anesthesia information management systems: past, present, and future of anesthesia records
TRANSCRIPT

MOUNT SINAI JOURNAL OF MEDICINE 79:154–165, 2012 154
Anesthesia Information ManagementSystems: Past, Present, and
Future of Anesthesia RecordsBassam Kadry, MD,1 William W. Feaster, MD, MBA,1 Alex Macario, MD, MBA,1
and Jesse M. Ehrenfeld, MD, MPH2
1Stanford University School of Medicine, Stanford, CA2Vanderbilt University, Nashville, TN
OUTLINE
ORIGINS OF ANESTHESIA RECORD
BENEFITS OF ANESTHESIA INFORMATION
MANAGEMENT SYSTEMS AS PUBLISHED IN
PEER-REVIEWED JOURNALS
ANESTHESIA INFORMATION MANAGEMENT SYSTEMS’INFLUENCE ON PERIOPERATIVE DOCUMENTATION
AND PATIENT COMMUNICATION
HEALTHCARE INFORMATION TECHNOLOGY AND
DOWNSIDE OF POOR SYSTEMS DESIGN
CONSUMER TECHNOLOGIES: RAISING EXPECTATIONS
FOR ANESTHESIA INFORMATION MANAGEMENT
SYSTEMS
ANESTHESIA INFORMATION MANAGEMENT SYSTEMS:
HELPING CLINICIANS CONVERT DATA INTO
KNOWLEDGE
UTILIZING ANESTHESIA INFORMATION MANAGEMENT
SYSTEMS FOR COMPARATIVE EFFECTIVENESS AND
TRANSLATIONAL RESEARCH
CHALLENGES OF USING ANESTHESIA INFORMATION
MANAGEMENT SYSTEMS DATA FOR ANALYSIS
CONCLUSION
Address Correspondence to:
Jesse EhrenfeldCenter for Evidence-Based Anesthesia
Vanderbilt UniversityNashville, TN
Email: [email protected]
ABSTRACT
Documenting a patient’s anesthetic in the medicalrecord is quite different from summarizing an officevisit, writing a surgical procedure note, or record-ing other clinical encounters. Some of the biggestdifferences are the frequent sampling of physiologicdata, volume of data, and diversity of data collected.The goal of the anesthesia record is to accuratelyand comprehensively capture a patient’s anestheticexperience in a succinct format. Having ready accessto physiologic trends is essential to allowing anesthe-siologists to make proper diagnoses and treatmentdecisions. Although the value provided by anesthesiainformation management systems and their func-tions may be different than other electronic healthrecords, the real benefits of an anesthesia informa-tion management system depend on having it fullyintegrated with the other health information technolo-gies. An anesthesia information management systemis built around the electronic anesthesia record andincorporates anesthesia-relevant data pulled fromdisparate systems such as laboratory, billing, imag-ing, communication, pharmacy, and scheduling. Theability of an anesthesia information managementsystem to collect data automatically enables anes-thesiologists to reliably create an accurate record atall times, regardless of other concurrent demands.These systems also have the potential to convertlarge volumes of data into actionable informationfor outcomes research and quality-improvement ini-tiatives. Developing a system to validate the datais crucial in conducting outcomes research usinglarge datasets. Technology innovations outside ofhealthcare, such as multitouch interfaces, near-instantsoftware response times, powerful but simple search
Published online in Wiley Online Library (wileyonlinelibrary.com).DOI:10.1002/msj.21281
© 2012 Mount Sinai School of Medicine

MOUNT SINAI JOURNAL OF MEDICINE 155
capabilities, and intuitive designs, have raised thebar for users’ expectations of health informationtechnology. Mt Sinai J Med 79:154–165, 2012. ©2012 Mount Sinai School of Medicine
Key Words: anesthesia information managementsystems, electronic medical record, operating roommanagement, outcomes research.
Although the traditional paper anesthesia record hasa unique format and structure that is generally ac-cepted by anesthesiologists, it may be challenging to
The goal of the anesthesia recordis to capture a patient’s response toanesthesia and surgery byrecording the procedures,physiologic changes, key events,and pharmacologicadministration that occurthroughout the perioperativeperiod.
understand for those not accustomed to its particularlayout. Documentation of a patient’s anesthetic isquite different from the documentation associatedwith an office visit or surgical procedure. Ultimately,the goal of the anesthesia record is to capturea patient’s response to anesthesia and surgery byrecording the procedures, physiologic changes, keyevents, and pharmacologic administration that occurthroughout the perioperative period.
ORIGINS OF ANESTHESIA RECORD
The paper anesthesia record has not changedfundamentally since its earliest inception in the 1890sby Dr Harvey Williams Cushing and Dr Ernest AmoryCodman (Figure 1).1,2 At the time, they documentedall the signs they could measure: pulse, temperature,and respirations. Their instinct to quantify theirefforts to help manage the patient is an importantprinciple–optimal management depends on accuratemeasurement.3–5 Since then, the anesthesia recordhas evolved to incorporate physiologic metricsmeasured by newer technologies (eg, pulse oximetry,end-tidal carbon dioxide [CO2]). However, the
A B
Fig 1. Ether chart and a modern-day anesthetic record. (A) The original Harvey Cushing Ether Chart from 1895.(B) Modern-day paper anesthesia record. Note the similarities in the metrics measured and in the layout of the2 documents. (Harvey Cushing Ether Chart courtesy of Massachusetts General Hospital Archives and SpecialCollections.)
DOI:10.1002/MSJ

156 B. KADRY ET AL.: ANESTHESIA INFORMATION MANAGEMENT SYSTEMS
original format remained unchanged: a longitudinalrecord of physiologic and pharmacologic data alongwith fundamental patient demographic information,anesthetic procedures, and key surgical or anestheticevents.
There is no other clinical setting in which suchan abundance of physiologic and pharmacologicdata is collected minute-to-minute. The hyperacuteperioperative environment necessitates such attentionto detail, given that a patient’s clinical conditioncan change within seconds. As with all patient datacollection, the sampling frequency of physiologicdata is dependent on the rate of change of thepatient’s clinical condition. The more critical thecondition, the more important it is to have a highersampling frequency of meaningful data such as vitalsigns, key laboratory values, or neurologic data (eg,pupil size).
There is no other clinical settingin which such an abundanceof physiologic and pharmacologicdata is collectedminute-to-minute.
Often during anesthesia, providers do not havesufficient time to confirm a diagnosis prior to makinga management decision. For example, if a patient has
Having ready access to physiologictrends (ie, a sudden decrease insaturation of peripheral oxygencoupled with an increase in peakairway pressures) and metrics isessential to allowinganesthesiologists to make properdiagnoses and treatmentdecisions.
an intraoperative pneumothorax, there may not beenough time to obtain a chest radiograph to confirmthe diagnosis. The anesthesiologist must assessincreased airway pressures, tachycardia, hypotension,and decreased breath sounds and proceed with chest-tube insertion if needed. Making the right treatmentdecision depends on making the correct diagnosisthrough clinical interpretation of the available data.Therefore, having ready access to physiologic trends(ie, a sudden decrease in saturation of peripheraloxygen [SpO2] coupled with an increase in peakairway pressures) and metrics is essential to allowing
anesthesiologists to make proper diagnoses andtreatment decisions. In addition to serving asofficial documentation of the anesthetic provided,the anesthesia record is designed to illustrate trendsgraphically, thereby making changes over time moreobvious to the clinician.
Anesthesia providers routinely monitor thefollowing continuous and frequently obtained metricsand waveform data:
• Heart rate.• Pulse oximetry.• Blood pressure.• Electrocardiogram.• End-tidal CO2.• Respiratory rate.• Airway pressure.• Tidal volume.• Temperature.• Volatile anesthetic concentration.• Central venous pressure.• Pulmonary artery pressure.
Although the paper anesthesia record hasserved well as a structure to temporally capturelarge amounts of physiologic, pharmacologic, andprocedure data, it has a number of limitations3,6–8:
• Recall bias occurs because the anesthesiologistcannot simultaneously write down the vital signsand deliver care to the patient. This limits therecord’s accuracy and can result in smoothing ofvital-sign data.
• Data can only be queried for outcomes research orquality-assurance purposes through manual chartreview.
• Records are often illegible or difficult to read.• Records may be lost or be otherwise inaccessible.• Incomplete documentation can limit charge
capture and billing opportunities.• Less medicolegal protection.
Anesthesia information management systems(AIMS) solve many of these problems. An AIMSinterfaces with multiple systems, but at its coreis the automated electronic anesthesia record. Anautomated anesthesia record allows for the collectionof physiologic data on a longitudinal record. AnAIMS is built around the electronic anesthesia recordand incorporates anesthesia-relevant data pulled fromdisparate systems within the hospital enterprise,such as laboratory, billing, imaging, communication,pharmacy, and scheduling systems. In additionto serving as an information hub for anesthesiaproviders, it allows for the documentation of key
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 157
perioperative events (eg, ‘‘incision,’’ ‘‘aortic cross-clamp,’’ or ‘‘end of procedure’’) to ultimately reflectthe patient’s entire procedural course.
An anesthesia informationmanagement system is builtaround the electronic anesthesiarecord and incorporatesanesthesia-relevant data pulledfrom disparate systems within thehospital enterprise, such aslaboratory, billing, imaging,communication, pharmacy, andscheduling systems.
The documentation of physiologic metrics bycomputers has been utilized since the 1970s.9 Themost obvious benefit of an automated anesthesiarecord is the ability to free up the anesthesia providerfrom manually transcribing physiologic and ventilatordata.10 Not only is the quality of data more accurate,
The most obvious benefit of anautomated anesthesia record isthe ability to free up the anesthesiaprovider from manuallytranscribing physiologic andventilator data. The ability of ananesthesia informationmanagement system to collectdata automatically enablesanesthesiologists to reliably createan accurate record at all times,regardless of the concurrentdemands on the provider.
but also it can be seamlessly recorded in real timeduring clinically sensitive times such as induction,emergence, resuscitation, and stabilization. Manualrecall and documentation of physiologic metrics onpaper records is inaccurate.11–14 Furthermore, duringtimes of clinical instability, requirements for patientcare often prohibit the manual transcription of data.However, the ability of an AIMS to collect dataautomatically enables anesthesiologists to reliablycreate an accurate record at all times, regardless ofthe concurrent demands on the provider. Finally, thismore accurate and complete measurement in many
cases results in better management. This is true forboth the individual care of patients as well as themanagement of entire operating suites. As a result,AIMS have gained significant importance because oftheir potential to improve operating-room efficiency,quality, and safety.6,15–18
BENEFITS OF ANESTHESIAINFORMATION MANAGEMENT
SYSTEMS AS PUBLISHED INPEER-REVIEWED JOURNALS
Anesthesia information management systems havebeen shown to have benefits in 7 key areas:
• Improved cost containment.• Improved operations management.• Improved reimbursement.• Improved quality of care.• Improved safety.• Improved translational research.• Improved documentation.
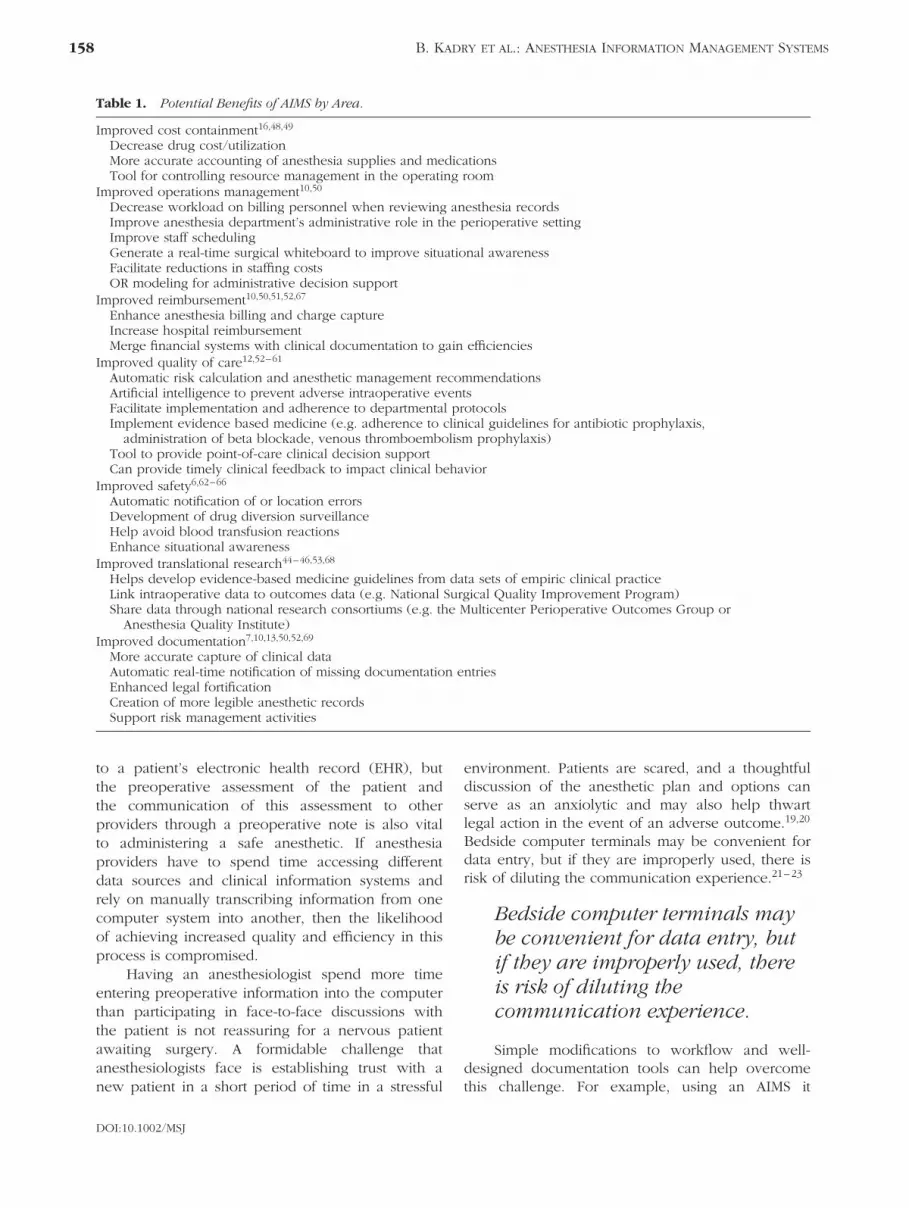
Each benefit depends on the particular perspective ofthe AIMS end user. The most obvious benefit to front-line clinicians is the automatic collection of vital signs,so that the anesthesiologist can focus on patient careduring sensitive times such as induction, emergence,and stabilization. To a departmental manager, anAIMS can help improve operations, scheduling,staffing, or even billing collections. For a quality-improvement officer, an AIMS can serve as a robustplatform for continuous quality improvement. Finally,the contemporaneous and objective physiologic datacaptured by an automated anesthesia record mayprovide a more credible medicolegal defense thana handwritten record generated by the anesthesiaprovider after the fact when an adverse outcomehas occurred. Table 1 outlines the potential benefitsof AIMS as demonstrated in the peer-reviewedliterature.
ANESTHESIA INFORMATIONMANAGEMENT SYSTEMS’
INFLUENCE ON PERIOPERATIVEDOCUMENTATION AND
PATIENT COMMUNICATION
A well-designed preoperative assessment tool isanother important aspect of anesthesia care. Not onlydoes it link preoperative anesthesia documentation
DOI:10.1002/MSJ
158 B. KADRY ET AL.: ANESTHESIA INFORMATION MANAGEMENT SYSTEMS
Table 1. Potential Benefits of AIMS by Area.
Improved cost containment16,48,49
Decrease drug cost/utilizationMore accurate accounting of anesthesia supplies and medicationsTool for controlling resource management in the operating room
Improved operations management10,50
Decrease workload on billing personnel when reviewing anesthesia recordsImprove anesthesia department’s administrative role in the perioperative settingImprove staff schedulingGenerate a real-time surgical whiteboard to improve situational awarenessFacilitate reductions in staffing costsOR modeling for administrative decision support
Improved reimbursement10,50,51,52,67
Enhance anesthesia billing and charge captureIncrease hospital reimbursementMerge financial systems with clinical documentation to gain efficiencies
Improved quality of care12,52–61
Automatic risk calculation and anesthetic management recommendationsArtificial intelligence to prevent adverse intraoperative eventsFacilitate implementation and adherence to departmental protocolsImplement evidence based medicine (e.g. adherence to clinical guidelines for antibiotic prophylaxis,
administration of beta blockade, venous thromboembolism prophylaxis)Tool to provide point-of-care clinical decision supportCan provide timely clinical feedback to impact clinical behavior
Improved safety6,62–66
Automatic notification of or location errorsDevelopment of drug diversion surveillanceHelp avoid blood transfusion reactionsEnhance situational awareness
Improved translational research44–46,53,68
Helps develop evidence-based medicine guidelines from data sets of empiric clinical practiceLink intraoperative data to outcomes data (e.g. National Surgical Quality Improvement Program)Share data through national research consortiums (e.g. the Multicenter Perioperative Outcomes Group or
Anesthesia Quality Institute)Improved documentation7,10,13,50,52,69
More accurate capture of clinical dataAutomatic real-time notification of missing documentation entriesEnhanced legal fortificationCreation of more legible anesthetic recordsSupport risk management activities
to a patient’s electronic health record (EHR), butthe preoperative assessment of the patient andthe communication of this assessment to otherproviders through a preoperative note is also vitalto administering a safe anesthetic. If anesthesiaproviders have to spend time accessing differentdata sources and clinical information systems andrely on manually transcribing information from onecomputer system into another, then the likelihoodof achieving increased quality and efficiency in thisprocess is compromised.
Having an anesthesiologist spend more timeentering preoperative information into the computerthan participating in face-to-face discussions withthe patient is not reassuring for a nervous patientawaiting surgery. A formidable challenge thatanesthesiologists face is establishing trust with anew patient in a short period of time in a stressful
environment. Patients are scared, and a thoughtfuldiscussion of the anesthetic plan and options canserve as an anxiolytic and may also help thwartlegal action in the event of an adverse outcome.19,20
Bedside computer terminals may be convenient fordata entry, but if they are improperly used, there isrisk of diluting the communication experience.21–23
Bedside computer terminals maybe convenient for data entry, butif they are improperly used, thereis risk of diluting thecommunication experience.
Simple modifications to workflow and well-designed documentation tools can help overcomethis challenge. For example, using an AIMS it
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 159
is possible to automatically send preoperativeinformation to the anesthesia provider assigned tothe case the night before. Another possibility is to usemobile devices to enhance acquisition and transfer ofpatient information. This is helpful, because one ofthe easiest methods anesthesiologists can use to helpalleviate patient anxiety is to convey prior knowledgeof the patient’s history during the initial encounter,and this can be facilitated by an AIMS.24–26
HEALTHCARE INFORMATIONTECHNOLOGY AND DOWNSIDE OF
POOR SYSTEMS DESIGN
The move to adopt ‘‘paperless’’ hospital informationsystems that create an EHR is prevalent in today’shealthcare environment. However, the informationoverload that these electronic records can generatecan also create an obstacle to achieving the goal thatthe EHR was intended to address in the first place:to improve the quality of care and patient safety.27,28
Furthermore, increased regulation to improve qualityhas paradoxically taken valuable resources awayfrom direct patient care and shifted them towardfulfilling administrative mandates to be consideredcompliant with regulatory bodies.
The preoperative anesthesia note can suffer thesame fate as other electronic documents within thepatient’s chart. Even though healthcare informationtechnology (HIT) is proposed to be a solution toan inefficient paper-based system, the reality is thatone computer keystroke can generate volumes ofclinically irrelevant information. Scrolling for pageson a computer screen that takes a few minutesto log into in a time-sensitive environment can beas much of a barrier to achieving quality care assifting through piles of paper. At least handwrittennotes, when legible and available, focus on pertinentinformation and can be written immediately. Thisproblem is exacerbated when the electronic chart hasto be printed for transfer of care to another clinician,service, or institution. Interoperability in theory isable to address this issue28; however, very fewsystems today are truly interoperable. Nonetheless,if HIT is to succeed, especially in the area of providerdocumentation, it must improve the natural clinicalworkflow and take into account human factors thatinfluence access to clinically relevant information.The hope is that HIT will ultimately enable cliniciansto make better decisions at the point of care byhaving faster, easier, and more complete access topertinent patient information. However, simply being
paperless does not equate to providing more efficientaccess to information.
Scrolling for pages on a computerscreen that takes a few minutes tolog into in a time-sensitiveenvironment can be as much of abarrier to achieving quality careas sifting through piles of paper.Thus, being paperless does notequate to providing more efficientaccess to information.
CONSUMER TECHNOLOGIES:RAISING EXPECTATIONS FORANESTHESIA INFORMATION
MANAGEMENT SYSTEMS
A usability gap exists between HIT and technologyin other industries.29–35 Human-factors engineeringtakes into account human capabilities in the designof a new technology.36–38 The discipline is buildingtraction in the technology industry, where theconsumer experience defines the success of theproduct or service. Novel innovations such asmultitouch interfaces, near-instant software responsetimes, powerful but simple search capabilities, andintuitive designs have raised the bar for users’expectations of technology. As AIMS evolve, itis likely that this gap will narrow and morerobust functional elements will be adopted. Thechallenge will be integrating various technologiesinto the overall AIMS architectures. Some future AIMSenhancements may include:
• Automatic escalation of care notifications forextremes in physiologic metrics.
• Automatic customized reports of outcomes ofinterest to authorized clinicians.
• Automatic risk stratification of patients based onknown risk factors.
• Automatic quality-assurance screening and report-ing.
• Use of color, text size, and stylized text featuresto distinguish computer-populated data frominformation manually entered by clinicians.
• Dynamic user interfaces that adjust based on datainputs.
• More usable output of printed anesthetic records.• Easy-to-use Web-based data warehouse queries by
authorized clinicians.
DOI:10.1002/MSJ

160 B. KADRY ET AL.: ANESTHESIA INFORMATION MANAGEMENT SYSTEMS
Knowledge Pyramid
Fig 2. Knowledge Pyramid illustrates how clinical data is converted into actionableinformation to treat a life-threatening intraoperative pneumothorax. Abbreviations:ACS, acute coronary syndrome; BP, blood pressure; Ddx, differential diagnosis; HR,heart rate; O2Sat, oxygen saturation; PAP, peak airway pressure; PTX, pneumothorax;RR, respiratory rate.
• Informed consent applications that can be accessedby patients at home or from bedside terminals.
• Integration of AIMS with hospital communicationsystems.
• Provision of digital files of anesthetic care that canbe uploaded into a personal health record.
• Real-time cost tabulation of anesthetic case.• Real-time handheld remote monitoring and
reporting.• Real-time location systems for tracking of patients,
clinicians, and equipment.• Web-based preoperative interview applications.
ANESTHESIA INFORMATIONMANAGEMENT SYSTEMS:
HELPING CLINICIANS CONVERTDATA INTO KNOWLEDGE
Converting data into action is a process that hasbeen extensively studied in other information-sciencedisciplines.18,39–43 Clinicians utilize the principlesbehind the ‘‘Knowledge Pyramid’’ when derivinga differential diagnosis and management strategy.Figure 2 illustrates how this principle is used tomanage an intraoperative pneumothorax.
Data are the foundation for knowledge.However, data by definition are without context and
are only useful if they are converted to information.Knowing how to use the information depends onappropriate knowledge structure. Ultimately, with
Data by definition are withoutcontext and are only useful if theyare converted to information.
experience, wise users of information know howto use data efficiently and effectively. So in theexample of a pneumothorax (Figure 2), one can seehow the data elements can be used to first assessthe clinical situation, then determine a diagnosis ofhighest likelihood and initiate appropriate treatment.
In anesthesia, the process of converting datainto knowledge is continuous and is the basis ofvigilant anesthetic care. Often, data are collected andin the process more data are needed to determinewhether a patient is safe or in danger. For example,in Figure 3, the patient’s heart rate is 135 beats perminute with a systolic blood pressure of 65 mmHg. While this may seem ominous, a key pieceof data is missing: the patient’s age. This exampleillustrates the importance of each data element. Inparticular, it shows how knowledge and wisdom helprefine which data elements are pertinent or irrelevantwhen determining an action plan. As EMRs becomemore prevalent, the new challenge will be converting
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 161
Fig 3. Utilizing data to drive action. Abbreviations: DBP, diastolic bloodpressure; ETCO2, end-tidal carbon dioxide; ETSev, end-tidal concentration ofsevoflurane; HR, heart rate; PAWP, peak airway pressure; Sat%, saturationpercentage; SBP, systolic blood pressure; Vt, tidal volume.
large volumes of data into meaningful information.Ultimately, the approach to doing so will utilize thesame principles behind the Knowledge Pyramid.
UTILIZING ANESTHESIAINFORMATION MANAGEMENT
SYSTEMS FORCOMPARATIVE EFFECTIVENESS AND
TRANSLATIONAL RESEARCH
The wealth of data stored in AIMS can offer insightinto the efficacy of perioperative care, and severalnational efforts have attempted to leverage this capa-bility. The American College of Surgeons recognizedthis potential and partnered with the AnesthesiaPatient Safety Foundation to study the feasibility ofincluding perioperative AIMS data into the Ameri-can College of Surgeons National Surgical QualityImprovement Program.44 These data would link thepreoperative patient risk factors, surgical factors, andadverse events following surgery. The technical chal-lenge of communicating both datasets is profound.Linking both records depends on using interoperabil-ity standards such as Systematized Nomenclature ofMedicine–Clinical Terms (SNOMED CT) and HealthLevel 7 Working Group for Generation of Anes-thesia Standards (HL7 WG GAS), as demonstratedby Walsh et al.44 The Multicenter Perioperative Out-comes Group based at the University of Michiganaggregates deidentified AIMS data from multiple insti-tutions to create a powerful research database.45,46
The American Society of Anesthesiologists, through
its Anesthesia Quality Institute (AQI), has also cre-ated a data warehouse to collect anesthesia dataand claims data, though often currently derived frombilling claims data and paper medical records ratherthan from an AIMS. Both organizations are workingtogether to import AIMS data directly into the AQIdata warehouse.
The benefit of aggregated AIMS data, as opposedto other clinical data, is its accuracy, granularity, andsheer volume. Such efforts to combine AIMS datafrom across institutions can help utilize the large vol-umes of available data to determine targets for futureresearch. The difficulty is delineating which anec-dotal methodologies are efficacious. The discoveryprocess is resource-intensive and time-consuming.Moreover, research funding is becoming more lim-ited. Therefore, organizations like the MulticenterPerioperative Outcomes Group or the AQI that cre-ate tools to assess relationships through queries oflarge datasets can guide researchers to targets worthyof exploration. The quicker the process, the fasteranecdotal information can be proven ineffective orbe incorporated as evidence-based medicine.
CHALLENGES OFUSING ANESTHESIA INFORMATIONMANAGEMENT SYSTEMS DATA FOR
ANALYSIS
There are several limitations of using any large datasetfor robust analytics. Sometimes important informationmay be hard to quantify and is consequently
DOI:10.1002/MSJ

162 B. KADRY ET AL.: ANESTHESIA INFORMATION MANAGEMENT SYSTEMS
overlooked.47 For data that are measured, confirmingtheir validity is important, because decisions based oninaccurate data can have bad consequences. Creatinga system of checks and balances to purge falsedata is essential to minimize poor data analysis. Forexample, if a pulse oximetry reading is 75% but thepulse oximetry waveform is poor, blood pressure isnormal, end-tidal CO2 is normal, and there is nochange in ventilation, then it is very likely that thepulse oximeter reading is artifactual 1. Whereas ina clinical situation this seems obvious, to a researchanalyst without the benefit of a clinical context it maynot.
Developing a system to validate data is thereforean important step in conducting outcomes researchusing large datasets. Another significant challenge forlarge datasets is that the distribution of data shouldideally represent the population at large, or at leastthe population of interest.
Developing a system to validatedata is an important step inconducting outcomes researchusing large datasets. Anothersignificant challenge for largedatasets is that the distributionof data should ideally representthe population at large, or at leastthe population of interest.
The validation process may take time but isimportant for further studies to be conducted usinga subset of the data. For example, the distributionof the age of patients in the dataset should resemblethe distribution of the entire population. Otherwise,the application of new insights as to how tooptimally treat patients as derived from the datasetmay not be applicable to the population at large.Confirming that the dataset is valid will help assessthe generalizability of outcomes research using largedatasets.
Identifying thresholds or definitions is verychallenging when conducting retrospective outcomesresearch. For example, troponin levels are a goodindicator of a myocardial event; but intraoperatively,anesthesiologists do not typically use this informationbecause they must act immediately. Anesthesiologistsoften do not have the time to wait for a laboratoryvalue, but they do have echocardiograms andother vital signs that can be used to establish adiagnosis and guide therapy. However, troponinlevels are often used to quantify whether or not
Table 2. Principles for Meaningful Outcomes Research70,71
Comprehensive data collectionValidation of dataClear definition of outcomes of interest (defined
numerators)Comprehensive collection of entire population (verified
denominators)Accurate relational mappingLogical and reproducible analysis
a patient had a myocardial event. Therefore, anintraoperative myocardial event may be difficultto ‘‘catch’’ retrospectively using an AIMS recordexclusively. More creative means to ‘‘catch’’ anevent may depend on a temporal mapping ofheart rate, blood pressure, electrocardiographicchanges, beta-blocker or nitroglycerin administration,or cardiology consultation in recovery. Moreover,the integration of the AIMS record with data froman inpatient laboratory system might help link asurgery with a myocardial event by evaluationfor increased troponin levels in the postoperativeperiod. Anesthesia information management systemsthat are part of a complete enterprise suiteoffer a compelling value proposition due to theirability to capture and analyze data across all caresettings. Furthermore, even among experts, reachingconsensus on specific definitions is difficult. Thismakes it difficult when analyzing large datasets,because specific thresholds need to be identified.Meaningful outcomes research requires agreementon the process of data collection, data validation,and clear definitions of outcomes, as shown inTable 2.
Meaningful outcomes researchrequires agreement on the processof data collection, data validation,and clear definitions of outcomes.
CONCLUSION
Although the paper record is relatively easy touse, the potential value brought by an AIMSmoves far beyond the simple automation of thepaper anesthesia record. To achieve all of thepotential benefits of the AIMS, however, it cannotexist as a stand-alone system. It must either beintegrated within an EHR or be able to automaticallyand bidirectionally communicate with one. Theexpansion of HIT without interoperability will likelyconvert inadequate paper documentation into more
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 163
legible, but still incomplete and ineffective, digitaldocumentation. In the future, AIMS will likely bemore intuitive to use, interoperable with hospital-based EHRs, and incorporate useful tools suchas decision support. These advances will likelyreduce barriers to AIMS adoption and accelerate theiradoption.
DISCLOSURES
Potential conflict of interest: Nothing to report.
REFERENCES
1. Bruce SS, Bruce JN. Harvey Cushing, neurosurgicalpioneer. Curr Surg 2005; 62: 138–140.
2. Molnar C, Nemes C, Szabo S, et al. Harvey Cushing,a pioneer of neuroanesthesia. J Anesth 2008; 22:483–486.
3. Blumenthal D. The future of quality measurement andmanagement in a transforming health care system.JAMA 1997; 278: 1622–1625.
4. Cerese J. Leveraging performance measurement andmanagement: the quality and efficiency edge. TopHealth Inf Manage 2001; 22: 73–78.
5. Kimberly JR. Assessing ‘‘quality’’ in health care: issuesin measurement and management. Int J Qual HealthCare 1997; 9: 161–162.
6. Balust J, Macario A. Can anesthesia informationmanagement systems improve quality in the surgicalsuite? Curr Opin Anaesthesiol 2009; 22: 215–222.
7. Ehrenfeld JM. Anesthesia Information ManagementSystems: a guide to their successful installation anduse. Anesthesiol News 2009; 9: 1–7.
8. Vigoda MM, Lubarsky DA. Failure to recognize loss ofincoming data in an anesthesia record-keeping systemmay have increased medical liability. Anesth Analg2006; 102: 1798–1802.
9. Daub D, Destunis S, Halbach M, et al. First experi-ences with a documentation system via display termi-nals. Acta Anaesthesiol Belg 1975; 23(suppl): 200–204.
10. Vigoda MM, Feinstein DM. Anesthesia informationmanagement systems. Adv Anesth 2008; 26: 121–136.
11. Benson M, Junger A, Fuchs C, et al. Using ananesthesia information management system to provea deficit in voluntary reporting of adverse events in aquality assurance program. J Clin Monit Comput 2000;16: 211–217.
12. Junger A, Hartmann B, Benson M, et al. The use ofan anesthesia information management system forprediction of antiemetic rescue treatment at thepostanesthesia care unit. Anesth Analg 2001; 92:1203–1209.
13. Reich DL, Kahn RA, Wax D, et al. Developmentof a module for point-of-care charge captureand submission using an anesthesia informationmanagement system. Anesthesiology 2006; 105:179–186.
14. Sanborn KV, Castro J, Kuroda M, et al. Detectionof intraoperative incidents by electronic scanning
of computerized anesthesia records: comparisonwith voluntary reporting. Anesthesiology 1996; 85:977–987.
15. Benson M, Junger A, Fuchs C, et al. Use of ananesthesia information management system (AIMS) toevaluate the physiologic effects of hypnotic agentsused to induce anesthesia. J Clin Monit Comput 2000;16: 183–190.
16. Coleman RL, Sanderson IC, Lubarsky DA. Anesthesiainformation management systems as a cost contain-ment tool. CRNA 1997; 8: 77–83.
17. Eden A, Grach M, Goldik Z, et al. The implementationof an anesthesia information management system. EurJ Anaesthesiol 2006; 23: 882–889.
18. Ehrenfeld JM, Epstein RH, Bader S, et al. Automaticnotifications mediated by anesthesia informationmanagement systems reduce the frequency ofprolonged gaps in blood pressure documentation.Anesth Analg 2011; 113: 356–363.
19. Hickson GB, Jenkins AD. Identifying and addressingcommunication failures as a means of reducingunnecessary malpractice claims. N C Med J 2007; 68:362–364.
20. Huntington B, Kuhn N. Communication gaffes: a rootcause of malpractice claims. Proc (Bayl Univ Med Cent)2003; 16: 157–161.
21. McCord G, Pendleton BF, Schrop SL, et al. Assess-ing the impact on patient-physician interaction whenphysicians use personal digital assistants: a Northeast-ern Ohio Network (NEON) study. J Am Board FamMed 2009; 22: 353–359.
22. Anderson JG, Rainey MR, Eysenbach G. The impact ofCyberHealthcare on the physician-patient relationship.J Med Syst 2003; 27: 67–84.
23. Rouf E, Whittle J, Lu N, et al. Computers in the examroom: differences in physician-patient interaction maybe due to physician experience. J Gen Intern Med2007; 22: 43–48.
24. Klafta JM, Roizen MF. Current understanding ofpatients’ attitudes toward and preparation foranesthesia: a review. Anesth Analg 1996; 83:1314–1321.
25. Nuebling M, Kindler CH, Langewitz W. Preoperativevisits in anesthesia: communication patterns andsequences: application of an explorative analysis.Patient Educ Couns 2004; 54: 379–381.
26. Orliaguet G. Preoperative information for paediatricpatients: the anaesthesiologist’s point of view [articlein French]. Ann Fr Anesth Reanim 2006; 25:451–457.
27. Boyer L, Renaud MH, Limousin S, et al. Perceptionand use of an electronic medical record system byprofessionals of a public psychiatric hospital [article inFrench]. Encephale 2009; 35: 454–460.
28. Van Vleck TT, Stein DM, Stetson PD, et al. Assessingdata relevance for automated generation of aclinical summary. AMIA Annu Symp Proc 2007;761–765.
29. Alamantariotou K, Zisi D. Consumer health informaticsand interactive visual learning tools for health. IntJ Electron Healthc 2010; 5: 414–424.
30. Bos L, Carroll D, Marsh A. The impatient patient. StudHealth Technol Inform 2008; 137: 1–13.
DOI:10.1002/MSJ

164 B. KADRY ET AL.: ANESTHESIA INFORMATION MANAGEMENT SYSTEMS
31. Cohen SB, Grote KD, Pietraszek WE, et al. Increasingconsumerism in healthcare through intelligent infor-mation technology. Am J Manag Care 2010; 16(12suppl HIT): SP37–SP43.
32. Haselkorn A, Coye MJ, Doarn CR. The future ofremote health services: summary of an expert paneldiscussion. Telemed J E Health 2007; 13: 341–347.
33. Ho J. Consumer health informatics. Stud HealthTechnol Inform 2010; 151: 185–194.
34. Nash M, Pestrue J, Geier P, et al. Leveraging infor-mation technology to drive improvement in patientsatisfaction. J Healthc Qual 2010; 32: 30–40.
35. Valimaki M, Nenonen H, Koivunen M, et al. Patients’perceptions of Internet usage and their opportunity toobtain health information. Med Inform Internet Med2007; 32: 305–314.
36. Elrod J, Androwich IM. Applying human factorsanalysis to the design of the electronic health record.Stud Health Technol Inform 2009; 146: 132–136.
37. Pelayo S, Bernonville S, Kolski C, et al. Applying aHuman Factors Engineering approach to healthcare ITapplications: example of a medication CPOE project.Stud Health Technol Inform 2009; 143: 334–339.
38. Santiago O, Li Q, Gagliano N, et al. Improving EMRusability: a method for both discovering andprioritizing improvements in EMR workflows basedon human factors engineering. AMIA Annu Symp Proc2006; 1086.
39. Bonniface L, Green L. Finding a new kind ofknowledge on the HeartNET website. Health Info LibrJ 2007; 24(suppl 1): 67–76.
40. Fleissner P, Hofkirchner W. The making of theinformation society: driving forces, ‘Leitbilder’ and theimperative for survival. Biosystems 1998; 46: 201–207.
41. Hollander MJ, Corbett C, Pallan P. Time for a paradigmshift: managing smarter by moving from data andinformation to knowledge and wisdom in healthcaredecision-making. Healthc Q 2010; 13: 49–54.
42. Wilkinson I. Dollar$ & $en$e. Part VI: Knowledgemanagement: the state of the art. Clin Leadersh ManagRev 2001; 15: 187–189.
43. Wilkinson I. Dollar$ & $en$e. Part IV: Measuring thevalue of people, structural, and customer capital. ClinLeadersh Manag Rev 2001; 15: 45–49.
44. Walsh JL, Hurrell MJ, Wu H, et al. Mapping anesthesiarecords to standard term enables inclusion of AIMSdata in the NSQIP database. Paper presented at:American Society of Anesthesiologists Annual Meeting;October 18 , 2009; New Orleans, LA.
45. Kheterpal S. Perioperative comparative effectivenessresearch: an opportunity calling. Anesthesiology 2009;111: 1180–1182.
46. Ramachandran SK, Kheterpal S. Outcomes researchusing quality improvement databases: evolvingopportunities and challenges. Anesthesiol Clin 2011;29: 71–81.
47. Rosenzweig P. Robert S. McNamara and the evolutionof modern management. Harvard Bus Rev. December1, 2010.
48. Junger A, Benson M, Quinzio L, et al. An AnesthesiaInformation Management System (AIMS) as a tool forcontrolling resource management of operating rooms.Methods Inf Med 2002; 41: 81–85.
49. Lubarsky DA, Sanderson IC, Gilbert WC, et al. Usingan anesthesia information management system as
a cost containment tool: description and validation.Anesthesiology 1997; 86: 1161–1169.
50. Egger Halbeis CB, Epstein RH. The value propositionof anesthesia information management systems.Anesthesiol Clin 2008; 26: 665–679, vi.
51. Sandberg WS, Sandberg EH, Seim AR, et al. Real-timechecking of electronic anesthesia records for doc-umentation errors and automatically text messagingclinicians improves quality of documentation. AnesthAnalg 2008; 106: 192–201.
52. Meyer-Jark T, Reissmann H, Schuster M, et al. Realisa-tion of material costs in anaesthesia: alternatives to thereimbursement via diagnosis-related groups [article inGerman]. Anaesthesist 2007; 56: 353–365.
53. Kheterpal S, Gupta R, Blum JM, et al. Electronicreminders improve procedure documentation com-pliance and professional fee reimbursement. AnesthAnalg 2007; 104: 592–597.
54. Jost A, Junger A, Zickmann B, et al. Potential benefitsof Anaesthesia Information Management Systemsfor multicentre data evaluation: risk calculation ofinotropic support in patients undergoing cardiacsurgery. Med Inform Internet Med 2003; 28: 7–19.
55. Kheterpal S, Han R, Tremper KK, et al. Incidence andpredictors of difficult and impossible mask ventilation.Anesthesiology 2006; 105: 885–891.
56. Ramachandran SK, Kheterpal S, Haas CF, et al. Auto-mated notification of suspected obstructive sleepapnea patients to the perioperative respiratory ther-apist: a pilot study. Respir Care 2010; 55: 414–418.
57. Wax DB, Beilin Y, Levin M, et al. The effect ofan interactive visual reminder in an anesthesiainformation management system on timeliness ofprophylactic antibiotic administration. Anesth Analg2007; 104: 1462–1466.
58. Rohrig R, Junger A, Hartmann B, et al. The incidenceand prediction of automatically detected intraoperativecardiovascular events in noncardiac surgery. AnesthAnalg 2004; 98: 569–577.
59. O’Reilly M, Talsma A, VanRiper S, et al. An anesthesiainformation system designed to provide physician-specific feedback improves timely administration ofprophylactic antibiotics. Anesth Analg 2006; 103:908–912.
60. Eden A, Pizov R, Toderis L, et al. The impact ofan electronic reminder on the use of alarms afterseparation from cardiopulmonary bypass. AnesthAnalg 2009; 108: 1203–1208.
61. Kooij FO, Klok T, Hollmann MW, et al. Decisionsupport increases guideline adherence for prescribingpostoperative nausea and vomiting prophylaxis.Anesth Analg 2008; 106: 893–898.
62. Nair BG, Newman SF, Peterson GN, et al. Feedbackmechanisms including real-time electronic alerts toachieve near 100% timely prophylactic antibioticadministration in surgical cases. Anesth Analg 2010;111: 1293–1300.
63. Epstein RH, Dexter F, Piotrowski E. Automated cor-rection of room location errors in anesthesia informa-tion management systems. Anesth Analg 2008; 107:965–971.
64. Epstein RH, Gratch DM, Grunwald Z. Development ofa scheduled drug diversion surveillance system basedon an analysis of atypical drug transactions. AnesthAnalg 2007; 105: 1053–1060.
DOI:10.1002/MSJ

MOUNT SINAI JOURNAL OF MEDICINE 165
65. Jiang M, Xing B, Sun Z, et al. A dynamic bloodinformation management system based on RFID. ConfProc IEEE Eng Med Biol Soc 2005; 1: 546–549.
66. Gaba DM. Anaesthesiology as a model for patientsafety in health care. BMJ 2000; 320: 785–788.
67. Muravchick S, Caldwell JE, Epstein RH, et al. Anes-thesia information management system implemen-tation: a practical guide. Anesth Analg 2008; 107:1598–1608.
68. Kheterpal S, Woodrum DT, Tremper KK. Too muchof a good thing is wonderful: observational data
for perioperative research. Anesthesiology 2009; 111:1183–1184.
69. Ehrenfeld JM, Rehman MA. Anesthesia informationmanagement systems: a review of functionality andinstallation considerations. J Clin Monit Comput 2011;25: 71–79.
70. Chumney EC, Simpson KN. Methods and Designs forOutcomes Research. Bethesda, MD: American Societyof Health-System Pharmacists; 2006.
71. Choy YC. Critical incident monitoring in anaesthesia.Med J Malaysia 2006; 61: 577–585.
DOI:10.1002/MSJ