nurse-surgeon object transfer: video analysis of communication and situation awareness in the...
TRANSCRIPT

1
POST-PRINT VERSION OF ARTICLE PUBLISHED IN INTERNATIONAL JOURNAL OF NURSING STUDIES (2014) 51, 1195-1206. Nurse-surgeon object transfer: Video analysis of communication and situation awareness in the operating theatre Terhi Korkiakangas, Sharon-Marie Weldon, Jeff Bezemer, & Roger Kneebone
Abstract Background. One of the most central collaborative tasks during surgical operations is the passing of objects, including instruments. Little is known about how nurses and surgeons achieve this. The aim of the present study was to explore what factors affect this routine-like task, resulting in fast or slow transfer of objects. Methods. A qualitative video study, informed by an observational ethnographic approach, was conducted in a major teaching hospital in the UK. A total of 20 general surgical operations were observed. In total, approximately 68 hours of video data have been reviewed. A subsample of 225 minutes has been analysed in detail using interactional video-analysis developed within the social sciences. Results. Two factors affecting object transfer were observed: 1) relative instrument trolley position; 2) alignment. The scrub nurse's instrument trolley position (close to vs. further back from the surgeon) and alignment (gaze direction) impacts on the communication with the surgeon, and consequently, on the speed of object transfer. When the scrub nurse was standing close to the surgeon, and "converged" to follow the surgeon's movements, the transfer occurred more seamlessly and faster (< 1.0 second) than when the scrub nurse was standing further back from the surgeon and did not follow the surgeon’s movements (>1.0 second). Conclusions. The smoothness of object transfer can be improved by adjusting the scrub nurse's instrument trolley position, enabling a better monitoring of surgeon’s bodily conduct and affording early orientation (awareness) to an upcoming request (changing situation). Object transfer is facilitated by the surgeon’s embodied practices, which can elicit the nurse’s attention to the request and, as a response, maximise a faster object transfer. A simple intervention to highlight the significance of these factors could improve communication in the operating theatre. Keywords Scrub nurse, surgeon, instrument trolley, body movement, communication, situation awareness 1. Introduction Health care professionals, such as surgeons and nurses, work in interprofessional teams. This seemingly obvious fact has crucial importance to patient safety (Kneebone and Fry, 2011), as adverse incidents in surgical operations are often the result of breakdowns in team communication (Aggarwal et al., 2004; Lingard et al., 2004). Research on interprofessional communication in the operating theatre has
2
drawn on different methodologies, including observational rating scales and interviews. Communication problems are frequently reported. According to Lingard et al. (2004), as much as 31% of all communications in the operating theatre could be categorised as failing some way. For example, information provided to colleagues can be inaccurate, delivered too late, or it fails to reach the individuals who need it, leaving issues unresolved until they become critical. In a recent systematic review, Weldon et al. (2013) found that there are not many video-based studies that elaborate on the actual, real-time communication behaviours in the operating theatre.
Communication breakdowns can have many consequences. They can cause delays that compromise the quality of patient care and the management of subsequent operations. As a result, delays in operations can incur substantial costs to hospitals (Wong et al., 2010). When an operation is in progress, surgeons and scrub nurses routinely exchange instruments, and this requires communication and alertness from both parties. Dropping instruments alone has been shown to extend operating time on average by 7.6 minutes (Khan et al., 2008). However, studies have not elaborated how non-vocal behaviours, such as eye-gaze and hand movements, might contribute to such incidents. Task-related communication is closely linked to situation awareness. This concept refers to a dynamic process of acquiring information from the immediate environment and responding accordingly to changing situations. There is no single definition of situation awareness but its understanding can be roughly divided into two concerns: the view of awareness primarily as a psychological, cognitive phenomenon (e.g., Endsley, 1995); or as a distributed awareness, involving interactions between people, artefacts, and the environment (Stanton et al., 2006). The widely cited model by Endsley involves three levels: perception of environmental elements in a time and space, understanding their meaning, and use of this information to predict events that are likely to happen. Anticipation is an important part of situation awareness, enabling an individual to respond rapidly to changing situations, and potentially preventing adverse incidents from occurring. Interpersonal communication and interaction with artefacts have also been suggested to impact the awareness of what is happening in one’s surroundings (Endesley & Jones, 2001). However, some researchers have called for a broader attention to these factors, so as to move the focus from individual cognition to collaboration (Salmon et al., 2008).
Coordination of activities is important for the efficient delivery of surgical operations. Therefore, understanding of situation awareness from the angle of communication becomes relevant. Bromiley (2008) notes how a lack of situation awareness and breakdowns in communication count as human factors that are present in fatal incidents in healthcare, but also in 75% of aviation accidents. A lapse in situation awareness can occur when attention is “fixated” and a professional fails to re-orient and to change a course of action (Bromiley, 2008). Situation awareness has particular relevance for scrub nurses. These nurses are “scrubbed up” to work within the sterile zone, and they continuously guard, count, and handle sterile instruments and items, such as swabs and syringes, on the instrument trolley. Their main task is to pass these items to the surgeon, ideally at the precise time of need, so as to avoid any
3
delays in the stages of an operation. Instrument exchange can be cognitively demanding, as the task requires constant vigilance and technical knowledge of the actual operation. Scrub nurses have to remain situationally aware to select the right instrument at the right time (Mitchell and Flin, 2008), and to "both think and remain ‘ahead’ of the surgeon" (Mitchell et al., 2011:822).
Situation awareness has been suggested to be one of the most important non-technical skills that scrub nurses have to master in the operating theatre (Mitchell and Flin, 2008). While such skills have been researched and assessed among surgeons (e.g. Non-Technical Skills for Surgeons [NOTSS], Yule et al., 2008), less is known about how nurses’ non-technical skills relate to situation awareness. Where nurses’ situation awareness has been examined more generally, these studies have tended to draw on cognitive assessments (Wright, 2009) and interviews (Mitchell et al., 2011). While these are important methods, they do not always reveal the details of actual interactions and how people display awareness of the events around them, as that is often beyond their awareness. Hence, operating theatre nurses often talk about a “tacit understanding” between colleagues (Gillespie et al., 2010, p. 736).
To address the relative lack of research on theatre nurses’ non-technical skills, The Scrub Practitioners’ List of Intraoperative Non-Technical Skills (SPLINTS) behavioural rating scale (Mitchell et al., 2012) has been recently developed. It focuses on the assessment of non-technical skills, situation awareness, communication and teamwork, and task management among scrub nurses. For example, the core category of situation awareness includes elements of “gathering information”, “recognising and understanding information” and “anticipating”, while two important elements of communication and teamwork are “exchanging information” and “coordinating with others”. Mitchell et al. showed that scrub practitioners have found the rating scale useful in assessing simulated scenarios representing good and bad practice in these core non-technical areas.
Some studies involving anaesthetists, surgeons and perfusionists (Fiouratou et al., 2010; Hazehurst et al., 2007; Parush et al., 2011) have considered situation awareness as a process where verbal communication and interaction with objects are paramount. Hazelhurst et al. show that vocal practices, such as requests and confirmations serve as important resources: A surgeon might ask a perfusionist to adjust the flow of fluids, and the perfusionist vocally confirms this after the adjustment has been done. The spoken clarification informs the surgeon that a transition to a new state has begun, establishing mutual understanding of the situation. Such research suggests that situation awareness can become “visible” through the study of actual interactions.
2. Researching communication through video Video offers an innovative way to examine communication that underpins situation awareness in a greater detail that has been done before. A study of collaboration in an organisational work environment has shown that activities of one colleague can unobtrusively encourage others to “notice” critical elements in the environment (Heath et al., 2002). In such cases, awareness is built in and through interactions with
4
others. Through video, real-time activities can be accessed repeatedly, so that their detailed scrutiny becomes possible. Communication through posture shifts, arm movements, gaze behaviours, and the like can be analysed on a second-by-second basis. Such detail would be difficult to recollect in interviews or to articulate in retrospective accounts when "the moment" has passed.
In a recent ethnographic study that employed video recordings as part of the observation of ward nurses' handover practices, Liu et al. (2012) described how the nurses routinely communicated through non-vocal means, such as by exchange of glances or gestures. Other studies (drawing on conversation analytic frameworks) in the operating theatre, or specifically in anaesthesia (Hindmarsh and Pilnick, 2007), have shown that bodily conduct is essential for effective collaboration and relate closely to the concept of awareness. Only a few studies have focused specifically on scrub nurses.
In an eye-tracking study of visual attention, Koh et al. (2011) reported that scrub nurses frequently used distinctly different visual sources of information for different tasks during an operation. The most frequently gazed areas were the operating field, patient's lower body, Mayo stand (a sterile tray on a stand for instruments that may be immediately needed by the surgeon; the tray is often positioned over the patient's lower body) and the main instrument trolley. The nurses’ attentiveness towards the operating field and the surgeon’s manual actions indicate that a gaze direction to these areas might be central for anticipating particular instrument needs at different stages of an operation (Koh et al., 2011).
This suggests that situation awareness and anticipation are processes that are visible and externalised in bodily conduct, as when one attends to a colleague’s manual actions. Through a close examination of video-recorded instrument transfer episodes, Sanchez Svensson et al. (2007a) noted also that the arrangement of surgical instruments on the instrument trolley embodies nurses’ awareness of surgeons’ needs during an operation. Furthermore, these authors demonstrated that,
[a]wareness does not simply rely on participants possessing the same information or knowledge about a particular activity but more on how they are able to contribute actively to the contingent organisation of awareness and interaction – in this case, the ways in which the participants in and through the grasping, handling, organisation and use of instruments can orientate prospectively to the upcoming actions and concerns of others. (p. 43)
Others have elaborated how the seemingly unproblematic instrument passing does not simply rest on the vocal requests (e.g., "Scissors, please") uttered by surgeons, but also on the simultaneous body movement and gaze practices that project the upcoming request to a nurse (Bezemer et al., 2011; also Koschmann et al., 2011). Bezemer et al. have shown how a surgeon can simultaneously engage in two different activities, knot tying and instrument exchange: scissors are requested exactly when needed through an arm movement towards the nurse. Likewise in other contexts, such as medical consultations (Heath, 1986), parties' orientation to body movements have been shown to push mutual engagement in motion.
Less is known about the ways in which scrub nurses, in particular, juggle different activities during operations, and how they display their awareness of the

5
surgeon's needs through their bodies. The focus on subtleties of behaviour offers practical value in improving communication, so that crucial tasks can be accomplished effectively. The present paper aims to address the gap of detailed video-based studies of situation awareness in the operating theatre. The analysis demonstrates how a scrub nurse and a surgeon build mutual awareness interactionally when exchanging syringes, scalpels, and swabs. The study elaborates on the link between body movement and situation awareness, and considers whether the relative proximity of the instrument trolley, the scrub nurse and the surgeon impacts on communication and the speed of object transfers.
3. Method
3.1. Methodological framework The current study is part of a video ethnographic research project examining communication in the operating theatre. The project was centrally concerned with how operating theatre team members communicate using different modes of communication (speech, gaze, movement, gesture, and handling of objects). Video ethnography was used to capture teamwork and communication events as they happened inside the operating theatre, and to record fleeting moments and detailed (vocal and non-vocal) aspects of communication that would be missed or forgotten otherwise.
Communication was analysed using video analysis (Heath et al., 2010) that draws on the framework of conversation analysis (CA) (Schegloff, 2007). This framework enabled the examination of why particular communication events happened and how they were organised. Video analysis proceeds through a detailed transcription of the actions that people perform - that is, it systematically describes and visualises a series of actions. People perform these actions through different forms of bodily conduct, such as speech, gesture, movement, and gaze (in medical contexts, see Heath, 1986). Interactional transcription and analysis renders visible how these actions are ordered as sequences: for instance, how an instrument request is made and followed by the provision of the instrument. Thus rather than considering the actions of the clinicians in isolation, it will be considered how each participant’s conduct emerges in relation to the actions of others. Such detailed description can make visible exactly how particular joint tasks, such as object exchanges, are achieved and sometimes not achieved. This framework was selected as it provides analytic tools for making situation awareness and tacit understanding visible in micro-level communication.
Field notes and brief informal interviews were conducted with the participants to support and to clarify observations. Two authors (TK [social interaction researcher with expertise in video analysis] and SMW [research nurse with background in operating theatre nursing]) were centrally involved in the data collection and analysis.
6
3.2. Data source
Operating theatre professionals were recruited from a UK health institution as part of a project funded by the Economic and Social Research Council (ESRC). Specific surgeons who were previously known to some members of the research team were first approached about participation in the observational study. Having gained these surgeons’ consent to observe their operations, two researchers (TK and SMW) from the team approached the theatre manager and gained her consent to attend the theatres and to observe (and eventually to film) operations. Theatre nurses, anaesthetists and operating department practitioners (ODP’s) were conveniently recruited. They were approached on the morning of a set of operations that the researchers attended to observe (consent was often gained continually due to a frequent rotation of staff). The researchers spent a month observing operations during which they familiarised themselves with the theatre staff. The surgeons, nurses, ODP’s, and anaesthetists were then separately consented to being filmed after the researchers had gradually introduced their wish to collect video data of teamwork in the operating theatres.
The project was granted the NHS Research Ethics Committee approval, as well as a Site Specific Assessment (SSA) approval at the participating NHS Trust. The study was conducted in accordance with the recommendations for physicians involved in research on human subjects adopted by the 18th World Medical Assembly, Helsinki 1964 and later revisions.
Video recordings of 20 operations were conducted over the period of three months in two different theatres, representing a mixture of open and laparoscopic procedures (see Table 1). In total, the data corpus involves approximately 68 hours of video recordings of three consultant surgeons (attending surgeons), three registrar surgeons (resident surgeons), five scrub nurses, six circulating nurses, three consultant anaesthetists and three ODP’s. In the current study, a subsample of two cases has been considered to examine instrument transfer episodes. This subsample includes two laparoscopic operations, with duration of 118 minutes (Case A; gastric banding) and 107 minutes (Case B; internal hernia repair), involving one consultant surgeon who was assisted by a different scrub nurse in both cases. The illustrative examples presented in this paper were taken from this subsample.
The two cases were selected for analysis following an initial stage of unmotivated looking (see Psathas, 1995) of the data. During this stage, the entire video corpus was viewed “openly”. That is, interactionally relevant phenomena were allowed to emerge from the data, as opposed to having preconceptions or hypotheses to guide the observations. It was noted that, in Case A and Case B, the instrument exchanges occurred differently, insofar as the former case was characterised as involving “smoother” exchanges than the latter case. It was decided to examine these cases more closely in order to understand the factors that appeared to impact this smoothness.
7
Table 1. Collected cases and types of operation observed.
Type of Operation Cases
Laparoscopic staging 4
Oesophogectomy 1
Laparoscopic sigmoidectomy 1
Laparscopic fundoplication 1
Laparoscopic gastric bypass Laparoscopic sleeve gastrectomy Laparoscopic gastric band Laparoscopic internal hernia repair Laparoscopic cholecystectomy Staging laparotomy Open hernia repair
1 3 2 2 2 2 1
Total 20
3.3. Data collection
The two researchers (TK and SMW), who jointly observed operations, recorded data with two tripod-mounted wide-angle HD Sony camcorders. The cameras were positioned so as to capture different viewpoints of the theatre. Two inconspicuous RevoLabs xTab wireless microphones were used for audio recording, worn by the consultant and the scrub nurses under their sterile gowns. Field notes were continually recorded during data collection and often included events not captured by the cameras. Participant interviews were conducted when the operating theatre members had a free moment and they were recorded with a Dictaphone.
3.4. Video analysis The analysis proceeded through a careful review of the video recordings. During the stage of unmotivated looking, recurring interactional phenomena were detected, which were subsequently subjected to in-depth, interactional video analysis (see the sections below and “Defining Analytical Focus”). Two authors (TK and SMW) re-inspected the entire video corpus, creating a detailed log of every form of interactional event (e.g., request, utterance, question, repetition, response; whether response was produced vocally or non-vocally; associated bodily conduct/position) from each team member, and linking these events with a unique time code identifier (using InqScribe software). The initial observations were then closely examined with
8
the logs, and selected examples were transcribed to enable a sequential analysis of the emerging actions (see below). It was observed that object exchange was a predominant feature of the scrub nurse-surgeon interactions, and that it involved both vocal and non-vocal communication. Transferring objects between colleagues is clearly a routine task, and the observations suggested that these exchanges often occurred in a smooth and timely manner at the research site. However, they were occasionally delayed or did not occur at all, resulting in a "no-exchange" whereby surgeons reached to the object themselves. It was decided to examine this variation in the apparent smoothness of object transfer in more detail in a subsample of two cases (see “Data Source” for information on case selection).
By focusing on the selected case examples, which involved re-playing of the selected video clips of object exchanges 25 times or more (often in slow motion; zooming in on the professionals’ face and hand areas), drafting of transcripts (see below) of the (selected) short item passing episodes, and timing of lapses between requests and responses, it was possible to examine the fine detail of surgeon and nurses’ conduct that seemed to explain some of the variation. In this paper, the transcripts has been synthesised into detailed descriptions of the passing episodes, and still images have been used to illustrate the key analytical moments. Object passings were described quantitatively in terms of their speed and qualitatively in terms of the interaction involved in the passings. The analysis was refined by the team of authors, who together reviewed the examples extracted from the subsample. The findings were further explored in a roundtable meeting involving some of the nurses and surgeons who were filmed as part of the research.
3.3. Defining Analytic Focus
The review of the video data rendered visible two basic interactional arrangements that scrub nurses adopted during surgical operations: alignment with the surgeon and the operating field and alignment with other people, objects and actions. These alignments were related to the nurses' gaze activities: whether they converged to gaze at the surgeon and the operating field, or whether they converged to attend other concerns, such as the instrument trolley or another nurse. A closer review suggested an association between these alignments and the relative position of the instrument trolley during an operation (see Table 2).
Interactions where the scrub nurse either converged or diverged with the operating surgeon, moments before an object exchange occurred, were then subjected to a more detailed video analysis in a subsample. The focus of the analysis was on the impact of these arrangements on the item passing episodes, namely whether the passings occurred ‘smoothly’ or less ‘smoothly’, and what in these arrangements appeared to account for the variation. The principle of sequential organisation of interactions, derived from the framework of conversation analysis (Schegloff, 2007), was used to inform the observations: when a request for an instrument or item was issued, a response was expected, and any delay in responsiveness could be some way problematic. Therefore the analysis was conducted to delineate the nurses’ behaviours
9
during the lapse between a request and a response (i.e., item passing) and just before a request had been issued, in order to examine the factors that seemed to impact on their fast or slow responsiveness to the requests. Furthermore, the ways in which surgeons constructed their requests were also considered as a factor that impacted on the nurses’ responsiveness to pass the requested items.
The quantitative rating was used to calculate the average speed of passings per case. The lapse of approximately one second was used as an indicative measure, based on the principle of “a standard maximum silence” of approximately one second in conversations (Jefferson, 1989). This principle, drawn from conversation analytic research, relates to an observation that a delay in responding to an initiating action is often taken to indicate some kind of interactional trouble (for example, problems of hearing or understanding with respect to the initiating action; disagreements with the prior turn, see Pomerantz, 1984). While previously used as a numerical indicator of silences in ordinary conversations, it was noted that the lapse of approximately one second was also applicable when distinguishing between fast and slow non-vocal responses (i.e., item passings) in the present study. Thus the speed of passings was measured in terms of the time lapse between the surgeon’s request for a passing and the scrub nurse’s response to that request. Passings taking less than a second were classified as ‘fast’, and passings taking a second or more were classified as ‘slow.’
The qualitative rating was used to map the different ways in which passings were achieved. Interaction was defined as the concerted actions of participants involved in passing of items. Interactions were described in terms of 1) the surgeon’s signalling of a request for a passing (i.e. the vocal and/or non-vocal means by which the request is articulated); 2) the scrub nurse’s focus of attention at the time of the signalling (i.e. the physical orientation of the scrub nurse); and 3) the scrub nurse’s response to the request for assistance. The contexts of item passings were also described, namely in terms of participants (scrub nurse, surgeons) and objects involved (e.g. syringe, instrument, swab) and their spatial arrangement (i.e. layout). Using this framework a detailed analysis of video recorded object passings was undertaken. Photo stills illustrate the key moments to provide access to the activities discussed in the analysis.
10
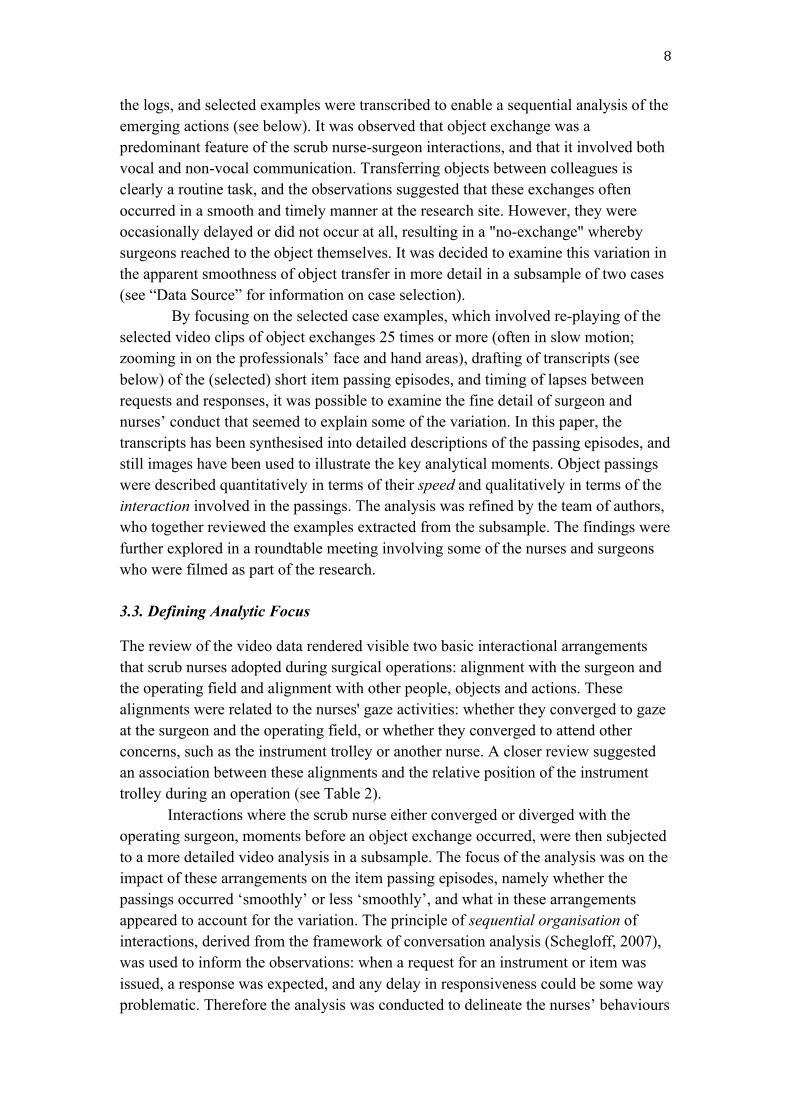
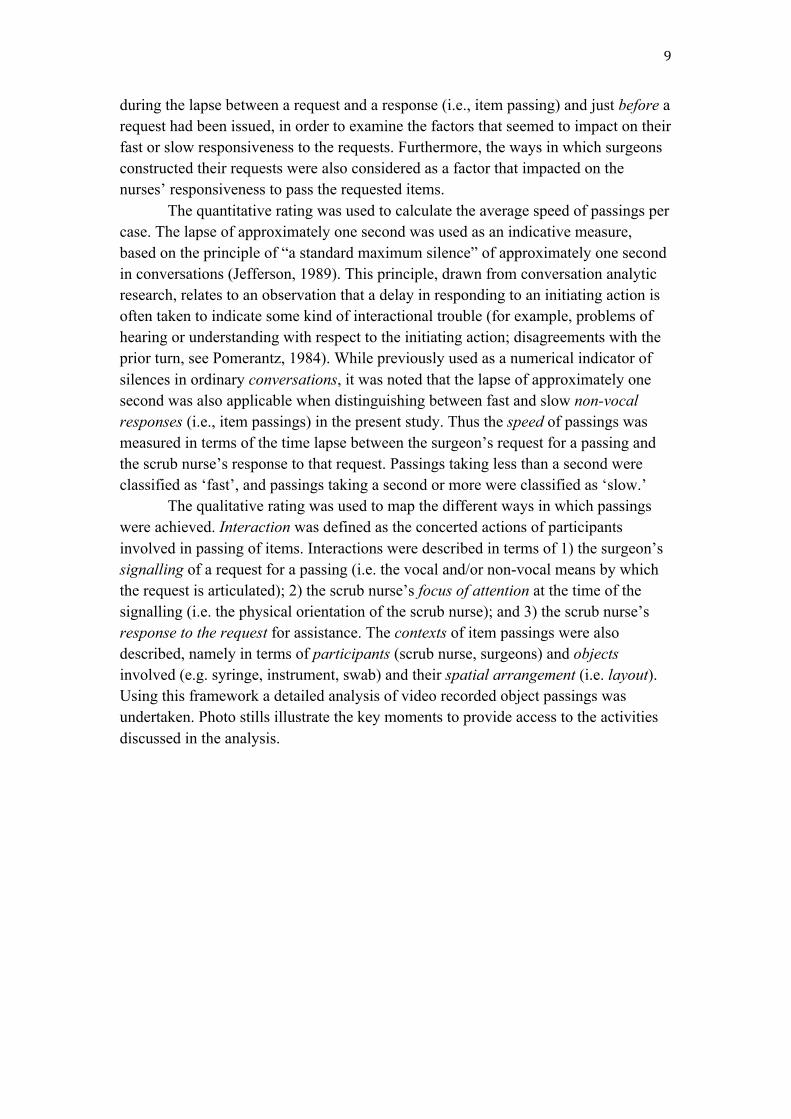
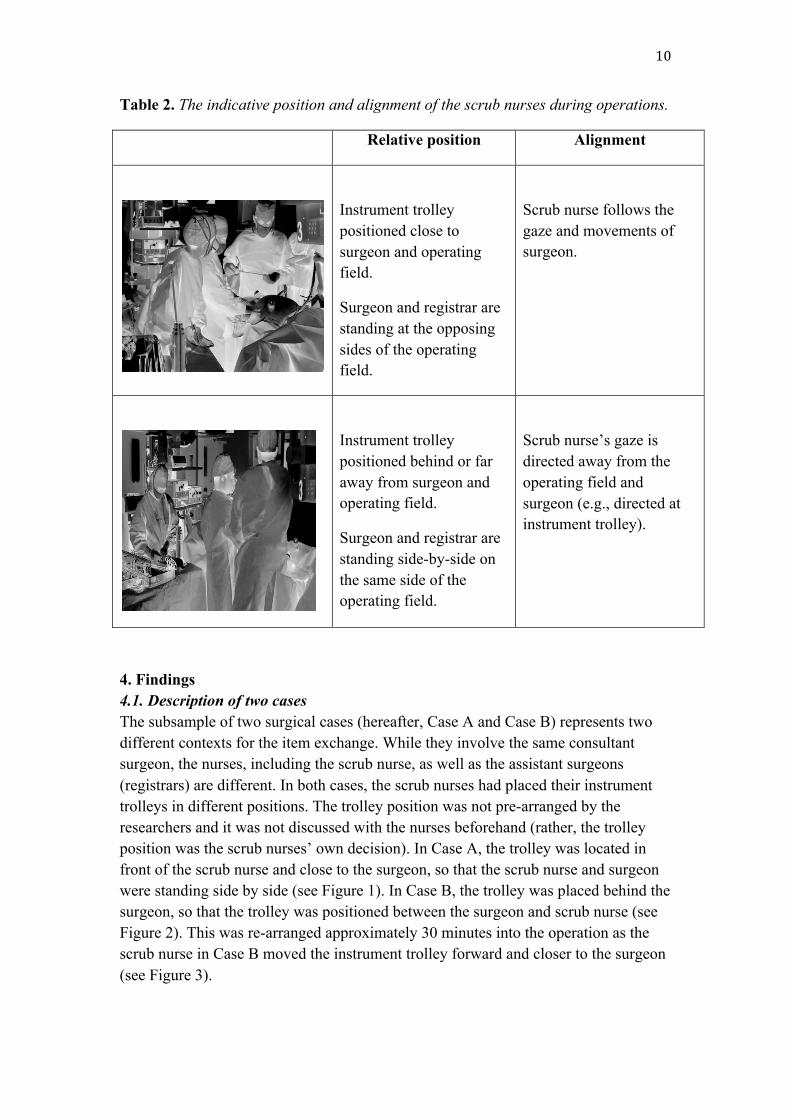
Table 2. The indicative position and alignment of the scrub nurses during operations.
Relative position Alignment
Instrument trolley positioned close to surgeon and operating field.
Surgeon and registrar are standing at the opposing sides of the operating field.
Scrub nurse follows the gaze and movements of surgeon.
Instrument trolley positioned behind or far away from surgeon and operating field.
Surgeon and registrar are standing side-by-side on the same side of the operating field.
Scrub nurse’s gaze is directed away from the operating field and surgeon (e.g., directed at instrument trolley).
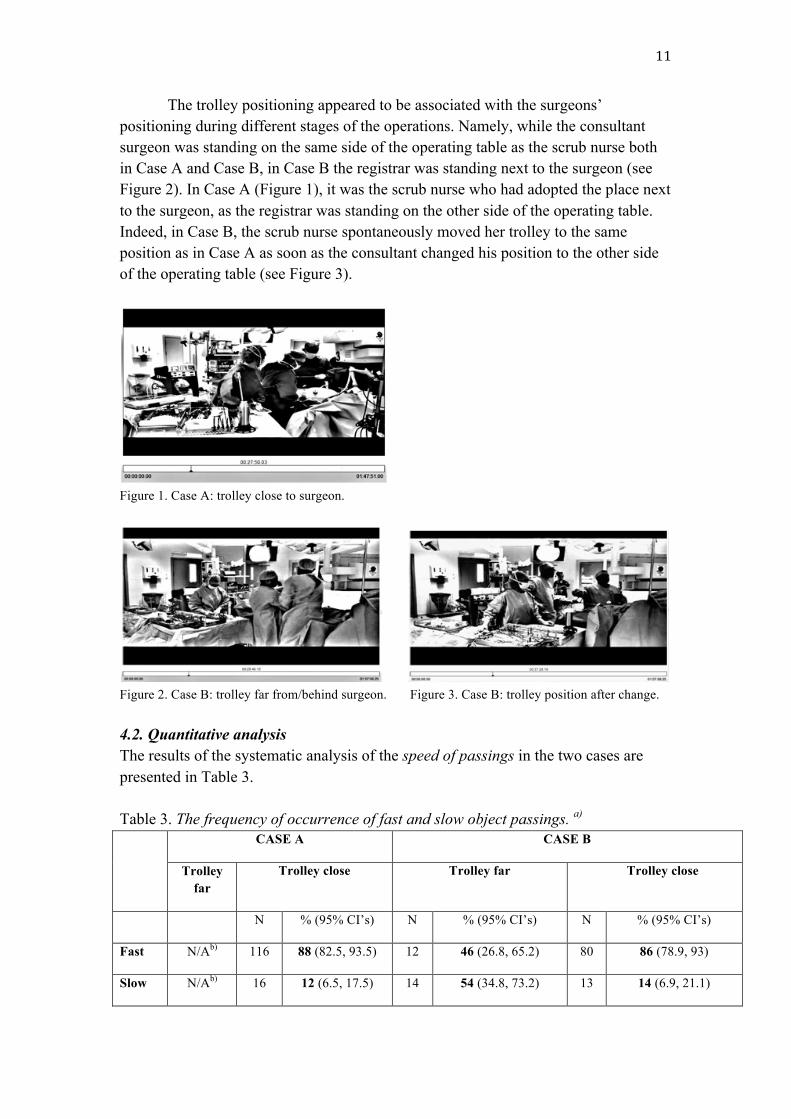
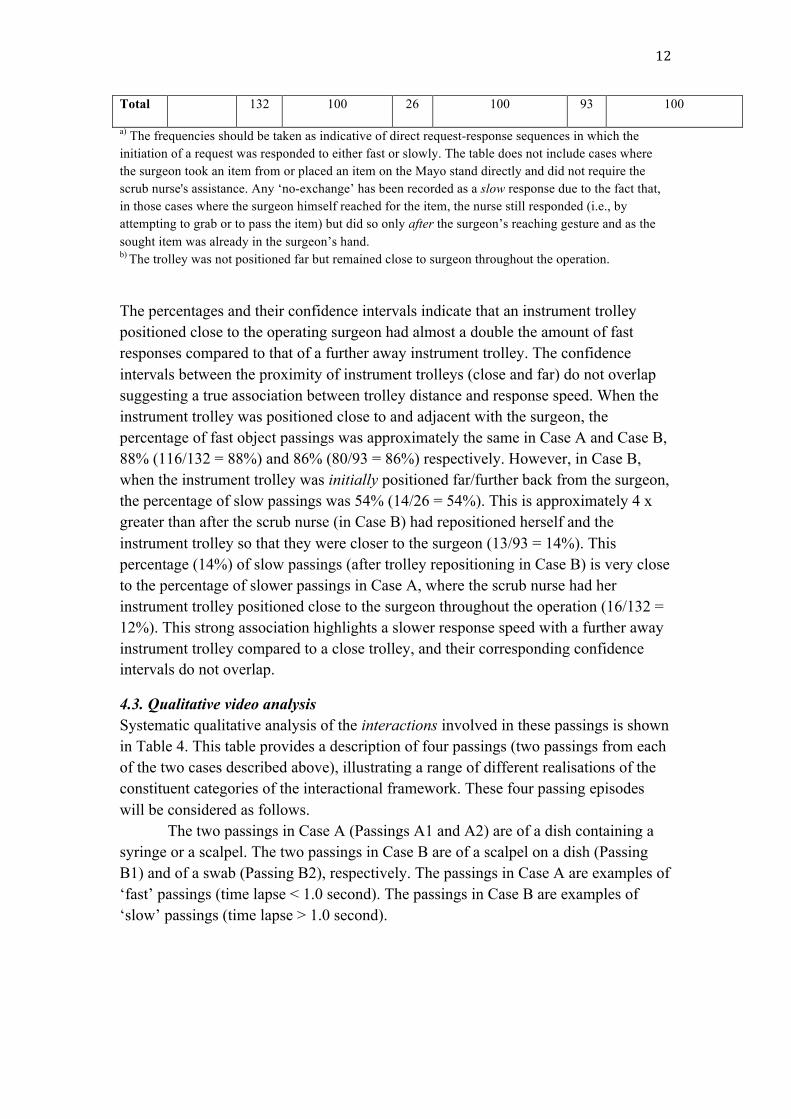
4. Findings 4.1. Description of two cases The subsample of two surgical cases (hereafter, Case A and Case B) represents two different contexts for the item exchange. While they involve the same consultant surgeon, the nurses, including the scrub nurse, as well as the assistant surgeons (registrars) are different. In both cases, the scrub nurses had placed their instrument trolleys in different positions. The trolley position was not pre-arranged by the researchers and it was not discussed with the nurses beforehand (rather, the trolley position was the scrub nurses’ own decision). In Case A, the trolley was located in front of the scrub nurse and close to the surgeon, so that the scrub nurse and surgeon were standing side by side (see Figure 1). In Case B, the trolley was placed behind the surgeon, so that the trolley was positioned between the surgeon and scrub nurse (see Figure 2). This was re-arranged approximately 30 minutes into the operation as the scrub nurse in Case B moved the instrument trolley forward and closer to the surgeon (see Figure 3).
11
The trolley positioning appeared to be associated with the surgeons’ positioning during different stages of the operations. Namely, while the consultant surgeon was standing on the same side of the operating table as the scrub nurse both in Case A and Case B, in Case B the registrar was standing next to the surgeon (see Figure 2). In Case A (Figure 1), it was the scrub nurse who had adopted the place next to the surgeon, as the registrar was standing on the other side of the operating table. Indeed, in Case B, the scrub nurse spontaneously moved her trolley to the same position as in Case A as soon as the consultant changed his position to the other side of the operating table (see Figure 3).
Figure 1. Case A: trolley close to surgeon.
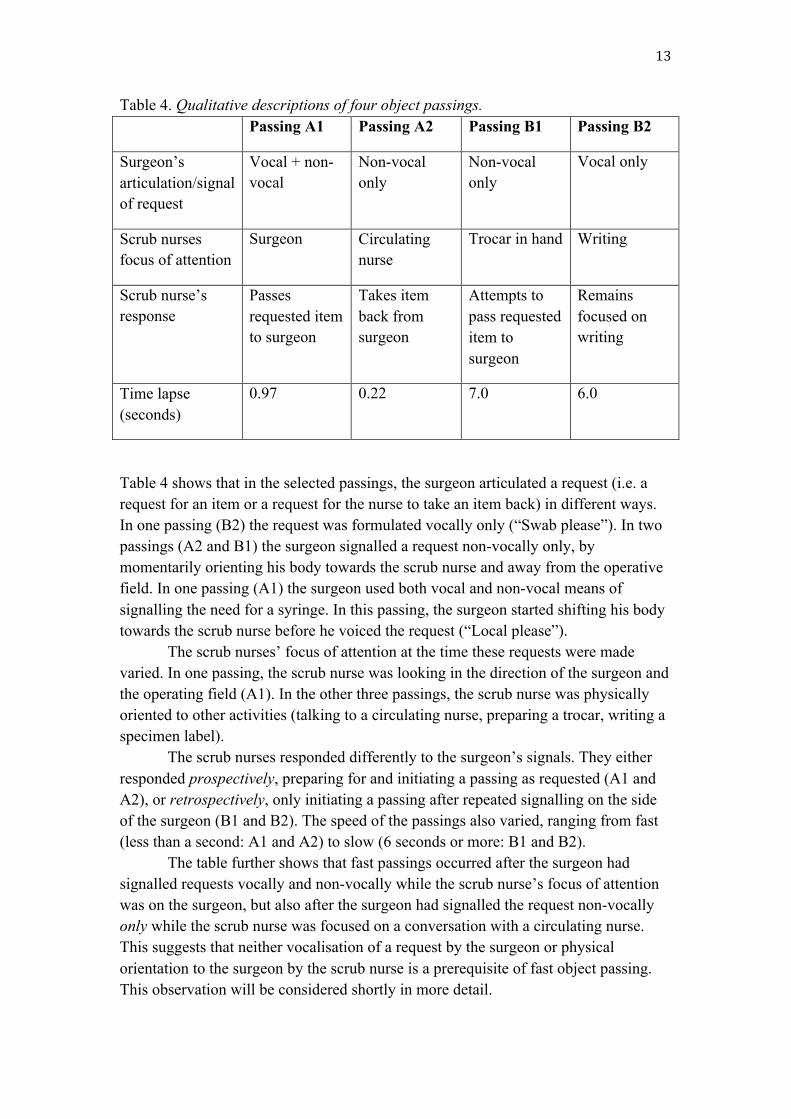
Figure 2. Case B: trolley far from/behind surgeon. Figure 3. Case B: trolley position after change. 4.2. Quantitative analysis The results of the systematic analysis of the speed of passings in the two cases are presented in Table 3. Table 3. The frequency of occurrence of fast and slow object passings. a) CASE A CASE B
Trolley far
Trolley close Trolley far Trolley close
N % (95% CI’s) N % (95% CI’s) N % (95% CI’s)
Fast N/Ab) 116 88 (82.5, 93.5) 12 46 (26.8, 65.2) 80 86 (78.9, 93)
Slow N/Ab) 16 12 (6.5, 17.5) 14 54 (34.8, 73.2) 13 14 (6.9, 21.1)
12
Total 132 100 26 100 93 100
a) The frequencies should be taken as indicative of direct request-response sequences in which the initiation of a request was responded to either fast or slowly. The table does not include cases where the surgeon took an item from or placed an item on the Mayo stand directly and did not require the scrub nurse's assistance. Any ‘no-exchange’ has been recorded as a slow response due to the fact that, in those cases where the surgeon himself reached for the item, the nurse still responded (i.e., by attempting to grab or to pass the item) but did so only after the surgeon’s reaching gesture and as the sought item was already in the surgeon’s hand. b) The trolley was not positioned far but remained close to surgeon throughout the operation.
The percentages and their confidence intervals indicate that an instrument trolley positioned close to the operating surgeon had almost a double the amount of fast responses compared to that of a further away instrument trolley. The confidence intervals between the proximity of instrument trolleys (close and far) do not overlap suggesting a true association between trolley distance and response speed. When the instrument trolley was positioned close to and adjacent with the surgeon, the percentage of fast object passings was approximately the same in Case A and Case B, 88% (116/132 = 88%) and 86% (80/93 = 86%) respectively. However, in Case B, when the instrument trolley was initially positioned far/further back from the surgeon, the percentage of slow passings was 54% (14/26 = 54%). This is approximately 4 x greater than after the scrub nurse (in Case B) had repositioned herself and the instrument trolley so that they were closer to the surgeon (13/93 = 14%). This percentage (14%) of slow passings (after trolley repositioning in Case B) is very close to the percentage of slower passings in Case A, where the scrub nurse had her instrument trolley positioned close to the surgeon throughout the operation (16/132 = 12%). This strong association highlights a slower response speed with a further away instrument trolley compared to a close trolley, and their corresponding confidence intervals do not overlap.
4.3. Qualitative video analysis Systematic qualitative analysis of the interactions involved in these passings is shown in Table 4. This table provides a description of four passings (two passings from each of the two cases described above), illustrating a range of different realisations of the constituent categories of the interactional framework. These four passing episodes will be considered as follows.
The two passings in Case A (Passings A1 and A2) are of a dish containing a syringe or a scalpel. The two passings in Case B are of a scalpel on a dish (Passing B1) and of a swab (Passing B2), respectively. The passings in Case A are examples of ‘fast’ passings (time lapse < 1.0 second). The passings in Case B are examples of ‘slow’ passings (time lapse > 1.0 second).
13
Table 4. Qualitative descriptions of four object passings. Passing A1 Passing A2 Passing B1 Passing B2
Surgeon’s articulation/signal of request
Vocal + non- vocal
Non-vocal only
Non-vocal only
Vocal only
Scrub nurses focus of attention
Surgeon Circulating nurse
Trocar in hand Writing
Scrub nurse’s response
Passes requested item to surgeon
Takes item back from surgeon
Attempts to pass requested item to surgeon
Remains focused on writing
Time lapse (seconds)
0.97 0.22 7.0 6.0
Table 4 shows that in the selected passings, the surgeon articulated a request (i.e. a request for an item or a request for the nurse to take an item back) in different ways. In one passing (B2) the request was formulated vocally only (“Swab please”). In two passings (A2 and B1) the surgeon signalled a request non-vocally only, by momentarily orienting his body towards the scrub nurse and away from the operative field. In one passing (A1) the surgeon used both vocal and non-vocal means of signalling the need for a syringe. In this passing, the surgeon started shifting his body towards the scrub nurse before he voiced the request (“Local please”). The scrub nurses’ focus of attention at the time these requests were made varied. In one passing, the scrub nurse was looking in the direction of the surgeon and the operating field (A1). In the other three passings, the scrub nurse was physically oriented to other activities (talking to a circulating nurse, preparing a trocar, writing a specimen label). The scrub nurses responded differently to the surgeon’s signals. They either responded prospectively, preparing for and initiating a passing as requested (A1 and A2), or retrospectively, only initiating a passing after repeated signalling on the side of the surgeon (B1 and B2). The speed of the passings also varied, ranging from fast (less than a second: A1 and A2) to slow (6 seconds or more: B1 and B2). The table further shows that fast passings occurred after the surgeon had signalled requests vocally and non-vocally while the scrub nurse’s focus of attention was on the surgeon, but also after the surgeon had signalled the request non-vocally only while the scrub nurse was focused on a conversation with a circulating nurse. This suggests that neither vocalisation of a request by the surgeon or physical orientation to the surgeon by the scrub nurse is a prerequisite of fast object passing. This observation will be considered shortly in more detail.
14
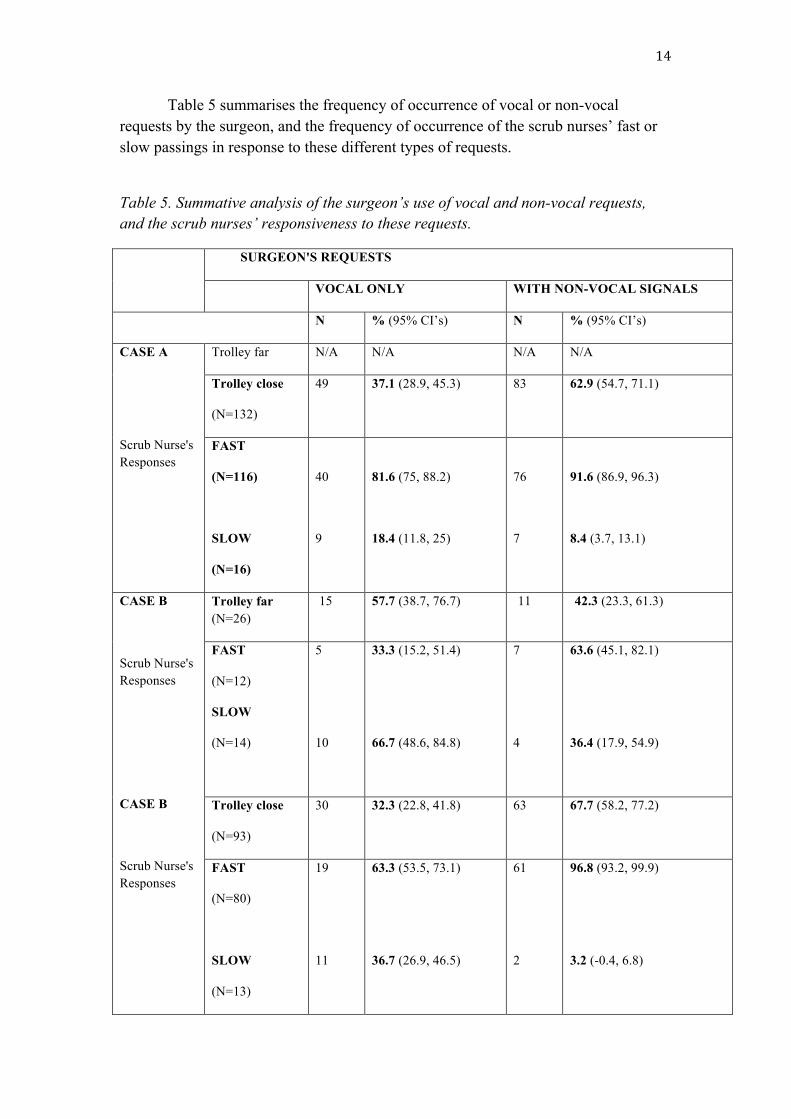
Table 5 summarises the frequency of occurrence of vocal or non-vocal requests by the surgeon, and the frequency of occurrence of the scrub nurses’ fast or slow passings in response to these different types of requests.
Table 5. Summative analysis of the surgeon’s use of vocal and non-vocal requests, and the scrub nurses’ responsiveness to these requests.
SURGEON'S REQUESTS
VOCAL ONLY WITH NON-VOCAL SIGNALS
N % (95% CI’s) N % (95% CI’s)
CASE A
Scrub Nurse's Responses
Trolley far N/A N/A N/A N/A
Trolley close
(N=132)
49 37.1 (28.9, 45.3) 83 62.9 (54.7, 71.1)
FAST
(N=116)
SLOW
(N=16)
40
9
81.6 (75, 88.2)
18.4 (11.8, 25)
76
7
91.6 (86.9, 96.3)
8.4 (3.7, 13.1)
CASE B
Scrub Nurse's Responses
CASE B
Scrub Nurse's Responses
Trolley far (N=26)
15 57.7 (38.7, 76.7) 11 42.3 (23.3, 61.3)
FAST
(N=12)
SLOW
(N=14)
5
10
33.3 (15.2, 51.4)
66.7 (48.6, 84.8)
7
4
63.6 (45.1, 82.1)
36.4 (17.9, 54.9)
Trolley close
(N=93)
30
32.3 (22.8, 41.8) 63
67.7 (58.2, 77.2)
FAST
(N=80)
SLOW
(N=13)
19
11
63.3 (53.5, 73.1)
36.7 (26.9, 46.5)
61
2
96.8 (93.2, 99.9)
3.2 (-0.4, 6.8)
15
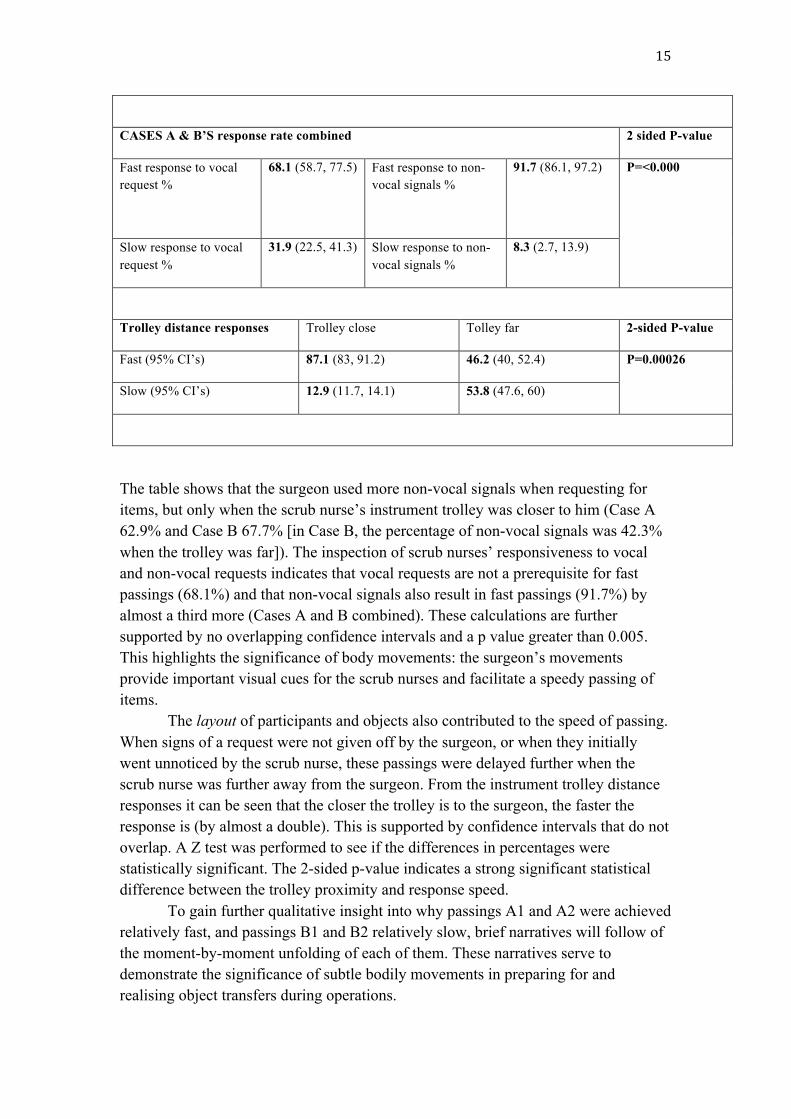
CASES A & B’S response rate combined 2 sided P-value
Fast response to vocal request %
68.1 (58.7, 77.5) Fast response to non-vocal signals %
91.7 (86.1, 97.2) P=<0.000
Slow response to vocal request %
31.9 (22.5, 41.3) Slow response to non-vocal signals %
8.3 (2.7, 13.9)
Trolley distance responses Trolley close Tolley far 2-sided P-value
Fast (95% CI’s) 87.1 (83, 91.2) 46.2 (40, 52.4) P=0.00026
Slow (95% CI’s) 12.9 (11.7, 14.1) 53.8 (47.6, 60)
The table shows that the surgeon used more non-vocal signals when requesting for items, but only when the scrub nurse’s instrument trolley was closer to him (Case A 62.9% and Case B 67.7% [in Case B, the percentage of non-vocal signals was 42.3% when the trolley was far]). The inspection of scrub nurses’ responsiveness to vocal and non-vocal requests indicates that vocal requests are not a prerequisite for fast passings (68.1%) and that non-vocal signals also result in fast passings (91.7%) by almost a third more (Cases A and B combined). These calculations are further supported by no overlapping confidence intervals and a p value greater than 0.005. This highlights the significance of body movements: the surgeon’s movements provide important visual cues for the scrub nurses and facilitate a speedy passing of items. The layout of participants and objects also contributed to the speed of passing. When signs of a request were not given off by the surgeon, or when they initially went unnoticed by the scrub nurse, these passings were delayed further when the scrub nurse was further away from the surgeon. From the instrument trolley distance responses it can be seen that the closer the trolley is to the surgeon, the faster the response is (by almost a double). This is supported by confidence intervals that do not overlap. A Z test was performed to see if the differences in percentages were statistically significant. The 2-sided p-value indicates a strong significant statistical difference between the trolley proximity and response speed. To gain further qualitative insight into why passings A1 and A2 were achieved relatively fast, and passings B1 and B2 relatively slow, brief narratives will follow of the moment-by-moment unfolding of each of them. These narratives serve to demonstrate the significance of subtle bodily movements in preparing for and realising object transfers during operations.

16
In Passing A1, the surgeon turned his upper body and uttered "Local please", while almost simultaneously the scrub nurse passed a kidney dish containing the requested syringe (Figure 4). It appears that in this instance the scrub nurse anticipated that local anaesthetic would be requested and took the surgeon’s posture shift as an early sign of the upcoming request.
Figure 4. Scrub nurse passes kidney dish in response to vocal and non-vocal signals from the surgeon (Passing A1). In Passing A2, the same scrub nurse’s attention was momentarily focused on the circulating nurse. Yet at the precise moment the consultant brought his posture up, she quickly shifted her gaze to him and placed her hands on the kidney dish on the instrument trolley (Figure 5). This shift in orientation suggests that while she was momentarily focused on something else, she was at the same time anticipating requests and able to pick up non-vocal signs of such requests, even though these signs were visible to her only peripherally.
Figure 5. Scrub nurse re-orients and holds kidney dish stand by in response to surgeon’s non-vocal signal (Passing A2). In Passing B1, a different scrub nurse (B) was preparing a trocar while the registrar signalled his need for an item on a kidney dish on the Mayo stand. The registrar extended his arm across the operating field and reached out to the kidney dish. Following these movements the scrub nurse shifted her orientation to the registrar, reaching over to the kidney dish in an attempt to assist with the item passing (Figure

17
6); yet she did so only after 2.0 seconds. This suggests that, in this instance, the scrub nurse neither anticipated nor picked up the early signs of the registrar’s request for a scalpel: her peripheral monitoring was not optimal. Furthermore, her positioning, with the instrument trolley almost out of reach, constrained the assistance she was eventually providing.
Figure 6. Scrub nurse reaches out to kidney dish on Mayo stand (Passing B1). In Passing B2, the scrub nurse was focused on writing a specimen label while the surgeon retracted a laparoscopic camera from the patient's abdomen and asked for a swab. Unlike in the other passings where he signalled the upcoming requests, on this occasion, he did not turn his body or gaze towards the scrub nurse. Following the vocalised request (“Swab please”) the scrub nurse shifted her attention to the surgeon, who by then had begun to reach for the swab (on the instrument trolley) himself (Figure 7). In this instance, the scrub nurse was unable to anticipate the request prior to it being vocalised as the surgeon did not give off any early non-vocal signs. At the same time, her positioning was hindering a speedy passing of the requested object for the surgeon.
Figure 7. Surgeon reaches out to a swab on instrument trolley (Passing B2). 5. Discussion A number of important theoretical, methodological and practical lessons can be drawn from the study. First, the analysis highlights the significance of the role of the scrub nurses’ and surgeons’ bodies in achieving object transfers. Body movements can make a colleague aware of what one is about to do next and consequently, what
18
contingencies this places on the other person (Hindmarsh & Pilnick 2007; Bezemer et al., 2011). This means that talk is not always needed, but rather attentiveness to non-vocal conduct is equally important. Through their hand and other body movements a surgeon can secure the availability of the scrub nurse for the upcoming request and thereby maximise the occurrence of a swift object passing. Minimal attention requests, such as a surgeon turning towards a scrub nurse, can be useful in seeking the orientation of the nurse who often has to divide their attention with several concerns at once. Thus while it is essential that surgeons and nurses both understand the detailed practices that can facilitate situation awareness, it is equally important that surgeons identify their own conduct that can facilitate, or hinder, communication with a scrub nurse.
In the present study, the scrub nurses’ embodiment of situation awareness contributed to the speed of instrument passing. However, the surgeon’s own actions contributed to the shaping of the situation so that his actions were noticed by the nurse. In the widely cited three-level model of situation awareness (Endsley, 1995) “noticing” has been highlighted as a prerequisite for subsequent understanding and action. Indeed, while the scrub nurses frequently oriented to multiple concerns at once, they were able to monitor the surgeon peripherally, understood what his movements were “about”, and responded by passing items. However, it would be simplistic to conclude that this accomplishment was primarily dependent on the nurses’ hidden cognitive processing. Rather, the present findings call for an interactional understanding of situation awareness where also “noticing” functions as a two-way process. That is, the surgeon’s non-vocal “signs” were important in eliciting the nurses’ attention to him. As such, the surgeon’s actions, movements, and occasional vocalisations were as important as the nurses’ orientation to them. In other studies, where situation awareness has been examined from the angle of distributed awareness, primacy has been given to vocal exchanges in the operating theatre (Fioratou et al., 2010; Hazelhurst et al., 2007; Parush et al., 2011). These studies have not elaborated on the interactional mechanisms with reference to non-vocal conduct, and how it unfolds on a second-by-second basis during naturalistic events. If situation awareness were treated purely as a cognitive state of an individual, it would be easy to overlook how particular environments and layouts impact this process. Previously Sanchez Svensson at al. (2007a) have considered how the arrangement of instruments on the trolley embodies awareness of “what is needed next” and the ease at which implements are exchanged between a nurse and a surgeon. The present analysis expands on this and highlights the role of the layout and proximity of people and objects around the operating table. Layout should be taken into account in order to maximise nurses' shared visual focus of the operating field. This suggests simple interventions to augment collaboration: Positioning the instrument trolley as close and adjacent as possible to the operating surgeon can help a nurse to swiftly respond to the anticipated object request as embodied in the surgeon’s movements. Simulation can be used to experiment with different spatial layouts, and to further examine the impact of proximity on communication and instrument transfer. Theatre nurses could safely explore the importance of sharing the
19
visual focus with the surgeon (often accomplished with side-by-side positioning), and the initial simulation trials have looked promising. This points to an important aspect for the training and professional development: In recognition of the implications of layout and proximity of people and objects around the operating table, the study recommends that surgical teams should discuss positioning prior to an operation.
Third, the analysis highlights the added value of using video in professional development. The monitoring of and responding to the bodily conduct of surgical colleagues could be taken as an indicator of “good practice” insofar as it embodies situation awareness. In the case of scrub nurses, situation awareness facilitates proactive behavior in instrument passing episodes, making them faster. A detailed examination of behaviours that are very subtle, but which crucially underpin communication, can suggest a change in practices deemed ineffective (Sanchez Svensson et al., 2007b; Heath et al., 2010). Often, for clinicians, any problems are more likely to be manifested as a general sense that an operation does not flow smoothly, rather than as a detailed awareness of what is causing the difficulty. It is only through a process of making visible the unspoken aspects of communication, such as orientation to movements and proximity of bodies, that participants can work out what is actually going on. By zooming in on moments that often go unnoticed trainees and professionals could examine questions such as “Did you notice how the scrub nurse responded quickly to the surgeon’s posture shift, which indicated her anticipation of a request for an instrument?” This way, the interactional mechanisms of situation awareness could be taught explicitly as part of training.
Detailed video-based studies can also contribute to research that measures team practices through observational rating scales, such as the SPLINTS (Mitchell et al., 2012). These rating scales have highlighted non-technical skills for safe and effective practice in the operating theatre. However, what is actually meant by “awareness” or “anticipation” has been rarely spelt out with a reference to real situated conduct. A detailed understanding of the factors that embody constructs, such as situation awareness, has direct relevance to the development of future assessment scales. Social scientific video studies could make a contribution to the refinement of existing scales so as to capture “micro-level” interactions. The present study has some limitations. Firstly, the interactions were filmed using two tripod-mounted video cameras placed at opposing ends of the operating theatre so as to capture a wide-angle view of the staff working in the theatre. In the current study, it was not possible to undertake eye-tracking measurements and consequently the determination of the scrub nurses’ eye-gaze direction can be sometimes a matter of judgement. However, video editing tools have been used to support observations by manually zooming in on the participants’ face and eye region where necessary. In further research, eye-tracing and interactional video analysis could be combined to examine nurses’ gaze patterns in response to particular body movements.
Secondly, the present study reports on the practices of two scrub nurses and one surgeon, which could place constraints on the extent to which the observations can be generalised. However, the case examples have been drawn from a wider

20
corpus of 20 operations involving different scrub nurses and surgeons where similar practices were observed. It should also be noted that the measured lapses of object passings in the two operations are approximate. The study does not suggest that smooth instrument transfers always occur within a second or so, as transfers can take a few seconds to complete. Further, some surgical instruments are larger or more complex than others, and consequently their handling can take longer. These are important considerations for a safe passing of objects between nurses and surgeons.
It is important to bear in mind that also the surgeons’ positioning during the operations can have an impact on the location where the scrub nurse can position their instrument trolley. Consequently, the surgeons’ positioning can occasionally hinder the nurse’s ability to monitor the procedure and the movements of the surgeon. Should these issues be recognised, re-positioning could avoid the risk of slowing down the operating time in terms of instrument transfer. Moreover, upon understanding the impact of movements and positioning, operating team members should explore how their bodies are important resources for communication. References Aggarwal, R., Undre, S., Moorthy, K., Vincent, C., Darzi A., 2004. The simulated
operating theatre: comprehensive training for surgical teams. Quality and Safety in Health Care 13(1), i27–i32.
Bezemer, J., Murtagh, G., Cope, A., Kress, G., Kneebone, R., 2011. “Scissors, please”: the practical accomplishment of surgical work in the operating theater. Symbolic Interaction 34(3), 398–414.
Bromiley, M., 2008. Have you ever made a mistake? A patient liaison group debate. Royal College of Anaesthetists Bulletin 48, 2442-5.
Endsley, M.R., 1995. Toward a theory of situation awareness in dynamic-systems. Human Factors 37(1), 32–64.
Endsley, M. R., Jones, W. M., 2001. A model of inter- and intrateam situation awareness: Implications for design, training and measurement. In: McNeese, M., Salas, E., Endsley, M. (Eds.), New trends in cooperative activities: Understanding system dynamics in complex environments. Human Factors and Ergonomics Society, Santa Monica, CA, pp. 46–67.
Fioratou, E., Flin, R., Glavin, R., Patey, R., 2010. Beyond monitoring: distributed situation awareness in anaesthesia. British Journal of Anaesthesia 105(1), 83-90.
Gillespie, B.M., Chaboyer, W., Longbottom, P., Wallis, M., 2010. The impact of organisational and individual factors on team communication in surgery: a qualitative study. International Journal of Nursing Studies 47(6), 732-741.
Hazlehurst, B., McMullen, C. K., Gorman, P. N., 2007. Distributed cognition in the heart room: How situation awareness arises from coordinated communications during cardiac surgery. Journal of Biomedical Informatics 40(5), 539-551.
Heath, C., 1986. Body movement and speech in medical interaction. Cambridge University Press, Cambridge.
Heath, C., Hindmarsh, Jon., Luff, P., 2010. Video in qualitative research: analysing social interaction in everyday life. Sage, Los Angeles.

21
Heath, C., Sanchez Svensson, M., Hindmarsh, J., Luff, P., Vom Lehn, D., 2002. Configuring awareness. Computer Supported Cooperative Work 11(3-4), 317-347.
Hindmarsh, J., Pilnick, A., 2007. Knowing bodies at work: embodiment and ephemeral teamwork in anaesthesia. Organization Studies 28(9), 1395-1416.
Jefferson, G., 1989. Preliminary notes on a possible metric which provides for a 'standard maximum' silence of approximately one second in conversation. In: Roger, D., Bull, P. (Eds.), Conversation: an interdisciplinary perspective. Multilingual Matters, Clevedon, pp. 166-96.
Khan, S. A., Kumar, A., Varshney, M. K., Trikha, V., Yadav, C., 2008. Accidentally falling instruments during orthopaedic surgery: Time to wake up! ANZ Journal of Surgery 78(9), 794–795.
Kneebone, R., Fry, H., 2011. The environment of surgical training and education. In: Fry, H., Kneebone, R. (Eds.), Surgical education: theorising the emerging domain. Springer, London, pp. 3-16.
Koh, R.Y.I, Park, T., Wickens, C.D., Ong, L.T., Chia, S.N., 2011. Differences in attentional strategise by novice and experienced operating theatre scrub nurses. Journal of Experimental Psychology: Applied 17(3), 233-246.
Koschmann, T., LeBaron, C., Goodwin, C., Feltovich, P., 2011. “Can you see the cystic artery yet?” A simple matter of trust. Journal of Pragmatics 43(2), 521-541.
Lingard, L., Espin, S., Whyte, S., Regehr, G., Baker, G. R., Reznick, R., Bohnen, J., Orser, B., Doran, D., Brober, E., 2004. Communication failures in the operating room: an observational classification of recurrent types and effects. Quality and Safety in Health Care 13(5), 330-334.
Liu, W., Manias, E., Gerdtz, M., 2012. Medication communication between nurses and patients during nursing handovers on medical wards: a critical ethnographic study. International Journal of Nursing Studies 49(8), 941-952.
Mitchell L. Flin R., 2008. Non-technical skills of the operating theatre scrub nurse: literature review. Journal of Advanced Nursing 63(1), 15–24.
Mitchell, L., Flin, R., Yule, S., Mitchell, J., Coutts, K., Youngson, G., 2011. Thinking ahead of the surgeon. An interview study to identify scrub nurses’ non-technical skills. International Journal of Nursing Studies 48(7), 818–828.
Mitchell, L., Flin, R., Yule, S., Mitchell, J., Coutts, K., Youngson, G., 2012. Evaluation of the scrub practitioners’ list of intraoperative non-technical skills (SPLINTS) system. International Journal of Nursing Studies 49(2), 201–211.
Parush, A., Kramer, C., Foster-Hunt, T., Momtahan, K., Hunter, A., Sohmer, B., 2011. Communication and team situation awareness in the OR: Implications for augmentative information display. Journal of Biomedical Informatics 44(3), 477–485.
Pomerantz, A., 1984. Agreeing and disagreeing with assessments: some features of preferred/dispreferred turn shapes. In: Atkinson J., Heritage, J.M. (Eds.),
22
Structures of Social Action. Cambridge University Press, Cambridge, pp. 55-101.
Psathas, G., 1995. Conversation analysis: The study of talk in interaction. Sage Publications, London.
Salmon, P. M., Stanton, N. A., Walker, G. H., Baber, C., Jenkins, D. P., McMaster, R., Young, M. S., 2008. What really is going on? Review of situation awareness models for individuals and teams. Theoretical Issues in Ergonomics Science 9(4), 297-323.
Sanchez Svensson, M., Heath, C., Luff, P., 2007a. Instrumental action: the timely exchange of implements during surgical operations. In: Bannon, L. et al., The Proceedings of the 10th European Conference on Computer Supported Cooperative Work. Springer-Verlag, London, pp. 41-61.
Sanchez Svensson, M., Heath, C., Luff, P., 2007b. Video and qualitative research: analysing medical practice and interaction. Medical Education 41(1), 109–116.
Stanton, N. A., Stewart, R., Harris, D., Houghton, R. J., Baber, C., McMaster, R., et al., 2006. Distributed situation awareness in dynamic systems: theoretical development and application of an ergonomics methodology. Ergonomics 49(12-13), 1288-1311.
Weldon, S.-M., Korkiakangas, T., Bezemer, J., Kneebone, R., 2013. Communication in the operating theatre. British Journal of Surgery, 100(13), 1677–1688.
Wong, J., Khu, K. J., Kaderali, Z., Bernstein, M., 2010. Delays in the operating room: signs of an imperfect system. Canadian Journal of Surgery 53(3), 189-195.
Wright S., 2009. Predictors of situation awareness in graduate student registered nurse anaesthetists. Virginia Commonwealth University, Richmond.
Yule, S., Flin, R., Paterson-Brown, S., Maran, N., Rowley, D.R., Youngson, G.G., 2008. Surgeons’ non-technical skills in the operating room: reliability testing of the NOTSS behaviour rating system. World Journal of Surgery 32, 548-556.