identification of overweight status is associated with higher rates of screening for comorbidities...
TRANSCRIPT

DOI: 10.1542/peds.2005-2867 2007;119;e148PediatricsBinns
Kimberley J. Dilley, Lisa A. Martin, Christine Sullivan, Roopa Seshadri and Helen J.for Comorbidities of Overweight in Pediatric Primary Care Practice
Identification of Overweight Status Is Associated With Higher Rates of Screening
http://pediatrics.aappublications.org/content/119/1/e148.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

ARTICLE
Identification of Overweight Status Is AssociatedWith Higher Rates of Screening for Comorbidities ofOverweight in Pediatric Primary Care PracticeKimberley J. Dilley, MD, MPHa,b, Lisa A. Martin, MD, MPHa,b, Christine Sullivan, MBA, MSc, Roopa Seshadri, PhDa,b,c, Helen J. Binns, MD, MPHa,b,c,
for the Pediatric Practice Research Group
aDepartment of Pediatrics, Children’s Memorial Hospital, Chicago, Illinois; bFeinberg School of Medicine, Northwestern University, Chicago, Illinois; cMary Ann andJ. Milburn Smith Child Health Research Program, Children’s Memorial Research Center, Chicago, Illinois
The authors have indicated they have no financial relationships relevant to this article to disclose.
ABSTRACT
OBJECTIVES. The goals were to determine whether primary care provider identifica-tion of children as overweight was associated with additional screening or referralsand whether the types and numbers of visits to primary care differed for over-weight and nonoverweight children.
METHODS. Sequential parents/guardians at 13 diverse pediatric practices completedan in-office survey addressing health habits and demographic features. Medicalrecords of each child from a sample of families were reviewed. Data were ab-stracted from the first visit and from all visits in the 14-month period before studyenrollment. Analyses were limited to children �2 years of age for whom BMIpercentile could be calculated.
RESULTS. The analytic sample included 1216 children (mean age: 7.9 years; 51%male) from 777 families (parents were 43% white, 18% black, 34% Hispanic, and5% other; 49% of families had a child receiving Medicaid/uninsured). Amongoverweight children (BMI of �95th percentile; n � 248), 28% had been identifiedas such in the record. Screening or referral for evaluation of comorbidities wasmore likely among overweight children who were identified in the record (54%)than among overweight children who were not identified (17%). Among childrenat risk of overweight (BMI of 85th to 94th percentile; n � 186), 5% had beenidentified as such in the record and overall 15% were screened/referred. In logisticregression modeling, the children identified as overweight/at risk of overweighthad 6 times greater odds of receiving any management for overweight.
CONCLUSIONS. Low rates of identification of overweight status and evaluation orreferrals for comorbidities were found. Identification of overweight status wasassociated with a greatly increased rate of screening for comorbidities.
www.pediatrics.org/cgi/doi/10.1542/peds.2005-2867
doi:10.1542/peds.2005-2867
Dr Martin’s current address is LoyolaUniversity, Stritch School of Medicine,Department of Pediatrics, 2160 S First Ave,Maywood, IL 60153.
KeyWordschildren, overweight, practice-basedresearch, screening
AbbreviationsAROW—at risk of overweightICC—intracluster correlationLR—logistic regressionOR—odds ratioHFHC—Healthy Families, Healthy Children:The Pediatrician’s RoleCI—confidence interval
Accepted for publication Jul 17, 2006
Address correspondence to Kimberley J. Dilley,MD, MPH, Children’s Memorial Hospital, 2300Children’s Plaza, Box 30, Chicago, IL 60614.E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005;Online, 1098-4275). Copyright © 2007 by theAmerican Academy of Pediatrics
e148 DILLEY et al at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

OBESITY IN CHILDREN is an increasing problem in theUnited States, mirroring similar increases in obe-
sity rates for adults in the United States and for popula-tions in other nations. An estimated 16.0% of US chil-dren and adolescents 6 to 19 years of age are overweight(BMI of �95th percentile), and 15.0% are at risk ofoverweight (AROW) (BMI of 85th to 94th percentile).1
Estimates are slightly lower for children 2 to 5 years ofage (10.3% overweight and 12.3% AROW).1 Not only isthe prevalence of childhood obesity increasing, but alsothere is a shift in weight distribution; obese children arefurther from their ideal body weights than ever before.2
Health care expenditures related to obesity are alsoincreasing. In the inpatient setting, 1.7% of all hospitalcosts for children between 1997 and 1999 were relatedto obesity.3 This number was �3 times the 0.43% foundbetween 1979 and 1981.4 Costs of outpatient care forobese children have not been reported, but we do knowthat reimbursement rates for outpatient treatment ofobese children are very low.5 Furthermore, althoughmany studies have documented higher rates of healthcare utilization and higher health care expenditures forobese adults, compared with nonobese adults,4,6–11 littleis known about whether health care utilization patternsin primary care settings differ for overweight children,compared with their nonoverweight counterparts.
Recommendations for the prevention,12 evaluation,and treatment13 of childhood obesity include a call forrepeated evaluations of a child’s nutritional status (ie, aninterpretation of weight in relation to height) by usingBMI calculations and percentile ranks for children thatare based on age and gender. The extent to which phy-sicians evaluate a child’s nutritional status annually inthis manner is not well known. Cross-sectional medicalrecord reviews in an academic primary care setting14 andan urban community health center that had introduceda type 2 diabetes mellitus screening protocol15 reportedidentification of obesity in �50% of health maintenancevisits in which the patient met objective criteria foroverweight. Lower rates of identification among AROWchildren (8%) were reported.15 Rates of documenteddiagnosis of overweight are lower (�20%) when AROWand overweight children are grouped together.16
It seems likely that identifying overweight andAROW children appropriately would foster evaluations,counseling, and treatments regarding health habits andcomorbid conditions. At the urban community healthcenter, children identified accurately as overweight weremore likely to receive counseling and type 2 diabetesscreening.15 Analysis of data from the National Ambula-tory Medical Care Survey and the National HospitalAmbulatory Medical Care Survey indicated that obesitywas diagnosed in only 0.93% of all well-child visits, amuch lower rate than would be expected on the basis ofoverweight prevalence.17 However, counseling regardingdiet and physical activity was more likely at visits at
which obesity was diagnosed.17 Another study that ex-amined data from both pediatric primary care and sub-specialty practices showed that the majority of children,especially younger children and those in the AROWcategory, were not diagnosed as overweight and did notreceive recommended screening.18 No studies to datehave examined health care utilization patterns for over-weight children in primary care settings. This study useda medical record review of visits to diverse primary carepediatric practices to examine the patterns of visits andcounseling for prevention or management of overweightand the patterns of additional evaluations provided tothose who met the criteria for overweight or AROWnutritional status classification.
METHODS
ParticipantsThirteen practices, which were members of the PediatricPractice Research Group, a practice-based, primary careresearch network,19 participated in study processes.These practices, including 6 private practices and 7health center/public health sites serving inner-city, low-income families, were recruited for participation in thestudy titled Healthy Families, Healthy Children: The Pe-diatrician’s Role (HFHC). The aims of HFHC were toexamine dissemination methods for practice systemschanges related to queries and counseling about tobaccousage and to evaluate family health habits and practicesystems related to general preventive evaluation andcounseling. Because HFHC included extensive parent-reported data both on family health habits and on pa-rental perceptions of the pediatrician’s role in healthpromotion counseling, we chose to examine the pediat-ric providers’ rates of evaluation of health status relatedto the weight of their pediatric patients. No specifichypothesis regarding the link between smoking house-holds and pediatric obesity was examined.
Individual study subjects entered the study in a2-stage process. First, a consecutive sample of parents/guardians of children who received care at the practicecompleted a baseline survey and provided signed con-sent for telephone follow-up contact and review of thepractice’s medical records for their children. Recruit-ment was accomplished between June 2002 and July2003 and occurred on 25 days at each practice. Of the6617 eligible subjects approached, 4218 (64%) signedconsent forms and completed a baseline survey. Of thosewho consented, a sample was selected for follow-upevaluation, including all families that reported house-hold tobacco use, those with missing information onhousehold tobacco use, and 1 randomly selected, non-smoking household per practice per recruitment day. At11 practices, the subjects for the current study includedthose who completed a first follow-up telephone call; at2 practices, all subjects selected for follow-up evaluation
PEDIATRICS Volume 119, Number 1, January 2007 e149 at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

(regardless of success with a first follow-up telephonecall) were included. This study was approved by theinstitutional review boards of the Children’s MemorialHospital and the Chicago Department of Public Health.
Data InstrumentsThe baseline survey collected data on demographic fea-tures, diet and activity habits of the respondent and anindex child (the oldest child in the office on the day ofthe survey), and household and personal smoking pat-terns. Demographic data included age and health insur-ance type of the index child and age, race/ethnicity, andeducation level of the respondent. Additional questionsaddressed the relationship between parent and childhealth habits and pediatricians’ role in counseling aboutparental health habits.
The retrospective medical record review began withan examination of the child’s initial visit and initialintake form (if available) for any family history of over-weight-related diagnoses (obesity, hypertension, heartdisease, or high cholesterol levels), asthma, or tobaccouse. Data were then collected by reviewing each visit fora 14-month period before and including visits occurringon the enrollment date. Overweight-related data col-lected from the provider notes and from laboratory re-sults sections of the chart are shown in Table 1. Corre-spondence sections of the records were also reviewed, tofacilitate assessment for specialist referrals. Chronic con-ditions expected to cause overweight, such as Prader-Willi syndrome, were noted if they appeared in anysection of the record that was reviewed. Data on respi-ratory-related symptoms, diagnoses, and treatmentswere also collected but are not reported here.
At each practice, a sample of �10% of medicalrecords were reviewed by Dr Dilley and either Dr Martinor another reviewer. Interrater reliability for individualitems within the medical record reviews had a � of0.687, with 95.7% agreement, for Drs Dilley and Martinand a � of 0.852, with 98.0% agreement, for Dr Dilleyand the other reviewer.
AnalysisOnly children �2 years of age within the medical recordreview period were included in analyses. Respondents’reports of race/ethnicity and the medical insurance sta-tus for the index child were assigned to all children inthe family. Height and weight data linked to age at thevisit and gender were used to calculate BMI, BMI per-centile, and BMI z score, based on national referencestandards, by using Epi Info (Centers for Disease Controland Prevention, Atlanta, GA). In analyses, overweightwas defined as �95th BMI percentile and AROW wasdefined as 85th to 94th BMI percentile.20 Each subjectchild was assigned to a BMI percentile group on the basisof the highest BMI obtained during the 14-month studyperiod. However, documentation of diagnoses, counsel-ing, laboratory tests, or referrals from any visit in thereview period was considered for reports of whether ornot these were provided. Bivariate analyses included �2,analysis of variance, and nonparametric tests, as appro-priate.
The first series of analyses described the prevalence ofoverweight and rates of physician documentation forchildren who were overweight or AROW. Factors fromthe record reviews (family history characteristics, childage group, and visit patterns) and parental surveys (eg,parent age group and race/ethnicity and child insurancetype) were examined for association with physician doc-umentation of an overweight diagnosis or concern aboutoverweight and provision of counseling or other assess-ments or referrals related to overweight. Multivariatelogistic regression (LR) models were developed to exam-ine the relative importance of the various factors asso-ciated with overweight identification and evaluation/referral for comorbid conditions. These models included4 categorical demographic variables (household tobaccouse, insurance status, race/ethnicity, and parent educa-tion) and 2 continuous variables (BMI percentile andchild age).
Next, multivariate LR modeling was used to examinewhat factors contributed to a high visit frequency (�3
TABLE 1 Data Collected in Medical Record Review
Category Elements
Visit type Health maintenance, other typeAnthropometric measurements Weight, heightDocumentation of concern for overweight ordiagnosis of overweight
Overweight, obesity, other (eg, weight of �95th percentile, increasedweight, discussed weight increase, watch weight gain)
Diagnoses of comorbid conditions Diabetes mellitus, hypertension, hyperlipidemia, sleep-related,orthopedic diagnoses, skin changes, psychosocial, other
Documentation of counseling regarding physicalactivity and diet
Any related notations
Laboratory tests to evaluate for comorbidconditions
Lipid levels, thyroid function, glucose level, insulin level, other (lateralneck radiograph for sleep apnea evaluation, liver function tests,sleep study)
Referrals related to comorbid conditions Nutrition, pulmonary, endocrine, orthopedics, other (otolaryngology,psychiatry)
e150 DILLEY et al at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

visits during the 14-month study period), to assesswhether overweight and AROW children would seekmore medical care, as has been shown for adults.4,6–11
The model included 4 categorical demographic variables(household tobacco use, insurance status, race/ethnicity,and parent education), 2 continuous variables (BMI per-centile and child age), and whether AROW/overweightwas identified by the provider.
To account for clustering of children within familiesand practices, multivariate LR models used the general-ized linear model with random effects approach,21 withSAS Proc Glimmix (SAS Institute, Cary, NC). Failure toaccount for clustering would mean that observed asso-ciations could be attributable simply to nonrandom dif-ferences between included clusters.
RESULTS
Demographic Features and Visit ContentAmong the families selected for medical record reviews,96% (1153 of 1198 families) had a record reviewed for�1 child (n � 2089 children), with 1940 children havinga visit in the review period. No subjects were found tohave chronic conditions expected to cause overweight;therefore, no exclusions for medical history were made.Seventy-five percent of children (n � 1453) with a visitin the period were �2 years of age at a visit, and 84% (n� 1216 children in 777 families) of those had a visit inthe review period at which height and weight wererecorded. Most respondents (46%) had 1 child in theanalysis (32% had 2 children and 22% had �3 chil-dren).
Twenty percent of children were overweight (15%AROW and 64% not overweight). Greater proportions
of overweight/AROW children were in nonwhite racial/ethnic groups and among those receiving Medicaid/un-insured (Table 2). The median number of visits per childwas 3 (range: 1–43 visits; 1 visit: 19%; 2 visits: 17%; 3visits: 18%; 4 visits: 14%; �5 visits: 32%), and 91% hada health maintenance visit in the review period; thesevalues did not vary according to BMI percentile group.Among children with simultaneous height and weightmeasurements, 18 AROW (10%) and 33 overweight(13%) children did not have a comprehensive healthmaintenance visit. Most children (70%) lived with asmoker, according to the study design. A greater per-centage of nonoverweight children (34%) lived in anonsmoking household, compared with AROW (21%)and overweight (25%) children (P � .0007).
Influence of BMI Percentile Group on Content of CareDocumentation of diagnosis of or concern about over-weight (defined as identification), as well as any man-agement related to overweight, was most commonlyfound for the overweight group of children (Table 3).Approximately one fourth of overweight and 15% ofAROW children had any management (defined as diag-nosis of a comorbid condition, any referral, or any test-ing related to overweight) for overweight. However,documentation of assessment or counseling provided atthe visit related to diet and physical activity did not differaccording to BMI percentile group status (Table 3).
A total of 13% of overweight children had any diag-nosis of a comorbid condition (�1% diabetes mellitus,�1% hypertension, 2% hyperlipidemia, 5% sleep-re-lated disorders, 6% orthopedic diagnoses, and 2% skinchanges). A comorbidity was more likely to be noted for
TABLE 2 Child Subject Characteristics (n � 1216)
Characteristic No. (%) P
Totala Not Overweight(n � 782)b
AROW(n � 186)b
Overweight(n � 248)b
Race/ethnicity (n � 1214) �.0001Black 231(19) 148 (64) 33 (14) 50 (22)White 531 (44) 392 (74) 68 (13) 71 (13)Hispanic 398 (33) 207 (52) 76 (19) 115 (29)Asian/other 54 (4) 34 (64) 9 (17) 11 (20)
Gender (n � 1216) .91Male 616 (51) 394 (64) 97 (16) 125 (20)Female 600 (49) 388 (65) 89 (15) 123 (21)
Age group (n � 1216) .592–5 y 480 (39) 318 (66) 66 (14) 96 (20)6–11 y 364 (30) 223 (61) 63 (17) 78 (21)�12 y 372 (31) 241 (65) 57 (15) 74 (20)
Insurance (n � 1213) �.0001Medicaid/uninsured 589 (49) 339 (58) 100 (17) 150 (25)Private/other 624 (51) 440 (71) 86 (14) 98 (16)
Totals may be different from 100% because of rounding.a Percentages in total column represent percentages of sample with data known; race data were missing for 2 subjects and insurance data for 3subjects.b Percentages represent proportions within the demographic subgroup that fall into each BMI percentile group.
PEDIATRICS Volume 119, Number 1, January 2007 e151 at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from
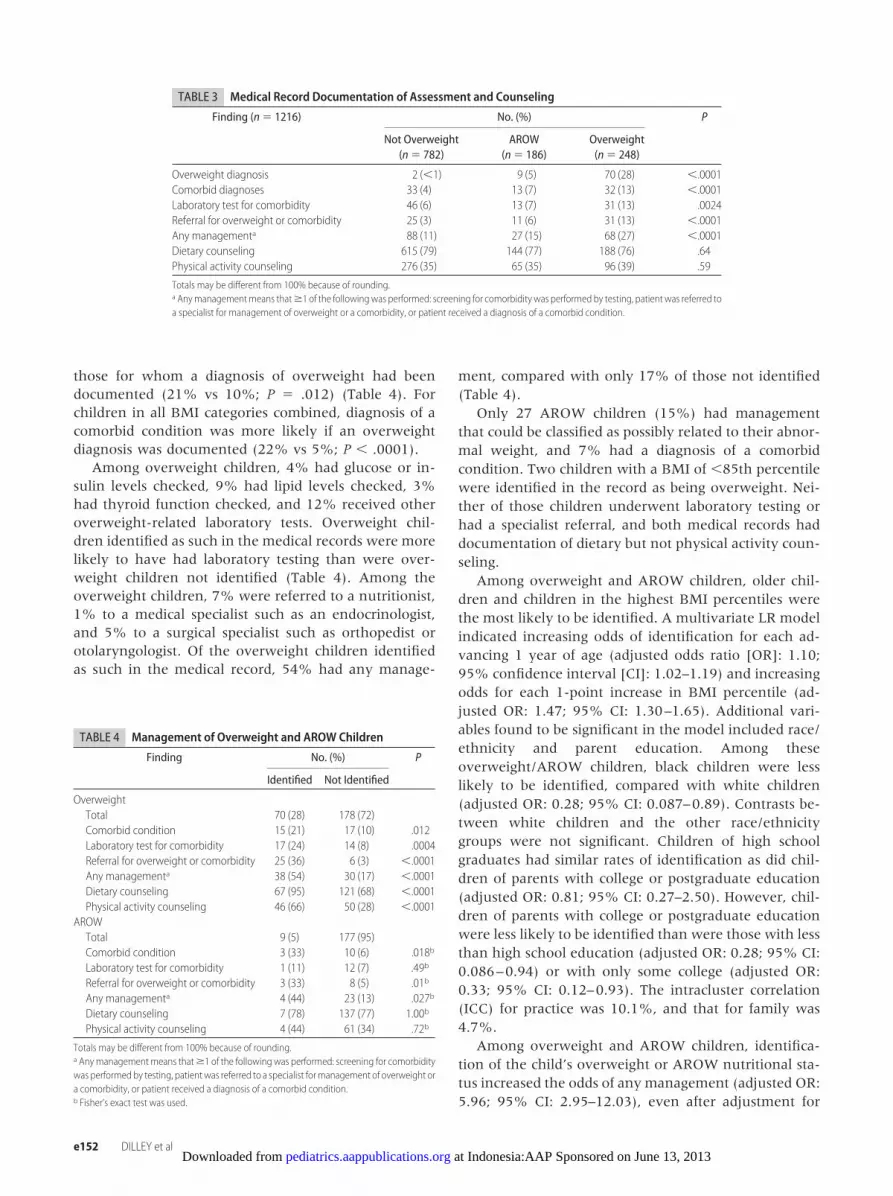
those for whom a diagnosis of overweight had beendocumented (21% vs 10%; P � .012) (Table 4). Forchildren in all BMI categories combined, diagnosis of acomorbid condition was more likely if an overweightdiagnosis was documented (22% vs 5%; P � .0001).
Among overweight children, 4% had glucose or in-sulin levels checked, 9% had lipid levels checked, 3%had thyroid function checked, and 12% received otheroverweight-related laboratory tests. Overweight chil-dren identified as such in the medical records were morelikely to have had laboratory testing than were over-weight children not identified (Table 4). Among theoverweight children, 7% were referred to a nutritionist,1% to a medical specialist such as an endocrinologist,and 5% to a surgical specialist such as orthopedist orotolaryngologist. Of the overweight children identifiedas such in the medical record, 54% had any manage-
ment, compared with only 17% of those not identified(Table 4).
Only 27 AROW children (15%) had managementthat could be classified as possibly related to their abnor-mal weight, and 7% had a diagnosis of a comorbidcondition. Two children with a BMI of �85th percentilewere identified in the record as being overweight. Nei-ther of those children underwent laboratory testing orhad a specialist referral, and both medical records haddocumentation of dietary but not physical activity coun-seling.
Among overweight and AROW children, older chil-dren and children in the highest BMI percentiles werethe most likely to be identified. A multivariate LR modelindicated increasing odds of identification for each ad-vancing 1 year of age (adjusted odds ratio [OR]: 1.10;95% confidence interval [CI]: 1.02–1.19) and increasingodds for each 1-point increase in BMI percentile (ad-justed OR: 1.47; 95% CI: 1.30–1.65). Additional vari-ables found to be significant in the model included race/ethnicity and parent education. Among theseoverweight/AROW children, black children were lesslikely to be identified, compared with white children(adjusted OR: 0.28; 95% CI: 0.087–0.89). Contrasts be-tween white children and the other race/ethnicitygroups were not significant. Children of high schoolgraduates had similar rates of identification as did chil-dren of parents with college or postgraduate education(adjusted OR: 0.81; 95% CI: 0.27–2.50). However, chil-dren of parents with college or postgraduate educationwere less likely to be identified than were those with lessthan high school education (adjusted OR: 0.28; 95% CI:0.086–0.94) or with only some college (adjusted OR:0.33; 95% CI: 0.12–0.93). The intracluster correlation(ICC) for practice was 10.1%, and that for family was4.7%.
Among overweight and AROW children, identifica-tion of the child’s overweight or AROW nutritional sta-tus increased the odds of any management (adjusted OR:5.96; 95% CI: 2.95–12.03), even after adjustment for
TABLE 3 Medical Record Documentation of Assessment and Counseling
Finding (n � 1216) No. (%) P
Not Overweight(n � 782)
AROW(n � 186)
Overweight(n � 248)
Overweight diagnosis 2 (�1) 9 (5) 70 (28) �.0001Comorbid diagnoses 33 (4) 13 (7) 32 (13) �.0001Laboratory test for comorbidity 46 (6) 13 (7) 31 (13) .0024Referral for overweight or comorbidity 25 (3) 11 (6) 31 (13) �.0001Any managementa 88 (11) 27 (15) 68 (27) �.0001Dietary counseling 615 (79) 144 (77) 188 (76) .64Physical activity counseling 276 (35) 65 (35) 96 (39) .59
Totals may be different from 100% because of rounding.a Anymanagementmeans that�1 of the followingwas performed: screening for comorbidity was performed by testing, patient was referred toa specialist for management of overweight or a comorbidity, or patient received a diagnosis of a comorbid condition.
TABLE 4 Management of Overweight and AROW Children
Finding No. (%) P
Identified Not Identified
OverweightTotal 70 (28) 178 (72)Comorbid condition 15 (21) 17 (10) .012Laboratory test for comorbidity 17 (24) 14 (8) .0004Referral for overweight or comorbidity 25 (36) 6 (3) �.0001Any managementa 38 (54) 30 (17) �.0001Dietary counseling 67 (95) 121 (68) �.0001Physical activity counseling 46 (66) 50 (28) �.0001
AROWTotal 9 (5) 177 (95)Comorbid condition 3 (33) 10 (6) .018b
Laboratory test for comorbidity 1 (11) 12 (7) .49b
Referral for overweight or comorbidity 3 (33) 8 (5) .01b
Any managementa 4 (44) 23 (13) .027b
Dietary counseling 7 (78) 137 (77) 1.00b
Physical activity counseling 4 (44) 61 (34) .72b
Totals may be different from 100% because of rounding.a Anymanagementmeans that�1 of the followingwas performed: screening for comorbiditywas performedby testing, patientwas referred to a specialist formanagement of overweight ora comorbidity, or patient received a diagnosis of a comorbid condition.b Fisher’s exact test was used.
e152 DILLEY et al at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

BMI percentile and child age. In this LR model, the oddsof any management increased with each 1-year increasein age (adjusted OR: 1.14; 95% CI: 1.07–1.22) and each1-point increase in BMI percentile (adjusted OR: 1.10;95% CI: 1.02–1.19). No other variables were significantin the model. The ICC for practice was 8.4%, and that forfamily was 28.0%.
Influence of BMI Percentile Group on Number of VisitsThe likelihood of having �3 visits (ie, a high number ofvisits) in the 14-month study period was examined todetermine whether overweight and AROW childrensought care more frequently. The odds of having a highnumber of visits were not affected by being in theAROW group (adjusted OR: 1.11; 95% CI: 0.77–1.60) oroverweight group (adjusted OR: 0.99; 95% CI: 0.68–1.42), compared with the normal-weight group.Younger children were slightly more likely to have �3visits (adjusted OR: 1.11; 95% CI: 1.08–1.15), and thoseidentified as overweight were marginally more likely tohave �3 visits (adjusted OR: 1.77; 95% CI: 1.00–3.14).Additional variables found to be significant in the modelincluded race/ethnicity and parent education. Childrenof black parents, compared with white parents, were lesslikely to have �3 visits (adjusted OR: 0.55; 95% CI:0.45–0.67). Children of parents with less than highschool education (OR: 0.46; 95% CI: 0.28–0.76) or highschool graduates (OR: 0.60; 95% CI: 0.39–0.93), but notthose with only some college (OR: 0.86; 95% CI: 0.59–1.26), were less likely than children of parents withcollege or postgraduate education to have �3 visits. TheICC for practice was 1.2%, and that for family was21.7%.
DISCUSSIONThis article demonstrates the significant relationship be-tween documentation of a diagnosis of or concern aboutoverweight in a child’s medical record and managementdecisions related to comorbid conditions. The resultslend support to the presumption that improved identifi-cation would lead to more comprehensive medical eval-uations of secondary effects in overweight children. Fur-thermore, it demonstrated that existing methods ofoverweight identification used at these practices at thetime of this study favored older and more overweightchildren, which points to the need for routine evaluationof all children. The strengths of the study include thelarge number of subjects from diverse practices, objec-tive calculation of BMI percentile values (to allow forassessment of missed diagnoses of overweight orAROW), and the analytic method to evaluate the effectsof the practice and family on identification and manage-ment of overweight. In addition, the examination of allvisits in a defined time period of �1 year and limiting ofthe sample to children with both weight and heightmeasurements available in that period allowed us to
draw conclusions based on complete data for childrenwho all had the opportunity for BMI interpretation andadditional management as indicated.
Use of objective data from the records to calculateBMI percentiles for age and gender yielded rates in thissample of 20% overweight and 15% AROW. Only 28%of the overweight children were identified as such bytheir providers, but identified children were more likelyto receive screening or referrals for comorbid conditions.Very few children in the AROW category were identifiedor had any management. Providers were more likely toidentify weight as a problem for older children and thosein the highest BMI percentiles, potentially missing im-portant opportunities for intervention or prevention atan early age and lower BMI.
Rates of identification of comorbid diagnoses thatmight be related to overweight were quite low for theoverweight and AROW children. This indicates eitherlow incidence of complications in the community sam-ple or underidentification of children with comorbiditiesactually occurring at expected rates.
Although rates of laboratory testing among the over-weight and AROW children were low, the expected rateis unclear, because it would not be expected that alloverweight children would necessarily have a laboratorytest in a specific 14-month period. Published recommen-dations for testing include (1) fasting glucose and insulinmeasurements for all overweight children and forAROW children with a family history of diabetes melli-tus or with other evidence of obesity complications,13 (2)lipid profiles for any child �2 years of age with a familyhistory of dyslipidemia or early cardiovascular disease orchildren with other risk factors, including obesity,22 and(3) evaluation for any medical causes of obesity as indi-cated by history and physical examination.13 No specificconsensus guidelines exist covering screening for nonal-coholic steatohepatitis. Notably absent from the guide-lines is comment on how often to retest children withpast normal laboratory results who remain overweight.
The children in this sample at �85th BMI percentile(overweight or AROW) were not more likely than theirnonoverweight counterparts to have �3 visits in a 14-month period. The fact that, unlike adults, overweightand AROW children are not presenting more frequentlyfor care suggests either that they are not experiencingcomplaints as a result of comorbid complications of obe-sity or that clinicians are not recommending or patientsare not completing more frequent follow-up evaluationsfor their weight. An alternative explanation could bethat not enough time elapsed between the identificationof patients as overweight and the end of the study periodfor assessment of the true impact. Because childrenwould be expected to have a health maintenance visitannually, each subject should have a BMI measurementand a health maintenance visit simultaneously. How-ever, 10% of AROW and 13% of overweight patients
PEDIATRICS Volume 119, Number 1, January 2007 e153 at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

who did have adequate data to allow BMI calculationnever had a health maintenance visit, which means thatheight and weight were instead measured simulta-neously at a focused visit, with the focus being weight-related in some but not all cases.
ICCs are used to account for sample designs in whichstudy subjects relate in some manner to other studysubjects. In this study, random-effects modeling wasnecessary, and reported ICCs provide information on thestrength of care delivery patterns according to practiceand family. We found practice decision-making out-comes to have ICCs as expected23 (10% for identificationof overweight and 10% for additional evaluation),whereas having a high number of visits had little prac-tice-related influence (ICC: 1%). Family influences werestrong for both frequent visits (ICC: 22%) and childrenhaving an additional evaluation (ICC: 28%). Family re-lationship had only a modest influence on identificationof children as overweight (ICC: 5%).
Potential limitations of this study include the use ofmedical record review data, which may not reflect allservices rendered or discussions held with patients, al-though record reviews do provide an improvement overadministrative data. In addition, only visits to the pri-mary care office were captured; therefore, it is possiblethat overweight children have increased or decreasedcontact with medical providers when specialty visits andacute care outside of the office are considered. Althoughrates of counseling regarding diet and physical activitywere high even for nonoverweight patients, the qualityand amount of such counseling could not be assessedaccurately from this record review. The 14-month studyperiod might not be optimal to capture all changes inmanagement that occur after a patient is identified bythe provider as overweight. BMI is only one of manypossible ways to assess nutritional status, and this studywas performed at a time when neither BMI nor anyother method of relating weight to height was usedroutinely in pediatric primary care. Because evaluationfor a comorbid condition was measured and likely oc-curred separately from provider identification of a pa-tient as overweight or AROW, these data may falselyinflate the impact that identification of overweight hason additional evaluation for comorbidities. The inclusionof a sample weighted to have high smoking rates couldhave introduced unmeasured bias. Finally, although rec-ommendations for screening for overweight patients ex-ist, the need for and frequency of rescreening that wouldbring overweight patients back to the office withoutexisting complications is not clear.
CONCLUSIONSOverweight children were frequently not identified assuch by their primary care providers. However, the chil-dren who were identified were far more likely to receivecounseling and additional evaluations, possibly only be-
cause they were in the highest range of BMI and wereconsidered at risk for complications by the providerwithout calculation of BMI. These findings indicate aneed for office systems incorporating routine growthinterpretation for identification of overweight children,to initiate prompt and early intervention with the po-tential to prevent comorbidities and persistence of over-weight into later life.
ACKNOWLEDGMENTSFunding for the Healthy Families, Healthy Children: ThePediatrician’s Role study was provided by the RobertWood Johnson Foundation, Substance Abuse Policy Re-search Program Grant 45645. Support was also providedby Health Resources and Services Administration Fac-ulty Development Grant D55HP00069 for Dr Dilley’sfellowship and Dr Binns’ supervision of the fellowshipprogram.
We thank the numerous research staff members, inparticular Robert S. Greenberg, MD, who provided helpwith medical record reviews and the many subjects whoparticipated in this project. In particular, we acknowl-edge the dedicated efforts of physicians and staff mem-bers of the following practices and the physicians whoguided study participation at their offices: Dianna Bro-gan, MD, Associated Pediatricians (Portage, IN); KathyShepherd, MD, Lisa McKenna, MD, Near North HealthServices (Chicago, IL); David Dobkin, MD, North Arling-ton Pediatrics (Arlington Heights, IL); Sara Naureckas,MD, Erie Family Health Center (Chicago, IL); DavidClaus, MD, Pedios (Oak Park, IL); Carl Toren, MD, MPH,Ramon Cabe, MD, Chicago Family Health Center (Chi-cago, IL): Barbara Bayldon, MD, Children’s MemorialPediatrics-Uptown (Chicago, IL); Judith Brown, MD, Pe-diatric Associates of Barrington (Barrington, IL); BruceRowell, MD, Lawndale Christian Health Center (Chi-cago, IL); George Harris, MD, Southwest Pediatrics (Pa-los Park, IL); Kamala Ghaey, MD, Kidz Health (Chicago,IL); W. Daniel Perez, MD, Abdul Bhurgri, MD, AlivioMedical Center (Chicago, IL); Judith Neafsey MD, Chi-cago Department of Public Health (Chicago, IL).
REFERENCES1. Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR,
Flegal KM. Prevalence of overweight and obesity among USchildren, adolescents, and adults, 1999–2002. JAMA. 2004;291:2847–2850
2. Serdula MK, Ivery D, Coates RJ, Freedman DS, Williamson DF,Byers T. Do obese children become obese adults? A review ofthe literature. Prev Med. 1993;22:167–177
3. Wang G, Dietz WH. Economic burden of obesity in youths aged6 to 17 years: 1979–1999. Pediatrics. 2002;109(5). Available at:www.pediatrics.org/cgi/content/full/109/5/e81
4. Sansone RA, Sansone LA, Wiederman MW. The relationshipbetween obesity and medical utilization among women in aprimary care setting. Int J Eat Disord. 1998;23:161–167
5. Tershakovec AM, Watson MH, Wenner WJ, Marx AL. Insur-
e154 DILLEY et al at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

ance reimbursement for the treatment of obesity in children.J Pediatr. 1999;134:573–578
6. Tucker LA, Clegg AG. Differences in health care costs andutilization among adults with selected lifestyle-related risk fac-tors. Am J Health Promot. 2002;16:225–233
7. Sturm R. The effects of obesity, smoking, and drinking onmedical problems and costs. Health Aff (Millwood). 2002;21:245–253
8. Guallar-Castillon P, Lopez Garcia E, Lozano Palacios L, et al.The relationship of overweight and obesity with subjectivehealth and use of health-care services among Spanish women.Int J Obes Metab Disord. 2002;26:247–252
9. Pronk NP, Tan AWH, O’Connor P. Obesity, fitness, willingnessto communicate and health care costs. Med Sci Sports Exerc.1999;31:1535–1543
10. Heithoff KA, Cuffel BJ, Kennedy S, Peters J. The associationbetween body mass and health care expenditures. Clin Ther.1997;19:811–820
11. Raebel MA, Malone DC, Conner DA, Xu S, Porter JA, Lanty FL.Health services use and health care costs of obese and non-obese individuals. Arch Intern Med. 2004;164:2135–2140
12. American Academy of Pediatrics, Committee on Nutrition. Pre-vention of pediatric overweight and obesity. Pediatrics. 2003;112:424–430
13. Barlow SE, Dietz WH. Obesity evaluation and treatment: ex-pert committee recommendations. Pediatrics. 1998;102(3).Available at: www.pediatrics.org/cgi/content/full/102/3/e29
14. O’Brien SH, Holubkov R, Reis EC. Identification, evaluation,and management of obesity in an academic primary care cen-ter. Pediatrics. 2004;114(2). Available at: www.pediatrics.org/cgi/content/full/114/2/e154
15. Drobac S, Brickman W, Smith T, Binns HJ. Evaluation of a type
2 diabetes screening protocol in an urban pediatric clinic. Pe-diatrics. 2004;114:141–148
16. Dorsey KB, Wells C, Krumholz HM, Concato JC. Diagnosis,evaluation, and treatment of childhood obesity in pediatricpractice. Arch Pediatr Adolesc Med. 2005;159:632–638
17. Cook S, Weitzman M, Auinger P, Barlow SE. Screening andcounseling associated with obesity diagnosis in a national sur-vey of ambulatory pediatric visits. Pediatrics. 2005;116:112–116
18. Riley MR, Bass NM, Rosenthal P, Merriman RB. Underdiagno-sis of pediatric obesity and underscreening for fatty liver dis-ease and metabolic syndrome by pediatricians and pediatricsubspecialists. J Pediatr. 2005;147:839–842
19. LeBailly S, Ariza A, Bayldon B, Binns HJ, Pediatric PracticeResearch Group. The origin and evolution of a regional pedi-atric practice-based research network: practical and method-ological lessons from the Pediatric Practice Research Group.Curr Probl Pediatr Adolesc Health Care. 2003;33:124–134
20. Himes JH, Dietz WH. Guidelines for overweight in adolescentpreventive services: recommendations from an expert commit-tee. Am J Clin Nutr. 1994;59:307–316
21. Wolfinger R, O’Connell M. Generalized linear mixed models: apseudo-likelihood approach. J Stat Comput Simul. 1993;48:233–243
22. Kavey RE, Daniels SR, Lauer RM, Atkins DL, Hayman LL,Taubert K. American Heart Association guidelines for primaryprevention of atherosclerotic cardiovascular diseases beginningin childhood. Circulation. 2003;107:1562–1566
23. Davis P, Gribben B, Lay-Yee R, Scott A. How much variation inclinical activity is there between general practitioners? A multi-level analysis of decision-making in primary care. J Health ServRes Policy. 2002;7:202–208
PEDIATRICS Volume 119, Number 1, January 2007 e155 at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2005-2867 2007;119;e148PediatricsBinns
Kimberley J. Dilley, Lisa A. Martin, Christine Sullivan, Roopa Seshadri and Helen J.for Comorbidities of Overweight in Pediatric Primary Care Practice
Identification of Overweight Status Is Associated With Higher Rates of Screening
ServicesUpdated Information &
tmlhttp://pediatrics.aappublications.org/content/119/1/e148.full.hincluding high resolution figures, can be found at:
References
tml#ref-list-1http://pediatrics.aappublications.org/content/119/1/e148.full.hat:This article cites 20 articles, 7 of which can be accessed free
Citations
tml#related-urlshttp://pediatrics.aappublications.org/content/119/1/e148.full.hThis article has been cited by 8 HighWire-hosted articles:
Subspecialty Collections
ubhttp://pediatrics.aappublications.org/cgi/collection/nutrition_sNutrition
ion:practice_management_subhttp://pediatrics.aappublications.org/cgi/collection/administratAdministration/Practice Managementthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
mlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhttables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2007 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Indonesia:AAP Sponsored on June 13, 2013pediatrics.aappublications.orgDownloaded from