medications as social phenomena
TRANSCRIPT
http://hea.sagepub.com
Health:
DOI: 10.1177/136345930100500403 2001; 5; 441 Health (London)
David Cohen, Michael McCubbin, Johanne Collin and Guilhème Pérodeau Medications as Social Phenomena
http://hea.sagepub.com/cgi/content/abstract/5/4/441 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Health: Additional services and information for
http://hea.sagepub.com/cgi/alerts Email Alerts:
http://hea.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.co.uk/journalsPermissions.navPermissions:
http://hea.sagepub.com/cgi/content/refs/5/4/441 Citations
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

Medications as socialphenomena
David CohenFlorida International University
Michael McCubbinUniversity of Regina
Johanne CollinUniversity of Montreal
Guilhème PérodeauUniversity of Quebec at Hull
ABSTRACT This article discusses medications as socially embeddedphenomena, using the class of psychoactive medications as a primaryexample. The analytical perspective is systemic, constructivist, and critical.We suggest that the ‘rational use of drugs’ paradigm fails to appreciate variouslegitimate rationalities motivating medication usages and is therefore inade-quate to understand the place of medications in society. Medications havecomplex life cycles, with diverse actors, social systems, and institutions deter-mining who uses what medications, how, when and why. Such understandingpermits analyzing medications simultaneously as entities and representations.We outline recent changes in usage patterns of psychoactive medications(notably prescriptions to children), in pharmaceutical marketing practices(notably direct-to-consumer advertising), and in the construction of knowl-edge about drugs (notably the role of the Internet in legitimating consumers’viewpoints). These changes indicate that medication life cycles evolve andmutate with social and technological change. These life cycles are viewed,then, as systems – part of other social, cultural, and economic systems, them-selves in constant change. This perspective provides fertile ground to raiseseveral research questions in order to understand better the nature of medi-cations, their effects, and their place in society.
KEYWORDS constructivism; critical analysis; general system theory; pharma-ceuticals; psychotropic medications; social change
ADDRESS David Cohen, School of Social Work, College of Health andUrban Affairs, Florida International University, University Park, 11200 S.W.8th St., Miami, Florida 33199, USA. [Tel: +1 305 348 4599; fax +1 305 3485313; e-mail: [email protected]]
ACKNOWLEDGEMENT This work was supported by grant 99-ER-3107 fromFonds FCAR, Quebec.
441
HealthCopyright © 2001
SAGE Publications (London,Thousand Oaks and New Delhi)
[1363–4593 (200110) 5:4]Vol 5(4): 441–469; 018997
03cohen (ds) 28/8/01 1:10 pm Page 441
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

Introduction
Medication use at the societal level is determined by much more than theoccurrence of ailments and the availability of pharmaceutical remedies todeal with these ailments. Numerous biological, psychological, social, eco-nomic, and cultural situations, all in constant interaction, affect the use ofprescribed medications (Bush and Osterweis, 1978; Vuckovic and Nichter,1997).1 Medications themselves are much more than material objects withphysiological effects; they are also representations that carry meanings andshape social relations as they evolve in conjunction with individuals andcollectivities (Montagne, 1996; Van der Geest et al., 1996). Hence, anattempt to comprehend medications and medication use in societies shouldbe informed by methods able to deal with complexity, given the wide varietyof interacting factors; with change, given the volatile nature of these factors;with social construction, given the preponderant role of human beliefs andjudgments; and, as we hope to show, with contradiction and paradox.
‘Systems thinking’ (Bowler, 1981) and constructivism (Gergen, 1985)share similar epistemological ground in recognizing that thought andbehavior are constructed in the exchange of symbols between individualsand collectivities. Yet, despite inroads made by these philosophies into mostareas of social science, the view of prescribed medication as a multifaceted,fluctuating, and mutating object has been virtually absent from the studyof medication consumption. Indeed, with a few notable exceptions,2 socialresearchers interested in medications have implicitly treated them in a wayquite consistent with the technocratic discourse – as technological productsto be consumed in satisfaction of precisely identified needs – and with itscompanion biomedical discourse – as tools of practitioners who possessspecialized knowledge to determine their appropriate use.
Our analytical perspective is critical3 because, first, we attempt to stepoutside the traditional biomedical/technological perspective, and the pro-fessional–patient dyad, in order to increase understanding of medicationsand their usages. Second, we attempt to consider power and interest distri-butions among actors involved with medications. Our perspective is alsoconstructivist, in the recognition that medications and medication usage areintertwined to form ‘social facts’ that are highly responsive to culture,history, and social context.
In this article, we aim to provide basic elements to inform an under-standing of medications as socially embedded phenomena. Severalexamples illustrating this understanding concern the class of psychoactive(psychotropic, psychiatric) medications,4 and this for several reasons. Thefirst is that the authors of this article have mostly studied psychoactive medi-cations. Another reason is that sociologists and anthropologists havestudied these particular medications more frequently than other classes ofdrugs. This is probably so because social and cultural factors associatedwith their use appear to be more obvious and less contested than for other
Health 5(4)
442
03cohen (ds) 28/8/01 1:10 pm Page 442
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

classes of medication. Indeed, most psychoactive drugs are prescribed totreat states with non-specific, uncertain, or speculative biological substrates.Their use encompasses a growing list of problems seen as real ‘mental ill-nesses,’ of difficulties viewed as deficits which might benefit from ‘cosmeticpsychopharmacology,’ as well as ordinary annoyances of daily life (Ehren-berg, 1995). Finally, use of psychoactive drugs continually transgresses tra-ditional boundaries (e.g. licit/illicit, medical/non-medical, moral/immoral)and may evoke extremely powerful institutionalized social responses (the‘war on drugs’). In other ways, usages of psychoactive drugs diverge fromthat of other medications. Only the effects of psychoactive drugs raise thequestion of addiction or dependence. One might also argue that only psy-choactive medications such as Valium or Prozac seem to attain status asgeneral cultural icons (but see more recently the case of the anti-impotencedrug Viagra). Given that their prescription is made on the basis of disturbedor disturbing behavior rather than altered bodily function, only psycho-active drugs appear to show dramatic expansions of use to populations previously untouched by such drugs, like children (see later). Other charac-teristics, such as the relatively high level of popular knowledge concerningtheir indications and effects, further distinguish psychoactive medicationsfrom the other broad classes of medications prescribed for numerous bodilyailments.
Besides obviously different indications and physiological effects, socio-logically relevant conceptual distinctions between any two drug classesmight appear upon closer inspection. However, we propose that despitetheir differences, all medications probably share fundamental similaritieswhich emerge when medications are approached from the analytical frame-work we present here. Our social scientific analysis is meant to encourageimaginative, heuristic, and socially useful sociological inquiry into theeffects, uses, and meanings of all classes of prescribed medications.
We begin by discussing why the traditional ‘rational use of drugs’ para-digm is inadequate for understanding the place of medications in society.This is so primarily because it fails to appreciate numerous competing andlegitimate rationalities that appear to motivate medication usages today.We then conceptualize medications as having a complex life cycle. Thisallows us to identify various types of actors, social systems, and institutionsthat play key technological and representational roles in determining whouses what medications, how, when, and why. Such understanding leads usto propose that medications need to be studied not just as technologicalproducts or medical substances but also as social and cultural phenomena.
We then outline changes in consumption patterns of psychoactive drugs,in pharmaceutical marketing practices, and in the construction of knowl-edge about drugs. Our observations serve to highlight how medication lifecycles mutate, adapt, and respond to social, economic, and technologicalchange. These life cycles are viewed, then, as systems – part of other social,cultural, and economic systems, themselves in constant change. We believe
Cohen et al.: Medications as Social Phenomena
443
03cohen (ds) 28/8/01 1:10 pm Page 443
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
this perspective provides fertile ground for the emergence of severalresearch questions in order to understand better the nature of medicationsand their place in society.
The rationalities of medication usages
A dominant normative framework to organize observations about pre-scribed medication use and to educate clinical practitioners remains that of‘rational use of drugs.’ This may be defined as the judicious prescription bywell-informed professionals of well-studied drugs to well-informed patientsfor well-defined conditions. Such use is defined by public health authori-ties and pharmaco-epidemiologists according to cost–benefit, necessity andefficiency criteria, ordinarily with respect to the first indications for apharmaceutical product when it enters the market (Sacristan, 1994). Thistechnicist version of rationality has been useful to analyze and interveneon issues such as access to ‘essential’ medications in developing countries(e.g. Laing, 1999), but it limits the understanding of contemporary medi-cation usages.
On the one hand, the rational use of drugs paradigm regards as ‘irra-tional’ many consumption behaviors which are quite prevalent. Amongpatients, these include self-medication, non-compliance with prescribedregimen, and polypharmacy (Vuckovic and Nichter, 1997). Among phys-icians, studies have revealed several types of seemingly irrational practices:failure to transmit necessary information to the patient and obtain informedconsent (Braddock et al., 1997), prescriptions for non-indicated (‘off-label’)purposes (Zito et al., 2000), reliance upon commercial rather than scien-tific sources of information (Wazana, 2000), polypharmacy (Meador, 1998),ignorance or non-conformity with recommendations from controlledstudies or practice guidelines (Cohen and Bisson, 1997; Butler et al., 1998),as well as failure to report suspected adverse effects – including extremelyserious ones – to public health authorities (Moore et al., 1998). Some ofthese practices, such as the last mentioned, are so widespread that their‘rational’ opposite is the rare exception.
Perhaps because of the above, several studies have taken a new look atpatient ‘compliance.’ Until recently, much literature in this field took forgranted that prescriptions are the function of unquestionable medicalexpertise (see Coambs et al., 1995). Some investigators focused onpatient–physician communication, hypothesizing that inadequate com-munication lies at the root of non-compliance (Roter and Frankel, 1992;Makoul et al., 1995; McGrath, 1999). Others examined the ‘rationality’ ofconsumers (Chinburapa et al., 1993) in order to understand why they donot follow medical advice that is ‘good’ for them. This body of researchreveals that far more may be understood about medication use than canbe modeled by the standard therapeutic relationship, in which the patientconsults an expert for specialized advice and brings no complementary
Health 5(4)
444
03cohen (ds) 28/8/01 1:10 pm Page 444
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

expertise. Under a still-dominant paternalist model for the patient–physician relationship, patients are viewed as passive and little inclined toinitiate their own therapeutic plans. This underestimates the constant delib-erations, adjustments, and changes, particularly among patients undergo-ing chronic drug treatment (Cohen and Karsenty, 1998).
By considering the actors’ subjectivity, as situated in a social context, wecan aim to appreciate a rationality which diverges from externally imposed‘objective’ scientific norms. This rationality is shaped by numerous factors,a brief list of which includes the inherently subjective basis of valuations ofalternative therapeutic outcomes, the uncertainty of these outcomes, theassessment of likelihoods of various outcomes, the willingness to acceptrisk and uncertainty (see Christensen-Szalanski and Bushyhead, 1988;Wolff, 1989). Physicians’ prescription decisions can also be influenced byfactors such as: a discomfort to refuse explicit or veiled patient requests,fear of losing the patient, diagnostic uncertainty and a hesitance to revealit (Gerrity et al., 1992; Butler et al., 1998; Collin et al., 1999; Damestoy etal., 1999). Thus, non-compliance – irrational from a medical standpoint –may express, as various authors have proposed, deliberate strategies bypatients to affirm their autonomy, to negotiate with physicians, or to rejectan attributed incapacity (Trostle, 1988; Fineman, 1991; Donovan and Blake,1992; Conrad, 1994; Collin, 1999).
An additional limitation of the rational use of drugs framework is itsusual focus on the most visible actors: prescribers and users of medication.However, as we discuss below, prescription, dispensation, and ingestioncomprise but few of many stages in a long process which involves manyother types of actors, whose actions reverberate throughout the entiresystem of drug use (Bernstein and Lennard, 1973). To the complexity ema-nating from this multiplicity of actors one may add the dynamism impliedby a conception of modern society and its institutions as resolutely ‘reflex-ive’ (Taylor, 1989; Giddens, 1990). The reflexive social order implies thatmost dimensions of social activity are subject to constant revision, in thelight of new information. As Williams and Calnan (1996) note, medicinebecomes a reflexive enterprise in terms of its knowledge, its social organiza-tion, and its daily practice, resulting in numerous practices that are some-times contradictory, such as high-tech ‘virtual’ medicine juxtaposed with‘holistic’ care. These simultaneous, fluctuating manifestations do not easilyfit within a ‘top-down’ paradigm of rational drug use.
In sum, understanding the various rationalities of medication usage andprescription well surpasses the signposts of a paradigm centered on amedical or even a therapeutic vision (Ehrenberg, 1995; Montagne, 1997).If this is the case, researchers ought to describe the individual and locallogics, representations, incentives, and constraints which motivate, justify,or perhaps explain diverse usages. Unfortunately, few such descriptionsexist. Even with respect to the use of psychoactive drugs, most studiesappear to be demographic, epidemiological, or correlational surveys. To be
Cohen et al.: Medications as Social Phenomena
445
03cohen (ds) 28/8/01 1:10 pm Page 445
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
sure, noteworthy, pioneering qualitative work on tranquilizers (reviews inGabe, 1991; Haafkens, 1997), antidepressants (Karp, 1996), or neuroleptics(Estroff, 1985; Rogers et al., 1998) has been conducted, though it has mostlysought patients’ perspectives. Studies on antibiotics have begun to explorephysicians’ and patients’ motives in prescribing or seeking prescriptionsdespite well-known evidence of antibiotics’ ineffectiveness in many con-ditions for which they are prescribed (Butler et al., 1998; Barden et al.,1998). Overall, however, the ‘rationality’ of the multiple strategies em-ployed by other actors, as influenced by their representations and socialinteractions, remains virtually unknown.
The life cycle of medications
As a therapeutic product, a particular drug follows a long and agitated tra-jectory (Pignarre, 1995). This may be considered its life cycle – from theinitial discovery or conception of a molecule to a substance’s eventualdisuse as a prescribed medication (Van der Geest et al., 1996). Few medi-cations remain in significant use as remedies for the class of problems forwhich they were initially indicated and marketed, after a few decades. It isnot uncommon for medications to experience rebirth as cultural attitudeschange or new uses are found for them. For example, once unrivalled asan over-the-counter analgesic, aspirin has been eclipsed by other painkillers– but it now holds a popular niche as a prophylactic agent for cardiovasculardisease (Jack, 1997). Even thalidomide, once the world’s most reviled medi-cation, recently returned to the market with new therapeutic indications(Raje and Anderson, 1999).
Between conception and death (or rebirth) a medication may be seen topass through several overlapping steps, including clinical trials, approvalfor use by regulatory agencies, approval for reimbursement by health andinsurance plans, marketing, promotion, prescription, consumption, andpost-marketing surveillance (Figure 1). In the initial steps of the life cycleas here conceived, a substance is merely a ‘molecule,’ then a ‘drug.’ Itsdesignation may be more attribute than property. Paradoxically, regardlessof its appearance as an ultra-sophisticated, extremely effective product ofrational and technological design, the modern drug may only take on theofficial appellation ‘medication’ or ‘medicine’ once it has proven itselfsuperior to inert placebo in a series of so-called ‘clinical trials.’ Of course,this speaks more about the nature and power of the ‘lowly’ placebo5 thanabout medications per se, though our point merely emphasizes that a sub-stance has to ‘earn’ the status of a medicinal product on the basis of chang-ing scientific and other criteria.
Each step or stage in the life cycle may be conceived as a mini-systemwith its own dynamics, which involve a context, a group of key actors, andvarious transactions among these actors. In addition to patients and phys-icians, pharmacists and nurses, these actors include investors and financial
Health 5(4)
446
03cohen (ds) 28/8/01 1:10 pm Page 446
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
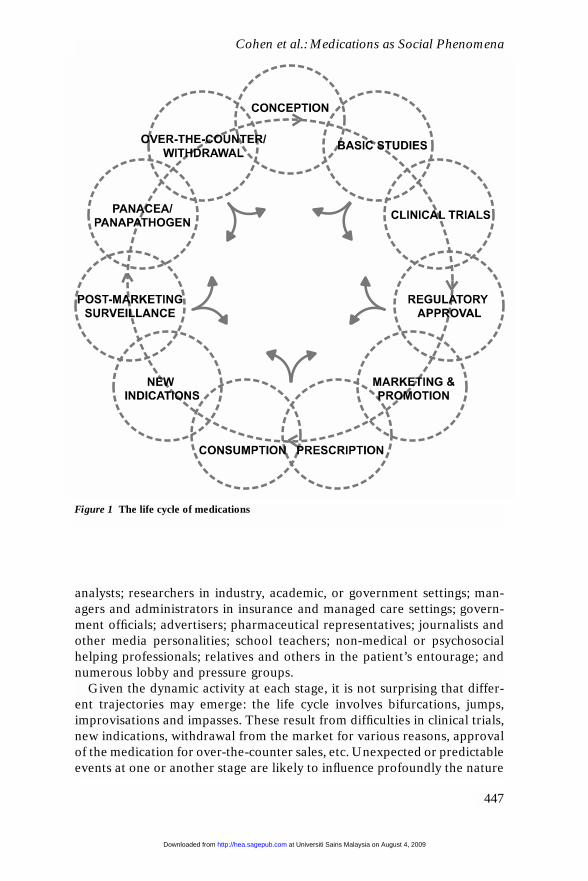
analysts; researchers in industry, academic, or government settings; man-agers and administrators in insurance and managed care settings; govern-ment officials; advertisers; pharmaceutical representatives; journalists andother media personalities; school teachers; non-medical or psychosocialhelping professionals; relatives and others in the patient’s entourage; andnumerous lobby and pressure groups.
Given the dynamic activity at each stage, it is not surprising that differ-ent trajectories may emerge: the life cycle involves bifurcations, jumps,improvisations and impasses. These result from difficulties in clinical trials,new indications, withdrawal from the market for various reasons, approvalof the medication for over-the-counter sales, etc. Unexpected or predictableevents at one or another stage are likely to influence profoundly the nature
Cohen et al.: Medications as Social Phenomena
447
Figure 1 The life cycle of medications
03cohen (ds) 28/8/01 1:10 pm Page 447
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
of the entire life cycle of the medication. Yet, the relationships betweensuch events and the overall fate of medications is little known, in partbecause researchers have generally failed to adopt such a comprehensive,‘biographical’ view of medications. In part also, it results from a lack ofaccess to information about the early stages of a drug’s life cycle, becauseof the simple fact that medications are the products of profit-making indus-tries intent on protecting their investments in a fiercely competitiveenvironment. Thus, a very large measure of proprietary activity and secrecycharacterizes the early stages of most medications’ life cycle, with infor-mation on these stages becoming available only at later stages, and then soonly partially.
For example, in most countries, negotiations between drug manu-facturers and regulatory agencies regarding the actual labeling of a drugand its clinical indications remain essentially inaccessible to researchers,clinicians, or even most public health authorities, except sometimes viafreedom of information laws. Although the secrecy is justified as a protec-tion for manufacturers’ commercial patents and intellectual property, muchof it undoubtedly stems from the well-known culture of secrecy that characterizes government and corporate operations. Undoubtedly, theextremely limited amount of information available about these transactionsimpacts on how the drug will be perceived and used by physicians andpatients in ordinary circumstances.
Another recent development illustrates potential changes in the life cycleof medications. In the last five years, a rapidly increasing proportion of sub-jects in clinical trials for new drugs are recruited via the offices of privatepractitioners, who receive financial rewards from drug manufacturers forthis purpose. This practice probably results from commercial incentives onmanufacturers to introduce products more quickly to the market, for whichthey must try to circumvent current monitoring and regulation of clinicaltrials by governments, universities, and ethics committees (Eichenwald andKolata, 1999). Repercussions of this new trend on other stages of a drug’slife cycle, and on other interacting systems such as patient–physicianrelationships, may be varied and numerous, and could be the subject offuture studies.
Finally, as Jacobs (1995) and Zarifian (1996) argue in the case of somenewer psychotropics, promotion of a drug by its manufacturer may actu-ally precede the clinical trials where the drug’s therapeutic effectivenessis presumably to be established. The promotion may involve funding professional committees working on the creation of a new psychiatricdiagnostic category listing specific target symptoms, treatment of whichthe new drug is then expected to improve. Or the promotion may involvefunding a lobby group of consumers or their relatives who will pressurehealth authorities to ease future bureaucratic hurdles which a new productis expected to face (Silverstein, 1999; O’Harrow, 2000). Hence, a modelof the life cycle of a medication must include individual behaviors,
Health 5(4)
448
03cohen (ds) 28/8/01 1:10 pm Page 448
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

institutional structures, sociohistorical tendencies – all in interaction overtime.
Drugs as social phenomena
The systemic view sketched above may help researchers detach themselvesfurther from a view of medications as ‘merely’ concrete, material objects.Because they are swallowed or injected inside physical bodies, it is initiallydifficult to consider how the effects of drugs resonate beyond an individualconsumer’s body or being, to shape social relations in families, groups, com-munities and larger societies – and in turn be shaped by these socialrelations. This insight is well understood in the study of illicit psychoactivesubstances (Stein, 1990), perhaps because their use is less mediated by pro-fessional expertise.
Is the physical/biologistic aspect of drugs’ nature fundamental? Perhaps,just as we may grasp the ‘essence’ of the body only by considering theexceedingly complex interweaving of agency and structure (e.g. Kelly andField, 1997), the ‘essence’ of drugs may be grasped by going beyond theirmaterial appearance. Studies of the placebo have long made use of thisinsight (Shapiro and Shapiro, 1997). Of course, the question of the essenceof drugs becomes exquisitely complex in the particular case of psychotropicdrugs, which by definition influence moods, thoughts, and behaviors of indi-viduals and have long sparked debate on the mind–body question (Huxley,1954).
One may analyze drugs as entities, as processes, and as representations,each in interaction with drug effects. In turn, drug effects might be per-ceived in the organic, personal, symbolic, social, and cultural realms (Bush,1977; Montagne, 1988, 1997). An analogy may be made with other commonbut nevertheless ‘charged’ objects, such as money, or automobiles. Forexample, though automobiles are obviously means of transportation, theyare just as evidently and simultaneously strategic commercial products, theplanet’s worst source of pollution, symbols of freedom and mobility – toname just a few of their intrinsic properties/ascribed attributes. Someauthors have explicitly analyzed the functions of written prescriptions, tran-quilizer tablets, and vitamins as modern-day talismans or amulets (Sands,1965; Rome, 1986; Olson, 1994). These analyses express the idea that thematerial nature of an object may matter less than its meanings in a complexweb of historically situated social interactions. A striking contemporaryillustration of this idea concerns cocaine and methylphenidate (Ritalin).These two stimulants may be observed to have virtually identical, inter-changeable physical and subjective effects in the short and long term onanimals and humans who ingest them (Volkow et al., 1995). Yet, they areclassified in law, medicine, public policy, and lay knowledge as radically dis-similar substances.
Like diamonds reflecting light, the ‘essence’ of medications changes
Cohen et al.: Medications as Social Phenomena
449
03cohen (ds) 28/8/01 1:10 pm Page 449
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
depending on one’s standpoint, and cannot quite be captured in a singleexpression. Thus, recognizing that drugs are concrete material objects doesnot prevent their simultaneous analysis as complex social phenomena,embedded in the web of individual and collective meanings and inter-actions. The following list identifies some themes for sociological inquiry:
1 medication as a primary tool in individual strategies for dealing withillness (emphasis on medication as a ‘pharmaceutical product’ withphysiological effects);
2 medication as interface between patients and physicians;3 medication as trigger for personal change – for example, as Karp (1996)
has shown, taking certain medications such as antidepressants may leadusers to undergo radical reinterpretations of their very sense of self, ina process akin to a religious conversion;
4 medication as a vehicle for various inter-related ideologies regardingthe body, health and illness, causality, personal responsibility (Nichterand Vuckovic, 1994);
5 psychoactive medication as an instrument of social control (Gabe andLipshitz-Phillips, 1984);
6 medication as cause and consequence of the medicalization of socialproblems (Kleinman and Cohen, 1991; Cohen, 1996);
7 ‘dangerous drugs’ or ‘approved medications’ (and their users) as reser-voirs of ‘badness’ or ‘goodness,’ respectively, for mainstream society(Szasz, 1974; Stein, 1990);
8 medication as a regulator of services and professional practices,diminishing or increasing the demand for these services (for example,by reducing the need for hospitalization or by increasing iatrogeniccasualties);
9 medication as locus of macro-regulation of actions taken by the state,the pharmaceutical industry, insurance companies, governments, pro-fessional and consumer associations (Bernstein and Lennard, 1973;Wertheimer and Smith, 1974; Davis, 1996);
10 medication as a vector of globalization (e.g. Bond, 1999) – given thatapproximately 15 countries sell most of the world’s drugs to all othercountries.
Changes in psychoactive medication usage patterns
Despite the long-standing centrality of drugs in healing practices in everysociety, the role of pharmaceuticals in modern medical care is gaining evenfurther prominence. For example, in Canada the proportion of totalnational health expenditures devoted to medications has risen from lessthan 9 percent in 1983 to 14.5 percent in 1997, when it surpassed for thefirst time spending on physician services (Buske, 2000). Yet, such develop-ments should not obscure the fact that the promotion of medications as
Health 5(4)
450
03cohen (ds) 28/8/01 1:10 pm Page 450
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
indispensable products has always been accompanied by doubts about theirsafety (Vuckovic and Nichter, 1997). Indeed, the contemporary triumph ofpharmaceuticals parallels a realization that even their proper use causesenough morbidity to rank adverse drug reactions in hospitalized patientsas the fourth leading cause of death in North America: Lazarou et al. (1998)estimated that 106,000 patients die and 2.2 million are injured yearly frommedication use, excluding errors, in the USA.
Large-scale longitudinal and international psychotropic consumptiontrend estimates are sparse and mostly document the situation in the USA:overall, they suggest that global and per capita usage in western countrieshave either remained stationary or decreased modestly during the 1970sand 1980s (Baum et al., 1988; Wysowski and Baum, 1991) but havemarkedly increased since the mid-1980s (Pincus et al., 1998). In the USA,managed care organizations such as health maintenance organizations(HMO) have probably contributed to this trend, to the extent that theyseek to limit their costs and see psychotropic drug use as less expensivethan personal contacts with caregivers. In addition, pharmaceutical com-panies have aggressively moved into the managed care business, where theycan promote their own products to HMO members.
At almost each decade since the 1930s, a different psychotropic drugappears to stand out in popularity, until professional disappointments andiatrogenic morbidities become noticeable or significant, and until a differ-ent candidate molecule is available to fill the coveted spot (Olivieri et al.,1986; Medawar, 1992; Cohen, 1996). With local variations, the large pro-portion of elderly and women users of psychotropics has remained stable.The most notable transformations in usage this past decade involve antide-pressants and psychostimulants, with a concomitant expansion of the marketto children. As noted in the introduction, this expansion clearly distinguishesthe use of psychotropics from that of other medications. In the class of anti-depressant drugs, the selective serotonin reuptake inhibitors (SSRIs) suchas Prozac are beginning to surpass in popularity the benzodiazepines, untilrecently the most prescribed psychotropics in the world (Pincus et al., 1998).This growth is not attributable to increased efficacy, since considerable evi-dence has failed to establish that the newer antidepressants are any moreeffective than the old or are better tolerated by users (Agency for HealthCare Policy and Research, 1999). Furthermore, research has also failed toestablish more than very modest support in short- and medium-term studiesfor antidepressants’ effectiveness in comparison with psychotherapy (Fisherand Greenberg, 1997; Antonuccio et al., 1999; Spiegel, 1999).
In North America, the 1990s have brought unprecedented growth in pre-scriptions to children, one sector of the population that appears to havebeen previously spared major exposure to prescribed psychotropics –though use of over-the-counter analgesics has long been significant (Koganet al., 1994). Medical visits in the USA resulting in psychostimulant pre-scriptions (most of which were for children) increased by more than 300
Cohen et al.: Medications as Social Phenomena
451
03cohen (ds) 28/8/01 1:10 pm Page 451
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
percent between 1985 and 1995 (Pincus et al., 1998). Psychotropic drugsare now being consumed by younger and younger children, for what areclearly unevaluated, ‘off label’ uses. In the USA such prescriptions to 2- to4-year-old children tripled between 1991 and 1995 (Zito et al., 2000). Inthat country, citing IMS Health, Diller (2000) reports the use of SSRIs inthe 7- to 12-year-old group to be up 151 percent between 1995 and 1999;for those under 6 years, the increase is 580 percent. For children under 18years, the use of ‘mood stabilizers’ other than lithium – mostly anticon-vulsant drugs – has grown 4000 percent and the use of newer neurolepticssuch as risperidone has grown nearly 300 percent. One may confidently esti-mate that 4 million American youths receive stimulants, 1 million receiveantidepressants, and nearly another million receive various other psycho-tropics.
Ironically, the growth in the consumption by children of prescribed stimu-lants has coincided with an escalation of the ‘war on drugs’ which especi-ally publicizes the dangers of illicitly used stimulants. In the USA, evenamphetamine, still viewed as a scourge in the drug abuse field (Baberg etal., 1996), is simultaneously one of the fastest-growing prescribed medi-cations for ‘attention deficit-hyperactivity disorder’ in children and adults.This is indicated by the popularity of Adderall, a mixture of pure amphet-amine salts. Made widely available on the US market in 1996, almost 3million prescriptions were dispensed during the first nine months of 1999only (Witte, 1999). This recalls but does not equal the huge popularity ofprescribed stimulants in that country during the 1950s and 1960s, thoughconsumers were mostly adults and ‘weight loss’ was a principal indication,until stimulants’ powerful potential to provoke dependence became widelyrecognized (Grinspoon and Hedblom, 1975). The possible relationshipbetween the resurgence of medical prescription of stimulants and the resur-gence of illicit stimulant use (Baberg et al., 1996) has not been explored.
The mass use of behavior-altering drugs with children remains confinedessentially to two countries in the world – Canada and the USA – whereit may represent an unprecedented experiment in social engineering. Toour knowledge, no researchers have investigated the sociocultural deter-minants of these practices. Rapid growth in stimulant use is now occurringin some other developed countries, especially the UK, though the differ-ences between the USA and Europe remain very large (International Nar-cotics Control Board, 2000). Interestingly, while the use of stimulants withchildren in France is extremely rare, studies have shown that the prescrip-tion of various tranquilizers to children for ‘sleep problems’ reached preva-lence hovering around 10 percent in the 1980s in some regions of thatcountry (Kopferschmitt et al., 1992).
The increased popularity and moral legitimacy of psychotropic drugs astreatments for emotional distress have also sparked developments such asthe drive among psychologists (at least in the USA and Canada) to obtainprescription privileges, similar to physicians, but for psychiatric drugs only.
Health 5(4)
452
03cohen (ds) 28/8/01 1:10 pm Page 452
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
This move represents a novel departure for psychology and has led tointense debates within that profession (Adams and Bieliauskas, 1994;Gutierrez and Silk, 1998) as well as fierce opposition from psychiatrists.
With cardiovascular and gastrointestinal medications, psychotropics areamong the three most prescribed drug classes in most post-industrialsocieties.6 This popularity, and the phenomenal financial returns on invest-ments from a few blockbuster drugs in the SSRI class, has spurred inten-sive efforts by pharmaceutical companies to market new products: in 2000some 103 molecules were under development as psychotropic candidates,particularly as anti-dementia drugs, antidepressants, anxiolytics or addic-tion treatments (Pharmaceutical Research and Manufacturers of America,2000).
Changes in pharmaceutical marketing practices
Among the many sociocultural determinants of the popularity of variousmedications, especially psychotropic medications, pharmaceutical market-ing practices have frequently been mentioned, although until a decade ago,there has been surprisingly little study of just how and to what extent thesepractices have impacted upon physicians (see Prather, 1991; review byLexchin, 1993). Recently, an exhaustive meta-analysis showed that mostgifts and incentives increase physician prescribing for the promoted drug,while simultaneously having a negative impact upon physicians’ knowledge(Wazana, 2000).
Advertisements in medical journals, visits to physicians using sophisti-cated persuasion techniques (Roughead et al., 1998), and symposia spon-sorship constitute the bulk of promotional activity. More recently, there hasbeen recent growing use of direct-to-consumer advertising (DTCA) inmass-media, a formerly prohibited practice but now fully allowed in theUSA and New Zealand and beginning in other western nations. In 1999,the pharmaceutical industry in the USA spent $13.9 billion on drug pro-motion, one-fifth more than the previous year. Of this amount, $1.8 billionwent to DTCA – triple what was spent three years before (IMS Health,2000b). Despite such estimates, total promotional spending remainsunknown because these data – if released by manufacturers – may be classi-fied under other less conspicuous headings; indications exist that pro-motional spending may approximate or even exceed true researchspending.
Direct-to-consumer advertising, via openly persuasive publicity slogans– mostly on television – or industry-funded ‘educational’ campaigns on theidentification and lifelong drug treatment of various troubles, is a harbin-ger for a major transformation in the significations and roles of medicationsin society – moving them even further out of the domain of medical mys-tique and into the mass market as lifestyle products. The transformation ofa prescription drug from strictly a tool of medical practice to a product that
Cohen et al.: Medications as Social Phenomena
453
03cohen (ds) 28/8/01 1:11 pm Page 453
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
may be sought or declined on the basis not only of ‘lay knowledge’ but,more precisely, consumer product knowledge, could have profound impli-cations given the ways in which such knowledge is obtained, perceived, andapplied. Direct-to-consumer advertising may also be expected to transformthe doctor–patient relationship as increasing numbers of patients arrive atthe consultation with not only explanatory frameworks regarding theirtroubles, but also the proposed solution: a prescription for a drug namedby the consumer (Lexchin, 1999). Studies suggest that most physiciansrespond positively to these requested prescriptions (Wilkes et al., 2000). Amarketing executive observes that ‘DTC advertising is now being used invirtually all phases of a product’s life cycle, from launch to patent expira-tion’ (cited in IMS Health, 2000b).
A major part of promotional activity in general is aimed not at con-sumers or medical prescribers, but at entire institutions: governments andother regulatory agencies, lobby groups concerned with specific illnesses,universities and other research bodies. Rarely is this promotional activitydescribed in the scientific literature though some serious independent orjournalistic investigations exist (e.g. Fried, 1998; Medawar, 1999; Silver-stein, 1999). The evidence is mounting, however, of persistent andexpanding influence of pharmaceutical companies in the formulation ofindustrial and health policies affecting their business, and in influencingwhat kind of research will be done, how it will be done, and how (orwhether) it will be reported (Medawar, 1992; Walker, 1994; Abraham,1995; Lehrman and Sharav, 1997). The title of a recent editorial in amedical journal illustrates growing medical concern over the issue: ‘Scien-tific harassment by pharmaceutical companies: Time to stop’ (Hailey,2000). In these circumstances, it remains an open question whether thepharmaceutical industry serves health systems or whether health systemsserve the pharmaceutical industry.
The Internet and changes in the construction of knowledgeabout medications
An exemplary sign of advanced modernity, the Internet has already sub-stantially altered the scientific and commercial stages of the life cyles of medi-cations (Cobert and Silvey, 1999; Henney et al., 1999) – and there is goodreason to believe that the interactive information revolution represented bythis new technology will alter the meanings and uses of medications beyondcurrent recognition. A major impact of the Internet has been to facilitate theconsumer’s participation as a prominent actor in the construction of knowl-edge about medications. This represents an enormous change within a healthcare system where such knowledge was strictly relegated to scientific, healthprofessional, government, and manufacturing experts. This may have beeneven more so with regard to psychiatric medications, used as they are –
Health 5(4)
454
03cohen (ds) 28/8/01 1:11 pm Page 454
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

especially over the long-term – by emotionally troubled persons who havebeen particularly powerless compared with other actors (Cohen and Mc-Cubbin, 1990; McCubbin and Cohen, 1996).
The Internet has made information from authorized sources increasinglyavailable to the general public, enabling patients to begin dialogue withphysicians at a much higher level. Goldsmith even suggests that physicians,who do not have time to search the Internet or analyze information fromit, might have to ‘rely on patients to update them on developments in theirown field, [which] is a stunning reversal of the traditional information flowin medicine’ (2000: 2). The Internet has also provided a means to createmutual support and interest groups in environments that allow for ano-nymity and relative safety in comparison with ‘real-life’ social circum-stances. Such forums, discussion lists, bulletin boards, news groups, ande-mail chains have clearly contributed to the emergence of the ‘consumer’class of users of mental health services: people who approach the ideal ofinformed consumers, who actively seek the best medications and the bestphysicians for dealing with their complex issues of treatment, advice, care,and support, who can ‘shop around’ for the best service, product, and price.Some Internet groups are categorized according to particular diagnoses andeven particular drugs. A participant may be struck by the detailed dailyexchange of experiences regarding different drugs, their perceived benefitsand side effects, withdrawal problems, and polypharmacy issues. Thenumbers of such groups, and interlocking participation within them, hasexploded into the hundreds, if not thousands.
In this new environment, radical innovations in knowledge constructionare possible. For example, within a few weeks following the introductionof a new psychotropic medication, hundreds of ordinary patients widelydispersed geographically will begin to provide their own detailed ‘productreports.’ Ironically, within these groups the problems of addiction and with-drawal are extremely well known and a constant topic of discussion, whilesuch issues are virtually unacknowledged by the manufacturers, regulators,and in the scientific literature (Medawar, 1997; Breggin and Cohen, 1999).Only a few years ago, to obtain a small fraction of such data – for example,bearing on withdrawal effects of a new psychiatric drug – would necessi-tate vast, costly studies in post-marketing surveillance, and only if the scien-tific, clinical, or public health interest was seriously piqued and sustainedin the first place. In sum, not only is knowledge on a medication’s effectssubject to ongoing revision, but today such knowledge must increasinglyaccommodate lay knowledge which – far from being hesitantly expressedin dyads of physician–patient or researcher–patient – possesses its ownchannels for direct, instant, and international diffusion.
This augmented participation of the consumer still is far from reachingequality with the traditional actors, who can mobilize resources far moreeffectively than consumers (Lenglet and Topuz, 1998). Yet, the traditionally
Cohen et al.: Medications as Social Phenomena
455
03cohen (ds) 28/8/01 1:11 pm Page 455
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

powerless ‘consumer movement’ may be approaching the levers of influencein the mental health and generally in the health care system, which couldgenerate unforeseen changes.
The availability of a multitude of Internet sites that carry various dis-courses on medications does have a dark side, as members of the publicmay confuse personal anecdotes and opinions with the results of scientificstudies. However, failure to consider scientific data and their uncertain-ties about the costs and benefits of various medications is not limited tothe lay public. Healy (1999), among others, suggests in the case of anti-depressants that professionals also may exaggerate the importance ofwidely disseminated personal narratives of healing and transformationrather than rely primarily upon sober analysis. But even published scien-tific studies of pharmaceuticals – presumably archetypes of balanced analy-sis – are regularly found to avoid reporting fundamental information,leading to exaggerated claims of efficacy and minimal adverse effects(Thornley and Adams, 1998). In sum, the Internet’s potential to ‘lead con-sumers astray’ is genuine – but this potential also serves to illustrate thatequally ‘dangerous’ though less studied incentives and constraints havealways operated and continue to operate upon all the actors involved inmaking decisions about drugs, not merely upon actors traditionally seenas ‘uninformed.’
Conclusion: exploring medications as social phenomena
Individuals use and professionals prescribe medications according to mean-ings – emanating from a complex psycho–socio–cultural matrix subject toconstant revision – which they attribute to health, illness, to the body, andto their identity. In turn, these meanings change as medications are usedand their effects resonate over time throughout individuals and collectivi-ties. This is particularly clear in the case of psychoactive medications. Inmany ways, however, psychoactive drugs share fundamental similaritieswith all medications and we believe that researchers would benefit fromapplying this insight to all medications.
In order to study medications as social phenomena, we favor an ana-lytical framework which is systemic, constructivist, and critical. Generalsystem theory (Sutherland, 1973) provides us with a ‘systems thinking’ per-spective which:
. . . is an epistemological perspective, sensitive to questions of context, structureand interaction such as complexity (multiple causality), dynamism (the import-ance of processes within the system and of the mutating nature of the system),uncertainty (actor choices are strategic due to the unknown future and the lackof transparency regarding the intentions of others), and holism (social systemsare viewed as ‘open’, being parts of larger systems). (McCubbin and Cohen,1999a: 60)
Health 5(4)
456
03cohen (ds) 28/8/01 1:11 pm Page 456
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

As an epistemological perspective, systems thinking embraces construc-tivism, supposing that apparently natural ‘reality’ and human experienceare created principally through sociocultural practices and mediated by lan-guage (Velody and Williams, 1998). Constructivism focuses on actors asinterpretors and active creators of knowledge, according to their experi-ence of the environment. To understand drugs, it is imperative to seize thesubjective narratives, discourses, and representations of the myriad actorswho make use of drugs (Montagne, 1997).
Finally, the framework is ‘critical,’ in that it steps out of a usual para-digm for studying medication use, and explicitly takes account of the distri-bution of power and interests among the actors directly or indirectlyinvolved in the phenomena of interest. Power and interests bear upon differential access to information and the ability to generate, circulate, orlegitimate particular discourses about medications and their effects(Medawar, 1992; Keen, 1998).
Several research avenues emerge from this framework. One point con-tinually stressed throughout this article concerns the involvement of numer-ous actors besides doctors and patients in the life cycle of medications, andthe fact that these actors’ motives and strategies as they interact with eachother remain virtually unknown. For example, studies are needed on howindividual officials in drug regulatory agencies construct notions such as‘risk,’ ‘harm,’ or ‘therapeutic,’ and how these personal constructions areassociated with various incentives and constraints operating upon theseindividuals in their networks. Another example concerns the impact offamily members or informal caregivers on medication use by the elderly.Countless epidemiological studies indicating high levels of use not alwaysjustified by state of health suggest that this avenue of research should bepursued more vigorously. Similarly, studies are needed of non-medicalhelping professionals’ attitudes and feelings about psychotropic medicationuse, and how these relate to power and ideological struggles in the mentalhealth field, and medication use by their clients.
On a broader level, more investigations are needed into the power of theeconomic multinationals (such as pharmaceutical companies) to shapesocial policies in various countries. This power is expanding in a globaleconomy and threatening the capacity of governments to regulate them(McCubbin, 1998). These policies involve drug regulation, access to drugs,drug advertising, and other policies created or altered in order to attractforeign investment. In the climate of globalization, economic power mayconstitute one of the greatest influences on the entire system of medicationuse and the life cycle of medications. For example, direct-to-consumer pro-motion of medications – strongly urged by drug manufacturers in countrieswhere it is not yet fully allowed – has the potential to modify profoundlyinstitutional, professional, and consumer attitudes and behaviors, likely inthe direction of increased brand-name medication usage. Many other issuesrequire examination, including the impact of DTCA on the provision of
Cohen et al.: Medications as Social Phenomena
457
03cohen (ds) 28/8/01 1:11 pm Page 457
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

independent information on drugs, on health-related behaviors, on the sup-pression of alternative treatments, on research funding.
The ideological and cultural dimensions of medication use deserve morestudy. For example, to what extent do systems of licit and illicit psycho-active drug use feed and impact upon each other? Prohibition of some psy-choactives nearly always goes hand in hand with promotion of some otherpsychoactives. Despite the porous, interactive features of these two seem-ingly disparate systems, we know of no serious attempts since Szasz (1974)to integrate observations about legal and illegal psychotropic drug use/pro-motion/prohibition in a single framework.
International differences in use of certain drugs, such as psychostimu-lants for children, deserve much closer examination than has been the caseup to now. These differences highlight how the social system of medicationuse interacts with other systems, such as public education and child care.In societies where economic development, access to technology, scientificworldviews, and adult psychoactive drug use are comparable – and whereclaims of concern for the needs and health of children are identical – themagnitude of contemporary differences between countries in the use ofbehavior-altering drugs among children is extremely intriguing. Within thefew societies where such use is common, differences between cultural orminority groups deserve more sophisticated investigations.
The need for well-founded figures on drug consumption is obvious. Cur-rently, researchers, and often, governments, depend on information fromcommercial sources or use outdated data to estimate prescription or con-sumption rates despite the rapidly changing patterns of use. In most coun-tries, independent sources of information on these patterns are lacking.This hampers relevant research and public health monitoring.
The veritable impact of iatrogenic effects of drugs is barely known. Thisignorance constitutes an inconspicuous but extremely powerful biastoward the ‘natural’ view of medications as primarily essential, lifesavingproducts and the intent of prescription as necessarily therapeutic. Theimpact of drug-related injuries in the social realm is also barely known orstudied. For example, psychotropic drugs are prescribed in order to modifybehavior by means of non-specific effects on the central nervous system,yet few researchers have studied the impact of these drugs on interpersonalprocesses (see Sice et al., 1975; Estroff, 1985; DeGiacomo et al., 1986).Since Illich’s (1976) discussions on the institutionalization of iatrogenesis,this topic has also been neglected. Drug-induced iatrogenesis may be con-ceived as a social system, and may be fruitfully investigated using insightsfrom constructivist and critical perspectives. For example, it is rarelyappreciated how even a seemingly fundamental pharmacological termsuch as ‘adverse effect’ may rest almost entirely on social construction(Cohen, 1997b).
Evaluating the impact of the Internet on numerous phases of the lifecycle of medications will undoubtedly spur several interesting studies.
Health 5(4)
458
03cohen (ds) 28/8/01 1:11 pm Page 458
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

Among its many effects, the Internet ostensibly removes an expert inter-mediary – such as a pharmacist or physician – from the physical, regulatory,and scientific ‘spaces’ between individuals and medications. The Internet(a new technology) helps to level the playing field between professionalsand clients, while changing how medications (an old technology) appear toall concerned. More direct access/relationships between individuals andmedications raises, as we have suggested, several research questions con-cerning all actors’ participation in the construction of knowledge and exper-tise about medications and all actors’ usages of medications as productsand as representations.
In this connection, the role of researchers and scientists in the life cyclesof different medications emphatically needs to be made more explicit.Scientists rarely view themselves as actors in the system, which allows themto exclude their own views and roles from their analyses. Given that a largeportion of drug research funding emanates directly or indirectly from thepharmaceutical industry, conflicts of interests remain understudied, as isthe fact that social researchers typically focus their attention on the visiblestages and transactions in drugs’ life cycles rather than question how andwhy other stages and transactions are less visible or studied.
In sum, we believe that thinking systemically about medications –described here as a necessarily critical and constructivist endeavor – raisesa number of interesting questions for research. A major challenge facingresearchers in this field is to relate the motives and reasonings expressedby the different actors involved in the life cycle of medications to observedtrends in the conception, promotion, prescription, consumption, and evalu-ation of medications in society. In turn, such analyses might reach moreprofound understandings by situating their results within the broader social,cultural, economic, and technological transformations and contradictionsat work as we begin another millennium.
Notes1. Each of the following factors and situations has been observed, in one or
another study, to be a significant predictor of medication use/prescription: age,gender, presenting complaints, physical condition, stress level, and attitudestoward medication (Pérodeau et al., 1992, 1996); perception of social network(Pérodeau and Galbaud du Fort, 2000); family structure (Mishara, 1997); socialrepresentations of health and illness (Morant, 1998); personal characteristics ofphysicians (Davidson et al., 1995); type of third-party payer (Sclar et al., 1998);cultural preferences for certain diagnoses and medications (Payer, 1990); newtechnologies and changed political and economic environments which affectmedication availability and determine its regulation (Davis, 1996); andpromotional practices by pharmaceutical manufacturers which – as we discuss inthis article – respond to and create professional and consumer demand.
2. In anthropology a small but thriving literature discusses the role, productionand use of drugs in third world countries; this work often incorporatesconsumers, sellers, healers, and producers in the same optic (Van der Geest et
Cohen et al.: Medications as Social Phenomena
459
03cohen (ds) 28/8/01 1:11 pm Page 459
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
al., 1996). In the case of psychotropic drugs in particular, an established butmarginalized literature critically evaluates the scientific claims made on behalfof drugs (e.g. Breggin, 1997; Cohen, 1997a; Antonuccio et al., 1999; Jacobs andCohen, 1999). These authors occasionally explain in political economy termsthe widespread acceptance of claims about drugs which contradict the scientificevidence (Cohen and McCubbin, 1990; Ray, 1991; Diller, 1996; DeGrandpre,1999; McCubbin and Cohen, 1999b). Extending on earlier studies of women andlong-term tranquilizer use, researchers continue to explore the perceptions ofconsumers of medication, largely in response to concerns about over-consumption, addiction, and iatrogenic effects (Searight, 1996; Haafkens, 1997).In response to ‘overprescription’ of antibiotics to children, researchers arebeginning to explore physicians’ and parents’ perceptions of these substances.
3. Our understanding of critical analysis is to attempt to step outside the dominantlogics and representations surrounding the object of study – indeed, to includethose logics and representations, and their historical construction, as part of theobject. This is consistent but not identical with ‘critical social theory’ whichensues from a long tradition of German epistemological thinking but which alsodemands and produces other forms of critique (Calhoun, 1995). However,‘stepping out’ of dominant discourses is not easy to do because the researchermay be enveloped by them to the point of not recognizing them. One approachis to adopt, at least for strategic purposes, an explicit standpoint which conflictswith some of the dominant beliefs; we do not do so in this article but do notdismiss its value in further pursuing the framework we present here. Anotherapproach is to construct an analysis from first principles: values (Prilleltensky,1996). This may reveal important inconsistencies in practices and discourse.Another approach is to analyze an object in terms of its power relations (e.g.Abraham, 1995; McCubbin and Cohen, 1996). This is always an implicit orexplicit element of our own analysis in this article.
4. By psychoactive or psychotropic medications we mean substances which actdirectly on the central nervous system and which physicians currently prescribein order to change moods, thoughts, or behavior. Also referred to as psychiatricmedications because as a rule their use receives first legitimation in psychiatry,they are mostly prescribed by primary care physicians (e.g. Ohayon et al., 1998).They include about 100 drugs typically regrouped under six labels:antipsychotics or neuroleptics; ‘mood stabilizers’ (lithium and anticonvulsants);antidepressants; ‘anxiolytics’ or tranquilizers or sleeping pills (mostlybenzodiazepines); psychostimulants; and, more recently, ‘cognition enhancers’used to treat mental symptoms of dementia.
5. The question of the placebo is a most complex one, given the demonstratedefficacy of placebos in numerous ailments, but also given the fact that placebosusually have to be believed in to work. In other words, the drug’s impact is notonly determined by the interaction of a chemical substance with the body, butalso by the expectations of the user and the deceptions of the provider. In thisconnection, inert placebos (e.g. sugar, yeast) may simply be controls for the‘normal state.’ To study better the effects of medications beyond placeboeffects, medications must be compared to ‘active’ placebos (e.g. atropine),substances which produce bodily changes (such as increased heartbeat orsweating) and thus which patients may ‘actively’ believe to be genuineremedies. In the few studies that use active placebos as controls, the relative
Health 5(4)
460
03cohen (ds) 28/8/01 1:11 pm Page 460
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
efficacy of the tested medication is typically much lower than in studies usinginert placebos (see, generally, Fisher and Greenberg, 1993).
6. IMS Health (2000a), a commercial company which tracks retail sales ofprescription drugs world-wide, lists 16 ‘therapeutic categories’ of medications,in decreasing order of sales in retail pharmacies for 12 months leading up toFebruary 2000: cardiovascular, alimentary/metabolism, central nervous system,anti-infectives, respiratory, genito-urinary, musculo-skeletal, cytostatics,dermatologicals, blood agents, sensory organs, diagnostic agents, hormones,miscellaneous, hospital solutions, parasitology.
ReferencesAbraham, J. (1995). Science, politics and the pharmaceutical industry: Controversy
and bias in drug regulation. London: UCL.Adams, K.M. and Bieliauskas, L.A. (1994). On perhaps becoming what you had
previously despised: Psychologists as prescribers of medication. Journal ofClinical Psychology in Medical Settings, 1, 189–97.
Agency for Health Care Policy and Research (AHCPR). (1999). Treatment ofdepression: Newer pharmacotherapies. Summary, evidence report/technologyassessment 7. Rockville, MD: AHCPR. Available at:http://www.ahcpr.gov/clinic/deprsumm.htm [accessed 13 July 2001].
Antonuccio, D., Danton, W.G., DeNelsky, G.Y., Greenberg, R.G. and Gordon, J.S.(1999). Raising questions about antidepressants. Psychotherapy andPsychosomatics, 68, 3–14.
Baberg, H.T., Nelesen, R.A. and Dimsdale, J.E. (1996). Amphetamine use: Returnof an old scourge in a consultation psychiatry setting. American Journal ofPsychiatry, 153, 789–93.
Barden, L.S., Dowell, S.F., Schwartz, B. and Lackey, C. (1998). Current attitudesregarding use of antimicrobial agents: Results from physician’s and parents’focus group discussions. Clinical Pediatrics, 37, 665–71.
Baum, C., Kennedy, D.L., Knapp, D.E., Juergens, J.P. and Faich, G.A. (1988).Prescription drug use in 1984 and changes over time. Medical Care, 26, 105–14.
Bernstein, A. and Lennard, H.L. (1973). The American way of drugging: Drugs,doctors and junkies. Society, May/June, 14–25.
Bond, P. (1999). Globalization, pharmaceutical pricing, and South African healthpolicy: Managing confrontation with US firms and politicians. InternationalJournal of Health Services, 29, 765–92.
Bowler, T.D. (1981). General systems thinking: Its scope and applicability. NewYork: North Holland.
Braddock, C.H., III, Fihn, S.D., Levinson, W., Jonson, A.R. and Pearlman, R.A.(1997). How doctors and patients discuss routine clinical decisions: Informeddecision making in the outpatient setting. Journal of General Internal Medicine,12, 339–45.
Breggin, P.R. (1997). Brain-disabling treatments in psychiatry: Drugs, electroshock,and the role of the FDA. New York: Springer.
Breggin, P.R. and Cohen, D. (1999). Your drug may be your problem: How andwhy to stop taking psychiatric medications. Cambridge, MA: Perseus.
Bush, P.J. (1977). Psychosocial aspects of medicine use. In A.I. Wertheimer andP.J. Bush (Eds.), Perspectives on medicines in society. Hamilton, IL: DrugIntelligence.
Cohen et al.: Medications as Social Phenomena
461
03cohen (ds) 28/8/01 1:11 pm Page 461
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
Bush, P.J. and Osterweis, M. (1978). Pathways to medicine use. Journal of Healthand Social Behavior, 19, 179–89.
Buske, L. (2000). Drug costs surpass spending on physicians. Canadian MedicalAssociation Journal, 162, 405–6.
Butler, C.C., Rollnick, S., Pill, R., Maggs-Rapport, F. and Stott, N. (1998).Understanding the culture of prescribing: Qualitative study of generalpractitioners’ and patients’ perceptions of antibiotics for sore throats. BMJ, 317,637–42.
Calhoun, C.J. (1995). Critical social theory: Culture, history, and the challenge ofdifference. Oxford: Blackwell.
Chinburapa, V., Larson, L.N. and Brucks, M. (1993). Physician prescribingdecisions: The effects of situational involvement and task complexity oninformation acquisition and decision making. Social Science & Medicine, 36,1473–82.
Christensen-Szalanski, J.J.J. and Bushyhead, J.B. (1988). Physicians’ use ofprobabilistic information in a real clinical setting. In J. Dowie and A. Elstein(Eds.), Professional judgment: A reader in clinical decision making. Cambridge:Cambridge University Press.
Coambs, R.B., Jensen, P., Hao Her, M., Ferguson, B.F., Larry, J.L., Wong, J.S.W. etal. (1995). Review of the scientific literature on the prevalence, consequences, andhealth costs of compliance and inappropriate use of prescription medication inCanada. Toronto: University of Toronto Press.
Cobert, B. and Silvey, J. (1999). The Internet and drug safety: What are theimplications for pharmacovigilance? Drug Safety, 20, 95–107.
Cohen, D. (1996). Les ‘nouveaux’ médicaments de l’esprit: Marche avant vers lepassé? (The ‘new’ mind drugs: Forward step into the past?) Sociologie etsociétés, 28, 17–34.
Cohen, D. (1997a). A critique of the use of neuroleptic drugs in psychiatry. In S.Fisher and R.P. Greenberg (Eds.), From placebo to panacea: Putting psychiatricdrugs to the test. New York: Wiley.
Cohen, D. (1997b). Psychiatrogenics: Introducing chlorpromazine in psychiatry.Review of Existential Psychology and Psychiatry, 23, 206–33.
Cohen, D. and Bisson, J. (1997). Médication neuroleptique et risque de dyskinésietardive: Une enquête auprès de psychiatres et d’omnipraticiens du Québec(Neuroleptic medication and the risk of tardive dyskinesia: A survey ofpsychiatrists and general practitioners in Québec). Santé mentale au Québec, 22,263–82.
Cohen, D. and Karsenty, S. (1998). Répresentations sociales des effets secondairesdes anxiolytiques: Une étude comparative Québec-France (Social representationsof the side effects of anxiolytics: A comparative Québec-France study).Montreal & Paris: GRASP & Hôpital La Salpêtrière.
Cohen, D. and McCubbin, M. (1990). The political economy of tardive dyskinesia:Asymmetries in power and responsibility. Journal of Mind and Behavior, 11,465–88.
Collin, J. (1999). Rationalité et irrationalité à l’origine des mésusages desmédicaments (Rationality and irrationality at the origin of medication misuse).Actualité et Dossiers en Santé Publique, 27, 55–8.
Collin, J., Damestoy, N. and Lalande, R. (1999). La construction d’une rationalité:Les médecins face à la prescription de psychotropes aux personnes âgées
Health 5(4)
462
03cohen (ds) 28/8/01 1:11 pm Page 462
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
(Constructing a rationality: Physicians and the prescription of psychotropics tothe elderly). Sciences Sociales et Santé, 17, 31–52.
Conrad, P. (1994). The meaning of medications: Another look at compliance. In P.Conrad and R. Kern (Eds.), The sociology of health and illness: Criticalperspectives. New York: St Martin’s.
Damestoy, N., Collin, J. and Lalande, R. (1999). Physicians’ perception ofpsychotropic medication prescriptions for elderly patients: Another perspective.Canadian Medical Association Journal, 161, 143–5.
Davidson, W., Molloy, W. and Bédard, M. (1995). Physician characteristics andprescribing for elderly people in New Brunswick: Relation to patient outcomes.Canadian Medical Association Journal, 152, 1227–34.
Davis, P. (1996). Contested ground: Public purpose and private interest in theregulation of prescription drugs. New York: Oxford University Press.
DeGiacomo, P., Silvestri, A., Pierri, G., Lefons, E. and Corfiati, L. (1986).Research on effects of psychodrugs on human interaction. Atheoretical/experimental approach. Acta Psychiatrica Scandinavica, 74,417–24.
DeGrandpre, R. (1999). Ritalin nation: Rapid-fire culture and the transformation ofhuman consciousness. New York: Norton.
Diller, L.H. (1996). The run on Ritalin: Attention-deficit disorder and stimulanttreatment in the 1990s. Hastings Center Report, March/April.
Diller, L.H. (2000). Kids on drugs: A behavioral pediatrician questions the wisdomof medicating our children. Salon Health and Body, 9 March. Available at:http://www.salon.com/health/feature/2000/03/09/kid_drugs/ [accessed 13 July2001].
Donovan, J.L. and Blake, D.R. (1992). Patient non-compliance: Deviance orreasoned decision-making? Social Science & Medicine, 34, 507–13.
Ehrenberg, A. (1995). L’individu incertain (The uncertain individual). Paris:Calmann-Lévy.
Eichenwald, K. and Kolata, G. (1999). Drug trials hide conflicts for doctors. NewYork Times, 16 May, 1.
Estroff, S.E. (1985). Making it crazy: An ethnography of psychiatric clients in anAmerican community. Berkeley, CA: University of California Press.
Fineman, H. (1991). The social construction of noncompliance. Sociology of Healthand Illness, 13, 354–74.
Fisher, S. and Greenberg, R.P. (1993). How sound is the double-blind design forevaluating psychotropic drugs? Journal of Nervous and Mental Disease, 181,345–50.
Fisher, S. and Greenberg, R.P., Eds. (1997). From placebo to panacea: Puttingpsychiatric drugs to the test. New York: Wiley.
Fried, S. (1998). Bitter pills: Inside the hazardous world of legal drugs. New York:Bantam.
Gabe, J., Ed. (1991). Understanding tranquilliser use: Contributions from the socialsciences. London: Tavistock/Routledge.
Gabe, J. and Lipshitz-Phillips, S. (1984). Tranquillisers as social control?Sociological Review, 36, 320–52.
Gergen, K.J. (1985). Social constructionist inquiry: Context and implications. InK.J. Gergen and K.E. Davis (Eds.), The social construction of the person. NewYork: Springer-Verlag.
Cohen et al.: Medications as Social Phenomena
463
03cohen (ds) 28/8/01 1:11 pm Page 463
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
Gerrity, M.S., Earp, J.A.L., DeVellis, R.F. and Light, D.W. (1992). Uncertainty andprofessional work: Perceptions of physicians in clinical practice. AmericanJournal of Sociology, 97, 1022–51.
Giddens, A. (1990). The consequences of modernity. Stanford, CA: StanfordUniversity Press.
Goldsmith, J. (2000). How will the Internet change our health system? HealthAffairs, March/April. Available at:http://www.projhope.org/HA/bonus/190112.htm [accessed 13 July 2001].
Grinspoon, L. and Hedblom, P. (1975). The speed culture: Amphetamine use andabuse in America. Cambridge, MA: Harvard University Press.
Gutierrez, P.M. and Silk, K.R. (1998). Prescription privileges for psychologists: Areview of the psychological literature. Professional Psychology-Research andPractice, 29, 213–22.
Haafkens, J. (1997). Rituals of silence. Long-term tranquilizer use by women in theNetherlands: A social case study. Amsterdam: University of the NetherlandsPress.
Hailey, D. (2000). Scientific harassment by pharmaceutical companies: Time tostop. Canadian Medical Association Journal, 162, 212–13.
Healy, D. (1999). The three faces of the antidepressants: A critical commentary onthe clinical-economic context of diagnosis. Journal of Nervous and MentalDisease, 187, 174–80.
Henney, J.E., Shuren, J.E., Nightingale, S.L. and McGinnis, T.J. (1999). Internetpurchases of prescription drugs: Buyer beware. Annals of Internal Medicine, 131,861–2.
Huxley, A. (1954). The doors of perception. London: Chatto & Windus.Illich, I. (1976). Medical nemesis: The expropriation of health. New York:
Pantheon.IMS Health. (2000a). IMS Health reports 10 percent growth in global retail drug
sales for 12 month period to February. Available athttp://www.imshealth.com/html/news_arc/ 04_20_2000_351.htm (accessed 5September 2000).
IMS Health. (2000b). IMS Health reports US pharmaceutical promotional spendingreached record $13.9 billion in 1999. Available at:http://www.imshealth.com/html/news_arc/ 04_20_2000_352.htm (accessed 5September 2000).
International Narcotics Control Board. (2000). Report of the InternationalNarcotics Control Board for 1999. New York: United Nations.
Jack, D.B. (1997). One hundred years of aspirin. Lancet, 350, 437–9.Jacobs, D.J. (1995). Psychiatric drugging: 40 years of pseudo-science, self-interest,
and indifference to harm. Journal of Mind and Behavior, 16, 421–70.Jacobs, D.J. and Cohen, D. (1999). What is really known about psychological
alterations produced by psychiatric drugs? International Journal of Risk andSafety in Medicine, 12, 37–47.
Karp, D.A. (1996). Speaking of sadness: Depression, disconnection, and themeanings of illness. New York: Oxford University Press.
Keen, E. (1998). Drugs, therapy, and professional power. Westport, CT: Praeger.Kelly, M.P. and Field, D. (1997). Body image and sociology: A reply to Simon
Williams. Sociology of Health and Illness, 19, 359–66.Kleinman, D.L. and Cohen, L.J. (1991). The decontextualization of mental illness:
Health 5(4)
464
03cohen (ds) 28/8/01 1:11 pm Page 464
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
The portrayal of work in psychiatric drug advertisements. Social Science &Medicine, 32, 867–74.
Kogan, M.D., Pappas, G., Yu, S.M. and Kotelchuk, M. (1994). Over-the-countermedication use among US preschool-age children. JAMA, 272, 1025–30.
Kopferschmitt, J., Meyer, P., Jaeger, A., Mantz, J.M. and Roos, M. (1992). Troublesdu sommeil et consommation de médicaments psychotropes chez l’enfant de sixans (Sleep disorders and consumption of psychotropic medications with respectto the six-year-old child). Revue d’épidémiologique et de Santé Publique, 40,467–71.
Laing, R. (1999). The world health and drug situation. International Journal of Riskand Safety in Medicine, 12, 51–7.
Lazarou, J., Pomeranz, B.H. and Corey, P. (1998). Incidence of adverse drugreactions in hospitalized patients. JAMA, 279, 1200–5.
Lehrman, N.S. and Sharav, V.H. (1997). Ethical problems in psychiatric research.Journal of Mental Health Administration, 24, 227–50.
Lenglet, R. and Topuz, B. (1998). Des lobbies contre la santé (Lobbies againsthealth). Paris: Syros.
Lexchin, J. (1993). Interactions between physicians and the pharmaceuticalindustry. Canadian Medical Association Journal, 149, 1401–7.
Lexchin, J. (1999). Direct-to-consumer advertising: Impact on patient expectationsregarding disease management. Disease Management and Health Outcomes, 5,273–83.
McCubbin, M. (1998). Global anarchy: Market failure, the prisoner’s dilemma, andsovereignty over health and social policy. Paper presented at Xth InternationalConference, International Association of Health Policy, Perugia, Italy. Availableat: http://www.mailbase.ac.uk/lists/radical-psychology-network/2000–02/0177.html [accessed 13 July 2001].
McCubbin, M. and Cohen, D. (1996). Extremely unbalanced: Interest divergenceand power disparities between clients and psychiatry. International Journal ofLaw and Psychiatry, 19, 1–25.
McCubbin, M. and Cohen, D. (1999a). A systemic and value-based approach tostrategic reform of the mental health system. Health Care Analysis, 7, 57–77.
McCubbin, M. and Cohen, D. (1999b). Empirical, ethical and political perspectiveson the use of methylphenidate. Ethical Human Sciences and Services, 1, 81–101.
McGrath, J.M. (1999). Physicians’ perspectives on communicating prescriptiondrug information. Qualitative Health Research, 9, 731–45.
Makoul, G., Arntson, P. and Schofield, T. (1995). Health promotion in primarycare: Physician–patient communication and decision making about prescriptionmedications. Social Science & Medicine, 41, 1241–54.
Meador, C.K. (1998). Polypharmacy: Old bad habits. Journal of the AmericanBoard of Family Practice, 11, 166–7.
Medawar, C. (1992). Power and dependence. London: Social Audit.Medawar, C. (1997). The antidepressant web. International Journal of Risk and
Safety in Medicine, 10, 75–126.Medawar, C. (1999). Direct-to-consumer advertising. Available at:
http://www.socialaudit.org.uk/5111-002.htm/#Dear [accessed 13 July 2001].Mishara, B. (1997). L’écologie familiale et la consommation de médicaments chez
les personnes âgées (Family ecology and the consumption of medications byelderly persons). Santé mentale au Québec, 22, 200–15.
Cohen et al.: Medications as Social Phenomena
465
03cohen (ds) 28/8/01 1:11 pm Page 465
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
Montagne, M. (1988). The metaphorical nature of drugs and drug-taking. SocialScience & Medicine, 26, 417–24.
Montagne, M. (1996). The Pharmakon phenomenon: Cultural conceptions ofdrugs and drug use. In P. Davis (Ed.), Contested ground: Public concern andprivate interest in the regulation of pharmaceuticals. New York: OxfordUniversity Press.
Montagne, M. (1997). De l’activité pharmacologique à l’usage des drogues: Laconstruction des connaissances sur les psychotropes (From pharmacologicalactivity to the use of drugs: The construction of knowledge about psychotropics).Santé mentale au Québec, 22, 149–63.
Moore, T.J., Psaty, B.M. and Furberg, C.D. (1998). Time to act on drug safety.JAMA, 279, 1571–3.
Morant, N. (1998). The social representations of mental ill-health in communitiesof mental health practitioners in the UK and France. Information sur lesSciences Sociales, 37, 663–85.
Nichter, M. and Vuckovic, N. (1994). Agenda for an anthropology ofpharmaceutical practice. Social Science & Medicine, 11, 1509–25.
O’Harrow, R., Jr (2000). Grass roots seeded by drugmaker. The Washington Post,12 September, A1.
Ohayon, M.M., Caulet, M., Priest, R.G. and Guilleminault, C. (1998). Psychotropicmedication consumption patterns in the UK general population. Journal ofClinical Epidemiology, 51, 273–83.
Olivieri, S., Cantopher, T. and Edwards, J.G. (1986). Two hundred years ofanxiolytic drug dependence. Neuropharmacology, 25, 669–70.
Olson, J.A. (1994). Vitamins: The tortuous path from needs to fantasies. Journal ofNutrition, 124, Supplement, S1771–S1776.
Payer, L. (1990). Medicine and culture: Notions of health and sickness in Britain,the US, France, and West Germany. London: Gollancz.
Pérodeau, G. and Galbaud du Fort, G. (2000). Psychotropic drug use and therelation between social support, life events and mental health in the elderly.Journal of Applied Gerontology, 19, 23–41.
Pérodeau, G., King, S. and Ostoj, M. (1992) Stress and psychotropic drug useamong the elderly: An exploratory model. Canadian Journal on Aging, 11,347–69.
Pérodeau, G., Jomphe-Hill, A., Hay-Paquin, L. and Amyot, E. (1996). Lespsychotropes et le vieillissement normal: Une perspective psychosociale etsocioéconomique (Psychotropics and normal aging: A psychosocial andsocioeconomic perspective). Canadian Journal on Aging, 15, 559–82.
Pharmaceutical Research and Manufacturers of America. (2000). New medicines indevelopment for mental illness. Available at:http://www.phrma.org/searchcures/newmeds/mentalill/surv2000/ [accessed 13July 2001].
Pignarre, P. (1995). Les deux médecines: Médicaments, psychotropes et suggestionthérapeutique (The two medicines: Medications, psychotropics, and therapeuticsuggestion). Paris: La Découverte.
Pincus, H.A., Tanielian, T.L., Marcus, S.C., Olfson, M., Zarin, D.A., Thompson, J.et al. (1998). Prescribing trends in psychotropic medications: Primary care,psychiatry, and other medical specialties. JAMA, 279, 526–31.
Prather, J. (1991). Decoding advertising: The role of communication studies in
Health 5(4)
466
03cohen (ds) 28/8/01 1:11 pm Page 466
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
explaining the popularity of tranquillisers. In J. Gabe (Ed.), Understandingtranquilliser use. London: Tavistock/Routledge.
Prilleltensky, I. (1996). Human, moral, and political values for an emancipatorypsychology. Humanist Psychologist, 24, 307–24.
Raje, N. and Anderson, K. (1999). Thalidomide: A revival story. New EnglandJournal of Medicine, 341, 1606–9.
Ray, L. (1991). The political economy of long-term minor tranquilliser use. In J.Gabe (Ed.), Understanding tranquilliser use. London: Tavistock/Routledge.
Rogers, A., Day, J.C., Williams, B., Randall, F., Wood, P., Healy, D. and Bentall,R.P. (1998). The meaning and management of neuroleptic medication: A studyof patients with a diagnosis of schizophrenia. Social Science and Medicine, 47,1313–23.
Rome, H.P. (1986). Personal reflections: The Rx as talisman. Psychiatric Annals,16, 566.
Roter, D.L. and Frankel, R. (1992). Quantitative and qualitative approaches to theevaluation of the medical dialogue. Social Science & Medicine, 34, 1097–103.
Roughead, E.E., Harvey, K.J. and Gilbert, A.L. (1998). Commercial detailingtechniques used by pharmaceutical representatives to influence prescribing.Australian and New Zealand Journal of Medicine, 28, 306–10.
Sacristan, J.A. (1994). Drug utilisation studies as tools in health economics.Pharmacoeconomics, 5, 299–312.
Sands, W.L. (1965). The tranquilizer tablet. Talisman for the 1960s. PsychiatricQuarterly, 39, 722–6.
Sclar, D.A., Robison, L.M., Skaer, T.L. and Galin, R.S. (1998). What factorsinfluence the prescribing of antidepressant pharmacotherapy? An assessment ofnational office-based encounters. International Journal of Psychiatry in Medicine,28, 407–19.
Searight, H.R. (1996). Perceptions of attention deficit/hyperactivity disorder andits treatment among children and adolescents. Journal of Medical Humanities,17, 51–61.
Shapiro, A.K. and Shapiro, E. (1997). The powerful placebo: From ancient priest tomodern physician. Baltimore, MD: Johns Hopkins University Press.
Sice, J., Levine, H.D., Levin, J. and Haertzen, C.A. (1975). Effects of personalinteractions and settings on subjective drug responses in small groups.Psychopharmacologia, 43, 181–6.
Silverstein, K. (1999). Prozac.org. Mother Jones, December, 18–19.Spiegel, D. (Ed.). (1999). Efficacy and cost-effectiveness of psychotherapy.
Washington, DC: American Psychiatric Press.Stein, H.F. (1990). In what systems do alcohol/chemical addictions make sense?
Clinical ideologies and practices as cultural metaphors. Social Science &Medicine, 30, 987–1000.
Sutherland, J.W. (1973). A general systems philosophy for the social and behavioralsciences. New York: Braziller.
Szasz, T.S. (1974). Ceremonial chemistry: The ritual persecution of drugs, addicts,and pushers. New York: Anchor.
Taylor, C. (1989). Sources of the self: The making of the modern identity.Cambridge, MA: Harvard University Press.
Thornley, B. and Adams, C. (1998). Content and quality of 2000 controlled trials inschizophrenia over 50 years. BMJ, 317, 1181–4.
Cohen et al.: Medications as Social Phenomena
467
03cohen (ds) 28/8/01 1:11 pm Page 467
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from
Trostle, J.A. (1988). Medical compliance as an ideology. Social Science & Medicine,27, 1299–308.
Van der Geest, S., Whyte, S.R. and Hardon, A. (1996). The anthropology ofpharmaceuticals: A biographical approach. Annual Review of Anthropology, 25,153–78.
Velody, I. and Williams, R., Eds. (1998). The politics of constructivism. London:Academy of Hebrew Language.
Volkow, N.D., Ding, Y., Fowler, J.S., Wang, G., Logan, J., Gatley, J.S., Dewey, S.,Ashby, C., Lieberman, J., Hitzemann, R. and Wolf, A.P. (1995). Ismethylphenidate like cocaine? Studies on their pharmacokinetics anddistribution in the human brain. Archives of General Psychiatry, 52, 456–63.
Vuckovic, N. and Nichter, M. (1997). Changing patterns of pharmaceutical practicein the United States. Social Science & Medicine, 44, 1285–302.
Walker, M.J. (1994). Dirty medicine: Science, big business and the assault on naturalhealth care, revised edn. London: Slingshot.
Wazana, A. (2000). Physicians and the pharmaceutical industry: Is a gift ever just agift? JAMA, 283, 373–80.
Wertheimer, A.I. and Smith, M.C., Eds. (1974). Pharmacy practice: Social andbehavioral aspects. London: University Park.
Wilkes, M.S., Bell, R.A. and Kravitz, R.L. (2000). Direct-to-consumer prescriptiondrug advertising: Trends, impact, and implications. Health Affairs, 19(2), 110–28.
Williams, S.J. and Calnan, M. (1996). The ‘limits’ of medicalization?: Modernmedicine and the lay populace in late modernity. Social Science & Medicine, 42,1609–20.
Witte, B. (1999). Judge cites hyperactivity drug in homicide acquittal. AssociatedPress dispatch, 25 October. Available at:www.abcnews.go.com/sections/living/DailyNews/ adderall991025.html [accessed13 July 2001].
Wolff, N. (1989). Professional uncertainty and physician medical decision-makingin a multiple treatment framework. Social Science & Medicine, 28, 99–107.
Wysowski, D.K. and Baum, C. (1991). Outpatient use of prescription sedative-hypnotic drugs in the United States, 1970 through 1989. Archives of InternalMedicine, 151, 1779–83.
Zarifian, E. (1996). Le prix du bien-être. Psychotropes et societé (The price of well-being. Psychotropics and society). Paris: Odile Jacob.
Zito, J.M., Safer, D.J., dosReis, S., Gardner, J.F., Boles, M. and Lynch, F. (2000).Trends in the prescribing of psychotropic medications to preschoolers. JAMA,283, 1025–30.
Author biographiesDAVID COHEN is Professor and Doctoral Program Coordinator, School of SocialWork, College of Health and Urban Affairs, Florida International University, andAssociate Researcher, Health and Prevention Social Research Group (GRASP),University of Montreal. He studies usages and representations of psychoactivedrugs, and has written on critical psychiatry, medicalization, iatrogenics, and psychi-atric medication withdrawal. He is now researching the prescription of behavior-altering drugs to children in different countries.
Health 5(4)
468
03cohen (ds) 28/8/01 1:11 pm Page 468
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from

MICHAEL MCCUBBIN is on the Research Faculty of the Saskatchewan PopulationHealth Evaluation and Research Unit, University of Regina, and is AssociateProfessor at GRASP, University of Montreal. He has a political science andeconomics background and researches mental health policy and politics, sociopo-litical aspects of psychoactive drug use, and the roles of power, powerlessness, andempowerment in pathways to population health, illness, and well-being.
JOHANNE COLLIN is Assistant Professor, Faculty of Pharmacy, and Researcher atGRASP, University of Montreal. Her research explores the cultural, social, andhistorical aspects of medication use, professional versus lay knowledge and attitudesabout medication, and the history of therapeutics and pharmacy.
GUILHÈME PÉRODEAU is Professor, Department of Psychology, University of Quebecat Hull, and Researcher at GRASP. Her background is in social psychology. Herresearch pertains to stress and coping among elders in relation to social and familynetworks and attitudes toward psychoactive drug use. She also studies work–familyconflict among female workers facing job and financial insecurity.
Cohen et al.: Medications as Social Phenomena
469
03cohen (ds) 28/8/01 1:11 pm Page 469
at Universiti Sains Malaysia on August 4, 2009 http://hea.sagepub.comDownloaded from