retinoblastoma in adults
TRANSCRIPT
409
CLINICAL PATHOLOGIC REVIEW
SURVEY OF OPHTHALMOLOGY
VOLUME 44
•
NUMBER 5
•
MARCH–APRIL 2000
© 2000 by Elsevier Science Inc. 0039-6257/00/$–see front matterAll rights reserved. PII S0039-6257(99)00132-0
DAVID APPLE AND MILTON BONIUK, EDITORS
Retinoblastoma in Adults: Report of Three Cases and Review of the Literature
Jyotirmay Biswas, MS,
1
Baskaran Mani, DO,
1
Mahesh P. Shanmugam, DO,
1
Dilip Patwardhan, MS,
2
K. S. Kumar, MS,
3
and Sengamedu S. Badrinath, FRCS(C)
1
1
Medical Research Foundation, Chennai, India,
2
Nandadeep Eye Hospital, Sangli, India, and
3
Narayana Nethralaya, Super Speciality Eye Hospital, Bangalore, India
Abstract.
Retinoblastoma usually presents in children younger than 5 years. To our knowledge, 20cases of retinoblastoma in adults (older than 20 years) have been reported in the literature. Of 173patients with histopathologically proven retinoblastoma seen in our institute, three were adults. All thepatients had endophytic tumors with vitreous seeds. Ultrasonography did not reveal calcification in twocases. Immunohistochemistry with neuron-specific enolase was used to confirm the diagnosis in twocases. All three patients ultimately required enucleation. None of the patients had been referred with adiagnosis of retinoblastoma. The diagnosis of retinoblastoma should be considered in cases of whitishmass lesion in the fundus of an adult. (
Surv Ophthalmol
44
:409–414, 2000. © 2000 by Elsevier ScienceInc. All rights reserved.)
Key words.
adult retinoblastoma
•
fine-needle aspiration biopsy
•
immunohistochemistry
•
neuron-specific enolase
•
retinoblastoma
•
ultrasonography
Retinoblastoma is the most common intraoculartumor in children. More than 90% of cases are diag-nosed before 5 years of age, and presentation of ret-inoblastoma in adults is rare.
22
Twenty cases of retin-oblastoma have been reported in patients who wereolder than 20 years at diagnosis
2–5,8–20,24,25
(Table 1);the oldest patient was a 74-year-old man.
5
We re-ported two cases of adult retinoblastoma in a peer-reviewed, nonindexed journal in 1996.
4
Since thenwe have seen another case of retinoblastoma in a 25-year-old female patient. This patient had no ocularcomplaints before the presentation. Herein, we re-port our three cases, which were seen in a referraleye institute in India during the last 11 years, and wereview the previous reports.
Case Reports
CASE 1
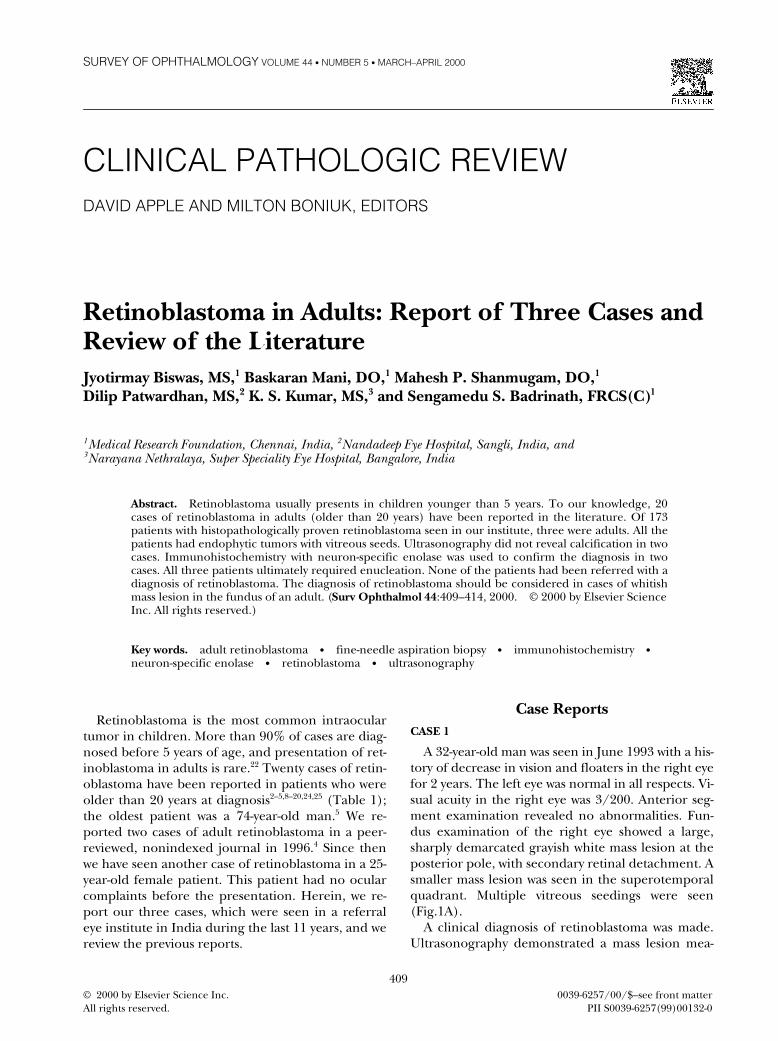
A 32-year-old man was seen in June 1993 with a his-tory of decrease in vision and floaters in the right eyefor 2 years. The left eye was normal in all respects. Vi-sual acuity in the right eye was 3/200. Anterior seg-ment examination revealed no abnormalities. Fun-dus examination of the right eye showed a large,sharply demarcated grayish white mass lesion at theposterior pole, with secondary retinal detachment. Asmaller mass lesion was seen in the superotemporalquadrant. Multiple vitreous seedings were seen(Fig.1A).
A clinical diagnosis of retinoblastoma was made.Ultrasonography demonstrated a mass lesion mea-

410 Surv Ophthalmol 44 (5) March–April 2000
BISWAS ET AL
suring 15
3
15
3
7.5 mm, of moderate to high re-flectivity, arising from the retina. Ultrasonographyindicated possible calcification (Fig. 1B). Computedtomography (CT) showed no evidence of calcifica-tion. Enucleation was performed. Grossly, the tumormeasured 10
3
8
3
8 mm. Histopathologic examina-tion confirmed the diagnosis of retinoblastoma, withfew Homer-Wright rosettes and occasional fleurettes(Fig. 1C). Immunohistochemical study with neuron-specific enolase was positive. On last follow-up exam-ination in June 1999, the socket was healthy, withoutany recurrence in the orbit.
CASE 2
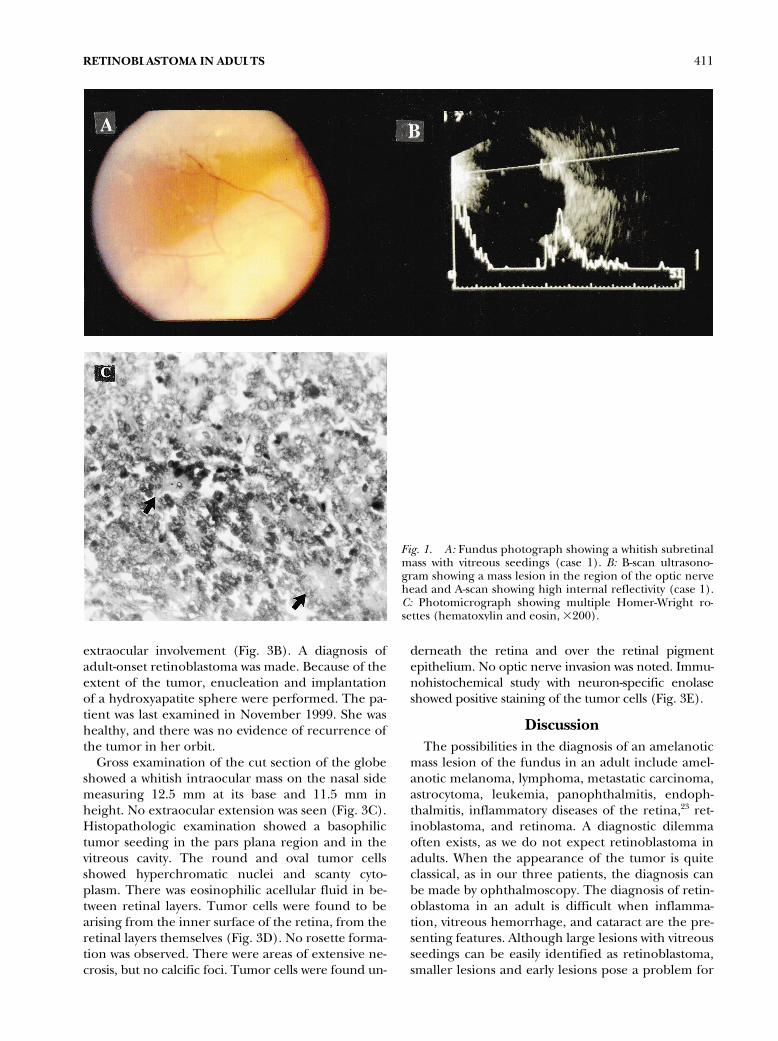
A 21-year-old man with a history of seeing blackspots in the right eye for 1 month had been treatedby his ophthalmologist with argon laser photocoagu-lation for suspected subretinal cysticercus. When thepatient was seen at Sankara Nethralaya, visual acuitywas 20/20 in both eyes.
The left eye was normal. There were retrolentalcells in the right eye. On fundus examination, a whit-ish, nodular, endophytic, vascularized mass lesion wasseen, which measured 3
3
5 mm, superotemporal tothe disk with multiple vitreous seedings (Fig. 2A). Ul-trasound showed the mass to be 3.7 mm thick. A trans-limbal intralesional biopsy revealed clumps of malig-nant cells with hyperchromatic nuclei and scantycytoplasm suggestive of retinoblastoma (Fig. 2B). Thepatient underwent external beam irradiation and acourse of chemotherapy, and the tumor regressed(Fig. 2C). The tumor showed activity after 18
months of therapy, and enucleation was performed.On histopathologic examination, the globe showedwell-differentiated endophytic retinoblastoma. Nooptic nerve invasion was seen.
CASE 3
A 25-year-old woman presented with complaints ofblurring of vision in the right eye of 1 month’s dura-tion in February 1998. Her father had died of gastriccarcinoma 3 years before. Other family memberswere healthy.
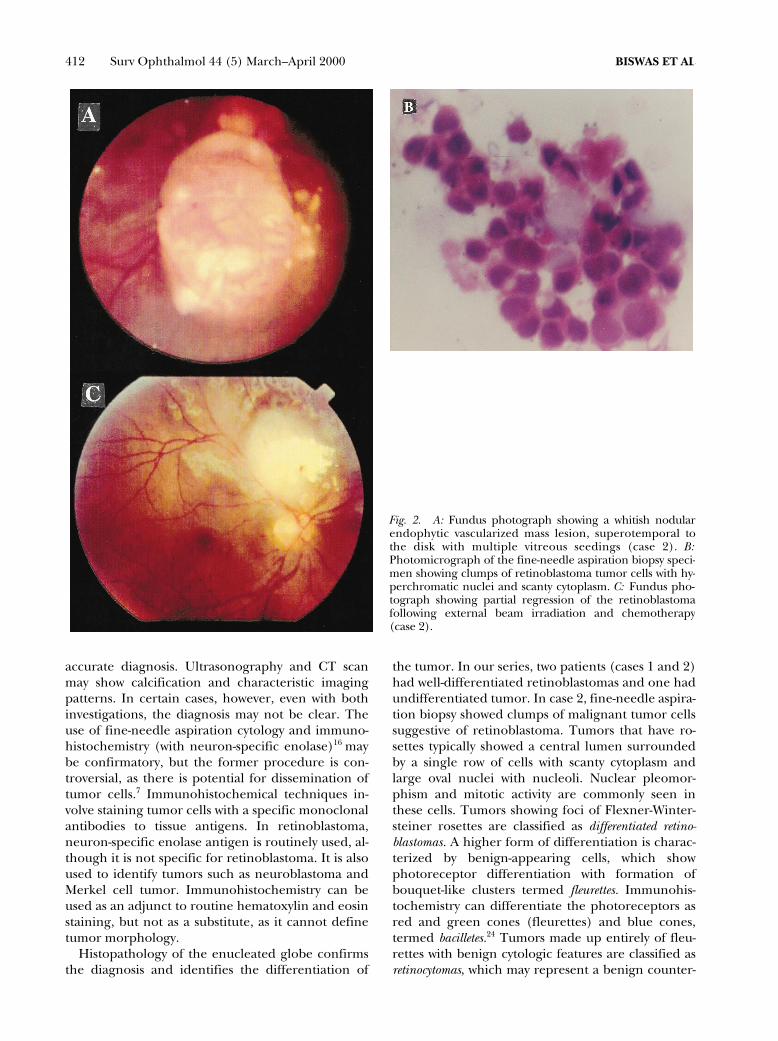
On examination, visual acuity in the right eye wasaccurate light projection, and in the left eye, 20/20.Extraocular movements were normal. There was noevidence of strabismus. The left eye was normal. Theright eye showed leukocoria and evidence of retro-lental cells on slit-lamp examination. Fundus exami-nation showed a large subretinal yellowish whitemass lesion located in the superonasal quadrant, as-sociated with secondary bullous retinal detachment(Fig. 3A). There were telangiectatic vessels in theretina. Multiple vitreous seedings were seen. Ultra-sound examination of the right eye disclosed moder-ately to highly reflective echoes in the vitreous cavity,subretinal mass in the superonasal quadrant, and to-tal bullous retinal detachment. There was no evi-dence of calcification or optic nerve involvement(Fig. 3B). Computed tomography of the orbits andbrain showed a soft tissue mass within the right globesuperomedially, abutting the retina and showing mildenhancement with a speck of calcification along withthe retinal detachment. There was no optic nerve or
TABLE 1
Clinical and Histopathologic Features in Reported Cases of Adult Retinoblastoma*
ReferenceYear of
publication Age/Sex Size (mm)Location of Tumor
in Fundus RosettesFollow-up
(mos.)
Maghy
10
1919 20/F Whole eye Whole eye FW 13Verhoeff
25
1929 48/M 10
3
15 Superonasal FW 6Rasmussen
19
1944 48/M 16
3
14 Anterior to the equator No NSO’Day
17
1948 29/M NS Anterior to the equator NS NSRychener
20
1948 33/F 6.5
3
7 Posterior pole FW NSArseni and Opresco
2
1959 53/M NS Posterior pole FW 3Mehra and Hamid
13
1961 45/M NS Anterior to the equator FW NSOhara et al
18
1963 43/F 3.8
3
3.8 Optic nerve head H NSMakley
11
1963 52/M 20
3
25 Whole eye FW 6Kremlicka and Roubkova
8
1975 42/M 8
3
18 Anterior to the equator FW NSBerkeley and Kalita
3
1977 60/M Whole eye Whole eye No NSTakahashi et al
24
1983 26/F NS Superior H 3Biswas et al
4
1996 32/M 10
3
8 Posterior pole H 1Biswas et al
4
1996 21/M 3
3
5 Superotemporal NS 24Nork et al
16
1996 29/F 8
3
10 Nasally B 132Mietz et al
14
1997 26/F 12
3
2 Anterior to the equator H 72Current case 2000 25/F 12.5
3
11. 5 Superonasal No 21
*Four other adult retinoblastoma cases have been reported in addition to the above cases.
5,9,12,15
We have excludedcases of spontaneously regressed retinoblastoma.
21
FW
5
Flexner-Wintersteiner rosettes; H
5
Homer-Wright’s rosettes; B
5
Bacilletes; NS
5
not stated.
RETINOBLASTOMA IN ADULTS
411
extraocular involvement (Fig. 3B). A diagnosis ofadult-onset retinoblastoma was made. Because of theextent of the tumor, enucleation and implantationof a hydroxyapatite sphere were performed. The pa-tient was last examined in November 1999. She washealthy, and there was no evidence of recurrence ofthe tumor in her orbit.
Gross examination of the cut section of the globeshowed a whitish intraocular mass on the nasal sidemeasuring 12.5 mm at its base and 11.5 mm inheight. No extraocular extension was seen (Fig. 3C).Histopathologic examination showed a basophilictumor seeding in the pars plana region and in thevitreous cavity. The round and oval tumor cellsshowed hyperchromatic nuclei and scanty cyto-plasm. There was eosinophilic acellular fluid in be-tween retinal layers. Tumor cells were found to bearising from the inner surface of the retina, from theretinal layers themselves (Fig. 3D). No rosette forma-tion was observed. There were areas of extensive ne-crosis, but no calcific foci. Tumor cells were found un-
derneath the retina and over the retinal pigmentepithelium. No optic nerve invasion was noted. Immu-nohistochemical study with neuron-specific enolaseshowed positive staining of the tumor cells (Fig. 3E).
Discussion
The possibilities in the diagnosis of an amelanoticmass lesion of the fundus in an adult include amel-anotic melanoma, lymphoma, metastatic carcinoma,astrocytoma, leukemia, panophthalmitis, endoph-thalmitis, inflammatory diseases of the retina,
23
ret-inoblastoma, and retinoma. A diagnostic dilemmaoften exists, as we do not expect retinoblastoma inadults. When the appearance of the tumor is quiteclassical, as in our three patients, the diagnosis canbe made by ophthalmoscopy. The diagnosis of retin-oblastoma in an adult is difficult when inflamma-tion, vitreous hemorrhage, and cataract are the pre-senting features. Although large lesions with vitreousseedings can be easily identified as retinoblastoma,smaller lesions and early lesions pose a problem for
Fig. 1. A: Fundus photograph showing a whitish subretinalmass with vitreous seedings (case 1). B: B-scan ultrasono-gram showing a mass lesion in the region of the optic nervehead and A-scan showing high internal reflectivity (case 1).C: Photomicrograph showing multiple Homer-Wright ro-settes (hematoxylin and eosin, 3200).
412 Surv Ophthalmol 44 (5) March–April 2000
BISWAS ET AL
accurate diagnosis. Ultrasonography and CT scanmay show calcification and characteristic imagingpatterns. In certain cases, however, even with bothinvestigations, the diagnosis may not be clear. Theuse of fine-needle aspiration cytology and immuno-histochemistry (with neuron-specific enolase)
16
maybe confirmatory, but the former procedure is con-troversial, as there is potential for dissemination oftumor cells.
7
Immunohistochemical techniques in-volve staining tumor cells with a specific monoclonalantibodies to tissue antigens. In retinoblastoma,neuron-specific enolase antigen is routinely used, al-though it is not specific for retinoblastoma. It is alsoused to identify tumors such as neuroblastoma andMerkel cell tumor. Immunohistochemistry can beused as an adjunct to routine hematoxylin and eosinstaining, but not as a substitute, as it cannot definetumor morphology.
Histopathology of the enucleated globe confirmsthe diagnosis and identifies the differentiation of
the tumor. In our series, two patients (cases 1 and 2)had well-differentiated retinoblastomas and one hadundifferentiated tumor. In case 2, fine-needle aspira-tion biopsy showed clumps of malignant tumor cellssuggestive of retinoblastoma. Tumors that have ro-settes typically showed a central lumen surroundedby a single row of cells with scanty cytoplasm andlarge oval nuclei with nucleoli. Nuclear pleomor-phism and mitotic activity are commonly seen inthese cells. Tumors showing foci of Flexner-Winter-steiner rosettes are classified as
differentiated retino-blastomas.
A higher form of differentiation is charac-terized by benign-appearing cells, which showphotoreceptor differentiation with formation ofbouquet-like clusters termed
fleurettes.
Immunohis-tochemistry can differentiate the photoreceptors asred and green cones (fleurettes) and blue cones,termed
bacilletes.
24
Tumors made up entirely of fleu-rettes with benign cytologic features are classified as
retinocytomas
, which may represent a benign counter-
Fig. 2. A: Fundus photograph showing a whitish nodularendophytic vascularized mass lesion, superotemporal tothe disk with multiple vitreous seedings (case 2). B:Photomicrograph of the fine-needle aspiration biopsy speci-men showing clumps of retinoblastoma tumor cells with hy-perchromatic nuclei and scanty cytoplasm. C: Fundus pho-tograph showing partial regression of the retinoblastomafollowing external beam irradiation and chemotherapy(case 2).
RETINOBLASTOMA IN ADULTS
413
part of retinoblastomas. Tumors devoid of Flexner-Wintersteiner rosettes and fleurettes are classified as
undifferentiated retinoblastomas.
Such tumors may con-tain Homer-Wright rosettes. These rosettes containfewer differentiated neoplastic cells and have no cen-tral lumen (seen in Flexner-Wintersteiner rosettes).
Almost all retinoblastomas in adults are sporadicand unilateral. Retinoblastoma normally is a rapidlygrowing tumor derived from embryonal retinal cells,which usually occur bilaterally in people predis-posed by a germline mutation with RB1 gene andunilaterally in people without this mutation.
Retinomas are clinically well-characterized quies-cent retinal masses, clearly linked to RB1 gene muta-tion, but they do not progress to malignant growth.There are few reports of retinoblastoma arising frompreviously documented retinoma or quiescent retin-oblastoma.
6
Normal fundi were not previously docu-
mented in our patients, so perhaps they did harbor aretinoma in which additional oncogenic mutationseventually occurred, leading to retinoblastoma tu-mor. This scenario is suggested by the observationthat all the reported cases are unilateral. It is un-known whether retinoblastomas can occur
de novo
inadults or whether they are preceded by a retinoma.
Enucleation was the primary treatment modalityin the majority of reported cases, as the lesions weredetected at a fairly advanced stage and each patienthad one normal unaffected eye. A few patients un-derwent external beam radiotherapy, as did one ofour patients, but the results were poor because ofthe advanced stage of the disease at diagnosis.
Our report of three cases indicates that, in thepresence of amelanotic whitish mass lesions in thefundus of an adult, one should consider the possibil-ity of retinoblastoma as a diagnosis. Ultrasound and
Fig. 3. A: Slit-lamp photograph showing a large whitish mass with secondary retinal detachment in the right eye (case 3)B: B-scan ultrasonogram showing a highly reflective mass lesion with secondary retinal detachment. Contrast CT scan showsa mass in the right globe superomedially with mild enhancement and a speck of calcification (case 3). C: Cut section of theglobe showing a white nasal intraocular mass and retinal detachment (case 3). D: Photomicrograph showing retinoblas-toma cells arising from the inner layer of the retina (hematoxylin and eosin, 3100; case 3). E: Immunohistochemical studywith neuron-specific enolase showing positive staining of the tumor cells (neuron-specific enolase, 3200; case 3).

414 Surv Ophthalmol 44 (5) March–April 2000
BISWAS ET AL
CT scan should be the first line of investigations. Ifdiagnostic confusion persists, fine-needle aspirationbiopsy of the mass can be advocated.
References
1. Abramson DH, Ellsworth RM, Grumbach N, et al: Retino-blastoma: correlation between age at diagnosis and survival.J Pediatr Ophthalmol Strabismus 23:174–7, 1986
2. Arseni C, Opresco I: An unusual case of retinoblastoma. AnnAnat Pathol 4:129–35, 1959
3. Berkeley JS, Kalita BC: Retinoblastoma in an adult [letter].Lancet 2:508–9, 1977
4. Biswas J, Shanmugam MP, Parikh S, et al: Retinoblastoma inadults: report of two cases with histopathologic correlation.Asia Pac J Ophthalmol 8:10–4, 1996
5. Finlay JR, Byron H: Retinoblastoma in the adult: review ofliterature and report of a case associated with benign mela-noma. Acta XIX Concilium Ophthalmologicum (NewDelhi) 2:1168–78, 1962
6. Gallie BL, Phillips RA, Ellsworth RM, et al: Significance of re-tinoma and phthisis bulbi for retinoblastoma. Ophthalmol-ogy 89:1393–9, 1982
7. Karcioglu ZA, Gordon RA, Karcioglu GL: Tumor seeding inocular fine needle aspiration biopsy. Ophthalmology 92:1763–7, 1985
8. Kremlicka L, Roubkova H: Retinoblastoma in an adult [inGerman]. Klin Monatsbl Augenheilkd 167:119–23, 1975
9. Lasch H: Ein Retinablastom rezidiz im Erwachsenenaiter.Klin Monatsbl Augenheilkd 144:268–72, 1964
10. Maghy C: A case of bilateral glioma of the retina in a girltwenty years of age in which the second eye was excised afteran interval of nearly eighteen years. Br J Ophthalmol 3:337–40, 1919
11. Makley TA Jr: Retinoblastoma in a 52-year-old man. ArchOphthalmol 69:325–27, 1963
12. McCrea WBE: Glioma of the retina: a review of twelve cases.Br J Ophthalmol 27:259–73, 1943
13. Mehra KS, Hamid S: Retinoblastoma in an adult. Am J Oph-thalmol 52:405–6, 1961
14. Mietz H, Hutton WL, Font RL: Unilateral retinoblastoma inan adult: report of a case and review of the literature [seecomments]. Ophthalmology 104:43–7, 1997
15. Neronova-Kotova LA: Case of retinoblastoma in an adult [inRussian]. Vestn Oftalmol 102:75, 1986
16. Nork TM, Millecchia LL, de Venecia GB, et al: Immunocy-tochemical features of retinoblastoma in an adult. ArchOphthalmol 114:1402–6, 1996
17. O’Day K: Two cases of choroidal melanoma with unusualhistories. Br J Ophthalmol 32:121–2, 1948
18. Ohara H, Akatuka S, Akutu S, Matui N: A case of retinoblas-toma in an aged woman. J Clin Ophthalmol 17:951–53, 1963
19. Rasmussen K: Retinoblastoma in a man aged forty-eight.Acta Ophthalmol (Copenh) 21:210–3, 1944
20. Rychener RO: Retinoblastoma in the adult. Trans Am Oph-thalmol Soc 46:318–26, 1948
21. Sanborn GE, Augsburger JJ, Shields JA: Spontaneous regres-sion of bilateral retinoblastoma. Br J Ophthalmol 66:685–90,1982
22. Shields CL, Shields JA, Shah P, et al: Retinoblastoma inolder children. Ophthalmology 98:395–9, 1991
23. Stafford WR, Yanoff M, Parnell BL: Retinoblastoma initiallymisdiagnosed as primary inflammation. Arch Ophthalmol73:771–3, 1969
24. Takahashi T, Tamura S, Inoue M, et al: Retinoblastoma in a26-year-old adult. Ophthalmology 90:179–83, 1983
25. Verhoeff FH: Retinoblastoma: report of a case in a man agedforty-eight. Arch Ophthalmol 2:643–650, 1929
We acknowledge Brenda L. Gallie, MD, Toronto, Ontario, Can-ada, for reviewing the manuscript and giving us valuable sugges-tions and guidance.
The authors have no proprietary or commercial interest in anyproduct or concept discussed in this article.
Reprint address: Jyotirmay Biswas, MS, 18 College Rd., Chen-nai, 600 006, India. E-mail: [email protected].