interactive session: equine ecg reading - vetfest
TRANSCRIPT

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Colin C. Schwarzwald, Prof. Dr. med. vet., PhD, Dipl. ACVIM & ECEIM Katharyn J. Mitchell, BVSc, DVCS, DVM, PhD, Dipl. ACVIM (LAIM)
Equine Hospital, Vetsuisse Faculty, University of Zurich Winterthurerstrasse 260, 8057 Zurich, ZH, Switzerland
INTRODUCTION Cardiac arrhythmias are common in horses. They can be observed at rest, during and after exercise, and under general anesthesia. Cardiac rate and rhythm disturbances can often be heard on auscultation, either isolated or in association with heart murmurs (most commonly caused by mitral or aortic regurgitation), but a definitive diagnosis of any arrhythmia or investigation of unexplained tachycardia or bradycardia is made by surface electrocardiography (ECG), telemetric ECG (during exercise), or 24-hour Holter ECG (for detection of paroxysmal or infrequent arrhythmias). The goals of the examination are to detect – and differentiate from each other – the most common physiologic and pathologic arrhythmias, assess their clinical relevance, determine their potential causes, and – if necessary – choose the appropriate management and treatment.
ANATOMICAL AND PHYSIOLOGICAL BASIS OF CARDIAC EXCITATION Impulse-forming and conduction system The specialized cardiac tissues forming the impulse-forming and conduction system consist of the sinoatrial node, internodal pathways, atrioventricular node, bundle of His, bundle branches, fascicles, and Purkinje system. The sinoatrial (SA) node represents the physiologic pacemaker. In the adult horse, it consists of a relatively large crescent-shaped structure located subepicardially, in the region of the terminal sulcus at the junction of the cranial vena cava and right atrium. The atrioventricular (AV) node is situated in the atrial septum, close to the orifice of the coronary sinus and at or slightly above the level of the septal tricuspid leaflet. The His-Purkinje system extends from the AV node to the ventricular septum and ventricular myocardium. Cardiac myocytes form a functional syncytium, which is excitable and able to conduct electrical impulses in response to stimulation by a natural or artificial pacemaker. Some specialized regions within the heart are capable of spontaneous depolarization and impulse formation independent of extrinsic stimulation or neural input. The sinoatrial node is the physiologic pacemaker of the heart, while the atrioventricular node and the Purkinje fibers can act as subsidiary (slower) pacemakers if the SA nodal activity becomes disturbed (e.g., sinus arrest) or impulse conduction to the lower areas of the heart becomes disrupted (e.g., 3rd degree AVB). The processes responsible for generation of electrical activity in the heart are caused by ion fluxes across the cell membrane. The local electrical activity in specific areas of the heart can be examined by intracardiac electrograms, while the sum of the electrical activity of all myocardial cells can be recorded non-invasively by a surface electrocardiogram (ECG). Cardiac activation The myocardial cells form a functional syncytium that allows the electrical impulse to spread through the heart. Intercellular connections, so called gap junctions (connexons), allow ionic currents to pass from cell to cell, so that depolarized cells act to stimulate and depolarize adjacent cells. Impulse conduction depends on active (action potential, ion currents) and passive properties (resistance, capacitance) of the conducting tissue, all of which can be modulated by physiologic regulatory systems or by pathologic processes.
324
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
The cardiac pacemaker, the SA node, is located at the junction of the cranial vena cava and right auricle; therefore, initial cardiac muscle depolarization develops across the right atrium. Activation waves spread through the atrial myocardial cells to the left atrium and towards the AV node. Specialized atrial muscle cells comprising internodal pathways and Bachman’s bundle facilitate transmission across the atria. The conduction across the AV nodal cells, between the low right atrium and Bundle of His, is very slow and subject to physiologic blockade resulting from vagal efferent activity. Conduction delay in the AV node allows for a coordinated, sequential atrio-ventricular pump function. Impulse conduction then proceeds at a greater velocity through the His bundle, the bundle branches, and the Purkinje system, which penetrates quite completely through the ventricular myocardium and ensures a coordinated ventricular activation path. The terms interventricular, intraventricular, and atrioventricular synchronization refer to the normal process of atrial and ventricular activation and contraction. Normal impulse conduction causes sequential contraction and relaxation of the atria and synchronized activation of the ventricles, assuring efficient cardiac pump function. Cardiac arrhythmias, especially those causing atrio-ventricular dissociation or abnormal ventricular activation, can cause dyssynergy with a resultant decrease in stroke volume. ELECTROPHYSIOLOGIC MECHANISMS OF COMMON ARRHYTHMIAS Three basic arrhythmogenic mechanisms are common to both atrial and ventricular arrhythmias: (1) Increased automaticity, (2) triggered activity due to afterdepolarizations, and (3) reentry circuits. Increased automaticity is caused by enhanced normal automaticity in the SA node or in subsidiary pacemakers or due to abnormal automaticity in pathologically altered conductive or myocardial tissue (e.g., due to ischemia). Sympathetic stimulation increases automaticity. Examples for increased automaticity are certain atrial and ventricular ectopic rhythms and accelerated idioventricular rhythms. Triggered activity is the result of afterdepolarizations that occur in association with a preceding impulse or series of impulses. Triggered activity is commonly characterized by a fixed coupling interval between the triggering beat and the triggered beat. Early afterdepolarizations (EADs) develop during the repolarization phase of the action potential and often arise at slow heart rates or after long pauses in the presence of interventions or conditions that prolong the action potential duration and the QT interval. EADs can induce ventricular arrhythmias such as torsades de pointes. Delayed afterdepolarizations (DADs) occur after complete repolarization. DADs are caused by intracellular calcium overload. Congestive heart failure may predispose to triggered activity. Arrhythmias most likely attributed to DADs include digoxin-induced arrhythmias (typically ventricular bigeminy) and certain catecholamine-dependent atrial and ventricular tachycardias. Reentrant excitation resulting from circus movement of electrical impulses is considered the most important arrhythmogenic mechanism. Reentry requires an adequate structural and/or functional substrate. Certain normal (e.g., AV node) or abnormal (e.g., accessory pathways) conductive pathways can serve as part of a reentrant circuit. A decrease in conduction velocity (e.g., in partially depolarized ischemic tissue), a shortening of the action potential duration and refractory period (e.g., high vagal tone), and an increase in myocardial mass (e.g., atrial enlargement due to mitral regurgitation) can predispose to reentrant arrhythmia. Furthermore, myocardial damage, ion channel abnormalities, or alterations in distribution and function of gap junctions (connexins) may increase the risk of reentry arrhythmias. Reentry is responsible for some forms of supraventricular and ventricular tachyarrhythmia, including AV nodal dependent supraventricular tachycardia, atrial flutter, some forms of ventricular tachycardia, and ventricular flutter/fibrillation. It is also considered the most important mechanism in the later phases of established atrial fibrillation (while ectopic activity and afterdepolarizations may be important triggers for the initiation and early persistence of AF).
325
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
ELECTROCARDIOGRAPHY The electrocardiogram is a tracing of the average electric potential generated by the heart muscle recorded throughout the different phases of the cardiac cycle and graphed in terms of voltage and time. Time is displayed along the x axis, and electrical potential is inscribed on the y axis of the ECG paper. Principles of recording and interpreting the ECG in the horse are similar to those for humans, dogs, and other species. The lead systems employed are identical, although some modified leads have been found to be useful in monitoring the cardiac rhythm of the horse. It is recommended that a consistent lead system (e.g., base-apex lead), paper speed (e.g., 25 mm/sec), and voltage calibration (e.g., 1 cm/mV) is used for routine ECGs in order to facilitate rapid recognition of normal and abnormal electrocardiographic patterns. Paper speed, voltage calibration, and (in selected cases) leads may then be adjusted as necessary to optimize the quality and diagnostic value of the recording. Indications for recording an ECG The indications for recording an ECG include:
• Arrhythmia heard on physical examination • Unexplained tachyarrhythmias or bradyarrhythmias • Poor performance or exercise intolerance • Evidence of moderate to severe structural heart disease potentially predisposing to
development of arrhythmias • Pre-purchase examination to confirm normal sinus rhythm or 2nd degree AV block • History of weakness or collapse • Monitoring heart rhythm as part of therapy (e.g. anti-arrhythmic therapy) • Monitoring heart rate to detect stress or pain (e.g. during hospital stay or transport)
Equipment ECG recorders With the large variety of medical technology available today, recording an ECG in a horse at rest, over prolonged periods of time, or during exercise is becoming more accessible to equine practitioners. Recordings can be obtained in field settings with handheld or easily attached ECG recording devices that can transmit digitalized data wirelessly and allow rapid sharing of data between colleagues for further analysis or second opinion. Short duration recordings can be easily obtained using hand held ECG recording devices (e.g. Alivecor Kardia Mobile ECG, Alivecor Inc), any variety of common monitoring devices used for anesthesia, or purpose-built ECG recorders (e.g. Televet 100, telemetric ECG system, Engel Engineering Service GmbH). Many of these devices display the ECG tracing on a monitor, smart phone, or tablet computer. It is mandatory for every device to contain some type of storage capability. Preferably, the device should store the data digitally, allowing the ECG to be post-processed, digitally analyzed, interpreted, or sent to an expert for analysis at a later time. Longer continuous recordings (e.g. longer than 5 min) require the use of an ambulatory device, which preferably records both locally (e.g. on an SD card) and remotely by sending the signal wirelessly to a storage device with display monitor. The most commonly used veterinary device for this purpose is the Televet recorder, while many human or small animal devices can be adapted for equine use. It is particularly important that the data from long-term ambulatory recordings be digitalized, stored, and available for further offline processing and analysis. This also allows the easy sharing of ECG recordings between individuals, which can be useful when a second opinion is required. Several products are currently being developed to improve the ease of ECG recording in horses, particularly during exercise. However, at this time, the Televet recorder is most commonly used and in the authors opinion, it remains the most reliable and easy to use product. It is important to note that the (veterinary) medical technology market has several heart rate monitors currently available, but these should not be confused with an ECG recording device. The heart rate monitors are supposed to detect RR intervals, but an
326

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
unknown amount of post processing occurs with the use of proprietary signal processing algorithms and filters to remove motion artefacts and arrhythmias. Accuracy and reliability of these devices cannot be easily verified by the user and some of them certainly do not provide accurate results in horses with arrhythmias or with exceptionally high heart rates during exercise. These devices provide no information on P-QRS-T morphology and should not be considered a substitute for an ECG recorder in the diagnosis and management of equine arrhythmias. They can however be useful (acknowledging their limitations), particularly for monitoring heart rates during exercise at home with the owner. Electrodes Short-term recordings can be obtained using crocodile clips attached on the ends of the ECG cables. However, this is not suitable to obtain longer-term recordings and some horses will not tolerate these being applied even for a short duration of time. Frequently, the application of water, normal saline, or alcohol to the skin/crocodile clips is required to ensure adequate contact and a good quality ECG recording. Self-adhesive gel patch electrodes provide a more comfortable alternative to crocodile clips and frequently remain in place for several hours of recording without issue. For longer duration (overnight) or exercising recordings, the sticky ECG electrodes can be further secured using self-adhesive foam patches or an elastic bandage applied on top. In most cases, it is not necessary to clip the coat, as long as the gel patch remains moist and the self-adhesive part of the electrode stays dry and provides sufficient adhesive strength. Occasionally, with a thick winter coat, it is necessary to clip the coat to provide better contact with the skin surface. It is essential for the coat to be dry (e.g. before exercise) when the sticky electrodes are applied, as they will not stick to a damp or wet surface.
Additional material For ambulatory recordings, it is necessary to affix the recording/transmitting device to the horse. This can be achieved by a reusable surcingle, purpose built for holding the device and the associated cables safely out of the way of damage, particularly if the horse lies down (e.g. Kruuse Televet Electrode support, Jørgen Kruuse A/S). Alternatively, the device can be affixed using single use, sticky elastic bandages. It is important that there is appropriate padding over the wither’s region, particularly if the device is to be worn overnight or for several days.
Lead placement Figure 1 shows the typical lead placement for a short duration, resting ECG recording. This is considered a ‘base-apex’ configuration, where either ‘Lead I’ (RALA) or ‘Lead II’ (RALL) can be chosen on the monitor to display the ECG trace. Figure 2 represents the typical P-QRS-T orientation when using this lead placement. Figure 3 displays the ‘modified base-apex’ configuration that the author typically uses for long-term ambulatory ECG recordings. With this configuration, ‘Lead I’ will highlight the atrial electrical activity, producing slightly magnified P waves to aid in the differentiation of atrial ectopic complexes. ‘Lead II’ will produce the typical ECG seen in Figure 2. ‘Lead III’ (LALL) will produce an alternative QRS configuration, which can aid in the detection of ventricular ectopic complexes. During exercise, the ECG electrodes can remain in the same position as described above (Figure 3) or can be moved to accommodate any equipment necessary (e.g. saddle, surcingle or harness, Figure 4). Figure 4C is a variation used particularly for lunging, treadmill, or ridden exercise. The downside of this lead configuration is that ‘Lead I’ and ‘Lead II‘ are very similar, which can make subtle changes in QRS configuration harder to identify but provides a ‘backup’ lead in case one electrode becomes dislodged during exercise.
327

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Optimization of recording quality Good quality ECG recordings are essential regardless of whether the ECG is recorded for 2 minutes, 24 hours, or during exercise. Careful attention to the placement of electrodes, ensuring adequate contact with the skin surface to optimally conduct the electrical signal, is critical. The use of additional adhesive material on top of the sticky electrode/lead unit can improve the robustness of the contact, particularly for longer duration recordings or situations where electrode contact may be disrupted (e.g. sweating during exercise). Frequent monitoring of the ECG recording quality is also important, so that any problems (e.g. electrodes coming off, batteries exhausted) can be identified and rapidly rectified without interfering with the diagnostic recording duration. If the ECG quality is suboptimal, then steps should be taken to problem solve the issue, checking the placement and contact of the electrodes (and replacing them where necessary), the placement of the surcingle and device, and the connection between the leads and recording device.
Figure 1. Positioning of the ECG electrodes to obtain a standard base-apex lead from a resting horse, useful to obtain short-term ECG recordings. The right arm electrode (RA) is placed on the right neck of the horse, while the left arm (LA) and left leg (LL) electrodes are placed on the left side of the horse over the apex of the heart. With this electrode configuration, both ‘Lead I’ (RALA) or ‘Lead II’ (RALL) can be chosen on the ECG recorder to display the base-apex ECG trace. RA, right arm electrode; LA, left arm electrode; LL, left leg (foot) electrode.
Figure 2. Typical base-apex ECG configuration. P, P wave; QRS, QRS complex and QRS duration; T, T wave; RR, RR interval; PQ, PQ interval; QT, QT interval.
Figure 3. Positioning of the ECG electrodes to obtain a modified base-apex recording from a resting horse. This configuration is useful, particularly for telemetric ECG monitoring or long-term (ambulatory, Holter) ECG recordings. RA, right arm electrode; LA, left arm electrode; LL, left leg (foot) electrode; N, neutral/ground electrode. In this example, the electrodes are colored for use with the Televet 100 recording system. Please note that the color system corresponds to the International Electrotechnical Commison (IEC) standard. Other devices might use a different color system (i.e. the one defined by the American Heart Association, where RA is white, LA is black, N is green, and LL is red).
328
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
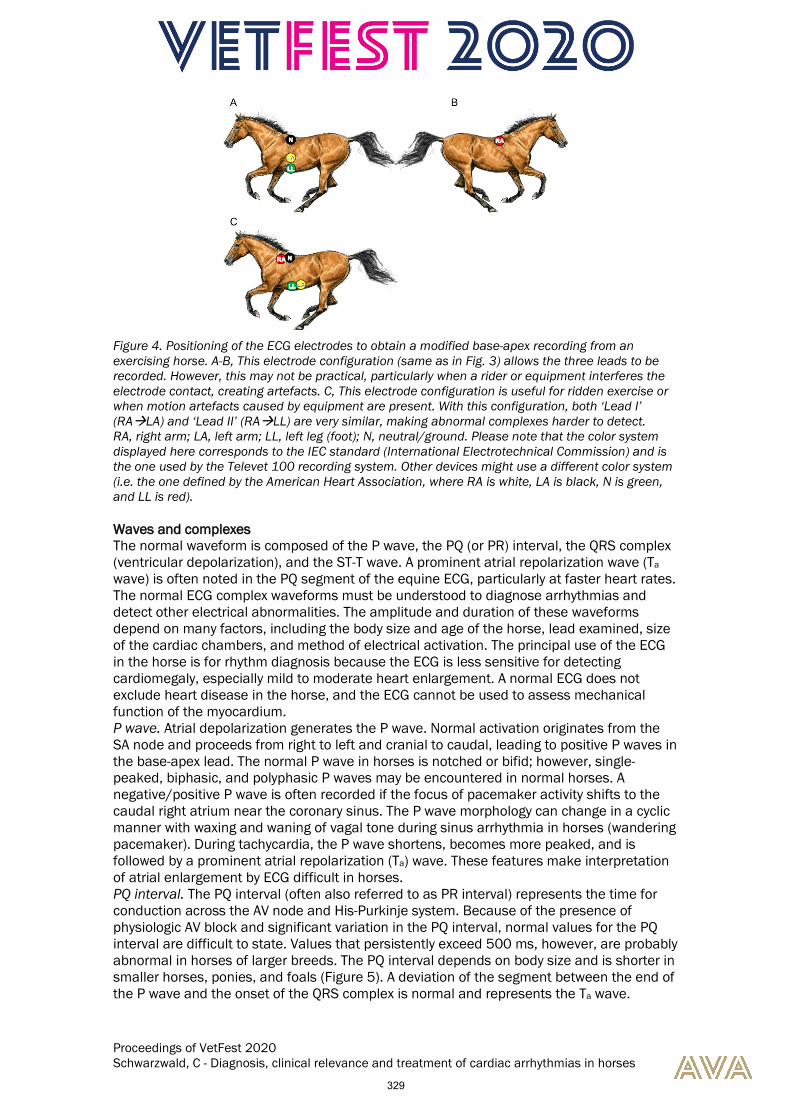
Figure 4. Positioning of the ECG electrodes to obtain a modified base-apex recording from an exercising horse. A-B, This electrode configuration (same as in Fig. 3) allows the three leads to be recorded. However, this may not be practical, particularly when a rider or equipment interferes the electrode contact, creating artefacts. C, This electrode configuration is useful for ridden exercise or when motion artefacts caused by equipment are present. With this configuration, both ‘Lead I’ (RALA) and ‘Lead II’ (RALL) are very similar, making abnormal complexes harder to detect. RA, right arm; LA, left arm; LL, left leg (foot); N, neutral/ground. Please note that the color system displayed here corresponds to the IEC standard (International Electrotechnical Commission) and is the one used by the Televet 100 recording system. Other devices might use a different color system (i.e. the one defined by the American Heart Association, where RA is white, LA is black, N is green, and LL is red).
Waves and complexes The normal waveform is composed of the P wave, the PQ (or PR) interval, the QRS complex (ventricular depolarization), and the ST-T wave. A prominent atrial repolarization wave (Ta wave) is often noted in the PQ segment of the equine ECG, particularly at faster heart rates. The normal ECG complex waveforms must be understood to diagnose arrhythmias and detect other electrical abnormalities. The amplitude and duration of these waveforms depend on many factors, including the body size and age of the horse, lead examined, size of the cardiac chambers, and method of electrical activation. The principal use of the ECG in the horse is for rhythm diagnosis because the ECG is less sensitive for detecting cardiomegaly, especially mild to moderate heart enlargement. A normal ECG does not exclude heart disease in the horse, and the ECG cannot be used to assess mechanical function of the myocardium. P wave. Atrial depolarization generates the P wave. Normal activation originates from the SA node and proceeds from right to left and cranial to caudal, leading to positive P waves in the base-apex lead. The normal P wave in horses is notched or bifid; however, single-peaked, biphasic, and polyphasic P waves may be encountered in normal horses. A negative/positive P wave is often recorded if the focus of pacemaker activity shifts to the caudal right atrium near the coronary sinus. The P wave morphology can change in a cyclic manner with waxing and waning of vagal tone during sinus arrhythmia in horses (wandering pacemaker). During tachycardia, the P wave shortens, becomes more peaked, and is followed by a prominent atrial repolarization (Ta) wave. These features make interpretation of atrial enlargement by ECG difficult in horses. PQ interval. The PQ interval (often also referred to as PR interval) represents the time for conduction across the AV node and His-Purkinje system. Because of the presence of physiologic AV block and significant variation in the PQ interval, normal values for the PQ interval are difficult to state. Values that persistently exceed 500 ms, however, are probably abnormal in horses of larger breeds. The PQ interval depends on body size and is shorter in smaller horses, ponies, and foals (Figure 5). A deviation of the segment between the end of the P wave and the onset of the QRS complex is normal and represents the Ta wave.
329
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Variation in the PQ interval often is unrelated to changes in ventilation but is often related to changes in blood pressure, heart rate, and autonomic tone. QRS complex. The QRS complex is variable in the horse. Because of complete penetration of the conduction system into the free walls of the ventricle, the ventricles are activated simultaneously with a burst of depolarization so that much of the divergent electromotive forces are cancelled. The commonly used base-apex monitor lead normally exhibits a prominent negative S wave (Figure 2). Axis deviations can be observed with cardiomegaly, cor pulmonale, conduction disturbances, and electrolyte imbalances. The conformation and axis of the QRS complex allows assessment of ventricular activation from ventricular ectopic foci. The duration of the QRS complex is determined by the propagation velocity of the impulse in the ventricular myocardium. Ectopic impulse formation, aberrant impulse conduction, partial membrane depolarization in diseased tissue, hyperkalemia, and drug-induced Na+ channel blockade (e.g., quinidine) can result in slowing of impulse conduction and widening of the QRS complex. However, the normal slur in the ST segment makes exact measurement of QRS duration difficult in most horses. ST-T wave. Repolarization of the ventricles begins at the end of the QRS complex (the J point) and extends to the end of the T wave. The T wave is often biphasic (positive-negative or negative-positive) in resting horses and its morphology may vary dramatically with changes in heart rate and autonomic tone. Although some authors have suggested that abnormalities of the ST-T indicate cardiac dysfunction, marked deviation of the ST segment and increased amplitude of the T wave are expected even in normal horses after exercise or excitement-induced tachycardia. However, progressive J point or ST deviation may also indicate myocardial ischemia. Enlargement of the T wave may develop with myocardial hypoxia or hyperkalemia. QT interval. The QT interval represents the total electrical activation-repolarization time, which is determined by the cellular action potential duration (APD) and the dispersion of the APD throughout the ventricular myocardium. The upper limits for the QT interval at resting heart rates are approximately 600 ms in adult horses (Figure 5) and 350–400 ms in foals. However, the QT interval shortens at higher heart rates and strongly depends on changes in autonomic tone. A variety of population-based or individual-based methods have been used in other species to correct for heart rate-related changes. Although some data are available for horses, correction formulas cannot be uniformly used for different populations or easily applied to individual horses. The diagnosis of QT prolongation in horses is further complicated by the commonly encountered difficulties to accurately detect the end of the T wave. Prolongation of the QT interval indicates delayed ventricular repolarization. Congenital (due to ion channel mutations) or acquired (due to drug effects on repolarizing currents) long QT syndrome (LQTS) associated with life-threatening cardiac arrhythmias and sudden death has not been well documented in horses. However, repolarizing currents in horses are similar to those in other species, and it has been suggested that horses may be at risk for acquired LQTS. Many drugs that potentially prolong cardiac repolarization in other species have also been used in horses, including quinidine, procainamide, flecainide, amiodarone, cisapride, metoclopramide, erythromycin, clarithromycin, fluconazole, trimethoprim-sulfamethoxazole, sevoflurane, and isoflurane. Quinidine-induced torsades de pointes, potentially related to drug-induced QT prolongation, have been reported in horses. The slow resting heart rate and the hypokalemia commonly associated with gastrointestinal disease in horses theoretically enhance the risk of drug-induced arrhythmias. It therefore seems advisable to consider potential proarrhythmic effects when QT-prolonging drugs are administered to horses at risk.
330
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Systematic evaluation of the electrocardiogram A systematic approach to ECG analysis should be undertaken and quantitative measures should be compared with normal values.
(1) Technical aspects: Paper speed (Standard: 25 or 50 mm/s), Calibration (Standard: 1 cm/mv), Lead (Standard: Base-Apex lead, with [+] electrode over the left apex (left chest, level of olecranon) and [–] electrode over the right jugular furrow; Alternatives: Einthoven I, II, III; Goldberger aVR, aVL, aVF; unipolar chest lead V10) (2) Artifacts: Electrical, motion, twitching, muscle tremor, equipment (3) Heart rate: Atrial and ventricular rate (e.g., count P waves and QRS-T complexes over 10 sec and multiply by 6) (4) Cardiac rhythm: Regular, regularly irregular, irregularly irregular Premature beats or pauses Atrial conduction, AV conduction sequence, ventricular conduction Site of abnormal impulse formation, myocardial fibrillation, or conduction Rate of abnormal impulse formation Conduction of abnormal impulses Coupling intervals, patterns, and repeating cycles (5) Waves / Complexes: P wave, PQ interval, QRS complex, ST segment, T wave, QT interval QRS morphology Association of P waves and QRS-T complexes (“for each P a QRS-T, for each QRS-T a P?”) (6) Miscellaneous: Electrical alternans, synchronous diaphragmatic contraction
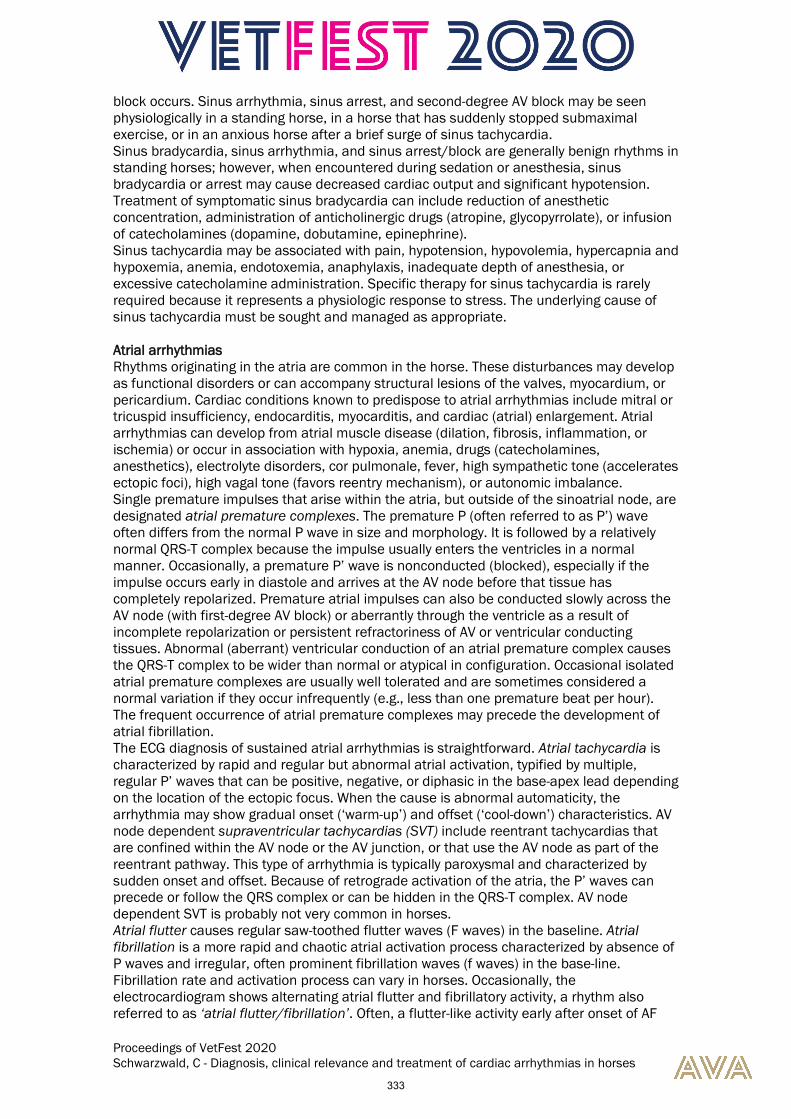
Normal heart rates and ECG time intervals for horses at rest
Breed HR (/min) PQ (ms) QRS (ms)* QT (ms) Adults Large breeds 26 – 50 200 – 500 80 – 140 360 – 600 Small breeds, Ponies 30 – 54 160 – 320 60 – 120 320 – 560 Large breed foals 1 – 7 d 14 d
100 – 140 80 – 130
100 – 180 100 – 190
50 – 80 60 – 80
200 – 350 230 – 350
Pony foals 1 – 30 d 60 d 90 d
70 – 145 60 – 95 50 – 85
90 – 130 110 – 150 130 – 170
25 – 70 30 – 70 50 – 80
180 – 370 220 – 420 310 – 390
* QRS duration is often difficult to determine due to the normal slur in the ST segment.
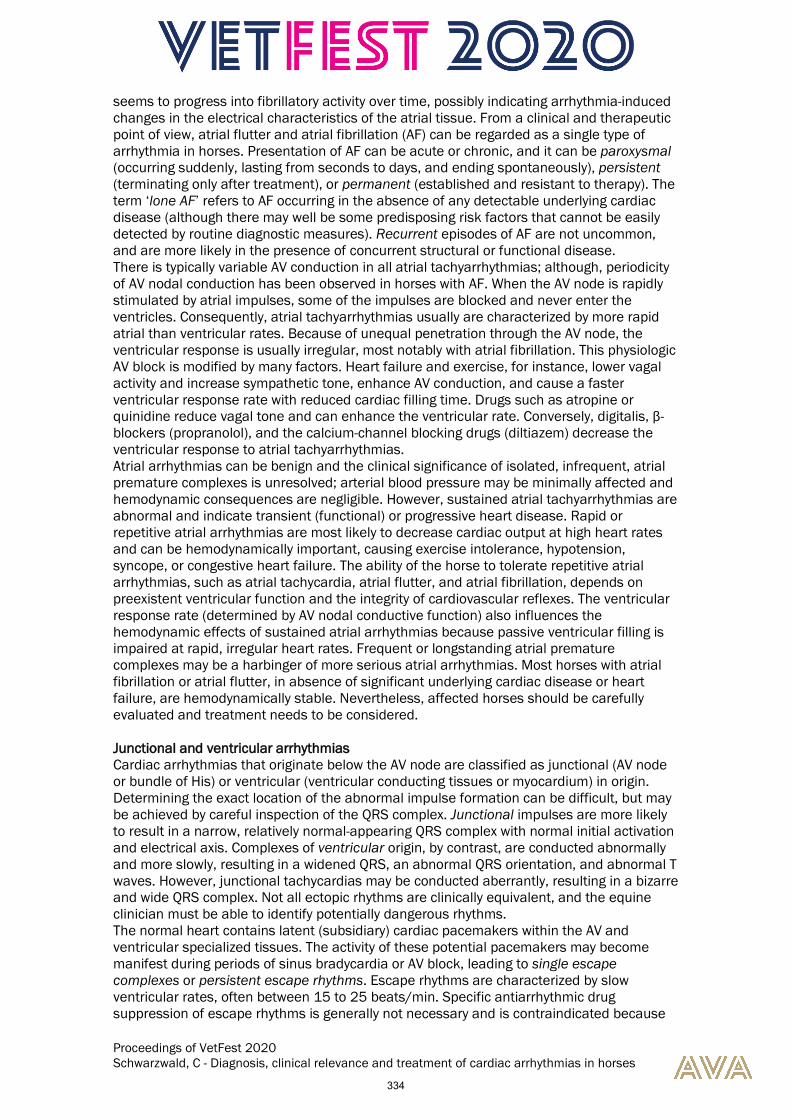
Figure 5: Scatter plots including the regression line and the 95% prediction band showing normal ranges for heart rate (HR), PQ interval, QRS duration and QT interval for different body size. The normal values for all time intervals for a specific BWT can be estimated based on the prediction band.
331

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
COMMON CARDIAC ARRHYTHMIAS
Cardiac arrhythmias are caused by disturbances in heart rate, rhythm, or conduction. Cardiac arrhythmias can be classified based on atrial and ventricular rate, anatomic origin of the impulse, method of impulse formation, and conduction sequence. A wide variety of cardiac arrhythmias have been recognized in horses, some of which are physiologic, and others that are potentially dangerous. Pathologic arrhythmias often develop in association with high sympathetic tone, fever, endotoxemia, sepsis, hypotension, electrolyte disorders, acidosis, hypoxemia, gastrointestinal disease, or severe pulmonary disease, and following administration of proarrhythmic drugs (e.g., digoxin, quinidine) or agents known to sensitize the heart to catecholamines (e.g., thiobarbiturates, halothane). Primary heart disease should be suspected if these secondary causes of arrhythmias can be ruled out. Of principal concern to the equine clinician are the hemodynamic consequences of arrhythmias (blood pressure, cardiac output, peripheral perfusion) and the potential for further electrical destabilization (malignant arrhythmias, myocardial fibrillation). Figure 6 provides a systematic overview of the most common cardiac arrhythmias in horses.
Figure 6. Systematic overview of the most common cardiac arrhythmias in horses. For ECG examples of the most common arrhythmias the reader is referred to the references listed below. The rhythms marked with * are considered physiologic. Sinus rhythms A number of physiologic sinus rhythms can be recognized in the horse. These can be explained by the impact of the autonomic nervous system on the sinoatrial node. Normal horses at rest demonstrate vagally mediated sinus bradycardia, sinus arrhythmia, or sinus block / sinus arrest (pause). Fear or sudden stimuli may provoke rapid withdrawal of vagal tone and sympathetic activation, resulting in sinus tachycardia. Atrioventricular conduction, generally, tends to follow sinus activity: during sinus tachycardia AV nodal conduction is facilitated and the PQ interval shortens, while during periods of progressive sinoatrial slowing AV nodal conduction is inhibited, the PQ interval prolongs, and second-degree AV
332
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
block occurs. Sinus arrhythmia, sinus arrest, and second-degree AV block may be seen physiologically in a standing horse, in a horse that has suddenly stopped submaximal exercise, or in an anxious horse after a brief surge of sinus tachycardia. Sinus bradycardia, sinus arrhythmia, and sinus arrest/block are generally benign rhythms in standing horses; however, when encountered during sedation or anesthesia, sinus bradycardia or arrest may cause decreased cardiac output and significant hypotension. Treatment of symptomatic sinus bradycardia can include reduction of anesthetic concentration, administration of anticholinergic drugs (atropine, glycopyrrolate), or infusion of catecholamines (dopamine, dobutamine, epinephrine). Sinus tachycardia may be associated with pain, hypotension, hypovolemia, hypercapnia and hypoxemia, anemia, endotoxemia, anaphylaxis, inadequate depth of anesthesia, or excessive catecholamine administration. Specific therapy for sinus tachycardia is rarely required because it represents a physiologic response to stress. The underlying cause of sinus tachycardia must be sought and managed as appropriate. Atrial arrhythmias Rhythms originating in the atria are common in the horse. These disturbances may develop as functional disorders or can accompany structural lesions of the valves, myocardium, or pericardium. Cardiac conditions known to predispose to atrial arrhythmias include mitral or tricuspid insufficiency, endocarditis, myocarditis, and cardiac (atrial) enlargement. Atrial arrhythmias can develop from atrial muscle disease (dilation, fibrosis, inflammation, or ischemia) or occur in association with hypoxia, anemia, drugs (catecholamines, anesthetics), electrolyte disorders, cor pulmonale, fever, high sympathetic tone (accelerates ectopic foci), high vagal tone (favors reentry mechanism), or autonomic imbalance. Single premature impulses that arise within the atria, but outside of the sinoatrial node, are designated atrial premature complexes. The premature P (often referred to as P’) wave often differs from the normal P wave in size and morphology. It is followed by a relatively normal QRS-T complex because the impulse usually enters the ventricles in a normal manner. Occasionally, a premature P’ wave is nonconducted (blocked), especially if the impulse occurs early in diastole and arrives at the AV node before that tissue has completely repolarized. Premature atrial impulses can also be conducted slowly across the AV node (with first-degree AV block) or aberrantly through the ventricle as a result of incomplete repolarization or persistent refractoriness of AV or ventricular conducting tissues. Abnormal (aberrant) ventricular conduction of an atrial premature complex causes the QRS-T complex to be wider than normal or atypical in configuration. Occasional isolated atrial premature complexes are usually well tolerated and are sometimes considered a normal variation if they occur infrequently (e.g., less than one premature beat per hour). The frequent occurrence of atrial premature complexes may precede the development of atrial fibrillation. The ECG diagnosis of sustained atrial arrhythmias is straightforward. Atrial tachycardia is characterized by rapid and regular but abnormal atrial activation, typified by multiple, regular P’ waves that can be positive, negative, or diphasic in the base-apex lead depending on the location of the ectopic focus. When the cause is abnormal automaticity, the arrhythmia may show gradual onset (‘warm-up’) and offset (‘cool-down’) characteristics. AV node dependent supraventricular tachycardias (SVT) include reentrant tachycardias that are confined within the AV node or the AV junction, or that use the AV node as part of the reentrant pathway. This type of arrhythmia is typically paroxysmal and characterized by sudden onset and offset. Because of retrograde activation of the atria, the P’ waves can precede or follow the QRS complex or can be hidden in the QRS-T complex. AV node dependent SVT is probably not very common in horses. Atrial flutter causes regular saw-toothed flutter waves (F waves) in the baseline. Atrial fibrillation is a more rapid and chaotic atrial activation process characterized by absence of P waves and irregular, often prominent fibrillation waves (f waves) in the base-line. Fibrillation rate and activation process can vary in horses. Occasionally, the electrocardiogram shows alternating atrial flutter and fibrillatory activity, a rhythm also referred to as ‘atrial flutter/fibrillation’. Often, a flutter-like activity early after onset of AF
333
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
seems to progress into fibrillatory activity over time, possibly indicating arrhythmia-induced changes in the electrical characteristics of the atrial tissue. From a clinical and therapeutic point of view, atrial flutter and atrial fibrillation (AF) can be regarded as a single type of arrhythmia in horses. Presentation of AF can be acute or chronic, and it can be paroxysmal (occurring suddenly, lasting from seconds to days, and ending spontaneously), persistent (terminating only after treatment), or permanent (established and resistant to therapy). The term ‘lone AF’ refers to AF occurring in the absence of any detectable underlying cardiac disease (although there may well be some predisposing risk factors that cannot be easily detected by routine diagnostic measures). Recurrent episodes of AF are not uncommon, and are more likely in the presence of concurrent structural or functional disease. There is typically variable AV conduction in all atrial tachyarrhythmias; although, periodicity of AV nodal conduction has been observed in horses with AF. When the AV node is rapidly stimulated by atrial impulses, some of the impulses are blocked and never enter the ventricles. Consequently, atrial tachyarrhythmias usually are characterized by more rapid atrial than ventricular rates. Because of unequal penetration through the AV node, the ventricular response is usually irregular, most notably with atrial fibrillation. This physiologic AV block is modified by many factors. Heart failure and exercise, for instance, lower vagal activity and increase sympathetic tone, enhance AV conduction, and cause a faster ventricular response rate with reduced cardiac filling time. Drugs such as atropine or quinidine reduce vagal tone and can enhance the ventricular rate. Conversely, digitalis, β-blockers (propranolol), and the calcium-channel blocking drugs (diltiazem) decrease the ventricular response to atrial tachyarrhythmias. Atrial arrhythmias can be benign and the clinical significance of isolated, infrequent, atrial premature complexes is unresolved; arterial blood pressure may be minimally affected and hemodynamic consequences are negligible. However, sustained atrial tachyarrhythmias are abnormal and indicate transient (functional) or progressive heart disease. Rapid or repetitive atrial arrhythmias are most likely to decrease cardiac output at high heart rates and can be hemodynamically important, causing exercise intolerance, hypotension, syncope, or congestive heart failure. The ability of the horse to tolerate repetitive atrial arrhythmias, such as atrial tachycardia, atrial flutter, and atrial fibrillation, depends on preexistent ventricular function and the integrity of cardiovascular reflexes. The ventricular response rate (determined by AV nodal conductive function) also influences the hemodynamic effects of sustained atrial arrhythmias because passive ventricular filling is impaired at rapid, irregular heart rates. Frequent or longstanding atrial premature complexes may be a harbinger of more serious atrial arrhythmias. Most horses with atrial fibrillation or atrial flutter, in absence of significant underlying cardiac disease or heart failure, are hemodynamically stable. Nevertheless, affected horses should be carefully evaluated and treatment needs to be considered. Junctional and ventricular arrhythmias Cardiac arrhythmias that originate below the AV node are classified as junctional (AV node or bundle of His) or ventricular (ventricular conducting tissues or myocardium) in origin. Determining the exact location of the abnormal impulse formation can be difficult, but may be achieved by careful inspection of the QRS complex. Junctional impulses are more likely to result in a narrow, relatively normal-appearing QRS complex with normal initial activation and electrical axis. Complexes of ventricular origin, by contrast, are conducted abnormally and more slowly, resulting in a widened QRS, an abnormal QRS orientation, and abnormal T waves. However, junctional tachycardias may be conducted aberrantly, resulting in a bizarre and wide QRS complex. Not all ectopic rhythms are clinically equivalent, and the equine clinician must be able to identify potentially dangerous rhythms. The normal heart contains latent (subsidiary) cardiac pacemakers within the AV and ventricular specialized tissues. The activity of these potential pacemakers may become manifest during periods of sinus bradycardia or AV block, leading to single escape complexes or persistent escape rhythms. Escape rhythms are characterized by slow ventricular rates, often between 15 to 25 beats/min. Specific antiarrhythmic drug suppression of escape rhythms is generally not necessary and is contraindicated because
334

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
these rhythms serve as rescue mechanisms for the heart. Instead, management of escape rhythms should be aimed at resolving the underlying cause of sinus bradycardia or AV block. Occasionally, the normal subsidiary pacemakers may be enhanced and discharge at a rate that is equal to or slightly above the sinoatrial rate (usually between 60 and 80 beats/min). The resulting rhythm is commonly referred to as accelerated idioventricular (idionodal) rhythm or slow ventricular tachycardia. Conditions that favor the development of accelerated idioventricular rhythms include gastrointestinal disease (possibly due to a combination of endotoxemia, autonomic imbalance, acid-base disturbances, and electrolyte abnormalities) and administration of anesthetics or catecholamines. Some combinations of preanesthetic drugs like xylazine and detomidine and anesthetic drugs (halothane) suppress SA function, potentially resulting in sinus bradycardia while enhancing the effects of catecholamines on latent junctional and ventricular pacemakers. Idioventricular rhythms are often quite regular and may be misdiagnosed as sinus tachycardia on auscultation or palpation of peripheral pulses. Persistent, unexplained mild to moderate tachycardia should therefore prompt an electrocardiographic examination to ascertain a correct rhythm diagnosis. However, accelerated idioventricular rhythms generally are of little clinical (electrophysiologic and hemodynamic) significance and resolve spontaneously with appropriate treatment of potential underlying conditions and reduction of anesthetic dosages. Electrolyte supplementation (potassium, magnesium) and correction of fluid deficits and acid-base disturbances may be beneficial. Lidocaine is sometimes administered as an intraoperative adjunct to general anesthesia, or it is used as an analgesic and prokinetic drug in the management of post-operative ileus; in these situations, its antiarrhythmic effects may provide some additional preventive or therapeutic benefits. Junctional and ventricular complexes that arise early relative to the next normal cardiac cycle are designated as premature junctional or ventricular complexes. They are often associated with administration of drugs (i.e. catecholamines, digoxin, halothane), sympathetic stimulation, electrolyte disturbances (i.e. hypokalemia, hypomagnesemia), acid-base disorders, ischemia, or inflammation. Premature complexes may occur as single events, couplets (pairs), triplets, or short runs. A rhythm characterized by sinus beats followed, at a fixed coupling interval, by premature ventricular beats is referred to as ventricular bigeminy. Repetitive ectopic complexes that occur in short bursts or runs are termed nonsustained or paroxysmal ventricular tachycardias. Sustained junctional and ventricular tachycardias may also occur. Ventricular tachycardias are referred to as uniform (monomorphic) if the QRS-T morphology of the ectopic beats is consistent throughout the recording, and as multiform (polymorphic) if two or more abnormal QRS-T configurations can be identified. Torsades de pointes represent a specific form of polymorphic ventricular tachycardia, characterized by progressive changes in QRS direction leading to a steady undulation in the QRS axis. Ventricular flutter and fibrillation are characterized by a chaotic ventricular activation pattern leading to uncoordinated undulations of the electrical baseline. Ventricular premature complexes and junctional arrhythmias are usually considered abnormal in the horse, although isolated ventricular ectopic complexes may be more common than recognized from routine ECG studies. The clinical relevance of an occasional junctional or ventricular premature complex in the horse is difficult to ascertain. Generally, persistent or repetitive junctional or ventricular rhythms are indicative of heart disease, systemic disease, or a drug-induced abnormality of cardiac rhythm. Ventricular tachycardia may be life threatening, if the arrhythmia is very rapid (e.g., above 180 beats/min), multiform (polymorphic, including torsades de pointes), or characterized by a short coupling interval with R-on-T phenomenon (R-on-T refers to premature complexes occurring on the peak of the preceding T wave). Ventricular tachycardia can progress into ventricular flutter or ventricular fibrillation, rhythms that commonly represent terminal events. Accelerated idionodal or idioventricular rhythms and junctional or ventricular tachycardias usually cause interference with AV conduction of normal sinoatrial impulses while leaving atrial activation unaffected. The resulting (independent) coexistence of the sinoatrial
335
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
activity (P wave) and the ectopic ventricular activity (QRS-T) is commonly referred to as AV dissociation. When the independent atrial and ventricular pacemaker foci discharge at similar rates, the P waves may appear to “march in and out” of the QRS complex. This phenomenon is called isorhythmic AV dissociation and is occasionally observed in adult horses. It rarely requires therapy because the ventricular rate is maintained near normal values. It is important to note that escape rhythms associated with sinus bradycardia or complete AV block also cause AV dissociation. Hence, ‘AV dissociation’ is a purely descriptive term of an ECG finding and neither characterizes the type and pathophysiologic mechanism of the arrhythmia nor determines the therapeutic approach. With sustained junctional or ventricular tachycardias, P waves may be identified but are not conducted and therefore not consistently associated with a QRS complex. Some P waves may be buried in the ectopic QRS-T complexes (especially at higher rates of ventricular activation), making their identification difficult. The use of ECG calipers helps determining the P-P interval and can greatly facilitate the identification of P waves. Occasionally, atrial impulses may be normally conducted, leading to capture beats or fusion beats. Capture beats are characterized by a normal P-QRS-T configuration, resulting from normal ventricular activation occurring before the ectopic focus discharges. Fusion beats are seen when both the conducted impulse and an ectopic impulse cause simultaneous ventricular activation, leading to a QRS-T morphology that represents the summation of a normal and an ectopic beat. Junctional and ventricular arrhythmias should be treated using antiarrhythmic drugs if there is clinical evidence of low cardiac output (e.g., weakness, pale mucous membranes, prolonged CRT, syncope), severe hypotension, or when premature complexes are frequent, multiform (polymorphic), rapid (> 100-120 beats/min), or show R-on-T characteristics. However, antiarrhythmic drugs may also cause considerable adverse (including proarrhythmic) effects and may only result in temporary conversion of ventricular tachycardia to normal sinus rhythm. In any case, ECG should be monitored and tissue oxygenation, electrolyte (potassium, magnesium), and acid-base status should be evaluated and corrected as appropriate. The prognosis is usually favorable for infrequent, single ectopic beats in the absence of other signs of significant cardiac disease, or for arrhythmias which can be attributed to a treatable underlying non-cardiac disease. The prognosis for sustained junctional or ventricular tachycardia is usually guarded, particularly if there is evidence of significant structural heart disease or congestive heart failure. The prognosis for multiform ventricular tachycardia or torsades de pointes is usually poor. Conduction disturbances Once a cardiac electrical impulse is formed, it is conducted rapidly throughout the heart. The sequence of cardiac electric activation is usually dictated by the specialized conducting tissues in the atria, the AV node, the bundle of His, the bundle branches, and the Purkinje fiber system. This conduction system permits orderly activation of atrial and ventricular muscle and provides the basis for effective mechanical activity of the heart. A variety of conduction disorders are recognized in horses, including SA nodal exit block, atrial standstill (usually due to hyperkalemia), AV block, bundle branch block, and ill-defined ventricular conduction disturbances. Sinoatrial block (SA nodal exit block) is considered physiologic in horses and is associated with a high vagal tone. Sinoatrial exit block is often seen with sinus bradycardia and AV block. Electrocardiographically it is characterized by a normal sinus rhythm interrupted by occasional pauses without detectable P-QRS-T activity. The differentiation between sinus arrest (sinus pause) and SA nodal exit block may be difficult based on a surface ECG and is clinically irrelevant. Delays in AV conduction are the most common conduction disorders in the horse. These are classified as first, second, and third degree (or complete). First-degree AV block occurs when the PQ interval exceeds the upper normal limit while the atrial impulse still transmits through the AV conduction system and activates the ventricle, causing a QRS complex. During second-degree AV block, some P waves are not conducted to the ventricles,
336
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
resulting in occasional P waves not followed by a QRS-T complex. Second-degree AV block following progressive prolongation of the PQ interval is classified as Mobitz type I (Wenckebach) block. Conversely, the AV block is termed Mobitz type II if the PQ interval is constant. Occurrence of two or more consecutive second-degree AV blocks in presence of a normal or slow sino-atrial rate is called high-grade (advanced) AV block. First- and second-degree AV block are considered normal variations in the horse. These rhythms are most often associated with high vagal tone and may be seen with sinus bradycardia and sinus arrhythmia, or during the recovery phase immediately after exercise. Second-degree AV block can usually be abolished during light exercise (spinning round, jogging, lunging, riding), stress, or with vagolytic drugs such as atropine or glycopyrrolate. If second-degree AV block persists despite exercise or vagolytic drugs, structural AV node disease should be suspected. Persistent high-grade second-degree AV block may progress into complete AV block. Third-degree or complete AV block is characterized by complete disruption of atrial to ventricular conduction, resulting in AV dissociation (see above). To prevent ventricular asystole, a junctional or ventricular escape rhythm must develop below the level of the AV block. The resulting ventricular activity (manifested by QRS complexes) is considerably slower than the atrial activity (manifested by P waves), and P waves are not related to QRS complexes. Complete AV block is usually persistent and indicative of organic heart disease or severe drug toxicity. Life-threatening AV block and other bradyarrhythmias occasionally occur in horses or foals with severe metabolic disturbances or structural cardiac disease. When high-grade second-degree or third-degree AV block develops, the clinical relevance depends, on the basic heart rate or the rate of the escape pacemaker. Immediate treatment (e.g., atropine, dobutamine, pacemaker) is required if severe hypotension develops. Intraventricular conduction disturbances or conduction blocks are less common in horses and more difficult to diagnose. Widening of the QRS complex and axis deviation are typical features. These abnormalities may also be found after atrial premature complexes, from overdosage with quinidine sulfate, or secondary to supraventricular tachycardias with rapid ventricular response. Pre-excitation or accelerated AV conduction has been reported sporadically in horses, but the clinical significance of this electrocardiographic abnormality has yet to be determined in horses. Ventricular preexcitation in humans and in dogs is often the result of an anomalous conducting pathway around the AV node, which causes early excitation of the ventricles and, under certain circumstances, can serve as a path for reentrant supraventricular tachycardias. ECG traces in horses occasionally show evidence of ventricular preexcitation and are characterized by a P-QRS-T relationship but with an extremely short PQ interval, early excitation of the ventricle characterized by a slurring of the initial QRS complex (a delta wave), and an overall widening of the QRS complex. Hyperkalemia most likely occurs in foals with uroperitoneum, in horses with acute renal failure and oliguria, during shock, after excessive intravenous potassium replacement, and in Quarter Horses with hyperkalemic periodic paralysis (HYPP). The cardiovascular manifestations of hyperkalemia include significant depression of atrial, atrioventricular, and ventricular conduction and shortening of ventricular repolarization. Experimentally, changes in the ECG are usually evident at potassium serum concentrations greater than 6 mEq/L, with severe changes evident when serum concentrations are between 8 to 10 mEq/L. Broadening and flattening of the P wave are the most consistently observed changes. Prolongation of the PQ interval and bradycardia develop, excitability decreases, and atrial standstill (sino-ventricular rhythm), characterized by complete absence of P waves, may be observed. Either inversion or enlargement (tenting) of the T waves is also likely. Marked widening of the QRS complex may be noted as near-lethal concentrations of potassium ion are approached. Ventricular asystole or fibrillation can develop. The QT interval is not a reliable indicator of induced hyperkalemia, and other electrolyte/acid-base alterations, including serum calcium and sodium, influence the effect of hyperkalemia on the heart. DEFINING SAFETY RISKS
337
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Of principal concern to the equine clinician are the hemodynamic consequences of arrhythmias (hypotension, low cardiac output, poor peripheral perfusion) and the potential for further electrical destabilization (malignant, potentially fatal arrhythmias). Generally, ventricular arrhythmias are of greater concern regarding performance capacity and safety of horses compared to supraventricular arrhythmias. Atrial fibrillation (AF), that was previously considered to be relatively benign, has now been shown to be frequently associated with very high heart rate responses to exercise (> 220 bpm) and with wide complex arrhythmia that is thought to pose the horse at a higher risk of collapse and sudden death. Defining the safety risks to the horse and to the rider or driver is critical in cases of ventricular ectopy. Generally, premature ventricular complexes (PVCs) are considered abnormal in the horse. They can occur at rest, during exercise, in association with aortic regurgitation and left ventricular enlargement, in association with atrial fibrillation, related to systemic disease or to conditions causing long QT interval. However, isolated PVCs may be more common than recognized from routine ECG studies, even in apparently healthy horses. Not all ectopic ventricular rhythms are considered equally dangerous and the complexity of ventricular arrhythmias is presumed to relate to the risk of hypotension, weakness, collapse and sudden cardiac death (SCD) because of ventricular fibrillation. However, risk stratification for ventricular arrhythmias is imperfect, particularly in horses with isolated PVCs at rest and/or during exercise. In the absence of clear evidence, recommendations should be biased toward safety, as opposed to maintaining athletic activity. Because safety is a concern with persistent atrial fibrillation, a horse with AF should be cardioverted or retired when the exercising HR during sustained maximal exercise exceeds 220 beats/min or if concurrent VA are detected during exercise or with sympathetic stimulation. Certainly, a history of collapse or co-existence of important structural heart disease (and cardiomegaly) raises great concern in a horse with PVCs. However, in the absence of obvious clinical signs or of serious structural heart disease, the risk of ventricular ectopy is usually defined by electrocardiographic characteristics, accepting the limitations of this analysis. This assessment includes timing, rate and morphology of the ectopic activity. As a general rule, ventricular arrhythmias should be considered complex or “malignant” and potentially life threatening, if they are characterized by one or more of the following criteria:
• Repetitive or sustained ectopic rhythms • Very rapid ventricular rate (exceeding 120 beats/min at rest) • Multiform or polymorphic QRS morphology (including torsades de pointes) • Short coupling interval with R-on-T phenomenon (i.e., PVCs occurring on the
peak of the preceding T wave) Complex ventricular arrhythmias can induce hemodynamic impairment resulting in clinical evidence of low cardiac output (e.g., weakness, stumbling, pale mucous membranes, prolonged CRT, syncope) and hypotension. Electrical instability is a particular concern in malignant ventricular arrhythmias and can cause ventricular tachycardia to progress into ventricular flutter or ventricular fibrillation. These commonly represent terminal events. Many cases with ventricular arrhythmia can be managed by treating the underlying disease and rest. Repeated or continuous ECG monitoring (to document progression of disease or resolution of arrhythmia) is recommended. Complex, “malignant” ventricular arrhythmias should be more aggressively managed by additional use of antiarrhythmic drugs. For general recommendations on management of athletic horses with atrial fibrillation and with ventricular arrhythmias, the readers are referred to the 2014 ACVIM/ECEIM Consensus Statement on Management of Equine Athletes with Cardiovascular Abnormalities (see references).
338
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
TREATMENT OF EQUINE ARRHYTHMIAS Compared to human medicine, the therapeutic options for the treatment of cardiac arrhythmias in horses are limited to a relatively small group of agents. Most recommendations for the use of antiarrhythmic drugs in horses are based on empirical data rather than scientific evidence, and the efficacy and safety of most drugs has not been well investigated in horses. In any instance, the benefits and potential risks of cardiovascular drug treatment should be carefully considered and treatment should be performed under close clinical supervision, electrocardiographic monitoring, monitoring of arterial blood pressures, and (where applicable) measurement of plasma or serum drug concentrations. Treatment of coexisting conditions, adequate hydration, support of cardio-respiratory function and peripheral perfusion, and correction of existing electrolyte (i.e., K+, Mg2+) and acid-base disturbances must precede or accompany antiarrhythmic drug treatment and can critically influence drug efficacy and incidence of adverse drug effects. Antiarrhythmic drugs Antiarrhythmics are commonly grouped according to the Vaughan Williams classification system that classifies the drugs into 6 classes (IA to IV), based on the primary mechanism of their antiarrhythmic effects. Some agents exert effects that are consistent with several classes (e.g., amiodarone), while other agents are not included in this classification (e.g., magnesium). It is important to realize that most antiarrhythmics may also exert proarrhythmic effects that can be detrimental to the horses’ health. For dose recommendations please see references listed below. Class IA: Quinidine, procainamide. Quinidine and procainamide are class IA sodium channel blockers that slow impulse conduction through the heart. They also inhibit repolarizing potassium currents, thereby prolonging the action potential duration and the QT interval and increasing the refractoriness of the myocardial cells. Furthermore, they exert anticholinergic and vasodilatory effects. Quinidine is primarily used for conversion of atrial flutter or atrial fibrillation (AF) to sinus rhythm, with a reported efficacy of up to 80-90%. Horses with AF and an increased resting heart rate, evidence of decreased left-ventricular systolic function (based on echocardiography) or congestive heart failure should be pre-treated with furosemide (to control edema) and digoxin (to control heart rate and improve systolic left-ventricular function) as necessary. Adverse effects are common, even at therapeutic plasma concentrations. Prolongation of the QRS complex of > 25% of baseline indicates toxic plasma concentrations (> 5 μg/mL). In horses with an accelerated atrioventricular conduction (heart rate > 100 beats/min), the rate may be controlled by intravenous administration of digoxin, diltiazem, or propranolol, under close monitoring of clinical response, ECG, and blood pressures. Diltiazem and propranolol may enhance hypotension and negative inotropism and should be administered with caution. If the rate is sustained in excess of 150 beats/min or severe hypotension occurs, administration of sodium bicarbonate (1 mEq/kg IV) should be considered to antagonize the sodium channel blocking effects of quinidine. Forced diuresis using fluids and diuretics may enhance renal excretion of the drug. Severe hypotension is treated with IV fluids/colloids and phenylephrine or norepinephrine. Ventricular arrhythmias are treated with lidocaine and magnesium sulfate. Hypokalemia and hypomagnesemia may increase the risk of torsades de pointes and should be prevented. The primary indication for the use of procainamide in horses is ventricular tachycardia, although procainamide may be effective against a wide spectrum of supraventricular and ventricular arrhythmias. The risk of adverse effects may be somewhat lower with procainamide compared to quinidine. Class IB: Lidocaine, phenytoin Lidocaine binds to inactivated sodium channels and inhibits membrane recovery after repolarization. Lidocaine acts preferentially at rapid heart rates and on the ischemic or
339
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
diseased (depolarized) myocardium, where it promotes conduction block and interrupts reentry arrhythmias. It does not prolong the action potential duration and QT interval. Lidocaine is the treatment of choice for ventricular arrhythmias in horses. Concurrent correction of electrolyte imbalances is important, as lidocaine is less effective with low extracellular potassium and magnesium concentrations. Lidocaine undergoes hepatic clearance and doses should be reduced (halved) in patients with poor liver blood flow (low cardiac output) or impaired liver function. Phenytoin acts similarly to lidocaine. It is primarily used for treatment of digitalis-induced arrhythmias, but has recently been advocated for use in horses with ventricular arrhythmias that are refractory to conventional treatment including lidocaine and procainamide. Class IC: Flecainide, propafenone Class IC antiarrhythmics are potent sodium channel inhibitors that slow impulse conduction through the heart and cause variable prolongation of the action potential duration and QT interval. They may be used to control supraventricular and ventricular arrhythmias resistant to other drugs. Specifically, flecainide has recently been proposed for treatment of acute AF in horses. However, it was shown to be ineffective in cases with chronic AF and was associated with potentially dangerous ventricular arrhythmias. Propafenone is a class IC agent that also exerts weak beta-blocking and L-type calcium channel blocking effects. It has been proposed for treatment of quinidine-induced ventricular tachycardia. Generally, class IC agents should be used with caution, as their efficacy and safety have not been fully investigated in horses. Class II: Propranolol Class II agents act by inhibition of β-adrenergic receptors. Different class II agents are characterized by varying receptor specificity, pharmacokinetic properties, and additional pharmacologic effects. Propranolol, a first-generation β-blocker that inhibits both (cardiac) β1- and (vascular and bronchial) β2-receptors, is the only class II agent that is occasionally used in horses to date. It has been proposed for ventricular rate control in horses with rapid supraventricular tachycardia or atrial flutter/fibrillation and for treatment of unresponsive supraventricular and ventricular arrhythmias. However, its efficacy as an antiarrhythmic drug in the horse has not been well established. The pharmacologic effects strongly depend on the level of sympathetic tone, which explains the wide variability of response observed during clinical use. It may therefore be most useful in cases of exercise (tachycardia)-induced arrhythmias. Class III: Sotalol, amiodarone, bretylium In human medicine, the attention has shifted from class I to class III agents due to their favorable effects on arrhythmias. However, all class III agents are potent potassium channel blockers that act by lengthening of the action potential duration and prolongation of the QT interval. This can lead to a predisposition to torsades de pointes, especially in the presence of hypokalemia, hypomagnesemia, or bradycardia. Sotalol is a potassium channel blocker that also exerts class II effects. Although not well described in the current literature, preliminary studies and clinical experience indicate that orally administered sotalol is well tolerated in horses. Since QT prolongation is a concern, monitoring of QT interval is recommended. Sotalol may be used for maintenance of sinus rhythm after successful cardioversion of atrial fibrillation and for chronic treatment of supraventricular and ventricular arrhythmias. Amiodarone is a potassium channel blocker that also exerts class I, II, and IV effects. It has recently been introduced in equine medicine as a new therapeutic option for treatment of atrial fibrillation. Although potentially effective in some cases, the long duration of treatment (up to 54 hours) and the high costs currently limit the use for routine treatment of AF in horses. Bretylium tosylate is a class III agent that also possesses indirect anti-adrenergic effects. It has been proposed for treatment of life-threatening ventricular tachycardia and ventricular fibrillation in horses. The use of the mixed class II/III agent sotalol and of pure class III agents such as ibutilide or dofetilide has not been described in horses, although they could potentially be efficacious for treatment of atrial fibrillation.
340

Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
Class IV: Diltiazem, verapamil Diltiazem and verapamil are L-type calcium channel blocking agents that primarily inhibit SA and AV nodal tissues and, to a lesser degree, act on vascular smooth muscle (vasodilation) and myocardium (negative inotropism). While the use of verapamil in horses is empirical, diltiazem was shown to be effective for acute ventricular rate control during treatment with quinidine in an equine pacing model of supraventricular tachycardia. Diltiazem is likely to be safe and more effective than digoxin for ventricular rate control in patients with atrial fibrillation. However, safety and efficacy of diltiazem for treatment naturally occurring AF have not been fully established to date, and the drug should be used with caution, considering potential adverse reactions. Magnesium sulfate Magnesium is a cofactor of the membrane Na+/K+-ATPase and plays an essential role in maintaining intracellular ion homeostasis and electrophysiological properties of cellular membranes. It also acts as a physiologic calcium channel inhibitor. Hypomagnesemia is a common finding in a variety of diseases, including heart failure. Magnesium deficiency (and potassium deficiency) predisposes to cardiac arrhythmias, and magnesium supplementation may be beneficial in the presence of cardiovascular diseases and arrhythmias. Magnesium sulfate (at higher doses) is also recommended for treatment of ventricular arrhythmias and is considered the drug of choice for torsades de pointes, even in patients with normomagnesemia. Unlike most other antiarrhythmic agents, magnesium does not exert significant proarrhythmic effects and is relatively safe to use. Digitalis glycosides: Digoxin Digoxin inhibits the membrane-bound Na+/K+-ATPase and causes an increase in intracellular sodium that promotes calcium influx through the Na+/Ca2+-exchanger. Digoxin thereby increases myocardial contractility (inotropy), but also increases the risk of arrhythmias. Furthermore, digoxin sensitizes the baroreceptors and thereby increases the parasympathetic and decreases the sympathetic tone. These autonomic effects, together with a modest direct depression of nodal tissues, suppress the impulse conduction in the atrioventricular node (negative dromotropic effect). In horses with atrial fibrillation (AF) and elevated resting heart rate or with sustained (supraventricular) tachycardia during quinidine treatment, digoxin is commonly used for ventricular rate control. Although not proven, digoxin may facilitate conversion of AF to sinus rhythm in some cases. Due to the variable pharmacokinetics and the narrow therapeutic window, therapeutic drug monitoring, individualized selection of a digoxin dosage regimen, and close monitoring of the clinical response is advisable. Due to the long half-life (16-29 hours), 3-6 days are required to achieve steady state conditions. The use of a loading dose is not recommended because of the increased chance of digoxin toxicity. Factors predisposing to digitalis toxicity include advanced heart disease, atrial fibrillation, impaired renal function, hypokalemia, hypomagnesemia, hypercalcemia, and hypoproteinemia. Quinidine decreases renal clearance and increases circulating blood digoxin concentrations, while phenylbutazone competes with protein binding sites and increases the free digoxin fraction. Anticholinergic (vagolytic) agents: Atropine, glycopyrrolate Atropine and glycopyrrolate competitively inhibit acetylcholine or other cholinergic stimulants at postganglionic parasympathetic effector sites. Pharmacologic effects are dose-related and include increase in sinus node activity and atrioventricular conduction, inhibition of salivation and bronchial secretions, and decrease of GI motility. Unlike sympathomimetics, vagolytic agents only minimally affect the ventricular myocardium and are less arrhythmogenic. Unlike atropine, glycopyrrolate does not cross the blood-brain barrier and crosses the placenta only marginally. Note that paradoxical parasympathomimetic effects can be seen at lower doses of atropine and glycopyrrolate;
341
Proceedings of VetFest 2020 Schwarzwald, C - Diagnosis, clinical relevance and treatment of cardiac arrhythmias in horses
therefore, dose recommendations should be followed and doses should not be uptitrated to effect. Transvenous electrical cardioversion of atrial fibrillation Transvenous electrical cardioversion (TVEC) of AF to sinus rhythm can be used for management of horses who respond adversely or inadequately to quinidine therapy. At some institutions, it has even become the primary method of treatment of AF. TVEC is a very effective non-pharmaceutical treatment option for AF. However, it requires special equipment and trained personnel and it is usually more expensive compared to conventional quinidine cardioversion. The procedure involves percutaneous, transvenous placement of two specialized electrode catheters into the left pulmonary artery and right atrial cavity, respectively. Catheter placement is done in the standing horse under sedation and local anesthesia. The catheters are guided by pressure monitoring through the catheter lumen and 2D echocardiographic imaging. Radiography is used to verify the placement of the catheters either before or preferably after induction of general anesthesia. Electrical cardioversion is very painful and must be performed under general anesthesia with the horse well-padded since the shock results in a sudden jolt of the body and limbs. After induction of general anesthesia, synchronized (i.e., concurrent with the QRS complex) electrical shocks are delivered every 2 min at increasing energy levels until conversion to sinus rhythm or until the maximum energy level of 360 J is reached. Cardioversion is usually achieved with a mean energy level around 170 Joules. Success rate varies highly between institutions and is likely dependent on the patient population. In young racehorses with ‘lone’ AF, a conversion rate of up to 98% has been reported. However, in an average hospital population of older horses of various breeds (incl. Warmbloods) with and without underlying structural heart disease, the conversion rate seems to be around 65%. For comparison, the average conversion rate using quinidine conversion is around 80-90%. To date, there has not been any formal comparison of the success rate of quinidine treatment vs. TVEC. The complications associated with TVEC appear to be quite low, but are finite related to general anesthesia or electrical shock. Mild increases in cardiac troponin I have been observed but are unlikely to be clinically relevant. Cardiovascular function under general anesthesia is generally well maintained, but a transient decrease in systemic blood pressure and episodes of bradycardia can be observed in some horses. A case of transient complete AV block has been reported and fatal ventricular arrhythmias after inadvertently shocking the T wave (vulnerable period) can rarely occur.
FURTHER READING − Keen JA. Examination of Horses with Cardiac Disease. Vet Clin North Am Equine Pract. 2019;35(1):23-42. − Mitchell KJ. Equine Electrocardiography. Vet Clin North Am Equine Pract. 2019;35(1):65-83. − van Loon G. Cardiac Arrhythmias in Horses. Vet Clin North Am Equine Pract. 2019;35(1):85-102. − Schwarzwald CC: Cardiovascular Diseases. In: Reed SM et al. (eds): Equine Internal Medicine, 4th ed. Saunders Elsevier,
2017: 387-541. − Schwarzwald CC et al.: The Cardiovascular System. In: Muir WW, Hubbell JAE (eds): Equine Anesthesia, 2nd ed. Elsevier
Saunders, 2009:37-100. − Schwarzwald CC: Cardiovascular Pharmacology. In: Robinson NE (ed): Current Therapy in Equine Medicine 6. Elsevier
Saunders, 2009:182-191. − Bowen IM: Cardiac Dysrhythmias. In: Robinson NE (ed): Current Therapy in Equine Medicine 5. Elsevier Saunders, 2003:
602-613. − Jesty SA, Reef VB: Cardiovascular System. In: Orsini JA, Divers TJ (eds): Equine Emergencies: Treatment and Procedures, 3rd
ed. Saunders Elsevier, 2008:60-100. − Marr CM, Bowen M (eds): Cardiology of the Horse. 2nd ed. Saunders Elsevier, 2010. − Reef VB, Bonagura J, Buhl R, McGurrin MK, Schwarzwald CC, van Loon G, et al. Recommendations for management of
equine athletes with cardiovascular abnormalities. J Vet Intern Med. 2014;28(3):749-61. − McGurrin MKJ, et al: Transvenous Electrical Cardioversion of Equine Atrial Fibrillation: Technical Considerations. J Vet Intern
Med 2005;19:695–702. CS/2020-06
342