pharmacokinetics, safety, and efficacy of bosentan in pediatric patients with pulmonary arterial...
TRANSCRIPT
CLINICAL TRIAL
Pharmacokinetics, safety, and efficacy ofbosentan in pediatric patients withpulmonary arterial hypertension
Background: Bosentan, a dual endothelin-receptor antagonist, is registered for the treatment of pulmonaryarterial hypertension. Little is known about the effects of bosentan in children. This study was conducted toinvestigate the pharmacokinetics, safety, and efficacy of bosentan in pediatric patients with pulmonary arterialhypertension.Methods: In this 2-center, open-label study, 19 pediatric patients with pulmonary arterial hypertension wereenrolled and stratified for body weight and epoprostenol use. Patients weighing between 10 and 20 kg,between 20 and 40 kg, or greater than 40 kg received a single dose of 31.25, 62.5, or 125 mg, respectively,on day 1, followed by 4 weeks of treatment with the initial dose. The dose was then up-titrated to the targetdose (31.25, 62.5, or 125 mg twice daily). Pharmacokinetic and hemodynamic parameters were obtained atbaseline and after 12 weeks of treatment. Six-minute walk distance and cardiopulmonary exercise testingresults were measured at baseline and at week 12 in children aged 8 years or older.Results: The variability in exposure among the 3 groups was less than 2-fold after single- and multiple-doseadministration. The exposure to bosentan decreased over time in all groups. The covariates body weight,gender, age, and the use of epoprostenol had no significant effect on the pharmacokinetics of bosentan.Bosentan produced hemodynamic improvement and was well tolerated. The mean change from baseline inmean pulmonary artery pressure was �8.0 mm Hg (95% confidence interval, �12.2 to �3.7 mm Hg), andthat in pulmonary vascular resistance index was �300 dyne · s · m2/cm5 (95% confidence interval, �576 to�24 dyne · s · m2/cm5 ).Conclusions: The pharmacokinetics of bosentan in pediatric patients with pulmonary arterial hypertensionand healthy adults are similar, and treatment with bosentan resulted in hemodynamic improvement. Theseresults suggest that the applied dosing regimens may be appropriate to treat pediatric patients. (ClinPharmacol Ther 2003;73:372-82.)
Robyn J. Barst, MD, Dunbar Ivy, MD, Jasper Dingemanse, PhD, Allison Widlitz, MS,PA, Kelly Schmitt, RN, Aimee Doran, RN, CPNP, Deborah Bingaman, RN, CPNP,Ngoc Nguyen, BS, Michael Gaitonde, MB, MRCP, and Paul L. M. van Giersbergen,PhD New York, NY, Denver, Colo, and Allschwil, Switzerland
Pulmonary arterial hypertension (PAH) is a rare anddebilitating disease associated with high morbidity and
mortality.1 The development of PAH may be primaryor related to systemic diseases such as scleroderma or
From the Division of Pediatric Cardiology, New York PresbyterianHospital, New York; University of Colorado Health SciencesCenter and Pediatric Heart Lung Center, Children’s Hospital, Den-ver; and Departments of Clinical Pharmacology and Medical Mar-keting, Actelion Pharmaceuticals Ltd, Allschwil.
Supported by Actelion Pharmaceuticals Ltd, Allschwil, Switzerland,and by grant No. MO1 RR00069, General Clinical Research Cen-ters Program, National Center for Research Resources, NationalInstitutes of Health, Bethesda, Md.
Received for publication Sept 25, 2002; accepted Jan 6, 2003.Reprint requests: Paul L. M. van Giersbergen, PhD, Actelion Phar-
maceuticals Ltd, Department of Clinical Pharmacology, Gewerbe-strasse 18, 4123, Allschwil, Switzerland.
E-mail: [email protected] © 2003 by the American Society for Clinical Pharmacol-
ogy & Therapeutics.0009-9236/2003/$30.00 � 0doi:10.1016/S0009-9236(03)00005-5
372

congenital heart defects.2-4 Despite differences in thepathogenesis of primary pulmonary hypertension andPAH related to other conditions, the pathologic char-acteristics have been found to be similar.5,6 Withouttransplantation (lung or heart-lung), prolonged PAHleads to increased pulmonary vascular resistance andprogressive right-sided heart failure and death. In gen-eral, the disease has similar characteristics in adults andchildren, but some differences exist, as recently re-viewed.7 The treatment options for PAH are limited,and despite therapy, most patients continue to havesymptoms and have a poor prognosis.8
Epoprostenol infusion has been shown to be effectivein improving the quality of life, exercise capacity, andsurvival rate in patients with severe PAH.9-11 Recently,the long-term effects of epoprostenol therapy have alsobeen investigated in pediatric patients with PAH relatedto congenital heart defects in whom conventional ther-apies failed.12 The benefit of epoprostenol treatmentwas similar to that reported for patients with primarypulmonary hypertension. However, epoprostenol treat-ment requires permanent, continuous intravenous infu-sion with a portable pump and thus is associated withpotentially life-threatening complications, as well asside effects related to epoprostenol.7
Endothelin (ET) is a promoter of cell proliferationand a potent vasoconstrictor. It is involved in endothe-lial dysfunction induced by prolonged increases in pul-monary pressure.13 Elevated levels of ET-1 have beenreported in both adults14 and pediatric patients15 andare correlated with the severity of PAH,14 suggestingthat ET receptor antagonism may be a promising ap-proach for the treatment of PAH. Bosentan is the firstorally active, nonpeptide, dual antagonist of ET recep-tors developed for PAH.16-18 It has been shown toefficaciously treat disease-related symptoms and toslow disease progression and was well tolerated in 2placebo-controlled trials in adult PAH patients.17,18 Inclinical practice, treatment with bosentan in adult pa-tients is initiated at 62.5 mg twice daily for 4 weeks,followed by up-titration to the maintenance dose of 125mg twice daily.
The pharmacokinetics of bosentan in healthy adultsubjects has been described previously19,20 and showsdose-proportionality up to oral doses of 600 mg, an oralbioavailability of 50%, a volume of distribution of 18L, a clearance of 8.2 L/h, and a half-life (t1/2) of 5.4hours. On multiple dosing, steady state is reached after3 to 5 days, and the area under the concentration-timecurve of bosentan is reduced by 40% to 50%.21-23 Thisreduction probably results from induction of metabo-lizing enzymes. Three metabolites have been identified,
as follows: the phenol metabolite (Ro 47-8634) formedvia cytochrome P450 (CYP) 3A4, the hydroxy metab-olite (Ro 48-5033) formed via CYP2C9 and CYP3A4,and the hydroxy-phenol metabolite (Ro 64-1056)formed via CYP2C9 and CYP3A4,20,21 of which onlyRo 48-5033 binds to ET receptors, albeit with a 2-foldlower affinity than bosentan (Actelion PharmaceuticalsLtd, data on file). Biliary excretion of the metabolites isthe main route of elimination.24
Thus far, no study has been performed evaluating theeffects of bosentan in children. This study was con-ducted to investigate the pharmacokinetics, efficacy,and safety of bosentan in pediatric PAH patients to givetreating physicians guidance for dose selection.Epoprostenol use was not allowed in the two phase 3trials of bosentan,17,18 but in clinical practice bothcompounds may sometimes be given concomitantly.Therefore in this study the concomitant administrationof bosentan and epoprostenol was also evaluated.
METHODSPatients. The target population for this study in-
cluded pediatric patients with PAH (World Health Or-ganization [WHO] functional class II or III), eitherprimary pulmonary hypertension or PAH related tocongenital heart defects. The study was conducted in 2centers, the University of Colorado Health SciencesCenter and Pediatric Heart Lung Center, Children’sHospital, Denver, Colo, and the Division of PediatricCardiology, New York Presbyterian Hospital, NewYork, NY, in full compliance with the principles of theDeclaration of Helsinki and its amendments. The ethicscommittees of both centers approved the study proto-col, and written informed consent and assent, if appro-priate, was obtained from a parent or legal guardianbefore any screening procedures were performed. Dur-ing the study, no concomitant medications with a pro-pensity to influence the pharmacokinetics of bosentan,such as inhibitors/inducers of CYP2C9 and CYP3A4,were allowed. Restrictions were applied regarding theintake of methylxanthine-containing beverages, as wellas the consumption of grapefruit (juice).
Study design. This was an open-label, noncon-trolled, single- and multiple-dose study conducted inpediatric PAH patients stratified by body weight andepoprostenol use. After a screening period of 3 to 21days, eligible patients were assigned to 1 of 3 dosingregimens on the basis of body weight (Table I). Theaim of these different regimens was to attain exposureto bosentan similar to that measured in adults. Patientswere hospitalized in the evening, and on the next day(day 1), they were treated with a single dose of oral
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 73, NUMBER 4 Barst et al 373

bosentan. On day 2, patients began daily treatment withthe initial dose for 4 weeks, after which the dosage wasincreased to twice the initial dose (target dose). At theweek 12 visit, patients were again hospitalized andtreated with a single bosentan dose. Hemodynamicassessments and WHO class were determined on day 1before the start of treatment and at week 12. In addition,exercise tests (6-minute walk test and cardiopulmonaryexercise testing with progressive cycle ergometry) wereperformed in patients aged 8 years or older. Safety wasevaluated by monitoring adverse events, laboratorytests, 12-lead electrocardiogram, vital signs, bodyweight, and premature discontinuations.
Blood sampling. On day 1 and during the week 12visit, blood samples (2 mL) were collected into ethyl-enediaminetetraacetic acid–containing tubes by veni-puncture or from an indwelling catheter without hepa-rin just before drug administration and at 1, 2.5, 4, 6, 9,12, 15, and 24 hours thereafter. Plasma was separatedand stored at �20°C pending analysis.
Bioanalytic methods. Plasma samples obtained wereanalyzed for bosentan and its 3 metabolites (the phenol,hydroxy, and hydroxy-phenol metabolites). A slightlymodified liquid chromatography method with tandemmass spectrometry detection was used, the details ofwhich have been described previously.25 The limit ofquantification was 1.0 ng/mL for bosentan and 2.0ng/mL for the 3 metabolites. The day-to-day coeffi-cients of variation varied between 4.1% and 8.4% forbosentan and its metabolites, and inaccuracy was lessthan 7%.
Pharmacokinetic and statistical evaluations. Thepharmacokinetic evaluation for bosentan and its metab-olites was performed by model-independent methods26
with the WinNonlin software package (version 3.3;Pharsight Corporation, Mountain View, Calif). Thepeak plasma concentration (Cmax) and time to Cmax
(tmax) were attained directly from the concentration-time data. The area under the plasma concentration–time curve during a dose interval (AUC�) and the AUCfrom time 0 to infinity [AUC(0-�)] were estimated withuse of the linear trapezoidal rule and extrapolation toinfinity when appropriate. The t1/2 was calculated asfollows: ln2/�z, in which �z is the terminal eliminationrate constant. Because of the lack of sufficient datapoints, �z for the metabolites could not be reliablyestimated. As a consequence, AUC(0-�) values are notreported for any of the metabolites. Pharmacokineticparameters were analyzed descriptively with the calcu-lation of geometric mean and 95% confidence intervalor, for tmax, median and range. Plasma concentrations infigures were expressed as arithmetic mean � SEM.
For comparison with previously obtained results inhealthy adult subjects and so that the effect of genderand epoprostenol use could be graphically explored,AUC values were corrected for either body weight ordose or both. Body weight correction was done bymultiplying individual AUC values by the correspond-ing body weight and then dividing by 70. Dose correc-tion was done by dividing individual AUC values bythe administered dose.
For exploration of the effect of different covariateson the pharmacokinetics of bosentan, several ANOVAsor analyses of covariance (ANCOVAs) were per-formed, with the dependent variable being either theln-transformed measurement or the untransformedmeasurement. Exploratory variables were as follows:dose, body weight, age, gender, and use of epoproste-nol. Depending on the type, ANOVA or ANCOVA wasperformed for Cmax and AUC of bosentan (separatelyfor the day 1 and week 12 determinations) (ie, if one ofthe variables was continuous, ANCOVA [dose, weight,age] was performed; otherwise, ANOVA [gender, useof epoprostenol] was performed). A stepwise,
Table I. Dosing regimens and mean doses per kilogram with ranges in parentheses for each body weight group
Body weightSingle dose (day 1
and at week 12 visit)Initial dose (day 2
through week 4 visit)Target dose (starting at
week 5)
�40 kgRegimen 125 mg 62.5 mg bid 125 mg bidMean and range 2.7 (2.3-3.1) mg/kg 1.4 (1.2-1.6) mg/kg bid 2.7 (2.3-3.1) mg/kg bid
�20 to 40 kgRegimen 62.5 mg 31.25 mg bid 62.5 mg bidMean and range 2.1 (1.7-2.8) mg/kg 1.0 (0.8-1.4) mg/kg bid 2.1 (1.7-2.8) mg/kg bid
10 to 20 kgRegimen 31.25 mg 31.25 mg qd 31.25 mg bidMean and range 1.9 (1.5-2.2) mg/kg 1.9 (1.5-2.2) mg/kg qd 1.9 (1.5-2.2) mg/kg bid
bid, Twice a day; qd, once a day.
CLINICAL PHARMACOLOGY & THERAPEUTICS374 Barst et al APRIL 2003
bottom-up procedure for the inclusion of exploratoryvariables was outlined before the analysis was per-formed. It consisted of first examining all variablesseparately and then taking significant variables into themodel together with the other variables.
Hemodynamic and exercise parameters were sum-marized descriptively as the change from baseline toweek 12. For exploratory purposes, P values weredetermined for the changes from baseline to week 12 byuse of the nonparametric paired signed rank test. He-modynamic parameters in the subgroups defined bywhether the patient was receiving concomitant epopro-stenol were analyzed descriptively. Changes in WHOclass were presented as numbers of patients. Safetyvariables, demographics, and baseline disease charac-teristics were analyzed descriptively.
The statistical analyses were performed with SAS,version 6.12 (SAS Institute, Cary, NC). A 2-tailed Pvalue was used, with the required level of significancebeing P � .05.
RESULTSPatient disposition. Nineteen children, aged 3 to 15
years, with primary pulmonary hypertension or PAHrelated to congenital heart disease were enrolled. Noneof the patients with congenital heart disease had theEisenmenger syndrome. At the time of enrollment, allpatients were in a clinically stable condition with nonew medications started within the previous 3 months.
In addition, no changes in medication doses were madeduring the month before enrollment (except for warfa-rin). Patients receiving epoprostenol were maintainedon stable doses for at least 3 months before enrollment.Concomitant PAH medications included epoprostenol(58%), warfarin (84%), supplemental oxygen (50%),furosemide (53%), digitalis (42%), and calcium chan-nel blockers (26%). The baseline characteristics of the19 patients enrolled in this study are shown in Table II.One patient in the group with low body weight wasprematurely discontinued from the study because of theoccurrence of adverse events and was not included inthe pharmacokinetic analyses. All other patients com-pleted the entire study in accordance with the protocoland were evaluable with regard to pharmacokinetics.
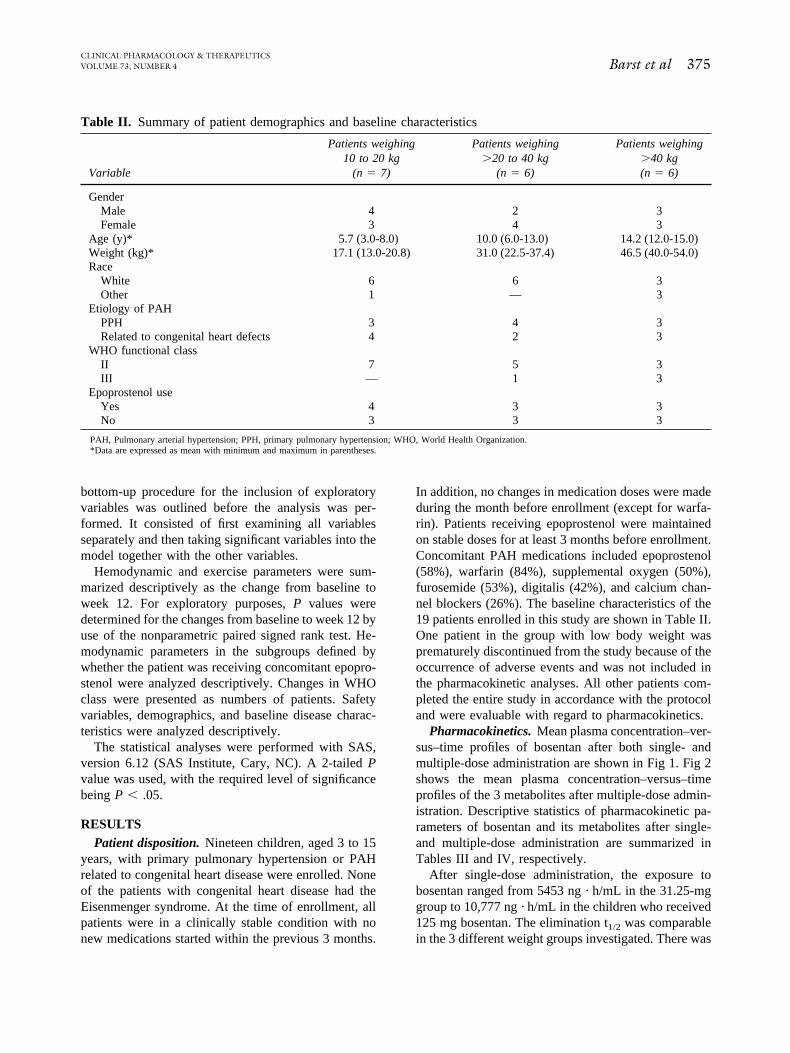
Pharmacokinetics. Mean plasma concentration–ver-sus–time profiles of bosentan after both single- andmultiple-dose administration are shown in Fig 1. Fig 2shows the mean plasma concentration–versus–timeprofiles of the 3 metabolites after multiple-dose admin-istration. Descriptive statistics of pharmacokinetic pa-rameters of bosentan and its metabolites after single-and multiple-dose administration are summarized inTables III and IV, respectively.
After single-dose administration, the exposure tobosentan ranged from 5453 ng · h/mL in the 31.25-mggroup to 10,777 ng · h/mL in the children who received125 mg bosentan. The elimination t1/2 was comparablein the 3 different weight groups investigated. There was
Table II. Summary of patient demographics and baseline characteristics
Variable
Patients weighing10 to 20 kg
(n 7)
Patients weighing�20 to 40 kg
(n 6)
Patients weighing�40 kg(n 6)
GenderMale 4 2 3Female 3 4 3
Age (y)* 5.7 (3.0-8.0) 10.0 (6.0-13.0) 14.2 (12.0-15.0)Weight (kg)* 17.1 (13.0-20.8) 31.0 (22.5-37.4) 46.5 (40.0-54.0)Race
White 6 6 3Other 1 — 3
Etiology of PAHPPH 3 4 3Related to congenital heart defects 4 2 3
WHO functional classII 7 5 3III — 1 3
Epoprostenol useYes 4 3 3No 3 3 3
PAH, Pulmonary arterial hypertension; PPH, primary pulmonary hypertension; WHO, World Health Organization.*Data are expressed as mean with minimum and maximum in parentheses.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 73, NUMBER 4 Barst et al 375
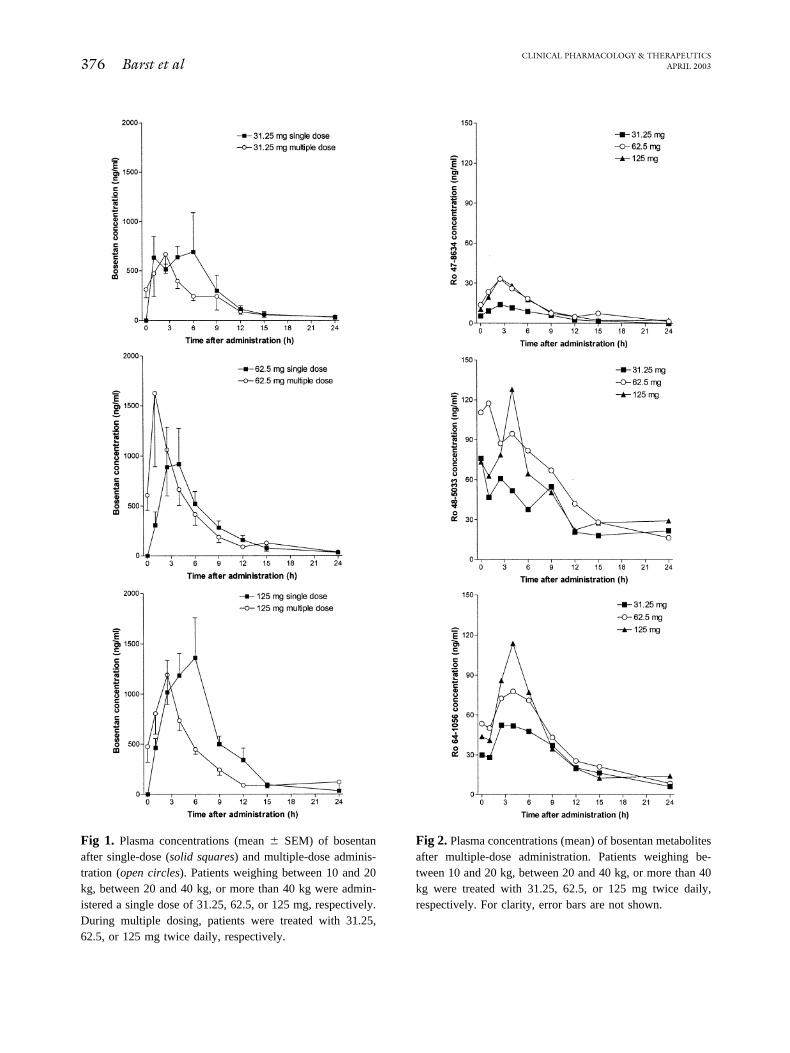
Fig 1. Plasma concentrations (mean � SEM) of bosentanafter single-dose (solid squares) and multiple-dose adminis-tration (open circles). Patients weighing between 10 and 20kg, between 20 and 40 kg, or more than 40 kg were admin-istered a single dose of 31.25, 62.5, or 125 mg, respectively.During multiple dosing, patients were treated with 31.25,62.5, or 125 mg twice daily, respectively.
Fig 2. Plasma concentrations (mean) of bosentan metabolitesafter multiple-dose administration. Patients weighing be-tween 10 and 20 kg, between 20 and 40 kg, or more than 40kg were treated with 31.25, 62.5, or 125 mg twice daily,respectively. For clarity, error bars are not shown.
CLINICAL PHARMACOLOGY & THERAPEUTICS376 Barst et al APRIL 2003
a trend for tmax to increase with dose. The exposure tothe 3 metabolites was low compared with bosentan,with Ro 48-5033 being the most prominent. Aftersingle-dose administration, the overall exposure to the3 metabolites did not exceed 19% of the exposure tobosentan (Table III).
After multiple-dose administration, the exposure tobosentan was reduced and ranged from 3496 ng · h/mLin the 31.25-mg group to 6124 ng · h/mL in the childrenwho received 125 mg bosentan. The extent of reductionwas similar in the children who received 125 mg twicea day (�43%) or 31.25 mg twice a day (�36%) and
Table III. Pharmacokinetic parameters of bosentan and its metabolites on day 1 (patients weighing between 10and 20 kg [n 6], between 20 and 40 kg [n 6], or more than 40 kg [n 6] were administered a single doseof 31.25, 62.5, or 125 mg, respectively)
Treatment AUC(0-�) (ng · h/mL) Cmax (ng/mL) tmax (h) t1/2 (h)
Bosentan31.25 mg 5,453 (56) 959 (69) 1.0 (1.0-6.0) 4.7 (40)62.5 mg 6,118 (55) 815 (108) 2.5 (1.0-4.0) 5.3 (35)125 mg 10,777 (32) 1,709 (39) 4.0 (2.5-6.0) 4.2 (44)
Ro 47-863431.25 mg 71.8 (45) 15.4 (45) 3.3 (2.5-6.0) ND62.5 mg 136 (72) 18.6 (91) 4.0 (2.5-12.0) ND125 mg 253 (52) 43.6 (48) 4.0 (2.5-6.0) ND
Ro 48-503331.25 mg 492 (80) 52.9 (73) 6.0 (4.0-12.3) ND62.5 mg 465 (86) 46.3 (110) 6.0 (4.0-15.0) ND125 mg 946 (60) 106 (89) 6.0 (4.0-6.9) ND
Ro 64-105631.25 mg 333 (35) 48.5 (34) 4.0 (2.5-6.0) ND62.5 mg 349 (105) 40.4 (116) 6.0 (4.0-12.0) ND125 mg 807 (52) 104 (58) 4.0 (4.0-6.0) ND
Data are expressed as geometric mean with percent coefficient of variation in parentheses or, for tmax, as median with range in parentheses. AUC(0-�), Area underplasma concentration–time curve from time 0 to infinity; Cmax, peak plasma concentration; tmax, time to peak plasma concentration; t1/2, half-life; ND, not determined.
Table IV. Pharmacokinetic parameters of bosentan and its metabolites at week-12 visit (patients weighingbetween 10 and 20 kg [n 6], between 20 and 40 kg [n 6], or more than 40 kg [n 6] were administeredmultiple doses of 31.25, 62.5, or 125 mg, respectively twice daily)
Treatment AUC� (ng · h/mL) Cmax (ng/mL) tmax (h) t1/2 (h)
Bosentan31.25 mg 3496 (49) 685 (77) 2.5 (0.0-9.0) 6.0 (61)62.5 mg 5428 (79) 1136 (85) 1.0 (0.0-2.5) 5.6 (25)125 mg 6124 (27) 1200 (50) 1.8 (1.0-6.0) 5.3 (38)
Ro 47-863431.25 mg 91.5 (38) 13.8 (34) 2.5 (1.0-9.0) ND62.5 mg 176 (81) 31.8 (72) 2.5 (1.0-15.0) ND125 mg 178 (64) 29.8 (71) 2.5 (2.5-4.0) ND
Ro 48-503331.25 mg 511 (41) 87.6 (46) 1.7 (0.0-9.2) ND62.5 mg 712 (115) 95.0 (103) 0.0 (0.0-3.8) ND125 mg 713 (53) 114 (86) 5.0 (0.0-9.0) ND
Ro 64-105631.25 mg 450 (37) 61.4 (43) 3.9 (0.0-9.0) ND62.5 mg 468 (141) 70.9 (111) 2.5 (0.0-6.0) ND125 mg 601 (70) 85.8 (98) 4.0 (0.0-6.0) ND
Data are expressed as geometric mean with percent coefficient of variation in parentheses or, for tmax, as median with range in parentheses. AUC�, Area under plasmaconcentration–time curve during a dose interval.
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 73, NUMBER 4 Barst et al 377
was less pronounced in the 62.5-mg twice-a-day group(�11%). In the latter group, 4 of 6 children did notshow a reduction in the exposure to bosentan. Cmax
values tended to decrease in the 31.25-mg twice-a-dayand 125-mg twice-a-day groups but increased in the62.5-mg twice-a-day group when compared withsingle-dose data. After multiple dosing, there was nolonger a trend for tmax to increase with dose. Actually,for both bosentan and its metabolites, there was atendency toward shorter tmax values after multiple dos-ing when compared with single-dose administration. Aswith single-dose administration, Ro 48-5033 was themost prominent metabolite after multiple-dose admin-istration, followed by Ro 64-1056 and Ro 47-8634. Theoverall exposure to the metabolites relative to bosentanwas slightly higher after multiple dosing (24%-30%)(Table IV).
The analysis of the effect of different covariables onthe pharmacokinetics of bosentan revealed that only
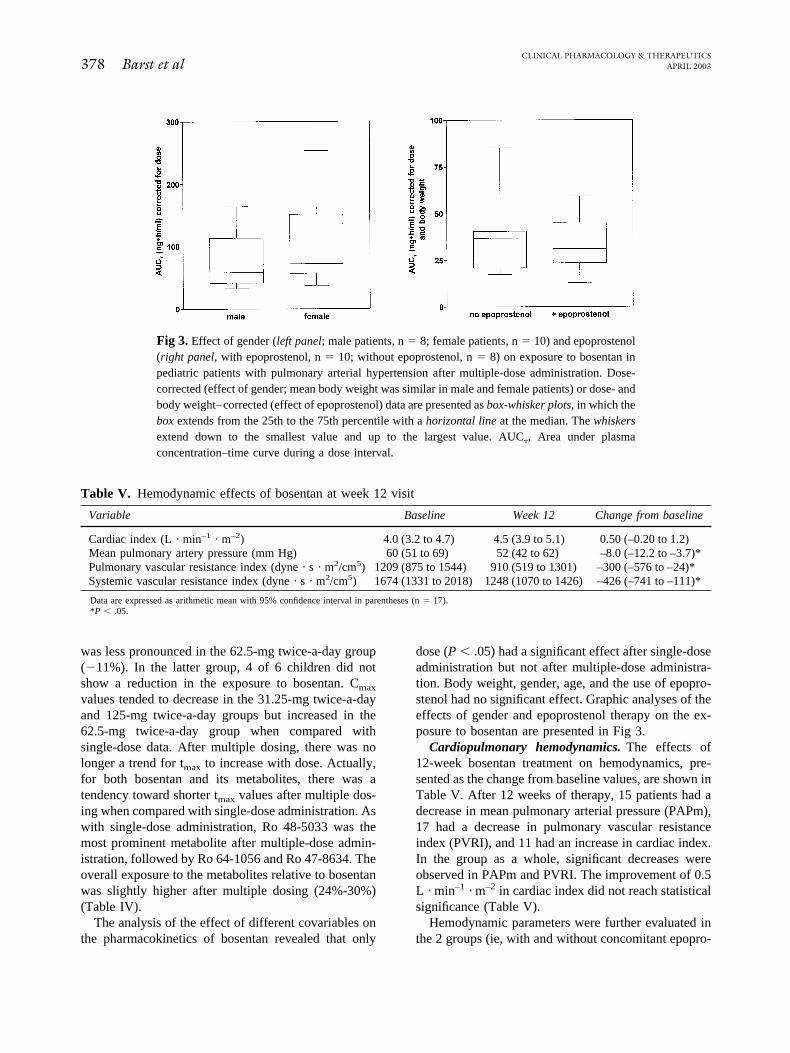
dose (P � .05) had a significant effect after single-doseadministration but not after multiple-dose administra-tion. Body weight, gender, age, and the use of epopro-stenol had no significant effect. Graphic analyses of theeffects of gender and epoprostenol therapy on the ex-posure to bosentan are presented in Fig 3.
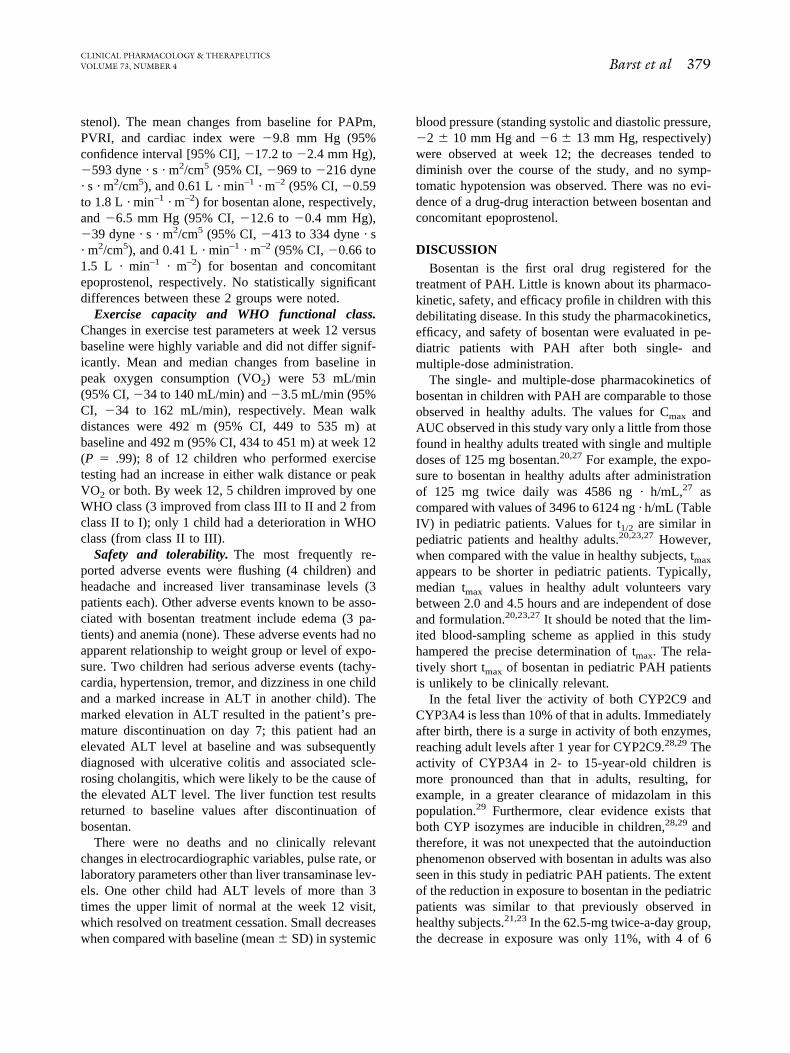
Cardiopulmonary hemodynamics. The effects of12-week bosentan treatment on hemodynamics, pre-sented as the change from baseline values, are shown inTable V. After 12 weeks of therapy, 15 patients had adecrease in mean pulmonary arterial pressure (PAPm),17 had a decrease in pulmonary vascular resistanceindex (PVRI), and 11 had an increase in cardiac index.In the group as a whole, significant decreases wereobserved in PAPm and PVRI. The improvement of 0.5L · min–1 · m–2 in cardiac index did not reach statisticalsignificance (Table V).
Hemodynamic parameters were further evaluated inthe 2 groups (ie, with and without concomitant epopro-
Fig 3. Effect of gender (left panel; male patients, n 8; female patients, n 10) and epoprostenol(right panel, with epoprostenol, n 10; without epoprostenol, n 8) on exposure to bosentan inpediatric patients with pulmonary arterial hypertension after multiple-dose administration. Dose-corrected (effect of gender; mean body weight was similar in male and female patients) or dose- andbody weight–corrected (effect of epoprostenol) data are presented as box-whisker plots, in which thebox extends from the 25th to the 75th percentile with a horizontal line at the median. The whiskersextend down to the smallest value and up to the largest value. AUC�, Area under plasmaconcentration–time curve during a dose interval.
Table V. Hemodynamic effects of bosentan at week 12 visit
Variable Baseline Week 12 Change from baseline
Cardiac index (L · min–1 · m–2) 4.0 (3.2 to 4.7) 4.5 (3.9 to 5.1) 0.50 (–0.20 to 1.2)Mean pulmonary artery pressure (mm Hg) 60 (51 to 69) 52 (42 to 62) –8.0 (–12.2 to –3.7)*Pulmonary vascular resistance index (dyne · s · m2/cm5) 1209 (875 to 1544) 910 (519 to 1301) –300 (–576 to –24)*Systemic vascular resistance index (dyne · s · m2/cm5) 1674 (1331 to 2018) 1248 (1070 to 1426) –426 (–741 to –111)*
Data are expressed as arithmetic mean with 95% confidence interval in parentheses (n 17).*P � .05.
CLINICAL PHARMACOLOGY & THERAPEUTICS378 Barst et al APRIL 2003
stenol). The mean changes from baseline for PAPm,PVRI, and cardiac index were �9.8 mm Hg (95%confidence interval [95% CI], �17.2 to �2.4 mm Hg),�593 dyne · s · m2/cm5 (95% CI, �969 to �216 dyne· s · m2/cm5), and 0.61 L · min–1 · m–2 (95% CI, �0.59to 1.8 L · min–1 · m–2) for bosentan alone, respectively,and �6.5 mm Hg (95% CI, �12.6 to �0.4 mm Hg),�39 dyne · s · m2/cm5 (95% CI, �413 to 334 dyne · s· m2/cm5), and 0.41 L · min–1 · m–2 (95% CI, �0.66 to1.5 L · min–1 · m–2) for bosentan and concomitantepoprostenol, respectively. No statistically significantdifferences between these 2 groups were noted.
Exercise capacity and WHO functional class.Changes in exercise test parameters at week 12 versusbaseline were highly variable and did not differ signif-icantly. Mean and median changes from baseline inpeak oxygen consumption (VO2) were 53 mL/min(95% CI, �34 to 140 mL/min) and �3.5 mL/min (95%CI, �34 to 162 mL/min), respectively. Mean walkdistances were 492 m (95% CI, 449 to 535 m) atbaseline and 492 m (95% CI, 434 to 451 m) at week 12(P .99); 8 of 12 children who performed exercisetesting had an increase in either walk distance or peakVO2 or both. By week 12, 5 children improved by oneWHO class (3 improved from class III to II and 2 fromclass II to I); only 1 child had a deterioration in WHOclass (from class II to III).
Safety and tolerability. The most frequently re-ported adverse events were flushing (4 children) andheadache and increased liver transaminase levels (3patients each). Other adverse events known to be asso-ciated with bosentan treatment include edema (3 pa-tients) and anemia (none). These adverse events had noapparent relationship to weight group or level of expo-sure. Two children had serious adverse events (tachy-cardia, hypertension, tremor, and dizziness in one childand a marked increase in ALT in another child). Themarked elevation in ALT resulted in the patient’s pre-mature discontinuation on day 7; this patient had anelevated ALT level at baseline and was subsequentlydiagnosed with ulcerative colitis and associated scle-rosing cholangitis, which were likely to be the cause ofthe elevated ALT level. The liver function test resultsreturned to baseline values after discontinuation ofbosentan.
There were no deaths and no clinically relevantchanges in electrocardiographic variables, pulse rate, orlaboratory parameters other than liver transaminase lev-els. One other child had ALT levels of more than 3times the upper limit of normal at the week 12 visit,which resolved on treatment cessation. Small decreaseswhen compared with baseline (mean � SD) in systemic
blood pressure (standing systolic and diastolic pressure,�2 � 10 mm Hg and �6 � 13 mm Hg, respectively)were observed at week 12; the decreases tended todiminish over the course of the study, and no symp-tomatic hypotension was observed. There was no evi-dence of a drug-drug interaction between bosentan andconcomitant epoprostenol.
DISCUSSIONBosentan is the first oral drug registered for the
treatment of PAH. Little is known about its pharmaco-kinetic, safety, and efficacy profile in children with thisdebilitating disease. In this study the pharmacokinetics,efficacy, and safety of bosentan were evaluated in pe-diatric patients with PAH after both single- andmultiple-dose administration.
The single- and multiple-dose pharmacokinetics ofbosentan in children with PAH are comparable to thoseobserved in healthy adults. The values for Cmax andAUC observed in this study vary only a little from thosefound in healthy adults treated with single and multipledoses of 125 mg bosentan.20,27 For example, the expo-sure to bosentan in healthy adults after administrationof 125 mg twice daily was 4586 ng · h/mL,27 ascompared with values of 3496 to 6124 ng · h/mL (TableIV) in pediatric patients. Values for t1/2 are similar inpediatric patients and healthy adults.20,23,27 However,when compared with the value in healthy subjects, tmax
appears to be shorter in pediatric patients. Typically,median tmax values in healthy adult volunteers varybetween 2.0 and 4.5 hours and are independent of doseand formulation.20,23,27 It should be noted that the lim-ited blood-sampling scheme as applied in this studyhampered the precise determination of tmax. The rela-tively short tmax of bosentan in pediatric PAH patientsis unlikely to be clinically relevant.
In the fetal liver the activity of both CYP2C9 andCYP3A4 is less than 10% of that in adults. Immediatelyafter birth, there is a surge in activity of both enzymes,reaching adult levels after 1 year for CYP2C9.28,29 Theactivity of CYP3A4 in 2- to 15-year-old children ismore pronounced than that in adults, resulting, forexample, in a greater clearance of midazolam in thispopulation.29 Furthermore, clear evidence exists thatboth CYP isozymes are inducible in children,28,29 andtherefore, it was not unexpected that the autoinductionphenomenon observed with bosentan in adults was alsoseen in this study in pediatric PAH patients. The extentof the reduction in exposure to bosentan in the pediatricpatients was similar to that previously observed inhealthy subjects.21,23 In the 62.5-mg twice-a-day group,the decrease in exposure was only 11%, with 4 of 6
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 73, NUMBER 4 Barst et al 379

children showing no decrease. This probably representsa chance finding, because a small reduction in exposureor no reduction has also been seen in some healthyadult subjects (Actelion Pharmaceuticals Ltd, data onfile).
PAH patients are frequently treated with digoxin,anticoagulants, calcium channel blockers, and diuretics.A number of these compounds are substrates of eitherCYP2C9 or CYP3A4 or both. In fact, drug-drug inter-action studies in healthy subjects have shown that con-comitant bosentan, when given at a dose of 500 mgtwice a day, may decrease plasma concentrations of R-and S-warfarin30 but had a negligible effect on digox-in.31 In the current study, 16 of 19 patients were takingwarfarin. Although the pharmacokinetics of warfarinwas not investigated, the fact that dose adjustments ofwarfarin were not needed is consistent with the absenceof a clinically relevant interaction, confirming previousobservations.32
About half of the patients in this study were under-going long-term continuous epoprostenol infusionwhile taking bosentan. Elimination of epoprostenol inhumans is characterized by extensive metabolism andthe formation of at least 16 metabolites, all retaining the6-keto-prostaglandin F structure. After intravenous ad-ministration of a radiolabeled dose, most of the drug-related material (82%) was found in the urine whereasbiliary excretion accounted for only 4% of the recov-ered radioactivity.33 Data from this study show thatepoprostenol had no statistically significant influenceon the pharmacokinetics of bosentan in the pediatricpopulation studied. On the basis of the markedly dif-ferent metabolism and excretion profiles of bosentanand epoprostenol, no pharmacokinetic interaction wasanticipated between these 2 drugs. However, epopro-stenol may influence the pharmacokinetics of otherdrugs by increasing gastrointestinal, liver, or kidneyblood flow. This mechanism may account for the de-crease in digoxin oral clearance observed in patientswith congestive heart failure receiving epoprostenol.34
After 12 weeks of therapy, bosentan was shown toimprove hemodynamic parameters in pediatric patientsto a similar extent as that demonstrated in adult pa-tients.17 In particular, PAPm and PVRI significantlyimproved. These results indicate that the doses ofbosentan used in this study appear to be appropriate forthe treatment of children with PAH. The limited dataavailable indicate that when bosentan was given con-comitantly to patients with or without stable epoproste-nol treatment it improved the hemodynamics in a sim-ilar fashion. These results suggest that the addition ofbosentan to epoprostenol may allow a subsequent de-
crease in epoprostenol dose, potentially decreasing theprostanoid-related side effects.
The lack of significant improvements in the exercisetest results is probably a result of the small number ofpatients evaluated, leading to high variability of thedata. Furthermore, the patients included in this studywere all in clinically stable condition (including WHOclass II children with baseline 6-minute walk distances�500 m), and the 6-minute walk test is considered amore robust tool in assessing more severely ill patients.This study was designed primarily as a pharmacoki-netic and safety-tolerability study, and efficacy evalu-ations were exploratory.
Bosentan was well tolerated in children with PAH,including those receiving concomitant epoprostenol.The safety and tolerability of bosentan were similar tothose described in previous studies with adult PAHpatients.17,18 No drug-drug interaction with epoproste-nol was observed.
Limitations of this open-label, noncontrolled studyincluded the lack of a placebo group, the small samplesize, and the heterogeneity of the patients studied. Ac-cording to the 1998 primary pulmonary hypertensionWHO classification guidelines,35 children with primarypulmonary hypertension and PAH related to congenitalheart disease are considered to have similar clinicalfeatures, as well as similar pulmonary vascularchanges. Therefore we elected to study this patientpopulation. In patients with PAH related to congenitalheart disease and who have left-to-right shunts, there isa risk of increasing the shunt (ie, increasing pulmonaryblood flow as a result of a decrease in pulmonaryvascular resistance). However, this occurrence can betreated with adjustment in diuretic therapy. This studydid not include patients with the Eisenmenger syn-drome; a separate study is necessary to evaluate theeffects of bosentan in these patients.
In conclusion, the pharmacokinetics of bosentan inpediatric PAH patients and healthy adults are similar.Furthermore, the safety and efficacy findings were sim-ilar to those observed in adult PAH patients. Theseresults may suggest that the applied dosing regimensare appropriate for treating pediatric patients with PAHwith a body weight above 10 kg.
References1. Rubin LJ. Primary pulmonary hypertension. N Engl
J Med 1997;336:111-7.2. Stupi AM, Steen VD, Owens GR, Barnes EL, Rodnan
GP, Medsger TAJ. Pulmonary hypertension in theCREST syndrome variant of systemic sclerosis. ArthritisRheum 1986;29:515-24.
CLINICAL PHARMACOLOGY & THERAPEUTICS380 Barst et al APRIL 2003
3. Bush A, Busst CM, Shinebourne EA. The use of oxygenand prostacyclin as pulmonary vasodilators in congenitalheart disease. Int J Cardiol 1985;9:267-74.
4. Ivy D. Diagnosis and treatment of severe pediatric pul-monary hypertension. Cardiol Rev 2001;9:227-37.
5. Wagenvoort CA, Wagenvoort N. Pathology of the Eisen-menger syndrome and primary pulmonary hypertension.Adv Cardiol 1974;11:123-30.
6. Ungerer RG, Tashkin DP, Furst D, Clements PJ, Gong HJr, Bein M, et al. Prevalence and clinical correlates ofpulmonary arterial hypertension in progressive systemicsclerosis. Am J Med 1983;75:65-74.
7. Haworth SG. Primary pulmonary hypertension in child-hood. Arch Dis Child 1998;79:452-5.
8. Berman Rosenzweig E, Barst RJ. Novel therapeutics forthe treatment of paediatric pulmonary arterial hyperten-sion. Expert Opin Investig Drugs 2001;10:811-23.
9. Barst RJ, Rubin LJ, McGoon MD, Caldwell EJ, LongWA, Levy PS. Survival in primary pulmonary hyperten-sion with long-term continuous intravenous prostacyclin.Ann Intern Med 1994;121:409-15.
10. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S,Badesch DB, et al. A comparison of continuous intrave-nous epoprostenol (prostacyclin) with conventional ther-apy for primary pulmonary hypertension. N Engl J Med1996;334:296-302.
11. Badesch DB, Tapson VF, McGoon MD, Brundage BH,Rubin LJ, Wigley FM, et al. Continuous intravenousepoprostenol for pulmonary hypertension due to thescleroderma spectrum of disease. A randomized, con-trolled trial. Ann Intern Med 2000;132:425-34.
12. Rosenzweig E, Kerstein D, Barst R. Long-term prosta-cyclin for pulmonary hypertension with associated con-genital heart defects. Circulation 1999;99:1858-65.
13. Luscher TF, Barton M. Endothelins and endothelin re-ceptor antagonists: therapeutic considerations for a novelclass of cardiovascular drugs. Circulation 2000;102:2434-40.
14. Galie N, Grigioni F, Bacchi-Reggiani K, Ussia GP, Par-langeli R, Catanzariti P, et al. Relation of endothelin-1 tosurvival in patients with primary pulmonary hypertension[abstract]. Eur J Clin Invest 1996;26(Suppl 1):273.
15. Allen SW, Chatfield BA, Koppenhafer SA, Schaffer MS,Wolfe RR, Abman SH. Circulating immunoreactiveendothelin-1 in children with pulmonary hypertension.Association with acute hypoxic pulmonary vasoreactiv-ity. Am Rev Respir Dis 1993;148:19-22.
16. Clozel M, Breu V, Gray GA, Kalina B, Loffler B-M,Burri K, et al. Pharmacological characterization of bosen-tan, a new potent orally active nonpeptide endothelinreceptor antagonist. J Pharmacol Exp Ther 1994;270:228-35.
17. Channick RN, Simonneau G, Sitbon O, Robbins IM,Frost A, Tapson VF, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary
hypertension: a randomised placebo-controlled study.Lancet 2001;358:1119-23.
18. Rubin LJ, Badesch DB, Barst R, Galie N, Black CM,Keogh A, et al. Bosentan therapy for pulmonary arterialhypertension. N Engl J Med 2002;346:896-903.
19. Weber C, Schmitt R, Birnboeck H, Hopfgartner G, vanMarle SP, Peeters PAM, et al. Pharmacokinetics andpharmacodynamics of the endothelin-receptor antagonistbosentan in healthy human subjects. Clin Pharmacol Ther1996;60:124-37.
20. Dingemanse J, Bodin F, Weidekamm E, Kutz K, VanGiersbergen P. Influence of food intake and formulationon the pharmacokinetics and metabolism of bosentan, adual endothelin receptor antagonist. J Clin Pharmacol2002;42:283-9.
21. Weber C, Schmitt R, Birnboeck H, Hopfgartner G, Egg-ers H, Meyer J, et al. Multiple-dose pharmacokinetics,safety, and tolerability of bosentan, an endothelin recep-tor antagonist, in healthy male volunteers. J Clin Phar-macol 1999;39:703-14.
22. Van Giersbergen PLM, Treiber A, Clozel M, Bodin F,Dingemanse J. In vivo and in vitro studies exploring thepharmacokinetic interaction between bosentan, a dualendothelin receptor antagonist, and glyburide. Clin Phar-macol Ther 2002;71:253-63.
23. Van Giersbergen PLM, Halabi A, Dingemanse J. Single-and multiple-dose pharmacokinetics of bosentan and itsinteraction with ketoconazole. Br J Clin Pharmacol 2002;53:589-95.
24. Weber C, Gasser R, Hopfgartner G. Absorption, excre-tion, and metabolism of the endothelin receptor antago-nist bosentan in healthy male subjects. Drug Metab Dis-pos 1999;27:810-5.
25. Lausecker B, Hess B, Fischer G, Mueller M, HopfgartnerG. Simultaneous determination of bosentan and its threemajor metabolites in various biological matrices and spe-cies using narrow bore liquid chromatography with ionspray tandem mass spectrometric detection. J Chro-matogr 2000;749:67-83.
26. Gibaldi M, Perrier D. Pharmacokinetics. 2nd ed. NewYork: Marcel Dekker; 1982.
27. Dingemanse J, Schaarschmidt D, van GiersbergenPLM. Investigation of the mutual pharmacokinetic in-teractions between bosentan, a dual endothelin recep-tor antagonist, and simvastatin. Clin Pharmacokinet2003;42:293-301.
28. Treluyer J-M, Gueret G, Cheron G, Sonnier M, CresteilT. Developmental expression of CYP2C and CYP2C-dependent activities in the human liver: in-vivo/in-vitrocorrelation and inducibility. Pharmacogenetics 1997;7:441-52.
29. de Wildt SN, Kearns GL, Leeder S, van den Anker JN.Cytochrome P450 3A. Ontogeny and drug disposition.Clin Pharmacokinet 1999;37:485-505.
30. Weber C, Banken L, Birnboeck H, Schulz R. Effect ofthe endothelin-receptor antagonist bosentan on the phar-
CLINICAL PHARMACOLOGY & THERAPEUTICSVOLUME 73, NUMBER 4 Barst et al 381

macokinetics and pharmacodynamics of warfarin. J ClinPharmacol 1999;39:847-54.
31. Weber C, Banken L, Birnboeck H, Nave S, Schulz R. Theeffect of bosentan on the pharmacokinetics of digoxin inhealthy male subjects. Br J Clin Pharmacol 1999;47:701-6.
32. Physicians’ desk reference 2002. Montvale (NJ): MedicalEconomics; 2002.
33. Brash AR, Jackson EK, Saggese CA, Lawson JA, OatesJA, Fitzgerald GA. Metabolic disposition of prostacyclinin humans. J Pharmacol Exp Ther 1983;226:78-87.
34. Carlton LD, Pollack GM, Brouwer KL. Physiologicpharmacokinetic modeling of gastrointestinal bloodflow as a rate-limiting step in the oral absorption ofdigoxin: implications for patients with congestiveheart failure receiving epoprostenol. J Pharm Sci 1996;85:473-7.
35. Tilton RG, Brock TA, Dixon RAF. Therapeutic potentialof endothelin receptor antagonists and nitric oxide donorsin pulmonary hypertension. Expert Opin Investig Drugs2001;10:1291-308.
CLINICAL PHARMACOLOGY & THERAPEUTICS382 Barst et al APRIL 2003