neointimal hyperplasia associated with synthetic hemodialysis grafts
TRANSCRIPT
Neointimal hyperplasia associated with synthetic hemodialysisgrafts
Li Li1, Christi M. Terry1, Yan-Ting E. Shiu2, and Alfred K. Cheung1,3
1 Department of Medicine, University of Utah, Salt Lake City, Utah, USA
2 Department of Bioengineering, University of Utah, Salt Lake City, Utah, USA
3 Medical Service, Veterans Affairs Salt Lake City Healthcare System, Salt Lake City, Utah, USA
AbstractStenosis is a major cause of failure of hemodialysis vascular grafts and is primarily caused byneointimal hyperplasia (NH) at the anastomoses. The objective of this article is to provide a scientificreview of the biology underlying this disorder and a critical review of the state-of-the-artinvestigational preventive strategies in order to stimulate further research in this exciting area. Thehistology of the NH shows myofibroblasts (that are probably derived from adventitial fibroblasts),extracellular matrices, pro-inflammatory cells including foreign-body giant cells, a variety of growthfactors and cytokines, and neovasculature. The contributing factors of the pathogenesis of NH includesurgical trauma, bioincompatibility of the synthetic graft, and the various mechanical stresses thatresult from luminal hypertension and compliance mismatch between the vessel wall and graft. Thesemechanical stimuli are focal in nature and may have a significant influence on the preferentiallocalization of the NH. Novel mechanical graft designs and local drug delivery strategies showpromise in animal models in preventing graft NH development. Successful prevention of graftstenosis would provide a superior alternative to the native fistula as hemodialysis vascular access.
Keywordshemodialysis; arteriovenous graft; stenosis; imaging; blood flow; hemodynamics
ARTERIOVENOUS GRAFTS AS HEMODIALYSIS VASCULAR ACCESSThe three major forms of vascular access used for chronic hemodialysis are the nativearteriovenous (AV) fistula, the synthetic AV graft, which is usually made of expandedpolytetrafluoroethylene (ePTFE), and the cuffed, tunneled central venous catheter. A well-functioning native fistula is the preferred choice of vascular access because it has the leastlong-term complications. The major drawback with the native fistula is the failure of manynew fistulas to develop into a usable access. The primary failure rate of native fistulas reportedin the literature varies between 20 and 50%.1 A randomized trial conducted by the NationalInstitutes of Health-sponsored Dialysis Access Consortium involving 758 patients recentlyreported a primary failure rate of approximately 60% at 6 months after the fistula creation. Thisrate was unaffected by a 6-week postoperative course of oral clopidogrel (preliminaryunpublished data from the National Institute of Diabetes and Digestive and Kidney Diseases
Correspondence: Alfred K. Cheung Research 151N, 500 Foothill Blvd., Salt Lake City, Utah 84148, USA E-mail:[email protected] the authors declared no competing interests.
NIH Public AccessAuthor ManuscriptKidney Int. Author manuscript; available in PMC 2008 November 1.
Published in final edited form as:Kidney Int. 2008 November ; 74(10): 1247–1261. doi:10.1038/ki.2008.318.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Dialysis Access Consortium Fistula Trial). The prevalence of AV fistula use is higher in Europeand Japan, even though their primary AV fistula failure rate is comparable with that in theUnited States.2–4 In addition, the dialysis blood flow rates vary among the United States,Europe, and Japan. Compared with 412 ml/min in the United States, the mean blood flow ratesin Europe and Japan were 300 and 197 ml/min, respectively,5 which may not be acceptable inmany US dialysis centers.
The high primary failure rate of native fistula has several consequences. More diagnostic andremedial procedures, such as fistulography and angioplasty, are performed. Multiple attemptsto create fistulas exhaust vascular sites and the patient’s tolerance. The need for central venouscatheters while waiting for the fistula to mature is prolonged, with their attendantcomplications. The initiative of increasing the rate of native fistula in the United States hasapparently led to increased catheter use. In fact, approximately 50% of patients begin chronichemodialysis with a central catheter.6 There are also long-term complications associated withnative fistulas, such as stenosis, although at lower rates than other forms of vascular access.7
The prevalence of the AV synthetic graft for hemodialysis has decreased in the United Statesin the last few years, concomitant with the increase in the use of native fistulas and catheters.However, synthetic grafts have an advantage in that they reliably provide high blood flow ratesshortly after placement, as they do not require maturation before use. The major problem withgrafts is stenosis followed by thrombosis and occlusion, which accounts for approximately85% of their failure.8 Early detection and angioplasty of stenosis do not improve the graftpatency (see ‘Treatment using angioplasty’ section). The successful prevention of stenosis istherefore essential for the longevity of AV synthetic grafts. Understanding the mechanismsthat lead to stenosis formation should facilitate the development of such preventive strategies.This article will review the pathogenesis of hemodialysis graft stenosis and describe promisingstrategies for its prevention.
PATHOLOGY OF HEMODIAYSIS GRAFT STENOSISIn AV PTFE grafts, stenosis occurs most commonly at the graft–venous anastomosis, the juxta-anastomotic venous segments (Figure 1a), and less frequently at the graft–arterial anastomosis.9–12 Other than the occasional kinking of the vessel or thrombus partially obstructing thelumen, stenosis almost always arises from progressive neointimal hyperplasia (NH). NH tendsto form in the ‘shoulder’ region within the lumen of the graft and in the ‘cushion’ region of thenative vessel (Figure 1b). Stenotic tissues obtained from the graft–venous anastomosis ofhuman AV ePTFE grafts showed an abundance of smooth muscle cells (SMC) and/ormyofibroblasts, accumulation of extracellular matrix, neovasculature within the NH andadventitia, and the presence of a macrophage layer lining the PTFE graft material. Variousgrowth factors, such as platelet-derived growth factor (PDGF), basic fibroblast growth factor,and vascular endothelial growth factor (VEGF), were conspicuous in the venous NH in patients.13,14 Similar pathology was found at the venous anastomosis in canine and porcine AV graftmodels, as reported by us and others.10,15–17
The proliferation and migration of medial SMCs have traditionally been considered to be theprimary cellular source in NH.17,18 The potential role of the adventitia has received attentiononly recently.16,19,20 Our results in a porcine AV ePTFE graft model support this notion.16 Cell proliferation activity was first detected in the adventitia of the venous anastomosis asearly as day 1 after graft implantation (Figure 2), followed by activities in the media. Cellproliferation in the neointima increased linearly only after 2 weeks. Most of the proliferatingcells were found to express smooth muscle α-actin, but not smoothelin or smooth musclemyosin heavy chain by immunohistochemistry, and were therefore identified asmyofibroblasts. Collectively, these results support the following paradigm. Within hours after
Li et al. Page 2
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

graft placement, adventitial fibroblasts are transformed into myofibroblasts. These adventitialmyofibroblasts then proliferate, and then migrate toward the vessel lumen, whereupon theydeposit extracellular matrix and serve as primary contributors to NH formation. Investigationof the pathology of NH in AV grafts has therefore enhanced our understanding of itspathogenesis and helped to direct the development of preventive strategies.
PATHOGENESIS OF HEMODIALYSIS GRAFT STENOSISThe pathogenic mechanisms of NH formation associated with AV ePTFE graft have not beendelineated to the same extent as that with arterial balloon injury or the arterial–arterial bypassePTFE graft. Multiple factors are believed to contribute to NH in the AV ePTFE graft, including(a) surgical trauma to the vessel during graft placement; (b) bioincompatibility of the ePTFEgraft material; (c) mechanical factors at the anastomoses; (d) endothelial dysfunction causedby uremia; and (e) vessel wall damage from repeated needle punctures for dialysis treatments.The effect of uremia on NH development has been discussed in other reviews.11,21 This reviewfocuses on the first three factors.
Surgical traumaArteriovenous graft placement surgery causes damage to the intima, media, and adventitia ofthe vessel. Manipulation during surgery causes vasospasm, ischemia, and changes inhemodynamic forces in the vessels, which likely contributes to NH development.22 Damageto the intima removes the protective endothelium and exposes the medial SMC directly to bloodflow and other procoagulant and proinflammatory blood constituents. The intact endotheliumsecretes prostacyclin (PGI2) and nitric oxide (NO), which are potent vasodilators.23 These twomolecules also inhibit platelet activation, aggregation, and adhesion to the endothelium orSMCs, which are likely early events in NH formation. NO also inhibits SMC proliferation andmigration.24,25 In addition, the adventitial layer is partially removed for creating theanastomosis during surgery. Depriving the vessel wall of oxygen and nutrients provided bythe adventitial vaso vasorum has been shown to enhance NH formation.26 Surgical traumaalso initiates the recruitment of inflammatory cells that release potent cytokines and promoteSMC migration and proliferation.22
BioincompatibilityClinical inflammation, as evident by erythema, edema, and tenderness in the skin overlyingthe graft, are common after surgical placement of grafts, often lasting 7–10 days.Histologically, macrophages have been observed in large numbers in the adventitial and mediallayers in the anastomotic tissues from AV ePTFE grafts collected from patients13,14 and fromporcine models of AV graft stenosis.10 In our porcine AV ePTFE graft model, the recruitmentof inflammatory cells, particularly neutrophils and macrophages, to the anastomosis occursvery early after graft placement (Terry CM et al, unpublished data). Another prominent celltype found at the anastomosis is the foreign-body giant cell. These cells arise from the fusionof macrophages and are a product of ‘frustrated phagocytosis’. Foreign-body giant cells andmacrophages are likely important contributors to NH development in AV grafts, through therelease of proinflammatory mediators such as cytokines, growth factors, matrixmetalloproteinases, and reactive oxygen species. In support of this notion, the macrophagesand foreign-body giant cells in the NH of porcine AV grafts have been found to express PDGF,FGF, and VEGF.13
In addition, we have observed an early and prolonged accumulation of T-lymphocytes thatmay participate in the development of graft NH by releasing cytokines such as tumor necrosisfactor-α. Tumor necrosis factor-α is known to recruit macrophages, induce matrixmetalloproteinases, and stimulate SMC and fibroblast migration.27,28 However, T-
Li et al. Page 3
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
lymphocytes may also attenuate SMC proliferation, as athymic rats and T-cell-depleted ratsdeveloped greater NH after balloon-catheter injury than normal animals.29 An explanation forthis potential inhibitory effect is the ability of T cells to produce interferon-γ that can inhibitSMC and fibroblast proliferation.29–31 However, the role of cytokines and T cells in NH iscomplex, and further work is needed to clarify their role in AV graft hyperplasia.
Dendritic cells, an antigen-presenting cell that activates T-lymphocytes, have been observedin arterial ePTFE patch grafts in a sheep model32 and in ePTFE grafts collected from humanpatients undergoing revision bypass operations.33–35 The role of dendritic cells inhemodialysis AV graft stenosis has not yet been reported.
In vitro studies have provided mechanistic insights on how ePTFE graft bioincompatibilitymay contribute to NH development. Conditioned media from human peripheral bloodmonocytes exposed to ePTFE graft material induces a significant increase in rat aortic SMCproliferation.36 Neutralizing antibodies to tumor necrosis factor-α inhibits this proliferativeresponse, suggesting that tumor necrosis factor-α plays a role in the mitogenic effect of theePTFE graft material per se. Conditioned media obtained from human peripheral bloodmonocytes maintained on ePTFE stimulated T-lymphocyte proliferation, probably through therelease of interleukin-1.37 Human macrophages maintained on ePTFE also released VEGFand angiopoiten-1 and stimulated the sprouting of capillaries from placental vessel fragmentsin vitro.38 Endothelialization of graft material is hypothesized to be inhibitory to NHdevelopment by tempering proliferation of the underlying SMCs and fibroblasts on the graftsurface. However, angiogenesis also provides blood supply to the NH. Thus, recruitment andactivation of macrophages and other inflammatory cells by the ePTFE material may contributeto neovascularization and thus promote NH development. Successfully addressing the issue ofbioincompatibility of ePTFE grafts could help alleviate NH development.
Mechanical factorsSeveral mechanical stresses are most likely involved in the NH development and its focal naturein the setting of AV ePTFE grafts. These include blood flow-induced stresses (for example,low fluid shear stress and increased wall stress at the NH-prone site)39,40 and non-flow-induced stresses (for example, wall stress concentrated at the suture line, increased wall stressdue to compliance mismatch of the elastic native tissue, and stiff graft/suture material).41,42
Low fluid shear stress—All cells in the vessel wall are constantly exposed to three typesof blood flow-induced mechanical stresses (Figure 3). (a) As the blood travels in the vessellumen, blood pressure exerts a stress perpendicular to the vessel wall. (b) Stretching of thecompliance vessel wall by the transmural pressure gradient causes circumferential wall stress,which is also known as ‘hoop stress’ or simply ‘wall stress’.43 (c) Fluid wall shear stress, orsimply ‘shear stress’, is the friction at the interface between luminal flowing blood and theapical surface of endothelial cells. Normally, only endothelial cells are directly exposed toluminal flow. In the event of denudement of the endothelial layer, however, SMC and evenfibroblasts can be exposed directly to luminal flow. This can occur after surgical trauma suchas AV grafting. These three types of hemodynamic stresses regulate the function and dynamicremodeling of the vascular wall, and also contribute to the development of pathologicalconditions.44–48
In contrast to that in a large straight vessel, blood flow is not laminar in the NH-prone sites ofthe graft–venous anastomosis and the juxta-anastomotic downstream venous segment. Bloodflow in these regions is far more complex and is characterized by flow separation (or flowsplit), stagnation, vortices (or eddies), turbulent flow, and low shear stress in different areas(Figure 4).49–53 Detailed flow information in these regions remains to be characterized, andthe majority of available flow data are derived from flow rates measured at a few locations
Li et al. Page 4
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

near or outside the anastomosis.39 Loth et al.54 used a realistic reconstruction of a canineiliofemoral PTFE graft model and computational fluid dynamic models, based on in vivo andin vitro hemodynamic measurements, to show an inverse correlation between wall shear stressand NH formation.
A strong association between low shear stress and atheroma formation with SMC proliferationwas first proposed in 1969.55 Since then, numerous subsequent cell culture, animal, andclinical studies have confirmed that physiologically high shear stress inhibits SMCproliferation, whereas low shear stress promotes SMC proliferation.56–60 High shear stressmay inhibit arterial SMC proliferation by upregulating transforming growth factor-β1 in anautocrine manner,60,61 whereas low shear stress induces arterial SMC proliferation byupregulating PDGF.56,57 It is unclear, however, if these findings are applicable to venousSMC. This question is important, as stenosis occurs more often at the venous than at the arterialanastomosis of the AV ePTFE graft. Furthermore, the complex flow pattern in the graft–venousanastomosis and the juxta-anastomotic segments exposes cells to abnormal temporal andspatial shear stress gradients. Although vein-wall vibration caused by flow-mediatedturbulence has been associated with enhanced mitogen-activated protein kinase activities in aporcine AV PTFE graft model,62 the effects of complex flow on arterial or venous SMC arenot completely known.63
In addition to its influence on SMC, low fluid shear stress may enhance the entrapment ofplatelets and leukocytes to the vessel wall in these regions.64 It is, however, controversial asto what level of fluid shear stress can entrap or activate circulating blood cells in vivo.65–71
Increased wall stress—Increased tensile wall stress at the graft anastomosis can result fromseveral mechanisms. The blood pressure and wall stress in veins are on the order of 103 and104 Pa, respectively, in healthy individuals.43 In the venous side of an AV graft, however,these values can increase 10-fold to levels that are comparable to arterial blood pressure (104
Pa) and arterial wall stress (105 Pa). There is a further elevation of wall stress at the graft-vesselanastomosis due to the compliance difference between the elastic native tissue and the lesscompliant graft and suture materials that is present in both arterial and venous sides of an AVePTFE graft. A relatively larger increase in wall stress in the venous side may render it moresusceptible to NH than the arterial side.
In contrast to the inverse relationship between fluid shear stress and cell proliferation, there isa positive, although nonlinear, relationship between tensile wall stress and cell proliferation.72–75 Although some investigators have questioned whether the enhanced proliferation is aresult of increased stress or the ensuing increased stiffness,76–78 it is generally accepted thatwall stress induces cell proliferation. From an engineering perspective, under normalconditions, cells appear to counteract an increase in tensile wall stress by increasing the tissuemass, thereby maintaining stress homeostasis. Such an adaptation is, however, not alwaysbeneficial and may contribute to pathological states. An example of this maladaptation iscardiac and vascular hypertrophy that is caused by chronic arterial hypertension.79 Numerouscell culture and animal studies have identified the growth factors and their receptors, signaltransduction pathways, and immediate genes that may participate in wall stress-induced arterialSMC proliferation. These studies generally showed that increased tensile wall stress activatesa transcription factor that reacts with a strain-responsive element in the promoter region of thePDGF gene,80 PDGF receptors,81,82 mitogen-activated protein kinase-mediated pathways,83–90 the prosurvival Akt pathway,91,92 and adenylyl cyclase93 in arterial SMC. It is alsounclear whether these findings are applicable to venous SMCs. Furthermore, in addition tocircumferential wall stress, stretching of the blood vessel wall also may result in longitudinaland radial wall stress, but their effects on SMC are unknown.
Li et al. Page 5
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
IMAGING NHColor Doppler ultrasonography
A number of imaging modalities are available for the evaluation of the hemodialysis AV graft.Color Doppler Ultrasonography (CDUS) is often the first-line method in the clinic, because itis noninvasive, widely available, and relatively inexpensive. CDUS provides the blood flowrate and the luminal diameter. However, operator skill can greatly influence the quality ofimages.94 In addition, CDUS does not detect the stenoses in central veins that are below theclavicle and can overestimate the stenotic lesions in the arterial anastomoses.95 CDUS alsodoes not provide as complete a global map of the vascular system as other techniques. However,Bacchini et al.96 reported the successful use of CDUS to guide the angioplasty of stenoticlesions in hemodialysis grafts.
Contrast digital subtraction angiographyDigital subtraction angiography (DSA) is the current gold standard for vascular access imagingand for guiding angioplasty. DSA provides a global and detailed vascular map of the lumen ina single plane. However, DSA exposes the patient to nephrotoxic radiocontrast agents and toradiation. In addition, as DSA provides only information about the vessel lumen but not thewall, vessel spasm that occurs spontaneously or induced by contrast can influence stenosisfindings.
Magnetic resonance imagingMagnetic resonance (MR) imaging techniques such as three-dimensional (3D) contrast-enhanced MR angiography (MRA), time-of-flight angiography, and cine phase-contrastangiography have been investigated for utility in preoperative vein mapping as well ashemodialysis AV graft surveillance.97,98 A detailed review of the utility of MR imaging inhemodialysis access management has been published.97 MR techniques can provide 2D (two-dimensional) and 3D images in any orientation, as well as blood flow information. The qualityof images obtained by 3D contrast-enhanced MRA, and interobserver agreement on stenosis,have been reported to be superior to those obtained by DSA,99 but it also results in a highernumber of false-positive stenotic lesions compared with DSA, presumably because of thecomplex flow patterns induced by the configuration of the conduit. The major drawbacks ofMRA for AV graft surveillance in the clinic are the expense, and the risks of developingnephrogenic systemic fibrosis from gadolinium-based contrast exposure.100
Magnetic resonance techniques can be very useful for research purposes. For example, we haverecently obtained high-resolution images of NH lesions in our porcine AV graft model usingMR without contrast.101 This technique allows the in vivo quantification of the NH volumewith repeated in vivo assessments over time that can be used as end points in the developmentof strategies to inhibit NH. Second, velocity-encoded cine phase-contrast MRA can providehighly resolved through-plane flow velocity patterns, and specific in-plane velocity patterns,in addition to blood volume flow rates. Fluid wall shear stress can then be calculated from thespace-averaged through-plane flow velocity. Misra et al.102 recently used cine-phase contrastMRA to show immediate and long-term increases in fluid wall shear stress at a location 2 cmdistal to the venous anastomosis of a porcine iliac artery-to-iliac vein ePTFE graft model.However, these data do not provide information about flow at the anastomosis itself where NHappears, or within other regions of the vein. We have used computational fluid dynamicmodeling to more completely predict flow patterns in our porcine AV graft model. In thesepreliminary studies, a 3D volumetric reconstruction of a graft-vein anastomosis was derivedfrom an in vivo MR image. Inflow values within the ePTFE graft were collected on the sameanimal using cine phase-contrast MRA. Computational fluid dynamic modeling was then usedto predict flow patterns on the basis of these in vivo values (Figure 4). These studies predict
Li et al. Page 6
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
very complex flow patterns at the venous anastomosis and the juxta-anastomotic regions ofthe vein. Analyzing such flow maps over time should help to further determine the effects ofblood flow on NH development and vice versa in specific locations of AV grafts.
Intravascular ultrasoundWith intravascular ultrasound (IVUS), an ultrasound transducer is introduced into the vascularaccess lumen and pulled along the vessel’s length, whereupon images of the vessel wall areobtained. Arbab-Zadeh et al.103 reported that IVUS was more sensitive than contrastangiography in detecting thrombus and graft deterioration from repeated needle puncture(roughening of luminal surface) in hemodialysis AV grafts. As it yields multiplane images,IVUS provides a more complete assessment of luminal diameters than DSA, which onlyprovides a single-plane image of the vessel lumen. Multiplane images are advantageousbecause the cross-sections of veins are typically elliptical in shape; further, NH may not involvethe complete circumference of the vessel.
Intravascular ultrasound has been found to be useful for evaluation of AV graft NH in animalmodels.104–106 Using this technique, the intima, media, and adventitia of the arterial wall canbe delineated. IVUS images of calcified regions of the vessel wall have been reported tocorrelate well with calcium quantification obtained by histological staining.107 A disadvantageis that IVUS provides only limited spatial resolution, making it difficult to determine the exactlocation of the obtained images along the length of the vessel. Precise spatial resolution canbe obtained if the progression of the ultrasound transducer is tracked by simultaneous biplaneangiography so that the IVUS images can be aligned with the vessel length.108 However, thisdual technique involves exposure of the patient to contrast and radiation and at this time is toocomplicated and expensive to be justified clinically.
Computerized tomographyRecently, findings of AV fistula stenosis using multislice computerized tomography (CT)angiography were shown to correlate well with those obtained by DSA.109 Ko et al.110reported that multidetector CT had high sensitivity compared with DSA in detecting stenoticlesions in AV fistulas and grafts. The production of 3D images is one advantage of CT scanningover DSA and CDUS. However, exposures to a significant amount of radiation and to iodinatedcontrast agents are disadvantages of CT scanning, similar to DSA.
TREATMENT USING ANGIOPLASTYThe current clinical treatment for AV graft stenosis is mainly percutaneous transluminalangioplasty (PTA). Early studies demonstrated that PTA was an effective treatment for alltypes of venous stenoses.7,111 Beathard111 reported an initial success rate of 94% and primarypatency rates at 90, 180, and 360 days of 90.6, 61.3, and 38.2%, respectively. Although PTAoften improved the blood flow, at least temporarily, the vascular wall injury produced by theballoon promotes hyperplasia and further stenosis, as seen in postangioplasty coronaryrestenosis.112 Histologically, markedly increased cell proliferation activity has been found inpostangioplasty restenotic lesions of AV fistula,113 which was much higher than that observedin primary stenotic lesions. In one clinical observational study, the 360-day primary patencyrate of forearm synthetic AV grafts was 40%, but after the second angioplasty, the patency ratewas only 25%. The 180-day patency rate following the third angioplasty was 0%.12 Thisaccelerated time course to stenosis after consecutive angioplasty procedures suggests thatangioplasty promotes NH formation. Indeed, most randomized clinical trials failed todemonstrate a benefit of routine monitoring of AV grafts with prophylactic PTA of stenoticlesions.114–117
Li et al. Page 7
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
To overcome the restenosis induced by PTA, various mechanical devices have been employed.Early clinical studies using bare metallic stents in conjunction with PTA have, however, yieldedlimited success because of the development of in-stent stenosis (that is, the ingrowth ofneointimal hyperplasic tissue through the mesh of a metallic stent).118 A recent retrospectivestudy examined in 51 patients the efficacy of stents made of nitinol or PTFE-encapsulated stentgrafts for the treatment of hemodialysis graft-related stenosis that had previously failed PTA.None of the stents used in that study were drug-eluting stents. Following PTA and insertion ofthe device, the primary patency of the nitinol stent or stent graft was 87% at 6 months, althoughthe primary patency of the entire vascular access was only 54%.119 A control group was notavailable for comparison in that study. Drug-eluting stents have been shown to be useful forthe prevention of coronary restenosis induced by PTA. In a porcine AV ePTFE graft model,rapamycin-eluting stents have also been shown to significantly reduce NH and increase graftdiameter and blood flow rate, compared with unstented grafts or grafts treated with bare-metalstents.120 There are, however, no clinical data using drug-eluting stents in conjunction withPTA to treat venous stenosis in hemodialysis vascular access.
PREVENTION STRATEGIESThe following discussion will explore approaches for NH prevention, although some of theseapproaches could also be potentially useful for regression of existing lesions (Table 1). Thesignificant progress that has been made in the understanding of its pathogenesis has led to thesuccessful employment of a number of agents to inhibit NH in various animal models, includingsome specifically in the hemodialysis AV graft setting. No therapy has proven effective inhemodialysis patients with AV grafts, although clinical trials conducted so far have been verylimited.
The optimum duration of the therapy would partly depend on the duration in which the graftis at risk for NH development. Foreign-body response, aberrant mechanical forces on thevascular wall, and repeated needle puncture are likely important on-going stimuli in thehemodialysis AV graft setting. This is in contrast to angioplasty-induced NH in the coronaryartery, in which the insult is transient. Therefore, preventive therapies would ideally becontinuous, as can theoretically be accomplished by the sustained release of a drug from areplenishable depot. Modification of the graft material or mechanical environment is also anattractive approach to inhibit NH development.
Mechanical designExpanded PTFE, polyethylene terephthalate (for example, Dacron), and polyurethane are themajor materials currently used for vascular prosthesis.121,122 ePTFE is preferred in partbecause of better surgical handling and lower rate of disintegration.122,123 ePTFE is a porousfluoropolymer produced by thermomechanical stretching, and its microstructure consists ofinterspaced solid nodes interconnected by small fibrils. The pore sizes average on the order of30 μm on the lumen surface in vascular applications. The addition of an external radial support(for example, coil or rings) enhances graft stability against compression and prevents kinkingat points of angulation.
Although ePTFE grafts have been used for many years, several problems remain. For example,because of the node-fibril structure, acute sealing of suture is difficult until tissue ingrowthoccurs to cover its surface. Furthermore, such microporous tubular structures tend to exhibitlow axial tear strength, so that a small tear tend to propagate along the axial length of the tube.These problems can be reduced by decreasing the pore size or density. However, smaller poresize inhibits tissue ingrowth through the pores, thus delaying integration of the graft with thesurrounding vascular tissue and decreasing the compliance of the graft, which wouldexacerbate the elasticity mismatch.124–126
Li et al. Page 8
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Elasticity mismatch between the stiff ePTFE graft and elastic native tissue is another majormechanical problem. The elastic modulus (or elastic stiffness) of the ePTFE graft wall is 4.06× 109 Pa, which is 1.6 times higher than the human coronary artery.127 Increasing the poresize and density can increase the compliance of the graft and enhance tissue ingrowth, but onlyat the expense of reducing overall tensile strength and the ability for the graft to retain sutures.Iterations of ePTFE (for example, a composite of ePTFE and polyurethane128) have beenstudied, but their usefulness remains to be explored.
Currently, the main approach to solve the elastic mismatch problem is to use natural, insteadof synthetic, material such as decellularized xenografts. Several hemodialysis grafts of bovineorigin are available commercially. Modified bovine carotid artery grafts have been used sincethe 1970s before ePTFE became available. Most retrospective studies suggest that ePTFEgrafts are superior to bovine artery grafts because the former are associated with less infectionand thrombosis and have a longer patency period.129–144 Decellularized xenografts madefrom bovine mesenteric veins145–148 or bovine ureters149,150 have become availablerecently. Some clinical studies have suggested that these new bovine grafts may offer a safealternative to patients who have a history of failed ePTFE grafts, but data are very limited.145 The major disadvantages of the bovine grafts include a lower overall mechanical strengthand more difficulty to repair when compared with synthetic grafts.
Expanded polytetrafluoroethylene grafts with various configurations have been designed toimprove the geometry at the anastomosis, thereby improving the blood flow patterns. Acommercially available modified ePTFE graft reinforced by a proprietary, cross-helicalnonporous ePTFE yarn wrap that covers 70% of the external graft surface, was proposed toenhance flow dynamics by preserving the graft luminal shape. Unfortunately, this design didnot prolong the graft patency in a clinical study.151 Another approach is to use tapered insteadof straight ePTFE grafts, where the graft’s luminal diameter decreases gradually from thevenous end to the arterial end. Such a design is based on the consideration that diametermismatch is an important factor contributing to abnormal flow patterns at the anastomoses.Limited clinical studies suggested that 8- to 6-mm tapered grafts improved primary patencyrate and decreased complications, compared with 6-mm straight grafts. Further studies arerequired to confirm these observations.152,153 Yet another approach is to create a cuffedgeometry made of ePTFE at the venous anastomosis to reduce regional turbulence, as venouscuffs seems to be beneficial in the arterial–arterial bypass ePTFE graft setting. However, it hasbeen suggested that the benefit associated with the vein cuff may be related to the presence ofvenous material, with improved wall compliance matching and other biological factors, ratherthan altered anastomotic geometry and hemodynamics, as CFE showed that anastomotichemodynamics are unchanged or worsened when vein cuffs are used.154–156 Anotherdisadvantage of the precuffed ePTFE graft is that it does not provide surgeons the flexibilityto trim the cuff to fit the native vessel during implantation. The cuff also increases the surfacearea that needs suturing, which in turn increases suture-line wall stress. Results from clinicalstudies comparing the cuffed and standard ePTFE hemodialysis grafts are conflicting.157,158
Surgical methods, such as suturing techniques41 and the angle of anastomosis,159 may playa role in attenuating the compliance mismatch problem.
Biological reagentsAntiproliferative drugs and biological reagents used to prevent NH can be delivered eithersystemically or locally. As NH is usually focal, although sometimes multifocal, and is relativelysmall and not malignant, local therapy is preferred because it would achieve a much higherconcentration at the target site with far fewer systemic side effects than systemic therapy. Anumber of biological reagents have been examined for efficacy against NH development in
Li et al. Page 9
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

AV grafts, including transfection of vessels with gene constructs that are antiproliferative andseeding of endothelial cells to grafts.
Antisense oligonucleotides—Antisense oligonucleotides (ODNs) can be used to inhibitDNA transcription, the production of mature mRNA, and protein synthesis. Antisense ODNsdirected against a number of proto-oncogenes and cell-cycle regulators, such as c-myc, c-myb, proliferating cell nuclear antigen, nuclear factor-κB, or different cyclin-dependentkinases, have been used to inhibit NH in arterial injury models.160–163 However, a clinicaltrial of intracoronary administration of antisense ODNs against c-myc immediately aftercoronary stenting failed to demonstrate the prevention of in-stent restenosis.164 There is noinformation on the usage of antisense ODN in AV graft models.
E2F decoy—Directly targeting E2F, a family of transcription factors important in cellreplication, by using decoy ODNs that bind E2F (E2F decoy) prevented NH in balloon-injuredcarotid arteries and vein interposition grafts in animal models.165–167 Earlier randomizedtrials conducted in patients undergoing peripheral arterial bypass (PREVENT I) or coronaryarterial bypass (PREVENT II) grafting with autologous veins have demonstrated thefeasibility, safety, and efficacy of using E2F decoy to prolong patency.168,169. Subsequentlarger randomized multicenter phase III trials, PREVENT III170 and PREVENT IV,171 failedto confirm the efficacy of E2F decoy in preventing vein bypass stenosis. A phase II clinicaltrial using E2F decoy to decrease NH in hemodialysis AV grafts is currently in progress.
Gene transfer—As surgical manipulation causes damage to the endothelium and theendothelium is important in regulating SMC growth, it has been hypothesized that rapid re-endothelialization of the vascular wall after injury may reduce restenosis. VEGF is a growthfactor family that induces endothelial cell proliferation and migration.172 Intravascularadenovirus-mediated VEGF-C gene transfer reduced NH in balloon-denuded rabbit aorta.173 In a rabbit carotid artery collar model, however, adventitial delivery of adenovirusesencoding VEGF-A and VEGF-D increased, rather than decreased, NH.174 Recently, ePTFEgrafts coated with VEGF-A in a fibrin matrix interposed in pig carotid arteries were also foundto enhance NH.175 Thus, maneuvers that are designed to inhibit NH by promotingendothelialization have yielded conflicting results. The effect of local delivery of VEGF bygene transfer has not yet been explored specifically in AV ePTFE grafts.
C-type natriuretic peptide is an endothelium-derived peptide with antiproliferative effects onSMC through the induction of cyclic guanosine monophosphate.176 Adenovirus-mediatedgene transfer of C-type natriuretic peptide was shown to inhibit NH in a rabbit jugular veininterpositional graft model.177 In a porcine AV ePTFE graft model, however, localoverexpression of C-type natriuretic peptide enhanced venous medial thickening but failed toinhibit NH.178 In another study, transduction of the external jugular vein with an adenoviralvector overexpressing the carboxyl terminus of the β-adrenergic receptor kinase, an inhibitorof G-protein signaling, significantly reduced NH at the venous anastomosis in a porcine AVePTFE graft model.179
Cell-based therapies—Several groups have reported cell-based therapies to inhibit NH inAV ePTFE graft models. In a porcine AV ePTFE graft model, Rotmans et al.180 evaluatedthe feasibility of capturing endothelial progenitor cells in vivo using anti-CD34 antibodiesimmobilized on ePTFE grafts. Despite the successful endothelialization using this technique,NH at the venous anastomosis increased substantially, instead of decreased, at 4 weeks afterimplantation.180 In another porcine AV ePTFE graft study, gelfoam matrices containingallogeneic porcine aortic endothelial cells were applied around the anastomoses and outflowvein. At 28 days after graft placement, venous lumen diameter and positive remodeling were
Li et al. Page 10
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
increased, but no significant decrease in NH was observed.181 These studies raise skepticismregarding the value of promoting endothelialization or endothelial functions in preventing NH.
Small-molecule drugsIf successful, small-molecule drugs have an advantage over biological reagents because theyare simpler and less likely to elicit host immunological responses. Local drug delivery can beachieved using several approaches: (1) coating of the graft with the drug; (2) placing a drug-coated stent intravascularly at the anastomosis; (3) injecting the drug into the vascular wall atthe anastomoses through an intravascular catheter; (4) placing a drug depot perivascularly atthe anastomoses. The latter has been accomplished by the placement or injection of a polymergel containing the drug15,182 or placing the drug in an impermeable wrap that encases theanastomoses.183,184 Hypothetically, the perivascular approach has a particular advantagebecause the drug will be in close proximity to the adventitial fibroblasts, which are consideredto be critical for NH formation. Below are several antiproliferative drugs that havedemonstrated efficacy in inhibiting NH in arterial-injury animal models. Some of these drugshave also been tested in AV ePTFE graft models by our group and other investigators.
Rapamycin (sirolimus)—Rapamycin is a macrocyclic triene antibiotic used clinically toinhibit T-lymphocyte activation and prevent allograft rejection. Rapamycin was also reportedto inhibit vascular SMC proliferation after balloon angioplasty.185–187 Rapymycin-coatedstents have been shown to be effective in decreasing major adverse cardiac events andrestenosis rates after angioplasty in patients with coronary disease (RAVEL, SIRIUS trials).188–191 In a porcine AV ePTFE graft model, rapamycin-eluting stents significantly reducedNH and increased graft diameter and blood flow rate, compared with unstented grafts or graftstreated with bare-metal stents.120 Although these studies are promising, this approach requiresan invasive procedure of placing a stent. Furthermore, drug release from coated stents is of alimited duration. The inability to replenish the drug depot in the stent may diminish theeffectiveness of this strategy in preventing NH development in AV grafts in which the stimuliare chronic. There are no clinical trials reported to date on hemodialysis AV grafts usingrapamycin-coated stents.
Paclitaxel—Paclitaxel inhibits cell division through stabilization of the mitotic spindle.192Local administration of paclitaxel by use of microporous intravascular balloons prevented NHformation in a rabbit carotid arterial-injury model.193 Several clinical trials (TAXUS I,ELUTES, ASPECT, TAXUS IV trials) have established the safety and efficacy of paclitaxel-coated stents in preventing restenosis in coronary arteries.194–197 Data from our laboratorydemonstrated that the perivascular sustained delivery of paclitaxel at the anastomoses using apolymer gel could inhibit NH in a canine AV ePTFE graft model.15 Coating of ePTFE graftswith paclitaxel has also been demonstrated to inhibit NH in a porcine model of AV graftstenosis, compared with uncoated grafts.198 Recently, paclitaxel-eluting wrap placed aroundthe anastomoses was reported to inhibit NH formation in sheep183 and porcine184 AV ePTFEgraft models. Clinical trials testing the efficacy of local delivery of paclitaxel using anytechnique have not been reported in hemodialysis AV grafts to date.
Dipyridamole—In addition to antiplatelet activity, dipyridamole also inhibits SMCproliferation in vitro, although the concentrations required for inhibition (IC50 values) areapproximately 1000-fold higher than those of rapamycin and paclitaxel.199,200 A smallclinical trial has suggested the efficacy of oral dipyridamole in decreasing PTFE graft occlusionin dialysis patients,201 but stenosis was not specifically examined in that study. A largemulticenter trial sponsored by the National Institutes of Health using the oral combination ofdipyridamole and aspirin in preventing AV graft failure in dialysis patients is ongoing.Continuous adventitial dipyridamole delivery using an osmotic pump inhibited NH formation
Li et al. Page 11
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
in rabbit artery-injury models.202 In contrast, there was no significant decrease in restenosisrates after coronary angioplasty using intracoronary dipyridamole in a small randomizedclinical trial.203 Furthermore, in our porcine AV ePTFE graft model, local perivascularsustained delivery of dipyridamole using a polymer gel applied at the anastomoses, even athigh dosages, was ineffective in inhibiting NH.204 This ineffectiveness of local delivery ofdipyridamole may be due to the relatively low antiproliferative potency of the drug againstvascular SMC, the short duration of release of the drug from the polymer gel because of thehydrophilic nature of the drug, or other factors.
Imatinib mesylate—Platelet-derived growth factor and its receptors are prominentlyexpressed in NH lesions of human vascular diseases and animal models. Previous studies havedemonstrated the efficacy of PDGF antibodies or PDGF-receptor antagonists in the preventionof NH in animal models of arterial injury or interposition grafts.205,206 Therefore, targetingPDGF and PDGF receptors is a logical strategy for NH inhibition associated with hemodialysisAV grafts. Imatinib mesylate is a low-molecular-weight inhibitor of the phosphotyrosinekinase activity of both PDGF receptor subtypes,207 as well as that of Bcr-Abl208 and c-kit.209 Imatinib is currently used clinically to treat several forms of malignancies.210,211 Thetherapeutic efficacy of imatinib has also been demonstrated in animal models of arterialproliferative diseases, including restenosis after balloon angioplasty,212 diet-inducedatherosclerosis,213 and post-transplant atherosclerosis of heart and aorta.214 Recently, oralimatinib has been shown to potentiate the effect of local intravascular transfection with theVEGF-C gene in reducing NH in hyperpcholesterolemic rabbits.215 Data from our laboratorydemonstrated the inhibitory effect of imatinib on both human arterial and venous SMC invitro, with the IC50 values being eightfold lower in the venous cells than in the arterial cells.216 Imatinib is therefore a promising drug for the prevention of hemodialysis AV graft stenosis.
IrradiationIn recent years, there has been intensive research on the use of ionizing radiation for inhibitionof NH. The main effect of vascular brachytherapy appears to be mediated by irradiation-induced DNA damage of vascular cells with consequent arrest at the G1 checkpoint andinduction of apoptosis through p53-induced p21 upregulation.217 Results from various animalmodels have clearly established that beta or gamma ionizing radiation inhibits restenosis afterangioplasty.218–220 Several clinical trials have also shown that intracoronary radiation is safeand effective for treatment of restenotic coronary arteries after angioplasty.221,222 In a porcinemodel of hemodialysis AV grafts, local delivery of gamma radiation reduced NH at the venousanastomosis.223 Despite these encouraging data, recent clinical trials in hemodialysis patientsfailed to demonstrate significant inhibition of stenosis by radiation treatment of native AVfistulas or ePTFE grafts.224,225
CONCLUSIONThe pathogenesis of NH associated with hemodialysis AV grafts is complex and likely involvessurgical manipulation of the tissues, material bioincompatibility, and mechanical factors,which could be aggravated by angioplasty of the stenosis. In contrast to post-coronaryangioplasty restenosis, the chronic nature of the stimuli in the AV graft likely requires strategiesthat provide chronic prevention. A large number of antiproliferative and immunomodulatingagents are already in use clinically for various proliferative and immunological disorders.Adoption of these agents, with the appropriate delivery platform, technique, and schedule,would likely be successful in preventing, and perhaps regressing, NH. As stenosis, andconsequentially occlusion, is the predominant cause of AV graft failure, successful preventionof this complication should make synthetic grafts a superior mode of hemodialysis vascularaccess to complement native fistulas.
Li et al. Page 12
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
AcknowledgementsThis work was supported by the National Heart, Lung, and Blood Institute (RO1HL67646), Medical and ResearchServices of the Department of Veterans Affairs, Dialysis Research Foundation and the National Kidney Foundationof Utah and Idaho. We gratefully acknowledge the work of Peter Vincent, M.S., and Spencer Sherwin, Ph.D., of theImperial College London for collaborations on the computational fluid dynamics modeling in the AV graft.
References1. Allon M, Robbin ML. Increasing arteriovenous fistulas in hemodialysis patients: problems and
solutions. Kidney Int 2002;62:1109–1124. [PubMed: 12234281]2. Pisoni RL, Young EW, Dykstra DM, et al. Vascular access use in Europe and the United States: results
from the DOPPS. Kidney Int 2002;61:305–316. [PubMed: 11786113]3. Rayner HC, Besarab A, Brown WW, et al. Vascular access results from the Dialysis Outcomes and
Practice Patterns Study (DOPPS): performance against Kidney Disease Outcomes Quality Initiative(K/DOQI) Clinical Practice Guidelines. Am J Kidney Dis 2004;44:22–26. [PubMed: 15486870]
4. Ravani P, Barrett B, Mandolfo S, et al. Factors associated with unsuccessful utilization and early failureof the arteriovenous fistula for hemodialysis. J Nephrol 2005;18:188–196. [PubMed: 15931647]
5. Saran R, Dykstra DM, Pisoni RL, et al. Timing of first cannulation and vascular access failure inhaemodialysis: an analysis of practice patterns at dialysis facilities in the DOPPS. Nephrol DialTransplant 2004;19:2334–2340. [PubMed: 15252160]
6. Lee H, Manns B, Taub K, et al. Cost analysis of ongoing care of patients with end-stage renal disease:the impact of dialysis modality and dialysis access. Am J Kidney Dis 2002;40:611–622. [PubMed:12200814]
7. Schwab SJ, Oliver MJ, Suhocki P, et al. Hemodialysis arteriovenous access: detection of stenosis andresponse to treatment by vascular access blood flow. Kidney Int 2001;59:358–362. [PubMed:11135091]
8. United States Renal Data System. 2007 USRDS Annual Report. 2007.9. Asif A, Gadalean FN, Merrill D, et al. Inflow stenosis in arteriovenous fistulas and grafts: a multicenter,
prospective study. Kidney Int 2005;67:1986–1992. [PubMed: 15840048]10. Kelly BS, Heffelfinger SC, Whiting JF, et al. Aggressive venous neointimal hyperplasia in a pig
model of arteriovenous graft stenosis. Kidney Int 2002;62:2272–2280. [PubMed: 12427156]11. Roy-Chaudhury P, Sukhatme VP, Cheung AK. Hemodialysis vascular access dysfunction: a cellular
and molecular viewpoint. J Am Soc Nephrol 2006;17:1112–1127. [PubMed: 16565259]12. Kanterman RY, Vesely TM, Pilgram TK, et al. Dialysis access grafts: anatomic location of venous
stenosis and results of angioplasty. Radiology 1995;195:135–139. [PubMed: 7892454]13. Roy-Chaudhury P, Kelly BS, Miller MA, et al. Venous neointimal hyperplasia in
polytetrafluoroethylene dialysis grafts. Kidney Int 2001;59:2325–2334. [PubMed: 11380837]14. Swedberg SH, Brown BG, Sigley R, et al. Intimal fibromuscular hyperplasia at the venous anastomosis
of PTFE grafts in hemodialysis patients. Clinical, immunocytochemical, light and electronmicroscopic assessment. Circulation 1989;80:1726–1736. [PubMed: 2688974]
15. Masaki T, Rathi R, Zentner G, et al. Inhibition of neointimal hyperplasia in vascular grafts by sustainedperivascular delivery of paclitaxel. Kidney Int 2004;66:2061–2069. [PubMed: 15496180]
16. Li L, Terry CM, Blumenthal DK, et al. Cellular and morphological changes during neointimalhyperplasia development in a porcine arteriovenous graft model. Nephrol Dial Transplant2007;22:3139–3146. [PubMed: 17602194]
17. Rotmans JI, Velema E, Verhagen HJ, et al. Rapid, arteriovenous graft failure due to intimalhyperplasia: a porcine, bilateral, carotid arteriovenous graft model. J Surg Res 2003;113:161–171.[PubMed: 12943826]
18. Schwartz SM, deBlois D, O’Brien ER. The intima. Soil for atherosclerosis and restenosis. Circ Res1995;77:445–465. [PubMed: 7641318]
19. Wilcox JN, Cipolla GD, Martin FH, et al. Contribution of adventitial myofibroblasts to vascularremodeling and lesion formation after experimental angioplasty in pig coronary arteries. Ann N YAcad Sci 1997;811:437–447. [PubMed: 9186621]
Li et al. Page 13
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
20. Misra S, Doherty MG, Woodrum D, et al. Adventitial remodeling with increased matrixmetalloproteinase-2 activity in a porcine arteriovenous polytetrafluoroethylene grafts. Kidney Int2005;68:2890–2900. [PubMed: 16316367]
21. Roy-Chaudhury P, Kelly BS, Melhem M, et al. Novel therapies for hemodialysis vascular accessdysfunction: fact or fiction! Blood Purif 2005;23:29–35. [PubMed: 15627734]
22. Mitra AK, Gangahar DM, Agrawal DK. Cellular, molecular and immunological mechanisms in thepathophysiology of vein graft intimal hyperplasia. Immunol Cell Biol 2006;84:115–124. [PubMed:16519729]
23. Radomski MW, Palmer RM, Moncada S. The anti-aggregating properties of vascular endothelium:interactions between prostacyclin and nitric oxide. Br J Pharmacol 1987;92:639–646. [PubMed:3322462]
24. Sarkar R, Meinberg EG, Stanley JC, et al. Nitric oxide reversibly inhibits the migration of culturedvascular smooth muscle cells. Circ Res 1996;78:225–230. [PubMed: 8575065]
25. Sarkar R, Webb RC. Does nitric oxide regulate smooth muscle cell proliferation? A critical appraisal.J Vasc Res 1998;35:135–142. [PubMed: 9647326]
26. McGeachie JK, Meagher S, Prendergast FJ. Vein-to-artery grafts: the long-term development ofneointimal hyperplasia and its relationship to vasa vasorum and sympathetic innervation. Aus N Z JSurg 1989;59:59–65.
27. Postlethwaite AE, Seyer JM. Stimulation of fibroblast chemotaxis by human recombinant tumornecrosis factor alpha (TNF-alpha) and a synthetic TNF-alpha 31–68 peptide. J Exp Med1990;172:1749–1756. [PubMed: 2258704]
28. Jovinge S, Hultgardh-Nilsson A, Regnstrom J, et al. Tumor necrosis factor-alpha activates smoothmuscle cell migration in culture and is expressed in the balloon-injured rat aorta. Arterioscler ThrombVasc Biol 1997;17:490–497. [PubMed: 9102167]
29. Hansson GK, Holm J, Holm S, et al. T lymphocytes inhibit the vascular response to injury. Proc NatlAcad Sci USA 1991;88:10530–10534. [PubMed: 1961717]
30. Robertson AK, Hansson GK. T cells in atherogenesis: for better or for worse? Arterioscler ThrombVasc Biol 2006;26:2421–2432. [PubMed: 16973967]
31. Duncan MR, Berman B. Gamma interferon is the lymphokine and beta interferon the monokineresponsible for inhibition of fibroblast collagen production and late but not early fibroblastproliferation. J Exp Med 1985;162:516–527. [PubMed: 2410528]
32. Bobryshev YV, Inder SJ, Cherian SM, et al. Colonisation of prosthetic grafts by immunocompetentcells in a sheep model. Cardiovasc Surg 2001;9:166–176. [PubMed: 11250186]
33. Inder SJ, Bobryshev YV, Cherian SM, et al. Identification of dendritic cells in ePTFE grafts explantedfrom humans. Cardiovasc Surg 2000;8:265–273. [PubMed: 10840203]
34. Cherian SM, Bobryshev YV, Inder SJ, et al. Involvement of dendritic cells in long-term aortocoronarysaphenous vein bypass graft failure. Cardiovasc Surg 1999;7:508–518. [PubMed: 10499893]
35. Cherian SM, Bobryshev YV, Inder SJ, et al. Dendritic cells in venous pathologies. Angiology1999;50:393–402. [PubMed: 10348427]
36. Mattana J, Effiong C, Kapasi A, et al. Leukocyte-polytetrafluoroethylene interaction enhancesproliferation of vascular smooth muscle cells via tumor necrosis factor-alpha secretion. Kidney Int1997;52:1478–1485. [PubMed: 9407493]
37. Miller KM, Anderson JM. Human monocyte/macrophage activation and interleukin 1 generation bybiomedical polymers. J Biomed Mater Res 1988;22:713–731. [PubMed: 3265135]
38. Dagtekin G, Schiffer R, Klein B, et al. Modulation of angiogenic functions in human macrophagesby biomaterials. Biomaterials 2003;24:3395–3401. [PubMed: 12809767]
39. Haruguchi H, Teraoka S. Intimal hyperplasia and hemodynamic factors in arterial bypass andarteriovenous grafts: a review. J Artif Organs 2003;6:227–235. [PubMed: 14691664]
40. Sivanesan S, How TV, Black RA, et al. Flow patterns in the radiocephalic arteriovenous fistula: anin vitro study. J Biomech 1999;32:915–925. [PubMed: 10460128]
41. Ballyk PD, Walsh C, Butany J, et al. Compliance mismatch may promote graft-artery intimalhyperplasia by altering suture-line stresses. J Biomech 1998;31:229–237. [PubMed: 9645537]
Li et al. Page 14
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

42. Hofer M, Rappitsch G, Perktold K, et al. Numerical study of wall mechanics and fluid dynamics inend-to-side anastomoses and correlation to intimal hyperplasia. J Biomech 1996;29:1297–1308.[PubMed: 8884475]
43. Fung, YC. Biomechanics: Mechanical Properties of Living Tissues. 2. Springer-Verlag; New York:1993.
44. Davies MG, Hagen PO. Pathophysiology of vein graft failure: a review. Eur J Vasc Endovasc Surg1995;9:7–18. [PubMed: 7664016]
45. Liu SQ. Biomechanical basis of vascular tissue engineering. Crit Rev Biomed Eng 1999;27:75–148.[PubMed: 10638850]
46. Kakisis JD, Liapis CD, Sumpio BE. Effects of cyclic strain on vascular cells. Endothelium2004;11:17–28. [PubMed: 15203876]
47. Davies PF, Polacek DC, Shi C, et al. The convergence of haemodynamics, genomics, and endothelialstructure in studies of the focal origin of atherosclerosis. Biorheology 2002;39:299–306. [PubMed:12122245]
48. Shiu, YT. Mechanical forces on cells. In: Bronzino, JD., editor. The Biomedical EngineeringHandbook: Tissue Engineering and Artificial Organs. 3. CRC Press Taylor & Francis Group, LLC;Boca Raton: 2006. p. 33.31-33.18.
49. Ene-Iordache B, Mosconi L, Remuzzi G, et al. Computational fluid dynamics of a vascular accesscase for hemodialysis. J Biomech Eng 2001;123:284–292. [PubMed: 11476373]
50. Krueger U, Zanow J, Scholz H. Comparison of two different arteriovenous anastomotic forms bynumerical 3D simulation of blood flow. Int J Angiol 2000;9:226–231. [PubMed: 11062312]
51. Krueger U, Zanow J, Scholz H. Computational fluid dynamics and vascular access. Artif Organs2002;26:571–575. [PubMed: 12081514]
52. Migliavacca F, Dubini G. Computational modeling of vascular anastomoses. Biomech ModelMechanobiol 2005;3:235–250. [PubMed: 15772842]
53. Van Tricht I, De Wachter D, Tordoir J, et al. Comparison of the hemodynamics in 6 and 4–7 mmhemodialysis grafts by means of CFD. J Biomech 2006;39:226–236. [PubMed: 16321624]
54. Loth F, Jones SA, Zarins CK, et al. Relative contribution of wall shear stress and injury in experimentalintimal thickening at PTFE end-to-side arterial anastomoses. J Biomech Eng 2002;124:44–51.[PubMed: 11871604]
55. Caro CG, Fitz-Gerald JM, Schroter RC. Arterial wall shear and distribution of early atheroma in man.Nature 1969;223:1159–1160. [PubMed: 5810692]
56. Kraiss LW, Geary RL, Mattsson EJ, et al. Acute reductions in blood flow and shear stress induceplatelet-derived growth factor-A expression in baboon prosthetic grafts. Circ Res 1996;79:45–53.[PubMed: 8925568]
57. Mondy JS, Lindner V, Miyashiro JK, et al. Platelet-derived growth factor ligand and receptorexpression in response to altered blood flow in vivo. Circ Res 1997;81:320–327. [PubMed: 9285633]
58. Sterpetti AV, Cucina A, D′Angelo LS, et al. Response of arterial smooth muscle cells to laminar flow.J Cardiovasc Surg 1992;33:619–624. [PubMed: 1447284]
59. Sterpetti AV, Cucina A, Santoro L, et al. Modulation of arterial smooth muscle cell growth byhaemodynamic forces. Eur J Vasc Surg 1992;6:16–20. [PubMed: 1555664]
60. Ueba H, Kawakami M, Yaginuma T. Shear stress as an inhibitor of vascular smooth muscle cellproliferation. Role of transforming growth factor-beta 1 and tissue-type plasminogen activator.Arterioscler Thromb Vasc Biol 1997;17:1512–1516. [PubMed: 9301628]
61. Song RH, Kocharyan HK, Fortunato JE, et al. Increased flow and shear stress enhance in vivotransforming growth factor-beta1 after experimental arterial injury. Arterioscler Thromb Vasc Biol2000;20:923–930. [PubMed: 10764655]
62. Loth F, Fischer PF, Arslan N, et al. Transitional flow at the venous anastomosis of an arteriovenousgraft: potential activation of the ERK1/2 mechanotransduction pathway. J Biomech Eng2003;125:49–61. [PubMed: 12661196]
63. Liu SQ, Tieche C, Tang D, et al. Pattern formation of vascular smooth muscle cells subject tononuniform fluid shear stress: role of PDGF-beta receptor and Src. Am J Physiol Heart Circ Physiol2003;285:H1081–H1090. [PubMed: 12738619]
Li et al. Page 15
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
64. Tarbell, JM.; Qui, Y. Arterial wall mass transport: the possible role of blood phase resistance in thelocalization of arterial disease. In: Bronzino, JD., editor. The Biomedical Engineering Handbook:Tissue Engineering and Artificial Organs. 3. CRC Press Taylor & Francis Group, LLC; Boca Raton:2006. p. 9.1-9.15.
65. Lipowsky HH, Riedel D, Shi GS. In vivo mechanical properties of leukocytes during adhesion tovenular endothelium. Biorheology 1991;28:53–64. [PubMed: 2049532]
66. House SD, Lipowsky HH. In vivo determination of the force of leukocyte-endothelium adhesion inthe mesenteric microvasculature of the cat. Circ Res 1988;63:658–668. [PubMed: 3409492]
67. Badimon L, Chesebro JH, Badimon JJ. Thrombus formation on ruptured atherosclerotic plaques andrethrombosis on evolving thrombi. Circulation 1992;86:III74–III85. [PubMed: 1424053]
68. Badimon JJ, Badimon L, Turitto VT, et al. Platelet deposition at high shear rates is enhanced by highplasma cholesterol levels. In vivo study in the rabbit model. Arterioscler Thromb 1991;11:395–402.[PubMed: 1998657]
69. Maalej N, Holden JE, Folts JD. Effect of shear stress on acute platelet thrombus formation in caninestenosed carotid arteries: an in vivo quantitative study. J Thromb Thrombolysis 1998;5:231–238.[PubMed: 10767119]
70. Maalej N, Folts JD. Increased shear stress overcomes the antithrombotic platelet inhibitory effect ofaspirin in stenosed dog coronary arteries. Circulation 1996;93:1201–1205. [PubMed: 8653842]
71. Bassiouny HS, Song RH, Kocharyan H, et al. Low flow enhances platelet activation after acuteexperimental arterial injury. J Vasc Surg 1998;27:910–918. [PubMed: 9620144]
72. Sumpio BE, Banes AJ. Response of porcine aortic smooth muscle cells to cyclic tensional deformationin culture. J Surg Res 1988;44:696–701. [PubMed: 3379947]
73. Mills I, Cohen CR, Kamal K, et al. Strain activation of bovine aortic smooth muscle cell proliferationand alignment: study of strain dependency and the role of protein kinase A and C signaling pathways.J Cell Physiol 1997;170:228–234. [PubMed: 9066778]
74. Li Q, Muragaki Y, Ueno H, et al. Stretch-induced proliferation of cultured vascular smooth musclecells and a possible involvement of local renin-angiotensin system and platelet-derived growth factor(PDGF). Hypertens Res 1997;20:217–223. [PubMed: 9328803]
75. Birukov KG, Shirinsky VP, Stepanova OV, et al. Stretch affects phenotype and proliferation ofvascular smooth muscle cells. Mol Cell Biochem 1995;144:131–139. [PubMed: 7623784]
76. Mizutani T, Haga H, Kawabata K. Cellular stiffness response to external deformation: tensionalhomeostasis in a single fibroblast. Cell Motil Cytoskeleton 2004;59:242–248. [PubMed: 15493061]
77. Maniotis AJ, Chen CS, Ingber DE. Demonstration of mechanical connections between integrins,cytoskeletal filaments, and nucleoplasm that stabilize nuclear structure. Proc Natl Acad Sci USA1997;94:849–854. [PubMed: 9023345]
78. Gladilin E, Micoulet A, Hosseini B, et al. 3D finite element analysis of uniaxial cell stretching: fromimage to insight. Phys Biol 2007;4:104–113. [PubMed: 17664655]
79. Ingber DE. Mechanobiology and diseases of mechanotransduction. Ann Med 2003;35:564–577.[PubMed: 14708967]
80. Wilson E, Vives F, Collins T, et al. Strain-responsive regions in the platelet-derived growth factor-A gene promoter. Hypertension 1998;31:170–175. [PubMed: 9453298]
81. Ma YH, Ling S, Ives HE. Mechanical strain increases PDGF-B and PDGF beta receptor expressionin vascular smooth muscle cells. Biochem Biophys Res Commun 1999;265:606–610. [PubMed:10558917]
82. Hu Y, Bock G, Wick G, et al. Activation of PDGF receptor alpha in vascular smooth muscle cells bymechanical stress. FASEB J 1998;12:1135–1142. [PubMed: 9737716]
83. Kawabe J, Okumura S, Lee MC, et al. Translocation of caveolin regulates stretch-induced ERKactivity in vascular smooth muscle cells. Am J Physiol Heart Circ Physiol 2004;286:H1845–H1852.[PubMed: 15072971]
84. Hamada K, Takuwa N, Yokoyama K, et al. Stretch activates Jun N-terminal kinase/stress-activatedprotein kinase in vascular smooth muscle cells through mechanisms involving autocrine ATPstimulation of purinoceptors. J Biol Chem 1998;273:6334–6340. [PubMed: 9497362]
Li et al. Page 16
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
85. Reusch HP, Chan G, Ives HE, et al. Activation of JNK/SAPK and ERK by mechanical strain invascular smooth muscle cells depends on extracellular matrix composition. Biochem Biophys ResCommun 1997;237:239–244. [PubMed: 9268693]
86. Zeidan A, Broman J, Hellstrand P, et al. Cholesterol dependence of vascular ERK1/2 activation andgrowth in response to stretch: role of endothelin-1. Arterioscler Thromb Vasc Biol 2003;23:1528–1534. [PubMed: 12907462]
87. Li W, Chen Q, Mills I, et al. Involvement of S6 kinase and p38 mitogen activated protein kinasepathways in strain-induced alignment and proliferation of bovine aortic smooth muscle cells. J CellPhysiol 2003;195:202–209. [PubMed: 12652647]
88. Darbeau MZ, Lutz RJ, Collins WE. Simulated lipoprotein transport in the wall of branched arteries.Asaio J 2000;46:669–678. [PubMed: 11110263]
89. Li C, Hu Y, Mayr M, et al. Cyclic strain stress-induced mitogen-activated protein kinase (MAPK)phosphatase 1 expression in vascular smooth muscle cells is regulated by Ras/Rac-MAPK pathways.J Biol Chem 1999;274:25273–25280. [PubMed: 10464250]
90. Kakisis JD, Pradhan S, Cordova A, et al. The role of STAT-3 in the mediation of smooth muscle cellresponse to cyclic strain. Int J Biochem Cell Biol 2005;37:1396–1406. [PubMed: 15833272]
91. Chen AH, Gortler DS, Kilaru S, et al. Cyclic strain activates the pro-survival Akt protein kinase inbovine aortic smooth muscle cells. Surgery 2001;130:378–381. [PubMed: 11490374]
92. Sedding DG, Seay U, Fink L, et al. Mechanosensitive p27Kip1 regulation and cell cycle entry invascular smooth muscle cells. Circulation 2003;108:616–622. [PubMed: 12835226]
93. Mills I, Letsou G, Rabban J, et al. Mechanosensitive adenylate cyclase activity in coronary vascularsmooth muscle cells. Biochem Biophys Res Commun 1990;171:143–147. [PubMed: 2393388]
94. Bay WH, Van Cleef S, Owens M. The hemodialysis access: preferences and concerns of patients,dialysis nurses and technicians, and physicians. Am J Nephrol 1998;18:379–383. [PubMed:9730560]
95. Dumars MC, Thompson WE, Bluth EI, et al. Management of suspected hemodialysis graftdysfunction: usefulness of diagnostic US. Radiology 2002;222:103–107. [PubMed: 11756712]
96. Bacchini G, Cappello A, La Milia V, et al. Color doppler ultrasonography imaging to guidetransluminal angioplasty of venous stenosis. Kidney Int 2000;58:1810–1813. [PubMed: 11012917]
97. Bakker CJ, Peeters JM, Bartels LW, et al. Magnetic resonance techniques in hemodialysis accessmanagement. J Vasc Access 2003;4:125–139. [PubMed: 17639491]
98. Zhang J, Hecht EM, Maldonado T, et al. Time-resolved 3D MR angiography with parallel imagingfor evaluation of hemodialysis fistulas and grafts: initial experience. AJR Am J Roentgenol2006;186:1436–1442. [PubMed: 16632742]
99. Planken RN, Tordoir JH, Dammers R, et al. Stenosis detection in forearm hemodialysis arteriovenousfistulae by multiphase contrast-enhanced magnetic resonance angiography: preliminary experience.J Magn Reson Imaging 2003;17:54–64. [PubMed: 12500274]
100. Deo A, Fogel M, Cowper SE. Nephrogenic systemic fibrosis: a population study examining therelationship of disease development to gadolinium exposure. Clin J Am Soc Nephrol 2007;2:264–267. [PubMed: 17699423]
101. Terry, cM; Goodrich, KC.; Hadley, JR., et al. No contrast, in vivo magnetic resonance imaging(MRI) of hemodialysis vascular access hyperplasia. J Am Soc Nephrol 2006;17:557A.
102. Misra S, Woodrum DA, Homburger J, et al. Assessment of wall shear stress changes in arteries andveins of arteriovenous polytetrafluoroethylene grafts using magnetic resonance imaging.Cardiovasc Intervent Radiol 2006;29:624–629. [PubMed: 16729233]
103. Arbab-Zadeh A, Mehta RL, Ziegler TW, et al. Hemodialysis access assessment with intravascularultrasound. Am J Kidney Dis 2002;39:813–823. [PubMed: 11920348]
104. Terry CM, Li L, Kuji T, et al. Intravascular ultrasound for imaging stenosis in a pig model ofhemodialysis grafts. J Am Soc Nephrol 2005;16:11A.
105. McLennan G, Trerotola SO, Forney M, et al. Short-term patency and safety of an expandedpolytetrafluoroethylene encapsulated endoluminal device at the venous anastomosis of a caninearteriovenous graft model. J Vasc Interv Radiol 2001;12:227–234. [PubMed: 11265888]
106. Johnson MS, McLennan G, Lalka SG, et al. The porcine hemodialysis access model. J Vasc IntervRadiol 2001;12:969–977. [PubMed: 11487678]
Li et al. Page 17
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

107. Kostamaa H, Donovan J, Kasaoka S, et al. Calcified plaque cross-sectional area in human arteries:correlation between intravascular ultrasound and undecalcified histology. Am Heart J1999;137:482–488. [PubMed: 10047630]
108. Weichert F, Wawro M, Muller H, et al. Registration of biplane angiography and intravascularultrasound for 3D vessel reconstruction. Methods Inf Med 2004;43:398–402. [PubMed: 15472753]
109. Ye C, Mao Z, Rong S, et al. Multislice computed tomographic angiography in evaluating dysfunctionof the vascular access in hemodialysis patients. Nephron 2006;104:c94–c100. [PubMed: 16785741]
110. Ko SF, Huang CC, Ng SH, et al. MDCT angiography for evaluation of the complete vascular treeof hemodialysis fistulas. AJR Am J Roentgenol 2005;185:1268–1274. [PubMed: 16247148]
111. Beathard GA. Percutaneous transvenous angioplasty in the treatment of vascular access stenosis.Kidney Int 1992;42:1390–1397. [PubMed: 1474770]
112. Jacobson GM, Dourron HM, Liu J, et al. Novel NAD(P)H oxidase inhibitor suppresses angioplasty-induced superoxide and neointimal hyperplasia of rat carotid artery. Circ Res 2003;92:637–643.[PubMed: 12609967]
113. Chang CJ, Ko PJ, Hsu LA, et al. Highly increased cell proliferation activity in the restenotichemodialysis vascular access after percutaneous transluminal angioplasty: implication inprevention of restenosis. Am J Kidney Dis 2004;43:74–84. [PubMed: 14712430]
114. Ram SJ, Work J, Caldito GC, et al. A randomized controlled trial of blood flow and stenosissurveillance of hemodialysis grafts. Kidney Int 2003;64:272–280. [PubMed: 12787419]
115. Dember LM, Holmberg EF, Kaufman JS. Randomized controlled trial of prophylactic repair ofhemodialysis arteriovenous graft stenosis. Kidney Int 2004;66:390–398. [PubMed: 15200448]
116. Moist LM, Churchill DN, House AA, et al. Regular monitoring of access flow compared withmonitoring of venous pressure fails to improve graft survival. J Am Soc Nephrol 2003;14:2645–2653. [PubMed: 14514744]
117. Robbin ML, Oser RF, Lee JY, et al. Randomized comparison of ultrasound surveillance and clinicalmonitoring on arteriovenous graft outcomes. Kidney Int 2006;69:730–735. [PubMed: 16518328]
118. Clark TW. Nitinol stents in hemodialysis access. J Vasc Interv Radiol 2004;15:1037–1040.[PubMed: 15466787]
119. Vesely TM, Amin MZ, Pilgram T. Use of stents and stent grafts to salvage angioplasty failures inpatients with hemodialysis grafts. Semin Dial 2008;21:100–104. [PubMed: 18251965]
120. Rotmans JI, Pattynama PM, Verhagen HJ, et al. Sirolimus-eluting stents to abolish intimalhyperplasia and improve flow in porcine arteriovenous grafts: a 4-week follow-up study. Circulation2005;111:1537–1542. [PubMed: 15781738]
121. Pasquinelli G, Freyrie A, Preda P, et al. Healing of prosthetic arterial grafts. Scanning Microsc1990;4:351–362. [PubMed: 2205909]
122. Schmedlen, RH.; Elbjeirami, WM.; Gobin, AS., et al. Tissue engineered vascualr grafts. In:Bronzino, JD., editor. The Biomedical Engineering Handbook: Tissue Engineering and ArtificialOrgans. 3. CRC Press Taylor & Francis Group, LLC; Boca Raton: 2006. p. 55.51-55.13.
123. Didisheim, P.; Watson, JT. Cadiovascular applications. In: Ratner, BD.; Hoffman, AS.; Schoen, FJ.;Lemons, JE., editors. Biomaterials Science: An Introduction to Materials in Medicine. AcademicPress; San Diego: 1996. p. 283-297.
124. Zhang Z, Wang Z, Liu S, et al. Pore size, tissue ingrowth, and endothelialization of small-diametermicroporous polyurethane vascular prostheses. Biomaterials 2004;25:177–187. [PubMed:14580921]
125. Voskerician G, Rodriguez A, Gingras PH. Macroporous condensed poly(tetra fluoro-ethylene). IIIn vivo effect on adhesion formation and tissue integration. J Biomed Mater Res A 2007;82:426–435. [PubMed: 17295248]
126. Legeais JM, Drubaix I, Briat B, et al. Influence of ePTFE polymer implant permeability on the rateand density of corneal extracellular matrix synthesis. J Biomed Mater Res 1997;36:49–54.[PubMed: 9212388]
127. Jorgensen CS, Paaske WP. Physical and mechanical properties of ePTFE stretch vascular graftsdetermined by time-resolved scanning acoustic microscopy. Eur J Vasc Endovasc Surg1998;15:416–422. [PubMed: 9633497]
Li et al. Page 18
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
128. Nakao A, Miyazaki M, Oka Y, et al. Creation and use of a composite polyurethane-expandedpolytetrafluoroethylene graft for hemodialysis access. Acta Med Okayama 2000;54:91–94.[PubMed: 10806530]
129. Guidoin R, Domurado D, Couture J, et al. Chemically processed bovine heterografts of the secondgeneration as arterial substitutes: a comparative evaluation of three commercial prostheses. JCardiovasc Surg 1989;30:202–209. [PubMed: 2708435]
130. Pare G, Guidoin R, Marois M, et al. (Evaluation of two commercial bovine vascular heterografts(author’s transl)). J Chir 1980;117:331–339.
131. Winsett OE, Wolma FJ. Complications of vascular access for hemodialysis. South Med J1985;78:513–517. [PubMed: 3992298]
132. Hurt AV, Batello-Cruz M, Skipper BJ, et al. Bovine carotid artery heterografts versuspolytetrafluoroethylene grafts. A prospective, randomized study. Am J Surg 1983;146:844–847.[PubMed: 6650773]
133. Brems J, Castaneda M, Garvin PJ. A five-year experience with the bovine heterograft for vascularaccess. Arch Surg 1986;121:941–944. [PubMed: 3729715]
134. Salmon P. Vascular access for hemodialysis using bovine heterografts and polytetrafluoroethyleneconduits. Can J Surg 1981;24:59–63. [PubMed: 7193074]
135. Oakes DD, Spees EK, Light JA, et al. A three year experience using modified bovine arterialheterografts for vascular access in patients requiring hemodialysis. Ann Surg 1978;187:423–429.[PubMed: 646481]
136. Wellington JL. Expanded polytetrafluoroethylene prosthetic grafts for blood access in patients ondialysis. Can J Surg 1978;21:420–422. [PubMed: 719565]
137. Haimov M, Burrows L, Schanzer H, et al. Experience with arterial substitutes in the construction ofvascular access for hemodialysis. J Cardiovasc Surg 1980;21:149–154. [PubMed: 7364857]
138. Doyle DL, Fry PD. Polytetrafluoroethylene and bovine grafts for vascular access in patients on long-term hemodialysis. Can J Surg 1982;25:379–382. [PubMed: 7093836]
139. Butler, HGr; Baker, LDJ.; Johnson, JM. Vascular access for chronic hemodialysis:polytetrafluoroethylene (PTFE) versus bovine heterograft. Am J Surg 1977;134:791–793.[PubMed: 339765]
140. Elliott MP, Gazzaniga AB, Thomas JM, et al. Use of expanded polytetrafluoroethylene grafts forvascular access in hemodialysis: laboratory and clinical evaluation. Am Surg 1977;43:455–459.[PubMed: 879604]
141. Pasternak BM, Paruk S, Kogan S, et al. A synthetic vascular conduit (expanded PTFE) forhemodialysis access–a preliminary report. Vasc Surg 1977;11:99–102. [PubMed: 616139]
142. Baker LDJ, Johnson JM, Goldfarb D. Expanded polytetrafluoroethylene (PTFE) subcutaneousarteriovenous conduit: an improved vascular access for chronic hemodialysis. Trans Am Soc ArtifIntern Organs 1976;22:382–387. [PubMed: 951854]
143. Harder F, Landmann J. Trends in access surgery for hemodialysis. Surg Annu 1984;16:135–149.[PubMed: 6729662]
144. Zincke H. Critical review of the use of carotid bovine grafts for hemodialysis. Eur Surg Res1976;8:189–195. [PubMed: 947757]
145. Katzman HE, Glickman MH, Schild AF, et al. Multicenter evaluation of the bovine mesenteric veinbioprostheses for hemodialysis access in patients with an earlier failed prosthetic graft. J Am CollSurg 2005;201:223–230. [PubMed: 16038820]
146. Tahami VB, Hakki H, Reber PU, et al. Polytetrafluoroethylene and bovine mesenterial vein graftsfor hemodialysis access: a comparative study. J Vasc Access 2007;8:17–20. [PubMed: 17393366]
147. Widmer MK, Aregger F, Stauffer E, et al. Intermediate outcome and risk factor assessment of bovinevascular heterografts used as AV-fistulas for hemodialysis access. Eur J Vasc Endovasc Surg2004;27:660–665. [PubMed: 15121120]
148. Hatzibaloglou A, Velissaris I, Kaitzis D, et al. ProCol vascular bioprosthesis for vascular access:midterm results. J Vasc Access 2004;5:16–18. [PubMed: 16596534]
149. Warakaulle DR, Evans AL, Cornall AJ, et al. Diagnostic imaging of and radiologic intervention forbovine ureter grafts used as a novel conduit for hemodialysis fistulas. AJR Am J Roentgenol2007;188:641–646. [PubMed: 17312048]
Li et al. Page 19
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
150. Darby CR, Roy D, Deardon D, et al. Depopulated bovine ureteric xenograft for complexhaemodialysis vascular access. Eur J Vasc Endovasc Surg 2006;31:181–186. [PubMed: 16129632]
151. Ko PJ, Hsieh HC, Chu JJ, et al. Patency rates and complications of Exxcel yarn-wrappedpolytetrafluoroethylene grafts versus Gore-tex stretch polytetrafluoroethylene grafts: a prospectivestudy. Surg Today 2004;34:409–412. [PubMed: 15108078]
152. Garcia-Pajares R, Polo JR, Flores A, et al. Upper arm polytetrafluoroethylene grafts for dialysisaccess. Analysis of two different graft sizes: 6 and 6–8 mm. Vasc Endovascular Surg 2003;37:335–343. [PubMed: 14528379]
153. Polo JR, Ligero JM, Diaz-Cartelle J, et al. Randomized comparison of 6-mm straight grafts versus6–8-mm tapered grafts for brachial-axillary dialysis access. J Vasc Surg 2004;40:319–324.[PubMed: 15297828]
154. Cole JS, Watterson JK, O′Reilly MJ. Is there a haemodynamic advantage associated with cuffedarterial anastomoses? J Biomech 2002;35:1337–1346. [PubMed: 12231279]
155. Cole JS, Wijesinghe LD, Watterson JK, et al. Computational and experimental simulations of thehaemodynamics at cuffed arterial bypass graft anastomoses. Proc Inst Mech Eng [H] 2002;216:135–143.
156. Kissin M, Kansal N, Pappas PJ, et al. Vein interposition cuffs decrease the intimal hyperplasticresponse of polytetrafluoroethylene bypass grafts. J Vasc Surg 2000;31:69–83. [PubMed:10642710]
157. Lin PH, Bush RL, Nguyen L, et al. Anastomotic strategies to improve hemodialysis access patency—a review. Vasc Endovascular Surg 2005;39:135–142. [PubMed: 15806274]
158. Berard X, Baste JC, Sassoust G, et al. [Retrospective study of the one-year patency of a cuffedpolytetrafluoroethylene Venaflo-type graft placed for venous hemodialysis access]. J Mal Vasc2003;28:73–78. [PubMed: 12750637]
159. Ojha M, Cobbold RS, Johnston KW. Influence of angle on wall shear stress distribution for an end-to-side anastomosis. J Vasc Surg 1994;19:1067–1073. [PubMed: 8201708]
160. Pollman MJ, Hall JL, Mann MJ, et al. Inhibition of neointimal cell bcl-x expression induces apoptosisand regression of vascular disease. Nat Med 1998;4:222–227. [PubMed: 9461197]
161. Morishita R, Higaki J, Tomita N, et al. Application of transcription factor ‘decoy’ strategy as meansof gene therapy and study of gene expression in cardiovascular disease. Circ Res 1998;82:1023–1028. [PubMed: 9622154]
162. Suzuki J, Isobe M, Morishita R, et al. Antisense Bcl-x oligonucleotide induces apoptosis and preventsarterial neointimal formation in murine cardiac allografts. Cardiovasc Res 2000;45:783–787.[PubMed: 10728401]
163. Suzuki J, Morishita R, Amano J, et al. Decoy against nuclear factor-kappa B attenuates myocardialcell infiltration and arterial neointimal formation in murine cardiac allografts. Gene Ther2000;7:1847–1852. [PubMed: 11110417]
164. Kutryk MJ, Foley DP, van den Brand M, et al. Local intracoronary administration of antisenseoligonucleotide against c-myc for the prevention of in-stent restenosis: results of the randomizedinvestigation by the Thoraxcenter of antisense DNA using local delivery and IVUS after coronarystenting (ITALICS) trial. J Am Coll Cardiol 2002;39:281–287. [PubMed: 11788220]
165. Morishita R, Gibbons GH, Horiuchi M, et al. A gene therapy strategy using a transcription factordecoy of the E2F binding site inhibits smooth muscle proliferation in vivo. Proc Natl Acad Sci USA1995;92:5855–5859. [PubMed: 7597041]
166. Ahn JD, Morishita R, Kaneda Y, et al. Novel E2F decoy oligodeoxynucleotides inhibit in vitrovascular smooth muscle cell proliferation and in vivo neointimal hyperplasia. Gene Ther2002;9:1682–1692. [PubMed: 12457282]
167. Hashiya N, Aoki M, Tachibana K, et al. Local delivery of E2F decoy oligodeoxynucleotides usingultrasound with microbubble agent (Optison) inhibits intimal hyperplasia after balloon injury in ratcarotid artery model. Biochem Biophys Res Commun 2004;317:508–514. [PubMed: 15063786]
168. Mann MJ, Whittemore AD, Donaldson MC, et al. Ex-vivo gene therapy of human vascular bypassgrafts with E2F decoy: the PREVENT single-centre, randomised, controlled trial. Lancet1999;354:1493–1498. [PubMed: 10551494]
Li et al. Page 20
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

169. Mann MJ, Dzau VJ. Therapeutic applications of transcription factor decoy oligonucleotides. J ClinInvest 2000;106:1071–1075. [PubMed: 11067859]
170. Conte MS, Bandyk DF, Clowes AW, et al. Results of PREVENT III: a multicenter, randomized trialof edifoligide for the prevention of vein graft failure in lower extremity bypass surgery. J Vasc Surg2006;43:742–751. 751. [PubMed: 16616230]
171. Alexander JH, Hafley G, Harrington RA, et al. Efficacy and safety of edifoligide, an E2Ftranscription factor decoy, for prevention of vein graft failure following coronary artery bypass graftsurgery: PREVENT IV: a randomized controlled trial. JAMA 2005;294:2446–2454. [PubMed:16287955]
172. Ferrara N. Molecular and biological properties of vascular endothelial growth factor. J Mol Med1999;77:527–543. [PubMed: 10494799]
173. Hiltunen MO, Laitinen M, Turunen MP, et al. Intravascular adenovirus-mediated VEGF-C genetransfer reduces neointima formation in balloon-denuded rabbit aorta. Circulation 2000;102:2262–2268. [PubMed: 11056103]
174. Bhardwaj S, Roy H, Heikura T, et al. VEGF-A, VEGF-D and VEGF-D(DeltaNDeltaC) inducedintimal hyperplasia in carotid arteries. Eur J Clin Investig 2005;35:669–676. [PubMed: 16269016]
175. Walpoth BH, Zammaretti P, Cikirikcioglu M, et al. Enhanced intimal thickening of expandedpolytetrafluoroethylene grafts coated with fibrin or fibrin-releasing vascular endothelial growthfactor in the pig carotid artery interposition model. J Thoracic Cardiovasc Surg 2007;133:1163–1170.
176. Komatsu Y, Itoh H, Suga S, et al. Regulation of endothelial production of C-type natriuretic peptidein coculture with vascular smooth muscle cells. Role of the vascular natriuretic peptide system invascular growth inhibition. Circ Res 1996;78:606–614. [PubMed: 8635218]
177. Ohno N, Itoh H, Ikeda T, et al. Accelerated reendothelialization with suppressed thrombogenicproperty and neointimal hyperplasia of rabbit jugular vein grafts by adenovirus-mediated genetransfer of C-type natriuretic peptide. Circulation 2002;105:1623–1626. [PubMed: 11940536]
178. Rotmans JI, Verhagen HJ, Velema E, et al. Local overexpression of C-type natriuretic peptideameliorates vascular adaptation of porcine hemodialysis grafts. Kidney Int 2004;65:1897–1905.[PubMed: 15086933]
179. Luo Z, Akita GY, Date T, et al. Adenovirus-mediated expression of beta-adrenergic receptor kinaseC-terminus reduces intimal hyperplasia and luminal stenosis of arteriovenouspolytetrafluoroethylene grafts in pigs. Circulation 2005;111:1679–1684. [PubMed: 15781730]
180. Rotmans JI, Heyligers JM, Verhagen HJ, et al. In vivo cell seeding with anti-CD34 antibodiessuccessfully accelerates endothelialization but stimulates intimal hyperplasia in porcinearteriovenous expanded polytetrafluoroethylene grafts. Circulation 2005;112:12–18. [PubMed:15983250]
181. Nugent HM, Sjin RT, White D, et al. Adventitial endothelial implants reduce matrixmetalloproteinase-2 expression and increase luminal diameter in porcine arteriovenous grafts. JVasc Surg 2007;46:548–556. [PubMed: 17826244]
182. Melhem M, Kelly B, Zhang J, et al. Development of a local perivascular paclitaxel delivery systemfor hemodialysis vascular access dysfunction: polymer preparation and in vitro activity. Blood Purif2006;24:289–298. [PubMed: 16465049]
183. Kohler TR, Toleikis PM, Gravett DM, et al. Inhibition of neointimal hyperplasia in a sheep modelof dialysis access failure with the bioabsorbable Vascular Wrap paclitaxel-eluting mesh. J VascSurg 2007;45:1029–1037. 1028. [PubMed: 17466798]
184. Kelly B, Melhem M, Zhang J, et al. Perivascular paclitaxel wraps block arteriovenous graft stenosisin a pig model. Nephrol Dial Transplant 2006;21:2425–2431. [PubMed: 16822794]
185. Gregory CR, Huie P, Billingham ME, et al. Rapamycin inhibits arterial intimal thickening causedby both alloimmune and mechanical injury. Its effect on cellular, growth factor, and cytokineresponse in injured vessels. Transplantation 1993;55:1409–1418. [PubMed: 8516827]
186. Braun-Dullaeus RC, Mann MJ, Seay U, et al. Cell cycle protein expression in vascular smoothmuscle cells in vitro and in vivo is regulated through phosphatidylinositol 3-kinase and mammaliantarget of rapamycin. Arterioscler Thromb Vasc Biol 2001;21:1152–1158. [PubMed: 11451744]
Li et al. Page 21
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
187. Gallo R, Padurean A, Jayaraman T, et al. Inhibition of intimal thickening after balloon angioplastyin porcine coronary arteries by targeting regulators of the cell cycle. Circulation 1999;99:2164–2170. [PubMed: 10217658]
188. Morice MC, Serruys PW, Sousa JE, et al. A randomized comparison of a sirolimus-eluting stentwith a standard stent for coronary revascularization. N Engl J Med 2002;346:1773–1780. [PubMed:12050336]
189. Fajadet J, Morice MC, Bode C, et al. Maintenance of long-term clinical benefit with sirolimus-eluting coronary stents: three-year results of the RAVEL trial. Circulation 2005;111:1040–1044.[PubMed: 15723977]
190. Morice MC, Serruys PW, Barragan P, et al. Long-term clinical outcomes with sirolimus-elutingcoronary stents: five-year results of the RAVEL trial. J Am Coll Cardiol 2007;50:1299–1304.[PubMed: 17903626]
191. Holmes DR Jr, Leon MB, Moses JW, et al. Analysis of 1-year clinical outcomes in the SIRIUS trial:a randomized trial of a sirolimus-eluting stent versus a standard stent in patients at high risk forcoronary restenosis. Circulation 2004;109:634–640. [PubMed: 14769686]
192. Jordan MA, Toso RJ, Thrower D, et al. Mechanism of mitotic block and inhibition of cellproliferation by taxol at low concentrations. Proc Natl Acad Sci USA 1993;90:9552–9556.[PubMed: 8105478]
193. Axel DI, Kunert W, Goggelmann C, et al. Paclitaxel inhibits arterial smooth muscle cell proliferationand migration in vitro and in vivo using local drug delivery. Circulation 1997;96:636–645. [PubMed:9244237]
194. Kaluza GL, Gershlick AH, Park SJ, et al. Comparison of neointimal formation in polymer-freepaclitaxel stents versus stainless stents (from the ASPECT and ELUTES randomized clinical trials).Am J Cardiol 2004;94:199–201. [PubMed: 15246901]
195. Gershlick A, De Scheerder I, Chevalier B, et al. Inhibition of restenosis with a paclitaxel-eluting,polymer-free coronary stent: the European evaLUation of pacliTaxel Eluting Stent (ELUTES) trial.Circulation 2004;109:487–493. [PubMed: 14744971]
196. Bullesfeld L, Gerckens U, Muller R, et al. Long-term evaluation of paclitaxel-coated stents fortreatment of native coronary lesions. First results of both the clinical and angiographic 18 monthfollow-up of TAXUS I. Z Kardiol 2003;92:825–832. [PubMed: 14579046]
197. Stone GW, Ellis SG, Cox DA, et al. One-year clinical results with the slow-release, polymer-based,paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation 2004;109:1942–1947. [PubMed:15078803]
198. Lee BH, Nam HY, Kwon T, et al. Paclitaxel-coated expanded polytetrafluoroethylene haemodialysisgrafts inhibit neointimal hyperplasia in porcine model of graft stenosis. Nephrol Dial Transplant2006;21:2432–2438. [PubMed: 16554328]
199. Himmelfarb J, Couper L. Dipyridamole inhibits PDGF- and bFGF-induced vascular smooth musclecell proliferation. Kidney Int 1997;52:1671–1677. [PubMed: 9407516]
200. Zhuplatov SB, Masaki T, Blumenthal DK, et al. Mechanism of dipyridamole′s action in inhibitionof venous and arterial smooth muscle cell proliferation. Basic Clin Pharmacol Toxicol 2006;99:431–439. [PubMed: 17169124]
201. Sreedhara R, Himmelfarb J, Lazarus JM, et al. Anti-platelet therapy in graft thrombosis: results ofa prospective, randomized, double-blind study. Kidney Int 1994;45:1477–1483. [PubMed:8072261]
202. Singh JP, Rothfuss KJ, Wiernicki TR, et al. Dipyridamole directly inhibits vascular smooth musclecell proliferation in vitro and in vivo: implications in the treatment of restenosis after angioplasty.J Am Coll Cardiol 1994;23:665–671. [PubMed: 8113550]
203. Heidland UE, Heintzen MP, Michel CJ, et al. Intracoronary administration of dipyridamole prior topercutaneous transluminal coronary angioplasty provides a protective effect exceeding that ofischemic preconditioning. Coron Artery Dis 2000;11:607–613. [PubMed: 11107508]
204. Kuji T, Masaki T, Goteti K, et al. Efficacy of local dipyridamole therapy in a porcine model ofarteriovenous graft stenosis. Kidney Int 2006;69:2179–2185. [PubMed: 16672912]
Li et al. Page 22
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
205. Rutherford C, Martin W, Salame M, et al. Substantial inhibition of neointimal response to ballooninjury in the rat carotid artery using a combination of antibodies to platelet-derived growth factor-BB and basic fibroblast growth factor. Atherosclerosis 1997;130:45–51. [PubMed: 9126647]
206. Davies MG, Owens EL, Mason DP, et al. Effect of platelet-derived growth factor receptor-alphaand -beta blockade on flow-induced neointimal formation in endothelialized baboon vascular grafts.Circ Res 2000;86:779–786. [PubMed: 10764412]
207. Buchdunger E, Cioffi CL, Law N, et al. Abl protein-tyrosine kinase inhibitor STI571 inhibits invitro signal transduction mediated by c-kit and platelet-derived growth factor receptors. J PharmacolExp Ther 2000;295:139–145. [PubMed: 10991971]
208. Druker BJ, Talpaz M, Resta DJ, et al. Efficacy and safety of a specific inhibitor of the BCR-ABLtyrosine kinase in chronic myeloid leukemia. N Engl J Med 2001;344:1031–1037. [PubMed:11287972]
209. Wang WL, Healy ME, Sattler M, et al. Growth inhibition and modulation of kinase pathways ofsmall cell lung cancer cell lines by the novel tyrosine kinase inhibitor STI 571. Oncogene2000;19:3521–3528. [PubMed: 10918610]
210. Shawver LK, Slamon D, Ullrich A. Smart drugs: tyrosine kinase inhibitors in cancer therapy. CancerCell 2002;1:117–123. [PubMed: 12086869]
211. Druker BJ. STI571 (Gleevec) as a paradigm for cancer therapy. Trends Mol Med 2002;8:S14–S18.[PubMed: 11927282]
212. Myllarniemi M, Frosen J, Calderon Ramirez LG, et al. Selective tyrosine kinase inhibitor for theplatelet-derived growth factor receptor in vitro inhibits smooth muscle cell proliferation afterreinjury of arterial intima in vivo. Cardiovasc Drugs Ther 1999;13:159–168. [PubMed: 10372232]
213. Boucher P, Gotthardt M, Li WP, et al. LRP: role in vascular wall integrity and protection fromatherosclerosis. Science 2003;300:329–332. [PubMed: 12690199]
214. Sihvola RK, Tikkanen JM, Krebs R, et al. Platelet-derived growth factor receptor inhibition reducesallograft arteriosclerosis of heart and aorta in cholesterol-fed rabbits. Transplantation 2003;75:334–339. [PubMed: 12589154]
215. Leppanen O, Rutanen J, Hiltunen MO, et al. Oral imatinib mesylate (STI571/gleevec) improves theefficacy of local intravascular vascular endothelial growth factor-C gene transfer in reducingneointimal growth in hypercholesterolemic rabbits. Circulation 2004;109:1140–1146. [PubMed:14769706]
216. Li L, Blumenthal DK, Masaki T, et al. Differential effects of imatinib on PDGF-induced proliferationand PDGF receptor signaling in human arterial and venous smooth muscle cells. J Cell Biochem2006;99:1553–1563. [PubMed: 16817200]
217. Scott S, O’Sullivan M, Hafizi S, et al. Human vascular smooth muscle cells from restenosis or in-stent stenosis sites demonstrate enhanced responses to p53: implications for brachytherapy and drugtreatment for restenosis. Circ Res 2002;90:398–404. [PubMed: 11884368]
218. Wiedermann JG, Marboe C, Amols H, et al. Intracoronary irradiation markedly reduces restenosisafter balloon angioplasty in a porcine model. J Am Coll Cardiol 1994;23:1491–1498. [PubMed:8176112]
219. Ducasse E, Cosset JM, Eschwege F, et al. External beam ionizing radiation for inhibition ofmyointimal hyperplasia after dilatation and anastomoses: experimental models and results. AnnVasc Surg 2004;18:108–114. [PubMed: 14727165]
220. Vodovotz Y, Waksman R, Kim WH, et al. Effects of intracoronary radiation on thrombosis afterballoon overstretch injury in the porcine model. Circulation 1999;100:2527–2533. [PubMed:10604891]
221. Grise MA, Massullo V, Jani S, et al. Five-year clinical follow-up after intracoronary radiation: resultsof a randomized clinical trial. Circulation 2002;105:2737–2740. [PubMed: 12057987]
222. Leon MB, Teirstein PS, Moses JW, et al. Localized intracoronary gamma-radiation therapy to inhibitthe recurrence of restenosis after stenting. N Engl J Med 2001;344:250–256. [PubMed: 11172151]
223. Sun S, Beitler JJ, Ohki T, et al. Inhibitory effect of brachytherapy on intimal hyperplasia inarteriovenous fistula. J Surg Res 2003;115:200–208. [PubMed: 14697284]
Li et al. Page 23
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

224. van Tongeren RB, Levendag PC, Coen VL, et al. External beam radiation therapy to preventanastomotic intimal hyperplasia in prosthetic arteriovenous fistulas: results of a randomized trial.Radiother Oncol 2003;69:73–77. [PubMed: 14597359]
225. Krueger K, Bendel M, Zaehringer M, et al. Centered endovascular irradiation to preventpostangioplasty restenosis of arteriovenous fistula in hemodialysis patients; Results of a feasibilitystudy. Cardiovasc Radiat Med 2004;5:1–8. [PubMed: 15275625]
Li et al. Page 24
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
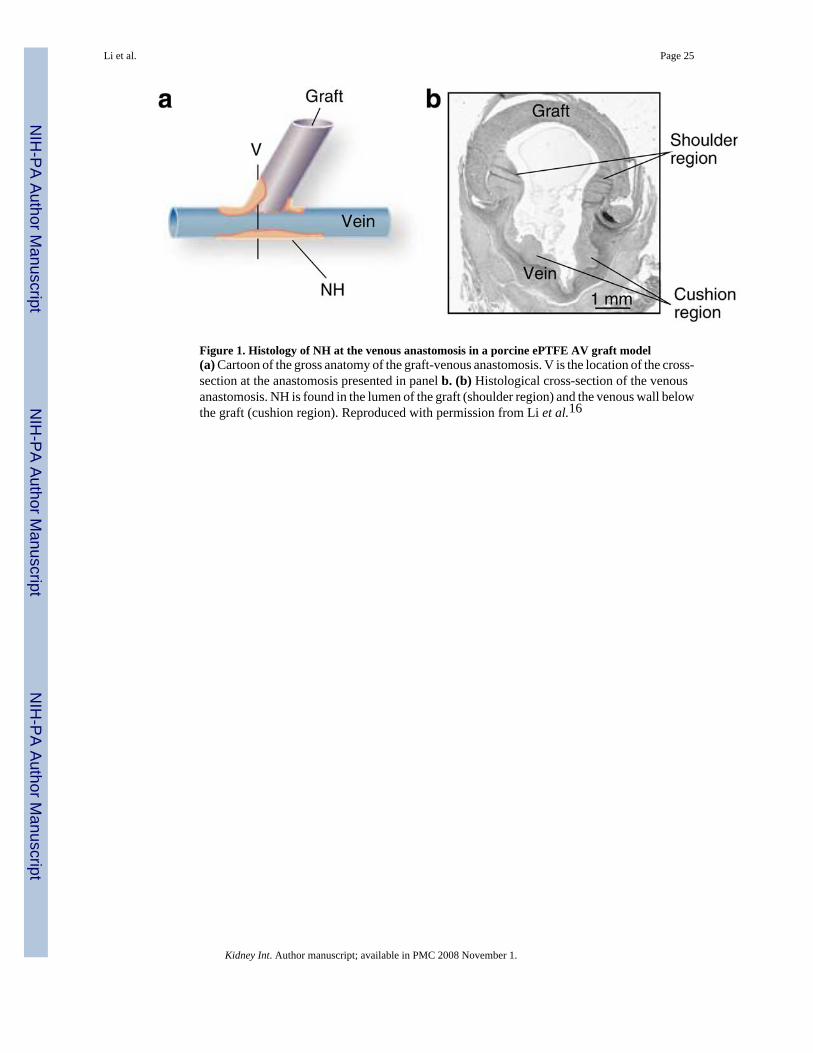
Figure 1. Histology of NH at the venous anastomosis in a porcine ePTFE AV graft model(a) Cartoon of the gross anatomy of the graft-venous anastomosis. V is the location of the cross-section at the anastomosis presented in panel b. (b) Histological cross-section of the venousanastomosis. NH is found in the lumen of the graft (shoulder region) and the venous wall belowthe graft (cushion region). Reproduced with permission from Li et al.16
Li et al. Page 25
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
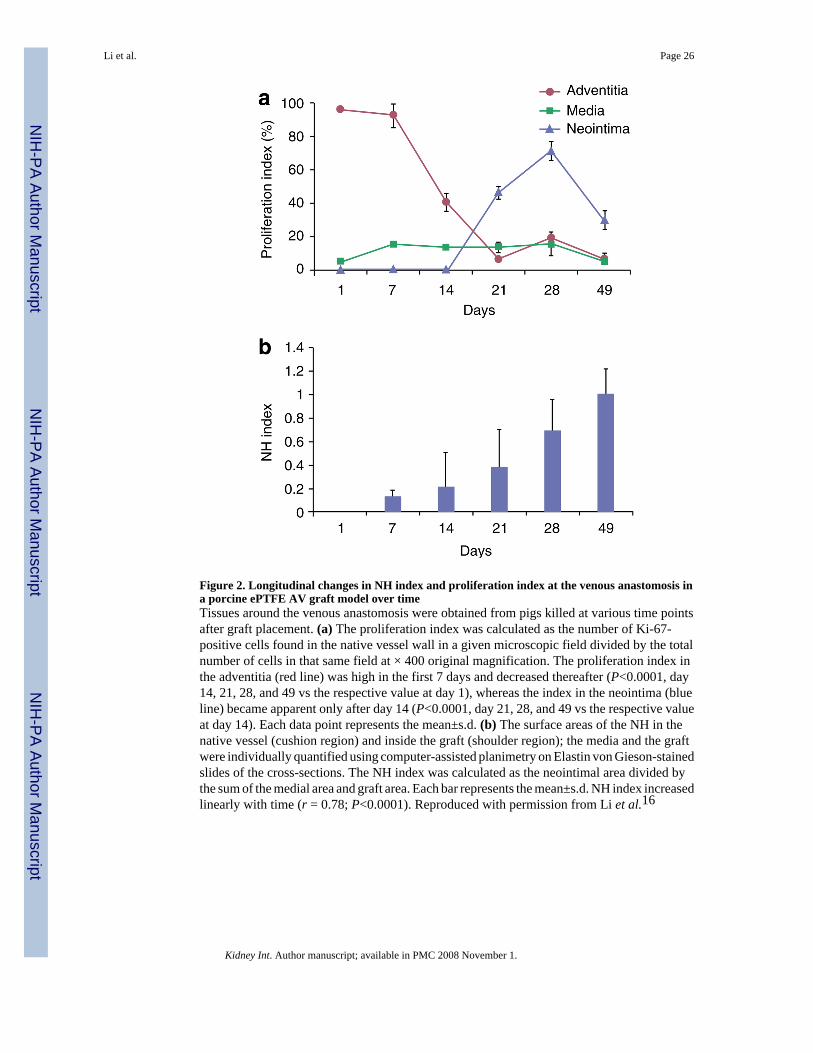
Figure 2. Longitudinal changes in NH index and proliferation index at the venous anastomosis ina porcine ePTFE AV graft model over timeTissues around the venous anastomosis were obtained from pigs killed at various time pointsafter graft placement. (a) The proliferation index was calculated as the number of Ki-67-positive cells found in the native vessel wall in a given microscopic field divided by the totalnumber of cells in that same field at × 400 original magnification. The proliferation index inthe adventitia (red line) was high in the first 7 days and decreased thereafter (P<0.0001, day14, 21, 28, and 49 vs the respective value at day 1), whereas the index in the neointima (blueline) became apparent only after day 14 (P<0.0001, day 21, 28, and 49 vs the respective valueat day 14). Each data point represents the mean±s.d. (b) The surface areas of the NH in thenative vessel (cushion region) and inside the graft (shoulder region); the media and the graftwere individually quantified using computer-assisted planimetry on Elastin von Gieson-stainedslides of the cross-sections. The NH index was calculated as the neointimal area divided bythe sum of the medial area and graft area. Each bar represents the mean±s.d. NH index increasedlinearly with time (r = 0.78; P<0.0001). Reproduced with permission from Li et al.16
Li et al. Page 26
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
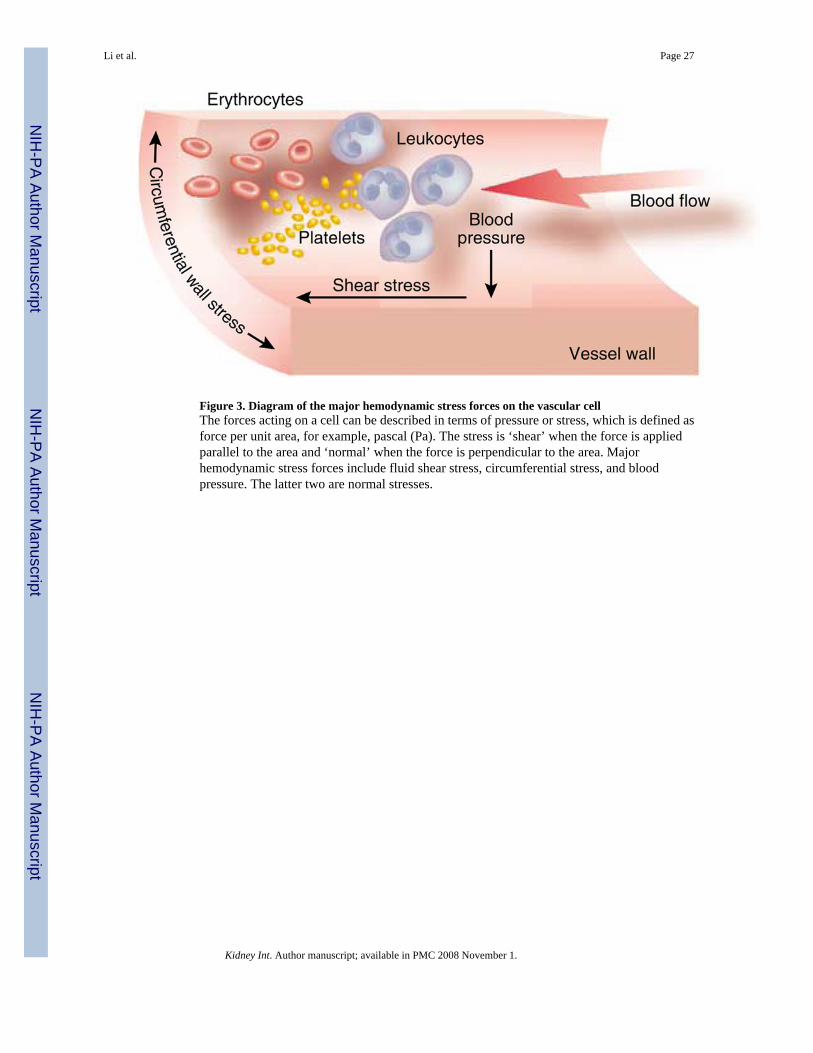
Figure 3. Diagram of the major hemodynamic stress forces on the vascular cellThe forces acting on a cell can be described in terms of pressure or stress, which is defined asforce per unit area, for example, pascal (Pa). The stress is ‘shear’ when the force is appliedparallel to the area and ‘normal’ when the force is perpendicular to the area. Majorhemodynamic stress forces include fluid shear stress, circumferential stress, and bloodpressure. The latter two are normal stresses.
Li et al. Page 27
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
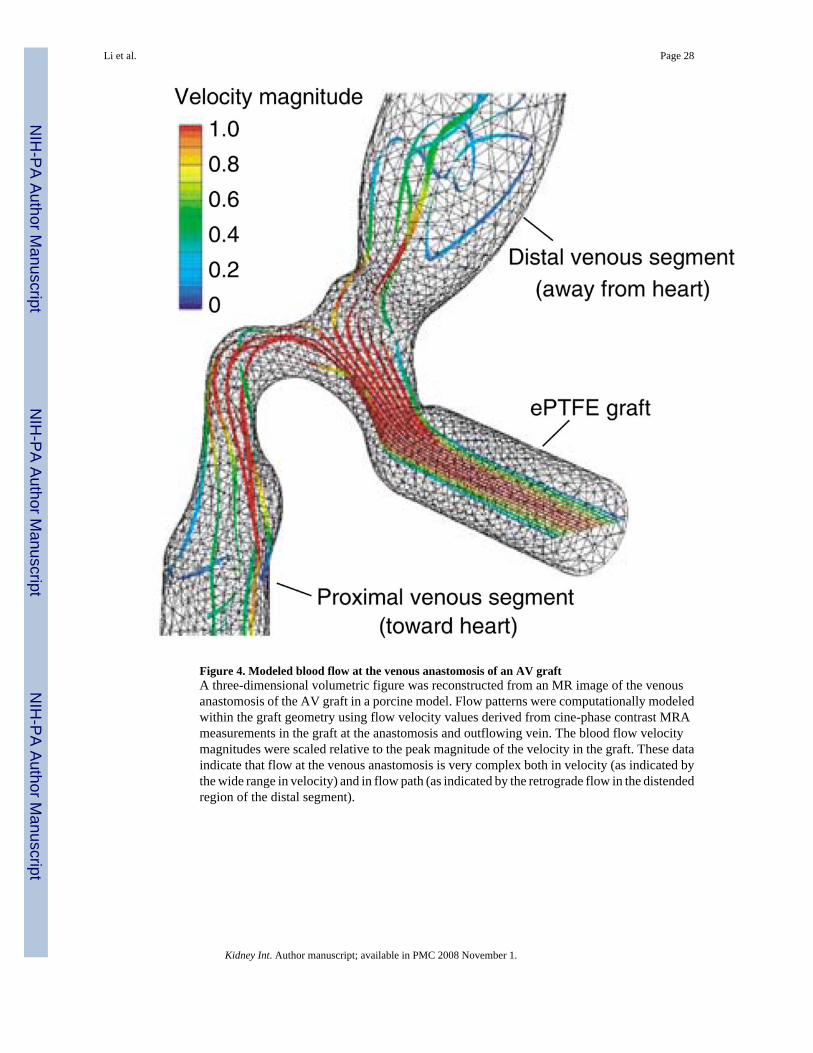
Figure 4. Modeled blood flow at the venous anastomosis of an AV graftA three-dimensional volumetric figure was reconstructed from an MR image of the venousanastomosis of the AV graft in a porcine model. Flow patterns were computationally modeledwithin the graft geometry using flow velocity values derived from cine-phase contrast MRAmeasurements in the graft at the anastomosis and outflowing vein. The blood flow velocitymagnitudes were scaled relative to the peak magnitude of the velocity in the graft. These dataindicate that flow at the venous anastomosis is very complex both in velocity (as indicated bythe wide range in velocity) and in flow path (as indicated by the retrograde flow in the distendedregion of the distal segment).
Li et al. Page 28
Kidney Int. Author manuscript; available in PMC 2008 November 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Li et al. Page 29
Table 1Preventive strategies for neointimal hyperplasia associated with synthetichemodialysis AV grafts
Strategy Mechanism of action Used in AV graft model(citation)
Mechanical design Tapered graft and precuffed graft Improve the geometry at anastomosis Yes152–158 Decellularized xenograft Improve elastic mismatch between graft and native vessel Yes145–150Biological reagents Antisense ODNs Inhibit DNA transcription, production of mRNA, and
synthesis of various proteinsNo
Decoy (E2F) Inhibit cell-cycle progression Yes11 Gene transfer VEGF Promote endothelialization No C-type natriuretic peptide Inhibit proliferation through cGMP induction Yes178 Cell-based therapies Endothelial progenitor cells Promote endothelialization of the graft surface Yes180 Endothelial cell implant using gelfoammatrices
Promote endothelial function Yes181
Small-molecule drugs Rapamycin Inhibit protein translation Yes120 Paclitaxel Inhibit mitosis by stabilizing microtubules Yes15,183,184,198 Dypiridamole Inhibit phosphodiesterase activity Yes204 Imatinib methylate Inhibit PDGF receptor activity NoIrradiation Induce DNA damage Yes223–225
AV, arteriovenous; cGMP, cyclic guanosine monophosphate; ODN, antisense oligonucleotide; PDGF, platelet-derived growth factor; VEGF, vascularendothelial growth factor.
Kidney Int. Author manuscript; available in PMC 2008 November 1.