hstp ii hmis tools hospital, heath center and
TRANSCRIPT

HSTP II HMIS TOOLSHOSPITAL, HEATH CENTER AND HEALTH POST
Content / Home
Pastoralist Registers, CHIS register, card and Tally sheets
Health Post Tools
TB and leprosy Registers
RMNCH Registers and Tally sheets
NTD
NCD Registers and Tally sheets
MSD Registers & Tally sheets
Malaria Register
HSS
HIV Registers & Tally sheets
Health center and Hospital HMIS Tools
Contents
Health center and Hospital HMIS Tools
Content / Home
HIV Registers & Tally sheetsContent / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital ART Register
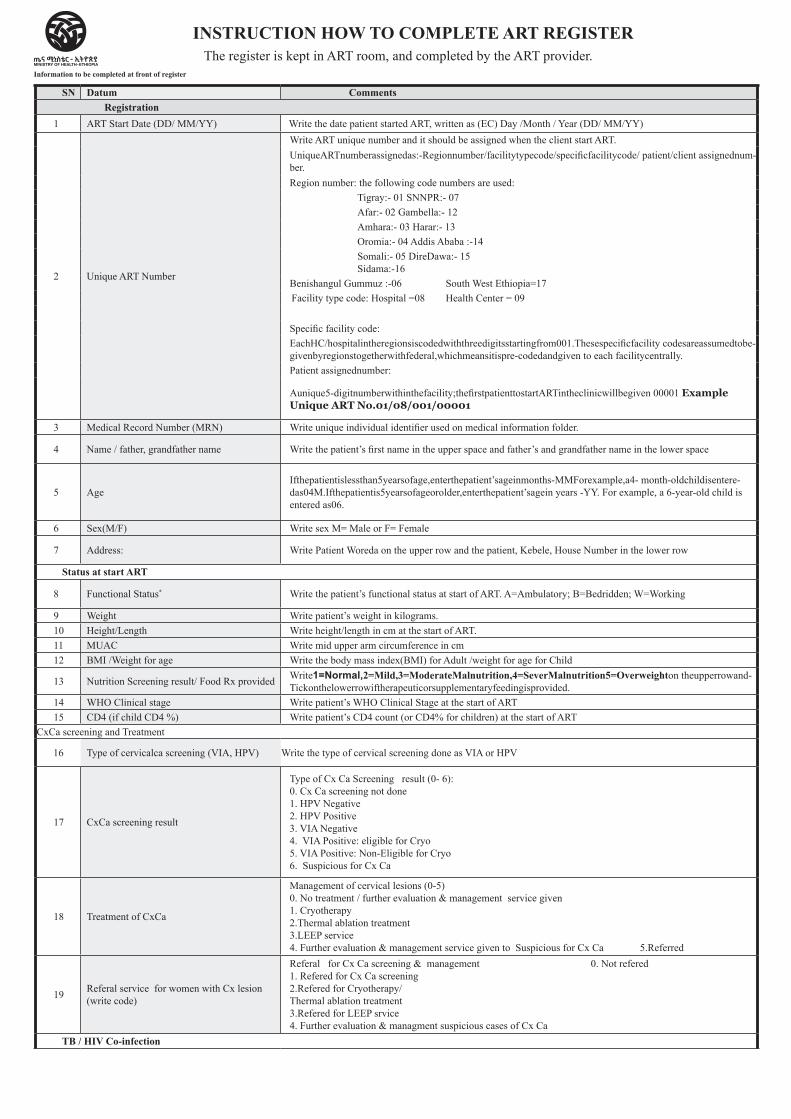
SN Datum CommentsRegistration
1 ART Start Date (DD/ MM/YY) Write the date patient started ART, written as (EC) Day /Month / Year (DD/ MM/YY)
2 Unique ART Number
Write ART unique number and it should be assigned when the client start ART.UniqueARTnumberassignedas:-Regionnumber/facilitytypecode/specificfacilitycode/ patient/client assignednum-ber.Region number: the following code numbers are used:
Tigray:- 01 SNNPR:- 07Afar:- 02 Gambella:- 12Amhara:- 03 Harar:- 13Oromia:- 04 Addis Ababa :-14Somali:- 05 DireDawa:- 15 Sidama:-16
Benishangul Gummuz :-06 South West Ethiopia=17 Facility type code: Hospital =08 Health Center = 09
Specific facility code:EachHC/hospitalintheregionsiscodedwiththreedigitsstartingfrom001.Thesespecificfacility codesareassumedtobe-givenbyregionstogetherwithfederal,whichmeansitispre-codedandgiven to each facilitycentrally.Patient assignednumber:
Aunique5-digitnumberwithinthefacility;thefirstpatienttostartARTintheclinicwillbegiven 00001 Example Unique ART No.01/08/001/00001
3 Medical Record Number (MRN) Write unique individual identifier used on medical information folder.
4 Name / father, grandfather name Write the patient’s first name in the upper space and father’s and grandfather name in the lower space
5 AgeIfthepatientislessthan5yearsofage,enterthepatient’sageinmonths-MMForexample,a4- month-oldchildisentere-das04M.Ifthepatientis5yearsofageorolder,enterthepatient’sagein years -YY. For example, a 6-year-old child is entered as06.
6 Sex(M/F) Write sex M= Male or F= Female
7 Address: Write Patient Woreda on the upper row and the patient, Kebele, House Number in the lower row
Status at start ART
8 Functional Status* Write the patient’s functional status at start of ART. A=Ambulatory; B=Bedridden; W=Working
9 Weight Write patient’s weight in kilograms.10 Height/Length Write height/length in cm at the start of ART.11 MUAC Write mid upper arm circumference in cm12 BMI /Weight for age Write the body mass index(BMI) for Adult /weight for age for Child
13 Nutrition Screening result/ Food Rx provided Write1=Normal,2=Mild,3=ModerateMalnutrition,4=SeverMalnutrition5=Overweighton theupperrowand-Tickonthelowerrowiftherapeuticorsupplementaryfeedingisprovided.
14 WHO Clinical stage Write patient’s WHO Clinical Stage at the start of ART15 CD4 (if child CD4 %) Write patient’s CD4 count (or CD4% for children) at the start of ART
CxCa screening and Treatment
16 Type of cervicalca screening (VIA, HPV) Write the type of cervical screening done as VIA or HPV
17 CxCa screening result
Type of Cx Ca Screening result (0- 6): 0. Cx Ca screening not done 1. HPV Negative 2. HPV Positive 3. VIA Negative 4. VIA Positive: eligible for Cryo 5. VIA Positive: Non-Eligible for Cryo 6. Suspicious for Cx Ca
18 Treatment of CxCa
Management of cervical lesions (0-5) 0. No treatment / further evaluation & management service given 1. Cryotherapy 2.Thermal ablation treatment 3.LEEP service 4. Further evaluation & management service given to Suspicious for Cx Ca 5.Referred
19 Referal service for women with Cx lesion (write code)
Referal for Cx Ca screening & management 0. Not refered 1. Refered for Cx Ca screening 2.Refered for Cryotherapy/ Thermal ablation treatment 3.Refered for LEEP srvice 4. Further evaluation & managment suspicious cases of Cx Ca
TB / HIV Co-infection
INSTRUCTION HOW TO COMPLETE ART REGISTERThe register is kept in ART room, and completed by the ART provider.
Information to be completed at front of register
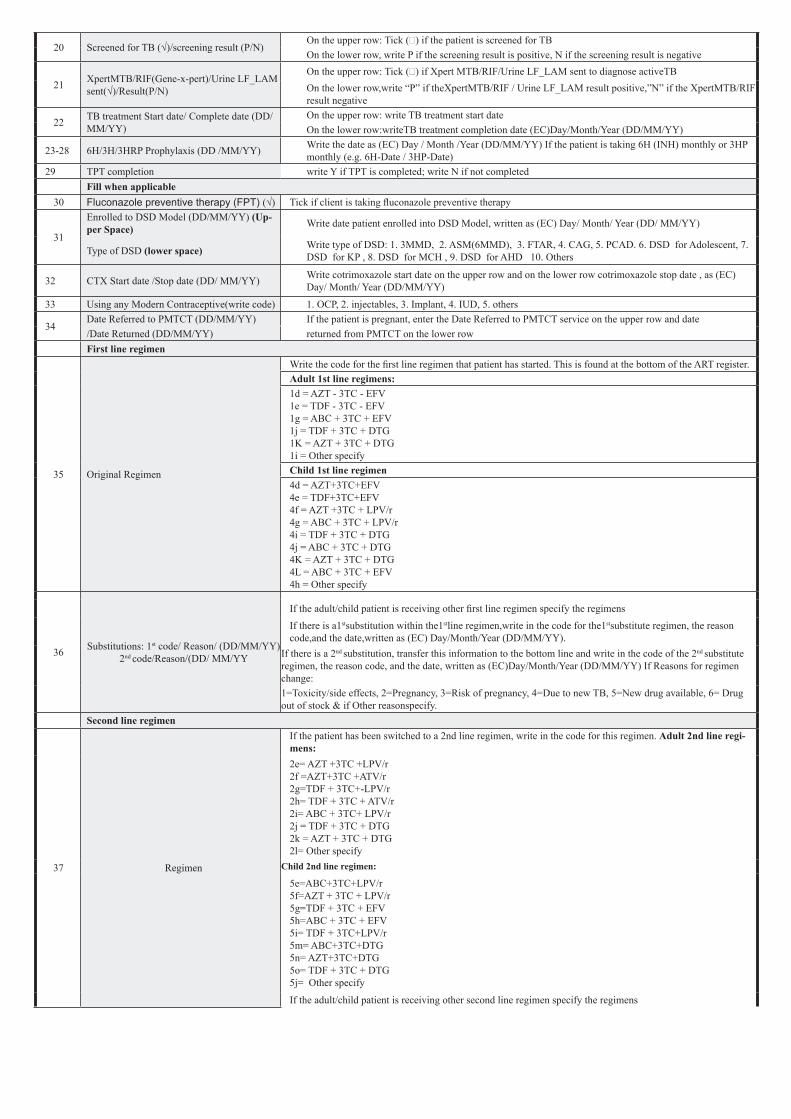
20 Screened for TB (√)/screening result (P/N)On the upper row: Tick (Ö) if the patient is screened for TBOn the lower row, write P if the screening result is positive, N if the screening result is negative
21 XpertMTB/RIF(Gene-x-pert)/Urine LF_LAM sent(√)/Result(P/N)
On the upper row: Tick (Ö) if Xpert MTB/RIF/Urine LF_LAM sent to diagnose activeTBOn the lower row,write “P” if theXpertMTB/RIF / Urine LF_LAM result positive,”N” if the XpertMTB/RIF result negative
22 TB treatment Start date/ Complete date (DD/MM/YY)
On the upper row: write TB treatment start dateOn the lower row:writeTB treatment completion date (EC)Day/Month/Year (DD/MM/YY)
23-28 6H/3H/3HRP Prophylaxis (DD /MM/YY) Write the date as (EC) Day / Month /Year (DD/MM/YY) If the patient is taking 6H (INH) monthly or 3HP monthly (e.g. 6H-Date / 3HP-Date)
29 TPT completion write Y if TPT is completed; write N if not completed Fill when applicable
30 Fluconazole preventive therapy (FPT) (√) Tick if client is taking fluconazole preventive therapy
31
Enrolled to DSD Model (DD/MM/YY) (Up-per Space) Write date patient enrolled into DSD Model, written as (EC) Day/ Month/ Year (DD/ MM/YY)
Type of DSD (lower space) Write type of DSD: 1. 3MMD, 2. ASM(6MMD), 3. FTAR, 4. CAG, 5. PCAD. 6. DSD for Adolescent, 7. DSD for KP , 8. DSD for MCH , 9. DSD for AHD 10. Others
32 CTX Start date /Stop date (DD/ MM/YY) Write cotrimoxazole start date on the upper row and on the lower row cotrimoxazole stop date , as (EC) Day/ Month/ Year (DD/MM/YY)
33 Using any Modern Contraceptive(write code) 1. OCP, 2. injectables, 3. Implant, 4. IUD, 5. others
34Date Referred to PMTCT (DD/MM/YY) If the patient is pregnant, enter the Date Referred to PMTCT service on the upper row and date/Date Returned (DD/MM/YY) returned from PMTCT on the lower rowFirst line regimen
35 Original Regimen
Write the code for the first line regimen that patient has started. This is found at the bottom of the ART register.Adult 1st line regimens:1d = AZT - 3TC - EFV 1e = TDF - 3TC - EFV 1g = ABC + 3TC + EFV 1j = TDF + 3TC + DTG 1K = AZT + 3TC + DTG 1i = Other specifyChild 1st line regimen 4d = AZT+3TC+EFV 4e = TDF+3TC+EFV 4f = AZT +3TC + LPV/r 4g = ABC + 3TC + LPV/r 4i = TDF + 3TC + DTG 4j = ABC + 3TC + DTG 4K = AZT + 3TC + DTG 4L = ABC + 3TC + EFV 4h = Other specify
36 Substitutions: 1st code/ Reason/ (DD/MM/YY) 2nd code/Reason/(DD/ MM/YY
If the adult/child patient is receiving other first line regimen specify the regimens
If there is a1stsubstitution within the1stline regimen,write in the code for the1stsubstitute regimen, the reason code,and the date,written as (EC) Day/Month/Year (DD/MM/YY).
If there is a 2nd substitution, transfer this information to the bottom line and write in the code of the 2nd substitute regimen, the reason code, and the date, written as (EC)Day/Month/Year (DD/MM/YY) If Reasons for regimen change:1=Toxicity/side effects, 2=Pregnancy, 3=Risk of pregnancy, 4=Due to new TB, 5=New drug available, 6= Drug out of stock & if Other reasonspecify.
Second line regimen
37 Regimen
If the patient has been switched to a 2nd line regimen, write in the code for this regimen. Adult 2nd line regi-mens:2e= AZT +3TC +LPV/r 2f =AZT+3TC +ATV/r 2g=TDF + 3TC+-LPV/r 2h= TDF + 3TC + ATV/r 2i= ABC + 3TC+ LPV/r 2j = TDF + 3TC + DTG 2k = AZT + 3TC + DTG 2l= Other specify
Child 2nd line regimen:
5e=ABC+3TC+LPV/r 5f=AZT + 3TC + LPV/r 5g=TDF + 3TC + EFV 5h=ABC + 3TC + EFV 5i= TDF + 3TC+LPV/r 5m= ABC+3TC+DTG 5n= AZT+3TC+DTG 5o= TDF + 3TC + DTG 5j= Other specify
If the adult/child patient is receiving other second line regimen specify the regimens
38 Switches:1stcode/Reason/(DD/MM/YY) 2nd-
code/Reason/(DD/MM/YY
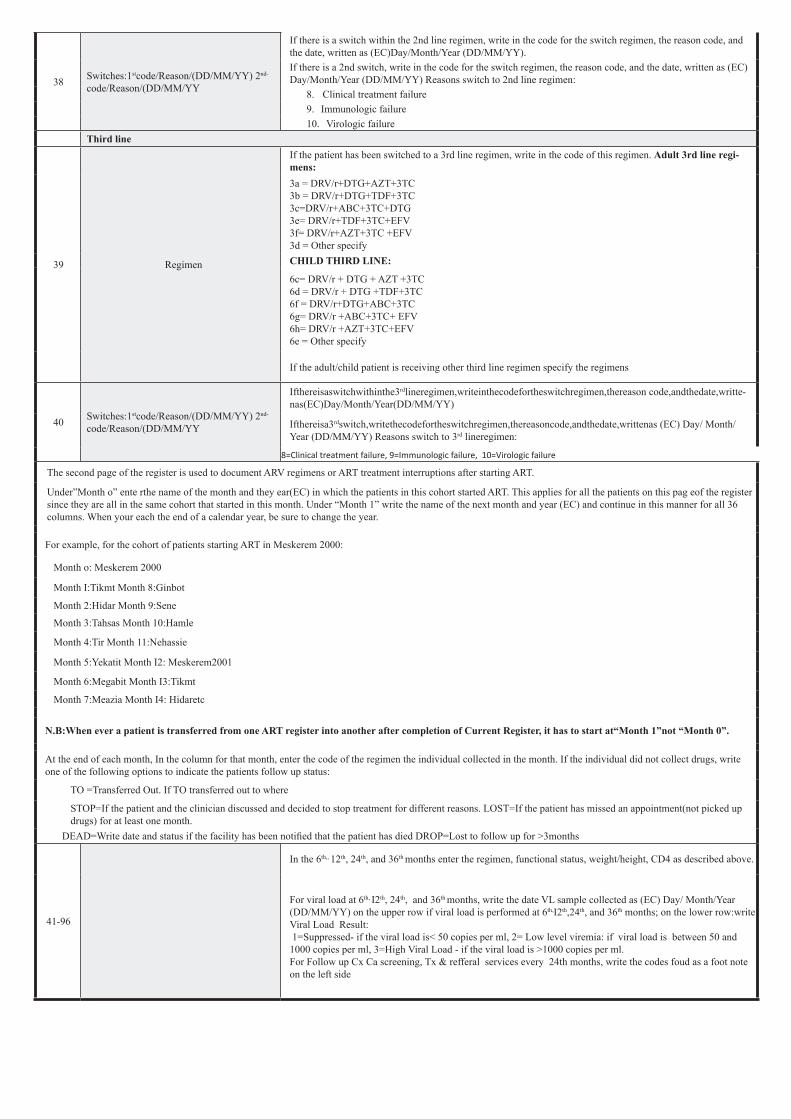
If there is a switch within the 2nd line regimen, write in the code for the switch regimen, the reason code, and the date, written as (EC)Day/Month/Year (DD/MM/YY).If there is a 2nd switch, write in the code for the switch regimen, the reason code, and the date, written as (EC) Day/Month/Year (DD/MM/YY) Reasons switch to 2nd line regimen:
8. Clinical treatment failure9. Immunologic failure10. Virologic failure
Third line
39 Regimen
If the patient has been switched to a 3rd line regimen, write in the code of this regimen. Adult 3rd line regi-mens:3a = DRV/r+DTG+AZT+3TC 3b = DRV/r+DTG+TDF+3TC 3c=DRV/r+ABC+3TC+DTG 3e= DRV/r+TDF+3TC+EFV 3f= DRV/r+AZT+3TC +EFV 3d = Other specifyCHILD THIRD LINE:
6c= DRV/r + DTG + AZT +3TC 6d = DRV/r + DTG +TDF+3TC 6f = DRV/r+DTG+ABC+3TC 6g= DRV/r +ABC+3TC+ EFV 6h= DRV/r +AZT+3TC+EFV 6e = Other specify
If the adult/child patient is receiving other third line regimen specify the regimens
40 Switches:1stcode/Reason/(DD/MM/YY) 2nd-
code/Reason/(DD/MM/YY
Ifthereisaswitchwithinthe3rdlineregimen,writeinthecodefortheswitchregimen,thereason code,andthedate,writte-nas(EC)Day/Month/Year(DD/MM/YY)
Ifthereisa3rdswitch,writethecodefortheswitchregimen,thereasoncode,andthedate,writtenas (EC) Day/ Month/ Year (DD/MM/YY) Reasons switch to 3rd lineregimen:
8=Clinical treatment failure, 9=Immunologic failure, 10=Virologic failure
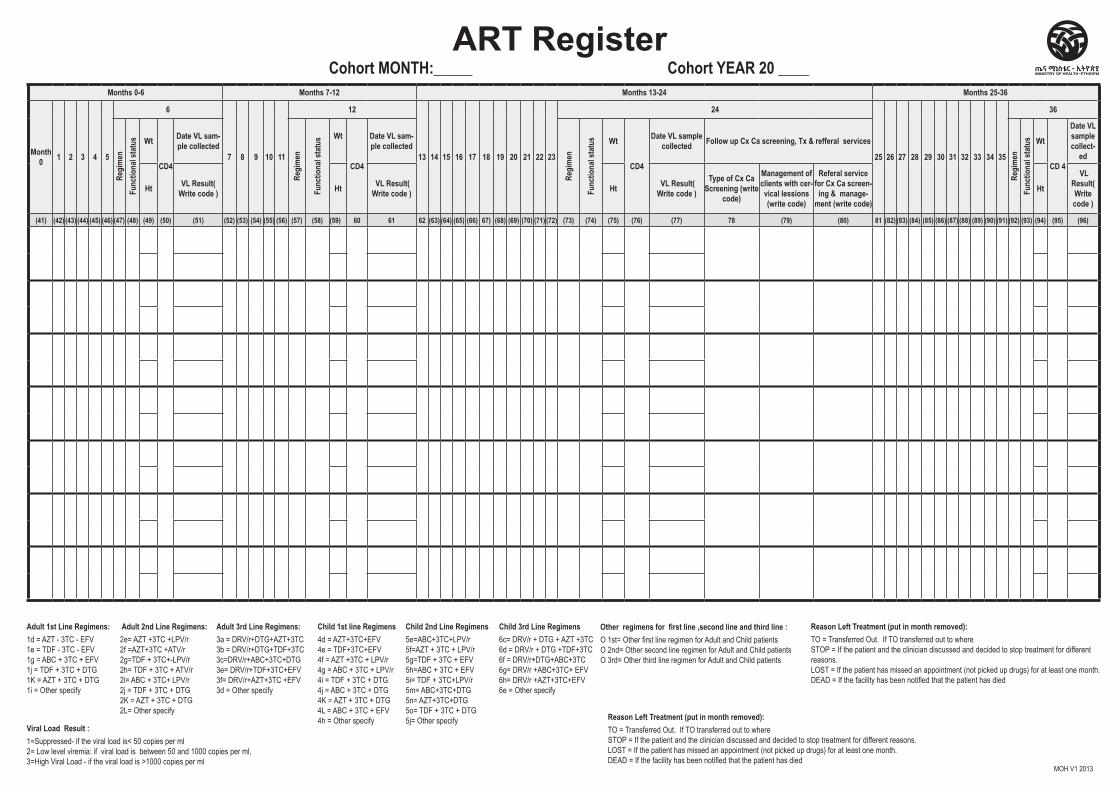
The second page of the register is used to document ARV regimens or ART treatment interruptions after starting ART.
Under”Month o” ente rthe name of the month and they ear(EC) in which the patients in this cohort started ART. This applies for all the patients on this pag eof the register since they are all in the same cohort that started in this month. Under “Month 1” write the name of the next month and year (EC) and continue in this manner for all 36 columns. When your each the end of a calendar year, be sure to change the year.
For example, for the cohort of patients starting ART in Meskerem 2000:
Month o: Meskerem 2000
Month I:Tikmt Month 8:Ginbot
Month 2:Hidar Month 9:Sene
Month 3:Tahsas Month 10:Hamle
Month 4:Tir Month 11:Nehassie
Month 5:Yekatit Month I2: Meskerem2001
Month 6:Megabit Month I3:Tikmt
Month 7:Meazia Month I4: Hidaretc
N.B:When ever a patient is transferred from one ART register into another after completion of Current Register, it has to start at“Month 1”not “Month 0”.
At the end of each month, In the column for that month, enter the code of the regimen the individual collected in the month. If the individual did not collect drugs, write one of the following options to indicate the patients follow up status:
TO =Transferred Out. If TO transferred out to where
STOP=If the patient and the clinician discussed and decided to stop treatment for different reasons. LOST=If the patient has missed an appointment(not picked up drugs) for at least one month.
DEAD=Write date and status if the facility has been notified that the patient has died DROP=Lost to follow up for >3months
41-96
In the 6th,, 12th, 24th, and 36th months enter the regimen, functional status, weight/height, CD4 as described above.
For viral load at 6th, I2th, 24th, and 36th months, write the date VL sample collected as (EC) Day/ Month/Year (DD/MM/YY) on the upper row if viral load is performed at 6th,I2th,24th, and 36th months; on the lower row:write Viral Load Result: 1=Suppressed- if the viral load is< 50 copies per ml, 2= Low level viremia: if viral load is between 50 and 1000 copies per ml, 3=High Viral Load - if the viral load is >1000 copies per ml. For Follow up Cx Ca screening, Tx & refferal services every 24th months, write the codes foud as a foot note on the left side
Registration Status at start ART Cx Ca screening, Tx & refferal services TB / HIV Coinfection
Fluc
onaz
ole p
reve
ntive
ther
apy
(FPT
) (√)
Fill when applicable 1st Line Regimen 2nd Line Regimen 3rd Line Regimen
ART Start Date
(DD/MM/YY)
Unique ART Num-ber
MRN
Name
Age Sex (M/F)
Woreda
Func
tiona
l Sta
tus*
Weig
ht
Heig
ht / L
engt
h
MUAC
(cm
)
BMI /W
eight
for A
geNu
tritio
n Sc
reen
ing
Resu
lt wr
ite
code
WHO
Clin
ical s
tage
CD4 (
if ch
ild C
D4 %
)
Type
of c
ervic
alca s
cree
ning
(V
IA, H
PV)
Cx C
a Scr
eeni
ng r
esul
t (wr
ite
code
) Ma
nage
men
t of c
lient
s with
ce
rvica
l less
ions
(writ
e cod
e)
Refe
ral s
ervic
e fo
r wom
en
with
Cx l
esio
ns (
write
code
)Sc
reen
ed fo
r TB
(√) GeneXpert
(1)/Urine LF-LAM (2)
sent (√) TB Tr
eatm
ent
Star
t dat
e (D
D/MM
/YY)
6H/3HP/3HR prophy-laxis
(DD/MM/YY)
TPT com-pleted (Y, N)
Enrolled to DSD Model (DD/MM/YY)
CTX Start date DD/MM/
YY)
Usin
g an
y Mod
ern
Cont
ra-
cept
ive (w
rite c
ode)
Date
Ref
erre
d to
PMT
CT
(DD/
MM/Y
Y)
Orig
inal
Regi
men
Substitutions 1st code /
Reason / (DD/MM/YY)
Regi
men
Switch 1st code / Reason /
(DD/MM/YY)
Regi
men
Switch 1st code / Reason / (DD/MM/
YY)
Father, Grandfather Name
Kebele HNo.
Food Rx (√)
Scre
enin
g re
sult
(P/N
)
Result (P/N)
Com
plet
e da
te (D
D/MM
/YY
)
Type of DSD( Write code )
Stop date (DD/MM/
YY) Date
Re-
turn
ed
(DD/
MM/Y
Y)
2nd code / Reason / (DD/
MM/YY)
2nd code / Reason /
(DD/MM/YY)
2nd code / Reason / (DD/MM/
YY)
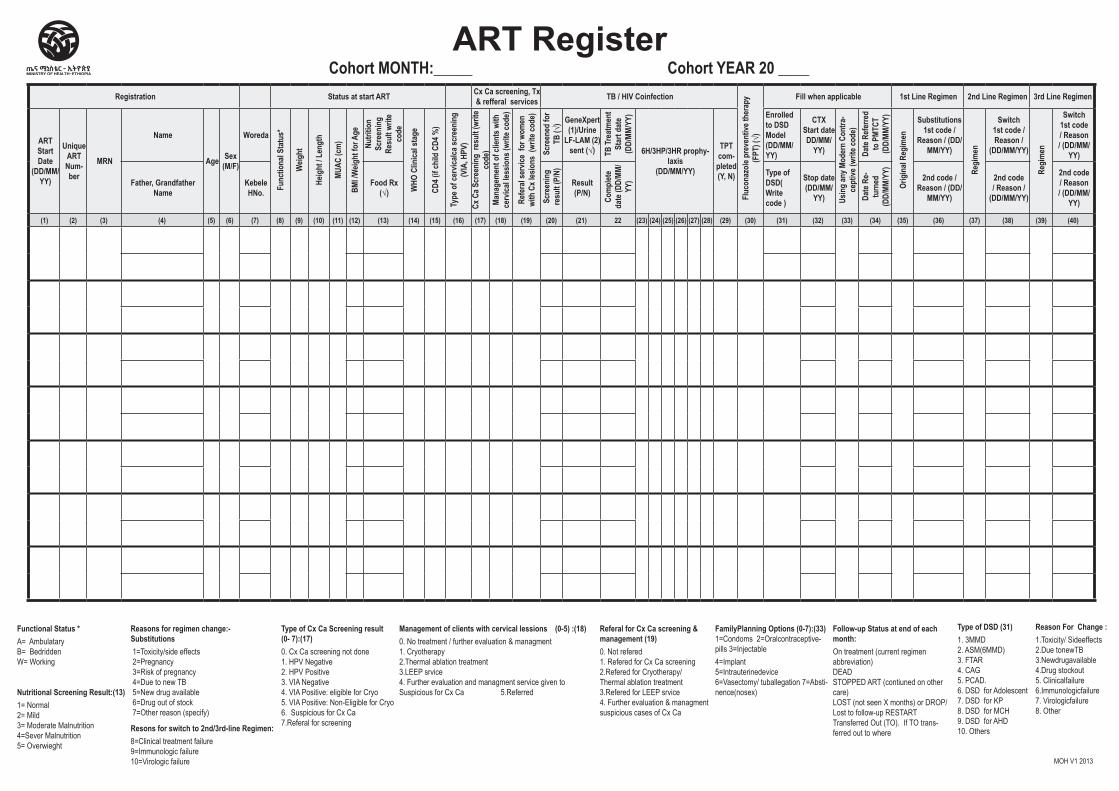
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) 22 (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40)
Cohort MONTH:_____ Cohort YEAR 20 ____ ART Register
Functional Status * A= AmbulataryB= BedriddenW= Working
Nutritional Screening Result:(13)1= Normal2= Mild3= Moderate Malnutrition4=Sever Malnutrition5= Overwieght
Reasons for regimen change:-Substitutions 1=Toxicity/side effects 2=Pregnancy 3=Risk of pregnancy 4=Due to new TB 5=New drug available 6=Drug out of stock 7=Other reason (specify)
Resons for switch to 2nd/3rd-line Regimen:8=Clinical treatment failure9=Immunologic failure10=Virologic failure
Type of Cx Ca Screening result (0- 7):(17)0. Cx Ca screening not done1. HPV Negative2. HPV Positive3. VIA Negative4. VIA Positive: eligible for Cryo5. VIA Positive: Non-Eligible for Cryo6. Suspicious for Cx Ca7.Referal for screening
Management of clients with cervical lessions (0-5) :(18) 0. No treatment / further evaluation & managment 1. Cryotherapy2.Thermal ablation treatment3.LEEP srvice4. Further evaluation and managment service given to Suspicious for Cx Ca 5.Referred
Referal for Cx Ca screening & management (19) 0. Not refered 1. Refered for Cx Ca screening 2.Refered for Cryotherapy/Thermal ablation treatment3.Refered for LEEP srvice4. Further evaluation & managment suspicious cases of Cx Ca
FamilyPlanning Options (0-7):(33) 1=Condoms 2=Oralcontraceptive-pills 3=Injectable 4=Implant 5=Intrauterinedevice6=Vasectomy/ tuballegation 7=Absti-nence(nosex)
Follow-up Status at end of each month:On treatment (current regimen abbreviation)DEAD STOPPED ART (contiuned on other care)LOST (not seen X months) or DROP/Lost to follow-up RESTARTTransferred Out (TO). If TO trans-ferred out to where
Type of DSD (31) 1. 3MMD 2. ASM(6MMD)3. FTAR 4. CAG 5. PCAD. 6. DSD for Adolescent7. DSD for KP 8. DSD for MCH 9. DSD for AHD 10. Others
Reason For Change :1.Toxicity/ Sideeffects2.Due tonewTB3.Newdrugavailable4.Drug stockout5. Clinicalfailure6.Immunologicfailure7. Virologicfailure 8. Other
MOH V1 2013
Cohort MONTH:_____ Cohort YEAR 20 ____ ART Register
Reason For Change :1.Toxicity/ Sideeffects2.Due tonewTB3.Newdrugavailable4.Drug stockout5. Clinicalfailure6.Immunologicfailure7. Virologicfailure 8. Other
Months 0-6 Months 7-12 Months 13-24 Months 25-36
Month 0 1 2 3 4 5
6
7 8 9 10 11
12
13 14 15 16 17 18 19 20 21 22 23
24
25 26 27 28 29 30 31 32 33 34 35
36Re
gim
enFu
nctio
nal s
tatu
s Wt
CD4
Date VL sam-ple collected
Regi
men
Func
tiona
l sta
tus Wt
CD4
Date VL sam-ple collected
Regi
men
Func
tiona
l sta
tus Wt
CD4
Date VL sample collected Follow up Cx Ca screening, Tx & refferal services
Regi
men
Func
tiona
l sta
tus Wt
CD 4
Date VL sample collect-
ed
Ht VL Result( Write code ) Ht VL Result(
Write code ) Ht VL Result( Write code )
Type of Cx Ca Screening (write
code)
Management of clients with cer-vical lessions (write code)
Referal service for Cx Ca screen-
ing & manage-ment (write code)
Ht
VL Result( Write code )
(41) (42) (43) (44) (45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) 60 61 62 (63) (64) (65) (66) 67) (68) (69) (70) (71) (72) (73) (74) (75) (76) (77) 78 (79) (80) 81 (82) (83) (84) (85) (86) (87) (88) (89) (90) (91) (92) (93) (94) (95) (96)
Adult 1st Line Regimens:1d = AZT - 3TC - EFV 1e = TDF - 3TC - EFV 1g = ABC + 3TC + EFV 1j = TDF + 3TC + DTG1K = AZT + 3TC + DTG1i = Other specify
Adult 2nd Line Regimens:2e= AZT +3TC +LPV/r 2f =AZT+3TC +ATV/r2g=TDF + 3TC+-LPV/r2h= TDF + 3TC + ATV/r2i= ABC + 3TC+ LPV/r2j = TDF + 3TC + DTG2K = AZT + 3TC + DTG2L= Other specify
Adult 3rd Line Regimens:3a = DRV/r+DTG+AZT+3TC3b = DRV/r+DTG+TDF+3TC3c=DRV/r+ABC+3TC+DTG3e= DRV/r+TDF+3TC+EFV 3f= DRV/r+AZT+3TC +EFV3d = Other specify
Child 1st line Regimens4d = AZT+3TC+EFV4e = TDF+3TC+EFV4f = AZT +3TC + LPV/r4g = ABC + 3TC + LPV/r4i = TDF + 3TC + DTG4j = ABC + 3TC + DTG4K = AZT + 3TC + DTG4L = ABC + 3TC + EFV4h = Other specify
Child 2nd Line Regimens5e=ABC+3TC+LPV/r5f=AZT + 3TC + LPV/r5g=TDF + 3TC + EFV5h=ABC + 3TC + EFV5i= TDF + 3TC+LPV/r5m= ABC+3TC+DTG5n= AZT+3TC+DTG5o= TDF + 3TC + DTG5j= Other specify
Child 3rd Line Regimens6c= DRV/r + DTG + AZT +3TC6d = DRV/r + DTG +TDF+3TC6f = DRV/r+DTG+ABC+3TC6g= DRV/r +ABC+3TC+ EFV6h= DRV/r +AZT+3TC+EFV6e = Other specify
Other regimens for first line ,second line and third line : O 1st= Other first line regimen for Adult and Child patients O 2nd= Other second line regimen for Adult and Child patients O 3rd= Other third line regimen for Adult and Child patients
Viral Load Result :1=Suppressed- if the viral load is< 50 copies per ml 2= Low level viremia: if viral load is between 50 and 1000 copies per ml, 3=High Viral Load - if the viral load is >1000 copies per ml
Reason Left Treatment (put in month removed):TO = Transferred Out. If TO transferred out to whereSTOP = If the patient and the clinician discussed and decided to stop treatment for different reasons.LOST = If the patient has missed an appointment (not picked up drugs) for at least one month.DEAD = If the facility has been notified that the patient has died
Reason Left Treatment (put in month removed):TO = Transferred Out. If TO transferred out to whereSTOP = If the patient and the clinician discussed and decided to stop treatment for different reasons.LOST = If the patient has missed an appointment (not picked up drugs) for at least one month.DEAD = If the facility has been notified that the patient has died
MOH V1 2013

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Differentiated Service Delivery (DSD)
Register
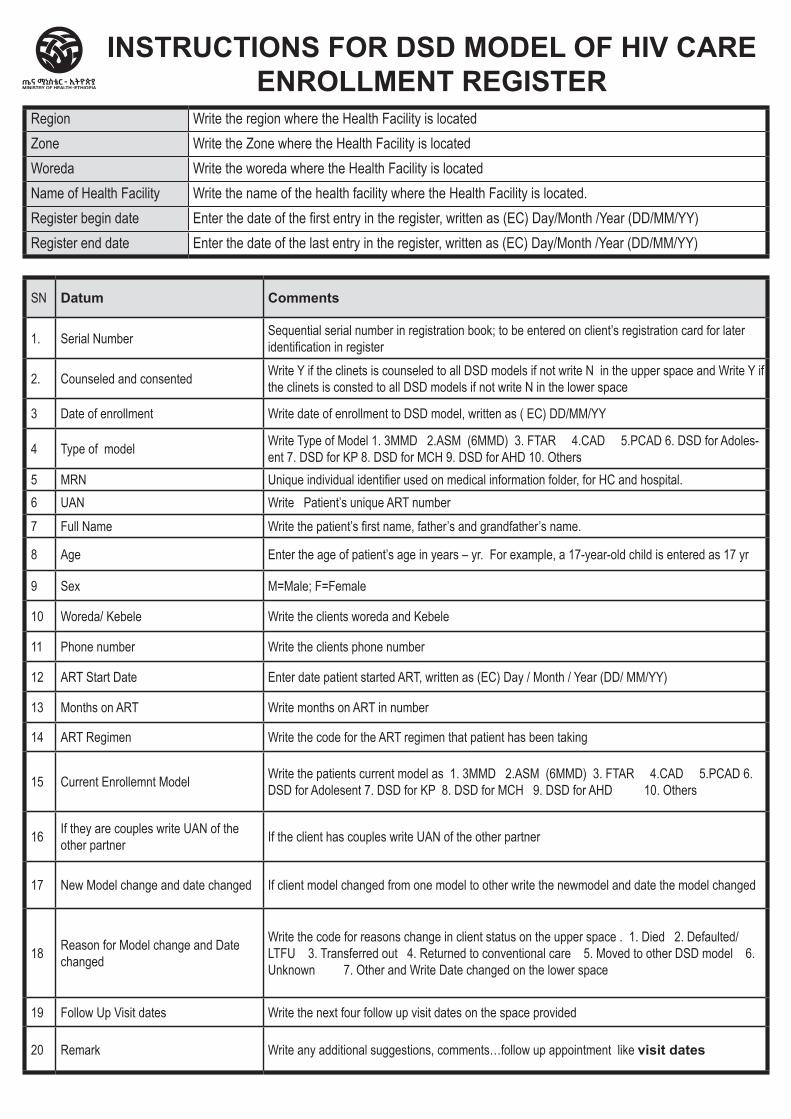
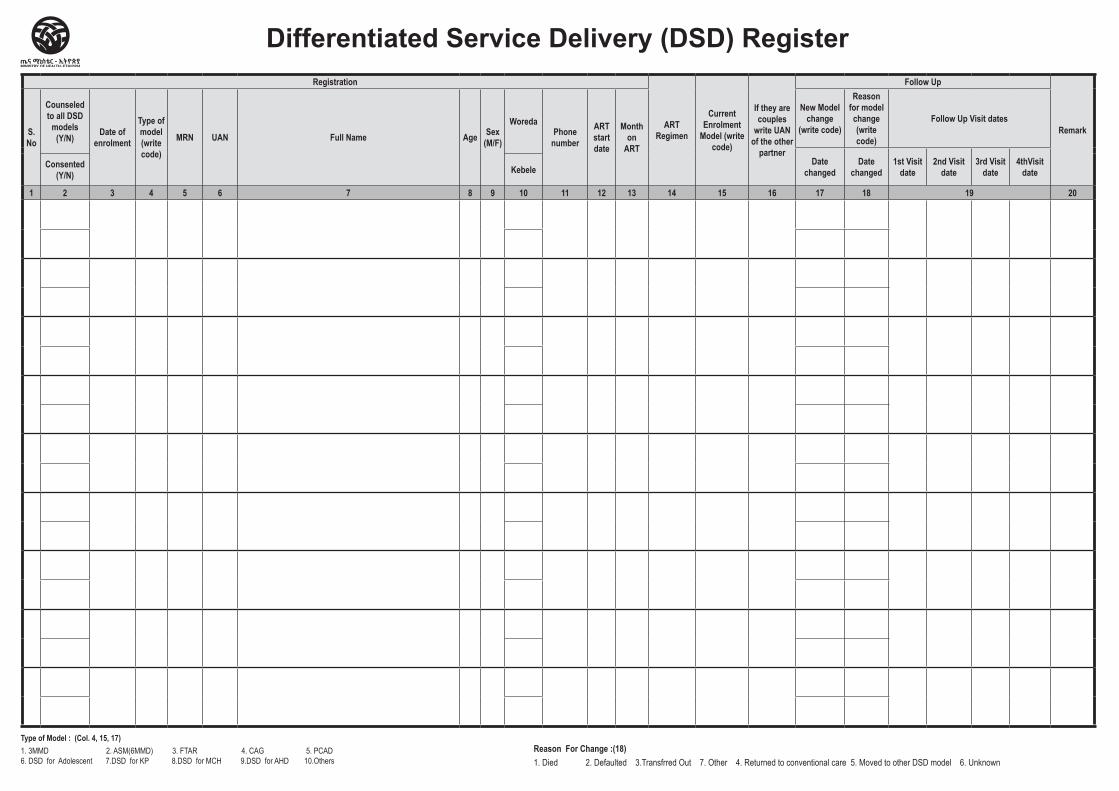
SN Datum Comments
1. Serial Number Sequential serial number in registration book; to be entered on client’s registration card for later identification in register
2. Counseled and consented Write Y if the clinets is counseled to all DSD models if not write N in the upper space and Write Y if the clinets is consted to all DSD models if not write N in the lower space
3 Date of enrollment Write date of enrollment to DSD model, written as ( EC) DD/MM/YY
4 Type of model Write Type of Model 1. 3MMD 2.ASM (6MMD) 3. FTAR 4.CAD 5.PCAD 6. DSD for Adoles-ent 7. DSD for KP 8. DSD for MCH 9. DSD for AHD 10. Others
5 MRN Unique individual identifier used on medical information folder, for HC and hospital.6 UAN Write Patient’s unique ART number 7 Full Name Write the patient’s first name, father’s and grandfather’s name.
8 Age Enter the age of patient’s age in years – yr. For example, a 17-year-old child is entered as 17 yr
9 Sex M=Male; F=Female
10 Woreda/ Kebele Write the clients woreda and Kebele
11 Phone number Write the clients phone number
12 ART Start Date Enter date patient started ART, written as (EC) Day / Month / Year (DD/ MM/YY)
13 Months on ART Write months on ART in number
14 ART Regimen Write the code for the ART regimen that patient has been taking
15 Current Enrollemnt Model Write the patients current model as 1. 3MMD 2.ASM (6MMD) 3. FTAR 4.CAD 5.PCAD 6. DSD for Adolesent 7. DSD for KP 8. DSD for MCH 9. DSD for AHD 10. Others
16 If they are couples write UAN of the other partner If the client has couples write UAN of the other partner
17 New Model change and date changed If client model changed from one model to other write the newmodel and date the model changed
18 Reason for Model change and Date changed
Write the code for reasons change in client status on the upper space . 1. Died 2. Defaulted/ LTFU 3. Transferred out 4. Returned to conventional care 5. Moved to other DSD model 6. Unknown 7. Other and Write Date changed on the lower space
19 Follow Up Visit dates Write the next four follow up visit dates on the space provided
20 Remark Write any additional suggestions, comments…follow up appointment like visit dates
INSTRUCTIONS FOR DSD MODEL OF HIV CARE ENROLLMENT REGISTER
Region Write the region where the Health Facility is locatedZone Write the Zone where the Health Facility is locatedWoreda Write the woreda where the Health Facility is locatedName of Health Facility Write the name of the health facility where the Health Facility is located.Register begin date Enter the date of the first entry in the register, written as (EC) Day/Month /Year (DD/MM/YY)Register end date Enter the date of the last entry in the register, written as (EC) Day/Month /Year (DD/MM/YY)
Registration
ART Regimen
Current Enrolment
Model (write code)
If they are couples
write UAN of the other
partner
Follow Up
RemarkS. No
Counseled to all DSD
models (Y/N) Date of
enrolment
Type of model (write code)
MRN UAN Full Name Age Sex (M/F)
Woreda Phone
number
ART start date
Month on
ART
New Model change
(write code)
Reason for model change (write code)
Follow Up Visit dates
Date changed
Date changed
1st Visit date
2nd Visit date
3rd Visit date
4thVisit date
Consented (Y/N) Kebele
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Differentiated Service Delivery (DSD) Register
Type of Model : (Col. 4, 15, 17)1. 3MMD 2. ASM(6MMD) 3. FTAR 4. CAG 5. PCAD 6. DSD for Adolescent 7.DSD for KP 8.DSD for MCH 9.DSD for AHD 10.Others
Reason For Change :(18) 1. Died 2. Defaulted 3.Transfrred Out 7. Other 4. Returned to conventional care 5. Moved to other DSD model 6. Unknown
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital HIV Care/ART Follow-Up Form
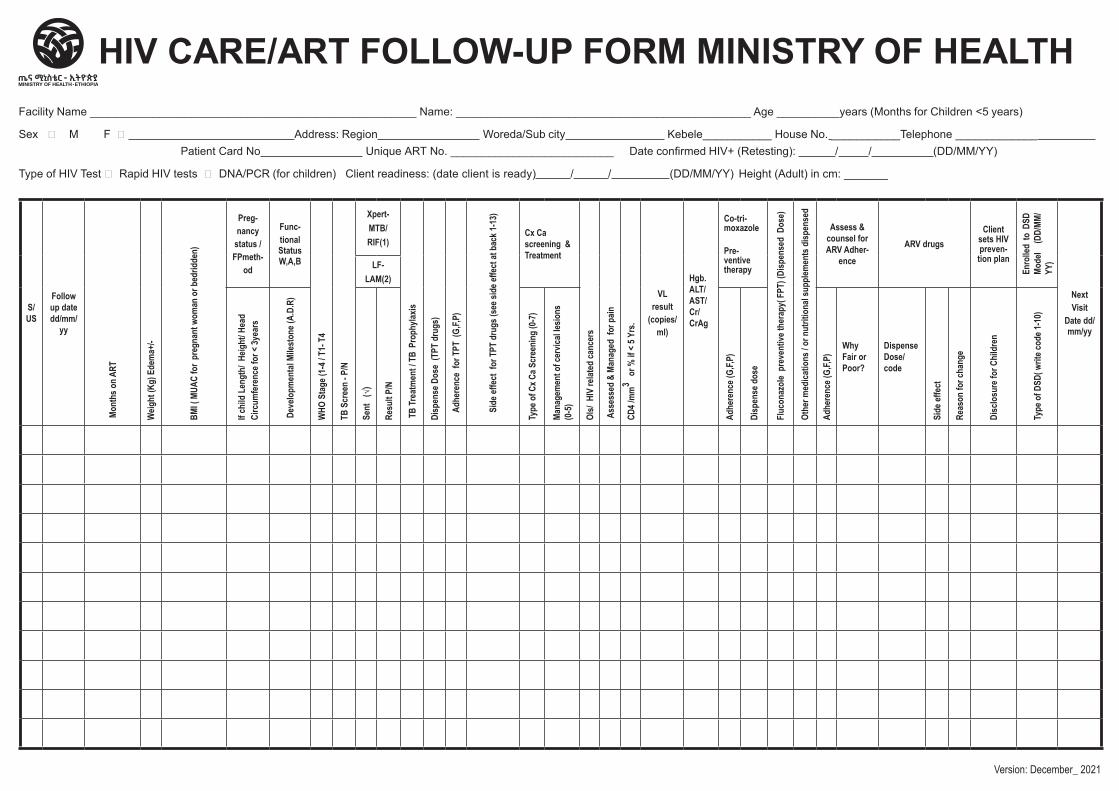
Facility Name ____________________________________________________ Name: _______________________________________________ Age __________years (Months for Children <5 years)
Sex M F Address: Region Woreda/Sub city Kebele___________ House No. ___________Telephone _____________ Patient Card No Unique ART No. __________________________ Date confirmed HIV+ (Retesting): / / (DD/MM/YY)
Type of HIV Test Rapid HIV tests DNA/PCR (for children) Client readiness: (date client is ready) / / (DD/MM/YY) Height (Adult) in cm: _______
HIV CARE/ART FOLLOW-UP FORM MINISTRY OF HEALTH
S/ US
Follow up date dd/mm/
yy
Mon
ths o
n ART
Weig
ht (K
g) E
dem
a+/-
BMI (
MUA
C fo
r pr
egna
nt w
oman
or b
edrid
den)
Preg-nancy
status /FPmeth-
od
Func-tional Status W,A,B
WHO
Sta
ge (1
-4 / T
1- T
4
TB S
cree
n - P
/N
Xpert-MTB/RIF(1)
TB
Trea
tmen
t / T
B Pr
ophy
laxis
Disp
ense
Dos
e (T
PT d
rugs
)
Adhe
renc
e fo
r TPT
(G,
F,P)
Side
effe
ct f
or T
PT d
rugs
(see
side
effe
ct at
bac
k 1-1
3)
Cx Ca screening & Treatment
OIs/
HIV
relat
ed ca
ncer
s
Ass
esse
d &
Mana
ged
for p
ain
CD4 /
mm
3 or
% if
< 5 Y
rs.
VL result
(copies/ml)
Hgb. ALT/ AST/ Cr/ CrAg
Co-tri-moxazole
Pre-ventive therapy
Fluc
onaz
ole
prev
entiv
e the
rapy
( FPT
) (Di
spen
sed
Dos
e)
Othe
r med
icatio
ns / o
r nut
ritio
nal s
uppl
emen
ts d
ispen
sed
Assess & counsel for ARV Adher-
ence
ARV drugsClient
sets HIV preven-tion plan
Enro
lled
to D
SD
Mode
l (D
D/MM
/YY
)
Next Visit
Date dd/mm/yy
LF-LAM(2)
If ch
ild L
engt
h/ H
eight
/ Hea
d Ci
rcum
fere
nce f
or <
3yea
rs
Dev
elopm
enta
l Mile
ston
e (A.
D.R)
Sent
(√)
Resu
lt P/
N
Type
of C
x Ca S
cree
ning
(0-7
)
Mana
gem
ent o
f cer
vical
lesio
ns
(0-5
)
Adhe
renc
e (G,
F,P)
Disp
ense
dos
e
Adhe
renc
e (G,
F,P)
Why Fair or Poor?
Dispense Dose/ code
Side
effe
ct
Reas
on fo
r cha
nge
Disc
losu
re fo
r Chi
ldre
n
Type
of D
SD( w
rite c
ode 1
-10)
Version: December_ 2021
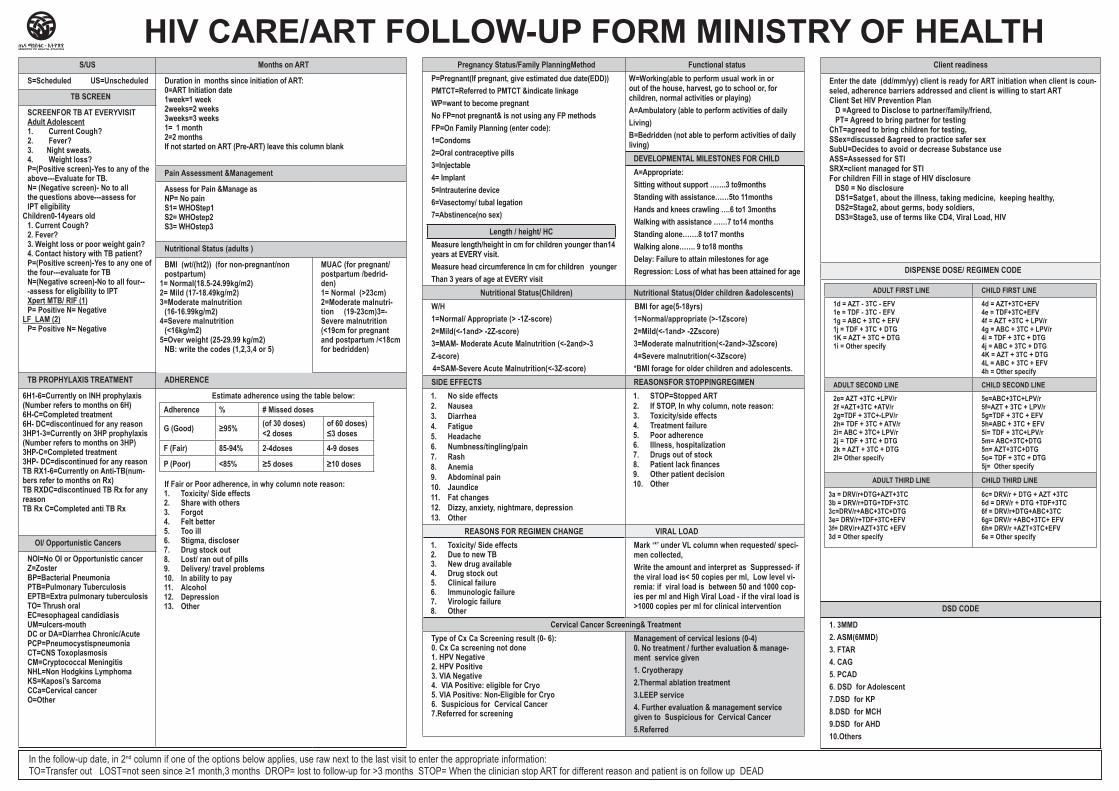
HIV CARE/ART FOLLOW-UP FORM MINISTRY OF HEALTHClient readiness
Enter the date (dd/mm/yy) client is ready for ART initiation when client is coun-seled, adherence barriers addressed and client is willing to start ART Client Set HIV Prevention Plan D =Agreed to Disclose to partner/family/friend, PT= Agreed to bring partner for testingChT=agreed to bring children for testing,SSex=discussed &agreed to practice safer sex SubU=Decides to avoid or decrease Substance use ASS=Assessed for STISRX=client managed for STIFor children Fill in stage of HIV disclosure DS0 = No disclosure DS1=Satge1, about the illness, taking medicine, keeping healthy, DS2=Stage2, about germs, body soldiers, DS3=Stage3, use of terms like CD4, Viral Load, HIV
DISPENSE DOSE/ REGIMEN CODE
ADULT FIRST LINE CHILD FIRST LINE
1d = AZT - 3TC - EFV1e = TDF - 3TC - EFV1g = ABC + 3TC + EFV1j = TDF + 3TC + DTG1K = AZT + 3TC + DTG1i = Other specify
4d = AZT+3TC+EFV4e = TDF+3TC+EFV4f = AZT +3TC + LPV/r4g = ABC + 3TC + LPV/r4i = TDF + 3TC + DTG4j = ABC + 3TC + DTG4K = AZT + 3TC + DTG4L = ABC + 3TC + EFV4h = Other specify
ADULT SECOND LINE CHILD SECOND LINE
2e= AZT +3TC +LPV/r 2f =AZT+3TC +ATV/r2g=TDF + 3TC+-LPV/r2h= TDF + 3TC + ATV/r2i= ABC + 3TC+ LPV/r2j = TDF + 3TC + DTG2k = AZT + 3TC + DTG2l= Other specify
5e=ABC+3TC+LPV/r5f=AZT + 3TC + LPV/r5g=TDF + 3TC + EFV5h=ABC + 3TC + EFV5i= TDF + 3TC+LPV/r5m= ABC+3TC+DTG5n= AZT+3TC+DTG5o= TDF + 3TC + DTG5j= Other specify
ADULT THIRD LINE CHILD THIRD LINE
3a = DRV/r+DTG+AZT+3TC3b = DRV/r+DTG+TDF+3TC3c=DRV/r+ABC+3TC+DTG3e= DRV/r+TDF+3TC+EFV 3f= DRV/r+AZT+3TC +EFV3d = Other specify
6c= DRV/r + DTG + AZT +3TC6d = DRV/r + DTG +TDF+3TC6f = DRV/r+DTG+ABC+3TC6g= DRV/r +ABC+3TC+ EFV6h= DRV/r +AZT+3TC+EFV 6e = Other specify
DSD CODE
1. 3MMD 2. ASM(6MMD)3. FTAR 4. CAG 5. PCAD 6. DSD for Adolescent 7.DSD for KP8.DSD for MCH9.DSD for AHD10.Others
S/US Months on ART
S=Scheduled US=Unscheduled Duration in months since initiation of ART:0=ART Initiation date1week=1 week2weeks=2 weeks3weeks=3 weeks1= 1 month2=2 monthsIf not started on ART (Pre-ART) leave this column blank
TB SCREEN
SCREENFOR TB AT EVERYVISITAdult Adolescent1. Current Cough?2. Fever?3. Night sweats.4. Weight loss?P=(Positive screen)-Yes to any of the above---Evaluate for TB.N= (Negative screen)- No to all the questions above---assess for IPT eligibility
Children0-14years old1. Current Cough?2. Fever?3. Weight loss or poor weight gain?4. Contact history with TB patient?P=(Positive screen)-Yes to any one of the four---evaluate for TBN=(Negative screen)-No to all four---assess for eligibility to IPT Xpert MTB/ RIF (1)P= Positive N= Negative
LF_LAM (2)P= Positive N= Negative
Pain Assessment &Management
Assess for Pain &Manage asNP= No painS1= WHOStep1S2= WHOstep2S3= WHOstep3
Nutritional Status (adults )
BMI (wt/(ht2)) (for non-pregnant/non postpartum)
1= Normal(18.5-24.99kg/m2)2= Mild (17-18.49kg/m2)3=Moderate malnutrition
(16-16.99kg/m2)4=Severe malnutrition
(<16kg/m2) 5=Over weight (25-29.99 kg/m2)
NB: write the codes (1,2,3,4 or 5)
MUAC (for pregnant/postpartum /bedrid-den) 1= Normal (>23cm)2=Moderate malnutri-tion (19-23cm)3=-Severe malnutrition (<19cm for pregnant and postpartum /<18cm for bedridden)
TB PROPHYLAXIS TREATMENT ADHERENCE
6H1-6=Currently on INH prophylaxis (Number refers to months on 6H) 6H-C=Completed treatment6H- DC=discontinued for any reason3HP1-3=Currently on 3HP prophylaxis (Number refers to months on 3HP) 3HP-C=Completed treatment3HP- DC=discontinued for any reasonTB RX1-6=Currently on Anti-TB(num-bers refer to months on Rx)TB RXDC=discontinued TB Rx for any reasonTB Rx C=Completed anti TB Rx
Estimate adherence using the table below:Adherence % # Missed doses
G (Good) ≥95% (of 30 doses)<2 doses
of 60 doses)≤3 doses
F (Fair) 85-94% 2-4doses 4-9 doses
P (Poor) <85% ≥5 doses ≥10 doses
If Fair or Poor adherence, in why column note reason:1. Toxicity/ Side effects2. Share with others3. Forgot4. Felt better5. Too ill6. Stigma, discloser7. Drug stock out8. Lost/ ran out of pills9. Delivery/ travel problems10. In ability to pay11. Alcohol12. Depression13. Other
OI/ Opportunistic Cancers
NOI=No OI or Opportunistic cancerZ=Zoster BP=Bacterial PneumoniaPTB=Pulmonary TuberculosisEPTB=Extra pulmonary tuberculosisTO= Thrush oral EC=esophageal candidiasisUM=ulcers-mouthDC or DA=Diarrhea Chronic/AcutePCP=PneumocystispneumoniaCT=CNS ToxoplasmosisCM=Cryptococcal Meningitis NHL=Non Hodgkins Lymphoma KS=Kaposi’s Sarcoma CCa=Cervical cancerO=Other
Pregnancy Status/Family PlanningMethod Functional statusP=Pregnant(If pregnant, give estimated due date(EDD))PMTCT=Referred to PMTCT &indicate linkageWP=want to become pregnantNo FP=not pregnant& is not using any FP methodsFP=On Family Planning (enter code):1=Condoms2=Oral contraceptive pills3=Injectable4= Implant5=Intrauterine device6=Vasectomy/ tubal legation7=Abstinence(no sex)
Length / height/ HCMeasure length/height in cm for children younger than14 years at EVERY visit.Measure head circumference In cm for children youngerThan 3 years of age at EVERY visit
W=Working(able to perform usual work in or out of the house, harvest, go to school or, for children, normal activities or playing)A=Ambulatory (able to perform activities of dailyLiving)B=Bedridden (not able to perform activities of daily living)
DEVELOPMENTAL MILESTONES FOR CHILDA=Appropriate:Sitting without support …….3 to9months Standing with assistance……5to 11months Hands and knees crawling ….6 to1 3months Walking with assistance ……7 to14 months Standing alone…….8 to17 monthsWalking alone……. 9 to18 monthsDelay: Failure to attain milestones for ageRegression: Loss of what has been attained for age
Nutritional Status(Children) Nutritional Status(Older children &adolescents)W/H1=Normal/ Appropriate (> -1Z-score)2=Mild(<-1and> -2Z-score)3=MAM- Moderate Acute Malnutrition (<-2and>-3Z-score)
4=SAM-Severe Acute Malnutrition(<-3Z-score)
BMI for age(5-18yrs)1=Normal/appropriate (>-1Zscore)2=Mild(<-1and> -2Zscore)3=Moderate malnutrition(<-2and>-3Zscore)4=Severe malnutrition(<-3Zscore)*BMI forage for older children and adolescents.
SIDE EFFECTS REASONSFOR STOPPINGREGIMEN1. No side effects2. Nausea3. Diarrhea4. Fatigue5. Headache6. Numbness/tingling/pain7. Rash8. Anemia9. Abdominal pain10. Jaundice11. Fat changes12. Dizzy, anxiety, nightmare, depression13. Other
1. STOP=Stopped ART2. If STOP, In why column, note reason:3. Toxicity/side effects4. Treatment failure5. Poor adherence6. Illness, hospitalization7. Drugs out of stock8. Patient lack finances9. Other patient decision10. Other
REASONS FOR REGIMEN CHANGE VIRAL LOAD1. Toxicity/ Side effects2. Due to new TB3. New drug available4. Drug stock out5. Clinical failure6. Immunologic failure7. Virologic failure8. Other
Mark ‘*’ under VL column when requested/ speci-men collected, Write the amount and interpret as Suppressed- if the viral load is< 50 copies per ml, Low level vi-remia: if viral load is between 50 and 1000 cop-ies per ml and High Viral Load - if the viral load is >1000 copies per ml for clinical intervention
Cervical Cancer Screening& Treatment Type of Cx Ca Screening result (0- 6):0. Cx Ca screening not done1. HPV Negative2. HPV Positive3. VIA Negative4. VIA Positive: eligible for Cryo5. VIA Positive: Non-Eligible for Cryo6. Suspicious for Cervical Cancer 7.Referred for screening
Management of cervical lesions (0-4) 0. No treatment / further evaluation & manage-ment service given1. Cryotherapy2.Thermal ablation treatment3.LEEP service4. Further evaluation & management service given to Suspicious for Cervical Cancer5.Referred
In the follow-up date, in 2nd column if one of the options below applies, use raw next to the last visit to enter the appropriate information:TO=Transfer out LOST=not seen since ≥1 month,3 months DROP= lost to follow-up for >3 months STOP= When the clinician stop ART for different reason and patient is on follow up DEAD
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
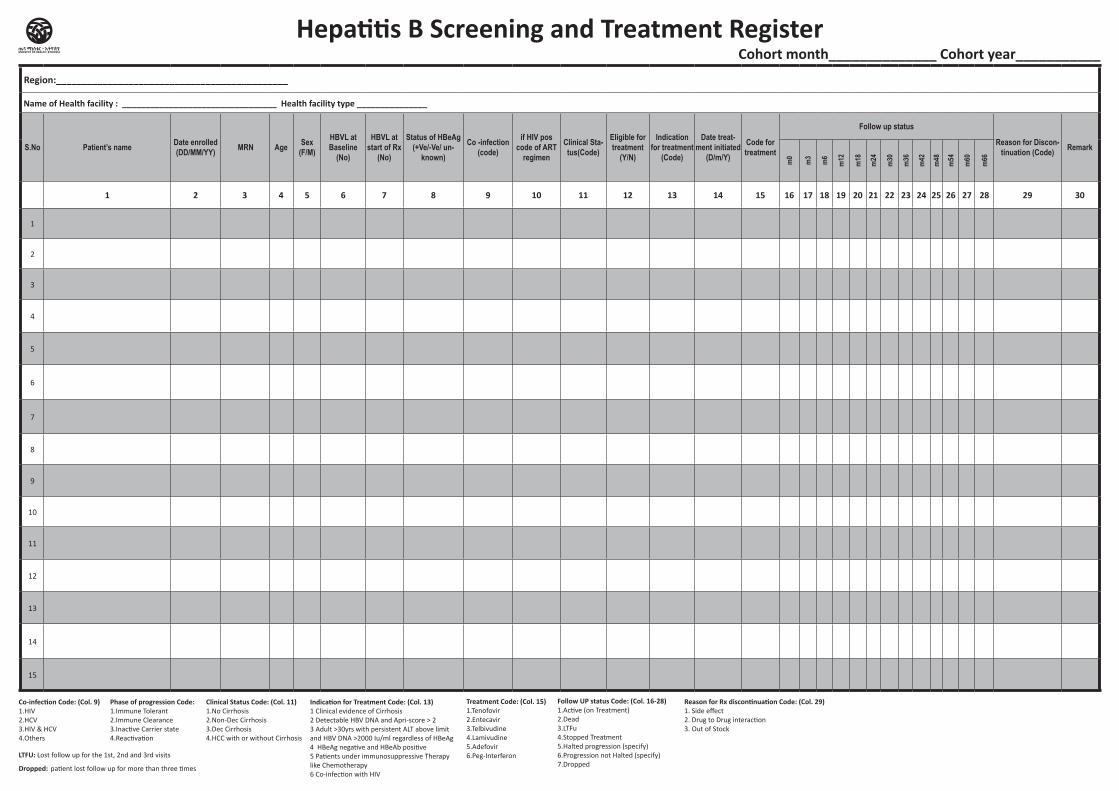
Hospital/Clinic Hepatitis B Screening and Treatment
Register
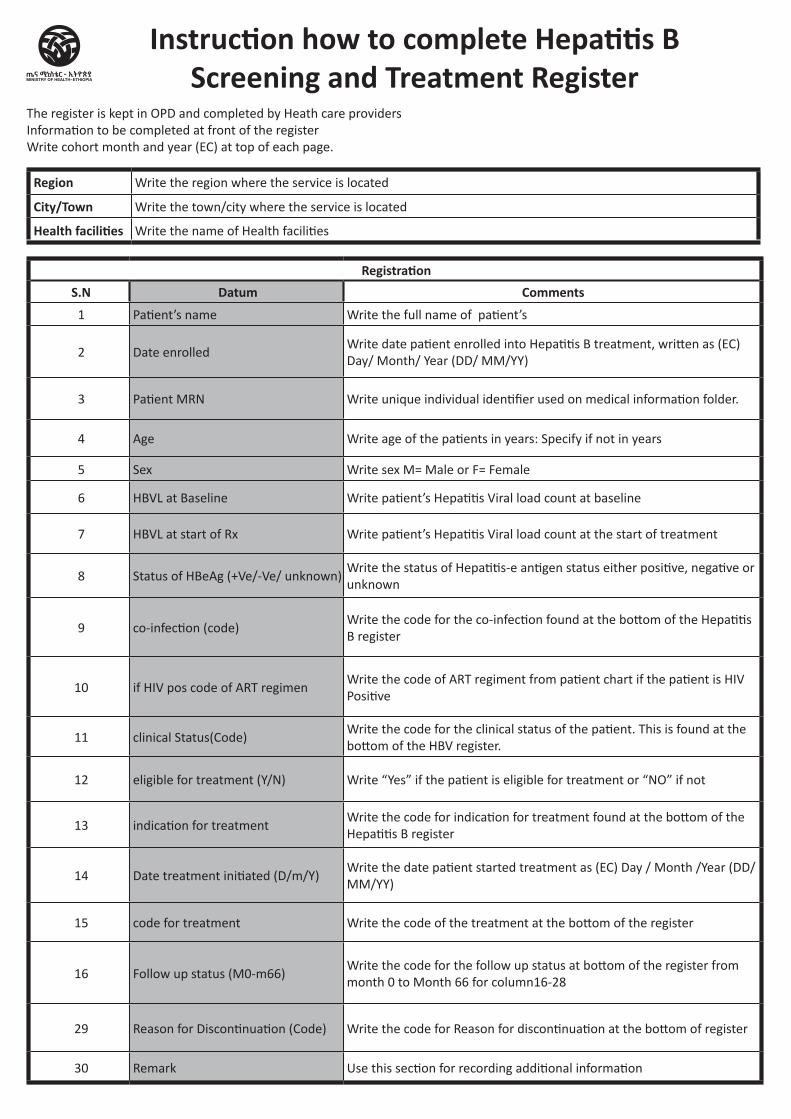
RegistrationS.N Datum Comments
1 Patient’s name Write the full name of patient’s
2 Date enrolledWrite date patient enrolled into Hepatitis B treatment, written as (EC) Day/ Month/ Year (DD/ MM/YY)
3 Patient MRN Write unique individual identifier used on medical information folder.
4 Age Write age of the patients in years: Specify if not in years
5 Sex Write sex M= Male or F= Female
6 HBVL at Baseline Write patient’s Hepatitis Viral load count at baseline
7 HBVL at start of Rx Write patient’s Hepatitis Viral load count at the start of treatment
8 Status of HBeAg (+Ve/-Ve/ unknown)Write the status of Hepatitis-e antigen status either positive, negative or unknown
9 co-infection (code)Write the code for the co-infection found at the bottom of the Hepatitis B register
10 if HIV pos code of ART regimenWrite the code of ART regiment from patient chart if the patient is HIV Positive
11 clinical Status(Code)Write the code for the clinical status of the patient. This is found at the bottom of the HBV register.
12 eligible for treatment (Y/N) Write “Yes” if the patient is eligible for treatment or “NO” if not
13 indication for treatmentWrite the code for indication for treatment found at the bottom of the Hepatitis B register
14 Date treatment initiated (D/m/Y)Write the date patient started treatment as (EC) Day / Month /Year (DD/MM/YY)
15 code for treatment Write the code of the treatment at the bottom of the register
16 Follow up status (M0-m66)Write the code for the follow up status at bottom of the register from month 0 to Month 66 for column16-28
29 Reason for Discontinuation (Code) Write the code for Reason for discontinuation at the bottom of register
30 Remark Use this section for recording additional information
Instruction how to complete Hepatitis B Screening and Treatment Register
The register is kept in OPD and completed by Heath care providersInformation to be completed at front of the registerWrite cohort month and year (EC) at top of each page.
Region Write the region where the service is located
City/Town Write the town/city where the service is located
Health facilities Write the name of Health facilities
Hepatitis B Screening and Treatment Register Cohort month______________ Cohort year___________
Region:_____________________________________________
Name of Health facility : _________________________________ Health facility type _______________
S.No Patient’s name Date enrolled (DD/MM/YY) MRN Age Sex
(F/M)
HBVL at Baseline
(No)
HBVL at start of Rx
(No)
Status of HBeAg (+Ve/-Ve/ un-
known)
Co -infection (code)
if HIV pos code of ART
regimen
Clinical Sta-tus(Code)
Eligible for treatment
(Y/N)
Indication for treatment
(Code)
Date treat-ment initiated
(D/m/Y)
Code for treatment
Follow up status
Reason for Discon-tinuation (Code) Remark
m0
m3
m6
m12
m18
m24
m30
m36
m42
m48
m54
m60
m66
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
Co-infection Code: (Col. 9)1.HIV2.HCV3.HIV & HCV4.Others
Phase of progression Code:1.Immune Tolerant2.Immune Clearance3.Inactive Carrier state4.Reactivation
Clinical Status Code: (Col. 11)1.No Cirrhosis2.Non-Dec Cirrhosis3.Dec Cirrhosis4.HCC with or without Cirrhosis
Indication for Treatment Code: (Col. 13)1 Clinical evidence of Cirrhosis 2 Detectable HBV DNA and Apri-score > 2 3 Adult >30yrs with persistent ALT above limit and HBV DNA >2000 Iu/ml regardless of HBeAg 4 HBeAg negative and HBeAb positive 5 Patients under immunosuppressive Therapy like Chemotherapy6 Co-infection with HIV
Treatment Code: (Col. 15)1.Tenofovir2.Entecavir3.Telbivudine4.Lamivudine5.Adefovir6.Peg-Interferon
Follow UP status Code: (Col. 16-28)1.Active (on Treatment)2.Dead3.LTFu4.Stopped Treatment5.Halted progression (specify)6.Progression not Halted (specify)7.Dropped
Reason for Rx discontinuation Code: (Col. 29)1. Side effect2. Drug to Drug interaction3. Out of Stock
LTFU: Lost follow up for the 1st, 2nd and 3rd visits
Dropped: patient lost follow up for more than three times
Health Center/Clinic / HospitalHCV Treatment Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
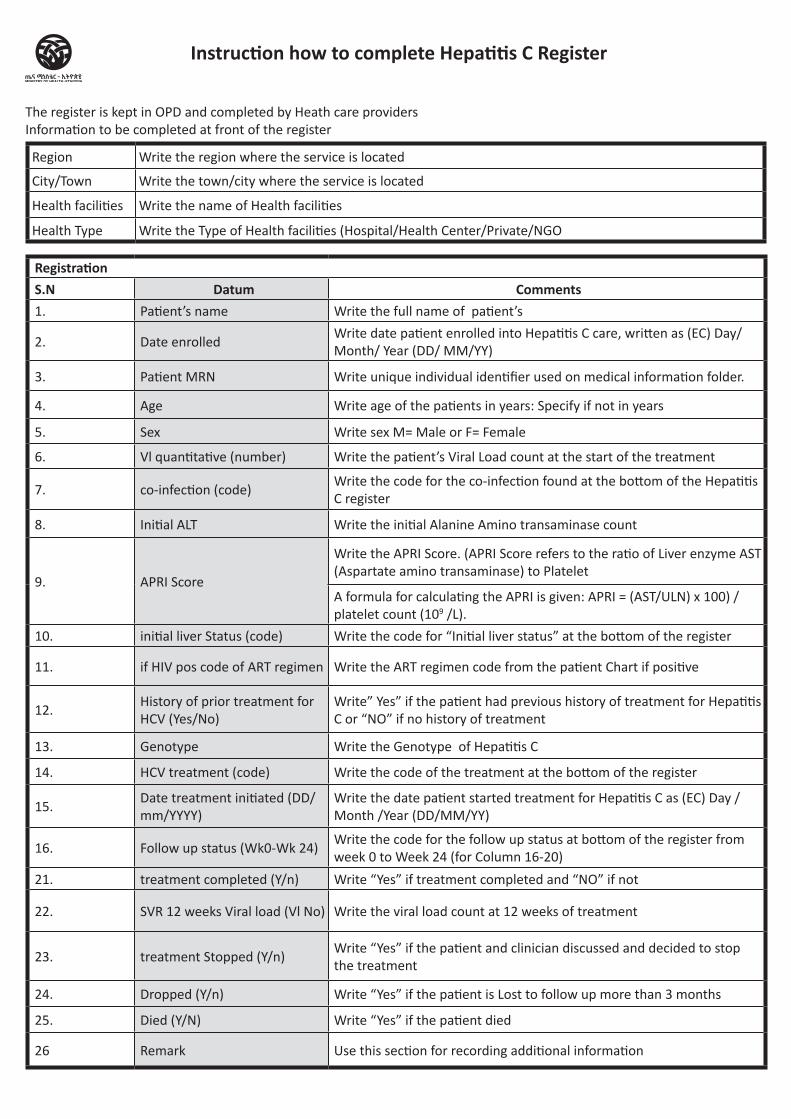
RegistrationS.N Datum Comments1. Patient’s name Write the full name of patient’s
2. Date enrolledWrite date patient enrolled into Hepatitis C care, written as (EC) Day/ Month/ Year (DD/ MM/YY)
3. Patient MRN Write unique individual identifier used on medical information folder.
4. Age Write age of the patients in years: Specify if not in years
5. Sex Write sex M= Male or F= Female
6. Vl quantitative (number) Write the patient’s Viral Load count at the start of the treatment
7. co-infection (code)Write the code for the co-infection found at the bottom of the Hepatitis C register
8. Initial ALT Write the initial Alanine Amino transaminase count
9. APRI Score
Write the APRI Score. (APRI Score refers to the ratio of Liver enzyme AST (Aspartate amino transaminase) to Platelet
A formula for calculating the APRI is given: APRI = (AST/ULN) x 100) / platelet count (109 /L).
10. initial liver Status (code) Write the code for “Initial liver status” at the bottom of the register
11. if HIV pos code of ART regimen Write the ART regimen code from the patient Chart if positive
12. History of prior treatment for HCV (Yes/No)
Write” Yes” if the patient had previous history of treatment for Hepatitis C or “NO” if no history of treatment
13. Genotype Write the Genotype of Hepatitis C
14. HCV treatment (code) Write the code of the treatment at the bottom of the register
15. Date treatment initiated (DD/ mm/YYYY)
Write the date patient started treatment for Hepatitis C as (EC) Day / Month /Year (DD/MM/YY)
16. Follow up status (Wk0-Wk 24)Write the code for the follow up status at bottom of the register from week 0 to Week 24 (for Column 16-20)
21. treatment completed (Y/n) Write “Yes” if treatment completed and “NO” if not
22. SVR 12 weeks Viral load (Vl No) Write the viral load count at 12 weeks of treatment
23. treatment Stopped (Y/n)Write “Yes” if the patient and clinician discussed and decided to stop the treatment
24. Dropped (Y/n) Write “Yes” if the patient is Lost to follow up more than 3 months
25. Died (Y/N) Write “Yes” if the patient died
26 Remark Use this section for recording additional information
Instruction how to complete Hepatitis C Register
The register is kept in OPD and completed by Heath care providersInformation to be completed at front of the register
Region Write the region where the service is located
City/Town Write the town/city where the service is located
Health facilities Write the name of Health facilities
Health Type Write the Type of Health facilities (Hospital/Health Center/Private/NGO
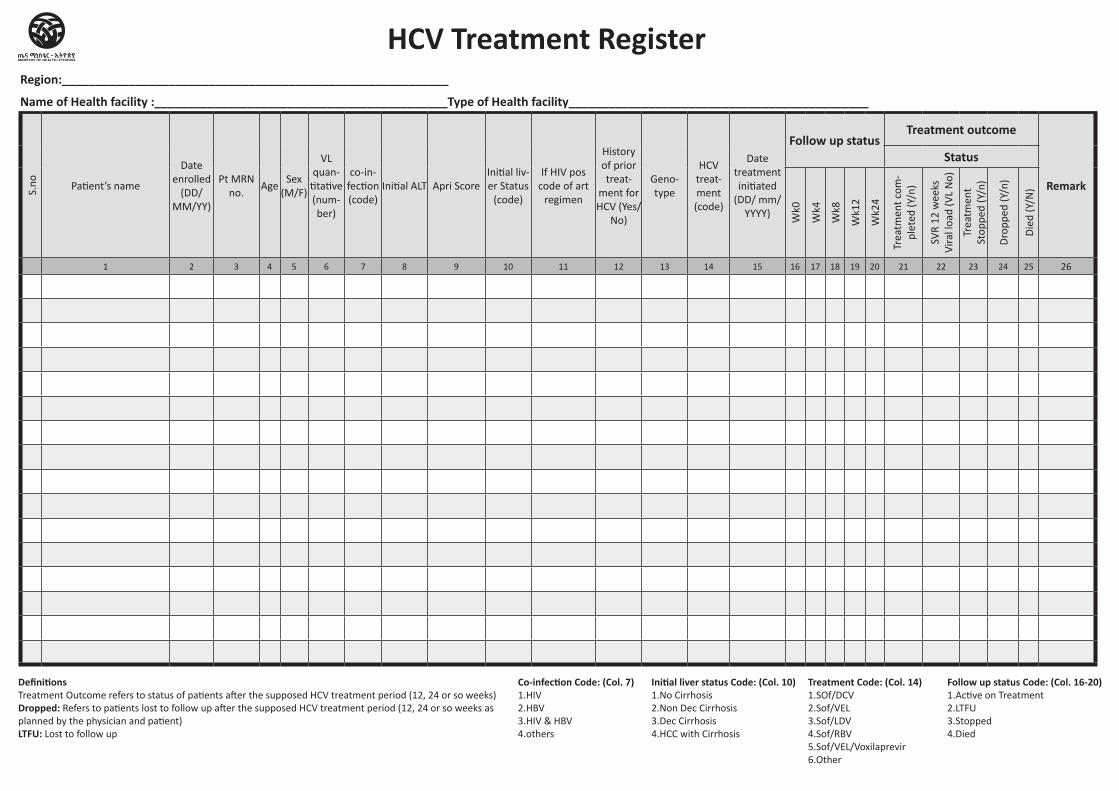
HCV Treatment Register
Definitions Treatment Outcome refers to status of patients after the supposed HCV treatment period (12, 24 or so weeks)Dropped: Refers to patients lost to follow up after the supposed HCV treatment period (12, 24 or so weeks as planned by the physician and patient)LTFU: Lost to follow up
Co-infection Code: (Col. 7)1.HIV2.HBV3.HIV & HBV4.others
Initial liver status Code: (Col. 10)1.No Cirrhosis2.Non Dec Cirrhosis3.Dec Cirrhosis4.HCC with Cirrhosis
Treatment Code: (Col. 14)1.SOf/DCV2.Sof/VEL3.Sof/LDV4.Sof/RBV5.Sof/VEL/Voxilaprevir6.Other
Follow up status Code: (Col. 16-20)1.Active on Treatment2.LTFU3.Stopped4.Died
Region:__________________________________________________________
Name of Health facility :____________________________________________Type of Health facility_____________________________________________
S.no Patient’s name
Date enrolled
(DD/MM/YY)
Pt MRN no.
AgeSex
(M/F)
VL quan-
titative (num-ber)
co-in-fection (code)
Initial ALT Apri ScoreInitial liv-er Status
(code)
If HIV pos code of art
regimen
History of prior treat-
ment for HCV (Yes/
No)
Geno-type
HCV treat-ment (code)
Date treatment initiated
(DD/ mm/YYYY)
Follow up statusTreatment outcome
Remark
Status
Wk0
Wk4
Wk8
Wk1
2
Wk2
4
Trea
tmen
t com
-pl
eted
(Y/n
)
SVR
12 w
eeks
Vi
ral l
oad
(VL
No)
Trea
tmen
t St
oppe
d (Y
/n)
Dro
pped
(Y/n
)
Die
d (Y
/N)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Health Center/Clinic / HospitalHIV Positive Clients’ Tracking
Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
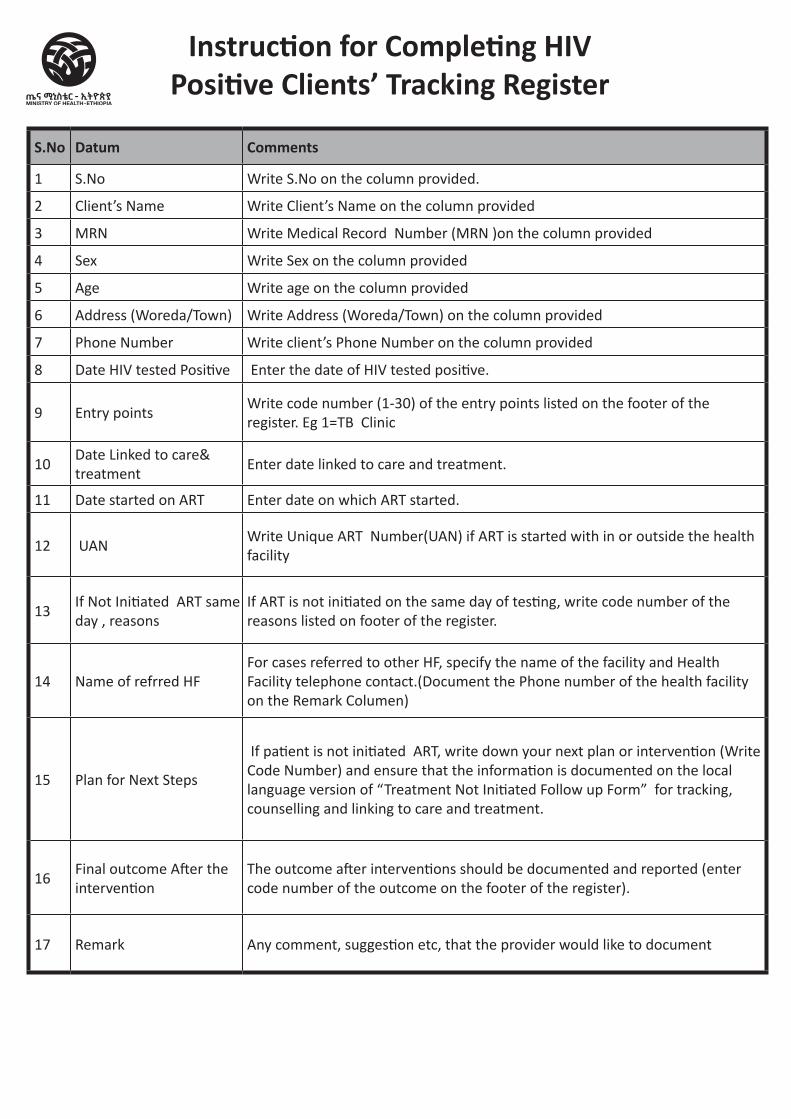
S.No Datum Comments
1 S.No Write S.No on the column provided.
2 Client’s Name Write Client’s Name on the column provided
3 MRN Write Medical Record Number (MRN )on the column provided
4 Sex Write Sex on the column provided
5 Age Write age on the column provided
6 Address (Woreda/Town) Write Address (Woreda/Town) on the column provided
7 Phone Number Write client’s Phone Number on the column provided
8 Date HIV tested Positive Enter the date of HIV tested positive.
9 Entry points Write code number (1-30) of the entry points listed on the footer of the register. Eg 1=TB Clinic
10Date Linked to care& treatment
Enter date linked to care and treatment.
11 Date started on ART Enter date on which ART started.
12 UANWrite Unique ART Number(UAN) if ART is started with in or outside the health facility
13If Not Initiated ART same day , reasons
If ART is not initiated on the same day of testing, write code number of the reasons listed on footer of the register.
14 Name of refrred HFFor cases referred to other HF, specify the name of the facility and Health Facility telephone contact.(Document the Phone number of the health facility on the Remark Columen)
15 Plan for Next Steps
If patient is not initiated ART, write down your next plan or intervention (Write Code Number) and ensure that the information is documented on the local language version of “Treatment Not Initiated Follow up Form” for tracking, counselling and linking to care and treatment.
16Final outcome After the intervention
The outcome after interventions should be documented and reported (enter code number of the outcome on the footer of the register).
17 Remark Any comment, suggestion etc, that the provider would like to document
Instruction for Completing HIV Positive Clients’ Tracking Register
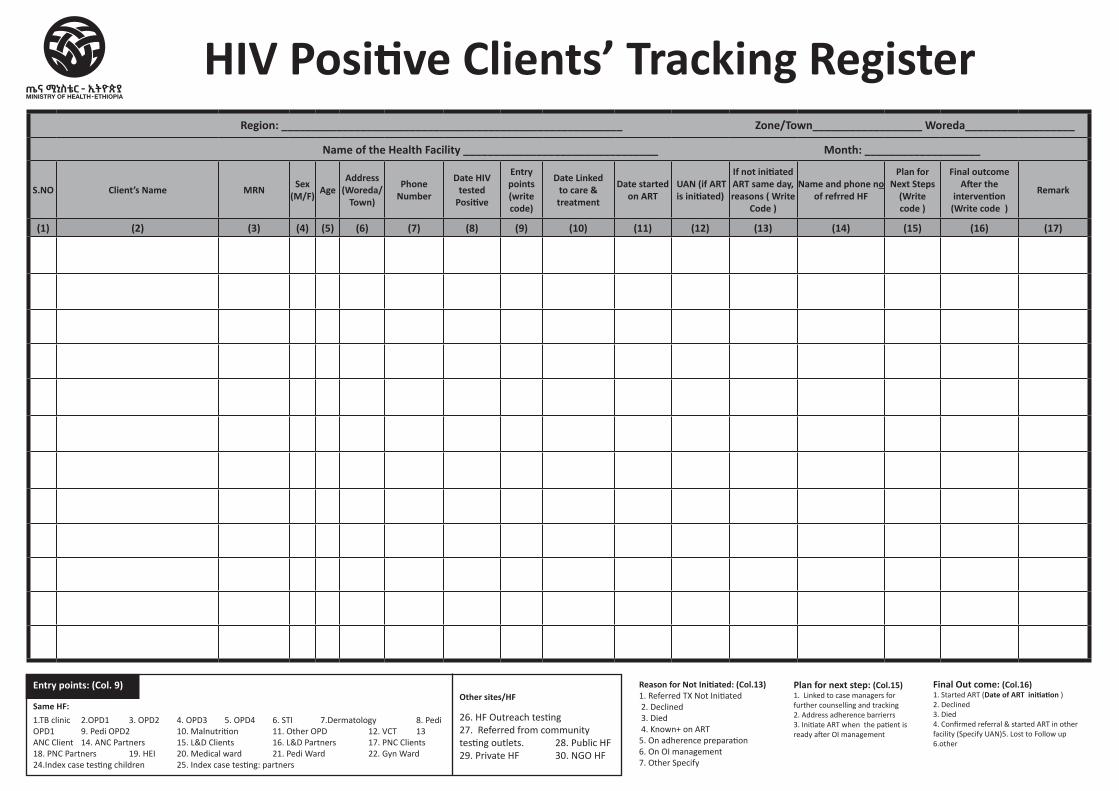
Region: ________________________________________________________ Zone/Town__________________ Woreda__________________
Name of the Health Facility ________________________________ Month: ___________________
S.NO Client’s Name MRN Sex(M/F) Age
Address (Woreda/
Town)
Phone Number
Date HIV tested
Positive
Entry points (write code)
Date Linked to care & treatment
Date started on ART
UAN (if ART is initiated)
If not initiated ART same day, reasons ( Write
Code )
Name and phone no of refrred HF
Plan for Next Steps
(Write code )
Final outcome After the
intervention (Write code )
Remark
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17)
HIV Positive Clients’ Tracking Register
1.TB clinic 2.OPD1 3. OPD2 4. OPD3 5. OPD4 6. STI 7.Dermatology 8. Pedi OPD1 9. Pedi OPD2 10. Malnutrition 11. Other OPD 12. VCT 13 ANC Client 14. ANC Partners 15. L&D Clients 16. L&D Partners 17. PNC Clients 18. PNC Partners 19. HEI 20. Medical ward 21. Pedi Ward 22. Gyn Ward 24.Index case testing children 25. Index case testing: partners
26. HF Outreach testing 27. Referred from community testing outlets. 28. Public HF 29. Private HF 30. NGO HF
Reason for Not Initiated: (Col.13)1. Referred TX Not Initiated 2. Declined 3. Died 4. Known+ on ART5. On adherence preparation6. On OI management 7. Other Specify
Plan for next step: (Col.15) 1. Linked to case managers for further counselling and tracking 2. Address adherence barrierrs 3. Initiate ART when the patient is ready after OI management
Final Out come: (Col.16) 1. Started ART (Date of ART initiation ) 2. Declined 3. Died 4. Confirmed referral & started ART in other facility (Specify UAN)5. Lost to Follow up 6.other
Entry points: (Col. 9)
Same HF:Other sites/HF
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital HIV Self Testing Register
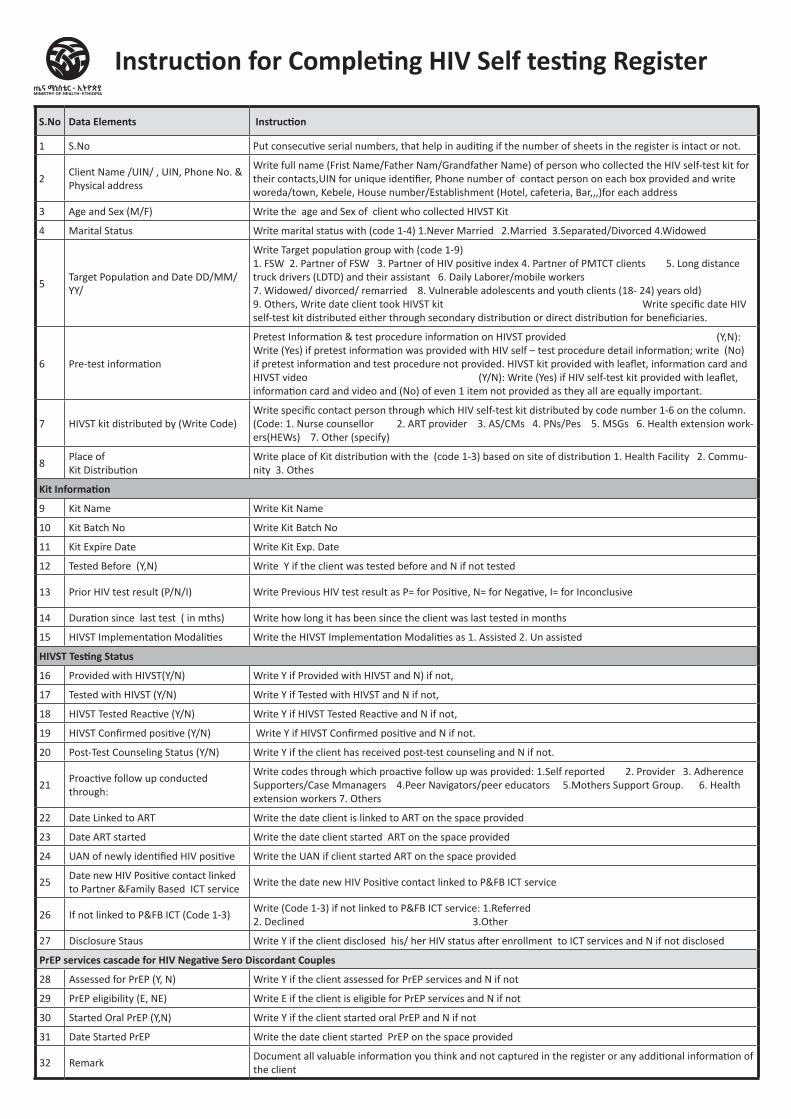
S.No Data Elements Instruction
1 S.No Put consecutive serial numbers, that help in auditing if the number of sheets in the register is intact or not.
2Client Name /UIN/ , UIN, Phone No. & Physical address
Write full name (Frist Name/Father Nam/Grandfather Name) of person who collected the HIV self-test kit for their contacts,UIN for unique identifier, Phone number of contact person on each box provided and write woreda/town, Kebele, House number/Establishment (Hotel, cafeteria, Bar,,,)for each address
3 Age and Sex (M/F) Write the age and Sex of client who collected HIVST Kit
4 Marital Status Write marital status with (code 1-4) 1.Never Married 2.Married 3.Separated/Divorced 4.Widowed
5Target Population and Date DD/MM/YY/
Write Target population group with (code 1-9) 1. FSW 2. Partner of FSW 3. Partner of HIV positive index 4. Partner of PMTCT clients 5. Long distance truck drivers (LDTD) and their assistant 6. Daily Laborer/mobile workers 7. Widowed/ divorced/ remarried 8. Vulnerable adolescents and youth clients (18- 24) years old) 9. Others, Write date client took HIVST kit Write specific date HIV self-test kit distributed either through secondary distribution or direct distribution for beneficiaries.
6 Pre-test information
Pretest Information & test procedure information on HIVST provided (Y,N): Write (Yes) if pretest information was provided with HIV self – test procedure detail information; write (No) if pretest information and test procedure not provided. HIVST kit provided with leaflet, information card and HIVST video (Y/N): Write (Yes) if HIV self-test kit provided with leaflet, information card and video and (No) of even 1 item not provided as they all are equally important.
7 HIVST kit distributed by (Write Code)Write specific contact person through which HIV self-test kit distributed by code number 1-6 on the column. (Code: 1. Nurse counsellor 2. ART provider 3. AS/CMs 4. PNs/Pes 5. MSGs 6. Health extension work-ers(HEWs) 7. Other (specify)
8Place of Kit Distribution
Write place of Kit distribution with the (code 1-3) based on site of distribution 1. Health Facility 2. Commu-nity 3. Othes
Kit Information
9 Kit Name Write Kit Name
10 Kit Batch No Write Kit Batch No
11 Kit Expire Date Write Kit Exp. Date
12 Tested Before (Y,N) Write Y if the client was tested before and N if not tested
13 Prior HIV test result (P/N/I) Write Previous HIV test result as P= for Positive, N= for Negative, I= for Inconclusive
14 Duration since last test ( in mths) Write how long it has been since the client was last tested in months
15 HIVST Implementation Modalities Write the HIVST Implementation Modalities as 1. Assisted 2. Un assisted
HIVST Testing Status
16 Provided with HIVST(Y/N) Write Y if Provided with HIVST and N) if not,
17 Tested with HIVST (Y/N) Write Y if Tested with HIVST and N if not,
18 HIVST Tested Reactive (Y/N) Write Y if HIVST Tested Reactive and N if not,
19 HIVST Confirmed positive (Y/N) Write Y if HIVST Confirmed positive and N if not.
20 Post-Test Counseling Status (Y/N) Write Y if the client has received post-test counseling and N if not.
21Proactive follow up conducted through:
Write codes through which proactive follow up was provided: 1.Self reported 2. Provider 3. Adherence Supporters/Case Mmanagers 4.Peer Navigators/peer educators 5.Mothers Support Group. 6. Health extension workers 7. Others
22 Date Linked to ART Write the date client is linked to ART on the space provided
23 Date ART started Write the date client started ART on the space provided
24 UAN of newly identified HIV positive Write the UAN if client started ART on the space provided
25Date new HIV Positive contact linked to Partner &Family Based ICT service
Write the date new HIV Positive contact linked to P&FB ICT service
26 If not linked to P&FB ICT (Code 1-3)Write (Code 1-3) if not linked to P&FB ICT service: 1.Referred 2. Declined 3.Other
27 Disclosure Staus Write Y if the client disclosed his/ her HIV status after enrollment to ICT services and N if not disclosed
PrEP services cascade for HIV Negative Sero Discordant Couples
28 Assessed for PrEP (Y, N) Write Y if the client assessed for PrEP services and N if not
29 PrEP eligibility (E, NE) Write E if the client is eligible for PrEP services and N if not
30 Started Oral PrEP (Y,N) Write Y if the client started oral PrEP and N if not
31 Date Started PrEP Write the date client started PrEP on the space provided
32 RemarkDocument all valuable information you think and not captured in the register or any additional information of the client
Instruction for Completing HIV Self testing Register
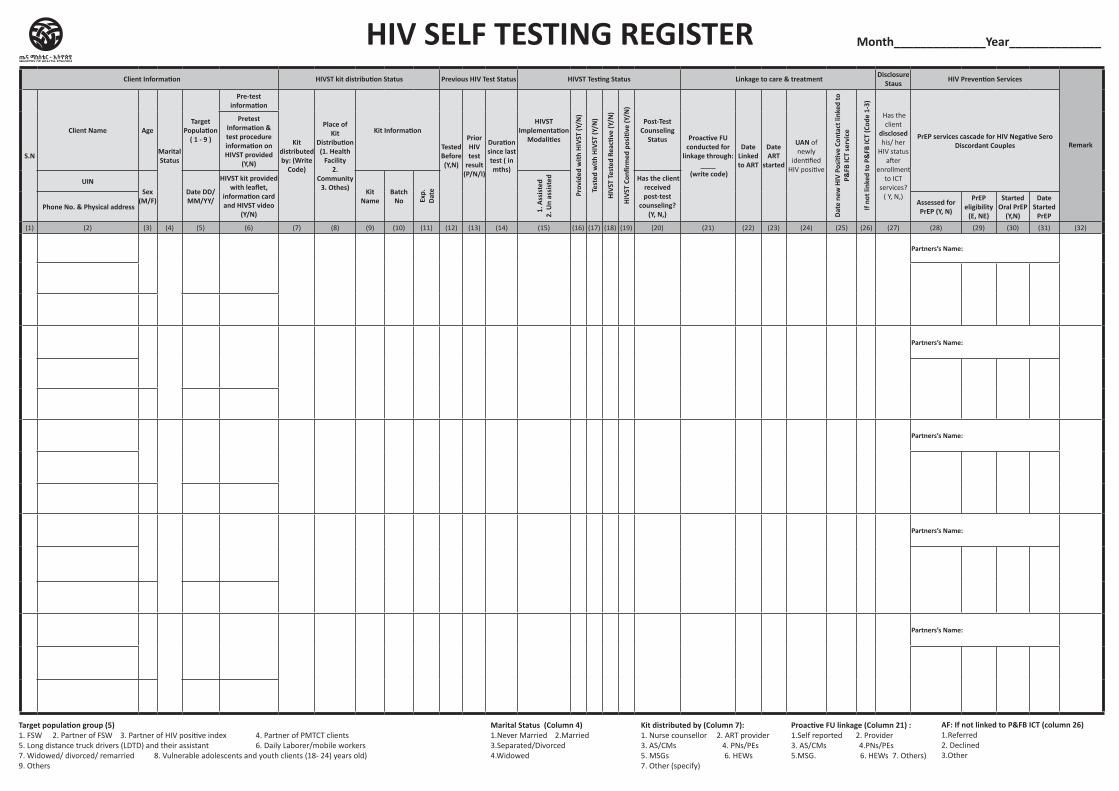
Client Information HIVST kit distribution Status Previous HIV Test Status HIVST Testing Status Linkage to care & treatment Disclosure Staus HIV Prevention Services
RemarkS.N
Client Name Age
Marital Status
Target Population
( 1 - 9 )
Pre-test information
Kit distributed by: (Write
Code)
Place of Kit
Distribution (1. Health
Facility 2.
Community 3. Othes)
Kit Information
Tested Before (Y,N)
Prior HIV test
result (P/N/I)
Duration since last test ( in mths)
HIVST Implementation
Modalities
Prov
ided
with
HIV
ST (Y
/N)
Test
ed w
ith H
IVST
(Y/N
)
HIVS
T Te
sted
Rea
ctive
(Y/N
)
HIVS
T Co
nfirm
ed p
ositi
ve (Y
/N)
Post-Test Counseling
Status Proactive FU conducted for
linkage through: ____
(write code)
Date Linked to ART
Date ART
started
UAN of newly
identified HIV positive
Date
new
HIV
Pos
itive
Con
tact
link
ed to
P&
FB IC
T se
rvic
e
If no
t lin
ked
to P
&FB
ICT
(Cod
e 1-
3)
Has the client
disclosed his/ her
HIV status after
enrollment to ICT
services? ( Y, N,)
PrEP services cascade for HIV Negative Sero Discordant Couples
Pretest Information & test procedure information on HIVST provided
(Y,N)
UINSex
(M/F)Date DD/MM/YY/
HIVST kit provided with leaflet,
information card and HIVST video
(Y/N)
Kit Name
Batch No Ex
p.
Date
1. A
ssis
ted
2. U
n as
sist
ed Has the client received post-test
counseling? (Y, N,)
Phone No. & Physical address Assessed for PrEP (Y, N)
PrEP eligibility
(E, NE)
Started Oral PrEP
(Y,N)
Date Started
PrEP (1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32)
Partners’s Name:
Partners’s Name:
Partners’s Name:
Partners’s Name:
Partners’s Name:
HIV SELF TESTING REGISTER
Target population group (5)1. FSW 2. Partner of FSW 3. Partner of HIV positive index 4. Partner of PMTCT clients 5. Long distance truck drivers (LDTD) and their assistant 6. Daily Laborer/mobile workers 7. Widowed/ divorced/ remarried 8. Vulnerable adolescents and youth clients (18- 24) years old) 9. Others
AF: If not linked to P&FB ICT (column 26)1.Referred2. Declined3.Other
Month______________Year______________
Marital Status (Column 4) 1.Never Married 2.Married3.Separated/Divorced4.Widowed
Kit distributed by (Column 7):1. Nurse counsellor 2. ART provider3. AS/CMs 4. PNs/PEs 5. MSGs 6. HEWs 7. Other (specify)
Proactive FU linkage (Column 21) :1.Self reported 2. Provider3. AS/CMs 4.PNs/PEs5.MSG. 6. HEWs 7. Others)
HIV Rapid Testing Logbook
HIV Rapid Testing Logbook
Region:________ Zone/Sub City:________ Woreda:________ Start Date : ____/___/___ End Date : ____/___/___ Health Facility Name: ______________ Testing Point Name: ______________ Logbook Number:____________
Instructions for HIV Rapid Testing Logbook
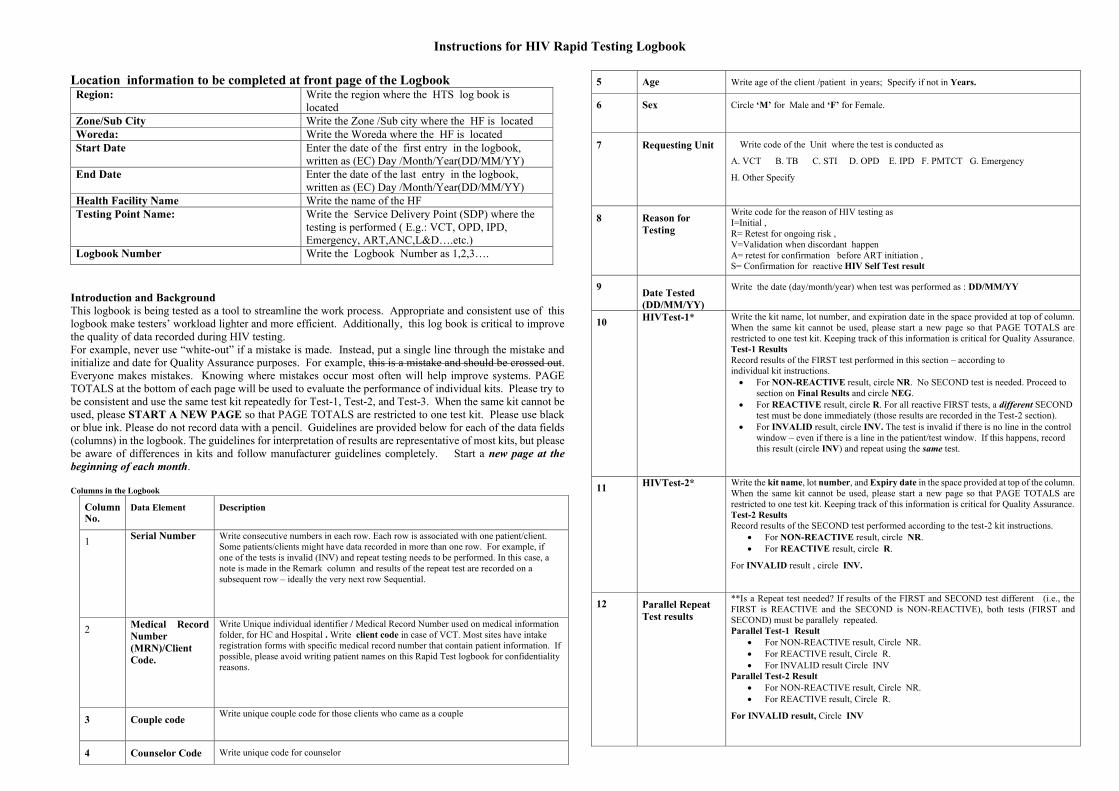
Location information to be completed at front page of the Logbook Region: Write the region where the HTS log book is
located Zone/Sub City Write the Zone /Sub city where the HF is located Woreda: Write the Woreda where the HF is located Start Date Enter the date of the first entry in the logbook,
written as (EC) Day /Month/Year(DD/MM/YY) End Date Enter the date of the last entry in the logbook,
written as (EC) Day /Month/Year(DD/MM/YY) Health Facility Name Write the name of the HF Testing Point Name: Write the Service Delivery Point (SDP) where the
testing is performed ( E.g.: VCT, OPD, IPD, Emergency, ART,ANC,L&D….etc.)
Logbook Number Write the Logbook Number as 1,2,3…. Introduction and Background This logbook is being tested as a tool to streamline the work process. Appropriate and consistent use of this logbook make testers’ workload lighter and more efficient. Additionally, this log book is critical to improve the quality of data recorded during HIV testing. For example, never use “white-out” if a mistake is made. Instead, put a single line through the mistake and initialize and date for Quality Assurance purposes. For example, this is a mistake and should be crossed out. Everyone makes mistakes. Knowing where mistakes occur most often will help improve systems. PAGE TOTALS at the bottom of each page will be used to evaluate the performance of individual kits. Please try to be consistent and use the same test kit repeatedly for Test-1, Test-2, and Test-3. When the same kit cannot be used, please START A NEW PAGE so that PAGE TOTALS are restricted to one test kit. Please use black or blue ink. Please do not record data with a pencil. Guidelines are provided below for each of the data fields (columns) in the logbook. The guidelines for interpretation of results are representative of most kits, but please be aware of differences in kits and follow manufacturer guidelines completely. Start a new page at the beginning of each month. Columns in the Logbook
Column No.
Data Element Description
1 Serial Number Write consecutive numbers in each row. Each row is associated with one patient/client. Some patients/clients might have data recorded in more than one row. For example, if one of the tests is invalid (INV) and repeat testing needs to be performed. In this case, a note is made in the Remark column and results of the repeat test are recorded on a subsequent row – ideally the very next row Sequential.
2 Medical Record Number (MRN)/Client Code.
Write Unique individual identifier / Medical Record Number used on medical information folder, for HC and Hospital . Write client code in case of VCT. Most sites have intake registration forms with specific medical record number that contain patient information. If possible, please avoid writing patient names on this Rapid Test logbook for confidentiality reasons.
3 Couple code Write unique couple code for those clients who came as a couple
4 Counselor Code Write unique code for counselor
5 Age Write age of the client /patient in years; Specify if not in Years.
6 Sex Circle ‘M’ for Male and ‘F’ for Female.
7 Requesting Unit
Write code of the Unit where the test is conducted as
A. VCT B. TB C. STI D. OPD E. IPD F. PMTCT G. Emergency
H. Other Specify
8 Reason for Testing
Write code for the reason of HIV testing as I=Initial , R= Retest for ongoing risk , V=Validation when discordant happen A= retest for confirmation before ART initiation , S= Confirmation for reactive HIV Self Test result
9 Date Tested (DD/MM/YY)
Write the date (day/month/year) when test was performed as : DD/MM/YY
10 HIVTest-1*
Write the kit name, lot number, and expiration date in the space provided at top of column. When the same kit cannot be used, please start a new page so that PAGE TOTALS are restricted to one test kit. Keeping track of this information is critical for Quality Assurance. Test-1 Results Record results of the FIRST test performed in this section – according to individual kit instructions. • For NON-REACTIVE result, circle NR. No SECOND test is needed. Proceed to
section on Final Results and circle NEG. • For REACTIVE result, circle R. For all reactive FIRST tests, a different SECOND
test must be done immediately (those results are recorded in the Test-2 section). • For INVALID result, circle INV. The test is invalid if there is no line in the control
window – even if there is a line in the patient/test window. If this happens, record this result (circle INV) and repeat using the same test.
11 HIVTest-2*
Write the kit name, lot number, and Expiry date in the space provided at top of the column. When the same kit cannot be used, please start a new page so that PAGE TOTALS are restricted to one test kit. Keeping track of this information is critical for Quality Assurance. Test-2 Results Record results of the SECOND test performed according to the test-2 kit instructions.
• For NON-REACTIVE result, circle NR. • For REACTIVE result, circle R.
For INVALID result , circle INV.
12 Parallel Repeat Test results
**Is a Repeat test needed? If results of the FIRST and SECOND test different (i.e., the FIRST is REACTIVE and the SECOND is NON-REACTIVE), both tests (FIRST and SECOND) must be parallely repeated. Parallel Test-1 Result
• For NON-REACTIVE result, Circle NR. • For REACTIVE result, Circle R. • For INVALID result Circle INV
Parallel Test-2 Result • For NON-REACTIVE result, Circle NR. • For REACTIVE result, Circle R.
For INVALID result, Circle INV
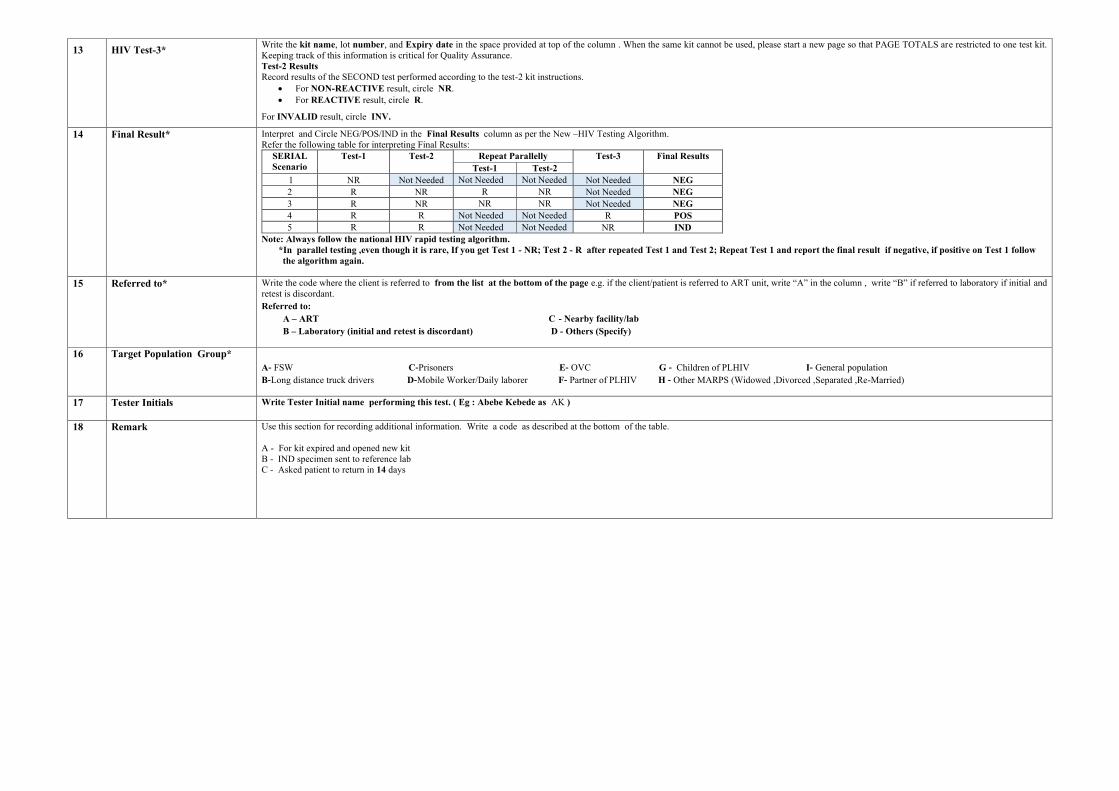
13 HIV Test-3* Write the kit name, lot number, and Expiry date in the space provided at top of the column . When the same kit cannot be used, please start a new page so that PAGE TOTALS are restricted to one test kit. Keeping track of this information is critical for Quality Assurance. Test-2 Results Record results of the SECOND test performed according to the test-2 kit instructions.
• For NON-REACTIVE result, circle NR. • For REACTIVE result, circle R.
For INVALID result, circle INV.
14 Final Result* Interpret and Circle NEG/POS/IND in the Final Results column as per the New –HIV Testing Algorithm. Refer the following table for interpreting Final Results:
SERIAL Scenario
Test-1 Test-2 Repeat Parallelly Test-3 Final Results Test-1 Test-2
1 NR Not Needed Not Needed Not Needed Not Needed NEG 2 R NR R NR Not Needed NEG 3 R NR NR NR Not Needed NEG 4 R R Not Needed Not Needed R POS 5 R R Not Needed Not Needed NR IND
Note: Always follow the national HIV rapid testing algorithm. *In parallel testing ,even though it is rare, If you get Test 1 - NR; Test 2 - R after repeated Test 1 and Test 2; Repeat Test 1 and report the final result if negative, if positive on Test 1 follow the algorithm again.
15 Referred to* Write the code where the client is referred to from the list at the bottom of the page e.g. if the client/patient is referred to ART unit, write “A” in the column , write “B” if referred to laboratory if initial and
retest is discordant. Referred to: A – ART C - Nearby facility/lab B – Laboratory (initial and retest is discordant) D - Others (Specify)
16 Target Population Group* A- FSW C-Prisoners E- OVC G - Children of PLHIV I- General population B-Long distance truck drivers D-Mobile Worker/Daily laborer F- Partner of PLHIV H - Other MARPS (Widowed ,Divorced ,Separated ,Re-Married)
17 Tester Initials
Write Tester Initial name performing this test. ( Eg : Abebe Kebede as AK )
18 Remark Use this section for recording additional information. Write a code as described at the bottom of the table. A - For kit expired and opened new kit B - IND specimen sent to reference lab C - Asked patient to return in 14 days
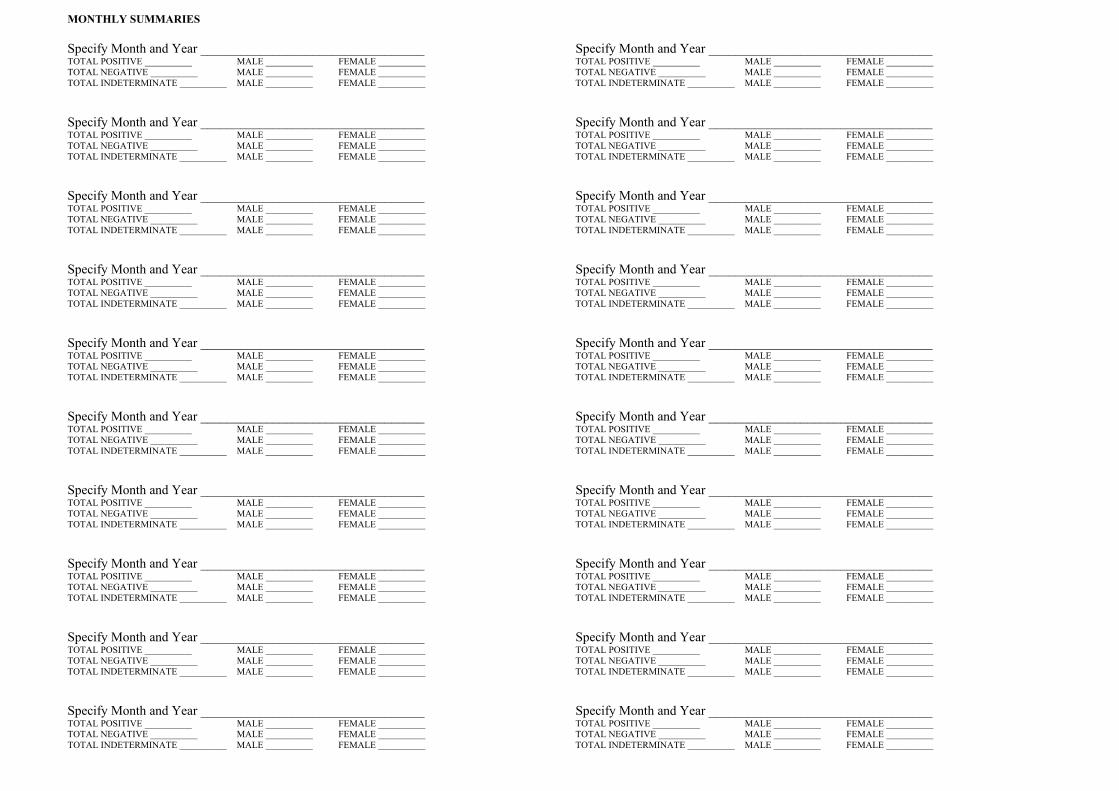
MONTHLY SUMMARIES Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ Specify Month and Year __________________________________ Specify Month and Year __________________________________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL POSITIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________ TOTAL NEGATIVE __________ MALE __________ FEMALE __________
TOTAL INDETERMINATE __________ MALE __________ FEMALE __________ TOTAL INDETERMINATE __________ MALE __________ FEMALE __________
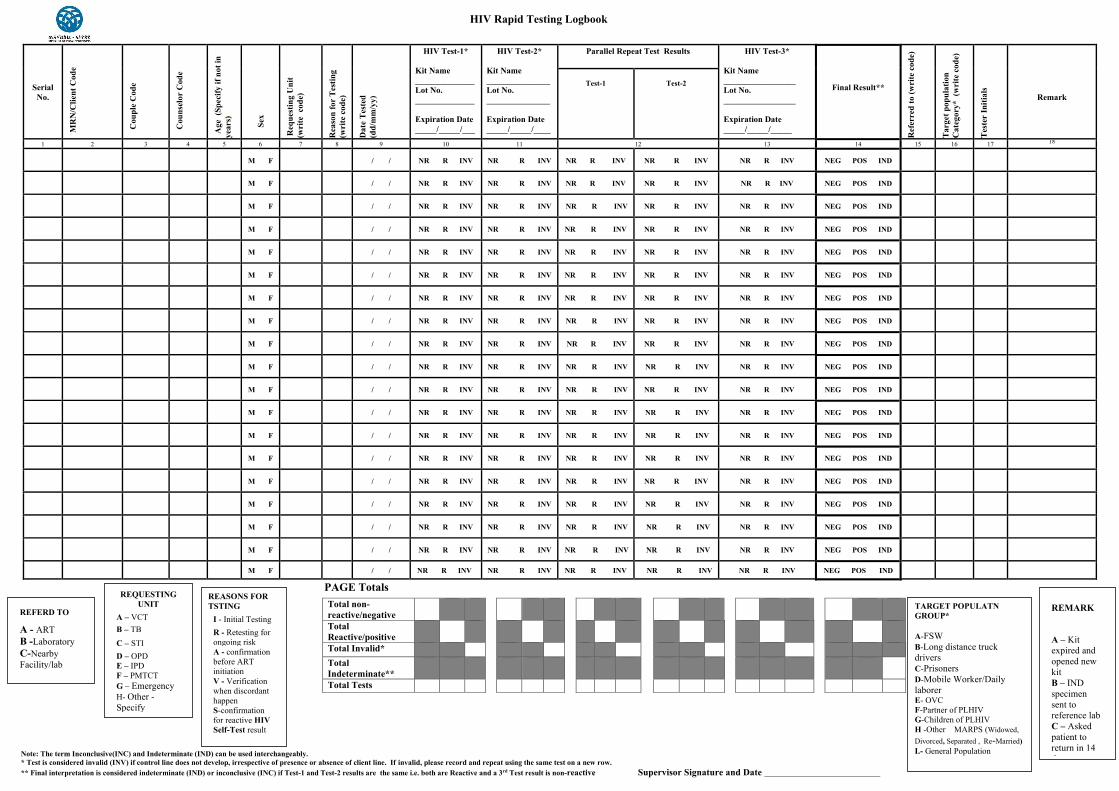
HIV Rapid Testing Logbook
PAGE Totals
Note: The term Inconclusive(INC) and Indeterminate (IND) can be used interchangeably. * Test is considered invalid (INV) if control line does not develop, irrespective of presence or absence of client line. If invalid, please record and repeat using the same test on a new row. ** Final interpretation is considered indeterminate (IND) or inconclusive (INC) if Test-1 and Test-2 results are the same i.e. both are Reactive and a 3rd Test result is non-reactive Supervisor Signature and Date
Serial No.
MR
N/C
lient
Cod
e
Cou
ple
Cod
e
Cou
nsel
or C
ode
Age
(Sp
ecify
if n
ot in
ye
ars)
S
ex
Req
uest
ing
Uni
t
(wri
te c
ode)
Rea
son
for
Tes
ting
(w
rite
cod
e)
Dat
e T
este
d
(dd/
mm
/yy)
HIV Test-1*
Kit Name ______________ Lot No. ______________ Expiration Date _____/_____/___
HIV Test-2*
Kit Name _______________ Lot No. _______________ Expiration Date _____/_____/____
Parallel Repeat Test Results HIV Test-3*
Kit Name _________________ Lot No. _________________ Expiration Date _____/_____/_____
Final Result**
Ref
erre
d to
(wri
te c
ode)
Tar
get p
opul
atio
n C
ateg
ory*
(w
rite
cod
e)
Tes
ter
Initi
als
Remark
Test-1
Test-2
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
M F / / NR R INV NR R INV NR R INV NR R INV NR R INV NEG POS IND
Total non-reactive/negative
Total Reactive/positive
Total Invalid* Total Indeterminate**
Total Tests
REFERD TO
A - ART B -Laboratory C-Nearby Facility/lab
REQUESTING UNIT
A – VCT B – TB C – STI D – OPD E – IPD F – PMTCT G – Emergency H- Other -Specify
TARGET POPULATN GROUP* A-FSW B-Long distance truck drivers C-Prisoners D-Mobile Worker/Daily laborer E- OVC F-Partner of PLHIV G-Children of PLHIV H -Other MARPS (Widowed, Divorced, Separated , Re-Married) I.- General Population
REMARK
A – Kit expired and opened new kit B – IND specimen sent to reference lab C – Asked patient to return in 14 days
REASONS FOR TSTING
I - Initial Testing R - Retesting for ongoing risk A - confirmation before ART initiation V - Verification when discordant happen S-confirmation for reactive HIV Self-Test result
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Index Case Testing Register
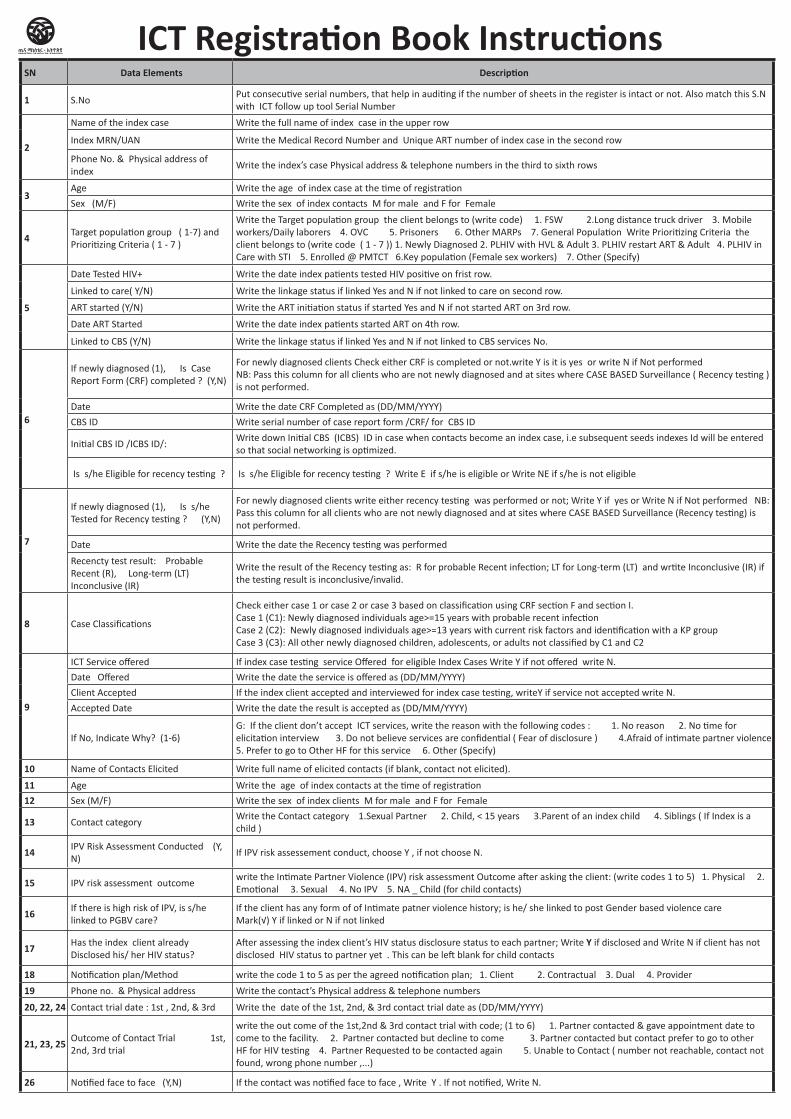
SN Data Elements Description
1 S.NoPut consecutive serial numbers, that help in auditing if the number of sheets in the register is intact or not. Also match this S.N with ICT follow up tool Serial Number
2
Name of the index case Write the full name of index case in the upper row
Index MRN/UAN Write the Medical Record Number and Unique ART number of index case in the second row
Phone No. & Physical address of index
Write the index’s case Physical address & telephone numbers in the third to sixth rows
3Age Write the age of index case at the time of registration
Sex (M/F) Write the sex of index contacts M for male and F for Female
4 Target population group ( 1-7) and Prioritizing Criteria ( 1 - 7 )
Write the Target population group the client belongs to (write code) 1. FSW 2.Long distance truck driver 3. Mobile workers/Daily laborers 4. OVC 5. Prisoners 6. Other MARPs 7. General Population Write Prioritizing Criteria the client belongs to (write code ( 1 - 7 )) 1. Newly Diagnosed 2. PLHIV with HVL & Adult 3. PLHIV restart ART & Adult 4. PLHIV in Care with STI 5. Enrolled @ PMTCT 6.Key population (Female sex workers) 7. Other (Specify)
5
Date Tested HIV+ Write the date index patients tested HIV positive on frist row.
Linked to care( Y/N) Write the linkage status if linked Yes and N if not linked to care on second row.
ART started (Y/N) Write the ART initiation status if started Yes and N if not started ART on 3rd row.
Date ART Started Write the date index patients started ART on 4th row.
Linked to CBS (Y/N) Write the linkage status if linked Yes and N if not linked to CBS services No.
6
If newly diagnosed (1), Is Case Report Form (CRF) completed ? (Y,N)
For newly diagnosed clients Check either CRF is completed or not.write Y is it is yes or write N if Not performed NB: Pass this column for all clients who are not newly diagnosed and at sites where CASE BASED Surveillance ( Recency testing ) is not performed.
Date Write the date CRF Completed as (DD/MM/YYYY)
CBS ID Write serial number of case report form /CRF/ for CBS ID
Initial CBS ID /ICBS ID/:Write down Initial CBS (ICBS) ID in case when contacts become an index case, i.e subsequent seeds indexes Id will be entered so that social networking is optimized.
Is s/he Eligible for recency testing ? Is s/he Eligible for recency testing ? Write E if s/he is eligible or Write NE if s/he is not eligible
7
If newly diagnosed (1), Is s/he Tested for Recency testing ? (Y,N)
For newly diagnosed clients write either recency testing was performed or not; Write Y if yes or Write N if Not performed NB: Pass this column for all clients who are not newly diagnosed and at sites where CASE BASED Surveillance (Recency testing) is not performed.
Date Write the date the Recency testing was performed
Recencty test result: Probable Recent (R), Long-term (LT) Inconclusive (IR)
Write the result of the Recency testing as: R for probable Recent infection; LT for Long-term (LT) and wrtite Inconclusive (IR) if the testing result is inconclusive/invalid.
8 Case Classifications
Check either case 1 or case 2 or case 3 based on classification using CRF section F and section I. Case 1 (C1): Newly diagnosed individuals age>=15 years with probable recent infection Case 2 (C2): Newly diagnosed individuals age>=13 years with current risk factors and identification with a KP group Case 3 (C3): All other newly diagnosed children, adolescents, or adults not classified by C1 and C2
9
ICT Service offered If index case testing service Offered for eligible Index Cases Write Y if not offered write N.
Date Offered Write the date the service is offered as (DD/MM/YYYY)
Client Accepted If the index client accepted and interviewed for index case testing, writeY if service not accepted write N.
Accepted Date Write the date the result is accepted as (DD/MM/YYYY)
If No, Indicate Why? (1-6) G: If the client don’t accept ICT services, write the reason with the following codes : 1. No reason 2. No time for elicitation interview 3. Do not believe services are confidential ( Fear of disclosure ) 4.Afraid of intimate partner violence 5. Prefer to go to Other HF for this service 6. Other (Specify)
10 Name of Contacts Elicited Write full name of elicited contacts (if blank, contact not elicited).
11 Age Write the age of index contacts at the time of registration
12 Sex (M/F) Write the sex of index clients M for male and F for Female
13 Contact category Write the Contact category 1.Sexual Partner 2. Child, < 15 years 3.Parent of an index child 4. Siblings ( If Index is a child )
14 IPV Risk Assessment Conducted (Y, N)
If IPV risk assessement conduct, choose Y , if not choose N.
15 IPV risk assessment outcome write the Intimate Partner Violence (IPV) risk assessment Outcome after asking the client: (write codes 1 to 5) 1. Physical 2. Emotional 3. Sexual 4. No IPV 5. NA _ Child (for child contacts)
16 If there is high risk of IPV, is s/he linked to PGBV care?
If the client has any form of of Intimate patner violence history; is he/ she linked to post Gender based violence care Mark(√) Y if linked or N if not linked
17 Has the index client already Disclosed his/ her HIV status?
After assessing the index client’s HIV status disclosure status to each partner; Write Y if disclosed and Write N if client has not disclosed HIV status to partner yet . This can be left blank for child contacts
18 Notification plan/Method write the code 1 to 5 as per the agreed notification plan; 1. Client 2. Contractual 3. Dual 4. Provider
19 Phone no. & Physical address Write the contact’s Physical address & telephone numbers
20, 22, 24 Contact trial date : 1st , 2nd, & 3rd Write the date of the 1st, 2nd, & 3rd contact trial date as (DD/MM/YYYY)
21, 23, 25 Outcome of Contact Trial 1st, 2nd, 3rd trial
write the out come of the 1st,2nd & 3rd contact trial with code; (1 to 6) 1. Partner contacted & gave appointment date to come to the facility. 2. Partner contacted but decline to come 3. Partner contacted but contact prefer to go to other HF for HIV testing 4. Partner Requested to be contacted again 5. Unable to Contact ( number not reachable, contact not found, wrong phone number ,...)
26 Notified face to face (Y,N) If the contact was notified face to face , Write Y . If not notified, Write N.
ICT Registration Book Instructions
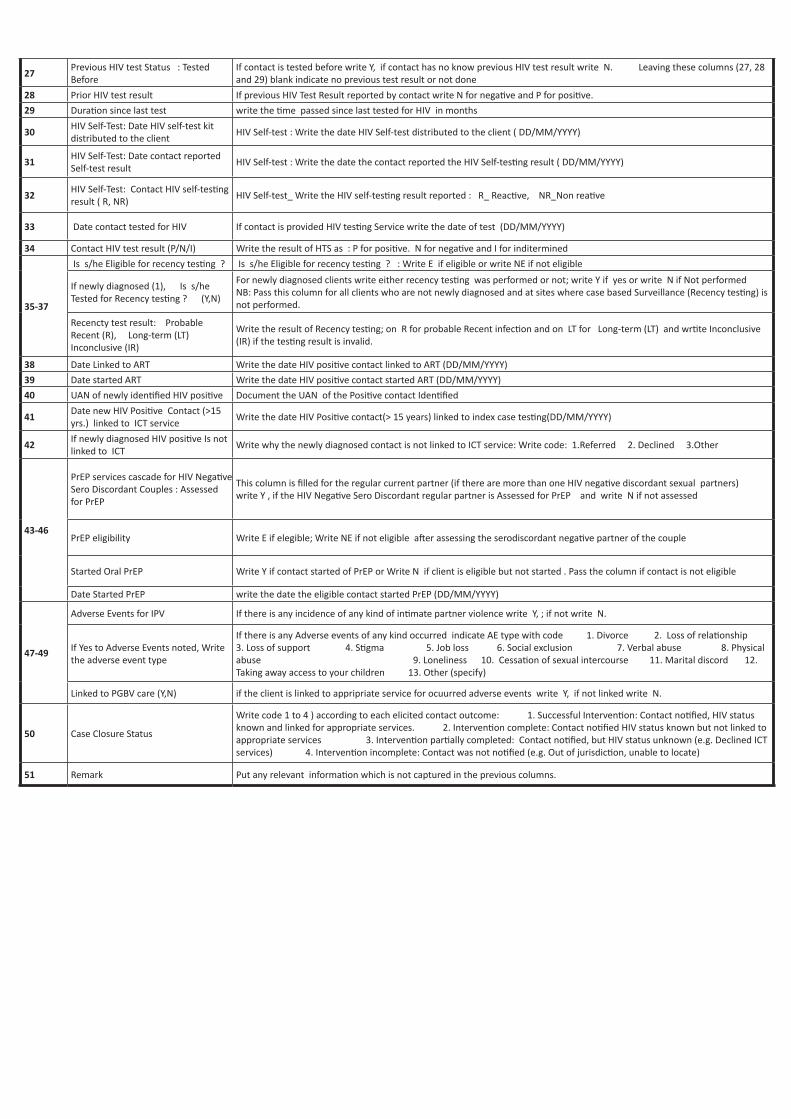
27 Previous HIV test Status : Tested Before
If contact is tested before write Y, if contact has no know previous HIV test result write N. Leaving these columns (27, 28 and 29) blank indicate no previous test result or not done
28 Prior HIV test result If previous HIV Test Result reported by contact write N for negative and P for positive.
29 Duration since last test write the time passed since last tested for HIV in months
30 HIV Self-Test: Date HIV self-test kit distributed to the client
HIV Self-test : Write the date HIV Self-test distributed to the client ( DD/MM/YYYY)
31 HIV Self-Test: Date contact reported Self-test result
HIV Self-test : Write the date the contact reported the HIV Self-testing result ( DD/MM/YYYY)
32 HIV Self-Test: Contact HIV self-testing result ( R, NR)
HIV Self-test_ Write the HIV self-testing result reported : R_ Reactive, NR_Non reative
33 Date contact tested for HIV If contact is provided HIV testing Service write the date of test (DD/MM/YYYY)
34 Contact HIV test result (P/N/I) Write the result of HTS as : P for positive. N for negative and I for inditermined
35-37
Is s/he Eligible for recency testing ? Is s/he Eligible for recency testing ? : Write E if eligible or write NE if not eligible
If newly diagnosed (1), Is s/he Tested for Recency testing ? (Y,N)
For newly diagnosed clients write either recency testing was performed or not; write Y if yes or write N if Not performed NB: Pass this column for all clients who are not newly diagnosed and at sites where case based Surveillance (Recency testing) is not performed.
Recencty test result: Probable Recent (R), Long-term (LT) Inconclusive (IR)
Write the result of Recency testing; on R for probable Recent infection and on LT for Long-term (LT) and wrtite Inconclusive (IR) if the testing result is invalid.
38 Date Linked to ART Write the date HIV positive contact linked to ART (DD/MM/YYYY)
39 Date started ART Write the date HIV positive contact started ART (DD/MM/YYYY)
40 UAN of newly identified HIV positive Document the UAN of the Positive contact Identified
41 Date new HIV Positive Contact (>15 yrs.) linked to ICT service
Write the date HIV Positive contact(> 15 years) linked to index case testing(DD/MM/YYYY)
42 If newly diagnosed HIV positive Is not linked to ICT
Write why the newly diagnosed contact is not linked to ICT service: Write code: 1.Referred 2. Declined 3.Other
43-46
PrEP services cascade for HIV Negative Sero Discordant Couples : Assessed for PrEP
This column is filled for the regular current partner (if there are more than one HIV negative discordant sexual partners) write Y , if the HIV Negative Sero Discordant regular partner is Assessed for PrEP and write N if not assessed
PrEP eligibility Write E if elegible; Write NE if not eligible after assessing the serodiscordant negative partner of the couple
Started Oral PrEP Write Y if contact started of PrEP or Write N if client is eligible but not started . Pass the column if contact is not eligible
Date Started PrEP write the date the eligible contact started PrEP (DD/MM/YYYY)
47-49
Adverse Events for IPV If there is any incidence of any kind of intimate partner violence write Y, ; if not write N.
If Yes to Adverse Events noted, Write the adverse event type
If there is any Adverse events of any kind occurred indicate AE type with code 1. Divorce 2. Loss of relationship 3. Loss of support 4. Stigma 5. Job loss 6. Social exclusion 7. Verbal abuse 8. Physical abuse 9. Loneliness 10. Cessation of sexual intercourse 11. Marital discord 12. Taking away access to your children 13. Other (specify)
Linked to PGBV care (Y,N) if the client is linked to appripriate service for ocuurred adverse events write Y, if not linked write N.
50 Case Closure Status
Write code 1 to 4 ) according to each elicited contact outcome: 1. Successful Intervention: Contact notified, HIV status known and linked for appropriate services. 2. Intervention complete: Contact notified HIV status known but not linked to appropriate services 3. Intervention partially completed: Contact notified, but HIV status unknown (e.g. Declined ICT services) 4. Intervention incomplete: Contact was not notified (e.g. Out of jurisdiction, unable to locate)
51 Remark Put any relevant information which is not captured in the previous columns.
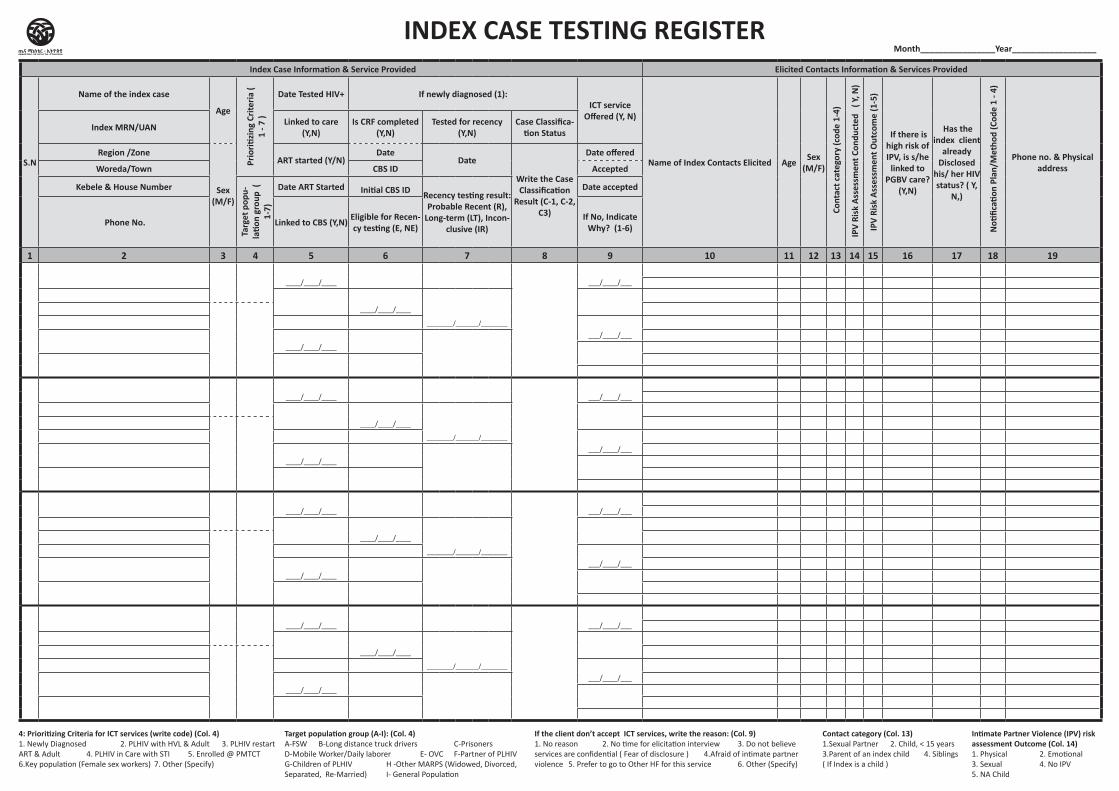
Index Case Information & Service Provided Elicited Contacts Information & Services Provided
RemarkS.N
Name of the index case
Age
Prio
ritizi
ng C
riter
ia (
1 - 7
)
Date Tested HIV+ If newly diagnosed (1): ICT service
Offered (Y, N)
Name of Index Contacts Elicited Age Sex (M/F)
Con
tact
cat
egor
y (c
ode
1-4)
IPV
Risk
Ass
essm
ent C
ondu
cted
( Y
, N)
IPV
Risk
Ass
essm
ent O
utco
me
(1-5
)
If there is high risk of IPV, is s/he
linked to PGBV care?
(Y,N)
Has the index client
already Disclosed
his/ her HIV status? ( Y,
N,)
N
otific
ation
Pla
n/M
etho
d (C
ode
1 - 4
)
Phone no. & Physical address
Outcome of Contact Trial
Noti-fied face to
face (Y,N)
Previous HIV Test Status HTS Provided RTRI for newly diagnosed HIV
positive contacts Linkage to care & treatment PrEP services cascade for HIV Negative Sero Discordant Couples Adverse Events monitoring
Case
clo
sure
stat
us (
code
1 to
4)
Index MRN/UAN Linked to care (Y,N)
Is CRF completed (Y,N)
Tested for recency (Y,N)
Case Classifica-tion Status 1st Trial 2nd Trial 3rd Trial
Test-ed Be-fore (Y,N)
Prio
r HIV
test
resu
lt (P
/N/I
)
Dura
tion
sinc
e la
st te
st (
in
mnt
h)
HIV Self-test National Algo-rithm
Is s/he Eligi-
ble for Recency testing ? (E, NE)
Is s/he Test-
ed for recency ? (Y,N)
Recency testing
result: Prob-able Recent
(R), Long-term (LT),
Inconclusive (IR)
Date Linked to ART
Date ART
started
UAN of new-ly identified HIV positive
Date
new
HIV
Pos
itive
Con
tact
lin
ked
to IC
T se
rvic
e
If no
t lin
ked
to I
CT (C
ode
1-3)
Assessed for PrEP
(Y, N)
PrEP el-igibility (E, NE)
Started Oral PrEP (Y,N)
Date started
PrEP
Adverse Events for IPV (Y,N)
If Y, AE type ( 1-13)
Linked to aprropriate
service (Y,N)
Region /Zone
Sex (M/F)
ART started (Y/N)Date
Date
Write the Case Classification
Result (C-1, C-2, C3)
Date offered
Date (D/M/Y)
Out
com
e ( 1
- 4)
Date (D/M/Y)
Out
com
e ( 1
- 4)
Date (D/M/Y)
Out
com
e ( 1
- 4) Date HIV
Self-test kit dis-
tributed (D/M/Y)
Date contact
reported self test result
(D/M/Y)
Cont
act H
IV S
elf-t
estin
g re
sult
(R/N
R) Date contact tested for HIV
(D/M/Y)
Cont
act H
IV te
st re
sult
(P/N
/I)
Woreda/Town CBS ID Accepted
Kebele & House Number
Targ
et p
opu-
latio
n gr
oup
( 1-
7)
Date ART Started Initial CBS ID Recency testing result: Probable Recent (R),
Long-term (LT), Incon-clusive (IR)
Date accepted
Phone No. Linked to CBS (Y,N) Eligible for Recen-cy testing (E, NE)
If No, Indicate Why? (1-6)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
4: Prioritizing Criteria for ICT services (write code) (Col. 4)1. Newly Diagnosed 2. PLHIV with HVL & Adult 3. PLHIV restart ART & Adult 4. PLHIV in Care with STI 5. Enrolled @ PMTCT 6.Key population (Female sex workers) 7. Other (Specify)
If the client don’t accept ICT services, write the reason: (Col. 9)1. No reason 2. No time for elicitation interview 3. Do not believe services are confidential ( Fear of disclosure ) 4.Afraid of intimate partner violence 5. Prefer to go to Other HF for this service 6. Other (Specify)
Contact category (Col. 13)1.Sexual Partner 2. Child, < 15 years 3.Parent of an index child 4. Siblings ( If Index is a child )
Intimate Partner Violence (IPV) risk assessment Outcome (Col. 14) 1. Physical 2. Emotional 3. Sexual 4. No IPV 5. NA Child
INDEX CASE TESTING REGISTERMonth________________Year__________________
Target population group (A-I): (Col. 4)A-FSW B-Long distance truck drivers C-PrisonersD-Mobile Worker/Daily laborer E- OVC F-Partner of PLHIV G-Children of PLHIV H -Other MARPS (Widowed, Divorced, Separated, Re-Married) I- General Population
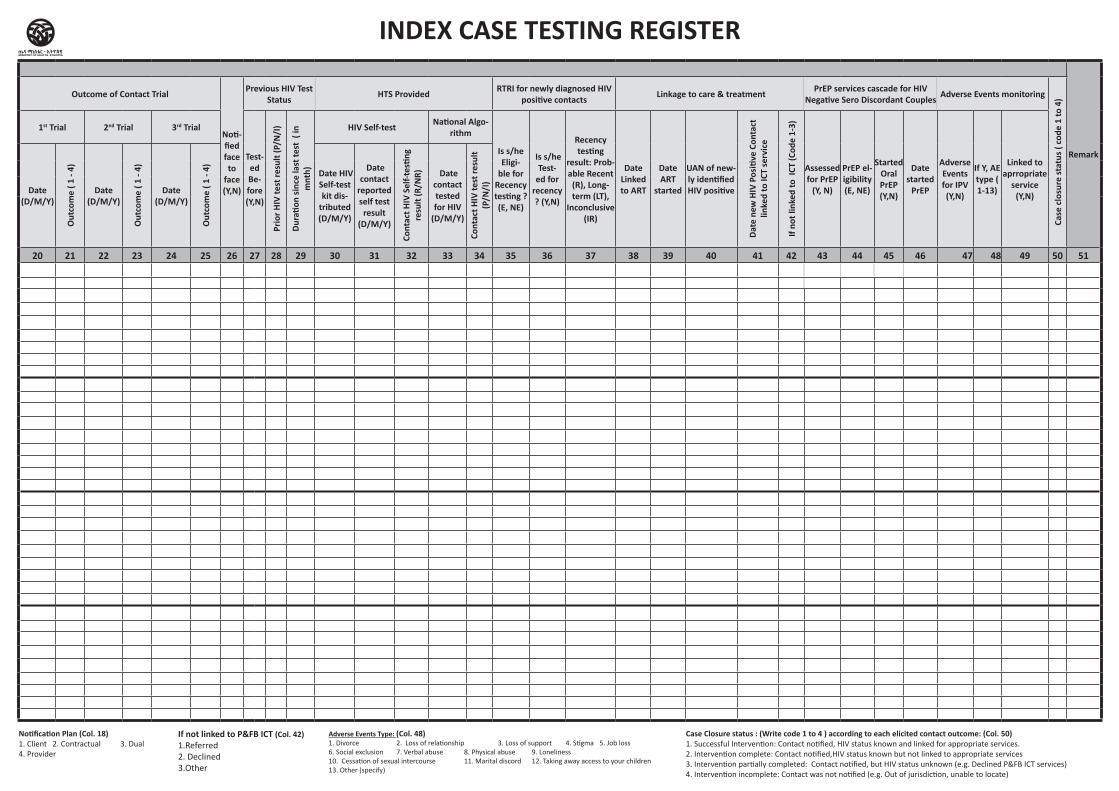
Index Case Information & Service Provided Elicited Contacts Information & Services Provided
RemarkS.N
Name of the index case
Age
Prio
ritizi
ng C
riter
ia (
1 - 7
)
Date Tested HIV+ If newly diagnosed (1): ICT service
Offered (Y, N)
Name of Index Contacts Elicited Age Sex (M/F)
Con
tact
cat
egor
y (c
ode
1-4)
IPV
Risk
Ass
essm
ent C
ondu
cted
( Y
, N)
IPV
Risk
Ass
essm
ent O
utco
me
(1-5
)
If there is high risk of IPV, is s/he
linked to PGBV care?
(Y,N)
Has the index client
already Disclosed
his/ her HIV status? ( Y,
N,)
N
otific
ation
Pla
n/M
etho
d (C
ode
1 - 4
)
Phone no. & Physical address
Outcome of Contact Trial
Noti-fied face to
face (Y,N)
Previous HIV Test Status HTS Provided RTRI for newly diagnosed HIV
positive contacts Linkage to care & treatment PrEP services cascade for HIV Negative Sero Discordant Couples Adverse Events monitoring
Case
clo
sure
stat
us (
code
1 to
4)
Index MRN/UAN Linked to care (Y,N)
Is CRF completed (Y,N)
Tested for recency (Y,N)
Case Classifica-tion Status 1st Trial 2nd Trial 3rd Trial
Test-ed Be-fore (Y,N)
Prio
r HIV
test
resu
lt (P
/N/I
)
Dura
tion
sinc
e la
st te
st (
in
mnt
h)
HIV Self-test National Algo-rithm
Is s/he Eligi-
ble for Recency testing ? (E, NE)
Is s/he Test-
ed for recency ? (Y,N)
Recency testing
result: Prob-able Recent
(R), Long-term (LT),
Inconclusive (IR)
Date Linked to ART
Date ART
started
UAN of new-ly identified HIV positive
Date
new
HIV
Pos
itive
Con
tact
lin
ked
to IC
T se
rvic
e
If no
t lin
ked
to I
CT (C
ode
1-3)
Assessed for PrEP
(Y, N)
PrEP el-igibility (E, NE)
Started Oral PrEP (Y,N)
Date started
PrEP
Adverse Events for IPV (Y,N)
If Y, AE type ( 1-13)
Linked to aprropriate
service (Y,N)
Region /Zone
Sex (M/F)
ART started (Y/N)Date
Date
Write the Case Classification
Result (C-1, C-2, C3)
Date offered
Date (D/M/Y)
Out
com
e ( 1
- 4)
Date (D/M/Y)
Out
com
e ( 1
- 4)
Date (D/M/Y)
Out
com
e ( 1
- 4) Date HIV
Self-test kit dis-
tributed (D/M/Y)
Date contact
reported self test result
(D/M/Y)
Cont
act H
IV S
elf-t
estin
g re
sult
(R/N
R) Date contact tested for HIV
(D/M/Y)
Cont
act H
IV te
st re
sult
(P/N
/I)
Woreda/Town CBS ID Accepted
Kebele & House Number
Targ
et p
opu-
latio
n gr
oup
( 1-
7)
Date ART Started Initial CBS ID Recency testing result: Probable Recent (R),
Long-term (LT), Incon-clusive (IR)
Date accepted
Phone No. Linked to CBS (Y,N) Eligible for Recen-cy testing (E, NE)
If No, Indicate Why? (1-6)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
____/____/____ ___/____/___
____/____/____
________/_______/________
___/____/___
____/____/____
Notification Plan (Col. 18) 1. Client 2. Contractual 3. Dual 4. Provider
If not linked to P&FB ICT (Col. 42)1.Referred2. Declined3.Other
Adverse Events Type: (Col. 48)1. Divorce 2. Loss of relationship 3. Loss of support 4. Stigma 5. Job loss 6. Social exclusion 7. Verbal abuse 8. Physical abuse 9. Loneliness 10. Cessation of sexual intercourse 11. Marital discord 12. Taking away access to your children 13. Other (specify)
Case Closure status : (Write code 1 to 4 ) according to each elicited contact outcome: (Col. 50)1. Successful Intervention: Contact notified, HIV status known and linked for appropriate services.2. Intervention complete: Contact notified,HIV status known but not linked to appropriate services3. Intervention partially completed: Contact notified, but HIV status unknown (e.g. Declined P&FB ICT services)4. Intervention incomplete: Contact was not notified (e.g. Out of jurisdiction, unable to locate)
INDEX CASE TESTING REGISTER
Health Center/Clinic / Hospital Post Exposure To HIV Prophylaxis
(PEP) Followup Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
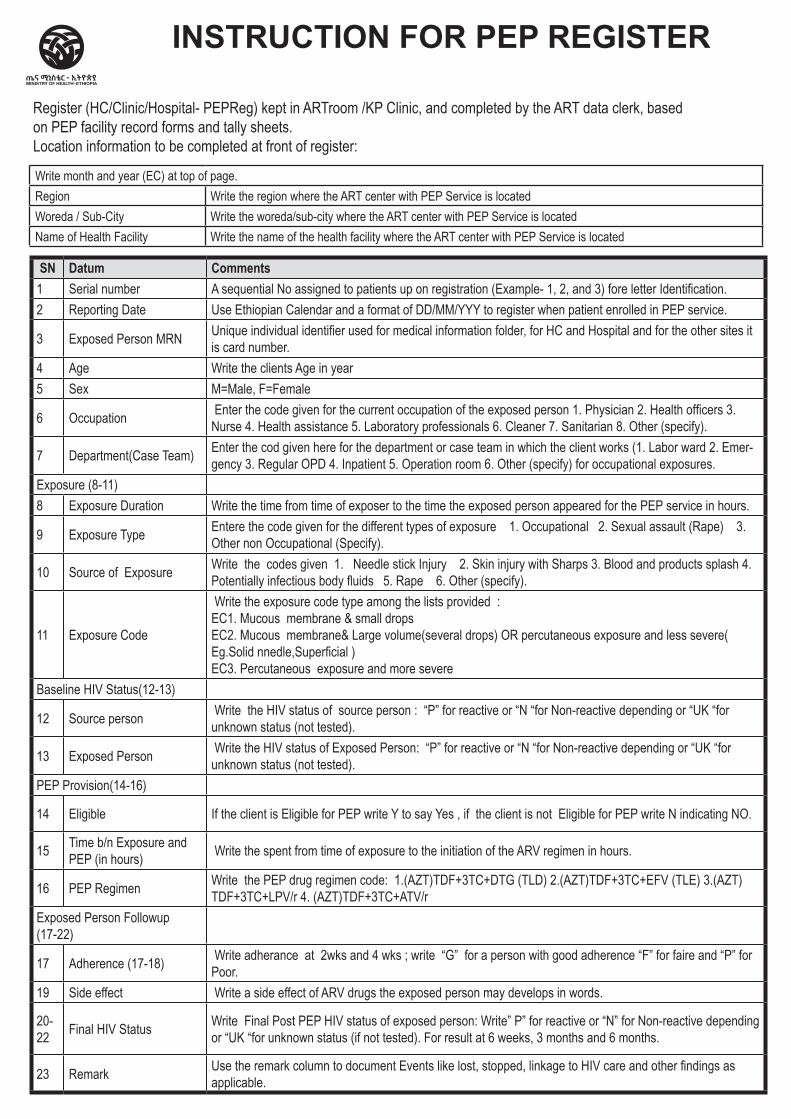
SN Datum Comments1 Serial number A sequential No assigned to patients up on registration (Example- 1, 2, and 3) fore letter Identification.2 Reporting Date Use Ethiopian Calendar and a format of DD/MM/YYY to register when patient enrolled in PEP service.
3 Exposed Person MRN Unique individual identifier used for medical information folder, for HC and Hospital and for the other sites it is card number.
4 Age Write the clients Age in year5 Sex M=Male, F=Female
6 Occupation Enter the code given for the current occupation of the exposed person 1. Physician 2. Health officers 3. Nurse 4. Health assistance 5. Laboratory professionals 6. Cleaner 7. Sanitarian 8. Other (specify).
7 Department(Case Team) Enter the cod given here for the department or case team in which the client works (1. Labor ward 2. Emer-gency 3. Regular OPD 4. Inpatient 5. Operation room 6. Other (specify) for occupational exposures.
Exposure (8-11)8 Exposure Duration Write the time from time of exposer to the time the exposed person appeared for the PEP service in hours.
9 Exposure Type Entere the code given for the different types of exposure 1. Occupational 2. Sexual assault (Rape) 3. Other non Occupational (Specify).
10 Source of Exposure Write the codes given 1. Needle stick Injury 2. Skin injury with Sharps 3. Blood and products splash 4. Potentially infectious body fluids 5. Rape 6. Other (specify).
11 Exposure Code
Write the exposure code type among the lists provided : EC1. Mucous membrane & small drops EC2. Mucous membrane& Large volume(several drops) OR percutaneous exposure and less severe( Eg.Solid nnedle,Superficial ) EC3. Percutaneous exposure and more severe
Baseline HIV Status(12-13)
12 Source person Write the HIV status of source person : “P” for reactive or “N “for Non-reactive depending or “UK “for unknown status (not tested).
13 Exposed Person Write the HIV status of Exposed Person: “P” for reactive or “N “for Non-reactive depending or “UK “for unknown status (not tested).
PEP Provision(14-16)
14 Eligible If the client is Eligible for PEP write Y to say Yes , if the client is not Eligible for PEP write N indicating NO.
15 Time b/n Exposure and PEP (in hours) Write the spent from time of exposure to the initiation of the ARV regimen in hours.
16 PEP Regimen Write the PEP drug regimen code: 1.(AZT)TDF+3TC+DTG (TLD) 2.(AZT)TDF+3TC+EFV (TLE) 3.(AZT)TDF+3TC+LPV/r 4. (AZT)TDF+3TC+ATV/r
Exposed Person Followup (17-22)
17 Adherence (17-18) Write adherance at 2wks and 4 wks ; write “G” for a person with good adherence “F” for faire and “P” for Poor.
19 Side effect Write a side effect of ARV drugs the exposed person may develops in words.
20-22 Final HIV Status Write Final Post PEP HIV status of exposed person: Write” P” for reactive or “N” for Non-reactive depending
or “UK “for unknown status (if not tested). For result at 6 weeks, 3 months and 6 months.
23 Remark Use the remark column to document Events like lost, stopped, linkage to HIV care and other findings as applicable.
INSTRUCTION FOR PEP REGISTER
Register (HC/Clinic/Hospital- PEPReg) kept in ARTroom /KP Clinic, and completed by the ART data clerk, based on PEP facility record forms and tally sheets.Location information to be completed at front of register:
Write month and year (EC) at top of page. Region Write the region where the ART center with PEP Service is locatedWoreda / Sub-City Write the woreda/sub-city where the ART center with PEP Service is locatedName of Health Facility Write the name of the health facility where the ART center with PEP Service is located
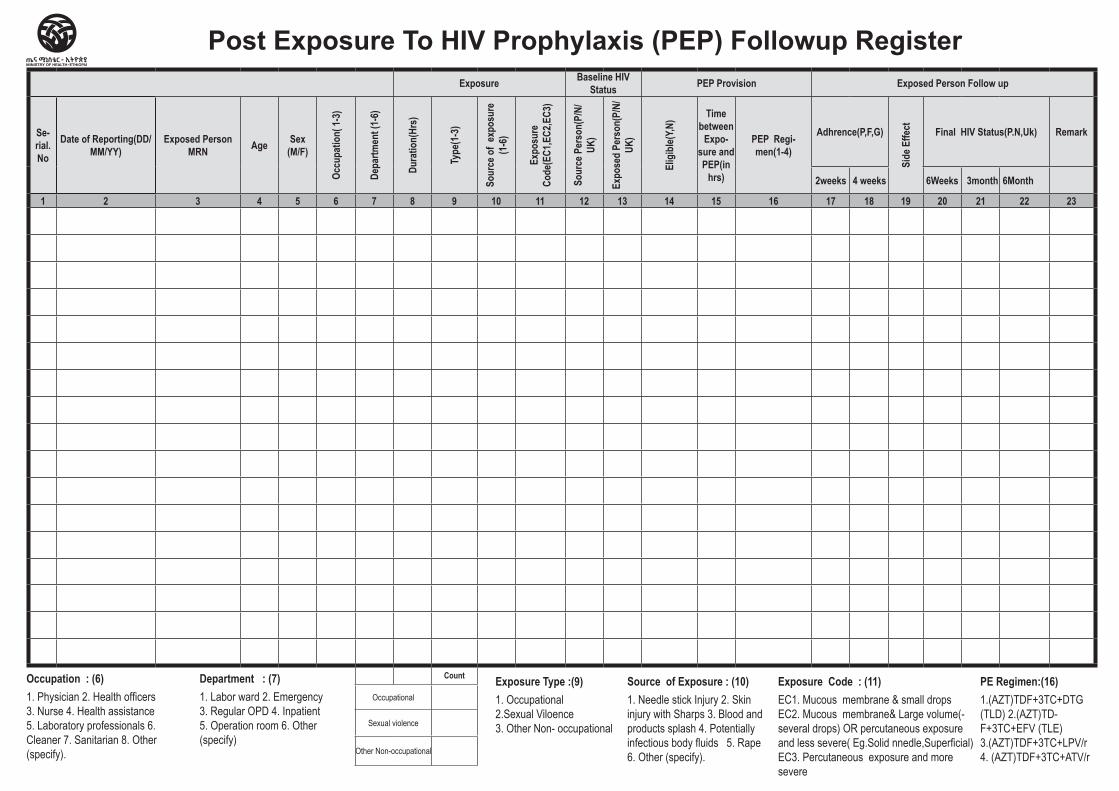
Exposure Baseline HIV Status PEP Provision Exposed Person Follow up
Se-rial. No
Date of Reporting(DD/MM/YY)
Exposed Person MRN Age Sex
(M/F)
Occu
patio
n( 1-
3)
Depa
rtmen
t (1-
6)
Dura
tion(
Hrs)
Type
(1-3
)
Sour
ce o
f ex
posu
re
(1-6
)
Expo
sure
Co
de(E
C1,E
C2,E
C3)
Sour
ce P
erso
n(P/
N/UK
)
Expo
sed
Pers
on(P
/N/
UK)
Elig
ible(
Y,N) Time
between Expo-
sure and PEP(in
hrs)
PEP Regi-men(1-4)
Adhrence(P,F,G)
Side
Effe
ct Final HIV Status(P.N,Uk) Remark
2weeks 4 weeks 6Weeks 3month 6Month
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23
Count
Occupational
Sexual violence
Other Non-occupational
Post Exposure To HIV Prophylaxis (PEP) Followup Register
Occupation : (6) 1. Physician 2. Health officers 3. Nurse 4. Health assistance 5. Laboratory professionals 6. Cleaner 7. Sanitarian 8. Other (specify).
Department : (7) 1. Labor ward 2. Emergency 3. Regular OPD 4. Inpatient 5. Operation room 6. Other (specify)
Exposure Type :(9)1. Occupational2.Sexual Viloence 3. Other Non- occupational
Source of Exposure : (10)1. Needle stick Injury 2. Skin injury with Sharps 3. Blood and products splash 4. Potentially infectious body fluids 5. Rape 6. Other (specify).
Exposure Code : (11)EC1. Mucous membrane & small drops EC2. Mucous membrane& Large volume(-several drops) OR percutaneous exposure and less severe( Eg.Solid nnedle,Superficial)EC3. Percutaneous exposure and more severe
PE Regimen:(16)1.(AZT)TDF+3TC+DTG (TLD) 2.(AZT)TD-F+3TC+EFV (TLE) 3.(AZT)TDF+3TC+LPV/r 4. (AZT)TDF+3TC+ATV/r
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital PrEP Register
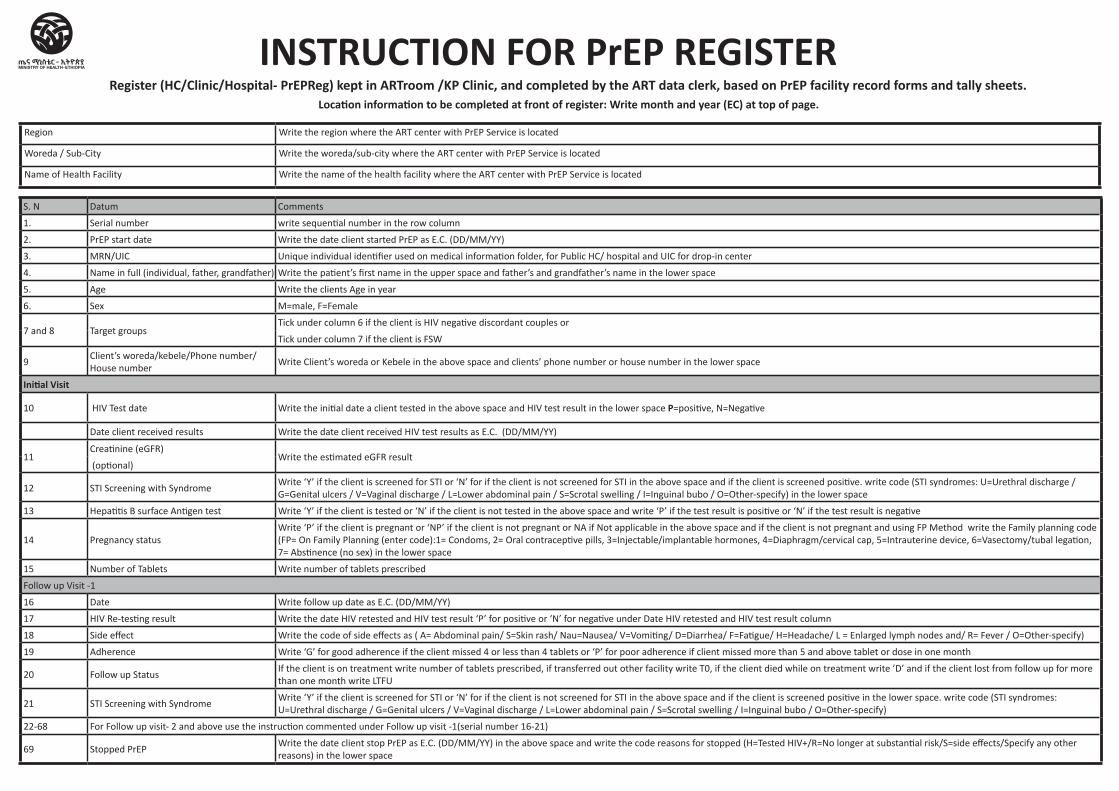
S. N Datum Comments
1. Serial number write sequential number in the row column
2. PrEP start date Write the date client started PrEP as E.C. (DD/MM/YY)
3. MRN/UIC Unique individual identifier used on medical information folder, for Public HC/ hospital and UIC for drop-in center
4. Name in full (individual, father, grandfather) Write the patient’s first name in the upper space and father’s and grandfather’s name in the lower space
5. Age Write the clients Age in year
6. Sex M=male, F=Female
7 and 8 Target groupsTick under column 6 if the client is HIV negative discordant couples or
Tick under column 7 if the client is FSW
9Client’s woreda/kebele/Phone number/House number
Write Client’s woreda or Kebele in the above space and clients’ phone number or house number in the lower space
Initial Visit
10 HIV Test date Write the initial date a client tested in the above space and HIV test result in the lower space P=positive, N=Negative
Date client received results Write the date client received HIV test results as E.C. (DD/MM/YY)
11Creatinine (eGFR)
Write the estimated eGFR result (optional)
12 STI Screening with SyndromeWrite ‘Y’ if the client is screened for STI or ‘N’ for if the client is not screened for STI in the above space and if the client is screened positive. write code (STI syndromes: U=Urethral discharge / G=Genital ulcers / V=Vaginal discharge / L=Lower abdominal pain / S=Scrotal swelling / I=Inguinal bubo / O=Other-specify) in the lower space
13 Hepatitis B surface Antigen test Write ‘Y’ if the client is tested or ‘N’ if the client is not tested in the above space and write ‘P’ if the test result is positive or ‘N’ if the test result is negative
14 Pregnancy statusWrite ‘P’ if the client is pregnant or ‘NP’ if the client is not pregnant or NA if Not applicable in the above space and if the client is not pregnant and using FP Method write the Family planning code (FP= On Family Planning (enter code):1= Condoms, 2= Oral contraceptive pills, 3=Injectable/implantable hormones, 4=Diaphragm/cervical cap, 5=Intrauterine device, 6=Vasectomy/tubal legation, 7= Abstinence (no sex) in the lower space
15 Number of Tablets Write number of tablets prescribed
Follow up Visit -1
16 Date Write follow up date as E.C. (DD/MM/YY)
17 HIV Re-testing result Write the date HIV retested and HIV test result ‘P’ for positive or ‘N’ for negative under Date HIV retested and HIV test result column
18 Side effect Write the code of side effects as ( A= Abdominal pain/ S=Skin rash/ Nau=Nausea/ V=Vomiting/ D=Diarrhea/ F=Fatigue/ H=Headache/ L = Enlarged lymph nodes and/ R= Fever / O=Other-specify)
19 Adherence Write ‘G’ for good adherence if the client missed 4 or less than 4 tablets or ‘P’ for poor adherence if client missed more than 5 and above tablet or dose in one month
20 Follow up StatusIf the client is on treatment write number of tablets prescribed, if transferred out other facility write T0, if the client died while on treatment write ’D’ and if the client lost from follow up for more than one month write LTFU
21 STI Screening with SyndromeWrite ‘Y’ if the client is screened for STI or ‘N’ for if the client is not screened for STI in the above space and if the client is screened positive in the lower space. write code (STI syndromes: U=Urethral discharge / G=Genital ulcers / V=Vaginal discharge / L=Lower abdominal pain / S=Scrotal swelling / I=Inguinal bubo / O=Other-specify)
22-68 For Follow up visit- 2 and above use the instruction commented under Follow up visit -1(serial number 16-21)
69 Stopped PrEPWrite the date client stop PrEP as E.C. (DD/MM/YY) in the above space and write the code reasons for stopped (H=Tested HIV+/R=No longer at substantial risk/S=side effects/Specify any other reasons) in the lower space
INSTRUCTION FOR PrEP REGISTERRegister (HC/Clinic/Hospital- PrEPReg) kept in ARTroom /KP Clinic, and completed by the ART data clerk, based on PrEP facility record forms and tally sheets.
Location information to be completed at front of register: Write month and year (EC) at top of page.
Region Write the region where the ART center with PrEP Service is located
Woreda / Sub-City Write the woreda/sub-city where the ART center with PrEP Service is located
Name of Health Facility Write the name of the health facility where the ART center with PrEP Service is located
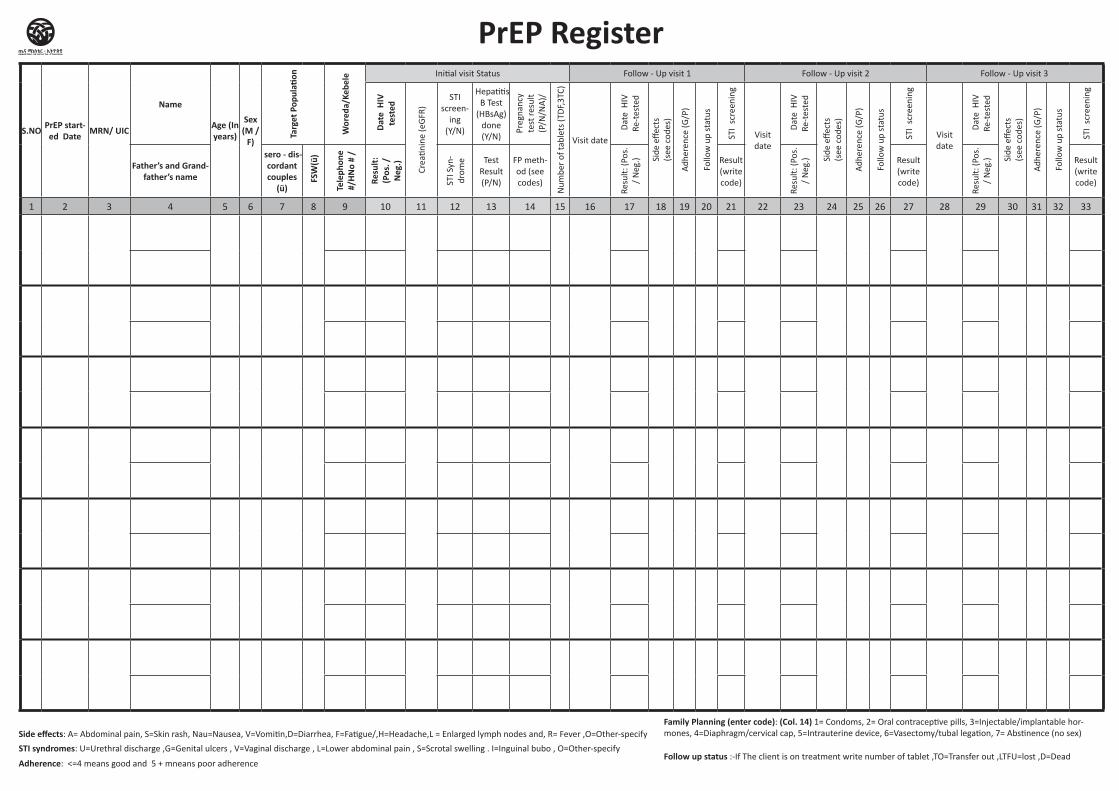
PrEP Register
Side effects: A= Abdominal pain, S=Skin rash, Nau=Nausea, V=Vomitin,D=Diarrhea, F=Fatigue/,H=Headache,L = Enlarged lymph nodes and, R= Fever ,O=Other-specifyFamily Planning (enter code): (Col. 14) 1= Condoms, 2= Oral contraceptive pills, 3=Injectable/implantable hor-mones, 4=Diaphragm/cervical cap, 5=Intrauterine device, 6=Vasectomy/tubal legation, 7= Abstinence (no sex)
STI syndromes: U=Urethral discharge ,G=Genital ulcers , V=Vaginal discharge , L=Lower abdominal pain , S=Scrotal swelling . I=Inguinal bubo , O=Other-specifyFollow up status :-If The client is on treatment write number of tablet ,TO=Transfer out ,LTFU=lost ,D=Dead
Adherence: <=4 means good and 5 + mneans poor adherence
S.NO PrEP start-ed Date MRN/ UIC
Name
Age (In years)
Sex (M /
F)
Targ
et P
opul
ation
Wor
eda/
Kebe
le Initial visit Status Follow - Up visit 1 Follow - Up visit 2 Follow - Up visit 3 Follow - Up visit 4 Follow - Up visit 5 Follow - Up visit 6 Follow - Up visit 7 Follow - Up visit 8 Stopped PrEP
Dat
e H
IV
test
ed
Crea
tinin
e (e
GFR
)
STI screen-
ing (Y/N)
Hepatitis B Test
(HBsAg) done (Y/N)
Preg
nanc
y te
st re
sult
(P/N
/NA
)/
Num
ber
of ta
blet
s (T
DF,
3TC)
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Date
Father’s and Grand-father’s name
sero - dis-cordant couples
(ü) FSW
(ü)
Tele
phon
e #/
HNo
# /
Resu
lt:
(Pos
. /
Neg
.)
STI S
yn-
drom
e Test Result (P/N)
FP meth-od (see codes)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code) Re
ason
s (s
ee c
odes
)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69
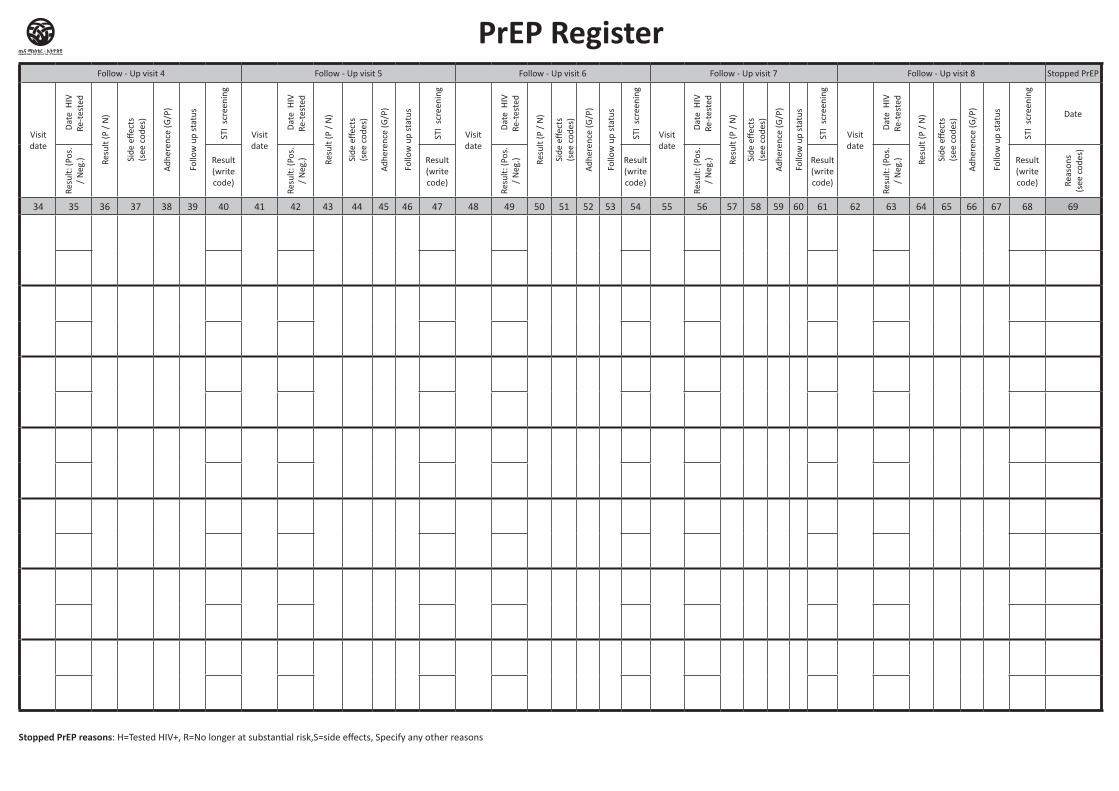
PrEP Register
Stopped PrEP reasons: H=Tested HIV+, R=No longer at substantial risk,S=side effects, Specify any other reasons
S.NO PrEP start-ed Date MRN/ UIC
Name
Age (In years)
Sex (M /
F)
Targ
et P
opul
ation
Wor
eda/
Kebe
le Initial visit Status Follow - Up visit 1 Follow - Up visit 2 Follow - Up visit 3 Follow - Up visit 4 Follow - Up visit 5 Follow - Up visit 6 Follow - Up visit 7 Follow - Up visit 8 Stopped PrEP
Dat
e H
IV
test
ed
Crea
tinin
e (e
GFR
)
STI screen-
ing (Y/N)
Hepatitis B Test
(HBsAg) done (Y/N)
Preg
nanc
y te
st re
sult
(P/N
/NA
)/
Num
ber
of ta
blet
s (T
DF,
3TC)
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Visit date
Dat
e H
IV
Re-t
este
d
Resu
lt (P
/ N
)
Side
effe
cts
(s
ee c
odes
)
Adh
eren
ce (G
/P)
Follo
w u
p st
atus
STI
scre
enin
g
Date
Father’s and Grand-father’s name
sero - dis-cordant couples
(ü) FSW
(ü)
Tele
phon
e #/
HNo
# /
Resu
lt:
(Pos
. /
Neg
.)
STI S
yn-
drom
e Test Result (P/N)
FP meth-od (see codes)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code)
Resu
lt: (P
os.
/ N
eg.) Result
(write code) Re
ason
s (s
ee c
odes
)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Clinical Care Tally
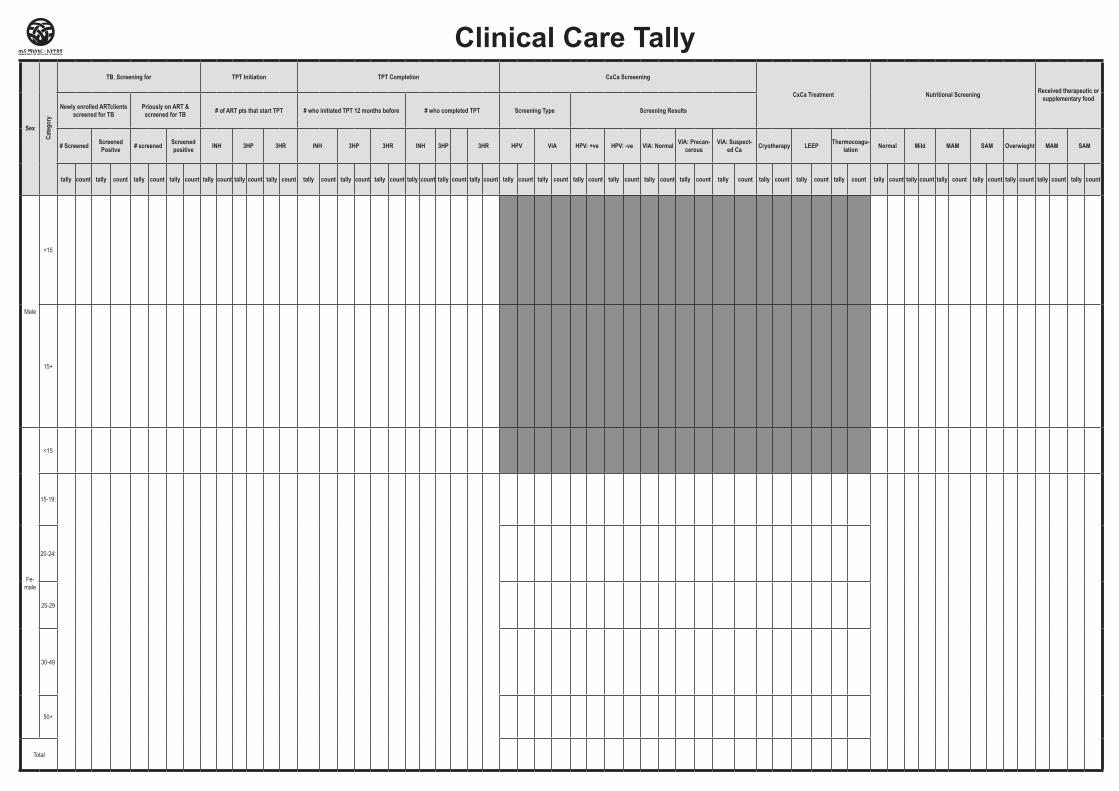
Sex
Cate
gory
TB_Screening for TPT Initiation TPT Completion CxCa Screeening
CxCa Treatment Nutritional Screening Received therapeutic or supplementary food
Newly enrolled ARTclients screened for TB
Priously on ART & screened for TB # of ART pts that start TPT # who initiated TPT 12 months before # who completed TPT Screening Type Screening Results
# Screened Screened Positve # screened Screened
positive INH 3HP 3HR INH 3HP 3HR INH 3HP 3HR HPV VIA HPV: +ve HPV: -ve VIA: Normal VIA: Precan-cerous
VIA: Suspect-ed Ca Cryotherapy LEEP Thermocoagu-
lation Normal Mild MAM SAM Overwieght MAM SAM
tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count
Male
<15
15+
Fe-male
<15
15-19:
20-24:
25-29
30-49
50+
Total
Clinical Care Tally
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Currently on ART by Regimens and
DSD Tally
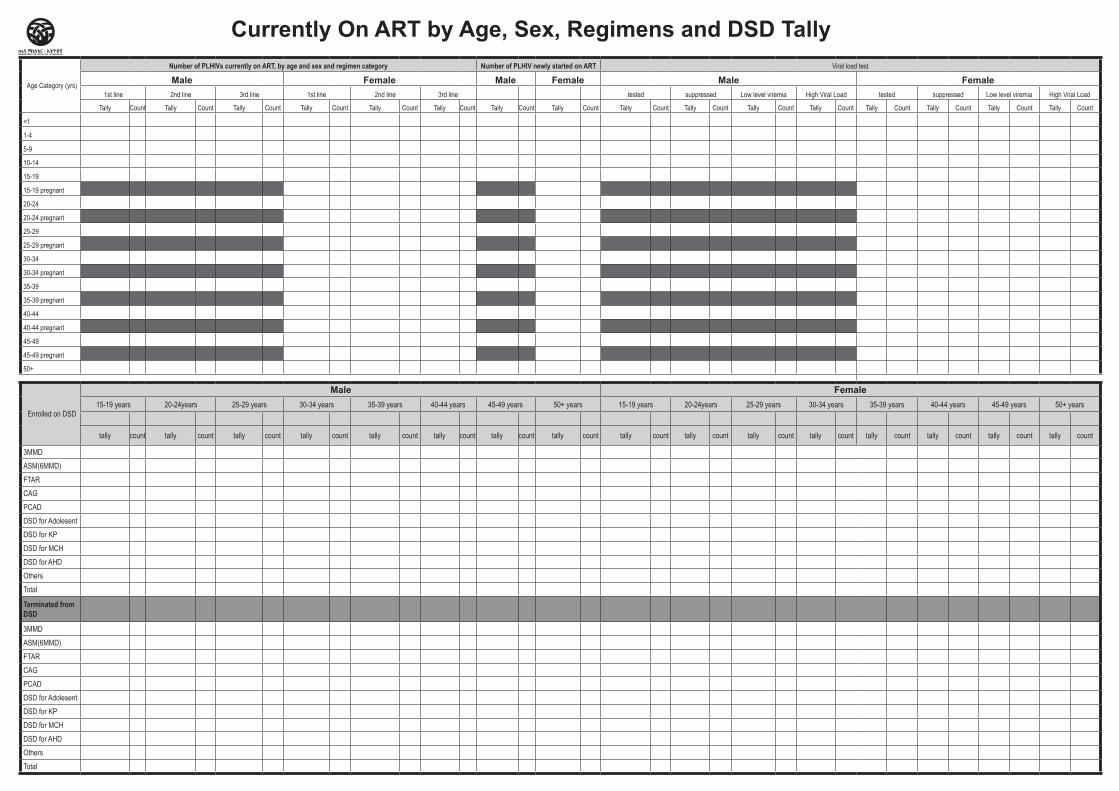
Age Category (yrs)
Number of PLHIVs currently on ART, by age and sex and regimen category Number of PLHIV newly started on ART Viral load test
Male Female Male Female Male Female1st line 2nd line 3rd line 1st line 2nd line 3rd line tested suppressed Low level viremia High Viral Load tested suppressed Low level viremia High Viral Load
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
<1
1-4
5-9
10-14
15-19
15-19 pregnant
20-24
20-24 pregnant
25-29
25-29 pregnant
30-34
30-34 pregnant
35-39
35-39 pregnant
40-44
40-44 pregnant
45-49
45-49 pregnant
50+
Enrolled on DSD
Male Female15-19 years 20-24years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ years 15-19 years 20-24years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ years
tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count
3MMD ASM(6MMD)FTARCAGPCADDSD for AdolesentDSD for KPDSD for MCHDSD for AHDOthers Total
Terminated from DSD
3MMD ASM(6MMD)FTARCAGPCADDSD for AdolesentDSD for KPDSD for MCHDSD for AHDOthers Total
Currently On ART by Age, Sex, Regimens and DSD Tally
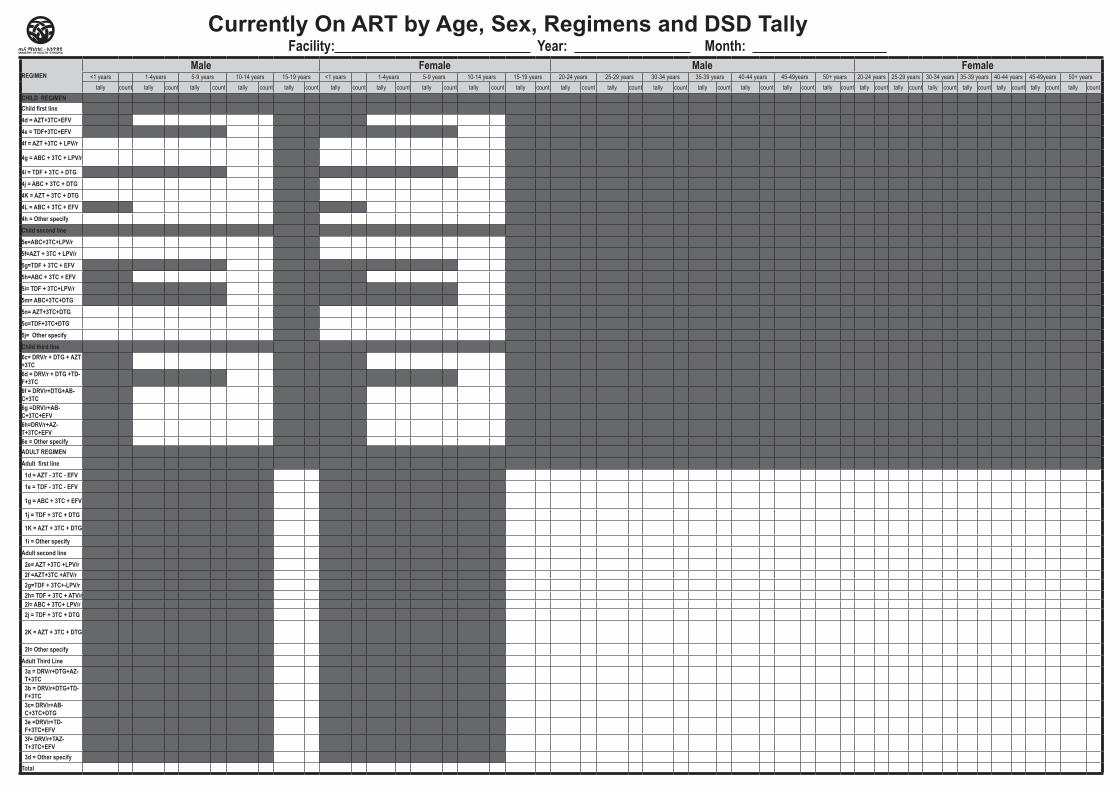
Currently On ART by Age, Sex, Regimens and DSD TallyFacility: Year: Month: _
REGIMENMale Female Male Female
<1 years 1-4years 5-9 years 10-14 years 15-19 years <1 years 1-4years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49years 50+ years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49years 50+ yearstally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count tally count
CHILD REGIMENChild first line 4d = AZT+3TC+EFV4e = TDF+3TC+EFV4f = AZT +3TC + LPV/r
4g = ABC + 3TC + LPV/r
4i = TDF + 3TC + DTG4j = ABC + 3TC + DTG4K = AZT + 3TC + DTG4L = ABC + 3TC + EFV4h = Other specifyChild second line5e=ABC+3TC+LPV/r5f=AZT + 3TC + LPV/r5g=TDF + 3TC + EFV5h=ABC + 3TC + EFV5i= TDF + 3TC+LPV/r5m= ABC+3TC+DTG5n= AZT+3TC+DTG5o=TDF+3TC+DTG5j= Other specifyChild third line6c= DRV/r + DTG + AZT +3TC6d = DRV/r + DTG +TD-F+3TC6f = DRV/r+DTG+AB-C+3TC6g =DRV/r+AB-C+3TC+EFV6h=DRV/r+AZ-T+3TC+EFV6e = Other specifyADULT REGIMENAdult first line
1d = AZT - 3TC - EFV 1e = TDF - 3TC - EFV
1g = ABC + 3TC + EFV
1j = TDF + 3TC + DTG
1K = AZT + 3TC + DTG
1i = Other specifyAdult second line
2e= AZT +3TC +LPV/r 2f =AZT+3TC +ATV/r2g=TDF + 3TC+-LPV/r2h= TDF + 3TC + ATV/r2i= ABC + 3TC+ LPV/r2j = TDF + 3TC + DTG
2K = AZT + 3TC + DTG
2l= Other specifyAdult Third Line
3a = DRV/r+DTG+AZ-T+3TC3b = DRV/r+DTG+TD-F+3TC3c= DRV/r+AB-C+3TC+DTG3e =DRV/r+TD-F+3TC+EFV3f= DRV/r+TAZ-T+3TC+EFV3d = Other specify
Total
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital HIV Testing Service Tally Sheet
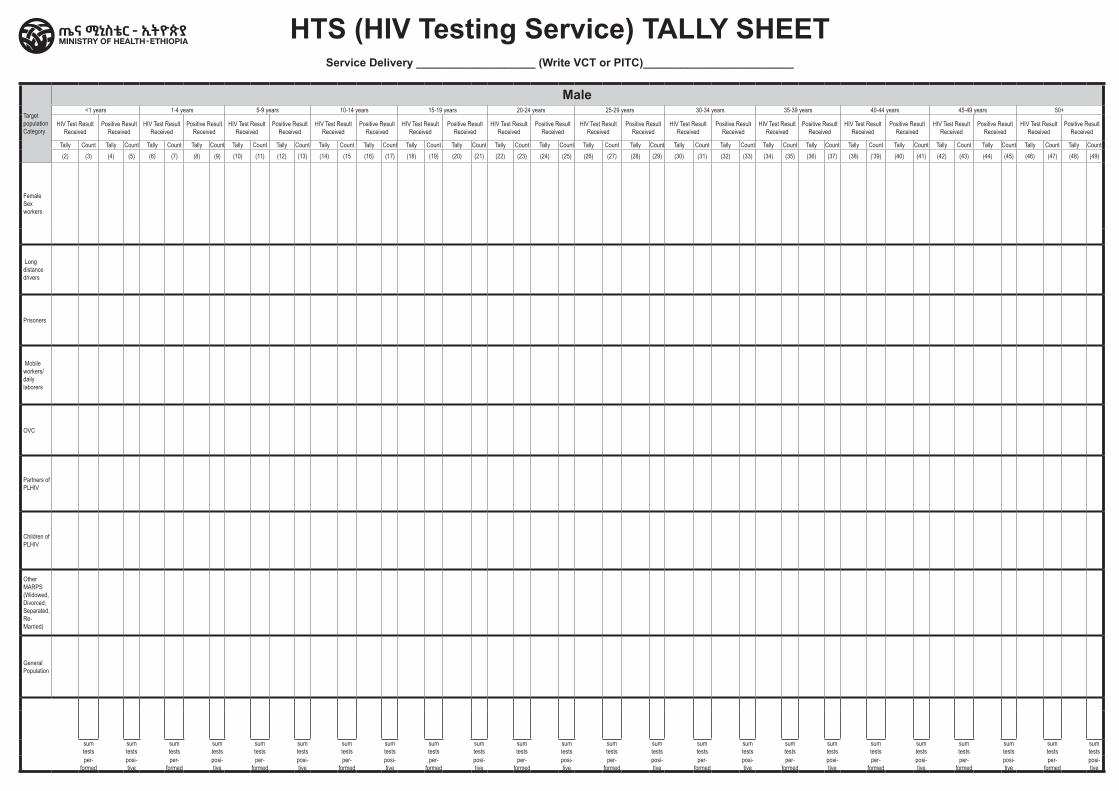
Target population Category
Male Female<1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ <1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ Years
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count(2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15 (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (‘39) (40) (41) (42) (43) (44) (45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) (60) (61) (62) (63) (64) (65) (66) (67) (68) (69) (70) (71) (72) (73) (74) (75) (76) (77) (78) (79) (80) (81) (82) (83) (84) (85) (86) (87) (88) (89) (90) (91) (92) (93) (94) (95) (96) (97)
Female Sex workers
Long distance drivers
Prisoners
Mobile workers/daily laborers
OVC
Partners of PLHIV
Children of PLHIV
Other MARPS (Widowed, Divorced, Separated, Re-Married)
General Population
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
HTS (HIV Testing Service) TALLY SHEETService Delivery ___________________ (Write VCT or PITC)________________________
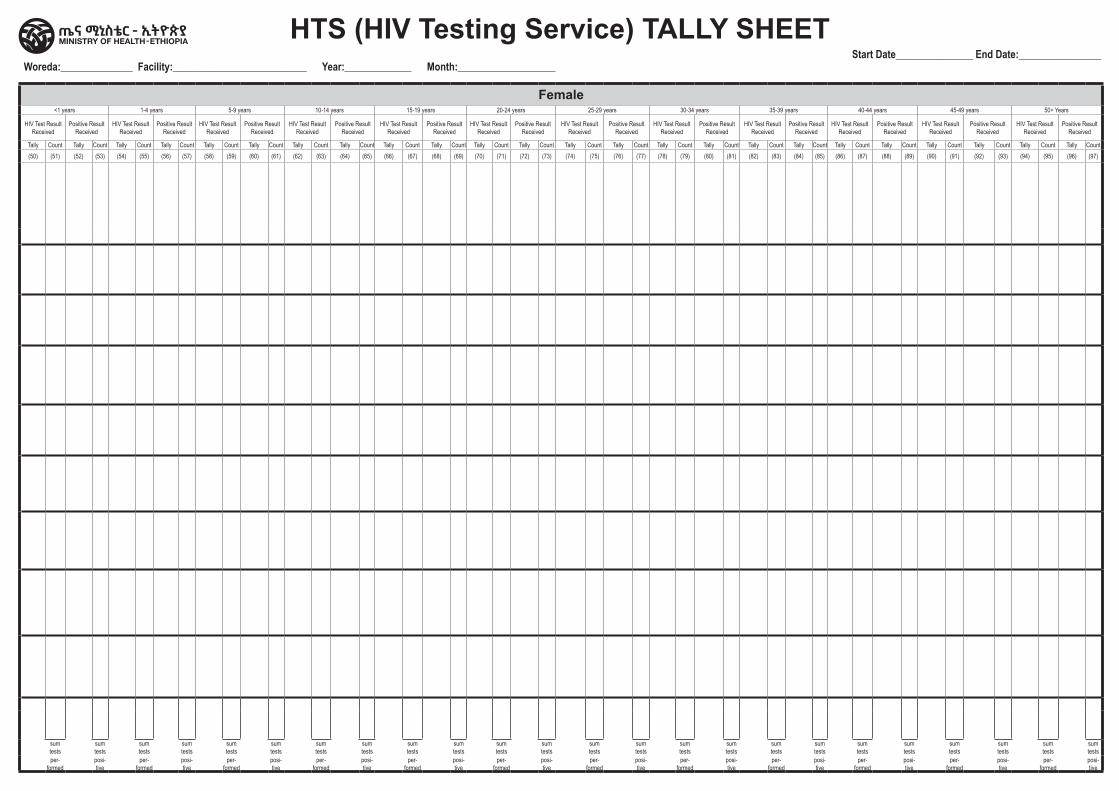
Target population Category
Male Female<1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ <1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ Years
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
HIV Test Result Received
Positive Result Received
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count(2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15 (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (‘39) (40) (41) (42) (43) (44) (45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) (60) (61) (62) (63) (64) (65) (66) (67) (68) (69) (70) (71) (72) (73) (74) (75) (76) (77) (78) (79) (80) (81) (82) (83) (84) (85) (86) (87) (88) (89) (90) (91) (92) (93) (94) (95) (96) (97)
Female Sex workers
Long distance drivers
Prisoners
Mobile workers/daily laborers
OVC
Partners of PLHIV
Children of PLHIV
Other MARPS (Widowed, Divorced, Separated, Re-Married)
General Population
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
sum tests
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
per-formed
posi-tive
HTS (HIV Testing Service) TALLY SHEET Woreda:______________ Facility:__________________________ Year:_____________ Month:___________________
Start Date_______________ End Date:________________
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital ICT Tally
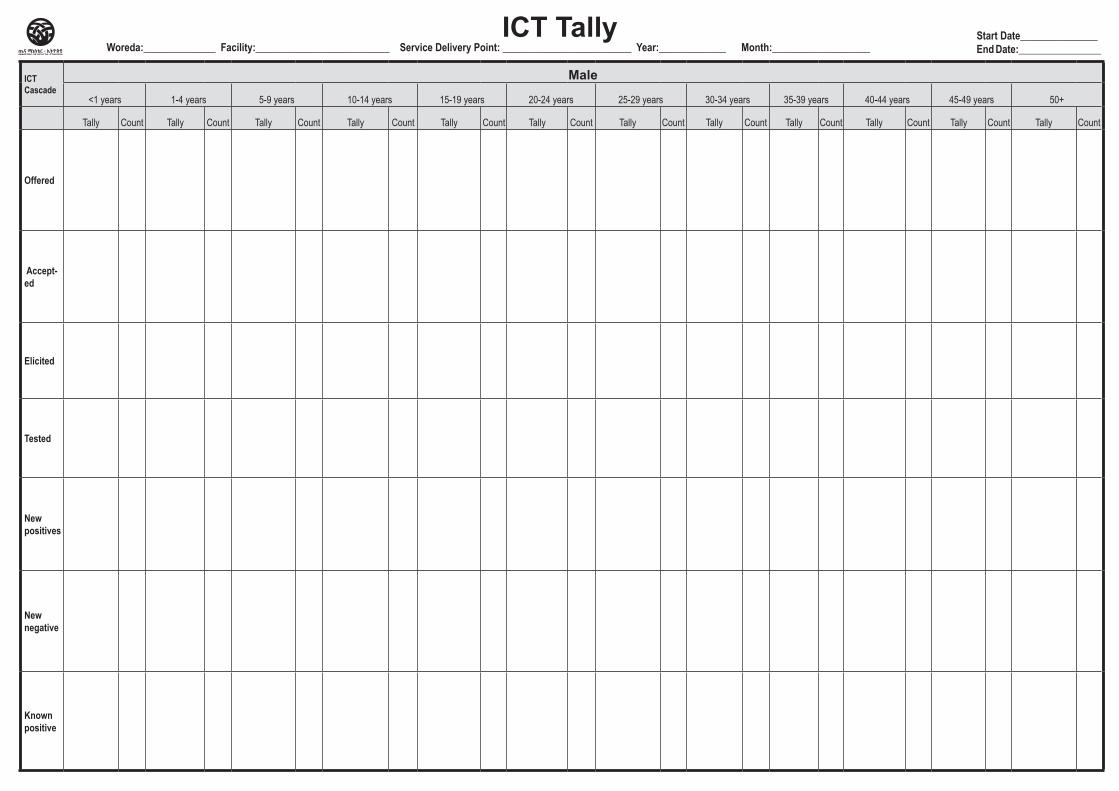
ICT Cascade
Male Female
Total
<1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ <1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
Offered
Accept-ed
Elicited
Tested
New positives
New negative
Known positive
Woreda:______________ Facility:__________________________ Service Delivery Point: _________________________ Year:_____________ Month:___________________Start Date_______________End Date:________________
ICT Tally
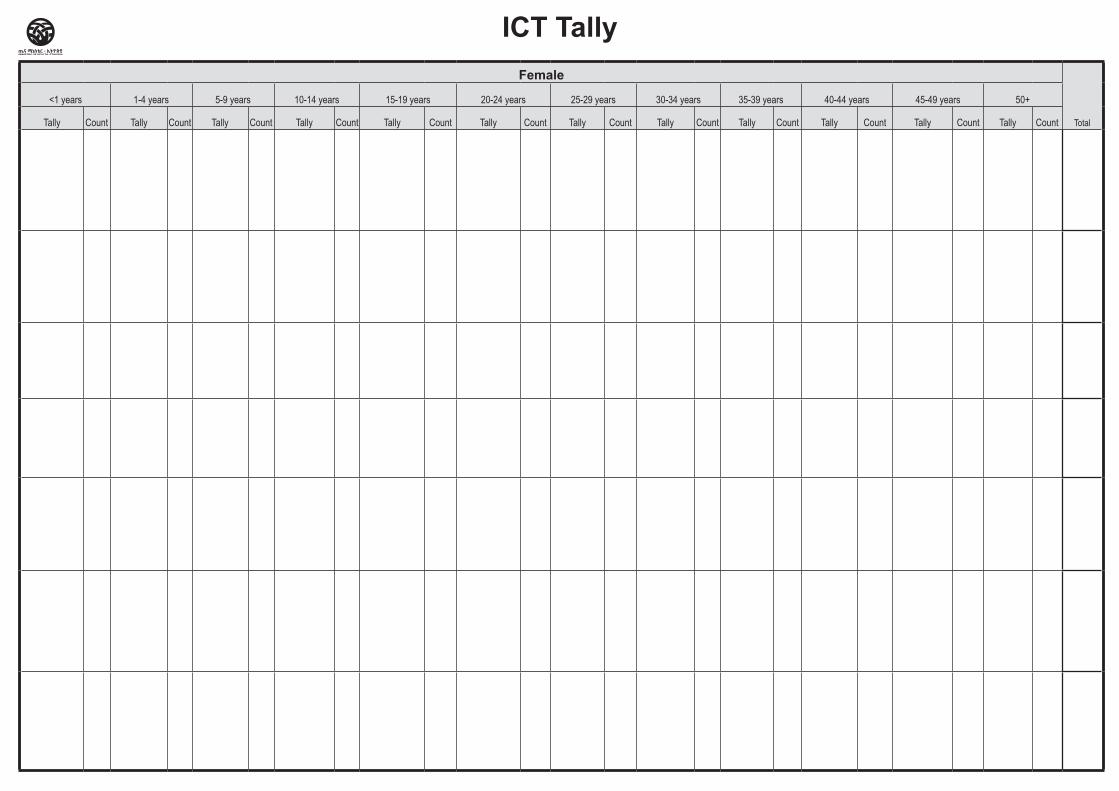
ICT Cascade
Male Female
Total
<1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+ <1 years 1-4 years 5-9 years 10-14 years 15-19 years 20-24 years 25-29 years 30-34 years 35-39 years 40-44 years 45-49 years 50+
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
Offered
Accept-ed
Elicited
Tested
New positives
New negative
Known positive
ICT Tally
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center/ HospitalDiseases Tally
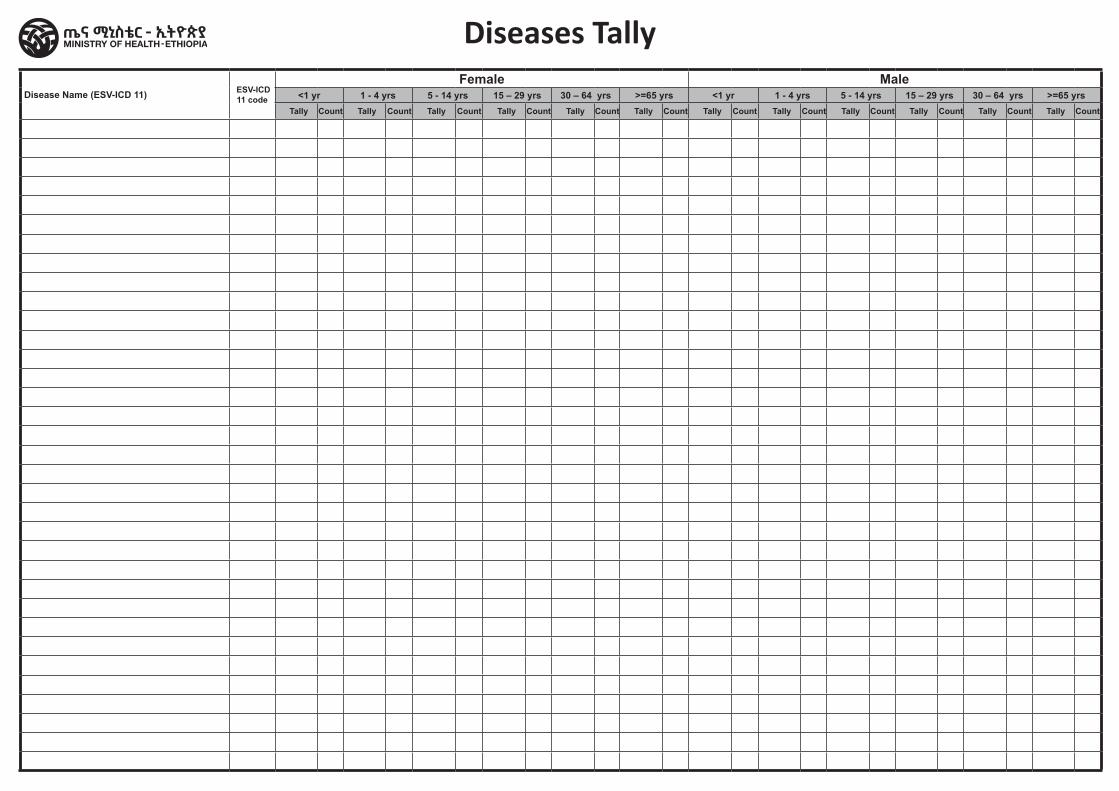
Disease Name (ESV-ICD 11) ESV-ICD 11 code
Female Male<1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs <1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
Diseases Tally

HSSContent / Home
Hospital Gender Based Violence Register
_______ _________________ ______________ ___________ __________ Region Sub-city/Woreda Health Facility Name Begin Date End Date
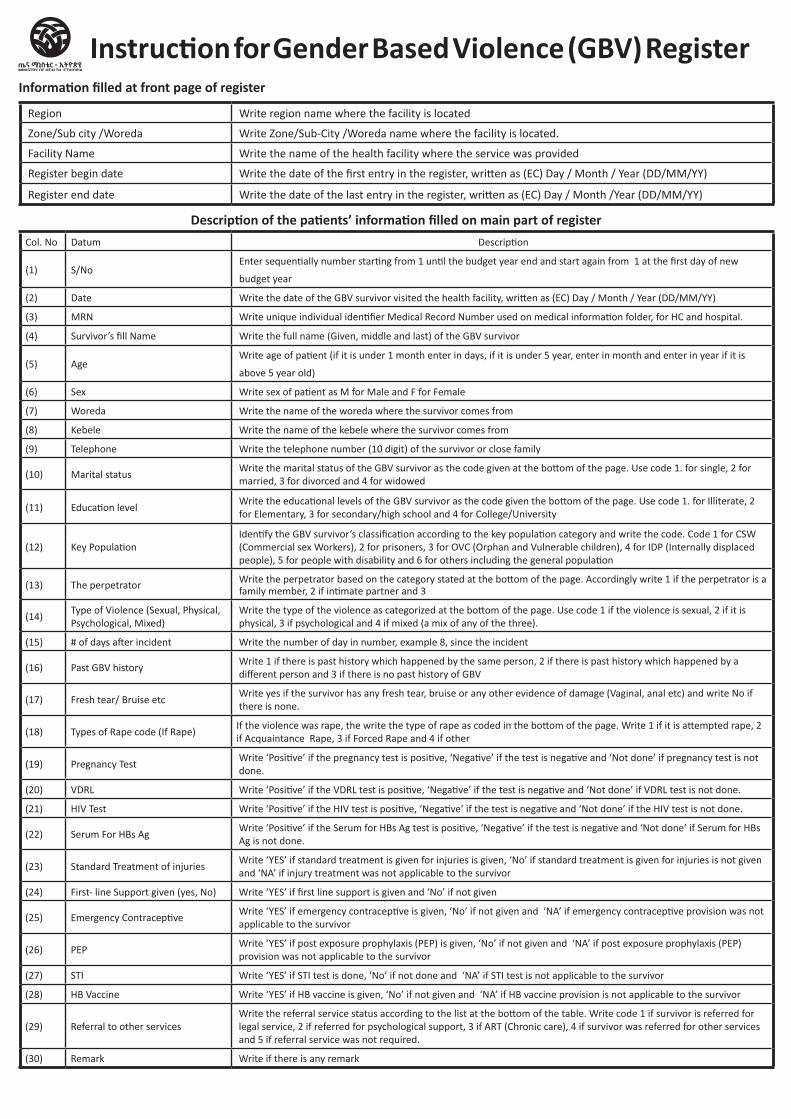
Description of the patients’ information filled on main part of registerCol. No Datum Description
(1) S/NoEnter sequentially number starting from 1 until the budget year end and start again from 1 at the first day of new
budget year
(2) Date Write the date of the GBV survivor visited the health facility, written as (EC) Day / Month / Year (DD/MM/YY)
(3) MRN Write unique individual identifier Medical Record Number used on medical information folder, for HC and hospital.
(4) Survivor’s fill Name Write the full name (Given, middle and last) of the GBV survivor
(5) AgeWrite age of patient (if it is under 1 month enter in days, if it is under 5 year, enter in month and enter in year if it is
above 5 year old)
(6) Sex Write sex of patient as M for Male and F for Female
(7) Woreda Write the name of the woreda where the survivor comes from
(8) Kebele Write the name of the kebele where the survivor comes from
(9) Telephone Write the telephone number (10 digit) of the survivor or close family
(10) Marital status Write the marital status of the GBV survivor as the code given at the bottom of the page. Use code 1. for single, 2 for married, 3 for divorced and 4 for widowed
(11) Education level Write the educational levels of the GBV survivor as the code given the bottom of the page. Use code 1. for Illiterate, 2 for Elementary, 3 for secondary/high school and 4 for College/University
(12) Key Population Identify the GBV survivor’s classification according to the key population category and write the code. Code 1 for CSW (Commercial sex Workers), 2 for prisoners, 3 for OVC (Orphan and Vulnerable children), 4 for IDP (Internally displaced people), 5 for people with disability and 6 for others including the general population
(13) The perpetrator Write the perpetrator based on the category stated at the bottom of the page. Accordingly write 1 if the perpetrator is a family member, 2 if intimate partner and 3
(14)Type of Violence (Sexual, Physical, Psychological, Mixed)
Write the type of the violence as categorized at the bottom of the page. Use code 1 if the violence is sexual, 2 if it is physical, 3 if psychological and 4 if mixed (a mix of any of the three).
(15) # of days after incident Write the number of day in number, example 8, since the incident
(16) Past GBV history Write 1 if there is past history which happened by the same person, 2 if there is past history which happened by a different person and 3 if there is no past history of GBV
(17) Fresh tear/ Bruise etc Write yes if the survivor has any fresh tear, bruise or any other evidence of damage (Vaginal, anal etc) and write No if there is none.
(18) Types of Rape code (If Rape)If the violence was rape, the write the type of rape as coded in the bottom of the page. Write 1 if it is attempted rape, 2 if Acquaintance Rape, 3 if Forced Rape and 4 if other
(19) Pregnancy Test Write ‘Positive’ if the pregnancy test is positive, ‘Negative’ if the test is negative and ‘Not done’ if pregnancy test is not done.
(20) VDRL Write ‘Positive’ if the VDRL test is positive, ‘Negative’ if the test is negative and ‘Not done’ if VDRL test is not done.
(21) HIV Test Write ‘Positive’ if the HIV test is positive, ‘Negative’ if the test is negative and ‘Not done’ if the HIV test is not done.
(22) Serum For HBs AgWrite ‘Positive’ if the Serum for HBs Ag test is positive, ‘Negative’ if the test is negative and ‘Not done’ if Serum for HBs Ag is not done.
(23) Standard Treatment of injuries Write ‘YES’ if standard treatment is given for injuries is given, ‘No’ if standard treatment is given for injuries is not given and ‘NA’ if injury treatment was not applicable to the survivor
(24) First- line Support given (yes, No) Write ‘YES’ if first line support is given and ‘No’ if not given
(25) Emergency ContraceptiveWrite ‘YES’ if emergency contraceptive is given, ‘No’ if not given and ‘NA’ if emergency contraceptive provision was not applicable to the survivor
(26) PEP Write ‘YES’ if post exposure prophylaxis (PEP) is given, ‘No’ if not given and ‘NA’ if post exposure prophylaxis (PEP) provision was not applicable to the survivor
(27) STI Write ‘YES’ if STI test is done, ‘No’ if not done and ‘NA’ if STI test is not applicable to the survivor
(28) HB Vaccine Write ‘YES’ if HB vaccine is given, ‘No’ if not given and ‘NA’ if HB vaccine provision is not applicable to the survivor
(29) Referral to other servicesWrite the referral service status according to the list at the bottom of the table. Write code 1 if survivor is referred for legal service, 2 if referred for psychological support, 3 if ART (Chronic care), 4 if survivor was referred for other services and 5 if referral service was not required.
(30) Remark Write if there is any remark
Instruction for Gender Based Violence (GBV) RegisterInformation filled at front page of register
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month /Year (DD/MM/YY)
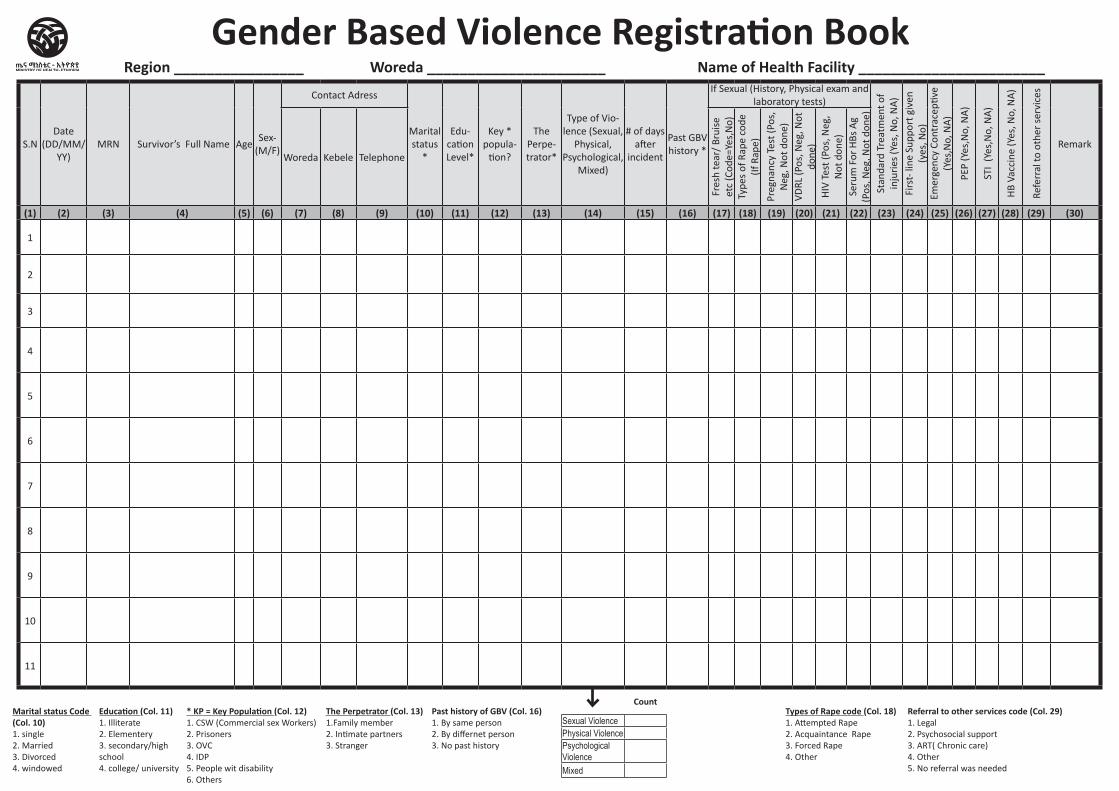
S.NDate
(DD/MM/YY)
MRN Survivor’s Full Name AgeSex-
(M/F)
Contact Adress
Marital status
*
Edu-cation Level*
Key * popula-
tion?
The Perpe-trator*
Type of Vio-lence (Sexual,
Physical, Psychological,
Mixed)
# of days after
incident
Past GBV history *
If Sexual (History, Physical exam and laboratory tests)
Stan
dard
Tre
atm
ent o
f in
juri
es (Y
es, N
o, N
A)
Firs
t- li
ne S
uppo
rt g
iven
(y
es, N
o)Em
erge
ncy
Cont
race
ptive
(Y
es,N
o, N
A)
PEP
(Yes
,No,
NA
)
STI
(Yes
,No,
NA
)
HB
Vacc
ine
(Yes
, No,
NA
)
Refe
rral
to o
ther
ser
vice
s
Remark Woreda Kebele Telephone
Fres
h te
ar/
Brui
se
etc
(Cod
e=Ye
s,N
o)
Type
s of
Rap
e co
de
(If R
ape)
Preg
nanc
y Te
st (P
os,
Neg
, Not
don
e)VD
RL (P
os, N
eg, N
ot
done
)H
IV T
est (
Pos,
Neg
, N
ot d
one)
Seru
m F
or H
Bs A
g (P
os, N
eg, N
ot d
one)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30)
1
2
3
4
5
6
7
8
9
10
11
Count
Sexual ViolencePhysical ViolencePsychological ViolenceMixed
Region ________________ Woreda ______________________ Name of Health Facility _______________________
* KP = Key Population (Col. 12)1. CSW (Commercial sex Workers)2. Prisoners 3. OVC4. IDP5. People wit disability6. Others
Types of Rape code (Col. 18)1. Attempted Rape 2. Acquaintance Rape 3. Forced Rape 4. Other
Marital status Code (Col. 10)1. single 2. Married 3. Divorced 4. windowed
Education (Col. 11)1. Illiterate 2. Elementery 3. secondary/high school4. college/ university
The Perpetrator (Col. 13)1.Family member 2. Intimate partners 3. Stranger
Past history of GBV (Col. 16)1. By same person2. By differnet person3. No past history
Referral to other services code (Col. 29)1. Legal2. Psychosocial support 3. ART( Chronic care)4. Other5. No referral was needed
Gender Based Violence Registration Book

_______ ___________ ______________ ________ ________
Region Zone/Sub city/Woreda Health Facility Name Begin Date End Date
Health center/Clinic/HospitalDrug Dispensing Register
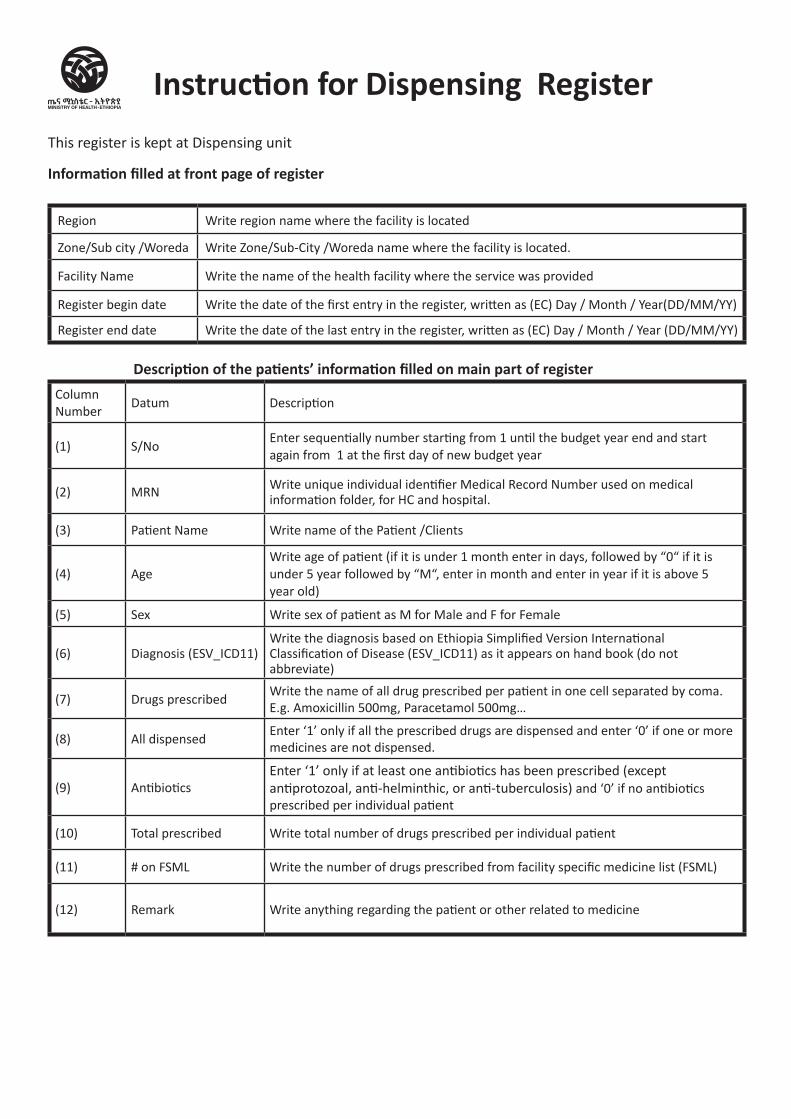
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
This register is kept at Dispensing unit
Information filled at front page of register
Description of the patients’ information filled on main part of registerColumnNumber
Datum Description
(1) S/NoEnter sequentially number starting from 1 until the budget year end and start again from 1 at the first day of new budget year
(2) MRN Write unique individual identifier Medical Record Number used on medical information folder, for HC and hospital.
(3) Patient Name Write name of the Patient /Clients
(4) AgeWrite age of patient (if it is under 1 month enter in days, followed by “0“ if it is under 5 year followed by “M“, enter in month and enter in year if it is above 5 year old)
(5) Sex Write sex of patient as M for Male and F for Female
(6) Diagnosis (ESV_ICD11)Write the diagnosis based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on hand book (do not abbreviate)
(7) Drugs prescribedWrite the name of all drug prescribed per patient in one cell separated by coma. E.g. Amoxicillin 500mg, Paracetamol 500mg…
(8) All dispensedEnter ‘1’ only if all the prescribed drugs are dispensed and enter ‘0’ if one or more medicines are not dispensed.
(9) AntibioticsEnter ‘1’ only if at least one antibiotics has been prescribed (except antiprotozoal, anti-helminthic, or anti-tuberculosis) and ‘0’ if no antibiotics prescribed per individual patient
(10) Total prescribed Write total number of drugs prescribed per individual patient
(11) # on FSML Write the number of drugs prescribed from facility specific medicine list (FSML)
(12) Remark Write anything regarding the patient or other related to medicine
Instruction for Dispensing Register
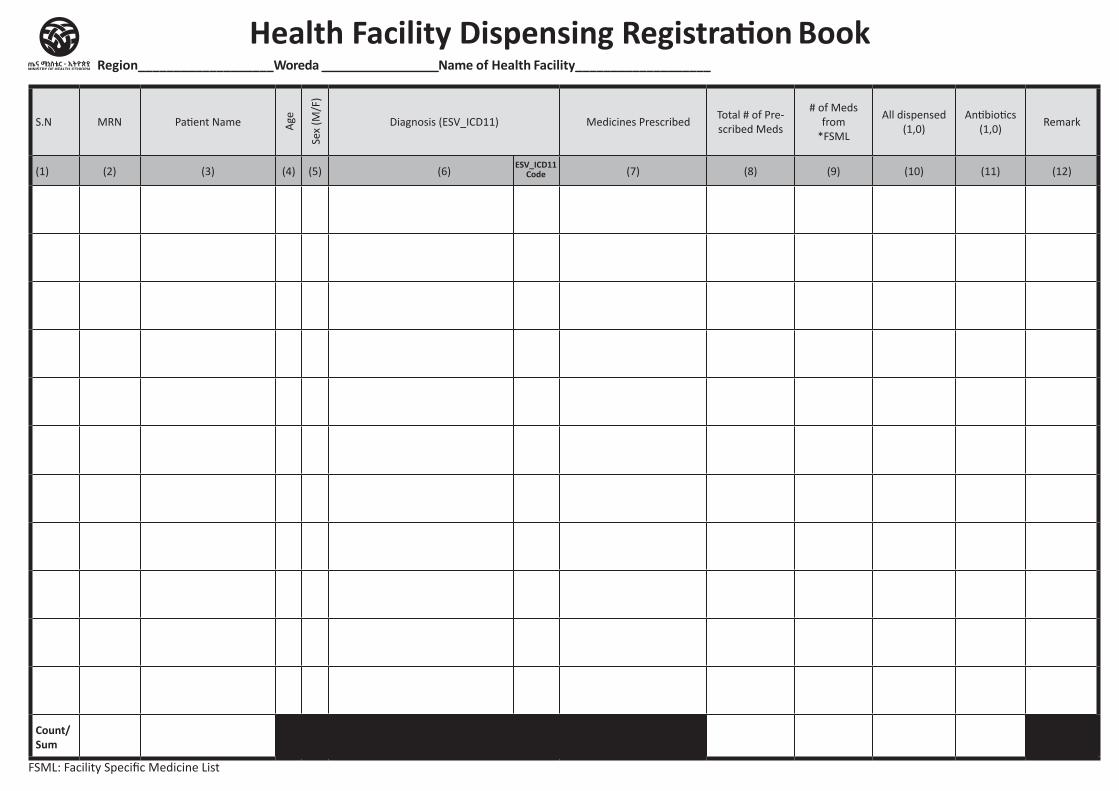
S.N MRN Patient Name Age
Sex
(M/F
)
Diagnosis (ESV_ICD11) Medicines PrescribedTotal # of Pre-scribed Meds
# of Meds from
*FSML
All dispensed (1,0)
Antibiotics (1,0)
Remark
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
Count/Sum
FSML: Facility Specific Medicine List
Health Facility Dispensing Registration BookRegion___________________Woreda _________________Name of Health Facility___________________
ESV_ICD11 Code
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Data Quality and Performance monitoring logbook Health center Level
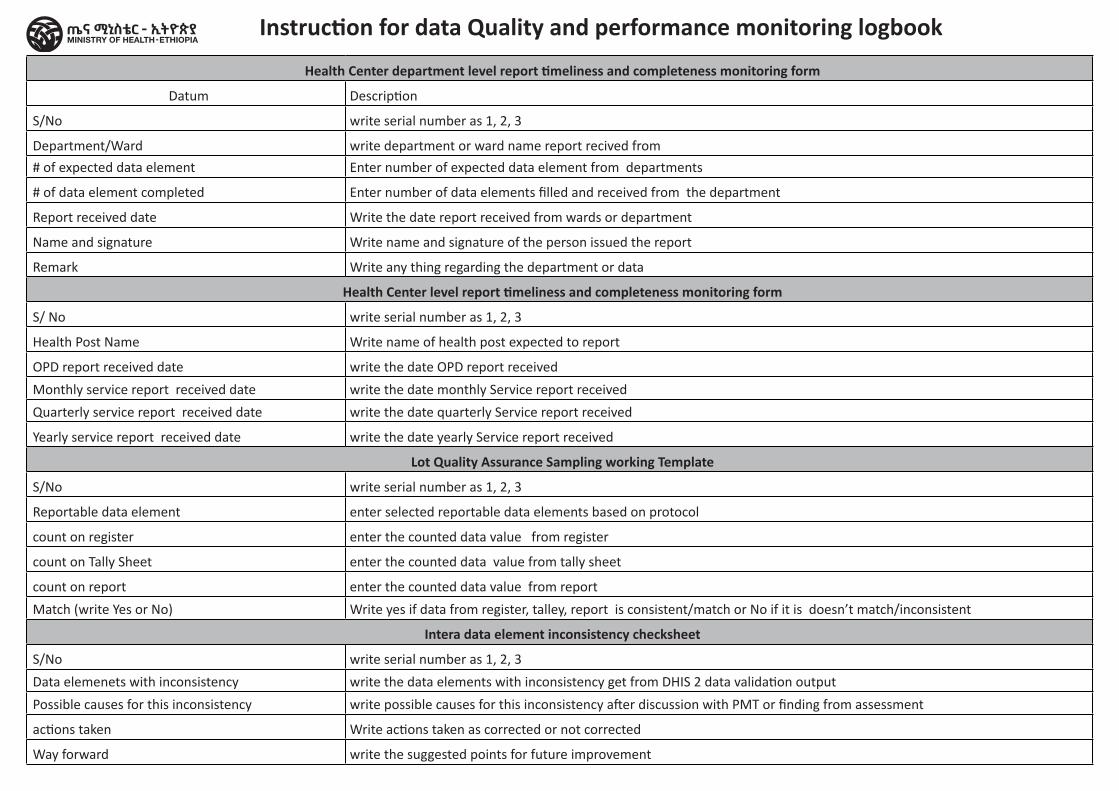
Health Center department level report timeliness and completeness monitoring form
Datum Description
S/No write serial number as 1, 2, 3
Department/Ward write department or ward name report recived from
# of expected data element Enter number of expected data element from departments
# of data element completed Enter number of data elements filled and received from the department
Report received date Write the date report received from wards or department
Name and signature Write name and signature of the person issued the report
Remark Write any thing regarding the department or data
Health Center level report timeliness and completeness monitoring form
S/ No write serial number as 1, 2, 3
Health Post Name Write name of health post expected to report
OPD report received date write the date OPD report received
Monthly service report received date write the date monthly Service report received
Quarterly service report received date write the date quarterly Service report received
Yearly service report received date write the date yearly Service report received
Lot Quality Assurance Sampling working Template
S/No write serial number as 1, 2, 3
Reportable data element enter selected reportable data elements based on protocol
count on register enter the counted data value from register
count on Tally Sheet enter the counted data value from tally sheet
count on report enter the counted data value from report
Match (write Yes or No) Write yes if data from register, talley, report is consistent/match or No if it is doesn’t match/inconsistent
Intera data element inconsistency checksheet
S/No write serial number as 1, 2, 3
Data elemenets with inconsistency write the data elements with inconsistency get from DHIS 2 data validation output
Possible causes for this inconsistency write possible causes for this inconsistency after discussion with PMT or finding from assessment
actions taken Write actions taken as corrected or not corrected
Way forward write the suggested points for future improvement
Instruction for data Quality and performance monitoring logbook
Month--------------------------------------------------Year-----------------------------------------------E.C
S/N Department/Ward # of Expected Data Element
# of Data Element Completed
Report Received Date Name and signature Remark
Total expected report from departmentsTotal received report during the given period from departmentsTotal report received timelyOverall report content completeness in %
Data quality monitoring logbook Health Center Department level report Timeliness and Completeness monitoring form
Health Center Name--------------------------------------
PHCU: ___________________ Woreda: _________________ Zone: __________________ Region: ______________________
Month _____________________________ Year _____________________ E.C
S/No Health Post Name Disease Report Received Date Monthly Service Report Received Date
Quarterly Service report Received date
Yearly Service Report Received Date
Total expected report from health Posts
Total received reported during the given period from health Posts
Total report received timely
Data Quality Monitoring logbookHealth Center Report Completeness and Timeliness Monitoring Sheet of Catchment Health Posts
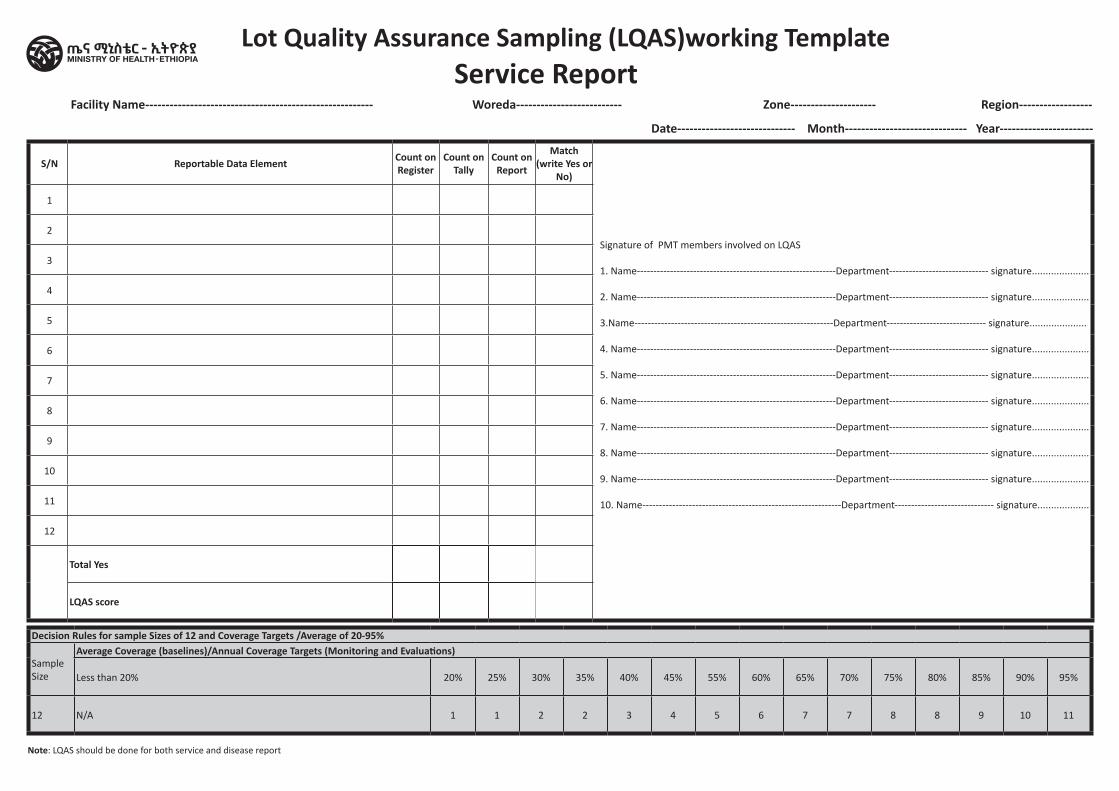
Lot Quality Assurance Sampling (LQAS)working TemplateService Report
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Note: LQAS should be done for both service and disease report
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
Date----------------------------- Month------------------------------ Year-----------------------
Facility Name-------------------------------------------------------- Woreda-------------------------- Zone--------------------- Region------------------
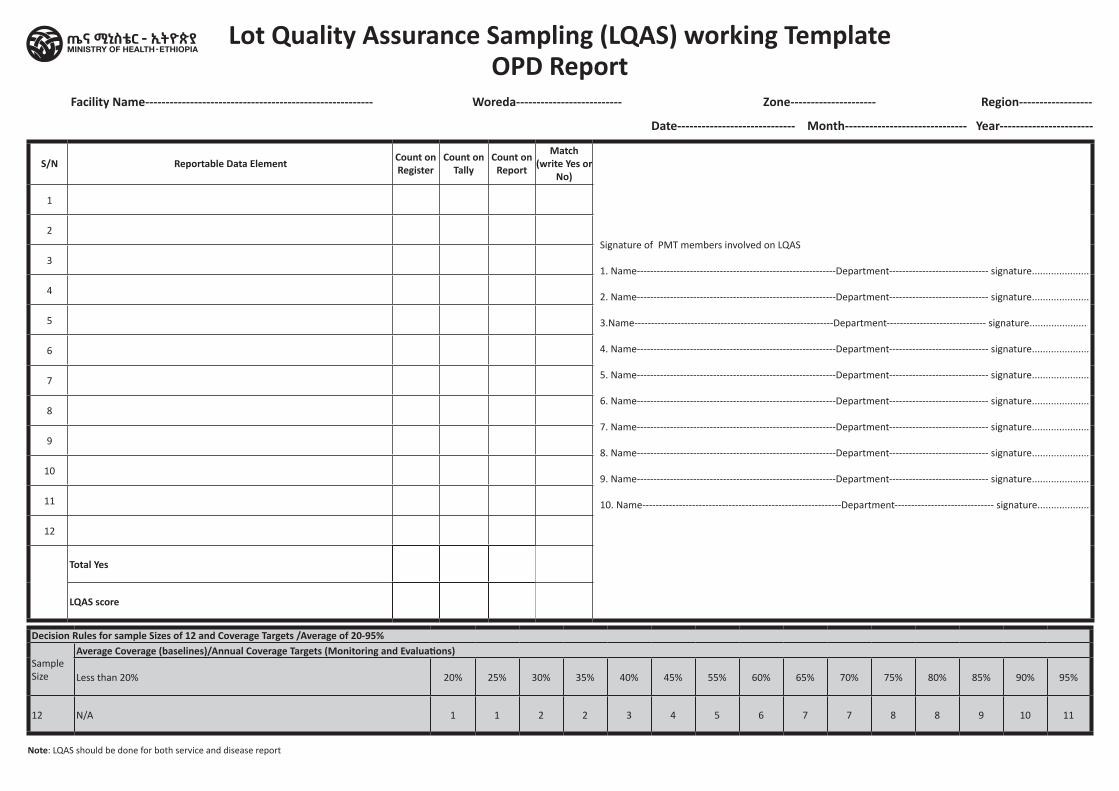
Lot Quality Assurance Sampling (LQAS) working TemplateOPD Report
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Note: LQAS should be done for both service and disease report
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
Date----------------------------- Month------------------------------ Year-----------------------
Facility Name-------------------------------------------------------- Woreda-------------------------- Zone--------------------- Region------------------
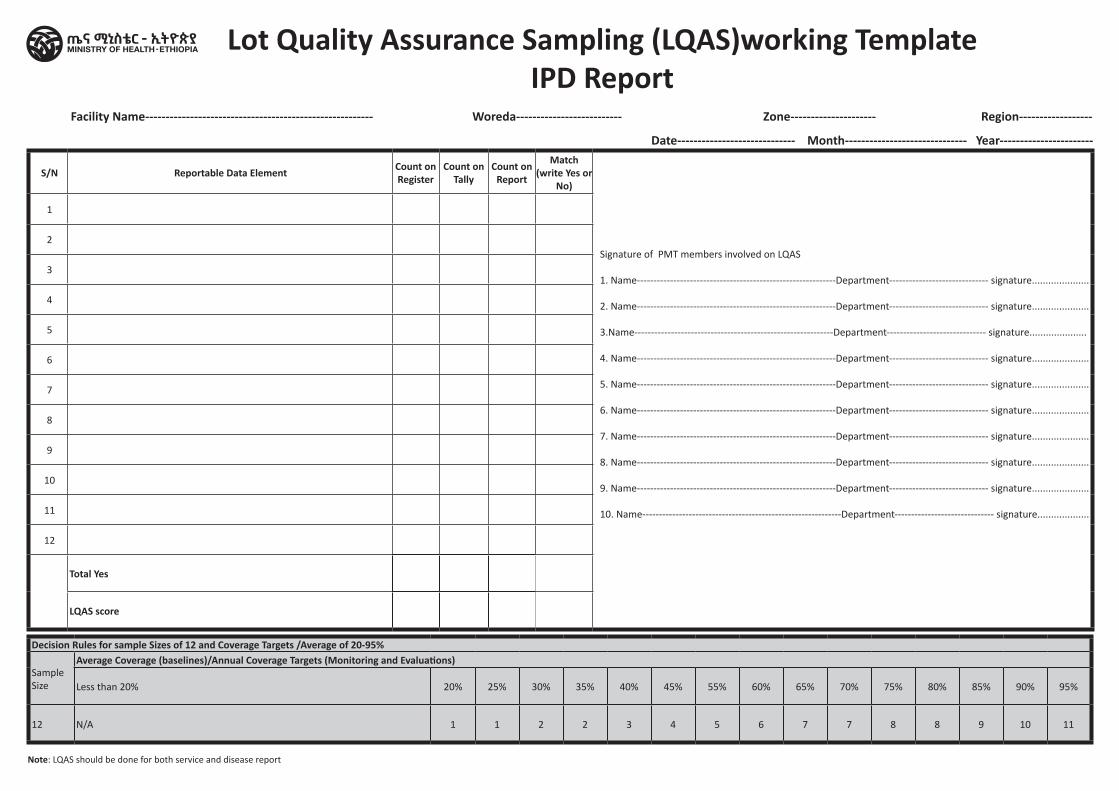
Lot Quality Assurance Sampling (LQAS)working Template IPD Report
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Date----------------------------- Month------------------------------ Year-----------------------
Facility Name-------------------------------------------------------- Woreda-------------------------- Zone--------------------- Region------------------
Note: LQAS should be done for both service and disease report
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
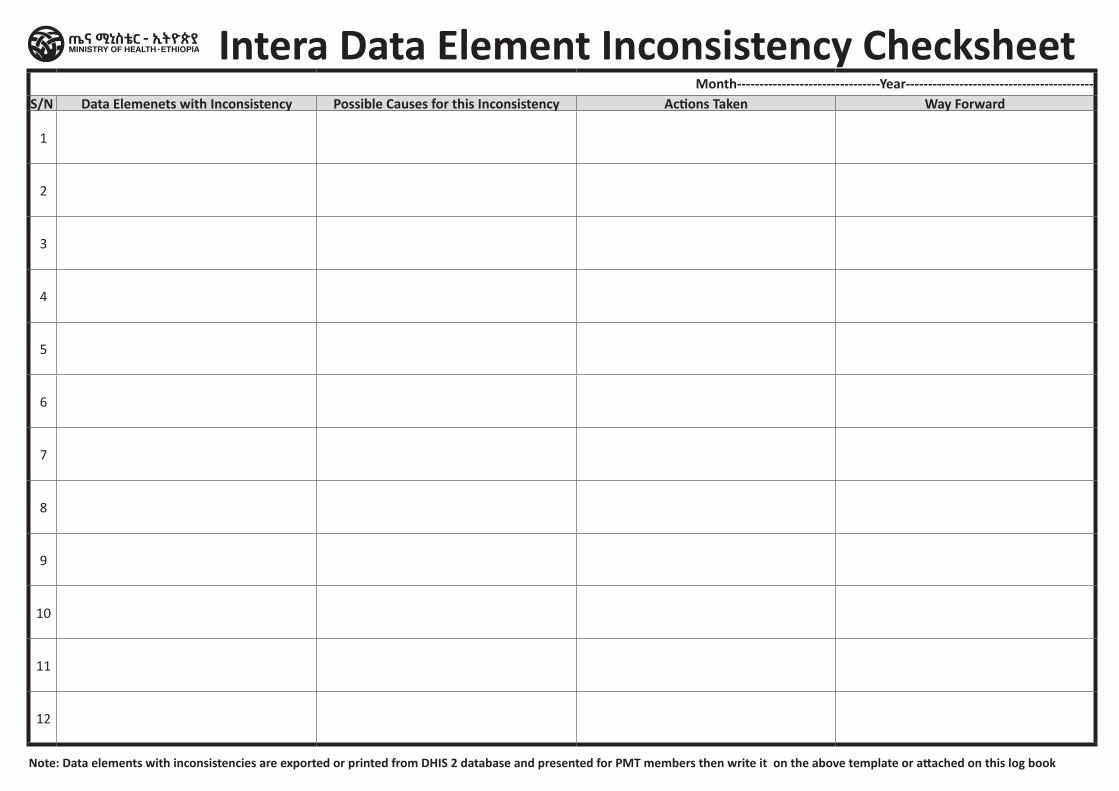
Month--------------------------------Year------------------------------------------S/N Data Elemenets with Inconsistency Possible Causes for this Inconsistency Actions Taken Way Forward
1
2
3
4
5
6
7
8
9
10
11
12
Note: Data elements with inconsistencies are exported or printed from DHIS 2 database and presented for PMT members then write it on the above template or attached on this log book
Intera Data Element Inconsistency Checksheet
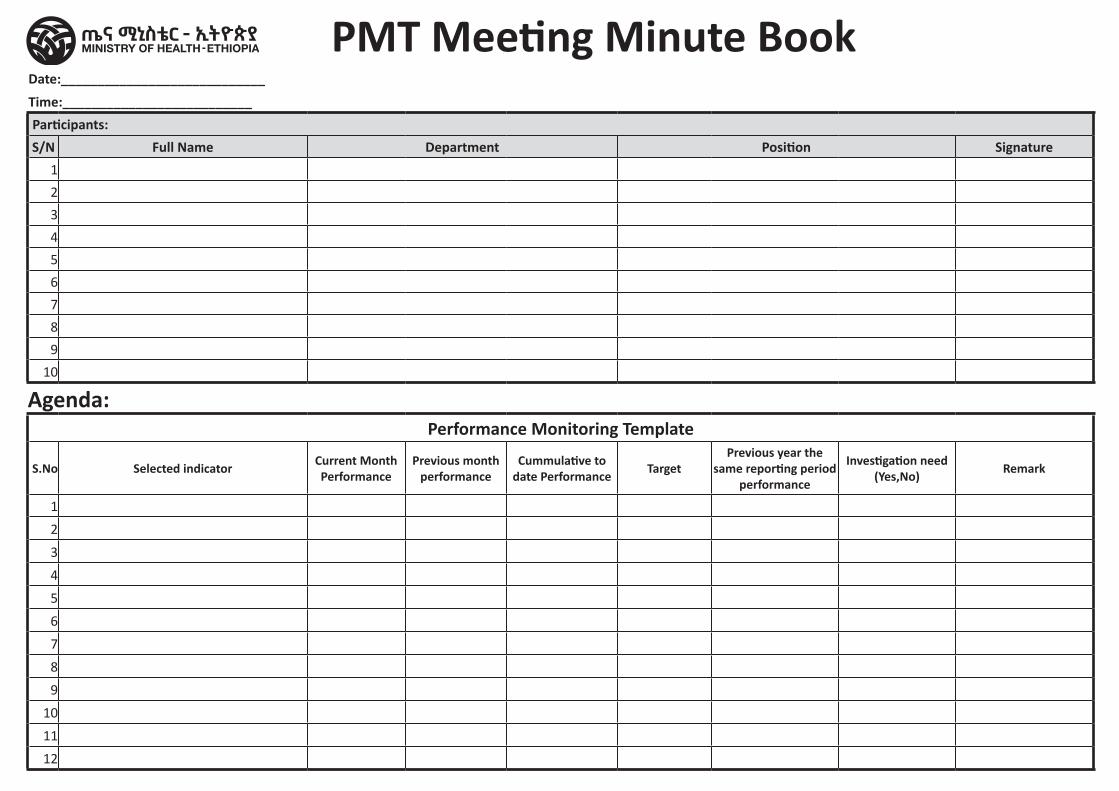
PMT Meeting Minute BookDate:____________________________Time:__________________________ Participants:S/N Full Name Department Position Signature
1
2
3
4
5
6
7
8
9
10
Agenda:Performance Monitoring Template
S.No Selected indicator Current Month Performance
Previous month performance
Cummulative to date Performance Target
Previous year the same reporting period
performance
Investigation need (Yes,No) Remark
1
2
3
4
5
6
7
8
9
10
11
12
Discussion on the Performance Finding
Discussion on the Data Quality
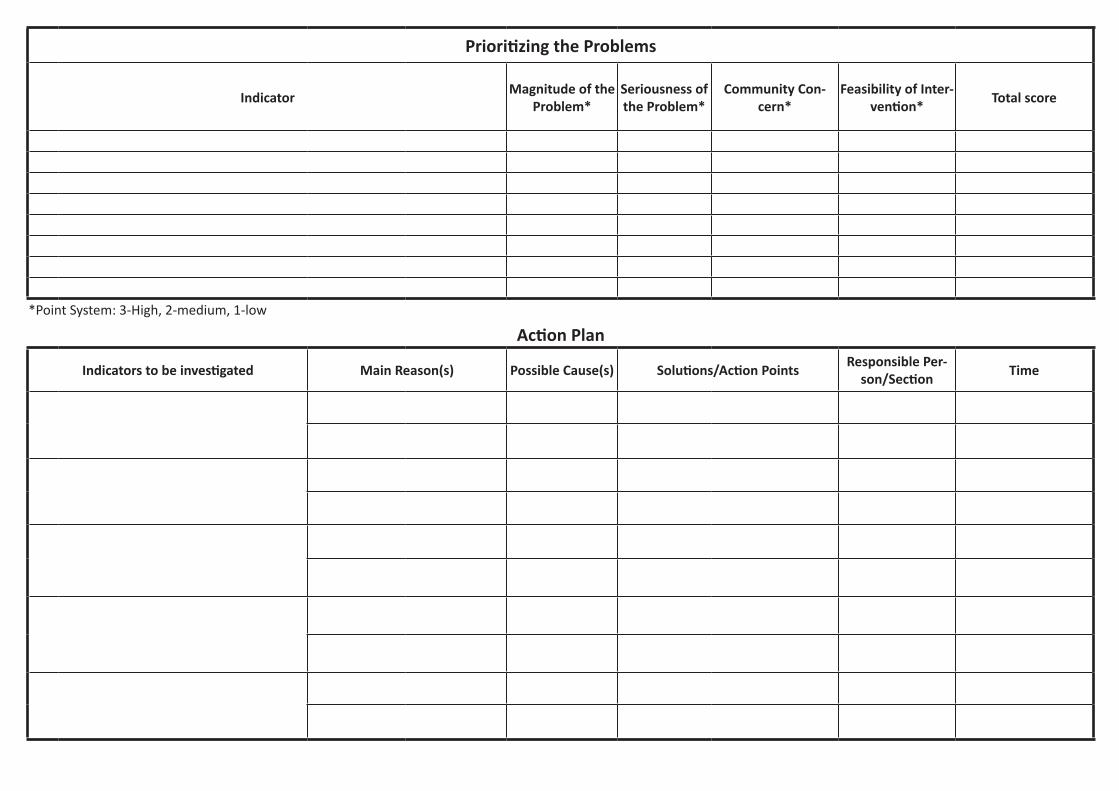
Prioritizing the Problems
Indicator Magnitude of the Problem*
Seriousness of the Problem*
Community Con-cern*
Feasibility of Inter-vention* Total score
*Point System: 3-High, 2-medium, 1-low
Action Plan
Indicators to be investigated Main Reason(s) Possible Cause(s) Solutions/Action Points Responsible Per-son/Section Time
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Data Quality and Performance monitoring logbook Hospital Level
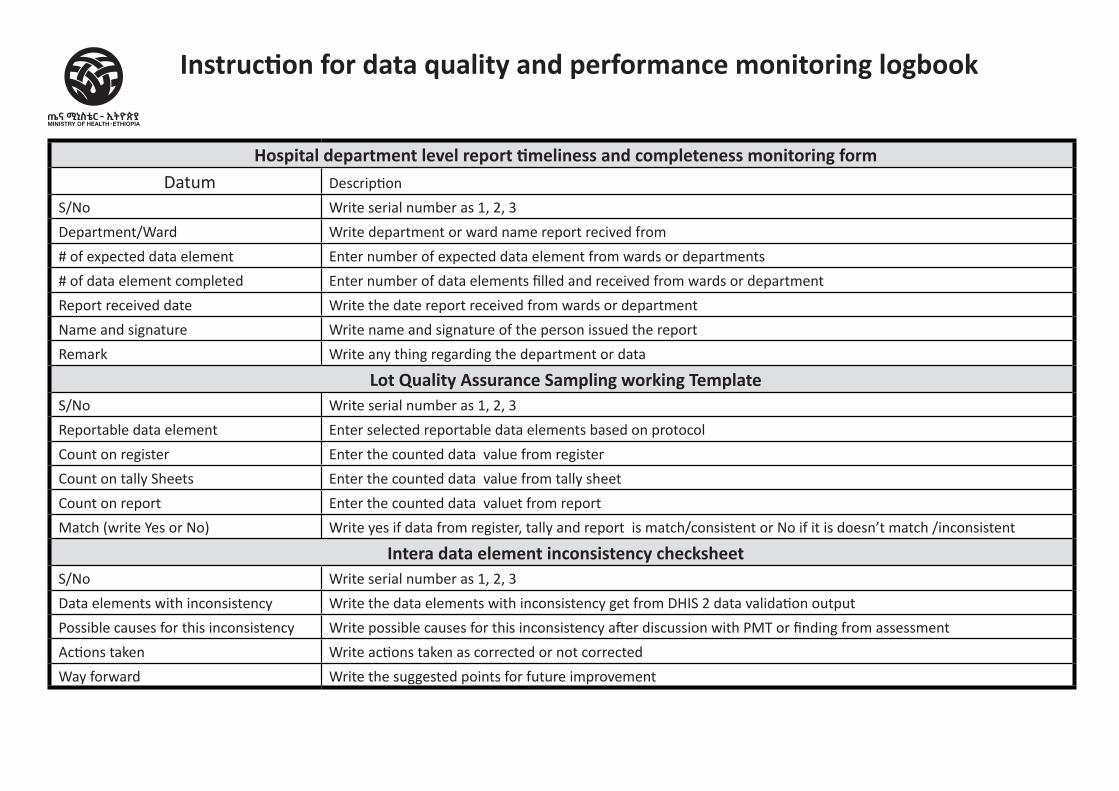
Hospital department level report timeliness and completeness monitoring formDatum Description
S/No Write serial number as 1, 2, 3
Department/Ward Write department or ward name report recived from
# of expected data element Enter number of expected data element from wards or departments
# of data element completed Enter number of data elements filled and received from wards or department
Report received date Write the date report received from wards or department
Name and signature Write name and signature of the person issued the report
Remark Write any thing regarding the department or data
Lot Quality Assurance Sampling working TemplateS/No Write serial number as 1, 2, 3
Reportable data element Enter selected reportable data elements based on protocol
Count on register Enter the counted data value from register
Count on tally Sheets Enter the counted data value from tally sheet
Count on report Enter the counted data valuet from report
Match (write Yes or No) Write yes if data from register, tally and report is match/consistent or No if it is doesn’t match /inconsistent
Intera data element inconsistency checksheetS/No Write serial number as 1, 2, 3
Data elements with inconsistency Write the data elements with inconsistency get from DHIS 2 data validation output
Possible causes for this inconsistency Write possible causes for this inconsistency after discussion with PMT or finding from assessment
Actions taken Write actions taken as corrected or not corrected
Way forward Write the suggested points for future improvement
Instruction for data quality and performance monitoring logbook
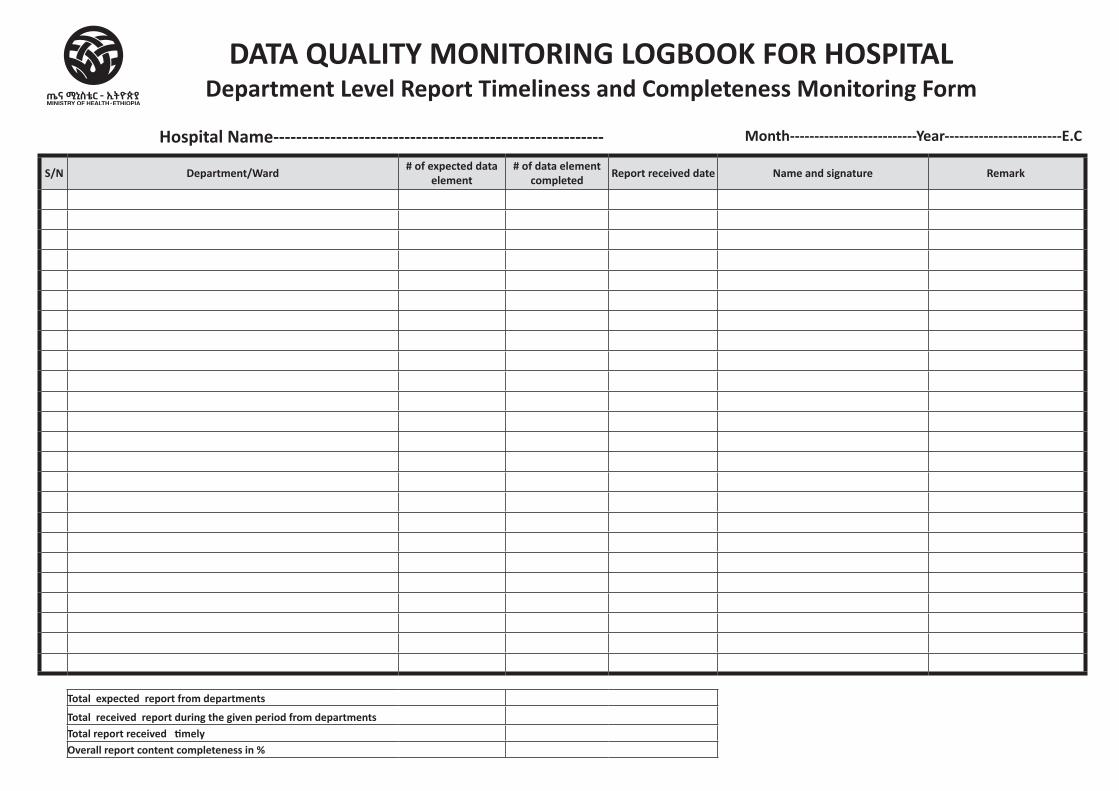
S/N Department/Ward # of expected data element
# of data element completed Report received date Name and signature Remark
Total expected report from departments
Total received report during the given period from departmentsTotal report received timelyOverall report content completeness in %
DATA QUALITY MONITORING LOGBOOK FOR HOSPITALDepartment Level Report Timeliness and Completeness Monitoring Form
Hospital Name---------------------------------------------------------- Month--------------------------Year------------------------E.C
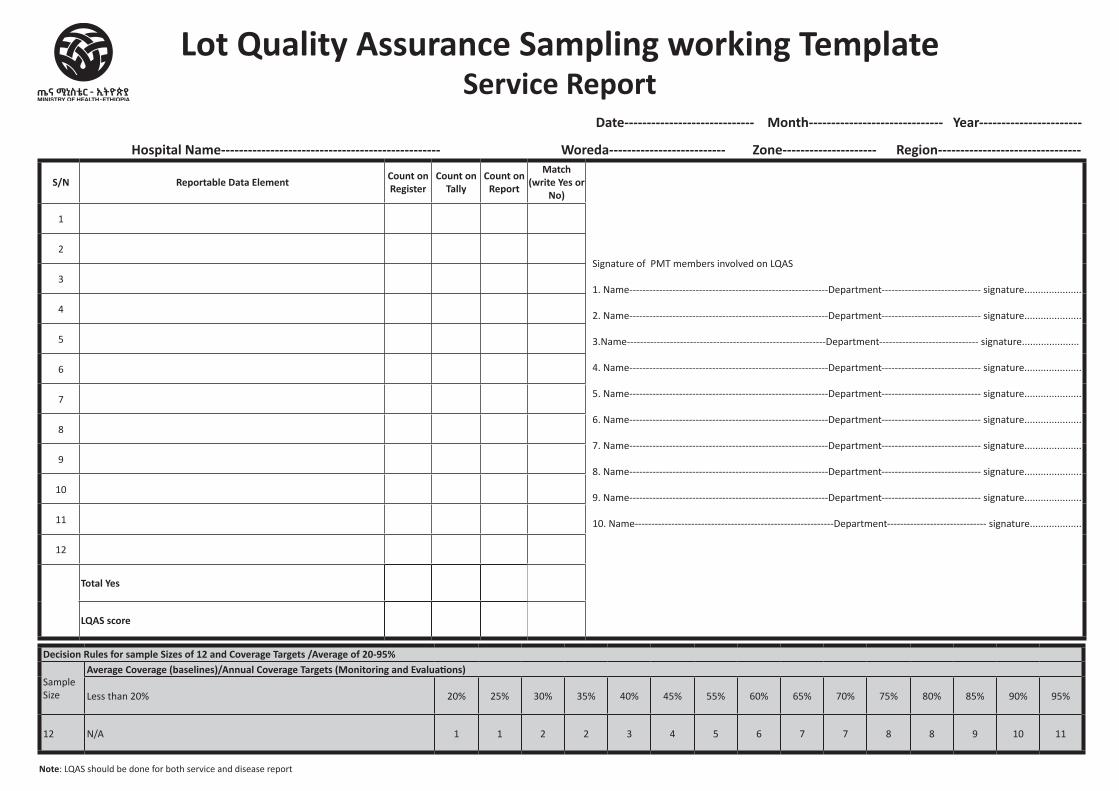
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Lot Quality Assurance Sampling working Template Service Report
Date----------------------------- Month------------------------------ Year-----------------------
Hospital Name------------------------------------------------- Woreda-------------------------- Zone--------------------- Region--------------------------------
Note: LQAS should be done for both service and disease report
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
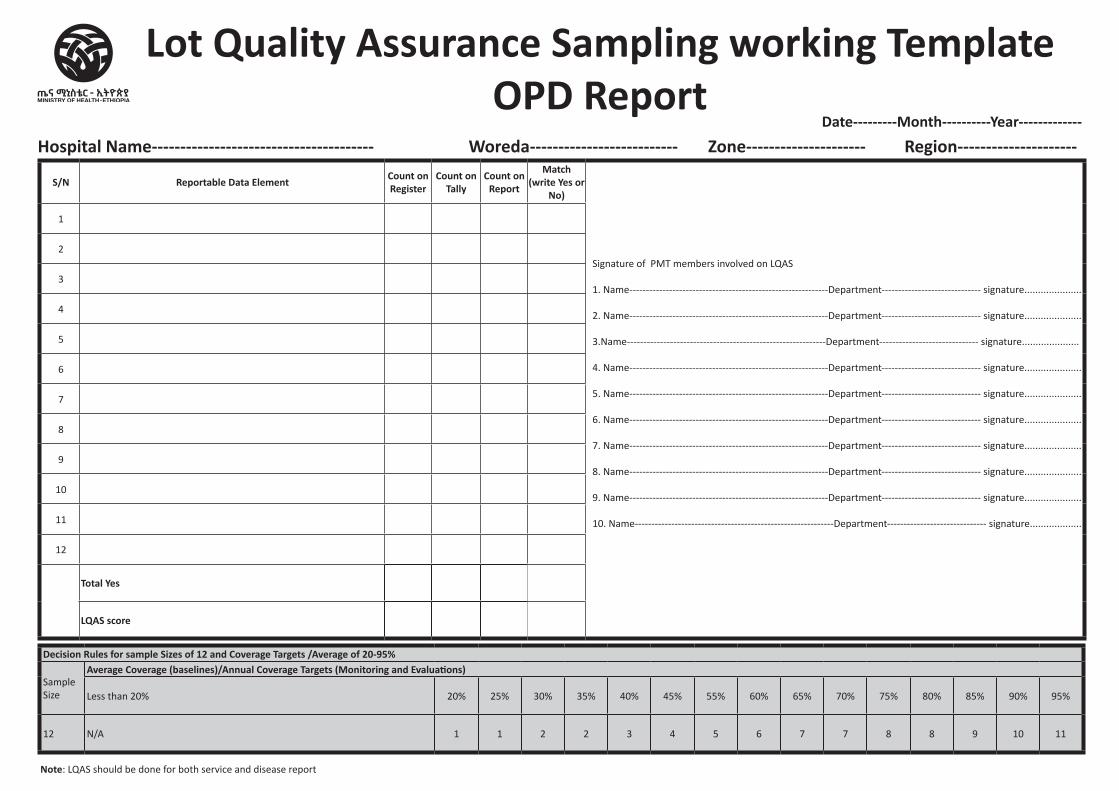
Lot Quality Assurance Sampling working Template OPD Report
Hospital Name--------------------------------------- Woreda-------------------------- Zone--------------------- Region---------------------Date---------Month----------Year-------------
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
Note: LQAS should be done for both service and disease report
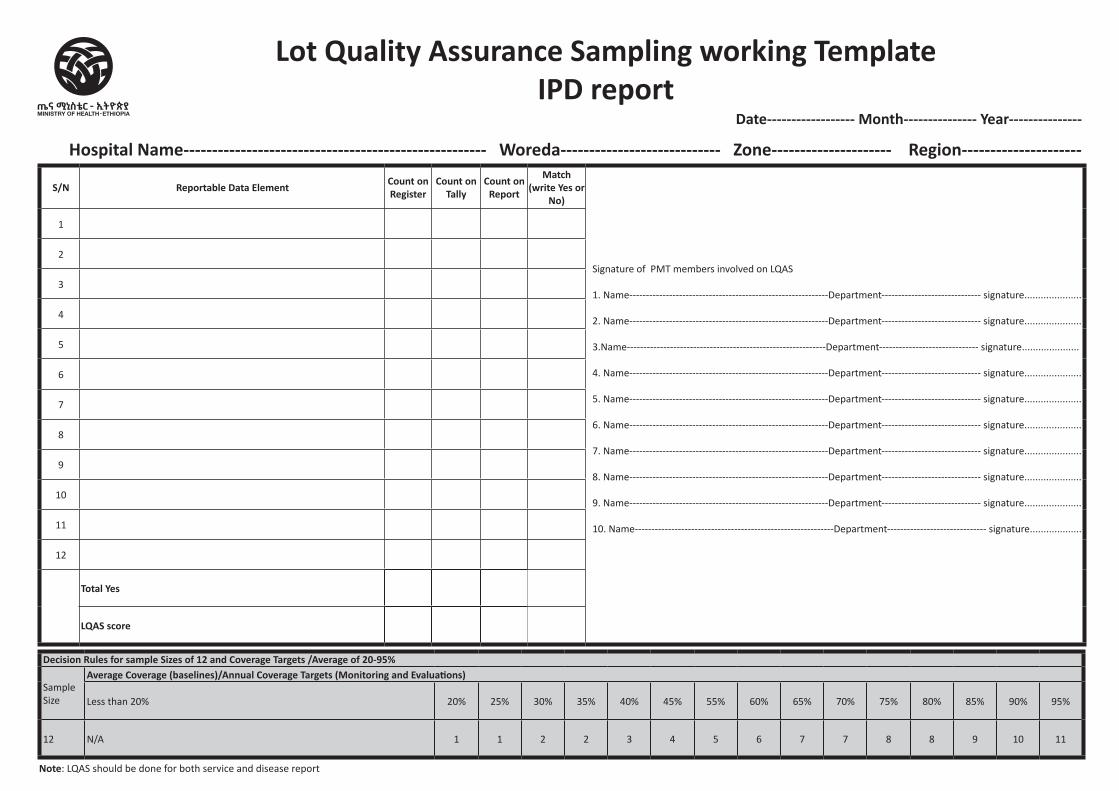
Lot Quality Assurance Sampling working Template IPD report
Hospital Name----------------------------------------------------- Woreda---------------------------- Zone--------------------- Region---------------------
Date------------------ Month--------------- Year---------------
S/N Reportable Data Element Count on Register
Count on Tally
Count on Report
Match (write Yes or
No)
Signature of PMT members involved on LQAS 1. Name------------------------------------------------------------Department------------------------------ signature..................... 2. Name------------------------------------------------------------Department------------------------------ signature..................... 3.Name------------------------------------------------------------Department------------------------------ signature..................... 4. Name------------------------------------------------------------Department------------------------------ signature..................... 5. Name------------------------------------------------------------Department------------------------------ signature..................... 6. Name------------------------------------------------------------Department------------------------------ signature..................... 7. Name------------------------------------------------------------Department------------------------------ signature..................... 8. Name------------------------------------------------------------Department------------------------------ signature..................... 9. Name------------------------------------------------------------Department------------------------------ signature..................... 10. Name------------------------------------------------------------Department------------------------------ signature...................
1
2
3
4
5
6
7
8
9
10
11
12
Total Yes
LQAS score
Decision Rules for sample Sizes of 12 and Coverage Targets /Average of 20-95%
Sample Size
Average Coverage (baselines)/Annual Coverage Targets (Monitoring and Evaluations)
Less than 20% 20% 25% 30% 35% 40% 45% 55% 60% 65% 70% 75% 80% 85% 90% 95%
12 N/A 1 1 2 2 3 4 5 6 7 7 8 8 9 10 11
Note: LQAS should be done for both service and disease report
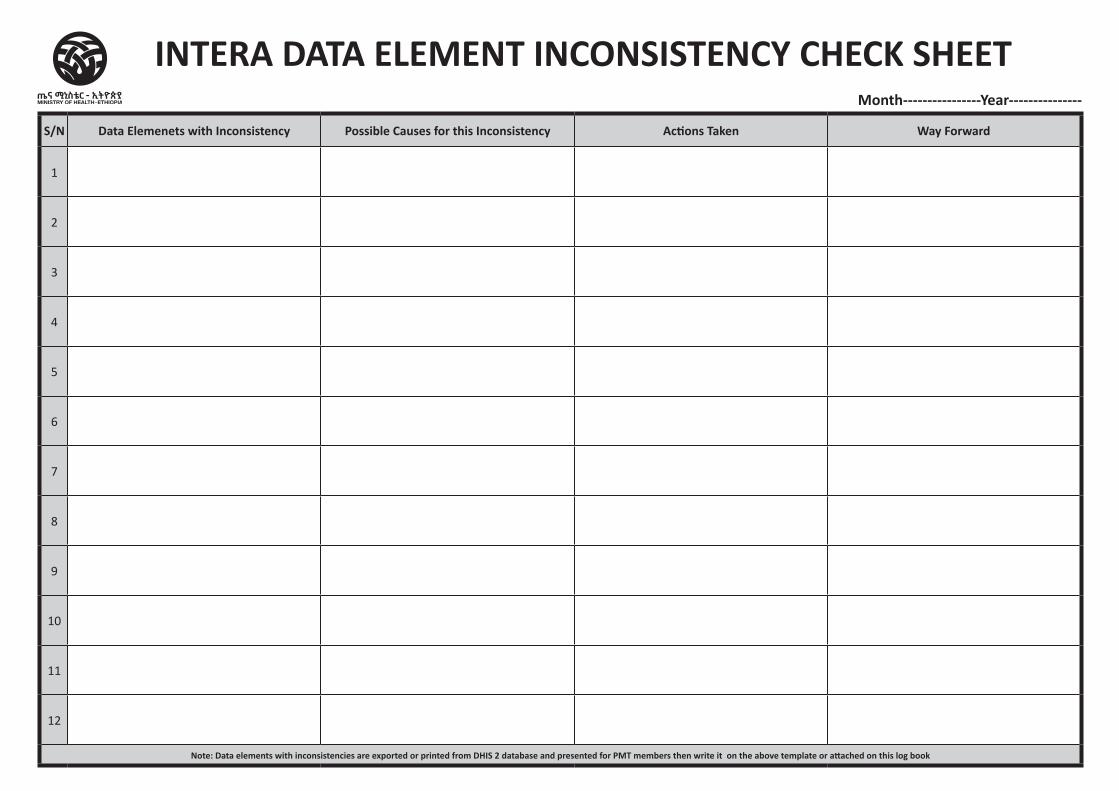
S/N Data Elemenets with Inconsistency Possible Causes for this Inconsistency Actions Taken Way Forward
1
2
3
4
5
6
7
8
9
10
11
12
Note: Data elements with inconsistencies are exported or printed from DHIS 2 database and presented for PMT members then write it on the above template or attached on this log book
INTERA DATA ELEMENT INCONSISTENCY CHECK SHEETMonth----------------Year---------------
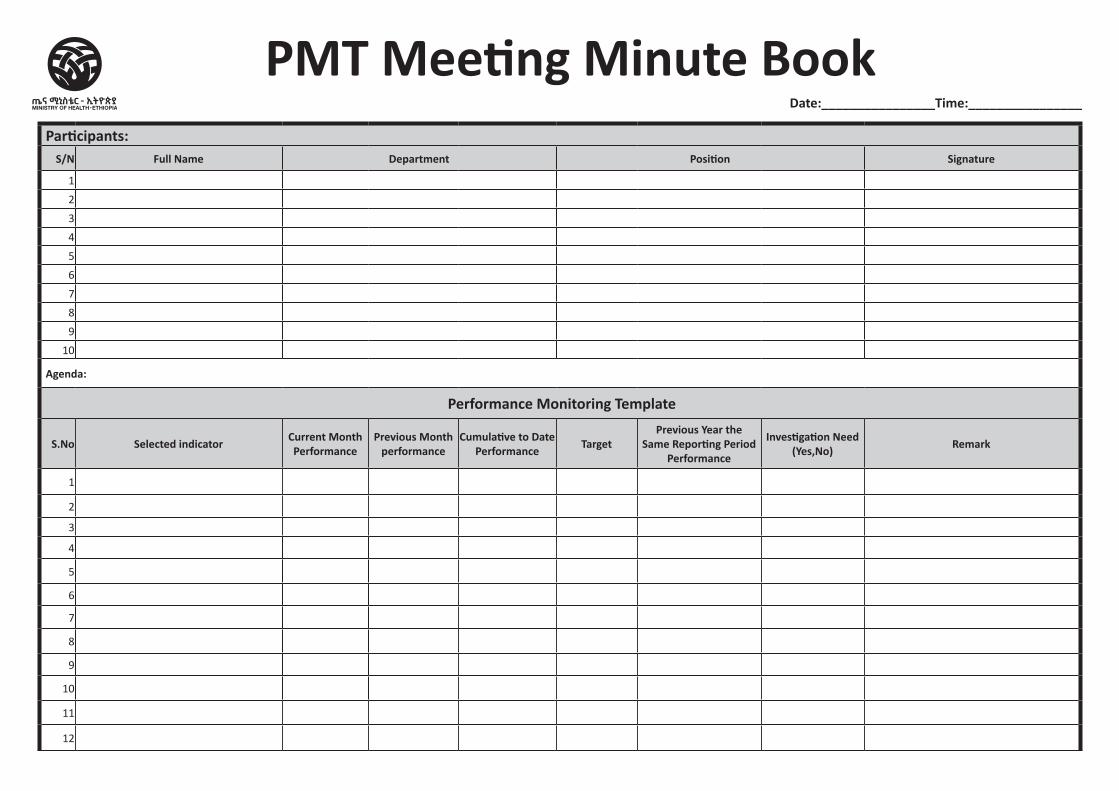
PMT Meeting Minute BookDate:________________Time:________________
Participants:S/N Full Name Department Position Signature
1
2
3
4
5
6
7
8
9
10
Agenda:
Performance Monitoring Template
S.No Selected indicator Current Month Performance
Previous Month performance
Cumulative to Date Performance Target
Previous Year the Same Reporting Period
Performance
Investigation Need (Yes,No) Remark
1
2
3
4
5
6
7
8
9
10
11
12
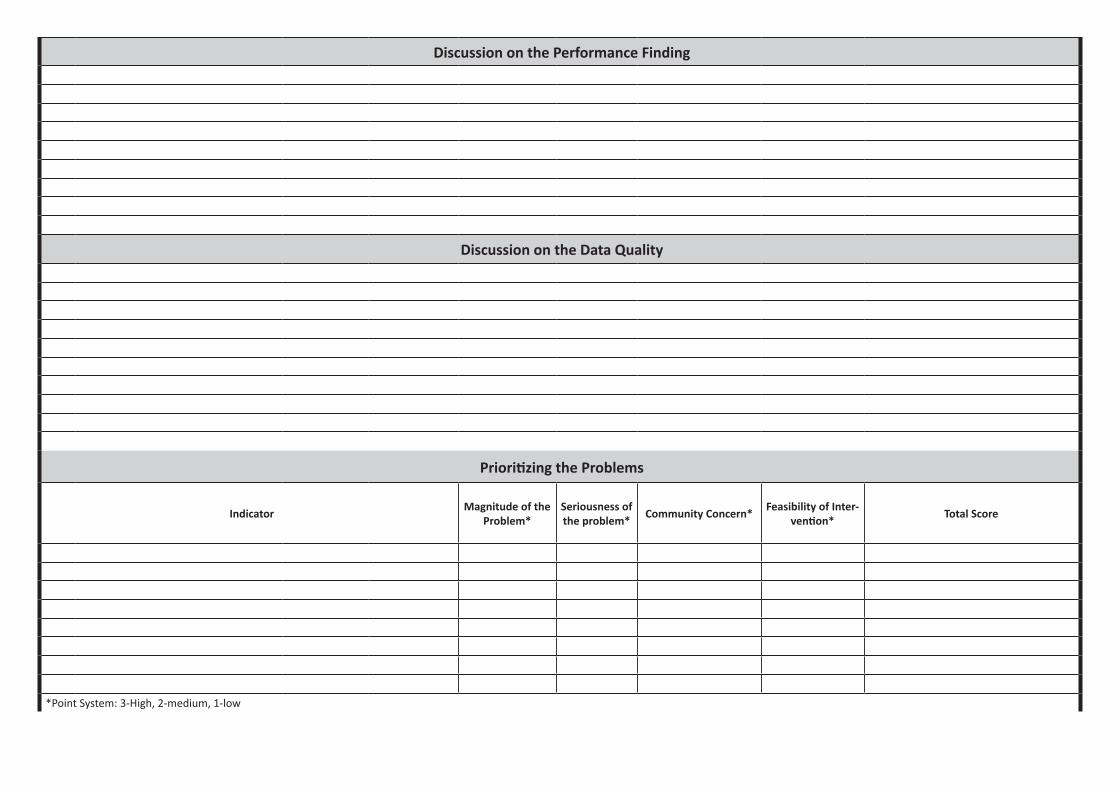
Discussion on the Performance Finding
Discussion on the Data Quality
Prioritizing the Problems
Indicator Magnitude of the Problem*
Seriousness of the problem* Community Concern* Feasibility of Inter-
vention* Total Score
*Point System: 3-High, 2-medium, 1-low
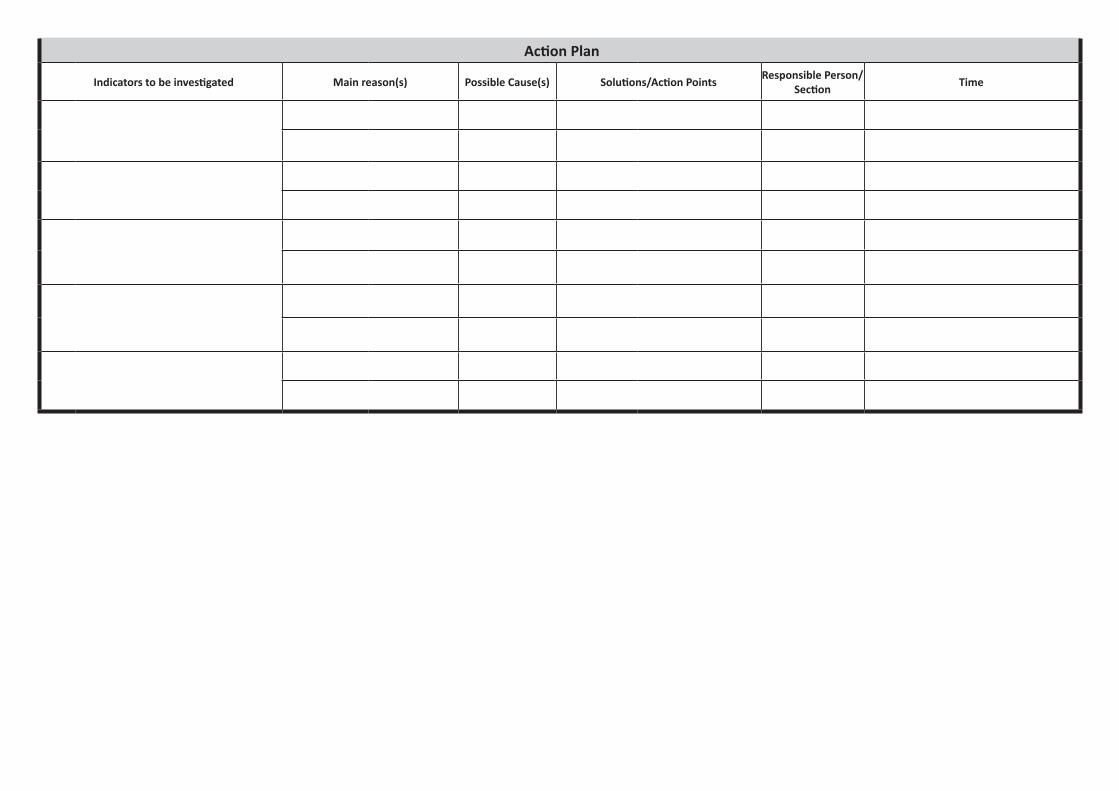
Action Plan
Indicators to be investigated Main reason(s) Possible Cause(s) Solutions/Action Points Responsible Person/Section Time
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Data Quality and Performance monitoring logbook Health Institution Level
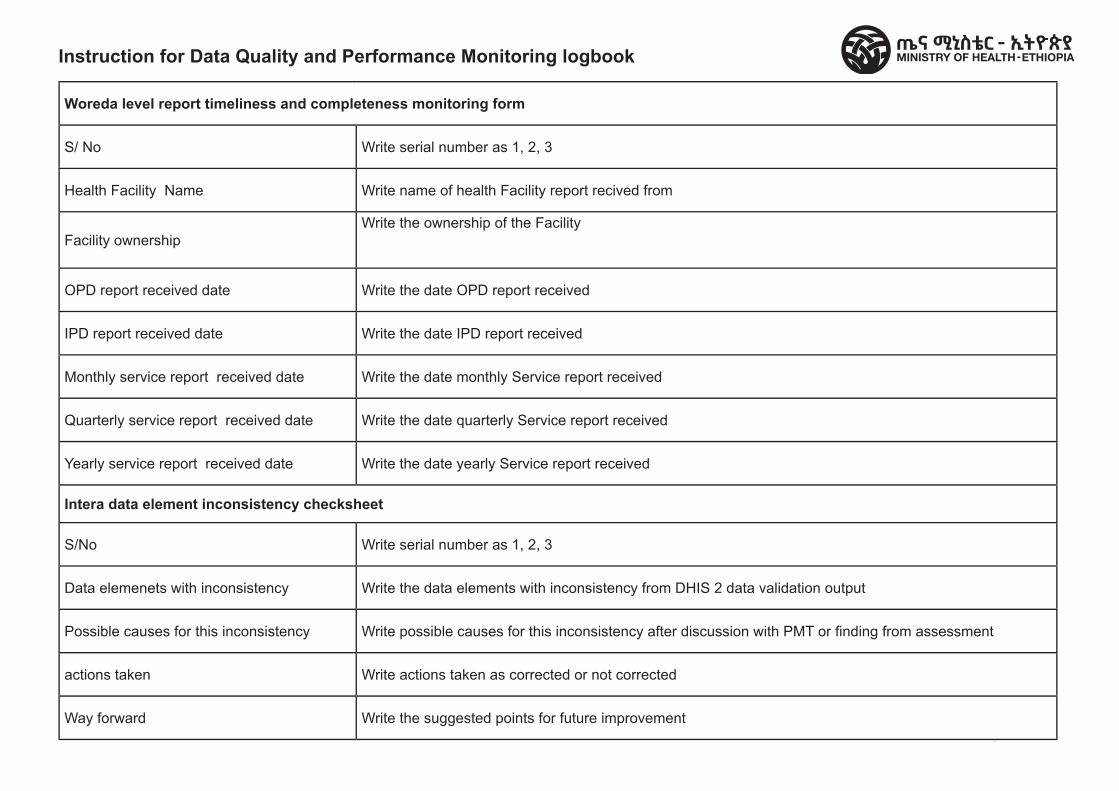
FMOH V1 2009
Instruction for Data Quality and Performance Monitoring logbookFederal Democratic Republic of Ethiopia Ministry of Health
Woreda level report timeliness and completeness monitoring form
S/ No Write serial number as 1, 2, 3
Health Facility Name Write name of health Facility report recived from
Facility ownershipWrite the ownership of the Facility
OPD report received date Write the date OPD report received
IPD report received date Write the date IPD report received
Monthly service report received date Write the date monthly Service report received
Quarterly service report received date Write the date quarterly Service report received
Yearly service report received date Write the date yearly Service report received
Intera data element inconsistency checksheet
S/No Write serial number as 1, 2, 3
Data elemenets with inconsistency Write the data elements with inconsistency from DHIS 2 data validation output
Possible causes for this inconsistency Write possible causes for this inconsistency after discussion with PMT or fi nding from assessment
actions taken Write actions taken as corrected or not corrected
Way forward Write the suggested points for future improvement
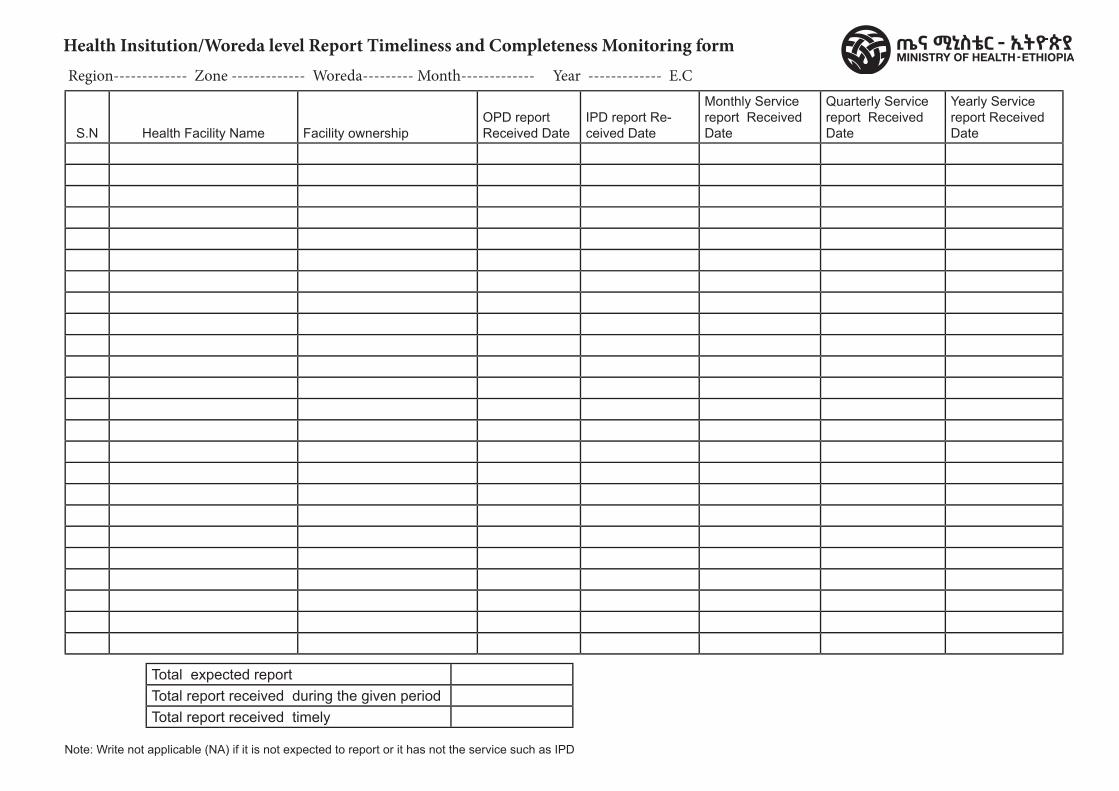
FMOH V1 2009
Health Insitution/Woreda level Report Timeliness and Completeness Monitoring form Region------------- Zone ------------- Woreda--------- Month------------- Year ------------- E.C
Note: Write not applicable (NA) if it is not expected to report or it has not the service such as IPD
S.N Health Facility Name Facility ownershipOPD report Received Date
IPD report Re-ceived Date
Monthly Service report Received Date
Quarterly Service report Received Date
Yearly Service report Received Date
Total expected reportTotal report received during the given periodTotal report received timely
Federal Democratic Republic of Ethiopia Ministry of Health
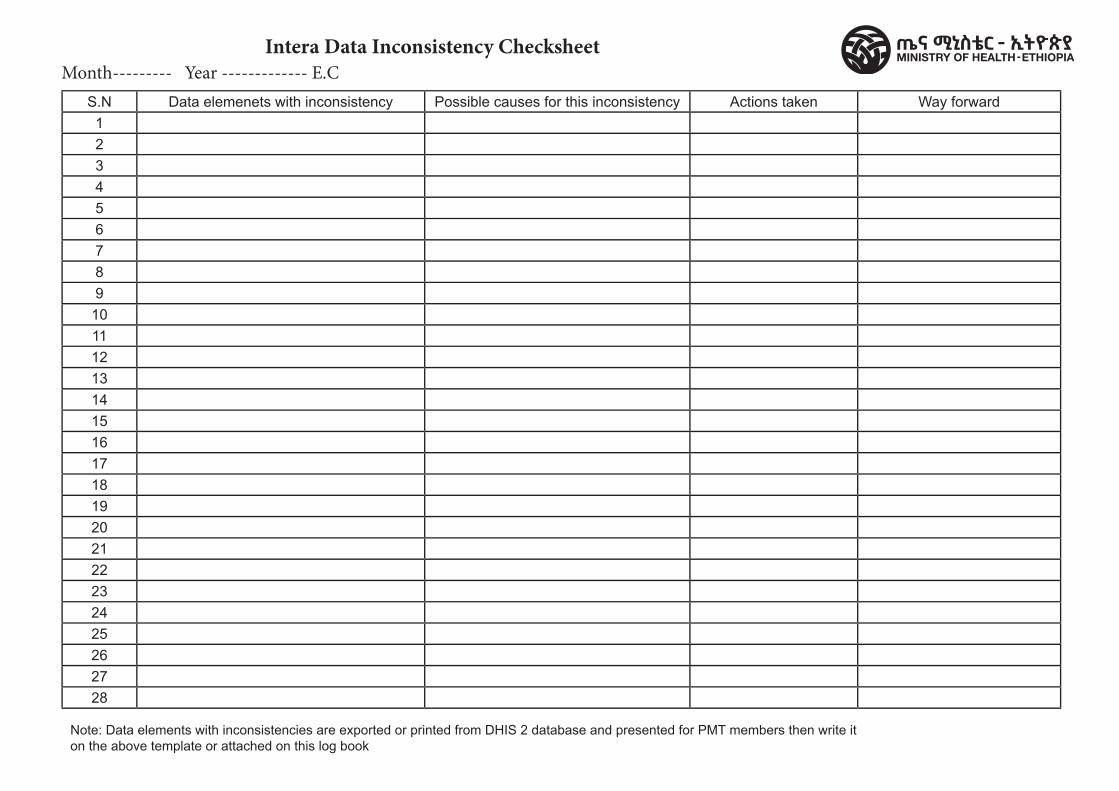
S.N Data elemenets with inconsistency Possible causes for this inconsistency Actions taken Way forward12345678910111213141516171819202122232425262728
FMOH V1 2009
Intera Data Inconsistency ChecksheetMonth--------- Year ------------- E.C
Note: Data elements with inconsistencies are exported or printed from DHIS 2 database and presented for PMT members then write it on the above template or attached on this log book
Federal Democratic Republic of Ethiopia Ministry of Health
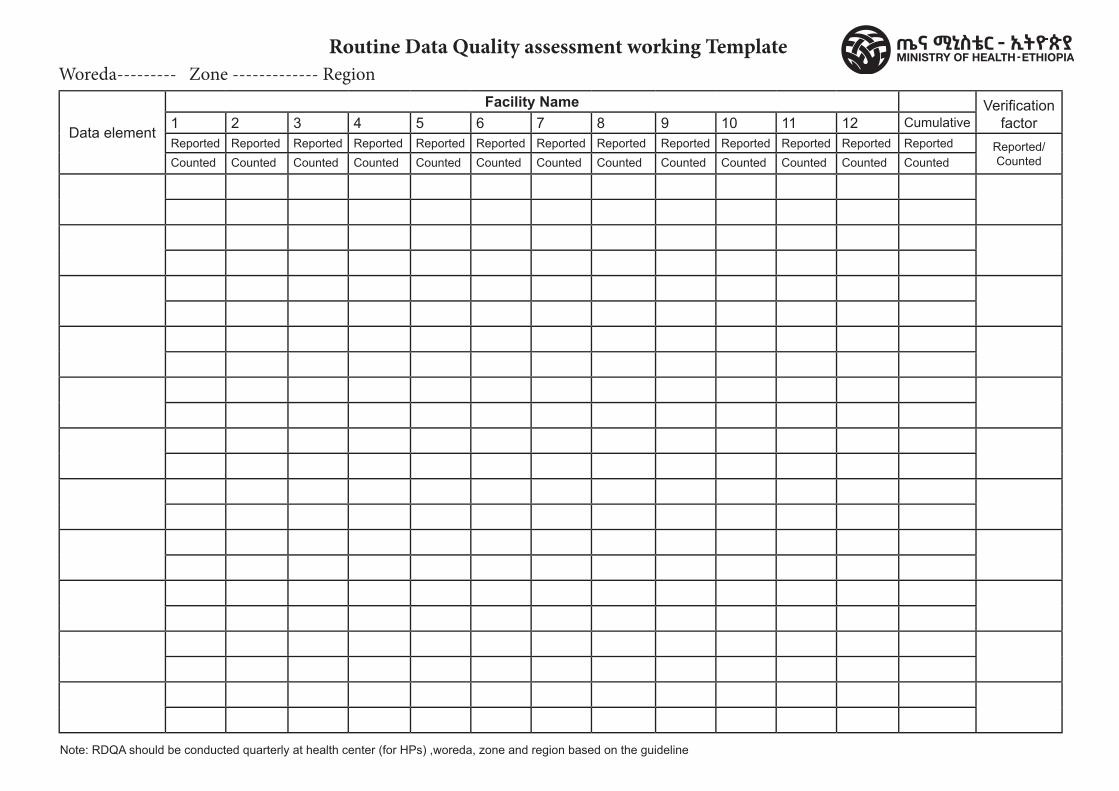
FMOH V1 2009
Routine Data Quality assessment working Template
Data element
Facility Name Verifi cation factor1 2 3 4 5 6 7 8 9 10 11 12 Cumulative
Reported Reported Reported Reported Reported Reported Reported Reported Reported Reported Reported Reported Reported Reported/CountedCounted Counted Counted Counted Counted Counted Counted Counted Counted Counted Counted Counted Counted
Woreda--------- Zone ------------- Region
Note: RDQA should be conducted quarterly at health center (for HPs) ,woreda, zone and region based on the guideline
Federal Democratic Republic of Ethiopia Ministry of Health
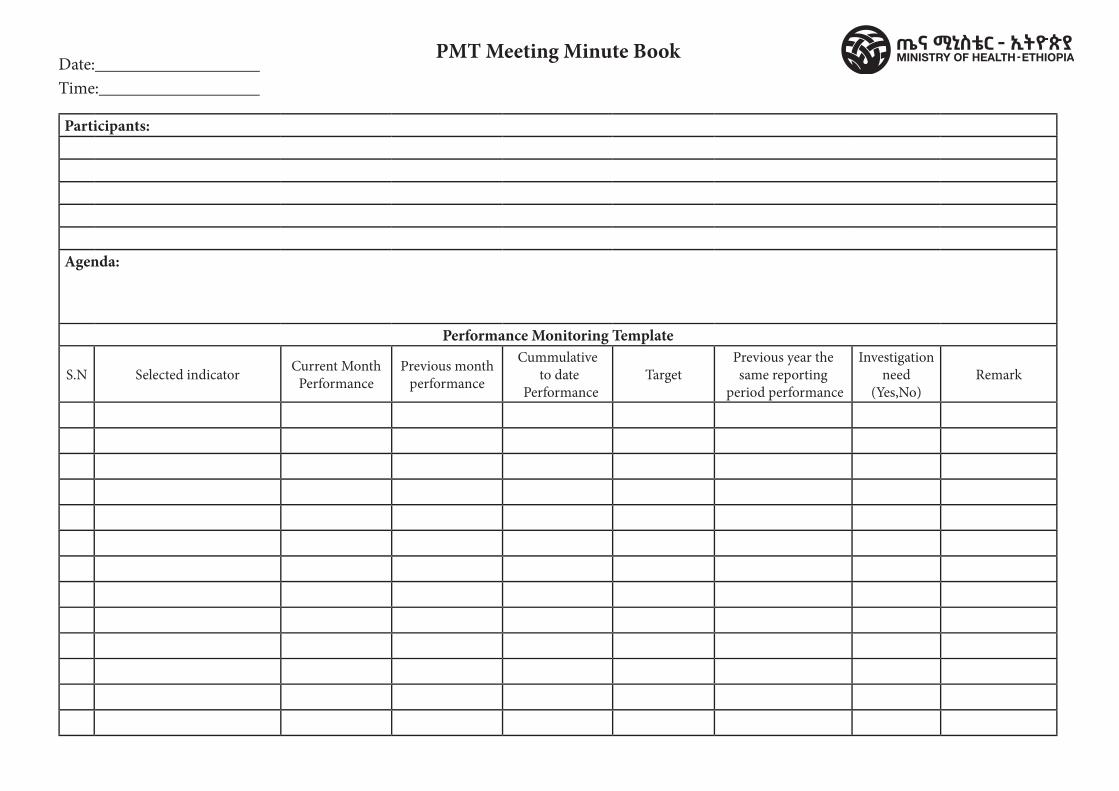
PMT Meeting Minute Book
FMOH V1 2009
Date: Time:
Participants:
Agenda:
Performance Monitoring Template
S.N Selected indicator Current Month Performance
Previous month performance
Cummulative to date
PerformanceTarget
Previous year the same reporting
period performance
Investigation need
(Yes,No)Remark
Federal Democratic Republic of Ethiopia Ministry of Health
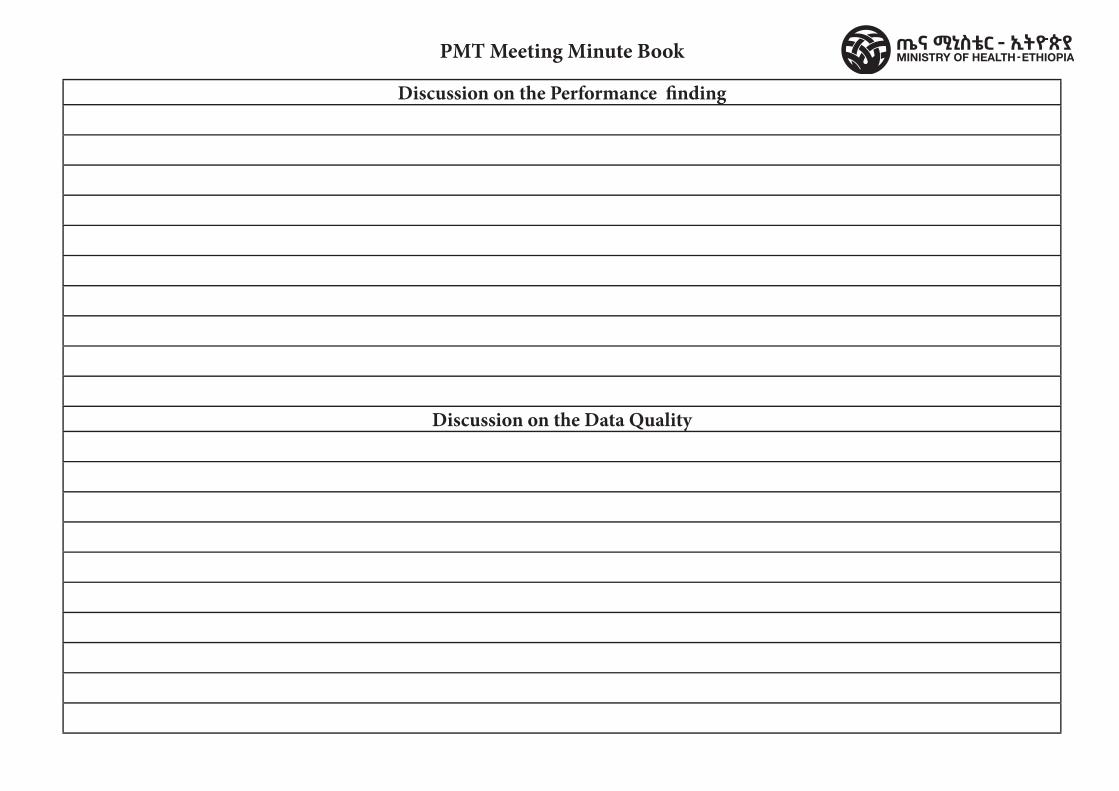
PMT Meeting Minute Book
FMOH V1 2009
Discussion on the Performance � nding
Discussion on the Data Quality
Federal Democratic Republic of Ethiopia Ministry of Health
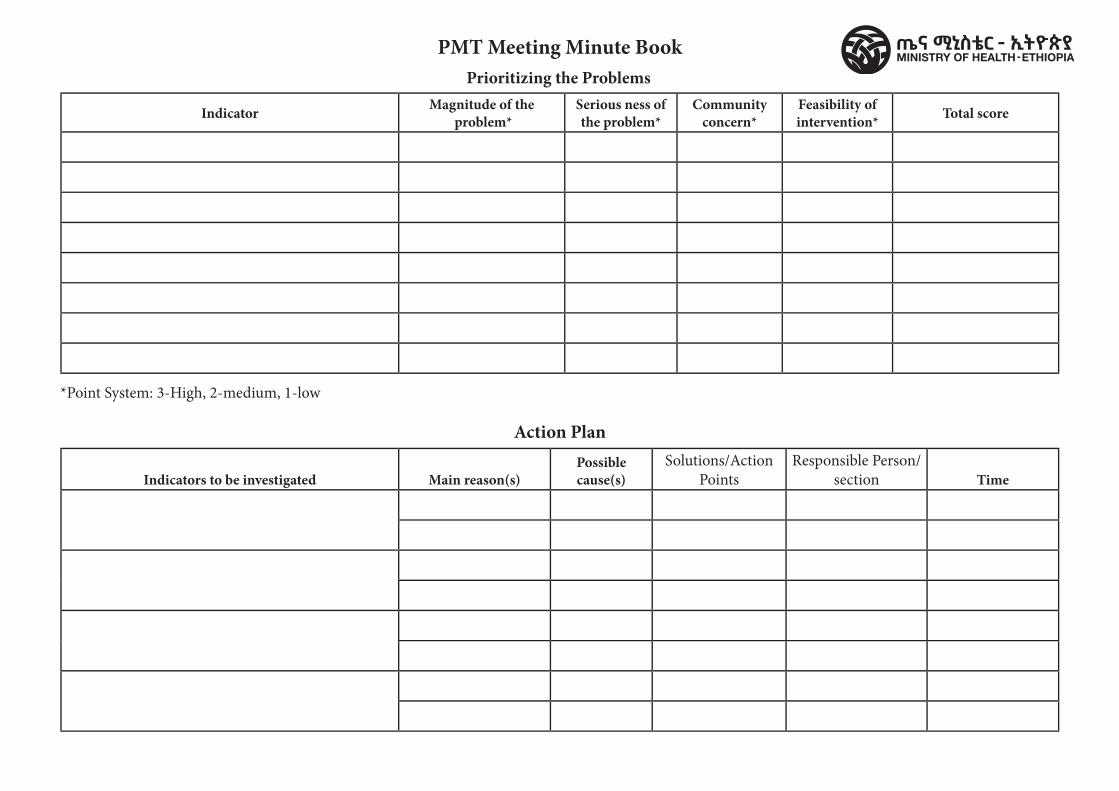
PMT Meeting Minute BookPrioritizing the Problems
FMOH V1 2009
Indicator Magnitude of the problem*
Serious ness of the problem*
Community concern*
Feasibility of intervention* Total score
Indicators to be investigated Main reason(s)Possible cause(s)
Solutions/Action Points
Responsible Person/section Time
Action Plan
*Point System: 3-High, 2-medium, 1-low
Federal Democratic Republic of Ethiopia Ministry of Health
Malaria RegisterContent / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center Malaria Screening and Investigation
Register
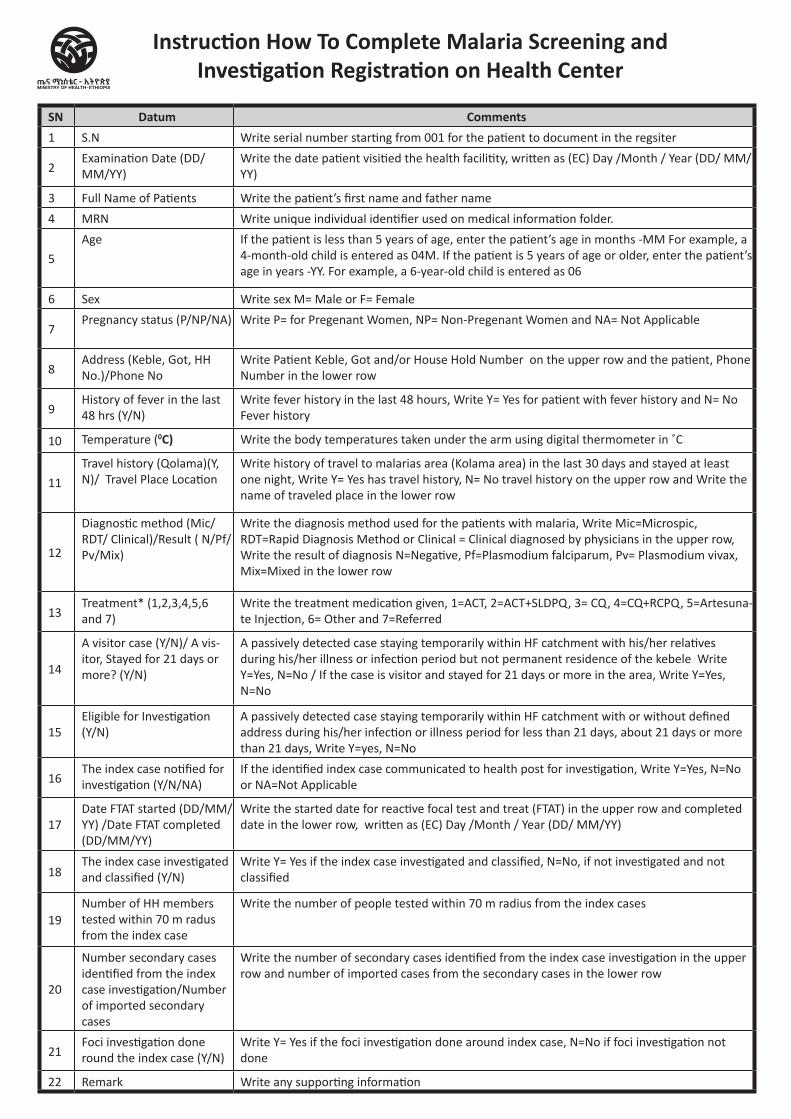
SN Datum Comments1 S.N Write serial number starting from 001 for the patient to document in the regsiter
2Examination Date (DD/MM/YY)
Write the date patient visitied the health facilitity, written as (EC) Day /Month / Year (DD/ MM/YY)
3 Full Name of Patients Write the patient’s first name and father name
4 MRN Write unique individual identifier used on medical information folder.
5
Age If the patient is less than 5 years of age, enter the patient’s age in months -MM For example, a 4-month-old child is entered as 04M. If the patient is 5 years of age or older, enter the patient’s age in years -YY. For example, a 6-year-old child is entered as 06
6 Sex Write sex M= Male or F= Female
7Pregnancy status (P/NP/NA) Write P= for Pregenant Women, NP= Non-Pregenant Women and NA= Not Applicable
8Address (Keble, Got, HH No.)/Phone No
Write Patient Keble, Got and/or House Hold Number on the upper row and the patient, Phone Number in the lower row
9History of fever in the last 48 hrs (Y/N)
Write fever history in the last 48 hours, Write Y= Yes for patient with fever history and N= No Fever history
10 Temperature (0C) Write the body temperatures taken under the arm using digital thermometer in ˚C
11
Travel history (Qolama)(Y, N)/ Travel Place Location
Write history of travel to malarias area (Kolama area) in the last 30 days and stayed at least one night, Write Y= Yes has travel history, N= No travel history on the upper row and Write the name of traveled place in the lower row
12
Diagnostic method (Mic/RDT/ Clinical)/Result ( N/Pf/Pv/Mix)
Write the diagnosis method used for the patients with malaria, Write Mic=Microspic, RDT=Rapid Diagnosis Method or Clinical = Clinical diagnosed by physicians in the upper row, Write the result of diagnosis N=Negative, Pf=Plasmodium falciparum, Pv= Plasmodium vivax, Mix=Mixed in the lower row
13Treatment* (1,2,3,4,5,6 and 7)
Write the treatment medication given, 1=ACT, 2=ACT+SLDPQ, 3= CQ, 4=CQ+RCPQ, 5=Artesuna-te Injection, 6= Other and 7=Referred
14
A visitor case (Y/N)/ A vis-itor, Stayed for 21 days or more? (Y/N)
A passively detected case staying temporarily within HF catchment with his/her relatives during his/her illness or infection period but not permanent residence of the kebele Write Y=Yes, N=No / If the case is visitor and stayed for 21 days or more in the area, Write Y=Yes, N=No
15Eligible for Investigation (Y/N)
A passively detected case staying temporarily within HF catchment with or without defined address during his/her infection or illness period for less than 21 days, about 21 days or more than 21 days, Write Y=yes, N=No
16The index case notified for investigation (Y/N/NA)
If the identified index case communicated to health post for investigation, Write Y=Yes, N=No or NA=Not Applicable
17Date FTAT started (DD/MM/YY) /Date FTAT completed (DD/MM/YY)
Write the started date for reactive focal test and treat (FTAT) in the upper row and completed date in the lower row, written as (EC) Day /Month / Year (DD/ MM/YY)
18The index case investigated and classified (Y/N)
Write Y= Yes if the index case investigated and classified, N=No, if not investigated and not classified
19Number of HH members tested within 70 m radus from the index case
Write the number of people tested within 70 m radius from the index cases
20
Number secondary cases identified from the index case investigation/Number of imported secondary cases
Write the number of secondary cases identified from the index case investigation in the upper row and number of imported cases from the secondary cases in the lower row
21Foci investigation done round the index case (Y/N)
Write Y= Yes if the foci investigation done around index case, N=No if foci investigation not done
22 Remark Write any supporting information
Instruction How To Complete Malaria Screening and Investigation Registration on Health Center
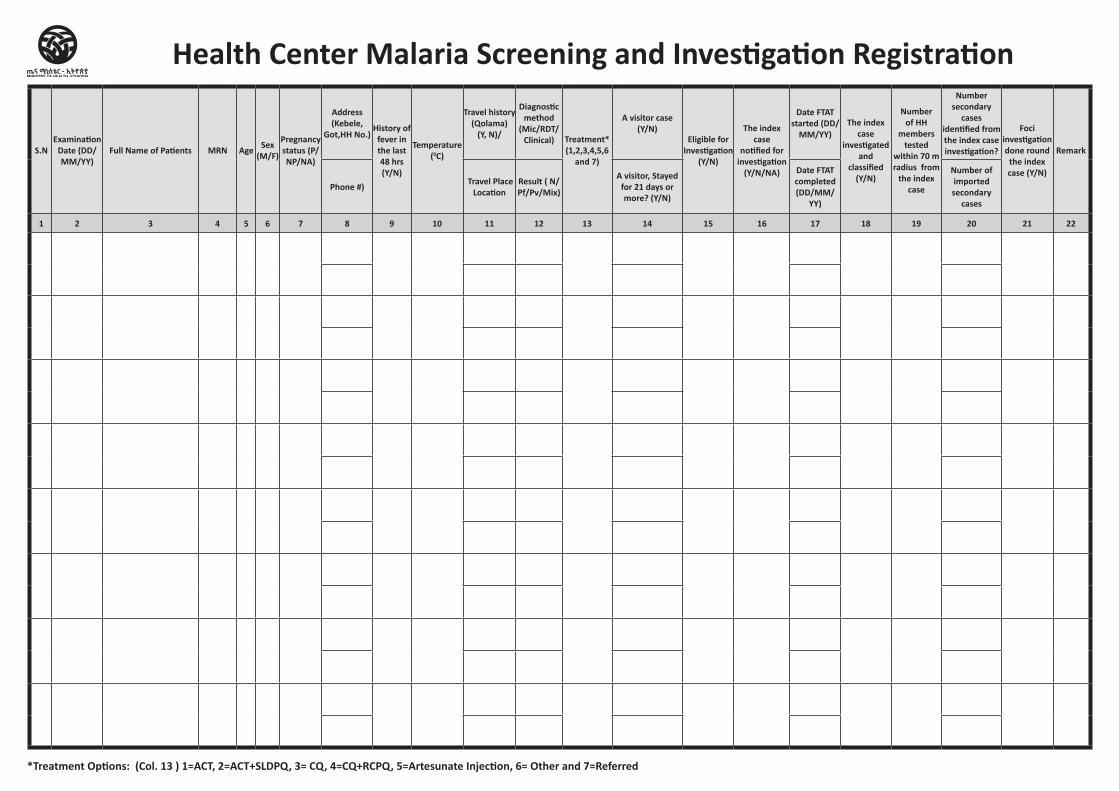
S.NExamination
Date (DD/MM/YY)
Full Name of Patients MRN Age Sex (M/F)
Pregnancy status (P/NP/NA)
Address (Kebele,
Got,HH No.)History of
fever in the last 48 hrs (Y/N)
Temperature (0C)
Travel history (Qolama)
(Y, N)/
Diagnostic method
(Mic/RDT/ Clinical) Treatment*
(1,2,3,4,5,6 and 7)
A visitor case (Y/N)
Eligible for Investigation
(Y/N)
The index case
notified for investigation
(Y/N/NA)
Date FTAT started (DD/
MM/YY) The index
case investigated
and classified
(Y/N)
Number of HH
members tested
within 70 m radius from
the index case
Number secondary
cases identified from the index case investigation?
Foci investigation done round
the index case (Y/N)
Remark
Phone #) Travel Place Location
Result ( N/Pf/Pv/Mix)
A visitor, Stayed for 21 days or more? (Y/N)
Date FTAT completed (DD/MM/
YY)
Number of imported secondary
cases
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Health Center Malaria Screening and Investigation Registration
*Treatment Options: (Col. 13 ) 1=ACT, 2=ACT+SLDPQ, 3= CQ, 4=CQ+RCPQ, 5=Artesunate Injection, 6= Other and 7=Referred
MSD Registers & Tally sheetsContent / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /WorHo & HospitalAmbulance Service Register
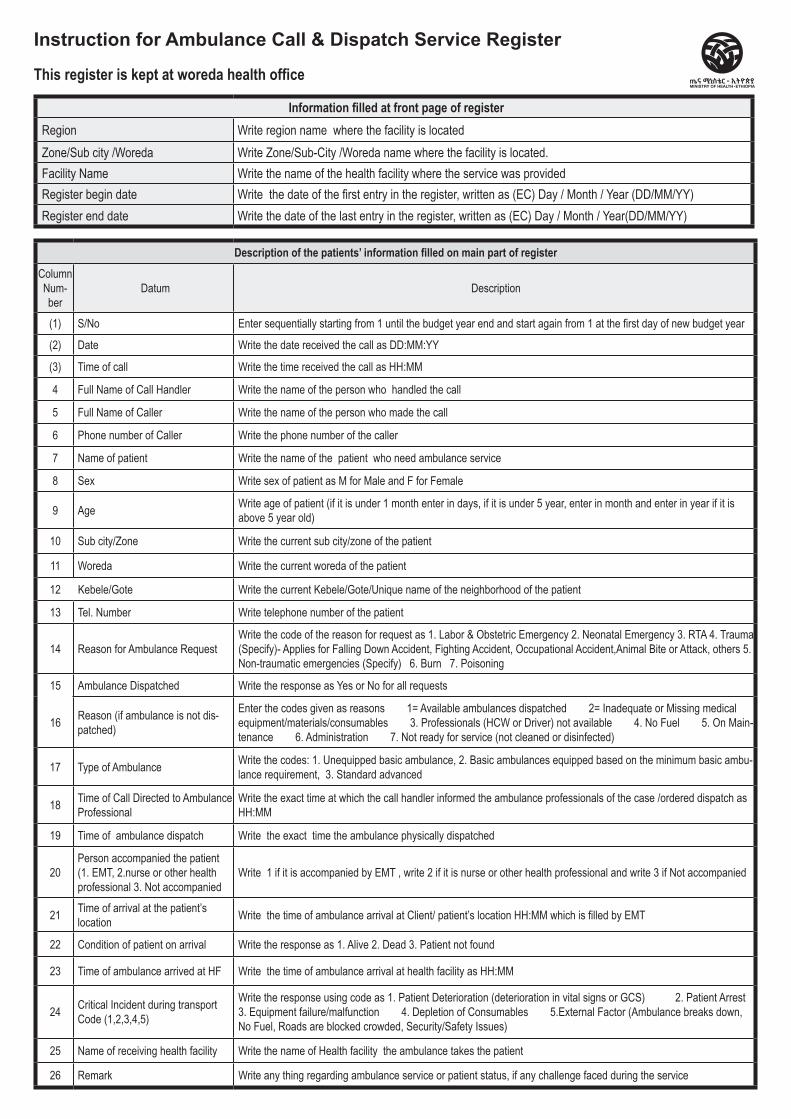
Description of the patients’ information filled on main part of registerColumn Num-ber
Datum Description
(1) S/No Enter sequentially starting from 1 until the budget year end and start again from 1 at the first day of new budget year
(2) Date Write the date received the call as DD:MM:YY
(3) Time of call Write the time received the call as HH:MM
4 Full Name of Call Handler Write the name of the person who handled the call
5 Full Name of Caller Write the name of the person who made the call
6 Phone number of Caller Write the phone number of the caller
7 Name of patient Write the name of the patient who need ambulance service
8 Sex Write sex of patient as M for Male and F for Female
9 Age Write age of patient (if it is under 1 month enter in days, if it is under 5 year, enter in month and enter in year if it is above 5 year old)
10 Sub city/Zone Write the current sub city/zone of the patient
11 Woreda Write the current woreda of the patient
12 Kebele/Gote Write the current Kebele/Gote/Unique name of the neighborhood of the patient
13 Tel. Number Write telephone number of the patient
14 Reason for Ambulance RequestWrite the code of the reason for request as 1. Labor & Obstetric Emergency 2. Neonatal Emergency 3. RTA 4. Trauma (Specify)- Applies for Falling Down Accident, Fighting Accident, Occupational Accident,Animal Bite or Attack, others 5. Non-traumatic emergencies (Specify) 6. Burn 7. Poisoning
15 Ambulance Dispatched Write the response as Yes or No for all requests
16 Reason (if ambulance is not dis-patched)
Enter the codes given as reasons 1= Available ambulances dispatched 2= Inadequate or Missing medical equipment/materials/consumables 3. Professionals (HCW or Driver) not available 4. No Fuel 5. On Main-tenance 6. Administration 7. Not ready for service (not cleaned or disinfected)
17 Type of Ambulance Write the codes: 1. Unequipped basic ambulance, 2. Basic ambulances equipped based on the minimum basic ambu-lance requirement, 3. Standard advanced
18 Time of Call Directed to Ambulance Professional
Write the exact time at which the call handler informed the ambulance professionals of the case /ordered dispatch as HH:MM
19 Time of ambulance dispatch Write the exact time the ambulance physically dispatched
20Person accompanied the patient (1. EMT, 2.nurse or other health professional 3. Not accompanied
Write 1 if it is accompanied by EMT , write 2 if it is nurse or other health professional and write 3 if Not accompanied
21 Time of arrival at the patient’s location Write the time of ambulance arrival at Client/ patient’s location HH:MM which is filled by EMT
22 Condition of patient on arrival Write the response as 1. Alive 2. Dead 3. Patient not found
23 Time of ambulance arrived at HF Write the time of ambulance arrival at health facility as HH:MM
24 Critical Incident during transportCode (1,2,3,4,5)
Write the response using code as 1. Patient Deterioration (deterioration in vital signs or GCS) 2. Patient Arrest 3. Equipment failure/malfunction 4. Depletion of Consumables 5.External Factor (Ambulance breaks down, No Fuel, Roads are blocked crowded, Security/Safety Issues)
25 Name of receiving health facility Write the name of Health facility the ambulance takes the patient
26 Remark Write any thing regarding ambulance service or patient status, if any challenge faced during the service
Instruction for Ambulance Call & Dispatch Service Register
This register is kept at woreda health office
Information filled at front page of registerRegion Write region name where the facility is locatedZone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Facility Name Write the name of the health facility where the service was providedRegister begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
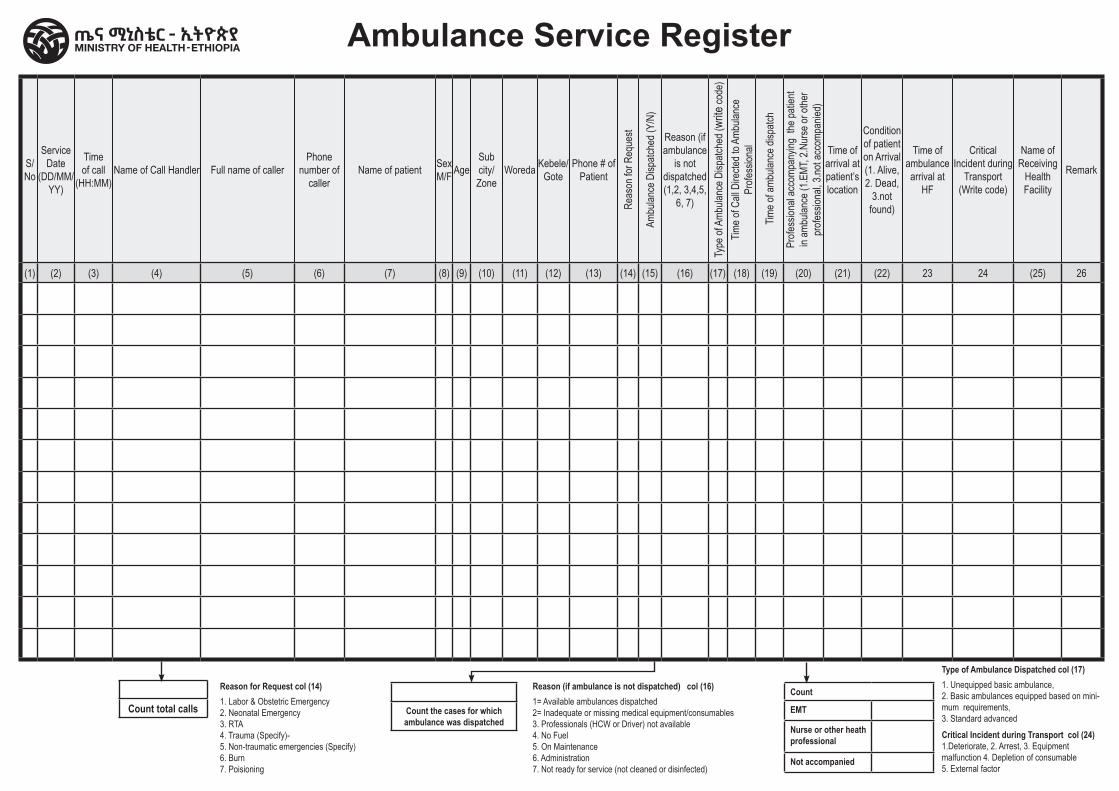
S/No
Service Date
(DD/MM/YY)
Time of call
(HH:MM)Name of Call Handler Full name of caller
Phone number of
callerName of patient Sex
M/F AgeSub city/Zone
Woreda Kebele/Gote
Phone # of Patient
Reas
on fo
r Req
uest
Ambu
lance
Disp
atche
d (Y/
N)
Reason (if ambulance
is not dispatched (1,2, 3,4,5,
6, 7)
Type
of A
mbula
nce D
ispatc
hed (
write
code
)Tim
e of C
all D
irecte
d to A
mbula
nce
Profe
ssion
al
Tim
e of a
mbula
nce d
ispatc
h
Profe
ssion
al ac
comp
anyin
g the
patie
nt in
ambu
lance
(1.E
MT, 2
.Nur
se or
othe
r pr
ofess
ional,
3.no
t acc
ompa
nied)
Time of arrival at patient’s location
Condition of patient on Arrival (1. Alive, 2. Dead,
3.not found)
Time of ambulance arrival at
HF
Critical Incident during
Transport (Write code)
Name of Receiving
Health Facility
Remark
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) 23 24 (25) 26
Ambulance Service Register
Count total calls
Reason for Request col (14)1. Labor & Obstetric Emergency2. Neonatal Emergency3. RTA4. Trauma (Specify)- 5. Non-traumatic emergencies (Specify)6. Burn7. Poisioning
Count the cases for which ambulance was dispatched
Reason (if ambulance is not dispatched) col (16)1= Available ambulances dispatched2= Inadequate or missing medical equipment/consumables3. Professionals (HCW or Driver) not available4. No Fuel5. On Maintenance6. Administration7. Not ready for service (not cleaned or disinfected)
Count
EMT
Nurse or other heath professional
Not accompanied
Type of Ambulance Dispatched col (17)1. Unequipped basic ambulance, 2. Basic ambulances equipped based on mini-mum requirements, 3. Standard advanced Critical Incident during Transport col (24) 1.Deteriorate, 2. Arrest, 3. Equipment malfunction 4. Depletion of consumable 5. External factor

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Special Center/ Hospital Assistive Technology Service Register
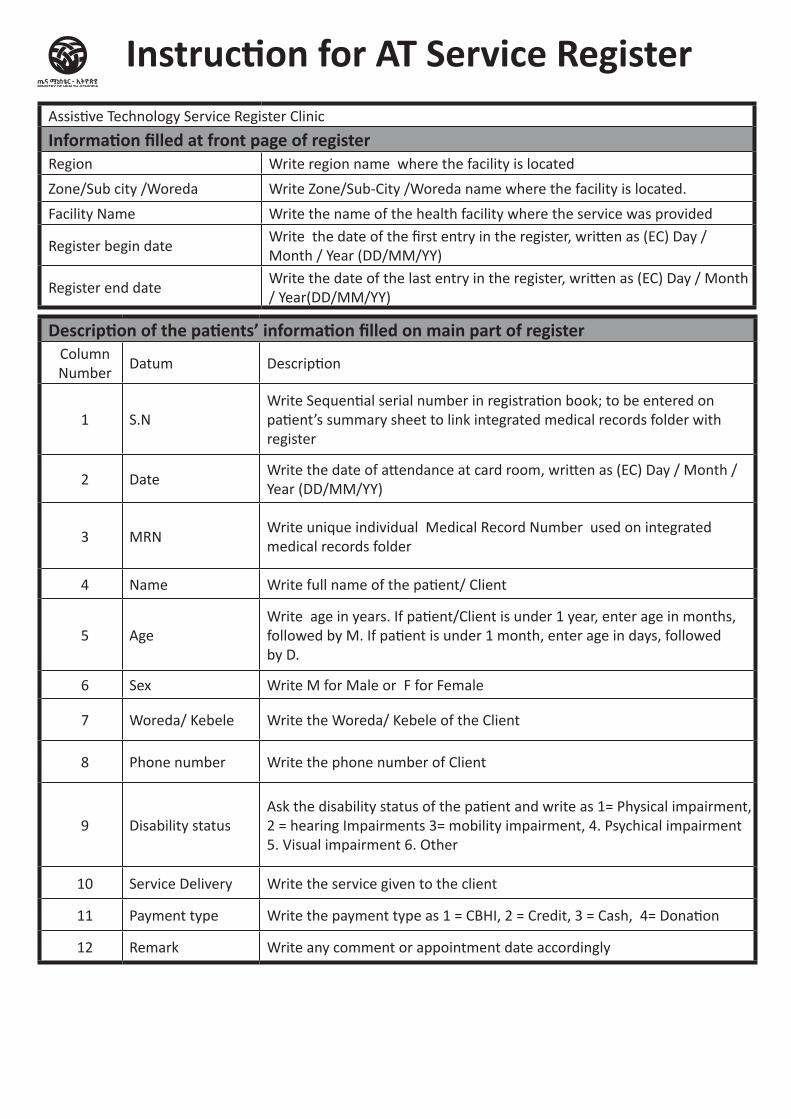
Description of the patients’ information filled on main part of registerColumn Number
Datum Description
1 S.NWrite Sequential serial number in registration book; to be entered on patient’s summary sheet to link integrated medical records folder with register
2 DateWrite the date of attendance at card room, written as (EC) Day / Month / Year (DD/MM/YY)
3 MRNWrite unique individual Medical Record Number used on integrated medical records folder
4 Name Write full name of the patient/ Client
5 AgeWrite age in years. If patient/Client is under 1 year, enter age in months, followed by M. If patient is under 1 month, enter age in days, followed by D.
6 Sex Write M for Male or F for Female
7 Woreda/ Kebele Write the Woreda/ Kebele of the Client
8 Phone number Write the phone number of Client
9 Disability status Ask the disability status of the patient and write as 1= Physical impairment, 2 = hearing Impairments 3= mobility impairment, 4. Psychical impairment 5. Visual impairment 6. Other
10 Service Delivery Write the service given to the client
11 Payment type Write the payment type as 1 = CBHI, 2 = Credit, 3 = Cash, 4= Donation
12 Remark Write any comment or appointment date accordingly
Instruction for AT Service RegisterAssistive Technology Service Register Clinic
Information filled at front page of registerRegion Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin dateWrite the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end dateWrite the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
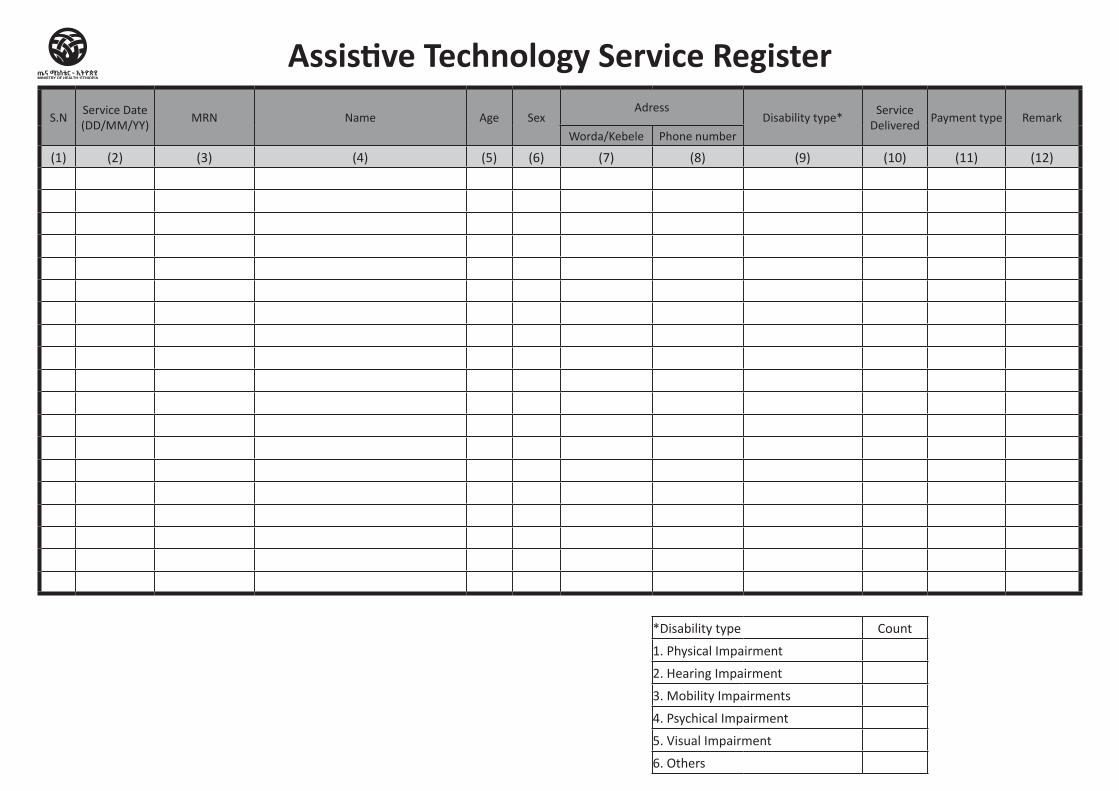
S.NService Date (DD/MM/YY)
MRN Name Age SexAdress
Disability type*Service
DeliveredPayment type Remark
Worda/Kebele Phone number
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
*Disability type Count
1. Physical Impairment
2. Hearing Impairment
3. Mobility Impairments
4. Psychical Impairment
5. Visual Impairment
6. Others
Assistive Technology Service Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital Central Register
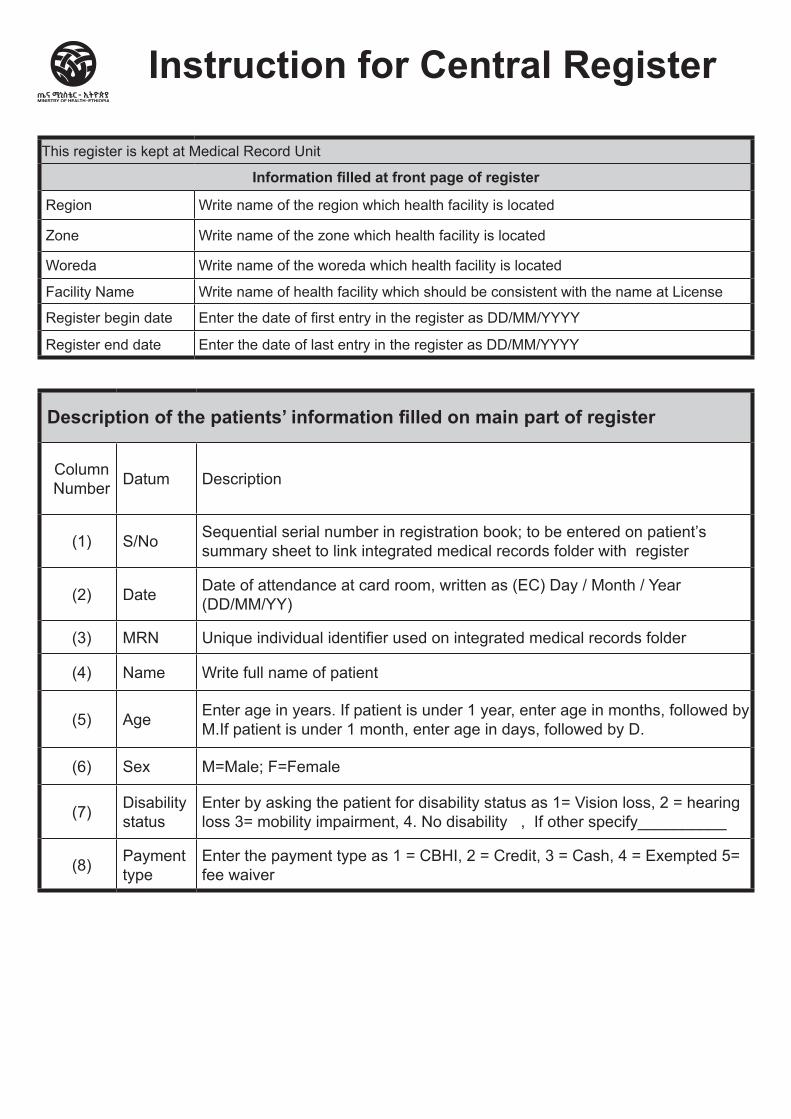
Description of the patients’ information filled on main part of register
Column Number Datum Description
(1) S/No Sequential serial number in registration book; to be entered on patient’s summary sheet to link integrated medical records folder with register
(2) Date Date of attendance at card room, written as (EC) Day / Month / Year (DD/MM/YY)
(3) MRN Unique individual identifier used on integrated medical records folder
(4) Name Write full name of patient
(5) Age Enter age in years. If patient is under 1 year, enter age in months, followed by M.If patient is under 1 month, enter age in days, followed by D.
(6) Sex M=Male; F=Female
(7) Disability status
Enter by asking the patient for disability status as 1= Vision loss, 2 = hearing loss 3= mobility impairment, 4. No disability , If other specify__________
(8) Payment type
Enter the payment type as 1 = CBHI, 2 = Credit, 3 = Cash, 4 = Exempted 5= fee waiver
Instruction for Central Register
This register is kept at Medical Record Unit
Information filled at front page of register
Region Write name of the region which health facility is located
Zone Write name of the zone which health facility is located
Woreda Write name of the woreda which health facility is located
Facility Name Write name of health facility which should be consistent with the name at License
Register begin date Enter the date of first entry in the register as DD/MM/YYYY
Register end date Enter the date of last entry in the register as DD/MM/YYYY
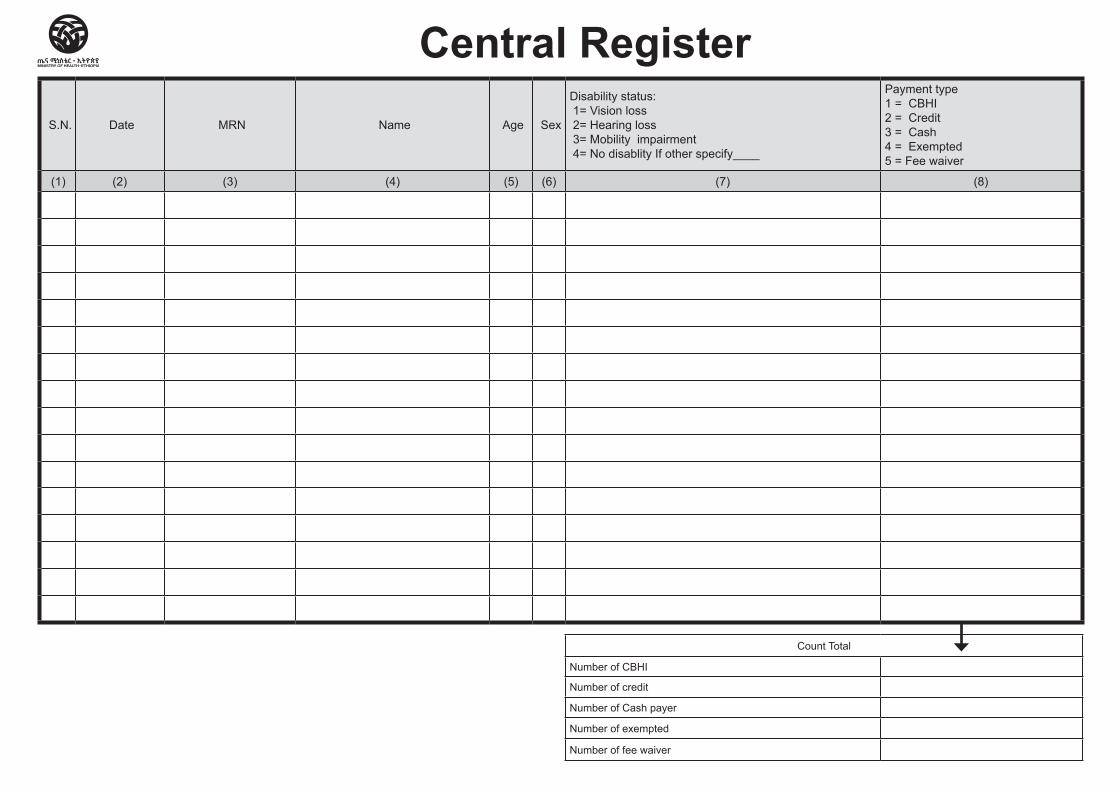
S.N. Date MRN Name Age Sex
Disability status: 1= Vision loss 2= Hearing loss 3= Mobility impairment 4= No disablity If other specify____
Payment type 1 = CBHI 2 = Credit 3 = Cash 4 = Exempted 5 = Fee waiver
(1) (2) (3) (4) (5) (6) (7) (8)
Count Total
Number of CBHI
Number of credit
Number of Cash payer
Number of exempted
Number of fee waiver
Central Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital Emergency Unit/ Department
Register
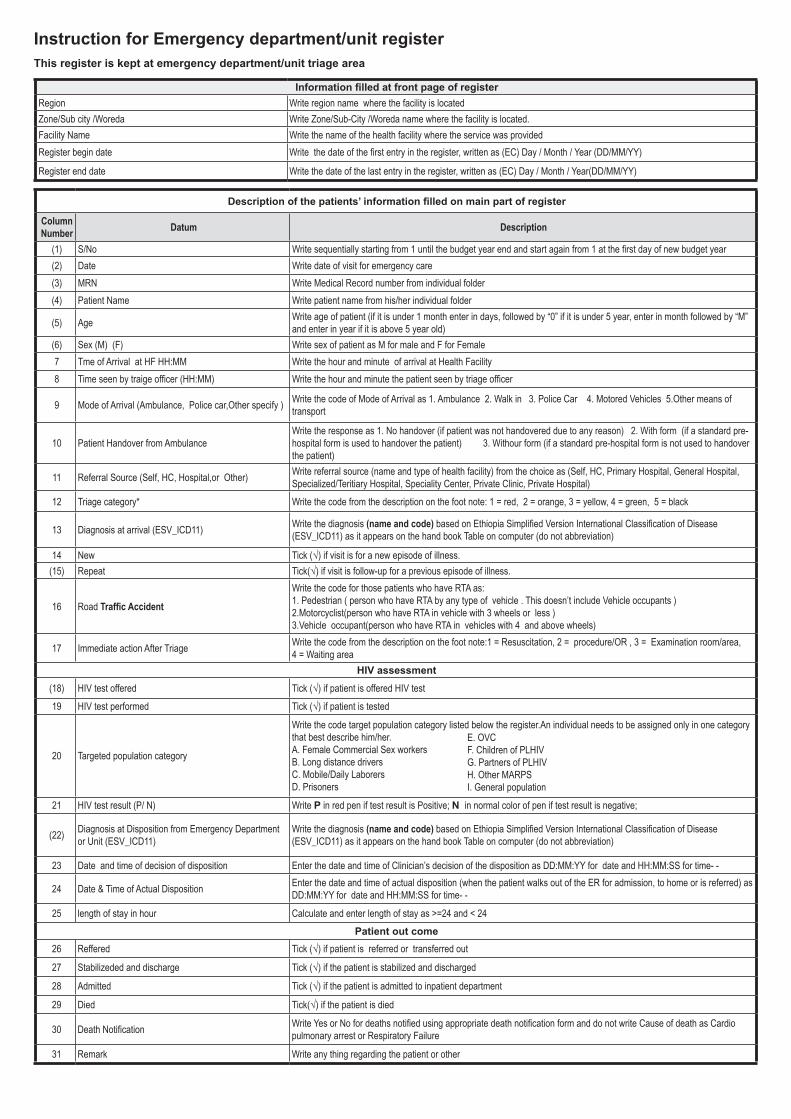
Description of the patients’ information filled on main part of register
Column Number Datum Description
(1) S/No Write sequentially starting from 1 until the budget year end and start again from 1 at the first day of new budget year(2) Date Write date of visit for emergency care(3) MRN Write Medical Record number from individual folder(4) Patient Name Write patient name from his/her individual folder
(5) Age Write age of patient (if it is under 1 month enter in days, followed by “0” if it is under 5 year, enter in month followed by “M” and enter in year if it is above 5 year old)
(6) Sex (M) (F) Write sex of patient as M for male and F for Female7 Tme of Arrival at HF HH:MM Write the hour and minute of arrival at Health Facility8 Time seen by traige officer (HH:MM) Write the hour and minute the patient seen by triage officer
9 Mode of Arrival (Ambulance, Police car,Other specify ) Write the code of Mode of Arrival as 1. Ambulance 2. Walk in 3. Police Car 4. Motored Vehicles 5.Other means of transport
10 Patient Handover from AmbulanceWrite the response as 1. No handover (if patient was not handovered due to any reason) 2. With form (if a standard pre-hospital form is used to handover the patient) 3. Withour form (if a standard pre-hospital form is not used to handover the patient)
11 Referral Source (Self, HC, Hospital,or Other) Write referral source (name and type of health facility) from the choice as (Self, HC, Primary Hospital, General Hospital, Specialized/Teritiary Hospital, Speciality Center, Private Clinic, Private Hospital)
12 Triage category* Write the code from the description on the foot note: 1 = red, 2 = orange, 3 = yellow, 4 = green, 5 = black
13 Diagnosis at arrival (ESV_ICD11) Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
14 New Tick (√) if visit is for a new episode of illness.(15) Repeat Tick(√) if visit is follow-up for a previous episode of illness.
16 Road Traffic Accident
Write the code for those patients who have RTA as: 1. Pedestrian ( person who have RTA by any type of vehicle . This doesn’t include Vehicle occupants ) 2.Motorcyclist(person who have RTA in vehicle with 3 wheels or less ) 3.Vehicle occupant(person who have RTA in vehicles with 4 and above wheels)
17 Immediate action After Triage Write the code from the description on the foot note:1 = Resuscitation, 2 = procedure/OR , 3 = Examination room/area, 4 = Waiting area
HIV assessment
(18) HIV test offered Tick (√) if patient is offered HIV test
19 HIV test performed Tick (√) if patient is tested
20 Targeted population category
Write the code target population category listed below the register.An individual needs to be assigned only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily Laborers D. Prisoners
21 HIV test result (P/ N) Write P in red pen if test result is Positive; N in normal color of pen if test result is negative;
(22) Diagnosis at Disposition from Emergency Department or Unit (ESV_ICD11)
Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
23 Date and time of decision of disposition Enter the date and time of Clinician’s decision of the disposition as DD:MM:YY for date and HH:MM:SS for time- -
24 Date & Time of Actual Disposition Enter the date and time of actual disposition (when the patient walks out of the ER for admission, to home or is referred) as DD:MM:YY for date and HH:MM:SS for time- -
25 length of stay in hour Calculate and enter length of stay as >=24 and < 24Patient out come
26 Reffered Tick (√) if patient is referred or transferred out
27 Stabilizeded and discharge Tick (√) if the patient is stabilized and discharged
28 Admitted Tick (√) if the patient is admitted to inpatient department
29 Died Tick(√) if the patient is died
30 Death Notification Write Yes or No for deaths notified using appropriate death notification form and do not write Cause of death as Cardio pulmonary arrest or Respiratory Failure
31 Remark Write any thing regarding the patient or other
Instruction for Emergency department/unit register This register is kept at emergency department/unit triage area
Information filled at front page of registerRegion Write region name where the facility is locatedZone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Facility Name Write the name of the health facility where the service was providedRegister begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
E. OVC F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
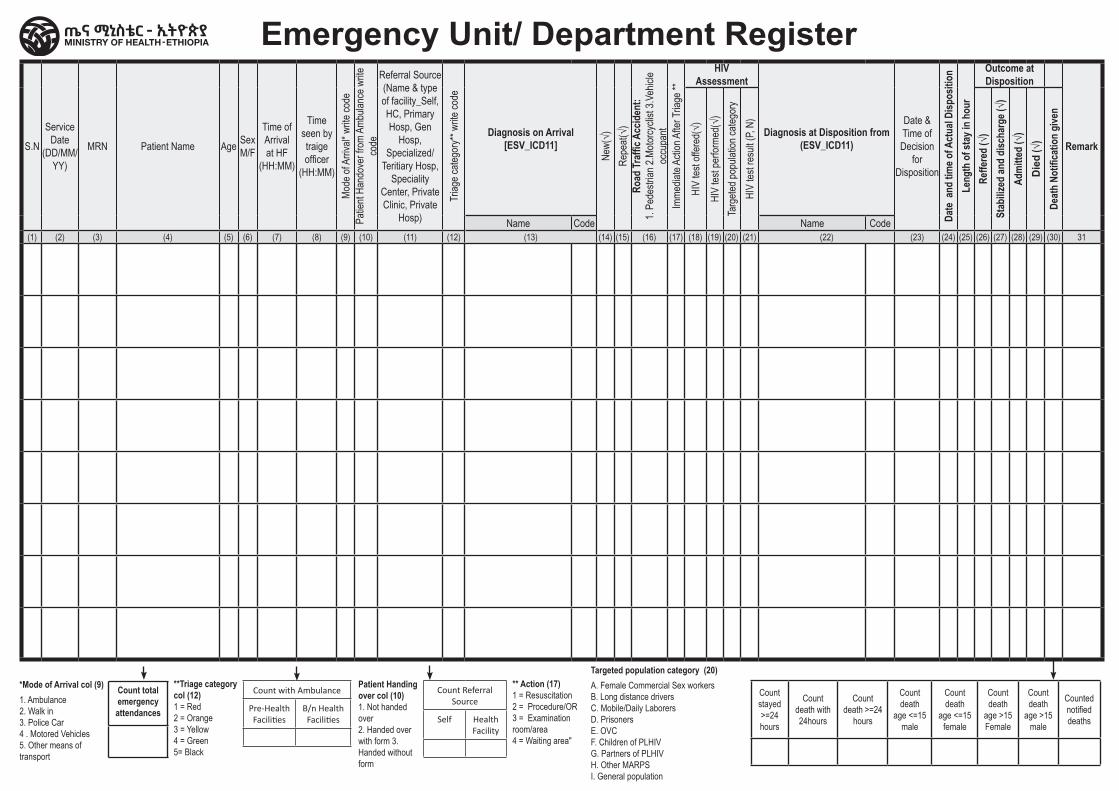
S.N
Service Date
(DD/MM/YY)
MRN Patient Name Age Sex M/F
Time ofArrival at HF
(HH:MM)
Time seen by traige officer
(HH:MM)
Mode
of A
rriva
l* wr
ite co
dePa
tient
Hand
over
from
Amb
ulanc
e write
co
de
Referral Source (Name & type of facility_Self, HC, Primary Hosp, Gen
Hosp, Specialized/
Teritiary Hosp, Speciality
Center, Private Clinic, Private
Hosp)
Triag
e cate
gory*
* write
code
Diagnosis on Arrival [ESV_ICD11]
New(
√)Re
peat(
√)Ro
ad Tr
affic
Acc
iden
t: 1.
Pede
strian
2.Mo
torcy
clist
3.Veh
icle
occu
pant
Imme
diate
Actio
n Afte
r Tria
ge **
HIV Assessment
Diagnosis at Disposition from (ESV_ICD11)
Date & Time of Decision
for Disposition
Date
and
tim
e of A
ctua
l Disp
ositi
onLe
ngth
of s
tay i
n ho
ur
Outcome at Disposition
Remark
HIV
test o
ffere
d(√)
HIV
test p
erfor
med(
√)Ta
rgete
d pop
ulatio
n cate
gory
HIV
test r
esult
(P, N
)
Reffe
red
(√)
Stab
ilized
and
disc
harg
e (√)
Adm
itted
(√)
Died
(√)
Deat
h No
tifica
tion
give
n
Name Code Name Code(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) 31
Emergency Unit/ Department Register
*Mode of Arrival col (9)1. Ambulance2. Walk in 3. Police Car4 . Motored Vehicles5. Other means of transport
Count total emergency
attendances
**Triage category col (12) 1 = Red 2 = Orange 3 = Yellow 4 = Green 5= Black
Patient Handing over col (10) 1. Not handed over 2. Handed over with form 3. Handed without form
** Action (17) 1 = Resuscitation 2 = Procedure/OR 3 = Examination room/area 4 = Waiting area"
Targeted population category (20)A. Female Commercial Sex workersB. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPSI. General population
Count stayed >=24 hours
Count death with 24hours
Count death >=24
hours
Count death
age <=15 male
Count death
age <=15 female
Count death
age >15 Female
Count death
age >15 male
Counted notified deaths
Count with Ambulance
Pre-Health Facilities
B/n Health Facilities
Count Referral Source
Self Health Facility
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Hospital Intensive Care Unit Register
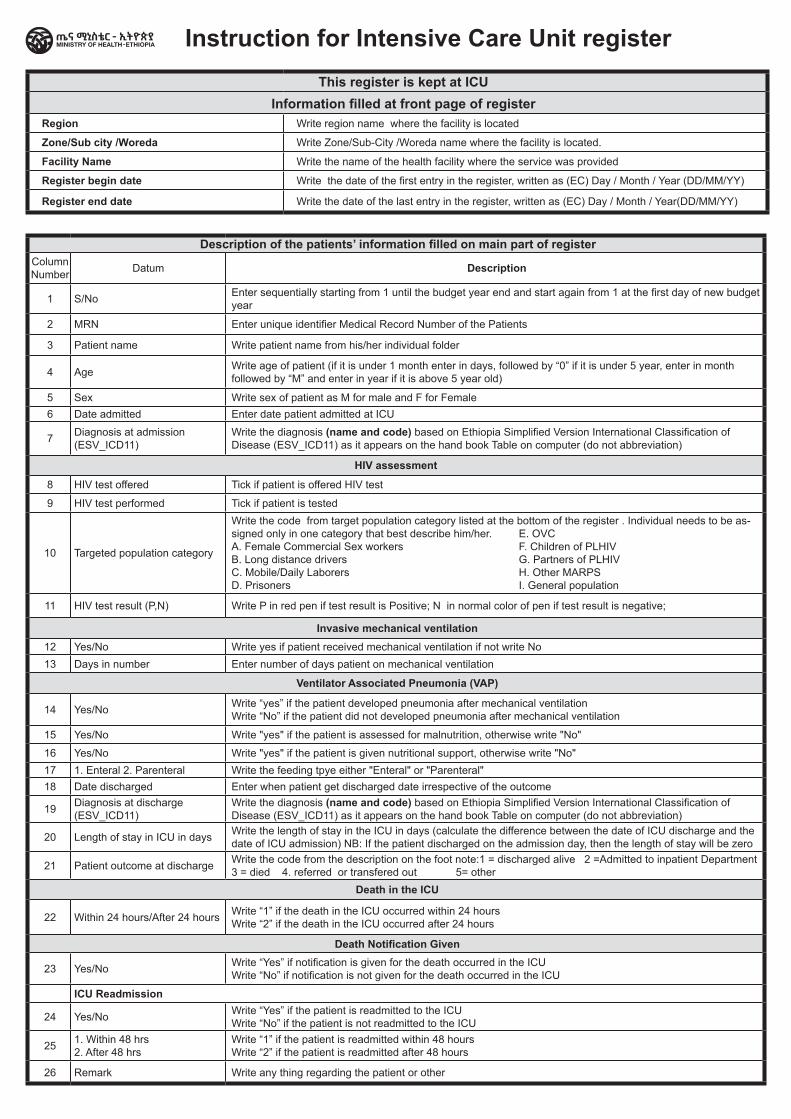
Description of the patients’ information filled on main part of registerColumn Number Datum Description
1 S/No Enter sequentially starting from 1 until the budget year end and start again from 1 at the first day of new budget year
2 MRN Enter unique identifier Medical Record Number of the Patients
3 Patient name Write patient name from his/her individual folder
4 Age Write age of patient (if it is under 1 month enter in days, followed by “0” if it is under 5 year, enter in month followed by “M” and enter in year if it is above 5 year old)
5 Sex Write sex of patient as M for male and F for Female6 Date admitted Enter date patient admitted at ICU
7 Diagnosis at admission (ESV_ICD11)
Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
HIV assessment
8 HIV test offered Tick if patient is offered HIV test
9 HIV test performed Tick if patient is tested
10 Targeted population category
Write the code from target population category listed at the bottom of the register . Individual needs to be as-signed only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily Laborers D. Prisoners
11 HIV test result (P,N) Write P in red pen if test result is Positive; N in normal color of pen if test result is negative;
Invasive mechanical ventilation12 Yes/No Write yes if patient received mechanical ventilation if not write No13 Days in number Enter number of days patient on mechanical ventilation
Ventilator Associated Pneumonia (VAP)
14 Yes/No Write “yes” if the patient developed pneumonia after mechanical ventilation Write “No” if the patient did not developed pneumonia after mechanical ventilation
15 Yes/No Write "yes" if the patient is assessed for malnutrition, otherwise write "No"
16 Yes/No Write "yes" if the patient is given nutritional support, otherwise write "No" 17 1. Enteral 2. Parenteral Write the feeding tpye either "Enteral" or "Parenteral" 18 Date discharged Enter when patient get discharged date irrespective of the outcome
19 Diagnosis at discharge(ESV_ICD11)
Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
20 Length of stay in ICU in days Write the length of stay in the ICU in days (calculate the difference between the date of ICU discharge and the date of ICU admission) NB: If the patient discharged on the admission day, then the length of stay will be zero
21 Patient outcome at discharge Write the code from the description on the foot note:1 = discharged alive 2 =Admitted to inpatient Department 3 = died 4. referred or transfered out 5= other
Death in the ICU
22 Within 24 hours/After 24 hours Write “1” if the death in the ICU occurred within 24 hours Write “2” if the death in the ICU occurred after 24 hours
Death Notification Given
23 Yes/No Write “Yes” if notification is given for the death occurred in the ICU Write “No” if notification is not given for the death occurred in the ICU
ICU Readmission
24 Yes/No Write “Yes” if the patient is readmitted to the ICU Write “No” if the patient is not readmitted to the ICU
25 1. Within 48 hrs 2. After 48 hrs
Write “1” if the patient is readmitted within 48 hours Write “2” if the patient is readmitted after 48 hours
26 Remark Write any thing regarding the patient or other
Instruction for Intensive Care Unit register
E. OVC F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
This register is kept at ICUInformation filled at front page of register
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
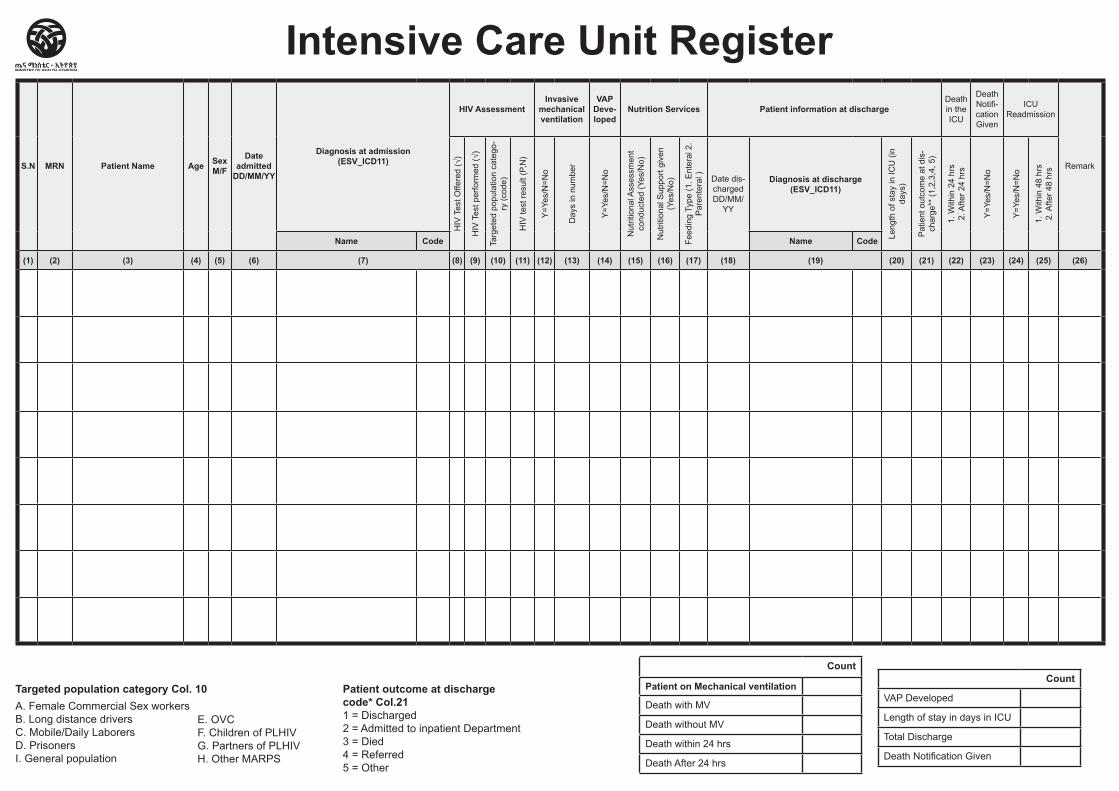
S.N MRN Patient Name Age SexM/F
Date admitted
DD/MM/YY
Diagnosis at admission (ESV_ICD11)
HIV AssessmentInvasive
mechanical ventilation
VAP Deve-loped
Nutrition Services Patient information at dischargeDeath in the ICU
Death Notifi-cation Given
ICU Readmission
Remark
HIV
Tes
t Offe
red
(√)
HIV
Tes
t per
form
ed (√
)
Targ
eted
pop
ulat
ion
cate
go-
ry (c
ode)
HIV
test
resu
lt (P
,N)
Y=Y
es/N
=No
Day
s in
num
ber
Y=Y
es/N
=No
Nut
ritio
nal A
sses
smen
t co
nduc
ted
(Yes
/No)
Nut
ritio
nal S
uppo
rt gi
ven
(Yes
/No)
Feed
ing
Type
(1. E
nter
al 2
. P
aren
tera
l ) Date dis-charged DD/MM/
YY
Diagnosis at discharge (ESV_ICD11)
Leng
th o
f sta
y in
ICU
(in
days
)
Pat
ient
out
com
e at
dis
-ch
arge
** (1
,2,3
,4, 5
)
1. W
ithin
24
hrs
2. A
fter 2
4 hr
s
Y=Y
es/N
=No
Y=Y
es/N
=No
1. W
ithin
48
hrs
2. A
fter 4
8 hr
s
Name Code Name Code
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26)
Intensive Care Unit Register
Targeted population category Col. 10 A. Female Commercial Sex workersB. Long distance driversC. Mobile/Daily LaborersD. PrisonersI. General population
Patient outcome at discharge code* Col.211 = Discharged 2 = Admitted to inpatient Department3 = Died 4 = Referred 5 = Other
Count
Patient on Mechanical ventilation
Death with MV
Death without MV
Death within 24 hrs
Death After 24 hrs
Count
VAP Developed
Length of stay in days in ICU
Total Discharge
Death Notification Given
E. OVC F. Children of PLHIVG. Partners of PLHIVH. Other MARPS
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital Admission/ Discharge Register
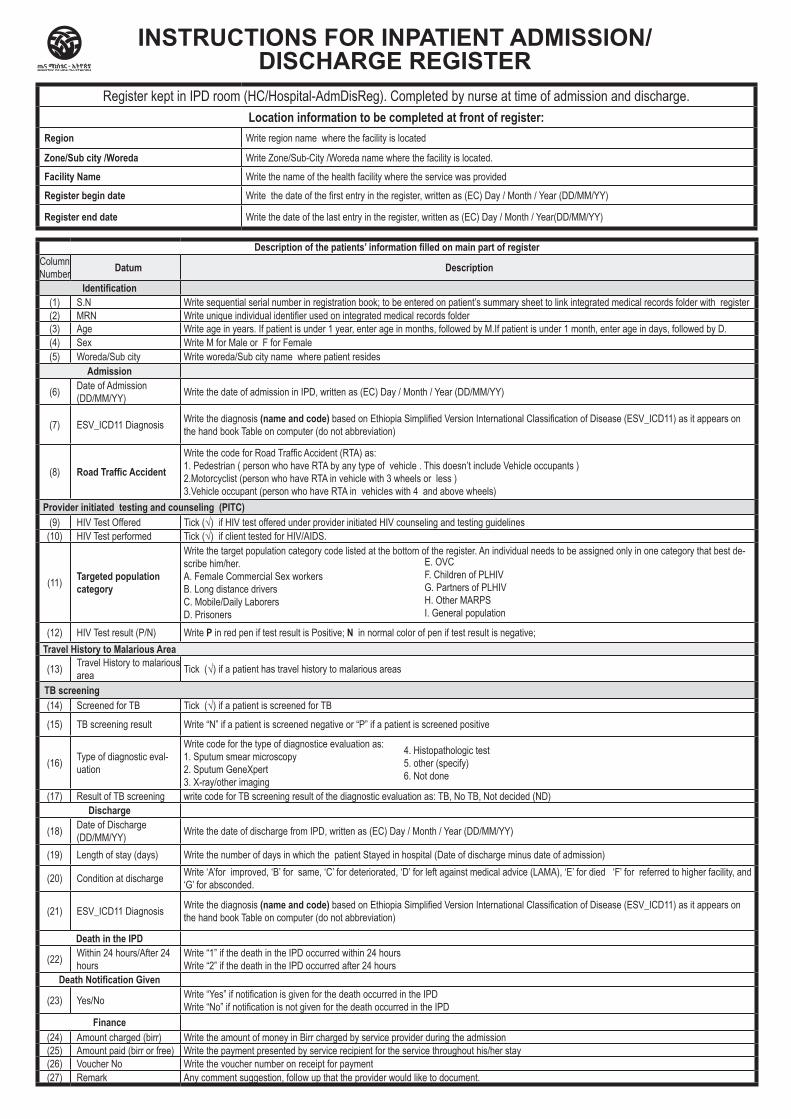
Description of the patients’ information filled on main part of registerColumn Number Datum Description
Identification(1) S.N Write sequential serial number in registration book; to be entered on patient’s summary sheet to link integrated medical records folder with register(2) MRN Write unique individual identifier used on integrated medical records folder(3) Age Write age in years. If patient is under 1 year, enter age in months, followed by M.If patient is under 1 month, enter age in days, followed by D.(4) Sex Write M for Male or F for Female(5) Woreda/Sub city Write woreda/Sub city name where patient resides
Admission
(6) Date of Admission (DD/MM/YY) Write the date of admission in IPD, written as (EC) Day / Month / Year (DD/MM/YY)
(7) ESV_ICD11 Diagnosis Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
(8) Road Traffic Accident
Write the code for Road Traffic Accident (RTA) as: 1. Pedestrian ( person who have RTA by any type of vehicle . This doesn’t include Vehicle occupants ) 2.Motorcyclist (person who have RTA in vehicle with 3 wheels or less ) 3.Vehicle occupant (person who have RTA in vehicles with 4 and above wheels)
Provider initiated testing and counseling (PITC)(9) HIV Test Offered Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines
(10) HIV Test performed Tick (√) if client tested for HIV/AIDS.
(11) Targeted population category
Write the target population category code listed at the bottom of the register. An individual needs to be assigned only in one category that best de-scribe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily Laborers D. Prisoners
(12) HIV Test result (P/N) Write P in red pen if test result is Positive; N in normal color of pen if test result is negative; Travel History to Malarious Area
(13) Travel History to malarious area Tick (√) if a patient has travel history to malarious areas
TB screening(14) Screened for TB Tick (√) if a patient is screened for TB
(15) TB screening result Write “N” if a patient is screened negative or “P” if a patient is screened positive
(16) Type of diagnostic eval-uation
Write code for the type of diagnostice evaluation as: 1. Sputum smear microscopy 2. Sputum GeneXpert 3. X-ray/other imaging
(17) Result of TB screening write code for TB screening result of the diagnostic evaluation as: TB, No TB, Not decided (ND)Discharge
(18) Date of Discharge (DD/MM/YY) Write the date of discharge from IPD, written as (EC) Day / Month / Year (DD/MM/YY)
(19) Length of stay (days) Write the number of days in which the patient Stayed in hospital (Date of discharge minus date of admission)
(20) Condition at discharge Write ‘A’for improved, ‘B’ for same, ‘C’ for deteriorated, ‘D’ for left against medical advice (LAMA), ‘E’ for died ‘F’ for referred to higher facility, and ‘G’ for absconded.
(21) ESV_ICD11 Diagnosis Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
Death in the IPD
(22) Within 24 hours/After 24 hours
Write “1” if the death in the IPD occurred within 24 hours Write “2” if the death in the IPD occurred after 24 hours
Death Notification Given
(23) Yes/No Write “Yes” if notification is given for the death occurred in the IPD Write “No” if notification is not given for the death occurred in the IPD
Finance(24) Amount charged (birr) Write the amount of money in Birr charged by service provider during the admission(25) Amount paid (birr or free) Write the payment presented by service recipient for the service throughout his/her stay(26) Voucher No Write the voucher number on receipt for payment(27) Remark Any comment suggestion, follow up that the provider would like to document.
INSTRUCTIONS FOR INPATIENT ADMISSION/DISCHARGE REGISTER
Register kept in IPD room (HC/Hospital-AdmDisReg). Completed by nurse at time of admission and discharge.Location information to be completed at front of register:
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
E. OVC F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
4. Histopathologic test 5. other (specify) 6. Not done
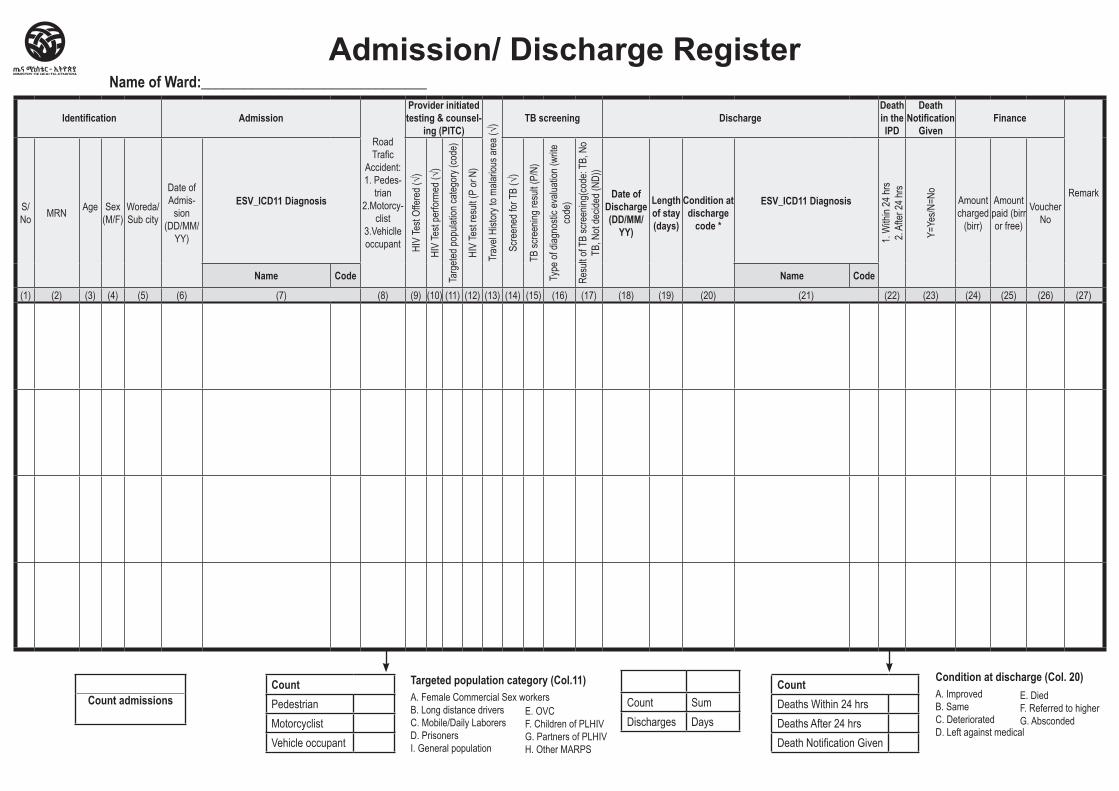
Identification Admission
Road Trafic
Accident: 1. Pedes-
trian 2.Motorcy-
clist 3.Vehiclle occupant
Provider initiated testing & counsel-
ing (PITC)
Trav
el Hi
story
to ma
lariou
s are
a (√)
TB screening DischargeDeath in the IPD
Death Notification
GivenFinance
RemarkS/No MRN Age Sex
(M/F)Woreda/Sub city
Date of Admis-
sion (DD/MM/
YY)
ESV_ICD11 Diagnosis
HIV
Test
Offer
ed (√
)
HIV
Test
perfo
rmed
(√)
Targ
eted p
opula
tion c
atego
ry (co
de)
HIV
Test
resu
lt (P
or N
)
Scre
ened
for T
B (√
)
TB sc
reen
ing re
sult (
P/N)
Type
of di
agno
stic e
valua
tion (
write
co
de)
Resu
lt of T
B sc
reen
ing(co
de: T
B, N
o TB
, Not
decid
ed (N
D))
Date of Discharge (DD/MM/
YY)
Length of stay (days)
Condition at discharge
code *
ESV_ICD11 Diagnosis
1. W
ithin
24 hr
s 2.
After
24 hr
s
Y=Ye
s/N=N
o
Amount charged
(birr)
Amount paid (birr or free)
Voucher No
Name Code Name Code
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27)
Admission/ Discharge RegisterName of Ward:_______________________________
Count admissionsCountPedestrianMotorcyclistVehicle occupant
CountDeaths Within 24 hrsDeaths After 24 hrsDeath Notification Given
Count SumDischarges Days
Targeted population category (Col.11)A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersI. General population
E. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
Condition at discharge (Col. 20)A. Improved B. Same C. Deteriorated D. Left against medical
E. Died F. Referred to higher G. Absconded
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Hospital Liaison Referral-in/out Register
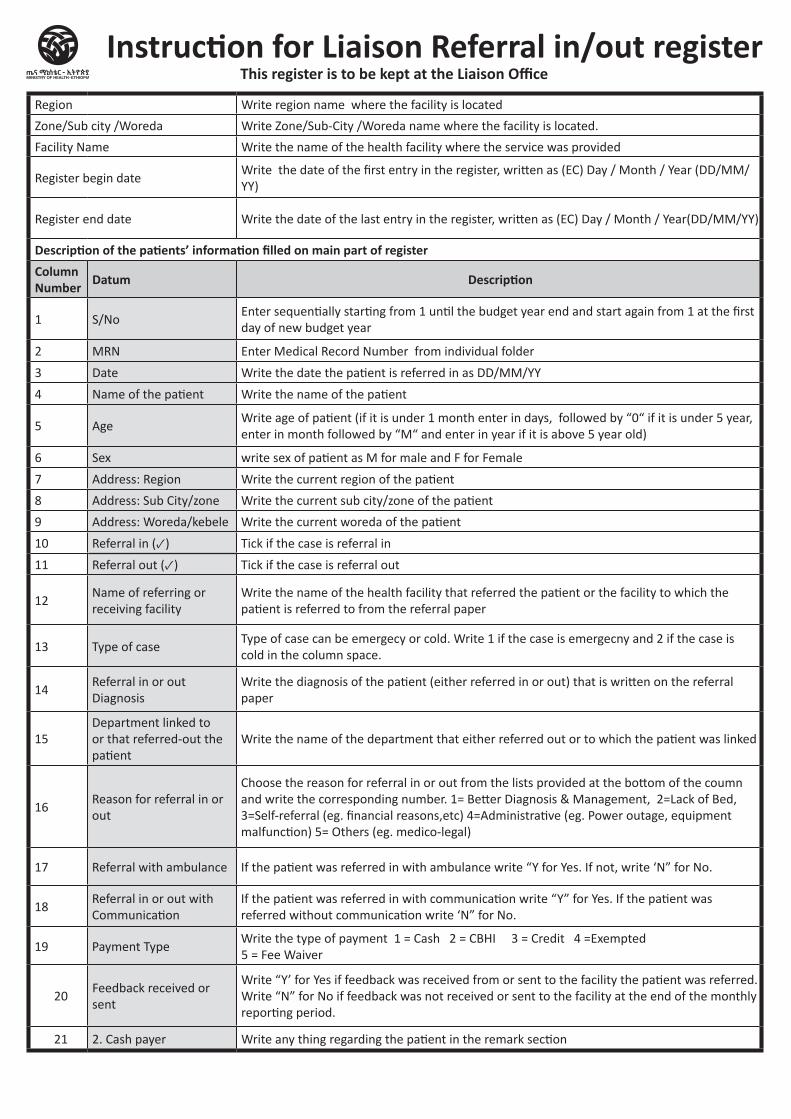
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin dateWrite the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Description of the patients’ information filled on main part of registerColumn Number Datum Description
1 S/NoEnter sequentially starting from 1 until the budget year end and start again from 1 at the first day of new budget year
2 MRN Enter Medical Record Number from individual folder
3 Date Write the date the patient is referred in as DD/MM/YY
4 Name of the patient Write the name of the patient
5 AgeWrite age of patient (if it is under 1 month enter in days, followed by “0“ if it is under 5 year, enter in month followed by “M“ and enter in year if it is above 5 year old)
6 Sex write sex of patient as M for male and F for Female
7 Address: Region Write the current region of the patient
8 Address: Sub City/zone Write the current sub city/zone of the patient
9 Address: Woreda/kebele Write the current woreda of the patient
10 Referral in (✓) Tick if the case is referral in
11 Referral out (✓) Tick if the case is referral out
12Name of referring or receiving facility
Write the name of the health facility that referred the patient or the facility to which the patient is referred to from the referral paper
13 Type of case Type of case can be emergecy or cold. Write 1 if the case is emergecny and 2 if the case is cold in the column space.
14Referral in or out Diagnosis
Write the diagnosis of the patient (either referred in or out) that is written on the referral paper
15Department linked to or that referred-out the patient
Write the name of the department that either referred out or to which the patient was linked
16Reason for referral in or out
Choose the reason for referral in or out from the lists provided at the bottom of the coumn and write the corresponding number. 1= Better Diagnosis & Management, 2=Lack of Bed, 3=Self-referral (eg. financial reasons,etc) 4=Administrative (eg. Power outage, equipment malfunction) 5= Others (eg. medico-legal)
17 Referral with ambulance If the patient was referred in with ambulance write “Y for Yes. If not, write ‘N” for No.
18Referral in or out with Communication
If the patient was referred in with communication write “Y” for Yes. If the patient was referred without communication write ‘N” for No.
19 Payment Type Write the type of payment 1 = Cash 2 = CBHI 3 = Credit 4 =Exempted 5 = Fee Waiver
20Feedback received or sent
Write “Y’ for Yes if feedback was received from or sent to the facility the patient was referred. Write “N” for No if feedback was not received or sent to the facility at the end of the monthly reporting period.
21 2. Cash payer Write any thing regarding the patient in the remark section
Instruction for Liaison Referral in/out registerThis register is to be kept at the Liaison Office
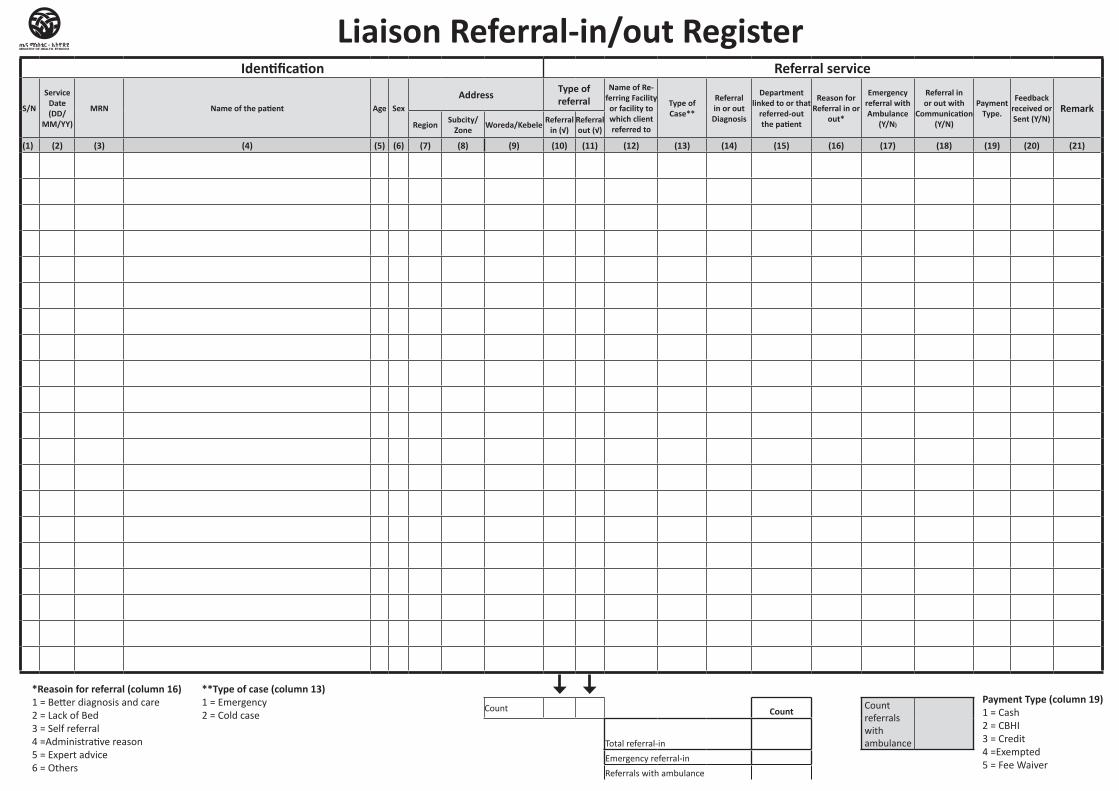
Identification Referral service
S/N
Service Date (DD/
MM/YY)
MRN Name of the patient Age SexAddress Type of
referral Name of Re-
ferring Facility or facility to which client referred to
Type of Case**
Referral in or out Diagnosis
Department linked to or that
referred-out the patient
Reason for Referral in or
out*
Emergency referral with Ambulance
(Y/N)
Referral in or out with
Communication (Y/N)
Payment Type.
Feedback received or Sent (Y/N)
Remark Region Subcity/
Zone Woreda/Kebele Referral in (√)
Referral out (√)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21)
Count Count Count referrals with ambulanceTotal referral-in
Emergency referral-in
Referrals with ambulance
Liaison Referral-in/out Register
*Reasoin for referral (column 16) 1 = Better diagnosis and care 2 = Lack of Bed 3 = Self referral 4 =Administrative reason 5 = Expert advice6 = Others
**Type of case (column 13) 1 = Emergency2 = Cold case
Payment Type (column 19) 1 = Cash 2 = CBHI 3 = Credit4 =Exempted5 = Fee Waiver
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital Out Patient Department Register
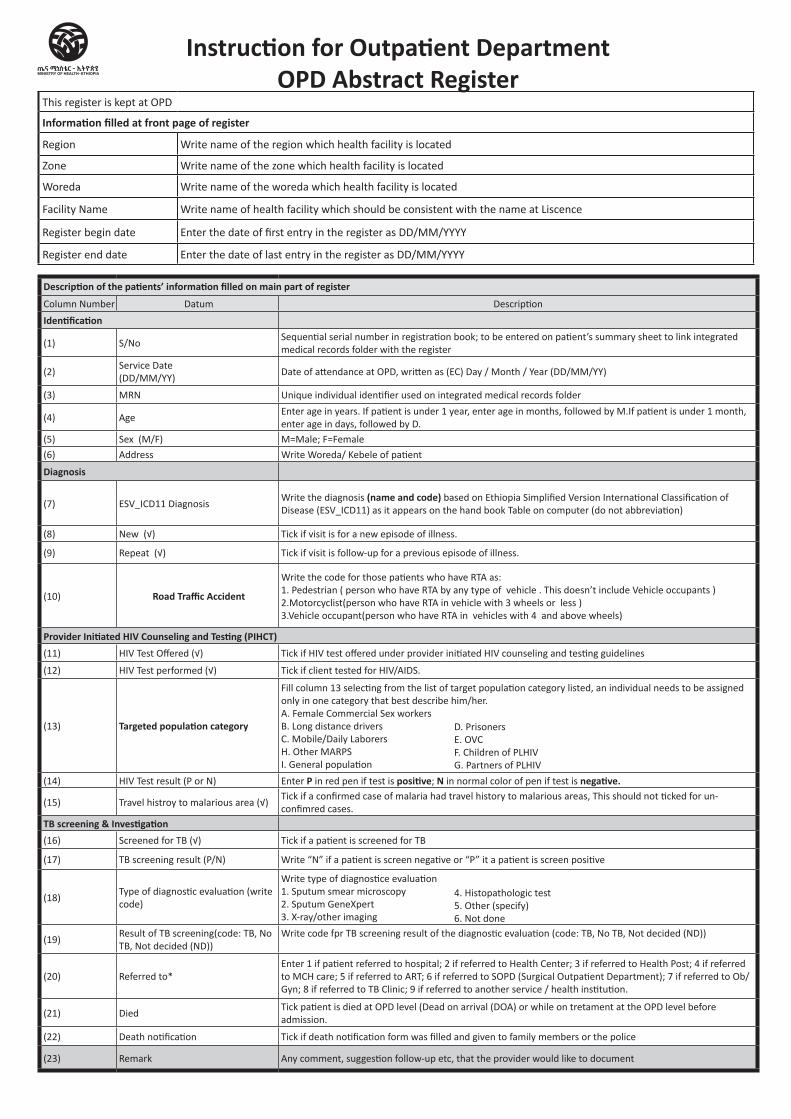
Instruction for Outpatient Department OPD Abstract Register
This register is kept at OPD
Information filled at front page of register
Region Write name of the region which health facility is located
Zone Write name of the zone which health facility is located
Woreda Write name of the woreda which health facility is located
Facility Name Write name of health facility which should be consistent with the name at Liscence
Register begin date Enter the date of first entry in the register as DD/MM/YYYY
Register end date Enter the date of last entry in the register as DD/MM/YYYY
Description of the patients’ information filled on main part of register
Column Number Datum Description
Identification
(1) S/NoSequential serial number in registration book; to be entered on patient’s summary sheet to link integrated medical records folder with the register
(2)Service Date (DD/MM/YY)
Date of attendance at OPD, written as (EC) Day / Month / Year (DD/MM/YY)
(3) MRN Unique individual identifier used on integrated medical records folder
(4) AgeEnter age in years. If patient is under 1 year, enter age in months, followed by M.If patient is under 1 month, enter age in days, followed by D.
(5) Sex (M/F) M=Male; F=Female
(6) Address Write Woreda/ Kebele of patient
Diagnosis
(7) ESV_ICD11 Diagnosis Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer (do not abbreviation)
(8) New (√) Tick if visit is for a new episode of illness.
(9) Repeat (√) Tick if visit is follow-up for a previous episode of illness.
(10) Road Traffic Accident
Write the code for those patients who have RTA as: 1. Pedestrian ( person who have RTA by any type of vehicle . This doesn’t include Vehicle occupants ) 2.Motorcyclist(person who have RTA in vehicle with 3 wheels or less ) 3.Vehicle occupant(person who have RTA in vehicles with 4 and above wheels)
Provider Initiated HIV Counseling and Testing (PIHCT) (11) HIV Test Offered (√) Tick if HIV test offered under provider initiated HIV counseling and testing guidelines
(12) HIV Test performed (√) Tick if client tested for HIV/AIDS.
(13) Targeted population category
Fill column 13 selecting from the list of target population category listed, an individual needs to be assigned only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily Laborers H. Other MARPS I. General population
(14) HIV Test result (P or N) Enter P in red pen if test is positive; N in normal color of pen if test is negative.
(15) Travel histroy to malarious area (√)Tick if a confirmed case of malaria had travel history to malarious areas, This should not ticked for un-confimred cases.
TB screening & Investigation(16) Screened for TB (√) Tick if a patient is screened for TB
(17) TB screening result (P/N) Write “N” if a patient is screen negative or “P” it a patient is screen positive
(18)Type of diagnostic evaluation (write code)
Write type of diagnostice evaluation 1. Sputum smear microscopy 2. Sputum GeneXpert 3. X-ray/other imaging
(19)Result of TB screening(code: TB, No TB, Not decided (ND))
Write code fpr TB screening result of the diagnostic evaluation (code: TB, No TB, Not decided (ND))
(20) Referred to*Enter 1 if patient referred to hospital; 2 if referred to Health Center; 3 if referred to Health Post; 4 if referred to MCH care; 5 if referred to ART; 6 if referred to SOPD (Surgical Outpatient Department); 7 if referred to Ob/Gyn; 8 if referred to TB Clinic; 9 if referred to another service / health institution.
(21) Died Tick patient is died at OPD level (Dead on arrival (DOA) or while on tretament at the OPD level before admission.
(22) Death notification Tick if death notification form was filled and given to family members or the police
(23) Remark Any comment, suggestion follow-up etc, that the provider would like to document
D. Prisoners E. OVC F. Children of PLHIV G. Partners of PLHIV
4. Histopathologic test 5. Other (specify) 6. Not done
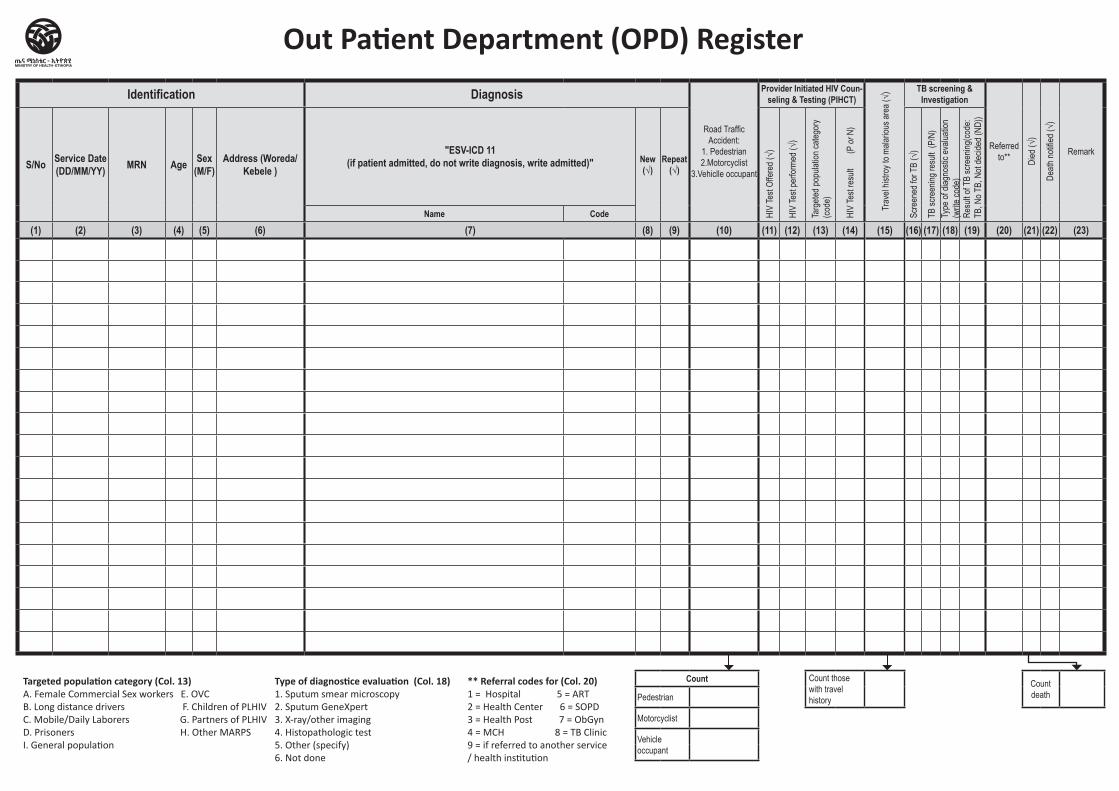
Identification Diagnosis
Road Traffic Accident:
1. Pedestrian 2.Motorcyclist
3.Vehiclle occupant
Provider Initiated HIV Coun-seling & Testing (PIHCT)
Trav
el his
troy t
o mala
rious
area
(√) TB screening &
Investigation
Referred to** Di
ed (√
)
Death
notifi
ed (√
)
RemarkS/No Service Date
(DD/MM/YY) MRN Age Sex (M/F)
Address (Woreda/ Kebele )
"ESV-ICD 11 (if patient admitted, do not write diagnosis, write admitted)" New
(√)Repeat
(√)
HIV
Test
Offer
ed (√
)
HIV
Test
perfo
rmed
(√)
Targ
eted p
opula
tion c
atego
ry (co
de)
HIV
Test
resu
lt
(P or
N)
Scre
ened
for T
B (√
)
TB sc
reen
ing re
sult
(P/N
)Ty
pe of
diag
nosti
c eva
luatio
n (w
rite co
de)
Resu
lt of T
B sc
reen
ing(co
de:
TB, N
o TB,
Not
decid
ed (N
D))
Name Code
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23)
Count Count those with travel history
Count deathPedestrian
Motorcyclist
Vehicle occupant
Out Patient Department (OPD) Register
Targeted population category (Col. 13)A. Female Commercial Sex workers E. OVC B. Long distance drivers F. Children of PLHIVC. Mobile/Daily Laborers G. Partners of PLHIVD. Prisoners H. Other MARPSI. General population
** Referral codes for (Col. 20) 1 = Hospital 5 = ART 2 = Health Center 6 = SOPD 3 = Health Post 7 = ObGyn 4 = MCH 8 = TB Clinic 9 = if referred to another service / health institution
Type of diagnostice evaluation (Col. 18)1. Sputum smear microscopy 2. Sputum GeneXpert 3. X-ray/other imaging 4. Histopathologic test5. Other (specify)6. Not done
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center/Clinic/Hospital Operation Register
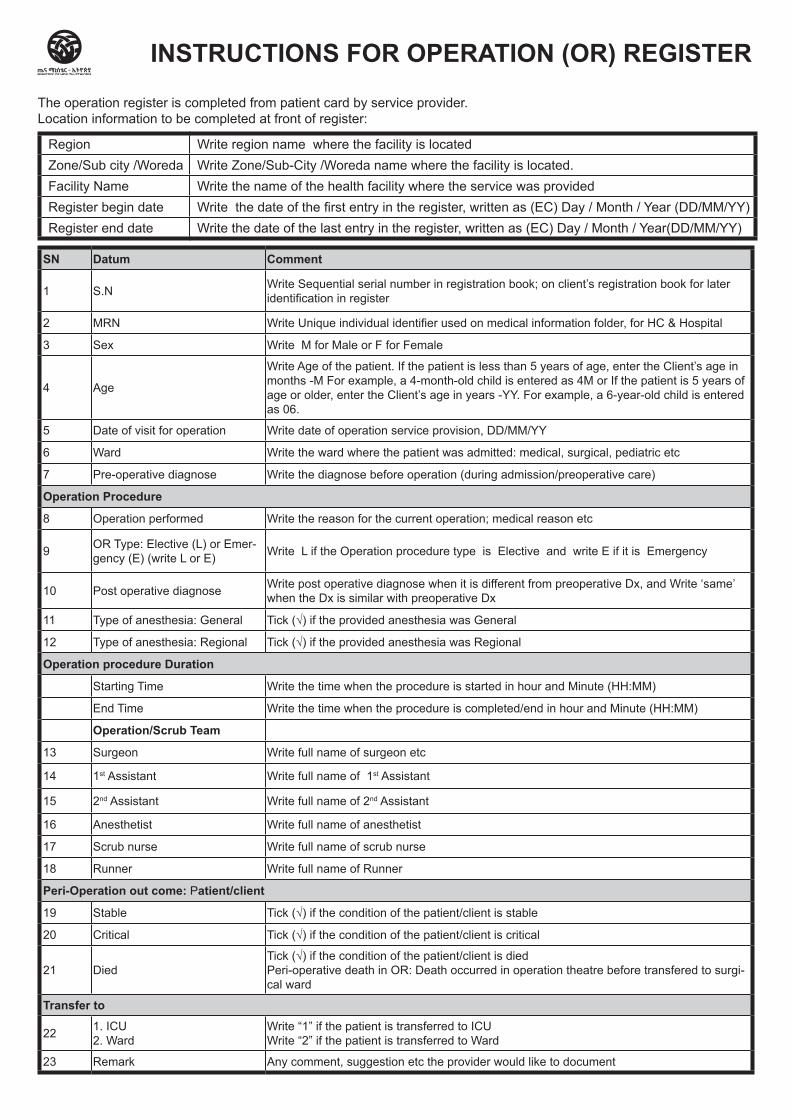
SN Datum Comment
1 S.N Write Sequential serial number in registration book; on client’s registration book for later identification in register
2 MRN Write Unique individual identifier used on medical information folder, for HC & Hospital
3 Sex Write M for Male or F for Female
4 Age
Write Age of the patient. If the patient is less than 5 years of age, enter the Client’s age in months -M For example, a 4-month-old child is entered as 4M or If the patient is 5 years of age or older, enter the Client’s age in years -YY. For example, a 6-year-old child is entered as 06.
5 Date of visit for operation Write date of operation service provision, DD/MM/YY
6 Ward Write the ward where the patient was admitted: medical, surgical, pediatric etc
7 Pre-operative diagnose Write the diagnose before operation (during admission/preoperative care)
Operation Procedure
8 Operation performed Write the reason for the current operation; medical reason etc
9 OR Type: Elective (L) or Emer-gency (E) (write L or E) Write L if the Operation procedure type is Elective and write E if it is Emergency
10 Post operative diagnose Write post operative diagnose when it is different from preoperative Dx, and Write ‘same’ when the Dx is similar with preoperative Dx
11 Type of anesthesia: General Tick (√) if the provided anesthesia was General
12 Type of anesthesia: Regional Tick (√) if the provided anesthesia was Regional
Operation procedure Duration
Starting Time Write the time when the procedure is started in hour and Minute (HH:MM)
End Time Write the time when the procedure is completed/end in hour and Minute (HH:MM)
Operation/Scrub Team
13 Surgeon Write full name of surgeon etc
14 1st Assistant Write full name of 1st Assistant
15 2nd Assistant Write full name of 2nd Assistant
16 Anesthetist Write full name of anesthetist
17 Scrub nurse Write full name of scrub nurse
18 Runner Write full name of Runner
Peri-Operation out come: Patient/client
19 Stable Tick (√) if the condition of the patient/client is stable
20 Critical Tick (√) if the condition of the patient/client is critical
21 Died Tick (√) if the condition of the patient/client is died Peri-operative death in OR: Death occurred in operation theatre before transfered to surgi-cal ward
Transfer to
22 1. ICU 2. Ward
Write “1” if the patient is transferred to ICU Write “2” if the patient is transferred to Ward
23 Remark Any comment, suggestion etc the provider would like to document
INSTRUCTIONS FOR OPERATION (OR) REGISTER
The operation register is completed from patient card by service provider.Location information to be completed at front of register:
Region Write region name where the facility is locatedZone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Facility Name Write the name of the health facility where the service was providedRegister begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
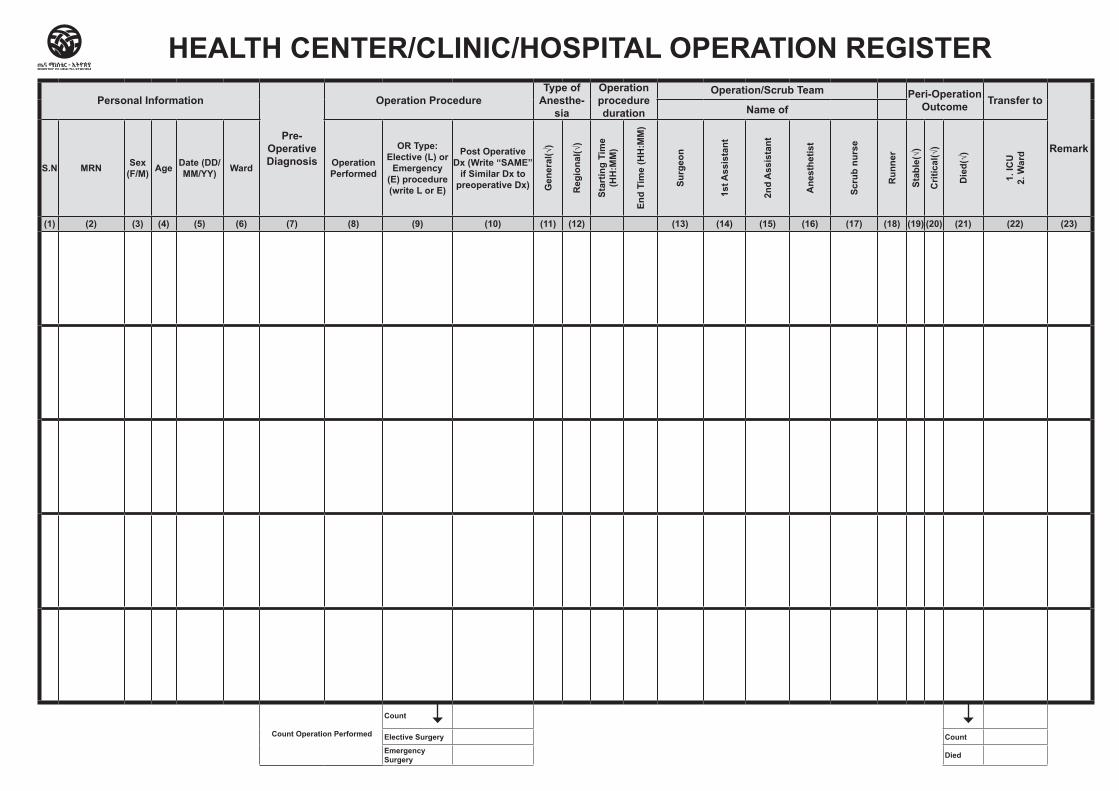
Personal Information
Pre-Operative Diagnosis
Operation ProcedureType of
Anesthe-sia
Operation procedure duration
Operation/Scrub Team Peri-Operation Outcome Transfer to
Remark
Name of
S.N MRN Sex (F/M) Age Date (DD/
MM/YY) Ward Operation Performed
OR Type: Elective (L) or
Emergency (E) procedure (write L or E)
Post Operative Dx (Write “SAME”
if Similar Dx to preoperative Dx) G
eneral(√)
Regional(√)
Star
ting
Tim
e (H
H:M
M)
End
Tim
e (H
H:M
M)
Surg
eon
1st A
ssis
tant
2nd
Ass
ista
nt
Ane
sthe
tist
Scru
b nu
rse
Run
ner
Stable(√)
Critical(√)
Died(√)
1. IC
U
2. W
ard
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23)
Count Operation Performed
Count
Elective Surgery Count
Emergency Surgery Died
HEALTH CENTER/CLINIC/HOSPITAL OPERATION REGISTER

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Hospital Surgery Register
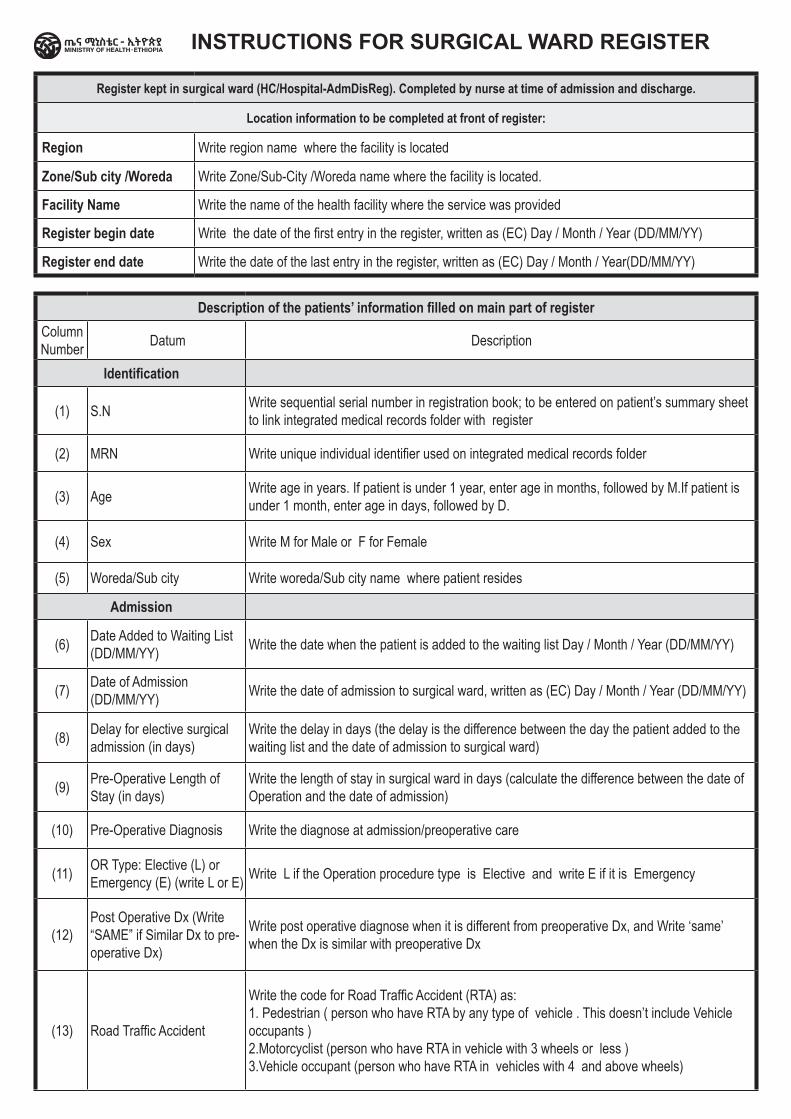
Description of the patients’ information filled on main part of registerColumn Number Datum Description
Identification
(1) S.N Write sequential serial number in registration book; to be entered on patient’s summary sheet to link integrated medical records folder with register
(2) MRN Write unique individual identifier used on integrated medical records folder
(3) Age Write age in years. If patient is under 1 year, enter age in months, followed by M.If patient is under 1 month, enter age in days, followed by D.
(4) Sex Write M for Male or F for Female
(5) Woreda/Sub city Write woreda/Sub city name where patient resides
Admission
(6) Date Added to Waiting List (DD/MM/YY) Write the date when the patient is added to the waiting list Day / Month / Year (DD/MM/YY)
(7) Date of Admission (DD/MM/YY) Write the date of admission to surgical ward, written as (EC) Day / Month / Year (DD/MM/YY)
(8) Delay for elective surgical admission (in days)
Write the delay in days (the delay is the difference between the day the patient added to the waiting list and the date of admission to surgical ward)
(9) Pre-Operative Length of Stay (in days)
Write the length of stay in surgical ward in days (calculate the difference between the date of Operation and the date of admission)
(10) Pre-Operative Diagnosis Write the diagnose at admission/preoperative care
(11) OR Type: Elective (L) or Emergency (E) (write L or E) Write L if the Operation procedure type is Elective and write E if it is Emergency
(12)Post Operative Dx (Write “SAME” if Similar Dx to pre-operative Dx)
Write post operative diagnose when it is different from preoperative Dx, and Write ‘same’ when the Dx is similar with preoperative Dx
(13) Road Traffic Accident
Write the code for Road Traffic Accident (RTA) as: 1. Pedestrian ( person who have RTA by any type of vehicle . This doesn’t include Vehicle occupants ) 2.Motorcyclist (person who have RTA in vehicle with 3 wheels or less ) 3.Vehicle occupant (person who have RTA in vehicles with 4 and above wheels)
INSTRUCTIONS FOR SURGICAL WARD REGISTER
Register kept in surgical ward (HC/Hospital-AdmDisReg). Completed by nurse at time of admission and discharge.
Location information to be completed at front of register:
Region Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
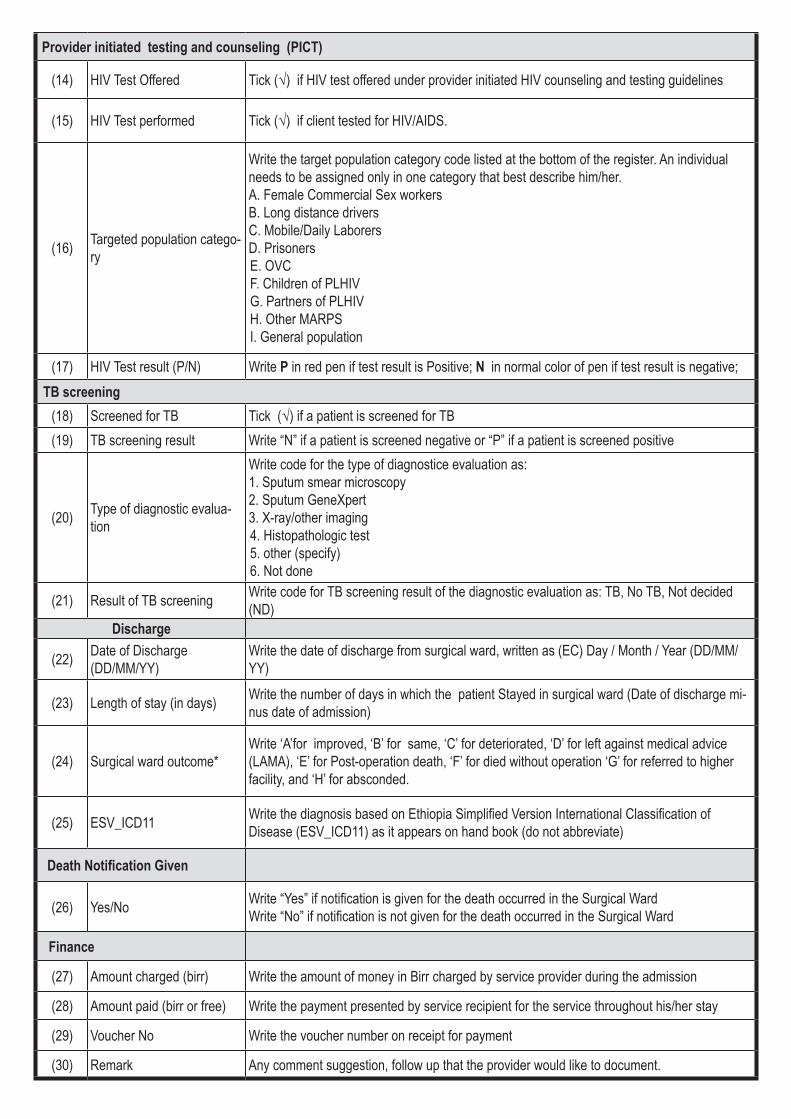
Provider initiated testing and counseling (PICT)
(14) HIV Test Offered Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines
(15) HIV Test performed Tick (√) if client tested for HIV/AIDS.
(16) Targeted population catego-ry
Write the target population category code listed at the bottom of the register. An individual needs to be assigned only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily Laborers D. PrisonersE. OVC F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
(17) HIV Test result (P/N) Write P in red pen if test result is Positive; N in normal color of pen if test result is negative; TB screening
(18) Screened for TB Tick (√) if a patient is screened for TB(19) TB screening result Write “N” if a patient is screened negative or “P” if a patient is screened positive
(20) Type of diagnostic evalua-tion
Write code for the type of diagnostice evaluation as: 1. Sputum smear microscopy 2. Sputum GeneXpert 3. X-ray/other imaging 4. Histopathologic test 5. other (specify) 6. Not done
(21) Result of TB screening Write code for TB screening result of the diagnostic evaluation as: TB, No TB, Not decided (ND)
Discharge
(22) Date of Discharge (DD/MM/YY)
Write the date of discharge from surgical ward, written as (EC) Day / Month / Year (DD/MM/YY)
(23) Length of stay (in days) Write the number of days in which the patient Stayed in surgical ward (Date of discharge mi-nus date of admission)
(24) Surgical ward outcome*Write ‘A’for improved, ‘B’ for same, ‘C’ for deteriorated, ‘D’ for left against medical advice (LAMA), ‘E’ for Post-operation death, ‘F’ for died without operation ‘G’ for referred to higher facility, and ‘H’ for absconded.
(25) ESV_ICD11 Write the diagnosis based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on hand book (do not abbreviate)
Death Notification Given
(26) Yes/No Write “Yes” if notification is given for the death occurred in the Surgical Ward Write “No” if notification is not given for the death occurred in the Surgical Ward
Finance
(27) Amount charged (birr) Write the amount of money in Birr charged by service provider during the admission
(28) Amount paid (birr or free) Write the payment presented by service recipient for the service throughout his/her stay
(29) Voucher No Write the voucher number on receipt for payment
(30) Remark Any comment suggestion, follow up that the provider would like to document.
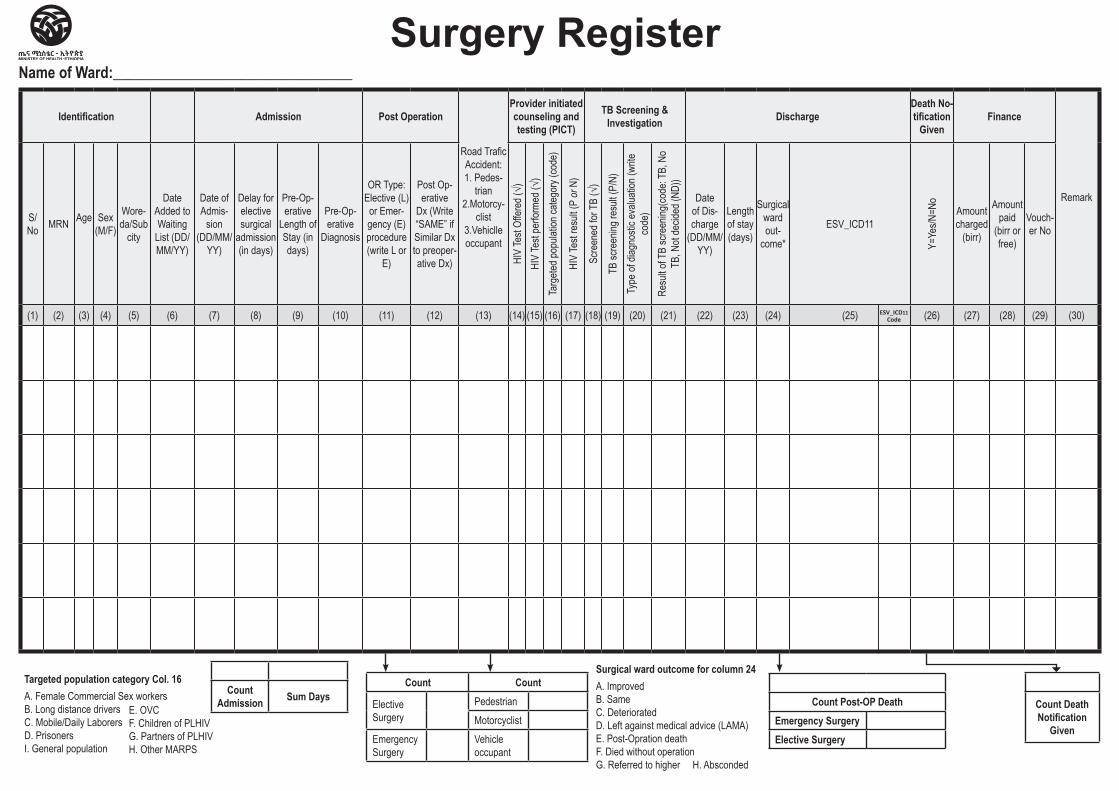
Identification Admission Post Operation
Road Trafic Accident: 1. Pedes-
trian 2.Motorcy-
clist 3.Vehiclle occupant
Provider initiated counseling and testing (PICT)
TB Screening & Investigation Discharge
Death No-tification
GivenFinance
Remark
S/No MRN Age Sex
(M/F)
Wore-da/Sub
city
Date Added to Waiting
List (DD/MM/YY)
Date of Admis-
sion (DD/MM/
YY)
Delay for elective surgical
admission (in days)
Pre-Op-erative
Length of Stay (in days)
Pre-Op-erative
Diagnosis
OR Type: Elective (L)
or Emer-gency (E) procedure (write L or
E)
Post Op-erative
Dx (Write “SAME” if Similar Dx to preoper-ative Dx) HI
V Te
st Of
fered
(√)
HIV
Test
perfo
rmed
(√)
Targ
eted p
opula
tion c
atego
ry (co
de)
HIV
Test
resu
lt (P
or N
)
Scre
ened
for T
B (√
)
TB sc
reen
ing re
sult (
P/N)
Type
of di
agno
stic e
valua
tion (
write
co
de)
Resu
lt of T
B sc
reen
ing(co
de: T
B, N
o TB
, Not
decid
ed (N
D))
Date of Dis-charge
(DD/MM/YY)
Length of stay (days)
Surgical ward out-
come*
ESV_ICD11
Y=Ye
s/N=N
o
Amount charged
(birr)
Amount paid
(birr or free)
Vouch-er No
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30)
Surgery RegisterName of Ward:________________________________
Targeted population category Col. 16 A. Female Commercial Sex workersB. Long distance driversC. Mobile/Daily LaborersD. PrisonersI. General population
E. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
Count Admission Sum Days Count Post-OP Death
Emergency SurgeryElective Surgery
Count Death Notification
Given
Count Count
Elective Surgery
PedestrianMotorcyclist
Emergency Surgery
Vehicle occupant
Surgical ward outcome for column 24A. Improved B. Same C. Deteriorated D. Left against medical advice (LAMA)E. Post-Opration deathF. Died without operationG. Referred to higher H. Absconded
ESV_ICD11 Code
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre/Clinic/HospitalClients waiting for Elective Surgery
Register
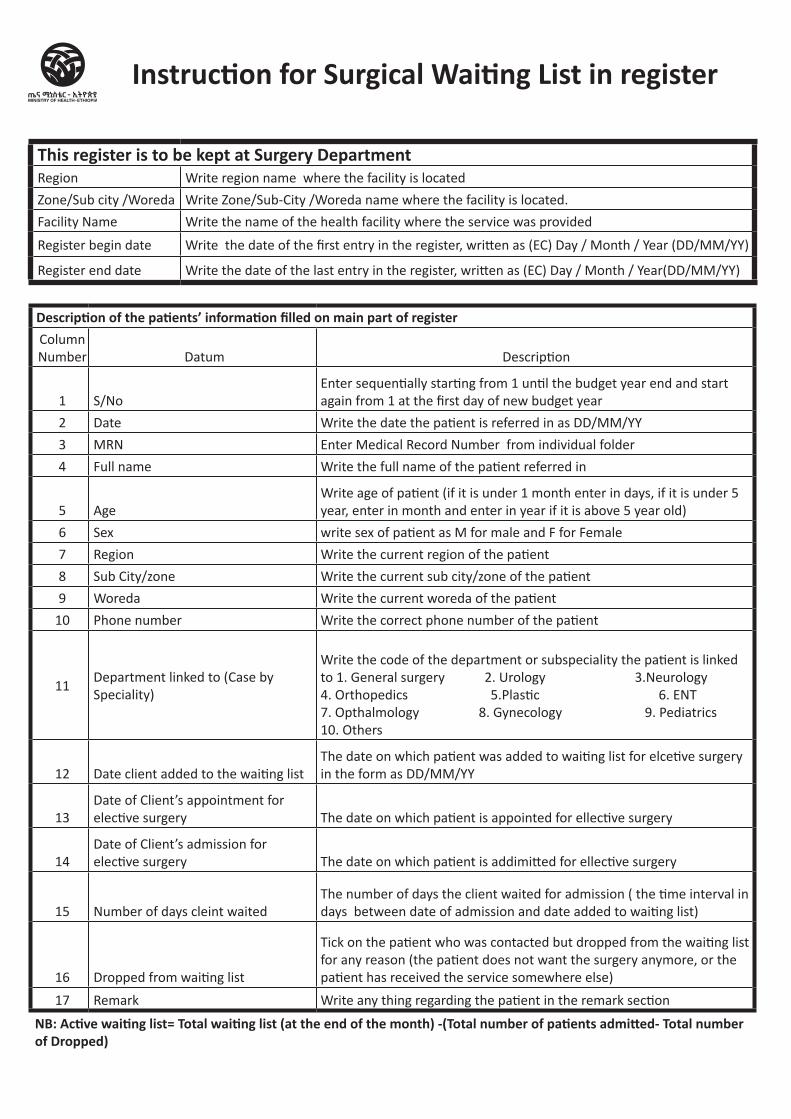
Instruction for Surgical Waiting List in register
Description of the patients’ information filled on main part of registerColumn Number Datum Description
1 S/NoEnter sequentially starting from 1 until the budget year end and start again from 1 at the first day of new budget year
2 Date Write the date the patient is referred in as DD/MM/YY
3 MRN Enter Medical Record Number from individual folder
4 Full name Write the full name of the patient referred in
5 AgeWrite age of patient (if it is under 1 month enter in days, if it is under 5 year, enter in month and enter in year if it is above 5 year old)
6 Sex write sex of patient as M for male and F for Female
7 Region Write the current region of the patient
8 Sub City/zone Write the current sub city/zone of the patient
9 Woreda Write the current woreda of the patient
10 Phone number Write the correct phone number of the patient
11Department linked to (Case by Speciality)
Write the code of the department or subspeciality the patient is linked to 1. General surgery 2. Urology 3.Neurology 4. Orthopedics 5.Plastic 6. ENT 7. Opthalmology 8. Gynecology 9. Pediatrics 10. Others
12 Date client added to the waiting listThe date on which patient was added to waiting list for elcetive surgery in the form as DD/MM/YY
13Date of Client’s appointment for elective surgery The date on which patient is appointed for ellective surgery
14Date of Client’s admission for elective surgery The date on which patient is addimitted for ellective surgery
15 Number of days cleint waitedThe number of days the client waited for admission ( the time interval in days between date of admission and date added to waiting list)
16 Dropped from waiting list
Tick on the patient who was contacted but dropped from the waiting list for any reason (the patient does not want the surgery anymore, or the patient has received the service somewhere else)
17 Remark Write any thing regarding the patient in the remark section
NB: Active waiting list= Total waiting list (at the end of the month) -(Total number of patients admitted- Total number of Dropped)
This register is to be kept at Surgery DepartmentRegion Write region name where the facility is located
Zone/Sub city /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Facility Name Write the name of the health facility where the service was provided
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
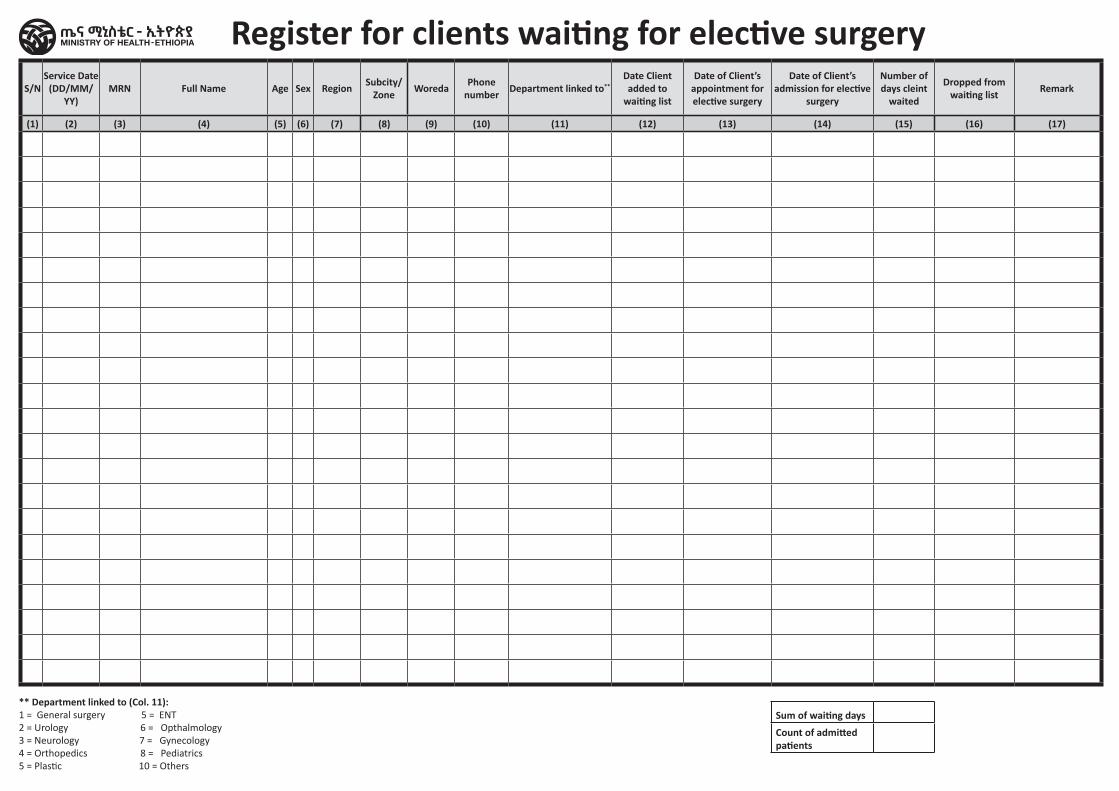
S/NService Date
(DD/MM/YY)
MRN Full Name Age Sex Region Subcity/ Zone Woreda Phone
number Department linked to**Date Client added to
waiting list
Date of Client’s appointment for elective surgery
Date of Client’s admission for elective
surgery
Number of days cleint
waited
Dropped from waiting list Remark
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17)
Sum of waiting days
Count of admitted patients
Register for clients waiting for elective surgery
** Department linked to (Col. 11): 1 = General surgery 5 = ENT 2 = Urology 6 = Opthalmology3 = Neurology 7 = Gynecology4 = Orthopedics 8 = Pediatrics5 = Plastic 10 = Others

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
HospitalAssistive Technology Service Tally Sheet
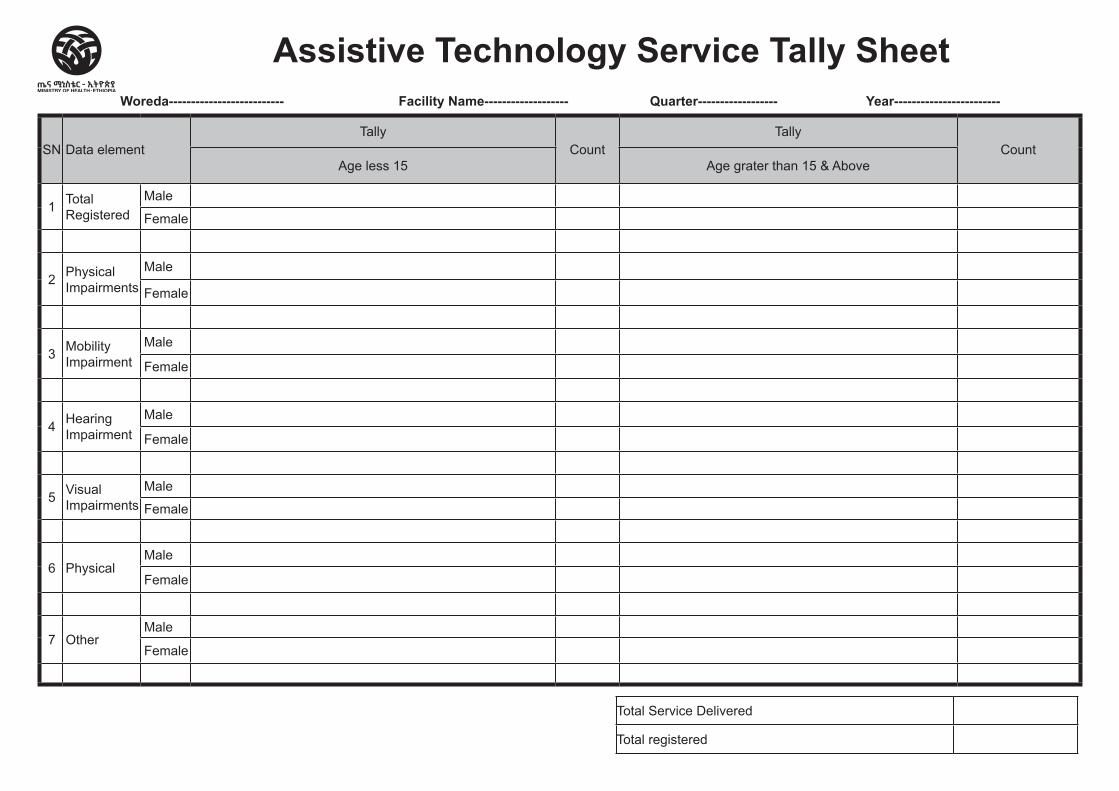
Woreda-------------------------- Facility Name------------------- Quarter------------------ Year------------------------
SN Data elementTally
CountTally
CountAge less 15 Age grater than 15 & Above
1 Total Registered
Male
Female
2 Physical Impairments
Male
Female
3 Mobility Impairment
Male
Female
4 Hearing Impairment
Male
Female
5 Visual Impairments
Male
Female
6 PhysicalMale
Female
7 OtherMale
Female
Assistive Technology Service Tally Sheet
Total Service Delivered
Total registered
Health Center/ Hospital Diseases Information Tally Sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
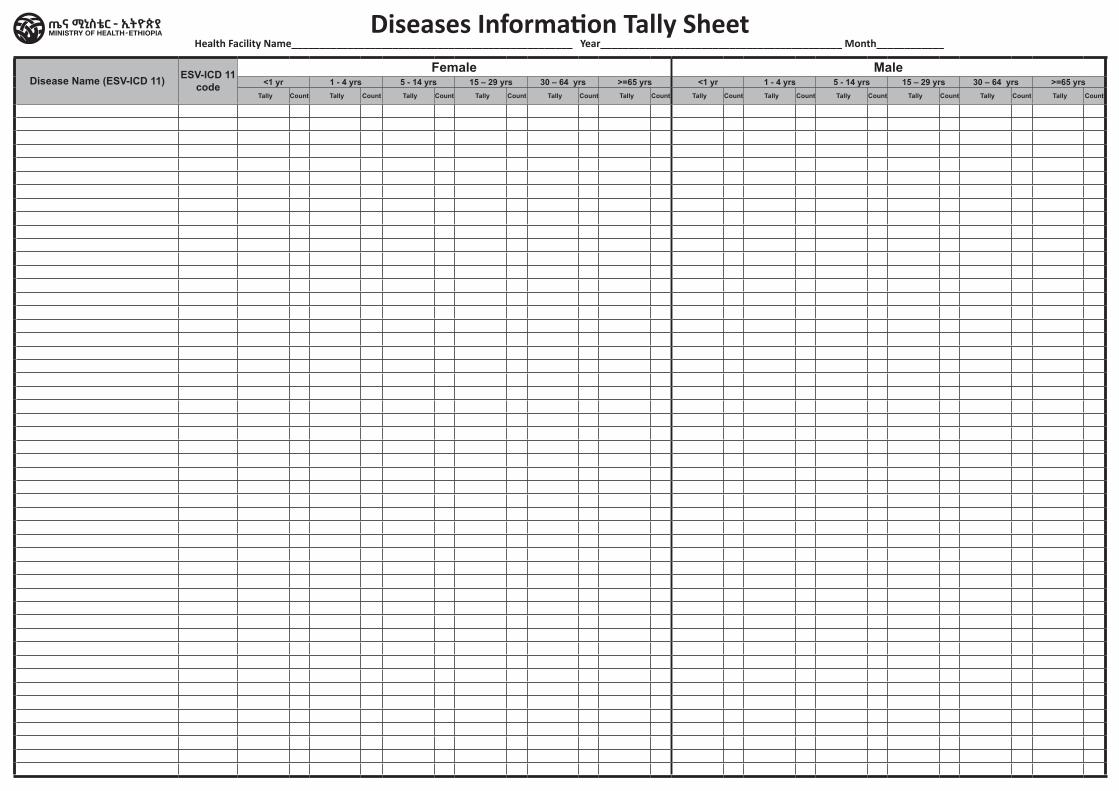
Disease Name (ESV-ICD 11) ESV-ICD 11 code
Female Male<1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs <1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs
Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
Diseases Information Tally SheetHealth Facility Name__________________________________________________ Year___________________________________________ Month____________
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital Tracer Drug Availability Tally Sheet
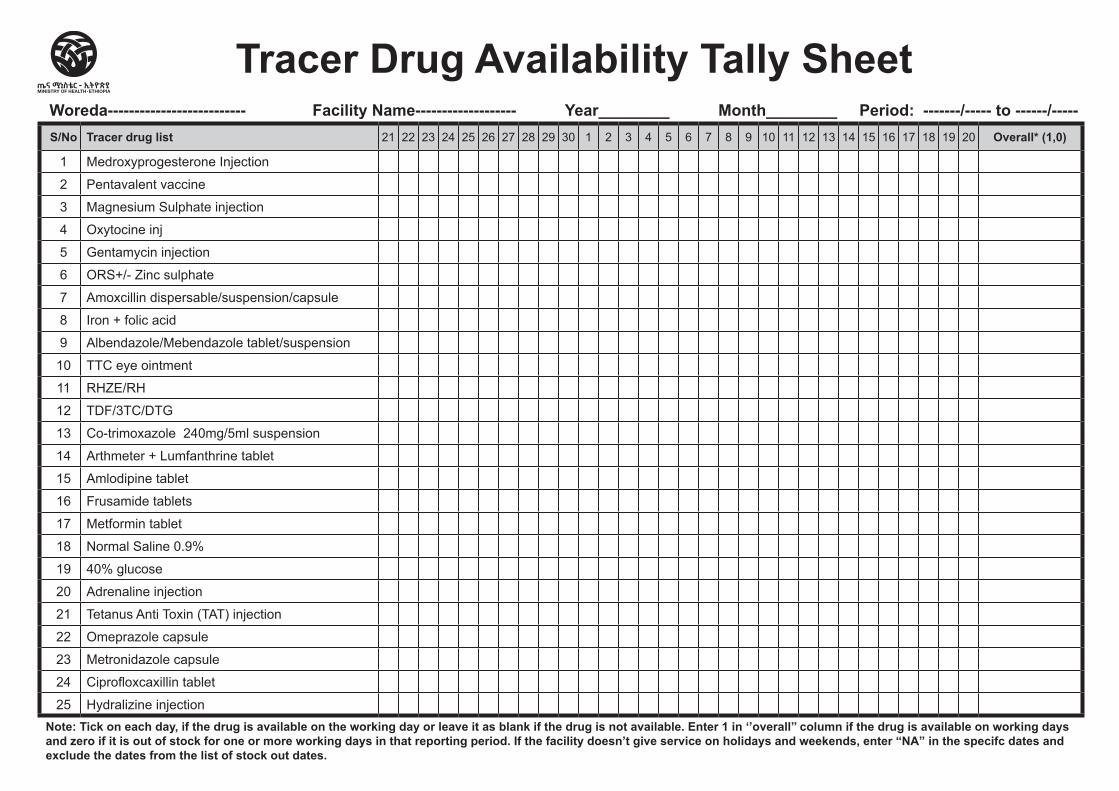
Woreda-------------------------- Facility Name------------------- Year________ Month________ Period: -------/----- to ------/-----S/No Tracer drug list 21 22 23 24 25 26 27 28 29 30 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 Overall* (1,0)
1 Medroxyprogesterone Injection
2 Pentavalent vaccine
3 Magnesium Sulphate injection
4 Oxytocine inj
5 Gentamycin injection
6 ORS+/- Zinc sulphate
7 Amoxcillin dispersable/suspension/capsule
8 Iron + folic acid
9 Albendazole/Mebendazole tablet/suspension
10 TTC eye ointment
11 RHZE/RH
12 TDF/3TC/DTG
13 Co-trimoxazole 240mg/5ml suspension
14 Arthmeter + Lumfanthrine tablet
15 Amlodipine tablet
16 Frusamide tablets
17 Metformin tablet
18 Normal Saline 0.9%
19 40% glucose
20 Adrenaline injection
21 Tetanus Anti Toxin (TAT) injection
22 Omeprazole capsule
23 Metronidazole capsule
24 Ciprofloxcaxillin tablet
25 Hydralizine injectionNote: Tick on each day, if the drug is available on the working day or leave it as blank if the drug is not available. Enter 1 in ‘’overall’’ column if the drug is available on working days and zero if it is out of stock for one or more working days in that reporting period. If the facility doesn’t give service on holidays and weekends, enter “NA” in the specifc dates and exclude the dates from the list of stock out dates.
Tracer Drug Availability Tally Sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health center/Clinic/Hospital ICU Service Tally Sheet
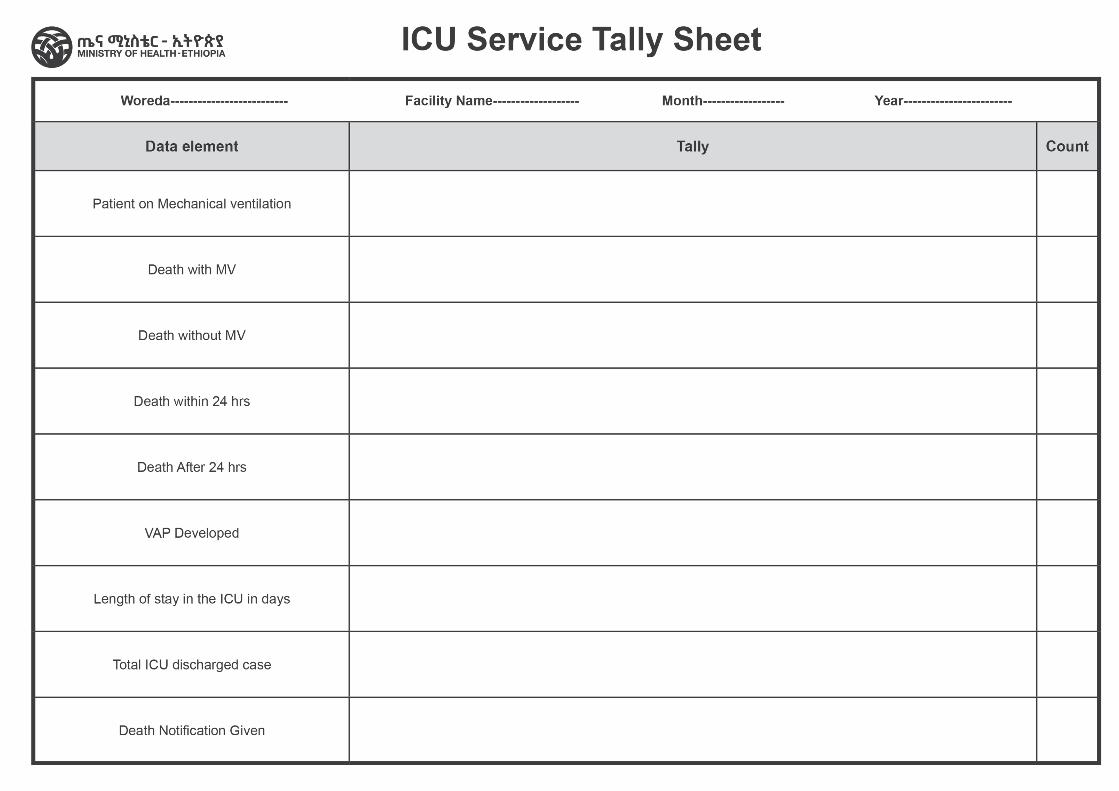
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ Hospital IPD Service Tally Sheet
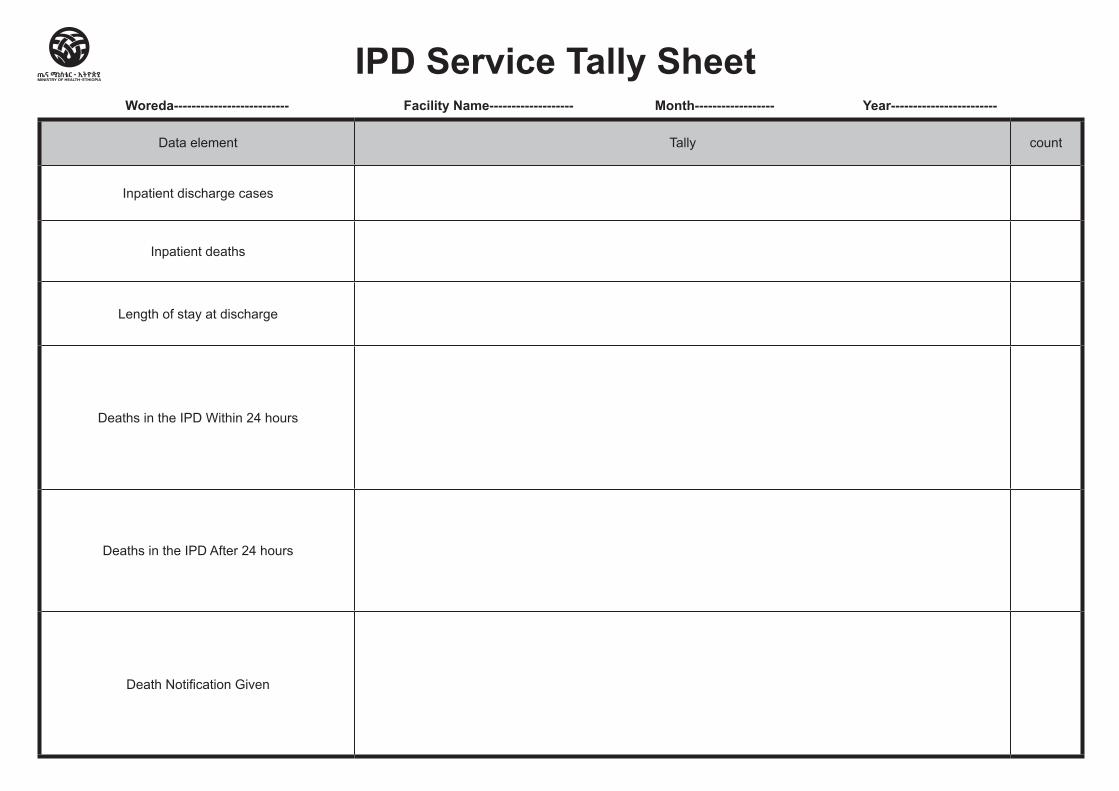
Woreda-------------------------- Facility Name------------------- Month------------------ Year------------------------
Data element Tally count
Inpatient discharge cases
Inpatient deaths
Length of stay at discharge
Deaths in the IPD Within 24 hours
Deaths in the IPD After 24 hours
Death Notification Given
IPD Service Tally Sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Center /Clinic/ HospitalPatient/Client Attendance Tally Sheet
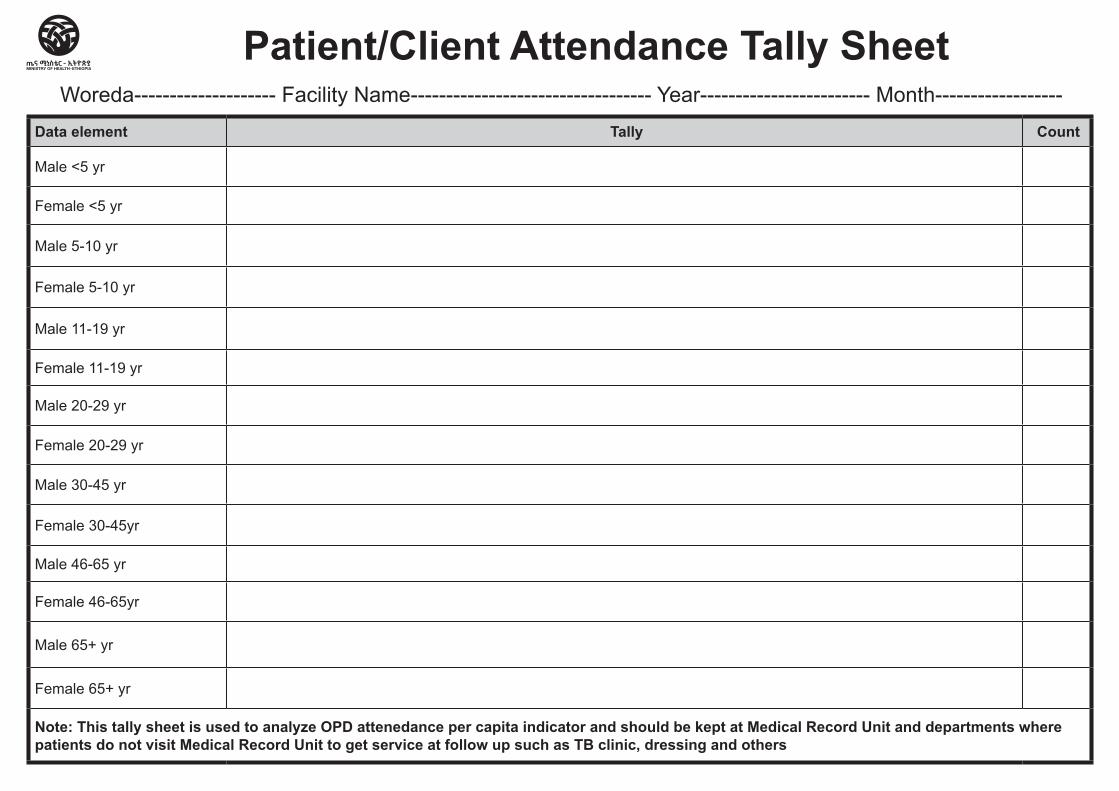
Data element Tally Count
Male <5 yr
Female <5 yr
Male 5-10 yr
Female 5-10 yr
Male 11-19 yr
Female 11-19 yr
Male 20-29 yr
Female 20-29 yr
Male 30-45 yr
Female 30-45yr
Male 46-65 yr
Female 46-65yr
Male 65+ yr
Female 65+ yr
Note: This tally sheet is used to analyze OPD attenedance per capita indicator and should be kept at Medical Record Unit and departments where patients do not visit Medical Record Unit to get service at follow up such as TB clinic, dressing and others
Patient/Client Attendance Tally SheetWoreda-------------------- Facility Name---------------------------------- Year------------------------ Month------------------
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
HospitalSurgical Waiting List Tally sheet
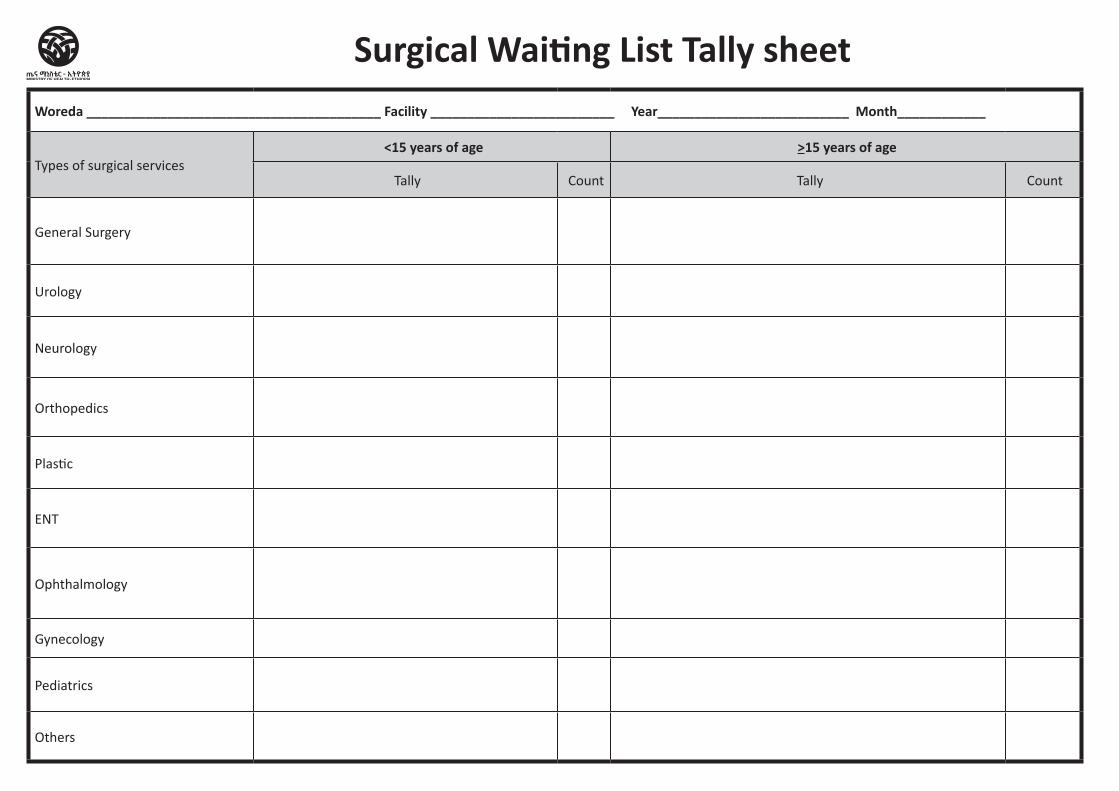
Woreda ________________________________________ Facility _________________________ Year__________________________ Month____________
Types of surgical services<15 years of age >15 years of age
Tally Count Tally Count
General Surgery
Urology
Neurology
Orthopedics
Plastic
ENT
Ophthalmology
Gynecology
Pediatrics
Others
Surgical Waiting List Tally sheet
NCD Registers and Tally sheets
Content / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Cervical Cancer Screening and
Treatment Register
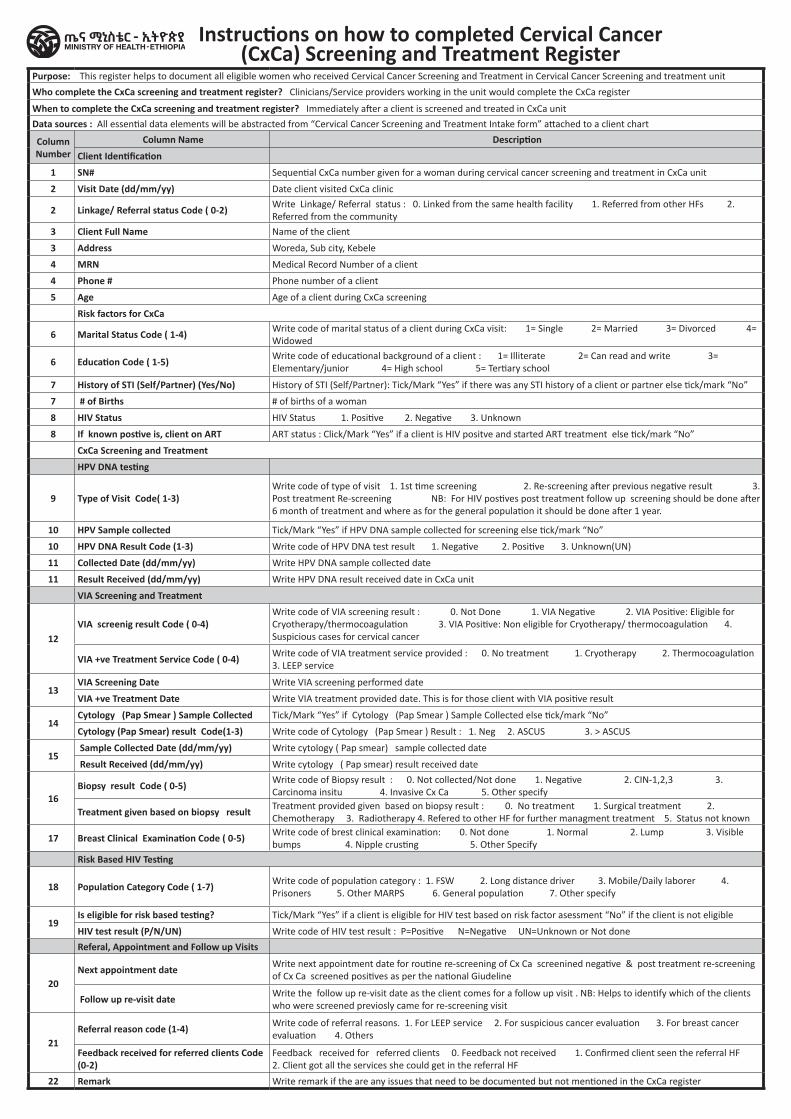
Purpose: This register helps to document all eligible women who received Cervical Cancer Screening and Treatment in Cervical Cancer Screening and treatment unit
Who complete the CxCa screening and treatment register? Clinicians/Service providers working in the unit would complete the CxCa register
When to complete the CxCa screening and treatment register? Immediately after a client is screened and treated in CxCa unit Data sources : All essential data elements will be abstracted from “Cervical Cancer Screening and Treatment Intake form” attached to a client chart
Column Number
Column Name Description
Client Identification
1 SN# Sequential CxCa number given for a woman during cervical cancer screening and treatment in CxCa unit
2 Visit Date (dd/mm/yy) Date client visited CxCa clinic
2 Linkage/ Referral status Code ( 0-2) Write Linkage/ Referral status : 0. Linked from the same health facility 1. Referred from other HFs 2. Referred from the community
3 Client Full Name Name of the client
3 Address Woreda, Sub city, Kebele
4 MRN Medical Record Number of a client
4 Phone # Phone number of a client
5 Age Age of a client during CxCa screening
Risk factors for CxCa
6 Marital Status Code ( 1-4) Write code of marital status of a client during CxCa visit: 1= Single 2= Married 3= Divorced 4= Widowed
6 Education Code ( 1-5) Write code of educational background of a client : 1= Illiterate 2= Can read and write 3= Elementary/junior 4= High school 5= Tertiary school
7 History of STI (Self/Partner) (Yes/No) History of STI (Self/Partner): Tick/Mark “Yes” if there was any STI history of a client or partner else tick/mark “No”
7 # of Births # of births of a woman
8 HIV Status HIV Status 1. Positive 2. Negative 3. Unknown
8 If known postive is, client on ART ART status : Click/Mark “Yes” if a client is HIV positve and started ART treatment else tick/mark “No”
CxCa Screening and Treatment
HPV DNA testing
9 Type of Visit Code( 1-3)Write code of type of visit 1. 1st time screening 2. Re-screening after previous negative result 3. Post treatment Re-screening NB: For HIV postives post treatment follow up screening should be done after 6 month of treatment and where as for the general population it should be done after 1 year.
10 HPV Sample collected Tick/Mark “Yes” if HPV DNA sample collected for screening else tick/mark “No”
10 HPV DNA Result Code (1-3) Write code of HPV DNA test result 1. Negative 2. Positive 3. Unknown(UN)
11 Collected Date (dd/mm/yy) Write HPV DNA sample collected date
11 Result Received (dd/mm/yy) Write HPV DNA result received date in CxCa unit
VIA Screening and Treatment
12VIA screenig result Code ( 0-4)
Write code of VIA screening result : 0. Not Done 1. VIA Negative 2. VIA Positive: Eligible for Cryotherapy/thermocoagulation 3. VIA Positive: Non eligible for Cryotherapy/ thermocoagulation 4. Suspicious cases for cervical cancer
VIA +ve Treatment Service Code ( 0-4) Write code of VIA treatment service provided : 0. No treatment 1. Cryotherapy 2. Thermocoagulation 3. LEEP service
13VIA Screening Date Write VIA screening performed date
VIA +ve Treatment Date Write VIA treatment provided date. This is for those client with VIA positive result
14Cytology (Pap Smear ) Sample Collected Tick/Mark “Yes” if Cytology (Pap Smear ) Sample Collected else tick/mark “No”
Cytology (Pap Smear) result Code(1-3) Write code of Cytology (Pap Smear ) Result : 1. Neg 2. ASCUS 3. > ASCUS
15 Sample Collected Date (dd/mm/yy) Write cytology ( Pap smear) sample collected date
Result Received (dd/mm/yy) Write cytology ( Pap smear) result received date
16Biopsy result Code ( 0-5) Write code of Biopsy result : 0. Not collected/Not done 1. Negative 2. CIN-1,2,3 3.
Carcinoma insitu 4. Invasive Cx Ca 5. Other specify
Treatment given based on biopsy result Treatment provided given based on biopsy result : 0. No treatment 1. Surgical treatment 2. Chemotherapy 3. Radiotherapy 4. Refered to other HF for further managment treatment 5. Status not known
17 Breast Clinical Examination Code ( 0-5) Write code of brest clinical examination: 0. Not done 1. Normal 2. Lump 3. Visible bumps 4. Nipple crusting 5. Other Specify
Risk Based HIV Testing
18 Population Category Code ( 1-7) Write code of population category : 1. FSW 2. Long distance driver 3. Mobile/Daily laborer 4. Prisoners 5. Other MARPS 6. General population 7. Other specify
19Is eligible for risk based testing? Tick/Mark “Yes” if a client is eligible for HIV test based on risk factor asessment “No” if the client is not eligible
HIV test result (P/N/UN) Write code of HIV test result : P=Positive N=Negative UN=Unknown or Not done
Referal, Appointment and Follow up Visits
20Next appointment date Write next appointment date for routine re-screening of Cx Ca screenined negative & post treatment re-screening
of Cx Ca screened positives as per the national Giudeline
Follow up re-visit date Write the follow up re-visit date as the client comes for a follow up visit . NB: Helps to identify which of the clients who were screened previosly came for re-screening visit
21Referral reason code (1-4) Write code of referral reasons. 1. For LEEP service 2. For suspicious cancer evaluation 3. For breast cancer
evaluation 4. Others
Feedback received for referred clients Code (0-2)
Feedback received for referred clients 0. Feedback not received 1. Confirmed client seen the referral HF 2. Client got all the services she could get in the referral HF
22 Remark Write remark if the are any issues that need to be documented but not mentioned in the CxCa register
Instructions on how to completed Cervical Cancer (CxCa) Screening and Treatment Register
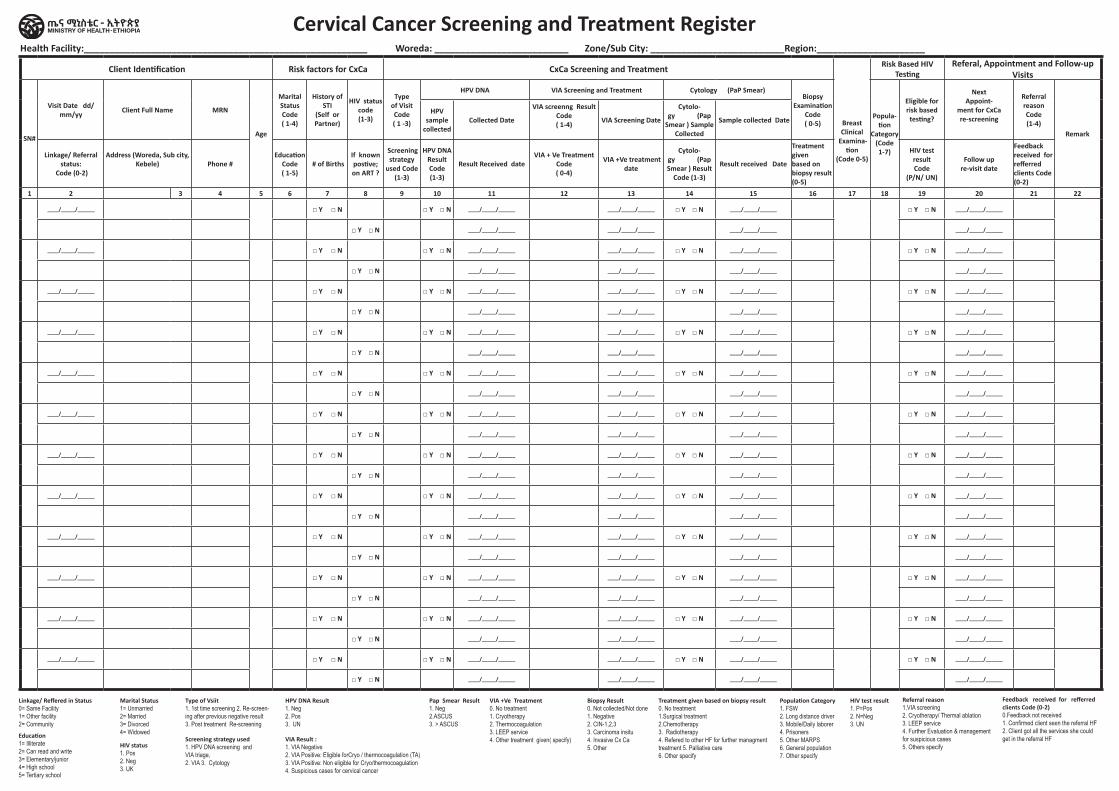
Health Facility:_______________________________________________________ Woreda: __________________________ Zone/Sub City: __________________________Region:_____________________
Client Identification Risk factors for CxCa CxCa Screening and Treatment
Breast Clinical
Examina-tion
(Code 0-5)
Risk Based HIV Testing
Referal, Appointment and Follow-up Visits
SN#
Visit Date dd/mm/yy Client Full Name MRN
Age
Marital Status Code ( 1-4)
History of
STI (Self or Partner)
HIV status code (1-3)
Type of Visit Code ( 1 -3)
HPV DNA VIA Screening and Treatment Cytology (PaP Smear)Biopsy
Examination Code ( 0-5)
Popula-tion
Category (Code 1-7)
Eligible for risk based testing?
Next Appoint-
ment for CxCa re-screening
Referral reason Code (1-4)
Remark
HPV sample
collectedCollected Date
VIA screenng Result Code ( 1-4) VIA Screening Date
Cytolo-gy (Pap
Smear ) Sample Collected
Sample collected Date
Linkage/ Referral status:
Code (0-2)
Address (Woreda, Sub city, Kebele) Phone #
Education Code ( 1-5)
# of BirthsIf known postive; on ART ?
Screening strategy
used Code (1-3)
HPV DNA Result Code (1-3)
Result Received dateVIA + Ve Treatment
Code ( 0-4)
VIA +Ve treatment date
Cytolo-gy (Pap Smear ) Result
Code (1-3)
Result received Date
Treatment given based on biopsy result (0-5)
HIV test result Code
(P/N/ UN)
Follow up re-visit date
Feedback received for refferred clients Code (0-2)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
____/_____/______ □ Y □ N □ Y □ N ____/_____/______ ____/_____/______ □ Y □ N ____/_____/______ □ Y □ N ____/_____/______
□ Y □ N ____/_____/______ ____/_____/______ ____/_____/______ ____/_____/______
Cervical Cancer Screening and Treatment Register
Linkage/ Reffered in Status 0= Same Facility 1= Other facility 2= CommunityEducation 1= Illiterate 2= Can read and write 3= Elementary/junior 4= High school 5= Tertiary school
Marital Status 1= Unmarried 2= Married 3= Divorced 4= Widowed
HIV status 1. Pos 2. Neg 3. UK
Type of Vsiit1. 1st time screening 2. Re-screen-ing after previous negative result 3. Post treatment Re-screening
Screening strategy used 1. HPV DNA screening and VIA triage, 2. VIA 3. Cytology
HPV DNA Result 1. Neg 2. Pos 3. UN
VIA Result : 1. VIA Negative 2. VIA Positive: Eligible forCryo / thermocoagulation (TA) 3. VIA Positive: Non eligible for Cryo/thermocoagulation 4. Suspicious cases for cervical cancer
VIA +Ve Treatment 0. No treatment 1. Cryotherapy 2. Thermocoagulation 3. LEEP service 4. Other treatment given( specify)
Pap Smear Result 1. Neg 2.ASCUS 3. > ASCUS
Biopsy Result 0. Not collected/Not done 1. Negative 2. CIN-1,2,3 3. Carcinoma insitu 4. Invasive Cx Ca 5. Other
Treatment given based on biopsy result 0. No treatment 1.Surgical treatment 2.Chemotherapy 3. Radiotherapy 4. Refered to other HF for further managment treatment 5. Palliative care 6. Other specify
Population Category 1. FSW 2. Long distance driver 3. Mobile/Daily laborer 4. Prisoners 5. Other MARPS 6. General population 7. Other specify
HIV test result 1. P=Pos 2. N=Neg 3. UN
Referral reason 1.VIA screening2. Cryotherapy/ Thermal ablation3. LEEP service4. Further Evaluation & management for suspicious cases 5. Others specify
Feedback received for refferred clients Code (0-2) 0.Feedback not received 1. Confirmed client seen the referral HF 2. Client got all the services she could get in the referral HF
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital HTN and DM Treatment Cohort
Register
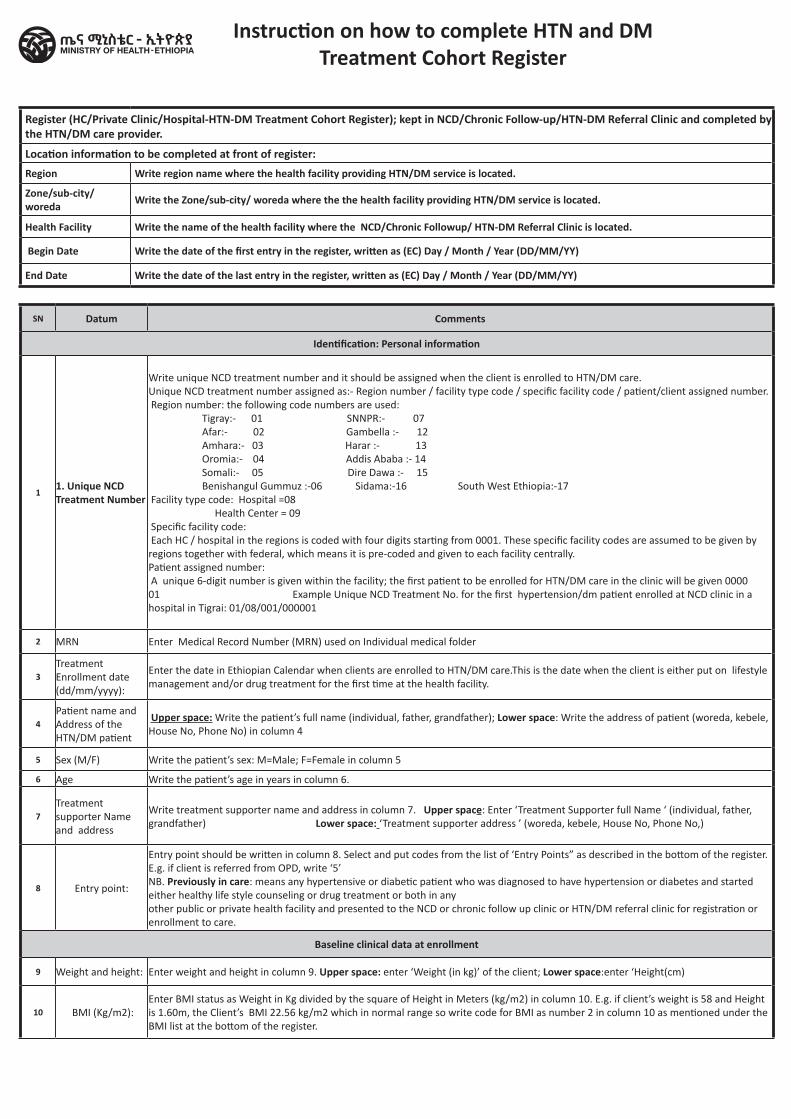
Instruction on how to complete HTN and DM Treatment Cohort Register
SN Datum Comments
Identification: Personal information
11. Unique NCD Treatment Number
Write unique NCD treatment number and it should be assigned when the client is enrolled to HTN/DM care. Unique NCD treatment number assigned as:- Region number / facility type code / specific facility code / patient/client assigned number. Region number: the following code numbers are used: Tigray:- 01 SNNPR:- 07 Afar:- 02 Gambella :- 12 Amhara:- 03 Harar :- 13 Oromia:- 04 Addis Ababa :- 14 Somali:- 05 Dire Dawa :- 15 Benishangul Gummuz :-06 Sidama:-16 South West Ethiopia:-17 Facility type code: Hospital =08 Health Center = 09 Specific facility code: Each HC / hospital in the regions is coded with four digits starting from 0001. These specific facility codes are assumed to be given by regions together with federal, which means it is pre-coded and given to each facility centrally. Patient assigned number: A unique 6-digit number is given within the facility; the first patient to be enrolled for HTN/DM care in the clinic will be given 000001 Example Unique NCD Treatment No. for the first hypertension/dm patient enrolled at NCD clinic in a hospital in Tigrai: 01/08/001/000001
2 MRN Enter Medical Record Number (MRN) used on Individual medical folder
3Treatment Enrollment date (dd/mm/yyyy):
Enter the date in Ethiopian Calendar when clients are enrolled to HTN/DM care.This is the date when the client is either put on lifestyle management and/or drug treatment for the first time at the health facility.
4Patient name and Address of the HTN/DM patient
Upper space: Write the patient’s full name (individual, father, grandfather); Lower space: Write the address of patient (woreda, kebele, House No, Phone No) in column 4
5 Sex (M/F) Write the patient’s sex: M=Male; F=Female in column 5
6 Age Write the patient’s age in years in column 6.
7Treatment supporter Name and address
Write treatment supporter name and address in column 7. Upper space: Enter ‘Treatment Supporter full Name ‘ (individual, father, grandfather) Lower space: ‘Treatment supporter address ’ (woreda, kebele, House No, Phone No,)
8 Entry point:
Entry point should be written in column 8. Select and put codes from the list of ‘Entry Points” as described in the bottom of the register. E.g. if client is referred from OPD, write ‘5’ NB. Previously in care: means any hypertensive or diabetic patient who was diagnosed to have hypertension or diabetes and started either healthy life style counseling or drug treatment or both in any other public or private health facility and presented to the NCD or chronic follow up clinic or HTN/DM referral clinic for registration or enrollment to care.
Baseline clinical data at enrollment
9 Weight and height: Enter weight and height in column 9. Upper space: enter ‘Weight (in kg)’ of the client; Lower space:enter ‘Height(cm)
10 BMI (Kg/m2):Enter BMI status as Weight in Kg divided by the square of Height in Meters (kg/m2) in column 10. E.g. if client’s weight is 58 and Height is 1.60m, the Client’s BMI 22.56 kg/m2 which in normal range so write code for BMI as number 2 in column 10 as mentioned under the BMI list at the bottom of the register.
Register (HC/Private Clinic/Hospital-HTN-DM Treatment Cohort Register); kept in NCD/Chronic Follow-up/HTN-DM Referral Clinic and completed by the HTN/DM care provider.
Location information to be completed at front of register:Region Write region name where the health facility providing HTN/DM service is located.
Zone/sub-city/ woreda Write the Zone/sub-city/ woreda where the the health facility providing HTN/DM service is located.
Health Facility Write the name of the health facility where the NCD/Chronic Followup/ HTN-DM Referral Clinic is located.
Begin Date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
End Date Write the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
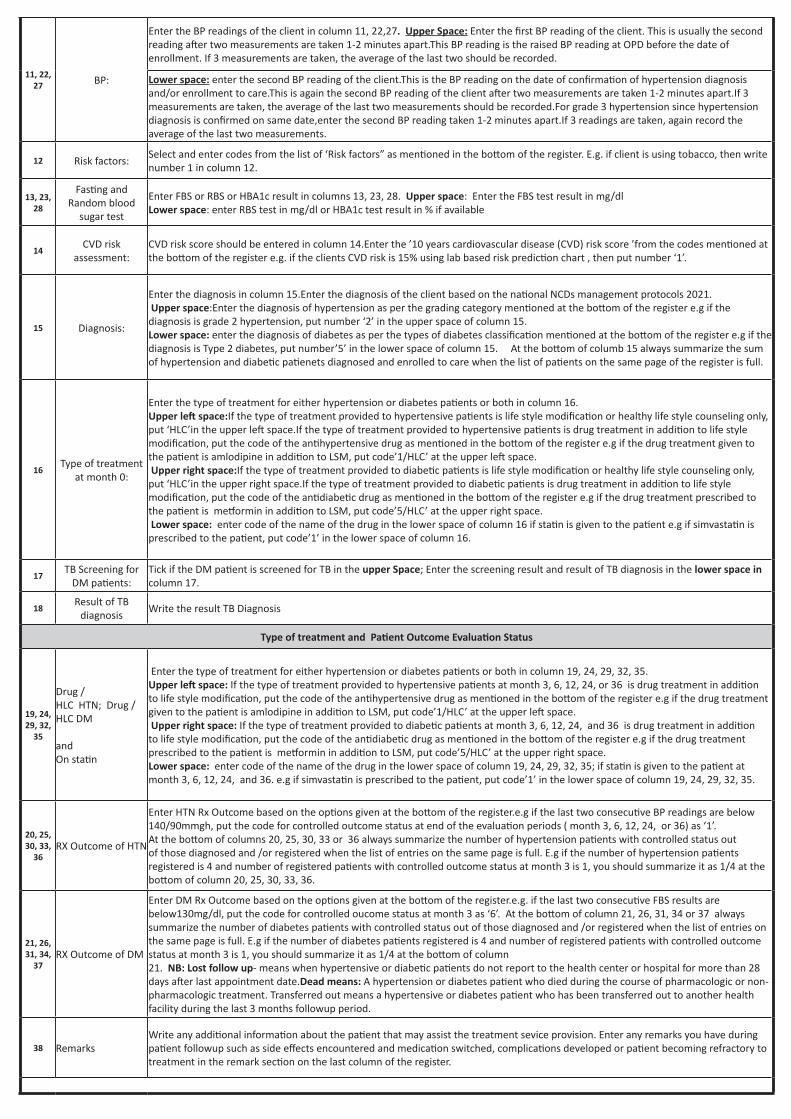
11, 22, 27 BP:
Enter the BP readings of the client in column 11, 22,27. Upper Space: Enter the first BP reading of the client. This is usually the second reading after two measurements are taken 1-2 minutes apart.This BP reading is the raised BP reading at OPD before the date of enrollment. If 3 measurements are taken, the average of the last two should be recorded.
Lower space: enter the second BP reading of the client.This is the BP reading on the date of confirmation of hypertension diagnosis and/or enrollment to care.This is again the second BP reading of the client after two measurements are taken 1-2 minutes apart.If 3 measurements are taken, the average of the last two measurements should be recorded.For grade 3 hypertension since hypertension diagnosis is confirmed on same date,enter the second BP reading taken 1-2 minutes apart.If 3 readings are taken, again record the average of the last two measurements.
12 Risk factors:Select and enter codes from the list of ‘Risk factors” as mentioned in the bottom of the register. E.g. if client is using tobacco, then write number 1 in column 12.
13, 23, 28
Fasting and Random blood
sugar test
Enter FBS or RBS or HBA1c result in columns 13, 23, 28. Upper space: Enter the FBS test result in mg/dl Lower space: enter RBS test in mg/dl or HBA1c test result in % if available
14CVD risk
assessment:CVD risk score should be entered in column 14.Enter the ’10 years cardiovascular disease (CVD) risk score ’from the codes mentioned at the bottom of the register e.g. if the clients CVD risk is 15% using lab based risk prediction chart , then put number ‘1’.
15 Diagnosis:
Enter the diagnosis in column 15.Enter the diagnosis of the client based on the national NCDs management protocols 2021. Upper space:Enter the diagnosis of hypertension as per the grading category mentioned at the bottom of the register e.g if the diagnosis is grade 2 hypertension, put number ‘2’ in the upper space of column 15. Lower space: enter the diagnosis of diabetes as per the types of diabetes classification mentioned at the bottom of the register e.g if the diagnosis is Type 2 diabetes, put number’5’ in the lower space of column 15. At the bottom of columb 15 always summarize the sum of hypertension and diabetic patienets diagnosed and enrolled to care when the list of patients on the same page of the register is full.
16Type of treatment
at month 0:
Enter the type of treatment for either hypertension or diabetes patients or both in column 16. Upper left space:If the type of treatment provided to hypertensive patients is life style modification or healthy life style counseling only, put ‘HLC’in the upper left space.If the type of treatment provided to hypertensive patients is drug treatment in addition to life style modification, put the code of the antihypertensive drug as mentioned in the bottom of the register e.g if the drug treatment given to the patient is amlodipine in addition to LSM, put code’1/HLC’ at the upper left space. Upper right space:If the type of treatment provided to diabetic patients is life style modification or healthy life style counseling only, put ‘HLC’in the upper right space.If the type of treatment provided to diabetic patients is drug treatment in addition to life style modification, put the code of the antidiabetic drug as mentioned in the bottom of the register e.g if the drug treatment prescribed to the patient is metformin in addition to LSM, put code’5/HLC’ at the upper right space. Lower space: enter code of the name of the drug in the lower space of column 16 if statin is given to the patient e.g if simvastatin is prescribed to the patient, put code’1’ in the lower space of column 16.
17TB Screening for
DM patients:Tick if the DM patient is screened for TB in the upper Space; Enter the screening result and result of TB diagnosis in the lower space in column 17.
18Result of TB
diagnosis Write the result TB Diagnosis
Type of treatment and Patient Outcome Evaluation Status
19, 24, 29, 32,
35
Drug / HLC HTN; Drug / HLC DM and On statin
Enter the type of treatment for either hypertension or diabetes patients or both in column 19, 24, 29, 32, 35. Upper left space: If the type of treatment provided to hypertensive patients at month 3, 6, 12, 24, or 36 is drug treatment in addition to life style modification, put the code of the antihypertensive drug as mentioned in the bottom of the register e.g if the drug treatment given to the patient is amlodipine in addition to LSM, put code’1/HLC’ at the upper left space. Upper right space: If the type of treatment provided to diabetic patients at month 3, 6, 12, 24, and 36 is drug treatment in addition to life style modification, put the code of the antidiabetic drug as mentioned in the bottom of the register e.g if the drug treatment prescribed to the patient is metformin in addition to LSM, put code’5/HLC’ at the upper right space. Lower space: enter code of the name of the drug in the lower space of column 19, 24, 29, 32, 35; if statin is given to the patient at month 3, 6, 12, 24, and 36. e.g if simvastatin is prescribed to the patient, put code’1’ in the lower space of column 19, 24, 29, 32, 35.
20, 25, 30, 33,
36RX Outcome of HTN
Enter HTN Rx Outcome based on the options given at the bottom of the register.e.g if the last two consecutive BP readings are below 140/90mmgh, put the code for controlled outcome status at end of the evaluation periods ( month 3, 6, 12, 24, or 36) as ‘1’. At the bottom of columns 20, 25, 30, 33 or 36 always summarize the number of hypertension patients with controlled status out of those diagnosed and /or registered when the list of entries on the same page is full. E.g if the number of hypertension patients registered is 4 and number of registered patients with controlled outcome status at month 3 is 1, you should summarize it as 1/4 at the bottom of column 20, 25, 30, 33, 36.
21, 26, 31, 34,
37RX Outcome of DM
Enter DM Rx Outcome based on the options given at the bottom of the register.e.g. if the last two consecutive FBS results are below130mg/dl, put the code for controlled oucome status at month 3 as ‘6’. At the bottom of column 21, 26, 31, 34 or 37 always summarize the number of diabetes patients with controlled status out of those diagnosed and /or registered when the list of entries on the same page is full. E.g if the number of diabetes patients registered is 4 and number of registered patients with controlled outcome status at month 3 is 1, you should summarize it as 1/4 at the bottom of column 21. NB: Lost follow up- means when hypertensive or diabetic patients do not report to the health center or hospital for more than 28 days after last appointment date.Dead means: A hypertension or diabetes patient who died during the course of pharmacologic or non-pharmacologic treatment. Transferred out means a hypertensive or diabetes patient who has been transferred out to another health facility during the last 3 months followup period.
38 RemarksWrite any additional information about the patient that may assist the treatment sevice provision. Enter any remarks you have during patient followup such as side effects encountered and medication switched, complications developed or patient becoming refractory to treatment in the remark section on the last column of the register.
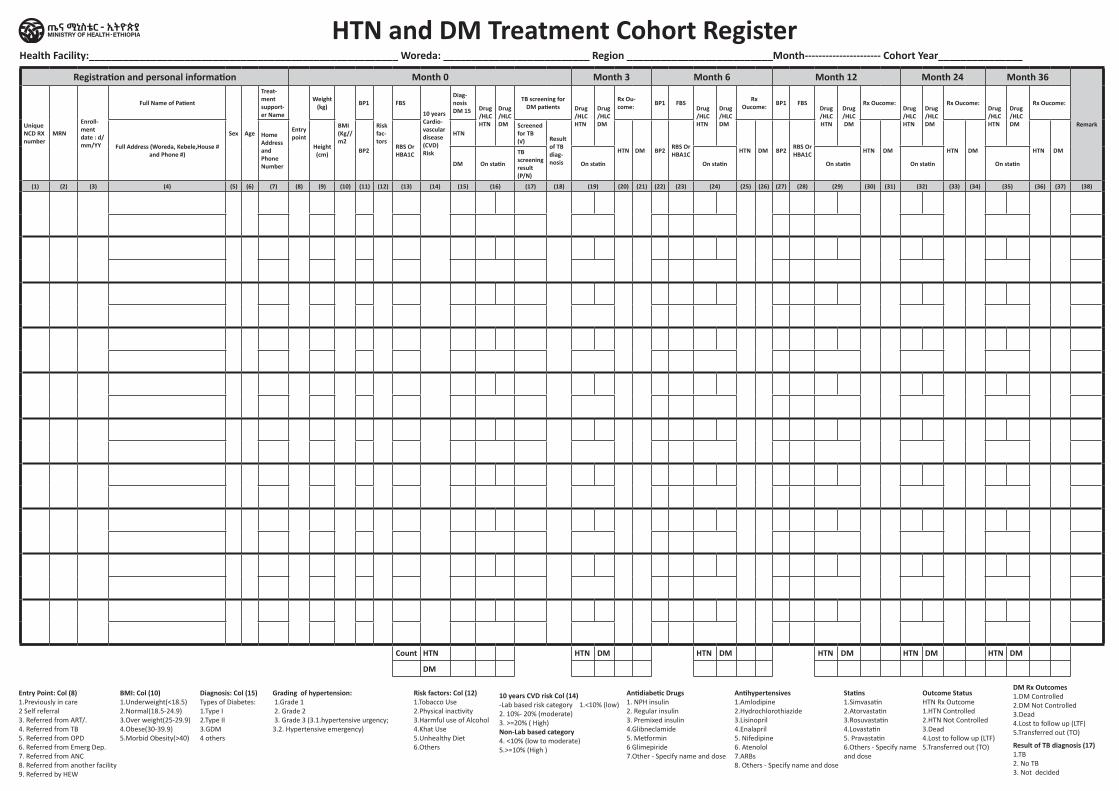
HTN and DM Treatment Cohort RegisterHealth Facility:_______________________________________________________ Woreda: __________________________ Region __________________________Month---------------------- Cohort Year_______________
Entry Point: Col (8)1.Previously in care2 Self referral3. Referred from ART/.4. Referred from TB5. Referred from OPD6. Referred from Emerg Dep.7. Referred from ANC8. Referred from another facility9. Referred by HEW
BMI: Col (10)1.Underweight(<18.5)2.Normal(18.5-24.9)3.Over weight(25-29.9)4.Obese(30-39.9)5.Morbid Obesity(>40)
Risk factors: Col (12)1.Tobacco Use2.Physical inactivity3.Harmful use of Alcohol4.Khat Use5.Unhealthy Diet6.Others
10 years CVD risk Col (14)-Lab based risk category 1.<10% (low)2. 10%- 20% (moderate)3. >=20% ( High)Non-Lab based category 4. <10% (low to moderate)5.>=10% (High )
Diagnosis: Col (15)Types of Diabetes:1.Type I2.Type II3.GDM4 others
Antidiabetic Drugs1. NPH insulin2. Regular insulin3. Premixed insulin4.Glibneclamide5. Metformin6 Glimepiride7.Other - Specify name and dose
Antihypertensives1.Amlodipine2.Hydrochlorothiazide3.Lisinopril4.Enalapril5. Nifedipine 6. Atenolol7.ARBs8. Others - Specify name and dose
Statins1.Simvasatin2.Atorvastatin3.Rosuvastatin4.Lovastatin5. Pravastatin 6.Others - Specify nameand dose
Outcome StatusHTN Rx Outcome1.HTN Controlled2.HTN Not Controlled3.Dead4.Lost to follow up (LTF)5.Transferred out (TO) Result of TB diagnosis (17)
1.TB2. No TB3. Not decided
DM Rx Outcomes1.DM Controlled2.DM Not Controlled3.Dead4.Lost to follow up (LTF)5.Transferred out (TO)
Grading of hypertension: 1.Grade 1 2. Grade 2 3. Grade 3 (3.1.hypertensive urgency; 3.2. Hypertensive emergency)
Registration and personal information Month 0 Month 3 Month 6 Month 12 Month 24 Month 36
RemarkUnique NCD RX number
MRN
Enroll-ment date : d/mm/YY
Full Name of Patient
Sex Age
Treat-ment support-er Name
Entry point
Weight (kg)
BMI (Kg//m2
BP1
Risk fac-tors
FBS
10 years Cardio-vascular disease (CVD) Risk
Diag-nosis DM 15 Drug
/HLC HTN
Drug /HLC DM
TB screening for DM patients Drug
/HLC HTN
Drug /HLC DM
Rx Ou-come: BP1 FBS
Drug /HLC HTN
Drug /HLC DM
Rx Oucome: BP1 FBS
Drug /HLC HTN
Drug /HLC DM
Rx Oucome:Drug /HLC HTN
Drug /HLC DM
Rx Oucome:Drug /HLC HTN
Drug /HLC DM
Rx Oucome:
Full Address (Woreda, Kebele,House # and Phone #)
Home Address and Phone Number
Height (cm) BP2 RBS Or
HBA1C
HTNScreened for TB (√) Result
of TB diag-nosis
HTN DM BP2 RBS Or HBA1C HTN DM BP2 RBS Or
HBA1C HTN DM HTN DM HTN DM
DM On statin
TB screening result (P/N)
On statin On statin On statin On statin On statin
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38)
Count HTN HTN DM HTN DM HTN DM HTN DM HTN DM
DM
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Mental Neurological and Substance
Use Disorder Treatment Register
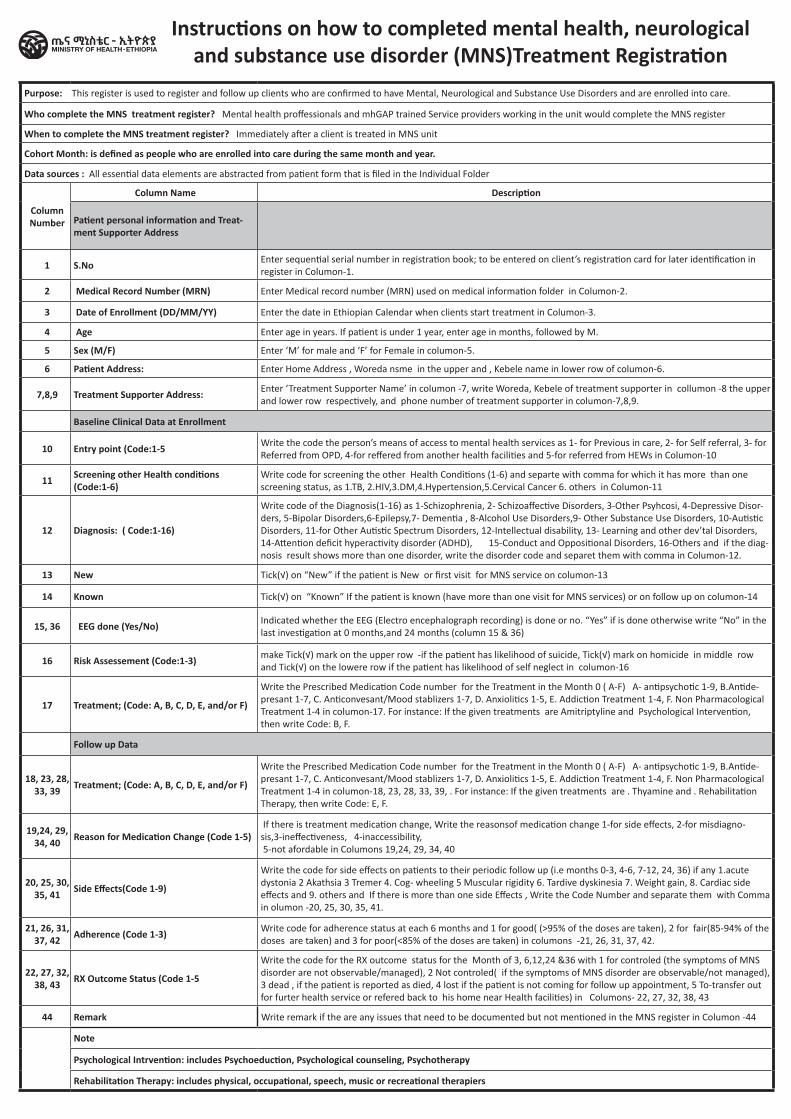
Purpose: This register is used to register and follow up clients who are confirmed to have Mental, Neurological and Substance Use Disorders and are enrolled into care.
Who complete the MNS treatment register? Mental health proffessionals and mhGAP trained Service providers working in the unit would complete the MNS register
When to complete the MNS treatment register? Immediately after a client is treated in MNS unit
Cohort Month: is defined as people who are enrolled into care during the same month and year.
Data sources : All essential data elements are abstracted from patient form that is filed in the Individual Folder
Column Number
Column Name Description
Patient personal information and Treat-ment Supporter Address
1 S.No Enter sequential serial number in registration book; to be entered on client’s registration card for later identification in register in Columon-1.
2 Medical Record Number (MRN) Enter Medical record number (MRN) used on medical information folder in Columon-2.
3 Date of Enrollment (DD/MM/YY) Enter the date in Ethiopian Calendar when clients start treatment in Columon-3.
4 Age Enter age in years. If patient is under 1 year, enter age in months, followed by M.
5 Sex (M/F) Enter ‘M’ for male and ‘F’ for Female in columon-5.
6 Patient Address: Enter Home Address , Woreda nsme in the upper and , Kebele name in lower row of columon-6.
7,8,9 Treatment Supporter Address: Enter ‘Treatment Supporter Name’ in columon -7, write Woreda, Kebele of treatment supporter in collumon -8 the upper and lower row respectively, and phone number of treatment supporter in columon-7,8,9.
Baseline Clinical Data at Enrollment
10 Entry point (Code:1-5 Write the code the person’s means of access to mental health services as 1- for Previous in care, 2- for Self referral, 3- for Referred from OPD, 4-for reffered from another health facilities and 5-for referred from HEWs in Columon-10
11 Screening other Health conditions (Code:1-6)
Write code for screening the other Health Conditions (1-6) and separte with comma for which it has more than one screening status, as 1.TB, 2.HIV,3.DM,4.Hypertension,5.Cervical Cancer 6. others in Columon-11
12 Diagnosis: ( Code:1-16)
Write code of the Diagnosis(1-16) as 1-Schizophrenia, 2- Schizoaffective Disorders, 3-Other Psyhcosi, 4-Depressive Disor-ders, 5-Bipolar Disorders,6-Epilepsy,7- Dementia , 8-Alcohol Use Disorders,9- Other Substance Use Disorders, 10-Autistic Disorders, 11-for Other Autistic Spectrum Disorders, 12-Intellectual disability, 13- Learning and other dev’tal Disorders, 14-Attention deficit hyperactivity disorder (ADHD), 15-Conduct and Oppositional Disorders, 16-Others and if the diag-nosis result shows more than one disorder, write the disorder code and separet them with comma in Columon-12.
13 New Tick(√) on “New” if the patient is New or first visit for MNS service on columon-13
14 Known Tick(√) on “Known” If the patient is known (have more than one visit for MNS services) or on follow up on columon-14
15, 36 EEG done (Yes/No) Indicated whether the EEG (Electro encephalograph recording) is done or no. “Yes” if is done otherwise write “No” in the last investigation at 0 months,and 24 months (column 15 & 36)
16 Risk Assessement (Code:1-3) make Tick(√) mark on the upper row -if the patient has likelihood of suicide, Tick(√) mark on homicide in middle row and Tick(√) on the lowere row if the patient has likelihood of self neglect in columon-16
17 Treatment; (Code: A, B, C, D, E, and/or F)
Write the Prescribed Medication Code number for the Treatment in the Month 0 ( A-F) A- antipsychotic 1-9, B.Antide-presant 1-7, C. Anticonvesant/Mood stablizers 1-7, D. Anxiolitics 1-5, E. Addiction Treatment 1-4, F. Non Pharmacological Treatment 1-4 in columon-17. For instance: If the given treatments are Amitriptyline and Psychological Intervention, then write Code: B, F.
Follow up Data
18, 23, 28, 33, 39 Treatment; (Code: A, B, C, D, E, and/or F)
Write the Prescribed Medication Code number for the Treatment in the Month 0 ( A-F) A- antipsychotic 1-9, B.Antide-presant 1-7, C. Anticonvesant/Mood stablizers 1-7, D. Anxiolitics 1-5, E. Addiction Treatment 1-4, F. Non Pharmacological Treatment 1-4 in columon-18, 23, 28, 33, 39, . For instance: If the given treatments are . Thyamine and . Rehabilitation Therapy, then write Code: E, F.
19,24, 29, 34, 40 Reason for Medication Change (Code 1-5)
If there is treatment medication change, Write the reasonsof medication change 1-for side effects, 2-for misdiagno-sis,3-ineffectiveness, 4-inaccessibility, 5-not afordable in Columons 19,24, 29, 34, 40
20, 25, 30, 35, 41 Side Effects(Code 1-9)
Write the code for side effects on patients to their periodic follow up (i.e months 0-3, 4-6, 7-12, 24, 36) if any 1.acute dystonia 2 Akathsia 3 Tremer 4. Cog- wheeling 5 Muscular rigidity 6. Tardive dyskinesia 7. Weight gain, 8. Cardiac side effects and 9. others and If there is more than one side Effects , Write the Code Number and separate them with Comma in olumon -20, 25, 30, 35, 41.
21, 26, 31, 37, 42 Adherence (Code 1-3) Write code for adherence status at each 6 months and 1 for good( (>95% of the doses are taken), 2 for fair(85-94% of the
doses are taken) and 3 for poor(<85% of the doses are taken) in columons -21, 26, 31, 37, 42.
22, 27, 32, 38, 43 RX Outcome Status (Code 1-5
Write the code for the RX outcome status for the Month of 3, 6,12,24 &36 with 1 for controled (the symptoms of MNS disorder are not observable/managed), 2 Not controled( if the symptoms of MNS disorder are observable/not managed), 3 dead , if the patient is reported as died, 4 lost if the patient is not coming for follow up appointment, 5 To-transfer out for furter health service or refered back to his home near Health facilities) in Columons- 22, 27, 32, 38, 43
44 Remark Write remark if the are any issues that need to be documented but not mentioned in the MNS register in Columon -44
Note
Psychological Intrvention: includes Psychoeduction, Psychological counseling, Psychotherapy
Rehabilitation Therapy: includes physical, occupational, speech, music or recreational therapiers
Instructions on how to completed mental health, neurological and substance use disorder (MNS)Treatment Registration
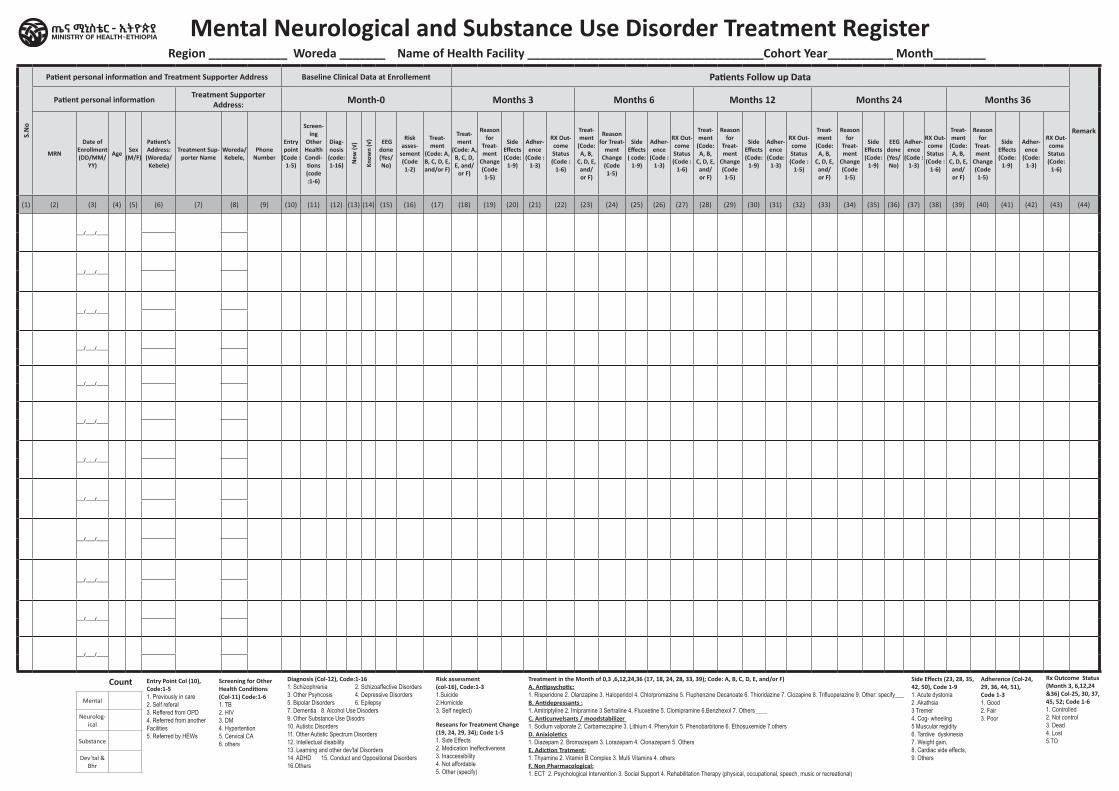
S.N
o
Patient personal information and Treatment Supporter Address Baseline Clinical Data at Enrollement Patients Follow up Data
Remark
Patient personal information Treatment Supporter Address: Month-0 Months 3 Months 6 Months 12 Months 24 Months 36
MRN
Date of Enrollment (DD/MM/
YY)
Age Sex (M/F)
Patient’s Address: (Woreda/ Kebele)
Treatment Sup-porter Name
Woreda/ Kebele,
Phone Number
Entry point
(Code : 1-5)
Screen-ing
Other Health Condi-tions (code :1-6)
Diag-nosis
(code: 1-16) N
ew (√
)
Know
n (√
) EEG done (Yes/No)
Risk asses-
sement (Code 1-2)
Treat-ment
(Code: A, B, C, D, E, and/or F)
Treat-ment
(Code: A, B, C, D, E, and/
or F)
Reason for
Treat-ment
Change (Code 1-5)
Side Effects (Code:
1-9)
Adher-ence
(Code : 1-3)
RX Out-come Status (Code :
1-6)
Treat-ment
(Code: A, B,
C, D, E, and/or F)
Reason for Treat-
ment Change (Code 1-5)
Side Effects ( code:
1-9)
Adher-ence
(Code : 1-3)
RX Out-come Status (Code :
1-6)
Treat-ment
(Code: A, B,
C, D, E, and/or F)
Reason for
Treat-ment
Change (Code 1-5)
Side Effects (Code:
1-9)
Adher-ence
(Code: 1-3)
RX Out-come Status (Code :
1-5)
Treat-ment
(Code: A, B,
C, D, E, and/or F)
Reason for
Treat-ment
Change (Code 1-5)
Side Effects (Code:
1-9)
EEG done (Yes/No)
Adher-ence
(Code : 1-3)
RX Out-come Status (Code :
1-6)
Treat-ment
(Code: A, B,
C, D, E, and/or F)
Reason for
Treat-ment
Change (Code 1-5)
Side Effects (Code:
1-9)
Adher-ence
(Code: 1-3)
RX Out-come Status (Code:
1-6)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44)
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
___/____/_____
Count
Mental
Neurolog-ical
Substance
Dev’tal & Bhr
Mental Neurological and Substance Use Disorder Treatment RegisterRegion ____________ Woreda _______ Name of Health Facility ____________________________________Cohort Year__________ Month________
Entry Point Col (10), Code:1-51. Previously in care2. Self referal 3. Reffered from OPD4. Referred from another Facilities5. Referred by HEWs
Screening for Other Health Conditions (Col-11) Code:1-61. TB 2. HIV3. DM 4. Hypertention 5. Cervical CA6. others
Diagnosis (Col-12), Code:1-161. Schizophrenia 2. Schizoaffective Disorders 3. Other Psyhcosis 4. Depressive Disorders 5. Bipolar Disorders 6. Epilepsy 7. Dementia 8. Alcohol Use Disoders 9. Other Substance Use Disodrs 10. Autistic Disorders 11. Other Autistic Spectrum Disorders 12. Intellectual disability 13. Learning and other dev'tal Disorders 14. ADHD 15. Conduct and Oppositional Disorders 16.Others
Risk assessment (col-16), Code:1-3 1.Suicide 2.Homicide3. Self neglect)
Reseans for Treatment Change (19, 24, 29, 34); Code 1-51. Side Effects 2. Medication Ineffectiveness3. Inaccessibility 4. Not affordable 5. Other (specify)
Treatment in the Month of 0,3 ,6,12,24,36 (17, 18, 24, 28, 33, 39); Code: A, B, C, D, E, and/or F)A. Antipsychotic: 1. Risperidone 2. Olanzapine 3. Haloperidol 4. Chlorpromazine 5. Fluphenzine Decanoate 6. Thioridazine 7. Clozapine 8. Trifluoperazine 9. Other: specify___ B. Antidepressants : 1. Amitriptyline 2. Imipramine 3 Sertraline 4. Fluoxetine 5. Clomipramine 6.Benzhexol 7. Others____ C. Anticunvelsants / moodstabilizer 1. Sodium valporate 2. Carbamezapine 3. Lithium 4. Phenytoin 5. Phenobarbitone 6. Ethosuxemide 7.others D. Anixioletics 1. Diazepam 2. Bromazepam 3. Lorazepam 4. Clonazepam 5. Others E. Adiction Tratment: 1. Thyamine 2. Vitamin B Complex 3. Multi Vitamins 4. others F. Non Pharmacological: 1. ECT 2. Psychological Intervention 3. Social Support 4. Rehabilitation Therapy (physical, occupational, speech, music or recreational)
Side Effects (23, 28, 35, 42, 50), Code 1-9 1. Acute dystonia 2 .Akathsia 3 Tremer 4. Cog- wheeling 5 Muscular regidity6. Tardive dyskinesia 7. Weight gain, 8. Cardiac side effects,9. Others
Adherence (Col-24, 29, 36, 44, 51), Code 1-31. Good 2. Fair 3. Poor
Rx Outcome Status (Month 3, 6,12,24 &36) Col-25, 30, 37, 45, 52; Code 1-6 1. Controlled 2. Not control 3. Dead 4. Lost 5.TO
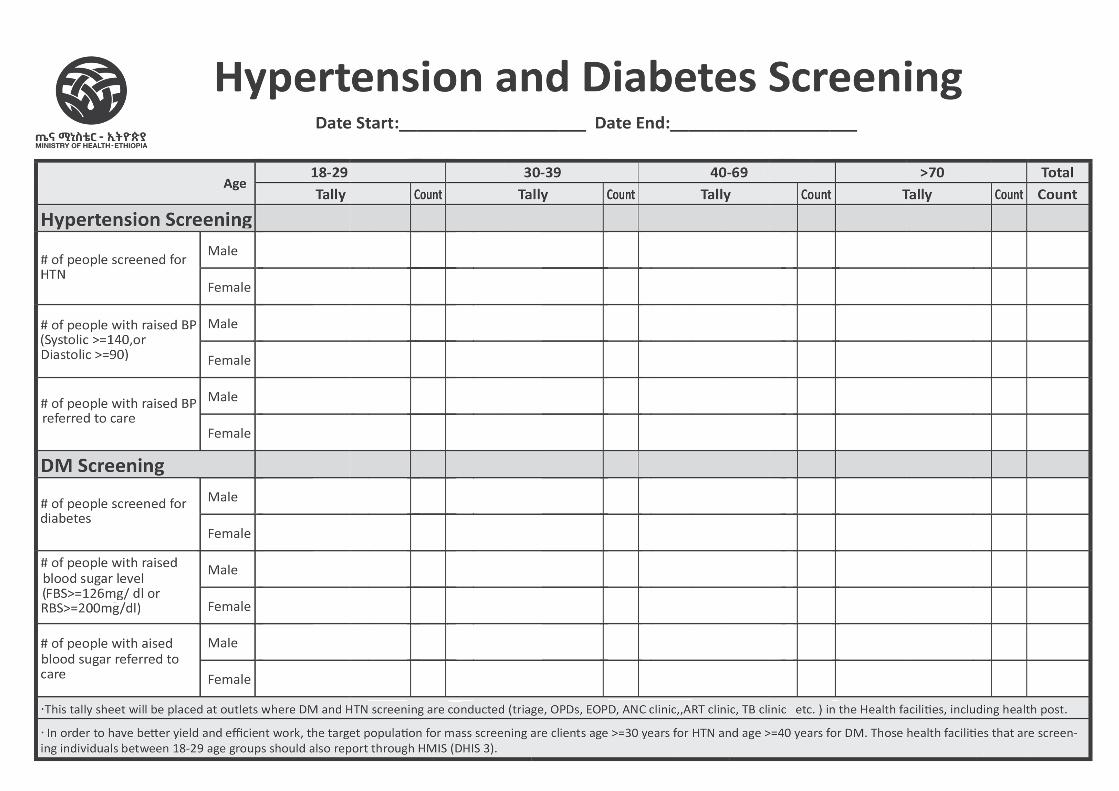
NTDContent / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Leishmanises Register
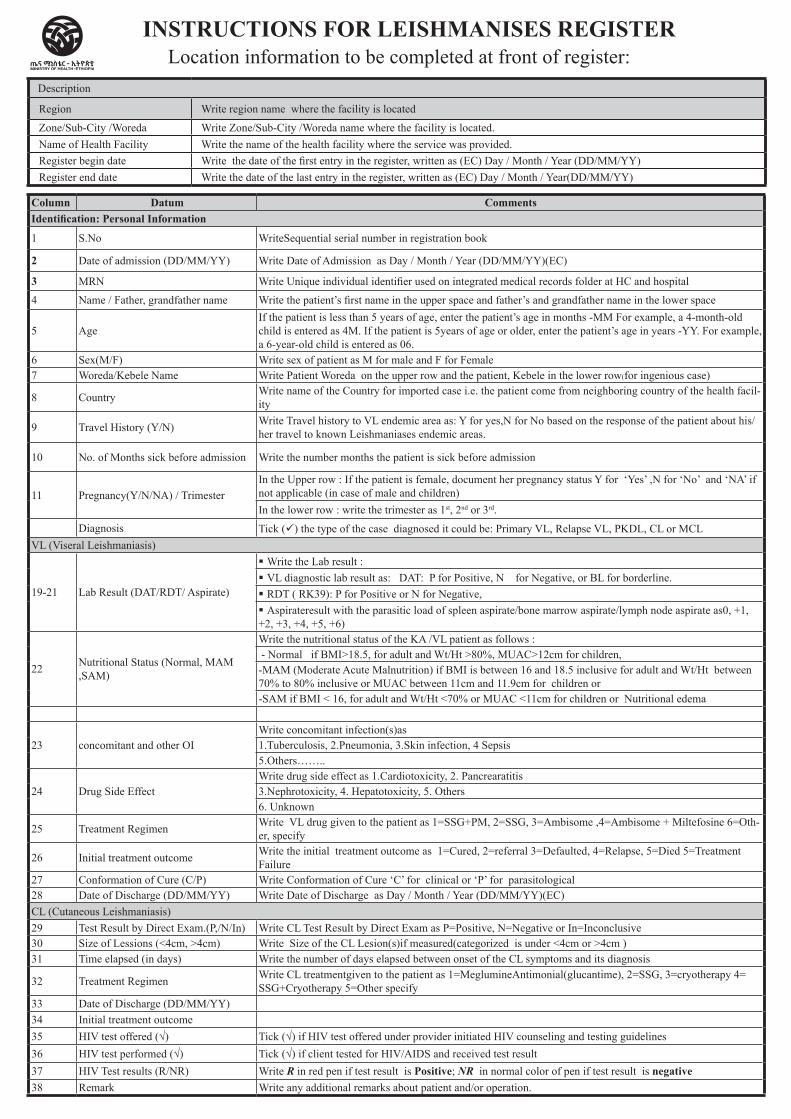
Column Datum CommentsIdentification: Personal Information
1 S.No WriteSequential serial number in registration book
2 Date of admission (DD/MM/YY) Write Date of Admission as Day / Month / Year (DD/MM/YY)(EC)
3 MRN Write Unique individual identifier used on integrated medical records folder at HC and hospital
4 Name / Father, grandfather name Write the patient’s first name in the upper space and father’s and grandfather name in the lower space
5 AgeIf the patient is less than 5 years of age, enter the patient’s age in months -MM For example, a 4-month-old child is entered as 4M. If the patient is 5years of age or older, enter the patient’s age in years -YY. For example, a 6-year-old child is entered as 06.
6 Sex(M/F) Write sex of patient as M for male and F for Female7 Woreda/Kebele Name Write Patient Woreda on the upper row and the patient, Kebele in the lower row(for ingenious case)
8 Country Write name of the Country for imported case i.e. the patient come from neighboring country of the health facil-ity
9 Travel History (Y/N) Write Travel history to VL endemic area as: Y for yes,N for No based on the response of the patient about his/her travel to known Leishmaniases endemic areas.
10 No. of Months sick before admission Write the number months the patient is sick before admission
11 Pregnancy(Y/N/NA) / TrimesterIn the Upper row : If the patient is female, document her pregnancy status Y for ‘Yes’ ,N for ‘No’ and ‘NA’ if not applicable (in case of male and children) In the lower row : write the trimester as 1st, 2nd or 3rd.
Diagnosis Tick (ü) the type of the case diagnosed it could be: Primary VL, Relapse VL, PKDL, CL or MCLVL (Viseral Leishmaniasis)
19-21 Lab Result (DAT/RDT/ Aspirate)
§ Write the Lab result : § VL diagnostic lab result as: DAT: P for Positive, N for Negative, or BL for borderline.§ RDT ( RK39): P for Positive or N for Negative, § Aspirateresult with the parasitic load of spleen aspirate/bone marrow aspirate/lymph node aspirate as0, +1, +2, +3, +4, +5, +6)
22 Nutritional Status (Normal, MAM ,SAM)
Write the nutritional status of the KA /VL patient as follows : - Normal if BMI>18.5, for adult and Wt/Ht >80%, MUAC>12cm for children, -MAM (Moderate Acute Malnutrition) if BMI is between 16 and 18.5 inclusive for adult and Wt/Ht between 70% to 80% inclusive or MUAC between 11cm and 11.9cm for children or -SAM if BMI < 16, for adult and Wt/Ht <70% or MUAC <11cm for children or Nutritional edema
23 concomitant and other OIWrite concomitant infection(s)as 1.Tuberculosis, 2.Pneumonia, 3.Skin infection, 4 Sepsis5.Others……..
24 Drug Side EffectWrite drug side effect as 1.Cardiotoxicity, 2. Pancrearatitis3.Nephrotoxicity, 4. Hepatotoxicity, 5. Others6. Unknown
25 Treatment Regimen Write VL drug given to the patient as 1=SSG+PM, 2=SSG, 3=Ambisome ,4=Ambisome + Miltefosine 6=Oth-er, specify
26 Initial treatment outcome Write the initial treatment outcome as 1=Cured, 2=referral 3=Defaulted, 4=Relapse, 5=Died 5=Treatment Failure
27 Conformation of Cure (C/P) Write Conformation of Cure ‘C’ for clinical or ‘P’ for parasitological28 Date of Discharge (DD/MM/YY) Write Date of Discharge as Day / Month / Year (DD/MM/YY)(EC)CL (Cutaneous Leishmaniasis)29 Test Result by Direct Exam.(P,/N/In) Write CL Test Result by Direct Exam as P=Positive, N=Negative or In=Inconclusive30 Size of Lessions (<4cm, >4cm) Write Size of the CL Lesion(s)if measured(categorized is under <4cm or >4cm )31 Time elapsed (in days) Write the number of days elapsed between onset of the CL symptoms and its diagnosis
32 Treatment Regimen Write CL treatmentgiven to the patient as 1=MeglumineAntimonial(glucantime), 2=SSG, 3=cryotherapy 4= SSG+Cryotherapy 5=Other specify
33 Date of Discharge (DD/MM/YY) 34 Initial treatment outcome35 HIV test offered (√) Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines36 HIV test performed (√) Tick (√) if client tested for HIV/AIDS and received test result37 HIV Test results (R/NR) Write R in red pen if test result is Positive; NR in normal color of pen if test result is negative38 Remark Write any additional remarks about patient and/or operation.
INSTRUCTIONS FOR LEISHMANISES REGISTERLocation information to be completed at front of register:
Description
Region Write region name where the facility is located
Zone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Name of Health Facility Write the name of the health facility where the service was provided.Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
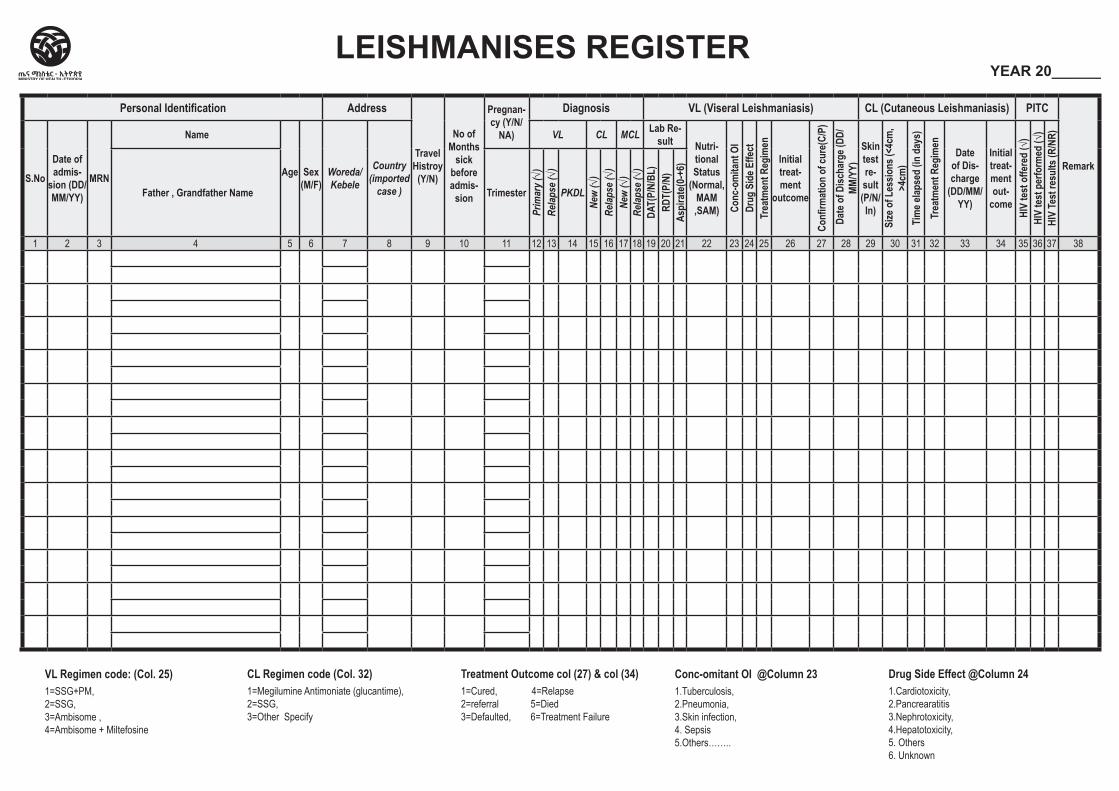
Personal Identification Address
Travel Histroy (Y/N)
No of Months
sick before admis-
sion
Pregnan-cy (Y/N/
NA)
Diagnosis VL (Viseral Leishmaniasis) CL (Cutaneous Leishmaniasis) PITC
RemarkS.No
Date of admis-
sion (DD/MM/YY)
MRN
Name
Age Sex (M/F)
Woreda/ Kebele
Country (imported
case )
VL CL MCL Lab Re-sult Nutri-
tional Status
(Normal, MAM ,SAM) Co
nc-o
mita
nt O
IDr
ug S
ide E
ffect
Trea
tmen
t Reg
imen
Initial treat-ment
outcome
Confi
rmat
ion
of cu
re(C
/P)
Dat
e of D
ischa
rge (
DD/
MM/Y
Y)
Skin test re-sult (P/N/In)
Size
of L
essio
ns (<
4cm
, >4
cm)
Tim
e elap
sed
(in d
ays)
Tr
eatm
ent R
egim
en
Date of Dis-charge
(DD/MM/YY)
Initial treat-ment out-
come
HIV
test
offe
red
(√)
HIV
test
per
form
ed (√
)HI
V Te
st re
sults
(R/N
R)
Father , Grandfather Name Trimester
Prim
ary (√)
Re
lapse
(√)
PKDL
New
(√)
Relap
se (√
)Ne
w (√
)Re
lapse
(√)
DAT(
P/N/
BL)
RDT(
P/N)
Aspi
rate
(0-+
6)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
LEISHMANISES REGISTER YEAR 20______
VL Regimen code: (Col. 25)1=SSG+PM, 2=SSG, 3=Ambisome ,4=Ambisome + Miltefosine
CL Regimen code (Col. 32)1=Megilumine Antimoniate (glucantime), 2=SSG, 3=Other Specify
Treatment Outcome col (27) & col (34)1=Cured, 4=Relapse2=referral 5=Died 3=Defaulted, 6=Treatment Failure
Conc-omitant OI @Column 23 1.Tuberculosis,2.Pneumonia,3.Skin infection,4. Sepsis5.Others……..
Drug Side Effect @Column 24 1.Cardiotoxicity,2.Pancrearatitis3.Nephrotoxicity,4.Hepatotoxicity,5. Others6. Unknown
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Hospital Trachomatous Trichiasis (TT)
Surgery Register
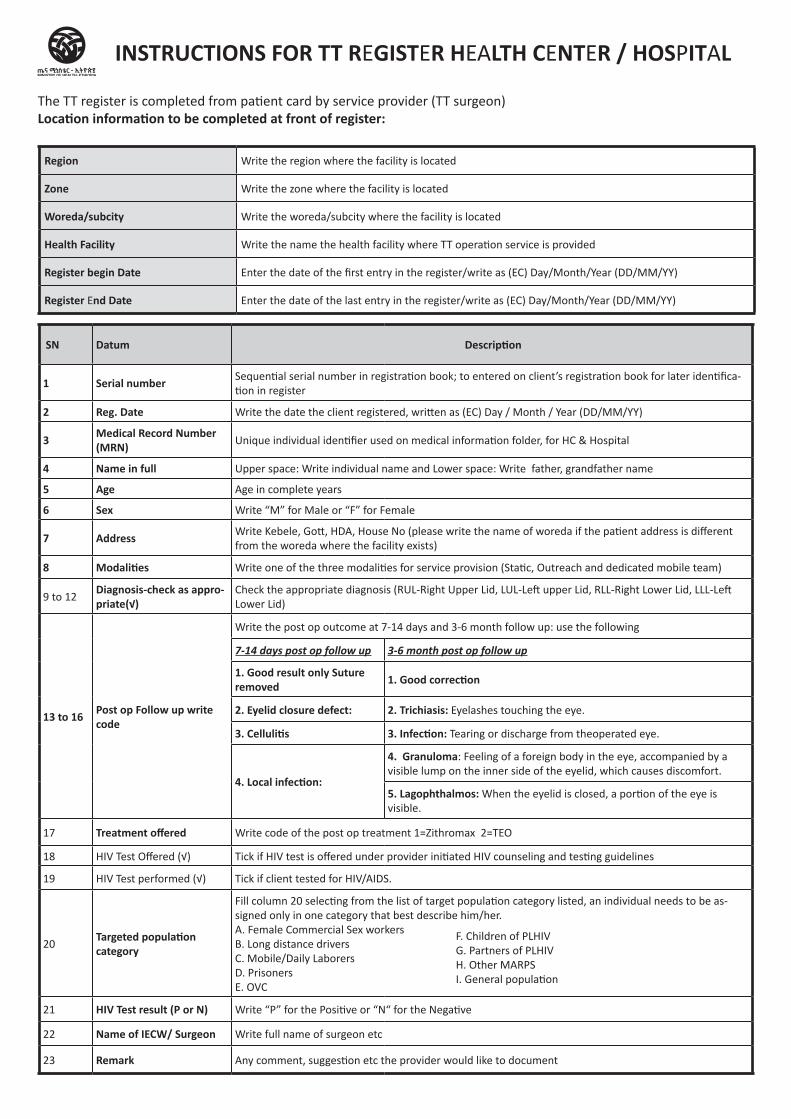
SN Datum Description
1 Serial number Sequential serial number in registration book; to entered on client’s registration book for later identifica-tion in register
2 Reg. Date Write the date the client registered, written as (EC) Day / Month / Year (DD/MM/YY)
3 Medical Record Number (MRN) Unique individual identifier used on medical information folder, for HC & Hospital
4 Name in full Upper space: Write individual name and Lower space: Write father, grandfather name
5 Age Age in complete years
6 Sex Write “M” for Male or “F” for Female
7 Address Write Kebele, Gott, HDA, House No (please write the name of woreda if the patient address is different from the woreda where the facility exists)
8 Modalities Write one of the three modalities for service provision (Static, Outreach and dedicated mobile team)
9 to 12Diagnosis-check as appro-priate(√)
Check the appropriate diagnosis (RUL-Right Upper Lid, LUL-Left upper Lid, RLL-Right Lower Lid, LLL-Left Lower Lid)
13 to 16 Post op Follow up write code
Write the post op outcome at 7-14 days and 3-6 month follow up: use the following
7-14 days post op follow up 3-6 month post op follow up
1. Good result only Suture removed 1. Good correction
2. Eyelid closure defect: 2. Trichiasis: Eyelashes touching the eye.
3. Cellulitis 3. Infection: Tearing or discharge from theoperated eye.
4. Local infection:
4. Granuloma: Feeling of a foreign body in the eye, accompanied by a visible lump on the inner side of the eyelid, which causes discomfort.
5. Lagophthalmos: When the eyelid is closed, a portion of the eye is visible.
17 Treatment offered Write code of the post op treatment 1=Zithromax 2=TEO
18 HIV Test Offered (√) Tick if HIV test is offered under provider initiated HIV counseling and testing guidelines
19 HIV Test performed (√) Tick if client tested for HIV/AIDS.
20Targeted population category
Fill column 20 selecting from the list of target population category listed, an individual needs to be as-signed only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance drivers C. Mobile/Daily LaborersD. Prisoners E. OVC
21 HIV Test result (P or N) Write “P” for the Positive or “N“ for the Negative
22 Name of IECW/ Surgeon Write full name of surgeon etc
23 Remark Any comment, suggestion etc the provider would like to document
INSTRUCTIONS FOR TT REGISTER HEALTH CENTER / HOSPITAL
The TT register is completed from patient card by service provider (TT surgeon)Location information to be completed at front of register:
Region Write the region where the facility is located
Zone Write the zone where the facility is located
Woreda/subcity Write the woreda/subcity where the facility is located
Health Facility Write the name the health facility where TT operation service is provided
Register begin Date Enter the date of the first entry in the register/write as (EC) Day/Month/Year (DD/MM/YY)
Register End Date Enter the date of the last entry in the register/write as (EC) Day/Month/Year (DD/MM/YY)
F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
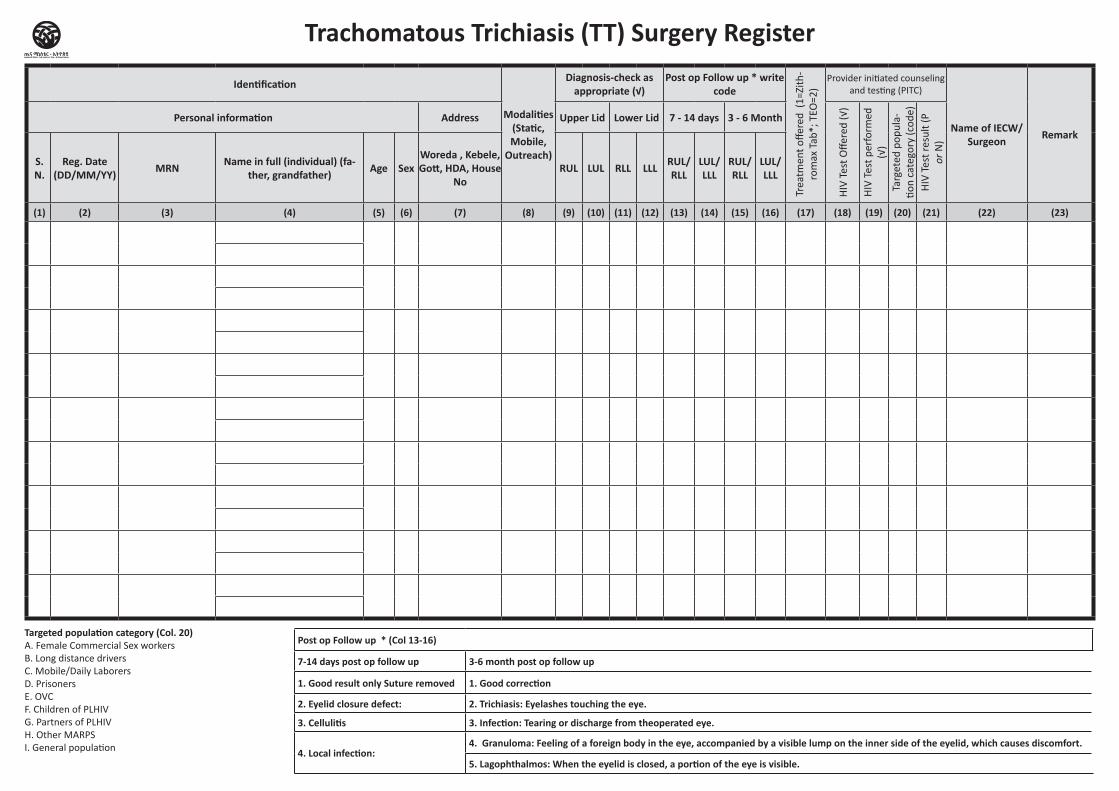
Identification
Modalities (Static, Mobile,
Outreach)
Diagnosis-check as appropriate (√)
Post op Follow up * write code
Trea
tmen
t offe
red
(1=Z
ith-
rom
ax T
ab*;
TEO
=2)
Provider initiated counseling and testing (PITC)
Name of IECW/ Surgeon Remark
Personal information Address Upper Lid Lower Lid 7 - 14 days 3 - 6 Month
HIV
Tes
t Offe
red
(√)
HIV
Tes
t per
form
ed
(√)
Targ
eted
pop
ula-
tion
cate
gory
(cod
e)H
IV T
est r
esul
t (P
or N
)
S. N.
Reg. Date (DD/MM/YY) MRN Name in full (individual) (fa-
ther, grandfather) Age SexWoreda , Kebele, Gott, HDA, House
NoRUL LUL RLL LLL RUL/
RLLLUL/LLL
RUL/RLL
LUL/LLL
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23)
Post op Follow up * (Col 13-16)
7-14 days post op follow up 3-6 month post op follow up
1. Good result only Suture removed 1. Good correction
2. Eyelid closure defect: 2. Trichiasis: Eyelashes touching the eye.
3. Cellulitis 3. Infection: Tearing or discharge from theoperated eye.
4. Local infection:4. Granuloma: Feeling of a foreign body in the eye, accompanied by a visible lump on the inner side of the eyelid, which causes discomfort.
5. Lagophthalmos: When the eyelid is closed, a portion of the eye is visible.
Targeted population category (Col. 20)A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPSI. General population
Trachomatous Trichiasis (TT) Surgery Register
RMNCH Registers and Tally sheets
Content / Home
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Family Planning Register
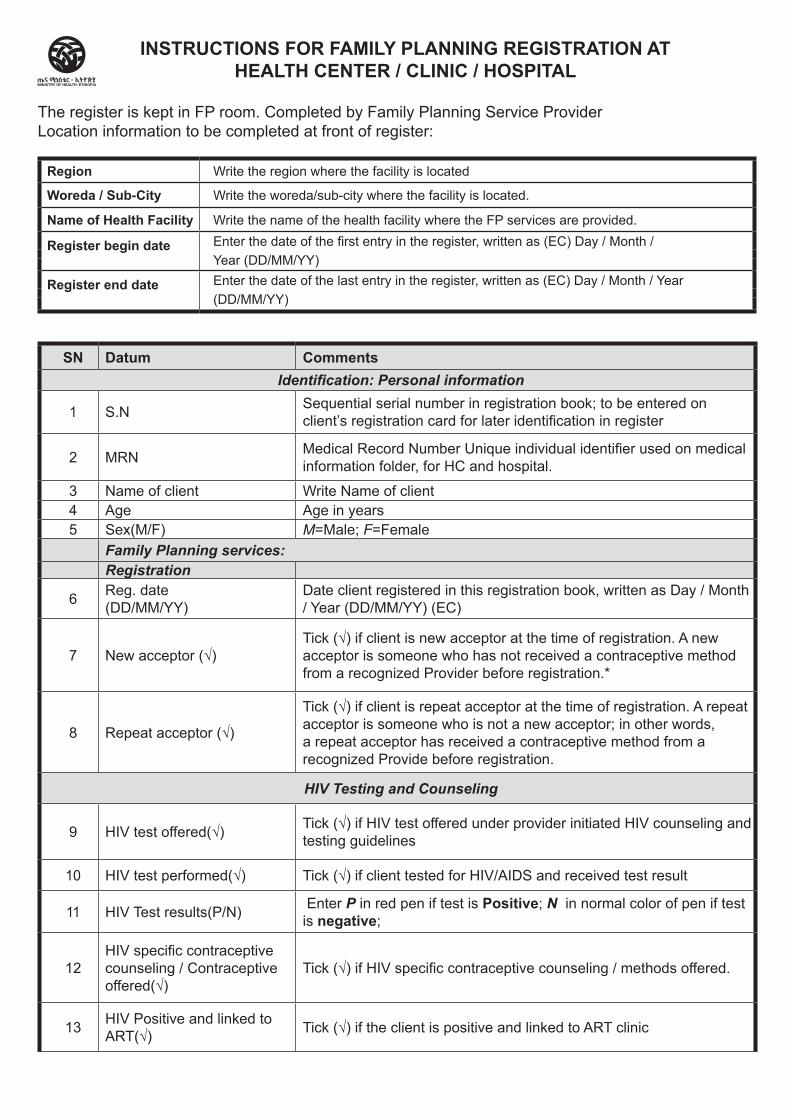
SN Datum CommentsIdentification: Personal information
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in register
2 MRN Medical Record Number Unique individual identifier used on medical information folder, for HC and hospital.
3 Name of client Write Name of client4 Age Age in years5 Sex(M/F) M=Male; F=Female
Family Planning services:Registration
6 Reg. date(DD/MM/YY)
Date client registered in this registration book, written as Day / Month / Year (DD/MM/YY) (EC)
7 New acceptor (√)Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.*
8 Repeat acceptor (√)
Tick (√) if client is repeat acceptor at the time of registration. A repeat acceptor is someone who is not a new acceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
HIV Testing and Counseling
9 HIV test offered(√) Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines
10 HIV test performed(√) Tick (√) if client tested for HIV/AIDS and received test result
11 HIV Test results(P/N) Enter P in red pen if test is Positive; N in normal color of pen if test is negative;
12HIV specific contraceptive counseling / Contraceptive offered(√)
Tick (√) if HIV specific contraceptive counseling / methods offered.
13 HIV Positive and linked to ART(√) Tick (√) if the client is positive and linked to ART clinic
The register is kept in FP room. Completed by Family Planning Service ProviderLocation information to be completed at front of register:
Region Write the region where the facility is located
Woreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility where the FP services are provided.
Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month /Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
INSTRUCTIONS FOR FAMILY PLANNING REGISTRATION ATHEALTH CENTER / CLINIC / HOSPITAL
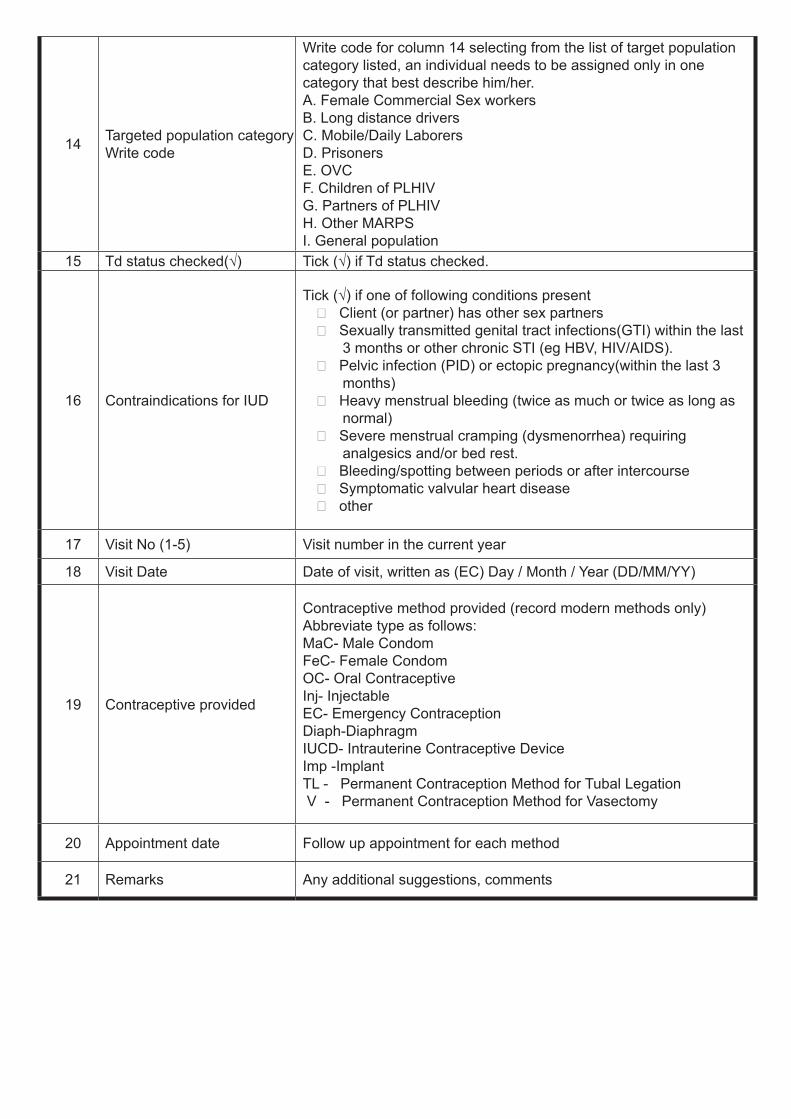
14 Targeted population category Write code
Write code for column 14 selecting from the list of target population category listed, an individual needs to be assigned only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPSI. General population
15 Td status checked(√) Tick (√) if Td status checked.
16 Contraindications for IUD
Tick (√) if one of following conditions present Client (or partner) has other sex partners Sexually transmitted genital tract infections(GTI) within the last
3 months or other chronic STI (eg HBV, HIV/AIDS). Pelvic infection (PID) or ectopic pregnancy(within the last 3
months) Heavy menstrual bleeding (twice as much or twice as long as
normal) Severe menstrual cramping (dysmenorrhea) requiring
analgesics and/or bed rest. Bleeding/spotting between periods or after intercourse Symptomatic valvular heart disease other
17 Visit No (1-5) Visit number in the current year
18 Visit Date Date of visit, written as (EC) Day / Month / Year (DD/MM/YY)
19 Contraceptive provided
Contraceptive method provided (record modern methods only) Abbreviate type as follows:MaC- Male CondomFeC- Female CondomOC- Oral ContraceptiveInj- InjectableEC- Emergency ContraceptionDiaph-DiaphragmIUCD- Intrauterine Contraceptive DeviceImp -Implant TL - Permanent Contraception Method for Tubal Legation V - Permanent Contraception Method for Vasectomy
20 Appointment date Follow up appointment for each method
21 Remarks Any additional suggestions, comments
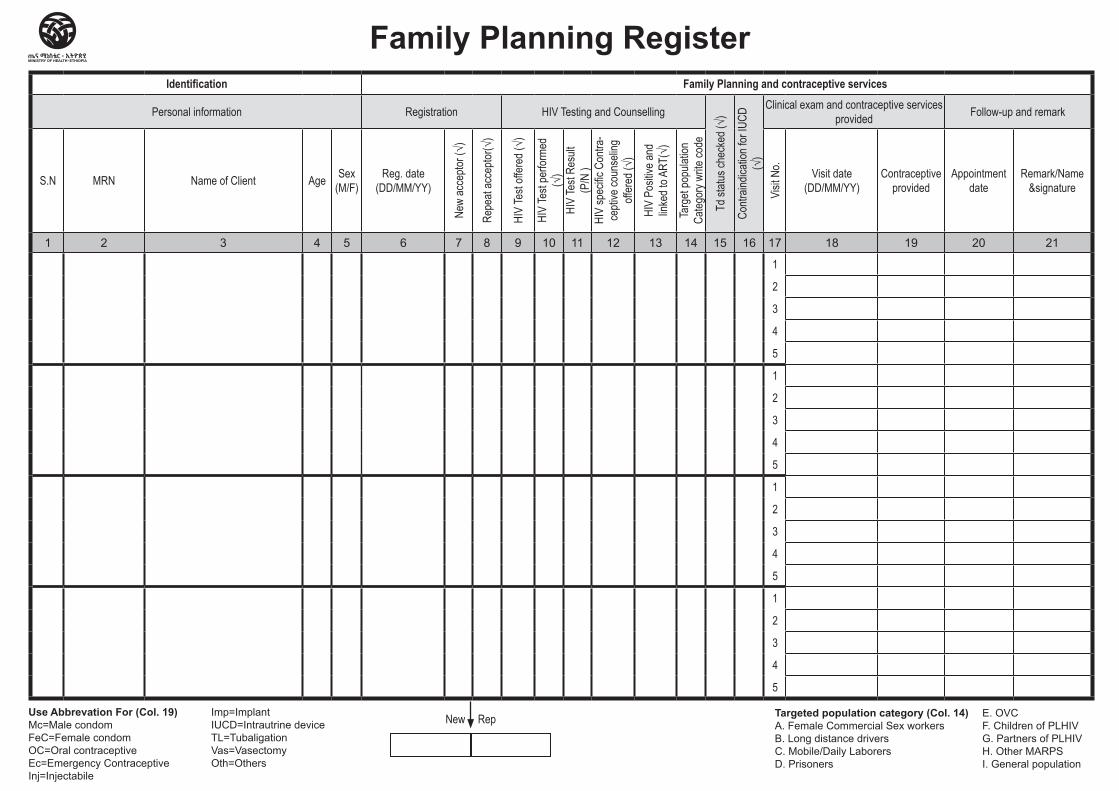
Identification Family Planning and contraceptive services
Personal information Registration HIV Testing and Counselling
Td st
atus c
heck
ed (√
)
Contr
aindic
ation
for I
UCD
(√)
Clinical exam and contraceptive services provided Follow-up and remark
S.N MRN Name of Client Age Sex (M/F)
Reg. date (DD/MM/YY)
New
acce
ptor (
√)
Repe
at ac
cepto
r(√)
HIV
Test
offer
ed (√
)
HIV
Test
perfo
rmed
(√
)HI
V Te
st Re
sult
(P/N
)HI
V sp
ecific
Con
tra-
cepti
ve co
unse
ling
offer
ed (√
)
HIV
Posit
ive an
d lin
ked t
o ART
(√)
Targ
et po
pulat
ion
Categ
ory w
rite co
de
Visit
No. Visit date
(DD/MM/YY)Contraceptive
providedAppointment
dateRemark/Name
&signature
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
New Rep
Family Planning Register
Use Abbrevation For (Col. 19) Mc=Male condom FeC=Female condom OC=Oral contraceptive Ec=Emergency Contraceptive Inj=Injectabile
Imp=Implant IUCD=Intrautrine device TL=Tubaligation Vas=Vasectomy Oth=Others
Targeted population category (Col. 14) A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. Prisoners
E. OVC F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Long Acting Family Planning Removal
Register
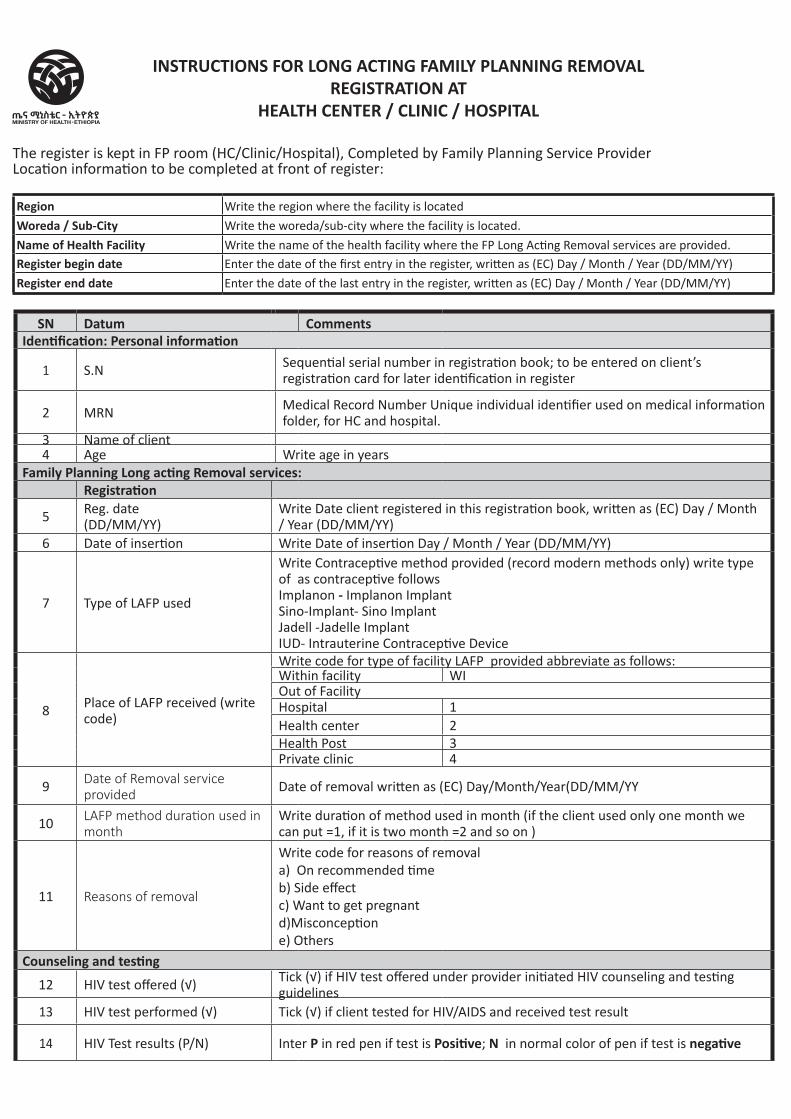
SN Datum CommentsIdentification: Personal information
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in register
2 MRN Medical Record Number Unique individual identifier used on medical information folder, for HC and hospital.
3 Name of client4 Age Write age in years
Family Planning Long acting Removal services:Registration
5 Reg. date(DD/MM/YY)
Write Date client registered in this registration book, written as (EC) Day / Month / Year (DD/MM/YY)
6 Date of insertion Write Date of insertion Day / Month / Year (DD/MM/YY)
7 Type of LAFP used
Write Contraceptive method provided (record modern methods only) write type of as contraceptive followsImplanon - Implanon ImplantSino-Implant- Sino ImplantJadell -Jadelle ImplantIUD- Intrauterine Contraceptive Device
8 Place of LAFP received (write code)
Write code for type of facility LAFP provided abbreviate as follows:Within facility WIOut of FacilityHospital 1Health center 2Health Post 3Private clinic 4
9 Date of Removal service provided Date of removal written as (EC) Day/Month/Year(DD/MM/YY
10 LAFP method duration used in month
Write duration of method used in month (if the client used only one month we can put =1, if it is two month =2 and so on )
11 Reasons of removal
Write code for reasons of removal a) On recommended timeb) Side effectc) Want to get pregnantd)Misconceptione) Others
Counseling and testing
12 HIV test offered (√) Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines
13 HIV test performed (√) Tick (√) if client tested for HIV/AIDS and received test result
14 HIV Test results (P/N) Inter P in red pen if test is Positive; N in normal color of pen if test is negative
INSTRUCTIONS FOR LONG ACTING FAMILY PLANNING REMOVAL REGISTRATION AT
HEALTH CENTER / CLINIC / HOSPITAL
The register is kept in FP room (HC/Clinic/Hospital), Completed by Family Planning Service ProviderLocation information to be completed at front of register:
Region Write the region where the facility is located
Woreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility where the FP Long Acting Removal services are provided.Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
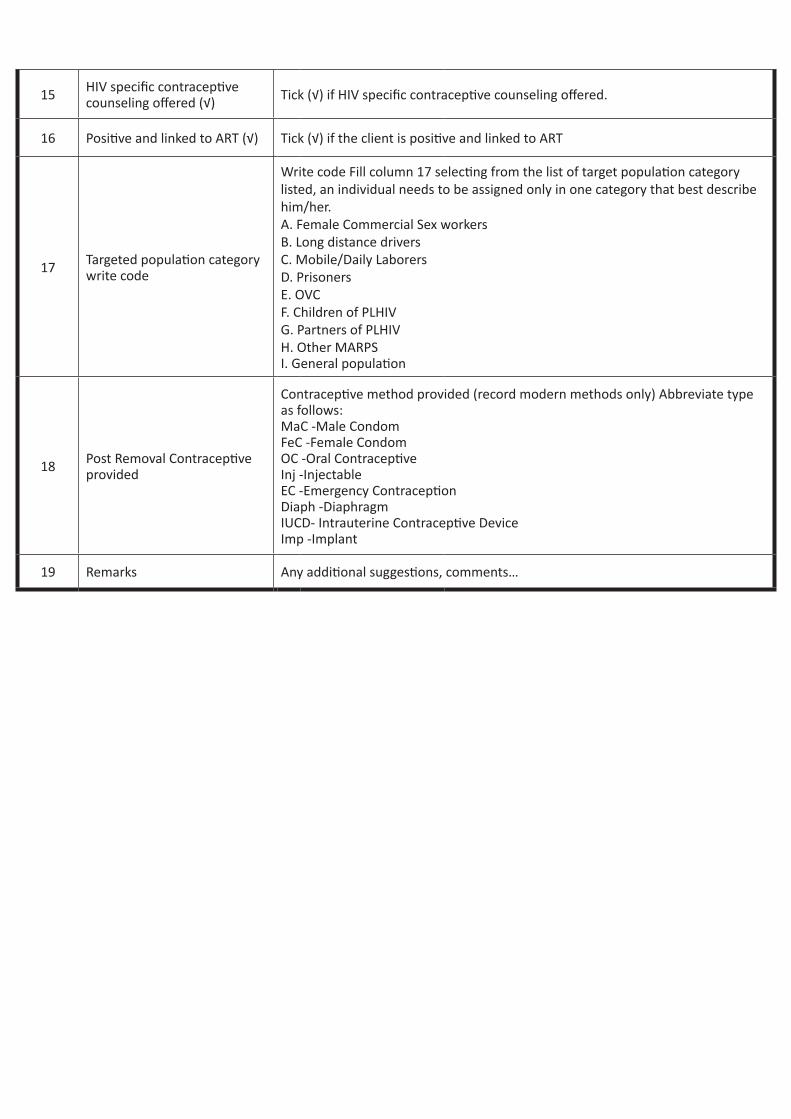
15 HIV specific contraceptive counseling offered (√) Tick (√) if HIV specific contraceptive counseling offered.
16 Positive and linked to ART (√) Tick (√) if the client is positive and linked to ART
17 Targeted population category write code
Write code Fill column 17 selecting from the list of target population category listed, an individual needs to be assigned only in one category that best describe him/her. A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPSI. General population
18 Post Removal Contraceptive provided
Contraceptive method provided (record modern methods only) Abbreviate type as follows:MaC -Male CondomFeC -Female CondomOC -Oral ContraceptiveInj -InjectableEC -Emergency ContraceptionDiaph -DiaphragmIUCD- Intrauterine Contraceptive DeviceImp -Implant
19 Remarks Any additional suggestions, comments…
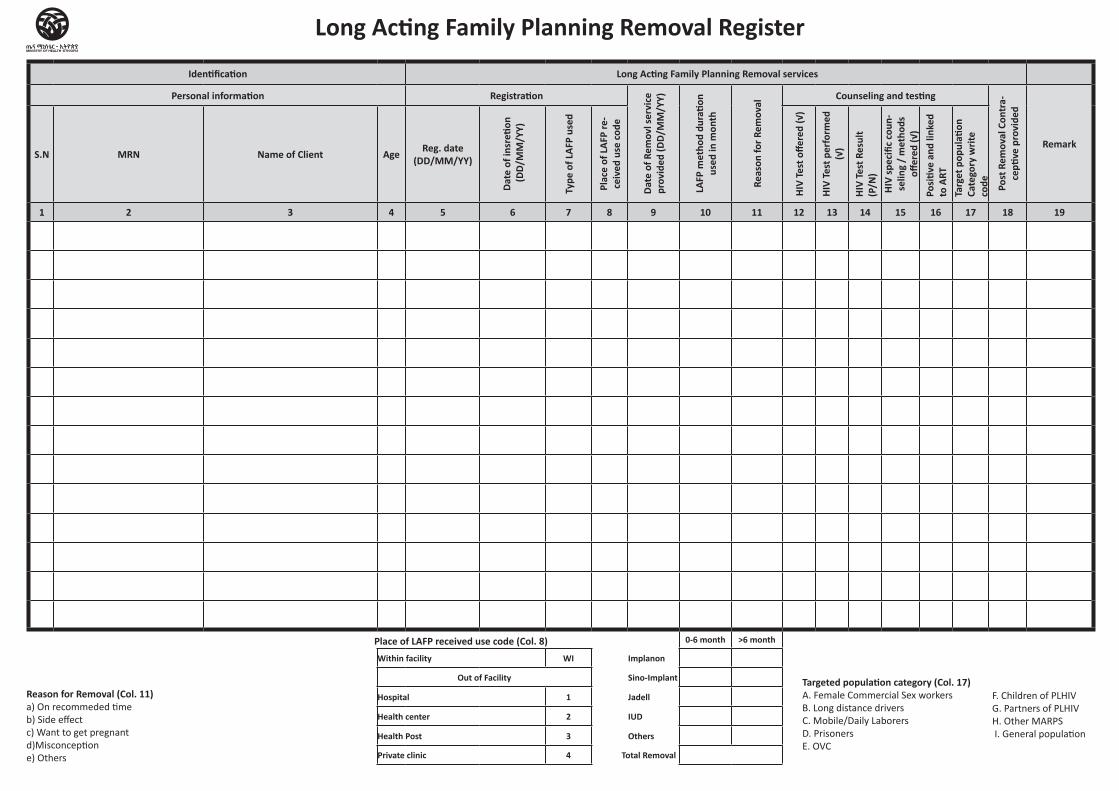
Identification Long Acting Family Planning Removal services
Personal information Registration
Date
of R
emov
l ser
vice
pr
ovid
ed (D
D/M
M/Y
Y)
LAFP
met
hod
dura
tion
used
in m
onth
Reas
on fo
r Rem
oval
Counseling and testing
Post
Rem
oval
Con
tra-
cepti
ve p
rovi
ded
RemarkS.N MRN Name of Client Age Reg. date
(DD/MM/YY)
Date
of i
nsre
tion
(DD/
MM
/YY)
Type
of L
AFP
used
Plac
e of
LAF
P re
-ce
ived
use
cod
e
HIV
Test
offe
red
(√)
HIV
Test
per
form
ed
(√)
HIV
Test
Res
ult
(P/N
)HI
V sp
ecifi
c co
un-
selin
g /
met
hods
off
ered
(√)
Posi
tive
and
linke
d to
ART
Targ
et p
opul
ation
Ca
tego
ry w
rite
code
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
0-6 month >6 month
Within facility WI Implanon
Out of Facility Sino-Implant
Hospital 1 Jadell
Health center 2 IUD
Health Post 3 Others
Private clinic 4 Total Removal
Long Acting Family Planning Removal Register
Reason for Removal (Col. 11)a) On recommeded time b) Side effect c) Want to get pregnant d)Misconception e) Others
F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
Targeted population category (Col. 17)A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVC
Place of LAFP received use code (Col. 8)
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Antenatal Care Register
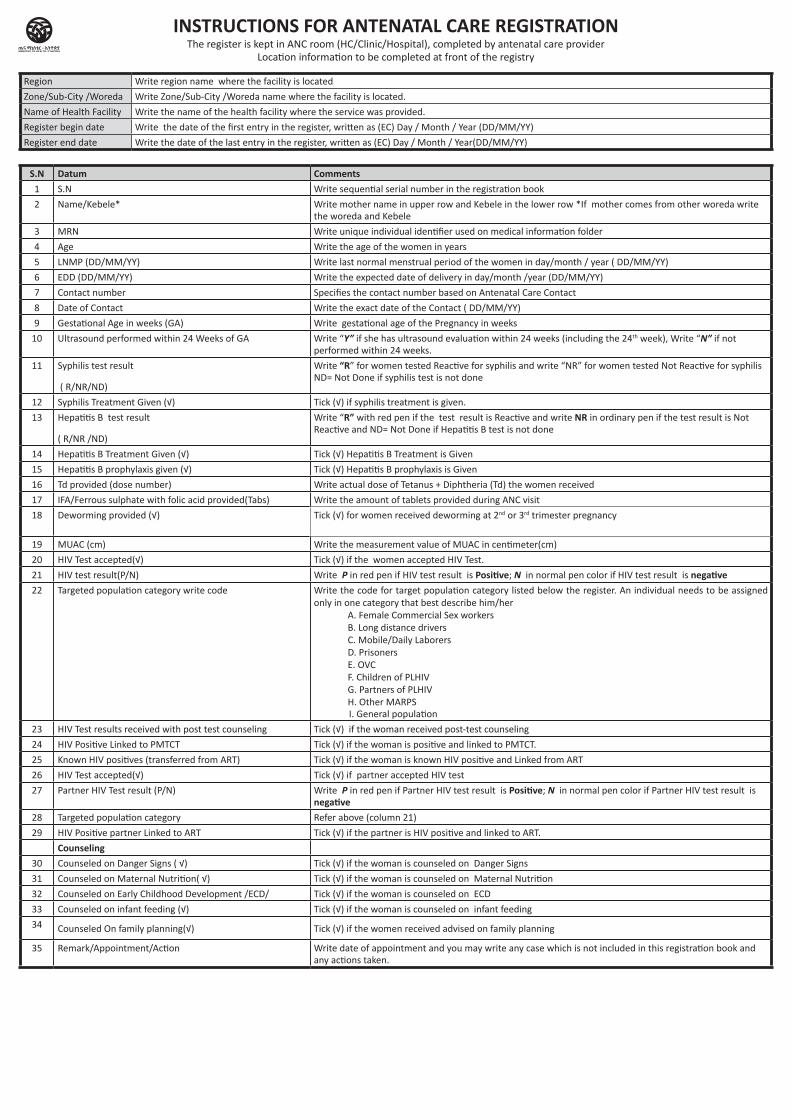
Region Write region name where the facility is located
Zone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Name of Health Facility Write the name of the health facility where the service was provided.
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
S.N Datum Comments 1 S.N Write sequential serial number in the registration book
2 Name/Kebele* Write mother name in upper row and Kebele in the lower row *If mother comes from other woreda write the woreda and Kebele
3 MRN Write unique individual identifier used on medical information folder
4 Age Write the age of the women in years
5 LNMP (DD/MM/YY) Write last normal menstrual period of the women in day/month / year ( DD/MM/YY)
6 EDD (DD/MM/YY) Write the expected date of delivery in day/month /year (DD/MM/YY)
7 Contact number Specifies the contact number based on Antenatal Care Contact
8 Date of Contact Write the exact date of the Contact ( DD/MM/YY)
9 Gestational Age in weeks (GA) Write gestational age of the Pregnancy in weeks
10 Ultrasound performed within 24 Weeks of GA Write “Y” if she has ultrasound evaluation within 24 weeks (including the 24th week), Write “N” if not performed within 24 weeks.
11 Syphilis test result
( R/NR/ND)
Write “R” for women tested Reactive for syphilis and write “NR” for women tested Not Reactive for syphilis ND= Not Done if syphilis test is not done
12 Syphilis Treatment Given (√) Tick (√) if syphilis treatment is given.
13 Hepatitis B test result
( R/NR /ND)
Write “R” with red pen if the test result is Reactive and write NR in ordinary pen if the test result is Not Reactive and ND= Not Done if Hepatitis B test is not done
14 Hepatitis B Treatment Given (√) Tick (√) Hepatitis B Treatment is Given
15 Hepatitis B prophylaxis given (√) Tick (√) Hepatitis B prophylaxis is Given
16 Td provided (dose number) Write actual dose of Tetanus + Diphtheria (Td) the women received
17 IFA/Ferrous sulphate with folic acid provided(Tabs) Write the amount of tablets provided during ANC visit
18 Deworming provided (√) Tick (√) for women received deworming at 2nd or 3rd trimester pregnancy
19 MUAC (cm) Write the measurement value of MUAC in centimeter(cm)
20 HIV Test accepted(√) Tick (√) if the women accepted HIV Test.
21 HIV test result(P/N) Write P in red pen if HIV test result is Positive; N in normal pen color if HIV test result is negative22 Targeted population category write code Write the code for target population category listed below the register. An individual needs to be assigned
only in one category that best describe him/her A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
I. General population
23 HIV Test results received with post test counseling Tick (√) if the woman received post-test counseling
24 HIV Positive Linked to PMTCT Tick (√) if the woman is positive and linked to PMTCT.
25 Known HIV positives (transferred from ART) Tick (√) if the woman is known HIV positive and Linked from ART
26 HIV Test accepted(√) Tick (√) if partner accepted HIV test
27 Partner HIV Test result (P/N) Write P in red pen if Partner HIV test result is Positive; N in normal pen color if Partner HIV test result is negative
28 Targeted population category Refer above (column 21)
29 HIV Positive partner Linked to ART Tick (√) if the partner is HIV positive and linked to ART.
Counseling30 Counseled on Danger Signs ( √) Tick (√) if the woman is counseled on Danger Signs
31 Counseled on Maternal Nutrition( √) Tick (√) if the woman is counseled on Maternal Nutrition
32 Counseled on Early Childhood Development /ECD/ Tick (√) if the woman is counseled on ECD
33 Counseled on infant feeding (√) Tick (√) if the woman is counseled on infant feeding
34 Counseled On family planning(√) Tick (√) if the women received advised on family planning
35 Remark/Appointment/Action Write date of appointment and you may write any case which is not included in this registration book and any actions taken.
INSTRUCTIONS FOR ANTENATAL CARE REGISTRATIONThe register is kept in ANC room (HC/Clinic/Hospital), completed by antenatal care provider
Location information to be completed at front of the registry
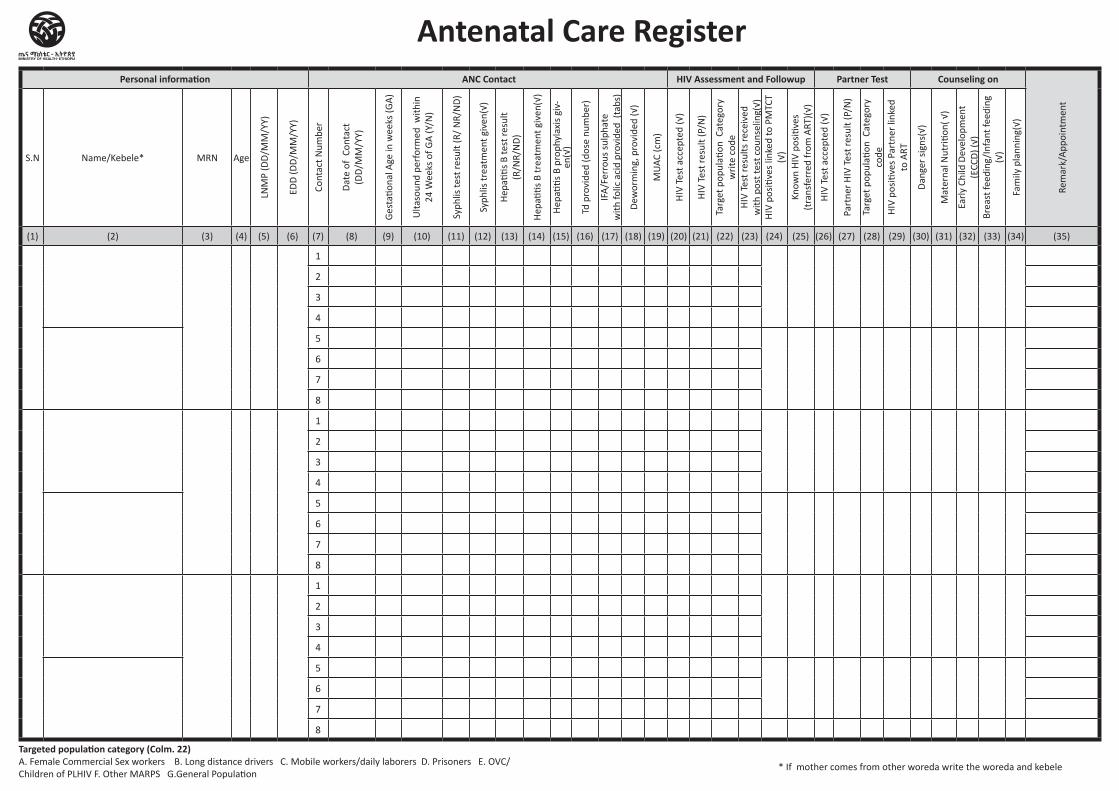
Personal information ANC Contact HIV Assessment and Followup Partner Test Counseling on
Rem
ark/
App
oint
men
t
S.N Name/Kebele* MRN Age
LNM
P (D
D/M
M/Y
Y)
EDD
(DD
/MM
/YY)
Cont
act N
umbe
r
Dat
e of
Con
tact
(D
D/M
M/Y
Y)
Ges
tatio
nal A
ge in
wee
ks (G
A)
Ulta
soun
d pe
rfor
med
with
in
24 W
eeks
of G
A (Y
/N)
Syph
lis te
st re
sult
(R/
NR/
ND
)
Syph
lis tr
eatm
ent g
iven
(√)
Hep
atitis
B te
st re
sult
(R
/NR/
ND
)
Hep
atitis
B tr
eatm
ent g
iven
(√)
Hep
atitis
B p
roph
ylax
is g
iv-
en(√
)
Td p
rovi
ded
(dos
e nu
mbe
r)
IFA
/Fer
rous
sul
phat
e
with
folic
aci
d pr
ovid
ed (
tabs
)
Dew
orm
ing,
pro
vide
d (√
)
MU
AC (c
m)
HIV
Tes
t acc
epte
d (√
)
HIV
Tes
t res
ult (
P/N
)
Targ
et p
opul
ation
Cat
egor
y w
rite
cod
e H
IV T
est r
esul
ts re
ceiv
ed
with
pos
t tes
t cou
nsel
ing(
√)H
IV p
ositi
ves
linke
d to
PM
TCT
(√)
Know
n H
IV p
ositi
ves
(t
rans
ferr
ed fr
om A
RT)(
√)
HIV
Tes
t acc
epte
d (√
)
Part
ner
HIV
Tes
t res
ult (
P/N
)
Targ
et p
opul
ation
Cat
egor
y co
de
HIV
pos
itive
s Pa
rtne
r lin
ked
to A
RT
Dan
ger
sign
s(√)
Mat
erna
l Nut
ritio
n( √
)
Earl
y Ch
ild D
evel
opm
ent
(ECC
D) (
√)Br
east
feed
ing/
Infa
nt fe
edin
g
(√)
Fam
ily p
lann
ing(
√)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35)
1
2
3
4
5
6
7
8
1
2
3
4
5
6
7
8
1
2
3
4
5
6
7
8
* If mother comes from other woreda write the woreda and kebele
Targeted population category (Colm. 22) A. Female Commercial Sex workers B. Long distance drivers C. Mobile workers/daily laborers D. Prisoners E. OVC/Children of PLHIV F. Other MARPS G.General Population
Antenatal Care Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Delivery Register
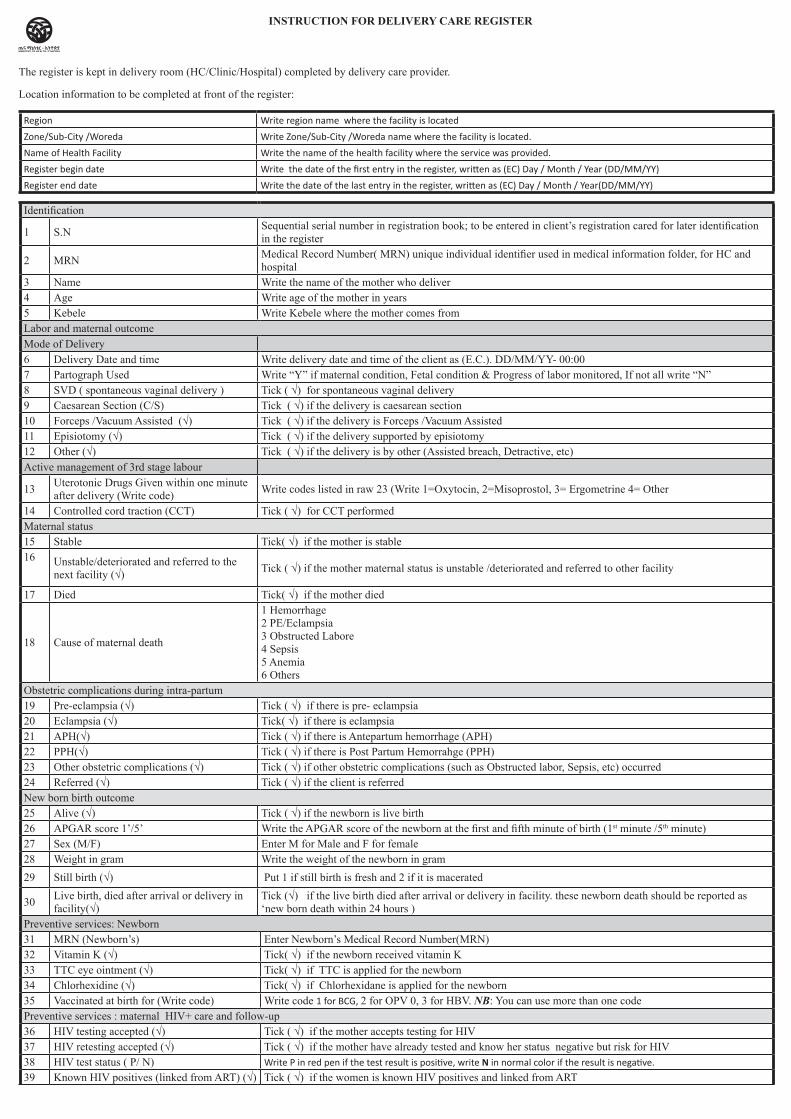
Identification
1 S.N Sequential serial number in registration book; to be entered in client’s registration cared for later identification in the register
2 MRN Medical Record Number( MRN) unique individual identifier used in medical information folder, for HC and hospital
3 Name Write the name of the mother who deliver4 Age Write age of the mother in years 5 Kebele Write Kebele where the mother comes fromLabor and maternal outcomeMode of Delivery6 Delivery Date and time Write delivery date and time of the client as (E.C.). DD/MM/YY- 00:007 Partograph Used Write “Y” if maternal condition, Fetal condition & Progress of labor monitored, If not all write “N”8 SVD ( spontaneous vaginal delivery ) Tick ( √) for spontaneous vaginal delivery 9 Caesarean Section (C/S) Tick ( √) if the delivery is caesarean section10 Forceps /Vacuum Assisted (√) Tick ( √) if the delivery is Forceps /Vacuum Assisted 11 Episiotomy (√) Tick ( √) if the delivery supported by episiotomy 12 Other (√) Tick ( √) if the delivery is by other (Assisted breach, Detractive, etc)Active management of 3rd stage labour
13 Uterotonic Drugs Given within one minute after delivery (Write code) Write codes listed in raw 23 (Write 1=Oxytocin, 2=Misoprostol, 3= Ergometrine 4= Other
14 Controlled cord traction (CCT) Tick ( √) for CCT performedMaternal status 15 Stable Tick( √) if the mother is stable 16 Unstable/deteriorated and referred to the
next facility (√) Tick ( √) if the mother maternal status is unstable /deteriorated and referred to other facility
17 Died Tick( √) if the mother died
18 Cause of maternal death
1 Hemorrhage2 PE/Eclampsia3 Obstructed Labore 4 Sepsis5 Anemia6 Others
Obstetric complications during intra-partum19 Pre-eclampsia (√) Tick ( √) if there is pre- eclampsia20 Eclampsia (√) Tick( √) if there is eclampsia 21 APH(√) Tick ( √) if there is Antepartum hemorrhage (APH)22 PPH(√) Tick ( √) if there is Post Partum Hemorrahge (PPH)23 Other obstetric complications (√) Tick ( √) if other obstetric complications (such as Obstructed labor, Sepsis, etc) occurred 24 Referred (√) Tick ( √) if the client is referred New born birth outcome 25 Alive (√) Tick ( √) if the newborn is live birth 26 APGAR score 1’/5’ Write the APGAR score of the newborn at the first and fifth minute of birth (1st minute /5th minute)27 Sex (M/F) Enter M for Male and F for female28 Weight in gram Write the weight of the newborn in gram29 Still birth (√) Put 1 if still birth is fresh and 2 if it is macerated
30 Live birth, died after arrival or delivery in facility(√)
Tick (√) if the live birth died after arrival or delivery in facility. these newborn death should be reported as ‘new born death within 24 hours )
Preventive services: Newborn 31 MRN (Newborn’s) Enter Newborn’s Medical Record Number(MRN) 32 Vitamin K (√) Tick( √) if the newborn received vitamin K33 TTC eye ointment (√) Tick( √) if TTC is applied for the newborn 34 Chlorhexidine (√) Tick( √) if Chlorhexidane is applied for the newborn 35 Vaccinated at birth for (Write code) Write code 1 for BCG, 2 for OPV 0, 3 for HBV. NB: You can use more than one codePreventive services : maternal HIV+ care and follow-up36 HIV testing accepted (√) Tick ( √) if the mother accepts testing for HIV 37 HIV retesting accepted (√) Tick ( √) if the mother have already tested and know her status negative but risk for HIV38 HIV test status ( P/ N) Write P in red pen if the test result is positive, write N in normal color if the result is negative.
39 Known HIV positives (linked from ART) (√) Tick ( √) if the women is known HIV positives and linked from ART
INSTRUCTION FOR DELIVERY CARE REGISTER
The register is kept in delivery room (HC/Clinic/Hospital) completed by delivery care provider.
Location information to be completed at front of the register:
Region Write region name where the facility is located
Zone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Name of Health Facility Write the name of the health facility where the service was provided.
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
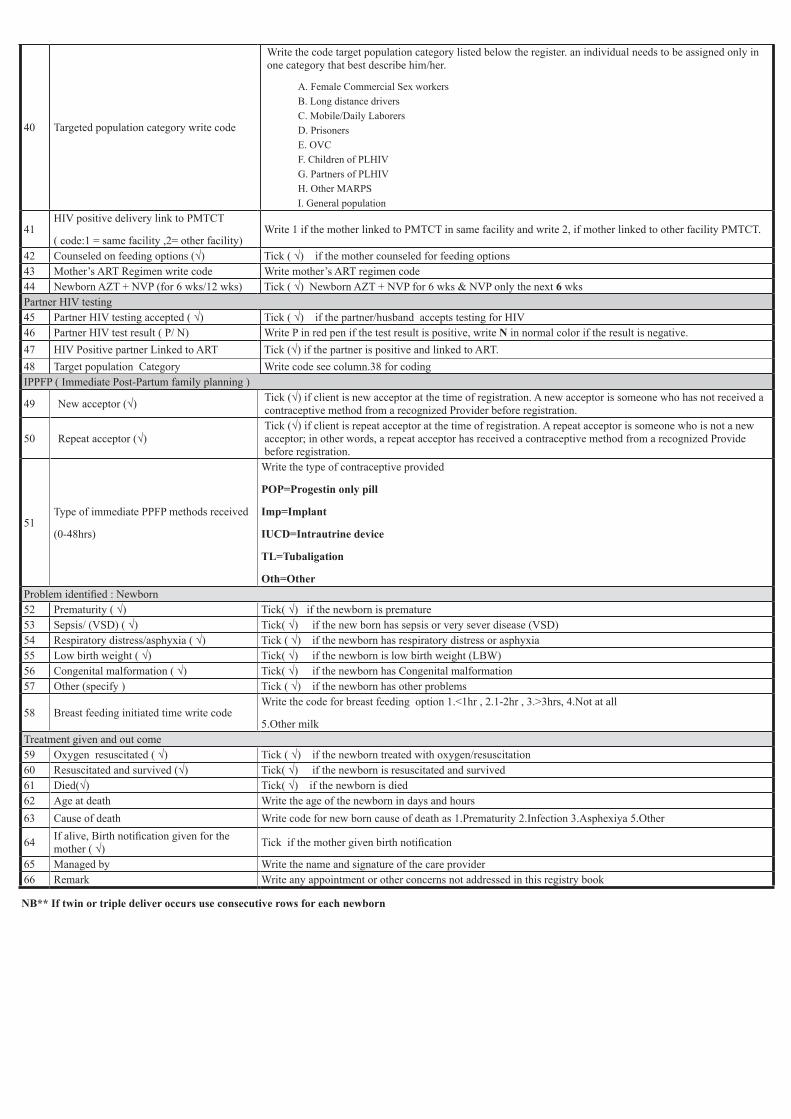
40 Targeted population category write code
Write the code target population category listed below the register. an individual needs to be assigned only in one category that best describe him/her.
A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
I. General population
41HIV positive delivery link to PMTCT
( code:1 = same facility ,2= other facility)Write 1 if the mother linked to PMTCT in same facility and write 2, if mother linked to other facility PMTCT.
42 Counseled on feeding options (√) Tick ( √) if the mother counseled for feeding options 43 Mother’s ART Regimen write code Write mother’s ART regimen code44 Newborn AZT + NVP (for 6 wks/12 wks) Tick ( √) Newborn AZT + NVP for 6 wks & NVP only the next 6 wksPartner HIV testing 45 Partner HIV testing accepted ( √) Tick ( √) if the partner/husband accepts testing for HIV 46 Partner HIV test result ( P/ N) Write P in red pen if the test result is positive, write N in normal color if the result is negative.47 HIV Positive partner Linked to ART Tick (√) if the partner is positive and linked to ART.48 Target population Category Write code see column.38 for codingIPPFP ( Immediate Post-Partum family planning )
49 New acceptor (√) Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.
50 Repeat acceptor (√)Tick (√) if client is repeat acceptor at the time of registration. A repeat acceptor is someone who is not a new acceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
51Type of immediate PPFP methods received
(0-48hrs)
Write the type of contraceptive provided
POP=Progestin only pill
Imp=Implant
IUCD=Intrautrine device
TL=Tubaligation
Oth=Other Problem identified : Newborn 52 Prematurity ( √) Tick( √) if the newborn is premature 53 Sepsis/ (VSD) ( √) Tick( √) if the new born has sepsis or very sever disease (VSD)54 Respiratory distress/asphyxia ( √) Tick ( √) if the newborn has respiratory distress or asphyxia55 Low birth weight ( √) Tick( √) if the newborn is low birth weight (LBW)56 Congenital malformation ( √) Tick( √) if the newborn has Congenital malformation 57 Other (specify ) Tick ( √) if the newborn has other problems
58 Breast feeding initiated time write codeWrite the code for breast feeding option 1.<1hr , 2.1-2hr , 3.>3hrs, 4.Not at all
5.Other milk Treatment given and out come59 Oxygen resuscitated ( √) Tick ( √) if the newborn treated with oxygen/resuscitation 60 Resuscitated and survived (√) Tick( √) if the newborn is resuscitated and survived61 Died(√) Tick( √) if the newborn is died62 Age at death Write the age of the newborn in days and hours 63 Cause of death Write code for new born cause of death as 1.Prematurity 2.Infection 3.Asphexiya 5.Other
64 If alive, Birth notification given for the mother ( √) Tick if the mother given birth notification
65 Managed by Write the name and signature of the care provider 66 Remark Write any appointment or other concerns not addressed in this registry book
NB** If twin or triple deliver occurs use consecutive rows for each newborn
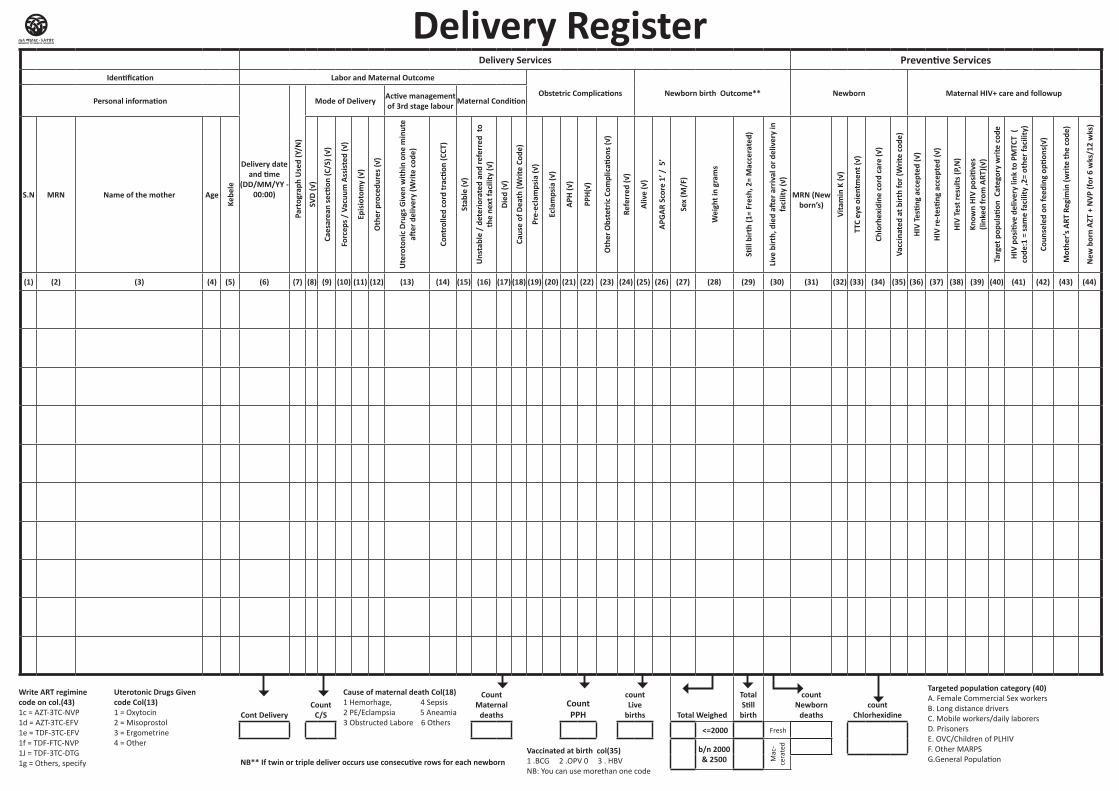
Delivery Services Preventive ServicesIdentification Labor and Maternal Outcome
Obstetric Complications Newborn birth Outcome** Newborn Maternal HIV+ care and followupPersonal information
Delivery date and time
(DD/MM/YY - 00:00)
Part
ogra
ph U
sed
(Y/N
)
Mode of Delivery Active management of 3rd stage labour Maternal Condition
S.N MRN Name of the mother Age
Kebe
le
SVD
(√)
Caes
area
n se
ction
(C/S
) (√)
Forc
eps /
Vac
uum
Ass
iste
d (√
)
Epis
ioto
my
(√)
Oth
er p
roce
dure
s (√)
Ute
roto
nic
Drug
s Giv
en w
ithin
one
min
ute
after
del
iver
y (W
rite
code
)
Cont
rolle
d co
rd tr
actio
n (C
CT)
Stab
le (√
)
Uns
tabl
e /
dete
riora
ted
and
refe
rred
to
the
next
faci
lity
(√)
Died
(√)
Caus
e of
Dea
th (W
rite
Code
)
Pre-
ecla
mps
ia (√
)
Ecla
mps
ia (√
)
APH
(√)
PPH(
√)
Oth
er O
bste
tric
Com
plic
ation
s (√)
Refe
rred
(√)
Aliv
e (√
)
APG
AR S
core
1’ /
5’
Sex
(M/F
)
Wei
ght i
n gr
ams
Still
birt
h (1
= Fr
esh,
2=
Mac
cera
ted)
Live
birt
h, d
ied
after
arr
ival
or d
eliv
ery
in
faci
lity
(√)
MRN (New
born’s)
Vita
min
K (√
)
TTC
eye
oien
tmen
t (√)
Chlo
rhex
idin
e co
rd c
are
(√)
Vacc
inat
ed a
t birt
h fo
r (W
rite
code
)
HIV
Testi
ng a
ccep
ted
(√)
HIV
re-t
estin
g ac
cept
ed (√
)
HIV
Test
resu
lts (P
,N)
Know
n HI
V po
sitiv
es
(link
ed fr
om A
RT)(√
)
Targ
et p
opul
ation
Cat
egor
y w
rite
code
HIV
posi
tive
deliv
ery
link
to P
MTC
T (
code
:1 =
sam
e fa
cilit
y ,2
= ot
her f
acili
ty)
Coun
sele
d on
feed
ing
optio
ns(√
)
Mot
her’s
ART
Reg
imin
(writ
e th
e co
de)
New
bor
n AZ
T +
NVP
(for
6 w
ks/1
2 w
ks)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44)
Cont DeliveryCount
C/S
Count Maternal
deathsCount PPH
count Live
births Total Weighed
Total Still
birth
count Newborn
deathscount
Chlorhexidine
<=2000 Fresh
b/n 2000 & 2500 M
ac-
cera
ted
Delivery Register
NB** If twin or triple deliver occurs use consecutive rows for each newborn
Cause of maternal death Col(18)1 Hemorhage, 4 Sepsis2 PE/Eclampsia 5 Aneamia3 Obstructed Labore 6 Others
Write ART regimine code on col.(43)1c = AZT-3TC-NVP1d = AZT-3TC-EFV1e = TDF-3TC-EFV1f = TDF-FTC-NVP1J = TDF-3TC-DTG 1g = Others, specify
Uterotonic Drugs Given code Col(13)1 = Oxytocin 2 = Misoprostol 3 = Ergometrine 4 = Other
Vaccinated at birth col(35)1 .BCG 2 .OPV 0 3 . HBV NB: You can use morethan one code
Targeted population category (40)A. Female Commercial Sex workers B. Long distance drivers C. Mobile workers/daily laborers D. Prisoners E. OVC/Children of PLHIVF. Other MARPS G.General Population
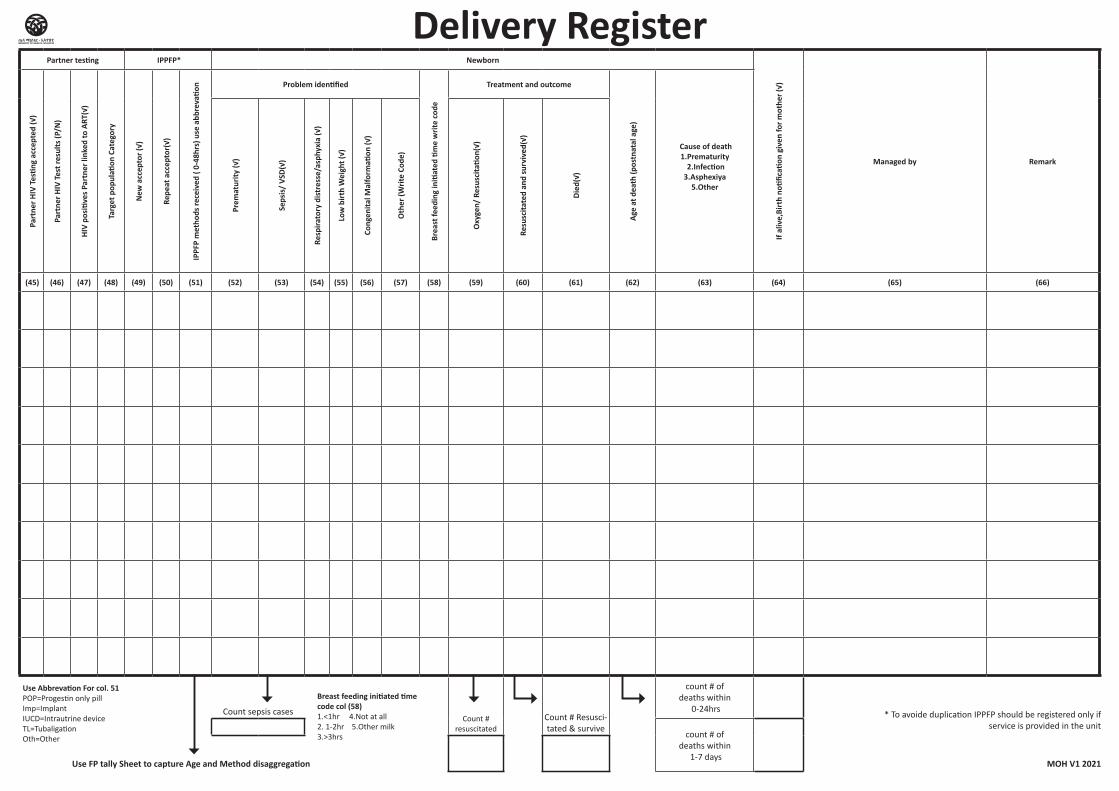
Delivery RegisterPartner testing IPPFP* Newborn
If al
ive,
Birt
h no
tifica
tion
give
n fo
r mot
her (
√)
Managed by Remark
Part
ner H
IV T
estin
g ac
cept
ed (√
)
Part
ner H
IV T
est r
esul
ts (P
/N)
HIV
posi
tives
Par
tner
link
ed to
ART
(√)
Targ
et p
opul
ation
Cat
egor
y
New
acc
epto
r (√)
Repe
at a
ccep
tor(
√)
IPPF
P m
etho
ds re
ceiv
ed (
0-48
hrs)
use
abb
reva
tion
Problem identified
Brea
st fe
edin
g in
itiat
ed ti
me
writ
e co
de
Treatment and outcome
Age
at d
eath
(pos
tnat
al a
ge)
Cause of death 1.Prematurity
2.Infection 3.Asphexiya
5.Other
Prem
atur
ity (√
)
Seps
is/
VSD(
√)
Resp
irato
ry d
istr
esse
/asp
hyxi
a (√
)
Low
birt
h W
eigh
t (√)
Cong
enita
l Mal
form
ation
(√)
Oth
er (W
rite
Code
)
Oxy
gen/
Res
usci
tatio
n(√)
Resu
scita
ted
and
surv
ived
(√)
Died
(√)
(45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) (60) (61) (62) (63) (64) (65) (66)
Count sepsis casesCount #
resuscitatedCount # Resusci-tated & survive
count # of deaths within
0-24hrs
count # of deaths within
1-7 days
Use FP tally Sheet to capture Age and Method disaggregation MOH V1 2021
Use Abbrevation For col. 51POP=Progestin only pillImp=ImplantIUCD=Intrautrine deviceTL=TubaligationOth=Other
Breast feeding initiated time code col (58)1.<1hr 4.Not at all 2. 1-2hr 5.Other milk3.>3hrs
* To avoide duplication IPPFP should be registered only if service is provided in the unit
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital PNC Register
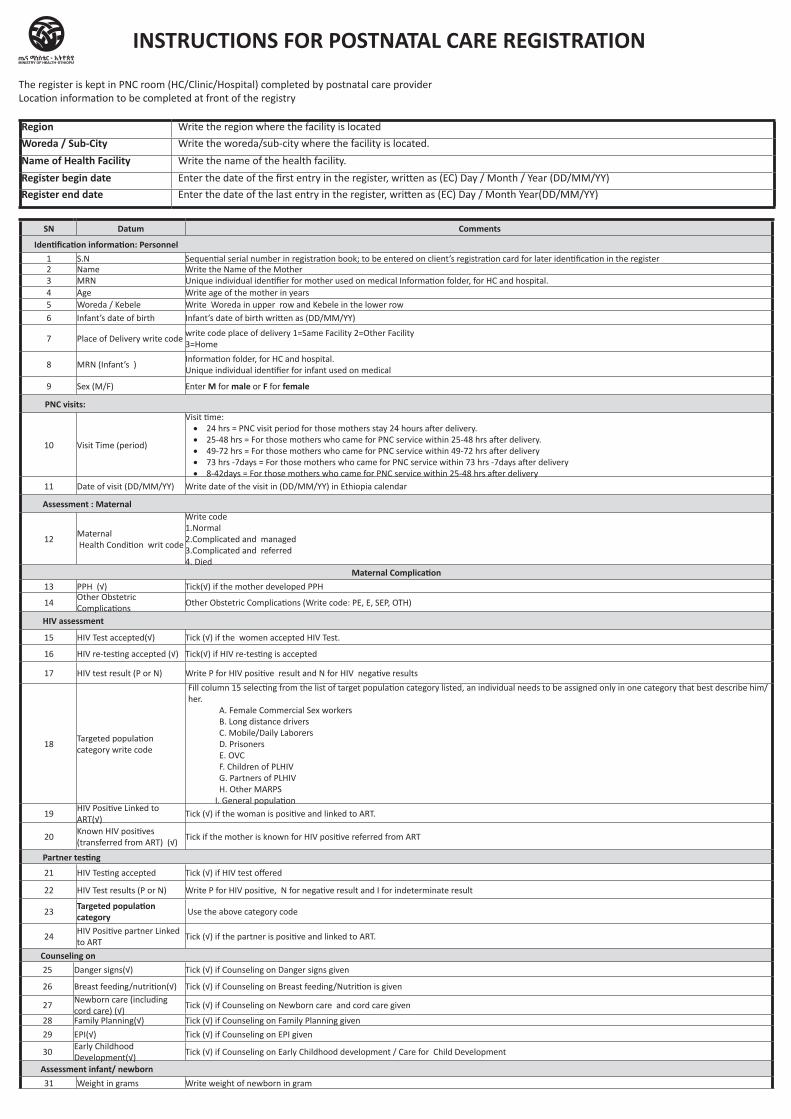
The register is kept in PNC room (HC/Clinic/Hospital) completed by postnatal care provider Location information to be completed at front of the registry
Region Write the region where the facility is located
Woreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility.
Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month Year(DD/MM/YY)
SN Datum Comments
Identification information: Personnel 1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in the register 2 Name Write the Name of the Mother 3 MRN Unique individual identifier for mother used on medical Information folder, for HC and hospital.4 Age Write age of the mother in years 5 Woreda / Kebele Write Woreda in upper row and Kebele in the lower row6 Infant’s date of birth Infant’s date of birth written as (DD/MM/YY)
7 Place of Delivery write codewrite code place of delivery 1=Same Facility 2=Other Facility3=Home
8 MRN (Infant’s )Information folder, for HC and hospital.Unique individual identifier for infant used on medical
9 Sex (M/F) Enter M for male or F for female
PNC visits:
10 Visit Time (period)
Visit time: • 24 hrs = PNC visit period for those mothers stay 24 hours after delivery. • 25-48 hrs = For those mothers who came for PNC service within 25-48 hrs after delivery. • 49-72 hrs = For those mothers who came for PNC service within 49-72 hrs after delivery• 73 hrs -7days = For those mothers who came for PNC service within 73 hrs -7days after delivery• 8-42days = For those mothers who came for PNC service within 25-48 hrs after delivery
11 Date of visit (DD/MM/YY) Write date of the visit in (DD/MM/YY) in Ethiopia calendar
Assessment : Maternal
12Maternal Health Condition writ code
Write code 1.Normal 2.Complicated and managed 3.Complicated and referred4. Died
Maternal Complication13 PPH (√) Tick(√) if the mother developed PPH
14Other Obstetric Complications
Other Obstetric Complications (Write code: PE, E, SEP, OTH)
HIV assessment
15 HIV Test accepted(√) Tick (√) if the women accepted HIV Test.
16 HIV re-testing accepted (√) Tick(√) if HIV re-testing is accepted
17 HIV test result (P or N) Write P for HIV positive result and N for HIV negative results
18Targeted population category write code
Fill column 15 selecting from the list of target population category listed, an individual needs to be assigned only in one category that best describe him/her.
A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
I. General population19
HIV Positive Linked to ART(√)
Tick (√) if the woman is positive and linked to ART.
20Known HIV positives (transferred from ART) (√)
Tick if the mother is known for HIV positive referred from ART
Partner testing
21 HIV Testing accepted Tick (√) if HIV test offered
22 HIV Test results (P or N) Write P for HIV positive, N for negative result and I for indeterminate result
23Targeted population category Use the above category code
24HIV Positive partner Linked to ART
Tick (√) if the partner is positive and linked to ART.
Counseling on25 Danger signs(√) Tick (√) if Counseling on Danger signs given
26 Breast feeding/nutrition(√) Tick (√) if Counseling on Breast feeding/Nutrition is given
27Newborn care (including cord care) (√)
Tick (√) if Counseling on Newborn care and cord care given
28 Family Planning(√) Tick (√) if Counseling on Family Planning given
29 EPI(√) Tick (√) if Counseling on EPI given
30Early Childhood Development(√)
Tick (√) if Counseling on Early Childhood development / Care for Child Development
Assessment infant/ newborn31 Weight in grams Write weight of newborn in gram
INSTRUCTIONS FOR POSTNATAL CARE REGISTRATION
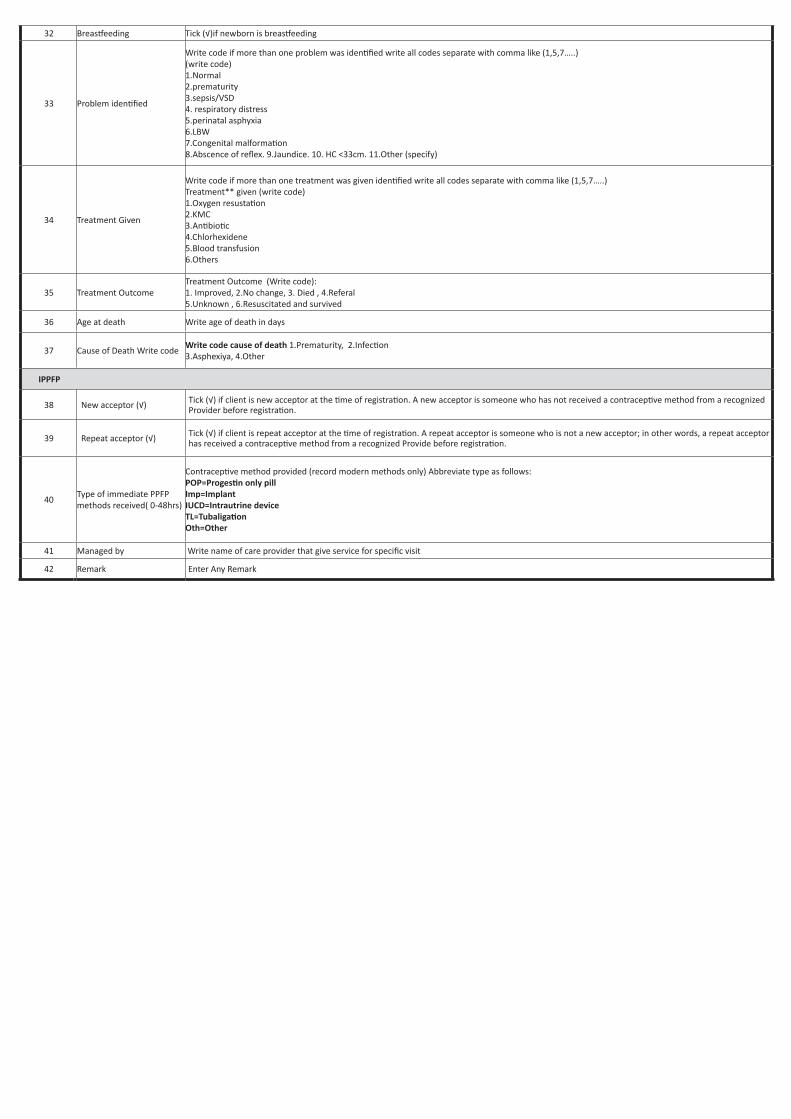
32 Breastfeeding Tick (√)if newborn is breastfeeding
33 Problem identified
Write code if more than one problem was identified write all codes separate with comma like (1,5,7…..) (write code) 1.Normal2.prematurity 3.sepsis/VSD4. respiratory distress5.perinatal asphyxia6.LBW7.Congenital malformation8.Abscence of reflex. 9.Jaundice. 10. HC <33cm. 11.Other (specify)
34 Treatment Given
Write code if more than one treatment was given identified write all codes separate with comma like (1,5,7…..)Treatment** given (write code)1.Oxygen resustation2.KMC3.Antibiotic4.Chlorhexidene5.Blood transfusion6.Others
35 Treatment OutcomeTreatment Outcome (Write code):1. Improved, 2.No change, 3. Died , 4.Referal 5.Unknown , 6.Resuscitated and survived
36 Age at death Write age of death in days
37 Cause of Death Write codeWrite code cause of death 1.Prematurity, 2.Infection3.Asphexiya, 4.Other
IPPFP
38 New acceptor (√) Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.
39 Repeat acceptor (√) Tick (√) if client is repeat acceptor at the time of registration. A repeat acceptor is someone who is not a new acceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
40Type of immediate PPFP methods received( 0-48hrs)
Contraceptive method provided (record modern methods only) Abbreviate type as follows:POP=Progestin only pillImp=ImplantIUCD=Intrautrine deviceTL=TubaligationOth=Other
41 Managed by Write name of care provider that give service for specific visit
42 Remark Enter Any Remark
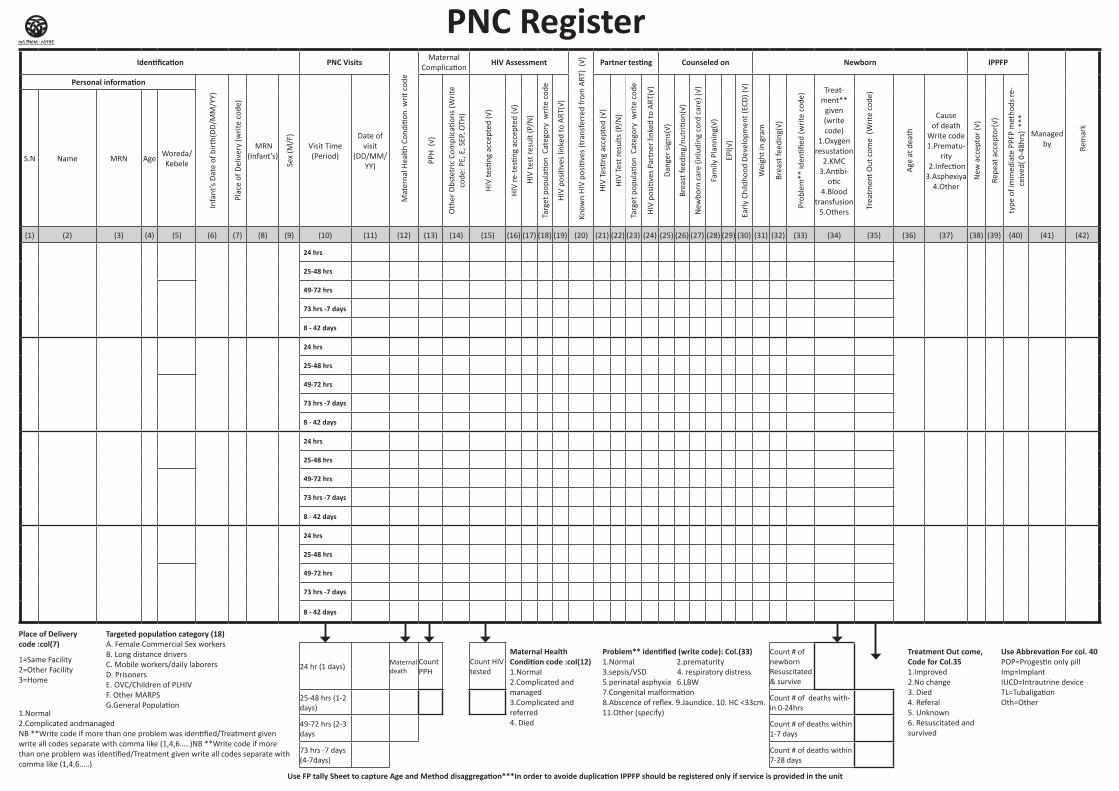
Identification PNC Visits
Mat
erna
l Hea
lth C
ondi
tion
wri
t cod
e
Maternal Complication
HIV Assessment
Know
n H
IV p
ositi
ves
(tra
nsfe
rred
from
ART
) (√
)
Partner testing Counseled on Newborn IPPFP
Managed by
Rem
ark
Personal information
Infa
nt’s
Dat
e of
bir
th(D
D/M
M/Y
Y)
Plac
e of
Del
iver
y (w
rite
cod
e)
MRN
(Infant’s)
Sex
(M/F
)
Visit Time (Period)
Date of visit
(DD/MM/YY) PP
H (
√)
Oth
er O
bste
tric
Com
plic
ation
s (W
rite
co
de: P
E, E
, SEP
, OTH
)
HIV
testi
ng a
ccep
ted
(√)
HIV
re-t
estin
g ac
cept
ed (√
)
HIV
test
resu
lt (P
/N)
Targ
et p
opul
ation
Cat
egor
y w
rite
cod
e
HIV
pos
itive
s lin
ked
to A
RT(√
)
HIV
Tes
ting
acce
pted
(√)
HIV
Tes
t res
ults
(P/N
)
Targ
et p
opul
ation
Cat
egor
y w
rite
cod
e
HIV
pos
itive
s Pa
rtne
r lin
ked
to A
RT(√
)
Dan
ger
sign
s(√)
Brea
st fe
edin
g/nu
triti
on(√
)
New
born
car
e (in
ludi
ng c
ord
care
) (√)
Fam
ily P
lann
ing(
√)
EPI(√
)
Earl
y Ch
ildho
od D
evel
opm
ent (
ECD
) (√)
Wei
ght i
n gr
am
Brea
st fe
edin
g(√)
Prob
lem
** id
entifi
ed (w
rite
cod
e) Treat-
ment** given (write code)
1.Oxygen resustation
2.KMC 3.Antibi-
otic 4.Blood
transfusion 5.Others
Trea
tmen
t Out
com
e (W
rite
cod
e)
Age
at d
eath
Cause of death
Write code 1.Prematu-
rity 2.Infection 3.Asphexiya
4.Other
New
acc
epto
r (√
)
Repe
at a
ccep
tor(
√)
type
of i
mm
edia
te P
PFP
met
hods
re-
ceiv
ed( 0
-48h
rs)
***
S.N Name MRN AgeWoreda/ Kebele
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42)
24 hrs
25-48 hrs
49-72 hrs
73 hrs -7 days
8 - 42 days
24 hrs
25-48 hrs
49-72 hrs
73 hrs -7 days
8 - 42 days
24 hrs
25-48 hrs
49-72 hrs
73 hrs -7 days
8 - 42 days
24 hrs
25-48 hrs
49-72 hrs
73 hrs -7 days
8 - 42 days
24 hr (1 days)Maternal death
Count PPH
Count HIV tested
Count # of newborn Resuscitated & survive
25-48 hrs (1-2 days)
Count # of deaths with-in 0-24hrs
49-72 hrs (2-3 days Count # of deaths within
1-7 days
73 hrs -7 days (4-7days)
Count # of deaths within 7-28 days
Use FP tally Sheet to capture Age and Method disaggregation***In order to avoide duplication IPPFP should be registered only if service is provided in the unit
Use Abbrevation For col. 40 POP=Progestin only pill Imp=Implant IUCD=Intrautrine device TL=Tubaligation Oth=Other
PNC Register
Place of Deliverycode :col(7)
1=Same Facility2=Other Facility3=Home
Targeted population category (18) A. Female Commercial Sex workers B. Long distance drivers C. Mobile workers/daily laborers D. Prisoners E. OVC/Children of PLHIVF. Other MARPS G.General Population
Maternal Health Condition code :col(12)1.Normal 2.Complicated and managed 3.Complicated and referred4. Died
1.Normal 2.Complicated andmanaged NB **Write code if more than one problem was identified/Treatment given write all codes separate with comma like (1,4,6…..)NB **Write code if more than one problem was identified/Treatment given write all codes separate with comma like (1,4,6…..)
Problem** identified (write code): Col.(33)1.Normal 2.prematurity 3.sepsis/VSD 4. respiratory distress5.perinatal asphyxia 6.LBW7.Congenital malformation8.Abscence of reflex. 9.Jaundice. 10. HC <33cm. 11.Other (specify)
Treatment Out come, Code for Col.351.Improved2.No change 3. Died 4. Referal 5. Unknown6. Resuscitated and survived
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital PMTCT Register
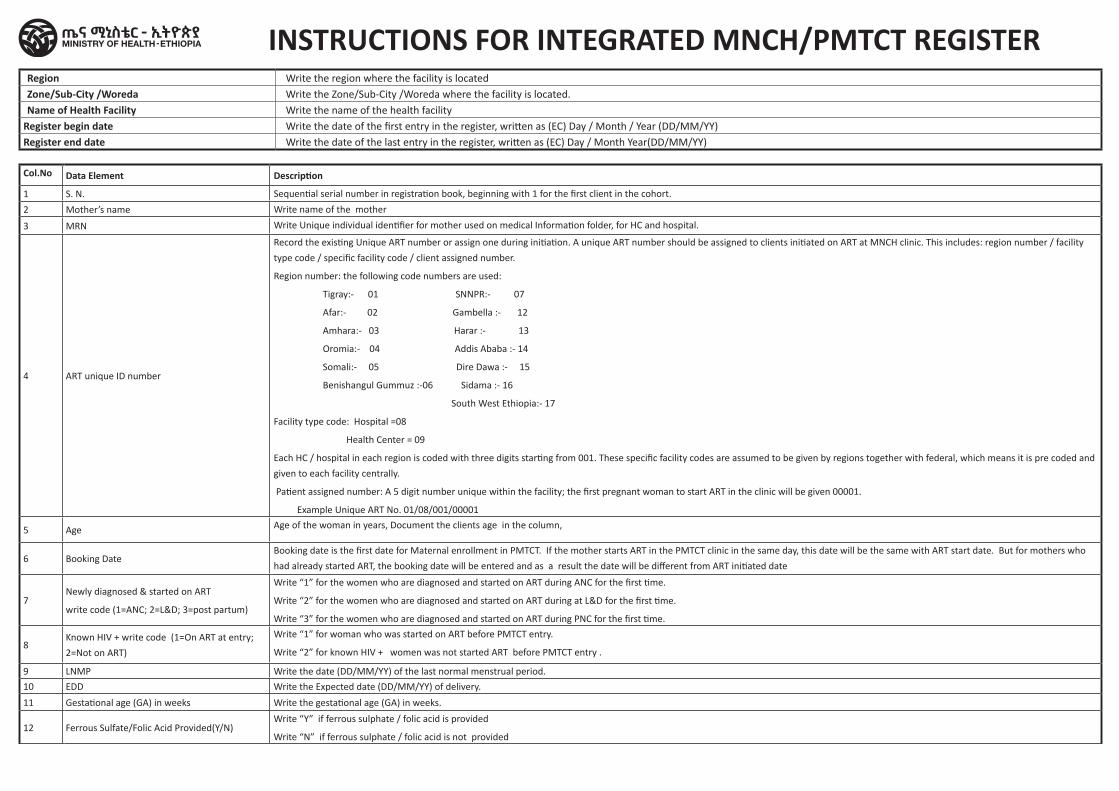
Col.No Data Element Description
1 S. N. Sequential serial number in registration book, beginning with 1 for the first client in the cohort.
2 Mother’s name Write name of the mother
3 MRN Write Unique individual identifier for mother used on medical Information folder, for HC and hospital.
4 ART unique ID number
Record the existing Unique ART number or assign one during initiation. A unique ART number should be assigned to clients initiated on ART at MNCH clinic. This includes: region number / facility
type code / specific facility code / client assigned number.
Region number: the following code numbers are used:
Tigray:- 01 SNNPR:- 07
Afar:- 02 Gambella :- 12
Amhara:- 03 Harar :- 13
Oromia:- 04 Addis Ababa :- 14
Somali:- 05 Dire Dawa :- 15
Benishangul Gummuz :-06 Sidama :- 16
South West Ethiopia:- 17
Facility type code: Hospital =08
Health Center = 09
Each HC / hospital in each region is coded with three digits starting from 001. These specific facility codes are assumed to be given by regions together with federal, which means it is pre coded and
given to each facility centrally.
Patient assigned number: A 5 digit number unique within the facility; the first pregnant woman to start ART in the clinic will be given 00001.
Example Unique ART No. 01/08/001/00001
5 Age Age of the woman in years, Document the clients age in the column,
6 Booking Date Booking date is the first date for Maternal enrollment in PMTCT. If the mother starts ART in the PMTCT clinic in the same day, this date will be the same with ART start date. But for mothers who
had already started ART, the booking date will be entered and as a result the date will be different from ART initiated date
7Newly diagnosed & started on ART
write code (1=ANC; 2=L&D; 3=post partum)
Write “1” for the women who are diagnosed and started on ART during ANC for the first time.
Write “2” for the women who are diagnosed and started on ART during at L&D for the first time.
Write “3” for the women who are diagnosed and started on ART during PNC for the first time.
8Known HIV + write code (1=On ART at entry;
2=Not on ART)
Write “1” for woman who was started on ART before PMTCT entry.
Write “2” for known HIV + women was not started ART before PMTCT entry .
9 LNMP Write the date (DD/MM/YY) of the last normal menstrual period.
10 EDD Write the Expected date (DD/MM/YY) of delivery.
11 Gestational age (GA) in weeks Write the gestational age (GA) in weeks.
12 Ferrous Sulfate/Folic Acid Provided(Y/N)Write “Y” if ferrous sulphate / folic acid is provided
Write “N” if ferrous sulphate / folic acid is not provided
INSTRUCTIONS FOR INTEGRATED MNCH/PMTCT REGISTERRegion Write the region where the facility is locatedZone/Sub-City /Woreda Write the Zone/Sub-City /Woreda where the facility is located.Name of Health Facility Write the name of the health facility
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month Year(DD/MM/YY)
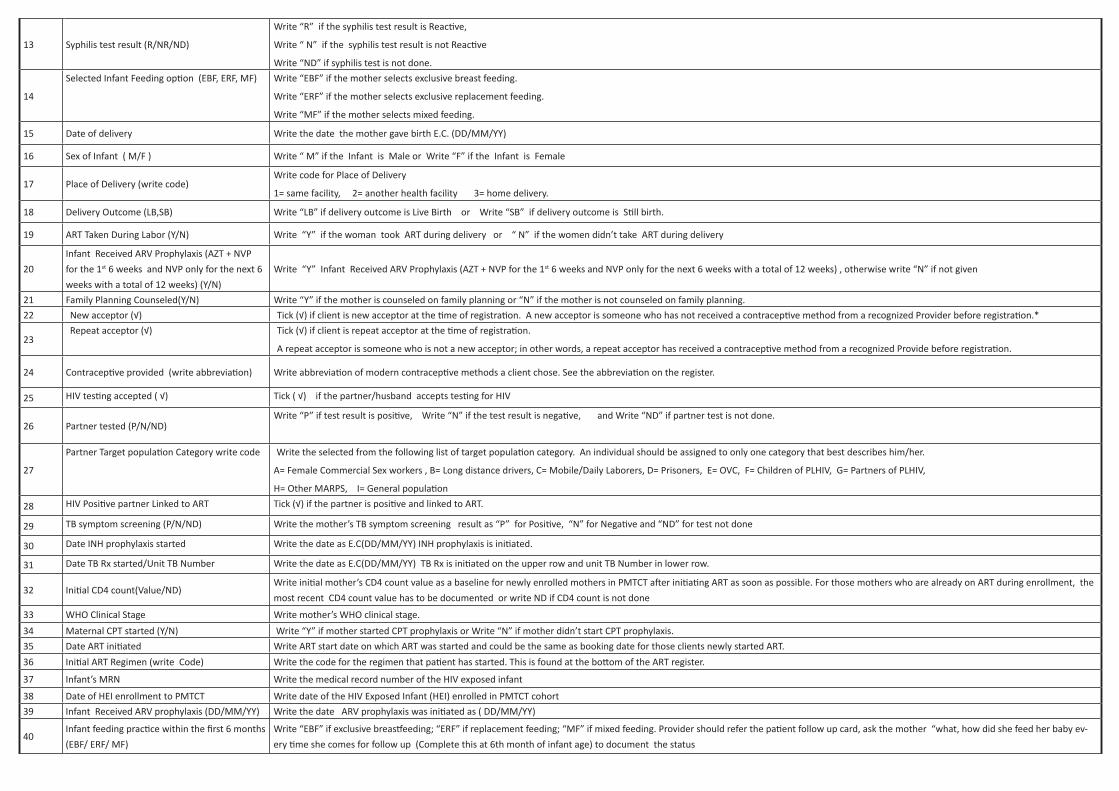
13 Syphilis test result (R/NR/ND)
Write “R” if the syphilis test result is Reactive,
Write “ N” if the syphilis test result is not Reactive
Write “ND” if syphilis test is not done.
14
Selected Infant Feeding option (EBF, ERF, MF) Write “EBF” if the mother selects exclusive breast feeding.
Write “ERF” if the mother selects exclusive replacement feeding.
Write “MF” if the mother selects mixed feeding.
15 Date of delivery Write the date the mother gave birth E.C. (DD/MM/YY)
16 Sex of Infant ( M/F ) Write “ M” if the Infant is Male or Write “F” if the Infant is Female
17 Place of Delivery (write code)Write code for Place of Delivery
1= same facility, 2= another health facility 3= home delivery.
18 Delivery Outcome (LB,SB) Write “LB” if delivery outcome is Live Birth or Write “SB” if delivery outcome is Still birth.
19 ART Taken During Labor (Y/N) Write “Y” if the woman took ART during delivery or “ N” if the women didn’t take ART during delivery
20
Infant Received ARV Prophylaxis (AZT + NVP
for the 1st 6 weeks and NVP only for the next 6
weeks with a total of 12 weeks) (Y/N)
Write “Y” Infant Received ARV Prophylaxis (AZT + NVP for the 1st 6 weeks and NVP only for the next 6 weeks with a total of 12 weeks) , otherwise write “N” if not given
21 Family Planning Counseled(Y/N) Write “Y” if the mother is counseled on family planning or “N” if the mother is not counseled on family planning.
22 New acceptor (√) Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.*
23Repeat acceptor (√) Tick (√) if client is repeat acceptor at the time of registration.
A repeat acceptor is someone who is not a new acceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
24 Contraceptive provided (write abbreviation) Write abbreviation of modern contraceptive methods a client chose. See the abbreviation on the register.
25 HIV testing accepted ( √) Tick ( √) if the partner/husband accepts testing for HIV
26 Partner tested (P/N/ND) Write “P” if test result is positive, Write “N” if the test result is negative, and Write “ND” if partner test is not done.
27
Partner Target population Category write code Write the selected from the following list of target population category. An individual should be assigned to only one category that best describes him/her.
A= Female Commercial Sex workers , B= Long distance drivers, C= Mobile/Daily Laborers, D= Prisoners, E= OVC, F= Children of PLHIV, G= Partners of PLHIV,
H= Other MARPS, I= General population
28 HIV Positive partner Linked to ART Tick (√) if the partner is positive and linked to ART.
29 TB symptom screening (P/N/ND) Write the mother’s TB symptom screening result as “P” for Positive, “N” for Negative and “ND” for test not done
30 Date INH prophylaxis started Write the date as E.C(DD/MM/YY) INH prophylaxis is initiated.
31 Date TB Rx started/Unit TB Number Write the date as E.C(DD/MM/YY) TB Rx is initiated on the upper row and unit TB Number in lower row.
32 Initial CD4 count(Value/ND)Write initial mother’s CD4 count value as a baseline for newly enrolled mothers in PMTCT after initiating ART as soon as possible. For those mothers who are already on ART during enrollment, the
most recent CD4 count value has to be documented or write ND if CD4 count is not done
33 WHO Clinical Stage Write mother’s WHO clinical stage.
34 Maternal CPT started (Y/N) Write “Y” if mother started CPT prophylaxis or Write “N” if mother didn’t start CPT prophylaxis.
35 Date ART initiated Write ART start date on which ART was started and could be the same as booking date for those clients newly started ART.
36 Initial ART Regimen (write Code) Write the code for the regimen that patient has started. This is found at the bottom of the ART register.
37 Infant’s MRN Write the medical record number of the HIV exposed infant
38 Date of HEI enrollment to PMTCT Write date of the HIV Exposed Infant (HEI) enrolled in PMTCT cohort
39 Infant Received ARV prophylaxis (DD/MM/YY) Write the date ARV prophylaxis was initiated as ( DD/MM/YY)
40Infant feeding practice within the first 6 months
(EBF/ ERF/ MF)
Write “EBF” if exclusive breastfeeding; “ERF” if replacement feeding; “MF” if mixed feeding. Provider should refer the patient follow up card, ask the mother “what, how did she feed her baby ev-
ery time she comes for follow up (Complete this at 6th month of infant age) to document the status
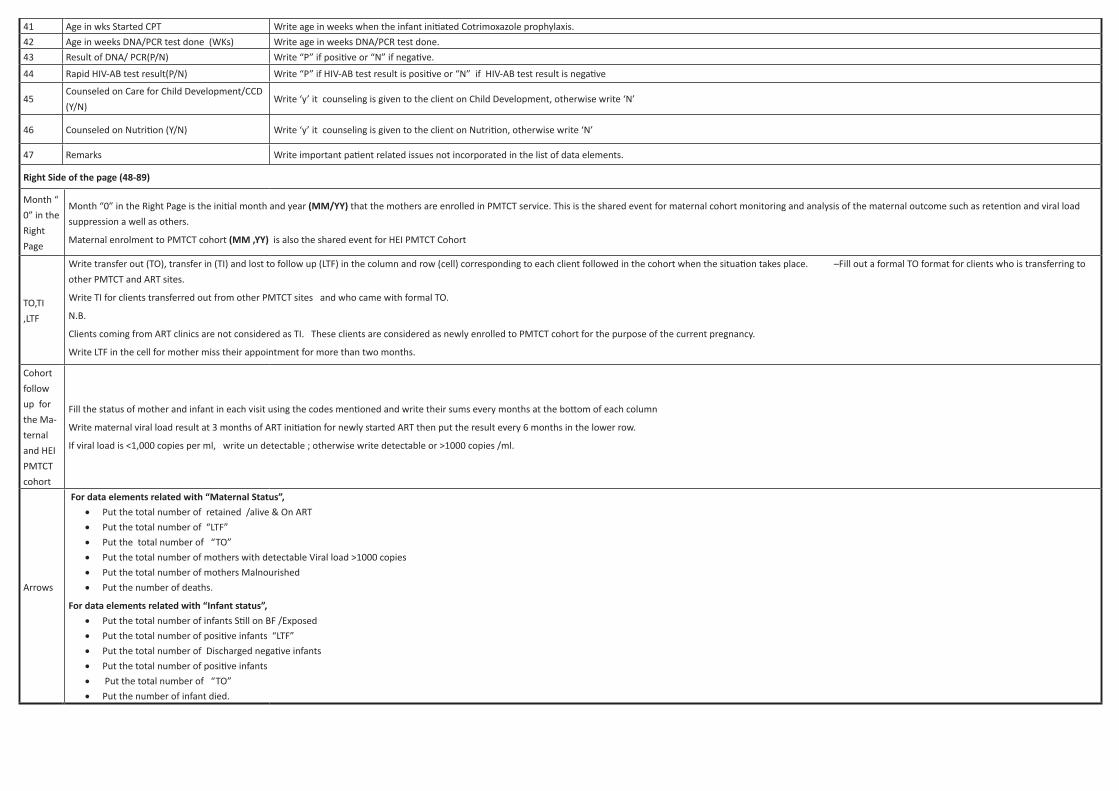
41 Age in wks Started CPT Write age in weeks when the infant initiated Cotrimoxazole prophylaxis.
42 Age in weeks DNA/PCR test done (WKs) Write age in weeks DNA/PCR test done.
43 Result of DNA/ PCR(P/N) Write “P” if positive or “N” if negative.
44 Rapid HIV-AB test result(P/N) Write “P” if HIV-AB test result is positive or “N” if HIV-AB test result is negative
45Counseled on Care for Child Development/CCD
(Y/N)Write ‘y’ it counseling is given to the client on Child Development, otherwise write ‘N’
46 Counseled on Nutrition (Y/N) Write ‘y’ it counseling is given to the client on Nutrition, otherwise write ‘N’
47 Remarks Write important patient related issues not incorporated in the list of data elements.
Right Side of the page (48-89)
Month “
0” in the
Right
Page
Month “0” in the Right Page is the initial month and year (MM/YY) that the mothers are enrolled in PMTCT service. This is the shared event for maternal cohort monitoring and analysis of the maternal outcome such as retention and viral load
suppression a well as others.
Maternal enrolment to PMTCT cohort (MM ,YY) is also the shared event for HEI PMTCT Cohort
TO,TI
,LTF
Write transfer out (TO), transfer in (TI) and lost to follow up (LTF) in the column and row (cell) corresponding to each client followed in the cohort when the situation takes place. –Fill out a formal TO format for clients who is transferring to
other PMTCT and ART sites.
Write TI for clients transferred out from other PMTCT sites and who came with formal TO.
N.B.
Clients coming from ART clinics are not considered as TI. These clients are considered as newly enrolled to PMTCT cohort for the purpose of the current pregnancy.
Write LTF in the cell for mother miss their appointment for more than two months.
Cohort
follow
up for
the Ma-
ternal
and HEI
PMTCT
cohort
Fill the status of mother and infant in each visit using the codes mentioned and write their sums every months at the bottom of each column
Write maternal viral load result at 3 months of ART initiation for newly started ART then put the result every 6 months in the lower row.
If viral load is <1,000 copies per ml, write un detectable ; otherwise write detectable or >1000 copies /ml.
Arrows
For data elements related with “Maternal Status”, • Put the total number of retained /alive & On ART
• Put the total number of “LTF”
• Put the total number of “TO”
• Put the total number of mothers with detectable Viral load >1000 copies
• Put the total number of mothers Malnourished
• Put the number of deaths.
For data elements related with “Infant status”, • Put the total number of infants Still on BF /Exposed
• Put the total number of positive infants “LTF”
• Put the total number of Discharged negative infants
• Put the total number of positive infants
• Put the total number of “TO”
• Put the number of infant died.
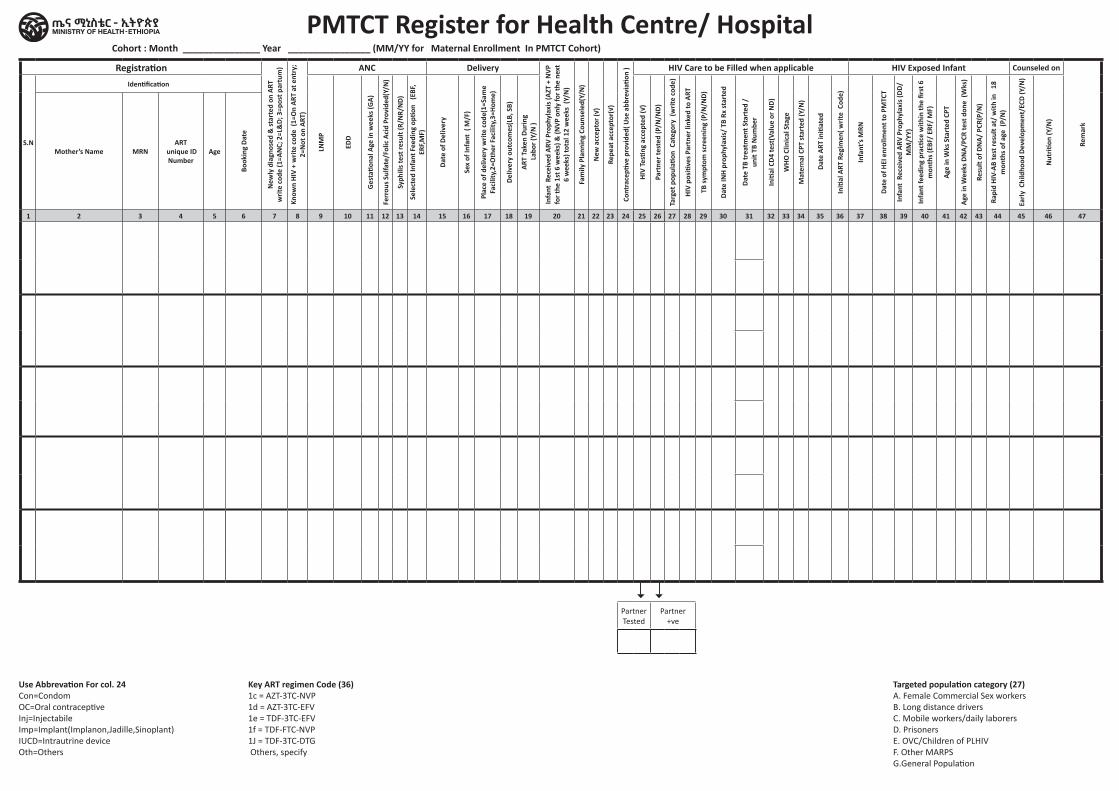
PMTCT Register for Health Centre/ HospitalRegistration
New
ly d
iagn
osed
& st
arte
d on
ART
w
rite
code
(1=A
NC;
2=L
&D;
3=p
ost p
artu
m)
Know
n HI
V +
writ
e co
de (
1=O
n AR
T at
ent
ry;
2=N
ot o
n AR
T)
ANC Delivery
Infa
nt R
ecei
ved
ARV
Prop
hyla
xis (
AZT
+ N
VP
for t
he 1
st 6
wee
ks) &
(NVP
onl
y fo
r the
nex
t 6
wee
ks) t
otal
12
wee
ks (
Y/N
)
Fam
ily P
lann
ing
Coun
sele
d(Y/
N)
New
acc
epto
r (√)
Repe
at a
ccep
tor(
√)
Cont
race
ptive
pro
vide
d( U
se a
bbre
viati
on ) HIV Care to be Filled when applicable HIV Exposed Infant Counseled on
Rem
ark
S.N
Identification
LNM
P
EDD
Ges
tatio
nal A
ge in
wee
ks (G
A)
Ferr
ous S
ulfa
te/F
olic
Aci
d Pr
ovid
ed(Y
/N)
Syph
ilis t
est r
esul
t (R/
NR/
ND)
Sele
cted
Infa
nt F
eedi
ng o
ption
(E
BF,
ERF,M
F)
Date
of D
eliv
ery
Sex
of In
fant
( M
/F)
Plac
e of
del
iver
y w
rite
code
(1=S
ame
Faci
lity,
2=O
ther
Fac
ility
,3=H
ome)
Deliv
ery
outc
omes
(LB,
SB)
ART
Take
n Du
ring
Lab
or (Y
/N )
HIV
Testi
ng a
ccep
ted
(√)
Part
ner t
este
d (P
/N/N
D)
Targ
et p
opul
ation
Cat
egor
y (w
rite
code
)
HIV
posi
tives
Par
tner
link
ed to
ART
TB sy
mpt
om sc
reen
ing
(P/N
/ND)
Date
INH
prop
hyla
xis/
TB
Rx st
arte
d
Date
TB
trea
tmen
t Sta
rted
/
unit
TB N
umbe
r
Initi
al C
D4 te
st(V
alue
or N
D)
WHO
Clin
ical
Sta
ge
Mat
erna
l CPT
star
ted
(Y/N
)
Dat
e AR
T in
itiat
ed
Initi
al A
RT R
egim
en( w
rite
Cod
e)
Infa
nt’s
MRN
Date
of H
EI e
nrol
lmen
t to
PMTC
T
Infa
nt R
ecei
ved
ARV
Prop
hyla
xis (
DD/
MM
/YY)
Infa
nt fe
edin
g pr
actic
e w
ithin
the
first
6
mon
ths (
EBF/
ERF
/ M
F)
Age
in W
ks S
tart
ed C
PT
Age
in W
eeks
DN
A/PC
R te
st d
one
(Wks
)
Resu
lt of
DN
A/ P
CR(P
/N)
Rapi
d HI
V-AB
test
resu
lt at
/ w
ith in
18
m
onth
s of a
ge (
P/N
)
Early
Chi
ldho
od D
evel
opm
ent/
ECD
(Y/N
)
Nut
rition
(Y/N
)
Mother’s Name MRN ART
unique ID Number
Age
Book
ing
Date
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47
Partner Tested
Partner +ve
Cohort : Month _______________ Year ________________ (MM/YY for Maternal Enrollment In PMTCT Cohort)
Use Abbrevation For col. 24Con=CondomOC=Oral contraceptiveInj=InjectabileImp=Implant(Implanon,Jadille,Sinoplant)IUCD=Intrautrine deviceOth=Others
Key ART regimen Code (36)1c = AZT-3TC-NVP1d = AZT-3TC-EFV1e = TDF-3TC-EFV1f = TDF-FTC-NVP1J = TDF-3TC-DTG Others, specify
Targeted population category (27)A. Female Commercial Sex workers B. Long distance drivers C. Mobile workers/daily laborers D. Prisoners E. OVC/Children of PLHIVF. Other MARPS G.General Population
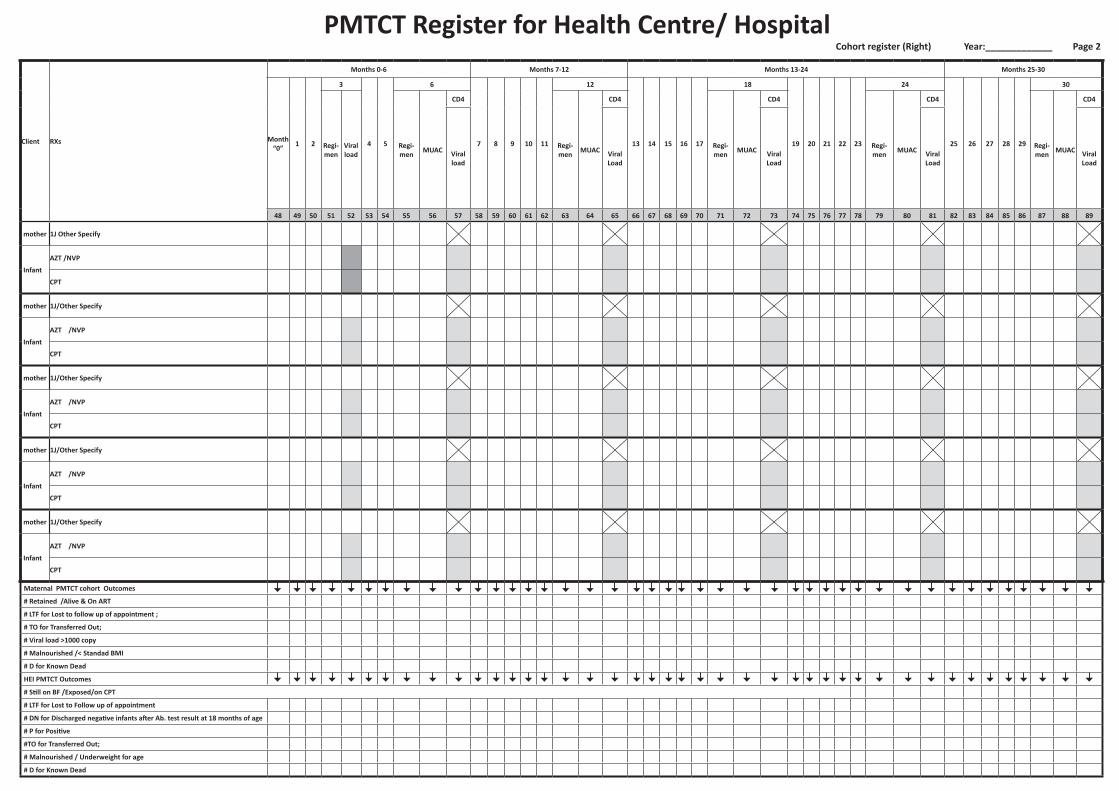
PMTCT Register for Health Centre/ Hospital
Client RXs
Months 0-6 Months 7-12 Months 13-24 Months 25-30
Month “0” 1 2
3
4 5
6
7 8 9 10 11
12
13 14 15 16 17
18
19 20 21 22 23
24
25 26 27 28 29
30
Regi-men
Viral load
Regi-men MUAC
CD4
Regi-men MUAC
CD4
Regi-men MUAC
CD4
Regi-men MUAC
CD4
Regi-men MUAC
CD4
Viral load
Viral Load
Viral Load
Viral Load
Viral Load
48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89
mother 1J Other Specify
Infant
AZT /NVP
CPT
mother 1J/Other Specify
Infant
AZT /NVP
CPT
mother 1J/Other Specify
Infant
AZT /NVP
CPT
mother 1J/Other Specify
Infant
AZT /NVP
CPT
mother 1J/Other Specify
Infant
AZT /NVP
CPT
Maternal PMTCT cohort Outcomes
# Retained /Alive & On ART
# LTF for Lost to follow up of appointment ;
# TO for Transferred Out;
# Viral load >1000 copy
# Malnourished /< Standad BMI
# D for Known Dead
HEI PMTCT Outcomes
# Still on BF /Exposed/on CPT
# LTF for Lost to Follow up of appointment
# DN for Discharged negative infants after Ab. test result at 18 months of age
# P for Positive
#TO for Transferred Out;
# Malnourished / Underweight for age
# D for Known Dead
Cohort register (Right) Year:_____________ Page 2
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Comprehensive Abortion Care
Services Register
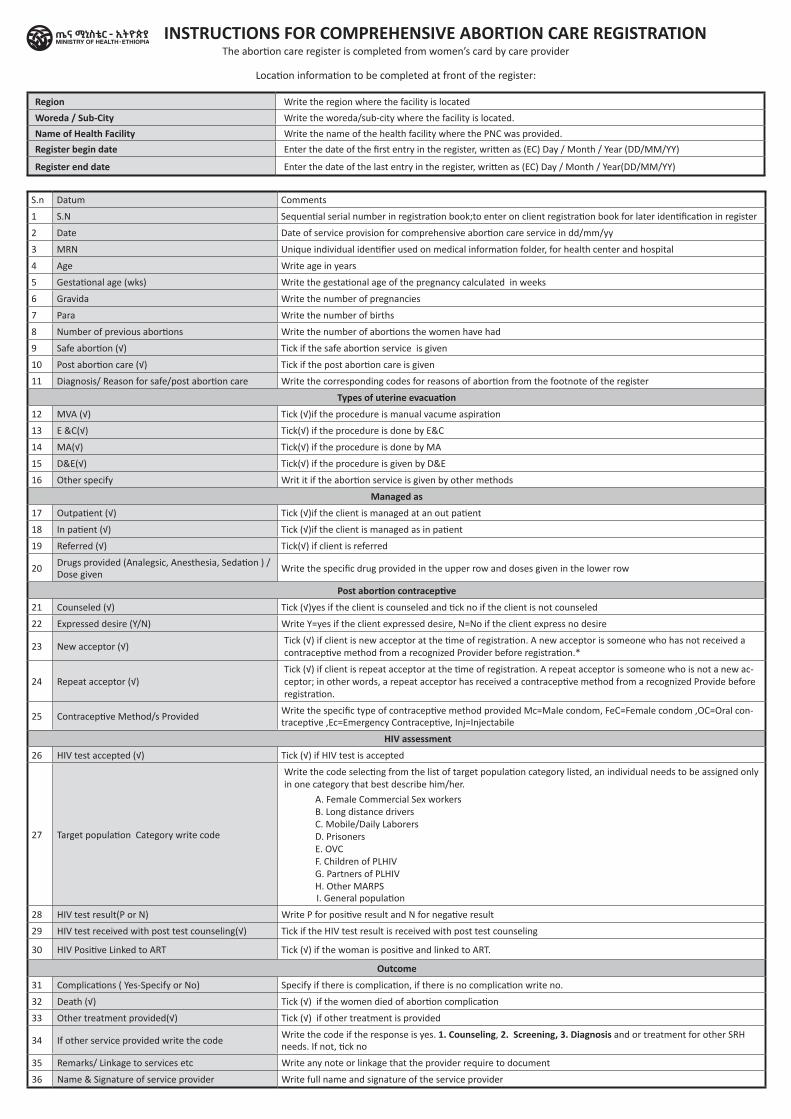
The abortion care register is completed from women’s card by care provider
Location information to be completed at front of the register:
Region Write the region where the facility is located
Woreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility where the PNC was provided.
Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
S.n Datum Comments
1 S.N Sequential serial number in registration book;to enter on client registration book for later identification in register
2 Date Date of service provision for comprehensive abortion care service in dd/mm/yy
3 MRN Unique individual identifier used on medical information folder, for health center and hospital
4 Age Write age in years
5 Gestational age (wks) Write the gestational age of the pregnancy calculated in weeks
6 Gravida Write the number of pregnancies
7 Para Write the number of births
8 Number of previous abortions Write the number of abortions the women have had
9 Safe abortion (√) Tick if the safe abortion service is given
10 Post abortion care (√) Tick if the post abortion care is given
11 Diagnosis/ Reason for safe/post abortion care Write the corresponding codes for reasons of abortion from the footnote of the register
Types of uterine evacuation
12 MVA (√) Tick (√)if the procedure is manual vacume aspiration
13 E &C(√) Tick(√) if the procedure is done by E&C
14 MA(√) Tick(√) if the procedure is done by MA
15 D&E(√) Tick(√) if the procedure is given by D&E
16 Other specify Writ it if the abortion service is given by other methods
Managed as
17 Outpatient (√) Tick (√)if the client is managed at an out patient
18 In patient (√) Tick (√)if the client is managed as in patient
19 Referred (√) Tick(√) if client is referred
20Drugs provided (Analegsic, Anesthesia, Sedation ) / Dose given
Write the specific drug provided in the upper row and doses given in the lower row
Post abortion contraceptive
21 Counseled (√) Tick (√)yes if the client is counseled and tick no if the client is not counseled
22 Expressed desire (Y/N) Write Y=yes if the client expressed desire, N=No if the client express no desire
23 New acceptor (√)Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.*
24 Repeat acceptor (√)Tick (√) if client is repeat acceptor at the time of registration. A repeat acceptor is someone who is not a new ac-ceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
25 Contraceptive Method/s ProvidedWrite the specific type of contraceptive method provided Mc=Male condom, FeC=Female condom ,OC=Oral con-traceptive ,Ec=Emergency Contraceptive, Inj=Injectabile
HIV assessment
26 HIV test accepted (√) Tick (√) if HIV test is accepted
27 Target population Category write code
Write the code selecting from the list of target population category listed, an individual needs to be assigned only in one category that best describe him/her.
A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS
I. General population
28 HIV test result(P or N) Write P for positive result and N for negative result
29 HIV test received with post test counseling(√) Tick if the HIV test result is received with post test counseling
30 HIV Positive Linked to ART Tick (√) if the woman is positive and linked to ART.
Outcome
31 Complications ( Yes-Specify or No) Specify if there is complication, if there is no complication write no.
32 Death (√) Tick (√) if the women died of abortion complication
33 Other treatment provided(√) Tick (√) if other treatment is provided
34 If other service provided write the codeWrite the code if the response is yes. 1. Counseling, 2. Screening, 3. Diagnosis and or treatment for other SRH needs. If not, tick no
35 Remarks/ Linkage to services etc Write any note or linkage that the provider require to document
36 Name & Signature of service provider Write full name and signature of the service provider
INSTRUCTIONS FOR COMPREHENSIVE ABORTION CARE REGISTRATION
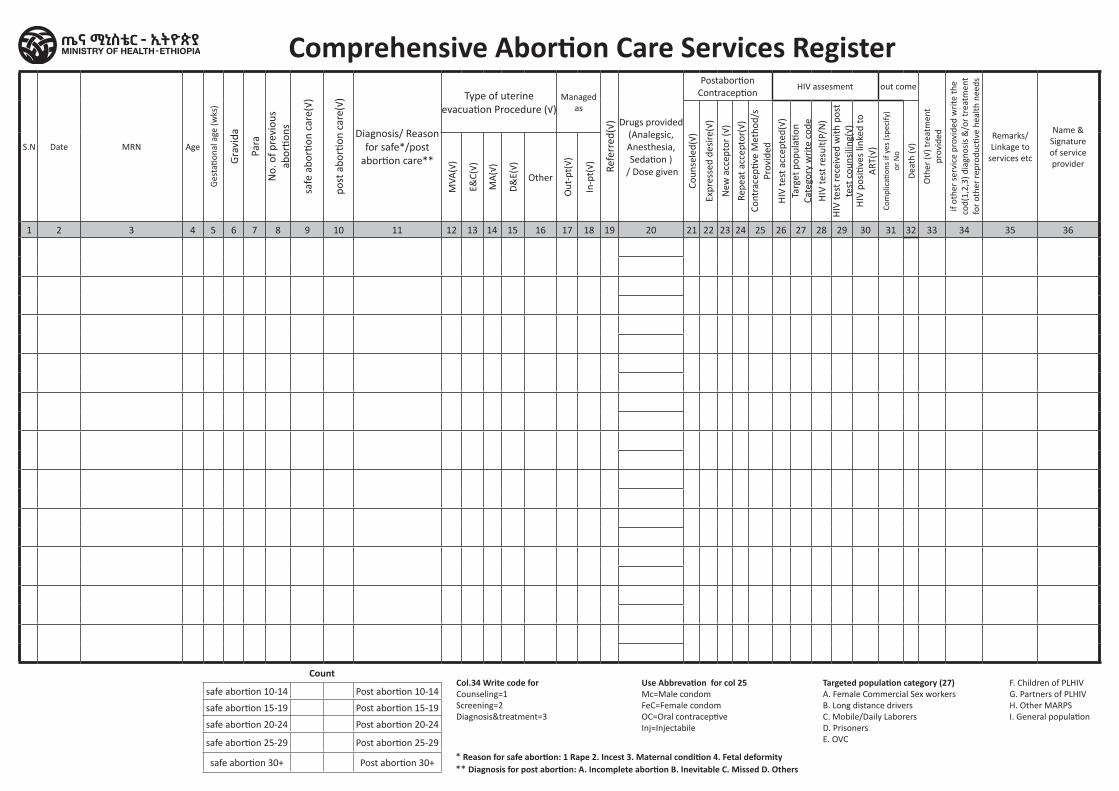
Comprehensive Abortion Care Services Register
S.N Date MRN Age
Ges
tatio
nal a
ge (w
ks)
Gra
vida
Para
No.
of p
revi
ous
ab
ortio
ns
safe
abo
rtion
car
e(√)
post
abo
rtion
car
e(√)
Diagnosis/ Reason for safe*/post
abortion care**
Type of uterine evacuation Procedure (√)
Managed as
Refe
rred
(√) Drugs provided
(Analegsic, Anesthesia, Sedation )
/ Dose given
Postabortion Contraception
HIV assesment out come
Oth
er (√
) tre
atm
ent
prov
ided
if ot
her
serv
ice
prov
ided
wri
te th
e co
d(1,
2,3)
dia
gnos
is &
/or
trea
tmen
t fo
r ot
her
repr
oduc
tive
heal
th n
eeds
Remarks/ Linkage to
services etc
Name & Signature of service provider
Coun
sele
d(√)
Expr
esse
d de
sire
(√)
New
acc
epto
r (√
)
Repe
at a
ccep
tor(
√)Co
ntra
cepti
ve M
etho
d/s
Prov
ided
HIV
test
acc
epte
d(√)
Targ
et p
opul
ation
Ca
tego
ry w
rite
cod
eH
IV te
st re
sult(
P/N
)H
IV te
st re
ceiv
ed w
ith p
ost
test
cou
nsili
ng(√
)H
IV p
ositi
ves
linke
d to
A
RT(√
)Co
mpl
icati
ons
if ye
s (s
peci
fy)
or N
o
Dea
th (√
)
MVA
(√)
E&C(
√)
MA
(√)
D&
E(√)
Other
Out
-pt(
√)
In-p
t(√)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36
Count
safe abortion 10-14 Post abortion 10-14
safe abortion 15-19 Post abortion 15-19
safe abortion 20-24 Post abortion 20-24
safe abortion 25-29 Post abortion 25-29
safe abortion 30+ Post abortion 30+
Use Abbrevation for col 25Mc=Male condomFeC=Female condomOC=Oral contraceptiveInj=Injectabile
Col.34 Write code for Counseling=1 Screening=2 Diagnosis&treatment=3
* Reason for safe abortion: 1 Rape 2. Incest 3. Maternal condition 4. Fetal deformity ** Diagnosis for post abortion: A. Incomplete abortion B. Inevitable C. Missed D. Others
Targeted population category (27)A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVC
F. Children of PLHIV G. Partners of PLHIV H. Other MARPS I. General population
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Routine Immunization Register
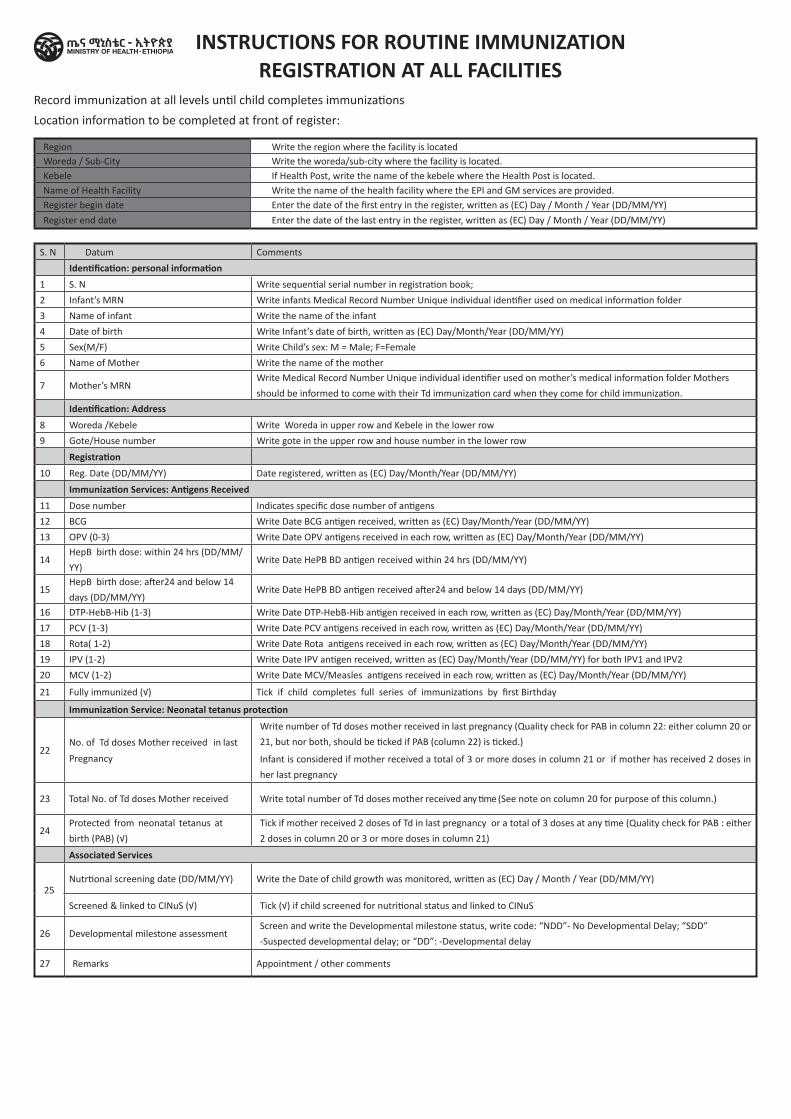
Region Write the region where the facility is locatedWoreda / Sub-City Write the woreda/sub-city where the facility is located.Kebele If Health Post, write the name of the kebele where the Health Post is located.Name of Health Facility Write the name of the health facility where the EPI and GM services are provided.Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
S. N Datum Comments
Identification: personal information 1 S. N Write sequential serial number in registration book;
2 Infant’s MRN Write infants Medical Record Number Unique individual identifier used on medical information folder
3 Name of infant Write the name of the infant
4 Date of birth Write Infant’s date of birth, written as (EC) Day/Month/Year (DD/MM/YY)
5 Sex(M/F) Write Child’s sex: M = Male; F=Female
6 Name of Mother Write the name of the mother
7 Mother’s MRNWrite Medical Record Number Unique individual identifier used on mother’s medical information folder Mothers
should be informed to come with their Td immunization card when they come for child immunization.
Identification: Address8 Woreda /Kebele Write Woreda in upper row and Kebele in the lower row
9 Gote/House number Write gote in the upper row and house number in the lower row
Registration 10 Reg. Date (DD/MM/YY) Date registered, written as (EC) Day/Month/Year (DD/MM/YY)
Immunization Services: Antigens Received 11 Dose number Indicates specific dose number of antigens
12 BCG Write Date BCG antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
13 OPV (0-3) Write Date OPV antigens received in each row, written as (EC) Day/Month/Year (DD/MM/YY)
14HepB birth dose: within 24 hrs (DD/MM/
YY)Write Date HePB BD antigen received within 24 hrs (DD/MM/YY)
15HepB birth dose: after24 and below 14
days (DD/MM/YY)Write Date HePB BD antigen received after24 and below 14 days (DD/MM/YY)
16 DTP-HebB-Hib (1-3) Write Date DTP-HebB-Hib antigen received in each row, written as (EC) Day/Month/Year (DD/MM/YY)
17 PCV (1-3) Write Date PCV antigens received in each row, written as (EC) Day/Month/Year (DD/MM/YY)
18 Rota( 1-2) Write Date Rota antigens received in each row, written as (EC) Day/Month/Year (DD/MM/YY)
19 IPV (1-2) Write Date IPV antigen received, written as (EC) Day/Month/Year (DD/MM/YY) for both IPV1 and IPV2
20 MCV (1-2) Write Date MCV/Measles antigens received in each row, written as (EC) Day/Month/Year (DD/MM/YY)
21 Fully immunized (√) Tick if child completes full series of immunizations by first Birthday
Immunization Service: Neonatal tetanus protection
22No. of Td doses Mother received in last
Pregnancy
Write number of Td doses mother received in last pregnancy (Quality check for PAB in column 22: either column 20 or
21, but nor both, should be ticked if PAB (column 22) is ticked.)
Infant is considered if mother received a total of 3 or more doses in column 21 or if mother has received 2 doses in
her last pregnancy
23 Total No. of Td doses Mother received Write total number of Td doses mother received any time (See note on column 20 for purpose of this column.)
24Protected from neonatal tetanus at
birth (PAB) (√)
Tick if mother received 2 doses of Td in last pregnancy or a total of 3 doses at any time (Quality check for PAB : either
2 doses in column 20 or 3 or more doses in column 21)
Associated Services
25Nutrtional screening date (DD/MM/YY) Write the Date of child growth was monitored, written as (EC) Day / Month / Year (DD/MM/YY)
Screened & linked to CINuS (√) Tick (√) if child screened for nutritional status and linked to CINuS
26 Developmental milestone assessmentScreen and write the Developmental milestone status, write code: “NDD”- No Developmental Delay; “SDD”
-Suspected developmental delay; or “DD”: -Developmental delay
27 Remarks Appointment / other comments
INSTRUCTIONS FOR ROUTINE IMMUNIZATION REGISTRATION AT ALL FACILITIES
Record immunization at all levels until child completes immunizations
Location information to be completed at front of register:
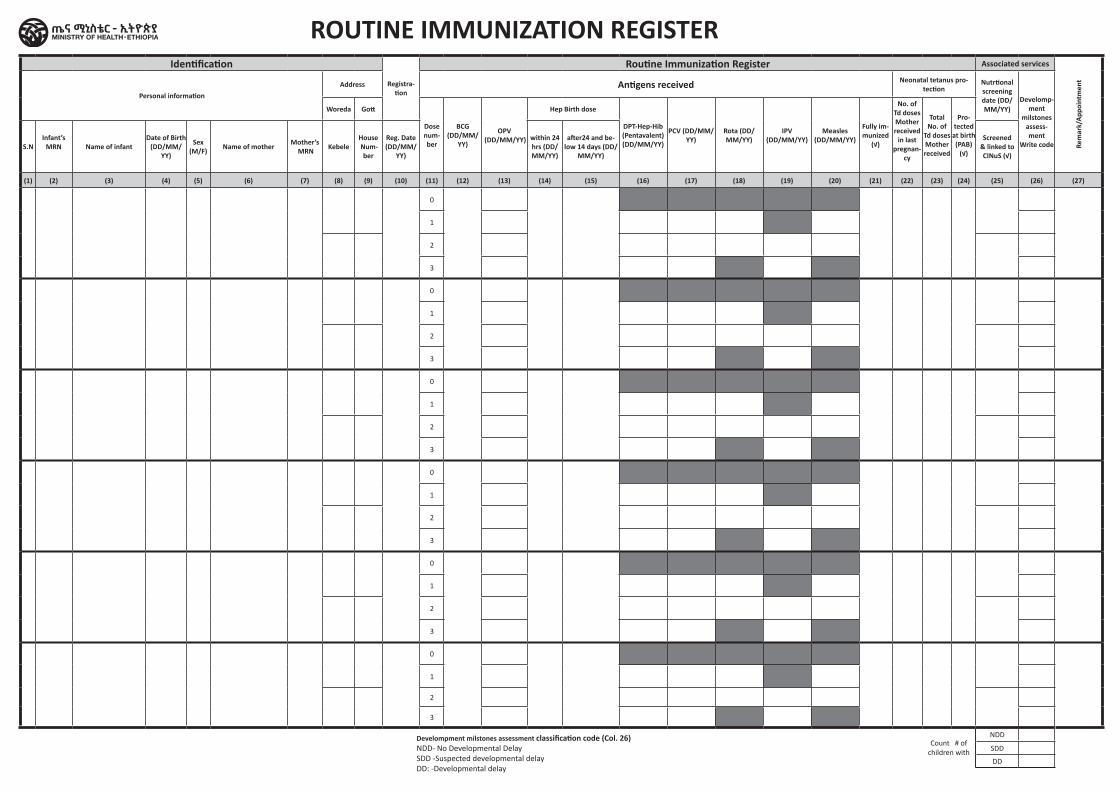
Identification
Registra-tion
Routine Immunization Register Associated services
Rem
ark/
Appo
intm
ent
Personal informationAddress Antigens received Neonatal tetanus pro-
tectionNutrtional screening date (DD/MM/YY)
Develomp-ment
milstones assess-ment
Write code
Woreda Gott
Dose num-ber
BCG (DD/MM/
YY)
OPV (DD/MM/YY)
Hep Birth dose
DPT-Hep-Hib (Pentavalent) (DD/MM/YY)
PCV (DD/MM/YY)
Rota (DD/MM/YY)
IPV (DD/MM/YY)
Measles (DD/MM/YY)
Fully im-munized
(√)
No. of Td doses Mother received
in last pregnan-
cy
Total No. of
Td doses Mother received
Pro-tected at birth (PAB)
(√)S.N
Infant’s MRN Name of infant
Date of Birth (DD/MM/
YY)
Sex (M/F) Name of mother Mother’s
MRN KebeleHouse Num-
ber
Reg. Date (DD/MM/
YY)
within 24 hrs (DD/MM/YY)
after24 and be-low 14 days (DD/
MM/YY)
Screened & linked to CINuS (√)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27)
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
0
1
2
3
Count # of children with
NDD SDD
DD
ROUTINE IMMUNIZATION REGISTER
Develompment milstones assessment classification code (Col. 26) NDD- No Developmental Delay SDD -Suspected developmental delay DD: -Developmental delay
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital HPV Immunization Register
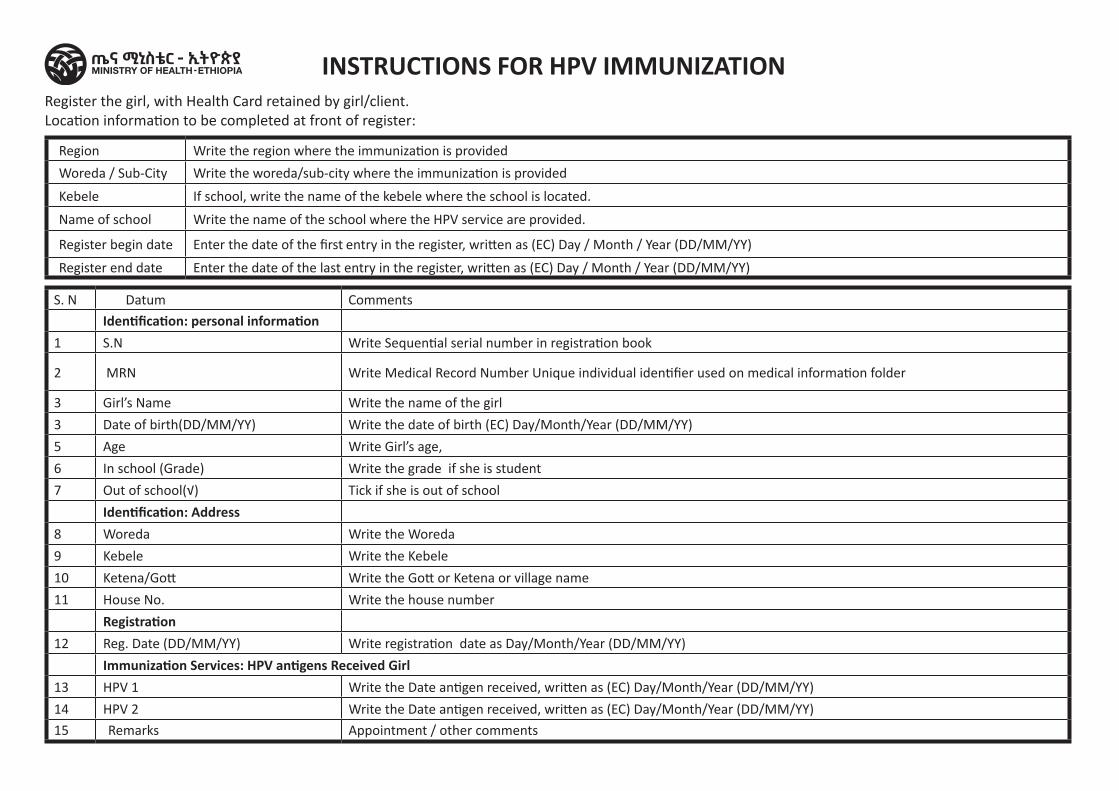
Region Write the region where the immunization is provided
Woreda / Sub-City Write the woreda/sub-city where the immunization is provided
Kebele If school, write the name of the kebele where the school is located.
Name of school Write the name of the school where the HPV service are provided.
Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
S. N Datum Comments
Identification: personal information 1 S.N Write Sequential serial number in registration book
2 MRN Write Medical Record Number Unique individual identifier used on medical information folder
3 Girl’s Name Write the name of the girl
3 Date of birth(DD/MM/YY) Write the date of birth (EC) Day/Month/Year (DD/MM/YY)
5 Age Write Girl’s age,
6 In school (Grade) Write the grade if she is student
7 Out of school(√) Tick if she is out of school
Identification: Address8 Woreda Write the Woreda
9 Kebele Write the Kebele
10 Ketena/Gott Write the Gott or Ketena or village name
11 House No. Write the house number
Registration 12 Reg. Date (DD/MM/YY) Write registration date as Day/Month/Year (DD/MM/YY)
Immunization Services: HPV antigens Received Girl 13 HPV 1 Write the Date antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
14 HPV 2 Write the Date antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
15 Remarks Appointment / other comments
INSTRUCTIONS FOR HPV IMMUNIZATIONRegister the girl, with Health Card retained by girl/client.Location information to be completed at front of register:
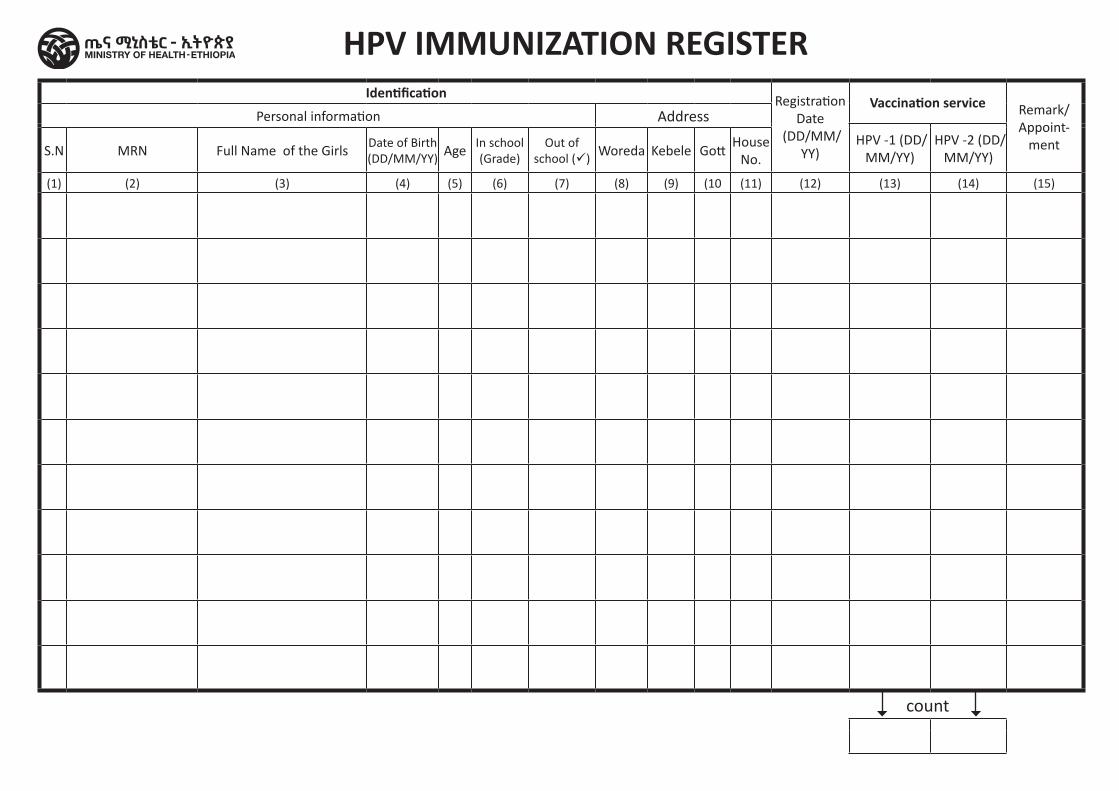
Identification Registration Date
(DD/MM/YY)
Vaccination service Remark/ Appoint-
ment
Personal information Address
HPV -1 (DD/MM/YY)
HPV -2 (DD/MM/YY)S.N MRN Full Name of the Girls
Date of Birth (DD/MM/YY) Age
In school (Grade)
Out of school (ü) Woreda Kebele Gott
House No.
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10 (11) (12) (13) (14) (15)
count
HPV IMMUNIZATION REGISTER
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Tetanus Diphtheria Register
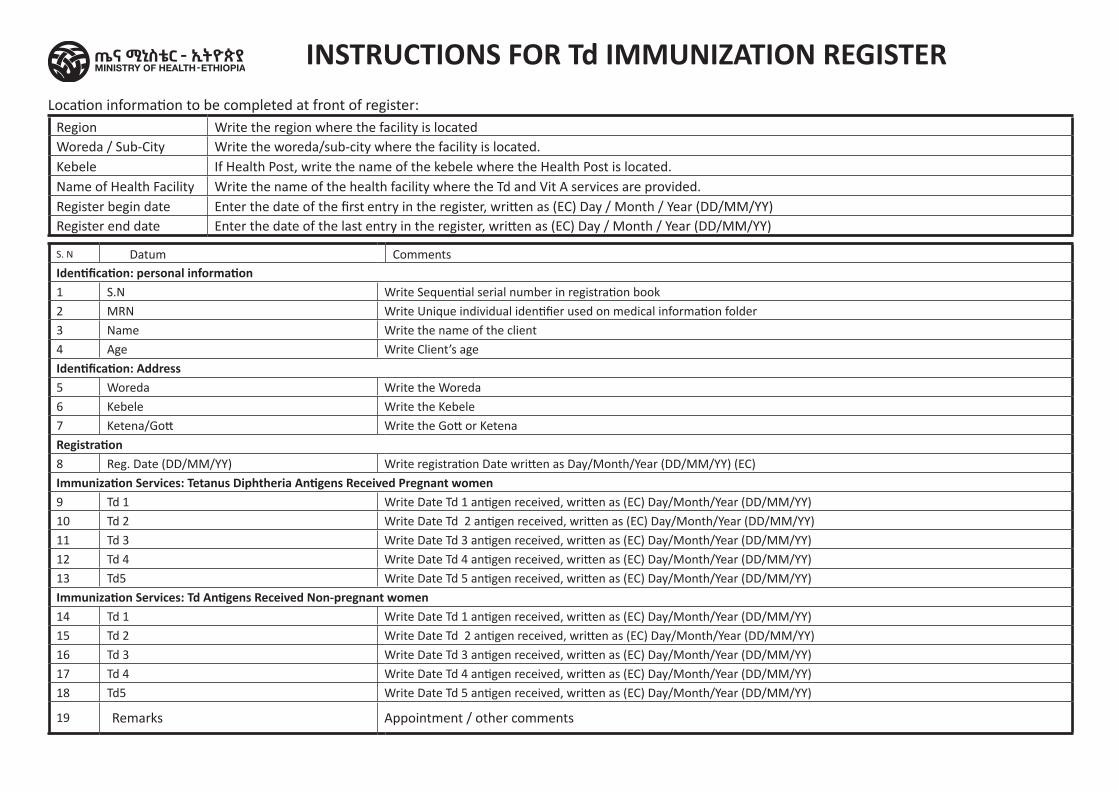
Location information to be completed at front of register:Region Write the region where the facility is locatedWoreda / Sub-City Write the woreda/sub-city where the facility is located.Kebele If Health Post, write the name of the kebele where the Health Post is located.Name of Health Facility Write the name of the health facility where the Td and Vit A services are provided.Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
S. N Datum CommentsIdentification: personal information 1 S.N Write Sequential serial number in registration book
2 MRN Write Unique individual identifier used on medical information folder
3 Name Write the name of the client
4 Age Write Client’s age
Identification: Address5 Woreda Write the Woreda
6 Kebele Write the Kebele
7 Ketena/Gott Write the Gott or Ketena
Registration 8 Reg. Date (DD/MM/YY) Write registration Date written as Day/Month/Year (DD/MM/YY) (EC)
Immunization Services: Tetanus Diphtheria Antigens Received Pregnant women9 Td 1 Write Date Td 1 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
10 Td 2 Write Date Td 2 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
11 Td 3 Write Date Td 3 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
12 Td 4 Write Date Td 4 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
13 Td5 Write Date Td 5 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
Immunization Services: Td Antigens Received Non-pregnant women14 Td 1 Write Date Td 1 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
15 Td 2 Write Date Td 2 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
16 Td 3 Write Date Td 3 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
17 Td 4 Write Date Td 4 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
18 Td5 Write Date Td 5 antigen received, written as (EC) Day/Month/Year (DD/MM/YY)
19 Remarks Appointment / other comments
INSTRUCTIONS FOR Td IMMUNIZATION REGISTER
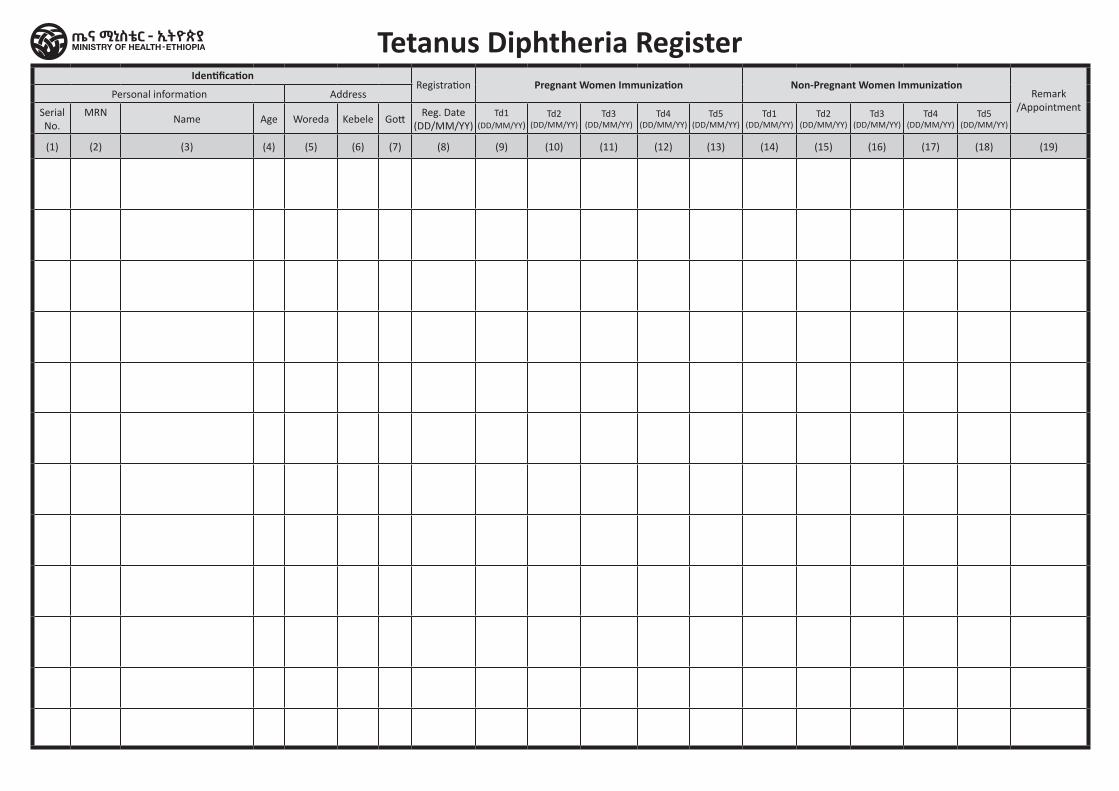
IdentificationRegistration Pregnant Women Immunization Non-Pregnant Women Immunization
Remark /Appointment
Personal information Address
Serial No.
MRN Name Age Woreda Kebele Gott
Reg. Date (DD/MM/YY)
Td1 (DD/MM/YY)
Td2 (DD/MM/YY)
Td3 (DD/MM/YY)
Td4 (DD/MM/YY)
Td5 (DD/MM/YY)
Td1 (DD/MM/YY)
Td2 (DD/MM/YY)
Td3 (DD/MM/YY)
Td4 (DD/MM/YY)
Td5 (DD/MM/YY)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19)
Tetanus Diphtheria Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Hospital / ClinicNeonatal Intensive Care Unit (NICU)
Register
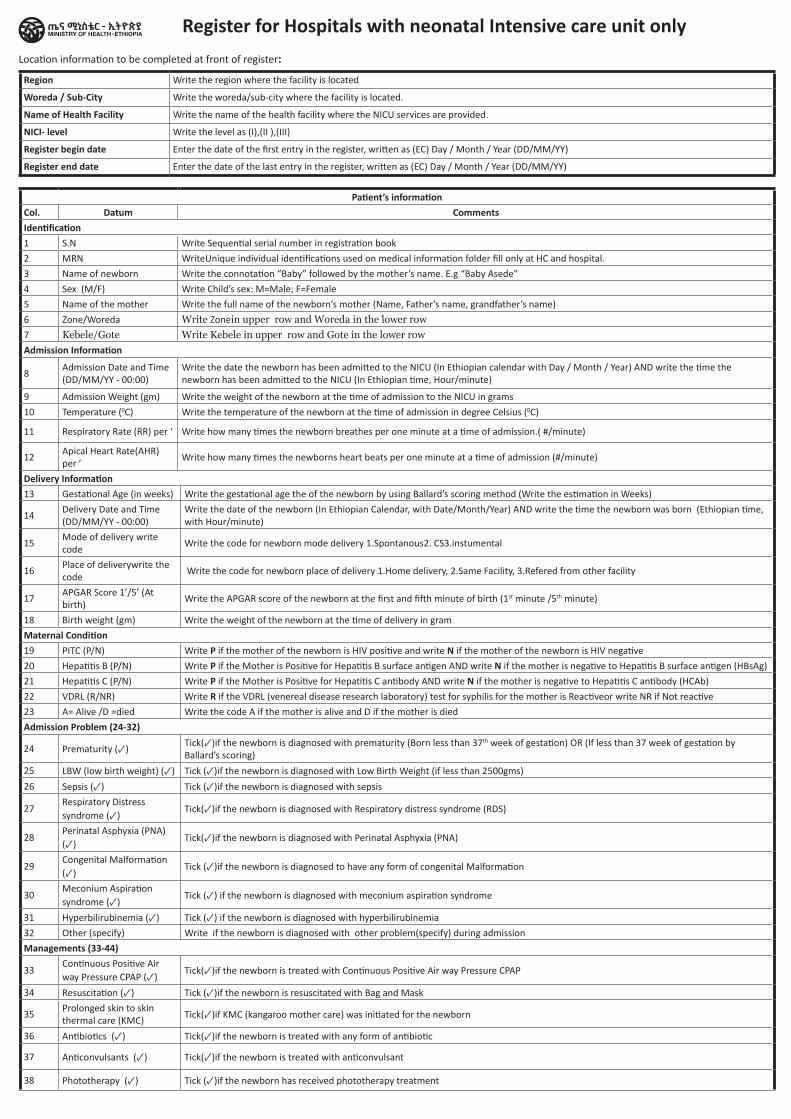
Register for Hospitals with neonatal Intensive care unit onlyLocation information to be completed at front of register:
Region Write the region where the facility is located
Woreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility where the NICU services are provided.
NICI- level Write the level as (I),(II ),(III)
Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Patient’s informationCol. Datum CommentsIdentification1 S.N Write Sequential serial number in registration book
2 MRN WriteUnique individual identifications used on medical information folder fill only at HC and hospital.
3 Name of newborn Write the connotation “Baby” followed by the mother’s name. E.g “Baby Asede”
4 Sex (M/F) Write Child’s sex: M=Male; F=Female
5 Name of the mother Write the full name of the newborn’s mother (Name, Father’s name, grandfather’s name)
6 Zone/Woreda Write Zonein upper row and Woreda in the lower row7 Kebele/Gote Write Kebele in upper row and Gote in the lower rowAdmission Information
8Admission Date and Time (DD/MM/YY - 00:00)
Write the date the newborn has been admitted to the NICU (In Ethiopian calendar with Day / Month / Year) AND write the time the newborn has been admitted to the NICU (In Ethiopian time, Hour/minute)
9 Admission Weight (gm) Write the weight of the newborn at the time of admission to the NICU in grams
10 Temperature (0C) Write the temperature of the newborn at the time of admission in degree Celsius (0C)
11 Respiratory Rate (RR) per ‘ Write how many times the newborn breathes per one minute at a time of admission.( #/minute)
12Apical Heart Rate(AHR) per ’
Write how many times the newborns heart beats per one minute at a time of admission (#/minute)
Delivery Information13 Gestational Age (in weeks) Write the gestational age the of the newborn by using Ballard’s scoring method (Write the estimation in Weeks)
14Delivery Date and Time (DD/MM/YY - 00:00)
Write the date of the newborn (In Ethiopian Calendar, with Date/Month/Year) AND write the time the newborn was born (Ethiopian time, with Hour/minute)
15Mode of delivery write code
Write the code for newborn mode delivery 1.Spontanous2. CS3.instumental
16Place of deliverywrite the code
Write the code for newborn place of delivery 1.Home delivery, 2.Same Facility, 3.Refered from other facility
17APGAR Score 1’/5’ (At birth)
Write the APGAR score of the newborn at the first and fifth minute of birth (1st minute /5th minute)
18 Birth weight (gm) Write the weight of the newborn at the time of delivery in gram
Maternal Condition19 PITC (P/N) Write P if the mother of the newborn is HIV positive and write N if the mother of the newborn is HIV negative
20 Hepatitis B (P/N) Write P if the Mother is Positive for Hepatitis B surface antigen AND write N if the mother is negative to Hepatitis B surface antigen (HBsAg)
21 Hepatitis C (P/N) Write P if the Mother is Positive for Hepatitis C antibody AND write N if the mother is negative to Hepatitis C antibody (HCAb)
22 VDRL (R/NR) Write R if the VDRL (venereal disease research laboratory) test for syphilis for the mother is Reactiveor write NR if Not reactive
23 A= Alive /D =died Write the code A if the mother is alive and D if the mother is died
Admission Problem (24-32)
24 Prematurity (✓)Tick(✓)if the newborn is diagnosed with prematurity (Born less than 37th week of gestation) OR (If less than 37 week of gestation by Ballard’s scoring)
25 LBW (low birth weight) (✓) Tick (✓)if the newborn is diagnosed with Low Birth Weight (if less than 2500gms)
26 Sepsis (✓) Tick (✓)if the newborn is diagnosed with sepsis
27Respiratory Distress syndrome (✓)
Tick(✓)if the newborn is diagnosed with Respiratory distress syndrome (RDS)
28Perinatal Asphyxia (PNA) (✓)
Tick(✓)if the newborn is diagnosed with Perinatal Asphyxia (PNA)
29Congenital Malformation (✓)
Tick (✓)if the newborn is diagnosed to have any form of congenital Malformation
30Meconium Aspiration syndrome (✓)
Tick (✓) if the newborn is diagnosed with meconium aspiration syndrome
31 Hyperbilirubinemia (✓) Tick (✓) if the newborn is diagnosed with hyperbilirubinemia
32 Other (specify) Write if the newborn is diagnosed with other problem(specify) during admission
Managements (33-44)
33Continuous Positive Air way Pressure CPAP (✓)
Tick(✓)if the newborn is treated with Continuous Positive Air way Pressure CPAP
34 Resuscitation (✓) Tick (✓)if the newborn is resuscitated with Bag and Mask
35Prolonged skin to skin thermal care (KMC)
Tick(✓)if KMC (kangaroo mother care) was initiated for the newborn
36 Antibiotics (✓) Tick(✓)if the newborn is treated with any form of antibiotic
37 Anticonvulsants (✓) Tick(✓)if the newborn is treated with anticonvulsant
38 Phototherapy (✓) Tick (✓)if the newborn has received phototherapy treatment
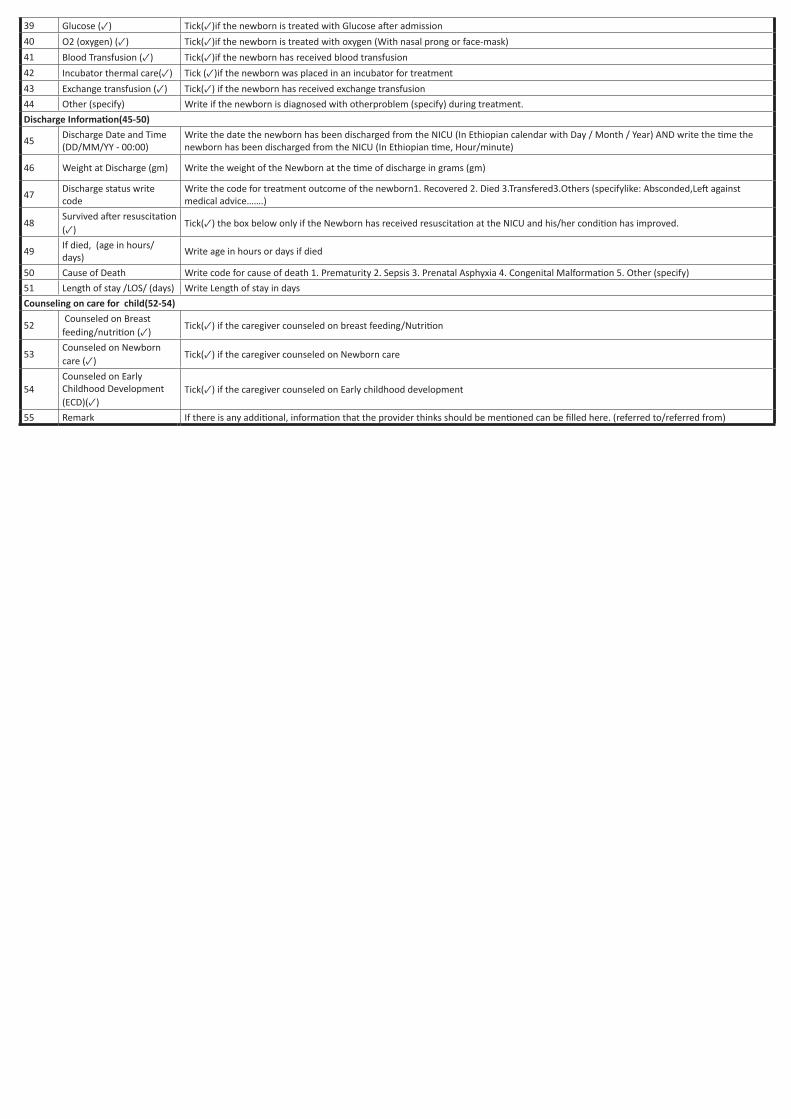
39 Glucose (✓) Tick(✓)if the newborn is treated with Glucose after admission
40 O2 (oxygen) (✓) Tick(✓)if the newborn is treated with oxygen (With nasal prong or face-mask)
41 Blood Transfusion (✓) Tick(✓)if the newborn has received blood transfusion
42 Incubator thermal care(✓) Tick (✓)if the newborn was placed in an incubator for treatment
43 Exchange transfusion (✓) Tick(✓) if the newborn has received exchange transfusion
44 Other (specify) Write if the newborn is diagnosed with otherproblem (specify) during treatment.
Discharge Information(45-50)
45Discharge Date and Time (DD/MM/YY - 00:00)
Write the date the newborn has been discharged from the NICU (In Ethiopian calendar with Day / Month / Year) AND write the time the newborn has been discharged from the NICU (In Ethiopian time, Hour/minute)
46 Weight at Discharge (gm) Write the weight of the Newborn at the time of discharge in grams (gm)
47Discharge status write code
Write the code for treatment outcome of the newborn1. Recovered 2. Died 3.Transfered3.Others (specifylike: Absconded,Left against medical advice…….)
48Survived after resuscitation (✓)
Tick(✓) the box below only if the Newborn has received resuscitation at the NICU and his/her condition has improved.
49If died, (age in hours/ days)
Write age in hours or days if died
50 Cause of Death Write code for cause of death 1. Prematurity 2. Sepsis 3. Prenatal Asphyxia 4. Congenital Malformation 5. Other (specify)
51 Length of stay /LOS/ (days) Write Length of stay in days
Counseling on care for child(52-54)
52 Counseled on Breast feeding/nutrition (✓)
Tick(✓) if the caregiver counseled on breast feeding/Nutrition
53Counseled on Newborn care (✓)
Tick(✓) if the caregiver counseled on Newborn care
54Counseled on Early Childhood Development (ECD)(✓)
Tick(✓) if the caregiver counseled on Early childhood development
55 Remark If there is any additional, information that the provider thinks should be mentioned can be filled here. (referred to/referred from)
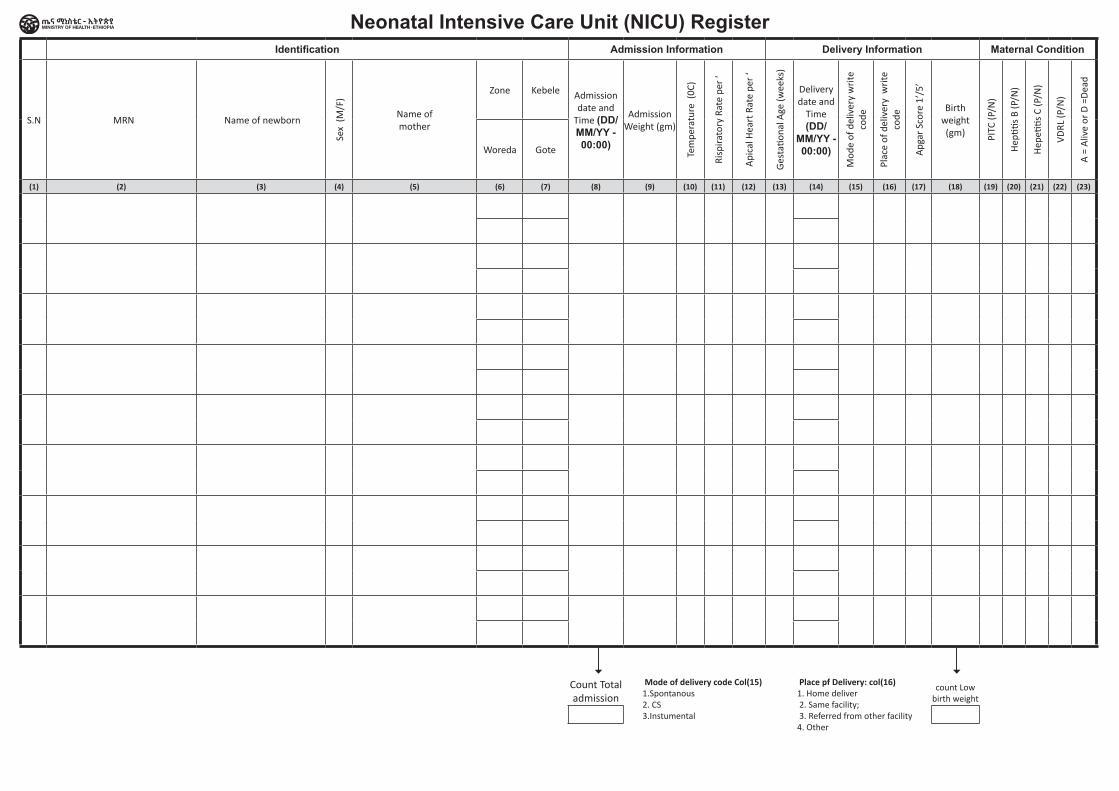
Identification Admission Information Delivery Information Maternal Condition
S.N MRN Name of newborn
Sex
(M/F
)
Name of mother
Zone Kebele Admission date and
Time (DD/MM/YY - 00:00)
Admission Weight (gm)
Tem
pera
ture
(0C
)
Risp
irato
ry R
ate
per
‘
Api
cal H
eart
Rat
e pe
r ‘
Ges
tatio
nal A
ge (w
eeks
)
Delivery date and
Time (DD/
MM/YY - 00:00)
Mod
e of
del
iver
y w
rite
co
de
Plac
e of
del
iver
y w
rite
co
de
Apg
ar S
core
1’/
5’
Birth weight (gm) PI
TC (P
/N)
Hep
titis
B (P
/N)
Hep
etitis
C (P
/N)
VDRL
(P/N
)
A =
Aliv
e or
D =
Dea
d
Woreda Gote
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23)
Count Total admission
count Low birth weight
Neonatal Intensive Care Unit (NICU) Register
Mode of delivery code Col(15)1.Spontanous2. CS3.Instumental
Place pf Delivery: col(16)1. Home deliver 2. Same facility; 3. Referred from other facility4. Other
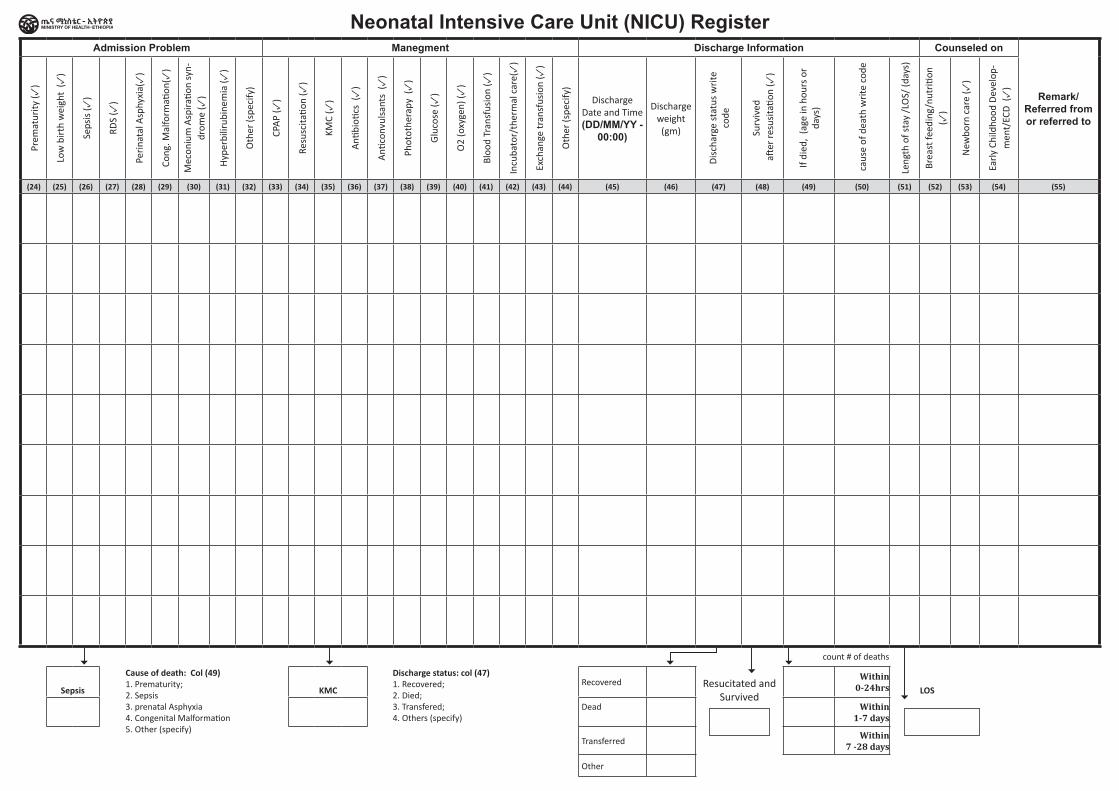
Neonatal Intensive Care Unit (NICU) RegisterAdmission Problem Manegment Discharge Information Counseled on
Remark/ Referred from or referred to
Prem
atur
ity (✓
)
Low
bir
th w
eigh
t ( ✓
)
Seps
is ( ✓
)
RDS
( ✓)
Peri
nata
l Asp
hyxi
a(✓
)
Cong
. Mal
form
ation
( ✓)
Mec
oniu
m A
spira
tion
syn-
drom
e (✓
)
Hyp
erbi
lirub
inem
ia (✓
)
Oth
er (s
peci
fy)
CPA
P (✓
)
Resu
scita
tion
( ✓)
KMC
( ✓)
Anti
bioti
cs (
✓)
Anti
conv
ulsa
nts
( ✓)
Phot
othe
rapy
(✓
)
Glu
cose
( ✓)
O2
(oxy
gen)
( ✓)
Bloo
d Tr
ansf
usio
n ( ✓
)
Incu
bato
r/th
erm
al c
are(
✓)
Exch
ange
tran
sfus
ion
( ✓)
Oth
er (s
peci
fy)
Discharge Date and Time (DD/MM/YY -
00:00)
Discharge weight (gm)
Dis
char
ge s
tatu
s w
rite
co
de
Surv
ived
a
fter
resu
sita
tion
( ✓)
If di
ed,
(age
in h
ours
or
days
)
cau
se o
f dea
th w
rite
cod
e
Leng
th o
f sta
y /L
OS/
(day
s)
Brea
st fe
edin
g/nu
triti
on
(✓)
New
born
car
e (✓
)
Earl
y Ch
ildho
od D
evel
op-
men
t/EC
D (
✓)
(24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44) (45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55)
count # of deaths
Sepsis KMCRecovered Resucitated and
Survived
Within 0-24hrs LOS
Dead Within 1-7 days
Transferred Within
7 -28 days
Other
Cause of death: Col (49)1. Prematurity; 2. Sepsis3. prenatal Asphyxia4. Congenital Malformation5. Other (specify)
Discharge status: col (47) 1. Recovered; 2. Died; 3. Transfered; 4. Others (specify)
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Integrated Management of New born and Childhood
Illness Register (2 to 59 Months) Register
1. A row separated by a hard line is for one patient. The very top row indicates which variable to fill, like name of patient, age, sex, weight, etc….
2. Some boxes are separated by dotted line. In these boxes two variables should be written. Example: in the first column, the first box is divided into two by dotted line. According to
the very top row, in the upper box the date of the visit should be filled and in the lower box the serial number should be filled. The same applies for the third, fourth and fifth columns.
In the third column name above and address below, in the fourth column age above and sex below, in the fifth column weight above and temperature below.
3. In the presenting complaint box the most important reason/s for the visit should be written clearly.
4. In the patient’s signs and symptom boxes all signs or symptoms the child has should be circled or written.
5. Write clearly in the columns for other problem, classification/s, medicine/s, referral, follow-up and other remarks.
6. Use all the information you noted to classify the child and provide medicine/s, referral or follow-up.
7. Do follow up to all sick young infants and children and document the outcome of your efforts
8. Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer
(do not abbreviation)
INSTRUCTION ON HOW TO COMPLETE THE UNDER-FIVE REGISTER
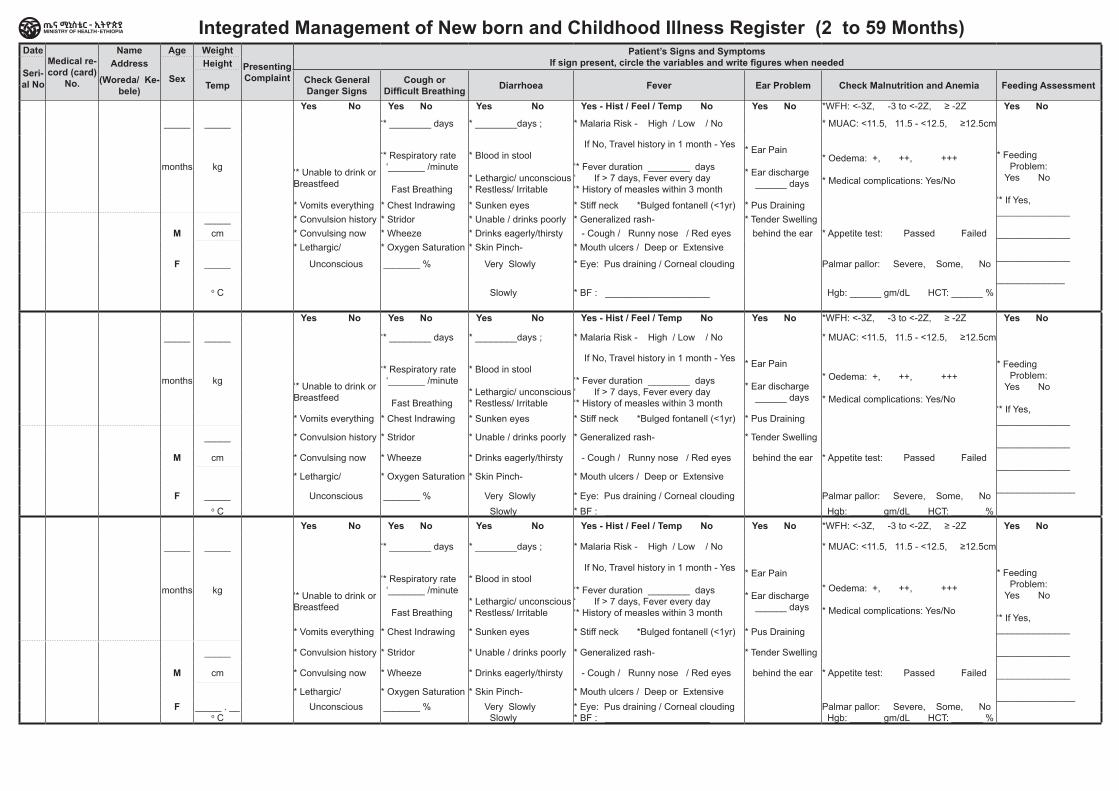
Integrated Management of New born and Childhood Illness Register (2 to 59 Months)Date
Medical re-cord (card)
No.
Name Age Weight
Presenting Complaint
Patient’s Signs and Symptoms If sign present, circle the variables and write figures when needed
Patient’s Signs and Symptoms If sign present, circle the variables and write figures when needed Other
Prob-lems
Classification
Treatment, Counsel and Follow Up [ESV_ICD11] Diagnosis
RemarksSeri-al No
Address Sex
Height Medicine (Name, Dose,
Schedule, Duration)
Counsel and Referral Follow up (Woreda/ Ke-
bele) Temp Check General Danger Signs
Cough or Difficult Breathing Diarrhoea Fever Ear Problem Check Malnutrition and Anemia Feeding Assessment HIV/AIDS Tuberculosis Development Immunization, Vit A
and Deworming Name CodeYes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother:
Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm
* Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _____________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No
* Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or Extensive
F _____ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No
o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
Yes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother: Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm * Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _______________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No * Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining
_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed
* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or Extensive
F _____ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
Yes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother: Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm * Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _______________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No * Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining
_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed
* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or ExtensiveF _____ . __ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No
o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
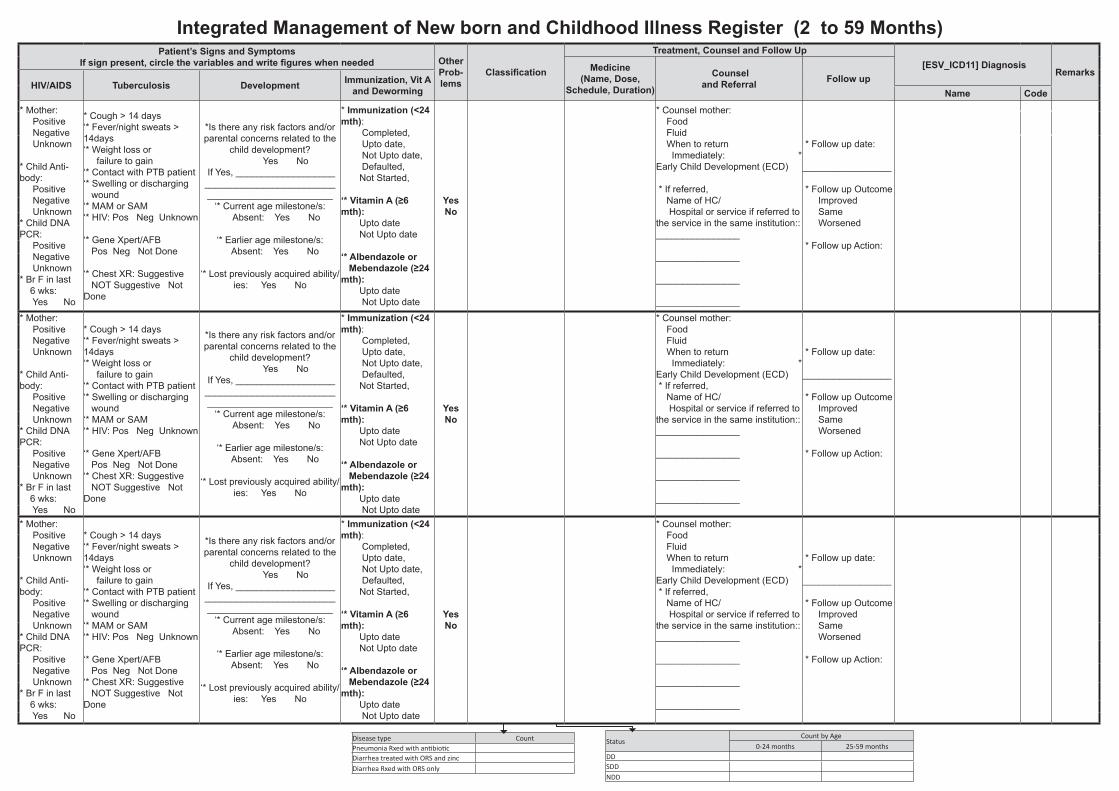
Integrated Management of New born and Childhood Illness Register (2 to 59 Months)Date
Medical re-cord (card)
No.
Name Age Weight
Presenting Complaint
Patient’s Signs and Symptoms If sign present, circle the variables and write figures when needed
Patient’s Signs and Symptoms If sign present, circle the variables and write figures when needed Other
Prob-lems
Classification
Treatment, Counsel and Follow Up [ESV_ICD11] Diagnosis
RemarksSeri-al No
Address Sex
Height Medicine (Name, Dose,
Schedule, Duration)
Counsel and Referral Follow up (Woreda/ Ke-
bele) Temp Check General Danger Signs
Cough or Difficult Breathing Diarrhoea Fever Ear Problem Check Malnutrition and Anemia Feeding Assessment HIV/AIDS Tuberculosis Development Immunization, Vit A
and Deworming Name CodeYes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother:
Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm
* Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _____________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No
* Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or Extensive
F _____ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No
o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
Yes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother: Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm * Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _______________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No * Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining
_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed
* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or Extensive
F _____ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
Yes No Yes No Yes No Yes - Hist / Feel / Temp No Yes No *WFH: <-3Z, -3 to <-2Z, ≥ -2Z Yes No * Mother: Positive Negative Unknown * Child Anti-body: Positive Negative Unknown * Child DNA PCR: Positive Negative Unknown * Br F in last 6 wks: Yes No
* Cough > 14 days ‘* Fever/night sweats > 14days ‘* Weight loss or failure to gain ‘* Contact with PTB patient ‘* Swelling or discharging wound ‘* MAM or SAM ‘* HIV: Pos Neg Unknown ‘* Gene Xpert/AFB Pos Neg Not Done ‘* Chest XR: Suggestive NOT Suggestive Not Done
*Is there any risk factors and/or parental concerns related to the
child development? Yes No
If Yes, ___________________ _________________________ ________________________
‘* Current age milestone/s: Absent: Yes No
‘* Earlier age milestone/s: Absent: Yes No
‘* Lost previously acquired ability/
ies: Yes No
* Immunization (<24 mth): Completed, Upto date, Not Upto date, Defaulted, Not Started, ‘* Vitamin A (≥6 mth): Upto date Not Upto date ‘* Albendazole or Mebendazole (≥24 mth): Upto date Not Upto date
Yes No
* Counsel mother: Food Fluid When to return Immediately: * Early Child Development (ECD) * If referred, Name of HC/ Hospital or service if referred to the service in the same institution:: ________________ ________________ ________________ ________________
* Follow up date: _________________ * Follow up Outcome Improved Same Worsened * Follow up Action:
_____ _____ ‘* ________ days * ________days ; * Malaria Risk - High / Low / No * MUAC: <11.5, 11.5 - <12.5, ≥12.5cm * Feeding Problem: Yes No ‘* If Yes, ______________ ______________ ______________ _______________
months kg
‘* Unable to drink or Breastfeed
‘* Respiratory rate ‘_______ /minute Fast Breathing
* Blood in stool * Lethargic/ unconscious * Restless/ Irritable
If No, Travel history in 1 month - Yes ‘* Fever duration ________ days ‘ If > 7 days, Fever every day ‘* History of measles within 3 month
* Ear Pain * Ear discharge ______ days
* Oedema: +, ++, +++ * Medical complications: Yes/No * Vomits everything * Chest Indrawing * Sunken eyes * Stiff neck *Bulged fontanell (<1yr) * Pus Draining
_____ * Convulsion history * Stridor * Unable / drinks poorly * Generalized rash- * Tender Swelling
M cm * Convulsing now * Wheeze * Drinks eagerly/thirsty - Cough / Runny nose / Red eyes behind the ear * Appetite test: Passed Failed
* Lethargic/ * Oxygen Saturation * Skin Pinch- * Mouth ulcers / Deep or ExtensiveF _____ . __ Unconscious _______ % Very Slowly * Eye: Pus draining / Corneal clouding Palmar pallor: Severe, Some, No
o C Slowly * BF : ____________________ Hgb: ______ gm/dL HCT: ______ %
Disease type CountPneumonia Rxed with antibiotic Diarrhea treated with ORS and zincDiarrhea Rxed with ORS only
StatusCount by Age
0-24 months 25-59 monthsDDSDDNDD
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Integrated Management of New born and Childhood
Illness Register (from 0-2 months)
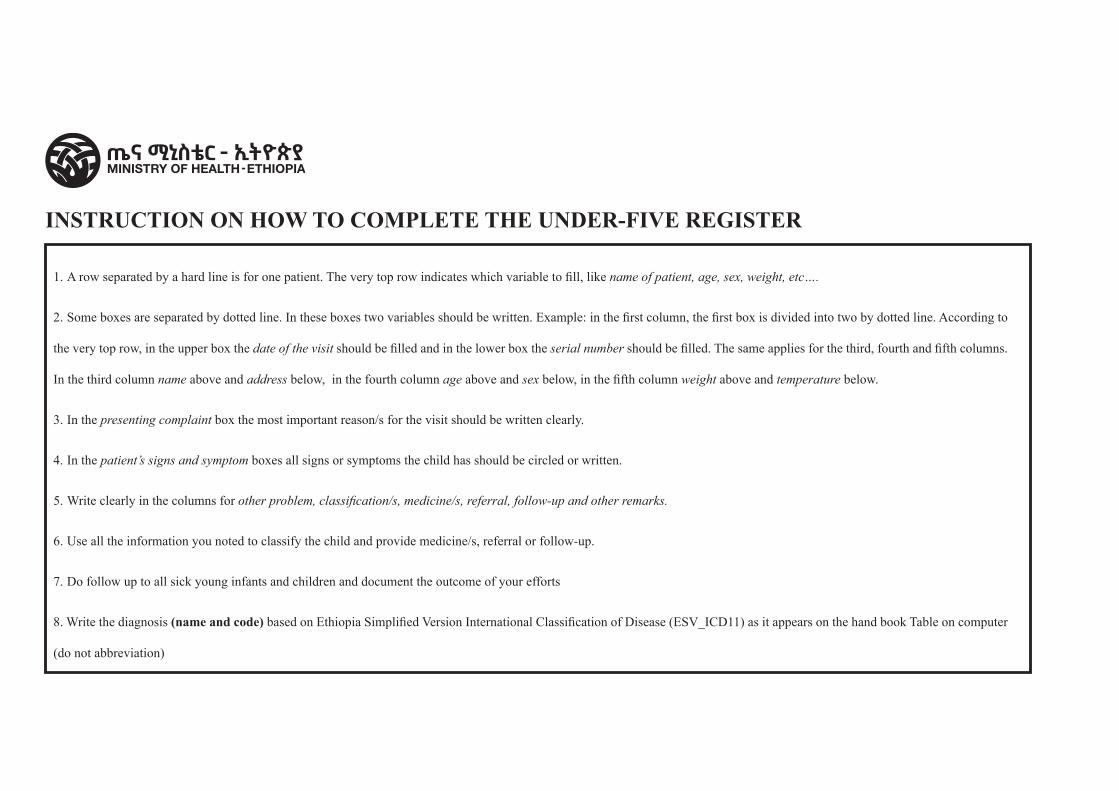
1. A row separated by a hard line is for one patient. The very top row indicates which variable to fill, like name of patient, age, sex, weight, etc….
2. Some boxes are separated by dotted line. In these boxes two variables should be written. Example: in the first column, the first box is divided into two by dotted line. According to
the very top row, in the upper box the date of the visit should be filled and in the lower box the serial number should be filled. The same applies for the third, fourth and fifth columns.
In the third column name above and address below, in the fourth column age above and sex below, in the fifth column weight above and temperature below.
3. In the presenting complaint box the most important reason/s for the visit should be written clearly.
4. In the patient’s signs and symptom boxes all signs or symptoms the child has should be circled or written.
5. Write clearly in the columns for other problem, classification/s, medicine/s, referral, follow-up and other remarks.
6. Use all the information you noted to classify the child and provide medicine/s, referral or follow-up.
7. Do follow up to all sick young infants and children and document the outcome of your efforts
8. Write the diagnosis (name and code) based on Ethiopia Simplified Version International Classification of Disease (ESV_ICD11) as it appears on the hand book Table on computer
(do not abbreviation)
INSTRUCTION ON HOW TO COMPLETE THE UNDER-FIVE REGISTER
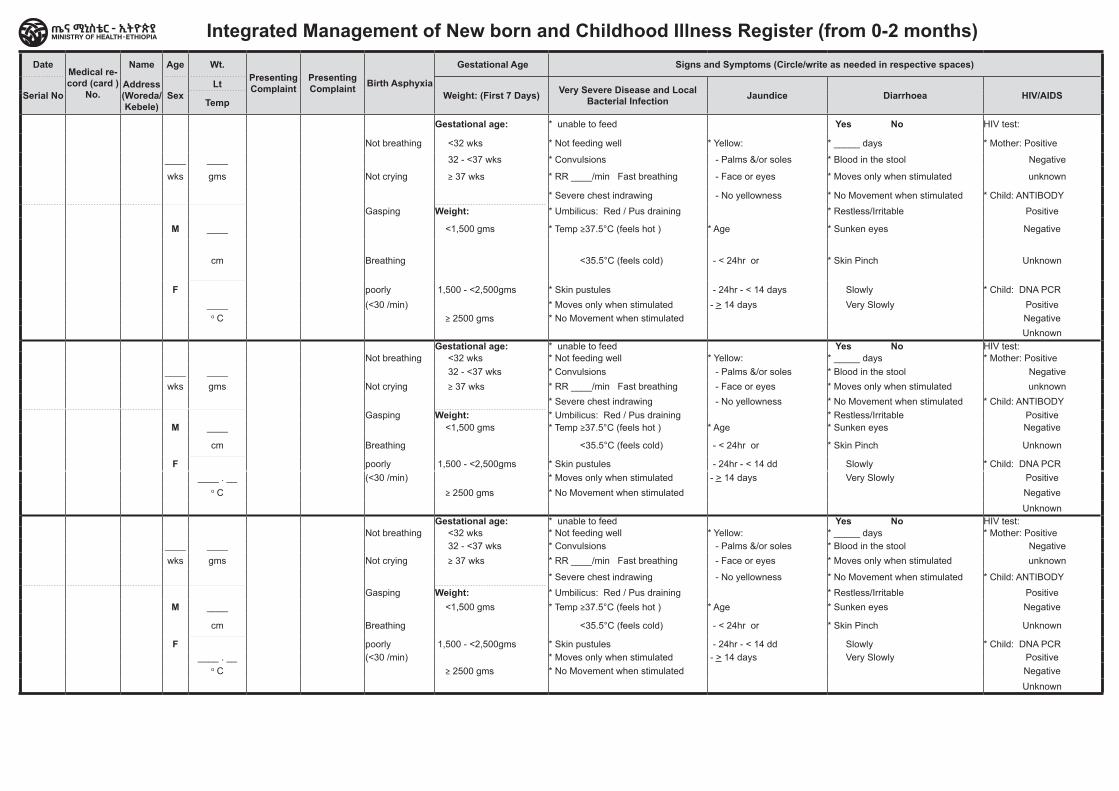
Integrated Management of New born and Childhood Illness Register (from 0-2 months) Date
Medical re-cord (card )
No.
Name Age Wt.Presenting Complaint
Presenting Complaint Birth Asphyxia
Gestational Age Signs and Symptoms (Circle/write as needed in respective spaces) Signs and Symptoms (Circle/write ...)Immuniza-tion Status
of Infant
Other ProblemsClassification
Treatment Follow up Date [ESV_ICD11] Diagnosis Remarks
Serial NoAddress (Woreda/ Kebele)
SexLt
Weight: (First 7 Days) Very Severe Disease and Local Bacterial Infection Jaundice Diarrhoea HIV/AIDS Feeding Problem (For Breast-
feeding ) Development problem Medicine (Name, Dose, Schedule, Duration) Counsel the Mother
Referred (Name of HC/
Hosp)Outcome
Temp Maternal Danger Signs (< 6wks) Name Code
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty
‘*Is there any risk factor and/or parental concern related to
the child development? Yes No
If Yes, ___________________
________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast
____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feeding
wks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * Improved
Gasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warm
M ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 days Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty‘*Is there any risk factor and/
or parental concern related to the child development?
Yes No If Yes,
___________________ ________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast ____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feedingwks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * ImprovedGasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warm
M ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 dd Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ . __ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty‘*Is there any risk factor and/
or parental concern related to the child development?
Yes No If Yes,
___________________ ________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast ____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feedingwks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * Improved
Gasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warmM ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 dd Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ . __ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
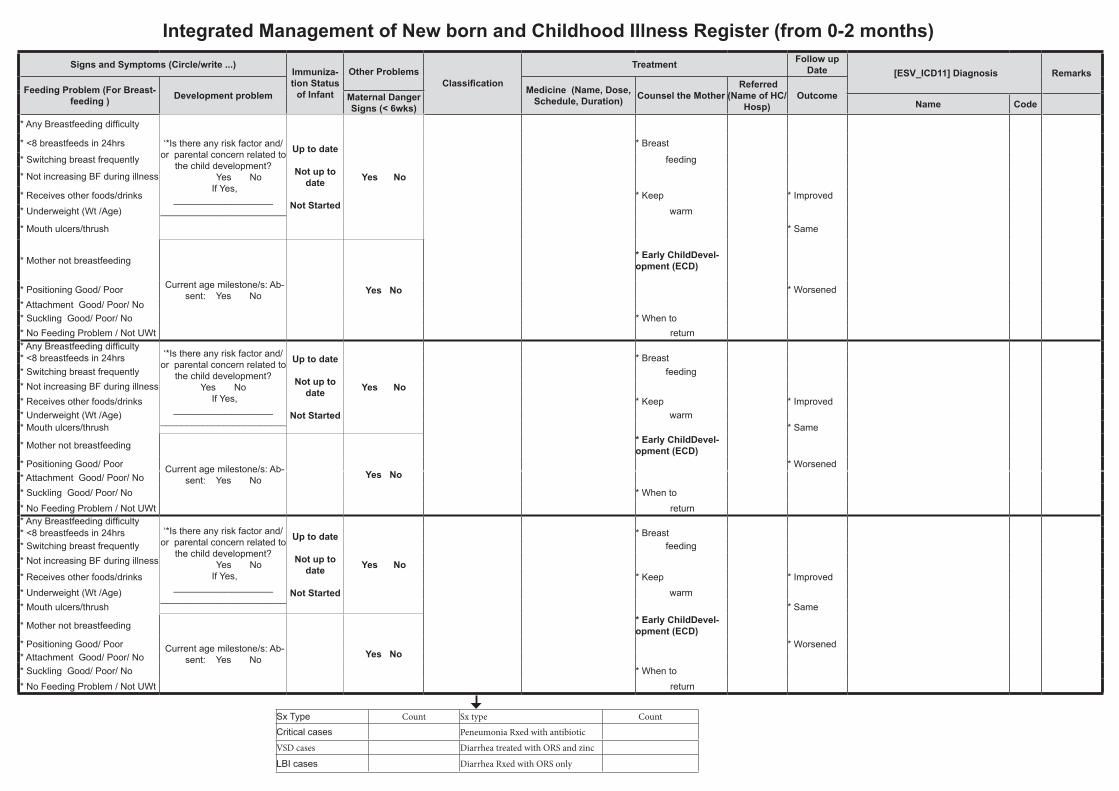
DateMedical re-cord (card )
No.
Name Age Wt.Presenting Complaint
Presenting Complaint Birth Asphyxia
Gestational Age Signs and Symptoms (Circle/write as needed in respective spaces) Signs and Symptoms (Circle/write ...)Immuniza-tion Status
of Infant
Other ProblemsClassification
Treatment Follow up Date [ESV_ICD11] Diagnosis Remarks
Serial NoAddress (Woreda/ Kebele)
SexLt
Weight: (First 7 Days) Very Severe Disease and Local Bacterial Infection Jaundice Diarrhoea HIV/AIDS Feeding Problem (For Breast-
feeding ) Development problem Medicine (Name, Dose, Schedule, Duration) Counsel the Mother
Referred (Name of HC/
Hosp)Outcome
Temp Maternal Danger Signs (< 6wks) Name Code
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty
‘*Is there any risk factor and/or parental concern related to
the child development? Yes No
If Yes, ___________________
________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast
____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feeding
wks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * Improved
Gasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warm
M ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 days Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty‘*Is there any risk factor and/
or parental concern related to the child development?
Yes No If Yes,
___________________ ________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast ____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feedingwks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * ImprovedGasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warm
M ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 dd Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ . __ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
Gestational age: * unable to feed Yes No HIV test: * Any Breastfeeding difficulty‘*Is there any risk factor and/
or parental concern related to the child development?
Yes No If Yes,
___________________ ________________________
Up to date
Not up to date
Not Started
Yes No
Not breathing <32 wks * Not feeding well * Yellow: * _____ days * Mother: Positive * <8 breastfeeds in 24hrs * Breast ____ ____ 32 - <37 wks * Convulsions - Palms &/or soles * Blood in the stool Negative * Switching breast frequently feedingwks gms Not crying ≥ 37 wks * RR ____/min Fast breathing - Face or eyes * Moves only when stimulated unknown * Not increasing BF during illness
* Severe chest indrawing - No yellowness * No Movement when stimulated * Child: ANTIBODY * Receives other foods/drinks * Keep * Improved
Gasping Weight: * Umbilicus: Red / Pus draining * Restless/Irritable Positive * Underweight (Wt /Age) warmM ____ <1,500 gms * Temp ≥37.5°C (feels hot ) * Age * Sunken eyes Negative * Mouth ulcers/thrush * Same
cm Breathing <35.5°C (feels cold) - < 24hr or * Skin Pinch Unknown * Mother not breastfeeding
Current age milestone/s: Ab-sent: Yes No Yes No
* Early ChildDevel-opment (ECD)
F poorly 1,500 - <2,500gms * Skin pustules - 24hr - < 14 dd Slowly * Child: DNA PCR * Positioning Good/ Poor * Worsened____ . __ (<30 /min) * Moves only when stimulated - > 14 days Very Slowly Positive * Attachment Good/ Poor/ No
o C ≥ 2500 gms * No Movement when stimulated Negative * Suckling Good/ Poor/ No * When to Unknown * No Feeding Problem / Not UWt return
Integrated Management of New born and Childhood Illness Register (from 0-2 months)
Sx Type Count Sx type Count
Critical cases Peneumonia Rxed with antibiotic
VSD cases Diarrhea treated with ORS and zinc
LBI cases Diarrhea Rxed with ORS only
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Adolescent Nutrition Register
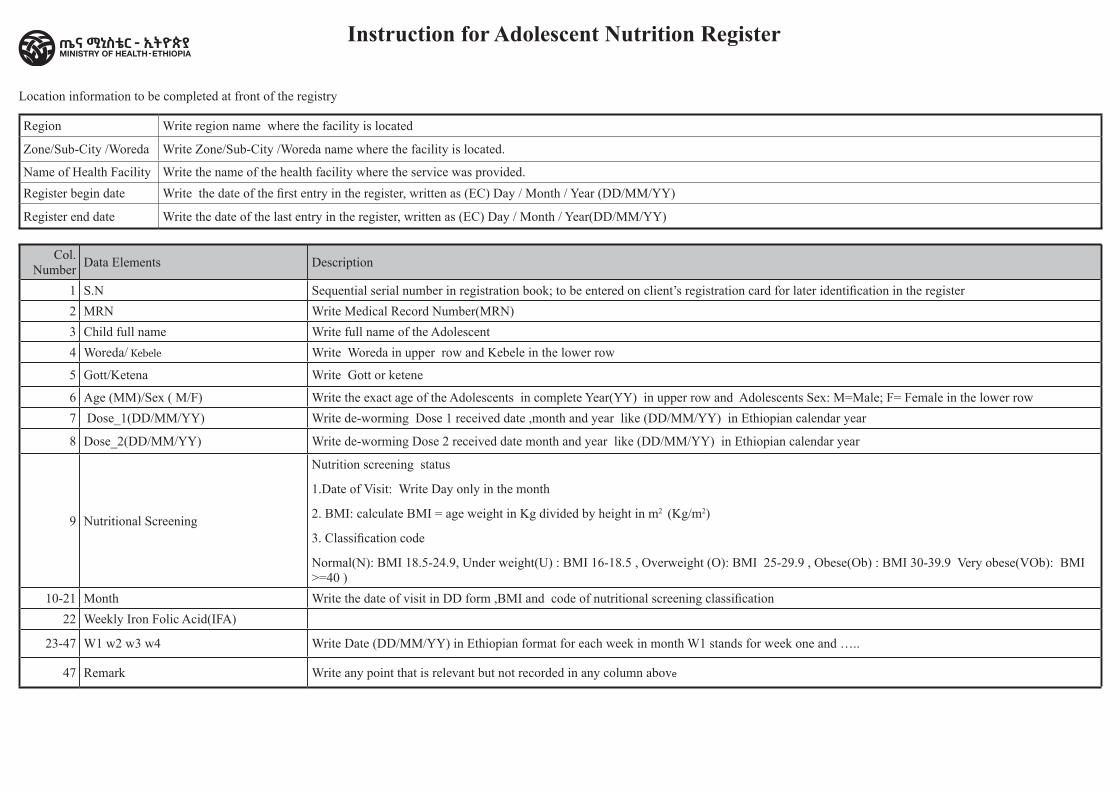
Location information to be completed at front of the registry
Region Write region name where the facility is located
Zone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Name of Health Facility Write the name of the health facility where the service was provided.Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Col. Number Data Elements Description
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in the register 2 MRN Write Medical Record Number(MRN) 3 Child full name Write full name of the Adolescent 4 Woreda/ Kebele Write Woreda in upper row and Kebele in the lower row
5 Gott/Ketena Write Gott or ketene
6 Age (MM)/Sex ( M/F) Write the exact age of the Adolescents in complete Year(YY) in upper row and Adolescents Sex: M=Male; F= Female in the lower row 7 Dose_1(DD/MM/YY) Write de-worming Dose 1 received date ,month and year like (DD/MM/YY) in Ethiopian calendar year
8 Dose_2(DD/MM/YY) Write de-worming Dose 2 received date month and year like (DD/MM/YY) in Ethiopian calendar year
9 Nutritional Screening
Nutrition screening status
1.Date of Visit: Write Day only in the month
2. BMI: calculate BMI = age weight in Kg divided by height in m2 (Kg/m2)
3. Classification code
Normal(N): BMI 18.5-24.9, Under weight(U) : BMI 16-18.5 , Overweight (O): BMI 25-29.9 , Obese(Ob) : BMI 30-39.9 Very obese(VOb): BMI >=40 )
10-21 Month Write the date of visit in DD form ,BMI and code of nutritional screening classification22 Weekly Iron Folic Acid(IFA)
23-47 W1 w2 w3 w4 Write Date (DD/MM/YY) in Ethiopian format for each week in month W1 stands for week one and …..
47 Remark Write any point that is relevant but not recorded in any column above
Instruction for Adolescent Nutrition Register
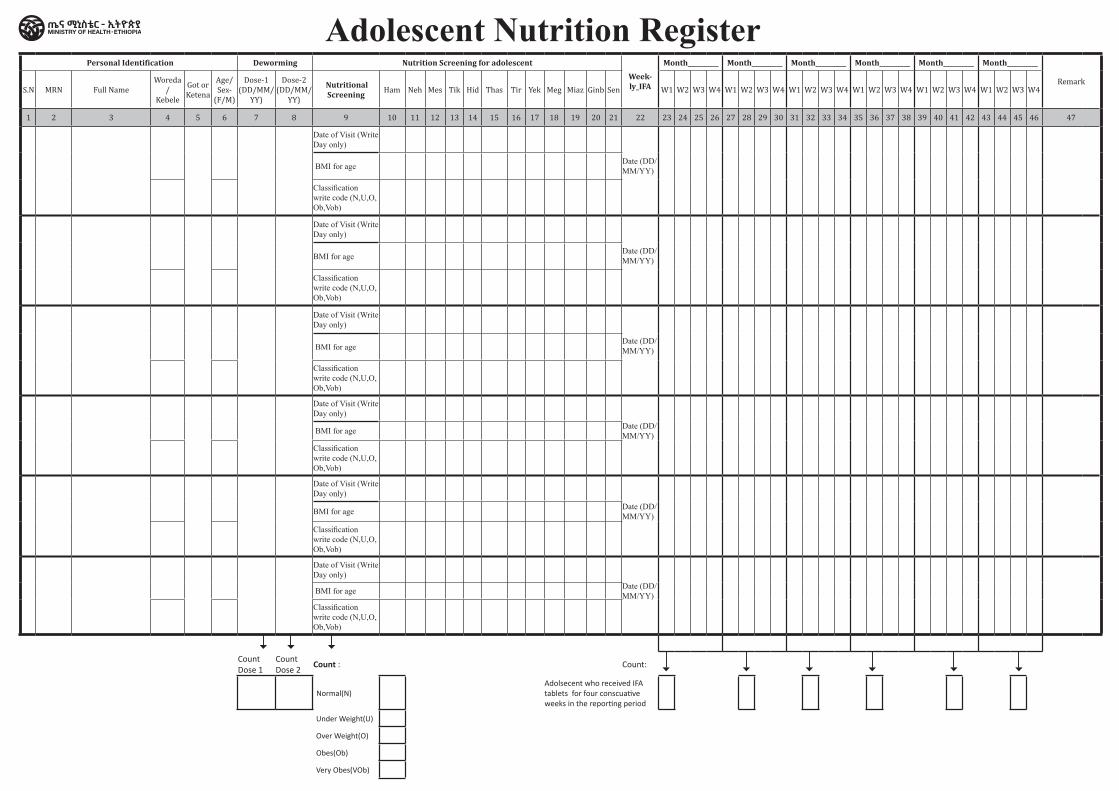
Personal Identification Deworming Nutrition Screening for adolescent Week-ly_IFA
Month__________ Month__________ Month__________ Month__________ Month__________ Month__________
RemarkS.N MRN Full Name
Woreda /
Kebele
Got or Ketena
Age/ Sex-
(F/M)
Dose-1 (DD/MM/
YY)
Dose-2 (DD/MM/
YY)
Nutritional Screening Ham Neh Mes Tik Hid Thas Tir Yek Meg Miaz Ginb Sen W1 W2 W3 W4 W1 W2 W3 W4 W1 W2 W3 W4 W1 W2 W3 W4 W1 W2 W3 W4 W1 W2 W3 W4
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Date of Visit (Write Day only)
Date (DD/MM/YY)
BMI for age
Classification write code (N,U,O, Ob,Vob)
Count Dose 1
Count Dose 2
Count : Count:
Normal(N)Adolsecent who received IFA tablets for four conscuative weeks in the reporting period
Under Weight(U)
Over Weight(O)
Obes(Ob)
Very Obes(VOb)
Adolescent Nutrition Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Integrated Adolescent and Youth
Health Service Register
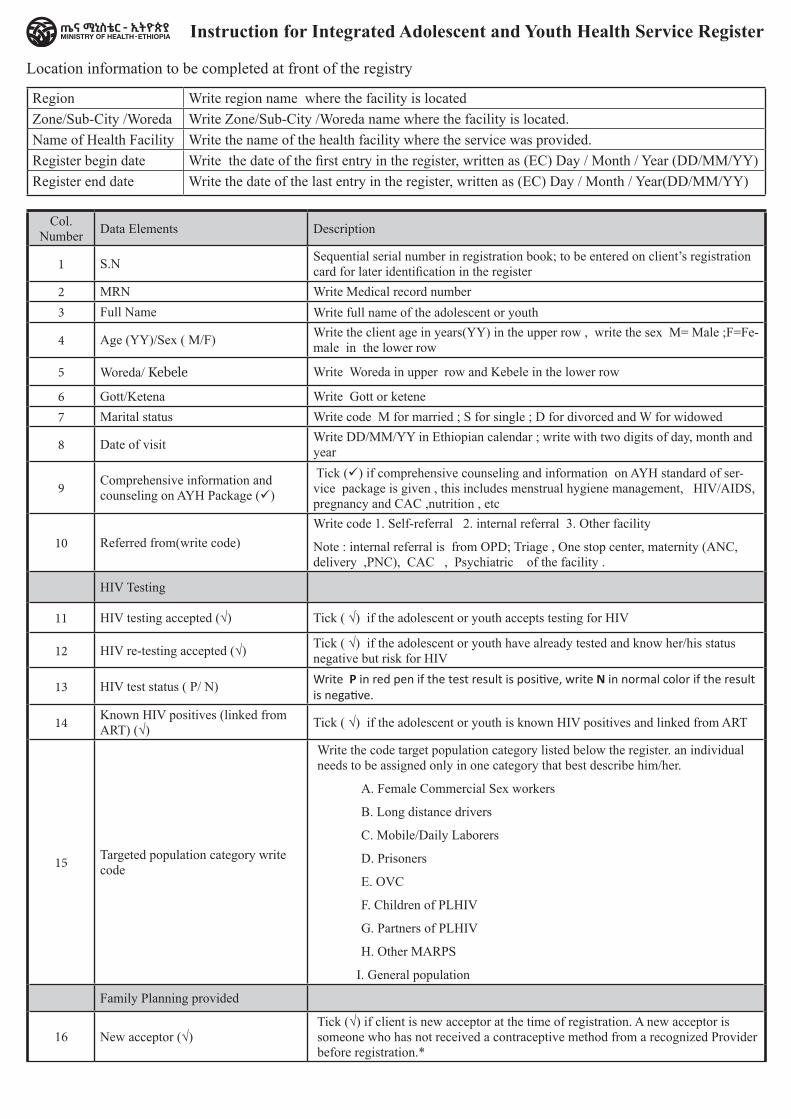
Location information to be completed at front of the registry
Region Write region name where the facility is locatedZone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Name of Health Facility Write the name of the health facility where the service was provided.Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Col. Number Data Elements Description
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in the register
2 MRN Write Medical record number3 Full Name Write full name of the adolescent or youth
4 Age (YY)/Sex ( M/F) Write the client age in years(YY) in the upper row , write the sex M= Male ;F=Fe-male in the lower row
5 Woreda/ Kebele Write Woreda in upper row and Kebele in the lower row
6 Gott/Ketena Write Gott or ketene 7 Marital status Write code M for married ; S for single ; D for divorced and W for widowed
8 Date of visit Write DD/MM/YY in Ethiopian calendar ; write with two digits of day, month and year
9 Comprehensive information and counseling on AYH Package ()
Tick () if comprehensive counseling and information on AYH standard of ser-vice package is given , this includes menstrual hygiene management, HIV/AIDS, pregnancy and CAC ,nutrition , etc
10 Referred from(write code)Write code 1. Self-referral 2. internal referral 3. Other facility
Note : internal referral is from OPD; Triage , One stop center, maternity (ANC, delivery ,PNC), CAC , Psychiatric of the facility .
HIV Testing
11 HIV testing accepted (√) Tick ( √) if the adolescent or youth accepts testing for HIV
12 HIV re-testing accepted (√) Tick ( √) if the adolescent or youth have already tested and know her/his status negative but risk for HIV
13 HIV test status ( P/ N) Write P in red pen if the test result is positive, write N in normal color if the result is negative.
14 Known HIV positives (linked from ART) (√) Tick ( √) if the adolescent or youth is known HIV positives and linked from ART
15 Targeted population category write code
Write the code target population category listed below the register. an individual needs to be assigned only in one category that best describe him/her.
A. Female Commercial Sex workers
B. Long distance drivers
C. Mobile/Daily Laborers
D. Prisoners
E. OVC
F. Children of PLHIV
G. Partners of PLHIV
H. Other MARPS
I. General population
Family Planning provided
16 New acceptor (√)Tick (√) if client is new acceptor at the time of registration. A new acceptor is someone who has not received a contraceptive method from a recognized Provider before registration.*
Instruction for Integrated Adolescent and Youth Health Service Register
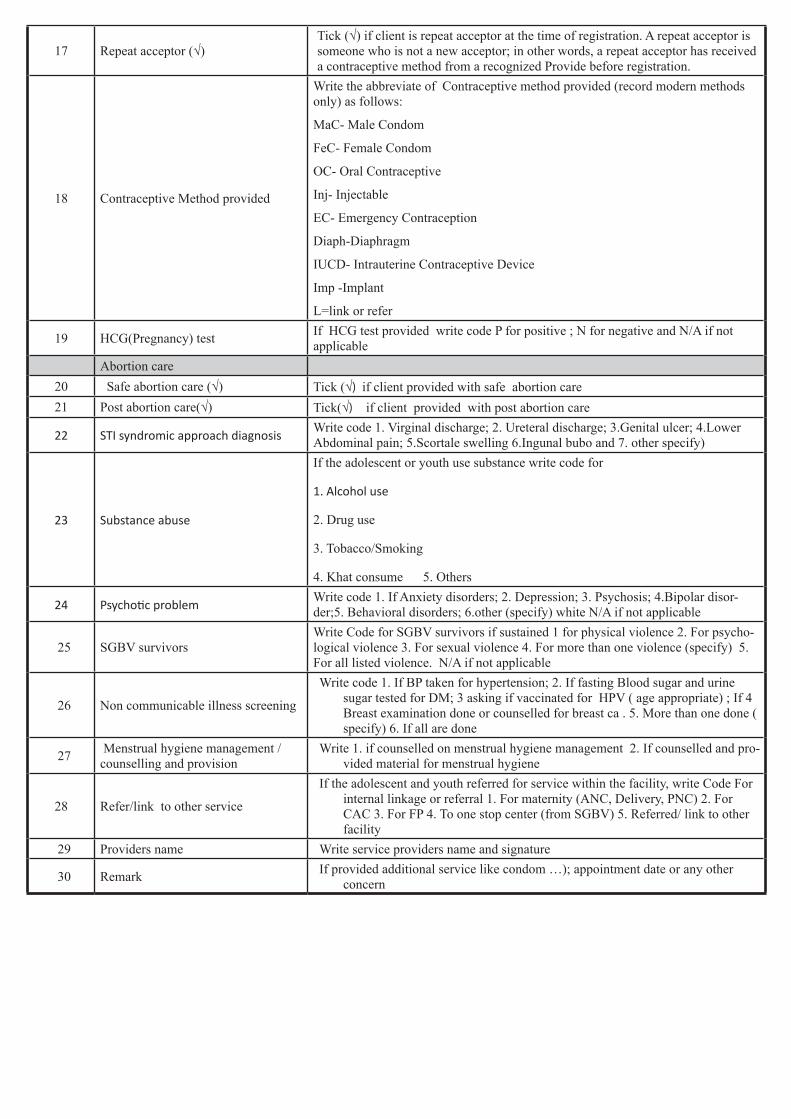
17 Repeat acceptor (√)Tick (√) if client is repeat acceptor at the time of registration. A repeat acceptor is someone who is not a new acceptor; in other words, a repeat acceptor has received a contraceptive method from a recognized Provide before registration.
18 Contraceptive Method provided
Write the abbreviate of Contraceptive method provided (record modern methods only) as follows:
MaC- Male Condom
FeC- Female Condom
OC- Oral Contraceptive
Inj- Injectable
EC- Emergency Contraception
Diaph-Diaphragm
IUCD- Intrauterine Contraceptive Device
Imp -Implant
L=link or refer
19 HCG(Pregnancy) test If HCG test provided write code P for positive ; N for negative and N/A if not applicable
Abortion care 20 Safe abortion care (√) Tick (√) if client provided with safe abortion care 21 Post abortion care(√) Tick(√) if client provided with post abortion care
22 STI syndromic approach diagnosis Write code 1. Virginal discharge; 2. Ureteral discharge; 3.Genital ulcer; 4.Lower Abdominal pain; 5.Scortale swelling 6.Ingunal bubo and 7. other specify)
23 Substance abuse
If the adolescent or youth use substance write code for
1. Alcohol use
2. Drug use
3. Tobacco/Smoking
4. Khat consume 5. Others
24 Psychotic problemWrite code 1. If Anxiety disorders; 2. Depression; 3. Psychosis; 4.Bipolar disor-der;5. Behavioral disorders; 6.other (specify) white N/A if not applicable
25 SGBV survivors Write Code for SGBV survivors if sustained 1 for physical violence 2. For psycho-logical violence 3. For sexual violence 4. For more than one violence (specify) 5. For all listed violence. N/A if not applicable
26 Non communicable illness screening
Write code 1. If BP taken for hypertension; 2. If fasting Blood sugar and urine sugar tested for DM; 3 asking if vaccinated for HPV ( age appropriate) ; If 4 Breast examination done or counselled for breast ca . 5. More than one done ( specify) 6. If all are done
27 Menstrual hygiene management /counselling and provision
Write 1. if counselled on menstrual hygiene management 2. If counselled and pro-vided material for menstrual hygiene
28 Refer/link to other service
If the adolescent and youth referred for service within the facility, write Code For internal linkage or referral 1. For maternity (ANC, Delivery, PNC) 2. For CAC 3. For FP 4. To one stop center (from SGBV) 5. Referred/ link to other facility
29 Providers name Write service providers name and signature
30 Remark If provided additional service like condom …); appointment date or any other concern
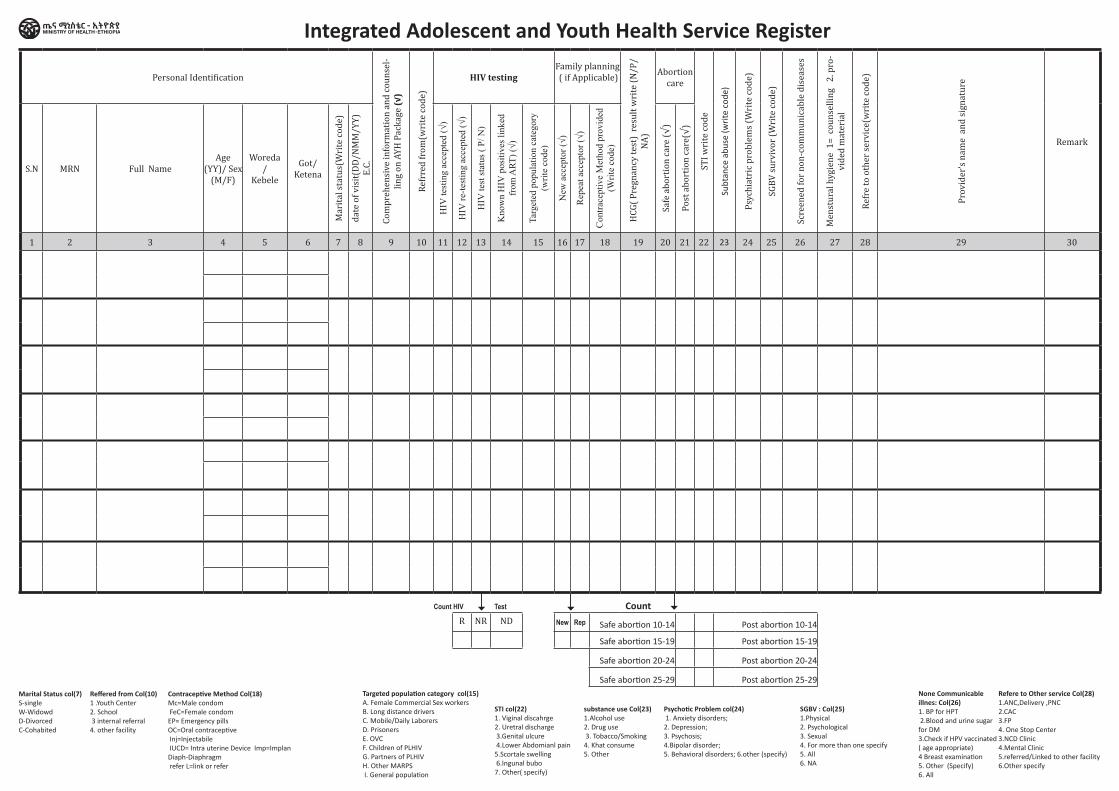
Personal Identification
Com
preh
ensi
ve in
form
atio
n an
d co
unse
l-lin
g on
AYH
Pac
kage
(√)
Refr
red
from
(wri
te co
de)
HIV testingFamily planning ( if Applicable)
HCG
( Pre
gnan
cy te
st)
resu
lt w
rite
(N/P
/NA
)
Abortion care
STI w
rite
code
Subt
ance
abu
se (w
rite
cod
e)
Psyc
hiat
ric p
robl
ems (
Wri
te co
de)
SGBV
surv
ivor
(Wri
te co
de)
Scre
ened
for n
on-c
omm
unic
able
dis
ease
s
Men
stur
al h
ygie
ne 1
= co
unse
lling
2. p
ro-
vide
d m
ater
ial
Refr
e to
oth
er se
rvic
e(w
rite
code
)
Prov
ider
’s na
me
and
sign
atur
e
Remark
S.N MRN Full NameAge
(YY)/ Sex (M/F)
Woreda /
Kebele
Got/ Ketena
Mar
ital s
tatu
s(W
rite
code
)
date
of v
isit(
DD/N
MM
/YY)
E.
C.
HIV
test
ing
acce
pted
(√)
HIV
re-te
stin
g ac
cept
ed (√
)
HIV
test
stat
us (
P/ N
)
Kno
wn
HIV
pos
itive
s lin
ked
from
ART
) (√)
Targ
eted
pop
ulat
ion
cate
gory
(w
rite
code
)
New
acc
epto
r (√)
Rep
eat a
ccep
tor (
√)
Con
trace
ptiv
e M
etho
d pr
ovid
ed
(Writ
e co
de)
Safe
abo
rtio
n ca
re (√
)
Post
abo
rtio
n ca
re(√
)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Count HIV Test CountR NR ND New Rep Safe abortion 10-14 Post abortion 10-14
Safe abortion 15-19 Post abortion 15-19
Safe abortion 20-24 Post abortion 20-24
Safe abortion 25-29 Post abortion 25-29
Marital Status col(7)S-singleW-WidowdD-DivorcedC-Cohabited
substance use Col(23)1.Alcohol use2. Drug use 3. Tobacco/Smoking 4. Khat consume 5. Other
Contraceptive Method Col(18)Mc=Male condom FeC=Female condom EP= Emergency pills OC=Oral contraceptive Inj=Injectabile IUCD= Intra uterine Device Imp=Implan Diaph-Diaphragm refer L=link or refer
Reffered from Col(10)1 .Youth Center 2. School 3 internal referral4. other facility
STI col(22)1. Viginal discahrge 2. Uretral discharge 3.Genital ulcure 4.Lower Abdomianl pain 5.Scortale swelling 6.Ingunal bubo 7. Other( specify)
None Communicable illnes: Col(26)1. BP for HPT 2.Blood and urine sugar for DM 3.Check if HPV vaccinated ( age appropriate) 4 Breast examination5. Other (Specify)6. All
Targeted population category col(15)A. Female Commercial Sex workers B. Long distance driversC. Mobile/Daily LaborersD. PrisonersE. OVCF. Children of PLHIVG. Partners of PLHIVH. Other MARPS I. General population
Psychotic Problem col(24) 1. Anxiety disorders; 2. Depression; 3. Psychosis; 4.Bipolar disorder;5. Behavioral disorders; 6.other (specify)
SGBV : Col(25)1.Physical 2. Psychological 3. Sexual 4. For more than one specify5. All6. NA
Refere to Other service Col(28)1.ANC,Delivery ,PNC2.CAC3.FP4. One Stop Center3.NCD Clinic4.Mental Clinic5.referred/Linked to other facility 6.Other specify
Integrated Adolescent and Youth Health Service Register

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital GMP and <5 years Nutrition
Screening Register
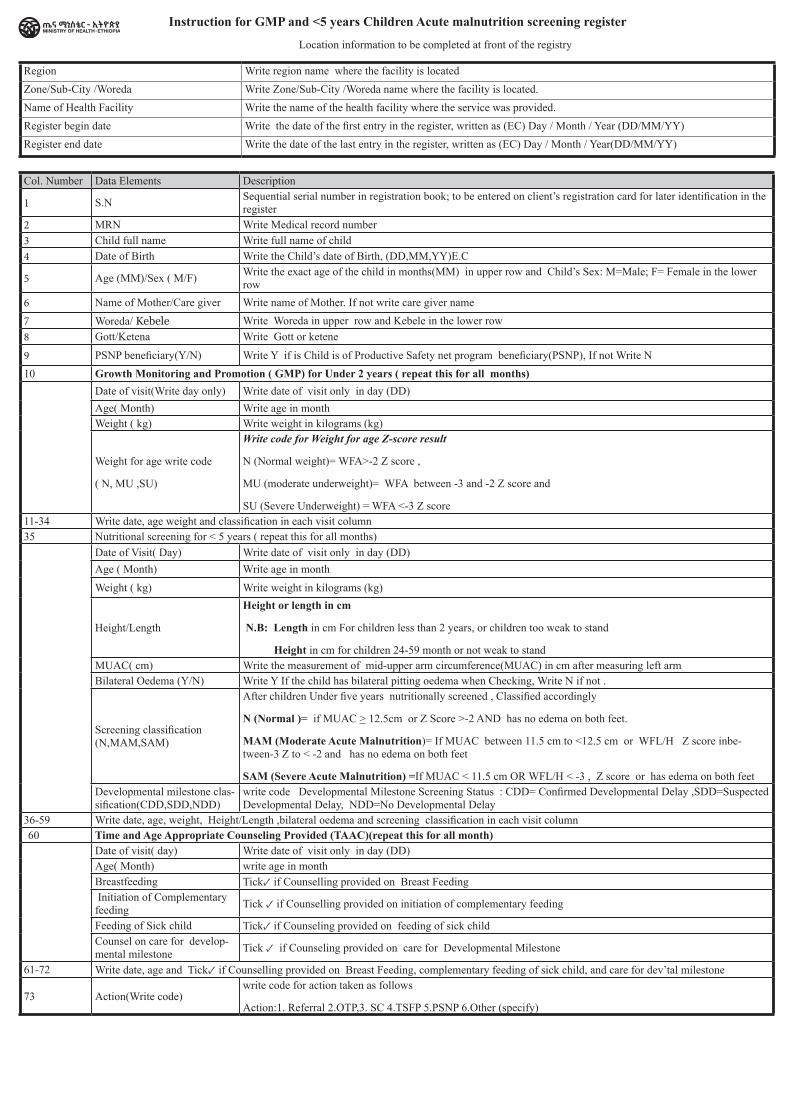
Instruction for GMP and <5 years Children Acute malnutrition screening register
Location information to be completed at front of the registry
Region Write region name where the facility is locatedZone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.Name of Health Facility Write the name of the health facility where the service was provided.Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Col. Number Data Elements Description
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in the register
2 MRN Write Medical record number3 Child full name Write full name of child4 Date of Birth Write the Child’s date of Birth, (DD,MM,YY)E.C
5 Age (MM)/Sex ( M/F) Write the exact age of the child in months(MM) in upper row and Child’s Sex: M=Male; F= Female in the lower row
6 Name of Mother/Care giver Write name of Mother. If not write care giver name7 Woreda/ Kebele Write Woreda in upper row and Kebele in the lower row8 Gott/Ketena Write Gott or ketene
9 PSNP beneficiary(Y/N) Write Y if is Child is of Productive Safety net program beneficiary(PSNP), If not Write N10 Growth Monitoring and Promotion ( GMP) for Under 2 years ( repeat this for all months)
Date of visit(Write day only) Write date of visit only in day (DD)Age( Month) Write age in monthWeight ( kg) Write weight in kilograms (kg)
Weight for age write code
( N, MU ,SU)
Write code for Weight for age Z-score result
N (Normal weight)= WFA>-2 Z score ,
MU (moderate underweight)= WFA between -3 and -2 Z score and
SU (Severe Underweight) = WFA <-3 Z score 11-34 Write date, age weight and classification in each visit column 35 Nutritional screening for < 5 years ( repeat this for all months)
Date of Visit( Day) Write date of visit only in day (DD)Age ( Month) Write age in month
Weight ( kg) Write weight in kilograms (kg)
Height/Length
Height or length in cm
N.B: Length in cm For children less than 2 years, or children too weak to stand
Height in cm for children 24-59 month or not weak to standMUAC( cm) Write the measurement of mid-upper arm circumference(MUAC) in cm after measuring left armBilateral Oedema (Y/N) Write Y If the child has bilateral pitting oedema when Checking, Write N if not .
Screening classification (N,MAM,SAM)
After children Under five years nutritionally screened , Classified accordingly
N (Normal )= if MUAC > 12.5cm or Z Score >-2 AND has no edema on both feet.
MAM (Moderate Acute Malnutrition)= If MUAC between 11.5 cm to <12.5 cm or WFL/H Z score inbe-tween-3 Z to < -2 and has no edema on both feet
SAM (Severe Acute Malnutrition) =If MUAC < 11.5 cm OR WFL/H < -3 , Z score or has edema on both feetDevelopmental milestone clas-sification(CDD,SDD,NDD)
write code Developmental Milestone Screening Status : CDD= Confirmed Developmental Delay ,SDD=Suspected Developmental Delay, NDD=No Developmental Delay
36-59 Write date, age, weight, Height/Length ,bilateral oedema and screening classification in each visit column60 Time and Age Appropriate Counseling Provided (TAAC)(repeat this for all month)
Date of visit( day) Write date of visit only in day (DD) Age( Month) write age in monthBreastfeeding Tick✓ if Counselling provided on Breast Feeding Initiation of Complementary feeding Tick ✓ if Counselling provided on initiation of complementary feeding
Feeding of Sick child Tick✓ if Counseling provided on feeding of sick child Counsel on care for develop-mental milestone Tick ✓ if Counseling provided on care for Developmental Milestone
61-72 Write date, age and Tick✓ if Counselling provided on Breast Feeding, complementary feeding of sick child, and care for dev’tal milestone
73 Action(Write code)write code for action taken as follows
Action:1. Referral 2.OTP,3. SC 4.TSFP 5.PSNP 6.Other (specify)
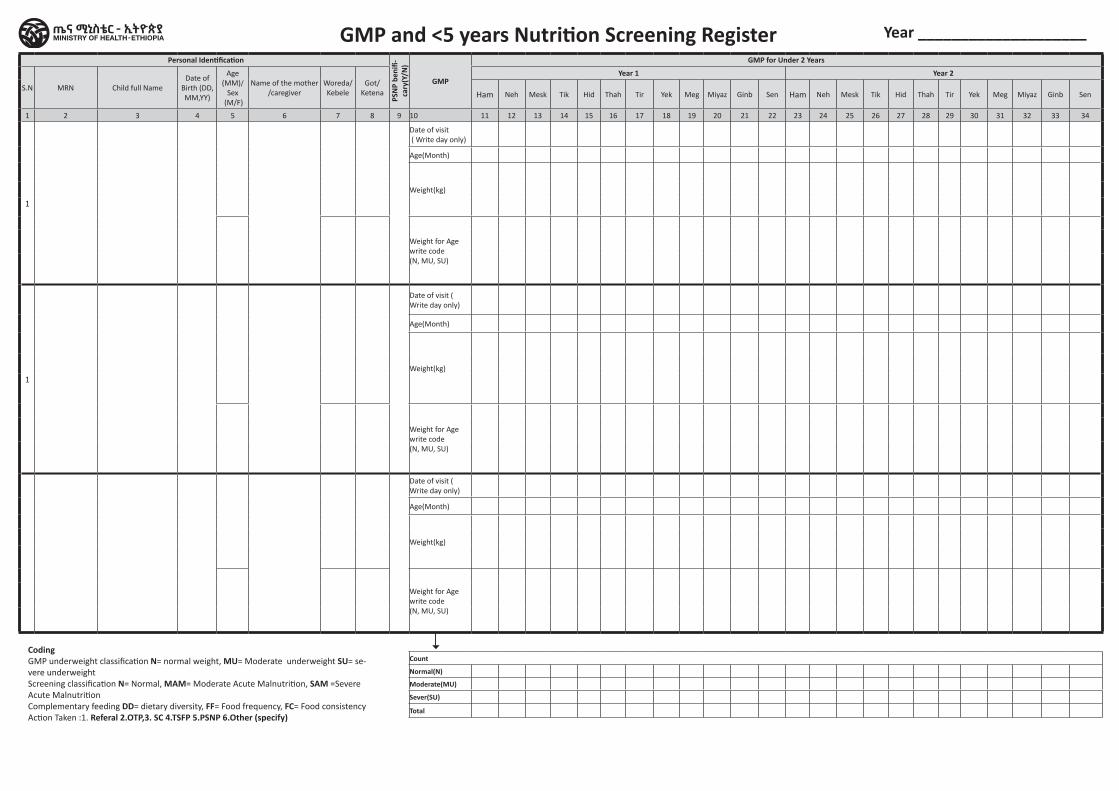
Personal Identification
PSN
P be
nifi-
cary
(Y/N
)
GMP
GMP for Under 2 YearsNutrition Screening and
Developmental milestone assessment U5
Nutrition Screening for under 5 years
Time and Age Approprite Councelling Provided (TAAC)
Time and Age Approprite Councelling Provided (TAAC)
Action(Write code)S.N MRN Child full Name
Date of Birth (DD,MM,YY)
Age(MM)/
Sex (M/F)
Name of the mother /caregiver
Woreda/ Kebele
Got/ Ketena
Year 1 Year 2 Year 1 Year 2
Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb SenHam Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73
1
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classification (N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
1
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classifica-tion(N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classifica-tion(N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
Count Count
Normal(N) Normal(N)
Moderate(MU) MAM
Sever(SU) SAM
Total ND
SD
DD
GMP and <5 years Nutrition Screening Register
CodingGMP underweight classification N= normal weight, MU= Moderate underweight SU= se-vere underweight Screening classification N= Normal, MAM= Moderate Acute Malnutrition, SAM =Severe Acute MalnutritionComplementary feeding DD= dietary diversity, FF= Food frequency, FC= Food consistencyAction Taken :1. Referal 2.OTP,3. SC 4.TSFP 5.PSNP 6.Other (specify)
Year ____________________
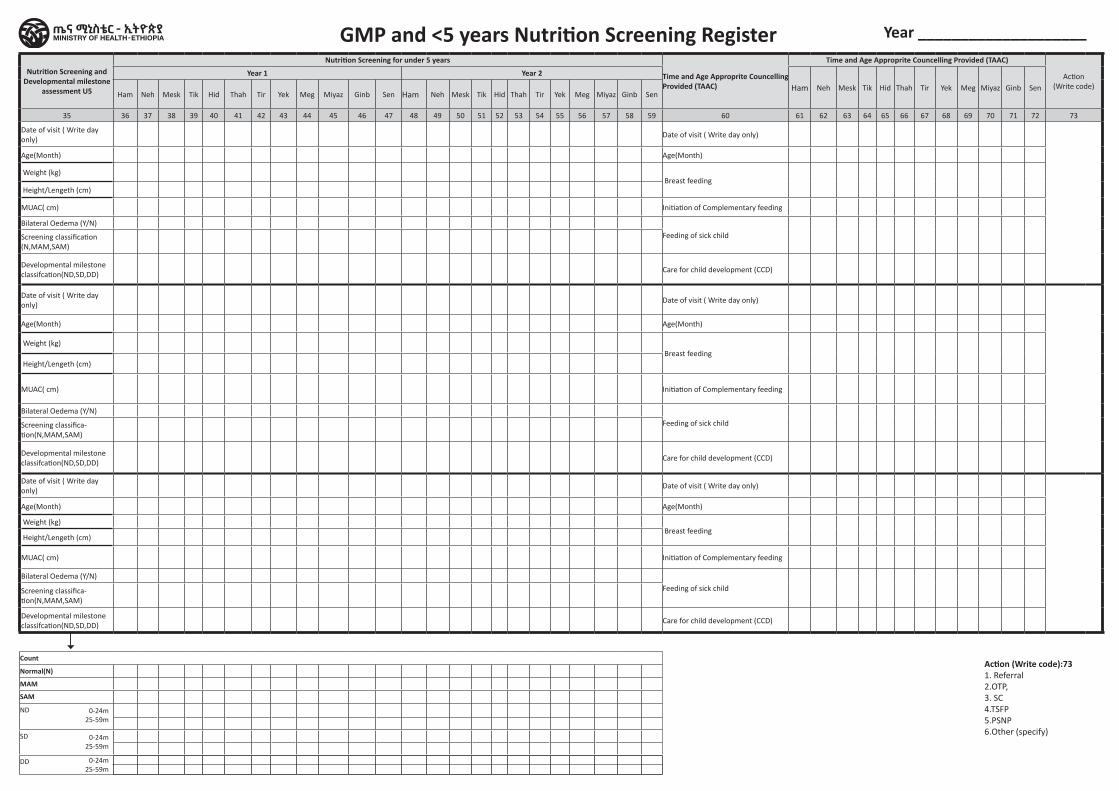
Personal Identification
PSN
P be
nifi-
cary
(Y/N
)
GMP
GMP for Under 2 YearsNutrition Screening and
Developmental milestone assessment U5
Nutrition Screening for under 5 years
Time and Age Approprite Councelling Provided (TAAC)
Time and Age Approprite Councelling Provided (TAAC)
Action(Write code)S.N MRN Child full Name
Date of Birth (DD,MM,YY)
Age(MM)/
Sex (M/F)
Name of the mother /caregiver
Woreda/ Kebele
Got/ Ketena
Year 1 Year 2 Year 1 Year 2
Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb SenHam Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen Ham Neh Mesk Tik Hid Thah Tir Yek Meg Miyaz Ginb Sen
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73
1
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classification (N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
1
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classifica-tion(N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
Date of visit ( Write day only)
Date of visit ( Write day only)
Date of visit ( Write day only)
Age(Month) Age(Month) Age(Month)
Weight(kg)
Weight (kg) Breast feeding
Height/Lengeth (cm)
MUAC( cm) Initiation of Complementary feeding
Weight for Age write code (N, MU, SU)
Bilateral Oedema (Y/N)
Feeding of sick childScreening classifica-tion(N,MAM,SAM)
Developmental milestone classifcation(ND,SD,DD)
Care for child development (CCD)
Count Count
Normal(N) Normal(N)
Moderate(MU) MAM
Sever(SU) SAM
Total ND
SD
DD
GMP and <5 years Nutrition Screening Register
Action (Write code):731. Referral 2.OTP,3. SC 4.TSFP 5.PSNP 6.Other (specify)
0-24m25-59m
0-24m25-59m
0-24m25-59m
Year ____________________
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Therapeutic Feeding Program
Register
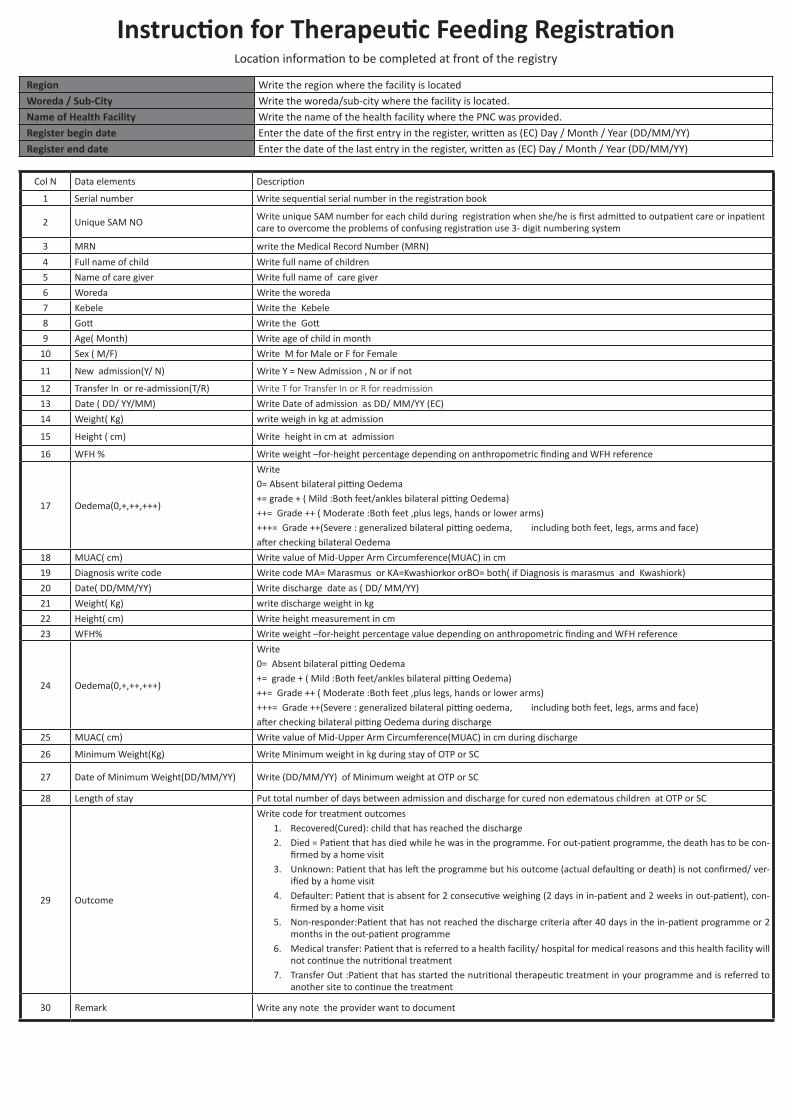
Instruction for Therapeutic Feeding RegistrationLocation information to be completed at front of the registry
Region Write the region where the facility is locatedWoreda / Sub-City Write the woreda/sub-city where the facility is located.Name of Health Facility Write the name of the health facility where the PNC was provided.Register begin date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Col N Data elements Description
1 Serial number Write sequential serial number in the registration book
2 Unique SAM NOWrite unique SAM number for each child during registration when she/he is first admitted to outpatient care or inpatient care to overcome the problems of confusing registration use 3- digit numbering system
3 MRN write the Medical Record Number (MRN)
4 Full name of child Write full name of children
5 Name of care giver Write full name of care giver
6 Woreda Write the woreda
7 Kebele Write the Kebele
8 Gott Write the Gott
9 Age( Month) Write age of child in month
10 Sex ( M/F) Write M for Male or F for Female
11 New admission(Y/ N) Write Y = New Admission , N or if not
12 Transfer In or re-admission(T/R) Write T for Transfer In or R for readmission 13 Date ( DD/ YY/MM) Write Date of admission as DD/ MM/YY (EC)
14 Weight( Kg) write weigh in kg at admission
15 Height ( cm) Write height in cm at admission
16 WFH % Write weight –for-height percentage depending on anthropometric finding and WFH reference
17 Oedema(0,+,++,+++)
Write 0= Absent bilateral pitting Oedema+= grade + ( Mild :Both feet/ankles bilateral pitting Oedema)++= Grade ++ ( Moderate :Both feet ,plus legs, hands or lower arms)+++= Grade ++(Severe : generalized bilateral pitting oedema, including both feet, legs, arms and face)after checking bilateral Oedema
18 MUAC( cm) Write value of Mid-Upper Arm Circumference(MUAC) in cm
19 Diagnosis write code Write code MA= Marasmus or KA=Kwashiorkor orBO= both( if Diagnosis is marasmus and Kwashiork)
20 Date( DD/MM/YY) Write discharge date as ( DD/ MM/YY)
21 Weight( Kg) write discharge weight in kg
22 Height( cm) Write height measurement in cm
23 WFH% Write weight –for-height percentage value depending on anthropometric finding and WFH reference
24 Oedema(0,+,++,+++)
Write 0= Absent bilateral pitting Oedema+= grade + ( Mild :Both feet/ankles bilateral pitting Oedema)++= Grade ++ ( Moderate :Both feet ,plus legs, hands or lower arms)+++= Grade ++(Severe : generalized bilateral pitting oedema, including both feet, legs, arms and face)after checking bilateral pitting Oedema during discharge
25 MUAC( cm) Write value of Mid-Upper Arm Circumference(MUAC) in cm during discharge
26 Minimum Weight(Kg) Write Minimum weight in kg during stay of OTP or SC
27 Date of Minimum Weight(DD/MM/YY) Write (DD/MM/YY) of Minimum weight at OTP or SC
28 Length of stay Put total number of days between admission and discharge for cured non edematous children at OTP or SC
29 Outcome
Write code for treatment outcomes1. Recovered(Cured): child that has reached the discharge 2. Died = Patient that has died while he was in the programme. For out-patient programme, the death has to be con-
firmed by a home visit3. Unknown: Patient that has left the programme but his outcome (actual defaulting or death) is not confirmed/ ver-
ified by a home visit4. Defaulter: Patient that is absent for 2 consecutive weighing (2 days in in-patient and 2 weeks in out-patient), con-
firmed by a home visit5. Non-responder:Patient that has not reached the discharge criteria after 40 days in the in-patient programme or 2
months in the out-patient programme6. Medical transfer: Patient that is referred to a health facility/ hospital for medical reasons and this health facility will
not continue the nutritional treatment7. Transfer Out :Patient that has started the nutritional therapeutic treatment in your programme and is referred to
another site to continue the treatment
30 Remark Write any note the provider want to document
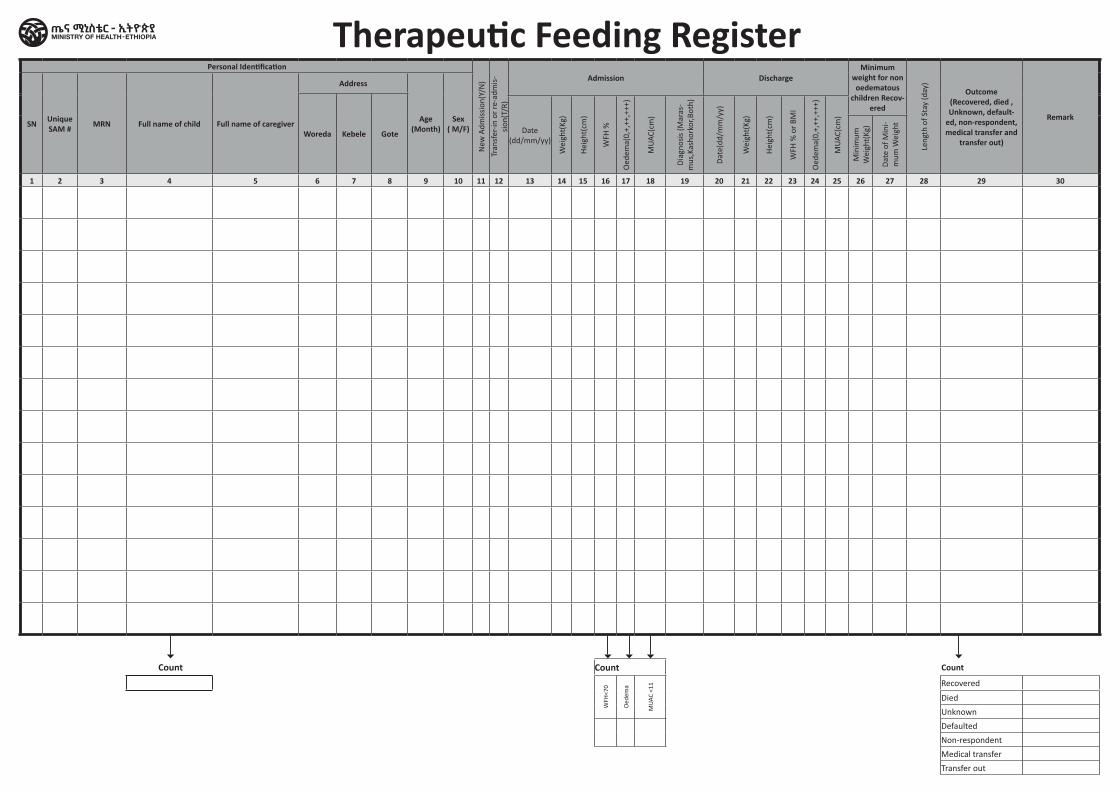
Personal Identification
New
Adm
issi
on(Y
/N)
Tran
sfer
-in o
r re
-adm
is-
sion
(T/R
)
Admission DischargeMinimum
weight for non oedematous
children Recov-ered
Leng
th o
f Sta
y (d
ay)
Outcome (Recovered, died , Unknown, default-
ed, non-respondent, medical transfer and
transfer out)
RemarkSN Unique
SAM # MRN Full name of child Full name of caregiver
Address
Age (Month)
Sex ( M/F)Woreda Kebele Gote Date
(dd/mm/yy)
Wei
ght(
Kg)
Hei
ght(
cm)
WFH
%
Oed
ema(
0,+,
++,+
++)
MU
AC(c
m)
Dia
gnos
is (M
aras
-m
us,K
asho
rkor
,Bot
h)
Dat
e(dd
/mm
/yy)
Wei
ght(
Kg)
Hei
ght(
cm)
WFH
% o
r BM
I
Oed
ema(
0,+,
++,+
++)
MU
AC(c
m)
Min
imum
W
eigh
t(Kg
)
Dat
e of
Min
i-m
um W
eigh
t
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Count Count
WFH
<70
Oed
ema
MU
AC <
11 Recovered
Died
Unknown
Defaulted
Non-respondent
Medical transfer
Transfer out
Therapeutic Feeding Register
Count
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Pregnant and Lactating Women (PLW)
Nutrition screening Register
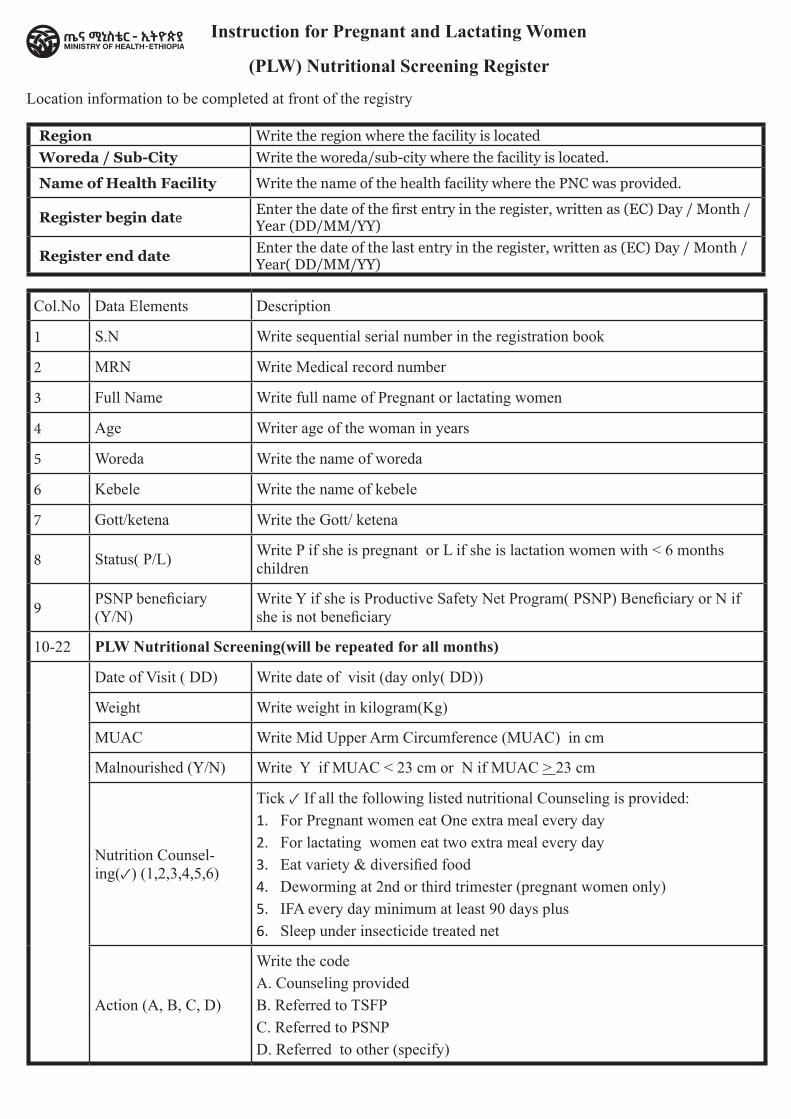
Col.No Data Elements Description
1 S.N Write sequential serial number in the registration book
2 MRN Write Medical record number
3 Full Name Write full name of Pregnant or lactating women
4 Age Writer age of the woman in years
5 Woreda Write the name of woreda
6 Kebele Write the name of kebele
7 Gott/ketena Write the Gott/ ketena
8 Status( P/L) Write P if she is pregnant or L if she is lactation women with < 6 months children
9 PSNP beneficiary (Y/N)
Write Y if she is Productive Safety Net Program( PSNP) Beneficiary or N if she is not beneficiary
10-22 PLW Nutritional Screening(will be repeated for all months)
Date of Visit ( DD) Write date of visit (day only( DD))
Weight Write weight in kilogram(Kg)
MUAC Write Mid Upper Arm Circumference (MUAC) in cm
Malnourished (Y/N) Write Y if MUAC < 23 cm or N if MUAC > 23 cm
Nutrition Counsel-ing(✓) (1,2,3,4,5,6)
Tick ✓ If all the following listed nutritional Counseling is provided:1. For Pregnant women eat One extra meal every day2. For lactating women eat two extra meal every day3. Eat variety & diversified food4. Deworming at 2nd or third trimester (pregnant women only)5. IFA every day minimum at least 90 days plus6. Sleep under insecticide treated net
Action (A, B, C, D)
Write the codeA. Counseling providedB. Referred to TSFPC. Referred to PSNPD. Referred to other (specify)
Instruction for Pregnant and Lactating Women
(PLW) Nutritional Screening Register
Location information to be completed at front of the registry
Region Write the region where the facility is locatedWoreda / Sub-City Write the woreda/sub-city where the facility is located.
Name of Health Facility Write the name of the health facility where the PNC was provided.
Register begin dateEnter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day / Month / Year( DD/MM/YY)
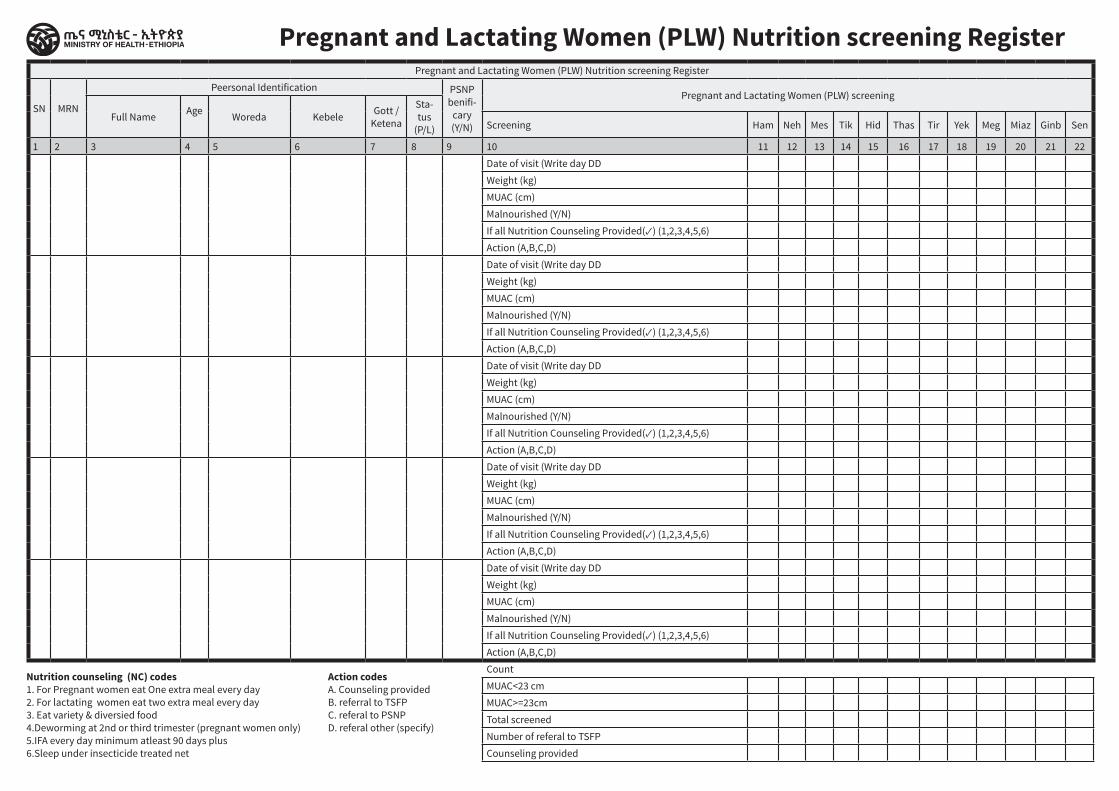
Pregnant and Lactating Women (PLW) Nutrition screening Register Pregnant and Lactating Women (PLW) Nutrition screening Register
SN MRN
Peersonal Identification PSNP benifi-
cary (Y/N)
Pregnant and Lactating Women (PLW) screening
Full Name Age Woreda Kebele Gott / Ketena
Sta-tus
(P/L) Screening Ham Neh Mes Tik Hid Thas Tir Yek Meg Miaz Ginb Sen
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22Date of visit (Write day DDWeight (kg)MUAC (cm)Malnourished (Y/N)If all Nutrition Counseling Provided(✓) (1,2,3,4,5,6)Action (A,B,C,D)Date of visit (Write day DDWeight (kg)MUAC (cm)Malnourished (Y/N)If all Nutrition Counseling Provided(✓) (1,2,3,4,5,6)Action (A,B,C,D)Date of visit (Write day DDWeight (kg)MUAC (cm)Malnourished (Y/N)If all Nutrition Counseling Provided(✓) (1,2,3,4,5,6)Action (A,B,C,D)Date of visit (Write day DDWeight (kg)MUAC (cm)Malnourished (Y/N)If all Nutrition Counseling Provided(✓) (1,2,3,4,5,6)Action (A,B,C,D)Date of visit (Write day DDWeight (kg)MUAC (cm)Malnourished (Y/N)If all Nutrition Counseling Provided(✓) (1,2,3,4,5,6)Action (A,B,C,D)CountMUAC<23 cmMUAC>=23cmTotal screenedNumber of referal to TSFP Counseling provided
Nutrition counseling (NC) codes1. For Pregnant women eat One extra meal every day2. For lactating women eat two extra meal every day3. Eat variety & diversied food4.Deworming at 2nd or third trimester (pregnant women only)5.IFA every day minimum atleast 90 days plus6.Sleep under insecticide treated net
Action codes A. Counseling providedB. referral to TSFPC. referal to PSNPD. referal other (specify)
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital MAM treatment for 6-59 months
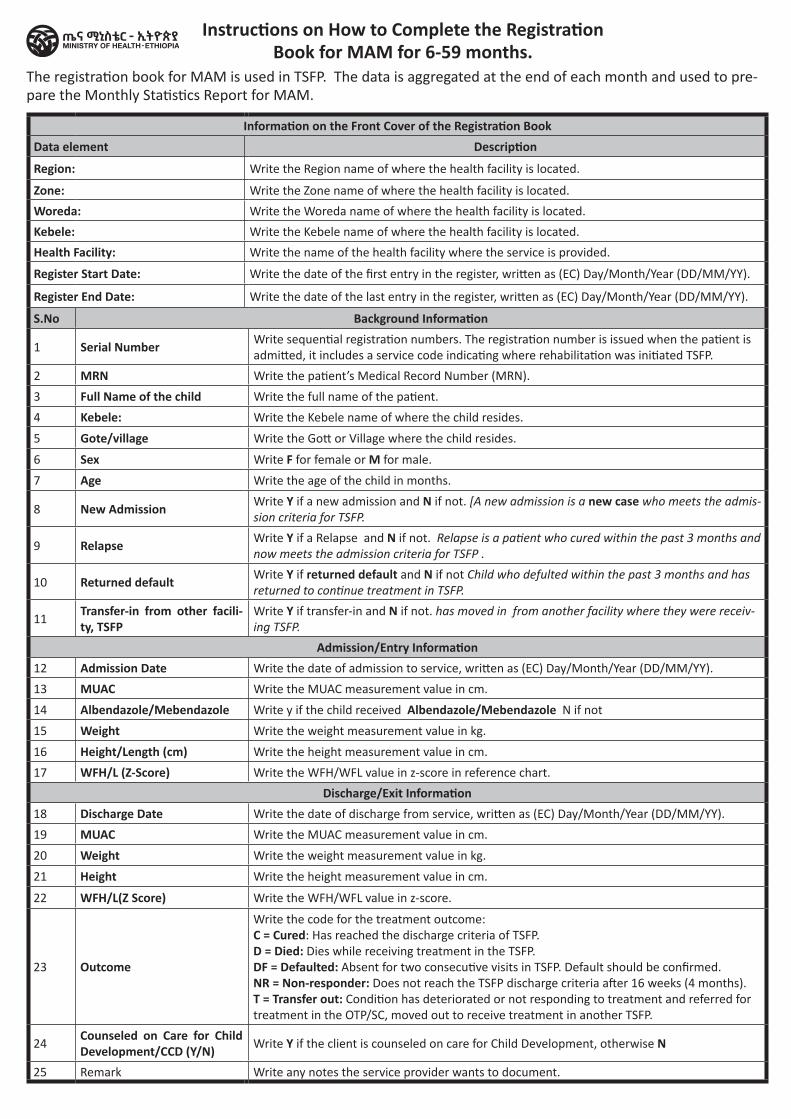
The registration book for MAM is used in TSFP. The data is aggregated at the end of each month and used to pre-pare the Monthly Statistics Report for MAM.
Information on the Front Cover of the Registration BookData element Description
Region: Write the Region name of where the health facility is located.
Zone: Write the Zone name of where the health facility is located.
Woreda: Write the Woreda name of where the health facility is located.
Kebele: Write the Kebele name of where the health facility is located.
Health Facility: Write the name of the health facility where the service is provided.
Register Start Date: Write the date of the first entry in the register, written as (EC) Day/Month/Year (DD/MM/YY).
Register End Date: Write the date of the last entry in the register, written as (EC) Day/Month/Year (DD/MM/YY).
S.No Background Information
1 Serial Number Write sequential registration numbers. The registration number is issued when the patient is admitted, it includes a service code indicating where rehabilitation was initiated TSFP.
2 MRN Write the patient’s Medical Record Number (MRN).
3 Full Name of the child Write the full name of the patient.
4 Kebele: Write the Kebele name of where the child resides.
5 Gote/village Write the Gott or Village where the child resides.
6 Sex Write F for female or M for male.
7 Age Write the age of the child in months.
8 New Admission Write Y if a new admission and N if not. [A new admission is a new case who meets the admis-sion criteria for TSFP.
9 Relapse Write Y if a Relapse and N if not. Relapse is a patient who cured within the past 3 months and now meets the admission criteria for TSFP .
10 Returned default Write Y if returned default and N if not Child who defulted within the past 3 months and has returned to continue treatment in TSFP.
11Transfer-in from other facili-ty, TSFP
Write Y if transfer-in and N if not. has moved in from another facility where they were receiv-ing TSFP.
Admission/Entry Information12 Admission Date Write the date of admission to service, written as (EC) Day/Month/Year (DD/MM/YY).
13 MUAC Write the MUAC measurement value in cm.
14 Albendazole/Mebendazole Write y if the child received Albendazole/Mebendazole N if not
15 Weight Write the weight measurement value in kg.
16 Height/Length (cm) Write the height measurement value in cm.
17 WFH/L (Z-Score) Write the WFH/WFL value in z-score in reference chart.
Discharge/Exit Information18 Discharge Date Write the date of discharge from service, written as (EC) Day/Month/Year (DD/MM/YY).
19 MUAC Write the MUAC measurement value in cm.
20 Weight Write the weight measurement value in kg.
21 Height Write the height measurement value in cm.
22 WFH/L(Z Score) Write the WFH/WFL value in z-score.
23 Outcome
Write the code for the treatment outcome: C = Cured: Has reached the discharge criteria of TSFP. D = Died: Dies while receiving treatment in the TSFP. DF = Defaulted: Absent for two consecutive visits in TSFP. Default should be confirmed. NR = Non-responder: Does not reach the TSFP discharge criteria after 16 weeks (4 months). T = Transfer out: Condition has deteriorated or not responding to treatment and referred for treatment in the OTP/SC, moved out to receive treatment in another TSFP.
24Counseled on Care for Child Development/CCD (Y/N) Write Y if the client is counseled on care for Child Development, otherwise N
25 Remark Write any notes the service provider wants to document.
Instructions on How to Complete the Registration Book for MAM for 6-59 months.
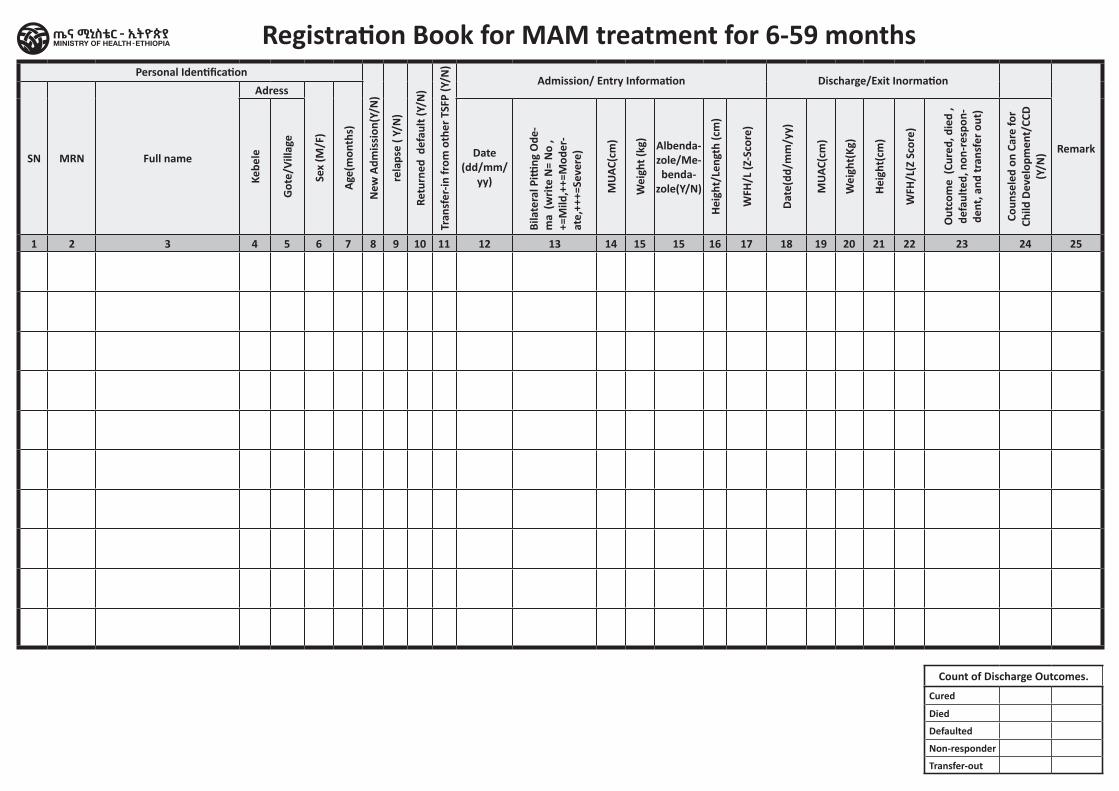
Personal Identification
New
Adm
issi
on(Y
/N)
rela
pse
( Y/N
)
Retu
rned
def
ault
(Y/N
)
Tran
sfer
-in fr
om o
ther
TSF
P (Y
/N)
Admission/ Entry Information Discharge/Exit Inormation
RemarkSN MRN Full name
Adress
Sex
(M/F
)
Age(
mon
ths)
Kebe
le
Got
e/Vi
llage
Date (dd/mm/
yy)
Bila
tera
l Pitti
ng O
de-
ma
(writ
e N
= N
o ,
+=M
ild,+
+=M
oder
-at
e,++
+=Se
vere
)
MUA
C(cm
)
Wei
ght (
kg)
Albenda-zole/Me-benda-
zole(Y/N)
Heig
ht/L
engt
h (c
m)
WFH
/L (Z
-Sco
re)
Date
(dd/
mm
/yy)
MUA
C(cm
)
Wei
ght(
Kg)
Heig
ht(c
m)
WFH
/L(Z
Sco
re)
Out
com
e (C
ured
, die
d ,
defa
ulte
d, n
on-r
espo
n-de
nt, a
nd tr
ansf
er o
ut)
Coun
sele
d on
Car
e fo
r Ch
ild D
evel
opm
ent/
CCD
(Y/N
)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 15 16 17 18 19 20 21 22 23 24 25
Count of Discharge Outcomes.
Cured
Died
Defaulted
Non-responder
Transfer-out
Registration Book for MAM treatment for 6-59 months
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital MAM treatment for Pregnant and
lactating women Register
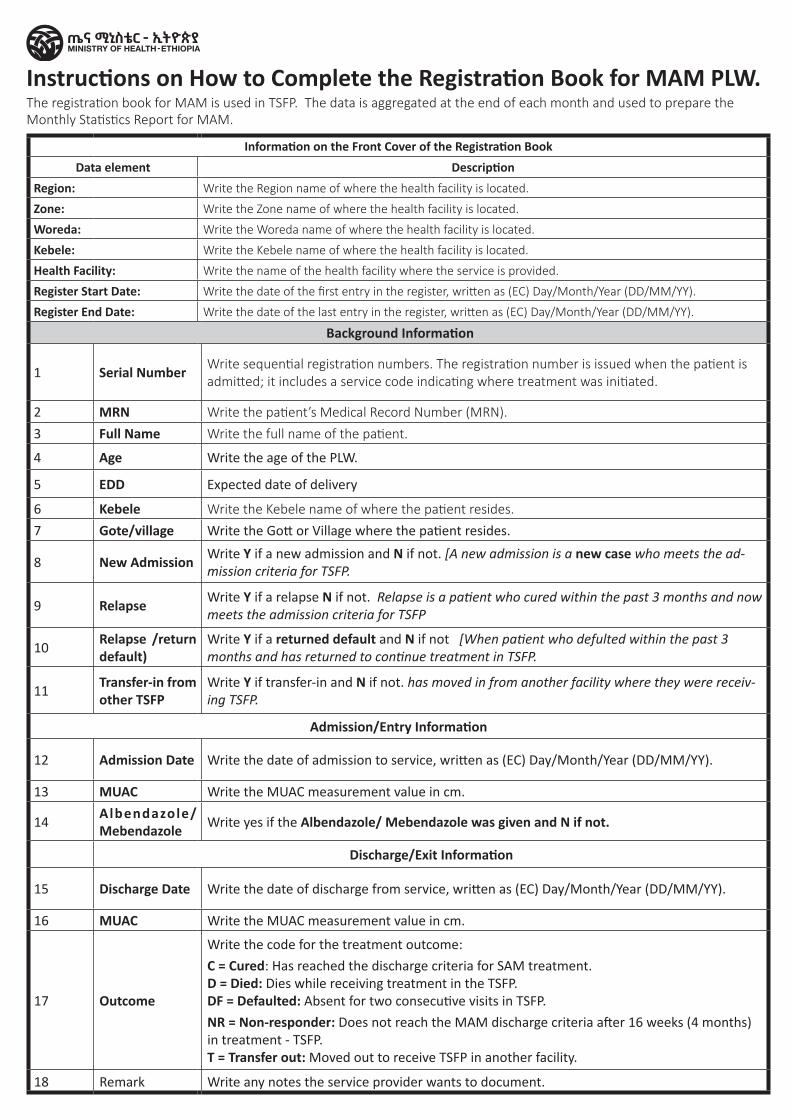
The registration book for MAM is used in TSFP. The data is aggregated at the end of each month and used to prepare the Monthly Statistics Report for MAM.
Information on the Front Cover of the Registration BookData element Description
Region: Write the Region name of where the health facility is located.
Zone: Write the Zone name of where the health facility is located.
Woreda: Write the Woreda name of where the health facility is located.
Kebele: Write the Kebele name of where the health facility is located.
Health Facility: Write the name of the health facility where the service is provided.
Register Start Date: Write the date of the first entry in the register, written as (EC) Day/Month/Year (DD/MM/YY).
Register End Date: Write the date of the last entry in the register, written as (EC) Day/Month/Year (DD/MM/YY).
Background Information
1 Serial Number Write sequential registration numbers. The registration number is issued when the patient is admitted; it includes a service code indicating where treatment was initiated.
2 MRN Write the patient’s Medical Record Number (MRN).3 Full Name Write the full name of the patient.
4 Age Write the age of the PLW.
5 EDD Expected date of delivery
6 Kebele Write the Kebele name of where the patient resides.7 Gote/village Write the Gott or Village where the patient resides.
8 New Admission Write Y if a new admission and N if not. [A new admission is a new case who meets the ad-mission criteria for TSFP.
9 Relapse Write Y if a relapse N if not. Relapse is a patient who cured within the past 3 months and now meets the admission criteria for TSFP
10Relapse /return default)
Write Y if a returned default and N if not [When patient who defulted within the past 3 months and has returned to continue treatment in TSFP.
11Transfer-in from other TSFP
Write Y if transfer-in and N if not. has moved in from another facility where they were receiv-ing TSFP.
Admission/Entry Information
12 Admission Date Write the date of admission to service, written as (EC) Day/Month/Year (DD/MM/YY).
13 MUAC Write the MUAC measurement value in cm.
14Albendazole/ Mebendazole Write yes if the Albendazole/ Mebendazole was given and N if not.
Discharge/Exit Information
15 Discharge Date Write the date of discharge from service, written as (EC) Day/Month/Year (DD/MM/YY).
16 MUAC Write the MUAC measurement value in cm.
17 Outcome
Write the code for the treatment outcome:
C = Cured: Has reached the discharge criteria for SAM treatment. D = Died: Dies while receiving treatment in the TSFP. DF = Defaulted: Absent for two consecutive visits in TSFP.
NR = Non-responder: Does not reach the MAM discharge criteria after 16 weeks (4 months) in treatment - TSFP. T = Transfer out: Moved out to receive TSFP in another facility.
18 Remark Write any notes the service provider wants to document.
Instructions on How to Complete the Registration Book for MAM PLW.
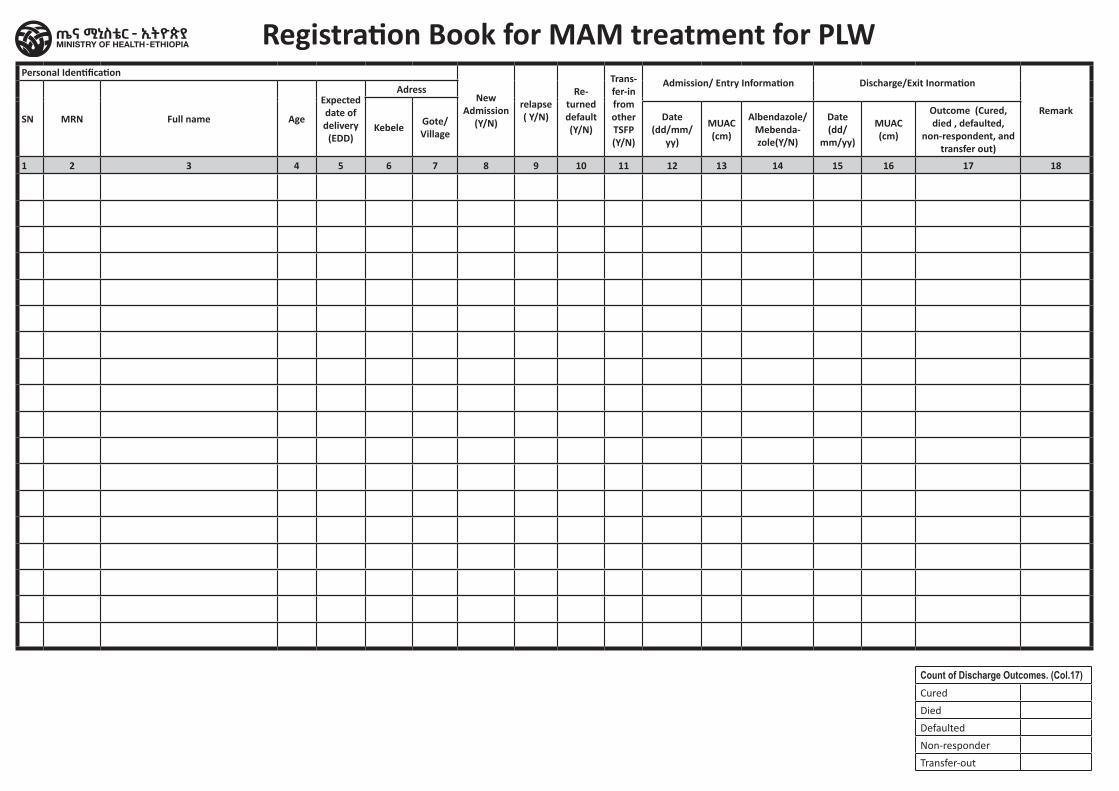
Personal Identification
New Admission
(Y/N)
relapse ( Y/N)
Re-turned default (Y/N)
Trans-fer-in from other TSFP (Y/N)
Admission/ Entry Information Discharge/Exit Inormation
RemarkSN MRN Full name Age
Expected date of delivery
(EDD)
Adress
Kebele Gote/Village
Date (dd/mm/
yy)
MUAC (cm)
Albendazole/ Mebenda-zole(Y/N)
Date (dd/
mm/yy)
MUAC (cm)
Outcome (Cured, died , defaulted,
non-respondent, and transfer out)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Count of Discharge Outcomes. (Col.17)Cured
Died
Defaulted
Non-responder
Transfer-out
Registration Book for MAM treatment for PLW
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Vitamin A Supplementation and Deworming
Register
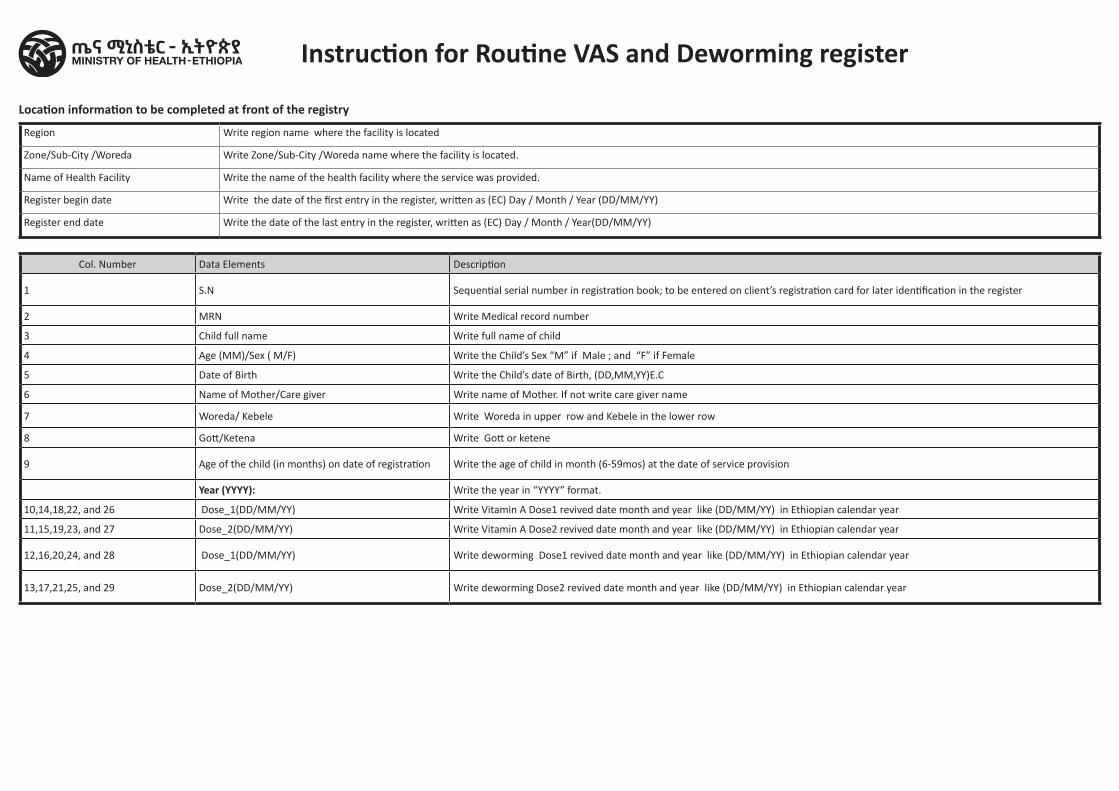
Region Write region name where the facility is located
Zone/Sub-City /Woreda Write Zone/Sub-City /Woreda name where the facility is located.
Name of Health Facility Write the name of the health facility where the service was provided.
Register begin date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register end date Write the date of the last entry in the register, written as (EC) Day / Month / Year(DD/MM/YY)
Col. Number Data Elements Description
1 S.N Sequential serial number in registration book; to be entered on client’s registration card for later identification in the register
2 MRN Write Medical record number
3 Child full name Write full name of child
4 Age (MM)/Sex ( M/F) Write the Child’s Sex “M” if Male ; and “F” if Female
5 Date of Birth Write the Child’s date of Birth, (DD,MM,YY)E.C
6 Name of Mother/Care giver Write name of Mother. If not write care giver name
7 Woreda/ Kebele Write Woreda in upper row and Kebele in the lower row
8 Gott/Ketena Write Gott or ketene
9 Age of the child (in months) on date of registration Write the age of child in month (6-59mos) at the date of service provision
Year (YYYY): Write the year in “YYYY” format.
10,14,18,22, and 26 Dose_1(DD/MM/YY) Write Vitamin A Dose1 revived date month and year like (DD/MM/YY) in Ethiopian calendar year
11,15,19,23, and 27 Dose_2(DD/MM/YY) Write Vitamin A Dose2 revived date month and year like (DD/MM/YY) in Ethiopian calendar year
12,16,20,24, and 28 Dose_1(DD/MM/YY) Write deworming Dose1 revived date month and year like (DD/MM/YY) in Ethiopian calendar year
13,17,21,25, and 29 Dose_2(DD/MM/YY) Write deworming Dose2 revived date month and year like (DD/MM/YY) in Ethiopian calendar year
Instruction for Routine VAS and Deworming register
Location information to be completed at front of the registry
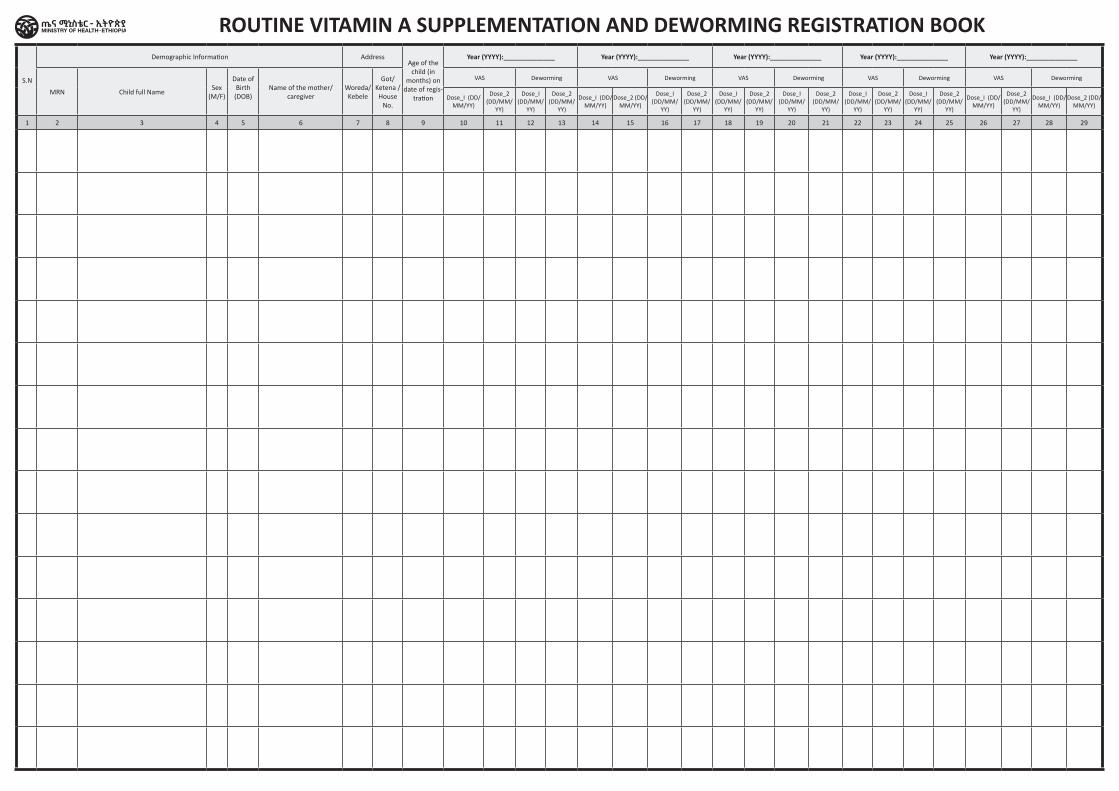
S.N
Demographic Information AddressAge of the
child (in months) on
date of regis-tration
Year (YYYY):______________ Year (YYYY):______________ Year (YYYY):______________ Year (YYYY):______________ Year (YYYY):______________
MRN Child full NameSex
(M/F)
Date of Birth (DOB)
Name of the mother/caregiver
Woreda/ Kebele
Got/Ketena /House
No.
VAS Deworming VAS Deworming VAS Deworming VAS Deworming VAS Deworming
Dose_I (DD/MM/YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/YY)
Dose_2 (DD/MM/YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/
YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/YY)
Dose_2 (DD/MM/
YY)
Dose_I (DD/MM/YY)
Dose_2 (DD/MM/YY)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29
ROUTINE VITAMIN A SUPPLEMENTATION AND DEWORMING REGISTRATION BOOK
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Abortion Care Tally Sheet
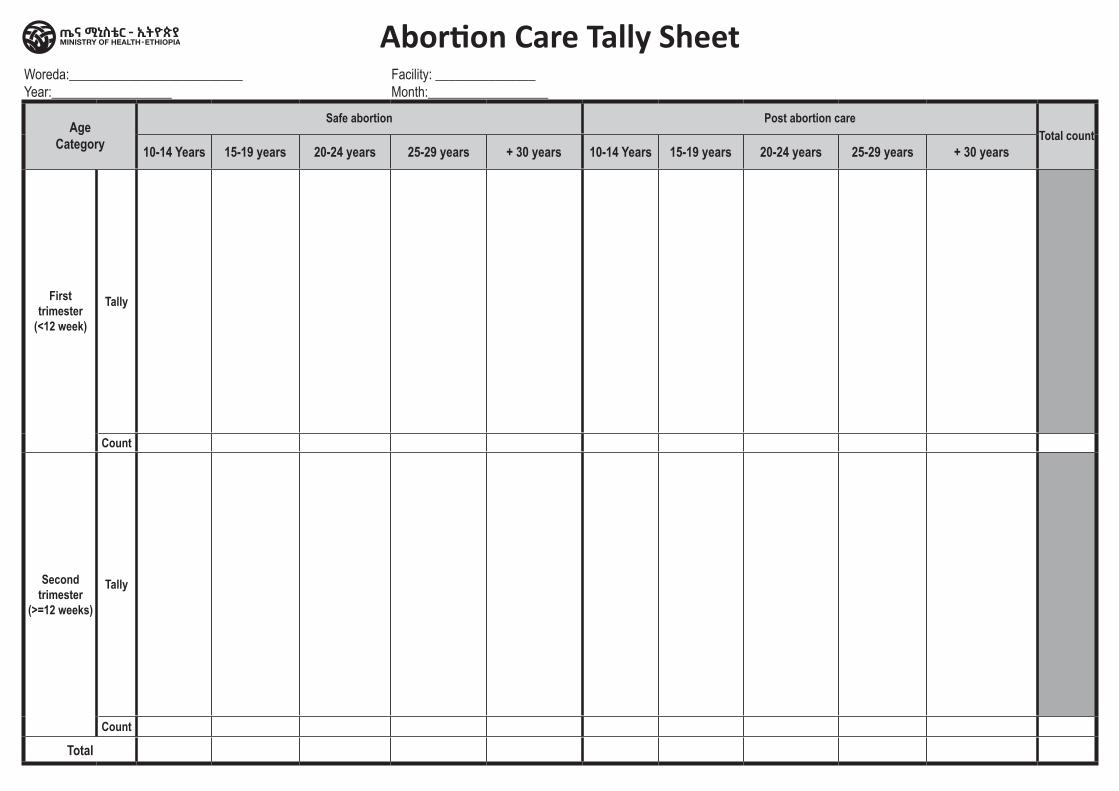
Abortion Care Tally SheetWoreda:__________________________Year:__________________
Facility: _______________ Month:__________________
Age Category
Safe abortion Post abortion careTotal count
10-14 Years 15-19 years 20-24 years 25-29 years + 30 years 10-14 Years 15-19 years 20-24 years 25-29 years + 30 years
First trimester
(<12 week)
Tally
Count
Second trimester
(>=12 weeks)
Tally
Count
Total
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Adolescent nutrition Service Tally
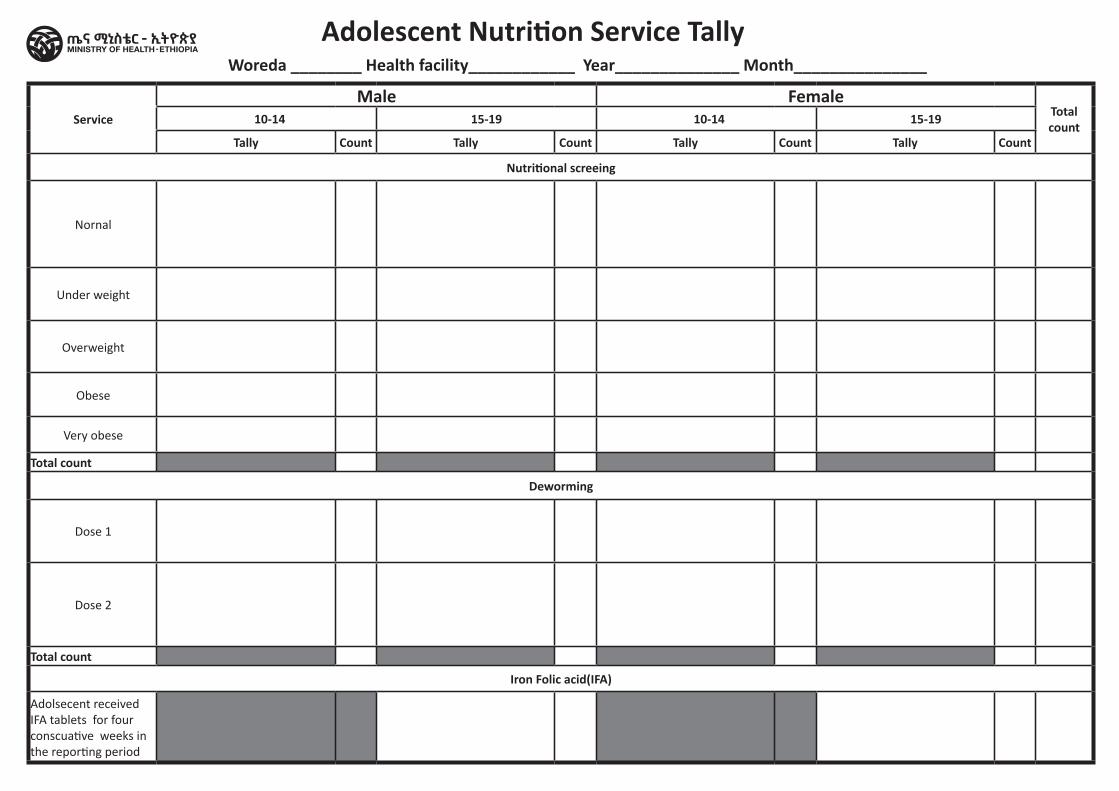
Adolescent Nutrition Service TallyWoreda ________ Health facility____________ Year______________ Month_______________
Service
Male FemaleTotal count 10-14 15-19 10-14 15-19
Tally Count Tally Count Tally Count Tally Count
Nutritional screeing
Nornal
Under weight
Overweight
Obese
Very obese
Total count
Deworming
Dose 1
Dose 2
Total count
Iron Folic acid(IFA)
Adolsecent received IFA tablets for four conscuative weeks in the reporting period
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital ANC Tally Sheet
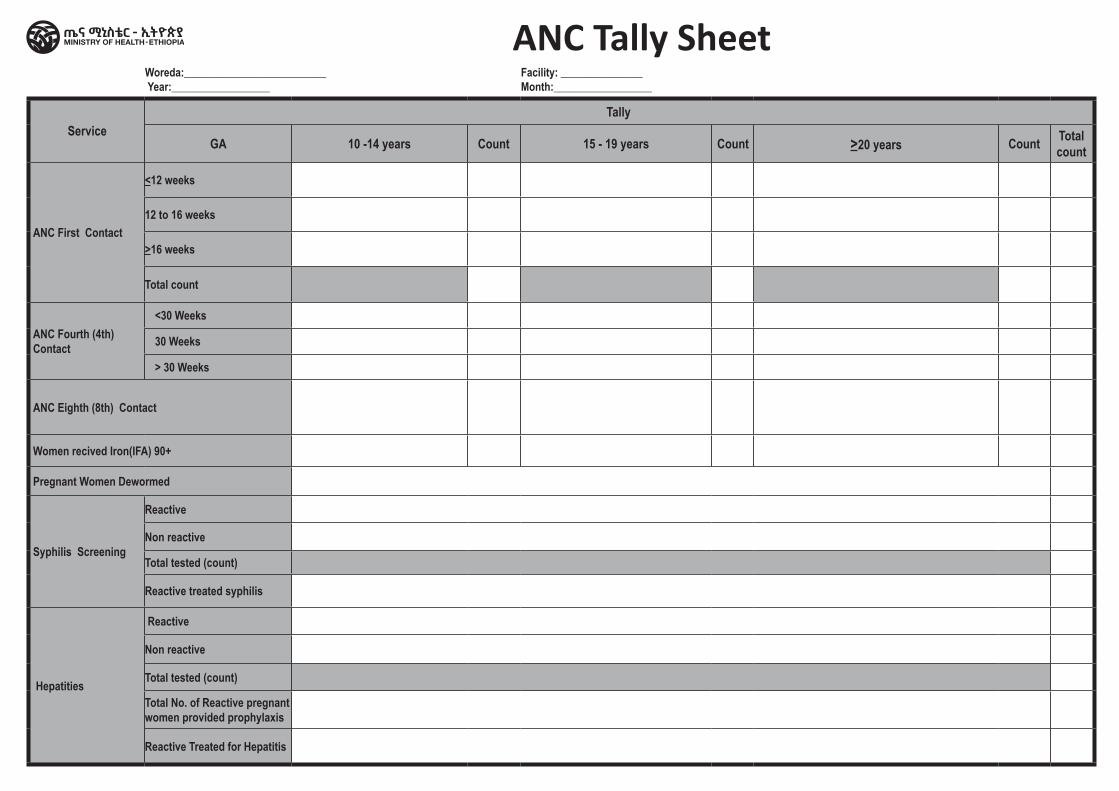
ANC Tally SheetWoreda:__________________________ Year:__________________
Facility: _______________ Month:__________________
Service Tally
GA 10 -14 years Count 15 - 19 years Count >20 years Count Total count
ANC First Contact
<12 weeks
12 to 16 weeks
>16 weeks
Total count
ANC Fourth (4th) Contact
<30 Weeks
30 Weeks
> 30 Weeks
ANC Eighth (8th) Contact
Women recived Iron(IFA) 90+
Pregnant Women Dewormed
Syphilis Screening
Reactive
Non reactive
Total tested (count)
Reactive treated syphilis
Hepatities
Reactive
Non reactive
Total tested (count)
Total No. of Reactive pregnant women provided prophylaxis
Reactive Treated for Hepatitis
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Comprehensive and Integrated Nutrition Service
for <5 years Tally Sheet
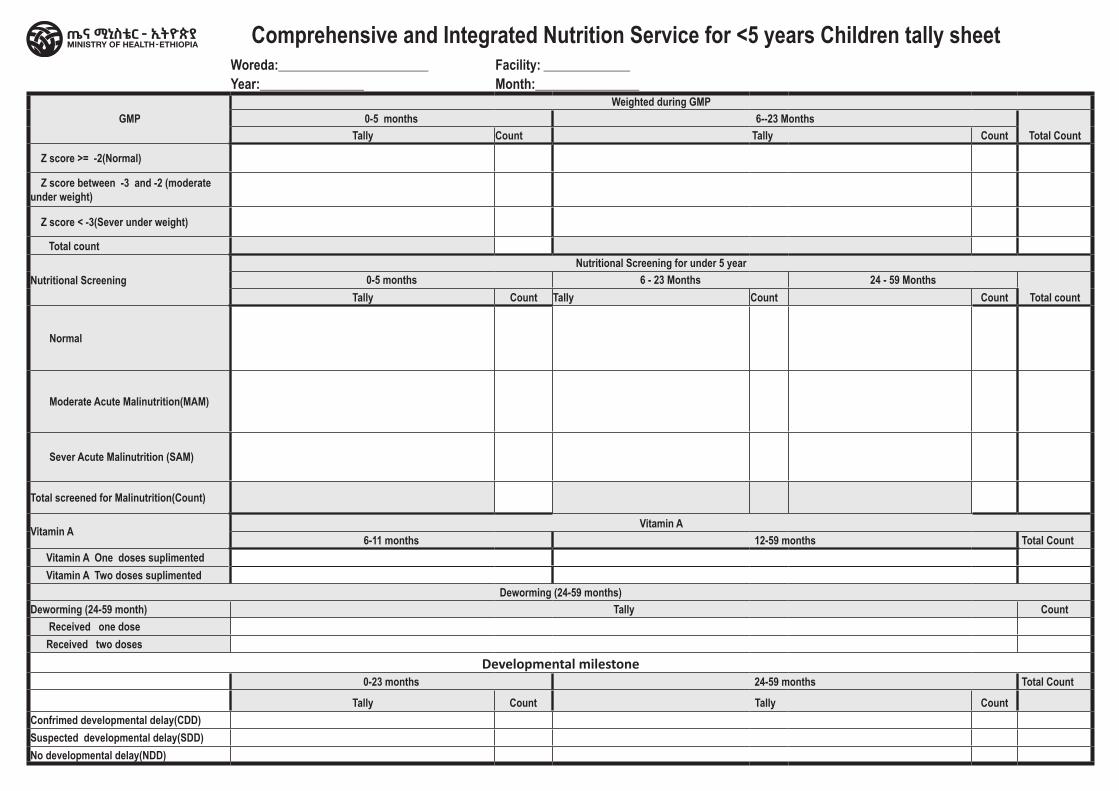
Woreda:__________________________ Facility: _______________ Year:__________________ Month:__________________
GMPWeighted during GMP
0-5 months 6--23 MonthsTotal CountTally Count Tally Count
Z score >= -2(Normal)
Z score between -3 and -2 (moderate under weight)
Z score < -3(Sever under weight)
Total count
Nutritional ScreeningNutritional Screening for under 5 year
0-5 months 6 - 23 Months 24 - 59 MonthsTotal countTally Count Tally Count Count
Normal
Moderate Acute Malinutrition(MAM)
Sever Acute Malinutrition (SAM)
Total screened for Malinutrition(Count)
Vitamin A Vitamin A 6-11 months 12-59 months Total Count
Vitamin A One doses suplimented Vitamin A Two doses suplimented
Deworming (24-59 months)Deworming (24-59 month) Tally Count Received one dose Received two doses
Developmental milestone0-23 months 24-59 months Total Count
Tally Count Tally CountConfrimed developmental delay(CDD)Suspected developmental delay(SDD)No developmental delay(NDD)
Comprehensive and Integrated Nutrition Service for <5 years Children tally sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Family Planning Dispensing Tally
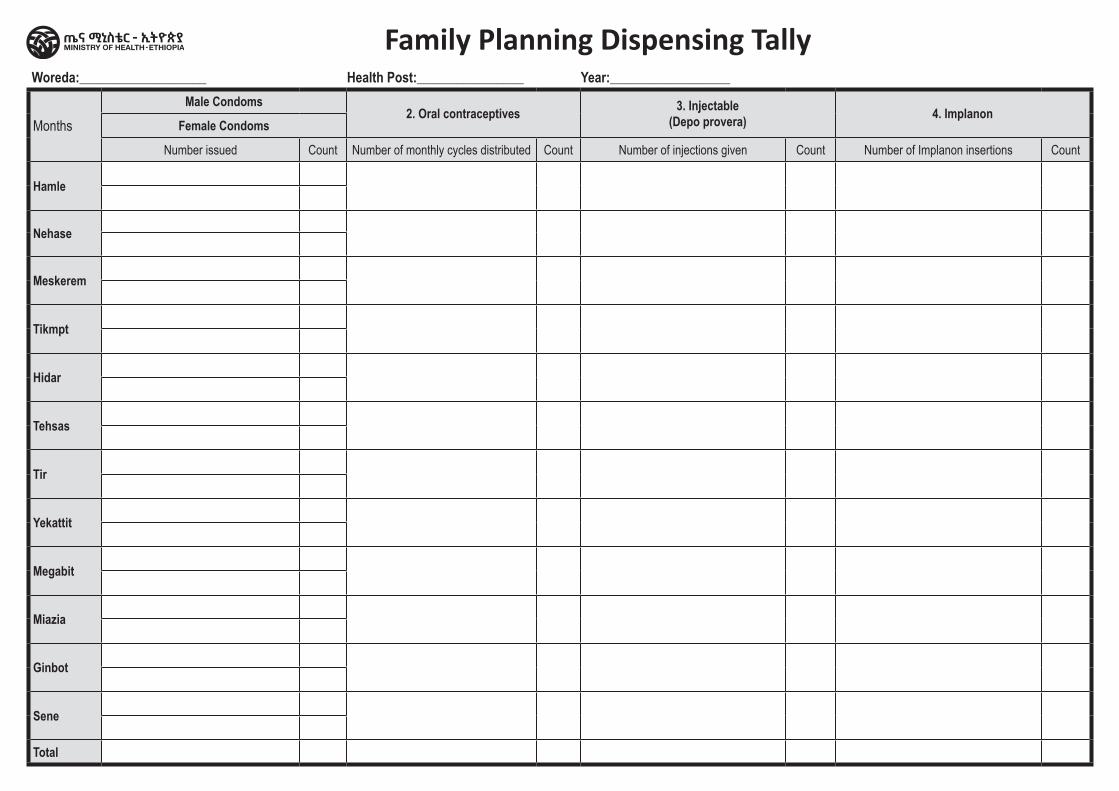
Woreda:___________________ Health Post:________________ Year:__________________
MonthsMale Condoms
2. Oral contraceptives 3. Injectable (Depo provera) 4. Implanon
Female Condoms
Number issued Count Number of monthly cycles distributed Count Number of injections given Count Number of Implanon insertions Count
Hamle
Nehase
Meskerem
Tikmpt
Hidar
Tehsas
Tir
Yekattit
Megabit
Miazia
Ginbot
Sene
Total
Family Planning Dispensing Tally
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Family Planning Service Tally
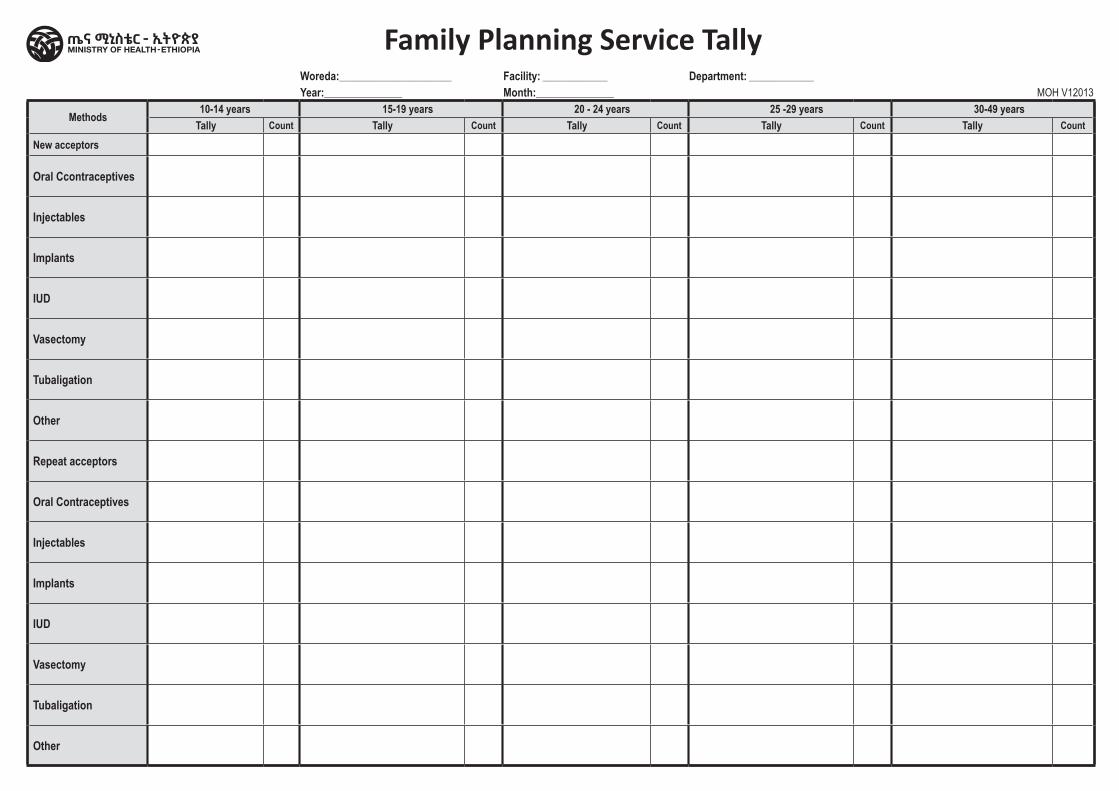
Woreda:__________________________ Facility: _______________ Department: _______________ Year:__________________ Month:__________________ MOH V12013
Methods 10-14 years 15-19 years 20 - 24 years 25 -29 years 30-49 yearsTally Count Tally Count Tally Count Tally Count Tally Count
New acceptors
Oral Ccontraceptives
Injectables
Implants
IUD
Vasectomy
Tubaligation
Other
Repeat acceptors
Oral Contraceptives
Injectables
Implants
IUD
Vasectomy
Tubaligation
Other
Family Planning Service Tally
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital PMTCT Tally Sheet
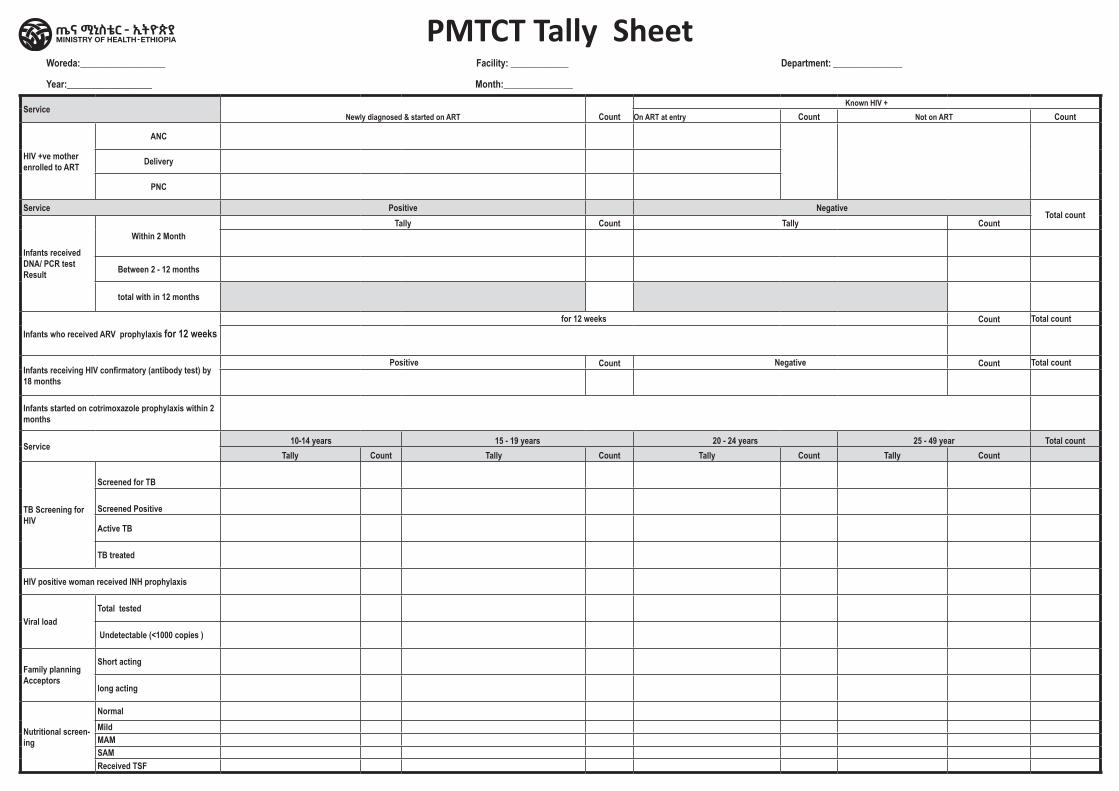
Woreda:__________________ Facility: _______________ Department: __________________
Year:__________________ Month:__________________
ServiceNewly diagnosed & started on ART Count
Known HIV +On ART at entry Count Not on ART Count
HIV +ve mother enrolled to ART
ANC
Delivery
PNC
Service Positive NegativeTotal count
Infants received DNA/ PCR test Result
Within 2 MonthTally Count Tally Count
Between 2 - 12 months
total with in 12 months
Infants who received ARV prophylaxis for 12 weeksfor 12 weeks Count Total count
Infants receiving HIV confirmatory (antibody test) by 18 months
Positive Count Negative Count Total count
Infants started on cotrimoxazole prophylaxis within 2 months
Service 10-14 years 15 - 19 years 20 - 24 years 25 - 49 year Total countTally Count Tally Count Tally Count Tally Count
TB Screening for HIV
Screened for TB
Screened Positive
Active TB
TB treated
HIV positive woman received INH prophylaxis
Viral load Total tested
Undetectable (<1000 copies )
Family planning Acceptors
Short acting
long acting
Nutritional screen-ing
NormalMildMAMSAMReceived TSF
PMTCT Tally Sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Pregnancy Test Tally Sheet
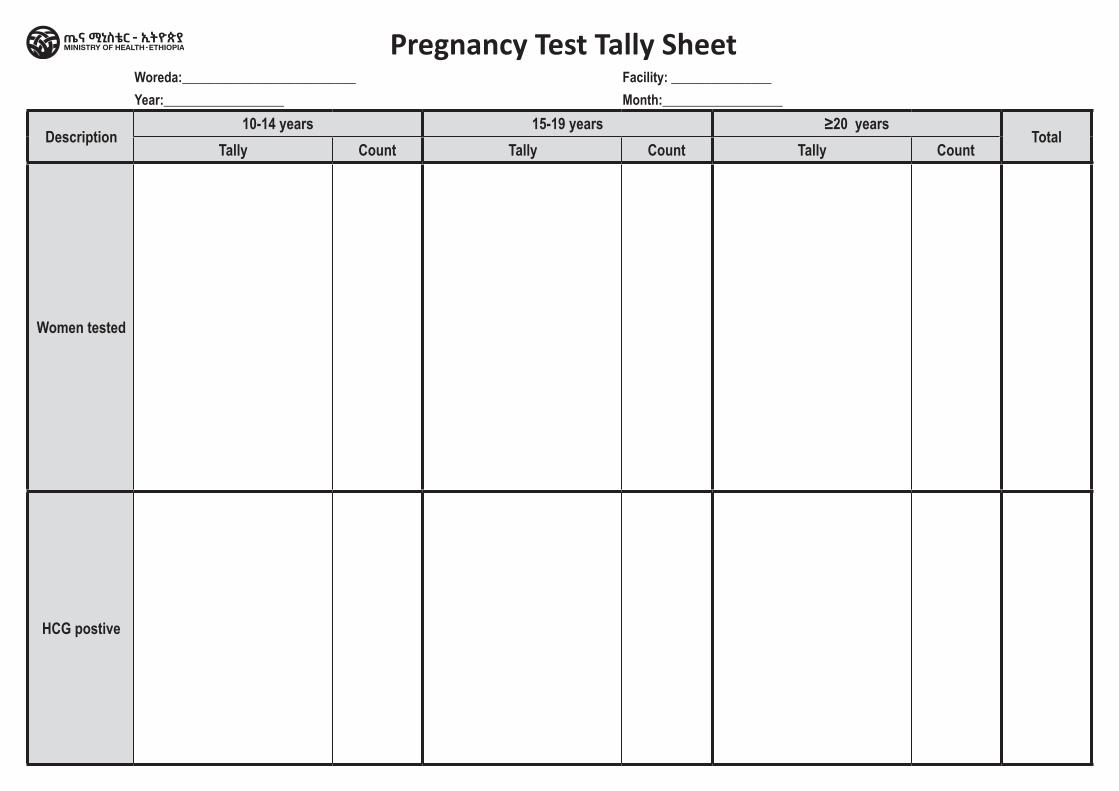
Woreda:__________________________ Facility: _______________ Year:__________________ Month:__________________
Description10-14 years 15-19 years ≥20 years
TotalTally Count Tally Count Tally Count
Women tested
HCG postive
Pregnancy Test Tally Sheet
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Routine Immunization Tally Sheet
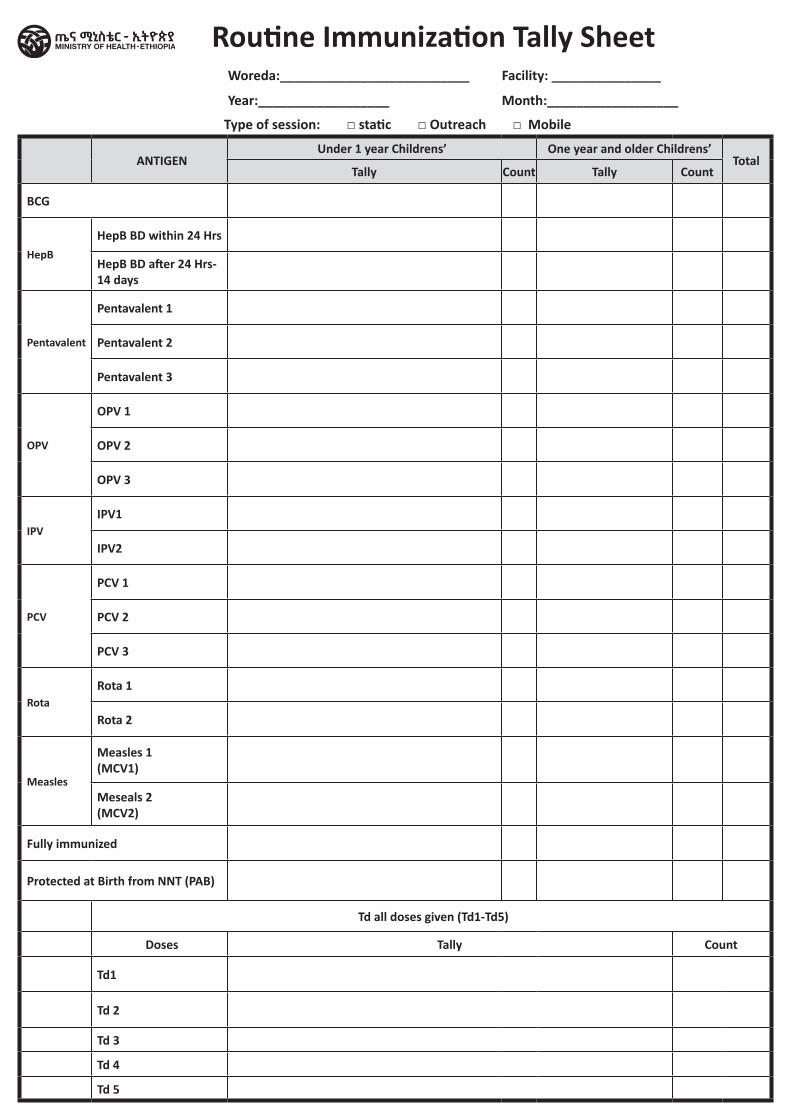
Woreda:__________________________ Facility: _______________
Year:__________________ Month:__________________
Type of session: □ static □ Outreach □ Mobile
ANTIGENUnder 1 year Childrens’ One year and older Childrens’
TotalTally Count Tally Count
BCG
HepBHepB BD within 24 Hrs
HepB BD after 24 Hrs-14 days
Pentavalent
Pentavalent 1
Pentavalent 2
Pentavalent 3
OPV
OPV 1
OPV 2
OPV 3
IPVIPV1
IPV2
PCV
PCV 1
PCV 2
PCV 3
RotaRota 1
Rota 2
Measles
Measles 1 (MCV1)
Meseals 2 (MCV2)
Fully immunized
Protected at Birth from NNT (PAB)
Td all doses given (Td1-Td5)
Doses Tally Count
Td1
Td 2
Td 3
Td 4
Td 5
Routine Immunization Tally Sheet
TB and leprosy RegistersContent / Home

Health Centre/Clinic/Hospital DR TB Follow up Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
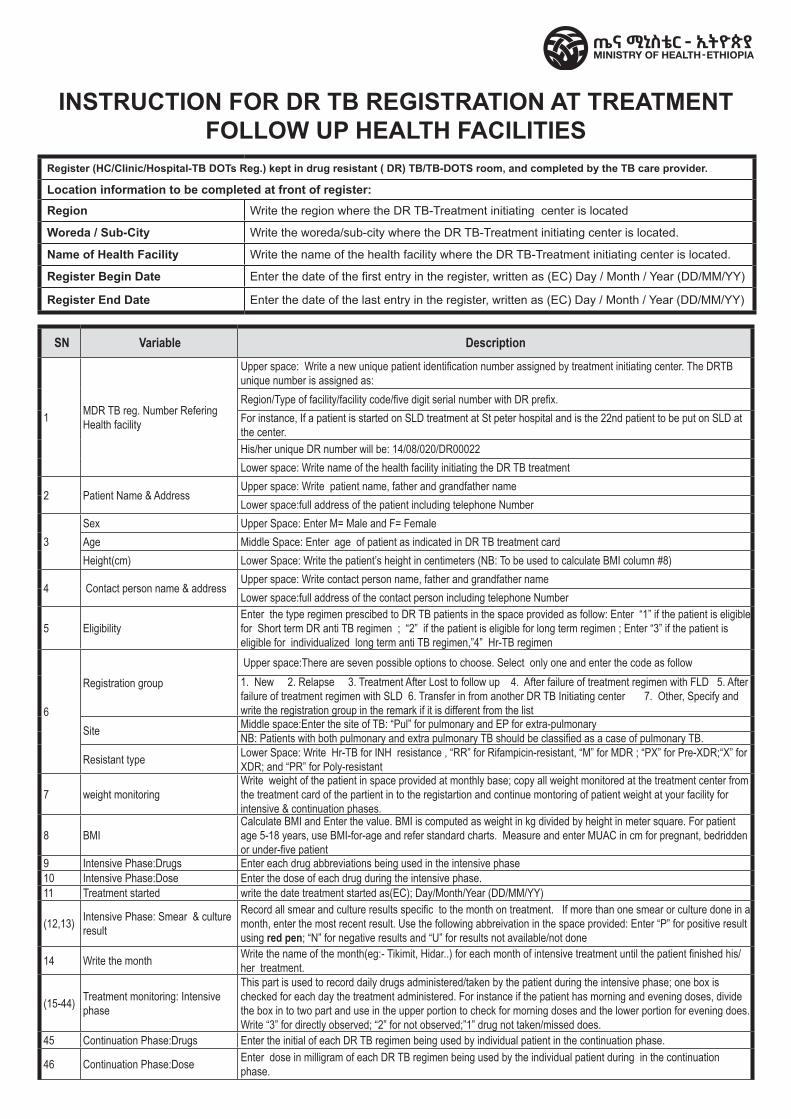
SN Variable Description
1 MDR TB reg. Number Refering Health facility
Upper space: Write a new unique patient identification number assigned by treatment initiating center. The DRTB unique number is assigned as:Region/Type of facility/facility code/five digit serial number with DR prefix.For instance, If a patient is started on SLD treatment at St peter hospital and is the 22nd patient to be put on SLD at the center.His/her unique DR number will be: 14/08/020/DR00022Lower space: Write name of the health facility initiating the DR TB treatment
2 Patient Name & AddressUpper space: Write patient name, father and grandfather nameLower space:full address of the patient including telephone Number
3Sex Upper Space: Enter M= Male and F= FemaleAge Middle Space: Enter age of patient as indicated in DR TB treatment cardHeight(cm) Lower Space: Write the patient’s height in centimeters (NB: To be used to calculate BMI column #8)
4 Contact person name & addressUpper space: Write contact person name, father and grandfather nameLower space:full address of the contact person including telephone Number
5 EligibilityEnter the type regimen prescibed to DR TB patients in the space provided as follow: Enter “1” if the patient is eligible for Short term DR anti TB regimen ; “2” if the patient is eligible for long term regimen ; Enter “3” if the patient is eligible for individualized long term anti TB regimen,”4” Hr-TB regimen
6
Registration group Upper space:There are seven possible options to choose. Select only one and enter the code as follow1. New 2. Relapse 3. Treatment After Lost to follow up 4. After failure of treatment regimen with FLD 5. After failure of treatment regimen with SLD 6. Transfer in from another DR TB Initiating center 7. Other, Specify and write the registration group in the remark if it is different from the list
Site Middle space:Enter the site of TB: “Pul” for pulmonary and EP for extra-pulmonary NB: Patients with both pulmonary and extra pulmonary TB should be classified as a case of pulmonary TB.
Resistant type Lower Space: Write Hr-TB for INH resistance , “RR” for Rifampicin-resistant, “M” for MDR ; “PX” for Pre-XDR;“X” for XDR; and “PR” for Poly-resistant
7 weight monitoring Write weight of the patient in space provided at monthly base; copy all weight monitored at the treatment center from the treatment card of the partient in to the registartion and continue montoring of patient weight at your facility for intensive & continuation phases.
8 BMICalculate BMI and Enter the value. BMI is computed as weight in kg divided by height in meter square. For patient age 5-18 years, use BMI-for-age and refer standard charts. Measure and enter MUAC in cm for pregnant, bedridden or under-five patient
9 Intensive Phase:Drugs Enter each drug abbreviations being used in the intensive phase 10 Intensive Phase:Dose Enter the dose of each drug during the intensive phase.11 Treatment started write the date treatment started as(EC); Day/Month/Year (DD/MM/YY)
(12,13) Intensive Phase: Smear & culture result
Record all smear and culture results specific to the month on treatment. If more than one smear or culture done in a month, enter the most recent result. Use the following abbreivation in the space provided: Enter “P” for positive result using red pen; “N” for negative results and “U” for results not available/not done
14 Write the month Write the name of the month(eg:- Tikimit, Hidar..) for each month of intensive treatment until the patient finished his/her treatment.
(15-44) Treatment monitoring: Intensive phase
This part is used to record daily drugs administered/taken by the patient during the intensive phase; one box is checked for each day the treatment administered. For instance if the patient has morning and evening doses, divide the box in to two part and use in the upper portion to check for morning doses and the lower portion for evening does. Write “3” for directly observed; “2” for not observed;”1” drug not taken/missed does.
45 Continuation Phase:Drugs Enter the initial of each DR TB regimen being used by individual patient in the continuation phase.
46 Continuation Phase:Dose Enter dose in milligram of each DR TB regimen being used by the individual patient during in the continuation phase.
INSTRUCTION FOR DR TB REGISTRATION AT TREATMENT FOLLOW UP HEALTH FACILITIES
Register (HC/Clinic/Hospital-TB DOTs Reg.) kept in drug resistant ( DR) TB/TB-DOTS room, and completed by the TB care provider.
Location information to be completed at front of register:
Region Write the region where the DR TB-Treatment initiating center is located
Woreda / Sub-City Write the woreda/sub-city where the DR TB-Treatment initiating center is located.
Name of Health Facility Write the name of the health facility where the DR TB-Treatment initiating center is located.
Register Begin Date Enter the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register End Date Enter the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
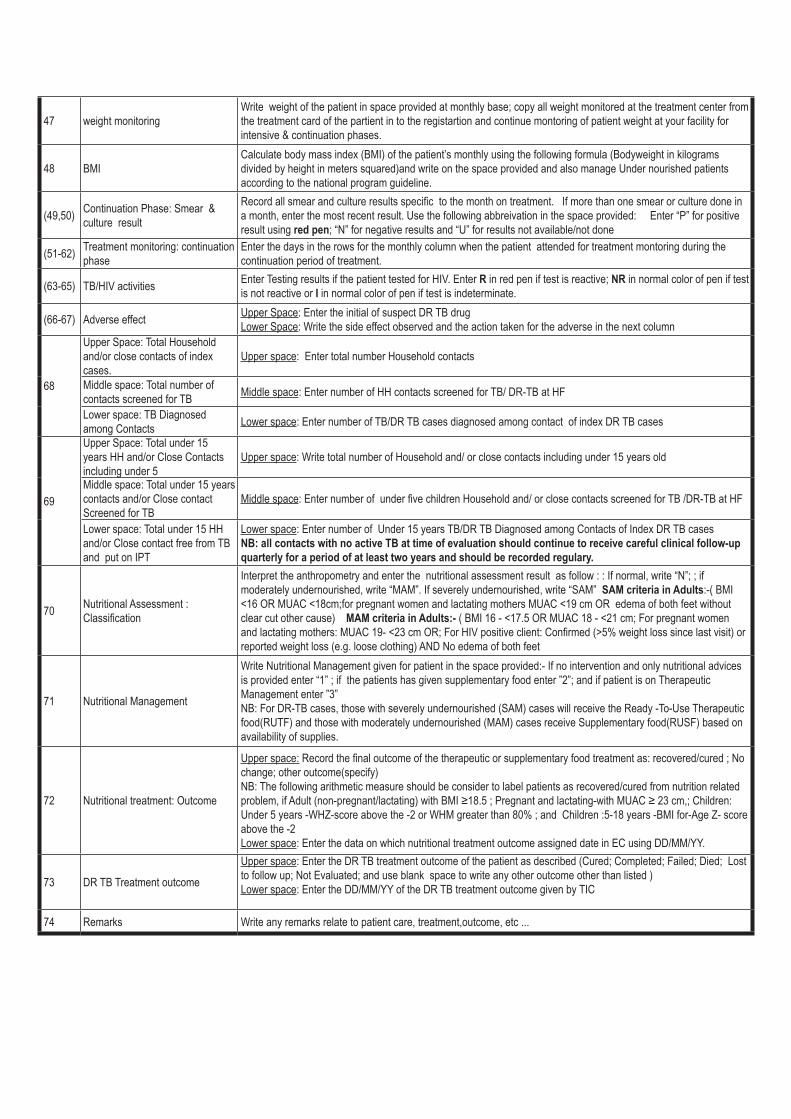
47 weight monitoring Write weight of the patient in space provided at monthly base; copy all weight monitored at the treatment center from the treatment card of the partient in to the registartion and continue montoring of patient weight at your facility for intensive & continuation phases.
48 BMICalculate body mass index (BMI) of the patient’s monthly using the following formula (Bodyweight in kilograms divided by height in meters squared)and write on the space provided and also manage Under nourished patients according to the national program guideline.
(49,50) Continuation Phase: Smear & culture result
Record all smear and culture results specific to the month on treatment. If more than one smear or culture done in a month, enter the most recent result. Use the following abbreivation in the space provided: Enter “P” for positive result using red pen; “N” for negative results and “U” for results not available/not done
(51-62) Treatment monitoring: continuation phase
Enter the days in the rows for the monthly column when the patient attended for treatment montoring during the continuation period of treatment.
(63-65) TB/HIV activities Enter Testing results if the patient tested for HIV. Enter R in red pen if test is reactive; NR in normal color of pen if test is not reactive or I in normal color of pen if test is indeterminate.
(66-67) Adverse effect Upper Space: Enter the initial of suspect DR TB drugLower Space: Write the side effect observed and the action taken for the adverse in the next column
68
Upper Space: Total Household and/or close contacts of index cases.
Upper space: Enter total number Household contacts
Middle space: Total number of contacts screened for TB Middle space: Enter number of HH contacts screened for TB/ DR-TB at HF
Lower space: TB Diagnosed among Contacts Lower space: Enter number of TB/DR TB cases diagnosed among contact of index DR TB cases
69
Upper Space: Total under 15 years HH and/or Close Contacts including under 5
Upper space: Write total number of Household and/ or close contacts including under 15 years old
Middle space: Total under 15 years contacts and/or Close contact Screened for TB
Middle space: Enter number of under five children Household and/ or close contacts screened for TB /DR-TB at HF
Lower space: Total under 15 HH and/or Close contact free from TB and put on IPT
Lower space: Enter number of Under 15 years TB/DR TB Diagnosed among Contacts of Index DR TB cases NB: all contacts with no active TB at time of evaluation should continue to receive careful clinical follow-up quarterly for a period of at least two years and should be recorded regulary.
70 Nutritional Assessment : Classification
Interpret the anthropometry and enter the nutritional assessment result as follow : : If normal, write “N”; ; if moderately undernourished, write “MAM”. If severely undernourished, write “SAM” SAM criteria in Adults:-( BMI <16 OR MUAC <18cm;for pregnant women and lactating mothers MUAC <19 cm OR edema of both feet without clear cut other cause) MAM criteria in Adults:- ( BMI 16 - <17.5 OR MUAC 18 - <21 cm; For pregnant women and lactating mothers: MUAC 19- <23 cm OR; For HIV positive client: Confirmed (>5% weight loss since last visit) or reported weight loss (e.g. loose clothing) AND No edema of both feet
71 Nutritional Management
Write Nutritional Management given for patient in the space provided:- If no intervention and only nutritional advices is provided enter “1” ; if the patients has given supplementary food enter ”2”; and if patient is on Therapeutic Management enter ”3” NB: For DR-TB cases, those with severely undernourished (SAM) cases will receive the Ready -To-Use Therapeutic food(RUTF) and those with moderately undernourished (MAM) cases receive Supplementary food(RUSF) based on availability of supplies.
72 Nutritional treatment: Outcome
Upper space: Record the final outcome of the therapeutic or supplementary food treatment as: recovered/cured ; No change; other outcome(specify) NB: The following arithmetic measure should be consider to label patients as recovered/cured from nutrition related problem, if Adult (non-pregnant/lactating) with BMI ≥18.5 ; Pregnant and lactating-with MUAC ≥ 23 cm,; Children: Under 5 years -WHZ-score above the -2 or WHM greater than 80% ; and Children :5-18 years -BMI for-Age Z- score above the -2 Lower space: Enter the data on which nutritional treatment outcome assigned date in EC using DD/MM/YY.
73 DR TB Treatment outcome
Upper space: Enter the DR TB treatment outcome of the patient as described (Cured; Completed; Failed; Died; Lost to follow up; Not Evaluated; and use blank space to write any other outcome other than listed ) Lower space: Enter the DD/MM/YY of the DR TB treatment outcome given by TIC
74 Remarks Write any remarks relate to patient care, treatment,outcome, etc ...
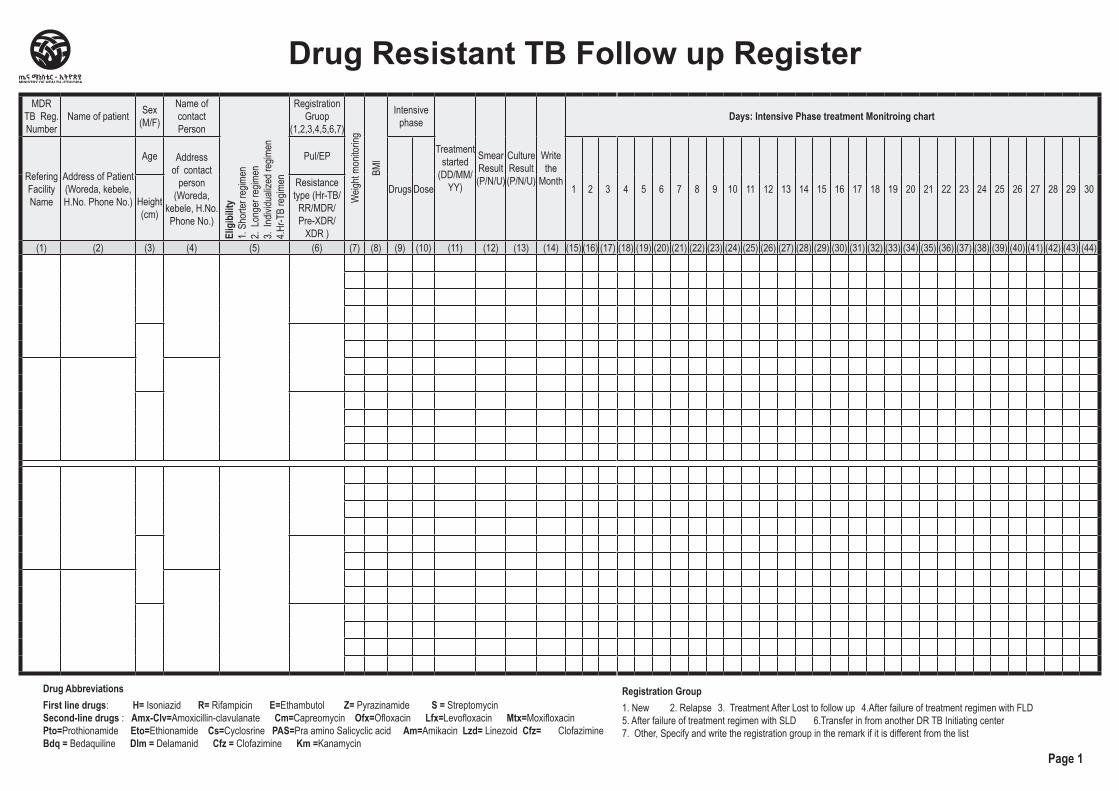
MDR TB Reg. Number
Name of patient Sex (M/F)
Name of contact Person
Elig
ibilit
y1.
Shor
ter re
gimen
2.
Long
er re
gimen
3.
Indiv
iduali
zed r
egim
en4.H
r-TB
regim
en
Registration Gruop
(1,2,3,4,5,6,7)
Weig
ht mo
nitor
ing
BMI
Intensive phase
Treatment started
(DD/MM/YY)
Smear Result (P/N/U)
Culture Result (P/N/U)
Write the
Month
Days: Intensive Phase treatment Monitroing chart
Refering Facility Name
Address of Patient (Woreda, kebele, H.No. Phone No.)
Age Address of contact
person (Woreda,
kebele, H.No. Phone No.)
Pul/EP
Drugs Dose 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30Height (cm)
Resistance type (Hr-TB/
RR/MDR/ Pre-XDR/
XDR )(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44)
Drug Resistant TB Follow up Register
Drug AbbreviationsFirst line drugs: H= Isoniazid R= Rifampicin E=Ethambutol Z= Pyrazinamide S = Streptomycin Second-line drugs : Amx-Clv=Amoxicillin-clavulanate Cm=Capreomycin Ofx=Ofloxacin Lfx=Levofloxacin Mtx=Moxifloxacin Pto=Prothionamide Eto=Ethionamide Cs=Cyclosrine PAS=Pra amino Salicyclic acid Am=Amikacin Lzd= Linezoid Cfz= Clofazimine Bdq = Bedaquiline Dlm = Delamanid Cfz = Clofazimine Km =Kanamycin
Registration Group1. New 2. Relapse 3. Treatment After Lost to follow up 4.After failure of treatment regimen with FLD 5. After failure of treatment regimen with SLD 6.Transfer in from another DR TB Initiating center 7. Other, Specify and write the registration group in the remark if it is different from the list
Page 1
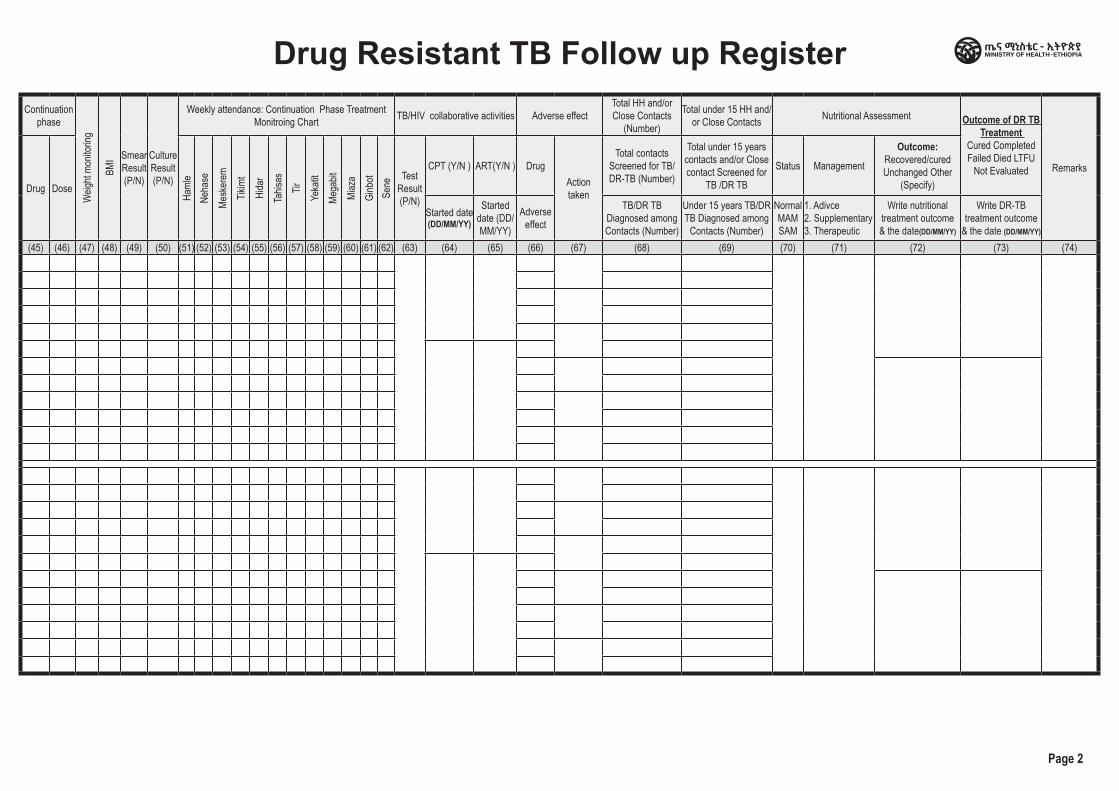
Continuation phase
Weig
ht mo
nitor
ing
BMI Smear
Result (P/N)
Culture Result (P/N)
Weekly attendance: Continuation Phase Treatment Monitroing Chart TB/HIV collaborative activities Adverse effect
Total HH and/or Close Contacts
(Number)
Total under 15 HH and/or Close Contacts Nutritional Assessment Outcome of DR TB
Treatment Cured Completed Failed Died LTFU
Not Evaluated Remarks
Drug DoseHa
mle
Neha
seMe
sker
emTik
imt
Hida
rTa
hisas
TirYe
katit
Mega
bitMi
aza
Ginb
otSe
ne Test
Result (P/N)
CPT (Y/N ) ART(Y/N ) Drug Action taken
Total contacts Screened for TB/ DR-TB (Number)
Total under 15 years contacts and/or Close contact Screened for
TB /DR TB
Status Management
Outcome: Recovered/cured Unchanged Other
(Specify)
Started date (DD/MM/YY)
Started date (DD/MM/YY)
Adverse effect
TB/DR TB Diagnosed among Contacts (Number)
Under 15 years TB/DR TB Diagnosed among
Contacts (Number)
Normal MAM SAM
1. Adivce2. Supplementary3. Therapeutic
Write nutritional treatment outcome & the date(DD/MM/YY)
Write DR-TB treatment outcome
& the date (DD/MM/YY)
(45) (46) (47) (48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) (60) (61) (62) (63) (64) (65) (66) (67) (68) (69) (70) (71) (72) (73) (74)
Drug Resistant TB Follow up Register
Page 2
Health Centre/Clinic/HospitalDrug Resistant TB Register
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
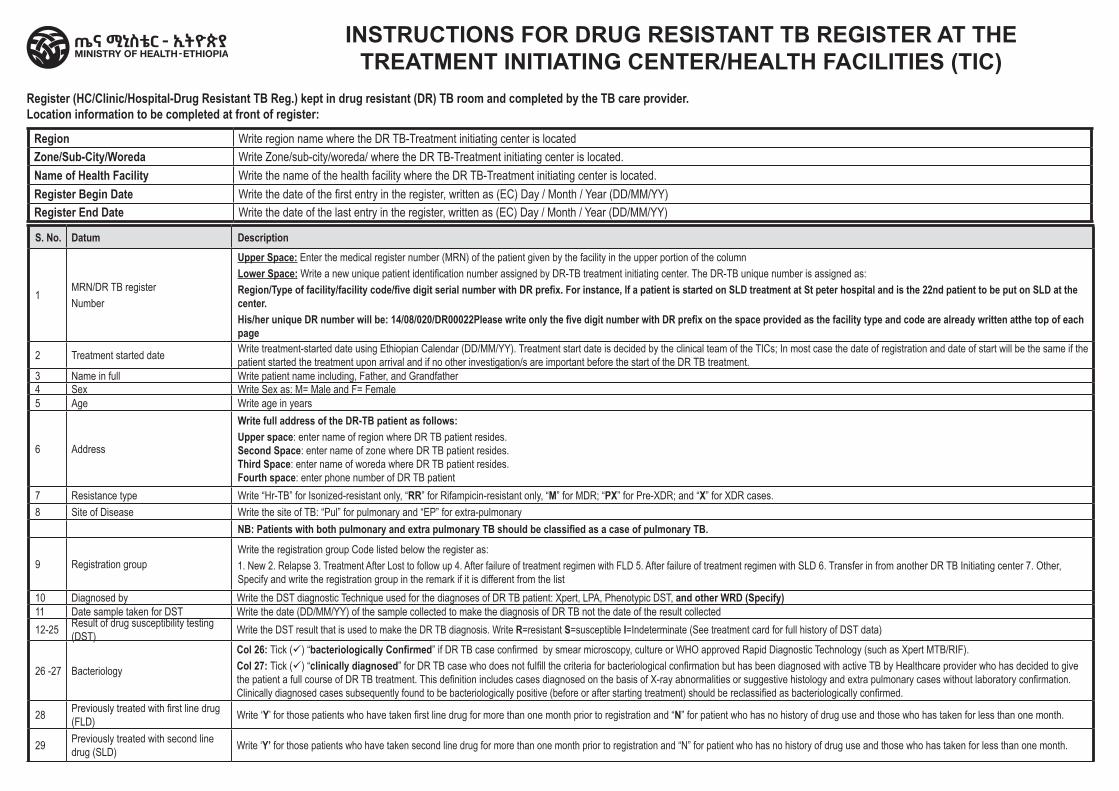
INSTRUCTIONS FOR DRUG RESISTANT TB REGISTER AT THE TREATMENT INITIATING CENTER/HEALTH FACILITIES (TIC)
Region Write region name where the DR TB-Treatment initiating center is locatedZone/Sub-City/Woreda Write Zone/sub-city/woreda/ where the DR TB-Treatment initiating center is located.Name of Health Facility Write the name of the health facility where the DR TB-Treatment initiating center is located.Register Begin Date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)Register End Date Write the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
Register (HC/Clinic/Hospital-Drug Resistant TB Reg.) kept in drug resistant (DR) TB room and completed by the TB care provider.Location information to be completed at front of register:
S. No. Datum Description
1MRN/DR TB registerNumber
Upper Space: Enter the medical register number (MRN) of the patient given by the facility in the upper portion of the columnLower Space: Write a new unique patient identification number assigned by DR-TB treatment initiating center. The DR-TB unique number is assigned as:Region/Type of facility/facility code/five digit serial number with DR prefix. For instance, If a patient is started on SLD treatment at St peter hospital and is the 22nd patient to be put on SLD at the center.His/her unique DR number will be: 14/08/020/DR00022Please write only the five digit number with DR prefix on the space provided as the facility type and code are already written atthe top of each page
2 Treatment started date Write treatment-started date using Ethiopian Calendar (DD/MM/YY). Treatment start date is decided by the clinical team of the TICs; In most case the date of registration and date of start will be the same if the patient started the treatment upon arrival and if no other investigation/s are important before the start of the DR TB treatment.
3 Name in full Write patient name including, Father, and Grandfather4 Sex Write Sex as: M= Male and F= Female5 Age Write age in years
6 Address
Write full address of the DR-TB patient as follows: Upper space: enter name of region where DR TB patient resides.Second Space: enter name of zone where DR TB patient resides.Third Space: enter name of woreda where DR TB patient resides.Fourth space: enter phone number of DR TB patient
7 Resistance type Write “Hr-TB” for Isonized-resistant only, “RR” for Rifampicin-resistant only, “M” for MDR; “PX” for Pre-XDR; and “X” for XDR cases.8 Site of Disease Write the site of TB: “Pul” for pulmonary and “EP” for extra-pulmonary
NB: Patients with both pulmonary and extra pulmonary TB should be classified as a case of pulmonary TB.
9 Registration groupWrite the registration group Code listed below the register as:1. New 2. Relapse 3. Treatment After Lost to follow up 4. After failure of treatment regimen with FLD 5. After failure of treatment regimen with SLD 6. Transfer in from another DR TB Initiating center 7. Other, Specify and write the registration group in the remark if it is different from the list
10 Diagnosed by Write the DST diagnostic Technique used for the diagnoses of DR TB patient: Xpert, LPA, Phenotypic DST, and other WRD (Specify)11 Date sample taken for DST Write the date (DD/MM/YY) of the sample collected to make the diagnosis of DR TB not the date of the result collected12-25 Result of drug susceptibility testing
(DST) Write the DST result that is used to make the DR TB diagnosis. Write R=resistant S=susceptible I=Indeterminate (See treatment card for full history of DST data)
26 -27 Bacteriology
Col 26: Tick (ü) “bacteriologically Confirmed” if DR TB case confirmed by smear microscopy, culture or WHO approved Rapid Diagnostic Technology (such as Xpert MTB/RIF).Col 27: Tick (ü) “clinically diagnosed” for DR TB case who does not fulfill the criteria for bacteriological confirmation but has been diagnosed with active TB by Healthcare provider who has decided to give the patient a full course of DR TB treatment. This definition includes cases diagnosed on the basis of X-ray abnormalities or suggestive histology and extra pulmonary cases without laboratory confirmation. Clinically diagnosed cases subsequently found to be bacteriologically positive (before or after starting treatment) should be reclassified as bacteriologically confirmed.
28 Previously treated with first line drug (FLD) Write ‘Y’ for those patients who have taken first line drug for more than one month prior to registration and “N” for patient who has no history of drug use and those who has taken for less than one month.
29 Previously treated with second line drug (SLD) Write ‘Y’ for those patients who have taken second line drug for more than one month prior to registration and “N” for patient who has no history of drug use and those who has taken for less than one month.
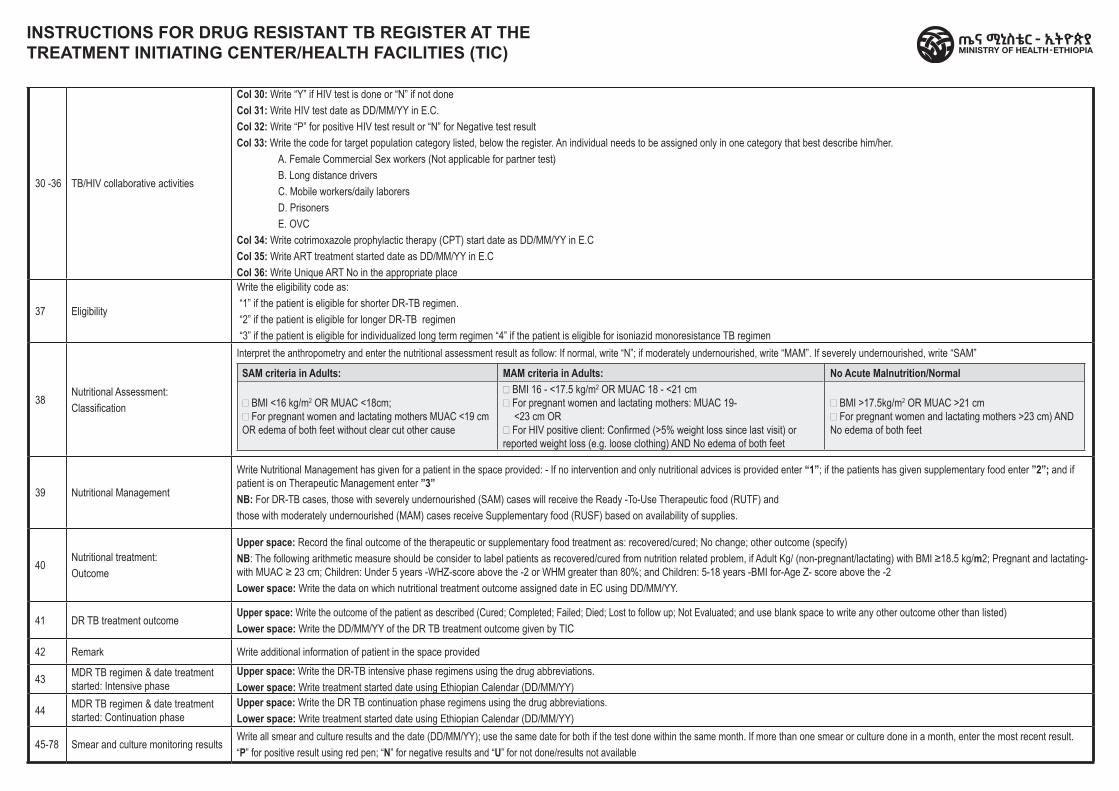
30 -36 TB/HIV collaborative activities
Col 30: Write “Y” if HIV test is done or “N” if not doneCol 31: Write HIV test date as DD/MM/YY in E.C.Col 32: Write “P” for positive HIV test result or “N” for Negative test resultCol 33: Write the code for target population category listed, below the register. An individual needs to be assigned only in one category that best describe him/her.
A. Female Commercial Sex workers (Not applicable for partner test)B. Long distance driversC. Mobile workers/daily laborersD. PrisonersE. OVC
Col 34: Write cotrimoxazole prophylactic therapy (CPT) start date as DD/MM/YY in E.CCol 35: Write ART treatment started date as DD/MM/YY in E.CCol 36: Write Unique ART No in the appropriate place
37 Eligibility
Write the eligibility code as:“1” if the patient is eligible for shorter DR-TB regimen.“2” if the patient is eligible for longer DR-TB regimen “3” if the patient is eligible for individualized long term regimen “4” if the patient is eligible for isoniazid monoresistance TB regimen
38Nutritional Assessment:Classification
Interpret the anthropometry and enter the nutritional assessment result as follow: If normal, write “N”; if moderately undernourished, write “MAM”. If severely undernourished, write “SAM”
SAM criteria in Adults: MAM criteria in Adults: No Acute Malnutrition/Normal
· BMI <16 kg/m2 OR MUAC <18cm;· For pregnant women and lactating mothers MUAC <19 cm OR edema of both feet without clear cut other cause
· BMI 16 - <17.5 kg/m2 OR MUAC 18 - <21 cm· For pregnant women and lactating mothers: MUAC 19-
<23 cm OR· For HIV positive client: Confirmed (>5% weight loss since last visit) or reported weight loss (e.g. loose clothing) AND No edema of both feet
· BMI >17.5kg/m2 OR MUAC >21 cm· For pregnant women and lactating mothers >23 cm) AND No edema of both feet
39 Nutritional Management
Write Nutritional Management has given for a patient in the space provided: - If no intervention and only nutritional advices is provided enter “1”; if the patients has given supplementary food enter ”2”; and if patient is on Therapeutic Management enter ”3” NB: For DR-TB cases, those with severely undernourished (SAM) cases will receive the Ready -To-Use Therapeutic food (RUTF) andthose with moderately undernourished (MAM) cases receive Supplementary food (RUSF) based on availability of supplies.
40Nutritional treatment:Outcome
Upper space: Record the final outcome of the therapeutic or supplementary food treatment as: recovered/cured; No change; other outcome (specify)NB: The following arithmetic measure should be consider to label patients as recovered/cured from nutrition related problem, if Adult Kg/ (non-pregnant/lactating) with BMI ≥18.5 kg/m2; Pregnant and lactating-with MUAC ≥ 23 cm; Children: Under 5 years -WHZ-score above the -2 or WHM greater than 80%; and Children: 5-18 years -BMI for-Age Z- score above the -2Lower space: Write the data on which nutritional treatment outcome assigned date in EC using DD/MM/YY.
41 DR TB treatment outcomeUpper space: Write the outcome of the patient as described (Cured; Completed; Failed; Died; Lost to follow up; Not Evaluated; and use blank space to write any other outcome other than listed)Lower space: Write the DD/MM/YY of the DR TB treatment outcome given by TIC
42 Remark Write additional information of patient in the space provided
43 MDR TB regimen & date treatment started: Intensive phase
Upper space: Write the DR-TB intensive phase regimens using the drug abbreviations.Lower space: Write treatment started date using Ethiopian Calendar (DD/MM/YY)
44 MDR TB regimen & date treatment started: Continuation phase
Upper space: Write the DR TB continuation phase regimens using the drug abbreviations.Lower space: Write treatment started date using Ethiopian Calendar (DD/MM/YY)
45-78 Smear and culture monitoring resultsWrite all smear and culture results and the date (DD/MM/YY); use the same date for both if the test done within the same month. If more than one smear or culture done in a month, enter the most recent result.“P” for positive result using red pen; “N” for negative results and “U” for not done/results not available
INSTRUCTIONS FOR DRUG RESISTANT TB REGISTER AT THE TREATMENT INITIATING CENTER/HEALTH FACILITIES (TIC)
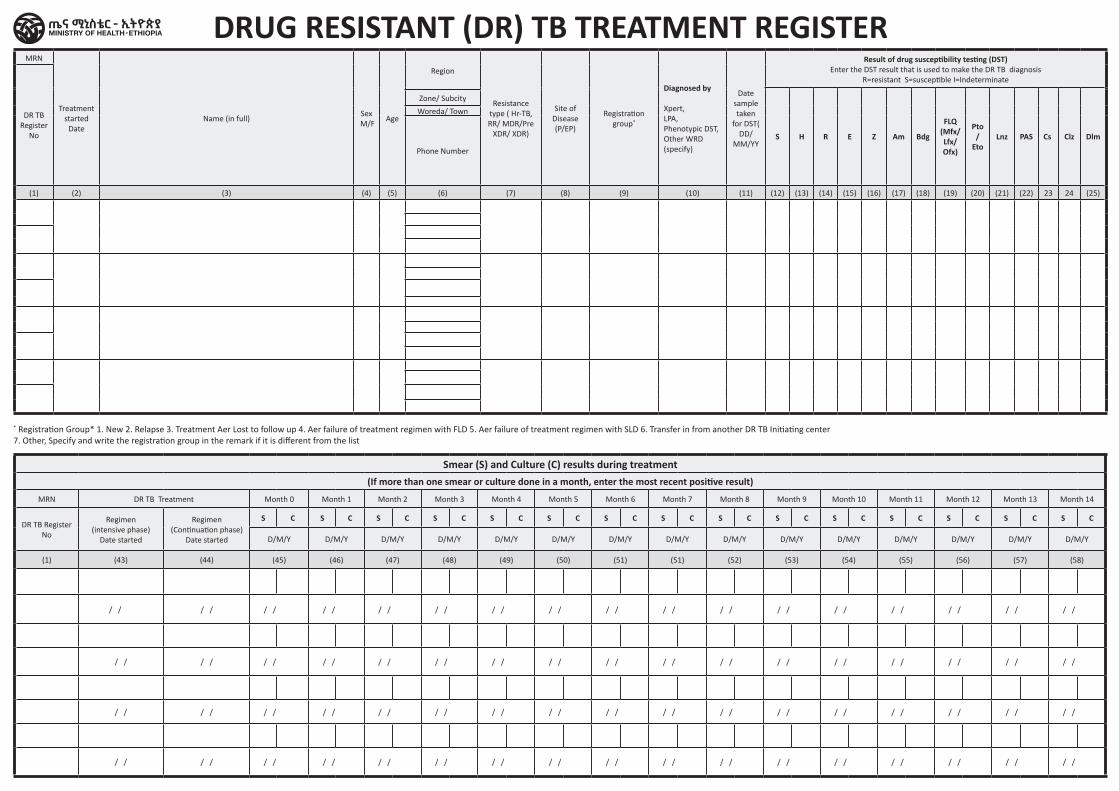
MRN
Treatment started
Date Name (in full)
Sex M/F
Age
Region
Resistance type ( Hr-TB, RR/ MDR/Pre
XDR/ XDR)
Site of Disease (P/EP)
Registration group*
Diagnosed by
Xpert, LPA, Phenotypic DST, Other WRD (specify)
Date sample taken
for DST( DD/
MM/YY
Result of drug susceptibility testing (DST)Enter the DST result that is used to make the DR TB diagnosis
R=resistant S=susceptible I=Indeterminate
DR TB Register
No S H R E Z Am Bdg
FLQ (Mfx/Lfx/ Ofx)
Pto /
EtoLnz PAS Cs Clz Dlm
Zone/ Subcity
Woreda/ Town
Phone Number
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) 23 24 (25)
* Registration Group* 1. New 2. Relapse 3. Treatment A er Lost to follow up 4. A er failure of treatment regimen with FLD 5. A er failure of treatment regimen with SLD 6. Transfer in from another DR TB Initiating center7. Other, Specify and write the registration group in the remark if it is different from the list
Smear (S) and Culture (C) results during treatment(If more than one smear or culture done in a month, enter the most recent positive result)
MRN DR TB Treatment Month 0 Month 1 Month 2 Month 3 Month 4 Month 5 Month 6 Month 7 Month 8 Month 9 Month 10 Month 11 Month 12 Month 13 Month 14
DR TB Register No
Regimen(intensive phase)
Date started
Regimen(Continuation phase)
Date started
S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C
D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y
(1) (43) (44) (45) (46) (47) (48) (49) (50) (51) (51) (52) (53) (54) (55) (56) (57) (58)
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
DRUG RESISTANT (DR) TB TREATMENT REGISTER
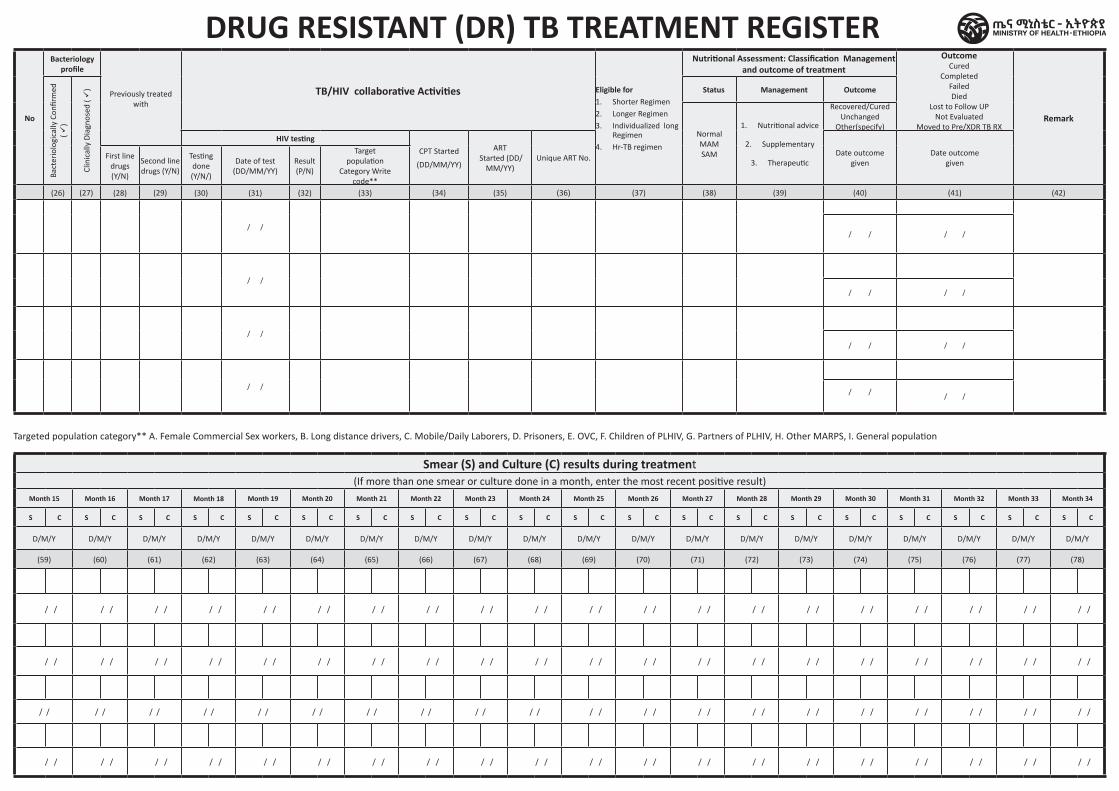
DRUG RESISTANT (DR) TB TREATMENT REGISTER
No
Bacteriology profile
Previously treated with
TB/HIV collaborative Activities Eligible for 1. Shorter Regimen 2. Longer Regimen 3. Individualized long
Regimen4. Hr-TB regimen
Nutritional Assessment: Classification Management and outcome of treatment
OutcomeCured
CompletedFailedDied
Lost to Follow UPNot Evaluated
Moved to Pre/XDR TB RXRemark
Bact
erio
logi
cally
Con
firm
ed
( ü)
Clin
ical
ly D
iagn
osed
( ü
) Status Management Outcome
NormalMAMSAM
1. Nutritional advice
2. Supplementary
3. Therapeutic
Recovered/CuredUnchanged
Other(specify)HIV testing
CPT Started
(DD/MM/YY)
ART Started (DD/
MM/YY)Unique ART No.
Date outcomegiven
Date outcome given
First line drugs (Y/N)
Second line drugs (Y/N)
Testing done (Y/N/)
Date of test(DD/MM/YY)
Result(P/N)
Targetpopulation
Category Writecode**
(26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42)
/ / / / / /
/ /
/ / / /
/ /
/ / / /
/ / / /
/ /
Targeted population category** A. Female Commercial Sex workers, B. Long distance drivers, C. Mobile/Daily Laborers, D. Prisoners, E. OVC, F. Children of PLHIV, G. Partners of PLHIV, H. Other MARPS, I. General population
Smear (S) and Culture (C) results during treatment(If more than one smear or culture done in a month, enter the most recent positive result)
Month 15 Month 16 Month 17 Month 18 Month 19 Month 20 Month 21 Month 22 Month 23 Month 24 Month 25 Month 26 Month 27 Month 28 Month 29 Month 30 Month 31 Month 32 Month 33 Month 34
S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C S C
D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y D/M/Y
(59) (60) (61) (62) (63) (64) (65) (66) (67) (68) (69) (70) (71) (72) (73) (74) (75) (76) (77) (78)
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
/ / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / / /
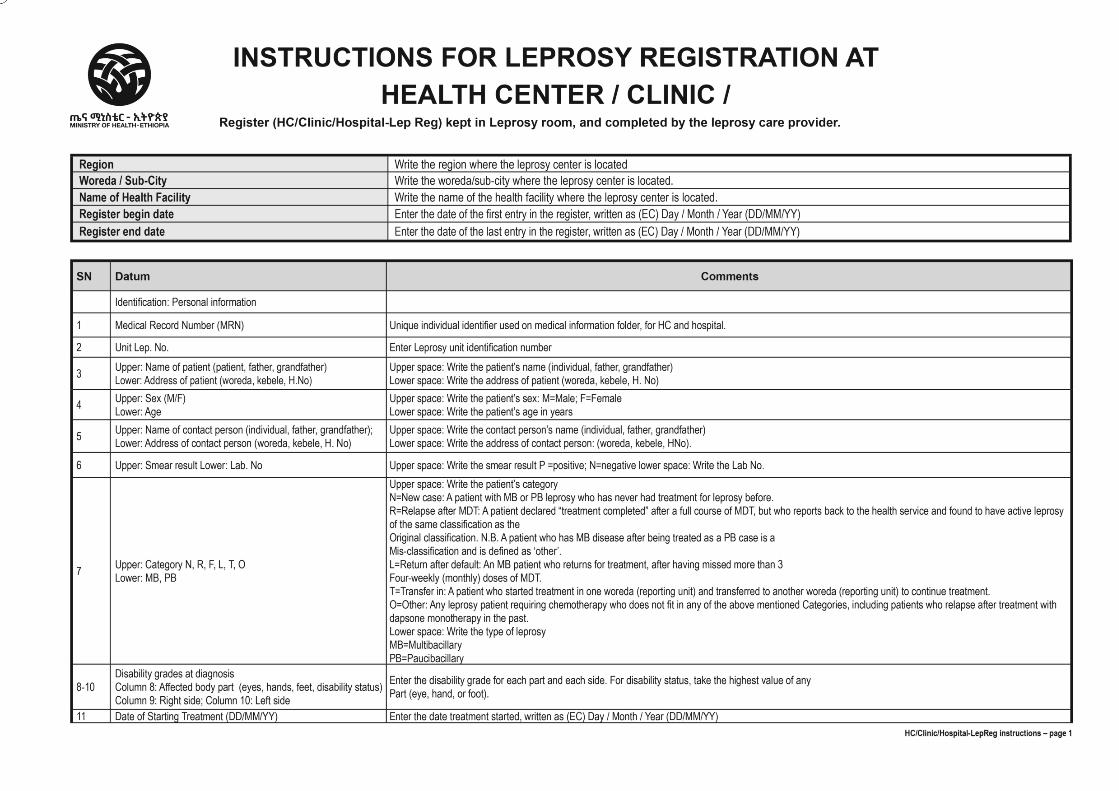
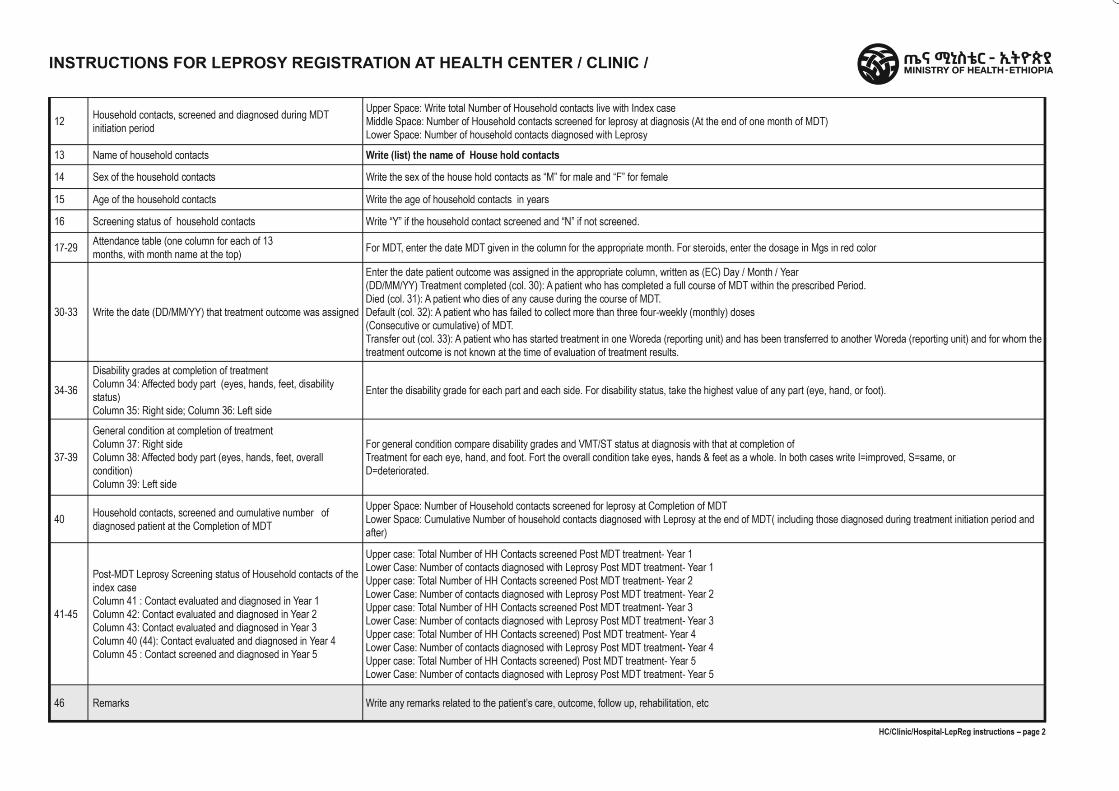
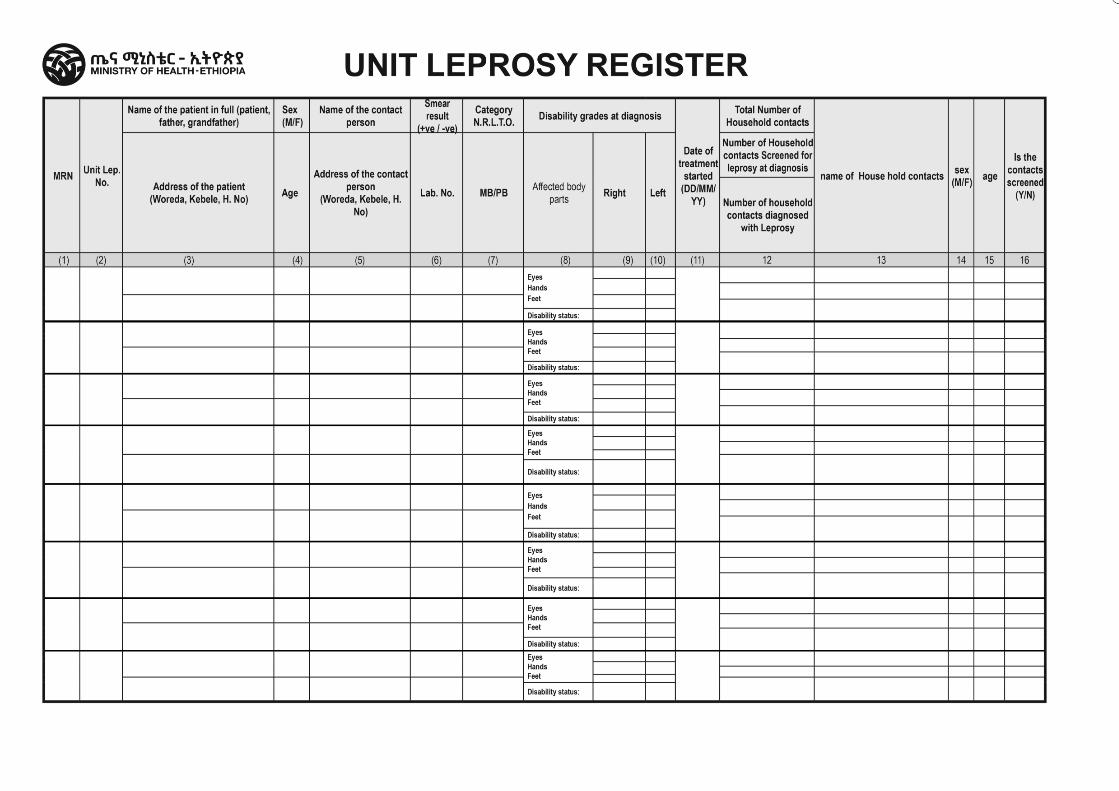
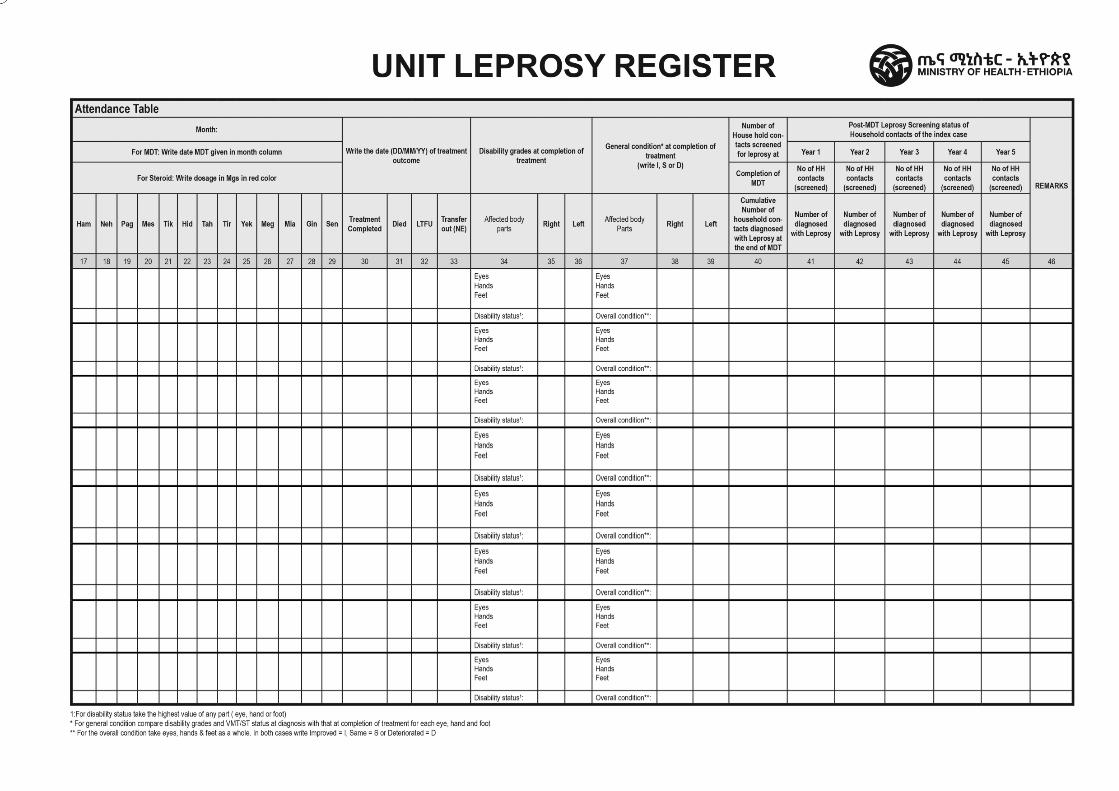
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Leprosy Register for Care After
Completion of Treatment Register
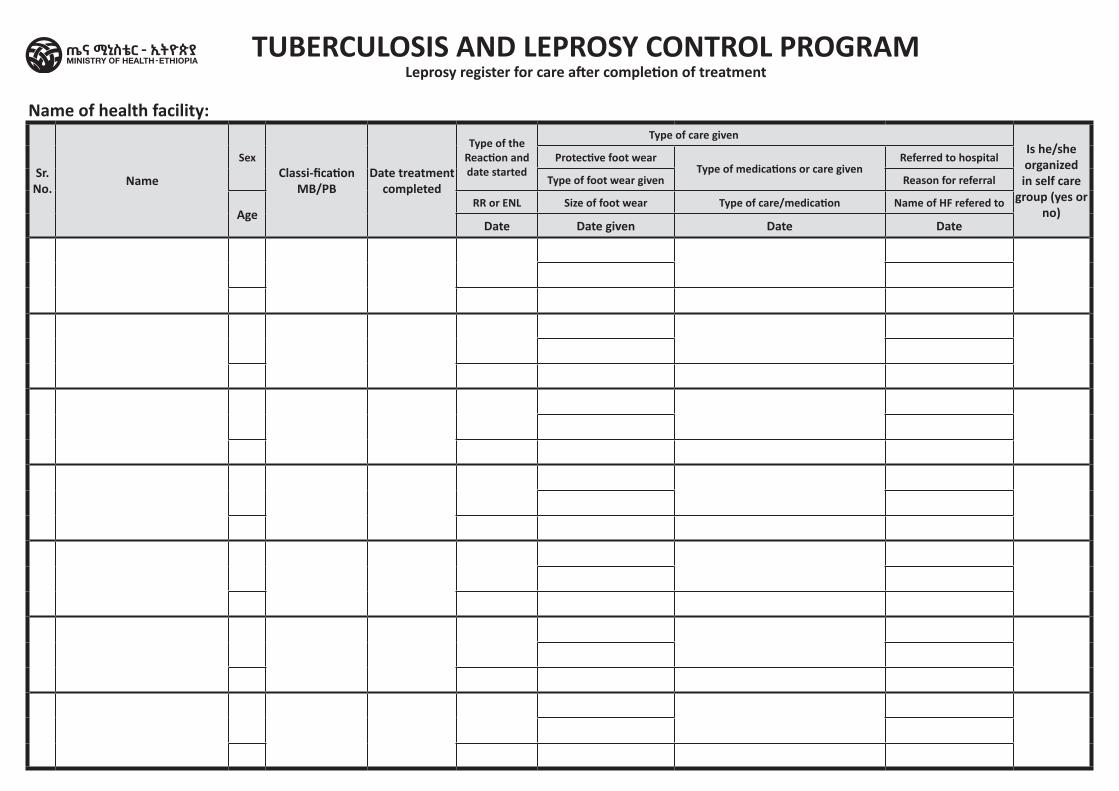
Name of health facility:
Sr. No. Name
SexClassi-fication
MB/PBDate treatment
completed
Type of the Reaction and date started
Type of care given Is he/she organized in self care
group (yes or no)
Protective foot wearType of medications or care given
Referred to hospital
Type of foot wear given Reason for referral
AgeRR or ENL Size of foot wear Type of care/medication Name of HF refered to
Date Date given Date Date
TUBERCULOSIS AND LEPROSY CONTROL PROGRAMLeprosy register for care after completion of treatment
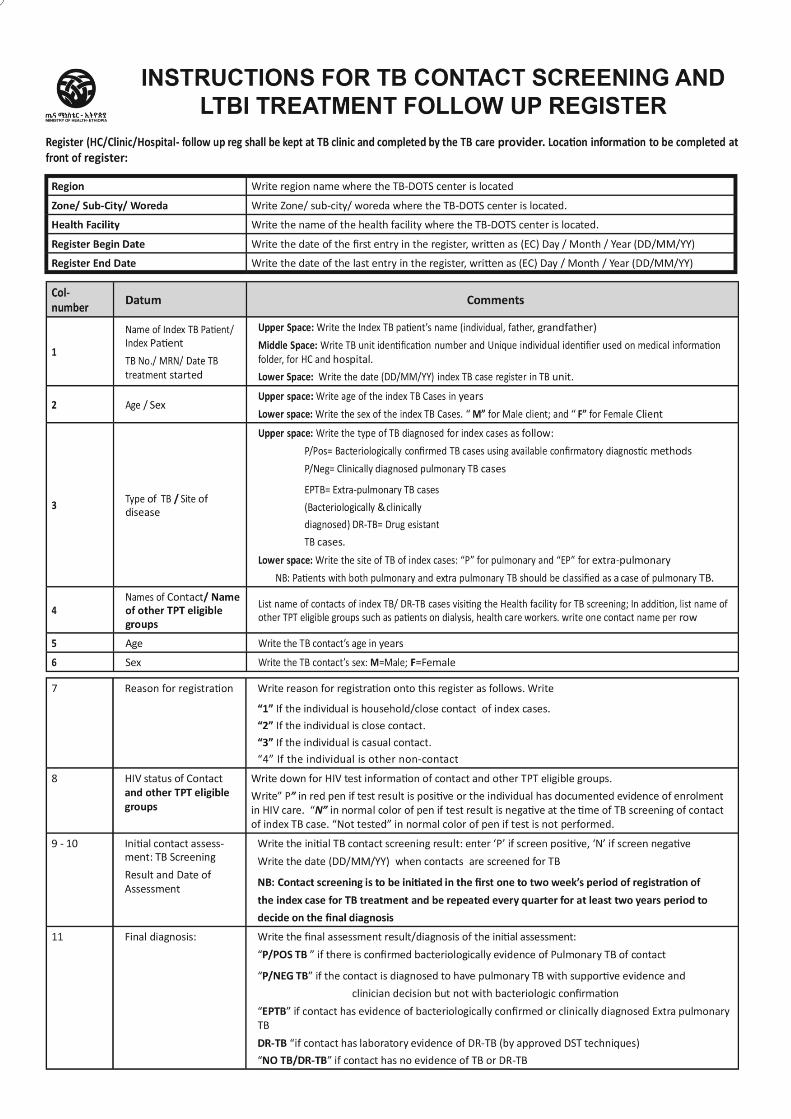
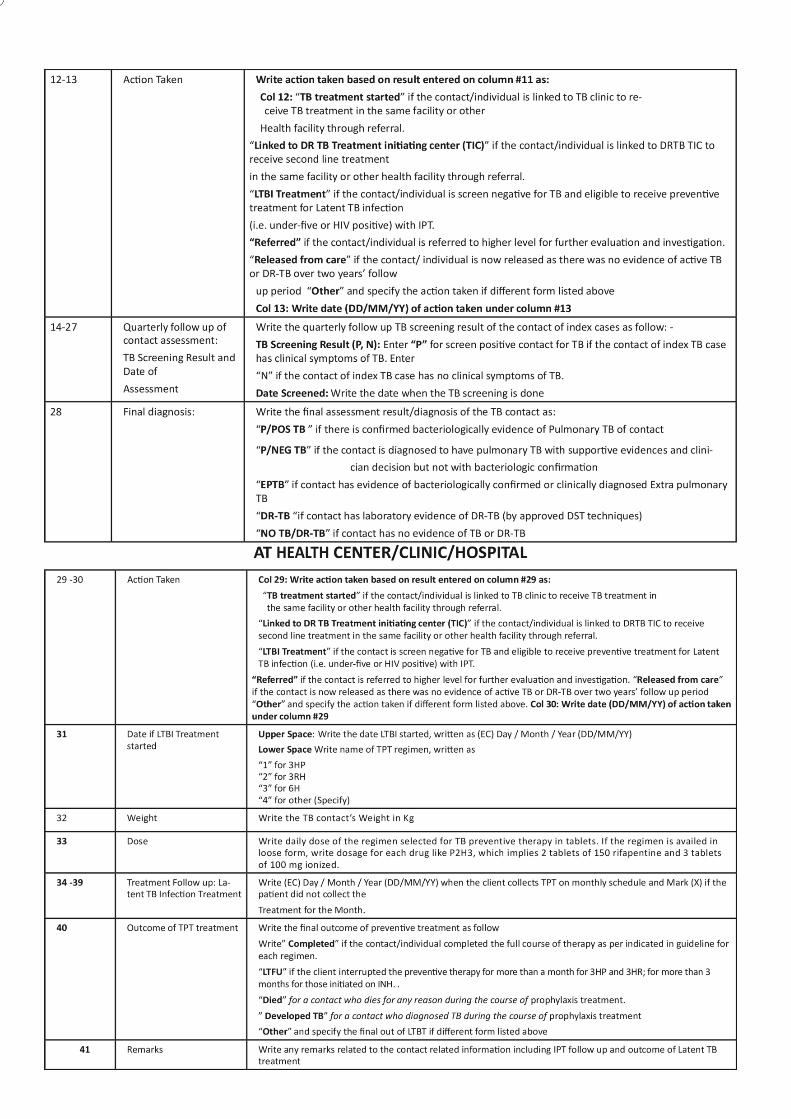
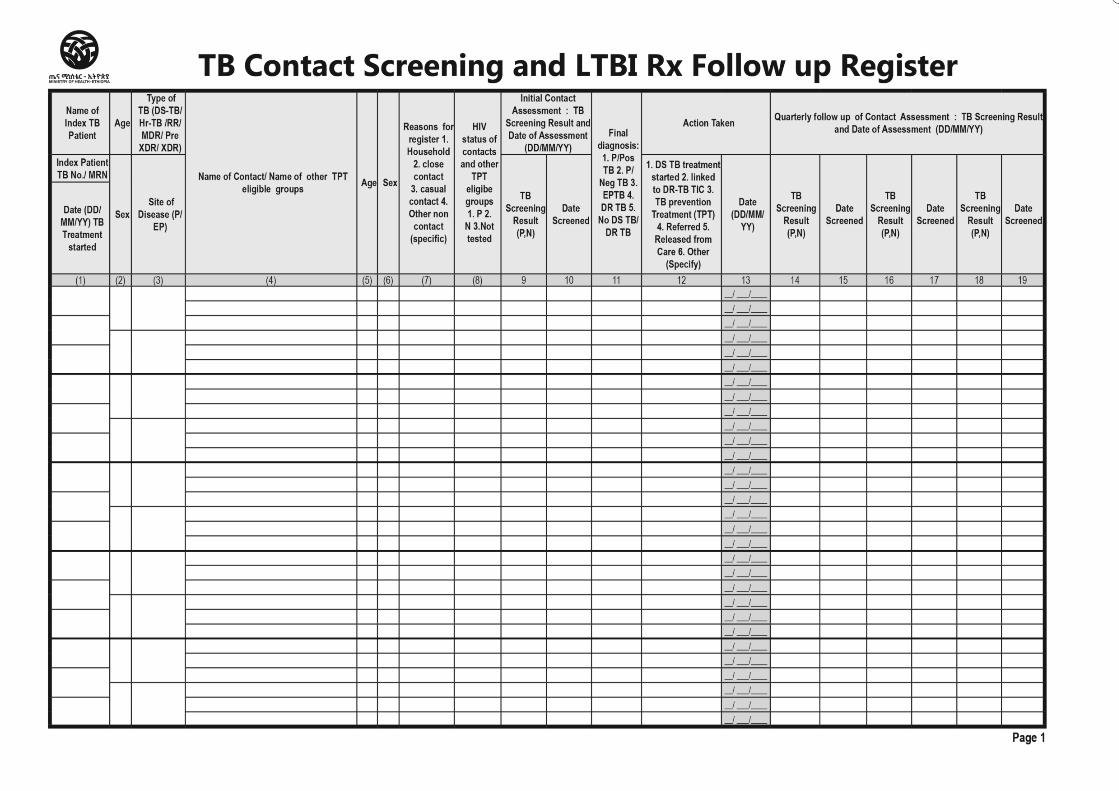
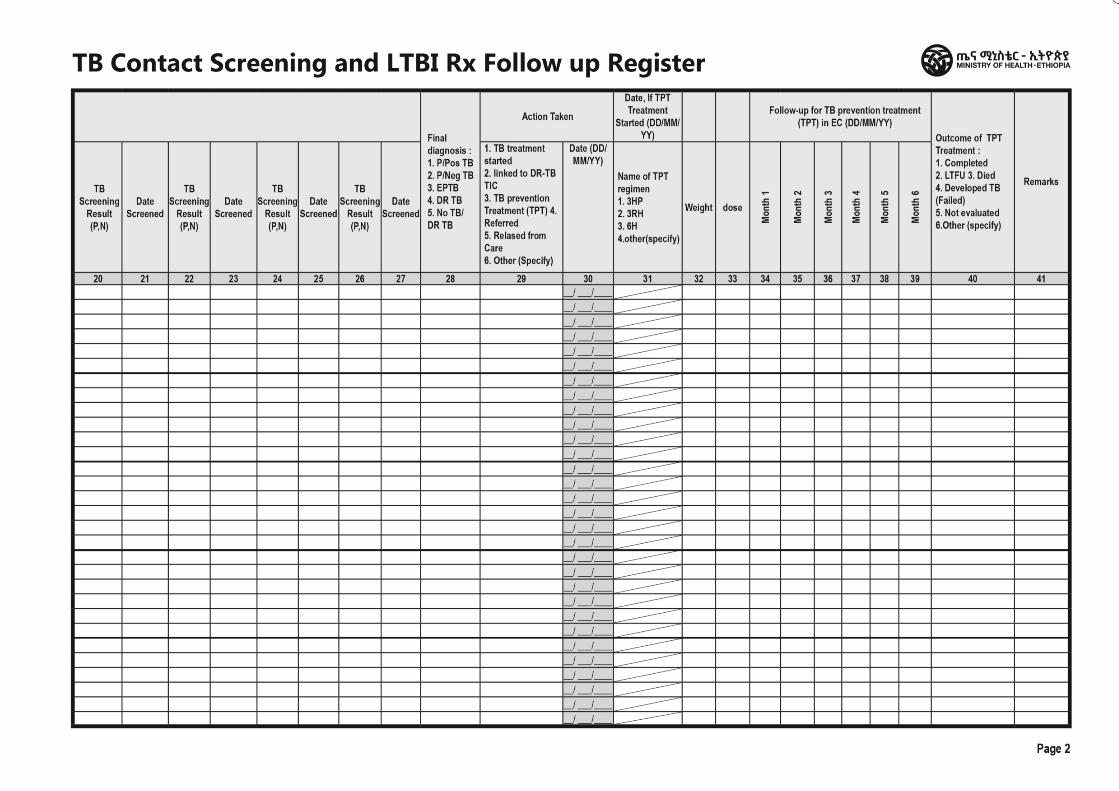
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Centre /Clinic/Hospital Unit TB Register
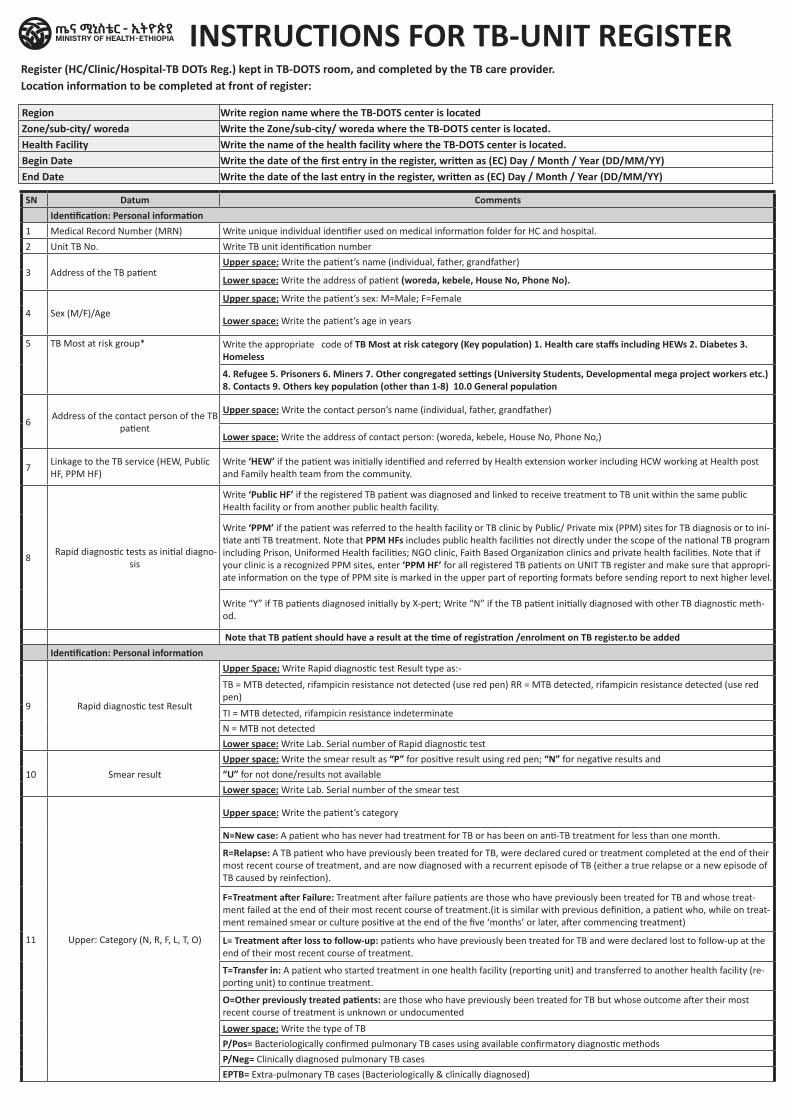
INSTRUCTIONS FOR TB-UNIT REGISTERRegister (HC/Clinic/Hospital-TB DOTs Reg.) kept in TB-DOTS room, and completed by the TB care provider.Location information to be completed at front of register:
Region Write region name where the TB-DOTS center is located Zone/sub-city/ woreda Write the Zone/sub-city/ woreda where the TB-DOTS center is located. Health Facility Write the name of the health facility where the TB-DOTS center is located. Begin Date Write the date of the first entry in the register, written as (EC) Day / Month / Year (DD/MM/YY) End Date Write the date of the last entry in the register, written as (EC) Day / Month / Year (DD/MM/YY)
SN Datum CommentsIdentification: Personal information
1 Medical Record Number (MRN) Write unique individual identifier used on medical information folder for HC and hospital.
2 Unit TB No. Write TB unit identification number
3 Address of the TB patientUpper space: Write the patient’s name (individual, father, grandfather)
Lower space: Write the address of patient (woreda, kebele, House No, Phone No).
4 Sex (M/F)/AgeUpper space: Write the patient’s sex: M=Male; F=Female
Lower space: Write the patient’s age in years
5 TB Most at risk group* Write the appropriate code of TB Most at risk category (Key population) 1. Health care staffs including HEWs 2. Diabetes 3. Homeless
4. Refugee 5. Prisoners 6. Miners 7. Other congregated settings (University Students, Developmental mega project workers etc.) 8. Contacts 9. Others key population (other than 1-8) 10.0 General population
6Address of the contact person of the TB
patient
Upper space: Write the contact person’s name (individual, father, grandfather)
Lower space: Write the address of contact person: (woreda, kebele, House No, Phone No,)
7Linkage to the TB service (HEW, Public HF, PPM HF)
Write ‘HEW’ if the patient was initially identified and referred by Health extension worker including HCW working at Health post and Family health team from the community.
8 Rapid diagnostic tests as initial diagno-
sis
Write ‘Public HF’ if the registered TB patient was diagnosed and linked to receive treatment to TB unit within the same public Health facility or from another public health facility.
Write ‘PPM’ if the patient was referred to the health facility or TB clinic by Public/ Private mix (PPM) sites for TB diagnosis or to ini-tiate anti TB treatment. Note that PPM HFs includes public health facilities not directly under the scope of the national TB program including Prison, Uniformed Health facilities; NGO clinic, Faith Based Organization clinics and private health facilities. Note that if your clinic is a recognized PPM sites, enter ‘PPM HF’ for all registered TB patients on UNIT TB register and make sure that appropri-ate information on the type of PPM site is marked in the upper part of reporting formats before sending report to next higher level.
Write “Y” if TB patients diagnosed initially by X-pert; Write “N” if the TB patient initially diagnosed with other TB diagnostic meth-od.
Note that TB patient should have a result at the time of registration /enrolment on TB register.to be addedIdentification: Personal information
9 Rapid diagnostic test Result
Upper Space: Write Rapid diagnostic test Result type as:-
TB = MTB detected, rifampicin resistance not detected (use red pen) RR = MTB detected, rifampicin resistance detected (use red pen)
TI = MTB detected, rifampicin resistance indeterminate
N = MTB not detected
Lower space: Write Lab. Serial number of Rapid diagnostic test
10 Smear result
Upper space: Write the smear result as “P” for positive result using red pen; “N” for negative results and
“U” for not done/results not available
Lower space: Write Lab. Serial number of the smear test
11 Upper: Category (N, R, F, L, T, O)
Upper space: Write the patient’s category
N=New case: A patient who has never had treatment for TB or has been on anti-TB treatment for less than one month.
R=Relapse: A TB patient who have previously been treated for TB, were declared cured or treatment completed at the end of their most recent course of treatment, and are now diagnosed with a recurrent episode of TB (either a true relapse or a new episode of TB caused by reinfection).
F=Treatment after Failure: Treatment after failure patients are those who have previously been treated for TB and whose treat-ment failed at the end of their most recent course of treatment.(it is similar with previous definition, a patient who, while on treat-ment remained smear or culture positive at the end of the five ‘months’ or later, after commencing treatment)
L= Treatment after loss to follow-up: patients who have previously been treated for TB and were declared lost to follow-up at the end of their most recent course of treatment.
T=Transfer in: A patient who started treatment in one health facility (reporting unit) and transferred to another health facility (re-porting unit) to continue treatment.
O=Other previously treated patients: are those who have previously been treated for TB but whose outcome after their most recent course of treatment is unknown or undocumented
Lower space: Write the type of TB
P/Pos= Bacteriologically confirmed pulmonary TB cases using available confirmatory diagnostic methods
P/Neg= Clinically diagnosed pulmonary TB cases
EPTB= Extra-pulmonary TB cases (Bacteriologically & clinically diagnosed)
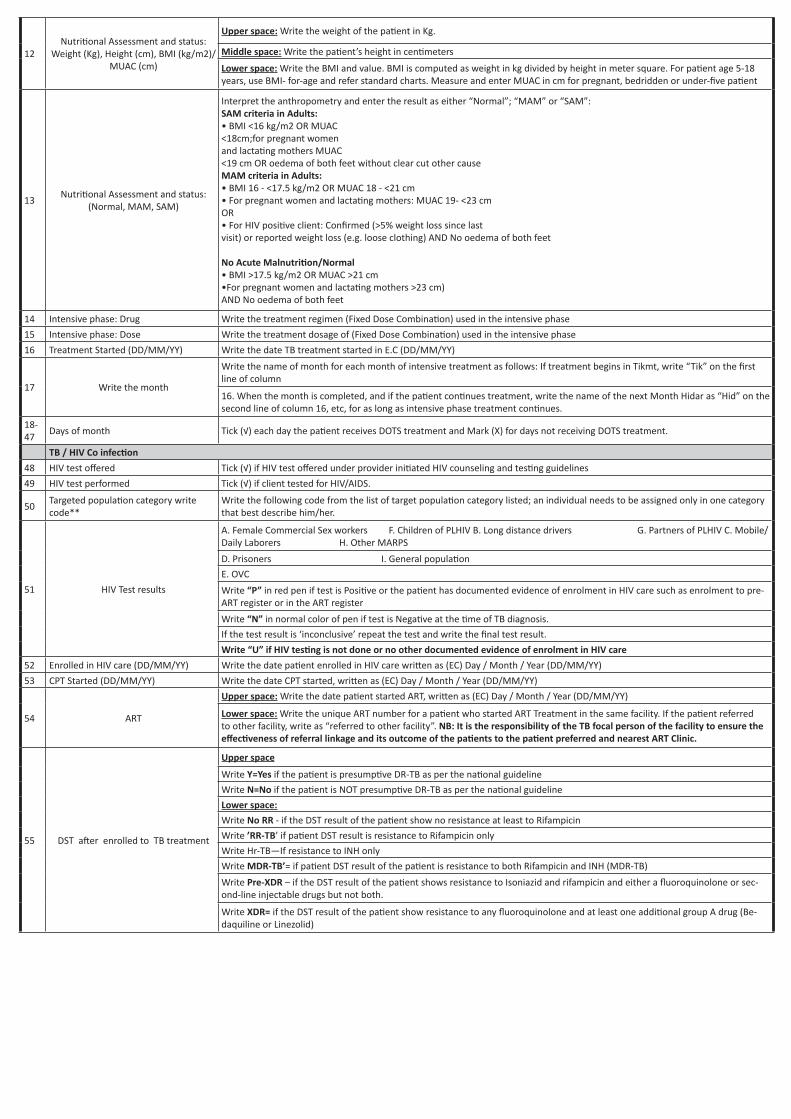
12Nutritional Assessment and status:
Weight (Kg), Height (cm), BMI (kg/m2)/MUAC (cm)
Upper space: Write the weight of the patient in Kg.
Middle space: Write the patient’s height in centimeters
Lower space: Write the BMI and value. BMI is computed as weight in kg divided by height in meter square. For patient age 5-18 years, use BMI- for-age and refer standard charts. Measure and enter MUAC in cm for pregnant, bedridden or under-five patient
13Nutritional Assessment and status:
(Normal, MAM, SAM)
Interpret the anthropometry and enter the result as either “Normal”; “MAM” or “SAM”: SAM criteria in Adults: • BMI <16 kg/m2 OR MUAC <18cm;for pregnant women and lactating mothers MUAC <19 cm OR oedema of both feet without clear cut other cause MAM criteria in Adults: • BMI 16 - <17.5 kg/m2 OR MUAC 18 - <21 cm • For pregnant women and lactating mothers: MUAC 19- <23 cm OR • For HIV positive client: Confirmed (>5% weight loss since last visit) or reported weight loss (e.g. loose clothing) AND No oedema of both feet No Acute Malnutrition/Normal • BMI >17.5 kg/m2 OR MUAC >21 cm •For pregnant women and lactating mothers >23 cm) AND No oedema of both feet
14 Intensive phase: Drug Write the treatment regimen (Fixed Dose Combination) used in the intensive phase
15 Intensive phase: Dose Write the treatment dosage of (Fixed Dose Combination) used in the intensive phase
16 Treatment Started (DD/MM/YY) Write the date TB treatment started in E.C (DD/MM/YY)
17 Write the month
Write the name of month for each month of intensive treatment as follows: If treatment begins in Tikmt, write “Tik” on the first line of column
16. When the month is completed, and if the patient continues treatment, write the name of the next Month Hidar as “Hid” on the second line of column 16, etc, for as long as intensive phase treatment continues.
18-47
Days of month Tick (√) each day the patient receives DOTS treatment and Mark (X) for days not receiving DOTS treatment.
TB / HIV Co infection48 HIV test offered Tick (√) if HIV test offered under provider initiated HIV counseling and testing guidelines
49 HIV test performed Tick (√) if client tested for HIV/AIDS.
50Targeted population category write code**
Write the following code from the list of target population category listed; an individual needs to be assigned only in one category that best describe him/her.
51 HIV Test results
A. Female Commercial Sex workers F. Children of PLHIV B. Long distance drivers G. Partners of PLHIV C. Mobile/Daily Laborers H. Other MARPS
D. Prisoners I. General population
E. OVC
Write “P” in red pen if test is Positive or the patient has documented evidence of enrolment in HIV care such as enrolment to pre-ART register or in the ART register
Write “N” in normal color of pen if test is Negative at the time of TB diagnosis.
If the test result is ‘inconclusive’ repeat the test and write the final test result.
Write “U” if HIV testing is not done or no other documented evidence of enrolment in HIV care52 Enrolled in HIV care (DD/MM/YY) Write the date patient enrolled in HIV care written as (EC) Day / Month / Year (DD/MM/YY)
53 CPT Started (DD/MM/YY) Write the date CPT started, written as (EC) Day / Month / Year (DD/MM/YY)
54 ART
Upper space: Write the date patient started ART, written as (EC) Day / Month / Year (DD/MM/YY)
Lower space: Write the unique ART number for a patient who started ART Treatment in the same facility. If the patient referred to other facility, write as “referred to other facility”. NB: It is the responsibility of the TB focal person of the facility to ensure the effectiveness of referral linkage and its outcome of the patients to the patient preferred and nearest ART Clinic.
55 DST after enrolled to TB treatment
Upper space
Write Y=Yes if the patient is presumptive DR-TB as per the national guideline
Write N=No if the patient is NOT presumptive DR-TB as per the national guideline
Lower space:Write No RR - if the DST result of the patient show no resistance at least to Rifampicin
Write ’RR-TB’ if patient DST result is resistance to Rifampicin only
Write Hr-TB—If resistance to INH only
Write MDR-TB’= if patient DST result of the patient is resistance to both Rifampicin and INH (MDR-TB)
Write Pre-XDR – if the DST result of the patient shows resistance to Isoniazid and rifampicin and either a fluoroquinolone or sec-ond-line injectable drugs but not both.
Write XDR= if the DST result of the patient show resistance to any fluoroquinolone and at least one additional group A drug (Be-daquiline or Linezolid)
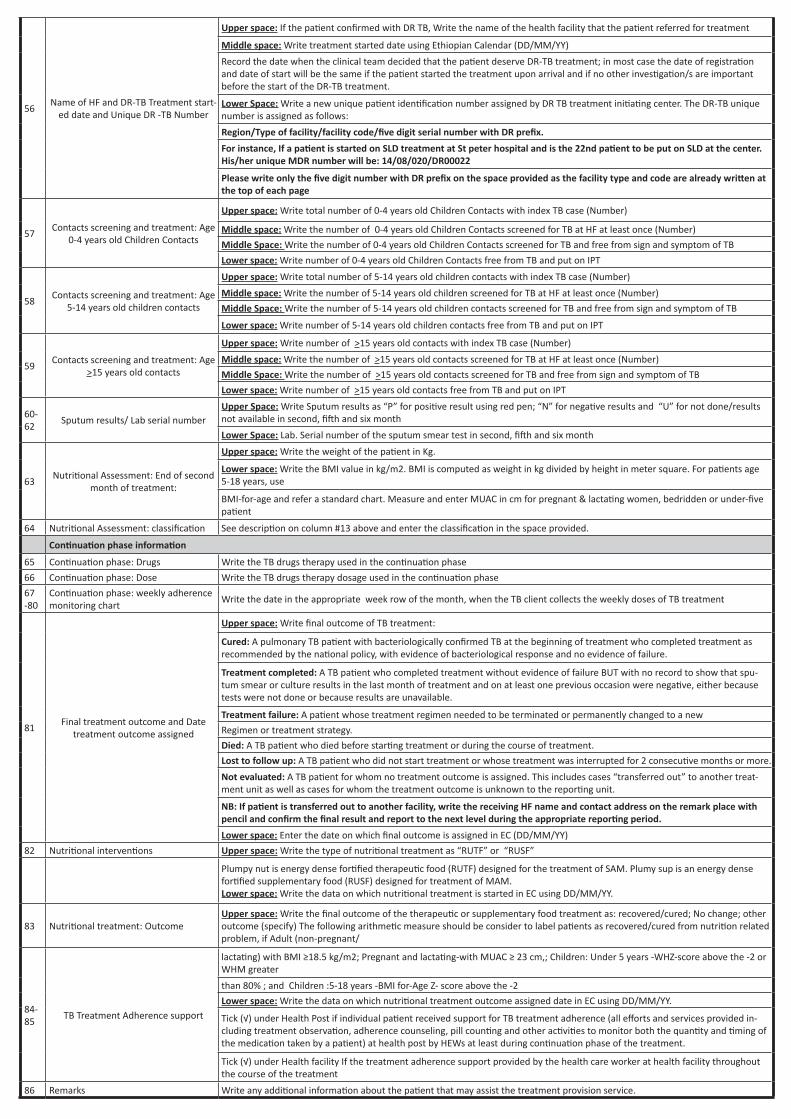
56Name of HF and DR-TB Treatment start-
ed date and Unique DR -TB Number
Upper space: If the patient confirmed with DR TB, Write the name of the health facility that the patient referred for treatment
Middle space: Write treatment started date using Ethiopian Calendar (DD/MM/YY)
Record the date when the clinical team decided that the patient deserve DR-TB treatment; in most case the date of registration and date of start will be the same if the patient started the treatment upon arrival and if no other investigation/s are important before the start of the DR-TB treatment.
Lower Space: Write a new unique patient identification number assigned by DR TB treatment initiating center. The DR-TB unique number is assigned as follows:
Region/Type of facility/facility code/five digit serial number with DR prefix.For instance, If a patient is started on SLD treatment at St peter hospital and is the 22nd patient to be put on SLD at the center. His/her unique MDR number will be: 14/08/020/DR00022
Please write only the five digit number with DR prefix on the space provided as the facility type and code are already written at the top of each page
57Contacts screening and treatment: Age
0-4 years old Children Contacts
Upper space: Write total number of 0-4 years old Children Contacts with index TB case (Number)
Middle space: Write the number of 0-4 years old Children Contacts screened for TB at HF at least once (Number)
Middle Space: Write the number of 0-4 years old Children Contacts screened for TB and free from sign and symptom of TB
Lower space: Write number of 0-4 years old Children Contacts free from TB and put on IPT
58Contacts screening and treatment: Age
5-14 years old children contacts
Upper space: Write total number of 5-14 years old children contacts with index TB case (Number)
Middle space: Write the number of 5-14 years old children screened for TB at HF at least once (Number)
Middle Space: Write the number of 5-14 years old children contacts screened for TB and free from sign and symptom of TB
Lower space: Write number of 5-14 years old children contacts free from TB and put on IPT
59Contacts screening and treatment: Age
>15 years old contacts
Upper space: Write number of >15 years old contacts with index TB case (Number)
Middle space: Write the number of >15 years old contacts screened for TB at HF at least once (Number)
Middle Space: Write the number of >15 years old contacts screened for TB and free from sign and symptom of TB
Lower space: Write number of >15 years old contacts free from TB and put on IPT
60-62
Sputum results/ Lab serial numberUpper Space: Write Sputum results as “P” for positive result using red pen; “N” for negative results and “U” for not done/results not available in second, fifth and six month
Lower Space: Lab. Serial number of the sputum smear test in second, fifth and six month
63Nutritional Assessment: End of second
month of treatment:
Upper space: Write the weight of the patient in Kg.
Lower space: Write the BMI value in kg/m2. BMI is computed as weight in kg divided by height in meter square. For patients age 5-18 years, use
BMI-for-age and refer a standard chart. Measure and enter MUAC in cm for pregnant & lactating women, bedridden or under-five patient
64 Nutritional Assessment: classification See description on column #13 above and enter the classification in the space provided.
Continuation phase information
65 Continuation phase: Drugs Write the TB drugs therapy used in the continuation phase
66 Continuation phase: Dose Write the TB drugs therapy dosage used in the continuation phase
67 -80
Continuation phase: weekly adherence monitoring chart
Write the date in the appropriate week row of the month, when the TB client collects the weekly doses of TB treatment
81Final treatment outcome and Date
treatment outcome assigned
Upper space: Write final outcome of TB treatment:
Cured: A pulmonary TB patient with bacteriologically confirmed TB at the beginning of treatment who completed treatment as recommended by the national policy, with evidence of bacteriological response and no evidence of failure.
Treatment completed: A TB patient who completed treatment without evidence of failure BUT with no record to show that spu-tum smear or culture results in the last month of treatment and on at least one previous occasion were negative, either because tests were not done or because results are unavailable.
Treatment failure: A patient whose treatment regimen needed to be terminated or permanently changed to a new
Regimen or treatment strategy.
Died: A TB patient who died before starting treatment or during the course of treatment.
Lost to follow up: A TB patient who did not start treatment or whose treatment was interrupted for 2 consecutive months or more.
Not evaluated: A TB patient for whom no treatment outcome is assigned. This includes cases “transferred out” to another treat-ment unit as well as cases for whom the treatment outcome is unknown to the reporting unit.
NB: If patient is transferred out to another facility, write the receiving HF name and contact address on the remark place with pencil and confirm the final result and report to the next level during the appropriate reporting period.Lower space: Enter the date on which final outcome is assigned in EC (DD/MM/YY)
82 Nutritional interventions Upper space: Write the type of nutritional treatment as “RUTF” or “RUSF”
Plumpy nut is energy dense fortified therapeutic food (RUTF) designed for the treatment of SAM. Plumy sup is an energy dense fortified supplementary food (RUSF) designed for treatment of MAM. Lower space: Write the data on which nutritional treatment is started in EC using DD/MM/YY.
83 Nutritional treatment: OutcomeUpper space: Write the final outcome of the therapeutic or supplementary food treatment as: recovered/cured; No change; other outcome (specify) The following arithmetic measure should be consider to label patients as recovered/cured from nutrition related problem, if Adult (non-pregnant/
84-85
TB Treatment Adherence support
lactating) with BMI ≥18.5 kg/m2; Pregnant and lactating-with MUAC ≥ 23 cm,; Children: Under 5 years -WHZ-score above the -2 or WHM greater
than 80% ; and Children :5-18 years -BMI for-Age Z- score above the -2
Lower space: Write the data on which nutritional treatment outcome assigned date in EC using DD/MM/YY.
Tick (√) under Health Post if individual patient received support for TB treatment adherence (all efforts and services provided in-cluding treatment observation, adherence counseling, pill counting and other activities to monitor both the quantity and timing of the medication taken by a patient) at health post by HEWs at least during continuation phase of the treatment.
Tick (√) under Health facility If the treatment adherence support provided by the health care worker at health facility throughout the course of the treatment
86 Remarks Write any additional information about the patient that may assist the treatment provision service.
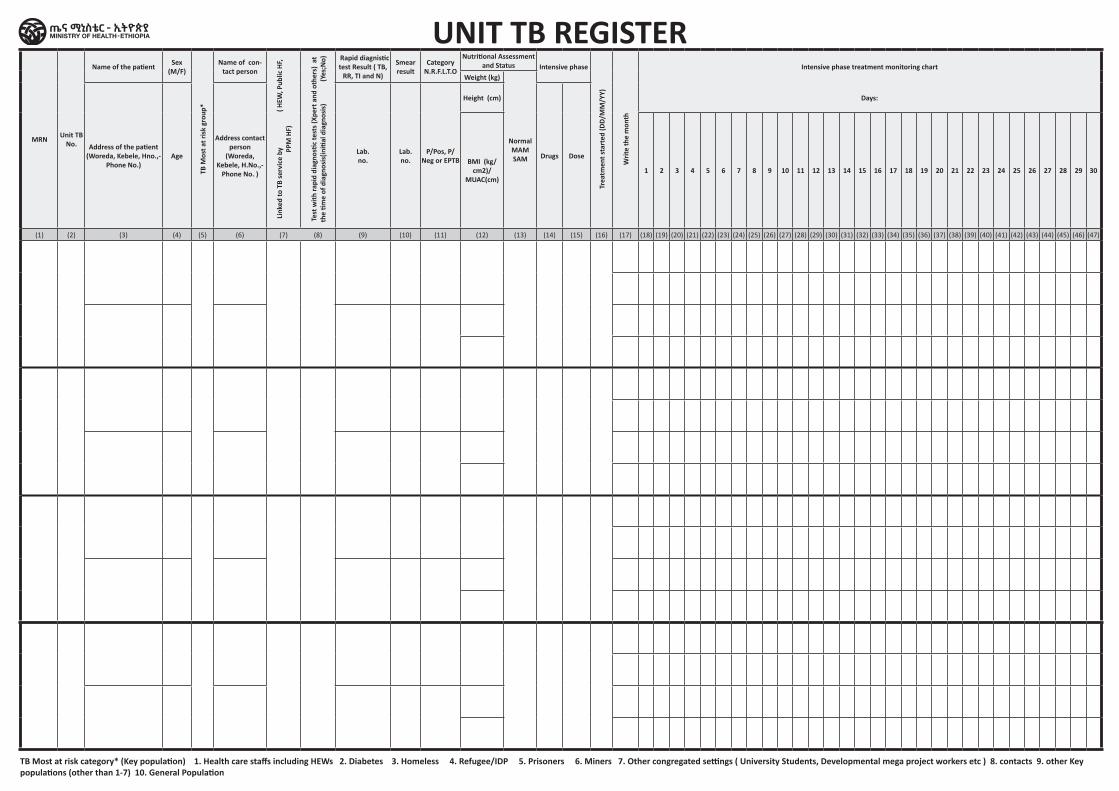
MRN Unit TB No.
Name of the patient Sex (M/F)
TB M
ost a
t ris
k gr
oup*
Name of con-tact person
Link
ed to
TB
serv
ice
by
( HEW
, Pub
lic H
F, PP
M H
F)
Test
with
rapi
d di
agno
stic
test
s (Xp
ert a
nd o
ther
s) a
t th
e tim
e of
dia
gnos
is(in
itial
dia
gnos
is)
(
Yes;
No) Rapid diagnistic
test Result ( TB, RR, TI and N)
Smear result
Category N.R.F.L.T.O
Nutritional Assessment and Status Intensive phase
Trea
tmen
t sta
rted
(DD/
MM
/YY)
Writ
e th
e m
onth
Intensive phase treatment monitoring chartWeight (kg)
Normal MAM SAM
Address of the patient (Woreda, Kebele, Hno.,-
Phone No.)Age
Address contact person
(Woreda, Kebele, H.No.,-
Phone No. )
Lab. no.
Lab. no.
P/Pos, P/Neg or EPTB
Height (cm)
Drugs Dose
Days:
BMI (kg/cm2)/
MUAC(cm)1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22) (23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44) (45) (46) (47)
TB Most at risk category* (Key population) 1. Health care staffs including HEWs 2. Diabetes 3. Homeless 4. Refugee/IDP 5. Prisoners 6. Miners 7. Other congregated settings ( University Students, Developmental mega project workers etc ) 8. contacts 9. other Key populations (other than 1-7) 10. General Population
UNIT TB REGISTER
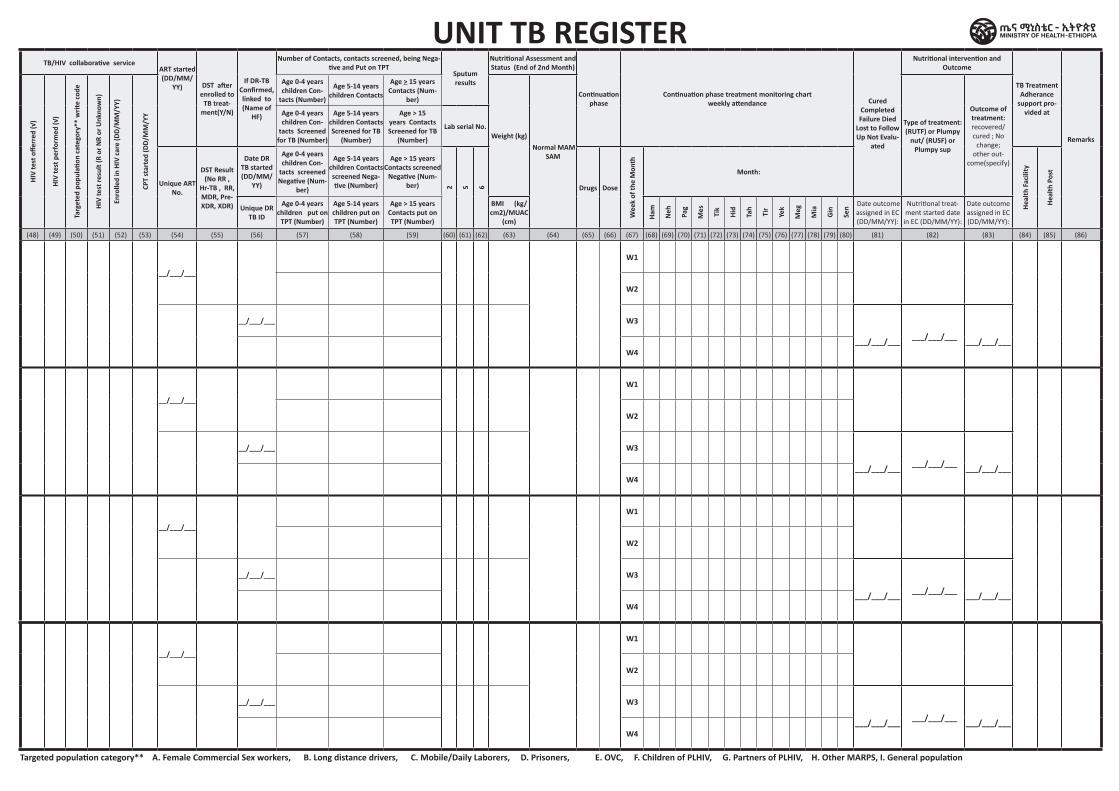
UNIT TB REGISTERTB/HIV collaborative service
ART started (DD/MM/
YY) DST after enrolled to
TB treat-ment(Y/N)
If DR-TB Confirmed, linked to (Name of
HF)
Number of Contacts, contacts screened, being Nega-tive and Put on TPT
Sputum results
Nutritional Assessment and Status (End of 2nd Month)
Continuation phase
Continuation phase treatment monitoring chart weekly attendance Cured
Completed Failure Died
Lost to Follow Up Not Evalu-
ated
Nutritional intervention and Outcome
TB Treatment Adherance
support pro-vided at
Remarks
HIV
test
offe
rred
(√)
HIV
test
per
form
ed (√
)
Targ
eted
pop
ulati
on c
ateg
ory*
* w
rite
code
HIV
test
resu
lt (R
or N
R or
Unk
now
n)
Enro
lled
in H
IV c
are
(DD/
MM
/YY)
CPT
star
ted
(DD/
MM
/YY
Age 0-4 years children Con-
tacts (Number)
Age 5-14 years children Contacts
Age > 15 years Contacts (Num-
ber)
Weight (kg) Normal MAM
SAM
Type of treatment: (RUTF) or Plumpy
nut/ (RUSF) or Plumpy sup
Outcome of treatment: recovered/cured ; No
change; other out-
come(specify)
Age 0-4 years children Con-
tacts Screened for TB (Number)
Age 5-14 years children Contacts Screened for TB
(Number)
Age > 15 years Contacts Screened for TB
(Number)
Lab serial No.
Unique ART No.
DST Result (No RR ,
Hr-TB , RR, MDR, Pre-XDR, XDR)
Date DR TB started (DD/MM/
YY)
Age 0-4 years children Con-
tacts screened Negative (Num-
ber)
Age 5-14 years children Contacts screened Nega-tive (Number)
Age > 15 years Contacts screened
Negative (Num-ber) 2 5 6 Drugs Dose
Wee
k of
the
Mon
th
Month:
Heal
th F
acili
ty
Heal
th P
ost
Unique DR TB ID
Age 0-4 years children put on
TPT (Number)
Age 5-14 years children put on TPT (Number)
Age > 15 years Contacts put on TPT (Number)
BMI (kg/cm2)/MUAC
(cm) Ham
Neh Pa
g
Mes Tik
Hid
Tah
Tir
Yek
Meg
Mia
Gin
Sen Date outcome
assigned in EC (DD/MM/YY):
Nutritional treat-ment started date
in EC (DD/MM/YY):
Date outcome assigned in EC (DD/MM/YY):
(48) (49) (50) (51) (52) (53) (54) (55) (56) (57) (58) (59) (60) (61) (62) (63) (64) (65) (66) (67) (68) (69) (70) (71) (72) (73) (74) (75) (76) (77) (78) (79) (80) (81) (82) (83) (84) (85) (86)
__/___/___
W1
W2
__/___/___ W3
___/___/___ ___/___/___ ___/___/___
W4
__/___/___
W1
W2
__/___/___ W3
___/___/___ ___/___/___ ___/___/___
W4
__/___/___
W1
W2
__/___/___ W3
___/___/___ ___/___/___ ___/___/___
W4
__/___/___
W1
W2
__/___/___ W3
___/___/___ ___/___/___ ___/___/___
W4
Targeted population category** A. Female Commercial Sex workers, B. Long distance drivers, C. Mobile/Daily Laborers, D. Prisoners, E. OVC, F. Children of PLHIV, G. Partners of PLHIV, H. Other MARPS, I. General population

Health Post ToolsContent / Home
Content / Home
Pastoralist Registers, CHIS register, card and Tally sheets
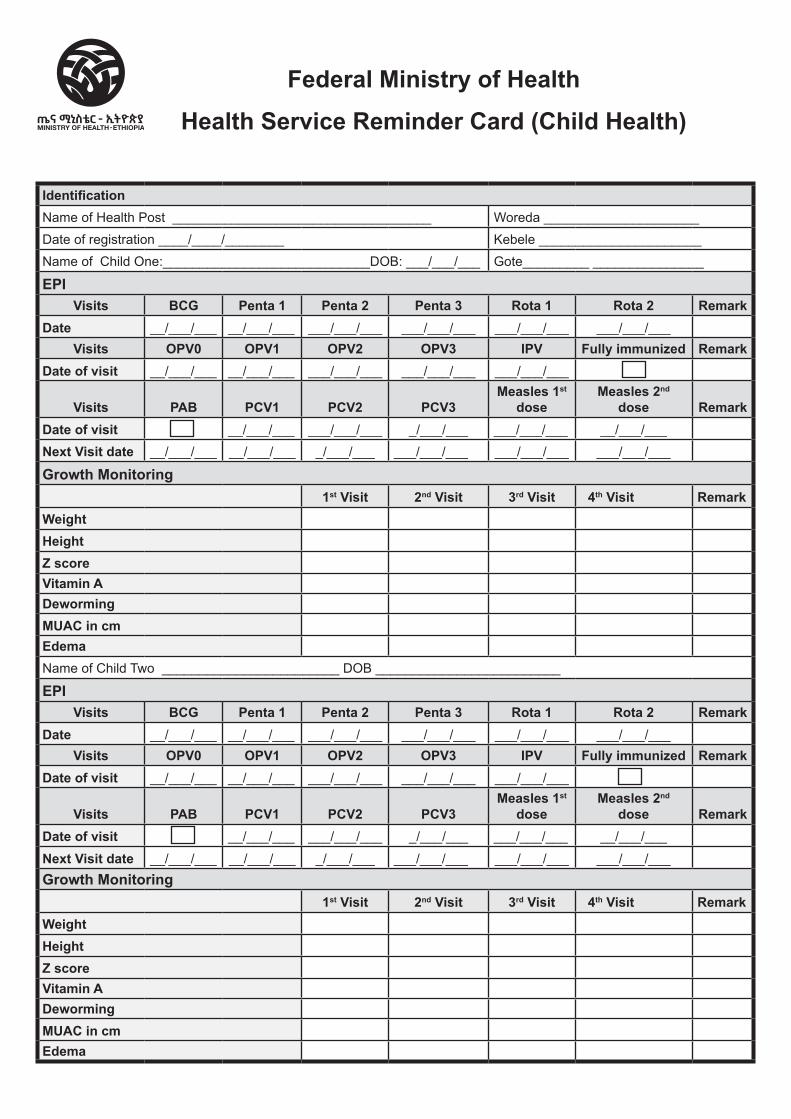
Federal Ministry of Health
Health Service Reminder Card (Child Health)
IdentificationName of Health Post ___________________________________ Woreda _____________________Date of registration ____/____/________ Kebele ______________________Name of Child One:____________________________DOB: ___/___/___ Gote_________ _______________
EPIVisits BCG Penta 1 Penta 2 Penta 3 Rota 1 Rota 2 Remark
Date __/___/___ __/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___Visits OPV0 OPV1 OPV2 OPV3 IPV Fully immunized Remark
Date of visit __/___/___ __/___/___ ___/___/___ ___/___/___ ___/___/___
Visits PAB PCV1 PCV2 PCV3Measles 1st
dose Measles 2nd
dose RemarkDate of visit __/___/___ ___/___/___ _/___/___ ___/___/___ __/___/___ Next Visit date __/___/___ __/___/___ _/___/___ ___/___/___ ___/___/___ ___/___/___
Growth Monitoring 1st Visit 2nd Visit 3rd Visit 4th Visit Remark
Weight Height Z score Vitamin A Deworming MUAC in cm Edema Name of Child Two ________________________ DOB _________________________
EPIVisits BCG Penta 1 Penta 2 Penta 3 Rota 1 Rota 2 Remark
Date __/___/___ __/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___Visits OPV0 OPV1 OPV2 OPV3 IPV Fully immunized Remark
Date of visit __/___/___ __/___/___ ___/___/___ ___/___/___ ___/___/___
Visits PAB PCV1 PCV2 PCV3Measles 1st
dose Measles 2nd
dose RemarkDate of visit __/___/___ ___/___/___ _/___/___ ___/___/___ __/___/___
Next Visit date __/___/___ __/___/___ _/___/___ ___/___/___ ___/___/___ ___/___/___Growth Monitoring
1st Visit 2nd Visit 3rd Visit 4th Visit RemarkWeight Height Z score Vitamin A Deworming MUAC in cm Edema
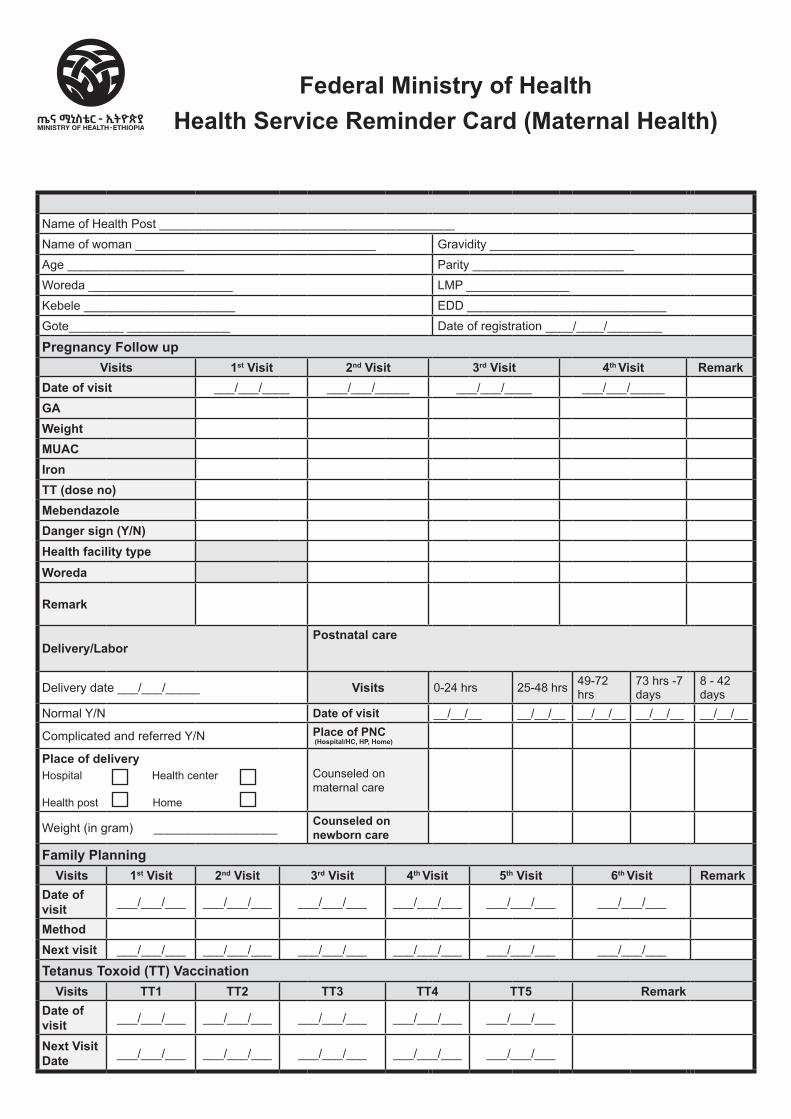
Federal Ministry of HealthHealth Service Reminder Card (Maternal Health)
Name of Health Post ___________________________________________Name of woman ___________________________________ Gravidity _____________________Age _________________ Parity ______________________Woreda _____________________ LMP _______________Kebele ______________________ EDD _____________________________Gote________ _______________ Date of registration ____/____/________
Pregnancy Follow upVisits 1st Visit 2nd Visit 3rd Visit 4th Visit Remark
Date of visit ___/___/____ ___/___/_____ ___/___/____ ___/___/_____
GA Weight MUAC Iron TT (dose no) Mebendazole Danger sign (Y/N)
Health facility type
Woreda
Remark
Delivery/LaborPostnatal care
Delivery date ___/___/_____ Visits 0-24 hrs 25-48 hrs 49-72 hrs
73 hrs -7 days
8 - 42 days
Normal Y/N Date of visit __/__/__ __/__/__ __/__/__ __/__/__ __/__/__
Complicated and referred Y/N Place of PNC (Hospital/HC, HP, Home)
Place of delivery Hospital Health center
Health post Home
Counseled on maternal care
Weight (in gram) __________________ Counseled on newborn care
Family PlanningVisits 1st Visit 2nd Visit 3rd Visit 4th Visit 5th Visit 6th Visit Remark
Date of visit ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___
Method
Next visit ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___
Tetanus Toxoid (TT) VaccinationVisits TT1 TT2 TT3 TT4 TT5 Remark
Date of visit ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___
Next Visit Date ___/___/___ ___/___/___ ___/___/___ ___/___/___ ___/___/___

Health PostCurative Care Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostCurative Care Register
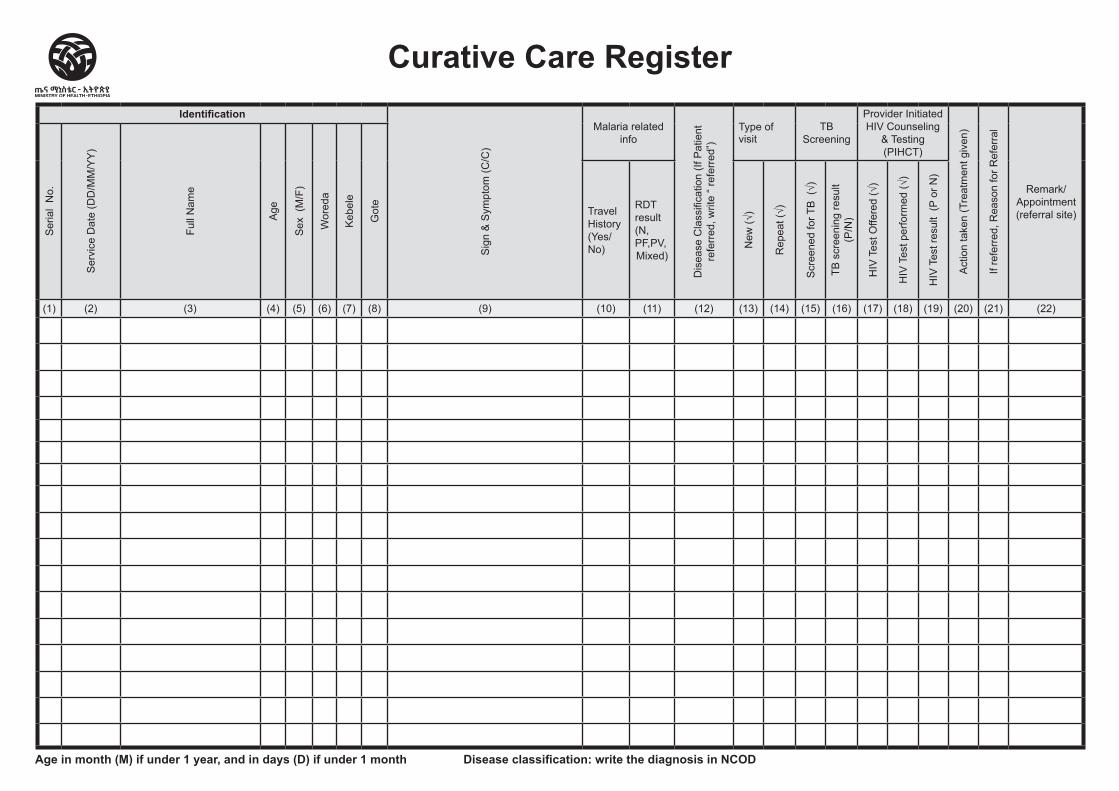
Identification
Sig
n &
Sym
ptom
(C/C
)
Malaria related info
Dis
ease
Cla
ssifi
catio
n (If
Pat
ient
re
ferr
ed, w
rite
“ ref
erre
d”)
Type of visit
TB Screening
Provider Initiated HIV Counseling
& Testing (PIHCT)
Act
ion
take
n (T
reat
men
t giv
en)
If re
ferr
ed, R
easo
n fo
r Ref
erra
l
Remark/ Appointment (referral site)
Ser
ial
No.
Ser
vice
Dat
e (D
D/M
M/Y
Y)
Full
Nam
e
Age
Sex
(M
/F)
Wor
eda
Keb
ele
Got
e
TravelHistory(Yes/No)
RDTresult(N,PF,PV,Mixed)
New
(√)
Rep
eat (
√)
Scr
eene
d fo
r TB
(√)
TB s
cree
ning
resu
lt (P
/N)
HIV
Tes
t Offe
red
(√)
HIV
Tes
t per
form
ed (√
)
HIV
Tes
t res
ult
(P o
r N)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22)
Curative Care Register
Age in month (M) if under 1 year, and in days (D) if under 1 month Disease classification: write the diagnosis in NCOD

Health PostDevelopmental Nutrition Service
Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health Post Developmental Nutrition Service
Register
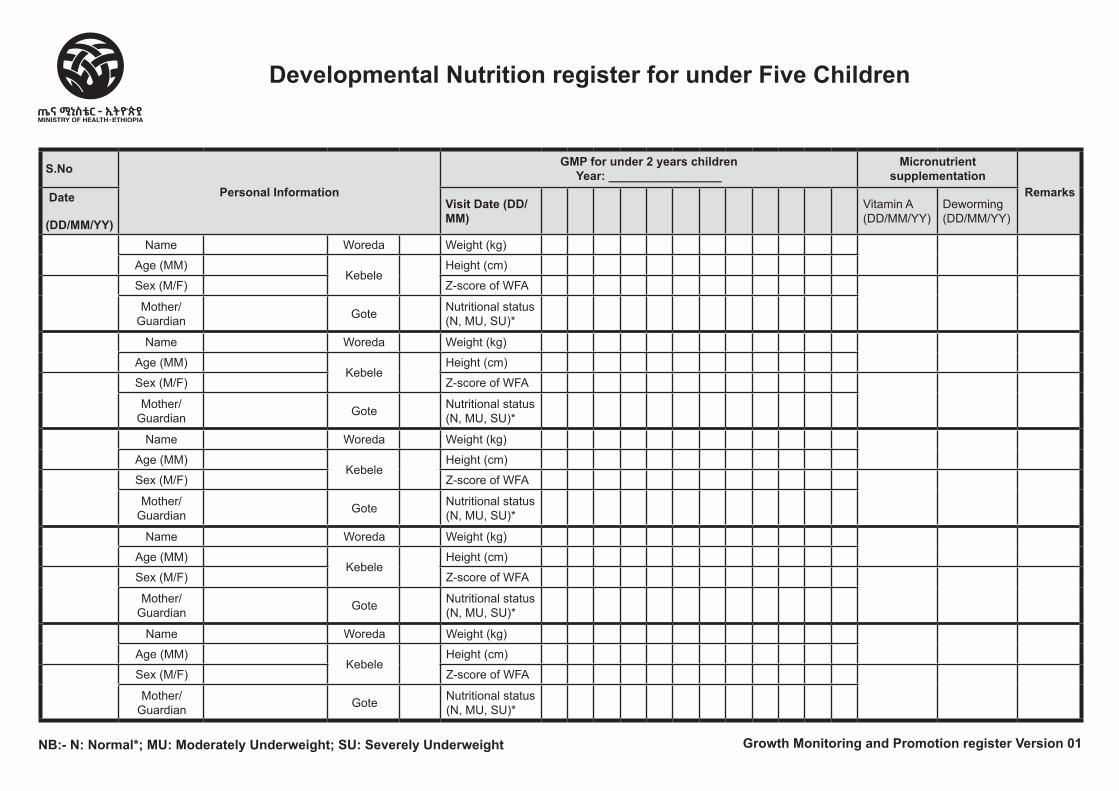
S.No
Personal Information
GMP for under 2 years children Year: _________________
Micronutrient supplementation
RemarksDate
(DD/MM/YY)
Visit Date (DD/MM) Vitamin A
(DD/MM/YY)Deworming (DD/MM/YY)
Name Woreda Weight (kg)
Age (MM)
Kebele Height (cm)
Sex (M/F) Z-score of WFA
Mother/Guardian Gote Nutritional status
(N, MU, SU)*
Name Woreda Weight (kg)
Age (MM)
Kebele Height (cm)
Sex (M/F) Z-score of WFA
Mother/Guardian Gote Nutritional status
(N, MU, SU)*
Name Woreda Weight (kg)
Age (MM)
Kebele Height (cm)
Sex (M/F) Z-score of WFA
Mother/Guardian Gote Nutritional status
(N, MU, SU)*
Name Woreda Weight (kg)
Age (MM)
Kebele Height (cm)
Sex (M/F) Z-score of WFA
Mother/Guardian Gote Nutritional status
(N, MU, SU)*
Name Woreda Weight (kg)
Age (MM)
Kebele Height (cm)
Sex (M/F) Z-score of WFA
Mother/Guardian Gote Nutritional status
(N, MU, SU)*
NB:- N: Normal*; MU: Moderately Underweight; SU: Severely Underweight Growth Monitoring and Promotion register Version 01
Developmental Nutrition register for under Five Children

Health PostExpanded Program of Immunization
(EPI) Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostExpanded Program of Immunization
(EPI) Register
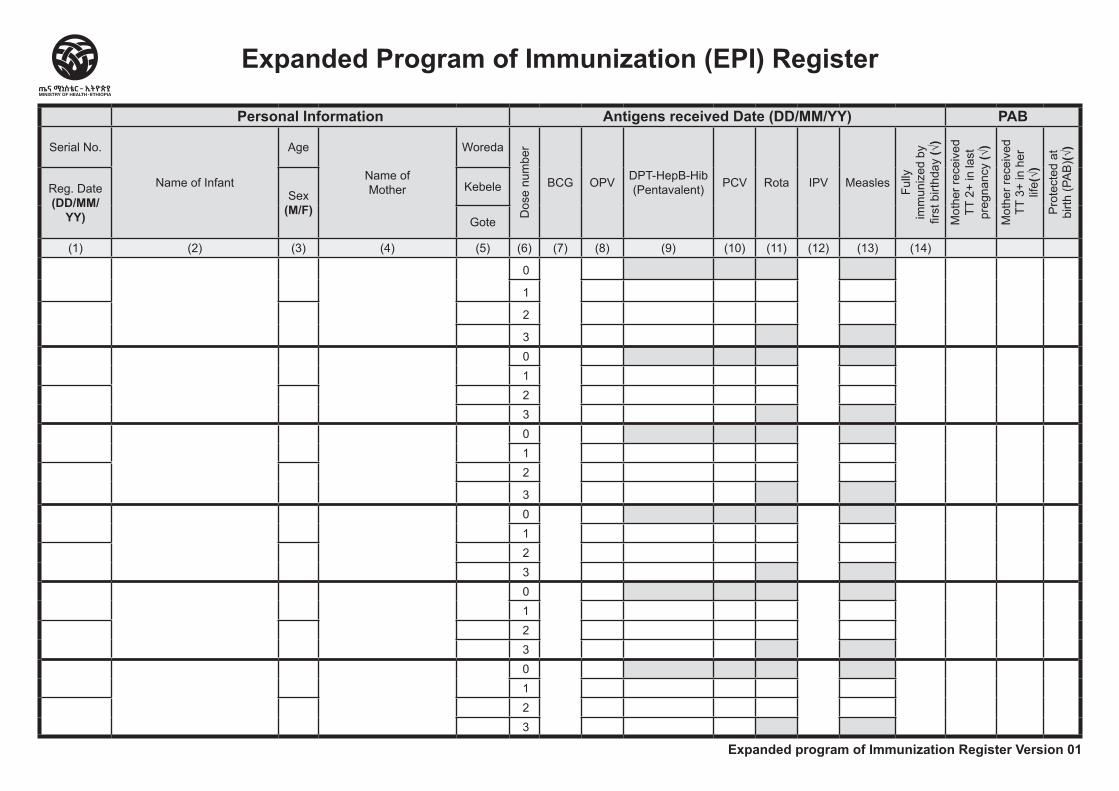
Personal Information Antigens received Date (DD/MM/YY) PAB
Serial No.
Name of Infant
Age
Name ofMother
Woreda
Dos
e nu
mbe
r
BCG OPV DPT-HepB-Hib (Pentavalent) PCV Rota IPV Measles
Fully
im
mun
ized
by
first
birt
hday
(√)
Mot
her r
ecei
ved
TT 2
+ in
last
pr
egna
ncy (√)
Mot
her r
ecei
ved
TT 3
+ in
her
lif
e(√)
Pro
tect
ed a
t bi
rth (P
AB
)(√)
Reg. Date(DD/MM/
YY)
Sex (M/F)
Kebele
Gote
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14)
0
1
2
3
0
1 2 3
0
1 2
3
0
1 2 3
0
1 2 3
0
1 2 3
Expanded program of Immunization Register Version 01
Expanded Program of Immunization (EPI) Register

Health PostFamily Planning (FP) Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostFamily Planning (FP) Register
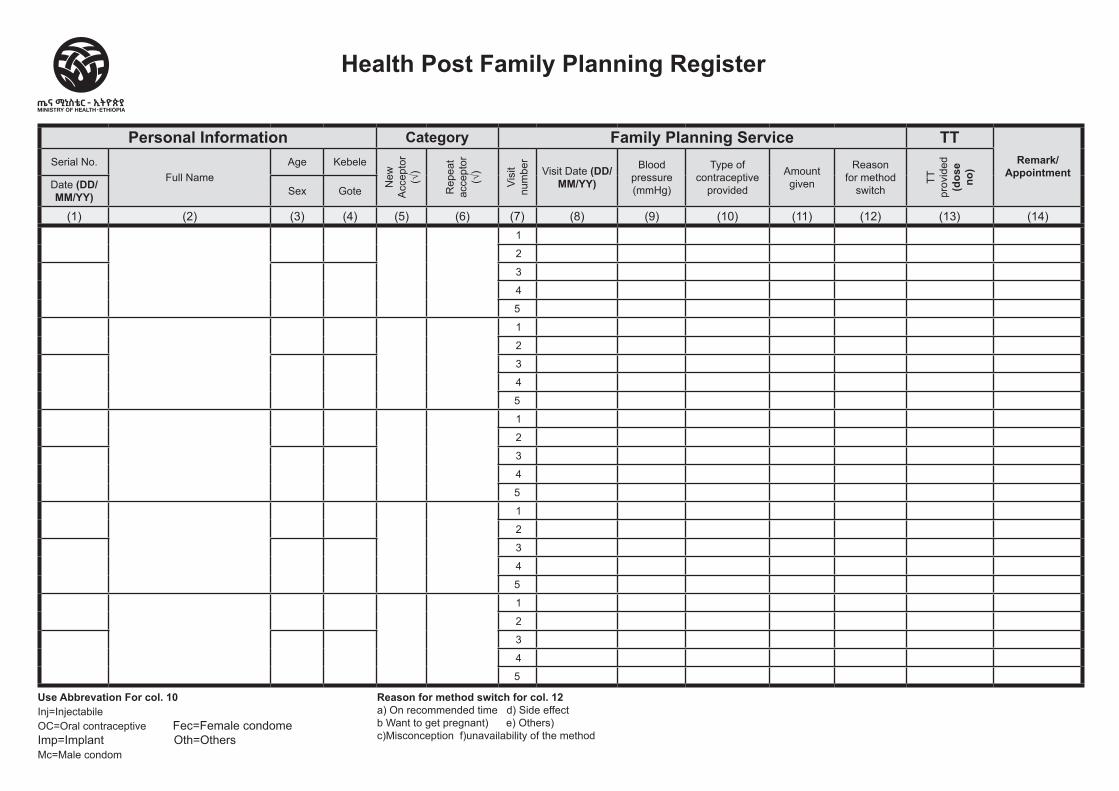
Health Post Family Planning Register
Personal Information Category Family Planning Service TT Remark/
AppointmentSerial No.
Full NameAge Kebele
New
A
ccep
tor
(√)
Rep
eat
acce
ptor
(√
)
Visi
t nu
mbe
r
Visit Date (DD/MM/YY)
Blood pressure (mmHg)
Type of contraceptive
provided
Amount given
Reason for method
switch
TT
prov
ided
(d
ose
no)
Date (DD/MM/YY) Sex Gote
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14)
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
Use Abbrevation For col. 10 Inj=Injectabile OC=Oral contraceptive Fec=Female condome Imp=Implant Oth=Others Mc=Male condom
Reason for method switch for col. 12a) On recommended time d) Side effectb Want to get pregnant) e) Others) c)Misconception f)unavailability of the method

Health PostMaternal and Newborn Health
(MNH) Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostMaternal and Newborn Health
(MNH) Register
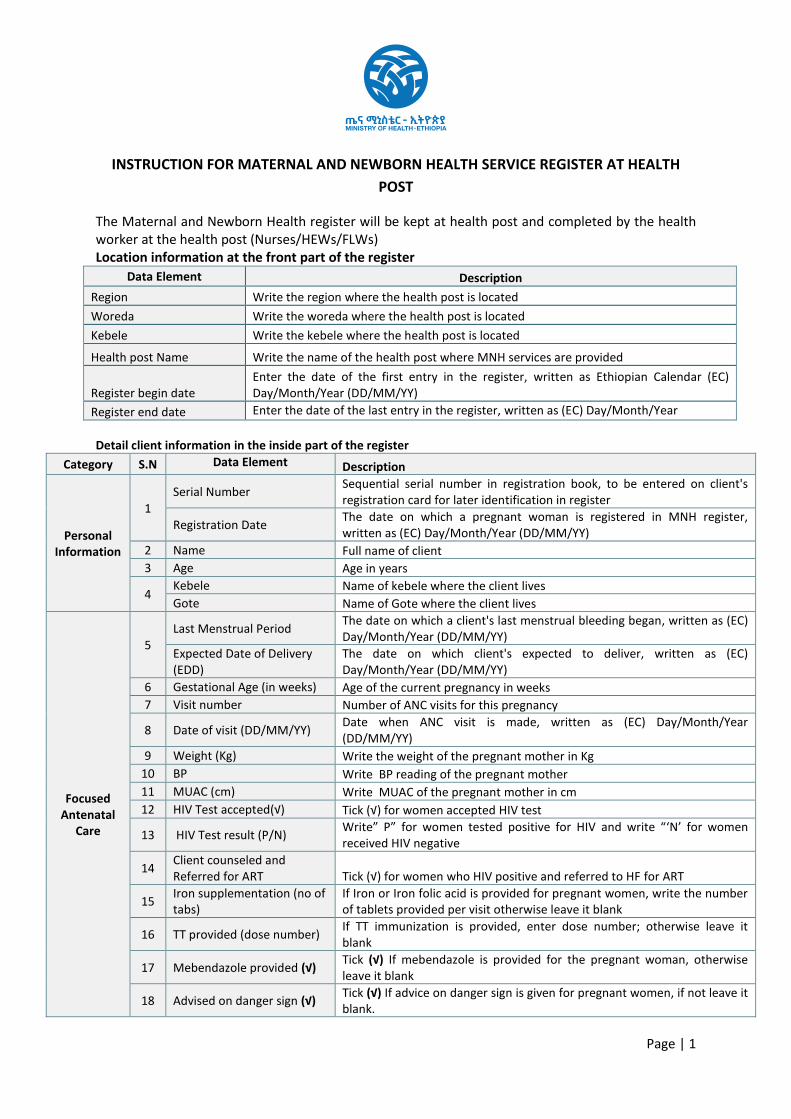
Page | 1
INSTRUCTION FOR MATERNAL AND NEWBORN HEALTH SERVICE REGISTER AT HEALTH POST
The Maternal and Newborn Health register will be kept at health post and completed by the health worker at the health post (Nurses/HEWs/FLWs) Location information at the front part of the register
Data Element Description Region Write the region where the health post is located Woreda Write the woreda where the health post is located Kebele Write the kebele where the health post is located Health post Name Write the name of the health post where MNH services are provided
Register begin date Enter the date of the first entry in the register, written as Ethiopian Calendar (EC) Day/Month/Year (DD/MM/YY)
Register end date Enter the date of the last entry in the register, written as (EC) Day/Month/Year (DD/MM/YY)
Detail client information in the inside part of the register Category S.N Data Element
Description
Personal Information
1 Serial Number Sequential serial number in registration book, to be entered on client's
registration card for later identification in register
Registration Date The date on which a pregnant woman is registered in MNH register, written as (EC) Day/Month/Year (DD/MM/YY)
2 Name Full name of client 3 Age Age in years
4 Kebele Name of kebele where the client lives Gote Name of Gote where the client lives
Focused Antenatal
Care
5 Last Menstrual Period The date on which a client's last menstrual bleeding began, written as (EC)
Day/Month/Year (DD/MM/YY) Expected Date of Delivery (EDD)
The date on which client's expected to deliver, written as (EC) Day/Month/Year (DD/MM/YY)
6 Gestational Age (in weeks) Age of the current pregnancy in weeks 7 Visit number Number of ANC visits for this pregnancy
8 Date of visit (DD/MM/YY) Date when ANC visit is made, written as (EC) Day/Month/Year (DD/MM/YY)
9 Weight (Kg) Write the weight of the pregnant mother in Kg 10 BP Write BP reading of the pregnant mother 11 MUAC (cm) Write MUAC of the pregnant mother in cm 12 HIV Test accepted(√) Tick (√) for women accepted HIV test
13 HIV Test result (P/N) Write” P” for women tested positive for HIV and write “‘N’ for women received HIV negative
14 Client counseled and Referred for ART Tick (√) for women who HIV positive and referred to HF for ART
15 Iron supplementation (no of tabs)
If Iron or Iron folic acid is provided for pregnant women, write the number of tablets provided per visit otherwise leave it blank
16 TT provided (dose number) If TT immunization is provided, enter dose number; otherwise leave it blank
17 Mebendazole provided (√) Tick (√) If mebendazole is provided for the pregnant woman, otherwise leave it blank
18 Advised on danger sign (√) Tick (√) If advice on danger sign is given for pregnant women, if not leave it blank.
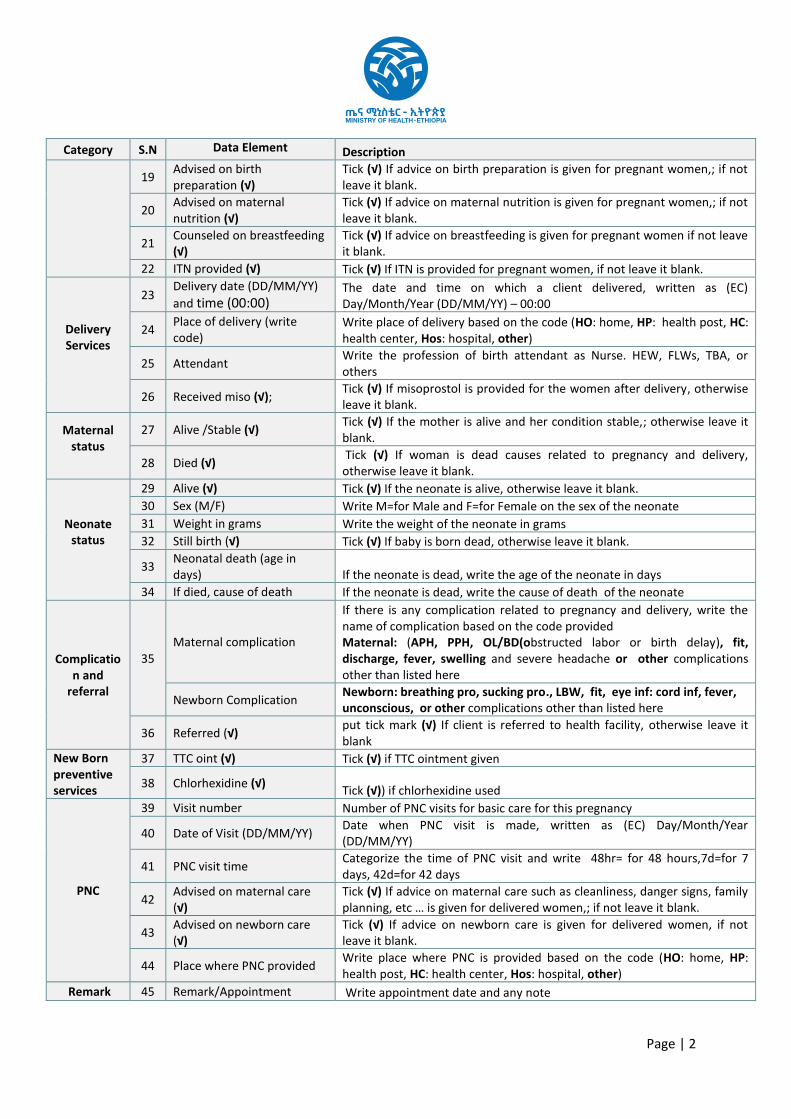
Page | 2
Category S.N Data Element
Description
19 Advised on birth preparation (√)
Tick (√) If advice on birth preparation is given for pregnant women,; if not leave it blank.
20 Advised on maternal nutrition (√)
Tick (√) If advice on maternal nutrition is given for pregnant women,; if not leave it blank.
21 Counseled on breastfeeding (√)
Tick (√) If advice on breastfeeding is given for pregnant women if not leave it blank.
22 ITN provided (√) Tick (√) If ITN is provided for pregnant women, if not leave it blank.
Delivery Services
23 Delivery date (DD/MM/YY) and time (00:00)
The date and time on which a client delivered, written as (EC) Day/Month/Year (DD/MM/YY) – 00:00
24 Place of delivery (write code)
Write place of delivery based on the code (HO: home, HP: health post, HC: health center, Hos: hospital, other)
25 Attendant Write the profession of birth attendant as Nurse. HEW, FLWs, TBA, or others
26 Received miso (√); Tick (√) If misoprostol is provided for the women after delivery, otherwise leave it blank.
Maternal status
27 Alive /Stable (√) Tick (√) If the mother is alive and her condition stable,; otherwise leave it blank.
28 Died (√) Tick (√) If woman is dead causes related to pregnancy and delivery, otherwise leave it blank.
Neonate status
29 Alive (√) Tick (√) If the neonate is alive, otherwise leave it blank. 30 Sex (M/F) Write M=for Male and F=for Female on the sex of the neonate 31 Weight in grams Write the weight of the neonate in grams 32 Still birth (√) Tick (√) If baby is born dead, otherwise leave it blank.
33 Neonatal death (age in days) If the neonate is dead, write the age of the neonate in days
34 If died, cause of death If the neonate is dead, write the cause of death of the neonate
Complication and
referral
35 Maternal complication
If there is any complication related to pregnancy and delivery, write the name of complication based on the code provided Maternal: (APH, PPH, OL/BD(obstructed labor or birth delay), fit, discharge, fever, swelling and severe headache or other complications other than listed here
Newborn Complication Newborn: breathing pro, sucking pro., LBW, fit, eye inf: cord inf, fever, unconscious, or other complications other than listed here
36 Referred (√) put tick mark (√) If client is referred to health facility, otherwise leave it blank
New Born preventive services
37 TTC oint (√) Tick (√) if TTC ointment given
38 Chlorhexidine (√) Tick (√)) if chlorhexidine used
PNC
39 Visit number Number of PNC visits for basic care for this pregnancy
40 Date of Visit (DD/MM/YY) Date when PNC visit is made, written as (EC) Day/Month/Year (DD/MM/YY)
41 PNC visit time Categorize the time of PNC visit and write 48hr= for 48 hours,7d=for 7 days, 42d=for 42 days
42 Advised on maternal care (√)
Tick (√) If advice on maternal care such as cleanliness, danger signs, family planning, etc … is given for delivered women,; if not leave it blank.
43 Advised on newborn care (√)
Tick (√) If advice on newborn care is given for delivered women, if not leave it blank.
44 Place where PNC provided Write place where PNC is provided based on the code (HO: home, HP: health post, HC: health center, Hos: hospital, other)
Remark 45 Remark/Appointment Write appointment date and any note
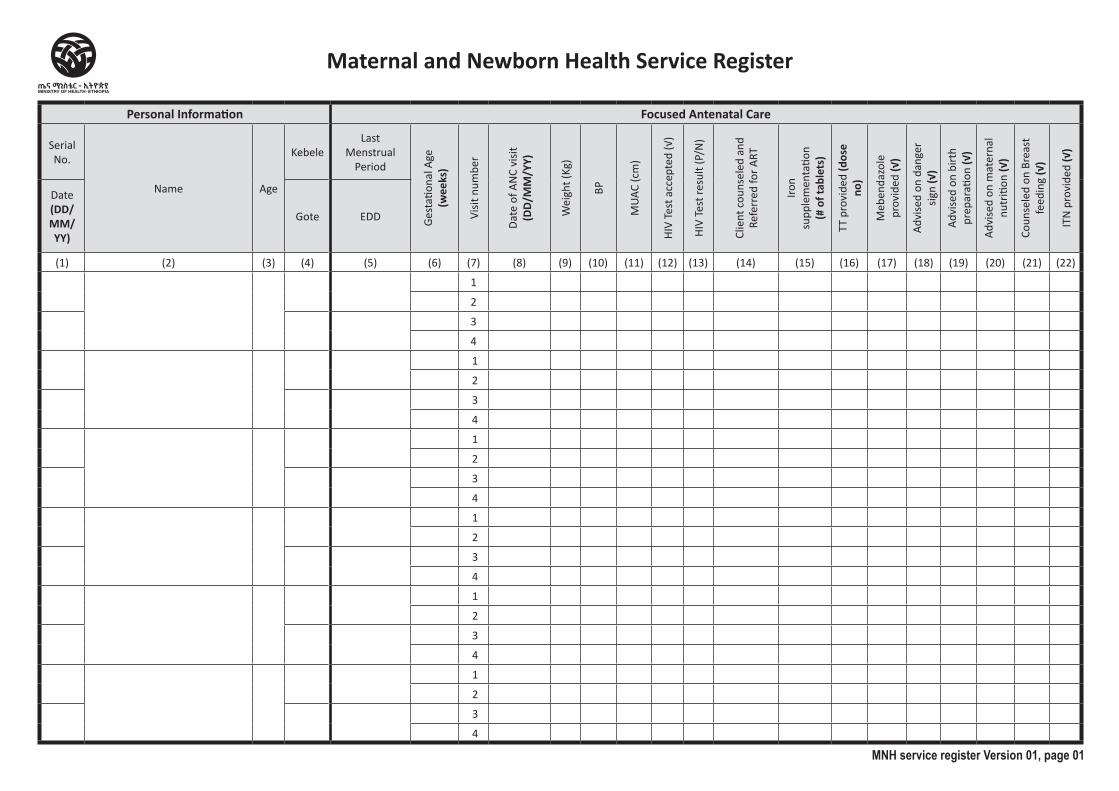
Personal Information Focused Antenatal Care
Serial No.
Name Age
KebeleLast
Menstrual Period
Gest
ation
al A
ge
(wee
ks)
Visit
num
ber
Date
of A
NC
visit
(D
D/M
M/Y
Y)
Wei
ght (
Kg)
BP
MUA
C (c
m)
HIV
Test
acc
epte
d (√
)
HIV
Test
resu
lt (P
/N)
Clie
nt c
ouns
eled
and
Re
ferr
ed fo
r ART
Iron
supp
lem
enta
tion
(# o
f tab
lets
)
TT p
rovi
ded
(dos
e no
)
Meb
enda
zole
pr
ovid
ed (√
)
Advi
sed
on d
ange
r sig
n (√
)
Advi
sed
on b
irth
prep
arati
on (√
)
Advi
sed
on m
ater
nal
nutr
ition
(√)
Coun
sele
d on
Bre
ast
feed
ing
(√)
ITN
pro
vide
d (√
)
Date(DD/MM/YY)
Gote EDD
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22)
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
1
2
3
4
MNH service register Version 01, page 01
Maternal and Newborn Health Service Register
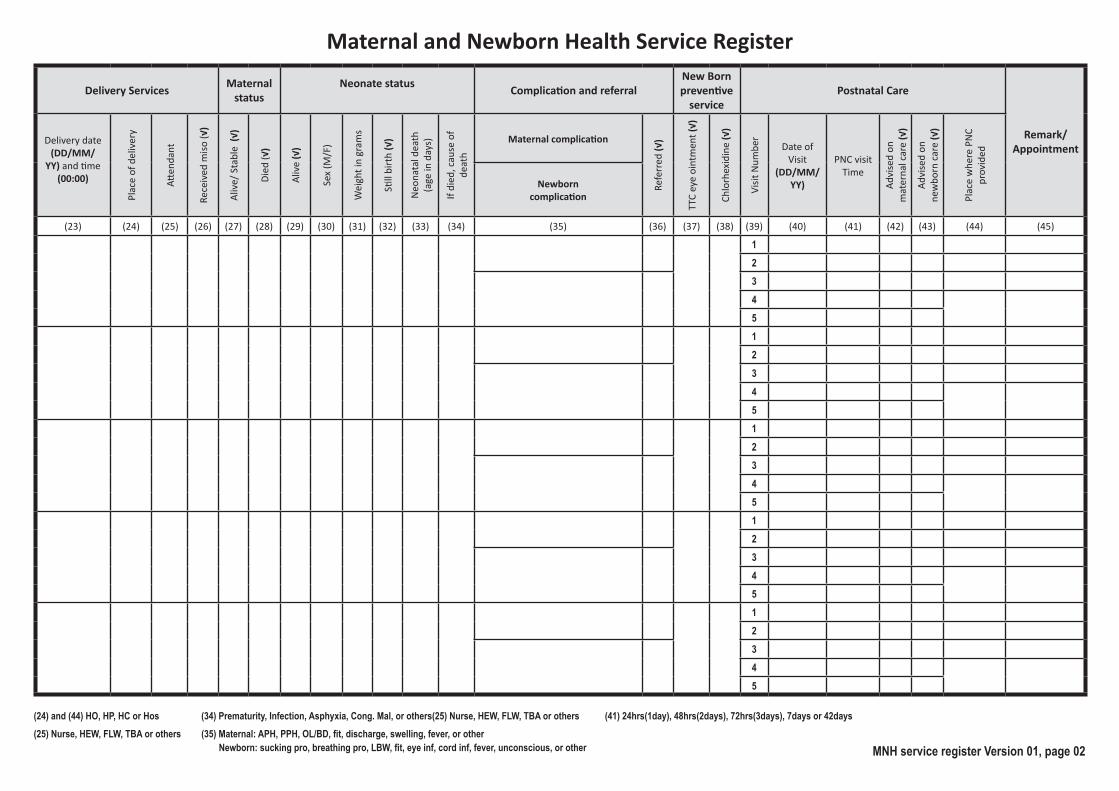
Maternal and Newborn Health Service Register
Delivery Services Maternal status
Neonate status Complication and referralNew Bornpreventive
servicePostnatal Care
Remark/ Appointment
Delivery date (DD/MM/
YY) and time (00:00)
Plac
e of
del
iver
y
Atten
dant
Rece
ived
miso
(√)
Aliv
e/ S
tabl
e (√
)
Died
(√)
Aliv
e (√
)
Sex
(M/F
)
Wei
ght i
n gr
ams
Still
birt
h (√
)
Neo
nata
l dea
th
(age
in d
ays)
If di
ed, c
ause
of
deat
h
Maternal complication
Refe
rred
(√)
TTC
eye
oint
men
t (√)
Chlo
rhex
idin
e (√
)
Visit
Num
ber
Date of Visit
(DD/MM/YY)
PNC visit Time
Advi
sed
on
mat
erna
l car
e (√
)
Advi
sed
on
new
born
car
e (√
)
Plac
e w
here
PN
C pr
ovid
ed
Newborncomplication
(23) (24) (25) (26) (27) (28) (29) (30) (31) (32) (33) (34) (35) (36) (37) (38) (39) (40) (41) (42) (43) (44) (45)
1234
512
3
4
5
1
2
3
4
5
1
2
3
4
5
1
2
3
4
5
(35) Maternal: APH, PPH, OL/BD, fit, discharge, swelling, fever, or other (41) 24hrs(1day), 48hrs(2days), 72hrs(3days), 7days or 42days
Newborn: sucking pro, breathing pro, LBW, fit, eye inf, cord inf, fever, unconscious, or other
(24) and (44) HO, HP, HC or Hos(25) Nurse, HEW, FLW, TBA or others
(34) Prematurity, Infection, Asphyxia, Cong. Mal, or others(25) Nurse, HEW, FLW, TBA or others
MNH service register Version 01, page 02

Health PostNTD Screening Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostNTD Screening Register
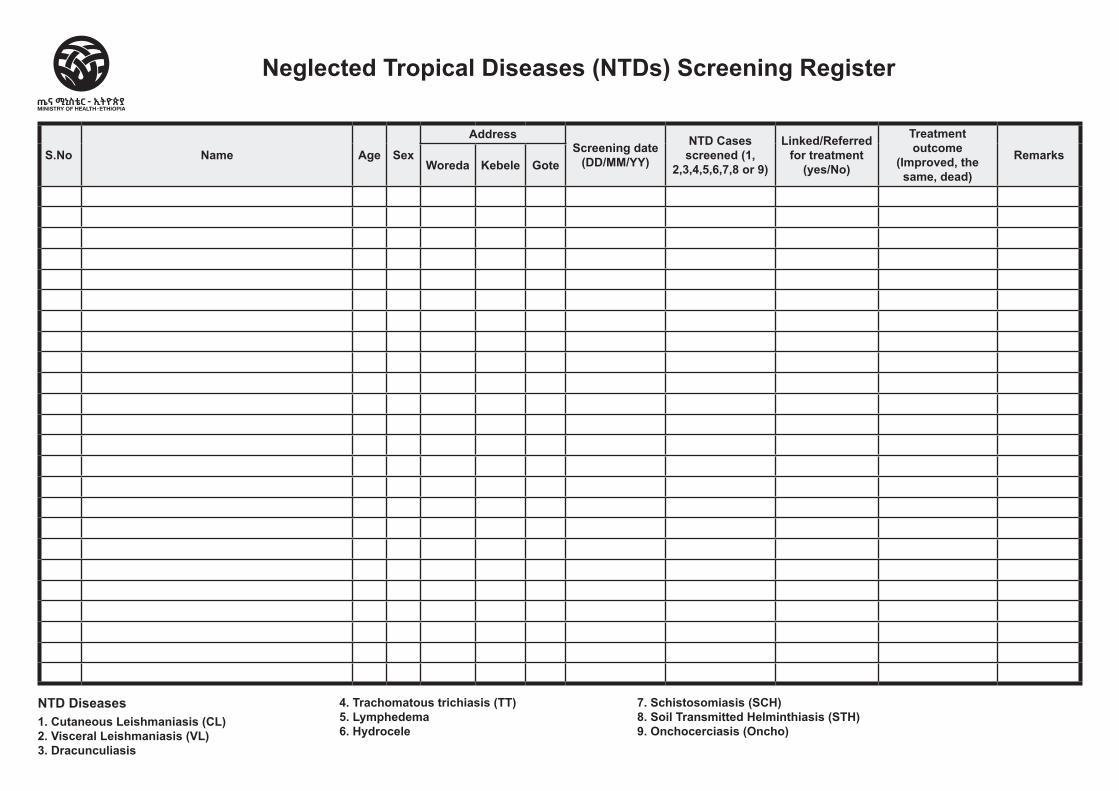
S.No Name Age Sex
AddressScreening date
(DD/MM/YY)
NTD Cases screened (1,
2,3,4,5,6,7,8 or 9)
Linked/Referred for treatment
(yes/No)
Treatment outcome
(Improved, the same, dead)
Remarks Woreda Kebele Gote
Neglected Tropical Diseases (NTDs) Screening Register
NTD Diseases1. Cutaneous Leishmaniasis (CL)2. Visceral Leishmaniasis (VL)3. Dracunculiasis
4. Trachomatous trichiasis (TT) 5. Lymphedema6. Hydrocele
7. Schistosomiasis (SCH)8. Soil Transmitted Helminthiasis (STH)9. Onchocerciasis (Oncho)
Health PostNutrition Screening and TFP Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostNutrition Screening and TFP Register
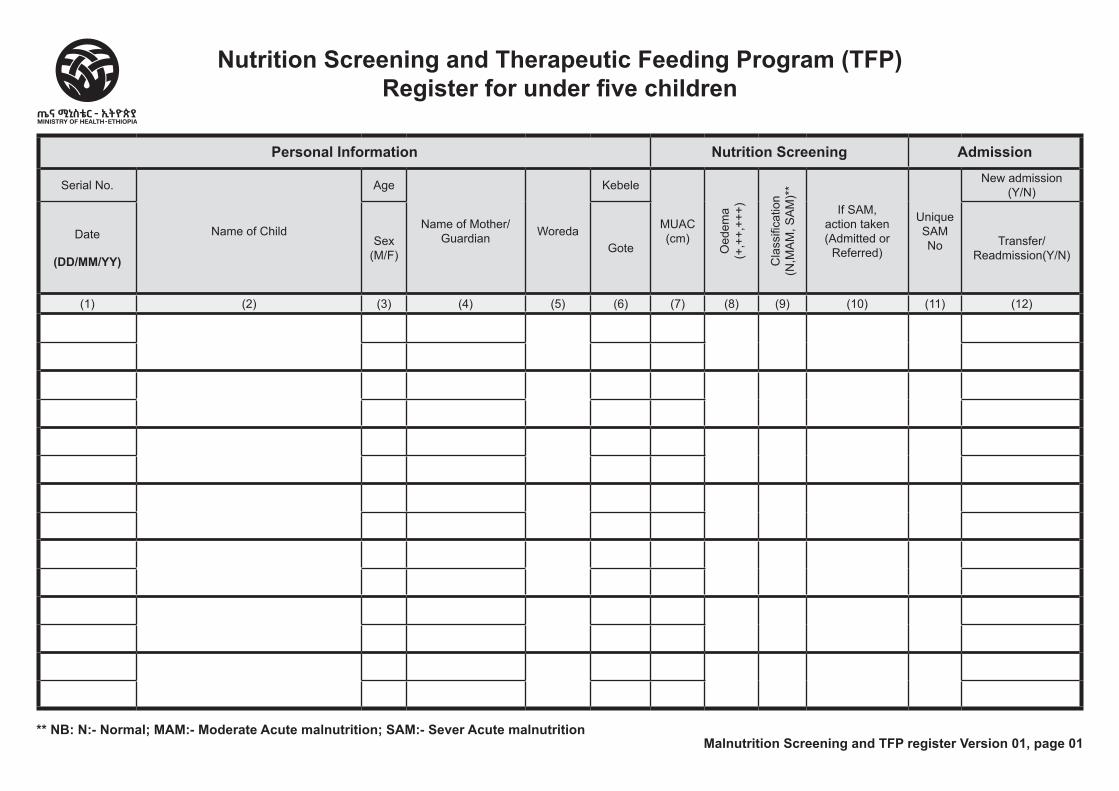
Malnutrition Screening and TFP register Version 01, page 01
Nutrition Screening and Therapeutic Feeding Program (TFP) Register for under five children
Personal Information Nutrition Screening Admission
Serial No.
Name of Child
Age
Name of Mother/Guardian Woreda
Kebele
MUAC (cm)
Oed
ema
(+,+
+,++
+)
Cla
ssifi
catio
n (N
,MA
M, S
AM
)**
If SAM, action taken (Admitted or
Referred)
Unique SAM No
New admission (Y/N)
Date
(DD/MM/YY)
Sex (M/F) Gote Transfer/
Readmission(Y/N)
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
** NB: N:- Normal; MAM:- Moderate Acute malnutrition; SAM:- Sever Acute malnutrition

Health PostPregnant and Lactating Mother
Nutrition Screening Register
Region Woreda Kebele Health Post Name
Begin Date End Date
Health PostPregnant and Lactating Mother
Nutrition Screening Register
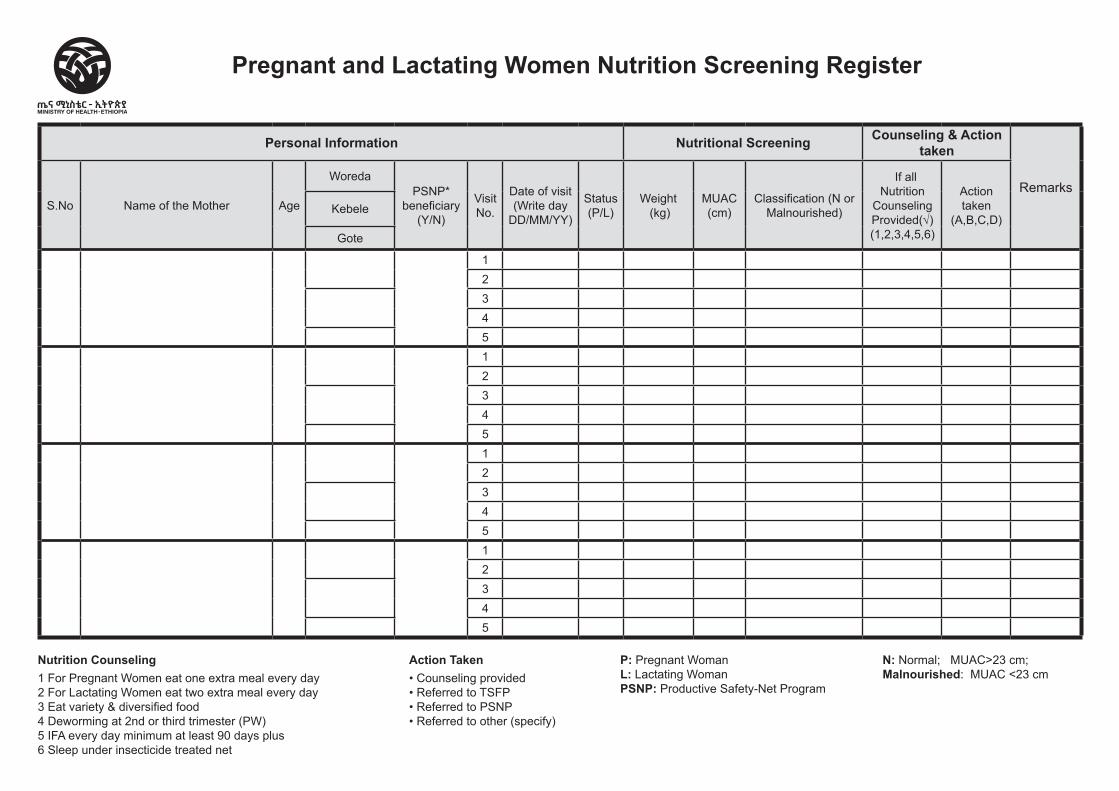
Personal Information Nutritional Screening Counseling & Action taken
RemarksS.No Name of the Mother Age
WoredaPSNP*
beneficiary (Y/N)
Visit No.
Date of visit (Write day
DD/MM/YY)
Status (P/L)
Weight (kg)
MUAC (cm)
Classification (N or Malnourished)
If all Nutrition
Counseling Provided(√) (1,2,3,4,5,6)
Action taken
(A,B,C,D)Kebele
Gote
1 2
3 4
5 1 2 3 4 5 1 2 34512345
Pregnant and Lactating Women Nutrition Screening Register
Nutrition Counseling1 For Pregnant Women eat one extra meal every day2 For Lactating Women eat two extra meal every day3 Eat variety & diversified food4 Deworming at 2nd or third trimester (PW)5 IFA every day minimum at least 90 days plus6 Sleep under insecticide treated net
Action Taken• Counseling provided• Referred to TSFP• Referred to PSNP• Referred to other (specify)
P: Pregnant WomanL: Lactating WomanPSNP: Productive Safety-Net Program
N: Normal; MUAC>23 cm;Malnourished: MUAC <23 cm
Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Post Malaria Screening and Investigation
Register
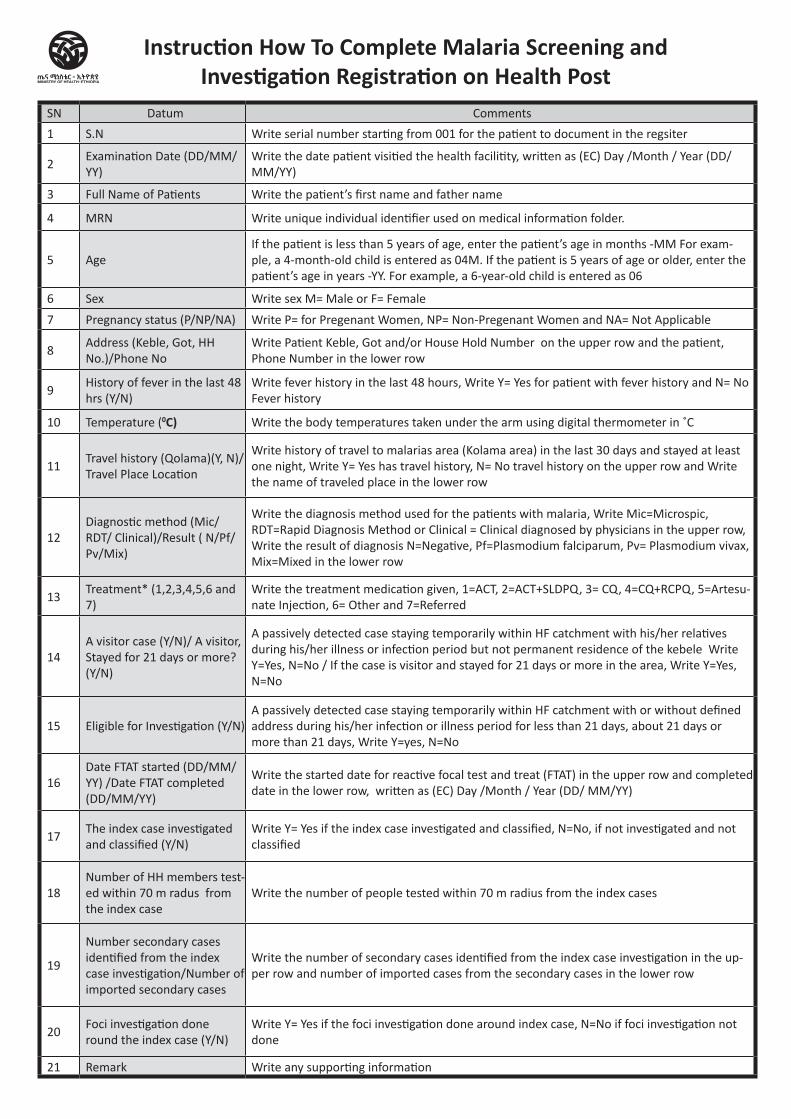
SN Datum Comments
1 S.N Write serial number starting from 001 for the patient to document in the regsiter
2Examination Date (DD/MM/YY)
Write the date patient visitied the health facilitity, written as (EC) Day /Month / Year (DD/ MM/YY)
3 Full Name of Patients Write the patient’s first name and father name
4 MRN Write unique individual identifier used on medical information folder.
5 AgeIf the patient is less than 5 years of age, enter the patient’s age in months -MM For exam-ple, a 4-month-old child is entered as 04M. If the patient is 5 years of age or older, enter the patient’s age in years -YY. For example, a 6-year-old child is entered as 06
6 Sex Write sex M= Male or F= Female
7 Pregnancy status (P/NP/NA) Write P= for Pregenant Women, NP= Non-Pregenant Women and NA= Not Applicable
8Address (Keble, Got, HH No.)/Phone No
Write Patient Keble, Got and/or House Hold Number on the upper row and the patient, Phone Number in the lower row
9History of fever in the last 48 hrs (Y/N)
Write fever history in the last 48 hours, Write Y= Yes for patient with fever history and N= No Fever history
10 Temperature (0C) Write the body temperatures taken under the arm using digital thermometer in ˚C
11Travel history (Qolama)(Y, N)/ Travel Place Location
Write history of travel to malarias area (Kolama area) in the last 30 days and stayed at least one night, Write Y= Yes has travel history, N= No travel history on the upper row and Write the name of traveled place in the lower row
12Diagnostic method (Mic/RDT/ Clinical)/Result ( N/Pf/Pv/Mix)
Write the diagnosis method used for the patients with malaria, Write Mic=Microspic, RDT=Rapid Diagnosis Method or Clinical = Clinical diagnosed by physicians in the upper row, Write the result of diagnosis N=Negative, Pf=Plasmodium falciparum, Pv= Plasmodium vivax, Mix=Mixed in the lower row
13Treatment* (1,2,3,4,5,6 and 7)
Write the treatment medication given, 1=ACT, 2=ACT+SLDPQ, 3= CQ, 4=CQ+RCPQ, 5=Artesu-nate Injection, 6= Other and 7=Referred
14A visitor case (Y/N)/ A visitor, Stayed for 21 days or more? (Y/N)
A passively detected case staying temporarily within HF catchment with his/her relatives during his/her illness or infection period but not permanent residence of the kebele Write Y=Yes, N=No / If the case is visitor and stayed for 21 days or more in the area, Write Y=Yes, N=No
15 Eligible for Investigation (Y/N) A passively detected case staying temporarily within HF catchment with or without defined address during his/her infection or illness period for less than 21 days, about 21 days or more than 21 days, Write Y=yes, N=No
16Date FTAT started (DD/MM/YY) /Date FTAT completed (DD/MM/YY)
Write the started date for reactive focal test and treat (FTAT) in the upper row and completed date in the lower row, written as (EC) Day /Month / Year (DD/ MM/YY)
17The index case investigated and classified (Y/N)
Write Y= Yes if the index case investigated and classified, N=No, if not investigated and not classified
18Number of HH members test-ed within 70 m radus from the index case
Write the number of people tested within 70 m radius from the index cases
19
Number secondary cases identified from the index case investigation/Number of imported secondary cases
Write the number of secondary cases identified from the index case investigation in the up-per row and number of imported cases from the secondary cases in the lower row
20Foci investigation done round the index case (Y/N)
Write Y= Yes if the foci investigation done around index case, N=No if foci investigation not done
21 Remark Write any supporting information
Instruction How To Complete Malaria Screening and Investigation Registration on Health Post
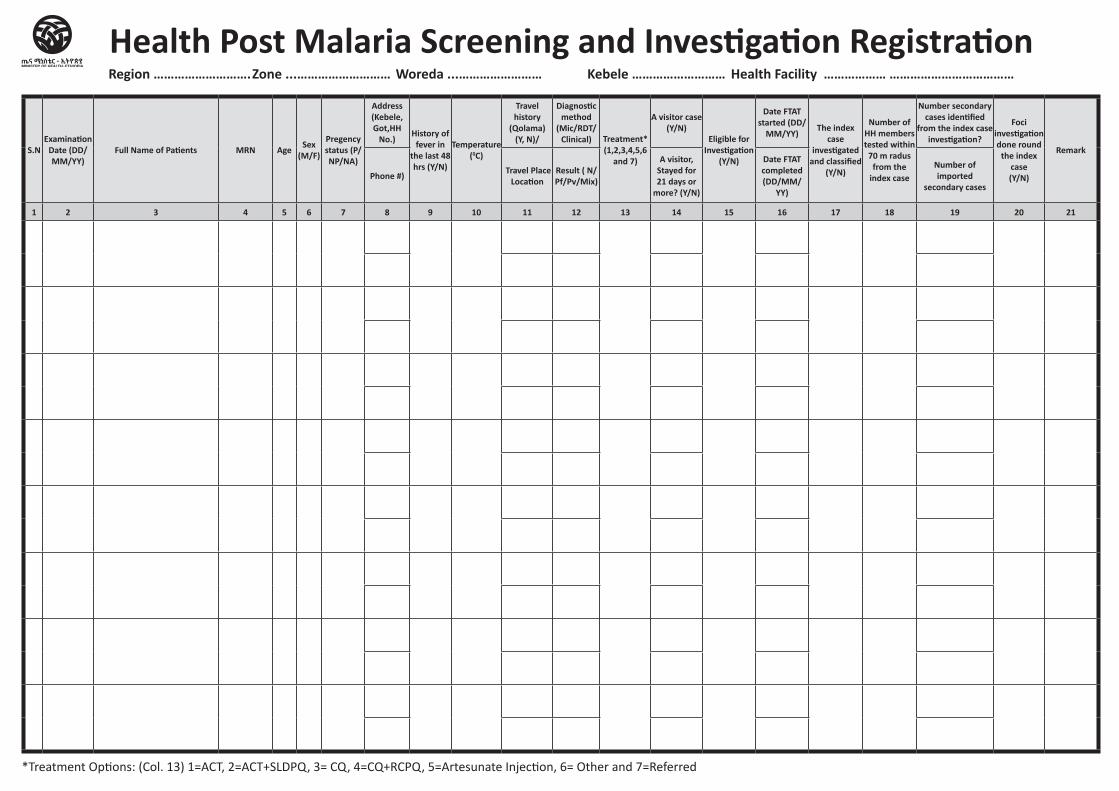
S.NExamination
Date (DD/MM/YY)
Full Name of Patients MRN Age Sex (M/F)
Pregency status (P/NP/NA)
Address (Kebele, Got,HH
No.)History of
fever in the last 48 hrs (Y/N)
Temperature (0C)
Travel history
(Qolama) (Y, N)/
Diagnostic method
(Mic/RDT/ Clinical) Treatment*
(1,2,3,4,5,6 and 7)
A visitor case (Y/N)
Eligible for Investigation
(Y/N)
Date FTAT started (DD/
MM/YY) The index
case investigated
and classified (Y/N)
Number of HH members tested within
70 m radus from the
index case
Number secondary cases identified
from the index case investigation?
Foci investigation done round
the index case (Y/N)
Remark
Phone #) Travel Place Location
Result ( N/Pf/Pv/Mix)
A visitor, Stayed for 21 days or
more? (Y/N)
Date FTAT completed (DD/MM/
YY)
Number of imported
secondary cases
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Health Post Malaria Screening and Investigation RegistrationRegion ………………………. Zone ...……………………… Woreda ...…………………… Kebele ……………………… Health Facility ……………… ………………………………
*Treatment Options: (Col. 13) 1=ACT, 2=ACT+SLDPQ, 3= CQ, 4=CQ+RCPQ, 5=Artesunate Injection, 6= Other and 7=Referred
ጤና ኬላ የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት
ህክምናና እንክብካቤ መዝገብ (ከሁለት ወር እስከ 59 ወር)
ክልል ዞን / ክፍለ ከተማ / ወረዳ የጤና ተቋሙ ስም የተጀመረበት ቀን ያልቀበት ቀን
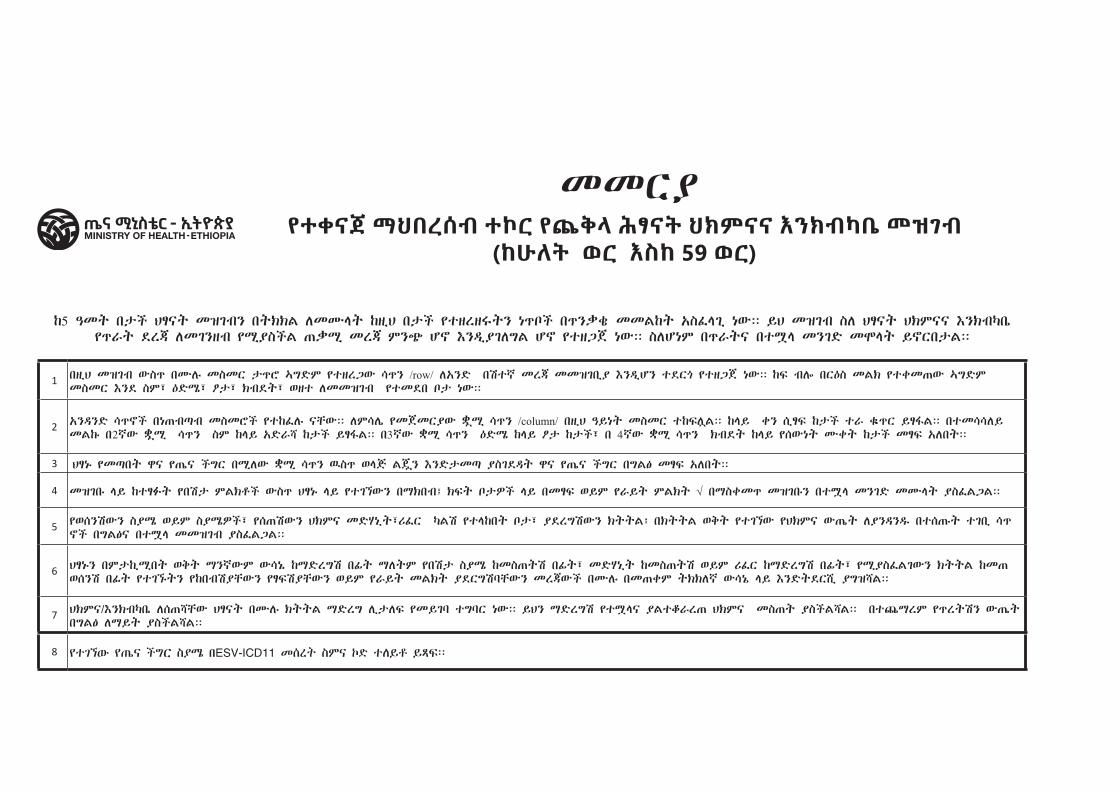
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና እንክብካቤ መዝገብ(ከሁለት ወር እስከ 59 ወር)
mmRÃ
k5 ›mT b¬C HÉÂT mZgBN bTKKL lmѧT kz!H b¬C ytzrz„TN n_ïC b_N”q& mmLkT xSf§g! nWÝÝ YH mZgB Sl HÉÂT HKM XNKBµb@ y_‰T dr© lmgNzB y¸ÃSCL -”¸ mr© MN+ çñ XNÄ!ÃglGL çñ ytzUj nWÝÝ SlçnM b_‰T btৠmNgD mä§T YñRb¬LÝÝ
1 bz!H mZgB WS_ bÑl# mSmR ¬_é ¨GDM ytzrUW ú_N /row/ lxND b>t¾ mr© mmZgb!à XNÄ!çN tdR¯ ytzUj nWÝÝ kF BlÖ bR:S mLK ytqm-W ¨GDM mSmR XNd SM½ :D»½ ò¬½ KBdT½ wzt lmmZgB ytmdb ï¬ nWÝÝ
2 xNÄND ú_ñC bn-BÈB mSméC ytkfl# ÂcWÝÝ lMúl@ ymjmRÃW Ì*¸ ú_N /column/ bz!H ›YnT mSmR tkFl*LÝÝ k§Y qN s!ÉF k¬C t‰ q$$$_R YÉÍLÝÝ btmúúlY mLk# b2¾W Ì*¸ ú_N SM k§Y xD‰š k¬C YÉÍLÝÝ b3¾W ̸ ú_N :D» k§Y ò¬ k¬C½ b 4¾W ̸ ú_N KBdT k§Y ysWnT ÑqT k¬C mÉF xlbTÝÝ
3 HÉn# ymÈbT ê y-@ CGR b¸lW ̸ ú_N ýS_ w§J Lj*N XND¬mÈ ÃSgdÄT ê y-@ CGR bGL} mÉF xlbTÝÝ
4 mZgb# §Y ktÉûT yb>¬ MLKèC WS_ HÉn# §Y ytgßWN b¥KbB¿ KFT ï¬ãC §Y bmÉF wYM y‰YT MLKT √ b¥Sqm_ mZgb#N btৠmNgD mѧT ÃSfLULÝÝ
5 ywsN>WN Sû wYM SûãC½ ys->WN HKM mD¦n!T½¶fR µL> yt§kbT ﬽ ÃdrG>WN KTTL¿ bKTTL wQT ytgßW yHKM W-@T lÃNÄNÇ bts-#T tgb! ú_ñC bGL} btৠmmZgB ÃSfLULÝÝ
6 HÉn#N bM¬k!¸bT wQT ¥N¾WM Wún@ k¥DrG> bðT ¥lTM yb>¬ Sû kmS-T> bðT½ mD¦n!T kmS-T> wYM ¶fR k¥DrG> bðT½ y¸ÃSfLgWN KTTL km-wsN> bðT ytgß#TN ykbB>ÃcWN yÉF>ÃcWN wYM y‰YT mLKT ÃdRG>ÆcWN mr©WC bÑl# bm-qM TKKl¾ Wún@ §Y XNDTdR¹! ÃGZšLÝÝ
7 HKM¼XNKBµb@ ls-šcW HÉÂT bÑl# KTTL ¥DrG l!¬lF ymYgÆ tGÆR nWÝÝ YHN ¥DrG> ytà§Â ÃLtö‰r- HKM mS-T ÃSCLšLÝÝ bt=¥rM y_rT>N W-@T bGL} l¥YT ÃSCLšLÝÝ
8 የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት ስምና ኮድ ተለይቶ ይጻፍ፡፡
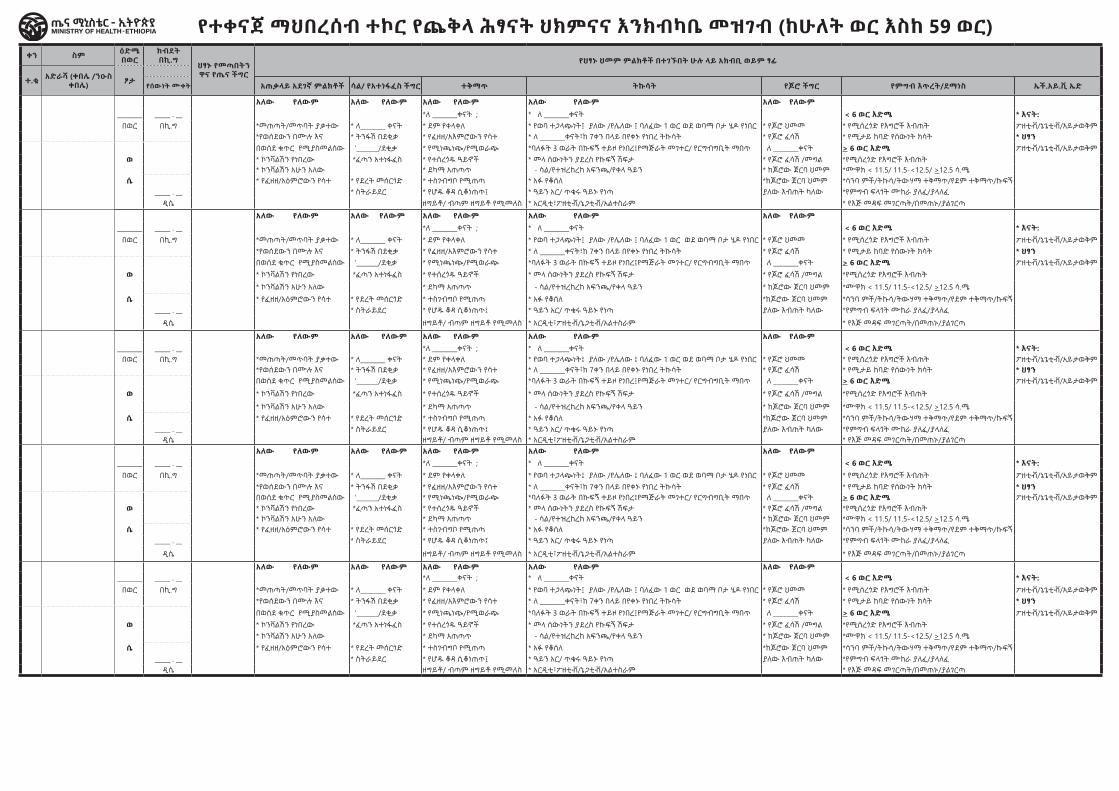
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና እንክብካቤ መዝገብ (ከሁለት ወር እስከ 59 ወር)ቀን ስም ዕድሜ
በወር ክብደት በኪ.ግ
ህፃኑ የመጣበትን ዋና የጤና ችግር
የህፃኑ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊ የህፃኑ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊቫይታሚን ኤ/እድሜ >
6 ወራት/ሌላ የጤና ችግር የተገኘው የጤና ችግር
ስያሜ
የተሠጠው ህክምና የክትትል ቀን የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት
አስተያየትተ.ቁ አድራሻ (ቀበሌ /ንዑስ
ቀበሌ) ፆታ የክትባት ሁኔታ ሜቤንዳዞል/
አልቤንዳዞል/ እድሜ ≥ 2 አመት
የተሠጠው መድሃኒት አወሳሰድ እናትን ማማከር
እሪፈር ከተባለ የተላከበት ተቋም ስም የተሠጠው አጭር የቀጠሮ
ቀን ውጤት የበሽታው ስም ኮድ
የሰውነት ሙቀት አጠቃላይ አደገኛ ምልክቶች ሳል/ የአተነፋፈስ ችግር ተቅማጥ ትኩሳት የጆሮ ችግር የምግብ እጥረት/ደማነስ ኤች.አይ.ቪ ኤድ ቴበርክሎሲስ/ቲቢ/ የእድገት ዳሰሳ / < 2 ዓመት/ የተላከበት ተቋም ስም
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለውበወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ
*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውበወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ
አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውበወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ
አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደ
ዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም ________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
Count 0-24 months 25-59 months
ተቅማጥን በ ORS and zinc የታከሙ -------
DD ተቅማጥን ORS ብቻ የታከሙ ----
SDD
NDD
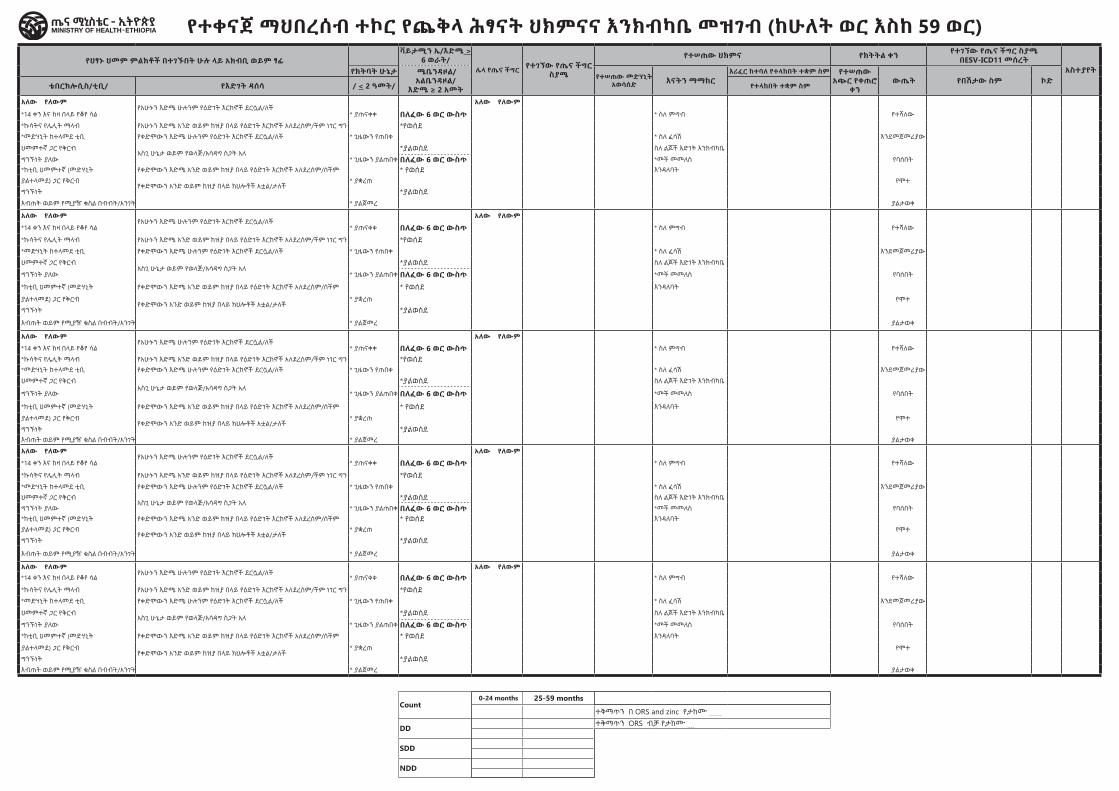
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና እንክብካቤ መዝገብ (ከሁለት ወር እስከ 59 ወር)ቀን ስም ዕድሜ
በወር ክብደት በኪ.ግ
ህፃኑ የመጣበትን ዋና የጤና ችግር
የህፃኑ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊ የህፃኑ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊቫይታሚን ኤ/እድሜ >
6 ወራት/ሌላ የጤና ችግር የተገኘው የጤና ችግር
ስያሜ
የተሠጠው ህክምና የክትትል ቀን የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት
አስተያየትተ.ቁ አድራሻ (ቀበሌ /ንዑስ
ቀበሌ) ፆታ የክትባት ሁኔታ ሜቤንዳዞል/
አልቤንዳዞል/ እድሜ ≥ 2 አመት
የተሠጠው መድሃኒት አወሳሰድ እናትን ማማከር
እሪፈር ከተባለ የተላከበት ተቋም ስም የተሠጠው አጭር የቀጠሮ
ቀን ውጤት የበሽታው ስም ኮድ
የሰውነት ሙቀት አጠቃላይ አደገኛ ምልክቶች ሳል/ የአተነፋፈስ ችግር ተቅማጥ ትኩሳት የጆሮ ችግር የምግብ እጥረት/ደማነስ ኤች.አይ.ቪ ኤድ ቴበርክሎሲስ/ቲቢ/ የእድገት ዳሰሳ / < 2 ዓመት/ የተላከበት ተቋም ስም
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለውበወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ
*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውበወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ
አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም
________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውበወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ
አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደ
ዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም አለው የለውም የአሁኑን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች
አለው የለውም ________ _____ . __ *ለ ________ቀናት ; * ለ ________ቀናት < 6 ወር እድሜ * እናት: *14 ቀን እና ከዛ በላይ የቆየ ሳል * ያጠናቀቀ በለፈው 6 ወር ውስጥ * ስለ ምግብ የተሻለው
በወር በኪ.ግ *መጠጣት/መጥባት ያቃተው * ለ________ ቀናት * ደም የቀላቀለ * የወባ ተጋላጭነት፤ ያለው /የሌለው ፤ ባለፈው 1 ወር ወደ ወባማ ቦታ ሄዶ የነበር * የጆሮ ህመመ * የሚሰረጎድ የእግሮች እብጠት ፖዘቲቭ/ኔጌቲቭ/አይታወቅም *ኩሳትና የሌሊት ማላብ የአሁኑን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ችም ነገር ግን *የወሰደ*የወሰደውን በሙሉ እና * ትንፋሽ በደቂቃ * የፈዘዘ/አእምሮውን የሳተ * ለ ________ቀናት፣ከ 7ቀን በላይ በየቀኑ የነበረ ትኩሳት * የጆሮ ፈሳሽ * የሚታይ ከባድ የሰውነት ክሳት * ህፃን *መድሃኒት ከተላመደ ቲቢ የቀድሞውን እድሜ ሁሉንም የዕድገት እርከኖች ደርሷል/ለች * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
በወሰደ ቁጥር የሚያስመልሰው ‘_______/ደቂቃ * የሚነጫነጭ/የሚወራጭ *ባለፉት 3 ወራት በኩፍኝ ተይዞ የነበረ፤የማጅራት መገተር/ የርግብግቢት ማበጥ ለ ________ቀናት > 6 ወር እድሜ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ህመምተኛ ጋር የቅርብ አስጊ ሁኔታ ወይም የወላጅ/አሳዳግ ስጋት አለ
*ያልወሰደ ስለ ልጆች እድገት እንክብካቤ
ወ * ኮንቫልሽን የነበረው *ፈጣን አተነፋፈስ * የተሰረጎዱ ዓይኖች * መላ ሰውነትን ያደረስ የኩፍኝ ሽፍታ * የጆሮ ፈሳሽ /መግል *የሚሰረጎድ የእግሮች እብጠት ግንኙነት ያለው * ጊዜውን ያልጠበቀ በለፈው 6 ወር ውስጥ *መች መመለስ የባሰበት
* ኮንቫልሽን አሁን አለው * ደካማ አጠጣጥ - ሳል/የተዝረከረከ አፍንጫ/የቀላ ዓይን * ከጆሮው ጀርባ ህመም *ሙዋክ < 11.5/ 11.5-<12.5/ >12.5 ሳ.ሜ *ከቲቢ ህመምተኛ (መድሃኒት የቀድሞውን እድሜ አንድ ወይም ከዝያ በላይ የዕድገት እርከኖች አለደረሰም/ሰችም * የወሰደ እንዳለባት
ሴ * የፈዘዘ/አዕምሮውን የሳተ * የደረት መሰርጎድ * ተስገብግቦ የሚጠጣ * አፉ የቆሰለ *ከጆሮው ጀርባ ህመም *ሳንባ ምች/ትኩሳ/ትውሃማ ተቅማጥ/የደም ተቅማጥ/ኩፍኝ ያልተላመደ) ጋር የቅርብየቀድሞውን አንድ ወይም ከዝያ በላይ ክህሎቶች አቷል/ታለች
* ያቋረጠ የሞተ
_____ . __ * ስትራይደር * የሆዱ ቆዳ ሲቆነጠጥ፤ * ዓይን አር/ ጥቁሩ ዓይኑ የነጣ ያለው እብጠት ካለው *የምግብ ፍላጎት ሙከራ ያለፈ/ያላለፈ ግንኙነት *ያልወሰደዲሴ ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ * አርዲቲ፣ፖዘቲቭ/ኔጋቲቭ/አልተስራም * የእጅ መዳፍ መገርጣት/በመጠኑ/ያልገርጣ እብጠት ወይም የሚያዥ ቁስል በብብት/አንገት * ያልጀመረ ያልታወቀ
Count 0-24 months 25-59 months
ተቅማጥን በ ORS and zinc የታከሙ -------
DD ተቅማጥን ORS ብቻ የታከሙ ----
SDD
NDD
ጤና ኬላ የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት
ህክምናና እንክብካቤ መዝገብ( ከሁለት ወር ዕድሜ በታች የሆኑ )
ክልል ዞን / ክፍለ ከተማ / ወረዳ የጤና ተቋሙ ስም የተጀመረበት ቀን ያልቀበት ቀን
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና እንክብካቤ መዝገብ( ከሁለት ወር ዕድሜ በታች የሆኑ )
mmRÃ
k5 ›mT b¬C HÉÂT mZgBN bTKKL lmѧT kz!H b¬C ytzrz„TN n_ïC b_N”q& mmLkT xSf§g! nWÝÝ YH mZgB Sl HÉÂT HKM XNKBµb@ y_‰T dr© lmgNzB y¸ÃSCL -”¸ mr© MN+ çñ XNÄ!ÃglGL çñ ytzUj nWÝÝ SlçnM b_‰T btৠmNgD mä§T YñRb¬LÝÝ
1 bz!H mZgB WS_ bÑl# mSmR ¬_é ¨GDM ytzrUW ú_N /row/ lxND b>t¾ mr© mmZgb!à XNÄ!çN tdR¯ ytzUj nWÝÝ kF BlÖ bR:S mLK ytqm-W ¨GDM mSmR XNd SM½ :D»½ ò¬½ KBdT½ wzt lmmZgB ytmdb ï¬ nWÝÝ
2 xNÄND ú_ñC bn-BÈB mSméC ytkfl# ÂcWÝÝ lMúl@ ymjmRÃW Ì*¸ ú_N /column/ bz!H ›YnT mSmR tkFl*LÝÝ k§Y qN s!ÉF k¬C t‰ q$$$_R YÉÍLÝÝ btmúúlY mLk# b2¾W Ì*¸ ú_N SM k§Y xD‰š k¬C YÉÍLÝÝ b3¾W ̸ ú_N :D» k§Y ò¬ k¬C½ b 4¾W ̸ ú_N KBdT k§Y ysWnT ÑqT k¬C mÉF xlbTÝÝ
3 HÉn# ymÈbT ê y-@ CGR b¸lW ̸ ú_N ýS_ w§J Lj*N XND¬mÈ ÃSgdÄT ê y-@ CGR bGL} mÉF xlbTÝÝ
4 mZgb# §Y ktÉûT yb>¬ MLKèC WS_ HÉn# §Y ytgßWN b¥KbB¿ KFT ï¬ãC §Y bmÉF wYM y‰YT MLKT √ b¥Sqm_ mZgb#N btৠmNgD mѧT ÃSfLULÝÝ
5 ywsN>WN Sû wYM SûãC½ ys->WN HKM mD¦n!T½¶fR µL> yt§kbT ﬽ ÃdrG>WN KTTL¿ bKTTL wQT ytgßW yHKM W-@T lÃNÄNÇ bts-#T tgb! ú_ñC bGL} btৠmmZgB ÃSfLULÝÝ
6 HÉn#N bM¬k!¸bT wQT ¥N¾WM Wún@ k¥DrG> bðT ¥lTM yb>¬ Sû kmS-T> bðT½ mD¦n!T kmS-T> wYM ¶fR k¥DrG> bðT½ y¸ÃSfLgWN KTTL km-wsN> bðT ytgß#TN ykbB>ÃcWN yÉF>ÃcWN wYM y‰YT mLKT ÃdRG>ÆcWN mr©WC bÑl# bm-qM TKKl¾ Wún@ §Y XNDTdR¹! ÃGZšLÝÝ
7 HKM¼XNKBµb@ ls-šcW HÉÂT bÑl# KTTL ¥DrG l!¬lF ymYgÆ tGÆR nWÝÝ YHN ¥DrG> ytà§Â ÃLtö‰r- HKM mS-T ÃSCLšLÝÝ bt=¥rM y_rT>N W-@T bGL} l¥YT ÃSCLšLÝÝ
8 የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት ስምና ኮድ ተለይቶ ይጻፍ፡፡
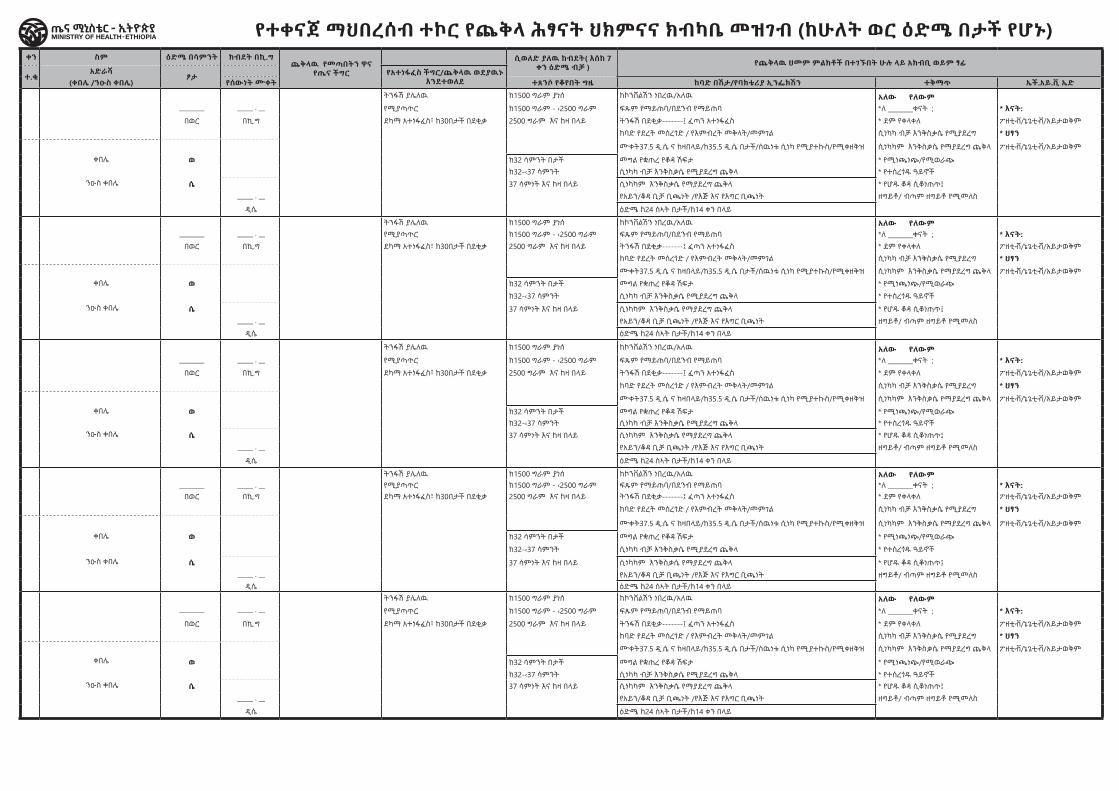
ቀን ስም ዕድሜ በሳምንት ክብደት በኪ.ግ ጨቅላዉ የመጣበትን ዋና
የጤና ችግር
ሲወለድ ያለዉ ከብደት( እሰከ 7 ቀን ዕድሜ ብቻ ) የጨቅላዉ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊ የጨቅላዉ ህመም ምልክቶች በተገኙበት
ሁሉ ላይ አክብቢ ወይም ፃፊ ሌላ የጤና ችግር የተገኘው የጤና ችግር ስያሜየተሠጠው ህክምና የክትትል ቀን የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት
አስተያየትተ.ቁ
አድራሻ ፆታ የአተነፋፈስ ችግር/ጨቅላዉ ወደያዉኑ
እንደተወለደየክትባት ሁኔታ
የተሠጠው መድሃኒት አወሳሰድ እናትን ማማከርእሪፈር ከተባለ የተላከበት ተቋም ስም የተሠጠው አጭር
የቀጠሮ ቀን ውጤት የበሽታው ስም ኮድ(ቀበሌ /ንዑስ ቀበሌ) የሰውነት ሙቀት ተጸንሶ የቆየበት ግዜ ከባድ በሽታ/የባክቴሪያ ኢንፌክሽን ተቅማጥ ኤች.አይ.ቪ ኤድ የአመጋገብ ችግር/ዝቅተኛ ክብደት የተላከበት ተቋም ስም
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤ
ቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበትከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት
ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብምዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤ
ቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበትከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት
ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀቁጥር ቁጥርእጅግ በጣም ከባደ በሽታ----------- ለሳምባ ምች የታከሙ ------------------- በጣም ከባደ በሽታ------------ ተቅማጥን በ ORS and zinc የታከሙ -------------------
የተወሰነ የባክቴሪያ ኢንፌክሽን----------- ተቅማጥን ORS ብቻ የታከሙ -------------------
የሳንምባ ምች ------------
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና ክብካቤ መዝገብ (ከሁለት ወር ዕድሜ በታች የሆኑ)
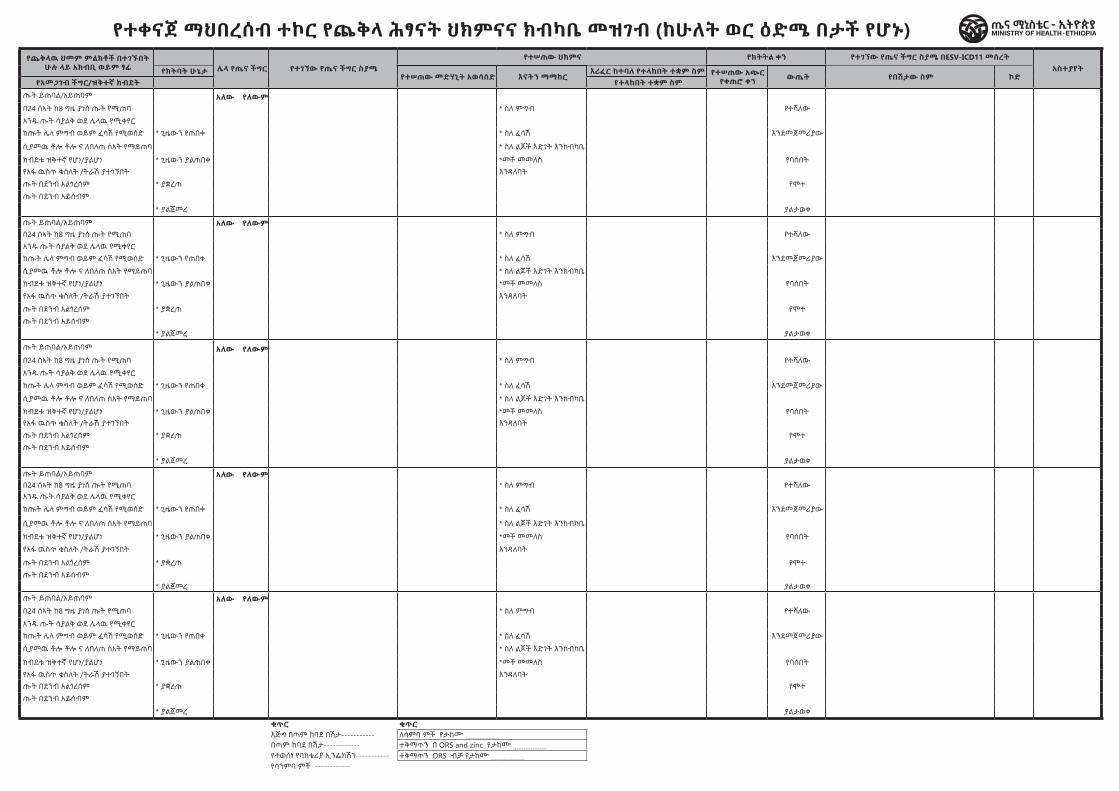
ቀን ስም ዕድሜ በሳምንት ክብደት በኪ.ግ ጨቅላዉ የመጣበትን ዋና
የጤና ችግር
ሲወለድ ያለዉ ከብደት( እሰከ 7 ቀን ዕድሜ ብቻ ) የጨቅላዉ ህመም ምልክቶች በተገኙበት ሁሉ ላይ አክብቢ ወይም ፃፊ የጨቅላዉ ህመም ምልክቶች በተገኙበት
ሁሉ ላይ አክብቢ ወይም ፃፊ ሌላ የጤና ችግር የተገኘው የጤና ችግር ስያሜየተሠጠው ህክምና የክትትል ቀን የተገኘው የጤና ችግር ስያሜ በESV-ICD11 መሰረት
አስተያየትተ.ቁ
አድራሻ ፆታ የአተነፋፈስ ችግር/ጨቅላዉ ወደያዉኑ
እንደተወለደየክትባት ሁኔታ
የተሠጠው መድሃኒት አወሳሰድ እናትን ማማከርእሪፈር ከተባለ የተላከበት ተቋም ስም የተሠጠው አጭር
የቀጠሮ ቀን ውጤት የበሽታው ስም ኮድ(ቀበሌ /ንዑስ ቀበሌ) የሰውነት ሙቀት ተጸንሶ የቆየበት ግዜ ከባድ በሽታ/የባክቴሪያ ኢንፌክሽን ተቅማጥ ኤች.አይ.ቪ ኤድ የአመጋገብ ችግር/ዝቅተኛ ክብደት የተላከበት ተቋም ስም
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤ
ቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበትከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት
ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያው
ሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበት
ከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ
_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብምዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀ
ትንፋሽ ያሌለዉ ከ1500 ግራም ያነሰ ከኮንቨልሽን ነበረዉ/አለዉ አለው የለውም ጡት ይጠባል/አይጠባም አለው የለውም ________ _____ . __ የሚያጣጥር ከ1500 ግራም - ‹2500 ግራም ፍጹም የማይጠባ/በደንብ የማይጠባ *ለ ________ቀናት ; * እናት: በ24 ሰኣት ከ8 ግዜ ያነሰ ጡት የሚጠባ * ስለ ምግብ የተሻለው
በወር በኪ.ግ ደካማ አተነፋፈስ፣ ከ30በታች በደቂቃ 2500 ግራም እና ከዛ በላይ ትንፋሽ በደቂቃ-------፤ ፈጣን አተነፋፈስ * ደም የቀላቀለ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም አንዱ ጡት ሳያልቅ ወደ ሌላዉ የሚቀየርከባድ የደረት መሰረጎድ / የእምብረት መቅላት/መምገል ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ * ህፃን ከጡት ሌላ ምግብ ወይም ፈሳሽ የሚወሰድ * ጊዜውን የጠበቀ * ስለ ፈሳሽ እንደመጀመሪያውሙቀት37.5 ዲ.ሴ ና ከዛበላይ/ከ35.5 ዲ.ሴ በታች/ሰዉነቱ ሲነካ የሚያተኩስ/የሚቀዘቅዝ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ ፖዘቲቭ/ኔጌቲቭ/አይታወቅም ሲያመዉ ቶሎ ቶሎ ና ለበለጠ ሰአት የማይጠባ * ስለ ልጆች እድገት እንክብካቤ
ቀበሌ ወ ከ32 ሳምንት በታች መግል የቋጠረ የቆዳ ሽፍታ * የሚነጫነጭ/የሚወራጭ ክብደቱ ዝቅተኛ የሆነ/ያልሆነ * ጊዜውን ያልጠበቀ *መች መመለስ የባሰበትከ32-‹37 ሳምንት ሲነካካ ብቻ እንቅስቃሴ የሚያደረግ ጨቅላ * የተሰረጎዱ ዓይኖች የአፋ ዉስጥ ቁስለት /ትራሽ ያተገኘበት እንዳለባት
ንዑስ ቀበሌ ሴ 37 ሳምነት እና ከዛ በላይ ሲነካካም እንቅስቃሴ የማያደረግ ጨቅላ * የሆዱ ቆዳ ሲቆነጠጥ፤ ጡት በደንብ አልጎረሰም * ያቋረጠ የሞተ_____ . __ የአይን/ቆዳ ቢቻ ቢጫነት /የእጅ እና የእግር ቢጫነት ዘግይቶ/ ብጣም ዘግይቶ የሚመለስ ጡት በደንብ አይሰብም
ዲሴ ዕድሜ ከ24 ሰኣት በታች/ከ14 ቀን በላይ * ያልጀመረ ያልታወቀቁጥር ቁጥርእጅግ በጣም ከባደ በሽታ----------- ለሳምባ ምች የታከሙ ------------------- በጣም ከባደ በሽታ------------ ተቅማጥን በ ORS and zinc የታከሙ -------------------
የተወሰነ የባክቴሪያ ኢንፌክሽን----------- ተቅማጥን ORS ብቻ የታከሙ -------------------
የሳንምባ ምች ------------
የተቀናጀ ማህበረሰብ ተኮር የጨቅላ ሕፃናት ህክምናና ክብካቤ መዝገብ (ከሁለት ወር ዕድሜ በታች የሆኑ)

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Post Integrated PC-NTD Elimination/
Control Program Treatment Register
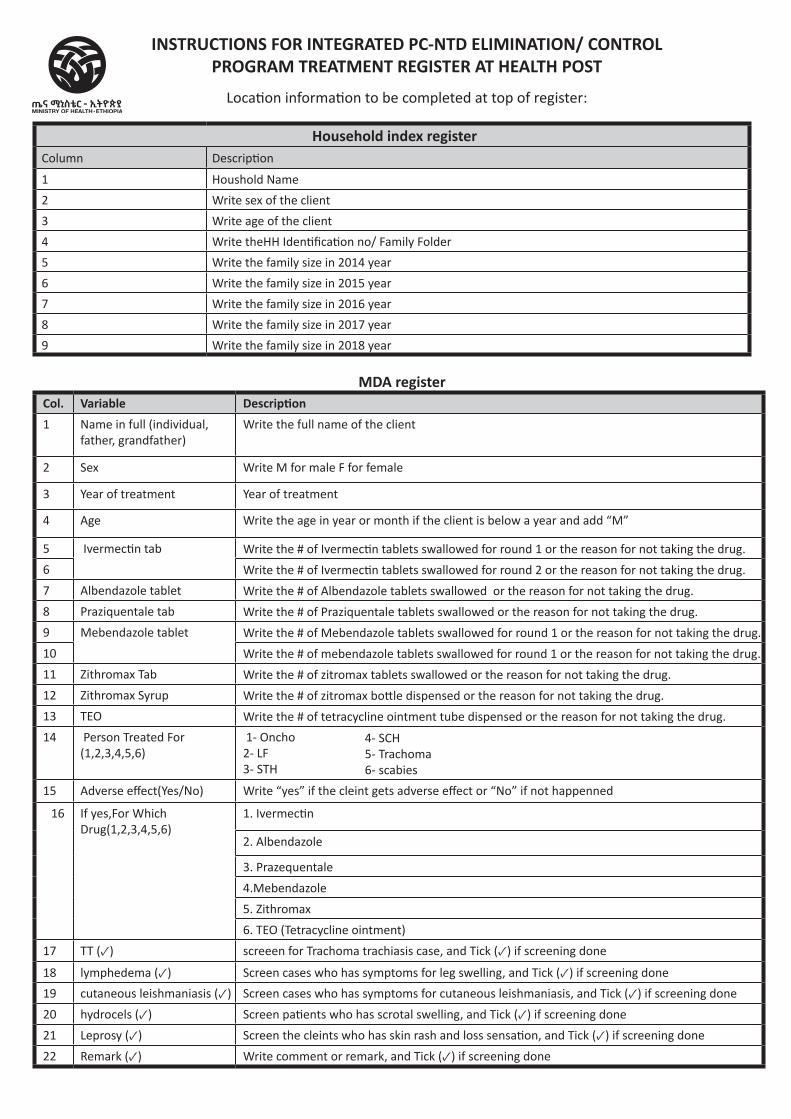
MDA register Col. Variable Description 1 Name in full (individual,
father, grandfather)Write the full name of the client
2 Sex Write M for male F for female
3 Year of treatment Year of treatment
4 Age Write the age in year or month if the client is below a year and add “M”
5 Ivermectin tab Write the # of Ivermectin tablets swallowed for round 1 or the reason for not taking the drug.
6 Write the # of Ivermectin tablets swallowed for round 2 or the reason for not taking the drug.
7 Albendazole tablet Write the # of Albendazole tablets swallowed or the reason for not taking the drug.
8 Praziquentale tab Write the # of Praziquentale tablets swallowed or the reason for not taking the drug.
9 Mebendazole tablet Write the # of Mebendazole tablets swallowed for round 1 or the reason for not taking the drug.
10 Write the # of mebendazole tablets swallowed for round 1 or the reason for not taking the drug.
11 Zithromax Tab Write the # of zitromax tablets swallowed or the reason for not taking the drug.
12 Zithromax Syrup Write the # of zitromax bottle dispensed or the reason for not taking the drug.
13 TEO Write the # of tetracycline ointment tube dispensed or the reason for not taking the drug.
14 Person Treated For (1,2,3,4,5,6)
1- Oncho 2- LF 3- STH
15 Adverse effect(Yes/No) Write “yes” if the cleint gets adverse effect or “No” if not happenned
16 If yes,For Which Drug(1,2,3,4,5,6)
1. Ivermectin
2. Albendazole
3. Prazequentale
4.Mebendazole
5. Zithromax
6. TEO (Tetracycline ointment)
17 TT (✓) screeen for Trachoma trachiasis case, and Tick (✓) if screening done
18 lymphedema (✓) Screen cases who has symptoms for leg swelling, and Tick (✓) if screening done
19 cutaneous leishmaniasis (✓) Screen cases who has symptoms for cutaneous leishmaniasis, and Tick (✓) if screening done
20 hydrocels (✓) Screen patients who has scrotal swelling, and Tick (✓) if screening done
21 Leprosy (✓) Screen the cleints who has skin rash and loss sensation, and Tick (✓) if screening done
22 Remark (✓) Write comment or remark, and Tick (✓) if screening done
INSTRUCTIONS FOR INTEGRATED PC-NTD ELIMINATION/ CONTROL PROGRAM TREATMENT REGISTER AT HEALTH POST
Location information to be completed at top of register:
Household index registerColumn Description
1 Houshold Name
2 Write sex of the client
3 Write age of the client
4 Write theHH Identification no/ Family Folder
5 Write the family size in 2014 year
6 Write the family size in 2015 year
7 Write the family size in 2016 year
8 Write the family size in 2017 year
9 Write the family size in 2018 year
4- SCH 5- Trachoma 6- scabies
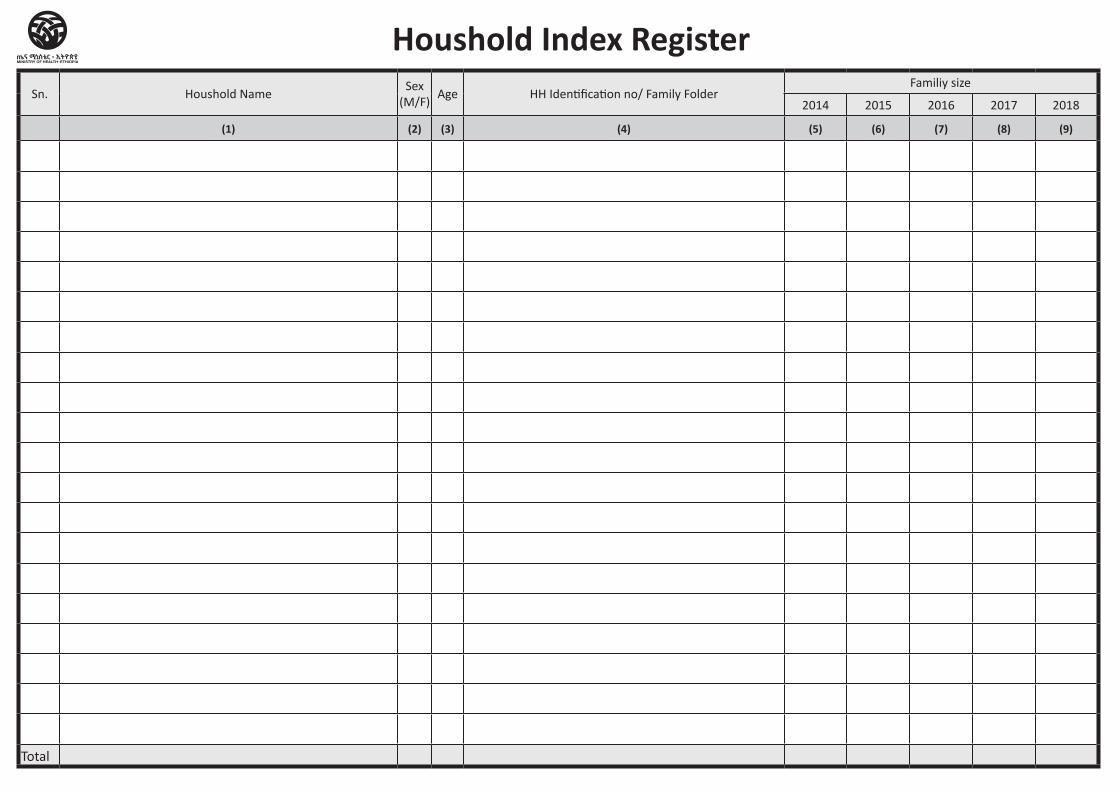
Sn. Houshold NameSex
(M/F)Age HH Identification no/ Family Folder
Familiy size
2014 2015 2016 2017 2018
(1) (2) (3) (4) (5) (6) (7) (8) (9)
Total
Houshold Index Register
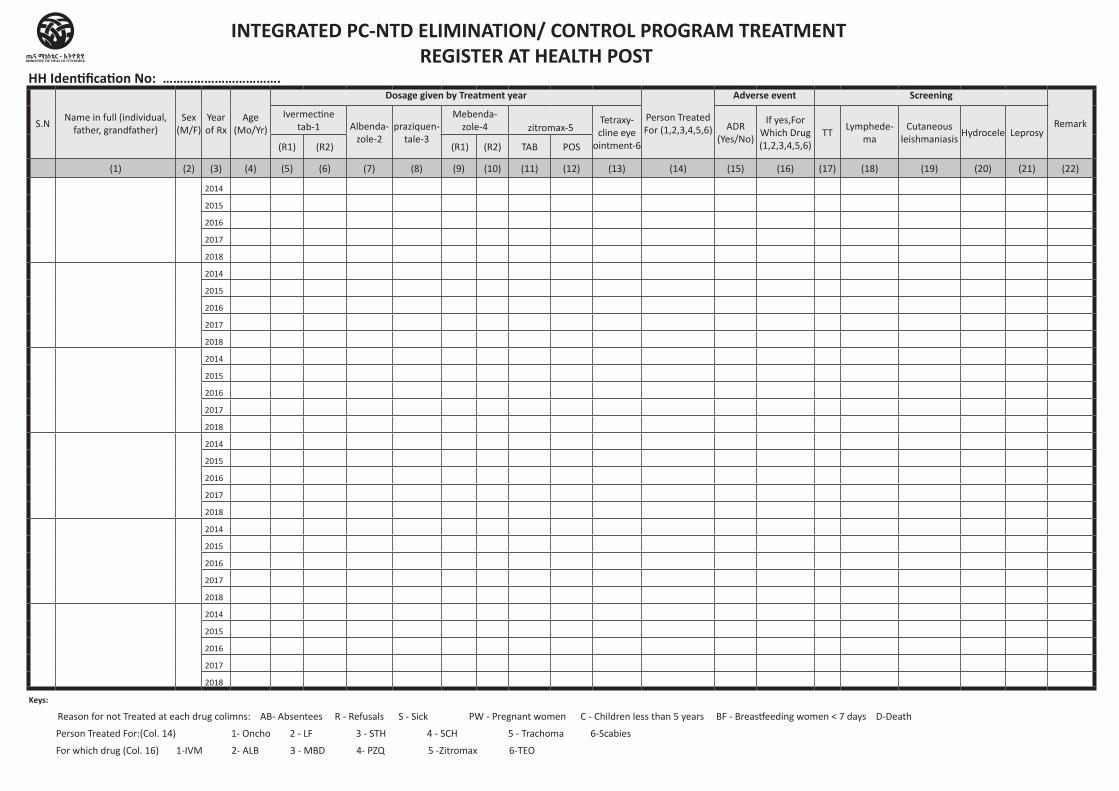
HH Identification No: …………………………….
S.NName in full (individual,
father, grandfather)Sex
(M/F)Year of Rx
Age (Mo/Yr)
Dosage given by Treatment year
Person Treated For (1,2,3,4,5,6)
Adverse event Screening
RemarkIvermectine
tab-1 Albenda-zole-2
praziquen-tale-3
Mebenda-zole-4 zitromax-5
Tetraxy-cline eye
ointment-6
ADR (Yes/No)
If yes,For Which Drug(1,2,3,4,5,6)
TTLymphede-
ma Cutaneous
leishmaniasisHydrocele Leprosy
(R1) (R2) (R1) (R2) TAB POS
(1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12) (13) (14) (15) (16) (17) (18) (19) (20) (21) (22)
2014
2015
2016
2017
2018
2014
2015
2016
2017
2018
2014
2015
2016
2017
2018
2014
2015
2016
2017
2018
2014
2015
2016
2017
2018
2014
2015
2016
2017
2018
Keys:
Reason for not Treated at each drug colimns: AB- Absentees R - Refusals S - Sick PW - Pregnant women C - Children less than 5 years BF - Breastfeeding women < 7 days D-Death
Person Treated For:(Col. 14) 1- Oncho 2 - LF 3 - STH 4 - SCH 5 - Trachoma 6-Scabies
For which drug (Col. 16) 1-IVM 2- ALB 3 - MBD 4- PZQ 5 -Zitromax 6-TEO
INTEGRATED PC-NTD ELIMINATION/ CONTROL PROGRAM TREATMENT REGISTER AT HEALTH POST

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Post Diseases Tally
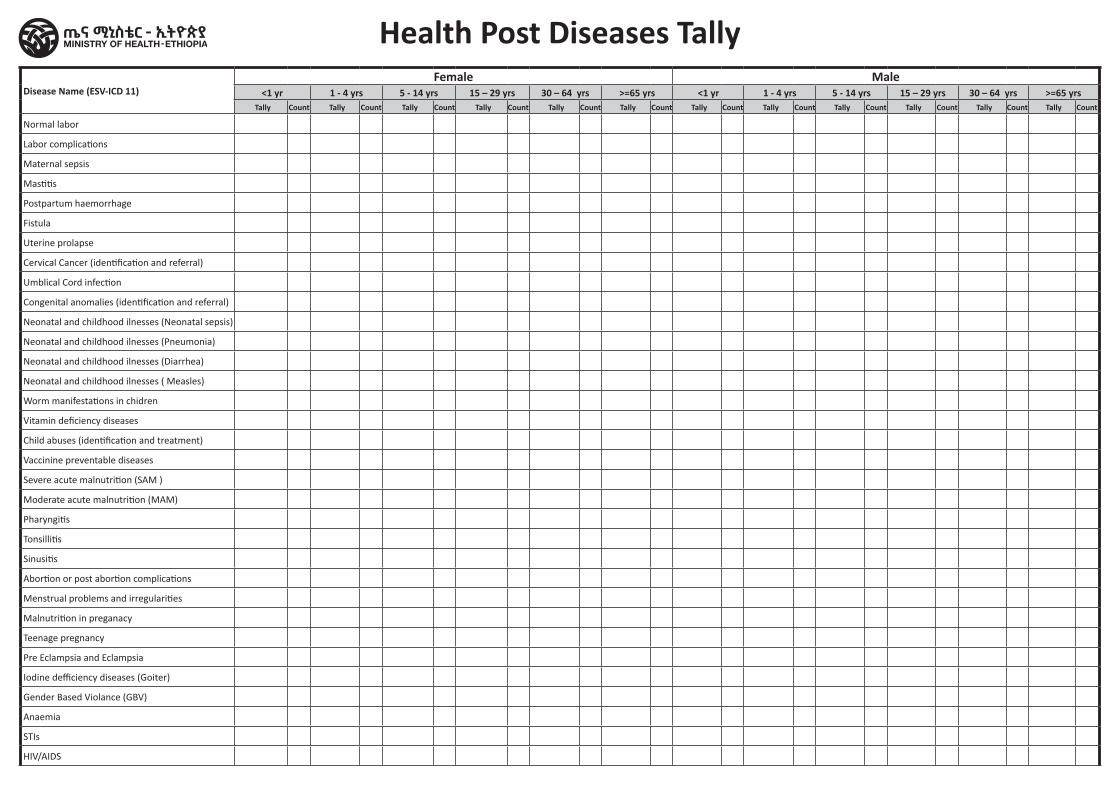
Disease Name (ESV-ICD 11)Female Male
<1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs <1 yr 1 - 4 yrs 5 - 14 yrs 15 – 29 yrs 30 – 64 yrs >=65 yrs Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count Tally Count
Normal labor
Labor complications
Maternal sepsis
Mastitis
Postpartum haemorrhage
Fistula
Uterine prolapse
Cervical Cancer (identification and referral)
Umblical Cord infection
Congenital anomalies (identification and referral)
Neonatal and childhood ilnesses (Neonatal sepsis)
Neonatal and childhood ilnesses (Pneumonia)
Neonatal and childhood ilnesses (Diarrhea)
Neonatal and childhood ilnesses ( Measles)
Worm manifestations in chidren
Vitamin deficiency diseases
Child abuses (identification and treatment)
Vaccinine preventable diseases
Severe acute malnutrition (SAM )
Moderate acute malnutrition (MAM)
Pharyngitis
Tonsillitis
Sinusitis
Abortion or post abortion complications
Menstrual problems and irregularities
Malnutrition in preganacy
Teenage pregnancy
Pre Eclampsia and Eclampsia
Iodine defficiency diseases (Goiter)
Gender Based Violance (GBV)
Anaemia
STIs
HIV/AIDS
Health Post Diseases Tally
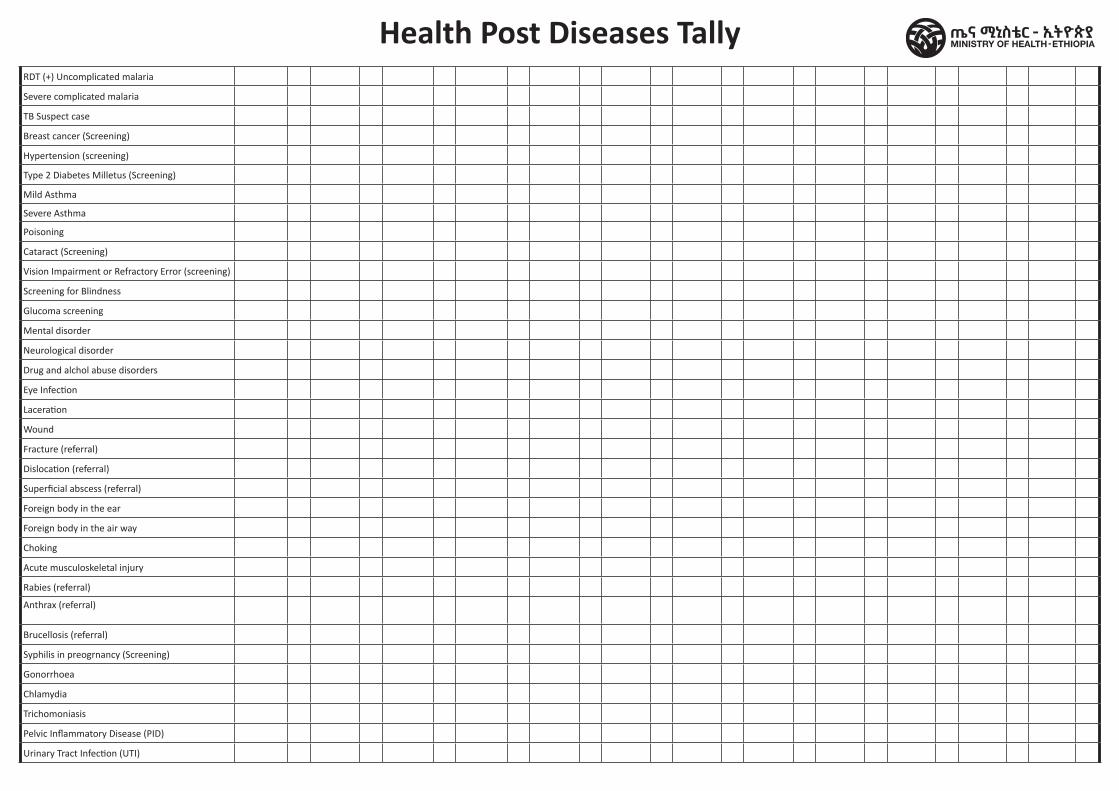
Health Post Diseases TallyRDT (+) Uncomplicated malaria
Severe complicated malaria
TB Suspect case
Breast cancer (Screening)
Hypertension (screening)
Type 2 Diabetes Milletus (Screening)
Mild Asthma
Severe Asthma
Poisoning
Cataract (Screening)
Vision Impairment or Refractory Error (screening)
Screening for Blindness
Glucoma screening
Mental disorder
Neurological disorder
Drug and alchol abuse disorders
Eye Infection
Laceration
Wound
Fracture (referral)
Dislocation (referral)
Superficial abscess (referral)
Foreign body in the ear
Foreign body in the air way
Choking
Acute musculoskeletal injury
Rabies (referral)
Anthrax (referral)
Brucellosis (referral)
Syphilis in preogrnancy (Screening)
Gonorrhoea
Chlamydia
Trichomoniasis
Pelvic Inflammatory Disease (PID)
Urinary Tract Infection (UTI)
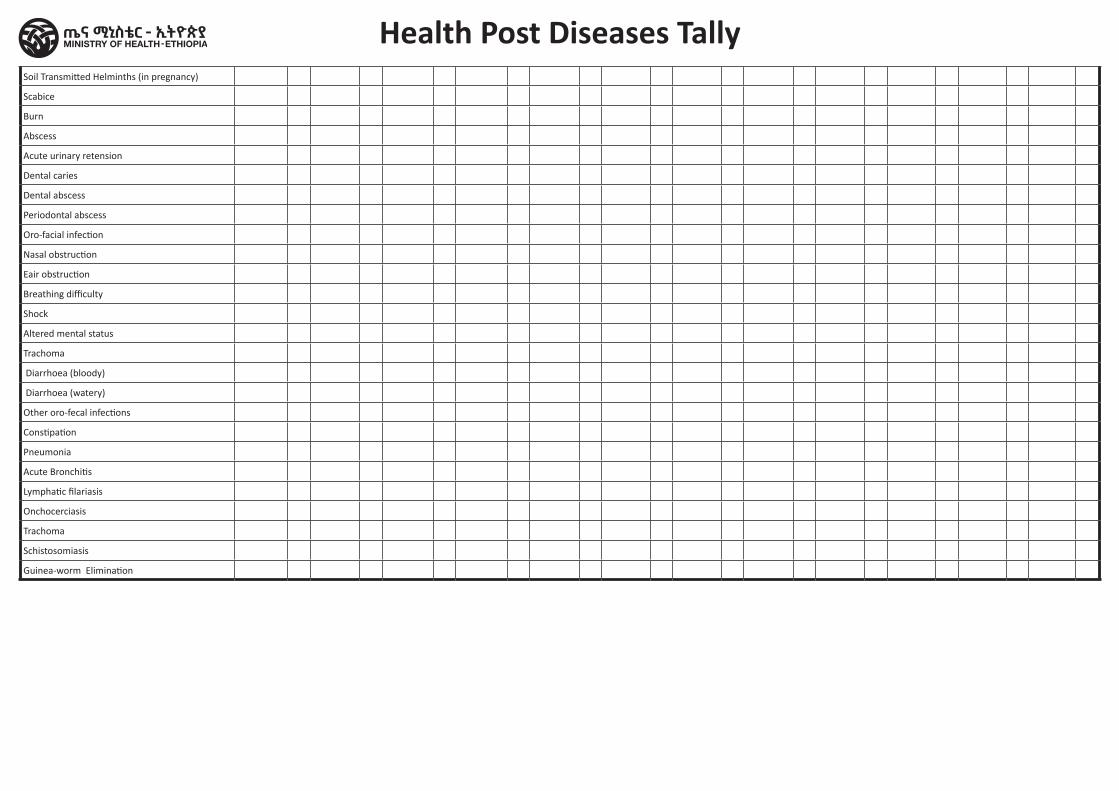
Soil Transmitted Helminths (in pregnancy)
Scabice
Burn
Abscess
Acute urinary retension
Dental caries
Dental abscess
Periodontal abscess
Oro-facial infection
Nasal obstruction
Eair obstruction
Breathing difficulty
Shock
Altered mental status
Trachoma
Diarrhoea (bloody)
Diarrhoea (watery)
Other oro-fecal infections
Constipation
Pneumonia
Acute Bronchitis
Lymphatic filariasis
Onchocerciasis
Trachoma
Schistosomiasis
Guinea-worm Elimination
Health Post Diseases Tally

Region Zone/Subcity/Woreda Health Facility Name Begin Date End Date
Health Post Service Delivery Tally
Health Post Monthly Service Delivery Tally
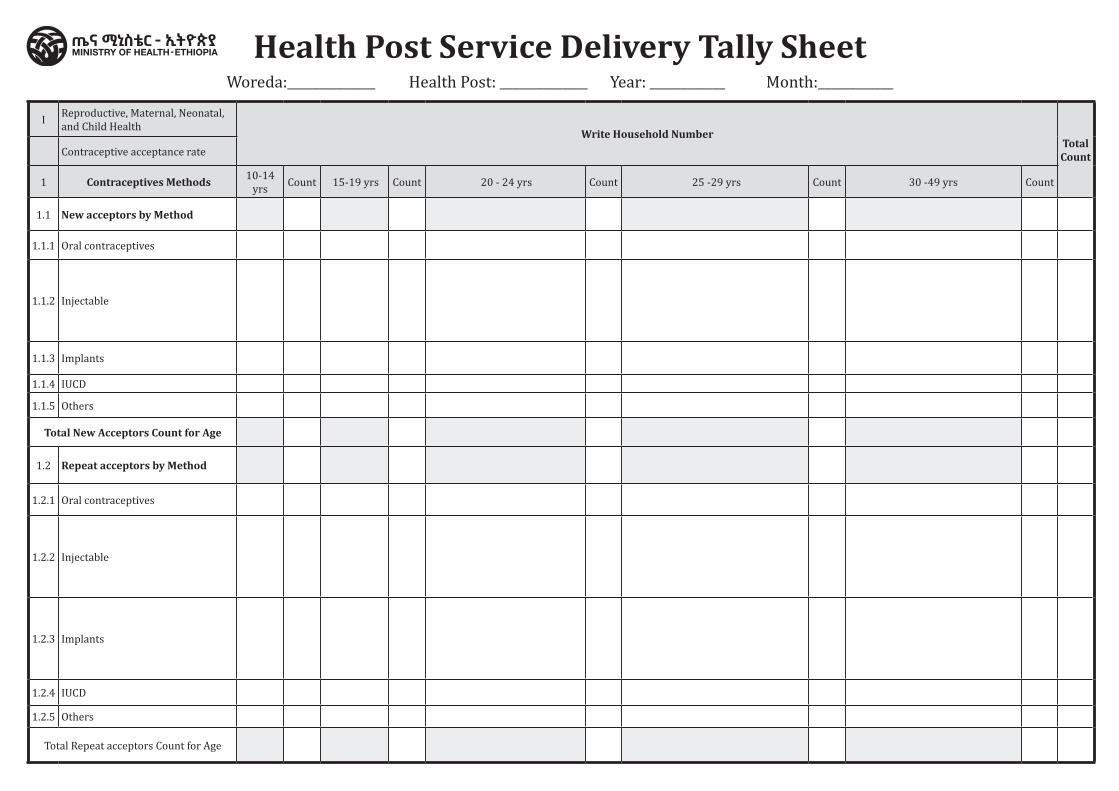
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
I Reproductive, Maternal, Neonatal, and Child Health
Write Household NumberTotal CountContraceptive acceptance rate
1 Contraceptives Methods 10-14 yrs Count 15-19 yrs Count 20 - 24 yrs Count 25 -29 yrs Count 30 -49 yrs Count
1.1 New acceptors by Method
1.1.1 Oral contraceptives
1.1.2 Injectable
1.1.3 Implants
1.1.4 IUCD
1.1.5 Others
Total New Acceptors Count for Age
1.2 Repeat acceptors by Method
1.2.1 Oral contraceptives
1.2.2 Injectable
1.2.3 Implants
1.2.4 IUCD
1.2.5 Others
Total Repeat acceptors Count for Age
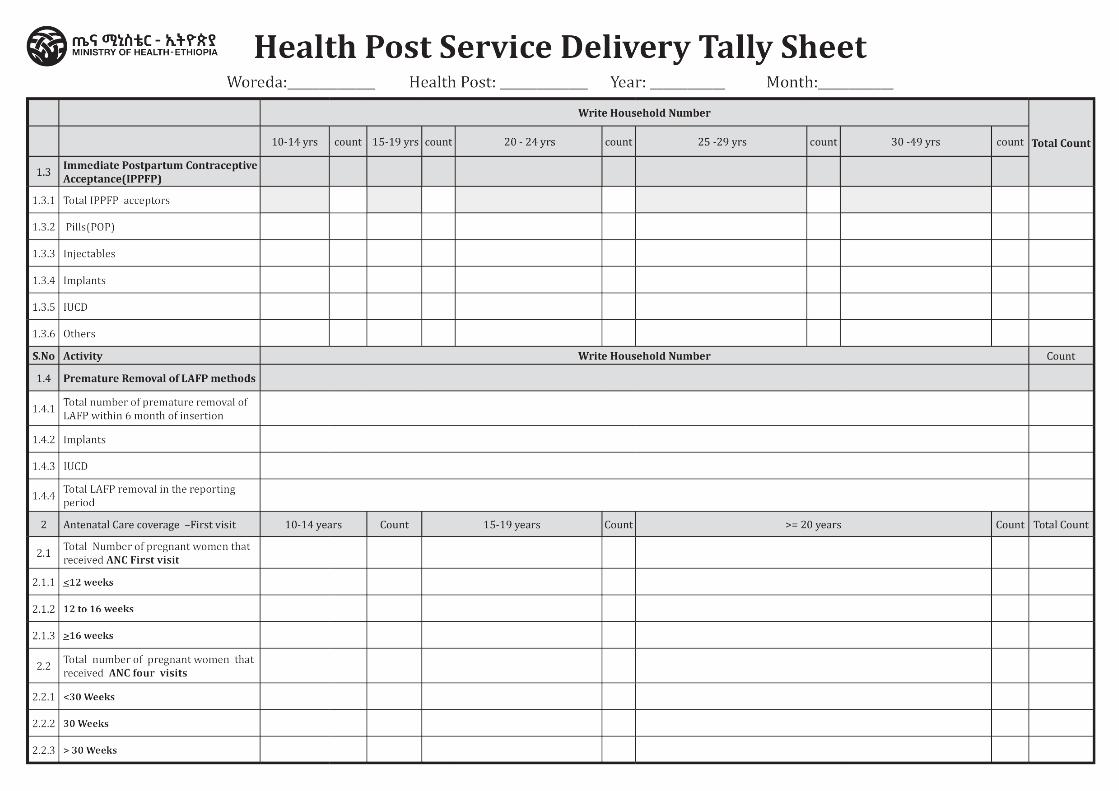
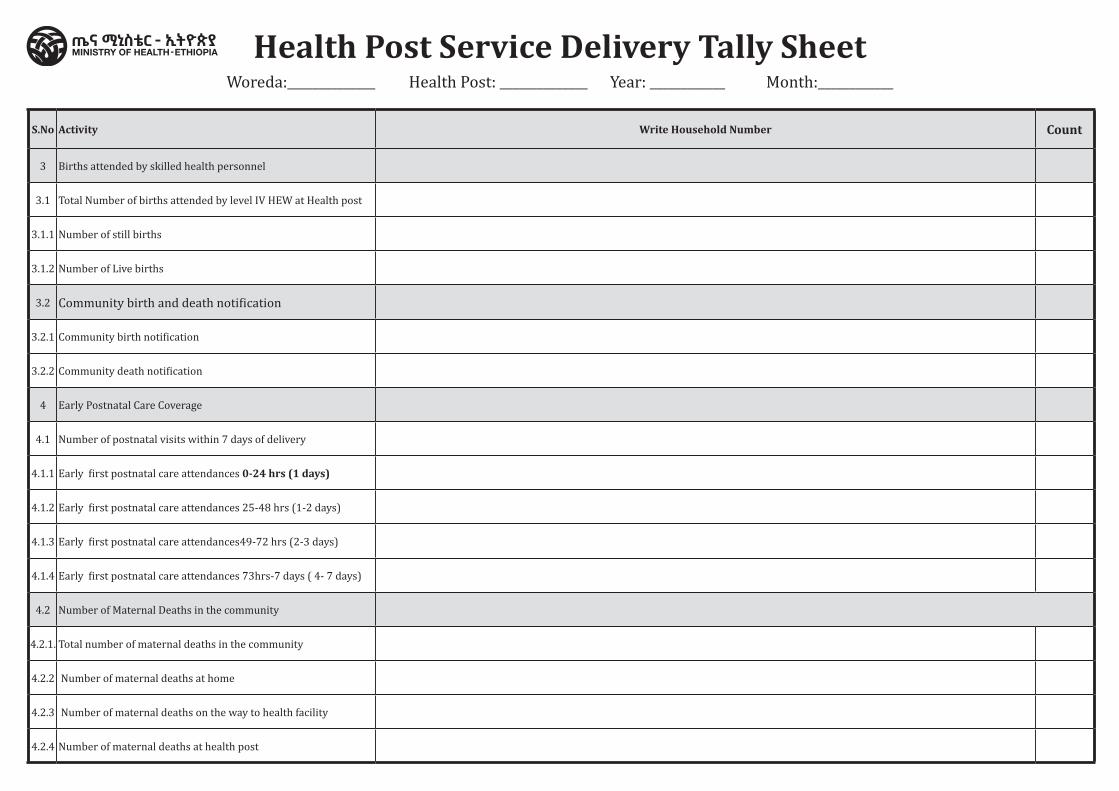
S.No Activity Write Household Number Count
3 Births attended by skilled health personnel
3.1 Total Number of births attended by level IV HEW at Health post
3.1.1 Number of still births
3.1.2 Number of Live births
3.2 Community birth and death notification
3.2.1 Community birth notification
3.2.2 Community death notification
4 Early Postnatal Care Coverage
4.1 Number of postnatal visits within 7 days of delivery
4.1.1 Early first postnatal care attendances 0-24 hrs (1 days)
4.1.2 Early first postnatal care attendances 25-48 hrs (1-2 days)
4.1.3 Early first postnatal care attendances49-72 hrs (2-3 days)
4.1.4 Early first postnatal care attendances 73hrs-7 days ( 4- 7 days)
4.2 Number of Maternal Deaths in the community
4.2.1. Total number of maternal deaths in the community
4.2.2 Number of maternal deaths at home
4.2.3 Number of maternal deaths on the way to health facility
4.2.4 Number of maternal deaths at health post
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
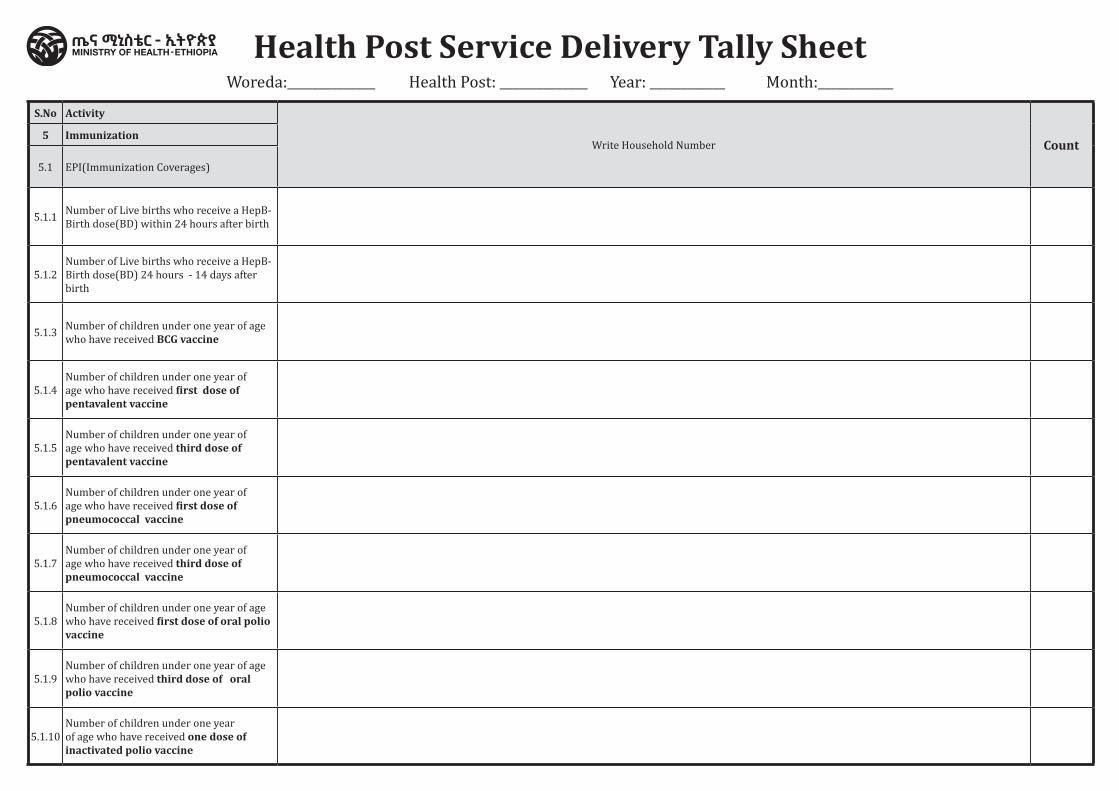
S.No Activity
Write Household Number Count5 Immunization
5.1 EPI(Immunization Coverages)
5.1.1 Number of Live births who receive a HepB-Birth dose(BD) within 24 hours after birth
5.1.2Number of Live births who receive a HepB-Birth dose(BD) 24 hours - 14 days after birth
5.1.3 Number of children under one year of age who have received BCG vaccine
5.1.4Number of children under one year of age who have received first dose of pentavalent vaccine
5.1.5Number of children under one year of age who have received third dose of pentavalent vaccine
5.1.6Number of children under one year of age who have received first dose of pneumococcal vaccine
5.1.7Number of children under one year of age who have received third dose of pneumococcal vaccine
5.1.8Number of children under one year of age who have received first dose of oral polio vaccine
5.1.9Number of children under one year of age who have received third dose of oral polio vaccine
5.1.10Number of children under one year of age who have received one dose of inactivated polio vaccine
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
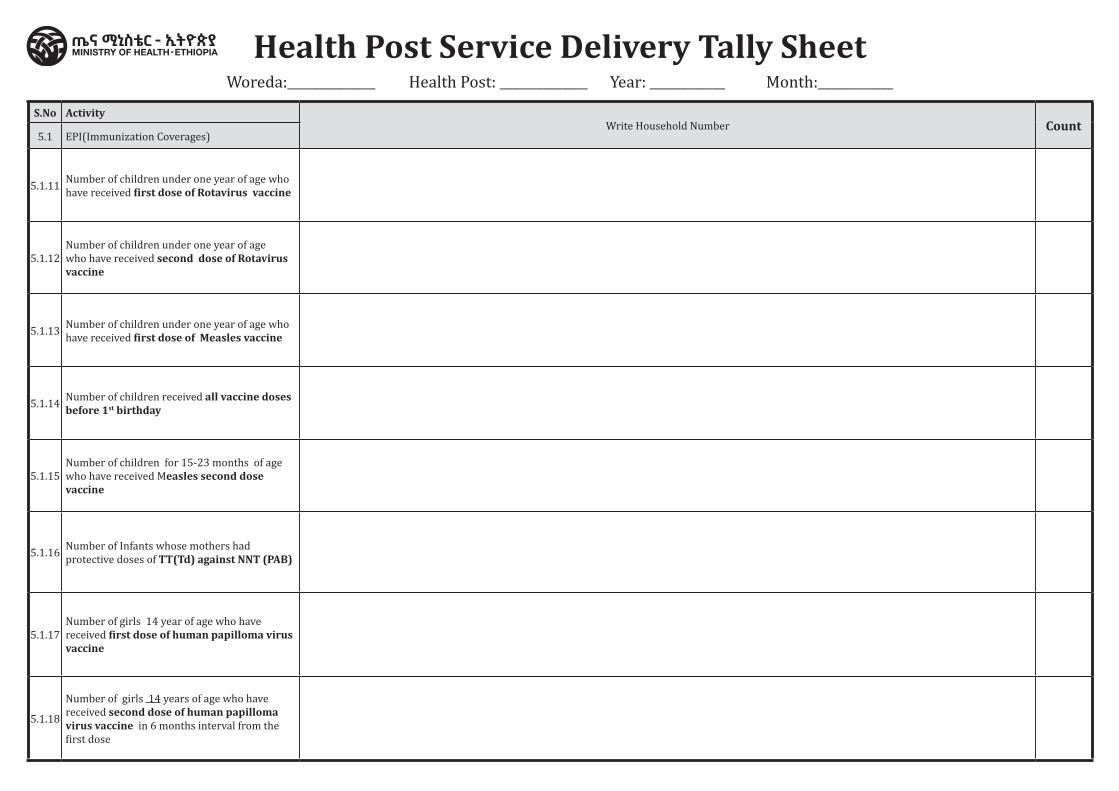
S.No ActivityWrite Household Number Count
5.1 EPI(Immunization Coverages)
5.1.11 Number of children under one year of age who have received first dose of Rotavirus vaccine
5.1.12Number of children under one year of age who have received second dose of Rotavirus vaccine
5.1.13 Number of children under one year of age who have received first dose of Measles vaccine
5.1.14 Number of children received all vaccine doses before 1st birthday
5.1.15Number of children for 15-23 months of age who have received Measles second dose vaccine
5.1.16 Number of Infants whose mothers had protective doses of TT(Td) against NNT (PAB)
5.1.17Number of girls 14 year of age who have received first dose of human papilloma virus vaccine
5.1.18Number of girls 14 years of age who have received second dose of human papilloma virus vaccine in 6 months interval from the first dose
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
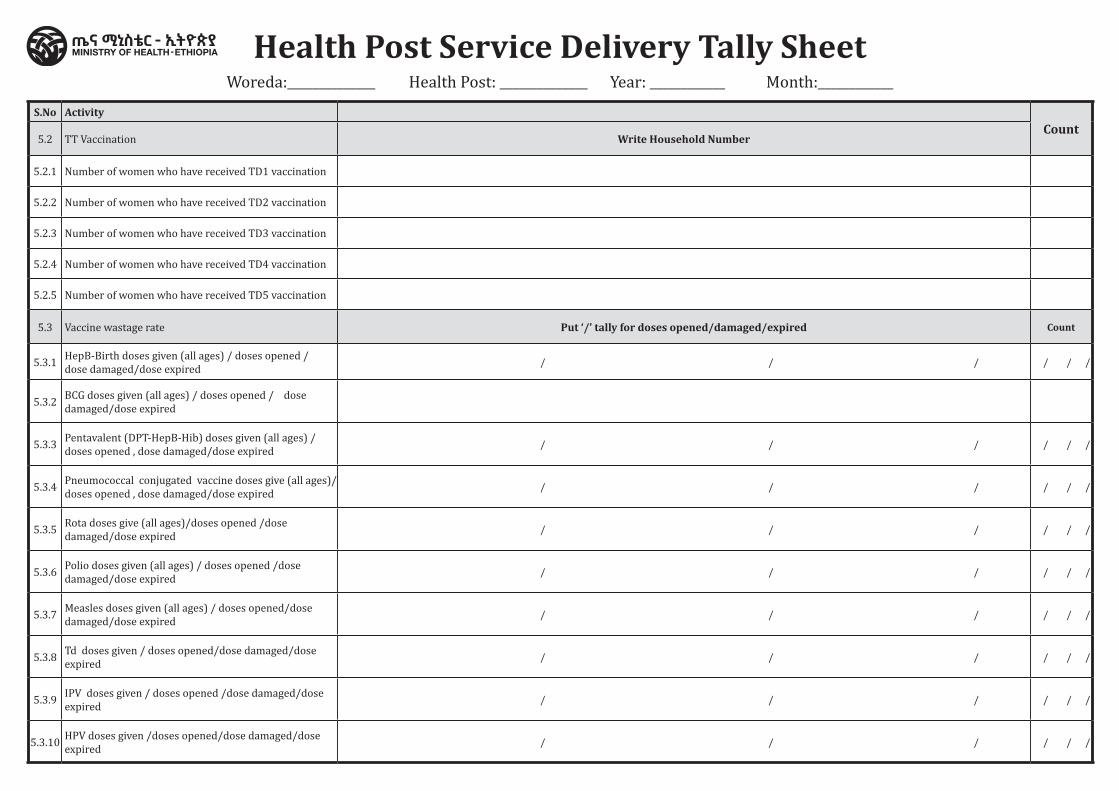
S.No ActivityCount
5.2 TT Vaccination Write Household Number
5.2.1 Number of women who have received TD1 vaccination
5.2.2 Number of women who have received TD2 vaccination
5.2.3 Number of women who have received TD3 vaccination
5.2.4 Number of women who have received TD4 vaccination
5.2.5 Number of women who have received TD5 vaccination
5.3 Vaccine wastage rate Put ‘/’ tally for doses opened/damaged/expired Count
5.3.1 HepB-Birth doses given (all ages) / doses opened / dose damaged/dose expired / / / / / /
5.3.2 BCG doses given (all ages) / doses opened / dose damaged/dose expired
5.3.3 Pentavalent (DPT-HepB-Hib) doses given (all ages) / doses opened , dose damaged/dose expired / / / / / /
5.3.4 Pneumococcal conjugated vaccine doses give (all ages)/doses opened , dose damaged/dose expired / / / / / /
5.3.5 Rota doses give (all ages)/doses opened /dose damaged/dose expired / / / / / /
5.3.6 Polio doses given (all ages) / doses opened /dose damaged/dose expired / / / / / /
5.3.7 Measles doses given (all ages) / doses opened/dose damaged/dose expired / / / / / /
5.3.8 Td doses given / doses opened/dose damaged/dose expired / / / / / /
5.3.9 IPV doses given / doses opened /dose damaged/dose expired / / / / / /
5.3.10 HPV doses given /doses opened/dose damaged/dose expired / / / / / /
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
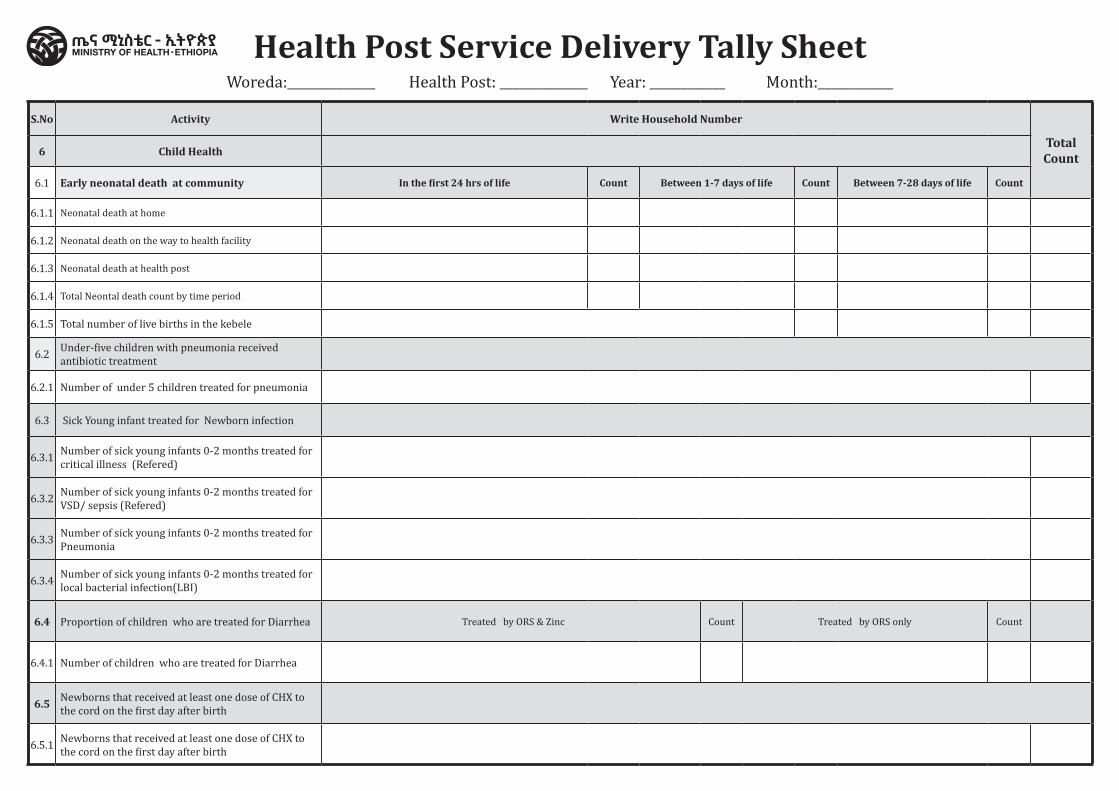
S.No Activity Write Household Number
Total Count6 Child Health
6.1 Early neonatal death at community In the first 24 hrs of life Count Between 1-7 days of life Count Between 7-28 days of life Count
6.1.1 Neonatal death at home
6.1.2 Neonatal death on the way to health facility
6.1.3 Neonatal death at health post
6.1.4 Total Neontal death count by time period
6.1.5 Total number of live births in the kebele
6.2 Under-five children with pneumonia received antibiotic treatment
6.2.1 Number of under 5 children treated for pneumonia
6.3 Sick Young infant treated for Newborn infection
6.3.1 Number of sick young infants 0-2 months treated for critical illness (Refered)
6.3.2 Number of sick young infants 0-2 months treated for VSD/ sepsis (Refered)
6.3.3 Number of sick young infants 0-2 months treated for Pneumonia
6.3.4 Number of sick young infants 0-2 months treated for local bacterial infection(LBI)
6.4 Proportion of children who are treated for Diarrhea Treated by ORS & Zinc Count Treated by ORS only Count
6.4.1 Number of children who are treated for Diarrhea
6.5 Newborns that received at least one dose of CHX to the cord on the first day after birth
6.5.1 Newborns that received at least one dose of CHX to the cord on the first day after birth
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
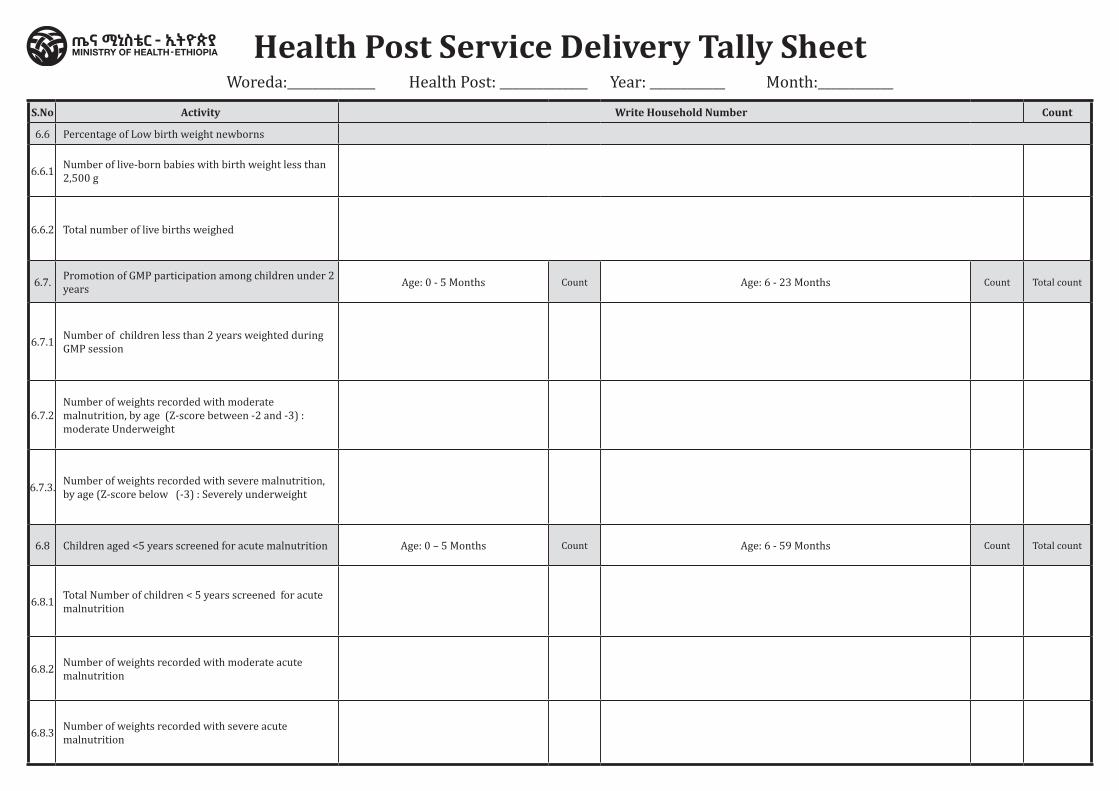
S.No Activity Write Household Number Count
6.6 Percentage of Low birth weight newborns
6.6.1 Number of live-born babies with birth weight less than 2,500 g
6.6.2 Total number of live births weighed
6.7. Promotion of GMP participation among children under 2 years Age: 0 - 5 Months Count Age: 6 - 23 Months Count Total count
6.7.1 Number of children less than 2 years weighted during GMP session
6.7.2Number of weights recorded with moderate malnutrition, by age (Z-score between -2 and -3) : moderate Underweight
6.7.3. Number of weights recorded with severe malnutrition, by age (Z-score below (-3) : Severely underweight
6.8 Children aged <5 years screened for acute malnutrition Age: 0 – 5 Months Count Age: 6 - 59 Months Count Total count
6.8.1 Total Number of children < 5 years screened for acute malnutrition
6.8.2 Number of weights recorded with moderate acute malnutrition
6.8.3 Number of weights recorded with severe acute malnutrition
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
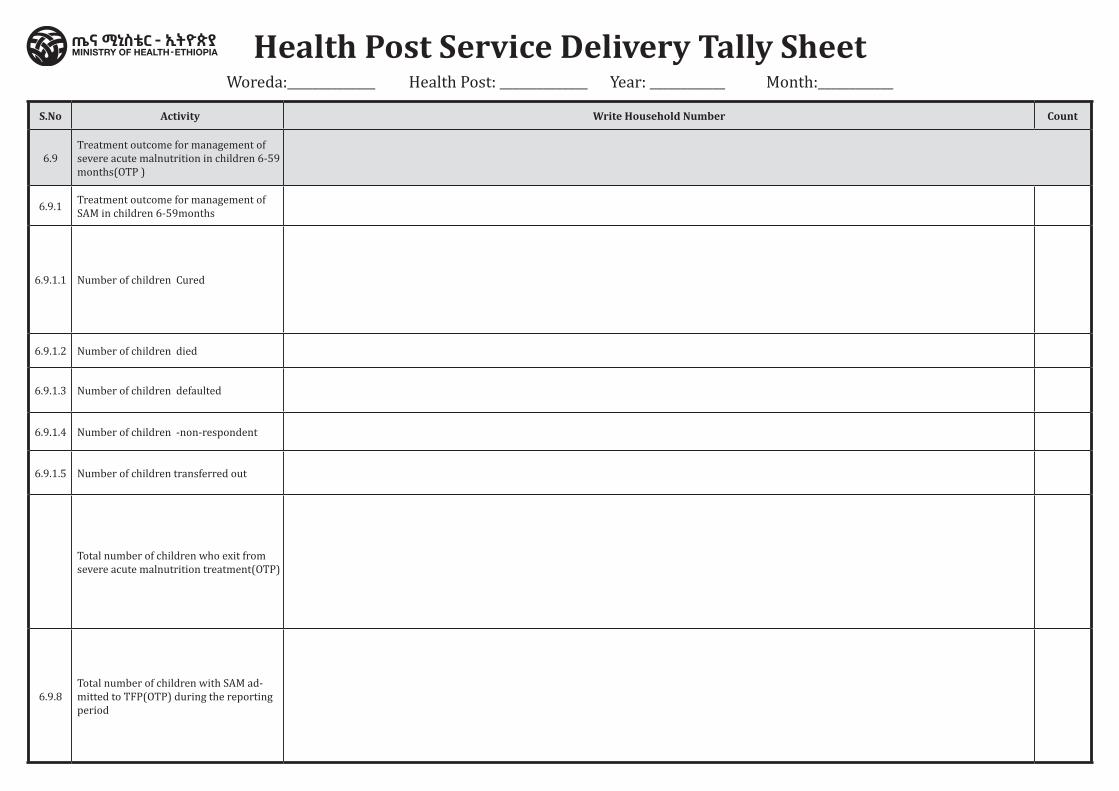
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
S.No Activity Write Household Number Count
6.9Treatment outcome for management of severe acute malnutrition in children 6-59 months(OTP )
6.9.1 Treatment outcome for management of SAM in children 6-59months
6.9.1.1 Number of children Cured
6.9.1.2 Number of children died
6.9.1.3 Number of children defaulted
6.9.1.4 Number of children -non-respondent
6.9.1.5 Number of children transferred out
Total number of children who exit from severe acute malnutrition treatment(OTP)
6.9.8Total number of children with SAM ad-mitted to TFP(OTP) during the reporting period
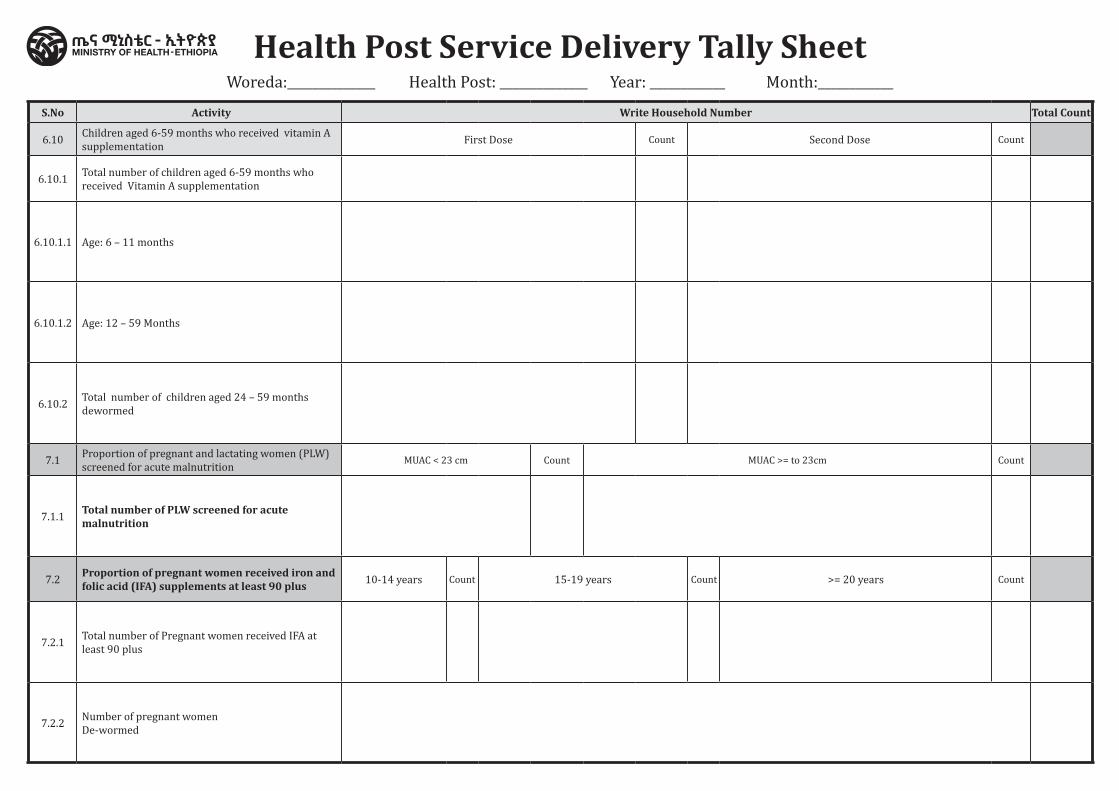
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
S.No Activity Write Household Number Total Count
6.10 Children aged 6-59 months who received vitamin A supplementation First Dose Count Second Dose Count
6.10.1 Total number of children aged 6-59 months who received Vitamin A supplementation
6.10.1.1 Age: 6 – 11 months
6.10.1.2 Age: 12 – 59 Months
6.10.2 Total number of children aged 24 – 59 months dewormed
7.1 Proportion of pregnant and lactating women (PLW) screened for acute malnutrition MUAC < 23 cm Count MUAC >= to 23cm Count
7.1.1 Total number of PLW screened for acute malnutrition
7.2 Proportion of pregnant women received iron and folic acid (IFA) supplements at least 90 plus 10-14 years Count 15-19 years Count >= 20 years Count
7.2.1 Total number of Pregnant women received IFA at least 90 plus
7.2.2 Number of pregnant women De-wormed
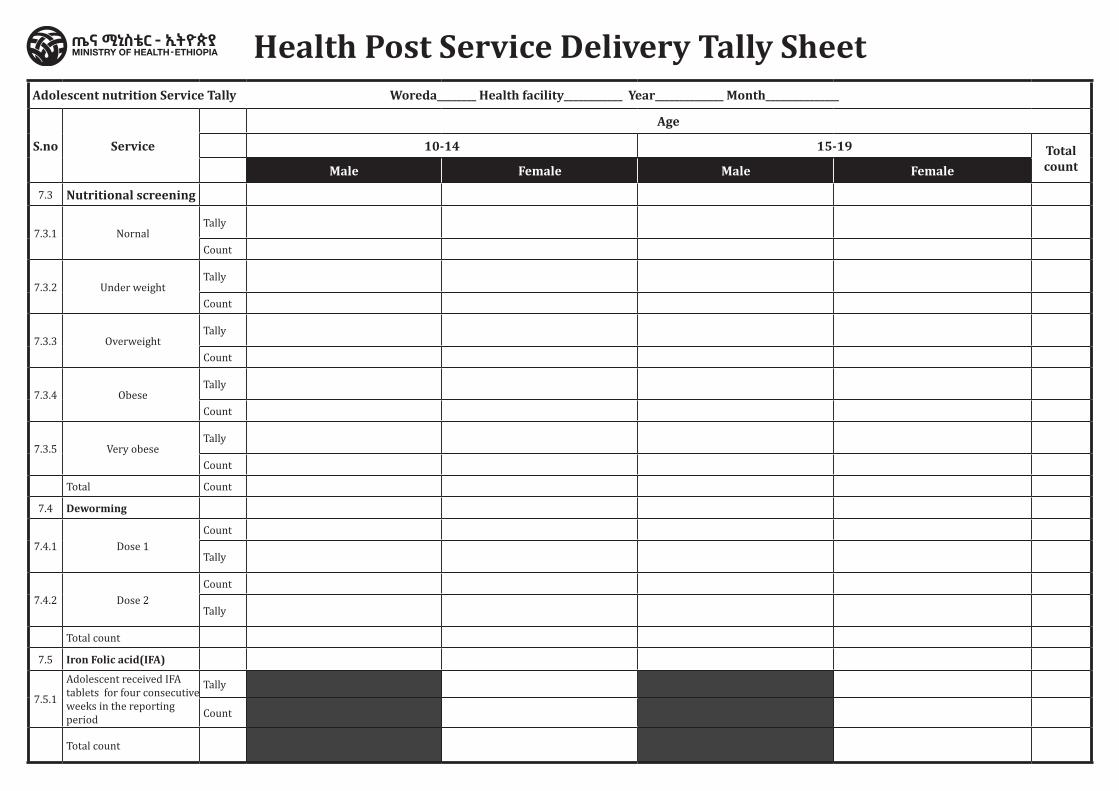
Adolescent nutrition Service Tally Woreda________ Health facility____________ Year______________ Month_______________
S.no Service
Age
10-14 15-19 Total countMale Female Male Female
7.3 Nutritional screening
7.3.1 NornalTally
Count
7.3.2 Under weightTally
Count
7.3.3 OverweightTally
Count
7.3.4 ObeseTally
Count
7.3.5 Very obeseTally
Count
Total Count
7.4 Deworming
7.4.1 Dose 1Count
Tally
7.4.2 Dose 2Count
Tally
Total count
7.5 Iron Folic acid(IFA)
7.5.1
Adolescent received IFA tablets for four consecutive weeks in the reporting period
Tally
Count
Total count
Health Post Service Delivery Tally Sheet
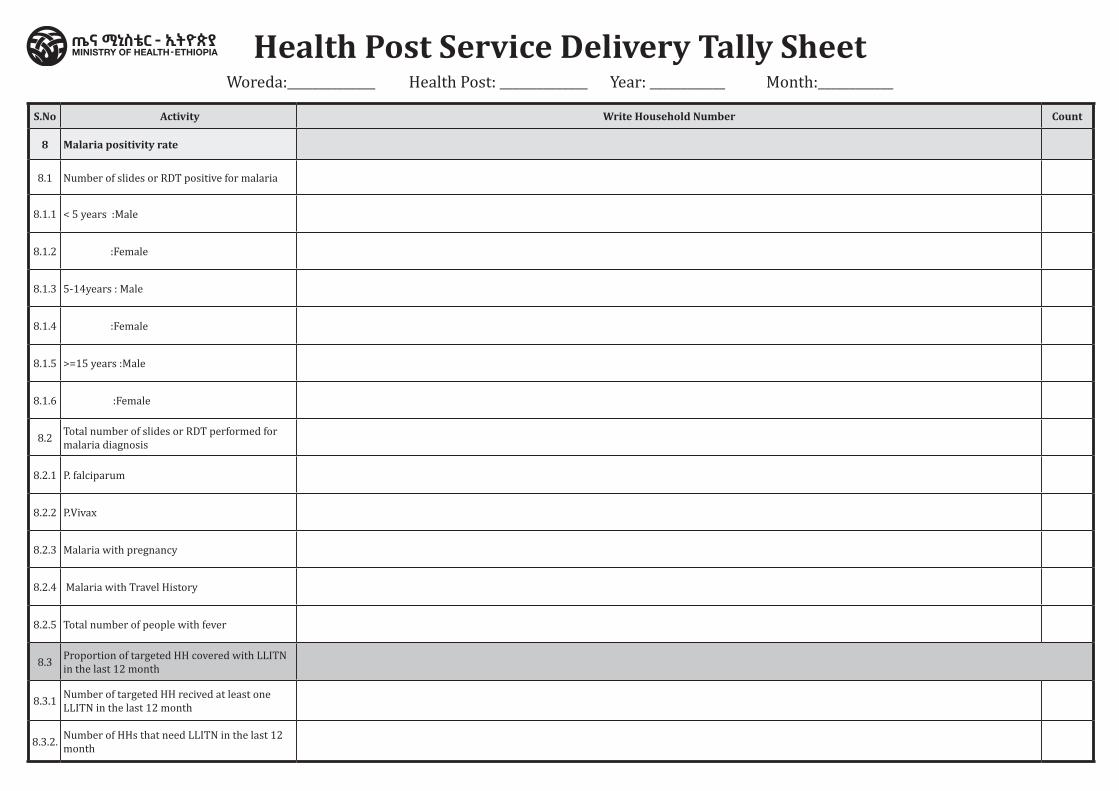
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
S.No Activity Write Household Number Count
8 Malaria positivity rate
8.1 Number of slides or RDT positive for malaria
8.1.1 < 5 years :Male
8.1.2 :Female
8.1.3 5-14years : Male
8.1.4 :Female
8.1.5 >=15 years :Male
8.1.6 :Female
8.2 Total number of slides or RDT performed for malaria diagnosis
8.2.1 P. falciparum
8.2.2 P.Vivax
8.2.3 Malaria with pregnancy
8.2.4 Malaria with Travel History
8.2.5 Total number of people with fever
8.3 Proportion of targeted HH covered with LLITN in the last 12 month
8.3.1 Number of targeted HH recived at least one LLITN in the last 12 month
8.3.2. Number of HHs that need LLITN in the last 12 month
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
S.No Activity Write Household Number Count
9 Outpatient attendance per capita
Male Count Female Count
9.1 Number of outpatient visits
9.1.1 OPD Visits < 5:
9.1.2 OPD visits 5-9:
9.1.3 OPD visits 11-19
9.1.4 OPD visits 20-29
9.1.5 OPD visits 30-45
9.1.6 OPD visits 46-65
9.1.7 OPD visits >=66
Health Post Service Delivery Tally SheetWoreda:______________ Health Post: ______________ Year: ____________ Month:____________
S.No Activity
Days of the reporting month(Write 1 if the drug is available for the day,if not write 0)
Write 1 if drug
available for 30 days / whenever needed ;if
not write 0
10 Essential drug availability
Months21 22 23 24 25 26 27 28 29 30 1 2 3 4 5 6 7 8 9 10 10 11 13 14 15 16 17 18 19 20
10.1 Amoxicillin dispersable tablet
10.2 Oral Rehydration Salts
10.3 Zinc dispersible tablet
10.4 Gentamycin Sulphate injection
10.5 Medroxyprogesterone Injection
10.6 Arthmeter + Lumfanthrine (Coartem) tablet (any packing)
10.7 Ferrous sulphate + folic acid
10.8 Albendazole tablet/suspension
11 Evidence Based Decision Making
11.1 Data quality assurance (LQAS) Score
11.2 Integrated Supportive supervision
11.3 Number of supervisory visits with written feedback received
11.4 Number supervisory visits expected in the reporting period

HSTP II HMIS TOOLSHOSPITAL, HEATH CENTER AND HEALTH POST
Content / Home