ratification of iatsic/who’s guidelines for essential trauma care assessment in the south american...
TRANSCRIPT

Ratification of IATSIC/WHO’s Guidelines for Essential TraumaCare Assessment in the South American Region
Michel B. Aboutanos • Francisco Mora •
Edgar Rodas • Juan Salamea • Marcelo Ochoa Parra •
Estuardo Salgado • Charlie Mock • Rao Ivatury
� Societe Internationale de Chirurgie 2010
Abstract
Background The purpose of the present study was to
evaluate the usefulness of the International Association for
Trauma Surgery and Intensive Care (IATSIC)/World
Health Organization (WHO)’s Guidelines for Essential
Trauma Care (EsTC Guidelines) in providing an interna-
tionally applicable and standardized template to assess
trauma care capabilities in the South American Region.
Methods Field assessment was conducted in seven
provinces (urban and rural, pop. 2,239,509) and 24 facili-
ties (5 large hospitals (LH); 15 small hospitals (SH); 4
basic hospitals (BH)) in Ecuador using EsTC criteria. A
total of 260 individual items in Human Resources
(HR– availability, clinical knowledge, skills) and physical
resources (PR) were evaluated via inspection, review of
local statistics, and administrative and staff interviews.
EsTC was evaluated on a scale as follows: 0 (absent);
1(inadequate; \ 50%); 2 (partly adequate [ 50%); 3 (ade-
quate–100%).
Results 210,045 Emergency Department (ED) visits and
61,365 (29%) ED trauma visits were recorded (incidence
rate 2,740/100,000 population). Deficits were noted in
prehospital trauma care (inadequate coordination, com-
munication), education and training (ATLS \ 30%, TNCC
0%), facility based trauma care (poor physical resources
[PR] and human resources [HR]), and quality assurance
(1/27 hospitals).
Conclusions The IATSIC/WHO EsTC Guidelines pro-
vide a simple and useful template to assess trauma care
capability in variable facilities and international settings,
and they could serve as a valuable tool for trauma sys-
tem development. Endorsement of EsTC Guidelines by the
Panamerican Health Organization and lead trauma
societies (the Panamerican Trauma Society) should be
considered.
Introduction
Trauma is a global epidemic, with 90% of the fatalities and
morbidities occurring in low and middle income countries
[1–3]. The region of the Americas accounts for 11% of the
global injury related mortality rate and 10% of the global
injury burden [4, 5].Injuries and non-communicable dis-
eases account for greater than 73% of deaths and 76% of
disability adjusted life years (DALYS) in the Latin
American region [2, 6]. This epidemiological transition has
been attributed to rapid urbanization and globalization of
the developing countries [6–8].
M. B. Aboutanos (&) � F. Mora � R. Ivatury
Department of Surgery, International Trauma System
Development Program, Virginia Commonwealth Medical
Center, 1200 East Broad Street, Richmond, VA 23298, USA
e-mail: [email protected]
E. Rodas
Department of Surgery, Broward General Medical Center,
303 SE 17th Street, Fort Lauderdale, FL 33316, USA
E. Rodas
Cinterandes Foundation, Av. Unidad Nacional and Gran
Colombia (Horizontes Building) 4th Floor # 404,
Cuenca, Ecuador
J. Salamea � M. O. Parra � E. Salgado
Ecuadorian Trauma Society, Cinterandes Foundation,
Av. Unidad Nacional and Gran Colombia (Horizontes Building)
4th Floor # 404, Cuenca, Ecuador
C. Mock
Department of Surgery, Harborview Injury Prevention and
Research Center, University of Washington, 325 Ninth Avenue,
Box 359960, Seattle, WA 98104, USA
123
World J Surg
DOI 10.1007/s00268-010-0716-9
However, because of the lack of appropriate injury
assessment tools in their respective countries, public health
officials and policy makers have failed to recognize trauma
as a serious public health issue [1, 7]. This is of signifi-
cance in the Latin region, especially in rural areas that
shoulder much of the burden of injury and where rapid
urbanization and development is ongoing without the cor-
responding improvement in infrastructure and health care
systems [9, 10]. Trauma care in rural areas of Latin
America remains rudimentary without appropriate injury
prevention and control efforts [11, 12]. Without appropri-
ate planning and organization no effective primary and
secondary prevention efforts can be carried out. The lack of
such planning and organization is highlighted by the World
Health Organization (WHO) as one of the primary reasons
for the health and injury outcome disparities between low-,
middle-, and high-income countries [13–15].
In response to the global burden of traumatic injuries,
significant efforts have been undertaken by WHO and the
International Association for Trauma and Surgical Inten-
sive Care (IATSIC) to delineate specific guidelines
regarding various injury prevention strategies that could be
implemented in developing nations [1, 16, 17]. The WHO/
IATSIC Guidelines for Essential Trauma Care (EsTC
Guidelines) are advocated to establish achievable and
affordable standards for the care of the injured patient
worldwide [18].
The EsTC Guidelines delineates eleven core essential
trauma care services that could, and should, be made
available to every injured person in the world. The EsTC
Guidelines additionally identified 260 individual items of
human resources (HR: knowledge, skills, training, staffing)
and physical resources (PR: equipment and supplies) that
would be needed to ensure these services are in place in
health facilities in countries at all economic levels.
The items are comprehensive, addressing both essential
and desirable elements at all levels of health care facilities
from rural health care clinics and hospitals, to larger spe-
cialty staffed hospitals and tertiary care facilities [18].
The EsTC Guidelines have been implemented in various
countries including Ghana, India, Vietnam, and Mexico
[19–23]. In the Latin American Region, the EsTC Guide-
lines were also adapted nationally and endorsed by the
Mexican Association for the Medicine and Surgery of
Trauma (AMMCT) [22, 23]. Additionally, in both Mexico
and Colombia recommendations contained in the WHO
Prehospital Trauma Care Systems were incorporated into
national legislation establishing standards for prehospital
care providers [22–24].
So far, the WHO/IATSIC EsTC Guidelines have not
been implemented regionally in South America. The pur-
pose of the present study was to carry out a comprehensive
regional assessment in a representative South American
region undergoing rapid urbanization and rural develop-
ment. This study was carried out jointly by the Ecuadorian
Trauma Society (ETS) and the International Trauma
System Development Program (ITSDP) of the Virginia
Commonwealth University (VCU), endorsed by the Pan-
american Trauma Society (PTS), the American Association
for the Surgery of Trauma (AAST), and approved by the
Ecuadorian Ministry of Health (EMH).
Methods
Site selection
According to the Pan American Health Organization,
Ecuador is experiencing one of the fastest urbanization
processes in the Andean region of South America [25]. We
selected the southeastern region of Ecuador, where large
urban and rural provinces are undergoing steady increase in
regional population and development with a 1.5% to 2.8%
estimated annual growth rate compared to the national
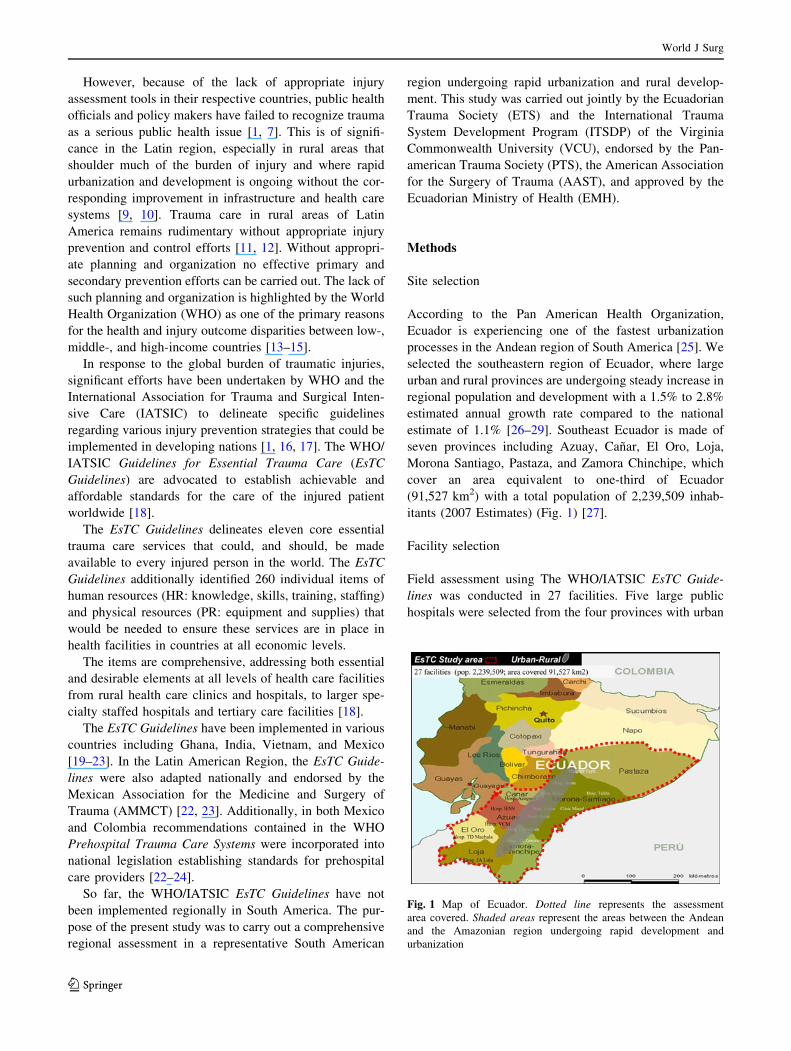
estimate of 1.1% [26–29]. Southeast Ecuador is made of
seven provinces including Azuay, Canar, El Oro, Loja,
Morona Santiago, Pastaza, and Zamora Chinchipe, which
cover an area equivalent to one-third of Ecuador
(91,527 km2) with a total population of 2,239,509 inhab-
itants (2007 Estimates) (Fig. 1) [27].
Facility selection
Field assessment using The WHO/IATSIC EsTC Guide-
lines was conducted in 27 facilities. Five large public
hospitals were selected from the four provinces with urban
Fig. 1 Map of Ecuador. Dotted line represents the assessment
area covered. Shaded areas represent the areas between the Andean
and the Amazonian region undergoing rapid development and
urbanization
World J Surg
123

centers (Azuay, Canar, El Oro, and Loja). These hospitals
are the tertiary care hospitals in the provincial capitals
responsible for the majority of trauma care in their
respective provinces. Other large hospitals that may occa-
sionally receive some trauma patients were not evaluated in
the study. Fifteen small general hospitals responsible for
significant trauma care were also selected from the Andean
province of Azuay and the Amazonian provinces of
Morona Santiago, Pastaza, and Zamora Chinchipe. The
small general hospitals were selected from representative
small towns and rural areas undergoing population growth,
rapid urbanization, and new road construction. Also
selected were seven representative rural clinics with high
trauma volumes from Azuay and Morona Santiago.
The EsTC Guidelinesemploys four categories for eval-
uation of trauma facilities: clinics, small hospitals staffed
with generalists, hospitals staffed with specialists, and
large hospitals serving as tertiary care facilities [18]. In
Ecuador, the small generalist-staffed hospitals are rare and
the majority of small hospitals involved with trauma care
have some degree of specialist staffing. Therefore, for this
study, only three facility levels were used: clinics, small
general hospitals, and large hospitals.
Assessment tools and process
The assessment tools used included two hospital assessment
forms provided by WHO, which were slightly modified and
adapted to the Ecuadorian circumstances (http://www.who.
int/violence_injury_prevention/services/traumacare/estc_
checklist.pdf). The first hospital form addressed the fol-
lowing criteria: (1) hospital type, (2) hospital size, (3)
trauma-related emergency visits and admissions, (4) staff
level of responders and their trauma care related training
and education (ATLS�, TNCC� or equivalents, in-service
training), and (5) staff availability [30, 31]. The assess-
ment form also evaluated the presence of trauma-related
quality improvement programs, trauma registry, contin-
uing medical education (CME) programs, and presence
and organization of ‘‘Trauma Teams’’ for acute resusci-
tation and management.
The second, more extensive assessment form employed
a 14-page checklist containing the 260 individual elements
suggested in the EsTC Guidelines, which address HR in
terms of availability, clinical knowledge, skills and train-
ing, and PR in terms of availability, operability, and
functionality. The elements were categorized as ‘‘not
applicable—NA’’ whenever an element was not relevant
for that level, ‘‘Absent—0’’ whenever an element was not
available, ‘‘Inadequate—1’’ when an element was not
available or when it was operational less than 50% of the
time, ‘‘Partly adequate—2’’ when an element was available
and operational greater than 50%, but not all, of the time,
and ‘‘Adequate—3’’ when an element was present and
available at all times.
To conduct the evaluation, permission was obtained from
all the provincial ministers of health. The facilities were
notified about the upcoming evaluation. All the evaluations
were performed in September 2007 by a team composed of
members from the VCU International Trauma System
Development Program (ITSDP) and the Ecuadorian
Trauma Society. The evaluation was carried out via
administrative and staff interviews of all individuals
involved in the care of the injured patient (nurses, residents,
physicians, supportive clerks, and technicians) from the
various services (general surgery, orthopedics, neurosur-
gery, emergency medicine, intensive and critical care,
radiology, pharmacy, and laboratory). To ensure the accu-
racy and completeness of the information, thorough walk-
throughs, inspections, and demonstrations of all supplies
and equipment were carried out, along with extensive
review of the ministry of health and hospital statistics. After
each facility evaluation, all information was reviewed by at
least two members of the team, and a second evaluation was
carried out to resolve any discrepancies if necessary.
Additionally all large hospitals and three small general
hospitals with large trauma services were re-visited at night
to verify the reported availability of staff, supportive ser-
vices, and machine operability.
Results
Facilities
Twenty-seven facilities were visited and evaluated. Despite
prior notification, only three hospitals made arrangements
for the visit. Therefore, the evaluation presented a more
accurate assessment of the daily operational capability of
each facility. Three of the clinics did not have enough staff
available to obtain a valid assessment and were excluded
from the study. This study was limited to the 24 facilities
where an adequate assessment could be obtained. Table 1
shows the type and size of the hospitals that were evaluated.
Overall, 210,045 emergency (ED) visits and 61,365
(29%) ED trauma visits per year (2006–2007) were
recorded. with an incidence rate of 2,740/100,000 inhab-
itants. The large urban hospitals had an average of 38,000
ED visits per year, which is equivalent to many U.S. urban
hospitals. One-third of these visits were trauma-related and
resulted in a 20% trauma admission rate. The small general
hospitals within areas undergoing rapid urbanization
showed a similar profile to urban hospitals, with a slightly
higher trauma admission rate (30%). The rural clinics had
fewer but still-significant numbers of trauma-related visits
(20%) (Table 1).
World J Surg
123
Prehospital and interhospital transport
Prehospital communication in the urban areas was noted to
be adequate. Major deficits were noted in interhospital
transfers at all levels. There was no effective coordination
or communication (no common communication channel, or
pre-existing agreements) between the facilities and no prior
notification of the patient’s transfer. Most of the ambulance
services for rural to urban areas were transport vehicles
devoid of any interhospital monitoring or paramedical care
services. All well-equipped ambulances were limited to the
provision of local services only. Fifteen of the twenty-five
ambulances inspected in the large and small facilities were
either nonfunctional or in repair.
Training and staffing
The large and small general hospitals were staffed by
physicians, nurses, and various specialists. The clinics were
staffed by health care promoters or general doctors with
very limited trauma training or resources (Table 2). None
of the physicians staffed the facilities full time. Most
physicians worked an average of 4 h per day at the public
hospitals. Nursing coverage, on the other hand, was more
comprehensive in all facilities, but incredibly limited in
trauma management. Specialty trained doctors were pres-
ent in the large and small general hospitals. However,
100% coverage of specialists in any setting was not pres-
ent. In one small general hospital representing the only
facility for trauma care in the province of Zamora-
Chinchipe, there was one general surgeon available for the
first two weeks of every month. Equally sparse in the small
general hospitals was the radiology staff (physicians and
technicians). In the province of Morona Santiago, trauma
care in six of the small hospitals was carried out without
diagnostic radiology support.
The level of preparation for essential trauma care was
alarmingly low in all settings (Table 2). The first responders
in the emergency rooms of the large hospitals and small
general hospitals were the interns, residents, and nurses.
The majority did not have trauma care training or education.
Less than 15% of physicians were trained in ATLS� or an
equivalent trauma course. No nurse had ever participated in
TNCC� or equivalent trauma care course for nurses. In the
large urban hospitals, few of the attending physicians and
administrators were ATLS� certified. However, they were
not involved in the initial management and resuscitation of
the injured patients. Most noted that ATLS� is expensive
and not feasible for most settings of the southeastern region
of Ecuador. In the small general hospitals, in-service trauma
education and training was minimal for both physicians and
nurses. The lack of adequate preparation and response and
the need for basic trauma care training was witnessed by the
authors (M.A., F.M.) during the inspection of a small pro-
vincial general hospital. Without any prehospital warning,
the emergency room was inundated by multiple casualties
from a motor vehicle crash. The response was marked by
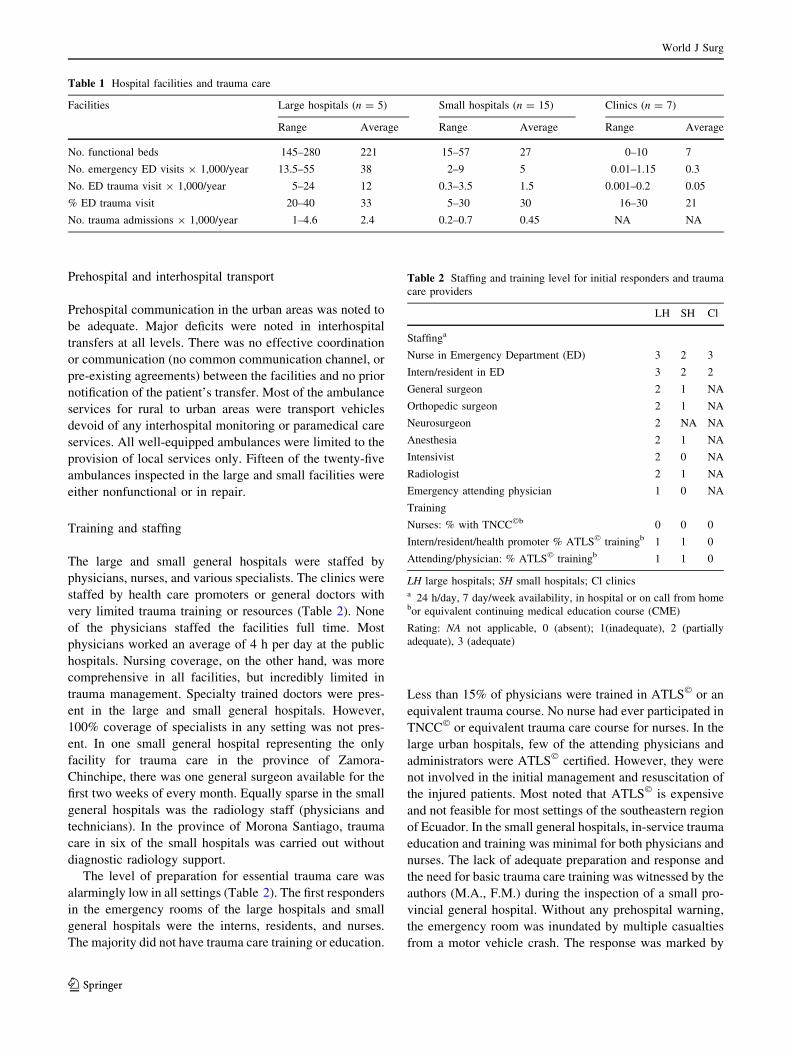
Table 1 Hospital facilities and trauma care
Facilities Large hospitals (n = 5) Small hospitals (n = 15) Clinics (n = 7)
Range Average Range Average Range Average
No. functional beds 145–280 221 15–57 27 0–10 7
No. emergency ED visits 9 1,000/year 13.5–55 38 2–9 5 0.01–1.15 0.3
No. ED trauma visit 9 1,000/year 5–24 12 0.3–3.5 1.5 0.001–0.2 0.05
% ED trauma visit 20–40 33 5–30 30 16–30 21
No. trauma admissions 9 1,000/year 1–4.6 2.4 0.2–0.7 0.45 NA NA
Table 2 Staffing and training level for initial responders and trauma
care providers
LH SH Cl
Staffinga
Nurse in Emergency Department (ED) 3 2 3
Intern/resident in ED 3 2 2
General surgeon 2 1 NA
Orthopedic surgeon 2 1 NA
Neurosurgeon 2 NA NA
Anesthesia 2 1 NA
Intensivist 2 0 NA
Radiologist 2 1 NA
Emergency attending physician 1 0 NA
Training
Nurses: % with TNCC�b 0 0 0
Intern/resident/health promoter % ATLS� trainingb 1 1 0
Attending/physician: % ATLS� trainingb 1 1 0
LH large hospitals; SH small hospitals; Cl clinicsa 24 h/day, 7 day/week availability, in hospital or on call from homebor equivalent continuing medical education course (CME)
Rating: NA not applicable, 0 (absent); 1(inadequate), 2 (partially
adequate), 3 (adequate)
World J Surg
123
disorganization, inappropriate resource utilization, and a
lack of systematic approach to the management of one and/
or multiple trauma patients.
In the clinics, the generalists and local health care
workers had significant knowledge and training in basic
primary care, but a disproportionately low level of knowl-
edge in basic injury mechanisms, trauma stabilization, and
referral.
Resources for essential trauma care
Human and physical resources for essential trauma care in
terms of airway, respiratory, and shock management are
summarized in Tables 3 and 4. Basic airway management
was adequate at the large urban hospitals. In the small
general hospitals, basic airway management was also
adequate in terms of skill and equipment. Advanced airway
management, however, in terms of endotracheal or surgical
airways were alarmingly deficient even in hospitals where
surgical specialties were present. This was not only due to
lack of equipment but also to lack of training. In some
small general hospitals, obtaining a definitive airway was
not a priority because there was lack of ventilators, critical
care capability, and timely transport.
In terms of respiratory support, 4 of the 5 large hospitals
had the training and equipment for sufficient management.
This was not the case in 13 of the small general hospitals
evaluated. For the treatment of a pneumothorax, the gen-
eralists and residents needed to wait for a surgical attending
to help in the placement of a chest tube. If the surgeon was
unavailable (nights and weekends), the patient was usually
transferred irrespective of the patient’s stability. Other
treatment measures, such as needle decompression or
placement of a Heimlich valve were not used in any hos-
pital evaluated. The majority of physicians and residents
attributed this to the lack of supplies for use in training and
acute events. However, during direct inspection all small
hospitals had chest tubes locked in inaccessible cabinets or
storage rooms. During the motor vehicle collision (MVC)
incident mentioned above, endotracheal tubes and Foley
catheters were modified and used as makeshift chest tubes),
with noted breakdown in sterility and loss of time.
Both large and small general hospitals had staff with
adequate knowledge and skills to control hemorrhage and
perform shock management. One common deficiency seen
throughout the southeastern region of Ecuador was the lack
of blood transfusion capabilities, especially during emer-
gencies and operative resuscitations. This was mainly
attributed to financial and logistical constraints. In the
urban areas, there was no formal process or agreement
between the hospitals and the local blood banks for a quick
supply of blood products. Additionally, blood needed to be
purchased by the patient prior to its administration. In the
urbanizing rural regions, no blood banks were available.
Finally, end-points of resuscitation in the small general
hospitals and one of the large hospitals were based on
blood pressure and urine output. Central venous pressure
measurement, lactate, and blood gases could not be per-
formed. Human and physical resources for essential trauma
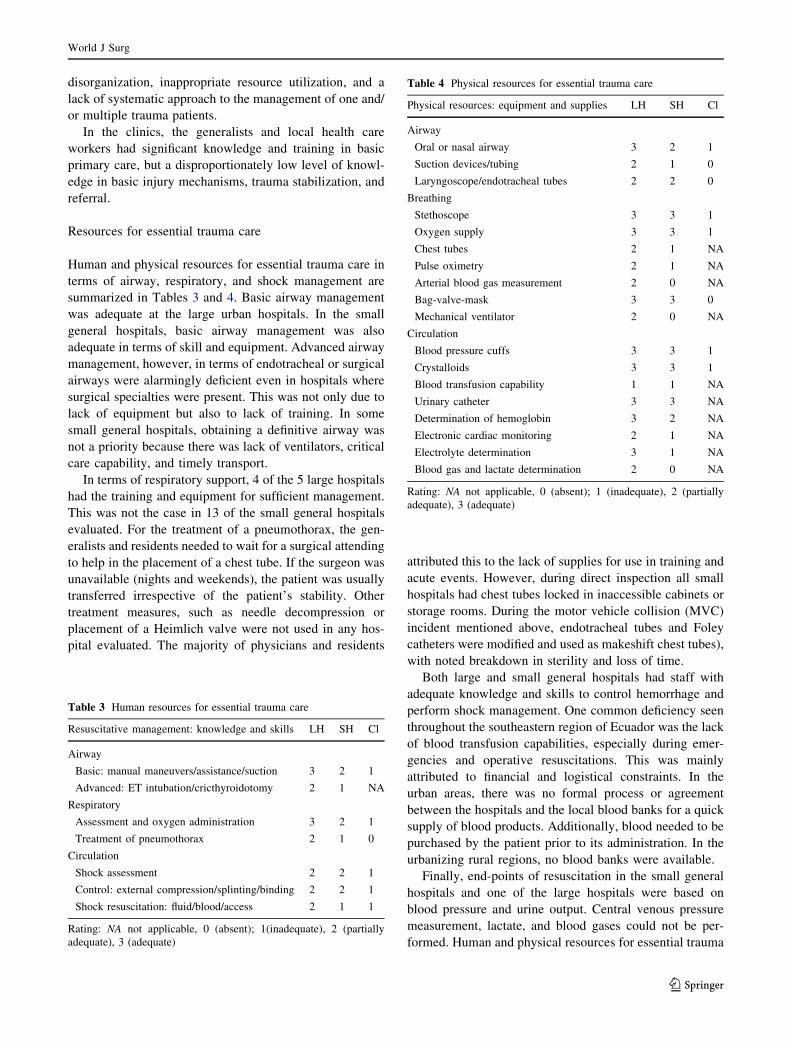
Table 3 Human resources for essential trauma care
Resuscitative management: knowledge and skills LH SH Cl
Airway
Basic: manual maneuvers/assistance/suction 3 2 1
Advanced: ET intubation/cricthyroidotomy 2 1 NA
Respiratory
Assessment and oxygen administration 3 2 1
Treatment of pneumothorax 2 1 0
Circulation
Shock assessment 2 2 1
Control: external compression/splinting/binding 2 2 1
Shock resuscitation: fluid/blood/access 2 1 1
Rating: NA not applicable, 0 (absent); 1(inadequate), 2 (partially
adequate), 3 (adequate)
Table 4 Physical resources for essential trauma care
Physical resources: equipment and supplies LH SH Cl
Airway
Oral or nasal airway 3 2 1
Suction devices/tubing 2 1 0
Laryngoscope/endotracheal tubes 2 2 0
Breathing
Stethoscope 3 3 1
Oxygen supply 3 3 1
Chest tubes 2 1 NA
Pulse oximetry 2 1 NA
Arterial blood gas measurement 2 0 NA
Bag-valve-mask 3 3 0
Mechanical ventilator 2 0 NA
Circulation
Blood pressure cuffs 3 3 1
Crystalloids 3 3 1
Blood transfusion capability 1 1 NA
Urinary catheter 3 3 NA
Determination of hemoglobin 3 2 NA
Electronic cardiac monitoring 2 1 NA
Electrolyte determination 3 1 NA
Blood gas and lactate determination 2 0 NA
Rating: NA not applicable, 0 (absent); 1 (inadequate), 2 (partially
adequate), 3 (adequate)
World J Surg
123
care in terms of airway management, respiratory support,
hemorrhage control, immobilization, and transfer were not
adequate at the clinic levels.
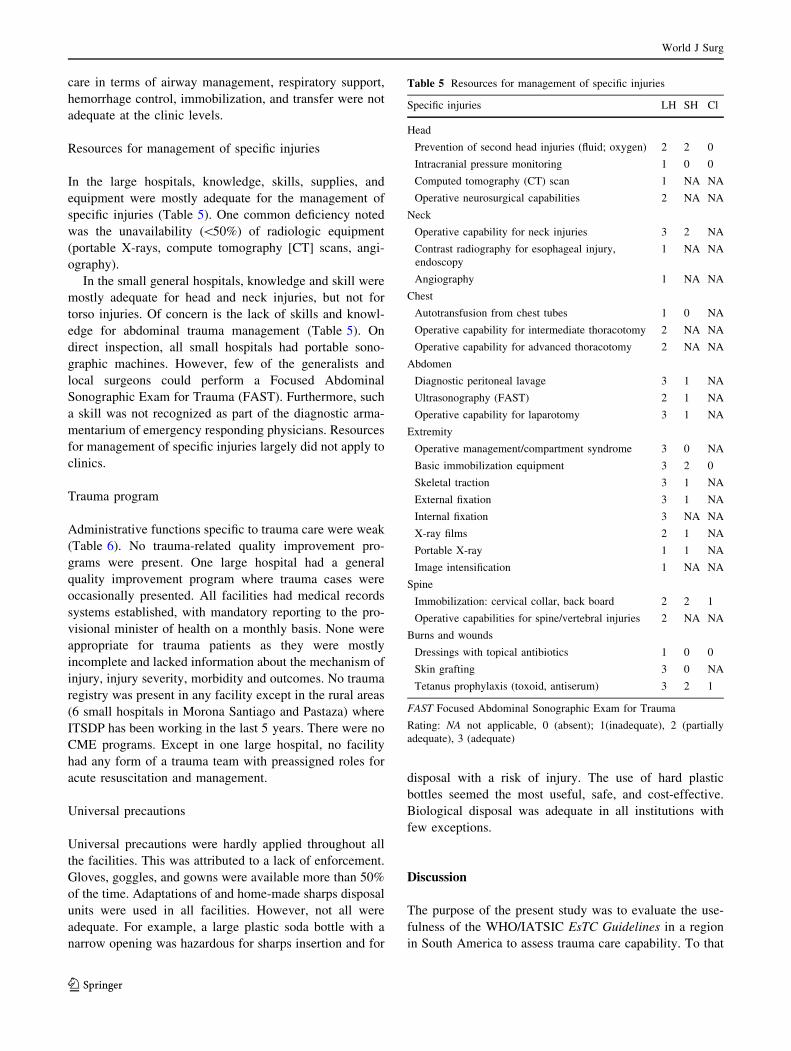
Resources for management of specific injuries
In the large hospitals, knowledge, skills, supplies, and
equipment were mostly adequate for the management of
specific injuries (Table 5). One common deficiency noted
was the unavailability (\50%) of radiologic equipment
(portable X-rays, compute tomography [CT] scans, angi-
ography).
In the small general hospitals, knowledge and skill were
mostly adequate for head and neck injuries, but not for
torso injuries. Of concern is the lack of skills and knowl-
edge for abdominal trauma management (Table 5). On
direct inspection, all small hospitals had portable sono-
graphic machines. However, few of the generalists and
local surgeons could perform a Focused Abdominal
Sonographic Exam for Trauma (FAST). Furthermore, such
a skill was not recognized as part of the diagnostic arma-
mentarium of emergency responding physicians. Resources
for management of specific injuries largely did not apply to
clinics.
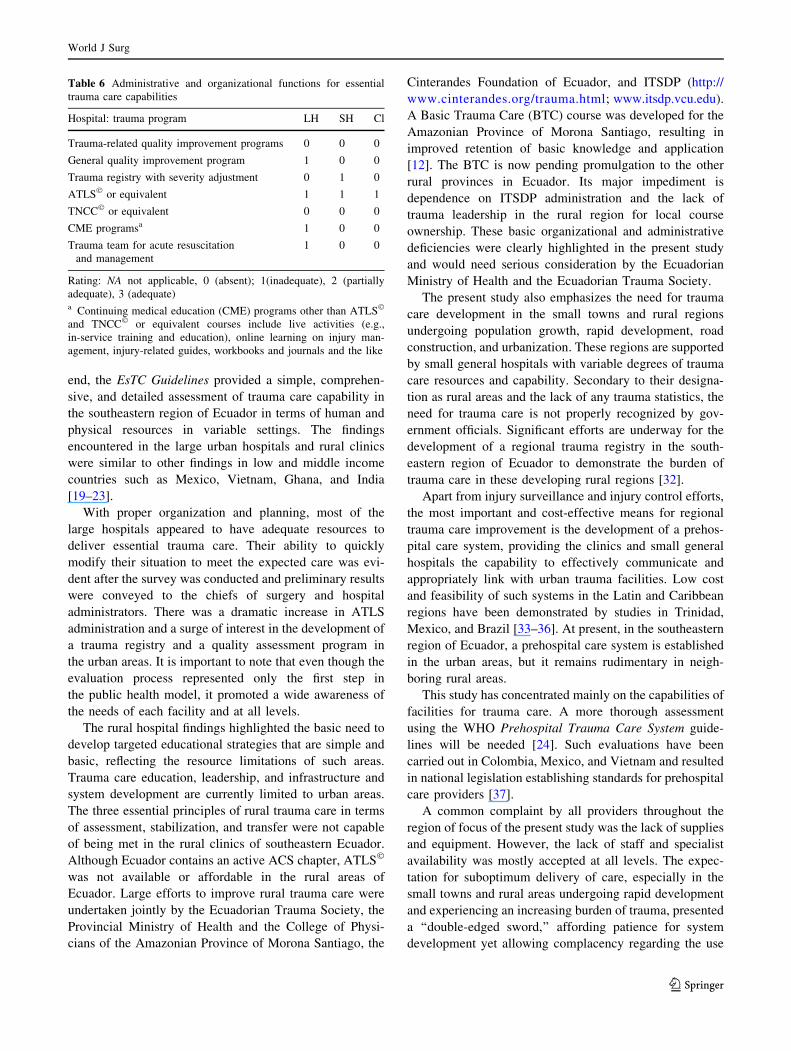
Trauma program
Administrative functions specific to trauma care were weak
(Table 6). No trauma-related quality improvement pro-
grams were present. One large hospital had a general
quality improvement program where trauma cases were
occasionally presented. All facilities had medical records
systems established, with mandatory reporting to the pro-
visional minister of health on a monthly basis. None were
appropriate for trauma patients as they were mostly
incomplete and lacked information about the mechanism of
injury, injury severity, morbidity and outcomes. No trauma
registry was present in any facility except in the rural areas
(6 small hospitals in Morona Santiago and Pastaza) where
ITSDP has been working in the last 5 years. There were no
CME programs. Except in one large hospital, no facility
had any form of a trauma team with preassigned roles for
acute resuscitation and management.
Universal precautions
Universal precautions were hardly applied throughout all
the facilities. This was attributed to a lack of enforcement.
Gloves, goggles, and gowns were available more than 50%
of the time. Adaptations of and home-made sharps disposal
units were used in all facilities. However, not all were
adequate. For example, a large plastic soda bottle with a
narrow opening was hazardous for sharps insertion and for
disposal with a risk of injury. The use of hard plastic
bottles seemed the most useful, safe, and cost-effective.
Biological disposal was adequate in all institutions with
few exceptions.
Discussion
The purpose of the present study was to evaluate the use-
fulness of the WHO/IATSIC EsTC Guidelines in a region
in South America to assess trauma care capability. To that
Table 5 Resources for management of specific injuries
Specific injuries LH SH Cl
Head
Prevention of second head injuries (fluid; oxygen) 2 2 0
Intracranial pressure monitoring 1 0 0
Computed tomography (CT) scan 1 NA NA
Operative neurosurgical capabilities 2 NA NA
Neck
Operative capability for neck injuries 3 2 NA
Contrast radiography for esophageal injury,
endoscopy
1 NA NA
Angiography 1 NA NA
Chest
Autotransfusion from chest tubes 1 0 NA
Operative capability for intermediate thoracotomy 2 NA NA
Operative capability for advanced thoracotomy 2 NA NA
Abdomen
Diagnostic peritoneal lavage 3 1 NA
Ultrasonography (FAST) 2 1 NA
Operative capability for laparotomy 3 1 NA
Extremity
Operative management/compartment syndrome 3 0 NA
Basic immobilization equipment 3 2 0
Skeletal traction 3 1 NA
External fixation 3 1 NA
Internal fixation 3 NA NA
X-ray films 2 1 NA
Portable X-ray 1 1 NA
Image intensification 1 NA NA
Spine
Immobilization: cervical collar, back board 2 2 1
Operative capabilities for spine/vertebral injuries 2 NA NA
Burns and wounds
Dressings with topical antibiotics 1 0 0
Skin grafting 3 0 NA
Tetanus prophylaxis (toxoid, antiserum) 3 2 1
FAST Focused Abdominal Sonographic Exam for Trauma
Rating: NA not applicable, 0 (absent); 1(inadequate), 2 (partially
adequate), 3 (adequate)
World J Surg
123
end, the EsTC Guidelines provided a simple, comprehen-
sive, and detailed assessment of trauma care capability in
the southeastern region of Ecuador in terms of human and
physical resources in variable settings. The findings
encountered in the large urban hospitals and rural clinics
were similar to other findings in low and middle income
countries such as Mexico, Vietnam, Ghana, and India
[19–23].
With proper organization and planning, most of the
large hospitals appeared to have adequate resources to
deliver essential trauma care. Their ability to quickly
modify their situation to meet the expected care was evi-
dent after the survey was conducted and preliminary results
were conveyed to the chiefs of surgery and hospital
administrators. There was a dramatic increase in ATLS
administration and a surge of interest in the development of
a trauma registry and a quality assessment program in
the urban areas. It is important to note that even though the
evaluation process represented only the first step in
the public health model, it promoted a wide awareness of
the needs of each facility and at all levels.
The rural hospital findings highlighted the basic need to
develop targeted educational strategies that are simple and
basic, reflecting the resource limitations of such areas.
Trauma care education, leadership, and infrastructure and
system development are currently limited to urban areas.
The three essential principles of rural trauma care in terms
of assessment, stabilization, and transfer were not capable
of being met in the rural clinics of southeastern Ecuador.
Although Ecuador contains an active ACS chapter, ATLS�
was not available or affordable in the rural areas of
Ecuador. Large efforts to improve rural trauma care were
undertaken jointly by the Ecuadorian Trauma Society, the
Provincial Ministry of Health and the College of Physi-
cians of the Amazonian Province of Morona Santiago, the
Cinterandes Foundation of Ecuador, and ITSDP (http://
www.cinterandes.org/trauma.html; www.itsdp.vcu.edu).
A Basic Trauma Care (BTC) course was developed for the
Amazonian Province of Morona Santiago, resulting in
improved retention of basic knowledge and application
[12]. The BTC is now pending promulgation to the other
rural provinces in Ecuador. Its major impediment is
dependence on ITSDP administration and the lack of
trauma leadership in the rural region for local course
ownership. These basic organizational and administrative
deficiencies were clearly highlighted in the present study
and would need serious consideration by the Ecuadorian
Ministry of Health and the Ecuadorian Trauma Society.
The present study also emphasizes the need for trauma
care development in the small towns and rural regions
undergoing population growth, rapid development, road
construction, and urbanization. These regions are supported
by small general hospitals with variable degrees of trauma
care resources and capability. Secondary to their designa-
tion as rural areas and the lack of any trauma statistics, the
need for trauma care is not properly recognized by gov-
ernment officials. Significant efforts are underway for the
development of a regional trauma registry in the south-
eastern region of Ecuador to demonstrate the burden of
trauma care in these developing rural regions [32].
Apart from injury surveillance and injury control efforts,
the most important and cost-effective means for regional
trauma care improvement is the development of a prehos-
pital care system, providing the clinics and small general
hospitals the capability to effectively communicate and
appropriately link with urban trauma facilities. Low cost
and feasibility of such systems in the Latin and Caribbean
regions have been demonstrated by studies in Trinidad,
Mexico, and Brazil [33–36]. At present, in the southeastern
region of Ecuador, a prehospital care system is established
in the urban areas, but it remains rudimentary in neigh-
boring rural areas.
This study has concentrated mainly on the capabilities of
facilities for trauma care. A more thorough assessment
using the WHO Prehospital Trauma Care System guide-
lines will be needed [24]. Such evaluations have been
carried out in Colombia, Mexico, and Vietnam and resulted
in national legislation establishing standards for prehospital
care providers [37].
A common complaint by all providers throughout the
region of focus of the present study was the lack of supplies
and equipment. However, the lack of staff and specialist
availability was mostly accepted at all levels. The expec-
tation for suboptimum delivery of care, especially in the
small towns and rural areas undergoing rapid development
and experiencing an increasing burden of trauma, presented
a ‘‘double-edged sword,’’ affording patience for system
development yet allowing complacency regarding the use
Table 6 Administrative and organizational functions for essential
trauma care capabilities
Hospital: trauma program LH SH Cl
Trauma-related quality improvement programs 0 0 0
General quality improvement program 1 0 0
Trauma registry with severity adjustment 0 1 0
ATLS� or equivalent 1 1 1
TNCC� or equivalent 0 0 0
CME programsa 1 0 0
Trauma team for acute resuscitation
and management
1 0 0
Rating: NA not applicable, 0 (absent); 1(inadequate), 2 (partially
adequate), 3 (adequate)a Continuing medical education (CME) programs other than ATLS�
and TNCC� or equivalent courses include live activities (e.g.,
in-service training and education), online learning on injury man-
agement, injury-related guides, workbooks and journals and the like
World J Surg
123

of basic, innovative, and cost effective measures. These
attitudes and perceptions can only be overcome with the
active involvement of trauma societies in educating trauma
care providers, average citizens, and policy makers regard-
ing the ‘‘essential rights of all trauma patients’’ as clearly
delineated in the EsTC Guidelines.
Additionally, the EsTC Guidelines provided specific
measures for the leaders in trauma care and for hospital
administrators as to how these guidelines can be achieved
and implemented in terms of improving trauma education,
in-service training, trauma team organization, development
of a trauma registry, and development of quality improve-
ment programs. All national trauma societies should take an
active advisory role to their provisional ministries of health
to help decide which elements delineated in the EsTC
Guidelines are essential and cost-effective, and can be
realistically assured to any injured patient at each facility
(Table 7).
The results of the present study were presented to the
Ecuadorian Trauma Society, the Ecuadorian National
Association of Rural Physicians, the Ecuadorian Chapter of
the American College of Surgeons, and the Ecuadorian
Ministry of Health. The EsTC Guidelines were endorsed by
members of the ETS, with plans to extend the assessment
to the remaining region of Ecuador. Additionally, a pro-
posal for trauma system development in Ecuador was
Table 7 Summary of
recommendationsPrehospital and inter-hospital transport
Improve prehospital and interfacility communication and transfer
Establish formal agreement and protocols for interfacility transfer
Define a core set of prehospital equipment and supplies for essential trauma care
Initiate cross training of prehospital personnel in urban and rural prehospital care
Rural clinics
Provide basic education in trauma definition, mechanism, and physiology
Provide targeted educational strategies and training initiatives to develop competency in basic trauma
care: assessment, stabilization, and transfer
Develop leadership training in organization and system development
Enhance coordination with urban facilities to improve transport and patient care
General and tertiary hospitals
Improve coordination and communication with prehospital and rural facilities
Improve capability for ED resuscitation and management
Redirect training resources toward first responders in ED
Develop targeted trauma education for nurses (TNCC or equivalent) and for residents and physicians
(ATLS or equivalent)
Enhance ‘‘Trauma Team’’ approach toward acute trauma resuscitation
Improve immediate accessibility to basic adjuncts for trauma care (airway adjuncts, chest tubes, X-rays,
ultrasound) and enhance capability for their use
Improve capability for surgical management of certain injuries: neck and abdomen
Administrative function per facility
Reorganization and planning for provision of essential trauma care within facility based
identified and documented local needs and resources
Develop a trauma registry with severity adjustment
Initiate trauma quality improvement programs focusing on preventable morbidity and mortality and
addressing correctable system and individual risk factors
Use of EsTC Guidelines to monitor improvement in trauma care capabilities
Require and subsidize CME programs for emergency and trauma care responders
Enforce universal precautions in all trauma care settings
Develop agreements with local blood banks for blood availability during emergencies and operative
resuscitations
Ecuadorian Trauma Society
Initiate targeted education for emergency care providers, hospital administrators, and policy makers on
‘‘essential rights of all injured patients’’ as delineated in the EsTC Guidelines
Define leadership positions and political advocacy plan for national, regional, and local promulgation of
the EsTC Guidelines
Advocate for health care policy development and national legislation to ensure universal provision of
essential trauma care as delineated in the EsTC Guidelines
World J Surg
123
jointly developed by the Ecuadorian Committee for the
Prevention, Management & Control of Injuries (CEP-
MCR), a joint committee composed of members of ETS
and the Ecuadorian ACS chapter, and VCU’s ITSDP and
submitted to the Ecuadorian Ministry of Health for con-
sideration. The objective is to incorporate the EsTC
Guidelines into national legislation and establish standards
for essential trauma care in all regions in Ecuador.
The methods and results of this study, along with similar
findings in Mexico and Colombia, regarding the effective
use of the EsTC Guidelines for trauma care prompted the
development of the Trauma System Committee (TSC) by
the Panamerican Trauma Society (PTS) [22, 37]. The PTS
serves as the ‘‘parent’’ organization for the various national
specialty societies dedicated to the care and management of
trauma patients in several countries, including Argentina,
Bolivia, Brazil, Canada, Chile, Colombia, Cuba, Ecuador,
Guatemala, Mexico, Panama, Paraguay, Peru, Uruguay,
and Venezuela. The objectives of the TSC include the
adaptation of the EsTC Guidelines to the Latin American
countries and their regional promulgation and implemen-
tation. This study does not reflect an assessment of other
areas or facilities throughout the entire South American
region. This endeavor is to be undertaken jointly with the
national trauma societies in collaboration with the Pan
American Health Organization (PAHO)/WHO.
Limitations to the present study include the fact that
skills assessments are mainly subjective. Thus documen-
tation of in-service training and presence of specialty care
was important. Also, improvement in physical resources
does not always equate with improvement in outcome.
However the availability of resources is integral to system
development and has been shown to improve trauma pro-
cesses and outcomes [38, 39].
Conclusions
The IATSIC/WHO EsTC Guidelines provide a simple and
useful template to assess trauma care capability in variable
facilities and international settings. The present study has
shown the usefulness of the EsTC Guidelines in various
economic settings and in various stages of development
and urbanization. This is important and increases the
ability of the EsTC Guidelines to provide an internationally
applicable and standardized template with which to assess
trauma care capabilities in the Latin American region. The
adaptation of the EsTC Guidelines for the Latin American
region and its joint endorsement by PAHO, the Panamer-
ican Trauma Society, and their respective national chapters
is the next important step for the promulgation of the EsTC
Guidelines throughout the Latin Region.
References
1. Hofman K, Primack A, Keusch G et al (2005) Addressing the
growing burden of trauma and injury in low- and middle-income
countries. Am J Public Health 95:13–17
2. Murray CJ, Lopez AD (1996) The global burden of disease: a
comprehensive assessment of mortality and disability from dis-
eases, injuries, and risk factors in 1990 and projected to 2020.
Harvard University Press, Cambridge, MA
3. Murray CJL, Lopez AD (1996) Global health statistics: a com-
pendium of incidence prevalence and mortality estimates for over
200 conditions. Harvard University Press, Cambridge, MA
4. Pan American Health Organization (2005) Regional Core Health
Data and Country Profile Initiative, 2000–2005. www.paho.org.
Accessed Nov 10 2005
5. World Health Organization (2004) The World Health Report
2004: changing history. WHO, Geneva, Switzerland
6. Perel P, Cases JP, Ortiz Z et al. (2006) Noncommunicable dis-
eases and injuries in Latin America and the Caribbean: time for
action. PLoS Med 3:e344
7. Fraade-Blanar L, Concha-Eastman A, Baker T (2007) Injury in
the Americas: the relative burden and challenge. Rev Panam
Salud Pub 22:254–259
8. Jamison DT, Mosley H (1991) Disease control priorities in
developing countries: health policy responses to epidemiological
changes. Am J Public Health 81:15–22
9. Fraser B (2005) Traffic accidents scar Latin America’s roads.
Lancet 366(9487):703–704
10. Tercero F, Andersson R, Pena R et al (2006) The epidemiology of
moderate and severe injuries in a Nicaraguan community: a
household-based survey. Public Health 120:106–114
11. Richman M, Shayne P, Heron S et al (2000) Injury control in
Honduras: a survey of injury mortality. Ann Emerg Med
36:333–339
12. Aboutanos MB, Rodas EB, Aboutanos SZ et al (2007) Trauma
education and care in the jungle of Ecuador, where there is no
advanced trauma life support. J Trauma 62:714–719
13. Mock C, Kobusingye O, Joshipura M et al (2005) Strengthening
trauma and critical care globally. Current Opin Crit Care
11:568–575
14. Aboutanos M, Areola-Risa C, Rodas EB (2009) Trauma care
system implementation & development in Latin America
[Implementacion y desarrollo de sistemas de atencion en trauma
en America Latina]. In: Ferrada R, Rodriguez A et al (eds)
Trauma-Sociedad Panamericana de Trauma, 2nd edn. Distribuna
Editorial Medica, Cali Colombia, pp 9–28
15. Joshipura M, Mock C, Goosen J et al (2004) Essential trauma
care: strengthening trauma systems around the world. Injury
35:841–845
16. Krug EG, Dahlberg LL, Mercy JA et al (eds) (2002) Violence and
health. World Health Organization, Geneva
17. Peden M, Scurfield R, Sleet D et al (eds) (2004) Road traffic
injury prevention. World Health Organization, Geneva
18. Mock C, Lormand JD, Goosen J et al (2004) Guidelines for
essential trauma care. World Health Organization, Geneva
19. Quansah R (2006) Essential trauma care in Ghana: adaptation and
implementation on the political tough road. World J Surg
30:934–939
20. Joshipura M (2006) Guidelines for essential trauma care: progress
in India. World J Surg 30:930–933
21. Son NT, Mock C (2006) Improvements in trauma care capabili-
ties in Vietnam through use of the WHO-IATSIC guidelines for
essential trauma care. Int J Injury Control Saf Promot 13:125–127
22. Arreola-Risa C, Mock C, Vega FR et al (2006) Evaluating trauma
care capabilities in Mexico with the World Health Organization’s
World J Surg
123

guidelines for essential trauma care publication. Rev Panam
Salud Pub 19:94–103
23. Mock C, Nguyen S, Quansah R et al (2006) Evaluation of trauma
care capabilities in four countries using the WHO-IATSIC
guidelines for essential trauma care. World J Surg 30:946–956
24. World Health Organization (2005) Prehospital trauma care sys-
tems. World Health Organization, Geneva
25. Pan American Health Organization (2007) Health in the Ameri-
cas, 2007. Volume II-Countries. Pan American Health Organi-
zation, Washington, pp 315–321
26. Population Division of the Department of Economic and Social
Affairs of the United Nations Secretariat, World Population
Prospects: The 2006 Revision and World Urbanization Prospects:
The 2007 Revision. http://esa.un.org/unup. Accessed September
03 2009
27. Proyeccion de la Poblacion Ecuatoriana, por Anos Calendario,
Segun Regiones y Provincias–Perıodo 2001–2010. Proyecto
‘‘Apoyo al Censo de Poblacion y Vivienda y al Fortalecimiento
del INEC.’’ Instituto Nacional de Estadısticas y Censos del
Ecuador. INEC–Ecuador’s National Institute for Statistics &
Census, 2004
28. Anuario de estadısticas de transporte (2006–2007) Instituto
Nacional de Estadısticas y Censos del Ecuador. INEC—Ecua-
dor’s National Institute for Statistics & Census
29. Proyectos de infraestructura para el transporte, construccion,
reconstruccion, mantenemineto y mejoramiento—Augosto 2009.
Ministerio de Transporte y Obras Publicas. Ecuador ‘s Ministry
of Transporte and Public Works
30. American College of Surgeons (2007) Advanced Trauma Life
Support (ATLS) Student Manual, 7th edn. American College of
Surgeons, Chicago
31. Emergency Nurse Association (2008) Trauma Nursing Core
Course (TNCC) Provider Manual, 6th edn. Emergency Nurse
Association, Des Plaines
32. Aboutanos M, Mora F, Duong M et al. (2007) Telemedicine
applications and rural system development in Latin America:
Ecuador’s experience. J Health Technol Appl. Accessed on line
Nov 15, 2009
33. Arreola-Risa C, Mock C, Padilla D et al (1995) Trauma care
systems in urban Latin America: the priorities should be pre-
hospital and emergency room management. J Trauma 39:
457–462
34. Marson A, Thomson J (2001) The influence of prehospital trauma
care on traffic accident mortality. J Trauma 50:917–921
35. Arreola-Risa C, Mock C, Herrera-Escamilla AJ et al (2004) Cost-
effectiveness and benefit of alternatives to improve training for
prehospital trauma care in Mexico. Prehospital Disaster Med
19:318–325
36. Ali J, Cohen R, Adam R et al (1997) Effect of the Prehospital
Trauma Life Support Program (PHTLS) on prehospital trauma
care. J Trauma 42:786–790
37. Mock C, Abantanga F, Goosen J et al (2009) Strengthening care
of injured children globally. Bull WHO 87:382–389
38. MacKenzie EJ, Rivara FP, Jurkovich GJ et al. (2006) A national
evaluation of the effect of trauma-center care on mortality.
N Engl J Med 26(354):366–378
39. Mann N, Mullins R, Mackenzie E et al (1999) A systematic
review of published evidence regarding trauma system effec-
tiveness. J Trauma 47:S23–S25
World J Surg
123