vascular news
TRANSCRIPT

CRESTfallen
sense at ESVS
carotid trials
updatePage 4
Cutting balloon
no better than
angioplastyPage 8
First drug-eluting
stent for the
superficial
femoral arteryPage 10
Venous News
Recovery rates:
Laser vs. surgeryPage 25
The place for
Daflon 500mgPage 26
Comment & analysis
William Gray:
Reading the
tea leavesPage 6
Janet Powell:
Where did all
the aneurysm
patients go?Page 14
Eric Chemla:
St George’s
Vascular Access
Day at CX 2010Page 16
1
November 2009ISSUE 44
The international newspaper for vascular specialists
I N T E R N A T I O N A L
ASTRAL trial results show nobenefit for renal artery stenting
Harry Hubert GraysonEastcott, the vascularsurgeon who first
published results on asuccessful carotid surgery, diedon 25 October 2009 in London,UK. “Felix” Eastcott was 92.
Eastcott and his team per-formed the carotid arteryreconstruction in a 66-year-oldwoman with transientischaemic attacks in May1954. They little realised thatthis was the beginning of thesurgical prevention of stroke,and that in the next twodecades carotid surgery was tobecome one of the most fre-quently performed vascularprocedures in the world.
Eastcott performed the pro-cedure on 19 May at St Mary’s
Hospital in London and report-ed the case in November 1954.The procedure is reported byJesse E Thompson, BaylorUniversity Medical Center,Dallas, USA, in the paper TheEvolution of Surgery for theTreatment and Prevention ofStroke: “The woman, havingsuffered 33 transient episodesof right hemiparesis, aphasia,and left amaurosis over a five-month period, was found tohave a severe stenosis of theleft carotid bifurcation after apercutaneous left carotid arte-riogram. With the patientunder general anaesthesia withhypothermia to 28°C by meansof ice bags for cerebral protec-tion, the bifurcation wasresected and blood flow
restored by end-to-end anasto-mosis between the commoncarotid and distal internalcarotid arteries. The carotid
was occluded for 28 minutes.The patient was completelyrelieved of her symptomsand was alive and well at theage of 86.”
In The epic 1954 operationthat led to one of surgery’smajor advances: carotidendarterectomy (Grand RoundsVol 4, 2004 e-Med), John EConnolly, professor of surgery,University of California,Irvine, USA, tells: “Pickering,Professor of Medicine at StMary’s (...) wisely obtained acarotid arteriogram whichshowed a significant stenosisof the left internal carotidartery. He then suggested to theProfessor of Surgery, CharlesRob, that the lesion might becorrected by surgery. Felix
Eastcott, who was hisAssistant Director, then per-formed the operation withoversight by Rob.”
The paper ‘Reconstruction ofinternal carotid artery in apatient with intermittent attacksof hemiplegia’ authored byEastcott, George WhitePickering and Charles G Robwas published in The Lancet inNovember 1954. The publica-tion gave the greatest impetusto the development of surgeryfor carotid occlusive disease.
Eastcott’s contributions to StMary’s Hospital is described byElsbeth Heaman in St Mary’s:The History of a LondonTeaching Hospital: “Eastcottwas born in Canada but raised
Felix Eastcott dies at age 92
Atherosclerotic renal arterystenosis is a commoncondition with an annual
mortality of approximately 16%per year. It is associated withhypertension and renal failurealthough it is not known if this is acausal relationship.
There have been three smallrandomised controlled trialscomparing angioplasty withbest medical treatment and nonehave been conclusive.
ASTRAL was set up in 2000to answer the question ofwhether stenting a renal arterystenosis would improve renalfunction and other cardiovascu-lar outcomes.
ASTRAL recruited 806
patients, making it the largestrenal revascularisation trial todate. Patients were largelyrecruited from the UK (53 cen-tres), Australia (three centres)and New Zealand (one centre).The majority of patients had>70% stenotic lesions with amean baseline creatinine ofapproximately 180umols/l(eGFR 40mls/min). Renal filtra-tion devices were not used.
Patients were randomised tobest medical treatment plusstenting or best medical treat-ment alone. Best medical treat-ment included antiplateletdrugs, statins and good bloodpressure control. Median fol-low-up was 34 months at thetime the data was locked.
There was no significant dif-ference in the rate of renaldecline between the twogroups, the mean difference inmean creatinine levels was only1.6umol/l lower in the stentingarm than the medical arm.Although the mean systolicblood pressure dropped overthe course of the trial, there wasno difference between the twoarms. Interestingly the diastolicblood pressure decreased sig-nificantly more in the medical
arm (p<0.03). The rate of renalevents (dialysis, nephrectomy,transplantation, dialysis anddeath from renal failure) wassimilar in both arms (p= 0.97).Cardiovascular events (myocar-
dial infarction, stroke, cardiacfailure, hospitalisation for angi-na, coronary revascularisationand peripheral arterial proce-dures) were again similar andnot significant (p=0.96). Therewas also no significant differ-ence in survival with 103deaths in the stent arm and 106in the medical arm, an overallfive-year mortality of about
40%. A per-protocol analysisalso failed to reveal any signifi-cant differences in any of theoutcome measures.
In the stenting arm, 23patients suffered 31 serious
complications including twodeaths, five significant acuterenal injuries, one renal arteryocclusion and three amputa-tions related to cholesterolembolisation.
In conclusion, ASTRALcould find no additional clinicalbenefit from renal artery stent-ing over and above best med-ical treatment at least in the
short term. There is also a smallbut not insignificant morbidityand mortality associated withrenal stenting in these arterio-pathic patients. The trial contin-ues to follow up the patients.
Some doctors have found theresults of ASTRAL difficult toaccept arguing that it is not theirexperience locally. Others citethe many papers which indicateup to a third of patients withrenal function improving afterstenting. ASTRAL also found asimilar proportion whose renalfunction improved but this fig-
The largest-ever randomised study evaluating theeffectiveness of catheter-based interventions inpatients with renal artery stenosis, the ASTRAL(Angioplasty and stent for renal artery lesions) trial,has shown that angioplasty and stenting offer nobenefit over medical therapy. The results arepublished in the 12 November issue of The NewEngland Journal of Medicine. Jon Moss, ASTRALjoint principal investigator (with Philip Kalra andKeith Wheatley) writes for Vascular News
BIBA Publishing
Continued on page 2
Continued on page 2Jon Moss
Felix Eastcott
“The largest renal revascularisation trial to dateshowed no difference in the rate of renal declinebetween the two groups”
www.vascularnews.com
WITH THIS ISSUE
SPECIALSUPPLEMENT

ure also applied to the medical arm suggestingthe stent has nothing to do with this improve-ment. This is one of the great strengths of a ran-domised controlled trial. Other critics ask aboutthe severity of the renal disease and degree ofstenosis in the ASTRAL patients.
When ASTRAL was set up the protocolspecified several subgroups, per cent stenosis,renal length, baseline renal function and rate ofdeterioration in renal function. Although thenumbers in each of these is understandablysmaller there were no significant differences tobe found. A post hoc subgroup analysis of the163 patients with either a single kidney orbilateral stenosis (>70%) again failed to showany significant between-group difference.Therefore although a large trail such asASTRAL may disguise a small subgroup whomay benefit from stenting, we were unable toidentify and such group.
It is important to understand that not everypatient with renal artery stenosis went intoASTRAL and the criteria for entry were simplythat the local team had to be “uncertain” as towhether stenting would be beneficial (a stipula-tion of any randomised controlled trial ethical-ly). Therefore patients with uncontrollablehypertension, acute renal failure and “flash”pulmonary oedema would have been unlikelyto be considered for ASTRAL in most centres.
The STAR trial conducted in Holland andalready published (2009) is a similar but smallerrandomised controlled trial (n=140). It alsofailed to find any improvement in renal functionwith stenting and reported a 3% procedure relat-ed mortality rate. The final and perhaps lastpiece of the jigsaw puzzle will come with thefindings of the awaited US CORAL trial.
Jon G Moss, Department of Radiology, NorthGlasgow University Hospitals, GartnavelGeneral Hospital, Glasgow, UK
November 2009
BIBA Publishing
Johannes Lammer, Vienna, Austria, principalinvestigator of the STRIDES trial spon-sored by Abbott Vascular, presented the six-
and 12-month results of the trial at CIRSE 2009,in Lisbon, Portugal.
“Dynalink E is a slow-eluting, self-expand-ing, drug-eluting stent releasing approximately80% of the drug over three months. There wassustained clinical benefit with improvement inRutherford-Becker clinical category in 80% ofpatients after 12 months and there were noobserved stent fractures after 12 months.
“A retrospective comparison to the historicalVIENNA Absolute trial suggested improvedpatency rate of Dynalink-E vs. bare metal at sixmonths. However, the improved patency ratewas not sustained at 12 months,” he said.
This follows the results of the SIROCCO IIstudy which showed that drug-eluting stents havedelayed, but failed to conquer restenosis in thesuperficial femoral artery. SIROCCO II(Sirolimus coated Cordis Smart nitinol self-expandable stent for the treatment of obstructivesuperficial femoral artery disease) confirmed theshort-term efficacy of the slower release formula-tion identified in SIROCCO I. It found good out-comes in the bare Smart stent arm of the trialwith an overall six-month angiographic pooledrestenosis rate of 11.6% (n=43) and an 18-monthrate of 22.2% (n=45). However, slower elutingdata pooled from SIROCCO I and II resulted inan early statistically significant difference in theprimary endpoint (mean stent diameter) showedthat this advantage was lost by 18 months.The STRIDES trial enrolled 104 patients at 14European sites, with a primary endpoint of in-stent restenosis in the superficial femoral arteryat six months. Secondary endpoints includeangiographic (X-ray) measurements of thechange in vessel lumen diameter between thetime immediately following stent placement andat 12 months, restenosis at 12 months, as well asfive-year clinical follow-up to track resolutionof peripheral artery disease symptoms, limbpreservation and patient survival.
The STRIDES trial enrolled complex patients,including 17% with critical limb ischaemia, 45%with total limb occlusions, 39% with lengthgreater than 10cm, 9.4% with restenosis and 78%with TASC C 2000 classification.
“This is a first-in-man evaluation of Dynalink-E in the superficial femoral arteries and the pur-pose of the first-in-human STRIDES trial was toevaluate the safety and efficacy of an everolimus-eluting nitinol stent for the treatment of superfi-cial femoral and proximal popliteal arterialocclusive disease,” Lammer said. “The superior
patency rate of the drug-eluting Dynalink-E stentwithin the first six months may be beneficial topatients with critical limb ischaemia to improveearly wound healing.”
Experts find that while drug-eluting stentsapproved for use today were designed with thecoronary arteries in mind, superficial femoralarteries in the leg present a different kind ofanatomy that can be challenging to treat becausere-obstruction of the vessel is a major concern.
The STRIDES trial is evaluating the use of aself-expanding stent system specifically designedto withstand normal leg movement, combinedwith the anti-proliferative drug everolimus, as a
longer-term treatment alternative for patientswith superficial femoral artery disease.
Johannes Lammer spoke to Vascular Newson the results of the STRIDES trial.
After the slightly disappointingSTRIDES results what are your viewson drug elution in the periphery?
JL: We have learned that the patency rates ofballoon angioplasty alone in superficial femoralarteries are poor (less than 50%). We have alsolearned that the patency rates of bare metalstents are significantly better than those ofballoon angioplasty, but they are not goodenough for patients with intermittentclaudication. Two-year patency rates of 50% to70% are certainly insufficient for patients withintermittent claudication. Therefore newstrategies are required. Drug-eluting balloonsand stents as well as covered stents are currentlyconcepts which may improve the patency ratesin superficial femoral artery obstructions.
What might be the future benefits ofdrug elution in the periphery?
JL: Drug-eluting balloons may improve thepatency rates for patients who have a goodangioplasty result without a residual stenosisand without flow limiting dissections.However, we know that at least 30% of patientswill have a poor balloon angioplasty result.These patients may need drug-eluting stents.The combination of bioabsorbable stents withdrug elution may be the ultimate concept.However, this is not available currently.
in the West Country, where two of his uncleswere medical men. Coming from a soccerschool, he played only third-string rugby at StMary’s, but he enjoyed the student life tremen-dously. While still an undergraduate, on theadvice of the physiology lecturer, he took hisPrimary FRCS, along with a few other students,‘the ones who were getting reasonable marks,and did not mind holding back our clinical workfor three months.’ When the war began, he wasevacuated to Hammersmith Hospital, where thepostgraduate atmosphere was enquiring ratherthan didactic, ‘just the opposite of Mary’s.’Astint as surgical registrar at Harefield provokedan interest in thoracic surgery.” Heaman saysthat, at the end of the war, Eastcott was invitedfor an exchange with the Peter Bent BrighamHospital in Boston, USA. “The Peter BentBrigham was a world-class centre for surgicalresearch, and by associating with it, St Mary’sjoined the vanguard of vascular surgery.
Eastcott was assigned to the laboratory of a bio-chemist-physiologist and introduced to CharlesHufnagel and David Hume, two great pioneersin transplantation surgery. By the end of theyear, Eastcott had done a hundred major graft-ing operations. Eastcott returned to St Mary’s asassistant director of the surgical unit in1950–51. However, few British surgeons wereperforming vascular surgery, and the field was
wide open. Under Rob and Eastcott, St Mary’sbecame an internationally famous centre forvascular surgery.”
The early days of carotid surgery
In 1948, Dos Santos had performed athrombendarterectomy of the femoral artery inLisbon and, in 1951, Miller Fisher, a neurologistfrom Montreal, had provoked the vascularsurgeons into attempting to overcome thefleeting symptoms of stroke by anastomosingthe patent branches of the external carotid arteryto the distal internal carotid artery. Certainly thisprocedure was performed in 1951 by CarreaMurphy and Molins and reported in 1955, butDeBakey performed carotid endarterectomy on7th August 1953. He did not publish the resultsfor a long time. The first published results on acarotid surgery were by Felix Eastcott inLondon in 1954. The procedure was performedat St Mary’s Hospital in early 1954 andpublished in The Lancet in November 1954.
Continued from page 1
Editorial comment by RogerGreenhalgh, editor-in-chief,Vascular News:We have waited for some time with batedbreath to see the rumoured results of theASTRAL trial which were given last springin the United States but just appear in print.It has to be said that whatever the cause ofthe delay, it is a pity because there has beengreat interest for some time but no data tocomment upon.It is very encouraging that the principal
investigator, Professor Jon Moss, has writtena review here which is greatly appreciated.I conclude that there is no evidence of
benefit with endovascular correction ofrenal artery stenosis. I sympathise with theinvestigators as the findings are counterintuitive just as some trials have turned out.EVAR 2 was one such. A certain result isexpected and clinicians can rightly questiona trial if it seems unlikely.We also need toassume that the results could be telling ussomething. There may be a subgroup as JonMoss implies but overall, the interventionhas not produced the expected result. Surelyit is obvious that a renal artery stenosis isbetter dilated to increase blood flow andproduce better renal function. Obvious butnot shown in this trial.I think I see why there was a delay in
publication. On one side or another of theeditorial process there has been checkingand double checking, but now we have it.
2
Johannes Lammer
Setback for drug elution in the peripheryas STRIDES follows SIROCCO
ASTRAL trialresults show nobenefit for renalartery stentingContinued from page 1
Felix Eastcott dies at age 92
Operating room during the carotid surgery in1954; back to camera is Eastcott


November 2009
BIBA Publishing
4
By Thomas Wyss
International CarotidStenting Study (ICSS)Jonathan Beard of the SheffieldVascular Institute, Sheffield, UK,started off with the safety results ofthe ICSS trial reporting on early out-come of patients with a symptomaticstenosis randomised for carotid arterystenting and endarterectomy. This trialhas been highlighted in the last issueof Vascular News following presenta-tion of results by Martin Brown at theEuropean Stroke Conference inStockholm, Sweden.
Over 800 patients in each groupwere analysed per protocol up to 30days post-procedure. “Not too manycrossovers, once the procedure was ini-tiated. However, 62 patients who wererandomised on duplex alone were thenfound to be unsuitable for stenting.“This tells you that you really shoulddo a magnetic resonance angiogrambefore deciding whether to randomise apatient. We know that now, we did not
know that then,” Beard said.Eighty five per cent of the patients
were treated within 30 days afterrandomisation. Primary short-termoutcome to 120 days post-randomisation showed a highlysignificant difference in stroke, deathand myocardial infarction rate of8.5% in the stenting group vs. 5.1%in the endarterectomy group (HR1.73, 1.18–2.52). Secondaryoutcomes were any stroke (7.7% inthe stenting group vs. 4% forendarterectomy) and all cause death(2.3% vs. 0.8%). Myocardialinfarction did not show a statisticallysignificant difference between thetwo groups.
“There is strong evidence thatendarterectomy is safer than stentingfor the primary outcome of anystroke, death or myocardialinfarction,” Beard said. This is mainlydriven, he added, by more fatalstrokes and more non-disablingstrokes lasting >7 days after stenting.Results from per protocol analysis and
a magnetic resonance imagingsubstudy (assessment of silentcerebral ischaemia) support the resultsfrom the intention to treat analyses.There is no clear benefit for cerebralprotection devices (filters) in asubgroup analysis.
Credentialing data of CREST
Thomas Brott of the Mayo Clinic inJacksonville, USA, was scheduled topresent the CREST data. His non-appearance and the sheer absence ofdata beyond the lead-in phase did raiseserious concerns. Despite the fact thatrandomisation stopped almost oneyear ago, safety data and 30-dayresults are still not available. NoAmerican investigator showed up togive the presentation. Henrik Sillesenof the University of Copenhagen,Denmark, kindly stepped in.
A credentialing phase was per-formed to ensure that the study com-pares the best surgical to best stentingability possible. This was a non-ran-domised phase, where procedural
indications, technique, and resultswere intensely scrutinised. The lead-in phase began in June 2000, and therandomisation in December 2000.Octogenarians were excluded laterbecause of safety. In January 2005,inclusion was extended to asympto-matic patients with stenosis ≥60%. Inthe CREST lead-in phase, 409patients were enrolled for stenting:stroke/death was 4.4% in total, and6% in symptomatic patients.Periprocedural stroke/death wasincreased when stenting was associat-ed with haemodynamic instability:11.4% vs. 4.1% (p=0.004). Women(37% of the lead-in cohort) showed a4.5% 30-day stroke/death rate com-pared to 4.2% in men.
In conclusion, the credentialingprocess has resulted in interventional-ists that have matched or exceededoutcomes achieved in other carotidartery stenting procedural reg-istries/trials. Additional knowledgewas gained on the importance ofhaemodynamic monitoring and man-
agement. Data is finally expected tobe presented by the investigators atthe end of 2009. During the discus-sion, Hans-Henning Eckstein,Munich, Germany, mentioned that,“From a researcher’s point of view, Ifind it really unacceptable, becausewe need those data. There is aresponsibility to the community.”Furthermore, the attendees ques-tioned the generalisability of theanticipated results because of theexclusion of octogenarians.
CAVATAS
Jonathan Beard also presented long-term results of the Carotid andVertebral Artery TransluminalAngioplasty Study (CAVATAS). It isthe first trial of endovasculartreatment vs. carotid endarterectomyfor symptomatic carotid stenosis. Alimitation is the relatively smallnumbers (roughly 250 in eachgroup). “The trial came in for somecriticism, mainly from Americans,regarding the high stroke and deathrate (10%). They then published theSAPPHIRE trial with pretty similarresults,” Beard said. There weredelays between randomisation andtreatment with quite a lot of the earlystrokes and deaths during this period.“After randomisation you need to geton with the treatment,” Beard added.
The pros of CAVATAS are long-term follow-up, annual duplexassessment of restenosis andangioplasty plus stenting. “It is theonly trial we have where we cancompare angioplasty vs. stenting,”Beard said. After eight years offollow-up, with a remainder of 21patients at risk in each group, carotidendarterectomy has a 30.2 %cumulative incidence of any stroke,transient ischaemic attack or amaurosis>30 days post-treatment, compared to36.9 % after endovascular treatment(HR 1.37, 95% CI 0.95–1.97).The rate of ≥70 % restenosis onultrasound, over five years after theprocedure, is three times morecommon after endovascular treatmentthan after endarterectomy. Stents havea lower restenosis rate than angioplasty(to five years). Furthermore, restenosisover ≥70% doubles the risk of anipsilateral neurological event. The riskof recurrent ipsilateral stroke is stillquite low.
In summary, continuing concernremains about long-term restenosisafter carotid artery stenting orangioplasty.
CRESTfallen sense at theESVS carotid trial sessionAbove all, the audience at the European Society for Vascular Surgery meeting, in Oslo, Norway, awaited the results of theCarotid Revascularization, Endarterectomy vs. Stenting Trial (CREST) by Thomas Brott but eventually heard that he would notspeak and no results were available. After the recent International Carotid Stenting Study, the results of CREST are eagerlyawaited. It is true to say the audience was crestfallen. Only the credentialing phase data were presented
Jonathan Beard Henrik Sillesen
The way we look at carotid artery plaques isvery old fashioned, Clark Zeebregts,University Medical Center in Groningen,
The Netherlands, said. Zeebregts provided aninsight into modern carotid artery plaque imagingtechniques at the European Society for VascularSurgery Annual Meeting in Oslo, Norway.“Asymptomatic today does not necessarily meanasymptomatic tomorrow,” he said.
According to Zeebregts, plaque vulnerabilityneeds to be predictable. Stable plaquecharacteristics have been identified as smoothmuscle cells, collagen, elastin, and calcification.Unstable plaque characteristics are inflammationof fibrous cap, lipid core, macrophages,neovascularisation, and intraplaquehaemorrhage. The contemporary modalities arecerebral angiography, duplex ultrasound andmagnetic resonance imaging and computedtomography angiography. However,identification of high-risk carotid plaques is a
key point. Plaque vulnerability rather than thedegree of stenosis might be important inpredicting the risk of events.
Biomarkers that can be targeted andvisualised by molecular imaging could provideinformation on inflammation, proteolysis,angiogenesis, hypoxia, and apoptosis. Forexample, inflammation can be visualised by18Fluorodeoxyglucose (FDG) – PositronEmission Tomography fused with magneticresonance imaging. There is presumably ahigher FDG uptake in symptomatic plaques, notverified yet. Proteolysis is involved in the earlystages of plaque development and the late stagesof plaque destabilisation. The proteolyticenzymes, e.g. matrix metalloproteinases andcathepsin cystein proteases can promote caperosion. Molecular imaging with a highlysensitive camera for molecular proteolytic stepscan reflect enzyme activity in hot spots of theplaque. Furthermore, this can lead to not only to
visualisation but even quantification ofproteolytic activity, Zeebregts said.
Hypoxia can possibly be visualised by directimaging of hypoxia markers (e.g. hypoxiainducible factor 1α). This has not beenperformed yet. Apoptosis is present in a necroticcore, containing lipids, dead cells and debris. Anuclear imaging tracer as Annexin A-5 can bindto phophatidylserine on the cell surface and canvisualise apoptosis. Bio-optical imaging hasbeen used in Groningen to locate sentinel lymphnodes in breast cancer patients using anintraoperative near infrared fluorescent imagingcamera. In the future, this could be used as akind of screening tool if available as a hand helddevice. Zeebregts hypothesises, “That thedegree of stenosis is less important than theplaque’s vulnerability.” The goal is to sort outwhich processes and biomarkers are mostprognostic for subsequent plaque rupture andthus superimposed thrombus.
Carotid plaque vulnerability may be key to predict risk
Clark Zeebregts

Over a dozen years ago, the seminaldiscussions regarding a randomised trialcomparing carotid endarterectomy with
carotid stenting in patients with severe carotidbifurcation stenosis and recent (<180 days)commenced. At the time carotid artery stentingwas a very novel (only practiced with anyfrequency since ~1995) percutaneous method ofcarotid revascularisation practiced by very fewexperienced sites or operators, with no dedicated(or nitinol) stent equipment, and no emboliprotection devices. Carotid endarterectomy wasan elegant, nearly half-century, well-establishedtherapy that at the time had recently been proveneffective over medical therapy in standard riskpatients. The data from the NACSET (1991) andACAS (1995) trial publications had solidlyestablished carotid endarterectomy as thestandard of care for symptomatic andasymptomatic patients, respectively. But carotidartery stenting had no such data on which to basea trial of standard risk patients: the majority ofcases that had been reported in the literaturewere in high surgical risk patients. Moreover thedevice system (stent and emboli protection) thatthe trial would ultimately use had very littlehuman experience, and actually did not complete
its pivotal FDA study until well after the start ofCREST (Carotid RevascularizationEndarterectomy vs. Stent Trial).
Trial design
These limitations in predicate carotid arterystenting data and lack of even phase I device dataaside, there was consensus among the organisersthat a randomised trial of symptomatic standardsurgical risk patients should and could beconstructed and completed. A statistical planincluded a 2,500 patient study conducted overfour years at 50 sites and powered (90%) todetect a >1.2% difference between the primaryendpoints. Unique in the CREST study designwas the a dual set of endpoints to address theneeds of the pivotal players: one for the sponsor(Abbott Vascular)/FDA for device approvalwhich was a standard non-inferiority at one yearof stenting and endarterectomy, and one for theNIH/NHLBI which was a superiority of a hazardratio on a multi-year basis of stenting overendarterectomy. While there is concern that acircumstance could arise that the outcome of thetrial might not be synchronous (e.g., having asuccessful non-inferiority outcome but failing onthe superiority outcome), the odds of this were
estimated at 1 in a 1,000.The first patient was enrolled in CREST in
2000, but in 2005 after four years and only ~20%of the planned population enrolled, the protocolwas amended to include asymptomatic patients inan effort to improve the tempo of recruitment. Inaddition site number was expanded to >100.While this had a very good effect on the pace ofthe study, and fortunately the split between symp-tomatic and asymptomatic patients was roughlyeven at the time the trial was completed, never-theless it will have consequences for the statisticsof the trial: since there will likely be fewer eventsin the overall population, the power to detect adifference between the two therapies will belower though probably not enough to limit theimpact of the results.
Impact of trial duration
Through the combined efforts of hundreds ofpeople and the solid support of the NIH/NHLBI,CREST completed enrolment in the summer of2008. Credit must be given to all of them formaintaining a strong commitment to thisimportant study, but most of all to the co-principleinvestigators, Robert Hobson (vascular surgery)and Thomas Brott (stroke neurology). Dr Hobsonunfortunately passed away during the trial, but theimportant work of completing the study is in thevery capable hands of Dr Brott, and trial resultsare expected to be made public at theInternational Stoke Meeting in February 2010.
During the course of this study, carotid arterystenting continued to evolve from both techni-cal/device as well as operator expertise andpatient selection perspectives. Specifically, at thestart of this study there were no US multicentrecontrolled data in carotid artery stenting nor anyFDA-approved carotid stent or embolic protec-tion systems; at the conclusion of CREST enrol-ment there were 10 successfully completed mul-ticentre pivotal trials, and almost as many FDAdevice approvals. It is clear from even a cursoryexamination of those trials that there has been arapid and significant temporal improvement instenting outcomes independent of devices, frominitial 30-day stroke and death rates in the 7–8%range to current rates of ~3%. Moreover, sincethe first device was approved in 2004 (coinci-dentally the same one used in the CREST) post-approval studies have also demonstrated a rapid
improvement outside the investigational centres,such that today carotid artery stenting outcomesin high surgical risk patients meet or better theAmerican Heart Association recommendationsfor outcomes in standard risk surgical patients.
Along the way, we have also identified predic-tors of outcomes in stenting (age, symptomaticstatus, specialty training) not previously recog-nized at the start of CREST. These were not builtinto CREST plan as prespecified analyses but willclearly have impact on its interpretation.
Ultimately, there may be very little effect ofthe duration of CREST and any interaction withthe evolution of carotid stenting outcomes andknowledge but it will be important to frame theresults on this background.
Importance of CREST
CREST is the largest study to assess carotidartery stenting and endarterectomy in arandomised prospective fashion, involved 224interventionalists and nearly 120 centres, and wasa multi-million dollar investment by the NIH so itis fair to ask what its relevance will be for thefield and its implications for patients care.
Previous outcomes in several European studiesof symptomatic patients have been less thanfavourable for stenting, and while there are widelyacknowledged limitations of the design and con-duct of those studies ranging from operator experi-ence to lack of embolic protection, they neverthe-less have had a significant negative impact oncarotid artery stenting worldwide. CREST was nothalted on the basis of these other study outcomesas the Data Safety Monitoring Board did not iden-tify any undo safety issues within CREST itself.Moreover we are in an impasse in this countryover coverage of carotid artery stenting by theCenters for Medicare and Medicaid Services ofdevices which have proven to be safe and effectivethrough FDA trials (and validated in post-approvalstudies), and nevertheless not a covered service forthe majority of Medicare beneficiaries who requireit. It is obvious that the results of CREST will addto the accumulating stenting data in a very mean-ingful way, comes at a critical juncture, anddepending on the outcome could significantly alterthe carotid therapeutic options for patients.
William A Gray, associate professor of ClinicalMedicine, Columbia University, New York, USA
November 2009
BIBA Publishing
6
The Centers for Medicare andMedicaid Services (CMS) haveruled against expanding cover-
age of carotid artery stenting in theUSA. In the decision released in earlySeptember, the CMS have alsorequested public comments on theproposed decision. After consideringthe public comments, the CMS willmake a final determination and issue afinal decision memorandum.
“We propose to make no changes incoverage of patient groups for percuta-neous transluminal angioplasty of thecarotid artery concurrent with stent-ing,” says the CMS decision. Theorgan proposed to retain the existingcoverage for the following with aslight revision to the language regard-ing embolic protection devices:� Patients who are at high risk for
carotid endarterectomy and whoalso have symptomatic carotidartery stenosis ≥70%. Coverage islimited to procedures performedusing FDA-approved carotid arterystenting systems and FDA-approved or cleared embolic protec-tion devices;
� Patients who are at high risk forcarotid endarterectomy and have
symptomatic carotid artery stenosisbetween 50% and 70%, in accor-dance with the Category B IDEclinical trials regulation (42 CFR405.201), as a routine cost underthe clinical trials policy (MedicareNCD Manual 310.1), or in accor-dance with the NCD on carotidartery stenting post-approval stud-ies (Medicare NCD Manual 20.7B);
� Patients who are at high risk forcarotid endarterectomy and haveasymptomatic carotid artery steno-sis ≥80%, in accordance with theCategory B IDE clinical trials regu-lation (42 CFR 405.201), as a rou-tine cost under the clinical trialspolicy (Medicare NCD Manual310.1), or in accordance with theNCD on carotid artery stentingpost- approval studies (MedicareNCD Manual 20.7B).
In March 2009, the Society forCardiovascular Angiography andInterventions asked the agency to con-sider new evidence that it believedwould support extending coveragepatients with symptomatic carotidartery stenosis of 50% to 60% orgreater outside of clinical studies. Thatevidence included research that was
only just published or under review forpublication at the time of the CMS’sprevious decision in October 2008 –results of the SAPPHIRE worldwidepostmarketing registry, the CAPTURE2 registry, and the EXACT registry.
But now, having reviewed this evi-dence, the CMS reviewers proposed“to make no changes in coverage ofpatient groups for percutaneous trans-luminal angioplasty of the carotidartery concurrent with stenting” and“to retain our existing coverage.” Theonly changes are some revisions tolanguage pertaining to embolic-protec-tion devices. Specifically, the revisednational coverage determination nowreads: “Coverage is limited to proce-dures performed using FDA-approvedcarotid artery stents and FDA-approved or -cleared embolic-protec-tion devices. The use of an FDA-approved or -clearedembolic-protection device is required.If deployment of the embolic-protec-tion device is not technically possible,then the procedure should be aborted,given the risks of (carotid artery stent-ing) without embolic protection.”
During the TCT conference, in SanFrancisco, Michael Jaff, associate pro-
fessor of medicine, Harvard MedicalSchool, and medical director, VascularCenter, Massachusetts GeneralHospital, Boston, USA, presented areview of the data on guidelines forcarotid stenting and commented on theCMS proposed decision.
“They make this decision based ontwo questions: ‘Is the evidence suffi-cient to conclude that carotid angio-plasty with stenting for asymptomaticpatients with 80% stenosis improvesoutcomes outside a clinical trial orpost-market surveillance study?’And,‘Is the evidence sufficient to concludethat carotid stenting for asymptomatic
patients with anatomic high risk and80% stenosis or symptomatic with 50to 75% stenosis improve outcomes?’Their answer is no, the data do notsupport that,” Jaff said. He continued:“How could they make such a deci-sion? They looked at a single publica-tion, an analysis of trials comparingendarterectomy and carotid stenting.And their conclusion is the results donot support a change in clinical prac-tice,” he said.
Jaff concluded that carotid stentingfor stroke prevention is comparable toendarterectomy for high-risk patientsand ACT 1, CREST, ACST 2, andSPACE trials will provide compar-isons between stenting and surgery forstandard-risk patients. Jaff alsoclaimed for additional data comparingstenting to contemporary medical ther-apy in both high- and standard-riskpatients. “Any comparisons must be‘apples with apples’, high risk withhigh risk, comparable operator train-ing, and same rigor of neuro assess-ment,” Jaff said.
There are currently seven carotidstent systems with premarket approvalfrom the FDA plus five distal filterembolic protection devices and onedistal balloon occlusion embolic pro-tection device with FDA 510(k) clear-ance. Recent FDA 510(k) clearedembolic protection devices includeone proximally placed flow reversalembolic protection device and one dis-tally placed filter with focal suction.
CMS rules against expandingcoverage for carotid stenting
Michael Jaff
Reading the tealeaves: Looking aheadto the outcomes andimpact of CREST
COMMENT & ANALYSIS
WILLIAMGRAY


November 2009
BIBA Publishing
8
The Crosser Catheter Systemwas found to be safe and feasi-ble in treating critical limb
ischaemia patients with peripheralchronic total occlusions, with a 30-day limb salvage rate of 90.3%.
Results of the CROSS (The CrosserCatheter to revascularise chronic totalocclusions to facilitate successful limbsalvage) multicentre registry were pre-sented by Raghotham Patlola,Cardiovascular Institute of the South,Lafayette, USA, at the TranscatheterCardiovascular Therapeutics confer-ence, in San Francisco.
Patlola said that “shockingly” pri-mary amputations are still the mostcommon critical limb ischaemia treat-ment, and in 2002–2003, 67% of theAmerican critical limb ischaemiapatients had primary amputation asinitial treatment. “More shockingly,50% of the primary amputations areperformed without angiography or asimple ankle brachial index test.”
Patlola reported his group 15-month experience with the CrosserCatheter System (FlowCardia), anovel chronic total occlusion crossingdevice now used as “first-line thera-py” in critical limb ischaemia. Thestudy was led by David E Allie,Louisiana Cardiovascular and LimbSalvage Center, Lafayette.
The Crosser utilises high frequency,mechanical vibration to facilitate pas-sage through blockages in the arteries.It is designed as a frontline therapy toenable central lumen crossing ofchronically occluded arteries.According to FlowCardia, over 7,500
Crosser procedures have been per-formed to date around the world.
“We theorised a centre lumenchronic total occlusion crossingwould offer technical and clinicaladvantages over traditional subadven-titial wire crossing facilitating treat-ment, optimising all definitive inter-ventional options, and potentiallyimproving outcomes therefore allow-ing treatment of the infrapoplitealslike the left anterior descendingartery,” Patlola said.
Between February 2008 and July2009, the CROSS critical limbischaemia registry analysed 269patients with 321 chronic total occlu-sions treated with the CrosserCatheter System as “front line thera-py”. Arteries treated included superfi-cial femoral 147 (45.7%), popliteal 44(13.7%), peroneal 35 (10.9%), anteri-or tibial 37 (11.5%), posterior tibial40 (12.5%), iliac 14 (4.4%) and com-mon femoral 4 (1.2%). In-stent occlu-
sions occurred in 44 of the 321 casestreated (16%).
The results showed that technicalsuccess of the device was achieved in269 out of 321 occlusions (83.8%).There were no clinically relevantcomplications. The average chronictotal occlusion length was 220.5 ±98.3mm. The mean Crosser actuationtime was 225 seconds (range 9–300).Crosser actuation time of <30 secondsoccurred in 68/321 (21.1%). The 30-day limb salvage rate was 280 of 321(90.3%). The average case total fluo-roscopic time was 23.5 ± 14.5 min-utes (9–61.5) and total proceduraltime was 91 ± 32 minutes (26–189).
“The Crosser is now our first-linetherapy in treating critical limbischaemia and has facilitated ourchronic total occlusion crossing strat-egy of centre lumen crossing as inte-gral to a more contemporary approachto treating “infrapopliteals like theleft anterior descending artery”.
CROSS: Treating popliteals like theleft anterior descending artery
Raghotham Patlola
He was reviewing the effectiveness ofcutting balloon angioplasty, and tolddelegates at the Transcatheter
Cardiovascular Therapeutics, San Francisco,USA, that the aims of cutting balloonangioplasty are to reduce the trauma, improveacute result, reduce stent frequency, and improvepatency, through a controlled incision of thevessel wall. “Because of the longitudinalincisions, cutting balloon angioplasty dilates thetarget vessel with less force than conventionalballoon angioplasty to potentially decrease thevessel wall trauma,” Minar said. Initially, thecutting balloon was used in haemodialysis accessmanagement and in lesions resistant to standardballoon angioplasty alone.
A non-randomised, comparative study ofshort- and mid-term primary patency rates ofcutting balloon angioplasty versus standard bal-loon angioplasty for failing infra-inguinal veingrafts (Vikram et al CardiovascularInterventional Radiology 2007; 30:607–610),concluded that cutting balloons offered no defi-nite advantage over standard balloon angioplasty.The primary patency rate at 12 months was 9/25(36%) for standard balloon angioplasty and 5/10(50%) for cutting balloon angioplasty (p=0.47).
Initial reports on the use of cutting balloonangioplasty for the treatment of obstructive ath-erosclerotic disease of the superficial femoralartery have revealed promising results. However,Minar reported, “data from randomised studies
involving comparisons between conventionalballoon angioplasty and cutting balloon angio-plasty in the coronary arteries have failed toprove the superiority of the cutting balloon pro-cedure.
In the randomised, controlled trial “De novosuperficial femoropopliteal artery lesions:Peripheral cutting balloon angioplasty andrestenosis rates”, from Amighi et al, published inRadiology in 2008, cutting balloon angioplastydid not prove to be superior to conventionalpercutaneous transluminal angioplasty, and evenincreased restenosis at six months.
In another study “Infrainguinal cutting balloonangioplasty in de novo arterial lesions involving128 consecutive patients with 203 lesions (183stenoses, 20 occlusions) Canaud et al (Journalof Vascular Surgery 2008; 48:1182–1188)concluded that cutting balloon angioplasty issafe and feasible for the treatment ofinfrainguinal arterial occlusive disease, withrelatively low mid-term restenosis ratescompared to other endovascular treatments. Theoverall primary patency rates at one and twoyears were 64.4% and 51.9%, respectively.
Cotroneo et al have also found positive resultsfor the technique. The non-randomised,restropective, single-centre study “Cuttingballoon vs. conventional angioplasty in shortfemoropopliteal arterial stenoses” (Journal ofEndovascular Therapy 2008; 15:283–291)involved 84 consecutive patients with a total of
142 focal (≤3cm), calcified femoropoplitealocclusive lesions. Forty patients (67 lesions)were treated with angioplasty, and 44 patients(75 lesions) underwent angioplasty with cuttingballoon. At 24 months, the primary patency ratewas 66.6% in the angioplasty group and 79.7%for the cutting balloon group (p<0.001).Cotroneo et al concluded that “Cutting balloonangioplasty seems to be a valuable tool in theendovascular treatment of short femoropoplitealstenotic lesions, achieving better patency atmidterm compared to conventional percutaneoustransluminal angioplasty.”
Minar also mentioned a prospective,randomised, single-centre, controlled pilot studyanalysing cutting balloon performance for in-stent restenosis. “Repeated conventional balloonangioplasty of in-stent restenosis is technicallyfeasible and mostly yields acceptable immediateresults. Unfortunately, the short and midtermrates of recurrent failure after repeat balloonangioplasty of in-stent restenosis remain high,”Minar said.
Dick et al (Radiology 2008; 248:297)concluded from their small randomised studythat “cutting balloon angioplasty failed to provesuperiority compared with balloon angioplastyfor treatment of femoropopliteal in-stentrestenosis in a pilot study. In restenotic lesionswith an average length of approximately 8cm,both treatment modalities yielded disappointingsix-month patency rates.”
Cutting balloons no better thanconventional angioplasty
Erich Minar
“Cutting balloon angioplasty has failed to demonstrate any advantage over balloon angioplasty with regard to reductionof restenosis in patients with de novo femoropopliteal or in-stent restenosis lesions in two small randomised trials,” saidErich Minar, Medical University Vienna, Austria
Vascular surgeons have thehighest market share, thelowest overall mortality and
morbidity rates for peripheral arterialinterventions, when compared tointerventional cardiologists andinterventional radiologists who alsoperform this procedure. MohammadH Eslami, associate professor ofvascular surgery at the University ofMassachusetts Medical School inWorcester, USA, and his colleaguesreported their findings in theNovember 2009 issue of the Journalof Vascular Surgery.
“With all three specialties involvedin peripheral arterial procedures,there has been a significant increaseof interventions which in certain loca-tions has led to significant ‘turf wars’as to who should perform them andwho should not,” said Eslami.
“Using the Nationwide InpatientSample our research team reviewed23,825 peripheral arterial interventioncases (about 75% of the providers’specialties) from 1998 to 2005,”added Eslami. “We found the marketshare for vascular surgeons increasedfrom 27% to 43%, while the cardiolo-gists’ share rose from 10% to 29%.The radiologists, who previouslyalmost exclusively used endovascularmethods to treat patients with periph-eral arterial disease, had their sharedecrease from 36% to 6%. A yearlypercentage of unidentified providersremained relatively stable with amedian value of 22%, and did notaffect the market share trends.”
The majority of all peripheral arte-
rial interventions (52.3%) were per-formed at teaching hospitals, wheretrends were even more pronounced,showing that market shares for vascu-lar surgeons and interventional cardi-ologist were higher, compared to theradiologists’ share which againreflected a decline. In these settings,the vascular surgeons’ market shareeven had a more robust rise duringthe study period (18% to 48%).
Researchers noted that in-hospitalmortality rates were highest for radi-ologists 2.1% vs. 1.2% for vascularsurgeons and 0.6% for interventionalcardiologists. When combing theoverall post-procedure iatrogenicarterial injuries and mortality, thevascular surgeon group was the low-est at 1.7%. The radiologists had 3%;cardiologists were at 3.04%.Compared with vascular surgeons,the mortality rate odds ratio was 1.62times higher for the radiologistgroup’s patients. The vascular sur-geons also had the lowest post-proce-dure iatrogenic arterial injuries at0.5% compared to the radiologists at0.9% and cardiologists at 1.3%.
Researchers noted that peripheralarterial intervention has increasedseven-fold from 1976 to 1996 forpatients with peripheral artery disease.
“We concluded vascular surgeonsare endovascularly-trained, and havebetter access to fluoroscopy units andbetter safety records; therefore theywill continue to increase their marketshare,” said Esalmi.
Source: Journal of Vascular Surgery
Vascular surgeons performmost peripheral interventions

November 2009
BIBA Publishing
10
Against thebackdrop ofthe disap-
pointing STRIDEStrial data, Cook Medicalhas launched the firstdrug-eluting stent foruse in the superficialfemoral artery inEurope. The commer-cial launch of ZilverPTX took place at theCIRSE annual meetingon 20 September 2009.
Zilver PTX iswidely expected toimprove the stan-dard of care formany patients withserious blockages inthe superficial femoralartery by creating a highlyeffective, completely new treat-ment option.
At CIRSE 2009, MichaelDake, Stanford School of
Medicine, Stanford, USA, pre-sented highly promising reg-istry data out to two years, butthis did not include patency as
an end-point
which willbe available
once the results ofthe USA randomised trial arepresented next year. The ZilverPTX registry is the largest reg-
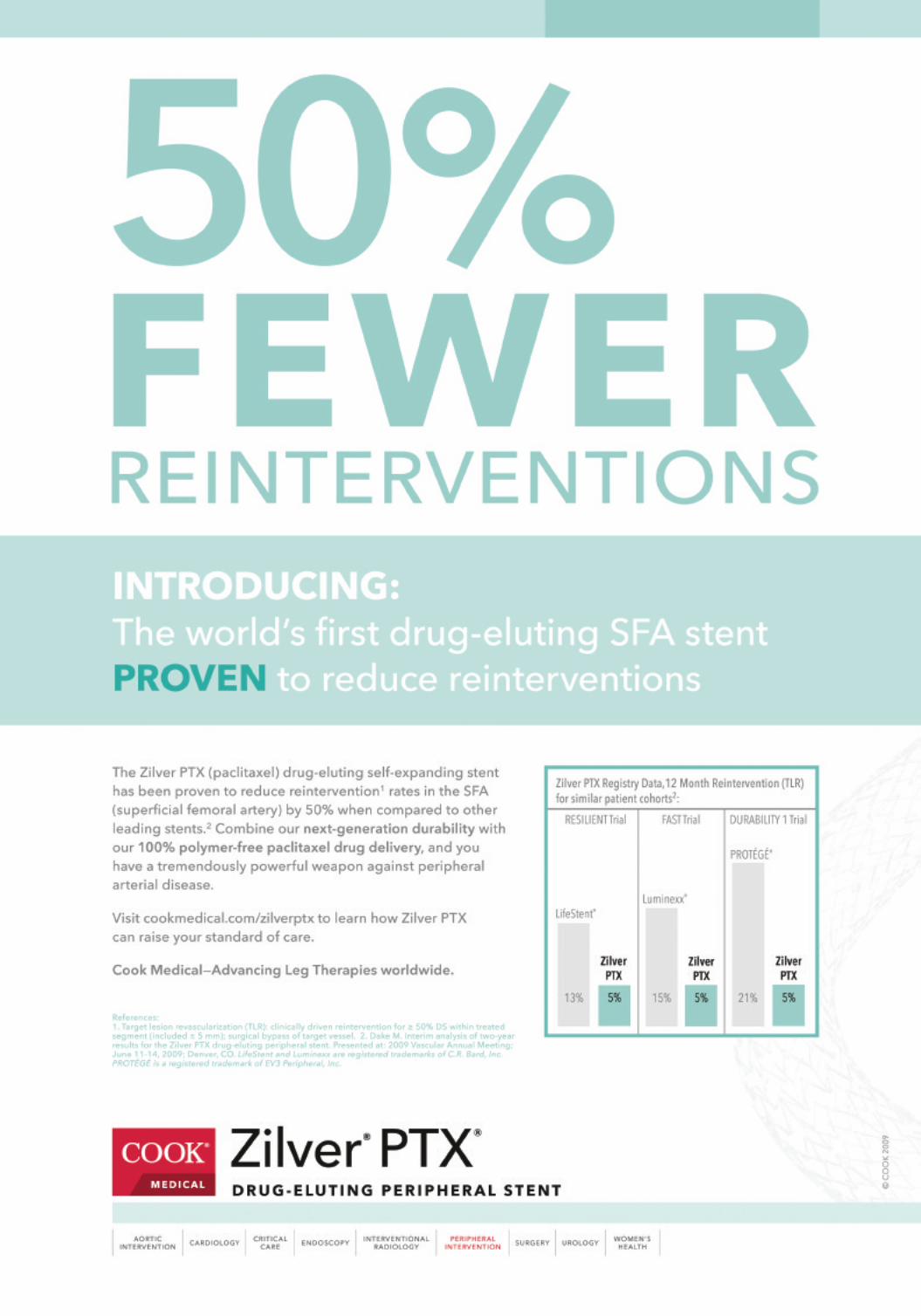
istry of its kind ever conduct-ed and results indicate thatthe Zilver PTX stent caneffectively bridge the gapbetween the patient resultsachieved using open surgicalbypass graft procedure.
In the largest clinical trialof its kind ever conducted, theZilver PTX stent was shown toeffectively bridge the gapbetween the patient resultsachieved using open surgicalbypass graft procedure – whichis typically more painful andrequires a longer hospital stayfor the patient – and the lesstraumatic, but typically less
effective, earlier minimallyinvasive treatment options forperipheral artery disease suchas balloon angioplasty and baremetal stenting, a press releasefrom the company said.
“With the Zilver PTX stent,Cook has introduced a truelandmark device that canreduce the number of peripher-al artery disease patients havingto endure the trauma of legamputations and bypass surger-ies,” explained Rob Lyles, vice-president and global leader ofCook’s peripheral interventionunit. “Clinically proven, poly-mer-free and exceptionallydurable, we expect the ZilverPTX stent to become the new
standard of care for peripheralartery disease in the superficialfemoral artery.”
The first drug-eluting stentapproved for treating peripheralartery disease in the superficialfemoral artery, the Zilver PTXstent first expands and holdsopen the artery to restore bloodflow. The device then deliversthe drug paclitaxel to the cellsin the vessel wall to reduce therisk of new blockages forming.In a major advance over previ-ous drug-eluting technologies,the Zilver PTX achieves target-ed drug delivery without usinga polymer to adhere the drug tothe stent body. This eliminatesthe potential patient risks asso-
ciated with polymer-coateddevices, including clot forma-tion and inflammation.
In an interview with VascularNews, Lyles indicated that Cookhad adopted a unique ‘afford-able innovation’ strategy toovercome potential financial orreimbursement barriers inEurope.
Cook Medical licenses therights to use paclitaxel onperipheral stents and othernoncoronary medical devicesfrom AngiotechPharmaceuticals of Vancouver,Canada. In the USA, ZilverPTX is an investigationaldevice not available for saleat this time.
First drug-eluting stentfor the superficialfemoral artery islaunched in Europe
Michael Dake
Cook Medical is collaboratingwith physicians around theworld to develop the
superficial femoral artery open-reg-istry using OpenDoor, the first-evertransparent clinical datamanagement suite.
Using an intuitive online webinterface called OpenDoor, clinicianscan track their patients, view themedical community’s trends intreating peripheral artery disease anddetermine the most effectivetreatment options for their patients.Transparency will be a centralobjective of the superficial femoralartery open registry, with results forall treatment types available toparticipating clinicians. This level oftransparency where all treatmentstypes are included, as well as real-time access could lead to a reductionin bias in the presentation of clinicaldata, and allow participatingclinicians access to real world patientresults. It will also provide a forumfor clinicians to communicate witheach other about superficial femoralartery treatments and outcomes.
The company says this observation-al registry will enable the exchange ofreal-world treatment results with otherclinicians to find the most effectiveoptions for patients, track patient out-comes and view community trends.OpenDoor assists with data visualisa-tion and analysis, while allowing clini-
cians to compare the outcomes of mul-tiple treatments, identify patient sub-sets and more. In addition, it couldhelp clinicians analyse with their prac-tice-specific data to monitor patientoutcomes.
The registry will collect clinicaldata including procedural and follow-
up information (out to five years).The data will be accessible within 30days of entry by the clinicians. It isintended to collect data on superficialfemoral artery cases including thosetreated with balloon angioplasty, baremetal stents, drug-eluting stents andsurgical intervention.
Features of OpenDoor:� Real-time data analysis� Data visualisation and analytics� Case portfolio management� Online forum for clinician collaboration� Resource library� Concierge service designed to assist clinicians with practice-specific
analyses
www.opendoor.cookmedical.com
Cook Medical developsclinical database on superficialfemoral artery treatments
Why do we need anotherdevice to treat superficialfemoral artery and
popliteal disease? Because currentdevices are not doing the job, dissec-tion rate is high, need for stenting isfrequent, and restenosis is prevalent,even with stenting, said JamesMargolis, Miami InternationalCardiology Consultants, Miami, USA.
Margolis presented individual andcombined results of two studies ofthe Guided Reshaping Technologysystem, from Minnow Medical, at theTranscatheter CardiovascularTherapeutics conference, in SanFrancisco, USA.
The Guided Reshaping Technologyconsists of a balloon angioplastycatheter designed to deliver radiofre-quency energy at non-ablative powerto dilate stenoses at low pressure,atraumatically reduce plaque, andlimit potential for restenosis in super-ficial femoral and popliteal arteries.
Margolis presented interim datafrom 78 patients showing 97.5 proce-dural success rate, improved ≥1Rutherford class at 94%, and that noadjunctive therapies, such as a stentor atherectomy were required. Noserious adverse events related to thedevice were reported. For thosepatients where interim six-month fol-low-up results are available, the datatrend to sustainable improvement.
“The early results are encouraging.
I am looking forward to seeing addi-tional data,” said Margolis. “TheGuided Reshaping Technology is fastand easy to use, and may become avaluable option to treat peripheralartery disease.”
The prospective, open-label, non-randomised study, which is being con-ducted at five sites in Germany, Chile,and Argentina, is assessing the safetyand effectiveness of the GRT systemin symptomatic patients with previ-ously untreated blockages in thepopliteal and superficial femoral arter-ies. The subjects are followed for sixmonths to determine clinical evidenceof restenosis. The company expects toreceive complete six-month follow-updata later this year. Minnow’s catheterreceived the CE mark in April 2009.
Plaques reduced withouttrauma using guidedreshaping system
James Margolis
The commercial launch of Cook Medical’s Zilver PTX took place at theCardiovascular and Interventional Radiological Society of Europe (CIRSE)meeting, in Lisbon, Portugal, in September

November 2009
BIBA Publishing
12
Endurant was designed toachieve ease of use andexpand the scope of
treatment of challenginganatomies. One of the new keyfeatures of Endurant is aunique design to conform tothe vascular anatomy of thepatient. Proximally, a coveredM-shaped stent reinforces theradial force on the neck andprovides sealing even inangulated and short necks. Thehydrophilic coating on the low-profile delivery system aims tofacilitate access in small andtortuous iliac arteries.
Medtronic’s commitment toevidence based medicine hasled to two projects: Firstly, theEndurant EU prospective mul-ticentre trial, which aimed toevaluate safety and efficacy ofthe device. Enrolment wascompleted in August 2008, andone-year follow-up was to becompleted before the end ofSeptember 2009 on 80 patients.Secondly, ENGAGE is thelargest industry-sponsoredprospective multicentre reg-istry of a stent graft everundertaken and aims to evalu-ate the device performanceover five years in a “realworld” setting. Eighty medicalcentres across six continentsare participating. The study isexpected to enrol 1,200patients.
What is your personalexperience with theEndurant stent graft?Has it allowed you toexpand the scope ofaortas treated with astent graft?Hence Verhagen: There are acouple of features that are areal improvement compared tostent grafts that were alreadyon the market at that time.What I particularly like is thesmaller sheath size of theintroducer. This definitelymakes a big difference. I havenot had an iliac issue since I
started using Endurant. Thistells you a lot. It is really moresmooth and easier to bring inthan the other stents. The otherthing I particularly like is thetop end of the stent graft: That
gives me the opportunity to putmy limits up a bit on what Ithink is suitable anatomy. So, Idefinitely treat shorter necksnow than I did before. Ofcourse, we only have experi-ence of one year and a couple
of months. So far, in my expe-rience, I have seen zero migra-tion and no problems withtreating shorter necks. This isjust a short time, but it is veryencouraging.
How does theintroducer size behavein very tortuous iliacarteries?
HV: Basically the same. If it isvery tortuous you need pusha-bility of the introduction sys-tem. This again, is better thanwhat we were used to, in myopinion. Tortuosity, whether itis narrow or not, is just not sucha big deal anymore. Especiallybecause the contralateral size isso small and one of the two ili-acs is usually pretty good. So,again, I have not declined onepatient on iliac anatomy.Yehuda Wolf: Predictably myexperience is similar because Iam using the same device.Maybe I would reiterate somepoints: Negotiation of iliacanatomy has stopped being aproblem, it is not an issue any-more. I really think the deviceis very flexible, and even themain body is so small andbehaves more like a flexiblecatheter/endovascular devicerather than like the stiff deviceswhich were available before. Soaccess and advancement in theiliac arteries has stopped beingan issue. Consequently, we now
do a large majority of casespercutaneously, since the small-er calibre makes negotiating theiliacs much easier. In theaneurysm neck, there is really asignificant improvement. Theway it appears after the deploy-
ment is truly impressive.Because the graft is flexible, itconforms to whatever deformi-ty you decide to tackleendovascularly. Plus you havea better feeling of control withthe capture mechanism anddelayed release of the
suprarenal crown and anchor-ing pins. Therefore, you canreally nail the graft downexactly where you want it. Thisis the reason why people feelmore comfortable addressingshorter necks.
It has definitely widenedthe variability of EVAR-treatable abdominalaortic aneurysms.
YW: It has enlarged the scopeof endovascular application.HV: Significantly, I think it is abig change. I have to stress thatas well. The preciseness of theproximal deployment is reallyon the millimetre. And that iswhat I particularly like.
Has it contributed to abetter outcome?
HV: Well, like I said, it is onlyjust over one year. So, that isnot very long of course. We canonly talk about the one-year
results, but the evaluation isongoing. I have not seen thefigures. I can only talk aboutmy own patients: There is nomigration, and there are notype I or III endoleaks. So far Ihave been really happy withthis device.
YW: I have an even shorter fol-low-up. We have only acute andearly midterm follow-up. But tosome extent even the short termfollow-up is important.Especially in the group of thevery old, let’s say octogenari-ans, what you are really lookingfor is to treat the aneurysmendovascularly without majoradverse events initially. This isnot to play down the long-termresults but for some of theabdominal aortic aneurysmpatients, the five- and 10-yearresults are not the most impor-tant thing. In the short term theresults seem very good.
Are you worried aboutsuprarenal deploymentwith wires across therenal artery orifices?
HV: Not at all. That is not anew concept. It has existed forabout 10 to 15 years. There hasbeen a lot of research on thatand I do not think there is anypaper that it is giving you badresults or kidney problems. So Iam not bothered. I am not con-cerned at all.
Could you comment onthe importance of theENGAGE study?
YW: Clinical evidence is obvi-
ously very important in all ofits aspects, this is clear cut. Ifwe are talking about theENGAGE study, it is a world-wide registry type, in a clinicalsetting in what we call the “realworld”, which is always differ-ent from the very strictly con-
trolled environment of a ran-domised controlled trial. It is animportant effort to take a lookand see what actually happenswith a device once it is on themarket. The goal is to recruit1,200 patients. Right now,enrolment is still below 100patients but proceeding beyondexpectations.HV: Clinical data are veryimportant. If I look at my ownpractice, I am treating youngerpatients with an endograft soclinical long-term data areextremely important. It is not aprospective trial; it is a registry,which is not the same. But it isprobably the best we that canhave for a long-term follow-up,so I am quite happy they decid-ed to do it.
Could you comment onthe Endurant EU trial?When will we have thefirst results?
HV: The results will be present-ed for the first time at CharingCross 2010 with 80 patients andone year follow-up.
We will be definitelylooking forward to theCharing CrossSymposium next year!
HV:Absolutely, so will I.
Results of the Endurant EU trialwill be unveiled at CX 2010
Hence Verhagen
Endurant
Yehuda Wolf
By Thomas Wyss
Medtronic celebrated the one year CE markand commercialisation anniversary of theEndurant abdominal stent graft at the AnnualMeeting of the European Society for VascularSurgery (ESVS) 2009 in Oslo, Norway.During the meeting, Vascular NewsInternational spoke to Hence Verhagen, ofthe Erasmus Medical Centre Rotterdam, TheNetherlands, principal investigator of theEndurant EU trial, and Yehuda Wolf, of theTel-Aviv Medical Centre, Israel, one of theseven members of the ENGAGE ExecutiveCommittee
“What I particularly like is the smaller sheath sizeof the introducer. This definitely makes a bigdifference. I have not had an iliac issue since Istarted using Endurant. This tells you a lot. It isreally more smooth and easier to bring in than theother stents” Hence Verhagen
“The device is very flexible, and even the mainbody is so small and behaves more like a flexiblecatheter/endovascular device rather than like thestiff devices which were available before”
Yehuda Wolf

BIBA Publishing
November 200914
CAESAR
The CAESAR trial, presented byPiergiorgio Cao, compared the poli-cies of early endovascular repair andsurveillance with aneurysm repair rec-ommended when either the aneurysmdiameter reached 5.5cm or there wasvery rapid aneurysm growth. Giventhe much lower operative mortalityrate associated with endovascular ver-sus open repair, it was possible thatthe findings of this trial might chal-lenge the current recommendationswhich emanate from the UK SmallAneurysm and ADAM trials of the1990s, when surveillance was com-pared with open repair. Both these tri-als showed the safety of a policy ofsurveillance until the aneurysm diam-eter reached 5.5cm. Subsequently this5.5cm threshold, before interventionis considered, has been used in sever-al national aneurysm screening pro-grammes
The CAESAR trial started in 2004,aiming to recruit 740 patients. In factrecruitment was too slow and the trialclosed with only 360 patients ran-domised and without showing any sur-vival benefit associated with a policyof early endovascular repair after threeyears of follow-up. This is hardly sur-prising; the trial is underpowered andpatients have not yet been followed-upfor the 54 months specified in thepower calculations. But why was thetrial presented now? The trial has suf-fered from both inadequate fundingand a lack of sufficient enthusiasmamongst clinicians. The trial, as pre-sented, also suffered from a lack ofinformation about the recruitment basefor the trial. How many patients wereconsidered? How many were ineligiblefor anatomical or other reasons? Such
facts should be reported for all trialsand perhaps we have to await thedetails of a publication to find out howgeneralisable the results might be. Inthe interim there is a suspicion thatonly a small proportion of screenedpatients were included in this trial.Nevertheless the authors must be con-gratulated that so many patientsadhered to trial protocol. Only 10 ofthe 76 aneurysm repairs in the surveil-lance group were against protocol andonly seven patients in the EVAR groupdid not undergo aneurysm repair, anoverall compliance of over 90%. Ofthe 360 patients randomised, hyperten-sion was the most common co-morbid-ity (in 75%) and only 4% of thepatients were female. Where did all thewomen go? It is possible that the lowrepresentation of women in this trialcontributed to the overall survival ratesof >90% at three years, which weresimilar in both randomised groups andthere were only two aneurysm rupturesin the surveillance group: women withsmall aneurysms appear to have aworse prognosis than men, including ahigher rupture rate. Few of thepatients lost their anatomical suitabilityfor EVAR during the surveillance peri-od but there were more adverse eventsin the EVAR group. By six monthsmore than 20% of the EVAR grouphad had a serious adverse event andnot until after three years was the rateof adverse events similar in the tworandomised groups.
The CAESAR trial did not showthat early EVAR can significantlyimprove the prognosis of patients withsmall aneurysms and the publicationplans were not revealed. The policy of“surveillance is best” for smallaneurysms still stands.
OVER
The issue about lack of generalisabili-ty also applies to the OVER trial, pre-sented by Frank Lederle. This trialhad a design similar to that of theEVAR 1 and DREAM trials. Althoughover 5,000 patients were consideredfor this trial, only 881 patients wererandomised. Some patients (n=834)had aneurysms too small, <5cm diam-eter, 450 patients refused randomisa-tion and another 2,702 withaneurysms ≥5cm in diameter wereineligible for anatomical reasons, sothat the trial represented only about20% of patients with aneurysms ofrelevant size.
The results of the OVER trial wereunsurprising and in line with those ofthe earlier trials EVAR 1 andDREAM, although the cohort ofpatients was >99% male and youngerand fitter than patients entered intothe EVAR 1 and DREAM trials. The30-day mortality rates were 0.5% and3% in the endovascular and openrepair groups respectively. For thistrial the low participation of women(<1%) is a direct result of the trialrecruitment base in VeteransAdministration hospitals.
Because the DREAM trial reportedno difference in overall mortality bytwo years, the OVER trial had delayedits first reporting until two-year follow-up was almost complete. Like theCAESAR trial, overall survival wasvery high and the leading cause ofdeath was cancer, perhaps the observa-tion that 41% of the patients were cur-rent smokers contributing to these can-cer deaths. At two years, there was nodifference in all cause mortality (withcumulative survival being 90% in theopen repair group and 93% in the
endovascular group) although the haz-ard ratio of 0.7 [95% CI 0.44–1.1]favoured endovascular repair. Therewere no differences in quality of lifebetween the two randomised groups atone year. We also were presented witha barrage of information about utilitiesand erectile dysfunction, mere sub-sidiary analyses of the main trial andtoo much information to assimilate inthis session. There was perhaps onesmall nugget of novel information:patients with pre-existing coronaryartery disease appeared to do betterwith endovascular repair, HR 0.5 [95%CI 0.2–1.0], although the results wereof borderline significance. Doubtlessthere will be lots more interestinginformation to come from this trial, themain results of which were publishedin JAMA on 14 October. We look for-ward to this and digesting the results atleisure.
AJAX
The final trial presented was theAJAX trial for ruptured aneurysm,presented by Ron Balm. This is pio-neering work from Amsterdam, butanother trial struggling for recruitmentand funding, although it was goodnews to hear that the Netherlands
Heart Foundation has supported theextension of this trial. Trial entrydepends on patients within the greaterAmsterdam area being anatomicallysuitable for emergency endovascularrepair, with patients then randomisedto either endovascular or open repair.Based on using a primary combinedendpoint of major morbidity and mor-tality, initial power calculations sug-gested that just 80 patients wererequired to show the benefit ofendovascular repair: endpoints in only40% of endovascular patients versus70% in the open surgery group. This
point has been reached... data assessedand a decision made to extend recruit-ment... there was no significant differ-ence after just 80 patients. Not onlyhas recruitment been extended toinclude 120 patients and plannedreporting after February 2011, but thepower calculation for the trial hasbeen revised to show a smaller differ-ence, now with the primary endpointoccurring in 65% of the open surgerygroup versus 40% in the endovasculargroup, albeit now with only a one-sided statistical test being used for thecalculation. Had a conventional two-sided test been used recruitmentwould need to be extended to about150 patients. Like the CAESAR trial,no information was presented aboutthe majority of patients assessed butconsidered ineligible for the trial(probably about two-thirds ofpatients). Again this is a trial repre-senting the minority of patients. Welook forward to hearing the results atESVS 2011.
So, we heard about three good trialswith the potential to yield importantresults but all having common prob-lems. These problems included worryabout the funding base to pursue the
trial to full recruitment in a speedymanner, potential lack of generalis-ability resulting in trials with limitedinfluence to alter clinical practice(largely because only a minority ofpatients are being recruited) and limit-ed recruiting base. Wake up, we needto work together to run large trials thatinclude the majority of patients(including women) and get theanswers to important policy issues forpatients and clinicians.
Janet Powell, Imperial College,London, UK
Where did all theaneurysm patients go?
COMMENT & ANALYSIS
JANETPOWELL
Abdominal aortic aneurysm (small, large and ruptured) was the subject of threerandomised trials presented in the special Saturday morning session at the EuropeanSociety for Vascular Surgery (ESVS) meeting in Oslo, Norway
Piergiorgio Cao
Ron Balm Frank Lederle


November 2009
BIBA Publishing
16
The St George’s vascular accessmeeting has been runningyearly successfully over the
past four years and is now approach-ing its fifth edition. The field of vas-cular access, although still veryyoung (the first arterio-venous fistulawas created in 1966), is evolving andchanging very rapidly. There are sev-eral reasons for this fast track evolu-tion towards becoming a major com-
ponent of vascular surgery:� As the number of haemodialysed
patients was predicted to increaseby 5% per annum until 2010where a steady state would beachieved, we have seen over thepast two years an 18% incrementeach year and absolutely no signof steady state loomingwhatsoever. This poses theproblem of the resources allocated
in terms of money but also interms of expertise. It seems nowcompletely unrealistic to confinethe practice of vascular accesssolely to a small group of renaltransplant surgeons; how wouldonly 100 individuals (renaltransplant surgeons in the UK)cater for almost 50,000 patientswith the kind of annual incrementdescribed above?
� The number of patients with type IIdiabetes has been estimated tobecome 350 million worldwide by2015, and it is now a requirementfor all our GPs to prevent chronicrenal failure by estimating theglomerular filtration rate of a target-ed group of their patients at risk.
� Vascular surgeons have seen thescope of their jobs changing dramat-ically over the past few years andthe number of open procedures hasdwindled to the benefit of complexendovascular procedures. The art ofvascular access remains very“open” and although endovascularoptions are always examined it isstill a very surgical specialty thathas now attracted significantly theattention of the vascular community.
� It is estimated that every singlepatient on haemodialysis needs anaverage of 1.5 surgical interven-tions per annum to service theirvascular access and to rescue itwhen failing. It is also widelyaccepted that for every 120patients on haemodialysis thereneeds to be a weekly operating listto create and service their vitalaccesses.
It seems therefore only natural thatfrom 2010, our St George’s vascularaccess meeting becomes part of theworldwide famous Charing CrossSymposium so that we could addressa much bigger audience and increasethe profile of our very popular butyet still small specialty.
We will hold our meeting on 12April 2010 on the Charing Crosscampus. It will be possible to registereither for the complete vascular andvascular access meetings or only forthe vascular access day should youfeel that only that part is relevant toyou and in this case the fees willremain those previously advertised onour website (£60, £80 or £150).
It is time now for our discipline toaddress to a much wider communityof doctors, nurses, carers etc as veryimportant challenges are afoot, whatcould be better than the Charing Crossvenue, experience or usual turnout tohelp increasing our profile?
Eric Chemla, consultant renaltransplant and vascular surgeon,chair of the Medicine andCardiovascular Sciences Division, StGeorge’s Healthcare NHS Trust
CX 2010 will host the 5thSt George’s Vascular AccessDay – It seems only natural!
COMMENT & ANALYSIS
ERICCHEMLA
It was a great privilege to be askedto give the inaugural Vollmarlecture at the Deutsche Geselschaft
fur Gefaeschirugie in Munich inOctober 2009.
The Joerg Vollmar stiftung is a fineornament at the DGG and very fittingsoon after the death of this great con-tributor to German vascular surgery.He was in his key post as Direktor derAbteilung Gefaess und ThoracicChirugie from 1970 till 1991.
My first question is why anEnglishman should give this but it issurely in recognition of the interna-tional status of Professor Vollmar.
Many advances occurred in vascu-lar surgery during his active life. FrauVollmar told me that he came to
London as a trainee in cardiothoracicsurgery and met professor CharlesRob in the early 1950s and from thatmoment, in London decided on afuture in vascular surgery. It shouldbe remembered that Cid dos Santoshad introduced endarterectomy in1948 and DeBakey applied this to thecarotid in August 1953. Nevertheless,it was Eastcott, Pickering and Rob in1954 who wrote first about a success-ful carotid procedure. It was an excit-ing place for a young man to be andJoerg Vollmar got interested. TheDacron era began from Houston inthese years and he went to that “vas-cular Mecca” also for training at thefeet of DeBakey who had in turn stud-ied in France and Germany and was a
fluent speaker of both languages.Ulm became the headquarters of
vascular surgery in Germany formany years. I well remember. As ayoung man, visiting the AustrianVascular Society in Salzburg in1977 and every paper was discussedby either Vollmar, van Dongan orDenck. It seemed to be a territorialissue with each having a circle ofinfluence, van Dongan in theGerman speaking world fromAmsterdam and Denck from Vienna.In the middle was Vollmar in Ulm.These pioneers were well travelledand very aware of internationaladvances. Their role was to bringback the tidings from afar and put thework of juniors into context.
It should not be forgotten that manyof these achievements were made inpost-war Germany which was dividedduring the Vollmar years. He was stillvery dominant in 1992 when wecelebrated the first East and WestGerman vascular meeting which tookplace in a very run-down Dresden.Vollmar will have heard with me aperformance of Zauberfloete whichwas put on for us by the Semper operon the Sunday night. It was aproduction in which Stasi were seen aspart of the Mozart nightmare. TheseGerman artistes were expressing theirfeelings in the only way they could andit brought tears to our eyes.
Vollmar was not known for evi-dence based results. These came afterhis time and it was my generationwho had the privilege of championingthese .I decided to ask myself whathas happened since 1992 and what
Vollmar would appreciate of it. Wehave the UK small aneurysm trial(UKSAT) which set the threshold forintervention for aortic aneurysm. Thiswas mirrored by ADAM with similarprotocol. Together, with high level ofevidence, we see that it is not neces-
sary to operate till an aorta reaches5.5cm. This was not proved until1998 when the UKSAT was reportedfirst (Figure 1). The two groups werefollowed for 12 years “to be sure thatno late benefit occurred in eitherarm.” (Figure 2)
This opened the door for aneurysmscreening and endovascular aneurysmrepair at a threshold of 5.5cm.EVAR 2 is unique but EVAR 1 is fol-lowed fortunately by DREAM, ACEand OVER.
The trials essentially ask a questionof what to do if either open repair orEVAR can be offered. Registriesalone are not enough. We had to com-pare like with like by random alloca-tion. This meant that surgeons like mehad to learn clinical trial technologyand surround themselves with statisti-cal advice and economic skills. It wasno longer an era for a surgeon to be
able to lead on his own.I will not repeat the results of trials
with which I have been associated asthey are in the literature. The purposeof this piece is to recognise thatVollmar made his enormouscontribution in a difficult time after thewar. He was a first generationEuropean pioneer and in my view theleader in his subject in Germany. It isimportant to recognise the prevailingattitudes at the time a great manachieves and only then is it put intocontext.
In short Joerg Vollmar launchedvascular surgery in Germany and it isfitting to establish this stiftung. Hisinfluence spanned the period whenWest Germany was separated from theeast block but he saw in the combinedGermany and was influential in it. Hewould love to have seen the evidencebase which we learned after his time. Itwas a great pleasure to recognise thisman in the inaugural lecture.
Roger Greenhalgh is the editor-in-chief of Vascular News
The inaugural JoergVollmar lecture
ROGERGREENHALGH
COMMENT & ANALYSIS
“Joerg Vollmar was a first generationEuropean pioneer and in my view theleader of his subject in Germany”
Figure 1 Figure 2


November 2009
BIBA Publishing
18
Patients with abdominal aorticaneurysm prefer future treat-ment with an endovascular
approach to open repair, said resultsfrom a study which was recently pub-lished online.
One hundred and sixty seven menwith asymptomatic small abdominalaortic aneurysm took part in a postalsurvey on the topic, in the UK. Thesurvey provides insight into patients’preferences, expectations and experi-ences on the two choices of treatmentavailable for abdominal aorticaneurysms.
Forty six per cent of the participantschose the endovascular approach,while 18% said they preferred opensurgery, say the researchers.Participants in the survey were askedabout their choice of treatment beforeand after receiving an informationpack describing the abdominal aorticaneurysm and available treatmentoptions.
The study titled ‘Patient Preferencefor Surgical Method of AbdominalAortic Aneurysm Repair: PostalSurvey,’ led by Justine A Reise,Vascular Surgery Research Group,Imperial College London, UK, waspublished online by the EuropeanJournal of Vascular and EndovascularSurgery.
Investigators sent participants in thesurvey a validated patient informationpack describing the background andnatural history of abdominal aorticaneurysm. It included a description ofboth endovascular and open repair andincorporated information on patientsuitability for each treatment, exactprocedural details, the associated bene-fits and disadvantages of each and the
most up to date published clinical trialevidence on the early and mid-termperformance results for each treatment.
The questions consisted of both pre-coded and free text questions groupedaccording to six themes: initial prefer-ence, current preference, the thingsthat are important to you, making adecision, your views of the informa-tion pack, and about you.
Patients’ characteristics
The age range of respondents was66–84 years and the majority (70%)was between 66 and 75. Almost allrespondents described themselves as‘white British’ (94%), 79% lived witha spouse or partner, nearly all (90%)were retired and 70% had left schoolat the age of 16 years or less. Almosttwo thirds (63%) reported that theyhad a longstanding illness, disabilityor condition which caused difficultywith routine activities in just over aquarter (28%) of respondents.
Only 16% of the patients had con-sidered the options for aneurysmrepair prior to receiving the surveyand even less (10%) had discussedthe options with a hospital doctor.Most (89%) had not received anywritten information about the twosurgical treatment options and twothirds had not received informationfrom other sources such as nurses,general practitioners, internet orfriends/family.
Investigators highlighted that afterreading the documentation posted,most participants wanted to be able todiscuss both of the options with theirclinician as they relied on the clinicianfor advice and guidance. “Sincepatients place great reliance on clini-
cian advice, it was important to conductthis survey in patients who had not yetbeen referred to a vascular surgeon orendovascular specialist,” they wrote.
“In this ‘naive’ situation, fewrespondents expressed a preferenceabout any necessary future treatment.Of those that did have an opinion,just 10 respondents (6%) were infavour of open repair (five definitelyand five to some extent) in contrast to28 respondents (17%) who favouredendovascular aneurysm repair (17definitely and 11 to some extent).Although 19 (11%) men were happywith either treatment; the majority ofrespondents (n=105, 63%) did notknow which they preferred.
After reading the information pack,the number of men preferring openrepair had increased to 30 (18%) (20definitely and 10 to some extent) andthose respondents preferring endovas-cular repair had increased to 77 (46%)(40 definitely and 37 to some extent);23 men (14%) were still happy witheither treatment. Only 34 respondents(20%) still did not know which treat-ment option they would prefer for anyfuture aneurysm repair.
Discussion with physician
“The response rate of 70% was verygood for a postal patient preferencestudy and was achieved by optimisedmethodology. Almost all participants
(92%) appreciated that the informationpack provided information to help sup-port them to discuss any decision aboutfuture surgical treatment options fortheir aneurysm. The pack was instru-mental in helping two thirds of respon-dents who initially did not have a pref-erence to go on to express an informedpreference,” the authors wrote.
“Participants showed a greaterdegree of preference for endovascularversus open repair before and afterreading the validated patient informa-tion pack; with informed respondentsmore than twice as likely to favourendovascular over open repair. Ofnote, respondents who expressed apreference for endovascular repairwere equally split in terms of thestrength of their preference (24% defi-nitely, 22% to some extent) in contrastto the smaller number who preferredopen repair but appeared more certainabout their choice (12%, 6%).
“Overall, informing patients abouttreatment options is likely to enhancethe patient-clinician relationship andlead to more effective patient-centredcare. Information received from avalidated information pack may beevaluated more objectively thanadvice from the treating physician.The information pack about interven-tions for aortic aneurysm facilitatedthe development of treatment prefer-ence by most patients, with endovas-cular repair being preferred over openrepair; even though most were pre-pared to comply with their cliniciansadvice. Such patient preferenceshould receive strong considerationin the continuing debate about thecost-effectiveness of endovascularrepair,” the authors wrote.
Patients prefer endovascular approach in aneurysm repair
Acute aortic dissectiontype A is a life-threat-ening emergency,
requiring immediate surgicalintervention. Controversyremains about acute medicalcare, including the diagnostics,peri-operative management,optimal surgical technique andpost-operative treatment. Theonly aspect all seem to agreeupon is the need for surgery.The aim of our registry was tooptimise the medical care ofacute aortic dissection type A-patients and thereby reducetheir morbidity and mortality.
To improve peri-operativemanagement, lots of data mustbe collected which can affect
the patient’s outcome. Toanalyse the underlying patholo-gy, we collected aetiologicaldata concerning the dissection(e.g. atherosclerosis, genetic,iatrogenic, systemic arterialhypertension, inflammatory oraneurysm/ectasia). Most of thecardiac centres use differentoperative and neuroprotectivestrategies. In accordance withthe literature, the most effectiveneuroprotective modalities arehypothermia and antegrade,selective perfusion of the brain.Which of these applied tech-niques and its combinationsachieve the best neurologicaloutcome? How deep shouldhypothermia be? These ques-
tions remain unanswered.Various cannulation and perfu-sion techniques such as retro-grade perfusion through thefemoral artery, selective ante-grade cerebral perfusion via thesubclavian or axillary artery,innominate or carotid artery orantegrade perfusion via directtrue lumen cannulation of theascending aorta or aortic archare possible alternatives appliedin the participating cardiac cen-tres. Which parameters influ-ence the initial, mid- and long-term survival of the patients?What are the predictors that maydetermine patient survival?These additional questionsremain unanswered as well.
Even recent studies cannotdefinitively define the best pos-sible surgical treatment, becausemost of these published retro-spective investigations havedescribed single-centre experi-ences. There are a variety ofoperative techniques available:supracoronary replacement ofascending aorta, valve-sparingprocedures (David-reimplanta-tion and Yacoub-remodellingtechnique), extending proce-dures of aortic arch anddescending aorta (e.g. partial,hemi or total aortic arch replace-ment, elephant-trunk, frozenelephant trunk and reconstruc-tion of the aortic valve orimplantation of a compositegraft). Due to the low level ofevidence of the available stud-ies, a closing recommendationfor the choice of a certain opera-tive strategy cannot be made.The decision as to which tech-nique is best for which patientremains an individual decision,considering the underlying aor-tic pathology and the extent ofacute aortic dissection type A,and each patient’s comorbiditiesand anatomical circumstances.Furthermore, the technical facil-ity in each cardiac centre, andthe staff’s experience concern-ing the operative strategies playa key role in the competentmanagement of patients withacute aortic dissection type A.Prospective analyses arerequired to support future evi-
dence-based individual deci-sions regarding the best-possibleoperative strategies and peri-operative management.
Nearly half of the patientswith acute aortic dissection typeA die without surgical treatmentwithin 48 hours. Only surgicalrepair of the ascending aorta,and occasionally aortic root,arch and descending aorticrepair can lead to a good long-term survival rate. Our web-based “GErman Registry forAcute Aortic Dissection type A(GERAADA)”, in which all sur-gically-treated patients could beincluded, was initiated by the“Working group for aortic sur-gery and interventional vascularsurgery” of the German Societyof Thoracic and CardiovascularSurgery (GSTCVS). In July2006, GERAADA was activatedfor all German, Austrian andSwiss heart centres on theGSTCVS homepage. Parametersconcerning surgical patientswith AADA have been collectedsince then. These data includeinformation about pre- and intra-operative patient status, pre-operative imaging, neuroprotec-tion, hypothermia, cannulationsite and perfusion technique,operative strategies, post-opera-tive complications, midtermresults and causes of death. Theaim of the registry is to gaininsight and knowledge whilecontinously improving surgicaltherapies and the peri-operative
management of patients withacute aortic dissection type A.
After successful presentationof our initial experience withGERAADA at national andinternational meetings, the wishto develop a “European Registryfor Aortic Diseases (EuRADa)”has been expressed. ThisEuropean database should col-lect parameters addressing allaortic diseases (dissection typeA and B, aneurysms, perforatingulcer, intramural wallhaematoma, traumatic aorticruptures, etc) and about allpotential treatment strategies(medical treatment, open surgi-cal, endovascular). In severaldiscussions with leading mem-bers of different national andEuropean societies, a commondeclaration of intent has beendrafted under the leadership ofthe Vascular Domain of theEuropean Association forCardiothoracic Surgeons to starta Europe-wide registry for aorticdiseases.
Ernst Weigang, Department ofCardiothoracic and VascularSurgery, University MedicalCenter of the JohannesGutenberg University Mainz,Mainz, Germany, for the GER-AADA study group and WorkingGroup for Aortic Surgery andInterventional Vascular Surgeryof the German Society forThoracic and CardiovascularSurgery
ERNST WEIGANG
From Germany to aEurope-wide registryfor aortic diseases
COMMENT & ANALYSIS
Definitely prefer open repair (12%)
Prefer open repair to some extent (6%)
Equally happy with either option (14%)
Definitely prefer EVAR (24%)
Prefer EVAR to some extent (22%)
Do not know/unsure (20%)
Missing/error (2%)
Preference towards open repair (18%)
Preference towards EVAR (46%)
Source: Imperial College, London
Results


When did you decide you wanted a career inmedicine and has it lived up to expectations?
The first memory I have of wanting to be a doctor was at theage of six. I do not think I knew why I wanted to be a doctorat that point, but I realised that I had a strong interest inmedicine. However, the focal aspects of my interest inmedicine have certainly changed over the years. I would saythat during college, medical school, residency and my career,I have fostered a great fascination with human physiology,imaging technology and engineering devices. It has been agreat joy to use these interests to develop new treatments thatwill hopefully improve the quality of people’s lives.
Why did you decide to specialise in vascularsurgery?
Well, this decision was subject to a bit of coincidence. Myfirst rotation as a resident was on the vascular surgical servicewith Drs DeWeese, Green and Ouriel at the University ofRochester. I remember my very first day of internship, DrOuriel quizzing my on some angiographic studies and I wasso proud of my ability to answer those questions. After that,they really cultivated my interest in diseases of the bloodvessels. This area of pathology fit in nicely with my interestin imaging and also in device design. The cumulative effectwas that of a snowball going down a mountain just gatheringmomentum and size in the process. It was really after my firstmonth of internship that I knew that I wanted to go intovascular surgery and to be honest I have never looked backsince that time, or regretted that decision.
On a professional level, what have been yourproudest moments?
I consider my proudest moments from a patient care standpointare when we are developing a new technique or using a newtype of device, and we have a successful outcome. Especiallywhen you sit and think about what the alternative method oftreatment would have been for that patient. For example, thefirst complex thoracoabdominal aneurysm we fixed with abranched graft was in a patient who had suffered two cardiacarrests during anaesthetic induction for attempted open repair.The advice provided by cardiology at that time, was not to useanaesthesia during his thoracoabdominal aneurysm repair. It isreally enjoyable when the patients appreciate this as well,although often patients do not have a comprehension of whatthe alternative treatments are like.
Another proud moment occurred this year when I receivedrecognition from my peers as to my accomplishments in medi-cine. I was awarded the Sam and Marie Miller Master ClinicianAward which is given to one physician a year from theCleveland Clinic who has demonstrated excellence in clinicalmedicine. Now, the Cleveland Clinic is an institution where it isvery easy to be a good clinician. You just have to know whatother good clinicians you can call when you have a problem.But, to be singled out by my peers at this institution was bothtouching and meaningful and on a professional level, meansmuch more than any title that I might earn after my name.
Finally, from a research standpoint, one of my proudestmoments is when I was able to work with my father and one ofhis graduate students named Vikash Goel, to the point of havinga joint patent and two papers published. It was very gratifying tosee both of our names in print in good journals, and on a patent,irrespective of the ultimate value of the endeavour.
Vascular surgery has undergone manychanges over the years – what do you thinkthe most fundamental changes have been?
Well, I would not characterise myself as a senior vascularsurgeon yet. I really grew up with endovascular being a part
of vascular surgery. In fact, I have very strong memories ofarguments during my residency and fellowship training inRochester about endovascular vs. open surgical therapeuticoptions. These arguments still go on, on a day to day basis,although the people have changed. But clearly, thetechnology that was once so cantankerous has become muchmore broadly accepted. I would say that the fundamentalchanges of vascular surgery are yet to come, and will involvea greater appreciation for non-invasive imaging, cross-sectional imaging techniques, tissue characterisation andmolecular genetics. Vascular surgery has certainly been oneof the few specialties that has embraced change rapidly andhas been able to morph itself to accommodate these newideas and philosophies. I hope that in the years to come, wecan all watch the field of vascular surgery continue to evolveinto a specialty that has even fewer boundaries and morepotential for significant changes in medicine.
Your professional training includes afellowship in interventional radiology. Whatinfluence did it have on your career?
Interestingly, when I was a general surgical resident, I had askedto have some dedicated training in interventional radiology. Atthat time, this concept was not met with great enthusiasm. I hadbeen following the career of Mike Dake over the years, andapproached him to see if further training under his guidance waspossible. That never really worked out, and when I returned froma visit with Dr Dake, I was greeted by Dr Green and Dr SeymourSchwartz at the University of Rochester who had met with thefolks in radiology and offered me the opportunity to do afellowship there in interventional radiology. This training wascritical to my medical education. It was really the detaileddisciplined training of learning radiology from the standpoint ofultrasound, computed tomography, magnetic resonance andinterventions during that year that honed my skills to allow meto have a different perspective of how patient care should beprovided in vascular surgery. This became particularly apparentwhen I went to Malmo, Sweden to train with Dr Krassi Ivancevand Dr Bengt Lindblad. In Malmo I received an opportunity toboth observe and participate in levels of care and interventionalprocedures that I had not thought existed anywhere at that time.So I would say that my radiology training had as much to dowith my professional career as my surgical training. It is reallythe mix of both, understanding radiology and understandingpatient care that provides me with a sound foundation formaking clinical decisions and also developing research concepts.
You have a number of patents registered.Which of them has had the greatest impact inthe treatment of vascular disease?
This is a hard question, because you really never know howvaluable patents are until many years after they are issued,and it also depends a bit on how you define vasculardisease. I actually think my most significant patent, is apatent that relates to heart valve treatment. And it doesnot stray far from concepts involved in endovasculargrafting. The heart valve technology that is existent todate relies on stents and valves and somehow they areattached together. And the technology that I haddeveloped here, and that we have implanted in onepatient, involves the separation of the concepts offixation, sealing and annular function. How those threeconcepts meld together into a device are the subject of apatent that I hope will have the greatest impact on thetreatment of patients with cardiovascular disease. Mypatents on branched graft technology, delivery systems,collaborations with people like David Hartley, MichaelLawrence-Brown, and Timothy Chutter, I think will all havesignificant impact, but clearly relate to a smaller segment ofthe population than those with valvular heart disease.
How do you see the performance offenestrated grafts, one of your areasof research?
Fenestrated grafts are one method bywhich aneurysm that involve or abutvisceral vessels can be treated.Although initially this was met withscepticism, we now have seven- andeight-year follow-up data on ourearly patients that show thetechnique to be surprisinglydurable. Ultimately I think itmakes sense to look at acomputed tomography scan anddetermine where the aorta ishealthy, and where the iliacarteries are healthy andrepair any disease from onehealthy segment to anotherhealthy segment,irrespective of whatbranches come off in theintervening segment. Thatmandates that these vesselsbe incorporated into the repairwith the use of eitherfenestrations or branches.Fenestrations are not conceptually anoptimal means of accommodating abranch, but they solve somefundamental problems that branchescannot. For example, they take up verylittle space, they are relatively easy to align,and devices that incorporate fenestrations canbe loaded in fairly small delivery systems.I think the true test of fenestrationswill be when the technique isdisseminated to treatpatients with thesecomplexaneurysms.Ultimately Ithink this isgoing tobe
Profile Roy GreenbergFrom fenestrated grafts, new medical devices and patents, Roy Greenberg, Cleveland Clinic,Cleveland, USA, is now also au fait with the Wii and talking about Pokemon, thanks to his children.He told Vascular News all about his fascination with human physiology, imaging, and fish tanks!
BIBA Publishing
November 200920

more successful than others believe largely because ofadvances in imaging technology that will make
this operation simpler. No longer will peoplebe forced to think in three dimensions
because we will be able to displayangiograms, and during operative
procedures, view the anatomy inthree dimensions and real-time.
Tell us about the mostmemorable case youhave ever treated?
It is very hard to narrow thatdown to one case. I have onepatient that I followed for manyyears, who presented in extremiswith an aortal bronchial fistula,ultimately requiring extracorporealmembrane oxygenation simply tokeep him alive. The aortalbronchial fistula formed afterseveral operations for childhoodcoarctation. We were able to treatthis with a stent graft and after 5–6days wean him off the echmo, treathim with antibiotics for a number
of months, as his lung abscessregressed, and watch him return to
health and relatively normal lung function.Over the years I have become friends with
him and his wife, and gotten to know a little bitof their family, and consequently, he is a very
memorable case. I have other patients like that too. Anumber of patients with connective tissue diseases who
are quite young, and are referred because they really do nothave any other options in terms of treatment. Some of those
memorable cases have really nice outcomes, and someof them are the saddest cases that I have ever beeninvolved in. But I guess it is the challenge of those
cases that makes this area of medicine the mostrewarding.
Who are the people who haveinfluenced you?
I think my father had the biggest influence on how Ithink. He has alwaysapproached thingswith an engineeringprospective, and itused to drive mecrazy when I wasa child and hewould help mewith mathhomework. Wewould alwayshave to go backto the very basics,but now, I realiseit is the verybasics that are themost important.And I will notforget thepeople thatreally taughtme a lot of thesurgicaltechniques that Iuse today on an
everyday basis, like Drs Green and Ouriel, training us on the useof sharp dissection instead of blunt dissection, and howimportant exposure was with respect to vascular surgery. Properexposure and the set-up of the field is probably one of thehardest things to train fellows today. And I have to credit DrIvancev with several pieces of advice that include two verymemorable sayings. The first is “pay attention to the very smalldetails, because it is the very small details that make adifference”, and that is clearly true in endovascular surgery aswell as vascular surgery. And the second, which is somethingthat many people laugh about, but is really true, is that “whenyou are nervous during a procedure, give the patient moreheparin”. Ironically, this is one of the fundamental differencesbetween vascular procedures and most other procedures, and Ifind that the fellows coming into our programme take a littlewhile to learn this. It is true from an endovascular prospectivebecause we have catheters and sheaths sitting in arteries forlonger periods of time, and it is true from an open perspectivebecause significant bleeding always results in a clampsomewhere, and then you do not want to propagate that problemwith more clotting, so I have to tell Krassi that he is right. If youare nervous, I would give more heparin. I would also have to saythat Dr Norman Hertzer had a significant influence on me interms of doing research as I saw him spending countless hoursgoing over his cases and results. I learned his underlyingphilosophy that “outcomes matter”. I hear myself saying it overand over again. And I would say that there is one more personthat had a lot of influence on me, and that would be Dr EdBevin. And although I cannot put a single line or saying tocrediting Dr Bevin with his methods of treatment or surgicaltechniques, it is his overall attitude that influenced me. He had acalm demeanour and appeared to be immune to political issues,allowing him to always put the patient and the individuals’interests of concern as the primary priority.
What are your current areas of research?
Well, they are really just evolutionary changes of my pastareas of research which include developing devices that areused to treat cardiovascular problems, developing imagingtechniques that can be used to facilitate diagnoses andimplantation of these devices, and the analysis of clinicalresults. Unfortunately, it is getting more and more difficult todo clinical research, at least in the United States. However, Ihope that this pendulum swing reverses, because it is theclinical research and as Dr Hertzer says “outcomes analysis”that makes the biggest difference. I think that our researchpatients probably get better treatment than other patientsbecause their progress and complications are so heavilyscrutinised. But I also think that we have learned from ourmistakes. Without paying careful attention in a systematicmanner to our outcomes, we will not learn from our mistakes.
Outside of medicine, what other interests doyou have?
My primary interests outside of medicine are my family. Mywife Alicia, and my two kids Zachary and Lucas. I love spendingtime with them and look forward to showing them how small theworld really is. I have actually become quite proficient at thingsthat are common in 5- and 7-year-old conversations, such asPokemon and playing the Wii, in addition to soccer and T-Ball. Iused to do a lot of diving, but since having children not of divingage, I have become more of a true fair weather diver, and have alot of fish tanks. They provide me a great deal of enjoyment bothto look at and learning about all of the details of how to keep fishand corals. I also like the outdoors, including camping, hikingand biking. And I do enjoy travelling. The world has beengetting smaller as you develop friends in more and morecountries. I find that my primary objective on a lot of trips hasfocused less on the specifics of a conference, but more in seeingthe colleagues that over the years I have gotten to know.
Education1992 MD, University of
Cincinnati College ofMedicine, Cincinnati,Ohio, USA
1987 BA, Cornell University,Ithaca, NY, USA
Employment history
� July 1999–Present – ClevelandClinic Foundation, StaffDepartments of VascularSurgery, Cardiothoracic Surgery and BiomedicalEngineering
� Associate Professor of Surgery, Cleveland ClinicLerner College of Medicine
� Director of Endovascular Research and PeripheralVascular Core Laboratory
Board certifications
� American Board of Surgery, certified 15 November1998 Recertified 1 December 2008
� American Board of Surgery in Vascular Surgery,certified 15 May 2001
Professional training
June 1998–June 1999Fellow in Vascular Surgery, The University ofRochester, Division of Vascular Surgery,Rochester, New York
January 1998–May 1998Endovascular Fellowship, LundUniversity/Malmo University, Department ofRadiology, Malmo, Sweden
1997–1998 Fellow in Interventional Radiology, Instructor,Vascular Surgery, The University of Rochester,Division of Vascular Surgery
1996–1997 Chief resident, Instructor in Surgery, TheUniversity of Rochester,
1992–1996 Intern, resident, and instructor in Surgery, TheUniversity of Rochester
Society memberships
Distinguished Fellow Society of Vascular Surgery, fellowof the American College of Surgeons, fellow of theAmerican College of Cardiology, fellow of the AmericanAssociation for Thoracic Surgeons,member of thePeripheral Vascular Surgery Society, member of theSociety of Interventional Radiology, Midwestern VascularSurgical Society (Chairman, Membership Committee),Ohio Chapter American College of Surgeons, andInternational Society of Endovascular Specialists.
Books and editorial activities
� Editor – Atlas of Endovascular Techniques. WBSaunders. In progress.
� Associate editor – Abdominal Aortic Aneurysm StentGrafts: The First Decade and Beyond. FuturaPublishing Company, NY. In Press.
� Section editor – Multidisciplinary Studies. TheRochester Manual. Laennec Publishers. 1996.� Editorial Boards: Journal of Endovascular Therapy,
Annals of Vascular Surgery, Cardiovascular Surgery,Endovascular Today, ISMICS/Innovations.
� Reviewer – Journal of Vascular Surgery, Journal ofEndovascular Therapy, Journal of the AmericanCollege of Surgeons, The Lancet, Circulation.
� Guest editor – Seminars in Vascular Surgery (June2009, Long Term Durability of Aortic Repair),Seminars in Vascular Surgery (June 2007, AorticDiseases), Saunders Atlas.
Numbers
� 134 published manuscripts, five manuscripts in press,and three submitted
� 30 book chapters published, three chapters in progress,and five in press
� 21 awards and honours� 10 cardiovascular summits organised� 16 US patents� Five physician sponsored investigational device
exemption studies
Fact File
BIBA Publishing
November 2009 21

November 2009
BIBA Publishing
22
Saving limbs is a key issue in vascular sur-gery. This complex and challenging topicis being addressed within the ilegx initia-
tive. Founded in 2008, this initiative aims toreduce the number of leg amputations. On 13–14October 2009, the second summit was held inMunich, just before the start of the annual meet-ing of the German Vascular Society – an excel-lent opportunity for everyone with particularinterest in limb salvage.
Despite important developments in the pre-vention of leg/tissue loss, the number of amputa-tions is still high across Europe. Ongoing rise inthe prevalence of diabetes has a major impact onamputation and survival. Consequences arisethrough clinical impact as well as socio-econom-ic effects. With a predicted 70% of cases beingpreventable there is great potential to reduce theamount of amputations. How can this be met?ilegx offers education and answers to such ques-tions. Nearly 300 delegates from a broad rangeof subspecialties attended: wound care special-ists, diabetologists, nurses, interventional radiol-
ogists, orthopaedists, vascular surgeons, derma-tologists, podiatrists, angiologists and manymore. One common goal!
Great interdisciplinarity makes up the unique
programme of the meeting. One and a half dayspacked with lectures from well respected spe-cialists from all over the world resulted in anintense course. First, presentations on a systemicapproach to the underlying aetiologies ofleg/foot tissue loss were held. New diagnostictools and techniques, differential diagnoses andexpert panel discussions were key features of it.The second part centred on the management ofthe different vascular and non-vascular origins oftissue loss. It was clearly shown that a singleapproach is insufficient. Moreover, the conceptof early referral, early intervention and earlyinfection control was highlighted. In order tooffer a variety of treatments, a compoundapproach with multiple disciplines is required.Aspects of creating such interdisciplinary teamsin hospitals were discussed in the third part ofthe meeting: How to establish a diabetic footprogramme, get people to work together in anambitious team to offer best practice to thepatient? Furthermore, experiences of differentspecialists reflect support and barriers of nation-al healthcare systems for such projects. It is veryinteresting to see what kinds of hurdles have to
be overcome in different settings.To illustrate the iLegx concept, an algorithm
was developed. It features a “wheel of knowl-edge” which facilitates the complexity andreminds the user of the inherent diversity of thematter. Hence, to reach the goal of saving legsthe wheel needs to be turned! In order toimprove care, awareness of the high rate ofamputation has to be spread to patients at riskand general practitioners. Furthermore, crossreferral among disciplines is needed. This con-tributes to improved patient management withless tissue loss. The broad spectrum of factorsthat play a vital role in the survival of tissuedemand interdisciplinarity. It is about anklebrachial index, diabetes, lymphatic disorders,venous and inflammatory causes and manymore. Nowadays, with more and more subspe-cialisation, the call for team work seems greaterthan ever. Only a holistic approach with special-ist opinions gathered can provide best practice. Itwas shown that centres with specialised woundcare/foot care teams were successful in loweringtheir amputation rate. Thus, the ilegx algorithmneeds to be spread. The overall striving atmos-phere of this meeting is an exceptional feature.The audience was keen on information.Condensed and dedicated education in a shorttime offers a powerful tool for professionalsinterested in limb salvage. Such a teaching andlearning conference is an important componentfor vascular surgeons in training and supports aprofessional approach to this difficult problem.Alertness, from the patient to the specialisedcentre, is the first step towards keeping the legs,but certainly not the last!
Thomas Wyss is a vascular fellow, ImperialCollege Vascular Surgery Research Group,London, UK
Read more about the symposium in the ilegxspecial supplement inserted in this issue ofVascular News.
ilegx: A vascularsurgeon in training’sperspective
COMMENT & ANALYSIS
THOMAS WYSS

November 2009
BIBA Publishing
23
Personal opinion on currentstate of carotid trials“Being partially retired from the full-time NHS, and innear full-time private practice, my medico-defensiveantennae are particularly sensitive to the happenings in theworld of carotid revascularisation. This is a crucial timefor evaluation of the relative merits of carotid stentingversus carotid thrombo-endarterectomy especially for tightsymptomatic carotid stenosis. (At present, we have nolevel I evidence for effectiveness of stenting pitted againstbest medical treatment for asymptomatic or symptomaticcarotid stenosis)
The literature abounds with level I evidence of thesuperiority of carotid endarterectomy over best medicaltreatment for both tight asymptomatic and tight sympto-matic carotid stenosis.
Over the last two years, level I studies from Germany,France and now from the United Kingdom have shown thatcarotid endarterectomy is not only not inferior to but supe-rior to stenting in terms of peri-procedural stroke andstroke/death. One previous level I study came out in favourof stenting when myocardial events detected by troponinchanges were used as adverse endpoints; and a furtherlevel I study (which was the predecessor of the presentInternational Carotid Stenting Study, ICSS) showed equiv-alence of stenting and endarterectomy. The last two men-tioned studies have been overtaken by technique anddevice advances and may be consigned to history.
The scene has been blurred by the publication of aprospective case-matched study of a mixed cohort of twothirds asymptomatic and one third symptomatic patientsprospectively allocated to stenting or endarterectomy butnot in a randomised fashion. Here the concept of “nonhigh-risk” and “broad risk” for stroke was introduced, andequivalence of stenting and endarterectomy was found.This was not level I evidence. In particular, the “melange”of symptomatic and asymptomatic makes the results diffi-cult to interpret.
Finally, there seems to be confusion over interpretationof the data in Vascular News issue 43. On page 2, there isexpression of surprise that low volume centres may havebetter results than high volume centres for carotid stentingand endarterectomy. Actually on careful perusal of thedata the following becomes apparent:� Centres performing high volumes of carotid stenting
and endarterectomy have better outcomes than lowvolume centres;
� In low volume centres, there appears to beequivalence of stenting and endarterectomy;
� In high volume centres, there is a significant benefitfor patients undergoing endarterectomy over stenting.At present:
� There is no evidence that stenting is superior to bestmedical treatment or endarterectomy;
� There is level I evidence that endarterectomy issuperior to best medical treatment for both tightsymptomatic stenosis and tight asymptomatic stenosis;
� There is level I evidence that endarterectomy is superiorto stenting for tight symptomatic stenosis at present;
� In low volume centres, stenting and endarterectomy areequally dangerous compared with high volume centres.However, no one should make assumptions that tech-
nology will not deliver a system that will allow carotidstenting to outperform endarterectomy in the future.”
Mohan Adiseshiah
Letter toVascular News
If you would like to comment onany of the stories published inVascular News, send an email [email protected]
Hybrid repair is one of the onlyoptions for patients with themost extensive and complex
thoracoabdominal aortic aneurysms. Inthis group, fenestrated/branched stent-grafting is not an option and opensurgery hazardous. A study publishedonline in the European Journal ofVascular and Endovascular Surgeryconcluded that early results of visceralhybrid repair in this high-risk groupare encouraging.
In this series, 118 consecutivepatients who underwent the procedureat three institutions in the UK andGermany (Imperial College HealthcareNHS Trust, London, and theUniversities of Munich andHeidelberg). All cases were reviewedby Susan Drinkwater and Michael
Jenkins, London, UK.Free ruptures were excluded from
the dataset, leaving 107 patients, 63%of whom were men. Mean age was 67years. Elective cases accounted for79.4% of those treated. There were 45Crawford type II, 32 type III, 11 type I,one each of type IV and type V, and 17“complex” thoracoabdominal aorticaneurysms treated. The complexaneurysms comprised nine dissections,three hourglass configurations, threefalse aneurysms, one mycoticaneurysm, and one extensivelyprogressing intramural haematoma.More than a quarter of the patients hadhad a previous thoracotomy for eithercardiac or open thoracic aortic surgery.
All patients underwent atransperitoneal abdominal procedure.
After debranching of the renal andvisceral arteries, endovascularexclusion of the thoracoabdominalaortic aneurysms was carried out. Theleft subclavian artery was covered in19 patients, 12 of whom underwent leftsubclavian artery revascularisation.Most patients (82 or 76.6%) underwentvisceral bypass grafting and aorticstent-grafting during a single operation.A total of 21 patients (19.6%) werestaged with a median interval betweenprocedures of 20 days; the remainingfour (3.7%) had successful visceralbypass grafting as part of a stagedprocedure but failed to proceed toaortic stent-grafting. Three patientsruptured, and one died of multiorganfailure while waiting for endovascularcompletion.
The full hybrid procedure wassuccessfully completed in 99 (92.5%)patients. In four patients, the procedurewas abandoned because of peri-operative instability; in four others,bypass was accomplished in a stagedfashion, but the patients neverproceeded to endovascularisation.
The overall 30-day mortality was14.9% (16 patients). Thirteen (12.1%)
experienced some degree of spinalcord ischaemia, nine of whom had fulland permanent paraplegia. Renalfailure occurred in 28 patients (26.2%)who required haemofiltration in theimmediate postoperative period; fourrequired long-term dialysis after theprocedure. Visceral/renal bypass graftpatency at 30 days was 86.9%(93/107); three patients developedbowel ischaemia requiring resection.
“The early results are acceptable in apatient cohort with few other options. Inhigh-risk patients in whom fenestratedor branched stent-grafting is not anoption, and open surgery hazardous, thevisceral hybrid represents a viable,robust, and transferable treatmentalternative. Therefore, in unfit patientswith a type I, II, or IIIthoracoabdominal aortic aneurysms, weoffer the visceral hybrid procedure inpreference to an open operation and forthe time being will continue to do so,”the authors concluded.
“Encouraging” results for hybrid repairin thoracoabdominal aortic aneurysms
Michael Jenkins


“Ahigh proportion ofpatients undergo-ing endovenous
laser ablation and phlebectomystill prefer general anaesthesia,particularly if they areyounger, having a bilateral pro-cedure or are troubled byaching varicosities rather thanulceration,” said P Sridhar,London, United Kingdom.
Speaking at the InternationalUnion of Phlebology meeting,Monaco, he told delegates thatthis preference for generalanaesthesia often reflectedpatients’ desire to avoid peri-operative discomfort and per-haps also a desire to achieveoptimal cosmesis.
The study titled, ‘Patientpreference for local or generalanaesthesia during endovenouslaser ablation and phlebectomyof symptomatic varicose veins’aimed to analyse the type ofanaesthesia preferred bypatients undergoing endove-nous laser ablation with phle-bectomy and the reasons fortheir choice.
“Endovenous laser ablationof varicose veins is often per-formed under local anaesthe-sia, but many patients still pre-fer general anaesthesia, ifgiven a choice,” Sridhar said.
In the study, 290 patientsunderwent unilateral (n=238)or bilateral (n=52) endovenous
laser ablation of incompetentsaphenous veins with simulta-neous avulsion of varicosities.Following informed consent,patients were given the optionof having either local anaesthe-sia with tumescent infiltrationor general anaesthesia. Sixweeks later ultrasound imagingwas performed and the needfor treatment of residual veinsdetermined. Patient experienceof their operation was deter-mined by questionnaire andtheir preference for either type
of anaesthesia was analysed.Results of the study showed
that all patients had successfulabolition of truncal reflux andonly two patients requiredpostoperative sclerotherapy.One hundred and sixty one(56%) elected to have localanaesthesia whilst 129 (44%)patients preferred generalanaesthesia.
“The median age of patientsundergoing endovenous laser
ablation under general anaes-thesia was lower than thosewho preferred local anaesthe-sia (47 vs. 63 years; p<0.01),and 62 of the 66 patients agedmore than 70 years of age hadlocal anaesthesia.
Sridhar said, “Patientsundergoing unilateral endove-nous laser ablation were morelikely to prefer local anaesthe-sia than those having bilateralprocedures (63% vs. 36%,p<0.01).
“Twenty one patients had
venous ulceration and theywere far more likely to chooselocal anaesthesia than the 269patients with varicose veins(90% vs 53%; p<0.001).Twenty four per cent ofpatients having local anaesthe-sia said they would prefer gen-eral anaesthesia if they were tohave a similar procedure againdue to anxiety or pain encoun-tered during the local anaesthe-sia procedure,” he said.
Office-based venoussurgery or not?
Is recovery after endovenous thermal ablation980nm laser vs. radiofrequency for endother-mal venous ablation of the greater saphenous
vein similar? “Yes”, say the results of a pilotstudy which will lead to a randomised, prospec-tive, single center study.
The study set out to compare the new cov-ered-tip laser fibre to the radiofrequencycatheter to determine if there was a differencein treatment outcomes for endovenous thermalablation of the vein.
Lowell Kabnick, New York, USA, told dele-gates at the International Union of Phlebology,Monaco, that, “Both the cover-tip fibre andradiofrequency electrode were effective intreating greater saphenous vein insufficiency.Comparing recovery surrogate markers, closurerates, pain and bruising, there was no differencein outcomes.”
Kabnick said, “We retrospectively reviewed49 patients (54 limbs) for ablation of thegreater saphenous vein, pain and bruising in therecovery period. Of these, 20 were treated with980nm endovenous laser and 34 patients weretreated with radiofrequency ablation. The samesurgeon performed all procedures.”
Investigators monitored all patients within72 hours to one week after the procedure with aduplex ultrasound. “Patients were required tofill out an analogue pain score for the firstseven days (scored by patients on a 10-pointanalogue pain scale) and have a digital pictureof the thigh taken at the postoperative visit,”said Kabnick
He told delegates, “The digital picturestaken were used to analyse the degree of ecchy-mosis on a five-point graded scale. Analysisand development of the bruising score was per-
formed by a nurse who was blinded to thedevice used.”
The 49 patients: 20 laser patients (18 femaleand two male; average age, 54.1); 30 radiofre-quency patients (22 female and eight male;average age, 58) completed treatment and fol-low-up examination. There was no statisticalsignificance for efficacy, analogue pain orbruising scores.
Kabnick also told delegates that a multicen-tre, prospective, randomised study is beingplanned to further evaluate these initial findingsand to look at venous severity scores and quali-ty of life changes.
Laser and radiofrequencyablation show similarrecovery rates
November 2009
Laser ablation more painful than highligation and stripping at two weeks
Andrew Bradbury, pro-fessor of vascularsugery, University of
Birmingham, and consultantvascular surgeon at the Heart ofEngland NHS FoundationTrust, Birmingham, UK, tolddelegates at the InternationalUnion of Phlebology meeting,in Monaco, that he has beenoffering ultrasound guidedfoam sclerotherapy for varicoseveins since 2001 and, to date,has treated around 1,000patients (1,500 procedures).
“We have found ultrasoundguided foam sclerotherapy tobe an extremely safe and cost-effective treatment for varicoseveins. It has largely replacedsurgery and the other minimal-ly invasive techniques, such asradiofrequency ablation andlaser, in our university depart-ment of vascular and endovas-cular surgery,” he said.
Foam sclerotherapy results inhigh levels of patient satisfac-tion, with most patients havingtheir expectations met in termsof symptom relief, cosmeticimprovement and other lifestyle
benefits. “These could, forexample include matters suchas choice of clothes, work per-formance, social and leisurepursuits, and relationships withlife partners,” he said.
Bradbury told delegates thathe had observed occlusionrates of 92.5%, 93.3% and82.5%, and an absence of vari-cose veins (in the patients’opinion) in 84.9%, 89.7% and84.8%, of the patients at one,six and 12 months.
“We have also seen rapidhealing and a low rate ofrecurrence in a small series ofpatients treated for open ulcersas well as a significantlyquicker return to normal activ-ities (e.g. work, driving, socialand leisure pursuits), and sig-nificantly less pain, bruisingand analgesia requirement,than after surgery with thistreatment,” he said.
Bradbury also shared thathis team had noted down sta-tistically significant improve-ments in both disease-specific(Aberdeen questionnaire) andgeneric health-related quality
of life (Short Form, SF-12) atone, six and 12 months.
A very low level of side-effects and complications hadbeen observed. In around1,500 treatments, the only seri-ous adverse events had beentwo cases of deep vein throm-bosis, five cases of transientvisual disturbance, two casesof procedure-induced migraineand one case of mild allergicreaction. “Up to 10–20% ofpatients get transient skin pig-mentation; thrombophlebitisrequiring treatment with non-steroidal anti-inflammatorydrugs and/or duplex guidedaspiration is seen in about 5%of patients,” he said.
The midterm results from arandomised clinical trialcomparing endovenous
laser ablation (980nm) versushigh ligation combined withstripping of the great saphenousvein show that both procedurescan be done safely under tumes-cent anaesthesia.
M Mooijj, Alkmaar, TheNetherlands, presented theresults of the data to delegatesat the International Union ofPhlebology conference,Monaco. “However, in the sec-ond postoperative week,endovenous laser ablation issignificantly more painful andresults in difficulty with dailyactivities, mobility and self-carecompared with high ligationand stripping,” he said.
Mooijj continued, “The studyaimed to identify the short andlong-term effects (10 years) ofendovenous laser ablation ver-sus high ligation combined withstripping of the great saphenousvein using local anaesthesia.The effects being studied withboth procedures were the clini-cal outcome, quality of life-assessment, recurrent varicosi-ties and neovascularisation.
Investigators in the studyincluded 120 patients (131legs). These were randomisedin the study from June 2007until 20 January 2009. Patientswere scored for pain (VisualAnalog Score), mobility, dailyactivities and daily care. Aduplex-scan was also per-formed on each visit. “CEAPclassification was determinedevery year. Complicationswere followed and analysed,”said Mooijj.
Researchers carried out strip-
ping in 69 legs, laser ablationon the other 62. Both groupswere homogenous for age, sex,body mass index and CEAP(range C2–C5). All procedureswere completed successfully.
“We found a significant andhigher postoperative pain scorein the laser ablation group afterone and two weeks (p<0.05).After one week, there was an
impediment in daily activities(p=0.007), mobility (p=0.000)and self-care (p=0.033) in theablation group. Cosmetic resultsas judged by the patients VisualAnalog Score were significantlyimproved and similar in bothgroups after six months(p<0.05). Duplex showed com-plete recanalisation andrenewed reflux of the greatersaphenous vein in one patienttreated with laser ablation,” saidMoiijj.
He also told delegates that in
both groups, two patients hadreflux in the groin of a side-branch originating from thefemoral vein. Two patients hada post-operative bleeding afterstripping. “After one yearCEAP improved evidently andequally for both groups, andonly one real recurrence wasobserved in the ablation groupbefore six months,” he said.
Foam sclerotherapy safe andcost-effective in experiencewith 1,000 patients
Lowell Kabnick
Andrew Bradbury
Twenty four per cent of patientswho had local anaesthesia saidthey would prefer generalanaesthesia if they were to have asimilar procedure again due toanxiety or pain
Laser ablation was significantlymore painful and resulted indifficulty with daily activities,mobility and self-care
BIBA Publishing

November 2009
BIBA Publishing
26
Compliance with use ofcompression stockings is animportant factor associated
with a successful outcome followingultrasound guided foam sclerotherapy,while gender is associated withcomplications, concluded a studyfrom the UK.
The study, ‘Ultrasound guided foamsclerotherapy for varicose veins:Factors associated with outcomes andcomplications’, presented at theEuropean Society for VascularSurgery (Oslo, Norway), highlightsthe need for discussion with patientsto emphasise the potential forcomplications of ultrasound guidedfoam sclerotherapy and compliancewith the use of compression stockingsafter the procedure.
“Ultrasound guided foamsclerotherapy has recently become anincreasingly popular treatment forvaricose veins. Although manypublished series detail the results offoam sclerotherapy, little is knownabout the factors which are associatedwith outcomes and complications,”
said Sarah Thomasset, Department ofVascular Surgery, King’s MillHospital, Nottinghamshire, UK.
The investigators reviewed aprospectively collected database ofultrasound guided foam sclerotherapyprocedures. A successful outcome wasdefined as complete occlusion of thetarget vein on duplex analysis at
follow-up. Eight factors were assessedto determine whether they wereassociated with outcomes andcomplications. These factors were: age(>65 years), gender, compliance withuse of post-procedure compressionstockings, previous varicose veinsurgery, single or multiple sites ofinjection, concentration of sclerosant
(<3%), volume of sclerosant (>10mls)and pre-procedure CEAP (>4).Statistical analysis was conductedusing the Chi-square test. P values ofless than 0.05 were deemed significant.
Between July 2007 and July 2009, atotal of 240 patients underwentultrasound guided foam sclerotherapy.Of these 131 (60 males, 71 females)have attended follow-up visits andhad a post-procedure duplex scan.Median age of patients was 55 years(range 18–80 years). Targets for foamsclerotherapy were long saphenousveins (n=75), small saphenous veins(n=13), accessory long saphenousveins (n=8), and reticular veins (n=5).The remaining procedures involvedother veins or more than a singletarget (n=30).
The median timing of follow-upwas three months (range 1.5–14months) with duplex scans revealingcomplete occlusion of the target veinin 79% of patients (n=104), partiallyoccluded vein in 14.5% of patients(n=19), and patent vein in 6% (n=8).
Complications were skin staining
(n=36, 27.4%), thrombophlebitis(n=24, 18.3%), pain (n=20, 15.2%),deep vein thrombosis (n=1, 0.76%),allergic reaction (n=1, 0.76%), andblistering (n=1, 0.76%). A total of 51patients experienced one or more ofthese complications.
The authors concluded thatultrasound foam sclerotherapy is aneffective and safe procedure for thetreatment of varicose veins. Of thevariables analysed, compliance withpost-procedure compression stockingswas the only factor associated with asuccessful outcome (p<0.05). Femalegender was the only factor associatedwith post-treatment complications,particularly skin staining (p<0.05).“With the exception of female gender,this series failed to identify any majorfactor associated with complicationsfollowing ultrasound guided foamsclerotherapy,” Thomasset said. “It isof absolute importance that patientsare given clear instructions regardingcompression hosiery and theimportance of adhering to these isemphasised,” she added.
Compression stockings and genderimportant for foam sclerotherapy success
Sarah Thomasset
The place of Daflon 500mgin guidelines andrecommendations
Andrew Nicolaides, from the VascularScreening and Diagnostic Centre,Nicosia, Cyprus, and emeritus
professor of vascular surgery, ImperialCollege, London, UK, presented a review ofrecent guidelines for venoactive drugs in thetreatment of symptoms, oedema and venousleg ulcer at the International Union ofPhlebology meeting, in Monaco.
Nicolaides explained to the conferencedelegates that a group of 14 experts, chosen tobe representative in the fields of angiology,dermatology, and vascular surgery, fromcountries in which venoactive drugs wereavailable and who had experience of theirclinical use, published the Siena consensuspaper on the efficacy of venoactive drugs inrelieving symptoms in 2005. Data fromrandomised, controlled trials were selectedand classified as Grade A (randomisedcontrolled trials with large sample sizes,meta-analyses with homogeneous results),Grade B (randomised controlled trials withsmall sample size), or Grade C (othercontrolled trials, non- randomised controlledtrials).
The experts agreed that venoactive drugswere indicated to relieve venous symptomsCEAP clinical class C0S through to painfulvenous ulcers (C6S). Micronised purifiedflavonoid fraction (Daflon 500 mg, Servier)was assigned Grade A in this indication,Nicolaides said.
Recommendation for oedema
Regarding oedema, Nicolaides continued,international guidelines on the management ofchronic venous disease used the same gradingsystem as that of the Siena experts. Outcomesincluded not only symptoms, but also oedemaand venous ulcer healing.
“When considering venoactive drugs, theguidelines largely summarised andendorsed the positive findings of the recent
Cochrane reviews and highlighted theevidence of efficacy of several venoactivedrugs in chronic venous disease-relatedoedema. Micronised purified flavonoidfraction was assigned Grade Arecommendation in venous symptoms andoedema, and as an adjunct to standardcompression treatment in the healing ofvenous ulcers,” Nicolaides said.
For venous leg ulcer, based on the GRADEsystem described by Guyatt, the recentguidelines of the American College of ChestPhysicians recommended micronised purifiedflavonoid fraction to be added to compression(Grade 2B) in the treatment of venous legulcers in patients with venousthromboembolic disease. In the last edition ofthe Handbook of Venous Disorders (2009), theuse of micronised purified flavonoid fractionin combination with compression inlongstanding or large venous ulcers wasrecommended (Grade 1B).
Andrew Nicolaides
More veins reopened afterlaser ablation than withsurgery at two years
Abolition of great saphenous vein refluxand improvement in quality of lifewere similar following high ligation
with stripping and endovenous laser therapyafter two years, Jan Christenson told delegatesat the International Union of Phlebologysymposium, in Monaco.
In the study titled ‘Prospective randomisedtrial comparing endovenous laser ablation andsurgery for treatment of primary greatsaphenous varicose veins – Two yearsfollow-up’, however, two great saphenousveins were found completely reopened andfour partially reopened following laser therapyat two years, which was significantly morethan following high ligation with stripping.
“Endovenous laser therapy for ablation ofthe great saphenous vein is thought to
minimise postoperative morbidity comparedwith high ligation and stripping. Only a fewrandomised trials have reported early results.This prospective randomised trial compareslaser therapy (980nm) and surgery results oneand two years following the intervention,”
Christenson, Division of CardiovascularSurgery, University Hospital of Geneva,Geneva University, Switzerland, said.
Patients with symptomatic varicose veinsdue to great saphenous vein insufficiencywere randomised to either high ligation andstripping (100 limbs) or endovenous laserablation (104 limbs). Four laser therapyprocedures failed and were excluded.Phlebectomy and ligature of incompetentperforators were performed wheneverindicated. Patients were examined by clinicalexamination and Duplex ultrasoundscanning preoperatively, at 12 days, one yearand two years postoperatively. Complicationrate, length of sick leave, Aberdeen VaricoseVein Score, venous clinical severity score andMedical outcome study SF-36 scores wererecorded. There was no differenceregarding patient demographics,CEAP-class, Widmer class or severity scoresbetween the groups.
According to Christenson, simultaneousinterventions did not differ between the groupsand sick leave time and postoperative pain wasreported the same. No major post-treatmentcomplications were recorded. “High ligationwith stripping induced significantly morepostoperative haematomas than laser therapy,while laser patients reported more bruising,”Christenson reported.
Follow-up at one year was 100% forsurgery and 99% for laser therapy. There weretwo laser therapy-great saphenous veinsreopened and three partially reopened. Ninetyeight per cent of the limbs in both groups weresymptom-free. Venous clinical severity score,Aberdeen Varicose Vein Score and SF-36 didnot reveal any group differences. At two yearspreliminary results on 83 and 71 limbsrespectively (surgery and laser therapy)showed one more laser therapy vein that wasfound partially opened.
The randomised trialresults showed thathigh ligation withstripping inducedsignificantly morepostoperativehaematomas thanlaser therapy, whilelaser patients reportedmore bruising

November 2009
BIBA Publishing
27
Isolated phlebectomy led toa modification in reflux inthe great saphenous vein,
with a significant reduction induration and peak velocity.The procedure also led to asignificant reduction in thegreat saphenous vein diameter.Together, these led to reductionin the volume of the reflux.
The refluxing volume couldbe the key point to explain theeffect of the ablation of thevaricose reservoir on thesaphenous reflux, according toPaul Pittaluga, Riviera VeineInstitut, Nice, France. Pittalugapresented data from “Theeffect of isolated phlebectomyon reflux and diameter of thegreat saphenous vein – Aprospective study” at theEuropean Society of VascularSurgery annual meeting inOslo, Norway, and at theInternational Union ofPhlebology meeting inMonaco.
Pittaluga conducted aprospective study to assess thehaemodynamic and anatomicconsequences of isolated phle-bectomy by analysing theduration and velocity of thesaphenous reflux and diame-ter. Fifty five legs in 54patients with varices and pres-ence of great saphenous
reflux, reaching or not reach-ing the saphenous junction,which were treated by isolatedphlebectomy (with the socalled ASVAL method) wereincluded. Of the 54 patients,24 were women and the meanage was 62.6 (37–83 years).The wide majority of patientshad symptomatic non-compli-cated varicose veins. Thestudy excluded patients previ-ously operated on for varicoseveins, cases of deep venousinsufficiency and limbs inwhich a reflux was present inboth great and small saphe-nous veins.
Reflux duration, peak refluxvelocity, and diameter of thegreat saphenous vein weremeasured using duplex ultra-sound pre-operatively and onemonth after procedure. Refluxduration was consideredabnormal if it lasted longerthan 0.5s. The diameter of thesaphenous vein was assessedwith five measurements fromthe junction to the calf.
“What has been the modifi-cation of the saphenous refluxin our study? A significantsaphenous reflux of more than0.5s was present in 50 casespre-operatively, while theduration was at the limit at0.5s in five cases. At the post-
operative control, the refluxwas significant in only 20cases, while there was nomore reflux in 35 cases. Thus,the reflux was abolished in 30out of 50 cases (60%),”Pittaluga said.
The modification of thereflux duration was highly sig-nificant with a mean reductionfrom 1.53s before the proce-dure to 0.81s at one month(p<0.0001). “This reductionwas obviously major for limbsin which the reflux has beenabolished, but even for limbsin which a reflux of more than0.5s was still present the mean
duration was significantlyreduced in more than 30%,”Pittaluga said.
The assessment of the peakreflux velocity also showed ahighly significant reductionwith a mean modificationchanging from 248.6mm/s pre-operatively to 119.5mm/s atone month. “Once again, thisreduction was significant evenif the reflux lasted more than0.5s at one month,” Pittalugaincluded. “Concerning thetransostial reflux, it was pres-ent in 20 out of 55 cases pre-operatively, whereas none ofthe limbs presented a trans-ostial reflux at one month afterthe procedure. Thus, the tran-sostial reflux was abolished inall cases in our study.”
Regarding modification inthe saphenous diameter,Pittaluga presented datashowing that the meandiameter was significantlyreduced at all levels ofmeasurement at one monthpost-operation. “It wasinteresting to see that,excluding the ostial, thecloser the level ofmeasurement was of thebottom, the reduction washigher, from 11.1% at the pre-ostial to 32% at the calf.”
“The ablation of thevaricose reservoir had asignificant haemodynamicconsequence on the refluxingsaphenous vein, with theabolition of the reflux in 60%of the cases for the wholecohort and in 100% for theostial reflux checked with theValsalva manoeuvre.
Other studies are requiredto confirm if the refluxingvolume is correlated to theclinical consequences of thereflux, said Pittaluga.
Isolated phlebectomyleads to reduction involume of reflux
Modification of the reflex duration
Pre-operative (s) At one month (s) Reduction p valueNo reflux at one month 1.0 0.31 70.2% <0.0001Reflux >0.5s at one month 2.5 1.67 32.7% <0.0001
Modification of peak reflux velocity
Pre-operative (mm/s) At one month (mm/s) Reduction p valueNo reflux at one month 236.7 82.1 70.2% <0.0001Reflux >0.5s at one month 269.2 185.0 32.5% 0.0006
Paul Pittaluga
Ten-year experience shows radiofrequencyand laser ablation are highly effective
Ten years of experience show thatendovenous ablation techniques arehighly effective for the treatment of
great and small saphenous veins with avery low incidence of side effects. RobertWeiss, Johns Hopkins University School ofMedicine, Baltimore, USA, and MarylandLaser, Skin & Vein Institute, Hunt Valley,USA, presented data from a decade ofexperience at the International Union ofPhlebology conference in Monaco.
Endovenous techniques were approvedin the USA in early 1999, Weiss told theconference delegates. “The technique usedinvolves single puncture, ultrasound guid-ance, large volume dilute local anaesthesia,no sedation with immediate ambulation.We use radiofrequency and 1320nm. Forradiofrequency, in 2007, we switched toClosureFast. For laser, we developed the1320nm to more selectively target water
instead of haemoglobin in an attempt toreduce endovascular and perivasular heatformation,” he said.
The purpose was to reduce risks of pain,hAematoma while increasing efficacy. For1320nm, an automatic pullback mechanismallows more uniform application of laserenergy. Patients were followed on a yearlybasis with a free ultrasound examination.Some 9% of patients returned with newperforating vein varicosities in the absenceof recurrent targeted saphenous veins.
The study has tracked over 600 patientsin the database. Overall success rate forpatients at 5–10 years is 91%, demonstrat-ed by absence of great saphenous vein orsmall saphenous vein. For five years orless, the success rate (as determined byultrasound disappearance of the targetedvein) is 95%. There was only one incidentof thrombosis, within six weeks of treat-
ment, extending into the common femoral,which occurred in 2000.
When segments of a great or smallsaphenous vein recanalised, of the 9% fail-ures, 2% were seen at six weeks, 6% at oneyear and 1% at two years. Post-operativepain was minimal with 84% experiencingno pain with either technique. In thepatients reporting mild pain or tenderness,only treated segments above the fasciawere involved.
In conclusion, Weiss said, both radiofre-quency and laser 1320nm, both of whichtarget water, not haemoglobin, are highlyeffective long term with a very low inci-dence of side effects. “The technique ofultrasound guided puncture under localanesthesia with immediate ambulation isvery safe and effective, and has replacedsurgical stripping. A decade of experiencevalidates endovenous ablation,” he said.

November 2009
BIBA Publishing
28
The Centre for Evidence BasedPurchasing (CEP) published itslong-awaited evidence review
on endovascular treatment of varicoseveins in August. CEP, now incorpo-rated into NICE, was established in2005 to provide impartial and objec-tive information about medical tech-nology to help the NHS make betterpurchasing decisions.
At the heart of its work is clinicaland cost effectiveness. Havingevolved from the former DeviceEvaluation Service, the centre hasover 30 years experience in evaluatingmedical devices.
This report draws its conclusionsfrom a systematic literature search anda survey of expert vascular surgicalopinion from across the UK.
Conclusions ofthe CEP report:
“Varicose veins cause major socio-economic and health problems. In theUK, varicose vein proceduresconsumed approximately £40 millionin 2005–6. Varicose veins are not anacute life-threatening condition but dohave an impact on quality of life andcan involve significant expenditure, inparticular in the provision of nursingcare for venous ulcers. Treatment ofvaricose veins gives a benefit topatients and both surgery and liquidsclerotherapy are well below theNational Institute for Health andClinical Excellence (NICE) thresholdof £30,000 per quality-adjusted lifeyear. This is also likely to be true forfoam sclerotherapy, radiofrequencyablation and endovenous laser ablation.
Surgery is the most commontreatment within the NHS at present.It is very effective in removingvaricose veins and has a high long-term success rate. Surgery in the UKis performed using general anaestheticin theatre. Patients may experiencesignificant bruising, post-procedurepain, and complications such as groin
infections. Return to work isfrequently reported as between oneand two weeks, or even more,resulting in a high social andeconomic cost to society.
Endovascular techniques offer analternative to surgery and NICE hasconcluded that they are sufficientlysafe and effective for use in the NHS.NICE recommends audit procedures
and patient information for foamsclerotherapy.
All the endovascular techniquesconsidered can be performed without ageneral anaesthetic. This frees theatres
for other surgical procedures and leadsto a, faster recovery, lower staff costs,reduced equipment needs and reducedward time pre and post procedure.They also give a quicker return to nor-mal activities.
Foam sclerotherapy is the cheapestprocedure and requires no specialequipment. It can be used on almostany patient, including those not suitedto general anaesthesia and those withtortuous veins. Its effects do not last aslong as other treatments, meaningrepeat procedures may be necessary.This reduces the overall cost effective-ness on foam sclerotherapy. It is lesspainful immediately after the proce-dure than surgery and allows a fasterreturn to normal activities, but maynot be as cosmetically pleasing assome other procedures. There are vari-ous side effects associated with foamsclerotherapy, some of which are seri-ous, although rare.
Although endovenous laser ablationand radiofrequency ablation are botheffective in the short term, there is alack of evidence for long-term results.They require capital investment andexpensive consumables. There is alack of robust UK evidence on costimplications. Patients may have afaster return to normal activitiesresulting in a cost saving to the widereconomy. Radiofrequency ablationstudies show a reduction in post-pro-cedure pain and bruising.
There is a significant potential toimprove both patient comfort postprocedure and recovery rates with allthe endovascular techniquesconsidered. There is also potential toreduce procedure costs, depending onindividual circumstances. There is alack of evidence for long-termefficacy. Foam sclerotherapy haspoorer long-term effectiveness thansurgery, while endovenous laserablation and radiofrequency ablationmay be similar to surgery in thisregard.”
Costs of minimally invasive treatmentfor varicose veins exposed
The Centre for Evidence BasedPurchasing (CEP) verdict isthat all the endovascular
techniques have the potential toimprove patient comfort post-procedure, recovery rates andprocedure costs. They identified ahigher rate of recurrence with foamsclerotherapy but both laser andradiofrequency ablation gave largelysimilar long-term recurrence ratescompared with surgery, and both havebetter immediate outcomes (less painand earlier return to work).
The report, however, identifieshuge differences in list pricesbetween suppliers. The only tworadiofrequency ablation suppliers inthe UK charge between £519(VNUS) and £350 (Olympus) per kitwhereas the increased competitionbetween laser suppliers has led toprices as low as £175 (SDL medical)up to £500 (Varilase). The CEPreport states that “The consumableitems are a significant cost and mustbe considered when choosing a laser
or radiofrequency generator. It maybe possible to use endovenous laserablation catheters from one supplierwith a different supplier’s generatorto achieve cost savings.”
This was a very rigorousassessment of both the economic andclinical effectiveness ofradiofrequency ablation, laser andfoam sclerotherapy undertaken by animpartial, well respected andexperienced scientific body. Theirconclusions tally with recentlypublished meta-analyses which showequivalent benefit of laser andradiofrequency over surgery andfoam sclerotherapy. In practice thereis no difference between all theradiofrequency and laser providers interms of clinical outcomes so thedecision as to what to purchase mustcome down to service and totallifetime costs which are basicallymaintenance and consumables.These vary dramatically betweenproviders. To secure best value formoney hospitals must go out to open
tender. These are not insignificantsavings; a large hospital undertaking200 cases per year can save over£300,000 over five years. Thesesavings can make a usefulcontribution to any department’s costimprovement targets.
Most of the studies on economicanalysis of the new endovenoustreatments are based on foreignhospitals whose costs are nottransferable to UK practice but doshow that even the most expensivetechnique (radiofrequency ablation)is cheaper than surgery when indirectcosts of productivity losses areincluded.
If, however, all 37,000 NHSvaricose vein procedures werereplaced by endovenous ablationusing the cheapest laser kits ratherthan radiofrequency ablation, theNHS would save £12,728,000 peryear in equipment savings alone.
David West, University Hospital ofNorth Staffordshire, UK
Huge variations in endovenouskit costs in the UK
COMMENT & ANALYSIS
DAVIDWEST
Less pain with bipolarradiofrequency obliteration
After one year, radiofrequencyobliteration is as effective and safe asendovenous laser therapy in treating
varicoses of great and small saphenous veinsunder tumescent anaesthesia, Jens Tesmann tolddelegates at the International Union ofPhlebology symposium, in Monaco.
“Less pain is induced by treatment withradiofrequency obliteration. Both methodsdeliver stable residual stumps,” Tesmann, of theCentre of Dermatology at Kurpark, Stuttgart,Germany, said.
The aim of this study was to compare theradiofrequency obliteration technique presentedin 2007 using a bipolar electrode catheter(Celon method) with laser ablation (810nm).“Comparative studies of bipolar and endove-nous laser treatment have not been reported sofar,” Tesmann said. “The objective was to com-pare bipolar radiofrequency obliteration withlaser ablation with emphasis on occlusion rates,side-effects and the stability of resulting stumpsas stump length is considered to be a risk factorfor recurrent varicoses after stripping.”
In this prospective study, 120 patients with
incompetent great or small saphenous veins weretreated by bipolar radiofrequency obliterationwith laser therapy using tumescent anaesthesia.The obliteration catheter and laser fibre tip werepositioned 1–1.5cm beyond the saphe-nofemoral/popliteal junction. Follow-up onocclusion rates and side-effects, measuring stumplength with duplex ultrasound, and performinglight reflexion rheography, was assessed at oneday, seven days, three months and one year.
At one year, occlusion rates of bipolarradiofrequency obliteration and endovenous lasertherapy were equal (95.5% vs. 97%) althoughsignificantly less energy had been applied byradiofrequency obliteration (LEED: 27.9 vs. 42.6J/cm). Functional outcome by light reflexionrheography did not differ significantly (28.7 vs.31.5s). Side-effects such as dyspigmentation(1.5% vs. 3%) were even, but patients treatedwith laser therapy suffered more pain in the firstweek (0% vs.16.4%). However, dysesthesiaswere more frequent in the bipolar radiofrequencyobliteration population (small saphenous vein:6% vs. 0%). Residual stumps were stable (12.3vs.14.3mm) with no significant differences.
Fewer complications withlaser than with surgery
Endovascular laser treatment results infewer complications than surgery andless time to recover than surgery, a
new study showed. Stefan Jianu,Proestetica Medical Centre, Department ofGeneral Surgery, Bucharest, Romania,presented the results at theInternational Union of Phlebology meeting,in Monaco.
This study was designed to evaluate theefficacy of endovascular laser treatmentcompared with surgery. “We randomised atotal of 945 patients with incompetent greatand small saphenous veins in two groups, 459with endovenous laser treatment and 486 withcrossectomy and saphenectomy. The patientswere submitted to a complete phebologicalexamination, including EchoDoppler andwere informed about both methods,” Jianusaid. The selection was based on the paymentability of the patients, with laser treatmentbeing considerably more expensive and notaccessible to almost half of the patients.
All the operations were performed underlocal tumescent anaesthesia, ambulatory-
endovenous laser treatment or phlebectomies,crossectomy and saphenectomy. The patientswere monitored clinically and byEchoDoppler at seven days, one month, threemonths, six months, one year and every sixmonths there after.
“Clinical recurrence at four years was 3%for the laser group and 4% for the surgicalgroup. The morbidity was very low for thelaser group, only 4%, with incidence ofindurations, pain, inflammation on the routeof the vein and small ecchymosis, withoutsuperficial burns, haematomas or deep veinthrombosis. Patients were able to return towork in 2–3 days,” Jianu said.
For the surgical group the morbidity was10%, with incidence of haematomas,paresthesias, infections of the wound, deepvein thrombosis (one case) and a number ofcases of ecchimosis and pain. The patientswere able to return to work at 5–7 days.
“We still need more time to evaluate thesituation, but it is clear that the future is notsurgery in the treatment of varicose veinsdisease,” Jianu said.

November 2009
BIBA Publishing
29
Cook launches NavAligndelivery system forinferior vena cava filtersPhysicians can now navigateeven the most tortuousanatomy with greater speed andsafety with the next-generationinferior vena cava filterdelivery system introduced inSeptember by Cook Medical atthe TranscatheterCardiovascular Therapeutics2009, in San Francisco, USA.The release of the NavAligndelivery system marks the 20thanniversary of Cook’s firstinferior vena cava filter, theBird’s Nest, and furtheradvances the treatment ofpulmonary embolism.
The NavAlign deliverysystem, available for both theCook Celect and Günther Tulipfilters, is designed to minimisetrauma and streamline filterplacement with featuresunavailable on any otherexisting deployment system. Ahaemostatic valve minimisesblood loss at the point of entry,
while a multipurpose dilatorhas radiopaque sizing bandsand flushing sideports thatdecrease fluoroscopy time andthe amount of contrast mediumrequired.
Clinical results forClariVein catheter forvaricose veinspresented
Results from the initial clinicaltrial of the ClariVein catheter,used in a new minimallyinvasive treatment for varicoseveins, were delivered at theXVIth World Meeting of theInternational Union ofPhlebology in Monaco inAugust and the 23rd AnnualMeeting of the EasternVascular Society inPhiladelphia in September.
Data were presented bySteve Elias, associate professorof Surgery at Mount SinaiHospital, NY and the directorof The Centers for VeinDisease at Mount Sinai andEnglewood Hospitals. Elias is
the principal investigator of thetrial, which was conducted atEnglewood Hospital andMedical Center, NJ. Thirtypatients were studied in thisinstitutional review board-regulated trial.
“Initial results were veryencouraging, and the successrates continue to be excellentas we follow patients over alonger period,” Elias said. “Thesuccess rates are equal to theearly results of radiofrequencyor laser treatment of greatsaphenous vein disease. Themain advantage is that thetechnique does not requiretumescence anesthesiainfusion, thus savingsignificant time and decreasingpatient discomfort. In addition,no generator is required andcapital and maintenance cost isreduced. This in-officeprocedure takes about 15minutes to perform and patientsresume normal activity thatday. All patients wouldrecommend the procedure toothers.”
The ClariVein catheteris a product ofVascular Insights.The company hasreceived 510(k)clearance from theFDA to marketClariVein forinfusion ofphysician-specifiedagents in theperipheral vasculature.The device combinesmechanical and chemicalmodalities to accomplishvein treatment in an in-office setting.
Sigvaris launchesUlceRx TherapySolution Kit forvenous leg ulcers
Sigvaris has launched theUlceRx Therapy Solution Kit, acompression stocking kit forthe treatment of venousleg ulcers. The kit con-sists of two underliner stock-ings and two 30–40 mmHggraduated medical compressionstockings, allowing the patientto wear one set while washingthe other.
In the study ‘The treatment
of venous leg ulcers with aspecifically designed compres-sion stocking kit’ (F Mariani etal; Phlebologie, September2008), 96.2% of the participat-ing patients achieved completeclosure of their wound with theuse of the UlceRx stocking kit(70% complete wound closurerate with traditional bandages)and healed ulcers up to 4cm indiameter twice as fast as com-pared to bandage wrapping.
Additionally, patients usingthe UlceRx therapy solutionreported that pain at night andin the morning was absent withthe use of Sigvaris UlceRx Kit,whereas patients using bandag-es experienced markedlystronger pain when bandageswere applied and removed, andwhile walking. This is notablebecause most patients sufferingfrom venous ulcers experiencesignificant, ongoing pain fromthe wound.
One of the pain-reducing fac-tors of the UlceRx TherapySolution Kit is the underlinerstocking that is made with cot-ton to soothe the wearer’s skin.The outerlayer fabric also pro-vides a “glide” which enablesthe outer stocking to be put onmore easily, reducing the painand discomfort of applyingcompression to a wound.
According to Sigvaris, theUlceRx Therapy Solution Kit isbest suited for the followingtypes of patients: a patient whocannot return on a regular basisto the medical clinic for band-age change, a patient who isexperiencing pain and/orswelling at night or in the morn-ing due to their venous legulcer, a patient who has noassistance at home for bandageapplication or removal, or homehealthcare patients, as bandagesused in wound care treatmentare normally changed twice perweek, and home health care isusually only covered by insur-ance for one weekly visit.
BioInvent recruits finalcohort for the phase IItrial of theanticoagulant TB-402
BioInvent Internationalannounced in September that ithas started recruitment of thethird and final cohort of 100patients for the phase II trial ofTB-402, a drug being devel-oped for the prevention of deepvein thrombosis.
The first two patient cohortsincluded 200 individuals intotal and the recruitment for thesecond cohort was concluded inAugust. The decision to startrecruitment of the third patientcohort follows a unanimousrecommendation from theexternal board monitoring theefficacy and safety of the study.
The phase II trial is an active(enoxaparin)-controlled, dose-escalating, multicentre,prospective, randomised, open
label trial evaluating TB-
402 for the prophylaxisof deep vein thrombosis afterknee surgery. The study willassess three different doses ofTB-402 given as a single intra-venous injection post kneereplacement surgery and thetrial will enrol 300 patients.The objective of the study is toassess the safety and efficacy ofthe three escalating doses ofTB-402. All the patients in thestudy will be monitored for aperiod of three months aftersurgery. TB-402 is developed incollaboration withThromboGenics NV.
TB-402 is a recombinanthuman monoclonal antibodythat partially inhibits FactorVIII, a key component of thecoagulation cascade. This novelmode of action is expected toreduce the risk of undesirablebleeding events, even at highdoses, as well as the need forpatient monitoring. These arethe two main drawbacks associ-ated with current anticoagu-lants. In addition, TB-402 is along-acting agent, which meansit could be given as a singledose after surgery to prevent
the development of deep veinthrombosis. This would be anattractive option, as all currentanticoagulant treatment optionsrequire daily treatment for up toseveral weeks.
F Care Systems NVshowcases the EVRF
F Care Systems NV showcasedthe EVRF (endovenousradiofrequency) system, used inthe treatment of varicose veinsis being showcased in a seriesof medical meetings in Europe.
According to F Care SystemsNV, with the new developedtechnology of the EVRF, newcatheters are used to treat veinsbetween 0.3 – 4mm. The com-pany has developed a newcatheter to introduce into a veinin order to coagulate it from theinside. These catheters haveunique characteristics like flex-ibility and a special rounded tipto make the treatment of vari-cose veins possible. Thesepatented catheters can only be
used on the EVRF
radiofrequencygenerator.The EVRF is a slick
designed machine thatallows the doctor to
treat varicose veins in theprivate cabinet or in the clin-
ic. The system can be set atdifferent frequencies and pulsesso that veins with differentdiameters can be treated. TheEVRF settings can be adaptedwith the touch screen which iseasy to use. With the touchscreen it is possible to choosebetween the transdermal appli-cation for small spider neavusor the endovenous applicationfor the big varicose veins.
The special designed handpiece allows the physician tointroduce the catheter easilyinto the vein.
The hand piece is sterile sofor each patient a new handpiece with catheter has to beused. The hand piece is madeout of light plastic and is dis-posable. Thanks to new andspecial molding technology thehand piece including thecatheter is very economicallypriced, according to the com-pany. The procedure comparedto sclerotherapy is about thesame cost.
The catheter has a specialmolded round tip whichimproves the gliding into thevein. The tip has been roundedso even when the vein is notstraight the catheter will followthe curve of the veins.
Product News
NavAlign
ClariVein catheter
EVRF

November 2009
BIBA Publishing
30
Janet T Powell of ImperialCollege, London, UK,held an inspiring
European Vascular Surgeonsin Training Honorary Lectureon behalf of Roger MGreenhalgh who was absentdue to illness. He had beenlooking forward very dearly tospeak to the young vascularsurgeons at the EuropeanSociety for Vascular SurgeryAnnual Meeting, in Oslo,Norway. He had viewed it as“The old professor lookingback, speaking to the youngvascular surgeons lookingforward”.
Powell followed with amemorable quote of
Greenhalgh: “Technicalmastery comes first, secondand third and awareness ofareas of change and advancefollows.” She went on to statethat, “Many of the keyinnovations and indications invascular surgery have beenestablished and evaluated inrandomised clinical trials andin this regard, vascular surgeryis perhaps foremost amongstthe surgical specialities withan extremely strong trackrecord in evidence basedmedicine and practice.” Shereflected on the history ofcarotid endarterectomy leadingto a plethora of trials and theireffect on practice. This
emphasised the importance oflevels of evidence from thetop of the pyramid withmultiple well conducted
randomised trials down to theimportant beginnings ofresearch with case historiesand simple observations. “Wenow have evidence for carotidendarterectomy from the verytop level with meta-analysesof randomised controlledtrials”. So, why do we actually
need randomised controlledtrials? Often, observationaltrials have been shown to bestrongly biased with enrolment
of selected subjects causingmajor problems. This has ledto false management andincorrect treatment of patients.But how do we know, when itis time to start a trial? “One ofthe first starting points is whenthere is a grey area ofuncertainty about the
treatment in question, e.g. isthere potential patient benefitor potential cost benefit?”Identifying and acting uponthese areas of uncertainty invascular surgery has definitelybeen a central inspiration toProfessor Greenhalgh.Looking at the different keytrials he has participated in,Professor Powell highlightedwhy some have altered clinicalpractice and why others havenot, often due to controversial
and sometimes unpopularresults. She emphasised, thatthe greatest impact comesfrom large, pragmaticrandomised trials. They setpolicy. Although they can bedifficult to interpret, one canuse them to indentifysubgroups. However, data can
also be misused. On the otherhand, small, clean randomisedtrials have less impact, sincethey reflect a selected cohortor subgroup, have largenumbers of excluded patientsand are not generalisable.
Briefly, Powell drewattention to the newly initiatedEurope-wide ImmediateManagement of Patient withRuptured Aneurysm: OpenVersus Endovascular Repair(IMPROVE) trial which willlook at emergency repair ofabdominal aortic aneurysmseither by endovascular or openrepair. It aims at answering avery important question:“Does a policy ofendovascular repair save livesin ruptured aneurysms incomparison to the standardtreatment of open surgicalrepair?” Thus, the quest fornew evidence is neverendingand the next generation ofsurgeons must rise to thechallenge of pursuing the besttreatments for their patients.
Clinical trials in vascularsurgery: Neverending quest fornew evidence
“I have saved more lives through time spent onclinical trials than on time spent treating patients”
Roger Greenhalgh
Will endovascular treatments cross the finalfrontier – the treatment of aortic arch disease?
Peter Harris, professor of endovascularsurgery at University College London, UK,told Vascular News that the objectives of
the meeting were to try and move theendovascular technologies on to deal with theremaining obstacles in the treatment of seriousaortic disease. “It is a very exciting area. Mostpeople would regard the arch of the aorta and theascending aorta as the final frontiers forendovascular treatments. We can treat theabdominal aorta, peripheral arteries and thecarotid arteries by endovascular means, thoughcurrent clinical evidence does not supportpreferential stenting of the carotid arteries. If wecould find minimally invasive endovasculartreatments for serious diseases that affect the aortaclose to the heart, it would make a big impact onthe survival of patients with these conditions.
“The size of the aorta, the very strong haemo-dynamic forces, the need to incorporate the criti-cal supra-aortic branches that supply the headand brain and also the closeness of the manipula-tions to the heart itself, are all very challenging,”he said. Currently the standard of care for dis-eases of the aortic arch and those affecting theascending aorta – principally aneurysms and dis-sections – is open surgery. But surgery in thisarea is also very challenging as it is associatedwith opening the chest, cardiopulmonary bypass,profound hypothermia and transient circulatoryarrest. In effect, the patient is put in a state ofsuspended animation. “If we select patients well,they do very well with open surgery. But becauseof the physical trauma associated with thisapproach, it is not an option for elderly patientsor for those with serious comorbidities, so theyare denied treatment,” Harris said.
“The endovascular option, on the other hand,has the potential to avoid the drawbacks of opensurgery. So far, we have treated only carefullyselected patients with arch aneuryms by endovas-cular means because one has to recognise thatwhat we are talking about is unproven therapy atthe moment, and we have to advance with caution.It would not be appropriate to treat a good-risk
patient with an unproven endovascular operationwhen we know that there is an alternative, opensurgery, with known risks and known outcomes.
“Even though endovascular treatments arevery much at an experimental stage, without anyestablished evidence-base to support their wide-spread use at present, there is great potential indiscussing options for overcoming the technicalbarriers that remain because the gains forpatients with these diseases will be considerable,if and when this is accomplished ,” said Harris.
“Multidisciplinary team working is likely to bea key factor in the achievement of our aims andthis is the principle behind the MultidisciplinaryEndovascular Team at University CollegeHospital (UCLH.MET) and the fully integratedmultispecialty faculty of this symposium that hasbrought together vascular and cardiac surgeons,interventional radiologists and cardiologists anddevice engineers to share their ideas,” he added.
First transfemoral endovascularrepair of the aortic arch in Montreal
Cherrie Abraham, vascular surgeon, McGillUniversity, Montreal, Canada, reported the resultsof his first transfemoral endovascular branchedgraft repair of the aortic arch using a novel designof branched endograft (Cook Medical).
He told Vascular News, “Currently, we usehybrid procedures, which are a combination ofopen and endovascular procedures. I thinkbranched graft endovascular repair is the newhorizon. All procedures will be done endovascu-larly once we have the right technology.”
“The patient who underwent this new procedurehad a distal transverse arch aneurysm, and theonly way to treat this by endovascular means wasto either place a stent graft in conjunction with anopen bypass of the carotid artery or to try a totallytransfemoral exclusion via a small incision in thegroin and small incisions in the arm. We were ableto do that and extend the branched graft into theartery supplying the brain with smaller coveredstents that were deployed via small incisions in theneck and arm. This patient did well; he was home
in about five days. To the best of my knowledge,this was the first time in the world this particulartype of branched graft was used, and I think wedid pretty well, all things considered. We onlyneed to make minor modifications, rather thangoing back to the drawing board.
“We are far off right now from having a com-pletely percutaneous procedure but it is notbeyond the realm of possibility,” said Abraham.
Challenges of treating archaneurysms by endovascular means
“Anatomical and haemodynamic conditions inthe aortic arch make stent graft orientation and
placement a challenge. Also, cerebral protectionremains a problem,” Krassi Ivancev, consultantradiologist, University College London Hospital,London, UK, told attendees.
Why is endovascular arch repair a challenge,questioned Ivancev. “From an anatomical pointof view, the short distance between the left sub-clavian artery and left common carotid artery,arch angulation and aortic size discrepancybetween the size of the ascending and descend-ing aorta make it a difficult region to stent.
“Technically, device delivery and orientationremain challenging. Physiologically, the need to
Peter Harris Krassi Ivancev
The London cardiovascular symposium focussed on new developments whichhave the potential to radically affect the treatment approaches to life-threatening diseases of the ascending aorta and arch. The coming of age ofendovascular treatments for these conditions, which represent some of themost severe challenges to conventional cardiovascular surgery, was discussedby participants from around the world
Continued on page 31

November 2009
BIBA Publishing
Will endovasculartreatments cross the finalfrontier – the treatment ofaortic arch disease?
protect cerebral perfusion and the high haemody-namic forces which are different from all otherareas, compound the challenge,” said Ivancev.
Open surgery still the best option
Robert Bonser, consultant cardiothoracicsurgeon, Birmingham, UK, told delegates thataortic arch repair was at this point in time, bestperformed, using open techniques.
“Open repair is the treatment of choice foraortic arch repair because other concomitant pro-cedures are often necessary, and it is neverrestricted by landing zone size or availability.The proximal aorta (ascending) is often too largeto consider stent deployment, even withdebranching techniques,” he said.
Bonser also drew attention to the fact thatopen surgery can be performed with excellentearly mortality rate and improving neurologicalmorbidity. “Long-term outcomes with surgeryare good and freedom from repair failure isexcellent,” he said.
Bonser concluded that, “Thoracic endovascu-lar repair may expand the pool of patients under-going treatments, but it is unlikely to subsumethe role of conventional surgery for proximalaortic problems.”
The importance of aortic curvature
“Aortic curvature may help to explain whynormal diameter aortas can dissect. It isrelatively more important than aortic diameter,blood pressure, cardiac output , beta-blocker useand patient size with regard to force acting onthe aortic wall,” Mike Poullis, consultantcardiothoracic surgeon, Liverpool Heart andChest Hospital, UK, told delegates.
Speaking on ascending aortic curvature as anindependent risk factor for type A dissection, hepresented a mathematical model for ascendinganeurysm formation. “Curvature also has majoreffects on the forces exerted on the aorta inpatients with Marfan’s syndrome,” he said.
“Aortic curvature increases the forces exertedon the ascending aorta by a factor of over 10-fold. Aortic curvature can cause patients with asystolic blood pressure of 80mmHg to havegreater forces exerted on their aorta despitesmaller diameters and lower cardiac outputs thanpatients with systolic blood pressures of120mmHg,” said Poullis who also said furtherclinical study was needed to validate results.
The London Cardiovascular Symposium wasorganised by the Vascular Medicine Section,Royal Society of Medicine and the UCLH.MET.It was supported by Cook Medical, Jotec andother companies.
31
Contrast-enhanced computed tomographyhas become the gold standard imagingmodality for surveillance following
endovascular aneurysm repair. However,ionising radiation and nephrotoxic contrast aremajor disadvantages of this technology.Contrast-enhanced ultrasound usesmicrobubbles as an intravenously administeredcontrast agent. These have a high degree ofechogenicity and potentially many applicationsin future medical imaging. The time and costeffectiveness are of great value, say somedoctors.
A systematic review and meta-analysis of therole of duplex ultrasound and contrast-enhanced ultrasound vs. computed tomographyfor the detection of endoleaks after EVAR waspresented at the European Society for VascularSurgery Annual Meeting in Oslo, Norway. Alan
Karthikesalingam and TA Mirza of CambridgeUniversity Hospital, Cambridge, UK, under-took an analysis of the evidence on the diag-nostic accuracy of duplex ultrasound and con-trast-enhanced ultrasound (non-nephrotoxic) todetect endoleaks.
To identify trials, Medline, Embase, trial reg-istries, conference proceedings and article ref-erence lists were searched. Twenty-one studiesin 2,567 patients compared duplex ultrasoundto computed tomography. The sensitivity fordetection of an endoleak was 0.69, and thespecificity 0.93. Seven studies in 285 patientscompared contrast-enhanced ultrasound tocomputed tomography: sensitivity 0.89, speci-ficity 0.92. There was significant heterogeneity.Karthikesalingam concluded that contrast-enhanced ultrasound is a highly sensitivemodality for endoleak detection. However,
duplex ultrasound has poor sensitivity. Moreevidence is needed for contrast-enhanced ultra-sound, but: “Do we need any imaging at all?What is the reintervention rate in asymptomaticpatients?” Karthikesalingam added.
The precise utility of postoperative surveil-lance after endovascular aneurysm repair andthe follow-up regimen needed is still unsettled.Louise Brown, Imperial College, questionedthe decision to set computed tomography as thegold standard. “This is arbitrary and based onconvention rather than solid evidence that com-puted tomography is better than ultrasound. Byreversing the analysis and setting ultrasound asthe gold standard would the results differ?” Theanswer to that was “No, we did not performthis analysis”.
Nevertheless, the results might be very inter-esting.
Is contrast-enhanced ultrasound reliable enoughfor the detection of endoleaks after EVAR?
Alan Karthikesalingam
Continued from page 30

November 2009
BIBA Publishing
32
First implant of nextgeneration ConformableGORE TAG in US trialIn October, Gore announcedthe first human implants of thenext generation ConformableGore TAG thoracic endopros-thesis for the treatment of tho-racic aortic aneurysms. Thefirst implants were performedby Joshua Rovin and EugeneMurphy, at Bayfront MedicalCenter and William McMillanand Scott Schultz, at NorthMemorial Medical Center.Rovin said, “It is exciting to bepart of the clinical trial for thenext generation ConformableGore TAG device.”
Gore received approval of aninvestigational device exemp-tion (IDE) from the FDA toinvestigate the use of the nextgeneration Conformable GoreTAG device. William Jordan,
from the University of Alabama,Birmingham will serve as thenational principal investigator inthe Conformable Gore TAGDevice in Thoracic AorticAneurysm Trial (Gore TAG 08-03). “This study will evaluatedevice performance across thewide portfolio of sizes availablewith the next generationConformable Gore TAGdevice,” said Jordan. The deviceportfolio includes device diame-ters ranging from 21 – 45mm aswell as tapered devices, and thestudy will investigate the treat-ment of patients with aorticdiameters of 16 – 42mm.
The commercially availableGore TAG thoracic endopros-thesis provides a minimallyinvasive option for safely andeffectively treating patients withaneurysms of the descendingthoracic aorta. It is comprised of
an ePTFE graft with an outerself-expanding nitinol supportstructure to combine both deviceflexibility and material durabili-ty. It received pre-marketapproval from the FDA in 2005.
In addition to thoracic aorticaneurysms, the ConformableGore TAG device has beenapproved to investigateendovascular repair of otheraetiologies including traumaticaortic transection and aorticdissection. Design enhance-ments include a modified stentframe, repositioned goldbands, and optimised graftmaterial.
Invatec receives FDAclearance for Mo.MaUltra Proximal CerebralProtection Device
Invatec has announced that ithas received 510(k) clearancefrom the FDA to market itsMo.Ma Ultra ProximalCerebral Protection Device foruse during carotid artery stent-ing. The device reduces andcaptures debris released duringthe stenting procedure to pre-vent it from traveling to thebrain, where it has the poten-tial to cause a stroke.
According to Invatec,Mo.Ma Ultra establishes full-time cerebral protection andcontrol during the carotid stent-ing procedure prior to crossingthe internal carotid arterylesion, thereby preventing dis-tal embolisation. Small bal-loons on the tip and proximalshaft are inflated in the external
carotid artery and the commoncarotid artery to suspend bloodflow during the stentingprocess. These balloons act likeendovascular surgical clamps,protecting the brain during theprocedure. However the easy-to-use percutaneous Mo.MaUltra requires no surgery.Guidewires, stents and ballooncatheters are used in this pro-tected environment to treat thetarget lesion through theMo.Ma Ultra Device, whichprovides stability, control andaccess to the internal carotidartery like a guiding catheter orsheath. The suspended blood isthen aspirated along with anyembolic debris to complete theprocedure safely.
L Nelson Hopkins, StateUniversity of New York inBuffalo, USA, and co-principalinvestigator of the ARMOURtrial stated, “Proximal embolicprotection is an importantadvance that gives us moreoptions in the treatment ofcarotid artery disease. TheMo.Ma Ultra combines theadvantages of carotidendarterectomy with the mini-mally invasive benefits ofcarotid artery stenting.”
Hopkins reported results ofthe pivotal, multi-centre, non-randomised ARMOUR trial atVIVA 2009 in Las Vegas duringthe conference’s late-breakingtrials session on 22 October.
Results of the 262-patientARMOUR trial support thesafety and effectiveness ofMo.Ma Ultra for patients at
high surgical risk for carotidendarterectomy undergoingstenting. Mo.Ma Ultra’s full-time protection and controlcontributed to a low 30-daystroke rate of 2.3% and majoradverse cardiac and cerebrovas-cular events (stroke, death andmyocardial infarction) rate of2.7% in the primary endpoint220-patient population set.“The primary endpoint resultsof the ARMOUR trial areimpressive and support the ben-efits of proximal protection. Welook forward to the availabilityof Mo.Ma Ultra in the US mar-ket,” said Gary Ansel,Riverside Methodist Hospital inColumbus, and co-principalinvestigator of ARMOUR.
Mo.Ma Ultra ProximalCerebral Protection Device isindicated as an embolic protec-tion system to contain andremove embolic material(thrombus/debris) while per-forming angioplasty andstenting proceduresinvolving lesionsof the internalcarotid arteryand/or the carotid bifurcation.The reference diameter of theexternal carotid artery shouldbe between 3–6mm and the ref-erence diameter of the commoncarotid artery should bebetween 5–13mm.
Invatec launches theREEF HP ballooncatheter in Europe
Invatec has announced theavailability of Reef HP, a per-
cutaneous transluminal angio-plasty balloon catheter, idealfor use in all peripheral highpressure dilatation procedures.The “lesion-specific” design ofthe balloon material is particu-larly useful in “hard-to-dilate”situations and the availabilityof variable shaft lengths meanthat the Reef HP is equallysuited to both arteriovenousshunts (50cm shaft), andperipheral applications(80/120cm shaft).
“The Reef HP is a robust andhighly stable balloon, capableof counter-acting even the mostsevere arterial lesions, withminimal slippage and a highpressure threshold,” said StefanWidensohler and AndreaVenturelli, co-founders ofInvatec.” It has a“lesion-specif-ic” design
that is ideal for usein dialysis patients whose
arteriovenous shunts often cre-ate short, fibrous, and hard-to-dilate lesions where the shunt isconnected to the native vessel.
The Reef HP balloon ismade from Invatec’s propri-etary Flexitec XF, a durablematerial with a large workingpressure range of up to 22 bar,offering complete control dur-ing high pressure procedures. Itis also a low compliant bal-loon, offering a uniform dilata-tion force and strong shaperetention to dilate resistivelesions with greater successand stability.
Product News
Conformable Gore TAG
Reef HP


November 2009
BIBA Publishing
34
Further positive Aorfixdata reported at CIRSEand TCTJohn Hardman, Royal UnitedHospital, Bath, UK, has pre-sented further positive datafrom the use of Aorfix(Lombard MedicalTechnologies) at the Cardiologyand Interventional RadiologySociety of Europe (CIRSE)congress. The same data wasalso presented at theTranscatheter CardiovascularTherapeutics (TCT) congress inSan Francisco, USA, by AlbertoCremonesi.
Hardman presented data fromLombard Medical’sRetrospective Aorfix DataRetrieval (RADAR) voluntaryregistry. At the time of theanalysis RADAR contained dataon 753 implants out of approxi-mately 1,000 performed to dateworldwide. The data for thosepatients where follow-up infor-mation was available, continuedto compare favourably withpublished data on the use ofother stent grafts. To September2009, all cause 30-day mortality(of those fit for open surgery)was 1.59% (n=753), stentmigration at 12 months was 0%(n=461), wire fracture at 12months was <0.25% (n=461),graft limb occlusion at 12months was <0.25% (n=461),aneurysm rupture at three yearswas 0.9% (n=106). This ruptureoccurred with a uni-iliac devicethat is no longer commerciallyavailable and in a patient whoopted not to undergo furtherintervention.
Endoleak rates at one yearwere presented for both normaland high-angle-neck aneurysmswith the incidence of type 1endoleaks being 1.3% (n=151)and 3.8% (n=104) respectively,demonstrating that Aorfix main-tains a good proximal seal evenin patients with tortuous anato-my that cannot be treated withany other licensed stent graft.
Hardman also presented theresults of the ARBITER 2 studythat supported approval inEurope of the unique labelclaim for Aorfix received inJune 2009, to treat patients withhigh-angle-neck aneurysms ofup to 90 degrees. The studywas of 30 patients withaneurysm neck-angles of 70-90° (mean 79°). A third ofpatients had severely tortuousiliac arteries. The resultsshowed that Aorfix was:� Successfully inserted in near-
ly all cases. There was oneearly mortality due to mis-placement of the graft result-ing in occlusion of the superi-or mesenteric artery.
� No graft related complica-tions or endoleaks reported atone month.
� No graft related complica-tions reported at six monthsand a late endoleak rate of7% represented two minortype 1a leaks that did notresult in expansion of theaneurysm sac or the require-ment for further interventionto date.Hardman commented: “The
RADAR patient cohort hasrevealed that Aorfix has goodclinical outcomes in terms ofclinical events, mortality rate,endoleaks, migration and frac-ture up to three years afterinsertion along with a very lowlimb occlusion rate. TheARBITER 2 data is alsoencouraging and demonstratesthe safety profile and good clin-ical outcomes of Aorfix in chal-lenging anatomy.”
Echoing the earlier presenta-tion at CIRSE, Cremonesi alsopresented the RADAR data tothe TCT audience. He empha-sised that there were no signifi-cant differences in operativerisk factors, such as blood lossand procedure time betweenhigh angle and low angle cases,underlining the success ofAorfix in extending EVAR sur-
gery to this group of patients.During the well attended
TCT session, William Gray(New York PresbyterianHospital) illustrated the needfor a flexible stent graft inhighly tortuous aortic anatomy.Mark Fillinger (Lebanon,USA), principal investigator ofthe US study of Aorfixdescribed the strengths of theimplant from his own experi-ence. He said: “The Pythagorasstudy is concentrating on themost challenging anatomy seenin abdominal aortic aneurysmsurgery; the company must bevery confident in their device todesign the study in this way.”Of several highly challengingcases illustrated, he concludedthat: “Aorfix is the onlyimplant that would haveworked in these anatomies”.Questioned by Gray about theavailability of full results of thePythagoras study, Fillingeradded: “We have more than100 high angle cases recruitedand need to submit 120. Weshould have all the data forsubmission to the FDA andpublication by the end of2010.”
Brij Maini (Harrisburg, PA)emphasised the controllabilityof Aorfix during deployment,commenting: “We need thisimplant for challenging cases.”
Aorfix is currently beingcommercialised in the EU, witha pivotal clinical trial ongoingin the USA.
On Saturday, 21 November,Brian Hopkinson, Nottingham,UK, will present “What is therole of a flexible kink-resistantstent graft: 7 year clinical expe-rience with Aorfix endograft forAAAs” at theVEITHsymposium, in NewYork, USA.
Medtronic receives CEmark and launches theCaptivia delivery system
Medtronic has announced CEmark and international launchof the Captivia Delivery Systemfor the Valiant Thoracic StentGraft, for the treatment ofaneurysms and other lesions ofthe thoracic aorta.
The Captivia DeliverySystem features tip capture forenhanced control of the Valiantstent graft during deploymentand a hydrophilic coating
applied to the graft cover tofacilitate iliac access anddelivery through patients’ vas-culature. The new ValiantCaptivia system enables physi-cians to treat a wide range ofanatomies with a highly con-formable stent graft, withaccuracy and ease of deliveryto achieve optimal clinicalresults. Both Valiant andCaptivia are investigational inthe United States, where theiruse is limited to clinical trialsapproved by the FDA.
Giovanni Torsello, chief ofvascular surgery at StFranziskus-Hospital inMuenster, Germany, per-formed the first Valiantimplantation with the Captiviasystem.
“The Captivia DeliverySystem’s tip capture featureprovides excellent control ofthe stent graft during deploy-ment, which is criticallyimportant when treatinglesions in the thoracic aorta,”Torsello said. “Its hydrophiliccoating has also made a signif-icant improvement in stentgraft delivery. These addedfeatures will provide greaterconfidence in physicians’ abili-ty to treat these very challeng-ing cases.”
Indicated for the treatmentof a variety of thoracic aorticlesions, the Valiant stent grafthas emerged as the minimallyinvasive “system of choice”for thoracic endovascular aor-tic repair outside the USA. Infour years of clinical experi-ence, more than 15,000patients worldwide havereceived the device.
Medtronic announcescompleting enrolmentin two Valiant trials
Medtronic has announced thecompletion of enrolments intwo separate clinical trialsstudying the use of theValiant Thoracic StentGraft System for treatingdescending thoracic aorticaneurysms and descendingthoracic aortic dissections,respectively. The Valiant deviceis Medtronic’s latest generationthoracic endograft designed forminimally-invasive treatment ofthoracic aortic diseases.
The VALOR II clinical trial,which enrolled 160 patients at
27 investigational sites in theUnited States, will examine thesafety and efficacy of Valiant intreating descending thoracicaortic aneurysms. The data fromthis trial will be used to supportapplication to the FDA for prod-uct approval in the USA.
The VIRTUE Registryenrolled 100 patients at 14 clini-cal centres in Western Europeand will evaluate the use of theValiant graft for the treatment ofdescending thoracic aortic dis-sections, or type B dissections.The Valiant Stent Graft hasbeen available outside the USsince 2005 for the treatment ofthoracic aortic aneurysms, dis-sections and other lesions. Theobjective of the VIRTUERegistry is to collect additionalhealth economic and clinicalperformance data on Valiant forthe treatment of acute dissec-tions, complicated or expandingsub-acute dissections andexpanding chronic dissections.
Abbott launches next-generation peripheralstent system in Europe
Abbott has announced theEuropean launch of its next-generation Omnilink ElitePeripheral Stent System for thetreatment of iliac artery disease.The Omnilink Elite is a premi-
um balloon expandable stentsystem that incorporatesAbbott’s latest stent andcatheter technologies. Thecobalt chromium stent used inthe system is designed to pro-vide excellent deliverability andflexibility without compromis-ing strength or visibility underX-ray. The device is designedand manufactured inRangendingen, Germany.
“Iliac stenting is an excellentfirst-line interventional treat-ment option for peripheralartery disease patients as it isless invasive than surgery andhas the potential to improvepatient outcomes. With its flexi-bility, deliverability, and lowprofile, the Omnilink Elite setsa new standard for ease-of-usein iliac treatment,” said ThomasJahnke, University HospitalSchleswig-Holstein in Kiel,Germany. “In addition, thistechnology has the potential toshorten procedure times in morechallenging cases, because thesystem uses a common sheathsize for all stents. This elimi-nates the need to switch to alarger sheath if a different sizestent system is needed duringthe procedure.”
Abbott is committed to mak-ing investments in endovasculartherapies and educational pro-grammes and to designing andconducting endovascular clini-cal trials. The company recentlyinitiated a clinical trial calledMOBILITY to study the com-pany’s investigational Omnilink
Elite and Absolute Pro periph-eral stent systems inpatients with iliac arterydisease in the US. In addi-
tion, the BRAVISSIMO trial,an investigator-sponsored studyconducted at multiple sites inEurope, will investigate long-term outcomes of Abbott’sAbsolute Pro and OmnilinkElite stent systems for the treat-ment of simple and complexlesions of the iliac artery. MarcBosiers, of the AZ Sint-Blasiusin Dendermonde, Belgium, isthe principal investigator of theBRAVISSIMO study.
Product NewsCaptivia Delivery System
Aorfix
Omnilink Elite

November 2009
BIBA Publishing
36
Jotec launches E-XLendoluminal aortic stentprosthesisJotec has launched its E-XLendoluminal aortic stent pros-thesis. The E-XL is a self-expandable nitinol stent pros-thesis especially designed forthe treatment of lesions of theaorta and vena cava in particu-lar in case of dissections orstenoses but also for endograftrepair. The device received theCE mark approval in May2009.
The unique design of the E-XL endoluminal stent prosthe-sis featuring flared end guaran-tees for optimal vessel fixation.The closed cell design of theends provides for high radialforce whereas the open-cellstructure in the middle partadds flexibility. The standardproduct portfolio comprisestwo different stent lengths andvarious diameters to matchindividual vascular anatomies.
Besides, the E-XL benefitsfrom a unique delivery systemin sizes as from 12F which pro-vides easy handling and secureapplication. The soft and atrau-matic tip allows for easy vesselcrossing whereas the especiallydeveloped sheath catheter guar-antees high flexibility andpushability. The patentedSqueeze-to-Release mechanismenables controlled release andprecise positioning of the stentprosthesis which is supportedby highly visible radiopaquemarkers at both ends of thestent prosthesis.
The first implantations of theE-XL were performed at SAnna Hospital Como, S CroceHospital Cuneo and at theGerman Heart Centre Berlin.
Verathon launchesthe new AortaScanAMI 9700
Verathon has launched the newAortaScan AMI 9700 aorticmeasurement instrument tohelp physicians identify thepresence of abdominal aorticaneurysms. Designed withemergency physicians,internists, and family practi-tioners in mind, the portableAortaScan AMI 9700 uses 3Dultrasound to quickly and non-invasively measure the diame-ter of the abdominal aorta with-out the need for a sonographer.The AortaScan AMI 9700 madeits official debut in October atthe American College ofEmergency Physicians confer-ence in Boston, USA.
The new AortaScan AMI9700 offers health careproviders a quick, accurate, andreliable instrument for theirEmergency Department. Theinstrument, which has anonboard video tutorial and doesnot require a sonographer, iseasy for nurses to learn and use.
In a primary care setting,with internists and family prac-titioners, the AortaScan AMI
9700 allows physicians to inte-grate abdominal aortic diameterexams into office visits. Theportable AMI 9700 is quick andeasy to use. Exam results canbe provided in a matter of min-utes during an office visit.When the scan button ispressed on the AortaScan AMI9700, the instrument measuresultrasonic reflections on multi-ple planes inside the body andproduces a three dimensionalimage. Based on this image, theAMI 9700 calculates and dis-plays the diameter of theabdominal aorta on the colourconsole, and offers aimingassistance to the user, on boththe probe and the console.
The AMI 9700 instrumentprovides a print out or it cansave exam data to an electronicmedical record via HIPAA-compliant ScanPoint onlineimaging technology. ScanPointtechnology provides the abilityto view, save and print examsas well as to quickly and easilycalibrate AortaScan instrumentsonline.
Invatec launches theMaris Plus self-expanding peripheralstent system
Invatec has launched its latestself-expanding peripheral stentsystem, Maris Plus. The MarisPlus stent has a “lesion-specif-ic” design with larger sizes tomeet the clinical requirementsof the iliac region. The MarisPlus becomes thesixth stent plat-form now mar-keted by Invatecfor the treatmentof peripheral arterydisease, greatly opti-mising visibility,flexibility and ease ofuse for the physician.
The Maris Plus isavailable in a 30–100mmlength with 9–12mm diam-eter, meeting the variableneeds of the iliac region. Thedistinct stent geometry allowsfor increased stability in thehip, yet it remains the mostflexible stent on the market.Additionally, larger and fullyintegrated tantalum markersgreatly enhance visibility forthe physician.
Invatec announcesworldwide launch ofFiberNet distal embolicprotection system
Invatec has introducedFiberNet, a 3-dimensional dis-tal embolic protection system(EPS) for carotid artery stent-ing with the lowest crossingprofile (0.031”) and highestperformance capabilities to themarket. Manufactured byLumen Biomedical, FiberNetcan provide superior deliver-ability and can be used in ves-sels ranging from 3.5 to 7mm.
With its unique design,FiberNet ensures excellent
atraumatic wall apposition. It isalso usable in the most complexvasculature formations, cap-tures micro-emboli as small as40µm via specially shapedPET-fibers and can aspiratethese emboli from the body,allowing for safe and easyretrieval.
The FiberNet embolic pro-tection system was evaluated inthe EPIC trial, a multicentreclinical study during carotidartery stenting of 237 high sur-gical risk patients with criticalartery stenosis demonstrating a30-day stroke rate of 2.1%, thelowest ever reported for a distalembolic protection device. TheFiberNet embolic protectionsystem captures microemboli toprevent fragments traveling tothe brain thus reducing the riskof ischaemic stroke. AndreaVenturelli and StefanWidensohler, co-founders ofInvatec said, “We are extremelyexcited about bringing thisadvancement in embolic pro-tection technology to theworldwide market and believeit sets a new performance stan-dard for distal embolic protec-tion of carotid artery stenting,further reducing the risk to thepatient. Our partnership with
Lumen represents atremendous opportunity toexpand our position in theendovascular field.”
“The FiberNetembolic protection sys-tem has several attrib-utes including ease ofuse, low profile, andthe ability to conformto an irregular sur-face in the vesselwall, all of whichhave contributedto the impressiveresults and safetyprofile that weobserved in the EPICtrial,” said SubbaraoMyla, medical director ofcardiovascular research andendovascular intervention atHoag Memorial Hospital inCalifornia and national princi-pal investigator for the trial.
“The device achieved the low-est stroke rate of any filter cur-rently available, makingFiberNet a top choice for physi-cians, and representing the nextgeneration in embolic protec-tion.”
Bolton Medicalannounces first US trialcase with new RelayPlus System
Bolton Medical announced inOctober 2009 the first use ofits new Relay Plus System inthe US Relay Clinical Trial.The case took place at theUniversity of PennsylvaniaMedical Center inPhiladelphia, USA.
Nimesh D Desai, Division ofCardiovascular Surgery, one ofthe surgeons who performedthe procedure, noted that thesurgery was successful and theRelay Plus System allowed foreasier access to the difficult-to-reach thoracic aorta. He com-mented that “the hydrophilicdual-sheath design in the RelayPlus makes this device highlyversatile in terms of tightaccess vessels, and the addi-tional sheath length providesbetter stability during graftdeployment.”
“The Relay Plus System hasa spiral support bar whichallows the graft to take the less-er curve without kinking andeliminates the notion of ‘bird-beaking’ gaps and ‘no-man’s
land’. The system also hassmaller caliber devices
(22mm) which allows forrepair of patients withsmaller diameter aor-tas,” said Grace JWang, Division ofVascular and
Endovascular Surgery,who also performed the
procedure.The Relay Plus System offersnew delivery system featuresto optimize navigation and isdesigned for use with theRelay Thoracic Stent-Graft.It was developed with feed-back from participatingphysicians and offers the fol-
lowing attributes:
� Hydrophilic coating on theouter sheath and tip for easierintroduction and advance-ment through the aorta;
� Longer 60cm braided outersheath with enhancedradiopacity and reinforcedpushrod to facilitate pusha-bility and visibility in chal-lenging aortic anatomies;
� New nitinol inner catheter toaid in the alignment of thedual sheath system;
� Streamlined tip-sheath transi-tion.Study investigator, Wilson
Szeto stated, “I have had fantas-tic results from the Relay trial.Here at University ofPennsylvania, we have had nomortalities, no stroke rate, andno vascular complications dur-ing the 2.5 years we have partic-ipated in the trial. BoltonMedical has really fine-tunedthe lessons learned from otherthoracic aortic aneurysm prod-ucts and incorporated them intoa great product.”
The Relay Plus System wasCE marked in March 2009. It
will be marketed along with theoriginal Relay Thoracic Stent-Graft System which waslaunched in Europe in 2005 andis well underway in clinical tri-als in the USA.
It is expected that by the endof 2009, more than 3,500 Relayand Relay NBS stent grafts willhave been implanted worldwide.
LeMaitre launchesthe UnBalloon Non-Occlusive ModelingCatheter
LeMaitre has launched the CEmarked UnBalloon Non-Occlusive Modeling Catheterrecently. Unlike a ballooncatheter, the UnBalloon allowsthe modeling of aortic stentgrafts without occluding bloodflow. The nitinol mesh expands,allowing modeling of the stent
graft snugly to the vessel wall.Blood flows freely, givingample time to model the stentgraft or repair an endoleakwhile minimising the risk ofstent graft migration.
The new UnBalloon featuresnon-occlusive nitinol meshdesign eliminates blood pres-sure spikes, radiopaque flexitipfor effective trackability, nitinolmesh design offers the radialforce of a balloon without theocclusion, nitinol mesh and tworadiopaque bands are highlyvisible under fluoroscopy with-out contrast, compatible with.035” and .038” guidewires foreffective trackability, and non-occlusive design which allowsthe physician to generate anappropriate range of force with-out risk of balloon burst.
Toshiba expandsavailability of imageprocessing forInfinix-i Line
Toshiba is expanding the avail-ability of next generationAdvanced Image Processing
(AIP) to more systems in theToshiba InfinixTM-i productline. Toshiba’s new AIP featureimproves patient care byincreasing the quality, sharp-ness, and image contrast duringinterventional procedures. Thisproprietary technology has vir-tually eliminated image lag,benefiting clinicians while guid-ing and deploying devices dur-ing fluoroscopy. The AIP furtherincreases image clarity duringinterventional procedures to cre-ate a safer, more time-efficientexam for the patient by reducingthe possibility of having to re-image the patient if the image isnot clear. Next generation AIP isparticularly beneficial for stentimplementation, patients withrapid heart rates or small tortu-ous arteries, bariatric patientsand emergency situations.
Product NewsJotec’s E-XL
FiberNet
Maris stent

November 2009
BIBA Publishing
38
21–22 NovemberEuropean Symposium on VascularInnovationsVelence, HungaryTel: +36 1 350 1854Fax: +36 1 350 0929Email: [email protected]: www.asszisztencia.hu/esvi
26–28 NovemberVascular SurgeryParis, FranceMarriott Rive GaucheTel: +33 (0)1 4909 5585Fax: +33 (0)1 4909 5318Email: [email protected]: www.vascular-research.org
4–5 DecemberICCA 2009 – International Courseon Carotid Angioplasty and OtherCerebrovascular InterventionsFrankfurt, GermanyTel: +49 69 8999 0507Fax +49 69 9794 7652Email: [email protected]: www.iccaonline.org
17–21 JanuaryISET – The InternationalSymposium on EndovascularTherapy
Hollywood, Florida, USAWestin DiplomatTel: +1 (305) 279 2263Fax: +1 (305) 279 8221Email: [email protected]: www.iset.org
22–23 JanuaryControversies & Updates in VascularSurgeryParis, FranceMarriott Rive GaucheTel: +33 (0)4 9109 7053Fax +33(0)4 9615 3308Email: [email protected]: www.cacvs.org
27–30 JanuaryLINC 2010 – Leipzig InterventionalCourseLeipzig, GermanyTel: +49 89 129 5440Fax: +49 89 139 36 704Email: [email protected]: www.leipzig-interventional-course.de
10–13 February22nd American Venous ForumAmelia Island, Florida, USATel: +1 (978) 744 5005Fax: +1 (978) 744 5029Email: [email protected]: www.veinforum.org
11–13 February10th JIM – Joint InterventionalMeetingRome, ItalyTel: +39 02 8905 3524Fax: +39 02 20 1395Email: [email protected]: www.jim-vascular.com
25–27 February14th European Vascular CourseMaastrich, The NetherlandsMECC MaastrichtTel: +31 73 700 3500Fax: +31 73 700 3505Email: [email protected]: www.cardiovascular-course.eu
28 February–4 MarchXXIII International Congress onEndovascular InterventionsScottsdale, Arizona, USATel: +1 (602) 604 5030Fax: +1 (602) 604 5020Email: [email protected]: www.endovascularcongress.org
18–20 MarchDFCon 2010 – Diabetic Foot GlobalConferenceLos Angeles, USARenaissance Hollywood Hotel
Tel: +1 (337) 235 6606Email: [email protected]: www.dfcon.com
21–25 AprilXXIV World Congress of theInternational Union of AngiologyBuenos Aires, ArgentinaSheraton Buenos Aires Hotel & ConventionCentreTel: +54 11 4777 9449Fax: +54 11 4771 1536Email: [email protected]: www.iua2010.com.ar
Calendar of Events
I N T E R N A T I O N A L
Sign up at
www.vascularnews.com
NEWS & VIEWSFOR
VASCULARSPECIALISTS
GET BREAKINGNEWS FAST!
Vascular News team
Editor-in-chief:Roger Greenhalgh
Publisher:Stephen Greenhalgh
Editor:Marcio [email protected]
Assistant editor:Lisa Glass
Editorial contribution:Thomas WyssUrmila Doraswami
Design:David Reekie
Layout:
Matt Hadfield
Advertising:Marianne [email protected]
Website:David Reekie
Please contact the VascularNews team with any news or ifyou would like to advertise in ourclassified section:
Tel: +44 (0)20 7736 8788Fax: +44 (0)20 7736 8283
Published by:
BIBA Medical,
44 Burlington Road, Fulham,
London SW6 4NX, UK
Tel: +44 (0) 20 7736 8788
Fax: +44 (0) 20 7736 8283
Printed by:Buxton Press
Next IssueJanuary 2010
To advertise vacancies for:Vascular technologyVascular radiologyVascular surgeryVascular nursingOr to advertise vascular meetings
Please contact:Vascular NewsBIBA Publishing,44 Burlington Road, Fulham,London SW6 4NX, UKTel: +44 (0)20 7736 8788Fax: +44 (0)20 7736 8283e-mail:[email protected] Vascular News youare guaranteed to reach 15,000
vascular specialists in Europe
and North America.
call for classified
©BIBAMedical Ltd, 2009All rights reserved.Printed by Buxton Press.Reprint requests and allcorrespondence regarding thenewspaper should be addressed tothe editor at the above address.
10–13 AprilCharing Cross 32ndInternational SymposiumLondon, UKImperial College
ContactTel: +44 (0)20 7736 8788Fax: +44 (0)20 7736 8283Email: [email protected]: www.cxsymposium.com
Hold the date!

I N T E R N A T I O N A L
Sign up at
www.vascularnews.com
NEWS & VIEWS FORVASCULAR SPECIALISTS
GET BREAKINGNEWS FAST!