relation of blast cell survival and proliferation to chemotherapy resistance in aml
TRANSCRIPT

Relation of blast cell survival and proliferationto chemotherapy resistance in AML
JAN M. NØRGAARD,1 SVEN T. LANGKJER,2 TORBEN PALSHOF,2 NIELS CLAUSEN,3 BENT PEDERSEN4
AND
PETER HOKLAND1 Departments of 1Medicine and Haematology, 2Oncology, 3Paediatrics, Danish Cancer Society,
and 4Department of Cytogenetics, Aarhus University Hospital, Aarhus, Denmark
Received 11 December 1995; accepted for publication 11 March 1996
Summary. We have investigated the in vitro blast cell survival(viability) and drug resistance to cytosine arabinoside (Ara-C), daunorubicin (Dau), mitoxantrone (Mitox) and aclarubi-cin (Acla) of fresh leukaemic blast cells from 80 patients withnewly diagnosed acute myeloid leukaemia (AML) employingthe semiautomated colourimetric MTT(3-[4,5-dimethylthia-zol-2-yl]-2,5-diphenyl tetrazolium bromide)-assay. In 15cases we concurrently investigated the relation between invitro blast cell survival (MTT assay) and blast cellproliferation (3H-thymidine incorporation) in the presenceand absence of myeloid growth factors (GFs) G-CSF, GM-CSFand IL-3 (individually and in combination). A highlysignificant correlation was found between blast cell survivaland blast cell proliferation (r � 0.87, P < 1� 10ÿ4).Furthermore, in 40 evaluable adult patients who completedintravenous induction chemotherapy and were evaluable forresponse to chemotherapy we found a positive correlationbetween in vitro blast survival (MTT assay) and response tochemotherapy with high blast survival being associatedwith poor response to chemotherapy (P � 0.05). Moreover,
in a multivariate analysis, high blast cell survival wassignificantly associated with high CD13 expression andmonocytic phenotype (P � 0.0003 and P � 0.02, respect-ively). Furthermore, we found an inverse relationshipbetween the baseline proliferation of the blasts and themagnitude of response to the GFs (P < 0.02), indicatingthat cells with low baseline proliferation were more readilystimulated by growth factors. Finally, we found a significantcorrelation between leukaemic cell survival and cellulardrug resistance towards Dau (P � 0.001) and Mitox(P � 0.03), but not towards Ara-C (P � 0.68) and Acla(P � 0.13). We conclude that high in vitro leukaemic cellsurvival is associated with drug resistance in vivo and invitro, and furthermore is correlated with high blast cellproliferation and some adverse prognostic factors previouslyidentified in AML.
Keywords: AML, drug resistance, cell survival, proliferation,myeloid growth factors.
Acute myeloid leukaemia (AML) is a potentially curabledisease with high-dose chemotherapeutic regimens inducingcomplete remission (CR) in up to 80% of patients, withsuperior results being obtained in the younger age group(Yates et al, 1982; Rees et al, 1986). However, even in theyounger age group the majority of patients will eventually dieof relapsing leukaemia within few years (Hamblin, 1992).
In an effort to improve diagnostic and prognosticprecision, a considerable number of prognostic factorshave, over the years, been identified in AML. These includeleucocyte count at presentation (Bell et al, 1982),
cytogenetic abnormalities (Yunis et al, 1984; Schiffer et al,1989), morphology (Mertelsmann et al, 1980; Swirsky et al,1986), immunological phenotype (IP) (Griffin et al, 1986;Kristensen & Hokland, 1991; Bradstock et al, 1994), and ahistory of prior myelodysplastic syndrome or chemotherapyfor other malignant diseases (Mertelsmann et al, 1980;Pedersen-Bjergaard et al, 1981; Hoyle et al, 1989; Gajewskiet al, 1989).
Recently, the in vitro proliferation and ability to formcolonies of AML blasts in the absence or presence ofexogenous myeloid growth factors have attracted consider-able interest (Young & Griffin, 1986; Kelleher et al, 1987;Budel et al, 1989; Lowenberg & Touw, 1993). It has, thus,been demonstratedthat the proliferative rate (Lowenberg et al,1993), the S-phase fraction (Vidriales et al, 1995), and the
British Journal of Haematology, 1996, 93, 888–897
888 # 1996 Blackwell Science Ltd
Correspondence: Dr Jan Maxwell Nørgaard, Medicinsk-Hæmatologiskafd., Aarhus Amtsygehus, Tage-Hansens Gade 2–4, DK-8000Aarhus C, Denmark.

889Blast Survival and Drug Resistance in AML
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
ability to form colonies in vitro (Hunter et al, 1993) are ofindependent prognostic significance in this disease. Althoughit is conceivable that the growth capacity of these cells in vitroreflects the regrowth capacity of the leukaemic cells in vivo,the lower CR rates which were demonstrated in two reports(Lowenberg et al, 1993; Hunter et al, 1993) are intriguing.These could, however, be due to rapid regrowth occurringquickly after cessation of chemotherapy or, alternatively, becaused by an increased drug resistance of the leukaemic cellsin such cases. Indirect evidence for the latter has recentlybeen provided by Bradbury et al (1994) who demonstratedincreased expression of the Bcl-2 protein in autonomouslygrowing AML cells, and by te Boekhorst et al (1995) whofound increased P-glycoprotein expression in AML cells withhigh proliferative capacity.
In addition, as apoptotic cell death – or absence ofapoptotic cell death – of neoplastic cells has emerged as animportant property, not only with respect to leukaemogenesis(or oncogenesis) (Williams et al, 1990; Hockenbery et al,1990; Yonish-Rouach et al, 1991; Campana et al, 1993;McGahon et al, 1994) but also regarding drug resistance invitro and in vivo (Lotem & Sachs, 1992; Greaves, 1993;Miyashita & Reed, 1993; Campos et al, 1994; Wattel et al,1994), we wished to investigate a tentative connectionbetween leukaemic cell survival, measured by the MTT assay(Mosmann, 1983; Sargent & Taylor, 1989; Pieters et al, 1991;Nørgaard et al, 1993) and proliferation in AML. Furthermore,we wished to investigate the relationship between leukaemiccell survival and drug resistance. We found a correlationbetween cell survival (MTT assay) and proliferation (3H-thymidine-incorporation assay) and demonstrate a correla-tion between leukaemic cell survival and drug resistance inthis disease. Furthermore, we observed an inverse relation-ship between baseline cellular proliferation and cellularresponsiveness to myeloid growth factors (3H-thymidine-incorporation assay), which indicates that responsiveness ofAML blasts to GFs is of significance with regard to drugresistance and treatment outcome in this disease.
MATERIALS AND METHODS
Patients and cytoreductive treatment. During a 48-monthperiod from April 1991 to March 1995 80 patients (age 0–86years, median 59.5) with newly diagnosedAML were includedin the study. Basic clinical data are listed in Table I. Thesepatients included four with AML following chemotherapyfor Hodgkin’s disease (two cases), for non-Hodgkin’s lym-phoma (one case) and polycythaemia vera (one case). Innine patients AML was preceded by well-documented
myelodysplastic syndromes of >2 months duration. Thediagnosis was based upon examination of peripheral bloodand bone marrow smears stained for routine histology andhistochemistry as well as on immunophenotypingcarried outas described below. Cases were subsequently classifiedaccording to the FAB (French–American–British) classifi-cation (Bennett et al, 1976, 1985, 1991). Followingchemotherapy, standard CALGB criteria were used forevaluation of response (Ellison et al, 1968).
Intravenous remission induction treatment was institutedin 56 patients. The remaining received either palliativechemotherapy (11 cases) or supportive treatment only (10cases). Three patients died before cytoreductive treatmentcould be instituted. 35 adult patients received the combi-nation of Acla and Ara-C (Acla 75 mg/m2 days 1–3 as i.v.bolus infusion and Ara-C 100 mg/m2 days 1–7 as continuousi.v. infusion) (Hansen et al, 1991). 14 were treated withsimilar 3� 7 or 2� 5 regimens, but with Acla substituted forMitox 12 mg/m2 for 2–3 d. One patient was treated withhigh-dose Ara-C 1 g/m2 as i.v. bolus infusion twice daily days1–4. The six paediatric patients included in this study weretreated with Ara-C, 6-thioguanine, doxorubicin, and etopo-side (Ara-C 200 mg/m2 days 1–4 as continuous i.v. infusion,6-thioguanine 100 mg/m2, twice daily days 1–4 p.o.,doxorubicin 75 mg/m2 day 5 as i.v. bolus infusion, etoposide100 mg/m2 days 1–4 as continuous i.v. infusion). In no casewas the treatment of the patients influenced by the drugresistance data obtained during the study.
Preparation of leukaemic cell suspensions and labelling withmonoclonal antibodies (MoAbs). Mononuclear cells fromheparinized peripheral blood and bone marrow sampleswere obtained by density gradient centrifugation on Ficoll-paque (1.077 g/ml, Pharmacia, Uppsala, Sweden). Theirimmunological phenotype was determined by indirectimmunofluorescence using flow cytometry as previouslydescribed (Madsen et al, 1995). All in vitro procedures ofpatient samples were performed according to protocolsapproved by the Ethical Committee for the County ofAarhus. The mononuclear cell suspensions contained 66–99% (median 89%) immature myeloid cells as judged byreactivity with one or more myeloid MoAbs, which alwaysincluded CD13, CD14 and CD33. In addition, an extendedimmunophenotyping including labelling for CD2, CD7, CD34and P-glycoprotein (P-GP) was performed using cryopre-served samples in 55/80 cases. 20% cells positive for agiven antibody was considered a positive staining exceptfor the P-GP-antibody for which 10% positive cells wasconsidered a positive staining. Cell viability was assessedbefore all these procedures with the trypan blue dye exclusionassay and was always >90%.
Cytogenetic analysis. Bone marrow cells from 70/80 caseswere cultured in medium RPMI 1640 with 15% fetal calfserum at 378C in an atmosphere enriched with 5% CO2
for approximately 30 h. Giemsa bands were produced inmetaphase chromosomes with Wright’s stain as describedelsewhere (Pedersen & Kerndrup, 1986). At least threemetaphases were required to produce meaningful cytogeneticanalysis and this number was obtained in 58 cases.The remaining (12) cases fewer than three karyotyped
Table I. Patient characteristics.
Gender 43 men, 37 womenAge Median 59.5, range 0–86 yearsLeucocyte count Median 41:7� 109/l, range 0:9–287� 109/lFAB type 5 M0; 18 M1; 27 M2; 1 M3; 23 M4; 5 M5; 1 M7

metaphases (five cases) or no metaphases found (seven cases)were not evaluable. Complex chromosomal aberrations weredefined as at least three aberrations per metaphase.
Cellular exposure to cytotoxic drugs. Ara-C and Acla werepurchased from Lundbeck (Valby, Denmark), Dau fromRhone-Poulenc Rorer (Birkerød, Denmark) and Mitox fromLederle (Copenhagen, Denmark). They were all diluted inmedium RPMI 1640 enriched with L-glutamine, 1% Hepesbuffer solution, antibiotics (penicillin 100 IU/ml, strepto-mycin 100�g/ml, and fungizone 0.25�g/ml), and 10%heat-inactivated fetal calf serum (FCS). Two batches of FCS(nos. 901112 and 30F7830S, Life Technologies, Roskilde,Denmark) found to be equally supportive of the blast cells inculture were used throughout the study. For each of thecytotoxic drugs eight dilution steps were employed. Maximaland minimal concentrations of the drugs were: Ara-C:0.2 mg/ml to 5 ng/ml, Dau: 20�g/ml to 8 pg/ml, Mitox:10�g/ml to 8 pg/ml, Acla: 4�g/ml to 0.1 ng/ml. 96-welledU-bottomed microtitre plates (Nunc, Roskilde, Denmark)were prepared with 100�l of the appropriately dilutedcytotoxic drug in each well, with control wells consistingof medium only. The prepared plates were sealed with plasticfoil and kept atÿ258C in the dark for a maximum of 3 monthsor until use.
Blast cell survival and drug resistance measured by the MTTassay. For the MTT assay, fresh leukaemic cells were placed inthe pre-prepared microtitre plates (2� 105 cells/well, totalvolume 200�l suspension/well) and incubated for 96 h.Following incubation, 50�l of a MTT (Sigma, St Louis, Mo.)solution (2 mg/ml in Hanks buffered saline solution (HBSS))was added to each well. During the following 6 h incubationat 378C, the purple formazan product formed by conversion ofthe yellowish MTT salt in the mitochondria of the viable cells(Huet et al, 1992). Its resulting precipitate was dissolved inacidified isopropanol and the amount of converted MTT wasquantified in an ELISA-reader (NJ-2000, TekNunc, Roskilde,Denmark) using 540 nm test and 750 nm referencewavelengths. Each data point was based on triplicatedeterminations of the absorbance for each dilution step.Dose–effect curves were computerized and fitted to asigmoidal mathematical model using the least squaresmethod (GraphPad Inplot, ver. 3.00, GraphPAD Software,San Diego, Calif.). The LC-50 value, which is the drugconcentration lethal to 50% of the cells, was derived fromeach computerized dose–effect curve.
Blast cells from bone marrow as well as from peripheralblood were subjected to viability measurements and drugresistance testing in 20 cases and in comparison found toexhibit similar survival and drug resistance patterns(P > 0.05, paired t-tests). When data from both bonemarrow and peripheral blood derived blasts were available,data from the most ‘pure’ of these blast cell suspensions werechosen for further analysis. In 19 cases cells were incubatedin culture flasks containing enriched RPMI medium at aconcentration of 1� 106 cells/ml for 48 h prior to plating inmicrotitre plates. This procedure did not significantlyinfluence blast cell survival and drug resistance resultsobtained after 96 h incubation in microtitre plates(P > 0.05, n � 10, paired t-tests).
3H-thymidine-incorporation assay and cellular response tomyeloid growth factors. For evaluation of the proliferativeresponse to myeloid growth factors, fresh leukaemic cells wereplated in U-bottomed microtitre plates at a concentration of2� 104 cells per well in 200�l RPMI 1640 medium enrichedas described earlier, with or without 100 ng/ml of thefollowing human recombinant growth factors, either indivi-dually or in combination: G-CSF (purchased from Roche,Hvidovre, Denmark), GM-CSF (purchased from Sandoz,Copenhagen, Denmark), IL-3 (a kind gift from Sandoz,Basel, Switzerland). The combination contained G-CSF50 ng/ml, GM-CSF 100 ng/ml, and IL-3 100 IU/ml(�10 ng/ml).
At the end of the 96 h incubation period, 1�Ci of 3H-labelled thymidine was added to each well before a further 8 hincubation period. After this the cells were harvested ontoglass-fibre filters using a semi-automated cell-harvester(Skatron, Lier, Norway). Finally, the incorporated thymidinewas counted in a Beckman automated scintillation counter(model LS 1801, Beckman Instruments, Fullerton, Calif.,U.S.A.).
Statistical analysis. Data sets with distributions compatiblewith Gaussian distribution (determined using the Kolmo-gorov-Smirnov (KS) test) were evaluated using parametricstatistical methods, i.e. paired t-test for paired and Student’st-test for unpaired data. Non-parametric test methods, i.e.Wilcoxon’s test for matched pairs and Mann-Whitney test,were used when data sets were not Gaussian distributed. Allstatistical calculations were performed with the statisticalsoftware program SPSS ver. 5.01 (SPSS Inc., Chicago, Ill.).Two-sided P values were used throughout.
RESULTS
Clinical response to chemotherapyThirty of the 35 patients receiving the Acla and Ara-C 3� 7intravenous remission induction regimen were evaluable forresponse to chemotherapy after the first cycle. 20 patientsentered CR, eight patients either obtained a partial remission(four cases) or showed no response (four cases). Sevenpatients died during the treatment or nadir periods. Amongthe latter, two were considered evaluable for response tochemotherapy according to the recommendations of Preisler(1980), with autopsies demonstrating that one patient stillhad overt leukaemia at day 16 after start of induction therapy,and in the other leukaemia could not be demonstrated at day14 after start of induction treatment. In the Acla and Ara-Ctreatment group a total of 25 (71%) patients eventuallyachieved CR. Ten patients receiving Mitox and Ara-Ctreatment were evaluable for response to chemotherapyafter the first cycle: four achieved CR, two achieved partialremission (PR), four had resistant disease (NR). Four patientssuffered early death during this treatment. Overall, sixpatients (43%) in this subgroup eventually achieved CR.Five of the six paediatric patients achieved CR after the firstinduction cycle; the remaining patient died after completingtwo cycles of induction therapy showing no sign of responseto therapy.
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
890 Jan M. Nørgaard et al

891Blast Survival and Drug Resistance in AML
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
Distribution of MTT activity values, LC-50 values, and 3H-thymidine countsA number of variables essential to this study including theMTT activity values, the LC-50 values (for Ara-C, Acla andDau), and the 3H-thymidine counts were found not to beGaussian distributed (P < 0.001, KS test, data not shown). Incontrast, their log10 transformed derivates were Gaussiandistributed (P > 0.05 KS test). The log transformed valuesfor Mitox, however, showed a slight departure fromGaussian distribution (P � 0.02, KS test). Therefore, asthe log transformed values of these variables wereclearly most compatible with a Gaussian (normal) distri-bution, the transformed values were used throughout infurther analysis.
Correlation of in vitro leukaemic cell survival to clinical response tochemotherapyAs can be seen from Fig 1, among the 46 patients evaluablefor clinical response to chemotherapy after the first cycle ofinduction therapy, the patients who did not achieve CR hadleukaemic cells with higher ability to survive (viability) invitro, compared to cells of patients who achieved CR(P � 0.02, t-test). This remained statistically significantwhen excluding the paediatric patients (n � 6), P � 0.05,but not when excluding both the paediatric patients and thepatients with secondary AML (n � 12), P � 0.2. However,since the mean difference in log MTT activity between the CRsubgroup and the non-CR subgroup remained largelyunchanged during exclusion of subgroups, the lack ofsignificance is probably a question of sample size.
Fig 1. Log MTT activity values of 46 patients evaluable for CR statusafter one induction cycle. Cells of patients who did not achieve CR(non-CR� NR� PR) had higher in vitro survival than the cells ofpatients who achieved CR (P � 0.02, t-test). Closed circles representsecondary AML cases; triangles represent paediatric cases. Horizontalbars indicate group means.
Fig 2. Correlation plot of DNA synthesis rate (thymidine incorpora-tion) versus cell survival (viability, MTT-assay) of AML blast cells,r � 0.87, n � 15.
Table II. Characteristics of cells used in experiments with and without myeloid growth factors added.
Sample Purity (%) Cell source* Patient age FAB type Leucocyte count†
1 96 BM 69 M2 4.62 92 PB 41 M4 52.23 98 BM 49 M1 193.54 93 PB 43 M2 61.75 89 BM 39 M1 112.76 96 BM 9 M1 39.77 96 PB 43 M1 168.28 90 PB 65 M1 36.19 91 PB 24 M2 139.9
10 92 PB 71 M2 192.811 96 PB 51 M5 166.612 88 PB 70 M4 56.113 94 PB 38 M2 163.914 98 PB 55 M1 85.715 94 BM 60 M2 17.9
* Cells isolated from peripheral blood (PB) or bone marrow (BM) samples.†�109cells/l.
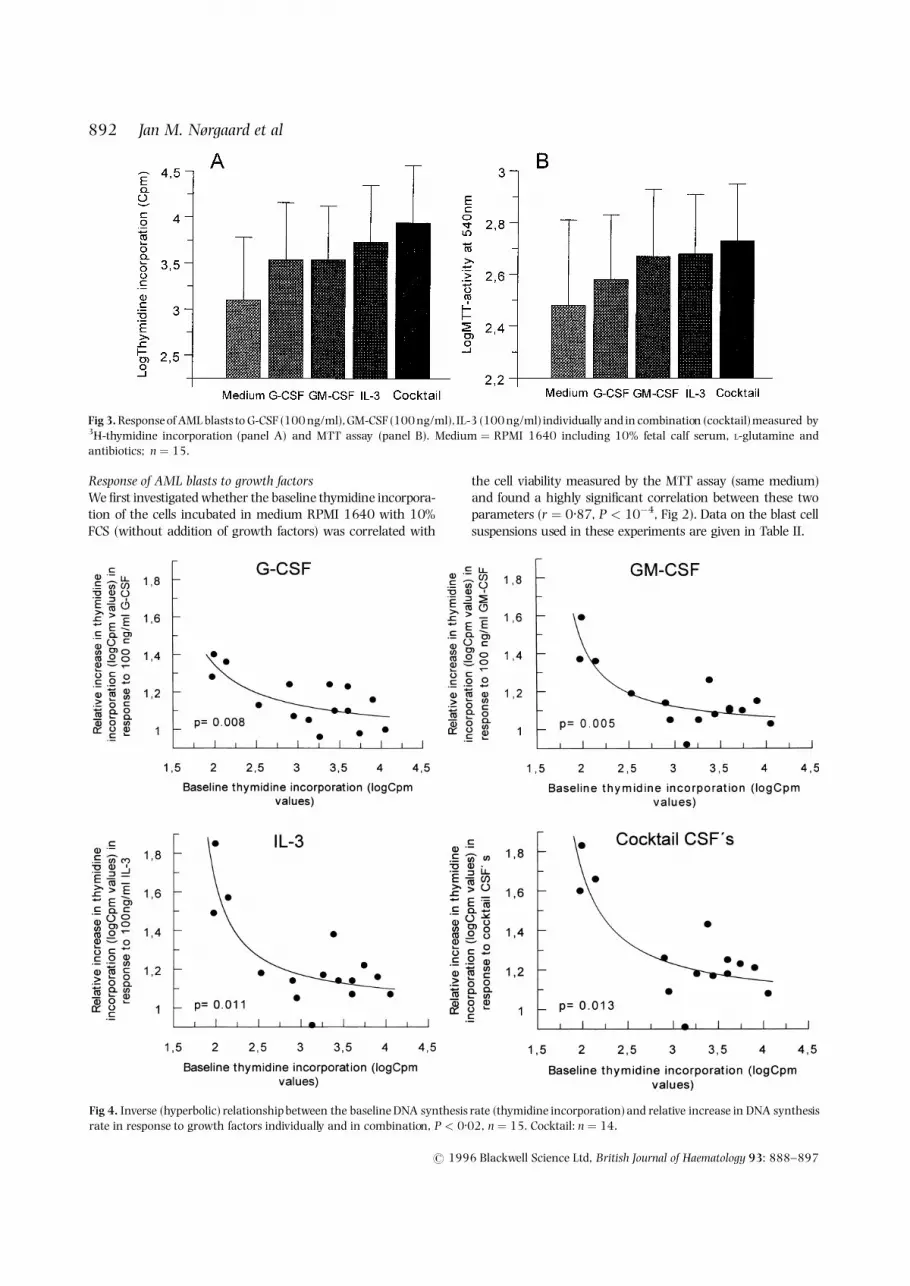
Response of AML blasts to growth factorsWe first investigated whether the baseline thymidine incorpora-tion of the cells incubated in medium RPMI 1640 with 10%FCS (without addition of growth factors) was correlated with
the cell viability measured by the MTT assay (same medium)and found a highly significant correlation between these twoparameters (r � 0.87, P < 10ÿ4, Fig 2). Data on the blast cellsuspensions used in these experiments are given in Table II.
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
892 Jan M. Nørgaard et al
Fig 3. Response of AML blasts to G-CSF (100 ng/ml), GM-CSF (100 ng/ml), IL-3 (100 ng/ml) individually and in combination (cocktail) measured by3H-thymidine incorporation (panel A) and MTT assay (panel B). Medium � RPMI 1640 including 10% fetal calf serum, L-glutamine andantibiotics; n � 15.
Fig 4. Inverse (hyperbolic) relationship between the baseline DNA synthesis rate (thymidine incorporation) and relative increase in DNA synthesisrate in response to growth factors individually and in combination, P < 0.02, n � 15. Cocktail: n � 14.

893Blast Survival and Drug Resistance in AML
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
We next investigated whether stimulation of the AMLblasts would be demonstrable in both the MTT- and the 3H-thymidine incorporation assays, and found that this was thecase. A breakdown of the data shown in Fig 3 revealed thataddition of the factors individually as well as in combinationresulted in degrees of stimulation, which could be demon-strated by both assays (P < 0.003, paired t-tests). We notedthat in both assays the stimulation of the cells by thecombination of factors (cocktail) was significantly greatercompared to stimulation by the factors individually(P < 0.05, paired t-test), with the exception that stimu-lation by the combination was not significantly higher thanthe stimulation by IL-3 alone in the MTT assay (P � 0.11).
Finally, we investigated the relation between the relativemagnitude of the response of the blasts to growth factorsindividually and in combination. The relative magnitude ofthe response to the myeloid growth factors, i.e. the ratiobetween the 3H-thymidine incorporation of stimulated cellsand of unstimulated cells (logCpm (with factors added)/logCpm (baseline)) was found to be inversely correlated to thebaseline thymidine incorporation (logCpm values) (P < 0.02,Fig 4).
Parameters correlated to leukaemic cell survivalA number of clinical and paraclinical parameters wereexamined in order to uncover possible correlations betweenthese parameters and leukaemic cell survival in vitro (TableIII). We found that CD13 expression (P � 0.0007, Fig 5) andpresence of a monocytic morphological phenotype (P � 0.02,Fig 6), i.e. FAB types M4 and M5, correlated with highleukaemic cell survival. These two parameters were in asubsequent multiple linear regression analysis found to be ofindependent significance with regard to high leukaemic cellsurvival (CD13; P � 0.0003, monocytic phenotype;P � 0.02). In contrast, gender, leucocyte count, age at
presentation, AML secondary to prior antineoplastic treatmentor MDS, complex karyotype, normal karyotype, CD2, CD7,CD14, CD33, CD34 and C-219 (P-glycoprotein) reactivitieswere not significantly correlated to leukaemic cell survival(P > 0.05). Throughout the analyses these patternsremained constant even after excluding the paediatric andsecondary AML cases.
Whereas monocytic phenotype was correlated with highleukaemic cell survival, the CD14 expression only showed atrend (P � 0.06) towards being correlated with leukaemiccell survival in the same manner. However, these twoparameters very strongly correlated as the 28 FAB M4 orM5 cases had significantly higher expression of CD14 thanthe 52 remaining cases (P � 0.0003, Mann-Whitney test).
Finally, we found that leukaemic cell survival wassignificantly correlated with drug resistance towards Dau(P � 0.001) and towards Mitox (P � 0.03), but was notTable III. Correlation between prognostic factors and in vitro
leukaemic cell survival: univariate analysis.
No. ofPrognostic factor evaluable r value(variable) patients* (Spearman) P value
Age 80 0.05 0.63Leucocyte count 80 0.15 0.15Secondary leukaemia 80 † 0.06Complex karyotype 58 † 0.22Normal karyotype 58 † 0.26Monocytic phenotype 80 † 0.02CD2 55 ÿ0.04 0.75CD7 55 ÿ0.06 0.67CD13 80 0.37 0.0007CD14 80 0.21 0.06CD33 80 0.1 0.39CD34 55 0.14 0.32P-glycoprotein expression 55 0.04 0.77
* Total number of evaluable patients in the whole group.† Evaluated using Student’s t-test.
Fig 5. Correlation between percentage of CD13 positive blast cells andsurvival (viability, MTT assay) in blast suspensions, n � 80, r � 0.39,P � 0.0006.
Fig 6. Correlation between AML phenotype and leukaemic cellsurvival (MTT assay). Monocytic cases (FAB M4 and M5, 28 cases)(�) had significantly higher blast cell survival than non-monocyticcases (FAB M0, M1, M2, M3, M7, 52 cases) (ÿ), P � 0.015, t-test.Horizontal bars indicate group means.

correlated with resistance towards Ara-C and Acla (Fig 7).These results remained statistically significant after excludingthe paediatric and secondary AML cases.
DISCUSSION
The results of this study link high leukaemic cell survival invitro to high drug resistance both in vitro and in vivo.Furthermore, they link high leukaemic cell survival to highproliferation and therefore suggest that the observed inferiorCR rates in patients whose leukaemic cells highly proliferate(autonomously) (Lowenberg et al, 1993; Hunter et al, 1993)are related to increased drug resistance and are not merely aconsequence of rapid leukaemic regrowth. The inverserelationship between autonomous growth and response togrowth factors, as demonstrated here, emphasizes that theresponse of AML cells to myeloid growth factors is animportant biological phenomenon with regard to regrowthpotential and to drug resistance.
Regarding the inverse relationship between autonomousgrowth and response to growth factors, a number of technical
aspects should, however, be taken into account beforeconsidering it an inherent property of the AML cells. Thus,the phenomenon observed with the 3H-thymidine-incorpora-tion assay could be due to ‘crowding’ or cellular overloadingin the test system. However, considering that stimulation ofthe leukaemic cells by the GFs could also be demonstratedwith the MTT assay at a cellular concentration 10 timeshigher than the ones used for the thymidine assay, this is notlikely to be the case. In addition, it could be shown that theadded amount of tritiated thymidine exceeded by far theamount which could be incorporated by the cells, whether GFstimulated or not. Finally, linearity of the liquid scintillationcounter over the several logs range of Cpms was confirmed(data not shown).
The molecular mechanisms which enable some AML cellsto survive and proliferate autonomously in vitro are not yetclarified, but autocrine and paracrine production of myeloidgrowth factors has been implicated in selected cases andappear to be plausible explanations for this phenomenon(Young & Griffin, 1986; Rogers et al, 1994). Furthermore, therelation between, on one hand, the ability of AML cells to
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
894 Jan M. Nørgaard et al
Fig 7. Correlation between leukaemic cell survival and in vitro cellular drug resistance (MTT assay). Dau: r � 0.40, P � 0.001, n � 63. Mitox:r � 0.28, P � 0.03, n � 61. Ara-C: r � 0.07, P � 0.56, n � 80. Acla: r � 0.17, P � 0.13, n � 80.

895Blast Survival and Drug Resistance in AML
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
proliferate and to form colonies in vitro, and, on the otherhand, the survival potential and ability to escape apoptoticdeath, is only sparsely investigated. From a biological point ofview it would be interesting to investigate in more detailwhether – as strongly indicated in this study – a closecorrelation can be demonstrated between proliferativepotential and ability to survive/escape apoptosis, becausethis would provide a link between the studies which havefocused on proliferative potential of AML cells and thosewhich have dealt with cell survival and apoptosis.
Considering the differences among the chemotherapeuticdrugs found in this study, it is quite conceivable that the anti-leukaemic activity of the S-phase-specific drug Ara-C does notappear to be decreased in highly viable (and thereby in highlyproliferating) leukaemic cells. Two opposing mechanismsmay well be operative here. On one hand, highly proliferatingcells are more susceptible to the cytotoxicity of this drug(Tafuri & Andreeff, 1990; Butturini et al, 1990; Brach et al,1990; Nørgaard et al, 1993; Tafuri et al, 1994). On the otherhand, protective mechanisms, which oppose cytotoxic(apoptotic) cell death such as DNA-repair mechanisms(Masuda et al, 1988), decreased action of p53 (Yonish-Rouach et al, 1991; Wattel et al, 1994), increased Bcl-2expression (Miyashita & Reed, 1993; Campos et al, 1993;Bradbury et al, 1994), increased P-glycoprotein expression (teBoekhorst et al, 1995) and others yet to be identified may wellbe operative in these cases.
Interestingly, the anthracycline Acla seems to represent anintermediate drug with a pattern which lies between Ara-Cand Dau (and Mitox) in this context. Although bothanthracyclines Acla and Dau intercalate with DNA theprimary intracellular targets responsible for their cytotoxiceffects are probably different ( Jensen et al, 1991). Thus, theprimary target for Dau is thought to be the nuclear enzymeTopoisomerase II (TOPO II) (Tewey et al, 1984; Bodley et al,1989) with which it interacts and produces DNA strand-breaks, which lead to cell death. In contrast, the primaryintracellular effect of Acla is more likely to be an inhibition ofRNA synthesis (Oki et al, 1981; Pedersen-Bjergaard et al,1984). Lack of cross-resistance between Acla and Dau haspreviously been demonstrated in both in vitro and in vivostudies of other groups. In the work of Pedersen-Bjergaard etal (1984) the activity of Acla as a single drug in patientspreviously treated with, and possibly refractory to, Dau andAra-C was demonstrated. Furthermore, using a panel of small-cell lung cancer cell lines, Jensen et al (1989) demonstrated lackof cross-resistance of Acla to Dau and doxorubicin, suggesting adifferent mechanism of action. Collectively, our own dataindirectly support the notion that Acla and Dau have differentmodes of intracellular action. Furthermore, they stronglysupport the proposal by Jensen et al (1989) that Mitox andDau have similar mechanisms of action.
There are at present two well-defined mechanisms ofresistance to the ‘classic’ anthracyclines (daunorubicin anddoxorubicin), the most well-known being related to the P-glycoprotein (also known as the multiple-drug resistanceprotein, or P-170), encoded for by the MDR-1 gene (Marie etal, 1991; Campos et al, 1992), which has been mapped to thelong arm of chromosome 7 (7q21-22) (Trent & Witkowski,
1987). This protein is considered to be an energy-dependent,blockable, drug efflux pump. The presence of this protein inAML has been associated with lower CR rates and shortersurvival, and has been shown to covariate with CD34expression but not CD13 and CD14 (Campos et al, 1992).The other drug-resistance mechanism is related to altered orreduced enzymatic activity of TOPO II (at-MDR) ( Jensen et al,1991). TOPO II exists in two known isoforms, the 170 kDTOPO II alpha, and the 180 kD TOPO II beta. The genes ofthese enzymes have recently been mapped to loci within17q21-22 (alpha isoform) (Smith et al, 1993) and to 3p24(beta isoform) ( Jenkins et al, 1992). In this respect, it isnoteworthy that ongoing studies in our laboratory suggestthat drug resistance towards two other TOPO II targeteddrugs doxorubicin (Dox) and etoposide (Eto) is correlated toleukaemic cell survival in a manner similar to that of Dau andMitox.
In conclusion, our present study indicates that twoparameters are associated with high in vitro survival of AMLblasts in vitro, namely, high CD13 expression and monocyticphenotype. This extends the findings of Griffin et al (1986) whodemonstrated that the presence of CD13 or CD14 on AMLblasts each were associated with inferior survival in patientstreated with Dau � Ara-C. In this context, it is also noteworthythat Lowenberg et al (1993) observed that FAB M4 and M5were significantly associated to high autonomous proliferationin vitro, and that Campos et al (1993) noted that high Bcl-2expression was associated with a monocytic phenotype.Therefore the present study adds the important finding thatin such cases the leukaemic cells have a higher ability to survivein vitro and that the leukaemic blasts in these cases have ahigher drug resistance in particular towards Dau and Mitoxwhich are both TOPO II targeted drugs.
ACKNOWLEDGMENTS
This work was supported by grants KFE-AA-36-93 and 94-100-30 from the Danish Cancer Society, by an educationalgrant from F. Hoffmann-La Roche, and by a grant from theMrs Agnes N. Anderssons Cancer Research Foundation.
The authors acknowledge the skilful technical assistance ofBirthe Høgh and Anni Krogh.
REFERENCES
Bell, R., Rohatiner, A.Z.S., Slevin, M.L., Ford, J.M., Dhaliwal, H.S.,Henry, G., Birkhead, B.G., Amess, J.A.L., Malpas, J.S. & Lister, T.A.(1982) Short-term treatment for acute myelogenous leukaemia.British Medical Journal, 284, 1221–1224.
Bennett, J.M., Catovsky, D., Daniel, M.T., Flandrin, G., Galton, D.A.G.,Gralnick, H.R. & Sultan, C. (1976) Proposals for the classification ofacute leukaemias. British Journal of Haematology, 33, 451–458.
Bennett, J.M., Catovsky, D., Daniel, M.T., Flandrin, G., Galton, D.A.G.,Gralnick, H.R. & Sultan C. (1985) Proposed revised criteria for theclassification of acute myeloid leukaemia. Annals of InternalMedicine, 103, 620–625.
Bennett, J.M., Catovsky, D., Daniel, M.T., Flandrin, G., Galton, D.A.G.,Gralnick, H.R. & Sultan, C. (1991) Proposal for the recognition ofminimally differentiated acute myeloid leukaemia (AML-M0).British Journal of Haematology, 78, 325–329.
Bodley, A., Liu, L.F., Israel, M., Seshadri, R., Koseki, Y., Giuliani, F.C.,

Kirschenbaum, S., Silber, R. & Potmesil, M. (1989) DNAtopoisomerase II-mediated interaction of doxorubicin and dau-norubicin congeners with DNA. Cancer Research, 49, 5969–5978.
Brach, M., Klein, H., Platzer, E., Mertelsmann, R. & Hermann, F.(1990) Effect of interleukin 3 on cytosine arabinoside-mediatedcytotoxicity of leukemia myeloblasts. Experimental Hematology, 18,748–753.
Bradbury, D., Zhu, Y-M. & Russell, N. (1994) Regulation of Bcl-2expression and apoptosis in acute myeloblastic leukemia cells bygranulocyte-macrophage colony-stimulating factor. Leukemia, 8,786–791.
Bradstock, K., Matthews, J., Benson, E., Page, F. & Bishop, J. (1994)Prognostic value of immunophenotyping in acute myeloidleukemia. Blood, 84, 1220–1225.
Budel, L.M., Touw, I.P., Delwel, R., Clark, S.C. & Lowenberg, B. (1989)Interleukin-3 and granulocyte-monocyte colony-stimulatingfactoron human acute myelocytic leukemia cells and relationship toproliferative response. Blood, 74, 565–571.
Butturini, A., Santucci, M.A., Gale, R.P., Perocco, P. & Tura, S. (1990)GM-CSF incubation prior to treatment with cytarabine ordoxorubicin enhances drug activity against AML cells in vitro:a model for leukemia chemotherapy. Leukemia Research, 14,743–749.
Campana, D., Coustan-Smith, E., Manabe, A., Buschle, M., Raimondi,S.C., Behm, F.G., Ashmun, R., Arico, M., Biondi, A. & Pui, C-H.(1993) Prolonged survival of B-lineage acute lymphoblasticleukemia cells is accompanied by overexpression of bcl-2 protein.Blood, 81, 1025–1031.
Campos, L., Guyotat, D., Archimbaud, E., Calmard-Oriol, P., Tsuruo,T., Troncy, J., Treille, D. & Fiere, D. (1992) Clinical significance ofmultidrug resistance p-glycoprotein expression on acute nonlym-phoblastic leukemia cells at diagnosis. Blood, 79, 473–476.
Campos, L., Rouault, J-P., Sabido, O., Oriol, P., Roubi, N., Vasselon, C.,Archimbaud, E,. Magaud, J-P. & Guyotat, D. (1993) Highexpression of bcl-2 protein in acute myeloid leukemia is associatedwith poor response to chemotherapy. Blood, 81, 3091–3096.
Campos, L., Sabido, O., Rouault, J-P. & Guyotat, D. (1994) Effects ofbcl-2 antisense oligodeoxynucleotides on in vitro proliferation andsurvival of normal marrow progenitors and leukemic cells. Blood,84, 595–600.
Ellison, R.R., Holland, J.F., Weil, M., Jacquillat, C., Boiron, M., Bernard,J., Sawitsky, A., Rosner, F., Gussof, B., Silver, R.T., Karansas, A.,Cuttner, J., Spurr, C.L., Hayes, D.M., Blom, J., Leone, L.A., Haurani,F., Kyle, R., Hutchison, J.L., Jackson Forcier, R. & Moon, J.H. (1968)Arabinosyl cytosine: useful agent in the treatment of acuteleukemia in adults. Blood, 32, 507–523.
Gajewski, J.L., Ho, W.G., Nimer, S.D., Hirji, K.F., Gekelman, L., Jacobs,A.D. & Champlin, R.E. (1989) Efficacy of intensive chemotherapyfor acute myelogenous leukemia associated with a preleukemicsyndrome. Journal of Clinical Oncology, 7, 1637–1645.
Greaves, M.F. (1993) Stem cell origins of leukaemia and curability.British Journal of Cancer, 67, 413–423.
Griffin, J.D., Davis, R., Nelson, D.A., Davey, F.R., Mayer, R.J., Schiffer,C., Ross McIntyre, O. & Bloomfield, C.D. (1986) Use of surfacemarker analysis to predict outcome of adult acute myeloblasticleukemia. Blood, 68, 1232–1241.
Hamblin, T. (1992) The treatment of acute myeloid leukemiapreceded by myelodysplastic syndrome. Leukemia Research, 16,101–108.
Hansen, O.P., Pedersen-Bjergaard, J., Ellegaard, J., Brincker, H.,Boesen, A.M., Christensen, B.E., Drivsholm, Aa., Hippe, E., Jans,H., Jensen, K.B., Killmann, S-Aa., Jensen, M.K., Karle, H., Laursen,B., Nielsen, J.B., Nissen, N.I. & Thorling, K. (1991) Aclarubicin plus
cytosine arabinoside versus daunorubicinplus cytosine arabinosidein previously untreated patients with acute myeloid leukemia: aDanish national phase III trial. Leukemia, 5, 510–516.
Hockenbery, D., Nunez, G., Milliman, C., Schreiber, R.D. & Korsmeyer,S.J. (1990) Bcl-2 is an inner mitochondrial membrane protein thatblocks programmed cell death. Nature, 348, 334–338.
Hoyle, C.F., de Bastos, M., Wheatley, K., Sherrington, P.D., Fischer, P.J.,Rees, J.K.H., Gray, R. & Hayhoe, F.G.J. (1989) AML associated withprevious cytotoxic therapy, MDS or myeloproliferative disorders:results from the MRC’s 9th AML trial. British Journal ofHaematology, 72, 45–53.
Huet, O., Petit, J.M., Ratinaud, H. & Julien, R. (1992) NADH-dependent dehydrogenase activity estimation by flow cytometricanalysis of 3-(4,5-dimethylthiazolyl-2-yl)-2,5-diphenyltetrazoliumbromide (MTT) reduction. Cytometry, 13, 532–539.
Hunter, A.E., Rogers, S.Y., Roberts, I.A.G., Barrett, J. & Russell, N.(1993) Autonomous growth of blast cells is associated withreduced survival in acute myeloblastic leukemia. Blood, 82, 899–903.
Jenkins, J.R., Ayton, P., Jones, T., Davies, S.L., Simmons, D.L., Harris,A.L., Sheer, D. & Hickson, I.D. (1992) Isolation of cDNA clonesencoding the � isoenzyme of human DNA topoisomerase II andlocalization of the gene to chromosome 3p24. Nucleic AcidsResearch, 20, 5587–5592.
Jensen, P.B., Vindeløv, L., Roed, H., Demant, E.J.F., Sehested, M.,Skovsgaard, T. & Hansen, H.H. (1989) In vitro evaluation of thepotential of aclarubicin in the treatment of small cell carcinoma ofthe lung (SCCL). British Journal of Cancer, 60, 838–844.
Jensen, P.B., Jensen, P.S., Demant, E.J.F., Friche, E., Sørensen, B.S.,Sehested, M., Wassermann, K., Vindeløv, L., Westergaard, O. &Hansen, H.H. (1991) Antagonistic effects of aclarubicin ondaunorubicin-induced cytotoxicity in human small cell lungcancer cells: relationship to DNA integrity and topoisomerase II.Cancer Research, 51, 5093–5099.
Kelleher, C., Miyauchi, J., Wong, G., Clark, S., Minden, M.D. &McCulloch, E.A. (1987) Synergism between recombinant growthfactors, GM-CSF and G-CSF acting on the blast cells of acutemyeloblastic leukemia. Blood, 69, 1498–1503.
Kristensen, J.S. & Hokland, P. (1991) Monoclonal antibodies inmyeloid diseases: prognostic use in acute myeloid leukemia.Leukemia Research, 15, 693–700.
Lotem, J. & Sachs, L. (1992) Hematopoietic cytokines inhibitapoptosis induced by transforming growth factor�1 and cancerchemotherapy compounds in myeloid leukemia cells. Blood, 80,1750–1757.
Lowenberg, B. & Touw, I.P. (1993) Hematopoietic growth factors andtheir receptors in acute leukemia. Blood, 81, 281–292.
Lowenberg, B., van Putten, W.L.J., Touw, I.P., Delwel, R. & Santini, V.(1993) Autonomous proliferation of leukemic cells in vitro as adeterminant of prognosis in adult acute myeloid leukemia. NewEngland Journal of Medicine, 328, 614–619.
Madsen, P.S., Hokland, P., Clausen, N., Ellegaard, J. & Hokland, M.(1995) Differential expression levels of the heat shock protein27 isoforms in pediatric normal, nonleukemic and commonacute lymphoblastic leukemia B-cell precursors. Blood, 85, 510–521.
Marie, J.P., Zittoun, R. & Sikic, B.I. (1991) Multidrug resistance (mdr1)gene expression in adult acute leukemias: correlation with treatmentoutcome and in vitro drug sensitivity. Blood, 78, 586–592.
Masuda, H., Ozols, R.F., Lai, G-M., Fojo, A., Rothenberg, M. &Hamilton, T.C. (1988) Increased DNA repair as a mechanism ofacquired resistance to cis-diamminedichloroplatinum(II) in humanovarian cancer cell lines. Cancer Research, 48, 5713–5716.
McGahon, A., Bissonnette, R., Schmitt, M., Cotter, K.M., Green, D.R. &
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
896 Jan M. Nørgaard et al

897Blast Survival and Drug Resistance in AML
# 1996 Blackwell Science Ltd, British Journal of Haematology 93: 888–897
Cotter, T.G. (1994) BCR-ABL maintains resistance of chronicleukemia cells to apoptotic cell death. Blood, 83, 1179–1187.
Mertelsmann, R., Thaler, H.T., To, L., Gee, T.S., McKenzie, S., Schauer,P., Friedman, A., Arlin, Z., Cirrincione, C. & Clarkson, B. (1980)Morphological classification, response to therapy, and survival in263 adult patients with acute non-lymphoblastic leukemia. Blood,56, 773–781.
Miyashita, T. & Reed, J.C. (1993) Bcl-2 oncoprotein blockschemotherapy-induced apoptosis in a human leukemia cell line.Blood, 81, 151–157.
Mosmann, T. (1983) Rapid colorimetric assay for cellular growth andsurvival: applicationto proliferationand cytotoxicity assays. Journalof Immunological Methods, 65, 55–63.
Nørgaard, J.M., Langkjer, S.T., Ellegaard, J., Palshof, T., Clausen, N. &Hokland, P. (1993) Synergistic and antagonistic effects of myeloidgrowth factors on in vitro cellular killing by cytotoxic drugs.Leukemia Research, 17, 689–694.
Oki, T., Takeuchi, T., Oka, S. & Umezawa, H. (1981) Newanthracycline antibiotic aclacinomycin A: experimental studiesand correlations with clinical trials. Recent Results in CancerResearch, 76, 21–40.
Pedersen-Bjergaard, J,, Brincker, H., Ellegaard, J., Drivsholm, A.,Freund, L., Jensen, K.B., Jensen, M.K. & Nissen, N.I. (1984)Aclarubicin in the treatment of acute nonlymphocytic leukemiarefractory to treatment with daunomycin and cytarabine: a phaseII trial. Cancer Treatment Reports, 68, 1233–1237.
Pedersen, B. & Kerndrup, G. (1986) Specific minor chromosomedeletions consistently occurring in myelodysplastic syndromes.Cancer Genetics and Cytogenetics, 23, 61–75.
Pedersen-Bjergaard, J., Philip, P., Mortensen, B.T., Ersbøll, J., Jensen,G., Panduro, J. & Thomsen, M. (1981) Acute nonlymphocyticleukemia, preleukemia, and acute myeloproliferative syndromesecondary to treatment of other malignant diseases: clinical andcytogenetic characteristics and results of in vitro culture of bonemarrow and HLA typing. Blood, 57, 712–723.
Pieters, R., Huismans, D.R., Loonen, A.H., Hahlen, K., van der Does-vanden Berg, A., van Vering, E.R. & Veerman, A.J.P. (1991) Relation ofcellular drug resistance to long-term clinical outcome in childhoodacute lymphoblastic leukaemia. Lancet, 338, 399–403.
Preisler, H.D. (1980) Prediction of response to chemotherapy in acutemyelocytic leukemia. Blood, 56, 361–367.
Rees, J.K.H., Gray, R.G., Swirsky, D. & Hayhoe, F.G.J. (1986) Principalresults of the Medical Research Council’s 8th acute myeloidleukaemia trial. Lancet, ii, 1236–1241.
Rogers, S.Y., Bradbury, D., Kozlowski, R. & Russell, N.H. (1994)Evidence for internal autocrine regulation of growth in acutemyeloblastic leukemia cells. Experimental Hematology, 22, 593–598.
Sargent, J.M. & Taylor, C.G. (1989) Appraisal of the MTT-assay as arapid test of chemosensitivity in acute myeloid leukaemia. BritishJournal of Cancer, 60, 206–210.
Schiffer, C.A., Lee, E.J., Tomiyasu, T., Wiernik, P.H. & Testa, J.R. (1989)Prognostic impact of cytogenetic abnormalities in patients with denovo acute nonlymphocytic leukemia. Blood, 73, 263–270.
Smith, K., Houlbrook, S., Greenall, M., Carmichael, J. & Harris, A.L.
(1993) Topoisomerase II� co-amplification with erbB2 in humanprimary breast cancer and breast cancer cell lines: relationship tom-AMSA and mitoxantrone sensitivity. Oncogene, 8, 933–938.
Swirsky, D.M., de Bastos, M., Parish, S.E., Rees, J.K.H. & Hayhoe, F.G.J.(1986) Features affecting outcome during remission induction ofacute myeloid leukaemia in 619 adult patients. British Journal ofHaematology, 64, 435–453.
Tafuri, A. & Andreeff, M. (1990) Kinetic rationale for cytokine-induced recruitment of myeloblastic leukemia followed by cycle-specific chemotherapy. Leukemia, 4, 826–834.
Tafuri, A., Lemoli, R.M., Chen, R., Gulati, S.C., Clarkson, B.D. &Andreeff, M. (1994) Combination of hematopoietic growthfactors containing IL-3 induce acute myeloid cell sensitizationto cycle specific and cycle non-specific drugs. Leukemia, 8,749–757.
te Boekhorst, P.A.W., Lowenberg, B., van Kapel, J., Nooter, K. &Sonneveld, P. (1995) Multidrug resistant cells with high prolif-erative capacity determine response to therapy in acute myeloidleukemia. Leukemia, 9, 1025–1031.
Tewey, K.M., Rowe, T.C., Yang, L., Halligan, B.D. & Liu, L.F. (1984)Adriamycin-induced DNA damage mediated by mammalian DNAtopoisomerase II. Science, 226, 466–468.
Trent, J.M. & Witkowski, C.M. (1987) Clarification of the chromoso-mal assignment of the human P-glycoprotein/MDR-1 gene:possible coincidence with the cystic fibrosis and c-met oncogene.Cancer Genetics and Cytogenetics, 26, 187–189.
Vidriales, M.B., Orfao, A., Lopez-Berges, M.C., Gonzalez, M., Lopez-Macedo, A., Ciudad, J., Lopez, A., Garcıa, M.A., Hernandez, J.H.,Borrego, D. & San Miguel, J.F. (1995) Prognostic value of S-phase cells in AML patients. British Journal of Haematology, 89,342–348.
Wattel, E., Preudhomme, C., Hecquet, B., Vanrumbeke, M., Quesnel,B., Dervite, I., Morel, P. & Fenaux, P. (1994) p53 mutations areassociated with resistance to chemotherapy and short survival inhematological malignancies. Blood, 84, 3148–3157.
Williams, G.T., Smith, C.A., Spooncer, E., Dexter, T.M. & Taylor, D.R.(1990) Haemopoietic colony stimulating factors promote cellsurvival by suppressing apoptosis. Nature, 343, 76–79.
Yates, J., Glidewell, O., Wiernik, P., Robert Cooper, M., Steinberg, D.,Dosik, H., Levy, R., Hoagland, C., Henry, P., Gottlieb, A., Cornell, C.,Berenberg, J., Hutchison, J.L., Raich, P., Nissen, N., Ellison, R.R.,Frelick, R., Watson James, G., Falkson, G., Silver, R.T., Haurani, F.,Green, M., Henderson, E., Leone, L. & Holland J.F. (1982) Cytosinearabinoside with daunorubicin or adriamycin for therapy of acutemyelocytic leukemia: a CALGB study. Blood, 60, 454–462.
Yonish-Rouach, E., Resnitzky, D., Lotem, J., Sachs, L., Kimchi, A. &Oren, M. (1991) Wild-type p53 induces apoptosis of myeloidleukaemic cells that is inhibited by interleukin-6. Nature, 352,345–347.
Young, D.C. & Griffin, J.D. (1986) Autocrine secretion of GM-CSF inacute myeloblastic leukemia. Blood, 68, 1178–1181.
Yunis, J.J., Brunning, R.D., Howe, R.B. & Lobell, M. (1984) Highresolution chromosomes as an independent prognostic indicator inadult acute nonlymphocytic leukemia. New England Journal ofMedicine, 311, 812–818.