pharmacokinetics of levetiracetam in neonates with seizures
TRANSCRIPT

Pharmacokinetics of Levetiracetam in Neonates with Seizures
A thesis submitted to the
Graduate School
of the University of Cincinnati
in partial fulfillment of the
requirements for the degree of
Master of Science in Clinical and Translational Research
in the Department of Environmental Health
of the College of Medicine
by
Stephanie Merhar
BA, University of Virginia
MD, University of Pennsylvania
June 2011
Committee Chair: Paul Succop, PhD

ii
ABSTRACT
Objective:
To evaluate the pharmacokinetics and adverse events of intravenous levetiracetam in treating
newborns with seizures.
Study design:
This was a prospective, open-label observational pharmacokinetic study in neonates ≥ 32 weeks
gestational age and ≤ 30 days of age with seizures persisting despite treatment with
phenobarbital. A loading dose of intravenous levetiracetam was given as per the prescribing
physician, followed by additional doses based on clinical response. Blood samples were
prospectively collected and analyzed for levetiracetam concentrations. Vital signs were
monitored during levetiracetam treatment, and safety and efficacy data were collected.
Results:
Eighteen patients (median 39 weeks gestation and 2 postnatal days) were included. Initial
loading doses ranged from 14.3-39.9 mg/kg. Median (range) clearance, volume of distribution,
and elimination half-life were 1.2 ml/min/kg (0.5-2.9), 0.89 L/kg (0.4-1.3), and 8.9 hours (3.2-
13.3), respectively. No adverse events related to levetiracetam were observed. Nine out of 18
patients required additional loading doses of levetiracetam to control their seizures.
Conclusions:
LEV clearance was lower, volume of distribution larger, and half life longer in neonates as
compared to older children. Given the increased volume of distribution and lower clearance in
neonates, we recommend a loading dose of at least 30 mg/kg, followed by maintenance dosing
every 8-12 hours.

iii
iv
ACKNOWLEDGMENTS
I would like to thank my mentors for this project, Kurt Schibler and Sander Vinks. I would also
like to thank all those who helped with planning and implementation, Paul Succop for his role as
my advisor, and most of all of the patients and families who took part in the study.

v
TABLE OF CONTENTS
Introduction……………………………………………………………………………………………1
Methods………………………………………………………………………………………………..2
Results……………………………………………………………………………………………….....4
Discussion……………………………………………………………………………………………..6
Bibliography…………………………………………………………………………………………..15
LIST OF TABLES/FIGURES
Table 1…………………………………………………………………………………………………11
Table 2…………………………………………………………………………………………………12
Figure 1………………………………………………………………………………………………...13
Figure 2………………………………………………………………………………………………...14

1
INTRODUCTION
Neonatal seizures are a common problem, affecting two to five per thousand infants in
the first month of life (1-3). Recent animal and human studies have shown that seizures can
harm the developing brain (4-6), reinforcing the current practice of treating electrographic
seizures in newborns. Phenobarbital, introduced in 1914, is still the most common medication
used to treat neonatal seizures (7). However, in the one randomized controlled trial on its use in
neonates, phenobarbital was effective in eliminating neonatal seizures only 43% of the time (8).
In addition, phenobarbital has been shown to cause neuronal apoptosis in rat pups (9,10), and
children receiving phenobarbital for febrile seizure prophylaxis were found to have decreased
cognitive ability and school achievement compared with those receiving placebo (11-13). For
these reasons, there has been considerable interest in recent years in developing new antiepileptic
medications for use in neonates.
Levetiracetam (Keppra®), introduced in 2000, is an anticonvulsant with a novel
mechanism of action that has been studied extensively in adults and older children (14-18).
Although its precise mechanism of action has not been fully established, levetiracetam is known
to bind to synaptic vesicle protein 2A in the central nervous system and does not appear to
directly affect the traditional excitatory and inhibitory neurotransmitter systems (18,19). Studies
in adults have shown that levetiracetam has linear pharmacokinetics (18), which means that
changes in dose result in proportional changes in drug concentration and exposure as measured
by the area under the concentration-time curve (AUC). Levetiracetam is mainly excreted by the
kidneys, and elimination correlates with creatinine clearance (18). The major metabolic pathway
is enzymatic hydrolysis by a plasma esterase (18). The volume of distribution of levetiracetam is
similar to total body water, and it has no documented clinically significant drug-drug interactions
2
(18).
Pharmacokinetic, safety, and efficacy trials have been performed in children down to 1
month of age (14-16,20,21). Case series have suggested that levetiracetam may be safe and
effective in the treatment of neonatal seizures (22-24), and a recent prospective study in 38 term
and preterm infants showed no adverse effects of a slow titration of levetiracetam (25). The aim
of our study was to determine the pharmacokinetics of levetiracetam and to gather preliminary
safety and efficacy in neonates with seizures.
METHODS
This study was conducted at Cincinnati Children's Hospital Medical Center and Good
Samaritan Hospital between October 2008 and June 2010. The institutional review board at each
hospital approved the protocol and written informed consent was obtained from the legal
guardian of all subjects. An investigational new drug application (IND) was obtained from the
FDA to perform this study.
Eligible neonates were ≤ 30 days old and ≥ 32 weeks gestational age, with seizures
requiring treatment with levetiracetam. Levetiracetam is often used as a second line medication
for the treatment of neonatal seizures in our institution. All subjects received at least 20 mg/kg
of phenobarbital before receiving levetiracetam. Exclusion criteria included birth weight < 2000
g and known creatinine ≥ 2.0 mg/dl.
Levetiracetam injection (100 mg/ml, UCB Pharma) was used for the initial loading dose
in all patients. Dosing was not specified in the protocol and was determined by the clinician
prescribing the drug. Levetiracetam was infused over 15 minutes as per package insert. Blood
sampling was conducted using a D-optimal sparse sampling design with three samples collected
in each patient (26). Patients were divided into three groups to obtain informative time points
3
over the entire dosing interval. Group 1 had samples drawn at 2-15 minutes, 1-2 hours, and 12
hours post infusion; Group 2 had samples drawn at 2-15 minutes, 2-4 hours, and 18 hours post
infusion, and Group 3 had samples drawn at 5-15 minutes, 4-8 hours, and 20-24 hours post
infusion.
In order to prevent metabolism by esterases in the test tube, the plasma was separated by
centrifugation directly after collection (27) and stored at -700 C until analysis. Levetiracetam
concentrations were determined by the Bioanalytical Core Laboratory at Georgetown University
using a validated liquid chromatography-electrospray tandem mass spectrometry assay (28). The
lower limit of detection of the assay was 0.1 µg/mL for plasma. Within-run and between-run
imprecision (n=10) for LEV controls ranged from 2.3%-4.7% and 3.4%-8.9%, respectively (29).
Non-linear mixed effects modeling (NONMEM, version 7.1, ICON Dev. Soln., Ellicott
City, MD) with PDx-Pop® (version 4.10, 2007 ICON Dev. Soln., Ellicott City, MD) interfaced
with Xpose® (version 4.0, release 6, update 1) was used to perform the pharmacokinetic
analyses. Individual Bayesian pharmacokinetic parameter estimates were calculated using
MW/PHARM (Version 3.60; MediWare, Groningen, The Netherlands) (30). The parameters of
interest were clearance, elimination half life, volume of distribution, and area under the curve at
2, 4, 6, 12, and 24 hours. SAS (Version 9.2, SAS Institute Inc, Cary, NC) was used to analyze
associations between demographic and pharmacokinetic parameters.
Safety assessments included a physical examination before and 24 hours after the loading
dose of levetiracetam and monitoring of vital signs (heart rate, respiratory rate, oxygen
saturation, and blood pressure) every 15 minutes for one hour after the loading dose and hourly
for 24 hours. All infants in the study had a renal panel, glucose, and electrolytes drawn before
receiving the initial dose of levetiracetam. Further labs were drawn for clinical reasons and were
4
recorded in the research record. Adverse events were reported by bedside nurse in response to
an open question about whether any problems were seen after the loading dose. Study subjects'
charts were reviewed at hospital discharge to identify any adverse events occurring during the 24
hours after the loading dose and during the remainder of the hospital stay.
Seizure frequency before and after the loading dose of levetiracetam was monitored
clinically or documented using full channel EEG at the discretion of the clinicians caring for the
patient. Further loading doses of levetiracetam were administered for the continuation of clinical
and/or electrographic seizures as per the discretion of the clinical team. Efficacy was coded as a
dichotomous variable: whether or not the infant required further loading doses of levetiracetam
after the initial loading dose. Statistical analysis for efficacy data was performed using SAS
(Version 9.2, SAS Institute Inc, Cary, NC).
RESULTS
A total of 21 infants who received levetiracetam for clinical and/or electrographic seizure
control were screened for the study from October 2008 to May 2010, and 19 of these infants
were enrolled in the study. The 2 patients who were not enrolled received levetiracetam before
consent could be obtained from the parents. One of the 19 subjects was excluded due to a lab
error resulting in only 2 usable samples. The resulting pharmacokinetic data consisted of 54
levetiracetam concentrations from 18 subjects. One patient was enrolled in the study at day of
life 30 but did not receive levetiracetam until day of life 32. This was not discovered until all
samples had been drawn, and the decision was made to include this patient in the final analysis.
The patient characteristics are summarized in table 1.
A loading dose of IV levetiracetam was administered at the discretion of the prescribing
physician. Loading doses ranged from 14.4-39.9 mg/kg. Further loading doses were
5
administered for the continuation of clinical and/or electrographic seizures as directed by the
clinical team caring for the patient. A maintenance dosing regimen of levetiracetam was
initiated in most cases, and was given IV during the study period in 17/18 patients. The first
maintenance dose was given 8-12 hours after the loading dose(s).
Pharmacokinetic modeling:
A two compartment model with first order elimination provided the best fit to the data.
The most significant covariates determined in the univariate analysis were weight, postmenstrual
age, serum creatinine, and creatinine clearance. After multivariate analysis, only weight and
creatinine clearance remained in the final model. Some unexplained variability remained in the
model (32-43%), which may be due to the small number of subjects with only 3 levetiracetam
concentrations per subject.
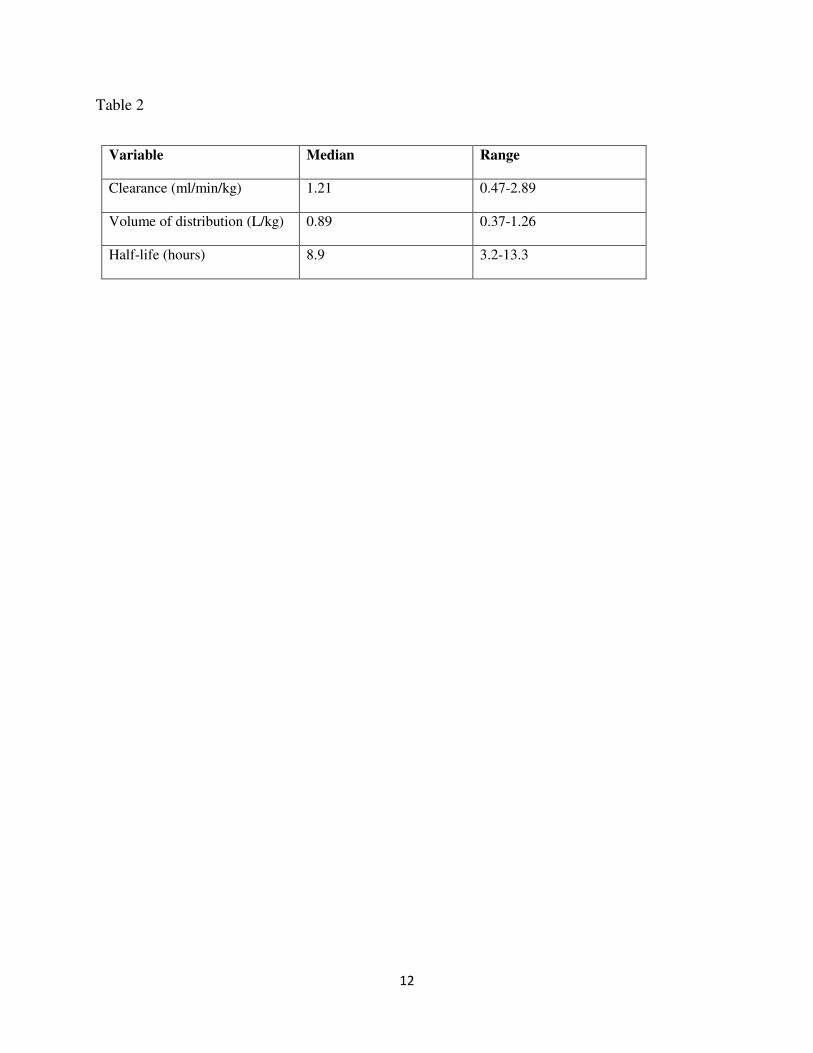
The parameter estimates from the base model were entered into MWPHARM to
determine the pharmacokinetic parameters for each individual subject, shown in table 2. The
median (range) Cmax as predicted by the model was 39.8 (14.8-91.9) mg/L. The highest
measured concentration measured in the study patients was 87.6 mg/L, 1 hour after a 30 mg/kg
dose. There was a significant linear relationship between serum creatinine and half life (Figure
1, Pearson correlation r = 0.67, p = 0.0002). Linear relationships were also found between serum
creatinine and levetiracetam clearance (r = -0.53, p = 0.02), and creatinine clearance and
levetiracetam clearance (r = 0.66, p = 0.003).
Safety and tolerability:
Levetiracetam was well tolerated in this population. No changes in vital signs or
laboratory parameters were observed. Several infants were noted to be somnolent in the 24
hours after levetiracetam administration. However, the majority of these infants were critically

6
ill and had received both phenobarbital and levetiracetam. The somnolence was recorded as
possibly related to levetiracetam administration.
One patient with overwhelming HSV infection died after withdrawal of support 24 hours
after receiving levetiracetam. One patient with severe HIE died after withdrawal of support 10
hours after receiving levetiracetam. These deaths were deemed not related to levetiracetam
administration.
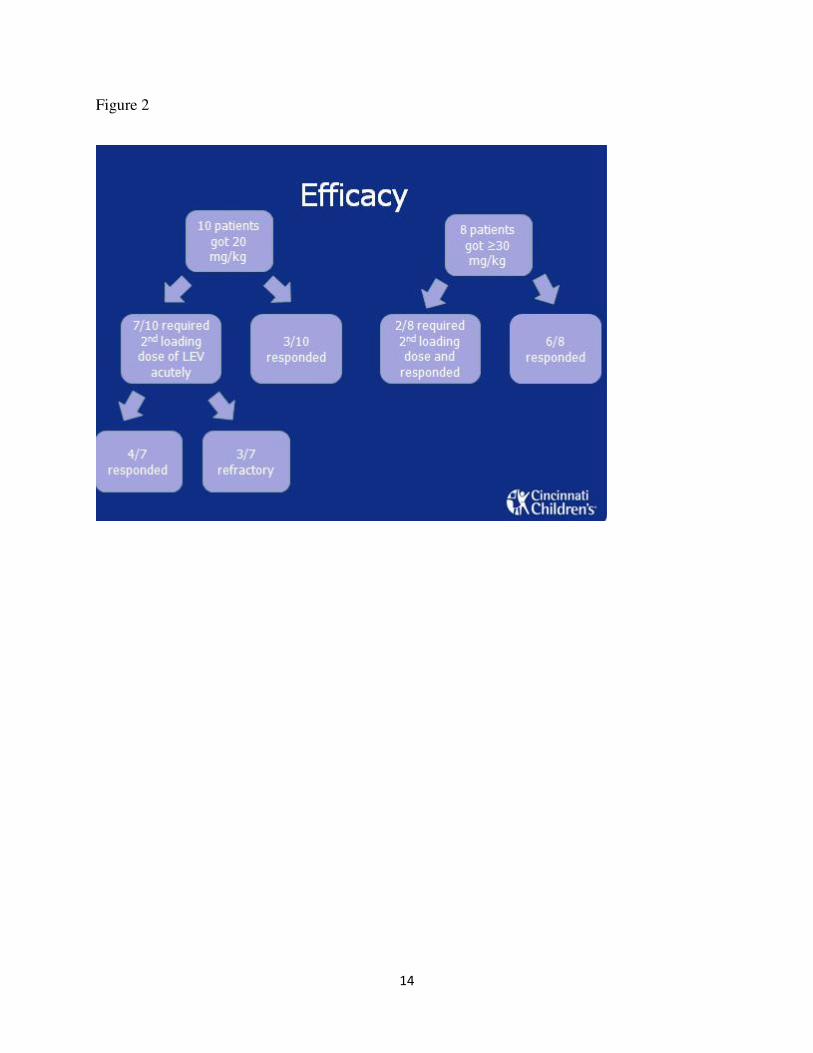
Efficacy:
This was designed as a pharmacokinetic study and was not sufficiently powered to
determine efficacy. Seizure frequency before and after the loading dose of levetiracetam was
monitored at the discretion of the clinicians caring for the patient. Nine of the 18 patients were
monitored by continuous full channel EEG during the initial loading dose of levetiracetam and
for at least 6 hours afterwards. Seven out of the 10 patients who received a 20 mg/kg loading
dose received a second loading dose of IV levetiracetam within 12 hours of the first due to
continued electrographic and/or clinical seizures. During the study period, clinical practice in
our institution changed to using a higher loading dose of levetiracetam (30 mg/kg instead of 20
mg/kg). This higher loading dose seemed to be more effective in stopping initial seizures (figure
2). A simple logistic regression model was constructed modeling the initial dose in mg/kg on
efficacy (whether the patient required a second dose of levetiracetam acutely to control
continued seizures) and the area under the ROC curve was reported. This simple model had an
area under the ROC curve of 0.77 (p = 0.10). Overall, after receiving levetiracetam, 15 out of
the 18 infants in the study (83%) did not require a third-line medication for seizure control.
DISCUSSION
7
The main objective of this study was to determine the pharmacokinetics of IV
levetiracetam in neonates with seizures. We found that levetiracetam pharmacokinetics were
different in this population than in adults and older children. The safety profile appeared to be
favorable with no serious adverse effects noted. Two deaths occurring in this critically ill study
population were deemed to be unrelated to levetiracetam treatment. We also found that
levetiracetam was effective for acute seizure control, with only 3 of the 18 infants requiring a
third line drug beyond phenobarbital and levetiracetam.
The pharmacokinetics of levetiracetam in adults and older children have been well
characterized. The half-life is 6-8 hours in adults (18) and 5-7 hours in older children (17,20).
In the only study that evaluated the pharmacokinetics of levetiracetam in neonates, the half life
was found to be 16-18 hours in newborn twins whose mother had received an oral dose of
levetiracetam 45 minutes prior to delivery (31). We found the median half-life of levetiracetam
to be 8.9 hours, which might be expected based on the lower clearance of levetiracetam in
neonates. The volume of distribution, the hypothetical volume in which an amount of drug
would need to be uniformly distributed to produce the observed blood concentration, is 0.5-0.7
L/kg in adults (32) and 0.6-0.7 L/kg in older children (17,20). The median volume of
distribution in our study was 0.89 L/kg. Because neonates have higher body water content than
adults and older children (as much as 85% total body water in preterm infants and 78% in full
term infants as compared to 60% in adults) (33) and levetiracetam distributes in parallel with
total body water, we would expect the volume of distribution to be higher in neonates than in
older children and adults.
Total body clearance of levetiracetam in adults is 0.96 ml/min/kg (18) and in children is
1.43-1.46 ml/min/kg (17,20). We found the clearance in neonates to be 1.21 ml/min/kg,

8
intermediate between adults and older children. Weight-adjusted clearance is often higher in
children than in adults, but models which allometrically scale clearance based on surface area or
the 3/4 power model often predict no difference in the size scaled clearance between these two
populations (34). Using the 3/4 power model, the standard clearance is 67.2 ml/min and the
clearance of neonates (with a mean weight of 3.3 kg, as in this study) is predicted to be 6.8
ml/min. The clearance of the neonates in this study was found to be 3 ml/min in the NONMEM
two compartment model and 4.2 ml/min in the MWPharm two compartment model, lower than
would be predicted using the 3/4 power model. Allometric scaling is able to correct for growth,
but does not correct for maturational differences in the population (34). Since clearance was
found to be lower in neonates than would be predicted using allometric scaling, we conclude that
the lower clearance of levetiracetam in this population is due to the lower GFR and possibly to
lower plasma esterase activity. In support of this conclusion, a significant linear relationship was
found between serum creatinine and levetiracetam clearance.
Based on the higher volume of distribution in neonates, the loading dose on a mg/kg basis
should be higher than in older children and adults. We found that a loading dose of 30 mg/kg
was more effective in controlling seizures than a loading dose of 20 mg/kg in our study
population. Due to the reduced clearance in neonates, the dosing interval may need to be
extended, at least until the GFR matures. Therefore, a twice daily dosing schedule may be more
appropriate than a three times daily schedule in neonates over the first several weeks of life. In
infants with reduced creatinine clearance, the dosing interval may need to be extended even
further.
Routine therapeutic drug monitoring has not been recommended for levetiracetam in the
past, as drug levels have not been found to correlate well with therapeutic efficacy (35,36). A
9
reference range of 12-46 mg/L has been proposed for adults with epilepsy (37), and most clinical
labs suggest similar reference ranges. Toxic levels have not been well established. The highest
concentration measured in our study was 87.6 mg/L and the highest Cmax predicted by the
model was 91.9 mg/L. No adverse effects were seen beyond mild somnolence even at these high
levels. Therapeutic drug monitoring may be useful in infants with impaired renal function, but
our study does not provide the data to support routine monitoring.
Infants in this study were closely monitored for 24 hours after the loading dose of
levetiracetam to assess for adverse events. Two subjects died after withdrawal of support due to
their severe underlying medical conditions during the 24 hours following levetiracetam
administration, but these deaths were not considered related to levetiracetam. Somnolence was
the only other adverse event recorded in subjects 24 hours after the dose that could possibly be
related to levetiracetam. The somnolence did not interfere with feeding or cause subjects to
require increased respiratory support. In older children, the main adverse events seen with
levetiracetam administration are somnolence, nervousness, dizziness, and irritability. In adults
and older children, small but statistically significant changes in hematologic parameters (RBC
count, mean hemoglobin, and WBC count) have been seen. These hematologic changes have not
been considered clinically significant by other investigators; therefore, we did not monitor
complete blood counts as part of the study. However, many of the infants in the study had
complete blood counts before and after receiving levetiracetam, and no changes were seen.
Although this study was not powered to determine efficacy, levetiracetam was considered
to be effective for acute seizure control in this population. In addition, as shown in figure 2, a
higher initial loading dose of 30 mg/kg appeared to be more effective than a loading dose of 20
mg/kg. When this relationship was examined with a simple logistic regression model, a trend
10
was found, but the study did not have sufficient power to detect statistical significance. Two
recent papers (24,25) have also suggested that levetiracetam is safe and effective in neonates.
These studies used lower doses (10 mg/kg BID), did not use continuous monitoring, and did not
include a control group.
This is the first pharmacokinetic study of levetiracetam in the neonatal population. We
were able to use a minimal sampling strategy to obtain pharmacokinetic parameters among
infants with variable seizure etiologies. The limitations of our study include the small sample
size with high interindividual variability. Although we intended to study preterm infants and
infants later in the first month of life, most of the patients in the study were full term and treated
with levetiracetam in the first two days of life. The pharmacokinetics of levetiracetam were
different in the neonatal population as compared to older children and adults, and in this small
study, levetiracetam was found to be safe and effective in the neonatal population. Future
investigations are needed to evaluate higher loading doses of levetiracetam in neonates, such as
the 50 mg/kg loading dose currently being used in older children with status epilepticus (38,39),
and to obtain more data on the steady state pharmacokinetics of levetiracetam in neonates.
Although levetiracetam appears to be effective in infants who have failed phenobarbital, more
information needs to be gathered on the efficacy of levetiracetam as a first line drug.

11
Table 1
Parameter n=18 % of total
Sex: Male
Female
10
8
56
44
Race: African-American
Caucasian
7
11
39
61
Cause of seizures: HIE1
Other2
6
12
33
67
Median Range
GA at birth (weeks) 38+6 35+2 - 41
Postnatal age (days) 2 0-32
Weight at time of dosing (kg) 3.5 2 – 4.4
Creatinine at time of dosing 0.7 0.2-1.6
1 HIE = hypoxic-ischemic encephalopathy
2 Other causes of seizures included ornithine transcarbamylase deficiency, hemimegalencephaly, cortical dysplasia,
perinatal stroke, herpes simplex virus, meningitis, birth trauma, kernicterus, and unknown (4 patients)
12
Table 2
Variable Median Range
Clearance (ml/min/kg) 1.21 0.47-2.89
Volume of distribution (L/kg) 0.89 0.37-1.26
Half-life (hours) 8.9 3.2-13.3

13
Figure 1
Creatinine (mg/dL)
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4 1.6 1.8
Half
-Lif
e (
h)
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
r=0.67, p=0.002
14
Figure 2

15
BIBLIOGRAPHY
1. Lanska MJ, Lanska DJ. Neonatal seizures in the united states: Results of the national hospital
discharge survey, 1980-1991. Neuroepidemiology. 1996;15(3):117-25.
2. Lanska MJ, Lanska DJ, Baumann RJ, Kryscio RJ. A population-based study of neonatal
seizures in fayette county, kentucky. Neurology. 1995 Apr;45(4):724-32.
3. Ronen GM, Penney S, Andrews W. The epidemiology of clinical neonatal seizures in
newfoundland: A population-based study. J Pediatr. 1999 Jan;134(1):71-5.
4. Holmes GL. Effects of seizures on brain development: Lessons from the laboratory. Pediatr
Neurol. 2005 Jul;33(1):1-11.
5. Miller SP, Weiss J, Barnwell A, Ferriero DM, Latal-Hajnal B, Ferrer-Rogers A, et al. Seizure-
associated brain injury in term newborns with perinatal asphyxia. Neurology. 2002 Feb
26;58(4):542-8.
6. Glass HC, Glidden D, Jeremy RJ, Barkovich AJ, Ferriero DM, Miller SP. Clinical neonatal
seizures are independently associated with outcome in infants at risk for hypoxic-ischemic brain
injury. J Pediatr. 2009 Sep;155(3):318-23.
7. Bartha AI, Shen J, Katz KH, Mischel RE, Yap KR, Ivacko JA, et al. Neonatal seizures:
Multicenter variability in current treatment practices. Pediatr Neurol. 2007 Aug;37(2):85-90.
8. Painter MJ, Scher MS, Stein AD, Armatti S, Wang Z, Gardiner JC, et al. Phenobarbital
compared with phenytoin for the treatment of neonatal seizures. N Engl J Med. 1999 Aug
12;341(7):485-9.
9. Bittigau P, Sifringer M, Genz K, Reith E, Pospischil D, Govindarajalu S, et al. Antiepileptic
drugs and apoptotic neurodegeneration in the developing brain. Proc Natl Acad Sci U S A. 2002
Nov 12;99(23):15089-94.
10. Diaz J, Schain RJ, Bailey BG. Phenobarbital-induced brain growth retardation in artificially
reared rat pups. Biol Neonate. 1977;32(1-2):77-82.
11. Vining EP, Mellitis ED, Dorsen MM, Cataldo MF, Quaskey SA, Spielberg SP, et al.
Psychologic and behavioral effects of antiepileptic drugs in children: A double-blind comparison
between phenobarbital and valproic acid. Pediatrics. 1987 Aug;80(2):165-74.
12. Farwell JR, Lee YJ, Hirtz DG, Sulzbacher SI, Ellenberg JH, Nelson KB. Phenobarbital for
febrile seizures--effects on intelligence and on seizure recurrence. N Engl J Med. 1990 Feb
8;322(6):364-9.
13. Sulzbacher S, Farwell JR, Temkin N, Lu AS, Hirtz DG. Late cognitive effects of early
treatment with phenobarbital. Clin Pediatr (Phila). 1999 Jul;38(7):387-94.
16
14. Grosso S, Cordelli DM, Franzoni E, Coppola G, Capovilla G, Zamponi N, et al. Efficacy and
safety of levetiracetam in infants and young children with refractory epilepsy. Seizure. 2007
Jun;16(4):345-50.
15. Grosso S, Franzoni E, Coppola G, Iannetti P, Verrotti A, Cordelli DM, et al. Efficacy and
safety of levetiracetam: An add-on trial in children with refractory epilepsy. Seizure. 2005
Jun;14(4):248-53.
16. Glauser TA, Pellock JM, Bebin EM, Fountain NB, Ritter FJ, Jensen CM, et al. Efficacy and
safety of levetiracetam in children with partial seizures: An open-label trial. Epilepsia. 2002
May;43(5):518-24.
17. Pellock JM, Glauser TA, Bebin EM, Fountain NB, Ritter FJ, Coupez RM, et al.
Pharmacokinetic study of levetiracetam in children. Epilepsia. 2001 Dec;42(12):1574-9.
18. UCB Pharma. Product information: Keppra (TM) levetiracetam. 2008.
19. Lynch BA, Lambeng N, Nocka K, Kensel-Hammes P, Bajjalieh SM, Matagne A, et al. The
synaptic vesicle protein SV2A is the binding site for the antiepileptic drug levetiracetam. Proc
Natl Acad Sci U S A. 2004 Jun 29;101(26):9861-6.
20. Glauser TA, Mitchell WG, Weinstock A, Bebin M, Chen D, Coupez R, et al.
Pharmacokinetics of levetiracetam in infants and young children with epilepsy. Epilepsia. 2007
Jun;48(6):1117-22.
21. Ng YT, Hastriter EV, Cardenas JF, Khoury EM, Chapman KE. Intravenous levetiracetam in
children with seizures: A prospective safety study. J Child Neurol. 2010 May;25(5):551-5.
22. Shoemaker MT, Rotenberg JS. Levetiracetam for the treatment of neonatal seizures. J Child
Neurol. 2007 Jan;22(1):95-8.
23. Krief P, Li K, Maytal J. Efficacy of levetiracetam in children with epilepsy younger than 2
years of age. J Child Neurol. 2008 May;23(5):582-4.
24. Furwentsches A, Bussmann C, Ramantani G, Ebinger F, Philippi H, Poschl J, et al.
Levetiracetam in the treatment of neonatal seizures: A pilot study. Seizure. 2010 Apr;19(3):185-
9.
25. Ramantani G, Ikonomidou C, Walter B, Rating D, Dinger J. Levetiracetam: Safety and
efficacy in neonatal seizures. Eur J Paediatr Neurol. 2010 Nov 18.
26. D'Argenio DZ. Optimal sampling times for pharmacokinetic experiments. J Pharmacokinet
Biopharm. 1981 Dec;9(6):739-56.
27. Patsalos PN, Ghattaura S, Ratnaraj N, Sander JW. In situ metabolism of levetiracetam in
blood of patients with epilepsy. Epilepsia. 2006 Nov;47(11):1818-21.

17
28. Guo T, Oswald LM, Mendu DR, Soldin SJ. Determination of levetiracetam in human
plasma/serum/saliva by liquid chromatography-electrospray tandem mass spectrometry. Clin
Chim Acta. 2007 Jan;375(1-2):115-8.
29. Mendu DR, Soldin SJ. Simultaneous determination of levetiracetam and its acid metabolite
(ucb L057) in serum/plasma by liquid chromatography tandem mass spectrometry. Clin
Biochem. 2010 Mar;43(4-5):485-9.
30. Proost JH, Meijer DK. MW/Pharm, an integrated software package for drug dosage regimen
calculation and therapeutic drug monitoring. Comput Biol Med. 1992 May;22(3):155-63.
31. Allegaert K, Lewi L, Naulaers G, Lagae L. Levetiracetam pharmacokinetics in neonates at
birth. Epilepsia. 2006 Jun;47(6):1068-9.
32. Patsalos PN. Clinical pharmacokinetics of levetiracetam. Clin Pharmacokinet.
2004;43(11):707-24.
33. Wojnar-Horton R, Kristensen J. Neonatology. In: Hughes J, Donnelly R, James-Chatgilaou
G, editors. Clinical Pharmacy: A Practical Approach. 2nd ed. Australia: Macmillan Publishers;
2001. p. 22.
34. Anderson BJ, Holford NH. Mechanism-based concepts of size and maturity in
pharmacokinetics. Annu Rev Pharmacol Toxicol. 2008;48:303-32.
35. Lancelin F, Franchon E, Kraoul L, Garciau I, Brovedani S, Tabaouti K, et al. Therapeutic
drug monitoring of levetiracetam by high-performance liquid chromatography with photodiode
array ultraviolet detection: Preliminary observations on correlation between plasma
concentration and clinical response in patients with refractory epilepsy. Ther Drug Monit. 2007
Oct;29(5):576-83.
36. Giroux PC, Salas-Prato M, Theoret Y, Carmant L. Levetiracetam in children with refractory
epilepsy: Lack of correlation between plasma concentration and efficacy. Seizure. 2009
Oct;18(8):559-63.
37. Leppik IE, Rarick JO, Walczak TS, Tran TA, White JR, Gumnit J. Effective levetiracetam
doses and serum concentrations: Age effects. Epilepsia. 2002;43(suppl 7):240.
38. Ng YT, Hastriter EV, Cardenas JF, Khoury EM, Chapman KE. Intravenous levetiracetam in
children with seizures: A prospective safety study. J Child Neurol. 2010 May;25(5):551-5.
39. Kirmani BF, Crisp ED, Kayani S, Rajab H. Role of intravenous levetiracetam in acute
seizure management of children. Pediatr Neurol. 2009 Jul;41(1):37-9.