redacted cto recall policy.doc.tif.pdf - whatdotheyknow
TRANSCRIPT
Camden and Islingto nN H S Foundation Trus t
Camden and Islington NHS Foundation Trus tLondon Boroughs of Camden and Islington Social Services Departments
London Ambulance ServiceMetropolitan Police in Camden and Islingto n
COMMUNITY TREATMENT ORDE R(CTO)
MENTAL HEALTH ACT 2007
RECALL POLICY
ACTION TO BE TAKENWHEN RECALLING A PATIENT
SUBJECT OF A COMMUNITY TREATMENT ORDE R
July 2008
S` Camden 4lSLlNGTONsupporting partnership in mental
+~ .R aw
MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
POLICY TITLE COMMUN ITY TRE ATME NT ORD E R (CTO) RECALL POLICY
PO L ICY REFERENCE MHA09
PO L ICY CATEGORY Clinica l
RE LEVANT TOAll Foundation Trust Staff and Local Authority Staff working in communityareas .
DATE PUB LISHED October 201 0
IMPLEMENTATION DATE October 201 0
DATE LAST REVIEWED N/A
NEXT REVIEW DATE September 201 0
RESPONSIB LE PERSON L:::=Criminal Justice Consultant
CONTACT DETAI LS 2
ACCOUNTABL E
DIRECTOR
APPROVED BY
Lis Jones , Director of Nursing
Signature and date
Area Mental Health Commi ttee ; Clinical Gove rnance Commi ttee (FoundationTrust) ; Social Servi ces for Camden and Islington .Date :
Date ...Version... Amendments
DOCUMENT HISTORY May 20081_
Dr Koye Odutoye, Natasha Sloman, (Criminal JusticeMEMBERSHIP OF THE 4PO L ICY REVIEW TEAM
Consultant) ,
Camden and Islington Police Liaison Groups ; Borough Management Groups ;
CONSU LTATION CMHTs; Local Authorities, London Ambulance service .
DISTRIBUTION ANDBRIEFING
This document will be circulated to all Directors and Managers who will be required to cascadethe information to members of their teams and to confirm receipt of the procedure and destructionof previous procedures/policies which this supersedes .
It will be available on the Intranet to all staff. Directors and managers will ensure that all staff arebriefed on its contents and on what it means for them .
DO NOT AMEND TH IS DOCUMENTFurther copies of this document can be found on the Care Trust Intranet .
CTO Recall Policy- 5' draft July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
Contents Page
Flowchart 1 - Summary of Action (Initial Recall) iiiFlowchart 2 - Summary of Action (Recall) ivFlowchart 3 - Summary of Action (Post-recall) v
PART I - RECALLING A PATIENT SUBJECT TO A CTO
1 .
2 .
3 .
4 .
5 .
6 .
7 .
8 .
9 .
Introduction
Guiding Principles
Role of Responsible Clinician
Role of Care Co-ordinator
Outcomes and resolutions
Role of the Metropolitan Police
Transport
Monitoring and Audit
Risk Assessment
1
2
3
3
6
6
7
8
9
PART II - APPENDICES AND REFERRALS
List of Appendices and References 1 0
APPENDIX 1
APPENDIX I I
APPENDIX III :
APPENDIX IV:
Extract from Mental Health Act 2007 (Section 17A)
Police Procedure For Patients who are deemed AWOLand Explanato ry Note
Application for Section 135(2) : Guidance Notes
Glossa ry and abbreviations
11
1 3
15
1 9
ii
CTO Recall Policy- 5' draft July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
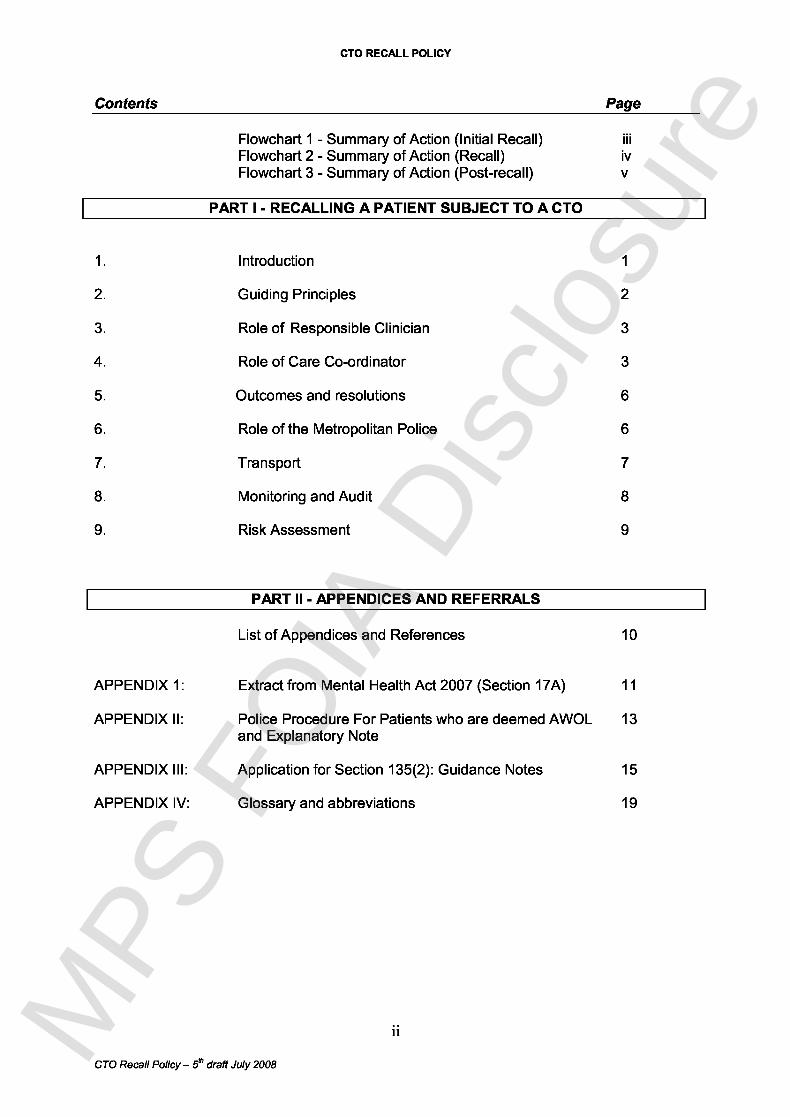
Patient notcompliant withd iscret i ona rycond i t ions
RECALL BEINGCONSIDERED
Patient notcompliant withMandatorycond itions
Not compliantwith condition s
Patient Informal persuasion fails .remains Deadline for section renewa lwell? or SOAD Assessment due .
Discharging CTO notdeemed aDDroDriate .
PatientRelapsing
Compliant withconditions
Informal Patient relapsed. Requires hospitalpersuasion. Incipient relapse. admissionConsider Risk behaviour.varying Meets recal lconditions? criter i aDischarge Refusing hospital admission
CTO if notpracticable.
VoluntaryRECALL DECISION MADE admission
(by RC i n consultat ion with CMHT keyworkerwho co -ord i nates the process . )
Serve Recall Notice
PATIENT CONTACTABLEArrange meeting & serve NoticeDirectly to patient.Recall deemed se rved i mmed iately .
Patient acceptsRecall :Arrange Hospital Bed .Transport to Hospitalin least restrictive waypossible bearing inmind risk assessment .
Patient goes AWOLfollow i ng Recall :FOLLOW HOSPITALAWOL POLICY
CTO Recall Policy - 5' draft July 2008
PATIENT NOT CONTACTABLENon -urgent cases : send Notice by 1S'class post to patient's last known address-Recall takes effect two "working days "after posting .
Urgent cases : Hand-deliver Notice toPatient's last known address-Recalltakes effect the next day after del i very .
Pat i ent does not comply with recall desp i tecont inued i nformal persuas ion . (The timeperiod for persuasion is at the discretion of theRC, ranging from one to several daysdepending on the degree of clinical urgency) .No response/not contactable .
Patient deemed AWOL .Arrange Hospital Bed .FOLLOW CTO RECALL / AWOLFLOWCHART 2
111MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
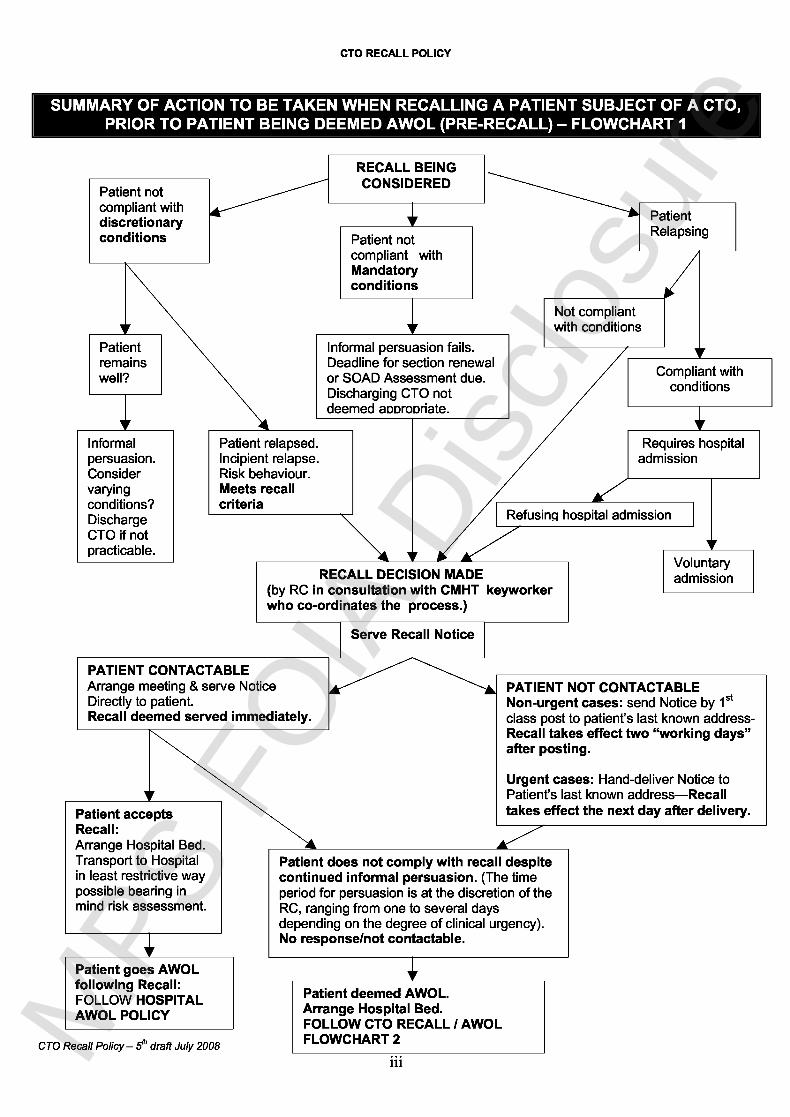
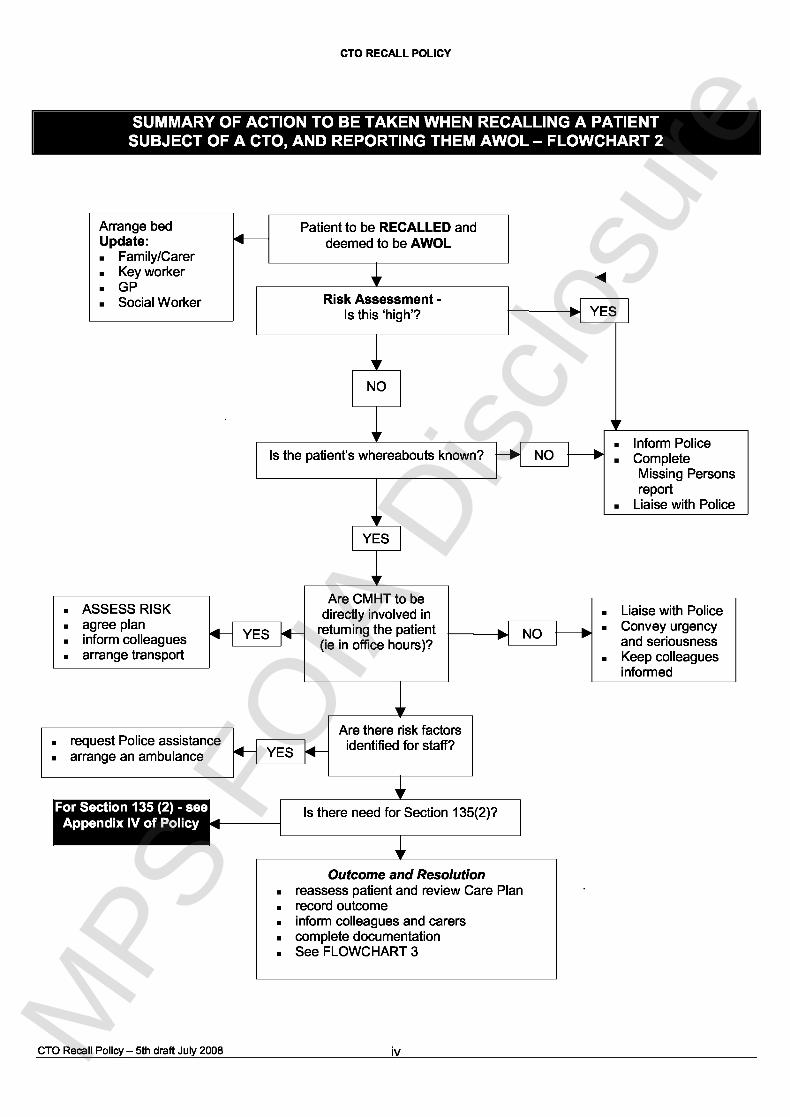
Arrange bedUpdate:
Family/CarerKey worker
. GPSocial Worker
NO
Patient to be RECALLED anddeemed to be AWOL
J
Risk Assessment -Is this `high'? YES
Is the patient's whereabouts known?Inform Police
NO CompleteMissing Person sreport
Liaise with Police
YES
ASSESS RISKagree planinform colleaguesarrange transport
Are CMHT to bedirectly involved in
YES returning the patient(ie in office hours)?
Liaise with PoliceNO Convey urgency
and seriousnessKeep colleaguesinformed
request Police assistancearrange an ambulance
Are there risk factorsYES identified for staff?
Is there need for Section 135(2)?
Outcome and Resolutionreassess patient and review Care Planrecord outcomeinform colleagues and carerscomplete documentationSee FLOWCHART 3
CTO Recall Policy - 5th draft July 2008 ivMPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
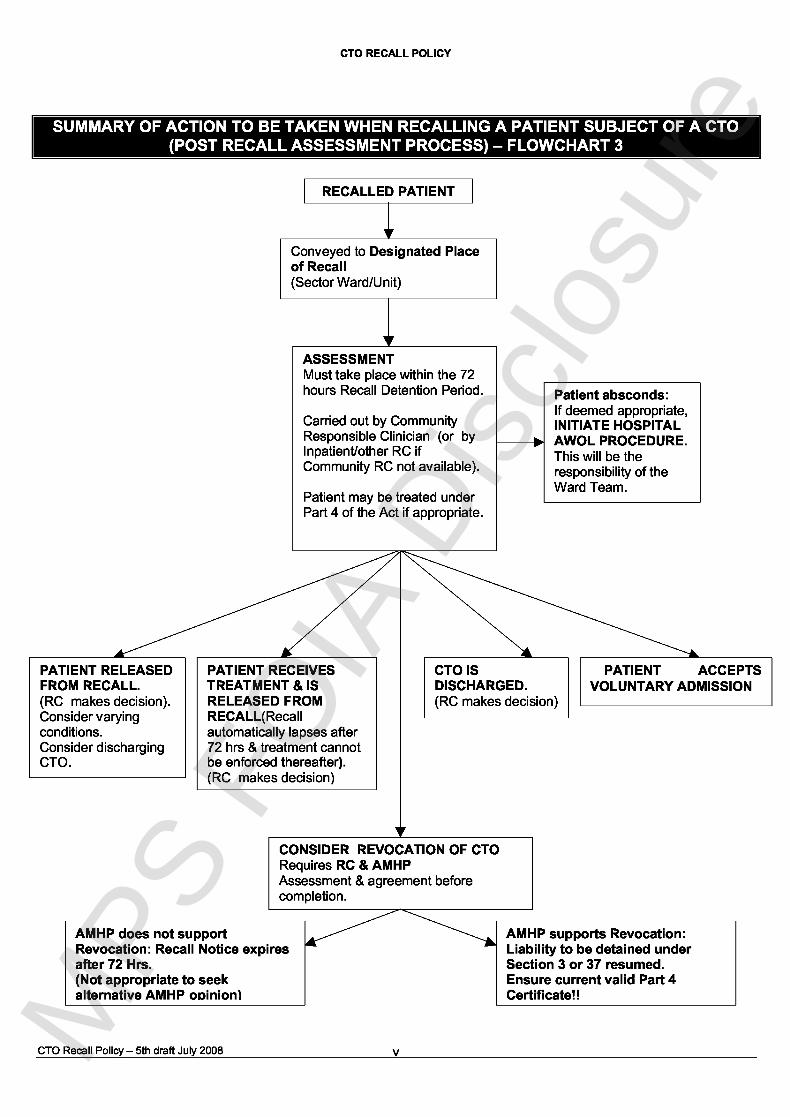
RECALLED PATIENT
Conveyed to Des ignated Placeof Recal l(Sector Ward/Unit)
ASSESSMENTMust take place within the 72hours Recall Detention Period .
Carried out by CommunityResponsible Clinician (or byInpatient/other RC ifCommunity RC not available) .
Patient may be treated underPart 4 of the Act if appropriate .
PATIENT RELEASEDFROM RECALL .(RC makes decision) .Consider varyingconditions .Consider dischargingCTO .
PATIENT RECEIVESTREATMENT & ISRELEASED FROMRECALL(Recallautomatically lapses after72 hrs & treatment cannotbe enforced thereafter) .(RC makes decision)
Patient absconds :If deemed appropriate,INITIATE HOSPITALAWOL PROCEDURE .This will be th eresponsibility of theWard Team.
CTOIS PATIENT ACCEPTSDISCHARGED . VOLUNTARY ADMISSION(RC makes decision )
CONSIDER REVOCATION OF CTORequires RC & AMH PAssessment & agreement beforecompletion .
AMHP does not supportRevocation : Recall Notice expiresafter 72 Hrs .(Not appropriate to seekalternative AMHP opinion)
AMHP supports Revocation :Liability to be detained underSection 3 or 37 resumed .Ensure current valid Part 4Certificate! !
CTO Recall Policy - 5th draft July 2008 vMPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
I PART I - RECALLING A PATIENT SUBJECT OF CTO
1 . INTRODUCTIO N
1 . 1 . This policy gives guidance on action to be taken when a patient , subject of a CTO , isrecalled (Section 17A , Mental Health Act 2007 - see Appendix I)L (Seeseparate/accompanying policy on Supe rv ised Community Treatment : Guidanceand Principles and Appendix II) .
1 . 2 . CTOs will most likely focus on higher risk , "revolving door" patients who are hard toengage and/or noncompliant with treatment so as to put themselves or others at risk .It is likely to include those on current extended Section 17 leave from hospital andthose on Section 25A Community Supervision Orders (which will be superseded) .
1 . 3 . Joint applications from the Responsible Clinician (RC) formerly the ResponsibleMedical Officer (RMO) and Approved Mental Health Professional (AMHP) formerlyApproved Social Worker (ASW) are both required to place a patient on a CTO . Thepatient will already be on a Section 3 (or 37) Hospital Treatment Order prior to beingplaced on a CTO .
1 .4 . In effect when a patient is placed on a CTO , the underlying Section 3 Order is"suspended ", lying inactive unless the CTO is revoked following recall of the patientwhen it is then reactivated .
1 . 5 . CTOs are initially renewable after six months , and yearly thereafter . As long as theCTO is in place , the underlying Section 3/37 Order remains suspended .
1 . 6 . If a patient fails to keep to the Mandato ry or Discretiona ry conditions of the CTO , theResponsible Clinician can decide to recall the patient . Patients who brea kDiscretiona ry Conditions must also fulfil the criteria of being an immediate o rimminent risk to themselves or others to justify recall . Frequent "routine" recall ofpatients who break Discretiona ry Conditions but are otherwise not unwell i sinappropriate . (The RC should reconsider the effectiveness and practicability of CTO sin such cases . )
1 . 7 . A patient must be served wri tten notice of recall to signal the recall process . I fdirectly/personally served to the patient , the notice takes immediate effect . If contactcannot be made with the patient , the written notice is then either hand-delivered o rsent by first-class post to the patient 's last known address . If hand-delivered , thenotice is deemed to be served (and takes effect) on the day after it is delivered-that is ,the day (which does not have to be a working day) beginning immediately afte rmidnight following delive ry . If sent by post , the notice is deemed served on th esecond working day after delive ry .
1 . 8 . A patient who is recalled and who fails to respond to the written notice or refuses toagree to return immediately to hospital is deemed AWOL . Recall proceduresinvolving the police can be commenced ONLY AFTER THE PATIENT HAS BEE NSERVED WRITTEN NOTICE OF RECALL . A discretiona ry time period (ranging fro mone to several days) may be allowed (at the RC 's discretion) for the patient torespond / comply with the Recall Directive before the recalled patient is deeme deffectively AWOL . (This time period may not apply if the situation is more urgent . )This means that the police will be notified only after the patient has been directl ygiven the notice (or it has been delivered to their address) and has failed to mak e
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
contact/failed to agree to return to hospital voluntarily within an agreed time period . Itis at this point that he/she is judged to be AWOL .
1 . 9 . Following the recall process , the Responsible Clinician (RC) has 72 hours with whichto assess the patient , leading to one of the following :• release of the patient (with , perhaps a review/revision of the agreed conditions) ;• revocation of the CTO and hospitalisation under the underlying section ;• treatment release of the patient ; or• complete discharge of the CTO/underlying section order .
1 . 10 . This policy describes best practice in responding to these situations so as to ensurethe safe return of patients to hospital . It describes the role and responsibilities ofeach se rv ice potentially involved in locating and returning patients to hospital . It hasbeen made as comprehensive as possible , but recognises that it cannot addres seve ry eventuality and that the needs of individual patients and the judgement an dexperience of professionals will influence the application of the policy . The policy wil lbe amended and revised in the light of experience .
1 .11 . This policy will form the basis of a joint working agreement between :• Camden and Islington NHS Foundation Trus t• Islington Social Services• Camden Social Service s• Metropolitan Police Borough Command Units (BCO) for Camden and Islingto n• London Ambulance Servic e
2. GUIDING PR IN CI PLES
2 . 1 Vulnerable patients , subject of CTOs , who are recalled may be at risk .
2 .2 Patients , subject of CTOs , are recalled to health and social services already involve din their care . Therefore the people best placed to respond to the needs of patient swill primarily be in these agencies , who will have a shared responsibility with th epolice for locating and returning patients to hospital . The Care Co-ordinator (or othe rteam member co-ordinating the recall process) must identify and book a bedbefore seeking police involvement . The bed will usually be in the relevant loca lmental health Inpatient unit (preferably on the relevant sector ward) but may be i nanother unit if the patient is believed to be outside the catchment area .
2 .3 The Metropolitan Police will assist in locating and returning patients, subject of CTOs ,who are recalled to hospital when there is genuine and serious concern that th eperson is an immediate risk to themselves or to others . The police will also routinelyassist in locating and returning those patients who break Mandatory Cond i t ions(and who are deemed AWOL) whether or not there are serious risk concerns . Thismay be done on a less urgent basis if there are no clinical/risk concerns .
2 . 4 These patients need to return to hospital as soon as possible in order that their careand treatment can continue , and this procedure needs to be undertaken with duerespect to their safety and dignity , as will as the safety and well being of carers andstaff .
2 .5 In appropriate cases , (ie those with significant risk to others and where the publicinterest outweighs the confidentiality imperative) , consideration should be given toinforming the Police when a patient is made subject of a CTO , for inclusion on th e
2
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
CRIMINT system . This information sharing could be helpful if a patient comes intocontact with the Police and the situation the Police encounter indicates a relapse /deterioration in mental health . It may also help facilitate a faster response . However ,the decision to share confidential information in this way will need to be carefullyconsidered on an individual case by case basis . For this purpose the Police can becontacted on the following email addresses :
6 or Camden ; and7 -for Islington .
2 .6 The agreed place for assessment of Recalled patients in Camden and Islington willbe the patient 's relevant sector Ward (or , if there is no bed available on the sectorward , another ward in the local unit) . However , patients may be recalled to otherwards within the trust as a last resort if there are bed shortages .
3. ROLE OF RESPONSIBLE CLINICIAN (RC)
3 . 1 A patient , subject of a CTO , may be recalled to hospital if their responsible cliniciandecides that they need to receive medical treatment for their mental disorder in ahospital and that , if they were not recalled to hospital for treatment , there would be arisk of harm to the patient ' s health or safety , or to other people .
3 . 2 There is also a power to recall a patient to hospital if they fail to comply with one ofthe mandato ry conditions of the order .
3 . 3 The RC may recall a patient by giving them written notice of recall using Form CT03 .A copy of the form must be sent to the managers of the hospital , the RC must also tellthose managers the name and address of the Responsible Hospital (RH) .
3 .4 The patient may be recalled to any hospital , not just the Responsible Hospital (RH) .In practice , a patient should not be recalled to any hospital unless it has bee nestablished that the target hospital can accept them - hospital managers are notobliged to accept patients just because a RC has issued a recall notice . In practice ,the Responsible Clinician will delegate the responsibility the securing of a bed and th eco-ordination of the recall process to the Care Co-ordinator (or other relevant tea mmember eg : the CMHT "Duty /Intake " team) .
3 . 5 A patient may be recalled even if they are already in hospital at the time . This couldhappen , for example , if a patient attends hospital either voluntarily or to comply with acondition of the CTO , but then refuses to accept the treatment the responsibl eclinician thinks is needed . If the patient , or someone else , would be at risk if thepatient does not have that treatment , the patient could be formally recalled to allowthe treatment to be given without the patient's consent .
4 . ROLE OF CARE CO -ORDINATOR
4 . 1 Care Co-ordinator under the Care Programme Approach (CPA) may come from arange of disciplines and settings . Most Care Co-ordinators are members of a CMHT .They may also be members of staff from residential se ttings in both the statuto ry andnon-statuto ry sector . In practice , patients subject to a CTO will usually have their car emanaged by a community mental health team (CMHT) under the Enhan ced CPAprocess . They will therefore have CMHT Care Co-ordinators . It is the responsibility o f
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
4 .2
the CMHT Care Co-ordinator to lead and co-ordinate action required to locate andreturn a patient , subject of a CTO , who has been recalled to a ward .
The Care Co-ordinator has a responsibility to assist in locating and returning thepatient to the hospital with due regard to staff safety and the well being of the patient .
4 .3 In the absence of the Care Co-ordinator , responsibility lies with the Team Manager ofthe Community Mental Health Team and to delegate responsibilities related to thisaction to other named team members .
4 . 4 Where appropriate and with due regard to local Health and Safety policies , the CareCo-ordinator will visit the patient at home or any other known location with the aim ofencouraging the patient to return to the ward . The patient should be conveyed tohospital in the least restrictive manner possible . If appropriate , the patient may beaccompanied by the Care Co-ordinator or a family member , carer or friend .
4 .5 Risk assessments will have been carried out on all patients in accordance with thecurrent Risk Assessment and Management Policy and the CPA Operational Policy .Patient care plans will reflect the level of risk identified for each individual .
4 .6
4 .7
4 .8
4 .9
Establish the last time that the patient was seen .
Scrutinise the care plan and other relevant documentation for an indication as to thepatient's whereabouts .
Contact the patient 's residence (if on the telephone) to attempt to establish contact .
If contact is not made at the patient 's residence then contact the identified relative ,carer or friend to whom they may have gone or who may know their whereabouts .
4 . 10 The Care Co-ordinator will ensure that there is a clear timescale to the recall process ,particularly with regard to when any Recall Notice takes effect and will also co-ordinate the delive ry of the Recall Notice to the patient .
4 . 11 Once it has been established that the patient has been recalled , and is considered tobe AWOL , the Care Co-ordinator will , in liaison with the RC , assess and determin ethe level of risk related to the patient . The degree of urgency in locating and returnin gthe patient to hospital will be communicated to other agencies involved . This RiskAssessment will take into account previous assessment of risk and managemen tplans , as well as the following specific factors relating to the person AWOL :
• any active symptoms which indicate an increased risk to self ;• risk to others ;• alcohol abuse ;• drug abuse ;• involvement in any incidents /unusual behaviour prior to recall ;• any family or social crises / events which might have bearing on their
whereabouts ;• age or physical condition which may increase risk ; and• details of whether they have been AWOL before including :
o the outcome ;o whether they come to any harm ;o where were they found ;o how did they return to the hospital ; and
4
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
o who was involved .
4 . 12 The above information will determine whether the person is low , medium or high ris kand will assist the Police when the missing person notification is made . There is aprofessional obligation to ensure that police are provided with relevant information a sappropriate where required in these cases . In high risk cases the Police should beinformed immediately , in medium and low risk cases this may be delayed . In additio nto an assessment of risk the Police will need the following information for thei rcomputerised Merlin system :
• name ;• date of birth ;• address and telephone number;• status under the Mental Health Act and expi ry date of Section ;• name and contact number of others involved , e . g . Care Co-ordinator , RC , GP ;
and• an accurate , updated physical description .
4 . 13 The ability of the Police to trace the patient may depend on this . The Police will alsoneed to know what action has already been undertaken to locate the patient .
4 . 14 The Care Co-ordinator must pre-confirm the place of Recall (ie ward bed) andprovide the police with the ward /unit details .
4 . 15 Police involvement in locating and assisting in returning the patient to the ward will bedependent on :
level of risk and urgency;risk of violence, self harm or harm to others ; andfailure of the patient to comply with Mandatory Cond it ions (ie to makethemselves available for medical examination when needed to for considerationof extending the CTO or, if necessary, to allow a Second Opinion AssessmentDoctor to provide a Part 4A certificate authorising treatment . )
NB : See APPEND IX II for the Police response in Cam den
4 . 16 The nearest relative is to be informed that the patient is now considered AWOL(statuto ry requirement of the Mental Health Act 1983 in relation to detained patients) .
4 . 17 Members of the family , friends or significant others are to be informed as appropriate ,with due regard to the patients ' previously expressed wishes /Advanced Directive .
4 . 18 Other agencies directly involved in the care of the patient , including the GP are to beinformed .
4 .19 Once the location of the patient is known, but the patient is refusing to a llow access,an app l ication under Section 135(2) of the Mental Health Act 1983 may be made(APPENDIX III ) .
4 .20 It is the Care Co -ordinator's responsibility to help ensure that the patient 'shome is locked and secured before they leave for hospital . If the police havehad to force entry to secure access to the patient , the Care Co-ordinator willalso need to ensure that appropr iate repa i rs are completed .
4 .21 When the patient is located out of area there may be occasions when an AWOLpatient has left the local area and it will not be possible for staff to undertake visits to
5
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
locate and return the patient . It is the responsibility of the Care Co-ordinator to liaisewith services local to the patient , and negotiate their assistance in locating andreturning the patient . When a patient is known to be at a particular address , contactwill be made with the local Social Services and the Police . They will agree a plan toreturn the patient. An ambulance must be used to transfer the patient to hospital .
4 .22 If there is a significant delay in arranging the transfer of the patient , it may benecessary to arrange for the patient to be seen and assessed overnight in a localmental health facility . After the patient has been assessed overnight it may bepossible to transfer the patient back by taxi , if their mental state is assessed as beingsufficiently stable .
4 .23 If the patient has been apprehended by the police in another area , the Care Co-ordinator will take responsibility for organising the transfer of the patient to thehospital . Appropriate statuto ry transfer forms will need to be filled .
4 . 24 When the patient is to be transferred directly from a police station , this must be byambulance .
5 . OUTCOMES AND RESOLUTION S
5 . 1 Once the patient 's whereabouts has become known and there has been a resolutio nof the AWOL situation , the following actions will be undertaken by the CareCo-ordinator, or delegated to another named member of staff on duty .
All relatives , carers , the GP and other agencies contacted during the recallprocess should be informed of the outcome .It is particularly important to inform the Poli ce as soon as possible as they maybe car ry ing out numerous lines of inqui ry including the interviewing of peopleknown to the patient .Details of the recall and any known factors which precipitated the recall must berecorded on the AWOL monitoring form and in medical and nursing records ,including the time contact was made with the next of kin , family, friends and otheragencies .
6 . ROLE OF THE METROPOLITAN POLIC E
6 . 1 The prima ry responsibility for locating and returning patients to the ward lies with theCare Co-ordinator.
6 . 2 Police intervention will be limited to those occasions where there is a risk of a breachof the peace involving violence or a threat of violence , or there may be a danger tothe public, or where a patient may be an immediate danger to themselves or wherethe patient has breached CTO Mandato ry Conditions and there is no realistic" informal" way of gett ing them to comply with the Recall Notice .
6 .3 The Police will attempt to locate an AWOL patient whose whereabouts is not known .If a recalled patient is reported missing to the local Police , the Police will grade theenqui ry according to the Risk Assessment . This will be done on the computerisedMerlin System . The grading will be either : high , medium or low . Enquiries will beinitiated which could include :
6
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
6 .4
• information passed to local officers and / or surrounding poli ce boroughs ;• circulation on the Police National Computer ;• visits to locations where intelligence suggests missing patient might be /has
been previously ; and• enquiries with relatives /friends .
The amount of resources given to the enqui ry will depend on the risk assessment andassociated grading .
6 .5 If a patient , subject of a CTO and who has been recalled , is found in a public pla ceand is considered to be presenting a risk to themselves or the public , the patient willbe transferred to the hospital by the Police under the provisions of Section 18 of theMental Health Act 1983 .
6 . 6 If the location of the patient is known , and steps are being taken to transfer the patientto hospital , the Police will respond to requests for assistance made by the Care Co-ordinator or delegated person .
6 .7 Police assistance shouldimmediate danger to thi sfor physical restraint .
be requested if there is evidence to suggest that there ispatient or others , a potential threat of violence or the need
6 .8 When requesting Police assistance , full information should be given of any potentialrisk factors which may be relevant to the safety of the patient , the public , or anyoneelse , including the Police , involved in the process - e . g . the possible involvement ofweapons or substance misuse . Sufficient notice should be given to the Police inorder that resources can be deployed effectively .
6 .9 Attending police officers will take the following actions .
• Consult and co-operate with the Care Co-ordinator , or other professionalspresent, in respect of requests over the method and timing of assistance .
• Preserve the peace and ensure public safety , assisting if the need for use ofrestraint may reasonably be anticipated .
• Help to effect the admission to hospital in a peaceful way , even by simply beingthere .
• Accompany the patient in the ambulance where judged necessa ry to preservethe peace and ensure public safety .
• Consult with other professionals involved to decide whether in extremecircumstances the Police van is the most appropriate means to transport thepatient to hospital .
• Where a ttending police officers assist in conveying the patient to the place ofRecall (hospital ward) , their input will cease at the point when the patient is safelyhanded over to ward staff .
6 . 10 When access is denied , the Police will assist in the execution of a warrant issuedunder Section 135(2) of the Mental Health Act 1983 (APPENDIX III) .
NB : Consideration should be given throughout to any Advanced Directive .
7
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
7. TRANSPORT
7 . 1 An ambulance is usually the preferred means of transfer to hospital . However , theremay be occasions when other forms of transport will be appropriate and expedient .Staff should not use their own transport . Judgements regarding transport should beclinically led .
7 .2 There may be circumstances when alternative transport arrangements may beacceptable if the patient is agreeable to transfer to hospital and there is no identifiedrisk either to members of staff or the patient .
7 . 3 Transfer in a police van should only be considered in ve ry exceptional circumstanceswhen restraint is required or the threat of violence is high .
7 .4 If the patient is sedated , an ambulance will be the only form of transport to be used .
7 . 5 To arrange an ambulance through the London Ambulance Service :
0 Ring 020 7827 4555 or 020 7827 4525 .
7 . 6 The following information will be required :
• name and address of the patient ;• the name of the Responsible Clinician / GP or AMHP / ASW ;• rendezvous point with other professionals involved ;• name and contact number for other professionals involved ;• an indication of the patient ' s condition (e . g . whether sedated , attitude to
readmission) ;• time of arrival of the ambulance ;• where the patient will be going ; and• whether there will be Police involvement .
7 .7 To arrange a taxi , contact the Administration Services Manager . The followinginformation will be required :
• name , status and place of work of the person requesting the taxi ;• address from which the member of staff and patient are to be collected ;• destination ; and• the expected time of arrival of the taxi to make the collection .
NB : The name of the patient must not be disclosed to the taxi firm .
7 . 8 Professionals involved must be confident that transferring the patient to hospital bytaxi does not pose a risk to the patient or to anyone else involved .
7 .9 Two members of staff should accompany the patient
8
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
8 . MONITORING AND AUDI T
8 . 1 The Camden and the Islington Police Liaison Groups will monitor the effectiveness ofservices responding to the needs of patients , subject of CTOs who have beenrecalled , and will review the impact of this policy on the welfare of those patients andon the use of limited resources .
8 . 2 The following factors will be monitored :• date and time of recall incidents ;• status of the patient ;• action taken monitored against policy guidelines ;• outcomes ; and• equality and diversity impact .
9 . RISK ASSESSMEN T
9 . 1 All decisions and the rationale for them must be recorded in the patient 's notes andcommunicated to other workers involved in the patient 's care , including the GP .
9 .2 When there is a resolution of events and decisions made about the futuremanagement of this patient , these must be communicated to other workers involvedin the patient's care , including the GP .
9 .3 If after assessing the level of risk , the Care Co-ordinator feels that this patient isvulnerable and at significant risk to themselves or to others , then the full proceduredetailed above should be implemented .
9
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
I PART II - APPENDICES AND REFEREN CES
APPENDIX I Extract from Mental health Act 2007 (Section 17A)
APPENDIX II Police Procedure For Patients who are deemed AWOL andExplanatory Note
APPENDIX III Application for Section 135(2) : Guidance Notes
APPENDIX IV Glossary and abbreviations
10
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL POLICY
APPENDIX I
Extract from Mental Health Act 2007 (Section 17A)
(1 ) The responsible clinician may by order in writing discharge a detained patient from hospital subject tohis being liable to recall in accordan ce with section 17E [below] .
(2 ) A detained patient is a patient who is liable to be detained in a hospital in pursuance of an application foradmission for treatment .
(3) An order under subsection (1) above is referred to in this Act as a "community treatment order" .
(4 ) The respon s ible clinician may not make a community treatmen t o rder unless-
(a) in his opinion, the relevant criteria are met ; and
(b) an approved mental health professional states in writing-
(i) that he agrees with that opinion ; and
(ii) that it is appropriate to make the order .
( 5 ) The relevan t criteria are-
(a) the patient is suffering from mental disorder of a nature or degree which makes it appropriate forhim to receive medical treatment ;
(b) it is necessary for his health or safety or for the protection of other persons that he shouldreceive such treatment;
(c) subject to his being liable to be recalled as mentioned in paragraph (d) below, such treatmentcan be provided without his continuing to be detained in a hospital ;
(d) it is necessary that the responsible clinician should be able to exercise the power under section17E(1) [below] to recall the patient to hospital ; and
(e) appropriate medical treatment is available for him .
(6 ) In determining whether the criterion in subsection (5 ) (d ) above is met, the responsible clinician shall , inpa rticular, consider, having regard to the patient ' s history of mental disorder and any other relevantfactors , what risk there would be of a deterioration of the patient 's condition if he were not detained in ahospital (as a result , for example , of his refusing or neglecting to receive the medical treatment herequires for his mental disorder) .
( 7 ) In this Act-
" community patient' means a patient in respect of whom a community treatment order is in force ;
"the community treatment order", in relation to such a patient , means the community treatmentorder in force in respect of him ; and
"the responsible hospital", in relation to such a patient , means the hospital in which he was liable tobe detained immediately before the community treatment order was made , subject to section 19A[below] .
1 1
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e

CTO RECALL PO LICY
12
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL POLICY
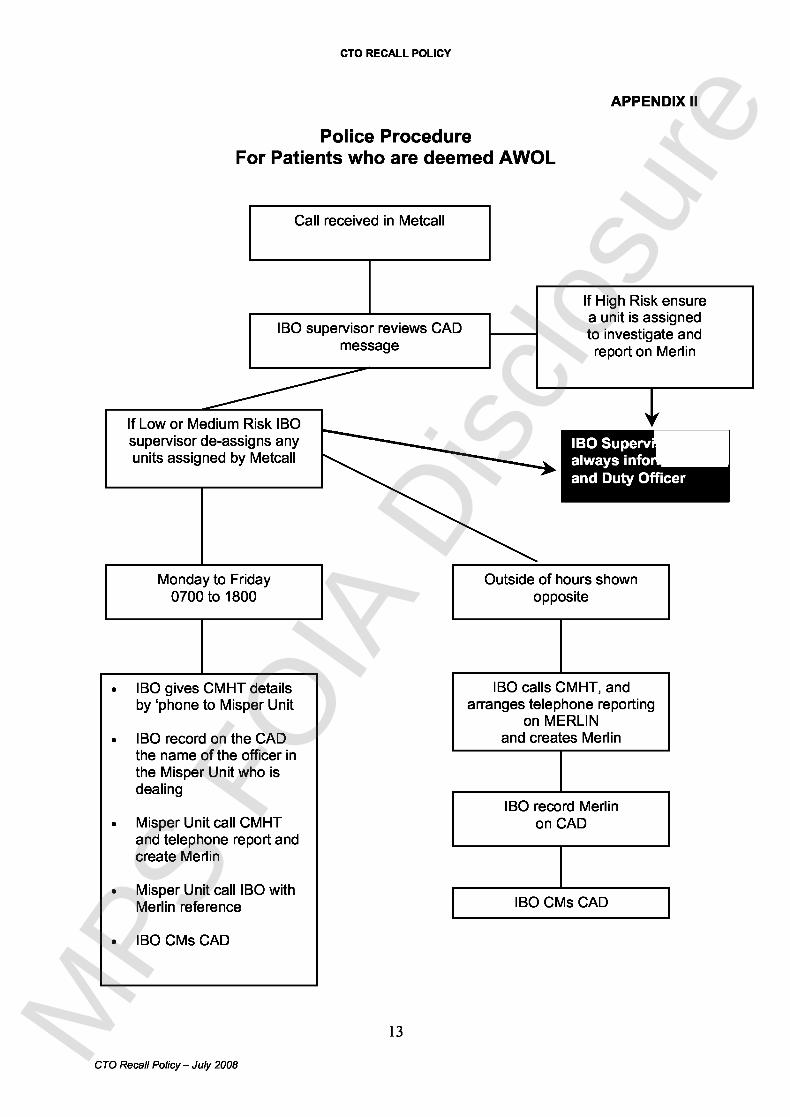
APPEND IX I I
Police ProcedureFor Patients who are deemed AWO L
Call received in Metcal l
IBO supervisor reviews CADmessage
If Low or Medium Risk IBOsupervisor de-assigns anyunits assigned by Metcal l
Monday to Friday0700 to 180 0
IBO gives CMHT detailsby ` phone to Misper Unit
IBO record on the CADthe name of the officer inthe Misper Unit who isdealing
Misper Unit call CMHTand telephone report andcreate Merli n
Misper Unit call IBO withMerlin reference
IBO CMs CAD
13
If High Risk ensurea unit is assignedto investigate an d
report on Merli n
IBO Superv=always info
and Duty Office r
Outside of hours shownopposite
IBO calls CMHT , andarranges telephone reporting
on MERLINand creates Merlin
IBO record Merlinon CAD
IBO CMs CAD
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
Camden and Islingto nNH S Foundation Trus t
Reporting Patients , who are deemed AWOL - Explanatory Note
The Camden and the Islington Police have a procedure for dealing with patients who aredeemed AWOL . This will ensure that delays caused by the MPS Metcall system procedures ,which require the attendance of police to all such calls , will be prevented . There will be agreater use of telephone reporting , with safeguards for out of hours cases .
This will not greatly affect the service the police are giving , it just means in the majority ofcases staff will get a telephone call instead of a police officer in person . The important issueis that staff must leave a "STAFFED " telephone number that will be answered when the IBOcall back .
An algorithm of the police procedure is attached for information and an explanation ofabbreviations/terminology is given below .
Abbreviations/terminology
CAD - (Computer Aided Despatch ) - the computerised messaging system used by thepolice to log and respond to calls for assistan ce .
CM - CAD terminology for `completed message ' .
IBO - (Integrated Borough Operations ) - the local borough `communications room ' .
Misper Unit - Police Missing Person Unit
MPS - Metropolitan Police Se rv ice
Merlin - computerised missing person system .
Metcall - A call centre system which covers a number of boroughs .
PS - Police Sergeant .
July 200814
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL POLICY
APPEND IX II I
Application for Section 135(2)
Guidance Notes for Camden & Islington Trust Staff
It is possible that there will be occasions when it may be necessa ry, in the interests of thepatient , to gain access by force to the premises where they are known to be . Theseinstances are likely to be rare , but when they occur, will reflect a degree of urgency andconcern which will require prompt and well co-ordinated action on the part of those involvedin the care of the patient . Early notification of the local police authorities is thereforeessential in order to plan a co-ordinated response .
Section 135(2) provides for the issue of a warrant to a po l ice officer to enter premises, usingforce if necessary, for the purposes of retaking a patient who is a l ready liable to bedetained .
Initiating 135(2)
Appl ications for a warrant, using Form M H 72 under Section 135(2) can be made by :
• approved Social Workers• any officer on the staff of the hospita l• by any constab l e• any person authorised in writing by the managers of the hospita l N B : Note that , for CTO
cases, it is the CMHT Care Co -ordinator who is likely to lead this process .
Any member of the Trust staff who may be required to make an app l ication under Section135(2) wi ll require authorisation in writing from the managers of the Trust . H ighburyMagistrates Court have agreed in writing to this procedure .
Prior to the app l ication for a warrant, a risk assessment shou ld be undertaken in consu ltationwith the Responsible C l inician, other medica l staff invo lved, a senior member of the nursingstaff (F Grade or above) and anyone e l se invo lved in the care of the patient . The decision toapp ly for a warrant under Section 135(2) shou l d be made by senior medica l and nursing staffwithin the Trust . App l ications shou l d be made by trained permanent members of staff .
For Trust staff, whether inpatient ward staff or CM HT staff members (for CTO cases), toapp ly for a warrant under Section 135(2) the fo llowing action must be taken :
• Liaise with the Events Office (Camden) / Duties Office (Islington) to inform them of theplan to apply for a warrant and request assistance .
Camden Events Office : 020 8733 6006 / $
• Liaise with relevant ward/local CMHTs to inform them of the plan and request assistanceas necessa ry .
• Contact the Clerk of the Court Magistrates Court to arrange to lay information on oathbefore a Justice of the Peace .
• Obtain from MH72 (Information in Support of an Application for Warrant to enter premisesand remove patient (Section 135(2)) - a supply of which are kept on the wards .
1 5
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
• Form M H 72 to be comp leted giving evidence/reasons to suspect that the criteria issatisfied in respect of the person - the person shou ld be named on the app l ication .
• Obtain written authorisation from Trust managers detai l ing the status of the app l icant,that they are authorised to `take or retake' the patient and the status of the personauthorising .
Within court hours (9.00 am - 4 .00 pm) an officer of the Trust or an Approved Socia l Workermay app ly for the warrant .
Documents to be taken to the Court
The fo llowing documentation is required :
• comp l eted Form M H72 (Supp l ies on the Ward with AWOL Po l icy) ;• obtain a letter of authorisation from, RMO / RC or Care Co-ordinator (a samp le letter is
shown be l ow) and• photo ID / name badge of staff member / UKCC Pin Card .
At the Magistrates Court
At the Court, ID and re levant papers need to be presented to the Clerk of the Court . It maya lso be worth asking the C lerk what exact procedures to fo llow e.g. which court to go to ;where to find the ` l ist caller' who needs to know why the app l icant is there so that the casecan be put on the l ist . The staff member wi ll be required to take the oath in front of amagistrate and may be questioned about the circumstances of the case .
Once the warrant has been issued and obtained
The fo llowing action is necessary :
• return to the hospital/CMHT base ;• liaise with the Police - (obtain a CAD Number for the assignment) - who will execute the
warrant ;• order an ambulance ;• alert and organise relevant workmen (e . g . Locksmiths) ; and• organise two staff members (may be ward staff and Care Co-ordinator) .
1 6
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
I SAMP LE LETTER
STRICTLYPRIVATE & CONFIDENTIA L
6 April 2008
The Justice of the Peace 'Highbu ry Corner Magistrates Court51 Holloway Roa dLondon N 7
TO WHOM IT MAY CONCERN
Re: Joe Public, 5 Station Road, Mayville N19
Detained under Section 3 Mental Health Act 1983Section Expires January 28 199 8
This is to confirm that the bearer of this letter , Josephine Briggs , Registered Mental HealthNurse , Pin Number . . . . . . . . . has authorisation to obtain a warrant to enable a constable toenter premises and retake the above named patient who absconded from Co ffman Ward atthe Psychiatric Ward on December 9 , 1997 .
Thank you for your co-operation in this matter .
Yours sincerely,
A .N . Othe rClinical Se rv ices Manager
Warrants need to be applied for at the Cou rt relevant to the patient's address . There may be specified times whenapplications are accepted e . g . 9 - 11 am . It is wort h checking this before going to cou rt in order to avoid unnecessa ry delays .
17
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL PO LICY
Additional Information
During out of hours , the Police will need to be given sufficient information so that a policeconstable may obtain a warrant from a magistrate .
Prior to removal of a patient under Section 135(2) , a minuted briefing meeting should beorganised between Trust staff , the Police and anyone else involved in this action .
In executing a warrant , the Police are in charge of the situation . Trust staff are there toadvise and assist the Police Officers . The Police at the scene are responsible for the safetyof the patient , staff , members of the public and their own offi cers .
When a patient is removed under Section 135(2) , they should be transferred back to hospitalin an ambulan ce .
Magistrates Court :
Highbu ry Corner Magistrates Court51 Holloway Roa dLondon N 7Tel : 020 7506 314 7
Police Stations :
Islington :Islington Control RoomIslington Police Station2 Tolpuddle Street , N1Tel : 020 7704 1212
18
Camden :Camden Control RoomKentish Town Police Station12A Holmes Road, NW5Tel : 020 7404 121 2
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e
CTO RECALL POLICY
APPENDIX IV
GLOSSARY AND ABBREVIATION S
Health
AMHP
ASW
AWOL
CMHT
CPA
C of P
CTO
MHA
PACE
RC
RH
SCT
SOAD
SpR
s12 docto r
CAD
CM
IBO
PS
Misper Unit
Merlin
Metcall
MPS
Approved Mental Health Professional
Approved Social Worker
Absent without leave
Community Mental Health Team
Care Programme Approac h
Code of Practice to The Mental Health Act 1983
Community Treatment Order
The Mental Health Act 1983
The Police and Criminal Evidence Act 1984
Responsible Clinicia n
Responsible Hospital
Supervised Community Treatment
Second Opinion Approved Doctor
Specialist Registrar in Psychiatry
A doctor approved under The Mental Health Act (section 12) ashaving specialist knowledge of psychiatr y
Police
Computer Aided Despatch - the computerised messaging systemused by the police to log and respond to calls for assistance .
CAD terminology for `completed message ' .
Integrated Borough Operations - the local borough ` communicationsroom ' .
Police Sergeant
Missing Person Unit
Computerised missing person system .
A call centre system which covers a number of boroughs .
Metropolitan Police Service
1 9
CTO Recall Policy - July 2008MPS
FO
IA D
iscl
osur
e