angioaccess for hemodialysis
TRANSCRIPT
IaadbtvSbyhM
mA1vacwsvaPia
E
N
ad
C0d
C
Angioaccess for Hemodialysis
n 1960, Quinton and colleagues created the first arteriovenous (AV)ccess by inserting Silastic tubes with Teflon tips directly into the radialrtery and cephalic vein.1 When the tubes were not connected to theialysis machine, they were joined by a U-shaped device that shuntedlood from the artery to the vein. Continuous blood flow prevented theubes from clotting and revolutionized dialysis by allowing repeatedascular access at the same anatomic site. The first patient treated with thecribner shunt spent the next 11 years on hemodialysis and marked theeginning of chronic renal replacement therapy. Today, more than 50ears later, more than 400,000 patients in the United States receiveemodialysis and the treatment of kidney failure accounts for 6% of alledicare spending.The evolution of chronic hemodialysis therapy parallels the advancesade in AV access. Brescia and colleagues described the first autogenousV fistula in the 1960s, and prosthetic AV grafts gained popularity in the970s.2 These techniques expanded the anatomic sites available forascular access and allowed more patients to receive long-term hemodi-lysis. Despite these advances, AV access remains the weakest link inhronic renal replacement therapy. Vascular access dysfunction interferesith dialysis, degrades the quality of life, and ultimately shortens the
urvival of patients with chronic kidney failure. Overcoming the limits ofascular access requires the concerted effort of all health care profession-ls involved in the care of patients with end stage renal disease (ESRD).atient preparation, surgical decision-making, dialysis monitoring, and
nterventional techniques all play a role in establishing a safe, effective,nd durable AV access.
stablishing Acute Dialysis Access
ontunneled Dialysis CathetersNontunneled dialysis catheters (NTDCs) provide short-term vascular
ccess. They can be inserted at the bedside and used immediately for
ialysis, making them a logical access choice for critically ill patientsurr Probl Surg 2011;48:443-517.011-3840/$36.00 � 0oi:10.1067/j.cpsurg.2011.03.002
urr Probl Surg, July 2011 443
wmvmvsPfgDrT
ppcavb
T
I
T
T
M
Ec
4
ith acute renal failure. The right internal jugular (IJ) vein represents theost common location for NTDCs, followed by either common femoral
ein. The drawbacks of NTDCs include their limited flow rates (250L/min) and susceptibility to infection or dislodgment.3,4 These disad-
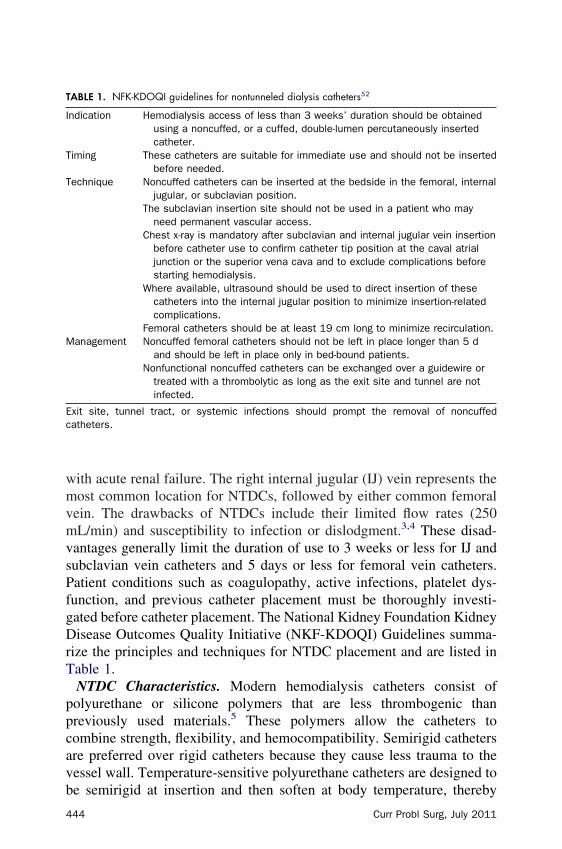
antages generally limit the duration of use to 3 weeks or less for IJ andubclavian vein catheters and 5 days or less for femoral vein catheters.atient conditions such as coagulopathy, active infections, platelet dys-unction, and previous catheter placement must be thoroughly investi-ated before catheter placement. The National Kidney Foundation Kidneyisease Outcomes Quality Initiative (NKF-KDOQI) Guidelines summa-
ize the principles and techniques for NTDC placement and are listed inable 1.NTDC Characteristics. Modern hemodialysis catheters consist ofolyurethane or silicone polymers that are less thrombogenic thanreviously used materials.5 These polymers allow the catheters toombine strength, flexibility, and hemocompatibility. Semirigid cathetersre preferred over rigid catheters because they cause less trauma to theessel wall. Temperature-sensitive polyurethane catheters are designed to
ABLE 1. NFK-KDOQI guidelines for nontunneled dialysis catheters52
ndication Hemodialysis access of less than 3 weeks’ duration should be obtainedusing a noncuffed, or a cuffed, double-lumen percutaneously insertedcatheter.
iming These catheters are suitable for immediate use and should not be insertedbefore needed.
echnique Noncuffed catheters can be inserted at the bedside in the femoral, internaljugular, or subclavian position.
The subclavian insertion site should not be used in a patient who mayneed permanent vascular access.
Chest x-ray is mandatory after subclavian and internal jugular vein insertionbefore catheter use to confirm catheter tip position at the caval atrialjunction or the superior vena cava and to exclude complications beforestarting hemodialysis.
Where available, ultrasound should be used to direct insertion of thesecatheters into the internal jugular position to minimize insertion-relatedcomplications.
Femoral catheters should be at least 19 cm long to minimize recirculation.anagement Noncuffed femoral catheters should not be left in place longer than 5 d
and should be left in place only in bed-bound patients.Nonfunctional noncuffed catheters can be exchanged over a guidewire or
treated with a thrombolytic as long as the exit site and tunnel are notinfected.
xit site, tunnel tract, or systemic infections should prompt the removal of noncuffedatheters.
e semirigid at insertion and then soften at body temperature, thereby
44 Curr Probl Surg, July 2011
fllcmTa2t
T
vccpa
Dc
T
I
T
T
C
C
C
urther minimizing vessel wall injury. The outer diameter of the dual-umen catheter ranges from 11 to 14 French, with the arterial and venousumens arranged side-by-side or coaxially. The arterial lumen ends 2 to 3m proximal to the venous lumen to reduce recirculation. Most companiesanufacture the catheters in 3 different lengths to suit the site of insertion.he right IJ vein typically requires a 15- to 16-cm catheter and the left IJnd subclavian veins require 19- to 20-cm catheters. In the femoral vein,4-cm catheters have been shown to reduce recirculation during intermit-ent hemodialysis (IHD) compared to shorter length femoral catheters.6
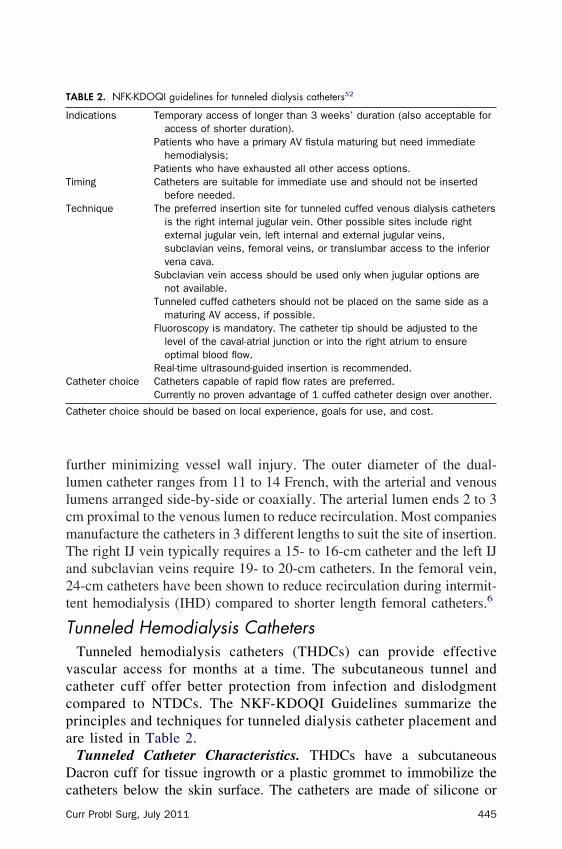
unneled Hemodialysis CathetersTunneled hemodialysis catheters (THDCs) can provide effectiveascular access for months at a time. The subcutaneous tunnel andatheter cuff offer better protection from infection and dislodgmentompared to NTDCs. The NKF-KDOQI Guidelines summarize therinciples and techniques for tunneled dialysis catheter placement andre listed in Table 2.Tunneled Catheter Characteristics. THDCs have a subcutaneousacron cuff for tissue ingrowth or a plastic grommet to immobilize the
ABLE 2. NFK-KDOQI guidelines for tunneled dialysis catheters52
ndications Temporary access of longer than 3 weeks’ duration (also acceptable foraccess of shorter duration).
Patients who have a primary AV fistula maturing but need immediatehemodialysis;
Patients who have exhausted all other access options.iming Catheters are suitable for immediate use and should not be inserted
before needed.echnique The preferred insertion site for tunneled cuffed venous dialysis catheters
is the right internal jugular vein. Other possible sites include rightexternal jugular vein, left internal and external jugular veins,subclavian veins, femoral veins, or translumbar access to the inferiorvena cava.
Subclavian vein access should be used only when jugular options arenot available.
Tunneled cuffed catheters should not be placed on the same side as amaturing AV access, if possible.
Fluoroscopy is mandatory. The catheter tip should be adjusted to thelevel of the caval-atrial junction or into the right atrium to ensureoptimal blood flow.
Real-time ultrasound-guided insertion is recommended.atheter choice Catheters capable of rapid flow rates are preferred.
Currently no proven advantage of 1 cuffed catheter design over another.
atheter choice should be based on local experience, goals for use, and cost.
atheters below the skin surface. The catheters are made of silicone or
urr Probl Surg, July 2011 445
onefsscw
FhU
4
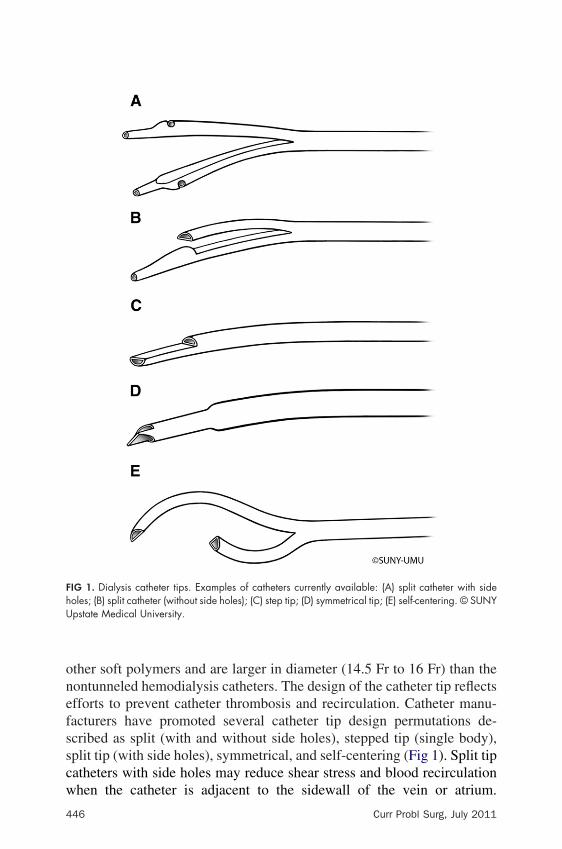
ther soft polymers and are larger in diameter (14.5 Fr to 16 Fr) than theontunneled hemodialysis catheters. The design of the catheter tip reflectsfforts to prevent catheter thrombosis and recirculation. Catheter manu-acturers have promoted several catheter tip design permutations de-cribed as split (with and without side holes), stepped tip (single body),plit tip (with side holes), symmetrical, and self-centering (Fig 1). Split tipatheters with side holes may reduce shear stress and blood recirculation
IG 1. Dialysis catheter tips. Examples of catheters currently available: (A) split catheter with sideoles; (B) split catheter (without side holes); (C) step tip; (D) symmetrical tip; (E) self-centering. © SUNYpstate Medical University.
hen the catheter is adjacent to the sidewall of the vein or atrium.
46 Curr Probl Surg, July 2011

Ttbrddwfa
dcSt(a
opcbccirbJifcMwco
T
cpar
C
rerotola and colleagues used ultrasonic flow monitors to show that splitip catheters had superior blood flow rates compared to step tip (singleody) catheters.7 The impact of these findings remains unclear since aeview by Ash failed to detect a long-term functional advantage amongifferent catheter designs.8 The side hole design of split catheters createsead space at the tip of the catheter and allows blood flow to enter andash out the catheter locking solution.9 This design flaw creates a nidus
or thrombus and infection, which may explain the catheter’s failure tochieve long-term functional superiority.10
In an animal model, a symmetrical tip catheter improved blood flow andecreased recirculation rates when compared to step tip catheters, butlinical trials in humans have failed to reproduce these findings.8
elf-centering catheters have a unique curved configuration of the distalip that keeps the lumens of the catheter centered in the superior vena cavaSVC). Preliminary clinical studies demonstrated high blood flow ratesnd no evidence of a fibrin sheath or thrombus.8
Catheter innovations that have targeted bacteremia, fibrin sheath devel-pment, and catheter dysfunction have met with mixed results. In arospective randomized study, Darouiche and colleagues showed thatatheters impregnated with minocycline and rifampin were less likely toe colonized with bacteria compared to catheters impregnated withhlorhexidine and silver sulfadiazine.11 Despite decreasing bacterialolonization, antimicrobial coatings of THDCs have had limited successn preventing bacteremia.12 These catheters may also incite an allergiceaction or encourage antibiotic resistance. Heparin-coated catheters haveeen developed to prevent thrombosis and fibrin sheath progression.13
ain and colleagues found that heparin-coated catheters reduced thencidence of catheter-related bacteremia but failed to improve catheterunction.14 Several other studies reported no difference in the rate ofatheter malfunction between heparin-coated and uncoated catheters.15
ojibian and colleagues have reported encouraging preliminary resultsith a newly designed heparin-coated THDC.16 Whether improved
atheter function depends on the method for heparin binding or the designf the catheter itself remains unclear.
echniquesInsertion of a NTDC can be performed at the bedside under sterile
onditions using the modified Seldinger technique. The right IJ veinrovides a direct path to the SVC, making it the preferred location fortemporary catheter. The left IJ vein has a more circuitous route to the
ight atrium, which can result in inadequate blood flow and catheter
urr Probl Surg, July 2011 447
mntvtf
oktTtashattFm
iilocvscipvanmavcmp
4
alfunction, especially in an unsedated, restless patient with frequenteck movements. The femoral veins rank ahead of the subclavian veins ashe next preferred location for a temporary catheter. Avoiding subclavianein instrumentation can minimize the risk of venous stenosis andhrombosis and preserve the ipsilateral upper extremity as a potential siteor permanent AV access in the future.The technical aspects of THDC insertion closely parallel those previ-usly outlined with a few special considerations. For IJ vein placement,eeping the needle puncture site low in the neck allows the catheter toake a gentle bend as it exits the subcutaneous tunnel and enters the vein.his technique can prevent kinking of the catheter, which invariably leads
o dysfunction. Bleeding around the catheter can be minimized by placingpursestring suture at the proposed catheter exit site before creating the
ubcutaneous tunnel.17 After micropuncture of the vein, fluoroscopy canelp choose the appropriate catheter length. The tip of the wire isdvanced under fluoroscopy to the desired catheter location; the wire ishen marked where it exits the skin, removed, and measured to determinehe distance from the caval-atrial junction to the vein puncture site.luoroscopy during and after catheter placement allows accurate place-ent of the catheter tip and ensures that the catheter is not kinked.Ultrasound guidance is the standard of care for all hemodialysis catheter
nsertions. Given the variability in venous anatomy, even experiencednterventionalists can have difficulty with “blind” central venous cannu-ation using only anatomic landmarks.6 In previous studies 28% to 35%f dialysis patients had significant vein abnormalities, including nonoc-lusive thrombus, venous stenosis, complete vein occlusion, and anatomicariation.18,19 A meta-analysis demonstrated that ultrasound guidanceignificantly reduced the risk of: insertion failure (relative risk [RR] 0.32),omplications from insertion (RR 0.22), and the need for multiplensertion attempts (RR 0.60).20 A more recent, prospective study of 900atients demonstrated that ultrasound-guided catheter placement in the IJein not only increased success rate and decreased complication rates, butlso reduced catheter-associated infections.21 Use of a micropunctureeedle, 5-French microsheath, and 0.018 wire for initial vein cannulationay decrease the risk of insertion-related injuries, such as inadvertent
rterial puncture and pneumothorax. During insertion of IJ and subclavianein catheters, continuous electrocardiographic monitoring can warn ofardiac dysrrhythmias induced by wire manipulation or catheter advance-ent. Before catheter use, a chest radiograph confirms the appropriate
osition of the catheter tip and evaluates for a pneumothorax.22
48 Curr Probl Surg, July 2011
G
Icnmcar0
ol0ropot
trhrceadFv
mdbcOefiad
C
eneral Catheter ComplicationsDialysis catheters can cause immediate or delayed complications.
mmediate complications result from injuries incurred at the time ofatheter insertion. Rare injuries, including brachial plexus and laryngealerve palsy, have also been reported.23 Ultrasound guidance appears toinimize the risk of injury during catheter insertion. Karakitsos and
olleagues compared ultrasound guidance to catheter placement usingnatomic landmarks. They found that ultrasound guidance significantlyeduced the rate of carotid injury (10.6% vs 1.1%), hematoma (8.4% vs.4%), hemothorax (1.7% vs 0%), and pneumothorax (2.4% vs 0%).21
Delayed catheter complications typically occur due to the accumulationf vessel trauma over time. Catheter erosion through the vein wall canead to cardiac tamponade or hemomediastinum, which complicates up to.5% of subclavian vein catheters.24,25 The endothelial injury incurred byepeated catheter motion and turbulent blood flow triggers a hyperplasticr thrombotic response in the form of venous stenosis or thrombosis. Arospective study of subclavian vein catheters reported a 28% incidencef associated venous stenosis and thrombosis, which was even higher inhe presence of infection.26
Dysfunctional catheters cannot provide sufficient blood flow for effec-ive dialysis. The minimal blood flow rate to sustain continuous renaleplacement therapy (CRRT) is 150 to 250 mL/min. IHD requires aigher rate of 200 to 300 mL/min and ambulatory dialysis patients needates above 300 mL/min with minimal recirculation. Multiple conditionsan cause catheter dysfunction, including intraluminal thrombosis, cath-ter kinking, catheter malposition, and the development of a fibrin sheathround the catheter or its tip. In addition to poor blood flow rates,ysfunctional catheters usually have high access pressure readings.emoral vein catheters have a higher rate of dysfunction compared to IJein catheters.27
For recently placed catheters, the cause of dysfunction usually involvesechanical obstruction or tip malposition. After 2 weeks, catheter
ysfunction is more likely due to progressive occlusion of the catheter tipy thrombus or fibrin. Fibrin sheaths start forming within 24 hours ofatheter placement and trap thrombus between the catheter and the sheath.ver 70% of fibrin sheaths contain organizing thrombus, which is in
ffect protected from endogenous fibrinolytic factors.28 The growth of thebrin sheath and associated thrombus impedes blood infusion and bloodspiration, leading to ineffective dialysis. Treatment options for catheter
ysfunction caused by fibrin sheaths include catheter exchange, balloonurr Probl Surg, July 2011 449
dbea
paecmcvctirc
n(mmosoCcde
lacocloaai
4
isruption, or sheath stripping. Studies comparing these strategies haveeen scarce and inconclusive. The NFK-KDOQI guidelines recommendxchange of the catheter and disruption of the fibrin sheath by balloonngioplasty.29
Recirculation describes what happens when blood being returned to theatient via the venous lumen of the catheter becomes entrained into therterial “draw” of the catheter and returns back to the dialysis machine. Inffect, blood recirculates from the outflow to the inflow part of theatheter, thereby reducing dialysis clearance. Recirculation becomesore pronounced at higher blood flow rates, making it a more important
omplication in IHD as opposed to CRRT. Functional IJ and subclavianenous catheters have low recirculation rates (�5%), while femoralatheters have higher rates, especially if the catheter is not long enougho reach the inferior vena cava.30,31 Inversion of the connecting linesncreases recirculation from 3% to 12%.32 For catheters in the SVC, highecirculation rates may improve if a new catheter is placed with its tiploser to or within the right atrium.Catheter thrombosis can impair or completely interrupt dialysis. In aonfunctioning catheter, a 2-mg infusion of tissue plasminogen activatortPA) in each lumen can usually reestablish blood flows greater than 200L/min. Daeihagh and colleagues reported that tPA treatment with aean dwell time of greater than 24 hours restored patency in 87% of
ccluded catheters.33 Patients who are receiving CRRT may only toleratehorter tPA dwell times before they must resume dialysis. A dwell timef 30 to 120 minutes was successful in 88% of 30 patients receivingRRT.34 Failure of tPA to restore patency warrants treatment with aatheter exchange over a wire or the placement of a new catheter at aifferent location. Guidewire exchange of a dysfunctional dialysis cath-ter does not appear to increase the risk of infection.35
Efforts to prevent catheter thrombosis have focused on the use ofocking solutions instilled into the catheter at the conclusion of hemodi-lysis. The most widely used solution has been unfractionated heparin inoncentrations ranging from 500 to 2500 IU/mL.6 In theory, the volumef locking solution should fill only the catheter itself, thereby preventingatheter thrombosis without causing systemic effects. In practice, theocking solution does not completely remain in the catheter and patientsften become systemically anticoagulated. Locking solutions that can acts both an anticoagulant and an antimicrobial have been developed toddress the thrombotic and infectious risk of catheters. Solutions consist-
ng of sodium citrate and antiseptic agents have shown promise in50 Curr Probl Surg, July 2011
dh
C
cfrrrdciisieG
lSmspnsreirifiaoccd
cw
C
ecreasing the risk of catheter infections and thrombosis compared toeparin locking solution.36
atheter InfectionsInfection ranks second only to cardiovascular disease as the leading
ause of death for dialysis patients.4,37 The majority of infections deriverom vascular access, with catheter use representing the highest overallisk factor.38 Compared to autogenous AV fistulas, catheters increase theisk of infection by 50%, and this risk more than doubles if catheters areequired in the first 6 months of dialysis. Infection can affect any type ofialysis catheter; however, NTDCs appear to be more susceptibleompared to THDCs (3.8-6.6 infection episodes/1000 days vs 1.6-5.5nfection episodes/1000 days).39 For NTDCs the rate of bacteremiancreases dramatically after 5 days for femoral catheters and after 21 daysubclavian and IJ vein placement. The most common microorganismssolated from catheter infections are Staphylococcus aureus, Staphylococcuspidermidis, and enterococcus.40 Other forms of skin bacteria as well asram-negative rods and Candida can also be found.Catheter infections begin with bacterial contamination of the catheter
umen or migration of skin bacteria onto the catheter through the exit site.everal clinical factors contribute to the risk of catheter-related bactere-ia, including number of infusion ports, frequency of manipulation,
everity of patient illness, catheter indwelling time, emergency accesslacement, and experience of the interventionist. Catheter location doesot appear to affect infection risk. Although nonrandomized studiesuggested an increased risk of infection for femoral vein catheters, aecent randomized, controlled study of 750 patients showed statisticallyquivalent infection rates for femoral and IJ vein catheters (2.3 vs 1.5nfections per 1000 catheter days for IJ and femoral vein catheters,espectively). In this study, NTDCs placed in obese patients (body massndex greater than 28.4) had a higher rate of bacterial colonization at theemoral site; however, this did not translate into a higher rate ofnfection.41 These studies highlight the importance of appropriate skinnd catheter care in preventing catheter infections. Betadine or antibioticintments on the catheter hubs and aseptic techniques for handling theatheter can minimize the risk of infection. Daily catheter dressinghanges with gauze should be performed instead of tight occlusiveressings, which can increase infection risk.6
Catheter-related infections range in severity from localized bacterialolonization to life-threatening systemic sepsis. Treatment strategies vary
ith the severity of the infection, the type of catheter involved, and theurr Probl Surg, July 2011 451

casawrcCr
d1iicrp
orTcphtstpphc
athacm
oi
4
linical presentation. Exit site infections manifest as erythema, crusting,nd exudate involving the skin around the catheter. They do not causeystemic illness and blood cultures remain negative. NTDCs with signs ofn exit site infection should be removed and replaced after 24 to 48 hoursith antibiotic coverage. Topical antibiotics and local site care can
esolve some exit infections in tunneled catheters. Drainage around theatheter from the tunnel should be cultured and treated with antibiotics.linical deterioration or failure to respond to these conservative measures
equires removal of the THDC.Bloodstream infections represent a potentially lethal complication ofialysis catheters and occur with an incidence of 1.5 to 5.5 episodes per000 catheter days.40,42 Risk factors for catheter-related bacteremianclude a history of IV drug abuse, prior episodes of bacteremia, andmmunosuppression. Diabetes, age, and gender have no association withatheter infection risk.42 Gram-positive bacteria cause most catheter-elated bloodstream infections followed by Gram-negative bacteria andolymicrobial infections.40
Left untreated, catheter-related bacteremia can lead to endocarditis,steomyelitis, sepsis, and death. These consequences can be prevented byecognizing and diagnosing bloodstream infections early in their course.he most common clinical scenario consists of the acute onset of fever,hills, or hypoglycemia. Older patients and patients who are immunosup-ressed may present with atypical signs, such as lethargy, confusion, andypothermia. Rarely, metastatic infections emerge as the first manifesta-ion of catheter-related bacteremia. Regardless of the specific presentingigns, all patients with catheters who do not have another explanation forheir symptoms are assumed to have a catheter-related infection untilroven otherwise. Paired quantitative cultures from the catheter and theeripheral circulation can help make the diagnosis. If the catheter culturesave 5- to 10-fold more bacterial colonies than the peripheral blood, theatheter is the most likely source of infection.43
All instances of catheter-related bacteremia require treatment withntibiotics initially directed at staphylococcus and streptococcus and thenailored to the culture results. Treatment should begin whether the patientas systemic signs or symptoms of illness. In some cases, antibioticslone resolve the infection. Marr and colleagues salvaged 12 of 38atheters (31%) with antibiotics alone and did not detect an increase inetastatic infectious complications.42
Antibiotics often fail to eradicate catheter-associated infections becausef the presence of biofilms on the catheter surface.44 Lack of clinical
mprovement after 36 hours of antibiotics mandates removal of the52 Curr Probl Surg, July 2011
iptdecgtwsse7cbcr
P
P
aCTrAsle
ppttmSst
o
C
nfected catheter with its adherent biofilm. Several studies support theractice of exchanging the infected catheter over a guidewire as long ashe infection does not involve the exit site or tunnel track. This approachoes not require negative blood cultures before performing the catheterxchange. In a 2-year prospective observational study of 114 patients,atheter-related bacteremia was managed with 1 of 3 methods: (1)uidewire exchange; (2) guidewire exchange with creation of a newunnel; or (3) catheter removal and replacement. The patients received 3eeks of antibiotic therapy and cure was defined as freedom from
ymptoms 45 days after stopping antibiotics. All 3 strategies hadatisfactory cure rates that were statistically equivalent: (1) guidewirexchange, 87.8%; (2) guidewire exchange with creation of a new tunnel,5%; and (3) catheter removal and replacement, 86.5%.45 Exchanging theatheter has the advantage of preserving a vascular access site, which cane a scarce resource in dialysis patients. Infections that persist afteratheter exchange should be treated by removing the catheter andeplacing it at a new site 2 days after obtaining a negative blood culture.
ermanent Hemodialysis Access Planning
atient PreparationIdeally, all patients with impending kidney failure would have an
utogenous AV fistula ready for dialysis and avoid a temporary catheter.atheters frequently clot, become infected, and destroy outflow veins.hese complications result in a higher rate of hospitalization and a higher
isk of death for patients who depend on catheters for dialysis.46,47
utogenous fistulas remain the first choice for AV access because of theiruperior safety, efficacy, and durability. Avoiding catheters and estab-ishing autogenous AV access requires a multidisciplinary approach thatmphasizes advanced planning and preparation.Preparation for AV access begins with patient education and veinreservation. Nephrologists and primary caregivers are in the bestosition to inform patients about the options for renal replacementherapy, including the advantages of autogenous AV access. Patients canake an active role in protecting their forearm and upper arm veins toaximize their chances for primary fistula placement and maturation.ubclavian vein catheters and peripherally inserted central cathetershould be avoided if possible because of their link to venous stenosis andhrombosis.48,49
Early referral to a vascular access surgeon increases a patient’s chances
f having a functional AV access before starting hemodialysis. Theurr Probl Surg, July 2011 453
mtrfigotIpit
aapao3e
mnwtddsfnvoaccs
ildsw
4
aturation period and primary failure rate of AV fistulas dictate the leadime required before dialysis begins. In the United States, the medianeported time for AV fistula maturation was 98 days and 20% to 54% ofstulas never mature.50,51 On the basis of these data, the NFK-KDOQIuidelines recommend AV fistula placement at least 6 months in advancef the anticipated need for dialysis.52 Early placement allows adequateime for AV fistula maturation, evaluation, and even revision if necessary.n contrast, prosthetic AV grafts are ready to use as soon as theostoperative edema resolves and the graft incorporates into the surround-ng tissue. Since most prosthetic grafts can be used within 2 to 3 weeks,hey require a surgery lead time of only 3 to 6 weeks.The history and physical examination helps individualize the AV
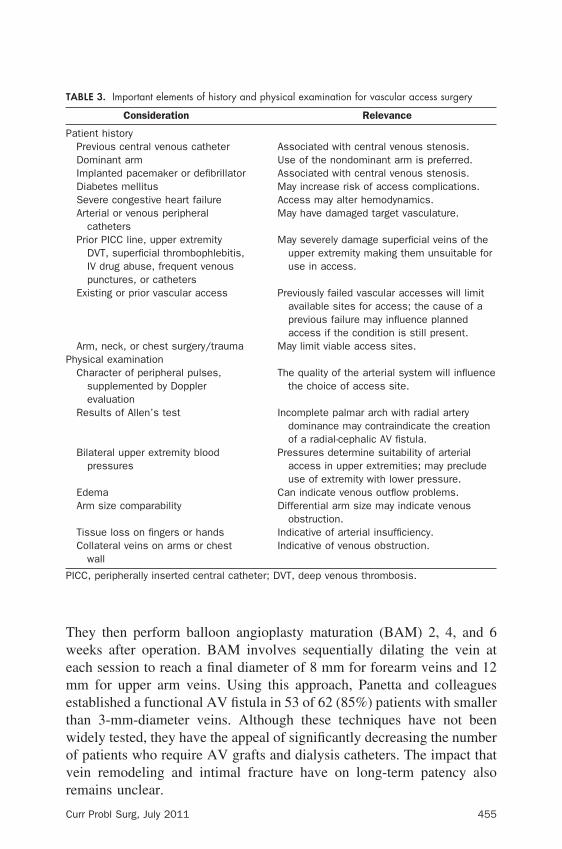
ccess treatment plan for each patient. The history should query forny conditions that could lead to access failure or complications. Aatient questionnaire or preprinted history can help cover all relevantspects of the patient’s history. The physical examination should focusn the patient’s venous, arterial, and cardiopulmonary systems. Tablesummarizes the most important points of the history and physical
xamination.The next step in preparation involves vascular imaging to determine theost appropriate site and type of AV access. Duplex ultrasound exami-
ations do not require contrast, making them ideal for evaluating patientsith residual kidney function. Preoperative duplex sonography records
he depth and caliber of the superficial venous system in addition toetecting evidence of previous phlebitis (eg, wall thickening, fillingefects, multiple tributaries, tortuosity). Continuous superficial veinegments greater than 2.5 mm in diameter are usually considered suitableor AV fistula creation. By identifying suitable superficial veins that areot apparent on physical examination, preoperative duplex ultrasoundein mapping increases the prevalence and improves the functionalutcome of AV fistulas.53,54 Duplex sonography is less sensitive andccurate for evaluating central veins. Patients with a history of multipleentral venous catheters or clinical signs of venous stenosis often requireontrast venography to determine the patency of the central venousystem.The push to increase the prevalence of autogenous access has sparked
nterest in using small-caliber veins for AV fistulas. Panetta and col-eagues have shown improved maturation using smaller than 3-mm-iameter veins for forearm and upper arm AV fistulas.55 At the time ofurgery they dilate the vein 1.0 to 1.5 mm larger than its starting diameter
ith an angioplasty balloon placed through the spatulated end of the vein.54 Curr Probl Surg, July 2011
Twemetwovr
T
P
P
P
C
hey then perform balloon angioplasty maturation (BAM) 2, 4, and 6eeks after operation. BAM involves sequentially dilating the vein at
ach session to reach a final diameter of 8 mm for forearm veins and 12m for upper arm veins. Using this approach, Panetta and colleagues
stablished a functional AV fistula in 53 of 62 (85%) patients with smallerhan 3-mm-diameter veins. Although these techniques have not beenidely tested, they have the appeal of significantly decreasing the numberf patients who require AV grafts and dialysis catheters. The impact thatein remodeling and intimal fracture have on long-term patency also
ABLE 3. Important elements of history and physical examination for vascular access surgery
Consideration Relevance
atient historyPrevious central venous catheter Associated with central venous stenosis.Dominant arm Use of the nondominant arm is preferred.Implanted pacemaker or defibrillator Associated with central venous stenosis.Diabetes mellitus May increase risk of access complications.Severe congestive heart failure Access may alter hemodynamics.Arterial or venous peripheral
cathetersMay have damaged target vasculature.
Prior PICC line, upper extremityDVT, superficial thrombophlebitis,IV drug abuse, frequent venouspunctures, or catheters
May severely damage superficial veins of theupper extremity making them unsuitable foruse in access.
Existing or prior vascular access Previously failed vascular accesses will limitavailable sites for access; the cause of aprevious failure may influence plannedaccess if the condition is still present.
Arm, neck, or chest surgery/trauma May limit viable access sites.hysical examinationCharacter of peripheral pulses,
supplemented by Dopplerevaluation
The quality of the arterial system will influencethe choice of access site.
Results of Allen’s test Incomplete palmar arch with radial arterydominance may contraindicate the creationof a radial-cephalic AV fistula.
Bilateral upper extremity bloodpressures
Pressures determine suitability of arterialaccess in upper extremities; may precludeuse of extremity with lower pressure.
Edema Can indicate venous outflow problems.Arm size comparability Differential arm size may indicate venous
obstruction.Tissue loss on fingers or hands Indicative of arterial insufficiency.Collateral veins on arms or chest
wallIndicative of venous obstruction.
ICC, peripherally inserted central catheter; DVT, deep venous thrombosis.
emains unclear.
urr Probl Surg, July 2011 455

O
asaaabopi
figmpcvfe
T
T
4
rder of Preference for AV AccessThe NFK-KDOQI guidelines set an order of preference for placing AV
ccess that reflects several underlying principles of vascular accessurgery: (1) always place a primary AV fistula when possible, and, if not,prosthetic AV graft; (2) move peripheral to central to preserve as many
ccess sites as possible, preferably in the nondominant extremity, andlternative sites (thigh, chest) used after all upper extremity sites haveeen exhausted; and (3) catheters should be avoided and only used if nother option is available. Based on these principles, the vascular accessreference list begins with the “snuff box” fistula at the base of the thumbn the nondominant arm and proceeds sequentially as outlined in Table 4.This order of preference places a high value on the advantages of AVstulas and minimizes their drawbacks (Table 5). The NFK-KDOQIuidelines acknowledge that rigid adherence to the order of preferenceay not be beneficial or cost-effective for all patients. Adopting the
hilosophy of “fistula first at all costs” can subject patients to prolongedatheter dependence with its attendant risks of bacteremia and centralenous stenosis. Vascular access planning must take into account severalactors, including whether dialysis has been initiated; the patient’s life
ABLE 4. Order of preference for vascular access52
1. Primary fistula (radio-cephalic) at the wrist or forearma) “Snuff box” fistulab) Wrist fistula (Brescia-Cimino)c) Mid-forearm fistula
2. Primary fistula at the elbowa) Brachial-cephalic AV fistulab) Brachial-basilic AV fistula
3. AV graft with synthetic or biologic materiala) Forearm loop AV graftb) Upper arm straight or loop AV graftc) Chest wall (“necklace”) or thigh AV graft
ABLE 5. Advantages and drawbacks of AV fistulas
Advantages Drawbacks
Superior patency Higher primary failure rateLower complication rate Failure to matureIncreased patient survival Long maturation timeLower hospitalization rate Increased need for temporary accessLower cost for implantation
and maintenanceMore difficult cannulation
xpectancy; whether the patient has had a previous failed vascular access;
56 Curr Probl Surg, July 2011
aoonp
T
m
F
kaa
cbaipchcc
taCadtmsppr
cta
C
nd the likelihood of fistula nonmaturation.56 Achieving the ultimate goalf a permanent, functional AV access may require deviating from therder of preference or using an AV graft as a bridge to an AV fistula. Theext section discusses the technical details and specific advantages anditfalls of each type of AV access.
echniquesThere are many AV access options for hemodialysis and some of theore common procedures are described.
orearm AV FistulasRadial-Cephalic AV Fistula. A radial-cephalic wrist AV fistula is alsonown as a Brescia-Cimino AV fistula and was first described by Bresciand colleagues in 1966.2 This fistula type has been described at thenatomical snuffbox or at the wrist.Technique Radial-Cephalic AV Wrist Fistula. Both the radial artery and
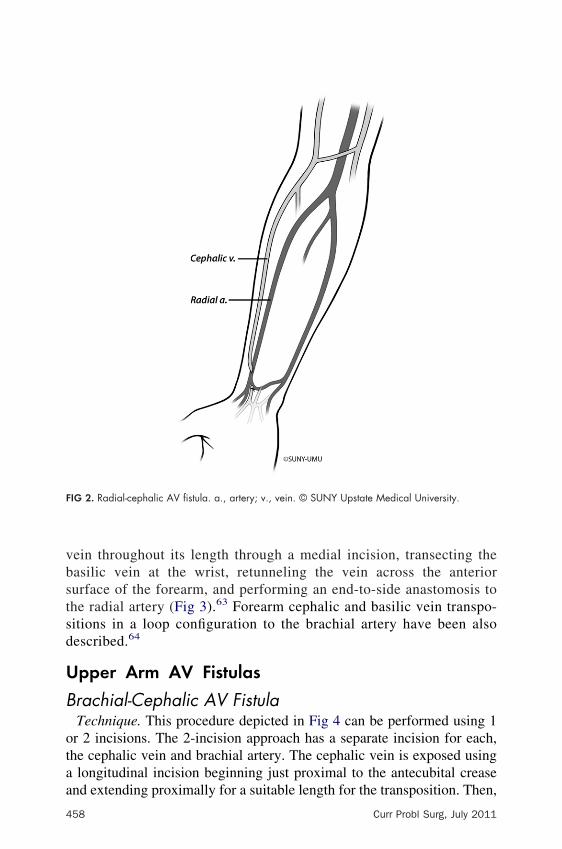
ephalic vein can be accessed through a single longitudinal incisionetween the 2 vessels (Fig 2). The structures in proximity to the vesselsre the median nerve and flexor carpi radialis tendon. The cephalic veins mobilized distally and an end-to-side anastomosis to the radial artery iserformed. Although a side-to-side anastomosis has been described, thisonfiguration can result in symptomatic venous hypertension (VH) in theand. To minimize the risk of hand ischemia, candidates for a radial-ephalic AV fistula should have a normal preoperative Allen’s testonfirming a patent palmar arch.Advantages and Drawbacks. The radial-cephalic AV fistula is a
echnically straightforward procedure and preserves other more proximalccess options. Radial-cephalic AV fistulas have few complications.annulation can sometimes be difficult secondary to less clearnatomic definition. Superficialization for easier cannulation has beenescribed.57,58 Compared to more proximally based configurations,he radial-cephalic AV fistula has a lower blood flow rate, andaturation can be slower. Radial-cephalic AV fistulas have been
hown to have a higher failure rate to mature in women, elderlyatients, and those with diabetes.59,60 The primary failure rate for allatients ranges from 15% to 24% and the 1-year cumulative patencyate is approximately 60%.61,62
Other Forearm Transpositions. Several other fistula types are lessommonly performed, but the access surgeon should still be aware ofhese options. One option is the basilic vein transposition to radial
rtery AV fistula. The basic technique involves mobilizing the basilicurr Probl Surg, July 2011 457
vbstsd
U
B
otaa
F
4
ein throughout its length through a medial incision, transecting theasilic vein at the wrist, retunneling the vein across the anteriorurface of the forearm, and performing an end-to-side anastomosis tohe radial artery (Fig 3).63 Forearm cephalic and basilic vein transpo-itions in a loop configuration to the brachial artery have been alsoescribed.64
pper Arm AV Fistulas
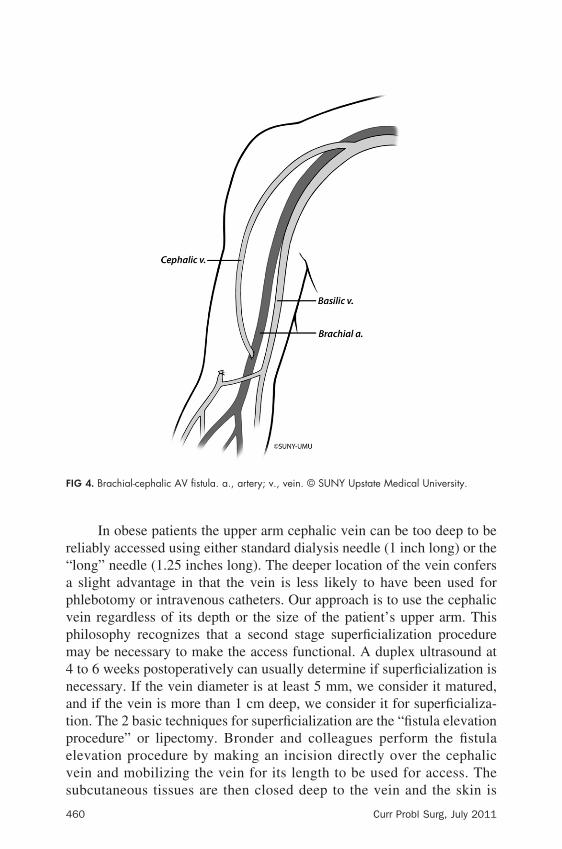
rachial-Cephalic AV FistulaTechnique. This procedure depicted in Fig 4 can be performed using 1r 2 incisions. The 2-incision approach has a separate incision for each,he cephalic vein and brachial artery. The cephalic vein is exposed using
longitudinal incision beginning just proximal to the antecubital crease
IG 2. Radial-cephalic AV fistula. a., artery; v., vein. © SUNY Upstate Medical University.
nd extending proximally for a suitable length for the transposition. Then,
58 Curr Probl Surg, July 2011

aisdtaa1ad
crlh
F
C
parallel shorter incision is made over the brachial artery and the arterys mobilized for a length just long enough to perform the anastomosis. Aubcutaneous tunnel connects the 2 incisions. The cephalic vein is thenivided near the antecubital fossa, brought through the subcutaneousunnel, and anastomosed end-to-side to the brachial artery. The 2-incisionpproach has the advantage of allowing more proximal exposure if thentecubital segment of the vein is fibrotic or the artery is diseased. The-incision approach involves exposing the cephalic vein and brachialrtery through a single oblique or transverse incision just proximal or justistal to the antecubital fossa.Advantages and Drawbacks. A brachial-cephalic AV fistula is a
ommonly performed access, which provides higher blood flow and moreeliable maturation than a wrist fistula.65 Because of its more proximalocation and greater blood flow, a brachial-cephalic AV fistula also has a
IG 3. Radial-basilic AV fistula. a., artery; v., vein. © SUNY Upstate Medical University.
igher incidence of edema and ischemic steal syndrome.
urr Probl Surg, July 2011 459
r“apvpm4natpevs
F
4
In obese patients the upper arm cephalic vein can be too deep to beeliably accessed using either standard dialysis needle (1 inch long) or thelong” needle (1.25 inches long). The deeper location of the vein confersslight advantage in that the vein is less likely to have been used for
hlebotomy or intravenous catheters. Our approach is to use the cephalicein regardless of its depth or the size of the patient’s upper arm. Thishilosophy recognizes that a second stage superficialization procedureay be necessary to make the access functional. A duplex ultrasound atto 6 weeks postoperatively can usually determine if superficialization is
ecessary. If the vein diameter is at least 5 mm, we consider it matured,nd if the vein is more than 1 cm deep, we consider it for superficializa-ion. The 2 basic techniques for superficialization are the “fistula elevationrocedure” or lipectomy. Bronder and colleagues perform the fistulalevation procedure by making an incision directly over the cephalicein and mobilizing the vein for its length to be used for access. The
IG 4. Brachial-cephalic AV fistula. a., artery; v., vein. © SUNY Upstate Medical University.
ubcutaneous tissues are then closed deep to the vein and the skin is
60 Curr Probl Surg, July 2011
cla
B
cp
necisitIsaso
abtdoplmwvfisripfiw
p
C
losed directly over the vein.58 Lipectomy using direct excision oriposuction has also been described to make AV fistulas moreccessible.66,67
rachial-Basilic AV FistulaTechnique. This access was initially described by Dagher and
olleagues in 1976, and it can be performed as a 1- or 2-stagerocedure.68
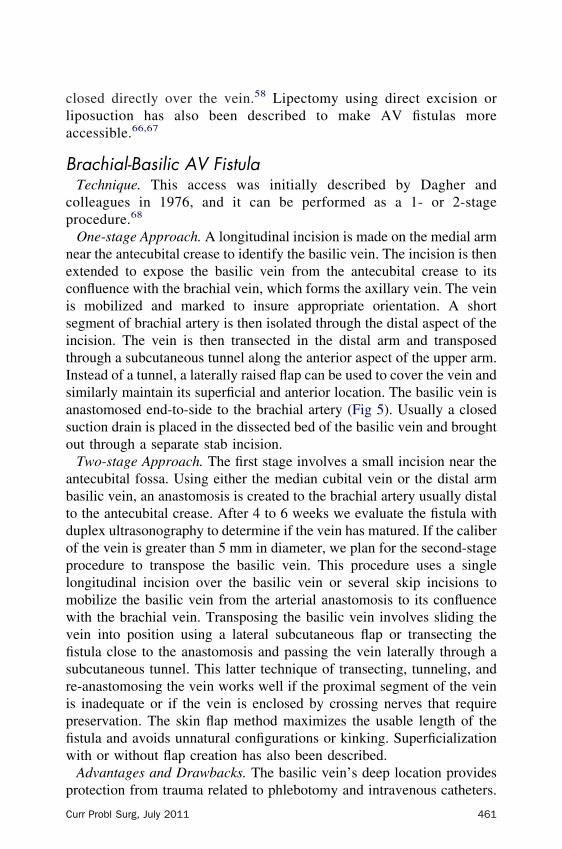
One-stage Approach. A longitudinal incision is made on the medial armear the antecubital crease to identify the basilic vein. The incision is thenxtended to expose the basilic vein from the antecubital crease to itsonfluence with the brachial vein, which forms the axillary vein. The veins mobilized and marked to insure appropriate orientation. A shortegment of brachial artery is then isolated through the distal aspect of thencision. The vein is then transected in the distal arm and transposedhrough a subcutaneous tunnel along the anterior aspect of the upper arm.nstead of a tunnel, a laterally raised flap can be used to cover the vein andimilarly maintain its superficial and anterior location. The basilic vein isnastomosed end-to-side to the brachial artery (Fig 5). Usually a closeduction drain is placed in the dissected bed of the basilic vein and broughtut through a separate stab incision.Two-stage Approach. The first stage involves a small incision near the
ntecubital fossa. Using either the median cubital vein or the distal armasilic vein, an anastomosis is created to the brachial artery usually distalo the antecubital crease. After 4 to 6 weeks we evaluate the fistula withuplex ultrasonography to determine if the vein has matured. If the caliberf the vein is greater than 5 mm in diameter, we plan for the second-stagerocedure to transpose the basilic vein. This procedure uses a singleongitudinal incision over the basilic vein or several skip incisions toobilize the basilic vein from the arterial anastomosis to its confluenceith the brachial vein. Transposing the basilic vein involves sliding theein into position using a lateral subcutaneous flap or transecting thestula close to the anastomosis and passing the vein laterally through aubcutaneous tunnel. This latter technique of transecting, tunneling, ande-anastomosing the vein works well if the proximal segment of the veins inadequate or if the vein is enclosed by crossing nerves that requirereservation. The skin flap method maximizes the usable length of thestula and avoids unnatural configurations or kinking. Superficializationith or without flap creation has also been described.Advantages and Drawbacks. The basilic vein’s deep location provides
rotection from trauma related to phlebotomy and intravenous catheters.urr Probl Surg, July 2011 461
Orsirtbrkaac
fip
F
4
ften, the basilic vein is the only upper extremity superficial vein thatemains patent in patients with previous access procedures. On the downide, brachial-basilic AV fistulas have a longer recovery time thatnvolves more postoperative edema and pain.69 They also carry a higherisk of developing ischemic steal syndrome compared to other accessypes.39 Transposing the basilic vein to facilitate needle cannulation cane technically challenging especially in cases involving an obese arm oredundant soft tissue. Positioning using the skin flap technique avoidsinking. The primary drawback of creating a flap is the increased risk ofn incisional complication. Superficialization with or without flap cre-tion has also been described, with mixed results in terms of patency andomplication rates.69,70
Several studies have confirmed the durability of brachial-basilic AVstulas. Hakaim and colleagues showed similar 18-month cumulative
IG 5. Brachial-basilic AV fistula. a., artery; v., vein. © SUNY Upstate Medical University.
atency rates for the brachial-basilic and the brachial-cephalic AV
62 Curr Probl Surg, July 2011
fic5bptptowsawp
A
atva
abAtaco
P
G
Ema(ccus
C
stulas, which were 79% and 78%, respectively.65 Humphries andolleagues demonstrated long-term patency rates of 84%, 73%, 73%, and2% at 1, 3, 5, and 10 years, respectively.70 Traditionally, the brachial-asilic AV fistula was performed as a 1-stage procedure, and 2-stagerocedures were reserved for small-caliber basilic veins whose matura-ion was questionable. Over time, the 2-stage approach has gainedopularity and several studies have demonstrated excellent results withhis technique and even improved patency rates.71-73 Another advantagef the 2-stage approach is that the first stage involves a small procedureith a short recovery time. If the fistula does not mature after the first
tage, patients will have avoided the larger transposition surgery with itsssociated longer incision and recovery time. These patients may be moreilling to undergo another procedure compared to patients who have arimary failure after the one stage approach.
ntecubital Level Vein to Brachial Artery AV FistulaTechnique. A transverse incision is made 1 fingerbreadth distal to the
ntecubital crease. The median antecubital vein is mobilized, taking careo protect its connections to both the cephalic and the basilic veins. Theein is then transected distally. Through the same incision the vein isnastomosed in an end-to-side fashion to the brachial artery (Fig 6).Advantages and Drawbacks. Depending on the venous anatomy at the
ntecubital fossa, the median antecubital vein can have connections tooth the cephalic and the basilic veins, thereby increasing venous outflow.n AV fistula using an antecubital vein may allow both the cephalic and
he basilic veins to mature at the same time. The venous anatomy maylso limit the fistula to only be to the cephalic or basilic veins. This fistulaonfiguration has been shown to be successful and may maximize accessptions.74,75
rosthetic AV Grafts
raft MaterialsA variety of materials have been used in the construction of AV grafts.xpanded polytetrafluoroethylene (PTFE) is the most commonly usedaterial. PTFE grafts should not be distended with saline under pressure
s this practice may predispose the grafts to excessive serous leaking“sweating”) and seroma formation. For the upper extremity the mostommon diameter is a 6-mm straight PTFE graft. The other commononfiguration is a 4- to 7-mm tapered graft with the smaller diameter endsed for the arterial anastomosis. The comments below presume a
tandard wall thickness PTFE graft.urr Probl Surg, July 2011 463

F
wcAtocdclgvcof
F
4
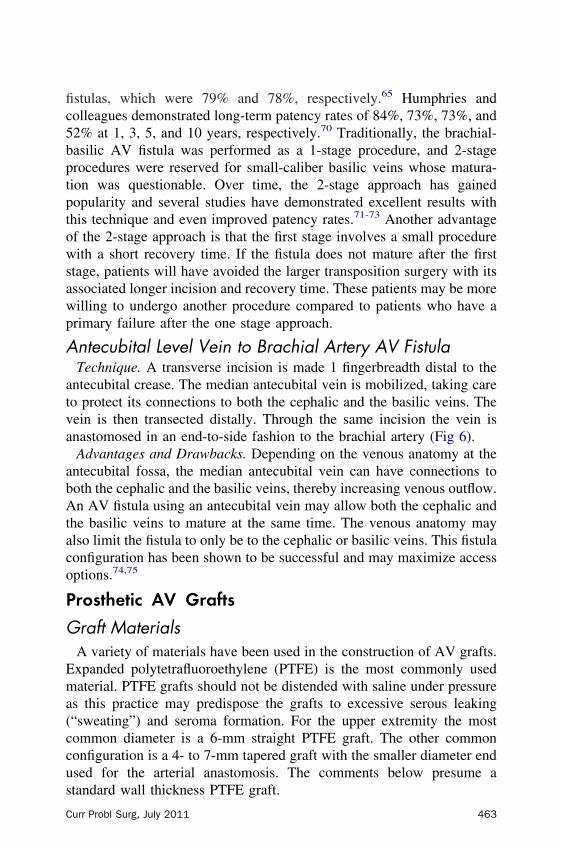
orearm Loop AV GraftTechnique. Forearm loop AV grafts originate in the antecubital fossaith the brachial artery providing arterial inflow (Fig 7). Venous outflow
an employ the cephalic, basilic, median antecubital, or brachial veins.n incision is made 1 to 2 cm distal to the antecubital crease, taking care
o preserve superficial veins and tributaries for potential use as venousutflow. After isolating the brachial artery and a suitable vein, a 2-cmounterincision (either vertical or transverse) is created on the mid toistal anterior forearm to facilitate the tunneling of the loop graftonfiguration. Using a semicircular tunneler maximizes the size of theoop while creating a uniform subcutaneous tunnel that decreases the riskraft kinking. After passing the graft through the tunnel, the arterial andenous anastomoses are performed in an end-to-side fashion. Beforeompleting the venous anastomosis, the graft is flushed. The subcutane-us layer is closed, followed by the skin closure. Because of the potential
IG 6. Brachial-antecubital vein AV fistula. a., artery; v., vein. © SUNY Upstate Medical University.
or edema, we recommend external skin stitches.
64 Curr Probl Surg, July 2011
U
taTvoTb
uaulcbbs
p
F
C
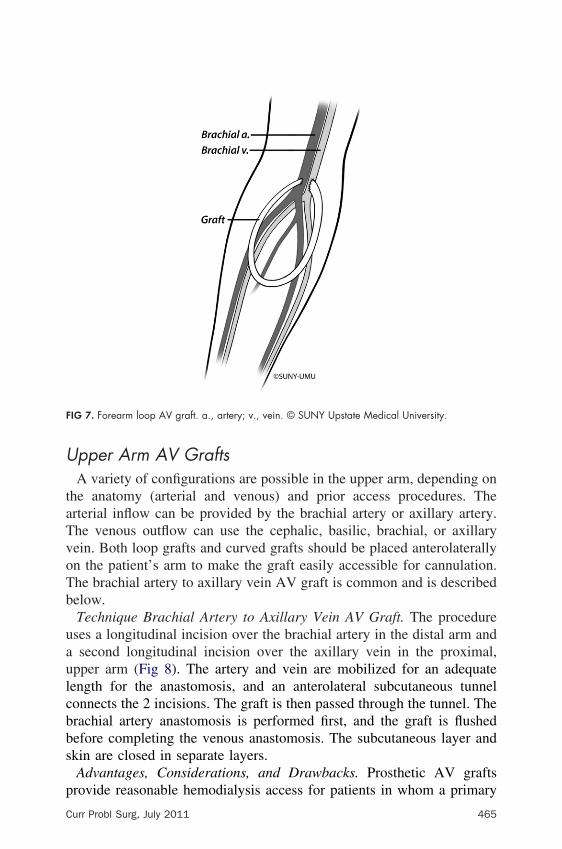
pper Arm AV GraftsA variety of configurations are possible in the upper arm, depending on
he anatomy (arterial and venous) and prior access procedures. Therterial inflow can be provided by the brachial artery or axillary artery.he venous outflow can use the cephalic, basilic, brachial, or axillaryein. Both loop grafts and curved grafts should be placed anterolaterallyn the patient’s arm to make the graft easily accessible for cannulation.he brachial artery to axillary vein AV graft is common and is describedelow.Technique Brachial Artery to Axillary Vein AV Graft. The procedureses a longitudinal incision over the brachial artery in the distal arm andsecond longitudinal incision over the axillary vein in the proximal,
pper arm (Fig 8). The artery and vein are mobilized for an adequateength for the anastomosis, and an anterolateral subcutaneous tunnelonnects the 2 incisions. The graft is then passed through the tunnel. Therachial artery anastomosis is performed first, and the graft is flushedefore completing the venous anastomosis. The subcutaneous layer andkin are closed in separate layers.Advantages, Considerations, and Drawbacks. Prosthetic AV grafts
IG 7. Forearm loop AV graft. a., artery; v., vein. © SUNY Upstate Medical University.
rovide reasonable hemodialysis access for patients in whom a primary
urr Probl Surg, July 2011 465
Ageoci
apAthA
F
4
V fistula is not possible. Patient anatomy generally determines the AVraft location and configuration. The lay of the graft should maximizease and surface area for needle access. Although prosthetic AV graftsffer technically easy cannulation and a shorter lag time from insertion tolinical use, these advantages are offset by a higher rate of thrombosis andnfection compared to autologous AV fistulas.52,76,77
The forearm loop AV graft and the straight arm AV grafts are commonnd are described above. Distally placed grafts preserve the moreroximal extremity access sites at the cost of lower blood flow rates.nother disadvantage of the forearm loop graft is edema and postopera-
ive pain. Although upper arm grafts have high blood flow rates, they alsoave a higher rate of hemodynamic steal syndrome compared to forearm
IG 8. Brachial-axillary AV graft. a., artery; v., vein. © SUNY Upstate Medical University.
V grafts.
66 Curr Probl Surg, July 2011
A
ltvwc
ivmpecPc
tftu
F
C
lternative Sites for AV AccessWhen the upper extremity options have been exhausted, other access
ocations and configurations are considered. A “necklace” AV graft useshe axillary artery for inflow and the contralateral axillary vein or jugularein for venous outflow.78 Since these grafts cross over the anterior chestall, they are not ideal for patients who may require a sternotomy for
ardiac revascularization in the future.Groin AV access sites have a higher incidence of infection and
schemia and should only be used if the upper extremities are not aiable option. The arterial circulation should be normal or haveinimal disease to create this type of access. In addition, some other
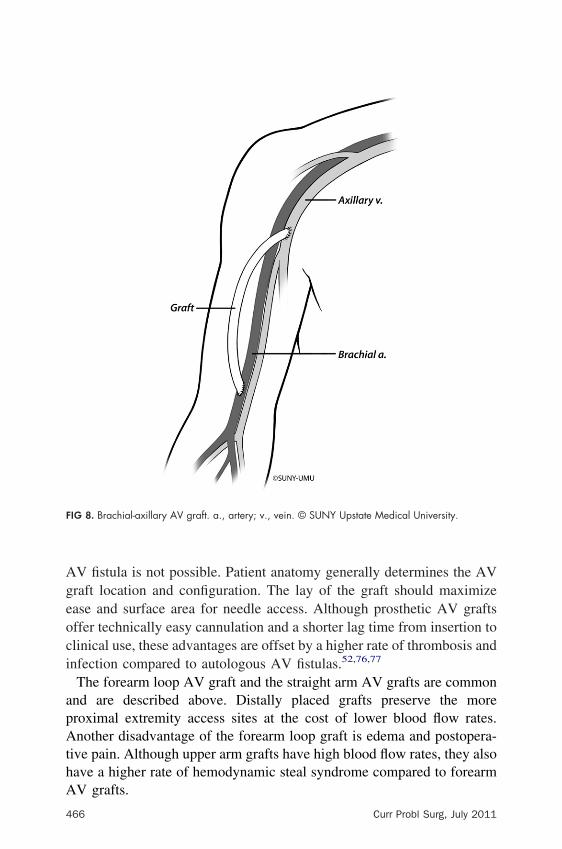
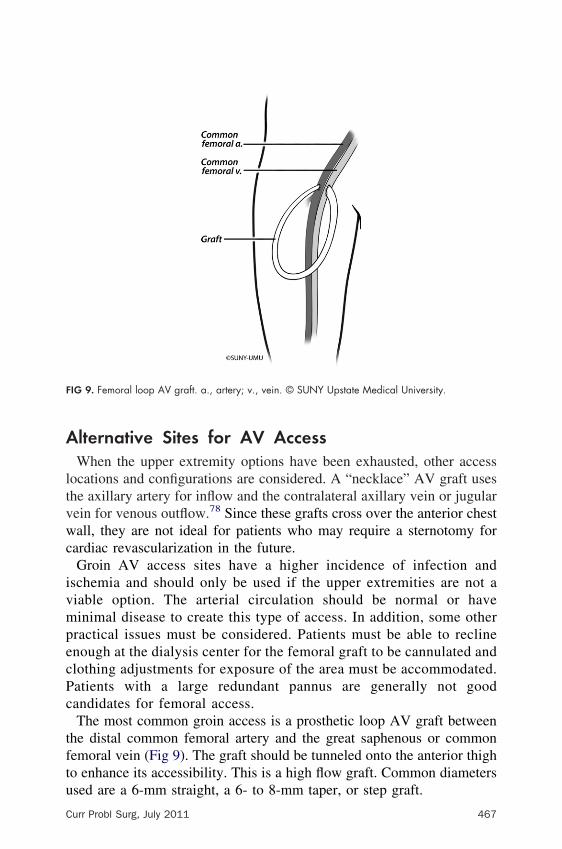
ractical issues must be considered. Patients must be able to reclinenough at the dialysis center for the femoral graft to be cannulated andlothing adjustments for exposure of the area must be accommodated.atients with a large redundant pannus are generally not goodandidates for femoral access.The most common groin access is a prosthetic loop AV graft between
he distal common femoral artery and the great saphenous or commonemoral vein (Fig 9). The graft should be tunneled onto the anterior thigho enhance its accessibility. This is a high flow graft. Common diameters
IG 9. Femoral loop AV graft. a., artery; v., vein. © SUNY Upstate Medical University.
sed are a 6-mm straight, a 6- to 8-mm taper, or step graft.
urr Probl Surg, July 2011 467
aecsadv
H
HAAap
FM
4
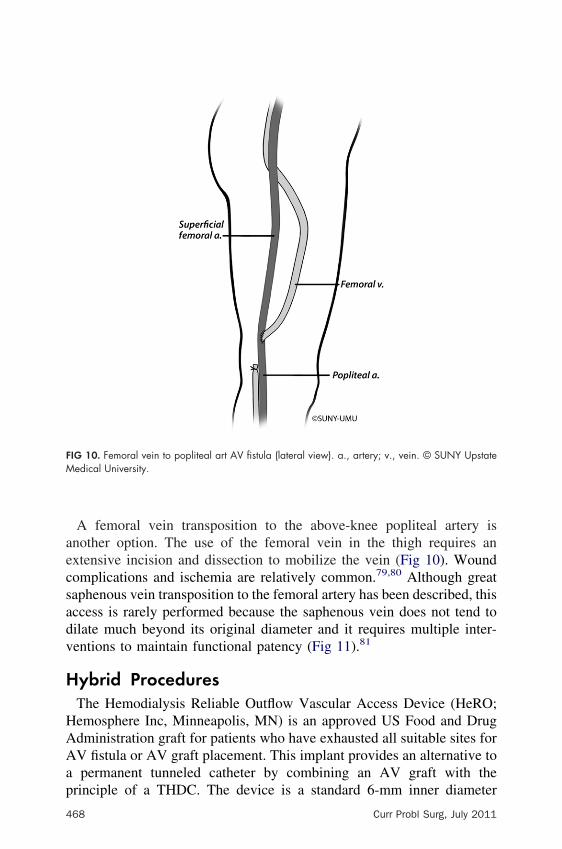
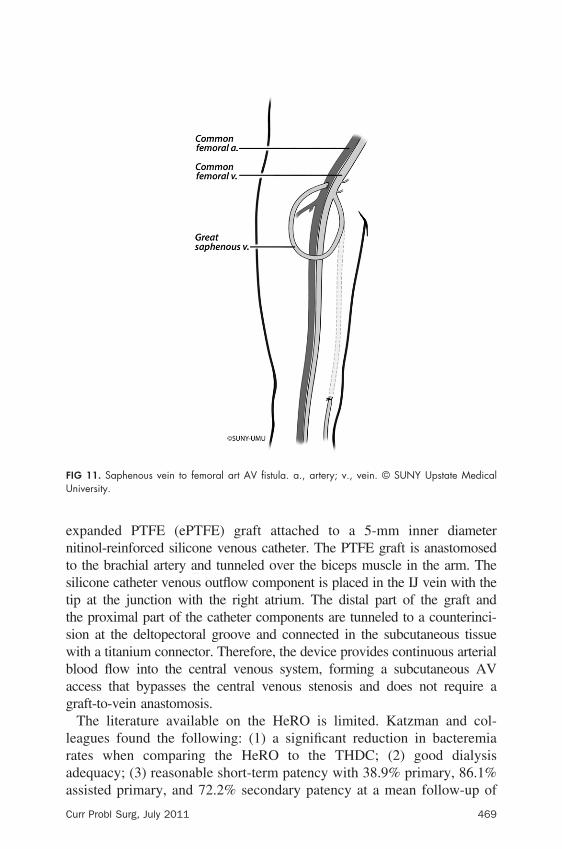
A femoral vein transposition to the above-knee popliteal artery isnother option. The use of the femoral vein in the thigh requires anxtensive incision and dissection to mobilize the vein (Fig 10). Woundomplications and ischemia are relatively common.79,80 Although greataphenous vein transposition to the femoral artery has been described, thisccess is rarely performed because the saphenous vein does not tend toilate much beyond its original diameter and it requires multiple inter-entions to maintain functional patency (Fig 11).81
ybrid ProceduresThe Hemodialysis Reliable Outflow Vascular Access Device (HeRO;emosphere Inc, Minneapolis, MN) is an approved US Food and Drugdministration graft for patients who have exhausted all suitable sites forV fistula or AV graft placement. This implant provides an alternative topermanent tunneled catheter by combining an AV graft with the
IG 10. Femoral vein to popliteal art AV fistula (lateral view). a., artery; v., vein. © SUNY Upstateedical University.
rinciple of a THDC. The device is a standard 6-mm inner diameter
68 Curr Probl Surg, July 2011
entsttswbag
lraa
FU
C
xpanded PTFE (ePTFE) graft attached to a 5-mm inner diameteritinol-reinforced silicone venous catheter. The PTFE graft is anastomosedo the brachial artery and tunneled over the biceps muscle in the arm. Theilicone catheter venous outflow component is placed in the IJ vein with theip at the junction with the right atrium. The distal part of the graft andhe proximal part of the catheter components are tunneled to a counterinci-ion at the deltopectoral groove and connected in the subcutaneous tissueith a titanium connector. Therefore, the device provides continuous arteriallood flow into the central venous system, forming a subcutaneous AVccess that bypasses the central venous stenosis and does not require araft-to-vein anastomosis.The literature available on the HeRO is limited. Katzman and col-
eagues found the following: (1) a significant reduction in bacteremiaates when comparing the HeRO to the THDC; (2) good dialysisdequacy; (3) reasonable short-term patency with 38.9% primary, 86.1%
IG 11. Saphenous vein to femoral art AV fistula. a., artery; v., vein. © SUNY Upstate Medicalniversity.
ssisted primary, and 72.2% secondary patency at a mean follow-up of
urr Probl Surg, July 2011 469

8pAp
SC
patsfroaa
Ttwwreoa
vulp
mm
V
R
fn
4
.6 months; and (4) reasonable intervention rates with an average of 2.5er year, which was comparable to AV grafts and lower than THDCs.82
lthough more studies are required, the HeRO device appears to be aromising form of alternative AV access.
urgical Techniques for AV Access—GeneralommentsAlthough specific surgical techniques can vary, several general princi-les play an important role in any type of vascular access surgery. Thenastomosis can be performed using a variety of different suturingechniques, including use of anastomotic clips. To minimize the risk ofteal, the anastomosis should be less than 1 cm in length. The arteriotomyor the anastomosis should be oriented to insure that the vein or graftemains in a natural position to avoid kinking. Accommodating the “lay”f the vein or graft may require an oblique rather than a longitudinalrteriotomy or an anastomosis on the side of the artery instead of itsnterior aspect.How the fistula or graft lays under the skin requires attention to detail.he location must be easily accessible and the overlying subcutaneous
issue cannot be too thick. Taking into account the position of the armhen the patient is receiving dialysis is important, particularly in a patientith redundant tissue in the upper arm. The arm position on the operating
oom table where the placement looks good is different when the arm isxtended more anteriorly as it would be in a dialysis chair. Redundancyr a very large arm sometimes makes the basilic vein hard to use forccess since it is not successfully shifted into a position for easy use.When performing AV access procedures, the degree of anticoagulationaries among surgeons. Surgeons vary their practice from full anticoag-lation, subtherapeutic systemic heparin, or heparinized saline infusedocally into the vessels. Part of the choice depends on the history of theatient and speed by which the anastomosis can be done.Maximizing venous outflow for AV access is advantageous. As long asaturation is not significantly inhibited, venous branches should beaintained to maximize venous outflow.
ascular Access Monitoring and Surveillance
ationaleVascular access may represent the single most important intervention
or patients with ESRD. Issues related to access placement and mainte-
ance are discussed elsewhere in this monograph. This section discusses70 Curr Probl Surg, July 2011

pdfstSciitca
M
dphaipt
mitAf
bavpvast
Aaa
C
recannulation evaluation of the access and reviews strategies foretecting access dysfunction to reduce morbidity and prevent accessailure. Although current literature lacks prospective clinical trials ortrong supportive data for a surveillance regimen, it is generally believedhat such a strategy is reasonable and will lead to improved outcomes.29,83
pecifically, early detection and correction of hemodynamically signifi-ant anatomic stenosis can improve long-term patency and reduce thencidence of acute thrombosis. As a consequence, quality of life andmproved dialysis for the patient may be appreciated. The issues relatedo “assessing the access,” with specific attention to maturation andannulation options, are reviewed first, after which the actual elements ofprospective monitoring program are presented.
aturation and CannulationThe time required from access creation to needle cannulation varies andepends on the type of AV access and the conduit material. Somerosthetic AV grafts tolerate cannulation 24 hours after placement;owever, PTFE, the most widely used AV graft conduit, usually requiresminimum of 2 weeks before it is ready for use. Clinical features that
ndicate an AV graft is ready for cannulation include the resolution ofostoperative swelling and inflammation and the ability to clearly palpatehe course of the graft.84
An autogenous AV fistula typically takes a minimum of 1 month andore often 3 to 4 months to fully mature. Maturation requires “arterial-
zation” of the venous conduit during which the diameter increases andhe vessel walls become stronger.85 The most useful tools in determiningV fistula maturity are the examiner’s fingertips, specifically assessing
or size, intensity of thrill, and elastic recoil of the palpated vessel.Patients have traditionally been advised to perform arm curls or squeezeall exercises to encourage AV fistula maturation. Although it has onlynecdotal evidence as support, the practice continues because it posesirtually no risk. Occasionally a tourniquet is used to increase backressure in the AV fistula and facilitate cannulation of a poorly definedein.86 In general, the need for a tourniquet should raise concern that theccess has not adequately matured. Prominent venous tributaries caniphon flow from the primary vein and may require ligation if they are felto be impeding fistula maturation.87
The “Rule of 6s” summarizes the most important features of a matureV fistula. A functional access should be at least 6 mm in diameter, havepalpable thrill extending at least 6 cm in length (ideally 10 cm), achieve
blood flow rate of 600 mL/min, and have clearly defined margins onurr Probl Surg, July 2011 471

ps
eofea6rfi
fpuerddivbfi
ccn
T
P
A
EE
E
N
C
4
hysical examination. The key physical examination characteristics of auccessful AV access are outlined in Table 6.A new access should be examined at every opportunity, at least with
very dialysis, and weekly before dialysis initiation. Because patients areften unfamiliar with self-assessment for AV access thrill and bruit, theserequent evaluations afford an opportunity for both patient education andarly detection of dysfunction. The routine examination includes evalu-tion for a soft pulse and a strong thrill at the anastomosis that extends forto 10 cm. Occlusion of venous outflow with digital pressure should
esult in an immediate diminution in pulse and thrill. Visual examinationor large venous branches forming collaterals and extremity edemandicative of proximal outflow obstruction should be noted.If the physical examination is abnormal, the patient should undergo
urther assessment to determine whether an intervention is warranted toromote AV access maturation. A duplex ultrasound can be particularlyseful for patients not yet on dialysis. Although this technique can overstimate stenosis, the ultrasound can give accurate information withegards to diameter, depth, presence of large side branches, and fillingefects and identify areas of significant turbulence. For a patient onialysis, a fistulogram offers a more definitive exam with the potential formmediate intervention. When identified, endovascular or surgical inte-entions can be performed to address abnormalities and are describedelow. A newer strategy to facilitate maturation of small-caliber AVstulas is the BAM procedure, which is described above.An established and mature AV access should be cannulated with
aution and by expert personnel when initially used. A specializedannulation team for each dialysis shift may allow focused expertise for
ABLE 6. Routine physical examination of the maturing AV access
Examination Significance
eripheral pulses Diminished pulses or cool distal digits suggestive ofsteal
llen test Positive findings suggestive of steal particularly withradial-cephalic fistula
valuation for unilateral edema Indicative of proximal obstruction to return flowxamination for collateral veins Venous tributaries indicate compromised drainage
outflowxamination for CHF Tachycardia and crackles indicative of high-output
cardiac failureeurologic examination Abnormal sensory or motor function indicative of more
than cutaneous nerve injury
HF, congestive heart failure.
ew or difficult to stick AV access and permits acquisition of experience
72 Curr Probl Surg, July 2011
ascimsiswrwtd
efifii
Fe
C
nd expertise that can then be conveyed in the form of regular patient andtaff education and orientation. A slowly maturing access may beannulated with a draw (or “arterial” side) needle if an existing catheters available for return (the “venous” side), allowing mildly acceleratedaturation with increased blood flow. The most common protocols use a
maller 17-G needle for the first 2 weeks of cannulation with a subsequentncrease weekly to 15-G needles. Cannulation needles are winged fortability and taping and have a safety housing to entrap the needle afterithdrawal from the patient. When using 17-G needles, the blood flow
ate should be reduced to 200 mL/min to avoid excessive turbulence,hich can damage the anastamosis or lead to hemolysis. Needles are
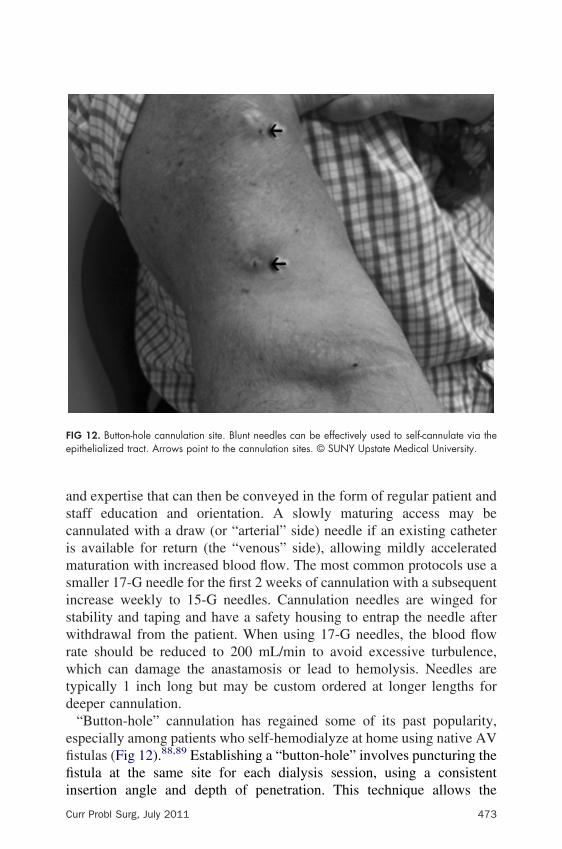
ypically 1 inch long but may be custom ordered at longer lengths foreeper cannulation.“Button-hole” cannulation has regained some of its past popularity,
specially among patients who self-hemodialyze at home using native AVstulas (Fig 12).88,89 Establishing a “button-hole” involves puncturing thestula at the same site for each dialysis session, using a consistent
IG 12. Button-hole cannulation site. Blunt needles can be effectively used to self-cannulate via thepithelialized tract. Arrows point to the cannulation sites. © SUNY Upstate Medical University.
nsertion angle and depth of penetration. This technique allows the
urr Probl Surg, July 2011 473

“waTefit
caapafoaceCtsghita
M
htmd
Aqceoet
4
constant sites” to epithelialize and develop a vascular wall flap. After 2eeks, patients can self-cannulate with specialized blunt needles with an
ntistick dull bevel that is inserted through the scar-tissue tunnel track.he technique has proven to have a high patient satisfaction rating and anxcellent safety profile. Hsiao and colleagues evaluated 104 button-holestulas with duplex ultrasound and found vascular dilation and intimal
hickening but no significant luminal stenosis at any access site.90
Site infiltration represents the single most common and significantomplication of cannulation. An episode of infiltration can be a dramaticcute event during dialysis where the blood pump speed is commonly sett 400 to 500 mL/min. Dialysis should immediately be halted, the needleulled, and digital pressure applied with 2 fingers to cover approximately1 inch radius directly over the bleeding hole. This provides hemostasis
or an anterior infiltrate, but it is usually ineffective in controlling a sider back-wall puncture. Some instances of slow infiltration, especiallyfter the patient has been systemically heparinized, may be managed withontinued dialysis and ice over the affected site with close monitoring forxpansion of the hematoma, in which case the dialysis must be stopped.are should be exercised to never apply pressure over an infiltrate while
he needles are still in situ because the risk of vessel laceration isignificant. Follow-up management should include close monitoring forraft thrombosis due to external compression of the AV access from theematoma. Finally, persistent slow bleeding, especially in a posterior wallnfiltrate, particularly in a thigh graft, can lead to catastrophic sequestra-ion of large amounts of blood and may require surgical intervention tochieve hemostasis.
ajor Elements of MonitoringDespite the fact that vascular access monitoring and early interventionave not been supported by strong data, experts in the field uniformly feelhis approach is both rational and reasonable in light of the considerableorbidity and cost—both financial and human—associated with access
ysfunction.An organized surveillance program begins with routine assessment ofV access and hemodialysis adequacy, from both a qualitative and auantitative standpoint. The first step in such a program is the identifi-ation of an access monitoring “team.” The team should be led by anxperienced facility access coordinator who has insight into the logisticsf access maintenance and familiarity with cannulation and the physicalxamination. Although debate concerning intervention options continues,
he skills required for the actual physical examination and clinical74 Curr Probl Surg, July 2011
ec
oidoidtioppdipaa
T
S
D
U
D
O
IE
A
Kr
C
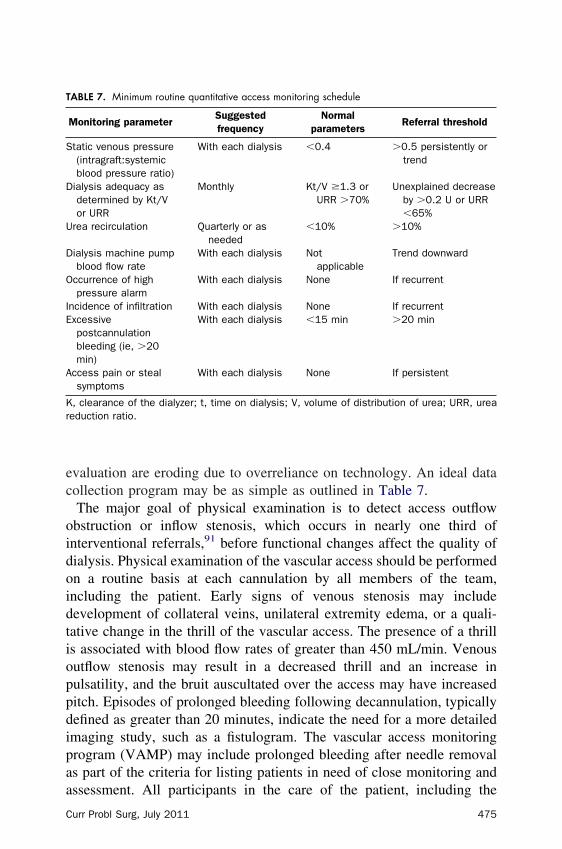
valuation are eroding due to overreliance on technology. An ideal dataollection program may be as simple as outlined in Table 7.The major goal of physical examination is to detect access outflowbstruction or inflow stenosis, which occurs in nearly one third ofnterventional referrals,91 before functional changes affect the quality ofialysis. Physical examination of the vascular access should be performedn a routine basis at each cannulation by all members of the team,ncluding the patient. Early signs of venous stenosis may includeevelopment of collateral veins, unilateral extremity edema, or a quali-ative change in the thrill of the vascular access. The presence of a thrills associated with blood flow rates of greater than 450 mL/min. Venousutflow stenosis may result in a decreased thrill and an increase inulsatility, and the bruit auscultated over the access may have increaseditch. Episodes of prolonged bleeding following decannulation, typicallyefined as greater than 20 minutes, indicate the need for a more detailedmaging study, such as a fistulogram. The vascular access monitoringrogram (VAMP) may include prolonged bleeding after needle removals part of the criteria for listing patients in need of close monitoring and
ABLE 7. Minimum routine quantitative access monitoring schedule
Monitoring parameterSuggestedfrequency
Normalparameters
Referral threshold
tatic venous pressure(intragraft:systemicblood pressure ratio)
With each dialysis �0.4 �0.5 persistently ortrend
ialysis adequacy asdetermined by Kt/Vor URR
Monthly Kt/V �1.3 orURR �70%
Unexplained decreaseby �0.2 U or URR�65%
rea recirculation Quarterly or asneeded
�10% �10%
ialysis machine pumpblood flow rate
With each dialysis Notapplicable
Trend downward
ccurrence of highpressure alarm
With each dialysis None If recurrent
ncidence of infiltration With each dialysis None If recurrentxcessivepostcannulationbleeding (ie, �20min)
With each dialysis �15 min �20 min
ccess pain or stealsymptoms
With each dialysis None If persistent
, clearance of the dialyzer; t, time on dialysis; V, volume of distribution of urea; URR, ureaeduction ratio.
ssessment. All participants in the care of the patient, including the
urr Probl Surg, July 2011 475

pi
arvhwm
bdTah(giatpcb
rcueicmstlsburbpr
4
hysician, nurse, patient care technician, and patients themselves, have anmportant role in the physical monitoring of access function.The preferred method of surveillance for detecting stenosis in AV grafts
nd fistulas uses a combination of intra-access flow monitoring andegular measures of direct static pressure. Nonstandardized dynamicenous pressures during actual pump function have not been validated;owever, these pressures may be useful to follow trends in a single patienthen performed sequentially with the same methodology. We recom-end continued use of the gold standard static venous pressure.Static venous pressure, measured routinely at the onset of dialysisefore the pump has been started, is simple and more standardized thanynamic venous pressure (obtained during actual dialysis pump function).he most commonly used measure is the ratio of venous outflow to meanrterial pressure, with low values reflecting the absence of stenosis andigh values suggestive of outflow obstruction. A normal measure is a ratiointragraft:systemic blood pressure) that is less than 0.4 and a valuereater than 0.5 is considered concerning. Several factors can result in ansolated abnormal value, the most important being needle placement (ie,gainst a vessel wall). It is therefore important to respond to trends overime rather than a single abnormal measurement. Decreased arterial sideressures are reflective of arterial inflow stenosis, a less commonondition that is also associated with reductions in overall intra-accesslood flow rates.The native AV fistula differs from an AV graft in that the pressure–flow
elationship evolves over several months, after which it remains relativelyonstant. Ultimate blood flow rates of 1000 mL/min or higher are notncommon and may increase the risk of high output cardiac failure,specially in upper arm AV fistulas. Blood flow in AV grafts increasesmmediately and pressures stabilize within weeks of placement. Venousollaterals associated with AV fistulas can make static pressure measure-ent an insensitive tool for detecting venous outflow stenosis. In this
cenario, venous back pressure does not necessarily increase because ofhe compensated flow provided by venous collaterals. In AV fistulas thatack venous collaterals, such as the transposed basilic vein, central venoustenosis results in a marked reduction in flow due to increased venousack-pressure. Hemodynamically, these AV fistulas behave more like anpper arm AV graft where increased static venous outflow pressures oreduced absolute flow indicate an anastomotic stenosis. For AV fistulas,lood flow rates less than 400 mL/min (certainly less than 200 mL/min)redict thrombosis, while AV grafts are at risk for thrombosis when flow
ates drop below 600 mL/min.9276 Curr Probl Surg, July 2011

ml“sdAsTedhstcug
flsfuflcuSfovdi
flishp
ceT
C
The assessment of recirculation using a non-urea-based dilutionalethod represents a useful strategy for monitoring AV fistulas. Recircu-
ation in an AV fistula occurs when blood flows retrograde from thevenous” to the “arterial” dialysis needles. In this scenario, dialyzer pumppeed is higher than actual net intra-access blood flow rate. Asescribed above, thrombosis occurs at much higher flow rates in anV graft compared to an AV fistula. Recirculation is therefore not
ensitive enough to detect critical reductions in flow for AV grafts.he results of blood laboratory work may indicate adequate dialysisven in the presence of access dysfunction and recirculation. Aiscrepancy between clinical findings (uremic symptoms, persistentyperkalemia, etc.) and the chemical measure of adequacy (Kt/V)uggests the presence of recirculation due to venous outflow obstruc-ion. Recirculation values are calculated by a simple formula usingoncentrations of urea in arterial and venous lines and may be orderedsing established procedure in all dialysis units. Recirculation valuesreater than 10% are considered abnormal.Several “investigational” techniques can measure and track accessow, which is considered one of the most sensitive and specificurveillance tools. Results of multiple recent studies, however, haveailed to demonstrate the predictive value of measuring access flowsing the currently available technology.87,93-96 All techniques forow surveillance require un-reimbursed time, in addition to labor andapital expense, forcing many dialysis units to abandon their use. Theltrasound dilution method using a saline bolus (Transonic; Transonicystems Inc, Ithaca, NY) has been studied extensively. Mathematicalormulas based on the Fick principle determine access flow via sensorsn arterial and venous lines following a saline injection. Absolutealues of flow less than 600 mL/min in the AV graft or a sequentialrop in flow rate by 15% have been reported to be associated with anncreased thrombosis risk.92,97
Other methods of flow surveillance that have been developed includeow dilution techniques with sodium, urea, or thermal methods, glucose
nfusion, differential electrical conductivity, variable flow Doppler ultra-ound, and magnetic resonance angiography. None of these techniquesas sufficient data support to warrant routine surveillance use in clinicalractice.98,99
The Society for Vascular Surgery recently published a meta-analysisomparing surveillance and clinical monitoring to determine the overallffect on the incidence of AV access thrombosis and abandonment.96
heir review of 9 studies (1363 patients) showed no significant overall
urr Probl Surg, July 2011 477

bpoat
tsiaqfifc
I
sWiwrrnbbcdn
piatdmg0r
4
enefit to surveillance followed by intervention. However, 3 studies (207atients) noted a 47% RR reduction in access thrombosis when a strategyf surveillance and intervention was specifically compared to observationlone. Based on these data, surveillance efforts may need to be targetedo specific patients at risk.The frequency of measurement is dependent on the patient’s propensity
o develop recurrent venous stenosis. Static flow pressure measurementshould be obtained with every treatment as they provide free, noninvasivenformation that is only useful when viewed over time. More detailedssessment of intra-access flow using tools may be obtained and trendeduarterly or more frequently in patients with recurrent problems. AVstula monitoring programs can be less aggressive in terms of intervalrequency because venous stenosis develops more slowly in AV fistulasompared to AV grafts.
ndications for Further Imaging or InterventionThe VAMP team should be charged with direct referral to corrective
ervices using an established algorithm and rational decision tree.100
aiting for additional physician assessment is typically not necessary nors it beneficial since the time delay to correction is usually associated withorse outcomes. The best approach for a VAMP team is to perform
outine longitudinal objective trend analysis that can prompt prospectiveeferral to an interventionalist. Single abnormal values are often related toeedle placement, vascular spasm, and other issues less likely to persist ore amenable to correction. Although pre-emptive intervention has noteen supported by prospective data, it appears to be a reasonable andost-effective approach. The significant morbidity associated with accessysfunction is unlikely to allow a truly blinded and controlled study in theear future.Verified abnormalities or trends in any of the monitoring or surveillancearameters previously discussed should prompt referral for access imag-ng and possible intervention. We recommend using cutoff objectiveccess flow rates when they drop to less than 600 mL/min in a graft or lesshan 400 mL/min in a fistula (flow rates are less helpful in the AV fistulasue to potential venous collateralization). Alternatively, a venous seg-ent static pressure to mean arterial pressure ratio greater than 0.5 in
rafts or fistulas or an arterial segment static pressure ratio greater than.75 in grafts should generate a referral if it is confirmed as a trend on
epeated measures.78 Curr Probl Surg, July 2011
SS
sBEcpcamtg
iseVdaeaa
M
spdsmTasa
alia
C
ummary of Vascular Access Monitoring andurveillanceThe main purpose for vascular access monitoring is to detect and correct
tenosis that may result in underdialysis or thrombosis of the AV access.oth occurrences are associated with significant morbidity and mortality.very access should be assessed for patency before each treatmentannulation. Education regarding AV access assessment, in particular thehysical examination, should be provided to the entire team, includingaregivers, trainees, and the patients themselves. An organized VAMPnd longitudinal data tracking should be instituted to follow trends andaintain continuous quality improvement (CQI). A thrombosis rate less
han 0.5 thrombotic episodes/patient-year at risk has been proposed as aoal by the National Kidney Foundation.29
At a minimum, AV access surveillance should include physical exam-nation and static venous pressure measurements. Direct measurement oftatic pressure should be made weekly or biweekly. Other indicators ofarly access dysfunction may also be tracked and discussed as part of theAMP in the medical record and with routine CQI. Robust prospectiveata in support of emerging and established technology for vascularccess monitoring do not currently exist. Although debate continues,arly referral and detection of patients for correction of stenosis throughppropriate intervention remains a goal worthy of a careful and rationalpproach.
aintenance of AV AccessAV access maintenance can affect the quality of life and ultimate
urvival of patients on hemodialysis. Interventions that preserve orrolong AV access function allow patients to continue life-sustainingialysis treatments, avoid the consequences of temporary catheters, andtay out of the hospital. Successful AV access maintenance programsust identify and effectively treat AV grafts and fistulas at risk for failure.he clinical examination and dialysis monitoring protocols usually triggerreferral for intervention as described in the previous section. This
ection discusses the treatment options for failing or ineffective AV graftsnd fistulas.Poor flow represents the most common reason for referring an AV
ccess for intervention. Determining the underlying cause of the flowimitation usually requires contrast fistulography to obtain completemaging from the arterial inflow to the central venous drainage. The
natomic picture provided by the fistulogram can be complemented withurr Probl Surg, July 2011 479
pspm
eatocrftovtteur
atdagIaibpspts
adfiI
4
hysiological insight obtained from access surveillance data or duplexonography. Although the requisite needle puncture classifies fistulogra-hy as invasive, it is usually combined with endovascular intervention,aking it both a diagnostic and a therapeutic procedure.The treatment of flow-limiting stenotic lesions engages in a never-
nding battle with intimal hyperplasia (IH). IH affects all forms of AVccess and can cause stenosis anywhere along the access circuit, includinghe anastomosis, along the course of the autologous fistula, venousutflow, and the central veins. Balloon angioplasty remains the mostommon form of treatment for IH-induced stenosis. Unlike atheroscle-otic disease, IH in the veins causes rubbery, fibrotic lesions that requireorceful dilatation with noncompliant, high-pressure balloons. Inflationimes of 2 to 3 minutes or longer may allow more vessel remodeling toccur and improve the immediate technical results. Unfortunately, theessel trauma incurred by this technique can trigger renewed IH, leadingo recurrent stenosis at the same location. Cutting balloon angioplasty wasouted as a method for controlling the dilation injury using an atherotomembedded in the balloon to score the fibrous lesion. This claim remainsnsupported as a recent study reported equivalent results for cutting andegular balloon angioplasty.101
Stenting can be useful when balloon angioplasty fails. As an implant-ble device, a stent can resolve elastic recoil and achieve immediateechnical success. Recurrent IH leading to in-stent restenosis limits theurability of stenting and explains why stents offer no significantdvantage over technically successful balloon angioplasty alone.52 Stentrafts consist of a prosthetic material covering the metal stent scaffolding.n theory, this prosthetic material could act as a barrier to tissue ingrowthnd decrease the risk of recurrent stenosis. Haskal and colleaguesnvestigated this hypothesis in their randomized trial of stent grafts vsalloon angioplasty for the treatment of venous outflow stenosis inrosthetic AV grafts. They found that patients treated with stent grafts haduperior access patency and longer freedom from reintervention com-ared to patients treated with balloon angioplasty alone.102 The results ofhis study may herald an expanded role for stent grafts at least in theituation of outflow stenoses in prosthetic AV grafts.Endovascular interventions have relegated surgery to second-line ther-
py for dysfunctional access. A stenotic lesion that completely resistsilation or rapidly recurs after endovascular treatment may be a candidateor surgical revision. Imaging of the entire flow circuit at the time ofntervention insures that the planned surgery addresses the culprit lesion.
n most cases, surgical options consist of patch angioplasty, interposition80 Curr Probl Surg, July 2011
gttrnip
V
Chhfsca
B
hbiland
toht(lbctpod
C
rafting, or jump grafting. Jump grafting excludes the stenotic segment athe cost of using up the more proximal vein(s). Patch angioplasty confineshe revision to the existing access by widening the area of stenosis. Theisk of recurrence may be higher after patch angioplasty because it doesot remove or exclude the local disease. The overall drawbacks of surgerynclude its invasiveness and the potential need for temporary catheterlacement.
ascular Access ComplicationsThe long-term success of hemodialysis depends on adequate AV access.omplications pose a constant threat and account for 15% to 20% ofospitalizations for patients with end-stage kidney disease who useemodialysis.37 The clinical impact of AV access complications rangesrom mild symptoms causing discomfort and inconvenience to cata-trophic conditions that endanger life and limb. Recognizing and treatingomplications can insure patient safety, improve quality of life measures,nd preserve AV access function.
leedingBleeding due to uremia can complicate vascular access surgery andemodialysis treatment. Although Morgagini recognized an associationetween kidney dysfunction and bleeding in 1764, the exact pathophys-ology remains unclear.103 The bleeding tendency in uremic patients mostikely results from multiple factors with platelet dysfunction, chronicnemia, and medication effects playing the most prominent roles. Aormal platelet count can, therefore, obfuscate an underlying functionalefect in the patient with ESRD.Normally, platelets adhere to exposed subendothelium, which triggers
heir activation and aggregation, culminating in the formation of ancclusive hemostatic plug. Uremia detracts from each step of thisemostatic cascade. Uremic platelets have decreased levels of glycopro-ein (GP) Ib and impaired binding of GP-IIb/IIIa to von Willebrand factorvWF), which decreases their ability to adhere to the subendothe-ium.104,105 Platelets from uremic patients fail to activate normallyecause they have less adenosine diphosphate (ADP) and serontininontent in their granules, and they release less ATP in response tohrombin.106 Uremia also distorts cytoskeletal proteins, which impairslatelet motility and aggregation.107 Overall, uremia undermines the rolef platelets in hemostasis by causing intrinsic platelet malfunction and
efective platelet–platelet and platelet–vessel wall interaction.urr Probl Surg, July 2011 481
pbtahas
uftbcad
pbfrpbRtbni
caumee
fiIlrr
4
Several studies point to anemia as an important determinant of therolonged bleeding time associated with uremia.108-110 Normally, redlood cells displace platelets to the periphery of the bloodstream so thathey are in close proximity to interact with the endothelium. In chronicnemia, the loss of red cell mass allows the blood elements to mix moreomogenously and platelets are evenly distributed in the bloodstream. Inddition to their rheologic effects, red blood cells also promote hemosta-is by releasing ADP and inactivating prostacyclin (a platelet inhibitor).Commonly used medications can contribute to ineffective hemostasis inremia. �-lactam antibiotics and cephalosporins accumulate in renalailure and interfere with ADP receptors and platelet membrane func-ion.111 Aspirin markedly prolongs the bleeding time in uremic patientsy a mechanism that appears to be distinct from its inhibition ofyclo-oxygenase. Among the anticoagulants, low molecular weight hep-rin and lepirudin are cleared by the kidneys and their doses can beifficult to titrate in patients with renal failure.112
Ensuring adequate hemodialysis, correcting chronic anemia, and stop-ing antithrombotic medications when feasible can minimize the risk ofleeding. Hemodialysis can be a two-edged sword: it improves plateletunction; however it may exacerbate bleeding if the dialysis sessionequires the use of anticoagulants. Raising the hematocrit to 30%romotes hemostasis by returning platelets to the periphery of theloodstream where they can more quickly interact with the endothelium.ecombinant human erythropoietin treatment plays an important role in
he treatment of chronic anemia for hemodialysis patients. In addition tooosting the hematocrit, recombinant human erythropoietin increases theumber of GP-IIb/IIIa receptors on platelets and enhances the thrombin-nduced phosphorylation of platelet proteins.105
Specific treatments to stop or prevent bleeding include desmopressin,ryoprecipitate, and estrogen. Desmopressin is a synthetic analog ofntidiuretic hormone that promotes the release of stored vWF.113 It issually given as a 0.3 �g/kg dose in 50 mL saline administered over 30inutes.114 Improved hemostasis occurs in approximately 1 hour; how-
ver, it has limited durability (4-6 hours) and repeat doses tend to be lessffective, thereby limiting its administration to emergent situations.115
Cryoprecipitate is a plasma derivative containing fibrinogen, vWF, andbronectin that has been used in the acute treatment of uremic bleeding.t has a rapid onset of action; however, its hemostatic effects usually lastess than 24 hours. Research on the effectiveness of cryoprecipitateemains scarce. One small study reported improved bleeding times and
educed bleeding complications in all 7 patients.116 A similar small82 Curr Probl Surg, July 2011
rsic
nadEdteh
ccsptbBsuwo
P
taamcccamt
cp
C
etrospective study reported that cryoprecipitate failed to achieve hemo-tasis in 3 of 5 patients with uremic bleeding.117 Inconsistent potency,nfectious risk, expense, and limited durability have relegated cryopre-ipitate to a second-line treatment for acute bleeding due to uremia.Estrogen therapy offers more sustained hemostatic control. An intrave-ous infusion of estrogen, 0.6 mg kg�1 d�1 for 4 to 5 days, starts to haven effect within 6 hours and provides improved hemostasis for up to 14ays.118 Oral estrogen therapy has a shorter duration of action of 5 days.strogen decreases bleeding risk by increasing platelet reactivity andecreasing nitric oxide generation by the endothelium.119 Estrogenherapy is equally effective in men and women. Because of inconsistentfficacy, estrogen is usually only used to treat chronic bleeding states thatave no clear option for definitive correction.The treatment of persistent bleeding at access sites depends on the
ircumstances. Needle hole bleeding with intact overlying skin can usually beontrolled with prolonged manual pressure or a hemostatic “figure of 8”titch with monofilament suture. If these measures fail, a percutaneouslylaced balloon can be inflated at the site of the bleeding to temporarilyamponade the hemorrhage. Preparations can then be made to exchange thealloon for an endoluminal stent graft or proceed to surgical revision.leeding associated with eroded skin or exposed conduit requires emergent
urgical intervention to excise the exposed conduit and reroute a new graftnder intact skin. Persistent bleeding that requires any form of interventionarrants evaluation for the underlying cause, which may include venousutflow obstruction, graft infection, or pseudoaneurysm.
seudoaneurysmPseudoaneurysms pose a thrombotic, infectious, and hemorrhagic risk
o patients receiving hemodialysis. Although pseudoaneurysms occur inutogenous AV fistulas, they are more common in prosthetic grafts withn estimated prevalence of 2% to 10%.120 A pseudoaneurysm usuallyanifests as a focal pulsatile mass. Duplex ultrasound scanning can
onfirm the diagnosis by demonstrating color flow within the mass andonnection to the access graft. Pseudoaneurysms that occur along theourse of the access graft typically represent puncture site injuries, whilenastomotic pseudoaneurysms usually result from infection. The treat-ent of a pseudoaneurysm depends on its etiology and location as well as
he type of access and clinical circumstances.Prosthetic graft degeneration combined with venous outflow obstruction
an lead to a cannulation site pseudoaneurysm. Expansion of the
seudoaneurysm causes necrosis of the overlying subcutaneous tissue andurr Probl Surg, July 2011 483
ssstsmwiswmSt
tavissptfapaottats
fclaTesp
4
kin resulting in multiple problems, including difficulty achieving hemo-tasis on needle withdrawal, spontaneous bleeding from cannulation sites,evere hemorrhage, and acute graft rupture. Treatment can vary accordingo the extent of the pseudoaneurysm and the condition of the overlyingkin. Small puncture site pseudoaneurysms can often be observed anday resolve without treatment. Enlarging pseudoaneurysms and thoseith compromised overlying skin warrant surgical intervention, which
nvolves pseudoaneurysm resection and interposition grafting around theite. In most cases, dialysis can continue through the uninvolved grafthile the new segment incorporates. A more extensive pseudoaneurysmay represent complete destruction of the anterior wall of the graft.urgical replacement in these cases will not allow continued dialysis
hrough the graft unless replacement is performed in stages.Stent graft placement offers an alternative to open surgery for the
reatment of AV graft pseudoaneurysms. Endovascular repair has theppeal of being able to exclude the pseudoaneurysm and address potentialenous outflow stenosis with one percutaneous intervention withoutnterrupting dialysis or requiring a temporary catheter placement. Severalmall series of endovascular therapy for pseudoaneurysms have appearedince the initial description in 1998.121 These reports document 100%rocedural success and excellent 30-day patency, which declines to 20%o 28% patency at 6 months.122,123 Durability remains an unresolved issueor stent graft interventions and has tempered some of the early enthusi-sm for this off-label technique. Stent grafts were not designed to beunctured by dialysis needles and several reports document stent damagend strut fracture from repeated cannulation.124 Stent grafts may not beptimal if there is a large pseudoaneurysm cavity with significant muralhrombus. Although the stent graft maintains access continuity, cannula-ion can be difficult due to the overlying pseudoaneurysm and itsssociated thrombus. In most cases, the limitations of endovascularherapy outweigh its advantages and it remains an inferior alternative tourgical revision.In autogenous fistulas, pseudoaneurysms may be difficult to distinguish
rom true venous aneurysms. Pseudoaneurysms generally occur withinannulation areas and result from repeated needle sticks in the sameocation, so-called “one site-itis.” Management involves abandoning therea and adhering to a rotating site or “rope ladder” cannulation strategy.he presence of a scab or extremely thin skin overlying the pseudoan-urysm mandates prompt intervention. Hemostasis may be tenuous in thiscenario and the patient is at risk for potentially fatal hemorrhage until the
seudoaneurysm is resected and the fistula is surgically revised.84 Curr Probl Surg, July 2011
soitmtcsh
I
faaitsfcemp5yt
etesnauianw
i
C
Diffuse enlargement of a long-standing autogenous AV fistula repre-ents a true aneurysm involving all layers of the access walls. If theverlying skin is intact and the aneurysm is free of layered thrombus,t will support continued dialysis and does not require intervention. Ifhe aneurysm causes obstructive problems from kinking or compro-ises the overlying skin, surgical revision may be required. In many cases,
he tortuous, aneurysmal area can be resected and continuity restored byreating an end-to-end anastomosis or interposition bypass between theegments. Diameter reduction procedures using a variety of techniquesave also reported good results and long-term durability.125
nfectionInfection ranks second only to thrombosis as the cause of AV access
ailure and follows cardiovascular disease as the leading cause of deathmong dialysis patients.126 Several factors conspire to make AV graftsnd fistulas vulnerable to infection. Uremia and renal failure causemmune dysfunction by impairing cellular immunity and reducing neu-rophil chemotaxis, phagocytosis, and bacterial killing. Immunosuppres-ion also results from conditions commonly associated with kidneyailure, including malnutrition, iron overload, and increased intracellularalcium. Hemodialysis itself poses a recurrent threat of infection sincevery session requires 2 needle punctures of the skin for access. Theicrobiology of access infections reflects the inherent risk in frequently
unctured subcutaneous AV grafts and fistulas. S. aureus accounts for0% to 70% of access infections followed by coagulase-negative staph-lococci and polymicrobial infections with multiple Gram-negative bac-eria.127
The diagnosis of hemodialysis access infection relies on the clinicalxamination. Explicit signs of infection include purulent drainage, a sinusract, or exposed access conduit. Localized findings of tenderness,rythema, and induration suggest an infection but may also occur in theetting of recent surgery or a cannulation site hematoma. Serial exami-ations and duplex ultrasound imaging may help differentiate an infectedccess from a hematoma or postsurgical fluid collection. The duplexltrasound examination can also help in treatment planning by ascertain-ng the full extent of the fluid collection.111 Indium-tagged imaging offerssensitive but nonspecific scan for infection. Inflammation from frequenteedle punctures and hematomas can generate false-positive results,hich limit the test’s accuracy.128
The management of access infections depends on several factors,
ncluding the type and functional status of the AV access, the extent ofurr Probl Surg, July 2011 485

ihaspssppacwr
1eatetcipIftolr
castpitosia
4
nfection, the bacterial etiology and the presenting symptoms. AV fistulasave the lowest rate of infections, and therefore, the least amount ofccumulated evidence comparing various treatment options. Cannulationite infections can be managed nonoperatively by stopping needleunctures at the site and resting the site. More extensive infections requireegmental ligation and resection. In some cases, the fistula can bealvaged by relocating the arterial anastomosis to a more proximal site orerforming an interposition autogenous bypass through clean tissuelanes.129 Fistula salvage should not be attempted for access infectionsssociated with bleeding or involving the arterial anastomosis. Theselinical scenarios generally require fistula ligation. All cases of infectionarrant broad spectrum antibiotic therapy for at least 6 weeks.130 The
esults of blood and tissue cultures can often refine the antibiotic choices.The incidence of infection for prosthetic AV grafts ranges from 3% to9%.120,131 Several clinical situations mandate complete or subtotal graftxcision, including systemic sepsis; graft occlusion; pseudomonas or otherggressive bacterial infection; the presence of fluid or purulence surroundinghe entire graft; and presence of an unincorporated graft. Complete graftxcision involves oversewing the outflow vein and removing the graft fromhe inflow artery. The arteriotomy at the site of the old anastomosis can belosed with an autogenous patch angioplasty. If the arterial anastomosis isntact, leaving a small cuff of prosthetic material on the artery to maintain itsatency and thereby avoid a potentially difficult dissection is acceptable.132
n cases of more severe infection with extensive tissue destruction, the onlyeasible option may be arterial ligation. Most patients can tolerate ligation ofhe radial artery or the brachial artery distal to the profunda brachial arteryrigin without requiring revascularization because of collateral flow. Thisimb will most likely not support a future AV access unless arterialeconstruction is eventually performed.Infection confined to a focal area along the body of the prosthetic graft
an be treated with segmental graft resection and bypass. The infectedrea of the bypass should be isolated with adhesive dressings beforeurgically exposing the incorporated prosthetic graft proximal and distalo the infected area. An interposition graft tunneled through clean tissuelanes restores graft continuity and preserves access patency. The bypassncisions should then be completely closed and covered before excisinghe infected portion of the graft through a separate incision. The successf segmental resection for graft infection depends on careful patientelection. Conditions that preclude the use of this treatment strategynclude systemic sepsis, aggressive bacterial species, and fluid tracking
round the entire graft.13386 Curr Probl Surg, July 2011
sisrgms
N
cbafpw
bNtcpssawhmac
pfitAafs
d
C
Nonfunctional grafts that were abandoned in the past retain theirusceptibility to infection and may be overlooked or ignored during thenitial diagnostic evaluation. Infection of a thrombosed prosthetic grafthould be suspected in the setting of unexplained systemic infection andesistance to epoeitin therapy. An 111indium-tagged white blood cell orallium scan can localize the abandoned access graft as site of inflam-ation. Removal of the infected graft provides definitive treatment and
hould restore the responsiveness to epoeitin.52
oninfectious Fluid CollectionsHematomas, seromas, and lymphoceles represent rare, relatively benign
omplications of AV access construction. Their clinical presentation cane similar to other more serious access complications, such as pseudo-neurysm, abscess, and infection. Successful management of nonin-ectious fluid collections depends on making an accurate diagnosis,reventing secondary infection, and proceeding with interventionhen appropriate.The clinical history of a difficult needle cannulation or prolongedleeding after decannulation supports the diagnosis of a hematoma.ewly created autogenous AV fistulas have an increased risk of hema-
oma formation because the walls of the vein are still thin. Likewise, earlyannulation (�2 weeks) of prosthetic AV grafts can lead to hemostaticroblems because the graft has not had time to incorporate into theurrounding subcutaneous tissue. Technical errors in needle cannulation,uch as posterior wall puncture, can be difficult to control with pressurend can lead to a hematoma. By checking for a persistent communicationith the AV access, a duplex ultrasound can distinguish between aematoma and a pseudoaneurysm. The extravasated blood causes ecchy-osis and soft tissue edema. Management usually consists of observation
nd resting the AV access if infiltration from the hematoma makes needleannulation extremely difficult.Seromas accumulate when serum-like fluid transudates through arosthetic graft. The persistent, sterile fluid is confined by a nonsecretory,brous pseudomembrane surrounding the graft.134 In the typical presen-
ation, a painless fluid collection slowly enlarges in the first month afterV graft placement. The collection usually centers on the arterial
nastomosis and occurs more commonly in upper arm grafts compared toorearm grafts.135 All prosthetic materials and AV graft configurations areusceptible to seroma formation.Several management options for a seroma have been reported with varying
egrees of success. Aspiration of the seroma can be useful to confirm theurr Probl Surg, July 2011 487
dabstt
tLoLnosll
I
pchsspsoatces
oupipgcB
4
iagnosis and evaluate for infection. When applied as a therapeutic strategy,spiration has the same clinical success rate as observation alone and haseen associated with an 8% rate of secondary infection or graft thrombo-is.136 Seroma excision and segmental replacement of the graft appears to behe most effective treatment. A different type of prosthetic should be tunneledhrough new tissue planes if possible.130
Disruption of the lymphatic channels during surgical dissection orunnel formation can result in lymphocele, lymphorrhea, or lymphedema.ymphoceles contain clear fluid and may be difficult to distinguish fromther fluid collections. Many small lymphoceles resolve spontaneously.ymphoceles that expand, communicate with the access, or drain exter-ally (lymphorrhea), respond to surgical intervention. Identifying andbliterating the source of the lymphatic drainage appears to be the besturgical strategy; however, the reported experience is limited.133 Diffuseymphedema of the extremity usually improves with time, elevation, andocalized compression in recalcitrant cases.
schemiaConstruction of an upper extremity AV access alters the blood flowatterns to the forearm and hand. Low resistance in the venous outflowauses reversal of flow in a portion of the arterial system. Most patientsave sufficiently large inflow arteries to compensate for this physiologicalteal phenomenon. Although pulse deficits and low digital blood pres-ures can be detected in 80% of patients after AV access, only 10% ofatients have any symptoms, most of which are mild and resolvepontaneously within several weeks.137,138 Symptomatic arterial stealccurs when blood flow is shunted from the tissue beds distal to therterial anastomosis and usually occurs in combination with 1 or more ofhe following clinical scenarios: arterial inflow stenosis; increased vas-ular resistance distal to the fistula; or increased access size leading toxtremely high access flow rates. Failure to recognize and treat arterialteal can lead to limb-threatening ischemia or permanent disability.Preoperative evaluation for risk factors and careful surgical planningffer the best strategies for preventing arterial steal. Impaired or marginalpper extremity arterial perfusion represents the underlying condition thatuts patients at risk for developing arterial steal. More susceptible groupsnclude women, elderly patients, diabetics, and patients with multiplerevious access procedures on the ipsilateral limb.139 Prosthetic AVrafts with brachial artery inflow have a higher risk for arterial stealompared to autogenous AV fistulas with a more distal donor artery.140
efore deciding on a surgical plan, all patients should have blood pressure
88 Curr Probl Surg, July 2011
mAifpupdte
1ovirosAppntm
pewelirdifPIlp
w
C
easurements in both upper extremities and an Allen’s test of both hands.blood pressure differential of more than 20 mm Hg suggests an arterial
nflow lesion that would need to be addressed if the limb were to be usedor access. An Allen’s test indicating an incomplete palmar arch shouldreclude creating access that is based off the radial artery unless thenderlying problem can be corrected first. Routine testing beyond thehysical examination does not help in predicting which patients willevelop arterial steal. More detailed imaging and noninvasive examina-ions should therefore be reserved for patients with abnormal physicalxamination findings.More than one half of patients who develop arterial steal do so withinmonth of the access creation. The clinical examination forms the basis
f diagnosis for arterial steal. Signs and symptoms of arterial steal canary in severity from a painless cool hand to muscle weakness orschemic tissue loss. On physical examination, an absent radial pulseepresents a nonspecific finding. Mattson noted an absent radial pulse inne third of 180 accesses, only 7 of which went on to develop arterialteal.141 Decreased hand perfusion that improves with compression of theV access provides more convincing and reliable evidence for theresence of steal. Several objective tests, such as color duplex ultrasound,hotoplethysmography, and pulse oximetry, can help confirm the diag-osis and differentiate arterial steal from conditions with similar symp-oms, such as nerve compression, tissue acidosis, VH, and ischemic
onomelic neuropathy (IMN).The initial management of arterial steal varies with the clinicalresentation. Tordoir and coworkers proposed standardizing limb isch-mia into the following stages139: stage I: mild—pale, blue, or cold handithout pain; absent radial pulse; stage II: moderate—pain during
xercise or hemodialysis; stage III: severe—pain at rest; and stage IV:imb threatening—ulcers, necrosis, gangrene. Patients with stage Ischemia can be observed with the expectation that the symptoms oftenesolve or stabilize without intervention. Stage II ischemia can quicklyeteriorate into more severe ischemia causing permanent damage. Non-nterventional management for these patients requires frequent, carefulollow-up to ensure that the patient’s symptoms are stable or improving.atients with progressive pain or numbness and patients with stage III andV ischemia require prompt intervention. Delaying intervention for asittle as 1 week has been associated with poor results and failure of theatient’s symptoms to improve.138
The ideal intervention for treating arterial steal restores hand perfusion,
hile preserving the function of the AV access. The choice of interven-urr Probl Surg, July 2011 489
tspirioct
saaiwshaipdian
i2oapimiabb
pAps
4
ion depends on several factors, including the cause of ischemia; theeverity of symptoms; the alternatives for dialysis access; and theatient’s medical comorbidities. Ligation of the AV access can be appliedn any clinical scenario and offers the most direct and reliable means ofestoring perfusion to the distal extremity and hand. Although it solves themmediate problem of ischemia, ligation creates the impending problemf establishing a new long-term AV access. This situation can behallenging because patients may have limited access sites remaining andhe risk of ischemia resurfaces with any future AV constructions.Banding offers a conceptually straightforward treatment for arterial
teal. Deliberately narrowing the AV graft just beyond the arterialnastomosis increases the resistance, thereby decreasing AV access flownd increasing perfusion to the distal extremity. The challenge of bandingnvolves determining how much narrowing will improve distal perfusionithout predisposing the AV access to thrombosis. Although a variety of
urgical techniques for banding have been proposed, the underlyingemodynamics of the procedure undermine its chance of success. Wixonnd colleagues reported that in large-caliber AV accesses, blood flow isndependent of access resistance and diameter. Flow is determinedrimarily by the relative resistances of the peripheral vascular bed, theonor artery, and the collateral circulation.142 Therefore, to limit flow byncreasing resistance, the conduit must be narrowed sufficiently to convert
large, flow-independent access to a small, flow-dependent access, theatural history of which is to thrombose.Distal revacularization and interval ligation (DRIL) has emerged as the
ntervention of choice for most cases of arterial steal. This procedure hascomponents: a bypass around the AV access anastomosis and ligation
f the native artery (most commonly the brachial artery) distal to the AVccess and proximal to the distal anastomosis of the bypass.143 The DRILrocedure is depicted in Fig 13. By acting as a low resistance collateraln parallel, the bypass reduces peripheral and systemic resistance andinimizes the ratio between systemic and access resistance. This change
n resistance decreases the proportion of blood flow diverted into theccess and increases the fraction flowing into the periphery. Ligating therachial artery further augments distal perfusion by eliminating reversedlood flow into the AV access.An arteriogram and catheter-directed pressure measurements facilitatereoperative planning for a DRIL procedure. The high capacitance of theV access creates an abrupt pressure dropoff that results in an area of lowressure in the adjacent proximal brachial artery. This so-called “pressure
ink” may be limited to the perianastomotic brachial artery or extend for90 Curr Probl Surg, July 2011
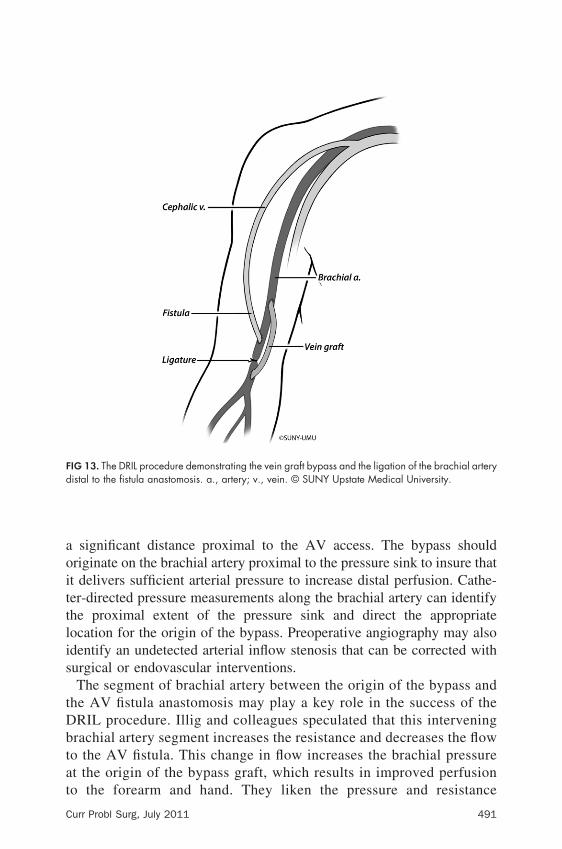
aoittlis
tDbtat
Fd
C
significant distance proximal to the AV access. The bypass shouldriginate on the brachial artery proximal to the pressure sink to insure thatt delivers sufficient arterial pressure to increase distal perfusion. Cathe-er-directed pressure measurements along the brachial artery can identifyhe proximal extent of the pressure sink and direct the appropriateocation for the origin of the bypass. Preoperative angiography may alsodentify an undetected arterial inflow stenosis that can be corrected withurgical or endovascular interventions.The segment of brachial artery between the origin of the bypass and
he AV fistula anastomosis may play a key role in the success of theRIL procedure. Illig and colleagues speculated that this interveningrachial artery segment increases the resistance and decreases the flowo the AV fistula. This change in flow increases the brachial pressuret the origin of the bypass graft, which results in improved perfusion
IG 13. The DRIL procedure demonstrating the vein graft bypass and the ligation of the brachial arteryistal to the fistula anastomosis. a., artery; v., vein. © SUNY Upstate Medical University.
o the forearm and hand. They liken the pressure and resistance
urr Probl Surg, July 2011 491
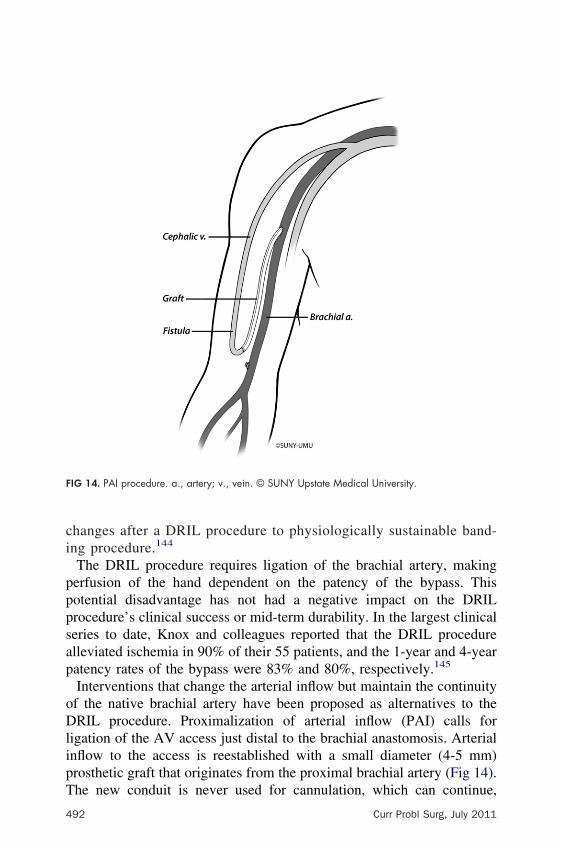
ci
pppsap
oDlipT
F
4
hanges after a DRIL procedure to physiologically sustainable band-ng procedure.144
The DRIL procedure requires ligation of the brachial artery, makingerfusion of the hand dependent on the patency of the bypass. Thisotential disadvantage has not had a negative impact on the DRILrocedure’s clinical success or mid-term durability. In the largest clinicaleries to date, Knox and colleagues reported that the DRIL procedurelleviated ischemia in 90% of their 55 patients, and the 1-year and 4-yearatency rates of the bypass were 83% and 80%, respectively.145
Interventions that change the arterial inflow but maintain the continuityf the native brachial artery have been proposed as alternatives to theRIL procedure. Proximalization of arterial inflow (PAI) calls for
igation of the AV access just distal to the brachial anastomosis. Arterialnflow to the access is reestablished with a small diameter (4-5 mm)rosthetic graft that originates from the proximal brachial artery (Fig 14).
IG 14. PAI procedure. a., artery; v., vein. © SUNY Upstate Medical University.
he new conduit is never used for cannulation, which can continue,
92 Curr Probl Surg, July 2011
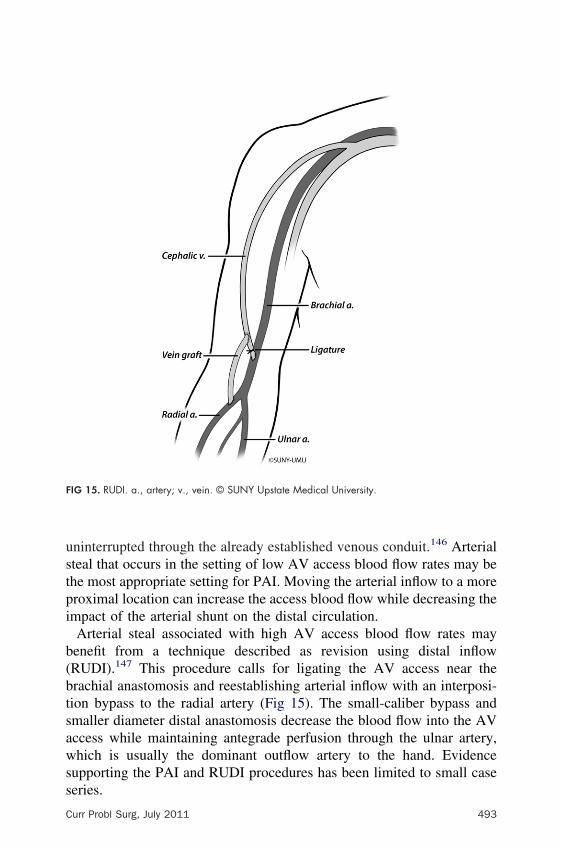
ustpi
b(btsawss
F
C
ninterrupted through the already established venous conduit.146 Arterialteal that occurs in the setting of low AV access blood flow rates may behe most appropriate setting for PAI. Moving the arterial inflow to a moreroximal location can increase the access blood flow while decreasing thempact of the arterial shunt on the distal circulation.Arterial steal associated with high AV access blood flow rates mayenefit from a technique described as revision using distal inflowRUDI).147 This procedure calls for ligating the AV access near therachial anastomosis and reestablishing arterial inflow with an interposi-ion bypass to the radial artery (Fig 15). The small-caliber bypass andmaller diameter distal anastomosis decrease the blood flow into the AVccess while maintaining antegrade perfusion through the ulnar artery,hich is usually the dominant outflow artery to the hand. Evidence
upporting the PAI and RUDI procedures has been limited to small case
IG 15. RUDI. a., artery; v., vein. © SUNY Upstate Medical University.
eries.
urr Probl Surg, July 2011 493
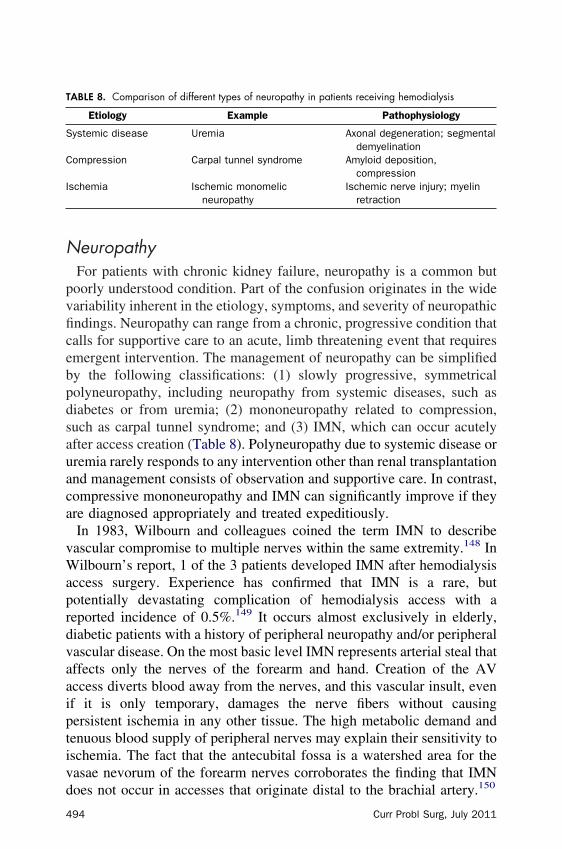
N
pvficebpdsauaca
vWaprdvaaiptivd
T
S
C
I
4
europathyFor patients with chronic kidney failure, neuropathy is a common butoorly understood condition. Part of the confusion originates in the wideariability inherent in the etiology, symptoms, and severity of neuropathicndings. Neuropathy can range from a chronic, progressive condition thatalls for supportive care to an acute, limb threatening event that requiresmergent intervention. The management of neuropathy can be simplifiedy the following classifications: (1) slowly progressive, symmetricalolyneuropathy, including neuropathy from systemic diseases, such asiabetes or from uremia; (2) mononeuropathy related to compression,uch as carpal tunnel syndrome; and (3) IMN, which can occur acutelyfter access creation (Table 8). Polyneuropathy due to systemic disease orremia rarely responds to any intervention other than renal transplantationnd management consists of observation and supportive care. In contrast,ompressive mononeuropathy and IMN can significantly improve if theyre diagnosed appropriately and treated expeditiously.In 1983, Wilbourn and colleagues coined the term IMN to describeascular compromise to multiple nerves within the same extremity.148 Inilbourn’s report, 1 of the 3 patients developed IMN after hemodialysis
ccess surgery. Experience has confirmed that IMN is a rare, butotentially devastating complication of hemodialysis access with aeported incidence of 0.5%.149 It occurs almost exclusively in elderly,iabetic patients with a history of peripheral neuropathy and/or peripheralascular disease. On the most basic level IMN represents arterial steal thatffects only the nerves of the forearm and hand. Creation of the AVccess diverts blood away from the nerves, and this vascular insult, evenf it is only temporary, damages the nerve fibers without causingersistent ischemia in any other tissue. The high metabolic demand andenuous blood supply of peripheral nerves may explain their sensitivity toschemia. The fact that the antecubital fossa is a watershed area for theasae nevorum of the forearm nerves corroborates the finding that IMN
ABLE 8. Comparison of different types of neuropathy in patients receiving hemodialysis
Etiology Example Pathophysiology
ystemic disease Uremia Axonal degeneration; segmentaldemyelination
ompression Carpal tunnel syndrome Amyloid deposition,compression
schemia Ischemic monomelicneuropathy
Ischemic nerve injury; myelinretraction
oes not occur in accesses that originate distal to the brachial artery.150
94 Curr Probl Surg, July 2011

afedtppcipDrfiiEtnb
ilihcbupfpwc
B
P
A
C
Symptoms of IMN usually start immediately after AV access surgerynd include pain, weakness, or paralysis of the muscles of the hand andorearm. Physical examination demonstrates sensory and motor loss thatqually involves the radial, median, and ulnar nerves. In the classicescription of IMN, the hand is warm with a palpable radial pulse andhere are no signs of ischemia. In practice, physical findings at the initialresentation can blur the distinction between IMN and arterial steal. Someatients with IMN have mild manifestations of distal ischemia, includingold fingers and an absent radial pulse. Sensorimotor loss may bencorrectly attributed to the after effects of regional anesthesia or patientositioning, further confusing and delaying the diagnosis of IMN.151
iagnostic testing can play a useful role if the diagnosis of IMN is noteadily apparent based on the characteristic clinical scenario and physicalndings. Normal creatine phosphokinase values and digital pressure
ndex greater than 0.3 support the diagnosis of IMN over arterial steal.lectromyographic findings in IMN demonstrate severe, acute denerva-
ion of all upper limb nerves. The denervation is more severe distally andormalizes proximally, implicating a more widespread process than coulde explained by a single-site infarction in a proximal nerve trunk.152
Successful treatment of IMN requires immediate correction of theschemic insult to the nerves of the forearm and hand. In most cases,igation of the fistula represents the most expeditious and acceptedntervention; however, successful techniques for revision of the fistulaave been described in case reports.153 In patients with IMN, early nerveonduction studies demonstrate that acute conduction blocks are causedy retraction of the myelin from the nodes of Ranvier. Myelin retraction,nlike demyelination, is a potentially reversible process if the ischemia isromptly corrected.154 Left untreated, IMN progresses to completeunctional loss of the hand and forearm and severe chronic pain. Evenrompt fistula ligation may not completely resolve the pain and muscleeakness of IMN.155 These patients may benefit from ongoing supportive
Symptoms Pattern Treatment
urning pain in feet; impairedsensation
Symmetrical Kidney transplant
ain, numbness, tingling (mediannerve distribution)
Unilateral orbilateral
Surgical decompression (carpaltunnel release)
cute pain, sensory loss (all 3nerves), weakness
Unilateral (sideof access)
AV access ligation
are measures, including pain management, range of motion exercises,
urr Probl Surg, July 2011 495
aip
ttoppntfiwcCtpc
pdatpdifschtanl
tifadp
4
nd desensitization therapy. Efforts to prevent IMN should focus ondentifying patients at risk and locating AV access inflow as distally asossible.An association between hemodialysis and nerve compression neuropa-
hy has been recognized for decades.156 Median nerve entrapment (carpalunnel syndrome) is the most common compressive neuropathy andccurs 10 times more frequently in dialysis patients compared to theopulation at large. Patients typically complain of pain, numbness, andaresthesias in the distribution of the median nerve that is more severe atight and during dialysis. Atrophy of the thenar muscles is a late findinghat can manifest as the inability to pinch between the thumb and indexnger. The likelihood of developing carpal tunnel syndrome increasesith the time spent on dialysis. After 5 years of dialysis the incidence of
arpal tunnel syndrome has been reported to be as high as 50%.157
oexisting systemic neuropathy can make the clinical diagnosis of carpalunnel syndrome difficult. In these cases, electrodiagnostic studies haveroven to be accurate adjunctive tests to differentiate between nerveompression mononeuropathy and systemic polyneuoropathy.158
Several factors can contribute to median nerve compression in dialysisatients and the pathogenesis of this condition has not been completelyefined. The failure of hemodialysis to clear �2-micorglobulin results inccumulation of �-amyloid in periarticular structures, including the carpalunnel. Significant �-amyloid accumulation typically occurs after a latenteriod of 6 to 8 years, which is consistent with the time for patients onialysis to develop carpal tunnel syndrome.159 Another hypothesismplicates the presence of an upper extremity AV access as a contributingactor to nerve compression. The AV access may create local conditions,uch as VH, hematoma formation, and nerve ischemia that result in nerveompression. Bicknell and colleagues questioned the validity of thisypothesis. They found that abnormal nerve function was independent ofhe side of the AV access and was just as common in peritoneal dialysiss it was in hemodialysis, suggesting that the development of compressiveeuropathy reflects a greater influence of systemic factors as opposed toocal conditions.160
Treatment of carpal tunnel syndrome involves transection of theransverse carpal ligament to decompress the median nerve. Surgicalntervention generally provides relief of pain and paresthesias. Motorunction represents a late manifestation of disease that rarely improvesfter decompression. Hirasawa and colleagues reported that surgicalecompression resulted in “good” relief of pain in 81%, relief of
aresthesias in 51%, and improvement in grip strength in 8%.161 Patients96 Curr Probl Surg, July 2011
wrrd(Safu
uApnosdlaswa
V
voAevapth
pvwvla
C
ith preoperative symptoms for more than 2 years had the poorestesponse to intervention. These findings emphasize the need for earlyecognition and treatment of nerve compression before it causes motorysfunction or permanent nerve damage. Ulnar nerve compressionGuyon’s syndrome) has also been reported in hemodialysis patients.162
ymptoms include pain and sensory loss in the ulnar distribution as wells weakness in abduction and adduction of the extended digits and weakorceful grasping. Treatment consists of decompression by transecting thelnar tunnel at the wrist.More than 50% of dialysis patients suffer from polyneuropathy due toremia, diabetes, or both.163 Although it is not a direct complication ofV access, polyneuropathy can delay intervention for conditions that areotentially correctable with surgery, including ischemic and compressiveeuropathy. Symptoms of polyneuropathy include burning dysesthesiasr lancinating pain and sensorimotor loss, which typically occur in aymmetrical pattern in the distal extremities. Physical examinationemonstrates loss of vibratory, light touch, and position sensation in theower extremities. Both uremic and diabetic neuropathy can affectutonomic nerves; however, diabetic patients are more likely to beymptomatic due to autonomic dysfunction. Electrodiagnostic tests,hich demonstrate slowing of sensory nerve conduction velocities, can
ssist with the diagnosis of polyneuropathy.
enous HypertensionVH develops when the arterial inflow from an AV access exceeds theenous outflow. In most cases, VH occurs in the setting of venous outflowbstruction and the 2 conditions share a strong association. A functionalV access can sustain a 10-fold increase in the arterial flow volume to the
xtremity.164 The combination of increased arterial inflow and obstructedenous outflow overwhelms the extremity’s compensatory mechanismsnd creates significant venous back pressure. This elevated venous backressure results in the clinical consequences of VH and outflow obstruc-ion, which can include extremity edema, venous reflux, inadequateemodialysis, and access failure.Venous obstruction is the most common condition that complicates thelacement of an upper extremity AV access. The sheer number of centralenous instrumentations performed on dialysis patients directly correlatesith the high incidence of venous stenosis and obstruction. All centralenous devices, including dialysis catheters, pacemaker and defibrillatoreads, and peripherally inserted central catheters lines, stimulate fibrosis
nd IH by the repeated trauma of the catheter contacting the vein wall.urr Probl Surg, July 2011 497
Tahcvoav
isamDvpmc
cc1geu
sSbfonceo
epmfla
4
he turbulence and vibration created by an ipsilateral extremity AVccess exacerbates the injury. Although subclavian vein catheters pose theighest risk for developing subsequent stenosis (50% incidence), anyatheter in any vein can cause venous stenosis or occlusion.165 Patenteins quickly become a scarce commodity among dialysis patients. Lossf a central draining vein can lead to abandonment of the extremity forny future AV access procedures, including placement of new centralenous catheters.Central venous stenosis or occlusion can be clinically silent, especially
n the absence of AV access flow. Before construction of an AV access,cars on the chest or arm may be the only clues to previous catheter usend subclinical venous obstruction. Ideally, these patients should have aore detailed imaging evaluation before undergoing AV access surgery.uplex ultrasound rarely provides a definitive assessment of the centralenous system and venography serves as a useful adjunct. If detectedreoperatively, the presence of central venous occlusion precludes place-ent of an ipsilateral extremity AV access unless the occlusion can be
orrected.Increased arterial inflow from a functional AV access can unmask
entral venous stenosis leading to VH. The symptoms of VH can belassified according to the following scale: grade 0, no symptoms; grade, mild symptoms, including discoloration and minimal extremity edema;rade 2, moderate symptoms of intermittent discomfort and severedema; grade 3, severe pain, edema, hyperpigmentation, and venouslceration.166
Edema represents the predominant symptom of VH and the nature andeverity of edema depends on the site of the venous obstruction.ubclavian vein stenosis or occlusion causes edema of the extremity andreast, while brachiocephalic vein stenosis impedes blood flow from theace as well as the upper extremity. Bilateral brachiocephalic veinbstructions or occlusion of the SVC can cause SVC syndrome. Facial,eck, and bilateral upper extremity edema, dyspnea, mental statushanges, and visual problems characterize SVC syndrome, which can bextremely disabling and even fatal if soft tissue edema causes airwaybstruction.167
Extremity edema due to VH can progress in a similar fashion to lowerxtremity chronic venous insufficiency. Physical findings include hyper-igmented, thickened, and indurated skin. Severe, long-standing casesay progress to ulceration. Venous outflow obstruction also diverts bloodow into patent venous tributaries, which results in incompetent valves
nd venous reflux. This flow pattern mirrors a common complication of98 Curr Probl Surg, July 2011
sbmefi
dpnofawwwtccdedi
fccibtapThoNh
isAt
C
ide-to-side fistulas, which can develop high volume retrograde flow. Inoth situations, the venous reflux adds to distal edema, which is usuallyost prominent in the index, middle, and ring fingers in the case of an
nd-to-side fistula and in the thumb and index finger in side-to-sidestulas.168
The time course of edema formation can determine the optimaliagnostic strategy. In the first 2 weeks after AV access surgery, mostatients experience mild limb edema. Whether this edema represents theormal postoperative course, a perioperative complication (hematoma),r VH can sometimes be difficult to determine. Duplex ultrasound isavored over contrast fistulography for imaging a newly created AVccess. A duplex ultrasound examination avoids needle cannulation,hich can damage a thin-walled vein and does not require giving contrastith patients who have yet to start dialysis. Edema that persists beyond 2eeks signifies central venous stenosis in approximately 25% of pa-
ients.169 In these patients, a fistulogram proves to be a superior imaginghoice compared to duplex ultrasound, which cannot directly evaluate theentral veins. Likewise, patients with long-standing AV access whoevelop arm swelling or elevated venous pressures on dialysis should bevaluated with fistulography. Extensive collateral vein development canecrease the accuracy of the velocity and color flow measurements usedn duplex imaging.Preventing VH begins by recognizing and minimizing the risk factors
or venous obstruction. In patients with renal insufficiency or failure,entral venous catheters of any kind should be avoided. Lacson andolleagues advocate the dual philosophy of “fistula first and catheter last”n response to the recent increase in catheter use that appears to be ayproduct of the fistula-promoting initiatives.170 Table 9 summarizesheir recommendations. Achieving the goal of less than 10% catheter uset the initiation of dialysis will require better adherence to theserinciples. In 2008, 30% of patients initiated dialysis with a catheter.124
he preoperative assessment for AV access placement should solicit aistory of past catheter use and identify physical signs of venousbstruction, including arm edema and prominent superficial veins. TheFK-KDOQI guidelines recommend venography for patients with aistory of an ipsilateral subclavian vein catheter.The fundamental problem of VH is excess arterial inflow coupled with
nadequate venous outflow. Treatment of VH must address at least oneide of this unbalanced equation. Treating excess arterial inflow requiresV access ligation, making it an unacceptable option in most cases. Most
reatment options target the relief of venous outflow obstruction. Endo-
urr Probl Surg, July 2011 499

vmOctt
viaUemrdhtto
irar
T
E
M
V
A
“
A
AC
5
ascular interventions have an acceptable technical success rate andediocre durability that can be improved with regular reintervention.pen surgery offers a potentially durable venous reconstruction at the
ost of a more invasive procedure. Well-established guidelines for thereatment of VH do not exist and the clinical scenario usually determineshe choice of therapy.Endovascular therapy offers a minimally invasive method of alleviatingenous outflow obstruction. The technical success of endovascularntervention depends on the ability to cross the stenosis or occlusion with
wire followed by balloon angioplasty to dilate the obstructed vein.nlike atherosclerotic arterial disease, stenotic venous lesions consist of
ndothelial hyperplasia and fibrous tissue.171 These histologic featuresay explain why venous stenoses tend to resist balloon angioplasty and
ecoil after dilation. Intravascular ultrasound performed after angioplastyemonstrated significant elastic recoil in 64% of patients.172 The use ofigh-pressure, noncompliant balloons can overcome some of the resis-ance to dilation. Selective stenting after balloon angioplasty attempts toreat the elastic recoil and may improve the immediate technical successf the procedure.Multiple studies confirm that endovascular therapy achieves excellent
nitial technical success, mediocre short-term primary patency, andeasonable mid-term-assisted patency. The initial success of balloonngioplasty for central venous stenosis ranges from 70% to 100%. A wide
ABLE 9. Conclusions of recommendations for “fistula first, catheter last”
Recommendation Rationale
arly referral to vascular accesssurgeon; (CKD Stage 4; GFR�30 mL/min)
Allow time for permanent AV access placement beforeinitiation of dialysis
ultidisciplinary team Establish timeline for catheter removal; insure activeparticipation of all dialysis caregivers; track clinicaloutcomes
ascular access coordinator Facilitate communication and planning between dialysiscenter, nephrologist, surgeon, and hospital
V fistula reevaluation 4-6 wkspostop
Determine maturation vs need for intervention
Bridge” therapy Peritoneal dialysis or AV grafts to avoid use of centralvenous catheters
V fistula maintenance Cannulation training, monitoring, and surveillance toprolong survival of existing AV fistulas
dapted with permission from Lacson et al.170
KD, chronic kidney disease; GFR, glomerular filtration rate; AV, arteriovenous.
ange of midterm patency results have been reported; however, most
00 Curr Probl Surg, July 2011
sR1srprifi7
ssadtIba1sssiFp
T
danuolpi
ibb
C
tudies document a primary patency of 60% to 70% at 6 months.173
epeat intervention can achieve symptomatic relief in 86% of patients atyear.174 The addition of stenting can increase the initial technical
uccess to 90% to 100%. Whether stenting improves mid-term outcomesemains unclear. Most studies have not demonstrated significantly betterrimary patency rates for stenting.175 Stents can trigger IH, causingestenosis at the shoulder of the stent or within the stent itself. Repeatntervention after stenting may be required in 62% of patients within therst 12 months and the assisted patency after stenting ranges from 46% to6%.176,177
Surgical options are tailored to the location of the lesion and the outflowources. Direct repairs reconstruct the SVC with an autogenous (spiraledaphenous or femoral vein graft) or prosthetic bypass to the righttrium.178,179 Although these procedures have proven to be effective andurable, the need for a thoracotomy and the associated morbidity limitsheir widespread use. Lesions of the central subclavian vein (medial to theJ) can be treated without a thoracotomy using an IJ to IJ crossoverypass.180 Likewise, subclavian vein lesions lateral to the IJ can beddressed with an extrathoracic IJ vein turndown to subclavian vein (Fig6) or an interposition subclavian to IJ vein bypass.181 The results ofurgical therapy come from relatively small case series. Most of thetudies report excellent clinical success rates with resolution of armwelling and preservation of the AV access. Mid- and long-term durabil-ty tends to reflect the results of interval interventions to maintain patency.or central venous reconstructions, the 4-year patency was 50% withrosthetic bypasses and 90% with autogenous conduits.182,183
hrombosisFrom a patient perspective, thrombosis represents one of the mostreaded complications. It is the most common cause of AV access lossnd even when successfully treated thrombosis interrupts routine dialysis,ecessitates invasive procedures, and often leads to hospitalization.184 Annderlying stenosis due to IH precipitates thrombosis in more than 85%f patients, highlighting the role of access flow surveillance.185 Other,ess common causes of thrombosis include hypotension, external com-ression, arterial inflow stenosis, pseudoaneurysm, and hypercoaguabil-ty.Thrombosis mandates treatment as quickly as possible. Delaying
ntervention allows the thrombus to grow and increases the contact timeetween the thrombus and the vessel wall. Thrombectomy procedures
ecome more difficult and less durable as time passes and this increasesurr Probl Surg, July 2011 501
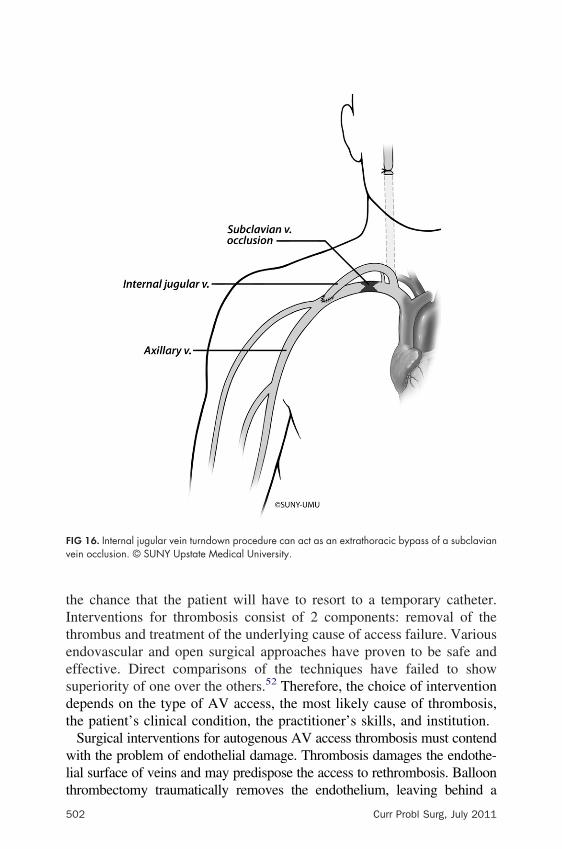
tIteesdt
wlt
Fv
5
he chance that the patient will have to resort to a temporary catheter.nterventions for thrombosis consist of 2 components: removal of thehrombus and treatment of the underlying cause of access failure. Variousndovascular and open surgical approaches have proven to be safe andffective. Direct comparisons of the techniques have failed to showuperiority of one over the others.52 Therefore, the choice of interventionepends on the type of AV access, the most likely cause of thrombosis,he patient’s clinical condition, the practitioner’s skills, and institution.Surgical interventions for autogenous AV access thrombosis must contendith the problem of endothelial damage. Thrombosis damages the endothe-
ial surface of veins and may predispose the access to rethrombosis. Balloon
IG 16. Internal jugular vein turndown procedure can act as an extrathoracic bypass of a subclavianein occlusion. © SUNY Upstate Medical University.
hrombectomy traumatically removes the endothelium, leaving behind a
02 Curr Probl Surg, July 2011
pdcIpsfa
bmdbpctpt6oy
belrssdtacpavp
mwso
C
otentially thrombogenic surface. This result probably accounts for theisappointing short-term outcomes achieved by surgical thrombectomy inombination with open or endovascular correction of an underlying stenosis.nitial technical success ranges from 50% to 70% and short-term primaryatency drops to 50% in small case series.186 Despite these modest results,urgical thrombectomy may be the preferred technique for thrombosis of aorearm AV fistula due to juxta-anastomotic stenosis. In these cases,nastomotic relocation can salvage the access.Endovascular therapy offers a relatively nontraumatic method of throm-us removal. Infusion of thrombolytics and a variety of percutaneousechanical thrombectomy devices can remove the thrombus without
irect endothelial contact. The entire procedure can remain percutaneousy treating the underlying stenosis with balloon angioplasty and/or stentlacement. By causing less trauma to the endothelium, this approachould, theoretically, translate into improved patency. In practice, thisechnique still suffers from poor primary patency results with a 6-monthrimary patency of 19% to 38% in reported case series. Repeat interven-ions have achieved a reasonable secondary patency of 74% and 69% atand 12 months, respectively.187 Convincing evidence to support the use
f more costly percutaneous thrombectomy devices instead of thrombol-sis and balloon angioplasty alone does not exist yet.Although prosthetic AV grafts thrombose more frequently, they have aetter response to thrombectomy compared to AV fistulas. Thrombus isasier to clear from prosthetic conduits for several reasons: no endothelialining to injure; uniform caliber; and they are able to be segmentallyeplaced if necessary. Open surgical treatment of AV graft thrombosistarts with surgical exposure of the graft and balloon thrombectomy. Theuspected cause of the thrombosis and potential need for revisionetermine the location of the incision. Once the graft has been cleared ofhrombus, contrast images should interrogate the access from the arterialnastomosis to the central veins. Intraoperative images can confirm theause of the thrombosis and uncover other pathology that could predis-ose the graft to recurrent thrombosis. In most cases, IH of the venousnastomosis proves to be the culprit lesion. Surgical options to treatenous outflow stenosis include revising the venous anastomosis with aatch angioplasty or performing a jump graft to a more proximal vein.The endovascular approach to thrombectomy relies on thrombolysis,echanical thrombectomy devices, and balloon angioplasty. The mostell-described technique begins with infusing tPA through crossed
heaths percutaneously placed into the clotted access. Balloon angioplasty
f the entire graft and venous outflow then debulks the thrombus andurr Probl Surg, July 2011 503
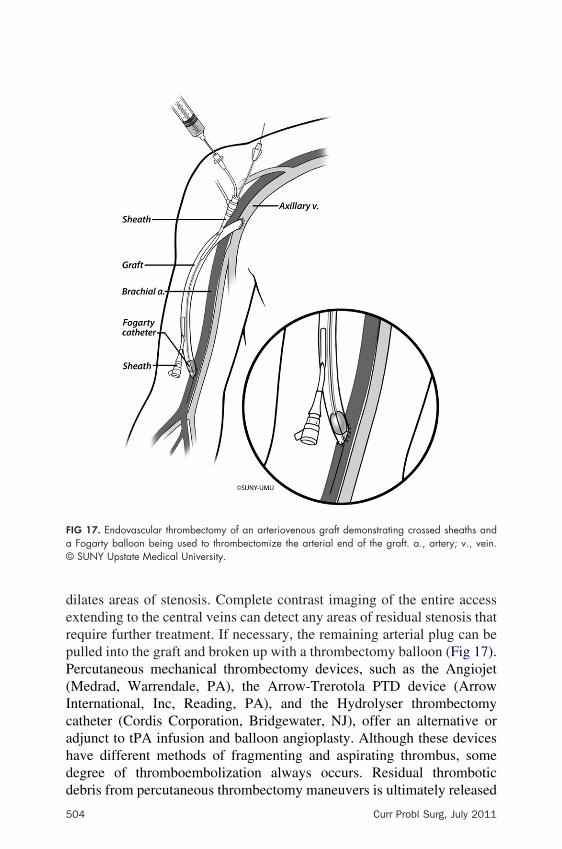
derpP(Icahdd
Fa©
5
ilates areas of stenosis. Complete contrast imaging of the entire accessxtending to the central veins can detect any areas of residual stenosis thatequire further treatment. If necessary, the remaining arterial plug can beulled into the graft and broken up with a thrombectomy balloon (Fig 17).ercutaneous mechanical thrombectomy devices, such as the AngiojetMedrad, Warrendale, PA), the Arrow-Trerotola PTD device (Arrownternational, Inc, Reading, PA), and the Hydrolyser thrombectomyatheter (Cordis Corporation, Bridgewater, NJ), offer an alternative ordjunct to tPA infusion and balloon angioplasty. Although these devicesave different methods of fragmenting and aspirating thrombus, someegree of thromboembolization always occurs. Residual thrombotic
IG 17. Endovascular thrombectomy of an arteriovenous graft demonstrating crossed sheaths andFogarty balloon being used to thrombectomize the arterial end of the graft. a., artery; v., vein.SUNY Upstate Medical University.
ebris from percutaneous thrombectomy maneuvers is ultimately released
04 Curr Probl Surg, July 2011

is
batmdStNatpfc
H
dLfmdthifl
apa(nvAp1pah
C
nto the pulmonary circulation; however, this event rarely has any clinicalequelae.188
Direct comparisons of surgical and percutaneous thrombectomy haveeen inconclusive. Despite a high rate of initial technical success, bothpproaches have poor short-term primary patency rates ranging from 30%o 50%.189,190 The minimally invasive appeal of endovascular treatment
ust be weighed against its reliance on thrombolytics, mechanicalevices, and balloon angioplasty to achieve adequate clot clearance.urgical therapy can achieve a more expeditious and complete thrombec-
omy at the cost of an incision and the need for graft revision. TheKF-DOQI guidelines established a benchmark of 40% primary patency
t 3 months for percutaneous thrombectomy. For surgical thrombectomy,he guidelines were set at 50% for 6-month and 40% for 12-monthrimary patency.52 The higher standard for surgical therapy reflects theact that most surgical procedures involve an access revision, whichonsumes “venous capital.”
igh-Output Cardiac FailureHigh-output cardiac failure occurs when symptoms of cardiac failureevelop in the presence of an above normal cardiac index (�2.3/min/m2). Although it has a simple definition, high-output cardiac
ailure proves to be difficult to diagnose in dialysis patients. Approxi-ately 31% to 36% of patients have cardiac failure at the initiation of
ialysis and an additional 25% of patients develop cardiac failure duringheir dialysis lifetime.191,192 The overwhelming majority of these patientsave cardiac failure due to conditions not related to high cardiac output,ncluding intrinsic heart disease, anemia, hypertension, dysrhythmias, anduid/electrolyte retention.In the classic clinical scenario, a patient with an extremely high-flow
utogenous AV fistula develops heart failure symptoms, including dys-nea on exertion, orthopnea, peripheral edema, pulmonary hypertension,nd tachycardia. Compression of the AV fistula may slow the heart rateNicoladoni-Barnham sign); however, this physical finding is not diag-ostic. The magnitude of AV access flow necessary to trigger heart failurearies widely depending on the patient. A well-trained athlete toleratedV fistula flow of 19 L/min before becoming symptomatic, whereas otheratients have developed heart failure with access flows as low as 0.8 to.0 L/min.193,194 Normalizing the AV access flow to the individualatient’s cardiac output appears to give the most accurate diagnosis. AVccess flow that exceeds 30% of the cardiac output correlates with a
igher risk of high-output cardiac failure.195 Although the clinicalurr Probl Surg, July 2011 505

pdr
owaicceotppc
nAfgscc(fwr
C
BaTyafi5hop
5
resentation and AV access flow ratio can be helpful, a definitiveiagnosis of high-output cardiac failure can only be made if the symptomsesolve with treatment.Pulmonary hypertension shares a strong association with high cardiacutput and has emerged as a common condition in the dialysis populationith a reported prevalence of 40%.196 The underlying pathophysiology
ppears to be an acquired dysfunction, likely related to a state of chronicnflammation, that prevents endothelial cells from adapting to increasedardiac output. This endothelial dysfunction appears to derive from aombination of renal failure, hemodialysis, AV access creation, andlevated cardiac output. Yigla and colleagues evaluated a wide spectrumf patients for pulmonary hypertension. They detected pulmonary hyper-ension in 37% of patients with AV access. None of the patients oneritoneal dialysis, and only 1 patient with renal insufficiency, hadulmonary hypertension.197 Although pulmonary hypertension signifi-antly decreases survival, it does respond to treatment.The only treatment options for high-output cardiac failure and pulmo-ary hypertension are to reduce flow through the AV fistula or ligate it.nastomotic revision and banding procedures have proven to be success-
ul in the treatment of high-output cardiac failure, which is surprisingiven their poor track record when applied to hemodynamic stealyndrome. Several small series have reported that banding improvedardiac function and preserved a functional AV access. Chemla andolleagues moved the arterial anastomosis to a more distal locationdistalization) and demonstrated 77% access patency and 100% heartailure symptom resolution.198 Ligation is usually reserved for patientsho no longer require hemodialysis, such as successful renal transplant
ecipients.
onclusionsVascular access has revolutionized the treatment of patients with ESRD.efore 1960, hemodialysis required surgical exposure of the vessels,llowing only a finite number of life-prolonging treatment sessions.oday, hemodialysis provides routine therapy that can sustain patients forears and even decades. Over the last 50 years, advances in vascularccess have expanded the scope of hemodialysis from 3 patients at therst dialysis center to 400,000 patients receiving treatment at more than000 dialysis centers in the United States. The safety, longevity, andappiness of these patients will depend on the function and reliabilityf their vascular access. Caring for this constantly growing dialysis
opulation calls for practitioners who excel in establishing and maintaining06 Curr Probl Surg, July 2011
vana
ATi
C
ascular access. We have highlighted the key elements to successful vascularccess, including patient preparation; surgical decision-making and tech-ique; surveillance and maintenance; and the recognition and management ofccess complications.
cknowledgmenthe authors thank Martha “Kit” Hefner for her efforts in creating the
llustrations used in this review.
REFERENCES1. Quinton W, Dillard D, Scribner BH. Cannulation of blood vessels for prolonged
hemodialysis. Trans Am Soc Artif Intern Organs 1960;6:104-13.2. Brescia MJ, Cimino JE, Appel K, et al. Chronic hemodialysis using venipuncture
and a surgically created arteriovenous fistula. N Engl J Med 1966;275:1089-92.3. Bander SJ, Schwab S. Central venous angioaccess for hemodialysis and its
complications. Semin Dial 1992;5:121-8.4. Fan PY, Schwab SJ. Vascular access: concepts for the 1990s. J Am Soc Nephrol
1992;3:1-11.5. Polderman KH, Girbes AJ. Central venous catheter use. Part 1: Mechanical
complications. Intensive Care Med 2002;28:1-17.6. Vijayan A. Vascular access for continuous renal replacement therapy. Semin Dial
2009;22:133-6.7. Trerotola SO, Shah H, Johnson M, et al. Randomized comparison of high-flow
versus conventional hemodialysis catheters. J Vasc Interv Radiol 1999;10:1032-8.8. Ash SR. Advances in tunneled central venous catheters for dialysis: design and
performance. Semin Dial 2008;21:504-15.9. Ash SR. Fluid mechanics and clinical success of central venous catheters for
dialysis—answers to simple but persisting problems. Semin Dial 2007;20:237-56.10. Tal MG, Peixoto AJ, Crowley ST, et al. Comparison of side hole versus non side
hole high flow hemodialysis catheters. Hemodial Int 2006;10:63-7.11. Darouiche RO, Raad HSO, II, Heard SO, et al. A comparison of two antimicrobial-
impregnated central venous catheters. Catheter Study Group. N Engl J Med1999;340:1-8.
12. Chan MR, Yevzlin AS. Tunneled dialysis catheters: recent trends and futuredirections. Adv Chronic Kidney Dis 2009;16:386-95.
13. Dwyer A. Surface-treated catheters—a review. Semin Dial 2008;21:542-6.14. Jain G, Allon M, Saddekni S, et al. Does heparin coating improve patency or reduce
infection of tunneled dialysis catheters? Clin J Am Soc Nephrol 2009;4:1787-90.15. Clark TW, Jacobs D, Charles HW, et al. Comparison of heparin-coated and
conventional split-tip hemodialysis catheters. Cardiovasc Interv Radiol 2009;32:703-6.
16. Mojibian H, Spector M, Ni N, et al. Initial clinical experience with a newheparin-coated chronic hemodialysis catheter. Hemodial Int 2009;13:329-34.
17. Kerr A, Pathalapati R, Qiuhu S, et al. Purse-string suture to prevent bleeding after
tunneled dialysis catheter insertion. J Vasc Interv Radiol 2008;19:1176-9.urr Probl Surg, July 2011 507
5
18. Forauer AR, Glockner JF. Importance of US findings in access planning during jugularvein hemodialysis catheter placements. J Vasc Interv Radiol 2000;11(2 Pt 1):233-8.
19. Lin BS, Kong CW, Tarng DC, et al. Anatomical variation of the internal jugularvein and its impact on temporary haemodialysis vascular access: an ultrasono-graphic survey in uraemic patients. Nephrol Dial Transplant 1998;13:134-8.
20. Randolph AG, Cook DJ, Gonzales CA, et al. Ultrasound guidance for placement ofcentral venous catheters: a meta-analysis of the literature. Crit Care Med1996;24:2053-8.
21. Karakitsos D, Labropoulos N, De Groot E, et al. Real-time ultrasound-guidedcatheterisation of the internal jugular vein: a prospective comparison with thelandmark technique in critical care patients. Crit Care 2006;10:R162.
22. Canaud B, Desmeules S, Klouche K, et al. Vascular access for dialysis in theintensive care unit. Best Pract Res Clin Anaesthesiol 2004;18:159-74.
23. Tarng DC, Huang TP, Lin KP. Brachial plexus compression due to subclavianpseudoaneurysm from cannulation of jugular vein hemodialysis catheter. Am JKidney Dis 1998;31:694-7.
24. Silberman H, Berne TV, Escandon R. Prospective evaluation of a double-lumensubclavian dialysis catheter for acute vascular access. Am Surg 1992;58:443-5.
25. Vanherweghem JL, Cabolet P, Dhaene M, et al. Complications related to subcla-vian catheters for hemodialysis. Report and review. Am J Nephrol 1986;6:339-45.
26. Hernández D, Díaz F, Rufino M, et al. Subclavian vascular access stenosis indialysis patients: natural history and risk factors. J Am Soc Nephrol 1998;9:1507-10.
27. Hryszko T, Brzosko S, Mazerska M, et al. Risk factors of nontunneled noncuffedhemodialysis catheter malfunction. A prospective study. Nephron Clin Pract2004;96:c43-7.
28. Suojanen JN, Brophy DP, Nasser I. Thrombus on indwelling central venouscatheters: the histopathology of “fibrin sheaths”. Cardiovasc Interv Radiol2000;23:194-7.
29. Vascular Access 2006 Work Group. Clinical practice guidelines for vascularaccess. Am J Kidney Dis 2006;48:S176-247.
30. Leblanc M, Fedak S, Mokris G, et al. Blood recirculation in temporary centralcatheters for acute hemodialysis. Clin Nephrol 1996;45:315-9.
31. Little MA, Conlon PJ, Walshe JJ. Access recirculation in temporary hemodialysiscatheters as measured by the saline dilution technique. Am J Kidney Dis2000;36:1135-9.
32. Level C, Lasseur C, Chauveau P, et al. Performance of twin central venouscatheters: influence of the inversion of inlet and outlet on recirculation. Blood Purif2002;20:182-8.
33. Daeihagh P, Jordan J, Chen J, et al. Efficacy of tissue plasminogen activatoradministration on patency of hemodialysis access catheters. Am J Kidney Dis2000;36:75-9.
34. Zacharias JM, Weatherston CP, Spewak CR, et al. Alteplase versus urokinase foroccluded hemodialysis catheters. Ann Pharmacother 2003;37:27-33.
35. Oliver MJ, Callery SM, Thorpe KE, et al. Risk of bacteremia from temporaryhemodialysis catheters by site of insertion and duration of use: a prospective study.
Kidney Int 2000;58:2543-5.08 Curr Probl Surg, July 2011
C
36. Sauer K, Steczko J, Ash SR. Effect of a solution containing citrate/methyleneblue/parabens on Staphylococcus aureus bacteria and biofilm, and comparison withvarious heparin solutions. J Antimicrob Chemother 2009;63:937-45.
37. Feldman HI, Kobrin S, Wasserstein A. Hemodialysis vascular access morbidity.J Am Soc Nephrol 1996;7:523-35.
38. Hoen B, Paul-Dauphin A, Hestin D, et al. A multicenter prospective study of riskfactors for bacteremia in chronic hemodialysis patients. J Am Soc Nephrol1998;9:869-76.
39. Vascular Access Work Group. Clinical practice guidelines for vascular access.Am J Kidney Dis 2006;48(Suppl 1):S248-73.
40. Saad TF. Bacteremia associated with tunneled, cuffed hemodialysis catheters. Am JKidney Dis 1999;34:1114-24.
41. Parienti JJ, Thirion M, Mégarbane B, et al. Femoral vs jugular venous catheter-ization and risk of nosocomial events in adults requiring acute renal replacementtherapy: a randomized controlled trial. JAMA 2008;299:2413-22.
42. Marr KA, Sexton DJ, Conlon PJ, et al. Catheter-related bacteremia and outcome ofattempted catheter salvage in patients undergoing hemodialysis. Ann Intern Med1997;127:275-80.
43. Fan ST, Teoh-Chan CH, Lau KF. Evaluation of central venous catheter sepsis bydifferential quantitative blood culture. Eur J Clin Microbiol Infect Dis1989;8:142-4.
44. Schwab SJ, Harrington JT, Singh A, et al. Vascular access for hemodialysis.Kidney Int 1999;55:2078-90.
45. Beathard GA. Management of bacteremia associated with tunneled-cuffed hemo-dialysis catheters. J Am Soc Nephrol 1999;10:1045-9.
46. Allon M, Daugirdas J, Depner TA, et al. Effect of change in vascular access onpatient mortality in hemodialysis patients. Am J Kidney Dis 2006;47:469-77.
47. Metcalfe W, Khan IH, Prescott GJ, et al. Hospitalization in the first year of renalreplacement therapy for end-stage renal disease. QJM 2003;96:899-909.
48. Spinowitz BS, Galler M, Golden RA, et al. Subclavian vein stenosis as acomplication of subclavian catheterization for hemodialysis. Arch Intern Med1987;147:305-7.
49. Abdullah BJ, Mohammad N, Sangkar JV, et al. Incidence of upper limb venousthrombosis associated with peripherally inserted central catheters (PICC). Br JRadiol 2005;78:596-600.
50. Rayner HC, Pisoni RL, Gillespie BW, et al. Creation, cannulation and survival ofarteriovenous fistulae: data from the Dialysis Outcomes and Practice PatternsStudy. Kidney Int 2003;63:323-30.
51. Fitzgerald JT, Schanzer A, Chin AI, et al. Outcomes of upper arm arteriovenousfistulas for maintenance hemodialysis access. Arch Surg 2004;139:201-8.
52. Besarab A, Work J; the Vascular Access Work Group. NKF-K/DOQI ClinicalPractice Guidelines for Vascular Access: update 2006. Am J Kidney Dis 2006;48(Suppl):S176-247.
53. Ferring M, Claridge M, Smith SA, et al. Routine preoperative vascular ultrasoundimproves patency and use of arteriovenous fistulas for hemodialysis: a randomized trial.Clin J Am Soc Nephrol 2010;5:2236-44.
54. Silva MB Jr, Hobson RW 2nd, Pappas PJ, et al. A strategy for increasing use of
urr Probl Surg, July 2011 509
5
autogenous hemodialysis access procedures: impact of preoperative noninvasiveevaluation. J Vasc Surg 1998;27:302-7 [Discussion 307-8].
55. De Marco Garcia LP, Davila-Santini LR, Feng Q, et al. Primary balloonangioplasty plus balloon angioplasty maturation to upgrade small-caliber veins (�3mm) for arteriovenous fistulas. J Vasc Surg 2010;52:139-44.
56. Allon M, Lok CE. Dialysis fistula or graft: the role for randomized clinicaltrials. Clin J Am Soc Nephrol 2010;5:2348-54.
57. Bourquelot P, Tawakol JB, Gaudric J, et al. Lipectomy as a new approach tosecondary procedure superficialization of direct autogenous forearm radial-cephalicarteriovenous accesses for hemodialysis. J Vasc Surg 2009;50:369-74, 374.e1.
58. Bronder CM, Cull DL, Kuper SG, et al. Fistula elevation procedure: experiencewith 295 consecutive cases during a 7-year period. J Am Coll Surg 2008;206:1076-81 [Discussion 1081-2].
59. Ernandez T, Saudan P, Berney T, et al. Risk factors for early failure of nativearteriovenous fistulas. Nephron Clin Pract 2005;101:c39-44.
60. Huijbregts HJ, Bots ML, Moll FL, et al. Hospital specific aspects predominantlydetermine primary failure of hemodialysis arteriovenous fistulas. J Vasc Surg2007;45:962-7.
61. Rooijens PPGM, Tordoir JHM, Stijnen T, et al. Radiocephalic wrist arteriovenousfistula for hemodialysis: meta-analysis indicates a high primary failure rate. Eur JVasc Endovasc Surg 2004;28:583-9.
62. Palder SB, Kirkman RL, Whittemore AD, et al. Vascular access for hemodialysis.Patency rates and results of revision. Ann Surg 1985;202:235-9.
63. Silva MB Jr, Hobson RW 2nd, Pappas PJ, et al. Vein transposition in the forearmfor autogenous hemodialysis access. J Vasc Surg 1997;26:981-6 [Discussion987-8].
64. Gefen JY, Fox D, Giangola G, et al. The transposed forearm loop arteriovenousfistula: a valuable option for primary hemodialysis access in diabetic patients. AnnVasc Surg 2002;16:89-94.
65. Hakaim AG, Nalbandian M, Scott T. Superior maturation and patency of primarybrachiocephalic and transposed basilic vein arteriovenous fistulae in patients withdiabetes. J Vasc Surg 1998;27:154-7.
66. Roberts C. Saving a brachiocephalic fistula using lipectomy. Nephrol Nurs J2005;32:331.
67. Causey MW, Quan R, Hamawy A, et al. Superficialization of arteriovenous fistulaeemploying minimally invasive liposuction. J Vasc Surg 2010;52:1397-400.
68. Dagher F, Gelber R, Ramos E, et al. The use of basilic vein and brachial artery asan A-V fistula for long term hemodialysis. J Surg Res 1976;20:373-6.
69. Hossny A. Brachiobasilic arteriovenous fistula: different surgical techniques andtheir effects on fistula patency and dialysis-related complications. J Vasc Surg2003;37:821-6.
70. Humphries AL Jr, Colborn GL, Wynn JJ. Elevated basilic vein arteriovenousfistula. Am J Surg 1999;177:489-91.
71. El Mallah S. Staged basilic vein transposition for dialysis angioaccess. Int Angiol1998;17:65-8.
72. Francis DM, Lu Y, Robertson AJ, et al. Two-stage brachiobasilic arteriovenous
fistula for chronic haemodialysis access. Aust NZ J Surg 2007;77:150-5.10 Curr Probl Surg, July 2011

C
73. Gonzalez E, Kashuk JL, Moore EE, et al. Two-stage brachial-basilic transpositionfistula provides superior patency rates for dialysis access in a safety-net population.Surgery 2010;148:687-93 [Discussion 693-94].
74. Bachleda P, Utikal P, Kojecky Z, et al. Autogenous arteriovenous elbow fistula forhaemodialysis and upper extremity ischemia. Biomed Pap Med Fac Univ PalackyOlomouc Czech Repub 2007;151:129-32.
75. Sparks SR, VanderLinden JL, Gnanadev DA, et al. Superior patency of perforatingantecubital vein arteriovenous fistulae for hemodialysis. Ann Vasc Surg 1997;11:165-7.
76. Gibson KD, Gillen DL, Caps MT, et al. Vascular access survival and incidence ofrevisions: a comparison of prosthetic grafts, simple autogenous fistulas, and venoustransposition fistulas from the United States Renal Data System Dialysis Morbidityand Mortality Study. J Vasc Surg 2001;34:694-700.
77. Kalman PG, Pope M, Bhola C, et al. A practical approach to vascular access forhemodialysis and predictors of success. J Vasc Surg 1999;30:727-33.
78. Morsy MA, Khan A, Chemla ES. Prosthetic axillary-axillary arteriovenous straightaccess (necklace graft) for difficult hemodialysis patients: a prospective single-center experience. J Vasc Surg 2008;48:1251-4, 1254.e1.
79. Gradman WS, Laub J, Cohen W. Femoral vein transposition for arteriovenoushemodialysis access: improved patient selection and intraoperative measuresreduce postoperative ischemia. J Vasc Surg 2005;41:279-84.
80. Gradman WS, Cohen W, Haji-Aghaii M. Arteriovenous fistula construction in thethigh with transposed superficial femoral vein: our initial experience. J Vasc Surg2001;33:968-75.
81. Pierre-Paul D, Williams S, Lee T, et al. Saphenous vein loop to femoral arteryarteriovenous fistula: a practical alternative. Ann Vasc Surg 2004;18:223-7.
82. Katzman HE, McLafferty RB, Ross JR, et al. Initial experience and outcome of anew hemodialysis access device for catheter-dependent patients. J Vasc Surg2009;50:600-7, 607.e1.
83. Allon M. Current management of vascular access. Clin J Am Soc Nephrol CJASN2007;2:786-800.
84. Miller PE, Tolwani A, Luscy CP, et al. Predictors of adequacy of arteriovenousfistulas in hemodialysis patients. Kidney Int 1999;56:275-80.
85. Schwartz SM, Reidy MA, O’Brien ER. Assessment of factors important inatherosclerotic occlusion and restenosis. Thromb Haemost 1995;74:541-51.
86. Leaf DA, MacRae HS, Grant E, et al. Isometric exercise increases the size of forearmveins in patients with chronic renal failure. Am J Med Sci 2003;325:115-9.
87. Sidawy A, Spergel L, Besarab A, et al. The Society for Vascular Surgery: Clinicalpractice guidelines for the surgical placement and maintenance of arteriovenoushemodialysis access. J Vasc Surg 2008;48:S2-S25.
88. van Loon MM, Goovaerts T, Kessels AG, et al. Buttonhole needling of haemodi-alysis arteriovenous fistulae results in less complications and interventions com-pared to the rope-ladder technique. Nephrol Dial Transplant Off Publ Eur DialTranspl Assoc European Renal Association 2010;25:225-30.
89. Marticorena RM, Hunter J, Cook R, et al. A simple method to create buttonholecannulation tracks in a busy hemodialysis unit. Hemodialysis Int International
Symposium On Home Hemodialysis 2009;13:316-21.urr Probl Surg, July 2011 511
1
1
1
1
1
1
1
1
1
1
1
5
90. Hsiao JF, Chou HH, Hsu LA, et al. Vascular changes at the puncture segments ofarteriovenous fistula for hemodialysis access. J Vasc Surg 2010;52:669-73.
91. Himmelfarb J, Dember LM, Dixon BS. Vascular Access. In: Chronic KidneyDisease, Dialysis, and Transplantation. 2nd edition. Philadelphia: WB Saunders,2005. p. 341-62.
92. Bosman PJ, Boereboom FT, Eikelboom BC, et al. Graft flow as a predictor ofthrombosis in hemodialysis grafts. Kidney Int 1998;54:1726-30.
93. Allon M, Robbin ML. Hemodialysis vascular access monitoring: current concepts.Hemodialysis Int Symp Home Hemodial 2009;13:153-62.
94. Polkinghorne KR. Does monthly native arteriovenous fistula blood-flow surveil-lance detect significant stenosis—a randomized controlled trial. Nephrol DialTransplant 2006;21:2498-506.
95. Henry ML. Routine surveillance in vascular access for hemodialysis. Eur J VascEndovasc Surg 2006;32:545-8.
96. Casey ET, Murad MH, Rizvi AZ, et al. Surveillance of arteriovenous hemodialysisaccess: a systematic review and meta-analysis. J Vasc Surg 2008;48(5 Suppl):S48-54.
97. Sullivan KL, Besarab A, Bonn J, et al. Hemodynamics of failing dialysis grafts.Radiology 1993;186:867-72.
98. Whittier WL, Mansy HA, Rutz DR, et al. Comparison of hemodialysis access flowmeasurements using flow dilution and in-line dialysance. ASAIO J 2009;55:369-72.
99. Soule JL, Henry ML. Noninvasive methods to identify early vascular accessdysfunction. Hemodialysis access: perspectives for current clinical practice, hemo-dialysis access. Perspect Curr Clin Pract 2007;20:164-6.
00. Plantinga LC, Jaar BG, Astor B, et al. Association of clinic vascular accessmonitoring practices with clinical outcomes in hemodialysis patients. Nephron ClinPractice 2006;104:c151-9.
01. Vesely TM, Siegel JB. Use of the peripheral cutting balloon to treat hemodialysis-related stenoses. J Vasc Interv Radiol 2005;16:1593-603.
02. Haskal ZJ, Trerotola S, Dolmatch B, et al. Stent graft versus balloon angioplasty forfailing dialysis-access grafts. N Engl J Med 2010;362:494-503.
03. Noris M, Remuzzi G. Uremic bleeding: closing the circle after 30 years ofcontroversies? Blood 1999;94:2569-74.
04. Sloand EM, Sloand JA, Prodouz K, et al. Reduction of platelet glycoprotein Ib inuraemia. Br J Haematol 1991;77:375-81.
05. Gawaz MP, Dobos G, Späth M, et al. Impaired function of platelet membraneglycoprotein IIb-IIIa in end-stage renal disease. J Am Soc Nephrol 1994;5:36-46.
06. Boccardo P, Remuzzi G, Galbusera M. Platelet dysfunction in renal failure. SeminThromb Hemost 2004;30:579-89.
07. Kaw D, Malhotra D. Platelet dysfunction and end-stage renal disease. Semin Dial2006;19:317-22.
08. Livio M, Gotti E, Marchesi D, et al. Uraemic bleeding: role of anaemia andbeneficial effect of red cell transfusions. Lancet 1982;2:1013-5.
09. Janssen MJ, van der Meulen J. The bleeding risk in chronic haemodialysis:preventive strategies in high-risk patients. Neth J Med 1996;48:198-207.
10. Sloand JA. Long-term therapy for uremic bleeding. Int J Artif Organs 1996;
19:439-40.12 Curr Probl Surg, July 2011
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
C
11. Andrassy K, Weischedel E, Ritz E, et al. Bleeding in uremic patients aftercarbenicillin. Thromb Haemost 1976;36:115-26.
12. Ng HJ, Koh LP, Lee LH. Successful control of postsurgical bleeding by recombi-nant factor VIIa in a renal failure patient given low molecular weight heparin andaspirin. Ann Hematol 2003;82:257-8.
13. Mannucci PM, Ruggeri ZM, Pareti FI, et al. 1-Deamino-8-d-arginine vasopressin:a new pharmacological approach to the management of haemophilia and vonWillebrands’ diseases. Lancet 1977;1:869-72.
14. Andrassy K, Ritz E. Uremia as a cause of bleeding. Am J Nephrol1985;5:313-9.
15. Canavese C, Salomone M, Pacitti A, et al. Reduced response of uraemic bleedingtime to repeated doses of desmopressin. Lancet 1985;1:867-8.
16. Janson PA, Jubelirer SJ, Weinstein MJ, et al. Treatment of the bleeding tendencyin uremia with cryoprecipitate. N Engl J Med 1980;303:1318-22.
17. Triulzi DJ, Blumberg N. Variability in response to cryoprecipitate treatment forhemostatic defects in uremia. Yale J Biol Med 1990;63:1-7.
18. Livio M, Mannucci PM, Viganò G, et al. Conjugated estrogens for the managementof bleeding associated with renal failure. N Engl J Med 1986;315:731-5.
19. Zoja C, Noris M, Corna D, et al. L-arginine, the precursor of nitric oxide, abolishesthe effect of estrogens on bleeding time in experimental uremia. Lab Invest1991;65:479-83.
20. Zibari GB, Rohr MS, Landreneau MD, et al. Complications from permanenthemodialysis vascular access. Surgery 1988;104:681-6.
21. Hausegger KA, Tiessenhausen K, Klimpfinger M, et al. Aneurysms of hemodial-ysis access grafts: treatment with covered stents: a report of three cases. CardiovascInterv Radiol 1998;21:334-7.
22. Barshes NR, Annambhotla S, Bechara C, et al. Endovascular repair of hemodialysisgraft-related pseudoaneurysm: an alternative treatment strategy in salvaging failingdialysis access. Vasc Endovasc Surg 2008;42:228-34.
23. Vesely TM. Use of stent grafts to repair hemodialysis graft-related pseudoaneu-rysms. J Vasc Interv Radiol 2005;16:1301-7.
24. Yevzlin AS, Schoenkerman AB, Gimelli G, et al. Arterial interventions inarteriovenous access and chronic kidney disease: a role for interventional neph-rologists. Semin Dial 2009;22:545-56.
25. Pierce GE, Thomas JH, Fenton JR. Novel repair of venous aneurysms secondary toarteriovenous dialysis fistulae. Vasc Endovasc Surg 2007;41:55-60.
26. US Renal Data System USRDS. 2010 Annual Data Report: Atlas of ChronicKidney Disease and End-Stage Renal Disease in the United States. Bethesda, MD:National Institutes of Health; National Institute of Diabetes and Digestive andKidney Diseases, 2010.
27. Tokars JI, Miller ER, Stein G. New national surveillance system for hemodialysis-associated infections: initial results. Am J Infect Control 2002;30:288-95.
28. Brunner MC, Mitchell RS, Baldwin JC, et al. Prosthetic graft infection: limitationsof indium white blood cell scanning. J Vasc Surg 1986;3:42-8.
29. Taylor B, Sigley RD, May KJ. Fate of infected and eroded hemodialysis grafts and
autogenous fistulas. Am J Surg 1993;165:632-6.urr Probl Surg, July 2011 513
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
5
30. Gray RJ, Sands JJ, editors. Dialysis access: A multidisciplinary approach. In:Stevenson KB, editor. Management of hemodialysis vascular access infection.Philadelphia, PA: Lippincott Williams & Wilkins, 2002.
31. Churchill DN, Taylor DW, Cook RJ, et al. Canadian Hemodialysis MorbidityStudy. Am J Kidney Dis 1992;19:214-34.
32. Ryan SV, Calligaro KD, Scharff J, et al. Management of infected prosthetic dialysisarteriovenous grafts. J Vasc Surg 2004;39:73-8.
33. Padberg FT Jr, Calligaro KD, Sidawy AN. Complications of arteriovenoushemodialysis access: recognition and management. J Vasc Surg 2008;48(Suppl5):55S-80S.
34. Borrero E, Doscher W. Chronic perigraft seromas in PTFE grafts. J CardiovascSurg [Torino] 1988;29:46-9.
35. Eid A, Lyass S. Acute perigraft seroma simulating anastomotic bleeding of a PTFEgraft applied as an arteriovenous shunt for hemodialysis. Ann Vasc Surg1996;10:290-1.
36. Dale WA, editor. Management of vascular surgical problems. In: Blumenberg RM,editor. Invited Commentary in Lymph Fistulas and Seromas. New York: McGraw-Hill,1985.
37. Duncan H, Ferguson L, Faris I. Incidence of the radial steal syndrome in patientswith Brescia fistula for hemodialysis: its clinical significance. J Vasc Surg1986;4:144-7.
38. Morsy AH, Kulbaski M, Chen C, et al. Incidence and characteristics of patientswith hand ischemia after a hemodialysis access procedure. J Surg Res 1998;74:8-10.
39. Tordoir JH, Dammers R, van der Sande FM. Upper extremity ischemia andhemodialysis vascular access. Eur J Vasc Endovasc Surg 2004;27:1-5.
40. Sivanesan S, How TV, Bakran A. Characterizing flow distributions in AV fistulaefor haemodialysis access. Nephrol Dial Transplant 1998;13:3108-10.
41. Mattson WJ. Recognition and treatment of vascular steal secondary to hemodialysisprostheses. Am J Surg 1987;154:198-201.
42. Wixon CL, Hughes JD, Mills JL. Understanding strategies for the treatment ofischemic steal syndrome after hemodialysis access. J Am Coll Surg 2000;191:301-10.
43. Schanzer H, Schwartz M, Harrington E, et al. Treatment of ischemia due to “steal”by arteriovenous fistula with distal artery ligation and revascularization. J VascSurg 1988;7:770-3.
44. Illig KA, Surowiec S, Shortell CK, et al. Hemodynamics of distal revascularization-interval ligation. Ann Vasc Surg 2005;19:199-207.
45. Knox RC, Berman SS, Hughes JD, et al. Distal revascularization-interval ligation:a durable and effective treatment for ischemic steal syndrome after hemodialysisaccess. J Vasc Surg 2002;36:250-5 [Discussion 256].
46. Zanow J, Kruger U, Scholz H. Proximalization of the arterial inflow: a newtechnique to treat access-related ischemia. J Vasc Surg 2006;43:1216-21 [Discus-sion 1221].
47. Mwipatayi BP, Bowles T, Balakrishnan S, et al. Ischemic steal syndrome: a caseseries and review of current management. Curr Surg 2006;63:130-5.
48. Wilbourn AJ, Furlan AJ, Hulley W, et al. Ischemic monomelic neuropathy.
Neurology 1983;33:447-51.14 Curr Probl Surg, July 2011
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
C
49. Ballard JL, Bunt TJ, Malone JM. Management of small artery vascular trauma.Am J Surg 1992;164:316-9.
50. Miles AM. Vascular steal syndrome and ischaemic monomelic neuropathy: twovariants of upper limb ischaemia after haemodialysis vascular access surgery.Nephrol Dial Transplant 1999;14:297-300.
51. Wodicka R, Isaacs J. Ischemic monomelic neuropathy. J Hand Surg Am2010;35:842-3.
52. Rogers NM, Lawton PD. Ischaemic monomelic neuropathy in a non-diabeticpatient following creation of an upper limb arteriovenous fistula. Nephrol DialTransplant 2007;22:933-5.
53. Thermann F, Brauckhoff M, Kornhuber M. Dialysis shunt-associated ischaemicmonomelic neuropathy: neurological recovery preserving the dialysis access.Nephrol Dial Transplant 2006;21:3334-6.
54. Kaku DA, Malamut RI, Frey DJ, et al. Conduction block as an early sign ofreversible injury in ischemic monomelic neuropathy. Neurology 1993;43:1126-30.
55. Miles AM. Upper limb ischemia after vascular access surgery: differentialdiagnosis and management. Semin Dial 2000;13:312-5.
56. Warren DJ, Otieno LS. Carpal tunnel syndrome in patients on intermittenthaemodialysis. Postgrad Med J 1975;51:450-2.
57. Halter SK, DeLisa JA, Stolov WC, et al. Carpal tunnel syndrome in chronic renaldialysis patients. Arch Phys Med Rehabil 1981;62:197-201.
58. Gousheh J, Iranpour A. Association between carpel tunnel syndrome and arterio-venous fistula in hemodialysis patients. Plast Reconstr Surg 2005;116:508-13.
59. Borman H, Akinbingol G, Maral T, et al. Entrapment neuropathy of the upperextremity in hemodialysis patients. Plast Reconstr Surg 2002;109:2598-9.
60. Bicknell JM, Lim AC, Raroque HG Jr, et al. Carpal tunnel syndrome, subclinicalmedian mononeuropathy, and peripheral polyneuropathy: common early compli-cations of chronic peritoneal dialysis and hemodialysis. Arch Phys Med Rehabil1991;72:378-81.
61. Hirasawa Y, Ogura T. Carpal tunnel syndrome in patients on long-term haemodi-alysis. Scand J Plast Reconstr Surg Hand Surg 2000;34:373-81.
62. Borgatti PP, Lusenti T, Franco V, et al. Guyon’s syndrome in a long-termhaemodialysis patient. Nephrol Dial Transplant 1991;6:734-5.
63. Pirzada NA, Morgenlander JC. Peripheral neuropathy in patients with chronic renalfailure. A treatable source of discomfort and disability. Postgrad Med 1997;102:249-50, 255-7, 261.
64. Begin V, Ethier J, Dumont M, et al. Prospective evaluation of the intra-access flowof recently created native arteriovenous fistulae. Am J Kidney Dis 2002;40:1277-82.
65. Bambauer R, Inniger R, Pirrung KJ, et al. Complications and side effects associatedwith large-bore catheters in the subclavian and internal jugular veins. Artif Organs1994;18:318-21.
66. Sidawy AN, Gray R, Besarab A, et al. Recommended standards for reports dealingwith arteriovenous hemodialysis accesses. J Vasc Surg 2002;35:603-10.
67. Agarwal AK, Patel BM, Haddad NJ. Central vein stenosis: a nephrologist’sperspective. Semin Dial 2007;20:53-62.
68. Deshmukh N, Reppert M. Venous ulceration of the hand secondary to a Cimino
fistula. Mil Med 1993;158:752-3.urr Probl Surg, July 2011 515
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
5
69. Surratt RS, Picus D, Hicks ME, et al. The importance of preoperative evaluation ofthe subclavian vein in dialysis access planning. AJR Am J Roentgenol1991;156:623-5.
70. Lacson E Jr, Lazarus JM, Himmelfarb J, et al. Balancing fistula first with catheterslast. Am J Kidney Dis 2007;50:379-95.
71. Gray RJ, Dolmatch BL, Buick MK. Directional atherectomy treatment for hemo-dialysis access: early results. J Vasc Interv Radiol 1992;3:497-503.
72. Davidson CJ, Newman GE, Sheikh KH, et al. Mechanisms of angioplasty inhemodialysis fistula stenoses evaluated by intravascular ultrasound. Kidney Int1991;40:91-5.
73. Maskova J, Komarkova J, Kivanek J, et al. Endovascular treatment of central veinstenoses and/or occlusions in hemodialysis patients. Cardiovasc Interv Radiol2003;26:27-30.
74. Wisselink W, Money SR, Becker MO, et al. Comparison of operative reconstruc-tion and percutaneous balloon dilatation for central venous obstruction. Am J Surg1993;166:200-4 [Discussion 204-5].
75. Bakken AM, Protack CD, Saad WE, et al. Long-term outcomes of primaryangioplasty and primary stenting of central venous stenosis in hemodialysispatients. J Vasc Surg 2007;45:776-83.
76. Oderich GS, Treiman GS, Schneider P, et al. Stent placement for treatment ofcentral and peripheral venous obstruction: a long-term multi-institutional experi-ence. J Vasc Surg 2000;32:760-9.
77. Bornak A, Wicky S, Ris HB, et al. Endovascular treatment of stenoses in thesuperior vena cava syndrome caused by non-tumoral lesions. Eur Radiol2003;13:950-6.
78. Doty DB, Baker WH. Bypass of superior vena cava with spiral vein graft. AnnThorac Surg 1976;22:490-3.
79. El-Sabrout RA, Duncan JM. Right atrial bypass grafting for central venousobstruction associated with dialysis access: another treatment option. J Vasc Surg1999;29:472-8.
80. Hoballah JJ, Eid GM, Nazzal MM, et al. Contralateral internal jugular veininterposition for salvage of a functioning arteriovenous fistula. Ann Vasc Surg2000;14:679-82.
81. Puskas JD, Gertler JP. Internal jugular to axillary vein bypass for subclavian veinthrombosis in the setting of brachial arteriovenous fistula. J Vasc Surg1994;19:939-42.
82. Rizvi AZ, Kalra M, Bjarnason H, et al. Benign superior vena cava syndrome:stenting is now the first line of treatment. J Vasc Surg 2008;47:372-80.
83. Kalra M, Gloviczki P, Andrews JC, et al. Open surgical and endovascular treatmentof superior vena cava syndrome caused by nonmalignant disease. J Vasc Surg2003;38:215-23.
84. Dossabhoy NR, Ram SJ, Nassar R, et al. Stenosis surveillance of hemodialysisgrafts by duplex ultrasound reduces hospitalizations and cost of care. Semin Dial2005;18:550-7.
85. Kanterman RY, Vesely TM, Pilgram TK, et al. Dialysis access grafts: anatomiclocation of venous stenosis and results of angioplasty. Radiology 1995;195:135-9.
86. Palmer RM, Cull DL, Kalbaugh C, et al. Is surgical thrombectomy to salvage failed
autogenous arteriovenous fistulae worthwhile? Am Surg 2006;72:1231-3.16 Curr Probl Surg, July 2011
1
1
1
1
1
1
1
1
1
1
1
1
C
87. Shatsky JB, Berns JS, Clark TW, et al. Single-center experience with theArrow-Trerotola Percutaneous Thrombectomy Device in the management ofthrombosed native dialysis fistulas. J Vasc Interv Radiol 2005;16:1605-11.
88. Smits HF, Van Rijk PP, Van Isselt JW, et al. Pulmonary embolism afterthrombolysis of hemodialysis grafts. J Am Soc Nephrol 1997;8:1458-61.
89. Beathard GA, Litchfield T, Physician Operators Forum of RMS Lifeline, Inc.Effectiveness and safety of dialysis vascular access procedures performed byinterventional nephrologists. Kidney Int 2004;66:1622-32.
90. Vogel PM, Bansal V, Marshall MW. Thrombosed hemodialysis grafts: lyse andwait with tissue plasminogen activator or urokinase compared to mechanicalthrombolysis with the Arrow-Trerotola Percutaneous Thrombolytic Device. J VascInterv Radiol 2001;12:1157-65.
91. Stack AG, Bloembergen WE. A cross-sectional study of the prevalence and clinicalcorrelates of congestive heart failure among incident US dialysis patients. Am JKidney Dis 2001;38:992-1000.
92. Harnett JD, Foley RN, Kent GM, et al. Congestive heart failure in dialysis patients:prevalence, incidence, prognosis and risk factors. Kidney Int 1995;47:884-90.
93. Young PR Jr, Rohr MS, Marterre WF Jr. High-output cardiac failure secondary toa brachiocephalic arteriovenous hemodialysis fistula: two cases. Am Surg1998;64:239-41.
94. Dikow R, Schwenger V, Zeier M, et al. Fistulas contribute to cardiac mortality inhemodialysis patients? Semin Dial 2002;15:14-7.
95. MacRae JM, Pandeya S, Humen DP, et al. Arteriovenous fistula-associatedhigh-output cardiac failure: a review of mechanisms. Am J Kidney Dis2004;43:e17-22.
96. Abassi Z, Nakhoul F, Khankin E, et al. Pulmonary hypertension in chronic dialysispatients with arteriovenous fistula: pathogenesis and therapeutic prospective. CurrOpin Nephrol Hypertens 2006;15:353-60.
97. Yigla M, Nakhoul F, Sabag A, et al. Pulmonary hypertension in patients withend-stage renal disease. Chest 2003;123:1577-82.
98. Chemla ES, Morsy M, Anderson L, et al. Inflow reduction by distalization ofanastomosis treats efficiently high-inflow high-cardiac output vascular access forhemodialysis. Semin Dial 2007;20:68-72.
urr Probl Surg, July 2011 517