myocapsular pectoralis major flap for pharyngeal reconstruction after cervical necrotizing fasciitis
TRANSCRIPT

LETTERS
GUIDELINESLetters to the Editor, discussingmaterial recently published inthe Journal, are welcome. Theywill have the best chance of ac-ceptance if they are receivedwithin 8 weeks of an article’s pub-lication. Letters to the Editormay be published with a re-
sponse from the authors of the article being discussed.Discussions beyond the initial letter and response will notbe published. Letters submitted pertaining to publishedDiscussions of articles will not be printed. Letters to theEditor are not usually peer reviewed, but the Journal mayinvite replies from the authors of the original publication.All Letters are published at the discretion of the Editor.
Authors will be listed in the order in which they appear inthe submission. Letters should be submitted electronicallyvia PRS’ enkwell, at www.editorialmanager.com/prs/.
We reserve the right to edit Letters to meet requirementsof space and format. Any financial interests relevant to thecontent of the correspondence must be disclosed. Submis-sion of a Letter constitutes permission for the AmericanSociety of Plastic Surgeons and its licensees and asignees topublish it in the Journal and in any other form or medium.
The views, opinions, and conclusions expressed in theLetters to the Editor represent the personal opinions of theindividual writers and not those of the publisher, the Edi-torial Board, or the sponsors of the Journal. Any stated views,opinions, and conclusions do not reflect the policy of any ofthe sponsoring organizations or of the institutions with whichthe writer is affiliated, and the publisher, the Editorial Board,and the sponsoring organizations assume no responsibilityfor the content of such correspondence.
Letters
Dr. Goldwyn and My FatherSir:
My father worked at Beth Israel Hospital in Boston,where Dr. Goldwyn spent most of his career. They
were at opposite ends of the hospital hierarchy totempole. I remember my father, a maintenance worker,telling me about a “new kid” he had met (his term forfresh new attending physicians). Needing a minorequipment repair, this new doctor was friendly, gra-cious, and appreciative. He sat with my father to prac-tice his passable German, and seemed most anxious tolearn about my father’s story of survival.
Dad barely escaped Germany to arrive at Ellis Islandliterally with the clothes on his back and a grapefruit inhis pocket. His family had their savings stolen and theirlives mercilessly ended. Working hard at a menial dayjob, his nights were spent learning English and a trade.Through sheer courage and will, he advanced his new skillsand was hired at Beth Israel Hospital, where he progressedto become chief electrician and maintenance officer. Dr.Goldwyn was sincerely proud of him, and my father, inturn, was fascinated by this highly intelligent, caring,
down-to-earth physician. They became friends. While incollege, my father asked me what I planned for an ulti-mate career. I suggested some options, but he told me “Iwant you to be just like Dr. Goldwyn.” I never woulddisagreewithmyfather.AlthoughIcertainlydidnotbecomejust like Dr. Goldwyn, I did become a plastic surgeon.
Among my most cherished memories was when, aspresident of the National Capital Society of Plastic Sur-geons, I had the honor to introduce Dr. Goldwyn as ourguest speaker. After his typically marvelous talk, I hadmy first opportunity to speak personally to this humblegiant in our field. He had no idea of the profound effecthe had had on my family. He expressed the enormousrespect he had for my father’s accomplishments, in-cluding raising two boys, one a distinguished professorof quantum mechanics and university dean, the othera plastic surgeon. He was genuinely saddened to learnthat Dad had passed on a few years earlier.
And now Dr. Goldwyn is also gone—but he left us awonderful legacy, a model to emulate. I do not believein an afterlife. I believe we live on in the memories ofthose that carry on living. In that sense, Dr. Goldwynwill be with us a long time. But also in that sense, withDr. Goldwyn’s passing, a little bit more of my father hasalso died. I miss them both dearly.DOI: 10.1097/PRS.0b013e3181f88df8
Peter Silversmith, [email protected]
Dr. Robert Goldwyn in South AmericaSir:
I cried when I learned that Dr. Goldwyn had died. Hecame to Chile as part of the faculty of the course called
Short-Scar Mammaplasty,1 presented in Santiago, Chile,in July of 2004. We had first asked Dr. Rod Rohrich tocome, but he suggested we contact Dr. Robert Goldwyn,who was then invited, and on the first day we met him, hetaught us about fraternity, fellowship, and friendship.
Dr. Goldwyn was empathetic with all of us here in Chile,because he understood our feelings in pretty much thesame way that we understood ourselves. He and hisextraordinary wife, Tanya, were the center of attention:He seemed to have known us all our lives; we werespellbound by his hilarious and mesmerizing conver-sations. He and Tanya gave us all time to speak and hadthe utmost respect for all members of the community.
During every day of his stay in Chile, he always madeus feel that he was glad to see us again in the morning.His lectures were shown in slides, and this contrastedwith what everyone else of the faculty was doing by usingPowerPoint and video presentations.
I remember his words that told us about how emo-tions can control actions and to think carefully whenmaking any type of criticism; he said that “life offersbetter solutions when we use objective logic to showother plastic surgeons that there are better ways ofdoing the same task that will enhance their success andproductivity in this profession.”Copyright ©2010 by the American Society of Plastic Surgeons
www.PRSJournal.com2274

He also spoke about respect and to treat others in adignified manner, especially in front of their plasticsurgery peers. No one had told us before, as Dr. Gold-wyn said, to “be responsible for your power, as one ofthe roles as a lecturer out of your country is to assessperformance, as some people will only want to talk totheir colleagues about what they are doing well.”
He spoke of what he had done wrong in plastic surgeryduring his life and made us understand that his trueexperience was the sum of his failures. Dr. Goldwyn spokeabout serving others and we felt in these words hisauthenticity.
He also mentioned his days as Editor-in-Chief ofPlastic and Reconstructive Surgery and said, “my practicalphilosophy was to focus on people who had chosen toserve first and then lead an expanding service with theobject of making sure that other plastic surgeons’ high-est priority needs were being served.”
He asked us about the roots of Chilean plastic sur-gery, in keeping with his exemplary work at the Na-tional Archives of Plastic Surgery (which he had in-spired) at the Harvard Medical School library, and hekindly asked us to provide him with old photographs ofChilean plastic surgery mentors and their operatingrooms; with this petition, he made us feel that we were“the South American plastic surgery kings.”
When we traveled to the wine country, he spokeabout the ethical backgrounds of cosmetic surgery, say-ing that “the essence of a surgeon is that he is a healer,and for this true healer there are questions about op-erating to save lives, to cure the patient and to alsoenhance the quality of the life of patients, and themodern plastic surgeon has all of these qualities.”
Dr. Goldwyn spoke to us about marketing and that,for him, it was fine, but his core thinking was aboutexperience, curiosity, and humanism and that thesebehaviors were the ones that the patient would neverforget. For Dr. Goldwyn, proficiency and ethics in plas-tic surgery spoke louder than marketing and Webpages.
Before Dr. Goldwyn came to Chile, I had judged himfor what he had, but after his visit, I judged him for whathe had not: self-interest, ego, and arrogance. After Dr.Goldwyn’s presentations in Chile, I saw his work as aselfless service, as if when it came time to take credit,he made himself invisible; as wanting nothing more thanto give people pride, to make people stand on their own,instead of trying to blind us with his brilliance. I truly feelblessed to have known Dr. Goldwyn and that he and hiswife Tanya felt good and cherished in Chile.DOI: 10.1097/PRS.0b013e3181f88e0b
Arturo S. Prado, M.D.Division of Plastic Surgery
School of MedicinePostgraduate School
University of ChileManquehue Norte 1701 ofic 210
VitacuraSantiago, Metropolitana, Chile
REFERENCE1. Prado A, Andrades P. Short-scar mammaplasty course in
Chile. Plast Reconstr Surg. 2005;116:1184–1186.
A Simple Suspension Technique in FacialParalysis Reanimation with Bone AnchorsSir:
We read with great interest the article by Terzis andOlivares1 about the results of surgery in facial
paralysis reanimation and further corrections. In thatarticle, the authors observe that secondary surgeryachieves appreciable results in all facial regions, up-grading symmetry and function. We applied a new sus-pension technique that uses a spinal needle and boneanchors to obtain midface suspension in facial palsy inadults, where nerve reconstruction is not advisable.
Under general or local anesthesia, a 3-mm incisionis performed laterally to the zygomatic muscle. A spinalneedle is then introduced through the nasolabial foldtoward the 3-mm incisions. The introduction should beperformed with a vertical zigzag maneuver, to penetratethe superficial musculoaponeurotic system (SMAS) sev-eral times. The spinal needle is then guided within 1 cmfrom the 3-mm incision.
The bioabsorbable anchor is then inserted and fixedin the zygomatic bone through the 3-mm incision(Fig. 1). The tip of the spinal needle is then eased outthrough the incision. One anchor thread is introducedin the needle and extracted at the needle hub (Fig. 2).This maneuver may be helped by the sucker, which caneasily catch and pull the thread throughout the needle.The spinal needle is then unthreaded (with the sutureinside) except for the last 5 mm; the needle is thenrotated and guided subcutaneously along the nasola-bial fold caudally for 1 cm. Here, the needle is rotatedand guided toward the cutaneous incision, penetratingthe SMAS as described previously. The suture thread isthen pulled out of the tip of the spinal needle through thecutaneous incision. (See Video, Supplemental DigitalContent 1, which demonstrates one thread being passedthrough the needle and extracted at the needle hub afterthe bone anchor has been placed and the spinal needlehas been introduced. The spinal needle is then un-threaded except for the last 5 mm; the needle is thenrotated and guided subcutaneously along the nasolabialfold caudally for 1 cm. Here, the needle is rotated andguided toward the cutaneous incision, penetrating the
Supplemental digital content is available forthis article. A direct URL citation appears inthe printed text; simply type the URL addressinto any Web browser to access this content. Aclickable link to the material is provided in theHTML text of this article on the Journal’s Website (www.PRSJournal.com).
Volume 126, Number 6 • Letters
2275

SMAS with a vertical zigzag maneuver. The suture threadis pulled out of the spinal needle through the cutaneousincision, http://links.lww.com/PRS/A245.)
Therefore, the thread describes subcutaneously anisosceles triangle, with the base in the nasolabial foldand the vertex corresponding to the 3-mm incision.The other thread of the anchor is tied to the first witha square knot and the SP is thus suspended.
In cases where greater suspension is required, two ormore passages could be performed. Although nerveanastomoses or nerve grafts are considered the firstchoice in treating facial nerve paralysis, the results canbe unsatisfactory. Sood et al.2 reported that 59.5 percentof patients report positive benefits after hypoglossal-to-facial nerve anastomosis. Moreover, dynamic reanimationrequires functional motor end plates, excluding patientswith old-age paralyses.
In contrast, suspension could be performed in thevast majority of cases using several materials (e.g., polypro-
pylene, polytetrafluoroethylene, dermal allografts, fascialata). Usually, suspensions are performed with suturepassers or endoscopic assistance3,4 that require longeroperative times and more invasive surgical tools.
This technique requires no more than one short inci-sion, having an optimal cosmetic result and being per-formed under local anesthesia. Only one anchor and justone knot could be performed, making this techniquequick and versatile. Moreover, the small caliber of thespinal needle allows the surgeon to easily pass severaltimes throughout the SMAS and prevents damage to thesurrounding tissues, being precise and safe.DOI: 10.1097/PRS.0b013e3181f619a8
Luciano A. Lanfranchi, M.D.
Riccardo Gazzola, M.D.
Matteo Marino, M.D.
Franz W. Baruffaldi Preis, M.D.Unit of Plastic and Reconstructive Surgery
IRCCS San Raffaele Hospital, andUnit of Plastic and Reconstructive Surgery
IRCCS Istituto Ortopedico GaleazziMilan, Italy
Correspondence to Dr. GazzolaDepartment of Plastic Surgery
IRCCS San Raffaele, MilanoVia Olgettina 60
20132 Milano, [email protected]
Fig. 1. The bioabsorbable anchor is inserted and fixed in the zy-gomatic bone through the 3-mm incision.
Fig. 2. One anchor thread is passed through the spinal needleand extracted at the needle hub. This maneuver could be helpedby the use of a sucker.
Video. Supplemental Digital Content 1 demonstrates onethread being passed through the needle and extracted at theneedle hub after placement of the bone anchor and introductionof the spinal needle. The spinal needle is then unthreaded exceptfor the last 5 mm; the needle is then rotated and guided subcu-taneously along the nasolabial fold caudally for 1 cm. Here, theneedle is rotated and guided toward the cutaneous incision, pen-etrating the SMAS with a vertical zigzag maneuver. The suturethread is pulled out of the spinal needle through the cutaneousincision, http://links.lww.com/PRS/A245 .
Plastic and Reconstructive Surgery • December 2010
2276
DISCLOSUREThe authors have no financial interest to declare in re-
lation to the content of this communication. No outside fund-ing was received.
PATIENT CONSENTThe patient provided written consent for the use of the
patient images.
REFERENCES1. Terzis JK, Olivares FS. Secondary surgery in adult facial pa-
ralysis reanimation. Plast Reconstr Surg. 2009;124:1916–1931.2. Sood S, Anthony R, Homer JJ, Van Hille P, Fenwick JD.
Hypoglossal-facial nerve anastomosis: Assessment of clini-cal results and patient benefit for facial nerve palsy follow-ing acoustic neuroma excision. Clin Otolaryngol Allied Sci.2000;25:219–226.
3. Alex JC, Nguyen DB. Multivectored suture suspension: A min-imally invasive technique for reanimation of the paralyzedface. Arch Facial Plast Surg. 2004;6:197–201.
4. Citarella ER, Sterodimas A, Green AC, Sinder R, Pitanguy I.Use of triple-convergence polypropylene thread for the aes-thetic correction of partial facial paralysis. Aesthetic Plast Surg.2008;32:688–691.
Eyelid Skin Necrosis with AccidentallyInjected FormaldehydeSir:
We read with interest the recent article by Lelli andLisman entitled “Blepharoplasty Complications”
(Plast Reconstr Surg. 2010;125:1007-1017).1 Althoughblepharoplasty is a common operation, because of thearea of operation being small, it should not be under-estimated, and the writers have emphasized this verywell in the article. We congratulate them.
However, the second named writer of the article andsome other writers have had a similar article publishedin 1997 in the journal Clinics in Plastic Surgery, in whichthey referred to a patient who was accidentally injectedwith formaldehyde rather than local anesthetics.2 In theold article, they mentioned that both upper and lowereyelids were defective (because of this injection) andthat they had to perform eight more operations torepair and reconstruct the injury. In this article, theymention having to perform four more operations. Wewould like to ask the following:
1. Is this a typographical error?2. If there is no such error, are these two different
patients?3. If these are two different patients, it is very sad
that such a terrible complication was experi-enced by the same team for the second time.
4. In the article, in the Eyelid Sloughing section, theauthors state that “eyelid necrosis has been re-ported sparingly and can follow inadvertent in-jection with formaldehyde or other substancesinstead of local anesthetic” but only refer to ref-erence 13. The reference numbered 13 is againwritten by the second author, this time along with
another first author. They could have at leastreferred to two sources in a case they use theword “sparingly” for, and the other source couldhave been the former article published in 1997.
5. Although it is understood that Dr. Lisman is awell-known author on this subject, we think itwould be more beneficial if he or she wrote moreconsistently, considering us old readers, rather thanhoping to come across new readers all the time.DOI: 10.1097/PRS.0b013e3181f61bdf
Mehmet Oguz Yenidunya, M.D., Ph.D.
Ozlem Gundeslioglu, M.D.
Onur Serin, M.D.Department of Plastic, Reconstructive, and Aesthetic
SurgeryMustafa Kemal University
School of MedicineHatay, Turkey
Correspondence to Dr. GundesliogluDepartment of Plastic, Reconstructive, and Aesthetic
SurgeryMustafa Kemal University
Antakya, Hatay, [email protected]
DISCLOSUREThe authors have no financial interest to declare in re-
lation to the content of this communication.
REFERENCES1. Lelli GJ, Lisman RD. Blepharoplasty complications. Plast Re-
constr Surg. 2010;125:1007–1017.2. Lisman RD, Hyde K, Smith B. Complications of blepharo-
plasty. Clin Plast Surg. 1988 ;15:309–335.
ReplySir:
Inadvertent injection of formaldehyde is an exceed-ingly rare but noteworthy complication of blepharo-plasty surgery. The case described in this article1 is theonly case of its type in the literature of which we areaware. That said, inadvertent injection of other sub-stances into the eyelid is plausible. This case was re-ferred to the senior author’s practice after this devas-tating complication occurred, and ultimately requiredfour reconstructive operations per eyelid (a total ofeight operations) to achieve the result shown in Figure7, c. The reference for this case was cited in our ref-erence list.2 Drs. Yenidunya, Gundeslioglu, and Serinshould be commended on their diligence in noticingthis typographical error.
We were initially invited by the editors of Plastic andReconstructive Surgery to write a summation of blepha-roplasty complications, which was slated for publicationin a blepharoplasty supplement to the Journal. Whenthe decision was made not to publish this supplement,the editors of the Journal requested that we submit thisarticle for routine publication. Many of the potential
Volume 126, Number 6 • Letters
2277

complications noted within the article are contempo-rary, but some, as in this example, are outstandingexamples of rare complications and are necessary toemphasize to all surgeons. The article is meant for anysurgeon who partakes in blepharoplasty surgery, as asound understanding of potential complications aroundthe ocular structures is imperative.DOI: 10.1097/PRS.0b013e3181f61bf2
Gary J. Lelli, Jr., M.D.Department of Ophthalmology
Division of Ophthalmic Plastic, Reconstructive, and OrbitalSurgery
New York Presbyterian HospitalWeill Cornell Medical Center
Richard D. Lisman, M.D.Department of Ophthalmology
Division of Ophthalmic Plastic, Reconstructive, and OrbitalSurgery
New York UniversityLangone Medical Center
New York, N.Y.
Correspondence to Dr. LismanDepartment of Ophthalmic Plastic Surgery
New York University Medical Center635 Park Avenue, Ground Floor
New York, N.Y. [email protected]
DISCLOSUREThe authors have no financial conflicts or interests to
report in association with the contents of this communication.
REFERENCES1. Lelli GJ, Lisman RD. Blepharoplasty complications. Plast Re-
constr Surg. 2010;125:1007–1017.2. Lisman RD, Hyde K, Smith B. Complications of blepharo-
plasty. Clin Plast Surg. 1988;15:309–335.
In Search of Suitable Indications for Homograftsand Allografts in Nasal AugmentationSir:
We had the great pleasure of reading the extremelyinformative article by Sajjadian et al. entitled
“Current Status of Grafts and Implants in Rhinoplasty:Part II. Homologous Grafts and Allogenic Implants” pub-lished in the March issue of the Journal. We congratulatethe authors for the brilliant and complete CME articlepublished on the alternatives to autografts.1
We would like to take the opportunity to furtherdiscuss the indications for homografts and allografts.The use of a number of grafts in primary (in the non-white or posttraumatic nose) and revision rhinoplastyhas become commonplace.2
As the authors rightly state, the main topic remainsto give appropriate indications for homografts and al-lografts, with priority given to autografts. In principle,the availability of autografts would avoid the use of ho-mologous grafts and allogenic implants; as a conse-quence, the surgeon plays a decisive role in graft selection.
Undoubtedly, homografts and allogenic implants doprovide a simple, fast, and “efficient” method of aug-mentation compared with autografts, which involve ad-ditional surgical procedures, extra operating time, co-morbidities, and surgical skills; in contrast, rejection,infection, mobility, dislocation, exposure, and extru-sion represent frequent and frightful complications ofsurgery. Use of allografts for structural support of thenasal framework often results in failure because ofthese complications, thus necessitating removal andreplacement with autografts.2,3
An exception is represented by skin substitutes: ho-mologous acellular dermis and a dermal regenerativetemplate can be used as a single layer or stacked inmultiple layers, depending on the degree of soft-tissuereplacement needed; these soft materials are used tocamouflage autografts and rough surfaces from previ-ous surgery but are not used for structural support.3Several implant materials have been used for nasalaugmentation: calcium ceramics (mainly hydroxyapa-tite), polymers (solid silicone implants; the liquid formis not U.S. Food and Drug Administration approved),polyethylene, polyesters, polytetrafluoroethylene, andpolymethylmethacrylate.
However, most reports in the literature share incom-plete follow-up of patients and no alloplastic materialhas yet proved successful, and the complication ratematches that of autografts, which are less prone to beextruded. In 1954, Peer noted that most allografts wereconstantly being buried by one group of surgeons andthen constantly being revived by another group of sur-geons after varying periods of time.4 In 1997, Collawnet al. discussed the increased use of autografts overallografts during a decade of experience.5
A variety of implant materials are available to shapeand augment the nose, but long-term retention andstability are poor and can depend on the recipient siteas well: the nasal tip is more predisposed to complicationbecause of its mobility; a surgical nose is predisposed toa higher complication rate because the impaired softtissues are scarred, less vascularized, and thinned.2,3,5
The most common cause of complications after nasalaugmentation with allografts is actually an improperpreoperative estimation of the risks of this type of sur-gery. The analysis of the quality and quantity of the skinand mucous membrane forming the implant bed andcovering the implant remains the main problem.2,3,5
We fully agree with Jack Sheen that “The rate ofcomplications is insignificant compared with the irre-versible tissue destruction that results in permanentdeformity to the patient. Any complication rate, how-ever small, cannot justify a procedure that is potentiallydisfiguring to patients when a better alternative is avail-able—the patient’s own tissues.”4 As stated by Sajjadianet al., our experience continues to support the conceptthat autografts are the material of choice even if theydo not always result in perfection and the absenceof complications.DOI: 10.1097/PRS.0b013e3181f61b3d
Plastic and Reconstructive Surgery • December 2010
2278

Tommaso Agostini, M.D.Department of Plastic and Reconstructive Surgery
University of FlorenceFlorence, Italy
Davide Lazzeri, M.D.
Christian Pascone, M.D.Burns and Plastic Surgery Unit
CisanelloPisa, Italy
Vittorugo Agostini, M.D.Department of Plastic and Reconstructive Surgery
University of FlorenceFlorence, Italy
Correspondence to Dr. Tommaso AgostiniDepartment of Plastic and Reconstructive Surgery
University of FlorenceFaculty of Medicine and Surgery
CTO-AOUCLargo Palagi
1-50100 Florence, [email protected]
DISCLOSUREThe authors have no financial interest to declare in re-
lation to the content of this communication.
REFERENCES1. Sajjadian A, Naghshineh N, Rubinstein R. Current status of
grafts and implants in rhinoplasty: Part II. Homologous graftsand allogenic implants. Plast Reconstr Surg. 2010;125:99e–109e.
2. Mathes SJ. Plastic surgery. In: Constantian MB, ed. ClosedRhinoplasty: Current Techniques, Theory, and Applications. Vol. 2,2nd ed. Philadelphia: Saunders Elsevier; 2006:517–572.
3. Mathes SJ. Plastic surgery. In: Constantian MB, ed. SecondaryRhinoplasty. Vol. 2, 2nd ed. Philadelphia: Saunders Elsevier;2006:765–799.
4. Rees DT, Baker CD, Tabbal N. Rhinoplasty: Problems and con-troversy. In: Sheen J, ed. A Clinical Assessment of Alloplastic Materialsin Secondary Rhinoplasty. St. Louis: Mosby; 1988:384–389.
5. Collawn SS, Fix RJ, Moore JR, Vasconez LO. Nasal cartilagegrafts: More than a decade of experience. Plast Reconstr Surg.1997;100:1547–1552.
ReplySir:
In response to the letter, “In Search of SuitableIndications for Homografts and Allografts in NasalAugmentation,” we would like to reiterate the thought-ful and accurate statements by Agostini and col-leagues with regard to the indications for the use ofautograft alternatives.
As the paradigm in rhinoplasty has shifted to one ofaugmentation, the search for grafting materials hasincreased. Especially in the secondary rhinoplasty orsaddle nose deformity patient, local options may beabsent. Furthermore, patient wishes, the desire forfaster recovery, or preexisting medical conditions maypreclude the use of autografts from sources other thanthe septum. Each donor site and graft presents with its
own unique properties with advantages and disadvan-tages. For example, the pain associated with iliac crestbone harvesting can be substantially greater than thatof the primary procedure. Though less morbid, auric-ular cartilage may not offer the physical propertiesdesired for support. Therefore, the search continuesfor an allograft with the desired physical properties,along with equivalent or lower infection, extrusion, andmalposition rates compared with autografts. However,until that is achieved, it is well documented that at thistime the role of allografts remains as a “last resort”source for grafts in nasal reconstruction.1,2
DOI: 10.1097/PRS.0b013e3181f61c2a
Ali Sajjadian, M.D.
Nima Naghshineh, M.D., M.Sc.
Roee Rubinstein, M.D.
Correspondence to Dr. Sajjadian496 Old Newport Boulevard, Suite 3
Newport Beach, Calif. [email protected]
REFERENCES1. Sajjadian A, Rubinstein R, Naghshineh N. Current status of
grafts and implants in rhinoplasty: Part I. Autologous grafts.Plast Reconstr Surg. 2010;125:40e–49e.
2. Sajjadian A, Naghshineh N, Rubinstein R. Current status ofgrafts and implants in rhinoplasty: Part II. Homologous graftsand allogenic implants. Plast Reconstr Surg. 2010;125:99e–119e.
Myocapsular Pectoralis Major Flap forPharyngeal Reconstruction after CervicalNecrotizing FasciitisSir:
We read with great interest the case described byHsu and Yu1 regarding complex salvage of failed
microvascular pharyngoesophageal reconstruction, andwe wanted to share our experience with a similar casein which we introduced a modification of the classicpectoralis major myocutaneous flap previously unde-scribed in the medical literature. A lot has been writtenabout pedicled and microvascular reconstructive op-tions in the head and neck area.2
As shown by the above-mentioned report, in cases ofirradiated or infected surgical fields, microvascular re-construction can be contraindicated, because of thehigher rate of pedicle thrombosis and total flap loss,and pedicled locoregional flaps should represent amore reliable option. Cervical necrotizing fasciitis is avery rare but life-threatening condition characterizedby necrosis of fascia and subcutaneous tissues, progress-ing rapidly to deeper structures and overlying skin.3 Inmost cases, debridement and reconstruction are per-formed at an early stage of the disease, on an emer-gency basis, when the patient’s life represents a priorityover functional restoration.
A 42-year-old female patient was referred to our de-partment for an abscess of the right cervical region. Six
Volume 126, Number 6 • Letters
2279

months earlier, she had undergone radical right mas-tectomy followed by immediate reconstruction with tis-sue-expander subpectoral placement. During chemo-therapy, a pneumococcal pneumonia with sepsisdeveloped. The subsequent tracheostomy was compli-cated by cervical necrotizing fasciitis, promoted byPseudomonas aeruginosa infection. Multiple surgical de-bridements were performed, resulting in the loss of thelateral right pharyngeal wall, epiglottis, and thyroidcartilages (Fig. 1, above). Local flaps were excluded inconsideration of the extensive involvement of cervicalsoft tissues. Free flaps were contraindicated for theabove-mentioned reasons. A classic pectoralis majormyocutaneous flap was impossible to raise because ofskin paddle unreliability caused by previous mastec-tomy. Thus, to solve this particular case, a modificationof the pectoralis major flap, the myocapsular pectoralismajor flap, was performed. Seven days before the pro-cedure, parotid glands were injected with 50 units ofbotulinum toxin to reduce sialorrhea.4 Therefore, aftertissue expander removal, a pedicled myocapsular pec-toralis major flap was raised, including part of the im-plant capsule on the inner surface of the muscular flap
(Fig. 1, below). The capsular layer was used to restore thecontinuity of the luminal mucosa, and the muscularside of the flap was used to reconstruct the full-thick-ness defect of the pharyngeal wall. No complicationswere encountered, and the exposed muscular surfacehealed by secondary intention (Fig. 2). A permanenttracheostomy was necessary in this case because of thedefinitive loss of epiglottis cartilage; nevertheless, thepatient restarted oral nutrition 2 months after the op-eration. Endoscopy confirmed the perfect integrationof capsular tissue with the surrounding mucosa, pre-venting the formation of strictures caused by abnormalscarring on the muscular side of the flap (Fig. 3).
This is the first report of the use of the breast implantcapsule in head and neck reconstruction. Capsular tis-sue has proven to be an adequate substitute for a pec-toral skin paddle in the event that it is unreliable. In
Fig. 1. (Above) Cervical and pharyngeal loss of substance afterdebridement. (Below) A pedicled myocapsular pectoralis majorflap has been raised.
Fig. 2. Results at 12 months postoperatively.
Fig. 3. One-year postoperative endoscopy shows integration ofthe capsular layer with the luminal mucosa (arrow on the transi-tion zone).
Plastic and Reconstructive Surgery • December 2010
2280

such a life-threatening case, locoregional pedicled flapsrepresent a safer option to avoid disastrous outcomes.DOI: 10.1097/PRS.0b013e3181f619c3
Paolo Persichetti, M.D., Ph.D.
Giovanni Francesco Marangi, M.D.
Pierluigi Gigliofiorito, M.D.
Francesco Segreto, M.S.
Beniamino Brunetti, M.D.Plastic and Reconstructive Surgery UnitCampus Bio-Medico University of Rome
Rome, Italy
Correspondence to Dr. MarangiDepartment of Plastic and Reconstructive Surgery
Via Alvaro del Portillo, 20000128 Rome, Italy
DISCLOSUREThe authors do not have any commercial associations that
might pose or create a conflict of interest with informationpresented in this communication. No intramural or extramu-ral funding supported any aspect of this work.
REFERENCES1. Hsu P, Yu P. Complex salvage of a failed pharyngoesophageal
reconstruction with impending airway disaster. Plast ReconstrSurg. 2010;125:208–210.
2. Alcalde JM, Gimeno-Vilar C, Montes-Jovellar L, Manrique R,Sanhueza I. Reconstruction of pharyngeal defects (in Spanish).Acta Otorrinolaringol Esp. 2009;60:283–290.
3. Ord R, Coletti D. Cervico-facial necrotizing fasciitis. Oral Dis.2009;15:133–141.
4. Laing TA, Laing ME, O’Sullivan ST. Botulinum toxin fortreatment of glandular hypersecretory disorders. J Plast Re-constr Aesthet Surg. 2008;61:1024–1028.
ReplySir:
Thank you for your comments on our article “Com-plex Salvage of a Failed Pharyngoesophageal Recon-struction with Impending Airway Disaster.”1 In yourletter, you presented a case with life-threatening ne-crotizing fasciitis in the neck with loss of the lateralpharyngeal wall, epiglottis, and thyroid cartilages.2 Thisdefect was reconstructed successfully with a pedicledpectoralis major muscle with the underlying submus-cular breast implant capsule lining the pharyngeal lu-men. Apparently, the capsule was successfully remuco-salized and prevented stenosis. Your case is anotherexcellent example of a “great save” with a pedicled flapfollowing a head and neck disaster. As you rightlypointed out, in the presence of an overwhelming in-fection such as in our case and yours, a free flap re-construction is usually not possible. Unlike in someother areas of the body where delayed reconstructionis appropriate, securing the airway and immediate cov-erage of important structures such as major arteries aremandatory in the head and neck region. The pectoralis
major muscle flap is the most commonly used pedicledregional flap for head and neck coverage. In femalepatients, including a skin paddle for pharyngeal recon-struction is not a good option because of its bulkinessand unreliability. Therefore, taking the muscle alonewith skin grafts may be a better option. The authorscleverly used a submuscular breast implant capsule for“lining,” which worked well. The well-formed capsulemost likely minimized the risk of stenosis, which is morelikely to occur when skin grafts are used for liningbecause of contracture. Therefore, a much larger lu-men should be created during skin graft reconstructionas was done in our case. A luminal stent such as theMontgomery salivary bypass tube is also helpful forminimizing contracture. The pectoralis major musclescan be thin, small, and short in some patients such asin obese women with lack of exercise. In our patient,the pectoralis muscles barely reach the upper neck. Inaddition, she had a much larger defect with exposureof major vessels in the upper chest and a large pha-ryngoesophageal and neck skin defect. Her pectoralismajor muscles were only large enough to cover thesemajor vessels in the upper chest and lower neck. Thus,the latissimus dorsi flap was needed for pharyngoe-sophageal and neck reconstruction. We have used thepedicled latissimus dorsi flap for similar defects in theneck and upper chest in another patient who had failedmultiple free flaps and bilateral pectoralis muscle flaps.I agree with the authors that locoregional pedicled flapscan be a lifeboat in these life-threatening situations.DOI: 10.1097/PRS.0b013e3181f61c3c
Peirong Yu, M.D.Department of Plastic Surgery, Unit 443
University of Texas M. D. Anderson Cancer Center1515 Holcombe Boulevard
Houston, Texas [email protected]
REFERENCES1. Hsu P, Yu P. Complex salvage of a failed pharyngoesophageal
reconstruction with impending airway disaster. Plast ReconstrSurg. 2010;125:208–210.
2. Persichetti P, Marangi GF, Gigliofiorito P, Segreto F, BrunettiB. Myocapsular pectoralis major flap for pharyngeal recon-struction after cervical necrotizing fascitis (Letter). Plast Re-constr Surg. 2010;126:2280–2281.
An Algorithmic Approach to BreastReconstruction Using Latissimus DorsiMusculocutaneous FlapsSir:
We read with interest the article by Durkin et al.1entitled “An Algorithmic Approach to Breast Re-
construction Using Latissimus Dorsi Musculocutane-ous Flaps.” We congratulate the authors for an excel-lent systematic evaluation of potential techniques forlatissimus dorsi breast reconstruction in patients witha variety of mastectomy defects and risk factors. Theirlogical approach is well structured in the planning of
Volume 126, Number 6 • Letters
2281

reconstruction for mastectomy defects with respectto the inframammary fold and designing the skinpedicle accordingly.
However, we would like to highlight the role of themuscle-sparing latissimus dorsi musculocutaneous flapas an addition to the algorithm, as it would offer morechoices to patients for reconstructive options and de-crease the complications encountered with traditionallatissimus dorsi flaps. The muscle-sparing latissimusdorsi technique for breast reconstruction has recentlybeen described,2,3 and we have been using this tech-nique for breast reconstruction for the past 3 years.
One of the principal drawbacks of the conventionallatissimus dorsi flap is donor-site seroma formation. Thiscomplication is nearly completely eliminated when pre-serving the bulk of the muscle in situ and reduces patienthospital stay, as the drains come out earlier.
We agree with and support the authors on the use ofan algorithmic approach to breast reconstruction. Wealso believe that the muscle-sparing latissimus dorsitechnique is an additional tool for breast reconstruc-tion and offers patients and surgeons more choices. Itsinclusion as an option would certainly strengthen theauthors’ algorithm.DOI: 10.1097/PRS.0b013e3181f61bcb
Anuj Mishra, M.R.C.S.
Philip Brackley, Ph.D., F.R.C.S.(Plast.)
Mandana Sigroudinia, M.R.C.S.
Azhar Iqbal, F.R.C.S.(Plast.)Department of Plastic and Reconstructive Surgery
Whiston HospitalLiverpool, United Kingdom
Correspondence to Dr. MishraDepartment of Plastic and Reconstructive Surgery
Whiston HospitalLiverpool, United Kingdom
REFERENCES1. Durkin AJ, Pierpont YN, Patel S, et al. An algorithmic ap-
proach to breast reconstruction using latissimus dorsi myo-cutaneous flaps. Plast Reconstr Surg. 2010;125:1318–1327.
2. Saint-Cyr M, Nagarkar P, Schaverien M, Dauwe P, Wong C,Rohrich RJ. The pedicled descending branch muscle-sparinglatissimus dorsi flap for breast reconstruction. Plast ReconstrSurg. 2009;123:13–24.
3. Brackley PT, Mishra A, Sigaroudina M, Iqbal A. Modifiedmuscle-sparing latissimus dorsi with implant for total breastreconstruction: Extending the boundaries. J Plast Reconstr Aes-thet Surg. 2010;63:1495–1502
Perforasomes, Venosomes, and Perfusion Zonesof the DIEAP FlapSir:
Kudos need to be extended to Saint-Cyr et al.1 fortheir recent publication “The Perforasome Theory:
Vascular Anatomy and Clinical Implications,” which cer-tainly should be a landmark article in the burgeoning
field of perforator flaps. Although intuitively many ofthe so-called gurus of perforator flaps have long un-derstood the concept and impact of the anatomicalcutaneous territory serviced by an individual perforatorand its relationship with adjacent perforasomes, this hadnot previously been so well defined with such an appro-priate appellation. The authors have subsequently ap-plied this theory to better describe the typical patterns ofcirculation to the lower abdomen,2 commonly used todayas a deep inferior epigastric artery perforator (DIEAP)free flap for autogenous breast reconstruction. On thebasis of their usual three- and four-dimensional ex vivocomputed tomographic angiography studies of selectedinjections of individual perforators, they concluded thatmedial row deep inferior epigastric artery perforators(zone I) capture the central abdomen with zones of pro-gressive perfusion following the schema of Hartrampf etal. and their unipedicled transverse rectus abdominismusculocutaneous flaps3 (i.e., zone II corresponded tothe territory of the contralateral deep inferior epigastricartery and zone III was the ipsilateral hemiabdomen lat-eral to zone I). If a lateral perforator was selected, thezones would be switched as originally described by Dinneret al.4 Physiologic studies by Holm et al.5 had also previ-ously assessed this perfusion sequence, but in vivo, usingdynamic laser fluorescence videoangiography with laser-induced fluorescence of indocyanine green. Their con-clusion suggested that only the schema of Dinner et al.4was correct, as perfusion across the midline was alwaysdelayed and less intense than in any territory on theipsilateral side.5 Unfortunately, the majority of their flapsmixed perforators from both deep inferior epigastric ar-tery branches.5
The role of any schema that would better explain theenigmas of the DIEAP flap must enhance its reliability,and this must be consistently reliable if it is to be prag-matic. The zones of perfusion according to both Har-trampf et al.3 and Dinner et al.4 were intended to reflectthe underlying angiosomes of the source vessels to thecorresponding skin territory of the lower abdomen.However, with perforator flaps, the interlinking per-forasomes do not necessarily follow the same princi-ples. Rozen et al.,6 also from individual perforator in-jection studies of the DIEAP flap, found results similarto those of Saint-Cyr et al.1 However, they concludedthat the so-called zone I of the angiosome principle ina perforator flap really represented two different per-forasomes, based on either a medial or lateral rowperforator. On this basis, the next captured skin region,corresponding to their zone II, would be the immedi-ately adjacent perforasome found in all directions (i.e.,both medial and lateral to the perforasome of the in-jected perforator). Zone III would be the next capturedperforasome(s), and zone IV the third captured terri-tory, which would be the most unreliable. Thus, ac-cording to Rozen et al.,6 a medial row perforator wouldcapture as zone II the contralateral medial row perfora-some and ipsilateral lateral row perforasome, whereas alateral row perforator would capture the ipsilateral medial
Plastic and Reconstructive Surgery • December 2010
2282

row perforasome and the ipsilateral superficial inferiorepigastric artery (SIEA) territory.
A recent clinical case further underscored our co-nundrum with perforator flaps. The central abdomenwas planned for unilateral breast reconstruction basedon a medial row perforator of the right rectus abdo-minis muscle identified using computed tomographicangiography. At the time of flap elevation, vascularclamps were affixed to several large left hemiabdomenperforators to assess the extent of perfusion only bythis selected perforator. Immediately on placement ofclamps, marked mottling was noted on the left side ofthe abdominal ellipse, starting at the boundary of thecontralateral lateral row perforators (Fig. 1). Much ofthis discoloration cleared rapidly by the time a photo-graph could be taken but was still readily apparent inthe most lateral aspect of zone IV. An intraoperativedecision was made to exclude that entire area andinstead keep completely the right hemiabdomen. Atthe time of excision of the mottled region, a mixture ofbright red and dark bleeding, consistent with the pres-ence of arterial perfusion but simultaneous venous con-gestion, was observed.
As Blondeel et al.7 first noted, and as subsequentlyconfirmed by Schaverien et al.8 and Rozen et al.,9 in-adequate venous outflow can really be the limiting fac-tor with perfusion of DIEAP flaps. Postulated mecha-nisms include the chosen venous perforator being toosmall, the absence of midline crossover veins except forindirect linking vessels at the subdermal plexus level,and oscillating veins connecting the superficial anddeep systems that usually would divert the normal sub-cutaneous venous flow into the deep inferior epigastricpedicle being too diminutive.9 In this clinical case, theobserved zones of perfusion actually appeared to followthis dictum in that they were most influenced by venous
Fig. 2. Zones of observed progressive perfusion by perfora-some: I, supplied by ipsilateral medial row DIEAP; II, immediatelyadjacent perforasomes captured by the ipsilateral medial rowDIEAP (i.e., the ipsilateral lateral row perforasome and the con-tralateral medial row perforasome); III, second captured perfora-some, the contralateral lateral row perforasome, with delayedvenous outflow; and IV, third captured perforasome, territory ofthe SIEA, with persistent venous congestion.
Fig. 3. The solitary perforatorof the zone I ipsilateral medial rowDIEAP.
Fig. 1. In situ DIEAP flap perfused by a solitary, medial row per-forator of the right hemiabdomen (arrow). Slowing resolvingmottling was observed in the lateral half of the contralateral side,starting overlying the lateral row perforasome and progressingto be most conspicuous in the most lateral aspect.
Volume 126, Number 6 • Letters
2283

perfusion or lack thereof, and not arterial perfusionthat traditionally has been the basis for devising sche-matics for this region (Figs. 2 and 3). To further con-fuse this issue, most of these proposals have reflectedonly the horizontal progression of perfusion in thelower abdomen. However, Keller10 found that inferiorsections even in so-called zone I had decreased tissueoxygen saturation, implying decreased perfusion. Onecould reasonably conclude that a very superior deepinferior epigastric artery perforator, especially in theextremely pendulous abdomen, may not capture allsequential perforasomes oriented in a vertical fashion.Taking all these nuances into consideration, oneshould assume that the optimal vascular configurationfor any DIEAP flap may require various combinationsof the superficial or deep systems, depending on whichis dominant for that individual.11 Any devised system ofschematics or theories must represent no more than arough guideline for the design and planning of aDIEAP flap. However, as with most perforator flaps, anindividualized approach to ensure accurate intraoper-ative mapping and reliable harvest of the flap depen-dent on the variability of the given perforator mustalways be carefully observed.6DOI: 10.1097/PRS.0b013e3181f61b26
Geoffrey G. Hallock, M.D.Division of Plastic Surgery
Sacred Heart Hospital and The Lehigh Valley HospitalAllentown, Pa.
St. Luke’s HospitalBethlehem, Pa.
Correspondence to Dr. Hallock1230 South Cedar Crest Boulevard, Suite 306
Allentown, Pa., [email protected]
DISCLOSUREThe author has no financial interest to declare in relation
to the content of this communication.
ACKNOWLEDGMENTDavid C. Rice, B.S., physician extender, Sacred
Heart Hospital, Allentown, and St. Luke’s Hospital,Bethlehem, Pennsylvania, assisted with the dissectionand microsurgery.
REFERENCES1. Saint-Cyr M, Wong C, Schaverien M, Mojallal A, Rohrich RJ.
The perforasome theory: Vascular anatomy and clinical im-plications. Plast Reconstr Surg. 2009;124:1529–1544.
2. Wong C, Saint-Cyr M, Mojallal A, et al. Perforasomes of theDIEP flap: Vascular anatomy of the lateral versus medial rowperforators and clinical implications. Plast Reconstr Surg.2010;125:772–782.
3. Hartrampf CR, Scheflan M, Black PW. Breast reconstructionwith a transverse abdominal island flap. Plast Reconstr Surg.1982;69:216–225.
4. Dinner MI, Dowden RV, Scheflan M. Refinements in the useof the transverse abdominal island flap for postmastectomyreconstruction. Ann Plast Surg. 1983;11:362–372.
5. Holm C, Mayr M, Hofter E, Ninkovic M. Perfusion zones ofthe DIEP flap revisited: A clinical study. Plast Reconstr Surg.2006;117:37–43.
6. Rozen WM, Ashton MW, Le Roux CM, Pan WR, Corlett RJ.The perforator angiosome: A new concept in the design ofdeep inferior epigastric artery perforator flaps for breastreconstruction. Microsurgery 2010;30:1–7.
7. Blondeel PN, Arnstein M, Verstraete K, et al. Venous con-gestion and blood flow in free transverse rectus abdominismyocutaneous and deep inferior epigastric perforator flaps.Plast Reconstr Surg. 2000;106:1295–1299.
8. Schaverien M, Saint-Cyr M, Arbique G, Brown SA. Arterialand venous anatomies of the deep inferior epigastric perfo-rator and superficial inferior epigastric artery flaps. PlastReconstr Surg. 2008;121:1909–1919.
9. Rozen WM, Pan WR, Le Roux CM, Taylor GI, Ashton MW. Thevenous anatomy of the anterior abdominal wall: An anatomicaland clinical study. Plast Reconstr Surg. 2009;124:848–853.
10. Keller A. Perfusion zones of the DIEP flap revisited: A clinicalstudy. Plast Reconstr Surg. 2006;118:1076–1077.
11. Brooks D, Buntic RF. Determination of the vascular config-uration in autogenous breast reconstruction using abdomi-nal tissue: Simple but not necessarily easy. Plast Reconstr Surg.2006;118:1665–1665.
ReplySir:
I thank Dr. Hallock for his comments on our previ-ous work with the deep inferior epigastric perforator(DIEP) flap vascular anatomy and perforasome theory.1,2
Each perforator has its own vascular territory (perfora-some) and will capture adjacent perforasomes in a vari-able fashion. Thus, with respect to perforator flaps, thefocus has now shifted from source artery vascular territory(angiosome) to the individual perforator vascular terri-tory (perforasome). More importantly, the number ofadjacent perforasomes that are perfused by means of themain perforator will dictate the overall vascular territoryand survivability of any given perforator flap. Traditionalclassification zones of perfusion for the lower abdomenare based entirely on source artery vascularity and theirangiosomes (e.g., transverse rectus abdominis musculo-cutaneus flap), and I agree with Drs. Hallock and Rozenthat they do not necessarily apply to perforator flaps. Inour previous studies,1–8 classic abdominal zones of perfu-sion according to Hartrampf et al.3 and Dinner et al.4 wereused to describe DIEP flap vascularity to keep the classi-fication simple and familiar.
The dominant perforators in the lower abdomen canbe found within the deep inferior epigastric artery (DIEA)medial row, and the most dominant medial perforatorsare found in the periumbilical region.8 I always try toharvest my DIEP flaps based on these perforators and willroutinely discard all of Hartrampf zone IV, half or one-third of zone III, and half of zone II (reminder:Hartrampf � zone II contralateral to the midline).
When looking at Hallock and Rozen’s perforatorperfusion classification scheme, this corresponds toperforator zones II, I, II, where zone I is supplied by themain medial perforator itself, and both adjacent per-forator zones II correspond to the contralateral medial
Plastic and Reconstructive Surgery • December 2010
2284

row and ipsilateral lateral row perforasomes (Fig. 1).For the DIEP flap, harvesting perforator zone I andboth adjacent perforator zones II can be consideredvery safe because only one adjacent perforasome isrecruited on both sides of the selected main perforator.Harvest of additional tissue is certainly possible and hasbeen reported (e.g., harvest of Hartrampf zones III andIV or, in other words, two or more adjacent perfora-somes recruited, e.g., perforasomes III, IV, and V) butcarries a higher risk of ischemia and venous congestion.Recruitment of additional perforasomes requires care-ful clinical evaluation, which can be facilitated by in-traoperative perfusion studies (e.g., laser-assisted indo-cyanine green angiography). The same can be said forharvest of a lateral row–based DIEP flap, where safeharvest can be expected with perfusion zones II, I, II,where zone II corresponds to the ipsilateral SIEA vas-cular territory, zone I the lateral row perforator, andzone II the ipsilateral medial row perforator. In lateralperforator–based DIEP flaps where zones II, I, II, areused, the perforator is safely centered within the flapand both single adjacent perforasomes are easily re-cruited (Fig. 2). In Dr. Hallock’s clinical example, asingle dominant medial perforator was used and dem-onstrated mottling at the boundary of the contralateralrow perforator with mixed arterial and venous bleedingwhen this area was excised. This area would correspondto perforator zones III and IV. No vascular compromiseis mentioned medial to the contralateral lateral row.This implies that perforator zones II, I, II were wellperfused, as was part of ipsilateral zone III, because theentire right hemiabdomen was used. This pattern ofperfusion for a single dominant medial row perforatoris predictable, safe, and confirmed by previous studies.2,6,8
Therefore, for any given perforator flap, flow fromthe main chosen perforator to adjacent perforators
Fig. 2. Perforasomes of a medial perforator– based DIEP flap.Zone I corresponds to the medial row perforator itself; zones II,the ipsilateral lateral row perforator and the contralateral medialrow perforator. Additional zones with higher degrees of variabil-ity include zones III, ipsilateral superficial inferior epigastric arteryvascular territory and contralateral lateral row perforator; andzone IV, contralateral superficial inferior epigastric artery vascu-lar territory.
Fig. 3. Harvest of a single dominant periumbilical medial rowperforator DIEP flap with perfusion and bright red bleeding up tozone IV.
Fig. 1. Perforasome classification of a lateral perforator– basedDIEP flap. Zone I corresponds to the lateral row perforator, andzones II correspond to the ipsilateral superficial inferior epigastricartery vascular territory and the ipsilateral medial row perforator.Additional zones with higher degrees of variability include zoneIII, contralateral medial row perforator; zone IV, contralateral lat-eral row perforator; and zone V, contralateral SIEA territory.
Volume 126, Number 6 • Letters
2285

(interperforator flow) occurs by means of direct andindirect linking vessels,1 and is dictated by multiplefactors such as perfusion pressure, perforator size, vas-cular resistance, and number and caliber of direct/indirect linking vessels. I agree with Drs. Hallock andRozen that perfusion decreases with each additionalperforasome recruited. Recruitment of two or moreadjacent perforasomes is possible but carries a higherrisk of venous congestion and arterial ischemia. Thisexplains why there can be variations in perforator flapperfusion and why careful clinical assessment alwaysremains important (Figs. 3 and 4).
DIEP Flap Zones of PerfusionA. Medial row DIEPII, I, II: very reliableIII*, II, I: very reliableIII*, II, I, II: reliableIII*, II, I, II, III: variableIII*, II, I, II, III, IV: variable*Third or half of zone III.
B. Lateral row DIEPII, I, II: very reliableII, I, II, III: variableII, I, II, III, IV: less reliableII, I, II, III, IV, V: much less reliable
DOI: 10.1097/PRS.0b013e3181fb7bad
Michel Saint-Cyr, M.D.Department of Plastic Surgery
University of Texas Southwestern Medical Center1801 Inwood Road
Dallas, Texas [email protected]
DISCLOSUREThe author has no financial conflict of interest to disclose.
REFERENCES1. Saint-Cyr M, Wong C, Schaverien M, Mojallal A, Rohrich RJ.
The perforasome theory: Vascular anatomy and clinical im-plications. Plast Reconstr Surg. 2009;124:1529–1544.
2. Wong C, Saint-Cyr M, Mojallal A, et al. Perforasomes of theDIEP flap: Vascular anatomy of the lateral versus medial rowperforators and clinical implications. Plast Reconstr Surg. 2010;125:772–782.
3. Hartrampf CR, Scheflan M, Black PW. Breast reconstructionwith a transverse abdominal island flap. Plast Reconstr Surg.1982;69:216–225.
4. Dinner MI, Dowden RV, Scheflan M. Refinements in the useof the transverse abdominal island flap for postmastectomyreconstruction. Ann Plast Surg. 1983;11:362–372.
5. Rozen WM, Ashton MW, Le Roux CM, Pan WR, Corlett RJ.The perforator angiosome: A new concept in the design ofdeep inferior epigastric artery perforator flaps for breast re-construction. Microsurgery 2010;30:1–7.
6. Schaverien M, Saint-Cyr M, Arbique G, Brown SA. Arterial andvenous anatomies of the deep inferior epigastric perforatorand superficial inferior epigastric artery flaps. Plast ReconstrSurg. 2008;121:1909–1919.
7. Wong C, Saint-Cyr M, Arbique G, et al. Three- and four-dimensional computed tomography angiographic studies of
commonly used abdominal flaps in breast reconstruction.Plast Reconstr Surg. 2009;124:18–27.
8. Bailey SH, Saint-Cyr M, Wong C, et al. The single dominantmedial row perforator DIEP flap in breast reconstruction:Three dimensional perforasome and clinical results. Plast Re-constr Surg. 2010;126:739–751.
Perforator Number Predicts Fat Necrosis in aProspective Analysis of Breast Reconstructionwith Free TRAM, DIEP, and SIEA FlapsSir:
We are writing regarding the interesting article byBaumann et al., “Perforator Number Predicts Fat
Necrosis in a Prospective Analysis of Breast Reconstruc-tion with Free TRAM, DIEP, and SIEA Flaps,” in whichsome exciting clinical observations have been madethat may shed further light on the physiology of deepinferior epigastric artery (DIEA) perforator flaps.1However, we would like to clarify some important an-atomical definitions made in the article that may havea substantial bearing on the ultimate interpretation ofthe findings.
Fig. 4. Intraoperativeflapinsettingwithuseofall fourzones,andpostoperative results 4 months later after revision surgery. Therewas some minor epidermolysis of the flap skin edge in zone IV,which healed with conservative treatment.
Plastic and Reconstructive Surgery • December 2010
2286

In their assessment of perforator flaps, the authorsinclude the superficial inferior epigastric artery (SIEA)flap, describing the flap as a perforator flap and statingthat the SIEA flap comprises “a single fasciocutaneousperforator.” We would like to make note of our ana-tomical findings of the SIEA, in which we assessed 500studies of the SIEA with imaging.2 In our experience,the SIEA does not “uniformly” lie deep to the Scarpafascia and in fact quite variably lies deep or superficialto the Scarpa fascia. Based on our studies, it wouldtherefore not be appropriate to call the SIEA flap aperforator flap at all. As such, to include the SIEA in thesame category as DIEA perforators is not appropriate,especially because even the SIEAs that are fasciocuta-neous perforators may not be functionally equivalent tomusculocutaneous perforators.
The authors also describe the SIEA territory, statingthat “SIEA flaps were included in this study as theycomprise the same anatomic territory of lower abdom-inal skin and subcutaneous fat as muscle-sparing TRAMand DIEP flaps.” This is certainly not true, with multiplecadaveric dissection and angiographic studies,3,4 andclinical injection and immunofluorescence studies,2,5,6
all showing that the anatomical studies of the DIEA andSIEA are absolutely distinct from one another (Fig. 1).7These studies have shown that the primary angiosomeof the SIEA is the region between the linea semilunarisand the anterior axillary line, whereas that of the DIEAis between the linea alba and the linea semilunaris,although interindividual variability certainly occurs. Thisfurther emphasizes that for the scientific purposes of ad-
dressing the primary aims of the study by Baumann et al.,it would be wise to exclude the data on the SIEA.
A last note on the methodology used by the authors inassessing perforator anatomy concerns the authorsstating that they counted the number of perforatorsintraoperatively, even where transverse rectus abdominismyocutaneous (TRAM) flaps were used. Furthermore,perforator size was assessed based on external diameters,as observed intraoperatively. Both of these techniquesseem difficult to achieve with substantial accuracy forinterpretation of results. In terms of counting perforatornumber in TRAM flaps, there may be many perforatorswithin the included muscle that are simply not seen in-traoperatively and missed in counting. We would suggestthat the use of preoperative imaging may substantiallyimprove the accuracy of this assessment. In our studies ofthe use of computed tomographic angiography, we havefound a near 100 percent positive predictive value forassessing perforator number with the use of computedtomographic angiography.8,9 Of additional note, the useof the external diameter of perforators is a poor re-flection of relative flow between perforators, as wallthickness varies substantially between individual perfo-rators, as does relative flow between two perforators ofthe same external diameter. Again, the use of flow-dependent imaging may be useful as an objective mea-sure of internal vessel diameter and relative flow,particularly with the use of color Doppler or duplexultrasonography or contrast computed tomographicangiography or magnetic resonance angiography.DOI: 10.1097/PRS.0b013e3181f61c04
Warren M. Rozen, M.B.B.S., B.Med.Sc.,P.G.Dip.Surg.Anat.
Iain S. Whitaker, M.B.B.Chir., Ph.D.
Daniel Chubb, M.B.B.S., B.Med.Sc.
Mark W. Ashton, M.B.B.S., M.D.Jack Brockhoff Reconstructive Plastic Surgery Research
UnitDepartment of Anatomy and Cell Biology
University of MelbourneParkville, Victoria, Australia
Correspondence to Dr. RozenJack Brockhoff Reconstructive Plastic Surgery Research
UnitRoom E533
Department of Anatomy and Cell BiologyUniversity of Melbourne
Parkville, Victoria 3050, [email protected]
DISCLOSUREThe authors have no financial interest to declare in re-
lation to the content of this communication.
REFERENCES1. Baumann DP, Lin HY, Chevray PM. Perforator number pre-
dicts fat necrosis in a prospective analysis of breast recon-struction with free TRAM, DIEP, and SIEA flaps. Plast ReconstrSurg. 2010;125:1335–1341.
Fig. 1. Computed tomographic angiogram with volume-ren-dered technique reformat of the vasculature of the anterior ab-dominal wall, demonstrating the differences between angio-some territories of deep inferior epigastric artery perforatorshighlighted in blue (perforators �1 mm) and yellow (perforators�1 mm) and the SIEA highlighted in white. (Reproduced withpermission from Rozen WM, Grinsell D, Koshima I, Ashton MW.Dominance between angiosome and perforator territories: Anew anatomical model for the design of perforator flaps. J Recon-str Microsurg. 2010;26:539 –545.
Volume 126, Number 6 • Letters
2287

2. Rozen WM, Chubb D, Grinsell D, et al. The variability of thesuperficial inferior epigastric artery (SIEA) and its angiosome:A clinical anatomical study. Microsurgery 2010;30:386–391.
3. Taylor GI. Blood supply of the abdomen revisited, with em-phasis of the superficial inferior epigastric artery (Discussion).Plast Reconstr Surg. 1984;74:667–670.
4. Taylor GI, Palmer JH. The vascular territories (angiosomes)of the body: Experimental study and clinical application. Br JPlast Surg. 1987;40:113–141.
5. Holm C, Mayr M, Hofter E, et al. Perfusion zones of the DIEP flaprevisited: A clinical study. Plast Reconstr Surg. 2006;117:37–43.
6. Holm C, Mayr M, Hofter E, Ninkovic M. The versatility of theSIEA flap: A clinical assessment of the vascular territory of thesuperficial epigastric inferior artery. J Plast Reconstr Aesthet Surg.2007;60:946–951.
7. Rozen WM, Grinsell D, Koshima I, Ashton MW. Dominancebetween angiosome and perforator territories: A new ana-tomical model for the design of perforator flaps. J ReconstrMicrosurg. 2010;26:539–545.
8. Rozen WM, Ashton MW, Stella DL, Phillips TJ, Grinsell D,Taylor GI. The accuracy of computed tomographic angiog-raphy for mapping the perforators of the deep inferior epi-gastric artery: A blinded, prospective cohort study. Plast Re-constr Surg. 2008;122:1003–1009.
9. Rozen WM, Ashton MW, Stella DL, Phillips TJ, Taylor GI. Theaccuracy of computed tomographic angiography for mappingthe perforators of the DIEA: A cadaveric study. Plast ReconstrSurg. 2008;122:363–369.
ReplySir:
We thank Drs. Rozen, Whitaker, Chubb, and Ashtonfor their letter1 and interest in our article2 showing theassociation of fat necrosis and the number of perfora-tors in free flaps from the lower abdomen used forbreast reconstruction, and their comments about per-forator flap anatomy. We agree that the superficialinferior epigastric artery (SIEA) flap is a fasciocutane-ous flap, not a perforator flap. We were very careful notto refer to the SIEA flap as a perforator flap in ourarticle.2 One must keep in mind that the purpose of ourarticle was to present the association we discoveredbetween the incidence of fat necrosis and the numberof perforators (either musculocutaneous or fasciocutane-ous) in free flaps from the lower abdomen when used forbreast reconstruction (see the first paragraph of the Pa-tients and Methods section of our article).2 We wanted tostudy the incidence of fat necrosis in lower abdominal freeflaps used for breast reconstruction, whether they areperforator (DIEP) flaps, musculocutaneous [muscle-spar-ing free transverse rectus abdominis musculocutaneous(TRAM)] flaps, or fasciocutaneous (SIEA) flaps. Our in-tent was not to study the territory of these flaps or theterritory of the angiosomes of perforators.
We made a carefully considered decision to includeSIEA flaps with DIEP and muscle-sparing free TRAMflaps in our study (see the third paragraph of the Dis-cussion section of our article).2 Neither SIEA flaps normuscle-sparing TRAM flaps are perforator flaps, butboth of these free flaps are used to reconstruct breastswith skin and subcutaneous tissue from the lower ab-
dominal donor site. We agree that the anatomical ter-ritory of the SIEA flap is distinct from the territory ofthe DIEP flap. However, their territories overlap to agreat extent. Moreover, we do not use an SIEA flapunless the SIEA vessels are large enough, and medialenough, to allow transfer of the identical paddle oflower abdominal skin and subcutaneous tissue re-quired for breast reconstruction as we would have har-vested had we used a DIEP flap or muscle-sparingTRAM flap in the same patient.
Dr. Rozen et al. state that in their experience theSIEA does not uniformly lie deep to the Scarpa fascia.The SIEA originates from the femoral artery, or froma common trunk with the deep circumflex iliac arteryoff the femoral artery, and therefore is necessarily uni-formly deep to the Scarpa fascia near its origin from thefemoral artery. The SIEA runs superiorly from its originwithin the anterior abdominal wall and, at some point,the SIEA or one of its branches pierces the Scarpa fasciafrom deep to superficial, but the SIEA always originatesdeep to the Scarpa fascia.
Dr. Rozen et al.1 questioned our methodology ofassessing perforators. Our flap selection algorithm is toattempt an SIEA flap first. If the SIEA vessels are in-adequate to support the required flap volume, we iden-tify and dissect all of the substantial perforators of theflap. If there are one or several dominant perforators,we usually use a DIEP flap. If the number and locationof perforators required to support the desired DIEPflap volume would lead to division of a substantialamount of rectus abdominis muscle fibers, we harvesta muscle-sparing TRAM flap. Therefore, all of the per-forators are identified and accounted for. We did notuse full-muscle-width free TRAM flaps, and there wasno undissected area of anterior rectus fascia of the flapsin which undetected perforators could have beenpresent. We do not believe that preoperative imagingwith computed tomographic angiography or other mo-dalities would have improved the accuracy of countingperforators in the muscle-sparing TRAM flaps.
Finally, we agree that assessing the external diameterof perforators is difficult to achieve with substantialaccuracy. For this reason, we based our major resultsand conclusions of our study on the number, and notsize, of perforators.DOI: 10.1097/PRS.0b013e3181f61c18
Pierre M. Chevray, M.D., Ph.D.Institute for Reconstructive Surgery
The Methodist Hospital
Donald P. Baumann, M.D.Department of Plastic Surgery
University of Texas M. D. Anderson Cancer CenterHouston, Texas
Correspondence to Dr. ChevrayDepartment of Surgery
Methodist Hospital6560 Fannin, Suite 800Houston, Texas 77030
Plastic and Reconstructive Surgery • December 2010
2288

REFERENCES1. Rozen WM, Whitaker IS, Chubb D, Ashton MW. Perforator
number predicts fat necrosis in a prospective analysis of breastreconstruction with free TRAM, DIEP, and SIEA flaps (Letter).Plast Reconstr Surg. 2010;126:2286–2288.
2. Baumann DP, Lin HY, Chevray PM. Perforator number pre-dicts fat necrosis in a prospective analysis of breast recon-struction with free TRAM, DIEP, and SIEA flaps. Plast ReconstrSurg. 2010;125:1335–1341.
Liponecrotic Pseudocysts following FatInjection into the BreastSir:
I read this article1 with the finding of liponecroticpseudocysts following fat injection into the breast
with interest. I also note that these were patients of aninstitution other than that of the authors. This type ofcomplication would probably not be found in the prac-tice of those skilled like Dr. Erol et al. I suspect thecomplications noted were more a matter of techniquethan a basic fault in the concept of fat transfer. In myseries of 650 cosmetic breast augmentations using fattransfer (autologous fat transplantation), there was a1.25 percent incidence of microcalcifications, all ofwhich were detectable only on follow-up mammogra-phy. Criteria that I have previously outlined were morethan sufficient to determine the benign nature of thesecalcifications, and no surgical interventions were nec-essary. I believe that in these cases the cause was simplythe excess of fat injected into a single site. Large de-posits of fat violate the original description of the tech-nique and are bound to result in necrosis and compli-cations such as were presented here. I agree with mostof Dr. Erol’s conclusions, but from my perspective, 29years is sufficient time for evaluation. Because fat trans-fer, in all of its applications, can offer so much benefit,it would be wiser to recommend a more widespreadteaching of the proper technique.2–7
DOI: 10.1097/PRS.0b013e3181f61b6b
Mel Bircoll, M.D.2700 Casiano Road
Los Angeles, Calif. [email protected]
REFERENCES1. Erol OO, Agaoglu G, Uysal AO. Liponecrotic pseudocysts fol-
lowing fat injection into the breast. Plast Reconstr Surg. 2010;125:168e–170e.
2. Bircoll MJ. Cosmetic breast augmentation utilizing autologousfat and liposuction techniques. Paper presented at: SecondAsian Congress of Plastic Surgery; May 1984; Bangkok andPattaya, Thailand.
3. Bircoll MJ. Cosmetic breast augmentation utilizing autologousfat and liposuction techniques. Plast Reconstr Surg. 1987;79:267–271.
4. Bircoll MJ. Autologous fat transplantation employing liposuc-tion techniques. Ann Plast Surg. 1987;18:327–329.
5. Bircoll MJ. Autologous fat transplantation: An evaluation of mi-crocalcification and fat cell survivability following (AFT) cos-metic breast augmentation. Am J Cosmet Surg. 1988;5:283–288.
6. Bircoll MJ. Innovations for fat transfer, fat storage, serial injec-tions and stem cell extraction from lipo-aspirate. Paper pre-sented at: American Society of Plastic Surgeons Perspectives andAdvances in Plastic Surgery; March 14–18, 2009; Vail, Colo.
7. Bircoll MJ. Innovations for fat transfer, fat storage and serialinjections for breast cancer prevention surgery. Paper pre-sented at: 29th Biennial Pan Pacific Plastic Surgery Congress;January 9–14, 2010; Honolulu, Hawaii.
Management of the Infected or Exposed BreastProsthesis: A Single Surgeon’s 15-YearExperience with 69 PatientsSir:
We read with great interest the article by Spear andSeruya1 about risk factors for failed breast im-
plant salvage. Understanding the risk factors for com-plications will help to improve the informed consentprocess and assist plastic surgeons and patients alikewith treatment decisions. Thus, this is a thoughtfularticle that should be relevant to many plastic surgeons.
Recently, there has been a resurgence of interest inoptions for implant salvage, and this article again il-lustrates the value of these methods. As the authorspoint out, there is still disagreement regarding theindications and the optimal timing. Furthermore, is-sues in management are complicated by an inability todetermine accurately the presence of an infection, thereluctance to operate on a patient who may not have aninfection, and unclear guidelines on optimal interven-tion. We agree that it would be valuable for plasticsurgeons to better define a set of guidelines addressingthese very issues, given the legal and economic issuesassociated with implant loss.
Another important issue is related to risk factors. Al-though the authors observed that radiotherapy or Staph-ylococcus aureus did not affect the success of device salvage,it has been our impression that this conclusion is attrib-utable to the limitation of the study. As the authorspointed out, the lack of statistical significance for specificrisk factors may stem from the sample size for subgroupanalysis rather than the true absence of a statistical dif-ference. In contrast, we believe that the main risk factorfor failed implant salvage is related to biofilm formation,characterized by the ability of bacteria to attach and growon inanimate surfaces, facilitated by the production ofadhesion molecules. Some studies demonstrated that dif-ferent strains of Staphylococcus differ in their ability toadhere to surfaces of foreign material and therefore differin their ability to produce biofilm.2 It is also widely ac-cepted that biofilm organisms living in their extracellularmatrix are much more resistant to the bactericidal effectsof antibiotics, in which they can tolerate antibiotics inconcentrations 10 to 1000 times greater than thoseneeded to kill their equivalent no-biofilm form.3
From a practical point of view, following implanta-tion of any surgical device, bacteria and host cells com-pete for colonization. If bacteria undergo biofilm for-mation, probably they will be able to evade the hostimmune response and become resistant to antibiotics,
Volume 126, Number 6 • Letters
2289

thus explaining the difficulty in eradicating such in-fections. Thus, given the ability of biofilms to favorbacterial survival, the rationale for removal of infecteddevices is provided.
We believe that the optimal treatment of breast implantinfections is not well established and is at best derivedfrom case studies. For suspected infections, cultureshould be obtained and empiric antibiotics directed at thepreviously mentioned organisms started. Response toantibiotics will determine whether surgical intervention isrequired. For persistent mild infections, local debridementwith closed-suction drainage may be successful.
In conclusion, the authors have performed a thought-ful study with a retrospective design. Although this studyhas limitations regarding its measures and analyses, theauthors described important risk factors that are relevantto the informed treatment decision-making process. Thevalidity of the results is dependent on the quality of themeasures along with statistical efforts to control forpotential biases. It is well understood that randomizedcontrolled trials are the standard means of producinghigh-level evidence. However, and especially in thebreast augmentation field, it is not always feasible toperform these trials when evaluating surgical treat-ments that are highly dependent on patient and sur-geon preferences. The authors are to be commendedfor their insightful approaches to these problems.DOI: 10.1097/PRS.0b013e3181f61b7d
Alexandre Mendonca Munhoz, M.D.
Rolf Gemperli, M.D., Ph.D.University of Sao Paulo
Sao Paulo, Brazil
Correspondence to Dr. MunhozDivision of Plastic Surgery
University of Sao Paulo School of MedicineRua Oscar Freire 1702 ap. 78
Sao Paulo, SP 05409-011, [email protected]
REFERENCES1. Spear SL, Seruya M. Management of the infected or exposed
breast prosthesis: A single surgeon’s 15-year experience with69 patients. Plast Reconstr Surg. 2010;125:1074–1084.
2. Schwank S, Rajacic Z, Zimmerli W, Blaser J. Impact of bacterialbiofilm formation on in vitro and in vivo activities of antibi-otics. Antimicrob Agents Chemother. 1998;42:895–898.
3. Jefferson KK. What drives bacteria to produce a biofilm? FEMSMicrobiol Lett. 2004;236:163–173.
Rib Fracture as a Complication of TissueExpansion in Breast ReconstructionSir:
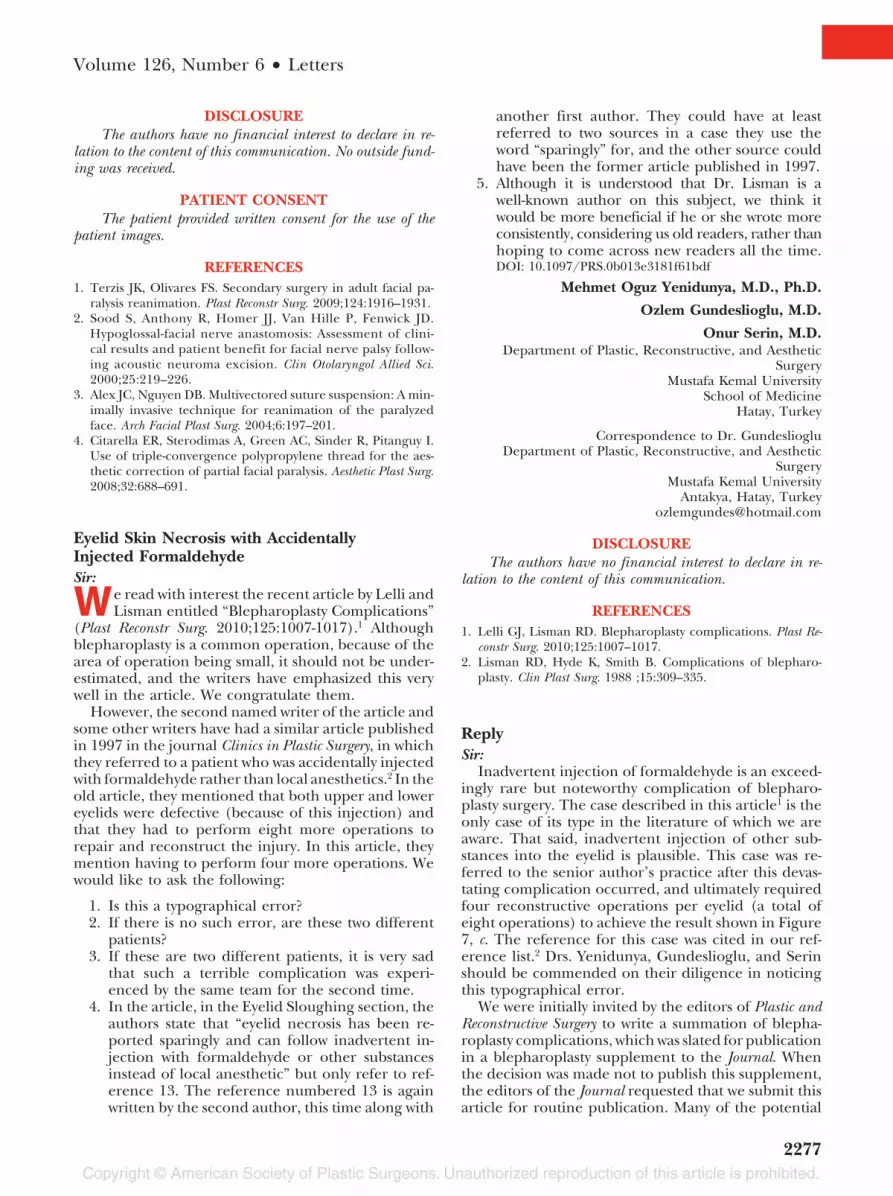
We read with great interest the article entitled “RibFractures: A Complication of Radiation Therapy
and Tissue Expansion for Breast Reconstruction” byTseng et al.1 We compliment the authors on their work.We totally agree with the recommendation that plasticsurgeons counsel patients requesting tissue expanders
in an irradiated field about the possibility of rib fractureand subsequent need to alter reconstructive plans. Wereport a case of two rib fractures subsequent to a breastreconstruction tissue expansion.
A 45-year-old woman was admitted for a skin expan-sion postmastectomy. A 500-cc tissue expander was im-planted in the submuscular plane. We inflated 50 cc ofsaline solution every week for 4 months. A total of 600 ccon each side was inflated. After 1 month, followinga sneeze, the patient reported sudden onset of chestpain under her left breast tissue expander. We removed100 cc of saline solution from the left skin expander,which resulted in improvement of the symptoms. After3 months, at periodic scintigraphic control, the ap-pearance of a “hot-spot” was observed on the costal leftbone (Fig. 1). A chest computed tomographic scan con-firmed the presence of left fourth and fifth rib fracturesand a moth-eaten appearance to the surrounding left ribs,consistent with postirradiation skeletal changes (Fig. 2).
After 2 months, the skin expander was replaced witha 450 mammary implant. No complication followed theoperation. At 2-year follow-up, the outcome was satis-factory to the patient.
We agree with the authors that caution should beused in skin expansion in postirradiation patients, whoare predisposed to a rib fracture more than nonirra-diated patients. We would argue for a slow skin expan-sion in postirradiation patients to avoid rib fracture. Inparticular, it is important to not overexpand the im-plant because of the high risk of rib fracture in thesepatients.2 We think that appropriate and well-per-formed planning in addition to a consent form is ap-propriate in irradiated patients before reconstructivesurgery with skin expansion.DOI: 10.1097/PRS.0b013e3181f61b56
Lucio Tirone, M.D.
Ivan La Rusca, M.D.
Fig. 1. Postoperative scintigraphic control showing appearanceof a hot-spot on the costal left bone.
Plastic and Reconstructive Surgery • December 2010
2290
Feliciano Ciccarelli, M.D.Plastic Surgery Unit
Villa dei Fiori HospitalNaples, Italy
Correspondence to Dr. La RuscaPlastic Surgery Unit
Villa dei Fiori HospitalVia San Domenico 80
Naples 80127, [email protected]
REFERENCES
1. Tseng J, Huang AH, Wong MS, Whetzel TP, Stevenson TR. Ribfractures: A complication of radiation therapy and tissue ex-pansion for breast reconstruction. Plast Reconstr Surg. 2010;125:65e–66e.
2. Fodor PB, Swistel AJ. Chest wall deformity following expan-sion of irradiated soft tissue for breast reconstruction. N Y StateJ Med. 1989;89:419–420.
Gynecomastia: Evolving Paradigm ofManagement and Comparison of TechniquesSir:
We read with interest the article by Petty et al.entitled “Gynecomastia: Evolving Paradigm of
Management and Comparison of Techniques.” Undera perfect title, we found this article precise and easy toread, most of all, because of its conclusion: arthroscopicmastectomy for gynecomastia is a safe and effectivetechnique, with excellent cosmetic results and an ac-ceptable complication rate. We found a major flaw inthis retrospective study, namely, “undercitation,” whichmany of us consider to be a serious offense in scientificmisconduct for not giving credit to previous publications.1,2
This operation, described in 2005 as an arthroscopicmastectomy for gynecomastia, was published before inthis same Journal (Techniques in Cosmetic Surgery)under the title “Minimal Surgical Access to Treat Gy-necomastia with the Use of a Power-Assisted Arthro-
Fig. 2. Chest computed tomographic scans showing presence of left fourth and fifth rib fractures and a moth-eaten appearance to the surrounding left ribs.
Volume 126, Number 6 • Letters
2291

scopic-Endoscopic Cartilage Shaver” by Prado andCastillo1 and assessed by another publication in 2009 byBenito-Ruiz et al.2
Without a better measure of the impact factor thatplaces Plastic and Reconstructive Surgery as a leader inpublications of our specialty in the world, the citationindex will continue to be used as a reflection of ajournal’s popularity.3 As a consequence, undercitationcould eventually affect the impression of this Journal.
Reviewers must take the responsibility of checkingevery citation reference, the accuracy of referencecontent, and the accuracy of cited material, and eval-uating possible missing citations, because the mostcrucial part of the review process is to “check theaccuracy of the content.” A big help for this job aresuch reference managers as Endnote/EndLink thatare related to PubMed/MEDLINE.DOI: 10.1097/PRS.0b013e3181f61b91
Arturo S. Prado, M.D.
Paulo Castillo, M.D.School of Medicine
Postgraduate SchoolPlastic Surgery
University of ChileSantiago, Chile
Correspondence to Dr. PradoDivision of Plastic Surgery
School of MedicinePostgraduate School
University of ChileManquehue Norte 1701 ofic 210
VitacuraSantiago, Metropolitana, Chile
DISCLOSUREThe authors have no financial interest to declare in re-
lation to the content of this communication.
REFERENCES1. Prado AC, Castillo PF. Minimal surgical access to treat gyneco-
mastia with the use of a power-assisted arthroscopic-endoscopiccartilage shaver. Plast Reconstr Surg. 2005;115:939–942.
2. Benito-Ruiz J, Raigosa M, Manzano M, Salvador L. Assessmentof a suction-assisted cartilage shaver plus liposuction for thetreatment of gynecomastia. Aesthet Surg J. 2009;29:302–309.
3. Chung KC. Value of citation numbers and impact factors foranalysis of plastic surgery research (Discussion). Plast ReconstrSurg. 2007;120:2092–2094.
Paradigm Misbehavior in the Evolving ParadigmSir:
I read with interest the article about gynecomastia byDr. Petty et al. in the May 2010 issue of Plastic and
Reconstructive Surgery.1 They indicated that they describea novel technique for the treatment of this condition.They claim that they have been using this techniquesince 1997, which consists of liposuction plus removalof the gland with an arthroscopic cartilage shaver.
Two former articles were absent from their refer-ences: those by Prado and Castillo2 and Benito-Ruiz etal.3 Prado and Castillo have to be credited as being thefirst authors to describe this technique in Plastic andReconstructive Surgery (and to my knowledge, this workwas presented at the Annual Meeting of the AmericanSociety for Aesthetic Plastic Surgery in Boston) and myteam and myself published our experience with thistechnique in a prospective research study to define itsindications in our hands. Reading Dr. Petty’s article, Ialso missed the revision by Hammond in Plastic andReconstructive Surgery in 2009.4
Moreover, the algorithm for treatment that they showat the end of their article is very similar to the one wepublished. I cannot understand how a colleague from aprestigious institution missed these former articles.DOI: 10.1097/PRS.0b013e3181f61bb8
Jesus Benito-Ruiz, Ph.D.Antiaging Group Barcelona
C/ Dr Carulla 12 Third FloorClınica Tres Torres
08017 Barcelona, [email protected]
REFERENCES1. Petty PM, Solomon M, Buchel EW, Tran NV. Gynecomastia:
Evolving paradigm of management and comparison of tech-niques. Plast Reconstr Surg. 2010;125:1301–1308.
2. Prado AC, Castillo PF. Minimal surgical access to treat gyneco-mastia with the use of a power assisted arthroscopic-endoscopiccartilage shaver. Plast Reconstr Surg. 2005;115:939–942.
3. Benito-Ruiz J, Raigosa M, Manzano M, Salvador L. Assessmentof a suction-assisted cartilage shaver plus liposuction for thetreatment of gynecomastia. Aesthet Surg J. 2009;29:302–309.
4. Hammond DC. Surgical correction of gynecomastia. Plast Re-constr Surg. 2009;124:61e–68e.
ReplySir:
I eagerly welcome the opportunity to respond to theletter written by Drs. Prado and Castillo concerning myarticle describing our experience at the Mayo Clinicwith arthroscopic mastectomy since 1997. This letter isalso a response to the comments by Dr. Benito-Ruizregarding our article in the May 2010 issue of Plastic andReconstructive Surgery.
The article contains the references appropriate to itscontent. Although one may appreciate the perceivedslight at a lack of reference, any attempt at systematicinclusion of every publication with any potential relevanceto an article would bring academic publishing to a grind-ing halt. The Journal shows a broadminded tolerancewhen it publishes the letter by Drs. Prado and Castillo.
As stated above, I developed this technique in 1997.All of the details of the day on which it occurred are stillvery clear in my mind. The decision to use an arthro-scopic debrider was a byproduct of a grand roundspresentation concerning liposuction that I gave whilea resident at The Johns Hopkins Medical Center in
Plastic and Reconstructive Surgery • December 2010
2292

1988. One of the endoscopic manufacturers had pro-duced a “liposhaver” attachment that was supposed tomake fat removal easier. The fact that it was a veryaggressive application for fat removal made me veryhesitant to want to use it for that purpose, but the seedof the concept had been sown with regard to its ulti-mate application.
In the mid 1990s, a number of articles had beenwritten about the removal of benign breast tissue frommen’s breasts using only liposuction equipment, withspecial sharp cannulas and/or in conjunction with ul-trasound. Those claims proved not to be useful forextremely firm breast tissue. I have noticed over thedecades that many declared advantages for new tech-niques in the plastic surgery literature fall somewhatshort of their initial lofty claims of superior outcomes,which accounts for a hesitancy on my own part to pub-lish before I am really sure that I have something ofsubstantial benefit to our plastic surgical colleagues.
During one of my efforts to remove breast tissue froma young man without using a periareolar incision andattempting to use only ultrasound and standard lipo-suction, it became clear that something else would berequired. I was operating in a room shared by orthope-dists, complete with arthroscopic equipment. The previ-ously mentioned liposhaver came to mind, and I found asmall orthopedic cartilage shaver that seemed appropri-ately similar. The settings on the shaver allow for clockwiseor counterclockwise rotation or an oscillating, “chewing”mode. None of the three choices of motion seemed to behelpful in this particular young man, so I asked to look atother, more aggressive, cutting-head options. At the time,the attachment we found was called a “gator” attachmentfor obvious reasons, with its serrated rows of teeth. WhenI ultimately turned the gator attachment on in oscillatingmode, the small, firm, white chunks of dense breast tissuefinally began their lovely little march down the suctiontubing toward the collecting canister. A battle was won; avery satisfying moment.
After a number of other successful uses of this tech-nique, I presented some preliminary findings in Janu-ary of 1998 at the 12th Annual Workshop in PlasticSurgery in Tortola, British Virgin Islands. During thesame year, we prepared a poster presentation for the16th Annual Lipoplasty Society meeting in Boston, Mas-sachusetts showing the details of the procedure. In Mayof 2003, I presented the technique to the 82nd AnnualMeeting of the American Association of Plastic Surgeonsin Baltimore, Maryland (a copy of the abstract is repro-duced below and easily verified). In March of 2009, wepresented the contents of the current article in questionto the American Association of Plastic Surgeons 88th An-nual Meeting in Rancho Mirage, California.
With regard to the publication of our technique, inlate 2004, we sent a manuscript to Plastic and Recon-structive Surgery describing the technique. Imagine mysurprise when Drs. Prado and Castillo’s publication wassubmitted and accepted just ahead of ours, claimingorigination of a technique that was essentially identicalto the one I had been describing in public forums since
1998, 1 year before their declared discovery and de-velopment of the application. I had my doubts as to“undercitation” and “scientific misconduct” on theirpart but kept them to myself. Rather than a letter ofindignation to the editors of Plastic and ReconstructiveSurgery, I simply decided that it would still be worth-while to publish our 12-year experience here at theMayo Clinic and compare it with the more standardtechniques performed at our institution during thesame time. Both the Association and Plastic and Recon-structive Surgery saw value in the contained informationand were kind enough to accept our presentation.
Had Dr. Prado or Dr. Castillo informed any aspect ofmy understanding or application of this technique, Iwould not only have listed their article in my referencesbut also praised their contribution in the body of myarticle. To have listed their article as contributing any-thing to what we have done here would have beenacademically dishonest.
In the future, should Dr. Prado or Dr. Castillo careto try to impugn my integrity or veracity concerning anyof my other academic activities or professional life, I willagain be happy to respond, but I believe this ratherthorough response closes the book on this ado.
Dr. Prado, believe me when I say, “I feel your pain.”Trust me when I say, “It gets better with time,” and, bythe way, I really appreciate the opportunity that youhave afforded me to unburden myself. Thank you.
ABSTRACTPurpose: A simple and reliable technique for re-
moval of breast tissue using a combination of ultra-sound, standard liposuction and an arthroscopic shaverthrough a remote incision is presented.
Methods & Procedures: Over the past five years, allpatients with gynecomastia presenting to this practicehave undergone subcutaneous mastectomy through re-mote incisions. The addition of a Linvatec arthroscopicshaver with a “gator” attachment has allowed for preciseremoval of tissue while avoiding visible peri-areolarscars in all cases. The procedure takes place in fourparts: (1) super-wet injection of dilute epinephrine andlidocaine, (2) ultrasound disruption of tissues, (3) stan-dard liposuction, and (4) removal of residual fibrousbreast tissue with the arthroscopic shaver.
Summary of Results: The addition of an arthro-scopic shaver to the practice of subcutaneous mastec-tomy has allowed for the procedure to be carried outthrough remote incisions in all gynecomastia patientstreated in this practice since 1997. The procedure hasbeen carried out with greater ease than the standardopen approach and allowed for more subtle, refinedresults. The average time of the procedure has beensimilar to that of open resection. Patient satisfaction hasbeen significantly higher. In the first 24 patients, therewas one hematoma early on in the series and a smallbuttonhole in the skin in yet another patient.
Conclusion: In all gynecomastia patients, without sig-nificant excess skin, subcutaneous mastectomy can easily
Volume 126, Number 6 • Letters
2293

be performed through a remote site. Peri-areolar inci-sions are no longer necessary. Outcomes are excellentwith high patient satisfaction. The learning cycle is short.DOI: 10.1097/PRS.0b013e3181f61de0
Paul M. Petty, M.D.Surgery
Mayo Clinic200 West 2nd Street SWRochester, Minn. 55905
An Alternative Technique Utilizing SerratusAnterior Fascia for Postmastectomy TissueExpander CoverageSir:
I would like to congratulate Dr. Saint-Cyr and col-leagues for revisiting a very important concept in
implant-based breast reconstruction: lateral cover-age of the tissue expander.1 The authors presenttheir technique for use of the serratus anterior fasciabased on a lateral pedicle. This not only providesadditional vascularized soft-tissue coverage under-neath the mastectomy flap, but also assists in main-tenance of expander position.
At our institution, we have similarly made it a pointto use this fascia when placing tissue expanders, with-out the additional use of acellular dermis. We agreethat this additional layer of vascularized tissue laterallyis beneficial, especially when the prosthetic underlies athin mastectomy flap.
Although achieving a similar degree of coverage asDr. Saint-Cyr and colleagues, we approach this dissec-tion in a slightly different fashion. We reported ourtechnique and the outcomes of 50 consecutive recon-structions using this technique in a recent issue ofPlastic and Reconstructive Surgery.2 In essence, the mid-portion of the pectoralis major is incised in the direc-tion of its fibers. Through this access point, a submus-cular pocket is developed in all directions. Laterally, thedissection continues beyond the lateral border of thepectoralis major, and as it proceeds, the serratus fasciais raised in continuity with this pocket. In this way, theborder between the pectoralis major and the serratusanterior fascia is not divided and thus does not requirerepair. The expander is placed into this pocket throughthe incision in the pectoralis major muscle.
In our hands, the benefit of this approach lies in thefact that the final step involves reapproximation of slips ofpectoralis major muscle to each other, rather than pec-toralis major to serratus fascia. As Dr. Saint-Cyr et al. alludeto in their article, this fascia can be thin in some patients.This method allows us to avoid having to directly repairthe fascia with sutures following expander placementand thus avoid potentially weakening it. The repair of thepectoralis major incision involves reapproximation of themore substantial muscle fibers to each other.
In the end, however, each of these techniques resultsin a fully vascularized pocket for the prosthetic. I
present this as an additional technique to achieve thesame excellent results that Dr. Saint-Cyr and colleagueshave been able to consistently achieve.DOI: 10.1097/PRS.0b013e3181f61da4
Hani Sbitany, M.D.University of Rochester
Rochester, N.Y.
Correspondence to Dr. Sbitany601 Elmwood Avenue, Box 661
Rochester, N.Y. [email protected]
REFERENCES1. Saint-Cyr M, Dauwe P, Wong C, Thakar H, Nagarkar P, Roh-
rich RJ. Use of the serratus anterior fascia flap for expandercoverage in breast reconstruction. Plast Reconstr Surg. 2010;125:1057–1064.
2. Sbitany H, Sandeen S, Amalfi AN, Davenport MS, LangsteinHN. Acellular dermis-assisted prosthetic breast reconstructionversus complete submuscular coverage: A head-to-head com-parison of outcomes. Plast Reconstr Surg. 2009;124:1735–1740.
ReplySir:
We would like to thank Dr. Sbitany for his commentsregarding our article on the use of the serratus anteriorfascia flap for lateral tissue expander coverage. We arein agreement that this fascia can be harvested in con-tinuity with the pectoralis major fascia when possible.1Criteria for using the approach, described by Dr. Sbi-tany, include continuity of fascia linking the serratusand pectoralis major muscles and continuity of thesubcutaneous tissue linking the inframammary fold tothe insertion of the pectoralis major muscle. In certaincases, the inframammary fold subcutaneous tissue link-ing the lower portion of the pectoralis major muscle hasbeen completely skeletonized following mastectomy.This results in discontinuity between the lower musclefibers of the pectoralis major and the inframammaryfold. The lower border of the pectoralis major musclemust then be sewn to the mastectomy skin flap subcu-taneous tissue and dermis, or a dermal allograft slingcan be used to reestablish continuity with the inframam-mary fold and allow precise tissue expander placement.We all too often encounter a scenario where there is alsolack of continuity between the fascia of the serratus andpectoralis major muscles laterally. Therefore, a pecto-ralis major–splitting technique with peripheral dissec-tion is not always feasible. In cases where continuitybetween serratus fascia and pectoralis major fascia hasbeen disrupted, or where the inferior fibers of thepectoralis major insert above the inframammary fold orhave been denuded of their overlying subcutaneoustissue, we are limited to having to elevate the serratusfascia independently from the pectoralis major fascia.In certain cases, we have also been able to elevate pec-toralis minor fascia in continuity with the serratus an-terior fascia or use the subpectoral fascia to provideadditional lateral tissue expander coverage. This pro-
Plastic and Reconstructive Surgery • December 2010
2294

vides well-vascularized tissue for lateral tissue expandercoverage, and as we mentioned in our previous publi-cations, can significantly limit the cost of dermal allo-graft use.2,3 Again, we would like to thank Dr. Sbitanyand colleagues for reporting their refinement in usingthe serratus anterior fascia for lateral tissue expandercoverage. This “no-touch,” minimally invasive tech-nique allows simple and readily available tissue for cov-erage over the lateral tissue expander, with minimalmorbidity. We are also advocates of using this tech-nique when the proper conditions exist which, as men-tioned previously, include a nonskeletonized breastpocket where fascial continuity is preserved betweenthe serratus and the pectoralis major muscles laterally,and where the inferior fibers of the pectoralis majormuscle have maintained their continuity with subcuta-neous tissue overlying the inframammary fold. Even ifthe inferior border of the pectoralis muscle is disin-serted, it is still kept in continuity with the inframam-mary fold by means of the overlying subcutaneoustissue bridge.DOI: 10.1097/PRS.0b013e3181f61e04
Michel Saint-Cyr, M.D.Department of Plastic Surgery
University of Texas Southwestern Medical Center1801 Inwood Road
Dallas, Texas [email protected]
DISCLOSUREThe author has no financial conflicts to disclose.
REFERENCES1. Sbitany H, Sandeen S, Amalfi AN, Davenport MS, Langstein
HN. Acellular dermis-assisted prosthetic breast reconstructionversus complete submuscular coverage: A head-to-head com-parison of outcomes. Plast Reconstr Surg. 2009;124:1735–1740.
2. Saint-Cyr M, Dauwe P, Wong C, Thakar H, Nagarkar P, Roh-rich RJ. Use of the serratus anterior fascia flap for expandercoverage in breast reconstruction. Plast Reconstr Surg. 2010;125:1057–1064.
3. Saint-Cyr M, Nagarkar P, Wong C, Thakar H, Dauwe P, Roh-rich RJ. The pedicled subpectoral fascia flap for expandercoverage in postmastectomy breast reconstruction: A noveltechnique. Plast Reconstr Surg. 2010;125:1328–1334.
Pedicled Perforator Flaps: A New Principle inReconstructive SurgerySir:
We read the article by Dr. Lee et al. on pedicledperforator flaps in the January of 2010 issue of
the Journal with great interest.1 Although we are pleasedto see that pedicled perforator flaps are receivinggreater attention, we feel that this article has potentiallyomitted any number of useful pedicled perforatorflaps. For example, we described the digital artery per-forator flap for fingertip reconstruction over 4 yearsago, and have further expanded the utility of this flapwith recently published modifications of our originaltechnique.2,3 Digital artery perforator flaps are pedicledrotational flaps based on perforators of the radial orulnar digital artery. They can be harvested as adiposal-only flaps or raised with full-thickness skin and subcu-taneous tissue, and are useful for reconstruction offingertip defects. A case example of this flap is pre-sented in Figure 1. The article would have further ben-efited readers by including the literature search criteriaused in construction of the “evolution of flap physiologyand reconstruction” database described in the abstractand by a formal reporting of these search results, neitherof which appears in the article. Strict reporting of searchcriteria and results would validate and aid in the con-struction of an atlas of pedicled perforator flaps which, assuggested by the authors and outlined in Table 1 of theirarticle,1 would benefit the clinician in designing recon-structions based on local anatomy. We applaud the au-thors for drawing attention to pedicled perforator flapsand look forward to future articles on the topic.DOI: 10.1097/PRS.0b013e3181f61ba4
Fig. 1. Digital artery perforator flap coverage of a long finger wound in a 68-year-old man following fingertip amputation with acircular saw. Flap elevation (left) and ulnar view of long-term result (right).
Volume 126, Number 6 • Letters
2295
Gerhard S. Mundinger, M.D.Division of Plastic and Reconstructive Surgery
The Johns Hopkins HospitalBaltimore, Md.
Mitsunaga Narushima, M.D.
Isao Koshima, M.D.Department of Plastic and Reconstructive Surgery
Tokyo University School of MedicineTokyo, Japan
Correspondence to Dr. NarushimaDepartment of Plastic and Reconstructive Surgery
Tokyo University School of Medicine7-3-1 Hongo Bunkyo-kuTokyo 113-0033, [email protected]
REFERENCES1. Lee BT, Lin SJ, Bar-Meir ED, Borud LJ, Upton J. Pedicled
perforator flaps: A new principle in reconstructive surgery.Plast Reconstr Surg. 2010;125:201–208.
2. Koshima I, Urushibara K, Fukuda N, et al. Digital artery per-forator flaps for fingertip reconstructions. Plast Reconstr Surg.2006;118:1579–1584.
3. Mitsunaga N, Mihara M, Koshima I, et al. Digital artery per-forator (DAP) flaps: Modifications for fingertip and fingerstump reconstruction. J Plast Reconstr Aesthet Surg. 2010;63:1312–1317.
ReplySir:
I thank Drs. Mundinger, Narushima, and Koshimafor their comments regarding our article, “PedicledPerforator Flaps: A New Principle in ReconstructiveSurgery.”1 The intent of the article was to consolidateand introduce to the readership the expanding field ofpedicled perforator flaps. The article was not meant tobe exhaustive, especially with the multitude of new flapsthat are being described on a monthly basis. We did,however, use exhaustive search criteria using variouskeywords through PubMed covering the past 30 years.
The important point, however, is the principle thatone can create a pedicled flap with an axial perforatorvessel at its base to improve reliability, rather than themethodology behind how one creates a laundry list offlaps. Despite that, the omission of the digital arteryperforator flap was an oversight, as this is clearly animportant contribution to the literature and the field.We would certainly include this flap in any atlas onwhich we embark in the future.DOI: 10.1097/PRS.0b013e3181f61dcc
Bernard T. Lee, M.D.Department of Surgery
Division of Plastic and Reconstructive SurgeryBeth Israel Deaconess Medical Center
Harvard Medical School110 Francis Street, Suite 5A
Boston, Mass. [email protected]
REFERENCE1. Lee BT, Lin SJ, Bar-Meir ED, Borud LJ, Upton J. Pedicled
perforator flaps: A new principle in reconstructive surgery.Plast Reconstr Surg. 2010;125:201–208.
Microvascular Anastomoses: A Series of 200Success StoriesSir:
We read with interest the article by Koizumi et al.entitled “Microvascular Anastomoses: A Series of
200 Success Stories” and congratulate them on their100 percent microvascular success rate in their mostrecent series.1 Their strategy for microvascular anasto-mosis is undoubtedly a very good guide. In our depart-ment too, experience has accumulated, and their strat-egy could be expanded to include the following:
• Complete preparation of both donor and recipientvessels before disconnecting the flap, to stabilize thevessels and to minimize “flap-off” time.
• The use of supports (e.g., rolled up theater drapes)to stabilize the hands and to reduce undesirablehand movements.
Although the skill and technical knowledge requiredof the surgeon during surgery is undoubted, we contendthat it is not the sole factor for microsurgical success.2,3
The physiologic condition of the patient is vital, and webelieve that keeping the patient warm, well perfused, andcomfortable throughout the perioperative period is cru-cial. We advocate that microsurgical cases:
• Are performed by a dedicated microsurgical team tooptimize familiarity with equipment and techniques.
• Are carried out in a warmed operating room (27°C).• Maintain a body core temperature at 38°C and core-
peripheral temperature difference less than 1°C.• Have regional anesthesia available where appropri-
ate, which can continue postoperatively.
Dedicated postoperative care is also essential. In a re-cent review of all (consecutive and unselected) free flaps(n � 2569) carried out in our unit between 1985 and2008, 327 free flaps were reexplored on 369 occasions.3 Inthis series, timing of reexploration was significant, withsuccessful reexplorations taking place at a mean � SE of19.4 � 2.5 hours compared with 56.1 � 10.5 hours forunsuccessful reexplorations (p � 0.001). Our work con-curs with other studies, in that the majority of flaps werereexplored in the first 24 hours, with most of these beingcarried out within the first 6 hours.4,5 The preoperativeclinical diagnosis for cause of the failing free flap was correctin over 90 percent of reexplorations. Therefore, the follow-ing are adopted in free-flap patients postoperatively:
• The patient is cared for in a warmed high-depen-dency care unit, ideally with continued review by thesame anesthetist.
Plastic and Reconstructive Surgery • December 2010
2296

• Initial flap observations are carried out every 15minutes by experienced nursing staff and continuewith hourly observations until 48 hours has passed.
• Invasive monitoring is removed when it is safe to do so.• Urgent surgical intervention is performed if flap
viability is in doubt, rather than waiting until theindication is absolute (in our series, 0.4 percent offlap reexplorations were negative, which we believeis acceptable if overall success rates are high3).
We believe that a “microsurgical culture” within aunit and availability of appropriate facilities are pivotalto microsurgical success. Patients and their flap(s)should have a period of very close observation postop-eratively, with a clinical model of flap monitoring at itscore. We also believe that careful perioperative man-agement of the patient (and flap) is as important as theskill of the surgeon in achieving consistently successfulfree tissue transfer.DOI: 10.1097/PRS.0b013e3181f61db6
Richard M. Pinder, M.R.C.S.
Robert I. Winterton, M.R.C.S.
Mark I. Liddington, F.R.C.S., F.R.C.S.(Plas.)
Simon P. Kay, F.R.C.S., F.R.C.S.(Plas.)Department of Plastic Surgery
Leeds General InfirmaryLeeds, United Kingdom
Correspondence to Dr. PinderDepartment of Plastic Surgery
Bradford Royal InfirmaryDuckworth Lane
Bradford BD9 6RJ, United [email protected]
DISCLOSUREThe authors have no financial interest to declare in relation
to the content of this communication.
REFERENCES1. Koizumi T, Nakagawa M, Nagamatsu S, Kayano S, Akazawa S.
Microvascular anastomoses: A series of 200 success stories.Plast Reconstr Surg. 2010;125:110e–111e.
2. Pinder RM, Hart A, Winterton RI, Yates A, Kay SP. Free tissuetransfers in the first 2 years of life: A successful cost effectiveand humane option. J Plast Reconstr Aesthet Surg. 2010;63:616–622.
3. Winterton RI, Pinder RM, Morritt AN, et al. Long term studyinto surgical re-exploration of the ‘free flap in difficulty.’J Plast Reconstr Aesthet Surg. 2010;63:1080–1086
4. Kroll SS, Schusterman MA, Reece GP, et al. Timing of pediclethrombosis and flap loss after free-tissue transfer. Plast ReconstrSurg. 1996;98:1230–1233.
5. Chen KT, Mardini S, Chuang DC, et al. Timing of presentation ofthe first signs of vascular compromise dictates the salvage outcomeof free flap transfers. Plast Reconstr Surg. 2007;120:187–195.
ReplySir:
We thank Pinder et al. for the insightful commentsmade in response to our article. We agree with their
microsurgical methods and believe that careful peri-operative management is very important. Keeping thepatient warm, well perfused, and comfortable through-out the perioperative period is favorable. Preventinghypothermia is particularly important for preventingsurgical-site infection.1 In addition, noninvasive objec-tive evaluations are necessary for flap management af-ter the operation. Our goal is to standardize the pin-prick test by introducing a fine-needle kit for themeasurement of blood glucose and determine whetherthere is bleeding in the flaps every 6 hours after theoperation.2,3 This will allow an evaluation of congestionbased on the amount and the color of hemorrhagecomparatively earlier than judging the tone change ofthe flap subjectively. A recent review of all microvas-cular anastomoses (n � 492) carried out in our insti-tution between 2002 and 2010 revealed that eight freeflaps were reexplored and six were total flap losses. Therate of total flap loss was 1.2 percent.DOI: 10.1097/PRS.0b013e3181f61df2
Takuya Koizumi, M.D.
Masahiro Nakagawa, M.D.
Shogo Nagamatsu, M.D.
Shuji Kayano, M.D.
Satoshi Akazawa, M.D.Division of Plastic and Reconstructive Surgery
Shizuoka Cancer Center HospitalShizuoka, Japan
Correspondence to Dr. KoizumiShizuoka Cancer Center Hospital
1007 ShimonagakuboNagaizumi-cho, Sunto-gunShizuoka 411-8777, Japan
REFERENCES1. Humphreys H. Preventing surgical site infection: Where now?
J Hosp Infect. 2009;73:316–322.2. Nakagawa M, et al. Pin prick test with blood collecting device
after free tissue transfer. J Jpn Soc Plast Reconstr Surg. 2006;26:269–271.
3. Iida T, et al. Standardization and characterization of the pin-prick test for monitoring circulatory status after free flap trans-fer. J Jpn Soc Reconstr Microsurg. 2007;20:40–45.
Antioxidants and Skin Care: The Essentials–-Old Wine in a New BottleSir:
A fter reading the article “Antioxidants and SkinCare: The Essentials” by Jeanette Graf,1 we are
happy to realize that our grandmothers have alwaysbeen making facials with the right constituents in theright proportions. The only difference was that they didnot have any scientific basis for their formulations. Thisarticle clearly elaborates the antioxidant properties ofthe naturally available fruits, vegetables, and wholegrains that have always been among the ingredients ofour age-old facials.
Volume 126, Number 6 • Letters
2297

The vegetable mask that has been traditionally usedfor oily skin contains tomatoes, which are rich in caro-tenoids; oatmeal powder, containing ferulic acid; curd,containing lactic acid, which is a chemical peel; cu-cumber; and mint leaves rich in vitamin C as antioxi-dants. Green tea facial, which is also quite ancient, hasnow been found to contain catechin, which is respon-sible for its antioxidant properties. The fruit facialscontain grape fruit, which is known to contain procya-nidin; lemon juice, which contains vitamin C; applecore, which contains vitamin C and phenols; and eggwhite, which is a skin tightener.
Honey and egg yolk have also been used in a varietyof facials, including the “egg yolk facial of ancientEgypt.” Much research has been conducted to discoverthe active ingredient in these natural food products.Honey2 is found to contain flavonoids, a polyphenol,and vitamin C, whereas yolks have been found to berich in carotenoids, which are antioxidants in general.In essence, it is the antioxidant action of these sourcesthat one is looking for while preparing antiaging solu-tions and that our ancestors had realized centuriesbefore, although they did not have the technology toprove it to the rest of the world.
Also, the “antioxidant cocktail” technology that isquoted in the article is a thing of the past, as thesefacials generally were made of a mixture of these con-stituents. Thus, I would like to conclude that beforeembarking on newer solutions to our old problems weshould work out the scientific basis of our age-old andtime-tested remedies because, for all that you know, theanswers may already be there.DOI: 10.1097/PRS.0b013e3181f61d8f
Sunil Choudhary, M.S., F.R.C.S.Ed.
Madhubari Vathulya, M.S., M.Ch.
Raghav Mantri, M.S., M.Ch.
Prateek Arora, M.S., M.Ch.
Satya Swarup Triparty, M.S., M.Ch.Department of Plastic Surgery
Max Institute of Aesthetic and Reconstructive Plastic SurgerySaket, New Delhi, India
Correspondence to Dr. ChoudharyMax Institute of Aesthetic and Reconstructive Plastic Surgery
Saket, New Delhi, [email protected]
REFERENCES1. Graf J. Antioxidants and skin care: The essentials. Plast Reconstr
Surg. 2010;125:378–383.2. Schramm DD, Karim M, Schrader HR, Holt RR, Cardetti M,
Keen CL. Honey with high levels of antioxidants can provideprotection to healthy human subjects. J Agric Food Chem. 2003;51:1732–1735.
ReplySir:
I quite agree with Dr. Choudhary that nature holdsmany answers to our health and well-being. Historically,some of the most important medications we have usedas healers have come from nature, such as digoxin fromthe foxglove plant and atropine from the belladonnaplant. The research and subsequent purification of thesemedications became an important part of our pharma-copoeia. However, I disagree with the idea that the anti-oxidant technology being used is outdated because of thehistoric use of food facials by our ancestors. For example,if we were to simply use green tea as a facial and did notlook further into the various catechins found in green tea,we would not know the clinical superiority of epigallo-catechin 3-gallate and its anticarcinogenic properties.Skin is a large organ and an organ of absorption andelimination, which makes its care far beyond cosmetic inimportance. Although we may look back romantically atthe vegetable masks that our grandmothers used, iden-tifying and purifying the active ingredients will be morebeneficial to the skin. The combination of scientificallypurified extracts from natural sources and technolog-ically advanced delivery systems is an essential part ofhealth and aesthetics.DOI: 10.1097/PRS.0b013e3181f61e16
Jeannette Graf, M.D., F.A.A.D.Dermatology
Mount Sinai Medical CenterNew York, N.Y.
Correspondence to Dr. GrafCenter for Aesthetic Dermatology
88 BayviewGreat Neck, N.Y. 11021
Plastic and Reconstructive Surgery • December 2010
2298