proliferative response in necrotising enterocolitis is insufficient to prevent disease progression
TRANSCRIPT

ORIGINAL ARTICLE
Daniela Vieten Æ Anthony Corfield Æ Pramila Ramani
Richard Spicer
Proliferative response in necrotising enterocolitis is insufficientto prevent disease progression
Published online: 10 November 2005� Springer-Verlag 2005
Abstract Necrotising enterocolitis (NEC) is character-ised by severe mucosal loss and therefore gastrointesti-nal (GI) cell proliferation is essential for survival,epithelial repair and recovery of function. Trefoil pep-tides play a key role in epithelial restitution and repair,and we previously reported a down-regulation of thesepeptides in NEC. Oral administration of epidermalgrowth factor has a protective effect in a rat model ofcolitis. These observations raised the question of a linkbetween the pathogenesis of NEC and decreasedmucosal cell proliferation. This study investigates thepattern of mucosal cell proliferation in the GI tract offetuses, normal neonatal controls, infants with NEC andthose recovering from NEC. Parents of neonates up to44 weeks’ gestation undergoing laparotomy and bowelresection were approached for consent. Bowel samplesfrom resection specimens, and GI tract extractions fromproducts of conception at termination of pregnancy,were fixed in formalin and then embedded in paraffinblocks. Patterns of small and large bowel mucosal pro-liferation were assessed by immunohistochemical stain-ing for Ki67. Seventeen foetal and 58 postnatal bowelsamples [34 with NEC (22 acute, 12 recovery) and 24controls] were analysed. The pattern of proliferationseen in the fetus and normal neonate was identical tothat in mature bowel. In NEC severe mucosal necrosis
was observed, but in viable crypts remaining, there wascrypt hyperplasia and a relative increase in the propor-tion of cells staining positive for Ki67. In those patientsrecovering from NEC the pattern of proliferation wasreturning towards the normal range. In those patientswith post-NEC strictures the recovery of normal bowelmorphology was delayed. In NEC there is massive lossof potential proliferative tissue. The remaining viabletissue shows an increase in proliferative activity in thesmall and large bowel. Failure of rapid regeneration offunctional mucosa may therefore be related to aninability of increased proliferative activity to match thelosses from the surface; alternatively there may be rapidproduction of immature, short-lived cells. This studyshows that the proliferative response, although present,is insufficient to rapidly reverse the mucosal insultobserved in NEC.
Keywords Ki-67 Æ Necrotising enterocolitis Æ Epithelialcell proliferation
Introduction
Necrotising enterocolitis (NEC) is an overwhelminggastrointestinal (GI) emergency in premature infants.With an annual incidence of 350 cases and a mortality of23% in the UK [7] it is the commonest emergencyaffecting premature neonates and a major cause ofmorbidity and mortality in neonatal intensive care units.The aetiology of NEC is multifactorial and its patho-genesis poorly understood [5]. The main lesion of NECis coagulative or ischaemic necrosis of the ileocolicregion, but the mechanism leading to necrosis is notknown. It is characterised by severe mucosal loss andtherefore GI epithelial cell proliferation is essential toepithelial repair and recovery of function and ultimatelyto survival of the bowel and the neonate.
The inflammation seen in the intestine of the majorityof NEC patients arises due to necrosis and bacterialproliferation. Current proposals for the chain of events
D. Vieten (&) Æ R. SpicerDepartment of Paediatric Surgery, Directorate of Children’sServices, Bristol Royal Hospital for Children, Paul O’GormanBuilding, Upper Maudlin Street, BS2 8BJ Bristol, UKE-mail: [email protected].: +44-117-3428825Fax: +44-117-9283525
A. CorfieldMucin Research Group, Clinical Science at South Bristol, BristolRoyal Infirmary, University of Bristol, Level 7, MarlboroughStreet, BS2 8HW Bristol, UK
P. RamaniDepartment of Paediatric Pathology, Division of Histopathology,Bristol Royal Infirmary, Level 9, Marlborough Street, BS2 8HWBristol, UK
Pediatr Surg Int (2006) 22: 50–56DOI 10.1007/s00383-005-1588-1

leading to NEC [5] identify mild postnatal infection orperinatal hypoxia resulting in low level mucosal damage.Formula feeding and bacterial proliferation allows theattachment of bacteria to the damaged and immaturemucosal barrier mucus and glycocalyx. This triggersrelease of tumour necrosis factor alpha (TNF-a) andplatelet activating factor (PAF) and leads to increasedepithelial permeability enabling the invasion and trans-location of bacteria and bacterial products from the gutlumen. The synergistic action of PAF with bacteriallipopolysaccharide and TNF-a causes a series ofinflammatory events [5]. Finally vasoconstriction occursand leads to ischaemia.
The GI tract is constantly confronted by a variety ofpotentially injurious agents, including acid, dietarycompounds, bacteria and bacterial toxins [9] Themucosal epithelium of the alimentary tract, a single layerof cells joined together by semi-permeable cell–celljunctions, forms a barrier to the broad spectrum ofnoxious substances present within the lumen. Rapidresealing of this barrier following even minor injury isessential to preservation of normal homeostasis [13].
The intestinal mucosa consists of a dynamic popu-lation of epithelial cells. Despite continued loss of ma-ture cells from villus tips in the small bowel and thelumenal surface in the colon, and their replacement fromthe crypts, the integrity of the mucosal barrier and itsfunctions are preserved. These processes require preciseregulation of proliferation and differentiation. Peptidegrowth factors play an important role in the regulationof epithelial homeostasis. Normal epithelial repair re-quires restitution and regeneration. Previous studieshave shown the ability of the GI tract to rapidly re-establish continuity of the surface epithelium afterextensive destruction such as in inflammatory boweldisease (IBD) by a process known as restitution. Thisinvolves migration of cells from the edge of the injuredarea across the basement membrane to cover the de-nuded area and re-establish surface-cell continuity. Thishappens within minutes to hours and does not dependon cellular proliferation. Brisk restitution after injurylimits fluid and electrolyte losses and prevents bacteriaand foreign antigens from the lumen reaching local andsystemic immune compartments [13].
Restitution is followed by and is a prerequisite forregeneration through cell proliferation and differentia-tion [9, 10]. Mucosal cell proliferation is essential for themaintenance of the integrity of the system and the pro-liferation rates of the GI tract are high, second only tothe haemopoietic system [15]. Cell division in the GItract is usually confined to an anatomically discretezone, the proliferative compartment at the base of thecrypts [15]. In the small intestine the normal villus:cryptratio is 3 or 4:1 and the proliferative zone (PZ) is re-stricted to the basal two-thirds of the crypt. In the colonthe crypts tend to be deeper compared to the small bo-wel and the PZ is restricted to the basal one-third to one-half of the crypt. The cell production rate in the GI tractcan be increased in response to injury by a number of
mechanisms: the cell cycle time can be reduced, thegrowth fraction can be increased by an upward exten-sion of the proliferative compartment and the crypt sizecan be increased. Increases in cell proliferation rates dueto varying combinations of the above mechanisms havebeen observed after intestinal resection [4], in coeliac [16]disease and following irradiation of the bowel [1].
Numerous agents, especially the secreted growthfactors: epidermal growth factor (EGF) and hepatocytegrowth factor (HGF) and transforming growth factor a(TGFa) may modulate the process of intestinal restitu-tion. Research in recent years indicates that trefoilproteins may play an essential role [13]. Recent researchby our group has demonstrated a down-regulation oftrefoil factor three (TFF3) expression, which may berelated to impaired mucosal regeneration [14]. There issome evidence that TFF3 acts in part through the epi-dermal growth factor receptor (EGFR). EGF is a potentgrowth factor and has been shown to have a protectiveeffect when given orally in a rat model of NEC [3].Human breast milk is the major source of EGF forneonates, which may in part explain the protective roleagainst NEC development [3]. This evidence raises thepossibility that the immature gut of premature neonatesmay lack the adequate reserve in proliferative capacityto counteract the rapid loss of epithelial cells seen inNEC.
The Ki-67 antigen is a nuclear protein, which hasbeen shown to be a reliable marker of cells within thecell cycle [11]. It is expressed by proliferating cells inall phases of the active cell cycle and is absent inresting (G0) cells. A monoclonal antibody against theKi-67 antigen (MIB-1) can be applied to paraffinembedded human tissues [8]. The growth fraction ofintestinal epithelial cells can therefore be assesed byimmunohistochemistry and the PZ can be locatedwithin the tissues.
The proliferative response of the intestinal epitheliumto NEC has not been investigated to date. It is possiblethat impaired mucosal regeneration due to inadequatereplacement of mature epithelial cells lost from thesurface contributes to the pathogenesis of NEC. The aimof this study is to investigate Ki-67 staining, to evaluatethe proliferative index (PI) and the distribution of pro-liferating cells in the GI tract of infants with NEC andnormal neonatal controls.
Materials and methods
Parents of all babies having a laparotomy in the neo-natal period (defined as up to 44 weeks gestation) andbowel resection were approached for written consent.We recruited 22 patients with NEC, 12 patients recov-ering from NEC (these patients required further lapa-rotomy for closure of stoma or resection of post-NECstrictures), 24 normal controls undergoing stoma for-mation or bowel resection in the neonatal period forHirschsprung’s disease, anorectal anomalies and gut
51

atresias. All bowel samples were taken from tissues re-moved for clinical purposes.
Foetal bowel samples were collected with maternalconsent from products of conception after vacuumsuction terminations of pregnancy.
Bowel specimens were fixed in formalin for 24 h andthen embedded in a paraffin block in an RNAse freemanner; 3 lm sections were cut from these blocks onto3-aminopropyltriethoxysilane (APES)-coated glassslides.
Sections of tonsil were used as positive tissue controlsand omission of primary antibody served as the negativecontrol.
Immunohistochemistry
Tissue sections were dewaxed in histoclear and rehy-drated to tap water through decreasing concentrationsof alcohols. Antigen retrieval was achieved by pressure-cooking tissue sections immersed in 10 mM citratebuffer at pH6.0 at 125�C for 4 min (Biocare MedicalPressure Cooker). Endogenous peroxidase activity wasblocked with 0.5% hydrogen peroxide solution indistilled water.
Tissue sections were then incubated with primarymonoclonal mouse anti-human MIB-1 antibody (Dako,High Wycombe, Bucks, UK) diluted in phosphate buf-fered saline at pH 7.0 (PBS). Table 1 shows the primaryantibody characteristics, the working dilution andincubation time.
Sections were washed in PBS after incubation inprimary antibody and then incubated in BioGenex Su-per EnhancerTM post-antibody blocking reagent(Launch Diagnostics, Kent, UK) for 20 min. After fur-ther washing in PBS the sections were incubated for20 min in BioGenex Polymer Horseradish PeroxidaseComplex (Launch Diagnostics, Kent, UK) followed by aPBS wash. Slides were developed with 3,3¢-diam-inobenzidine (BioGenex DAB substrate, Launch Diag-nostics, Kent, UK) for 10 min and counterstained withMayer’s haematoxylin. Slides were then dehydratedthrough increasing concentrations of alcohol to xyleneand coverslip mounted with DPX.
Scoring of tissues for immunostaining was performedby conventional light microscopy. In foetal sections thePI (number of positive stained cells/total cells counted)was determined by counting the proportion of positivelystained cells in ten high-powered fields (objective ·40,diameter of field 400 lm).
In neonatal colonic sections the average crypt depthwas evaluated by counting the number of cells from thebase of the crypt to the surface. The PI was defined asthe proportion of Ki-67 positive cells per crypt. Tencrypts were assessed in each section. The distribution ofproliferating cells within each crypt was also noted. Inaddition in small bowel sections the villus-length:crypt-depth ratio was assessed.
Statistical analysis of results was performed by uni-variate ANOVA and the disease groups were subject topost hoc analysis by Scheffe test using SPSS for Win-dows version 12 (SPSS inc., Chicago, IL, USA).
Results
All foetal bowel samples were collected from foetuses ofless than 13 weeks gestation as routine terminations ofpregnancy are not performed after the first trimester atour institution. Seventeen foetal bowel samples wereobtained of which 15 were suitable for analysis (10+3
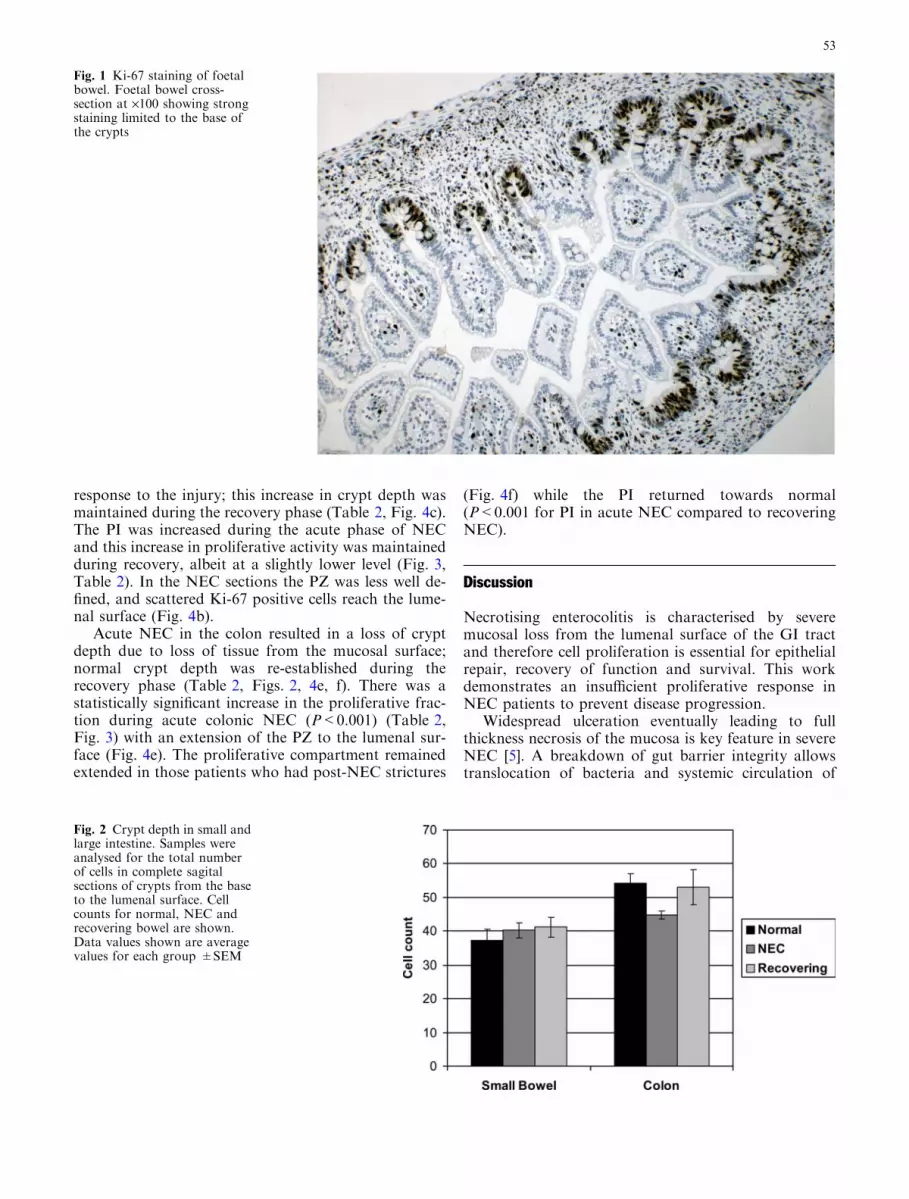
n=3, 10+4 n=2, 10+5 n=2, 11+2 n=3, 11+5 n=4,12+4 n=1). The average PI for the foetal sections was0.55. Positively stained cells were observed mainly liningthe circumference of the cross-sections of foetal (seeFig. 1) bowel in those areas corresponding to the base ofcrypts in mature bowel. The PI was similar to that seenin mature small bowel.
The neonatal samples were allocated to three groups.Group A included all patients with histologically con-firmed NEC, group B patients recovering from NEC(requiring repeat laparotomy for closure of stoma orresection of post-NEC strictures) and group C includedall normal neonatal controls (infants undergoing stomaformation or bowel resection in the neonatal period forHirschsprung’s disease, anorectal anomalies or intestinalatresias). There were 22, 12 and 24 patients in thegroups, respectively. Two patients with NEC were ex-cluded from the analysis as the sections were completelydenuded of mucosa.
The average gestational ages at birth were 28+5, 29and 36+5 in groups A, B and C, respectively, and themean age at the time of surgery was 16, 55 and 22.5 daysin the three groups. All neonatal tissue samples exam-ined were from either the ileum or the colon. For pur-poses of analysis the sections were further divided intosmall and large intestinal samples. Table 2 summarisesthe details of the patient groups and the staining results.
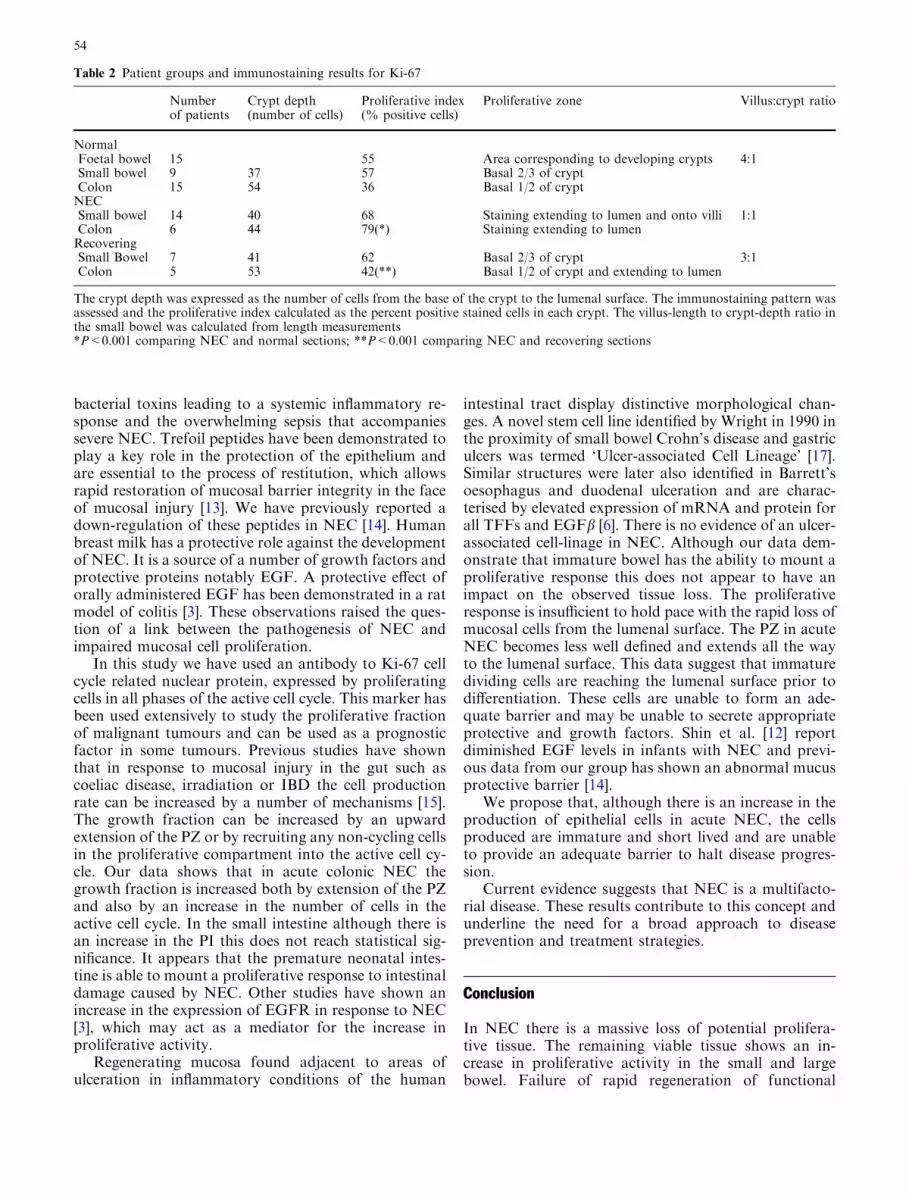
In the normal neonatal small and large intestine(Figs. 2, 3) the pattern of proliferation and the fractionof dividing cells was similar to that seen in mature bowelwhile the crypt depth in neonatal bowel was reducedcompared with adult bowel [2] Ki-67 positivity wasobserved at the base of the crypts in both small and largebowel (Fig. 4a, d).
In small bowel NEC there was loss of villus heightreducing the average villus-length to crypt-depth ratiofrom 4:1 to 1:1 (Table 2). The crypt depth was increasedin NEC, which may indicate crypt hyperplasia in
Table 1 Ki-67 antibody. Characteristics, dilution and incubationtime used for immunohistochemical methodologies in immuno-staining
Antigen Primaryantibody
Workingdilution
Incubationtime
Ki-67 MIB-1 mouse monoclonal 1:200 40 min
52
response to the injury; this increase in crypt depth wasmaintained during the recovery phase (Table 2, Fig. 4c).The PI was increased during the acute phase of NECand this increase in proliferative activity was maintainedduring recovery, albeit at a slightly lower level (Fig. 3,Table 2). In the NEC sections the PZ was less well de-fined, and scattered Ki-67 positive cells reach the lume-nal surface (Fig. 4b).
Acute NEC in the colon resulted in a loss of cryptdepth due to loss of tissue from the mucosal surface;normal crypt depth was re-established during therecovery phase (Table 2, Figs. 2, 4e, f). There was astatistically significant increase in the proliferative frac-tion during acute colonic NEC (P<0.001) (Table 2,Fig. 3) with an extension of the PZ to the lumenal sur-face (Fig. 4e). The proliferative compartment remainedextended in those patients who had post-NEC strictures
(Fig. 4f) while the PI returned towards normal(P<0.001 for PI in acute NEC compared to recoveringNEC).
Discussion
Necrotising enterocolitis is characterised by severemucosal loss from the lumenal surface of the GI tractand therefore cell proliferation is essential for epithelialrepair, recovery of function and survival. This workdemonstrates an insufficient proliferative response inNEC patients to prevent disease progression.
Widespread ulceration eventually leading to fullthickness necrosis of the mucosa is key feature in severeNEC [5]. A breakdown of gut barrier integrity allowstranslocation of bacteria and systemic circulation of
Fig. 1 Ki-67 staining of foetalbowel. Foetal bowel cross-section at ·100 showing strongstaining limited to the base ofthe crypts
Fig. 2 Crypt depth in small andlarge intestine. Samples wereanalysed for the total numberof cells in complete sagitalsections of crypts from the baseto the lumenal surface. Cellcounts for normal, NEC andrecovering bowel are shown.Data values shown are averagevalues for each group ±SEM
53
bacterial toxins leading to a systemic inflammatory re-sponse and the overwhelming sepsis that accompaniessevere NEC. Trefoil peptides have been demonstrated toplay a key role in the protection of the epithelium andare essential to the process of restitution, which allowsrapid restoration of mucosal barrier integrity in the faceof mucosal injury [13]. We have previously reported adown-regulation of these peptides in NEC [14]. Humanbreast milk has a protective role against the developmentof NEC. It is a source of a number of growth factors andprotective proteins notably EGF. A protective effect oforally administered EGF has been demonstrated in a ratmodel of colitis [3]. These observations raised the ques-tion of a link between the pathogenesis of NEC andimpaired mucosal cell proliferation.
In this study we have used an antibody to Ki-67 cellcycle related nuclear protein, expressed by proliferatingcells in all phases of the active cell cycle. This marker hasbeen used extensively to study the proliferative fractionof malignant tumours and can be used as a prognosticfactor in some tumours. Previous studies have shownthat in response to mucosal injury in the gut such ascoeliac disease, irradiation or IBD the cell productionrate can be increased by a number of mechanisms [15].The growth fraction can be increased by an upwardextension of the PZ or by recruiting any non-cycling cellsin the proliferative compartment into the active cell cy-cle. Our data shows that in acute colonic NEC thegrowth fraction is increased both by extension of the PZand also by an increase in the number of cells in theactive cell cycle. In the small intestine although there isan increase in the PI this does not reach statistical sig-nificance. It appears that the premature neonatal intes-tine is able to mount a proliferative response to intestinaldamage caused by NEC. Other studies have shown anincrease in the expression of EGFR in response to NEC[3], which may act as a mediator for the increase inproliferative activity.
Regenerating mucosa found adjacent to areas ofulceration in inflammatory conditions of the human
intestinal tract display distinctive morphological chan-ges. A novel stem cell line identified by Wright in 1990 inthe proximity of small bowel Crohn’s disease and gastriculcers was termed ‘Ulcer-associated Cell Lineage’ [17].Similar structures were later also identified in Barrett’soesophagus and duodenal ulceration and are charac-terised by elevated expression of mRNA and protein forall TFFs and EGFb [6]. There is no evidence of an ulcer-associated cell-linage in NEC. Although our data dem-onstrate that immature bowel has the ability to mount aproliferative response this does not appear to have animpact on the observed tissue loss. The proliferativeresponse is insufficient to hold pace with the rapid loss ofmucosal cells from the lumenal surface. The PZ in acuteNEC becomes less well defined and extends all the wayto the lumenal surface. This data suggest that immaturedividing cells are reaching the lumenal surface prior todifferentiation. These cells are unable to form an ade-quate barrier and may be unable to secrete appropriateprotective and growth factors. Shin et al. [12] reportdiminished EGF levels in infants with NEC and previ-ous data from our group has shown an abnormal mucusprotective barrier [14].
We propose that, although there is an increase in theproduction of epithelial cells in acute NEC, the cellsproduced are immature and short lived and are unableto provide an adequate barrier to halt disease progres-sion.
Current evidence suggests that NEC is a multifacto-rial disease. These results contribute to this concept andunderline the need for a broad approach to diseaseprevention and treatment strategies.
Conclusion
In NEC there is a massive loss of potential prolifera-tive tissue. The remaining viable tissue shows an in-crease in proliferative activity in the small and largebowel. Failure of rapid regeneration of functional
Table 2 Patient groups and immunostaining results for Ki-67
Numberof patients
Crypt depth(number of cells)
Proliferative index(% positive cells)
Proliferative zone Villus:crypt ratio
NormalFoetal bowel 15 55 Area corresponding to developing crypts 4:1Small bowel 9 37 57 Basal 2/3 of cryptColon 15 54 36 Basal 1/2 of cryptNECSmall bowel 14 40 68 Staining extending to lumen and onto villi 1:1Colon 6 44 79(*) Staining extending to lumenRecoveringSmall Bowel 7 41 62 Basal 2/3 of crypt 3:1Colon 5 53 42(**) Basal 1/2 of crypt and extending to lumen
The crypt depth was expressed as the number of cells from the base of the crypt to the lumenal surface. The immunostaining pattern wasassessed and the proliferative index calculated as the percent positive stained cells in each crypt. The villus-length to crypt-depth ratio inthe small bowel was calculated from length measurements*P<0.001 comparing NEC and normal sections; **P<0.001 comparing NEC and recovering sections
54

mucosa may therefore be related to an inability ofincreased proliferative activity to match the losses fromthe surface; alternatively there may be rapid produc-tion of immature, short-lived cells. Stimulation ofproliferative activity alone is unlikely to expedite therecovery from NEC; the replacement of cells lost fromthe surface must consist of mature cells that are ableto form and secrete a functional protective barrier.This study shows that the proliferative response, al-though present, is insufficient to rapidly reverse themucosal insult observed in NEC.
Acknowledgements We would like to thank Miss. Sharman Chaterfor assistance with the immunostaining and Dr. Amanda Williamsfor help with the statistical analysis and creation of the figures.
References
1. Cairnie AB (1967) Cell proliferation studies in the intestinalepithelium of the rat: response to continuous irradiation. Ra-diat Res 32:240–264
2. Day DW, Jass JR, Price AB, Shepherd NA, Sloan JM, TalbotIC, Warren BF, Williams GT (2003) Morson and Dawson’sgastrointestinal pathology, 4th edn. Blackwell, Oxford
Fig. 3 Proliferative index for foetal bowel and small and largeneonatal intestine. The proportion of cells staining positive for Ki-67 per crypt was measured and the proliferative index (PI)calculated (Ki-67 positive cells/total number of cells in crypt). PI
for normal, NEC and recovering groups are shown. Foetal PIscores were calculated by counting the number of positive cells per200 cells in ten high-powered fields. Data values shown are averagevalues for each group ±SEM
Fig. 4 Ki-67 staining ofneonatal small and largeintestine. Examples of stainingfor normal (a, d), NEC (b, e)and recovering (c, f) groups areshown. Immunostaining ofsmall bowel at ·100 (a–c) andcolon at ·100 (d–f) isdemonstrated. The bars infigure d indicate the total cryptdepth shown in black and theproliferative zone shown in red
55

3. Dvorak B, Halpern MD, Holebec H, Williams CS, McWilliamDL, Dominguez JA, Stepankova R, Payne CM, McCluskey RS(2002) Epidermal growth factor reduces the development ofnecrotizing enterocolitis in a neonatal rat model. Am J PhysiolGastrointest Liver Physiol 282:G156–G164
4. Hanson WR, Osborne JW, Sharp JG (1977) Compensation bythe residual intestine after intestinal resection in the rat.I. Influence of amount of tissue removed. Gastroenterology72:692–700
5. Hsueh W, Caplan MS, Qu X-W, Tan X-D, de Plaen IG,Gonzalez-Crussi F (2002) Neonatal necrotising enterocolitis:clinical considerations and pathogenic concepts. Pediatr DevPathol 6:6–23
6. Longman RJ, Thomas MG, Poulsom R (1999) Trefoil peptidesand surgical disease. Br J Surg 86:740–748
7. Lucas A (1997) BPSU British Paediatric Surveillance Unitannual report. Commun Dis Rep CDR Wkly 7:453–456
8. McCormick D, Chong H, Hobbs C, Datta C, Hall PA (1993)Detection of the Ki67 antigen in fixed and wax embeddedsections with the monoclonal antibody MIB1. Histopathology22:355–360
9. Podolsky DK (1999) Mucosal immunity and inflammation. V.Innate mechanisms of mucosal defense and repair: the bestoffense is a good defense. Am J Physiol 277:G495–G499
10. Podolsky DK (2000) Mechanisms of regulatory peptide actionin the gastrointestinal tract: trefoil peptides. J Gastroenterol35:69–74
11. Scott RJ, Hall PA, Haldane JS, van Noorden S, Price Y, LaneDP, Wright NA (1991) A comparison of immunohistochemicalmarkers of cell proliferation with experimentally determinedgrowth fraction. J Pathol 165:173–178
12. Shin CE, Falcone RAJ, Stuart L, Erwin CR, Warner BW(2000) Diminished epidermal growth factor levels in infantswith necrotizing enterocolitis. J Pediatr Surg 35:173–177
13. Taupin D, Podolsky DK (2003) Trefoil factors: initiators ofmucosal healing. Nat Rev Mol Cell Biol 4:721–734
14. Vieten D, Corfield A, Carroll D, Ramani P, Spicer (2005)Impaired mucosal regeneration in neonatal necrotisingenterocolitis. Pediatr Surg Int 21:153–160
15. Wong WM, Wright NA (1999) Cell proliferation in gastroin-testinal mucosa. J Clin Path 52:321–333
16. Wright NA, Watson AL, Morley A, Appleton D, Marks J(1973) Cell kinetics in flat (avillous) mucosa of the human smallintestine. Gut 14:701–710
17. Wright NA, Elia G, Pike C (1990) Induction of a novel epi-dermal growth factor-secreting cell lineage by mucosal ulcera-tion in gastrointestinal stem cells. Nature 343:82–85
56