated and effectively localized to the tumor in vivo." One patient, with recurrent breast cancer on the chest wall, had a temporary, complete remission." In our initial pharmacokinetic studies in patients, L6 la- beled with I 3 l I delivered sufficient amounts of radioac- tivity to tumors to be of therapeutic interest when 200 mg or more unlabeled antibody was preinfused.' Prom- ising results have been observed in a Phase I therapy study in which patients with advanced breast cancer were given therapeutic doses of l3lI-1abeled ChL6.11,12
A Phase 1 study in nine patients with monthly cy- cles of I3lI ChL6 after a 2-day infusion of 200 mg/day of L6 or ChL6 indicated that 60 mCi/m2 I3'I ChL6 was the maximum tolerated dose without stem cell or marrow s u p p ~ r t . ' ~ ~ ' ~ More than 5o0/o of these rapidly deteriorating patients had measurable tumor regres- sion. Strikingly, several patients with superficial tumors had evidence for inflammatory reactions manifested by warmth, erythema, or tenderness in areas of adenocarci- noma within a few hours of infusion of antibody. These findings led to a study of several parameters of biologic systems activation associated with 1311 ChL6 treatment. In this study, we examined complement activation, in- terleukin 1 (IL-l), IL-2, and IL-2 receptor levels in serum, serum albumin, tumor uptake and radiation dose, and the role of possible synergy between the bio- logic systems and the radiation leading to therapeutic responses.
Materials and Methods
Patient Population
The information presented here was obtained from two groups of patients. Most of the data were from nine patients treated on the initial arm of an 13'1 ChL6 ther-
apy study under a physician-sponsored Food & Drug Administration Investigational New Drug. They were dosed for imaging and therapy studies on sequential days, and the 24-hour tumor uptake and blood clear- ances of the imaging and therapy doses were com- pared. A second group of eight patients had partici- pated in a previously reported pharmacokinetic anti- body dose escalation imaging study with L6.' All patients in both groups had advanced metastatic breast cancer that was L6 positive (more than 70% of cells strongly reactive) by immunopathology performed on fresh or frozen tissue. Aggressive standard therapy had failed and the patients had rapidly progressing disease.
The therapy study had been devised to assess the toxicity of the radiopharmaceutical and determine the maximum tolerated dose (MTD) when a minimum of two doses were given at 1-month intervals. Six of the nine patients (aged 29-78) had metastatic cancer in su- perficial lymph nodes or skin and subcutaneous lesions that facilitated gamma camera computerized imaging to obtain accurate quantitation of tumor uptake. Other sites of significant tumor involvement were bone, liver, mesentery, lung, the contralateral breast, and chest wall. Each patient could receive up to four doses of 13'1 ChL6, and a total of 20 therapeutic doses was actually given to the nine patients. Palpable lesions were mea- sured with calipers before the first treatment, at fre- quent intervals thereafter, and immediately before each subsequent treatment. Serial photographs of superficial dlsease on the chest wall were also obtained. X-ray computed tomography (CT) or magnetic resonance imaging (MRI) were used to follow tumor size in non- palpable areas at appropriate intervals. Tumor size was calculated from data obtained pretherapy and postther- apy by the sum of the products of the longest diameter and the greatest perpendicular diameter (L X W) of all measurable lesions.
Blood samples from the group of patients on the pharmacokinetic antibody dose escalation study was used to evaluate cytokine activity before and after infu- sion of mouse L6.9 Two patients were studied at each dose level of 50,100,150,200, and 400 mg. This patient group was included in this study to evaluate the effect of the smaller amounts of L6 on cytokine response.
Monoclonal Antibody
The mouse MoAb L6, an IgG2a antibody, targets a membrane-bound antigen found on human adenocarci- noma cells of the lung, colon, ovary, and breast.' It pos- sesses tumoricidal activity both by antibody-dependent cellular cytotoxicity (ADCC) in the presence of human peripheral blood mononuclear cells and by comple- ment-dependent cytotoxicity (CDC) in the presence of

Biologic Window for Chimeric LG/DeNardo et al. 1025
human complement.2 A chimeric human-mouse anti- body was produced using recombinant DNA technol- ogy in which mouse constant domains C-G2a and C- kappa were replaced by the human C-GI and C- kappa.14 Chimeric and mouse L6 antibodies bind adenocarcinoma cells with the same avidity, but ChL6 is 50-100 times more effective at mediating ADCC in ~ i t r o . ~ , ’ ~ Following studies that demonstrated favorable pharmacokinetic characteristics in m i ~ e , ~ , ’ ~ this anti- body was chosen for human use because of the poten- tial for superior biologic activity and high tumor immu- noreactivity .
Radiopharmaceu ticals
L6 and ChL6 MoAb were obtained in a sterile, pyro- gen-free form from Bristol-Myers Squibb Pharmaceuti- cal Research Institute (Seattle, WA). All radiopharma- ceutical preparations were carried out in a shielded lami- nar air flow glove box using sterile techniques. The chloramine-T method was used for radioiodination, and the final product was assured to be sterile and apyrogenic.” L6 and ChL6 were radiolabeled at a level of 10 mCi 1311/mg of L6 or ChL6, and the product was adjusted to 1 mCi 1311/ml with normal saline containing 10% (wt/vol) human serum albumin (HSA). High-per- formance liquid chromatography (TSK 3000) and cellu- lose acetate electrophoresis were used to document that 95% or more of the radioactivity was associated with the antibody, and a binding assay with live cells was used to document that immunoreactive binding of the labeled L6 or ChL6 to the cell surface target was 75% or greater. l8
Imaging and Therapy Infusion
The L6 dose escalation pharmacokinetic study used preinfusions of 50, 100, 150, 200, or 400 mg L6 fol- lowed by 10 mCi 1311 L6, and demonstrated a change in the pharmacokinetics of I 3 l I L6 with variation in the L6 antibody dose up to the 200 mg level.’ Cytokine activity in blood samples obtained before infusion and 0-4 hours after infusion in this patient group were obtained to evaluate the effect of the lower antibody doses on biologic response.
This previous pharmacokinetic study of murine L6 in breast cancer patients showed the need to give a 200- mg infusion of unconjugated antibody before the 1311- labeled antibody to detect tumors by imaging, maxi- mize the circulation time of 1311-ChL6, and to minimize lung uptake.’ Therefore, in the 13’1 ChL6 therapy group, imaging and therapy doses were given on sequential days after slow infusion of 200 mg L6 and 20 mg ChL6 in the first 3 patients” and 200 mg of ChL6 in the next 6
patients. No difference in the response (cytokine, com- plement, albumin, tumor regression) of patients receiv- ing L6 compared with ChL6 was observed. In all nine patients, a therapy cycle consisted of an imaging study (dose 1) that was performed the day before the thera- peutic dose (dose 2). In 4 of the 20 treatment cycles in these nine patients, the imaging study was omitted be- cause of a low-level HAMA (1 patient, third and fourth cycle) or because of the patient’s condition (2 patients, second cycle for each). Therapy cycles were given as close to monthly intervals as permitted by the patient’s peripheral blood counts. Dose levels of 20 (1 patient) or 60 (8 patients) mCi/m2 were used as the initial therapy dose and adjusted downward for subsequent doses if necessitated by Grade 3 or 4 hematologic toxicity. Be- cause the specific activity of the 1311-ChL6 or 13’I-L6 was approximately 10 mCi/mg antibody, an imaging dose contained approximately 1 mg of antibody and a ther- apy dose contained 3-15 mg of antibody. These amounts of antibody were probably not biologically sig- nificant relative to the amount of antibody adminis- tered during the pre-infusion.
Quantitative Imaging
After each imaging and therapy dose, quantitative gamma camera imaging was performed immediately, at 3 hours, and at 24 hours after infusion of 1311. This was continued for 4-7 additional days for therapy doses to obtain pharmacokinetics for dosimetric ana ly~ i s . ’ ’~~~ To obtain radiopharmaceutical uptake in areas of superfi- cial tumor, irregular regions of interest (ROIs) were drawn manually with a light pen on the image to out- line each of the areas of tumor. A corresponding mirrored background ROI was defined in the same manner on the contralateral side of the patient, or a comparable area if there was tumor in the contralateral region. The counts from each tumor after background subtraction were converted to percent injected dose us- ing a sensitivity measured with a 10 ml volume of 1311 solution. Because all of the tumors were superficial, no attenuation correction was used. The values at 24 hours after imaging dose were compared with the values 24 hours after therapy dose with and without coincidence correction (Fig. 1). This method of quantitation has been validated by comparing gamma camera quantita- tion of superficial melanoma before and after excision, and the agreement was found to be within lo%.*’ Cor- rections for coincidence in the images obtained after therapeutic doses of 13’1 were made by determining the fractional count losses for a standard imaged simulta- neously and using the reciprocal of this fraction to make the corrections.
1026 CANCER Supplement February 1, 2994, Volume 73, No. 3
1 2 3 4 s 6 7 e 9 10 i t i z 13 14 15 16 17 in 19 20 zi lndhldual Tumors
U U - + + L _ - 6 L - - l 1
Patients
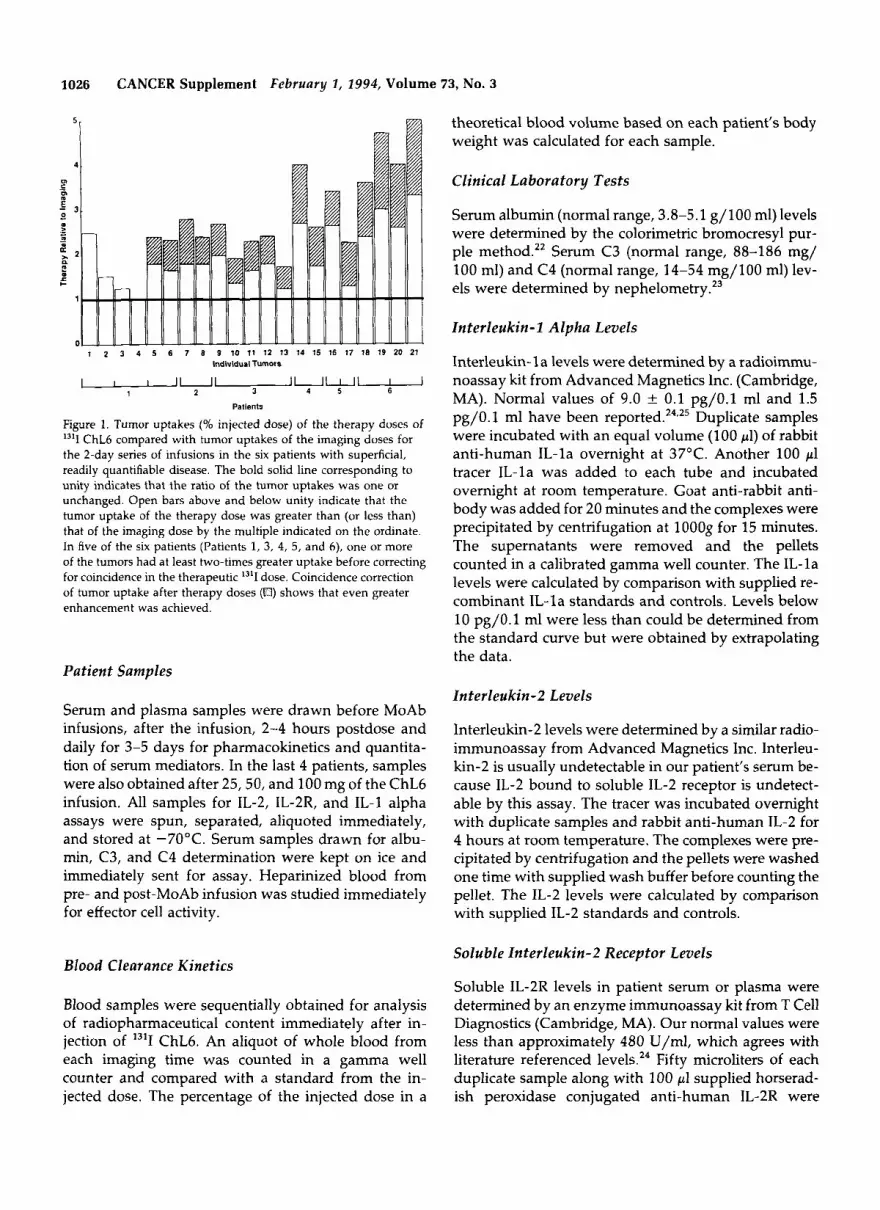
Figure 1. Tumor uptakes (% injected dose) of the therapy doses of 13'1 ChL6 compared with tumor uptakes of the imaging doses for the 2-day series of infusions in the six patients with superficial, readily quantifiable disease. The bold solid line corresponding to unity indicates that the ratio of the tumor uptakes was one or unchanged. Open bars above and below unity indicate that the tumor uptake of the therapy dose was greater than (or less than) that of the imaging dose by the multiple indicated on the ordinate. In five of the six patients (Patients 1, 3, 4, 5, and 6), one or more of the tumors had at least two-times greater uptake before correcting for coincidence in the therapeutic 13'1 dose. Coincidence correction of tumor uptake after therapy doses (El) shows that even greater enhancement was achieved.
theoretical blood volume based on each patient's body weight was calculated for each sample.
Clinical Laboratory Tests
Serum albumin (normal range, 3.8-5.1 g/100 ml) levels were determined by the colorimetric bromocresyl pur- ple method." Serum C3 (normal range, 88-186 mg/ 100 ml) and C4 (normal range, 14-54 mg/100 ml) lev- els were determined by nephel~metry.'~
Interleukin-1 Alpha Levels
Interleukin- l a levels were determined by a radioimmu- noassay kit from Advanced Magnetics Inc. (Cambridge, MA). Normal values of 9.0 k 0.1 pg/O.l ml and 1.5 pg/O. 1 ml have been reported.24e25 Duplicate samples were incubated with an equal volume (100 pl) of rabbit anti-human IL-la overnight at 37°C. Another 100 pl tracer IL-la was added to each tube and incubated overnight at room temperature. Goat anti-rabbit anti- body was added for 20 minutes and the complexes were precipitated by centrifugation at 1000s for 15 minutes. The supernatants were removed and the pellets counted in a calibrated gamma well counter. The IL-la levels were calculated by comparison with supplied re- combinant IL- l a standards and controls. Levels below 10 pg/O.l ml were less than could be determined from the standard curve but were obtained by extrapolating the data.
Patient Samples Interleukin-2 Levels
Serum and plasma samples were drawn before MoAb infusions, after the infusion, 2-4 hours postdose and daily for 3-5 days for pharmacokinetics and quantita- tion of serum mediators. In the last 4 patients, samples were also obtained after 25,50, and 100 mg of the ChL6 infusion. All samples for IL-2, IL-2R, and IL-1 alpha assays were spun, separated, aliquoted immediately, and stored at -70°C. Serum samples drawn for albu- min, C3, and C4 determination were kept on ice and immediately sent for assay. Heparinized blood from pre- and post-MoAb infusion was studied immediately for effector cell activity.
Blood Clearance Kinetics
Blood samples were sequentially obtained for analysis of radiopharmaceutical content immediately after in- jection of l3*I ChL6. An aliquot of whole blood from each imaging time was counted in a gamma well counter and compared with a standard from the in- jected dose. The percentage of the injected dose in a
Interleukin-2 levels were determined by a similar radio- immunoassay from Advanced Magnetics Inc. Interleu- kin-2 is usually undetectable in our patient's serum be- cause IL-2 bound to soluble IL-2 receptor is undetect- able by this assay. The tracer was incubated overnight with duplicate samples and rabbit anti-human IL-2 for 4 hours at room temperature. The complexes were pre- cipitated by centrifugation and the pellets were washed one time with supplied wash buffer before counting the pellet. The IL-2 levels were calculated by comparison with supplied IL-2 standards and controls.
Soluble Interleukin-2 Receptor Levels
Soluble IL-2R levels in patient serum or plasma were determined by an enzyme immunoassay kit from T Cell Diagnostics (Cambridge, MA). Our normal values were less than approximately 480 U/ml, which agrees with literature referenced levels.24 Fifty microliters of each duplicate sample along with 100 pl supplied horserad- ish peroxidase conjugated anti-human IL-2R were

Biologic Window for Chimeric LG/DeNardo et al. 1027
added to duplicate wells in a 96-well microtiter plate already coated with another anti-human IL-2R mono- clonal antibody that recognizes a nonoverlapping epi- tope. After incubation for 3 hours at room temperature, the wells were washed 3 times and 100 pl chromogen was added to each well and allowed to develop for 30 minutes. The reaction was stopped with 50 pl 2N sul- furic acid and the absorbance read at 490 nm. The sIL- 2R level was determined by comparison with recombi- nant sIL-2R standards and controls supplied by the manufacturer.
Antibody Dependent Cellular Cytotoxicity
For this assay both monocytes and large granular lym- phocytes (NK [natural killer]-enriched cells) were used as effector cells. These populations were purified from peripheral blood by density centrifugation on a Ficoll- Histopaque gradient.26 Mononuclear cells were resus- pended in medium and added to 96-well plates such that the number of monocytes would be fixed at an effector:target (E:T) ratio of 5:l. After 90 minutes at 37"C, the nonadherent cells were plated into another 96-well plate so that the E:T ratio was 20:l. The nonad- herent fraction was considered to be enriched for natu- ral killer cells. The tumor target cells, HBT3477, a hu- man mammary tumor cell line, were labeled with "Cr and then washed extensively before adding to the ef- fector cells in the presence of monoclonal antibody L6 at 1 &ml. The MoAb was present for the duration of the assay. Direct cytolysis of target cells without added exogenous L6 was also measured. After 18 hours of incubation, supernatants were harvested and radioac- tivity measured in a gamma counter. Cytotoxicity was determined by the amount of 51Cr released from the target cells destroyed by effector cells and calculated as previously described." In this experiment, samples from eight patients were used.
Results
Six of the nine treated patients responded with decrease in tumor size of at least 30% (Table l).12*13 The maxi- mum injected dose had been 60 mCi 1311 ChL6/mZ. In the nine patients who received sequential imaging and therapy doses, six had metastatic disease in superficial areas distinct from blood pool structures. Uptake in these tumors 24 hours after injection of the initial I3'I ChL6 dose (imaging) was compared with that for each tumor 24 hours after the second l3II ChL6 injection (therapy dose) (Fig. 1). Even before correction for coinci- dence for the therapy doses, mean tumor uptakes in each patient was almost double in five of the six pa- tients when compared with those after the imaging
Table 1. Number of Treatment Doses of 1311 ChL6 and the Responses of the 9 Therapy Patients
Peak IL-2R Patient no. No. of doses Response ratiost
PR PR NR NR PR* SR NR P SR
3.7 5.6 4.4 3.3 1.9 1.5 2 .3 1.7 2.2 2.7 2.6 2.3 2.3 2.3 1.2 1.3 2.9 2.3
PR: partial response, 2 50% sum of products of tumor L and W; SR: some response, decrease by < 50% and 2 30% sum of products of tumor L and W; NR: no response, decrease by < 30% and progression of I 25% in any existing lesion; P: progression, increased by > 25% in any existing lesion.
Skin erythema fluctuations not weighted. t Peak IL-2R ratios for 24 hr after first and second infusion levels of first ther- apy cycle to baseline level.
doses. After coincidence correction, the difference in tumor uptakes between the imaging and therapy doses was greater yet. In these six patients, blood clearances of the imaging and therapy doses were comparable to each other and in eight of their 10 two-dose cycles, the 24-hour percent ID of therapy dose in blood only ranged from +4 to -3% above or below the imagng dose 24-hour blood percent ID. On two occasions, this difference was 8% (Patient 3, Cycle 1) and 10% (Patient 6, Cycle 2) between the 24-hour blood injected dose levels. Thus, differences in blood clearances did not ac- count for the enhanced tumor uptake of the therapy doses.
To determine if the apparent increase in tumor up- take for therapeutic doses compared with the imaging doses was a significant finding, data from the initial study on each of the six patients was tested using the sign test. If a patient had more than one tumor, the median ratio (%ID therapy/%ID imaging) among all tumors was used. The results for the six patients then were evaluated. If therapy %ID was not different from imaging %ID, you would expect the median to be 1.
There is an average 1.974-fold increase in %ID/tu- mor during our six patients' initial therapy dose of L6 compared with their initial imaging dose using camera data that is not coincidence corrected. Using coinci- dence correction on the same data due to the higher therapy count rates compared with imaging, there is an average 2.864-fold increase in %ID/tumor. The proba- bility that all six patients have values greater than 1 is (0.5)6 = 0.016. Thus, the hypothesis test of no differ- ence would be rejected.
In the nine therapy patients, C3, C4, and albumin levels decreased during both L6 and ChL6 infusions
1028 CANCER Supplement February 1, 2994, Volume 73, No. 3
5 1€4 5 160 I40
120 110
00
and remained below normal for hours to days after ther- :I apy (Figs. 2, 3). Patients in the antibody dose escalation study receiving preload doses of 50,100, 150, or 200 mg
;; F;;:
4 130 4
i 3 ' 5
80 6 8 of L6 did not demonstrate a significant increase in their
IL-2 receptor level unless 150 mg or more had been : 80 Y -.
70 a given. A decrease was demonstrated in those patients 2 8o 2 6 4 2 a
receiving only 50 mg (Fig. 4). The nine patients receiv-
demonstrated a dose- and time-dependent pattern of lo I0
60 40
PO
24 48 72 120 144 ;& $-72n̂ -o6120 1 U 14
uI
1 3 0 1 ing imaging and therapy infusions on sequential days
soluble IL-2 receutor levels in serum when compared with their preinfusion baseline level (Fig. 5). In only two patients, IL-2 levels were found to be elevated shortly after initiation of the infusion of L6 or ChL6. Interleukin-2 levels, however, could not be detected by this assay once the IL-2 receptor level had increased.
150
130
Levels of IL-la varied in the 9 therapy patients, but many decreased after the initial 200 mg of L6 or ChL6 (Fig. 6). Levels below 10 pg/O.l ml were less than could be determined from the standard curve but were ob- tained by extrapolation of the data. One patient had no measurable IL-la throughout.
To determine whether the mononuclear cells from patients as compared with normal volunteers were acti- vated before infusion with L6 or whether either L6 or ChL6 enhanced cytolysis, ADCC was measured (Fig.
I W[ 12 60 40 30 PO 10 0
1m I S 0 140
130
110 I20 - tm 8
- E
90 ' 5 I 80
70 a 60
60 40
7). Monocytes from the breast cancer patients were not spontaneously cytolytic toward the mammary tumor 1 3 0 1
20 20 cell line. After infusion of either L6 or ChL6, levels of lo 10
Pre-cold Ab Post-cold Ab Day 1
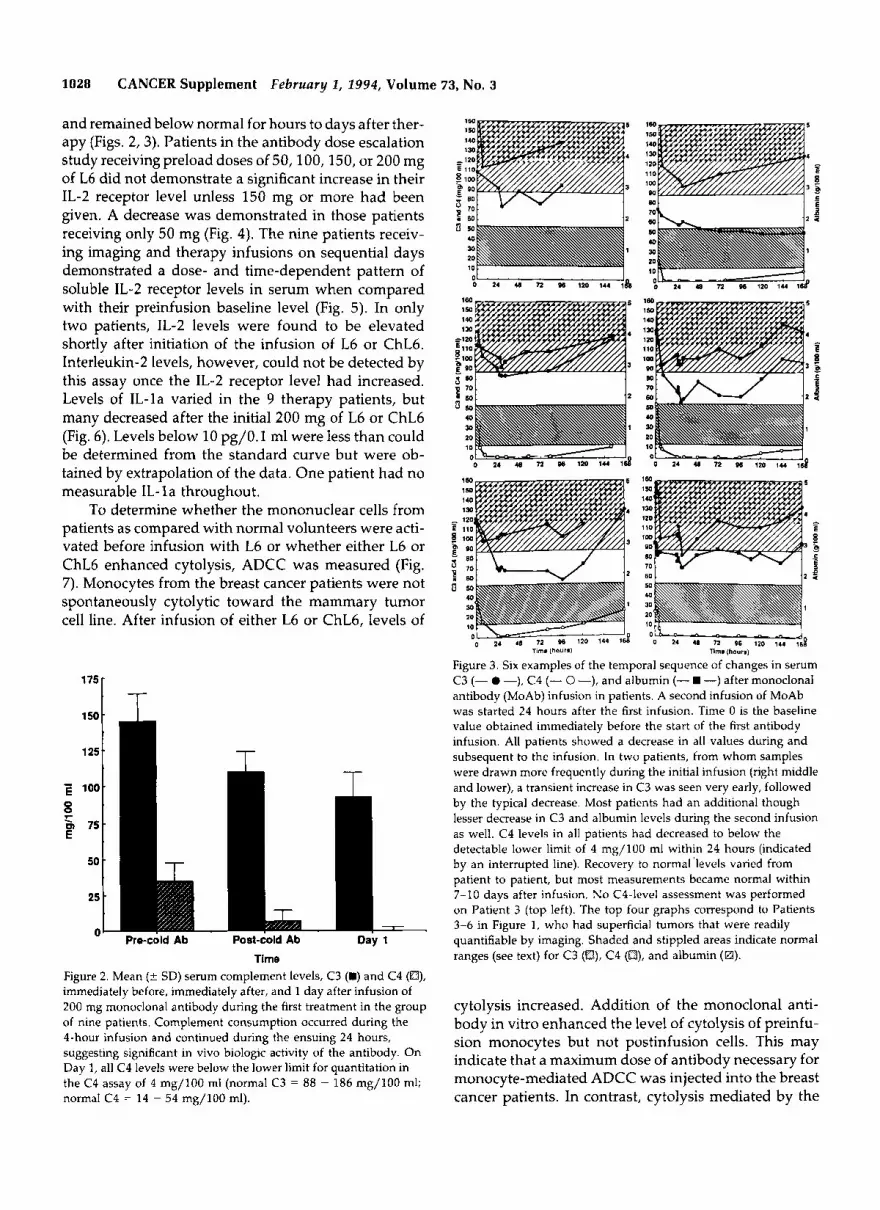
Time Figure 2. Mean (t SD) serum complement levels, C3 (B) and C4 (O), immediately before, immediately after, and 1 day after infusion of 200 mg monoclonal antibody during the first treatment in the group of nine patients. Complement consumption occurred during the 4-hour infusion and continued during the ensuing 24 hours, suggesting significant in vivo biologic activity of the antibody. On Day 1, all C4 levels were below the lower limit for quantitation in the C4 assay of 4 mg/100 ml (normal C3 = 88 - 186 mg/100 ml; normal C4 = 14 - 54 mg/100 ml).
' 0 OIL " - - 96 120 1.4 168 0 24 U 72 96 120 7;. $1
Tim.(hourrl nm. (hour.)
Figure 3. Six examples of the temporal sequence of changes in serum C3 (- 0 -), C4 (- 0 -), and albumin (- -) after monoclonal antibody (MoAb) infusion in patients. A second infusion of MoAb was started 24 hours after the first infusion. Time 0 is the baseline value obtained immediately before the start of the first antibody infusion. All patients showed a decrease in all values during and subsequent to the infusion. In two patients, from whom samples were drawn more frequently during the initial infusion (right middle and lower), a transient increase in C3 was seen very early, followed by the typical decrease. Most patients had an additional though lesser decrease in C3 and albumin levels during the second infusion as well. C4 levels in all patients had decreased to below the detectable lower limit of 4 mg/100 ml within 24 hours (indicated by an interrupted line). Recovery to normal 'levels varied from patient to patient, but most measurements became normal within 7-10 days after infusion. No C4-level assessment was performed on Patient 3 (top left). The top four graphs correspond to Patients 3-6 in Figure 1, who had superficial tumors that were readily quantifiable by imaging. Shaded and stippled areas indicate normal ranges (see text) for C3 (a), C4 (El), and albumin (H).
cytolysis increased. Addition of the monoclonal anti- body in vitro enhanced the level of cytolysis of preinfu- sion monocytes but not postinfusion cells. This may indicate that a maximum dose of antibody necessary for monocyte-mediated ADCC was injected into the breast cancer patients. In contrast, cytolysis mediated by the
Biologic Window for Chimeric LGIDeNardo et al . 1029
NK-enriched fraction was higher with cells obtained after infusion of ChL6 than before infusion of any anti- body, hut increased in all assays irrespective of whether the antibody was added in vivo or in vitro. Thus, the presence of L6 or ChL6 enhanced cytolysis mediated by the NK-enriched fraction of cells.
A
" 5
f f 4
Discussion
Tumor-targeted therapy with MoAb-based pharma- ceuticals has an exciting potential for therapy. Never- theless, results in clinical therapy trials of unconjugated
trast, radioimmunoconjugates have enjoyed success in several clinical trials in lymphoma and l e ~ k e m i a . ~ ~ - ~ ~ Using 1311 ChL6 radioimmunoconjugate, we have dem- onstrated measurable tumor regression in patients with advanced breast The L6 and ChL6 antibod- ies were chosen because they have ADCC and CDC activity in vitro that led us to expect some inflammatory response at the tumor site and in turn enhanced deliv- ery of radioimmunoconjugate because of increased vas- cular permeability. This hypothesis was derived from our experiences with lymphoma patients that received therapy with 13'I-Lym-l, a mouse IgG2a biologically active monoclonal antibody. Several of these lym-
antibodies have only shown minimal success. In con- 'bra i o i b o 200 1-;31 Pra 5b roo 260 1. i3 i 0.; 3 ~ . ; 8 1 rng mp mp ChL6 2 mp rng mp ChL6
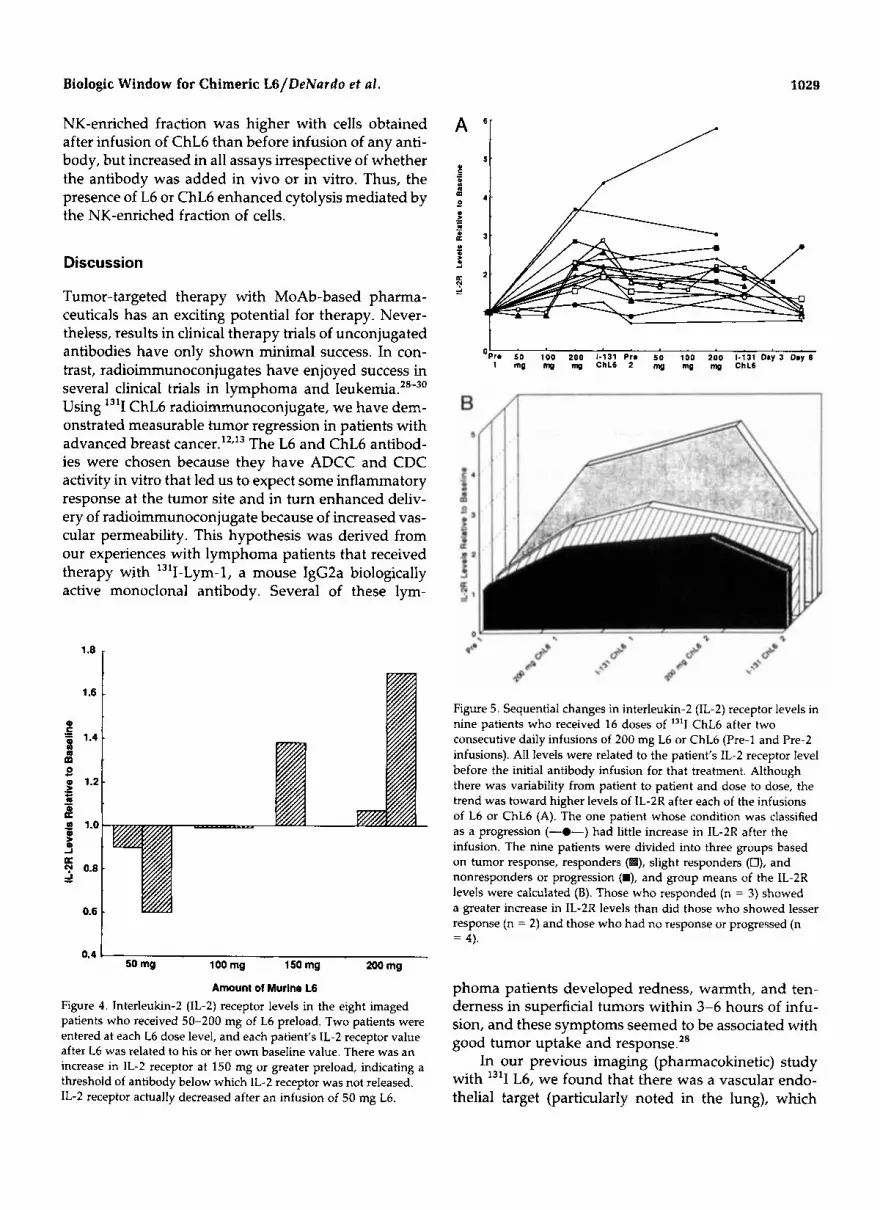
Figure 5. Sequential changes in interleukin-2 (IL-2) receptor levels in nine patients who received 16 doses of "'I ChL6 after two consecutive daily infusions of 200 mg L6 or ChL6 (Pre-1 and Pre-2 infusions). All levels were related to the patient's IL-2 receptor level before the initial antibody infusion for that treatment. Although there was variability from patient to patient and dose to dose, the trend was toward higher levels of IL-2R after each of the infusions of L6 or ChL6 (A). The one patient whose condition was classified as a progression (-0-) had little increase in IL-2R after the infusion. The nine patients were divided into three groups based on tumor response, responders ( ), slight responders (0), and nonresponders or progression (B), and group means of the IL-2R levels were calculated (B). Those who responded (n = 3) showed a greater increase in IL-2R levels than did those who showed lesser response (n = 2) and those who had no response or progressed (n = 4).
0.4 I 50 mg 100 mg 150 mg 200 mg
Amount of Murlne L6 Figure 4. Interleukin-2 (1L-2) receptor levels in the eight imaged patients who received 50-200 mg of L6 preload. Two patients were entered at each L6 dose level, and each patient's IL-2 receptor value after L6 was related to his or her own baseline value. There was an increase in 1L-2 receptor at 150 mg or greater preload, indicating a threshold of antibody below which IL-2 receptor was not released. IL-2 receptor actually decreased after an infusion of 50 mg L6.
phoma patients developed redness, warmth, and ten- derness in superficial tumors within 3-6 hours of infu- sion, and these symptoms seemed to be associated with good tumor uptake and response.28
In our previous imaging (pharmacokinetic) study with I3'I L6, we found that there was a vascular endo- thelial target (particularly noted in the lung), which

1030 CANCER Supplement February 1, 2994, Volume 73, No. 3
2oF\
r I \ \
Pro Post Post Imaging Dose
Therapy Dose
Figure 6. Levels of interleukin-1 alpha varied in nine therapy patients, but many decreased after the initial 200 mg of L6 or ChL6. Levels below 10 pg/O.l ml were too low to be determined from the standard curve but were obtained from extrapolated data. One patient had no measurable interleukin-1 alpha throughout.
could be coated with 200 mg of unlabeled L6. That enabled a subsequent dose of 13'1 L6 to reach extravas- cular breast cancer metastases in quantities that allowed tumor visualization by imaging.' We have shown in this report that 50-100 mg of L6 or ChL6, an amount that coats the antigen targets on vascular endothelium, also activates the classical complement cascade with a de- crease in C3 and C4. Soluble IL-2 receptor is not re- leased in amounts above preinfusion baseline levels unless 150 mg or greater of L6 or ChL6 is infused, how- ever. Furthermore, in those imaging patients who re- ceived only 50 or 100 mg of L6, IL-2 receptor was not released even 4-5 hours after the end of infusion. All but one patient receiving more than 150 mg L6 or ChL6 had an increased IL-2 receptor level within that time frame. The exceptional patient was the only one whose tumor progressed during the first month posttherapy. In these patients, the increase in serum IL-2 receptor level was dose and time dependent. Because a sufficient L6 dose was necessary to saturate vascular endothelial targets and escape to the extravascular space before an increase in serum IL-2 receptor was detectable, it seems likely that IL-2R or an intermediate cytokine trigger was released from cells at extravascular sites. One can pos- tulate these cells may be tumor-infiltrating lympho- cytes (TILs), cells in lymph nodes, or cells in lymphatic vessels. Further study is needed to evaluate these hy- potheses.
When patients are divided into three groups based on their clinical response to I3'I L6/ChL6 therapy (Ta- ble l), the mean IL-2 receptor elevation stimulated by treatment corresponded to the clinical response of each
group of patients. Greater IL-2 receptor increase corre- sponded to better response to treatment. Although the numbers are small, it is intriguing to speculate that some degree of biologic activity related to IL-2R release increased vascular permeability and helped create the observed clinical response. The patient who progressed despite 13'1 ChL6 therapy showed no increase in IL-2 receptor during the therapeutic cycle, and the three pa- tients in the "no response" group had the least increase in IL-2 receptor.
Serum C3 and C4 levels decreased after 50 mg or less of L6 or ChL6 with a correlative decrease in serum albumin in most patients. The amount of intravenous saline required to maintain blood pressure during these infusions and the rapid initial decrease followed by a protracted decrease in serum albumin without clinical evidence for pulmonary edema support the concept that general increased vascular permeability occurred (Table 2). Enhanced tumor accumulation after the ther- apy dose of 13'1 ChL6 compared with the imaging dose of 13'1 ChL6 suggests that the accentuated vascular leak indicated in some patients by further decrease in serum albumin concentration after the second (therapy dose) infusion allowed a greater amount of radiolabeled anti- body to accumulate at the tumor during the time of high blood concentration of the therapy dose. Theoretically this may be greater in tumored areas if the local warmth
NK-enriched (+I exogenousL6
Monocytes (+) exogrnous L6
Monocytcs NK-enriched cells 40 -
30 -
T
Pre-infusion Post L6 infusion Post ChL6 infusion
Figure 7. Direct cytolysis and antibody-dependent cellular cytotoxicity by monocytes and natural killer cells collected before and after infusion of L6 or ChL6 into breast cancer patients. Cytolysis of human mammary tumor cells, HBT3477, was measured in the presence or absence of exogenous L6 antibody: monocytes with L6 (O), monocytes without L6 ( ), natural killer cells with L6 (O), and natural killer cells without L6 (m).

Biologic Window for Chimeric LG/DeNardo et al . 1031
Table 2. Albumin Levels in Patients Immediately Before Initial L6 or ChLG Infusion and at the Time of the 1311 ChLG Therapy Dose
Serum albumin level @/lo0 ml) Volume of Increase in Plasma distribution volume of
Patient no. Pre-L6 infusion Post second infusion volume (ml) of albumin distribution
1 4.0 3.0 2468 3290 822 2 4.0 3.5 2327 2659 332 3 3.7 2.3 2438 3913 1475 4 3.7 1.8 2814 5784 2970 5 3.7 3.2 3217 3719 502 6 3.7 2.8 3069 4055 986 7 3.4 2.1 2668 4320 1652 8 3.0 2.2 4096 5585 1489 9 4.6 3.6 4022 5139 1117
Plasma volume was calculated based on body weight and pretreatment peripheral blood hematocrit. The volume of distribution was calculated using the plasma volume and the theoretical increase in volume needed to achieve the dilution of serum albumin after the second infusion at the time of the 1311-Ch-L6 therapy dose.
and tenderness found clinically relates to more cytokine and NK cell activity.
In this small group of patients, there was less corre- lation among enhancement of superficial tumor uptake, estimated tumor radiation dose, and patients obtaining the best response. As previously reported,"*'* the esti- mated tumor radiation dose was quite variable, ranging from 3 to 70 rads/mCi injected 1311, but Patients I, 2, and 5 (Table 1) with the best response had calculated tumor rad doses from low to middle of this range, whereas Patients 3 and 4 having higher calculated rad/ tumor doses demonstrated less response.
In conclusion, these findings suggest that the bio- logic activity of L6 and ChL6 in vivo was responsible for enhanced tumor uptake of I 3 l I ChL6 in many of our patients secondary to transient, increased vascular per- meability without significant adverse clinical sequelae. Complement activation and IL-2 receptor release may have been triggered by separate mechanisms. Tumor response was seen more frequently in this study than in any previously reported study using radioimmunocon- jugates in solid tumors. Because of the correlation of IL-2R increase to the later tumor response and the rela- tively low calculated radiation dose in several respond- ing tumors, we postulate that responses may have been secondary to synergy between enhanced delivery of the targeted radiation and sensitizing effects on tumor caused by activated effector cell mechanisms. The pos- tulate is further supported by clinical studies of L6 and ChL6 alone with minimal to no therapeutic response."
References
1. Hellstrom I, Horn D, Linsley P, Brown JP, Brankovan V, Hell- strom KE. Monoclonal antibodies raised against human lung carcinomas. Cancer Res 1986; 46:3917-23.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Hellstrom I, Beaumier PL, Hellstrom KE. Antitumor effects of L6, an IgG2a antibody that reacts with most human carcinomas. Proc Natl Acad Sci U S A 1986; 83:7059-63. Adams GP, DeNardo SJ, Amin A, Kroger LA, DeNardo GL, Hellstrom I, et al. Comparison of the pharmacokinetics in mice and the biological activity of murine L6 and human-mouse chi- meric ChL6 antibody. Antibody Imiiiunoconj Radiopharni 1992;
Rosenbaum LC, Neuwelt EA, Van To1 HH, Loh YP, Verbalis JG, Hellstrom I, et al. Expression of neurophysin-related precursor in cell membranes of a small-cell lung carcinoma. Proc Natl Acad Sci U S A 1990; 87:9928-32. Marken JS, Schieven GL, Hellstrom I, Hellstrom KE, Aruffo A. Cloning and expression of the tumor-associated antigen L6. Proc Natl Acad Sci U S A 1992; 89:3503-7. Hotta H, Ross AH, Huebner K, Isobe M, Wendeborn 5, Chao MV, et al. Molecular cloning and characteristics of an antigen associated with early stages of melanoma tumor progression. Cancer Res 1988; 48:2955-62. Metzelaar MJ, Wijnaard PLJ, Peters PJ, Sixma JJ, Nieuwenhuis HK, Clevers HC. CD63 antigen: a novel lysosomal membrane glycoprotein, cloned by a screening procedure for intracellular antigens in eukaryotic cells. Biol Chen7 1991; 266:3239-45. Szala S, Kasai Y, Steplewski 2, Rodeck U, Koprowski H, Linnen- bach AJ. Molecular cloning of a cDNA for the human tumor-as- sociated antigen CO-029 and identification of related trans- membrane antigens. Proc Natl Acad Sci U S A 1990; 87:6833-7. DeNardo SJ, O'Grady LF, Macey DJ, Kroger LA, DeNardo GL, Lamborn KR, et al. Quantitative imaging of mouse L-6 monoclo- nal antibody in breast cancer patients to develop a therapeutic strategy. Nucl Med Biol 1991; 18:621-31. Goodman GE, Hellstrom I, Brodzinsky L, Nicaise C, Kulander B, Hummel D, et al. Phase I trial of murine monoclonal antibody L6 in breast, colon, ovarian, and lung cancer. J Clin Oncol 1990; 8:1083-92. DeNardo SJ, Warhoe KA, O'Grady LF, Hellstrom I, Hellstrom KE, Mills SL, et al. Radioimmunotherapy for breast cancer: treatment of a patients with I3'l L6 chimeric monoclonal anti- body. J n f j Biol Markers 1991; 6:221-230. DeNardo SJ, Warhoe KA, O'Grady LF, DeNardo GL, Hellstrom I, Hellstrom KE, et al. Radioimmunotherapy with '"I chimeric L-6 in advanced breast cancer. In: Ceriani RL, editor. Breast epithelial antigens. New York: Plenum Press, 1991: 227-32.
5:81-95.
1032 CANCER Supplement February 1, 2994, Volume 73, No. 3
13.
14.
15.
16.
17.
18.
19.
20
21
DeNardo SJ, O'Grady LF, Kramer EL, Richman CM, Warhoe KA, Salako QA, et al. Radioimmunotherapy in breast cancer: current results in phase 1 protocols. Clin Nttcl Med 1992; 17:761. Fell HP, Gayle MA, Yelton D, Lipsich L, Schieven GL, Marken IS, et al. Chimeric L6 anti-tumor antibody: genomic construc- tion, expression, and characterization of the antigen binding site. I Biol Chem 1992; 267:15552-8. Liu AY, Robinson RR, Hellstrom KE, Murray ED Jr, Chang CP, Hellstrom I. Chimeric mouse-human IgGl antibody that can mediate lysis of cancer cells. Proc Natl Acad Sci U S A 1987; 84:3439-43. Lavie E, Beaumier PL, Brodzinsky L, Hellstrom KE, Hellstrom I . Evaluation of L6, an anti-carcinoma murine monoclonal anti- body in tumor-bearing nude mice. Radiother Oncol 1989;
DeNardo SJ. DeNardo GL, Peng J-S. Pharmaceutical quality control for radiolabeled monoclonal antibodies and their frag- ments. A m ] Ph!/siol Imaging 1989; 4:39-44. DeNardo SJ, Peng J-S, DeNardo GL, Mills SL, Epstein AL. lmmu- nochemical aspects of monoclonal antibodies important for ra- diopharmaceutical development. Int I Radiat Appl Instrum [B]
DeNardo GL, DeNardo SJ, Macey DJ, Mills SL. Quantitative pharmacokinetics of radiolabeled monoclonal antibodies in pa- tients. In: Srivastava SC, editor. Radiolabeled monoclonal anti- bodies for imaging and therapy. New York: Plenum Press, 1988:
Macey DJ, DeNardo GL, DeNardo SJ. A treatment planning pro- gram for radioimmunotherapy. In: Vaeth JM, Meyer JL, editors. Frontiers of radiation therapy and oncology. Basel: S. Karger,
Macey DJ, DeNardo SJ, DeNardo GL, Goodnight JK, Unger MW. Uptake of In-1 11 labeled monoclonal antibody ZME-018
15:295-305.
1986; 13:303-10.
293-310.
1990: 123-31.
22.
23.
24.
25.
26.
27.
28.
29.
30
as a function of tumor size in a patient with melanoma. A m I Physiol Imaging 1988; 3:l-6. Louderback A, Mealy EH, Wiernik PH. A new dye-binding tech- nique using bromocresyl purple for determination of albumin in serum. Clin Chem 1968; 14:793-4. Yam P, Petz LD, Cooper NR. The relationship between hemo- lytic and immunodiffusion methods for measurement of C4 in patients with immunologic disorders. A m J Clin Pathol 1975;
Linde A, Anderson B, Svenson SB, Ahrne H, Carlsson M, Fors- berg P, et al. Serum levels of lymphokines and soluble cellular receptors in primary Epstein-Barr virus infection and in patients with chronic fatigue syndrome. ]Infect Dis 1992; 165:994-1000. Wolf RE, Brelsford WG, Hall VC, Adams SB. Cytokines and soluble interlukin 2 receptors in rheumatoid arthritis. I Rheunta-
Kleinerman ES, Erickson KL, Schroit AJ, Fogler WE, Fidler IJ. Activation of tumoricidal properties in human blood monocytes by liposomes containing lipophilic muramyl peptide. Cancer Res
Somers SD, Erickson KL. Regulation of murine macrophage function by IL-4: Activation of macrophages by a T-T cell hybrid- oma is due to IL-4. Cell Zmmunol 1989; 122:178-87. DeNardo SJ, DeNardo GL, O'Grady LF. Treatment of B cell ma- lignancies with "'I-Lym-l monoclonal antibodies. In t \ Cancer
Press OW, Early JF, Badger CC, Martin PL, Appelbaum FR, Levy R, et al. Treatment of refractory non-Hodgkin's lymphoma with radiolabeled MB-1 (anti-CD37) antibody. ] Clin Oncol 1989;
Scheinberg DA, Lovett D, Divgi CR, Graham MC, Berman E, Pentlow K, et al. A phase 1 trial of monoclonal antibody M195 in acute myelogenous leukemia: specific bone marrow targeting and internalization of radionuclide. I Clin Oncol 1991; 9:478-90.
64~351-7.
t ~ l 1992; 19~524-8.
1983; 43:2010-4.
(SUPPI) 1988; 3:96-101.
7: 1027-38.