long-term outcomes of surgical tongue reduction in beckwith-wiedemann syndrome
TRANSCRIPT
PEDIATRIC/CRANIOFACIAL
Long-Term Outcomes of Surgical TongueReduction in Beckwith–Wiedemann Syndrome
Jillian K. Tomlinson,M.B.B.S., Dip. Anat.
Sue A. Morse, B.App.Sci.(Speech Path.)
Simon P. L. Bernard,F.R.A.C.S.
Andrew L. Greensmith,F.R.A.C.S.
John G. Meara, F.R.A.C.S.,M.B.A.
Melbourne, Australia
Background: Surgical tongue reduction is often performed in Beckwith–Wiede-mann syndrome when macroglossia results in abnormal tongue function orcosmesis; however, no published studies have examined the long-term outcomesof this procedure.Methods: Patients older than 18 years with Beckwith–Wiedemann syndromewho had previously undergone surgical tongue reduction at the Royal Chil-dren’s Hospital in Melbourne underwent assessment of speech and tonguefunction, mobility, sensation, and cosmesis. These assessments were performedby questionnaire on 11 subjects and by formal medical and speech pathologyreview in four of these 11 subjects.Results: Eleven patients aged 19 to 31 years completed responses by means ofquestionnaire. The most common self-reported abnormalities were continueddisproportionate tongue bulk (91 percent), abnormal tongue appearance (82percent), specific speech sound errors (73 percent), and a short tongue tip (55percent). Formal assessments investigated speech, swallowing, taste, and tonguemobility in four quite different subjects. One of these four subjects had nodetectable deficits in tongue function. All 11 patients were of normal intelli-gence and did not report significant difficulties in their day-to-day life that wereattributable to their macroglossia or tongue reduction surgery.Conclusions: Pediatric patients with symptomatic macroglossia requiring sur-gical tongue reduction may not achieve complete normality in tongue functionand appearance in adulthood. It is important that surgical tongue reductionaddresses the global nature of the macroglossia and aims to retain a taperedtongue tip with length sufficient to permit normal tongue movements. (Plast.Reconstr. Surg. 119: 992, 2007.)
Beckwith–Wiedemann syndrome is an over-growth disorder initially described by Beck-with in 19631 and Wiedemann in 1964.2 It
has a prevalence of 0.07 per 1000 births3,4 and istypically characterized by exomphalos, macroglos-sia, and gigantism (thus its previous name of EMGsyndrome). The syndrome results from chromo-somal changes in the imprinted 11p15.5 regionthat cause increased levels of the fetal growth fac-tor insulin-like growth factor 2. Fifteen percent ofcases are familial and 85 percent are sporadic.4,5
Other clinical and histologic features frequentlyassociated with Beckwith–Wiedemann syndromeinclude neonatal hypoglycemia, renal abnormali-ties, visceromegaly, hemihypertrophy, nevus flam-
meus of the forehead, and an increased incidenceof childhood neoplasms.
Macroglossia is seen in 80 to 99 percent of pa-tients with Beckwith–Wiedemann syndrome4,6–8;surgical tongue reduction (partial glossectomy)aims to correct macroglossia to confer normaltongue function and appearance. Not all patientswith Beckwith–Wiedemann syndrome will requiretongue reduction, as the condition is not pheno-typically homogenous and, often, mildly symptom-atic macroglossia will improve without interventionas a result of normal mandibular and skeletalgrowth. The indications for surgical tongue reduc-tion are airway obstruction, swallowing problemswith failure to thrive, dental deformities, articula-tion disorders, recurrent lingual trauma, inabilityto achieve oral competency, persistent drooling,and cosmetic concerns.
PATIENTS AND METHODSEthics approval for the study was granted by
the Royal Children’s Hospital Ethics and Research
From the Department of Plastic and Maxillofacial Surgery,Royal Children’s Hospital.Received for publication June 6, 2005; accepted August 31,2005.Copyright ©2007 by the American Society of Plastic Surgeons
DOI: 10.1097/01.prs.0000252256.77086.67
www.PRSJournal.com992

Department. The subject group consisted of pa-tients with Beckwith–Wiedemann syndrome whowere older than 18 years and had undergone sur-gical tongue reduction at the Royal Children’sHospital after 1970. A medical records search wasperformed and histories of patients coded as hav-ing “Beckwith syndrome” or “Beckwith–Wiede-mann syndrome” were examined to identify pa-tients who had also undergone surgical tonguereduction. Medical records of patients born be-fore 1970 were not examined because of differ-ences in coding before this time and the diffi-culties of obtaining archived records. Patientsyounger than 18 years were excluded to ensurethat all subjects had finished mandibular growthand to streamline consent processes for both sub-jects and controls.
Eleven of 19 patients eligible for inclusion inthe study were located and agreed to participate inthe study. Eight of 19 patients either could not betraced or did not return the survey forms. Sixty-sixuniversity students of a similar age constituted thecontrol group.
Informed consent was obtained and subjectswere asked to complete a questionnaire by indi-cating agreement or disagreement with 35 state-ments regarding tongue mobility, function, taste,sensation, speech, and cosmesis. Information re-garding dental deformities and sleep apnea wasnot sought. If a respondent failed to mark a re-sponse for a question, that individual’s responsewas excluded from analysis of that question. Sta-tistical analysis was carried out with Yates correc-tion for chi-square, with p � 0.05 considered sig-nificant.
Patients were invited to undergo further as-sessments of taste, speech, and tongue mobility atthe Royal Children’s Hospital. Of the 11 subjectswho completed the survey, four attended for fur-ther assessments; only six of the 11 subjects livedwithin 350 km of Royal Children’s Hospital.
Taste assessment was performed with solutionsof 0.9% normal saline, lemon juice (Berri LemonSqueeze, Berri Ltd., Carlton, Victoria, Australia),sterile water, 1:6 diluted artificial sweetener (Liq-uid Splenda; McNeill Nutritionals, Ft. Washing-ton, Pa.), white vinegar (Cornwall’s White Vine-gar; Meadow Lea Foods Ltd., Mascot, New SouthWales, Australia), peppermint essence (Queen Es-sence; Queen Fine Foods Pty Ltd., Alderley,Queensland, Australia), and aniseed essence(Queen Essence; Queen Fine Foods Pty Ltd). Sub-jects sampled each solution in turn by placing acotton bud soaked in solution on the tongue. Sub-jects were asked to describe the taste and to state
whether the solution was salty, sweet, bitter, sour,or had no identifiable taste. Subjects were thenasked to identify the substance. Two attempts werepermitted with each solution; subjects were askedto describe the taste of the solution after eachattempt.
Subjects had a speech assessment conductedby an experienced speech pathologist. Assess-ments were videotaped and reviewed by one ad-ditional speech pathologist. The speech sound er-ror pattern was assessed with the ArticulationSurvey.9 Speech errors were assessed in both read-ing, free speech, and conversational contexts. In-telligibility and diadochokinetic ability were as-sessed with subtests of the Frenchay DysarthriaProfile.10 Chewing and swallowing motions wereassessed by observing staged consumption of drybiscuits and of water.
Tongue mobility was assessed by observingeach subject’s ability to maneuver the tongue tipwithin and outside the oral cavity. In situationswhere the position of the tongue tip could not beviewed by an observer, the subject was asked toself-report ability to perform the maneuver.
RESULTSSurvey Responses
The 11 subjects were six men and five womenaged from 19 to 31 years, with a mean age of 24.7years. The average age of the control group was20.5 years, ranging from 18 to 27 years (Table 1).Twelve of the 13 operations involved a form ofanterior wedge resection; in seven of 12, tissue wasalso excised from the central tongue (Table 2).Nine subjects underwent a single tongue reduc-tion operation; two subjects had two tongue re-duction operations. The subjects’ ages at the timeof surgery ranged between 3.5 and 38.5 months;the median age at the time of surgery was 11.5months. Surgery had been performed by one of sixsurgeons (Table 3).
Selected questionnaire responses are listed inTable 4. Subjects’ responses differed significantlyfrom controls with regard to tongue cosmesis andfunction during eating and speech. Subjects weremore likely to report frequently biting their
Table 1. Demographics
Subjects Controls
No. 11 66Male-to-female ratio 6:5 30:36Age, years
Mean 24.7 20.5Range 19–31 18–27
Volume 119, Number 3 • Surgical Tongue Reduction
993
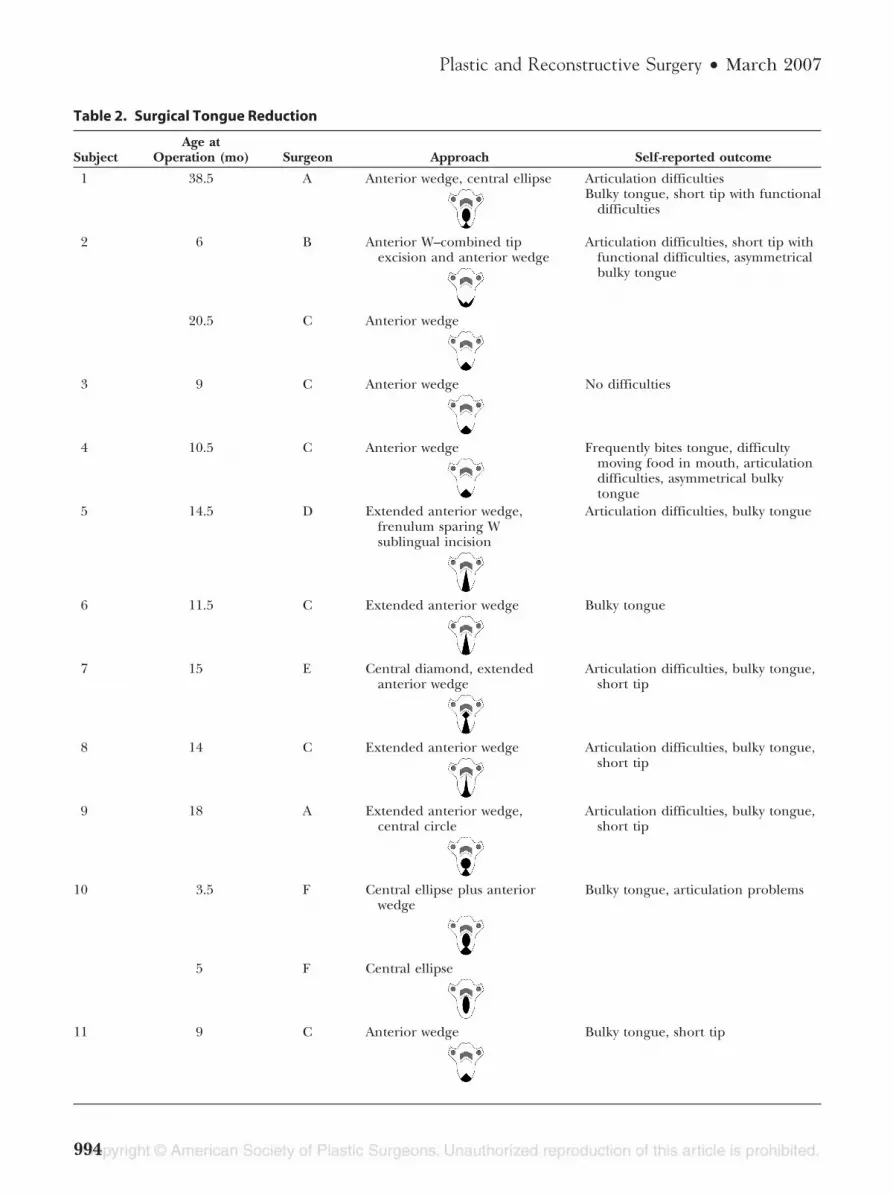
Table 2. Surgical Tongue Reduction
SubjectAge at
Operation (mo) Surgeon Approach Self-reported outcome
1 38.5 A Anterior wedge, central ellipse Articulation difficultiesBulky tongue, short tip with functional
difficulties
2 6 B Anterior W–combined tipexcision and anterior wedge
Articulation difficulties, short tip withfunctional difficulties, asymmetricalbulky tongue
20.5 C Anterior wedge
3 9 C Anterior wedge No difficulties
4 10.5 C Anterior wedge Frequently bites tongue, difficultymoving food in mouth, articulationdifficulties, asymmetrical bulkytongue
5 14.5 D Extended anterior wedge,frenulum sparing Wsublingual incision
Articulation difficulties, bulky tongue
6 11.5 C Extended anterior wedge Bulky tongue
7 15 E Central diamond, extendedanterior wedge
Articulation difficulties, bulky tongue,short tip
8 14 C Extended anterior wedge Articulation difficulties, bulky tongue,short tip
9 18 A Extended anterior wedge,central circle
Articulation difficulties, bulky tongue,short tip
10 3.5 F Central ellipse plus anteriorwedge
Bulky tongue, articulation problems
5 F Central ellipse
11 9 C Anterior wedge Bulky tongue, short tip
Plastic and Reconstructive Surgery • March 2007
994
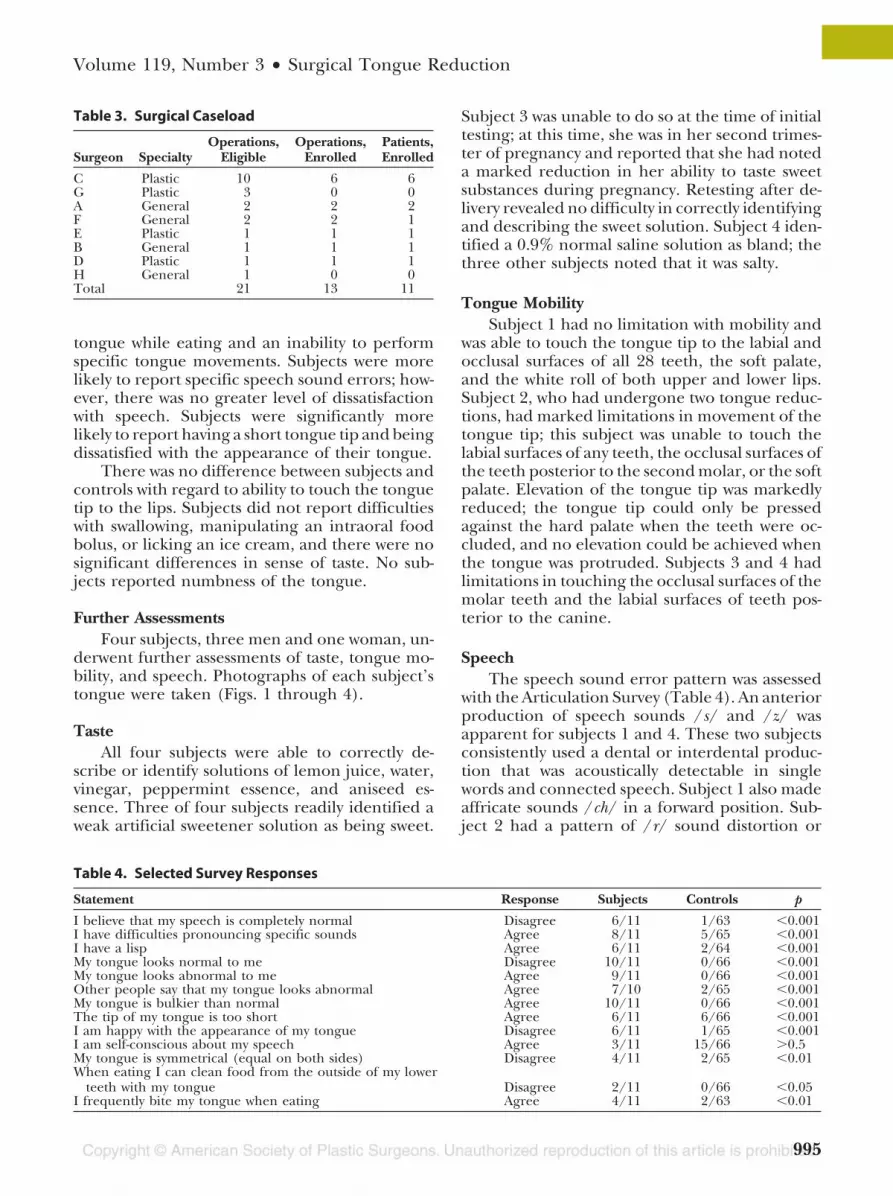
tongue while eating and an inability to performspecific tongue movements. Subjects were morelikely to report specific speech sound errors; how-ever, there was no greater level of dissatisfactionwith speech. Subjects were significantly morelikely to report having a short tongue tip and beingdissatisfied with the appearance of their tongue.
There was no difference between subjects andcontrols with regard to ability to touch the tonguetip to the lips. Subjects did not report difficultieswith swallowing, manipulating an intraoral foodbolus, or licking an ice cream, and there were nosignificant differences in sense of taste. No sub-jects reported numbness of the tongue.
Further AssessmentsFour subjects, three men and one woman, un-
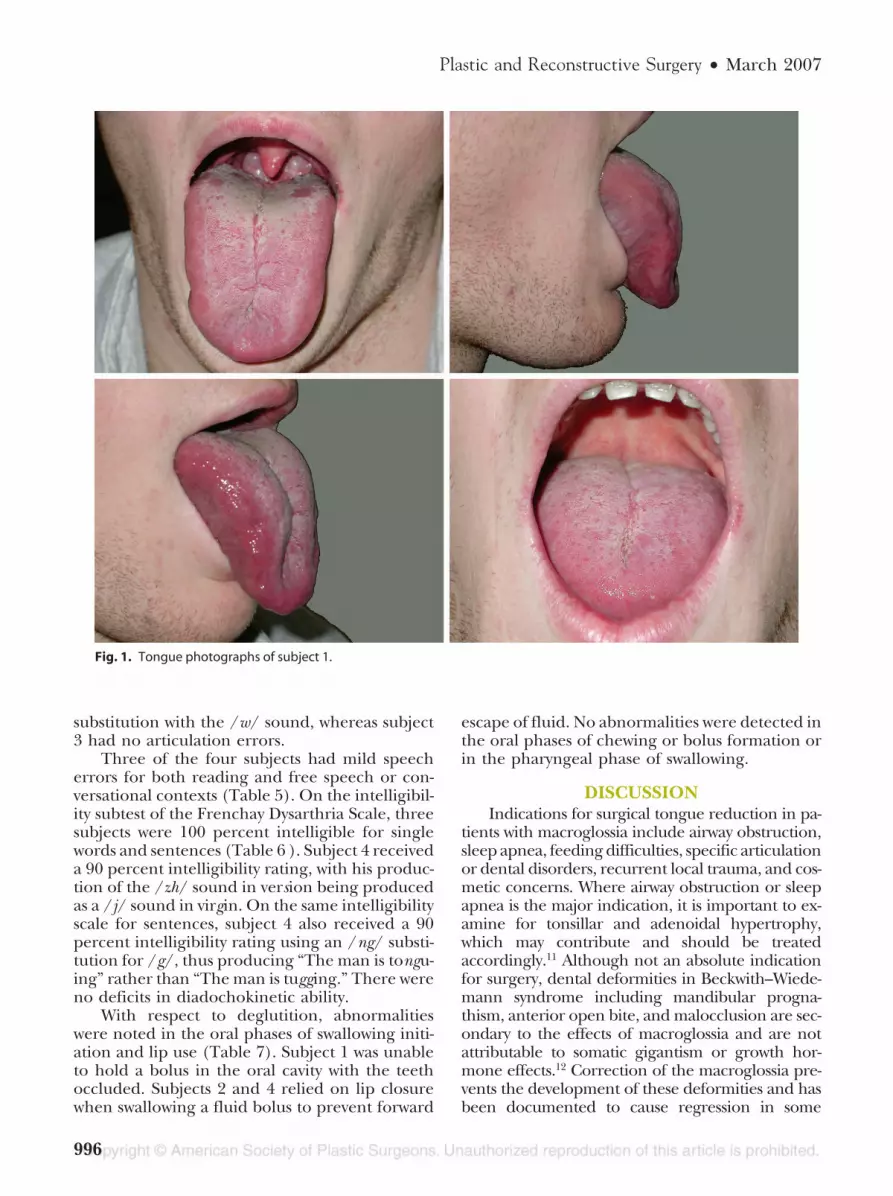
derwent further assessments of taste, tongue mo-bility, and speech. Photographs of each subject’stongue were taken (Figs. 1 through 4).
TasteAll four subjects were able to correctly de-
scribe or identify solutions of lemon juice, water,vinegar, peppermint essence, and aniseed es-sence. Three of four subjects readily identified aweak artificial sweetener solution as being sweet.
Subject 3 was unable to do so at the time of initialtesting; at this time, she was in her second trimes-ter of pregnancy and reported that she had noteda marked reduction in her ability to taste sweetsubstances during pregnancy. Retesting after de-livery revealed no difficulty in correctly identifyingand describing the sweet solution. Subject 4 iden-tified a 0.9% normal saline solution as bland; thethree other subjects noted that it was salty.
Tongue MobilitySubject 1 had no limitation with mobility and
was able to touch the tongue tip to the labial andocclusal surfaces of all 28 teeth, the soft palate,and the white roll of both upper and lower lips.Subject 2, who had undergone two tongue reduc-tions, had marked limitations in movement of thetongue tip; this subject was unable to touch thelabial surfaces of any teeth, the occlusal surfaces ofthe teeth posterior to the second molar, or the softpalate. Elevation of the tongue tip was markedlyreduced; the tongue tip could only be pressedagainst the hard palate when the teeth were oc-cluded, and no elevation could be achieved whenthe tongue was protruded. Subjects 3 and 4 hadlimitations in touching the occlusal surfaces of themolar teeth and the labial surfaces of teeth pos-terior to the canine.
SpeechThe speech sound error pattern was assessed
with the Articulation Survey (Table 4). An anteriorproduction of speech sounds /s/ and /z/ wasapparent for subjects 1 and 4. These two subjectsconsistently used a dental or interdental produc-tion that was acoustically detectable in singlewords and connected speech. Subject 1 also madeaffricate sounds /ch/ in a forward position. Sub-ject 2 had a pattern of /r/ sound distortion or
Table 3. Surgical Caseload
Surgeon SpecialtyOperations,
EligibleOperations,
EnrolledPatients,Enrolled
C Plastic 10 6 6G Plastic 3 0 0A General 2 2 2F General 2 2 1E Plastic 1 1 1B General 1 1 1D Plastic 1 1 1H General 1 0 0Total 21 13 11
Table 4. Selected Survey Responses
Statement Response Subjects Controls p
I believe that my speech is completely normal Disagree 6/11 1/63 �0.001I have difficulties pronouncing specific sounds Agree 8/11 5/65 �0.001I have a lisp Agree 6/11 2/64 �0.001My tongue looks normal to me Disagree 10/11 0/66 �0.001My tongue looks abnormal to me Agree 9/11 0/66 �0.001Other people say that my tongue looks abnormal Agree 7/10 2/65 �0.001My tongue is bulkier than normal Agree 10/11 0/66 �0.001The tip of my tongue is too short Agree 6/11 6/66 �0.001I am happy with the appearance of my tongue Disagree 6/11 1/65 �0.001I am self-conscious about my speech Agree 3/11 15/66 �0.5My tongue is symmetrical (equal on both sides) Disagree 4/11 2/65 �0.01When eating I can clean food from the outside of my lower
teeth with my tongue Disagree 2/11 0/66 �0.05I frequently bite my tongue when eating Agree 4/11 2/63 �0.01
Volume 119, Number 3 • Surgical Tongue Reduction
995
substitution with the /w/ sound, whereas subject3 had no articulation errors.
Three of the four subjects had mild speecherrors for both reading and free speech or con-versational contexts (Table 5). On the intelligibil-ity subtest of the Frenchay Dysarthria Scale, threesubjects were 100 percent intelligible for singlewords and sentences (Table 6 ). Subject 4 receiveda 90 percent intelligibility rating, with his produc-tion of the /zh/ sound in version being producedas a /j/ sound in virgin. On the same intelligibilityscale for sentences, subject 4 also received a 90percent intelligibility rating using an /ng/ substi-tution for /g/, thus producing “The man is tongu-ing” rather than “The man is tugging.” There wereno deficits in diadochokinetic ability.
With respect to deglutition, abnormalitieswere noted in the oral phases of swallowing initi-ation and lip use (Table 7). Subject 1 was unableto hold a bolus in the oral cavity with the teethoccluded. Subjects 2 and 4 relied on lip closurewhen swallowing a fluid bolus to prevent forward
escape of fluid. No abnormalities were detected inthe oral phases of chewing or bolus formation orin the pharyngeal phase of swallowing.
DISCUSSIONIndications for surgical tongue reduction in pa-
tients with macroglossia include airway obstruction,sleep apnea, feeding difficulties, specific articulationor dental disorders, recurrent local trauma, and cos-metic concerns. Where airway obstruction or sleepapnea is the major indication, it is important to ex-amine for tonsillar and adenoidal hypertrophy,which may contribute and should be treatedaccordingly.11 Although not an absolute indicationfor surgery, dental deformities in Beckwith–Wiede-mann syndrome including mandibular progna-thism, anterior open bite, and malocclusion are sec-ondary to the effects of macroglossia and are notattributable to somatic gigantism or growth hor-mone effects.12 Correction of the macroglossia pre-vents the development of these deformities and hasbeen documented to cause regression in some
Fig. 1. Tongue photographs of subject 1.
Plastic and Reconstructive Surgery • March 2007
996

cases.12–15 Speech may also be improved followingcorrection of macroglossia.16 In severe cases, desic-cation of the protruding tongue can occur and in-ability to achieve oral competence can result indrooling. Tongue protrusion may give the appear-ance of mental retardation, which can cause tre-mendous distress to patients and families and resultin poor bonding with parents, social ostracism, andlow self-esteem.
Not all patients with Beckwith–Wiedemannsyndrome will require tongue reduction, as thecondition is not phenotypically homogenous and,often, mild degrees of macroglossia will improvewithout intervention as a result of normal man-dibular and skeletal growth. Histologic examina-tion of tongue tissue in Beckwith–Wiedemann syn-drome invariably demonstrates microscopicallynormal muscle and nerve fibers17 and thus surgicalreduction is theoretically curative with adequateresection. Nevertheless, extensive resection risksdamage to the neurovascular bundles, and theglobal nature of the macroglossia poses difficultiesin creating a normal tongue.
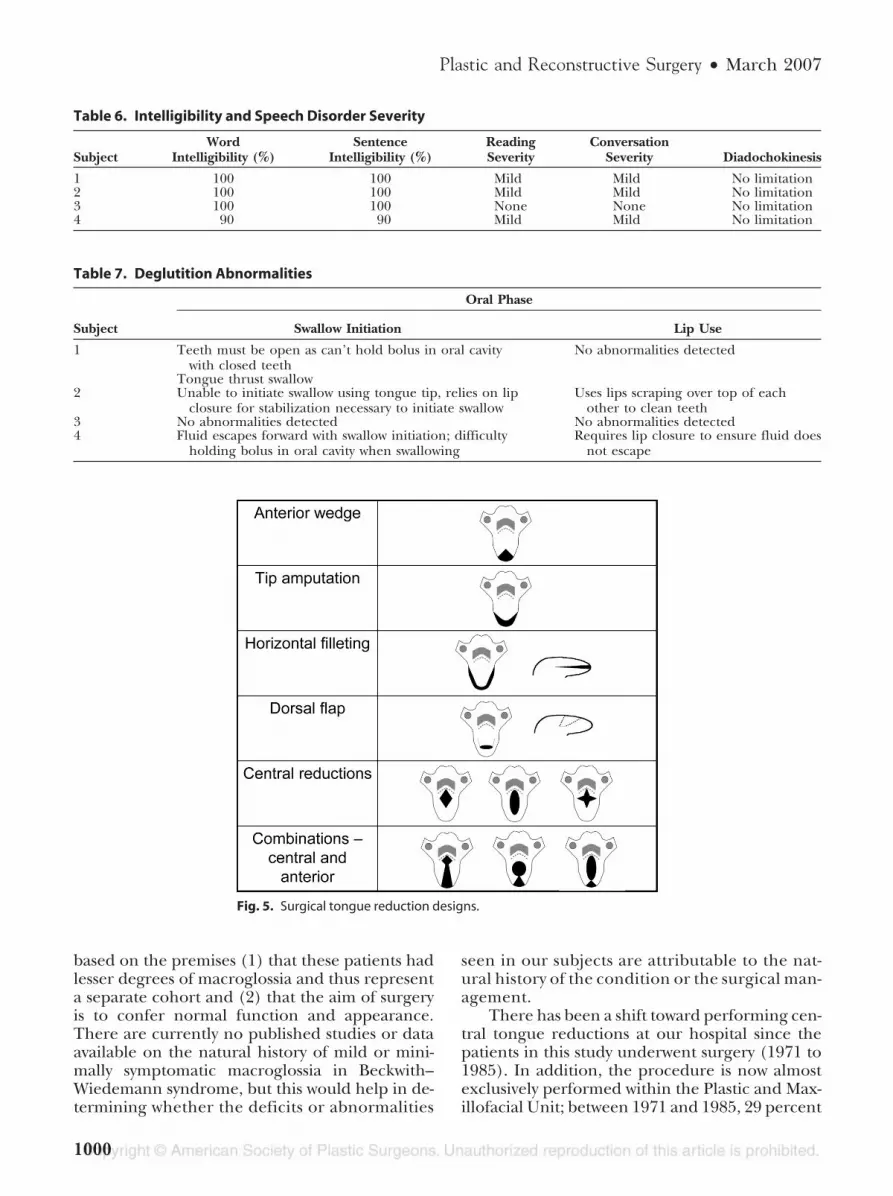
Surgical approaches include the anteriorwedge reduction, tip amputation, central reduc-tion, marginal resection, and dorsal flap excision.Combinations of these are also used, for example,in a keyhole reduction (Fig. 5). Anterior wedgereductions and tip amputations reduce tonguelength; central reductions and dorsal flap tech-niques address the bulk of the tongue base. Mar-ginal resection reduces tongue width and lengthbut cannot address height.
Various authors have suggested that the ante-rior wedge produces suboptimal results and riskscreating a shortened, ankylosed tongue.18,19 Theprevalence of enlarged tongues and short tonguetips in this study supports the view that excessivetongue bulk in Beckwith–Wiedemann syndrome isbetter treated with central tongue reduction, com-bined with additional methods as required toachieve normal tongue length. This is particularlyimportant when more than one operative inter-vention is undertaken; sequential anterior wedgereductions should be performed only with ex-treme care. Notably, however, the one subject in
Fig. 2. Tongue photographs of subject 2.
Volume 119, Number 3 • Surgical Tongue Reduction
997
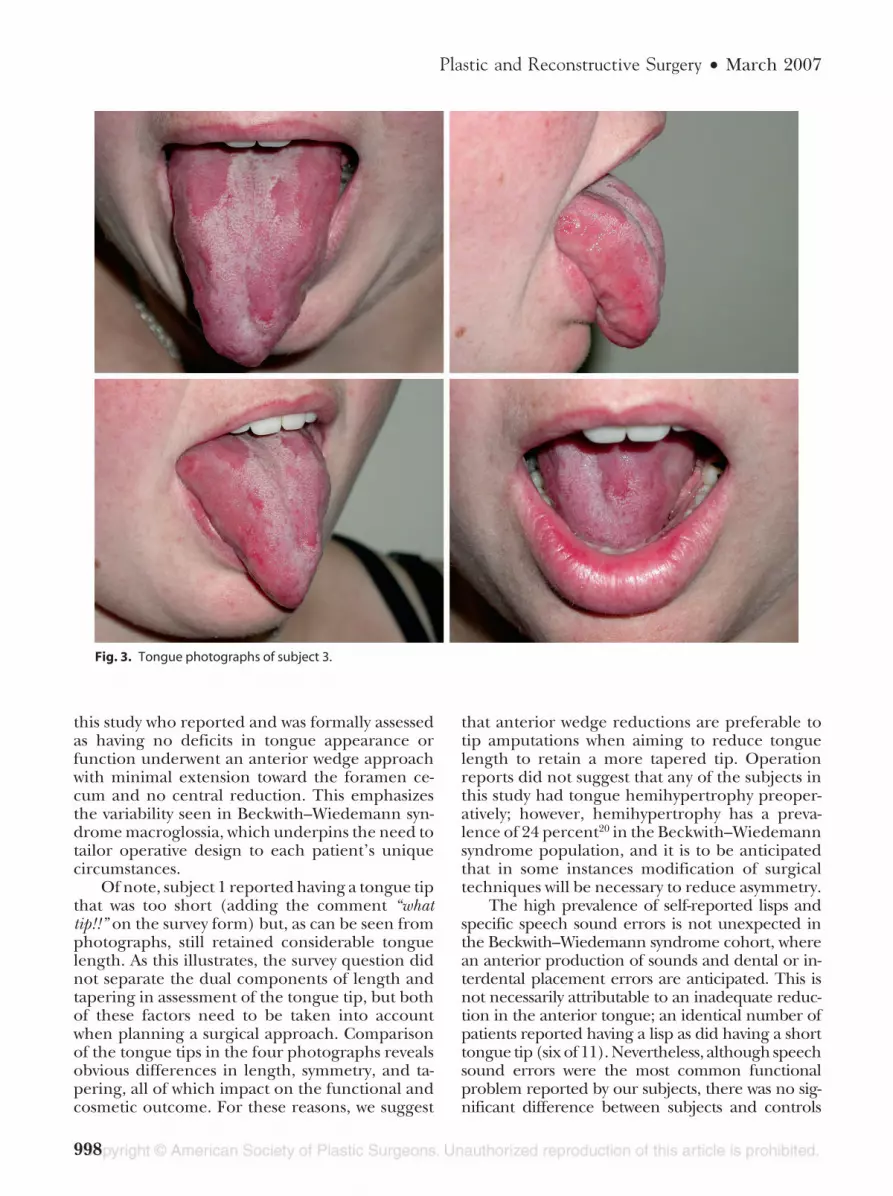
this study who reported and was formally assessedas having no deficits in tongue appearance orfunction underwent an anterior wedge approachwith minimal extension toward the foramen ce-cum and no central reduction. This emphasizesthe variability seen in Beckwith–Wiedemann syn-drome macroglossia, which underpins the need totailor operative design to each patient’s uniquecircumstances.
Of note, subject 1 reported having a tongue tipthat was too short (adding the comment “whattip!!” on the survey form) but, as can be seen fromphotographs, still retained considerable tonguelength. As this illustrates, the survey question didnot separate the dual components of length andtapering in assessment of the tongue tip, but bothof these factors need to be taken into accountwhen planning a surgical approach. Comparisonof the tongue tips in the four photographs revealsobvious differences in length, symmetry, and ta-pering, all of which impact on the functional andcosmetic outcome. For these reasons, we suggest
that anterior wedge reductions are preferable totip amputations when aiming to reduce tonguelength to retain a more tapered tip. Operationreports did not suggest that any of the subjects inthis study had tongue hemihypertrophy preoper-atively; however, hemihypertrophy has a preva-lence of 24 percent20 in the Beckwith–Wiedemannsyndrome population, and it is to be anticipatedthat in some instances modification of surgicaltechniques will be necessary to reduce asymmetry.
The high prevalence of self-reported lisps andspecific speech sound errors is not unexpected inthe Beckwith–Wiedemann syndrome cohort, wherean anterior production of sounds and dental or in-terdental placement errors are anticipated. This isnot necessarily attributable to an inadequate reduc-tion in the anterior tongue; an identical number ofpatients reported having a lisp as did having a shorttongue tip (six of 11). Nevertheless, although speechsound errors were the most common functionalproblem reported by our subjects, there was no sig-nificant difference between subjects and controls
Fig. 3. Tongue photographs of subject 3.
Plastic and Reconstructive Surgery • March 2007
998

with regard to self-consciousness about speech. Sub-jects reported that they did not experience any dif-ficulties in verbal communication, either whenspeaking face-to-face or by means of telephone, andfrequently were employed in occupations thatrequire high levels of verbal communication.The errors, although prevalent, were not con-sidered to have a significant subjective or ob-jective impact on daily life.
Three of the four subjects formally assesseddemonstrated abnormalities of the oral phase of
swallowing, and these results suggest that the dis-proportionate tongue bulk reported by 10 of the11 subjects by means of questionnaire frequentlymandates functional adaptations. The inability ofsubject 1 to hold a bolus in the oral cavity with theteeth occluded illustrates the degree of bulk thatremained following a combined anterior and cen-tral tongue reduction; this is also evident in pho-tographs (Fig. 1).
The decision not to use conservatively man-aged patients as a control group in this study was
Fig. 4. Tongue photographs of subject 4.
Table 5. Speech Error: Self-Description and Formal Assessment
Subject Self-DescriptionSpeech
Sound Error Error Type
1 Lisp; tongue always protruding; problems with multiples/s/ or /ch/ sounds
/s//z//ch/
Dental or interdental placement
2 Deliberate speaker; lisp with /f/ for /th/ substitution /r/ /w/ substitution or /r/distortion
Vowel distortion3 No concerns, talkative person None None4 Shy, lazy speaker, mumbler /s/ Dental placement
/z/
Volume 119, Number 3 • Surgical Tongue Reduction
999
based on the premises (1) that these patients hadlesser degrees of macroglossia and thus representa separate cohort and (2) that the aim of surgeryis to confer normal function and appearance.There are currently no published studies or dataavailable on the natural history of mild or mini-mally symptomatic macroglossia in Beckwith–Wiedemann syndrome, but this would help in de-termining whether the deficits or abnormalities
seen in our subjects are attributable to the nat-ural history of the condition or the surgical man-agement.
There has been a shift toward performing cen-tral tongue reductions at our hospital since thepatients in this study underwent surgery (1971 to1985). In addition, the procedure is now almostexclusively performed within the Plastic and Max-illofacial Unit; between 1971 and 1985, 29 percent
Table 6. Intelligibility and Speech Disorder Severity
SubjectWord
Intelligibility (%)Sentence
Intelligibility (%)ReadingSeverity
ConversationSeverity Diadochokinesis
1 100 100 Mild Mild No limitation2 100 100 Mild Mild No limitation3 100 100 None None No limitation4 90 90 Mild Mild No limitation
Table 7. Deglutition Abnormalities
Oral Phase
Subject Swallow Initiation Lip Use
1 Teeth must be open as can’t hold bolus in oral cavitywith closed teeth
No abnormalities detected
Tongue thrust swallow2 Unable to initiate swallow using tongue tip, relies on lip
closure for stabilization necessary to initiate swallowUses lips scraping over top of each
other to clean teeth3 No abnormalities detected No abnormalities detected4 Fluid escapes forward with swallow initiation; difficulty
holding bolus in oral cavity when swallowingRequires lip closure to ensure fluid does
not escape
Fig. 5. Surgical tongue reduction designs.
Plastic and Reconstructive Surgery • March 2007
1000

of procedures were performed by a pediatric gen-eral surgeon. For these reasons, we anticipate thatthe long-term outcomes of patients treated in thepast two decades may differ from those seen in thisstudy. There is little information available aboutthe long-term outcomes of central tongue reduc-tions, and follow-up of patients who underwentsurgery after 1985 will be important in assessingwhether this newer technique results in improvedoutcomes when compared with the subjects re-viewed in this study. At the present time, an in-sufficient number of these younger patients havecompleted mandibular growth, so their assess-ment results cannot be properly compared withthe present cohort.
Most of the tongue reduction operations inour study were performed for failure of oral com-petence, drooling, and tongue protrusion. Theexceptions were subjects 2 and 10, both of whomhad severe macroglossia and underwent two op-erative reductions. Subject 2 underwent initial sur-gery at age 6 months for macroglossia associatedwith swallowing difficulties and failure to thrive,and again at 20.5 months for persistent failure toachieve oral competence. Subject 10 underwentinitial reduction at 3.5 months for failure to thrivethat was attributed to a combination of chronicairway obstruction and swallowing difficulties. Thetongue had noticeably increased in size sincebirth. After a combined central and anteriortongue reduction, the patient failed multiple trialsof extubation because of airway obstruction thatwas attributed to residual posterior tongue bulk.For this reason, a second tongue reduction wasperformed at 5 months of age and the child wassuccessfully extubated 3 days later.
These two patients illustrate the intuitive viewthat severe macroglossia, which tends to present atan earlier age with airway compromise or feedingdifficulties, is a more difficult management prob-lem than lesser degrees of macroglossia, whichtend to present with oral incompetence, drooling,or tongue protrusion. Long-term outcomes oftongue function in these patients are also likely tobe poorer, as a significantly greater proportion ofthe tongue must be resected. Although surgerycan and should be delayed well past the age of 6months in the majority of cases, gross macroglossiamay require earlier tongue reduction, as a suc-cessful reduction may negate the need for a sur-gical airway or prolonged nasogastric feeding.Nevertheless, earlier intervention carries in-creased anesthetic and airway risks,13 and there isalso a risk of significant regrowth of the tonguepostoperatively,21 as insulin-like growth factor 2 is
still circulating in relatively high levels in the neo-natal period. This increases the likelihood thatpatients will require an additional surgical tonguereduction at a later age, and given that early re-duction does not always achieve its aims, it may beadvisable to manage some patients’ airway andfeeding difficulties with surgical tracheostomy andnasogastric feeding to delay tongue reduction un-til a later age. Staged reductions may also improvelong-term outcomes in these patients. Regardless,gross macroglossia in the neonate remains a dif-ficult management problem, even for experi-enced practitioners with a full range of options ofreduction techniques.
To optimize results, surgeons should carefullyassess each patient preoperatively and intraoper-atively to select an operative approach that willappropriately address the issues of bulk andlength. Central tongue reductions are preferredto anterior wedge reductions, although certainlythe latter can have excellent outcomes in selectedcases. Anterior wedge reductions, when performed,should have a narrow base to retain a tapered tipto the tongue.
We do not routinely use elective tracheostomy,particularly when surgery is performed for mildmacroglossia. Perioperatively, we administer sys-temic steroids to reduce the risk of edema andwe monitor all patients in an intensive care unitsetting postoperatively because of the risk of air-way obstruction. Careful monitoring of blood glu-cose levels is required, as patients with Beckwith–Wiedemann syndrome are at risk of hypoglycemiawhen fasting. Incision margins are marked withink, and local infiltration with a vasoconstrictiveagent is used to reduce intraoperative bloodloss. Use of a laser also provides good intraop-erative hemostasis and should be consideredwhen the facilities permit and the clinician isfamiliar with its use. A stay suture is an invalu-able aid in drawing the tongue forward so thatthe posterior tongue can be accessed, and thiscan be left in situ for 24 to 48 hours postoper-atively to assist in airway management in theevent of sudden airway compromise.
CONCLUSIONSPediatric patients with symptomatic macro-
glossia and Beckwith–Wiedemann syndrome whoundergo surgical tongue reduction are unlikely tohave completely normal tongue function and ap-pearance as adults. The most prevalent abnormal-ity is that of continued disproportionate tonguebulk, and many patients report having a shorttongue tip. Specific speech sound errors are very
Volume 119, Number 3 • Surgical Tongue Reduction
1001

common but do not result in significant levels ofself-consciousness about speech or affect day-to-day interactions. It is important that the surgicaltechnique used addresses the global nature of themacroglossia and aims to retain a tapered tonguetip with length sufficient to permit normal tonguemovements.
John G. Meara, F.R.A.C.S., M.B.A.Department of Plastic and Maxillofacial Surgery
Royal Children’s HospitalFlemington Road
Parkville, Victoria 3052, [email protected]
DISCLOSURENone of the authors has a financial interest in any
of the products devices, or drugs mentioned in this article.
REFERENCES1. Beckwith, J. B. Extreme cytomegaly of the adrenal fetal cor-
tex, omphalocele, hyperplasia of the kidneys and pancreas,and Leydig-cell hyperplasia: Another syndrome? Presentedat the Annual Meeting of the Western Society for PaediatricResearch, Los Angeles, Calif., November of 1963.
2. Wiedemann, H. R. Complexe malformatif familial avechernie ombilicale et macroglossie: un “syndrome nouveau”?J. Genet. Hum. 13: 223, 1964.
3. Higurashi, M., Iijima, K., Sugimoto, Y., et al. The birth prev-alence of malformation syndromes in Tokyo infants: Surveyof 14,430 newborn infants. Am. J. Med. Genet. 6: 189, 1980.
4. Elliot, M., and Maher, E. R. Beckwith–Wiedemann syn-drome. J. Med. Genet. 31: 560, 1994.
5. Lodeiro, J. G., Byers, J., III, Chuipek, S., and Feinstein, S. J.Prenatal diagnosis and perinatal management of the Beck-with–Wiedemann syndrome: A case and review. Am. J. Peri-natol. 6: 446, 1989.
6. Engstrom, W., Lindham, S., and Schofield, P. Beckwith–Wiedemann syndrome. Eur. J. Pediatr. 147: 450, 1998.
7. Filippi, G., and McKusick, V. A. The Beckwith–Wiedemann syn-drome (the exomphalos-macroglossia-gigantism syndrome): Re-port of two cases and review of the literature. Medicine 49: 279,1970.
8. Sotelo-Avila, C., Gonzalez-Crussi, F., and Fowler, J. W. Com-plete and incomplete forms of Beckwith–Wiedemann syn-drome: Their oncogenic potential. J. Pediatr. 96: 47, 1980.
9. Aitkin, J., and Fisher, N. T. Articulation Survey. Melbourne,Australia: Royal Children’s Hospital Melbourne, 1996.
10. Enderby, P. The Frenchay Dysarthria Assessment. San Diego,Calif.: College Hill Press, 1983.
11. Rimmell, F. L., Shapiro, A. M., Shoemaker, D. L., and Kenna,M. A. Head and neck manifestations of Beckwith–Wiede-mann syndrome. Otolaryngol. Head Neck Surg. 113: 262, 1995.
12. Menard, R. M., Delaire, J., and Schendel, S. A. Treatment ofthe craniofacial complications of Beckwith–Wiedemann syn-drome. Plast. Reconstr. Surg. 96: 27, 1995.
13. Shafer, A. D. Primary macroglossia. Clin. Paediatr. 7: 357, 1968.14. Schwenzer, N., Voy, E., and Neimczyk, H. Effect of tongue
reduction on the orthodontic and surgical treatment of dys-gnathia. J. Maxillofac. Surg. 5: 15, 1977.
15. Maisel, D. O. Spontaneous regression of anterior open bitefollowing treatment of macroglossia. Br. J. Plast. Surg. 32: 309,1979.
16. Siddiqui, A., and Pensler, J. M. The efficacy of tongue re-section in treatment of symptomatic macroglossia in thechild. Ann. Plast. Surg. 25: 14, 1990.
17. Sokolski, P. M., Ogle, R. G., and Waite, D. E. Surgical cor-rection of macroglossia in Beckwith–Wiedemann syndrome.J. Oral Surg. 36: 212, 1978.
18. Mixter, R. C., Ewanowski, S. J., and Carson, L. V. Centraltongue reduction for macroglossia. Plast. Reconstr. Surg. 91:1159, 1993.
19. Kacker, A., Honrado, C., Martin, D., and Ward, R. Tonguereduction in Beckwith–Wiedemann syndrome. Int. J. Pediatr.Otorhinolaryngol. 53: 1, 2000.
20. Elliott, M., Bayly, R., Cole, T., Temple, I. K., and Maher, E.R. Clinical features and natural history of Beckwith–Wiede-mann syndrome: Presentation of 74 new cases. Clin. Genet. 46:168, 1994.
21. Kopriva, D., and Classen, D. A. Regrowth of tongue followingreduction glossoplasty in the neonatal period for Beckwith–Wiedemann macroglossia. J. Otolaryngol. 27: 232, 1998.
Plastic and Reconstructive Surgery • March 2007
1002