periodontal pathogenesis, immunity and autoimmune diseases
TRANSCRIPT
PERIODONTAL PATHOGENESIS,
IMMUNITY and AUTOIMMUNE DISEASES
By Dr. Stephen B. Weinmann
Microorganisms Associated with Various
Forms of Periodontal Disease
HEALTH
1) Actinomyces Naeslundii
2) Actinomyces Viscosus
3) Rothia Dentocariosa
4) Veillonella Parvula
5) Streptococcus Uberis
6) Streptococcus Sanguis
7) Streptococcus Mitis
Experimental Gingivitis (supragingival)
1) Actinomyces Israelii
2) Actinomyces Viscosus
Experimental Gingivitis (subgingival) ANUG
Bacteroides
1) Actinomyces Viscosus Intermedius or
2) Actinomyces Naeslundii Prevotella
3) Fusobacterium Nucleatum intermedia
4) Streptococcus Auginosus
5) Lactobacillus Sp.
6) Treponema Sp.
7) Veillonella Parvula [1]
Localized Juvenile
Periodontitis
Actinobacillus
Actinomycetem-
comitans
Bacteroides
Intermedius or
Chronic Gingivitis Prevotella
Intermedia
1) Actinomyces Israelii Capnocytophaga
2) Actinomyces Naeslundii Ochracea
3) Actinomyces Viscosus Eikinella
4) Bacteroides Intermedius Corrodens
5) Campylobacter Sputorum
6) Capnocytophaga Gingivalis
7) Capnocytophaga Ochracea
8) Fusobacterium Nucleatum
9) Streptococcus Sanguis
10) Streptococcus Uberis
11) Veillonella Parvula
[2]
Adult Periodontitis
1) Bacteroides Capillus
2) Bacteroides Forsythus
3) Bacteroides Gingivalis
4) Bacteroides Intermedius or Prevotella Intermedia
5) Eikinella Corrodens
6) Eubacterium Brachy
7) Eubacterium Nodatum
8) Eubacterium Timidum
9) Fusobacterium Nucleatum
10) Lactobacillus Minitus
11) Selenomonas Sputigena
12)Streptococcus Intermedius
13) Wolinella Recta or Campylobacter Rectus
A source of microorganisms (reservoir) Infectious disease; and, infection
connotes the occurrence of colonization accompanied by an immune response.1
Potential pathogens can be transferred by direct (insects, animals, people),
Or indirect paths (water, soil).
Periodontal Diseases are produced by endogenous organisms derived from
exogenous organisms may be comprised of one or many clonal types.
[3]

Putative periodontal pathogens are genetically heterogeneous and consist of
many clonal types. 1
A common genotyping is restriction endonuclease analysis (REA), which is a
method of DNA fingerprinting for a bacterial species using enzymes to cleave
genomic DNA between specific sequences of nucleotide base pairs.
These fragments are separated by gel electrophoresis & stained with ethidium
bromide resulting in a banding pattern representing the DNA fingerprint using
laser densitometry.1
The potential exists that infection may be spread by dental instruments from one
site to another within the oral cavity; such as, Streptococcus Mutans,
Actinobacillus Actinomycetemcomitans. Periodontal probes even transfer
pathogens from diseased to healthy sites.
Spouses may be at risk for being colonized by pathogens if the mate is infected;
but the chances are low. 1-4
If a child harbors a pathogen, at least one of the parents will usually exhibit the
same genotype of bacteria. Transmission of pathogens is more common than
previously thought. But, between siblings is difficult to verify. 1
Animals can be sources of bacterial transfer.
Saliva is a major vector for bacterial transfer. 11
[4]
Contagious leads one to think in terms that pathogens are easily communicable
and easily induce disease.
Specific subgingival bacteria are the primary risk factor for developing disease.1
Most Periodontal Disease is due to microorganisms. The primary defense
mechanism against these microorganisms is the epithelial attachment. The
epithelial attachment has two layers (the Stratum Germinativum & the Stratum
Spinosum); and, the epithelial attachment adheres cell to cell. There is no
organic attachment as advocated by Dr. B. Orban; however, there is a cementing
attachment which binds one cell to another. This cementing attachment is
believed to be a protein-linked polysaccharide that is a sticky, mucilaginous
substance that helps neighboring cells to adhere to each other. Certain drugs,
such as Cortisone, the integrity of the cementing substance and a in the
production of epithelial cells hyperplasia. As the intercellular cementing
substance breaks down a “splitting” of the cells occurs; and, the epithelial cells
proliferate & migrate. Once “splitting” of the epithelial structure occurs the
collagen fibers & the ground substance become adversely effected.
Of the more than 250 bacterial species that may colonize the gingival crevice in
humans, only 10 or so appear to be involved in periodontal disease. According to
Clark & Loe they are as follows: 5
[5]
1) Actinobacillus Actinomycetemcomitans, 2) Treponema Denticola, 3)
Eikinella Corrodens, 4) Bacteroides Gracilis, 5) Eubacterium species, 6)
Wolinella Recta, 7) Capnocytophaga species, 8) Prevotella Intermedia, & 9)
Black-pigmented Bacteroides species including Porphyromonas Gingivalis.
When host cell membranes are injured a process called the ARACHIDONIC
ACID CASCADE 7,8 results. The biologically active products in this cascade are
Leukotrienes, Prostaglandins, Thromboxane, and other products. The effects are
the attraction of phagocytic cells and enhanced vascular permeability; allowing
the influx of serum factors (antibodies & complement) destruction of localized
microorganisms and the potentially toxic products of microbial metabolism.
There are potentially harmful effects to the periodontal tissues that cause
mucosal edema, bone resorption, and collagenase (digests connective tissue
fibers) creating part of the periodontal pathology. The primary phagocytic cells 6-10
derived from the Leukotrienes are polymorphonuclear neutrophils (PMNs) and
macrophages. The PMNs make up 50-70% of the circulating leukocytes and
originate in the bone marrow from pluripotential stem cells induced to
differentiate by colony-stimulating factors (CSFs).
[6]
There are three phases of microbial attack by neutrophils (1) chemotaxis
(directed movement of an attractant substance toward a target organism), (2)
phagocytosis (engulfment of the microbe), and (3) microbial killing (a chemical
attack on the ingested microorganisms by bactericidal proteins,
myeloperoxidase, and cathepsins and the formation of oxygen-free radicals
(superoxide & hydroxyl ion). Chemotaxis 6-10 involves the margination of
circulating neutrophils along the endothelial lining of the postcapillary venules,
their penetration through the vascular wall, and their directed migration toward
the extravascular source of the infection. The initial adhesion of neutrophils to the
vascular endothelium is mediated by surface glycoproteins (CD11/CD18), which
bind to adhesion molecules on activated endothelium (ICAM-1, ELAM-1).
Leukocyte proteases are responsible for the production of complement-derived
chemotaxins. The serum-complement system is composed of more than twenty
serum proteins which when activated have potent biological effects. There are 2
main pathways that the proteins of the complement system are activated. These
are the classical pathway (binding of antibody to bacterial cell wall surfaces)
and the alternate pathway (activated by endotoxins of certain gram- bacteria).
Meanwhile, lipoxygenases mediate production of arachidonic acid-derived
leukotrienes & hydroxyacids.
[7]
OPSONIMS 7-10 (proteins that coat microorganisms & promote their avid uptake
by neutrophils) is made up of complement fragment C3b, fibronectin (a large
plasma protein), and immunoglobulins. These substances adhere to
microorganisms & promote binding to C3b & Fc receptors on the neutrophils
plasma membrane. The microbial activity of neutrophils involves two interacting
functions: degranulation and activation of the respiratory burst.
NEUTROPHILS 6-10 (polymorphonuclear leukocytes or PMNs) have two sets of
cytoplasmic granules. The azurophilic granules contain acid hydrolases,
lysozyme, neutral proteases(Cathepsin G & Elastase), myeloperoxidase, & basic
proteins. Specific granules contain lysozyme, transcobalamin III, apolactoferrin,
collagenase, & The C5 cleaving protease which aid in the digestion of the
bacterial cell wall, degrade cellular debris, dissolve connective tissue, and bind
substances like iron that are useful in bacterial metabolism. Neutrophils are the
circulating white cells needed for phagocytosis and proteolysis by which bacteria,
cellular debris, and solid particles are destroyed and removed. They are the
primary effector cells of the acute inflammatory response & contain potent
antibacterial peptides called defensins. Neutrophils posses receptors for the
metabolites of the complement molecule C3, complement receptors CR1, CR3,
CR4, C5, C5aR, and the IgG antibody (FcR) that enable neutrophils to participate
in phagocytosis.
[8]
MAST CELLS 6-10,12,13 are a constituent of connective tissue containing large
basophilic granules that contain Serotonin, heparin, histamine, & bradykinin all of
which are released from the mast cell in response to injury & infection. Histamine
causes blood vessels to dilate and become more permeable allowing an influx of
serum & serum factors into local tissue spaces. Serotonin is a naturally occurring
derivative of tryptophan found in platelets and is released upon injury to blood
vessel walls. It acts as a vasoconstrictor. Heparin is a naturally occurring
mucopolysaccharide that acts as an antithrombin factor preventing intravascular
clotting. It is found mostly around connective tissue surrounding capillaries.
Bradykinin is a peptide of nonprotein origin comprised of 9 amino acid residues
produced from 2-globulin by kallikrein and acts as a potent vasodilator.
Bradykinins and other kinins both directly & indirectly affect the renal secretion of
salt and water. Mast cells 14-16 possess receptors for C3a, C5a, and the antibody
molecules IgE (FcR) and IgG (FcR). Mast cells can synthesize other
inflammatory mediators such as SRS-A, TNF-, and leukotriene C4.
The IMMUNE SYSTEM 6-10 is a network of interacting cellular & soluble
components. Its function is to distinguish entities within the body as “self” or
“nonself” and to eliminate those that are “nonself”. Microorganisms are the
primary “nonself” entities, but neoplasms, transplants, foreign substances, &
implants are also important.
[9]
Two mechanisms enable the immune system to function: (1) NONSPECIFIC
(innate) IMMUNITY and (2) the SPECIFIC (adaptive) IMMUNITY. Nonspecific
immunity is present at birth, does not develop memory, & needs no previous
encounter with the offending substance. The cellular components are (1) the
phagocytic system whose function is to ingest / digest invading microorganisms,
and (2) Natural Killer (NK) cells whose function is to kill some tumors,
microorganisms, and virally infected cells. NK cells possess Killer Inhibitory
Receptors (KIR) and Killer Activating Receptors (KAR). Phagocytes include
neutrophils, monocytes, & macrophages. CYTOKINES are nonimmunoglobulin
polypeptides secreted by monocytes & lymphocytes in response to interaction a
nonspecific antigen (Ag), a specific antigen (Ag), or a nonspecific soluble
stimulus (endotoxins, other cytokines). Cytokines affect the magnitude of
inflammatory or immune responses. Specific (adaptive) Immunity has the ability
to learn, to adapt, and memory. The cellular component is the lymphocyte; the
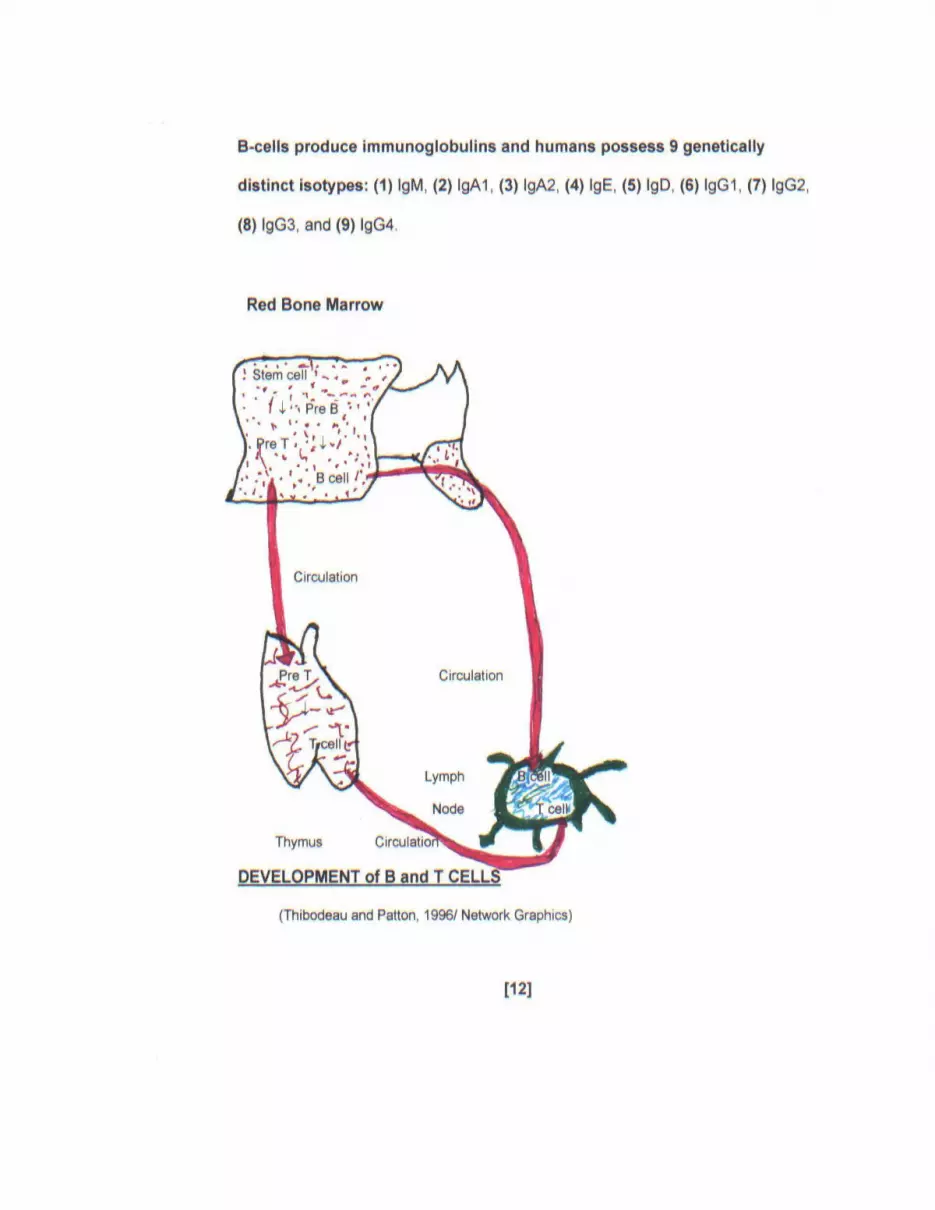
soluble components are the immunoglobulins (Igs). The lymphocytes are divided
into two subsets: (1) the T- lymphocytes (Thymus- derived), & (2) the B-
lymphocytes (bone marrow derived). The T- lymphocyte is responsible cellular
immune responses and acts in rejection of graft tissues & organ transplants, the
production of lymphokines such as (1) osteoclast-activating factor [OAF] that has
the ability to cause bone resorption;
[10]
(2) Macrophage migration inhibitory factor (MIF) which the migration of
Macrophages Phagocytic efficiency; (3) chemo-attractiveness for phagocytic
cells, (4) toxicity for fibroblast cells; and, (5) protection of host cells from viral
infections. Another important function of T cells is called “helper T cell” which
promotes the immune response of other lymphocytes to foreign antigens by
releasing soluble proteins called helper factors. It is the subpopulation of “helper”
T-cells that are affected by the Human Immunodeficiency Virus (HIV). The T cell
induces B-cell activation. CD4 and CD8 are T-cell coreceptors.
Immunosuppressants block the intracellular processes of T-cell activation. Both
Cyclosporin A and Tacrolimus bind and activate immunophilins causing their
immunosuppressive effects.
The B-lymphocyte is responsible for the humoral immune response. It originates
in bone marrow; and, is a precursor of the plasma cell which release antibodies
and memory cells that provide a rapid response if the same antigen is
encountered again. Since factors involved in hypersensitivity reactions (i.e.
Calciphylaxis, activated compliment factors) have been observed in periodontal
tissues and in the crevicular fluids and may play a role in the pathogenesis of
periodontal disease. Defense mechanisms are constantly active in moderating
the effects of bacteria & their products upon the threat to periodontal health.
[11]
CYTOKINES 6-10 are divided into several groups as follows: (1) interleukins (IL),
(2) interferons (IFN), (3) tumor necrosis factors (TNF), (4) colony-stimulating
factors (CSF), (5) transforming growth factors (TGF), and (6) chemokines. A brief
discussion will be entered into here since they are discussed in detail elsewhere.
They activate oxidative metabolism.
INTERLEUKINS are a large group of cytokines produced mainly by T cells. Most
interleukins influence other cells to divide & differentiate. They are grouped as
interleukin-1 (IL-1) through interleukins-18 (IL-18).
INTERFERONS are a natural cellular protein formed when cells are exposed to a
virus or another foreign particle of nucleic acid. They induce the production of
translation inhibitory protein (TIP) in noninfected cells. TIP blocks translation of
viral ribonucleic acid giving other cells protection against the original & other
viruses. Interferon is species specific. They are listed as IFN- , IFN- , and IFN-
; or, as Interferon alpha-2a, recombinant; Interferon alpha-2b, recombinant; &
Interferon beta-1a.
TUMOR NECROSING FACTOR (TNF) is a natural body protein & can be
synthetically produced possessing anticancer properties. Adverse effects are
shock & cachexia. They are listed as TNF- and TNF- .
COLONY-STIMULATING FACTORS (CSF) is important for cells to be able to
pass a restriction point in their reproductive cycle. After cells have entered the
deoxyribonucleic acid synthesis phase it is no longer needed. They are listed as
(1) GM-CSF, (2) G-CSF, and (3) M-CSF.
[13]
TRANSFORMING GROWTH FACTOR (TGF) is a group of proteins produced by
the cells of a tumor that cause a disorderly increase in the number of cells. TGF-
induces angiogenesis, keratinocyte proliferation, bone resorption, and tumor
growth. TGF- induces fibroblast proliferation, synthesis of collagen &
fibronectin, enhances angiogenesis & wound healing, and inhibits CTL (cytotoxic
T lymphocytes), NK (natural killer), LAK (lymphokines-activated killers), and T &
B CELL proliferation.
CHEMOKINES are a new family of cytokines. They induce chemotaxis and
migration of leukocyte subsets. They are called (1) C, (2) C-C, (3) C-X-C, &
C-X3-C. Their major effects are: C--- induces chemotaxis of T & NK cells; C-C---
induces chemotaxis of T & NK cells, basophils, & eosinophils; C-X-C induces
chemotaxis of T cells, mast cells, monocytes, and eosinophils;
C-X3-C has not been well clarified at this point. Some of the receptors on
chemokines may serve as coreceptors for entry of HIV into
monocytes/macrophages.
[14]
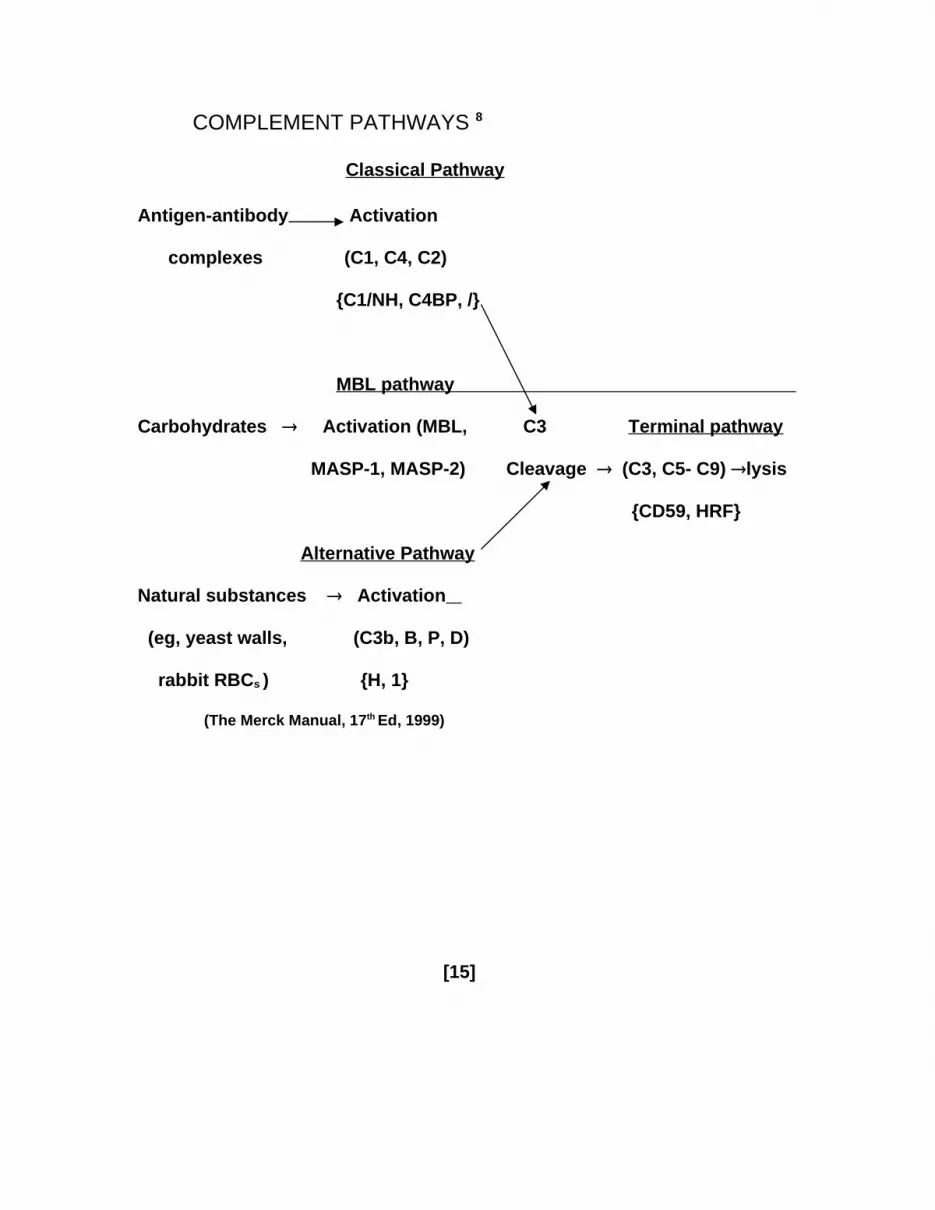
COMPLEMENT PATHWAYS 8
Classical Pathway
Antigen-antibody Activation
complexes (C1, C4, C2)
{C1/NH, C4BP, /}
MBL pathway
Carbohydrates Activation (MBL, C3 Terminal pathway
MASP-1, MASP-2) Cleavage (C3, C5- C9) lysis
{CD59, HRF}
Alternative Pathway
Natural substances Activation
(eg, yeast walls, (C3b, B, P, D)
rabbit RBCs ) {H, 1}
(The Merck Manual, 17th Ed, 1999)
[15]
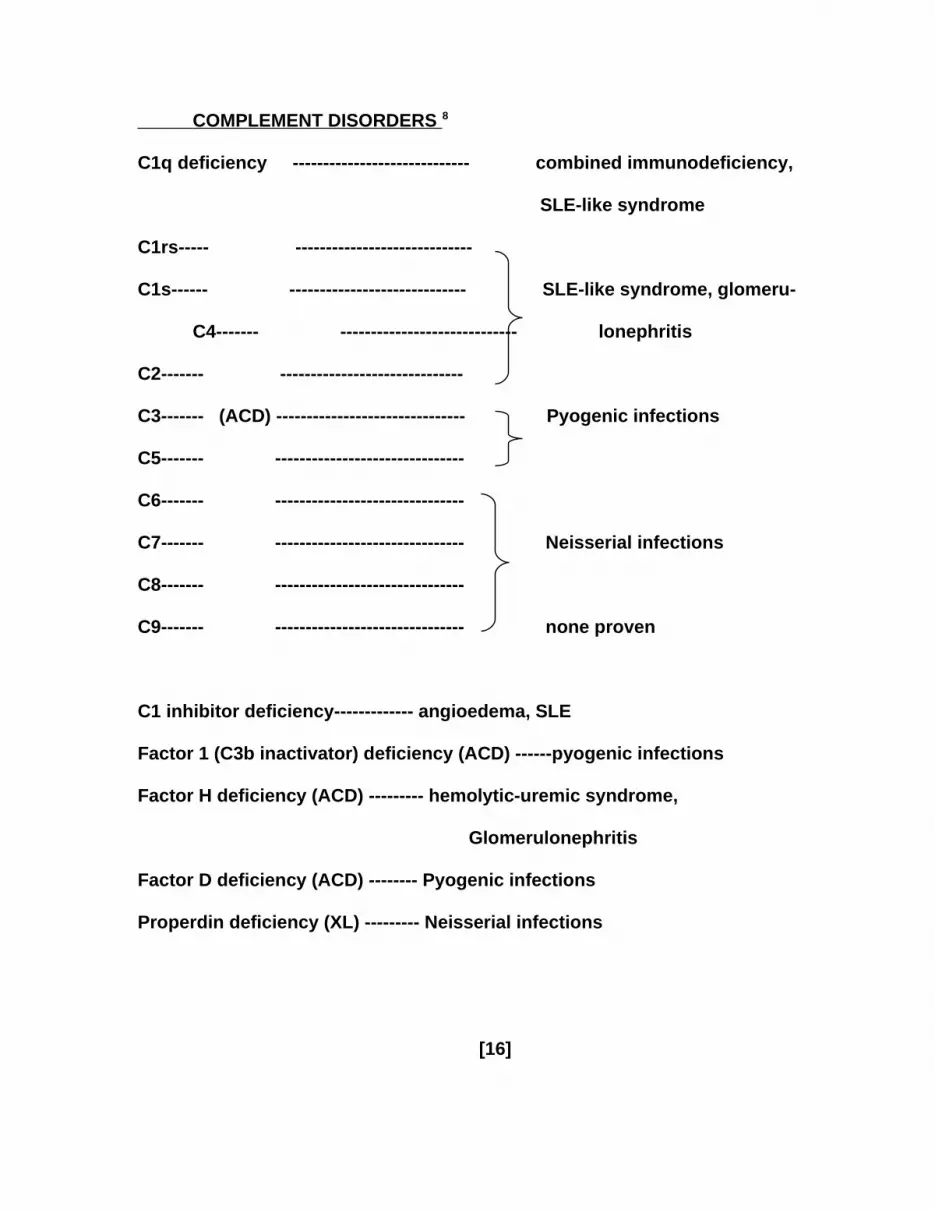
COMPLEMENT DISORDERS 8
C1q deficiency ----------------------------- combined immunodeficiency,
SLE-like syndrome
C1rs----- -----------------------------
C1s------ ----------------------------- SLE-like syndrome, glomeru-
C4------- ----------------------------- lonephritis
C2------- ------------------------------
C3------- (ACD) ------------------------------- Pyogenic infections
C5------- -------------------------------
C6------- -------------------------------
C7------- ------------------------------- Neisserial infections
C8------- -------------------------------
C9------- ------------------------------- none proven
C1 inhibitor deficiency------------- angioedema, SLE
Factor 1 (C3b inactivator) deficiency (ACD) ------pyogenic infections
Factor H deficiency (ACD) --------- hemolytic-uremic syndrome,
Glomerulonephritis
Factor D deficiency (ACD) -------- Pyogenic infections
Properdin deficiency (XL) --------- Neisserial infections
[16]
IMMUNODEFICIENCY DISEASES
DISORDERS with INCREASED SUSCEPTIBILITY to UNUSUAL
INFECTIONS:
8-10, 17
1) Primary Immunodeficiencies 2) Foreign Bodies
X- linked agammaglobulinemia Central venous catheter
DiGeorge anomaly Ventricular shunts
Chronic granulomatous disease Artificial heart valves
C3 deficiency Urinary catheter
Aspirated foreign bodies
3) Unusual Microbiological Factors 4) Obstructive Disorders
Chronic infections Bronchial asthma
Continuous reinfection Allergic rhinitis
Antibiotic overgrowth Cystic fibrosis
Contaminated water supply Urethral stenosis
Contaminated inhalation equipment Bronchiectasis
Blocked Eustachian
Tube
5) Circulatory & Systemic Disorders 6) Integumentary defects
Diabetes Mellitus Burns
Sickle Cell Disease Skull fractures
Nephrosis Midline sinus tracts
Varicose veins Ciliary abnormalities
[17]
(Circulatory & Systemic Disorders—cont.) (Integumentary defects)
Congenital Cardiac Disease Eczema
7) Secondary Immunodeficiencies
Lymphoma
Splenectomy
Immunosuppressive therapy
Chronic viral diseases
Malnutrition
Prematurity
Uremia
Protein-losing enteropathy
PRIMARY IMMUNODEFICIENCY DISORDERS and associated findings: 8
T-cell (cellular) deficiencies
1) Predominant T-cell deficiency
DiGeorge anomaly (hypocalcemia, heart disease, aortic arch
Abnormalities, peculiar facies).
Chronic mucocutaneous candidiasis (endocrinopathies,
Thrush, & nail dystrophy).
Combined Immunodeficiency with Igs or Nezelof syndrome
(Bronchiectasis, diarrhea, & Thrush).
[18]
[T-cell (cellular) deficiencies—cont.]
Nucleoside phosphorylase deficiency (AR)
Natural killer cell deficiency (severe herpes viral infection).
Idiopathic CD4 lymphocytopenia (often asymptomatic).
2) Combined T- & B-cell deficiencies
XL lymphoproliferative syndrome (severe Epstein-Barr).
Wiskott-Aldrich Syndrome (XL) {eczema,thrombocytopenia,
Melena, & draining ears}.
Short-limbed dwarfism (cartilage-hair Hypoplasia, severe
Varicella).
Reticular Dysgenesis (pancytopenia).
Ataxia-telangiectasia (AR)-{dermatitis, Neurologic decline,
Sinopulmonary infections, & telangiectasia}.
Bare lymphocyte Syndrome (absence of HLA).
Adenosine deaminase deficiency (AR)-{skeletal abnormality}
Severe combined immunodeficiency (AR or XL)- {diarrhea,
Pneumonia, thrush, & failure to thrive}.
3) B-cell (antibody) deficiencies
X-linked agammaglobulinemia (Pyogenic infection after
Age 6, paralytic disease after oral polio
Immunization).
[19]
[B-cell (antibody) deficiencies—cont.]
Transient hypogammaglobulinemia of infancy (prematurity).
Common variable immunodeficiency (autoimmunity,
Splenomegally, malabsorption, & sinopulmon-
ary infections).
Immunodeficiency with thymoma (aplastic anemia).
Ig deficiency with hyper-IgM (XL)-{neutropenia and lymph-
Adenopathy}.
IgA deficiency (autoimmunity, respiratory or food allergy,
Respiratory infection often asymptomatic).
IgG subclass deficiencies (IgA deficiency).
Antibody deficiency with normal or elevated Igs (not proven).
4) Phagocytic disorders
Defects of cell movement
Hyperimmunoglobulinemia E syndrome (staph. Infections,
Eczema, & dermatitis, & course facial features).
Leukocyte adhesion defect type 1 (AR)-{prolonged attach-
ment of umbilical cord, leukocytosis, periodontitis).
Defects of microbial activity
Chediak-Higashi Syndrome (AR)-{giant granules of neutro-
phils, oculocutaneous albinism, neutropenia, and
recurrent infections}.
[20]
[Phagocytic Disorders—cont.]
Myeloperoxidase deficiency (AR)- {not proven}
Neutrophil G6PD deficiency (not proven)
Chronic granulomatous disease (XL or AR)- {lymphadenop-
athy, dermatitis, antral obstruction, small bone
osteomyelitis, & pneumonias}.
Abbreviations:
XL= X-linked Ig= immunoglobulins AR= autosomal recessive
ACD= autosomal codominant AD= autosomal dominant
SECONDARY IMMUNODEFICIENCY DISORDERS 8
Heredity & Metabolic Diseases Infectious Diseases
1) Down Syndrome 1) Congenital Rubella
2) Uremia 2) Measles
3) Diabetes Mellitus 3) Varicella Zoster
4) Malnutrition 4) HIV infection
5) Sickle cell disease 5) Cytomegalovirus (CMV)
6) Myotonic dystrophy 6) Infectious Mononucleosis
7) Protein-losing enteropathies 7) Acute bacterial disease
8) Nephrotic syndrome 8) Severe mycobacterial/
9) Vitamin deficiencies fungal disease
10)Mineral deficiencies [21]
Infiltrative/ Hematologic Diseases Immunosuppressive agents
1) Sarcoidosis 1) Anti-T-cell monoclonal
2) Hodgkin’s disease/Lymphoma antibodies
3) Histocytosis 2) Anti-lymphocyte globulin
4) Myeloma 3) Anti- thymocyte globulin
5) Leukemia 4) Radiation
6) Agranulocytosis 5) Corticosteroids
7) Aplastic anemia 6) Immunosuppressive
drugs
Miscellaneous
1) Aging
2) Anticonvulscent drugs
3) Graft-vs-Host disease [GVHD] (maculopapular rash, lymphadenopathy,
hepatosplenomegally, & alopecia).
4) Alcoholic Cirrhosis
5) SLE
6) Chronic Active Hepatitis
[22]
PROGNOSIS OF PRIMARY IMMUNODEFICIENCIES 8
Poor
X-linked lymphoproliferative syndrome (highly sensitive EBV infections)
Ataxia-telangiectasia (Cerebellar ataxia, telangiectasia of conjunctiva &
Skin, recurrent sino-pulmonary infections, & variable immuno-
logic disease).
Wiskott-Aldrich syndrome (eczema, recurrent infection, & thrombocyto-
penia).
Leukocyte-adhesion deficiency (disorder of WBC, poor wound healing,
leukocytosis, periodontitis, progressive necrotic soft tissue
infection, & delayed umbilical cord detachment).
Severe combined Immunodeficiencies (hereditary deficiency T- & B-cell
Systems, lymphoid aplasia, & thymic dysplasia).
Guarded
Hyper-IgE syndrome (recurrent staphylococcal infections of the skin, &
highly elevated IgE levels).
DiGeorge anomaly (absence/Hypoplasia of the parathyroid & thymus
glands, partial or complete T-cell immunodeficiency, &
near normal or normal B-cell immunity).
Hyper-IgM syndrome (elevated levels of IgM, decreased levels of IgA & IgG,
Susceptibility to infection, & intermittent neutropenia).
[23]
[Miscellaneous—cont.]
Chronic granulomatous disease (disorder of WBCs bactericidal function,
hypergammaglobulinemia, anemia, leukocytosis, & wide-
spread granulomatous lesions of the skin, lungs, and lymph
nodes).
Common variable immunodeficiency (decreased Ig & antibody levels &
Recurrent bacterial infections).
Good
IgG subclass deficiency (an antibody deficiency associated with
susceptibility to infections).
Complement deficiencies
Chronic mucocutaneous candidiasis (persistant Candidia infections of the
nails, skin, scalp, & mucous membranes often associated
with endocrinopathies mostly hypoparathyroidism and
hypoadrenalism).
Selective IgA deficiency ( IgA with normal levels of Igs).
Transient hypogammaglobulinemia (self-limited antibody deficiency).
X-linked agammaglobulinemia (panhypogammaglobulinemia, low or
abscent B cells, intact cellular immunity, and the onset of
infections after age 6).
[24]
AUTOIMMUNE DISORDERS 8,10, 17 are disorders in which the immune
system produces autoantibodies to an endogenous antigen resulting in injury to
the tissues involved by forming antibodies against the body’s own cells.
Autoantigens normally present in the internal cells stimulate the development of
autoantibodies act against the internal cell to cause localized and systemic
reactions resulting in a variety of diseases. The diseases most often considered
in autoimmune disorders are:
1) Hashimoto’s Thyroiditis, 2) SLE, 3) Goodpasture’s syndrome, 4)
Pemphigus, 5) Graves’ Disease, 6) Myasthenia Gravis, 7) Rheumatoid
Arthritis (RA), 8) Polymyositis, 9) Idiopathic Addison’s Disease, 10)
Bullous Pemphigoid, 11) Sjogren’s Syndrome, 12) Vitiligo, 13) Vasculitis,
and 14) some endocrinopathies.
Hashimoto’s Thyroiditis: is associated with antibodies to thyroglobulin, a
second colloid antigen, the microsomes of thyroid epithelial cells, and a thyroid
cell surface antigen. This disease is 20x more prevalent in women than in men.
The goiter is asymptomatic, but there is difficulty in swallowing, a feeling of local
pressure, the thymus is usually enlarged, & regional lymph nodes are
hyperplastic. Other names for this disease are Hashimoto’s Disease,
Lymphocytic Thyroiditis, Struma Lymphomatosis, & Hashimoto’s Struma.
[25]
Systemic Lupus Erythematosis (SLE) is an example of collagen disease
affecting many systems of the body. The pathologic characteristics are severe
Vasculitis, renal involvement, & lesions of the skin & nervous system. Viral
infection or dysfunction of the immune system may be the cause of this disease.
It is 4x more common in women than in men. The erythematous rash (“butterfly
rash”) over the nose & malar eminences,
fatigue, weakness, loss of weight, photosensitivity, fever, alopecia, & skin lesions
spreading to the mucous membranes. Also, pleuritis, glomerulonephritis,
peritonitis, pericarditis, neuritis, & anemia may be involved. Immunofluorescence
shows the presence of IgM, IgA, IgG, C3, & fibrinogen in the basement
membrane zone.
Goodpasture’s Syndrome is a chronic relapsing pulmonary hemosiderosis
associated with glomerulonehritis characterized by a cough with hemoptysis,
anemia, dyspnea, & progressive renal failure. The severe cases may be treated
by hemodialysis and kidney transplantation. It is characterized by circulating anti-
glomerular basement membrane antibodies in the blood and linear deposition of
immunoglobulins & complement in the glomerular basement membrane causing
pulmonary hemorrhage with progressive glomerulonephritis. This syndrome can
be rapidly fatal with pulmonary hemorrhage and respiratory failure as the cause
of death.
[26]
Pemphigus is a severe disease of the skin & mucous membranes characterized
by intraepidermal bullae and extensive erosions on apparently healthy skin &
mucous membranes. In active Pemphigus the serum & skin readily demonstrate
IgG antibodies binding to the site of the epidermal damage. The primary lesions
are flaccid bullae that upon pealing off leave painful erosions. The lesions may
be localized to the face and may need to be differentiated from Seborrheic
Dermatitis or Subacute Cutaneous Lupus Erythematosis; as well as, Exfoliative
Dermatitis. In addition, there are other disease entities that should be ruled out.
They are Bullous Pemphigoid, Benign Mucosal Pemphigoid, drug eruptions,
Erythema Multiforme, Dermatitis Herpetiformis, & Bullous Contact Dermatitis. In
Pemphigus Vulgaris the epidermis is easily detached from the underlying skin
(Nikolsky’s sign) & biopsy yields suprabasal epidermal cell separation. This
separation does not occur in Pemphigus Foliaceus in the suprabasal region, but
it does occur in the upper layers of the stratum spinosum or stratum granulosum.
Another test (Tzanck cell) shows the presence of acantholytic cells, typical of
Pemphigus. Cicatricial Pemphigoid [CP] (Benign Mucous Membrane
Pemphigoid) is a chronic
vesiculobullous autoimmune disorder with the most common clinical feature
being Desquamative Gingivitis (Nikolsky’s sign).
[27]
Direct immunofluorescence (DIF) is of great diagnostic value, since in CP, DIF of
mucosal biopsies reveal IgG, C3, & other Ig & fibrin deposits. Sometimes IgA &
IgM may be present.
GRAVES’ DISEASE is a disorder characterized by hyperthyroidism, enlarged
thyroid gland, exopthalmus (protrusion of the eyes), familial, autoimmune, 5x
more common in women than in men, exacerbated by stress or emotional upset,
nervousness, hand tremors, weight loss, fatigue, breathlessness, palpitations,
tachycardia, frontal bossing, heat intolerance, metabolic rate, gastrointestinal
motility, enlarged thymus, hyperplasia of the lymph nodes, blurred or double
vision, localized edema, atrial arrythmias, & osteoporosis. This disease is also
called Exopthalmic Goiter, Toxic Goiter, Thyrotoxicosis, or Diffuse Toxic Goiter.
Graves’ disease is caused by an antibody directed against the TSH receptor on
the thyroid follicular cell (TRAb).
MYASTHENIA GRAVIS is characterized by chronic fatigue, muscle weakness
(face & throat) due to the inability of neural receptors at the myoneural junction to
depolarize due to a of acetylcholine bringing about the loss or dysfunction of
acetylcholine receptors.
[28]
The onset of symptoms are: 1) Ptosis of the upper eyelids, 2) diplopia,
weakness of the facial muscles, 3) muscle fatigability, 4) dysarthria, 5)
dysphagia, proximal limb weakness, 6) severe quadriperesis may develop, 7)
voice changes, 8) nasal regurgitation, & 9) choking. In Ocular Myasthenia Gravis
only the extraocular muscles are involved.
RHEUMATOID ARTHRITIS (RA) is a chronic, inflammatory, destructive,
deforming collagen disease. It is characterized by symmetric synovial
inflammation leading to thickening of the synovium and swelling of the joint.
Other names used for RA are; Atrophic Arthritis, Ankylosing Spondylitis, Juvenile
Arthritis, & Arthritis Deformens. Some Immunologic abnormalities (immune
complexes, plasma cells antibodies (rheumatoid factor [RF]), lymphocytes
primarily T-helper cells pro-inflammatory cytokines, TNFs, CSFs, all contribute
to increased number of lining cells that produce collagenase & stromelysin
contributing to cartilage destruction, & interleukins-1 lymphocyte production &
prostaglandins.
Hyperplastic synovial tissue (pannus) may erode cartilage & ligaments. The signs
& symptoms include: 1) joint tenderness, 2) synovial thickening, 3) hands, feet,
wrists, ankles primarily involved, 4) stiffness, 5) fatigue, 6) malaise, 7)
deformities, 8) flexion contractures, & 9) ruptured popliteal cysts that can mimic
deep vein thrombosis (DVT).
[29]
SLE may mimic RA, and polymyositis, polyarteritis, progressive systemic
sclerosis, and dermatomyositis all have to be differentiated from RA.
GOUT is a recurrent form of chronic arthritis of peripheral joints that may be
precipitated by minor trauma, overindulgence in purine-rich foods, too much
alcohol, fatigue, & emotional stress. Signs resemble an acute infection—swelling,
warmth, redness, tenderness, fever, tachycardia, chills, malaise, & leukocytosis.
POLYMYOSITIS is a connective tissue disease having degenerative and
inflammatory changes in the muscles; and, also in the skin (dermatomyositis).
Pain, insomnia, edema, deformity, sweating, and tension accompany
Polymyositis. Deposits of IgM, IgG, and picornavirus-like substances have been
found in muscle cells. The disease is most common between ages 5-15 & 40-60.
The disease is characterized by proximal muscle weakness, tenderness, pain,
rash, polyarthralgias, Raynaud’s phenomenon, dysphagia, pulmonary disease,
fever, fatigue, & weight loss. There is nonhistone ANAs.
IDIOPATHIC ADDISON’S DISEASE (IAD) is caused by complete or partial
failure of the adrenocortical function resulting from autoimmune process,
infection, neoplasm, or hemorrhage in the gland.
[30]
Characteristics of this disease are 1) bronze pigmentation of the skin & mucous
membrane, 2) weakness, 3) anorexia, 4) dehydration, 5) weight loss, 6)
decreased endurance, 7) GIT disturbances, 8) anxiety, 9) depression, & 10)
decreased tolerance to cold. There is an increased need for salt,
mineralocorticoids, & glucocorticoids from the increase in stress. IAD exhibits
humoral & cell-mediated cytotoxicity.
SJOGREN’S SYNDROME (SS) is an Immunologic disorder characterized by
deficient moisture production of the lacrimal (causing desiccation of the cornea &
conjunctiva), salivary (causing dental disorders), and other glands resulting in
dryness of the mouth, eyes, and other mucous membranes including vaginal
dryness. There are also loss of taste and smell. Sjogren’s syndrome is often
associated with Rheumatoid Arthritis, Waldenstrom’s Macroglobulinemia,
Lymphoma, and Raynaud’s phenomenon. Immunological tests that should be
done are antithyroid antibodies, immunoglobulins & gammaglobulins, rheumatoid
factors (RFs), cryoglobulins, and Sjogren’s antibodies [called SS-A & SS-B]. The
salivary & lacrimal glands are infiltrated with CD4+ T cells and some B cells. The
T- cells inflammatory cytokines (interleukins-2, interferon ). SS is an
autoimmune disease characterized by keratoconjunctivitis sicca (KCS) and
xerostomia. Retroviruses and Epstein-Barr virus have been implicated in the
etiology of SS.
[31]
Organ System Conditions in SS are:
1) SKIN (dry, sweat, Vasculitis, purpura)
2) SALIVARY & LACRIMAL GLANDS (enlarged, xerostomia, atrophy,
keratoconjunctivitis)
3) GASTROINTESTINAL TRACT ( dental caries, oral candidiasis,
hypochlorhydria, hepatomegaly, splenomegally, biliary cirrhosis)
4) RESPIRATORY (rhinitis, pharyngitis, obstructive pulmonary disease)
5) CARDIOVASCULAR SYSTEM (Raynaud’s disease, LE)
6) MUSCULOSKELETAL SYSTEM (RA)
7) HEMATOPOETIC SYSTEM (megaloblastic anemia, microcytic-
hypochromic anemia, leukopenia, hypergammaglobulinemia,
hypersedimentation).
VASCULITIS is an inflammatory condition of the blood vessels (allergic
vasculitis, segmented hyalinizing Vasculitis, necrotizing Vasculitis). The
predominant inflammatory cells are PMNs. Some diseases connected to
vasculitic disorders are: 1) Henoch-Schoelein Syndrome, 2) Pseudomonas
septicemia, 3) drug-induced vasculitis, 4) Erythema nodosum, 5) polyarteritis
nodosa, 6) Temporal arteritis, & 7) Takayasu’s arteritis. IgG & complements are
commonly found in vessel walls.
VITILIGO is a benign skin disease consisting of irregular patches of various sizes
completely lacking any pigment with hyperpigmented borders.
[32]
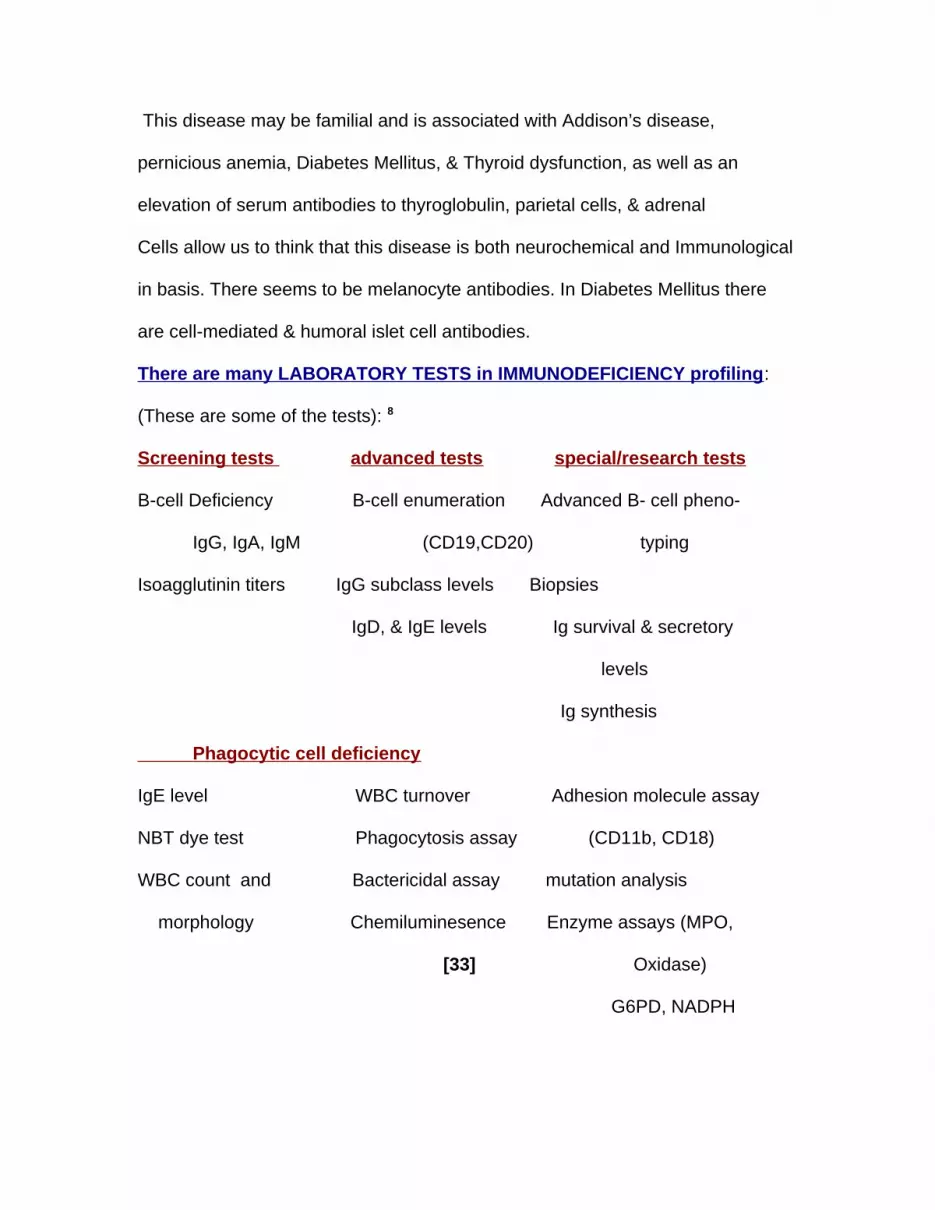
This disease may be familial and is associated with Addison’s disease,
pernicious anemia, Diabetes Mellitus, & Thyroid dysfunction, as well as an
elevation of serum antibodies to thyroglobulin, parietal cells, & adrenal
Cells allow us to think that this disease is both neurochemical and Immunological
in basis. There seems to be melanocyte antibodies. In Diabetes Mellitus there
are cell-mediated & humoral islet cell antibodies.
There are many LABORATORY TESTS in IMMUNODEFICIENCY profiling:
(These are some of the tests): 8
Screening tests advanced tests special/research tests
B-cell Deficiency B-cell enumeration Advanced B- cell pheno-
IgG, IgA, IgM (CD19,CD20) typing
Isoagglutinin titers IgG subclass levels Biopsies
IgD, & IgE levels Ig survival & secretory
levels
Ig synthesis
Phagocytic cell deficiency
IgE level WBC turnover Adhesion molecule assay
NBT dye test Phagocytosis assay (CD11b, CD18)
WBC count and Bactericidal assay mutation analysis
morphology Chemiluminesence Enzyme assays (MPO,
[33] Oxidase)
G6PD, NADPH
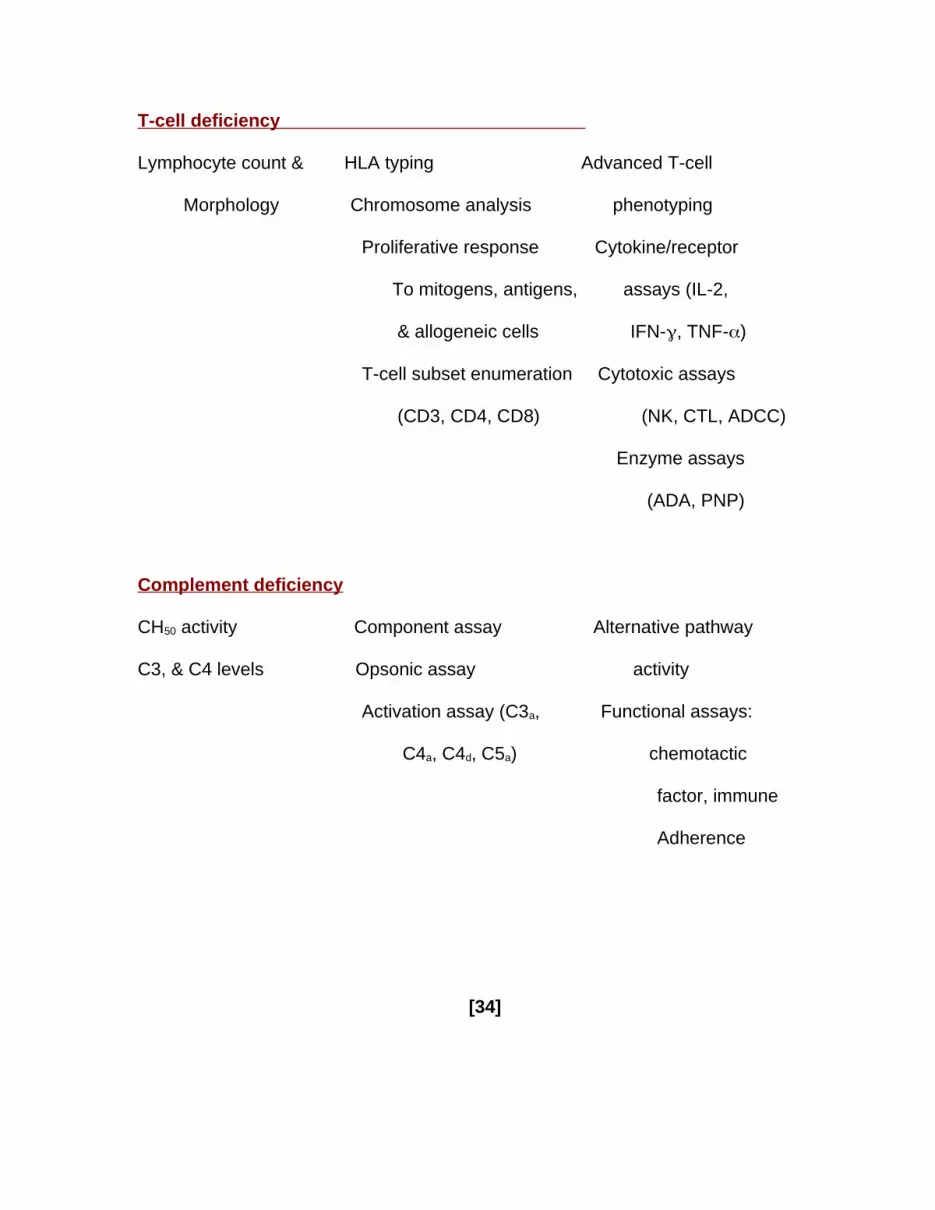
T-cell deficiency
Lymphocyte count & HLA typing Advanced T-cell
Morphology Chromosome analysis phenotyping
Proliferative response Cytokine/receptor
To mitogens, antigens, assays (IL-2,
& allogeneic cells IFN-, TNF-)
T-cell subset enumeration Cytotoxic assays
(CD3, CD4, CD8) (NK, CTL, ADCC)
Enzyme assays
(ADA, PNP)
Complement deficiency
CH50 activity Component assay Alternative pathway
C3, & C4 levels Opsonic assay activity
Activation assay (C3a, Functional assays:
C4a, C4d, C5a) chemotactic
factor, immune
Adherence
[34]
MUCOCUTANEOUS DISORDERS & PERIODONTAL PATIENTS: some brief
Autoimmune relationships: 8,10,17
Cicatricial Pemphigoid (CP) with DIF of mucosal biopsies there are IgG, C3, fibrin
deposits, & other IgG deposits in the basement membrane zone (BMZ). It is
possible that a BMZ antigen initiates a reaction of unknown stimulus triggering an
immunogenic signal in the antigen activating the B-cell immune system and the
synthesis of IgG antibodies initiating the complement activation.
Pemphigus Foliaceus (PF) by using indirect immunofluorescence (IIF) circulating
IgG autoantibodies primarily; however, IgA & IgM may also be present. Also, C3
must be present in the epithelial intercellular spaces.
Systemic Lupus Erythematosis (SLE) with DIF of the BMZ there are deposits of
IgM, IgA, IgG, C3, & fibrinogen. There is a predominance of T-cells; and, an
immunocytochemical analysis of the oral mucosa & the skin yield HLA-DR
antigen expression on keratinocytes.
Acquired Immunodeficiency Syndrome (AIDS) or (HIV): the best predictors of the
onset of AIDS are the total number of circulating CD4+ lymphocytes or CD4 count
and the level of HIV RNA in plasma (viral load). The disruption of T-lymphocytes
results in B-cell disregulation. Suppressor/ Cytotoxic CD8+ lymphocytes in HIV
infection. IgG & IgA antibody levels are increased in this disease. In 1980 AIDS
was referred to as Gay Related Immune Deficiency (GRID).
[35]
AIDS is often accompanied by a progressive decline in CD4 immune cells, which
is a marker for immune suppression. A healthy person may have a high T4 count
& a low T8 cell count; but, with AIDS the T4 count is low & the T8 count is high.
Patients with AIDS are usually deficient in iron, zinc, folic acid (B9), selenium,
pyridoxine (B6), cyanocobalamin (B12), beta- carotene (vit. A), tocopherol (vit. E),
thiamine (B1), riboflavin (B2), Pantothenic acid (B5), and ascorbic acid (vit. C).
Therefore, supplementation with these minerals and vitamins can be beneficial to
AIDS patients. Of course, this would be in conjunction with routine AIDS
treatment.
MEDIATORS of BONE RESORPTION: 18
BONE STIMULATORS BONE INHIBITORS
Interleukin-1 (IL-1) Interferon gamma (IFN)
Interleukin- 6 (IL-6) Osteoprotegerin (OPG)
Tumor Necrosing Factor (TNF) Estrogens
Parathyroid Hormone (PTH) Androgens
PTH-related Protein (PTHrP) Calcitonin (CT)
Prostaglandin E2 (PGE2) Cyclosporin
Macrophage-colony stimulating
Factor (M-CSF)
Receptor activator of NFkB (RANK)
RANK Ligand (RANKL)
1,25 dihydroxyvitamin D3 (vitamin D)
[36]
The gingival crevicular fluid (GCF) contains biochemical mediators (IL-1 ,
IL-1 , IL- 6, & TNF- ) that can show the metabolic status of the tissues of
the periodontium. These cytokines reflect the following:
1) Periodontal inflammation IL-1.
2) IL-1 levels after periodontal therapy.
3) IL-1 is synergistic with TNF- (lymphotoxin) in stimulating bone
resorption.
4) IL-1 alveolar bone loss.
5) levels of IL-1 & IL- 6 are associated with Eikenella Corrodens &
Prevotella Intermedia and continuous loss of attachment and bone.
6) IL- 6 levels are associated with continually progressing periodontitis.
7) levels of estrogen are associated with levels of bone resorbing
cytokines.
8) levels of PGE2 attachment & bone loss.
9) alkaline phosphatase (ALP) in GCF is higher than in serum.
10) collagenases (Elastase, Stromelysin, Collagenase) associated with
bone loss, inflammation, & probing depth.
11) Collagenase- 2 & Collagenase- 3 reflect peri-implant osteolysis.
12) Osteonectin (ON or SPARC) is elevated in sites with severe periodontitis
& in GCF.
[37]
13) Osteopontin (OPN) is related to probing depth & attachment loss.
14) Osteocalcin (OCN) not established in human GCF; but only in animal
experimental periodontitis.
15) Estrogen deficiency leads to accelerated bone loss.
16) Estrogen replacement therapy (ERT) gingival bleeding, & decreases
attachment loss.
17) Osteoprotegerin (OPG) can inhibit osteoclastic differentiation and
function.
18) When cells show two factors (bone morphogenetic protein- 4 [BMP-4], &
vascular endothelial growth factor [VEGF]) this causes an increase in
bone density.
19) Localized Aggressive Periodontitis (LAgP) is connected to some
functional abnormalities of neutrophils and there is severe periodontal
breakdown. These functional abnormalities are:
a) phagocytosis
b) killing of Actinobacillus Actinomycetemcomitans
c) Impaired leukotriene B4 (LTB4 ) synthesis
d) superoxide production
e) Chemotaxis
f) receptor expression
20) TNF- suppresses insulin action by its specific receptor activating
insulin resistance. [38]
21) TNF- produced by adipose tissue of obese patients is a risk factor for
periodontal inflammation, & TNF- stimulates osteoclasts to activate
bone resorption.
22) TNF stimulates lipolysis in adipocytes to release free fatty acids that may
induce insulin resistance.
23) TNF induces intracellular hydrogen peroxide, which inhibits tyrosine
phosphorylation of Insulin Receptor Substrate-1 (IRS-1).
24) TNF- vascular endothelial growth factor (VEGF) in human
Periodontal ligament (HPDL) cells angiogenesis in
Periodontitis.
25) ROXITHROMYCIN (RXM) inhibits TNF- mediated VEGF induction;
Perhaps another way to help treat periodontitis.
26) IL- 1(specific cytokine), IL- 10(a regulatory cytokine), IL- 8, &
RANTES (chemokines) is related to the development of chronic adult
periodontitis.
[39]
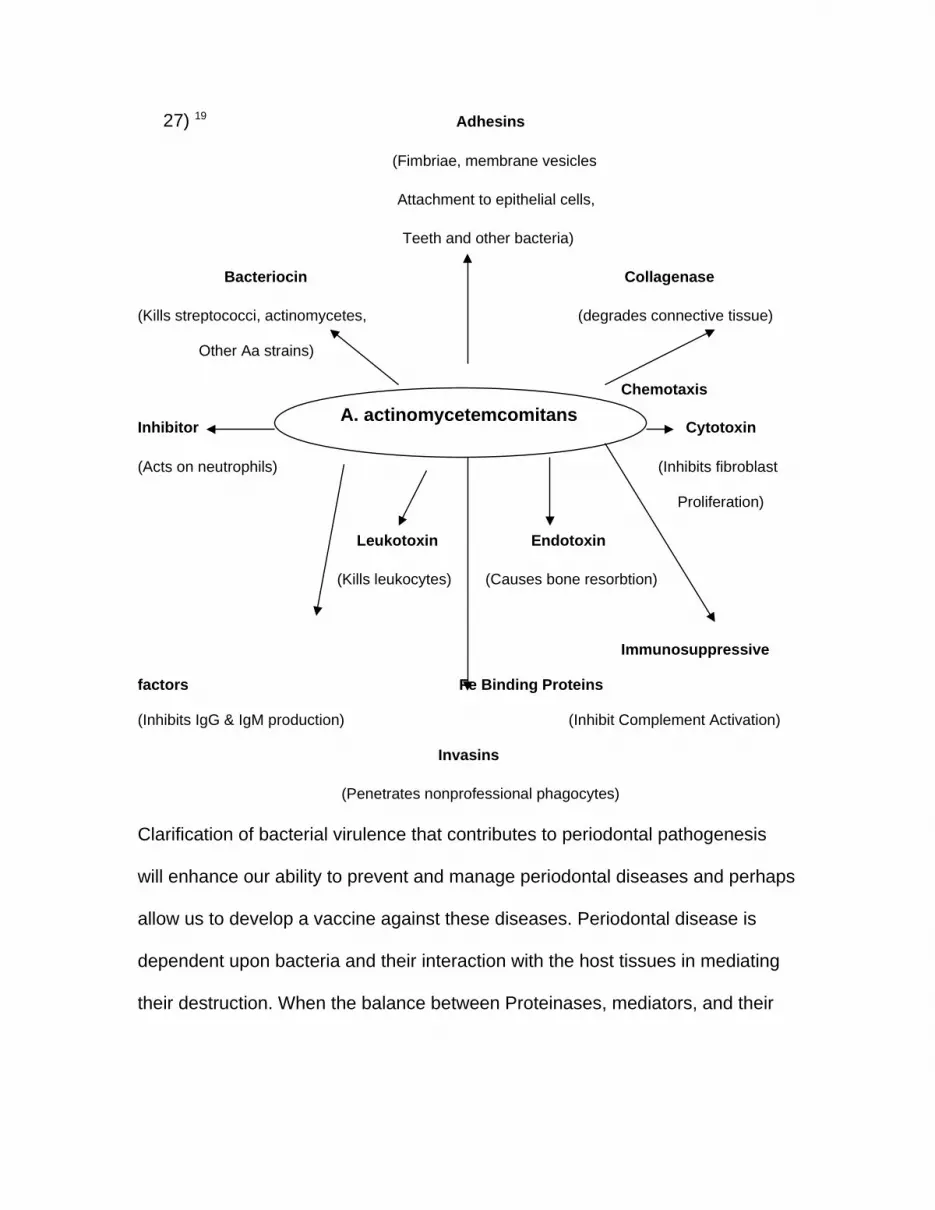
27) 19 Adhesins
(Fimbriae, membrane vesicles
Attachment to epithelial cells,
Teeth and other bacteria)
Bacteriocin Collagenase
(Kills streptococci, actinomycetes, (degrades connective tissue)
Other Aa strains)
Chemotaxis
Inhibitor A. actinomycetemcomitans Cytotoxin
(Acts on neutrophils) (Inhibits fibroblast
Proliferation)
Leukotoxin Endotoxin
(Kills leukocytes) (Causes bone resorbtion)
Immunosuppressive
factors Fe Binding Proteins
(Inhibits IgG & IgM production) (Inhibit Complement Activation)
Invasins
(Penetrates nonprofessional phagocytes)
Clarification of bacterial virulence that contributes to periodontal pathogenesis
will enhance our ability to prevent and manage periodontal diseases and perhaps
allow us to develop a vaccine against these diseases. Periodontal disease is
dependent upon bacteria and their interaction with the host tissues in mediating
their destruction. When the balance between Proteinases, mediators, and their
A. actinomycetemcomitans
[40]
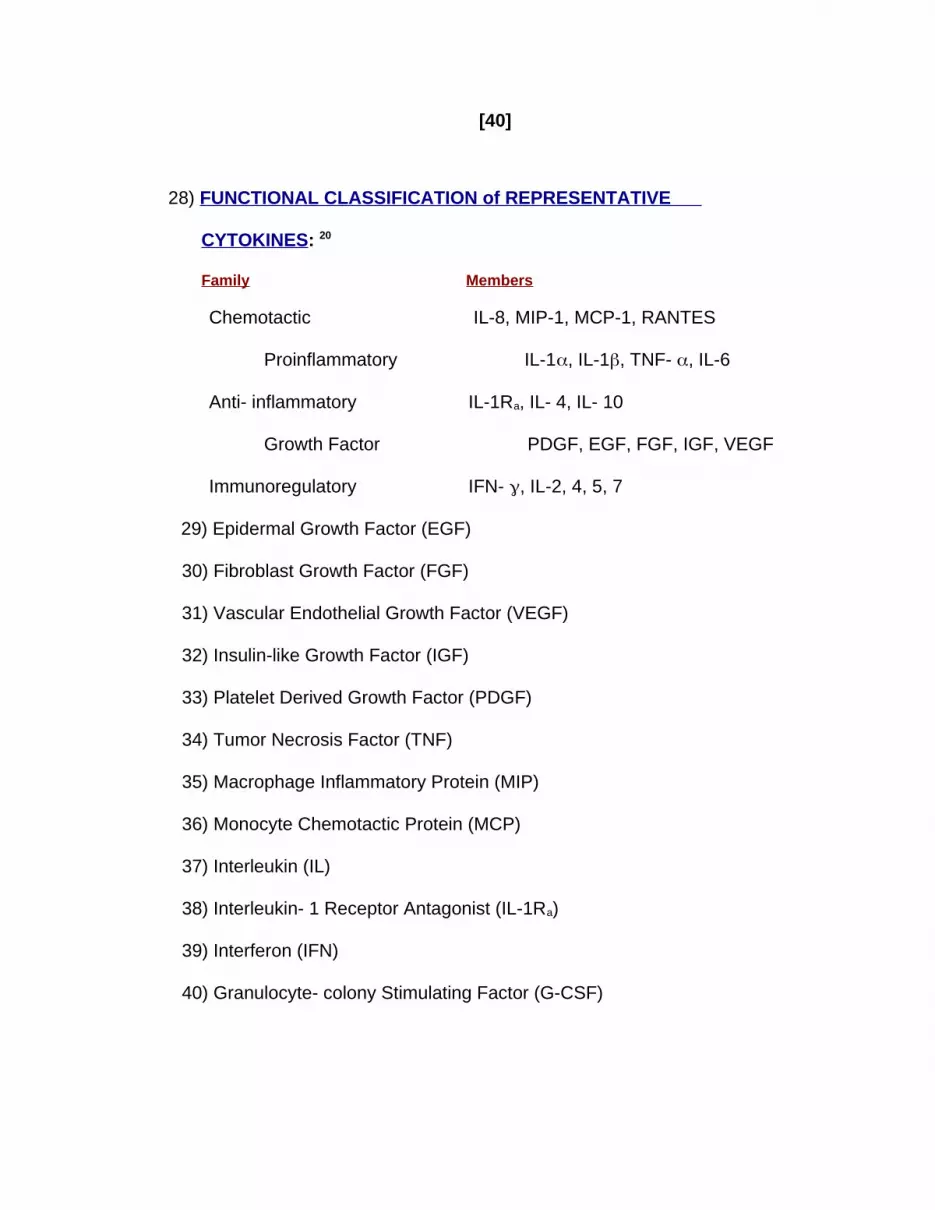
28) FUNCTIONAL CLASSIFICATION of REPRESENTATIVE
CYTOKINES: 20
Family Members
Chemotactic IL-8, MIP-1, MCP-1, RANTES
Proinflammatory IL-1, IL-1, TNF- , IL-6
Anti- inflammatory IL-1Ra, IL- 4, IL- 10
Growth Factor PDGF, EGF, FGF, IGF, VEGF
Immunoregulatory IFN- , IL-2, 4, 5, 7
29) Epidermal Growth Factor (EGF)
30) Fibroblast Growth Factor (FGF)
31) Vascular Endothelial Growth Factor (VEGF)
32) Insulin-like Growth Factor (IGF)
33) Platelet Derived Growth Factor (PDGF)
34) Tumor Necrosis Factor (TNF)
35) Macrophage Inflammatory Protein (MIP)
36) Monocyte Chemotactic Protein (MCP)
37) Interleukin (IL)
38) Interleukin- 1 Receptor Antagonist (IL-1Ra)
39) Interferon (IFN)
40) Granulocyte- colony Stimulating Factor (G-CSF)
[41]
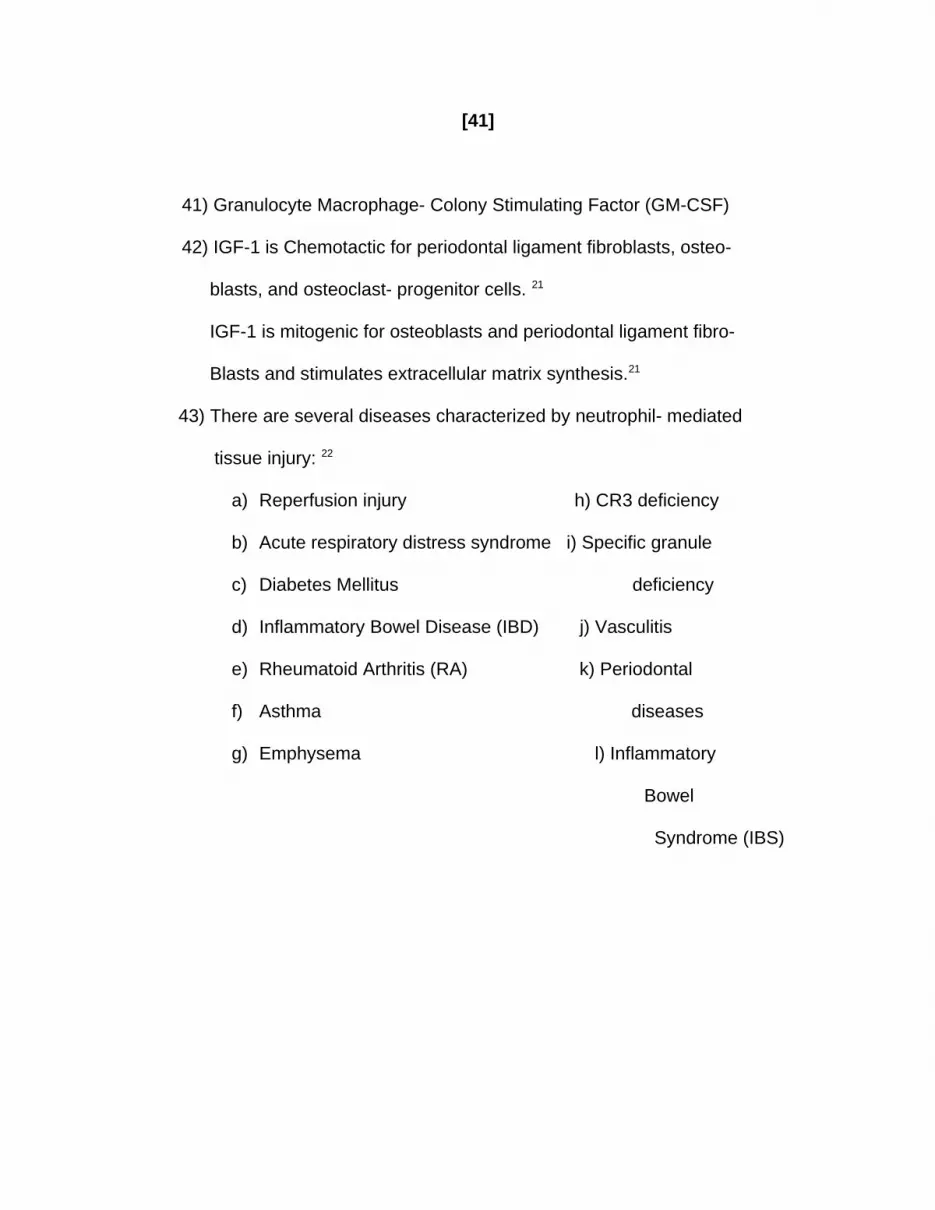
41) Granulocyte Macrophage- Colony Stimulating Factor (GM-CSF)
42) IGF-1 is Chemotactic for periodontal ligament fibroblasts, osteo-
blasts, and osteoclast- progenitor cells. 21
IGF-1 is mitogenic for osteoblasts and periodontal ligament fibro-
Blasts and stimulates extracellular matrix synthesis.21
43) There are several diseases characterized by neutrophil- mediated
tissue injury: 22
a) Reperfusion injury h) CR3 deficiency
b) Acute respiratory distress syndrome i) Specific granule
c) Diabetes Mellitus deficiency
d) Inflammatory Bowel Disease (IBD) j) Vasculitis
e) Rheumatoid Arthritis (RA) k) Periodontal
f) Asthma diseases
g) Emphysema l) Inflammatory
Bowel
Syndrome (IBS)
[42]
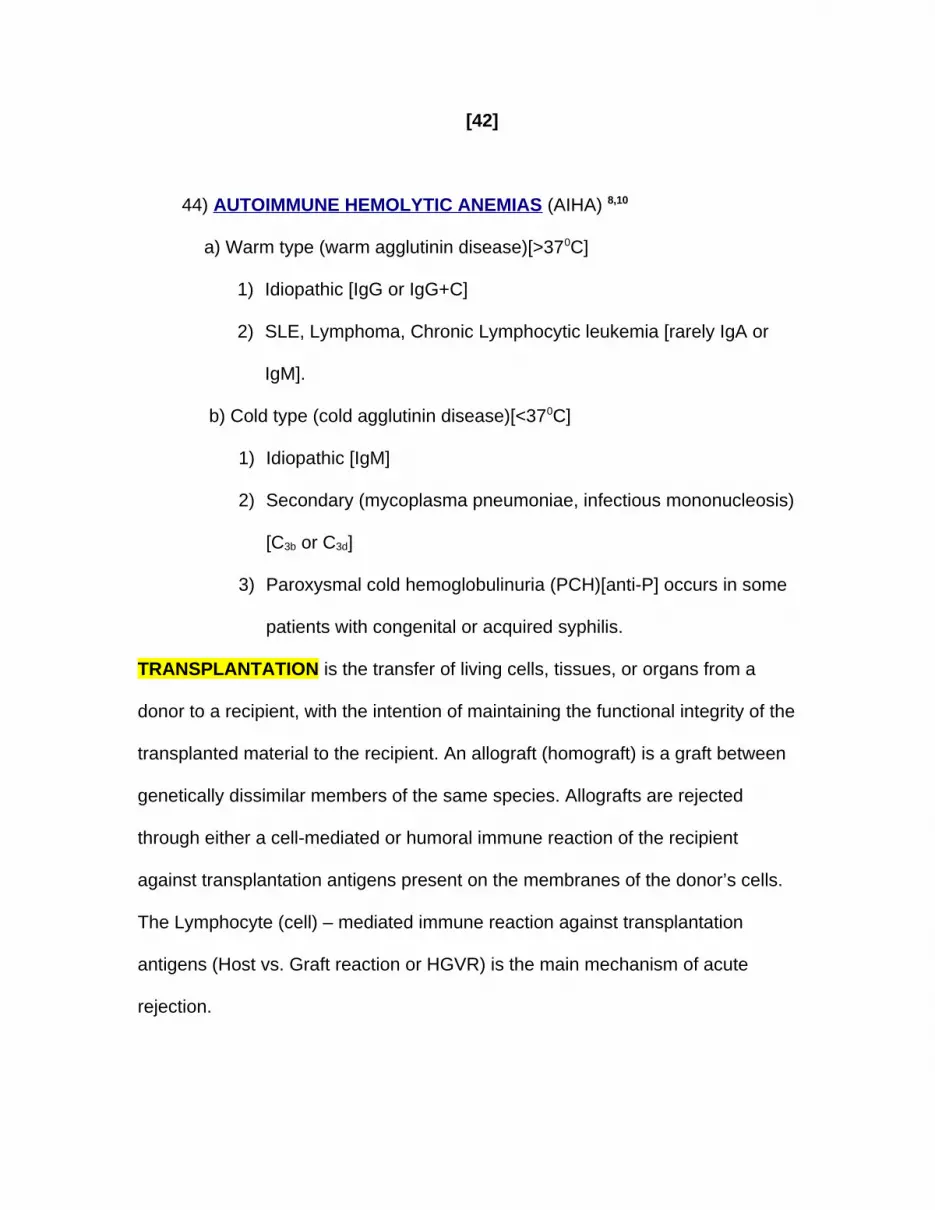
44) AUTOIMMUNE HEMOLYTIC ANEMIAS (AIHA) 8,10
a) Warm type (warm agglutinin disease)[>370C]
1) Idiopathic [IgG or IgG+C]
2) SLE, Lymphoma, Chronic Lymphocytic leukemia [rarely IgA or
IgM].
b) Cold type (cold agglutinin disease)[<370C]
1) Idiopathic [IgM]
2) Secondary (mycoplasma pneumoniae, infectious mononucleosis)
[C3b or C3d]
3) Paroxysmal cold hemoglobulinuria (PCH)[anti-P] occurs in some
patients with congenital or acquired syphilis.
TRANSPLANTATION is the transfer of living cells, tissues, or organs from a
donor to a recipient, with the intention of maintaining the functional integrity of the
transplanted material to the recipient. An allograft (homograft) is a graft between
genetically dissimilar members of the same species. Allografts are rejected
through either a cell-mediated or humoral immune reaction of the recipient
against transplantation antigens present on the membranes of the donor’s cells.
The Lymphocyte (cell) – mediated immune reaction against transplantation
antigens (Host vs. Graft reaction or HGVR) is the main mechanism of acute
rejection.
[43]
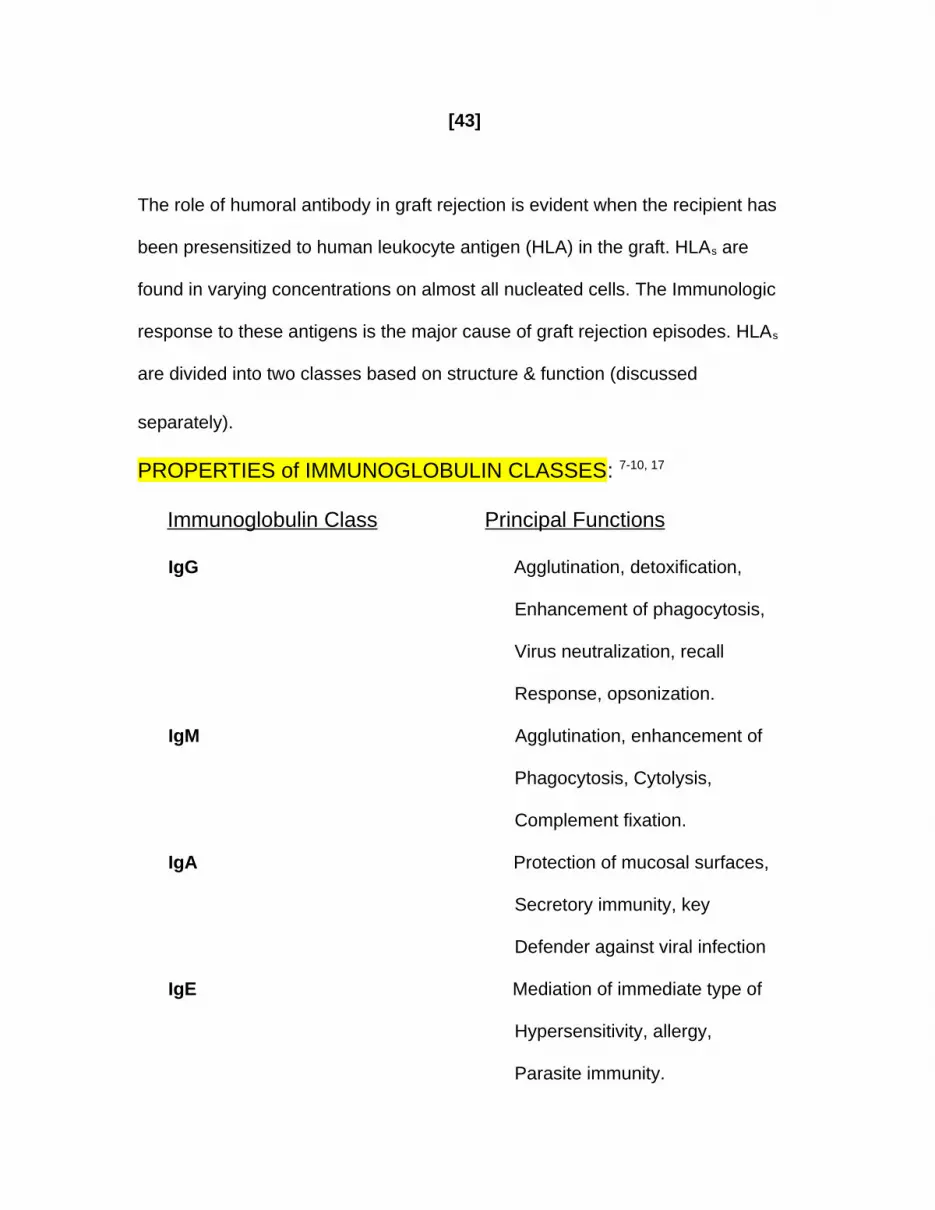
The role of humoral antibody in graft rejection is evident when the recipient has
been presensitized to human leukocyte antigen (HLA) in the graft. HLAs are
found in varying concentrations on almost all nucleated cells. The Immunologic
response to these antigens is the major cause of graft rejection episodes. HLAs
are divided into two classes based on structure & function (discussed
separately).
PROPERTIES of IMMUNOGLOBULIN CLASSES: 7-10, 17
Immunoglobulin Class Principal Functions
IgG Agglutination, detoxification,
Enhancement of phagocytosis,
Virus neutralization, recall
Response, opsonization.
IgM Agglutination, enhancement of
Phagocytosis, Cytolysis,
Complement fixation.
IgA Protection of mucosal surfaces,
Secretory immunity, key
Defender against viral infection
IgE Mediation of immediate type of
Hypersensitivity, allergy,
Parasite immunity.
[44]
IgD Control of lymphocytic activa-
Tion and suppression.
INFECTIONS in PATIENTS with IMPAIRED CELL- MEDIATED IMMUNITY: 8-
10, 17
Bacteria: Viruses:
Listeria Monocytogenes Herpes Simplex
Nocardia Varicella- zoster
Mycobacterium Tuberculosis Cytomegalovirus
Nontuberculosis Mycobacteria
Legionella Pneumophila
Fungi: Protozoa:
Histoplasma Cryptosporidium species
Coccidioides Toxoplasma gondii
Cryptococcus Pneumocystis carinii
Candida
Aspergillus
Zygomycetes
IMMUNOSUPPRESSIVE DRUGS:
Prednisolone (IV) [a Corticosteroid] {a glucocorticoids}.
Azathiopine (an antimetabolite) [orally or IV].
Cyclophosphamide (an alkylating agent) is used when the patient is not tolerating
Azathriopine.
[45]
Cyclosporine [CsA] (a fungal metabolite) [spares the bone marrow & acts to
inhibit T- cell proliferation & activation].
Tacrolimus (used for liver transplant patients). When substituted for CsA in cases
of gingival overgrowth (GE) there is a reduction in GE.
Antilymphocyte globulin (ALG) [used as an adjunct in chemotherapy].
Antithymocyte globulin (ATG) [used as an adjunct in chemotherapy].
Monoclonal antibodies {MOAB} (the murine monoclonal antibody – OKT3- can
reverse rejection by binding to T- cell antigen- receptor complex [TCR/CD3].
Irradiation is of limited use in transplantation.
C- REACTIVE PROTEIN, IL- 6, & Neutrophils if elevated in humans are
considered to be indicators as risk factors for cardiovascular diseases.
PORPHYROMONAS GINGIVALIS if elevated in humans is also
considered to be an indicator for cardiovascular diseases (CVDs). P.Gingivalis is
also known to activate human gingival epithelial cells, spleen cells, and
peripheral blood monocytes the release of IL-1, IL- 6, IL- 8, & TNF- .
TNF- produced by the adipose tissue of obese patients is a risk factor
for periodontal inflammation; and, TNF- produced due to periodontal
inflammation may influence insulin sensitivity in both obese and type 2 diabetic
patients.
[46]
HUMAN GINGIVAL FIBROBLASTS (HGF) can be targets for TNF- & IL-
1 I in periodontal diseases. An important effect of IL-1 and TNF- is to
stimulate fibroblasts production of metalloproteinase (MMP) & stromelysin
(MMP- 3), which degrade components of the extracellular matrix in rheumatoid
arthritis & periodontitis. Both TNF- & IL- 1 induce bone resorption. Excess IL-
6 is produced in chronic periodontitis. Anti-
cytokine therapy can reduce inflammation, but the immune system is also
downregulated the risk of bacterial infections. Is the cure worth the
hardships? Only when we can control both (inflammation & the chance for
bacterial infection)!
GINGIPAINS 23 are trypsin- like cysteineproteinases produced by Porphyromonas
Gingivalis (P. Gingivalis) that is a major contributor to periodontitis. Gingipains
degrade macrophage CD14 and inhibit activation of leukocytes through
lipopolysaccharide (LPS) receptors sustaining the colonization of P. Gingivalis. 24
There are three Gingipains (HRgpA, RgpB, & Kgp) that have received the bulk of
the current research. A vaccination may be beneficial in treating periodontitis.
[47]
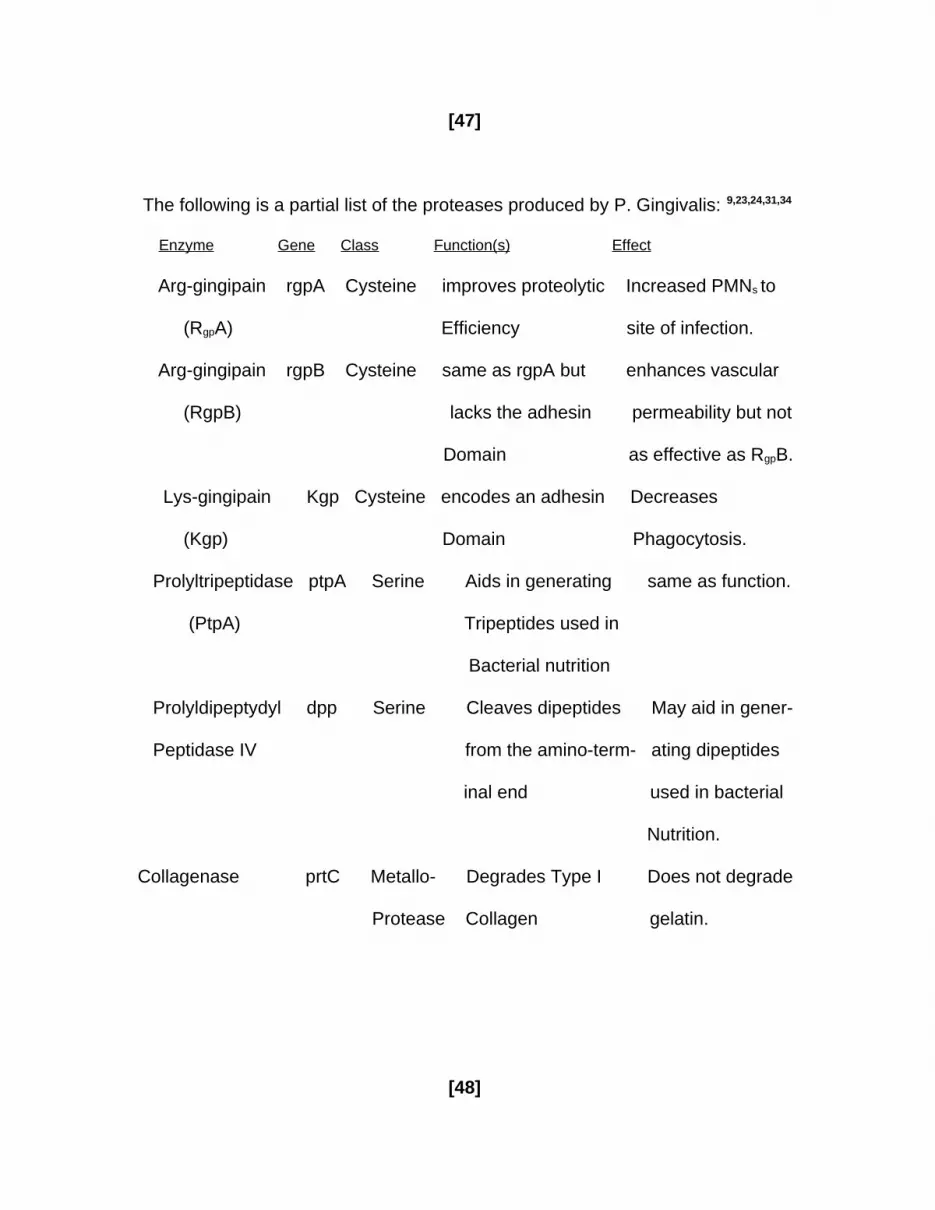
The following is a partial list of the proteases produced by P. Gingivalis: 9,23,24,31,34
Enzyme Gene Class Function(s) Effect
Arg-gingipain rgpA Cysteine improves proteolytic Increased PMNs to
(RgpA) Efficiency site of infection.
Arg-gingipain rgpB Cysteine same as rgpA but enhances vascular
(RgpB) lacks the adhesin permeability but not
Domain as effective as RgpB.
Lys-gingipain Kgp Cysteine encodes an adhesin Decreases
(Kgp) Domain Phagocytosis.
Prolyltripeptidase ptpA Serine Aids in generating same as function.
(PtpA) Tripeptides used in
Bacterial nutrition
Prolyldipeptydyl dpp Serine Cleaves dipeptides May aid in gener-
Peptidase IV from the amino-term- ating dipeptides
inal end used in bacterial
Nutrition.
Collagenase prtC Metallo- Degrades Type I Does not degrade
Protease Collagen gelatin.
[48]
Other Conditions Associated with Immunologic Defects:
1) Linear IgA Disease with DIF shows linear deposits of IgA at the epithelial-
connective tissue junction.
2) Discoid Lupus Erythematosis (DLE) with DIF shows positive, granular-
linear basement membrane (BM) deposits of Ig.
3) Systemic Lupus Erythematosis (SLE) with DIF shows the same as DLE.
4) Lichen Planus shows no immunoglobulins, complements (coarse granular
deposits, & usually fibrinogen.
5) Benign Lymphoepithelial Lesion (Mikulicz’s Disease) has excess T-helper
cells that stimulate B- cell antibody activity.
6) Macroglobulinemia shows IgM deposits. A malignant plasma cell
dyscrasia of B cells that normally synthesize & secrete IgM.
Treatment is with plasmaphoresis, alkylating agents (chlorambucil),
Melphalan or Cyclophosphamide, Prednisone, Fludarabine, &/or 2-
chlorodeoxyadenosine may be used.
7) Multiple Myeloma shows IgG, IgA, light-chains (Bence – Jones protein)
only, IgD & IgE are non-secretory. Treatment is with alkylating agents,
prednisone, & local radiation.
8) Nonhereditary Primary Systemic Amyloidosis shows light-chains (Bence –
Jones protein) only, but on occasion intact immunoglobulin molecules
(IgG, IgA, IgD, IgM).
[49]
9) Heavy Chain Malignant Plasma Cell Dyscrasias may show:
a) IgG heavy- chain () disease (elderly patients). Treatment
With alkylating drugs (vincristine), corticosteroids, and x-rays.
b) IgA heavy- chain () disease (Middle East children). Treatment
is with broad- spectrum antibiotics, Corticosteroids, and Cytotoxic
drugs.
c) IgM heavy- chain () disease (chronic lymphocytic leukemia).
Treatment is symptomatic. Almost as rare as IgD form.
d) IgD heavy- chain () disease (rare). Treatment is symptomatic.
Currently only 2 cases have been confirmed through 1998.
10) Minor Apthous Ulcers shows a defect in their cell- mediated
response. T4 helper/inducer lymphocytes are seen in early stages.
Basal cells express HLA-DR antigens. These are associated with
Crohn’s Disease.
11) Major Aphthous Ulcers (Periadenitis Mucosa Necrotica Recurrens or
PMNR) shows the same Immunologic responses as in cases of Minor
Aphthous Ulcers except that the lesions may appear for 6 weeks rather
than 7- 10 days.
12) Herpetiform Aphthous Ulcers shows T4 lymphocytes and
eventually more T8 lymphocytes than T4 lymphocytes. Macrophages
and Mast cells are common at the ulcer base. Healing occurs in 1- 2
weeks.
[50]
13) Becket’s Syndrome is an immune dysfunction accompanied by
vasculitis. Human Leukocyte Antigen (HLA- B51) is frequently present.
SALIVARY GLAND DISEASES:
1) Mikulicz’s Disease or Benign Lymphoepithelial Lesion may be unilateral
or bilateral in appearance with both dry mouth and dry eyes. T- helper
cells are in excess & stimulate B- cell antibody activity.
2) Sialadenitis is benign, painful, & swelling occurs involving one or more of
the salivary glands.
3) Sjogren’s Syndrome primarily affects women age 40 & is an
Immunologic disorder abnormal dryness of the mouth, eyes, & other
mucous membranes.
4) Immunologically CD4 & T- cells are abundant along with some
B-cells. (See Pg 17 for additional information).
5) Xerostomia (or Dry Mouth) is caused by cessation of normal salivary
secretion. This is a symptom of many diseases (diabetes, hysteria, acute
infections, Sjogren’s Syndrome, paralysis of the facial nerves, & adverse drug
reactions to antihistamines, antidepressants, antihypertensives, neuroleptics, and
parasympatholytics). Medications beneficial to relieving dry mouth are
Pilocarpine, Cevimeline, & Crystalline Maltose. Chewing gum has a tendency to
improve salivary flow.
6) Sialolithiasis is accompanied by swelling that increases at mealtime
or when eating a pickle. Located primarily in the floor of the mouth. Stone
formation either single or multiple are formed in these glands. [51]
SALIVARY IgA (Secretory immunoglobulin A or SIgA) is an antibody produced by
the body and found in all bodily secretions in the mucous membranes, lining the
intestines, in the bronchi, in saliva, and in tears. By combining with a protein in
the mucosa it defends body surfaces against invading microorganisms. The
synthesis of SIgA depends on locally activated CD4+ T cells. A deficiency in CD4+
T cells causes abnormalities in mucosal immune function including secretory
immunity. SIgA phagocytosis, and level of experimental clinical gingivitis.
SIgA inhibits the adherence of microorganisms to epithelial cells decreasing
mucosal infections. Patients with high levels of salivary IgA reactive with bacteria
in dental plaque may show a slower development of clinical experimental
gingivitis .25 Salivary IgA inhibits the adherence of microorganisms on epithelial
cells preventing mucosal infections 26. CD8 lymphocytosis syndrome (DILS) is a
subset of HIV disease; while, in Sjogren’s syndrome there is a predominance of
CD4 cells 27. In Necrotizing Ulcerative Periodontitis (NUP) there is an increase in
specific IgA output 28.
ENZYMES PRODUCED by PERIODONTAL MICROORGANISMS: 9
These enzymes appear to degrade almost all host tissues and intercellular matrix
molecules 29-34. (Modified April 2003 by Weinmann, SB).
Bacterial Enzyme Species Tissues Degraded
1) Collagenase P. Gingivalis Monocytes, PMNs function,
A. Actinomycetemcomitans neutrophil collagenase
MMP-8, bone resorption,
Depolymerizes collagen
Fibers. [52]
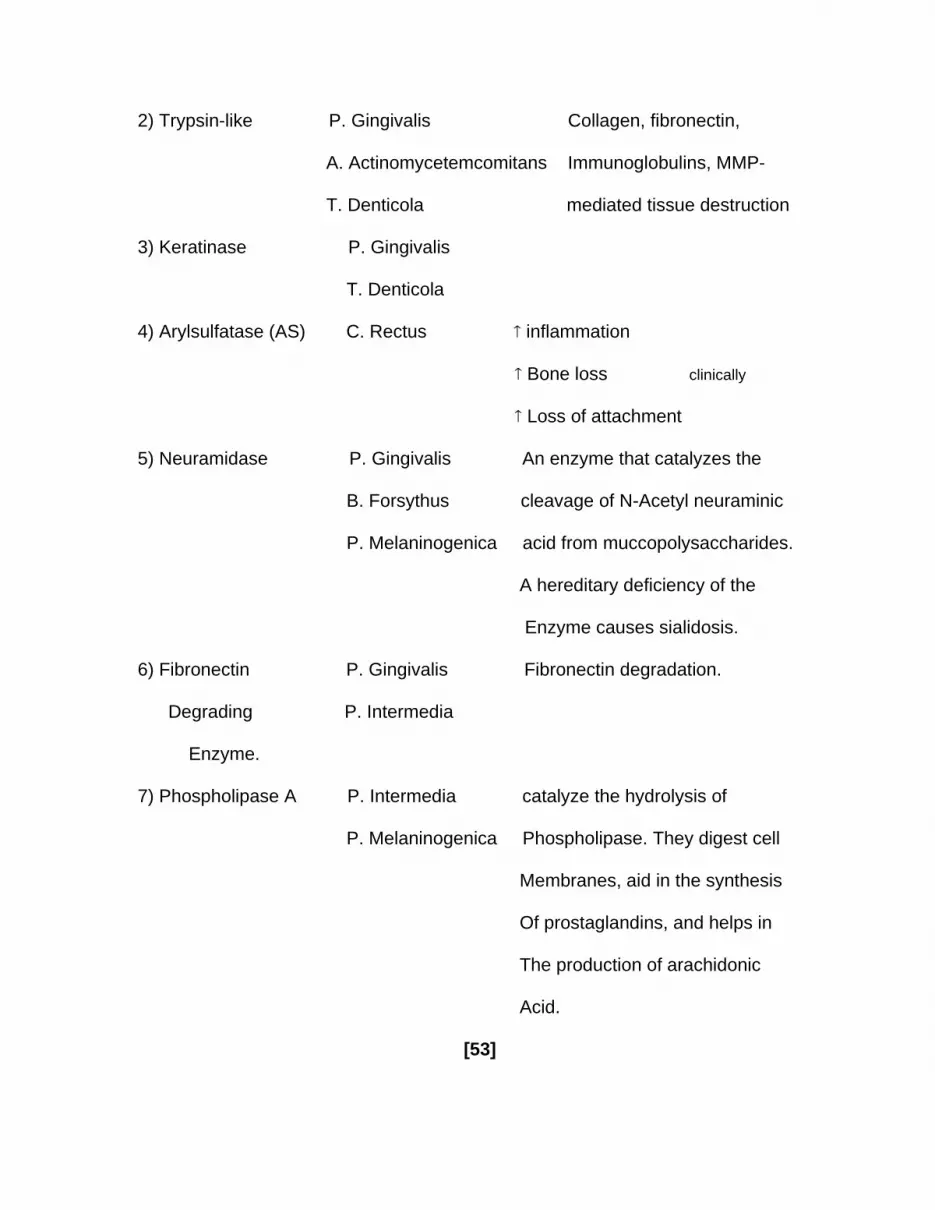
2) Trypsin-like P. Gingivalis Collagen, fibronectin,
A. Actinomycetemcomitans Immunoglobulins, MMP-
T. Denticola mediated tissue destruction
3) Keratinase P. Gingivalis
T. Denticola
4) Arylsulfatase (AS) C. Rectus inflammation
Bone loss clinically
Loss of attachment
5) Neuramidase P. Gingivalis An enzyme that catalyzes the
B. Forsythus cleavage of N-Acetyl neuraminic
P. Melaninogenica acid from muccopolysaccharides.
A hereditary deficiency of the
Enzyme causes sialidosis.
6) Fibronectin P. Gingivalis Fibronectin degradation.
Degrading P. Intermedia
Enzyme.
7) Phospholipase A P. Intermedia catalyze the hydrolysis of
P. Melaninogenica Phospholipase. They digest cell
Membranes, aid in the synthesis
Of prostaglandins, and helps in
The production of arachidonic
Acid.
[53]

Clarification of bacterial virulence that contributes to periodontal pathogenesis
will enhance our ability to prevent and manage periodontal diseases and perhaps
allow us to develop a vaccine against these diseases. Periodontal disease is
dependent upon bacteria and their interaction with the host tissues in mediating
their destruction. When the balance between Proteinases, mediators, and their
inhibitors (produced by host tissue cells) occurs net loss of tissue (active
periodontal disease) is the predominant result.
[56]

METABOLIC INTERACTIONS from BACTERIAL SPECIES found in DENTAL
PLAQUE may be schematically illustrated showing the intricate
interrelationship as follows: 9, 36-39
Streptococcus p-amino benzoate Streptococcus mutans
Actinomyces
CO2 Capnocytophaga
Lactate NH4+
Veillonella H2
Formate
Menadione Fusobacterium
Campylobacter
Protoheme Treponema
Succinate
Isobutyrate
Porphyromonas Gingivalis
Prevotella intermedia
Hemin -Globulin
Host [57]
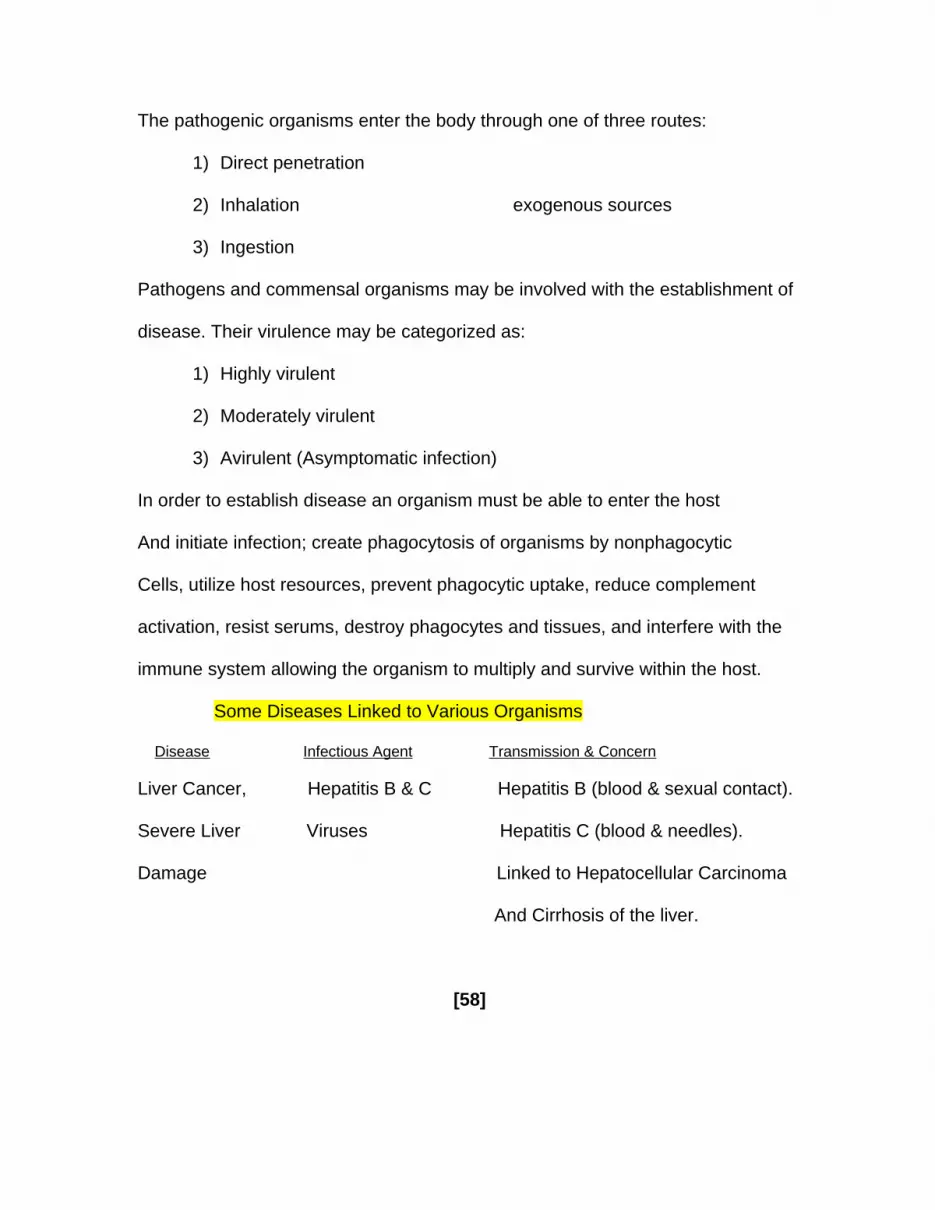
The pathogenic organisms enter the body through one of three routes:
1) Direct penetration
2) Inhalation exogenous sources
3) Ingestion
Pathogens and commensal organisms may be involved with the establishment of
disease. Their virulence may be categorized as:
1) Highly virulent
2) Moderately virulent
3) Avirulent (Asymptomatic infection)
In order to establish disease an organism must be able to enter the host
And initiate infection; create phagocytosis of organisms by nonphagocytic
Cells, utilize host resources, prevent phagocytic uptake, reduce complement
activation, resist serums, destroy phagocytes and tissues, and interfere with the
immune system allowing the organism to multiply and survive within the host.
Some Diseases Linked to Various Organisms
Disease Infectious Agent Transmission & Concern
Liver Cancer, Hepatitis B & C Hepatitis B (blood & sexual contact).
Severe Liver Viruses Hepatitis C (blood & needles).
Damage Linked to Hepatocellular Carcinoma
And Cirrhosis of the liver.
[58]

Some Diseases Linked to Various Organisms—cont.
Disease Infectious Agent Transmission & Concern
Ulcers, Stomach Helicobacter Pyloris 90% of peptic ulcer cases are
Cancer related to H. Pylori and Gastric
Cancer, but complete under-
Standing of H. Pylori’s spreading.
Heart Disease, Periodontitis Periodontal pathogens inhabit the
Premature Babies, mouth & transmitted via the saliva.
Stroke Risk factor for heart disease and
Premature birth.
Anal Cancer Sexually Transmitted Direct sexual contact during anal,
Diseases vaginal, and oral sex—primary
HPV.
Cervical Cancer Human Papilloma Direct sexual contact with an
Virus infected carrier.
Adult T-cell Human T-cell HTLV-1 can be transmitted thru
Leukemia Lymphotrophic blood, sexual contact, and mother
Virus to child. Common in Japan and
The Carribean.
Heart attacks, Chlamydia, Chlamydia spreads like a cold.
Clogged arteries Pneumoniae, There is a possible link to heart
Cytomegalovirus attacks & Atherosclerosis.
[59]
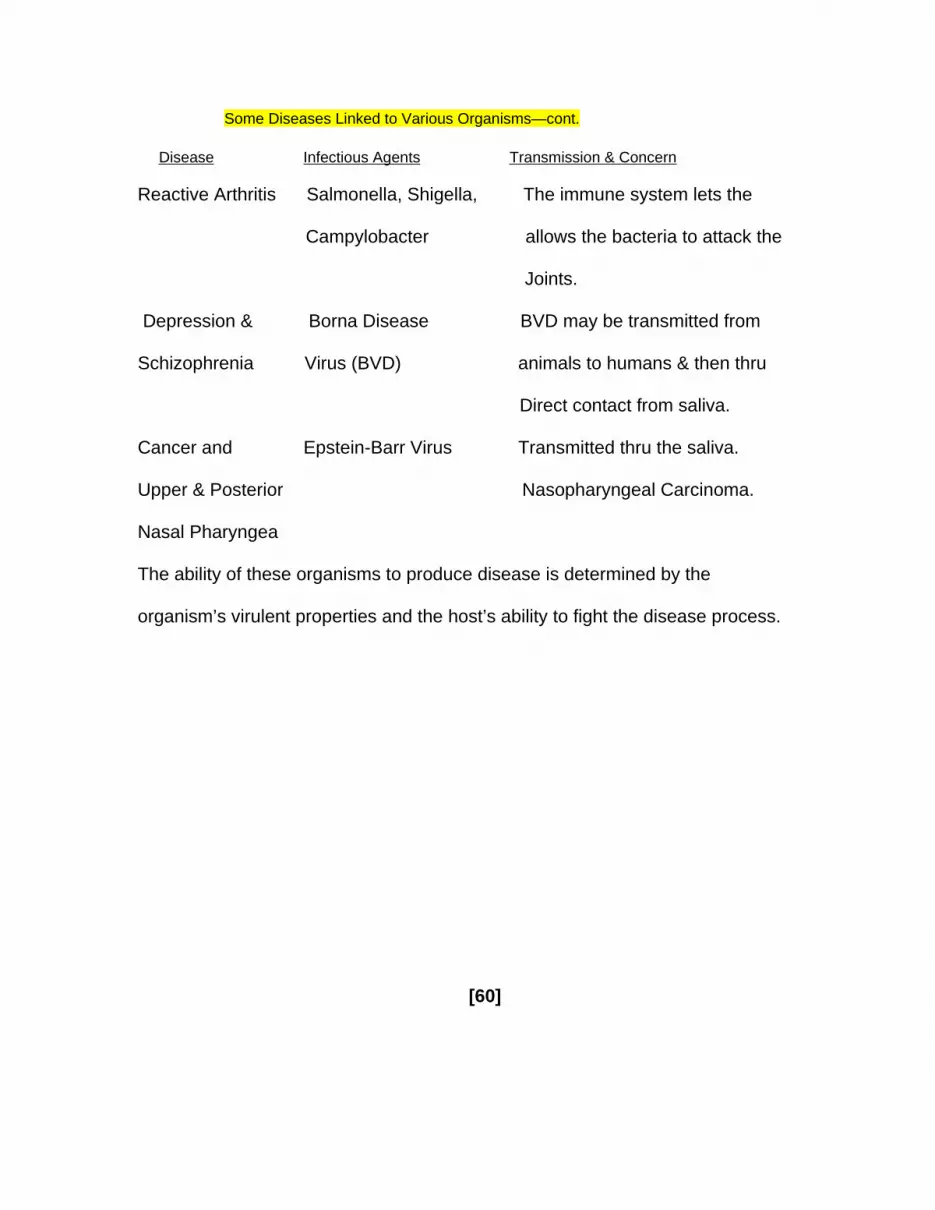
Some Diseases Linked to Various Organisms—cont.
Disease Infectious Agents Transmission & Concern
Reactive Arthritis Salmonella, Shigella, The immune system lets the
Campylobacter allows the bacteria to attack the
Joints.
Depression & Borna Disease BVD may be transmitted from
Schizophrenia Virus (BVD) animals to humans & then thru
Direct contact from saliva.
Cancer and Epstein-Barr Virus Transmitted thru the saliva.
Upper & Posterior Nasopharyngeal Carcinoma.
Nasal Pharyngea
The ability of these organisms to produce disease is determined by the
organism’s virulent properties and the host’s ability to fight the disease process.
[60]
REFERENCES
1) Greenstein G; Lamster IB: Bacterial Transmission in Periodontal
Diseases: A Critical Review. Jnl Periodontol 68(5): 421-431, 1997.
2) Von Steenbergen TJM; Petit MDA; et al: Transmission of Porphyromonas
Gingivalis between spouses. Jnl Clin Periodontol 20: 340-345, 1993.
3) Preus HR; Zambon JJ; et al: The distribution and Transmission of
Actinobacillus Actinomycetemcomitans in families with established adult
Periodontitis. Jnl Periodontol 65: 2-7, 1994.
4) Saarela M; von Troil-Linden B; et al: Transmission of oral bacterial
Species between spouses. Oral Microbiol Immunol 8: 349-353, 1993.
5) Clark WB; Loe H: Mechanisms of Initiation and progression of periodontal
Disease. Periodontology 2000. 2: 72-82, 1993.
6) International Conference on Research in The Biology of Periodontal
Disease. Pp 195-210, June 12-15, 1977.
7) Fedi PF Jr: The Periodontic Syllabus. 2nd Ed. Lea & Febiger, 1989.
8) The Merck Manual of Diagnosis and Therapy. Merck Research
Laboratories. 17th Ed, 1999.
9) Newman MG; Takei HH; Carranza FA (Eds): Carranza’s Clinical
Periodontology. 9th Ed. WB Saunders Company, 2002.
10) Andreolli TE; Bennett JC; Carpenter CCJ; Plum F; Smith LH Jr (Eds): Cecil
Essentials of Medicine. 3rd Ed. WB Saunders Company, 1993.
[61]
11) Petit MDA; von Steenbergen TJM; et al: Prevalence of periodontitis and
Suspected periodontal pathogens in families of adult periodontitis patients.
Jnl Clin Periodontol 21: 76-85, 1994.
12) Selye H: The Mast Cells. Butterworths, 1965.
13) Holroyd S: Wynn RL: Clinical Pharmacology in dental practice. 3rd Ed. CV
Mosby Company, 1983.
14) Thorlacius H; Raud J; et al: Mast cell activation induces P-selectin-
Dependent leukocyte rolling and adhesion in post-capillary venules in vivo.
Bichem Biophys Res Commun 203: 1043, 1994.
15) Malanuya, B; Ikeda T; et al: Mast cell modulation of neutrophil influx and
Bacterial clearance at sites of infection through TNF-alpha. Nature 381: 77,
1996.
16) Gaboury JP; Johnston B; et al: Mechanism underlying acute mast cell-
Induced leukocyte rolling and adhesion in vivo. Jnl Immunol 154: 804,
1995.
17) Regezi JA; Sciubba J: Oral Pathology Clinical-pathologic Correlations.
2nd Ed. WB Saunders Company, 1993.
18) McCauley LK; Nohutcu RM: Mediators of periodontal osseous destruction
And Remodeling: Principles and Implications for Diagnosis and Therapy.
Jnl Periodontol 73(11): 1377-1391, 2002.
[62]
19) Nishimura F; Iwamoto Y; et al: Periodontal disease and Diabetes Mellitus:
The role of Tumor Necrosis Factor- in a 2-way relationship. Jnl
Periodontol 74 (1): 97-102, 2003.
20) Takashiba S;Naruishi K; et al: Perspective of cytokine regulation for
Periodontal treatment: Fibroblast biology. Jnl Periodontol 74 (1): 103-
110, 2003.
21) Oringer RJ: Biological Mediators for Periodontal and Bone Regeneration.
The Compendium 23(6): 501-516, 2002.
22) Kantarci A; Oyaizu K; Van Dyke TE: Neutrophil-mediated tissue injury in
Periodontal Disease Pathogenesis: Findings from Localized Aggressive
Periodontitis. Jnl Periodontol 74(1): 66-75, 2003. Modified slightly by
Weinmann, SB; April 2003.
23) Travis J; Banbula A; Potempa J: The role of bacterial and host Proteinases
In Periodontal Disease. In: Langer J; Ansorge S (Eds): Cellular Peptidases
In Immune Functions and Diseases. 2. New York, Kluwer Academic/
Plenum, 2000.
24) Sugawara S; Nemoto E; et al: Proteolysis of Human Monocyte CD14 by
Cysteine Proteinases (gingipains) from P. Gingivalis leading to
Lippopolysaccharide hyporesponsiveness. Jnl Immunol 165: 411, 2000.
[63]
25) Schenck K; Popplesdorf D; et al: Salivary IgA antibodies reactive with
Bacteria from dental plaque are associated with susceptibility to
Experimental Gingivitis. Jnl Clin Periodontol 20: 411-417, 1993.
26) Challacombe SJ: Immunologic aspects of oral candidiasis. Oral Surg Oral
Med Oral Pathol 78: 205-210, 1994.
27) Mandel L: Salivary glands-HIV disease. Salivary gland center (SGC)
Newsletter, April 2002.
28) Myint MM; Steinsvoll S; et al: Salivary IgA responses to bacteria in dental
Plaque as related to periodontal and HIV infection status. Eur Jnl Oral Sci
105: 562-570, 1997.
29) Ding Y; Uitto VJ; et al: Membrane components of Treponema denticola
Trigger proteinase release from human polymorphonuclear leukocytes.
Jnl Dent Res 75: 1986, 1996.
30) Curtis MA; Kuramitsu HK; et al: Molecular genetics and nomenclature of
Proteases of Porphyromonas Gingivalis. Jnl Periodontal Res 34: 464,1999.
31) Kuramitsu HK: Proteases of Porphyromonas Gingivalis: What don’t they
do? Oral Microbiol Immunol 13: 263, 1998.
32) Lamster IB; Celenti R; Ebersole JL: The relationship of serum IgG antibody
Titers to periodontal pathogens to indicators of the host response to
Crevicular fluid. Jnl Clin Periodontol 17: 419-425, 1990.
[64]
33) Oshrain RL; Lamster IB; et al: Arylsulfatase activity in human gingival
Crevicular fluid. Arch Oral Biol 29: 399-402, 198
34) Banbula A; Mak P; et al: Prolyl tripeptidyl peptidase from polyphormonas
Gingivalis – A novel enzyme with possible pathological implications for the
Development of periodontitis. Jnl Biol Chem 274: 9246, 1999.
35) Fives-Taylor P; Meyer D; Mintz K: Virulence factors of the periodontopath-
ogen Actinobacillus Actinomycetemcomitans. Jnl Periodontol 67: 291-
297, 1996.
36) Carlsson J: Microbiology of plaque associated periodontal disease. In:
Lindhe J (Ed): Textbook of Clinical Periodontology, ed 1. Munksgaard
International Publishing, 1983.
37) Grenier D: Nutritional interaction between two suspected
Periodontopathogens, Treponema denticola and Porphyromonas
Gingivalis. Infect Immun 60: 5298, 1992.
38) Loesche WJ: Importance of nutrition in gingival crevice microbial ecology.
Periodontics 6: 245, 1968.
39) Walden WC; Hentges DJ: Differential effects of oxygen and oxidation-
Reduction potential on the multiplication of three species of anaerobic
Intestinal bacteria. Applied Microbiol 30: 781, 1975.
[65]