quantification of distal antral contractile motility in healthy human stomach with magnetic...
TRANSCRIPT

Original Research
Quantification of Distal Antral Contractile Motilityin Healthy Human Stomach with MagneticResonance Imaging
Monika A. Kwiatek, BASc (Hons),1* Andreas Steingoetter, PhD,2 Anupam Pal, PhD,3
Dieter Menne, PhD,4 James G. Brasseur, PhD,3 Geoffrey S. Hebbard, MD, PhD,5
Peter Boesiger, PhD,2 Miriam Thumshirn, MD,1 Michael Fried, MD,1 andWerner Schwizer, MD1
Purpose: To quantify healthy postprandial: 1) propagation,periodicity, geometry, and percentage occlusion by distalantral contraction waves (ACWs); and 2) changes in ACWactivity in relationship to gastric emptying (GE).
Materials and Methods: Using 1.5-T MR scanner, ninehealthy fasted volunteers were examined in the right decu-bitus position after ingestion of 500 mL of 10% glucose (200kcal) with 500 �M Gd-DOTA. Total gastric (TGV) and mealvolumes (MV) were assessed every five minutes for 90 min-utes, in and interspersed with dynamic scan sequences(duration: 2.78 minutes) providing detailed images of distalACWs.
Results: TGV increased by 738 � 38 mL after ingestion (t0),subsequently decreasing in parallel to GE. The mean GErate and half-emptying time were 24 � 3 mL/5 minutes and71 � 6 minutes, respectively. Accompanying ACWs reacheda periodicity of 23 � 2 seconds at t35 and propagated at anunvarying speed of 0.27 � 0.01 cm/second. Their ampli-tude of 0.70 � 0.08 cm was constant, but the width de-creased along the antral wall by 6 � 2%/cm (P � 0.003).ACWs were nonocclusive (percentage occlusion 58.1 �5.9%, t0 at the pylorus) with a reduction in occlusion awayfrom the pylorus (P � 0.001). No propagation and geometrycharacteristics of ACWs correlated with the changes of MV(mL/5 minutes; R2 � 0.05).
Conclusion: Our results indicate that ACWs are not im-perative for emptying of liquids. This study provides a de-tailed quantitative reference for MRI inquiries into pharma-cologically- and pathologically-altered gastric motility.
Key Words: antral contraction waves; computerized anal-ysis; gastric emptying; gastric motility; MRIJ. Magn. Reson. Imaging 2006;24:1101–1109.© 2006 Wiley-Liss, Inc.
INVESTIGATIONS INTO THE MECHANISMS drivinggastric emptying have allowed better understanding ofpathophysiology of certain gastrointestinal disordersand consequences of surgical and/or pharmacologicalinterventions. Particular attention has been devoted togastric motility. Taken as the final expression of com-plex neurohormonal interactions, gastric motility iscentral to effective controlled delivery of ingested foodand oral medications for subsequent duodenal absorp-tion.
Liquid emptying has been largely attributed to toniccontraction of the gastric fundus, creating an overallpressure gradient across the pylorus, controlling liquidemptying during periods of pyloric opening (1–3). Re-cent studies have concluded that the primary purposesof phasic distal antral contraction waves (ACWs) aremixing of gastric content and triturating of solids (4–6).However, it has also been argued that ACWs contributeto the rate of liquid gastric emptying (4,7,8) and thegeneration of pulsatile emptying patterns (1,3,9,10). Al-though ACWs may contribute to and modulate theemptying process, they may not be necessarily relatedto or required for gastric outflow (5,6,11). Prokineticmedications stimulating antral contractility, applied fortreatment of gastroparesis, support this hypothesis.Their efficacy is modest and results of clinical studiesare controversial (12). Hence, the contribution of ACWsto gastric emptying of liquids remains unclear.
Detailed quantification of propagation, geometry, andocclusive characteristics of ACWs in a normal physio-logical state, and modulation by drug or disease, may
1Division of Gastroenterology and Hepatology, University Hospital Zu-rich, Zurich, Switzerland.2Institute of Biomedical Engineering, Swiss Federal Institute of Tech-nology (ETH) Zurich, Zurich, Switzerland.3Department of Mechanical Engineering, The Pennsylvania State Uni-versity, University Park, Pennsylvania, USA.4Menne Biomed, Tubingen, Germany5Department of Gastroenterology, The Royal Melbourne Hospital, Mel-bourne, Australia.Contract grant sponsor: Swiss National Science Foundation; Contractgrant number: 32.54056.98.*Address reprint requests to: M.K., Division of Gastroenterology, Depart-ment of Internal Medicine, University Hospital Zurich, Raemistrasse 100,8091 Zurich, Switzerland. E-mail: [email protected] October 31, 2005; Accepted July 27, 2006DOI 10.1002/jmri.20738Published online 9 October 2006 in Wiley InterScience (www.interscience.wiley.com).
JOURNAL OF MAGNETIC RESONANCE IMAGING 24:1101–1109 (2006)
© 2006 Wiley-Liss, Inc. 1101

offer new insight into the relative contribution of peri-staltic activity to gastric emptying. Accurate quantifica-tion, however, is difficult. MRI has progressed to allownoninvasive recording of antral motility with high spa-tiotemporal resolution (13,14). Coupled with advancedcomputer-based image analysis, MRI can provide quan-titative detail on gastric motor function. Such quanti-tative detail is lacking in the current literature. An invivo quantification is necessary for complete under-standing of the role of distal antral motility in gastrictrituration, mixing, and emptying, as well as the con-sequences of the alteration of antral motility by nutri-ents, drugs, and disease, enhancement of future drugdesign, and clinical treatment, as well as for computermodeling of gastric function. Currently, the only modal-ity available for precise quantification of ACW motility isstate-of-the-art time-resolved MRI coupled with pur-pose-written image analysis requiring a combination ofexperimental and numerical expertise.
The aims of this study were 1) to quantify accuratelydistal ACW motility, specifically propagation, fre-quency, geometry, and extent of antral occlusion in thepresence of a nutrient liquid, and 2) to quantify changesin ACW activity over the postprandial period in relation-ship to patterns of liquid gastric emptying in health.
MATERIALS AND METHODS
Subjects and Protocol
Nine healthy subjects (four males, aged 23–42 years,body-mass index [BMI]: 19–29 kg/m2) participated inthe study. All subjects gave written informed consent.The study protocol was approved by the local ethicscommittee.
Following an eight-hour fast, subjects ingested 500mL of 10% liquid glucose (200 kcal), labeled with 0.5mmol/liter Gd-DOTA (Dotarem; Laboratorie Guerbet,Aulnay-sous-Bois, France) in the right decubitus posi-tion. Postprandial stomach volume (total gastric vol-ume; TGV), gastric contents (meal volume; MV), anddistal antral peristaltic activity were assessed over 90minutes with volunteers remaining in the right decub-itus position.
MRI
Studies were performed using a 1.5-T whole body MRIsystem (1.5 T Intera, Philips Medical System, Best, TheNetherlands). Two different types of scans were applied:1) a “volume scan,” covering the complete stomach vol-ume, to assess TGV and MV, and 2) a “motility scan,”dynamically imaging three longitudinal sectionsthrough the gastroduodenal region, to assess antropy-loroduodenal luminal wall motion with a focus on distalACWs. Six rectangular surface coils (height � 20 cm,width � 10 cm), fixed around the abdomen and con-nected to six independent receive channels were usedfor signal detection.
Volume Scan
Gastric volumes were assessed using a balancedsteady-state free precession (b-SSFP) imaging tech-
nique (TE/TR � 1.9/4.0 msec; flip angle � 35°). A totalof 40 sagittal and 15 transverse image slices were ac-quired in 23 seconds with a slice thickness of 5 mm,field of view (FOV) � 400 mm, and matrix size � 256 �205 pixels (spatial resolution: 1.56 � 1.95 � 5 mm3). Toavoid motion artifact, volunteers were asked to holdtheir breath in expiration during the length of eachvolume measurement. Volume scans were performedevery five minutes.
Motility Scan
ACWs were assessed using a dynamic b-SSFP imagingtechnique accelerated with the sensitivity encoding(SENSE) parallel imaging technique (15) (TE/TR � 1.8/4.0 msec; flip angle � 35°; SENSE reduction factor �1.6). A total of 120 consecutive scans were acquiredover a period of 2.78 minutes (167 seconds). Each scanimaged three oblique coronal or sagittal image planes(depending on the volunteer’s anatomy) of slice thick-ness � 8 mm, FOV � 400 mm, and matrix size � 256 �205 (spatial resolution � 1.56 � 1.95 � 8.0 mm3).Dynamic imaging was performed during normalbreathing. Motility scans were performed one minute(preparation time) after each completed volume scan.
Data Analysis
Volume Scan
TGV was evaluated by semiautomatically outlining thecontour of the gastric wall within each slice using the“Spline_p” procedure within the IDL 5.5 library (Re-search Systems Inc., Boulder, CO, USA), which per-forms a parametric cubic spline interpolation betweenuser-defined points. The segmented area within eachslice was multiplied by the slice thickness and all “slicevolumes” were added to calculate the stomach volume.Since intragastric air (black) and labeled liquid meal(bright signal) had a distinct contrast, a manually se-lected intensity threshold was used to determine andcompute MV. Volume analysis was performed using anin-house-written software package implemented in IDL5.5 (14).
Motility Scan
Details of gastric motility were computed using customdesigned image analysis software based on Matlab 6.5(Mathworks Inc., Natick, MA, USA). Each dynamic MRImotility sequence was analyzed frame by frame to followpropagating indentations on the walls of the distal an-trum, which denoted ACWs. The image analysis de-scribed below is illustrated in Fig. 1.
From the three slices of every MRI motility scan, animage plane was chosen that best displayed the antro-pyloroduodenal axis and the propagating ACWs (Fig.1a). The pylorus was located and marked on the appro-priate image plane and tracked through the dynamicimage sequence by finding the maximum correlationbetween two consecutive images calculated over anarea of 20 � 20 pixels around the marked location. Along axis was drawn through the center of the visibleportion of the antrum (Fig. 1b). The position of thepylorus was the anchoring point for the central axis.
1102 Kwiatek et al.
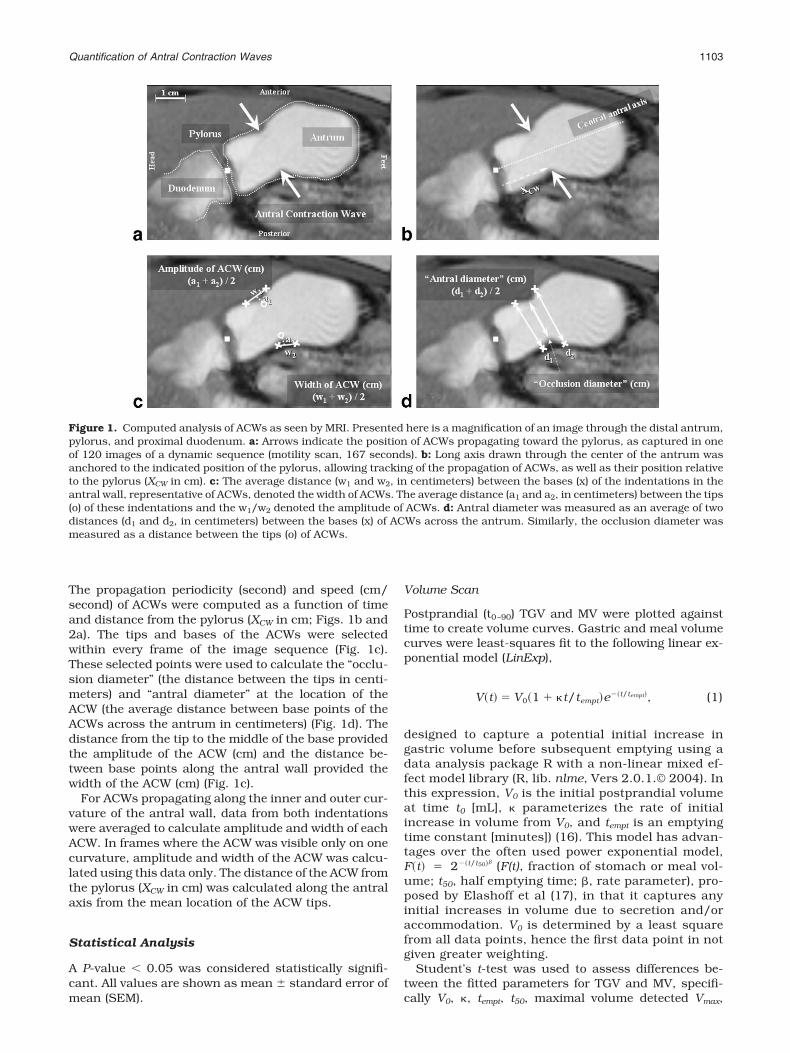
The propagation periodicity (second) and speed (cm/second) of ACWs were computed as a function of timeand distance from the pylorus (XCW in cm; Figs. 1b and2a). The tips and bases of the ACWs were selectedwithin every frame of the image sequence (Fig. 1c).These selected points were used to calculate the “occlu-sion diameter” (the distance between the tips in centi-meters) and “antral diameter” at the location of theACW (the average distance between base points of theACWs across the antrum in centimeters) (Fig. 1d). Thedistance from the tip to the middle of the base providedthe amplitude of the ACW (cm) and the distance be-tween base points along the antral wall provided thewidth of the ACW (cm) (Fig. 1c).
For ACWs propagating along the inner and outer cur-vature of the antral wall, data from both indentationswere averaged to calculate amplitude and width of eachACW. In frames where the ACW was visible only on onecurvature, amplitude and width of the ACW was calcu-lated using this data only. The distance of the ACW fromthe pylorus (XCW in cm) was calculated along the antralaxis from the mean location of the ACW tips.
Statistical Analysis
A P-value � 0.05 was considered statistically signifi-cant. All values are shown as mean � standard error ofmean (SEM).
Volume Scan
Postprandial (t0–90) TGV and MV were plotted againsttime to create volume curves. Gastric and meal volumecurves were least-squares fit to the following linear ex-ponential model (LinExp),
V�t� � V0�1 � �t/tempt�e�t/tempt�, (1)
designed to capture a potential initial increase ingastric volume before subsequent emptying using adata analysis package R with a non-linear mixed ef-fect model library (R, lib. nlme, Vers 2.0.1.© 2004). Inthis expression, V0 is the initial postprandial volumeat time t0 [mL], � parameterizes the rate of initialincrease in volume from V0, and tempt is an emptyingtime constant [minutes]) (16). This model has advan-tages over the often used power exponential model,F�t� � 2�t/t50�� (F(t), fraction of stomach or meal vol-ume; t50, half emptying time; , rate parameter), pro-posed by Elashoff et al (17), in that it captures anyinitial increases in volume due to secretion and/oraccommodation. V0 is determined by a least squarefrom all data points, hence the first data point in notgiven greater weighting.
Student’s t-test was used to assess differences be-tween the fitted parameters for TGV and MV, specifi-cally V0, �, tempt, t50, maximal volume detected Vmax,
Figure 1. Computed analysis of ACWs as seen by MRI. Presented here is a magnification of an image through the distal antrum,pylorus, and proximal duodenum. a: Arrows indicate the position of ACWs propagating toward the pylorus, as captured in oneof 120 images of a dynamic sequence (motility scan, 167 seconds). b: Long axis drawn through the center of the antrum wasanchored to the indicated position of the pylorus, allowing tracking of the propagation of ACWs, as well as their position relativeto the pylorus (XCW in cm). c: The average distance (w1 and w2, in centimeters) between the bases (x) of the indentations in theantral wall, representative of ACWs, denoted the width of ACWs. The average distance (a1 and a2, in centimeters) between the tips(o) of these indentations and the w1/w2 denoted the amplitude of ACWs. d: Antral diameter was measured as an average of twodistances (d1 and d2, in centimeters) between the bases (x) of ACWs across the antrum. Similarly, the occlusion diameter wasmeasured as a distance between the tips (o) of ACWs.
Quantification of Antral Contraction Waves 1103
changes in volumes detected �V, and the time periodfrom initial to maximal volume �t.
Nonmodeled MV changes within five-minute intervals(mL/5 minutes) were correlated with characteristics ofACWs (percent occlusion, amplitude, and width) de-scribed below.
Student’s t-test and correlations were assessed usingGraphPad Prism version 4.00 for Windows statisticalpackage (GraphPad Software, San Diego, CA, USA; ww-w.graphpad.com).
Motility Scan
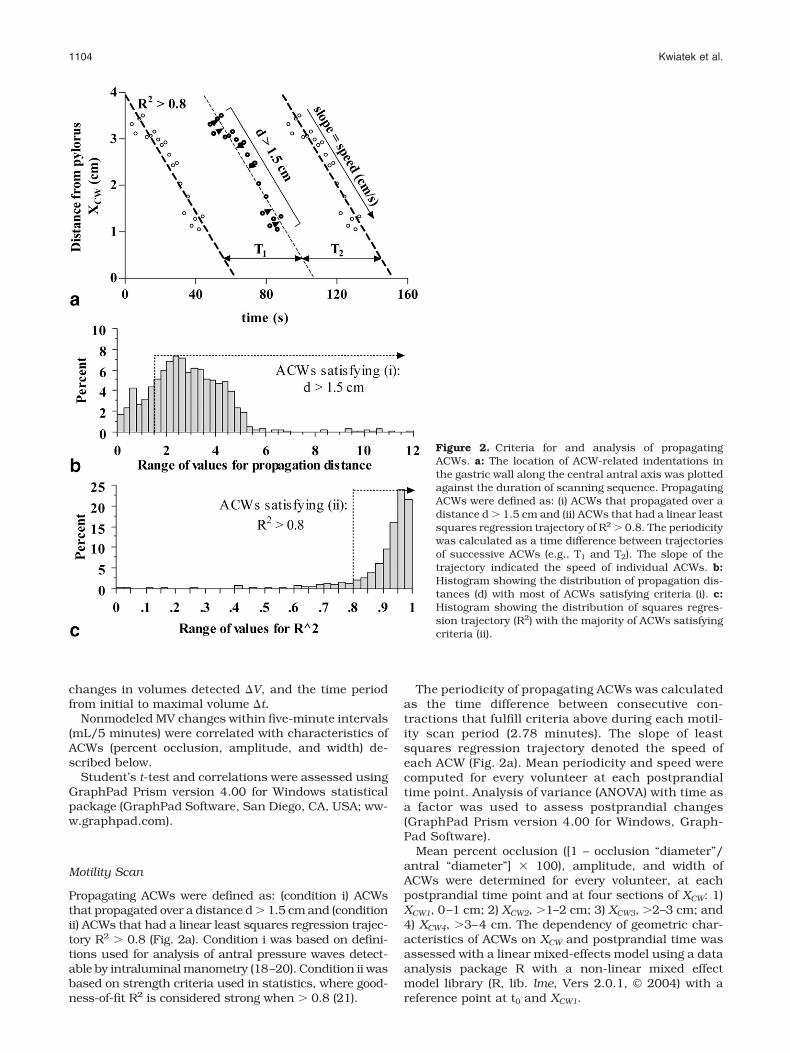
Propagating ACWs were defined as: (condition i) ACWsthat propagated over a distance d � 1.5 cm and (conditionii) ACWs that had a linear least squares regression trajec-tory R2 � 0.8 (Fig. 2a). Condition i was based on defini-tions used for analysis of antral pressure waves detect-able by intraluminal manometry (18–20). Condition ii wasbased on strength criteria used in statistics, where good-ness-of-fit R2 is considered strong when � 0.8 (21).
The periodicity of propagating ACWs was calculatedas the time difference between consecutive con-tractions that fulfill criteria above during each motil-ity scan period (2.78 minutes). The slope of leastsquares regression trajectory denoted the speed ofeach ACW (Fig. 2a). Mean periodicity and speed werecomputed for every volunteer at each postprandialtime point. Analysis of variance (ANOVA) with time asa factor was used to assess postprandial changes(GraphPad Prism version 4.00 for Windows, Graph-Pad Software).
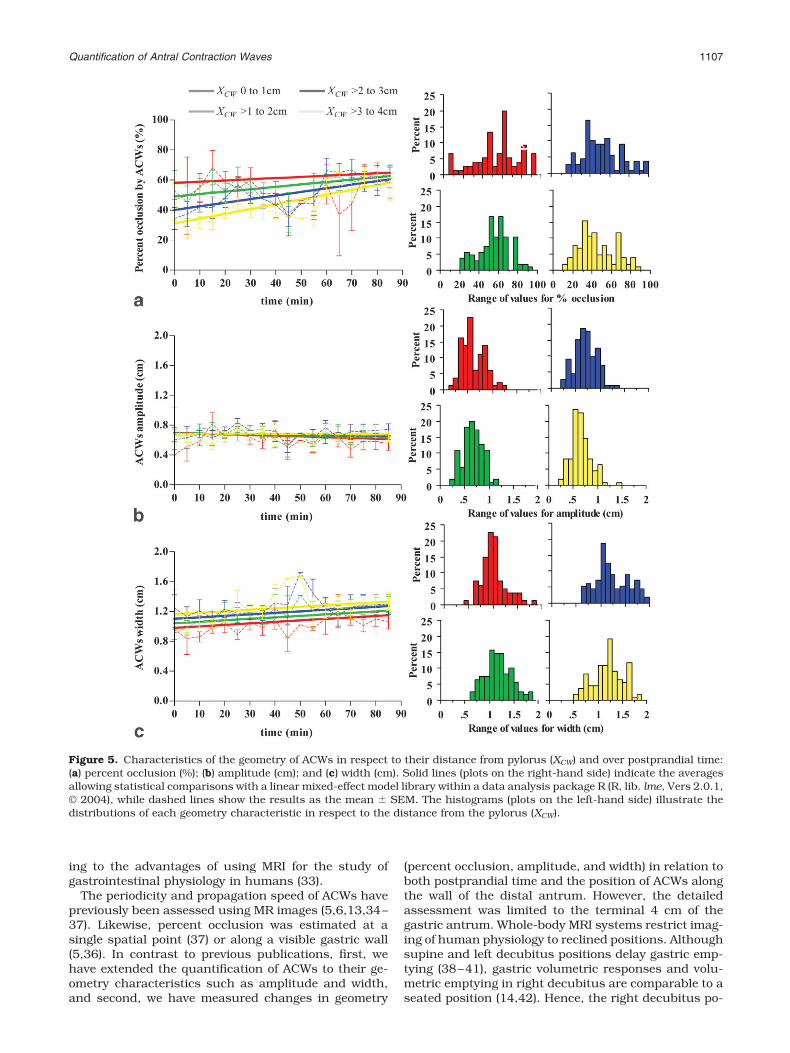
Mean percent occlusion ([1 – occlusion “diameter”/antral “diameter”] � 100), amplitude, and width ofACWs were determined for every volunteer, at eachpostprandial time point and at four sections of XCW: 1)XCW1, 0–1 cm; 2) XCW2, �1–2 cm; 3) XCW3, �2–3 cm; and4) XCW4, �3–4 cm. The dependency of geometric char-acteristics of ACWs on XCW and postprandial time wasassessed with a linear mixed-effects model using a dataanalysis package R with a non-linear mixed effectmodel library (R, lib. lme, Vers 2.0.1, © 2004) with areference point at t0 and XCW1.
Figure 2. Criteria for and analysis of propagatingACWs. a: The location of ACW-related indentations inthe gastric wall along the central antral axis was plottedagainst the duration of scanning sequence. PropagatingACWs were defined as: (i) ACWs that propagated over adistance d � 1.5 cm and (ii) ACWs that had a linear leastsquares regression trajectory of R2 � 0.8. The periodicitywas calculated as a time difference between trajectoriesof successive ACWs (e.g., T1 and T2). The slope of thetrajectory indicated the speed of individual ACWs. b:Histogram showing the distribution of propagation dis-tances (d) with most of ACWs satisfying criteria (i). c:Histogram showing the distribution of squares regres-sion trajectory (R2) with the majority of ACWs satisfyingcriteria (ii).
1104 Kwiatek et al.

RESULTS
Total Gastric Volume, Gastric Emptying, andRates of Gastric Emptying
Modeled postprandial TGV and MV are shown in Fig. 3with key parameters detailed in Table 1. Ingestion of thetest meal resulted in greater initial postprandial TGV thanMV (�V: Vpreingestion3 V0 and V0). The dynamics of subse-quent increase to maximal volume were comparable (�V:V03 Vmax and �), but the time required for TGV to reachmaximal volume (�t: V0 3 Vmax) was significantly longerthan for the meal. Greater V0 and delayed rise to Vmax
translated into longer t50 and tempt for TGV than for MV.The mean emptying rate was 24 � 3 mL/5 minutes (ap-proximate equivalent of 2 kcal/minute).
Propagation Characteristics of Distal ACWs
Of 900 ACWs detected over a total of 349 minutes,82% propagated over d � 1.5 cm (Fig. 2b), 88% had alinear least squares regression trajectory of R2 � 0.8
(Fig. 2c), and 77% satisfied both criteria for propagatingACWs.
There was a decrease in the periodicity of consecu-tive propagating ACWs from 40 � 2 seconds at t0, to23 � 2 seconds at t35 (P � 0.0004; Fig. 4a; top),reflected by the histogram of periodicities beingskewed to the right (Fig. 4a; bottom). This change wasnot complemented by a change in propagation speedof ACWs (P � 0.33; Fig. 4b; top), despite the broadrange of speeds recorded during the analysis (Fig. 4bbottom). The overall mean speed was 0.27 � 0.01cm/second. On average, ACWs terminated 1.17 �0.02 cm before reaching the pylorus; 43% and 50% ofanalyzed ACWs stopped at XCW1 and XCW2, respec-tively.
Geometry of Distal ACWs
ACWs were largely nonlumen occlusive (Fig. 5a;right). The modeled percent of occlusion was greatestcloser to the pylorus (XCW1); at proximal XCW, percent-age of occlusion increased during emptying, resultingin the greatest divergence of modeled results at t0,
from 58.1 � 5.9% at XCW1 by 8.4 � 1.5%/cm (Fig. 5a;left). Statistically, the percent of occlusion dependedon both the distance from the pylorus (XCW) and thepostprandial time (P � 0.04), but the distance fromthe pylorus (XCW) was the main modulating factor (P �0.001).
The amplitude of ACW indentations was 0.70 �0.08 cm, at the reference point of t0 and XCW1 (Fig. 5b;left) with constant range of values across distancesfrom pylorus (Fig. 5b; right). The amplitude did notalter over XCW and the entire postprandial time (P �0.65).
The width of ACWs was greater that their amplitude(P � 0.0001; 0.97 � 0.06 cm at t0 and XCW1). The widthof ACWs decreased on approach to the pylorus (P �0.003) by approximately 6 � 2%/cm (Fig. 5c; left) witha broadening spread of values at XCW3 and XCW4 (Fig. 5c;right), but not over postprandial time.
Figure 3. Average total gastric (TGV) and meal volumecurves (MV) of nine subjects following ingestion of anutrient liquid (10% glucose, 500 mL, 200 kcal) in theright decubitus position. Average stomach and meal vol-umes were computed from the averaged coefficients,estimated in the overall fit to the linear exponentialmodel (LinExp). Nonmodeled TGV and MV (both) areshown as mean � SEM.
Table 1Parameters of Volumetric Responses of the Stomach (TGV) andVolumetric Gastric Emptying (MV) Following Ingestion of 500 mLof 10% Glucose (200 kcal)
Total gastricvolume(TGV)
Mealvolume(MV)
P value
�V: Vpre-ingestion3V0 738 � 38 500 � 13 0.0009*V0 (mL) 890 � 45 528 � 13 0.0002*Vmax (mL) 941 � 46 564 � 21 0.0001*� 1.4 � 0.1 1.4 � 0.1 0.67�V: V03Vmax (mL) 51 � 21 36 � 15 0.25�t: V03Vmax (minutes) 14 � 4 8 � 3 0.02*t50 (minutes) 119 � 12 71 � 6 0.0005*tempt (minute–1) 60 � 6 35 � 3 0.0006*
*P � 0.05 TGV vs. MV was statistically significant.Vpreingestion � volume prior in drinking the test meal, V0 � volumeimmediately after completed ingestion, Vmax � maximal volumereached subsequently to V0, � � initial rate of volume increase, t50 �half-emptying time, tempt � emptying time constant, MV � mealvolume, TGV � total gastric volume.
Quantification of Antral Contraction Waves 1105

Correlation Between Distal ACWs and Rates ofGastric Emptying
Although the association between the rate of emptying(mL/5 minutes) and percent occlusion was significant(P � 0.02), its magnitude was negligible (R2 � 0.04). Themagnitude of association between the rate of emptyingand amplitude or width of ACWs was also minor (R2 �0.001 or R2 � 0.001, respectively), but in contrast topercent occlusion, it was insignificant (P � 0.83 or P �0.65, respectively).
DISCUSSION
In this study, we utilized the current advances in MRimaging and analysis technology for comprehensive as-sessment of postprandial gastric motor function over aprolonged period. Fast acquisition of images with highspatiotemporal resolution allowed virtually simulta-neous assessment of postprandial gastric volume re-sponses and distal ACWs. For the first time, using pur-pose-written software, characteristics such as thepropagation and geometry of ACWs were quantified indetail. Following ingestion of a liquid meal (10% glu-cose), the periodicity of ACWs was initially high, subse-quently reaching a constant periodicity approximatingpacesetter frequency ( 20 seconds � 3 ACWs/minute)without significant alteration in the propagation speed.ACWs were largely nonlumen occlusive (percent occlu-sion � 70%). The increasing occlusion of ACWs on ap-proach to the pylorus and over postprandial time maybe attributed to narrowing of the antrum closer to thepylorus, rather than amplification of their amplitude.None of the characteristics of ACWs correlated with therate of gastric emptying, while the gastric volume re-sponses and patterns of emptying paralleled eachother, indicating that ACWs are not essential for liquidemptying.
The “gold standards” for assessing motility of thestomach are gastric barostat and intraluminal manom-etry. These techniques are limited to either the proximal(barostat measures of compliance and tonicity) or distalstomach (manometry measures of antral contractility)and are incapable of simultaneous estimation of gastricemptying. Barostat is invasive, uncomfortable, and dif-ficult to use in the presence of a meal, hence, it not onlyaffects normal mechanosensory physiology (22,23), butrepeated measurements are poorly tolerated. Manome-try is also invasive and has reduced sensitivity for de-tection of nonlumen occlusive contractions in the gas-tric antrum (3,5,6,24). Imaging methods provide anoninvasive alternative. Scintigraphy estimates pat-terns of gastric emptying and antral motility (24); singlephoton emission computed tomography (SPECT) hasbeen validated against the barostat for measuring vol-ume responses of the stomach wall (25–27); the rate ofemptying can be estimated based on gastric volume orantral cross-section measurement done by ultrasound(US) (28–30) which is also used to evaluate antral mo-tility (9,11,31,32). MRI has the advantage of a largeFOV, allowing instantaneous and concurrent assess-ment of gastric volume responses and emptying, as wellas related antral motility with good spatial resolution.Similarly to US, which has comparable image quality,MRI is still limited to a two-dimensional acquisitionapproach to preserve the required temporal resolutionof approximately one second per measurement. How-ever, with the advent of multiple coil arrays and theongoing optimization of parallel imaging techniques,faster image acquisition and larger volume coveragewithout significant loss in image quality will soon befeasible on most MRI systems. Moreover, the recentlyintroduced k-t BLAST or k-t SENSE dynamic acquisi-tion schemes promise the possibility of three-dimen-sional dynamic imaging of the abdominal region, add-
Figure 4. Propagation characteristics of ACWs are shown asmean � SEM. a: The periodicity of ACWs was prolonged im-mediately after ingestion before being establishing at one every 20 seconds (top panel). A histogram of distribution (bottompanel) shows most ACWs occurred with a periodicity of a gas-tric pacesetter (one every 20 seconds � 3 ACWs perminute). b: Once present, on average, ACWs always moved ata constant speed over the 4 cm proximal to the pylorus (toppanel). However, the distribution of speeds was varied (bottompanel).
1106 Kwiatek et al.
ing to the advantages of using MRI for the study ofgastrointestinal physiology in humans (33).
The periodicity and propagation speed of ACWs havepreviously been assessed using MR images (5,6,13,34–37). Likewise, percent occlusion was estimated at asingle spatial point (37) or along a visible gastric wall(5,36). In contrast to previous publications, first, wehave extended the quantification of ACWs to their ge-ometry characteristics such as amplitude and width,and second, we have measured changes in geometry
(percent occlusion, amplitude, and width) in relation toboth postprandial time and the position of ACWs alongthe wall of the distal antrum. However, the detailedassessment was limited to the terminal 4 cm of thegastric antrum. Whole-body MRI systems restrict imag-ing of human physiology to reclined positions. Althoughsupine and left decubitus positions delay gastric emp-tying (38–41), gastric volumetric responses and volu-metric emptying in right decubitus are comparable to aseated position (14,42). Hence, the right decubitus po-
Figure 5. Characteristics of the geometry of ACWs in respect to their distance from pylorus (XCW) and over postprandial time:(a) percent occlusion (%); (b) amplitude (cm); and (c) width (cm). Solid lines (plots on the right-hand side) indicate the averagesallowing statistical comparisons with a linear mixed-effect model library within a data analysis package R (R, lib. lme, Vers 2.0.1,© 2004), while dashed lines show the results as the mean � SEM. The histograms (plots on the left-hand side) illustrate thedistributions of each geometry characteristic in respect to the distance from the pylorus (XCW).
Quantification of Antral Contraction Waves 1107

sition, as used here, is to a large extent representative ofthe typical postprandial habitus. The tradeoff is a pro-nounced curvature between the proximal and distalstomach compared to the seated position, which fur-ther hinders capturing a cross-section including thefundus, incisura, and pyloric sphincter for completequantification of motility. We have optimized image ac-quisition to visualize the pylorus, as the least mobilegastrointestinal structure (43). Hence, we could localizedistal ACWs during propagation and their point of ter-mination with reference to the pylorus, but were con-sequently unable to see their origin.
Previous combined findings of semi- and quantitativeanalysis of MRI and scintigraphy after intraduodenalnutrient infusion (2.1 kcal/minute) and ingestion ofliquid or even solids were that ACWs occurred at meanperiodicity and speed approximating 20 seconds and0.3 cm/second, respectively, with occlusion magnituderemaining below 70%, which was inversely related tothe distance of an ACW from the pylorus and antralfilling (5,6,14,24,36,37). However, none of the studiespresented all the above features at once and in detail,including dynamics over extended postprandial time.With our current methodology, we were able to addressthese issues, broaden the scope of analyzable charac-teristics of distal ACWs, and relate them to gastric emp-tying.
The initial decrease in periodicity of ACWs suggests aregulation phase in the emptying process and has alsobeen observed in other MRI studies using liquids andsemisolid meals (13,37,44). This finding coincides withthe increase in meal and stomach volume. The relation-ship between these two phenomena and the effect ofdifferent initial emptying patterns or gastric secretionwere not examined and remain speculative. Furtherspecifically designed studies are needed to examine thisinterrelation. However, the majority of the postprandialtime, the propagation periodicity and speed of ACWsremained constant, while the geometric characteristicswere unrelated to the volume of the 10% glucose liquidemptying during five-minute intervals. This contrastswith the initial conclusions of animal studies, in whichan electromagnetic flowmeter was used to measure vol-umes of gastric outflow. After intragastric infusion ofsaline, events of outflow usually coincided with antralcontractions (1,8,45). This has often been taken as anassociation between phasic motility of the distal stom-ach and gastric emptying, as well as an explanation ofthe pulsatile nature of gastric outflow. However, outflowand antral contractions were not necessarily initiatedtogether (8,46), although antral contractions aug-mented the volume of each saline pulse (8,45–47). Inhumans, most US studies consistently provide resultsindicative of varied association between antral contrac-tions and transpyloric flow. Gastric outflow occurs bothprior to or after occlusive antral contractions, as well asduring their absence or lack of termination at the pylo-rus, with episodes of reflux from the duodenum appear-ing during times of antral activity (31,32,48–50). Infact, the fluctuations across the pylorus, of gastric out-flow and reflux, are greater than the frequency of antralcontractions (11). Hence, our findings from statisticalanalysis of MRI data support the above indications that
distal ACWs are not central to the emptying of liquids,although they may still play a role in a complex inter-action between gastric and duodenal motility to effectemptying—a conclusion also reached with statisticalanalysis of high-resolution manometry data of theantropyloric region (6). Moreover, our volumetric datashowed parallels in the dynamics of TGV and MV, indi-cating involvement of other motility mechanisms (i.e.,tonic motility and/or pyloric resistance). Concurrentintraluminal and pyloric pressure readings in furtherstudies may assist in differentiating whether the emp-tying process is controlled by tonic pressurization (i.e.,stomach drives emptying) or by pyloric modulation (i.e.,stomach follows meal).
In conclusion, distal antral contraction waves are notimperative for gastric emptying of liquids. The maincontrol is provided by gastric pressurization and/orpyloric resistance. For 10% glucose, distal ACWs areexclusively nonoccluding with initially long periodicity,but have constant speed and amplitude along with de-creasing width when propagating to the pylorus. Theconstant amplitude indicates that observed changes inpercent occlusion are affected by morphology of antraldiameter. Improvements in MRI allow detailed quanti-tative computer analysis of propagation and geometrycharacteristics of ACWs with relation to volumetric gas-tric responses and emptying in healthy patients. Thestudy established a reference for future studies analyz-ing altered gastric motility under pharmacological mod-ulation, with either prokinetic medications or in rela-tion to formulations affecting gastric relaxation, or inpatients with disturbed gastric motility, such as sub-groups of patients with functional dyspepsia or gastro-paresis. Further studies establishing the proposedtechnology and additional automation of image analy-sis will be necessary to establish the method in thediagnostic setting.
ACKNOWLEDGMENTS
We thank Mrs. Bernadette Stutz, Dr. Heiko Fruehauf,Dr. Oliver Goetze, and Mr. Reto Treier for their clinicaland technical assistance.
REFERENCES1. Paterson C, Anvari M, Tougas G, Huizinga J. Determinants of oc-
currence and volume of transpyloric flow during gastric emptying ofliquids in dogs: importance of vagal input. Dig Dis Sci 2000;45:1509–1516.
2. Pal A, Indireshkumar K, Schwizer W, Abrahamsson B, Fried M,Brasseur JG. Gastric flow and mixing studied using computer sim-ulation. Proc R Soc Lond B Biol Sci 2004;271:2587–2594.
3. Hausken T, Mundt M, Samsom M. Low antroduodenal pressuregradients are responsible for gastric emptying of a low-caloric liquidmeal in humans. Neurogastroenterol Motil 2002;14:97–105.
4. Camilleri M, Malagelada JR, Brown ML, Becker G, Zinsmeister AR.Relation between antral motility and gastric emptying of solids andliquids in humans. Am J Physiol 1985;249(Pt 1):G580–G585.
5. Faas H, Hebbard GS, Feinle C, et al. Pressure-geometry relation-ship in the antroduodenal region in humans. Am J Physiol 2001;281:G1214–G1220.
6. Indireshkumar K, Brasseur JG, Faas H, et al. Relative contribu-tions of “pressure pump” and “peristaltic pump” to gastric empty-ing. Am J Physiol 2000;278:G604–G616.
7. Miller J, Kauffman G, Elashoff J, Ohashi H, Carter D, Meyer JH.Search for resistances controlling canine gastric emptying of liquidmeals. Am J Physiol 1981;241:G403–G415.
1108 Kwiatek et al.
8. Malbert C, Mathis C. Antropyloric modulation of transpyloric flowof liquids in pigs. Gastroenterol 1994;107:37–46.
9. Hausken T, Gilja O, Odegaard S, Berstad A. Flow across the humanpylorus soon after ingestion of food, studied with duplex sonogra-phy. Effect of glyceryl trinitrate. Scan J Gastroenterol 1998;33:484–490.
10. Malbert C, Ruckebusch Y. Gastroduodenal motor activity associ-ated with gastric emptying rate in sheep. J Physiol (Lond) 1988;401:227–239.
11. King P, Adam R, Pryde A, McDicken W, Heading R. Relationships ofhuman antroduodenal motility and transpyloric fluid movement:non-invasive observations with real-time ultrasound. Gut 1984;25:1384–1391.
12. Talley NJ. Diabetic gastropathy and prokinetics. Am J Gastroen-terol 2003;98:264–271.
13. Ajaj W, Lauenstein T, Papanikolaou N, et al. Real-time high-reso-lution MRI for the assessment of gastric motility: pre- and postp-harmacological stimuli. J Magn Reson Imaging 2004;19:453–458.
14. Treier R, Steingoetter A, Weishaupt D, et al. Gastric motor functionand emptying in the right decubitus and seated body position asassessed by magnetic resonance imaging. J Magn Reson Imaging2006;23:331–338.
15. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE:sensitivity encoding for fast MRI. Magn Reson Med 1999;42:952–962.
16. Goetze O, Menne D, Kwiatek M, et al. Modeling of gastric volumedata to assess gastric accommodation and emptying following in-gestion of liquid meals. Neurogastroenterol Motil 2005;17(Suppl2):29.
17. Elashoff J, Reedy T, Meyer J. Analysis of gastric emptying data.Gastroenterol 1982;83:1306–1312.
18. Rayner CK, Su YC, Doran SM, Jones KL, Malbert CH, Horowitz M.The stimulation of antral motility by erythromycin is attenuated byhyperglycemia. Am J Gastroenterol 2000;95:2233–2241.
19. Sun WM, Smout A, Malbert C, et al. Relationship between surfaceelectrogastrography and antropyloric pressures. Am J Physiol1995;268(Pt 1):G424–G430.
20. Verghagen MA, Samsom M, Smout JP. Effects of intraduodenalglucose infusion on gastric myoelectrical activity and antropylo-roduodenal motility. Am J Physiol 1998;274(Pt 1):G1038–G1044.
21. Hopkins WG. A new view of statistics. Internet Society for SportScience; http://www.sportsci.org/resource/stats; 2000.
22. Mundt MW, Hausken T, Samsom M. Effect of intragastric barostatbag on proximal and distal gastric accommodation in response toliquid meal. Am J Physiol 2002;283:G681–G686.
23. Ropert A, des Varannes SB, Bizais Y, Roze C, Galmiche JP. Simul-taneous assessment of liquid emptying and proximal gastric tonein humans. Gastroenterol 1993;105:667–674.
24. Jones K, Edelbroek M, Horowitz M, et al. Evaluation of antralmotility in humans using manometry and scintigraphy. Gut 1995;37:643–648.
25. Kim DY, Myung SJ, Camilleri M. Novel testing of human gastric motorand sensory functions: rationale, methods, and potential applicationsin clinical practice. Am J Gastroenterol 2000;95:3365–3373.
26. Kuiken SD, Samsom M, Camilleri M, et al. Development of a test tomeasure gastric accommodation in humans. Am J Physiol 1999;277(Pt 1):G1217–G1221.
27. Bouras EP, Delgado-Aros S, Camilleri M, et al. SPECT imaging ofthe stomach: comparison with barostat, and effects of sex, age,body mass index, and fundoplication. Single photon emission com-puted tomography. Gut 2002;51:781–786.
28. Bolondi L, Bortolotti M, Santi V, Calletti T, Gaiani S, Labo G.Measurement of gastric emptying time by real-time ultrasonogra-phy. Gastroenterol 1985;89:752–759.
29. Berstad A, Hausken T, Gilja O, Hveem K, Nesje L, Odegaard S.Ultrasonography of the human stomach. Scan J GastoenterolSuppl 1996;220:75–82.
30. Gilja OH, Detmer PR, Jong JM, et al. Intragastric distribution andgastric emptying assessed by three-dimensional ultrasonography.Gastroenterol 1997;113:38–49.
31. Kwiatek MA, Hebbard GS. Patterns of transpyloric flow followingingestion of nutrient and non-nutrient liquids. Gastroenterology2000;118(Suppl):A414.
32. Pallotta N, Cicala M, Frandina C, Corazziari E. Antro-pyloric con-tractile patterns and transpyloric flow after meal ingestion in hu-mans. Am J Gastroenterol 1998;93:2513–2522.
33. Tsao J, Boesiger P, Pruessmann KP. k-t BLAST and k-t SENSE:dynamic MRI with high frame rate exploiting spatiotemporal cor-relations. Magn Reson Med 2003;50:1031–1042.
34. Marciani L, Gowland PA, Fillery-Travis A, et al. Assessment ofantral grinding of a model solid meal with echo-planar imaging.Am J Physiol 2001;280:G844–G849.
35. Marciani L, Young P, Wright J, et al. Antral motility measurementsby magnetic resonance imaging. Neurogastroenterol Motil 2001;13:511–518.
36. Borovicka J, Lehmann R, Kunz P, et al. Evaluation of gastric emp-tying and motility in diabetic gastroparesis with magnetic reso-nance imaging: effects of cisapride. Am J Gastroenterol 1999;94:2866–2873.
37. Schwizer W, Fraser R, Borovicka J, et al. Measurement of proximaland distal gastric motility with magnetic resonance imaging. Am JPhysiol 1996;271(Pt 1):G217–G222.
38. Anvari M, Horowitz M, Fraser R, et al. Effects of posture on gastricemptying of nonnutrient liquids and antropyloroduodenal motility.Am J Physiol 1995;268(Pt 1):G868–G871.
39. Horowitz M, Jones K, Edelbroek MAL, Smout AJPM, Read NW. Theeffect of posture on gastric emptying and intragastric distributionof oil and aqueous meal components and appetite. Gastroenterol-ogy 1993;105:382–390.
40. Moore JG, Datz FL, Christian PE, Greenberg E, Alazraki N. Effect ofbody posture on radionuclide measurements of gastric emptying.Dig Dis Sci 1988;33:1592–1595.
41. Spiegel TA, Fried H, Hubert CD, Peikin SR, Siegel JA, Zeiger LS.Effect of posture on gastric emptying and satiety ratings after anutritive liquid and solid meal. Am J Physiol 2000;279:R684–R694.
42. Omari TI, Rommel N, Staunton E, et al. Paradoxical impact of bodypositioning on gastroesophageal reflux and gastric emptying in thepremature neonate. J Pediatr 2004;145:194–200.
43. Gray H. Gray’s anatomy. New York: Churchill Livingstone; 1995. p1753–1763.
44. Kunz P, Feinle C, Schwizer W, Fried M, Boesiger P. Assessment ofgastric motor function during the emptying of solid and liquidmeals in humans by MRI. J Magn Reson Imaging 1999;9:75–80.
45. Malbert C, Ruckebusch Y. Duodenal bulb control of the flow rate ofdigesta in the fasted and fed dog. J Physiol (Lond) 1989;409:371–384.
46. Malbert C, Ruckebusch Y. Relationships between pressure andflow across the gastroduodenal junction in dogs. Am J Physiol1991;260(Pt 1):G653–G657.
47. Treacy PJ, Jamieson GG, Dent J. Pyloric motor function duringemptying of a liquid meal from the stomach in the conscious pig.J Physiol (Lond) 1990;422:523–538.
48. Hausken T, Li X, Goldman B, Leotta D, Odegaard S, Martin R.Quantification of gastric emptying and duodenogastric refluxstroke volumes using three-dimensional guided digital color Dopp-ler imaging. Eur J Ultrasound 2001;13:205–213.
49. King P, Pryde A, Heading R. Effect of alterations in test meal com-position on episodic transpyloric fluid movement in humans. DigDis Sci 1988;33:1537–1543.
50. Hausken T, Odegaard S, Matre K, Berstad A. Antroduodenal mo-tility and movements of luminal contents studied by duplex sonog-raphy. Gastroenterology 1992;102:1583–1590.
Quantification of Antral Contraction Waves 1109