questionnaire pack - whatdotheyknow
TRANSCRIPT
USection 1: Confirmation of Appointment (T0)
UI confirm that I would like an appointment at the Nottingham Gender Clinic
Name (in Capitals):
To register with the clinic we require the following details:
Home telephone: Mobile telephone:
Can we leave a message on your phone? Yes No
Email address:
GP Name:
Surgery Address:
Surgery telephone number:
NHS number (this is a 10 digit number that is available from your GP
Date of Birth
d d m m y y y y
Please tell us of any physical or other special need requirements:
Have you changed your name by Deed Poll or by Statutory Declaration?
Yes □ No
UIf yes:U □ Included
USection 2: Personal Details
1. Age: ………………..
2. Biological Gender □ Male □ Female
3. Ethnic origin: (Please tick the appropriate box)
White Black Caribbean Black African Black Other Indian Pakistani
Bangladeshi Chinese Other Ethnic Group (Please
specify) ……………………………………..
4. Employment status: (Please tick the appropriate box)
Employed full-time Employed part-time Student Volunteer work Housewife/husband
Disabled Unemployed Retired Other (Please specify)
……………………………………..
If in work, please state how many weekly hours undertaken:……..
5. Civil status: (Please tick the appropriate box)
Single, never married Married/Civil partnership Separated / Divorced
Co-habiting / partner Widowed Other (Please specify)
....................................................
6. Do you have any children? □ Yes □ No
If Yes, how many? ………………
Please state their ages …………………………
7. Living situation: (Please tick the appropriate box)
With family of origin Alone Share with non-partner/s With partner only With partner and child/ren With child/ren only Other (Please specify)
………………………………
8. Religion (please specify) ……………………………………………
9. Do you smoke? □ Yes □ No
10. Age when you were first referred to UanyU gender clinic: ...................................
11. Age of coming out ……………….. □ Not applicable
13. Age of transition ………………… □ Not applicable
14. How would you describe your gender identity?
I identify as a man
I identify as a woman
I identify partly as a man, and partly as a woman
I identify neither as a man, nor as a woman
I don’t know what my gender identity is (yet) or I am questioning my gender identity
Other (please specify) ……………………..…….
15. How do you identify yourself?
□ Trans* □ Gender neutral / neutrois
□ Trans □ Non-binary gender
□ Transvestite □ Pangender
□ Transgender □ Bigender
□ Transsexual □ Genderqueer
□ Androgynous □ I don’t know
□ Cisgender (you are content to remain the gender you were assigned at birth)
Other (please specify) ..............................................................................................
16. Current stage of gender programme: (Please tick all that apply))
Assessment period □ In ‘Real Life Experience’/ treatment program
Post-surgery
17. Are you currently using any hormones?
□ yes □ No
If yes: how did you obtain the hormones?
□ Internet □ Friends/family □ From a doctor (Dr Name: ) □ Other……………………………………………..
18. Have you undergone any sex reassignment surgery? (Please tick the appropriate box
Yes (Please give details in the box below) □ No
Type of surgery: Date (month/year):
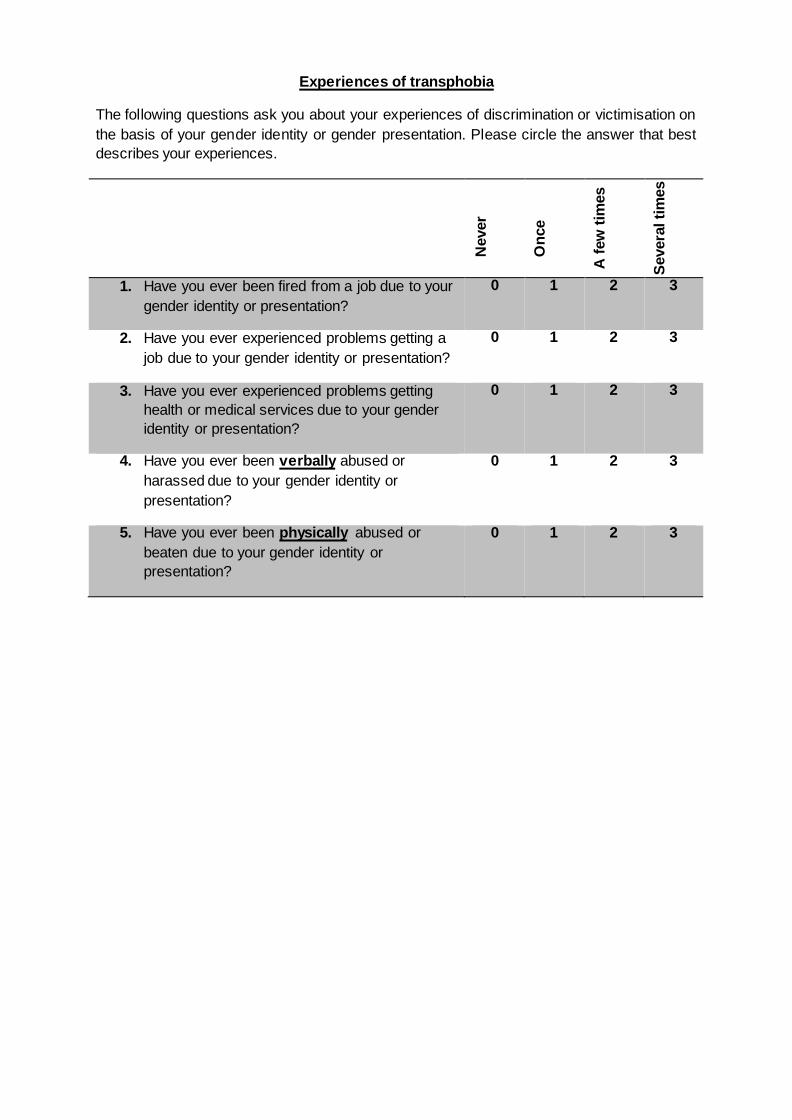
UExperiences of transphobia
The following questions ask you about your experiences of discrimination or victimisation on the basis of your gender identity or gender presentation. Please circle the answer that best describes your experiences.
N
ever
O
nce
A fe
w ti
mes
Seve
ral t
imes
1. Have you ever been fired from a job due to your gender identity or presentation?
0 1 2 3
2. Have you ever experienced problems getting a job due to your gender identity or presentation?
0 1 2 3
3. Have you ever experienced problems getting health or medical services due to your gender identity or presentation?
0 1 2 3
4. Have you ever been UverballyU abused or harassed due to your gender identity or presentation?
0 1 2 3
5. Have you ever been UphysicallyU abused or beaten due to your gender identity or presentation?
0 1 2 3
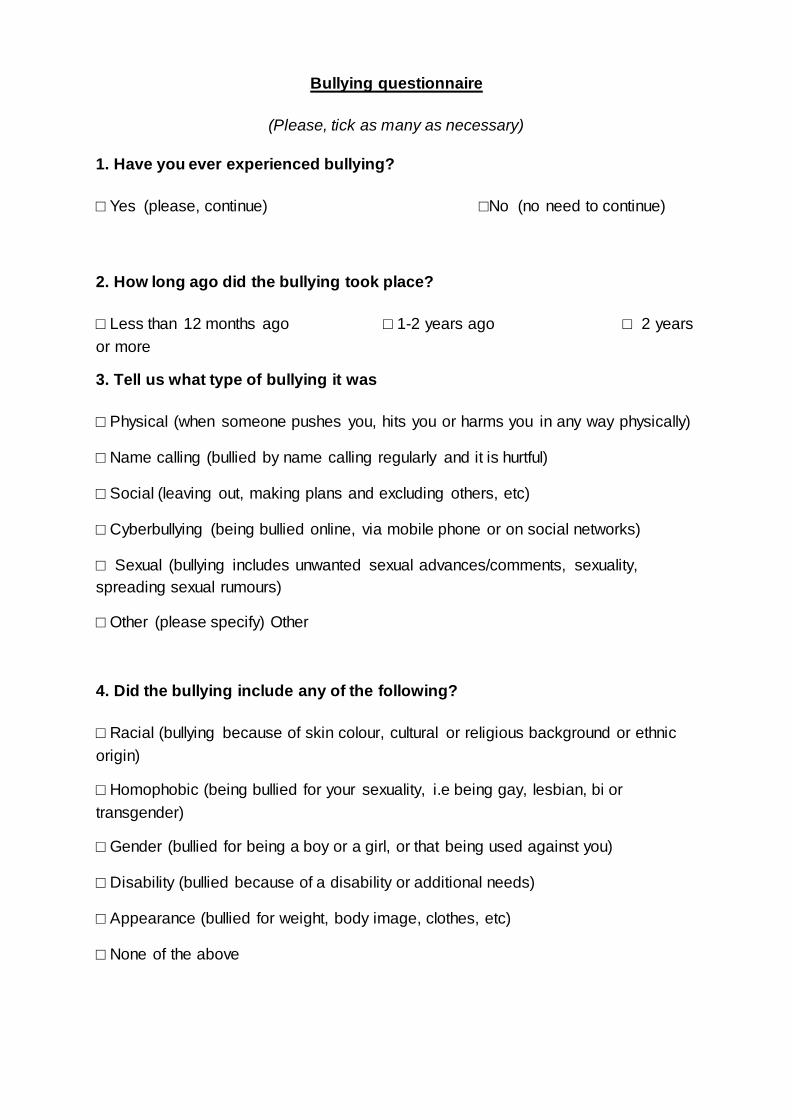
UBullying questionnaire
(Please, tick as many as necessary)
1. Have you ever experienced bullying?
□ Yes (please, continue) □No (no need to continue)
2. How long ago did the bullying took place?
□ Less than 12 months ago □ 1-2 years ago □ 2 years or more
3. Tell us what type of bullying it was
□ Physical (when someone pushes you, hits you or harms you in any way physically)
□ Name calling (bullied by name calling regularly and it is hurtful)
□ Social (leaving out, making plans and excluding others, etc)
□ Cyberbullying (being bullied online, via mobile phone or on social networks)
□ Sexual (bullying includes unwanted sexual advances/comments, sexuality, spreading sexual rumours)
□ Other (please specify) Other
4. Did the bullying include any of the following?
□ Racial (bullying because of skin colour, cultural or religious background or ethnic origin)
□ Homophobic (being bullied for your sexuality, i.e being gay, lesbian, bi or transgender)
□ Gender (bullied for being a boy or a girl, or that being used against you)
□ Disability (bullied because of a disability or additional needs)
□ Appearance (bullied for weight, body image, clothes, etc)
□ None of the above
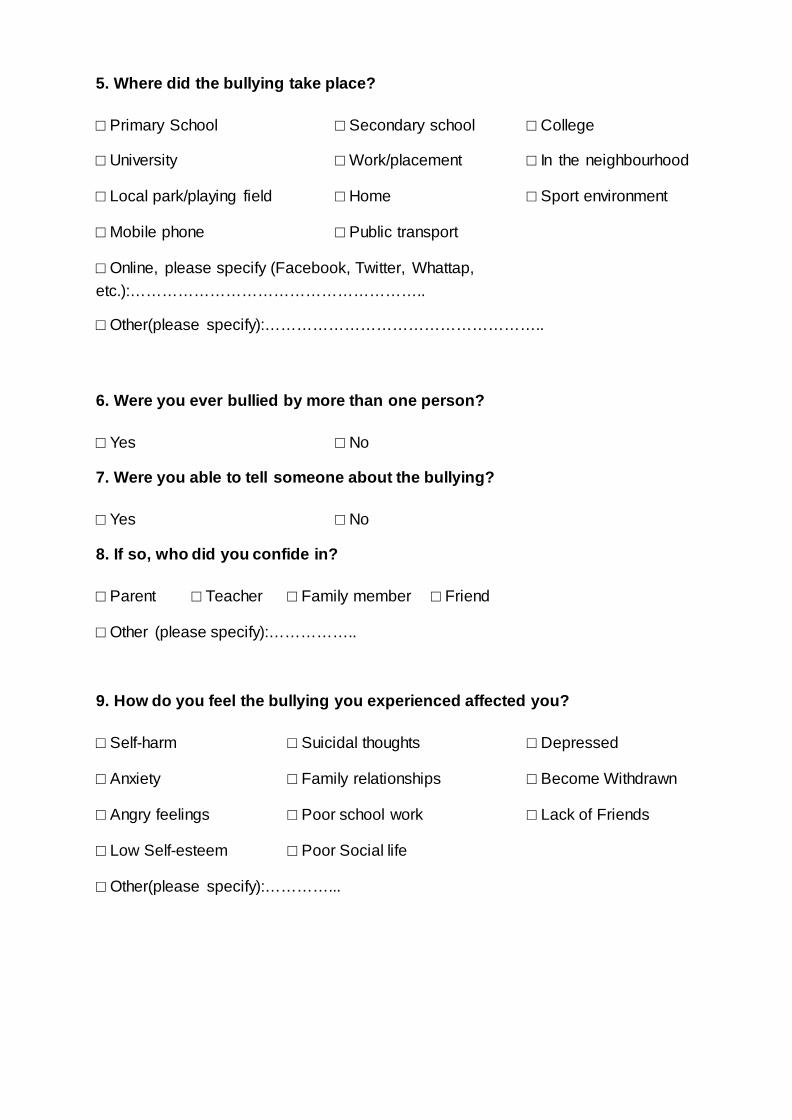
5. Where did the bullying take place?
□ Primary School □ Secondary school □ College
□ University □ Work/placement □ In the neighbourhood
□ Local park/playing field □ Home □ Sport environment
□ Mobile phone □ Public transport
□ Online, please specify (Facebook, Twitter, Whattap, etc.):………………………………………………..
□ Other(please specify):……………………………………………..
6. Were you ever bullied by more than one person?
□ Yes □ No
7. Were you able to tell someone about the bullying?
□ Yes □ No
8. If so, who did you confide in?
□ Parent □ Teacher □ Family member □ Friend
□ Other (please specify):……………..
9. How do you feel the bullying you experienced affected you?
□ Self-harm □ Suicidal thoughts □ Depressed
□ Anxiety □ Family relationships □ Become Withdrawn
□ Angry feelings □ Poor school work □ Lack of Friends
□ Low Self-esteem □ Poor Social life
□ Other(please specify):…………...
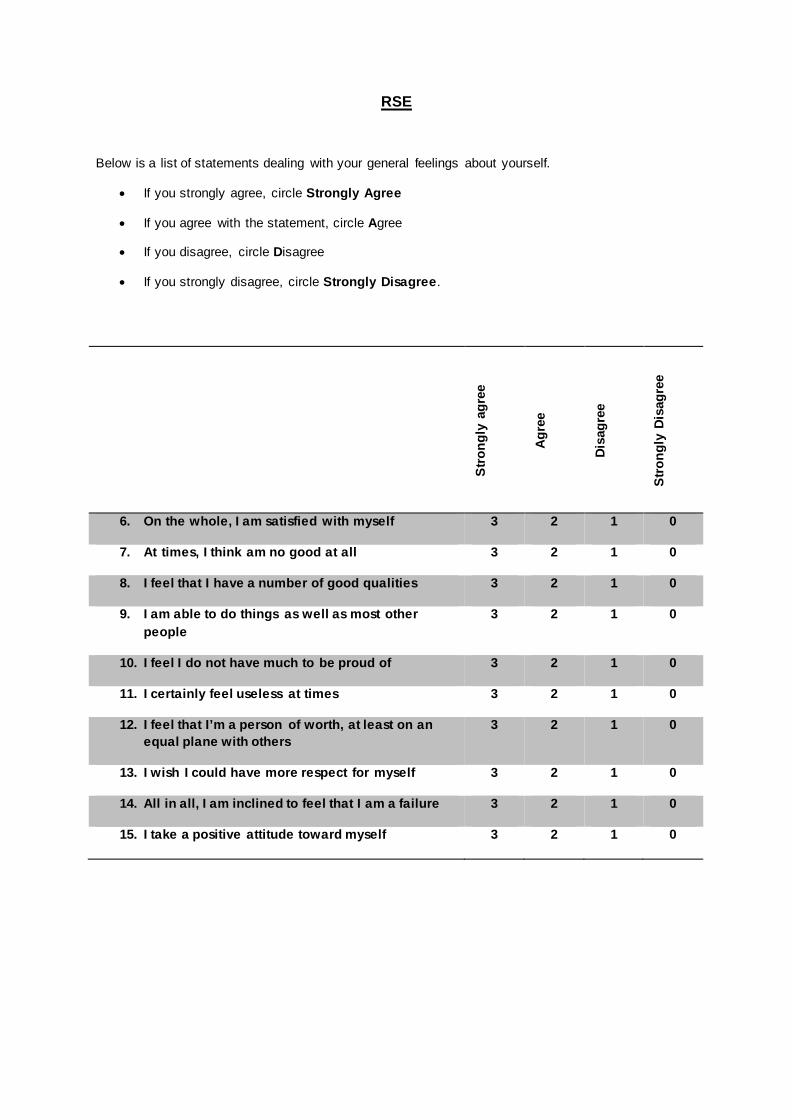
URSE
Below is a list of statements dealing with your general feelings about yourself.
• If you strongly agree, circle Strongly Agree
• If you agree with the statement, circle Agree
• If you disagree, circle Disagree
• If you strongly disagree, circle Strongly Disagree.
Stro
ngly
agr
ee
Agre
e
Disa
gree
Stro
ngly
Dis
agre
e
6. On the whole, I am satisfied with myself 3 2 1 0
7. At times, I think am no good at all 3 2 1 0
8. I feel that I have a number of good qualities 3 2 1 0
9. I am able to do things as well as most other people
3 2 1 0
10. I feel I do not have much to be proud of 3 2 1 0
11. I certainly feel useless at times 3 2 1 0
12. I feel that I’m a person of worth, at least on an equal plane with others
3 2 1 0
13. I wish I could have more respect for myself 3 2 1 0
14. All in all, I am inclined to feel that I am a failure 3 2 1 0
15. I take a positive attitude toward myself 3 2 1 0
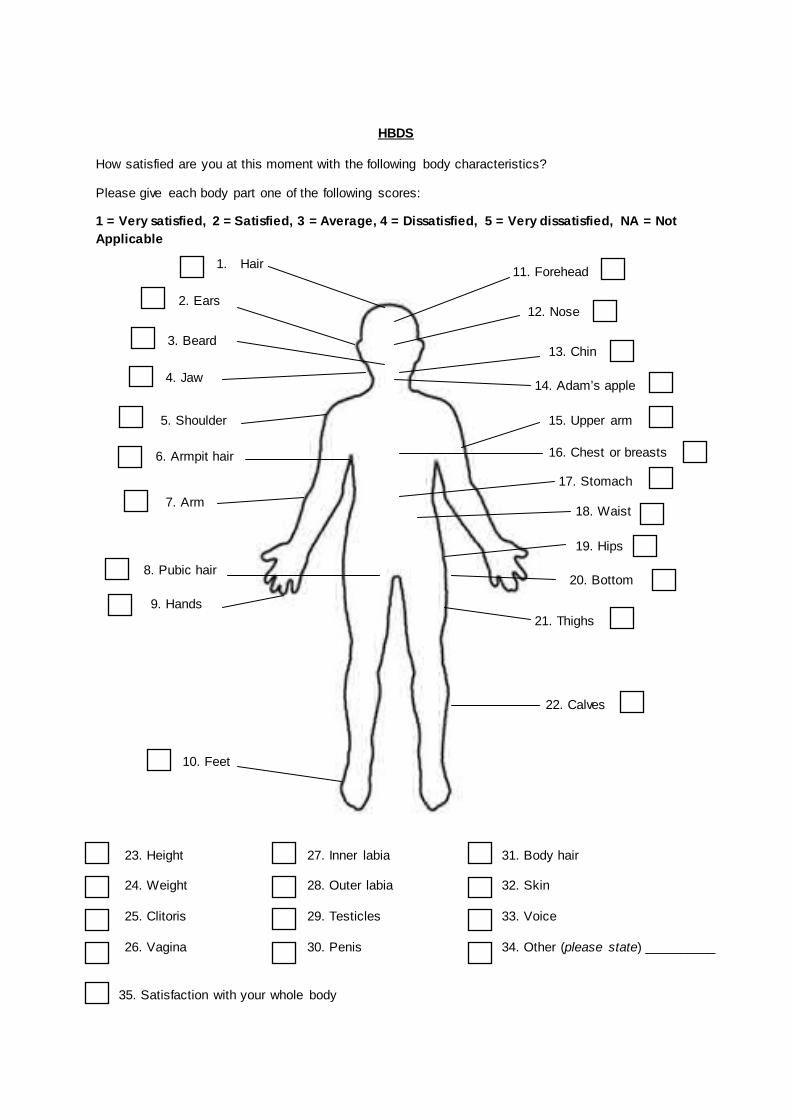
UHBDS
How satisfied are you at this moment with the following body characteristics?
Please give each body part one of the following scores:
1 = Very satisfied, 2 = Satisfied, 3 = Average, 4 = Dissatisfied, 5 = Very dissatisfied, NA = Not Applicable
1. Hair
2. Ears
3. Beard
4. Jaw
5. Shoulder
6. Armpit hair
7. Arm
8. Pubic hair
9. Hands
10. Feet
11. Forehead
12. Nose
13. Chin
14. Adam’s apple
15. Upper arm t
16. Chest or breasts
17. Stomach
18. Waist
19. Hips
20. Bottom
21. Thighs
22. Calves
23. Height
24. Weight
25. Clitoris
26. Vagina
27. Inner labia
28. Outer labia
29. Testicles
30. Penis
31. Body hair
32. Skin
33. Voice
34. Other (please state) __________
35. Satisfaction with your whole body
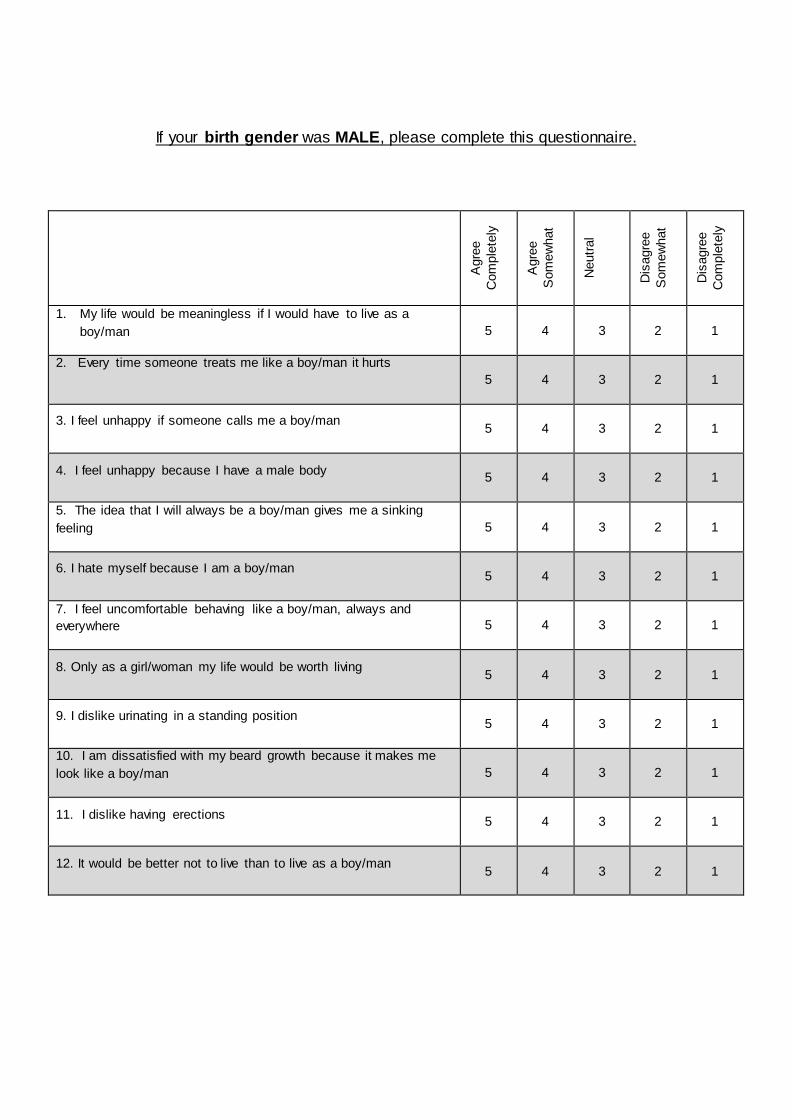
UIf your birth gender was MALE, please complete this questionnaire.
Agr
ee
Com
plet
ely
Agr
ee
Som
ewha
t
Neu
tral
Dis
agre
e S
omew
hat
Dis
agre
e C
ompl
etel
y
1. My life would be meaningless if I would have to live as a boy/man 5 4 3 2 1
2. Every time someone treats me like a boy/man it hurts 5 4 3 2 1
3. I feel unhappy if someone calls me a boy/man 5 4 3 2 1
4. I feel unhappy because I have a male body 5 4 3 2 1
5. The idea that I will always be a boy/man gives me a sinking feeling 5 4 3 2 1
6. I hate myself because I am a boy/man 5 4 3 2 1
7. I feel uncomfortable behaving like a boy/man, always and everywhere 5 4 3 2 1
8. Only as a girl/woman my life would be worth living 5 4 3 2 1
9. I dislike urinating in a standing position 5 4 3 2 1
10. I am dissatisfied with my beard growth because it makes me look like a boy/man 5 4 3 2 1
11. I dislike having erections 5 4 3 2 1
12. It would be better not to live than to live as a boy/man 5 4 3 2 1
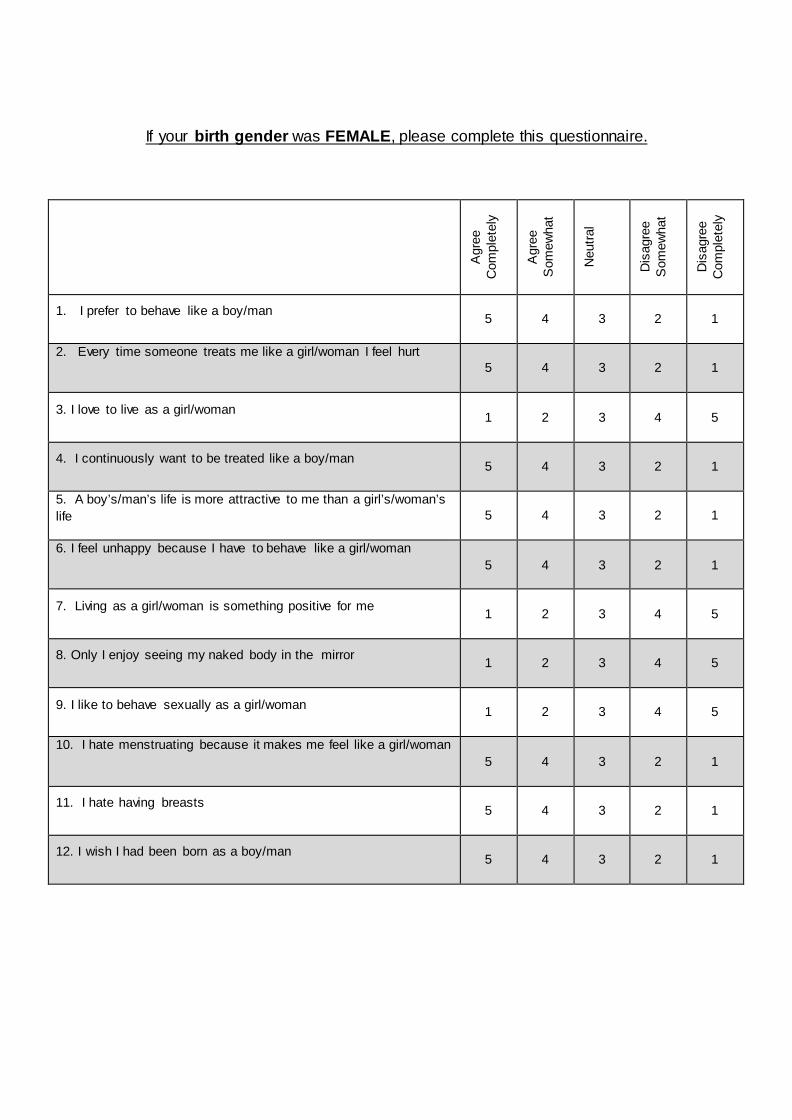
UIf your birth gender was FEMALE, please complete this questionnaire.
Agr
ee
Com
plet
ely
Agr
ee
Som
ewha
t
Neu
tral
Dis
agre
e S
omew
hat
Dis
agre
e C
ompl
etel
y
1. I prefer to behave like a boy/man 5 4 3 2 1
2. Every time someone treats me like a girl/woman I feel hurt 5 4 3 2 1
3. I love to live as a girl/woman 1 2 3 4 5
4. I continuously want to be treated like a boy/man 5 4 3 2 1
5. A boy’s/man’s life is more attractive to me than a girl’s/woman’s life 5 4 3 2 1
6. I feel unhappy because I have to behave like a girl/woman 5 4 3 2 1
7. Living as a girl/woman is something positive for me 1 2 3 4 5
8. Only I enjoy seeing my naked body in the mirror 1 2 3 4 5
9. I like to behave sexually as a girl/woman 1 2 3 4 5
10. I hate menstruating because it makes me feel like a girl/woman 5 4 3 2 1
11. I hate having breasts 5 4 3 2 1
12. I wish I had been born as a boy/man 5 4 3 2 1
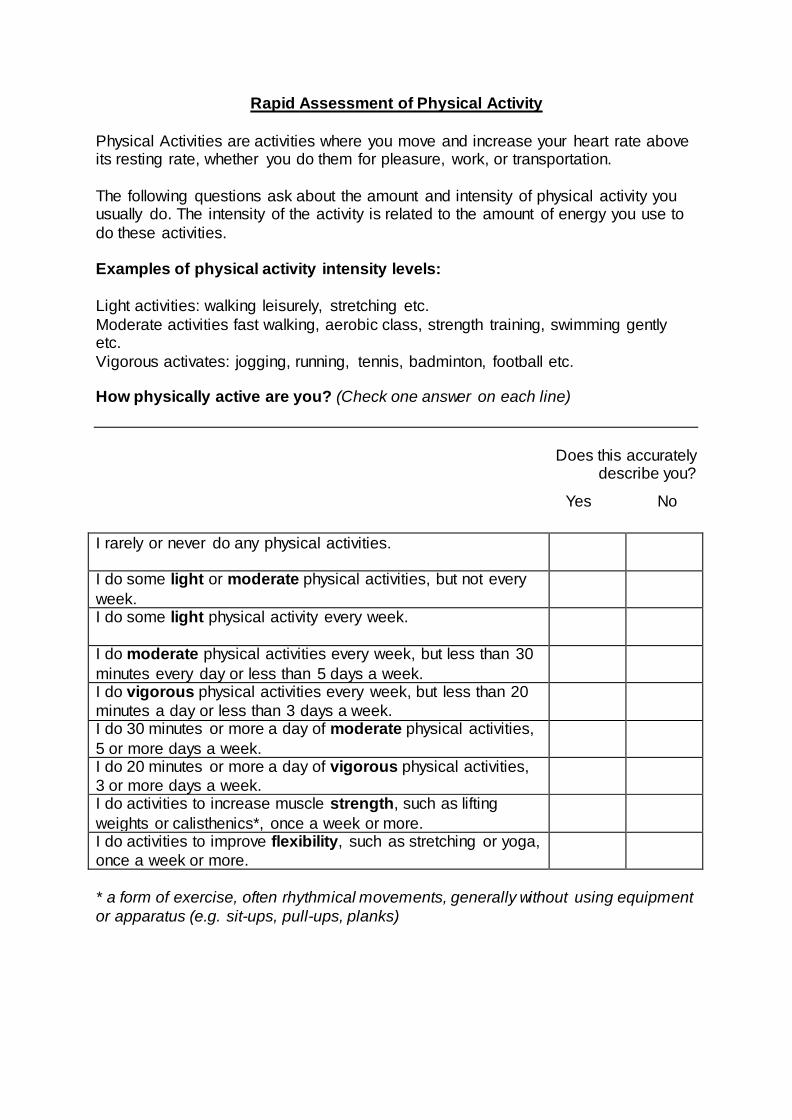
URapid Assessment of Physical Activity
Physical Activities are activities where you move and increase your heart rate above its resting rate, whether you do them for pleasure, work, or transportation. The following questions ask about the amount and intensity of physical activity you usually do. The intensity of the activity is related to the amount of energy you use to do these activities. Examples of physical activity intensity levels: Light activities: walking leisurely, stretching etc. Moderate activities fast walking, aerobic class, strength training, swimming gently etc. Vigorous activates: jogging, running, tennis, badminton, football etc. How physically active are you? (Check one answer on each line)
Does this accurately describe you?
* a form of exercise, often rhythmical movements, generally without using equipment or apparatus (e.g. sit-ups, pull-ups, planks)
I rarely or never do any physical activities.
I do some light or moderate physical activities, but not every week.
I do some light physical activity every week.
I do moderate physical activities every week, but less than 30 minutes every day or less than 5 days a week.
I do vigorous physical activities every week, but less than 20 minutes a day or less than 3 days a week.
I do 30 minutes or more a day of moderate physical activities, 5 or more days a week.
I do 20 minutes or more a day of vigorous physical activities, 3 or more days a week.
I do activities to increase muscle strength, such as lifting weights or calisthenics*, once a week or more.
I do activities to improve flexibility, such as stretching or yoga, once a week or more.
Yes No
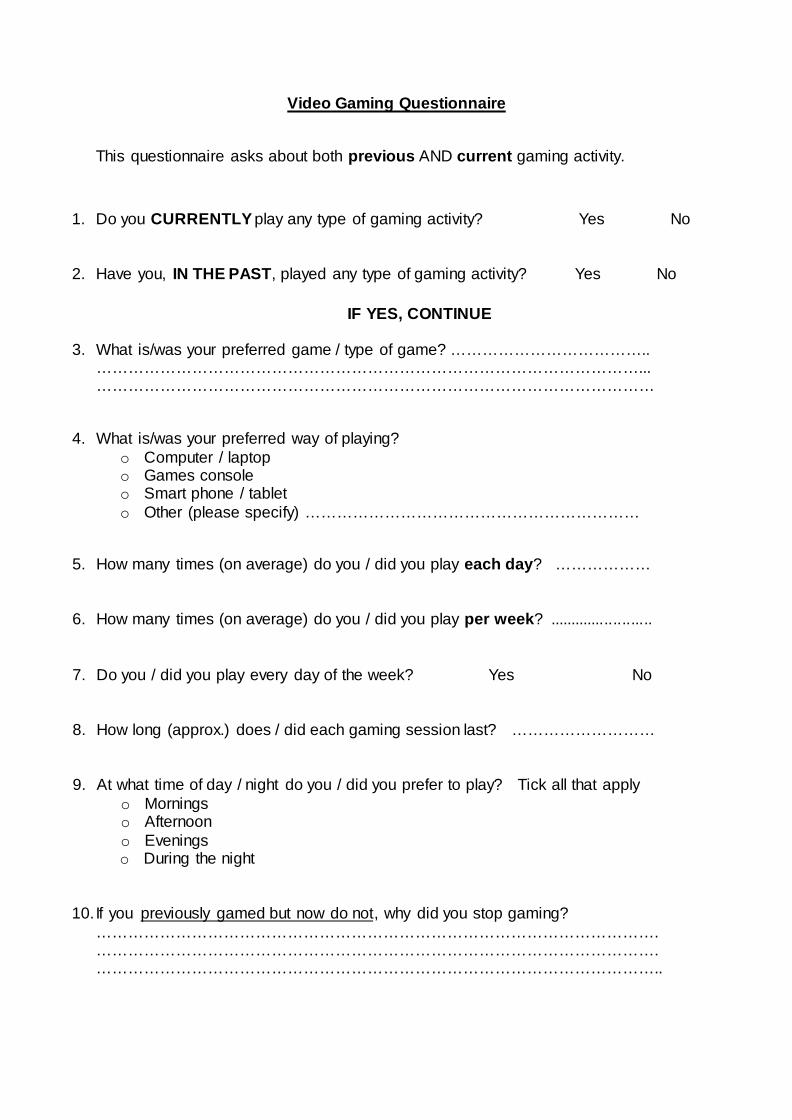
UVideo Gaming Questionnaire
This questionnaire asks about both previous AND current gaming activity.
1. Do you CURRENTLY play any type of gaming activity? Yes No
2. Have you, IN THE PAST, played any type of gaming activity? Yes No
IF YES, CONTINUE
3. What is/was your preferred game / type of game? ……………………………….. …………………………………………………………………………………………... ……………………………………………………………………………………………
4. What is/was your preferred way of playing? o Computer / laptop o Games console o Smart phone / tablet o Other (please specify) ………………………………………………………
5. How many times (on average) do you / did you play each day? ………………
6. How many times (on average) do you / did you play per week? ........................
7. Do you / did you play every day of the week? Yes No
8. How long (approx.) does / did each gaming session last? ………………………
9. At what time of day / night do you / did you prefer to play? Tick all that apply o Mornings o Afternoon o Evenings o During the night
10. If you Upreviously gamed but now do notU, why did you stop gaming? ……………………………………………………………………………………………. ……………………………………………………………………………………………. ……………………………………………………………………………………………..
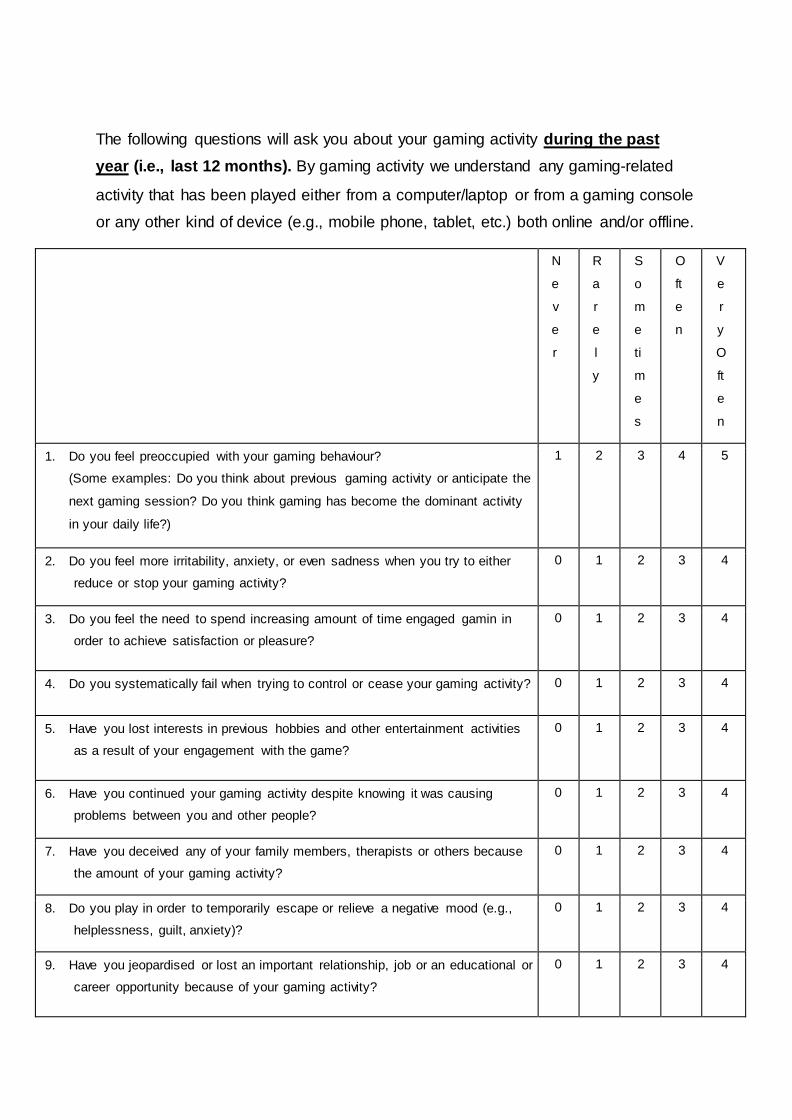
The following questions will ask you about your gaming activity Uduring the past yearU (i.e., last 12 months). By gaming activity we understand any gaming-related
activity that has been played either from a computer/laptop or from a gaming console
or any other kind of device (e.g., mobile phone, tablet, etc.) both online and/or offline.
N
e
v
e
r
R
a
r
e
l
y
S
o
m
e
ti
m
e
s
O
ft
e
n
V
e
r
y
O
ft
e
n
1. Do you feel preoccupied with your gaming behaviour?
(Some examples: Do you think about previous gaming activity or anticipate the
next gaming session? Do you think gaming has become the dominant activity
in your daily life?)
1 2 3 4 5
2. Do you feel more irritability, anxiety, or even sadness when you try to either
reduce or stop your gaming activity? 0 1 2 3 4
3. Do you feel the need to spend increasing amount of time engaged gamin in
order to achieve satisfaction or pleasure? 0 1 2 3 4
4. Do you systematically fail when trying to control or cease your gaming activity? 0 1 2 3 4
5. Have you lost interests in previous hobbies and other entertainment activities
as a result of your engagement with the game? 0 1 2 3 4
6. Have you continued your gaming activity despite knowing it was causing
problems between you and other people? 0 1 2 3 4
7. Have you deceived any of your family members, therapists or others because
the amount of your gaming activity? 0 1 2 3 4
8. Do you play in order to temporarily escape or relieve a negative mood (e.g.,
helplessness, guilt, anxiety)? 0 1 2 3 4
9. Have you jeopardised or lost an important relationship, job or an educational or
career opportunity because of your gaming activity? 0 1 2 3 4
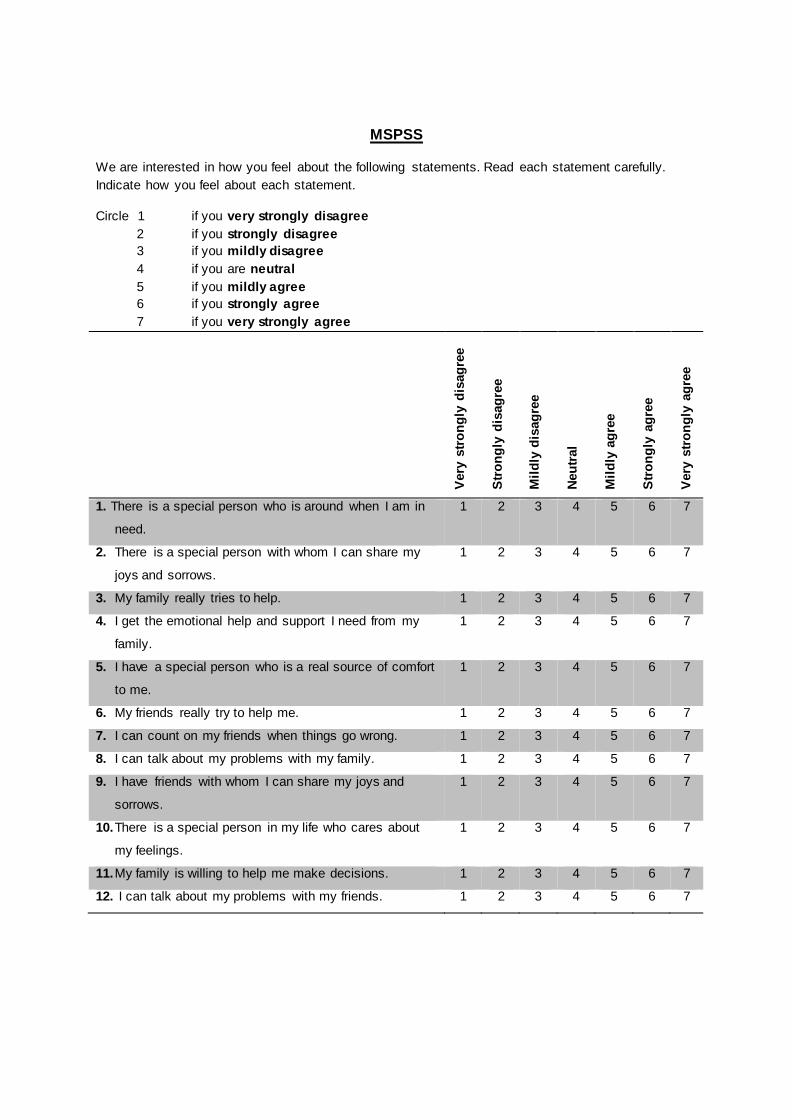
UMSPSS
We are interested in how you feel about the following statements. Read each statement carefully. Indicate how you feel about each statement.
Circle 1 if you very strongly disagree 2 if you strongly disagree 3 if you mildly disagree 4 if you are neutral 5 if you mildly agree 6 if you strongly agree 7 if you very strongly agree
Very
stro
ngly
dis
agre
e
Stro
ngly
dis
agre
e
Mild
ly d
isag
ree
Neut
ral
Mild
ly a
gree
Stro
ngly
agr
ee
Very
stro
ngly
agr
ee
1. There is a special person who is around when I am in
need.
1 2 3 4 5 6 7
2. There is a special person with whom I can share my
joys and sorrows.
1 2 3 4 5 6 7
3. My family really tries to help. 1 2 3 4 5 6 7
4. I get the emotional help and support I need from my
family.
1 2 3 4 5 6 7
5. I have a special person who is a real source of comfort
to me.
1 2 3 4 5 6 7
6. My friends really try to help me. 1 2 3 4 5 6 7
7. I can count on my friends when things go wrong. 1 2 3 4 5 6 7
8. I can talk about my problems with my family. 1 2 3 4 5 6 7
9. I have friends with whom I can share my joys and
sorrows.
1 2 3 4 5 6 7
10.There is a special person in my life who cares about
my feelings.
1 2 3 4 5 6 7
11.My family is willing to help me make decisions. 1 2 3 4 5 6 7
12. I can talk about my problems with my friends. 1 2 3 4 5 6 7
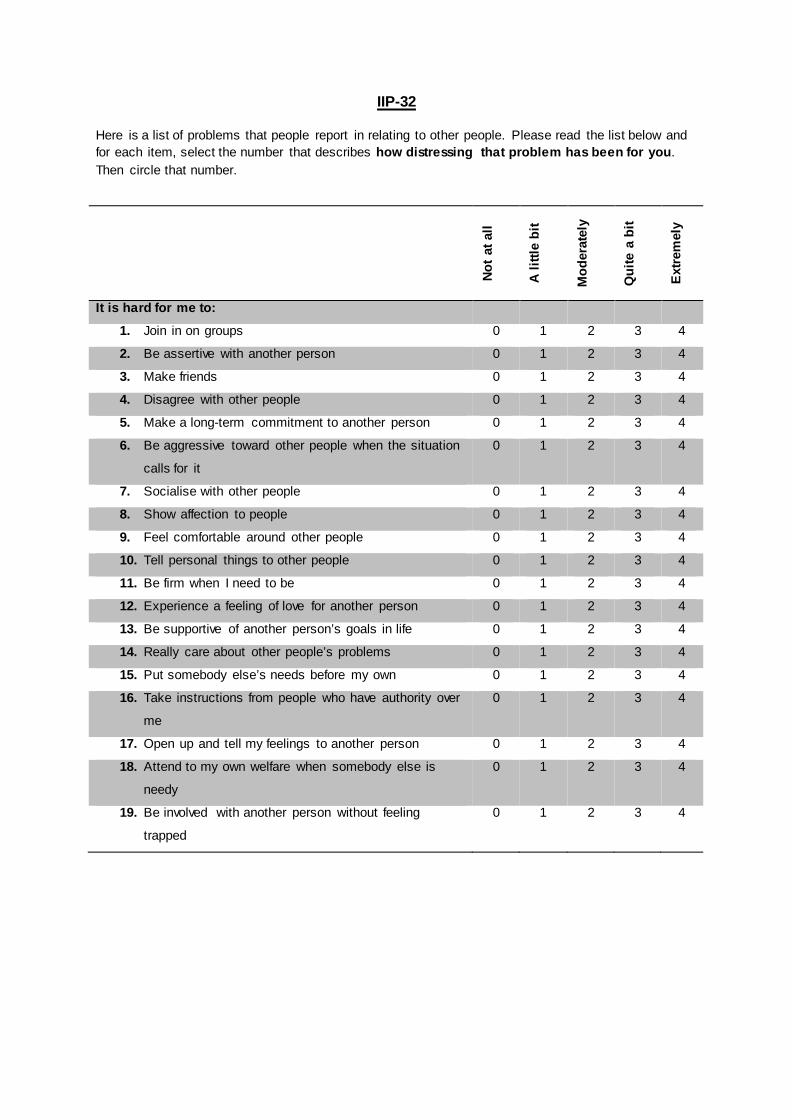
UIIP-32
Here is a list of problems that people report in relating to other people. Please read the list below and for each item, select the number that describes how distressing that problem has been for you. Then circle that number.
Not a
t all
A lit
tle b
it
Mod
erat
ely
Qui
te a
bit
Extre
mel
y
It is hard for me to:
1. Join in on groups 0 1 2 3 4
2. Be assertive with another person 0 1 2 3 4
3. Make friends 0 1 2 3 4
4. Disagree with other people 0 1 2 3 4
5. Make a long-term commitment to another person 0 1 2 3 4
6. Be aggressive toward other people when the situation
calls for it
0 1 2 3 4
7. Socialise with other people 0 1 2 3 4
8. Show affection to people 0 1 2 3 4
9. Feel comfortable around other people 0 1 2 3 4
10. Tell personal things to other people 0 1 2 3 4
11. Be firm when I need to be 0 1 2 3 4
12. Experience a feeling of love for another person 0 1 2 3 4
13. Be supportive of another person’s goals in life 0 1 2 3 4
14. Really care about other people’s problems 0 1 2 3 4
15. Put somebody else’s needs before my own 0 1 2 3 4
16. Take instructions from people who have authority over
me
0 1 2 3 4
17. Open up and tell my feelings to another person 0 1 2 3 4
18. Attend to my own welfare when somebody else is
needy
0 1 2 3 4
19. Be involved with another person without feeling
trapped
0 1 2 3 4
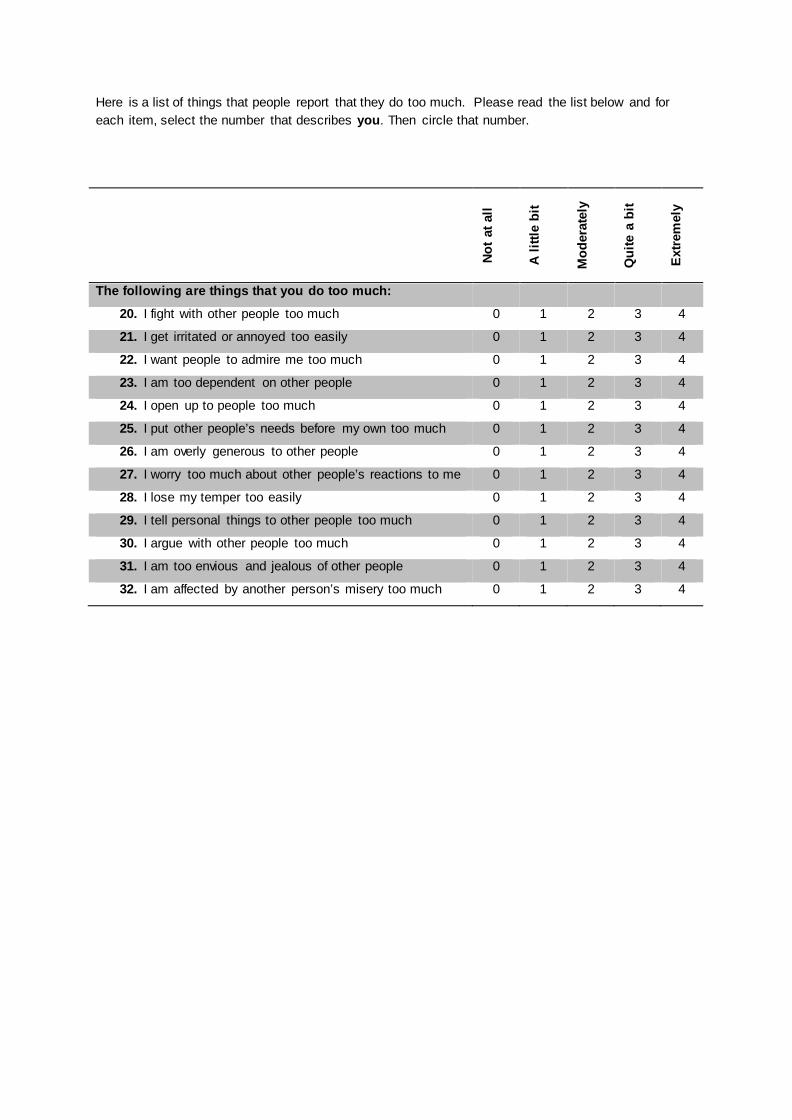
Here is a list of things that people report that they do too much. Please read the list below and for each item, select the number that describes you. Then circle that number.
Not a
t all
A lit
tle b
it
Mod
erat
ely
Qui
te a
bit
Extre
mel
y
The following are things that you do too much:
20. I fight with other people too much 0 1 2 3 4
21. I get irritated or annoyed too easily 0 1 2 3 4
22. I want people to admire me too much 0 1 2 3 4
23. I am too dependent on other people 0 1 2 3 4
24. I open up to people too much 0 1 2 3 4
25. I put other people’s needs before my own too much 0 1 2 3 4
26. I am overly generous to other people 0 1 2 3 4
27. I worry too much about other people’s reactions to me 0 1 2 3 4
28. I lose my temper too easily 0 1 2 3 4
29. I tell personal things to other people too much 0 1 2 3 4
30. I argue with other people too much 0 1 2 3 4
31. I am too envious and jealous of other people 0 1 2 3 4
32. I am affected by another person’s misery too much 0 1 2 3 4
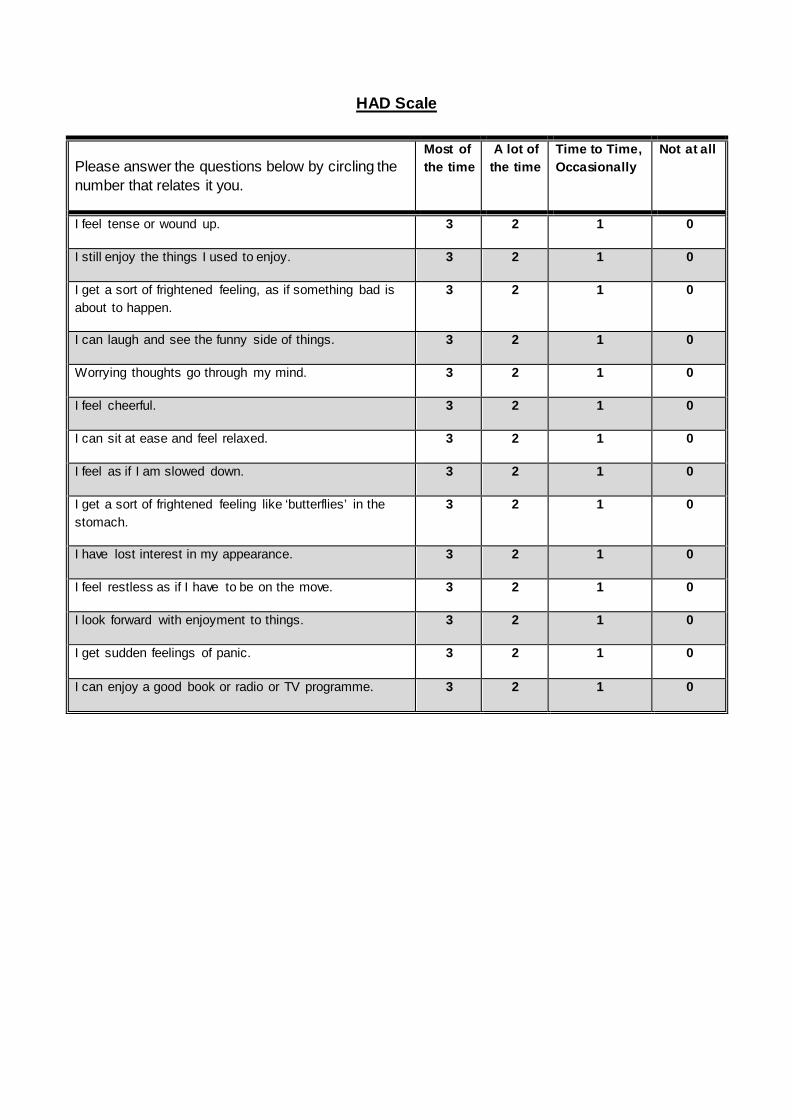
UHAD Scale
Please answer the questions below by circling the number that relates it you.
Most of the time
A lot of the time
Time to Time, Occasionally
Not at all
I feel tense or wound up. 3 2 1 0
I still enjoy the things I used to enjoy. 3 2 1 0
I get a sort of frightened feeling, as if something bad is about to happen.
3 2 1 0
I can laugh and see the funny side of things. 3 2 1 0
Worrying thoughts go through my mind. 3 2 1 0
I feel cheerful. 3 2 1 0
I can sit at ease and feel relaxed. 3 2 1 0
I feel as if I am slowed down. 3 2 1 0
I get a sort of frightened feeling like ‘butterflies’ in the stomach.
3 2 1 0
I have lost interest in my appearance. 3 2 1 0
I feel restless as if I have to be on the move. 3 2 1 0
I look forward with enjoyment to things. 3 2 1 0
I get sudden feelings of panic. 3 2 1 0
I can enjoy a good book or radio or TV programme. 3 2 1 0
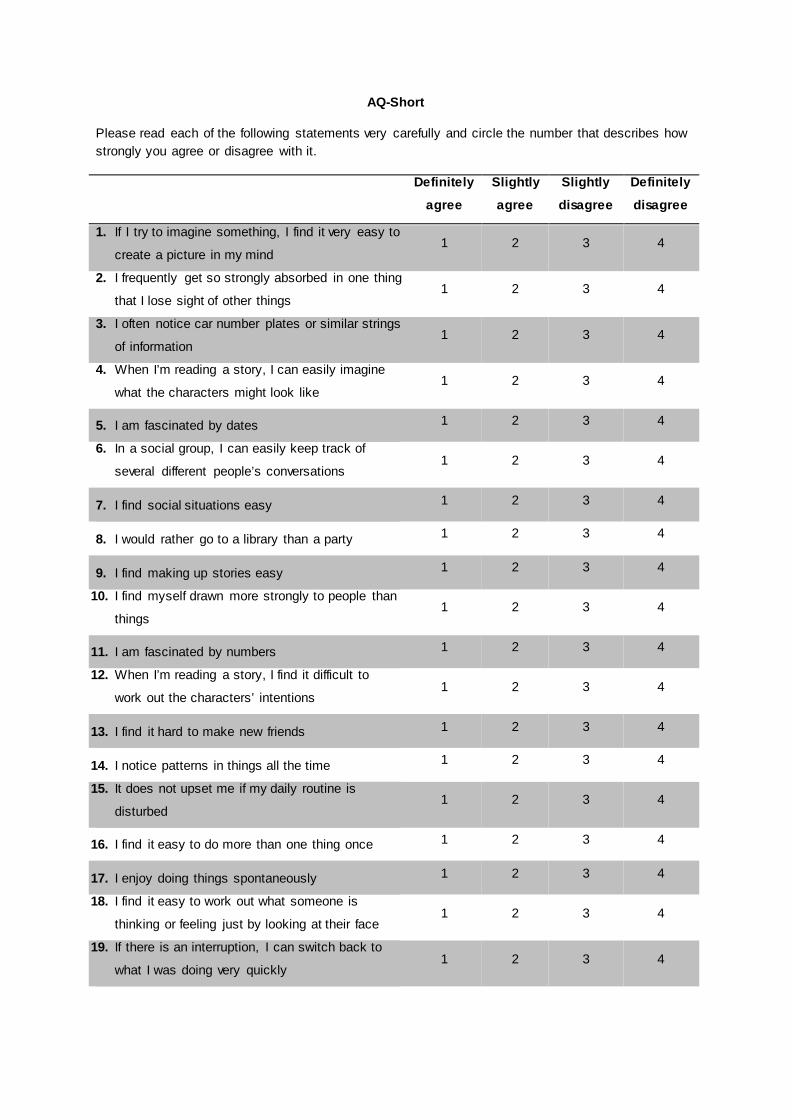
AQ-Short
Please read each of the following statements very carefully and circle the number that describes how strongly you agree or disagree with it.
Definitely
agree
Slightly
agree
Slightly
disagree
Definitely
disagree
1. If I try to imagine something, I find it very easy to
create a picture in my mind 1 2 3 4
2. I frequently get so strongly absorbed in one thing
that I lose sight of other things 1 2 3 4
3. I often notice car number plates or similar strings
of information 1 2 3 4
4. When I’m reading a story, I can easily imagine
what the characters might look like 1 2 3 4
5. I am fascinated by dates 1 2 3 4
6. In a social group, I can easily keep track of
several different people’s conversations 1 2 3 4
7. I find social situations easy 1 2 3 4
8. I would rather go to a library than a party 1 2 3 4
9. I find making up stories easy 1 2 3 4
10. I find myself drawn more strongly to people than
things 1 2 3 4
11. I am fascinated by numbers 1 2 3 4
12. When I’m reading a story, I find it difficult to
work out the characters’ intentions 1 2 3 4
13. I find it hard to make new friends 1 2 3 4
14. I notice patterns in things all the time 1 2 3 4
15. It does not upset me if my daily routine is
disturbed 1 2 3 4
16. I find it easy to do more than one thing once 1 2 3 4
17. I enjoy doing things spontaneously 1 2 3 4
18. I find it easy to work out what someone is
thinking or feeling just by looking at their face 1 2 3 4
19. If there is an interruption, I can switch back to
what I was doing very quickly 1 2 3 4
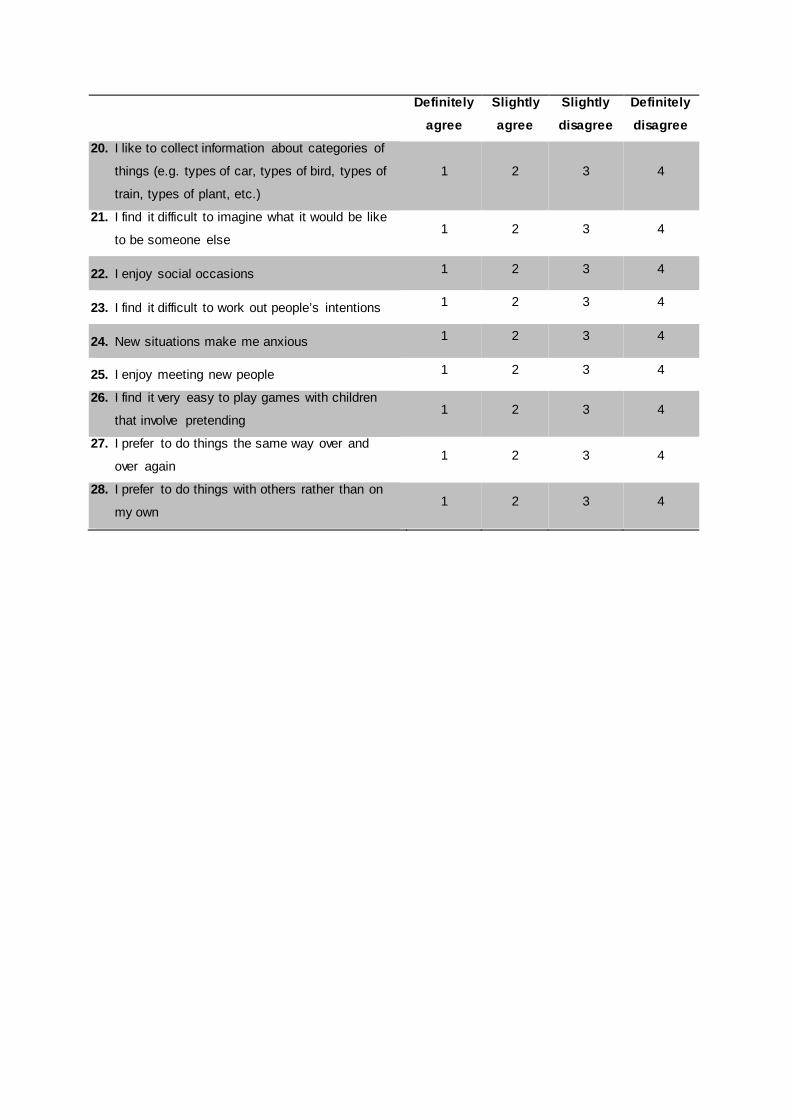
Definitely
agree
Slightly
agree
Slightly
disagree
Definitely
disagree
20. I like to collect information about categories of
things (e.g. types of car, types of bird, types of
train, types of plant, etc.)
1 2 3 4
21. I find it difficult to imagine what it would be like
to be someone else 1 2 3 4
22. I enjoy social occasions 1 2 3 4
23. I find it difficult to work out people’s intentions 1 2 3 4
24. New situations make me anxious 1 2 3 4
25. I enjoy meeting new people 1 2 3 4
26. I find it very easy to play games with children
that involve pretending 1 2 3 4
27. I prefer to do things the same way over and
over again 1 2 3 4
28. I prefer to do things with others rather than on
my own 1 2 3 4
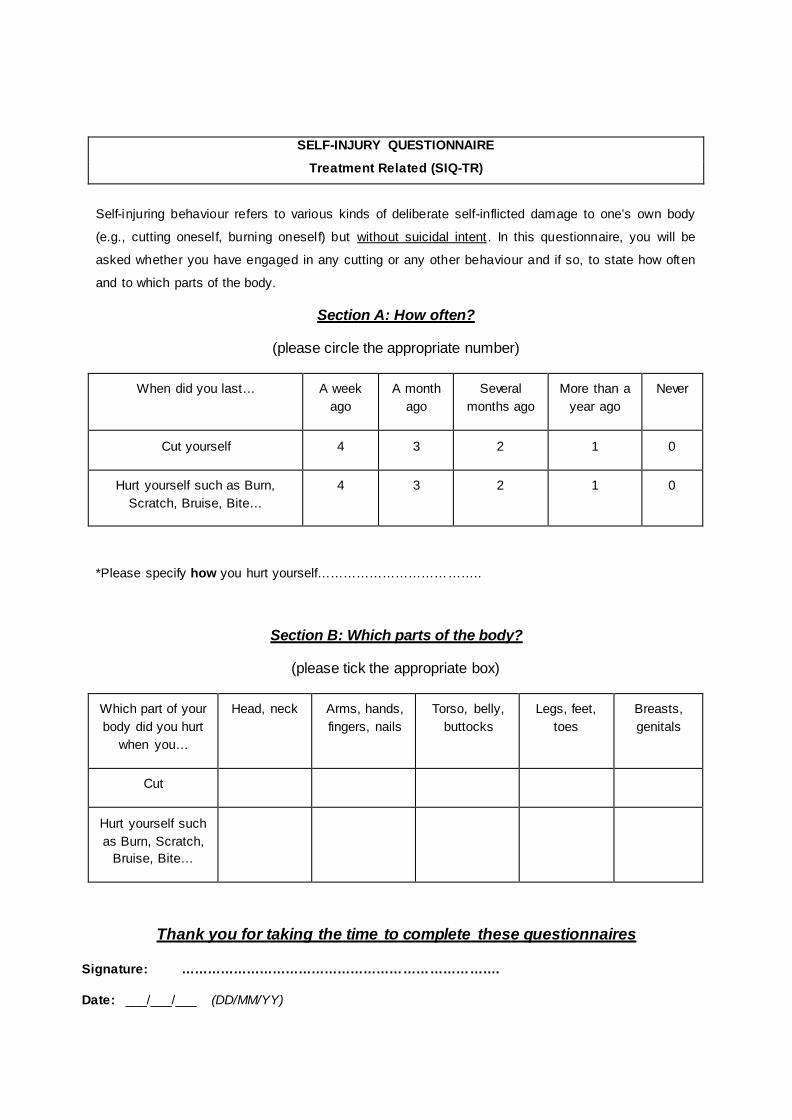
SELF-INJURY QUESTIONNAIRE
Treatment Related (SIQ-TR)
Self-injuring behaviour refers to various kinds of deliberate self-inflicted damage to one’s own body
(e.g., cutting oneself, burning oneself) but Uwithout suicidal intent U. In this questionnaire, you will be
asked whether you have engaged in any cutting or any other behaviour and if so, to state how often
and to which parts of the body.
USection A: How often?
(please circle the appropriate number)
When did you last… A week ago
A month ago
Several months ago
More than a year ago
Never
Cut yourself 4 3 2 1 0
Hurt yourself such as Burn, Scratch, Bruise, Bite…
4 3 2 1 0
*Please specify how you hurt yourself………………………………..
USection B: Which parts of the body?
(please tick the appropriate box)
Which part of your body did you hurt
when you…
Head, neck Arms, hands, fingers, nails
Torso, belly, buttocks
Legs, feet, toes
Breasts, genitals
Cut
Hurt yourself such as Burn, Scratch,
Bruise, Bite…
UThank you for taking the time to complete these questionnaires
Signature: ……………………………………………………………….
Date: ___/___/___ (DD/MM/YY)
THE QUESTIONNAIRES YOU HAVE JUST
COMPLETED ARE AN IMPORTANT PART OF YOUR ASSESSMENT
BUT
WE WOULD LIKE TO ASK YOUR PERMISSION TO USE THE INFORMATION FROM THOSE
QUESTIONNAIRES ANONIMOUSLY ALSO FOR A RESEARCH PROJECT.
THIS RESEARCH AIMS TO INVESTIGATE HOW THE TREATMENT FOR GENDER DYSPHORIA HELPS (OR
NOT) PEOPLE.
Please read the information sheet at the end of this package. If you are happy for us to use the information from the
questionnaires anonymously for this project, please sign the consent form and sent it back to us with all the questionnaires
Thank you
Clinical correlates and outcomes of treatment for trans people
INFORMED CONSENT
(to be completed after Participant Information Sheet has been read)
Please read the following carefully. Please initial each box and sign at the bottom to show you have read and understood what is expected of you. I hereby give my consent to participate in the questionnaire study clinical correlates and outcomes of treatment at the Nottingham Centre for Gender Dysphoria. I confirm that: The purpose and details of the study have been explained to me in the attached information sheet. I understand that this study is designed to further scientific knowledge and that all procedures have been approved by the regional Ethics Committee.
I have read and understood the Patient Information Sheet
I have been informed that my participation in the study will involve completing a set of questionnaires and that my responses will be kept anonymous and confidential.
I understand that relevant sections of my medical notes and data collected during this study may be looked at by individuals from the Nottingham Centre for Gender Dysphoria, where it is relevant to my taking part in this research. I give permission for these individuals to have access to my records.
I understand that I am under no obligation to take part in the study; I have the right to withdraw at any stage for any reason; and that I will not be required to explain my reasons for withdrawing.
Your name
Your Signature
Date

Patient Information Sheet
(Please retain this information sheet for your own reference)
Clinical correlates and outcomes of treatment for trans people
Introduction You are invited to take part in our research project. Please read this information sheet carefully. It is important for you to understand why the research is being done and what it would involve if you agree to take part. If you have any questions please contact one of the researchers – contact details are at the end of this sheet. Please take time to consider whether or not you wish to take part. What is the purpose of this study? The purpose of this research study is to identify what influence treatment has on the overall quality of life, mental health, self-esteem, body image, social support and interpersonal function of people with gender dysphoria. People who have gender dysphoria face a number of difficulties unique to their gender identity or gender presentation. These difficulties can be alleviated through treatment, including hormone therapy and gender surgery. This study will help researchers and clinicians better understand the role hormone treatment plays in the overall treatment pathway of people with gender dysphoria. Why have I been chosen? All patients attending the Nottingham Gender Clinic will be invited to take part in this research project. We need to know how they were before treatment, after hormones and after surgery. You have been invited to take part because you meet the recruitment criteria for the research project. Who is organising the study? This research is being organised by Dr Walter Pierre Bouman, Lead Clinician, Christina Richards, Senior Specialist Psychology Associate, Dr Meghan Thurston, Research Associate, and Professor Jon Arcelus, Head of Research at the Nottingham Centre for Gender Dysphoria. Do I have to take part? Your help in the study is entirely voluntary. If you do not want to take part, you do not have to give a reason. If you do take part and later decide to withdraw from the study, you have the right to have your data withdrawn and destroyed at any time up until publication. You do not have to give a reason to withdraw. What do I have to do? If you have any questions or concerns, please do not hesitate to contact the researchers before proceeding (contact details are provided at the end of this sheet).
If you are interested in taking part and have no further questions, you will first need to sign the consent form enclosed in this pack. The pack contains several questionnaires related to outcome measures for you to complete. This should take you approximately one hour. To return your questionnaire pack, please use the stamped and addressed envelope provided or hand it in to your clinician in person. What are the possible disadvantages of taking part? These questionnaires should not cause you any comfort or distress. However, if you do feel distressed at any point during the study we would strongly advise you to talk to your clinician. Alternatively you may wish to speak to your local GP or The Samaritans (telephone no. 08457 909090). If you decide not to take part in the study, your decision will in no way affect your care at the Nottingham Centre for Gender Dysphoria. What are the possible benefits of taking part? There are no benefits of participating in this study but your participation in this study may help clinicians and researchers understand what the influence is of treatment on quality of life, mental health, self-esteem, body image, social support and interpersonal function of people with gender dysphoria. If you wish to receive a summary of the study’s findings on completion of the project, you may request this from the researcher via email. Will my taking part in this study be kept confidential? All information given will be kept strictly confidential and will only be accessible to the clinical team at the Nottingham Centre for Gender Dysphoria. All questionnaire data entered into the research database will be assigned a unique identifier code to achieve anonymity. Completed questionnaire packs and consent forms will be separated and stored in a locked filing cabinet at the Nottingham Centre for Gender Dysphoria. These will be stored for ten years following completion of the study and destroyed thereafter. The procedure for handling, processing, storage and destruction of your data will be compliant with the data Protection Act 1998. What happens if I don’t want to carry on with the study? You can withdraw from the study at any time without giving a reason for doing so. If you wish to withdraw, your data will be discarded from the study and subsequently destroyed. Again this decision will not affect your care at the Nottingham Centre for Gender Dysphoria. What will happen to the results of the research study? The study’s findings will be shared with the clinical team at the Nottingham Centre for Gender Dysphoria and may be published in academic journals and presented at research conferences. Also a summary of the study’s findings will be made available on request to participants on completion of the study. Who has reviewed the study? This study has been reviewed and was given a favourable ethical opinion for conduct by the regional NHS Research and Ethics Committee.
What if I have any other questions or concerns? If you have any questions or concerns about this study, please contact one of the researchers. Dr Walter Bouman, Head of Service Professor Jon Arcelus Nottingham Centre for Gender Dysphoria 3 Oxford Street, Nottingham NG1 5BH Telephone: 0115 876 0160 If you would like independent advice about taking part in research, you may wish to contact Patient Advice Liaison Service (PALS): Tel: 0800 015 3367 Website: Uwww.pals.nhs.ukU (for general information only)
Thank you for taking the time to read this information sheet and for considering taking part in the study. Please retain this information sheet for
future reference.