quantification of gas denucleation and thrombogenicity of vascular grafts
TRANSCRIPT

Quantification of gas denucleation and thrombogenicity of vascular grafts"
Christopher V. Bemen>$ Richard D. Vann? Kim E. Koger,' and Bruce KlitzmantT5,' 'Plastic Surgery Research Laboratories, #E G. Hall Hyperbaric Laboratory, Department of Anesthesiology, and §Division of Physiology, Duke University Medical Center, Durham, North Carolina 27710
In vitro methods were developed to mea- sure the air content of vascular graft walls and the thrombogenicity of this air. Gas content (volume %) of expanded polyte- trafluoroethylene (ePTFE) grafts from dif- ferent sources ranged from 75.5 a 0.4% to 61.8 k 0.3%. Exposure of Vitagraft ePTFE to a vacuum prior to saline immersion re- placed 87.5% of the gas nuclei with saline (denucleation). Acetone and ethanol im- mersion produced 98.9% and 94.3% denu- cleation, respectively. Denucleation was essentially complete when vacuum expo- sure was followed by hydrostatic pressure
treatment at 500 psig or greater. The in- f luence of gas content on thrombogenicity was determined by immersing graft sam- ples in whole canine blood and weighing the adherent thrombus. Denucleation sig- nificantly reduced adherent thrombus weight compared with control grafts ( p < 0.001). Air in Vitagraft walls was responsible for 84% of the adherent thrombus weight at four minutes. The de- scribed methods could be employed to as- sess the hemocompatibility of various biomaterials.
INTRODUCTION
Biomaterials used in the production of vascular prostheses are inherently thrombogenic.' Heparin bonding, endothelial cell seeding, and the use of local and systemic antiplatelet agents are several methods that improve hem~compatibility.~~ One component of thrombogenicity that is of ten over- looked is the blood-gas interface. Gas was first found to cause blood damage in bubble oxygenators as the result of the interfacial denaturation of globular plasma protein^."^ This denaturation results in the activation of platelets, com- plement, and fibrinogen:-lo Madras et al. demonstrated that air trapped in sur- face imperfections will persist indefinitely on hydrophobic surfaces and may require prolonged times to dissolve on hydrophilic surfaces." Such air may be present at any material-blood interface.
Expanded polytetraf luoroethylene (ePTFE) grafts were first used clinically by Soyer in 1972 and currently have widespread applicability in vascular re-
*No benefit of any kind will be received either directly or indirectly by the author(s), although this work was funded in part by Bard Cardiosurgery, Inc., Billerica, MA.
'To whom correspondence should be addressed at Plastic Surgery Research Labora- tories, P. 0. Box 3906, Duke University Medical Center, Durham, North Carolina 27710.
Journal of Biomedical Materials Research, Vol. 25, 373-386 (1991) 0 1991 John Wiley & Sons, Inc. CCC 0021-9304/91/030373-14$04.00

374 BENSEN ET AL.
construction. A limiting factor, however, is their high rate of thrombosis. Ex- panded PTFE grafts were found to have a gas content of 70% air by volume.’2 Thus, blood in contact with ePTFE is exposed to a composite surface of bub- bles or ”gas nuclei” and ePTFE fibrils. The removal of these gas nuclei has been called denucleation. Several techniques, including immersion in ethanol, acetone, and vacuum, have been employed to denucleate biomateri- als.8,11,12 Recent studies in rats have demonstrated a profound increase in pa- tency of l-mm-I.D. ePTFE microvascular grafts denucleated by hydrostatic pres~ure.’”~
There is currently no method for systematically quantifying the efficacy of denucleation or assessing the consequent reduction of thrombogenicity. The purposes of these studies were to quantify the gas content of six types of vas- cular grafts, the efficiency of denucleation methods, and the effect of denu- cleation on the thrombogenicity of Vitagraf t.
MATERIALS A N D METHODS
Methods of gas denucleation
Graft samples measuring 4 mm I.D. X 1.0 cm long were weighed to the nearest 0.0001 g and placed in 10-mL Vacutainer (Becton Dickinson, Ruther- ford, NJ) tubes. For acetone or ethanol treatment, tubes were filled with 5 mL of liquid for 15 min and vigorously rinsed with distilled water. For vacuum treatment, a small vacuum pump reduced the absolute pressure in the Vacu- tainer to 4 mm Hg as a “pretreatment” to eliminate most of the gas. The pump was connected to a 21-gauge needle inserted in the rubber stopper. After vacuum exposure for 1 min, the tube was filled with physiologic saline de- gassed by boiling through a water seal as described by Do~g1as.l~
For pressure denucleation, tubes were exposed to vacuum and then placed in a hydrostatic pressure chamber and subjected to 100, 200, 300, 400, 500, 1000,2000,4000,6000, or 20,000 psig for a period of 1 min.
Determination of degree of denucleation
1. Qualitative analysis
Graft samples in tubes filled with degassed saline were subjected to a 4 mm Hg vacuum and observed for surface air bubbles. Bubbling was inter- preted as an indication that grafts were not totally denucleated. If no bubbles appeared on the graft surfaces, denucleation was considered complete.
2. Quantitative analysis
(a) Buoyancy method: Graft samples were suspended from a support tower (Fig. 1) by a single strand of 5-0 nylon suture and submerged in a beaker of

QUANTIFICATION OF DEN UCLEATION AND T HROMBOGENICITY 375
Support Tower
lcm Graft -
, _(Turntable
Analyt ical Balance - w Laboratory Jack
Figure 1. Schematic diagram of the apparatus for gravimetric assessment of thrombogenicity.
physiologic saline. Grafts were anchored by a small washer. The apparatus was weighed on an analytical balance accurate to 0.0001 g. The washer weight was subtracted to obtain the underwater weight of the graft. The graft was weighed before and after denucleation and the volumes of the graft ma- terial and air were determined by Archimedes’ principle (see Appendix). Air volume could be resolved to 100 nL, which corresponds to 0.15% denucleation in a 1-cm length of graft.
(b) Photometry: The transmittance of white light was measured through 10 control grafts and 10 grafts denucleated at 20,000 psig. Graft samples were placed on microscope slides on the stage of a Zeiss ACM microscope and illu- minated from below hith a 100-W halogen lamp. Light transmittance was measured through a UD20 objective at a magnification of approximately 300X using a Hamamatsu model 1P21 photomultiplier tube.
Gas content of vascular prostheses
For comparison with Vitagraft ePTFE, the gas content was determined for naked and albumin-coated Dacron (Bard Cardiosurgery, Inc., Billerica, MA), naked polyurethane (Corvita, Inc., Miami, FL), and other ePTFE grafts made by Impra, Inc. (Tempe, AZ) and W. L. Gore, Inc. (Flagstaff, AZ).
Renucleation
Renucleation is the regeneration of gas nuclei on the surface or in the ma- trix of a denucleated graft. Renucleation occurs if the graft is exposed to air or immersed in a gas-saturated solution. Quantitatively, renucleation is the percentage of original air regained following complete denucleation. Renu- cleation was measured in the conditions described below.

376 BENSEN ET AL.
1. Shelf life
Five 2-cm lengths of denucleated graft were stored at atmospheric pressure in 10-mL Vacutainer tubes filled with distilled water. The volume of air in each sample was measured after eight months of storage using Archimedes’ principle.
2. Intraoperafive renucleation
To simulate various conditions that might be encountered during surgical implantation, three groups of 10 I-cm denucleated grafts were removed from their saline-filled tubes and placed on a lab counter in room air. The tempera- ture was 22°C and the relative humidity was approximately 70%. The per- centage renucleation was measured after 2 h. The three conditions under which renucleation was assessed included intermittently immersed, nonim- mersed, and gauze wrapped. The intermittently immersed grafts were sub- merged in normal saline for 30 s every 15 min, nonimmersed grafts were allowed to dry in air with no saline immersion, and gauze-wrapped grafts were covered with wet 2 x 2 gauze pads and irrigated with normal saline every 15 min.
Scanning electron microscopy
Structural changes in ePTFE that occurred as a result of denucleation were examined with scanning electron microscopy. Grafts denucleated by either acetone immersion or vacuum followed by 20,000 psig were immersed in ethanol, and allowed to dry. Control and dried denucleated grafts were sput- ter coated with gold. Micrographs of the graft sample luminal surface were taken at magnifications of 1 0 0 0 ~ and 2 0 0 0 ~ .
Gravimetric assessment of thrombogenicity
The thrombogenicity of vascular graft materials was assessed using a method in which the weight of an adherent thrombus was measured as a function of time. A wooden support tower (Fig. 1) was constructed and covered with several coats of polyurethane sealant to minimize changes in hydration and weight. A small plexiglass rod hung from a cantilevered wooden arm connected to the top of the tower. A segment of graft material 4 mm I.D. x 1.0 cm long was placed over the rod leaving only the exterior graft surface exposed. The support structure rested on an analytical balance accurate to 0.0001 g. Directly under the graft on a platform was a 1-mL poly- carbonate test tube that rotated at 6 rpm to prevent thrombus from simulta- neously adhering to both the graft and the sides of the tube. The platform could be raised or lowered to completely immerse the graft in the tube.

QUANTIFICATION OF DENUCLEATION AND THROMBOGENICITY 377
A thrombogenicity test began by weighing the graft and support structure in air. The graft was then immersed in saline for 15 s, removed, and touched to the side of the test tube to remove loose fluid adhering to the graft. The weight was again recorded. The saline immersion was performed to ensure that all easily wetted surfaces were exposed to water. A similar submersion in canine whole blood immediately followed the saline immersion. The graft was immersed for 15 s, removed, and the scale was tared to establish an ini- tial weight. The graft was again immersed in blood and subsequently re- moved for 10 s and weighed at 4,5,6, 7, and 8 min. Preliminary experiments indicated that measurable thrombosis occurred after 4 min.
Blood was drawn from 20-kg mongrel dogs into standard blue-top Vacu- tainer tubes containing buffered sodium citrate. Experiments were per- formed within 24 h of collections. The citrate was reversed just prior to the assay by adding 0.07 mL of 0.025M calcium chloride to 0.7 mL of blood for a 1 : 10 ratio.
The thrombogenicity of Vitagraft ePTFE was determined at four degrees of denucleation: undenucleated (CONTROL, n = lo), denucleated by 4 mm Hg vacuum only (VACUUM, n = 10) partially denucleated at 100 psig (PAR- TIAL, n = lo), and completely denucleated at 20,000 psig (TOTAL, n = 10).
Statistics
Differences between groups were evaluated using a Wilcoxon Rank Sum test with a p value of 0.05 or less required for statistical significance.
RESULTS
Gas denucleation
All denucleation methods caused grafts to change from opaque white to translucent gray as previously rep~rted.”””’~ Acetone or ethanol treatments produced a more uniform change to a translucent appearance than pressure treatments. However, small bubbles formed on these grafts when placed in water. Preliminary studies indicated that vacuum and vacuum plus pressure denucleation caused a 10-20% decrease in graft length due to a reduction of the internodal distance. No measurable shortening occurred in grafts denu- cleated in acetone or ethanol. Grafts used in this study had various pretreat- ment lengths in order to assure uniform 1-cm lengths following treatment.
Determination of degree of denucleation
1. Qualitative analysis
When exposed to vacuum (4 mm Hg), untreated grafts bubbled violently. Partially denucleated grafts (100 psig-500 psig) produced only small bubbles.

378 BENSEN ET AL.
C 100- .- 0 c m a, 0 3 C a,
-
n c 90-
2 c al a, a C m
80
No bubbles were observed on the completely denucleated grafts (500 psig or greater).
- /I n=5 n=5 n=5 n.5 n.5
T n.15 -
, /*
2. Quantitative analysis
(a) Buoyancy method (Archimedes’ Principle): Graft buoyancy decreased as the denucleation pressure increased (Fig. 2). Denucleation was 97.4% complete with a pressure treatment of 100 psig and indistinguishable from 100% with pressure treatments of 500 psig or greater. Grafts denucleated by ethanol im- mersion had a mean denucleation of 94.3%. Grafts denucleated by acetone immersion had a significantly higher denucleation of 98.9% ( p < 0.05).
(b) Photometry: The light transmittance of control grafts was 8.88 f 0.70%. After denucleation at 20,000 psig, transmittance significantly increased to 41.70 t 0.81% ( p < 0.001).
Gas content of vascular prostheses
These results indicate that there is a wide range in gas content of commonly used vascular prostheses on submersion in water. Vitagraft ePTFE was 75.5 f 0.4% air (n = 20), Gore-tex ePTFE 69.2 f 0.3% (n = 5), Impra ePTFE 61.8 t 0.3% (n = lo), Corvita naked polyurethane 30.2 f 0.3% (n = 5), naked Dacron 7.6 4 0.7% (n = lo), and albumin-coated Dacron 2.4 -+ 0.3% (n = 10).
Renucleation
1. Shelflife
The data indicate that an average of 0.01 f 0.01% renucleation occurred over the 8-month test period. Since the resolution of the method was 0.15%, no detectable renucleation occurred when grafts were immersed during storage.

QUANTIFICATION OF DEN UCL EAT ION AND THROMBOGENICITY
t .- 0 (d - Q) 80 0 3 c
c
0" 6 0 - c. K Q1 40 2
20 W
c a s o
379
loo+- """""-..---.-- - :+ '. intermittently Immersed '. '. '. '. - '. '.
'*'. '. '.\. Non-immersed '. x. '. -
t p<O.OOl vs. non-immersed x. t p<O.OOl vs. immersed '. '. '.
=.= '.
L , i
2. In t raoperat ive renucleat ion
The results of the simulated surgical setting are summarized in Figure 3. These data demonstrate that intermittent immersion dramatically reduced graft renucleation from 89% to 3.4%. Wrapping the grafts in wet gauze fur- ther reduced renucleation significantly to only 1.4% ( p < 0.001).
Scanning electron microscopy
Figure 4 shows that denucleation caused a reduction in internodal dis- tance. This is consistent with the observed overall shortening of the grafts. The closer nodes appear to allow the fibrils to clump together into bundles, resulting in large, irregularly spaced pores between the nodes. The large pores appear to be more numerous in the pressure denucleated grafts.
Gravimetric assessment of thrombogenicity
Figure 5a indicates that both partially (100 psig) and totally (20,000 psig) denucleated grafts had significantly less adherent thrombus than the control and vacuum denucleated grafts. Differences between partially and totally de- nucleated grafts were not significant. At 4 min, vacuum denucleated grafts had significantly less thrombus than control grafts. In Figure 5b, the thrombus weights of Figure 5a are plotted against the percentage denucleation from Figure 2. Figure 5b shows that the removal of air from the graft results in progressive and significant reduction in adherent thrombus weight.
DISCUSSION

380 BENSEN ET AL.
Figure 4. Scanning electron micrographs of Gore-tex ePTFE: (A) control, (B) denucleated with acetone, and (C) denucleated with vacuum followed by 20,000 psig. Note the shortened internodal distance, clumped fibrils, and large pores with vacuum plus pressure denucleation. White calibration bars are 10 pm.

QUANTIFICATION OF DENUCLEATION AND THROMBOGENICITY
200
l60 E
.- Q, 120
v
E
s u) 3 80 n E 2
40
0
381
- + Control - ---O-- Vacuum --t- 100 pslg
. . . . o... 20,000 pslg pc0.005 vs control
t pc0.05 vs vacuum -
-
-
I
- 150 c-
~ .......... a.
6 mlnutes %* I-.-.-.- ------.---.-.-._._._.___ '.
4 minutes %
------. 5 minutes
' 8
o-.-.-.-.-.-.-.-.-.-.-.-.-.-.-.-.-.-.-.o
................................................. ...
L 0, .- 2 100 v) 3 D
50 2 r I-
n 0 10 20 30 40 50 60 70 80 90 100
Percent Denucleation (b)
Figure 5. (A) Gravimetric assessment of thrombus adhesion to 4-mm-I.D. Vitagraft ePTFE. Adherent thrombus weight was measured to the nearest 0.0001 g every minute from 4 to 8 min following immersion in canine blood. At 4 min the mean thrombus weight on the control grafts was 6 times that of the weight on denucleated grafts. (B) The effect of percentage de- nucleation on thrombogenicity. Corresponding data from Figures 2 and 5(a) are shown for control, vacuum only, partial (100 psig), and complete (20,000 psig) denucleation.
Air content was measured in Vitagraft ePTFE which had been denucleated by vacuum, hydrostatic pressure, or immersion in acetone or ethanol. Thrombo- genicity was determined after hydrostatic pressure denucleation of Vitagraf t.
Fluids tend to enter the pores of a graft through the process of ~apillarity.'~ Expanded PTFE is hydrophobic and little capillary rise occurs upon immer- sion in water. This difficulty can be overcome by using vacuum and hydro- static pressure to force water into the graft matrix. Degassed water acts as a
382 BENSEN ET AL.
diffusion sink for adjacent gas. Thus, the air is likely first displaced and then dissolved.
When surface tension between air and a fluid is low, capillary rise is high, surfaces are easily wetted, and fluid infiltration is extensive. The mutual affinity between ePTFE and organic solvents such as acetone and ethanol al- lows these liquids to readily enter the graft matrix. Immersion in acetone has an advantage over pressure treatment in that 97.4% denucleation can be achieved without vacuum and pressure equipment. Acetone- and ethanol- treated grafts must be rinsed before surgical implantation, however, and small bubbles were observed to form when these grafts were immersed in de- gassed distilled water. Although we are uncertain of the thrombotic effect of these bubbles, we construe this effect to indicate incomplete denucleation.
The 10-20% decrease in graft length and reduction in internodal distance following vacuum and pressure treatment is a consequence of compression when the vacutainer is filled with water. Compression occurs because surface tension prevents water from entering the pores. The grafts can be restored to their original length by gentle stretching under water to avoid renucleation.
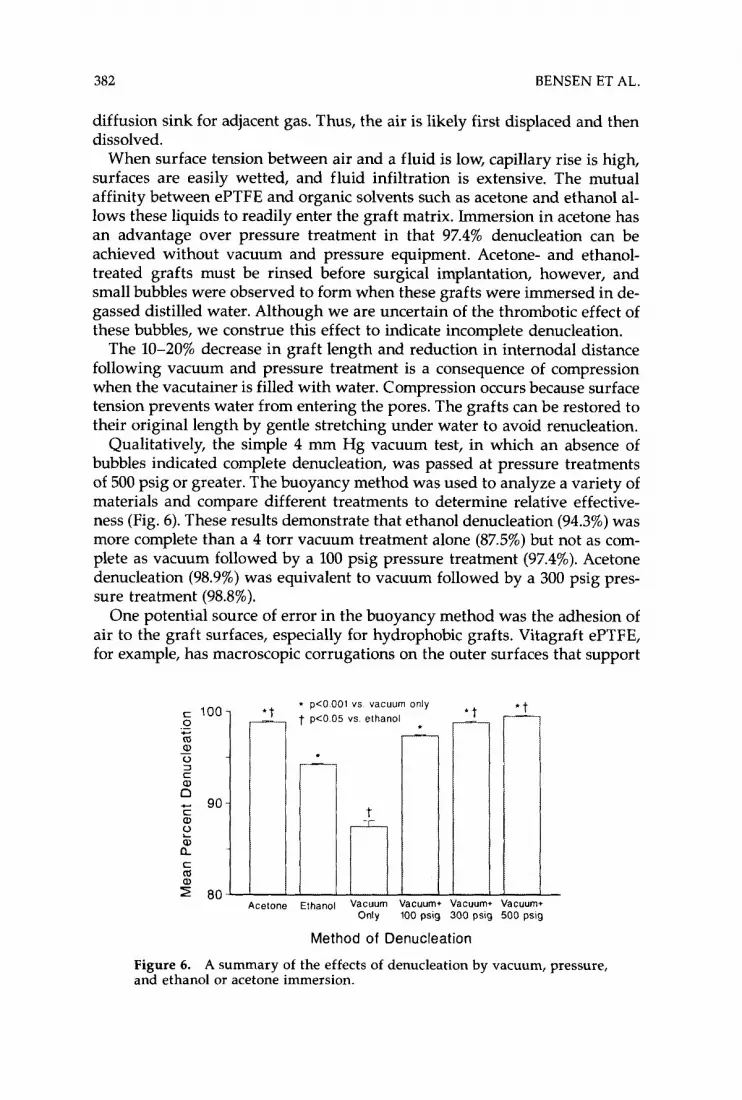
Qualitatively, the simple 4 mm Hg vacuum test, in which an absence of bubbles indicated complete denucleation, was passed at pressure treatments of 500 psig or greater. The buoyancy method was used to analyze a variety of materials and compare different treatments to determine relative effective- ness (Fig. 6). These results demonstrate that ethanol denucleation (94.3%) was more complete than a 4 torr vacuum treatment alone (87.5%) but not as com- plete as vacuum followed by a 100 psig pressure treatment (97.4%). Acetone denucleation (98.9%) was equivalent to vacuum followed by a 300 psig pres- sure treatment (98.8%).
One potential source of error in the buoyancy method was the adhesion of air to the graft surfaces, especially for hydrophobic grafts. Vitagraft ePTFE, for example, has macroscopic corrugations on the outer surfaces that support
* p<O 001 vs vacuum only t pCOO5 vs ethanol
- Acetone Ethanol Vacuum Vacuum* Vacuum. Vacuum+
Only 100 psig 300 psig 500 psig
Method of Denucleation
Figure 6. A summary of the effects of denucleation by vacuum, pressure, and ethanol or acetone immersion.

QUANTIFICATION OF DENUCLEATION AND THROMBOGENICITY 383
a large volume of air relative to its matrix volume. This unique structure results in the graft being completely enveloped by a stratum of air when im- mersed in water. Vigorous underwater agitation removed most of the adher- ent air, but it was impossible to determine how much surface air remained. This could account for the unusually high measured gas content value for Vitagraft compared to the other ePTFE materials.
The photometry results demonstrated a fivefold change in transmit- tance between control and pressure denucleated Vitagraf t ePTFE. The change from opaque to translucent as a result of denucleation can be quantified to assess the degree of denucleation. Photometric methods might be used to quantify the degree of denucleation.
There was wide variability in the gas content of the prostheses currently used for vascular reconstruction. Vitagraft, for example, has more than 20 times as much gas as albumin-coated Dacron. This suggests that denucle- ation may greatly benefit some biomaterials, while the effect on others may be minimal.
No measurable renucleation occurred over 8 months of storage. Should longer periods result in significant renucleation, storage under partial vacuum might be beneficial.
It is inevitable that grafts will have some air exposure and renucleation during an implant procedure. Severe renucleation could be avoided by wrap- ping denucleated grafts in gauze that is periodically irrigated. The 1.4% renu- cleation of gauze-wrapped grafts (Fig. 3) would have little effect on graft thrombogenicity (Fig. 5).
The scanning electron micrographs revealed a decrease in internodal dis- tance, which correlated well with the observed overall gross decrease in length. As a result of the closer nodes, the relative length of the fibrils in- creased, allowing the fibrils to clump together and enlarge some of the pores. From these studies, it cannot be determined whether the fibril clumping was a direct unavoidable result of the shortening, or if the clumping was an arti- fact of the drying process necessary for scanning electron microscopy. In the undenucleated grafts, the drying might not generate clumping since the inner fibrillar surfaces would not contain water and would not have the surface tension tending to pull fibrils together. Conversely, the denucleated grafts, particularly the grafts treated with pressure, would have all inner surfaces wetted. The subsequent drying would create shrinking droplets with a high surface tension, which would tend to pull fibrils together and lead to fibrillar clumping and some enlarged pores. The enlarged pores, if present in the de- nucleated grafts, could contribute to the increase in weeping of blood ob- served following implantati~n.'~
Denucleation of Vitagraft delayed the onset and rate of thrombus adhesion, which is consistent with recent in vivo studie~.'~,'~ Interestingly, the rates of adhesion above 40 mg were similar for all degrees of denucleation, which may reflect the blood-ePTFE interaction occurring only during the initial thrombus development. Subsequent clotting reflects blood-thrombus interac- tion and is independent of the initiating events.

384 BENSEN ET AL.
Several sources of variability were identified for the gravimetric thrombo- genicity assessment. First, there was a marked increase in the coagulability of blood during the interval between the collection of blood and assay. For ex- ample, blood collected within two hours of an assay could take 7 min before measurable thrombus adhered to the graft. However, if the same blood sam- ple was used 24 h later, significant thrombus adhered to the graft as early as 4 min. Additionally, blood samples collected from the same animal on differ- ent days often had a variability of several minutes in measured thrombo- genicity. The thrombogenicity of blood from different animals had even greater variability. Consequently, blood was obtained from a single collection from one animal for all thrombogenicity data reported. Results from experi- ments using other blood samples were qualitatively similar to those reported here. To further reduce variability, the grafts were assessed in sets where one graft from each treatment group was measured before continuing to the sec- ond graft from each treatment group.
A second source of variability was the exposure of the graft to air during weighing which may have minimized any differences in thrombogenicity or increased the variability. In future studies, it is possible that weight measure- ment at a single time, such as 6 min, could increase the sensitivity of the gravimetric technique by eliminating the effects of repeated air exposure.
Finally, there is the possibility that the presence of a Langmuir film at the air-blood interface could have affected the results. However, the only differ- ence between the experimental conditions was the amount of air in the graft matrix. Therefore, the effect of the Langmuir film, if any, should be a con- stant factor in each condition and should not alter the conclusions. A similar case may arise during in vivo implantation where Langmuir films could form at the blood-air interface. The effects of this film are unknown and warrant further investigation.
In summary, the continuum of gas denucleation and the resulting reduc- tion in thrombogenicity can be quantified using gravimetric techniques. Air is clearly thrombogenic and has been largely overlooked in the design and implementation of most cardiovascular prostheses. The techniques described herein could be applied to a variety of biomaterials and antithrombotic pro- cedures for which the effects of denucleation have yet to be determined. Pressure is an effective method of denucleation and in the future could be used to integrate antithrombotics, thrombolytics, or antibiotics with various biomaterials."
The excellent assistance of Mr. Matthew Bielefeld in assembling the photometer is ac- knowledged. We are grateful to Mr. Tony Almon for his assistance in graft denucle- ation and to Dr. Donald Serafin of the Division of Plastic Surgery, Duke University Medical Center, for his advice and support during this project. We would also like to thank Ms. Judy Parker of the clinical coagulation laboratory, Duke University Medical Center, for her advice on the handling and preparation of blood used in the study. We are especially indebted to Dr. Wayne Gerth of the Division of Physiology, Duke Uni- versity Medical Center, for his technical advice and use of his hyperbaric chamber fa- cilities. Without his assistance, this work would not have been possible. The Vitagraft ePTFE and Dacron graft materials were provided by Bard Cardiosurgery, lnc., Billerica, MA. The Impra ePTFE was donated by Impra, Inc., Tempe, AZ. The Gore-tex ePTFE

QUANTIFICATION OF DENUCLEATION AND THROMBOGENICITY 385
was donated and the SEM was performed by W. L. Gore & Assoc., Flagstaff, AZ. The naked polyurethane was donated by Corvita Corp., Miami, FL. This work was funded in part by Bard Cardiosurgery, Inc., Billerica, MA.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
P. M. Galletti, ”Applications of plastics in membrane oxygenators,” J. Biomed. Muter. Res. Symp., 5, 129-134 (1971). C. 0. Esquivel, C. J. Bjorck, S. E. Bergentz, et al., ”Reduced thrombo- genic characteristics of expanded polytetrafluoroethylene and poly- urethane arterial grafts after heparin bonding,” Surgery, 95, 102-107 (1984). M. B. Herring, R. Dilley, R. A. Jersild, Jr., et al., ”Seeding arterial pros- theses with vascular endothelium. The nature of the lining,” Ann.
R. M. Green, L. R. Roedersheimer, and J. A. DeWeese, ”Effects of aspirin and dipyridamole on expanded polytetrafluoroethylene graft patency,” Surgery, 92, 1016-1026 (1982). B. T. Allen, R. E. Sparks, M. J. Welch, et al., “Reduction of platelet de- position on vascular grafts using an antiplatelet graft coating tech- nique,“ J. Surg. Res., 36, 80-88 (1984). W. H. Lee Jr., D. Krumhaar, E. W. Fonkalsrud, O.A. Schjeide, and J. V. Maloney Jr., ”Denaturation of plasma proteins as a cause of morbidity and death after intracardiac operations,” Surgery, 50,29-39 (1961). W. H. Lee Jr., and P. Hairston, ”Structural effects on blood proteins at the gas-blood interface,” Fed. Proc., 30, 1615-1622 (1971). C. A. Ward, B. Ruegsegger, D. Stanga, et al., “Reduction in platelet ad- hesion to biomaterials by removal of gas nuclei,” Trans. Am. SOC. Arfif. Intern. Organs, 20, 77-84 (1974). G. A. Herzlinger and R. D. Cumming, ”Role of complement activation in cell adhesion to polymer blood contact surfaces,” Trans. Am. SOC. Artq. Intern. Organs, 26, 165-171 (1980). C. A. Ward, D. Stanga, B. J. Zdasiuk, et al., ”Effect of air nuclei on the adsorption of fibrinogen to silicone rubber,” Ann. Biomed. Eng., 7, 451- 469 (1979). P. N. Madras, W. R. Johnson, and C. A. Ward, ”Enhancement of throm- bus formation by vascular prostheses,” Can. J. Surg., 23,544-546 (1980). L. A. Trudell, L. Boudreau, J. M. Van De Water, et al., “Alcohol-treated PTFE vascular grafts,” Trans. Am. SOC. Arfif. Intern. Organs, 24, 320-323 (1978). C. P. Demas, R.D. Vann, E. F. Ritter, R. S. Sepka, B. Klitzman, and W. J. Barwick, “Decreased thrombogenicity of vascular prostheses follow- ing gas denucleation by hydrostatic pressure,“ Plasf. Reconstr. Surg., 82,
E. F. Ritter, R.D. Vann, C. W. Wyble, W. J. Barwick, and B. Klitzman, “Hydrostatic pressure reduces thrombogenicity of polytetrafluo- roethylene vascular grafts,” Am. J. Physiol., in press. E. Douglas, ”Solubilities of oxygen argon, and nitrogen in distilled water,” J. Phys. Chern., 68,169-174 (1964). K. E. Koger, C.V. Bensen, R.D. Vann, H. G. Clark, and B. Klitzman, ”Decreased thrombogenicity of biomaterial with chitosan,” FASEB J., 3, A1391 (1989). N. K. Adam, The Physics and Chemistry of Surfuces, Dover Publications, Inc., New York, 1968, pp. 8-12.
Surg, 190,84-90 (1979).
1042-1045 (1988).
Received November 15,1989 Accepted September 5, 1990

386 BENSEN ET AL.
APPENDIX: DETERMINATION OF GAS VOLUME IN ePTFE GRAFT MATERIAL
Archimedes’ principle states that the weight of an object under water is equal to its weight in air minus the weight of water it displaces. By partition- ing the volume of displaced water into a volume of solid graft material and air trapped in the graft matrix, the underwater weight is given by
U = W - D(V + A) , (1) where
U = Underwater or buoyant weight of graft, W = Weight of graft in air, D = Density of water, V = Volume of solid graft material, and A = Volume of air trapped in the graft.
Rearranging,
When A = 0 in the case of a completely denucleated graft, Eq. (2) becomes
(w - u d >
D V =
where & = Underwater weight of a completely denucleated graft. Substituting Eq. (3) into Eq. (2) and solving for A,
(3)
Thus, by measuring the graft weight in air and the underwater weight be- fore and after denucleation, Eq. (4) defines the volume of air in the graft and Eq. (3) defines the volume of solid graft material. Percent denucleation can be estimated from Eq. (3) as one minus the ratio of air in the graft after a treat- ment “x” to air in the graft before treatment. Expressed as a percentage, this quantity is
Where
and U, = Underwater weight of graft treated to x pressure,
U, = Underwater weight of control graft. In application, a graft is weighed under water before a denucleation treat-
ment (U), after treatment “x” (Ux) , and after complete denucleation (&). Consistent with Figure 2, the weight of the completely denucleated graft was determined after vacuum treatment at 4 mm Hg followed by pressure treat- ment at 20,000 psig.