part 2: history of 20th century neurology: decade by decade
TRANSCRIPT

PART 2: History of 20th CenturyNeurology: Decade by Decade
Kenneth Tyler, MD, George K. York, MD, David A. Steinberg, MD, Michael S. Okun, MD,Michelle Steinbach, MD, Richard Satran, MD, Edward J. Fine, MD, Tara Manteghi, BA, BS,
Thomas P. Bleck, MD, Jerry W. Swanson, MD, Shrikant Mishra, MD, MS, Kimford J. Meador, MD,David B. Clifford, MD, James F. Toole, MD, and Lella Melson
Neurology in the 1900s: 1900–1909H. Richard Tyler, MDThe first decade of the 20th century (1900–1909) sawdramatic changes and advances in virtually every aspectof neurology. The basic science framework for neurologywas solidified by fundamental advances in neurophysiol-ogy, led by Sir Charles Sherrington and his collabora-tors. Equally important advances were made in the studyof the histology and pathology of the nervous system byCajal and others (Tables 1 and 2). The clinical spectrumof neurology was broadened and enriched by many con-tributions still remembered eponymously today (see Ta-ble 1). A very subjective and selective selection of addi-tional landmark contributions in different fields ofneurology are listed in Table 2. Prominent among thesewere the studies that led to Nobel Prizes for Pavlov in1904 on digestive physiology and to Golgi and Cajal in1906 for their work on the neuron theory.
Few neurodiagnostic tests were available to cliniciansin the first decade of the 20th century, with arteriog-
Fig 3. Neurosurgery became an active specialty in parallel tothe development of medical neurology. This photograph showsHorsley at the National Hospital, Queen Square, London in1906. Horsley is shown on the far right of the photographawaiting the start of the surgical procedure. His apparent bulkis because of the fact that he is wearing a large antisepticdressing beneath his coat as a preoperative treatment for hisown appendix removal the next day. (From Habib AA,Mozaffar T. Brain Abscess. Arch Neurology2001;58(8):1302–4).
Fig 1. Sir Charles Sherrington shown as a young man was apre-eminent neurophysiologist of the first decade of the 20thcentury. The Integrative Action of the Nervous System,published in 1906, was a landmark in the history of science.Sherrington received the Nobel Prize in 1932 for physiology.
Fig 2. Santiago Ramon y Cajal (1852–1934). This photographof Cajal was taken in 1899 at the time of his visit to theUnited States to lecture at the Decennial Celebration of ClarkUniversity in Worcester, Massachusetts. Cajal shared the NobelPrize in 1906 with Golgi for his work on the structure of thenervous system. He was instrumental in providing clear histolog-ical proof that nerve cells were discrete cellular units whose pro-cesses were interconnected at synapses (“neuron doctrine”) ratherthan through a continuous reticular net. Cajal’s illustration ofthe giant pyramidal cells shown here from the motor cortex of a20-day-old infant is from his lecture at Clark University in1899.
© 2003 Wiley-Liss, Inc. S27

raphy, ventriculography, myelography, and electroen-cephalography all still in the future. One of the mostimportant early tests was the examination of the cere-brospinal fluid, first attempted by Corning (1855) andintroduced in modern form by Quincke (1891). Sev-eral contributions related to cerebrospinal fluid and itsphysiology and pathology appeared during this decade
(see Cushing, Froin, Sicard, Wasserman in Tables 1and 2).
A quick world tour of leading neurological centers inthe first decade of the 20th century would have shownthat American neurology largely revolved around Phil-adelphia, New York, and Boston. Leading neurologicalfigures included such giants as Silas Weir Mitchell
Table 1. Some Famous Eponyms
Author Date Contribution
J. J. Dejerine 1900 Description of olivopontocerebellar atrophyH. W. Cushing 1902–3 Studies on intracranial hypertension and associated blood pressure changesG. Froin 1903 Description of extreme cerebrospinal fluid protein elevation with spinal
blockH. Lundborg 1903 Description of progressive myoclonic epilepsyE. Marchiafava and A. Bignami 1903 Description of abnormalities in the corpus callosum in Italian red wine
drinkersG. Gradenigo 1904 Description of syndrome of facial pain and VIth nerve palsy with
inflammation of the apex of the temporal boneJ. J. Dejerine and G. Roussy 1906 Description of thalamic pain syndromeJ. Ramsay Hunt 1907 Description of herpetic infection of the geniculate ganglionG. Holmes 1907 Familial cerebellar degenerationL. Merzbacher 1908 Description of a form of infantile leukodystrophyC. F. Hoover 1908 New sign for detecting malingering involving leg weaknessJ. Brudzinski 1909 Leg sign in meningitis
Table 2. Some Notable Contributions
Author Date Contribution
H. Head 1900 Map of human dermatomes based on pattern of shingles eruptionsH. K. Liepmann 1900 Description of apraxiaP. E. Flechsig 1901 Studies on developmental patterns of cerebral myelinizationP. Marie 1901 Description of lacunar stateW. R. Gowers 1902 Description of distal myopathyI. P. Pavlov 1902 Studies on digestive glandsJ. A. Sicard 1902 Monograph on cerebrospinal fluidC. S. Sherrington and A. S. F.
Grunbaum (Leyton)1902–3 Studies on physiology of cerebral cortex in apes
J. F. F. Babinski 1903 Studies on reflexes (l’abduction des orteils)P. T. Herring 1903 Studies on cervical sympathetic systemA. Alzheimer 1904 Description of pathological changes in presenile dementiaT. R. Elliott 1904–5 Work on action of “adrenalin”G. Holmes 1904 Monograph on symptomatology of cerebellar tumorsI. P. Pavlov 1904 Nobel Prize for studies of digestive physiologyA. Pick 1905 Description of apraxiaC. Golgi and S. Ramon y Cajal 1906 Share Nobel Prize for studies on neuronal staining and neuron
theoryP. Marie 1906 Studies on aphasiaC. S. Sherrington 1906 Publication of Integrative Action of the Nervous SystemA. von Wasserman 1906 Test for syphilisW. R. Gowers 1907 Publication of the Borderland of EpilepsyR. Barany 1906–7 Monographs on vestibular physiologyR. G. Harrison 1907–8 Studies on developing nerve fibers and neurogenesisC. E. Beevor 1908 Papers on cerebral arterial supply and vascular territoriesS. Flexner 1908 Serum treatment of meningococcal meningitisA. E. Garrod 1908 Croonian Lectures on “Inborn Errors of Metabolism”W. H. Rivers and H. Head 1908 Experiments on human nerve division (on Head)J. F. F. Babinski 1909 Studies on cerebellar functionK. Landsteiner and E. Popper 1909 Studies on virology and pathogenesis of acute poliomyelitisK. Lucas 1909 All or none contraction of skeletal muscle
S28 Annals of Neurology Vol 53 (suppl 4) 2003
(elected for the second time to the ANA’s presidencyin 1909), Charles K. Mills (ANA President in 1924)and William Spiller (ANA President in 1905) in Phil-adelphia, and James Jackson Putnam (ANA Presidentin 1888) in Boston. A notable landmark during thisdecade was the creation of the New York NeurologicalInstitute (1909). English neurology was in the midst ofa generational change as William Gowers (1845–1915), Hughlings Jackson (1835–1911), C. E. Beevor(1854–1908), and Henry Bastian (1837–1915) wereentering the end of their active careers, and a new gen-eration of leaders that included Henry Head (1861–1940), Gordon Holmes (1876–1966), and S. A. Kin-near Wilson (1878–1937) was emerging. French neur-ology was dominated by Charcot’s successors includingVulpian’s students, Dejerine (1849–1917), PierreMarie (1853–1940), and J. F. F. Babinski (1857–1932). In Germany, William Erb (1840–1921) and H.Oppenheim (1858–1918) were leading figures.
Neurology in the 1910s: 1910–1919George K. York, MD and David A. Steinberg, MDNeurologists began the decade 1910 to 1919 optimis-tically, in the conviction of the primacy of science.They ended the decade discouraged and uncertain. Inbetween, they participated in a war unparalleled in fu-tility.
In the beginning of the decade, amid studies of neu-rosyphilis and brain tumors, the American Neurologi-cal Association engaged in a contentious debate aboutthe place of Freudian psychoanalysis in the practice of
neurology. As practical physicians, many neurologistsfound the time required for couch therapy onerous.Harvey Cushing, Ramsay Hunt, Bernard Sachs, FosterKennedy, and Charles Dana presented important pa-pers at nearly every annual meeting of the ANA. Wil-liam Osler, Adolph Meyer, and James Jackson Putnamgraced the masthead of the Journal of Nervous andMental Disease, joining Transactions of the AmericanNeurological Association as two official organs of theANA. Clinical, pathological, and methodological stud-ies were to be found in the pages of the internationaljournals Brain, Revue Neurologique, and the Archiv furPsychiatire und Nervenkrankenheiten. In 1912, S. A.Kinnier Wilson published his classic description ofhepatolenticular degeneration. As the cataclysm of warapproached, Robert Barany was awarded the 1914 No-bel Prize for physiology or medicine for his work onthe vestibular system.
As the American Civil War had provided Silas WeirMitchell with a rich source of patients with nerve in-jury, so the outbreak of hostilities in August 1914 gave
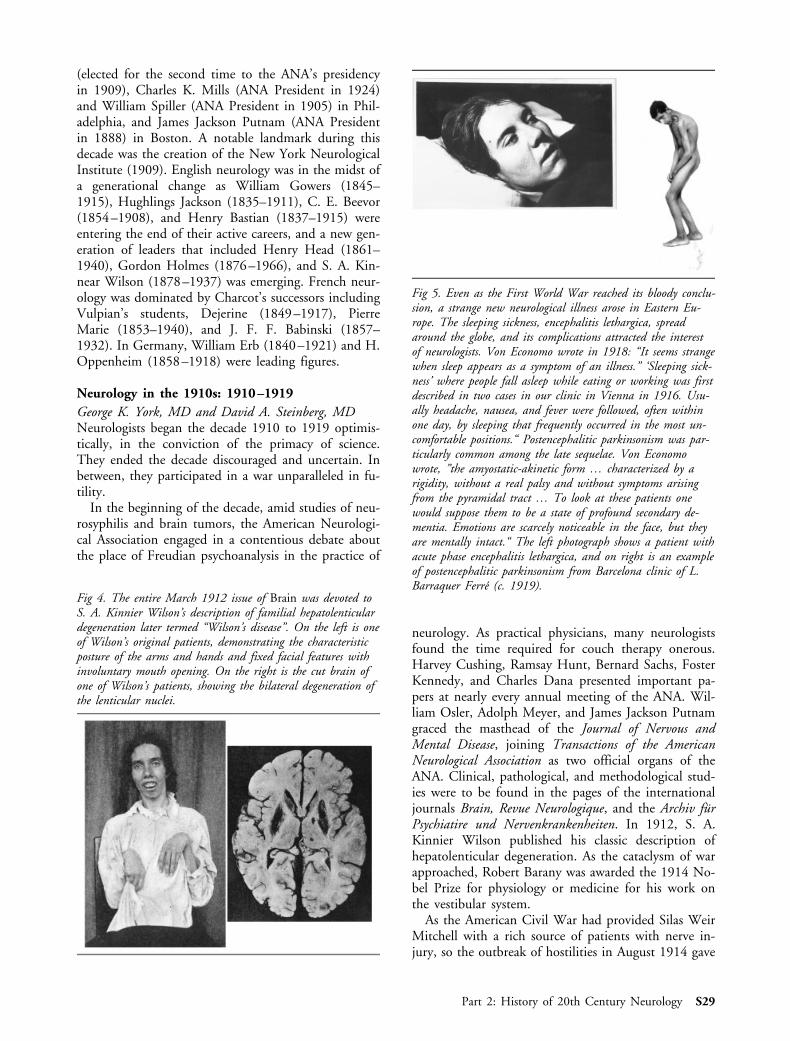
Fig 4. The entire March 1912 issue of Brain was devoted toS. A. Kinnier Wilson’s description of familial hepatolenticulardegeneration later termed “Wilson’s disease”. On the left is oneof Wilson’s original patients, demonstrating the characteristicposture of the arms and hands and fixed facial features withinvoluntary mouth opening. On the right is the cut brain ofone of Wilson’s patients, showing the bilateral degeneration ofthe lenticular nuclei.
Fig 5. Even as the First World War reached its bloody conclu-sion, a strange new neurological illness arose in Eastern Eu-rope. The sleeping sickness, encephalitis lethargica, spreadaround the globe, and its complications attracted the interestof neurologists. Von Economo wrote in 1918: “It seems strangewhen sleep appears as a symptom of an illness.” ‘Sleeping sick-ness’ where people fall asleep while eating or working was firstdescribed in two cases in our clinic in Vienna in 1916. Usu-ally headache, nausea, and fever were followed, often withinone day, by sleeping that frequently occurred in the most un-comfortable positions.“ Postencephalitic parkinsonism was par-ticularly common among the late sequelae. Von Economowrote, ”the amyostatic-akinetic form … characterized by arigidity, without a real palsy and without symptoms arisingfrom the pyramidal tract … To look at these patients onewould suppose them to be a state of profound secondary de-mentia. Emotions are scarcely noticeable in the face, but theyare mentally intact.“ The left photograph shows a patient withacute phase encephalitis lethargica, and on right is an exampleof postencephalitic parkinsonism from Barcelona clinic of L.Barraquer Ferre (c. 1919).
Part 2: History of 20th Century Neurology S29

neurologists an unmatched, if unwanted, research op-portunity. Technological advances in the treatment ofshock and the prevention of infection meant that manymore people survived war wounds. Neurologists madeuse of this gruesome natural experiment to learn theimpact that bullets, bombs, and shrapnel had on thehuman nervous system, including wounds of the cere-bellum and spinal cord. Trench warfare also generatedmany soldiers with unexplained tremor, blindness, andparaplegia, known collectively as shell shock. Debatingthe neurology of shell shock, some members of theANA claimed that it is the “neurology of degeneracy,”caused by pre-existing psychological inadequacy. Othermore sensitive members observed that shell shock wasinduced by experiences of unimaginable horror, that itcould occur in anyone, and that its origin lay in thepsychological conflict between the sense of duty andthe instinct for self-preservation. Twenty-nine membersof the ANA were commissioned in the armed servicesin World War I, and the US Army created a divisionof Neurology and Psychiatry, headed by Pearce Bailey,to supervise the examination of recruits and the reha-bilitation of the wounded. Henry Head, in an addressdelivered 3 days after the armistice, recalled the oppres-sive horror of the previous 4 years. He observed thatthe cataclysmic events of the war had shaken theyounger generation’s belief in the pervasive positivismof the old order. Saying that the charm of neurologylies in the way it forces us into daily contact with prin-ciples, he called for an end to the obsessive study ofstatic anatomical and topographical detail and a returnto the neurophysiological principles of Sherrington andHughlings Jackson.
Encephalitis lethargica spread from its outbreak inVienna in 1917 to engulf the world, leaving in its wakepostencephalitic parkinsonism. Influenza struck themalnourished and fractured world in 1919, killing 20million people, twice as many as had perished in thewar. Postwar neurology also considered the topics ofracial hygiene and constitutional criminality, topicsthat would soon be used to justify atrocity and anni-hilation. Behind it all, the greatest scientific minds ofthe century explored the physics of the atom and theuniverse.
Neurology in the 1920s: 1920–1929Michael S. Okun, MD and Michelle Steinbach, MDThe “roaring twenties” were a colorful decade filledwith jazz, the flappers, motion pictures, and radio. Atthe end of the decade, Herbert Hoover occupied theWhite House and the world helplessly watched theAmerican stock market tumble, setting into motion theGreat Depression. Violent mob wars and the St. Val-entine’s Day Massacre made names like Al Capone andMachine Gun McGurn commonplace in American
households. Mies van der Rohe’s international style ofarchitecture became the modern contemporary look forAmerican society.
The 1920s represented a decade of discovery and in-novation in neurology and the neurosciences. The my-elogram, angiogram, electroencephalogram, and elec-tromyogram were all introduced in a span of less than
Fig 6. This famous photo appeared in Egas Moniz’ 1927original article detailing the world’s first experience with ahuman carotid angiogram. Pictured in the lower left of thephotograph is the needle, which is being used for a direct ca-rotid injection of dye.
Fig 7. Harvey Cushing, the world’s leading neurosurgeon, pic-tured in 1929. His multiple publications on the pituitarygland in JAMA and other journals coupled with his 1926test, The Third Circulation, made his contributions to neurol-ogy seminal.
S30 Annals of Neurology Vol 53 (suppl 4) 2003

10 years. In 1929, acetylcholine was isolated and thedata on the first human electroencephalogram werepublished.
In the 1920s, neurology was a division of internalmedicine or psychiatry. Except at the University ofPennsylvania, Columbia, Harvard, and a select fewother medical institutions, neurology struggled to es-tablish and retain an identity. A singular advance camefrom a 1928 endowment from the Rockefeller Foun-dation to the Boston City Hospital. The endowmentwas specifically outlined to develop a full-time teachingand education unit of medical neurology. This modelwas progressively adopted during the 1930s as moredepartments of neurology were established in theUnited States.
On the international level, the neurological worldgathered in Paris in 1925 to commemorate the cente-nary of the birth of the founding father of clinical neu-rology, Jean-Martin Charcot. The meeting was orga-nized by the French Neurological Society but drew aninternational list of participants and speakers. Majortopics of discussions included the disorders closelylinked to Charcot himself including amyotrophic lat-eral sclerosis, tabes dorsalis, multiple sclerosis, andclinical-anatomical correlations.
Neurology in the 1930s: 1930–1939Richard Satran, MDThe decade of the 1930s was heralded by severe globaleconomic hardship and progressive dictatorial central-ization of power in Italy and Germany. The eventualoutcome of the Great Depression was uncertain, andthere was increasing anxiety regarding Germany’s an-nexation and acquisition of territory.
In the United States, neurologists and psychiatristshad concerns about postgraduate training. Neurologistswere not enthusiastic about the growth of their spe-cialty, partly because of the lack of therapies for neu-rological diseases. Both specialties believed that im-proving postgraduate training and certification wouldenhance the status of specialists. Despite their historyof professional disagreements and different orientations
Fig 8. In 1929, Dale and Dudley cut the fresh spleen of oxinto three to four strips, minced it, and stored it overnight inalcohol. It was filtered and condensed, and alcohol was addedagain. Ether and water layers were evaporated and acetylcho-line was finally isolated. The picture shows Dale and Dudley’soriginal measurements.
Fig 9. Hans Berger’s publication, On the Electroencephalo-gram of Man, in 1929 changed neurophysiology forever. Pic-tured are one of the first human electroencephalograms, HansBerger’s laboratory, and some of his original notes.
Fig 10. Mainly as the result of the efforts of Dr Clarence O.Cheney, aided by the National Committee for Mental Hy-giene, an accreditation body was incorporated on October 19,1934, under the title American Board of Psychiatry and Neu-rology. On October 20, 1934, a meeting of the Board washeld in New York, at which all the members were present.Officers were elected and by-laws were adopted. The officerswere H. Douglas Singer, president; C. Macfie Campbell, vice-president; and Walter Freeman, secretary and treasurer. (Mod-ified from News and Comment. Arch Neurol Psychiat 1934;32:1064).
Part 2: History of 20th Century Neurology S31

toward mind and brain relationships, representatives ofthe Section of Nervous and Mental Disease of theAmerican Medical Association (AMA), American Neu-rological Association (ANA), and the American Psychi-atric Association (APA) participated in discussions thatled to the formation of the single board, the AmericanBoard of Psychiatry and Neurology in 1934.
Committees of the ANA during this decade studieddiverse programs and issues ranging from long-termfollow-up of multiple sclerosis patients, contraception,teaching in state hospitals, and prevention of crime. Ata time when an active sterilization program existed inGermany to, according to its supporters, ensure Ger-manic racial purity and superiority, a detailed study
was conducted of eugenical sterilization in the UnitedStates. The recommendations presented to the ANAdiffered from those used to justify the program in Ger-many. (see Fig 13 legend).
In 1932, the United States Public Health Service be-gan what became known as the Tuskegee Experimentto observe the natural history of untreated latent syph-ilis in Macon County, Alabama, and periodic reportswere published. A cohort of 408 black men with syph-ilis and 196 black male controls were enrolled. Thethen current therapies of fever, mercury, and bismuthwere supervised by general practitioners or syphilolo-gists and usually not by neurologists or psychiatrists.Forty years elapsed before the study was brought topublic attention by a critical national press and ad-dressed by Congress. The natural history of syphilis
Fig 11. H. Houston Merritt and Tracy J. Putnam developedphenytoin in 1938 and established a new era of anticonvul-sant neurotherapeutics. Adapted from Landmark article Sept17, 1938: Merritt HH, Putnam TJ. Sodium diphenyl hydan-toinate in the treatment of convulsive disorders. JAMA 1984;251:1062–1067.
Fig 12. Egas Moniz studied the effects of frontal lobe abla-tions during the 1930s and introduced lobectomy surgery tothe United States via his American colleagues, Walter Free-man and James Watts. Egas Moniz is shown placing the em-blem of the Lisbon Academy of Sciences around the neck ofWalter Freeman in 1948. Also shown is a photograph ofJames W Watts at Yale in 1933.
Fig 13. Recommendations of the ANA Committee for the In-vestigation of Eugenical Sterilization. This report was pub-lished in 1936 and offered the following recommendations. (1)Sterilization should be voluntary and carried out only withpatient consent. (2) The administration of sterilization lawsshould be in the hands of one or more boards possessing specialtraining in this area. Candidates for sterilization should beconsidered individually rather than as groups. (3) Sterilizationcan be recommended in certain hereditary diseases of the ner-vous system. These include Huntington’s chorea, familial Frie-dreich’s ataxia, and hereditary optic atrophy. In addition, alsoin special or selective situations sterilization may be indicatedin familial feeblemindedness, dementia praecox (schizophre-nia), manic-depressive psychosis, and epilepsy. Sterilization inepileptics with infrequent seizures and an “intact personality”should not be performed. (From Myerson A, Ayer JB, PutnamTH, et al. Eugenical sterilization. A reorientation of the prob-lem. American Neurological Association. New York: Mac-millan, 1936).
S32 Annals of Neurology Vol 53 (suppl 4) 2003

and its treatment, racism, informed consent, and fail-ure to treat despite the availability of penicillin werereviewed. Eventually, follow-up care was provided forthe survivors and their families, and in 1997 PresidentClinton gave an official apology on behalf of theUnited States.
Although there had been some successful reports us-ing sulfonamide drugs in the treatment of infectiousdisease, the number of patients and long-term post-therapy observations were few. In 1937, an untestedsulfanilamide preparation containing diethylene glycolcaused more than 73 deaths in this country. An imme-diate review by the federal government led to legisla-tion to correct deficiencies in the preparation, safetytesting, labeling, distribution, and marketing of certaindrugs.
The electroencephalogram observations, which HansBerger, the German psychiatrist, began in the 1920s,were confirmed by Adrian and Matthews in 1933.There was intense study of the generation of electricalactivity in the brain, its changes at successive ages, andalterations in different physiological states and in ner-vous system diseases. In the United States, there wasparticular interest in epilepsy.
Merritt and Putnam in their search for a nontoxicanticonvulsant drug tested more than 700 substances
by studying the elevation of seizure threshold uponelectrical stimulation in the brain of animals. Some hy-dantoin and dione compounds were found to have an-tiepileptic potential. In 1938, they described their re-markable results using phenytoin to treat major,absence, and psychic equivalent seizures. Their discov-ery ranked as the first major successful medical treat-ment for epilepsy in the 20th century.
In England, Mary Walker in a short letter to theeditor of the Lancet in 1934 reported the successfultreatment of myasthenia gravis with physostigmine.The following year, Viets and Schwab described theuse of the prostigmine test in the diagnosis of myas-thenia.
In 1935, Moniz of Portugal was impressed by thereport of behavioral changes in chimpanzees after fron-tal lobe ablations. No psychotropic drugs were avail-able then to control the behavior of severely disturbedpatients. Moniz and Lima, first with alcohol injectionsand later a leucotome, interrupted the frontothalamicpathways of 20 mentally ill patients and described theirresults. In 1937, Freeman and Watts introduced theoperation in this country. Thousands of surgeries weredone, although there was some physician resistance tothe procedure. The years, which followed, clarified themerits and deficiencies of this operation for whichMoniz received a Nobel Prize.
Although the 1930s were bleak, stressful, and uncer-tain, important changes in neurology took place. In ad-dition to providing financial assistance, the governmentbecame more involved with medical care. These discov-eries and laboratory investigations during this periodnot only strengthened the specialty but brought neu-rology in the United States to a position of interna-tional stature.
Neurology in the 1940s: 1940–1949Edward J. Fine, MD and Tara Manteghi, BA, BSIn 1940, Panzer divisions of the Nazi German Reichinvaded Western Europe in blitzkrieg attacks, drivingthe Allied Forces from the continent. Isolationists at-tempted to keep the United States out of World WarII. Foster Kennedy, in his 1940 presidential address,urged members of the ANA, to “be strong, to endure,and … make a new world robustly believing in ourpower for reason and for … virtue.” At that meeting,H. Houston Merritt presented data to demonstratethat molecules which contained a malonyl ring linkedto an aromatic nucleus had antiseizure properties, suchas diphenylhydantoin.
Japanese air forces bombed Pearl Harbor on Decem-ber 7, 1941 and shattered our isolated nation’s tran-quility. The following day, the US Congress declaredwar on Japan; the ANA would not meet again until1946.
Fig 14. Elixir sulfanilamide became one of the most impor-tant therapeutic advances of the 1930s, although contaminateddrug batches were associated with death and high morbidity.Shown is a label from a 1-gallon bottle of elixir sulfanil-amide. Disclosure of diethylene glycol is not present. Adaptedfrom Leech PN. Special article from the American MedicalAssociation Chemical Laboratory. Elixir of sulfanilamide—Massengil chemical, pharmacologic, pathologic and necropsyreports; preliminary toxicity reports on dielthylene glycol andsulfanilamide. JAMA 1937;109:1531–1539.
Part 2: History of 20th Century Neurology S33

On June 6, 1944, British and American troops in-vaded Normandy with a bold amphibious assault onOmaha, Utah, and Juno Beaches. This invasion turnedthe course of World War II. Nazi forces made a sui-cidal last stand at the Battle of the Bulge in December1944 and when defeated were driven into retreat.
The American public felt the impact of neurologicaldisease when US President Franklin D. Roosevelt diedsuddenly on April 12, 1945, from cerebral hemorrhage.He had suffered from uncontrolled hypertension andhad been paraplegic from 1921 caused by paralytic po-liomyelitis. While French, English, and Americantroops surrounded Berlin from the West, Russiantroops fought the Nazis on the streets of Berlin. OnApril 30, 1945, Adolph Hitler committed suicide witha gunshot wound to his head. The Nazis uncondition-ally surrendered on May 7, 1945.
During 1945, the majority of neurological publica-tions in the Allied Countries related to war injuries,aviation medicine, and clinical neurophysiology. DerekDenny-Brown (1901–1981) immigrated to the UnitedStates from England to become Physician-in-Chief ofthe Harvard Neurology Service at Boston City Hospi-tal in 1941. He and Doherty stretched peroneal nervesof anesthetized cats and produced epineural hemor-rhages, swollen axis cylinders, and beading of the my-elin. Their observations accounted for the peripheralnerve dysfunction from high-velocity gunshot woundsthat passed through adjacent tissue.
W. K. Stewart of the British Royal Air Force andcolleagues endured severe acceleration in flight to dis-cover that temporary loss of vision (blacking out) wascaused by blood pooling in leg veins. This discoverywas applied to construct “G-suits” that compressed pi-lot’s leg veins and increased return of venous blood.
In 1945, Herbert Jasper (1906–) and William Cone(1897–1959) of the Montreal Neurological Institutetested soldiers with electromyogram for suspected nerveinjuries. They confirmed that fibrillation potentialsarose from single fibers of denervated muscles. Jasperand Cone determined that polyphasic potentials, 5 to15 milliseconds in duration, were recorded in reinner-vated muscles.
Victims of the Nazi killing machine did not die en-tirely in vain; from Leo Alexander’s testimony in 1946,responsible scientists devised the Declaration of Hel-sinki recommendations to prevent harmful experimen-tation without informed consent.
In 1947, George Dawson recorded evoked responsesfrom the scalp of humans in response to somatosensorystimuli. In 1949, Dawson constructed a signal averagerto extract minute potentials from unrelated electronicnoise.
In 1948, Bardeen, Brattain, and Schockley invented
Fig 15. A. B. Baler, R. DeJong, F. Forster, and A. Sahs wereresponsible for the founding of the American Academy of Neu-rology and became known as “the Four Horsemen.”
Fig 16. Mary A. B. Brazier, MD (1908–1998) used surfaceelectromyogram to demonstrate that patients with neurotictremor had irregular patterns of activation in agonist andantagonist muscles, firing in synchronous or diffuse bursts at 6to 10Hz. The tremor of Parkinson’s disease had a pattern of4-7Hz bursts, alternating between agonist and antagonists.
Fig 17. In 1941, Birdsey Renshaw, PhD (1908–1948) dem-onstrated that alpha motor neurons could be inhibited by an-tidromic impulses. He postulated that recurrent axon collater-als inhibited alpha motor neurons. In 1946, Birdsey Renshawrecorded trains of discharges from interneurons that were acti-vated by centripetal stimulation applied to the ventral roots.
S34 Annals of Neurology Vol 53 (suppl 4) 2003

the transistor from which they developed solid statejunctional semiconductors. Small, stable amplifierswere constructed with these components, to replacebulky and fragile vacuum tube electroencephalogramamplifiers.
Dr Forster recalled that A. B. Baker was spurred bya query from one of his residents, who asked “how canI join a neurology society?” A. B. Baker began his cam-paign for an inclusive neurological academy that wouldserve members from the beginning of residencythrough emeritus status and provide educational op-portunities to level the playing field by providingcourses to overcome weaknesses in training programs.He recruited other young neurologists including Rus-sell DeJong of University of Michigan, Francis Forsterthen of Thomas Jefferson University (Philadelphia),and Adolph Sahs of University of Iowa. Baker andthese three colleagues became known as “the FourHorsemen” of the American Academy of Neurology.An organizational meeting was held in the Stevens Ho-tel in Chicago in 1947. The first scientific meeting ofthe Academy was held at French Lick, a spa in Indianain 1948. Some members had apprehension that an in-ternecine struggle would develop between the two so-cieties. But as A. R. Vonderahe of the University ofCincinnati pointed out, the organizations had differentbut compatible missions. He likened the Academy tothe US House of Representatives and the AmericanNeurological Association to the Senate. These societies’symbiotic existence and cooperation resulted in rapidgrowth and refinement of American neurology (FrancisForster, personal observations, January 23, 2000).
Neurology in the 1950s: 1950–1959Thomas P. Bleck, MDAlthough the decade of the 1950s is sometimes ideal-ized as a period of quiet before the explosive eventsthat characterized the 1960s, it was actually a time oftremendous, if evolutionary, social change. This wastrue for American neurology as well. In 1950, theAmerican Neurological Association had 233 activemembers. In 1959, there were 223. Although thesenumbers suggest that the profession was static duringthis period, it was in fact a time of tremendous growthand vitality.
The overarching medical achievement of the decadewas the development of a vaccine for poliomyelitis.This disease had become epidemic in the UnitedStates, and by the early 1950s there were 25 cases per100,000 population. The disease had also shifted to af-fect older children and young adults. With the releaseof Jonas Salk’s vaccine in 1955, the incidence fell toless than 0.5 cases per 100,000 by the end of the de-cade. Polio has since been eradicated in the WesternHemisphere and we hope will soon join smallpox as aformer scourge of humanity.
Care for patients with polio occupied a substantialportion of a neurologist’s time in the 1950s. The poliopatient in an iron lung frequently received “principalcare” from a neurologist. In an era of rotating intern-ships and fewer specialists, it was not uncommon forneurologists to perform whatever surgical proceduresthe patient might require, in some cases including tra-cheostomy, rigid bronchoscopy, and appendectomy.
Some of the pathophysiological concepts that remainmost important in the current practice of neurologyemerged during the 1950s. Among many, perhaps themost seminal was C. Miller Fisher’s description of ca-rotid thrombosis as a cause of stroke. The role of in-tracranial pressure disturbances in many disease statesbecame clearer. After the description of the reticularactivating system in 1949, many publications exploredthe clinical consequences of brainstem lesions. Most ofthese explorations were of necessity autopsy studies,but many were very insightful and have been con-firmed by more contemporary techniques.
A text on modern trends in neurology published in1957 opened with a chapter on “Recent advances inthe anatomy of the nervous system,” something we areunlikely to see again. Cerebrovascular disorders occupya substantial portion of the text. Despite the introduc-tion of phenothiazines, a chapter on “Neurosurgicaltreatment of disorders of the affect” noted that suchprocedures were still in use and still useful. Anotherchapter summarized the role of hippocampal sclerosisin epilepsy, a topic still of research interest today.
Neurologists of the 1950s saw very few new thera-pies added to their armamentarium. Phenytoin andphenobarbital remained the mainstays of treatment forepilepsy. “Me, too” drugs were a phenomenon of thatdecade as well as today, with derivative drugs such as
Fig 18. Arguable, this text from the 1950s remains the mostimportant source in neurology. The clinical descriptions, andtheir correlations with electroencephalography, contain the nu-cleus of most of the subsequent advances in both the under-standing of epilepsy syndromes and their surgical management.
Part 2: History of 20th Century Neurology S35

ethotoin being introduced. Great fanfare greeted theintroduction of the succinimides, derived from pheno-barbital; today, only ethosuximide remains.
The 1958 edition of Harrison’s Principles of InternalMedicine (of which Raymond Adams was the neurolog-ical editor) includes a 40-page chapter on cerebrovas-cular disease; about two pages are devoted to therapy,and most of the comments discourage use of the pop-ular treatments of the era. However, it does contain therecommendation that “patients with a stroke as the re-sult of an ischemic infarction should remain horizontalin bed for 7 to 10 days initially,” suggesting that man-aged care had yet to become a fixture. (Most of thecerebrovascular diagrams in the current edition of Ad-ams, Victor, and Ropper’s Principles of Neurology arealready present in this edition of Harrison’s text.) Thediscussion of multiple sclerosis declares that “ACTHand cortisone appear to be of no value.” Therapy forParkinson’s disease is limited to anticholinergic agents,although the results of surgical lesions “in or near theglobus pallidus” are said to be encouraging. The dis-cussion of dementia does not mention therapy. In con-trast with our current mania for evidence-based medi-cine, the text is peppered with recommendations basedupon the fact that an author has always or never founda particular treatment or test to be useful. A text onmyasthenia from 1958 declares that “early reports oncortisone and ACTH which showed favorable results”were subsequently disproved. Thymectomy was recom-mended, but as an alternative one might denervate thecarotid sinus.
Neurology was still a small field at the start of the1950s and was still viewed as a part of psychiatry bymany. A. B. Baker estimated that in 1952 there wereless than 250 true neurologists in the United States.There were 15 neurological training programs, and lessthan half of the 79 medical schools had a neurologycourse taught by a neurologist. In 1953, the NationalInstitute of Neurologic Disease and Blindness beganfunding training grants in neurology; by the end of thedecade, there were 111 supported training programsfunded by a 3 million dollar budget. Approximatelyhalf of these programs were housed in independentneurology departments.
A national commission on residency training sug-gested that each resident should admit a minimum of“three or four new patients per week” and manage aservice of about eight to ten patients. In the outpatientclinic, where a trainee was to spend a fifth of his time,one new and two return patients were to be seen in ahalf-day session. Attending supervision was to take atleast 12 hours per week in the first 2 years, and 4hours per week in the final year. All trainees were ex-pected to be proficient in the following procedures:lumbar and cisternal punctures, subdural taps in in-fants, pneumoencephalography, myelography, arteriog-
raphy, psychological testing, testing of special senses,and electroencephalography.
The 1950s were a time of great concern about the“Red Menace” and the potential for subversion athome. Although it is sometimes difficult now to sepa-rate which individuals and trends represented true con-cern about this possibility and which were attempts toexploit public concern, it is certain that this topic ex-erted a tremendous influence on the tenor of the de-cade. Neurology was not immune to these forces. Ananalysis of “Communist interrogation and indoctrina-tion of ‘enemies of the state’” was a prominent paperin the neurological section of the Archives of Neurologyand Psychiatry in 1956. Viewed in the light of thepresent day, many of the authors’ contentions aboutthe how “brainwashing” worked seem to be biased byantipathy against the victims of this technique.
Neurology in the 1960s: 1960–1969Jerry W. Swanson, MDThe 1960s were characterized by change and turmoil.Soon after the dawn of the decade, John F. Kennedywas elected President of the United States. He inspiredgreat hope at his inauguration, but his life was cutshort by assassin. Later in the decade, further violentacts would strike down the Reverend Martin LutherKing Jr. and Senator Robert F. Kennedy. Neurologi-cally, these events awakened a heightened sensibility toissues of brain death and neurotrauma.
The decade was characterized by intensification ofthe Cold War with the Soviet Union and its allies. Anattempt to contain communism in Asia resulted in USintervention in Vietnam; by 1968, US troop strengthin Southeast Asia reached 550,000. Neurologists servedin the medical corps, usually as members of combinedneuropsychiatric staffs. The first use of herbicides be-gan in 1962 and culminated in the vast spraying ofAgent Orange and other products by the late 1960s.Concerns of neurotoxicity and other sequelae of expo-sure arose later. The Vietnam conflict, combined withracial strife, greatly divided the United States. Asyoung baby boomers took to the streets to protest,
Fig 19. Levodopa was introduced by Birkmayer and Hornyk-iewicz in 1961. Its efficacy was subsequently confirmed byBarbeau and colleagues and Cotzias and colleagues. This fig-ure shows the effect of levodopa on the handwriting of anearly Parkinson’s disease patient treated with levodopa. Sample(A) shows the patient’s handwriting before being treated withlevodopa and (B) shows the same patient’s handwriting aftertreatment with levodopa.
S36 Annals of Neurology Vol 53 (suppl 4) 2003

many also embraced a counterculture that includedhallucinogenic drugs, several associated with specificneurological syndromes.
Major events included the development of microsur-gical techniques in neurosurgery, and the first humanheart transplant. The US Surgeon General also an-nounced that cigarette smoking was a major healthhazard. Landmark Medicare legislation became law andprovided insurance for medical care to millions of el-derly Americans. Such provisions would have a far-reaching impact on the practice of neurologists who
Fig 20. This photograph of several ANA members was takenon the Boardwalk in Atlantic City during the annual ANAmeeting in 1964. From left to right: D. Denny Brown, SidGilman, Bob Feldman, and Joe Vandermuelan. (Photographcourtesy of Bob Feldman, Boston University School of Medi-cine, Boston, MA).
Fig 21. Symptomatic occult hydrocephalus and its successfultreatment was described by R. D. Adams and colleagues inthis 1965 issue of the New England Journal of Medicine.(From Adams RD, Fisher CM, Hakim S, et al. Symptomaticoccult hydrocephalus with “normal” cerebral spinal fluid pres-sure: a treatable syndrome. N Engl J Med 1965;273:117–126.)
Fig 22. The clinical and pathological description of progressivesupranuclear palsy was published by Steele, Richardson, andOlszewski in 1964.
Fig 23. Microneurosurgery was pioneered by M. GaziYasargil, a technique which would revolutionize neurologicalsurgery. (Photo of Professor R. M. P. Donaghy and Yasargilfrom Neurosurgery 1999;45:1035).
Part 2: History of 20th Century Neurology S37

dealt increasingly with the problems of chronic ill-nesses.
Perhaps most symbolic of America’s will to accom-plishment and discovery was the exploration of space.Early in the decade, humans first left the atmosphereand before its conclusion, the first human walked onthe earth’s moon. Understanding the nervous system inresponse to gravitational alterations, pressure variances,and isolation were key factors in this exploration effort.
Neurology in the 1970s: 1970–1979Shrikant Mishra, MD, MSThe 1970s witnessed tremendous growth in the basicand clinical fields of neurology involving patient care,education, and research. Specific areas of great discov-ery included the basic neurobiological, neurophysiolog-ical, neuroimaging, neuroimmunological, and neuro-pharmacological fields. In addition, many importanttreatment modalities for neurological disorders such asParkinson’s disease, stroke, epilepsy, myasthenia gravis,and muscle disorders were developed during this de-cade. The 1970s also saw growth in neurological edu-cation and organizational development exemplified bythe growth of the National Institutes of Health (NIH),the awarding of Nobel prizes in the field of neuro-science, and the founding of the Society of Neuro-science.
The most significant scientific discovery of this de-cade was in the field of neuroimaging involving the
development of computerized axial tomography (CAT)scan, magnetic resonance imaging (MRI) scan, positronemission tomography (PET), and single-photon emis-sion tomography (SPECT) scans.
In 1972, G. N. Hounsfield of EMI Limited of Lon-don, England, first produced the prototype of CATscans. The original concept of axial tomography was,however, developed by William H. Oldendorf manyyears before this event. Felix Bloch and Robert Purcellindependently described the phenomenon of nuclearmagnetic resonance in 1946, but P. C. Lauterbur de-scribed the use of linear gradients to localize signals in
Fig 24. The immunological basis of myasthenia gravis wasposited based on the animal models developed with�-bungarotoxin and the development of acetylcholine receptorantigens. Top photo shows a rabbit with “floppy” ears after aninjection of receptor antigens. Bottom photo shows the samerabbit after receiving edrophonium.
Fig 25. In 1972, G. N. Hounsfield of EMI Limited of Lon-don first produced the prototype of the CAT scan. The origi-nal concept of axial tomography was developed by W. Olden-dorf several years prior to the 1970s. (A) Portrait ofOldendorf (left) and Hounsfield (right) receiving the Ziedsesde Plantes Award in 1974. (B) Prototype of an early CTscanner developed by Oldendorf.
Fig 26. Hugo Moser discovered the fatty acid abnormalityresponsible for adrenoleukodystrophy and developed the modali-ties for therapeutic intervention. This therapy was popularizedin the film Lorenzo’s Oil.
S38 Annals of Neurology Vol 53 (suppl 4) 2003

1973. Physicists described more elaborate methods forimaging, and, in 1972, the physician, R. Damadian,developed ideas and patented the concept in theUnited States. Throughout the 1970s, MRI was pri-marily a research tool with its clinical application oc-curring in the 1980s. PET scan was originally de-scribed in 1952, but the prohibitive cost of cyclotronand its upkeep prevented its clinical use until the de-velopment of newer PET scan technology is 1974. Ini-tial clinical experience with 18F-flurodeoxyglucose fordetermination of local cerebral utilization by emissioncomputed tomography occurred in 1977.
Other advances in central nervous system studies in-cluded the introduction of combined carbidopa/levo-dopa in 1973, which permitted high dopaminergic ac-tivation for Parkinson’s disease patients without severenausea or other peripheral side effects. The major ad-vances is cerebrovascular neurology included improve-ment in diagnosis due to CAT scan and the Canadiancooperative study demonstrating the efficacy of aspirinin transient ischemic attack in male patients. Major ad-vances in epilepsy included a uniform internationalclassification of epilepsy, and the identification of ge-netic and other causative factors in temporal lobe epi-lepsy.
Major discoveries in central nervous system, periph-eral nervous system, and muscle tissue chemistries oc-curred in the 1970s. Key enzymes responsible for var-ious lipid storage disorders such as hexosaminidase Aand B and many biochemical abnormalities associatedwith peroxisomal disorders were identified. In 1973,Moser and colleagues discovered the abnormalities inlong chain fatty acids as the cause of the geneticallyinherited adrenoleukodystrophy. Also during this de-cade, genetically determined muscle disorders were de-fined and explored, particularly in the metabolic andmitochondrial myopathies. Muscle carnitine was iden-tified by Andrew Engel and Carado Angilini, and car-nitine palmitoyltransferase deficiency was identified byMauro, Slavatore, and colleagues. Many other mito-chondrial disorders such as cytochrome c oxidase defi-ciency and pathogenesis of malignant hyperthermia wasdelineated.
Drachman, Engel, and other colleagues revolution-ized concepts on the pathogenesis of myasthenia graviswhen they demonstrated abnormalities in postsynapticmembrane function. They used �-bungarotoxin as anexperimental model to define behavioral, physiological,and structural events consequent to blockade of nico-tine cholinergic receptors. Studies of myasthenia gravisas an autoimmune antibody disorder opened the gatefor diagnosis through antibody assays and for treatmentthrough immunomodification.
Neurology in the 1980s: 1980–1989Kimford J. Meador, MDComputerized tomographic (CT) x-ray imaging of thebrain was the foremost advance in neurology in the1970s, and the next decade saw widespread clinical ap-plication of this technique to the diagnosis of intracra-nial lesions. Despite an initial controversy over thecosts of CT, the utility and cost effectiveness of CTbecame readily apparent. CT scanners were commonplace across the United States by the early 1980s, andmultiple articles on clinical correlations with CT werebeing published. During this decade, the revolution incerebral imaging escalated, and positron emission to-mography (PET) was being used to explore cerebralblood flow and metabolism. The initial functional im-aging techniques from the 1970s using xenon regionalcerebral blood flow were advanced using PET, and, in1981, Phelps and colleagues demonstrated PET activa-tion of the primary and association visual cortices tovisual stimuli. Nuclear magnetic resonance (NMR)spectroscopy was increasingly used to detect metabolicand chemical changes in disease states. In 1980, thefirst topographic NMR images were performed in vivoin humans, and the ability of NMR to detect patho-logical structural changes had been demonstrated.Within the next few years, NMR was renamed mag-netic resonance imaging (MRI), and the technologyadvanced rapidly providing high-resolution images ofthe brain. MRI quickly gained widespread applicationto the diagnosis and management of neurological dis-eases.
New technologies including recombinant DNA andrapid DNA sequencing were creating a revolution in
Fig 27. Air-cooled four-coiled solenoid used in original NMRtomography of the brain (1980). (From Holland GN, MooreWS, Hawkes RC. Nuclear magnetic resonance tomography ofthe brain. J Comput Assist Tomogr 1980;4:1–3.)
Part 2: History of 20th Century Neurology S39

biology. The techniques to reveal gene structure weresoon directed at the evaluation of patients with geneticand metabolic disorders. One of the first major break-throughs in neurology was the discovery in 1983 of apolymorphic DNA marker indicating the chromosomallocalization of the genetic defect in Huntington’s dis-ease.
Other important events and advances in neurologyduring this period included an improved understand-ing of neuroimmunology (e.g., the mechanisms under-lying paraneoplastic syndromes), the first reports of ac-quired immune deficiency syndrome and its
complications, identification of an infectious protein(i.e., prion) causing a spongiform encephalopathy, ap-plication of antiplatelet agents for stroke, and the in-creased use of neurosonographic techniques in themanagement of stroke. Research in parkinsonism wasenhanced when clinical observations in drug abuse pa-tients led to the discovery that a metabolite of MPTPselectively damages cells in the substantia nigra. Therewas also a renewed interest in epilepsy surgery andgrowth in video electroencephalogram monitoringunits, the delineation of a theory concerning domi-nance of the right brain for directed attention, and in-creasing research efforts on Alzheimer’s disease as a re-sult of the evolving recognition of its impact onsociety.
Advances in medical technology created new ethicalproblems. In the early 1980s, neurologists were at theforefront of developing criteria for the determination ofbrain death and of persistent vegetative state. Neurol-ogists also were involved in developing a consensus forappropriate management of patients with persistentvegetative state. Their efforts directly affected legal rul-ings as evidenced by the Amicus briefs filed by neurol-ogists in the mid-1980s concerning the withdrawal ofnutrition and hydration in the cases of Brophy andCruzan. The NIH imposed a ban on the use of itsfunds for fetal tissue transplant research. Congress be-came interested in reducing graduate education fund-ing and controlling the physician workforce. Debateswere raised in the literature concerning the appropriatesize of the neurological workforce. As a result of thisand related factors, the major neurological organiza-tions substantially increased their legislative activitiesfor funding and educational issues. One result was that
Fig 28. In 1980, the first topographic NMR images were per-formed in vivo in humans, and the ability of NMR to detectpathological structural changes had been demonstrated. Withinthe next few years, the technology advanced rapidly providinghigh-resolution images of the brain. MRI quickly gained wide-spread application to the diagnosis and management of neuro-logical diseases. First published tomographic NMR images ofthe human brain: February 1980. (From Holland GN,Moore WS, Hawkes RC. Nuclear magnetic resonance tomog-raphy of the brain. J Comput Asssist Tomogr 1980;4:1–3.)
Fig 29. A portion of the pedigree of the Venezuelan familyfrom the Lake Maracaibo region, which was studied in thediscovery of a polymorphic DNA marker genetically linked toHuntington’s disease. The discovery represented an interna-tional collaboration between multiple groups of clinicians andbasic scientists. (From Guesella JF, Wexler NS, ConneallyPM, et al. A polymorphic DNA marker genetically linked toHuntington’s disease. Nature 1983;306:234–238.)
Fig 30. Insignia of “Decade of the Brain” was developed in1989 for the subsequent decade.
S40 Annals of Neurology Vol 53 (suppl 4) 2003

President George H. Bush signed a congressional reso-lution on July 25, 1989 designating the years 1990 to2000 as the “Decade of the Brain.”
Neurology in the 1990s: 1990–1999David B. Clifford, MDProgress in neurology during the 1990s was markedby continuing explosions in knowledge about the un-derlying biology of neurological disease and by an in-creasing pace of translation of progress “at the bench”to applications in human beings. The decade of the1990s marked a period when scientifically demon-strated new efficacious therapeutic options were atlast a fact for several major neurological problems,further obliterating the image of the neurologist asdiagnostician with little of therapeutic value to offerthe patient.
In the 1990s, cerebrovascular accidents were themost common destructive neurological events, result-ing in around half of the neurology hospital admis-sions in major hospitals. In 1995, the first effectiveintervention for a stroke in progress was demon-strated by Marler and colleagues. Their demonstra-tion that tissue plasminogen activator administratedto appropriately selected subjects early in the courseof a stroke, could significantly reduce the permanentinjury marked an important milestone in neurology.
This observation resulted in increasing focus of neu-rologists on immediate responsiveness with diagnosticand therapeutic teams and in a major public cam-paign to alert the public of the critical importance ofprompt medical treatment for a “brain attack.” Earlyevaluation of strokes also set the stage for anticipatedinterventions based on the cellular biology of tissuedamage during ischemia. Cellular mechanisms ofdeath by necrosis and apoptosis were actively studied,leading to the hope that further protection of thebrain would soon be possible. Tools to rapidly recog-nize areas of ischemia, most prominently the recentdevelopment of diffusion and perfusion weightedmagnetic resonance scanning, also gave promise ofmore powerful studies of acute ischemia based onquantitative knowledge of brain at risk. The decadeclearly provided a powerful springboard that shouldlift stroke out of the category of an extremely com-mon, yet untreatable human catastrophe.
The decade of the 1990s was also marked by tre-mendous progress in application of human genetics toneurological diseases. Perhaps the most striking break-through came with the report of the gene locus associ-ated with development of Huntington’s disease in1983 by Guesella and colleagues. However, this hasbeen followed during this decade by a torrent of ob-servations touching virtually every corner of neurologyof neurodegenerative conditions. Genetic links of im-portance to Alzheimer’s disease, multiple disorders withtrinucleotide repeats, Parkinson’s disease, and motorneuron diseases have been discovered. An intense na-tional program to map the entire human genome wasinitiated in this decade and promises to be the corner-
Fig 31. Neurosurgical interventions to assist the control ofparkinsonism and other movement disorders have gained re-newed importance in this decade as illustrated by developmentof ablative pallidotomy procedures (top) as well as introductionof stimulation of the subthalamic nucleus (bottom). Themounting scientific interest in most effective treatment of Par-kinson’s disease promises to be fueled in the coming years bycongressional support of earmarked funding to pursue the op-portunity in this area of neurology.
Fig 32. The Nobel Prize in Medicine was given to ANAmember and neurologist, Dr Stanley Prusiner for his workdiscovering and describing prions. This important expansion ofmechanisms of human and animal diseases is relevant to agrowing number of important progressive and fatal conditions.Prusiner is shown presenting his findings at the ANA meetingin Seattle in October 1999. The other two panels shows anartist’s conception of the formation of abnormal prion proteinmolecules, which lead eventually to molecular aggregation intovisible deposits of amyloid in the brain by processes yet to bedetermined. (Middle and right illustrations published in BrMed Journal 1998;317:1688–1692 with permission from theBMJ Publishing Group. Illustration courtesy of WGBH/NOVA, Boston and BBC/HORIZON, London).
Part 2: History of 20th Century Neurology S41

stone for tremendous progress in the new millennium,unleashing a vast amount of information that can beused creatively to understand and combat neurologicalillnesses.
Conceptual advances in the spectrum of humandiseases are rare. Neurologist and ANA member Stan-ley Prusiner’s discovery and description of prions asagents of human and animal diseases, most promi-nently Creutzfeldt–Jakob disease and bovine spongi-form encephalopathy, was recognized by the NobelPrize in Medicine in 1997. Prusiner’s honor wascelebrated at the 1999 ANA meeting in Seattle whenPrusiner delivered the F. E. Bennett Lecture. Hiscontinuing elucidation of the prion and its role incausing neurological disease promise opportunities todevelop therapy to stop these devastating fatal ill-nesses.
Whereas multiple sclerosis is another major neuro-logical illness, until very recently, none of hundredsof proposed treatments had survived the scrutiny ofappropriately designed controlled trials. This distress-ing lack of demonstrable treatments ended in 1993with the report of interferon-� as a treatment for re-lapsing remitting multiple sclerosis. Although the fullimplications of ongoing therapy remained to be ex-plored fully, it was clear that at last a therapy wasavailable that alters the course of this disabling neu-rological disease. Multiple reports further character-ized the contribution of interferon—�. A second classof agents, including glatiramer acetate, quickly wasadded to a growing armamentarium of effective treat-ments that should improve the prognosis for this ill-ness. Once again, a part of the breakthrough was
technological use of magnetic resonance imaging, thathighlighted the dynamic pathophysiology underlyingclinical multiple sclerosis symptoms, and provided aquantitative measure of disease activity enabling effec-tive measurement of the impact of therapeutic inter-ventions.
As the decade closed, Parkinson’s disease also drewto the center of a national effort to focus researchfunding on a disabling neurological condition thatappeared to be yielding to scientific probing. Politicalaction by advocates rallying behind the name of Stew-art Udall successfully lobbied Congress to focus fund-ing on this area of neuroscience. This was justified bythe important progress and the belief that concertedscientific efforts will yield substantial benefits in thenear future. During the 1990s, much progress oc-curred in the area of Parkinson’s disease. Multicenterclinical trials were efficiently organized to developtherapy that provided better control of parkinsoniansymptoms and suggested ways to slow the rate of pro-gression of this degenerative condition. Althoughpharmacotherapy remained the most widely usedmeans of coping with this illness, the decade saw aresurgence of interest in both lesioning and deep-brain stimulation as exciting and useful adjuncts topharmacotherapy. These neurosurgical approacheswere based on developing pathophysiological knowl-edge of motor circuits in the brain and were furtherexplored in animal models through recent availabilityof MPTP models of parkinsonism. The genetic andbiological underpinning of this syndrome was alsoyielding to application of genetic techniques andpainstaking evaluation of familial cohorts.
Another area in which intersection of public interestand scientific opportunity promised rapid and impor-tant progress was in the treatment of spinal cord dis-eases and other traumatic brain injuries. Actor Chris-topher Reeve deserves much credit for using his tragicaccident resulting in a spinal cord lesion to rally scien-tific interest and funding sources to focus on neurolog-ical injury. The rapidly expanding knowledge of mech-anisms of tissue damage and the hope that neurologicalrepair might be spurred by application of modern tech-nology including stem cells set the stage for tremen-dous progress bettering the outcome of these tragic in-juries. Stem cells appeared as one of the mostpromising breakthroughs of the decade offering newhope for treatments of degenerative and traumaticbrain injuries.
Toward the 21st CenturyJames F. Toole, MD and Lella MelsonAs the 21st century begins, neurology finds itself in apivotal evolutionary point in its history. Breakthroughdiscoveries linked to molecular biology and genetic en-
Fig 33. The figures show a scanning electron micrographicimage of entire embryoid body (right) and embryonic stemcell derived neurons (left) stained with �-tubulin III after 9days in vitro. Recognition of the potential of stem cell useand increased awareness of regenerative properties of the ner-vous system fuel a growing interest in neurorehabilitation fornumerous neurological conditions. (Figures courtesy of DrJohn McDonald, Washington University School of Medi-cine).
S42 Annals of Neurology Vol 53 (suppl 4) 2003
gineering apply themselves directly to the nervous sys-tem. For the first time, the gamut of neurodegenerativeand hereditometabolic disorders can be approachedwith techniques envisioned to offer focused and evencurative therapies. Information technology, nowadapted to the scientific and medical arenas, opens ho-rizons for increasingly more efficient transfer of dataand for the development of neurological teaching tech-niques never before available.
In 1996, there were approximately 12,500 active USneurologists, fulfilling roughly 10,000 full-time equiv-alents involved in patient care. Based on data generatedby the American Academy of Neurology, by 2020, thisnumber is expected to expand to approximately 12,000full-time equivalents. The demand for care will increaseas well, though the factors that influence this evolu-tion, an aging population, economic growth, new tech-nology, and the influence of managed care, make pre-diction hazardous. There are approximately 450neurology residency positions available in the UnitedStates at this time, but the number is estimated to de-crease over the next two decades. Furthermore, the rawnumbers and percentages of US graduates choosingneurology will likely remain stable or shrink slightly,creating a hiatus between manpower and need for spe-cial neurological care.
The challenge of training these new neurologists iscurrently debated, often with disagreements betweengeneral neurologists in practice and subspecialists inteaching centers, residents, and fellows. As a unifiedforce, neurologists surveyed by the American Academyof Neurology oppose a fifth year of general neurologytraining and a yearly competency examination for the21st century. However, subspecialists strongly favor theconcept of developing subspecialty certification proce-dures even though this is not supported by generalists.
Whereas current specialty certification exists in Neuro-physiology and Child Neurology, movements to ex-pand this process to cerebrovascular neurology, behav-ioral neurology, and movement disorders will bedebated in the first decade of the century.
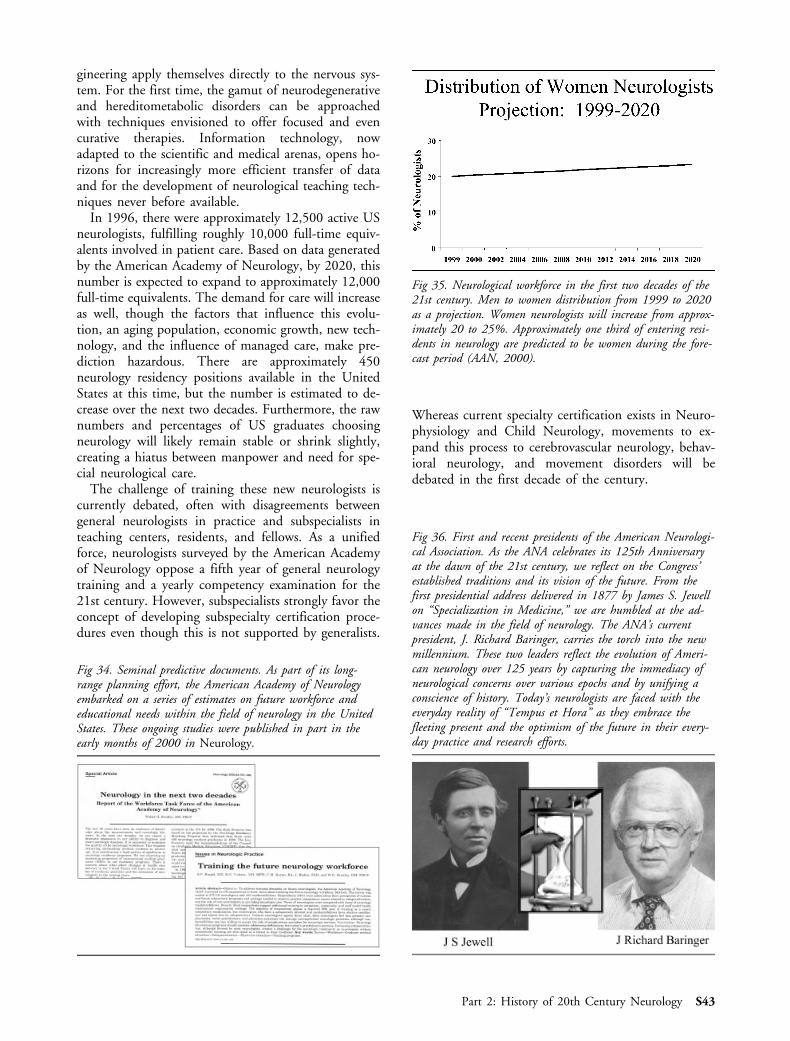
Fig 35. Neurological workforce in the first two decades of the21st century. Men to women distribution from 1999 to 2020as a projection. Women neurologists will increase from approx-imately 20 to 25%. Approximately one third of entering resi-dents in neurology are predicted to be women during the fore-cast period (AAN, 2000).
Fig 36. First and recent presidents of the American Neurologi-cal Association. As the ANA celebrates its 125th Anniversaryat the dawn of the 21st century, we reflect on the Congress’established traditions and its vision of the future. From thefirst presidential address delivered in 1877 by James S. Jewellon “Specialization in Medicine,” we are humbled at the ad-vances made in the field of neurology. The ANA’s currentpresident, J. Richard Baringer, carries the torch into the newmillennium. These two leaders reflect the evolution of Ameri-can neurology over 125 years by capturing the immediacy ofneurological concerns over various epochs and by unifying aconscience of history. Today’s neurologists are faced with theeveryday reality of “Tempus et Hora” as they embrace thefleeting present and the optimism of the future in their every-day practice and research efforts.
Fig 34. Seminal predictive documents. As part of its long-range planning effort, the American Academy of Neurologyembarked on a series of estimates on future workforce andeducational needs within the field of neurology in the UnitedStates. These ongoing studies were published in part in theearly months of 2000 in Neurology.
Part 2: History of 20th Century Neurology S43

Part 2 Bibliographic Sources1900–1909DeJong RN. A history of American neurology. New York: RavenPress, 1982.
Finger S. Origins of neuroscience. A history of explorations intobrain function. New York: Oxford University Press, 1994.
Sherrington, C. The integrative action of the nervous system. NewHaven: Yale University Press, 1906.
1910–1919Rhein JHW. Central pain. A pathological study of eight cases.J Nerv Mental Dis 1912;39:661–676.
Knauer A, Maloney WJMA. The cephalograph: a new instrumentfor recording and controlling head movements. J Nerv Mental Dis1914;41:75–80.
Transactions of the American Neurological Association. 36th An-nual Meeting, Washington DC, May 2–4, 1910. J Nerv MentalDis, 1911.
1920–1929Berger H. Uber das Electrekephalogramm des Menschen. ArchPscyiatr Nervenkr 1929;87:527–570.
Cushing H. The pituitary body and its disorders; clinical states pro-duced by disorders of the hypophysis cerebri. Philadelphia: Lippin-cott, 1912.
Cushing H. Disorders of the pituitary gland. JAMA 1921;75:25.
1930–1939News and Comments. American Board of Psychiatry and Neurol-ogy, Inc. Arch Neurol Psychiat 1934;32:1064.
Freeman W. The psychiatrist personalities and patterns. New York:Grune and Stratton, 1968.
Gibbs FA, Gibbs EL, Lennox WG. Cerebral dysrhythmias of epi-lepsy. Measures for their control. Arch Neurol Psychiat 1938;39:298–314.
Leech P. Special article from the American Medical AssociationChemical Laboratory. Elixir of sulfanilamide Massengill. JAMA1937;109:1531–1539.
Lennox WG, Lennox MA. Epilepsy and related disorders. Vol 2.Boston: Little, Brown, 1960.
Putnam TJ. The demonstration of specific anticonvulsant action ofdiphenyl hydantoin and related compounds. In: Discoveries in bio-logical psychiatry. Ayd FJ, Blackwell B, eds. Philadelphia: Lippin-cott, 1970.
Merrit HH, Putnam TJ. Sodium diphenyl hydantoinate in thetreatment of convulsive disorders. JAMA 1938;111:1068–1073.
Myerson A, Ayer JB, Putnam TJ, et al. Eugenical sterilization. Areorientation of the problem. American Neurological Association.New York: Macmillan, 1936.
The Tuskegee study: the 30th year of observation. Summaryadapted from Rockwell DH, Yobs AR, Moore MB. The Tuskegeestudy of untreated syphilis. Arch Int Med 1964;114:792–798.
Viets HR, Schwab RS. Prostigmin in the diagnosis of myastheniagravis. N Eng J Med 1935;213:1280–1283.
1940–1949Jasper HH. Diffuse projection systems: the integrative action of thethalamic reticular system. Electroenceph Clin Neurophysiol 1949;1:405–419.
Penfield W. The cerebral cortex and consciousness. Harvey Lect1936–1937;32:35–69.
Penfield W, Rasmussen AT. The cerebral cortex of man. New York:Macmillan, 1950.
Renshaw B, Forbes A, Morison BR. Activity in isocortex andhippocampus; electrical studies with microelectrodes. J Neuro-physiol 1940;3:74–105.
1950–1959Bernhard CG, Bohm E, Hojeberg S. A new treatment of status epi-lepticus. Intravenous injections of a local anesthetic (lidocaine).AMA Arch Neurol Psychiatr 1955;74:208–214.
Narabayash H, Okuma T, Shikiba S. Procaine oil blocking of theglobus pallidus. AMA Arch Neurol Psychiatr 1956;75:36–48.
Adams RD, Victor M, Mancall EL. Central pontine myelinolysis.AMA Arch Neurol Psychiatr 1959;81:154–172.
Landau WM, Clare MH. The plantar reflex in man, with specialreference to some condition where the exterior response is unexpect-edly absent. Brain 1959;82:321–355.
Jervis GA, McAllister FF, Hogg BM, Deterling RA. Revasculariza-tion of the brain in mental defectives. Neurology 1953;3:871–878.
Madonick MJ. Statistical control studies in neurology. III. TheHoffmann sign. AMA Arch Neurol Psychiatr 1952;68:109–115.
Fisher M. Occulsion of the internal carotid artery. AMA Arch Neu-rol Psychiatr 1951;65:346–377.
Rosomoff HL. Hypothermia and cerebral vascular lesions. II. Ex-perimental middle cerebral artery interruption followed by induc-tion of hypothermia. AMA Arch Neurol Psychiatr 1957;78:454–464.
Penfield W, Jasper H. Epilepsy and the functional anatomy of thehuman brain. Boston: Little, Brown, 1954.
1960–1969Mackay RP, Wortis SB, Sugar O, eds. The yearbook of neurology,psychiatry and neurosurgery (1961–1962 yearbook series). Chicago:Yearbook Medical Publishers, 1962.
Kimball RW, Friedman AP, Vallejo E. Effect of serotonin in mi-graine patients. Neurology 1960;10:107–111.
Cotzias GC, Vanwoert H, Schiffer LM. Aromatic amino acids inmodification of parkinsonism. N Engl J Med 1967;276:377.
Zu Rhein GM, Chou S. Particles resembling papova viruses in hu-man cerebral demyelinating disease. Science 1965;148:1477–1479.
Yasargil MG. A legacy of microneurosurgery: memoirs, lessons andaxioms. Neurosurgery 1999;45:1025–1092.
Milner B. Effects of different brain lesions on card sorting. The roleof the frontal lobes. Arch Neurol 1963;9:90–96.
Kurtzke JF. On the evaluation of disability in multiple sclerosis.Neurology 1961;11:686–694.
Steele JC, Richardson JC, Olszewski J. Progressive SupranuclearPalsy. Arch Neurol 1964;10:333–359.
Elmquist D, Lambert EH. Detailed analysis of neuromuscular trans-mission in a patient with the myasthenic syndrome sometimes as-sociated with bronchial carcinoma. Mayo Clin Proc 1968;43:689–712.
Adams RD, Fisher CM, Hakim S, et al. Symptomatic occult hy-drocephalus with “normal” cerebral spinal fluid pressure: a treatablesyndrome. N Engl J Med 1965;273:117–126.
1970–1979Di Mauro S, Melis-Di Mauro PM. muscle carnitine palmityl-transferase deficiency and myoglobinuria. Science 1973;182:929.
Engel AG, Angelini C. Carnitine deficiency of human skeletal mus-cle with associated lipid storage myopthy: a new syndrome. Science1973;173:899.
S44 Annals of Neurology Vol 53 (suppl 4) 2003

Hounsfield GN. Computerized transverse axial scanning (tomogra-phy) I. Description of system. Br J Radiol 1973;46:1016–1022.
Kawamura N, Moser HW, Kishimoto Y, et al. Excess C-26 fattyacid in culture skin fibroblasts from adrenoleucodyatrophy anda-drenomyeloneuropathy patients. Trans Am Neurol Assoc 1978;103:113–115.
Kuhl DE, Phelps ME, Hoffman EJ, et al. Initial clinical experiencewith 18 F-2-fluoro-2 deolxy-D-glucose for determination of local ce-rebral utilization by emission computed tomography. Acta NeurolScand 1977;56(suppl 64):178–179.
Lauterbur PC. Image formation by induced local interactions. Ex-amples employing nuclear magnetic resonance. Nature 1973;242:190–191.
Oldendorf WH. The quest for an image of brain. A brief historicaland technical review of brain imaging techniques. Neurology 1978;28:517–533.
Oldendorf WH. isolated flying-spot detection of radiodensitydiscontinuities: displaying the internal structural pattern of a com-plex object. Trans Biomed Electron 1961;8:68–72.
1980–1989Guesella JF, Wexler NS, Conneally PM, et al. A polymorphic DNAmarker genetically linked to Huntington’s disease. Nature 1983;306:234–238.
Calne DB, Langston JW, Martin WRW, et al. Positron emissiontomography after MPTP: observations relating to the cause of Par-kinson’s disease. Nature 1985;317:246–248.
Holland GN, Moore WS, Hawkes RC. Nuclear magnetic resonancetomography of the brain. J Comput Assist Tomogr 1980;4:1–3.
Marx JL. NMR opens a new window into the body. The use ofnuclear magnetic resonance for medical diagnosis hovers on thebrink of practical application. Science 1980;17:302–305.
Prusnier SB. Novel proteinaceous infectious particles cause scrapie.Science 1982;216:136–144.
Sato S, Long RL, Porter RJ. Monitoring at the National Institute ofNeurological and Communicative Disorders and Stroke. In: Got-man J, Ives JR, Gloor P, eds. Long-term monitoring in epilepsy.Electroenceph Clin Neurophysiol 1985;37(suppl):415–422.
Snider WD, Simpson DM, Nielsen S, et al. Neurological compli-cations of acquired immune deficiency syndrome: analysis of 50 pa-tients. Ann Neurol 1983;14:403–418.
Whitehouse PJ, Price DL, Clark AW, et al. Alzheimer’s disease: ev-idence for selective loss of cholinergic neurons in the nucleus basalis.Ann Neurol 1981;10:122–126.
1990–1999The IFNB Multiple Sclerosis Study Group. Interferon Beta-lb iseffective in relapsing-remitting multiple sclerosis. I. Clinical resultsof a multicenter, randomized, double-blind, placebo-controlled trial.Neurology 1993;43:655–661.
Brown P, Raymond B. Clinical review. 1755 and all that: a histor-ical primer of transmissible spongiform encephalopathy. Br Med J1998;317:1688–1692.
Gusella JF, Wexler NS, Connally PM, et al. A polymorphic DNAmarker genetically linked to Huntington’s disease. Nature 1983;306:234–238.
Larner AJ, Farmer SF. Clinical review. Recent advances: neurology.Br Med J 1999;319:362–366.
Marler JA. The National Institute of Neurological Disorders andStroke rt-PA Stroke Study Group. Tissue plasminogen activator foracute ischemic stroke. N Engl J Med 1995;333:1581–1587.
Martin JB. Mechanism of disease: molecular basis of the neurode-generative disorders. N Engl J Med 1999;340:1970–1980.
Mehler M, Kessler JA. Progenitor cell biology: implications for neu-ral regeneration. Arch Neurol 1999;56:780–784.
Toward the 21st CenturyAgid Y. Will neurological practice be different during the 21st cen-tury? Arch Neurol 2000;57:56–57.
Ausman JI. Achievements of the last century in neurosurgery and aview to the 21st century. Arch Neurol 2000;57:61–62.
Bradley WG. Neurology in the next two decades. Report of theworkforce task force of the American Academy of Neurology. Neu-rology 2000;54:787–789.
Fathallah-Shaykh HM. Fiction, reality, and molecular neurology.Arch Neurol 2000;57:63–64.
Menken M. Medical and neurologic education at the millennium.Arch Neurol 2000;57:62–63.
Piradov MA. Neurology at the millennium. Arch Neurol 2000;57:60.
Ringel SP, Vickrey BG, Keran CM, et al. Training the future neu-rology workforce. Neurology 2000;54:480–484.
Rosenberg, RN. The Brain Code in Health and Disease. Arch Neu-rol 2000;57:50–51.
Rowland LP. A century and a half of modern neurology, a decade ofthe brain, and the millennium. Arch Neurol 2000;57:52.
Toole JF. Stroke research and the 21st century. Arch Neurol 2000;57:55.
Swift T. Advances in neurology in the 20th century. Arch Neurol2000;57:60–61.
Part 2: History of 20th Century Neurology S45