scimitar syndrome presenting in adults
TRANSCRIPT

J CARD SURG2008;23:63-78
REDDY, ET AL.REGIONAL RECONSTITUTION OF IMA
63
CASE REPORTS
Regional Variation in theReconstitution of Flow in theInternal MammaryArtery Graft
Proddutur R. Reddy, M.D.,∗ MamdouhBakhos, M.D.,† and Ferdinand Leya,M.D.∗
∗Department of Medicine, Division ofCardiology; and †Department of Thoracicand Cardiovascular Surgery, LoyolaUniversity Medical Center, Maywood, Illinois
ABSTRACT We report an 81-year-old man withcoronary artery disease and bypass surgery witha sequential internal mammary artery (IMA) to thediagonal and then the anterior descending, whodeveloped regional variations in the flow throughhis arterial conduit. Four years after his initialsurgery, he developed atresia of the proximal seg-ment of the arterial conduit due to competitiveflow. After reoperation, the patient reconstitutedflow in his proximal segment, but developed atre-sia of the distal segment. We describe for thefirst time, regional variation in arterial conduit pa-tency and discuss factors controlling patency in thesequential arterial conduit. doi: 10.1111/j.1540-8191.2007.00492.x (J Card Surg 2008;23:63-65)
The internal mammary artery (IMA) has properties
unique from saphenous vein grafts (SVG) that distin-
guish it as the ideal bypass conduit. Atresia of arterial
grafts after thrombosis or low flow states has been
previously described, including its reversal to patent
flow.1 We describe for the first time a case demon-
strating regional patency and regional reconstitution in
a sequential IMA conduit.
CASE REPORT
An 81-year-old man was evaluated and treated at an
outside hospital in 2000 for dyspnea on exertion and
fatigue. Cardiac catheterization revealed a normal left
ventricle but severe mitral regurgitation (MR) and triple
vessel coronary disease. He underwent mitral annu-
loplasty and bypass surgery including a sequential in-
ternal mammary artery (IMA) to the first diagonal (D1)
Address for correspondence: Proddutur R. Reddy, M.D., Department
of Medicine, Division of Cardiology, Loyola University Medical Center,
Bld. 110, Room 6231, 2160 S. First Ave., Maywood, IL 60153. Fax:
708-327-2771; e-mail: Dr [email protected]
No funding was involved in this work.
There is no conflict of interest with any of the authors.
branch then to the left anterior descending (LAD) artery.
Four years later, he presented to our hospital with recur-
rent symptoms. Cardiac catheterization revealed mildly
dilated left ventricle with preserved ejection fraction,
severe MR, severe tricuspid regurgitation, and moder-
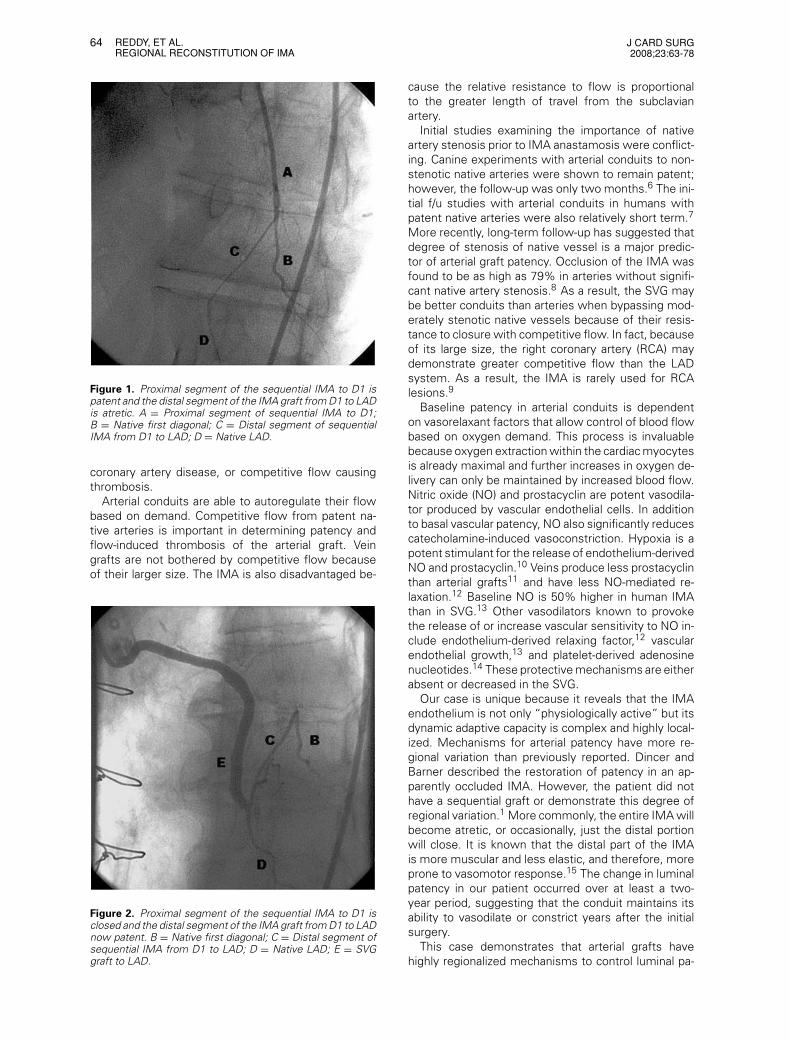
ate coronary artery disease. The IMA graft to D1 was
patent, but the sequential segment of the IMA from
D1 to LAD had become atretic (Fig. 1). The patient un-
derwent a second operation with mitral and tricuspid
valve repair and single vessel bypass with saphenous
vein grafts (SVG) to the mid-LAD (distal to the previous
IMA graft). Most recently, the patient presented again
with symptoms of dyspnea on exertion and fatigue.
Cardiac catheterization revealed mild MR, mild aortic
stenosis, and moderate coronary artery disease. The
diagonal was occluded proximally, the mid-LAD steno-
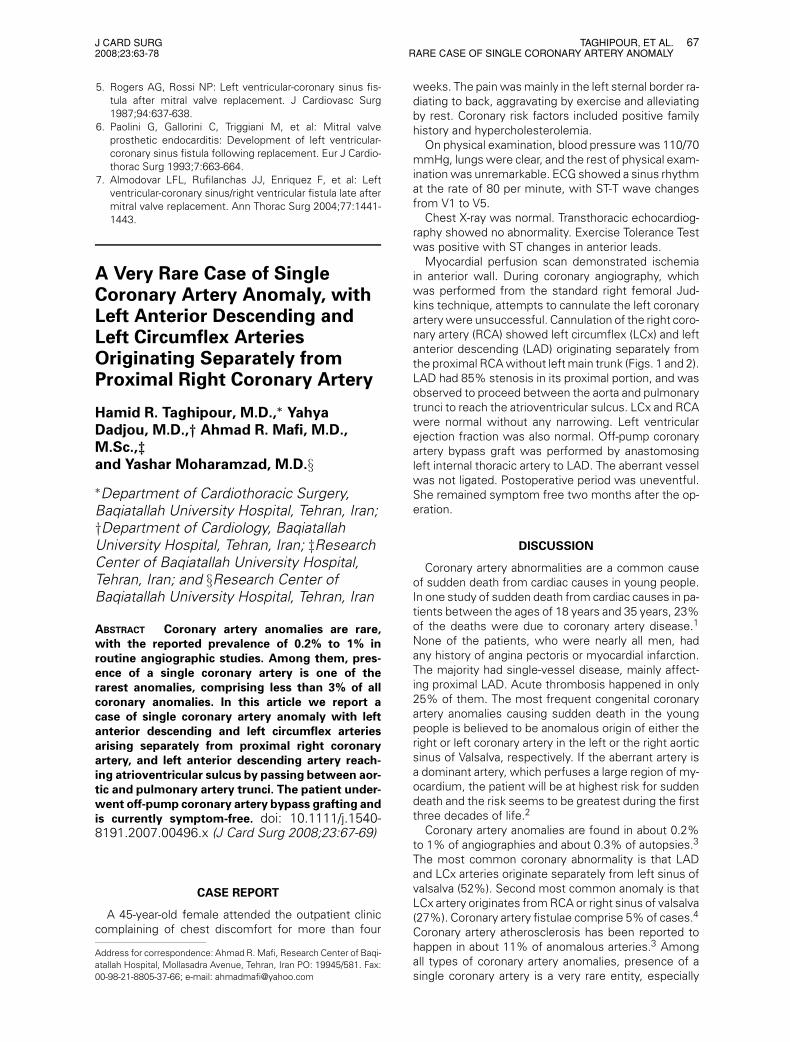
sis worsened, and the SVG’s were patent. The proximal
IMA segment grafted to D1 had now become atretic,
but the distal IMA segment connecting D1 to LAD was
now widely patent (Fig. 2) with reverse flow from the
well-perfused LAD toward D1.
The atretic distal internal thoracic artery (IMA) seg-
ment was likely due to competitive flow from the na-
tive LAD. The larger SVG to LAD had significantly more
blood flow to supply not only the LAD territory, but also
the D1. As a result, the proximal IMA now became
atretic while the distal IMA was reconstituted.
DISCUSSION
The IMA has vascular properties unlike the SVG that
give them long-term patency advantages. The patency
rates of the IMA approaches 99% at one year and
from 85% to 95% in 10 years.2 Unlike arterial conduits,
SVG’s are more susceptible to intimal hyperplasia, ar-
teriosclerosis, progressive stenosis, thrombus forma-
tion, and occlusion. The one-year patency rates are
from 80% to 90%. However, this significantly decrease
thereafter: 1% to 2% per year occlusion rate for the
first five years up to 4% to 5% occlusion rate from
years 5 through 10. Overall the 10-year patency rates
of SVG’s are only 60% and only 30% of those are free
of any stenosis.3 These advantages in patency have led
to better survival and freedom from ischemic events in
patients with multiple grafts including the IMA.4 The
use of the IMA, particularly to the LAD, is the standard
of care.
Because of improved patency rates, the IMA is se-
quentially grafted to one or more diagonal branches
and occasionally to two sites on the LAD. This prac-
tice has been proven effective and is practiced by
many surgeons;5 however, the greatest risk is the
potential to jeopardize the distal IMA, which is usually
the most important anastamosis. IMA failures are infre-
quent and most often occur due to intimal compromise
and thrombosis secondary to faulty technique, severe
64 REDDY, ET AL.REGIONAL RECONSTITUTION OF IMA
J CARD SURG2008;23:63-78
Figure 1. Proximal segment of the sequential IMA to D1 ispatent and the distal segment of the IMA graft from D1 to LADis atretic. A = Proximal segment of sequential IMA to D1;B = Native first diagonal; C = Distal segment of sequentialIMA from D1 to LAD; D = Native LAD.
coronary artery disease, or competitive flow causing
thrombosis.
Arterial conduits are able to autoregulate their flow
based on demand. Competitive flow from patent na-
tive arteries is important in determining patency and
flow-induced thrombosis of the arterial graft. Vein
grafts are not bothered by competitive flow because
of their larger size. The IMA is also disadvantaged be-
Figure 2. Proximal segment of the sequential IMA to D1 isclosed and the distal segment of the IMA graft from D1 to LADnow patent. B = Native first diagonal; C = Distal segment ofsequential IMA from D1 to LAD; D = Native LAD; E = SVGgraft to LAD.
cause the relative resistance to flow is proportional
to the greater length of travel from the subclavian
artery.
Initial studies examining the importance of native
artery stenosis prior to IMA anastamosis were conflict-
ing. Canine experiments with arterial conduits to non-
stenotic native arteries were shown to remain patent;
however, the follow-up was only two months.6 The ini-
tial f/u studies with arterial conduits in humans with
patent native arteries were also relatively short term.7
More recently, long-term follow-up has suggested that
degree of stenosis of native vessel is a major predic-
tor of arterial graft patency. Occlusion of the IMA was
found to be as high as 79% in arteries without signifi-
cant native artery stenosis.8 As a result, the SVG may
be better conduits than arteries when bypassing mod-
erately stenotic native vessels because of their resis-
tance to closure with competitive flow. In fact, because
of its large size, the right coronary artery (RCA) may
demonstrate greater competitive flow than the LAD
system. As a result, the IMA is rarely used for RCA
lesions.9
Baseline patency in arterial conduits is dependent
on vasorelaxant factors that allow control of blood flow
based on oxygen demand. This process is invaluable
because oxygen extraction within the cardiac myocytes
is already maximal and further increases in oxygen de-
livery can only be maintained by increased blood flow.
Nitric oxide (NO) and prostacyclin are potent vasodila-
tor produced by vascular endothelial cells. In addition
to basal vascular patency, NO also significantly reduces
catecholamine-induced vasoconstriction. Hypoxia is a
potent stimulant for the release of endothelium-derived
NO and prostacyclin.10 Veins produce less prostacyclin
than arterial grafts11 and have less NO-mediated re-
laxation.12 Baseline NO is 50% higher in human IMA
than in SVG.13 Other vasodilators known to provoke
the release of or increase vascular sensitivity to NO in-
clude endothelium-derived relaxing factor,12 vascular
endothelial growth,13 and platelet-derived adenosine
nucleotides.14 These protective mechanisms are either
absent or decreased in the SVG.
Our case is unique because it reveals that the IMA
endothelium is not only “physiologically active” but its
dynamic adaptive capacity is complex and highly local-
ized. Mechanisms for arterial patency have more re-
gional variation than previously reported. Dincer and
Barner described the restoration of patency in an ap-
parently occluded IMA. However, the patient did not
have a sequential graft or demonstrate this degree of
regional variation.1 More commonly, the entire IMA will
become atretic, or occasionally, just the distal portion
will close. It is known that the distal part of the IMA
is more muscular and less elastic, and therefore, more
prone to vasomotor response.15 The change in luminal
patency in our patient occurred over at least a two-
year period, suggesting that the conduit maintains its
ability to vasodilate or constrict years after the initial
surgery.
This case demonstrates that arterial grafts have
highly regionalized mechanisms to control luminal pa-

J CARD SURG2008;23:63-78
MACKIE AND CLEMENTSLEFT VENTRICULAR TO CORONARY SINUS FISTULA
65
tency that remain viable for years. Further investi-
gation into the mechanism and extent of regional-
ity may clinically improve grafting patterns and our
understanding of hemodynamic effects on vascular
physiology.
REFERENCES
1. Dincer B, Barner HB: The “occluded” internal mammary
artery graft: Restoration of patency after apparent occlu-
sion associated with progression of coronary disease. J
Thorac Cardiovasc Surg 1983;85(2):318-320.
2. Tatoulis J, Buxton BF, Fuller JA: Patencies of 2127 arte-
rial to coronary conduits over 15 years. Ann Thorac Surg
2004;77:93-101.
3. Fitzgibbon GM, Kafka HP, Leach AJ, et al: Coronary by-
pass graft fate and patient outcome: Angiographic follow-
up of 5,065 grafts related to survival and reoperation
in 1,388 patients during 25 years. J Am Coll Cardiol
1996;28:616-626.
4. Cameron A, Davis KB, Green G, et al: Coronary bypass
surgery with internal-artery-grafts on 10-year survival and
other cardiac events. N Eng J Med 1986;314:1-6.
5. Dion R, Glineur D, Derouck D, et al: Long-term clinical
and angiographic follow-up of sequential internal thoracic
artery grafting. Europ J Cardiothorac Surg 2000;17:407-
414.
6. Lust RM, Zeri RS, Spence PA, et al: Effect of chronic
native flow competition on internal thoracic artery grafts.
Ann Thorac Surg 1994;57:45-50.
7. Sabik JF, Lytle BW, Blackstone EH, et al: Does compet-
itive flow reduce internal thoracic artery graft patency?
Ann Thorac Surg 2003;76:1490-1497.
8. Berger A, MacCarthy PA, Siebert U, et al: Long-term pa-
tency of internal mammary artery bypass grafts. Circula-
tion 2004;110(2 Suppl):II-36-II-40.
9. Sabik JF, Lytle BW, Blackstone EH, et al: Comparison
of saphenous vein and internal thoracic artery graft pa-
tency in coronary system. Ann Thorac Surg 2005;79:544-
551.
10. Pearson PJ, Evora PR, Discigil B, et al: Hypoxia in-
creases vasodilator release from internal mammary artery
and saphenous vein grafts. Ann Thorac Surg 1998
May;65(5):1220-1225.
11. Chaikhouni A, Crawford FA, Kochel PJ, et al: Human in-
ternal mammary artery produces more prostacyclin than
saphenous vein. J Thorac Cardiovasc Surg 1986;92:88-
91.
12. Luscher TF, Diederich D, Siebenmann R, et al: Differ-
ences between endothelium-dependent relaxation in ar-
terial and in venous coronary bypass grafts. N Eng J Med
1988;319(8):462-467.
13. Broeders MA, Doevendans PA, Maessen JG, et al: The
human internal thoracic artery releases more nitric oxide
in response to vascular endothelial growth factor than
the human saphenous vein. J Thorac Cardiovasc Surg
2001;122:305-309.
14. Yang Z, Luscher TF: Basic cellular mechanisms of
coronary bypass graft disease. Eur Heart J 1993;14(1
Suppl):193-197.
15. Angelini GD, Bryan AJ, Dion R: Surgical anatomy and
histological characteristics. In Van Son JA, Smedts FM
(eds): Arterial Conduits in Myocardial Revascularization.
1st ed. New York: Oxford University Press; 1996, pp.
13-22.
Left Ventricular to CoronarySinus Fistula Following MultipleMitral Valve ReplacementSurgeries
Benjamin D. Mackie, M.D.,∗ and StephenJ. Clements, M.D.†∗Department of Medicine, J. Willis HurstInternal Medicine Residency Program,Emory University School of Medicine,Atlanta, Georgia; and †Division ofCardiology, Department of Medicine, EmoryUniversity School of Medicine, Atlanta,Georgia
ABSTRACT Development of left ventricular to coro-nary sinus fistula is a rare complication of mitralvalve surgery. Three of the seven previously re-ported cases occurred following multiple valve re-placement surgeries, all of which were thought tobe secondary to a complication of surgery and allwere treated with surgical closure of the fistula.We report a case of left ventricular to coronary si-nus fistula occurring after two mitral valve replace-ment surgeries that was treated medically withfavorable long-term results. doi: 10.1111/j.1540-8191.2007.00491.x (J Card Surg 2008;23:65-67)
Frank Gerbode first described congenital left ventric-
ular to right atrial shunts in 1958. However, Chambers
and Rogers were the first to describe a left ventricular
to coronary sinus fistula following mitral valve replace-
ment in 1972.1,2 Since that time, additional cases have
been reported; taken together they suggest a greater
risk of fistula formation following multiple mitral valve
replacement surgeries and/or after excessive debride-
ment of the mitral valve annulus.3-7 Our case describes
a patient with late development, five years out from the
second mitral valve replacement, of a left ventricular to
coronary sinus fistula who presented with a two-month
history of increased dyspnea on exertion and new car-
diac murmur.
CASE REPORT
A 77-year-old female, with no previous cardiac his-
tory, originally presented with ruptured chordae ten-
dinae and underwent mitral valve replacement with
a 29 mm Hancock tissue valve at that time. She did
well postoperatively until four years later, when she
developed severe mitral regurgitation requiring a sec-
ond valve replacement, again with a 29 mm Hancock
valve. The postoperative course was uneventful except
Address for correspondence: Benjamin D. Mackie, 69 Jesse Hill Drive,
Atlanta, GA 30303. Fax: 404-778-3508; e-mail: [email protected]

66 MACKIE AND CLEMENTSLEFT VENTRICULAR TO CORONARY SINUS FISTULA
J CARD SURG2008;23:63-78
Figure 1. Cardiac angiography showing origin of LV to coro-nary sinus fistula depicted by the white arrow. Other struc-tures include the right atrium = RA; coronary sinus = CS;right ventricle = RV; metallic ring of Hancock valve in the mi-tral position = MV; and ascending aorta = Ao.
for bradycardia for which a permanent pacemaker was
placed.
A year later, she presented with increasing dys-
pnea on exertion, shortness of breath at rest, and
fatigue. Physical exam showed a blood pressure of
152/78 mmHg, pulse of 80 beats/min, respiratory rate
of 20 breaths/min, and a temperature of 96.5 ◦F. She
was in no acute distress. Cardiac auscultation revealed
a regular rate and rhythm, normal S1 and S2 with a III/VI
holosystolic murmur loudest at the left lower sternal
border and apex, radiating to the neck and axilla. Vis-
ible jugular venous distention to the angle of her jaw
at 45 degrees was observed and hepatojugular reflux
was present. Lung fields were clear to auscultation.
Abdominal exam showed right upper quadrant tender-
ness and a liver spanning 8 cm. Trace pretibial edema
was present.
Electrocardiogram showed a paced rhythm. Chest
X-ray showed mild cardiomegaly and left atrial enlarge-
ment. Routine labs were within normal limits.
Further evaluation with cardiac catheterization re-
vealed a fistula between the posterior left ventricular
wall and the coronary sinus leading to opacification of
the coronary sinus, the right atrium, and both cavae
(Fig. 1). The shunt ratio was 1.75/1 and pulmonary
artery pressures were 45/18 mmHg with a mean pul-
monary capillary wedge pressure of 16 mmHg without
a large v-wave. Left ventricular ejection fraction was
65%.
Following cardiac catheterization, a transthoracic
echocardiogram showed a high-velocity jet inferior to
the mitral valve and high-velocity systolic flow into the
coronary sinus and right atrium, both consistent with a
left ventricular to coronary sinus fistula. The patient im-
proved symptomatically with optimization of her blood
pressure, diuresis, and the addition of verapamil to her
medical regimen. She deferred any additional surgeries
and continued to do well for 16 years when she died
of another cause.
DISCUSSION
This case illustrates a very rare, yet significant, com-
plication following mitral valve replacement surgery.
The increased pulmonary pressures, illustrating mild
pulmonary hypertension, provide the physiological
explanation behind the patients presenting clinical
symptoms. Even though all previously reported cases
were treated with surgical closure; this patient was ad-
equately managed with medical therapy alone since her
frail health caused her to decline surgery.
The decision to treat medically versus surgically
should be individualized taking into account the pa-
tients age, degree of pulmonary hypertension, and
other medical comorbidities. However, surgical inter-
vention should remain the definitive therapy.
Two etiologies have been postulated to account for
the formation of left ventricular to coronary sinus fistula
formation following mitral valve replacement surgery.
The first is direct injury during surgery leading to forma-
tion of a fistulous tract. Second is injury to the posterior
ventricular wall, inferior to the mitral valve leaflets, sec-
ondary to excessive debridement of a usually calcified
mitral valve annulus. This predisposes to spontaneous
dissection and eventually results in fistula formation.6
In our case, fistula formation was likely the result of the
second etiology described above based upon the dis-
tant chronological relationship between valve replace-
ment surgery and fistula recognition.
Obviously, the exact time of fistula development can-
not be determined, but can be estimated based upon
time of clinical presentation.
Even though uncommon, left ventricular to coronary
sinus fistula should be a diagnosis of consideration in
patients who have undergone multiple mitral valve re-
placement surgeries and present with symptoms con-
sistent with pulmonary congestion. One needs a high
index of suspicion to make this diagnosis clinically. The
murmur created from the fistula closely mimics that
of mitral regurgitation, and the presenting symptoms
are those of heart failure. In all reported cases, angio-
graphic visualization, echocardiographic evaluation, or
direct surgical visualization/palpation has been required
to confirm the diagnosis. All patients responded well
to repeat surgery. Based upon the small number of
reported cases in the literature, we feel that postop-
erative left ventricular to coronary sinus fistula carries
a favorable prognosis if diagnosed in a timely fashion,
but does require repeat surgery in most cases.
REFERENCES
1. Gerbode F, Hultgren H, Melrose D, et al: Syndrome of left
ventricular-right atrial shunt. Ann Surg 1958;148:433.
2. Chambers RL, Rodgers MA: Left ventricular-to-coronary-
vein fistula following mitral valve replacement. Ann Thorac
Surg 1972;14:305-308.
3. Miller DC, Schapira JN, Stinson EB, et al: Left ventricular-
coronary sinus fistula following repeated mitral valve re-
placements. J Thorac Cardiovasc Surg 1978;76:43-45.
4. Morritt GN, Jamieson MPG, Irwing JB, Marquis RM, Wal-
baum PR: Development of left ventricular-coronary sinus
fistula following replacement of mitral valve prosthesis. J
Thorac Cardiovasc Surg 1978;76:381-384.
J CARD SURG2008;23:63-78
TAGHIPOUR, ET AL.RARE CASE OF SINGLE CORONARY ARTERY ANOMALY
67
5. Rogers AG, Rossi NP: Left ventricular-coronary sinus fis-
tula after mitral valve replacement. J Cardiovasc Surg
1987;94:637-638.
6. Paolini G, Gallorini C, Triggiani M, et al: Mitral valve
prosthetic endocarditis: Development of left ventricular-
coronary sinus fistula following replacement. Eur J Cardio-
thorac Surg 1993;7:663-664.
7. Almodovar LFL, Rufilanchas JJ, Enriquez F, et al: Left
ventricular-coronary sinus/right ventricular fistula late after
mitral valve replacement. Ann Thorac Surg 2004;77:1441-
1443.
A Very Rare Case of SingleCoronary Artery Anomaly, withLeft Anterior Descending andLeft Circumflex ArteriesOriginating Separately fromProximal Right Coronary Artery
Hamid R. Taghipour, M.D.,∗ YahyaDadjou, M.D.,† Ahmad R. Mafi, M.D.,M.Sc.,‡and Yashar Moharamzad, M.D.§∗Department of Cardiothoracic Surgery,Baqiatallah University Hospital, Tehran, Iran;†Department of Cardiology, BaqiatallahUniversity Hospital, Tehran, Iran; ‡ResearchCenter of Baqiatallah University Hospital,Tehran, Iran; and §Research Center ofBaqiatallah University Hospital, Tehran, Iran
ABSTRACT Coronary artery anomalies are rare,with the reported prevalence of 0.2% to 1% inroutine angiographic studies. Among them, pres-ence of a single coronary artery is one of therarest anomalies, comprising less than 3% of allcoronary anomalies. In this article we report acase of single coronary artery anomaly with leftanterior descending and left circumflex arteriesarising separately from proximal right coronaryartery, and left anterior descending artery reach-ing atrioventricular sulcus by passing between aor-tic and pulmonary artery trunci. The patient under-went off-pump coronary artery bypass grafting andis currently symptom-free. doi: 10.1111/j.1540-8191.2007.00496.x (J Card Surg 2008;23:67-69)
CASE REPORT
A 45-year-old female attended the outpatient clinic
complaining of chest discomfort for more than four
Address for correspondence: Ahmad R. Mafi, Research Center of Baqi-
atallah Hospital, Mollasadra Avenue, Tehran, Iran PO: 19945/581. Fax:
00-98-21-8805-37-66; e-mail: [email protected]
weeks. The pain was mainly in the left sternal border ra-
diating to back, aggravating by exercise and alleviating
by rest. Coronary risk factors included positive family
history and hypercholesterolemia.
On physical examination, blood pressure was 110/70
mmHg, lungs were clear, and the rest of physical exam-
ination was unremarkable. ECG showed a sinus rhythm
at the rate of 80 per minute, with ST-T wave changes
from V1 to V5.
Chest X-ray was normal. Transthoracic echocardiog-
raphy showed no abnormality. Exercise Tolerance Test
was positive with ST changes in anterior leads.
Myocardial perfusion scan demonstrated ischemia
in anterior wall. During coronary angiography, which
was performed from the standard right femoral Jud-
kins technique, attempts to cannulate the left coronary
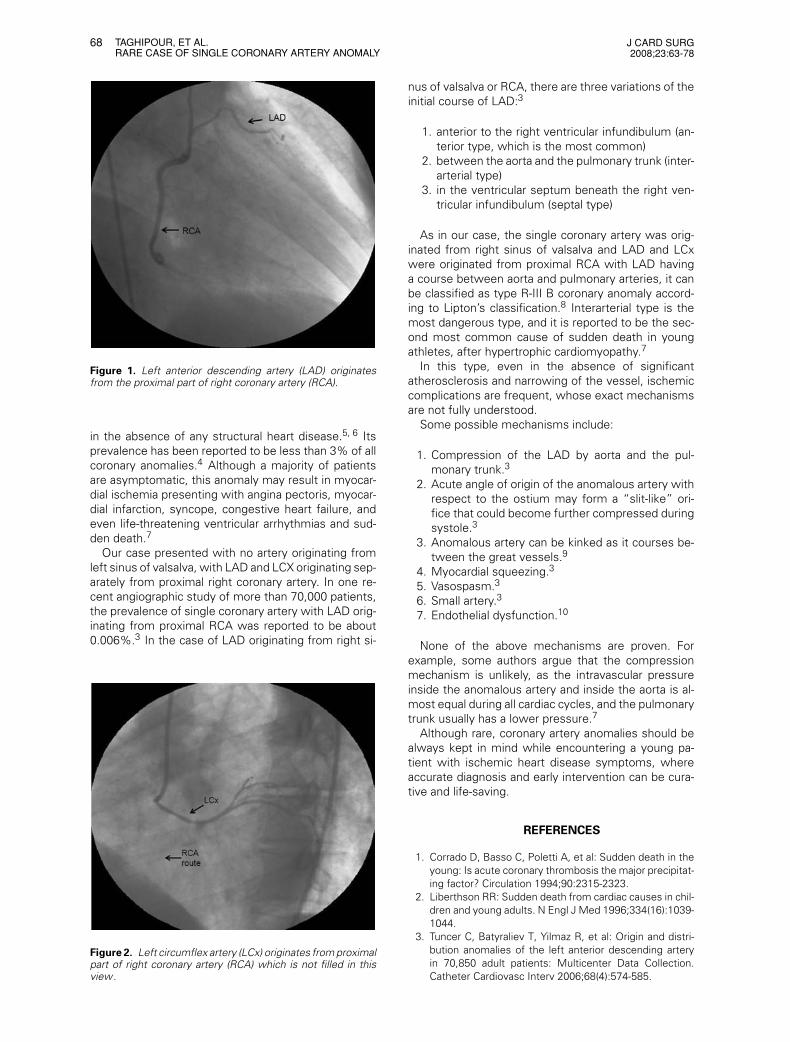
artery were unsuccessful. Cannulation of the right coro-
nary artery (RCA) showed left circumflex (LCx) and left
anterior descending (LAD) originating separately from
the proximal RCA without left main trunk (Figs. 1 and 2).
LAD had 85% stenosis in its proximal portion, and was
observed to proceed between the aorta and pulmonary
trunci to reach the atrioventricular sulcus. LCx and RCA
were normal without any narrowing. Left ventricular
ejection fraction was also normal. Off-pump coronary
artery bypass graft was performed by anastomosing
left internal thoracic artery to LAD. The aberrant vessel
was not ligated. Postoperative period was uneventful.
She remained symptom free two months after the op-
eration.
DISCUSSION
Coronary artery abnormalities are a common cause
of sudden death from cardiac causes in young people.
In one study of sudden death from cardiac causes in pa-
tients between the ages of 18 years and 35 years, 23%
of the deaths were due to coronary artery disease.1
None of the patients, who were nearly all men, had
any history of angina pectoris or myocardial infarction.
The majority had single-vessel disease, mainly affect-
ing proximal LAD. Acute thrombosis happened in only
25% of them. The most frequent congenital coronary
artery anomalies causing sudden death in the young
people is believed to be anomalous origin of either the
right or left coronary artery in the left or the right aortic
sinus of Valsalva, respectively. If the aberrant artery is
a dominant artery, which perfuses a large region of my-
ocardium, the patient will be at highest risk for sudden
death and the risk seems to be greatest during the first
three decades of life.2
Coronary artery anomalies are found in about 0.2%
to 1% of angiographies and about 0.3% of autopsies.3
The most common coronary abnormality is that LAD
and LCx arteries originate separately from left sinus of
valsalva (52%). Second most common anomaly is that
LCx artery originates from RCA or right sinus of valsalva
(27%). Coronary artery fistulae comprise 5% of cases.4
Coronary artery atherosclerosis has been reported to
happen in about 11% of anomalous arteries.3 Among
all types of coronary artery anomalies, presence of a
single coronary artery is a very rare entity, especially
68 TAGHIPOUR, ET AL.RARE CASE OF SINGLE CORONARY ARTERY ANOMALY
J CARD SURG2008;23:63-78
Figure 1. Left anterior descending artery (LAD) originatesfrom the proximal part of right coronary artery (RCA).
in the absence of any structural heart disease.5, 6 Its
prevalence has been reported to be less than 3% of all
coronary anomalies.4 Although a majority of patients
are asymptomatic, this anomaly may result in myocar-
dial ischemia presenting with angina pectoris, myocar-
dial infarction, syncope, congestive heart failure, and
even life-threatening ventricular arrhythmias and sud-
den death.7
Our case presented with no artery originating from
left sinus of valsalva, with LAD and LCX originating sep-
arately from proximal right coronary artery. In one re-
cent angiographic study of more than 70,000 patients,
the prevalence of single coronary artery with LAD orig-
inating from proximal RCA was reported to be about
0.006%.3 In the case of LAD originating from right si-
Figure 2. Left circumflex artery (LCx) originates from proximalpart of right coronary artery (RCA) which is not filled in thisview .
nus of valsalva or RCA, there are three variations of the
initial course of LAD:3
1. anterior to the right ventricular infundibulum (an-
terior type, which is the most common)
2. between the aorta and the pulmonary trunk (inter-
arterial type)
3. in the ventricular septum beneath the right ven-
tricular infundibulum (septal type)
As in our case, the single coronary artery was orig-
inated from right sinus of valsalva and LAD and LCx
were originated from proximal RCA with LAD having
a course between aorta and pulmonary arteries, it can
be classified as type R-III B coronary anomaly accord-
ing to Lipton’s classification.8 Interarterial type is the
most dangerous type, and it is reported to be the sec-
ond most common cause of sudden death in young
athletes, after hypertrophic cardiomyopathy.7
In this type, even in the absence of significant
atherosclerosis and narrowing of the vessel, ischemic
complications are frequent, whose exact mechanisms
are not fully understood.
Some possible mechanisms include:
1. Compression of the LAD by aorta and the pul-
monary trunk.3
2. Acute angle of origin of the anomalous artery with
respect to the ostium may form a “slit-like” ori-
fice that could become further compressed during
systole.3
3. Anomalous artery can be kinked as it courses be-
tween the great vessels.9
4. Myocardial squeezing.3
5. Vasospasm.3
6. Small artery.3
7. Endothelial dysfunction.10
None of the above mechanisms are proven. For
example, some authors argue that the compression
mechanism is unlikely, as the intravascular pressure
inside the anomalous artery and inside the aorta is al-
most equal during all cardiac cycles, and the pulmonary
trunk usually has a lower pressure.7
Although rare, coronary artery anomalies should be
always kept in mind while encountering a young pa-
tient with ischemic heart disease symptoms, where
accurate diagnosis and early intervention can be cura-
tive and life-saving.
REFERENCES
1. Corrado D, Basso C, Poletti A, et al: Sudden death in the
young: Is acute coronary thrombosis the major precipitat-
ing factor? Circulation 1994;90:2315-2323.
2. Liberthson RR: Sudden death from cardiac causes in chil-
dren and young adults. N Engl J Med 1996;334(16):1039-
1044.
3. Tuncer C, Batyraliev T, Yilmaz R, et al: Origin and distri-
bution anomalies of the left anterior descending artery
in 70,850 adult patients: Multicenter Data Collection.
Catheter Cardiovasc Interv 2006;68(4):574-585.

J CARD SURG2008;23:63-78
CHRISTIANSEN, ET AL.SURGERY FOR CORONARY ANEURYSM
69
4. Kosar F, Ermis N, Erdil N, et al: Anomalous LAD and CX
artery arising separately from the proximal right coronary
artery:-A case report of single coronary artery with coro-
nary artery disease. J Card Surg 2006;21(3):309-312.
5. Surucu H, Okudan S, Tatli E: Rare coronary artery
anomaly: A single coronary artery arising from the
right sinus of Valsalva. Anadolu Kardiyol Derg 2007;7(1):
113-114.
6. Namboodiri N, Harikrishnan S, Tharakan JA: Case reports:
Single coronary artery from right aortic sinus with sep-
tal course of left anterior descending artery and left cir-
cumflex artery as continuation of right coronary artery: A
hitherto unreported coronary anomaly. J Invasive Cardiol
2007;19(4):E102-E103.
7. Vianna CB, Gonzalez MM, Dallan LA, et al: Anomalous
coronary artery causing transmural ischaemia and ven-
tricular tachycardia in a high school athlete. Resuscitation
2007, doi:10.1016/j.resuscitation.2006.11.012.
8. Lipton MJ, Barry WH, Obrez I, et al: Isolated single coro-
nary artery: Diagnosis, angiographic classification, and
clinical significance. Radiology 1979;130(1):39-47.
9. Davis JA, Cecchin F, Jones TK, et al: Major coronary
artery anomalies in a pediatric population: Incidence and
clinical importance. J Am Coll Cardiol 2001;37(2):593-
597.
10. Tuncer C, Gokce M, Sokmen G: An anomalous left
main coronary artery with coronary torsion originat-
ing from the right sinus Valsalva. Int J Cardiol 2007,
doi:10.1016/j.ijcard.2006.11.198.
Surgical Management of a LeftMain Stem Coronary ArteryAneurysm
S. Christiansen, M.D., A. Klocke, M.D., A.Hoffman, M.D., and R. Autschbach, M.D.
Department of Cardiothoracic Surgery,University of Aachen, Aachen, Germany
ABSTRACT Left main stem aneurysms are rarely de-scribed and the optimal treatment is controver-sially discussed. A majority of these patients un-dergo medical treatment with antiplatelet or anti-coagulation drugs. Surgery is just recommendedin symptomatic patients or when there is the riskof thromboembolic events or rupture. We reporton a 51-year-old patient suffering from intermit-tent angina pectoris in whom an aneurysm of theleft main stem was diagnosed by coronary an-giography. The patient underwent successful sur-gical management with aneurysm closure and re-construction of the left main stem by a segmentof the great saphenous vein. This report summa-rizes the main treatment options for left main
Address for correspondence: PD Dr. med. S. Christiansen, Depart-
ment of Cardiothoracic Surgery, University of Aachen, Pauwelsstr.
30, 52074 Aachen, Germany. Fax: +49-241-80-82454; e-mail:
stem aneurysms and discusses the role of cardiacsurgery for this rare disease. doi: 10.1111/j.1540-8191.2007.00498.x (J Card Surg 2008;23:69-70)
Coronary artery aneurysms are defined as coronary
dilatation exceeding the diameter of the normal coro-
nary artery or the patient’s largest coronary vessel by
1.5 times.1 The incidence varies from 1.5% to 5% with
left main stem aneurysms often associated with two-
or three-vessel disease being extremely rare [0.1%].1-3
Coronary aneurysms may be caused by atheroscle-
rosis, Kawasaki’s disease, coronary angioplasty (bal-
loon, laser, atherectomy), arteritis, dissection, trauma,
connective tissue disorders, and metastatic tumors
or may be a congenital disorder.1,4 Here, we report
on a patient with a probably atherosclerotic left main
stem aneurysm undergoing surgical treatment and
discuss the various therapeutic options for this rare
disease.
CASE REPORT
A 51-year-old male patient was admitted to our de-
partment due to instable angina pectoris with typical
chest pain radiating into the left arm. The symptoms
were independent from physical activity and occurred
irregular and unpredictable. The coronary angiography
did not reveal any high-grade stenoses of the right or
left coronary artery except a proximal 50% stenosis of
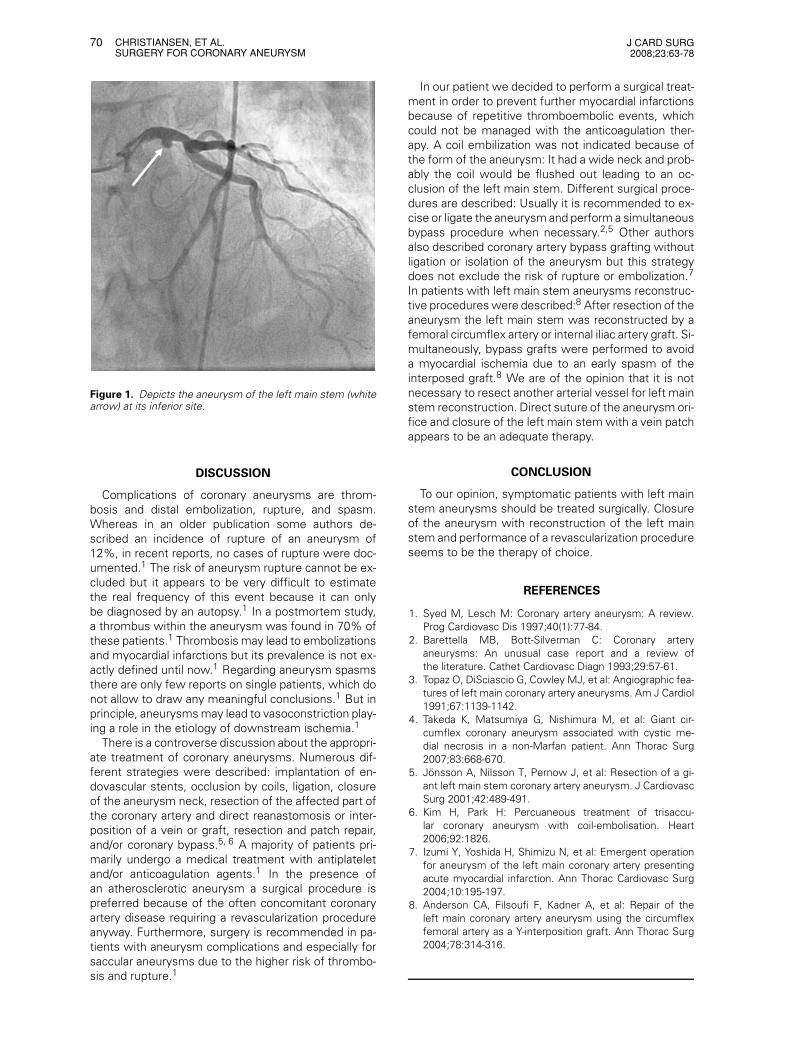
the first marginal branch. Surprisingly, we also found
an aneurysm of the left main stem (Fig.1).
The left ventricular function was not impaired un-
til now as demonstrated by the ventriculography and
a transthoracic echocardiography. The patient was
treated with acetylsalicylic acid and phenprocoumon
but the symptoms persisted. It was hypothesized that
the symptoms were caused by repetitive minor em-
bolizations from the aneurysm despite the anticoagu-
lation therapy. Therefore, we decided to operate the
patient to exclude the aneurysm as source of the em-
boli to avoid further myocardial infarctions.
After median sternotomy, the heart-lung-machine
was instituted via the ascending aorta and the right
atrium and cardioplegia was administered. The main
pulmonary artery was divided and the aorta incised into
the left main stem till the bifurcation into the left an-
terior descending coronary artery and the circumflex
artery. The aneurysm was situated in the middle of the
left main stem at the inferior site and was closed by a
suture. The incision of the left main stem was closed
with a vein patch from the great saphenous vein, which
was also used for closure of the aortotomy. Further-
more, a vein graft to the first marginal branch was con-
structed. After extensive deairing and weaning from
cardiopulmonary bypass the procedure was finished.
The intraoperative angiography demonstrated a com-
plete exclusion of the aneurysm and a patent vein graft.
The patient was extubated on the same day. The post-
operative recovery was uneventful and the patient was
discharged home six days later.
70 CHRISTIANSEN, ET AL.SURGERY FOR CORONARY ANEURYSM
J CARD SURG2008;23:63-78
Figure 1. Depicts the aneurysm of the left main stem (whitearrow) at its inferior site.
DISCUSSION
Complications of coronary aneurysms are throm-
bosis and distal embolization, rupture, and spasm.
Whereas in an older publication some authors de-
scribed an incidence of rupture of an aneurysm of
12%, in recent reports, no cases of rupture were doc-
umented.1 The risk of aneurysm rupture cannot be ex-
cluded but it appears to be very difficult to estimate
the real frequency of this event because it can only
be diagnosed by an autopsy.1 In a postmortem study,
a thrombus within the aneurysm was found in 70% of
these patients.1 Thrombosis may lead to embolizations
and myocardial infarctions but its prevalence is not ex-
actly defined until now.1 Regarding aneurysm spasms
there are only few reports on single patients, which do
not allow to draw any meaningful conclusions.1 But in
principle, aneurysms may lead to vasoconstriction play-
ing a role in the etiology of downstream ischemia.1
There is a controverse discussion about the appropri-
ate treatment of coronary aneurysms. Numerous dif-
ferent strategies were described: implantation of en-
dovascular stents, occlusion by coils, ligation, closure
of the aneurysm neck, resection of the affected part of
the coronary artery and direct reanastomosis or inter-
position of a vein or graft, resection and patch repair,
and/or coronary bypass.5, 6 A majority of patients pri-
marily undergo a medical treatment with antiplatelet
and/or anticoagulation agents.1 In the presence of
an atherosclerotic aneurysm a surgical procedure is
preferred because of the often concomitant coronary
artery disease requiring a revascularization procedure
anyway. Furthermore, surgery is recommended in pa-
tients with aneurysm complications and especially for
saccular aneurysms due to the higher risk of thrombo-
sis and rupture.1
In our patient we decided to perform a surgical treat-
ment in order to prevent further myocardial infarctions
because of repetitive thromboembolic events, which
could not be managed with the anticoagulation ther-
apy. A coil embilization was not indicated because of
the form of the aneurysm: It had a wide neck and prob-
ably the coil would be flushed out leading to an oc-
clusion of the left main stem. Different surgical proce-
dures are described: Usually it is recommended to ex-
cise or ligate the aneurysm and perform a simultaneous
bypass procedure when necessary.2,5 Other authors
also described coronary artery bypass grafting without
ligation or isolation of the aneurysm but this strategy
does not exclude the risk of rupture or embolization.7
In patients with left main stem aneurysms reconstruc-
tive procedures were described:8 After resection of the
aneurysm the left main stem was reconstructed by a
femoral circumflex artery or internal iliac artery graft. Si-
multaneously, bypass grafts were performed to avoid
a myocardial ischemia due to an early spasm of the
interposed graft.8 We are of the opinion that it is not
necessary to resect another arterial vessel for left main
stem reconstruction. Direct suture of the aneurysm ori-
fice and closure of the left main stem with a vein patch
appears to be an adequate therapy.
CONCLUSION
To our opinion, symptomatic patients with left main
stem aneurysms should be treated surgically. Closure
of the aneurysm with reconstruction of the left main
stem and performance of a revascularization procedure
seems to be the therapy of choice.
REFERENCES
1. Syed M, Lesch M: Coronary artery aneurysm: A review.
Prog Cardiovasc Dis 1997;40(1):77-84.
2. Barettella MB, Bott-Silverman C: Coronary artery
aneurysms: An unusual case report and a review of
the literature. Cathet Cardiovasc Diagn 1993;29:57-61.
3. Topaz O, DiSciascio G, Cowley MJ, et al: Angiographic fea-
tures of left main coronary artery aneurysms. Am J Cardiol
1991;67:1139-1142.
4. Takeda K, Matsumiya G, Nishimura M, et al: Giant cir-
cumflex coronary aneurysm associated with cystic me-
dial necrosis in a non-Marfan patient. Ann Thorac Surg
2007;83:668-670.
5. Jonsson A, Nilsson T, Pernow J, et al: Resection of a gi-
ant left main stem coronary artery aneurysm. J Cardiovasc
Surg 2001;42:489-491.
6. Kim H, Park H: Percuaneous treatment of trisaccu-
lar coronary aneurysm with coil-embolisation. Heart
2006;92:1826.
7. Izumi Y, Yoshida H, Shimizu N, et al: Emergent operation
for aneurysm of the left main coronary artery presenting
acute myocardial infarction. Ann Thorac Cardiovasc Surg
2004;10:195-197.
8. Anderson CA, Filsoufi F, Kadner A, et al: Repair of the
left main coronary artery aneurysm using the circumflex
femoral artery as a Y-interposition graft. Ann Thorac Surg
2004;78:314-316.

J CARD SURG2008;23:63-78
TJANG, ET AL.SCIMITAR SYNDROME IN ADULTS
71
Scimitar Syndrome Presentingin Adults
Yanto Sandy Tjang, M.D., M.B.A., M.P.H.,M.Sc., D.Sc., F.I.C.S.,∗ Ute Blanz, M.D.,∗
Stanley Kirana, M.D.,† and Reiner Korfer,M.D., Ph.D.∗
∗Department of Thoracic and CardiovascularSurgery, Heart and Diabetes CenterNRW/Ruhr-University Hospital of Bochum,Bad Oeynhausen, Germany; and †DiabetesCenter, Heart and Diabetes CenterNRW/Ruhr-University Hospital of Bochum,Bad Oeynhausen, Germany
ABSTRACT Scimitar syndrome is a rare and com-plex congenital anomaly, which is characterizedby the image of a Turkish sword on the chestX-ray. Very few cases in adults are reported inthe literature. The long-term results of scimitarsyndrome after surgical correction remain disap-pointing. We report an adult patient with scimitarsyndrome undergoing surgery at our center. doi:10.1111/j.1540-8191.2007.00497.x (J Card Surg2008;23:71-72)
Scimitar syndrome is a rare and complex congenital
anomaly, mostly associated with a variety of thoracic
abnormalities. The anomalous pulmonary venous re-
turn of all or most of the right lung to the inferior vena
cava just below or above the right hemidiaphragm cre-
ates the image of a Turkish sword on the chest X-ray.
Very few cases presenting in adults are reported. The
long-term results of scimitar syndrome after surgical
correction remain disappointing. We report an adult pa-
tient with scimitar syndrome undergoing surgery at our
center.
CASE REPORT
A 19-year-old female was admitted to our center for
systolic murmur. Medical history revealed syncope at
11 years old. No recurrent pneumonia or cyanosis ex-
isted. Physical examination revealed no other abnor-
malities. The ECG showed right axis deviation with right
ventricular hypertrophy. The chest X-ray demonstrated
dextroposition of the heart with an irregular shadow
in the right lower lung field and increased vascularity
in the right lung. Cardiac catheterization revealed mod-
erate elevation of right heart pressure. Ejection frac-
tion and pulmonary artery pressures were normal. The
scimitar vein resulted in an estimated left/right shunt
volume of 43% (Qp/Qs = 1.8:1). There was no evi-
dence of atrial septal defect. Magnetic resonance imag-
ing demonstrated an anomalous venous drainage of
Address for correspondence: Yanto Sandy Tjang, M.D., M.B.A., M.P.H.,
M.Sc., D.Sc., F.I.C.S., Wielandstrasse 11, 32545 Bad Oeynhausen,
Germany. Fax: +49-5731-971820; e-mail: [email protected]
the right lung to the subphrenic inferior vena cava, con-
firming the diagnosis of scimitar syndrome (Fig. 1). The
patient underwent surgery via median sternotomy. The
scimitar vein was identified in the right hemithorax and
followed distally below the diaphragm. Due to close
proximity of the hepatic vein confluence and the infe-
rior vena cava, the latter could not be snared in order to
isolate the venous return to the right atrium. The entire
surgical procedure was performed under hypothermic
circulatory arrest at 18◦C. The right atrium was incised
to create an atrial septal defect. Surgical repair was
performed by baffling the orifice of the scimitar vein
from its entry into the inferior vena cava to the cre-
ated atrial septal defect using a large diameter of au-
tologous pericardium. The postoperative course was
uneventful. Four years after surgery, the patient was
completely free of symptoms. Echocardiography re-
vealed no stenosis of the intraatrial tunnel.
DISCUSSION
Scimitar syndrome occurs in 1–3/1,00,000 live
births.1 Described by Cooper in 1836, the term “scimi-
tar” was firstly used by Halasz in 1956.2 The age at pre-
sentation varies. The mean age of diagnosis is seven
months.3 This malformation is classically divided into
infant and adult forms.1,4 Infant patients typically have
features of congestive heart failure due to significant
left/right shunt from the anomalous pulmonary venous
drainage or more commonly from an additional cardiac
defect such as atrial septal defect. Older children and
adults may have symptoms and the diagnosis may be
made by chest X-ray demonstrating the scimitar sign
in as many as 70% of patients.5 Cardiac catheteriza-
tion should always be performed to confirm the diag-
nosis, identify the specific course of the anomalous
pulmonary venous drainage, determine the presence
of scimitar vein stenosis and pulmonary hypertension,
measure the degree of left/right shunt, and detect any
associated cardiac abnormalities.5 Computed tomogra-
phy, angiography, and magnetic resonance imaging are
helpful if the scimitar vein is obscured by the overlying
cardiac shadow, particularly when cardiac dextroposi-
tion is pronounced.
Surgical intervention is indicated for: (1) large left/
right shunt exceeding 50%, resulting in pulmonary hy-
pertension and heart failure; and (2) lung sequestration
and/or recurrent right-sided chest infection.6 Some re-
pair options include the creation of a long baffle from
the orifice of the scimitar vein within the inferior vena
cava to the atrial septal defect that directs the anoma-
lous pulmonary venous flow to the left atrium,7 divi-
sion with reimplantation of the scimitar vein into the
right atrium with an intraatrial baffle that directs blood
flow through an atrial septal defect to the left atrium,8
partitioning of the inferior vena cava into anterior and
posterior compartments with a pericardial baffle that
channels pulmonary venous blood flow directly into
the left atrium,9 or direct anastomosis of the divided
scimitar vein to the left atrium.5 In general, the long-
term results of scimitar syndrome after surgical correc-
tion remain disappointing. Stenosis of the intracardiac

72 MARISCALCO, ET AL.ECHOCARDIOGRAPHY IN CORONARY ANEURYSM
J CARD SURG2008;23:63-78
Figure 1. Anomalous venous drainage of the right lung to thesubphrenic inferior vena cava.
baffle often develops, and thrombosis of the anasto-
mosis can lead to immediate infarction of the right
lung, pulmonary hypertension, and cataclysmic hemop-
tysis.10 In our case, we attempted to create a large
diameter of intraatrial pericardial baffle to enable im-
provement in hemodynamic conditions. We believed it
could prevent early restenosis and thrombosis of the
anastomosis. Our follow-up at four years after surgery
revealed an encouraging result.
REFERENCES
1. Dupuis C, Charaf LA, Breviere GM, et al: The “adult” form
of the scimitar syndrome. Am J Cardiol 1992;70(4):502-
507.
2. Holt PD, Berdon WE, Marans Z, et al: Scimitar vein drain-
ing to the left atrium and a historical review of the scimitar
syndrome. Pediatr Radiol 2004;34(5):409-413.
3. Najm HK, Williams WG, Coles JG, et al: Scimitar syn-
drome: Twenty years’ experience and results of repair. J
Thorac Cardiovasc Surg 1996;112(5):1161-1168.
4. Dupuis C, Charaf LA, Breviere GM, et al: “Infantile” form
of the scimitar syndrome with pulmonary hypertension.
Am J Cardiol 1993;71(15):1326-1330.
5. Brown JW, Ruzmetov M, Minnich DJ, et al: Surgical man-
agement of scimitar syndromeAn alternative approach. J
Thorac Cardiovasc Surg 2003;125(2):238-245.
6. Schramel FM, Westermann CJ, Knaepen PJ, et al: The
scimitar syndrome: Clinical spectrum and surgical treat-
ment. Eur Respir J 1995;8(2):196-201.
7. Zubiate P, Kay JH: Surgical correction of anomalous pul-
monary venous connection. Ann Surg 1962;156:234-250.
8. Shumaker HB Jr, Judd D: Partial anomalous pulmonary
venous return with reference to drainage into the inferior
vena cava and to an intact atrial septum. J Cardiovasc
Surg 1964;5:271-278.
9. Calhoun RF, Mee RB: A novel operative approach to scim-
itar syndrome. Ann Thorac Surg 2003;76(1):301-303.
10. Reddy R, Shah R, Thorpe JA, et al: Scimitar syndrome:
A rare cause of haemoptysis. Eur J Cardiothorac Surg
2002;22(5):821.
Transthoracic Echocardiographyis Adequate for the Diagnosisof Right Coronary ArteryAneurysms
Giovanni Mariscalco, M.D.,∗ FaustoSessa, M.D.,† Davide Vanoli, M.D.,‡Vittorio Mantovani, M.D., Ph.D,∗
Ferrarese Sandro, M.D.,∗ and AndreaSala, M.D.∗
∗Department of Surgical Sciences, CardiacSurgery Division, Varese University Hospital,Italy; †Department of Pathology, ClinicalInstitute Multimedica Holding Santa Mana,Castellanza, University of Insubria, Varese,Italy; and ‡Department of ClinicalPhysiology, Heart Center, University ofNorthern Sweden, Umea, Sweden
ABSTRACT Coronary artery aneurysms (CAA) arerare but potentially fatal pathologies. This case wasreferred to our Unit after occasional echocardio-graphic finding of an intracardiac mass. A new de-tailed transthoracic echocardiogram was decisivefor a diagnosis of a large CAA of the right coro-nary artery, compressing and dislocating the rightatrium. Transesophageal echocardiography wasnot performed because of the data obtained. Thediagnosis was confirmed by cardiac catheteriza-tion. The patient was managed with a surgical pro-cedure. doi: 10.1111/j.1540-8191.2007.00500.x (JCard Surg 2008;23:72-74)
BACKGROUND
Coronary artery aneurysms (CAA) are rare patholo-
gies, appearing on only 0.3% to 4.9% of coronary
angiograms.1 Spontaneous rupture, myocardial infarc-
tion, and thrombotic or embolic events can complicate
CAA.2-4 The diagnosis is most often an unexpected
finding at cardiac catheterization.5
This report shows that transthoracic echocardiogra-
phy provides sufficient information for a reliable diag-
nosis of a right CAA.
Address for correspondence: Dr. Giovanni Mariscalco, Department
of Surgical Sciences, Cardiac Division, Varese University Hospital,
21100 Varese, Italy. Fax: +39-0332-264394; e-mail: giovanimariscalco@
yahoo.it
J CARD SURG2008;23:63-78
MARISCALCO, ET AL.ECHOCARDIOGRAPHY IN CORONARY ANEURYSM
73
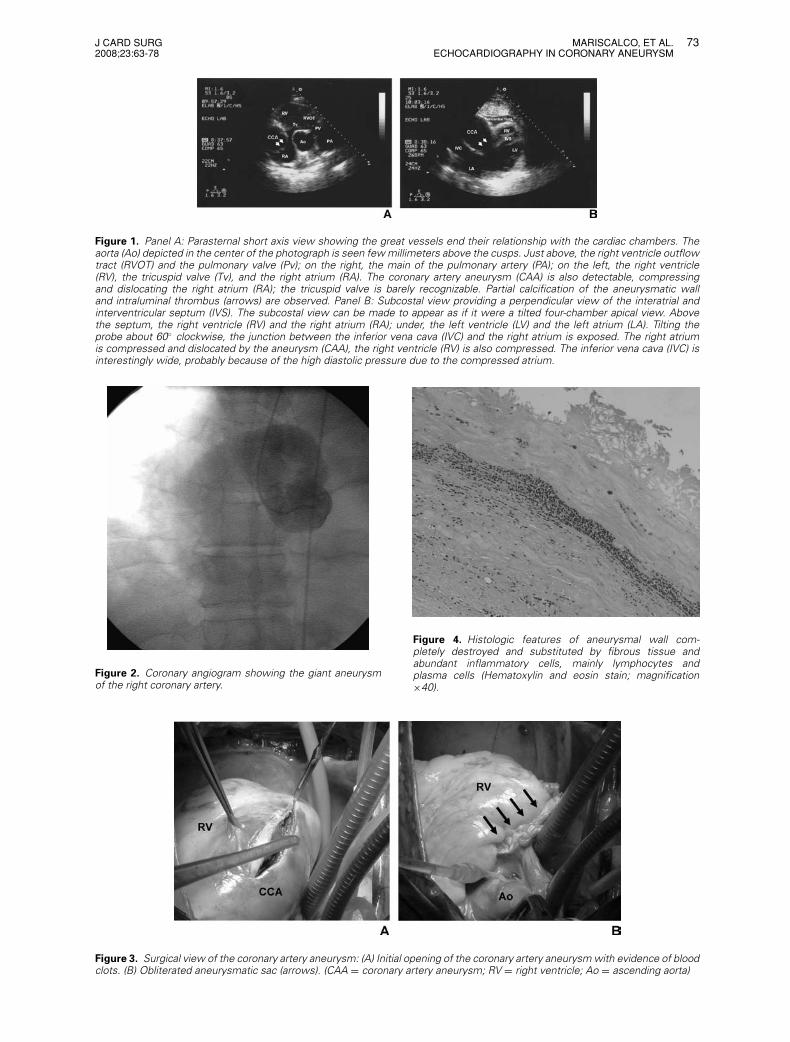
Figure 1. Panel A: Parasternal short axis view showing the great vessels end their relationship with the cardiac chambers. Theaorta (Ao) depicted in the center of the photograph is seen few millimeters above the cusps. Just above, the right ventricle outflowtract (RVOT) and the pulmonary valve (Pv); on the right, the main of the pulmonary artery (PA); on the left, the right ventricle(RV), the tricuspid valve (Tv), and the right atrium (RA). The coronary artery aneurysm (CAA) is also detectable, compressingand dislocating the right atrium (RA); the tricuspid valve is barely recognizable. Partial calcification of the aneurysmatic walland intraluminal thrombus (arrows) are observed. Panel B: Subcostal view providing a perpendicular view of the interatrial andinterventricular septum (IVS). The subcostal view can be made to appear as if it were a tilted four-chamber apical view. Abovethe septum, the right ventricle (RV) and the right atrium (RA); under, the left ventricle (LV) and the left atrium (LA). Tilting theprobe about 60◦ clockwise, the junction between the inferior vena cava (IVC) and the right atrium is exposed. The right atriumis compressed and dislocated by the aneurysm (CAA), the right ventricle (RV) is also compressed. The inferior vena cava (IVC) isinterestingly wide, probably because of the high diastolic pressure due to the compressed atrium.
Figure 2. Coronary angiogram showing the giant aneurysmof the right coronary artery.
Figure 3. Surgical view of the coronary artery aneurysm: (A) Initial opening of the coronary artery aneurysm with evidence of bloodclots. (B) Obliterated aneurysmatic sac (arrows). (CAA = coronary artery aneurysm; RV = right ventricle; Ao = ascending aorta)
Figure 4. Histologic features of aneurysmal wall com-pletely destroyed and substituted by fibrous tissue andabundant inflammatory cells, mainly lymphocytes andplasma cells (Hematoxylin and eosin stain; magnification×40).

74 MARISCALCO, ET AL.ECHOCARDIOGRAPHY IN CORONARY ANEURYSM
J CARD SURG2008;23:63-78
CASE SUMMARY
A 61-year-old man with an occasional echocardio-
graphic finding of a mass compressing the right atrium
was referred to our department. The patient was
asymptomatic for angina and without signs of conges-
tive heart failure. Electrocardiogram and blood analy-
sis values were normal, chest-X-ray demonstrated car-
diomegaly.
A new transthoracic echocardiogram was per-
formed, revealing decisive data for the presence of
a CAA involving the right coronary artery (RCA) and
confirming the compression and dislocation of the
right atrium. Partial calcifications of the aneurysmatic
wall and an intraluminal thrombus were also detected
(Fig. 1). Mild left ventricular dysfunction, with an es-
timated ejection fraction of 45%, and a moderate re-
gurgitation of the tricuspid valve were observed. The
specificity of the transthoracic pictures made trans-
esophageal echocardiography unnecessary. The diag-
nosis was confirmed by cardiac catheterization. A very
large and partially thrombosed CAA involving the right
coronary artery (RCA) was discovered (8 × 6 × 8 cm),
with occlusion of the middle RCA tract (Fig. 2). Critical
stenosis of the proximal left anterior descending artery
(LAD) and left circumflex (LCx) occlusion were also re-
vealed.
Surgical treatment was undertaken. Median ster-
notomy and moderately hypothermic (32 ◦C) cardiopul-
monary bypass were employed; the procedure was
done in a standardized fashion with ascending aortic
cannulation and two-stage venous cannulation of the
right atrium. The CAA was identified and longitudinally
incised in order to remove blood clots and verify the
absence of anomalous communications between the
aneurysm and the cardiac chambers (Fig. 3). The prox-
imal and distal openings were identified and occluded.
The sac was obliterated with running sutures (Fig. 3).
Finally, a saphenous bypass graft was performed dis-
tally to the excluded aneurysm. Myocardial revascular-
ization was completed by grafting the left internal tho-
racic artery to the LAD and a saphenous vein graft to
the LCx artery.
Histopathologic analysis was also obtained, revealing
atherosclerotic alteration of the vessel (Fig. 4).
DISCUSSION
CAA is a dilatation that exceeds 1.5 times the di-
ameter of a normal adjacent coronary artery.2 This
disease is a rare entity with a poor prognosis if un-
treated.1-4 Patients with aneurysmal disease have a
higher incidence of acute myocardial infarction (AMI)
and reduced survival as compared with unaffected
patients.2
The proximal and middle segments of the right coro-
nary artery are frequently involved locations.2 The most
common etiology is atherosclerotic, and destruction
of the vessel media is the usual histologic feature.2,5
Histologic and clinical studies suggest that these pro-
cesses are similar to those occurring in abdominal aor-
tic aneurysm (AAA).5,6
No clinical picture is specifically suggestive of a
CAA diagnosis.5 Angina and dyspnea are usually en-
countered in this disease.7 In cases of giant CAAs
(diameter >50 mm), chest discomfort, pain, and pal-
pitations can also be reported.8 CAAs are basically di-
agnosed as an incidental finding in coronary angiogra-
phy, which provides useful information regarding size,
shape, and location of the aneurysms.7 Angiography,
transesophageal echocardiography, and magnetic
resonance imaging can be used for the diagnosis and
follow-up of such aneurysms.9 To our knowledge, this
report is the first documentation of CAA in which
transthoracic echocardiography provided decisive infor-
mation regarding the aneurysmatic involvement of a
RCA.
According to Biglioli et al.,10 surgery is mandatory
when the aneurysm is three to four times larger
than the original vessel diameter. This is a critical
size for uncontrolled progression.10 Hence, because
of the aneurysm size and the above-mentioned com-
plications, surgical correction as mandatory in our
case.
REFERENCES
1. Lenihan DJ, Zeman HS, Collins GJ: Left main coronary
artery aneurysm in association with severe atheroscle-
rosis: A case report and review of the literature. Cathet
Cardiovasc Diagn 1991;23:28-31.
2. Swaye PS, Fisher LD, Litwin P, et al: Aneurysmal coronary
artery disease. Circulation 1983;67:134-138.
3. Virmani R, Robinowitz M, Atkinson JB, et al: Acquired
coronary arterial aneurysms: An autopsy study of 52 pa-
tients. Hum Pathol 1986;17:575-583.
4. Anabtawi IN, de Leon JA: Arteriosclerotic aneurysms
of the coronary arteries. J Thorac Cardiovasc Surg
1974;68:226-228.
5. Mariscalco G, Mantovani V, Ferrarese S, et al: Coronary
artery aneurysm: Management and association with ab-
dominal aortic aneurysm. Cardiovasc Pathol 2006;15:100-
104.
6. Kishi K, Ito S, Hiasa Y: Risk factors and incidence of
coronary artery lesions in patients with abdominal aortic
aneurysms. Intern Med 1997;36:384-388.
7. LaMendola CL, Culliford AT, Harris LJ, et al: Multi-
ple aneurysms of the coronary arteries in a patient
with systemic aneurysmal disease. Ann Thorac Surg
1990;49:1009-1010.
8. Tunick PA, Slater J, Kronzon I, et al: Discrete atheroscle-
rotic coronary artery aneurysms: A study of 20 patients:
J Am Coll Cardiol 1990;15:279-282.
9. Selke KG, Vemulapalli P, Brodarick SA, et al: Giant coro-
nary artery aneurysm: Detection with echocardiography,
computed tomography, and magnetic resonance imag-
ing. Am Heart J 1991;121:1544-1547.
10. Biglioli P, Alamanni F, Antona C, et al: Aneurysms of the
coronary arteries: One case report. Thorac Cardiovasc
Surg 1988;36:239-240.

J CARD SURG2008;23:63-78
RAFFA, ET AL.PFO CLOSURE DEVICE COMPLICATION
75
Minimally InvasiveVideo-Assisted Surgery forIatrogenic Aortic Root-to-RightAtrium Fistula After IncompletePercutaneous Occlusionof Patent Foramen Ovale: CaseReport and Review of theLiterature
Giuseppe M. Raffa, M.D.,∗ CarloPellegrini, M.D., Ph.D.,∗ Salvatore Lentini,M.D.,†Sossio Perrotta, M.D.,† Fabrizio Tancredi,M.D.,† Roberto Gaeta, M.D.,†and Mario Vigano, M.D.∗,‡
∗Department of Cardiac Surgery, Universityof Pavia, Pavia, Italy; †Department ofCardiac Surgery, University of Messina,Messina, Italy; and ‡Department of CardiacSurgery, Foundation IRCCS Policlinico “SanMatteo” Hospital, Pavia, Italy
ABSTRACT Background: The foramen ovale re-mains patent in about 25% of the population. Para-doxical embolism through a patent foramen ovale(PFO) may produce ischemic events. The closure ofa PFO may prevent recurrence of cerebrovascularevents. Percutaneous closure of a PFO is now-a-days a standard procedure and it appears to carrya low rate of complications. A surgical approach, insome cases, may be needed. Methods: A patientunderwent percutaneous closure of PFO. Therewas a residual shunt after the procedure and a fis-tula between the aortic root-to-right atrium wassubsequently discovered. Surgery was carried outusing a “Port-Access technique” through a rightanterior minithoracotomy. Results: Postoperativecourse was uneventful. Complete obliteration ofthe fistula was achieved. Conclusion: Minimally in-vasive surgery may be effective to treat PFO oreven complications after previous percutaneous at-tempts of closure. An aesthetically acceptable con-clusion, especially in young female patients, and avery low rate of morbidity may be accomplished.doi: 10.1111/j.1540-8191.2007.00483.x (J CardSurg 2008;23:75-78)
Address for correspondence: Giuseppe Raffa, Department of Cardio-
thoracic Surgery, University of Pavia, Pavia, Italy, Piazzale Golgi 2, 27100
Pavia, Italy. Fax: +39-090-2217086; e-mail: [email protected]
Foramen ovale remains patent throughout adulthood
in approximately 25% of the general population, repre-
senting the most commonly persistent abnormality of
fetal origin. Patent foramen ovale along with other atrial
septal defects is responsible for cerebrovascular mor-
bidity and reduction in life expectancy.1 Paradoxical em-
bolism through a PFO may produce ischemic events in
patients with cryptogenic stroke. Patients with a PFO
after cerebral, coronary, or systemic embolic events
of presumed paradoxical origin are at risk for recur-
rent thromboembolism. Closure of PFO is considered,
by some authors, as the most effective procedure in
stroke prevention.2-4
Therapeutic options include either percutaneous ap-
proach with specifically designed devices or surgical
treatment. Despite that percutaneous interventions are
well accepted by patients, complications rate is not
negligible5 and in some cases surgery may be needed
to manage any drawbacks.
MATERIALS AND METHODS: CASE REPORT
A 35-year-old lady was presented at our institution
both for surgical correction of an iatrogenic aortic root-
to-right atrium fistula and definitive closure of a residual
PFO.
History: the patient was affected with two acute neu-
rologic events, likely to be on ischemic grounds, re-
spectively eight and nine years before admission to
our institution. She had residual right eye motility im-
pairment and right-side hypostenia as neurologic se-
quelae. The patient was first started on oral anticoagu-
lant therapy. Later on, seven years after the last stroke,
she experienced recurrent headache episodes; there-
fore, she underwent further medical investigations. A
transesophageal echocardiography (TEE) at that time
revealed a PFO associated with aneurysm of the inter-
atrial septum. Bidirectional shunting was detected by
doppler echocardiography. Because of that the patient
underwent, in other institution, percutaneous closure
of the PFO by a 30 mm Cardia ® Starr device occluder
(Cardia Inc. Burnsville, MN, USA). Six months later, a
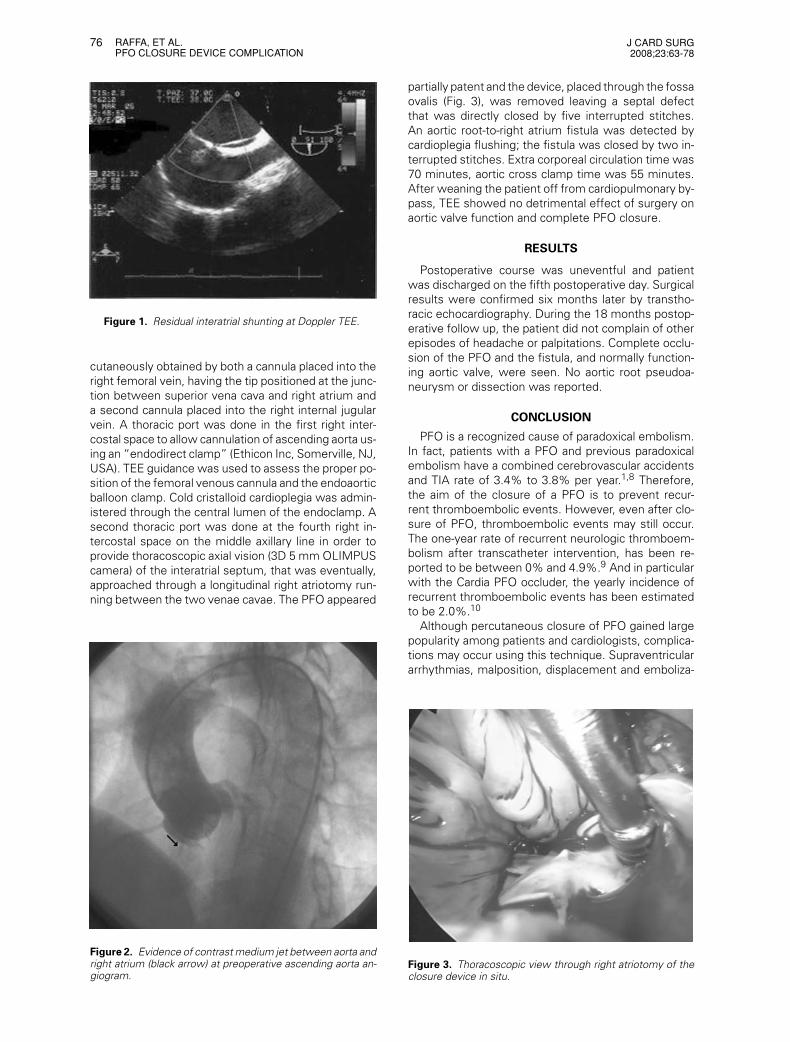
transthoracic echocardiogram and a TEE demonstrated
an incomplete PFO obliteration with residual bidirec-
tional shunting, (Fig. 1) and a fistula between the aortic
root and the right atrium. At first, medical treatment of
this complication was attempted by holding the anti-
coagulant therapy as described by other authors6,7 but
this did not succeed. The patient was then admitted
to our institution two months later. She was mostly
complaining of both dyspnea and palpitations. Holter
monitoring showed the presence of frequent atrial pre-
mature beats and runs of atrial tachycardia. By TEE the
fistula was located in the noncoronary sinus of the aor-
tic root, close to the commissure to the right sinus. No
interference on aortic valve function was noted. Preop-
erative angiogram of ascending aorta confirmed TEE
findings (Fig. 2).
Surgical procedure: Minimally invasive surgery was
performed through a minithoracotomy in the fourth
right intercostal space using a Port-Access technique
by a skin incision of 4.5 cm. Venous drainage was per-
76 RAFFA, ET AL.PFO CLOSURE DEVICE COMPLICATION
J CARD SURG2008;23:63-78
Figure 1. Residual interatrial shunting at Doppler TEE.
cutaneously obtained by both a cannula placed into the
right femoral vein, having the tip positioned at the junc-
tion between superior vena cava and right atrium and
a second cannula placed into the right internal jugular
vein. A thoracic port was done in the first right inter-
costal space to allow cannulation of ascending aorta us-
ing an “endodirect clamp” (Ethicon Inc, Somerville, NJ,
USA). TEE guidance was used to assess the proper po-
sition of the femoral venous cannula and the endoaortic
balloon clamp. Cold cristalloid cardioplegia was admin-
istered through the central lumen of the endoclamp. A
second thoracic port was done at the fourth right in-
tercostal space on the middle axillary line in order to
provide thoracoscopic axial vision (3D 5 mm OLIMPUS
camera) of the interatrial septum, that was eventually,
approached through a longitudinal right atriotomy run-
ning between the two venae cavae. The PFO appeared
Figure 2. Evidence of contrast medium jet between aorta andright atrium (black arrow) at preoperative ascending aorta an-giogram.
partially patent and the device, placed through the fossa
ovalis (Fig. 3), was removed leaving a septal defect
that was directly closed by five interrupted stitches.
An aortic root-to-right atrium fistula was detected by
cardioplegia flushing; the fistula was closed by two in-
terrupted stitches. Extra corporeal circulation time was
70 minutes, aortic cross clamp time was 55 minutes.
After weaning the patient off from cardiopulmonary by-
pass, TEE showed no detrimental effect of surgery on
aortic valve function and complete PFO closure.
RESULTS
Postoperative course was uneventful and patient
was discharged on the fifth postoperative day. Surgical
results were confirmed six months later by transtho-
racic echocardiography. During the 18 months postop-
erative follow up, the patient did not complain of other
episodes of headache or palpitations. Complete occlu-
sion of the PFO and the fistula, and normally function-
ing aortic valve, were seen. No aortic root pseudoa-
neurysm or dissection was reported.
CONCLUSION
PFO is a recognized cause of paradoxical embolism.
In fact, patients with a PFO and previous paradoxical
embolism have a combined cerebrovascular accidents
and TIA rate of 3.4% to 3.8% per year.1,8 Therefore,
the aim of the closure of a PFO is to prevent recur-
rent thromboembolic events. However, even after clo-
sure of PFO, thromboembolic events may still occur.
The one-year rate of recurrent neurologic thromboem-
bolism after transcatheter intervention, has been re-
ported to be between 0% and 4.9%.9 And in particular
with the Cardia PFO occluder, the yearly incidence of
recurrent thromboembolic events has been estimated
to be 2.0%.10
Although percutaneous closure of PFO gained large
popularity among patients and cardiologists, complica-
tions may occur using this technique. Supraventricular
arrhythmias, malposition, displacement and emboliza-
Figure 3. Thoracoscopic view through right atriotomy of theclosure device in situ.

J CARD SURG2008;23:63-78
RAFFA, ET AL.PFO CLOSURE DEVICE COMPLICATION
77
tion of the device, pericardial tamponade, local vascu-
lar complications, thrombus apposition on the device,
early and late residual shunting, fractures of device
arms, transient ST elevation, ventricular fibrillation, and
perforation of left atrium may be seen after percuta-
neous treatment.11
Early and late cardiac perforations are considered the
most severe complications.12 Trepels et al. described
the first case of cardiac perforation using the Amplatzer
device in 2003.13 This rare complication occurs pre-
dominantly in the anterosuperior atrial wall and adjacent
to the aorta.12 Moreover, with the same device risk of
erosion of the atrial wall is estimated to be 0.1%.14
Baykut et al. the treated on an emergency basis a late
perforation of the aortic root by an atrial septal defect
occlusion device 4 years after the percutaneous proce-
dure.15
The first case of aortic root-to-right atrium fistula with
Amplatzer septal occluder requiring surgical treatment
was reported by Chun et al. in 2003.16-18 There are
also reports of surgical repair of aortic root-to-left atrium
fistula following percutaneous closure in an adult19,20
and in a child.21 Till date, to the best of our knowledge,
there are ten reports of an aortic root to atrium fistula
(Table 1). On this ground, we believe that a strict long-
term follow-up of those patients is mandatory.
Two fistulas had a spontaneous closure and the
other eight were repaired surgically. Surgical treat-
ment was performed either by a right anterolateral tho-
racothomy22 or a standard longitudinal median ster-
notomy.23 In some cases, as for perforations, the clin-
ical status of a patient affected with a fistula required
an urgent operation.17,19,20,23
As different from previously reported cases,6,7 in our
patient, the withdrawal of oral medical therapy did not
provide spontaneous closure of the communication.
From the anatomic point of view, we believe that this
type of complication is probably the consequence of a
particular anatomic pattern, that is, when the area of
the “torus aorticus” is quite bulging within the right
atrium, and when the plane of PFO is not well aligned
TABLE 1Review of the Literature
Diagnosis AfterAuthor Device Fistula Percoutaneous Closure Treatment
Aggoun et al. 200219 Amplatzer Ao-La 21 days Surgery
Chun et al. 200315 Amplatzer Ao-Ra 3 months Surgery
Stauffer et al. 20046 PFO Star Ao-Ra 1 month Spontaneous closurea
Knirsch et at. 200520 Amplatzer Ao-La 28 days Surgery
Mello et al. 200518 Amplatzer Ao-La 6 months Surgery
Meier et al. 20057 PFO Star Ao-Ra 1 year Spontaneous closureb
Jang et al. 200516 Amplatzer Ao-Ra 2 months Surgery
Grayburn et al 200517 Amplatzer Ao-Ra 2 years Surgery
Lange et al. 200622 Cardia Star Ao-Ra 28 days Surgery
Sauer et al. 200623 Amplatzer Ao-Ra 1 day Surgery
Ao-La = aorta to left atrium fistula; Ao-Ra: aorta to right atrium fistula.aAfter one month of suspension of anticoagulant treatment.bAfter two years of suspension of antiaggregant treatment.
with it. Moreover, a diminutive aortic rim may play an
important role.24
In order to minimize the rate of complications of per-
cutaneous closure of PFO a careful selection of patients
on the basis of morphology and location of the intera-
trial defect (dimensions of border and distance from
intra-atrial structures) is required.
Even considering the continuing refinement of per-
cutaneous procedures, surgical closure of PFO should
be considered in all cases that not adhere to the selec-
tion criteria.
The surgical closure of a PFO is a low-risk and highly
successful procedure with a low probability of residual
shunt, short hospital stay, and excellent long-term re-
sults.25 Some authors even describe less hospital cost
associated with surgical treatment.26
However, many patients are not keen on having a
long residual scar in the sternal region because of
cosmetic dissatisfaction, and this is true especially in
young asymptomatic female patients.
To minimize surgical trauma and improve cos-
metic results, different minimally invasive surgical ap-
proaches have been described, both, for cosmetic rea-
son and further reduction of the already fair morbidity
of traditional surgery.27,28
In particular, minimally invasive cardiac surgery by
means of Port-Access technique is probably associated
with reduced postoperative hospital stay and costs,
better postoperative chest function, improved cosmet-
ics results, and early return to full activities.29
We have been routinely using this technique in our
Institution since 1997, and till February 2006, have
treated by this means, 875 patients (mostly affected by
mitral valve disease), and, among those, we operated
on 108 patients for abnormalities of the atrial septum.
In front of a wide-accepted procedure such as percu-
taneous closure of a PFO there is a not negligible risk
of related complications.5,9
Among the surgical options used to repair any ad-
verse event, particular attention should be paid to min-
imally invasive video-assisted surgery.

78 RAFFA, ET AL.PFO CLOSURE DEVICE COMPLICATION
J CARD SURG2008;23:63-78
The 35-year-old women in this report, even after a
complication such as aortic root to right atrium fistula
following an incomplete percutaneous closure of the
PFO, had the benefit of a definitive correction of these
defects, along with a cosmetically satisfactory result.
Therefore, we suggest, after any failed percutaneous
procedure, to consider this surgical approach in order
to offer the patient a chance of treatment characterized
by trivial risks, fast recovery, and satisfactory aesthetic
results.
Therefore, we suggest to consider this type of ap-
proach when we want to offer the patient benefits in
terms of aesthetic results and faster postoperative re-
covery after any failed percutaneous treatment.
REFERENCES
1. Mas JL, Zuber M: French Study Group on Patent Foramen
Ovale, and Atrial Septal Aneurysm. Recurrent cerebrovas-
cular events in patients with patent foramen ovale, atrial
septal aneurysm, or both and cryptogenic stroke or tran-
sient ischemic attack. Am Heart J 1995;130:1083-1088.
2. Bruch L, Parisi A, Grad MO, et al: Transcatheter closure
of interatrial communications for secondary prevention of
paradoxical embolism: Single-center experience. Circula-
tion 2002;105:2845-2848.
3. Kiblawi FM, Sommer RJ, Levchuck SG: Transcatheter clo-
sure of patent foramen ovale in older adults. Catheter
Cardiovasc Interv 2006;68:136-142.
4. Bartz PJ, Cetta F, Cabalka AK, et al: Paradoxical emboli
in children and young adults: Role of atrial septal defect
and patent foramen ovale device closure. Mayo Clin Proc
2006;81:615-618.
5. Chessa M, Carminati M, Butera G, et al: Early and
late complications associated with transcatheter occlu-
sion of secundum atrial septal defect. J Am Coll Cardiol
2002;39:1061-1065.
6. Stauffer JC, Serra M, Juillard JM, et al: Percutaneous clo-
sure of patent foramen ovale: Preliminary experience with
the PFO Star. Arch Mal Coeur Vaiss 2004;97:37-41.
7. Meier JM, Nasratullah M, Eeckhout E: Late spontaneous
resolution of iatrogenic fistula between right atrium and
aorta secondary to percutaneous closure of patent fora-
men ovale. Eur J Echocardiogr 2005; [Epub ahead of
print]
8. Bogousslavsky J, Garazi S, Jeanrenaud X, et al: Lausanne
Stroke with Paradoxical Embolism Study Group. Stroke
recurrence in patients with patent foramen ovale: The
Lausanne Study. Neurology 1996;46:1301-1305.
9. Khairy P, O’Donnell CP, Landzberg MJ: Transcatheter clo-
sure versus medical therapy of patent foramen ovale and
presumed paradoxical thromboemboli. Ann Intern Med
2003;139:753-760.
10. Spies C, Strasheim R, Timmermanns I, et al: Patent fora-
men ovale closure in patients with cryptogenic thrombo-
embolic events using the Cardia PFO occluder. Eur Heart
J. 2006;27:365-371.
11. Chan KC, Godman MJ, Walsh K, et al: Transcatheter clo-
sure of atrial septal defect and interatrial communications
with a new self expanding nitinol double disc device (Am-
platzer septal occluder): multicentre UK experience. Heart
1999;82:300-306.
12. Divekar A, Gaamangwe T, Shaikh N, et al: Cardiac per-
foration after device closure of atrial septal defects
with the Amplatzer septal occluder. J Am Coll Cardiol.
2005;45:1213-1218.
13. Trepels T, Zeplin H, Sievert H, et al: Cardiac perforation
following transcatheter PFO closure. Catheter Cardiovasc
Interv. 2003;58:111-113.
14. Amin Z, Hijazi ZM, Bass JL, et al: Erosion of Amplatzer
septal occluder device after closure of secundum atrial
septal defects: review of registry of complications and
recommendations to minimize future risk. Catheter Car-
diovasc Interv. 2004;63:496-502.
15. Baykut D, Doerge SE, Grapow M, et al: Late perforation of
the aortic root by an atrial septal defect occlusion device.
Ann Thorac Surg 2005;79:e28.
16. Chun DS, Turrentine MW, Moustapha A, et al: Develop-
ment of aorta-to-right atrial fistula following closure of se-
cundum atrial septal defect using the Amplatzer septal
occluder. Catheter Cardiovasc Interv 2003;58:246-251.
17. Jang GY, Lee JY, Kim SJ, et al: Aorta to right atrial fistula
following transcatheter closure of an atrial septal defect.
Am J Cardiol 2005;96:1605-1606. Epub 2005 Oct 14.
18. Grayburn PA, Schwartz B, Anwar A, et al: Migration of an
amplatzer septal occluder device for closure of atrial sep-
tal defect into the ascending aorta with formation of an
aorta-to-right atrial fistula. J Cardiol 2005;96:1607-1609.
Epub 2005 Oct 14.
19. Mello DM, Fahey J, Kopf GS: Repair of aortic-left atrial fis-
tula following the transcatheter closure of an atrial septal
defect. Ann Thorac Surg 2005;80:1495-1498.
20. Aggoun Y, Gallet B, Acar P, et al: Perforation of the
aorta after percutaneous closure of an atrial septal defect
with an Amplatz prosthesis, presenting with acute severe
hemolysis. Arch Mal Coeur Vaiss 2002;95:479-482.
21. Knirsch W, Dodge-Khatami A, Balmer C, et al: Aortic
sinus-left atrial fistula after interventional closure of atrial
septal defect. Catheter Cardiovasc Interv 2005;66:10-13.
22. Lange SA, Schoen SP, Braun MU, et al: Perforation of
aortic root as secondary complication after implantation
of patent foramen ovale occlusion device in a 31-year-old
woman. J Interv Cardiol 2006;19:166-169.
23. Sauer HH, Ntalakoura K, Haun C, et al: Early cardiac per-
foration after atrial septal defect closure with the Am-
platzer septal occluder. Ann Thorac Surg 2006;81:2312-
2313.
24. Du ZD, Koening P, Cao QL, et al: Comparison of tran-
scatheter closure of secundum atrial septal defect us-
ing the Amplatzer septal occluder associated with defi-
cient versus sufficient rims. Am J Cardiol 2002;90:865-
869.
25. Murphy JG, Gersh BJ, McGoon MD, et al: Long term
outcome after surgical repair of isolated atrial septal
defect. Follow up at 27 to 32 years. NJ Engl J Med
1990;323:1645-1650.
26. Vida VL, Barnoya J, O’Connell M, et al: Surgical ver-
sus percutaneous occlusion of ostium secundum atrial
septal defects: results and cost-effective considerations
in a low-income country. J Am Coll Cardiol 2006;47:326-
31.
27. Dearani JA, Ugurlu BS, Danielson GK, et al: Surgical
patent foramen ovale closure for prevention of paradox-
ical embolism-related cerebrovascular ischemic events.
Circulation 1999;100:II171-5.
28. Berger F, Vogel M, Alexi-Meskishvili V, et al: Comparison
of results and complications of surgical and Amplatzer de-
vice closure of atrial septal defects. J Thorac Cardiovasc
Surg 1999;118:674-80.
29. Spreafico P, Rinaldi M, Alloni A, et al: Minimally inva-
sive closure of patent foramen ovale through port-access
surgery. Neurol Sci 2003;24(Suppl 1):S20-S22.