pediatric anesthesia - dräger
TRANSCRIPT
Pediatric Anesthesia
Pedi
atri
c An
esth
esia
-Fib
le
Dr. K. RuppDr. J. HolzkiDr. T. FischerDr. C. Keller
22222
Dr. Katrin RuppDräger Medizintechnik GmbHMoislinger Allee 53-55D-23542 Lübeck
With special thanks to the following people for their kind assistance:Dr. J. HolzkiKinderklinik Köln (Children’s Hospital, Cologne)Amsterdamstraße 59D-50735 Köln
Dr. T. FischerDeutsches Herzzentrum Berlin(German Center for Cardiology, Berlin)Augustenbürgerplatz 1D-13353 Berlin
Dr. C. KellerKlinik für Anästhesie und Allgemeine Intensivmedizin(Clinic for Anesthesiology and General Intensive Care Medicine)Leopold-Franzens-Universität InnsbruckAnichstraße 35A-6020 Innsbruck
Dräger Medizintechnik GmbH reserves all rights to this publication,especially as pertaining to its duplication and distribution. No part ofthis publication may be reprinted or saved through any means,mechanical, electrical/electronic or photographic, without theexpressed written consent of the Dräger Medizintechnik GmbH.
E-Mail: [email protected]
ISBN 3-926762-48-9
translated by: L.A. Weaver
Author:
33333
Pediatric Anesthesia

44444
Important Information:Medical knowledge is constantly changing as a result ofresearch and clinical testing. The editors and authors ofthis primer have taken great care to ensure that theinformation and therapeutic details contained hereincorrespond to the most up-to-date research results(especially as pertains to indications, dosages andundesirable side effects), they cannot, however, guaranteethis. Those persons using this book as a reference areadvised to carefully peruse all instructions included withmedications used and to make all decisions pertaining todosage or application at their own discretion.
The Editors October, 1999
55555
Table of Contents
1. Introduction 8
2. Special Anatomical and Physiological Features 122.1 Breathing 13
2.1.1 Anatomical Fundamentals 13of the Respiratory Tract
2.1.2 Controlling the Respiratory Process 152.1.3 Respiratory Mechanics 172.1.4 Pulmonary Volumes 192.1.5 Surfactant 232.1.6 Oxygen Requirements 242.1.7 Extrapulmonary Oxygen Toxicity 26
2.2 The Heart and Circulatory System 272.2.1 The Fetal Circulatory System 272.2.2 The Heart 292.2.3 Blood Volume and Blood Pressure 302.2.4 Hemoglobin Contents 31
2.3 Temperature Regulation 322.4 The Balance between Water and Electrolytes 35
3. Anesthetic Agents 373.1 Inhalation Anesthesia 383.2 Interactions with Soda Lime 453.3 Intravenous Anesthesia 493.4 Muscle Relaxants 51
4. Anesthesia Accessories 534.1 Masks 544.2 Tubes 554.3 Laryngeal Masks 58
66666
5. Ventilation in Pediatric Anesthesia 605.1 Mechanical Modes of Ventilation 61
5.1.1 The Ventilation Mode IPPV 615.1.2 The Ventilation Mode SIMV 635.1.3 The Ventilation Mode PCV 64
5.2 Ventilation Parameters 735.3 Breathing Systems 78
5.3.1 Flow-controlled 79Non-rebreathing Systems
5.3.2 Valve-controlled 86Non-rebreathing Systems
5.3.3 Partial Rebreathing Systems(Semi-closed Breathing Systems) 87
5.3.4 Complete Rebreathing Systems(Closed Systems) 89
5.4 Characteristics of Ventilation forPediatric Anesthesia 90
5.4.1 Manual and Mechanical Ventilation for 90Neonates and Infants
5.4.2 Respirator Requirements for Children 925.4.3 The Fresh-gas Decoupler 945.4.4 Compliance Compensation 965.4.5 Dead Space Volume 98
5.5 Anesthetic Machines 995.5.1 Cato/Cicero EM 995.5.2 Julian 1015.5.3 PhysioFlex 102
5.6 Monitoring 1085.6.1 The Stethoscope 1095.6.2 Pulse Oximetry 1105.6.3 Measuring Body Temperature 1135.6.4 Measuring Blood Pressure(NiBP/iBP) 1155.6.5 The ECG 118
77777
5.6.6 Capnography 1205.6.7 Measuring Respiratory Pressure 1255.6.8 Volumetry 1265.6.9 Measuring the Concentration 127
of Anesthetic Agent5.6.10 Measuring the Inspiratory 128
Oxygen Concentration5.6.11 Oxygen Uptake 1295.6.12 Anesthetic Agent Uptake 130
5.7 Low-flow Anesthesia 1325.7.1 The Wash-in/Wash-out Rate 137
of Anesthetic Agent5.8 Breathing Gas Conditioning
for Anesthetic Ventilation Systems 142
6. Bibliography 151
7. Practical Application 1617.1 Anesthetic Ventilation for Infants 161
and Small ChildrenDr. J. HolzkiChildren’s Clinic, Cologne, Germany
7.2 PCV during Pediatric Cardio-anesthesia 176Dr. T. FischerGerman Heart Center, Berlin
7.3 Using a Laryngeal Mask for Pediatric Anesthesia 185Dr. C. KellerLeopold-Franzens University, Innsbruck
8. Abbreviations 193
9. Index 196
88888
1. Introduction
Childrenpose many questions
for anesthetists.
99999
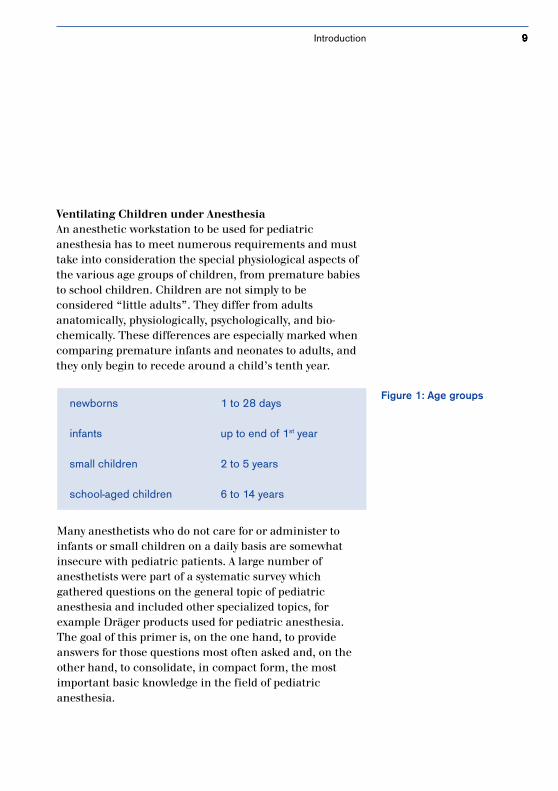
Figure 1: Age groupsnewborns 1 to 28 days
infants up to end of 1st year
small children 2 to 5 years
school-aged children 6 to 14 years
Ventilating Children under AnesthesiaAn anesthetic workstation to be used for pediatricanesthesia has to meet numerous requirements and musttake into consideration the special physiological aspects ofthe various age groups of children, from premature babiesto school children. Children are not simply to beconsidered “little adults”. They differ from adultsanatomically, physiologically, psychologically, and bio-chemically. These differences are especially marked whencomparing premature infants and neonates to adults, andthey only begin to recede around a child’s tenth year.
Many anesthetists who do not care for or administer toinfants or small children on a daily basis are somewhatinsecure with pediatric patients. A large number ofanesthetists were part of a systematic survey whichgathered questions on the general topic of pediatricanesthesia and included other specialized topics, forexample Dräger products used for pediatric anesthesia.The goal of this primer is, on the one hand, to provideanswers for those questions most often asked and, on theother hand, to consolidate, in compact form, the mostimportant basic knowledge in the field of pediatricanesthesia.
Introduction
1010101010
It is not the intent of this primer to replace other textbooks,but rather to supplement known textbooks by providinginformation on practical applications for pediatricanesthesia. Concrete examples for application topics likeanesthetic ventilation for small children, pressure-controlled ventilation (PCV), and laryngeal mask usage inpediatric anesthesia, help complete this primer.
The following complex questions on the topics of anestheticmachines, accessories, special physiological featuresand anesthetics shall be addressed:
• Are the latest anesthetic machines able to ventilateusing a pressure-controlled ventilation mode (PCV)?(p. 64)
• What are the advantages of pressure-controlledventilation over volume-controlled ventilation? (p. 64)
• Which ventilation parameter settings should be selectedfor which age group? (p. 73)
• Does it make sense to use PEEP, on principle, for eachand every case of newborn ventilation? (p. 75)
• What usage problems are associated with non-rebreathing systems? (p. 79)
• What features does an efficient pediatric respiratorhave? (p. 92)
• How does dead space volume affect ventilation? (p. 98)• How low is the minimum tidal volume which an
anesthetic machine can apply? (p.␣ 99)• What are the advantages of closed-system ventilation for
pediatric anesthesia? (p.␣ 104)• What kind of monitoring is used for pediatric anesthesia
and what special features are available for this agegroup? (p. 108)
Introduction
1111111111
• How much is volume-controlled or, respectively,pressure-controlled ventilation affected by a siphoninggas measurement procedure during side-streamcapnography? (p. 123)
• Can low-flow anesthesia be carried out for pediatricanesthesia? (p. 132)
• How quickly does the system react to changes inconcentration (wash-in/wash-out rate)? (p. 137)
• Why is it necessary to condition breathing gases forchildren (p. 143), and which types of breathing gashumidification should be used for which age group?(p. 144)
• Which oxygen concentration is dangerous for neonates?(p. 26)
• How high are the anesthetic MAC values for children?(p. 39)
• How do inhalation anesthetics interact with soda lime(p. 46) and how can this be prevented? (p. 48)
• When would one use intravenous anesthesia on childreninstead of inhalation anesthesia? (p.␣ 50)
• When is intubation preferred to mask anesthesia forpediatric anesthesia? (p. 54)
• What are the advantages and disadvantages of laryngealmask usage? (p. 59)
These questions shall appear on those pages, indicated bythe blue italicized page numbers behind the questions.
Introduction
1212121212
2. Special Anatomical andPhysiological Features
The “little” patientsshould not be considered
“miniature adults”.
1313131313
2.1 1.1 Breathing
2.1.1 Anatomical Fundamentals of the Respiratory TractKnowing the differences between the respiratory tract of achild and that of an adult is essential for anesthetists inorder for them to safely administer anesthesia.
• A child’s nostrils, oropharynx and trachea are relativelynarrow (see Figure 2). Breathing can be hindered byirritation of the mucous membrane due to edema build-up in this area.
• The trachea is short – it only measures approximately4cm from the larynx to the carina – and has a narrowdiameter of 6 mm.
• The tongue is relatively large and tends to fall backwardsunder anesthesia.
• Neonates, infants and small children have a very softthorax compared to their lungs. The thorax is relativelyshort. The ribs run horizontally and not diagonally, as isthe case with adults. The intercostal muscles areimmature.
• The salivary secretions of children are more pronouncedthan those of adults.
• The larynx of a child is more ventrally located and onlevel with the third to fourth (neck) vertebrae, thusabout a whole vertebrae higher than that of an adult.Until the age of 8 to 10 years, the most narrow point is avery sensitive mucous membrane on level with thelarynx cartilage and not, as is the case with adults, withthe glottis.
• The epiglottis is relatively large and shaped like a U.• The size of the tonsils and the adenoid in children can
complicate the intubation process.
Special Anatomical and Physiological Features

1414141414
Figure 2: Sagittal tomogramof a newborn and an adult
adult infant
nasal cavity upperairway
lowerairway
oral cavity
windpipe
epiglottis
• Infants breath through their nose until they reach anage of 5 months. Inserting a stomach probe through thenose can be a massive respiratory hindrance.
Special Anatomical and Physiological Features
1515151515
2.1.2 Controlling the Respiratory ProcessThe respiratory process of both premature newborns andneonates, like that of adults, is essentially controlled bychanges in paCO2, paO2 and pH (see Figure 3). The hypoxiabreathing regulation of newborns is not, however, fullydeveloped; right after birth, the oxygen receptors and theirfunctions are immature. The paCO2 and paO2 values ofnewborns and infants are lower than those of adults untilthe end of their first year.
Premature infants often experience respiratory arrest(apnea) either at regular (periodical breathing) orirregular intervals. Periodical breathing is considered anepisode of 3 or more respiratory pauses of at least 3seconds. Normal breathing periods of less than 20 secondsaccompany these. Apnea phases can be due to a centralproblem (no physical breathing exertion) or, less often,caused by an obstruction (no flow despite physicalbreathing exertion). In addition, there are mixed forms ofboth. Nevertheless, these breathing abnormalities are notusually dangerous. Respiratory arrest can, however, lead todecreased O2 partial pressure in the blood and can causebradycardia if the length of such a phase is longer than 30seconds.
Infants react to hypoxia biphasically. First there is a 30second increase in minute volume, followed by hypo-ventilation or apnea. If hypothermia or hypoglycemiaoccurs simultaneously, hypoventilation is the immediateresult. An adequate reaction to lack of oxygen on the part ofthe child can only be observed 2 to 4 weeks after birth.
Special Anatomical and Physiological Features
1616161616
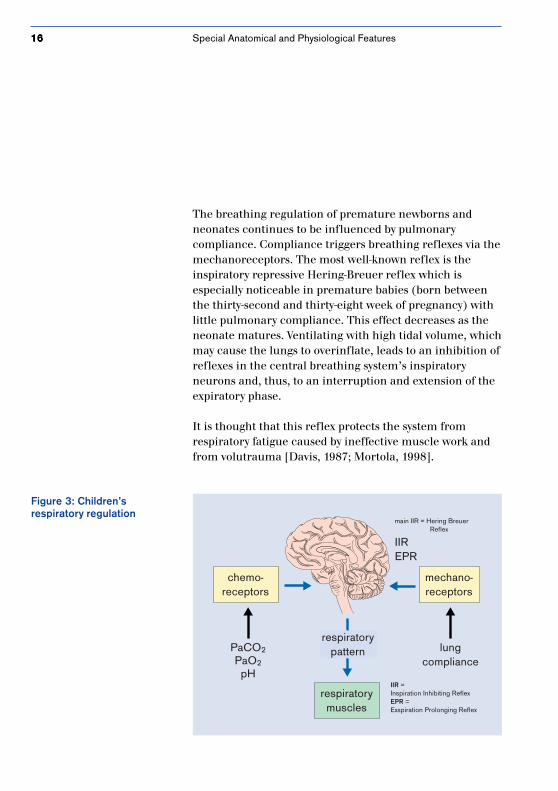
The breathing regulation of premature newborns andneonates continues to be influenced by pulmonarycompliance. Compliance triggers breathing reflexes via themechanoreceptors. The most well-known reflex is theinspiratory repressive Hering-Breuer reflex which isespecially noticeable in premature babies (born betweenthe thirty-second and thirty-eight week of pregnancy) withlittle pulmonary compliance. This effect decreases as theneonate matures. Ventilating with high tidal volume, whichmay cause the lungs to overinflate, leads to an inhibition ofreflexes in the central breathing system’s inspiratoryneurons and, thus, to an interruption and extension of theexpiratory phase.
It is thought that this reflex protects the system fromrespiratory fatigue caused by ineffective muscle work andfrom volutrauma [Davis, 1987; Mortola, 1998].
Figure 3: Children’srespiratory regulation
chemo-receptors
mechano-receptors
respiratorypattern
respiratorymuscles
PaCO2
PaO2
pH
lungcompliance
main IIR = Hering Breuer Reflex
IIREPR
IIR = Inspiration Inhibiting ReflexEPR = Exspiration Prolonging Reflex
Special Anatomical and Physiological Features
1717171717
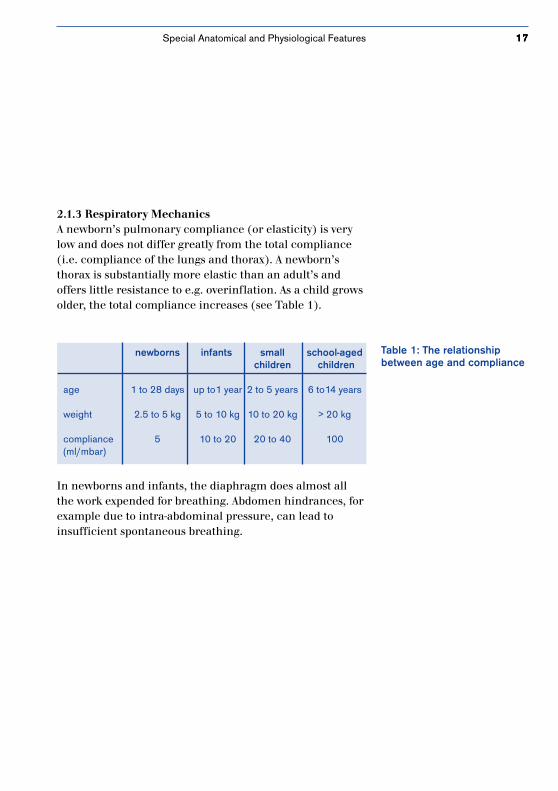
2.1.3 Respiratory MechanicsA newborn’s pulmonary compliance (or elasticity) is verylow and does not differ greatly from the total compliance(i.e. compliance of the lungs and thorax). A newborn’sthorax is substantially more elastic than an adult’s andoffers little resistance to e.g. overinflation. As a child growsolder, the total compliance increases (see Table 1).
Table 1: The relationshipbetween age and compliance
In newborns and infants, the diaphragm does almost allthe work expended for breathing. Abdomen hindrances, forexample due to intra-abdominal pressure, can lead toinsufficient spontaneous breathing.
newborns infants small school-agedchildren children
age 1 to 28 days up to1 year 2 to 5 years 6 to14 years
weight 2.5 to 5 kg 5 to 10 kg 10 to 20 kg > 20 kg
compliance 5 10 to 20 20 to 40 100(ml/mbar)
Special Anatomical and Physiological Features
1818181818
Pulmonary compliance can be reduced due to manycauses, for example:
parenchyma changes• bronchopneumonia• pulmonary edema• ARDS• fibrosis
functional surfactant disorders• alveolar pulmonary edema• atelectasis• aspiration• RDS/ARDS
reduced volume• pneumothorax• raised diaphragm
[Oczenski, 1997]
Special Anatomical and Physiological Features
1919191919
totalcapacity
inspiratoryreserve volume
inspiratorycapacity
vitalcapacity
tidalvolume
expiratoryreserve volume
residualvolume
functionalresidualcapacity
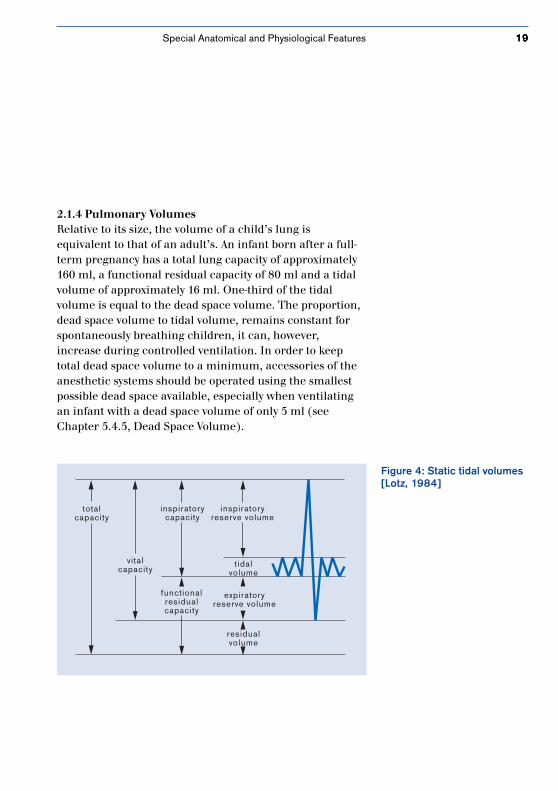
2.1.4 Pulmonary VolumesRelative to its size, the volume of a child’s lung isequivalent to that of an adult’s. An infant born after a full-term pregnancy has a total lung capacity of approximately160 ml, a functional residual capacity of 80 ml and a tidalvolume of approximately 16 ml. One-third of the tidalvolume is equal to the dead space volume. The proportion,dead space volume to tidal volume, remains constant forspontaneously breathing children, it can, however,increase during controlled ventilation. In order to keeptotal dead space volume to a minimum, accessories of theanesthetic systems should be operated using the smallestpossible dead space available, especially when ventilatingan infant with a dead space volume of only 5 ml (seeChapter 5.4.5, Dead Space Volume).
Figure 4: Static tidal volumes[Lotz, 1984]
Special Anatomical and Physiological Features
2020202020
The following static tidal volumes can be distinguished:
• total capacity (TC): includes total air volume in thelungs after a maximal inspiratory phase (TC = FRC + IC)
• vital capacity (VC): the maximum volume which can beexhaled after a maximal inspiratory phase(VC = ERV + IC)
• residual volume (RV): the volume remaining in thelungs after a maximal expiratory phase
• functional residual capacity (FRC): the volumeremaining in the lungs after a normal expiratory phase(FRC = RV + ERV)
• expiratory reserve volume (ERV): additional volumewhich can be exhaled after a normal expiratory phase
• tidal volume (VT): the volume normally inspired andexpired
• inspiratory capacity (IC): the maximum volume whichcan be inspired (IC = VT + IRV)
• inspiratory reserve volume (IRV): additional volumewhich can be inspired after a normal inspiratory phase
In addition to the above tidal volumes, closing volume isimportant (see Table 2). Although all respiratory paths areopen in a completely filled lung, decreasing expiratoryvolume may cause peripheral paths to become blocked.The closing volume of infants and small children is ratherlarge compared to that of adults. It could exceed thefunctional residual capacity and, during normalventilation, impair tidal volume.
Special Anatomical and Physiological Features

2121212121
Intubation eliminates physiologically intrinsic PEEP in thelarynx area, which counteracts peripheral respiratory pathblockage. Autogenic PEEP can be compensated for in mostanesthetic machines by using a slightly extrinsic PEEP ofabout 3 mbar, or by implementing the system ALICE [auto-matic lung inflation control effect] (see page 104).
The alveolar ventilation (ventilation of the alveoli for thepurpose of pulmonary/blood gas exchanges) of a child, 100to 150 ml/kg/min, is twice as high as that of an adult. Thisis achieved mainly through an increased respiratory rate,not through increased tidal volume (VT). The ratio ofalveolar ventilation to functional residual capacity is 5:1 forinfants and 1.5:1 for adults. As a result, the functional resi-dual capacity of an infant is only a slight “buffer” againstfluctuations of breathing gas and anesthetic agentconcentrations so that changes in anesthetic agentconcentrations are reflected very quickly in the arterialblood gas values.
Any reduction in functional residual capacity, e.g. byanesthetics, can lead to blockage in the smaller paths ofthe respiratory tract, uneven breathing gas distribution,and hypoxemia.
Special Anatomical and Physiological Features
2222222222
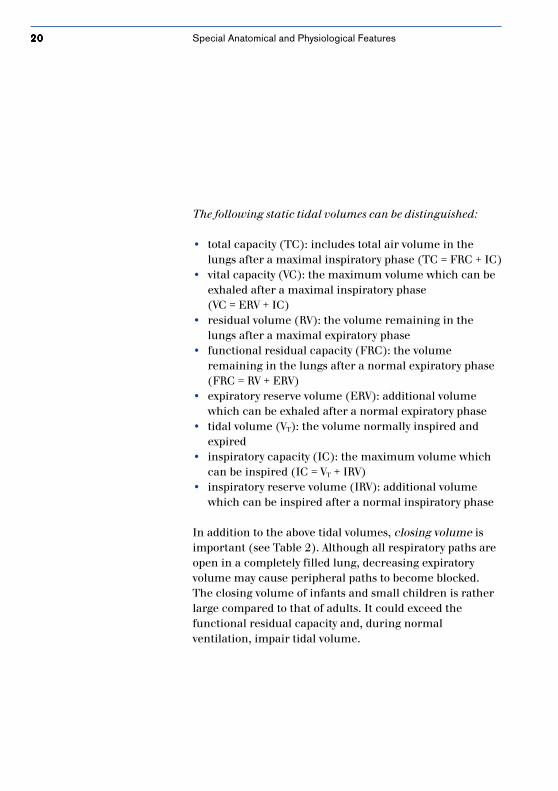
Table 2: Average respiratoryrates, tidal volumes andresistance values accordingto age
Respiratory resistance in newborns is high. This is due tothe smallness of the inside diameter of the nostrils, theminute diameter of the smaller bronchi and low tidalvolume. During an operation, significant fluctuations inrespiratory resistance can occur. For example, bronchialdilatatorical effects from volatile anesthetics reducerespiratory resistance while even the slightest swelling oraccumulation of fluids in the respiratory tract, or thetiniest obstruction in the tube area can increase total flowresistance.
newborns infants small school-agedchildren children
age 1 to 28 days up to 1 year 2 to 5 years 6 to 14 years
weight 2.5 to 5 kg 5 to 10 kg 10 to 20 kg > 20 kg
respiratory rate(min-1) 40 to 60 30 to 60 30 to 40 12 to 20
tidalvolume(ml kg -1) 8 to 10 8 to 10 8 to 10 8 to 10
resistance(mbar L -1 s) 40 20 to 30 20 1 to 2
Special Anatomical and Physiological Features

2323232323
2.1.5 SurfactantSurfactant is a surface-active substance found on thealveolar surface which is synthesized by type 2 alveolar cellsand released during inspiration. Surfactant mainly consistsof lipoproteins made of lecithin. It stabilizes the alveoli andprevents them from collapsing during the expiratory phase.In addition to this, surfactant reduces the risk of too littleventilation and atelectasis build-up. Premature newbornssuffer from respiratory distress syndrome (RDS) becausetheir surfactant is not yet mature; surfactant first maturesin the thirty-fifth and thirty-sixth weeks of pregnancy.Although hypo- and hyperoxia, acidosis and hyperthermiacan affect surfactant development, the anesthetic agents ofinhalation anesthesia seem to have little influence onsurfactant production. Those newborns with insufficientsurfactant will have a considerable amount of trouble withpulmonary gas exchange. These children usually requireventilation.
When premature newborns are treated with surfactant,functional residual capacity (FRC) builds up during thefirst 6 to 12 hours after application. The dynamiccompliance of the lungs can only increase after this timelapse has occurred. It is important to monitor tidal volumeand reduce pressure simultaneous to applying surfactantin order to prevent potential pneumothorax build-up. Anysurfactant already generated can be destroyed again bydelivering 100 % oxygen, by aspiration pneumonia or byventilating too aggressively, e.g. by applying a tidal volumewhich is too high.
Special Anatomical and Physiological Features
2424242424
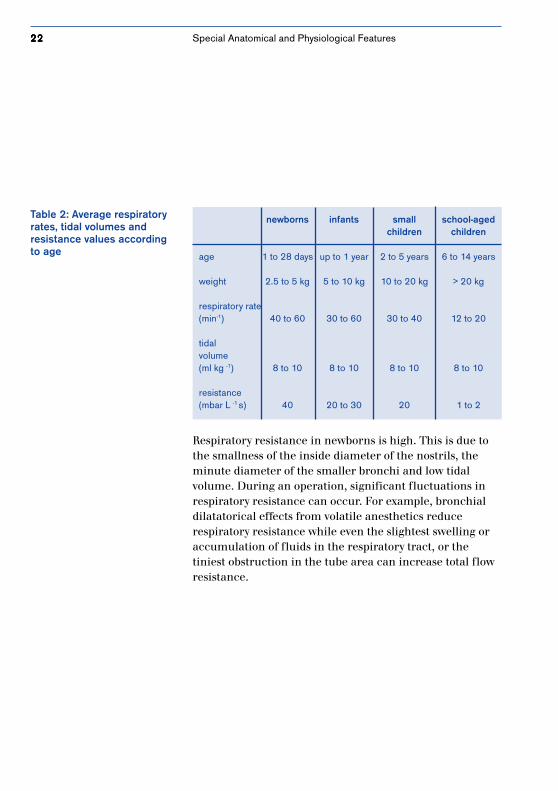
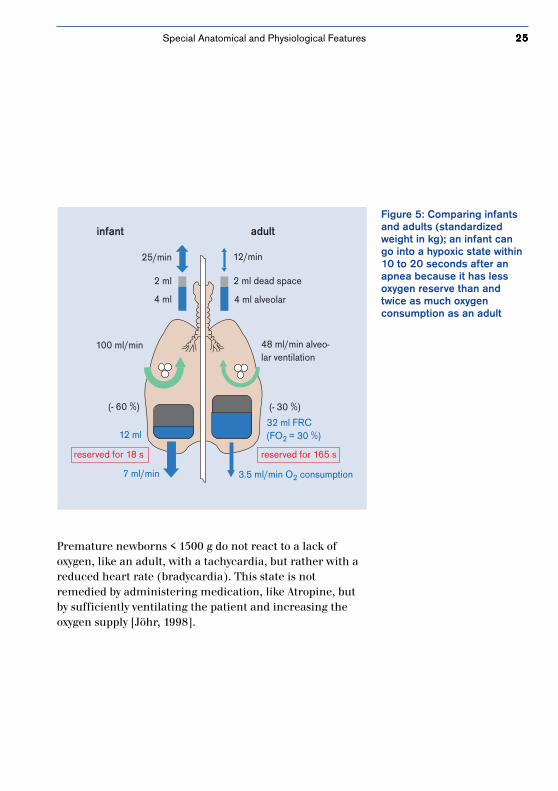
2.1.6 Oxygen RequirementsAt 7 ml/kg x min, the oxygen needs of a neonate or apremature newborn are about twice as high as that of anadult (see Table 3). At the same time, the level of oxygenconsumption depends on the child’s state of health, bodilymaturity, and stress due to cold. For example, post-operativehypothermia causes an increase of 15 to 16 ml/kg x min,whereas the oxygen required under anesthesia decreases asthe body temperature sinks.
Table 3: Interdependency ofoxygen consumption andfunctional residual capacity tobody weight
Newborns and infants are significantly more susceptible tohypoxia than adults because of higher oxygen consumptionlevels, higher alveolar ventilation (twice that of adults),and little functional residual capacity; the latter is reducedeven more after anesthetics have been administered (60 %vs. 30 %). The small oxygen reserve available to a newbornor small child is quickly used up; hypoxia can occur within10 to 20 seconds after an apnea. For comparison, an adulthas a length of tolerance of 2 to 3 minutes (see Figure 5)[Frei, 1994].
oxygen consumption functionalresidual capacity
5 kg 9 ml/kg x min 10 ml/kg
10 kg 7 ml/kg x min 15 ml/kg
20 kg 6 ml/kg x min 30 ml/kg
adults 3.5 ml/kg x min
Special Anatomical and Physiological Features
2525252525
Figure 5: Comparing infantsand adults (standardizedweight in kg); an infant cango into a hypoxic state within10 to 20 seconds after anapnea because it has lessoxygen reserve than andtwice as much oxygenconsumption as an adult
infant adult
25/min
2 ml
4 ml
100 ml/min
(- 60 %)
12 ml
reserved for 18 s
7 ml/min
12/min
2 ml dead space
4 ml alveolar
48 ml/min alveo-lar ventilation
(- 30 %)
32 ml FRC (FO2 = 30 %)
3.5 ml/min O2 consumption
reserved for 165 s
Premature newborns < 1500 g do not react to a lack ofoxygen, like an adult, with a tachycardia, but rather with areduced heart rate (bradycardia). This state is notremedied by administering medication, like Atropine, butby sufficiently ventilating the patient and increasing theoxygen supply [Jöhr, 1998].
Special Anatomical and Physiological Features

2626262626
2.1.7 Extrapulmonary Oxygen ToxicityTheir immature state and contact with partial oxygen pres-sures which are too high put premature infants at risk ofgoing blind (retinopathy of prematurity). This risk increa-ses with the degree of immaturity, the duration of oxygenapplication and the height of the partial pressures.Premature infants born before the forty-forth week ofpregnancy and exposed to a paO2 of more than 80␣ mmHgfor more than 3 hours, or a paO2 of more than 150 mmHgfor more than 2 hours, are in acute danger [Shann, 1988].For this age group, an oxygen saturation level of 90 to 95␣ %should be targeted using pulse oximetry in order to avoidpaO2 values of > 70 mmHg (see the oxygen disassociationcurve for premature infants on page 111).
The risk of damaging the retina by excessive partialpressure depends on age and is almost non-existent whenpremature infants reach the infant stage.
Which oxygen concentrationis dangerous for prematureinfants?
Special Anatomical and Physiological Features

2727272727
2.2 The Heart and Circulatory System
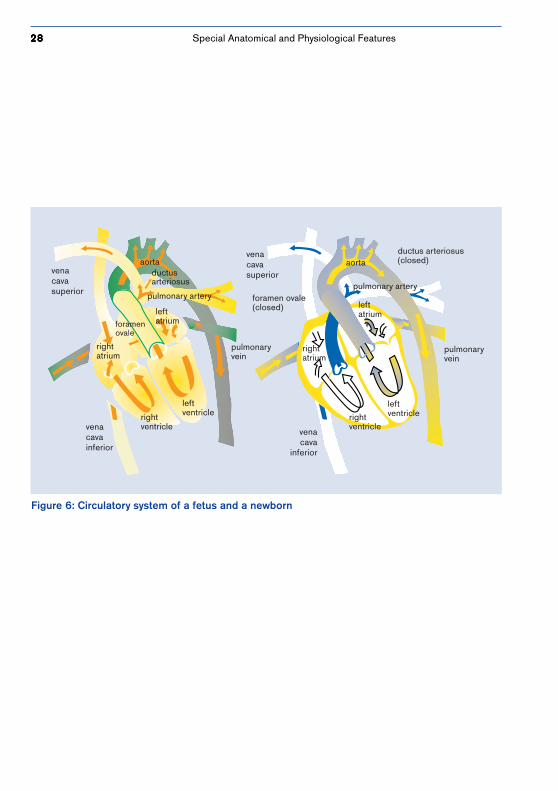
2.2.1 The Fetal Circulatory SystemThe lungs of a fetus are not ventilated before birth and areonly supplied with very little blood. Oxygen-enriched bloodis carried from the placenta of the mother through thevena cava inferior to the right atrium. The main portion ofthis blood flows through the foramen ovale directly into theleft atrium without being mixed with other blood. It istransported to the brain through the aorta ascendens andthe carotid artery while blood pushed from the rightventricle is pumped into the aorta through the ductusarteriosus. All this causes high pulmonary tissue resistanceto be present, with a right-to-left shunt via the ductusarteriosus and the foramen ovale (see Figure 6).
Lung tissue resistance decreases shortly after birth as aresult of lung expansion and an increased paO2 value in thealveoli. The result is functional blockage of the ductus andthe foramen ovale. After only 6 to 18 weeks, this blockagebecomes permanent. Before this, however, the ductus of anewborn can be reopened by acidosis and/or hypoxia.
Special Anatomical and Physiological Features
2828282828
Figure 6: Circulatory system of a fetus and a newborn
venacavasuperior
rightatrium
rightventricle vena
cavainferior
leftventricle
foramenovale
aorta
leftatrium
ductusarteriosus
pulmonary artery
pulmonaryvein
venacavasuperior
foramen ovale(closed)
rightatrium
rightventricle
leftventricle
pulmonaryvein
aortaductus arteriosus(closed)
pulmonary artery
leftatrium
venacava
inferior
Special Anatomical and Physiological Features
2929292929
2.2.2 The HeartThe heart of a newborn has fewer contractile elementsthan that of an adult. Because the metabolic rate is raised,cardiac output is relatively high: infants 200 ml/kg/min;adults 70 ml/kg/min. Cardiac output can only beincreased by increasing the heart rate. Systolic dischargecannot be increased significantly.
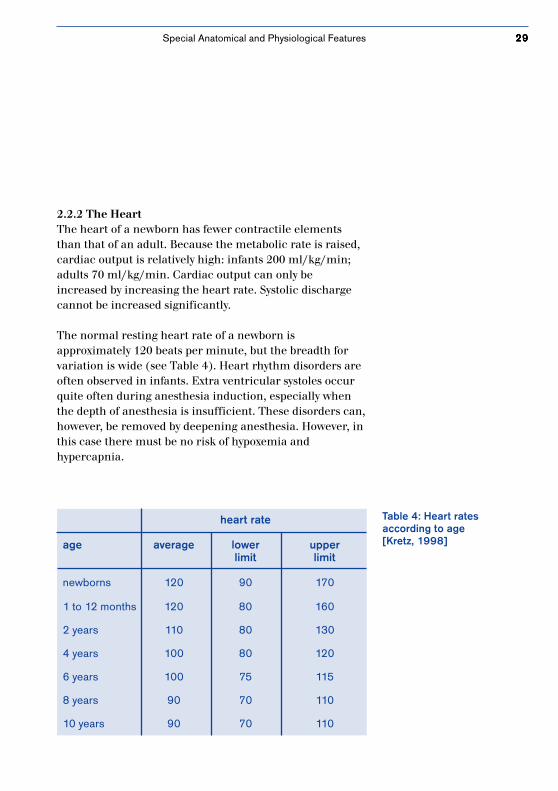
The normal resting heart rate of a newborn isapproximately 120 beats per minute, but the breadth forvariation is wide (see Table 4). Heart rhythm disorders areoften observed in infants. Extra ventricular systoles occurquite often during anesthesia induction, especially whenthe depth of anesthesia is insufficient. These disorders can,however, be removed by deepening anesthesia. However, inthis case there must be no risk of hypoxemia andhypercapnia.
Table 4: Heart ratesaccording to age[Kretz, 1998]
heart rate
age average lower upperlimit limit
newborns 120 90 170
1 to 12 months 120 80 160
2 years 110 80 130
4 years 100 80 120
6 years 100 75 115
8 years 90 70 110
10 years 90 70 110
Special Anatomical and Physiological Features
3030303030
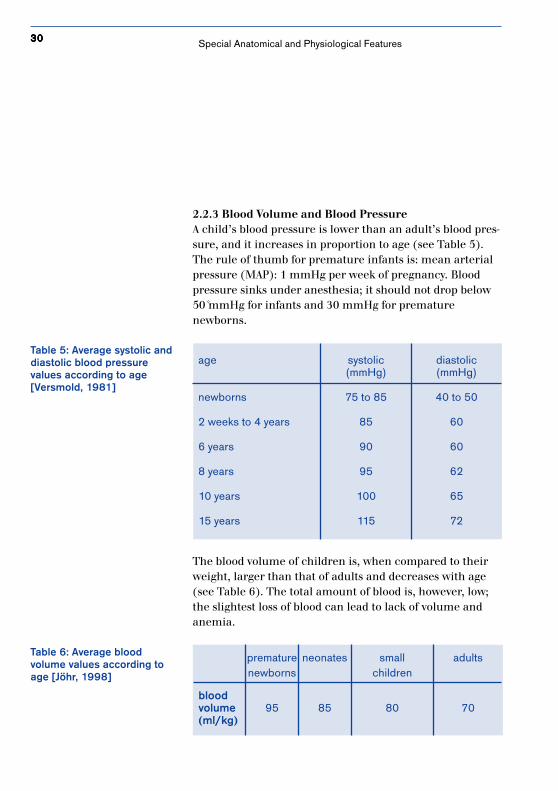
2.2.3 Blood Volume and Blood PressureA child’s blood pressure is lower than an adult’s blood pres-sure, and it increases in proportion to age (see Table 5).The rule of thumb for premature infants is: mean arterialpressure (MAP): 1 mmHg per week of pregnancy. Bloodpressure sinks under anesthesia; it should not drop below50␣ mmHg for infants and 30 mmHg for prematurenewborns.
age systolic diastolic(mmHg) (mmHg)
newborns 75 to 85 40 to 50
2 weeks to 4 years 85 60
6 years 90 60
8 years 95 62
10 years 100 65
15 years 115 72
The blood volume of children is, when compared to theirweight, larger than that of adults and decreases with age(see Table 6). The total amount of blood is, however, low;the slightest loss of blood can lead to lack of volume andanemia.
Table 5: Average systolic anddiastolic blood pressurevalues according to age[Versmold, 1981]
Table 6: Average bloodvolume values according toage [Jöhr, 1998]
premature neonates small adultsnewborns children
bloodvolume 95 85 80 70(ml/kg)
Special Anatomical and Physiological Features
3131313131
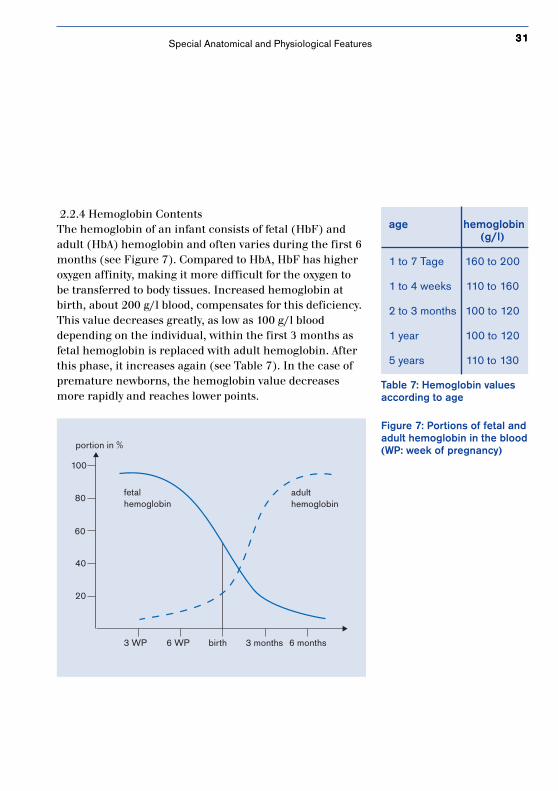
2.2.4 Hemoglobin ContentsThe hemoglobin of an infant consists of fetal (HbF) andadult (HbA) hemoglobin and often varies during the first 6months (see Figure 7). Compared to HbA, HbF has higheroxygen affinity, making it more difficult for the oxygen tobe transferred to body tissues. Increased hemoglobin atbirth, about 200 g/l blood, compensates for this deficiency.This value decreases greatly, as low as 100 g/l blooddepending on the individual, within the first 3 months asfetal hemoglobin is replaced with adult hemoglobin. Afterthis phase, it increases again (see Table 7). In the case ofpremature newborns, the hemoglobin value decreasesmore rapidly and reaches lower points.
Figure 7: Portions of fetal andadult hemoglobin in the blood(WP: week of pregnancy)
Table 7: Hemoglobin valuesaccording to age
age hemoglobin(g/l)
1 to 7 Tage 160 to 200
1 to 4 weeks 110 to 160
2 to 3 months 100 to 120
1 year 100 to 120
5 years 110 to 130
3 WP 6 WP birth 3 months 6 months
40
20
60
80
100
portion in %
fetalhemoglobin
adulthemoglobin
Special Anatomical and Physiological Features
3232323232 Special Anatomical and Physiological Features
2.3 Temperature RegulationOne of the anesthetist’s main tasks during anesthesia ismaintaining the patient’s body temperature. Infants andsmall children are especially susceptible to hypothermiaboth during and after an operation. Children absorb andgive off heat more quickly than adults because they have arelatively large body surface compared to their size andbecause their skin is thin and has little subcutaneous fat.
Infants and small children are not able to produce heat byshivering. Postoperative shivering appears only at about sixyears. Unil then, heat is produced by increasingmetabolism, for which so-called “brown adipose tissue” isbroken down.
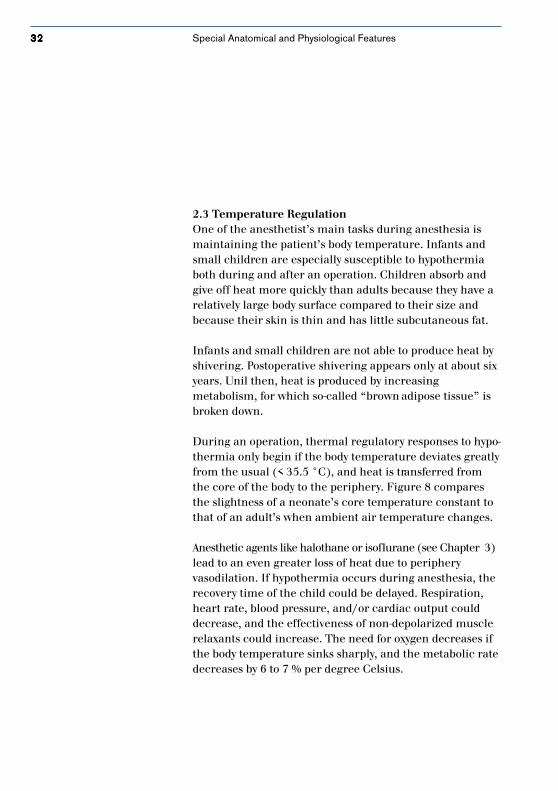
During an operation, thermal regulatory responses to hypo-thermia only begin if the body temperature deviates greatlyfrom the usual (< 35.5 °C), and heat is transferred fromthe core of the body to the periphery. Figure 8 comparesthe slightness of a neonate’s core temperature constant tothat of an adult’s when ambient air temperature changes.
Anesthetic agents like halothane or isoflurane (see Chapter 3)lead to an even greater loss of heat due to peripheryvasodilation. If hypothermia occurs during anesthesia, therecovery time of the child could be delayed. Respiration,heart rate, blood pressure, and/or cardiac output coulddecrease, and the effectiveness of non-depolarized musclerelaxants could increase. The need for oxygen decreases ifthe body temperature sinks sharply, and the metabolic ratedecreases by 6 to 7 % per degree Celsius.
3333333333
Figure 8: Changes in coretemperature for prematureinfants and adults
37
30
˚C
core temperature
hypothermia thermoneutral zone hyperthermia ˚C
ambient temperature
37
30
˚C
core temperature
hypothermia
thermoneutral zone
hyperthermia ˚C
ambient temperature
The Core Temperature of an Adult
The Core Temperatue of a Premature Infant
Special Anatomical and Physiological Features
3434343434
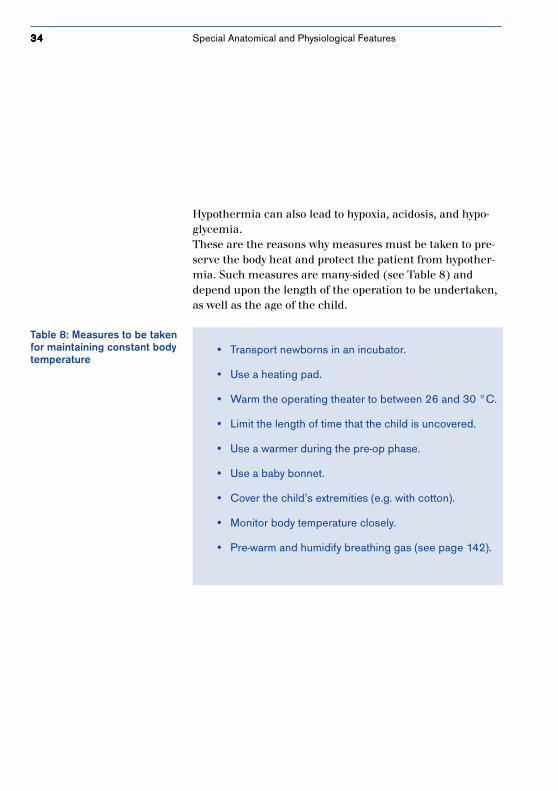
Table 8: Measures to be takenfor maintaining constant bodytemperature
• Transport newborns in an incubator.
• Use a heating pad.
• Warm the operating theater to between 26 and 30 °C.
• Limit the length of time that the child is uncovered.
• Use a warmer during the pre-op phase.
• Use a baby bonnet.
• Cover the child’s extremities (e.g. with cotton).
• Monitor body temperature closely.
• Pre-warm and humidify breathing gas (see page 142).
Hypothermia can also lead to hypoxia, acidosis, and hypo-glycemia.These are the reasons why measures must be taken to pre-serve the body heat and protect the patient from hypother-mia. Such measures are many-sided (see Table 8) anddepend upon the length of the operation to be undertaken,as well as the age of the child.
Special Anatomical and Physiological Features
3535353535
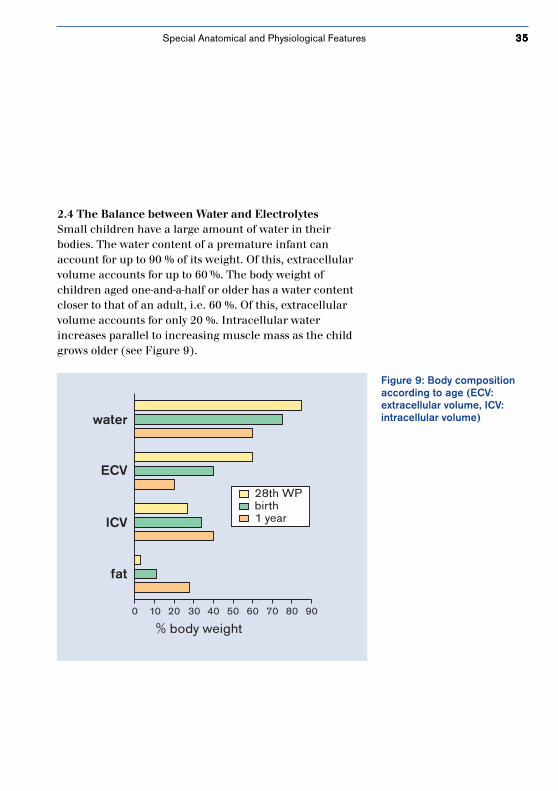
Figure 9: Body compositionaccording to age (ECV:extracellular volume, ICV:intracellular volume)
0 10 20 30 40 50 60 8070 90
% body weight
water
ECV
ICV
fat
28th WPbirth1 year
2.4 The Balance between Water and ElectrolytesSmall children have a large amount of water in theirbodies. The water content of a premature infant canaccount for up to 90 % of its weight. Of this, extracellularvolume accounts for up to 60␣ %. The body weight ofchildren aged one-and-a-half or older has a water contentcloser to that of an adult, i.e. 60 %. Of this, extracellularvolume accounts for only 20 %. Intracellular waterincreases parallel to increasing muscle mass as the childgrows older (see Figure 9).
Special Anatomical and Physiological Features
3636363636
weight liquid requirements
adults 70 kg 1.5 ml/kg/h
school-aged 50 kg 2.0 ml/kg/hchildren 20 kg 3.5 ml/kg/h
small children 13 kg 4.0 mg/kg/h
infants 10 kg 5.0 ml/kg/h
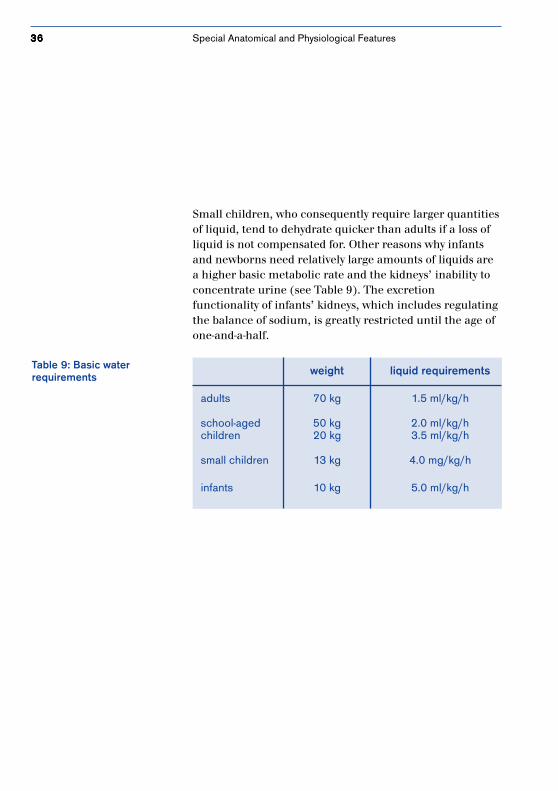
Table 9: Basic waterrequirements
Small children, who consequently require larger quantitiesof liquid, tend to dehydrate quicker than adults if a loss ofliquid is not compensated for. Other reasons why infantsand newborns need relatively large amounts of liquids area higher basic metabolic rate and the kidneys’ inability toconcentrate urine (see Table 9). The excretionfunctionality of infants’ kidneys, which includes regulatingthe balance of sodium, is greatly restricted until the age ofone-and-a-half.
Special Anatomical and Physiological Features
3737373737
3. Anesthetic Agents
A suitable choice of anesthetic agentsis adapted especially for little patients.

3838383838 Anesthetic Agents
3.1 Inhalation AnesthesiaMany anesthesiologists consider inhalation anesthesia theideal method of application for children. Whenadministering anesthetic agents and other medication,anesthetists need to bear in mind that dosages cannot betransferred from adults to newborns and small childrenone-to-one. Reasons for this include the varying nature ofthe absorption and distribution of anesthetic agent in achild, as well as the child’s metabolism.
Newborns and small children absorb anesthetics fasterthan adults due to a high alveolar ventilation rate and asmaller blood-gas distribution coefficient for anestheticagent (less blood solubility). For example, a newborn’sblood-gas distribution coefficient for halothane, enfluraneand isoflurane is 18 % lower than a young adult’s (20 to 40years old), and for small children it is stall a good 12␣ %lower.
The distribution of anesthetic agent is influenced by alarge amount of extracellular space and a difference inmembrane permeability (immature blood/brain barriers).The metabolic rate for anesthetic agent (passing throughthe liver) is often slower because the metabolic paths ofnewborns are immature.
3939393939
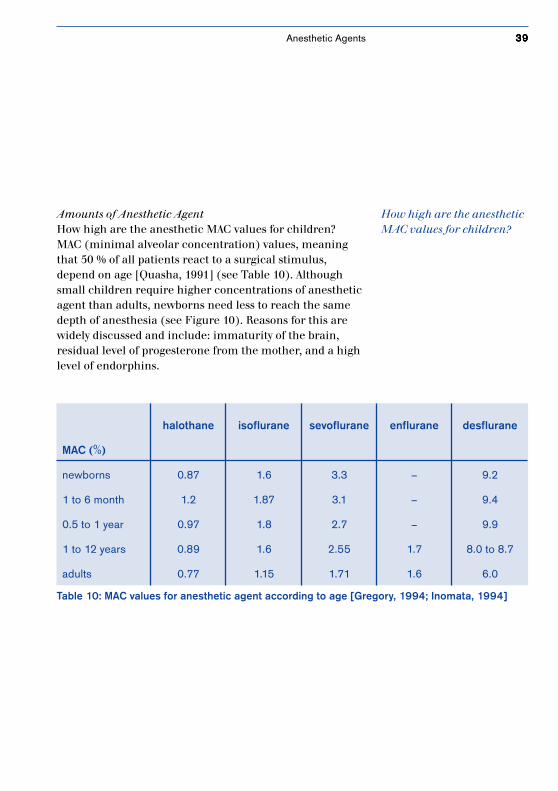
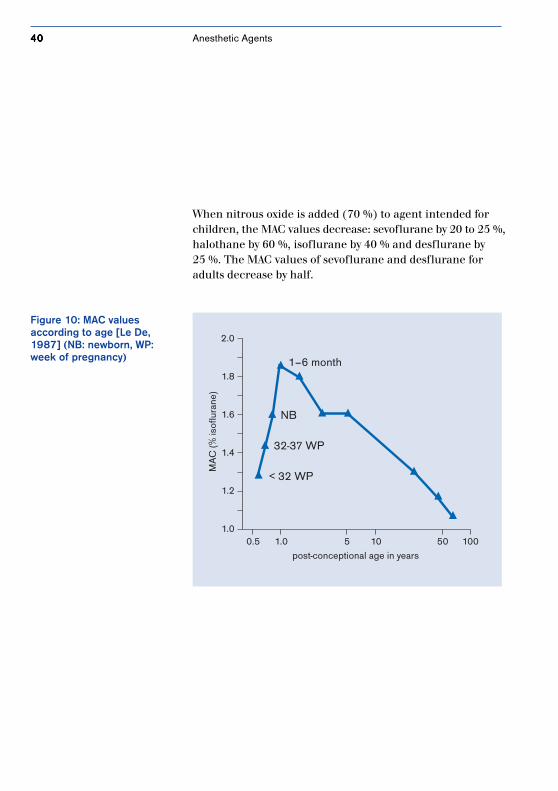
Amounts of Anesthetic AgentHow high are the anesthetic MAC values for children?MAC (minimal alveolar concentration) values, meaningthat 50 % of all patients react to a surgical stimulus,depend on age [Quasha, 1991] (see Table 10). Althoughsmall children require higher concentrations of anestheticagent than adults, newborns need less to reach the samedepth of anesthesia (see Figure 10). Reasons for this arewidely discussed and include: immaturity of the brain,residual level of progesterone from the mother, and a highlevel of endorphins.
Table 10: MAC values for anesthetic agent according to age [Gregory, 1994; Inomata, 1994]
halothane isoflurane sevoflurane enflurane desflurane
MAC (%)
newborns 0.87 1.6 3.3 – 9.2
1 to 6 month 1.2 1.87 3.1 – 9.4
0.5 to 1 year 0.97 1.8 2.7 – 9.9
1 to 12 years 0.89 1.6 2.55 1.7 8.0 to 8.7
adults 0.77 1.15 1.71 1.6 6.0
How high are the anestheticMAC values for children?
Anesthetic Agents
4040404040
When nitrous oxide is added (70 %) to agent intended forchildren, the MAC values decrease: sevoflurane by 20 to 25 %,halothane by 60 %, isoflurane by 40 % and desflurane by25 %. The MAC values of sevoflurane and desflurane foradults decrease by half.
1.0
1.2
1.4
1.6
1.8
2.0
0.5 1.0 5 10 50 100
1–6 month
NB
32-37 WP
< 32 WP
MA
C (%
isof
lura
ne)
post-conceptional age in years
Figure 10: MAC valuesaccording to age [Le De,1987] (NB: newborn, WP:week of pregnancy)
Anesthetic Agents

4141414141
Nitrous OxideNitrous oxide, a rather odorless gas with good analgesicproperties, is used as a supplement in general anesthesia.It is not a potent anesthetic (MAC 105 %) and has, byreason of its low solubility in the blood, a very rapid wash-in/wash-out rate. Nitrous oxide, which has little effect onthe functionality of the circulatory system, should not beused on newborns and children with pulmonary infectionssince, in this case, it could trigger so-called diffusionhypoxia. In addition, it could be contraindicate ofheightened intracranial pressure or marked ileus [Loop].
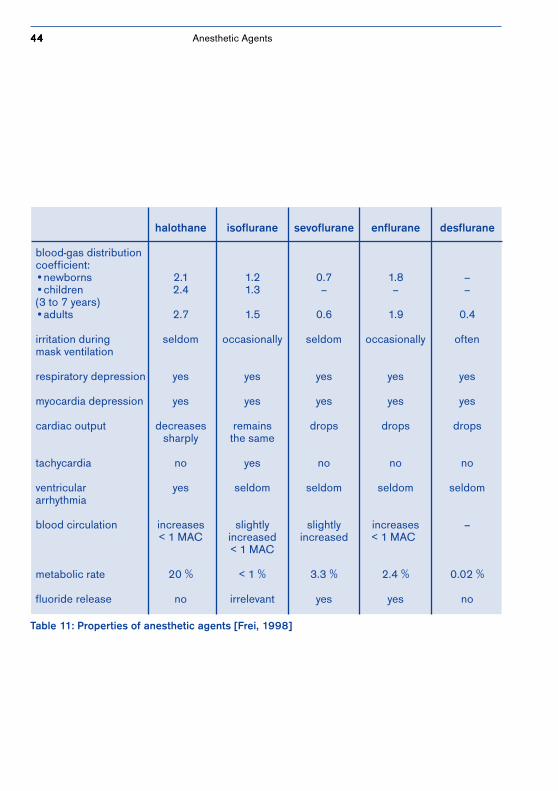
HalothaneNext to nitrous oxide, halothane remains the most widelyused anesthetic agent in pediatric anesthesia. Reasonsgiven for halothane’s suitability for children include theability to introduce the mask agreeably due to a pleasant,non-pungent smell, potency and price. Halothane does,however, have a grave side-effect: the myocardium’sincreased sensitiveness to circulating catecholamines. Thiscan lead to increased occurrences of intra-operativearrhythmia. In addition, halothane can cause liver damagein adult patients. Indications of liver damage to pediatricpatients repeatedly under anesthesia are, however,considerably lower and furthermore, are considered to be ajustifiable risk in most cases [Conzen, 1998]. Otherproperties of this agent are described in Table 11and compared to the other four anesthetic agents.
Anesthetic Agents

4242424242
IsofluraneThe use of isoflurane in pediatric patients is controversial.Isoflurane, which irritates the respiratory tract, often leadsto laryngospasms in children who have not received pre-medication prior to the induction phase. This gas is, thus,used less often for initiating anesthesia in pediatricpatients and more often for maintaining a specific depth ofanesthesia. Due to its low metabolic rate of 0.2 %,isoflurane is the preferred anesthetic agent for childrenwith marked liver damage.
SevofluraneIn 1995, anesthetists began using another inhalationanesthetic, sevoflurane, for pediatric anesthesia. Thisanesthetic gas, as pleasant smelling as halothane, does notirritate the respiratory tract and has little effect on thecardio-circulatory system. A lower blood-gas distributioncoefficient means that anesthetic induction and therecovery phase are shorter with sevoflurane than withhalothane, and pediatric patients have less postoperativenausea and vomiting. The shortened recovery time coupledwith a more rapid recovery of perception, may produce astate of restlessness [Holzki, 1999].
EnfluraneEnflurane is not widely used in pediatric anesthesia due topossible epileptic effects, a great depression of breathing,higher fluoride concentrations and an ether-like smell.This gas is more potent than sevoflurane but less so thanhalothane.
Anesthetic Agents

4343434343
DesfluraneDesflurane, less potent than other gases (MAC 8-9 %), has(like sevoflurane) a low blood-gas distribution coefficientand, thus, allows for quicker and more exact adaptation tothe depth of anesthesia. Quick gas induction and speedyremoval from the blood are the reasons for this. Comparedto sevoflurane, however, desflurane is not very suitable formask induction in pediatric anesthesia because of itsether-like smell. This is why desflurane is the preferredagent used for maintaining general anesthesia duringpediatric anesthesia rather than for an inhalationinduction. It is also especially suitable for prolongedanesthesia because it has the lowest fatty tissue/blooddistribution coefficient of all five gases. Side-effects includerespiratory tract irritation, apnea and laryngospasms[Mielke, 1998].
XenonWhen considering the odorless, colorless inert gas xenon,the question arises as to whether this gas could be the idealanesthetic agent of the future. The properties of this inertgas are considered excellent. Low solubility (blood-gasdistribution coefficient: 0.14) means that the induction/removal phase is very short. When a mixture of 30 Vol. %oxygen and 70 Vol. % xenon is used, the analgesic effect isexcellent. In addition, xenon has no effect on thehemodynamics or compliance of the lungs. Xenon is alsoconsidered environmentally friendly. Since this gas is onlyavailable in limited quantities, its use is extremely costly.Means must be found to scavenge the gas by using specialscavenging equipment or it must be sparingly used (forexample by implementing a closed rebreathing system).Xenon is not yet registered nor is it validated for pediatricanesthesia.
Anesthetic Agents
4444444444
Table 11: Properties of anesthetic agents [Frei, 1998]
halothane isoflurane sevoflurane enflurane desflurane
blood-gas distributioncoefficient:•newborns 2.1 1.2 0.7 1.8 –•children 2.4 1.3 – – –(3 to 7 years)•adults 2.7 1.5 0.6 1.9 0.4
irritation during seldom occasionally seldom occasionally oftenmask ventilation
respiratory depression yes yes yes yes yes
myocardia depression yes yes yes yes yes
cardiac output decreases remains drops drops dropssharply the same
tachycardia no yes no no no
ventricular yes seldom seldom seldom seldomarrhythmia
blood circulation increases slightly slightly increases –< 1 MAC increased increased < 1 MAC
< 1 MAC
metabolic rate 20 % < 1 % 3.3 % 2.4 % 0.02 %
fluoride release no irrelevant yes yes no
Anesthetic Agents

4545454545
3.2 Interactions with Soda LimeThe fact that patient gas is rebreathed in partial and closedre-breathing systems makes it imperative that CO2 be safelyeliminated. To achieve this, an absorber filled with sodalime is built into the breathing circuit. Soda lime used, forexample, in Germany Drägersorb 800 Plus, is composed of75 to 85 % calcium hydroxide, 1 to 4 % nitrous hydroxideand 14 to 18 % water (soda lime). Barium lime, usedalmost exclusively in the USA, is made up of 65 % calciumhydroxide, 1 to 4 % potassium hydroxide, and about 35 %barium hydroxide which binds approximately 15 %constitutional water. Both kinds have a colored indicatorwhich allows the anesthetist to see when the absorbershould be replaced.
The neutralization reaction begins with carbonic acidbeing formed from expiratory carbon dioxide and water.After that, nitrous carbonate is created from nitroushydroxide, which then combines with calcium hydroxide tomake a calcium carbonate. This process releases nitroushydroxide, allowing new reactions with carbon dioxide totake place [Förster, 1999].
Since carbon dioxide can only be absorbed if soda lime isavailable in a hydrated form, Drägersorb 800 or 800 Plus,for example, is provided with a moisture level of 14 to 18␣ %.Carbon dioxide cannot be eliminated if the level ofmoisture falls below 4 %.
Anesthetic Agents

4646464646
If the soda lime dries out, regardless of the type of sodalime or the type of inhalation anesthetic used, undesiredreactions are generally the result, but which kind dependson the degree of dryness. Typical reactions includereduced CO2 absorption, the formation of carbonmonoxide, absorption and decomposition of anestheticagent, increased heat in the absorber and, thus, higherbreathing gas temperatures.
These reactions could endanger the pediatric patient withcarbon monoxide poisoning, a depth of anesthesia which istoo shallow, and/or respiratory tract burns.Using moist soda lime can, however, also lead to by-products of decomposition. The most well-known productof the decomposition of sevoflurane is so-called CompoundA (see Figure 10). This compound is a nephrotoxic vinylether. The amount of concentration generated depends onthe type of soda lime used, the temperature of and level ofmoisture in the soda lime, the amount of fresh-gas flow,and the composition and concentration of the gas.
Several factors favorable to Compound A generationinclude:
• higher interaction with barium lime than withsoda lime
• increased bonding during low-flow and minimal flowanesthesia
• high temperatures (= increased production of CO2)• reduced level of moisture in CO2 absorber
How do inhalationanesthetics interact withsoda lime?
Anesthetic Agents
4747474747
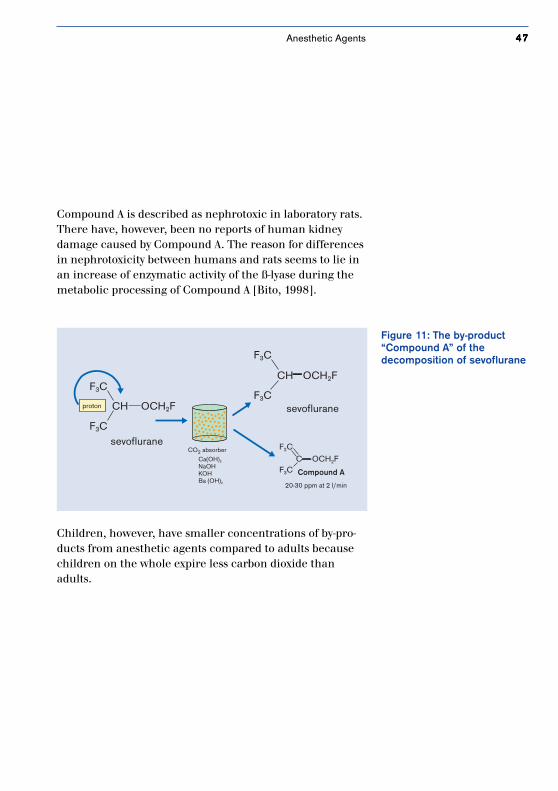
Compound A is described as nephrotoxic in laboratory rats.There have, however, been no reports of human kidneydamage caused by Compound A. The reason for differencesin nephrotoxicity between humans and rats seems to lie inan increase of enzymatic activity of the ß-lyase during themetabolic processing of Compound A [Bito, 1998].
Figure 11: The by-product“Compound A” of thedecomposition of sevoflurane
Children, however, have smaller concentrations of by-pro-ducts from anesthetic agents compared to adults becausechildren on the whole expire less carbon dioxide thanadults.
sevoflurane
CH OCH2F
F3C
F3C
proton
CO2 absorber
Ca(OH)2
NaOHKOHBa (OH)2
F3C
F3C
CH OCH2F
sevoflurane
F2C
F3CC OCH2F
Compound A
20-30 ppm at 2 l/min
Anesthetic Agents
4848484848
Tips for Soda Lime UsageThe Dräger Medizintechnik GmbH and the DGAI [GermanAssociation of Anesthesiology and Intensive Care] recom-mend the following measures be taken to prevent soda limefrom drying out [Union information, 1999]:
• Change soda lime routinely according to the indicatoror CO2 measurement.
• Close the precision needle valves carefully after everyanesthesia case.
• For those anesthetic devices not intended to be usedfor a long period of time, the absorber should be leftempty after the device has been serviced.
• When drying out the breathing system and therespirator, the absorber, filled with soda lime, has to beremoved from the system and sealed using theappropriate air-tight covers.
• It is not advised that the soda lime be moistened bypouring water over it or spraying it with water.
Changing the chemical make-up of Drägersorb 800 Plus,available since the beginning of 1999, has allowed thedevelopment of undesired by-products like Compound Aand carbon monoxide to be greatly reduced.
How can interactionsbetween soda lime andinhalation anesthetics beprevented?
Anesthetic Agents

4949494949
3.3 Intravenous AnesthesiaNumerous clinics and hospitals prefer to use intravenousmethods, with continuous intravenous injections ofanesthetics, for administering anesthetics and maintainingdepth of anesthesia. One of the reasons for this is thatpersonnel in the operating room cannot be exposed tovolatile anesthetic agents during mask anesthesia or fromleaking endotracheal tubes. Other reasons being discussedare the advantages of increased safety and the more rapidinduction associated with intravenous anesthesia, as wellas fewer incidents of excitation and laryngospasms.
One of the hypnotics most frequently used for intravenousanesthesia is Propofol (Disoprivan®). Anesthetists who usePropofol must, however, take the following into consid-eration: dosages for children and adults differ greatlybecause children have smaller amounts of fat and muscle—this corresponds to their weight— and lower levels ofplasma protein. An infusion of approximately 3 to 5 mg/kgis used for pediatric anesthesia induction and around 5 to15 mg/kg/h for maintaining depth of anesthesia.
Some of the side effects of Propofol described are pain ofinjection, lowered blood pressure, and bradycardia. Thefrequency of bradycardia incidents in children is about 10to 20 % higher than in adults. These side effects can beimportant when one considers that the cardiac output ofinfants and small children is mainly controlled by theirheart rate and that baroreceptor functions are not yetmarked.
Anesthetic Agents
5050505050
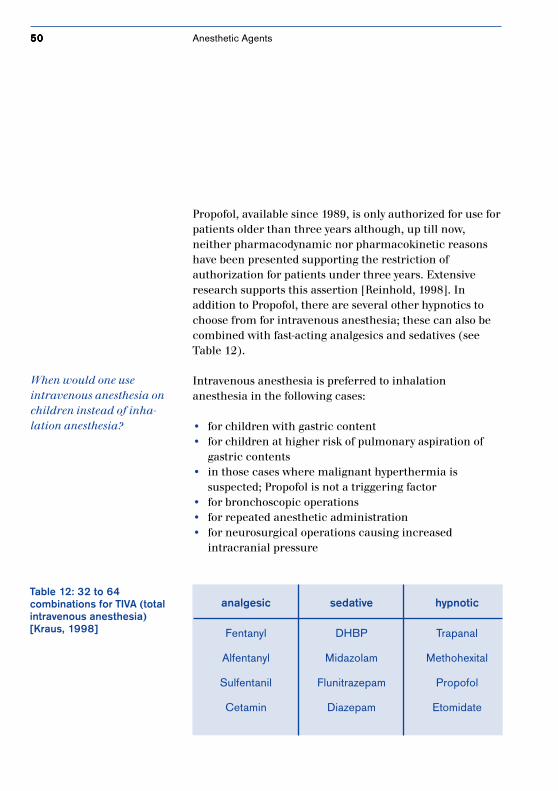
Propofol, available since 1989, is only authorized for use forpatients older than three years although, up till now,neither pharmacodynamic nor pharmacokinetic reasonshave been presented supporting the restriction ofauthorization for patients under three years. Extensiveresearch supports this assertion [Reinhold, 1998]. Inaddition to Propofol, there are several other hypnotics tochoose from for intravenous anesthesia; these can also becombined with fast-acting analgesics and sedatives (seeTable 12).
Intravenous anesthesia is preferred to inhalationanesthesia in the following cases:
• for children with gastric content• for children at higher risk of pulmonary aspiration of
gastric contents• in those cases where malignant hyperthermia is
suspected; Propofol is not a triggering factor• for bronchoscopic operations• for repeated anesthetic administration• for neurosurgical operations causing increased
intracranial pressure
Table 12: 32 to 64combinations for TIVA (totalintravenous anesthesia)[Kraus, 1998]
analgesic sedative hypnotic
Fentanyl DHBP Trapanal
Alfentanyl Midazolam Methohexital
Sulfentanil Flunitrazepam Propofol
Cetamin Diazepam Etomidate
When would one useintravenous anesthesia onchildren instead of inha-lation anesthesia?
Anesthetic Agents

5151515151
3.4 Muscle RelaxantsThe pharmaceutical kinetics and dynamics of musclerelaxants in children differ considerably from those inadults.
• A larger distribution volume leads to lower plasma levelsdespite an equal dosage of muscle relaxants.
• Motor endplates and contractile elements of the musclecells are at different levels of maturity and the release ofacetylcholine is limited.
• The time it takes muscle relaxants to become effectivein children varies greatly.
• The elimination of muscle relaxants takes place moreslowly due to immature kidneys and liver.
• Muscle fatigue has been observed in infants youngerthan 2 months, even without the presence of musclerelaxants [Diefenbach, 1998].
SuccinylcholineSuccinylcholine is used for endotracheal intubation. Inorder to obtain the same degree of relaxation, childrenneed higher doses of fast-acting depolarizing relaxants thanadults because of their weight. Infants are given infusionsof 2 mg/kg and older children 1.5 mg/kg.
Administering succinylcholine to children can lead to life-threatening complications like bradycardia, asystole, stiffmuscles, and muscle fiber decomposition withmyoglobinemia and malignant hyperthermia.
Anesthetic Agents
5252525252
dosage fordosage fordosage fordosage fordosage for repeatedrepeatedrepeatedrepeatedrepeated length oflength oflength oflength oflength of sidesidesidesidesideintubationintubationintubationintubationintubation dosagesdosagesdosagesdosagesdosages effectivenesseffectivenesseffectivenesseffectivenesseffectiveness effectseffectseffectseffectseffects(mg/kg) (mg/kg) (min)(min)(min)(min)(min)
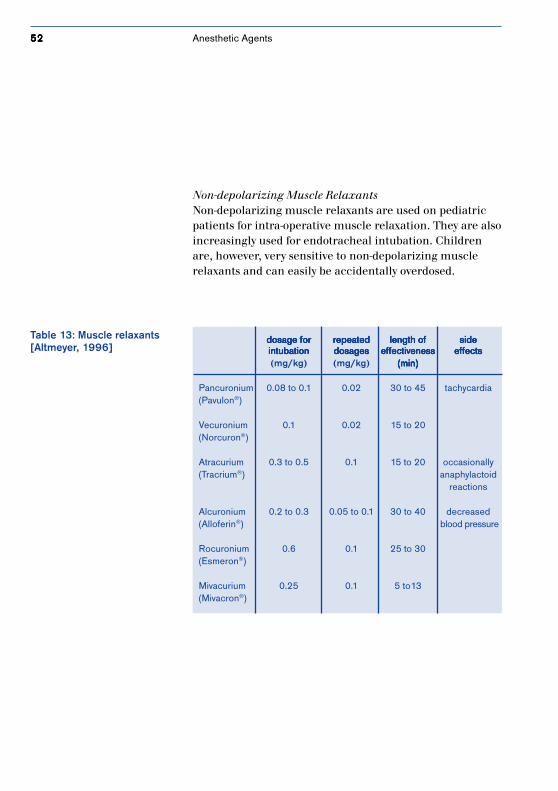
Pancuronium 0.08 to 0.1 0.02 30 to 45 tachycardia(Pavulon®)
Vecuronium 0.1 0.02 15 to 20(Norcuron®)
Atracurium 0.3 to 0.5 0.1 15 to 20 occasionally(Tracrium®) anaphylactoid
reactions
Alcuronium 0.2 to 0.3 0.05 to 0.1 30 to 40 decreased(Alloferin®) blood pressure
Rocuronium 0.6 0.1 25 to 30(Esmeron®)
Mivacurium 0.25 0.1 5 to13(Mivacron®)
Table 13: Muscle relaxants[Altmeyer, 1996]
Non-depolarizing Muscle RelaxantsNon-depolarizing muscle relaxants are used on pediatricpatients for intra-operative muscle relaxation. They are alsoincreasingly used for endotracheal intubation. Childrenare, however, very sensitive to non-depolarizing musclerelaxants and can easily be accidentally overdosed.
Anesthetic Agents
5353535353
4. Anesthesia Accessories
A large assortment ofanesthesia accessories,
specially made to meet the needs of children,is available for all sorts of use.
5454545454 Anesthetic Accessories
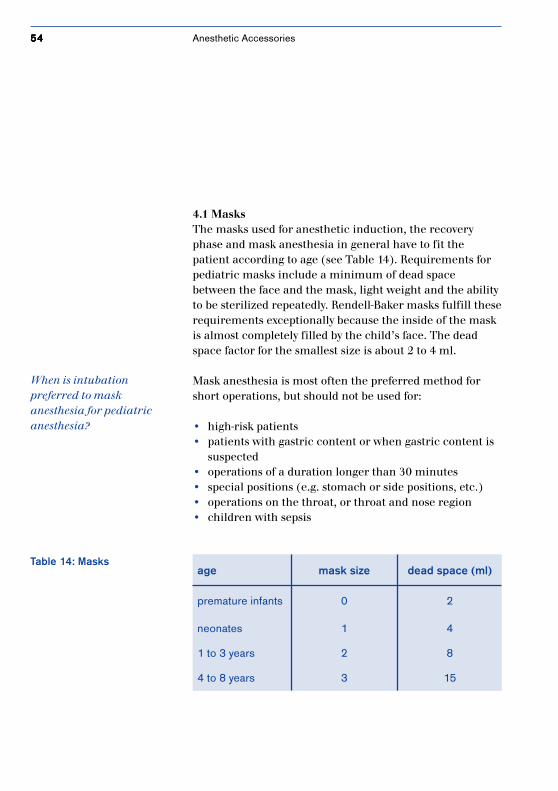
4.1 MasksThe masks used for anesthetic induction, the recoveryphase and mask anesthesia in general have to fit thepatient according to age (see Table 14). Requirements forpediatric masks include a minimum of dead spacebetween the face and the mask, light weight and the abilityto be sterilized repeatedly. Rendell-Baker masks fulfill theserequirements exceptionally because the inside of the maskis almost completely filled by the child’s face. The deadspace factor for the smallest size is about 2 to 4 ml.
Mask anesthesia is most often the preferred method forshort operations, but should not be used for:
• high-risk patients• patients with gastric content or when gastric content is
suspected• operations of a duration longer than 30 minutes• special positions (e.g. stomach or side positions, etc.)• operations on the throat, or throat and nose region• children with sepsis
Table 14: Masksage mask size dead space (ml)
premature infants 0 2
neonates 1 4
1 to 3 years 2 8
4 to 8 years 3 15
When is intubationpreferred to maskanesthesia for pediatricanesthesia?

5555555555Anesthetic Accessories
4.2 TubesAuxiliary equipment for respirators includes throat,tracheal and nasopharyngeal tubes.
Throat TubesThe Guedel tube, oropharyngeally inserted, helps keep therespiratory tract open and is available for pediatric patientsin three different sizes. It should be noted that by using aGuedel tube which is too small, the root of the tonguecould drop backwards. If a Guedel tube which is too large isused, the epiglottis could be closed off from the trachea.
Tracheal TubesThin-walled non-recyclable tubes made from PVCs areoften used for pediatric endotracheal tubes. In order toprevent cuff pressure from damaging the tracheal mucusmembrane, only uncuffed tubes are used on children aged8 or younger. In emergency situations, the throat isenlarged with the aide of special wadding, or the nextlarger size is used.
Air leakage during ventilation should be less for those tubeswithout cuffs. Leak rates for any given tube should bewithin a range of 10 to 20 % of the applied minute volume,and if respiratory pressure values are >20 mbar, theanesthetist should be able to hear the sound of leakage. Ifthere is no leaking noise, a smaller tube should be used[Eberhard, 1998].
The black mark on the tip of the tube indicates how deepintubation should be; the mark should be positioned belowthe vocal chords.
5656565656
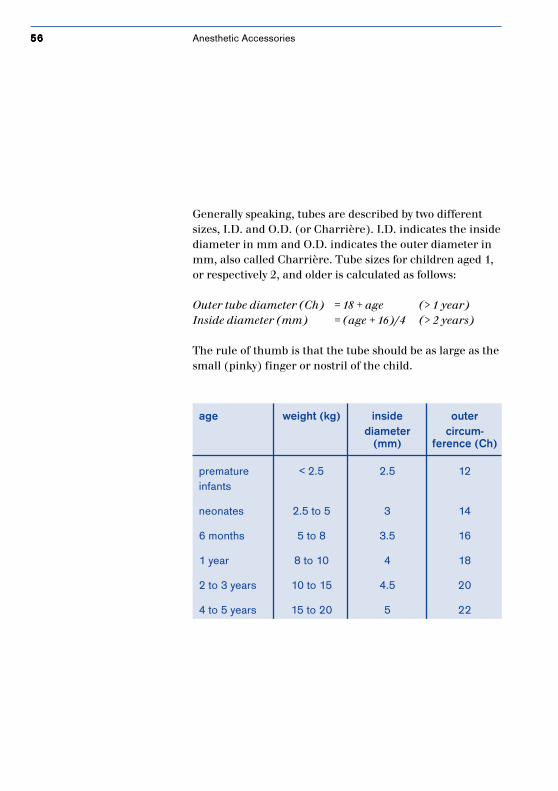
Generally speaking, tubes are described by two differentsizes, I.D. and O.D. (or Charrière). I.D. indicates the insidediameter in mm and O.D. indicates the outer diameter inmm, also called Charrière. Tube sizes for children aged 1,or respectively 2, and older is calculated as follows:
Outer tube diameter (Ch) = 18 + age (> 1 year)Inside diameter (mm) = (age + 16)/4 (> 2 years)
The rule of thumb is that the tube should be as large as thesmall (pinky) finger or nostril of the child.
age weight (kg) inside outerdiameter circum-
(mm) ference (Ch)
premature < 2.5 2.5 12infants
neonates 2.5 to 5 3 14
6 months 5 to 8 3.5 16
1 year 8 to 10 4 18
2 to 3 years 10 to 15 4.5 20
4 to 5 years 15 to 20 5 22
Anesthetic Accessories
5757575757
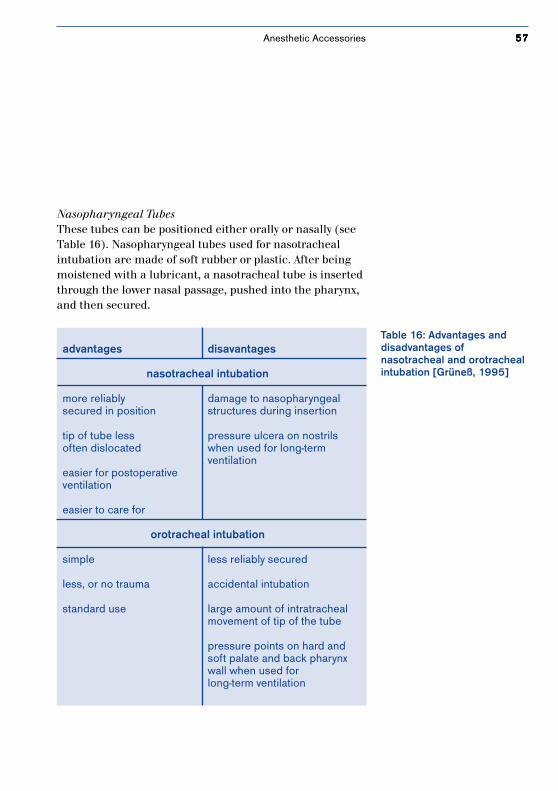
Nasopharyngeal TubesThese tubes can be positioned either orally or nasally (seeTable 16). Nasopharyngeal tubes used for nasotrachealintubation are made of soft rubber or plastic. After beingmoistened with a lubricant, a nasotracheal tube is insertedthrough the lower nasal passage, pushed into the pharynx,and then secured.
Table 16: Advantages anddisadvantages ofnasotracheal and orotrachealintubation [Grüneß, 1995]
advantages disavantages
nasotracheal intubation
more reliably damage to nasopharyngealsecured in position structures during insertion
tip of tube less pressure ulcera on nostrilsoften dislocated when used for long-term
ventilationeasier for postoperativeventilation
easier to care for
orotracheal intubation
simple less reliably secured
less, or no trauma accidental intubation
standard use large amount of intratrachealmovement of tip of the tube
pressure points on hard andsoft palate and back pharynxwall when used forlong-term ventilation
Anesthetic Accessories

5858585858
4.3 Laryngeal MasksLaryngeal masks have found world-wide acceptance, evenin pediatric anesthesia. They represent a compromisebetween face masks and endotracheal intubation. As is thecase with endotracheal intubation, the hands of theanesthtetist are free to perform other tasks, but mucusmembranes in the larynx and trachea are not irritated (seeTable 17). These masks are inserted under inhalationanesthesia or after intravenous anesthesia induction. Afterthe correct position has been obtained, the cuff is filledwith air until there is no leakage. Monitoring is doneacoustically: a respiratory pressure value of 20 mmHgshould not produce any sound of leakage.
Chapter 7.3 describes in detail how laryngeal masks areused.
Anesthetic Accessories
5959595959
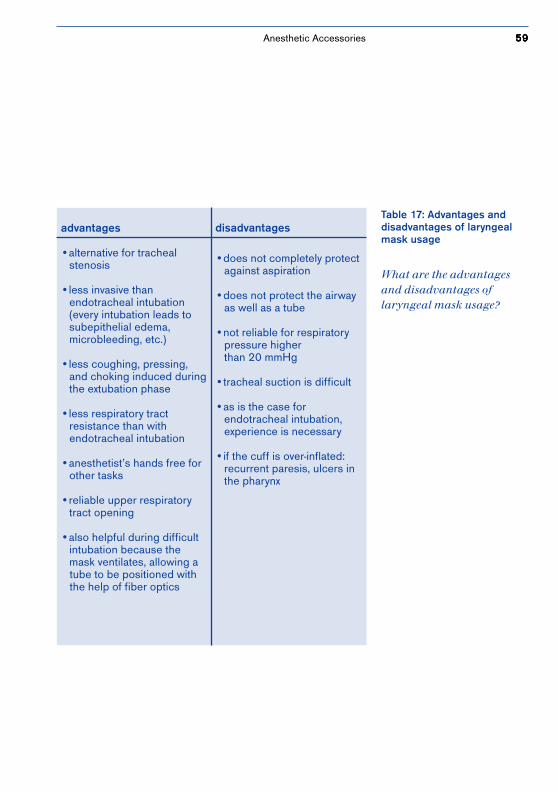
Table 17: Advantages anddisadvantages of laryngealmask usage
advantages
•alternative for tracheal stenosis
•less invasive than endotracheal intubation (every intubation leads to subepithelial edema, microbleeding, etc.)
•less coughing, pressing, and choking induced during the extubation phase
•less respiratory tract resistance than with endotracheal intubation
•anesthetist’s hands free for other tasks
•reliable upper respiratory tract opening
•also helpful during difficult intubation because the mask ventilates, allowing a tube to be positioned with the help of fiber optics
disadvantages
•does not completely protect against aspiration
•does not protect the airway as well as a tube
•not reliable for respiratory pressure higher than 20 mmHg
•tracheal suction is difficult
•as is the case for endotracheal intubation, experience is necessary
•if the cuff is over-inflated: recurrent paresis, ulcers in the pharynx
What are the advantagesand disadvantages oflaryngeal mask usage?
Anesthetic Accessories
6060606060
5. Ventilation in PediatricAnesthesia
Choosing the mostsuitable form of ventilation
ensures the mostgentle treatment possible.
6161616161Ventilation in Pediatric Anesthesia
5.1 Mechanical Modes of VentilationAll known ventilation modes used in pediatric anesthesiacome from adult anesthesia. These modes include theconventional forms of ventilation, IPPV and SIMV, as well asthe latest, PCV.
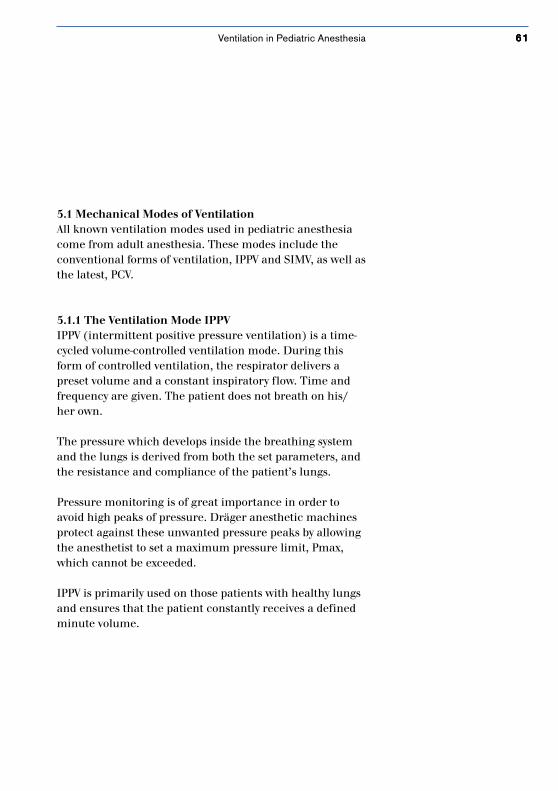
5.1.1 The Ventilation Mode IPPVIPPV (intermittent positive pressure ventilation) is a time-cycled volume-controlled ventilation mode. During thisform of controlled ventilation, the respirator delivers apreset volume and a constant inspiratory flow. Time andfrequency are given. The patient does not breath on his/her own.
The pressure which develops inside the breathing systemand the lungs is derived from both the set parameters, andthe resistance and compliance of the patient’s lungs.
Pressure monitoring is of great importance in order toavoid high peaks of pressure. Dräger anesthetic machinesprotect against these unwanted pressure peaks by allowingthe anesthetist to set a maximum pressure limit, Pmax,which cannot be exceeded.
IPPV is primarily used on those patients with healthy lungsand ensures that the patient constantly receives a definedminute volume.
6262626262
Figure 12: Pressure and flowcurves during IPPV pressure
time
IPPV Mode
flow
time
0
PPeak
PPlat
PEEP
TI TE
TIP
1/frequency
Ventilation in Pediatric Anesthesia
6363636363
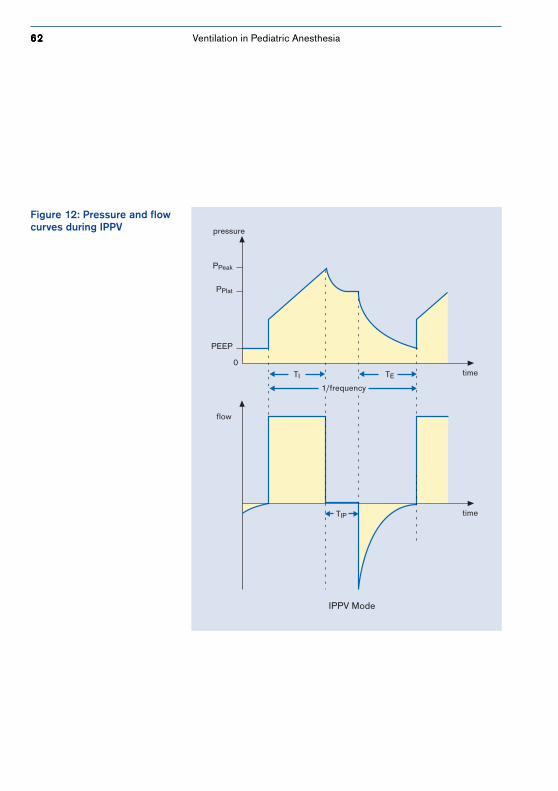
5.1.2. The Ventilation Mode SIMVSIMV (synchronized intermittent mandatory ventilation) isa mixture of spontaneous breathing and controlledventilation in which the respiratory strokes of therespirator are synchronized with those of the patient. Thepatient is able to breath spontaneously in regular,predetermined intervals. Mandatory ventilation strokesensure that a minimum in ventilation is fulfilled withinthese intervals. Mechanical respiratory strokes aretriggered by the patient; that means they take place withina timeframe anticipated by the patient and his/herinspiratory efforts, not during the unsynchronized deliveryof respiratory strokes. SIMV is used in pediatric anesthesia,for instance, during the recovery phase.
Figure 13: Pressure and flow curves during SIMV
1/frequency
time
pressure
timeframe
0
- 0.5 mbarconstanttrigger
artificialrespiration
spontaneousbreathing
TIP
TI TE
artificialrespiration
SIMV
Ventilation in Pediatric Anesthesia

6464646464
5.1.3 The Ventilation Mode PCVIn addition to volume-controlled ventilation, the latestanesthetic machines from Dräger come with a pressure-controlled ventilation mode. Pressure-controlled ventilation(PCV) is not, however, the successor to volume-controlledventilation. It is ideal not only for adult anesthesia, but forgeneral use in pediatric anesthesia as well. The lungs ofchildren are susceptible to overinflation during anesthesia.Reasons for this include insufficient flexibility of thealveoli, shallow breaths and an elastic thorax.Having a set maximum pressure, which makes it possible tolimit the amount of pressure going into the respiratorytract, minimizes the risk of barotrauma and helps avoidpressure peaks. Barotrauma could occur during IPPV as aresult of an inspiratory flow which is too high, secretiondeposits, or bronchospasm.
The major advantage of PCV over volume-controlled modes(IPPV) in conventional partial rebreathing systems is inbeing able to use uncuffed endotracheal tubes for neonatesand small children, which allow large amounts of leakage(> 20 % of the minute volume). By increasing the flow tomaintain the set pressure, losses caused by leakage areautomatically compensated for to a certain degree. But notonly is tube leakage counteracted, leakage caused by thelungs (e.g. lung fistulas) are also counteracted.
In addition, gas distribution disorders within the lungs canbe better compensated for in PCV than in IPPV.
Are the latest anestheticmachines able to ventilateusing a pressure-controlledventilation mode (PCV)?
What are the advantages ofpressure-controlledventilation over volume-controlled ventilation?
Ventilation in Pediatric Anesthesia
6565656565
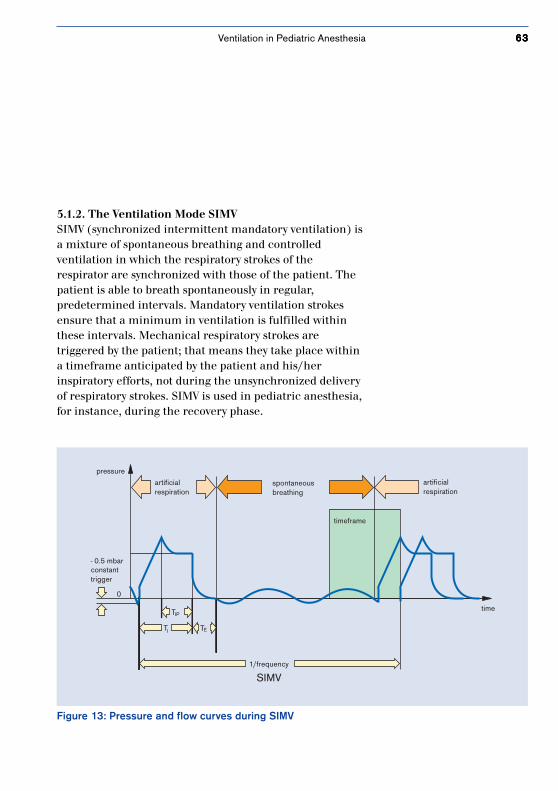
Figure 14: Different effectson inhomogeneous lungsduring ventilation in thevolume and pressure-controlled ventilation mode
Paw(mbar)
Paw(mbar)
time time
lung with stenosisnormal lung
volume-controlledventilation
pressure-controlledventilation
normal lung is overinflated both lungs receive the sameamount of pressure
If the lungs are inhomogeneous, conventional volume-controlled ventilation overinflates the normally healthylung and underinflates the obstructed areas (see Figure14).This results in temporary pressure differences in and diffe-rent levels of volume throughout the lungs, which areexposed to great mechanical loads.
PCV ensures that the lungs fill more evenly and that thehealthy lung is not damaged by excess pressure.
Ventilation in Pediatric Anesthesia
6666666666
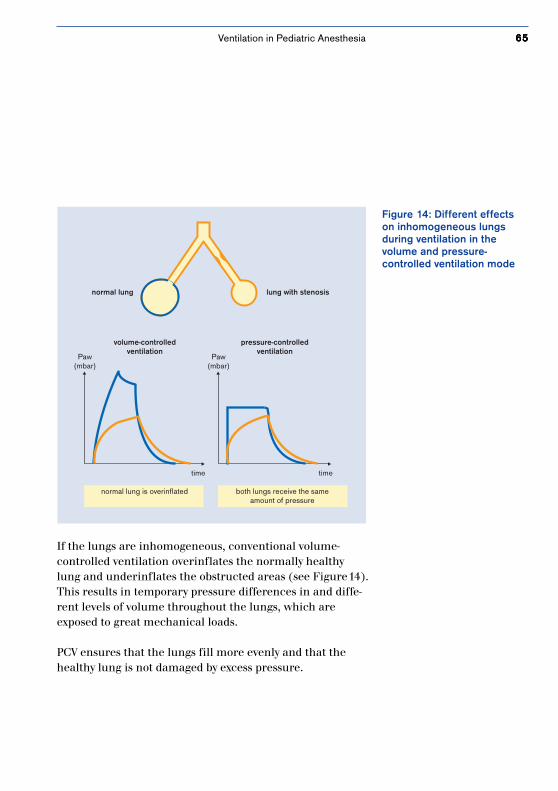
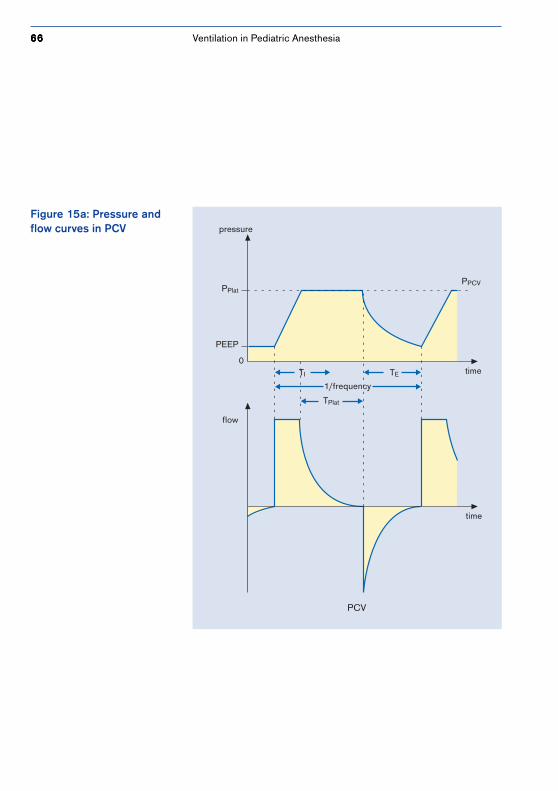
Figure 15a: Pressure andflow curves in PCV pressure
time
PCV
flow
time
0
PPlat
PEEP
TI TE
1/frequency
TPlat
PPCV
Ventilation in Pediatric Anesthesia

6767676767
Today’s Dräger respirators initially deliver constant inspira-tory flow, and do so until the PCV pressure limit has beenreached. The inspiratory flow is then decelerated for therest of the inspiratory phase (see Figure 15a). Sincepressure is constant, the more the lung fills, the more theinspiratory flow decreases. At the end of inspiration,pressure in the lungs equals the pressure in the breathingsystem and there is no more flow.
The Dräger pressure-controlled ventilation mode distingu-ishes itself from that of other manufacturers in that itoffers variable inspiratory flow setting. This feature allowsthe inspiratory flow to be set as low as possible in order toprovide the most homogeneous ventilation possible. Lowflow rates produce less turbulence and thus, provide bettergas distribution.
The volume delivered in PCV is not set directly, it is derivedfrom the set pressure (PPCV* ), the level of PEEP and thepatient’s lung compliance in a linear volume-pressurerange:Vpat = Cpat (PPCV – PEEP)
Every individual change in pressure or level of PEEPchanges the tidal volume (see Figure 15b and 15c).
* Respiratory pressure is marked as the absolute Pmax in the Julian anesthetic workstation and as the relative dPi (pressure difference above PEEP) in PhysioFlex.
Ventilation in Pediatric Anesthesia
6868686868
That means:• An increase in PEEP with a fixed PPCV reduces the vol-
ume. Volume only remains constant if PEEP and PPCV
are changed simultaneously.• The amount of volume delivered is influenced by each
and every change in compliance which occurs, e.g. as aresult of physical movement, opening the thorax, theeffects of medication, or varying lengths of ventilation.This increases the importance of monitoring the expira-tory volume.
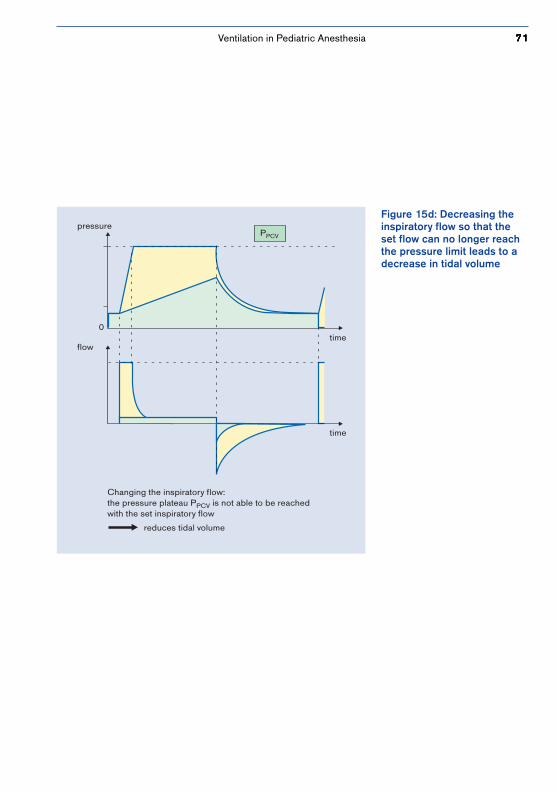
It is important to note that a variation in the inspiratoryflow can lead to a decrease in tidal volume if the set flowdoes not reach the pressure limit (see Figure 15d). Achange in frequency on the device does not lead to tidalvolume deviations provided that the expiratory phase islong enough and that the inspiratory flow is large enoughto reach the plateau curve needed to drive PCV.
If PCV is used on the anesthetic workstation PhysioFlex, afew minor differences in philosophy should be noted ascompared to other Dräger anesthetic machines. Ventilationparameters for PCV on this device include the setrespiratory pressure dPi, the tidal volume minimallyrequired (VT min), frequency, the I:E ratio and PEEP. Thecourse of the inspiratory phase does not need to be set bythe user, the system calculates this from dynamic lungcompliance.
Ventilation in Pediatric Anesthesia
6969696969
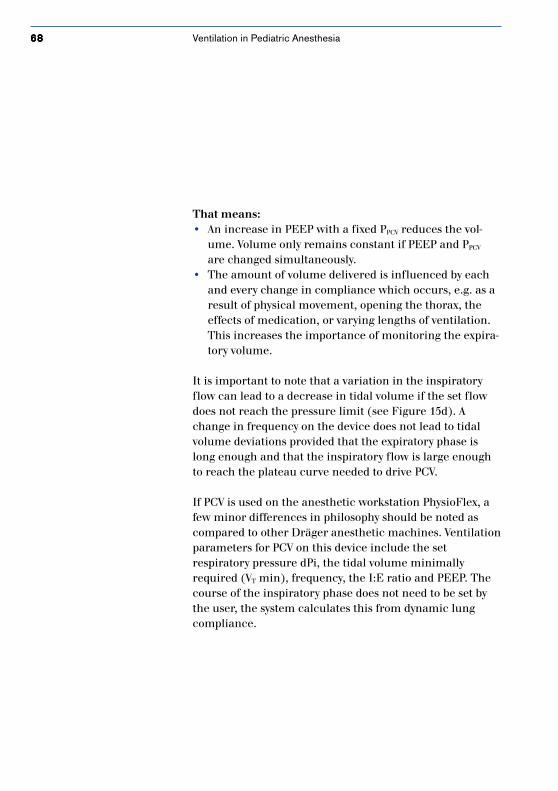
Figure 15b: Increasing onlythe pressure limit withoutsimultaneously increasing thePEEP level causes the tidalvolume to increase
flow
time
time
PPCV
V
pressure
PPCV
0
increasing the pressure limit
increase in tidal volume
Ventilation in Pediatric Anesthesia
7070707070
pressure
timeflow
time
PEEP
V
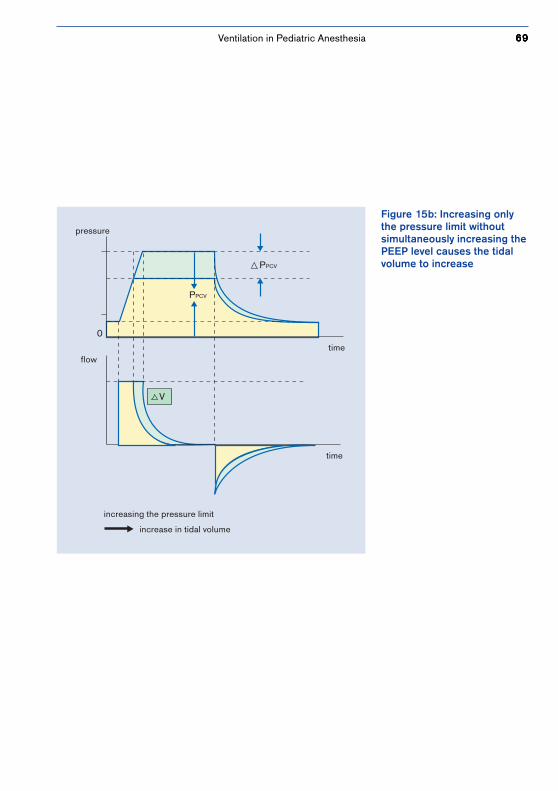
increasing the PEEP
reduces tidal volume
0
Figure 15c: Increasing thePEEP level without simultan-eously increasing thepressure limit causes the tidalvolume to decrease
Ventilation in Pediatric Anesthesia
7171717171
Figure 15d: Decreasing theinspiratory flow so that theset flow can no longer reachthe pressure limit leads to adecrease in tidal volume
pressure
timeflow
time
Changing the inspiratory flow:the pressure plateau PPCV is not able to be reachedwith the set inspiratory flow
reduces tidal volume
PPCV
0
Ventilation in Pediatric Anesthesia
7272727272
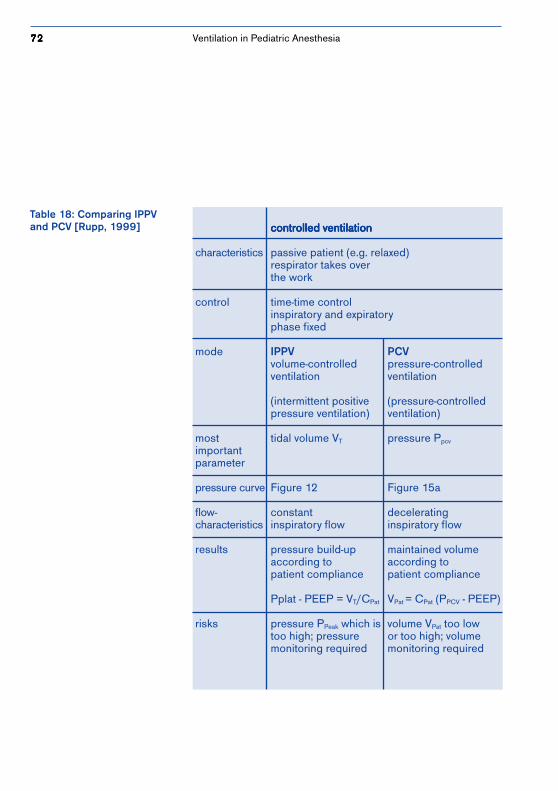
Table 18: Comparing IPPVand PCV [Rupp, 1999] controlled ventilationcontrolled ventilationcontrolled ventilationcontrolled ventilationcontrolled ventilation
characteristics passive patient (e.g. relaxed)respirator takes overthe work
control time-time controlinspiratory and expiratoryphase fixed
mode IPPV PCVvolume-controlled pressure-controlledventilation ventilation
(intermittent positive (pressure-controlledpressure ventilation) ventilation)
most tidal volume VT pressure Ppcv
importantparameter
pressure curve Figure 12 Figure 15a
flow- constant deceleratingcharacteristics inspiratory flow inspiratory flow
results pressure build-up maintained volumeaccording to according topatient compliance patient compliance
Pplat - PEEP = VT/CPat VPat = CPat (PPCV - PEEP)
risks pressure PPeak which is volume VPat too lowtoo high; pressure or too high; volumemonitoring required monitoring required
Ventilation in Pediatric Anesthesia
7373737373
5.2 Ventilation ParametersIn order to maintain or to improve the pulmonary gasexchange of a child, the initial ventilation parametersmust be adjusted to each given situation on the variousanesthetic workstations (see Tables 19 and 20).
Alveolar ventilation and thus, pulmonary gas exchange, canbe improved by using high tidal volumes withcorrespondingly low respiratory frequencies. At the sametime however, the rise in mean respiratory pressure mustbe monitored since it can have negative effects on thecirculatory system and alveolar perfusion. By increasingthe respiratory rate and maintaining minute volume, deadspace ventilation increases. Infants are usually ventilatedwith a frequency of 20 to 30/min and small children with afrequency of 15 to 20/min. In volume.-controlledventilation, tidal volume can be set directly, while inpressure-controlled ventilation the desired tidal volume isinfluenced by the patient’s respiratory characteristics(compliance) and by pressure (see Chapter 5.1,Mechanical Forms of Ventilation).
Tidal volumes of 4 to 6 ml/kg for premature infants and 6to 8 ml/kg for neonates are recommended. Tidal volumesettings are monitored, among others, by the resultingetCO2 and capillary CO2 values which should be around35 to 40 mmHg.
As several studies have shown, the use of high peakpressures is more advantageous for lungs with poorcompliance than the use of high tidal volumes. The lattercan easily lead to the tearing of individual elastic alveoli[Bancalari, 1980].
Which ventilationparameter settings shouldbe selected for which agegroup?
Ventilation in Pediatric Anesthesia
7474747474
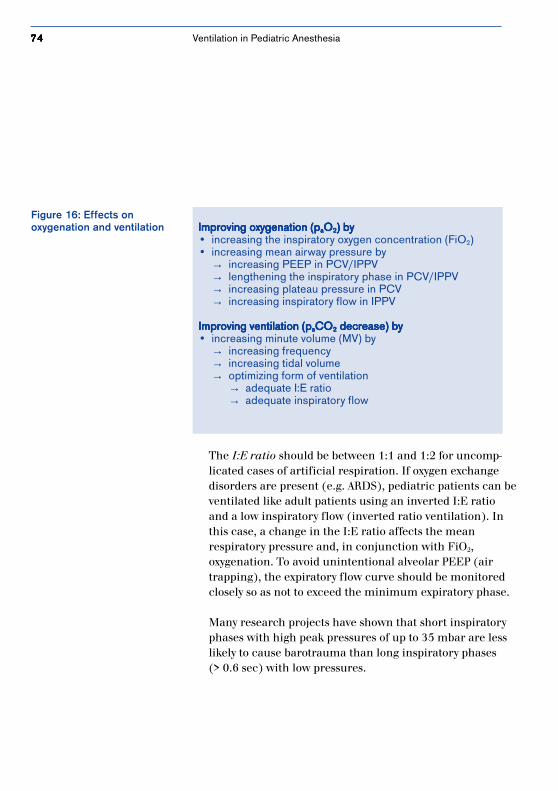
The I:E ratio should be between 1:1 and 1:2 for uncomp-licated cases of artificial respiration. If oxygen exchangedisorders are present (e.g. ARDS), pediatric patients can beventilated like adult patients using an inverted I:E ratioand a low inspiratory flow (inverted ratio ventilation). Inthis case, a change in the I:E ratio affects the meanrespiratory pressure and, in conjunction with FiO2,oxygenation. To avoid unintentional alveolar PEEP (airtrapping), the expiratory flow curve should be monitoredclosely so as not to exceed the minimum expiratory phase.
Many research projects have shown that short inspiratoryphases with high peak pressures of up to 35 mbar are lesslikely to cause barotrauma than long inspiratory phases(> 0.6 sec) with low pressures.
Figure 16: Effects onoxygenation and ventilation Improving oxygenation (pImproving oxygenation (pImproving oxygenation (pImproving oxygenation (pImproving oxygenation (paaaaaOOOOO22222) by) by) by) by) by
• increasing the inspiratory oxygen concentration (FiO2)• increasing mean airway pressure by
→ increasing PEEP in PCV/IPPV→ lengthening the inspiratory phase in PCV/IPPV→ increasing plateau pressure in PCV→ increasing inspiratory flow in IPPV
Improving ventilation (p Improving ventilation (p Improving ventilation (p Improving ventilation (p Improving ventilation (paaaaaCOCOCOCOCO22222 decrease) by decrease) by decrease) by decrease) by decrease) by• increasing minute volume (MV) by
→ increasing frequency→ increasing tidal volume→ optimizing form of ventilation
→ adequate I:E ratio→ adequate inspiratory flow
Ventilation in Pediatric Anesthesia
7575757575
Physiologically, premature infants and newborns build up aphysiologic PEEP in the larynx area during expirationwhich is then eliminated by intubation. By setting the posi-tive end-expiratory pressure (PEEP), the risk of bronchialcollapse which is easily triggered by high closing volume—is reduced. Short expirations phases (caused by ”invertedratio ventilation,” or high respiratory frequencies) alsogenerate automatic PEEP. PEEP does not triggeratelectasis, instead it keeps the alveoli which have been re-opened through high inspiratory pressure or throughprolonged inspiratory phases from collapsing again. Inaddition, PEEP helps increase the functional residual capa-city (FRC).
In a study of Motoyama, ventilating with a PEEP of 5 mbarincreased the FRC of intubated or anesthetized infants by28␣ % as compared to ventilating them without PEEP.
Depending on the child’s oxygenation level, PEEP pressureis set to between 4 and 8 mbar and, in extreme situations,to 10 mbar. Higher levels are not normally tolerated bypediatric patients. Changing the setting should take placein increments of 1 to 2 mbar. One side-effect of ventilatingwith PEEP is the disruption of the cardiac and circulatorysystems, e.g. a decrease in cardiac output due to alessening in venous return flows and cardiac compression.
For cases of heart defects with minimum pulmonary bloodcirculation, a PEEP of > 2 mbar should be avoided. In addi-tion to this, there is also the risk of overinflating the alveoliof damaged lungs with varying areas of distribution (e.g.bronchial stenosis).
Does it make sense to usePEEP, on principle, for eachand every case of newbornventilation?
Ventilation in Pediatric Anesthesia

7676767676
Peak pressures affect alveolar ventilation via paCO2 duringartificial respiration and depend on resistance,compliance, inspiratory flow and tidal volume. Pressurelimiting is of utmost importance in volume-controlledventilation modes to reduce the risk of alveolaroverinflation. Peak pressure should not be set higher than20 to 25 mbar. Peak pressures of > 35 mbar should beavoided altogether since the risk of brain hemorrhageincreases [Bancalari, 1980]. Peak pressures of between 6and 8 mbar are usually sufficient for ventilating prematureinfants under 1000 g. Changes to the setting should bemade in increments of 2 mbar.
While the inspiratory flow is regulated directly in pressure-controlled ventilation modes, it can only be indirectly regu-lated in IPPV through the I:E ratio, Tip:Ti and therespiratory rate. If, during pressure-controlled ventilation,the inspiratory flow chosen is too low, the desired volumecannot be delivered in the preset time and artificialrespiration will be insufficient. The steepness of the rise inpressure increases in IPPV as the inspiratory flowincreases, and peak pressure increases simultaneously. Inorder to protect small pediatric patients, a stenosis alarm istriggered whenever respiratory pressure reaches the setupper limit. Usually, an inspiratory flow of 4 to 10 ml/minis sufficient for infants.
Ventilation in Pediatric Anesthesia
7777777777
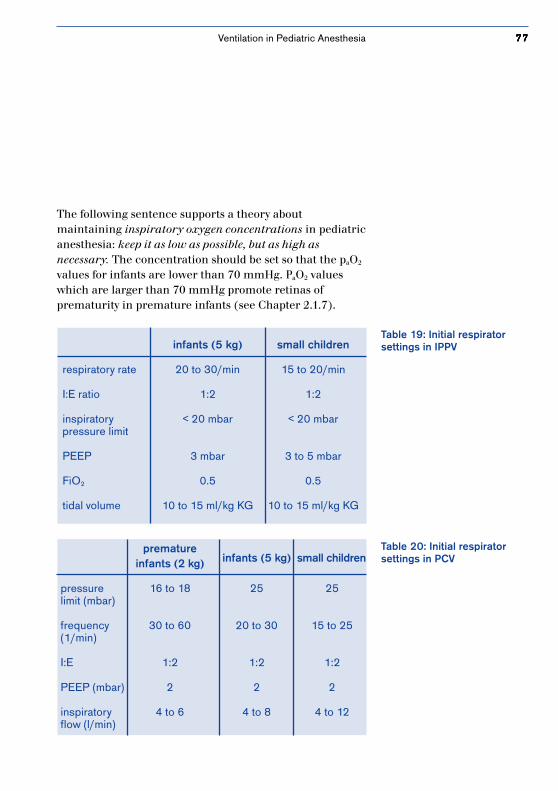
The following sentence supports a theory aboutmaintaining inspiratory oxygen concentrations in pediatricanesthesia: keep it as low as possible, but as high asnecessary. The concentration should be set so that the paO2
values for infants are lower than 70 mmHg. PaO2 valueswhich are larger than 70 mmHg promote retinas ofprematurity in premature infants (see Chapter 2.1.7).
Table 19: Initial respiratorsettings in IPPVinfants (5 kg) small children
respiratory rate 20 to 30/min 15 to 20/min
I:E ratio 1:2 1:2
inspiratory < 20 mbar < 20 mbar pressure limit
PEEP 3 mbar 3 to 5 mbar
FiO2 0.5 0.5
tidal volume 10 to 15 ml/kg KG 10 to 15 ml/kg KG
Table 20: Initial respiratorsettings in PCV
prematureinfants (2 kg) infants (5 kg) small children
pressure 16 to 18 25 25limit (mbar)
frequency 30 to 60 20 to 30 15 to 25(1/min)
I:E 1:2 1:2 1:2
PEEP (mbar) 2 2 2
inspiratory 4 to 6 4 to 8 4 to 12flow (l/min)
Ventilation in Pediatric Anesthesia
7878787878
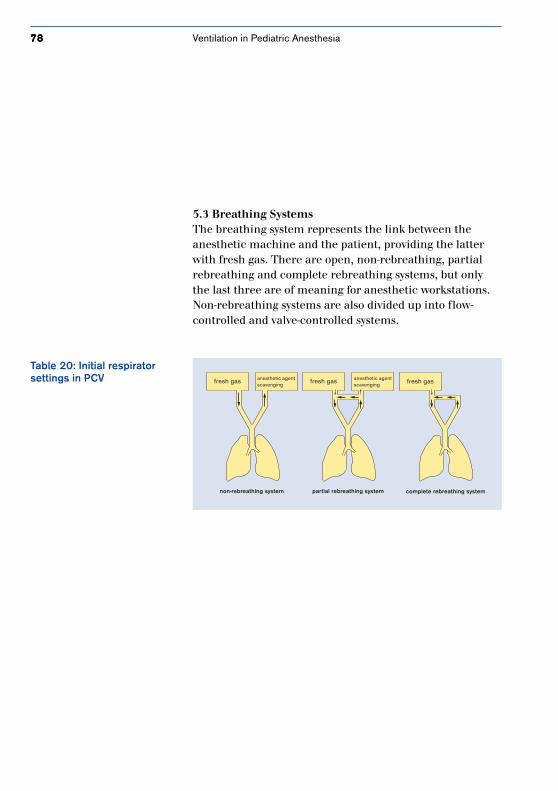
5.3 Breathing SystemsThe breathing system represents the link between theanesthetic machine and the patient, providing the latterwith fresh gas. There are open, non-rebreathing, partialrebreathing and complete rebreathing systems, but onlythe last three are of meaning for anesthetic workstations.Non-rebreathing systems are also divided up into flow-controlled and valve-controlled systems.
Table 20: Initial respiratorsettings in PCV fresh gasfresh gasfresh gas anesthetic agent
scavenginganesthetic agentscavenging
non-rebreathing system partial rebreathing system complete rebreathing system
Ventilation in Pediatric Anesthesia
7979797979
5.3.1 Flow-controlled Non-rebreathing SystemsVarious kinds of breathing systems are used in pediatricanesthesia. Different flow-controlled non-rebreathingsystems on the market include modifications of the so-called Ayre T-piece, like the Kuhn System, the Bain Systemand the Jackson-Rees System. These non-rebreathingsystems are characterized by the fact that they have neithernon-rebreathing valves nor apparatus for absorbing carbondioxide, part of the expiratory gas. These systems are sim-ple and light-weight, they have little dead space and,because they do without inspiratory and expiratory valves,there is a minimum of airway resistance.The biggest problem with these systems is a high fresh-gasflow, which has to be kept high in order to be able toprevent the possibility of rebreathing. If the fresh-gas flowis too low, CO2 can accumulate in the expiratory hoseduring expiration and be taken up by the patient duringthe inspiratory phase. It is recommended that the fresh-gasflow be 2 to 3 times higher than the estimated minutevolume (see Table 21).
These systems are only used for infants and small childrenbecause the fresh-gas consumption of older children isconnected with a higher degree of risk to OR personneland thus, not tolerable [Altemeyer, 1993].
Many anesthesiologists feel that the high fresh-gas flow,active in addition to the actual tidal volume, isproblematic. Studies from Wawersik and Schreiber showthat the use of non-rebreathing systems for anestheticventilation almost always leads to hyperventilation with acarbon dioxide partial pressure of < 30 mmHg [Wawersik,1976] or 18 to 25 mmHg [Schreiber, 1994].
What usage problems areassociated with non-rebreathing systems?
Ventilation in Pediatric Anesthesia
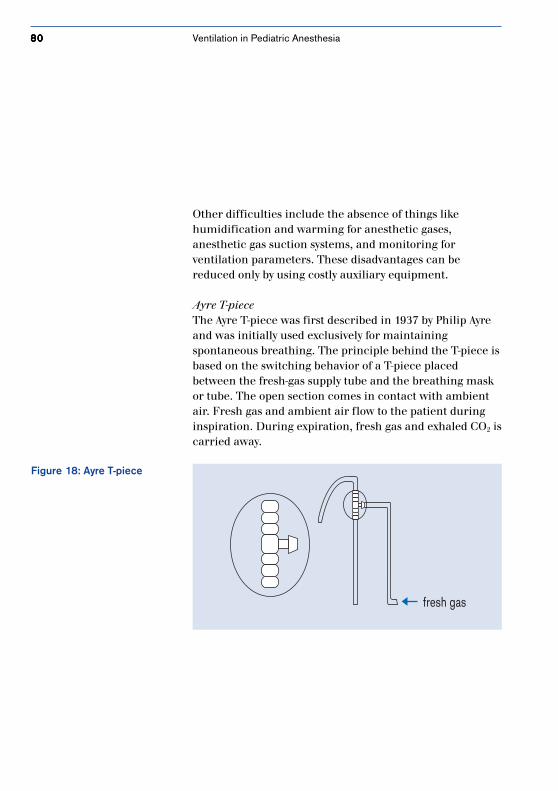
8080808080
Figure 18: Ayre T-piece
fresh gas
Other difficulties include the absence of things likehumidification and warming for anesthetic gases,anesthetic gas suction systems, and monitoring forventilation parameters. These disadvantages can bereduced only by using costly auxiliary equipment.
Ayre T-pieceThe Ayre T-piece was first described in 1937 by Philip Ayreand was initially used exclusively for maintainingspontaneous breathing. The principle behind the T-piece isbased on the switching behavior of a T-piece placedbetween the fresh-gas supply tube and the breathing maskor tube. The open section comes in contact with ambientair. Fresh gas and ambient air flow to the patient duringinspiration. During expiration, fresh gas and exhaled CO2 iscarried away.
Ventilation in Pediatric Anesthesia

8181818181
Figure 19: Jackson-Reessystem
Jackson-Rees SystemThis system represents the first modification of the T-piece.The expiratory hose was lengthened and has a bag on oneend with an opening. This construction allows systemvolume to become greater than tidal volume inpediatric patients. During spontaneous breathing,system is comparable to the T-piece. Assisted ventilation isperformed by closing the open end of the bag with thethumb and forefinger and compressing the bag.
Ventilation in Pediatric Anesthesia

8282828282
Kuhn SystemThe Kuhn system can be used for both spontaneous breath-ing and for manual anesthetic ventilation. Compared to theJackson-Rees system, the Kuhn system has less apparatusdead space (there is a special fresh-gas supply tube guide inthe corner piece) and less flow resistance duringexpiration. The system should only be used on childrenweighing less than 15 kg. The anesthetic workstations Cice-ro EM, Cato and Julian from Dräger also provide this formof manual ventilation in a non-rebreathing system; theyalso monitor respiratory pressure, the delivered O2
concentration and —if possible— the concentration ofanesthetic gases. The system has two advantages: thepossiblity of quickly adjusting the gas concentrationdelivered and little expiratory resistance.
Ventilation in Pediatric Anesthesia
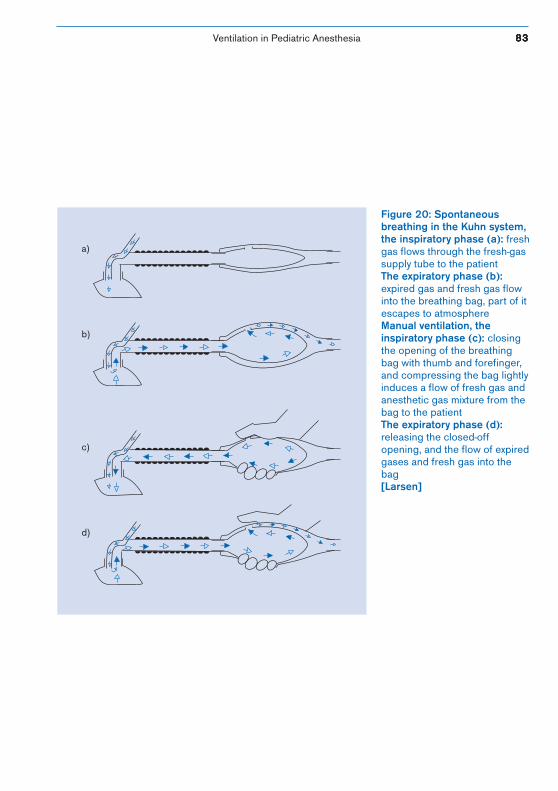
Ventilation in Pediatric Anesthesia
Figure 20: Spontaneousbreathing in the Kuhn system,the inspiratory phase (a): freshgas flows through the fresh-gassupply tube to the patientThe expiratory phase (b):expired gas and fresh gas flowinto the breathing bag, part of itescapes to atmosphereManual ventilation, theinspiratory phase (c): closingthe opening of the breathingbag with thumb and forefinger,and compressing the bag lightlyinduces a flow of fresh gas andanesthetic gas mixture from thebag to the patientThe expiratory phase (d):releasing the closed-offopening, and the flow of expiredgases and fresh gas into thebag[Larsen]
a)
b)
c)
d)
8383838383
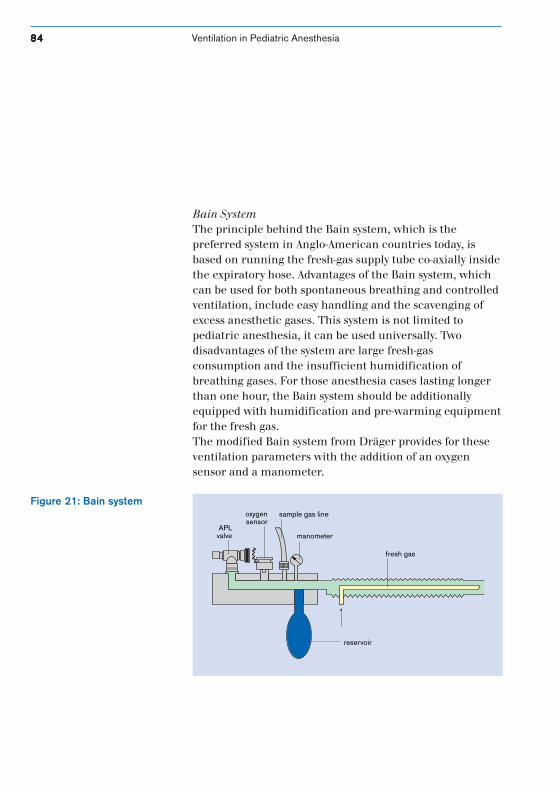
8484848484 Ventilation in Pediatric Anesthesia
Bain SystemThe principle behind the Bain system, which is thepreferred system in Anglo-American countries today, isbased on running the fresh-gas supply tube co-axially insidethe expiratory hose. Advantages of the Bain system, whichcan be used for both spontaneous breathing and controlledventilation, include easy handling and the scavenging ofexcess anesthetic gases. This system is not limited topediatric anesthesia, it can be used universally. Twodisadvantages of the system are large fresh-gasconsumption and the insufficient humidification ofbreathing gases. For those anesthesia cases lasting longerthan one hour, the Bain system should be additionallyequipped with humidification and pre-warming equipmentfor the fresh gas.The modified Bain system from Dräger provides for theseventilation parameters with the addition of an oxygensensor and a manometer.
Figure 21: Bain system
reservoir
fresh gas
manometer
sample gas lineoxygensensor
APLvalve
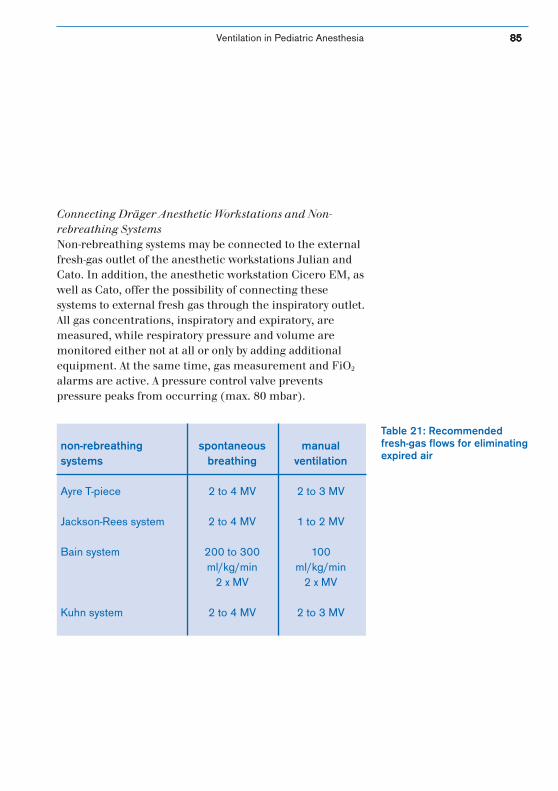
Ventilation in Pediatric Anesthesia 8585858585
Connecting Dräger Anesthetic Workstations and Non-rebreathing SystemsNon-rebreathing systems may be connected to the externalfresh-gas outlet of the anesthetic workstations Julian andCato. In addition, the anesthetic workstation Cicero EM, aswell as Cato, offer the possibility of connecting thesesystems to external fresh gas through the inspiratory outlet.All gas concentrations, inspiratory and expiratory, aremeasured, while respiratory pressure and volume aremonitored either not at all or only by adding additionalequipment. At the same time, gas measurement and FiO2
alarms are active. A pressure control valve preventspressure peaks from occurring (max. 80 mbar).
Table 21: Recommendedfresh-gas flows for eliminatingexpired air
non-rebreathing spontaneous manualsystems breathing ventilation
Ayre T-piece 2 to 4 MV 2 to 3 MV
Jackson-Rees system 2 to 4 MV 1 to 2 MV
Bain system 200 to 300 100ml/kg/min ml/kg/min
2 x MV 2 x MV
Kuhn system 2 to 4 MV 2 to 3 MV
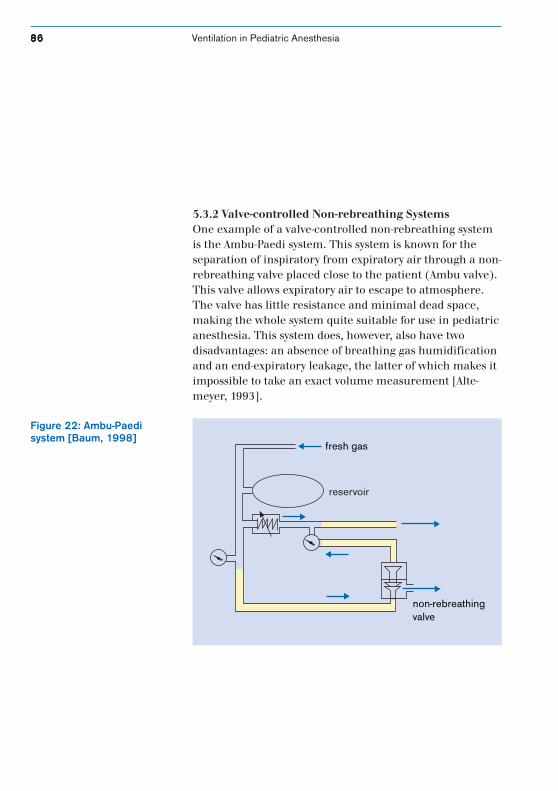
8686868686 Ventilation in Pediatric Anesthesia
5.3.2 Valve-controlled Non-rebreathing SystemsOne example of a valve-controlled non-rebreathing systemis the Ambu-Paedi system. This system is known for theseparation of inspiratory from expiratory air through a non-rebreathing valve placed close to the patient (Ambu valve).This valve allows expiratory air to escape to atmosphere.The valve has little resistance and minimal dead space,making the whole system quite suitable for use in pediatricanesthesia. This system does, however, also have twodisadvantages: an absence of breathing gas humidificationand an end-expiratory leakage, the latter of which makes itimpossible to take an exact volume measurement [Alte-meyer, 1993].
Figure 22: Ambu-Paedisystem [Baum, 1998]
fresh gas
non-rebreathingvalve
reservoir
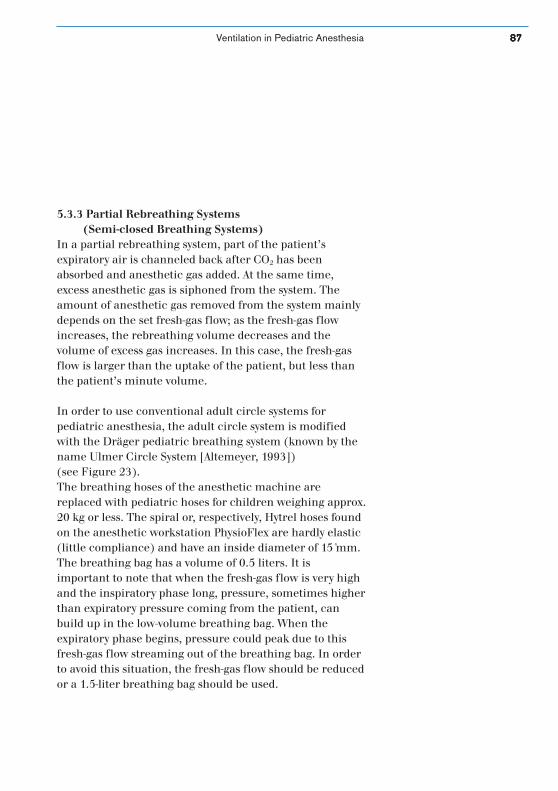
Ventilation in Pediatric Anesthesia 8787878787
5.3.3 Partial Rebreathing Systems(Semi-closed Breathing Systems)
In a partial rebreathing system, part of the patient’sexpiratory air is channeled back after CO2 has beenabsorbed and anesthetic gas added. At the same time,excess anesthetic gas is siphoned from the system. Theamount of anesthetic gas removed from the system mainlydepends on the set fresh-gas flow; as the fresh-gas flowincreases, the rebreathing volume decreases and thevolume of excess gas increases. In this case, the fresh-gasflow is larger than the uptake of the patient, but less thanthe patient’s minute volume.
In order to use conventional adult circle systems forpediatric anesthesia, the adult circle system is modifiedwith the Dräger pediatric breathing system (known by thename Ulmer Circle System [Altemeyer, 1993])(see Figure 23).The breathing hoses of the anesthetic machine arereplaced with pediatric hoses for children weighing approx.20 kg or less. The spiral or, respectively, Hytrel hoses foundon the anesthetic workstation PhysioFlex are hardly elastic(little compliance) and have an inside diameter of 15␣ mm.The breathing bag has a volume of 0.5 liters. It isimportant to note that when the fresh-gas flow is very highand the inspiratory phase long, pressure, sometimes higherthan expiratory pressure coming from the patient, canbuild up in the low-volume breathing bag. When theexpiratory phase begins, pressure could peak due to thisfresh-gas flow streaming out of the breathing bag. In orderto avoid this situation, the fresh-gas flow should be reducedor a 1.5-liter breathing bag should be used.
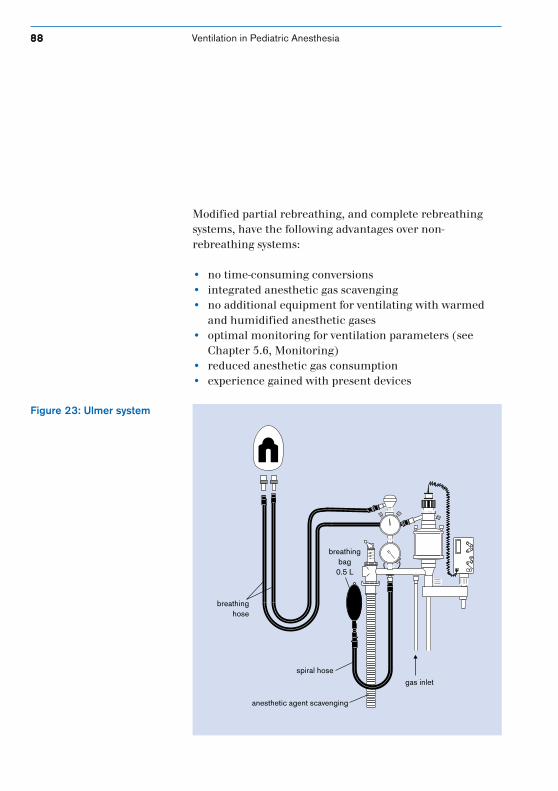
8888888888 Ventilation in Pediatric Anesthesia
Modified partial rebreathing, and complete rebreathingsystems, have the following advantages over non-rebreathing systems:
• no time-consuming conversions• integrated anesthetic gas scavenging• no additional equipment for ventilating with warmed
and humidified anesthetic gases• optimal monitoring for ventilation parameters (see
Chapter 5.6, Monitoring)• reduced anesthetic gas consumption• experience gained with present devices
Figure 23: Ulmer system
510
30
7050
max. 134 C
breathinghose
breathingbag
0.5 L
spiral hose
anesthetic agent scavenging
gas inlet

Ventilation in Pediatric Anesthesia 8989898989
The effectiveness of non-rebreathing systems and pediatriccircle systems has been compared in several studies.Stevenson, for instance, has varied inspiratory peakpressures, respiratory frequencies and lung compliance toshow that, during pressure-controlled ventilation, the Bainsystem has no advantage over the circle system [Stevenson,1999]. In another study, Schreiber researched theinfluence of the Kuhn system and the pediatric circlesystem on the oxygenation and ventilation of infants duringmask or intubation anesthesia using transcutaneous paO2
and paCO2 measurements. This study went on to show thatthe type of anesthetic procedure influences oxygenationdifferently, but the circle system proved itself superior tothe non-rebreathing system [Schreiber, 1994].
5.3.4 Complete Rebreathing Systems(Closed Systems)
In a complete rebreathing system, also known as a closedsystem, the total amount of gas expired from the patient ischanneled back to the patient in the subsequentinspiratory phase after carbon dioxide has been eliminatedfrom that gas. The fresh-gas volume corresponds to theamount of oxygen required for a child’s metabolism andthe amount of anesthetics taken in by the body (seeChapter 5.5.3, PhysioFlex).

9090909090 Ventilation in Pediatric Anesthesia
5.4 Characteristics of Ventilation for Pediatric Anesthesia
5.4.1 Manual and Mechanical Ventilation for Neonates and Infants
Many publications describe neonates and infants as beingbetter off with manual than with mechanical ventilation.Reasons given for this include the fact that an anesthetist’strained hand can more quickly detect changes inrespiratory compliance than a machine can and thatsuitable respirators or the necessary respiratorymonitoring is unavailable. A study from Spears simulatedchanges in respiratory compliance, like occlusions of thetracheal tube, on a test lung which was connected to eitherthe Mapleson D system or a pediatric breathing system.This study proved that even experienced anesthetist’swere not always able to identify these changes [Spears,1991], but even the tiniest unidentified changes incompliance can lead to serious ventilation changes anddisturbances in oxygenation for pediatric patients.
In comparison, mechanical ventilation maintainsconsistent ventilation while keeping the anesthetist’shands free for other important tasks.

Ventilation in Pediatric Anesthesia 9191919191
The biggest advantage of volume-controlled ventilation(IPPV) over manual ventilation is the consistency of thevolume delivered by the respirator. Even changes in patientcompliance occurring, for instance, as a result of theoperation can be compensated for by the anestheticmachine’s so-called compliance compensation (seeChapter 5.4.3), thus avoiding a change in tidal volume.Large changes in compliance are reflected in a change ofairway pressure and immediately displayed for theanesthetist.
Using pressure-controlled ventilation also means thatvarious kinds of leakage will be identified and, usually,compensated for completely.
9292929292 Ventilation in Pediatric Anesthesia
5.4.2 Respirator Requirements for ChildrenThe goal of each and every ventilation case is to providesufficient oxygenation (paO2) and ventilation (paCO2) withas little mean pressure as possible in order to protect lungtissue from damage. At the same time, healthy lungs shouldbe protected from overinflation and collapsed lungs shouldbe re-opened. This means that respirators have to meetmany demanding requirements, especially in pediatricanesthesia. These requirements are best met by four of thelatest Dräger anesthetic machines mostly used in adultanesthesia, but also in pediatric anesthesia. The anestheticmachines include the anesthesia workstations Julian, Cice-ro EM (US brand name Narkomed 6000), Cato andPhysioFlex.
• controlled/mechanical ventilation• volume-constant, pressure-limited ventilation• applicable low tidal volumes• frequency variations: 6 to 60/min• a variable I:E ratio• PEEP up to 15 mbar• sufficient breathing gas humidification and
pre-warming• low respirator compliance (> 0.5 ml/mbar)• flow variance (4 to 20 l/min)• alarms for disconnection and excess pressure• monitoring for oxygen, pressure, volume, CO2 and agent
concentration
Which features does anefficient pediatricrespirator have?

Ventilation in Pediatric Anesthesia 9393939393
All of the above anesthetic devices from Dräger maintainvolume-constant ventilation independent of respiratoryrate, I:E ratio and fresh-gas flows by means of fresh-gasdecoupling and compliance compensation [Schirmer, 1992and 1994].
Many anesthetic machines from other manufacturerscouple a change in fresh-gas flow, several ventilationparameters or patient compliance with a change in thetidal volume delivered by the respirator. This undesiredinfluence is especially relevant for pediatric patients sinceit can lead to hypo- and hyperventilation if the errorpercentage of the delivered minute volume is very large.
Generally speaking, all respirators used for pediatricanesthesia should be equipped with at least a pressurelimiting device to protect the sensitive lungs of pediatricpatients. This requirement is met, for instance, by theanesthetic machine Fabius from Dräger.

9494949494 Ventilation in Pediatric Anesthesia
5.4.3 The Fresh-gas DecouplerThe fact that fresh gas is not continuously admitted to thebreathing system during the expiratory phase (fresh-gasdecoupling) ensures that the applied tidal volume (VT) isnot influenced by the fresh-gas flow during the inspiratoryphase. During the inspiratory phase, a valve ensures thatfresh-gas delivery is decoupled from the patient.
Fresh gas is only fed into the breathing system of theanesthetic workstation Julian during the expiratory phasein IPPV. The anesthetic machines Cicero EM and Cato, onthe other hand, store fresh gas in the reservoir during theinspiratory phase for the next respiratory stroke. Then,during the expiratory phase, this stored volume goesdirectly into the system. All breathing systems have aminute volume thus independent of the fresh-gas flow. Inconventional breathing systems without fresh-gasdecouplers, gas continually flows into the breathing systemindependent of inspiration or expiration. In addition to bagvolume, fresh gas also flows to the patient during theinspiratory phase. When the fresh-gas flow decreases in asystem without a fresh-gas decoupler, the set tidal volumedecreases and the applied minute volume is reduced. Thishas a drastic effect on pediatric patients, because alveolarventilation can be reduced by some 50 % (risk of hypoxia),although only about 30 % of the tidal volume is missing[Fösel, 1991].
If there is no fresh-gas decoupler and a high fresh-gas flowis set, the pressure curve continually rises, during theplateau phase, reflecting a rise in pressure and in this wayacquires a second peak pressure (see Figure 24).
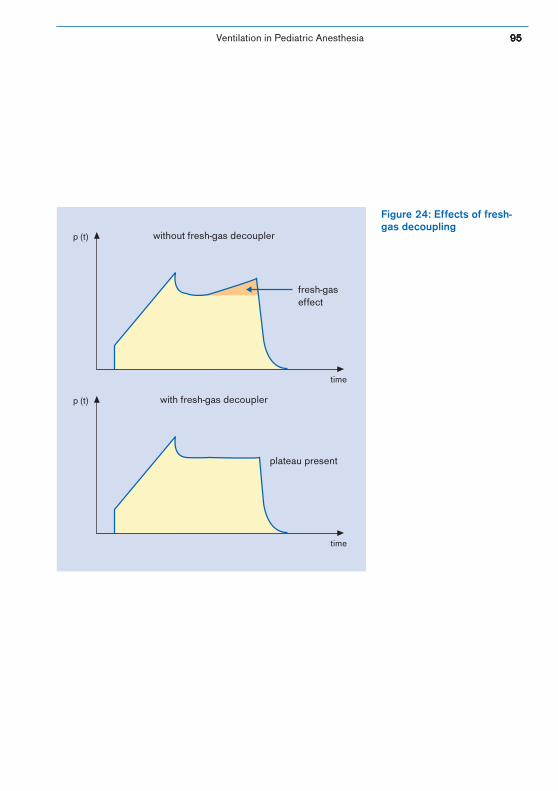
Ventilation in Pediatric Anesthesia 9595959595
without fresh-gas decoupler
with fresh-gas decoupler
p (t)
time
p (t)
time
fresh-gaseffect
plateau present
Figure 24: Effects of fresh-gas decoupling

9696969696 Ventilation in Pediatric Anesthesia
5.4.4 Compliance CompensationWhen ventilating premature infants and newborns withconventional respirators, large discrepancies can be seenbetween the set tidal volume of the device and thatdelivered to the lungs of the patient. This can have seriousconsequences for the already low pediatric tidal volumes.
A rise in inspiratory pressure compresses the gas withinand expands the breathing hoses of those parts of therespirator which carry gas. This means that part of thetidal volume sent from the respirator to the system does notreach the pediatric patient. The level of this compressedvolume depends on the compressed volume of thebreathing system (absorber, hoses, bellows), on theproportion of internal device compliance to patientcompliance, and on peak pressure (see Figure 25).
Dräger anesthetic machines carry out compliancecompensation automatically and allow for volume lost inthe breathing system and the hoses. This information isprovided in the power-on self test of the devices, saving theanesthetist the trouble of having to calculate complianceand pressure values in order to apply the desired tidalvolume. In addition, the anesthetist simultaneouslyreceives leak information from the automatic leak test,carried out on the entire breathing system.
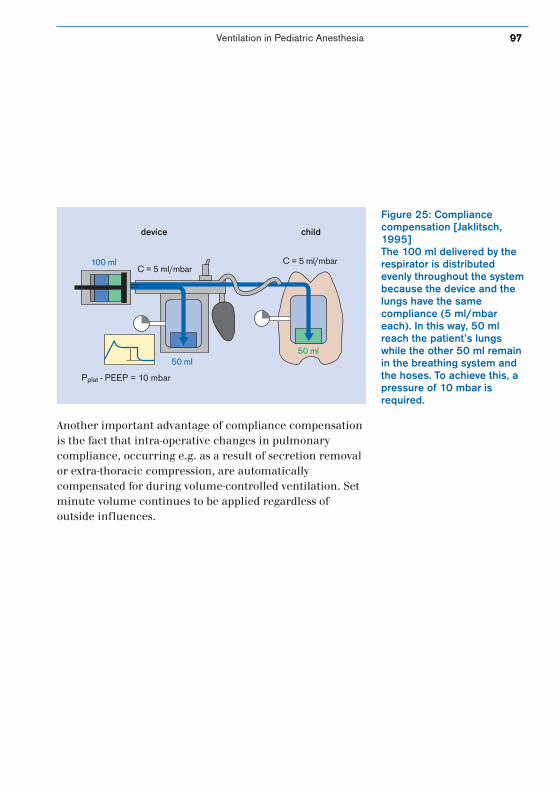
Ventilation in Pediatric Anesthesia 9797979797
Figure 25: Compliancecompensation [Jaklitsch,1995]The 100 ml delivered by therespirator is distributedevenly throughout the systembecause the device and thelungs have the samecompliance (5 ml/mbareach). In this way, 50 mlreach the patient’s lungswhile the other 50 ml remainin the breathing system andthe hoses. To achieve this, apressure of 10 mbar isrequired.
Pplat - PEEP = 10 mbar
C = 5 ml/mbar
50 ml50 ml
100 mlC = 5 ml/mbar
device child
Another important advantage of compliance compensationis the fact that intra-operative changes in pulmonarycompliance, occurring e.g. as a result of secretion removalor extra-thoracic compression, are automaticallycompensated for during volume-controlled ventilation. Setminute volume continues to be applied regardless ofoutside influences.

9898989898 Ventilation in Pediatric Anesthesia
5.4.5 Dead Space VolumeReducing dead space volume —that part of tidal volumewhich is not involved in the gas exchange— is an especiallyimportant concern when using anesthetic systems for pedi-atric anesthesia. Compared to adults, premature infantsand newborns, especially, have a much more unfavorableratio of tidal volume to dead space. Since a large portion oftidal volume is used for flushing the anatomical dead space(the airway up to where the alveoli begin), ventilating withtoo little tidal volume could mean that CO2 is ineffectivelyexchanged despite this age group’s high respiratory rate.The anatomical dead space for each respiratory stroke is 2ml/kg. In addition to the anatomical dead space,physiological and apparatus dead space must also be takeninto consideration. Physiological dead space refers to thealveoli ventilated but not perfused, and apparatus deadspace includes the individual components of the devicewhich are between the Y-piece and the alveoli. Theseindividual components include the Y-piece itself, the tube,tube adapters, or the alternative to that, the mask.Apparatus dead space can increase even more with the useof filters (bacterial or HME filters, see Chapter 5.8,Breathing Gas Conditioning) or, if the anesthetic machineis from another manufacturer, flow sensors orcapnography sensors (see Chapter 5.6.6, Capnography).Thus, it is important that the anesthetist choose suitableaccessories to reduce dead space. The Dräger anestheticdevices Cicero EM, Cato, PhysioFlex and Julian are markedby a significant lack of apparatus dead space volume. Thepediatric Y-piece has both optimal form and size, andincludes a connection for capnography sample lines so thatother adapters with additional dead space need not beused.
How does dead spacevolume affect ventilation?
Ventilation in Pediatric Anesthesia 9999999999
5.5 Anesthetic Machines
5.5.1 Cicero EM/CatoThe anesthetic workstations Cicero EM and Cato areequipped with an electrically driven piston respirator and afresh-gas decoupler, as well as a very tight breathing systemwhich supports both low-flow or minimal flow anesthesia.The tightness of the breathing system is determined duringan automatic power-on self test. The respirator in thesedevices can be operated in the following modes: manual/spontaneous, IPPV, SIMV, and PCV. It also supportsprecision ventilation for even the lowest tidal volumes (upto 10 ml in IPPV) and at high respiratory rates (up to 80/min). The machines have standard features including thepreviously mentioned dynamic compliance correctionwhich automatically and continuously adjusts itself to thechosen system configuration [Feldman, 1999].
The smallest tidal volumes can be reached with PCV whereleakage is also compensated for. The respirator providesoptimal breathing gas pre-warming through a heatingelement in the breathing system. If heatable hoses areused, the condition of the breathing gas can be improvedeven more (see Chapter 5.8).
The difference between the Cicero EM and Cato devices isboth in monitoring equipment and in the dimensions ofintegration. Cicero EM offers a large portion ofintegration. By integrating monitoring for breathing gasand hemodynamics, the pediatric patient can be monitoredin the best way possible –especially if the appropriate limitsare set according to each individual case. In order tosimplify the extensiveness of these settings, the Cicero EMsystem screen allows the user, one time only, to change theconfiguration of a specific set of limits.
Cato
How low is the minimumtidal volume which ananesthetic machine canapply?
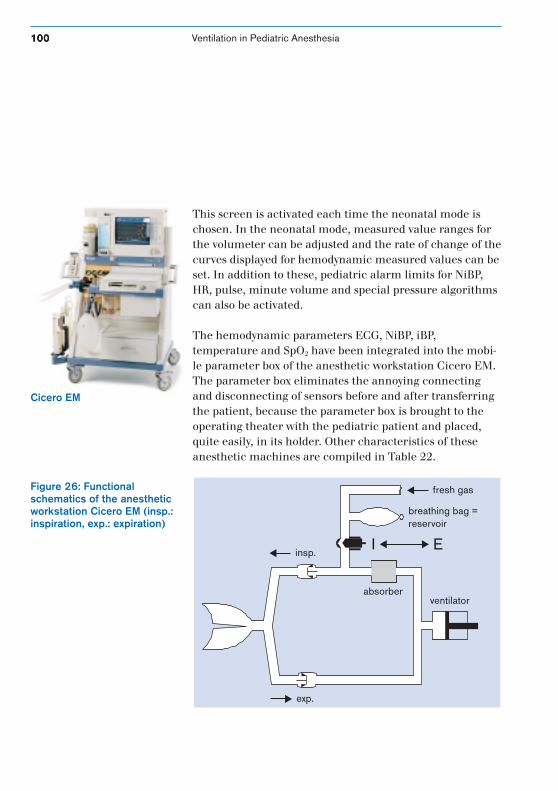
100100100100100 Ventilation in Pediatric Anesthesia
This screen is activated each time the neonatal mode ischosen. In the neonatal mode, measured value ranges forthe volumeter can be adjusted and the rate of change of thecurves displayed for hemodynamic measured values can beset. In addition to these, pediatric alarm limits for NiBP,HR, pulse, minute volume and special pressure algorithmscan also be activated.
The hemodynamic parameters ECG, NiBP, iBP,temperature and SpO2 have been integrated into the mobi-le parameter box of the anesthetic workstation Cicero EM.The parameter box eliminates the annoying connectingand disconnecting of sensors before and after transferringthe patient, because the parameter box is brought to theoperating theater with the pediatric patient and placed,quite easily, in its holder. Other characteristics of theseanesthetic machines are compiled in Table 22.
Figure 26: Functionalschematics of the anestheticworkstation Cicero EM (insp.:inspiration, exp.: expiration)
insp.
exp.
absorberventilator
fresh gas
breathing bag = reservoir
EI
Cicero EM
Ventilation in Pediatric Anesthesia 101101101101101
5.5.2 JulianThe anesthetic workstation Julian has been ergonomicallyoptimized and comes equipped with an electronicallycontrolled, pneumatically driven membrane and aheatable breathing system. This system was developed to bea rebreathing system, optimized for low-flow anesthesiaand able to be operated in the minimal flow range. A highlevel of system tightness and electronic fresh-gas deliverymake it possible to make precision settings for very smallflows and to change quickly between high and low flows.Gas delivery is not controlled by mechanical flowmetersbut rather by an electronically controlled mixer for whichthe anesthetist only has to set the oxygen and carrier gasconcentrations and the fresh-gas flow.
In order to prevent the amount of volume delivered in IPPVfrom changing when the fresh-gas flow is changed andthus to keep the amount of CO2 exhaled by the patientconstant, the respirator in Julian has a fresh-gas decouplerjust like the respirators of Cicero EM and Cato. Here too,dynamic compliance compensation is carried out parallelto changing patient compliance. The respirator can beoperated in three different modes: manual/spontaneous,IPPV and PCV.
Julian
102102102102102 Ventilation in Pediatric Anesthesia
5.5.3 PhysioFlexPhysioFlex is the only anesthetic machine which allowsquantitative inhalation anesthesia to be carried out in aclosed system; that means the gas uptake of the patient,eventual losses due to leakage and the amount of gasdelivered are all balanced. The heart of this anestheticmachine, the ventilator, is a system designed withmembrane chambers with a volumetric capacity of 625 mleach, connected in parallel. According to the selected tidalvolume, one or more membrane chambers are in use par-allel to the breathing circuit. These chambers are thepneumatic drive for the respirator and the manualventilation circuit including the hand bag which isseparated from the completely closed breathing circuit.A blower, built into the breathing circuit, produces a highflow of 70 l/min in the system. This causes the circulatinganesthetic gas to flow in one direction only (without returnflow), while enabling rapid gas mixing and CO2
elimination. CO2 is eliminated by a CO2 absorber,integrated in the circle system.
The closed system has three electronic feedback controlcircuits integrated with each other for O2 concentration,volatile anesthetic agents concentration and system volume(carrier gas). The O2 concentration is kept constant withinthe O2 control circuit by continuous paramagneticmeasurements. If the oxygen concentration decreases as aresult of patient uptake, oxygen will be added to the systemuntil the measured oxygen value reaches the set value. Inaddition to this, end-tidal agent concentration isdetermined by an infrared measuring bench andmaintained by injecting liquid volatile agent. In order toreduce or completely flush out anesthetic agent, the systemis equipped with an charcoal filter.
PhysioFlex
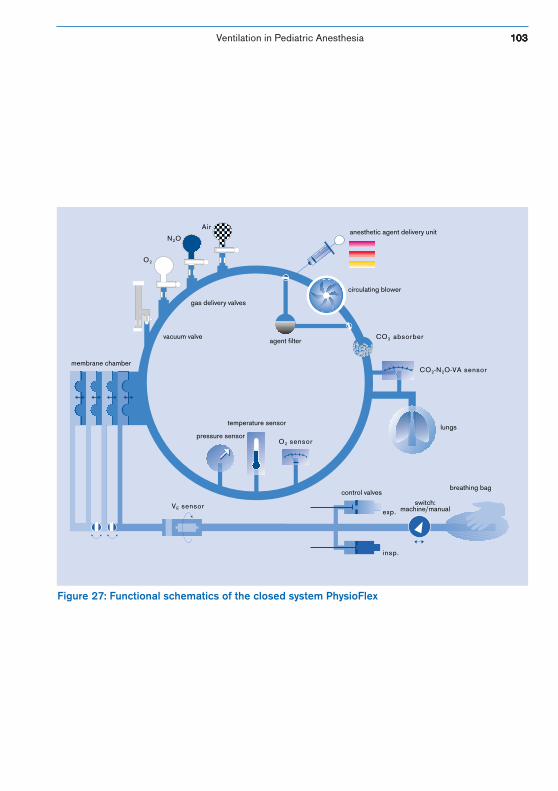
Ventilation in Pediatric Anesthesia 103103103103103
Figure 27: Functional schematics of the closed system PhysioFlex
N2O
O2
agent filterCO2 absorber
circulating blower
anesthetic agent delivery unit
gas delivery valves
vacuum valve
membrane chamber
pressure sensor
temperature sensor
O2 sensor
control valves
exp.
insp.
lungs
VE sensor
CO2-N2O-VA sensor
Air
breathing bag
switch:machine/manual

104104104104104 Ventilation in Pediatric Anesthesia
Carrier gas is controlled within the system’s volumecontrol circuit, and the membrane’s position right afterthe patient’s inspiratory phase is used as a reference pointfor control. The patient’s carrier gas uptake does notreturn the chamber to its original position by the end ofexpiration, so carrier gas is added to the system until thatoriginal position is attained. The amount of carrier gasdelivered then equals patient uptake since oxygen andvolatile agent are added in small doses within thisconcentration. In addition, this control system cancompensate for leakage of up to 15 l/min which come frome.g. using unblocked tubes.
The end-expiratory control circuit for volatile anestheticagents is carried out in a closed system for those pediatricpatients being ventilated through intubation or laryngealmasks. When mask ventilation is being carried out, theinspiratory control circuit is operated using an increasedfresh-gas flow of at least 600 ml/min because end-tidalvolume measurements are not available.
Due to physiological factors, children build up anautogenic PEEP in the larynx area during expiration. Thisdevelops along the closed vocal chords as a result ofexpiration itself and a narrow nasal passage. In order tomaintain physiological control over the expiratory phase,PhysioFlex was equipped with the so-called ALICE systemwhich simulates the function of the vocal chords (ALICE =automatic lung inflation control effect). Autogenic PEEP(or intrinsic PEEP) helps avoid end-expiratory alveolarcollapse during expiration in IPPV or PCV which is causedby the high closing volume of pediatric patients. It alsohelps preserve functional residual capacity (optimizing thesurface available for gas exchange).
What are the advantages ofclosed-system ventilation forpediatric anesthesia?
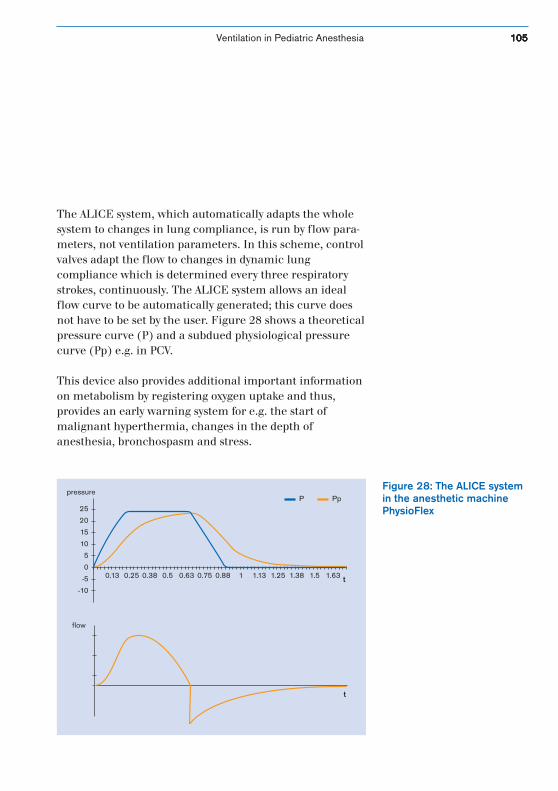
Ventilation in Pediatric Anesthesia 105105105105105
The ALICE system, which automatically adapts the wholesystem to changes in lung compliance, is run by flow para-meters, not ventilation parameters. In this scheme, controlvalves adapt the flow to changes in dynamic lungcompliance which is determined every three respiratorystrokes, continuously. The ALICE system allows an idealflow curve to be automatically generated; this curve doesnot have to be set by the user. Figure 28 shows a theoreticalpressure curve (P) and a subdued physiological pressurecurve (Pp) e.g. in PCV.
This device also provides additional important informationon metabolism by registering oxygen uptake and thus,provides an early warning system for e.g. the start ofmalignant hyperthermia, changes in the depth ofanesthesia, bronchospasm and stress.
Figure 28: The ALICE systemin the anesthetic machinePhysioFlex
0.13 0.25 0.38 0.5 0.63 0.75 0.88 1 1.13 1.25 1.38 1.5 1.63 t
25
20
15
10
5
0
-5
-10
P Pp
t
pressure
flow
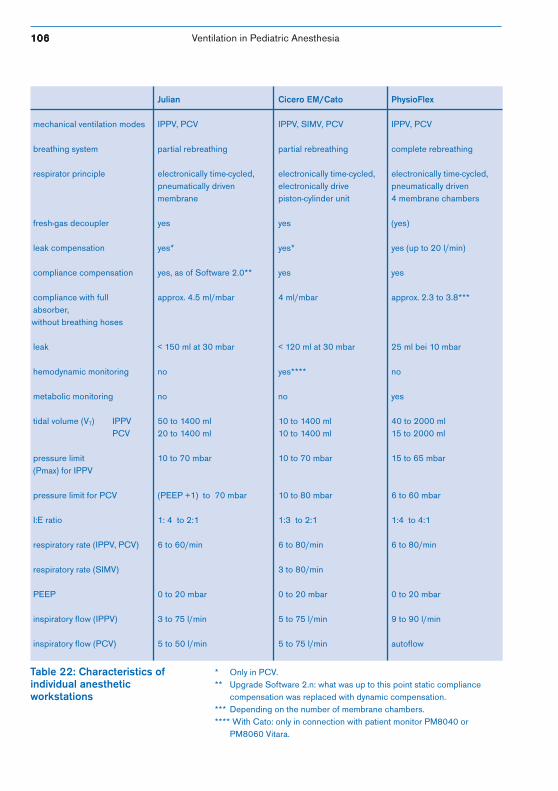
106106106106106 Ventilation in Pediatric Anesthesia
Table 22: Characteristics ofindividual anestheticworkstations
* Only in PCV.** Upgrade Software 2.n: what was up to this point static compliance
compensation was replaced with dynamic compensation.*** Depending on the number of membrane chambers.**** With Cato: only in connection with patient monitor PM8040 or
PM8060 Vitara.
Julian Cicero EM/Cato PhysioFlex
mechanical ventilation modes IPPV, PCV IPPV, SIMV, PCV IPPV, PCV
breathing system partial rebreathing partial rebreathing complete rebreathing
respirator principle electronically time-cycled, electronically time-cycled, electronically time-cycled,pneumatically driven electronically drive pneumatically drivenmembrane piston-cylinder unit 4 membrane chambers
fresh-gas decoupler yes yes (yes)
leak compensation yes* yes* yes (up to 20 l/min)
compliance compensation yes, as of Software 2.0** yes yes
compliance with full approx. 4.5 ml/mbar 4 ml/mbar approx. 2.3 to 3.8***absorber,
without breathing hoses
leak < 150 ml at 30 mbar < 120 ml at 30 mbar 25 ml bei 10 mbar
hemodynamic monitoring no yes**** no
metabolic monitoring no no yes
tidal volume (VT) IPPV 50 to 1400 ml 10 to 1400 ml 40 to 2000 mlPCV 20 to 1400 ml 10 to 1400 ml 15 to 2000 ml
pressure limit 10 to 70 mbar 10 to 70 mbar 15 to 65 mbar(Pmax) for IPPV
pressure limit for PCV (PEEP +1) to 70 mbar 10 to 80 mbar 6 to 60 mbar
I:E ratio 1: 4 to 2:1 1:3 to 2:1 1:4 to 4:1
respiratory rate (IPPV, PCV) 6 to 60/min 6 to 80/min 6 to 80/min
respiratory rate (SIMV) 3 to 80/min
PEEP 0 to 20 mbar 0 to 20 mbar 0 to 20 mbar
inspiratory flow (IPPV) 3 to 75 l/min 5 to 75 l/min 9 to 90 l/min
inspiratory flow (PCV) 5 to 50 l/min 5 to 75 l/min autoflow
Ventilation in Pediatric Anesthesia 107107107107107
Children, like all patients,require careful,
considerate monitoring.

108108108108108 Ventilation in Pediatric Anesthesia
5.6 MonitoringThe anesthetist receives information about the patient’sstate of health by monitoring skin color and respiration.With the aid of the stethoscope, the anesthetist can observethorax movement and auscultation of the lungs (tubedislocation). In addition to this, device-specific informationis of great importance. All breathing gas monitoring isintegrated into the anesthetic workstation and includesairway pressure, minute volume, breathing gastemperature, O2, CO2 and N2O concentrations, as well asthe concentrations of each of the anesthetic agents.Hemodynamic monitoring, the extent of which varies inthe anesthetic workstations Cicero EM, Cato, Julian andPhysioFlex (see Table 24), is important for pediatricmonitoring. In contrast to adults, children have high heartrates, low systolic discharge and low blood pressure. Adecrease in the heart rate of a pediatric patient is, forinstance, often a sign of hypoxia; this can also beinterpolated from a decrease in functional oxygensaturation, SpO2.
The following are used for monitoring purposes:
• stethoscope• pulse oximetry• body temperature• blood pressure (NiBP, iBP)• ECG• capnography• pressure measurements• volumetry• anesthetic agent concentration• inspiratory oxygen concentration
What kind of monitoring isused for pediatricanesthesia and what specialfeatures are available forthis age group?
Ventilation in Pediatric Anesthesia 109109109109109
The closed-system anesthetic workstation PhysioFlex hasbeen extended to include a special feature for monitoringthe metabolic rate of pediatric patients by using theparameters:• oxygen/N2O uptake• anesthetic agent uptake
Other clinical monitoring, depending on the operation,includes urine sampling, blood-gas analyses and acid-baseparameters, or other hemodynamic monitoring likerelaxometry and EEG.
5.6.1 The StethoscopeAt present, the stethoscope is used in every case of pediatricanesthesia. It can be placed at either a precordial position(above the top left side of the thorax) or an esophagealposition, and is used to monitor cardiac rhythm andbreathing. Accidental stomach inflation and air embolismscan also be determined with the stethoscope. The loudnessand tone of the heartbeats provide information on thefullness and contractional force of the heart.

110110110110110 Ventilation in Pediatric Anesthesia
5.6.2 Pulse OximetryThis non-invasive standard process is used to continuouslymeasure the arterial oxygen saturation level of eachpediatric patient undergoing anesthesia, even neonates.Hypoxia, which occurs during anesthesia rather frequentlyin pediatric patients of less than two years, can be detectedearly with the help of pulse oximetry, making the earlydetection of acute oxygenation disorders also possible[Cote, 1991]. In most intra-operative cases, pulse oximetryhas replaced transcutaneous oxygen measurementsbecause the exactness of measurement of thetranscutaneous method is influenced by such factors asblood circulation in the skin, hypothermia, andhypovolemia. Hyperoxia is the exception to this since itcannot be detected with pulse oximetry.
In some cases, the oxygen saturation level of thehemoglobin measured with pulse oximetry and the oxygenpartial pressure (paO2) from the blood gas analysis do notconcur exactly. There are many factors which affectoxygen’s affinity for hemoglobin and thus cause a shift inthe oxygen-binding curve to the right or left (see Figure29). A curve shifted to the left represents a high level ofoxygen affinity, as is the case in hypothermia and alkalosis,and when a high level of fetal hemoglobin is present. Acurve shifted to the right, meaning that oxygen delivery isfacilitated, is caused, for instance, by acidosis or anincrease in concentration of 2.3 diphosphoglycerate(DPG).
To avoid a paO2 of > 70 mmHg and thus, the risk ofretinopathy of prematurity, the oxygen saturation level ofpremature infants and neonates should not exceed 90 to95 % (see Figure 30 and Chapter 2.1.7, ExtrapulmonaryOxygen Toxicity).
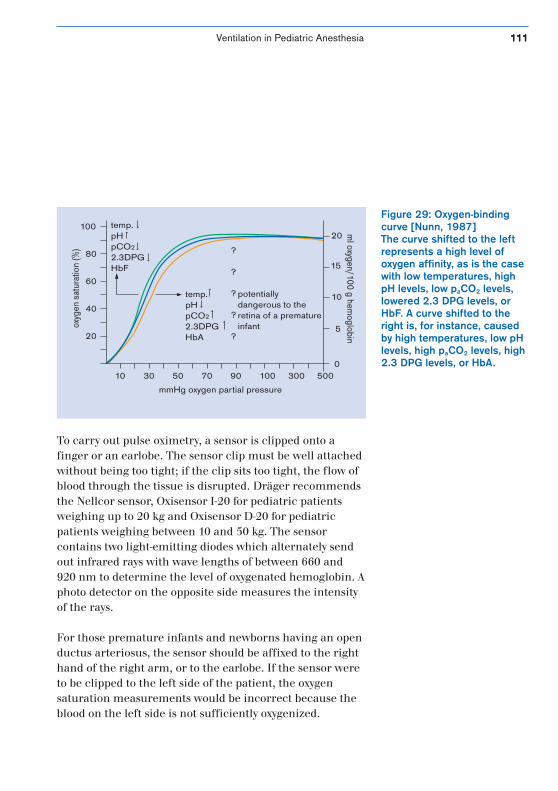
Ventilation in Pediatric Anesthesia 111111111111111
To carry out pulse oximetry, a sensor is clipped onto afinger or an earlobe. The sensor clip must be well attachedwithout being too tight; if the clip sits too tight, the flow ofblood through the tissue is disrupted. Dräger recommendsthe Nellcor sensor, Oxisensor I-20 for pediatric patientsweighing up to 20 kg and Oxisensor D-20 for pediatricpatients weighing between 10 and 50 kg. The sensorcontains two light-emitting diodes which alternately sendout infrared rays with wave lengths of between 660 and920 nm to determine the level of oxygenated hemoglobin. Aphoto detector on the opposite side measures the intensityof the rays.
For those premature infants and newborns having an openductus arteriosus, the sensor should be affixed to the righthand of the right arm, or to the earlobe. If the sensor wereto be clipped to the left side of the patient, the oxygensaturation measurements would be incorrect because theblood on the left side is not sufficiently oxygenized.
0
5
10
15
20
20
10 30 50 70 90 100 300 500
40
60
80
100 temp.pHpCO2
2.3DPGHbF
temp.pHpCO2
2.3DPGHbA
potentiallydangerous to theretina of a prematureinfant
mmHg oxygen partial pressure
ml oxygen/100 g hem
oglobin
oxyg
en s
atur
atio
n (%
) ?
?
?
?
?
Figure 29: Oxygen-bindingcurve [Nunn, 1987]The curve shifted to the leftrepresents a high level ofoxygen affinity, as is the casewith low temperatures, highpH levels, low paCO2 levels,lowered 2.3 DPG levels, orHbF. A curve shifted to theright is, for instance, causedby high temperatures, low pHlevels, high paCO2 levels, high2.3 DPG levels, or HbA.
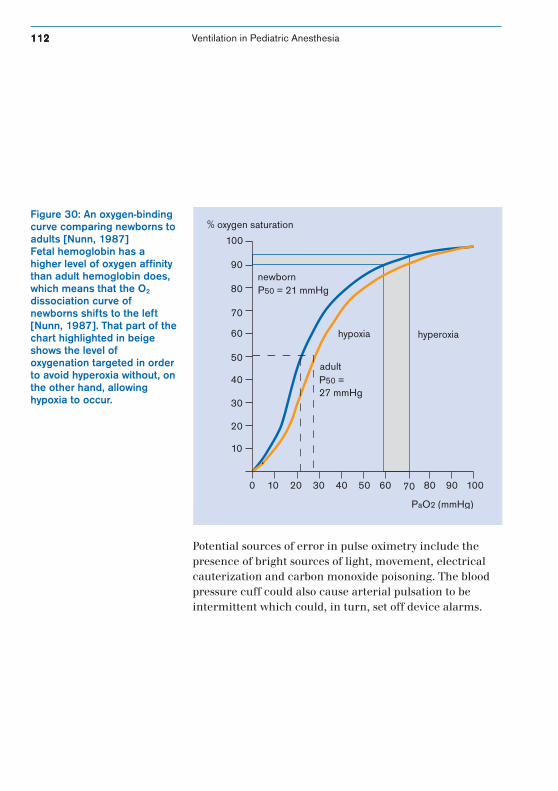
112112112112112 Ventilation in Pediatric Anesthesia
Potential sources of error in pulse oximetry include thepresence of bright sources of light, movement, electricalcauterization and carbon monoxide poisoning. The bloodpressure cuff could also cause arterial pulsation to beintermittent which could, in turn, set off device alarms.
Figure 30: An oxygen-bindingcurve comparing newborns toadults [Nunn, 1987]Fetal hemoglobin has ahigher level of oxygen affinitythan adult hemoglobin does,which means that the O2
dissociation curve ofnewborns shifts to the left[Nunn, 1987]. That part of thechart highlighted in beigeshows the level ofoxygenation targeted in orderto avoid hyperoxia without, onthe other hand, allowinghypoxia to occur.
newbornP50 = 21 mmHg
hypoxia
adult
hyperoxia
PaO2 (mmHg)
P50 = 27 mmHg
10
0 10 20 30 40 50 60 70 80 90 100
20
30
40
50
60
70
80
90
100
% oxygen saturation
Ventilation in Pediatric Anesthesia 113113113113113
5.6.3 Measuring Body TemperatureChildren, whose body surface is relatively large, absorb andgive off heat more quickly than adults. Newborns, infantsand small children are at risk of hypothermia during theperioperative phase because most anesthetic agentssuppress the reflexes which, in children, are responsiblefor maintaining body temperature. Additional warmth canalso be lost if the breathing gas to be inspired is notoptimally warmed and humidified (see Chapter 5.8,Breathing Gas Conditioning). To protect pediatric patients,measures must be taken to preserve heat and thusmaintain body temperature during anesthesia (see page34).
The targeted temperature for a pediatric patient is between36 and 37.5 °C. Caution is called for if the patient’stemperature falls below 35.5 °C. Infants often react toabnormally low temperatures with postoperativerespiratory depression. Oxygen consumption increases asthe result of an increase in the metabolic rate which,again, can cause serious problems because an increase inthe pediatric patient’s cardiac output is limited. Because ofthe risk of hypoventilation occurring in hypothermicpediatric patients, children are ventilated from the end ofthe operation until their body temperature has returned tonormal. At the time of extubation, the pediatric patient’sbody temperature should not be below 36 °C.

114114114114114 Ventilation in Pediatric Anesthesia
The body temperature of a pediatric patient should bemonitored at least during those operations expected to lastlonger than 30 minutes. Premature newborns and neo-nates undergoing surgery should have their temperaturesmonitored regardless of the length of the operation.
Body temperature may be taken rectally, nasopharyngeallyor esophageally. If the esophageal method is used onpediatric patients, the measurement must be taken in thedistal esophagus since the temperature there is less likelyto be affected by breathing gases coming from the trachea.The nasopharyngeal probe could cause lesions of the nasalpassage’s mucus membrane which could lead to postopera-tive respiratory complications.
In addition to body temperature measuring equipment,three different temperature probes from Dräger make itpossible to determine airway temperature and peripheralskin temperatures.
Ventilation in Pediatric Anesthesia 115115115115115
5.6.4 Measuring Blood Pressure (NiBP/iBP)The non-invasive oscillatory method for measuring bloodpressure (NiBP), highly reliable and exact, providesvaluable information on the state of the pediatriccirculatory system. This information is based onrecognizing the fact that changes in blood pressure can bemeasured by using an inflated cuff which partially closesoff the arteries through which the blood must flow.Registering the first oscillation of the arteries determinessystolic blood pressure, the maximum number ofoscillations determines arterial mean pressure, and thediastolic pressure can be determined from that point atwhich the oscillations can no longer be made out.
When using the non-invasive blood pressure monitoringmethod, it is important to have the right size cuff to ensureexactness of measurement and the pediatric patient’s well-being. The Dräger monitoring systems are equipped withan adaptable cuff for use on neonates and children. Whenusing the optimal cuff width of 1.2 x the diameter of theupper arm, the care person should make sure the cuff isnot too wide because if it is, the values calculated could betoo low. Incorrect blood pressure values can also be causedby movement.
The neonatal mode of the Dräger monitoring systemsmeasures the initial and maximum cuff pressures of thisage group, calculates the maximum measuring period anddisplays alarm limits.

116116116116116 Ventilation in Pediatric Anesthesia
Blood pressure must be taken invasively in order for it to beregistered continuously and beat-for-beat. Pressure built upin the artery as a result of blood being pumped out of theheart is transferred through an arterial cannule to themembrane of a pressure recorder, changed into an electricsignal and, in this form, sent to an amplifier. The invasivelyrecorded blood pressure is then displayed on the screen ofthe monitoring unit as both a digital reading and a curve.
Invasive blood pressure measurements (iBP) are mainlyused in those pediatric operations which will most likelyinclude large fluid transfusions, respiratory disorders orinstability of the circulatory system, since hemodynamicdisorders can be ascertained more quickly with thismethod.
The invasive method can be used to take arterial bloodpressure, central venous pressure and pulmonary arterypressure.
The arterial blood pressure measuring method is used inpediatric anesthesia for, among other things, neurologicalor cardiac surgery, for children suffering multiple traumaor who are septic. The arterial blood pressure curve shouldrun biphasic if the patient is stable, otherwise the curve issubdued or compressed (see Figure 31). A subdued line isusually caused by air bubbles or blockage in the system. Inthis case, the systolic pressure measurement is too low andthe diastolic pressure measurement too high. If the probelines are too long, the curve is compressed [Larsen].
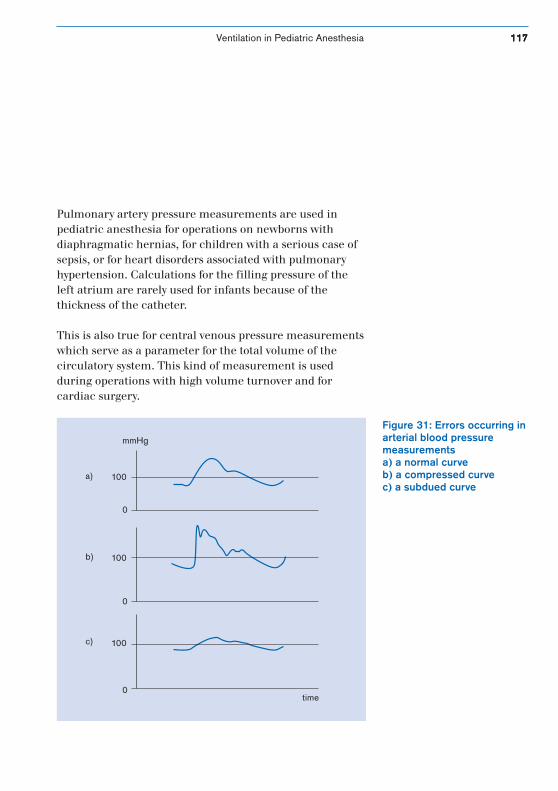
Ventilation in Pediatric Anesthesia 117117117117117
Pulmonary artery pressure measurements are used inpediatric anesthesia for operations on newborns withdiaphragmatic hernias, for children with a serious case ofsepsis, or for heart disorders associated with pulmonaryhypertension. Calculations for the filling pressure of theleft atrium are rarely used for infants because of thethickness of the catheter.
This is also true for central venous pressure measurementswhich serve as a parameter for the total volume of thecirculatory system. This kind of measurement is usedduring operations with high volume turnover and forcardiac surgery.
Figure 31: Errors occurring inarterial blood pressuremeasurementsa) a normal curveb) a compressed curvec) a subdued curve
100
mmHg
100
100
0
0
0
a)
b)
c)
time
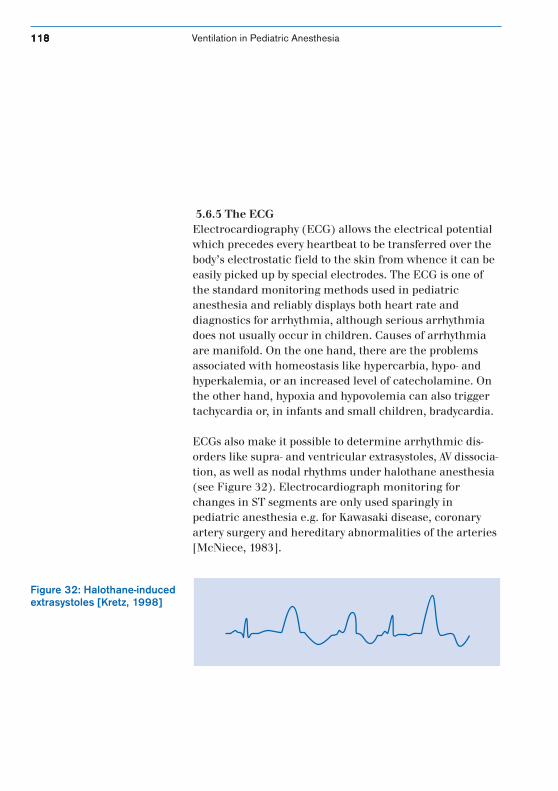
118118118118118 Ventilation in Pediatric Anesthesia
5.6.5 The ECGElectrocardiography (ECG) allows the electrical potentialwhich precedes every heartbeat to be transferred over thebody’s electrostatic field to the skin from whence it can beeasily picked up by special electrodes. The ECG is one ofthe standard monitoring methods used in pediatricanesthesia and reliably displays both heart rate anddiagnostics for arrhythmia, although serious arrhythmiadoes not usually occur in children. Causes of arrhythmiaare manifold. On the one hand, there are the problemsassociated with homeostasis like hypercarbia, hypo- andhyperkalemia, or an increased level of catecholamine. Onthe other hand, hypoxia and hypovolemia can also triggertachycardia or, in infants and small children, bradycardia.
ECGs also make it possible to determine arrhythmic dis-orders like supra- and ventricular extrasystoles, AV dissocia-tion, as well as nodal rhythms under halothane anesthesia(see Figure 32). Electrocardiograph monitoring forchanges in ST segments are only used sparingly inpediatric anesthesia e.g. for Kawasaki disease, coronaryartery surgery and hereditary abnormalities of the arteries[McNiece, 1983].
Figure 32: Halothane-inducedextrasystoles [Kretz, 1998]
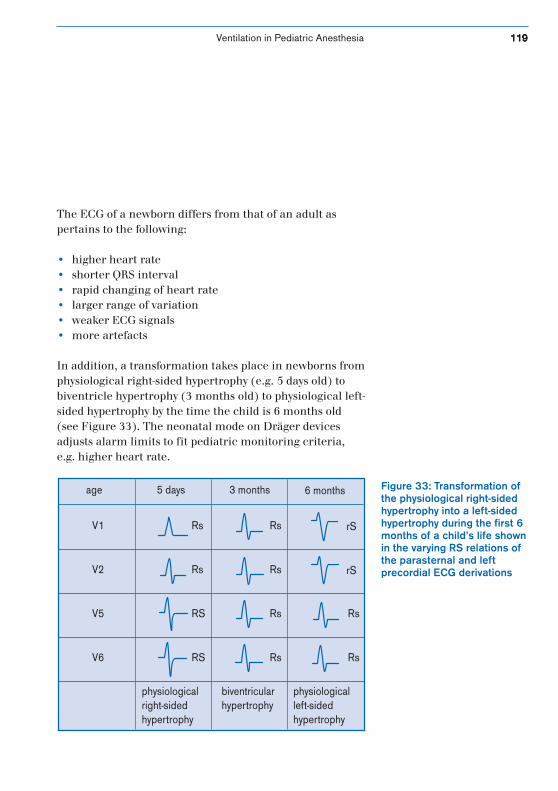
Ventilation in Pediatric Anesthesia 119119119119119
The ECG of a newborn differs from that of an adult aspertains to the following:
• higher heart rate• shorter QRS interval• rapid changing of heart rate• larger range of variation• weaker ECG signals• more artefacts
In addition, a transformation takes place in newborns fromphysiological right-sided hypertrophy (e.g. 5 days old) tobiventricle hypertrophy (3 months old) to physiological left-sided hypertrophy by the time the child is 6 months old(see Figure 33). The neonatal mode on Dräger devicesadjusts alarm limits to fit pediatric monitoring criteria,e.g. higher heart rate.
Figure 33: Transformation ofthe physiological right-sidedhypertrophy into a left-sidedhypertrophy during the first 6months of a child’s life shownin the varying RS relations ofthe parasternal and leftprecordial ECG derivations
age 5 days 3 months 6 months
V1 Rs Rs
Rs
Rs
Rs
rS
rS
Rs
Rs
Rs
RS
RS
V2
V5
V6
physiologicalright-sidedhypertrophy
biventricularhypertrophy
physiologicalleft-sidedhypertrophy
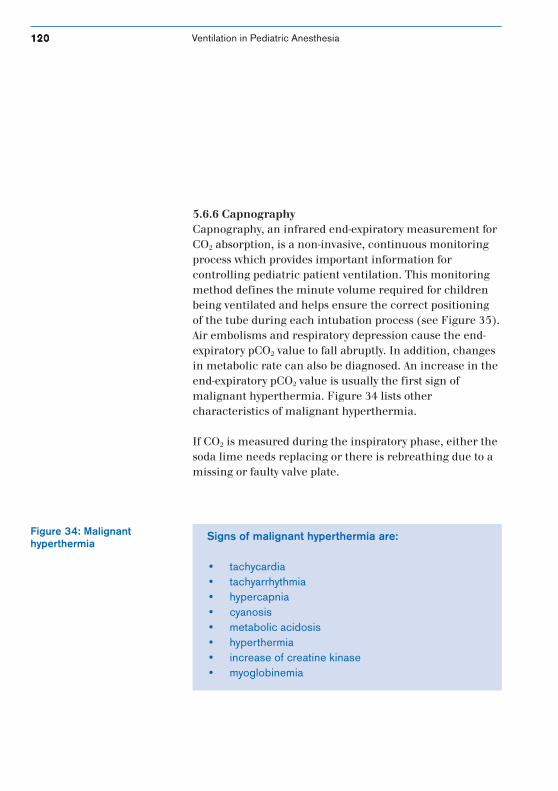
120120120120120 Ventilation in Pediatric Anesthesia
Figure 34: Malignanthyperthermia
5.6.6 CapnographyCapnography, an infrared end-expiratory measurement forCO2 absorption, is a non-invasive, continuous monitoringprocess which provides important information forcontrolling pediatric patient ventilation. This monitoringmethod defines the minute volume required for childrenbeing ventilated and helps ensure the correct positioningof the tube during each intubation process (see Figure 35).Air embolisms and respiratory depression cause the end-expiratory pCO2 value to fall abruptly. In addition, changesin metabolic rate can also be diagnosed. An increase in theend-expiratory pCO2 value is usually the first sign ofmalignant hyperthermia. Figure 34 lists othercharacteristics of malignant hyperthermia.
If CO2 is measured during the inspiratory phase, either thesoda lime needs replacing or there is rebreathing due to amissing or faulty valve plate.
Signs of malignant hyperthermia are:
• tachycardia• tachyarrhythmia• hypercapnia• cyanosis• metabolic acidosis• hyperthermia• increase of creatine kinase• myoglobinemia
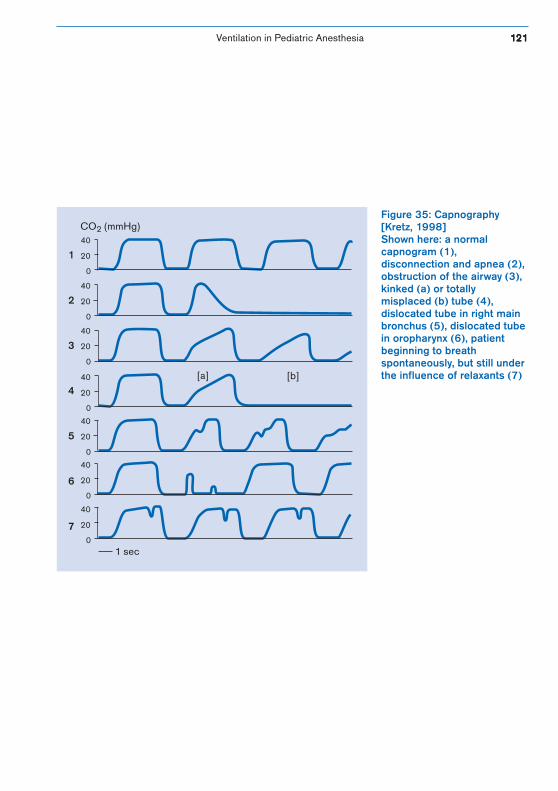
Ventilation in Pediatric Anesthesia 121121121121121
40
40
40
40
40
40
40
20
20
20
20
20
20
20
0
0
0
0
0
0
0
CO (mmHg)2
1 sec
1
2
3
4
5
6
7
[a] [b]
Figure 35: Capnography[Kretz, 1998]Shown here: a normalcapnogram (1),disconnection and apnea (2),obstruction of the airway (3),kinked (a) or totallymisplaced (b) tube (4),dislocated tube in right mainbronchus (5), dislocated tubein oropharynx (6), patientbeginning to breathspontaneously, but still underthe influence of relaxants (7)

122122122122122 Ventilation in Pediatric Anesthesia
There are two different measuring methods forcapnography: the mainstream or flow-through method,and the side-stream or aspirating method. The so-calledmainstream capnography takes a measurement directlyfrom the main respiratory flow, whereas a side-streamcapnography removes sample gas from the breathingcircuit and analyzes it on the outside. The biggest disadvan-tage of the mainstream method, which otherwise providesgood results without a latent period, is increased deadspace. Aside from that, the weight of the sensors --attachedclose to the tube-- is considered troublesome and thesensors themselves can damage the skin with the heat theyproduce.
Otherwise very handy, some publications point out a disad-vantage of side-stream capnography as its having slurredcurves the quality of which depends on the length andcondition of the sample hose and on the ascension rate ofthe capnogram. To ensure reliable measurements from theDräger side-stream capnography, sample gas is taken frombetween the distal end of the tube and the Y-piece. In orderto reduce dead space, the sample gas line has been inte-grated into the Y-piece; it is not, as used to be the case, aseparate T-piece.
There is a scavenger integrated into the breathing systemwhich returns the sample gas to the system so that minutevolume is not effected. This is especially good for pediatricpatients who would otherwise react poorly to minutevolume reductions. If a sample gas scavenger was notconnected to the system, the amount of tidal volumedelivered to a child’s lungs would typically be reduced by 5to 10 percent.

Ventilation in Pediatric Anesthesia 123123123123123
A suction rate of 200 ml/min should be set for measuringCO2, especially when treating pediatric patients, in order toregister the capnograph signal which changes rapidly athigher respiratory rates. The suction rate affects the rate ofincrease t10-90; this is the time it takes the capnograph todisplay a change in concentration of 10 % to 90 %. Thiswould be about 0.3 seconds at a suction rate of 200 ml/minon the anesthetic workstations Cicero EM and Julian. Ifthe suction rate is 60 ml/min, the capnogram signal wouldbe delayed relative to that, i.e. the rate of increase t10-90
would rise from 0.3 sec to 1 sec [Jaklitsch, 1995]. Thisproduces a sine-like CO2 curve and an iCO2 which would betoo high compared to the capillary CO2 level (see Figure36).
For it to be reliable, the capnogram can only be used inpartial rebreathing, closed or non-rebreathing systems withnon-rebreathing valves. Non-rebreathing systems withoutnon-rebreathing valves (Kuhn, Bain) could cause problemsbecause fresh gas and expiratory gas could mix. In thiscase, sample gas has to be taken from a place close to thetip of the tube, otherwise the etCO2 value will be too low.
How much is volume-controlled or, respectively,pressure-controlled venti-lation affected by a gasmeasurement procedureduring side-streamcapnography?
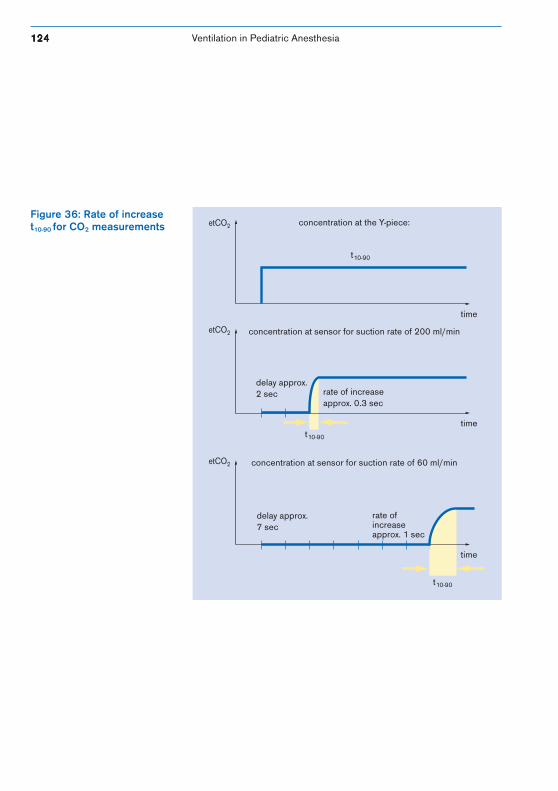
124124124124124 Ventilation in Pediatric Anesthesia
Figure 36: Rate of increaset10-90 for CO2 measurements
time
time
time
delay approx.2 sec rate of increase
approx. 0.3 sec
t10-90
delay approx.7 sec
t10-90
t10-90
concentration at the Y-piece:
concentration at sensor for suction rate of 60 ml/min
concentration at sensor for suction rate of 200 ml/min
etCO2
etCO2
etCO2
rate ofincreaseapprox. 1 sec
Ventilation in Pediatric Anesthesia 125125125125125
5.6.7 Measuring Respiratory PressureRespiratory pressure (PAW) is an important parameter forregistering changes in lung compliance, lung resistance,and for registering obstructions and disconnection. Arespiratory pressure of up to 20 mbar can be obtained inthe lungs of a healthy infant, but if there is an obstruction,this value would be exceeded. If something has becomedisconnected, it can be recognized by observing that the setlower pressure limit value no longer runs periodically inboth directions.
Anesthetic machines from Dräger are equipped with asafety valve to limit pressure and thus protect the patientfrom barotrauma.
Current non-rebreathing systems are not equipped tomeasure respiratory pressure so they have to be modifiedaccordingly.

126126126126126 Ventilation in Pediatric Anesthesia
5.6.8 VolumetryThe anesthetic workstations Cicero EM, Cato, Julian andPhysioFlex from Dräger offer a volumeter function whichprecisely monitors the expiratory volume (VT) of everybreath during spontaneous, manual or volume-controlledventilation. The function itself adds up the individual tidalvolumes over one minute, allowing the spontaneousventilation used to be judged accordingly.
In contrast to PhysioFlex, which incorporates a capacitivemeasuring principle for its volumetric measurements, theother anesthetic machines mentioned above use a hot-wireanemometer procedure. In this procedure, a very thinplatinum wire is heated to a temperature of about 180 °Cusing electric current. If gas flows past it, the wire cools.The larger the volume is that flows past per unit of time,the faster the wire cools. If the temperature of the platin-um wire is kept constant by using a control loop, theelectric current required to maintain this constant can beused as a point of reference for the gas flow. For example, ahigh flow rate requires a high level of electric current inorder to keep the temperature constant. The volume isobtained by electronically integrating the strength ofcurrent over a period of time.
This measurement is not affected by gases with differentproperties (density, viscosity, conductivity) since it iscorrected by an internal algorithm. Non-rebreathingsystems do not have a practical method of determiningexpiratory volume (see Table 23, page 130).
Ventilation in Pediatric Anesthesia 127127127127127
5.6.9 Measuring the Concentration of Anesthetic AgentIn order to recognize a under- or overdose of anestheticagent, the inspiratory agent concentration is measured.Three light wave lengths of the infrared zone are employedto register the volume concentrations of the five volatileanesthetic agents available. Anesthetic agent is identifiedand its concentration calculated from the strength ofabsorption of these three wave lengths.
The Dräger anesthetic workstations Cicero EM, Cato andJulian, and as of 2000 PhysioFlex too, are equipped with anautomatic anesthetic agent detector. A change inanesthetic agent, which often takes place during pediatricanesthesia between the induction phase and the phase ofmaintaining depth of anesthesia, causes the agent to be ina mixed state for a short period of time. This mixed state isregistered by the anesthetic workstations Cicero EM, Cato,PhysioFlex* and Julian** and its primary component isidentified and quantified. In such cases, the accuracy ofthe measurement can be limited.
The anesthetic workstation Julian** also allows anestheticagent to be automatically set and delivered according toage-related MAC values.
* As of 2000.
** With software version 3.0.
128128128128128 Ventilation in Pediatric Anesthesia
5.6.10 Measuring the Inspiratory Oxygen ConcentrationUsing an oxygen probe based on principles of galvanic or,as is the case for PhysioFlex, paramagnetic cells, theinspiratory oxygen concentration can be easily determinedin partial rebreathing and closed systems.
Oxygen is measured in the fresh-gas flow of non-rebreathing systems. In such systems, if the fresh-gas flowis too low, partial rebreathing could result, causing theoxygen portion of the inspiratory gas mixture to be lowerthan that of the fresh-gas phase.
Both inspiratory and expiratory oxygen concentrations aredisplayed on the screen of the anesthetic workstationsCicero EM, Cato, PhysioFlex and Julian.

Ventilation in Pediatric Anesthesia 129129129129129
5.6.11 Oxygen UptakeWhen the anesthetic workstations Cicero EM, Cato and/orJulian are used, the anesthetist manually determines theamount of breathing gas and anesthetic agent in the freshgas (carrier gas) using preset values. In comparison, theclosed system PhysioFlex controls breathing gases andanesthetic agent on its own, depending on the patientuptake, which changes continuously.
With a paramagnetic oxygen analyzer, the oxygenconcentration within the breathing circuit is continuallymeasured. The device compares the measured value withthe set value for oxygen concentration. If the measuredvalue is lower, PhysioFlex uses an oxygen valve to measureand deliver the amount of oxygen needed to reach the setvalue.
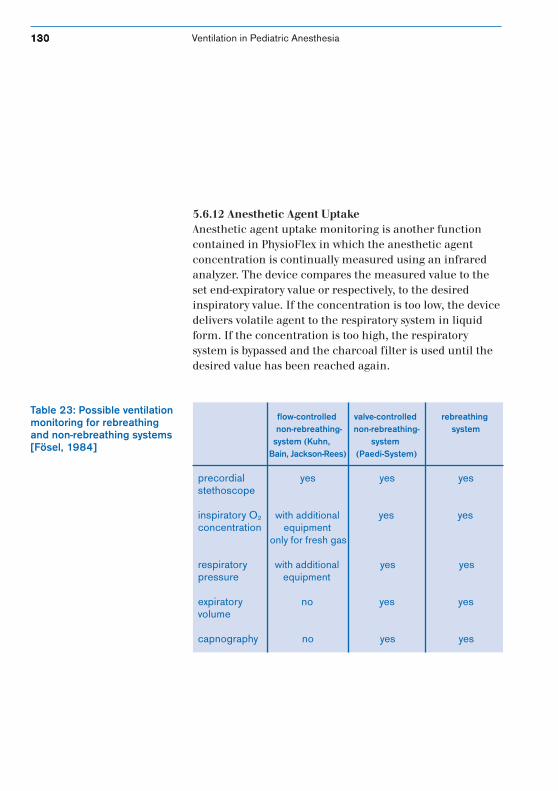
130130130130130 Ventilation in Pediatric Anesthesia
5.6.12 Anesthetic Agent UptakeAnesthetic agent uptake monitoring is another functioncontained in PhysioFlex in which the anesthetic agentconcentration is continually measured using an infraredanalyzer. The device compares the measured value to theset end-expiratory value or respectively, to the desiredinspiratory value. If the concentration is too low, the devicedelivers volatile agent to the respiratory system in liquidform. If the concentration is too high, the respiratorysystem is bypassed and the charcoal filter is used until thedesired value has been reached again.
Table 23: Possible ventilationmonitoring for rebreathingand non-rebreathing systems[Fösel, 1984]
flow-controlled valve-controlled rebreathing non-rebreathing- non-rebreathing- system system (Kuhn, system Bain, Jackson-Rees) (Paedi-System)
precordial yes yes yesstethoscope
inspiratory O2 with additional yes yesconcentration equipment only for fresh gas
respiratory with additional yes yespressure equipment
expiratory no yes yesvolume
capnography no yes yes
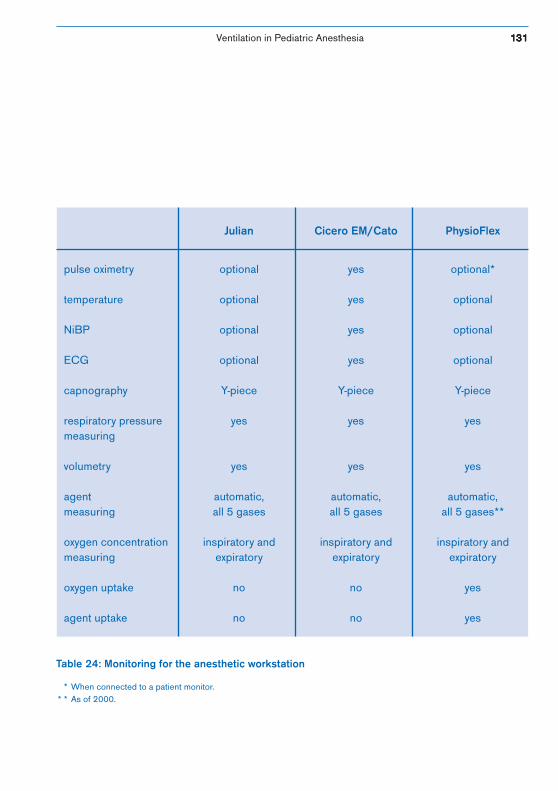
Ventilation in Pediatric Anesthesia 131131131131131
Julian Cicero EM/Cato PhysioFlex
pulse oximetry optional yes optional*
temperature optional yes optional
NiBP optional yes optional
ECG optional yes optional
capnography Y-piece Y-piece Y-piece
respiratory pressure yes yes yesmeasuring
volumetry yes yes yes
agent automatic, automatic, automatic,measuring all 5 gases all 5 gases all 5 gases**
oxygen concentration inspiratory and inspiratory and inspiratory andmeasuring expiratory expiratory expiratory
oxygen uptake no no yes
agent uptake no no yes
Table 24: Monitoring for the anesthetic workstation
* When connected to a patient monitor.* * As of 2000.
132132132132132 Ventilation in Pediatric Anesthesia
5.7 Low-flow AnesthesiaFor years now several publications have providedinformation on low-flow techniques for pediatricanesthesia in which the fresh-gas flow is reduced to < 20 %of the minute volume. Children provide ideal anatomicalconditions for carrying out anesthesia with reduced fresh-gas flows. The respiratory system of a pediatric patientequilibrates more quickly with anesthetic gases due to theslightness of the patient’s weight which has lower oxygenconsumption, absorbs less nitrous oxide and retains lessdissolved nitrogen within the body itself, and due to the factthat the anesthetic agent has little room for distribution[Weiser, 1993].
Pediatric anesthesia using a fresh-gas flow of 1 l/min and0.5 l/min corresponds to the definition of adult low-flowor, respectively, minimal flow anesthesia. Since these twoterms refer to the fresh-gas flow and the level ofrebreathing associated with a particular level, a minimalflow situation is not present even when the fresh-gas inputis 0.5 l/min for an infant of e.g. 5 kg. This fresh-gas flowstill replaces half of the infant’s minute volume.
The advantages of low-flow adult anesthesia are simultan-eously the advantages of low-flow pediatric anesthesia, likereduced environmental stress due to anesthetic agentvapors, reduced costs, and improved breathing gascondition.
Nevertheless, there are still hardly any studies available onlow-flow pediatric anesthesia with flow rates lower than1 l/min.
Can low-flow anesthesia becarried out for pediatricanesthesia?
Ventilation in Pediatric Anesthesia 133133133133133
This might be due to historical, traditional reservationswhich exist and claim that low-flow anesthesia for smallchildren can only be carried out using flow-controlledrebreathing systems, or that the performance features ofan adult respirator cannot satisfy the demands of pediatricanesthesia [Wieser, 1993]. In order to ensure that low-flowanesthesia is safe for pediatric anesthesia, demands on theanesthetic machines involved, like system tightness andprecision, have been increased considerably.
The modern anesthetic workstations from Dräger: Julian,Cato, Cicero EM and PhysioFlex, equipped with pediatriccircle systems, exceed these demands. The already highdegree of system tightness is checked using self testsequences automatically carried out. If leakage occurs, theanesthetist receives a message on the display screen,or it is compensated for in the conventional partialrebreathing systems in PCV or, in the closed systemPhysioFlex, in IPPV also. The compliance compensationfunction included in all four anesthetic workstations allowshose compliance to be compensated for provides precisiontidal volume settings of 10, 40 or 50 ml in IPPV.
Extensive monitoring for anesthetic agent, inspiratoryoxygen concentration, minute volume, oxygen saturation,CO2 and pressure is another important componentrequired for carrying out low-flow anesthesia. The fresh-gas decoupling function lets the anesthetist reduce thefresh-gas flow to operate in the low-flow or minimal flowmode without having to worry about the effect of the fresh-gas flow on the applied tidal volume [Baum, 1998].

134134134134134 Ventilation in Pediatric Anesthesia
The econometer, an integrated part of the anesthetic work-station Cicero EM, provides the anesthetist with additionalsupport for judging the balance of fresh gas (see Figure37). The fill level of the system is monitored and excessfresh gas is displayed on the screen as a bar diagram. Thisdisplay provides a basis which the anesthetist can use toreduce the fresh-gas flow to the necessary amount, thusincreasing the efficiency of modern anesthetic concepts.
The latest studies from e.g. Peters, Gebhardt and Igarashipoint out that low-flow anesthetist can be safely carried outfor pediatric anesthesia [Peters, 1998; Gebhardt, 1999;Igarashi, 1998]. Peters comments on the fact that hypoxiaand significant CO2 rebreathing could not be proven tooccur during anesthesia procedures for which the Drägeranesthetic workstations Cicero EM and Cato were used onchildren weighing between 2 and 6 kg (at a flow of 0.6 l/min). To reduce the risk of a decrease in FiO2, the oxygenconsumption of the child was added to the initial fresh-gascomposition calculation.
Mask anesthesia with low fresh-gas flows is usuallyperformed only by those anesthetists acquainted withthe procedure. Low-flow anesthesia with laryngeal masksfor airway protection can be carried out without causingproblems. The tightness of a correctly positioned laryngealmask allows for controlled ventilation in many cases[Möllhoff]. Even the use of an endotracheal tube without acuff does not exclude the possibility of well-adapted flowreduction if the size of the tube is correctly chosen,particularly since the total gas uptake of an infant or asmall child is very low and thus, the level of excess gascomparatively high [Baum, 1998].
Figure 37: Econometer
fresh-gas excess
trend
none little great
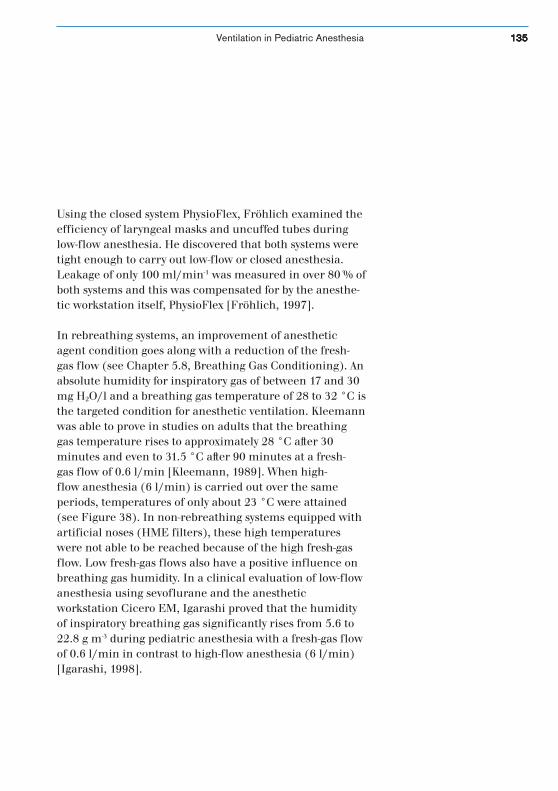
Ventilation in Pediatric Anesthesia 135135135135135
Using the closed system PhysioFlex, Fröhlich examined theefficiency of laryngeal masks and uncuffed tubes duringlow-flow anesthesia. He discovered that both systems weretight enough to carry out low-flow or closed anesthesia.Leakage of only 100 ml/min-1 was measured in over 80␣ % ofboth systems and this was compensated for by the anesthe-tic workstation itself, PhysioFlex [Fröhlich, 1997].
In rebreathing systems, an improvement of anestheticagent condition goes along with a reduction of the fresh-gas flow (see Chapter 5.8, Breathing Gas Conditioning). Anabsolute humidity for inspiratory gas of between 17 and 30mg H2O/l and a breathing gas temperature of 28 to 32 °C isthe targeted condition for anesthetic ventilation. Kleemannwas able to prove in studies on adults that the breathinggas temperature rises to approximately 28 °C after 30minutes and even to 31.5 °C after 90 minutes at a fresh-gas flow of 0.6 l/min [Kleemann, 1989]. When high-flow anesthesia (6 l/min) is carried out over the sameperiods, temperatures of only about 23 °C were attained(see Figure 38). In non-rebreathing systems equipped withartificial noses (HME filters), these high temperatureswere not able to be reached because of the high fresh-gasflow. Low fresh-gas flows also have a positive influence onbreathing gas humidity. In a clinical evaluation of low-flowanesthesia using sevoflurane and the anestheticworkstation Cicero EM, Igarashi proved that the humidityof inspiratory breathing gas significantly rises from 5.6 to22.8 g m-3 during pediatric anesthesia with a fresh-gas flowof 0.6 l/min in contrast to high-flow anesthesia (6 l/min)[Igarashi, 1998].
136136136136136 Ventilation in Pediatric Anesthesia
Figure 38: Interdependenceof breathing gas temper-atures and fresh-gas flow[Baum, 1998]
15 30 45 60 75 90 105 12020
22
24
26
28
30
32
0.6 l/min3.0 l/min
1.5 l/min6.0 l/min
min
°C
Ventilation in Pediatric Anesthesia 137137137137137
5.7.1 The Wash-in/Wash-out Rate of Anesthetic AgentThe principles of carrying out low-flow pediatricanesthesia as pertains to induction, maintaining depth ofanesthesia and the recovery phase do not differ from thoseof adult anesthesia.
It is extremely important to consider time constants whencontrolling inhalation anesthesia, especially low-flowanesthesia. What exactly is meant by the term ”timeconstant”? The time constant of an anesthetic machinedescribes the time it takes a change in fresh-gasconcentration to initiate a change in inspiratoryconcentrations in the anesthetic machine. This constantdepends on device volume, pulmonary volume, the amountof gas delivered with the fresh-gas flow, and individualconsumption of this gas.
device volume + pulmonary volumetime constant:
fresh-gas flow – patient uptake
When the fresh-gas flow is reduced in a partial rebreathingsystem, the sluggishness of the system increasesconsiderably; this can be best shown by comparing high-flowand minimal flow anesthesia (0.5 l/min) (see Figure 39).During low-flow or minimal flow anesthesia, drasticchanges in the fresh-gas concentration can also lead todelays in the course of changes in inspiratory and expiratoryanesthetic agent concentrations within the anestheticsystem.
How quickly does the systemreact to changes inconcentration (wash-in/wash-out rate)?

138138138138138 Ventilation in Pediatric Anesthesia
A short time constant leads to rapid changes in anestheticagent concentrations within the system. The time constantcan only be shortened by changing the amount of agentvapor delivered to the breathing system with the fresh gas.With conventional anesthetic agents like halothane,isoflurane, and enflurane, this can only be improved byincreasing the fresh-gas flow. The newer anesthetic agentsdesflurane and sevoflurane have low uptakes due onlyto their specific pharmacodynamic and pharmacokineticcharacteristics. If maximum concentrations are used, thetime constant can also be decreased for low fresh-gas flows[Baum, 1998].
When considering the above, it should not be forgotten thatthe course of wash-in and wash-out processes for anestheticagents differs greatly between partial rebreathing systemsand complete rebreathing systems (closed systems). Theclosed system of the anesthetic workstation PhysioFlex doesnot require high fresh-gas flows to wash gases into thesystem. Independently controlled doses of oxygen, carriergas and anesthetic agent, as well as rapid mixing withinthe circuit due to a blower, produce a very small timeconstant and a closed circuit shortly after induction. Afterthe volatile gases have been injected into the system, achild’s end-tidal volume concentration can be reachedwithin 4 minutes, regardless of the fresh-gas flow (seeFigure 40). Removing or reducing the anesthetic gasconcentration also takes place without a high flow phase.The low fresh-gas flow remains unchanged and theanesthetic gases are quickly eliminated by the charcoalfilter found in the bypass. The desired value for anestheticagent concentration is reached within one minute ofchanging the set value.
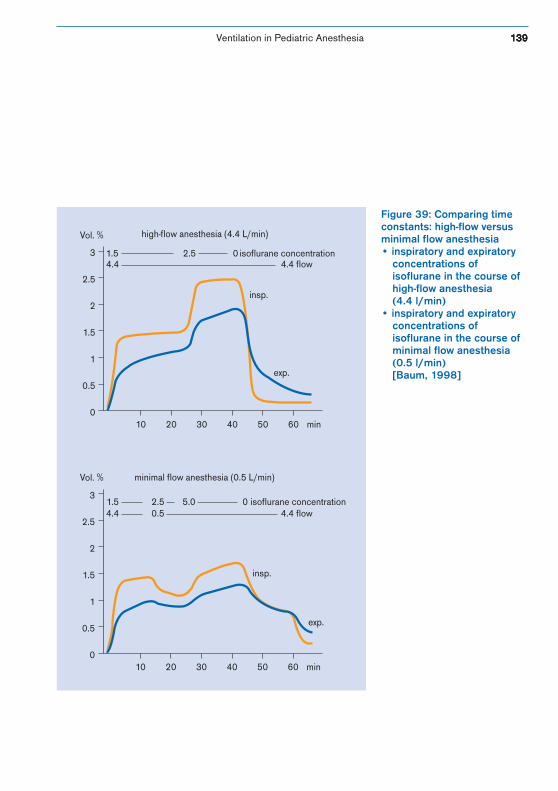
Ventilation in Pediatric Anesthesia 139139139139139
Figure 39: Comparing timeconstants: high-flow versusminimal flow anesthesia• inspiratory and expiratory
concentrations ofisoflurane in the course ofhigh-flow anesthesia(4.4␣ l/min)
• inspiratory and expiratoryconcentrations ofisoflurane in the course ofminimal flow anesthesia(0.5 l/min)[Baum, 1998]
0
0.5
1
1.5
2
2.5
3
10 20 30 40 50 60 min
1.5 2.5 0 isoflurane concentration
high-flow anesthesia (4.4 L/min)
0
0.5
1
1.5
2
2.5
3
10 20 30 40 50 60 min
minimal flow anesthesia (0.5 L/min)
1.5 2.5 5.0 04.4 0.5 4.4 flow
4.4 4.4 flow
isoflurane concentration
Vol. %
Vol. %
insp.
insp.
exp.
exp.
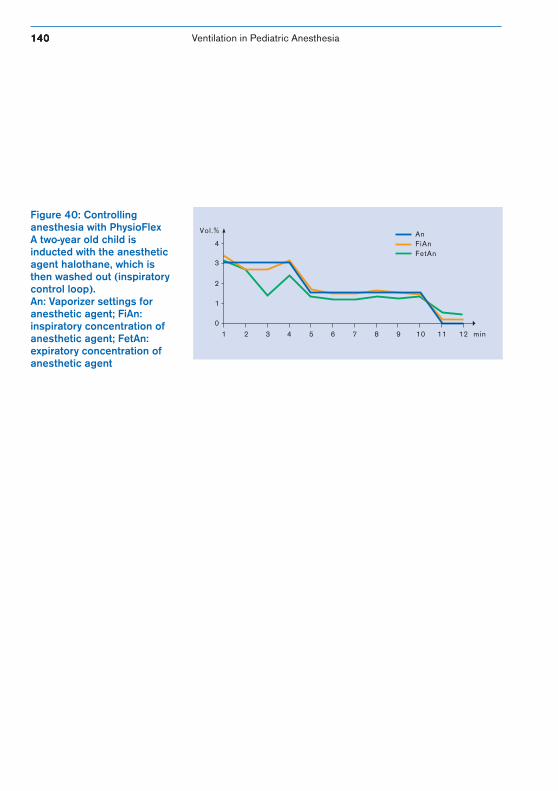
140140140140140 Ventilation in Pediatric Anesthesia
Figure 40: Controllinganesthesia with PhysioFlexA two-year old child isinducted with the anestheticagent halothane, which isthen washed out (inspiratorycontrol loop).An: Vaporizer settings foranesthetic agent; FiAn:inspiratory concentration ofanesthetic agent; FetAn:expiratory concentration ofanesthetic agent
4
Vol.%
3
2
1
0
1 2 3 4 5 6 7 8 9 10 11 12 min
AnFiAnFetAn
Ventilation in Pediatric Anesthesia 141141141141141
Children require anoptimal environment,
adapted to meet their special needs.
142142142142142 Ventilation in Pediatric Anesthesia
5.8 Breathing Gas Conditioning for Anesthetic Ventilation Systems
During natural respiration, the air breathed is warmedand moistened on its way through the nose, throat andwindpipe. About three-fourths of this warmth and moistureis provided by the mucus membrane of the nose andthroat, the remaining fourth comes from the windpipe.The upper airway also serves as an initial air filter,removing particles from the inspired air by way of nasalhair. If, despite this filtering, foreign debris finds its way tothe respiratory tract, mucus encircles it, transports ittoward the larynx via cilia and expels it by sneezing.
Endotracheal intubation bypasses the upper airway and itswarming/moistening function (see Figure 41). If measuresare not taken to compensate for this lost warmth andmoisture, the lower airway could dry out [BGM].
This could lead to the following:
• secretion thickening• reduced cilia movement• mucus blocking lower airway and tube• atelectasis build-up from secretion blockage in
bronchia, lung infections• necrosis build-up in respiratory organs
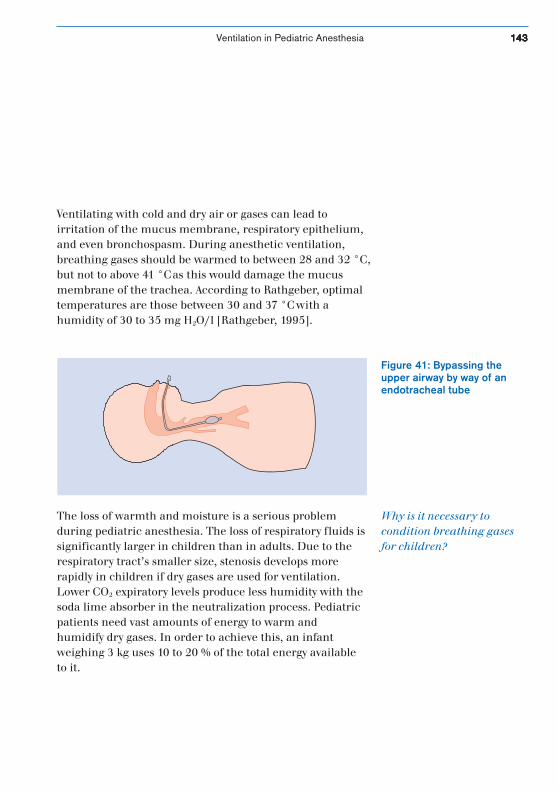
Ventilation in Pediatric Anesthesia 143143143143143
Ventilating with cold and dry air or gases can lead toirritation of the mucus membrane, respiratory epithelium,and even bronchospasm. During anesthetic ventilation,breathing gases should be warmed to between 28 and 32 °C,but not to above 41 °C as this would damage the mucusmembrane of the trachea. According to Rathgeber, optimaltemperatures are those between 30 and 37 °C with ahumidity of 30 to 35 mg H2O/l [Rathgeber, 1995].
Figure 41: Bypassing theupper airway by way of anendotracheal tube
The loss of warmth and moisture is a serious problemduring pediatric anesthesia. The loss of respiratory fluids issignificantly larger in children than in adults. Due to therespiratory tract’s smaller size, stenosis develops morerapidly in children if dry gases are used for ventilation.Lower CO2 expiratory levels produce less humidity with thesoda lime absorber in the neutralization process. Pediatricpatients need vast amounts of energy to warm andhumidify dry gases. In order to achieve this, an infantweighing 3 kg uses 10 to 20 % of the total energy availableto it.
Why is it necessary tocondition breathing gasesfor children?

144144144144144 Ventilation in Pediatric Anesthesia
Often, the only way to prevent hypothermia in pediatricpatients, whose compensation mechanism for temperatureregulation is immature, is to actively warm and humidifythe breathing gases (see Table 25, Advantages anddisadvantages of various humidifiers). If the operationbeing performed is of a short duration (up to one hour)and has a low fresh-gas flow (10 % of minute volume), arelative humidity of 60 % can be achieved with partialrebreathing systems not having an active moisteningfeature. If the operation is longer, active humidification isdefinitely an advantage. This is why the anestheticworkstations Cicero EM, Cato and Julian have integratedbreathing gas warmers and offer optional connections forartificial noses, heatable hoses, or active breathing gashumidifiers. In addition, anesthetic gases are conditionedby the fresh-gas flow (see page 135), and the amount ofrebreathing is calculated.
The breathing gas humidifier works according to theprinciples of an atomizer or nebulizer. Atomizers producean aerosol by atomizing. In a nebulizer, breathing gas flowsthrough a humidifier chamber and is added to watersteam. When it leaves the humidifier, the breathing gas iswarmer than the desired tube temperature, but it cools asit passes through the hose system, which means the watercondenses. Heatable hose systems counteract this andavoid both a loss of warmth and condensation.
Which type of breathing gashumidification should beused for which age group?
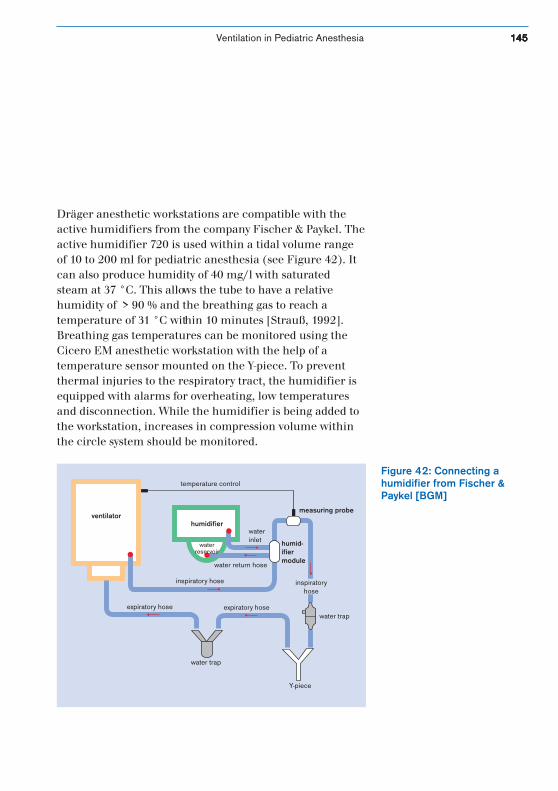
Ventilation in Pediatric Anesthesia 145145145145145
Dräger anesthetic workstations are compatible with theactive humidifiers from the company Fischer & Paykel. Theactive humidifier 720 is used within a tidal volume rangeof 10 to 200 ml for pediatric anesthesia (see Figure 42). Itcan also produce humidity of 40 mg/l with saturatedsteam at 37 °C. This allows the tube to have a relativehumidity of > 90 % and the breathing gas to reach atemperature of 31 °C within 10 minutes [Strauß, 1992].Breathing gas temperatures can be monitored using theCicero EM anesthetic workstation with the help of atemperature sensor mounted on the Y-piece. To preventthermal injuries to the respiratory tract, the humidifier isequipped with alarms for overheating, low temperaturesand disconnection. While the humidifier is being added tothe workstation, increases in compression volume withinthe circle system should be monitored.
Figure 42: Connecting ahumidifier from Fischer &Paykel [BGM]
ventilatorhumidifier
temperature control
measuring probe
humid-ifiermodule
inspiratory hose
expiratory hose expiratory hosewater trap
water trap
Y-piece
water return hose
waterinlet
inspiratoryhose
waterreservoir

146146146146146 Ventilation in Pediatric Anesthesia
Heat and moisture exchangers (HME), also called artificialnoses, offer a passive alternative to active breathing gasconditioning. They are made of various materials likecellulose, or polyurethane or polyethylene onto whichhydroscopic substances have been cultured.
HME absorb warmth and moisture given off by thepatient’s lungs during expiration and store it (see Figure43). During inspiration, this is then carried back to thelungs. HME are placed between the Y-piece and the tubeand thus increase dead space ventilation (up to 150 mldepending on the manufacturer). They should never beused in combination with active breathing gas humidifiersor medication nebulizers because this would greatlyincrease the risk of increased respiratory resistance andcould lead to complete blockage. There is contradictoryinformation about the tidal volume which must beguaranteed if an artificial nose is to be used on pediatricpatients. This information depends both on themanufacturer and the type of filter.
The Humid Vent Mini from the Gibeck-Dryden Corp. isoften used for pediatric anesthesia. This filter is well-known for its very low dead space volume (2.4 ml at thetube-breathing system connection) and high efficiency.According to the manufacturer, the filter can be used in atidal volume range of 10 to 50 ml and produces a humidityof 30 mg/H2O at a VT of 20 ml.
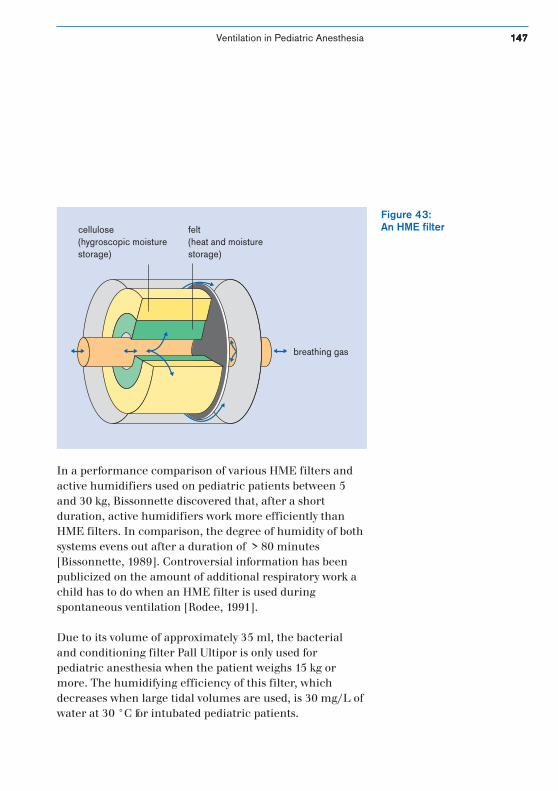
Ventilation in Pediatric Anesthesia 147147147147147
cellulose(hygroscopic moisturestorage)
felt(heat and moisturestorage)
breathing gas
Figure 43:An HME filter
In a performance comparison of various HME filters andactive humidifiers used on pediatric patients between 5and 30 kg, Bissonnette discovered that, after a shortduration, active humidifiers work more efficiently thanHME filters. In comparison, the degree of humidity of bothsystems evens out after a duration of > 80 minutes[Bissonnette, 1989]. Controversial information has beenpublicized on the amount of additional respiratory work achild has to do when an HME filter is used duringspontaneous ventilation [Rodee, 1991].
Due to its volume of approximately 35 ml, the bacterialand conditioning filter Pall Ultipor is only used forpediatric anesthesia when the patient weighs 15 kg ormore. The humidifying efficiency of this filter, whichdecreases when large tidal volumes are used, is 30 mg/L ofwater at 30 °C for intubated pediatric patients.
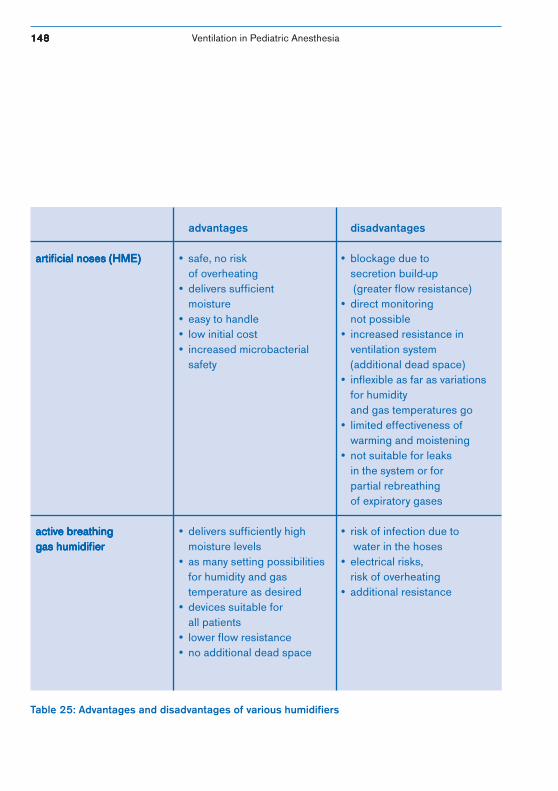
148148148148148 Ventilation in Pediatric Anesthesia
advantages disadvantages
artificial noses (HME)artificial noses (HME)artificial noses (HME)artificial noses (HME)artificial noses (HME) • safe, no risk • blockage due toof overheating secretion build-up
• delivers sufficient (greater flow resistance)moisture • direct monitoring
• easy to handle not possible• low initial cost • increased resistance in• increased microbacterial ventilation system
safety (additional dead space)• inflexible as far as variations
for humidityand gas temperatures go
• limited effectiveness ofwarming and moistening
• not suitable for leaksin the system or forpartial rebreathingof expiratory gases
active breathingactive breathingactive breathingactive breathingactive breathing • delivers sufficiently high • risk of infection due togas humidifiergas humidifiergas humidifiergas humidifiergas humidifier moisture levels water in the hoses
• as many setting possibilities • electrical risks,for humidity and gas risk of overheatingtemperature as desired • additional resistance
• devices suitable forall patients
• lower flow resistance• no additional dead space
Table 25: Advantages and disadvantages of various humidifiers

Ventilation in Pediatric Anesthesia 149149149149149
Heatable HosesAn alternative to the active humidifier is the passive condi-tioner in the form of heatable hoses; these have recentlybeen made available for the anesthetic workstations CiceroEM and Cato for use on both pediatric and adult patients.Initial research on heatable hoses tested on adultsindicates an obvious improvement to breathing gascondition during low-flow anesthesia. For example,Baum showed that, after the breathing system was pre-warmed and moistened by a previous anesthesia, the levelof humidity --already high at 25 mg H2O (at the beginningof anesthesia)-- was able to be raised to 30 and 35 mg H2O(within one hour) using heatable hoses. Temperaturesreached the optimal range of 30 to 37 °C man y timesduring this time. There was no condensation found in thehoses [Baum, 1999].
In addition to the conditioning effect described above,using heatable hoses also provides the advantages of easyhandling and an easy preparation phase. A quick responsetime of five minutes for the hose warming unit was also, inanother study, proven to be advantageous with regard tothe quick dynamics of body temperature during open-heartsurgery on pediatric patients (see Chapter 7.2, PCV duringPediatric Cardio-anesthesia).

150150150150150 Ventilation in Pediatric Anesthesia
The slight loss of gas to environment inherent in the closedsystem PhysioFlex limits consumption of cold, dry fresh gasduring anesthesia. The high blower-supported flow ratealso has a thermal stabilizing function and thus optimizesthe heat-moisture profile. Wissing reported a humiditylevel of 20 mg H2O/l within 10 minutes of beginninganesthesia, and this level was able to be increased shortlythereafter to between 25 and 30 mg H20/l. A systemtemperature of approximately 34 °C and high humidityremain nearly constant due to an efficient CO2 absorber.Thus, this system does not need an additional HME filter oran active humidifier.
Ventilation in Pediatric Anesthesia 151151151151151
6. Bibliography
Altemeyer, K.-H., Th. Fösel, E. Breucking, F. W. Ahnefeld.Narkosen im Kindesalter. Rüsch, 1996.
Altemeyer, K.-H.:Narkosebeatmung-Prinzipien.Workshop: AK Kinderanästhesie der DGAI 1991.In: Beatmung von Kindern in Anästhesie und Intensivmedi-zin.T. Fösel, G. Kraus. Springer: 1993. p. 36 – 49.Atemkalk: Hinweise zu korrektem Umgang und fachgerech-ter Nutzung. Verbandsmitteilungen: Anästhesiologie &Intensivmedizin 6, 1999. 40: 507 – 509.
Badgwell, J. M., J. Tapper.Ventilating the Pediatric Patient in the Operating Room.Clinical Practice Bulletin 6.Dräger Medizintechnik GmbH: 1998.
Baum, J.Die Inhalationsnarkose mit niedrigem Frischgasfluß.Thieme: 1998.
Bengtson, J. P., H. Sonander, O. Stenquist.Preservation of Humidity and Heat of Respiratory Gasesduring Anaesthesia – A Laboratory Investigation.Acta Anaesthesiol Scand, 1987. 31: 127 – 131.
BGM.Atemluft-Befeuchtung in Theorie und Praxis.Bürk Gesellschaft für Vertrieb und Service von medizini-schen Geräten mbH.
Bissonnette, B., D. I. Sessler.Passive or Active Inspired Gas Humification Increases Ther-mal Steady State Temperatures in Anesthetized Infants.Anesth Analg, 1989. 69: 783 – 787.

152152152152152 Ventilation in Pediatric AnesthesiaBibliography
Bito, H., Y. Ikeuchi, K. Ikeda.Effects of the Water Content of Soda Lime on Compound AConcentration in the Anesthesia Circuit in SevofluraneAnesthesia.Anesthesiology, 1998. 88 (1): 66 – 70.
Conzen, P.Muß Halothan ersetzt werden?Workshop: Neue Pharmaka und Techniken in der Kinder-anästhesie. W. Funk and H. Hollnberger. Springer: 1998.
Cote, C. J., E. A. Goldstein, M. A. Cote.A Single-blind Study of Combined Pulse Oximetry inChildren.Anesthesiology, 1991. 74: 980 – 987.
Davis, G. M., M. A. Bureau.Pulmonary and Chest Wall Mechanics in the Control ofRespiration in the Newborn.Clinics in Perinatology, 1987. 5: 51 – 79.
Diefenbach, C.Pharmakologie von Muskelrelaxanzien im Kindesalter.Workshop: Neue Pharmaka und Techniken in der Kinder-anästhesie. W. Funk and H. Hollnberger. Springer: 1998.
Eberhard, M., R. Schäfer .Klinikleitfaden Anästhesie.Gustav Fischer Verlag: 1998.
Engström, Edith.Die natürliche Befeuchtung.Gambro Engström
Ventilation in Pediatric Anesthesia 153153153153153Bibliography
Feldman.Pediatric Ventilation using the Narkomed 6000.Clinical Practice Bulletin 7.Dräger Medizintechnik GmbH: 1998.
Förster, H.Das Soda lime-Problem.Anaesthesist, 1999. 48: 409 – 416.
Fösel, Th., G.-B. Kraus.Beatmung von Kindern in Anästhesie und Intensivmedizin.Springer Verlag: 1993.
Fösel, T., K.-H. Altemeyer, H. Heinrich, P. Lotz.Möglichkeiten und Grenzen der Ventilationsüberwachungbei Narkosen von Säuglingen und Kleinkindern.Anaesthesist, 1984. 33: 31 – 38.
Frei, F. J., C. Johmarker, O. Werner.Kinderanästhesie.Springer Verlag: 1994.
Frei, Ummenhofer.Besonderheiten bei der Prä-Oxygenierung von Kindern.Anästhesiol. Intensivmed. Schmerzther.,1994. 29: 233 – 235.
Fröhlich, D., B. Schwall, W. Funk, J. Hobbhahn.Laryngeal mask airway and uncuffed tracheal tubes areequally effective for low flow or closed system anaesthesia inchildren.British Journal of Anaesthesia, 1997. 79: 289 – 292.
154154154154154 Ventilation in Pediatric AnesthesiaBibliography
Funk, W., H. Hollnberger.Sevofluran in der Kinderanästhesie.Neue Pharmaka und Techniken in der Kinderanästhesie.Springer Verlag: 1998.
Gebhardt, R., U. K. Weiser.Anaesthesiol Reanim, 1999. 24 (2): 41 – 6.
Gregory, G. A.Pediatric Anesthesia.Churchill Livingstone: 1994.
Grüneß, V., W. Wilhelm, Th. Fösel.Besonderheiten der endotrachealen Intubation beim Kind.Anästhesiol. Intensivmed. Notfallmed. Schmerzther., 1995.30: 479 – 482.
Holzki, J.Changing Aspects of Sevoflurane in Paediatric Anaesthsia:1975-99.Paediatric Anaesthesia, 1999. 9: 283 – 286.
Huehns, E. R., E. M. Shooter.Human Hemoglobins.J. Med Genet 2, 1965. p. 48.
Igarashi, M., H. Watanabe, H. Iwasaki, A. Namiki.Clinical Evaluation of Low-flow Sevoflurane Anesthesia forPediatric Patients.Acta Anaesthesiologica Scandinavica, 1999. 43: 19 – 23.
Inomata, S., S. Watanabe, M. Taguchi, M. Okada.End-tidal sevoflurane Concentration for Tracheal Intubati-on and Minimum Alveolar Concentration in PediatricPatients.Anesthesiology, 1994. 80: 93 – 96.

Ventilation in Pediatric Anesthesia 155155155155155Bibliography
Jaklitsch, R.Der integrierte Arbeitsplatz für die Kinderanästhesie.Dräger Medizintechnik aktuell. 2/95.
Jöhr, M.Kinderanästhesie.Gustav Fischer Verlag: 1998.
Kleemann, P. P.Tierexperimentelle und klinische Untersuchungen zumStellenwert der Klimatisierung anästhetischerGase im narkosekreissystem bei Langzeiteingriffen.Wissenschaftliche Verlagsabteilung. Abbott GmbH:Wiesbaden, 1989.
Kleemann, P. P.The Climatisation of Anesthetic Gases under Conditions ofHigh Flow to Low Flow.Anaesthesist, 1989. Nov/38 (11): 639 – 41.
Krane, Haberkern, Jacobsen.Postoperative Apnea, Bradycardia and OxygenDesaturation in Formerly Premature Infants; ProspectiveComparison of Spinal and General Anesthesia.Pediatric Anesthesia 80, 1995. 80: 7 – 13.
Kraus, G.Konzepte der totalen intravenösen Anästhesie (TIVA).Workshop: Neue Pharmaka und Techniken in der Kinder-anästhesie. W. Funk and H. Hollnberger.Springer: 1998.
Kretz, F.-J.Sicherheitsaspekte in der Kinderanästhesie.Kinderkrankenschwester 13. 1994: 9.
156156156156156 Ventilation in Pediatric AnesthesiaBibliography
Kretz, F.-J.Anästhesie, Intensiv- und Notfallmedizin bei Kindern.Thieme.
Larsen.Anästhesie.Urban & Schwarzenberg.
Le Dez, K. M., Lerman J.The Minimum Alveolar Concentration of Isoflurane inPreterm Neonates.Anesthesiology, 1987. 67: 301 – 307.
Lotz, P., E. Siegel, D. Spilker.Grundbegriffe der Beatmung.GIT Verlag: Darmstadt, 1984.
Loop, T.Inhalationsanästhesie bei Kindern.Pharmacia & Upjohn.
McNiece, W. L., G. Krishna.Kawasaki Disease: A Disease with Anesthetic Implications.Anesthesiology, 1983. 58: 269 – 271.
Mielke, L., R. Hipp, S. Hargasser, E. Entholzner.Desfluran in der Kinderanästhesie.Workshop: Neue Pharmaka und Techniken in der Kinder-anästhesie. W. Funk and H. Hollnberger.Springer: 1998.
Möllhoff, Th., G. Burgard, Th. Prien.Low-flow Anästhesie während der Beatmung mit derlaryngealen Maske.Anästhesie – allgemein. p. 141.
Ventilation in Pediatric Anesthesia 157157157157157Bibliography
Mortola, J. P.Mechanics of Breathing:Fetal and Neonatal Physiology.Philadelphia, 1998. p. 1118 – 29.
Nunn, J. F.Applied Respiratory Physiology.Butterworths: London, 1987.
Oczenski, W., A. Werba, H. Andel.Breathing and Mechanical Support.Blackwell-MZV: 1997.
Peters, J. W. B., J. Bezstarosti-Van Eeden, W. Erdmann,E E. Meursing.Safety and Efficacy of Semi-closed Circle Ventilation inSmall Infants.Paediatric Anaesthesia, 1998. 8: 299 – 304.
Quasha, A. L., E. L. Eger, J. H. Tinker.Determinations and Applications of MAC.Anesthesiology, 1991. 53: 315 – 334.
Rathgeber, J.Praxis der maschinellen Beatmung.MCN-Verlag: 1990.
Rathgeber, J.Grundlagen und Methoden der Atemgasklimatisierung inder Intensivmedizin.Intensivmedizin, 1995. 32: 448 – 456.
Reinhold, P., G. Kraus, E. Schüttler.Propofol zur Narkose und Kurzzeitsedierung.Anaesthesist, 1998. 47: 229 – 237.

158158158158158 Ventilation in Pediatric AnesthesiaBibliography
Rodee, W. D., M. J. Banner, N. Gravenstein.Variation in Imposed Work of Breathing with Heat andMoisture Exchangers.Anesth Analg, 1989. 72: 226.
Rupp, K., E. Siegel.Atempause?Dräger Medizintechnik aktuell 1/98.
Schäfer, R., Barthel M. Gerlach, P. Schmucker.Auswirkungen endoskopischer Operationstechniken beiKindern auf die Beatmung.Anästhesiol. Intensivmed. Notfallmed. Schmerzther., 1997.32: 343 – 347.
Schirmer, U., M. Schreiber, A. Goertz, W. Schütz, M.Georgieff, Rockemann.Einfluß von Störungen der Lungencompliance auf die Venti-lation von Neugeborenen.Anaesthesist, 1994. 43: 521 – 527.
Schirmer, U., J. Villwock, T. Fösel, M. Schreiber, A. Goertz,M. Georgieff.Untersuchung von Einflußgrößen auf das abgegebene Hub-volumen.Anästhesist, 1992. 41: 785 – 789.
Schreiber, G., W. Heß, A. Marichal.Der Einfluß verschiedener Narkosebeatmungsverfahren aufOxygenierung und Ventilation von Säuglingen.Anaesthesist, 1994. 43: 510 – 520.

Ventilation in Pediatric Anesthesia 159159159159159Bibliography
Shann, F., S. Gatchalian, R. Hutchinson.Nasopharyngeal Oxygen in Children.Lancet, 1988. 2: 1238 – 1240.
Spears, R. S., A. Yeh, D. M. Fischer.The Educated Hand: Can Anesthesiologists Assess Changesin Neonatal Pulmonary Compliance Manually?Anesthesiology, 1991. 75: 693 – 696.
Stevenson, G. W., M. Tobin, B. Horn, E. Chen, S. C. Hall, C.J. Cote.An Adult System Versus a Bain System:Comparative Ability to Deliver Minute Ventilation to anInfant Lung Model with Pressure-limited Ventilation.Anesth Analg, 1999. 88: 527 – 530.
Strauß, Hausdörfer, Hagemann, Schröder.Klimatisierung anästhetischer Gase während Säuglings-narkosen mit dem Anästhesiearbeitsplatz Cicero.Anaesthesist, 1992. 41: 534 – 538.
Suprane.Edmond I Eger II.Pharmacia & Upjohn: 1994.
Versmold, H. T.Pediatrics, 1981. 67: 607.

160160160160160 Ventilation in Pediatric AnesthesiaBibliography
Wawersik, J.Respiratorische Probleme bei der Säuglingsnarkose.In: Der Risikopatient in der Anästhesie. 2. RespiratorischeStörungen.F.W. Ahnefeld, H. Bergmann, C. Burri, W. Dick, M.Halmugyi, E. Rügheimer,eds. Springer Verlag: Klinische Anästhesiologie und Inten-sivmedizin, 1976. 12: 163 – 177.
Weiser, U.-K.Praktische Erfahrungen mit Narkoseverfahren bei redu-ziertem Frischgasflow.In: Beatmung von Kindern in Anästhesie und Intensivmedi-zin. T. Fösel, G. Kraus, eds.Springer: 1993. p. 36 – 49.

Ventilation in Pediatric Anesthesia 161161161161161
7.1 Anesthetic Ventilation for Infants and Small ChildrenDr. Holzki, Children’s Clinic, Cologne, Germany
Ventilating premature infants, newborns and smallchildren during an operation, whether an operation ofshort or long duration, usually means ventilating lungswhich are not only immature, but also often anatomicallymodified as a result of some damage, be it from maturingtoo quickly, a lack of surfactant, oxygen use or long-termventilation.
Ventilating these pediatric patients calls not only for a tech-nique which will ensure that the patient survives theanesthesia, it also calls for a technique which neitherstresses the very vulnerable lungs of these childrenunnecessarily, nor worsens the lungs’ already damagedstructure. Even inadequate ventilation of short durationduring anesthesia can lengthen the process of weaningpediatric patients from the respirator by days or weeks.
Otherwise “healthy” premature infants and “normal”newborns also have immature lung structures. The countof alveoli, for instance, is about 50 million for a full-termnewborn; this number increases during the first month toabout 150 million (1). The amount of surfactant, thatsubstance which keeps the alveoli from collapsing, isusually insufficient and it can be very easily destroyed byhigh concentrations of oxygen, infections of the bronchialmucus membrane and lung tissue (e.g. aspirationpneumonia), as well as manipulation of the respiratorytract. Atelectasis development leads to insufficientventilation which in turn necessitates artificial respiration.
7. Practical Application

162162162162162 Ventilation in Pediatric Anesthesia
If these immature lungs have to be ventilated incombination with anesthetics, the anesthesia itself couldcause additional problems, like reducing the functionalresidual capacity of the lungs (FRC), disturbing thedistribution process of ventilation and perfusion in manyparts of the lungs, thus increasing the physiological deadspace to the point that anesthetic ventilation must beinitiated using a tidal volume of 10 to 15 ml/kg. This isclearly a higher value than that of spontaneous breathing(2). If inadequate ventilation techniques are applied, aboveall inadequate pressure-volume loads, a vicious circle ofdamage may occur in which structural changes of lungtissue, or even a cor pulmonale, could lead to death (3).
About the twenty-fifth week after conception, a prematureinfant is able to breath, spontaneously, sufficiently. Eachventilation process required, even if it only has to becarried out as a result of apnea, meets with alveoli ofvarying compliance, reduced elastic fibers with insufficientsurfactant, a very fragile ductus alveolares structure, and avery elastic rib cage which yields without resistance to theinspiratory pressure of the respirator. These pooranatomical conditions can lead to regional overinflation,tears in the ductus alveolares and subsequent interstitialemphysema. These sorts of damage necessitate higherconcentrations of oxygen and can, in the end, lead tochronic lung damage called bronchopulmonary dysplasia(BPD (4)), (Figure 1).
Practical Application
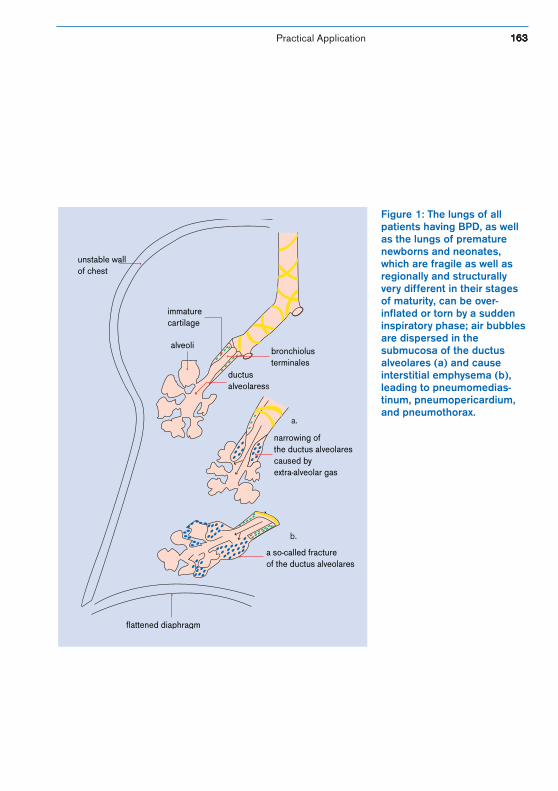
Ventilation in Pediatric Anesthesia 163163163163163
Figure 1: The lungs of allpatients having BPD, as wellas the lungs of prematurenewborns and neonates,which are fragile as well asregionally and structurallyvery different in their stagesof maturity, can be over-inflated or torn by a suddeninspiratory phase; air bubblesare dispersed in thesubmucosa of the ductusalveolares (a) and causeinterstitial emphysema (b),leading to pneumomedias-tinum, pneumopericardium,and pneumothorax.
Practical Application
alveolibronchiolusterminales
ductusalveolaress
immaturecartilage
narrowing ofthe ductus alveolarescaused byextra-alveolar gas
a so-called fractureof the ductus alveolares
flattened diaphragm
unstable wallof chest
a.
b.
164164164164164 Ventilation in Pediatric Anesthesia
Danger to the lungs does decrease as the pediatric patientmatures, but the strategies necessary to avoid causing BPDremain relevant for children of all ages, especially duringanesthesia.
In some rare cases, premature infants and newborns canonly undergo anesthesia if a lack of surfactant has beenreplaced by artificial means. Since a single surfactantadministration is often not enough to stabilize the alveolifor good, it is of utmost importance to ensure that thelungs provide sufficient gas exchange several hours prior tothe operation, for if a relapse occurs during anesthesia, theconsequences can be deadly.
Even if the individual patho-physiological steps leading tothe development of chronic lung diseases are still the topicof controversial discussion, the importance of ventilationas a prime factor leading to damage in the form of BPD isno longer contested. An incorrect ventilation technique canstop the process of alveolar development. For this reason,only that ventilation technique is acceptable which causesthe least baro- or volume trauma for each respectivepatient.
When the thorax of a premature infant is open, even theslightest regional overinflation of the lungs can be seenon X-rays for weeks (a personal observation). Thisdemonstrates the importance of a good ventilation strategyfor pediatric anesthesia, especially for the youngest ofpediatric patients, and even if the anesthesia is only part ofwhat is already long-term ventilation.
Practical Application
Ventilation in Pediatric Anesthesia 165165165165165
A pediatric anesthetist is confronted with a variety ofpatients and, in addition to immature lungs, must oftencontend with disturbances in respiratory regulation,atelectasis due to aspiration pneumonia, occasionalesophagotracheal fistulas, hypoplastic lungs, or thoraxdeformations which, initially, do not cause any damage tothe tissue structure of the lungs. The pediatric anesthetistmust inevitably, for these cases also, use internationallyestablished standards for neonatal ventilation duringanesthesia.
From the very beginning of IMV ventilation for babies, theprimary, most adequate method of artificial ventilation ofpediatric patients was, and still is, the kind of ventilationwhich allows the inspiratory and expiratory phases, and setpressure to be individually controlled. After the epoch-making discovery by Gregory in 1971 (5), the use ofcontinuously applied airway pressure (CPAP) between 2and 10 cm H2O has become a basic rule to be usedwhenever premature infants or newborns are ventilated.This means that there is a continuous flow of gas duringventilation, even during expiration, which maintainspreviously set positive airway pressure and prevents thealveoli from collapsing. This method allows the patient totake a spontaneous breath at any time. This form of venti-lation was titled “intermittent mandatory ventilation”, orIMV, and is the basic form of ventilating today(Figure 2).
Practical Application
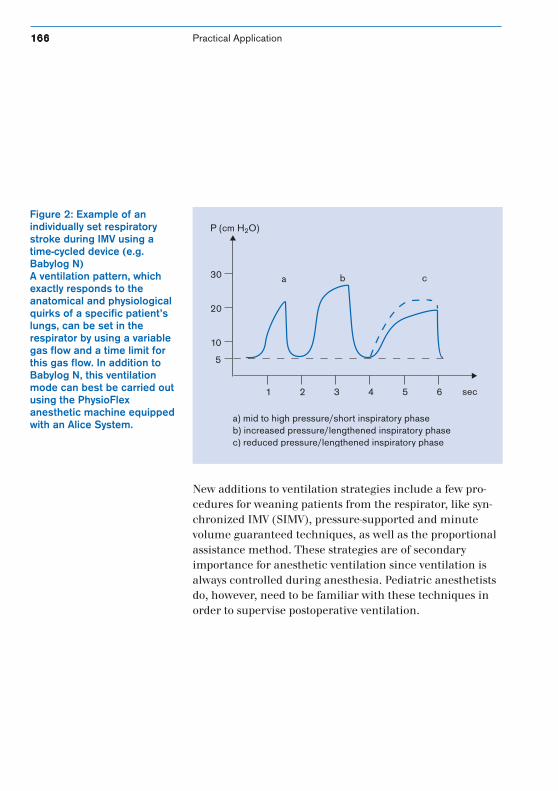
166166166166166 Ventilation in Pediatric Anesthesia
20
30
P (cm H2O)
10
5
1 2 3 4 5 6 sec
a) mid to high pressure/short inspiratory phaseb) increased pressure/lengthened inspiratory phasec) reduced pressure/lengthened inspiratory phase
a b c
New additions to ventilation strategies include a few pro-cedures for weaning patients from the respirator, like syn-chronized IMV (SIMV), pressure-supported and minutevolume guaranteed techniques, as well as the proportionalassistance method. These strategies are of secondaryimportance for anesthetic ventilation since ventilation isalways controlled during anesthesia. Pediatric anesthetistsdo, however, need to be familiar with these techniques inorder to supervise postoperative ventilation.
Figure 2: Example of anindividually set respiratorystroke during IMV using atime-cycled device (e.g.Babylog N)A ventilation pattern, whichexactly responds to theanatomical and physiologicalquirks of a specific patient’slungs, can be set in therespirator by using a variablegas flow and a time limit forthis gas flow. In addition toBabylog N, this ventilationmode can best be carried outusing the PhysioFlexanesthetic machine equippedwith an Alice System.
Practical Application
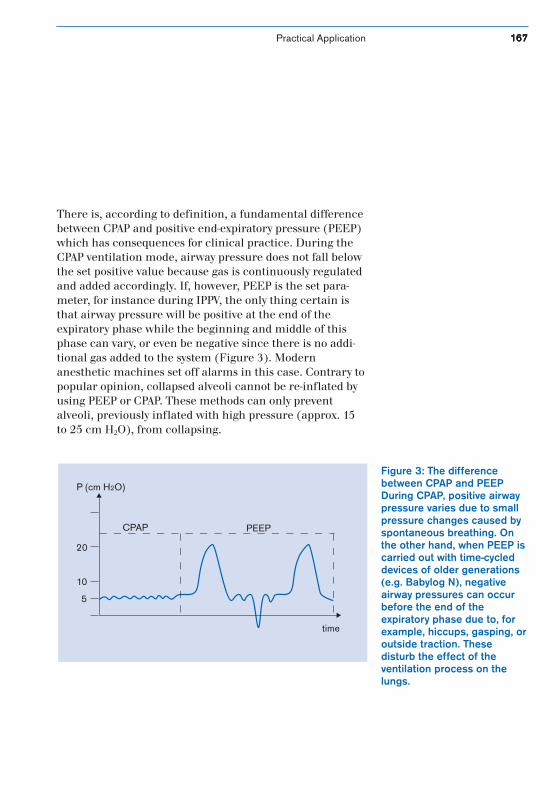
Ventilation in Pediatric Anesthesia 167167167167167
There is, according to definition, a fundamental differencebetween CPAP and positive end-expiratory pressure (PEEP)which has consequences for clinical practice. During theCPAP ventilation mode, airway pressure does not fall belowthe set positive value because gas is continuously regulatedand added accordingly. If, however, PEEP is the set para-meter, for instance during IPPV, the only thing certain isthat airway pressure will be positive at the end of theexpiratory phase while the beginning and middle of thisphase can vary, or even be negative since there is no addi-tional gas added to the system (Figure 3). Modernanesthetic machines set off alarms in this case. Contrary topopular opinion, collapsed alveoli cannot be re-inflated byusing PEEP or CPAP. These methods can only preventalveoli, previously inflated with high pressure (approx. 15to 25 cm H2O), from collapsing.
Figure 3: The differencebetween CPAP and PEEPDuring CPAP, positive airwaypressure varies due to smallpressure changes caused byspontaneous breathing. Onthe other hand, when PEEP iscarried out with time-cycleddevices of older generations(e.g. Babylog N), negativeairway pressures can occurbefore the end of theexpiratory phase due to, forexample, hiccups, gasping, oroutside traction. Thesedisturb the effect of theventilation process on thelungs.
5
10
20
P (cm H2O)
time
CPAP PEEP
Practical Application
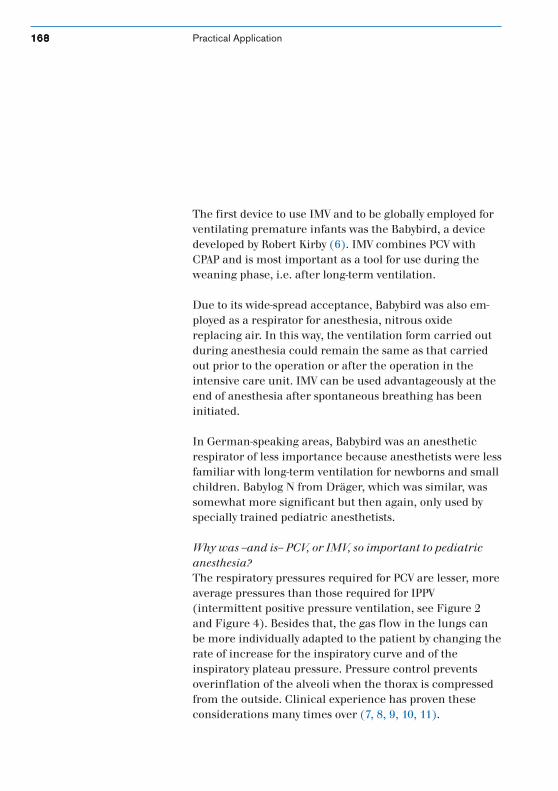
168168168168168 Ventilation in Pediatric Anesthesia
The first device to use IMV and to be globally employed forventilating premature infants was the Babybird, a devicedeveloped by Robert Kirby (6). IMV combines PCV withCPAP and is most important as a tool for use during theweaning phase, i.e. after long-term ventilation.
Due to its wide-spread acceptance, Babybird was also em-ployed as a respirator for anesthesia, nitrous oxidereplacing air. In this way, the ventilation form carried outduring anesthesia could remain the same as that carriedout prior to the operation or after the operation in theintensive care unit. IMV can be used advantageously at theend of anesthesia after spontaneous breathing has beeninitiated.
In German-speaking areas, Babybird was an anestheticrespirator of less importance because anesthetists were lessfamiliar with long-term ventilation for newborns and smallchildren. Babylog N from Dräger, which was similar, wassomewhat more significant but then again, only used byspecially trained pediatric anesthetists.
Why was --and is-- PCV, or IMV, so important to pediatricanesthesia?The respiratory pressures required for PCV are lesser, moreaverage pressures than those required for IPPV(intermittent positive pressure ventilation, see Figure 2and Figure 4). Besides that, the gas flow in the lungs canbe more individually adapted to the patient by changing therate of increase for the inspiratory curve and of theinspiratory plateau pressure. Pressure control preventsoverinflation of the alveoli when the thorax is compressedfrom the outside. Clinical experience has proven theseconsiderations many times over (7, 8, 9, 10, 11).
Practical Application
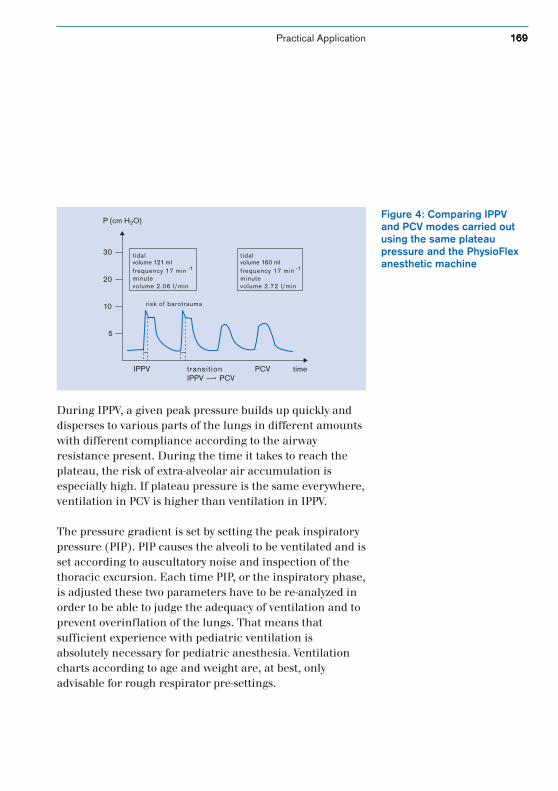
Ventilation in Pediatric Anesthesia 169169169169169
During IPPV, a given peak pressure builds up quickly anddisperses to various parts of the lungs in different amountswith different compliance according to the airwayresistance present. During the time it takes to reach theplateau, the risk of extra-alveolar air accumulation isespecially high. If plateau pressure is the same everywhere,ventilation in PCV is higher than ventilation in IPPV.
The pressure gradient is set by setting the peak inspiratorypressure (PIP). PIP causes the alveoli to be ventilated and isset according to auscultatory noise and inspection of thethoracic excursion. Each time PIP, or the inspiratory phase,is adjusted these two parameters have to be re-analyzed inorder to be able to judge the adequacy of ventilation and toprevent overinflation of the lungs. That means thatsufficient experience with pediatric ventilation isabsolutely necessary for pediatric anesthesia. Ventilationcharts according to age and weight are, at best, onlyadvisable for rough respirator pre-settings.
Figure 4: Comparing IPPVand PCV modes carried outusing the same plateaupressure and the PhysioFlexanesthetic machine
P (cm H2O)
transitionIPPV PCV
5
10
20
30
IPPV PCV time
risk of barotrauma
tidalvolume 160 mlfrequency 17 min -1
minutevolume 2.72 l/min
tidalvolume 121 mlfrequency 17 min -1
minutevolume 2.06 l/min
Practical Application

170170170170170 Ventilation in Pediatric Anesthesia
If tidal volume is preset on a volume-controlled respirator,the effects of ventilation on lung structure can only bepoorly assessed. As early as 1977, Kirby pointed out thatvolume-controlled ventilation is unfavorable for very youngchildren whose very small respiratory tract has to receiveand cushion crucial respiratory pressure (“volumecontrolled is a myth in neonatal ventilation,” (12)). Thisstatement is supported by an observation of D. Null whohas very often seen tears in mucus membrane at theterminal respiratory tract which he describes as “fracturesof the ductus alveolares” (13). Apparently, volume-controlled ventilation has often left the lung structure in astate of overinflation, interstitial emphysema, or withinfections caused by trauma and recorded as a BPD(Figure 5).
Regardless of the type of ventilation, PEEP should be set towithin a range of 2 to 5 cm H20 in order to prevent thealveoli from collapsing during expiration. PEEPcorresponds to CPAP during controlled ventilation on arelaxed patient. A higher PEEP (6 to 12 cm H20) canimpede compliance and thus, hinder ventilation if theindications which make such a high value necessary arenot absolutely clear. PIP increases during volume-controlled ventilation.
Practical Application
Ventilation in Pediatric Anesthesia 171171171171171
Figure 5: X-rays of the thoraxes of threeinfants• Bronchopulmonary dysplasia after
several weeks of ventilation (a)• Pneumomediastinum and
pneumothorax, left, during IPPV (b)• Pneumopericardium during IPPV (c)These kinds of ventilation complicationswere seen on a daily basis before IMVbecame the more common practice(1975 – 1977) as a result of IPPV used onvery young children.
Practical Application

172172172172172 Ventilation in Pediatric Anesthesia
The respiratory rate changes the ventilation rate of thealveoli, but it also changes the ratio of inspiratory toexpiratory time (I:E ratio). There is a sufficient amount ofempirical numbers available for and helpful in setting therespiratory rate for the lungs of a newborn. Rates greaterthan 60/min can easily lead to air being trapped and, thus,to barotrauma. The I:E ratio is not a good parameter forregulating ventilation and oxygenation on very youngchildren due to their erratic respiratory rates. Adapting anactual inspiratory phase to the needs of individual lungshas proven to be much better. It has also been empiricallyproven that inspiratory phases longer than 0.6 seconds onlyincrease oxygenation temporarily, but then they can oftenlead to pneumothorax due to reduced venous backflowwhile inspiratory phases shorter than 0.2 seconds oftenprovide only partial ventilation to the alveoli.
Those who wish to carry out optimal anesthetic ventilationon pediatric patients inevitably have to learn thefundamentals of neonatal ventilation techniques and thenapply them to situations in the operating theater.Throughout an operation, additional techniques andmonitoring parameters are desirable to provide more exactindications of how the lungs are actually functioning anda clear picture of the concentrations of anesthetic gases,which should not escape into the operating theater at all ifpossible.
Practical Application
Ventilation in Pediatric Anesthesia 173173173173173
Today, the question is which anesthetic respirator shouldbe used to ventilate premature infants and newborns in thefuture? Older devices like Babylog N are not equipped withthe gas monitoring necessary for the future and, at thesame time, the latest generation of neonatal respiratorscannot be adapted for anesthetic use.
The PhysioFlex anesthetic system provides one possibility,even if it is not yet ready to use on premature infants.Technological development, already proven exceptional forpatients weighing over 5 kilograms, is underway forpatients under 3 kilograms. Using PhysioFlex with asoftware program for ventilating small children, PCV canbe carried out in this closed system which is almostequivalent to regular IMV. The end-expiratory CO2
measurement lies below the known limits for youngchildren, but if ventilation is carried out almost leak-free,oxygen consumption is measured indirectly. Thismeasurement can provide the anesthetist with valuableinformation which was, up till now, not available duringanesthesia. For instance, an acute increase in oxygenconsumption could be an indication of insufficient depthof anesthesia or it could be --depending on the patient’sstate of health-- an indication of an imminent asthmaattack (personal observation).
One can hope that closed-system PCV is available in thenear future for use on premature infants.
Anesthetic ventilation for pediatric patients will most likelyalways prove a great challenge to all practicinganesthetists.
Practical Application

174174174174174 Ventilation in Pediatric AnesthesiaPractical Application
Bibliography
(1) Langston, C., et al.Human Lung Growth in Late Gestation and in the Neonate.Am Rev Resp Dis, 1984. 129: 607 – 611.
(2) Motoyama, E. K.Respiratory Physiology in Infants and Children.In: Anesthesia for Infants and Children.6th edition. E. K. Motoyama, P. J. Davis, eds. 1996. p. 11 – 68.
(3) Bancalari, E.Neonatal Chronic Lung Disease.In: Neonatal-Perinatal Medicine. 6th edition. A. A. Fanaroff, R. J. Martin, eds.Mosby: St. Louis, 1997. p. 1074 – 1089.
(4) Martin, R. J., Fanaroff, A. A.The Respiratory Distress Syndrome and its Management.In: Neonatal-Perinatal Medicine. 6th edition.A. A. Fanaroff, R. J. Martin, eds. 1998. p. 1018 – 1028.
(5) Gregory, G. A., J. A. Kitterman, R. H. Phibbs, et al.Treatment of the Idiopathic Respiratory Distress Syndromewith Continuous Positive Airway Pressure.New England Journal of Medicine, 1971. 284: 1333 – 1339.
(6) Kirby, R. R.Design of Mechanical Ventilators.D. W. Thibeault, G. A. Gregory, eds. Addison-WesleyPublishing Co.: Menlo Park, Ca., 1979. p. 154 – 167.
Ventilation in Pediatric Anesthesia 175175175175175Practical Application
(7) Reynolds, E. O. R., et al.Improved Prognosis of Infants Mechanically Ventilated forHyaline Membrane Disease.Arch Dis Child, 1970. 49: 505 – 510.
(8) Boros, S. J.Variations in Inspiratory : Expiratory Ratio and AirwayPressure Wave Form during Mechanical Ventilation: TheSignificance of Mean Airway Pressure.J Pediatr., 1979. 94: 114 – 119.
(9) Bancalari, E., J. C. Sinclair.In: Effective Care of the Newborn Infant.J. C. Sinclair, ed. Oxford University Press:New York, 1992.
(10) Carlo, W. A., R. J. Martin, A. A. Fanaroff.Assisted Ventilation and Complications ofRespiratory Distress.In: Neonatal-Perinatal Medicine. 6th edition. A. A.Fanaroff, R. J. Martin, eds. Mosby: St. Louis, 1998. p.1028 – 1036.
(11) Holzki, J.Kongressberichte über das 4.–26. Neonatal and InfantRespiratory Symposium. AINS: 1977 – 1999.
(12) Kirby, R.In: Kongressbericht über das 4. Neonatal and InfantRespiratory Symposium. J. Holzki, ed.Prakt Anästh, 1977. 12: 541–555.
(13) Null, D. M.In: Kongressbericht über das 20. Neonatal and InfantRespiratory Symposium. J. Holzki, ed.AINS: 1993. 28: 394 – 397.
176176176176176 Ventilation in Pediatric Anesthesia
7.2 PCV during Pediatric Cardio-anesthesiaDr. Fischer, German Center for Cardiology, Berlin
Pediatric cardio-anesthesia has a spectrum which includescorrecting congenital defects (cyanotic, acyanotic),transplantation surgery (heart and lung) and relatedillnesses (e.g. cystic fibrosis, Wilson-Mikity syndrome), bothby employing and not employing extracorporeal circulation(ECC). Extracardia deformities (VACTERL association,asplenia syndrome, Ivemark’s syndrome), which usually goalong with a congenital defect, are particularly challengingto anesthetists.
Since the heart and lungs represent a single functioningunit, mechanical ventilation has an effect on (partially)varying hemodynamics (e.g. fontanel hemodynamics),before and after correcting a congenital defect, whichshould not be underestimated.
Using ECC to correct congenital defects, which could leadto capillary leak syndrome (alveolar capillary leakage), alsoplaces additional emphasis on the necessity of sufficientventilation.
Practical Application

Ventilation in Pediatric Anesthesia 177177177177177
As a result of this, the following prerequisites for anestheticrespirators can be derived:
• large variables for tidal volume and respiratory rate dueto greater distribution of age
• low dead space volume• avoiding high ventilating pressures (e.g. fontanel opera-
tive procedures)• reliable monitoring for ventilation parameters and
capnography (pulmonary hypertension caused byhypoventilation)
• valid capnogram for regulating pulmonary vascularresistance (e.g. HLHS, shunt defects)
• sufficient breathing gas conditioning
In the past, pressure and time-cycled respirators (Bird®,Penlon®, Babylog N®) were used for mechanical ventilationin pediatric cardio-anesthesia. The disadvantage of theserespirators --the volumes provided were inconsistent-- wascompensated for by the introduction of volume- and time-cycled devices in the middle of the 1980s (SERVO 900®,Sulla 800®). These devices, developed for adult patients, do,however, have a few disadvantages when used for pediatricanesthesia, like large dead space volume and compressiblevolume. The latest generation of anesthetic machines (Ci-cero®, Cato®, Julian®, Aestiva®, Kion®) allow anesthetists touse both pressure- and volume-controlled ventilationmodes.
Practical Application
178178178178178 Ventilation in Pediatric Anesthesia
At our Heart Center, we use a Cato-PCV anestheticrespirator (from Dräger, Germany) which has active hosewarming (see the section on Conditioning Breathing Gasfor Children). The properties associated with the variousventilation forms (IPPV/VCV, PCV) were discussed in aprevious chapter (see Chapter 5.1, Mechanical Forms ofVentilation). As far as the form of ventilation is concerned,we use volume-controlled ventilation (IPPV, VT 10 to 1400ml, respiratory rate 6 to 80) before employingextracorporeal circulation and PCV afterwards.
Advantages of the PCV ventilation mode
• lower respiratory pressure (approx. 2 mbar under IPPVpeak pressure)
• no accidental overinflation of the lungs when thethorax is open
• better alveolar recruitment due to decelerated flow
Disadvantages of the PCV ventilation mode
• VT changes when thorax compliance is changed(surgical manipulation, closed thorax), Pmax is thesame for both
For this reason, when pressure-controlled ventilation isused, alarm limits (MV) should be set conservatively andthe tidal volume should be continuously displayed by thevolumeter.
Practical Application
Ventilation in Pediatric Anesthesia 179179179179179
PCV is used either before or after ECC for ductus ligationand pulmonary diseases which can severely influencehemodynamics as a result of high peak pressures occurringduring ventilation (restrictive lung disease, after fontaneloperative procedures).
Special features of these two forms of ventilation can besummed up as follows:
Volume-controlled and time-cycled ventilation (VCV)The greatest disadvantage of VCV is limited consistency intidal volume (tube leakage) which puts the patient at riskof barotrauma due to a change in pulmonary compliance,an increase of compression volume due to the deteriorationof pulmonary compliance, and lung overinflation. By intro-ducing static compliance correction, it is at least possible toset a simple tidal volume.
Pressure-controlled and time-cycled ventilation (PCV)The advantages of PCV include avoiding peak pressuresduring ventilation (barotrauma), decelerating flow,compensating for tube leakage, and providing staticcompliance for newborns and infants with low tidalvolumes. The big disadvantage caused by the dependencybetween tidal volume and a varying lung compliancerequires the anesthetist to be very attentive to the situation,but can be controlled by using adequate monitoring (VT,MV).
Practical Application
180180180180180 Ventilation in Pediatric Anesthesia
Conditioning Breathing Gas for ChildrenIn a joint venture with Dräger of Lübeck, Germany, ourHeart Center integrated a heatable hose system into therespirator system of a Cato anesthetic workstation. Atemperature sensor was added to the inspiratory hose at apoint close to the patient, and a bacterial filter was addedto the inspiratory and expiratory limbs of the circle system.
Over a period of six months, this hose system was used in261 congenital defects operations. The ages of the pediatricpatients were less than five (0 to 5 years), and a largeportion of these children (> 60 %) were younger than threemonths. The minute volume was between 1 and 2 l/min.Since sevoflurane was always used, low-flow anesthesia wasnot used and the MV fresh-gas flow was adaptedaccordingly up to a maximum of 2 l/min.
The aim of this research into usability was to find an easy-to-handle hose warmer which sufficiently humidifiesbreathing gas, not putting the small patients atunnecessary risk.
ResultsThe hose system, used over six months in 261 operations,did not fail unexpectedly. Breathing gas temperatures,central and peripheral body temperature and roomtemperature were recorded for 20 children with the hosewarming system and for 10 children without it.
Practical Application
Ventilation in Pediatric Anesthesia 181181181181181
As far as body temperature dynamics during open-heartsurgery are concerned (cooling down to a bodytemperature of 16 °C, warming up to 36 °C due to heart-lung machines, room temperatures originally at 16 °C andafter ECC up to 22 °C), the hose warmer was able to adjustthe hoses sufficiently within five minutes without anydangerous ”hot spots” appearing. The course of theoperation being smooth, all 20 children had constant bodytemperatures before and after ECC. Breathing gastemperatures before ECC (room temperature at 16 °C), aswell as after ECC (room temperature at 22 °C), were at30 °C within five minutes of IPPV beginning (withtemperatures ranging between 28 and 32 °C). In com-parison, the circle system itself warms up without the inte-grated hose system only after 30 minutes and only up to amaximum of 22 °C (temperatures here range between 20and 24 °C) and it exhibits condensation build-up after oneto two hours of anesthesia administration, indicating thatthe pediatric patient has suffered loss of liquid and loss ofwater.
Advantages of active hose warming systems over activehumidification systems
• easy to handle and clean• rapid rise in temperature without hot spots appearing
during high-flow pediatric anesthesia (fresh-gas flow 2 l/min)• reduced risk of disconnection• by not having condensation, no bacterial contamination
or drowning of pediatric patient• cost reductions through recycling
Practical Application

182182182182182 Ventilation in Pediatric Anesthesia
Advantages of active hose warming systems over heat-moisture exchangers (HME)
• dead space does not increase• airway resistance does not increase• no secretion and/or tube obstructions• quick reactions• cost reducing
In conclusion one could say that PCV is highly valued, as faras the quality of ventilation is concerned, for ventilatingcritically ill infants and children.
Practical Application
Ventilation in Pediatric Anesthesia 183183183183183Practical Application
Bibliography
Bernstein, G., et al.Airway Leak Size in Neonates and Autocycling of ThreeFlow-triggered Ventilators.Crit Care Med., 1995. 23 (10): 1739 – 44.
Bourdelles, G., L. Mier, B. Fiquet, G. Saumon, D. Dreyfuss.Comparison of the Effect of Heat and Moisture Exchangersand Heated Humidifiers on Ventilation and Gas Exchangeduring Weaning Trials from Mechanical Ventilation.Chest, 1996. 110: 1294 – 98.
Konrad, F., M. Mezody, A. Goertz, T. Marx, M. Georgieff.Einfluß eines Wärme und Feuchtigkeitsaustauscher(HME) auf den bronchialen Schleimtransport im Rück-atemnarkosesystem.Anaesthesist, 1996. 45: 802 – 06.
Nikitin, E. S., et al.The Use of a Pressure Support Ventilation Regimen in theRecovery of Spontaneous Respiration after HeartOperations.Anesthesiol Reanimatol, 1998. 8 (4): 31 – 6.
Marini, J. J.New Options for the Ventilatory Management ofAcute Lung Injury.New Horizons: 1993. 1: 489 – 503.

184184184184184 Ventilation in Pediatric AnesthesiaPractical Application
Martin, L. D., et al.New Approaches to Ventilation in Infants and Children.Curr Opin Pediatr., 1995. 7: 253.
Pollak, M. M., et al.Pneumothorax and Pneumomediastinum during PediatricMechanical Ventilation.Crit Care Med., 1979. 7: 536 – 539.
Rathgeber, J., W. Weyland, T. Bettka, K. Züchner, D. Kettler.Is Reduction of Intraoperative Heat Loss and Managementof Hypothermic Patients with Anesthetics Gas ClimateAdvisable? Heat and Humidity Exchangers vs. Humidifiersin a Functional Lung Model.Anaesthesist, 1996. 45: 807 – 13.
Rawlings, D. J., et al.The Siemens-Elema Servo Ventilator 900 B for the Manage-ment of Newborns with Severe Respiratory DistressSyndrome.Crit Care Med., 1980. 8 (5): 307 – 11.
Sugg, B. R., et al.The Penlon Oxford Ventilator. A New Ventilator for Adultor Pediatric Use.Anaesthesia, 1976. 31(9): 1234 – 44.

Ventilation in Pediatric Anesthesia 185185185185185
7.3 Using a Laryngeal Mask for Pediatric AnesthesiaDr. Keller, Leopold-Franzens University, Innsbruck
In 1981, Archie Brain, a British anesthesiologist, developedthe laryngeal mask (LMA) within the scope of a researchproject at the Royal London Hospital which aimed atfinding a user-friendlier airway than the face mask and aless invasive one than the endotracheal tube. Within thelast eight years, the LMA has become a universal airwaygenerally used for performing routine pediatric anesthesia.The LMA, available in various sizes (see below, Table 1), isused in 30 to 60 % of all anesthesia cases. It is usedparticularly for those cases which require a face mask, butnot for those cases in which an endotracheal tube isadvisable. Those factors indicating an unfavorable situationfor LMA use are described further below.
To date, the LMA has been handled in more than 1,600publications and used on more than 50 million anesthesiapatients (pediatric and adult) in at least 90 countries. Inmore than six years, there have been no know reports ofdeath caused by the use of the laryngeal mask.
Practical Application
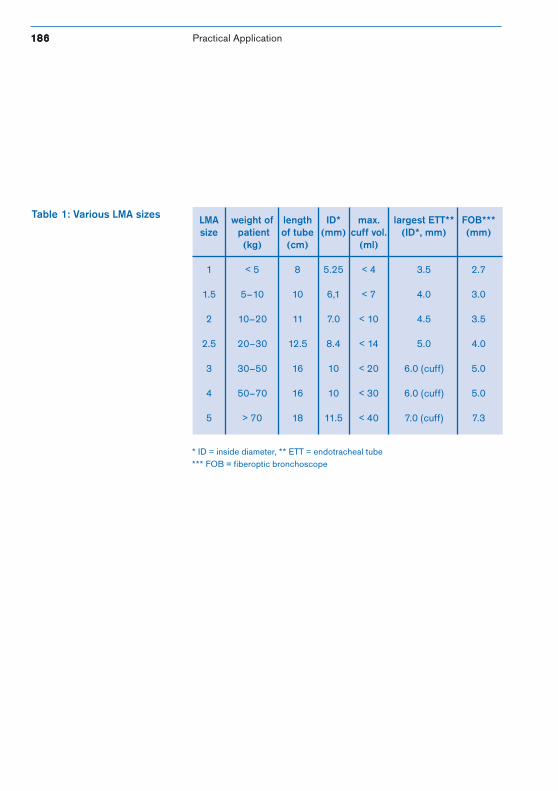
186186186186186 Ventilation in Pediatric Anesthesia
Table 1: Various LMA sizes LMA weight of length ID* max. largest ETT** FOB***size patient of tube (mm) cuff vol. (ID*, mm) (mm)
(kg) (cm) (ml)
1 < 5 8 5.25 < 4 3.5 2.7
1.5 5–10 10 6,1 < 7 4.0 3.0
2 10–20 11 7.0 < 10 4.5 3.5
2.5 20–30 12.5 8.4 < 14 5.0 4.0
3 30–50 16 10 < 20 6.0 (cuff) 5.0
4 50–70 16 10 < 30 6.0 (cuff) 5.0
5 > 70 18 11.5 < 40 7.0 (cuff) 7.3
* ID = inside diameter, ** ETT = endotracheal tube*** FOB = fiberoptic bronchoscope
Practical Application
Ventilation in Pediatric Anesthesia 187187187187187
Contraindications for Pediatric LMAs
Patient-related factors which increase the risk of aspiration:• gastric content• upper gastrointestinal pathology• pathological obesity• large amounts of pain• anamnesis unattainable• gastrointestinal obstructions• residual gastric content or delayed reduction due to
opiates
Operation-related factors which increase the risk ofpulmonary aspiration:• upper stomach surgery• peritoneal traction• increased intra-abdominal pressure• head tilted back in the extreme
High respiratory pressure (> 20 mbar):• low lung and thorax compliance• high airway resistance• pathological glottis (ray treatment of the larynx or
pharynx)• intrathoracic surgery
Pathological mouth or pharynx (for example,anamnestical radiotherapy)
Blood anamnesis (relative)
Practical Application

188188188188188 Ventilation in Pediatric Anesthesia
Anesthesia InductionIf added to an induction dose, Propofol subdues pharyngealand laryngeal activity more than Thiopental and it is consi-dered an excellent induction agent. Taguchi and colleagueshave shown that a lower sevoflurane MAC value is requiredwhile LMAs are being positioned on pediatric patients thanis the case when an endotracheal tube is being inserted.
Laryngeal Mask InsertionThe ideal patient position for inserting an LMA is an exten-ded head and flexed neck, the classic “sniff-the-morning-air” position. This position is attained by tilting the head ofthe patient backwards and downward during the insertionmovement using the non-dominant hand. LMA insertioncan be compared to the act of swallowing. The mask can beinserted blind and without administering musclerelaxants, and a collision with the front of the pharynx withits numerous nerve endings is simultaneously avoided.When a person swallows, the tongue pushes nourishmentalong the curved wall made up of the palate and the backpart of the pharynx and then pushes it down. An LMAinsertion is accomplished in a similar way: the index fingerpushes the mask upwards, thus imitating the tongue whenit pushes the food along the palate. That means that theanesthetist holds his finger pointed toward his bellybuttonthroughout the insertion maneuver. The mask iscompletely inserted as soon as definite resistance isnoticeable. This resistance is the result of the tip of themask meeting the top of the esophageal sphincter. Themost common error made during the insertion phase isthat the centrifugal force of the index finger exertedagainst the curve of the hard palate and the back of theoropharynx is not kept constant long enough for the LMA toreach the hypopharynx.
Practical Application
Ventilation in Pediatric Anesthesia 189189189189189
It is important to differentiate between pressure in thecuff, the pressure the cuff places on the mucosa, and theairway pressure which could be the source of leakage. Oneof the LMA cuff’s most important functions duringspontaneous breathing is to protect the larynx fromoropharyngeal secretions. In order to carry out thisfunction, an oropharyngeal pressure of up to 10 mbar isnecessary. Tension in the cuff should be checked regularly.It could become necessary to let off slight amounts of airbecause the pressure in the cuff increases as a result ofnitrous oxide diffusion.
Maintaining Depth of AnesthesiaA combination of regional and inhalation anesthesia (O2/N2O, sevoflurane or isoflurane) for spontaneous breathingwith inspiratory pressure support (“hand on the bag”) orpure CPAP ventilation is most common. At the same timehowever, most children with no gastric content can bemechanically ventilated in the IPPV mode over the LMAusing normal lung compliance with a maximum airwaypeak pressure of approx. 20 mbar (see below, Table 2,Dräger respirator setups). Having a low-pressure sealmeans that tidal volume is about 6 – 8 ml kg1 and that theinspiratory flow should be reduced in order to ensure safeand sufficient ventilation. An epigastria auscultationshould be performed on all children to prevent stomachinsufflation. Several large-scale studies have confirmed thesafeness of using IPPV with the LMA on both adults andchildren. A meta-analysis of 547 publications dealing withLMAs did not show any correlation between IPPV andpulmonary aspiration, either in patients from LMA studiesor in patients from case reports on aspiration.
Practical Application
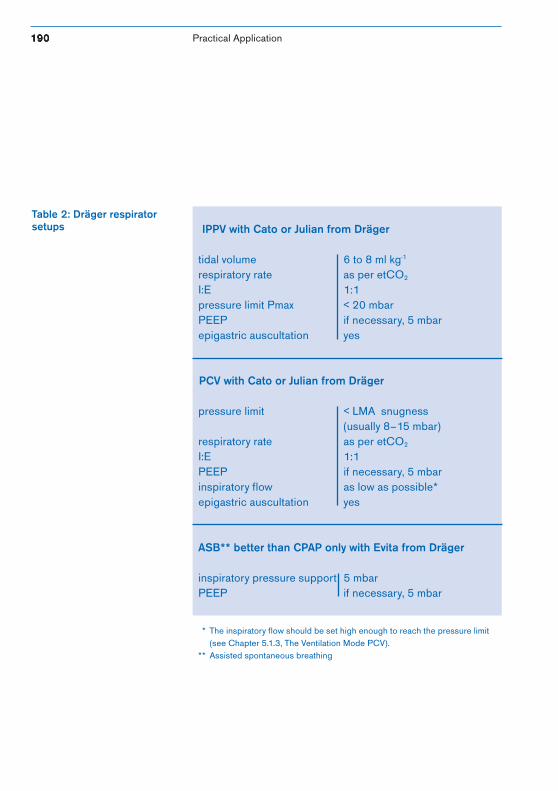
190190190190190 Ventilation in Pediatric Anesthesia
Table 2: Dräger respiratorsetups IPPV with Cato or Julian from Dräger
tidal volume 6 to 8 ml kg-1
respiratory rate as per etCO2
I:E 1:1pressure limit Pmax < 20 mbarPEEP if necessary, 5 mbarepigastric auscultation yes
PCV with Cato or Julian from Dräger
pressure limit < LMA snugness(usually 8–15 mbar)
respiratory rate as per etCO2
I:E 1:1PEEP if necessary, 5 mbarinspiratory flow as low as possible*epigastric auscultation yes
ASB** better than CPAP only with Evita from Dräger
inspiratory pressure support 5 mbarPEEP if necessary, 5 mbar
* The inspiratory flow should be set high enough to reach the pressure limit(see Chapter 5.1.3, The Ventilation Mode PCV).
** Assisted spontaneous breathing
Practical Application
Ventilation in Pediatric Anesthesia 191191191191191
Removing the LMAThe LMA may be removed when the pediatric patient isstill under anesthesia or awake, and while the patient islaying on its back or side. The mask should not be removedwhen the patient is going through a transition stage as thiscould lead to laryngospasm, coughing or choking. Thechild should not be disturbed by the LMA when waking up.It is not necessary to use suction to remove secretionsaround the upper pharynx since they will not enter thelarynx unless the cuff is unblocked before the LMA isremoved. The cuff should be unblocked at the same timethe LMA is removed.
Advantages and Disadvantages of Usingthe Laryngeal MaskAdvantages of the laryngeal mask over the face maskinclude the availability of a freer respiratory tract whichfrees the hands of the anesthetist for other important tasks,like administering medication and preparingdocumentation. It is also easier to obtain an effective, air-tight closure which facilitates ventilation and improvesmonitoring for breathing gas mixtures and low-flowanesthesia. The quality of the airway is generallyunaffected by anatomical factors which complicate matterswhen a face mask is used, i.e. due to the patient’s beingtoothless or having a beard or being a newborn. Using anLMA as opposed to a face mask does not require personnelwhich is still being trained or does not yet have a lot ofclinical experience to be extremely skilled.
Practical Application

192192192192192 Ventilation in Pediatric Anesthesia
Comparative analyses of face masks report that hypoxia israre in conjunction with the LMA. In addition, LMAs offerdirect access to the glottis without sacrificing control of theairway and thus, make it easier to see and get at both thevocal chords and a larger part of the respiratory tract. TheLMA also poses less environmental risk to the operatingtheater and recovery room.The advantages of the laryngeal mask as compared to thetracheal tube include being able to do withoutlaryngoscopy, being less invasive to the respiratory tract,avoiding the risks associated with endobronchial oresophageal intubation, being able to do without musclerelaxants, and relieving local tissue of a good portion oftrauma. Learning to position a laryngeal mask is easy and,generally speaking, not associated with those factors whichmake inserting an endotracheal tube difficult. Pediatricpatients tolerate an LMA at a more shallow depth ofanesthesia than they do an endotracheal tube and areusually awake before they resist the LMA. Incidences ofcoughing, choking and holding of breath during thewaking phase are reduced. Inserting and removing theLMA have a minimum effect on cardiovascular reactionsand intra-ocular pressure. Barotrauma is not common withan LMA. The biggest disadvantage of the LMA compared tothe endotracheal tube is that the LMA does not provide anyprotection against aspiration.
Practical Application
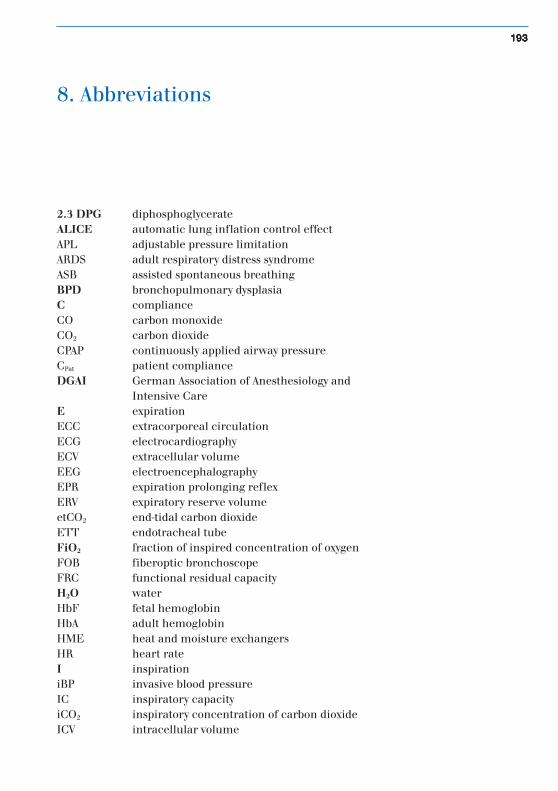
Ventilation in Pediatric Anesthesia 193193193193193
8. Abbreviations
2.3 DPG diphosphoglycerateALICE automatic lung inflation control effectAPL adjustable pressure limitationARDS adult respiratory distress syndromeASB assisted spontaneous breathingBPD bronchopulmonary dysplasiaC complianceCO carbon monoxideCO2 carbon dioxideCPAP continuously applied airway pressureCPat patient complianceDGAI German Association of Anesthesiology and
Intensive CareE expirationECC extracorporeal circulationECG electrocardiographyECV extracellular volumeEEG electroencephalographyEPR expiration prolonging reflexERV expiratory reserve volumeetCO2 end-tidal carbon dioxideETT endotracheal tubeFiO2 fraction of inspired concentration of oxygenFOB fiberoptic bronchoscopeFRC functional residual capacityH2O waterHbF fetal hemoglobinHbA adult hemoglobinHME heat and moisture exchangersHR heart rateI inspirationiBP invasive blood pressureIC inspiratory capacityiCO2 inspiratory concentration of carbon dioxideICV intracellular volume
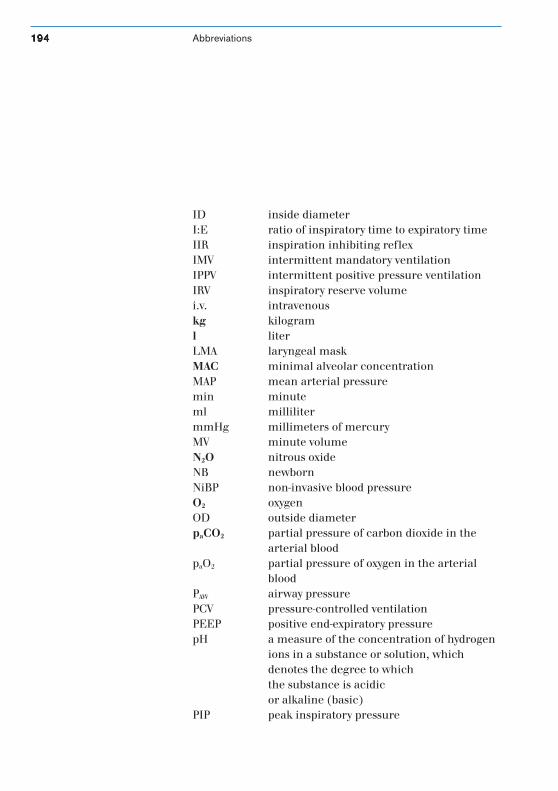
194194194194194 Ventilation in Pediatric Anesthesia
ID inside diameterI:E ratio of inspiratory time to expiratory timeIIR inspiration inhibiting reflexIMV intermittent mandatory ventilationIPPV intermittent positive pressure ventilationIRV inspiratory reserve volumei.v. intravenouskg kilograml literLMA laryngeal maskMAC minimal alveolar concentrationMAP mean arterial pressuremin minuteml millilitermmHg millimeters of mercuryMV minute volumeN2O nitrous oxideNB newbornNiBP non-invasive blood pressureO2 oxygenOD outside diameterpaCO2 partial pressure of carbon dioxide in the
arterial bloodpaO2 partial pressure of oxygen in the arterial
bloodPAW airway pressurePCV pressure-controlled ventilationPEEP positive end-expiratory pressurepH a measure of the concentration of hydrogen
ions in a substance or solution, whichdenotes the degree to whichthe substance is acidicor alkaline (basic)
PIP peak inspiratory pressure
Abbreviations
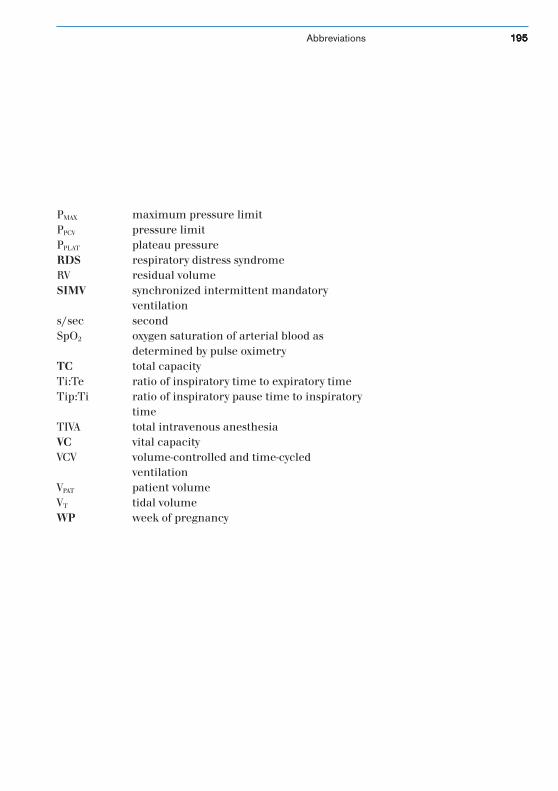
Ventilation in Pediatric Anesthesia 195195195195195
PMAX maximum pressure limitPPCV pressure limitPPLAT plateau pressureRDS respiratory distress syndromeRV residual volumeSIMV synchronized intermittent mandatory
ventilations/sec secondSpO2 oxygen saturation of arterial blood as
determined by pulse oximetryTC total capacityTi:Te ratio of inspiratory time to expiratory timeTip:Ti ratio of inspiratory pause time to inspiratory
timeTIVA total intravenous anesthesiaVC vital capacityVCV volume-controlled and time-cycled
ventilationVPAT patient volumeVT tidal volumeWP week of pregnancy
Abbreviations
196196196196196 Ventilation in Pediatric Anesthesia
9. Index
ALICE 21, 104, 166alveolar ventilation 21, 73, 76, 169, 172Ambu-Paedi System 86anesthetic agent 44, 46-48, 132, 137anesthetic agent measuring 108, 127anesthetic agent uptake 102, 109, 130Ayre T-piece 85, 131Bain System 79, 84, 85balance of water 89blood pressure 30, 100, 115, 116, 131blood volume 30body temperature 24, 32, 34breathing gas conditioning 113, 135, 142, 148breathing gas humidifier 144-146, 148capnography 98, 120-123, 130, 131Cato 85, 92, 94, 99, 106, 131, 133Cicero EM 85, 92, 94, 99, 106, 131, 133, 134closing volume 20, 75complete rebreathing system (closed system) 89compliance 16, 17-18, 61, 67, 68, 73, 76, 91, 97compliance compensation 91, 96, 97, 106, 133dead space volume 19, 54, 79, 98, 122, 177, 182desflurane 39, 40, 43, 44Disoprivan 49ductus botalli 27, 28electrocardiography (ECG) 100, 108, 118, 119, 131electrolyte 35enflurane 38, 39, 42, 44extrapulmonary oxygen toxicity 26, 110FiO2 74, 77, 108, 131foramen ovale 27, 28fresh-gas decoupler 93, 94, 95, 106, 133functional residual capacity (FRC) 20, 23, 75, 162halothane 32, 39, 40, 41, 44, 118
Ventilation in Pediatric Anesthesia 197197197197197Index
heart 27, 29, 75, 118heart rate 29,32,118,119heatable hoses 149, 180-182heat and moisture exchanger (HME) 146-148, 150, 182hemoglobin 31, 111, 112hypoxia 15, 24, 27, 112I:E ratio 74inspiratory flow 61, 67, 72, 76, 92, 106intermittent mandatory ventilation (IMV) 165intermittent positive pressure ventilation (IPPV) 91, 106, 168, 169intravenous anesthesia 49isoflurane 32, 38, 39, 42, 44Jackson-Rees 79, 81Julian 85, 92, 94, 99, 106, 127, 131, 133Kuhn System 79, 82, 85, 89, 130laryngeal mask (LMA) 54, 185-192leakage 55, 64, 91, 96, 104, 106, 133low-flow anesthesia 132-135, 137malignant hypothermia 50, 51, 105, 120manual ventilation 85, 90-91mask 54, 89, 98measuring body temperature 113measuring FiO2 128mechanical ventilation 61, 90mechanics of ventilation 17minimal alveolar concentration (MAC) 39, 127minute volume (MV) 74, 87, 94, 120, 122muscle relaxant 51nitrous oxide 40, 41non-rebreathing system 78, 79, 85, 86, 88, 123, 130oxygen-binding curve 110-112oxygen consumption 24, 32, 113
198198198198198 Ventilation in Pediatric AnesthesiaIndex
oxygen toxicity 26oxygen uptake 129partial rebreathing system 87PhysioFlex 89, 92, 102-106, 109, 129, 130positive end-expiratory pressure (PEEP) 21, 67, 75, 92, 104, 167, 170pressure-controlled ventilation (PCV) 64-72, 77, 106, 133, 149, 168,178, 179pressure limit 76, 77Propofol 49pulmonary volume 19pulse oximetry 26, 108, 110-112rebreathing system 87-88, 130regulating body temperature 32resistance 22, 61respiratory rate 21-22, 73, 77, 89, 93, 98, 106, 123respiratory resistance 22retinopathy of prematurity 26, 110sevoflurane 39, 40, 42, 44, 46soda lime 45-48, 120stethoscope 108, 109, 130surfactant 18, 23, 161, 169synchronized intermittent mandatory ventilation (SIMV) 63, 106tidal volume 19, 22, 67, 73, 94, 96, 146, 179time constant 137total intravenous anesthesia (TIVA) 50tube 55-57, 134ventilation control 15ventilation parameter 73volumetry 108, 126, 131xenon 43

Ventilation in Pediatric Anesthesia 199199199199199Stichworte

200200200200200 Ventilation in Pediatric Anesthesia
Dräger Medizintechnik GmbHMoislinger Allee 53 - 55D-23542 LübeckTel. +49 451 8 82 - 34 75Fax +49 451 8 82 - 27 93http://www.draeger.com
90 9
7 53
5 •
L/L
/040
0D •
Pri
nted
in G
erm
any
• Ä
nder
unge
n vo
rbeh
alte
n! •
chl
orfr
ei –
um
wel
tfre
undl
ich
As of August 2015:Dräger Medical GmbH changes to Drägerwerk AG & Co. KGaA.
Dräger Medical GmbH