pectoralis major rupture in athletes: footprint technique and results
TRANSCRIPT
Editorial Manager(tm) for Techniques in Shoulder and Elbow Surgery Manuscript Draft Manuscript Number: Title: Pectoralis major rupture in athletes; Footprint technique and results. Article Type: Technique Keywords: Pectoralis major rupture, Surgical technique, Suture Anchors, Double row, Results, Athletes, Foot print Corresponding Author: Mr L Funk, FRCS (T&O), FFSEM (UK) Corresponding Author's Institution: Wrightington Hospital First Author: NH Shah, MSc, FRCS (T&O) Order of Authors: NH Shah, MSc, FRCS (T&O); R Badge , MRCS; S Talwalkar , FRCS (T&O); L Funk, FRCS (T&O), FFSEM (UK) Manuscript Region of Origin: UNITED KINGDOM Abstract: Over a two year period, ten male athletes underwent repair of the pectoralis major tendon using a double row surgical technique employing three bone anchors to produce a foot print repair of the pectoralis major tendon. The mean patient age was 33.9 years (23-46 years). The mean time between surgery and the original injury was 11.6 weeks (1- 48 weeks). Outcome measures included patient satisfaction, bench press strength, pain and cosmesis. The average follow up was 20.3 months (12-39). Eight patients had pain prior to surgery and all patients were not satisfied with the appearance of their chest. The average loss of bench press strength was 75% preoperatively. At the final follow up, none of the patients complained of any pain while one patient reported mild pain. Nine were satisfied with the appearance. The average improvement in bench press strength was 90%. One patient developed a deep infection requiring a further washout and antibiotics. No re-rupture was seen amongst any of our patients. There was no difference in outcomes between the early and late repairs in all the criteria. In conclusion, satisfactory results can be achieved with a suture-anchor footprint repair technique of the pectoralis major strength athletes with return to previous sports and strength.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
1
TITLE
Pectoralis major rupture in athletes; Footprint technique and results.
AUTHORS
Shah NH; MSc, FRCS (T&O), Upper Limb Fellow
Badge R; MRCS, Clinical Research Fellow
Talwalkar S; FRCS (T&O), Upper Limb Fellow
Funk L; FRCS (T&O), FFSEM (UK), Consultant Shoulder & Upper Limb Surgeon
INSTITUTION
Upper Limb Unit, Wrightington Hospital
Hall Lane, Appley Bridge, Lancashire, England, WN6 9EP
CORRESPONDING ADDRESS
Lennard Funk, 120 Princess Road, Manchester, M15 5AT, UK
Tel: +44 161 227 0027
Email: [email protected]
SHORT TITLE
Footprint technique for pectoralis major repair
DISCLOSURE OF FUNDING AND CONFLICT OF INTEREST
We declare no conflict of interest neither we received any funding from any organization.
Manuscript (All Manuscript Text Pages, including Title Page, References and Figure Legends)

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
2
ABSTRACT
Over a two year period, ten male athletes underwent repair of the pectoralis major tendon
using a double row surgical technique employing three bone anchors to produce a foot
print repair of the pectoralis major tendon.
The mean patient age was 33.9 years (23-46 years). The mean time between surgery and
the original injury was 11.6 weeks (1- 48 weeks). Outcome measures included patient
satisfaction, bench press strength, pain and cosmesis. The average follow up was 20.3
months (12-39).
Eight patients had pain prior to surgery and all patients were not satisfied with the
appearance of their chest. The average loss of bench press strength was 75%
preoperatively. At the final follow up, none of the patients complained of any pain while
one patient reported mild pain. Nine were satisfied with the appearance. The average
improvement in bench press strength was 90%. One patient developed a deep infection
requiring a further washout and antibiotics. No re-rupture was seen amongst any of our
patients. There was no difference in outcomes between the early and late repairs in all the
criteria.
In conclusion, satisfactory results can be achieved with a suture-anchor footprint repair
technique of the pectoralis major strength athletes with return to previous sports and
strength.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
3
INTRODUCTION
Muscle injury may vary from minor strains to a complete disruption of fibres. These
injuries involve different locations within the musculotendinous unit; including the site of
origin, within the muscle belly itself, at the musculotendinous junction and complete
tendinous avulsion from the bone. Tendon avulsion from the bony insertion usually
occurs when a maximally contracted muscle is subjected to an overwhelming force [1].
Injury to the pectoralis major muscle is usually caused by a sudden forceful overload of
the maximally contracted muscle, which usually involves the application of an
overwhelming extension force to the maximally contracted pectoralis major muscle.
Hence, this eccentric contraction of the muscle with the arm in the adducted and extended
position leads to a complete avulsion from the bone [2, 3].
Rupture of the pectoralis major is a relatively uncommon injury first being reported in
1822 [4]. Since then more than 200 cases have been reported in literature so far, however
most of these cases have been described in the last 25 years due to the increasing
popularity and involvement in competitive sports. The most common mechanism of
injury tends to be weight lifting [2]. Most of these injuries occurred in men during their
third and fourth decades [3]. The single most common mechanism for pectoralis major
rupture has been the bench press exercise [5, 6, 7, 8].
There are many published repair techniques including bony tunnels [2, 6, 8, 9, 10, 11,
12], pull out wires [13], staples [14], cancellous screw [15] and suture anchors [3, 11, 16,
17]. All have had satisfactory results.We used a new double row surgical technique using

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
4
three bone anchors to produce a large foot print of the pectoralis major tendon on the
humeral shaft. Here, we present the result of our new surgical technique for the repair of
the pectoralis tendon rupture in strength athletes.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
5
MATERIAL AND METHODS
Between June 2005 and September 2007, senior author (LF) performed surgical repair of
the distal end of the pectoralis major tendon in ten male athletes. Six patients had seen
other surgeons previously and had been advised non-operative treatment. One had had an
exploration and attempted repair before presenting to us.
Patients were assessed subjectively for pain, appearance and strength. We used the same
outcome criteria as previously described [2]. Appearance of the chest was assessed by a
visual analogue scale ranging from 0 (completely unsatisfied with the appearance of the
chest in the mirror) to 10 (complete satisfaction with the appearance of the chest). Pain
was also measured on a visual analogue scale ranging from 0 (no pain) to 10 (severe
pain). Shoulder strength was determined by asking the patients to estimate the percentage
of normal shoulder strength which they had prior to injury.
We used the Tietjen classification [18] for the management of the pectoralis major tears.
All patients had type 3-D (complete tears at the tendon level), which was confirmed intra-
operatively. Diagnosis was made with history and clinical examination. Magnetic
resonance imaging (MRI) scans were obtained for five of the patients, but the diagnosis
was predominantly a clinical diagnosis and therefore not required.
Operative Details
Surgery was performed under general anaesthetic with an interscalene block and
additional local anaesthesia for the axillary incision. Patients were placed in a supine
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
6
position with their arm on a short arm table. After preparing the whole upper limb and
ipsilateral anterior chest wall, isolation draping was performed to allow the free
movement of the arm and full exposure of the affected anterior chest wall. In some cases
the opposite chest wall was also prepared and exposed to ensure good cosmetic symmetry
post-repair.
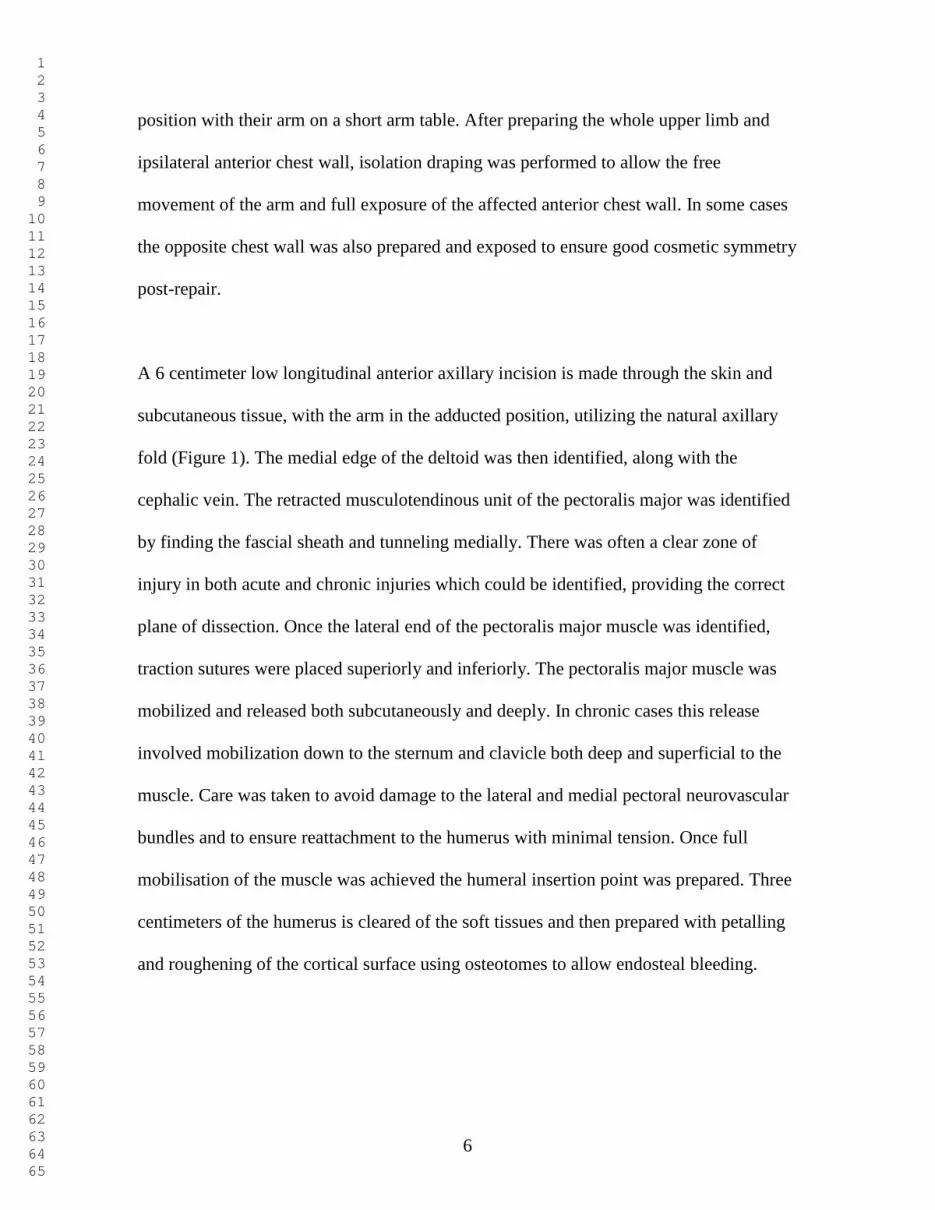
A 6 centimeter low longitudinal anterior axillary incision is made through the skin and
subcutaneous tissue, with the arm in the adducted position, utilizing the natural axillary
fold (Figure 1). The medial edge of the deltoid was then identified, along with the
cephalic vein. The retracted musculotendinous unit of the pectoralis major was identified
by finding the fascial sheath and tunneling medially. There was often a clear zone of
injury in both acute and chronic injuries which could be identified, providing the correct
plane of dissection. Once the lateral end of the pectoralis major muscle was identified,
traction sutures were placed superiorly and inferiorly. The pectoralis major muscle was
mobilized and released both subcutaneously and deeply. In chronic cases this release
involved mobilization down to the sternum and clavicle both deep and superficial to the
muscle. Care was taken to avoid damage to the lateral and medial pectoral neurovascular
bundles and to ensure reattachment to the humerus with minimal tension. Once full
mobilisation of the muscle was achieved the humeral insertion point was prepared. Three
centimeters of the humerus is cleared of the soft tissues and then prepared with petalling
and roughening of the cortical surface using osteotomes to allow endosteal bleeding.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
7
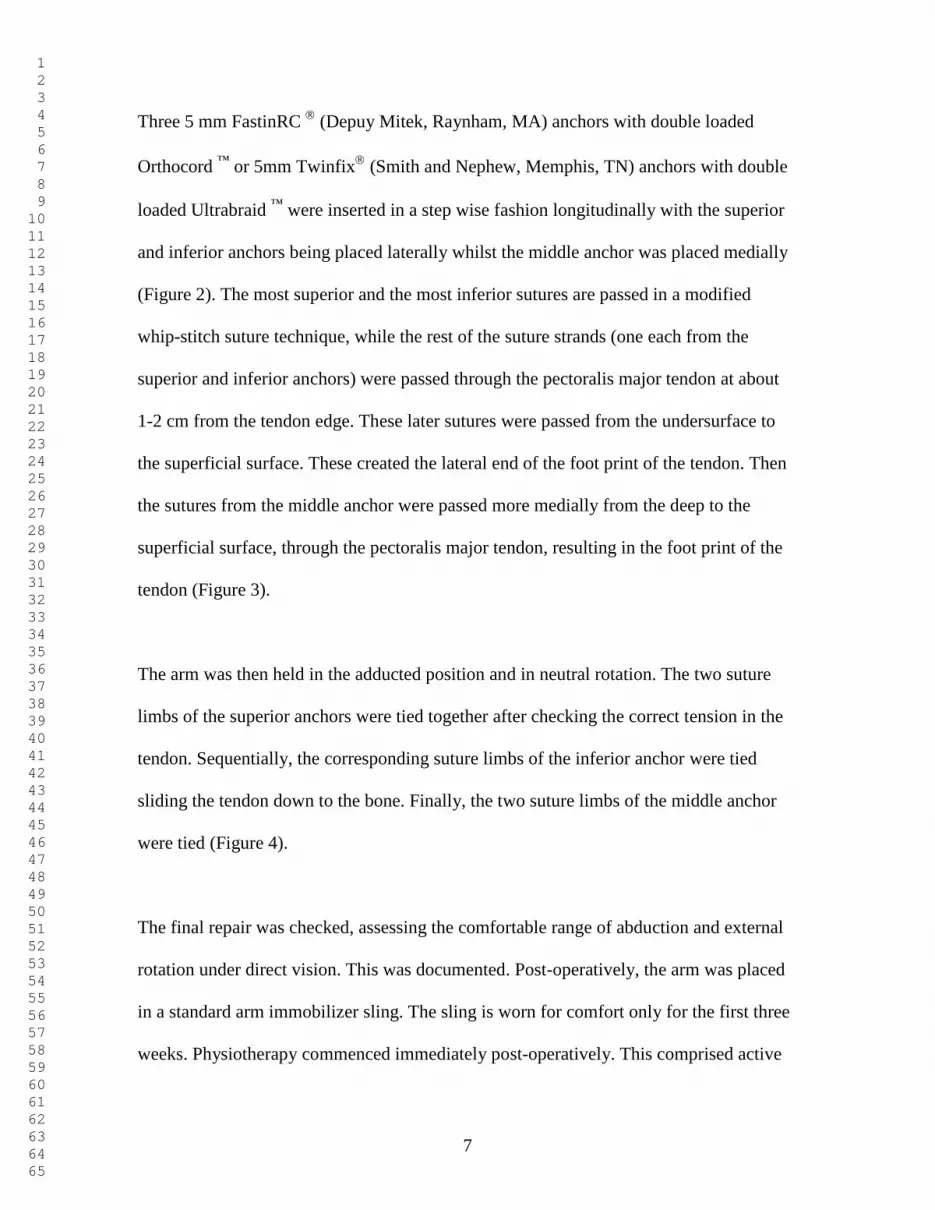
Three 5 mm FastinRC
(Depuy Mitek, Raynham, MA) anchors with double loaded
Orthocord ™
or 5mm Twinfix
(Smith and Nephew, Memphis, TN) anchors with double
loaded Ultrabraid ™
were inserted in a step wise fashion longitudinally with the superior
and inferior anchors being placed laterally whilst the middle anchor was placed medially
(Figure 2). The most superior and the most inferior sutures are passed in a modified
whip-stitch suture technique, while the rest of the suture strands (one each from the
superior and inferior anchors) were passed through the pectoralis major tendon at about
1-2 cm from the tendon edge. These later sutures were passed from the undersurface to
the superficial surface. These created the lateral end of the foot print of the tendon. Then
the sutures from the middle anchor were passed more medially from the deep to the
superficial surface, through the pectoralis major tendon, resulting in the foot print of the
tendon (Figure 3).
The arm was then held in the adducted position and in neutral rotation. The two suture
limbs of the superior anchors were tied together after checking the correct tension in the
tendon. Sequentially, the corresponding suture limbs of the inferior anchor were tied
sliding the tendon down to the bone. Finally, the two suture limbs of the middle anchor
were tied (Figure 4).
The final repair was checked, assessing the comfortable range of abduction and external
rotation under direct vision. This was documented. Post-operatively, the arm was placed
in a standard arm immobilizer sling. The sling is worn for comfort only for the first three
weeks. Physiotherapy commenced immediately post-operatively. This comprised active

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
8
assisted mobilisation within the safe zone (as dictated by the range post-repair and patient
tolerance) under the direct supervision of a physiotherapist. During this time forced
external rotation, abduction and resisted adduction of the shoulder was not performed.
The sling was weaned by three weeks. After three weeks, active movements were
introduced and were progressed to increase the range of movement in all directions, as
tolerated by the patient and under strict supervision. Exercises which combined
isometrics, closed chain exercises, proprioceptive and core stability exercises were an
essential part of the rehabilitation from early post-operatively, using the senior author’s
guidelines [19]. Sports specific props were encouraged early in the regimen. This
progressed to open chain exercises from approximately three to six weeks and then light
active resistance activities.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
9
RESULTS
All ten patients were male athletes with a mean age of 33.9 years (23-46 years). The
average follow up was 20.3 months (12-39). The mean time between surgery and original
injury was 11.6 weeks (1- 48 weeks). Four patients claimed that they were using anabolic
steroids. None of the patients were lost in follow-up. Five patients had incurred the injury
on the dominant side while another five patients sustained the injury on the non-dominant
side. Mean time between injury and surgery was 11.6 weeks (1- 48 weeks). Details of the
sports involved and the mechanism of injury are presented in table 1 & 2. One patient had
previously undergone an exploration and attempted repair a few months prior to
presentation to us.
Pain
Pre-operatively two patients complained of severe pain, five reported moderate pain and
one experienced mild pain while another two did not complain of pain either at rest or
with activity. After the surgical repair and at their last follow up, nine patients did not
complain of any pain while one patient experienced mild pain on moving their arm across
the body. None of the patients reported any pain on pushing weights away from the body.
Appearance
Pre-operatively all ten patients were unsatisfied with the cosmetic appearance of their
chest. Two patients were totally unsatisfied. Average pre-operative score was 4.1 for the
appearance (0-7 range). However, after the surgical repair eight patients were completely
satisfied with the appearance of their chest (Figure 5 & 6); one patient was unsatisfied

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
10
while one patient was moderately satisfied. Average post op score was 6.8 (1-10 range), a
40% improvement.
Strength
Prior to the surgical repair, average loss of strength was 75% (range 50-100%). However,
after the repair average post-op strength was 90% of normal for that patient.
Re-ruptures
No clinical re-ruptures were seen at their final follow up visit. Four of the patients had
follow-up magnetic resonance imaging (MRI) scans. One patient had a scan report that
was equivocal, but clinically appeared intact.
There was no difference in outcomes between the early and late repairs in all the criteria.
Complications
One patient, who had undergone previous exploration and repair of the pectoralis major
tendon, developed a deep wound infection which required a wound washout and a course
of antibiotics. He made a full recovery.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
11
DISCUSSION
After a pectoralis major tendon rupture some patients, especially the elderly or those with
low physical demands, are able to return to normal activities of daily living without
surgical repair. However strength athletes require full pectoralis major muscle strength
and bodybuilders require pectoralis major symmetry to continue their pre-injury sports.
Non-operative treatment has been shown to lead to a significant loss of strength of
adduction especially active people. Previous studies have shown that patients who have
had their pectoralis major muscle repaired have less pain, experience a subjective and
objective improvement in strength, and are happier with their outcome when compared
with similar patients who have not had a repair [2, 20, 21, 22, 23].
A meta-analysis by Bak et al [21] on pectoralis major muscle injuries revealed that 88%
of patients had excellent or good results after surgical repair compared with 27% for
patients treated non-operatively. Hanna et al [20] reported a series of 22 pectoralis major
ruptures, of which 10 underwent surgical repair while 12 were treated non-operatively.
They concluded that patients who had surgical repair had a better functional outcome as
99% strength recovery was seen among patients who had surgical repair while 56 %
strength recovery was seen among patients who had non-operative treatment. Petilon et al
[3] recommended surgical repair for all complete distal tears to regain full strength and
function and also to reduce cosmetic deformity. Kakwani et al [17] reported good to
excellent results in 92% patients after surgical treatment in their series of 13 athletes with
a complete pectoralis major rupture.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
12
All previous studies have used bone sutures or single row anchor techniques. Double row
techniques and very strong suture anchor and suture technology has led to much stronger
fixations in rotator cuff repairs. We have therefore adapted this for pectoralis major
repairs thus allowing more confidence in a faster rehabilitation and return to sports and
activities.
Our results are comparable to others and demonstrate that the surgical technique that we
have used in athletes is safe, reliable and can produce high patient satisfaction
accompanied with excellent pain relief and cosmetic results. The complication rate in our
study was low and we had no re- ruptures at a 20 month review.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
13
REFERENCES
1. D'Alessandro DF, Shields CL Jr, Tibone JE et al. Repair of distal biceps tendon
ruptures in athletes. Am J Sports Med. 1993; 21(1):114-9.
2. Schepsis AA, Grafe MW, Jones HP et al. Rupture of the pectoralis major muscle.
Outcome after repair of acute and chronic injuries. Am J Sports Med. 2000;
28(1):9-15.
3. Petilon J, Carr DR, Sekiya JK et al. Pectoralis major muscle injuries: evaluation
and management. J Am Acad Orthop Surg. 2005; 13(1):59-68.
4. Patissier P. Traite des Maladies des Artisans. Paris. 1882; 162–165.
5. Jones M, Matthews J. Rupture of pectoralis major in weight lifters: a case report
and review of the literature. Injury.1988; 19(3):219.
6. Kretzler HH Jr, Richardson AB. Rupture of the pectoralis major muscle. Am J
Sports Med. 1989; 17(4): 453–458.
7. Purnell R. Ruptur of pectoralis major muscle: a complication. Injury.
1988;19(4):284
8. Wolfe SW, Wickiewicz TL, Cavanaugh JT. Ruptures of the pectoralis major
muscle: An anatomic and clinical analysis. Am J Sports Med. 1992; 20(5): 587–
593.
9. Stein BES, Potter HG, Wickiewicz TL. Repair of chronic pectoralis major
ruptures. Tech Shoulder & Elbow Surg.2002; 3(3):174-179.
10. Orava S, Sorasto A, Aalto K et al. Total rupture of pectoralis major muscle in
athletes. Int J Sports Med. 1984; 5(5):272-4.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
14
11. Aärimaa V, Rantanen J, Heikkilä J et al. Rupture of the pectoralis major muscle.
Am J Sports Med. 2004; 32(5):1256-62.
12. Park JY, Espiniella JL. Rupture of pectoralis major muscle. A case report and
review of literature. J Bone Joint Surg Am. 1970; 52(3):577-81.
13. McEntire JE, Hess WE, Coleman SS. Rupture of the pectoralis major muscle. A
report of eleven injuries and review of fifty six. J Bone Joint Surg Am. 1972;
54(5):1040-6.
14. Egan T, Hall H. Avulsion of the pectoralis major tendon in a weight lifter: repair
using a barbed staple. Can J Surg.1987; 30(6):434-435.
15. Quinlan JF, Molloy M, Hurson BJ. Pectoralis major tendon ruptures: when to
operate. Br J Sports Med. 2002; 36(3):226-8.
16. Miller MD, Johnson DL, Fu FH et al. Rupture of the pectoralis major muscle in a
collegiate football player. Use of magnetic resonance imaging in early diagnosis.
Am J Sports Med. 1993; 21(3):475-7.
17. Kakwani RG, Matthews JJ, Kumar KM et al. Rupture of the pectoralis major
muscle: surgical treatment in athletes. Int Orthop. 2007; 31(2):159-63.
18. Tietjen R. Closed injuries of pectoralis major muscle. J Trauma. 1980; 20(3):262-
264.
19. Funk L, Tatlow K, Leftley C et al. Shoulderdoc Shoulder Exercise Book.
Published by Shoulderdoc Ltd. 2008. ISBN: 978-0-9561396-0-3
20. Hanna CM, Glenny AB, Stanley SN et al. Pectoralis major tears: Comparison of
surgical and conservative treatment. Br J Sports Med. 2001; 35(3):202-206.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
15
21. Bak K, Cameron EA, Henderson IJ. Rupture of the pectoralis major: A
metaanalysis of 112 cases. Knee Surg Sports Traumatol Arthrosc. 2000;
8(2):113-119.
22. Rijnberg WJ, van Linge B. Rupture of the pectoralis major muscle in body-
builders. Arch Orthop Trauma Surg. 1993; 112(2):104-5.
23. Pavlik A, Csépai D, Berkes I. Surgical treatment of pectoralis major rupture in
athletes. Knee Surg Sports Traumatol Arthrosc. 1998; 6(2):129-33.

1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65
16
FIGURE LEGENDS
Fig 1. Low longitudinal anterior axillary incision
Fig 2. Three anchors placed in a step wise longitudinal pattern lateral to biceps
Fig 3. Sutures passed 1-2 cm from the edge of the tendon
Fig 4. Final position after suture tying
Fig 5. Final appearance
Fig 6. Final appearance

1
TABLE 1
Sports Number of patients
Body builder 4
Weight lifter 2
Professional rugby league player 2
Martial arts 1
Climber 1
TABLE 2
Mechanism of injury Number of patients
Bench press 5
Dumbbell flies 2
Fall 2
Direct impact 1
Table (NO Excel Files! Submit as MS Word)

Fig 1. Low longitudinal anterior axillary
incision
Figure (TIF or EPS files. 300 ppi Images or 1200 ppi Line-Art)

Fig 2. Three anchors placed in a step
wise longitudinal pattern lateral to
biceps
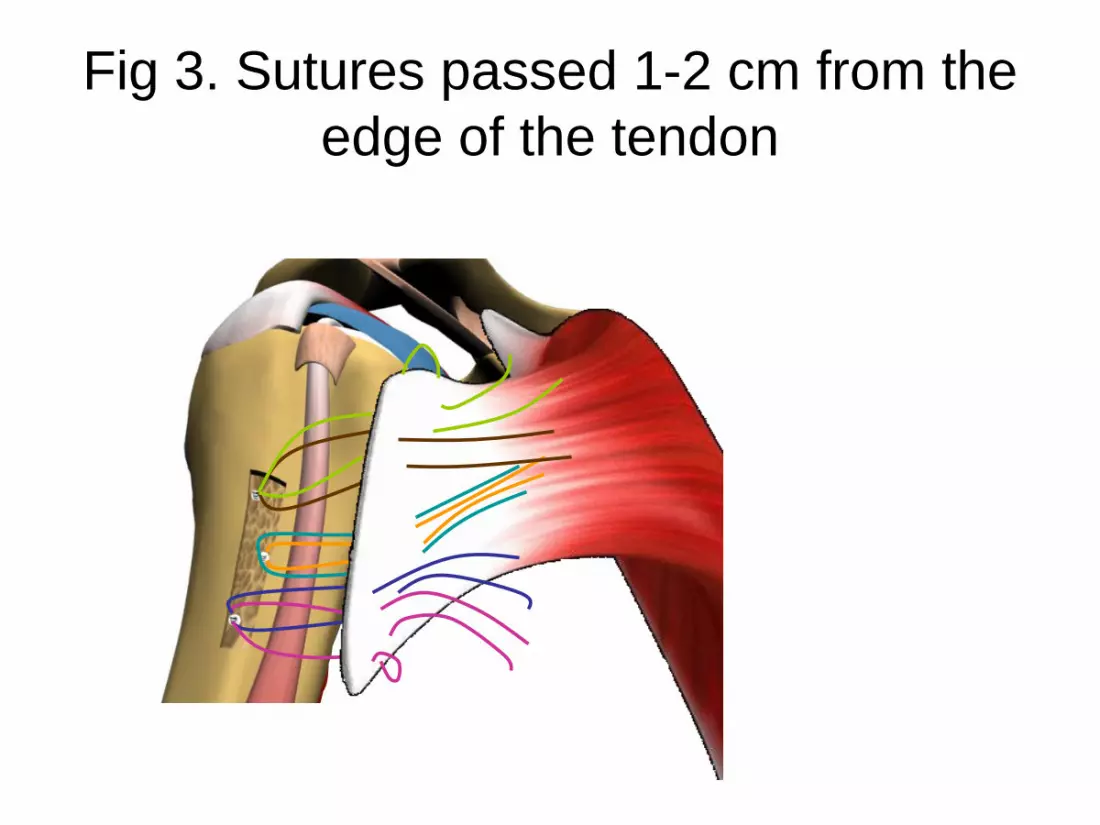
Fig 3. Sutures passed 1-2 cm from the
edge of the tendon
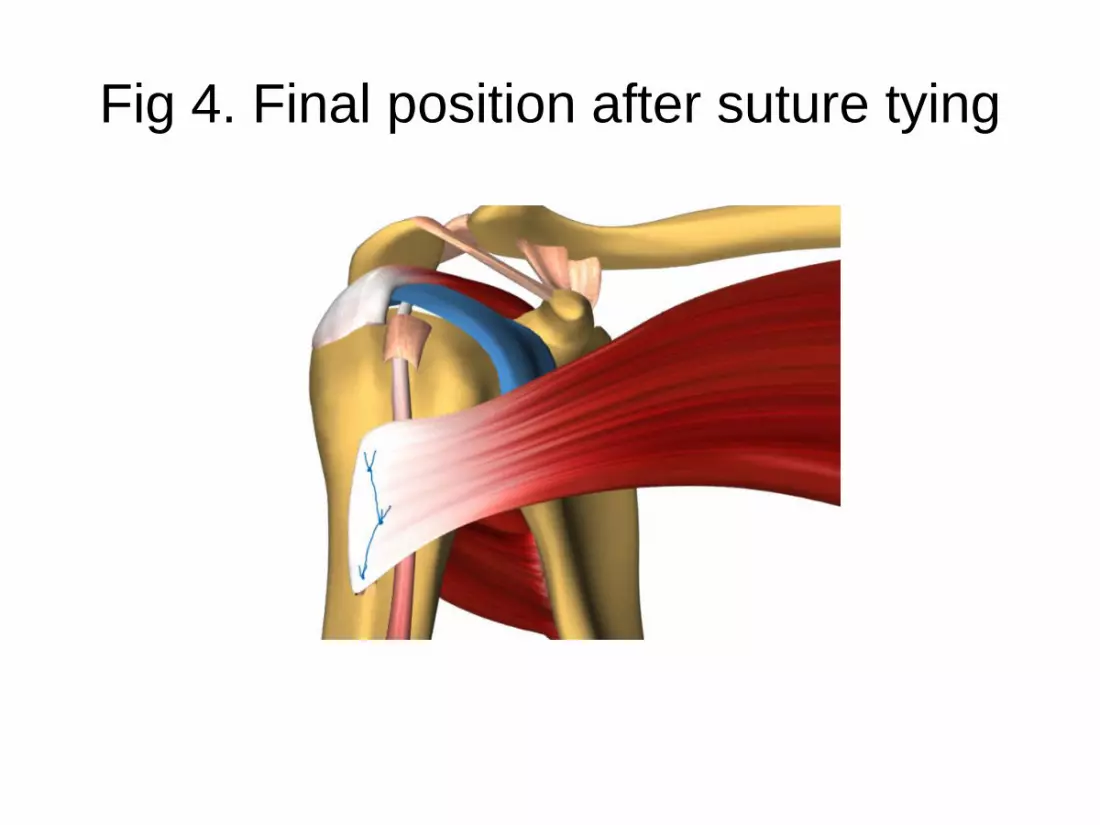
Fig 4. Final position after suture tying

Fig 5. Final appearance
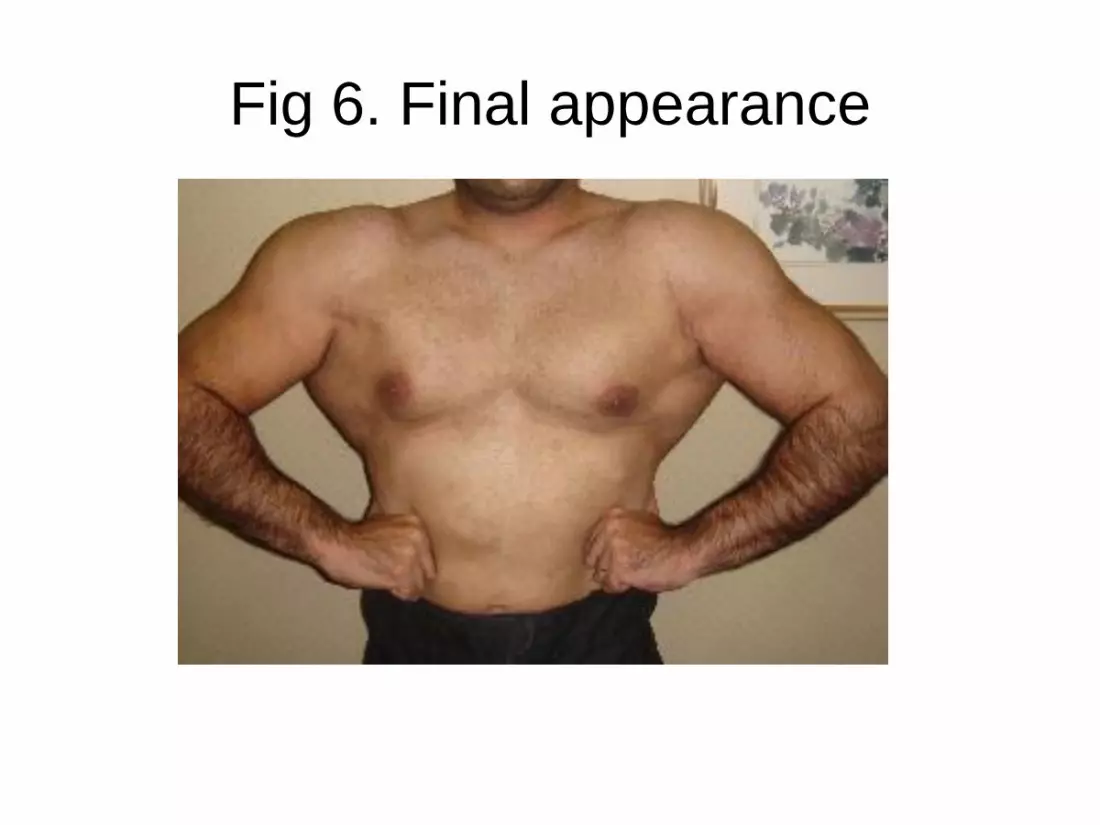
Fig 6. Final appearance