navigating the neck: landmarks and danger points
TRANSCRIPT

Navigating the Neck:Landmarks and Danger Points
Dr. Elisabeth Ference and Dr. Jose DutraNovember 20, 2014
Northwestern Feinberg School of MedicineDepartment of Otolaryngology- Head and Neck Surgery

Overview
Locating cranial nerves VII, IX-XII
Important Anatomic Relationships: Carotid Artery, Erb’s Point, Thyrocervical Trunk
Neck Level INeck Level IIa&bNeck Level IVNeck Level V
Drawings from Netter and Photos from OR unless otherwise specified
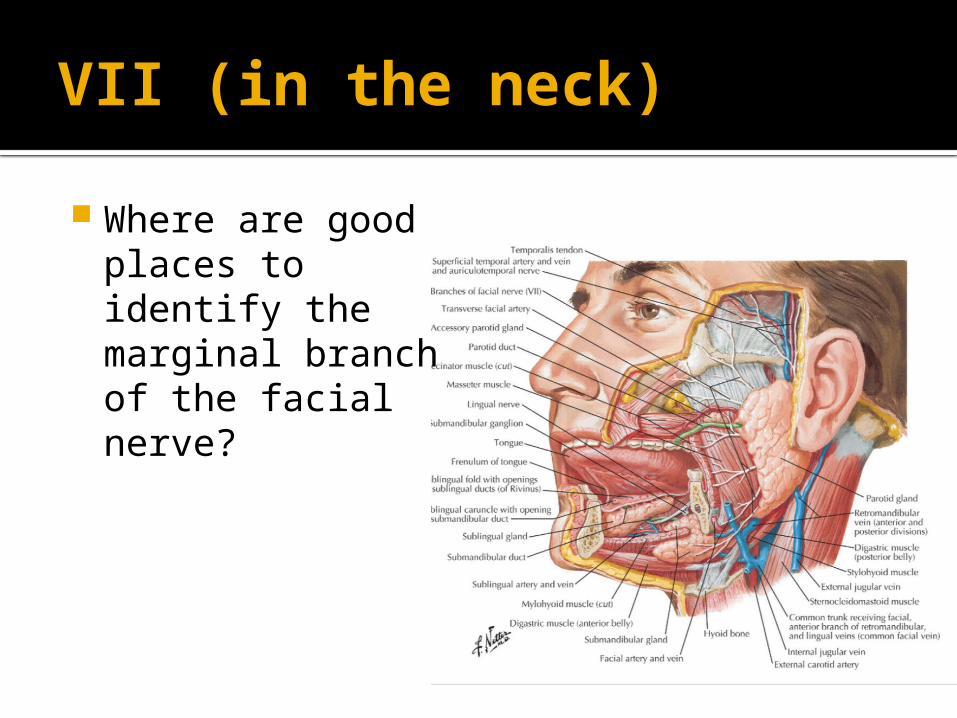
VII (in the neck) Where are good places to identify the marginal branch of the facial nerve?

VII (in the neck) ~ 1 cm anterior and inferior to angle of mandible
At the mandibular notch Within the fascia of the submandibular gland (superficial level of deep cervical fascia)
Superficial to adventitia of the facial vein Facial vein can be divided where it crosses the posterior digastric and elevated to protect the nerve
Møller, M. N., & Sørensen, C. H. (2012)
IX
What muscle does the glossopharyngeal nerve travel with and innervate?

IX Leave the posterior fossa through the jugular foramen
Lies with the stylopharyngeus (which it innervates)
Muscle and nerve enter pharynx between the lower fibers of the superior pharyngeal constrictor and upper fibers of the middle constrictor

X: SLN At what level does the superior laryngeal nerve divide?

X: SLN Divides just posterior and inferior to the greater cornu of the hyoid External follows the superior thyroid artery on the inferior constrictor muscle until it enters the cricothyroid
Internal branch follows the superior laryngeal branch of the superior thyroid artery until it pierces the lateral thyrohyoid membrane

X: Cernea Classification for EBSLN (based on Superior Thyroid Artery)
Type 1: cross behind superior thyroid artery greater than 1 cm above the upper border of the thyroid gland 68%
Type 2a: cross within 1 cm of the upper border of the thyroid 11%
Type 2b: cross below the upper border of the gland 14%, Vulnerable to injury when ligating the superior thyroid vascular pedicle
Ozlugedik, S., Acar, H. I., Apaydin, N., Tekdemir, I., Elhan, A., & Comert, A. (2007).
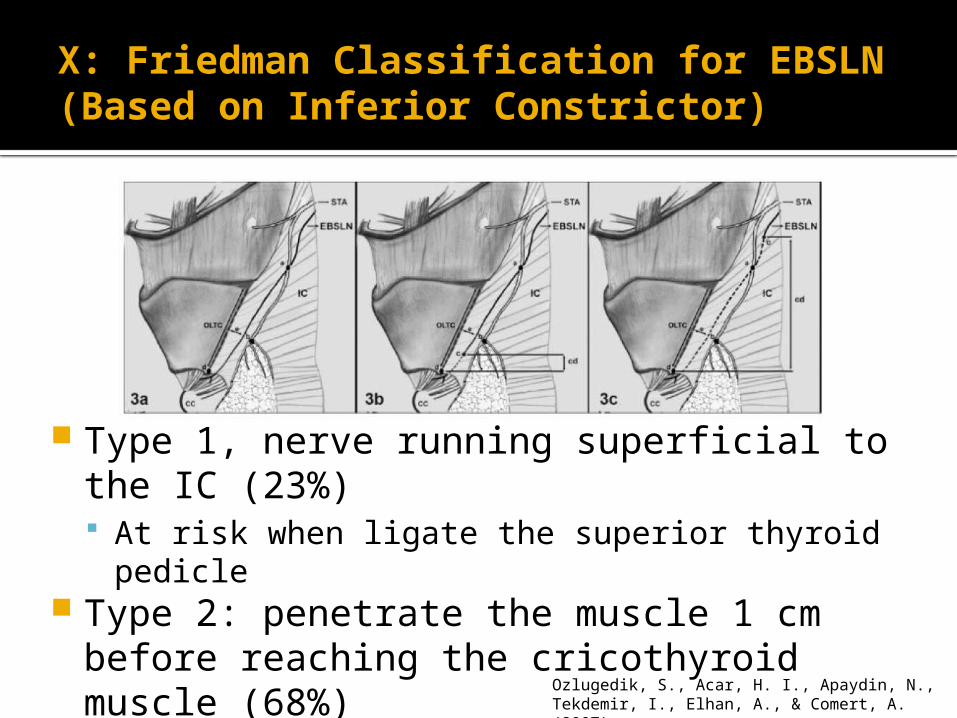
X: Friedman Classification for EBSLN (Based on Inferior Constrictor)
Type 1, nerve running superficial to the IC (23%) At risk when ligate the superior thyroid pedicle
Type 2: penetrate the muscle 1 cm before reaching the cricothyroid muscle (68%)
Type 3: nerve runs deep into the IC (10%)
Ozlugedik, S., Acar, H. I., Apaydin, N., Tekdemir, I., Elhan, A., & Comert, A. (2007).
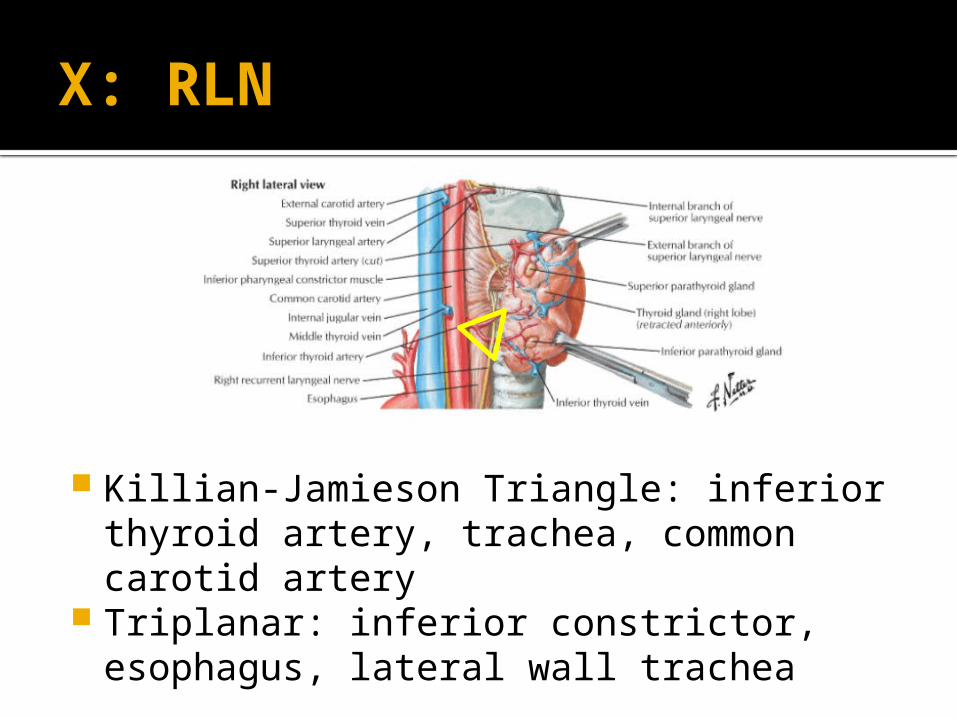
X: RLN
Killian-Jamieson Triangle: inferior thyroid artery, trachea, common carotid artery
Triplanar: inferior constrictor, esophagus, lateral wall trachea

X: Zuckerkandl Process
Mohebati, A., & Shaha, A. R. (2012).
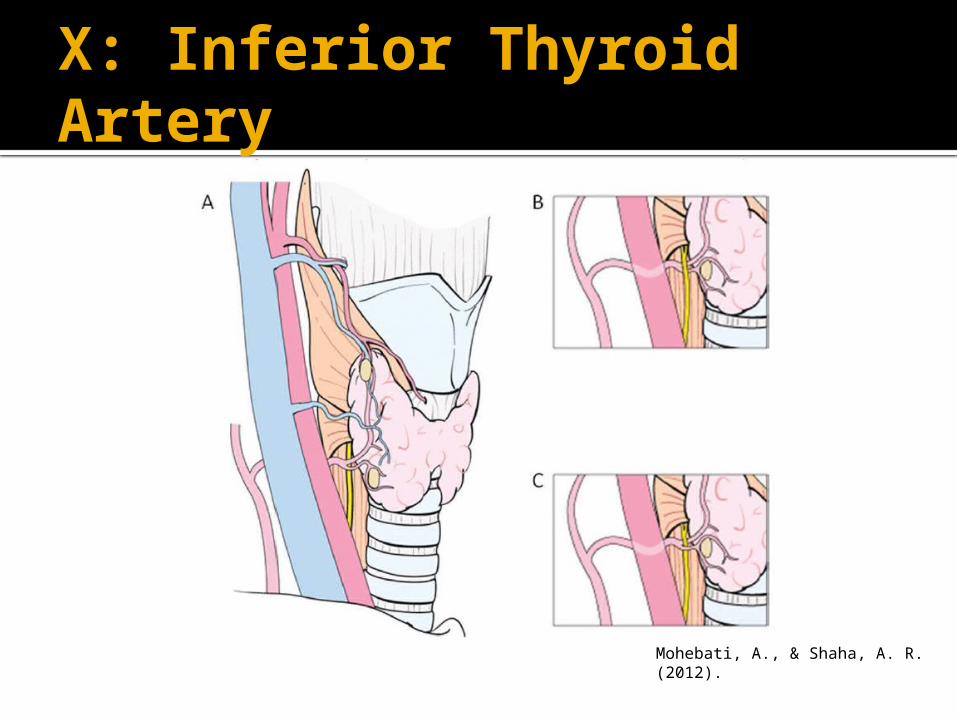
X: Inferior Thyroid Artery
Mohebati, A., & Shaha, A. R. (2012).

XI
What characterizes shoulder syndrome from spinal accessory nerve paralysis?

XI
Shoulder syndrome: pain, stiffness, drooping, limited abduction and flexion, aberrant scapular rotation (scapular winging)
http://www.msdlatinamerica.com/ebooks/PracticalOrthopaedicSportsMedicineArthrocopy/sid169169.html

Examination for XI Injury Weak head turn Weak shoulder shrug (may be preserved based on levator function)
Weakness of shoulder abduction past 90 degrees Requires upward rotation of the scapula by the trapezius
Note: more distal injury may spare function to SCM
Trapezius derives varying levels of innervation directly from cervical roots so function may not be completely absent http://
nervesurgery.wustl.edu/so/CaseStudies/2011/110325-1/Pages/default.aspx
XI
Name 4 places to find XI:

XI Retract posterior belly of the digastric superiorly, where it crosses superficial to the IJV Anterior to lateral process of C1
~4cm below the mastoid tip where penetrates the deep portion of SCM
The posterior border of the SCM ~1-2 cm superior to Erb’s Point
At penetration into the trapezius Lloyd, S. (2007).

XI Where is XI relative to the IJV?
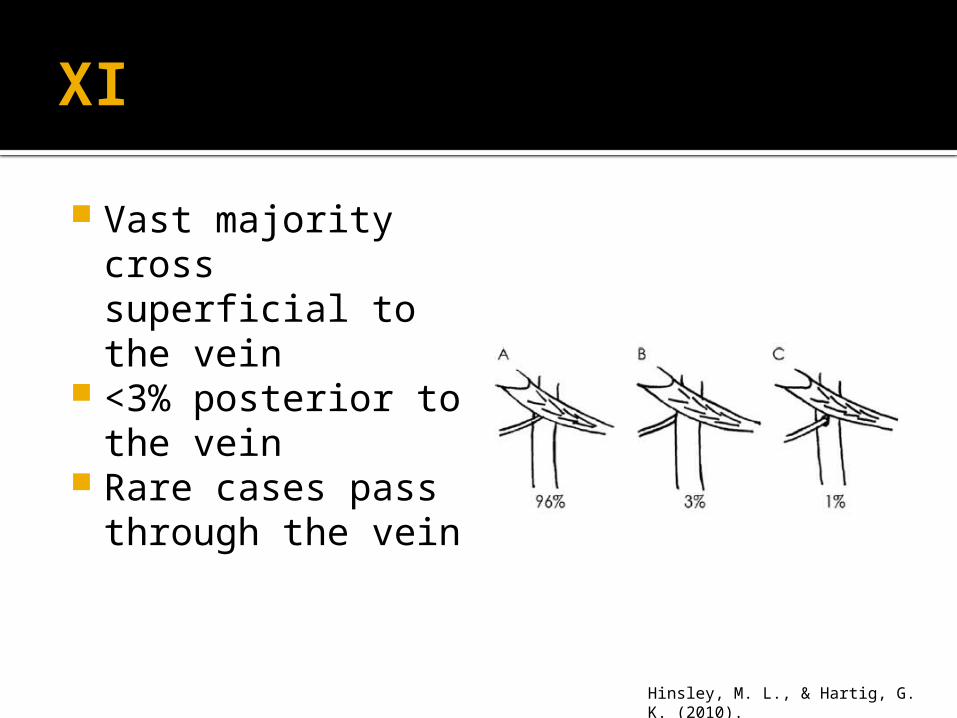
XI Vast majority cross superficial to the vein
<3% posterior to the vein
Rare cases pass through the vein
Hinsley, M. L., & Hartig, G. K. (2010).
XII
Where does the hypoglossal nerve cross the ECA?
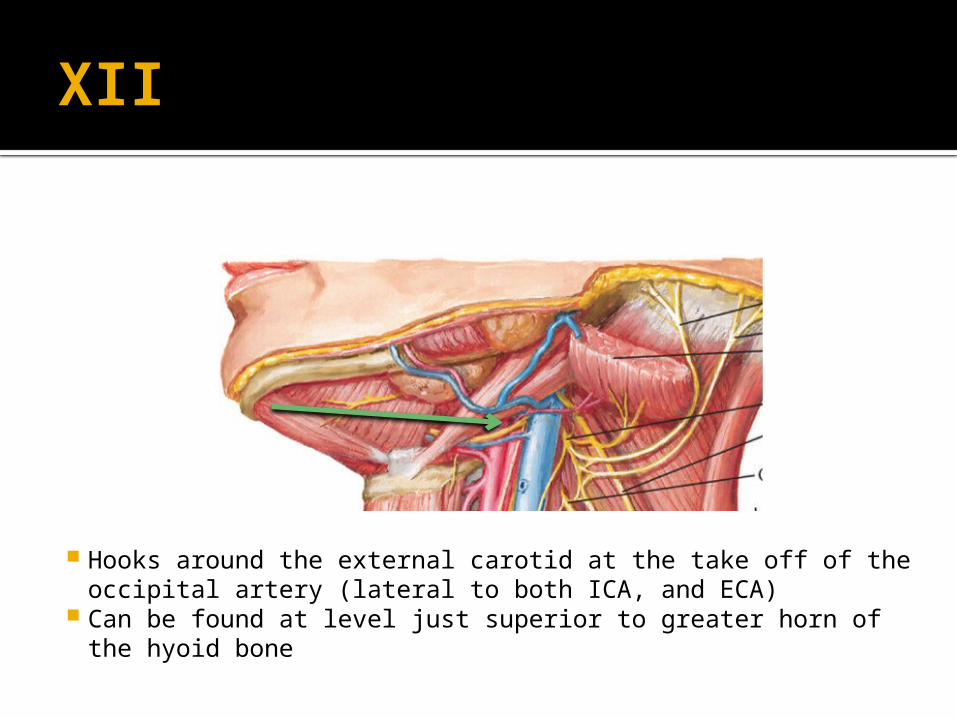
XII
Hooks around the external carotid at the take off of the occipital artery (lateral to both ICA, and ECA)
Can be found at level just superior to greater horn of the hyoid bone
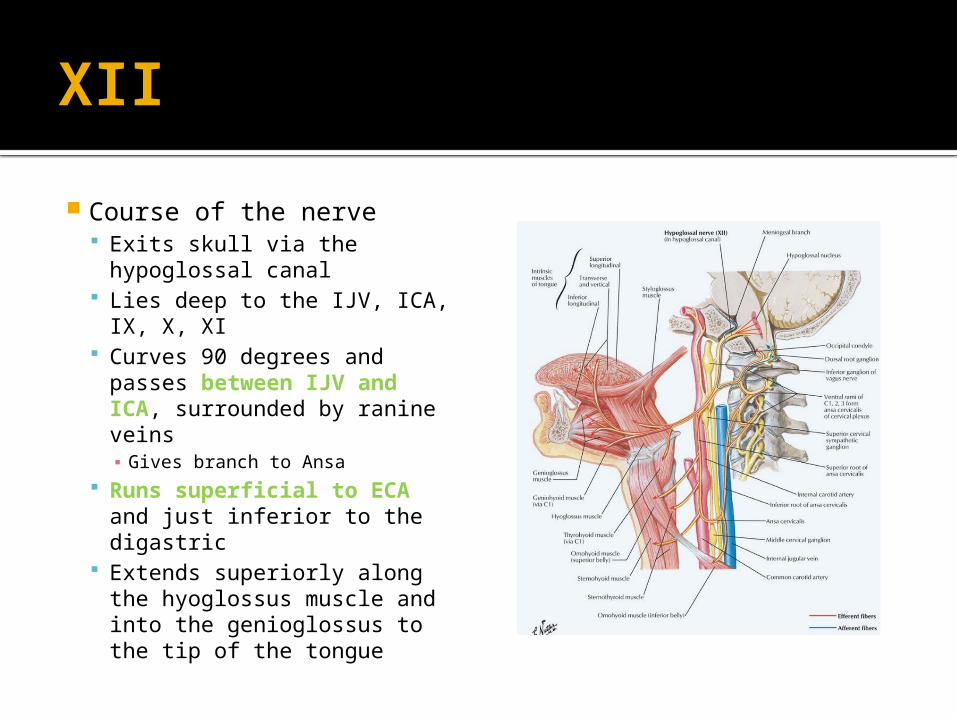
XII Course of the nerve
Exits skull via the hypoglossal canal
Lies deep to the IJV, ICA, IX, X, XI
Curves 90 degrees and passes between IJV and ICA, surrounded by ranine veins▪ Gives branch to Ansa
Runs superficial to ECA and just inferior to the digastric
Extends superiorly along the hyoglossus muscle and into the genioglossus to the tip of the tongue

XII
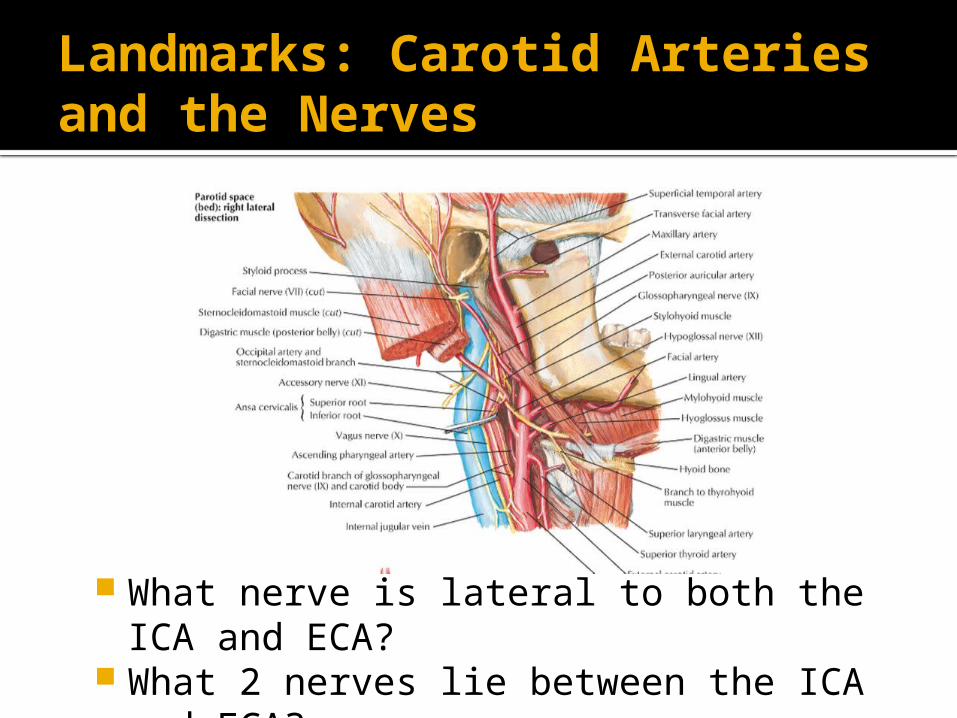
Landmarks: Carotid Arteries and the Nerves
What nerve is lateral to both the ICA and ECA?
What 2 nerves lie between the ICA and ECA?

CN XII is lateral to both ICA and ECA CN IX and pharyngeal portion of X lie between ICA and ECA
Landmarks: Carotid Arteries and the Nerves

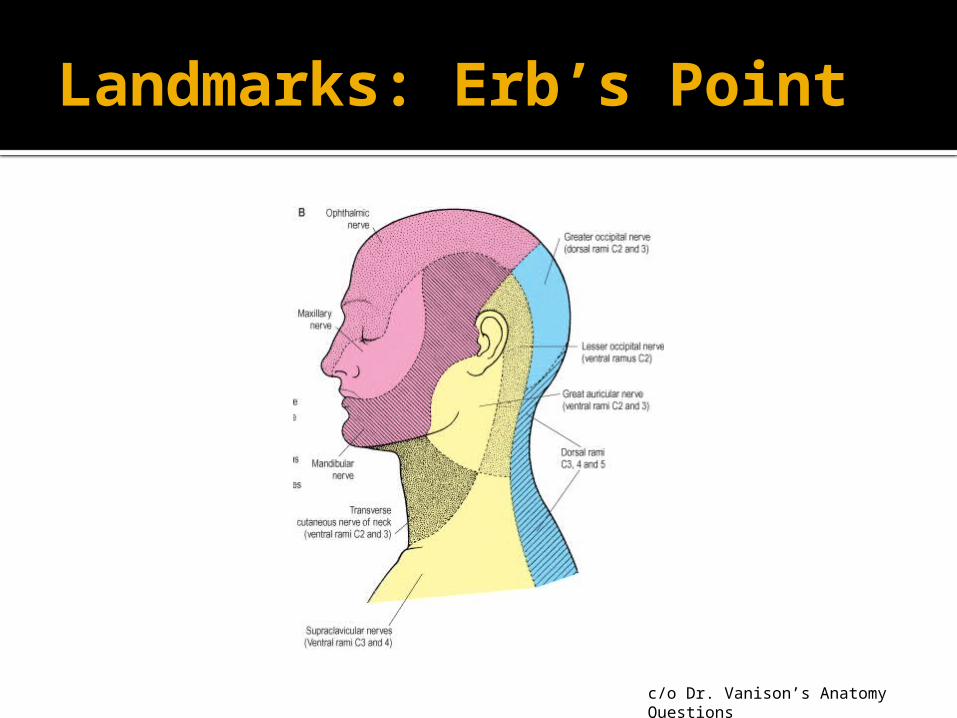
Landmarks: Erb’s Point What nerve is demarcated by * ?
*
Lesser Occipital
Greater Auricular
Supraclavicular
c/o Dr. Vanison’s Anatomy Questions
Landmarks: Erb’s Point
c/o Dr. Vanison’s Anatomy Questions

Landmarks: Thyrocervical TrunkWhat arteries cross the phrenic nerve laterally?

Landmarks: Thyrocervical Trunk
Tranverse cervical and suprascapular arteries course laterally over the surface fo the phrenic nerves
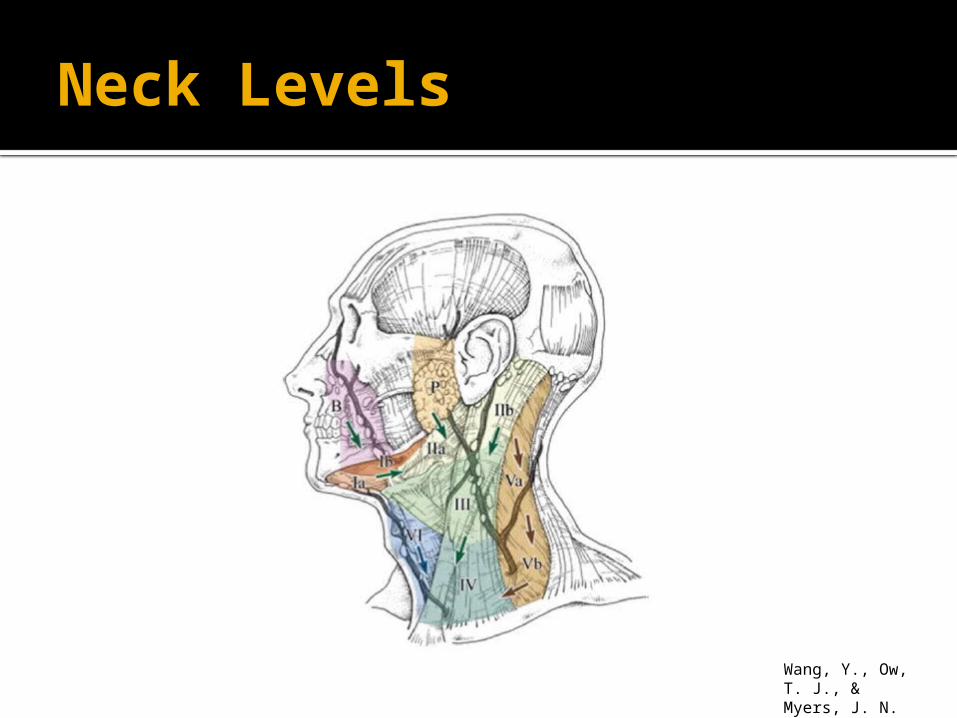
Neck Levels
Wang, Y., Ow, T. J., & Myers, J. N. (2012).
Level I
What are the boundaries of Ia?Ib?

Level I
Wang, Y., Ow, T. J., & Myers, J. N. (2012).

Level I
What is the clinical significance of levels Ia and Ib (ie when do you dissect Ia)?

Level I Drainage patterns Ia: lower lip, floor of mouth, ventral tongue
Ib: all other oral cavity subsites
Wang, Y., Ow, T. J., & Myers, J. N. (2012).

Level I What is the order of important structures, from inferior to superior, that you find going under the mylohyoid when you lift up the submandibular gland?
123
4
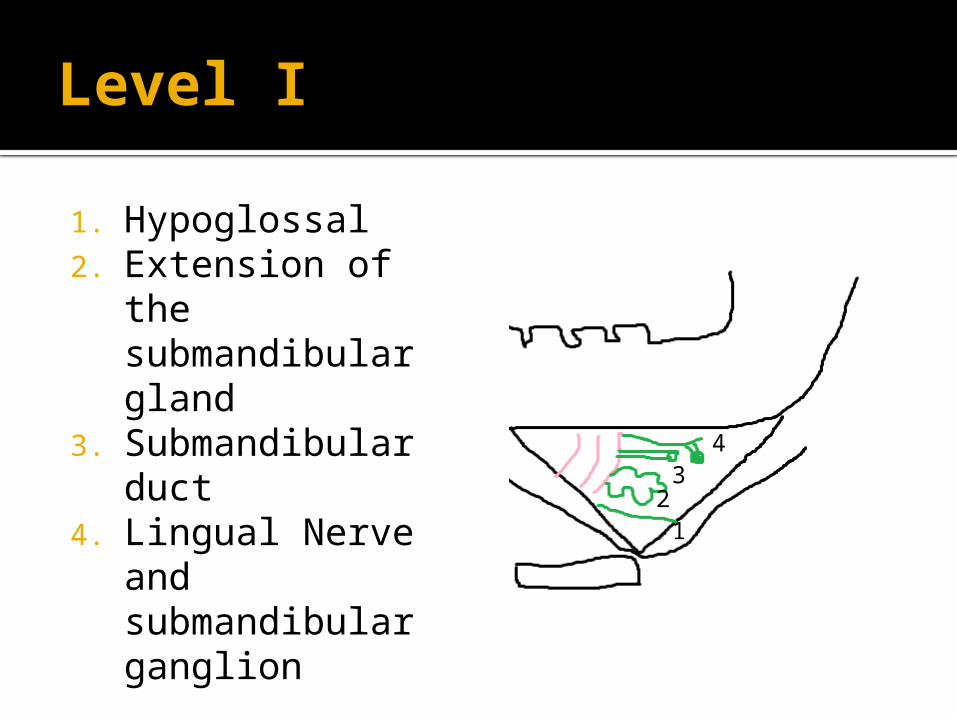
Level I
1. Hypoglossal2. Extension of
the submandibular gland
3. Submandibular duct
4. Lingual Nerve and submandibular ganglion
123
4

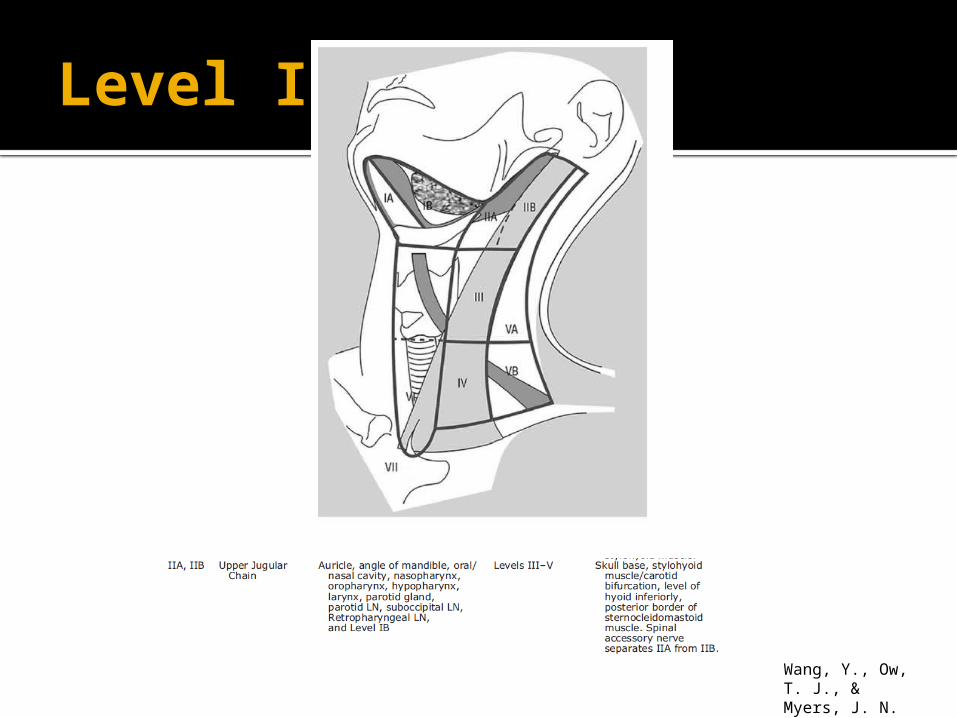
Level II
What are the boundaries of II? What structure divides it into a and b?
Level I
Wang, Y., Ow, T. J., & Myers, J. N. (2012).
Level IIa&b
What is the clinical significance between IIa and IIb (ie when do you dissect IIB)?
Level IIa&b
IIB: oropharynx and nasopharynx drain to IIB Therefore should mobilize XI
Oral cavity, larynx and hypopharynx first drain to IIa prior to IIb May not be necessary to dissect IIb if IIa not involved

Level IIa&b
Where is the jugulodigastric lymph node?

Level IIa&b
Level II node where IJV crossed by the posterior belly of the digastric Normal size <= 1.5 cm Other neck nodes should be < 1 cm

Level IIa&b

Level IIa&b What is deep to the posterior belly of the digastric?
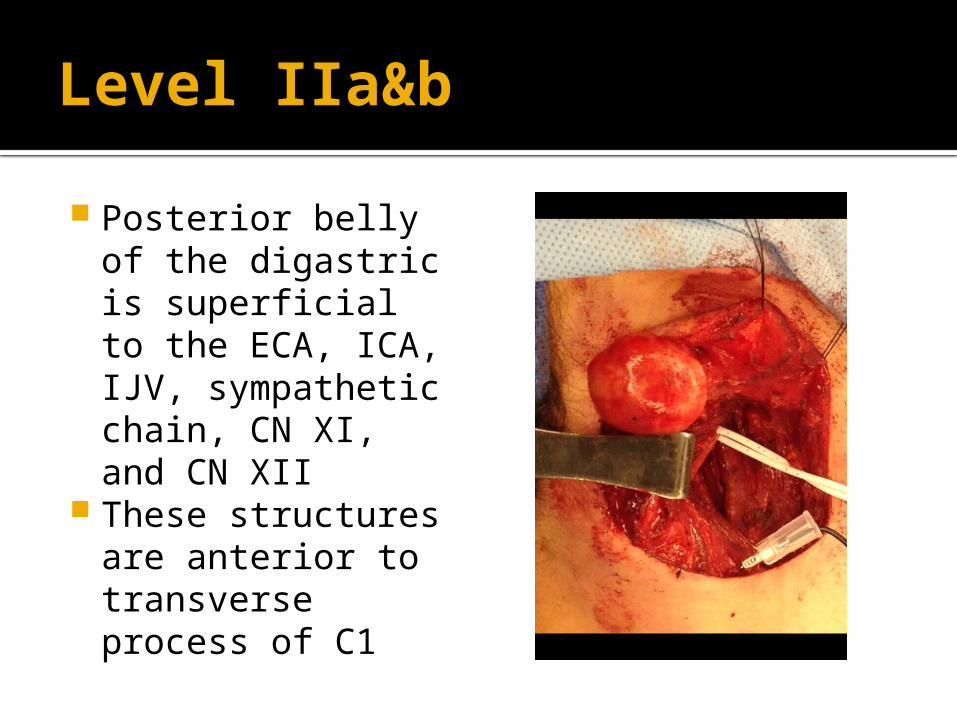
Level IIa&b Posterior belly of the digastric is superficial to the ECA, ICA, IJV, sympathetic chain, CN XI, and CN XII
These structures are anterior to transverse process of C1
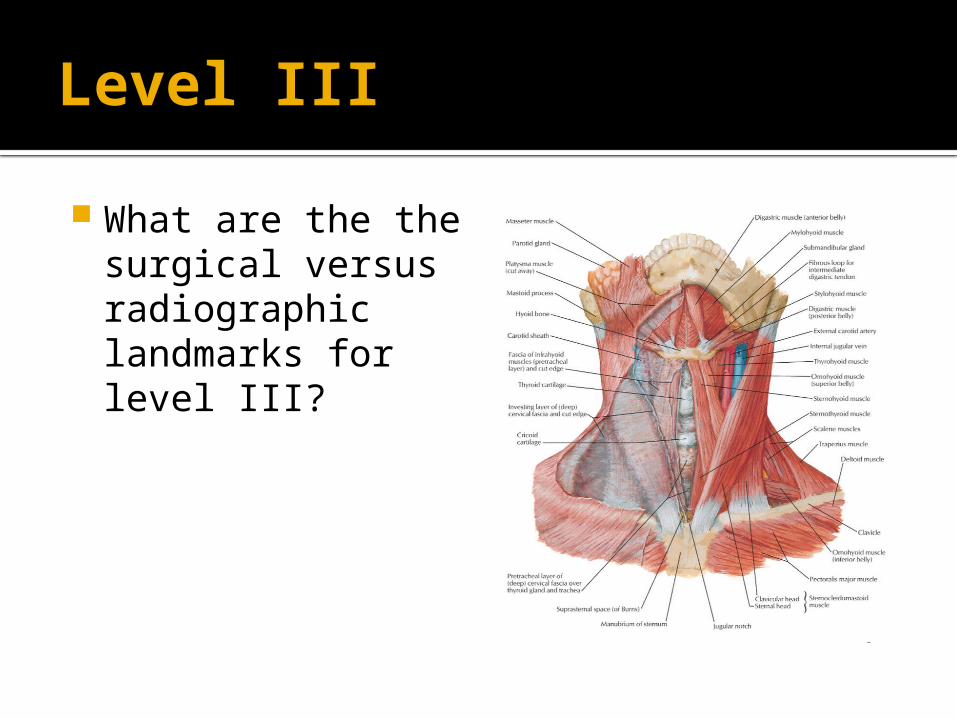
Level III What are the the surgical versus radiographic landmarks for level III?

Level III Surgical: carotid bifurcation to the omohyoid
Radiologic: hyoid bone to inferior border of the cricoid
Wang, Y., Ow, T. J., & Myers, J. N. (2012).
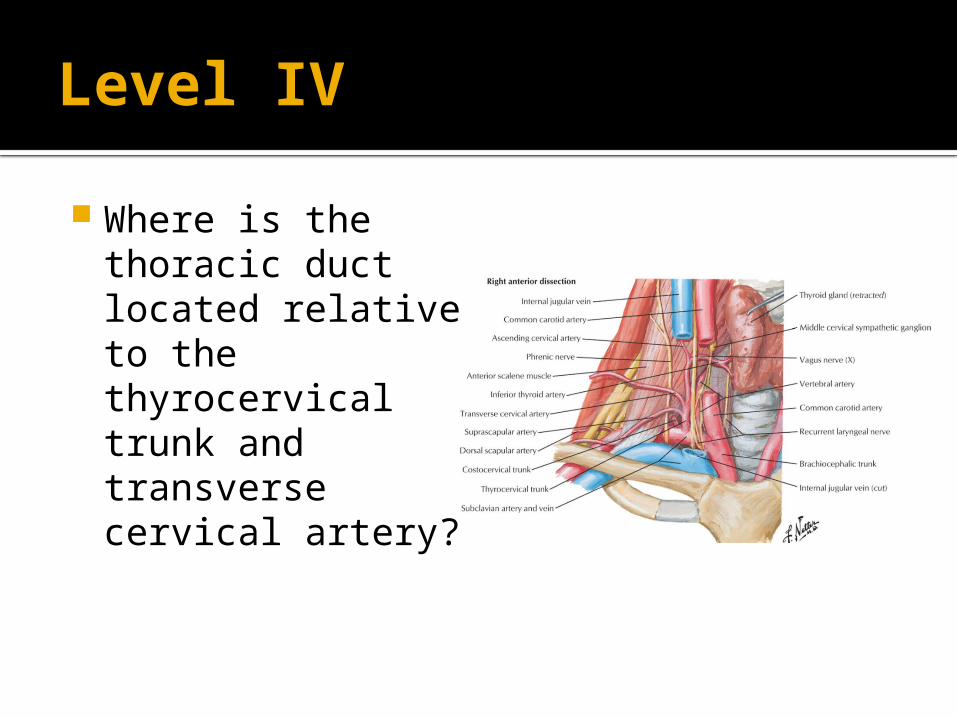
Level IV Where is the thoracic duct located relative to the thyrocervical trunk and transverse cervical artery?

Level IV Thoracic Duct
Superficial to the vertebral artery/vein and thyrocervical trunk
Lies at medial border of anterior scalene left neck, just anterior to the phrenic nerve
Joins venous system at the left internal jugular and left subclavian vein intersection
Also lymphatic drainage into IJV-subclavian junction on right!

Thoracic Duct Injury Non-surgical options (low output < 500 mL/day) Low-fat diet w/ medium-chain triglycerides
TPN Careful monitoring fluid and electrolytes
Drainage of leakage Somatostatin analogs such as octreotide
Negative pressure wound therapy
Surgical Options (> 1L/day, persistant) Percutaneous lymphography-guided thoracic duct cannulation/embolization
Surgical repair Closure by locoregional flaps
VATS/thoracotomy/pleuro-desis/pleura-venous or pleura-peritoneal shunts

Level V
What are the boundaries of level V?

Level V Boundaries: SCM, trapezius, clavicle
Divided by omohyoid Occipital Triangle
Supraclavicular triangle
Wang, Y., Ow, T. J., & Myers, J. N. (2012).
Level V What is deep to the posterior belly of the omohyoid
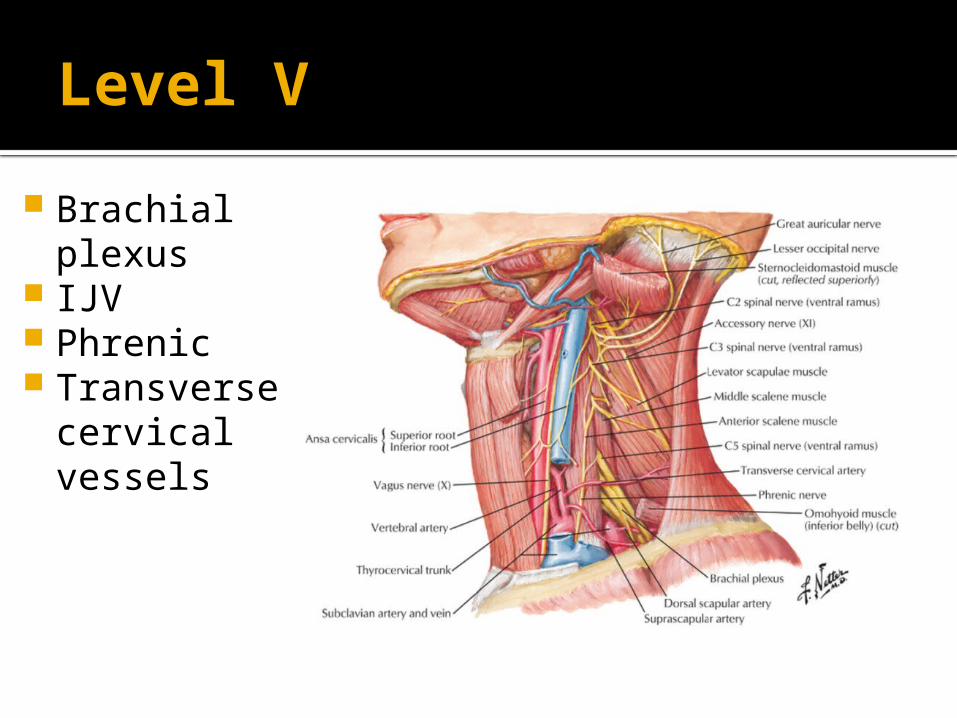
Level V Brachial plexus
IJV Phrenic Transverse cervical vessels
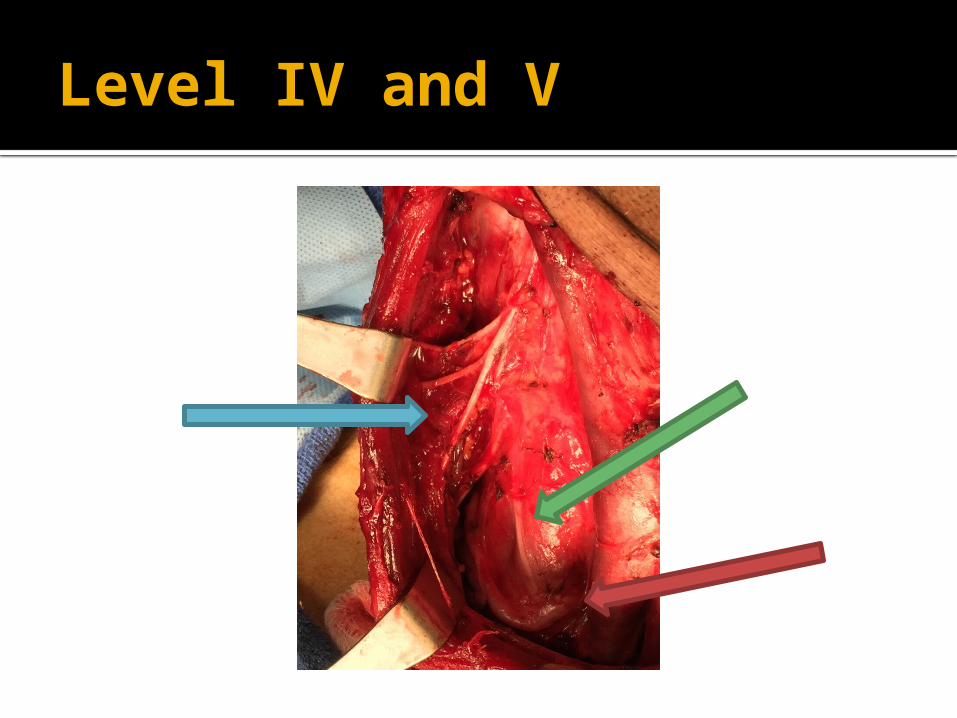
Level IV and V

Level IV and V
Cervical Roots
Phrenic Nerve
Transverse Cervical Artery and
Vein

ReferencesBatstone, M. D., Scott, B., Lowe, D., & Rogers, S. N. (2009). Marginal mandibular nerve injury during neck dissection and its impact on patient perception of appearance. Head & Neck, 31(5), 673–8. doi:10.1002/hed.21013
Cernea, C. R., Ferraz, A. R., Nishio, S., Dutra, A., Hojaij, F. C., & dos Santos, L. R. (n.d.). Surgical anatomy of the external branch of the superior laryngeal nerve. Head & Neck, 14(5), 380–3. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/1399571
Friedman, M., LoSavio, P., & Ibrahim, H. (2002). Superior laryngeal nerve identification and preservation in thyroidectomy. Archives of Otolaryngology--Head & Neck Surgery, 128(3), 296–303. Retrieved from http://www.ncbi.nlm.nih.gov/pubmed/11886347
Fujimura, I., de Souza, R. R., de Carvalho, C. A. F., & Rodrigues, A. J. (1990). A method for locating the marginal mandibular branch of the facial nerve in the neck. Clinical Anatomy, 3(2), 143–147. doi:10.1002/ca.980030207
Hinsley, M. L., & Hartig, G. K. (2010). Anatomic relationship between the spinal accessory nerve and internal jugular vein in the upper neck. Otolaryngology--Head and Neck Surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery, 143(2), 239–41. doi:10.1016/j.otohns.2010.03.033
Lloyd, S. (2007). Accessory nerve: anatomy and surgical identification. The Journal of Laryngology and Otology, 121(12), 1118–25. doi:10.1017/S0022215107000461
Mohebati, A., & Shaha, A. R. (2012). Anatomy of thyroid and parathyroid glands and neurovascular relations. Clinical Anatomy (New York, N.Y.), 25(1), 19–31. doi:10.1002/ca.21220
Møller, M. N., & Sørensen, C. H. (2012). Risk of marginal mandibular nerve injury in neck dissection. European Archives of Oto-Rhino-Laryngology : Official Journal of the European Federation of Oto-Rhino-Laryngological Societies (EUFOS) : Affiliated with the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery, 269(2), 601–5. doi:10.1007/s00405-011-1610-2
Ozlugedik, S., Acar, H. I., Apaydin, N., Tekdemir, I., Elhan, A., & Comert, A. (2007). Surgical anatomy of the external branch of the superior laryngeal nerve. Clinical Anatomy (New York, N.Y.), 20(4), 387–91. doi:10.1002/ca.20399
Robbins, K. T., Shaha, A. R., Medina, J. E., Califano, J. A., Wolf, G. T., Ferlito, A., … Day, T. A. (2008). Consensus statement on the classification and terminology of neck dissection. Archives of Otolaryngology--Head & Neck Surgery, 134(5), 536–8. doi:10.1001/archotol.134.5.536
Sheahan, P., & Murphy, M. S. (2011). Thyroid Tubercle of Zuckerkandl: importance in thyroid surgery. The Laryngoscope, 121(11), 2335–7. doi:10.1002/lary.22188
Shin, J., & Cunningham, M. (n.d.). Otolaryngology Prep and Practice. San Diege: Plural Publishing.Wang, Y., Ow, T. J., & Myers, J. N. (2012). Pathways for cervical metastasis in malignant neoplasms of the head and neck region. Clinical Anatomy (New York, N.Y.), 25(1), 54–71. doi:10.1002/ca.21249
Questions?