integrated treatment programs for individuals with concurrent substance use disorders and trauma...
TRANSCRIPT

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Regular article
Integrated treatment programs for individuals with concurrentsubstance use disorders and trauma experiences: A systematic
review and meta-analysis
Iris Torchalla, (Ph.D.) a,⁎,1, Liz Nosen, (M.A.) b,Hajera Rostam, (M.A.) c, Patrice Allen, (M.A.) a,2
aBritish Columbia Centre of Excellence for Women's Health, 311-4500 Oak Street, Vancouver, BC, Canada V6H 3N1bUniversity of British Columbia, Department of Psychology, 2136 West Mall, Vancouver, BC, Canada V6T 1Z4
cUniversity of British Columbia, Department of Counselling Psychology, 2125 Main Mall, Vancouver, BC, V6T 1Z4, Canada
Received 18 May 2011; received in revised form 23 August 2011; accepted 15 September 2011
Abstract
The purpose of this study was to examine the evidence of psychotherapeutic integrated treatment (IT) programs for individuals withconcurrent substance use disorders and trauma histories. Electronic searches of Cochrane Central Register of Controlled Trials, MEDLINE,Web of knowledge, PubMed, PsycINFO, CINAHL, PILOTS, and EMBASE identified 17 IT trials (9 controlled trials). Both narrative reviewand meta-analysis indicate that IT effectively reduces trauma symptoms and substance abuse from pretreatment to longest follow-up.However, IT and nonintegrated programs appear to produce similar declines in symptoms. Methodological issues limiting the current bodyof work and recommendations for future research are discussed. Well-designed randomized controlled trials are clearly needed, particularlylarge sample studies evaluating understudied IT programs and exposure-based approaches. © 2012 Elsevier Inc. All rights reserved.
Keywords: Integrated treatment; Psychiatric comorbidity; Substance use disorders; Trauma; Meta-analysis
1. Introduction
The co-occurrence of substance use disorder (SUD) andposttraumatic stress disorder (PTSD) represents a growingarea of concern for researchers, policy makers, and treatmentproviders. Estimates of PTSD prevalence rates amongindividuals presenting for SUD treatment range from 20%to 38% (Najavits, Gastfriend, et al., 1998; Reynolds et al.,2005), with lifetime prevalence rates between 30% and 52%(Back et al., 2000; Clark, Masson, Delucchi, Hall, & Sees,
2001; Reynolds et al., 2005). Histories of traumatic events(i.e., with or without PTSD diagnosis) are considerably morecommon and are reported by as many as 90% of some SUDsamples (Brown, Stout, & Mueller, 1999).
PTSD appears to be a risk factor for later substance use. Inthe National Comorbidity Study, 51.9% of men and 27.9% ofwomen with PTSD had a concurrent alcohol use disordercompared with 34.4% of men and 13.5% of women withoutPTSD (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995).Following up on the same sample, PTSD diagnosis pros-pectively predicted new onset of alcohol and drug depen-dence 10 years later (Swendsen et al., 2010). Similarly, astudy of young adults without preexisting drug dependencefound that individuals with PTSD experienced a nearly five-fold higher incidence of drug abuse or dependence at the12-month follow-up compared with those who were notexposed to trauma (Reed, Anthony, & Breslau, 2007). Thisevidence supports a self-medication model, whereby indivi-duals with PTSD use substances to regulate distress and other
Journal of Substance Abuse Treatment 42 (2012) 65–77
⁎ Corresponding author. Centre for Health Evaluation and OutcomeSciences (CHEOS); 620B-1081 Burrard Street, Vancouver, BC, CanadaV6Z 1Y6. Tel.: +1 604 682 2344x66329; fax: +1 604 806 8674.
E-mail address: [email protected] (I. Torchalla).1 Iris Torchalla is now at the Centre for Health Evaluation and Outcome
Sciences, St. Paul's Hospital, 620B-1081 Burrard Street, Vancouver, BC,V6Z 1Y6, Canada.
2 Patrice Allen is now at the BC Mental Health and Addiction Services,2601 Lougheed Highway, Coquitlam, BC, V3C 4J2, Canada.
0740-5472/11/$ – see front matter © 2012 Elsevier Inc. All rights reserved.doi:10.1016/j.jsat.2011.09.001

Author's personal copy
symptoms (Khantzian, 1997). Consistent with this idea,Ouimette, Read, Wade, and Tirone (2010) found that weeklyfluctuations in PTSD symptoms predicted concurrent cocaineand subsequent opioid use among individuals receivingoutpatient SUD treatment. Other causal pathways have alsobeen suggested, including the hypotheses that substance abusemay increase the risk of exposure to traumatic events, thatsubstance users may be more likely to develop PTSDfollowing exposure to a traumatic event, and that a thirdvariable may predispose an individual to both substance abuseand PTSD (Chilcoat & Breslau, 1998; Coffey, Read, &Norberg, 2008; Kilpatrick, Resnick, Saunders, & Best, 1998).
Individuals with concurrent PTSD and SUD tend to presentwith a more complicated clinical picture, experiencing moresevere symptoms (Driessen et al., 2008), higher rates ofadditional psychiatric disorders (Brady, Killeen, Saladin,Dansky, & Becker, 1994), and poorer physical health (Tate,Norman, McQuaid, & Brown, 2007) than individuals withoutthis comorbidity. Clients with PTSD also do not appear tobenefit optimally from standard SUD intervention programs;they demonstrate poorer treatment outcome and higher relapserates than substance-abusing individuals without PTSD (Mills,Teesson, Ross, Darke, & Shanahan, 2005; Norman, Tate,Anderson, &Brown, 2007; Ouimette, Finney, &Moos, 1999).Furthermore, persistence of PTSD symptoms in SUD clientspredicted substance use over a 6-month follow-up period(Read, Brown, & Kahler, 2004). On the other hand, attendingPTSD treatment following discharge from a substance abusetreatment program has been associated with long-term SUDremission in individuals with SUD/PTSD comorbidity(Ouimette, Moos, & Finney, 2000, 2003).
In view of such findings, it is recommended that assessmentand treatment address both conditions to fullymeet the needs ofthis population (Ruzek, Polusny, & Abueg, 1998). Treatmentapproaches that aim at addressing both PTSD and SUD arebased on sequential, parallel, or integrated models. Insequential interventions, clients receive treatment for onedisorder and are subsequently referred to another service toreceive treatment for the other disorder. Typically, PTSDtreatment is provided following SUD treatment, based on theassumption that PTSD treatment is too challenging for activesubstance users and can only be successfully implemented afterabstinence fromsubstances has been achieved and stabilized. Inparallel interventions, SUD is treated within an SUD program,and PTSD is concurrently treatedwithin a PTSDprogram. Likein the sequential model, both interventions are provided indifferent facilities and by different clinicians/teams. In contrast,integrated programs treat both disorders simultaneously withinthe same service by the same (team of) clinicians (Donald,Dower, & Kavanagh, 2005; Drake et al., 2001).
In recent years researchers have developed a number ofintegrated models for the treatment of concurrent trauma/PTSD and substance abuse and empirical tests of suchintegrated treatment (IT) programs have proliferated gradu-ally. Enthusiasm for these protocols is widespread; integrat-ed approaches are being highly recommended to address
PTSD-SUD comorbidity (Back, Waldrop, Brady, & Hien,2006; Finkelstein et al., 2004). Although number of studiesfocusing on developing an evidence base for IT models havebeen conducted and several narrative reviews of ITs forcomorbid SUDs and PTSD have recently become available(e.g., Jennings, 2004; Riggs & Foa, 2008), no studies haveattempted to summarize the findings as a whole using sys-tematic and empirical methods. Understanding the currentempirical status of integrated PSD-SUD treatments isessential for making best practice recommendations and forguiding future work in this area. Substance abuse and mentalhealth service systems are traditionally disconnected and themajority of counselors in both systems do not receivespecialized dual-disorder training (Ridgely, Goldman, &Willenbring, 1990). At present, it is unclear whether revisionand adaptation of these existing service frameworks isrequired to provide effective treatment for individuals withPTSD/SUD or whether improving collaboration between theseparate services is sufficient.
Accordingly, the current work represents a systematic re-view of clinical trials that evaluated the effects of integratedpsychotherapy models for individuals with concurrent traumaand SUDs. We were interested in two primary researchquestions. First, are IT programs effective in reducing trauma-related symptoms and substance use? Second, do IT programsreduce these symptoms and behaviors to a greater extent thantraditional non-IT programs? Both narrative review and meta-analysis were used to answer these questions.
2. Materials and methods
2.1. Selection criteria
We included all English-language studies that quanti-tatively evaluated the outcome of psychotherapeutic integratedsubstance use and trauma programs. Case studies and un-published reports were excluded; the search was not restrictedby publication date. At minimum, all study participants wererequired to both (a) meet diagnostic criteria for substanceabuse or dependence and/or be seeking SUD treatment and (b)report a history of psychological trauma and/or the presence ofPTSD symptoms. Integrated psychotherapeutic treatmentwas defined as a coordinated and simultaneous focus onboth substance use and trauma issues within the same serviceand by the same (team of) clinicians. Studies were excluded ifeither substance use or trauma was treated solely bydetoxification or pharmacotherapy (although concurrentpharmacotherapy was permitted). Studies were required toreport quantitative substance use and/or trauma symptomseverity outcomes; type of measure (e.g., self-report vs.biochemical validation) however was not restricted. Studiesreporting only on other outcomes relevant to clinical care (e.g.,cost-effectiveness, attrition, client satisfaction), baselinecharacteristics of the sample, or investigations of treatmentmechanisms (e.g., order of symptom improvement,
66 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
moderating effects) were excluded. When multiple eligiblearticles stemmed from the same data set, one representativearticle was selected to reduce biases and redundancies in themeta-analysis; the first study to present treatment outcome datafrom the longest follow-up period was selected as therepresentative article. Reanalyses, secondary analyses, andsubsample analyses of original data were excluded.
2.2. Search strategy
Studies were identified by searching electronic databasesand scanning reference lists of identified articles, reviews ofsubstance use and trauma comorbidity, and Web sites ofpublished IT programs. Electronic searches were conductedin Cochrane Central Register of Controlled Trials (CEN-TRAL), MEDLINE, Web of knowledge, PubMed, Psy-cINFO, CINAHL, PILOTS, and EMBASE. We searched forthe following terms in titles, abstracts, and keywords:trauma or ptsd or posttraumatic stress disorder or acutestress disorder; addiction or substance use or substanceabuse or substance dependence or alcohol or alcohol abuseor alcohol dependence; and treatment or therapy or inter-vention. The most recent full search was conducted in June2010. All articles meeting the broad inclusion criteria werereviewed and evaluated for eligibility by at least tworeviewers. Uncertainty regarding study eligibility wasresolved by consensus among all authors.
2.3. Risk of bias assessment and data extraction
For each study, an author extracted information needed forthe qualitative and quantitative analyses using a standardizedform, which was subsequently reviewed and confirmed byanother author. To identify the risk of bias associated withindividual studies, two researchers also independentlyassessed each selected article using the McMaster UniversityQuality Assessment Tool for Quantitative Studies (QAT;Thomas, 1998). The QAT has been recommended for use insystematic reviews that include nonrandomized interventionstudies (Deeks et al., 2003). Six individual study components(study design, selection bias, confounders, blinding, datacollection, and withdrawals and dropouts) are rated as strong,moderate, orweak using standardized guidelines; these ratingsare combined to provide a global rating of methodologicalquality. Following the guidelines provided by the QAT, studydesigns were classified as a “randomized controlled trial,”“controlled clinical trial” (if randomization method was notdescribed, or randomization sequence did not result in equaland unpredictable chances of receiving each intervention),“cohort analytic study” (allocating individuals to interventionswas not under the control of the investigators), and “cohortstudy” (no control group). Both randomized controlled andcontrolled clinical trials received a strong design rating,whereas cohort analytic and cohort studies received a mode-rate rating. Disagreements between the reviewers werediscussed among the team and resolved by consensus.
2.4. Meta-analytic procedures
Meta-analysis was used to corroborate narrative impres-sions. Two analyses (one for each symptom cluster) examinedwhether IT effectively reduced SUD and PTSD symptomsover time (within-group comparisons). Dependent-sampleeffect sizes (ESs) comparing baseline symptoms with those atthe longest available follow-up point for the IT group werecomputed for each study. Analyses focusing on end-of-treatment outcomes are not presented in this article butproduced similar results. To examine whether IT relievessymptoms more effectively than non-IT interventions, twoadditional meta-analyses compared IT with control conditionson SUD and PTSD outcomes at the longest available follow-up point (between-group comparisons). We used the Metaforpackage for R (Viechtbauer, 2010) to estimate random effectsmodels (DerSimonian & Laird, 1986). After computingoverall ESs, potential for publication bias was examined viafunnel plots (a plot of effect vs. sample sizes). The trim-and-fillmethod (Duval & Tweedie, 2000) was used to estimateadjusted ESs. The underlying assumption of thismethod is thatasymmetrical funnel plots indicate a possible publication bias.The trim-and-fill method removes (“trims”) the studies causingfunnel plot asymmetry, uses the trimmed funnel plot toestimate the “true center” of the funnel, and replaces (“fills”)the omitted studies and their missing counterparts around thecenter (Duval & Tweedie, 2000).
In some studies, SUD or trauma symptoms were assessedusing multiple measures. To avoid violations of statisticalindependence assumptions, it is necessary that each studyonly contributes one ES per construct. To facilitate this,preference was given to established measures on continuousscales (e.g., Addictions Severity Index, Clinician-Adminis-tered PTSD Scale (CAPS) total score) over single-item,unpublished, researcher-created or binary measures (e.g.,days drinking in past month); the latter outcomes were usedsolely in the absence of other measures (applicable for threestudies, all SUD abstinence rates). Aggregate ESs were thencalculated by averaging the ESs of relevant measures(Hunter & Schmidt, 2004).
ES calculations are based on formulas from Lipsey andWilson (2001). The ES for within-group IT comparisons wasthe standardized mean gain based on Becker (1988),calculated as
ESsg =PxT2 − PxT1
sp
where xPT2 and xPT1 are the means at follow-up and baselinewithin the IT group, respectively, and sp is the pooledstandard deviation. Standard error of ESsg is
SEsg =
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi2 1 − rð Þ
n+
ES2sg2n
s
where n is the common sample size, and r is the correlationbetween T1 and T2 scores (estimated via test–retestcorrelations from examinations of measure psychometrics).
67I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
The ES comparing IT with non-IT treatments is thestandardized mean difference. It was calculated directly,when possible, as
ESsm =PxIT − PxCG
sp
in which xPIT is the mean of the IT group at the longestfollow-up point, xPCG is the mean of the comparison group,and sp is the pooled standard deviation. Standard error ofESsm is calculated as
SEsm =
ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffinIT + nCGnITnCG
+ES2sm
2 nIT + nCGð Þ:s
When insufficient statistics were reported, the ES wasestimated using available data. For dichotomous outcomes,0.5 was added to any cell frequencies equal to zero (Fleiss,1994); logit transformations were applied to permit compar-ison with interval-based ESs (Lipsey & Wilson, 2001).Results reported only as nonsignificant were coded as ES =0.00; unclear effects (e.g., when results were amalgamatedacross groups) were omitted from analyses. Hedges andOlkin's (1985) correction for small sample bias was appliedto all ESs. In all instances, positive ESs represented im-provement over time or superiority of IT; negative ESsrepresented worsening of symptoms over time or superiorityof non-IT.
Studentized deleted residuals (±1.96), COVRATIOs (b1),and DFBETAS (N1) were used to identify influential outliers(Viechtbauer & Cheung, 2010). One outlying PTSD ES(from Hien et al., 2009) was reduced in magnitude justenough to improve model fit (changed from d = 1.43 to d =1.30). To note, direction and significance of results were thesame before and after this adjustment. In meta-analysis,outlying sample sizes can also disproportionately affect re-sults. As such, the extremely large sample size of one study(N = 1,481; Morrissey et al., 2005) was winsorized (to n =355) to prevent outcomes from being unduly dominated bya single trial. Results affected by this change are noted in theresults as relevant.
3. Results
3.1. Study identification
The literature search identified a combined database of1,300 potentially relevant, nonduplicate abstracts. A total of1,087 were removed because they were clearly unrelated toour research question based on the title or abstract. Of theremaining articles, 51 were studies involving integratedSUD–PTSD treatment, 27 of which met our eligibilitycriteria. Of these, 9 reports stemmed from the Women, Co-occurring Disorders and Violence Study (WCDVS);Morrissey et al. (2005) was selected to represent thisdata set in the meta-analysis. Three articles stemmed from the
National Institute on Drug Abuse Women and Trauma Study(WTS); Hien et al. (2009) was chosen to represent these data.The WCDVS and WTS subsample and secondary analyseswere not included in the tables or meta-analysis, butqualifying results are discussed in the narrative reviewwhen relevant. Hence, a total of 17 independent studies areincluded in the review and analyses.
3.2. Study characteristics
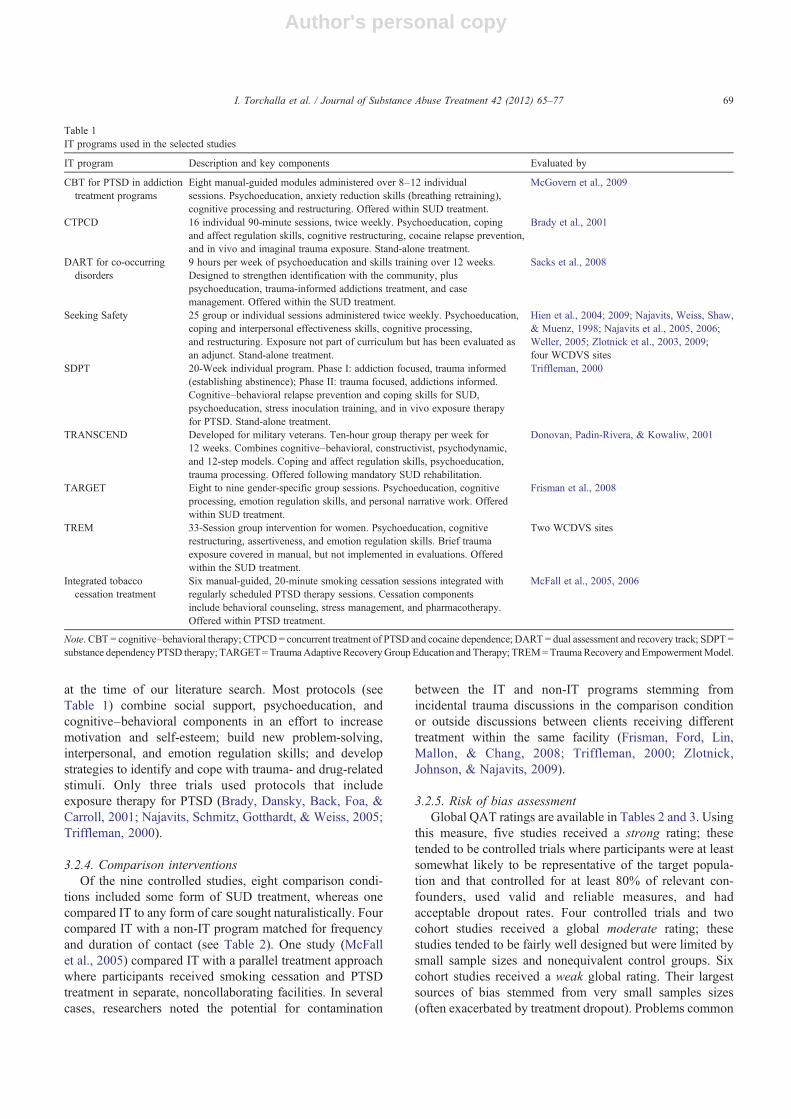
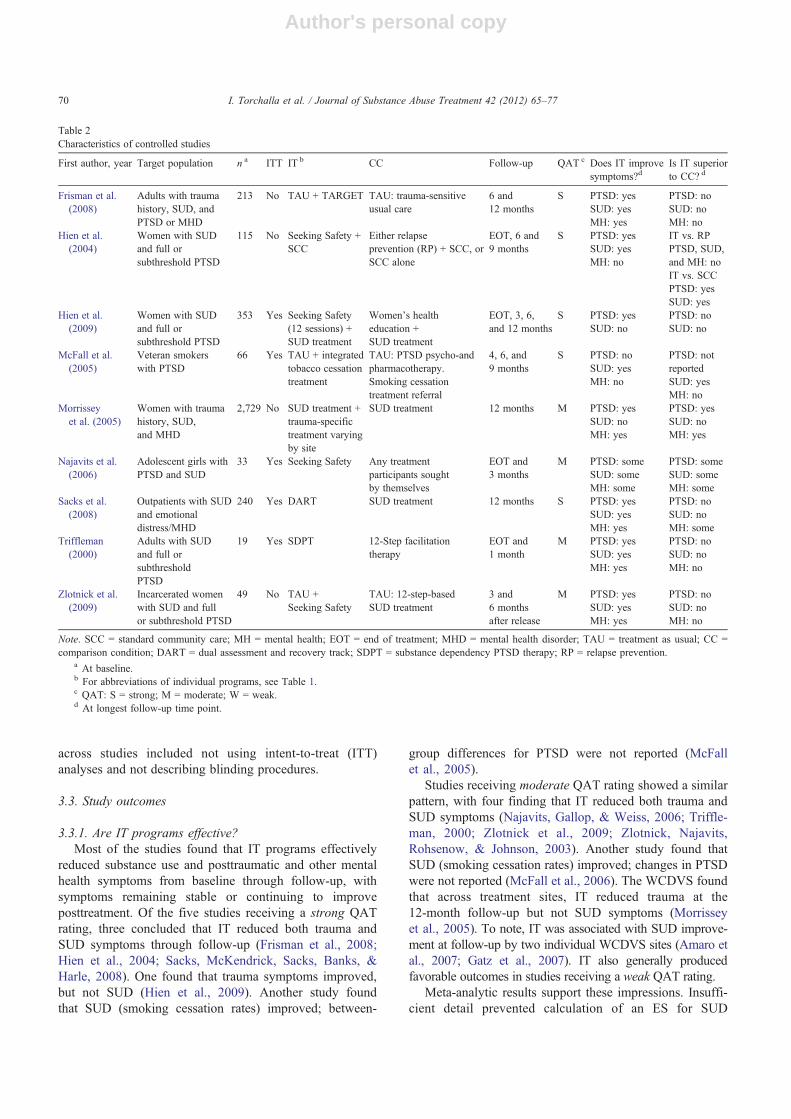
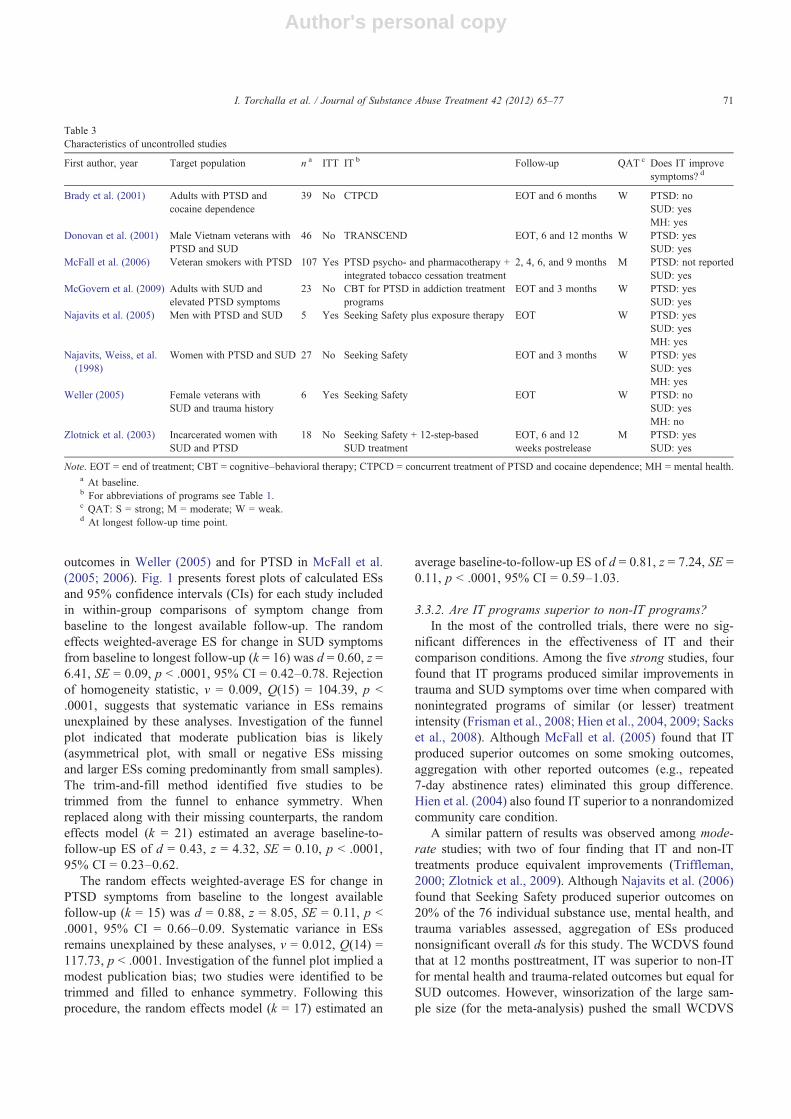
Treatment models and programs employed in their ori-ginal or modified form are presented in Table 1. Character-istics of the individual studies are presented in Tables 2(controlled studies) and 3 (cohort studies).
3.2.1. MethodsOf the nine controlled studies, only one (Hien et al., 2009)
qualified as a randomized controlled trial (RCT) accordingto the QAT because for several trials, randomization wasnot described in sufficient detail to permit classification asan RCT. Accordingly, seven were categorized as controlledclinical trials, one of which included an additional non-randomized comparison group (Hien, Cohen, Miele, Litt, &Capstick, 2004).1 The WCDVS used a cohort analyticdesign where each IT treatment site selected its owncomparison site, and participants were not allocated totreatment. All eight of the uncontrolled studies were cohortdesigns. All studies used structured interviews and/orestablished questionnaires for symptom assessment. Elevenstudies also verified self-reported substance use with bio-chemical measures.
3.2.2. ParticipantsBaseline sample sizes ranged from 19 to 2,729 in studies
that included a control group and from 5 to 107 in the cohortstudies. Nine studies had women-only samples, 2 had men-only samples, and 6 had mixed-gender samples. A fewstudies targeted specific subgroups, including veterans, in-carcerated women, and adolescents. Most of the studiesincluded participants who had either drug use disorder oralcohol use disorder or both (as indicated with “SUD” in thesecond column in Tables 2 and 3). Three studies focused onthe treatment of specific SUDs (i.e., smoking in 2 studies andcocaine dependence in 1 study). Although 14 studies re-quired participants to fulfill SUD diagnostic criteria, only8 (2 controlled trials) required full PTSD diagnosis.
3.2.3. Integrated interventionsInterventions were primarily based in SUD treatment
facilities in the United States. Treatment providers werepredominantly master's level addiction or mental healthcounselors or graduate/postdoctoral students. All curriculawere manualized; all manuals except two (McFall et al.,2006, 2005; McGovern et al., 2009) had been published
1 Meta-analytic results include only the randomized group.
68 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77
Author's personal copy
at the time of our literature search. Most protocols (seeTable 1) combine social support, psychoeducation, andcognitive–behavioral components in an effort to increasemotivation and self-esteem; build new problem-solving,interpersonal, and emotion regulation skills; and developstrategies to identify and cope with trauma- and drug-relatedstimuli. Only three trials used protocols that includeexposure therapy for PTSD (Brady, Dansky, Back, Foa, &Carroll, 2001; Najavits, Schmitz, Gotthardt, & Weiss, 2005;Triffleman, 2000).
3.2.4. Comparison interventionsOf the nine controlled studies, eight comparison condi-
tions included some form of SUD treatment, whereas onecompared IT to any form of care sought naturalistically. Fourcompared IT with a non-IT program matched for frequencyand duration of contact (see Table 2). One study (McFallet al., 2005) compared IT with a parallel treatment approachwhere participants received smoking cessation and PTSDtreatment in separate, noncollaborating facilities. In severalcases, researchers noted the potential for contamination
between the IT and non-IT programs stemming fromincidental trauma discussions in the comparison conditionor outside discussions between clients receiving differenttreatment within the same facility (Frisman, Ford, Lin,Mallon, & Chang, 2008; Triffleman, 2000; Zlotnick,Johnson, & Najavits, 2009).
3.2.5. Risk of bias assessmentGlobal QAT ratings are available in Tables 2 and 3. Using
this measure, five studies received a strong rating; thesetended to be controlled trials where participants were at leastsomewhat likely to be representative of the target popula-tion and that controlled for at least 80% of relevant con-founders, used valid and reliable measures, and hadacceptable dropout rates. Four controlled trials and twocohort studies received a global moderate rating; thesestudies tended to be fairly well designed but were limited bysmall sample sizes and nonequivalent control groups. Sixcohort studies received a weak global rating. Their largestsources of bias stemmed from very small samples sizes(often exacerbated by treatment dropout). Problems common
Table 1IT programs used in the selected studies
IT program Description and key components Evaluated by
CBT for PTSD in addictiontreatment programs
Eight manual-guided modules administered over 8–12 individualsessions. Psychoeducation, anxiety reduction skills (breathing retraining),cognitive processing and restructuring. Offered within SUD treatment.
McGovern et al., 2009
CTPCD 16 individual 90-minute sessions, twice weekly. Psychoeducation, copingand affect regulation skills, cognitive restructuring, cocaine relapse prevention,and in vivo and imaginal trauma exposure. Stand-alone treatment.
Brady et al., 2001
DART for co-occurringdisorders
9 hours per week of psychoeducation and skills training over 12 weeks.Designed to strengthen identification with the community, pluspsychoeducation, trauma-informed addictions treatment, and casemanagement. Offered within the SUD treatment.
Sacks et al., 2008
Seeking Safety 25 group or individual sessions administered twice weekly. Psychoeducation,coping and interpersonal effectiveness skills, cognitive processing,and restructuring. Exposure not part of curriculum but has been evaluated asan adjunct. Stand-alone treatment.
Hien et al., 2004; 2009; Najavits, Weiss, Shaw,& Muenz, 1998; Najavits et al., 2005, 2006;Weller, 2005; Zlotnick et al., 2003, 2009;four WCDVS sites
SDPT 20-Week individual program. Phase I: addiction focused, trauma informed(establishing abstinence); Phase II: trauma focused, addictions informed.Cognitive–behavioral relapse prevention and coping skills for SUD,psychoeducation, stress inoculation training, and in vivo exposure therapyfor PTSD. Stand-alone treatment.
Triffleman, 2000
TRANSCEND Developed for military veterans. Ten-hour group therapy per week for12 weeks. Combines cognitive–behavioral, constructivist, psychodynamic,and 12-step models. Coping and affect regulation skills, psychoeducation,trauma processing. Offered following mandatory SUD rehabilitation.
Donovan, Padin-Rivera, & Kowaliw, 2001
TARGET Eight to nine gender-specific group sessions. Psychoeducation, cognitiveprocessing, emotion regulation skills, and personal narrative work. Offeredwithin SUD treatment.
Frisman et al., 2008
TREM 33-Session group intervention for women. Psychoeducation, cognitiverestructuring, assertiveness, and emotion regulation skills. Brief traumaexposure covered in manual, but not implemented in evaluations. Offeredwithin the SUD treatment.
Two WCDVS sites
Integrated tobaccocessation treatment
Six manual-guided, 20-minute smoking cessation sessions integrated withregularly scheduled PTSD therapy sessions. Cessation componentsinclude behavioral counseling, stress management, and pharmacotherapy.Offered within PTSD treatment.
McFall et al., 2005, 2006
Note. CBT = cognitive–behavioral therapy; CTPCD= concurrent treatment of PTSD and cocaine dependence; DART = dual assessment and recovery track; SDPT =substance dependency PTSD therapy; TARGET=TraumaAdaptiveRecoveryGroup Education and Therapy; TREM=TraumaRecovery andEmpowermentModel.
69I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77
Author's personal copy
across studies included not using intent-to-treat (ITT)analyses and not describing blinding procedures.
3.3. Study outcomes
3.3.1. Are IT programs effective?Most of the studies found that IT programs effectively
reduced substance use and posttraumatic and other mentalhealth symptoms from baseline through follow-up, withsymptoms remaining stable or continuing to improveposttreatment. Of the five studies receiving a strong QATrating, three concluded that IT reduced both trauma andSUD symptoms through follow-up (Frisman et al., 2008;Hien et al., 2004; Sacks, McKendrick, Sacks, Banks, &Harle, 2008). One found that trauma symptoms improved,but not SUD (Hien et al., 2009). Another study foundthat SUD (smoking cessation rates) improved; between-
group differences for PTSD were not reported (McFallet al., 2005).
Studies receiving moderate QAT rating showed a similarpattern, with four finding that IT reduced both trauma andSUD symptoms (Najavits, Gallop, & Weiss, 2006; Triffle-man, 2000; Zlotnick et al., 2009; Zlotnick, Najavits,Rohsenow, & Johnson, 2003). Another study found thatSUD (smoking cessation rates) improved; changes in PTSDwere not reported (McFall et al., 2006). The WCDVS foundthat across treatment sites, IT reduced trauma at the12-month follow-up but not SUD symptoms (Morrisseyet al., 2005). To note, IT was associated with SUD improve-ment at follow-up by two individual WCDVS sites (Amaro etal., 2007; Gatz et al., 2007). IT also generally producedfavorable outcomes in studies receiving a weak QAT rating.
Meta-analytic results support these impressions. Insuffi-cient detail prevented calculation of an ES for SUD
Table 2Characteristics of controlled studies
First author, year Target population n a ITT IT b CC Follow-up QAT c Does IT improvesymptoms?d
Is IT superiorto CC? d
Frisman et al.(2008)
Adults with traumahistory, SUD, andPTSD or MHD
213 No TAU + TARGET TAU: trauma-sensitiveusual care
6 and12 months
S PTSD: yesSUD: yesMH: yes
PTSD: noSUD: noMH: no
Hien et al.(2004)
Women with SUDand full orsubthreshold PTSD
115 No Seeking Safety +SCC
Either relapseprevention (RP) + SCC, orSCC alone
EOT, 6 and9 months
S PTSD: yesSUD: yesMH: no
IT vs. RPPTSD, SUD,and MH: noIT vs. SCCPTSD: yesSUD: yes
Hien et al.(2009)
Women with SUDand full orsubthreshold PTSD
353 Yes Seeking Safety(12 sessions) +SUD treatment
Women's healtheducation +SUD treatment
EOT, 3, 6,and 12 months
S PTSD: yesSUD: no
PTSD: noSUD: no
McFall et al.(2005)
Veteran smokerswith PTSD
66 Yes TAU + integratedtobacco cessationtreatment
TAU: PTSD psycho-andpharmacotherapy.Smoking cessationtreatment referral
4, 6, and9 months
S PTSD: noSUD: yesMH: no
PTSD: notreportedSUD: yesMH: no
Morrisseyet al. (2005)
Women with traumahistory, SUD,and MHD
2,729 No SUD treatment +trauma-specifictreatment varyingby site
SUD treatment 12 months M PTSD: yesSUD: noMH: yes
PTSD: yesSUD: noMH: yes
Najavits et al.(2006)
Adolescent girls withPTSD and SUD
33 Yes Seeking Safety Any treatmentparticipants soughtby themselves
EOT and3 months
M PTSD: someSUD: someMH: some
PTSD: someSUD: someMH: some
Sacks et al.(2008)
Outpatients with SUDand emotionaldistress/MHD
240 Yes DART SUD treatment 12 months S PTSD: yesSUD: yesMH: yes
PTSD: noSUD: noMH: some
Triffleman(2000)
Adults with SUDand full orsubthresholdPTSD
19 Yes SDPT 12-Step facilitationtherapy
EOT and1 month
M PTSD: yesSUD: yesMH: yes
PTSD: noSUD: noMH: no
Zlotnick et al.(2009)
Incarcerated womenwith SUD and fullor subthreshold PTSD
49 No TAU +Seeking Safety
TAU: 12-step-basedSUD treatment
3 and6 monthsafter release
M PTSD: yesSUD: yesMH: yes
PTSD: noSUD: noMH: no
Note. SCC = standard community care; MH = mental health; EOT = end of treatment; MHD = mental health disorder; TAU = treatment as usual; CC =comparison condition; DART = dual assessment and recovery track; SDPT = substance dependency PTSD therapy; RP = relapse prevention.
a At baseline.b For abbreviations of individual programs, see Table 1.c QAT: S = strong; M = moderate; W = weak.d At longest follow-up time point.
70 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77
Author's personal copy
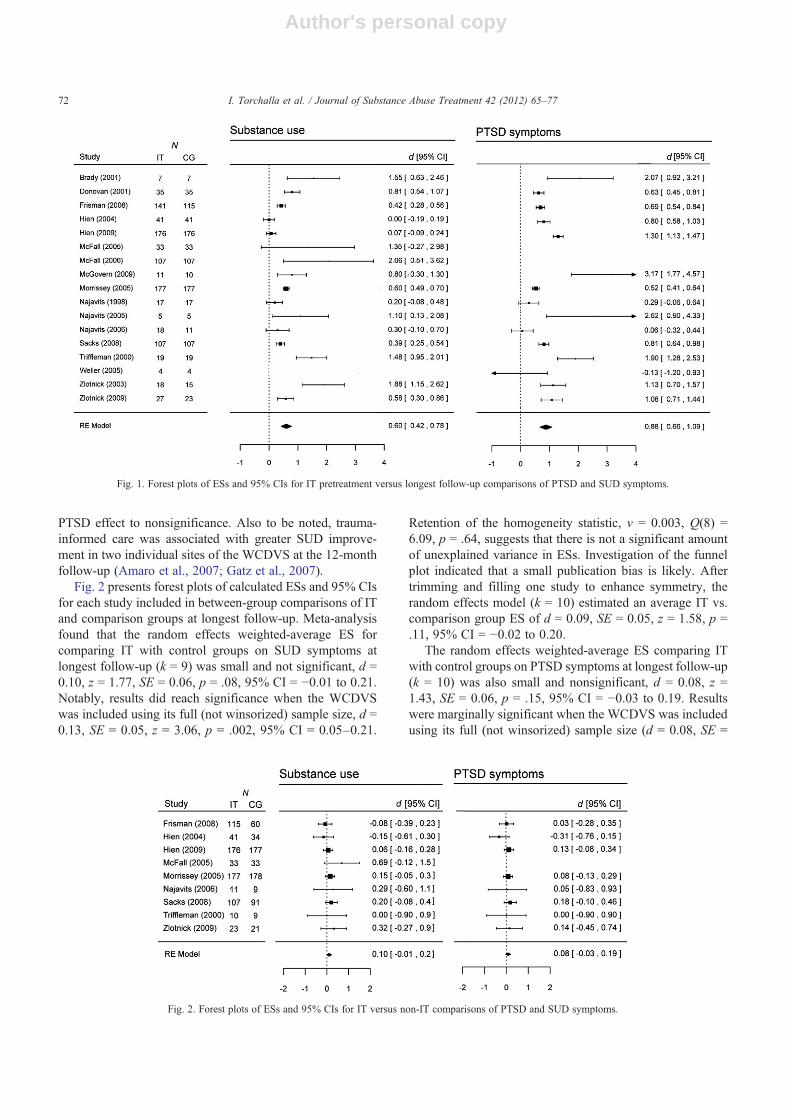
outcomes in Weller (2005) and for PTSD in McFall et al.(2005; 2006). Fig. 1 presents forest plots of calculated ESsand 95% confidence intervals (CIs) for each study includedin within-group comparisons of symptom change frombaseline to the longest available follow-up. The randomeffects weighted-average ES for change in SUD symptomsfrom baseline to longest follow-up (k = 16) was d = 0.60, z =6.41, SE = 0.09, p b .0001, 95% CI = 0.42–0.78. Rejectionof homogeneity statistic, v = 0.009, Q(15) = 104.39, p b.0001, suggests that systematic variance in ESs remainsunexplained by these analyses. Investigation of the funnelplot indicated that moderate publication bias is likely(asymmetrical plot, with small or negative ESs missingand larger ESs coming predominantly from small samples).The trim-and-fill method identified five studies to betrimmed from the funnel to enhance symmetry. Whenreplaced along with their missing counterparts, the randomeffects model (k = 21) estimated an average baseline-to-follow-up ES of d = 0.43, z = 4.32, SE = 0.10, p b .0001,95% CI = 0.23–0.62.
The random effects weighted-average ES for change inPTSD symptoms from baseline to the longest availablefollow-up (k = 15) was d = 0.88, z = 8.05, SE = 0.11, p b.0001, 95% CI = 0.66–0.09. Systematic variance in ESsremains unexplained by these analyses, v = 0.012, Q(14) =117.73, p b .0001. Investigation of the funnel plot implied amodest publication bias; two studies were identified to betrimmed and filled to enhance symmetry. Following thisprocedure, the random effects model (k = 17) estimated an
average baseline-to-follow-up ES of d = 0.81, z = 7.24, SE =0.11, p b .0001, 95% CI = 0.59–1.03.
3.3.2. Are IT programs superior to non-IT programs?In the most of the controlled trials, there were no sig-
nificant differences in the effectiveness of IT and theircomparison conditions. Among the five strong studies, fourfound that IT programs produced similar improvements intrauma and SUD symptoms over time when compared withnonintegrated programs of similar (or lesser) treatmentintensity (Frisman et al., 2008; Hien et al., 2004, 2009; Sackset al., 2008). Although McFall et al. (2005) found that ITproduced superior outcomes on some smoking outcomes,aggregation with other reported outcomes (e.g., repeated7-day abstinence rates) eliminated this group difference.Hien et al. (2004) also found IT superior to a nonrandomizedcommunity care condition.
A similar pattern of results was observed among mode-rate studies; with two of four finding that IT and non-ITtreatments produce equivalent improvements (Triffleman,2000; Zlotnick et al., 2009). Although Najavits et al. (2006)found that Seeking Safety produced superior outcomes on20% of the 76 individual substance use, mental health, andtrauma variables assessed, aggregation of ESs producednonsignificant overall ds for this study. The WCDVS foundthat at 12 months posttreatment, IT was superior to non-ITfor mental health and trauma-related outcomes but equal forSUD outcomes. However, winsorization of the large sam-ple size (for the meta-analysis) pushed the small WCDVS
Table 3Characteristics of uncontrolled studies
First author, year Target population n a ITT IT b Follow-up QAT c Does IT improvesymptoms? d
Brady et al. (2001) Adults with PTSD andcocaine dependence
39 No CTPCD EOT and 6 months W PTSD: noSUD: yesMH: yes
Donovan et al. (2001) Male Vietnam veterans withPTSD and SUD
46 No TRANSCEND EOT, 6 and 12 months W PTSD: yesSUD: yes
McFall et al. (2006) Veteran smokers with PTSD 107 Yes PTSD psycho- and pharmacotherapy +integrated tobacco cessation treatment
2, 4, 6, and 9 months M PTSD: not reportedSUD: yes
McGovern et al. (2009) Adults with SUD andelevated PTSD symptoms
23 No CBT for PTSD in addiction treatmentprograms
EOT and 3 months W PTSD: yesSUD: yes
Najavits et al. (2005) Men with PTSD and SUD 5 Yes Seeking Safety plus exposure therapy EOT W PTSD: yesSUD: yesMH: yes
Najavits, Weiss, et al.(1998)
Women with PTSD and SUD 27 No Seeking Safety EOT and 3 months W PTSD: yesSUD: yesMH: yes
Weller (2005) Female veterans withSUD and trauma history
6 Yes Seeking Safety EOT W PTSD: noSUD: yesMH: no
Zlotnick et al. (2003) Incarcerated women withSUD and PTSD
18 No Seeking Safety + 12-step-basedSUD treatment
EOT, 6 and 12weeks postrelease
M PTSD: yesSUD: yes
Note. EOT = end of treatment; CBT = cognitive–behavioral therapy; CTPCD = concurrent treatment of PTSD and cocaine dependence; MH = mental health.a At baseline.b For abbreviations of programs see Table 1.c QAT: S = strong; M = moderate; W = weak.d At longest follow-up time point.
71I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77
Author's personal copy
PTSD effect to nonsignificance. Also to be noted, trauma-informed care was associated with greater SUD improve-ment in two individual sites of the WCDVS at the 12-monthfollow-up (Amaro et al., 2007; Gatz et al., 2007).
Fig. 2 presents forest plots of calculated ESs and 95% CIsfor each study included in between-group comparisons of ITand comparison groups at longest follow-up. Meta-analysisfound that the random effects weighted-average ES forcomparing IT with control groups on SUD symptoms atlongest follow-up (k = 9) was small and not significant, d =0.10, z = 1.77, SE = 0.06, p = .08, 95% CI = −0.01 to 0.21.Notably, results did reach significance when the WCDVSwas included using its full (not winsorized) sample size, d =0.13, SE = 0.05, z = 3.06, p = .002, 95% CI = 0.05–0.21.
Retention of the homogeneity statistic, v = 0.003, Q(8) =6.09, p = .64, suggests that there is not a significant amountof unexplained variance in ESs. Investigation of the funnelplot indicated that a small publication bias is likely. Aftertrimming and filling one study to enhance symmetry, therandom effects model (k = 10) estimated an average IT vs.comparison group ES of d = 0.09, SE = 0.05, z = 1.58, p =.11, 95% CI = −0.02 to 0.20.
The random effects weighted-average ES comparing ITwith control groups on PTSD symptoms at longest follow-up(k = 10) was also small and nonsignificant, d = 0.08, z =1.43, SE = 0.06, p = .15, 95% CI = −0.03 to 0.19. Resultswere marginally significant when the WCDVS was includedusing its full (not winsorized) sample size (d = 0.08, SE =
Fig. 1. Forest plots of ESs and 95% CIs for IT pretreatment versus longest follow-up comparisons of PTSD and SUD symptoms.
Fig. 2. Forest plots of ESs and 95% CIs for IT versus non-IT comparisons of PTSD and SUD symptoms.
72 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
0.04, z = 1.96, p = .05, 95% CI = 0.0001–0.16). Homo-geneity was not rejected, v = 0.003, Q(7) = 3.58, p = .82.Investigation of the funnel plot indicated that a smallpublication bias is likely. After trimming and filling onestudy to enhance symmetry, the random effects model (k =10) estimated a marginally significant average ES of d =0.11, SE = 0.06, z = 1.97, p = .05, 95% CI = 0.0005–0.22.
4. Discussion
This is the first study to our knowledge that systematicallyreviewed and quantitatively evaluated the effects of inte-grated trauma and substance abuse service models on PTSDand SUD symptoms. Of the 17 trials identified, most of thestudies found that IT effectively reduced PTSD and SUDsymptoms over time. Meta-analyses confirmed this resultacross studies; IT was associated with large reductions inboth SUD and PTSD symptoms from baseline throughfollow-up (overall ds of 0.60 and 0.88, respectively). How-ever, at present, there is insufficient evidence to concludethat IT is any more effective than nonintegrated programs.Specifically, most studies (particularly those using strongermethods) found that IT and non-IT conditions producedsimilar reductions in PTSD and SUD symptoms. Meta-analyses comparing IT and non-IT groups on symptoms atlongest follow-up also produced small, nonsignificant ESsfor both PTSD (d = 0.10) and SUD (d = 0.08). The equiva-lency of IT and non-IT groups should be interpreted withcaution, given the small number of high-quality studies.Indeed, estimations of between-group effects after account-ing for publication bias suggested that PTSD symptoms werereduced marginally more by IT than non-IT. Calculationsthat included the WCDVS (Morrissey et al., 2005) at fullsample size (not winsorized) also pushed the group dif-ferences to significance for both PTSD and SUD symptoms(in favor of IT). Even so, ESs were small in all cases (dsranging from 0.08 to 0.13), suggesting that the superiority ofIT is slight either way.
Our study adds to emerging evaluations of IT programsfor individuals with concurrent disorders. Its overall findingis in line with two recent systematic reviews, which con-cluded that although IT is a promising approach for thetreatment of concurrent disorders, empirical evidence for thesuperiority of IT compared with non-IT is lacking. Speci-fically, these reviews failed to find evidence that IT issuperior to non-IT programs for individuals with SUD andcomorbid general mental health disorders (Donald et al.,2005) or individuals with SUD and any type of anxiety ordepressive disorder (Hesse, 2009). This study adds to thesefindings by specifically focusing on treatments for SUD andPTSD (as opposed to more general psychological condi-tions) and by using systematic, quantitative methods to sup-plement narrative impressions.
Equivalence in outcomes is surprising given the strongrationale for IT programs. If we assume that IT is truly no
more or less effective, it may be because non-IT sincidentally alleviate PTSD symptoms through nonspecifictreatment characteristics (e.g., therapeutic alliance), general-ization of non-trauma-specific skills (e.g., relaxation,emotion regulation, problem solving), reductions in co-occurring SUD, or simple regression to the mean. Indeed,these may actually be the active mechanisms of change in ITrather than any trauma-specific treatment components.Indeed, many IT programs had a greater treatment intensity,frequency, and/or duration than comparison programs,which could explain some instances in which IT appearssuperior. They also tended to use more structured protocolsand more carefully trained clinicians. Clearly, equating thesenonspecific factors will be essential for future work. Thatbeing said, it is premature to conclude that IT is not asuperior treatment based on the current state of the literature.
Several methodological issues may at least partly con-tribute to failures to detect between-group differences intreatment efficacy. First, the overall quality of the evidencebase is an issue. Only five studies included in this reviewreceived a strong quality rating based on the QAT. Second,studies were limited by small sample sizes, and many maynot have the appropriate statistical power to reliably detectexisting advantages of IT versus non-IT. Nonequivalentcontrol groups, poor control of confounders, and a lack ofassessor blinding further limited the remaining studies.Although we acknowledge that carrying out treatmentstudies with individuals with psychiatric comorbidities isextremely challenging (due to difficulties recruiting, engag-ing, and retaining clients in treatment; maintaining contactfor follow-up; etc.), more well-designed, randomized controltrials using large samples are definitely needed to move thefield forward.
Second, intended differences between IT and non-IT pro-tocols were minimal in some trials. Incidental traumadiscussion in control groups, for example, was a source ofcontamination in several studies (Frisman et al., 2008;Triffleman, 2000; Zlotnick et al., 2009). Limited IT “dosage”was also common. Frisman et al. (2008), for example, foundthat only 27% of their participants received a full course ofTrauma Adaptive Recovery Group Education and Therapy(TARGET). Hien et al. (2009) found that participantsattended only 6 of 12 Seeking Safety sessions on average,with only 12% attending all 12 sessions. Similarly, Najavitset al. (2006) found that participants attended an average of11.78 of 25 Seeking Safety sessions, only 1.33 of which weretrauma-focused discussion. Such results confirm that thetreatment of individuals with concurrent disorders ischallenged by difficulties in engaging and keeping them inrecovery programs, and strategies to enhance treatment moti-vation in this population are underresearched and not wellunderstood (DiClemente, Nidecker, & Bellack, 2008).Although most studies find that attrition rates do not differfor IT versus non-IT, further investigation of ways to maxi-mize IT viability and participants' motivation, retention, andcompliance may be warranted. It will also be critical for
73I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
future IT trials to demonstrate that participants allocatedto receive IT actually received a qualitatively different type oftherapy in a sufficient dosage to effect anticipated changes.Similarly, unintended attention to trauma issues in compar-ison groups should be assessed and controlled when possible.
Related to this issue, assessment bias may also have beenintroduced by uniform assessment of psychiatric symptomsat follow-up. It may be that IT interventions resulted in anincreased awareness of emotional responses and traumasymptoms compared with treatment that did not addresstrauma/PTSD. As a consequence, trauma symptoms mayhave been more salient for individuals who attended IT;hence, they may have been more likely than non-IT par-ticipants to report such symptoms at follow-up. Alterna-tively, repeated assessment of trauma symptoms duringnon-IT interventions could have increased participants'resolve to work on improving these symptoms via othermeans (e.g., discussing trauma issues with peers). Researchexamining the impact of measurement on trauma symptomswould be valuable toward clarifying the extent to whichassessment bias helps explain treatment equivalency.
Fourth, heterogeneity in samples may be obfuscatingtreatment differences. For example, although evidence sug-gests that women with less severe PTSD symptoms do notbenefit from IT as much as those with more severe symptoms(Cusack, Morrissey, & Ellis, 2008), only two controlledtrials required all participants to meet full diagnostic criteriafor PTSD (McFall et al., 2005; Najavits et al., 2006). Otherstudies indicated that IT may be more effective for White (vs.non-White) men (Frisman et al., 2008) and for womenmandated (vs. volunteering) for treatment (Clark & Young,2009). Furthermore, the type of substance may be impor-tant. Research suggests that women misusing alcohol mayhave more benefits from IT than women using other sub-stances (Hien, Campbell, Ruglass, Hu, & Killeen, 2010).However, only three studies in our review targetedindividuals with specific SUDs (i.e., smokers and cocaine-dependent persons), whereas the remaining studies includedindividuals who met criteria for any SUD. Other factors,such as whether participants were required to be abstinentat the time of admission or not, may also be relevant. Un-fortunately, most studies did not include sufficient samplesizes to permit subgroup analysis. Future studies are en-couraged to present analyses and/or separate ESs for gender,ethnicity, and substance-related subgroups to promote betterunderstanding of this issue.
Finally, if specific IT programs are more or less effectivethan others, heterogeneity in protocols may also be an issue.One limitation of our study is that by analyzing the differentIT programs altogether, we are assuming that theoretically,they all have similar efficacy. However, programs variedconsiderably on how IT was delivered (e.g., number ofsessions, content of treatment manual, level of integration,handling of substance use/relapse). There are several reason-able arguments about why and under which circumstancesone type of program may be more effective than another. For
example, in the WCDVS, the ESs were substantially greaterin sites where women in the IT intervention condition(relative to those in the comparison condition) reportedgreater integration of mental health, trauma, and substanceuse issues (Ellis & Morrissey, 2009).
In addition, nine different IT programs were investigatedin this study, not including the variety used solely at aWCDVS site. Unfortunately, most programs have only beenevaluated by one or two studies, making it difficult todetermine relative efficacy. Only Seeking Safety was inves-tigated multiple times; studies using this paradigm appearedto find reductions in symptoms similar to nonintegratedinterventions. Problematically, despite strong evidence forthe efficacy of exposure-based treatment for PTSD (Bradley,Greene, Russ, Dutra, & Westen, 2005; Powers, Halpern,Ferenschak, Gillihan, & Foa, 2010), only one controlled(Triffleman, 2000) and two uncontrolled (Brady et al., 2001;Najavits et al., 2005) IT trials contained imaginal and/or invivo trauma exposure components. Further work in this areais sorely needed; recommendations for successfully inte-grating SUD and exposure therapies are available in Hensleeand Coffey (2010). Greater attention to pharmacotherapyoptions is also warranted. Only a few studies have examinedthe efficacy of specific pharmaceuticals as a stand-alonetreatment for concurrent PTSD and SUD, and not one hasexamined the efficacy of medication in supporting psycho-therapeutic interventions. In a recent review of the literature,Norman et al. (2011) concluded that medications targetingthe serotonin or dopamine system warrant further attentionin well-conducted studies with large samples and rigorousscientific methods. Finally, it may also be useful to explorethe integration of SUD treatment with intensive, longer termtherapy programs such as dialectical behavior therapy.
5. Conclusions and recommendations
Given the high concurrence rates of PTSD and SUD(Kessler et al., 1995), as well as indications that PTSDsymptoms precipitate substance use (Ouimette et al., 2010),the rationale for integrated trauma and SUD interventionsis strong. Development and evaluation of various ITs haveprogressed gradually over the past decade. Overall, ITappears to effectively reduce trauma and SUD symptoms,but there is insufficient evidence to support its superiorityover nonintegrated programs. We found no evidence that ITis harmful or less effective than nonintegrated programs.Thus, the existing evidence base suggests that both inte-grated and nonintegrated programs are viable and effectivetreatment options. Clinicians currently considering whichtreatment approach to take may wish to base their decisionson factors like client preference, program availability, andexpense. That said, it is critical not to discount the pre-liminary, rather limited state of the existing body of litera-ture because these recommendations may change withfurther research. In particular, more methodologically
74 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
rigorous randomized control trials are required to clarify therelative efficacy of integrated programs. Particular attentionshould be devoted to maximizing intended differencesbetween IT and non-IT programs (e.g., ensuring adequateIT dosage, minimizing contamination), evaluating under-studied IT programs, incorporating and evaluating exposure-based paradigms, developing innovative approaches toincrease treatment engagement, and using suitable samples(e.g., clients with PTSD diagnoses, ns large enough topermit subgroup analysis). More funding should be dedi-cated to support the implementation of studies addressingthese challenging methodological issues.
Acknowledgments
This study was partly supported by a development fundthrough the BC Mental Health and Addictions ResearchNetwork. Iris Torchalla, Liz Nosen, and Hajera Rostam werepartly supported through research fellowships at the In-tersections of Mental Health Perspectives in AddictionsResearch Training, a training program funded by theCanadian Institutes of Health Research.
References
Amaro, H., Dai, J., Arévalo, S., Acevedo, A., Matsumoto, A., Nieves, R., &Prado, G. (2007). Effects of integrated trauma treatment on outcomes ina racially/ethnically diverse sample of women in urban community-based substance abuse treatment. Journal of Urban Health, 84,508–522, doi:10.1007/s11524-007-9160-z.
Back, S. E., Dansky, B. S., Coffey, SF, Saladin, M. E., Sonne, S., & Brady,K. T. (2000). Cocaine dependence with and without post-traumatic stressdisorder: A comparison of substance use, trauma history and psychiatriccomorbidity. The American Journal on Addictions, 9, 51–62, doi:10.1080/10550490050172227.
Back, S. E., Waldrop, A. E., Brady, K. T., & Hien, D. (2006). Evidenced-based time-limited treatment of co-occurring substance-use disordersand civilian-related posttraumatic stress disorder. Brief Treatment andCrisis Intervention, 6, 283–294, doi:10.1093/brief-treatment/mhl013.
Becker, B. J. (1988). Synthesizing standardized mean-change measures.British Journal of Mathematical & Statistical Psychology, 41, 257–278.
Bradley, R., Greene, J., Russ, E., Dutra, L., & Westen, D. (2005). A multi-dimensional meta-analysis of psychotherapy for PTSD. The AmericanJournal of Psychiatry, 162, 214–227, doi:10.1176/appi.ajp.162.2.214.
Brady, K. T., Dansky, B. S., Back, S. E., Foa, E. B., & Carroll, K. M. (2001).Exposure therapy in the treatment of PTSD among cocaine-dependentindividuals: Preliminary findings. Journal of Substance Abuse Treat-ment, 21, 47–54, doi:10.1016/S0740-5472(01)00182-9.
Brady, K. T., Killeen, T., Saladin, M. E., Dansky, B., & Becker, S. (1994).Comorbid substance abuse and posttraumatic stress disorder. TheAmerican Journal on Addictions, 3, 160–164, doi:10.1111/j.1521-0391.1994.tb00383.x.
Brown, P. J., Stout, R. L., & Mueller, T. (1999). Substance use disorder andposttraumatic stress disorder comorbidity: Addiction and psychiatrictreatment rates. Psychology of Addictive Behaviors, 13, 115–122, doi:10.1037/0893-164X.13.2.115.
Chilcoat, H. D., & Breslau, N. (1998). Investigations of causal pathwaysbetween PTSD and drug use disorders. Addictive Behaviors, 23,827–840, doi:10.1016/S0306-4603(98)00069-0.
Clark, C., & Young, M. S. (2009). Outcomes of mandated treatmentfor women with histories of abuse and co-occurring disorders. Journal
of Substance Abuse Treatment, 37, 346–352, doi:10.1016/j.jsat.2009.03.011.
Clark, H.W.,Masson, C. L., Delucchi, K. L., Hall, S.M., & Sees, K. L. (2001).Violent traumatic events and drug abuse severity. Journal of SubstanceAbuse Treatment, 20, 121–127, doi:10.1016/S0740-5472(00)00156-2.
Coffey, C. F., Read, J. P., & Norberg, M. M. (2008). Posttraumatic stressdisorder and substance use disorder: Neuroimaging, neuroendocrine, andpsychophysiological findings. In S. H. Stewart, & P. J. Conrod (Eds.),Anxiety and substance use disorders. The vicious cycle of comorbidity(pp. 37–57). New York, NY: Springer Sciences + Business Media.
Cusack, K. J., Morrissey, J. P., & Ellis, A. R. (2008). Targeting trauma-related interventions and improving outcomes for women with co-occurring disorders. Administration and Policy in Mental Health, 35,147–158, doi:10.1007/s10488-007-0150-y.
Deeks, J. J., Dinnes, J., D'Amico, R., Sowden, A. J., Sakarovitch, C., Song,F., et al. (2003). Evaluating non-randomised intervention studies. HealthTechnology Assessment, 7, iii–x, 1–173.
DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials. Con-trolled Clinical Trials, 7, 177–188, doi:10.1016/0197-2456(86)90046-2.
DiClemente, C. C., Nidecker, M., & Bellack, A. S. (2008). Motivation andthe stages of change among individuals with severe mental illness andsubstance abuse disorders. Journal of Substance Abuse Treatment, 34,25–35, doi:10.1016/j.jsat.2006.12.034.
Donald, M., Dower, J., & Kavanagh, D. (2005). Integrated versus non-integrated management and care for clients with co-occurring mentalhealth and substance use disorders: A qualitative systematic review ofrandomised controlled trials. Social Science & Medicine, 60,1371–1383, doi:10.1016/j.socscimed.2004.06.052.
Donovan, B., Padin-Rivera, E., & Kowaliw, S. (2001). “Transcend”:Initial outcomes from a posttraumatic stress disorder/substanceabuse treatment program. Journal of Traumatic Stress, 14, 757–772,doi:10.1023/A:1013094206154.
Drake, R. E., Essock, S. M., Shaner, A., Carey, K. B., Minkoff, K., Kola, L.,et al. (2001). Implementing dual diagnosis services for clients withsevere mental illness. Psychiatric Services, 52, 469–476, doi:10.1176/appi.ps.52.4.469.
Driessen, M., Schulte, S., Luedecke, C., Schaefer, I., Sutmann, F., Ohlmeier,M., et al. (2008). Trauma and PTSD in patients with alcohol, drug, ordual dependence: A multi-center study. Alcoholism, Clinical andExperimental Research, 32, 481–488, doi:10.1111/j.1530-0277.2007.00591.x.
Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel-plot-basedmethod of testing and adjusting for publication bias in meta-analysis.Biometrics, 56, 455–463, doi:10.1111/j.0006-341X.2000.00455.x.
Ellis, A. R., & Morrissey, J. P. (2009). Assessing multiple outcomes forwomen with co-occurring disorders and trauma in a multi-site trial: Apropensity score approach. Administration and Policy in Mental Health,36, 123–132, doi:10.1007/s10488-009-0204-4.
Finkelstein, N., VandeMark, N., Fallot, R., Brown, V., Cadiz, S., &Heckman, J. (2004). Enhancing substance abuse recovery throughintegrated trauma treatment. Sarasota, FL: National Trauma Consor-tium, Center for Substance Abuse Treatment.
Fleiss, J. L. (1994). Measures of effect size for categorical data. In H. M.Cooper, & L. V. Hedges (Eds.), The Handbook of research synthesis.New York: Russell Sage Foundation.
Frisman, L., Ford, J., Lin, H. -J., Mallon, S., & Chang, R. (2008). Outcomesof trauma treatment using the TARGET model. Journal of Groups inAddiction & Recovery, 3, 285, doi:10.1080/15560350802424910.
Gatz, M., Brown, V., Hennigan, K., Rechberger, E., O'Keefe, M., Rose,T., & Bjelajac, P. (2007). Effectiveness of an integrated, trauma-informed approach to treating women with co-occurring disorders andhistories of trauma: The Los Angeles site experience. Journal ofCommunity Psychology, 35, 863–878, doi:10.1002/jcop.20186.
Hedges, L., & Olkin, I. (1985). Statistical methods for meta-analysis.Orlando: Academic Press.
Henslee, A. M., & Coffey, S. F. (2010). Exposure therapy for posttraumaticstress disorder in a residential substance use treatment facility.
75I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
Professional Psychology, Research and Practice, 41, 34–40, doi:10.1037/a0018235.
Hesse, M. (2009). Integrated psychological treatment for substance use andco-morbid anxiety or depression vs. treatment for substance use alone. Asystematic review of the published literature. BMC Psychiatry, 9, 6, doi:10.1186/1471-244X-9-6.
Hien, D. A., Campbell, A. N. C., Ruglass, L. M., Hu, M. C., & Killeen, T.(2010). The role of alcohol misuse in PTSD outcomes for women incommunity treatment: A secondary analysis of NIDA's Women andTrauma Study. Drug and Alcohol Dependence, 111, 114–119, doi:10.1016/j.drugalcdep.2010.04.011.
Hien, D. A., Cohen, L. R., Miele, G. M., Litt, L. C., & Capstick, C. (2004).Promising treatments for women with comorbid PTSD and substanceuse disorders. The American Journal of Psychiatry, 161, 1426–1432,doi:10.1176/appi.ajp.161.8.1426.
Hien, D. A., Wells, E. A., Jiang, H., Suarez-Morales, L., Campbell, A. N. C.,Cohen, L. R., et al. (2009). Multisite randomized trial of behavioralinterventions for women with co-occurring PTSD and substance usedisorders. Journal of Consulting and Clinical Psychology, 77, 607–619,doi:10.1037/a0016227.
Hunter, J. E., & Schmidt, F. L. (2004). Methods of meta-analysis:Correcting error and bias in research findings , 2nd ed). ThousandOaks, CA: SAGE.
Jennings, A. (2004). Models for developing trauma-informed behavioral-health systems and trauma-specific services. National Association ofMental Health Program Directors, National Technical AssistanceCenter for State Mental Health Planning 2004. National Associationof State Mental Health Program Directors (NASMHPD) and NationalTechnical Assistance Center for State Mental Health Planning (NTAC).Retrieved from http://theannainstitute.org/MDT.pdf.
Kessler, RC, Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995).Posttraumatic stress disorder in the National Comorbidity Survey. Arc-hives of General Psychiatry, 52, 1048–1060.
Khantzian, E. J. (1997). The self-medication hypothesis of substance usedisorders: A reconsideration and recent applications. Harvard Review ofPsychiatry, 4, 231–244, doi:10.3109/10673229709030550.
Kilpatrick, D. G., Resnick, H. S., Saunders, B. E., & Best, C. L. (1998).Victimization, posttraumatic stress disorder, and substance use andabuse among women. In C. L. Wetherington, & A. B. Roman (Eds.),Drug addiction research and the health of women, NIH PublicationNo. 98-4290 (pp. 285–307). Rockville, MD: U. S. Department of Healthand Human Services.
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Appliedsocial research methods series (Vol. 49). Thousand Oaks, CA.
McFall, M., Atkins, D. C., Yoshimoto, D., Thompson, C. E., Kanter, E.,Malte, C. A., et al. (2006). Integrating tobacco cessation treatmentinto mental health care for patients with posttraumatic stress disorder.The American Journal on Addictions, 15, 336–344, doi:10.1080/10550490600859892.
McFall, M., Saxon, A. J., Thompson, C. E., Yoshimoto, D., Malte, C., Straits-Troster, K., et al. (2005). Improving the rates of quitting smoking forveterans with posttraumatic stress disorder. The American Journal ofPsychiatry, 162, 1311–1319, doi:10.1176/appi.ajp.162.7.1311.
McGovern, M. P., Lambert-Harris, C., Acquilano, S., Xie, H., Alterman, A.I., & Weiss, R. D. (2009). A cognitive behavioral therapy for co-occurring substance use and posttraumatic stress disorders. AddictiveBehaviors, 34, 892–897, doi:10.1016/j.addbeh.2009.03.009.
Mills, K. L., Teesson, M., Ross, J., Darke, S., & Shanahan, M. (2005). Thecosts and outcomes of treatment for opioid dependence associated withposttraumatic stress disorder. Psychiatric Services, 56, 940–945, doi:10.1176/appi.ps.56.8.940.
Morrissey, J. P., Jackson, E. W., Ellis, A. R., Amaro, H., Brown, V. B., &Najavits, L. M. (2005). Twelve-month outcomes of trauma-informedinterventions for women with co-occurring disorders. PsychiatricServices, 56, 1213–1222, doi:10.1176/appi.ps.56.10.1213.
Najavits, L. M., Gallop, R. D., & Weiss, R. D. (2006). Seeking Safetytherapy for adolescent girls with PTSD and substance use disorder: A
randomized controlled trial. The Journal of Behavioral Health Servicesand Research, 33, 453–463, doi:10.1007/s11414-006-9034-2.
Najavits, L. M., Gastfriend, D. R., Barber, J. P., Reif, S., Muenz, L. R.,Blaine, J., et al. (1998). Cocaine dependence with and without PTSDamong subjects in the National Institute on Drug Abuse CollaborativeCocaine Treatment Study. The American Journal of Psychiatry, 155,214–219.
Najavits, L. M., Schmitz, M., Gotthardt, S., & Weiss, R. D. (2005). SeekingSafety plus exposure therapy: An outcome study on dual diagnosis men.Journal of Psychoactive Drugs, 37, 425–435.
Najavits, L. M., Weiss, R. D., Shaw, S. R., & Muenz, L. R.. (1998).“Seeking Safety”: Outcome of a new cognitive–behavioral psychother-apy for women with posttraumatic stress disorder and substancedependence. Journal of Traumatic Stress, 11, 437–456, doi:10.1023/A:1024496427434.
Norman, S. B., Myers, U. S., Wilkins, K. C., Goldsmith, A. A., Hristova, V.,Huang, Z., et al. (2011). Review of biological mechanisms andpharmacological treatments of comorbid PTSD and substance usedisorder. Neuropharmacology, doi:10.1016/j.neuropharm.2011.04.032.
Norman, S. B., Tate, S. R., Anderson, K. G., & Brown, S. A.. (2007). Dotrauma history and PTSD symptoms influence addiction relapse context?Drug and Alcohol Dependence, 90, 89–96, doi:10.1016/j.drugalcdep.2007.03.002.
Ouimette, P. C., Finney, J. W., & Moos, R. H. (1999). Two-yearposttreatment functioning and coping of substance abuse patients withposttraumatic stress disorder. Psychology of Addictive Behaviors, 13,105–114, doi:10.1037/0893-164X.13.2.105.
Ouimette, P. C., Moos, R. H., & Finney, J. W. (2000). Two-year mentalhealth service use and course of remission in patients with substance useand posttraumatic stress disorders. Journal of Studies on Alcohol, 61,247–253.
Ouimette, P. C., Moos, R. H., & Finney, J. W. (2003). PTSD treatment and5-year remission among patients with substance use and posttraumaticstress disorders. Journal of Consulting and Clinical Psychology, 71,410–414, doi:10.1037/0022-006X.71.2.410.
Ouimette, P., Read, J. P., Wade, M., & Tirone, V. (2010). Modelingassociations between posttraumatic stress symptoms and substance use.Addictive Behaviors, 35, 64–67, doi:10.1016/j.addbeh.2009.08.009.
Powers, M. B., Halpern, J. M., Ferenschak, M. P., Gillihan, S. J., & Foa, E.B. (2010). A meta-analytic review of prolonged exposure forposttraumatic stress disorder. Clinical Psychology Review, 30,635–641, doi:10.1016/j.cpr.2010.04.007.
Read, J. P., Brown, P. J., & Kahler, C. W. (2004). Substance use andposttraumatic stress disorders: Symptom interplay and effects onoutcome. Addictive Behaviors, 29, 1665–1672, doi:10.1016/j.addbeh.2004.02.061.
Reed, P. L., Anthony, J. C., & Breslau, N. (2007). Incidence of drugproblems in young adults exposed to trauma and posttraumaticstress disorder: Do early life experiences and predispositions matter?Archives of General Psychiatry, 64, 1435–1442, doi:10.1001/archpsyc.64.12.1435.
Reynolds, M., Mezey, G., Chapman, M., Wheeler, M., Drummond, C., &Baldacchino, A. (2005). Co-morbid post-traumatic stress disorder in asubstance misusing clinical population. Drug and Alcohol Dependence,77, 251–258, doi:10.1016/j.drugalcdep.2004.08.017.
Ridgely, M. S., Goldman, H. H., & Willenbring, M. (1990). Barriers to thecare of persons with dual diagnoses: Organizational and financing issues.Schizophrenia Bulletin, 16, 123–132, doi:10.1093/schbul/16.1.123.
Riggs, D. S., & Foa, E. B. (2008). Treatment for co-morbid posttraumaticstress disorder and substance use disorders. In S. H. Stewart, & P. J.Conrod (Eds.), Anxiety and substance use disorders (pp. 119–137).New York: Springer.
Ruzek, J. I., Polusny, M. A., & Abueg, F. R. (1998). Assessment andtreatment of concurrent posttraumatic stress disorder and substanceabuse. In V. M. Follette, J. I. Ruzek, & F. R. Abueg (Eds.), Cognitive–behavioral therapies for trauma (pp. 226–255). New York, NY: TheGuilford Press.
76 I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77

Author's personal copy
Sacks, S., McKendrick, K., Sacks, J. Y., Banks, S., & Harle, M. (2008).Enhanced outpatient treatment for co-occurring disorders: Main out-comes. Journal of Substance Abuse Treatment, 34, 48–60, doi:10.1016/j.jsat.2007.01.009.
Swendsen, J., Conway, K. P., Degenhardt, L., Glantz, M., Jin, R.,Merikangas, K. R., et al. (2010). Mental disorders as risk factors forsubstance use, abuse and dependence: Results from the 10-year follow-up of the National Comorbidity Survey. Addiction, 105, 1117–1128,doi:10.1111/j.1360-0443.2010.02902.x.
Tate, S. R., Norman, S. B., McQuaid, J. R., & Brown, S. A. (2007). Healthproblems of substance-dependent veterans with and those withouttrauma history. Journal of Substance Abuse Treatment, 33, 25–32, doi:10.1016/j.jsat.2006.11.006.
Thomas, H.. (1998). Quality assessment tool for quantitative studies.Effective Public Health Practice Project. Retrieved from http://www.nccmt.ca/registry/view/eng/14.html.
Triffleman, E.. (2000). Gender differences in a controlled pilot study ofpsychosocial treatments in substance dependent patients with post-
traumatic stress disorder—Design considerations and outcomes. Alco-holism Treatment Quarterly, 18, 113, doi:10.1300/J020v18n03_10.
Viechtbauer, W. (2010). Conducting meta-analyses in R with the Metaforpackage. Journal of Statistical Software, 36, 1–48.
Viechtbauer, W., & Cheung, M. W. L. (2010). Outlier and influencediagnostics for meta-analysis. Research Synthesis Methods, 1, 112–125,doi:10.1002/jrsm.11.
Weller, L. A. (2005). Group therapy to treat substance use and traumaticsymptoms in female veterans. Federal Practicioner, 22, 27–38.
Zlotnick, C., Johnson, J., & Najavits, L. M. (2009). Randomized controlledpilot study of cognitive–behavioral therapy in a sample of incarceratedwomen with substance use disorder and PTSD. Behavior Therapy, 40,325–336, doi:10.1016/j.beth.2008.09.004.
Zlotnick, C., Najavits, L. M., Rohsenow, D. J., & Johnson, D. M. (2003). Acognitive–behavioral treatment for incarcerated women with substanceabuse disorder and posttraumatic stress disorder: Findings from a pilotstudy. Journal of Substance Abuse Treatment, 25, 99–105, doi:10.1016/S0740-5472(03)00106-5.
77I. Torchalla et al. / Journal of Substance Abuse Treatment 42 (2012) 65–77